

About This Board Review Set
This is Part 255 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 255
This module focuses heavily on: Ankle, Arthroplasty, Dislocation, Fracture, Knee, Nerve, Revision, Shoulder.
Sample Questions from This Set
Sample Question 1: Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy? Review Topic...
Sample Question 2: Ayearoldwomanundergoesrevisiontotalkneearthroplastyfortibialcomponentasepticloosening.Sheisconcernedaboutrecurrentloosening,andtibialstemfixationoptionsduringrevisionarereviewed. Figurebelowdisplaysaradiographoftherevisiontechniqueusedforth...
Sample Question 3: A 60-year-old right hand-dominant women fell on her outstretched arm and sustained an anterior shoulder dislocation. The shoulder is reduced in the emergency department and she is seen for follow-up 1 week later wearing a sling. Examination...
Sample Question 4: Figures A through C are the radiograph and CT scans of a 42-year-old man who sustained an injury to both of his ankles and underwent surgical repair 2 weeks prior to presentation to your office. One ankle is healing well. On thecontralatera...
Sample Question 5: Figures 5a and 5b show the radiographs of a 21 -year-old wrestler who reports that his leg was rolled over while wrestling. The patient has decreased sensation and function in the distribution of the peroneal nerve, and he has absent pulses...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy? Review Topic
Explanation
Question 2
A year old woman undergoes revision total knee arthroplasty for tibial component aseptic loosening. She is concerned about recurrent loosening, and tibial stem fixation options during revision are reviewed. Figure below displays a radiograph of the revision technique used for this patient. What is the incidence of intraoperative tibial shaft fracture that is associated with this type of revision surgery?
Explanation
Using press-fit tibial stems during a hybrid revision total knee arthroplasty is associated with a 3% to 5% incidence of intraoperative tibial shaft fracture. Diaphyseal fixation of press-fit stems has the advantage of setting component alignment, dispersing forces on the proximal tibia, and offers excellent clinical results. The disadvantages include proximal and distal tibia anatomic mismatch and tibial shaft fracture. Cipriano and associates reported a tibial shaft fracture incidence of 4.9% in a series of 420 consecutive
knee revisions. All fractures healed with nonsurgical management, and none led to implant loosening. In this patient, it is important to recognize on the radiograph that this technique is a hybrid method of revision total knee arthroplasty, with cementation along the tibial tray and metaphysis and with press-fit fixation of the diaphyseal engaging stem. Then, it is important to know the risk and management of intraoperative diaphyseal tibial fractures. Cemented tibial stems are associated with a low rate of intraoperative fracture, because the implant is typically undersized to allow for an appropriate cement mantle. Option C is incorrect, because this revision is not cemented. Option A underestimates the incidence of fracture,
whereas D overestimates the rate of fracture.
Question 3
A 60-year-old right hand-dominant women fell on her outstretched arm and sustained an anterior shoulder dislocation. The shoulder is reduced in the emergency department and she is seen for follow-up 1 week later wearing a sling. Examination reveals that she has significant difficulty raising her arm in forward elevation and has excessive external rotation compared to the contralateral shoulder. What is the next most appropriate step in management? Review Topic
Explanation
in management should be MRI. If the findings are negative, suspicion of nerve injury should lead to electromyography.
Question 4
Figures A through C are the radiograph and CT scans of a 42-year-old man who sustained an injury to both of his ankles and underwent surgical repair 2 weeks prior to presentation to your office. One ankle is healing well. On the contralateral side, he reports pain and restricted ankle range of motion. Management should consist of

Explanation
Question 5
Figures 5a and 5b show the radiographs of a 21 -year-old wrestler who reports that his leg was rolled over while wrestling. The patient has decreased sensation and function in the distribution of the peroneal nerve, and he has absent pulses. What is the most appropriate initial management at this time?
Explanation
intervention of the artery, but documentation with studies would be appropriate. Delayed reconstruction of injured structures is appropriate.
REFERENCES: Fanelli GC, Orcutt DR, Edson CJ: The multiple- ligament injured knee: Evaluation, treatment, and results. Arthroscopy 2005;21:471 -486.
McDonough EB Jr, Wojtys EM: Multiligamentous injuries of the knee and associated vascular injuries.
Am J Sports Med 2009;37:156-159.
Wascher DC: High-velocity knee dislocation with vascular injury: Treatment principles. Clin Sports Med 2000;19:457-477.
Question 6
The main advantage of surgical repair of an acute Achilles tendon rupture, when compared with nonsurgical management, is reduced
Explanation
REFERENCES: Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036.
Cetti R, Christensen SE, Ejsted R, Jensen NM, Jorgensen U: Operative versus nonoperative treatment of Achilles tendon rupture: A prospective randomized study and review of the literature. Am J Sports Med 1993;21:791-799.
Nistor L: Surgical and non-surgical treatment of Achilles tendon rupture. J Bone Joint Surg Am 1981;63:394-399.
Question 7
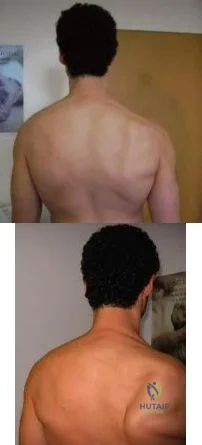
A 49-year-old male presents with right shoulder pain and weakness after undergoing open cervical lymph node biopsy approximately one year ago. A pertinent finding from the physical exam is seen in Figure A, with the patients arms by his side. Physical exam finding with the arms in a position of 90 degrees of forward elevation and 10 degrees of external rotation are shown in Figure B. What nerve is most likely injured? Review Topic
Explanation
The spinal accessory nerve is fundamental to scapulothoracic function and essential for scapulohumeral rhythm. This nerve is vulnerable along its superficial course. The majority of injuries to the spinal accessory nerve are iatrogenic and occur secondary to head and neck surgery. There is often a marked delay in recognition and initiating treatment. Surgical treatment with the Eden-Lange transfer lateralizes the levator scapulae and rhomboids (transfer from medial border to lateral border)
Camp et al. reviewed the results of 111 patients who underwent operative management of a lesion to the spinal accessory nerve. They found that the majority (~80%) of injuries were sustained iatrogenically and that diagnosis was delayed for approximately 12 months.
Pikkarainen et al. reviewed the natural history of isolated serratus palsy. They found that symptoms mostly recover in 2 years, but at least one-fourth of the patients will have long-lasting symptoms, especially pain.
Figure A depicts a patient with lateral scapular winging. Figure B demonstrates physical exam of this patient with their arms in a position of 90 degrees of forward elevation and 10 degrees of external rotation. Illustration A highlights the difference between medial and lateral scapular winging. Illustration B depicts another example of a patient with lateral scapular winging.
Incorrect Answers:
An injury to the long thoracic nerve would result in serratus anterior palsy which would lead to MEDIAL scapular winging.
An injury to the suprascapular nerve would result in weakness and wasting of the supraspinatus and/or infraspinatus.
An injury to the axillary nerve would result in deltoid muscle weakness.
An injury to the thoracodorsal nerve would result in latissimus dorsi weakness and would not cause scapular winging
Question 8
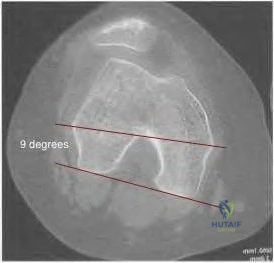
98 degrees (range, 0 degrees to 9 degrees). In knees with varus joint lines
Explanation
Question 9
A 65-year-old woman with rheumatoid arthritis is unable to actively extend her index, middle, ring, and little fingers secondary to tendon rupture. In performing a flexor digitorum sublimis (FDS) of the middle/ring finger to extensor digitorum communis (EDC) transfer to restore active metacarpophalangeal (MCP) joint extension, the FDS should be passed
Explanation
Question 10
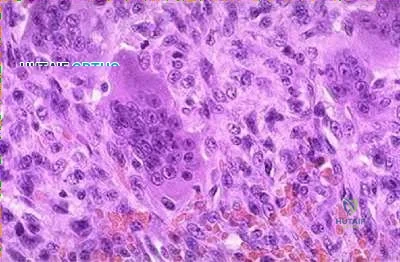
Metastatic disease of several cancers create lytic lesions because these cancers:
Explanation
Cancers that originate or metastasize to bone can be blastic, lytic, or mixed when viewed on radiographs. Lytic lesions appear radiolucent due to bone resorption that occurs around the cancer cells. This is secondary to direct production and release of RANKL by the cancer cells themselves. RANKL then stimulates osteoclastogenesis and an increase in local bone resorption. Denosumab is a monoclonal antibody against RANKL that has been shown to decrease rates of pathologic fractures.
Lynch et al. review the progression of metastatic disease. They note that cancer cells can stimulate both osteogenesis and osteolysis, and that this pathologic increase in bone matrix turnover is what allows the cancer to progressively expand or metastasize to distant sites. They discuss the role of matrix metalloproteinases as primary regulators of this process.
Illustration A is a diagram illustrating how the binding of RANKL to receptors on the surface of osteoclast precursors activates them and begins the process of bone resorption. Cancer cells can directly produce RANKL thus increasing the rate of local bone resorption.
Incorrect Answers:
Question 11
A 10-year-old boy has had a prominent scapula for the past year. He reports crepitus and aching over the area, but only when he is active. A radiograph and CT scans are shown in Figures 37a through 37c. What is the most likely diagnosis?
Explanation
REFERENCE: Schmade GA, Conrad EV III, Raskind WH: The natural history of hereditary multiple exostoses. J Bone Joint Surg Am 1994;76:986-992.
Question 12
A 32-year-old volleyball player has dull posterior shoulder pain. An examination reveals moderate external rotation weakness with his arm at his side but normal strength on supraspinatus isolation. Deltoid and supraspinatus bulk appear normal, although there appears to be mild infraspinatus atrophy. Sensation is normal throughout the shoulder and shoulder girdle. What is the most likely diagnosis?
Explanation
Question 13
Giant cell tumors of bone can occur in many different areas throughout the body. All of the following are common locations for giant cell tumors of bone EXCEPT?
Explanation
Giant cell tumors are one of the more common tumors in young adults 22-40 years of age. There is much argument as to whether giant cell tumors arise in the metaphysis or the epiphysis, but most authors agree that giant cell tumors are very uncommon in the diaphysis. The most common sites of giant cell tumors in bone, which are the distal radius, sacrum, distal femur, proximal tibia and proximal humerus. Treatment typically involves intralesional curettage with adjuvant treatment (e.g., phenol, hydrogen peroxide, argon beam, etc).
Williams et al undertook a prospective study to evaulate the recurrence rate of giant cell tumors of the hand and they found that soft tissue extension of the tumor significantly increased the rate of local recurrence. This finding is significant because multiple previous studies have demonstrated similar higher recurrence rates for giant cell tumors with soft tissue extension in other areas like around the knee and the distal radius.
Illustration A are radiographs classic for a giant cell tumor showing a large lytic metaphseal-epiphyseal lesion in the distal femur. Illustration B is an axial CT of the distal femur showing the lytic giant cell tumor, abutting and fracturing the subchondral bone. Illustration C is histology classic for a giant cell tumor where the nuclei of the multi-nucleated giant cells look identical to the nuclei of the stromal cells.
Incorrect Answers:


What is the most appropriate treatment for a 65-year-old female with a 100-pack-year tobacco history who presents with a new painful lytic lesion in her femoral diaphysis?
Antegrade femoral nailing with reamings sent to pathology for analysis
Antegrade femoral nailing with adjuvant radiotherapy to the lesion 3
. Minimally invasive plating of the femur for stabilization and open cementation of the lesion
Referral to medical oncology for chemo-radiotherapy
Lesion biopsy with further treatment based on the results of the biopsy
New lesions which are not diagnosed by imaging and require surgical intervention need to have an appropriate biopsy with treatment dictated by the results of the biopsy. While this patient has a significant tobacco history, incorrect treatment of this lytic bone lesion could affect both her overall morbidity and mortality. As an example, a lytic high-grade chondrosarcoma may look exactly like a metastatic lesion but requires wide surgical excision, not just stabilization of an impending pathological fracture. Intramedullary nailing of a chondrosarcoma would spread the tumor the entire length of the bone and likely require a major amputation, not a limb salvage operation.
A 14-year-old child is referred to your office for evaluation of a tibia lesion found incidentally after a minor ankle injury. A radiograph of the child's ankle is shown in Figure A. What treatment do you suggest?

Endocrine consultation secondary to associated endocrine abnormalities
Surgical consultation secondary to associated gastrointestional cancers
Short leg cast and non-weight bearing for a minimum of 6 weeks
Open biopsy and tumor staging
Routine followup of tibial lesion
The radiograph is classic for a non-ossifying fibroma given the classic eccentric position, sclerotic margin, and benign appearance. Other than routine followup for the tibial lesion, this child requires no subsequent treatment. Marks and Bauer review the diagnosis, imaging, and treatment of many different fibrous tumors of bone and review the diagnostic imaging criteria specific to each subclass of bony fibrous tumors.
The chromosomal translocation t(X;18)is found in which of the following conditions?
Myxoid liposarcoma
Synovial Sarcoma
Osteosarcoma
Ewing's Sarcoma
Clear cell sarcoma
Synovial sarcoma is a rare soft tissue sarcoma with biphasic features of both spindle cell and epithelial differentiation. Synovial sarcoma is a rare high-grade tumor that spreads along fascial planes and, thus, can be much more widespread than apparent on initial evaluation. Males are more commonly affected than females with a ratio of 1.1:1. Synovial sarcoma is characterized by a specific chromosomal translocation t(X;18)(p11;q11) that is observed in more than 90% of cases. The t(X;18)(p11;q11) translocation fuses the SYT gene from chromosome 18 to either of 2 homologous genes at Xp11, either SSX1 or SSX2. The fusion proteins SYT-SSX1 and SYT-SSX2 function as aberrant transcriptional regulators, resulting in either activation of protooncogenes or inhibition of tumor suppressor genes.
Kawai et al found that SYT-SSX fusion transcripts are a defining diagnostic marker of synovial sarcomas. These fusion transcripts may yield important independent prognostic information and provide important information for different types of treatment.
Incorrect Answers
Question 14
An otherwise healthy 78-year-old woman has low back and buttock pain. Rectal examination reveals a large sacral mass. Figures 7a and 7b show a CT scan and a sagittal MRI scan of the lumbosacral spine. A biopsy specimen is shown in Figure 7c. What is the most likely diagnosis?
Explanation
REFERENCES: Mindell ER: Chordoma. J Bone Joint Surg Am 1981;63:501-505.
Samson IR, Springfield DS, Suit HD, Mankin HJ: Operative treatment of sacrococcygeal chordoma: A review of twenty-one cases. J Bone Joint Surg Am 1993;75:1476-1484.
Question 15
In the first dorsal compartment of the wrist, what tendon most frequently contains multiple slips?
Explanation
REFERENCES: Jackson WT, Viegas SF, Coon TM, Stimpson KD, Frogameni AD, Simpson JM: Anatomical variations in the first extensor compartment of the wrist: A clinical and anatomical study. J Bone Joint Surg Am 1986;68:923-926.
Minamikawa Y, Peimer CA, Cox WL, Sherwin FS: DeQuervain’s syndrome: Surgical and anatomical studies of the fibro-osseous canal. Orthopedics 1991;14:545-549.
Question 16
A football player injures his knee when he is tackled and falls awkwardly. He does not note any discreet “pop,” but pain prevents him from returning to the game. An effusion is noted the following day and an MRI scan is ordered. Selected images are shown in Figures 1 through 3. Based on these images, physical examination findings likely include

Explanation
Question 17
What is the most appropriate orthotic management for the lesion shown in Figure 6?
Explanation
REFERENCE: Rudicel SA: Intractable plantar keratoses, in Gould J (ed): Operative Foot Surgery. Philadelphia, PA, WB Saunders, 1994, p 70.
Question 18
An 18-year-old hockey player sustains an acute anterior shoulder dislocation that requires manual reduction. At arthroscopy, the lesion shown in Figure 24 will be observed in what percent of patients?
Explanation
REFERENCES: Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
Baker CL, Uribe JW, Whitman C: Arthroscopic evaluation of acute initial anterior shoulder dislocations. Am J Sports Med 1990;18:25-28.
Question 19
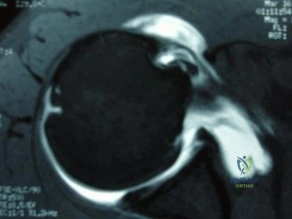
A 41-year-old male truck driver fell off his truck and tried to break his fall by holding on to the side of the door with his left arm. His MRI is depicted in Figures A. Which of the following special tests would most likely be positive on physical examination? Review Topic
Explanation
While the subscapularis is the largest of the rotator cuff muscles, the relative
prevalence of injuries to the subscapularis tendon has only recently been recognized. The primary function of the subscapularis is to internally rotate the humerus. Patients with such injury often present with anterior shoulder pain, and increased external rotation compared to the contralateral limb. It is often associated with medial subluxation of the long head of biceps. A number of special tests have been developed to help aid in the clinical diagnosis of this injury including the belly press, lift off and bear hug tests.
Gerber et al. demonstrated the efficacy of a simple clinical maneuver called the ‘lift-off test’ to reliably diagnose or exclude clinically relevant rupture of the subscapularis tendon in 16 patients.
Barth et al. evaluated the diagnostic value of three clinical tests commonly used to diagnose subscapularis tendon tears; the lift-off test, belly-press test, and bear-hug test. They found that the lift-off test was the most difficult for patients to perform. However, when it was performed and found to be positive, it was 74% sensitive of very severe tears. They also found that the bear hug test was the most sensitive of all tests (82%).
Figures A shows an axial MRI arthrogram showing a subscapularis tear with dislocation of the biceps tendon. Illustration A demonstrates how to perform the bear hug test.
Incorrect Answers:
Question 20
-Four months after injury, the tibia is showing evidence of slow healing on radiographs. What is the optimal treatment for this potential nonunion?
Explanation
This patient is unstable and is not a good candidate for Early Total Care (ETC) and therefore should be managed by the tenets of Damage Control Orthopaedics (DCO). Débridement and external fixation is preferable for this patient. Intramedullary nails would be a component of ETC. Calcaneal traction is not considered ideal because it does not allow the patient to travel as easily. The S.P.R.I.N.T. study concluded that while reamed nails may offer benefit in closed fractures, there was no difference between reamed or unreamed nails in the treatment of open fractures of the tibia. Uniplanar external fixation and tibial plating are not considered the best options for open tibia fractures. Additional findings of the S.P.R.I.N.T. study conclude that delaying surgical intervention for at least 6 months after injury may reduce the need for reoperation.
Question 21
Which of the following best characterizes the antigenicity of allograft bone?
Explanation
REFERENCES: Crawford MJ, Swenson CL, Arnoczky SP, et al: Lyophilization does not inactivate infectious retrovirus in systemically infected bone and tendon allografts. Am J Sports Med 2004;32:580-586.
Stevenson S, Li XQ, Davy DT, et al: Critical biological determinants of incorporation of non-vascularized cortical bone grafts: Quantification of a complex process and structure. J Bone Joint Surg Am 1997;79:1-16.
Simon SR (eds): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 277-320.
Question 22
When comparing the overall outcomes of surgical versus nonsurgical treatment of stable thoracolumbar burst fractures in patients without neurologic injury, 5 years following injury, the principle differences lie in Review Topic
Explanation
Question 23
The artery located within the substance of the coracoacromial ligament is a branch of what artery?
Explanation
REFERENCES: Esch JC, Baker CL: The shoulder and elbow, in Whipple TL (ed): Arthroscopic Surgery. Philadelphia, PA, JB Lippincott, 1993, pp 65-66.
Woodburne RT (ed): Essentials of Human Anatomy, ed 2. New York, NY, Oxford University Press, 1983, pp 75-76.
Question 24
Which of the following indicates resolution of a postoperative wound infection? Review Topic
Explanation
Question 25
In the pediatric population, CECS most commonly presents in females involved in running sports. In this cohort, recurrence occurs at a rate of 18%. Wound complications are the next most common at a rate of 11.2%. A 15-year-old male ice hockey player is hit in the chest by a puck and immediately falls to the ground unconscious. What has been shown to predict survival in the treatment of this condition?
Explanation
against ventricular fibrillation. The velocity of the projectile (most commonly baseball, hockey puck or lacrosse ball) has also not been shown to alter survival.
Question 26
A 29-year-old patient sustains a closed, displaced joint depression intra-articular calcaneus fracture. In discussing potential complications of surgical intervention through an extensile lateral approach, which of the following is considered the most common complication following surgery?
Explanation
REFERENCES: Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.
Sanders RW, Clare MP: Fractures of the calcaneus, in Bucholz RW, Heckman JD,
Court-Brown C (eds): Rockwood and Green’s Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2293-2336.
Question 27
A 16-year-old girl has had anterior leg pain and a mass for the past 8 months. Figures 2a and 2b show a radiograph and an H & E histologic specimen. Which of the following disorders is believed to be a precursor of this lesion?
Explanation
REFERENCE: Springfield DS, Rosenberg AE, Mankin HJ, et al: Relationship between osteofibrous dysplasia and adamantinoma. Clin Orthop 1994;309:234-244.
Question 28
When compared with patients having a body mass index (BMI) lower than 35, patients with a BMI above 40 who undergo primary total hip arthroplasty (THA) and total knee arthroplasty (TKA) are likely to have
Explanation
The obesity epidemic is increasing, and the number of patients with a BMI higher than 35 undergoing THA and TKA also is growing. Controversy exists over the optimal BMI cutoff and the ability to perform joint replacements safely in patients who are morbidly obese. Several clinical series and national database analyses have shown that morbidly obese patients undergoing THA or TKA are at increased risk for wound complications as well as 30-day and 90-day readmissions. These patients’ incisions are typically larger because of the size of the soft-tissue envelope. Although the clinical scores following successful THA or TKA often are lower than the scores of controls, the overall changes in clinical function and satisfaction are equivalent in nonobese and obese patients.
Question 29
A 16-year-old girl has a painful foot mass. A radiograph, MRI scan, and biopsy specimens are shown in Figures 35a through 35d. What is the most likely diagnosis?
Explanation
REFERENCES: Ghert MA, Scully SP, Harrelson JM: Pigmented villonodular synovitis of the foot and ankle: A review of six cases. Foot Ankle Int 1999;20:326-330.
Jones BC, Sundaram M, Kransdorf MJ: Synovial sarcoma: MR imaging findings in 34 patients. Am J Roentgenol 1993;161:827-830.
Sartoris DJ, Resnick D: Magnetic resonance imaging of pediatric foot and ankle disorders. J Foot Surg 1990;29:489-494.
Scully SP, Temple HT, Harrelson JM: Synovial sarcoma of the foot and ankle. Clin Orthop 1999;364:220-226.
Question 30
An active 68-year-old woman undergoes an uncomplicated rotator cuff repair with a double-row construct using biocomposite knotless anchors. At her two month follow up, she is noted to have increased shoulder pain, weakness and limited motion. Imaging reveals failure of the rotator cuff repair. What is the most likely mechanism of failure? Review Topic
Explanation
The overall complication rate of arthroscopic RCR is roughly 10%. Failed RCR most commonly results from failure to heal (19-94%) secondary to poor rotator cuff tissue, insufficient vascularity or poor bone quality. Other causes of RCR failure include surgical complications (deltoid disruption, infection, foreign body reaction, stiffness, neurologic injury), diagnostic errors (missed lesions of the rotator interval, long head of biceps or subscapularis tear), and technical errors (excessive tension due to lack of proper tissue mobilization, anchor pull out secondary to improper anchor placement).
George et al evaluated the causes of failed RCR and results of revision RCR. While results of revision RCR are inferior to primary RCR, arthroscopic repair yields > 60% good or excellent results. Risk factors for poor results following revision RCR include poor tissue quality, detachment of the deltoid origin and multiple previous surgeries.
Diduch et al reviewed the design and composition of various anchors used in arthroscopic shoulder surgery. Current advancements in the field include high-strength polyethylene sutures, new biocompatible anchor materials (PEEK, biocomposite) and modified designs including knotless systems. With improved strength of the current anchors and repair constructs, the most common mode of arthroscopic RCR failure is now related to tissue failure occurring at the tissue-anchor interface.
Cole et al discussed the different primary rotator cuff repair constructs, including single row, double row, transosseous and transosseous equivalent. The authors concluded that construct selection depends on tear acuity, size and tissue quality. For acute tears < 12mm in anteroposterior length, single-row configuration likely has sufficient strength to maintain the repair and promote healing. For more chronic tears, poor tissue quality, or tears > 12-15mm in the anteroposterior dimension, the authors recommend double-row or transosseous-equivalent repair to better restore the anatomic footprint and provide optimal mechanical stability to achieve healing.
Illustration A is an algorithm from George et al detailing the decision-making process when considering revision RCR for a symptomatic failed RCR.
Incorrect Responses
Question 31
-This boy’s parents are eager to get him back on the field as soon as possible. What is the most appropriate treatment option?
Explanation
Although a recent increase in the number of pitches may have contributed to this patient’s development of little leaguer’s shoulder, the most significant overall factor is age. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress, and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Genetic factors and gender have not been studied in association with little leaguer’s shoulder. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms.Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to baseline pitching is implemented until the patient is back to baseline. This protocol has a long-term success rate exceeding 90%.

Question 32
A 57-year-old man involved in a motor vehicle accident sustains an injury to his right shoulder. A spot AP radiograph is shown in Figure 34. What is the next most appropriate step in the orthopaedic management of this patient? Review Topic

Explanation
Question 33
Which of the following methods is considered effective in decreasing the dislocation rate following a total hip arthroplasty using a posterior approach to the hip?
Explanation
REFERENCES: Pellicci PM, Bostrom M, Poss R: Posterior approach to total hip replacement using enhanced posterior soft tissue repair. Clin Orthop 1998;355:224-228.
Morrey BF: Difficult complications after hip joint replacement: Dislocation. Clin Orthop 1997;344:179-187.
Question 34
An 80-year-old right-hand dominant male presents to clinic with 1 month of left shoulder pain. He has crepitance as well as a positive drop arm test on exam. Radiographs are significant for moderate glenohumeral arthritis and MRI demonstrates Goutallier Stage IV fatty infiltration of the rotator cuff. Which of the following is NOT an appropriate option for treatment of this condition? Review Topic
Explanation
The optimal management of patients with irreparable rotator cuff tears with glenohumeral osteoarthritis is not well defined in literature. Initial management should involve conservative measures, including injection of corticosteroids, physical therapy, activity modification, and NSAIDs, with consideration of operative intervention in those that fail a trial of nonoperative management.
Laudicina et al review the management of irreparable rotator cuff tears in the setting of glenohumeral osteoarthritis(OA). NSAIDs, corticosteroid injection, activity modification, and physical therapy are mainstays of nonoperative treatment. Failure of conservative management may lead to operative intervention. The authors endorse that hemiarthroplasty is currently the procedure of choice for patients with moderate to severe glenohumeral OA and irreparable cuff tears.
Izquierdo et al provide a clinical practice guideline of the treatment of glenohumeral osteoarthritis based on systematic review. Nine of 16 addressed recommendations were inconclusive, illustrating that the management of glenohumeral osteoarthritis remains controversial. The single moderate-rated recommendation was for the use of total shoulder arthroplasty (TSA) rather than hemiarthroplasty. The two recommendations reached by consensus include use of perioperative mechanical and/or chemical DVT prophylaxis for shoulder arthroplasty patients and that TSA should be avoided in patients with glenohumeral OA with irreparable rotator cuff tear.
Illustration A demonstrates the Goutallier staging system of rotator cuff tears.
Incorrect Answers:
Question 35
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the Review Topic
Explanation
Question 36
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with
Explanation
REFERENCES: Bokor DJ, Conboy VB, Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br 1999;81:93-96.
Wolf EM, Cheng JC, Dickson K: Humeral avulsion of the inferior glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Question 37
A 47-year-old woman has had left medial clavicle pain for the past 6 months. History is remarkable for mediastinal non-Hodgkin’s lymphoma, treated with mantel radiation 22 years ago. A radiograph, CT scan, MRI scan, and a biopsy specimen are shown in Figures 68a through 68d. What is the most likely diagnosis?
Explanation
REFERENCES: Shaheen M, Deheshi BM, Riad S, et al: Prognosis of radiation-induced bone sarcoma is similar to primary osteosarcoma. Clin Orthop Relat Res 2006;450:76-81.
Tabone MD, Terrier P, Pacquement H, et al: Outcome of radiation-related osteosarcoma after treatment of childhood and adolescent cancer: A study of 23 cases. J Clin Oncol 1999;17:2789-2795.
Question 38
A 48-year-old man has recurrent right knee pain. Figure 52a shows the sagittal proton density T2-weighted MRI scan, and Figure 52b shows the sagittal T2-weighted MRI scan at the same level. The arrow is pointing to a
Explanation
REFERENCES: Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Mink JH, Deutsch AL: The knee, in MRI of the Musculoskeletal System, ed 1. New York, NY, Raven Press, 1990, pp 251-387.
Question 39
Locked plating techniques have been shown to have biomechanical advantages over standard plating in which of the following scenarios?
Explanation
REFERENCES: Zlowodzki M, Williamson S, Cole PA, et al: Biomechanical evaluation of the less invasive stabilization system, angled blade plate, and retrograde intramedullary nail for the internal fixation of distal femur fractures. J Orthop Trauma 2004;18:494-502.
Comparison of the AO Locking Plate with the Standard Limited-Contact Dynamic Compression Plate (LC-DCP) for Fixation of Osteoporotic Humeral Shaft Fractures. David J. Hak, MD, MBA; Scott J. Hazelwood, PhD. OTA Book of Abstracts 2003.
Question 40
Figure 163 is the radiograph of an 81-year-old man who had primary total hip arthroplasty 12 years ago and now has a 3-month history of left hip weight-bearing thigh pain. The appropriate treatment at this time is
Explanation
This patient has a loose cemented femoral component. The implant has subsided and the femur has remodeled into a varus position. Although the component may be removable without an extended trochanteric osteotomy, the varus bow of the femur will not allow distal fixation without use of an extended trochanteric osteotomy. The acetabular component appears
to be well fixed, and, as a result, should be retained in this older patient. An evaluation of stability could lead to possible revision of the acetabulum, and implants should be available.
Question 41
Figure 12 shows the radiograph of a 55-year-old man who has severe, painful osteoarthritis of the left hip and is scheduled to undergo a left total hip arthroplasty. History reveals that he underwent a right total hip arthroplasty 5 years ago that remains pain-free. Based on the preoperative radiograph, the patient is at greatest risk for what complication?
Explanation
REFERENCE: Ranawat CS, Rodriguez JA: Functional leg-length inequality following total hip arthroplasty. J Arthroplasty 1997;12:359-364.
Question 42
Collagen orientation is parallel to the joint surface in what articular cartilage zone?
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 498-499.
Mankin HJ, Mow VC, Buckwalter JA: Articular cartilage structure, composition, and function, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006,
in press.
Question 43
What is the most common reason for reoperation in total knee arthroplasty?
Explanation
REFERENCES: Blasier RB, Matthews LS: Complications of prosthetic knee arthroplasty, in Epps CH (ed): Complications in Orthopaedic Surgery. Philadelphia, PA, JP Lippincott, 1994, pp 1066-1069.
Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620.
Wilson MG, Kelley K, Thornhill TS : Infection as a complication of total knee-replacement arthroplasty: Risk factors and treatment in sixty-seven cases. J Bone Joint Surg Am 1990;72:878-883.
Question 44
Which specific legislative Act in the United States was created to require reporting of annual monetary gifts or compensation of more than $10 by orthopaedic implant companies to physicians?
Explanation
Under this Act, all manufacturers of drugs and devices covered under Medicare, Medicaid, and SCHIP are obliged to federally report payments beyond $10 annually to physicians and academic centers. The Act was first introduced in 2007, enacted in 2010, and in 2014 the first data (from 2012) was reported publicly online in the Open Payment Program of the Centers for Medicare and Medicaid Services website.
Samuel et al analyze orthopedic surgeons available data from the Sunshine Act regarding industry payments and find over 110 million USD paid to approximately 15,000 orthopedic surgeons over the 5-month study period. No long term data exists to determine if these payments have any affect in healthcare.
Incorrect Answers:
Question 45
- Which of the following procedures is associated with the highest risk of osteonecrosis of the metatarsal head?
Explanation
Question 46
A 15-year-old boy has a fracture of the proximal tibia extending from the apophysis of the tubercle up through the posterior part of the proximal tibial epiphysis and into the joint. What is the most likely mechanism of injury?
Explanation
Question 47
Figure 20 shows the radiograph of a 21-year-old college basketball player who jammed his left index finger on the rim. He reports pain and tenderness over the dorsum of the distal interphalangeal (DIP) joint. Examination reveals that he is unable to actively extend the DIP joint; however, the skin is intact. Management should consist of
Explanation
REFERENCES: Crawford GP: The molded polyethylene splint for mallet finger deformities.
J Hand Surg Am 1984;9:231-237.
Wehbe MA, Schneider LH: Mallet fractures. J Bone Joint Surg Am 1984;66:658-669.
Question 48
An 18-month-old boy has 45 degrees of kyphosis in the thoracolumbar spine secondary to type I congenital kyphosis. Examination reveals that he is neurologically intact, and an MRI scan shows no evidence of intraspinal pathology. Management should consist of
Explanation
REFERENCES: Winter RB: Congenital Deformities of the Spine. New York, NY, Thieme-Stratton, 1983, pp 229-261.
Winter RB, Moe JH: The results of spinal arthrodesis for congenital spinal deformity in patients younger than five years old. J Bone Joint Surg Am 1982;64:419-432.
Question 49
Which of the following properties apply to the human meniscus when compared with articular cartilage?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 3-23.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, AAOS, 1999, pp 349-354.
Question 50
..The optimal method to treat a recurrent presentation of pigmented villonodular synovitis (PVNS) with diffuse joint involvement in a 24-year-old woman with pain and symptomatic effusions is
Explanation

Question 51
A 77-year-old woman who underwent total knee arthroplasty 16 years ago now reports pain, swelling, and notable crepitation with range of motion. AP, lateral, and Merchant radiographs are shown in Figures 54a through 54c. What is the most likely diagnosis?
Explanation
REFERENCES: Poss R (ed): Orthopaedic Knowledge Update 3. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, pp 590-593.
Leopold SS, Berger RA, Patterson L, et al: Serum titanium level for diagnosis of a failed metal-backed patellar component. J Arthroplasty 2000;15:938-943.
Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1993, pp 613-614.
Question 52
A 6-year-old African-American boy with sickle cell disease has had pain and limited use of his right arm for the past 3 days. History reveals that he sustained a humeral fracture approximately 3 years ago. A lateral radiograph is shown in Figure 25. Based on these findings, a presumptive diagnosis of chronic osteomyelitis is made. What are the two most likely organisms?
Explanation
REFERENCES: Piehl FC, David RJ, Prugh SI: Osteomyelitis in sickle cell disease. J Pediatr Orthop 1993;13:225-227.
Givner LB, Luddy RE, Schwartz AD: Etiology of osteomyelitis in patients with major sickle hemoglobinopathies. J Pediatr 1981;99:411-413.
Epps CH Jr, Bryant DD III, Coles MJ, Castro O: Osteomyelitis in patients who have sickle-cell disease: Diagnosis and management. J Bone Joint Surg Am 1991;73:1281-1294.
Lovell and Winter’s Pediatric Orthopaedics, ed 4, 1996.
Question 53
Figures 48a through 48c show the lateral radiograph and MRI scans of a 60-year-old man who has had pain in his thigh for 1 month. The next most appropriate step in management should consist of
Explanation
REFERENCES: Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Rougraff BT, Kneisl JS, Simon MA: Skeletal metastases of unknown origin: A prospective study of a diagnostic strategy. J Bone Joint Surg Am 1993;75:1276-1281.
Question 54
An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes
Explanation
REFERENCE: Rettig ME, Raskin KB: Galeazzi fracture-dislocation: A new treatment-oriented classification. J Hand Surg Am 2001;26:228-235.
Question 55
A 30-year-old patient is indicated for distal femoral osteotomy. This procedure results in survivorship with
Explanation
Distal femoral varus osteotomy (DFVO) is intended for patients younger than age 50, more active patients with isolated lateral compartment arthritis and valgus malalignment. Although the knee functional score improves at 1-year follow-up, the function scores significantly deteriorate at 10-year follow-up. At 15-year follow-up, the knee function further declines, resulting in an overall failure rate of 48.5%. DFVO provides longer lasting benefit in patients with better presurgical knee function.
Total knee arthroplasty following DFVO provides improved function and successful outcomes. Standard posterior stabilized components provide satisfactory stability after appropriate ligament balancing without the need for stemmed or highly constrained implants for most patients.

CLINICAL SITUATION FOR QUESTIONS 65 THROUGH 67
Figures 65a and 65b are the radiographs of an 80-year-old woman with long-standing knee pain who has failed nonsurgical treatment that includes a structured physical therapy program, nonsteroidal anti-inflammatory medications, and intra-articular steroid injections. Her radiographs reveal significant degenerative changes. She has experienced some cognitive decline during the last several years and poorly tolerates pain medications, but she remains very active.
Question 56
A 5-year-old boy has had right hip pain and a limp for the past 3 months. Examination of the right hip reveals irritability and restricted abduction and internal rotation. AP and lateral radiographs of the hips are shown in Figures 31a and 31b. Initial management should consist of
Explanation
REFERENCES: Herring JA: The treatment of Legg-Calve-Perthes disease: A critical review of the literature. J Bone Joint Surg Am 1994;76:448-458.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 161-166.
Question 57
-Which gene mutation is associated with the condition shown in Figures a and b?

Explanation

Question 58
What structure (arrow) is shown in Figure 24?
Explanation
REFERENCES: Onibokun A, Khoo LT, Holly L: Anterior retroperitoneal approach to the lumbar spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 101-105.
Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.
Question 59
A 6-month-old child is seen in the emergency department with a spiral fracture of the tibia. The parents are vague about the etiology of the injury. There is no family history of a bone disease. In addition to casting of the fracture, initial management should include Review Topic
Explanation
(SBQ13PE.60) If a child develops dynamic supination after treatment of idiopathic clubfoot with Ponseti casting, at what age would it be appropriate to consider transfer of the tibialis anterior tendon to the lateral dorsum of the foot? Review Topic
In the first six months of life, immediately following failed cast treatment
12 months
4 years
12 years
15 years
Tibialis tendon transfer to the dorsum of the foot should be performed to address dynamic supination when the lateral cuneiform has ossified. This is typically after at least 2 years of age and usually not before age 3.
Question 60
A 62-year-old woman has advanced osteoarthritis of the knee that has been refractory to nonsurgical treatment. She wishes to discuss total knee arthroplasty. She reports a lifelong history of intolerance to most jewelry and is concerned about having an allergic reaction to the metallic knee implant.Hypersensitivity to metal implants is usually classified as what type of Gell-Coombs reaction?
Explanation
Question 61
Figure 11 shows the lateral radiograph of a 16-year-old boy who has been unable to participate in sports activities because of pain in the anterior aspect of the knee. He states that the pain is aching in nature and is located in the region of the tibial tuberosity. He denies having joint effusion or symptoms of instability. Management should consist of
Explanation
REFERENCES: Flowers MJ, Bhadreshwar DR: Tibial tuberosity excision for symptomatic Osgood-Schlatter disease. J Pediatr Orthop 1995;15:292-297.
Greene WB: Osteochondrosis and tibia vara, in Canale ST, Beaty JH (eds): Operative Pediatric Orthopaedics, ed 2. Philadelphia, Pa, Mosby, 1995, pp 804-854.
Question 62
Which of the following is considered a risk factor for the development of low back pain?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 627-643.
Question 63
Commotio cordis is best treated with
Explanation
REFERENCES: McCrory P: Commotio cordis. Br J Sports Med 2002;36:236-237.
Boden BP, Tacchetti R, Mueller FO: Catastrophic injuries in high school and college baseball players. Am J Sports Med 2004;32:1189-1196.
Question 64
When comparing arthroscopic lavage and knee debridement with placebo in patients with chronic symptomatic osteoarthritis, what outcome has been demonstrated?
Explanation
Excluding a diagnosis of meniscal tear, loose body, or mechanical derangement, treating knee osteoarthritis of indeterminate cause with arthroscopic lavage and debridement has been found to provide no discernable benefit to offset the risk of surgery. The effects of arthroscopy have not been clinically significant in the vast majority of patient-oriented outcomes measures for pain and function at multiple
times between 1 week and 2 years after surgery.
Question 65
An MRI scan
Explanation
Question 66
A year-old woman is referred for evaluation of a painful knee replacement. She underwent total knee arthroplasty (TKA) more than 1 year ago without perioperative complications but has had consistent pain since the surgery. The patient’s preoperative radiographs and postoperative radiographs are shown in Figures below. Examination reveals medial laxity during valgus stress testing and range of motion of 0° to 70°. Her erythrocyte sedimentation rate and C-reactive protein level are normal. What is the best next step?
Explanation
The radiographs show substantial valgus malalignment of the femoral component, with lateral mechanical axis deviation. Clinically, by examination she displays instability and stiffness as a result. Revision knee replacement is appropriate and should consist of total revision to stemmed femoral and tibial components with a varus-valgus constrained insert, given the likely attenuation of the medial collateral ligament. Open debridement with ligament balancing and polyethylene exchange do not address the underlying cause and are inappropriate. Distal femoral osteotomy is not useful in the setting of previous total knee replacement.
Nonsurgical treatment with an unloader brace would be ineffective in correcting the alignment.
Question 67
Venous thromboembolism may occur after total joint arthroplasty. The risk of this complication is elevated in patients with
Explanation
Obesity, a prior history of venous thromboembolism, and metabolic syndrome have all been associated with an increased risk of thromboembolism. A recent meta-analysis showed that diabetes had no significant relationship with venous thromboembolism following hip or knee arthroplasty. Tranexamic acid is an antifibrinolytic agent that has been shown to reduce blood loss substantially following hip and knee arthroplasty. It has also been shown to be safe in patients with severe medial comorbidities and a prior history of venous thromboembolism.
Question 68
An 11-year-old female gymnast has had gradually increasing right wrist pain for the past 6 months. Examination reveals normal range of motion and strength. Moderate tenderness is present over the distal radius. AP radiographs will most likely show
Explanation
REFERENCES: Mandelbaum BR, Bartolozzi AR, Davis CA, Teurlings L, Bragonier B: Wrist pain syndrome in the gymnast: Pathogenetic, diagnostic, and therapeutic consideration. Am J Sports Med 1989;17:305-317.
Roy S, Caine D, Singer KM: Stress changes of the distal radial epiphysis in young gymnasts: A report of twenty-one cases and a review of the literature. Am J Sports Med 1985;13:301-308.
Question 69
-A likely candidate for treatment with a thoracic lumbosacral orthosis scoliosis brace is seen in
Explanation

Question 70
Figure 38a shows the radiograph of a 12-year-old boy who underwent a reamed intramedullary nailing for a closed femoral shaft fracture. One year after rod removal, he reports groin pain. A current radiograph is shown in Figure 38b. The findings are most likely the result of
Explanation
REFERENCES: Letts M, Jarvis J, Lawton L, et al: Complications of rigid intramedullary rodding of femoral shaft fractures in children. J Trauma 2002;52:504-516.
Stans AA, Morrissy RT, Renwick SE: Femoral shaft fracture treatment in patients age 6 to 16 years. J Pediatr Orthop 1999;19:222-228.
Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop 1997;338:60-73.
Beaty JH, Austin SM, Warner WC, et al: Interlocking intramedullary nailing of femoral-shaft fractures in adolescents: Preliminary results and complications. J Pediatr Orthop
1994;14:178-183.
Question 71
Figures below depict the radiographs obtained from a 60-year-old man with instability and pain 1 year after primary right total knee arthroplasty. He states that he had surgery on two occasions for a tendon rupture that was repaired with sutures but that his knee popped again, and now the leg is unable to hold his weight. On examination, he is in no acute distress. His height is 6'3", and he weighs 240 pounds. He is ambulatory with crutches. Range of motion of the right knee is 50° to 120° actively and 0° to 120° passively. More than 10° of varus/valgus laxity and more than 5 mm of anteroposterior drawer are present. A palpable defect is observed in the tissue just proximal to the patella. The incision is well healed. The erythrocyte sedimentation rate is 46 mm/h (reference range 0 to 20 mm/h) and the C-reactive protein level is 2.04 mg/L (reference range 0.08 to 3.1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1% neutrophils. No growth of organisms is seen on routine culture. What is the best next step?

Explanation
This patient has a chronic quadriceps tendon rupture after total knee arthroplasty. Two previous primary repair attempts have failed, which is not surprising based on the poor results of primary repair reported in the literature. The patient also has an unstable knee and will require revision of some or all of the prosthesis to achieve a stable knee. Revision total knee arthroplasty with extensor mechanism allograft allows an allograft reconstruction of the ruptured quadriceps tendon. The other option is to utilize a synthetic mesh extensor mechanism reconstruction. These are likely to have the best result in this situation. Revision total knee arthroplasty with liner change and primary quadriceps repair is not the best form of management, because it involves a third attempt at primary tendon repair, which will likely fail again. Resection knee arthroplasty and arthrodesis with antegrade nail is a possible option but is not the best, because it would likely make driving and other daily activities difficult. Two-stage revision total
knee arthroplasty with extensor mechanism allograft is not the best option because the laboratory results show no signs of infection, so a single-stage procedure is preferred.
Question 72
Figures below depict the radiographs obtained from a 76-year-old woman who comes to the emergency department after experiencing a fall. She is an unassisted community ambulator with a history of right hip pain. What is the most appropriate surgical treatment for this fracture?
Explanation
This patient has pre-existing right hip osteoarthritis. The most correct option for the treatment of this active patient is a right total hip arthroplasty. Hemiarthroplasty would not address the patient's pain from osteoarthritis, and open reduction and internal fixation would not fix the femoral head issue or the
osteoarthritis.
Question 73
Which of the following is considered the best method for the prevention of wrong-site surgery?
Explanation
REFERENCES: DeGiovanni CW, Kang L, Manuel J: Patient compliance in avoiding wrong site surgery. J Bone Joint Surg Am 2003;85:815-819.
American Academy of Orthopaedic Surgeons. Advisory Statement: Wrong-site Surgery. Document 1015, 2002 Sept. www.aaos.org/wordhtml/papers/advismt/wrong.htm.
Question 74
A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?
Explanation
REFERENCES: Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Sanders R: Displaced intraarticular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.
Sanders R, Fortin P, DiPasquale T, et al: Operative treatment in 120 displaced intra-articular calcaneal fractures: Results using a prognostic computed tomography scan classification. Clin Orthop Relat Res 1993;290:87-95.
Question 75
A 3-year-old child sustains a T2/T3 fracture-dislocation with complete paraplegia secondary to a car accident in which the child was an unrestrained passenger. What is the likelihood that this child will develop subsequent spinal deformity in the future? Review Topic
Explanation
Question 76
What is the most appropriate indication for replantation in an otherwise healthy 35-year-old man?
Explanation
the thumb, are a relative contraindication for replantation. Replantations at the level of the proximal phalanx lead to poor motion of the proximal interphalangeal joint. In a healthy
active adult, an amputation through the wrist is an appropriate situation to proceed with a replantation. A transverse forearm amputation is a good indication with a warm ischemia time
of less than 6 hours.
REFERENCES: Urbaniak JR: Replantation, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1085.
Boulas HJ: Amputations of the fingers and hand: Indications for replantation. J Am Acad Orthop Surg 1998;6:100-105.
Question 77
The husband of a 22-year-old woman has hypophosphatemic rickets. The woman has no orthopaedic abnormalities, but she is concerned about her chances of having a child with the same disease. What should they be told regarding this disorder?
Explanation
REFERENCES: Herring JA: Metabolic and endocrine bone diseases, in Tachdjian’s Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743.
Sillence DO: Disorders of bone density, volume, and mineralization, in Rimoin DL, Conner JM, Pyerite RE, et al (eds): Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002.
Staheli LT: Practice of Pediatric Orthopedics. Philadelphia, PA, Lippincott Williams & Wilkins, 2001.
Question 78
A 29-year-old man sustained an injury when he was playing basketball, landing on his left knee while jumping for a rebound. He had vague pain in the anterior aspect of the knee for several weeks. The initial radiographs were negative with the exception of a large traumatic effusion. Examination reveals no apparent ligament instability but a significant extension lag of 30 degrees. There was a palpable defect above the superior pole of the patella. What is the most appropriate management? Review Topic
Explanation
Question 79
- A 40-year old man has limited, painful motion in dorsiflexion at the metatarsophalangeal (MTP) joint of the right great toe, despite nonsurgical treatment. Radiographs show dorsal and medial osteophytes and minimal narrowing of the articular space. Treatment should consist of
Explanation
Question 80
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk? Review Topic
Explanation
(SBQ13PE.27) A 15-year-old male patient presents requesting clearance to perform in the Special Olympics. He has had abnormal facies, has had mental developmental delay and cytogenetic analysis confirmed abnormalities on chromosome 21. Orthopaedically, he has been treated in the past for an elbow dislocation as well as bilateral patellar dislocation. He has already visited his cardiologist and endocrinologist and has been cleared. He has no complaints, denies any pain, difficulties with walking and reports that his training has been going well. What is the next best step? Review Topic
With a normal physical exam, patient can be cleared for participation
MRI bilateral knees and elbow to ensure no ligamentous injury
Referral to a neurologist for clearance
Lateral cervical spine flexion and extension radiographs
AP pelvis radiograph
Ruling-out C1-C2 instability with flexion/extension radiographs is necessary prior to any spine surgery or participation in sports in patients with Down's Syndrome.
Patients with Down's Syndrome typically present with generalized ligamentous laxity and decreased tone. Thus, dislocations (elbow or patella) along with asymptomatic instability in the cervical spine can commonly occur. Imaging analysis is necessary prior to sports participation.
McKay et al. performed a systematic review to summarize all congenital causes of cervical instability. They found in Down's patients, cervical instability due to ligamentous laxity is found mostly at C1-2. They recommend asymptomatic patients
with an ADI <4.5mm can resume unrestricted activities, while asymptomatic patients between 4.5-10mm should not participate in contact sports. With ADI >10mm OR symptoms/cord changes on MRI, surgery is recommended. Symptomatic patients with ADI between 4.5-10mm should be observed with activity restriction.
Dedlow et al. outlines the most recent 2011 update and guidelines for cervical instability in Down's syndrome patients. One of the major highlighted changes is the emphasis placed on radiographic re-examination, regardless of prior clearance. Re-examination should occur prior to participation in sports and/or the onset of new symptoms.
Illustrations A, B and C highlight the C1-2 instability on flexion-extension lateral radiographs. Careful attention can be placed on the relationship of the anterior arch of C1 and the dens (Illustration C). This allows for the measurements of ADI and the space available for the cord (SAC), which is highlighted in Illustration D.
Incorrect answers:
Question 81
A 17-year-old girl with a history of Scheuermann's kyphosis has a fixed thoracic deformity of 80 degrees. There was no correction of her deformity on supine hyperextension radiographs. What is the most appropriate treatment? Review Topic
Explanation
Question 82
A 72-year-old woman is evaluated for sacrococcygeal pain sustained after a twisting injury. Radiographic and MRI evaluation confirms the presence of a nondisplaced fracture at the sacrococcygeal junction. Over a 3-week period, the pain has gotten significantly better. No additional lesions or injuries are noted. Laboratory studies show a serum calcium level of 8.8 mg/dL (normal 8.6-10.3 mg/dL) and a 25-OH Vitamin D level of 14 ng/mL (normal 30-80 ng/mL). What is the most appropriate treatment for this patient?
Explanation
Question 83
An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis? Review Topic
Explanation
(SBQ07SM.48) Carbohydrate loading is a common practice among endurance athletes that works by what mechanism? Review Topic
Increasing serum fructose levels
Maximizing stored muscle glycogen for endurance after 90 minutes of exercise
Diuresis
Decreasing serum glucose levels
Maximizing stored liver glycogen for endurance after 60 minutes of exercise
Carbohydrate loading is a strategy that involves changes to training and nutrition which can maximize muscle glycogen stores prior to endurance exercise lasting longer than 90 minutes.
There continues to be varying scientific opinions as to whether athletes should eat low vs. high glycemic index foods, and how this will affect the amount that the serum glucose levels rise. Fructose is able to be converted to glycogen in the liver but not muscle, therefore high-fructose containing foods are suboptimal. This practice is recommended for athletes participating in events that are longer than 90 minutes (after the bodies normal supply of glycogen is depleted).
Coyle et al. analyzed 10 trained cyclists who performed two bicycle ergometer exercise tests 1 wk apart. They found that blood glucose concentration was 20-40% higher during the exercise after carbohydrate ingestion than during the exercise without carbohydrate feeding. The exercise-induced decrease in plasma insulin was prevented by carbohydrate feeding. Ultimately, fatigue was postponed by carbohydrate feeding during exercise in seven out of the ten subjects.
Costill et al. examined the effect of carbohydrates on muscle glycogen resynthesis in trained runners and found that muscle glycogen levels could be normalized with the proper use of carbohydrates after strenuous activity.
Sherman et al. used muscle biopsies to determine the effects of moderate- or high-carbohydrate diets on muscle glycogen and performance in runners and cyclists over 7 consecutive days of training. They found that a high carbohydrate diet restored muscle glycogen to more normal levels than a moderate carbohydrate diet but did not find any difference in the effect on performance.
Illustration A is a graph depicting the typical carbohydrate depletion/loading regimen that endurance athletes utilize to maximize muscle glycogen stores prior to endurance exercise. This typically involves a hard workout followed by three days of a low-carb diet, another hard workout, and another three days of a high-carb diet.
Incorrect
Question 84
In a patient with rheumatoid arthritis of the wrist, which of the following extensor tendons is most at risk of rupture?
Explanation
REFERENCES: Vaughan-Jackson OJ: Rupture of extensor tendons by attrition at the inferior radioulnar joint: A report of two cases. J Bone Joint Surg Br 1948;30:528-530.
Papp SR, Athwal GS, Pichora DR: The rheumatoid wrist. J Am Acad Orthop Surg
2006;14:65-77.
Question 85
A 35-year-old man sustained the closed injury shown in Figure 52 in his dominant extremity. Neurologic function is normal. Treatment should consist of
Explanation
REFERENCES: Sarmiento A, Zagorski JB, Zych GA, et al: Functional bracing for the treatment of fractures of the humeral diaphysis. J Bone Joint Surg Am 2000;82:478-486.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 267.
Question 86
Tension band wire fixation is best indicated for which of the following types of olecranon fractures?
Explanation
Question 87
03 Figure 33 shows the radiograph of a 48-year-old man who sustained a fracturedislocation of his dominant arm and a significant head injury in a fall from a roof. Eight days after injury he is medically cleared for surgery. Treatment should consist of

Explanation
proximal humerus, with what appears to be a head-splitting component. Answer 1
(rotator cuff repair) is certainly not indicated yet – maybe as a secondary procedure
once the bone is healed, or as a subsequent procedure while dealing with the fracture.
Similar to question #109, there is no need to resurface the glenoid unless we have
evidence of significant degenerative changes, which we don’t. ORIF of head-splitting
fractures hasn’t had any promising results, and AVN is always an issue here. Both
articles referenced discuss the outcomes of acute hemiarthroplasty in the
treatment of 3- and 4-part proximal humerus fractures versus late replacement for
failed non-operative treatment, and the benefits of early management in regards
to difficulty of procedure, post-operative pain, and functional ROM/strength outcomes. Arthrodesis is a viable option, but not with the good results of hemiarthroplasty as evidenced here.
Goldman RT, Koval KJ, Cumom F, Gallagher MA, Zuckerman JD: Functional outcome after humeral head replacement for acute three- and four-part proximal humeral fractures. J Shoulder Elbow Surg 1995;4:81-86.
Norris TR, Green A, McGuigan FX: Late prosthetic shoulder arthroplasty for displaced proximal humerus fracture. J Shoulder Elbow Surg 1995;4:271-280.
back to this question next question
Question 88
The spread of malignant cells to the vertebrae is often through
Explanation
REFERENCE: Batson OV: The function of the vertebral veins and their role in the spread of metastases. Ann Surg 1940;112:138-149.
Question 89
A 59-year-old woman with a history of osteoporosis is involved in a high-speed motor vehicle accident, resulting in left hip pain and deformity. The initial radiograph from the trauma bay is shown in Figure 1. Postreduction CT is shown in Figures 2 through 4. What is the most appropriate definitive surgical treatment?
Explanation
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
Question 90
1mg/L (normal 1-3mg/L). Knee aspiration yields WBC of 673 cells/mm(3) with 30% polymorphonucleocytes, and a negative gram stain. There is no surrounding erythema but there is a 1cm area at the inferior aspect of the wound that has a large amount of serous drainage able to be expressed. She has a painless range of motion is 0° to 117°. What would be the next most appropriate step in management?
Explanation
Malinzak et al performed a Level 4 review of 8494 patients undergoing a total knee arthroplasty. They found that patients with a body mass index greater
than 50 had an increased odds ratio of infection of 21.3 (P < .0001). Diabetic patients were 3 times as likely to become infected compared to nondiabetic patients (P = .0027).
Rasul et al performed a Level 4 review of 24 patients for a duration of 2 years with total knee arthroplasty infections. They found that patients with chronic (>1 month) deep infections were successfully treated 75% with debridement, intravenous antibiotics, tobramycin-impregnated polymethylmethacrylate beads, and delayed exchange arthroplasty with mean interval of staged reimplantation being 8 weeks.
OrthoCash 2020
A 47-year-old man presents with 1 week of left leg pain. 6 months prior he underwent a vascularized free-fibula bone graft from his left leg to his right hip for avascular necrosis. The pain is located at the level of his donor site and is worse with weight-bearing and relieved by rest. Physical exam shows focal tenderness over his tibia. A lateral radiograph from the day of presentation is shown in Figure A. WBC, ESR, and CRP are all within normal limits. What is the next best step in management to confirm the diagnosis?

Compartment pressure measurements
CT scan
MRI scan
Ultrasound to rule out deep abscess
Bone biopsy
The clinical presentation is suspicious for a stress fracture of the tibia following free-fibula bone grafting. If plain radiographs are negative, more sensitive imaging such as a MRI or bone scan should be performed.
Tibial stress fractures are a known complication following free-fibula bone grafting. Radiographs may be normal (as is the case in figure A), or might show the "dreaded black line" and/or new periosteal bone formation. If a stress fracture is confirmed with imaging, appropriate management would then consist of protective weight bearing until symptoms subside.
Pacifico et al detail a case report of tibial stress fractures after vascularised free-fibula graft to the mandible. They report non-traumatic stress fracture to the tibia following a vascularised free-fibula graft is an uncommon but important complication.
Ivey et al detail a case report of a tibial stress fracture after vascularised free-fibula graft for repair of non-union of the humerus.
Emery et al report a case-series of 5 patients who sustained tibial stress fractures after a graft had been obtained from the ipsilateral fibula for use in anterior reconstruction of the spine. They theorize that the increased load the tibia bears as a result of the missing fibular graft may result in stress fractures.
Illustration A shows new periosteal bone formation on the lateral cortex of the tibia consistent with a stress fracture.
Incorrect Answer Choices:
1: While compartment syndrome is on the differential diagnosis, his signs and symptoms are not most consistent with that diagnosis.
2: While CT scan may show evidence of a stress fracture, MRI/bone scans have been shown to be superior methods for detection.
4: As infectious laboratories are normal, an ultrasound to rule out a deep abscess would likely be negative.
5: Bone biopsy is not appropriate without evidence of a lesion or concern for
osteomyelitis.

OrthoCash 2020
A 65-year-old female with a history of developmental dysplasia of the hip (DDH) undergoes a total hip arthroplasty (THA) utlizing a posterior approach. Following THA, she notices an inability to dorsiflex the ankle of her operative extremity. Her pre-operative and postoperative radiographs are seen in figues A and B. Which of the following intra-operative techniques could have avoided this complication in this patient?

Utilization of an anterior approach
Modular components
Use of a larger femoral head
Femoral shortening osteotomy
Acetabular osteotomy
Patients with DDH undergoing THA are at risk for post-operative sciatic nerve palsy due to intra-operative limb lengthening which increases tension on the sciatic nerve. Appropriate management after discovering a sciatic nerve palsy
after surgery should include immediate knee flexion and hip extension to decrease tension on the sciatic nerve. Sciatic nerve palsy following THA most commonly only affects the common peroneal nerve branch, and spares the tibial nerve and can present as an inability to dorsiflex and evert the ankle.
Farrell et al retrospectively looked at the risk factors for motor nerve palsy after THA. They found while motor nerve palsy is uncommon following primary THA, it can be a devastating complication. Some risk factors include: preoperative diagnosis of developmental dysplasia of the hip, posttraumatic arthritis, the use of a posterior approach, lengthening of the extremity, and use of an uncemented femoral implant. In their review, many of the motor nerve deficits did not fully resolve.
Barrack et al reviewed neurovascular complications following THA. They stated that sciatic nerve injury is the most common nerve injury following THA utilizing a posterior approach. In comparison, femoral nerve injury is much less common and is usually from an anterior approach.
OrthoCash 2020
A cane held in the contralateral hand reduces joint reactive forces through the affected hip approximately 50% by which of the following mechanisms?
Reducing hip abductor muscle pull
Increasing hip flexor muscle pull
Moving the center of rotation for the femoroacetabular joint
Increasing joint congruence at the femoroacetabular joint
Moving the center of gravity posterior to the second sacral vertebra Corrent answer: 1
A cane held in the contralateral hand reduces joint reactive forces through the affected hip up to 50% by reducing abductor muscle pull.
A cane create an additional force that keeps the pelvis level in the face of gravity's tendency to adduct the hip during unilateral stance. The cane's force must substitute for the hip abductors of the affected hip and creates a moment arm that is relatively long and originates on the side opposite the hip whose abductor muscles are weak. Additionally, the person needs adequate strength in the muscles of the wrist, elbow, shoulder girdle, and trunk.
Brand and Crowninshield performed a 3-dimensional hip joint reactive force evaluation of 4 different groups of patients. The groups included normal
subjects, preoperative THA subjects walking without a cane, preoperative THA subjects walking with a cane, and subjects following total hip reconstruction. Each of the 3 groups evaluated without the cane had statistically similar hip joint reactive forces. The preoperative THA subjects walking with a cane and significantly lower joint reactive forces (approximately 60%).
The article by Blount was named by JBJS as a "Classics in JBJS" in 2003. It is a commentary encouraging the use of canes by describing how the biomechanics of the hip joint are altered while using a cane.
Illustration A shows some of the mathematics behind cane use.
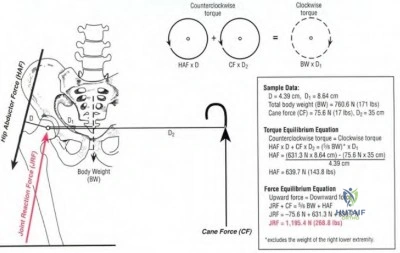
OrthoCash 2020
Which of the following is an example of an antalgic gait pattern not typically seen in clinical practice?
Patient's knee is maintained in slight flexion throughout the stance period for ipsilateral knee arthritis
Patient's contralateral step length is shortened with ipsilateral ankle arthritis
Patient leans their trunk laterally over the painful leg during stance phase with ipsilateral hip arthritis
Patient ambulates on their toes with an ipsilateral calcaneal stress fracture
Patient ambulates predominately through the heel for ipsilateral knee arthritis
The term antalgic gait is non-specific and describes any gait abnormality resulting from pain. A patient with knee arthritis maintains slight flexion throughout the gait cycle. This compensatory knee flexion is exacerbated if the patient has a concomitant effusion in the knee as flexion reduces tension on
the knee joint capsule. Gait compensation for knee arthritis also involves toe walking on the affected side, reducing the stride length, and reducing time of weight bearing on the painful leg.
Gok et al performed a case-control gait analysis study of 13 patients with OA and 13 normal patients. They found that walking velocity, cadence and stride length were reduced in the OA group and that the overall stance phase was prolonged in the OA group. They concluded that computerized gait analysis can be used to reveal various mechanical abnormalities accompanying arthrosis of the knee joint at an early stage.
Cole and Harner present Level 5 evidence about knee arthritis in the active patient. They stress that weightbearing radiographs are important in the diagnosis of arthritis. They also discuss the importance of looking for medial or lateral thrusts during gait and dynamic gait changes such as quadriceps avoidance or out-toeing.
Incorrect Answers:
OrthoCash 2020
A 78-year-old male falls at home four months following a right total hip arthroplasty. Right leg deformity, pain, and inability to bear weight are present on physical exam. An injury radiograph is provided in Figure A, while radiographs taken immediately following the initial total hip arthroplasty are provided in Figures B and C. The patient denies any prodromal groin pain prior to his fall. Which of the following is the best treatment option?

Traction for 6 weeks followed by slow return to weight bearing
Open reduction and internal fixation
Revision to a long, cementless femoral stem
Revision to a long, cementless stem with strut allograft
Revision to a long, cemented stem Corrent answer: 2
The clinical presentation and radiograph are consistent with a Vancouver B1 periprosthetic femur fracture. The stem appears stable within the femur, and there is no evidence of subsidence with comparison to the initial post-THA radiographs. This fracture pattern is best treated with internal fixation.
Illustrations A and B are radiographs of this patient following fixation. Illustrations C and D show bone healing at 2 years following the fracture.
Duwelius et al report on 33 periprosthetic femur fractures. All fractures that demonstrated a stable stem at the time of surgery were treated with internal fixation, while those that were unstable were treated with a long, cementless revision femoral stem. At 2.5 years complications were minimal and the patients had regained their pre-fracture level of function.
The review article by Kelley outlines the evaluation, classification, and treatment of periprosthetic femur fractures reinforcing the importance of stem stability within the femur. Periprosthetic fractures around a hemiarthroplasty should be treated with the same algorithm. However, if the patient had antecedent groin pain, then conversion to a total hip arthroplasty should be considered to prevent continued groin pain.

OrthoCash 2020
A 64-year-old male underwent the procedure shown in Figures A and B 7 weeks ago. He complains of difficulty with going down stairs. He reports no pain and denies constitutional symptoms. On examination the incision is well healed and no effusion is present. He is able to perform a straight leg raise with 5/5 strength. He lacks 2 degrees of terminal extension and has 80 degrees of active flexion. The knee is stable to varus and valgus stress testing at extension and mid flexion. His C-reactive protein and erythrocyte sedimentation rate are normal. What is the next most appropriate step in management?

Manipulation under anesthesia
Cortisone injection followed by physical therapy for quadriceps strengthening
Aspiration to evaluate for septic arthritis
Revise femoral component by downsizing A-P diameter
Revise tibial component and add 5 degrees of posterior tibial slope Corrent answer: 1
The history, physical examination, laboratory studies, and imaging are consistent with a total knee arthroplasty patient with arthrofibrosis. The next most appropriate option includes a manipulation under anesthesia to increase the patient's flexion.
Maloney presents Level 4 evidence discussing TKA postoperative arthrofibrosis. They report that manipulation under anesthesia was successful in improving flexion from an average of 67 degrees premanipulation to 111 degrees
postmanipulation.
Keating et al report Level 4 evidence of 113 patients that underwent manipulation following TKA. They found that 90% of the patients achieved improvement of ultimate knee flexion following manipulation. The average improvement in flexion from the measurement made before manipulation to that recorded at the five-year follow-up was 35 degrees.
OrthoCash 2020
Which of the following total hip arthroplasty patients appropriately meets the criteria for a surgical debridement with isolated femoral head and polyethylene liner exchange?
Prosthesis infection of 4 months duration
Prosthesis infection 8 weeks following implantation
Prosthesis infection 3 days following a systemic infection
Acetabular component loosening due to osteolysis
Vancouver Type A periprosthetic fracture.
Femoral head and polyethylene liner exchange is an appropriate treatment for the acutely infected arthroplasty. Acute infection has been defined as 3-6 weeks following surgery or following a systemic infection depending on the literature source. Subacute and chronic infections must be treated with a complete explant and exchange of all components. (One-stage or two-stage is controversial).
Salvati et al review the management of total hip arthroplasty infection. Most importantly, the pathogen must be isolated to direct antibiotic treatment. The acuity of the infection must also be recognized to direct surgical management.
OrthoCash 2020
A 54-year-old woman is at physical therapy 3 months after a total knee arthroplasty when she feels a pop and develops increased pain in her knee. She continues therapy for another 3 months but reports weakness and frequent buckling. On exam, she has full passive extension but a 60 degree extensor lag. A lateral radiograph is shown in Figure A. What is the treatment of choice?

Reconstruction with a bone-tendon allograft
Repair augmented with hamstring autograft
Continued therapy and strengthening
Arthrodesis
Treatment with orthotics for support Corrent answer: 1
The patient has a chronic patellar tendon rupture following a TKA with marked extensor lag and patella alta on radiograph. A study by Barrack et al concluded that allograft reconstruction for the chronically-disrupted extensor mechanism after TKA could restore active extension and improve ambulatory function. In chronic cases, primary repair with or without local tissue augmentation have had disappointing results. Extensor mechanism injuries after TKA was reviewed by Parker et al. Patellar tendon ruptures are rare complications after TKA with an incidence reported <2.5%. Quadriceps tendon ruptures are even more rare with an incidence ~1%.
OrthoCash 2020
When compared to the standard medial parapatellar approach for revision total knee arthroplasties, the oblique rectus snip approach
showed impairment in which of the following post-operative outcomes?
range-of-motion
patient satisfaction
pain
WOMAC function score
no difference in outcomes Corrent answer: 5
Meek et al compared the rectus snip to a standard medial parapatellar approach for revision total knee arthroplasty. The WOMAC function, pain, stiffness and satisfaction scores demonstrated no statistical difference. They concluded that use of a rectus snip as an extensile procedure had no adverse effect on outcome.
OrthoCash 2020
What is the range of pore size of cementless porous implants to allow for optimal bony ingrowth?
Less than 1 micron
50 to 400 microns
1,000 to 5,000 microns
10,000 to 50,000 microns
100,000 to 500,000 microns
The range of 50 to 400 microns is the optimal pore size for cementless porous implants to allow for optimal bony ingrowth.
Bobyn et al looked at the optimum pore size for fixation of porous surfaced metallic implants. Four different pore sizes were examined and placed in canine femurs for 4, 8, and 12 weeks and tested to measure the shear strength based on pore sizes. A pore size of 50 to 400 microns provided the maximum fixation strength in the shortest time period (8 weeks), implying maximal bony ingrowth.
Pilliar et al discussed two independent canine studies which showed that initial implant movement relative to host bone can result in attachment by a nonmineralized fibrous connective tissue layer. They state that implant movement of greater than 150 microns leads to fibrous ingrowth.
Jasty et al implanted porous-coated implants in the distal femoral metaphyses of twenty dogs and subjected them to zero, twenty, forty, or 150 micrometers of oscillatory motion. They found that that the implants that had been subjected to 150 micrometers of motion were surrounded by dense fibrous tissue.
OrthoCash 2020
An active 73-year-old male presents with progressive pain and instability 15 years after undergoing a left total knee arthroplasty. He denies any recent trauma. A comprehensive workup for infection is negative. What is the most appropriate management of this patient?

Protected weight bearing for 6 weeks
Revision total knee arthroplasty
Bisphosphonate therapy
Routine follow-up in 1 year
Polyethylene liner exchange and bone grafting Corrent answer: 2
This patient has evidence of periarticular osteolysis and component loosening around a previous total knee arthroplasty. He is symptomatic and would benefit from revision total knee arthroplasty (TKA).
Osteolysis is one of the leading causes for late reoperation in patients who undergo TKA. Osteolysis occurs as the result of a foreign body response to particulate wear debris from the prosthetic joint. These particles consist of polyethylene, polymethylmethacrylate cement, and metal, all of which have been shown to elicit a distinct inflammatory response. Once the particles are generated from and around the implant, they become phagocytosed by macrophages and giant cells in the synovial or periprosthetic tissue. These cells, in turn, become activated and can directly or indirectly cause osteolysis. The femur is prone to osteolysis in the region of the femoral condyles and near the attachments of the collateral ligaments of the femur. Osteolysis around the tibia tends to occur along the periphery of the component or along the access channels to the cancellous bone.
Maloney & Rosenberg reviewed the management and outcome of periprosthetic osteolysis around hip and knee implants. They recommended surgical intervention for periprosthetic osteolysis around a TKA with (1) first-time presentation of advanced osteolysis in the presence of an identifiable cause of wear particle production or in the presence of associated bone loss that places the structural integrity of the bone or fixation of the components at risk, (2) bearing surface wear in the presence of impending wear-through or related mechanical symptoms, (3) progressive osteolysis in an active individual, and (4) symptoms of wear debris-related synovitis that are refractory to conservative treatment.
Griffin et al. evaluated the results of isolated polyethylene exchange for wear and/or osteolysis in 68 press-fit condylar TKAs from four centers. At a minimum of 24 months after polyethylene exchange surgery, there were 11 failures (16.2%).
Gupta et al. discuss the etiology, diagnosis, contributing factors, and management of osteolysis as it relates to TKAs. They recommend that if the patient is asymptomatic with minimal osteolysis on plain radiographs, regular
follow-up at 6 months to 1 year with medical management including calcium and bisphosphonates would be adequate. If the patient becomes symptomatic or the osteolysis is progressive, then early liner exchange with or without tibial baseplate exchange is considered.
Figure A & B are AP and lateral radiographs of periarticular osteolysis and component loosening. Illustration A is an AP and lateral radiograph of the revision TKA.
Incorrect Answers:

OrthoCash 2020
Which of the following statements is true regarding the thirty-year follow-up data obtained from the Charnley "low-friction" total hip arthroplasty?
Acetabular component failure was the least common reason for revision surgery
The number of revisions required for periprosthetic fractures was higher than that for deep infections
Acetabular component failure was a more common reason for revision than deep infection
Femoral component failure was a more common reason for revision than acetabular component failure
Deep infection was the most common reason for revision Corrent answer: 3
Failure of the acetabular component was the most common reason for revision at thirty-years for the Charnley "low-friction" total hip arthroplasty.
The Charnley low-friction torque arthroplasty was introduced in 1962. It consisted of a 22mm diameter metal head, a cemented femoral component, and a cemented ultra-high-molecular-weight polyethylene acetabular component. Overall, the results were very good at thirty years with only 11.8% requiring revision.
Charnley et al. in 1972 reported the 4-7 year results of 379 "low-friction" total hip arthroplasties. Overall, their short-term results were very good with only 2 loose acetabular components, 0 loose femoral components, and 1 late dislocation.
Wroblewski et al. in 2009 reported the 30 year follow-up of 110 patients who underwent the "low-friction" total hip arthroplasty. 13 hips (11.8%) had to be revised. Of these, 5 were for problems with the acetabular component, 4 were for loosening of both components, 2 were for deep infection, 1 was from a loose femoral component, and 1 was from a fractured femoral component.
Illustration A shows a radiograph after a Charnley low-friction total hip arthroplasty. Note the all poly-ethylene acetabular component. Illustration B shows the components used for the operation.
Incorrect Answers:

OrthoCash 2020
A 71 year old gentleman underwent left total hip arthroplasty 10 years ago. Eighteen months ago he began having hip and thigh pain. Over the past 6 weeks, the pain has become excruciating and he has been unable to ambulate, even with the aid of a walker. He has mild pain with passive internal and external rotation of the hip. He is unable to ambulate in the office. Laboratory values are notable for a WBC of 10,300, CRP of 0.2, and ESR of 13. A radiograph is provided in figure A. Which of the following is the best treatment option?

Radionuclide bone scan and MRI
Open reduction internal fixation with a cable plate and allograft strut
Revision arthroplasty with a fully coated cementless stem, cable wiring, and bone graft
Revision arthroplasty with a modular, tapered stem and bone grafting of the diaphyseal fixation
Revision arthroplasty with a total femur prosthesis Corrent answer: 3
The radiograph is consistent with a periprosthetic femur fracture, with a loose femoral stem, and a Paprosky IIIA femoral defect. This is best treated with a fully-coated cementless stem with metaphyseal onlay allograft.
Paprosky devised a classification for femoral bone loss following THA. The classification is as follows:
Type I: minimal metaphyseal bone loss and intact diaphyseal fixation Type II: extensive metaphyseal bone loss with intact diaphyseal fixation
Type IIIA: severe metaphyseal bone loss with greater than 4 cm of diaphyseal bone preservation for distal fixation.
Type IIIB: severe metaphyseal bone loss and less than 4 cm of diaphyseal
bone preservation for distal fixation
Type IV: extensive metaphyseal and diaphyseal bone loss.
Type IIIA may be treated with a fully coated stem. Type IIIB should consider a tapered, modular stem and/or bone grafting. Type IV likely needs a megaprosthesis. In this patient, given the preserved diaphyseal bone, revision arthroplasty with a fully coated femoral stem is the most appropriate treatment.
The Sporer article reviews a case series of patients undergoing revision hip arthroplasty for femoral bone loss. Type IIIB defects with a femoral canal less than 19 mm may be treated with a fully porous-coated stem. However, patients with Type IIIB defect and a cavernous canal greater than 19 mm or a Type IV defect may need a modular tapered stem or a bone grafting procedure.
The Paprosky article summarizes his classification of femoral bone loss in revision hip arthroplasty and provides an algorithm for treatment. Extensively porous-coated, diaphyseal filling femoral components showed excellent results in Paprosky IIIA defects.
Radiograph A shows a total hip arthroplasty with severe metaphyseal bone loss and a supportive diaphysis.
Incorrect Answers:
OrthoCash 2020
A 74-year-old man presents with start-up thigh pain following a total hip replacement 10 years ago. Immediate post-operative radiograph is shown in Figure A. A current radiograph is shown in Figure B. Aspiration of the hip yields 1,005 white blood cells/ml. ESR is 12 (normal <40) and CRP is 0.4 (normal <1.2). Which of the following is the most appropriate management at this time?
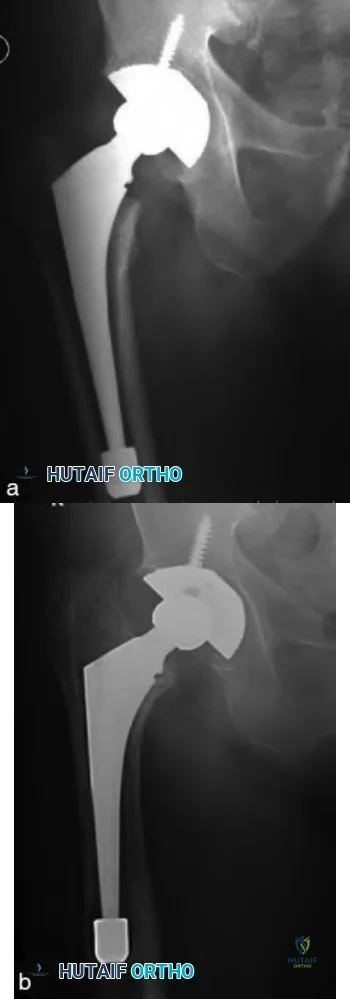
Revision of the femoral component to an uncemented, long, fully porous-coated stem
Revision of the femoral component to a cemented stem
Revision of the femoral component to an allograft prosthetic composite
Revision of the femoral component to a proximal femoral replacement
Removal of prosthesis with insertion of antibiotic spacer Corrent answer: 1
The clinical presentation is consistent with symptomatic, aseptic femoral component loosening with no evidence of femoral bone defects. Appropriate management consists of revision of the femoral component to an uncemented, fully porous-coated stem.
Aseptic loosening remains one of the most common indications for revision total hip arthroplasty. After infection has been ruled-out, management is determined by gauging the patients symptoms, the rate of progression of the subsidence, and the amount of femoral bone loss. Uncemented revision femoral components have shown superior results to cemented revision femoral components in the long-term. In the setting of Paprosky Type I, II, and IIIA defects of the femur, revision to an uncemented, fully porous-coated stem is advised.
Moreland et al. review the results of 134 patients (137 hips) who underwent revision arthroplasty with an extensively porous-coated cobalt chrome femoral prosthesis. At a mean follow-up of 9.3 years, only 10 (7%) had to removed for any reason.
Sporer et al. review the results of fully porous-coated stems, impaction bone grafting, and modular tapered stems for Paprosky III and IV femoral defects. They found a high rate of failure with fully porous-coated stems when used in patients with Type IIIB defects >19mm and Type IV defects. They attribute these failures to instability and the inability to eliminate micromotion.
Figure A shows a cementless, metaphyseal engaging femoral component in good alignment. Figure B is a post-operative radiograph from 10 years later showing significant subsidence of the femoral component.
Incorrect Answers:
OrthoCash 2020
A 72-year old female who underwent an uncemented right total hip arthroplasty 2 years ago complains of right hip pain after a fall. Figure A shows her current radiograph. Which acetabular bone defect classification and treatment option best describes this scenario?

AAOS Type III - anti-protrusio cage with augmentation and a posterior column plate
AAOS Type IV - anti-protrusio cage with screw fixation and a posterior column plate
AAOS Type II - jumbo cup with augmentation and a posterior column plate
AAOS Type I - total acetabular allograft with a cemented cup
AAOS Type II - custom triflange acetabular component Corrent answer: 2
Figure A shows pelvic discontinuity, which is consistent with a AAOS Type IV defect. Acetabular antiprotrusio cage with screw fixation and a posterior column plate is a reasonable treatment option for this condition.
Acetabular bone loss following total hip arthroplasty is a challenging problem with a wide variety of treatment options available. The two most widely accepted classification systems are the AAOS and Paprosky classifications.
AAOS type I defects are segmental, type II are cavitary, type III are combined cavitary and segmental, type IV is discontinuity, and type V is arthrodesis. All of the treatment options listed above are described for pelvic discontinuity,
with none being described as superior.
DeBoer et al. describe the results of 28 patients with pelvic discontinuity treated with a custom-made porous-coated triflange acetabular prosthesis. 20 of these patients were followed for 10 years. There were no re-operations, 5 hip dislocations, 1 sciatic nerve palsy, and an average improvement in the Harris hip score from 41 to 80.
Paprosky et al. retrospectively reviewed patients who had an acetabular revision using a trabecular metal acetabular component for a pelvic discontinuity and compared these patients with a cohort of patients who had a previous reconstruction for a pelvic discontinuity using an acetabular cage.
They found a decreased incidence of pain and need for walking aids in those patients who had revision with a trabecular metal acetabular component.
Figure A shows pelvic discontinuity, likely acute given the lack of associated bony defects and recent fall. Illustration A details the AAOS hip acetabular defect classification and Illustration B is the often cited Paprosky classification.
Incorrect Answers:

OrthoCash 2020
Which of the following is indicative of type 1 collagen breakdown and can be utilized as a marker of bone turnover?
Increased urinary N-telopeptide
Increased urinary cAMP and phosphate
Increased urinary phosphoethanolamine
Increased urinary Bence Jones proteins
Increased serum bone sialoprotein Corrent answer: 1
Urinary N-telopeptide is a marker of increased bone turnover and is a breakdown product of Type 1 collagen.
Increased serum alkaline phosphatase level and increased urinary markers of N-telopeptide, hydroxylproline, deoxypyridinoline indicate high bone turnover and can be seen in metabolic bone diseases such as Paget's disease.
von Schewelov et al. reviewed 160 patients that underwent total hip replacements and examined their urine specimens to see if N-telopeptide levels correlated to periprosthetic osteolysis. They found that n-telopeptide levels were 1/3 higher in the patients that had evidence of osteolysis. N-
telopeptide release and annual wear were both associated with increased prevalence of osteolysis in the study.
Illustration A shows a radiograph of Pagets disease of the femur, an example of a condition where there is an increased level of N-telopeptide in the urine. Illustration B is a radiograph showing periprosthetic osteolysis, another condition where there is an increased level of N-telopeptide in the urine.
Incorrect Answers:
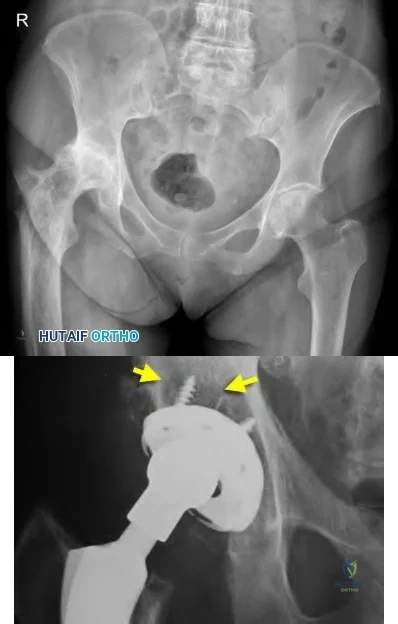
OrthoCash 2020
A 78-year-old female undergoes total hip arthroplasty through a minimally invasive surgical approach. During insertion of a metaphyseal fixation stem with a cementless press-fit technique, a crack in the calcar is identified. The stem is removed, two cable wires are passed around the calcar, and the same stem is reinserted. Which of the following statements is true?
The patient should be advised she is at greater risk of stem subsidence and early revision
Female sex is a risk factor for intraoperative calcar fracture
A better outcome would be expected if a long-stem diaphyseal fixation stem had been inserted after recognition of the calcar fracture
Cementless press-fit technique is not a risk factor for intraoperative fracture
Minimally invasive surgical approach is not a risk factor for intraoperative fracture
Of the statements listed, the only true statement is that female gender is a risk factor for intraoperative calcar fracture.
Calcar fractures are a documented complication of total hip arthroplasty. Studies have shown that successful outcomes can be achieved with stem removal, cable wiring of the calcar, and re-insertion of the primary stem.
Berend et al. reviewed a series of 58 total hip arthroplasties who sustained an intraoperative calcar fracture. All were treated with cable wiring of the calcar and stem insertion. The authors report no femoral component subsidence or failure otherwise at 16 year follow-up.
Graw et al. review a series of 46 revision THA's. Of the 46, fifteen underwent primary THA through a minimally invasive technique. The average length of time from primary THA to revision was 1.4 years for the minimally invasive group versus 14.7 years for the traditional exposure THA's. The authors conclude minimally invasive THA is a risk for early revision.
Davidson et al. review intraoperative periprosthetic hip fractures. "Risk factors for intraoperative periprosthetic fractures include the use of minimally invasive techniques; the use of press-fit cementless stems; revision operations, especially when a long cementless stem is used or when a short stem with impaction allografting is used; female sex; metabolic bone disease; bone diseases leading to altered morphology such as Paget disease; and technical errors at the time of the operation." The authors summarize techniques for treatment and postulate that long term outcome is unaffected when the intraoperative fracture is identified and treated appropriately.
Illustration A shows a nondisplaced calcar crack that was treated with a single Luque wire.
Incorrect Answers:

OrthoCash 2020
Which of the following types of prosthetic designs, seen in figures A-E, has been shown to have a high rate of loosening secondary to overconstraint?

Figure C shows an example of an Walldius hinge total knee prosthesis. This design had a higher rate of aseptic loosening (up to 20%) secondary to a high-degree of constraint.
Constraint is defined as the effect of the elements of knee implant design that provides the stability needed to counteract forces about the knee after arthroplasty in the presence of a deficient soft-tissue envelope. While increasing component constraint increases the stability of the knee, it also transmits forces to the fixation and implant interfaces, which may lead to premature aseptic loosening. First-generation total knee hinged prostheses were highly constrained devices that only allowed a single axis of rotation.
Lombardi et al. provide an Instructional Course Lecture on the different prosthetic designs in total knee arthroplasty. They argue that PCL sacrificing implants are more appropriate than cruciate-retaining implants in rheumatoid arthritis, previous patellectomy, previous high tibial osteotomy or distal femoral osteotomy, and in cases where the PCL is absent secondary to trauma.
Morgan et al. discuss constraint in primary total knee arthroplasty. They argue that a hinge total knee arthroplasty should be reserved for severe instability, elderly patients with comminuted distal femur fractures, patients with
extensor-mechanism disruption and unstable knees, and those with substantial bone loss not amenable to augmentation.
Figure C shows an example of a Walldius hinged prosthesis.
Illustration A shows an intra-operative example of a constrained-hinged knee prosthesis. Note the link between the tibial and femoral components, which differentiates it from a constrained, non-hinged prosthesis.
Incorrect Answers: The following responses are incorrect as they all have lower rates of aseptic loosening than than varus/valgus constrained prostheses or hinged designs.

OrthoCash 2020
A 28-year-old football player sustains a contact knee injury while being tackled. On physical exam, he has a 1A Lachman, and a normal McMurray test. His posterior drawer, dial, and varus stress tests are normal. He has pain and 5mm opening on valgus stress at 30 degrees of flexion. Which statement is true regarding the injured structure?
Resides between layers 1 and 2 on medial side of knee
Inserts onto Gerdy's tubercle
Originates slightly posterior and proximal to the medial epicondyle
Courses intraarticularly thru hiatus of lateral meniscus
Has an attachment between adductor tubercle and medial epicondyle at Schöttle's point
The clinical presentation is consistent with an injury to the superficial medial collateral ligament (MCL) of the knee, which originates slightly posterior and proximal to the medial epicondyle.
The superficial portion of the MCL is the primary stabilizer to valgus stress at all angles, contributing 57% and 78% of medial stability at 5 degrees and 25 degrees of knee flexion, respectively. Anatomic studies have shown that the superficial MCL originates approximately 3.2 mm proximal and 4.8 mm posterior from the medial femoral epicondyle and inserts into the periosteum of the proximal tibia (deep to pes anserinus). The superficial MCL lies in layer 2, just deep to gracilis and semitendinosus tendons.
Wijdicks et al. (2009) looked at radiographic identification of the primary medial knee structures including the superficial MCL. On the lateral radiograph, they found that the attachment of the superficial MCL was an average of 6.0 mm from the medial epicondyle.
Wijdicks et al. (2010) reviewed injuries to the MCL and associated medial structures of the knee. They state that physical examination is the initial method of choice for the diagnosis of medial knee injuries through the application of a valgus load both at full knee extension and between 20 degrees and 30 degrees of knee flexion. Treatment of isolated grade-III injuries to the MCL, or such injuries combined with an anterior cruciate ligament tear, should start with nonoperative treatment of the MCL due to high rates of success with nonoperative treatment. If operative treatment is required, an anatomic repair or reconstruction is recommended.
Illustration A shows the femoral and tibial attachments of the superficial MCL. Illustration B shows the osseous landmarks and attachments of medial knee structures (AT, adductor tubercle; GT, gastrocnemius tubercle; ME, medial epicondyle; AMT, adductor magnus tubercle; MGT, medial gastrocnemius tendon; sMCL, superficial MCL; MPFL, medial patellofemoral ligament; POL, posterior oblique ligament).
Incorrect Answers:
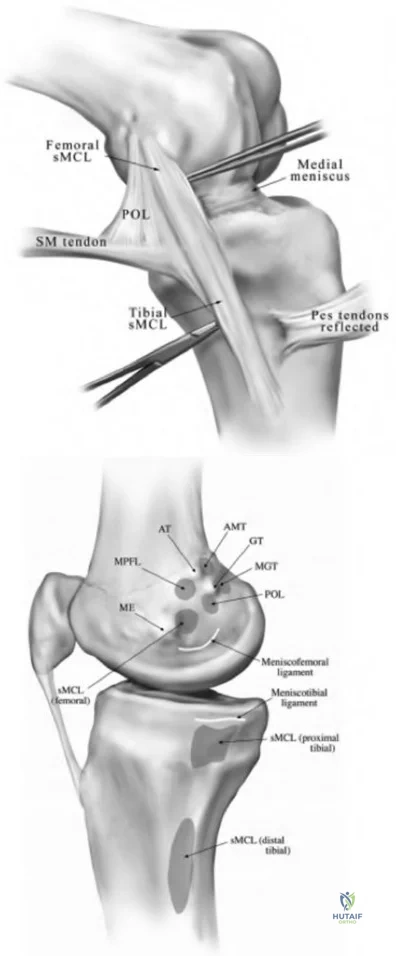
OrthoCash 2020
Which of the following best describes normal tibio-femoral joint kinematics ?
The femur undergoes internal rotation with knee flexion
The lateral femoral condyle remains stationary on the lateral tibia plateau during knee flexion from 0 to 120 degrees
The tibia undergoes internal rotation with knee flexion
The medial femoral condyle moves posteriorly on the medial tibial plateau during knee flexion from 0 to 120 degrees
Beyond 120 degrees of flexion only the lateral femoral condyle participates in femoral rollback
Tibia is subjected to internal rotation with knee flexion and the tibia EXternally rotates on femur as the knee EXtends.
The axis of rotation shifts posterior on the lateral condyle with knee flexion. Flexion and extension at the knee occur about a constantly changing center of rotation (polycentric rotation).
Freeman et al. conducted a biomechanical experiment and found that the medial femoral condyle does not move much from 0 to 120 degrees of flexion. They also found that the lateral femoral condyle and the contact area between that condyle and the tibia move posteriorly and tibial internal rotation occurs with knee flexion. They found that from 120 degrees to full flexion both condyles participate in "roll back".
Illustration A shows why the screw-home mechanism occurs. The medial tibial plateau is longer than the lateral tibial plateau, leading to external rotation of the tibia during extension as the femoral condyle rotates about the tibia. Video V shows an example of external tibial rotation during extension.
Incorrect Answers:
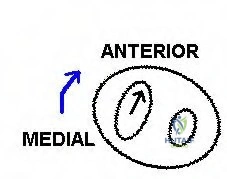
OrthoCash 2020
Which of the following molecules is associated with macrophage induced osteolysis surrounding orthopaedic implants?
BMP-7
IL-10
SOX-9
Osteoprotegrin
IL-1
Of the options provided, IL-1 is most associated with macrophage induced osteolysis surrounding orthopaedic implants.
Macrophages initiate the inflammatory cascade associated with aseptic loosening of orthopaedic implants by secreting platelet-derived growth factor (PDGF), prostaglandin E2 (PGE2), TNF-alpha, IL-1, and IL-6.
Archibeck et al. state the primary cells involved in the process of periprosthetic loosening include the macrophage, osteoblast, fibroblast, and osteoclast. They report the chemical mediators that are responsible for the cellular interactions and effects on bone primarily include PGE2, TNF-alpha, IL-1, and IL-6.
Drees et al. discuss the molecular pathway of aseptic loosening of orthopedic implants. They describe the following steps: 1) Wear debris particles released at the cement–bone interface attract macrophages, which, in turn, are stimulated to produce proinflammatory mediators and proteolytic enzymes; 2) RANKL, TNF-alpha, IL-1, IL-6, IL-17, and M-CSF mediate the differentiation of myeloid precursor cells into multinucleated osteoclasts, which release cathepsin K and acid and cause resorption lacunae; 3) Mesenchymal cells (prosthesis-loosening fibroblasts) present at the bone surface contribute actively to bone resorption.
Illustration A shows the pathway described by Drees et al.
Incorrect Answers
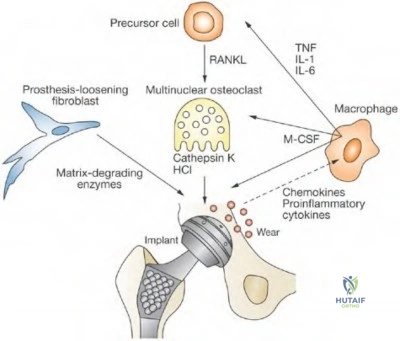
OrthoCash 2020
Which of the following templates, seen in Figures A-E, will increase the offset while keeping the leg lengths the same?

If the total hip prosthesis is inserted according to the template in Figure E, the offset will be increased, while the leg lengths will remain unchanged.
Restoration of limb length is essential following total hip arthroplasty. The amount of limb-length change will be the vertical distance between the center of rotation of the femoral component and the center of rotation of the acetabular component. Thus, when the femoral center of rotation on templating is inferior to that of the acetabular component, the limb will be shortened. Restoring femoral offset is also important. If the center of rotation of the prosthetic head lies lateral to that of the cup on templating, the reconstruction will produce decreased offset.
Scheerlinck et al. present a stepwise approach to hip templating through four steps. Step 1 involves identifying landmarks, step 2 involves assessing the
quality of the radiograph, step 3 identifies mechanical references, and step 4 optimizes implant positioning.
Tripuraneni et al. discuss the common errors encountered when templating for total hip arthroplasty. They found the most common error was excessive limb lengthening and incomplete medialization of the acetabular component.
Della Valle et al. review hip templating. They stress the importance of preoperative planning, but also discuss the importance of tactile feedback during the surgery in choosing the correct implants.
Illustration A shows a table of how offset and leg lengths can be changed through positioning and selection of components.
Incorrect Answers:
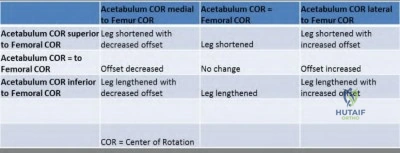
OrthoCash 2020
A 91-year-old male with a history of chronic leukemia and dementia falls and sustains the hip fracture shown in Figure A. He undergoes a hemiarthroplasty through a posterior approach. A postoperative radiograph is shown in Figure B. Three weeks later he dislocates the hip arising from the toilet seat. A radiograph is shown in Figure C. The patient undergoes a closed reduction and is placed in a hip abduction brace. Post reduction radiograph is shown in Figure D. One month later he returns to clinic complaining of pain and inability to bear weight through the leg. A radiograph of the hip is included in Figure E. Which of the following factors has MOST likely contributed to the instability of the hip hemiarthroplasty?

Femoral stem subsidence
Increased offset
Inadequate femoral stem neck length
Patient's dementia status
Patient's gender
The most likely contributing factor to the instability include the patient's dementia.
Sultan et al use a basic science model to show liners with elevated rims placed in the posterior superior quadrant allow greater range of motion to dislocation than standard liners. They also show that 32 mm heads have greater range of motion to dislocation compared to 28 mm heads.
Morrey et al reviewed a series of 19,680 primary THA's for late dislocation (first dislocation greater than 5 years after surgery). 165 hips (0.8%) had a late dislocation. Factors associated with late dislocation include implant malposition, neurologic decline, trauma, and polyethylene wear.
Figure A shows a femoral neck fracture. Figures B and D show a hip hemiarthroplasty in appropriate position. Figure C and E show a dislocated hip hemiarthroplasty
This patient's instability was managed by converting the hip hemiarthroplasty to a total hip arthroplasty with a constrained liner as shown in illustration A. No further instability episodes occurred following the revision.
Incorrect Answers:

OrthoCash 2020
What surgeon is credited for designing the prosthesis seen in Figure A?
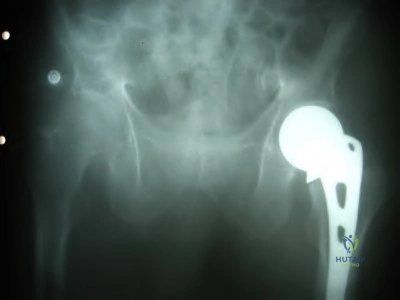
John Charnley
San Baw
Sir Harry Platt
Austin T. Moore
Charles Frederick Thackray Corrent answer: 4
Figure A shows an example of an Austin-Moore hemiarthroplasty.
Austin Moore developed the most popular long-stemmed prosthesis in the 1950s. The Austin-Moore prosthesis was a large, uncemented femoral stem that didn't use polyethylene. The Austin-Moore prosthesis had fenestrations for self-locking which later became the impetus for biological fixation. These implants were originally used to treat hip fractures and certain cases of degenerative arthritis. Later, in the 1960s, John Charnley introduced the idea of replacing the eroded acetabulum with a Teflon component.
Moore et al. describe the first metallic hip replacement surgery in 1940. The patient had a proximal femoral resection for a giant cell tumor. The original prosthesis he designed was a proximal femoral replacement, with a large fixed head, made of the Cobalt-Chrome alloy Vitallium.
Charnley et al. discuss the long-term results (up to 7 years) of the "low-friction" total hip arthroplasty. Infection rate was 3.8%, late mechanical failure was 1.3%, and most patients had excellent pain relief.
Figure A shows a radiograph of an Austin-Moore hemiarthroplasty. Illustration A shows an Austin-Moore prosthesis. Illustration B shows an example of Charnley's "low-friction" total hip arthroplasty, with a stainless steel head and
stem and a polyethylene acetabular component.
Incorrect Answers:
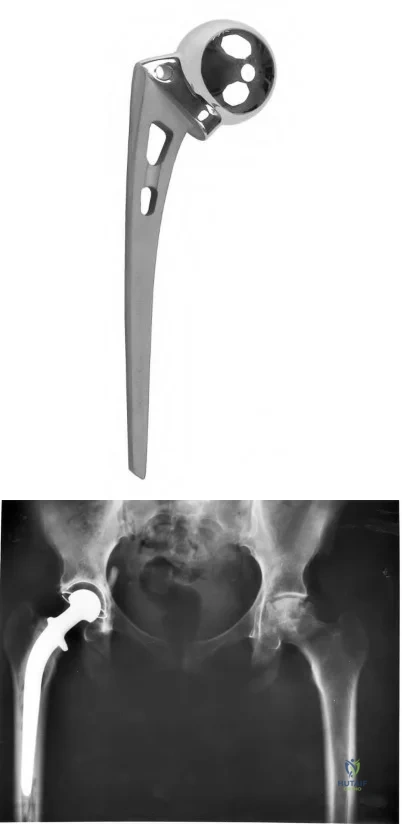
OrthoCash 2020
A 45-year-old man has had the gait disturbance shown in Video A ever since a total hip replacement two years ago. Since then he has undergone physical therapy and nerve exploration without any clinical improvement. Extensive AFO bracing was attempted but was not tolerated by the patient. A recent ankle radiograph is shown in Figure
A. The Silfverskiold test reveals dorsiflexion of 20 degrees with knee flexion, and 10 degrees with full knee extension. The results of muscle
testing using a Cybex dynamometer are shown in Figure B. What is the most appropriate next step in in treatment.
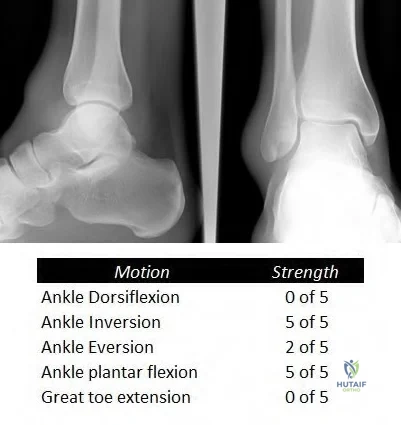
Ankle arthrodesis in 30 degrees of dorsiflexion
Posterior tibial tendon transfer to the lateral cuneiform through the interosseous membrane
Split anterior tibial tendon transfer to the cuboid
Peroneus longus transfer to the navicular and gastrocnemius recession
Flexor hallucis transfer to the navicular and tendo Achilles lengthening (TAL) Corrent answer: 2
The clinical presentation is consistent with a sciatic neuropathy following THA in a patient that does not tolerate AFO bracing. Posterior tibialis tendon transfer is the next most appropriate step in treatment.
Sciatic neuropathy, especially involving the common peroneal branch, is a known complication of total hip arthroplasty. Typically a patient is adequately treated with an AFO. In some clinical situations an AFO is not tolerated, and a tendon transfer is required. The posterior tibial tendon is the most commonly used donor muscle. A tendon transfer is feasible only if the tendon possesses at least 4/5 power. There is a loss of 1 MRC grade of strength following transfer.
Rodriguez et al. retrospectively reviewed the results of the Bridle procedure 10 patients (11 feet) with a foot drop. The Bridle procedure consists of a posterior tibial tendon transfer through the interosseous membrane to the dorsum of the foot with a dual anastomosis to the tendon of the anterior tibial and a rerouted peroneus longus in front of the lateral malleolus. In their study all 11 feet were brace-free at final followup at 6.68 years.
Yeap et al. retrospectively reviewed 12 patients who were treated with tibialis posterior tendon transfer for footdrop. They found good/excellent patient satisfaction in 10/12 patients. Additionally they found favorable variables for a good outcome include common peroneal nerve palsy over sciatic nerve palsy, male gender less than 30 years of age.
Figure V is a Video that shows a right footdrop with high steppage gait. Figure A shows normal ankle radiographs. Figure B shows the results of dynamometer testing described above. Illustration A shows the Bridle procedure. The left panel shows how the tibialis posterior tendon (C) is tunneled through the interosseous membrane and through a slit in the tibialis anterior tendon (A) and inserted into the second cuneiform. The peroneus longus (B) is also transected and the distal stump is routed anterior the lateral malleolus and anastomosed to the tibialis anterior and tibialis posterior (at the slit where it passes through the tibialis anterior). The right panel shows retrieval of the tibialis posterior tendon above the ankle and passage through a window in the interosseous membrane.
Incorrect Answers:
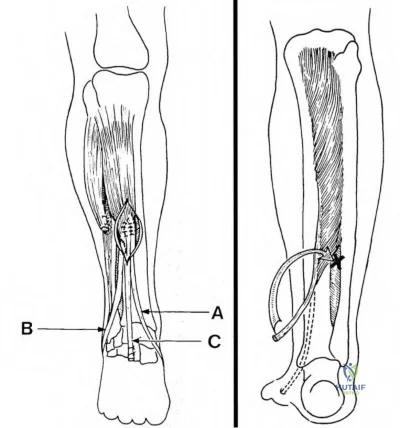
OrthoCash 2020
Which of the following variables is associated with elevated serum metal ion levels following metal-on-metal hip resurfacing arthroplasty?
Smaller implant diameter
Smaller acetabular cup abduction angle
Higher postoperative functional scores
Severe preoperative osteoarthritis
Anteversion of acetabular cup between 10 and 20 degrees Corrent answer: 1
Smaller femoral head diameter is associated with elevated serum metal ion levels with metal-on-metal hip resurfacing arthroplasty.
Metal-on-metal (MOM) hip resurfacing arthroplasty has the advantage of better wear properties (lower linear wear rate and volume of particles) than metal on polyethylene. However, elevated serum metal ion levels is one of the negatives which has received much attention recently. Studies have found smaller implant diameter and acetabular cup abduction angle >55 degrees are associated with elevated serum metal ion levels. Cup abduction angles of greater than 55 degrees lead to a more vertical cup and edge loading.
Desy et al. found that smaller implant diameter, larger cup inclination, and lower postoperative functional scores are associated with increased cobalt and chromium levels after metal-on-metal hip resurfacing. They found that severity of preoperative osteoarthritis, acetabular version, femoral stem-shaft and valgus angle, and anterior orientation of the femoral component had no effect on the circulating metal ion levels.
DeHaan et al. obtained serum ion levels in 214 MOM resurfacing patients at least 1 year following surgery. They found that cup abduction angles greater than 55 degrees combined with smaller component sizes led to edge loading and elevated ion levels.
Illustration A shows how a metal-on-metal prosthesis design allows you to have a larger femoral head as opposed to a metal on polyethylene design (example in THA). Illustrations B and C show a photo of a metal on metal resurfacing implant and radiographs of the implant.
Incorrect Answers:
2: Elevated cup abduction angle leads to elevated serum metal ions.
3: Higher postoperative functional scores have not been shown to increase serum metal ions.
4: Severity of pre-operative arthritis has not been associated with increased serum metal ions.
5: Anteversion of the acetabular cup between 10 and 20 degrees has not been shown to increase serum metal ions.
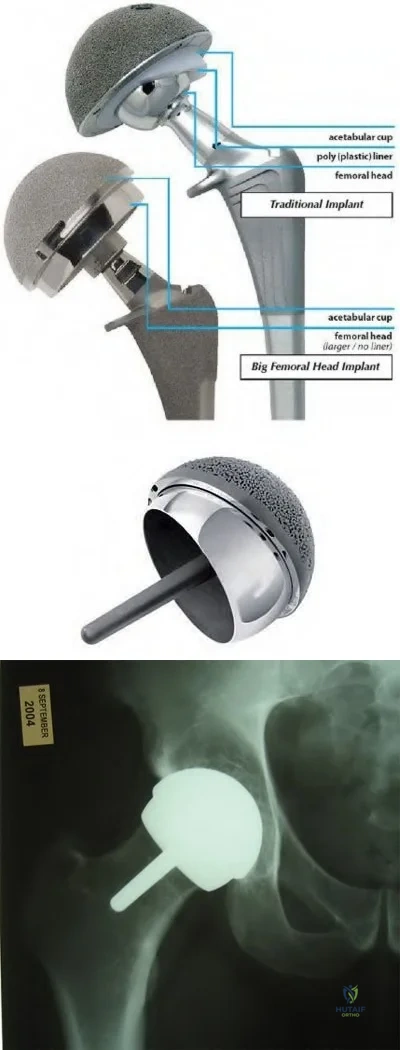
OrthoCash 2020
Which of the following intra-operative steps would put a patient at risk for lateral patellar maltracking during total knee arthroplasty (TKA)?
External rotation of the femoral component
Medial placement of the patellar component
Internal rotation of the tibial component
Lateral translation of the femoral component
Superior placement of the patellar component Corrent answer: 3
Internal rotation of the tibial component increases the Q angle and causes an increased risk of lateral patellar maltracking.
During TKA, useful techniques that help prevent patellar maltracking include: external rotation of the femoral and tibial components, lateral translation of the femoral component, and medial placement of the patellar component.
In an instructional course lecture, McPherson looked at patellar tracking in primary TKA. He reviews the concept of patellofemoral maltracking, the importance of the Q angle, mechanical alignment, femoral component rotation, tibial component positioning, patellar component positioning, patellar height, and patellar resurfacing as factors related to patellofemoral tracking.
Bengs et al. studied the effect of patellar thickness on intra-operative knee flexion and patellar tracking during PCL retaining TKAs. Using 2mm increments (2-8 mm), passive knee flexion was recorded and gross mechanics of patellofemoral tracking were assessed. On average, passive knee flexion decreased 3 degrees for every 2-mm increment of patellar thickness, there was no gross effect on patellar subluxation or tilt.
Illustration A shows how internal rotation of the tibial component would increase the Q angle, and thus be more likely to have lateral patellar maltracking.
Incorrect answers:
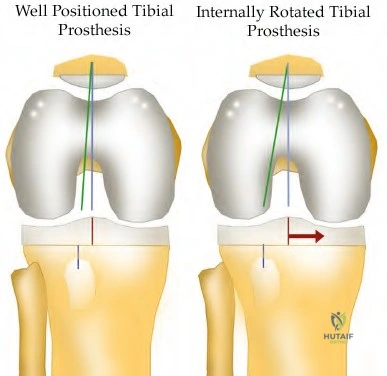
OrthoCash 2020
A patient undergoes a primary total hip arthroplasty with a highly cross-linked ultra-high molecular weight (UHMW) polyethylene acetabular liner. In comparison to a 28mm femoral head, a 32mm femoral head will provide which of the following?
Increased risk of dislocation
Decreased range of motion
Decreased risk of osteolysis
Equivalent wear rate of the polyethylene acetabular liner
Increased risk of periprosthetic fracture Corrent answer: 4
Wear rates of highly cross-linked UHMW polyethylene liners are independent of femoral head size between 22 and 46 mm in diameter.
While the wear rates of old polyethylene liners increased with increasing femoral head size, wear rates of the new highly cross-linked UHMW polyethylene liners have shown to be independent of head size. This is extremely advantageous, as increasing the femoral head size improves range of motion and increases jump distance, thereby decreasing dislocation rates.
Geller et al. report a prospective series of 42 patients that had a total hip arthroplasty with a highly cross-linked UHMW polyethylene liner and a femoral head >32 mm in diameter. After three years, there were no cases of osteolysis or failure due to aseptic loosening.
Muratoglu et al. studied the wear rates of several polyethylene liners with varying femoral head sizes. In the highly cross-linked UHMW polyethylene group, wear rates were independent of femoral head size.
Illustration A shows how increasing femoral head size increases the jump distance required for dislocation.
Incorrect Answers:
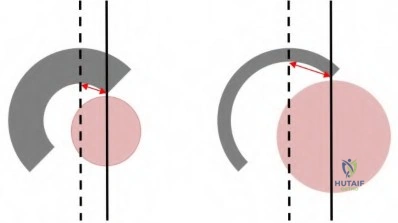
OrthoCash 2020
A 56-year-old male undergoes an uncomplicated revision total knee arthroplasty. Post-operatively, he is noted to have a foot drop that has persisted despite conservative management including bracing and physical therapy. At two months, the patient undergoes external neurolysis with no improvement in function. At 18 months follow-up, he demonstrates passive ankle dorsiflexion 10 degrees past neutral, complete absence of active dorsiflexion, and 5/5 inversion strength. Which of the following is the most appropriate treatment at this time?
Continue Ankle-foot orthosis (AFO) and physical therapy
Repeat neurolysis with possible nerve repair
Peroneus tertius transfer
Peroneus tertius transfer with achilles tendon lengthening
Posterior tibial tendon transfer to dorsum of foot Corrent answer: 5
A peroneal nerve palsy (with intact posterior tibial tendon strength) that has failed conservative management is best treated with a posterior tibial tendon transfer to the dorsum of the foot.
Peroneal nerve palsy following total knee arthroplasty or knee dislocation is a potentially devastating complication that may lead to lack of active dorsiflexion and a compensatory steppage gait pattern. Initial management consists of an ankle-foot orthosis (AFO) and physical therapy to maintain passive ankle dorsiflexion. If nerve function fails to return during the course of conservative management and the patient demonstrates intact posterior tibialis muscle strength, posterior tibial tendon transfer to the dorsum of the foot has been shown to improve functional outcomes and eliminate the need for continued bracing. The most common procedure for posterior tibial tendon transfer involves transferring the tendon through the interosseous membrane and inserting the tendon onto the lateral cuneiform.
Prahinski et al. review the results of 10 patients at 61 months' follow-up who underwent the Bridle transfer (posterior tibialis transfer through interosseous membrane and peroneus longus to front of lateral malleolus) for peroneal nerve palsies. They conclude the Bridle procedure is adequate for return to function in low-demand individuals, but may fail over time in those who return to vigorous physical activity.
Rodriguez et al. review the results of 10 patients who underwent the Bridle procedure for peroneal nerve palsy in an attempt to balance their foot and
provide dorsiflexion. All of their patients were brace free at an average followup of 6.8 years.
Video V shows the clinical results 10 weeks after transfer of the tibialis posterior tendon for a drop foot.
Incorrect Answers:
OrthoCash 2020
An 82-year-old male sustains a ground level fall and sustains the injury shown in Figure A. Which of the following treatment methods is most appropriate for treating this injury?

Closed reduction and functional bracing
Open reduction and fixation with a plate with screws and cerclage cables
Open reduction and fixation with a cortical allograft strut and cerclage cables
Revision hip arthroplasty with bridging of the fracture with a plate with screws and cerclage cables
Total femoral replacement Corrent answer: 2
This fracture pattern is typically referred to as an interprosthetic fracture; this is increasing in incidence due to increasing numbers of patients with ipsilateral hip and knee arthroplasty.
The first reference by Ricci et al reviewed 50 Vancouver B1 fractures treated with a lateral plate without allograft. They reported 100% union rate at a mean of 12 weeks and only one deep infection. Nearly 75% of patients were able to return to their baseline ambulatory status.
The second reference by Ricci et al reviewed 59 patients with periprosthetic femur fractures (THA or TKA) treated with ORIF without bone grafting. They report 58/59 patients healed after the index procedure and 49/59 were able to
return to their baseline functional level.
The reference by Fulkerson et al reported on 24 patients who underwent LISS plate fixation of periprosthetic femur fractures around well-fixed THA or TKA. They reported union in 21/24 at a mean of 6.2 months, with only one failure of fixation. They note that percutaneous fixation is effective although technically demanding.
Figure A shows an interprosthetic femur fracture between well-fixed hip and knee arthroplasties.
Incorrect Answers:
OrthoCash 2020
A 62-year-old female undergoes an uncomplicated primary total knee replacement. Her knee range-of-motion pre-operatively was 0-135 degrees of flexion. Which of the following is true regarding the immediate post-operative use of a continuous passive motion machine in this patient?
Reduced risk of venous thromboembolism
No long-term difference in ROM compared to patients not using CPM
Increased passive knee flexion at 6 months
Increased length of hospitalization
Decreased risk of surgical site infection Corrent answer: 2
The use of a continuous passive motion (CPM) machine following primary total knee arthroplasty has not shown any long-term benefits with regards to
range-of-motion.
The concept of CPM was created by Dr. Robert Salter in 1970 and is currently being used in select patients following total knee replacement, ACL
reconstruction, and a variety of other procedures about the knee. In theory, the CPM allows for movement of synovial fluid to allow for better diffusion of nutrients into damaged cartilage. Additionally, it has been thought to prevent fibrous scar tissue formation about the joint. While some studies have shown increased early active knee flexion at two weeks, these results were not significant at later follow-up. Controversy exists as to whether these small benefits offset the patient inconvenience and expense of the CPM.
Lotke et al. expolre the effects of tourniquets and CPM machines in 121 patients undergoing total knee arthroplasty. They found that immediate CPM combined with intraoperative release of the tourniquet increased blood loss. The patients with the least amount of blood loss had the tourniquet released after a compressive dressing was applied and in whom CPM was delayed for a few days.
Bourne et al. perform a meta-analysis on the effectiveness of CPM following total knee arthroplasty. They found the CPM plus physical therapy increased active knee flexion more than physical therapy alone 2 weeks after surgery with a decreased length of hospitalization. The benefits of increased active knee flexion were not maintained after 2 weeks.
Illustration A shows an example of a CPM machine. Incorrect Answers:
from available RCTs to conclude that CPM reduces the risk of venous thromboembolism following total knee arthroplasty.

OrthoCash 2020
A 67-year-old female complains of anterior groin pain one year following a primary, uncemented total hip arthroplasty. The pain is exacerbated when she tries to climb stairs or get up from a seated position. She denies any recent fevers or chills. On physical exam, the pain is reproduced with resisted seated hip flexion. Laboratory analysis, including WBC, ESR, and CRP are within normal limits. Radiographs reveal that the components are appropriately positioned without evidence of loosening or fracture. Which of the following is the most appropriate at this time?
Revision of the acetabular component
Image-guided diagnostic injection of lidocaine into the iliopsoas tendon sheath
Hip aspiration
Bone scan
Conservative management including activity modifications, NSAIDs, and physical therapy
The patients history and physical exam are most consistent with iliopsoas impingement. This diagnosis is most reliably confirmed with a diagnostic/therapeutic injection of steroid or lidocaine into the iliopsoas tendon sheath.
Iliopsoas tendinitis following total hip arthroplasty is an uncommon but treatable cause of anterior groin pain following total hip arthroplasty. The true incidence is unknown, but some studies suggest it is the cause of a painful
total hip arthroplasty in up to 4.3% of cases. Potential causes include a malpositioned acetabular component, excessively long screws, limb length discrepancy, or retained cement. Diagnosis is confirmed by injecting the iliopsoas tendon sheath. Most cases are refractory to conservative management and often require surgical intervention. In the case of a malpositioned acetabular component, revision to a more agreeable position is advisable. In the absence of a defined etiology, iliopsoas tendon release offers adequate pain relief and return to function in a majority of patients.
Lachiewicz et al. review anterior iliopsoas impingement after total hip arthroplasty. They state that most patients with iliopsoas impingement often require surgical treatment, with options including iliopsoas tendon release or resection, removal of protruding cement or screws, and acetabular revision.
O' Sullivan et al. review 16 cases of iliopsoas impingement following primary total hip arthroplasty. Only 1 of the cases was secondary to a malpositioned acetabular component, with the other 15 cases being attributed to altered anatomy of the iliopsoas tendon as a result of the surgery. These 15 patients underwent iliopsoas tendon release, and all had improvement in pain and function following surgery.
Nunley et al. review 27 patients with a presumed diagnosis of iliopsoas impingement following total hip arthroplasty who were treated with fluoroscopically guided injections of the iliopsoas bursa. The average modified Harris hip score in the patients who underwent injection improved, however, 30% required an additional injection and 22% underwent surgical release for continued pain.
Illustration A shows a flouroscopic injection into the iliopsoas tendon sheath. Incorrect Answers:
revision of the acetabular component without a confirmed diagnosis is not advisable.
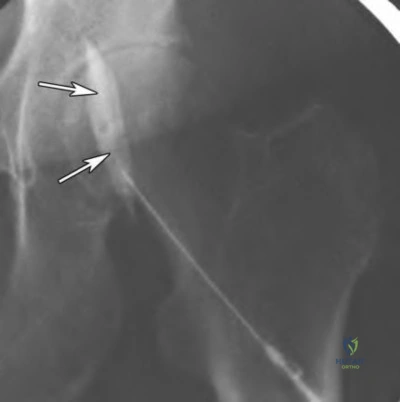
OrthoCash 2020
A 72-year-old female underwent an uncomplicated primary total hip replacement 18 years ago. Current radiographs reveal the abnormality shown in Figure A. Which of the following cell types (Figures B-F) is implicated in the process shown by the arrow?

Figure F shows an example of a macrophage, which is a key mediator in the osteolytic process shown in Figure A.
Osteolysis is the end result of a biologic process that begins when the number of wear particles following a joint replacement overwhelms the body's capacity to clear them from circulation. The residual particles are phagocytosed by macrophages, which then release an array of cytokines and other inflammatory mediators that recruit osteoclasts to resorb bone.
Gupta et al. review osteolysis following total knee arthroplasty, including etiology, diagnosis, and management. Amongst other things, they highlight the importance of design changes to minimize osteolysis including highly cross-linked polyethylene and alternative bearing materials.
Ren et al. performed a study where they implanted a hollow titanium rod into the distal femur and pumped polyethylene particles into the femoral bone marrow cavity. They found that macrophage migration occurs at a systemic (rather than local) level, and that the recruitment of macrophages led to localized osteolysis.
Holt et al. review the biology behind aseptic osteolysis. Specifically, they highlight the importance of the RANK-RANKL-OPG pathway as the final
common pathway to osteoclastogenesis, and the possibility of eliminating osteolysis by blocking this pathway. AMG-162 is a human immunoglobulin monoclonal antibody with a high affinity for RANKL, and studies are currently being undertaken to determine its safety and efficacy.
Figure F shows an example of a macrophage, which may be identified by its irregular shape and phagocytic inclusions. Illustration A shows the pathway by which marcrophages induce osteolysis following a joint replacement surgery.
Incorrect Answers:
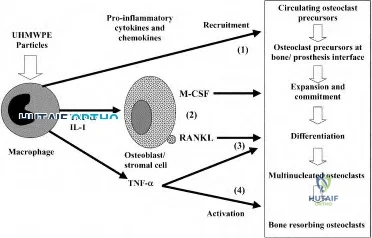
OrthoCash 2020
A 45-year-old with a history of sickle cell anemia reports hip pain for the past 6 months. A radiograph of the affected hip is shown in Figure A. Which of the following interventions has been shown to have the best outcomes in this patient population?

Observation
Bisphosphonates
Hemi-arthroplasty
Uncemented metal on polyethylene total hip arthroplasty
Cemented metal on polyethylene total hip arthroplasty Corrent answer: 4
Based on the radiographs and current literature, the best intervention is an uncemented metal on polyethylene total hip arthroplasty.
Avascular necrosis of the hip may be idiopathic in nature or associated with alcoholism, steroid use, or as in this case, sickle cell anemia. The Ficat staging system is used to classify avascular necrosis of the hip. Changes in treatment are driven by development of symptoms as well as the development of subchondral bone collapse (Ficat Stage 3). In those with with femoral head flattening (Ficat Stage 4) and acetabular degenerative changes (Ficat Stage 5), total hip replacement has good to excellent outcomes.
Mont et al. review surgical options for avascular necrosis of the hip. Head preserving procedures are generally reserved for those patients where the femoral head has not collapsed. Collapse and associated arthritis warrant utilization of arthroplasty procedures.
Mont et al. conducted a systematic review to better delineate the symptomatic progression of asymptomatic avascular necrosis of the hip. They found that patients with sickle cell disease have the highest rate of progression to
collapse. Medium sized, laterally located lesions were associated with a higher frequency of collapse and joint preserving procedures are recommended for these.
Figure A shows radiograph of a patient with avascular necrosis; note the femoral head flattening, narrowing of the joint space and acetabular sclerosis.
Incorrect Answers:
OrthoCash 2020
The function of which of the following structures is to resist internal tibial rotation with the knee in full extension?
Anterior cruciate ligament
Iliotibial band
Popliteus tendon
Popliteofibular ligament
Posterior oblique ligament Corrent answer: 5
The primary function of the posterior oblique ligament is to resist internal tibial rotation with the knee in full extension.
The posterior oblique ligament is a structure within the posteromedial corner of the knee, with attachments proximally to the adductor tubercle of the femur and distally to the tibia/posterior knee capsule. The posterior oblique ligament and posteromedial capsule play a significant role in the prevention of additional posterior tibial translation in the knee in the setting of posterior cruciate ligament injury. They also act to resist internal tibial rotation with the knee in full extension.
Griffith et al. reports that the posterior oblique ligament provides significant resistance to valgus and internal rotation forces with knee extension. They used a cadaver model and demonstrated that the superficial MCL resists valgus and external rotation forces more than the posterior oblique ligament, while the posterior oblique ligament is more involved in resisting internal rotation.
Tibor et al. reviews the anatomy of the posteromedial corner of the knee. They report that failing to recognize injury to these structures may cause failure of cruciate ligament reconstruction surgery, and that reconstruction or repair of the posteromedial corner may be indicated in the face of multiple ligament injuries.
Illustration A shows the posteromedial corner of the knee, including the posterior oblique ligament.
Incorrect answers:
4: These structures are not primary restraints to internal tibial rotation in full extension.
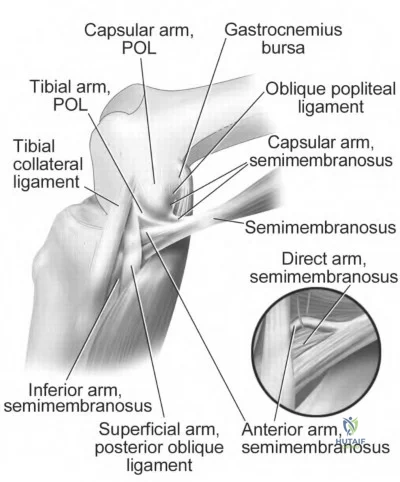
OrthoCash 2020
Increasing the porosity of a cement spacer for an infected total knee arthroplasty leads to which of the following?
Increased strength
Increased elution of antibiotics
Increased cement density
Improved cement-prosthesis bonding
Increased reinfection rate Corrent answer: 2
Elution of an antibiotic is increased with increased porosity of a cement spacer. This porosity increase can be obtained with hand mixing and avoiding the use of a vacuum-type mixing device.
Joseph et al. reviews antibiotic-impregnated cement in hip arthroplasty. They note that use of this cement in one- or two-stage revisions has lowered reinfection rates, with the spacers acting to reduce dead space while stabilizing the joint.
Cui et al. reviews antibiotic impregnated cement for TKA and THA. They report that use of greater than 2 grams of antibiotic per 40 gram unit of cement weakens the cement and that use of two antibiotics in conjunction may potentially increase elution.
The reference by Stevens et al compared Simplex and Palacos bone cement in regards to elution in a TKA mold model. They found that initial as well as weekly (9 weeks total) elution rates were greater in the Palacos spacers than the Simplex models. They recommend use of the Palacos cement in TKA model to target antimicrobial delivery while limiting the potential for systemic antibiotic-related toxicity.
Illustrations A and B show an antibiotic spacer in a two-stage revision TKA. Illustration C shows a PROSTALAC in a two-stage revision THA.
Incorrect Answers:

OrthoCash 2020
A 65-year-old patient was treated with an open reduction/internal fixation for a left femoral neck fracture sustained 25 years ago. Five years ago he developed hip pain and was converted to a left hip hemiarthroplasty. He presents with complaints of groin pain for the past 6 weeks. A recent radiograph is shown in Figure A. The patient’s physical exam is limited secondary to pain. Serum laboratory values are WBC-8.0, ESR-20, CRP-0.5. A synovial fluid aspirate of the hip demonstrates < 500 cells (60% PMN). What is the most likely cause of this patient's symptoms?

Acetabular protrusio
Infected hip hemiarthroplasty
Lumbar radiculopathy
Impingement of the hip hemiarthroplasty
Iliopsoas tendinitis
Based on the history, radiographs, and laboratory values, the patient has developed failure of his hip hemiarthroplasty. At this point in time he warrants a conversion to a total hip arthroplasty.
Avascular necrosis (AVN) of the femoral head after traumatic injury to the femoral neck occurs at an incidence of 10-45%. Although the risk increases with failure to anatomically reduce the fractue, it can still occur in non displaced settings. Treatment of avascular necrosis in older patients includes hip hemiarthroplasty or a total hip replacement. With the former, development of acetabular protrusio can contribute to groin symptoms. Functional outcomes have been reported to be higher in those receiving total hip replacement for AVN of the femoral head.
Lee et al. prospectively compared the use of bipolar hip hemiarthroplasty versus total hip arthroplasty for advanced stages of AVN of the femoral head (Ficat Stage 3). Total hip scores were most improved in the total hip arthroplasty group. Migration of the outer head in the hemiarthroplasty group was seen in 23% of patients. They recommend use of a total hip arthroplasty in patients with Ficat Stage 3 AVN of the femoral head
Ito et al. evaluated the outcomes of patients who underwent bipolar hemiarthroplasties for femoral head avascular necrosis. They found that proximal migration and acetabular degeneration were risk factors for groin symptoms. They also found that outcomes were inferior to patients who had undergone total hip arthroplasty for AVN of the femoral head. They recommend use of total hip arthroplasty in advanced osteonecrosis of the femoral head
Diwanji et al. evaluated outcomes of patients who underwent a conversion from a bipolar hip arthroplasty to total hip arthroplasty in 25 patients. Thirteen (52%) patients were revised to THA because of acetabular erosions. Follow up was completed for an average of 7.2 years. At final follow-up, they found improvement of the Harris Hip Scores and improvement of the pain portion of the WOMAC index. They recommend use of total hip replacement as an option to salvage failed bipolar hip hemiarthroplasty
Figure A shows the radiograph of a hip hemiarthroplasty where acetabular protrusion has developed.
Incorrect Answers
OrthoCash 2020
A 38-year-old female patient presents to your office three years after a hip resurfacing. She complains of worsening left hip discomfort for the last 6 months. Her ESR is 12 (normal 0-20) and CRP is 1.2 (0-5). A radiograph and axial and coronal MRI scans are shown in Figures A, B, and C. What is the most likely diagnosis?
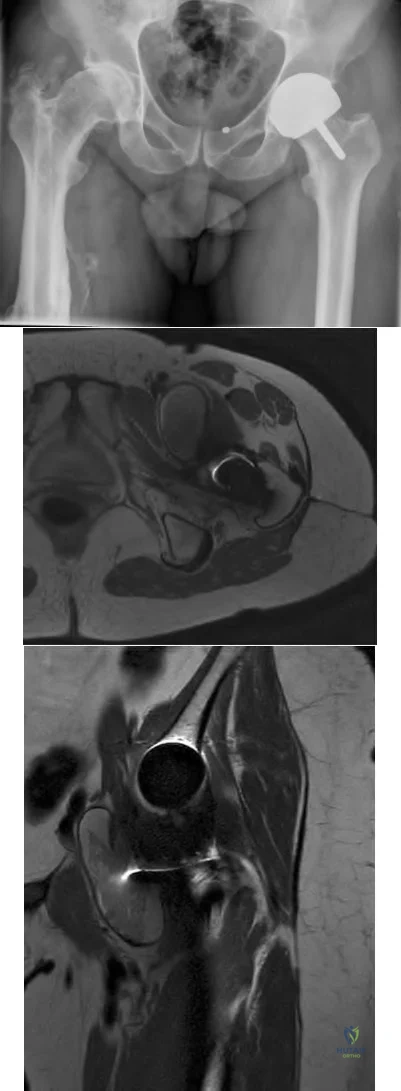
Infection
Type I Hypersensitivity reaction
Femoral neck fracture
Prosthesis Loosening
Pseudotumor
The clinical presentation is consistent with a young woman who has developed a symptomatic pseudotumor following hip resurfacing. Her hip discomfort is related to a mass that has developed around the left hip.
Pseudotumors, also referred to as Aseptic Lymphocyte-Dominated Vascular-Associated Lesions (ALVAL), are sterile inflammatory lesions that most commonly occur from metal-on-metal articulations. They occur at an incidence of 0-39% with metal-on-metal resurfacing hip components. The exact mechanishm of formation is unclear, however excessive wear is considered the initiating process, leading to the release of microscopic metal particles. These are cytotoxic to macrophages once phagozytised, leading to necrosis within the lesions and the development of semi-solid or fluid-filled masses around the implant. Lymphocytes are thought to be responsible for the tissue reaction.
Patients often do not complain of pain, but present with a mass around the hip that causes discomfort.
Hart et al. performed a case-control study comparing patients with well-functioning metal-on-metal hip resurfacing to those who have painful prostheses. They found no significant difference between the painfree and painful groups with MRI diagnosed pseudtumors (61% vs. 57%). They concluded that the presence of a pseudotumor should not automatically necessitate revision surgery.
Daniel et al. reviewed the current concepts surrounding pseudotumor. Risk factors associated with pseudotumor formation and failure are female gender, age under 40, hip dysplasia, metal hypersensitivity, and small components.
Larger components have been found to decrease the risk of failure.
Figure A is an AP pelvis radiograph of a patient following a left hip resurfacing surgery. Figures B and C are axial and coronal MR images demonstrating a large pseudotumor around the left hip resurfacing. Illustrations A and B identify the large pseudotumor as outlined in red.
Incorrect Answers:
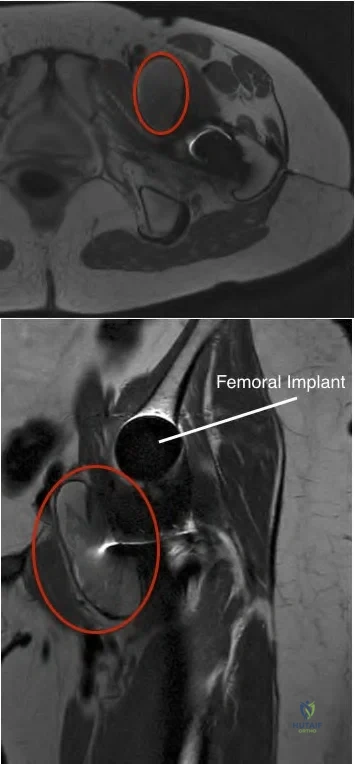
OrthoCash 2020
After total hip arthroplasty (THA) for osteoarthritis a patient is unable to dorsiflex her ankle or extend her great toe. She is treated conservatively with an orthosis and after 3 months on physical therapy she ambulates with a "slapping gait." What is the most appropriate next treatment option?
MRI of her spine
Ankle Fusion
Continue Ankle-Foot Orthosis
Revision total hip arthroplasty
Sural nerve grafting Corrent answer: 3
The patient has suffered from a peroneal nerve injury most likely from errant retractor placement during the hip replacement resulting in a foot drop. The most appropriate next treatment is an ankle-foot orthosis.
The ankle joint of an ankle-foot orthoses (AFOs) should restrict plantarflexion to prevent foot drop during the swing phase. In a patient who can not actively dorsiflex the foot the AFO keeps the foot in a neutral position during gait allowing for uninterrupted swing during ambulation.
Park et al reviewed common peroneal nerve injury after THA. Only one-half of the patients in the study who developed common peroneal nerve palsy following total hip arthroplasty recovered fully. The mean time to recovery was approximately one year for partial peroneal palsy and one and one-half years for complete palsy. Obesity adversely influenced the nerve recovery. Thus, at 3 months, the nerve should continue to be monitored and the use of an AFO would assist in ambulation.
Yokoyama et al. developed an AFO with an oil damper to adjust the plantarflexion resistive moment as excessive plantarflexion resistance will cause excessive knee flexion during the stance phase. They found the AFO with the oil damper achieved sufficient plantarflexion of the ankle and mild flexion of the knee by adjusting a proper plantarflexion resistive moment during initial stance phase, and provided a more comfortable gait than did the traditional AFOs.
Illustration A shows the location of the sciatic nerve relative to the short external rotators when performing a posterior approach to the hip.
Incorrect Answers:
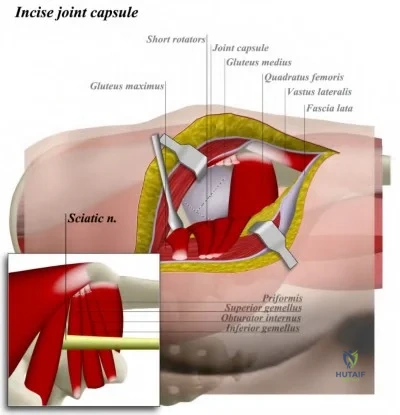
OrthoCash 2020
Which of the following statements is true about racial disparities in total joint arthroplasty?
The rate of surgical intervention for African American males is lower than white or Hispanic males
The rate of surgical intervention for Hispanics is higher than that for whites
The rate of surgical intervention for white males is lower than for African American males
There is no difference in the rate of surgical intervention between whites, Hispanics, or African Americans
The rate of surgical intervention is equal for Hispanic and white males Corrent answer: 1
The rate of surgical intervention for African American males is lower than either white or Hispanic males.
Numerous studies have shown clear racial disparities in the utilization of total joint arthroplasty for the treatment of osteoarthritis. African American and Hispanic patients undergo total joint arthroplasty at a rate much lower than
white patients, even in areas where insurance coverage is more equitable. Currently, little is known about the reasons for such disparities.
Skinner et al. reviewed the Medicare claims between 1998 through 2000 to determine any racial or ethnic disparities amongst patients undergoing total knee arthroplasty. Amongst other things, they showed that the arthroplasty rates for black men were consistently lower than white men in nearly every region.
Nelson reviews health disparities in orthopaedic surgery. Amongst other things, they discuss how African American patients and white patients perceive the same pain and functional limitations for similar radiographic disease. Thus, ethnic differences in perception of symptoms cannot explan the racial disparities noted in total joint arthroplasty.
Incorrect Answers:
OrthoCash 2020
A 65-year-old man presents with aseptic loosening 3 years after total knee arthroplasty. The surgeon reviews radiographs of his knee and takes him to the operating room for revision total knee arthroplasty. During surgery, the exposure technique shown in Figure A is used. Which of the following radiographs (Figures B-F) has the greatest likelihood of needing this exposure technique?

Figure A shows a tibial tubercle osteotomy (TTO). Patella baja (Figure D) is an indication for a TTO.
In revision total knee arthroplasty (TKA), surgical exposure should be extensile. Different exposure techniques have been described (see below). Patella baja may indicate that there is patellar tendon contracture. In this instance, a TTO can be used to prevent inadvertent patellar tendon avulsion which is difficult to repair and may lead to loss of function. Further, proximal transfer of the osteotomized tibial tubercle may be used to correct patella baja, bearing in mind that excessive superior translation alters the mechanics of the knee by making the quadriceps less efficient.
Younger et al. reviewed surgical approaches in revision TKA. They include quadriceps snip, patellar turndown, TTO, femoral peel, medial epicondylar osteotomy and quadriceps myocutaneous approach.
Mendes et al. reviewed the results of TTO in revision TKA. They advocate TTO for cases where the patellar cannot be retracted laterally with knee in 90deg of flexion. Complications include nonunion, tubercle fragment fracture and displacement, and tibial metaphyseal fracture (at the level of the distal cut of the osteotomy).
Della Valle et al. reviewed surgical approaches for revision TKA. They advocate TTO because repair is stronger than patellar turndown, there is less tension on the tibial tubercle in flexion than on the quadriceps tendon, and where multiple operations are required (as multiple VY approaches lead to excessive scar, making the approach difficult) or where stemmed tibial components need to be removed.
Illustration A shows tibial tubercle osteotomy hinged on a lateral periosteal flap. Illustration B shows quadriceps snip. Illustration C shows patellar turndown. Illustration D shows medial epicondyle osteotomy.
Incorrect Answers
situation.
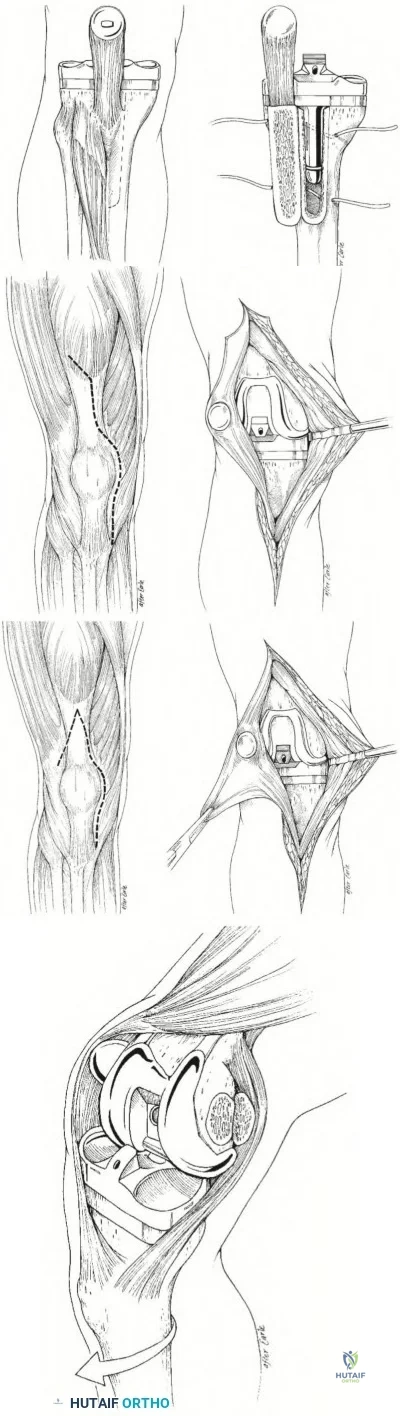
OrthoCash 2020
Which of the following is the most common intraoperative complication in a patient with sickle cell disease undergoing a total hip arthroplasty?
Periprosthetic fracture distal to the implant
Iatrogenic fracture causing pelvic discontinuity
Perforation of the femoral canal
Cardiac arrest from fat embolization to lungs
Injury to the sciatic nerve Corrent answer: 3
Perforation of the femoral canal during preparation of the femur is not an uncommon complication, with rates ranging from 4.9-18.2%.
While total hip arthroplasty is extremely effective for pain relief in patients with osteonecrosis of the hip secondary to sickle cell disease, the procedure carries a higher rate of complications compared with non-sickle cell disease patients. Particular attention should be given to the preparation of the femur as femoral medullary widening from chronic marrow hyperplasia adjacent to patchy areas of dense sclerosis can make preparation of the canal difficult.
Some surgeons prefer to ream over a guide-wire to avoid perforation.
Jeong et al. reviewed total hip arthroplasty in patients with sickle cell disease. Amongst other things, they discuss the difficulties associated with preparation of the femoral canal, quoting a perforation rate between 4.9-18.2%. They also state there are no prospective studies comparing cementless to cemented THA, but retrospective data has shown promising results with cementless components.
Hernigou et al. retrospectively reviewed 244 patients with sickle cell disease that underwent cemented total hip arthroplasty. They had a 3% infection rate, a relatively low rate of revision for aseptic loosening, and a 27% rate of medical complications. Overall, they viewed their results as favorable.
Illustration A shows a patient with bilateral AVN secondary to sickle cell disease. Note the areas of patchy dense sclerosis in the metaphyseal region of the proximal femur.
Incorrect Answers:
to be more common in this patient population. The rate of post-operative hematoma causing sciatic nerve dysfunction may be higher in this patient population.

OrthoCash 2020
A 63-year-old patient presents with periprosthetic joint infection 3 years after primary total knee arthroplasty. A radiograph of her knee is seen in Figure A. She undergoes 2-stage revision total knee arthroplasty. Radiographs taken at the time of explantation are seen in Figure B. An articulating antibiotic spacer is placed. Two months later, she is deemed to be free of infection and is taken to the operating room for the second stage operation. Intraoperatively, it is noted that the collaterals are intact and the previous tibial tubercle osteotomy had healed. What is the most appropriate surgical strategy at this point?

Address epiphyseal defects with impaction particulate bone grafting
Address metaphyseal defects with structural allograft and uncemented, unstemmed implants
Address metaphyseal defects with uncemented, porous metaphyseal
sleeves and uncemented, stemmed implants
Address diaphyseal defects with porous metal cones and uncemented, stemmed implants
Address diaphyseal defects with cemented stemmed implants Corrent answer: 3
This patient has massive metaphyseal defects following resection of primary TKA implants. Metaphyseal defects may be addressed with uncemented, porous metaphyseal sleeves and uncemented stemmed implants.
In revision settings, metaphyseal bone is often deficient. The Anderson Orthopaedic Research Institute classification (AORI) is most commonly used to classify defects. Stemmed implants are necessary to divert stress away from deficient metaphyseal defects to structurally sound cortical bone. These may be cemented or uncemented.
Haidukewych et al. reviewed metaphyseal fixation in revision TKA. For large defects, they advocate structural allograft, porous metal cones, and stepped metaphyseal sleeves.
Bush et al. reviewed managing bone loss in TKA. They cautioned that joint line elevation, distal femoral bone loss, and femoral prosthesis downsizing leads to flexion instability. They advocate cement filling for Type I defects, modular augments for Type 2, impaction grafting for Type 1 or 3, structural allograft for Types 2 and 3, metaphyseal filling or megaprosthesis for Type 3, including porous metal implants.
Figure A shows an infected primary TKA with a stemmed tibial component with medial augments. This suggests that the revision implant will require at least a stemmed, augmented component. Figure B shows massive metaphyseal defects (AORI Type 2) at the time of explantation. Illustration A comprises postop images of osseointegrated metaphyseal sleeves and stemmed implants. Illustration B depicts the AORI classification (see Review Topic for detailed description). Images courtesy of Haidukewych et al (Ref 1).
Incorrect Answers:
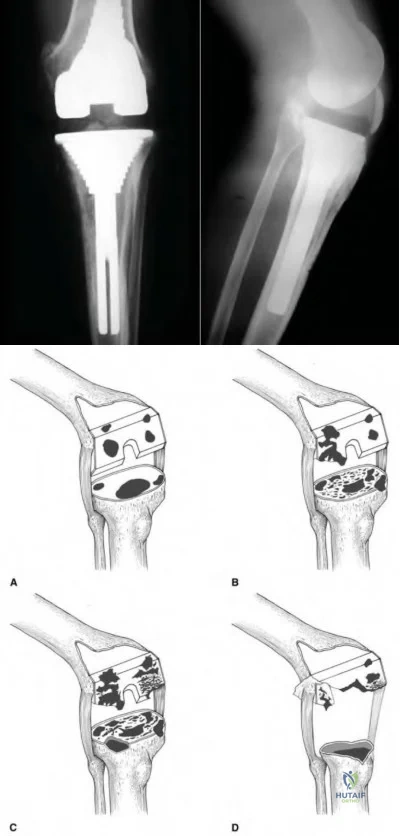
OrthoCash 2020
During templating for a total hip arthroplasty, placing the femoral head center of rotation directly superior to the center of rotation of the acetabular component will have which of the following effects?
Increase offset
Decrease limb length
Decrease offset
Increase limb length
No change in length or offset Corrent answer: 4
Placing the femoral head center of rotation directly superior (above) the acetabular center of rotation will lengthen the limb without changing offset.
When templating the femoral component for a total hip arthroplasty, it is imperative to restore limb length and offset. To change limb length, the femoral component center of rotation (COR) can be adjusted in a superior or inferior direction. If the femoral component COR is superior to the acetabular component COR, the limb will be lengthened (as in the example above).
Conversely, if the femoral component COR is inferior to the acetabular component COR, the hip will be shortened. A change in offset will be determined by the medial/lateral relationship between the acetabular and femoral components. In the example above, the COR of the femoral component is directly above the COR of the acetabular component. In this situation, there is no change in offset.
Merle et al. performed a retrospective cohort study to identify differences in femoral offset as measured on an AP pelvis radiograph, AP hip radiograph, and a CT scan. They found that femoral offset is significantly underestimated on AP radiographs of the pelvis. In contrast, AP radiographs of the hip are much more accurate in representing true offset.
Della Valle et al. review the importance of preoperative planning prior to total hip arthroplasty. While they mention that templating can be very accurate, determination of stem and cup size should also be determined by tactile feedback during broaching and reaming.
Illustration A shows the femoral head COR inferior to the acetabular COR. This will result in a decreased limb length.
Incorrect Answers:

OrthoCash 2020
Which of the following intra-operative errors most commonly leads to patellar maltracking during a total knee arthroplasty?
Using the gap balancing technique instead of measured resection technique
Internal rotation of the femoral component
External rotation of the tibial component
Lateralization of the femoral prosthesis
Overresection of the patella
Internal rotation of the femoral component increases the Q-angle and will increase the likelihood of patellar maltracking.
Patellar maltracking is one of the most common complications following a total knee arthroplasty. Any alteration that results in increased lateral retinaculum tension or an increased Q-angle may lead to patellofemoral instability.
Common causes include internal rotation of the femoral or tibial components, medialization of the femoral component, and placement of the patellar prosthesis on the lateral border of the patella. If a patient presents with postoperative maltracking and component rotation is thought to be the cause, a CT scan is the diagnostic study of choice.
Rhoads et al. analyze 7 cadaveric specimens to define the kinematics of the intact knee and to evaluate the effects of prosthetic replacement on those kinematics. Amongst other things, they showed that lateralization of the femoral component improved patellar tracking and prevented dislocation.
Malo et al. review patellar maltracking following a total knee replacement. They discuss the importance of externally rotating the femoral component on the femur relative to the posterior articular condyles to establish a rectangular and balanced flexion gap and to accommodate central patellar tracking.
Illustration A shows how an internally rotated femoral component displaces the patella medially. The blue line is a straight line upwards from the tibial tubercle, and the green line represents a line from the tibial tubercle to the center of the patella. The difference between the blue and green lines in the internally rotated prosthesis is the amount the patella has displaced medially. If you deviate the patella medially, this increases the Q-angle and could lead to patellar maltracking in a total knee replacement.
Incorrect Answers:
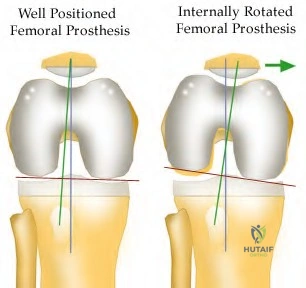
OrthoCash 2020
When performing a total knee arthroplasty on a 60-year-old female patient, a surgeon chooses not to resurface the patella. Instead, he performs a patelloplasty by excising the marginal osteophytes and reshaping the patella. All of the following statements comparing the results of patelloplasty to patella resurfacing are true EXCEPT:
There is no difference in relative risk of anterior knee pain.
There is no difference in relative risk for revision surgery involving the tibial and femoral components.
There is an increased risk that she will need secondary resurfacing.
No difference in rates of patellar avascular necrosis or patellar tendon injury.
Total knee arthroplasty improved function regardless of whether the patella was resurfaced.
In TKA with an unresurfaced patella, there is an increased risk of anterior knee pain and secondary resurfacing.
Surgeons can choose to resurface or not resurface all patellae, or selectively resurface patellae. In unresurfaced patellae, they may perform a patelloplasty (excise marginal osteophytes and reshape the patella). Unresurfaced patellae have increased risk of anterior knee pain requiring secondary resurfacing.
Indications for resurfacing include inflammatory arthritis, patella maltracking, patellofemoral osteoarthritis as the main indication for TKA.
Meneghini et al. reviewed the literature on patellar resurfacing. Prospective, randomized studies show conflicting results with regards to satisfaction rates between groups. Meta-analyses show increased risk of re-operation and anterior knee pain in the unresurfaced group.
Parvizi et al. performed meta-analysis on 1519 knees. They found there was
(1) lower relative risk of re-operation (resurfaced group), (2) lower relative risk of anterior knee pain (resurfaced group), (3) increased rate of secondary resurfacing (unresurfaced group), (4) no difference in patient satisfaction, (5) TKA improved function regardless of whether the patella was resurfaced, (6) no difference in complications.
Incorrect Answers:
OrthoCash 2020
A 55-year-old patient returns for followup 2 years after a left ceramic-on-ceramic total hip arthroplasty. He has no pain or symptoms of instability. The video in Figure V shows him ascending stairs. All of the following factors may contribute to this phenomenon EXCEPT
Impingement
Edge-loading
Loss of fluid film lubrication.
Third-body particles
Subclinical infection
The clinical presentation is consistent for prosthesis squeaking following a THA. Squeaking is multifactorial and may include impingement, edge-loading, loss of fluid film lubrication, and third-body particles. Subclinical infection does not play a role in squeaking.
Squeaking is defined as a high-pitched, audible sound occurring during movement of the hip. In ceramic-on-ceramic (COC) hips, the incidence is 0.5-10%. The incidence of revision because of squeaking is 0.5%. Squeaking is less common in metal-on-metal bearing surfaces (4-5%).
Chevilotte et al. reviewed COC bearing surfaces. They found that without lubrication, squeaking occurred with normal gait, high load, stripe wear, material transfer, edge wear and microfractures. In contrast, with lubrication, squeaking only occurred with material transfer.
Finkbone et al. reviewed COC total hip arthroplasty in patients <20-years-old after 52-month (average) follow-up. They found that survival rate was 96% with 1 revision for a loose acetabular component (failure of bone ingrowth). They found no cases of osteolysis, which can theoretically occur because of stripe wear, or femoral neck-on-liner impingement.
Walter et al. reviewed squeaking hips. They found that this phenomenon is associated with (1) walking, bending, rising (cyclical gait movements or extreme flexion), (2) maloriented acetabular components, (3) impingement,
(4) third-body particles, (5) edge loading, (6) loss of fluid film lubrication and
(7) thin, flexible (titanium) stem.
The video shows squeaking of a left total hip arthroplasty during hip extension from a flexed position. This is consistent with edge loading. Illustration A shows superior edge loading in the walking position. The arrow represents the loading force. The superolateral edge of the liner is in contact with the superior surface of the head. The dark area (area of edge loading) is anteverted with respect to a line of latitude (dark line) on the head. Illustration B shows posterior edge loading in the bending position. The arrow represents the loading force. The posterior edge of the liner is in contact with the superior surface of the head. The shaded area represents the area of edge loading and the dark stripe indicates wear on the femoral head.
Incorrect Answers:
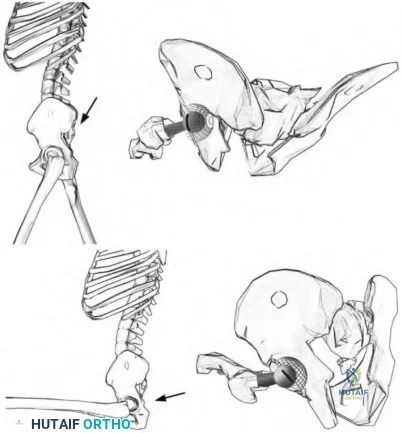
OrthoCash 2020
Figure A shows the image of a 72-year-old male who sustained a fall from standing. Past medical history is significant for hypertension. He was a community ambulator without the use of a cane or walker prior to the fall. During the operation, he is noted to have a well-fixed acetabular component without significant wear of his polyethylene liner, but his femoral component is easily extractable. Which of the following correctly pairs his Vancouver classification and appropriate surgical intervention?
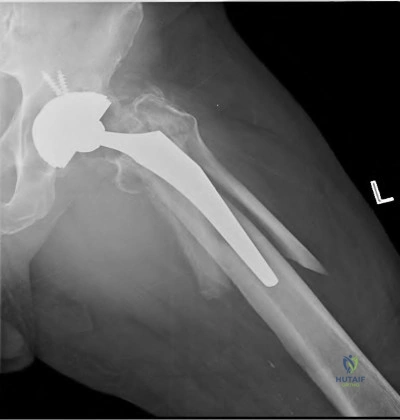
Vancouver A, Revision of femoral component to cemented stem with fixation of the fracture
Vancouver B1, Revision of femoral component to cemented stem with fixation of the fracture
Vanvouver B1, Revision of femoral component to a long, porous-coated, cementless stem with fixation of the fracture
Vancouver B2, Fixation of the fracture with a plate and cerclage wires
Vancouver B2, Revision of femoral component to a long, porous-coated, cementless stem with fixation of the fracture
Figure A shows a Vancouver B fracture around the femoral prosthesis. Because the prosthesis is noted to be loose during the operation, it is classified as a Vancouver B2 fracture. The most appropriate operation would be revision of the femoral component to a long, porous-coated, cementless stem in addition to fixation of fracture with a plate and cerclage wires.
According to the Vancouver classification, a type B2 fracture occurs around or just distal to a loose femoral stem with adequate proximal bone. Revision of the femoral component is necessary, with uncemented stems showing superior clinical results to cemented stems in most studies. The revision prosthesis should bypass the distal fracture by 2 cortical widths.
Corten et al. reviewed thirty-one patients with Vancouver B2 fractures that
were treated with a long cemented stem with additional allograft or plate fixation. At 46 months, none of the implants had to be revised, but it should be noted that 43% of the patients died within the first year.
Mulay et al. reviewed 24 patients with Vancouver B2 and B3 fractures managed with a cementless, tapered, fluted, and distally fixed stem. 91% of fractures united uneventfully. Complications included dislocations (5), nonunions (2), and infection (1).
Springer et al. review 116 patients with Vanvouver B fractures treated with revision of the femoral component. The uncemented, extensively porous-coated implants had the highest likelihood of stable fixation and were not associated with any nonunions.
Illustration A reviews the Vancouver classification for periprosthetic femur fractures. Illustration B shows a post-operative radiograph following a Vancouver B2 fracture. In this case, a trochanteric plate with cerclage wires was used to fix the fracture. A long-stemmed, porous-coated, cementless femoral prosthesis was used for the revision.
Incorrect Answers:
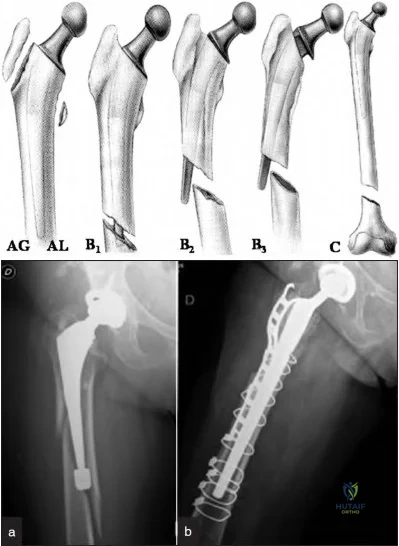
OrthoCash 2020
A 56-year-old male undergoes revision of his right hip arthroplasty for acute pain and radiographs suggestive of ceramic femoral head fracture. At the time of the revision, multiple fragments of the ceramic femoral head were seen in the joint and soft tissues. The components were noted to be in good position. He was copiously irrigated and the ceramic head was exchanged with a metallic femoral head. 12 months later, the patient presents with insidious onset right groin pain. Radiographs show no gross abnormalities without signs of loosening. Which of the following is the most likely cause of the patient's pain?
Periprosthetic infection
Massive third body wear
Pseudotumor formation
Soft tissue metallosis
Iliopsoas tendonitis
The most likely cause of the patient's pain is massive third body wear caused by retained ceramic fragments.
Cermamic femoral head fractures create many fragments that are difficult to extract at the time of revision surgery. During the revision surgery, it is imperative to remove all fragments that can be visualized. Despite a thorough debridement, microscopic fragments will still remain. These particles may cause pain through the creation of an inflammatory response in the tissues.
Exchange of the femoral head should be performed with another ceramic head, as opposed to a metal head. If a metal head is used, abrasive wear will ensue as the microscopic fragments will scratch the femoral head due to differences in hardness.
Traina et al. describe their experiences with revision of ceramic components. Most commonly, fractures of ceramic components occur as a result of trauma, dislocation, or errors in operative technique. These include head-neck taper mismatch, impacting the ceramic head with too much force, debris, and intraoperative damage to the metal neck taper.
Hannouche et al. review ceramics in total hip replacement. They state that if the ceramic is properly manufactured, it can be a highly effective, low-wear solution for the young patient in need of a total hip replacement.
Illustration A shows the typical ceramic femoral head used for a total hip arthroplasty. Illustration B shows a fractured ceramic head in many pieces.
Incorrect Answers:

OrthoCash 2020
Figure A and B are radiographs of a 77-year-old patient presenting with right hip and upper thigh pain for the past 3 months. He is an avid golfer and plans to travel south for 6 months on a golf tour. He denies fever, chills or weight loss. His past medical history includes hypertension and a right total hip replacement 15 years ago. Physical examination reveals minimal pain with range of motion. ESR=10 (normal range 0-20) and CRP=4 (normal range 0-10). He does not want any further surgery. The patient is at the highest risk of which complication with non-operative care?

Infection
Pseudotumour formation
Periprosthetic femoral fracture
Periprosthetic acetabular fracture
Dislocation
This patient has presented with significant osteolysis and aseptic loosening of his femoral THA component. If untreated, he is at an increased risk of a periprosthetic femur fracture.
Indications for surgery for periprosthetic osteolysis include: pathological fracture, impending pathological fracture, symptomatic THA with evidence of osteolysis, and extensive osteolysis that would compromise revision surgery in the future. The goal of surgery is to remove the loose component, repair/bypass/replace bone deficiency, and obtain stable component fixation.
Robbins et al. reviewed the causes of pain in THA. They report that hip pain can originate from the implant, soft tissue, or bone. The use of laboratory tests (e.g. ESR/CRP), radiographic and fluoroscopic imaging, hip aspirate, contrast arthrography and local anesthetic injections can help to determine the origin of pain.
Ollivere et al. report that the most frequent cause of failure after total hip replacement in all reported arthroplasty registries is periprosthetic osteolysis. Osteolysis occurs with the activation of macrophages and a complex biological cascade that results in bone loss.
Hirakawa et al. analyzed the circumstances around retrieved failed THA components. They showed that cement mantle defects, noncircumferential porous coatings, and screw holes are risk factors for osteolysis. They conclude by saying that the formation of a granulomatous tissue that ultimately invades the bone-implant interface is the final step in the pathogenesis of aseptic loosening.
Figure A and B show AP and lateral views of a right THA. The femoral stem shows gross loosening in all zones. Subsidence is obvious with a high-riding greater trochanter. The lateral cement mantle is fractured. There is endosteal erosion distally with the tip of the stem showing radiographic toggle.
Incorrect Answers:
osteolysis, but it remains well fixed. Acetabular fractures are less likely when there is minimal osteolysis.
OrthoCash 2020
A 60-year-old woman undergoes a total knee arthroplasty for end-stage osteoarthritis. Preoperative knee range of motion is 5 to 100 degrees. Postoperatively, she experiences reduced range of motion. She is scheduled to undergo manipulation under anesthesia. In which of the following scenarios is this procedure best indicated?
Knee range of motion 0 to 60 degrees at 2 months postoperatively
Knee range of motion 0 to 60 degrees at 8 months postoperatively
Knee range of motion 30 to 120 degrees at 2 months postoperatively
Knee range of motion 30 to 120 degrees at 8 months postoperatively
Knee range of motion 30 to 120 degrees at 2 weeks postoperatively
Manipulation under anesthesia (MUA) can achieve the greatest gains in flexion when performed for patients with less than 90 degrees of flexion within the first three months.
There are many risk factors for postoperative stiffness, the most important being preoperative stiffness. MUA is indicated when flexion is less than 90 degrees. Flexion gains are generally greater when applied early (6-12 weeks postoperatively) rather than late (>12 weeks). In cases with late-presenting stiffness (>12wks), MUA may still be attempted. Failed MUA is addressed with arthroscopic or open adhesiolysis +/- MUA, quadricepsplasty, or component revision.
Namba et al. compared the results of early (<90 days) vs late (>90 days) MUA. They found that: (1) knee flexion improved a mean of 32 deg and 20 deg after early and late MUA respectively, (2) extension improved in the early MUA group, but not the late MUA group, and (3) pain improved after early but not late MUA. Despite early MUA being more desirable, the authors state that patients with limited flexion at 6-12 months may still benefit from late MUA.
Keating et al. assessed the outcomes of MUA in 113 knees at a mean of 10 weeks after surgery. They found that (1) 90% of patients achieved
improvement in knee flexion of 35 degrees at 5 year followup, (2) there was no difference in flexion gains between early (<12 weeks) and late (>12 weeks) MUA and (3) patients treated with MUA had better pain control than those without MUA. They concluded that manipulation can result in significant and lasting improvement in knee flexion.
Incorrect Answers
OrthoCash 2020
A 62-year-old man is scheduled for a total knee arthroplasty. In his pre-operative office visit, he asks questions about different tibial components. You tell him that compared with the tibial component shown in Figure A, the tibial component shown in Figure B:
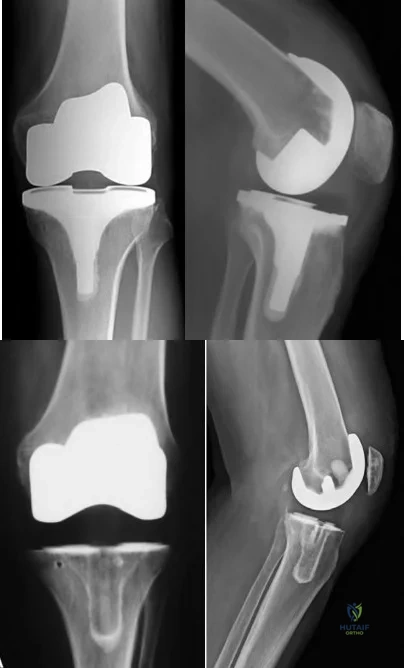
Is less expensive
Has greater durability
Has greater instability because of its monobloc nature
Provides improved short-term functional status, but no difference in long term functional status
Is associated with fewer adverse events because of easier implantation Corrent answer: 1
Figure B shows an all-polyethylene tibia (APT) component, which is $470 to
$1650 less expensive than metal-backed tibia (MBT) designs.
It was traditionally thought that modular MBT may have lower survivorship (compared to APT) because of locking mechanism dysfunction, breakage,
backside wear, and osteolysis. However, many studies now show the two to be comparable, with the only difference being that APT are less expensive.
Voight et al. performed a systematic review comparing APT and MBT. They found that the former was cheaper. There was no difference in adverse events, durability (need for revision or radiographic failure) at 2, 10, and 15 years, and functional status at 2, 8, and 10 years.
Toman et al. compared APT and MBT retrospectively. They found that APT implants perform as well as MBT implants in patients with BMI <37.5. There were 4 tibial implant failures in the MBT group in patients BMI >40.
Dalury et al. examined APT performance in obese patients (125 knees) after a minimum of 7 years. There were no implant failures. There were 5 nonprogressive tibial radiolucencies and 1 case of nonprogressive osteolysis.
Figure A shows a cemented metal-backed tibia component. Figure B shows a cemented all-polyethylene tibia component.
Incorrect Answers:
OrthoCash 2020
Figures A and B show pre- and post-operative radiographs of a sedentary 75-year-old female who underwent surgery on her left hip. Based on the radiographic findings, what was the most likely indication for revision surgery?
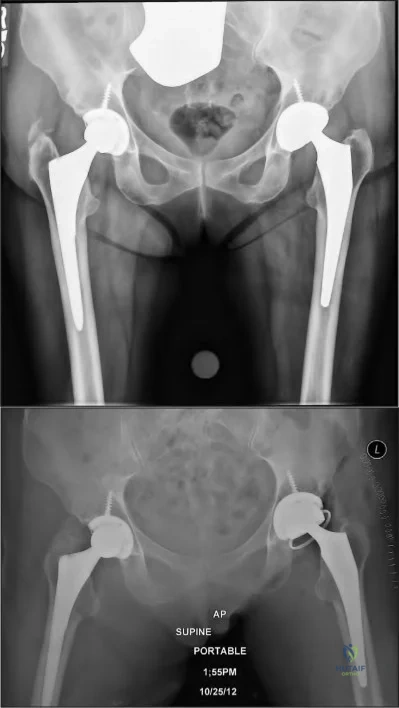
Left acetabular fracture
Left acetabular cup osteolysis
Left femoral stem osteolysis
Left hip instability
Left femoral stem valgus malalignment Corrent answer: 4
Figure A shows a left total hip arthroplasty with eccentric polyethylene wear. Figure B shows that her left hip was revised to a constrained acetabular liner, most likely a result of recurrent instability.
Revision strategies for hip instability are typically directed at correcting the underlying cause of instability. For example, instability most commonly occurs as a result of poor implant design, positioning or loosening, or the loss of soft-tissue function or tensioning. Operative strategies are designed to correct these etiologies by repositioning or exchanging components, integrating modular designs and improving soft tissue tensioning, etc. Constrained acetabular liners are often used in conjunction with these modalities to address the problem of recurrent instability relating to soft tissue deficiency and dysfunction in the affected hip.
Alberton et al. retrospectively reviewed 1548 revision arthroplasties for the incidence of dislocation. They found the overall dislocation rate to be 7.8%. Factors contributing to increased dislocations were found to be trochanteric non-unions, femoral heads <28mm in diameter and extensive soft-tissue dissection. Protective factors were modular acetabular components or liners, larger femoral heads >28mm and re-establishing abductor tensioning.
Paterno et al. retrospectively reviewed 438 primary and 181 revision total hip arthroplasties for patient factors contributing to dislocation. They found an overall dislocation rate of 6%. 23% of patients with a history of excessive intake of alcoholic beverages (more than six ounces a day) had at least one dislocation. There was no relationship between the variables of age, gender, obesity, or preoperative diagnosis and the incidence of dislocation.
Figure A shows bilateral primary cementless, nonconstrained total hip replacements. The left hip shows eccentric femoral head placement within the acetabulum indicative of eccentric polyethylene wear. Figure B shows the conversion to a constrained, dual-mobility, polyethylene liner. The overall metal component position appears satisfactory.
Incorrect Answers:
OrthoCash 2020
A 62-year-old woman is brought to the emergency room after falling down a flight of stairs. Prior to her fall, she had no knee pain and was a community ambulator without assistance. Intraoperatively,
it is determined that the implants are well-fixed. What is the best next treatment step to optimize her quality of life?

Closed reduction and long leg casting at 20 degrees of flexion for 6 weeks, followed by hinged-knee brace for 6 weeks.
Open reduction and internal fixation with a distal femoral locking plate
Open reduction and internal fixation with a condylar buttress plate
Distal femoral replacement arthroplasty
Closed reduction and fixation with an antegrade intramedullary nail Corrent answer: 2
This patient has a displaced far-distal supracondylar fracture around a stable TKA femoral component. Locked plating is the best option for management of this fracture.
Surgical fixation of periprosthetic fractures around a stable femoral component is challenging. Locked plating allows for multiple angle-stable fixation points around stems and lugs and does not depend on TKA design or quality of distal bone stock for fixation. Su Type I fractures may be treated with retrograde or antegrade intramedullary nailing. Type II fractures require retrograde intramedullary nailing or fixed-angle plating. Type III fractures require fixation with a fixed-angle device or revision arthroplasty when bone stock is poor.
Ricci et al. evaluated indirect reduction and locked lateral plating of Vancouver B1 THA fractures without allograft struts. They found that all fractures healed with satisfactory alignment and without implant loosening at an average of 12 weeks. They recommend this technique for stable Vancouver B1 fractures.
Streubel et al. examined the outcomes of locked plating in treatment of extreme distal periprosthetic supracondylar fractures located proximal to the flange (Su Types I and II) compared with fractures distal to the flange (Su Type III, see Illustration B). They found no difference in delayed union, nonunion, infection and failure rates between the 2 groups.
Figure A shows a Su Type III periprosthetic fracture around a TKA femoral component. Illustration A shows fixation of the same fracture with a distal femur locking plate. Illustration B shows the Su classification of fractures around the femoral component (Type I, proximal to the femoral component; Type II, starting at the anterior flange and extending proximally; Type III, fracture line distal to the anterior flange).
Incorrect Answers

OrthoCash 2020
Which of the following fractures would most likely require revision arthroplasty with a long-stemmed, uncemented prosthesis?

Figure B shows a Vancouver B2 periprosthetic femur fracture with an unstable femoral stem that requires revision arthroplasty with a long-stemmed prosthesis.
The Vancouver classification for periprosthetic femur fractures can help guide treatment of these challenging problems. Vancouver A fractures involve the greater and lesser trochanter and can be initially managed with non-operative measures. Vancouver B fractures occur around the stem and are broken down into B1 (stable prosthesis), B2 (unstable prosthesis) and B3 (poor proximal bone quality) fractures. B1 fractures may be treated with internal fixation, B2 fractures require a revision arthroplasty, and B3 fractures often require more advanced reconstruction with a proximal femoral replacement versus revision with a distally fixed prosthesis. Vancouver C fractures occur distal to the stem and require internal fixation.
Springer et al. reviewed 118 patients who underwent revision arthroplasty for Vancouver B2 periprosthetic fractures. They had a 90% survival rate at 5-years and a 79.2% survival rate at 10-years. The most common reasons for revision were loosening, infection, and non-union.
Illustration A shows the Vancouver classification of periprosthetic fractures about the femur.
Incorrect Answers:
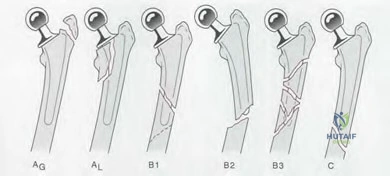
OrthoCash 2020
A 65-year-old female sustains a periprosthetic supracondylar femur fracture proximal to a well-fixed implant. She undergoes direct reduction and locked plating with a titanium distal femoral locking plate via an extensile lateral approach. At 9 months post-operatively, weightbearing is at 50% and is painful. Examination reveals mild swelling and warmth around the distal incision. Erythrocyte sedimentation rate and C-reactive protein are normal. Radiographs taken 9 months post-operatively are shown in Figure A. Which of the following may have increased the risk of this complication?
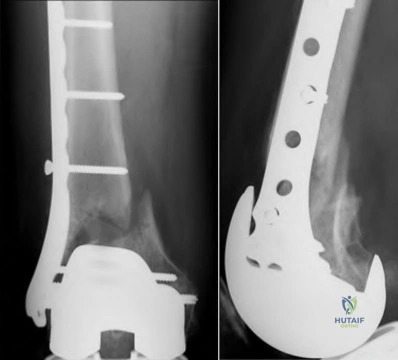
Neglecting to add topical rhBMP-2 on a carrier-scaffold
Neglecting to use lag screws and cerclage cables
Locked plating instead of locked antegrade nailing
Use of a titanium plate instead of a stainless steel plate
Use of an extensile lateral approach instead of a submuscular approach Corrent answer: 5
A submuscular approach has been shown to have less risk of nonunion than an extensile lateral approach. There is less disruption of soft tissue attachments and devitalization of fracture fragments with the submuscular approach.
The risks for periprosthetic fractures include notching, knee stiffness, osteoporosis, poor mobility and falls. The risk is higher in females and after revision surgery. The treatment of periprosthetic supracondylar fractures depends on the location of the fracture, fixation of the implant, and bone stock.
Hoffman et al. retrospectively reviewed 36 periprosthetic supracondylar femur fractures treated with locked plating. They found that submuscular plating had reduced nonunion risk compared to an extensive lateral approach. They recommend indirect reduction and submuscular plating to reduce the incidence of nonunion.
Hou et al. retrospectively reviewed 53 fractures fixed with retrograde nailing
(18) and locked plating (34). They found no difference in blood loss, time to union, operating time and hospital stay. They believe locked plating can
provide the same favorable results as retrograde nailing and recommend this technique for most patients and prosthetic designs.
Figure A shows nonunion and surrounding osteopenia after locked plating of a periprosthetic supracondylar fracture. Illustration A shows management of these fractures according to the Su classification.
Incorrect Answers
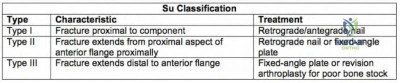
OrthoCash 2020
Immediately following a total hip arthroplasty (THA), a healthy 55-year-old patient is unable to dorsiflex her ankle or extend her great toe. After 4 weeks she continues to ambulate with a "slapping gait." Examination reveals passive ankle joint dorsiflexion to 10 degrees. What is the most appropriate next treatment option?
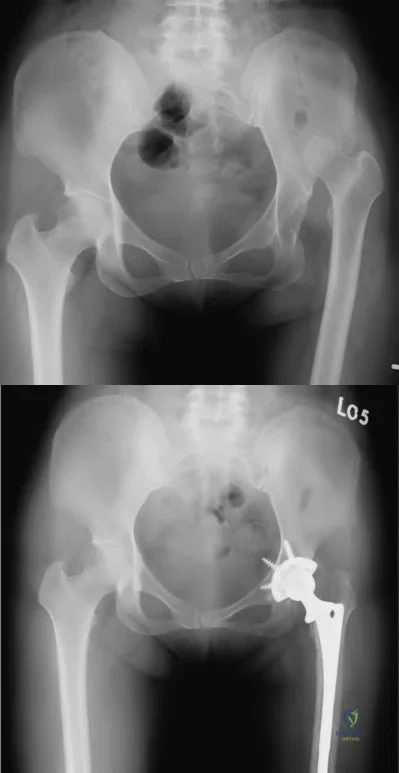
MRI of her spine and pelvis
Revision total hip arthroplasty
Ankle-foot orthosis
Posterior tibial tendon transfer to navicular bone
Neurology consult
This patient is presenting with foot drop after a THA for hip dysplasia (Crowe 4). The most appropriate treatment at this stage would be providing her with an ankle foot orthosis (AFO) for mobility.
Sciatic nerve injury after THA is an uncommon and difficult situation to manage. Patients with DDH that have undergone a large limb-lengthening procedure are at a greater risk due to the significant stretch of the sciatic nerve. Intra-operative procedures that have been shown to prevent this outcome include good pre-operative planning, limb lengthening <3 cm, subtrochanteric osteotomy, intra-operative wake-up test, and downsizing implant components if presenting with deficits peri-operatively. An ankle-foot orthosis may be used for foot drop when surgery is not warranted or during neurologic recovery.
Prahinski et al. reviewed the Bridle transfer for paresis of the anterior and lateral compartment musculature. Indications for the procedure include no neurological recovery for at least 18 months after injury or 18 months after the most recent attempt at exploration or repair of the nerve.
Electrodiagnostic changes must indicate permanent damage. In addition, there must be good passive range of motion, with at least 90° of dorsiflexion.
Edwards et al. reported on twenty-three peroneal and sciatic nerve palsies that occurred in patients following total hip arthroplasty. They showed that peroneal nerve palsy occurred with an average lengthening of 2.7 cm (1.9 cm-3.7 cm) in comparison with 4.4 cm (4.0 cm-5.1 cm) for sciatic nerve palsies.
Figure A and B show pre- and post-operative images of a patient with severe hip dysplasia treated with primary total hip arthroplasty.
Incorrect Answers:
OrthoCash 2020
A 60-year-old male with history of renal transplantation and previous intravenous drug abuse undergoes total knee arthroplasty. Two years later, he begins to have mild knee pain and low-grade swelling that persists for 10 months before he finally comes to the emergency room. Examination reveals no fever. Range of motion is 5 to 70 degrees. Erythrocyte sedimentation rate is 22mm/h, and C-reactive protein is 0.8mg/L. Knee aspiration reveals 12,000/mm3 nucleated cells with 76% neutrophils. Gram stain is negative and aerobic and anaerobic cultures are negative after 4 days in culture. His symptoms do not resolve after 5 days of empiric intravenous antibiotics and he is taken to the operating room for arthroscopic irrigation and debridement. Operative synovial tissue cultures are shown in Figure A. What is the best next step?
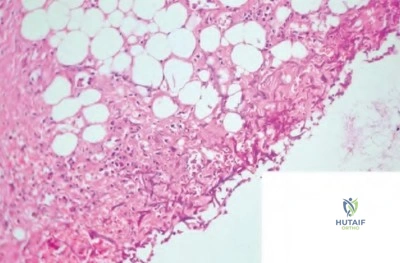
Cessation of immunosuppressant medication, lifelong antimycobacterial suppression
Open irrigation and debridement, implant retention and lifelong antifungal suppression
Open irrigation and debridement, resection arthroplasty, antimycobacterial drugs for 6 to 12 months
Open irrigation and debridement, single-stage exchange, antifungal drugs for 6 to 12 months
Open irrigation and debridement, two-stage exchange, antifungal drugs for 6 to 12 months
This patient has a fungal prosthetic joint infection (PJI) with Candida albicans. Optimal treatment involves resection arthroplasty, delayed reimplantation
arthroplasty, and antifungal drugs for 6-12 months.
Fungal PJI are uncommon. Risk factors include immune suppression and systemic illness e.g. diabetes and chronic renal failure. Candida species is usually the causative organism. The infection is usually indolent and systemic symptoms (e.g. fever) may be absent. ESR and CRP may be only minimally elevated. Two-stage exchange arthroplasty is standard of care.
Phelan et al. described delayed reimplantation in 10 patients with fungal PJI. They found that the median time from resection to reimplantation arthroplasty was 9 and 2 months for total hip and total knee arthroplasty respectively. Two patients had recurrence of infection. They recommend antifungal therapy and delayed reimplantation arthroplasty after confirmation of an infection-free period as the best chance for cure.
Azzam et al. retrospectively reviewed arthroplasty database data to identify 31 fungal PJIs in 6 centers. Delayed implantation was performed in 19 of 29 patients who underwent resection arthroplasty at an average of 7 months.
They recommend two-stage exchange arthroplasty as the treatment of choice, addition of antibacterial drugs to the cement spacer to prevent superinfection, antifungal drugs for 6-12 months, repeat joint aspirations prior to reimplantation, and optimization of host nutritional status prior to reimplantation.
Figure A is a high-powered micrograph showing synovial tissue covered by fibrinopurulent exudates containing fungal colonies of Candida albicans.
Incorrect Answers:
OrthoCash 2020
Which of the following non-operative treatments for osteoarthritis has the best evidence to support its use?
Combination of supervised and home exercise programs
Hyaluronic acid injections
Lateral heel wedge
Acetaminophen
Glucosamine
Of the options listed, a combination of home and supervised exercise has the best supporting evidence for the treatment of osteoarthritis.
The AAOS has recently developed guidelines for the treatment of osteoarthritis. Therapies that are recommended by the AAOS include weight loss, home and supervised exercise programs, and NSAIDs/tramadol.
Therapies that remain inconclusive (lack of supporting evidence) include electrotherapeutic modalities, manual therapy, bracing, acetaminophen/opiods, steroid injections and PRP. Glucosamine, lateral heel wedges and hyaluronic acid injections are not recommended, as current literature has shown them to be ineffective. Keep in mind that these guidelines are subject to change as new literature is published.
Zhang et al. present a systematic review of the literature on arthritis management in the three years following the original OA Research Society International (OARSI) guidelines published in 2006. While weight loss showed an increase in effectiveness with the addition of new studies, electromagnetic therapy, glucosamine, chondroitin sulfate, and hyaluronic acid injections showed a decrease in effectiveness.
Incorrect Answers:
OrthoCash 2020
Figure A shows the 2 bundles of the ACL dissected from a cadaveric knee off their bony attachments. They are labeled Bundle A and Bundle B, respectively. Which of the following is true?

The tibial attachment of Bundle A is anterior to Bundle B. In extension, Bundle B is loose and Bundle A is tight.
The tibial attachment of Bundle A is anterior to Bundle B. In flexion, Bundle B is loose and Bundle A is tight.
The tibial attachment of Bundle B is anterior to Bundle A. In flexion, Bundle B is loose and Bundle A is tight.
The tibial attachment of Bundle B is anterior to Bundle A. In flexion, Bundle A is loose and Bundle B is tight.
The tibial attachment of Bundle B is anterior to Bundle A. In extension, Bundle A is loose and Bundle B is tight.
Bundle A is the anteromedial (AM) bundle, which is longer, and is tight in flexion. Bundle B is the posterolateral (PL) bundle, which is shorter, and is loose in flexion. The AM bundle is attached anterior to the PL bundle on the tibia.
The ACL is comprised of 2 bundles. The AM bundle is longer than the PL bundle. Their names reflect their relative anatomic positions on the tibial insertion site. On the femur, the AM bundle begins at the proximal-anterior aspect of the femoral insertion site, while the PL bundle begins at the posterior-inferior part. In flexion, the AM bundle is tight and the PL bundle is loose. In extension, the AM bundle is loose and the PL bundle is tight.
Bicer et al. reviewed the anatomy of the ACL. They found that the AM bundle was longer (32mm) compared with the PL bundle (18mm). PL bundle carries greater force near full extension, and the AM bundle carries greater force after 15-45° of flexion. Under combined rotatory loads (valgus and internal tibial torque at knee flexion >30°), the AM bundle bore more force than the PL bundle.
Figure A shows the 2 bundles of the ACL. The AM bundle is longer than the PL bundle. The oft referred to length of ACL refers mainly to the length of the AM bundle. Illustrations A and B show the spatial relationships of the AM and PL bundles in a cadaveric knee. Illustration C shows the relative positions of the attachments of each bundle.
Incorrect Answers:
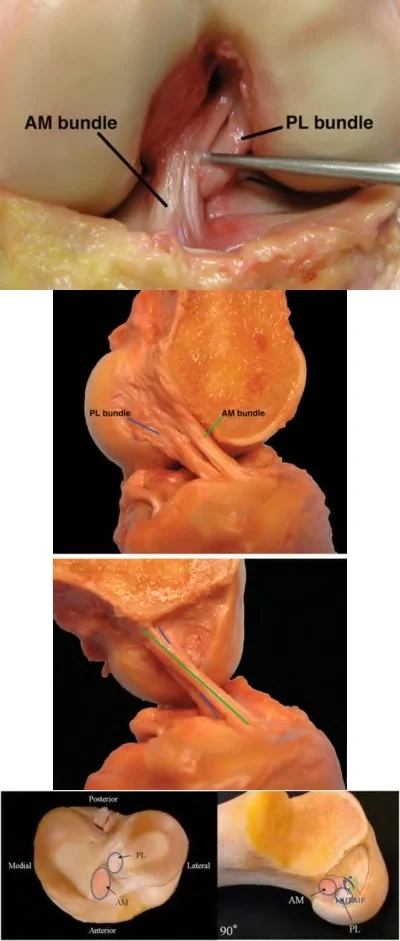
OrthoCash 2020
An 83-year-old man, who had a total hip arthroplasty performed 13 years ago, is referred to your office for evaluation. He reports worsening groin pain over the past year, which has been increasing in frequency. Prior to this past year, he had no other complaints. His current radiograph is shown in Figure A. If he continues to ambulate with this implant, he is at greatest risk for which of the following?

Infection
Acetabular component loosening
Femoral component loosening
Dislocation
Periprosthetic fracture
The patient has eccentric polyethylene wear secondary to component malpositioning. He is at highest risk for dislocation.
Late dislocation following total hip arthroplasty(THA) can occur and has a high recurrence rate, thereafter. Risk factors include eccentric polyethylene, THA at an early age, neurologic decline or associated neurologic conditions (i.e.
Parkinson's disease), or associated trauma.
Parvizi et al. noted in this instructional course lecture that eccentric, excessive polyethylene wear is one of the most common reasons for late, recurrent dislocation. Revision is recommended.
Pulido et al. in this review, reiterated that polyethylene wear can lead to increased inflammation, capsular distention, and instability, increasing risk for dislocation.
von Knoch et al. reviewing over 500 dislocated hips, also noted that eccentric wear was one of major causes linked to late dislocation.
Figure A. exhibits a left total hip arthroplasty with eccentric wear. Incorrect answers:
OrthoCash 2020
Figure A shows a radiograph of a 62-year-old female that underwent a left total hip arthroplasty 5 years ago. She presents to your office with insidious onset of left groin and buttock pain. She denies trauma, fever or chills. On physical examination, her left hip has mild pain with range of motion. She has a normal gait cycle, normal power across the hip and her vitals signs are stable. A left hip aspirate was performed and results are shown in Figure B. What is the most likely cause of her hip pain?
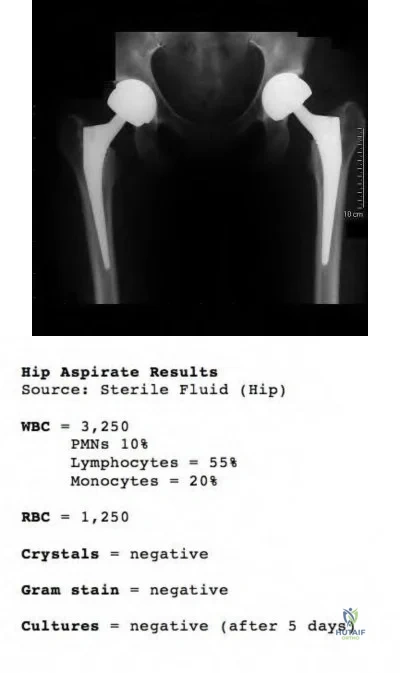
Periprosthetic bacterial hip infection
Periprosthetic hip fracture
Large-particle wear debris disease
Pseudotumor hypersensitivity response
Abductor tendon tear Corrent answer: 4
This patient is presenting with a metal induced system hypersensitivity response in the setting of a metal-on-metal total hip arthroplasty.
A hip aspiration of a painful THR is a very useful investigation for the work up of infection, having a sensitivity of 75-85% and specificity of 85-100% for
infection. Metal-on-metal THA may mimic infection as aspirate results will often show increased inflammatory infiltrate, with synovial WBC counts in the thousands. However, infected THA are more likely to produce higher percentages of PMNs (>70%) in comparison to hypersensitivity reactions/ adverse reaction to metal debris, which are more likely to produce a higher percentage of lymphocytes (>40%).
Campbell et al. looked at the histological features of pseudotumor-like tissues from metal-on-metal hips. They found that the patients with hip pain and suspected metal sensitivity had fewer metal particles but more aseptic lymphocytic vasculitis-associated lesions compared to patients with evidence of metallic wear. They concluded that pseudotumors occur more because of a hypersensitivity reaction than particle wear.
Kwon et al. examined a small cohort of patients with metal-on-metal hip arthroplasties to investigate the incidence and level of metal-induced systemic hypersensitivity. They found that lymphocyte reactivity to Co, Cr, and Ni did not significantly differ in patients with pseudotumors compared to those patients without pseudotumors. This suggests that systemic hypersensitivity type IV reactions may not be the dominant biological reaction involved in the occurrence of the soft tissue pseudotumors.
Figure A shows a patient with bilateral metal-on-metal total hip arthroplasties. There are no identifiable fractures. The position of the left acetabular cup is slightly vertical, which can increase edge loading and particle wear. Figure B shows the results from the hip aspirate.
Incorrect Answers:
OrthoCash 2020
A 72-year-old patient is scheduled to undergo revision total hip arthroplasty. A 3D-model of the patient's hemipelvis is constructed for pre-operative planning and is shown in Figure A. A custom-designed implant shown in Figure B is created. Which of the following is TRUE of the planned reconstruction?

The implant is a bilobed cup.
The most common complication is dislocation.
The acetabular defect can be classified as AAOS Type V.
Radiation-compromised bone stock is a contraindication.
The winged profile of the implant facilitates insertion through both anterior and anterolateral approaches.
The patient has pelvic discontinuity that will be reconstructed with a custom triflange acetabular component. Dislocation is the most common complication.
Custom triflange acetabular components are indicated for severe acetabular bone loss and pelvic discontinuity that are not amenable to treatment with off-the-shelf implants such as reconstruction plates, jumbo cups and antiprotrusio cages. Dislocation is common and possible etiologies include extensive dissection, less reliable soft tissue repair, deficient abductors/trochanteric nonunion, superior gluteal nerve stretch neuropraxia, and surgeon reluctance to use constrained liners in the face of poor bone stock.
Christie et al. reviewed reconstruction with the triflange cup in 78 hips with AAOS Type III (combined deficiency) or Type IV (pelvic discontinuity) defects. They found improvement in Harris hip scores, limp, need for walking aids.
Dislocation was the most common complication (15.6%, 12 patients), and half of these patients (6/12) needed re-operation for recurrent dislocation. They recommend the triflange cup for difficult reconstructions involving severe bone loss.
Taunton et al. reviewed 57 patients with pelvic discontinuity treated with a custom triflange component. They found that 21% developed instability (10 required revision, and 2 treated nonoperatively). Of note, 51% had preop trochanteric escape (nonunion of the greater trochanter to the femoral component or femur with >1cm of displacement. They recommend the custom triflange implant for discontinuity as it provides predictable midterm fixation and consistent healing.
Figure A is a 3D hemipelvis model generated by stereolithography from a patient’s CT scan. It shows massive bone loss and pelvic discontinuity. Figure B is a custom hydroxyapatite (HA)-coated porous triflange acetabular prosthesis with ilial and ischial screw holes. Illustration A shows a bilobed cup and its appearance on an AP radiograph.
Incorrect Answers:
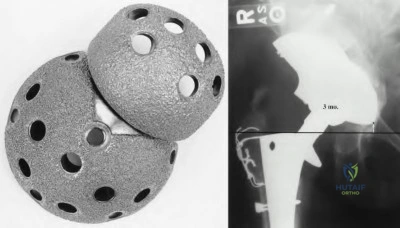
OrthoCash 2020
All of the following are risk factors for wear-related failure in total knee arthroplasty when using a polyethylene liner that underwent sterilization via gamma irradiation in air EXCEPT?
Increasing shelf age of polyethylene liner
Younger age of patient
Male gender
Posterior cruciate retaining knee design
Use of a rough tibial baseplate Corrent answer: 4
Increasing shelf age, younger age, male gender, and a rough tibial baseplate are all risk factors for wear-related failure in total knee arthroplasty when using a polyethylene liner. Posterior cruciate retaining knee design is not a documented risk factor.
Fehring et al reviewed 2091 TKA using the Press fit condylar system and noted that the 13-year survivorship for all patients was 82.6% with a 8.3% prevalence of wear-related failure. Cox hazards analysis revealed five variables that were correlated with wear-related failure: patient age, patient gender, polyethylene sheet vendor, polyethylene finishing method, and polyethylene shelf age. They were unable to identify one factor as the defining reason for these wear-related failures. They cautioned that these findings may only be specific to inserts that underwent sterilization via gamma irradiation in air.
Collier et al followed 365 TKA (PCL-retaining) for 5-10 yrs and noted that
factors related to polyethylene insert osteolysis included advanced shelf age, sterilization method, and the material from which it was machined. Osteolysis was identified in 34% with an insert that had been gamma-irradiated in air and affixed to a rough baseplate surface, but only 9% when the insert had been gamma-irradiated in an inert gas or not irradiated at all and joined to a polished surface.
OrthoCash 2020
A 65-year-old healthy patient fell 18 years after a total hip arthroplasty and sustained the fracture shown in Figure A. Which of the following would be the most appropriate treatment?

Percutaneous locked plating
Open reduction internal fixation with a cable plate and allograft strut
Revision to a long femoral stem with allograft bone
Revision to a cemented revision femoral stem that bypasses the fracture site by 5 cm
Three months of non-weight bearing Corrent answer: 3
The Vancouver classification of periprosthetic femur fractures is based on the fracture site, implant stability, and remaining bone stock. The patient in the question has a type B3 fracture. The cemented stem is loose and there is very poor remaining bone stock. He should be treated with a long, cementless
revision stem with biplanar strut grafts. A tumor prosthesis or allograft-prosthesis composite would be alternate possibilities. Illustrations A and B are a diagram and table of the Vancouver classification of periprosthetic hip fractures.
Springer, et al. looked at the results and complications of revision total hip arthroplasty for the treatment of acute Vancouver type-B periprosthetic femoral fracture. In their series they treated these fractures in multiple ways, including cemented stems, uncemented stems, allograft-prosthetic composite, or tumor prosthesis. They concluded that the best results were with an uncemented, porous coated femoral stem, and the most common cause of revision was loosening.
Parvizi, et al. concluded that due to the poor bone quality and delayed healing of older patients & their periprosthetic fractures that it is imperative that a strong mechanical construct be achieved in the treatment of these fractures. They “advocate the use of numerous screws with purchase of at least ten cortices and reinforcement of fixation with biplanar strut allografts whenever possible. When a revision stem is used, we ensure that adequate diaphyseal fixation is obtained and the fracture is traversed by at least 5 to 8 cm.”
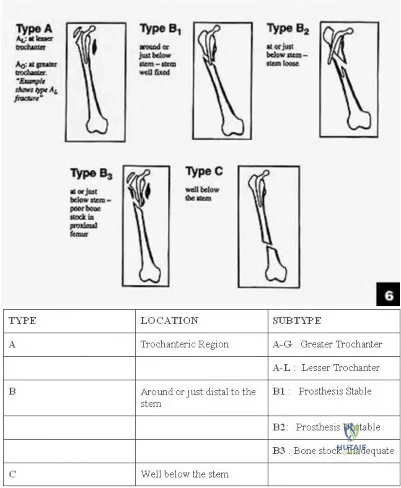
OrthoCash 2020
A 85-year-old man who underwent hemiarthroplasty 5 years ago now complains of thigh pain for the past four months. Laboratory studies show a normal white blood cell count (WBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). An aspiration of the hip is performed and is negative for infection. A radiograph is shown in Figure A. Which of the following is the best management option for the femoral implant?

Bone scan to look for loosening
Touch down weight bearing and physical therapy
Revision with a tumor prosthesis
Revision of femoral component with metaphyseal cement fixation of the stem
Revision to a cementless femoral component with diaphyseal press-fit fixation of the stem
The radiograph shows lucency around the femoral stem cement mantle consistent with loosening. There is bone loss in the proximal femur. Diaphyseal fixation is the best option from the choices available. Revision to a cementless femoral stem is the most appropriate management.
Paprosky et al. described their results of revision to cementless femoral components and report 95% survivorship with a minimum of 10 years follow
up.
Haydon et al showed that despite historical literature discouraging the use of cemented femurs for revision, in their experience cemented femoral revision had 91% survivorship when the cause was aseptic loosening. They found early generation cementing techniques, poor cement mantle, poor bone quality, age of less than 60, and male gender to be risk factors for failure in cemented revisions.
OrthoCash 2020
Figure A is a diagram showing the medial side of the knee. During a total knee arthroplasty, proximal tibia resection results in the transection of the ligament in Figure A along the red line. Intraoperative examination reveals coronal plane instability. What are the best next steps?

Use of the implant shown in Figure B, and use of a hinged knee brace postoperatively
Suture repair of the torn ligament, use of the implant shown in Figure C
Use of the implant shown in Figure D, and use of a knee immobilizer postoperatively
Suture repair of the torn ligament, use of the implant shown in Figure D, and use of a hinged knee brace postoperatively
Use of the implant shown in Figure C alone Corrent answer: 4
This patient has intraoperative midsubstance transection of the MCL. MCL repair, use of either a CR or PS implant, and postoperative knee bracing for 6 weeks is recommended. A possible alternative is the use of an unlinked constrained implant.
The MCL is likely to be compromised by medially placed retractors or during medial subperiosteal elevation (tibial avulsion) or injured by oscillating saw-blade during the tibial or posterior femoral condyle cut. There is no consensus for the treatment of intraoperative rupture. Acceptable salvage options include
(1) direct repair (heavy sutures for midsubstance rupture, and suture anchors for tibial sleeve avusions) and postop knee bracing for 6 weeks with either CR or PS implants, or (2) use of unlinked constrained implants with or without repair.
Lee and Lotke reviewed 37 patients with intraoperative MCL injury out of 1478 patients. They attempted repair in 14 patients, and increased constraint in 30
patients. They found higher failure rates (regardless of MCL repair technique) for cruciate retaining components. They recommend use of an unlinked constrained prosthesis (with or without ligament repair), especially for midsubstance injuries.
Leopold et al. reviewed 16 MCL injuries in 600 knees. They performed suture or suture anchor repair and used a hinged knee brace for 6 weeks postoperatively. All limbs were stable and did not require bracing beyond 6 weeks, demonstrated acceptable alignment, and did not require revision at 45 months. They recommend the use of primary MCL repair or reattachment and postoperative bracing instead of implants with increased constraint.
Figure A shows MCL transection in its midsubstance. Figure B shows a cruciate retaining implant. Figure C shows a hinged knee prosthesis (linked constrained implant). Figure D shows a posterior stabilized implant. Illustration A shows an unlinked constrained implant.
Incorrect Answers:

OrthoCash 2020
A 65-year-old woman complains of intermittent knee pain 12 years after a total knee arthroplasty. She has no history of fever or recent infections. Radiographs are shown in Figures A and B. Examination reveals minimal warmth and a moderate knee effusion. Range of motion is 5 to 100 degrees bilaterally. The C-reactive protein level is 15 mg/L (normal, 0.0-0.8mg/L), and erythrocyte sedimentation rate is 45mm/h (normal, 0-10mm/h). Arthrocentesis reveals 7500 white blood cells and 90% neutrophils. Gram stain is negative. Cultures are negative at 3 days. What is the next best step?

MRI with metal subtraction protocol
Arthroscopic debridement
Open debridement and polyethylene liner exchange
Single-stage revision total knee arthroplasty (TKA)
Explantation of components with two-stage revision TKA Corrent answer: 5
By the updated 2018 Musculoskeletal Infection Society (MSIS) criteria, this presentation is consistent with a diagnosis of periprosthetic joint infection (PJI). The patient has an elevated CRP (2), ESR (1), synovial WBC >3,000 (3), and >80% PMNs (2), for a total of 8 points. Given the chronicity of the infection, the patietn would be a candidate for two-stage revision.
This patient has clinical signs of PJI such as elevated laboratory values and radiographs suggestive of implant loosening. Even in the absence of positive cultures, the next most supported step in management if two-stage revision with explantation of the prosthesis and insertion of an antibiotic spacer.
Intraoperative cultures should be taken to guide post-operative antibiotic treatment.
Parvizi et al. recently released the updated 2018 MSI crtieria for diagnosis of PJI. The updated criteria (Illustration A) included new diagnostic tests and studies from the seven-year period since the previous criteria were established. Alpha defensin was a new addition. The two major criteria remained, each individually diagnostic of PJI. However the minor crtieria were broken down into pre-operative and intra-operative. The authors showed that a total of 6 points or more had a 97.7% SN and 99.5% SP for PJI.
Huang et al. retrospectively reported the infection control rates in 2-stage exchanges in 55 patients, and compared culture-negative cases with 295 culture-positive cases. They found that infection control in culture-negative cases was 73% at 1-year. Infection control rates were similar in culture-negative and culture-positive cases, and that infection-free survival is highest after 2-stage exchange with postoperative vancomycin. They recommend 2-stage exchange with postoperative vancomycin.
Buller et al. retrospectively assessed traits that would predict the success of debridement and liner exchange for 62 hips and 247 knees. They found that 149 (48.2%) cases failed to eradicate infection. Risks for recurrent infection include longer symptom, higher ESR, previous PJI or infection in the same joint, and an infection by a group 1 (MRSA, VRE, and methicillin-resistant S. epidermidis) or group 2 (MSSA or methicillin-sensitive coagulase-negative Staphylococcus) organism.
Della Valle et al. discuss the AAOS recommendations on diagnosis of periprosthetic hip and knee infections. They recommend repeat hip and knee aspirations when there is discrepancy between probability of PJI and initial aspiration culture result.
Aggarwal et al. prospectively compared the yield of intraoperative tissue and swab cultures in 74 hip, 43 knee, 30 septic and 87 aseptic cases. They found that tissue cultures had higher sensitivity, specificity, positive and negative predictive values for identifying PJI. Swab cultures had higher false positive and negative values. They recommend not using swab cultures, and only using tissue cultures.
Figures A and B are AP and lateral radiographs showing areas of bony erosion suggestive of loosening of the femoral and tibial components.
Illustration A is the 2018 MSIS criteria with point values.
Incorrect Answers:
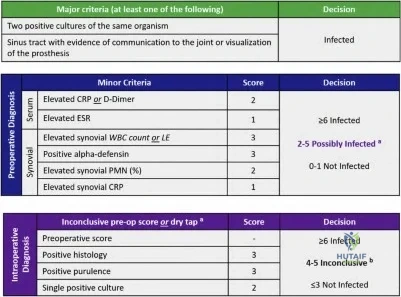
OrthoCash 2020
What are the affects on limb-length and offset according to the total hip arthroplasty template shown in Figure A?

Limb-length will stay the same, offset will be increased
Limb-length will be decreased, offset will be increased
Limb-length will stay the same, offset will be decreased
Limb-length will be increased, offset will be increased
No change in either limb-length or offset Corrent answer: 1
In Figure A, the center of rotation of the femoral component lies medial to the center of rotation of the acetabular component. If these components are implanted as shown, the offset will be increased and the leg-lengths will remain equal.
Offset and leg-length changes during templating and insertion of a total hip replacement are determined by the changes in the center of rotation (COR) of the femur relative to the acetabulum. If changes are made in the horizontal plane (x-axis), a change in offset will occur. If changes are made in the vertical plane (y-axis), changes in leg-lengths will occur. If the femoral COR is templated superior to the acetabular COR, the leg will be lengthened. In
contrast, if the femoral COR is templated inferior to the acetabular COR, the leg will be shortened. For offset, the same principles apply. If the femoral COR is templated medial to the acetabular COR, offset will be increased. In contrast, if the femoral COR is templated lateral to the acetabular COR, offset will be decreased. One should aim to restore native offset and leg-lengths in uncomplicated primary total hip arthroplasty.
Merle et al. retrospectively reviewed 152 patients to evaluate femoral offset on an AP pelvis and AP hip radiograph compared to a CT scan of the affected hip. They found that AP pelvis radiograph underestimated femoral offset by 13% when compared to a CT scan. In contrast, the AP hip radiograph showed no difference when compared to the CT scan. They recommend obtaining AP of the hip prior to templating for accurate assessment of femoral offset.
Della Valle et al. review preoperative planning for total hip arthroplasty. While they state that templating has a high predictive value in achieving the desired plan, the surgeon should always be prepared to make intraoperative adjustments based on tactile feedback.
Illustration A shows an example where leg-length will be shortened (femoral COR is inferior to acetabular COR) and offset will stay the same (femoral COR and acetabular COR are in the same horizontal plane). Illustration B is a table which summarizes the points we have discussed.
Incorrect Answers:

OrthoCash 2020
A 65-year-old patient is diagnosed with a periprosthetic joint infection 6 years after total knee arthroplasty. He recalls a history of knee realignment surgery many years prior. Examination reveals lateral patellar tracking and passive flexion to 65 degrees. A recent radiograph is shown in Figure A. During the exposure for explantation, a standard medial parapatellar approach is performed through the previous incision. It is found that adequate knee flexion to allow exposure of the prosthesis cannot be achieved even after release of the lateral gutters and excision of the scar. Which surgical exposure technique (depicted in Figures B through F) would provide the best
surgical exposure for the procedure and preserve the blood supply to the patella?

Fig B
Fig C
Fig D
Fig E
Fig F
A tibial tubercle osteotomy (TTO) would provide the best surgical exposure without compromising patellar blood supply. This patient has patella baja arising from previous high tibial osteotomy, with a scarred, contracted patellar tendon leading to knee stiffness.
A TTO is able to provide good exposure while protecting the extensor mechanism and preventing inadvertent avulsion of a contracted patellar tendon. Further, proximal transfer of the osteotomized tibial tubercle may be used to correct patella baja, bearing in mind that excessive superior translation alters the mechanics of the knee by making the quadriceps less efficient.
Mendes et al. used TTO for surgical exposure in 67 knees undergoing revision TKA. There were good-excellent knee scores at 30 months in 87%. There were no patellofemoral complications, no component malalignments, and no avulsions of the patellar tendon occurred. They advocate TTO for cases where the patellar cannot be retracted laterally with knee in 90deg of flexion.
Whiteside described a series of TTO in 136 TKA. At 2 years, mean range of motion was 94deg. There were 2 tibial tubercle avulsion fractures and 3 tibial fractures (2 in a patient with Charcot arthropathy, and 1 following manipulation after open adhesiolysis. He advises using stemmed tibial components in patients with insensate knees and in cases where manipulation is expected.
Figure A is a lateral radiograph showing severe patella baja. Figure D shows a TTO. See below for Figures B, C, E and F. Illustration A shows the surgical technique for TTO. The distal saw cut angles out of the anterior cortex at a gentle angle to reduce the stress riser effect and risk of postoperative tibial stress fracture.
Incorrect Answers:
sufficient in the presence of severe patellar baja and patellar tendon contracture.
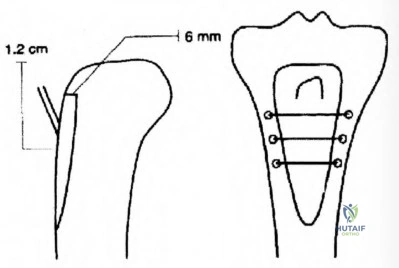
OrthoCash 2020
Figure A show pre- and post-operative radiographs, from left to right respectively, of a 79-year-old male that underwent revision total hip arthroplasty 2 years ago. He presents today for consultation after 4 episodes of right hip dislocation within the past 6 months. Physical examination reveals a trendelenburg gait with no clinical or radiographic limb length discrepancy. An Infection work-up is negative. Results from a CT scan are shown in Figure B. What would be the best treatment option?
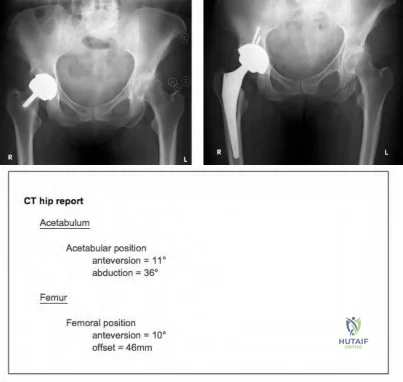
Physiotherapy and application of abductor brace
Revision arthroplasty to medialize the cementless cup and surgical repair of the abductor tendon
Revision arthroplasty to a constrained polyethylene liner
Revision arthroplasty to a femoral component with extended offset
Revision arthroplasty to a large ceramic femoral head and offset polyethylene cup
On the left, Figure A shows a metal-on-metal (MOM) bearing hip resurfacing. On the right, Figure A shows a large head, uncemented metal-on-polyethylene (MOP) total hip replacement. In this setting, the most appropriate treatment option would be revision arthroplasty with constrained polyethylene liner.
Constrained liners should be reserved for patients demonstrating recurrent instability despite treatment with a large femoral head. Other indications include elderly patients who do not require implant longevity or have a low functional demand, as well as patients with deficient or non-repairable abductor mechanisms.
Sikes et al. report on the results of a series of 41 patients (52 hips) with recurrent dislocations. They recommend that large femoral heads (LFH) be used as a first-line treatment in high-risk patients (patients of any age with dementia, neuromuscular disability, and inability to comply with precautions). Constrained liners should be reserved for patients demonstrating recurrent
instability despite treatment with an LFH.
Kilampali et al. reviewed late instability of bilateral metal on metal hip resurfacings. They suggest that late instability of hip resurfacing should raise concerns relating to possible local tissue reaction and muscle damage.
Concerning features include steeply-inclined acetabular components a large abduction angle of more than 55 degrees along with a combination of small size component.
Figure A shows an image of a revised socket which was performed to convert the MOM THA to a MOP THA. Figure B shows normal parameters of THA components. The recommendation for acetabular position is anteversion 20° ± 10° and abduction 45° ± 10°. For the femur, recommendations are 10°- 15° of anteversion and 41mm - 45mm of offset.
Incorrect Answers:
OrthoCash 2020
Which of the following has been shown to increase the rate of failure of cemented femoral components in total hip arthroplasty?
Stems that are precoated with polymethylmethacrylate
Calcar contact of the collar
Smoother implant corners
Cement mantle of 2 millimeters
Stem material with a Young's modulus higher than 115 GPa Corrent answer: 1
Precoating a stem with PMMA adds an additional inferface at risk of failure.
Stiffer stem materials (higher Young's modulus) improve performance. Titanium has a Young's modulus of 115 GPa with alloy and stainless steel
having a higher Young's modulus than titanium. Calcar collar contact adds minimal strength to the construct, but does not lead to premature failure. Smoother corners decrease the rate of failure since they decrease stress risers. The ideal cement mantle is ~2mm. Obtaining less than this would decrease the strength of the construct.
OrthoCash 2020
An 80-year-old male sustains a fall down the stairs and presents with knee swelling. He is a community ambulator who does not use walking aids. Injury radiographs are shown in Figures A and B. What is the next best step?

Intramedullary nailing
Locked plating
Long leg casting
External fixation
Revision total knee arthroplasty Corrent answer: 5
This patient sustained a periprosthetic femoral fracture around the femoral component which is now loose. Revision of the femoral component is necessary.
Various classifications exist for periprosthetic fractures around TKA. In general, for the femoral component, treatment depends on fracture displacement, fracture location, bone stock, and whether the component is loose. For loose femoral components, revision TKA using distal femoral replacement prosthesis is an option.
Kim et al. proposed a new classification for periprosthetic fractures. Type IA fractures (good bone stock, well fixed, nondisplaced or easily reducible) are managed conservatively. Type IB fractures (good bone stock, well fixed, irreducible closed) are managed with reduction and fixation. Type II fractures (good bone stock, reducible, loose or malpositioned components) are managed with revision. Type III fractures (poor bone stock, loose or malpositioned components) are treated with distal femoral replacement.
Johnston et al. reviewed the options for treating periprosthetic fractures about the knee. They advocate revision of the femoral component when the prosthesis is loose, where there is poor bone stock, or insufficient bone to gain purchase for locked plates or distal locking screws of intramedullary nails.
Nauth et al. review the current concepts in treatment of periprosthetic fractures. They prefer minimally invasive locked plating unless the fracture is significantly proximal to the anterior flange and amenable to retrograde intramedullary nailing. Then they choose nails with options for distal interlocking screws and locking condylar bolts. In extreme osteopenia, they use intramedullary fibular strut allografts (with locked plating). For loose prostheses or poor bone stock, they perform alloprosthetic composite in younger patients and a distal femoral replacement in elderly patients.
Figures A and B are AP and lateral radiographs showing periprosthetic femoral fracture around a loose femoral component. Illustrations A and B are postoperative radiographs showing revision to a hinged prosthesis with long-stemmed components. Illustration C shows Kim' proposed classification of
periprosthetic fractures around the femoral component of a TKA.
Incorrect Answers:

OrthoCash 2020
Utility of the implant seen in Figure A would be best considered in which of the following revision total hip arthroplasty scenarios?
Minimal acetabular deformity, intact rim
Superior acetabular bone lysis with intact superior rim
Localized acetabular destruction of medial wall
Absent superior acetabular rim, superolateral migration
Significant acetabular bone loss, pelvic discontinuity Corrent answer: 5
Paprosky Type 3B acetabular bone defects describes significant acetabular bone loss, with pelvic discontinuity. Type 3 defects often require reconstruction cages (as seen in Figure A) or acetabular distraction techniques
to treat severe bone loss with an associated pelvic discontinuity.
Deficient acetabular bone stock poses a technical challenge in hip arthroplasty surgery. Paprosky classification for acetabular bone loss to helps guide treatment for revision total hip arthroplasty. The classification is as follows:
Type 1: Minimal deformity, intact rim
Type 2A: Superior bone lysis with intact superior rim Type 2B: Absent superior rim, superolateral migration Type 2C: Localized destruction of medial wall
Type 3A: Significant bone loss, superolateral cup migration Type 3B: Significant bone loss, pelvic discontinuity
Sheth et al. reviewed acetabular bone loss in revision total hip arthroplasty. They state that Paprosky Type 1 and 2 defects can usually be managed with porous-coated hemisphere cup secured with screws. Type 3 defects require reconstruction cages to protect with cups and structural augments or custom triflange implants.
Taunton et al. investigated clinical outcomes and cost-effectiveness of using a custom triflange acetabular component to treat pelvic discontinuity in revision THA. They found satisfactory clinical outcomes (81% had a stable triflange component with healed pelvic discontinuity) and cost equivalence with Trabecular Metal cup-cage constructs.
Figure A shows a lateral image of the pelvis with a reconstruction cage and cup construct. Illustration A shows an illustration of the Paprosky classification. Illustration B shows a table of the Saleh/Gross classification. Illustration C shows a table of the AAOS classification.
Incorrect Answers:
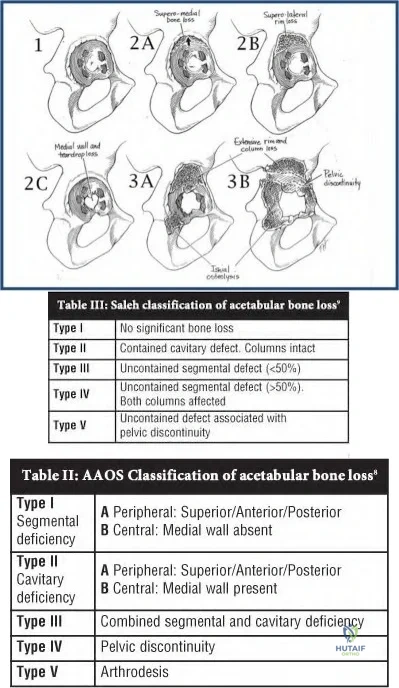
OrthoCash 2020
A 65-year-old male who had a total knee arthroplasty 8 years ago comes into the office with worsening knee pain. The orthopaedic surgeon is concerned about infection and aspirates the knee. Which of the following are the lowest laboratory values from a synovial aspirate suggestive of infection?
WBC of 500 cells/ml and PMN 25%
WBC of 1,000 cells/ml and PMN 25%
WBC of 1,500 cells/ml and PMN 70%
WBC of 5,000 cells/ml and PMN 70%
WBC of 25,000 cells/ml and PMN 70%
WBC of 1,500 cells/ml and PMN 70% indicates the lowest synovial aspirate suggestive of infection.
Mason et al in 2003 reviewed 440 revision TKA's of which 86 had preoperative aspirations. The aspirations yield 55 aseptic failures and 31 septic failures. The mean WBC of the aseptic group was 645 cells/mm(3) compared to 25,951 cells/mm(3) for the septic group (P=<.001). The mean percentage of polymorphonuclear cells (PMNs) was statistically higher in the septic group compared with the aseptic group (72.8% vs 27.3%; P=<.001). With these results, the authors concluded that aspirates with a WBC count greater than 2,500 and 60% PMNs are highly suggestive of infection.
However, in a more recent and larger study, Ghanem et al reviewed 161 infected TKA's vs 268 aseptic failures and concluded that aspiration with WBC of >1100 cells/mm3 and PMN > 64% are suggestive of infection. When both tests yielded results below their cutoff values, the negative predictive value was 98.2% (95% confidence interval, 95.5% to 99.5%), whereas when both tests yielded results greater, infection was confirmed in 98.6% (95% confidence interval, 94.9% to 99.8%) of the cases. Thus, according to the most recent literature, WBC >1100 and PMN > 64% should be considered suggestive of infection in a TKA.
OrthoCash 2020
A 50-year-old man with a past medical history significant for diabetes and end-stage renal disease presents with a chief complaint of instability 6-months following a total knee arthroplasty. Preoperative radiographs are shown in Figures A-C. Physical exam at that time was notable for a large effusion, maltracking patella, extensor lag of 15 degrees, medial instability, and gross laxity to anterior and posterior forces. The procedure was uncomplicated, and was completed using a posterior-stabilized prosthesis with tibial augements and uncemented intramedullary rods in both the femur and tibia. Which of the following surgical techniques should have been implemented to avoid this complication?

Cementing the intramedullary rods in the tibia and femur
Explant with placement of an antibiotic spacer
Taking 5mm of extra bone from the distal femur to elevate the joint line
Use of a hinged total knee arthroplasty
Taking 5mm of extra bone from the tibia to distalize the joint line Corrent answer: 4
The patient has a neuropathic joint with ligamentous instability and a maltracking patella. The appropriate procedure would have included use of a hinged total knee arthroplasty.
Choosing the appropriate constraint during a total knee arthroplasty ensures the best possible outcome. Hinged total knee arthroplasty prostheses are indicated in the setting of global instability, massive bone loss in a neuropathic joint, oncologic procedures, and hyperextension instability. In a hinged prosthesis, the tibial and femoral components are linked with an axle that restricts varus/valgus and translational stresses. While hinged prostheses are useful in the setting of major revision surgery, they are at increased risk for aseptic loosening due to the high degree of constraint inherent to the device.
Petrou et al. review the results of 100 primary cemented rotating-hinge total knee arthroplasty at 7- to 15-years. At 15 years, survival was 96.1%.
Complications included DVT (n=3), skin necrosis (n=2), subcutaneous hematoma (n=5), intra-operative fracture of either the femur or tibia (n=4), and early infection (n=2).
Figures A-C show a neuropathic joint with considerable lateral bone loss and a frankly dislocated patella. Illustration A shows an example of a hinged total knee arthroplasty. Note how the tibial and femoral components are linked using an axle.
Incorrect Answers:

OrthoCash 2020
A 63-year-old man returns for follow-up 4 years after metal-on-metal left total hip arthroplasty complaining of mild chronic hip pain with ambulation. He is afebrile and ESR and CRP are within normal limits. Radiograph of the left hip is shown in Figure A. What is the best next step?

Anti-inflammatory medication
Serum cobalt and chromium levels
MRI with metal subtraction
Physical therapy
Revision hip arthroplasty Corrent answer: 2
Metal-on-metal total hip arthroplasties (THA) have been associated with complications presumably due to metal debris and toxicity. Serum cobalt and chromium levels are recommended as part of follow-up evaluation for patients with metal-on-metal hips, even when asymptomatic.
Many patients with metal-on-metal hips have been found to have elevated serum cobalt and chromium levels, for which MR with metal subtraction is recommended to look for pseudotumors and other pathologies. These solid or cystic masses are thought to be related to metal debris and macrophage infiltration and may be associated with pain in some patients.
Lombardi et al summarize and present on behalf of The Hip Society an algorithmic approach to evaluating and treating patients with metal-on-metal THA in follow-up. They state the goals of care as determining the etiology of any pain, managing any intrinsic problems with the arthroplasty, and reassuring/observing when appropriate. They organize the types of patients seen in followup and components of the evaluation.
Chang et al evaluate the correlation between symptoms and MRI findings and report that symptomatic patients tend to have bone marrow edema and tendon tearing on MRI. They report a 69% prevalence of pseudotumors on MRI after metal-on-metal hip arthroplasty, but did not find a correlation between pseudotumor presence and pain.
Hayter et al focus on MRI findings in symptomatic (painful) patients with metal-on-metal THA in a review including 31 hip resurfacing and 29 THA. In the THA group, they report 86% rate of synovitis, 10% extracapsular disease, and 24% osteolysis, with no statistically significant difference in rates between resurfacing and THA.
Figure A is an AP view radiograph of a left hip after metal-on-metal total hip arthroplasty with components well positioned and no osteolysis.
Illustrations A and B from Lombardi et al depict a recommended algorithm for the workup and management of symptomatic and asymptomatic patients, respectively, with metal-on-metal THA.
Incorrect Answers:
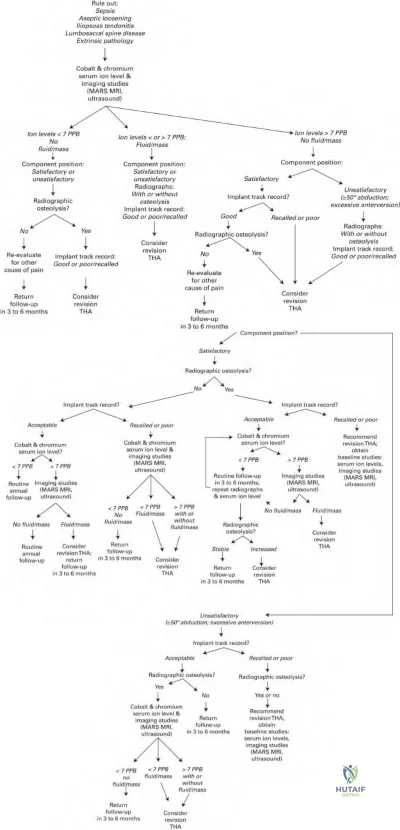
OrthoCash 2020
A 72-year-old woman sustains a fall onto her knee three years after an uncomplicated total knee replacement. The fracture pattern is seen in Figure A. The operative note reveals that a cemented patellar component was used. On exam, she has a large effusion and an
inability to straight leg raise. If the patellar component is well fixed, what is the best treatment option?

Patellectomy
Extensor mechanism allograft
Revision of the patellar component with cement and bone grafting of any residual defect
Open reduction and internal fixation of the patella fracture
Non-operative treatment in a knee brace locked in extension for 6 weeks Corrent answer: 4
Displaced, periprosthetic patella fractures with a deficient extensor mechanism and adequate bone stock are best treated with open reduction and suture or implant fixation.
Periprosthetic patella fractures are a rare, but potentially devastating complication associated with total knee arthroplasty. When evaluating patella fractures, it is important to consider 1) is the extensor mechanism intact, 2) is the patellar component well fixed or loose, and 3) is there sufficient bone stock remaining. Stable implants with an intact extensor mechanism should almost exclusively be treated non-operatively in a brace. In contrast, a deficient
extensor mechanism is an absolute indication for surgical management.
Adigweme et al. review the epidemiology, diagnosis, and treatment of periprosthetic patella fractures. When analyzing patella fractures, they suggest treatment should be based on fracture severity, remaining bone stock, patellar component stability, as well as extensor mechanism function.
Sarmah et al. review periprosthetic fracture around total knee arthroplasty. They provide an algorithm for treatment of periprosthetic patella fractures based on displacement, viability of remaining bone stock, and fracture type.
Figure A is a preoperative lateral radiograph showing a periprosthetic patellar fracture. The distal fragment is comminuted and separated from the proximal fragment by approximately 15 mm. The patellar component appears to be well fixed. Illustration A is intraoperative photograph showing the threads of the suture anchors in the proximal fragment passing through the tunnels in the distal fragment and exiting at the inferior pole of the patella. Illustration B demonstrates anatomical reduction after the knots were tied at the inferior pole of the patella. Illustration C is a lateral x-ray 1 year postoperatively showing fracture union.
Incorrect Answers:
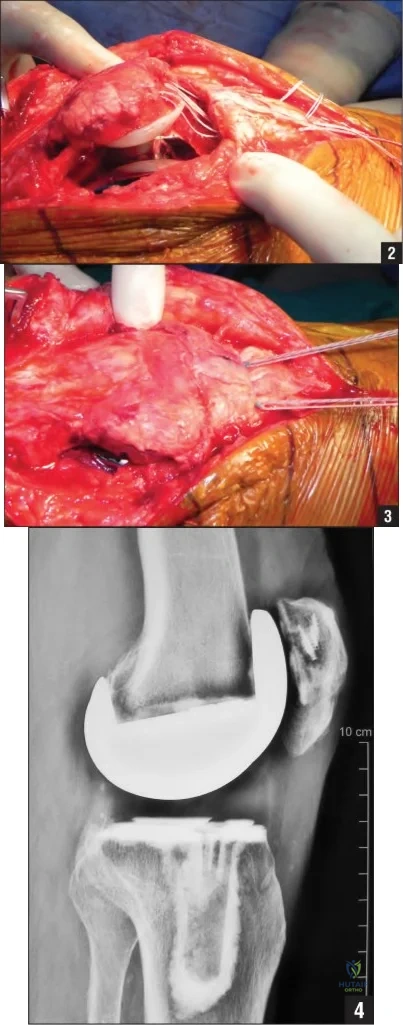
OrthoCash 2020
Knee pain and osteoarthritis are associated with "metabolic syndrome." All of the following are included in the collection of risk factors known as "metabolic syndrome" EXCEPT:
Peripheral vascular disease
Dyslipidemia
Hypertension
Impaired glucose tolerance
Central obesity
Peripheral vascular disease (PVD) may develop in patients with metabolic syndrome. However, no direct relationship between metabolic syndrome and PVD is known, and it is not a part of metabolic syndrome itself. Metabolic syndrome has been shown to be associated with knee pain and development of knee osteoarthritis (OA).
Metabolic syndrome is a collection of medical comorbidities that are known to
be risk factors for developing cardiovascular disease. Metabolic syndrome includes central (abdominal) obesity, dyslipidemia (high triglycerides and low-density lipoproteins), high blood pressure, and elevated fasting glucose levels. There is an increased prevalence of knee pain (and OA) among patients with metabolic syndrome. It is felt that the most important contributing factor to knee pain and OA in metabolic syndrome is obesity. Patients presenting with knee pain or OA and the risk factors included in metabolic syndrome should be counseled on the need to control those risk factors.
Inoue et al. present a study comparing metabolic syndrome and knee OA in a Japanese population. They found that knee OA and metabolic syndrome were highly correlated in females, but not in males.
Engström et al. present a study comparing metabolic syndrome with hip and knee OA. They found no relationship to hip OA, but did find a strong correlation between patients with metabolic syndrome and risk of developing knee arthritis. Patient BMI was the most predictive factor. They also compared prevalence of knee OA to CRP levels, but found no significant relationship.
Incorrect answers:
OrthoCash 2020
A 75-year-old male presents with recurrent dislocations of this left hip. He underwent bilateral total hip arthroplasties 12 and 8 years ago. There were no early post-operative complications with either hip. Despite a total of 5 dislocations in 6 months, he does not have pain or weakness across the left hip. On examination, there is a healthy appearing left lateral scar, equal limb lengths, normal gait and full abductor strength. Radiographs of the pelvis are shown in Figure A. His laboratory results show an erythrocyte sedimentation rate of 8 mm/h (reference range, 0-20 mm/h), and C-reactive protein of 3 mg/L (reference range, 0-5.0 mg/L). A hip aspirate culture is negative. What is the next best management option for this patient?

Magnetic resonance imaging of left hip to exclude an abductor muscle tear
Re-aspiration of left hip to exclude a subclinical infection
Continued observation for trochanteric bursitis
Supervised physiotherapy and gait training for abductor strengthening
Left revision total hip arthroplasty for polyethylene wear Corrent answer: 5
This patient presents with recurrent late hip instability with radiographic evidence of eccentric polyethylene wear. The best treatment option for this patient would be revision total hip arthroplasty (THA).
The etiology of late instability includes polyethylene wear, component malpositioning or loosening, trauma, infection or deterioration in neurological status of the patient. Identifying the cause of late instability will require a thorough work up. A good history, examination and scrutiny of radiographs can identify most causes. Advanced imaging may be requires when bone or soft-tissue pathology is suspected or radiographic evidence of osteolysis or malpositioning needs further assessment. Blood work to assess for an acute inflammatory response (ESR and CRP) should be ordered routinely as elevated markers may indicate an underlying infection.
Parvizi et al. evaluated the outcome of revision arthroplasty for polyethylene wear presenting as late dislocation. They found that revision surgery restored stability to eighteen of the twenty-two patients. Surgical treatment options may include liner-only exchange (contained or unconstrained) +/- soft-tissue repair, or revision of one or all components.
Berry et al. evaluated the long-term risk of dislocation in 6,623 consecutive primary total hip arthroplasties with a Charnley prosthesis. They found a 7% incidence of late dislocation at 25 years compared to 1% after 5 years.
Patients at highest risk were females, patients with osteonecrosis of the femoral head or an acute fracture, and nonunion of the proximal part of the femur.
Figure A shows an AP pelvis with bilateral, uncemented, total hip arthroplasties. There is eccentric wear of the left acetabular component. No fracture or loosening of the components can be identified. The components appear well-positioned.
Incorrect Answers:
This patient has no pain or weakness in the affected hip. Therefore, soft tissues can be evaluated intra-operatively during the revision THA procedure. Answer 2: A hip aspirate would not be warranted. There are no risk factors for infection in this patient (for example, no pain, no early wound complications or antibiotics, etc). Additionally, his inflammatory markers are normal.
OrthoCash 2020
A 58-year-old woman undergoes a total knee arthroplasty with a posterior stabilized design. Two years later, she returns with recurrent sterile joint effusions, a sensation of instability without giving way and difficulty with ascending and descending stairs. Examination reveals diffuse tenderness around the pes anserinus and peripatellar region, and increased anterior tibial translation most notable at 90° of flexion. Radiographs demonstrate well cemented implants with 5° of posterior tibial slope. Figure A represents a femoral cutting block with lines 1 through 5 corresponding to femoral bone cuts. The most likely cause of her symptoms is over-resection at:

Resection line 1
Resection line 2
Resection line 3
Resection line 4
Resection line 5
Over-resection of the posterior femoral condyles (resection line 2) in posterior-stabilized (PS) TKA leads to flexion instability without frank dislocation.
There are 7 bone cuts in a total knee replacement. The posterior condylar cut determines the flexion gap. Flexion instability in PS knees arises because of an enlarged flexion gap (excessive posterior condylar resection, or increased tibial slope), allowing anterior tibial translation, which is pathognomonic. There will not be posterior subluxation because of the cam-post design. Symptoms include sensation of instability without giving way, especially with stair climbing, recurrent knee effusions, and diffuse knee pain. Signs include anterior tibial translation at 90° flexion, tenderness at multiple sites (including pes anserinus, peripatellar, posterior hamstrings), and effusion. Revision surgery is indicated for symptomatic patients.
Clarke et al. reviewed flexion instability after primary TKA. They caution that most cases arise from failure to create symmetric balanced flexion and extension spaces. Treatment is usually revision TKA using the same principles. If this is not possible, increased constraint is required (constrained condylar prosthesis or hinged prosthesis).
Schwab et al. reviewed flexion instability without dislocation in PS knees in 10 patients. Revision surgery focused on flexion-extension gap balancing and filling the enlarged flexion gaps and successfully relieved pain, and improved stability to anterior tibial translation. Flexion space reconstruction includes using a larger femoral component or posterior augments. Isolated polyethylene exchange is not recommended.
Figure A shows a 5-in-1 cutting block with anterior femoral cut (line 1), posterior femoral cut (line 2), posterior chamfer cut (line 3), anterior chamfer cut (line 4), and distal femoral cut (line 5). Of note, most TKA systems have a 4-in-1 cutting block and the distal femoral cut is made separately. Illustration A shows restoration of the posterior condylar offset (line A) with the femoral component (line B).
Incorrect Answers
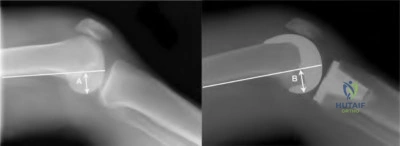
OrthoCash 2020
Which of the following is true regarding intra-operative fractures during total knee arthroplasty?
They occur more commonly in cruciate-retaining total knee replacements
Fractures of the medial femoral condyle are the most common fracture type
Fractures of the patella are the most common fracture type
Most can be treated without additional fixation at the time of surgery
Tibial fractures are more common than femoral fractures Corrent answer: 2
Fractures of the medial femoral condyle are the most common type of intraoperative fracture during a total knee arthroplasty.
Intra-operative fractures during total knee replacement are rare, but usually requiring alterations in surgical technique once they occur. The most common time for fractures to occur is during exposure and bone preparation, with fracture during trialing being the next most common. Fractures occur more commonly in posterior cruciate substituting designs, likely due the box cut.
Osteoporosis, female gender, chronic steroid use, advanced age, rheumatoid arthritis, and neurologic disorders are risk factors for post-operative fracture, but are also thought to be risk factors for intra-operative fractures.
Alden et al. reviewed 17,389 primary TKAs and found an intra-operative fracture rate of 0.39%. Of the 67 fractures, 49 were femur fractures, 18 were tibia fractures, and none were patella fractures. They recommend careful surgical technique in patients at high risk for fracture to avoid such a complication.
Sharkey et al. reviewed 10 intra-operative femoral fractures during primary, cementless total hip arthroplasty. They matched these with 20 patients who did not have this complication. At follow-up, there were no differences found between the two groups.
Incorrect Answers:
OrthoCash 2020
A 68-year-old male complains of increasing medial sided knee pain and buckling. The pain is exacerbated by sharp turns while
running. He undergoes knee arthroscopy. Recent radiographs and an arthroscopic photograph of the medial compartment are shown in Figure A. His pain has worsened since the arthroscopy. Which of the following images (Figures B through F) represents the best treatment recommendation for this patient?

This patient has isolated medial compartment osteoarthritis with Outerbridge IV medial compartment cartilage wear on arthroscopy. The best surgical option is a medial unicompartmental knee arthroplasty (UKA).
Indications for UKA include range of motion >100deg with <5deg flexion contracture, angular deformity <15deg valgus or <5deg varus that is passively correctable to neutral. Relative contra-indications include younger patients (age <60), obesity (BMI >30), and ACL deficiency in medial UKA. Asymptomatic patellofemoral chondromalacia is not a contraindication. In general, a UKA is preferred for older, less active patients with minimal varus, more severe arthritis, and no/little knee instability. A HTO is preferred for younger, active patients, with milder arthritis, more malalignment, and AP instability.
Steadman et al. retrospectively examined outcomes of TKA after arthroscopic treatment of OA in 73 patients. They found that mean survival time (conversion to TKA) after arthroscopy was 6.8 years (5.7 years in patients with Kellgren-Lawrence grade 4, and 7.5 years in those with grade 3). They conclude that in patients who want to avoid TKA, arthroscopy may help postpone TKA.
LaPrade et al. examined the results of proximal tibial opening wedge
osteotomies in 47 patients <55 years old with medial compartment osteoarthritis (OA) and genu varus. They found that there was improvement in knee scores and the mechanical axis at 3.6 years. They recommend this technique for patients with medial compartment OA and malalignment.
Figure A is a composite image showing isolated medial compartment osteoarthritis, and Outerbridge IV cartilage wear with large areas of visible subchondral bone. (See below for Figures B through F). Illustration A is a table comparing the indications of HTO vs UKA.
Incorrect Answers:
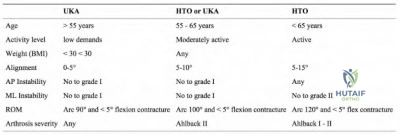
OrthoCash 2020
A 58-year-old female, with a BMI of 34 kg/m2, underwent a total knee arthroplasty for osteoarthritis 6 weeks ago. She has been participating in supervised rehabilitation since the procedure. Her preoperative, intra-operative and 6 week post-operative knee flexion are shown in Figure A. Current radiographs are shown in Figure B. What is the best step in management?

Convert to a resurfaced patella
Downsize the polyethylene liner
Arthroscopic lysis of adhesions and release of posterior capsule
Continuous passive motion at home for two weeks
Manipulation under anesthesia Corrent answer: 5
This patient has early post-operative stiffness after total knee arthroplasty (TKA). The next best step would be manipulation under anesthesia.
Management of stiffness following TKA can be challenging. The standard initial treatment option for post-operative knee stiffness is physical therapy. When this fails to achieve knee range of motion (ROM) greater than or equal to 90°, alternative treatment modalities should be considered, such as knee manipulation under anesthesia (MUA). MUA is a non-invasive treatment shown to achieve dramatic improvement in knee flexion during the early postoperative period (usually considered less than three months). Periprosthetic fracture during manipulation is rare, with an overall incidence less than 1%.
Issa et al. examined a cohort of patients that underwent MUA after TKA. At a mean follow-up of 51 months (range, 24 to 85 months), the mean gain in flexion in the MUA cohort was 33° (range, 5° to 65°). There was one periprosthetic fracture in 134 patients. The authors noted a significant improvement in ROM from pre-manipulation values.
Manrique et al. reviewed stiffness after total knee arthroplasty. MUA may be considered within the first three months after the index TKA if physical therapy fails to improve the ROM. Beyond this point, consideration should be given to surgical intervention such as lysis of adhesions, either arthroscopic or open.
Maniar et al. looked at the effectiveness of continuous passive motion immediately after TKA. A total of 84 patients were allocated to no CPM; 1 day CPM; or 3 day CPM. They found that continuous passive motion immediately after TKA did not improve short or mid-term knee ROM.
Figure B shows a cruciate sacrificing total knee arthroplasty with implants in a good position.
Incorrect Answers:
OrthoCash 2020
Which of the following fracture patterns (Figures A-E) would require revision of the femoral component to a long-stemmed, cementless prosthesis?

Figure C depicts a Vancouver B2 periprosthetic fracture, which is optimally treated with a long-stem, fully porous-coated, revision femoral prosthesis.
The Vancouver classification for total hip periprosthetic femoral fractures takes into account the three most important factors in management of these injuries: the site of the fracture, the stability of the femoral component, and the quality of the surrounding femoral bone stock. Type A fractures include those involving the lesser trochanter or the greater trochanter. Type B fractures occur around the stem or just below it. More specifically, B1 fractures have a well fixed stem, B2 fractures have a loose stem but good proximal bone stock and B3 fractures have a loose stem with proximal bone that is of poor quality or severely comminuted. Type C fractures are well below the tip of the femoral stem.
O'Shea et al. assessed the outcome of patients with Vancouver type B2 and B3 periprosthetic fractures treated with femoral revision using an uncemented extensively porous-coated implant. Union of the fracture was successfully achieved in 20 of the 22 patients. Overall, they found good early survival rates and a low incidence of nonunion using this implant.
Figure A depicts a radiograph of a Vancouver type C periprosthetic femur fracture, occurring distal to the stem of the total hip arthroplasty. Figure B demonstrates a Vancouver type A periprosthetic fracture of the greater trochanter. Figure C is an x-ray of a Vancouver type B2 periprosthetic fracture adjacent to the stem with an unstable implant, but adequate bone stock.
Figure D depicts a radiograph of a Vancouver type C periprosthetic femur fracture, occurring distal to the stem of the total hip arthroplasty. Figure E is a Vancouver type B1 periprosthetic fracture at the level of the stem that is well fixed. Illustration A shows a table summarizing the Vancouver classification of periprosthetic femur fractures and the corresponding management options.
Incorrect Answers:
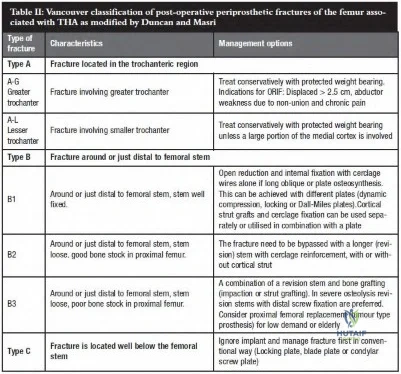
OrthoCash 2020
Which of the following maneuvers places the obturator artery at greatest risk during a total hip arthroplasty?
Placement of a posterior retractor along the posterior wall
Placement of an acetabular screw in the posterior-superior quadrant
Placement of an inferior retractor under the transverse acetabular ligament
Placement of an acetabular screw in the anterior-superior quadrant
Placement of an anterior retractor along the anterior wall Corrent answer: 3
Damage to the obturator artery most commonly occurs from placement of an inferior retractor inferior to the transverse acetabular ligament (into the obtrator foramen), and/or placement of an acetabular screw in the anterior-inferior quadrant.
Vascular injury during total hip arthroplasty is a rare but devastating complication with a reported incidence of 0.1%-0.2%. The obturator artery travels along the quadrilateral surface of the acetabulum and exits the pelvis at the superolateral corner of the obturator foramen. If the vessel is severely
damaged and bleeding cannot be controlled, ligation of the internal iliac artery has been reported.
Nachbur et al. report on 15 cases of severe arterial injury during hip reconstructive surgery over a period of 8 years. The most common injury was injury to the external iliac artery, the common femoral artery, or main branches of the lateral and medial circumflex femoral artery. These were thought to be caused by the tip of a narrow-pointed Hohmann retractor used for exposure of the hip joint.
Rue et al. review neurovascular injuries during total hip arthroplasty. Among other things, they recommend against placement of screws in the anterior-superior quadrant, prudent retractor placement, and avoiding excessive tension on the sciatic nerve.
Della Valle and Di Cesare review complications resulting from total hip replacement. They state that injury to the obturator artery can occur with acetabular screw fixation in the antero-inferior quadrant or from retractors placed underneath the transverse acetabular ligament.
Illustration A shows the obturator artery as it exits the pelvis at the superolateral corner of the obturator foramen. Illustration B reviews acetabular screw placement and the structures at risk in each quadrant.
Incorrect Answers:
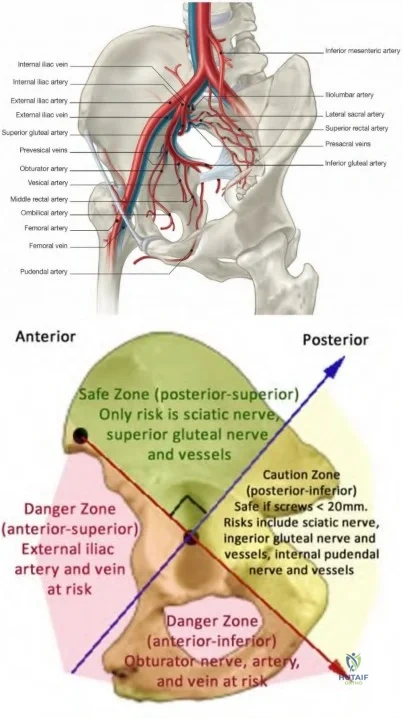
OrthoCash 2020
A 65-year-old male sustains a fall onto his left hip 3 years after a total hip arthroplasty. A radiograph taken at the emergency room is shown in Figure A. What is the next best step?

Open reduction and internal fixation with locked plates and cables through an extensile approach
Revision with a proximally porous-coated stem
Revision with an extensively porous-coated stem
Nonoperative management
Minimally invasive plate osteosynthesis Corrent answer: 3
The patient has a Vancouver B2 periprosthetic fracture. There is a loose stem that should be treated with revision to an extensively coated stem that bypasses the fracture site.
Revision of the femoral component is recommended for Vancouver B2 and B3 periprosthetic fractures. Type B1 fractures are treated with ORIF and stem retention, and proximally deficient B3 fractures may be treated with alloprosthetic composites or tumor prostheses.
Springer et al. retrospectively reviewed 118 hips with Vancouver B fractures. Seventy-seven percent of 30 extensively coated stems, 60% of 42 cemented stems, 36% of 28 proximally coated stems, and 61% of 18 tumor prosthesis/allo-prosthetic composite stems were well fixed and demonstrated
fracture union. Nonunion and loosening were the most common complications. They recommend extensively porous-coated stems for better results.
Haidukewych et al. review revision of periprosthetic fractures. They found that most acetabular components are well fixed. When the distal fragment has parallel endosteal cortices with >=5 cm of tubular diaphysis (usually with a diameter of <18 mm), they recommend an extensively coated, uncemented, monoblock long-stemmed prosthesis. If the distal diaphysis is divergent, has
<5 cm of parallel endosteal cortex, or large endosteal diameters, a fluted, grit-blasted, titanium, tapered modular stem can be used.
Figure A shows Vancouver B2 fracture. The stem has subsided relative to the proximal fracture fragment, indicating that it is loose. Illustration A shows revision of the same fracture with an extensively porous-coated stem.
Illustration B shows the endoskeleton technique using an osteotomy to split the proximal fragment coronally for stem removal, followed by insertion of a modular, fluted, tapered stem and cerclage fixation of the proximal fragments.
Incorrect Answers:
Question 91
A 58-year-old woman is seen in the emergency department after falling at home. History reveals that she underwent right total knee arthroplasty 2 years ago. Radiographs are shown in Figures 56a and 56b. What is the most appropriate treatment?
Explanation
REFERENCES: Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209.
Raab GE, Davis CM III: Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty 2005;20:984-989.
Tharani R, Nakasone C, Vince KG: Periprosthetic fractures after total knee arhtroplasty.
J Arthroplasty 2005;20:27-32.
Question 92
A high school football player asks you about an oral supplement that increases body mass and improves sprint times. He would like to use it to improve performance. What is the most likely agent?
Explanation
REFERENCES: McGuine TA, Sullivan JC, Bernhardt DT: Creatine supplementation in high school football players. Clin J Sports Med 2001 ;11:247-253.
Rawson ES, Gunn B, Clarkson PM: The effects of creatine supplementation on exercise-induced muscle damage. J Strength Cond Res 2001; 15:178-184.
Branch JD: Effect of creatine supplementation on body composition and performance: A meta-analysis.
Int J Sport Nutr Exerc Metab 2003;13:198-226.
Question 93
A newborn has an anterolateral bow of the tibia and a duplication of the great toe. Which of the following conditions will develop as the infant grows?
Explanation
REFERENCE: Weaver KM, Henry GW, Reinker KA: Unilateral duplication of the great toe with anterolateral tibial bowing. J Pediatr Orthop 1996;16:73-77.
Question 94
An 8-year-old boy sustains injuries to his head, abdomen, and left lower extremity after being struck by a truck. In the emergency department, his mental status deteriorates and he is intubated after assessment reveals a Glasgow Coma Scale score of 3; the score subsequently improves to 10. A CT scan reveals a right parietal intracranial hemorrhage, and an abdominal ultrasound reveals free fluid. Prior to an emergency laparotomy, the swollen left thigh is evaluated. Radiographs reveal a transverse fracture of the mid-diaphysis. Management of the fracture should consist of
Explanation
REFERENCES: Tolo VT: Management of the multiply injured child, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996,
pp 83-95.
Heinrich SD, Drvaric DM, Darr K, MacEwen GD: The operative stabilization of pediatric diaphyseal femur fractures with flexible intramedullary nails: A prospective analysis. J Pediatr Orthop 1994;14:501-507.
Question 95
In a fracture such as the one shown in Figure 16 (Salter-Harris type I fracture of the distal femur), which of the following best describes the location of the fracture?
Explanation
REFERENCES: Smith DG, Geist RW, Cooperman DR: Microscopic examination of a naturally occurring epiphyseal plate fracture. J Pediatr Orthop 1985;5:306-308.
Jaramillo D, Kammen BF, Shapiro F: Cartilaginous path of physeal fracture separations: Evaluation with MR
imaging: An experimental study with histologic correlation in rabbits. Radiology 2000;215:504-511. Question 17
A 14-year-old boy has had a 3-month history of low back pain with no known trauma. The pain is worse with activity and relieved by rest, although he does report difficulty with prolonged sitting in school.
The patient was on the football team but stopped participating because of the back pain during football practice. He reports no history of radicular pain and denies any numbness, tingling, or weakness in the legs.
Neurologic examination is normal. Back examination reveals slight tenderness over the lower back area but no swelling or skin defects. Strength testing is 5 over 5 in the lower extremities and the straight leg raise test is negative. Back range of motion is nearly full, but back extension is painful. The hamstrings are slightly tight. Initial radiographs, including AP, lateral and oblique views, are negative. What is the best test to determine the patient’s diagnosis?
Flexion and extension lateral radiographs
MRI
Myelogram
Diskogram
Bone scan with SPECT PREFERRED RESPONSE: 5
DISCUSSION: A bone scan with SPECT is very sensitive and specific for spondylolysis not seen on initial
radiographs. MRI can sometimes visualize spondylolysis, but it is not as sensitive nor as specific as a bone scan with SPECT. Flexion and extension views have no role in the evaluation of the patient who presents with classic spondylolysis-type symptoms. The most sensitive physical examination finding is pain with back extension. Oblique radiographs can be obtained, but they are not as sensitive or specific as a bone scan with SPECT. The patient does not have any signs of a disk problem; therefore, an evaluation of the disk is not helpful.
REFERENCES: Hu SS, Tribus CB, Diab M, et al: Spondylolisthesis and spondylolysis. J Bone Joint Surg Am 2008;90:656-671.
Lawrence JP, Greene HS, Grauer JN: Back pain in athletes. J Am Acad Orthop Surg 2006;14:726-735.
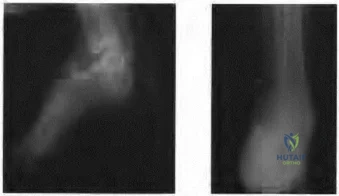
Figure 18a Figure 18b
Question 96
If a surgeon inadvertently burrs through the midlateral wall of C5 during a anterior corpectomy, what structure is at greatest risk for injury?
Explanation
REFERENCES: Pfeifer BA, Freidberg SR, Jewell ER: Repair of injured vertebral artery in anterior cervical procedures. Spine 1994;19:1471-1474.
Gerszten PC, Welch WC, King JT: Quality of life assessment in patients undergoing nucleoplasty-based percutaneous discectomy. J Neurosurg Spine 2006;4:36-42.
Question 97
Figure A shows the operative technique used during arthroscopic repair of 25-year-old male patient with vague shoulder pain. The glenoid rim was prepared using the drill bit insertion angles as shown. Three suture anchors, measuring 14mm in length were inserted 4-6 mm deep to the surface. What structure is at the highest risk with this technique? Review Topic
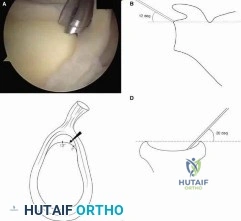
Explanation
At the scapular spine level, the suprascapular nerve is approximately 1.5-2.0 cm from the glenoid cortex. This places the nerve at risk of injury during shoulder surgery, and injuries have been described. Arthroscopic SLAP repair is known to be a safe and relatively simple procedure. However, deep drilling or anchor insertion from the anterior or anteriosuperior portal during SLAP repair can place the suprascapular nerve at risk of iatrogenic injury.
Morgan et al. performed a cadaveric study to compare the risk of injury to the suprascapular nerve during suture anchor placement in the glenoid when using an anterosuperior portal versus a rotator interval portal. Standard 3 × 14 mm suture anchors were placed in the glenoid rim (1 o’clock, 11 o’clock, and 10 o’clock positions for the right shoulder). They showed that the distance from the far-posterior anchor tip to the suprascapular nerve averaged 8 mm (range, 3.4 to 14 mm) for the anterosuperior portal and 2.1 mm (range, 0 to 5.5 mm) for the rotator interval portal (P = .001).
Koh et al. evaluated the risk of suprascapular nerve injury during the drilling and anchor insertion for anterior SLAP repair. They inserted 1 suture anchor
arthroscopically from the anterior portal at 00:30-1:00 o’clock in right shoulders (11-11:30 in left). Using a mean drill depth was 14.2 (±2.8) mm, all suture anchors perforated the glenoid wall and the tips were measured to be approx. 3.1 (±2.7) mm from the suprascapular nerve.
Figure A shows an arthroscopic view and corresponding schematic image of arthroscopic drill position for SLAP repair. Illustration A shows the close proximity of anchor tip to the suprascapular nerve, as the nerve nerve enters the supraspinatus fossa below the superior transverse scapular ligament and then enters the infraspinatus fossa between the neck of the scapula and base of the spine of the scapula.
Incorrect Answers:
(SBQ11UE.106) A 60 year-old diabetic man presents with increasing right shoulder pain and stiffness for 10 weeks. He works as a lawyer and has been treating the pain with non-steroidal anti-inflammatory drugs with little improvement. He had a previous injury to his right shoulder 15 years ago while playing hockey, but cannot recall any recent precipitants for this presentation. Physical examination shows significant reduction in right shoulder range of motion, with the greatest loss in external rotation. His MRI images are seen in Figures A-C. What would be the most appropriate treatment? Review Topic

Open supraspinatus cuff repair
Arthroscopic supraspinatus cuff repair
Reverse shoulder arthroplasty
Arthroscopic posterior capsular release
Physical therapy and medical management
The patient is presenting with right shoulder adhesive capsulitis. The most appropriate treatment at this time would be physical therapy and medical management (i.e., nonsteroidal anti-inflammatories +/- intra-articular steroid injections).
Adhesive capsulitis (aka frozen shoulder) is defined by pain and loss of both active and passive motion, especially loss of external rotation in comparison to the contralateral side. Risk factors include diabetes, thyroid disease, age, previous surgery and prolonged immobilization. Initial treatment options include NSAIDs, physical therapy, and intra-articular steroid injections. Surgical treatment is not commonly recommended, but may be used late in the course to address residual stiffness if extensive therapy has failed.
Griggs et al. prospectively reviewed seventy-five consecutive patients (seventy-seven shoulders) with adhesive capsulitis. They showed that 90 percent of the patients reported a satisfactory outcome with shoulder stretching exercises. However, male gender and diabetes mellitus were associated with worse motion at the final evaluation.
Hannafin et al. reviewed the treatment options for adhesive capsulitis. They suggest
that benign neglect, home-based and supervised physical therapy, and intra-articular corticosteroid injections should be considered in the early treatment of adhesive capsulitis. Duration of treatment should be considered for at least 3 months before more aggressive treatments are considered.
Levine et al. retrospectively reviewed the treatment and outcome of 234 patients with adhesive capsulitis. No significant difference was found for success of nonoperative treatment versus operative treatment or patient gender. With supervised treatment, most patients with adhesive capsulitis experience resolution with nonoperative measures in a relatively short period.
Figures A (Sagittal oblique T1 MRI), and Figure B (coronal oblique fat-saturated T2 MRI) show the anterior rotator cuff interval in the right shoulder demonstrate high-signal soft tissue thickening of the coracohumeral ligament (arrow). Figure C (Coronal oblique fat-saturated T2 MRI) demonstrates a thickened inferior glenohumeral ligament of the right shoulder.
Incorrect Answers:
Question 98
A 43-year-old man sustained a closed, intra-articular pilon fracture. It has now been 1 year since he underwent open reduction and internal fixation. Which of the following statements most accurately describes his perceived outcome?
Explanation
REFERENCE: Marsh JL, Weigel DP, Dirschl DR: Tibial plafond fractures: How do these ankles function over time? J Bone Joint Surg Am 2003;85:287-295.
Question 99
006%-3.4 %. The typical skin flora includes staph and strep as well as P. acnes, which has a propensity for the shoulder. Because it is an anaerobic organism, cultures may only become positive after 7-21 days.
Explanation
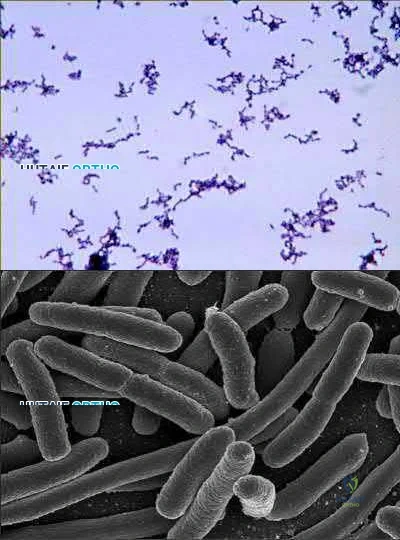
A 47-year-old, healthy, active patient presents with a sub-acute, full-thickness supraspinatus tear. His physical examination reveals significant weakness and pain with abduction. There was no glenohumeral instability. Radiographs demonstrate a type 1 acromion. An MRI scan shows a crescent shaped tear with 2-cm of tendinous retraction and no tendinous fatty changes. A subacromial corticosteroid injection 6 weeks ago provided him with 24 hours of pain relief but no improvement in strength. What would be the most appropriate treatment option?
Repeat subacromial corticosteriod injection

Biological augmentation of rotator cuff with porcine small intestine xenograft Rotator cuff repair

Rotator cuff repair plus acromioplasty

Rotator cuff repair, remplissage procedure, bicep tenodesis and distal clavicle excision
This patient has an isolated supraspinatus rotator cuff tear with symptomatic weakness. The most appropriate treatment would be isolated rotator cuff repair.
The primary purpose of rotator cuff repair is to restore muscle function. Secondary outcomes include reduction of pain and prevention of irreversible cuff changes, specifically muscular atrophy. Non-operative treatment ( exercise, therapy and pain medications) are recommended for partial thickness tears. The indication of surgical repair includes, isolated supraspinatus weakness +/- pain
that correlates with MRI imaging of a respective full thickness tear. Routine acrominoplasty is not recommended in conjunction with rotator cuff repair, especially with no previous symptoms of impingement.
Pedowitz et al. developed clinical practice guidelines for the treatment of rotator cuff pathology. The strongest supporting evidence in current literature was given a grade of 'moderate' with four treatment recommendations. These were,
Exercise and non-steroidal anti-inflammatory drugs can be used to manage partial thickness tears,

Routine acromioplasty is not required the time of cuff repair,

Non-cross-linked, porcine small intestine submucosal xenograft patches should not be used to manage cuff tears, and

Surgeons can advise patients that workers' compensation status correlates with a less favorable outcome after rotator cuff surgery.
Illustration A shows the different shapes of rotator cuff tears. Incorrect Answers:
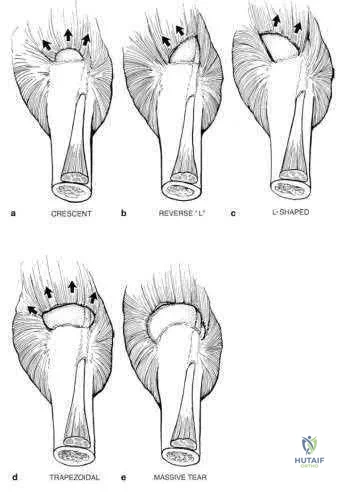
A 12-year-old baseball pitcher describes progressive worsening of medial elbow pain on
his throwing side. Examination reveals normal elbow range of motion. He is tender over the medial elbow to palpation. A dynamic ultrasound of his elbow shows no evidence of medial widening with valgus stress. His radiograph is shown in Figure A and an MRI is shown in Figure B. What is the most likely cause of his symptoms?

Displaced medial epicondyle avulsion fracture Medial apophysitis

Medial ulnar collateral ligament tear

Valgus extension overload with olecranon osteophytes Ulnar neuritis
The clinical presentation is consistent with Little League Elbow caused by medial apophysitis. Little League elbow is a general term explaining medial elbow pain in adolescent pitchers. The underlying pathology can include medial epicondyle stress fractures, avulsion fractures of the medial epicondyle, ulnar collateral ligament (UCL) injuries, or medial epicondyle apophysitis. In order to identify the underlying cause it is important to first rule out injury to the MCL by looking for medial widening on stress radiographs or dynamic ultrasound, or valgus instability on physical exam. Radiographs are useful to look for avulsion fractures or subtle physeal widening commonly seen with apophysitis.
Wei et al. obtained radiographs and magnetic resonance imaging on nine adolescent pitchers with a clinical diagnosis of Little League Elbow. They found radiographic findings in 4/9 and MRI findings in 6/9 patients. They emphasized that the MRI did not change management in any patients. Cain et al. review the different elbow conditions seen in throwing athletes. They emphasize the need to understand the underlying pathophysiology in order to treat and make appropriate changes to the biomechanics of the pitching technique.
Figure A shows an AP radiograph with slight widening of the apophysis, but no evidence of avulsion fracture. Figure B is an MRI which shows signal consistent with edema of the medial epicondyle apophysis.
Incorrect Answers:
The other responses are all typical throwing elbow conditions, but are much less common than apophysitis in the adolescent thrower.
What is the primary function of the structure labeled with an asterisk in Figure A?
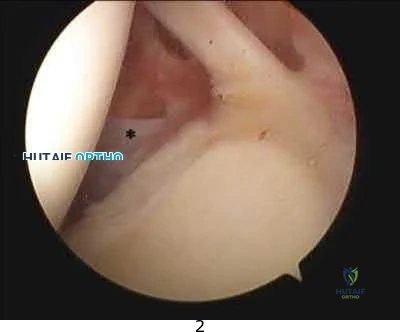
Prevents inferior translation of the humerus with the arm by the side Provides internal rotation of the humerus

Prevents anterior translation of the humerus with the arm in 45 degrees of abduction Prevents anterior translation of the humerus with the arm in 90 degrees of abduction Provides supination of the forearm and elbow flexion
The labeled structure is the middle glenohumeral ligament (MGHL) of the shoulder. The primary function of the MGHL is to prevent anterior translation of the humeral head with the arm in 45-60 degrees of abduction.
This structure originates from the glenoid labrum and inserts medial to the lesser tuberosity running obliquely across the subscapularis. The size of the structure may be variable and there are recognized normal anatomic variants ( including a cord like MGHL in the Buford complex). It is important to be able to recognize the MGHL and differentiate this from the subscapularis, IGHL, SGHL, and other intraarticular structures in the shoulder to be able to perform effective and precise arthroscopic procedures.
Burkhart et al. describe the function of the glenohumeral ligaments in anterior shoulder instability, noting that the MGHL provides a restraint to anterior translation with the arm in 45-60 degrees of abduction.
Wang et al. discuss microdamage to the inferior glenohumeral ligament from a basic science perspective, indicating that over time it may stretch and compromise it's function in restraining humeral translation.
Figure A is an arthroscopic image of the intraarticular structures of the shoulder with an asterisk on the MGHL.
Incorrect Answers (these are labeled on Illustration A, with the exception of the subscapularis which is difficult to visualize):

In which of the following clinical circumstances would it be appropriate to eccentrically ream the anterior glenoid?

year-old male undergoing a shoulder arthroplasty due to rotator cuff arthropathy 65-year-old female with a glenoid retroversion of 13-degrees undergoing shoulder arthroplasty

year-old female with humeral anteversion of 13-degrees undergoing shoulder arthroplasty

year-old female with glenoid retroversion of 25-degrees undergoing shoulder arthroplasty

year-old male with significant glenoid bone stock deficiency and severe osteoarthritis
The surgeon should consider eccentrically reaming the anterior glenoid when performing a total shoulder arthroplasty on a patient with a retroverted glenoid due to posterior deficiency associated with osteoarthritic changes which is most consistent with answer choice #2.
Normal version of the glenoid is 0-3 degrees of retroversion, but when doing a total shoulder the goal should be to place the glenoid component in neutral to slight anteversion. Reaming the anterior glenoid to neutral is a technique to be considered by the operative surgeon when presented with a patient undergoing total shoulder arthroplasty with a retroverted glenoid, as failure to perform this step increases the chance for glenoid loosening. If reaming down the anterior glenoid will take away too much bone stock (down to the coracoid process), one may consider bone grafting the posterior glenoid. To perform a total shoulder arthroplasty patients will need a functioning rotator cuff and appropriate glenoid bone stock.
Clavert et al. performed cadaveric analysis to simulate glenoid retroversion of greater than 15 degrees and found that retroversion to this degree cannot be safely corrected with eccentric anterior reaming when using a glenoid component with peripheral pegs due to penetration into the glenoid vault.
Nowak et al. used 3D-CT models of patients with advanced shoulder osteoarthritis with varying degrees of glenoid retroversion and simulated glenoid resurfacing. They found that smaller size glenoid components may allow for greater version correction when using in-line pegged components, as they would be less likely to result in peg penetration.
Illustration A shows >25 degrees of glenoid retroversion seen by axial radiograph of the shoulder in a patient with advanced osteoarthritis. In this case, anterior glenoid reaming is not the correct answer and a posterior glenoid allograft reconstruction would be appropriate.
Incorrect Answers:
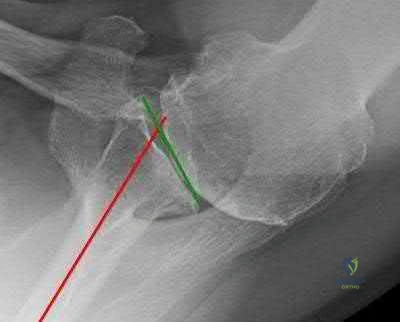
A 44-year-old left-hand dominant carpenter experienced immediate left elbow pain after trying to stop a heavy object from falling two days ago. Figure A shows a clinical image of the patient upon presentation. Physical exam shows full strength with wrist flexion, wrist extension, and pronation, but notable weakness with supination of the forearm. Sensory exam shows no deficits in the forearm or hand. There is a negative milking maneuver test and a positive hook test. Radiographs are shown in Figure B. What is the next most appropriate step in management?

Sling use as needed for comfort and progressive physical therapy Allograft reconstruction of the distal biceps tendon

Ulnar collateral ligament reconstruction Distal biceps tendon avulsion repair Brachioradialis and ECRB avulsion repair
Distal biceps tendon avulsion repair is the most appropriate next step in management.
Distal biceps tendon ruptures occur most commonly in middle-aged men and usually involve the dominant extremity. The mechanism of injury is usually a single traumatic event with eccentric force on the flexed elbow.
Sutton et al. authored a Level 5 review of distal biceps tendon ruptures. They discuss that nonsurgical management of distal biceps tears is appropriate in the low-demand or medically ill patient. Surgical repair improves elbow flexion strength by 30% and supination strength by 40% compared to nonoperative management.
O'Driscoll et al. conducted a Level 2 study examining the accuracy of the hook test for distal biceps rupture diagnosis. They found that the hook test was abnormal in 33 of 33 (100%) patients with complete biceps avulsions, and intact in 12 of 12 (100%) with partial detachments.
Figure A is a clinical image demonstrating ecchymosis in the distal arm and antecubital fossa. Figure B shows normal elbow radiographs. Illustration A shows a normal hook test with an intact distal biceps insertion.
Incorrect Answers:

Early reverse total shoulder designs (before the development of the Grammont-style prosthesis) had a high failure rate due to early loosening of the glenoid component. What biomechanical feature accounted for this problem?

Glenoid component did not have a neck Humeral component too horizontal Center of rotation too lateral

Center of rotation too anterior Center of rotation too inferior
Early reverse ball-and-socket designs failed because their center of rotation remained lateral to the scapula, which limited motion and produced excessive torque on the glenoid component, leading to early loosening. The first modern reverse prosthesis was designed by Paul Grammont. According to Boileau et al., Grammont's design "introduced 2 major innovations (1) a large glenoid hemisphere with no neck and (2) a small humeral cup almost horizontally oriented with a nonanatomic inclination of 155 degrees, covering less than half of the glenosphere. This design medializes the center of rotation compared to earlier versions which minimizes torque on the glenoid component. Furthermore, the humerus is lowered relative to the acromion, restoring and even increasing deltoid tension. The Grammont reverse prosthesis imposes a new biomechanical environment for the deltoid muscle to act, thus allowing it to compensate for the deficient rotator cuff muscles." According to Gerber, "moving the center of rotation more medial and distal as well as implanting a large glenoid hemisphere that articulates with a humeral cup in 155 degrees of valgus are the biomechanical keys to sometimes spectacular short- to midterm results".
Which of the following preoperative factors is a contraindication to total shoulder arthroplasty?

Passive external rotation less than 10 degrees Eccentric posterior glenoid erosion

A 2-cm full-thickness supraspinatus tendon tear Inflammatory arthritis

A preganglionic brachial plexus injury
A preganglionic brachial plexus palsy, otherwise known as a root avulsion injury, presents with a flail arm and has a poor prognosis for recovery of motor function. Patients with brachial plexus palsies are not candidates for total shoulder arthroplasty due to the substantial motor and sensory deficits associated with these injuries.
In contrast, patients with a preoperative loss of passive external rotation, posterior glenoid erosion, a reparable full-thickness rotator cuff tear isolated to the supraspinatus tendon, and inflammatory arthritis are not contraindicated for a total shoulder arthroplasty.
Iannotti et al. performed a Level I prospective study in 118 patients who underwent either a total shoulder arthroplasty or a shoulder hemiarthroplasty for primary osteoarthritis. The presence of a reparable full-thickness rotator cuff tear did not adversely affect outcomes in either group but rather provided better active external rotation in the cohort receiving total shoulder arthroplasties. The authors concluded that a reparable tear of supraspinatus is not a contraindication to the use of a glenoid component.
Norris et al. compared outcomes of total shoulder arthroplasty and hemiarthroplasty performed for primary osteoarthritis in 160 patients. There were no differences in postoperative pain, function, ASES scores, or range of motion between groups for patients with reparable rotator cuff tears. The authors concluded that minor thinning and small tears of the rotator cuff can be adequately addressed at the time of surgery without adversely affecting outcomes.
Illustration A is a cervical T2 axial MRI which shows a cervical root avulsion, a form of preganglionic brachial plexus injury. Notice the perineural hyperintensity.
Incorrect Answers:
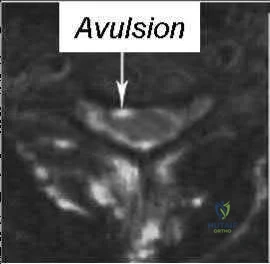
A 42-year-old male sustains a flail chest injury and subsequently undergoes operative stabilization of his chest wall. At first follow-up, the inferior angle of his ipsilateral scapula translates medially with any attempt at overhead activity. Injury to which of the following structures would cause this abnormality?

Spinal accessory nerve C8 and T1 nerve roots

Upper and lower subscapular nerves Thoracodorsal nerve

Long thoracic nerve
The clinical vignette describes medial scapular winging, which is seen after injury to the long thoracic nerve.
Medial scapular winging due to a long thoracic nerve palsy can be seen after repetitive stretching in athletes, with direct compression injury, or even iatrogenically during surgical procedures to the lateral thorax. Injury to the long thoracic nerve will eliminate the function of the serratus anterior,
which acts to protract the scapula laterally and upward and stabilize the vertebral border of scapula. This results in upper extremity weakness in forward elevation or abduction as the scapula is not stabilized against the thorax.
Meininger et al. report that lesions of the long thoracic nerve and spinal accessory nerves are the most common cause of scapular winging, although numerous underlying etiologies have been described. They report patients describe diffuse neck pain, shoulder girdle discomfort, upper back pain, and weakness with abduction and overhead activities. They also report that most cases are treated nonsurgically.
Wiater et al. review injuries to the spinal accessory nerve which causes dysfunction of the trapezius and subsequent lateral scapular winging. They note that the superficial course of the spinal accessory nerve in the posterior cervical triangle makes it susceptible to injury, and iatrogenic injury to the nerve after a surgical procedure is one of the most common causes of trapezius palsy. Most injuries are treated nonoperatively, but the Eden-Lange procedure, in which the insertions of the levator scapulae, rhomboideus minor, and rhomboideus major muscles are transferred, relieves pain, corrects deformity, and improves function in patients with irreparable injury to the spinal accessory nerve.
Illustration A shows a clinical photo of medial scapular winging, while illustration B shows a clinical photo of lateral scapular winging. Illustration C shows the long thoracic nerve during a rib fixation procedure, with the nerve sitting directly on top of the serratus anterior. The trapezius is overlying the scapula at the bottom of the photo, and the patient's head is to the right of the photo. Incorrect Answers:

A patient sustains a distal biceps brachii tendon rupture. If treated non-operatively, the greatest loss of strength would be seen with which activity?

Forearm supination Forearm pronation

Elbow flexion

Shoulder forward flexion Shoulder internal rotation
While both elbow flexion and forearm supination strength are affected, there is a greater percentage loss of supination strength. Patients may complain of weakness and fatigue with rotational activities such as using a screwdriver. The primary elbow flexor is actually the brachialis, and therefore less weakness in flexion is reported.
Patterson reviewed distal biceps ruptures and found nonsurgical treatments had 21 55% loss of supination strength and 8 36% loss of flexion strength.
Klonz reviewed anatomic and non-anatomic repairs and found better results with anatomic repairs with 91% return of supination strength and 96% return of flexion strength. Supination strength after nonanatomic repair did not improve in 4 of 8 patients (42%-56% of the uninjured arm).
A 27-year-old right hand dominant construction worker falls off a scaffold onto his outstretched arm. Figure A exhibits the radiograph taken at a local emergency room.
Following treatment, he is placed in a sling and follows up at your office two weeks later. He complains of a feeling that his arm is going to 'pop out'. Which specific physical examination finding is likely to be present?

Hornblower's Test Jobe's Test

Apprehension Sign with shoulder abducted and externally rotated Speed's Test

Kim's Test
The patient suffered a posterior shoulder dislocation, likely injuring the posterior capsule and/or labrum. Out of all the answer choices, Kim's test assesses posterior structures. Thus, Kim's test is the physical examination finding most likely to be present.
Posterior dislocations occur less frequently than anterior dislocations, and are often missed. Following closed reduction, persistent instability can occur, usually associated with posterior capsular or labral pathology. Posteriorly directed provocative maneuvers, such as the Kim test can be positive.
Robinson et al. performed an epidemiologic analysis on 120 posterior dislocations. Recurrent instability occurred at a rate of 17.7%. Risk factors for recurrent instability included age less than 40-years-old, dislocation during seizure, and a large reverse Hill-sachs (>1.5 cm3). Kim et al. describe the Kim lesion, a separation between the posteroinferior labrum and the articular cartilage without complete detachment of the labrum, which cause persistent posterior instability.
Figure A depicts a posterior dislocation on xray. Illustration A depicts the Kim test, which is performed by having the patient seated, arm at 90° abduction, followed by flexing the shoulder to 45° forward flexion while simultaneously applying axial load on the elbow and posterior-inferior force on the upper humerus. The test is positive when there is pain. Video 1 depicts the proper way to perform a Kim Test.
Incorrect answers:
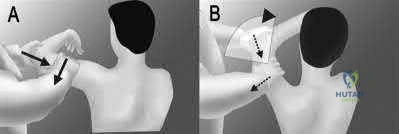
A 27-year-old male bodybuilder presents to the office with vague, deep shoulder pain and weakness with his bench press. His examination is somewhat difficult due to his large size, but no significant abnormal findings are noted. Radiographs are normal, and an MRI arthrogram is shown in Figure A. Which of the following is the most likely etiology of his complaints?

Pectoralis major rupture Supraspinatus partial thickness tear SLAP lesion

Tendonitis of the long head of the biceps Posterior labral tear
The clinical presentation and MRI are consistent with a Posterior labral tear.
Posterior labral tears are commonly seen in individuals that have repeated posteriorly-directed stress across their glenohumeral joint (football linemen, bodybuilders). These patients will often present with ill-described pain deep in their shoulder joint, along with decreases in shoulder strength. Focused shoulder examinations, such as the Jahnke Jerk Test or Push-pull test, can elicit pain from posterior labral tears; however, the sensitivity and specificity of these tests remain under question.
Mair et al. reviewed the outcome of posterior labral injuries in nine athletes who underwent arthroscopic repair with a bioabsorbable tack after failure of conservative management; all were
able to return to contact sports. They note that posteriorly applied forces can result in a shear-type vector that can cause posterior labral tears without capsular injury.
Bradley et al. reviewed 91 athletes with unidirectional recurrent posterior shoulder instability that were treated with an arthroscopic posterior capsulolabral reconstruction. They found that significant improvements in stability, pain, and function at a mean of 27 months postoperatively. Eightynine percent of the patients were able to return to their sport.
Figure A shows an axial MRI arthrogram of the shoulder with a posterior labral tear and an associated paralabral cyst. Illustration A is another axial shoulder MRI arthrogram cut showing a posterior labral tear (red arrow) and an associated paralabral cyst (yellow arrows).
Incorrect Answers:
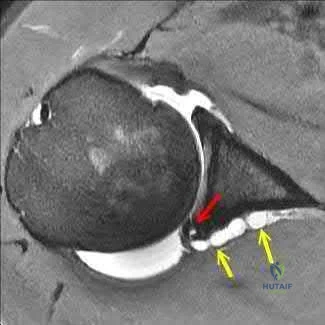
A patient sustains a full thickness tear of their teres minor. Which of the following test/signs would most likely be positive in this patient?

Jobe's test Belly press test

Internal rotation lag sign Hornblower's sign Hawkin's sign
Hornblower's test is completed by asking the patient to hold their shoulder in 90 degrees of abduction and 90 degrees of external rotation. The test is positive if the arm falls into internal rotation or they are unable to actively externally rotate against resistance. This suggests teres minor pathology.
There are various tests/signs used by clinicians to detect rotator cuff pathology. The teres minor is innervated by the axillary nerve and functions to externally rotate the humerus. The hornblower's test/sign has various descriptions, but all act to determine external rotation weakness. In addition to being sensitive and specific for teres minor pathology, it can also be positive with posterior supraspinatus tears.
Walch et al. review 54 patients that underwent repair of combined supraspinatus and infraspinatus rotator-cuff tears. They found that the hornblower's sign was highly sensitive and specific for irreparable degeneration of the teres minor, while the dropping-sign was highly sensitive and specific for irreparable degeneration of the infraspinatus.
Hertel et al. prospectively review 100 patients with painful shoulders and impingement syndrome. They compared various lag signs (ERLS-external rotation lag sign, IRLS-internal rotation lag sign, drop sign) to the Jobe and lift-off signs. The ERLS was less sensitive but more specific than the
Jobe sign for the supraspinatus/infraspinatus. The drop sign was the least sensitive but was as specific as the ERLS. The IRLS was as specific but more sensitive than the lift-off sign for subscapularis tears.
Illustration A shows another variation of the hornblower's sign as originally desbribed by Arthui et

positive if the patient is unable to do this without abducting the affected arm and demonstrates the difficulty in raising the hand to the mouth in the absence of external rotation of the shoulder. The video provided shows how to perform both variations of the hornblower's test.
Incorrect Answers:

Reverse total shoulder arthroplasty combined with latissimus dorsi transfer would be
most appropriate for which of the following patients?
year-old male with post-traumatic shoulder arthritis after a four-part proximal humerus fracture with no motor dysfunction

year-old male with grade 4 shoulder arthritis with severe deltoid muscle dysfunction secondary to a stroke

year-old female with significant rotator cuff arthropathy, a negative Hornblower sign and less than 5 degrees of external rotation lag

year-old female with pseudoparesis of anterior elevation and external rotation, narrowing of gleno-humeral joint and acetabularization of the acromion

year-old male with grade 4 shoulder arthritis and an isolated supraspinatus tear
Reverse total shoulder arthroplasty combined with latissimus dorsi transfer would be most appropriate in a patient with pseudoparesis of anterior elevation and external rotation, in the setting of shoulder arthritis (narrowing of glenohumeral joint and acetabularization of the acromion).
Combining a latissimus dorsi tendon transfers with reverse total shoulder arthroplasty (R-TSA) helps to restore control of active external rotation. Dysfunction with external rotation can be determined clinically with external rotation lag sign, a positive Hornblower's sign, and radiographically with fatty degeneration of the teres minor classified as stage 2 or greater according to the system of Goutallier et al. or Fuchs et al.
Gerber et al. found that R-TSA with combined lat dorsi transfer yielded minimal improvements in external rotation ROM (13 deg to 19 deg) compared to increases in shoulder ROM in flexion (94 deg to 137 deg) and abduction (87 deg to 145 deg), with this procedure.
Boileau et al. examined 17 consecutive patients treated with reverse shoulder arthroplasty and latissimus dorsi and teres major transfer (L'Episcopo). They found that external rotation increased from -21 degrees to 13 degrees (+34 degrees ). They recommend transferring both the LD and TM, rather than the LD alone as it results in better active external rotation.
Illustration A is a radiograph showing a right reverse total shoulder replacement. Illustration B shows a cadaveric image of the positioning of the latissimus dorsi tendon transfer prior to implantation of the reverse total shoulder components.
Incorrect Answers
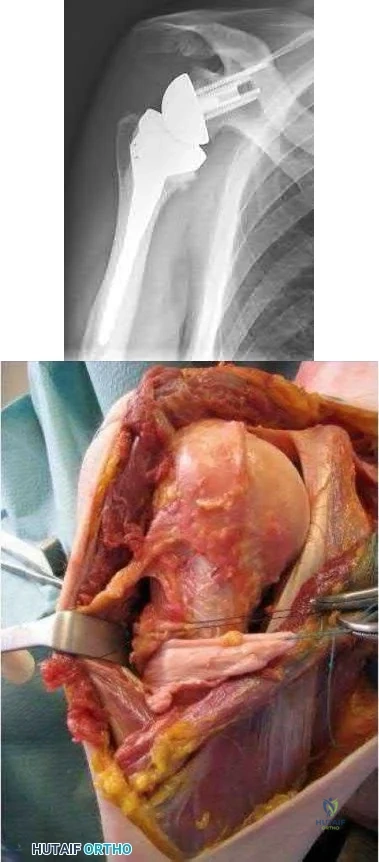
Figure A and B are MRI images of a 42-year-old male with symptoms of right shoulder neuropathy. If this patient has an abnormality detected on EMG and nerve conduction testing, which of the following nerves is most likely to be involved?
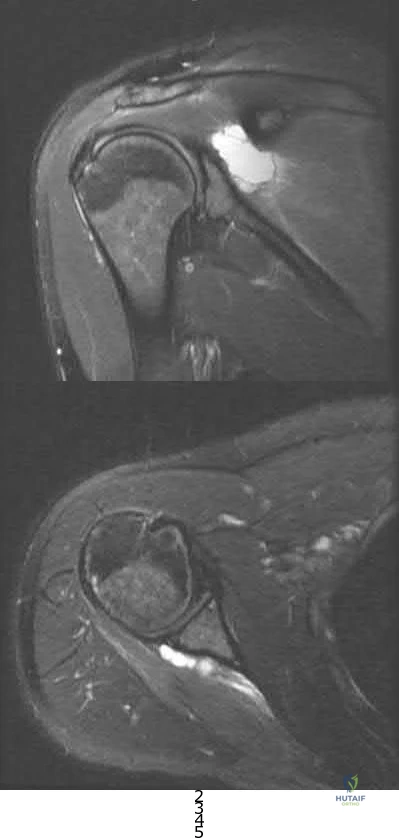
Subscapular nerve Axillary nerve Musculocutaneous nerve Suprascapular nerve Long thoracic nerve
This patient is presenting with suprascapular nerve compression secondary to a spinoglenoid cyst. Injuries of the posterior shoulder joint capsule or posterior-superior labrum can result in spinoglenoid cysts. They may lead to suprascapular nerve palsy.
Patients will present with characteristic findings of external rotation
( infraspinatus) weakness when the cyst is isolated in the spinoglenoid notch. If the cyst is located in the suprascapular notch, both external rotation weakness and abduction (supraspinatus) weakness will be present. Electromyography and MRI are the investigations of choice in depicting the etiology of this mononeuropathy.
Piatt et al. found posterosuperior labral tears in 65/73 patients who had spinoglenoid notch cysts. All patients presented with should pain and weakness. Patients undergoing surgical intervention by drainage or excision +/- arthroscopic labral repair had a better outcome than non-operative care.
Westerheide et al. reported fourteen patients who underwent arthroscopic decompression of ganglion cysts associated with suprascapular neuropathy. All patients had a labral tear intraoperatively with arthroscopic drainage and labral repair. There was not recurrence at an average of 51 months of followup.
Piasecki et al. reviewed suprascapular neuropathy. Causes include:nerve entrapment along this path, particularly at the vulnerable suprascapular and spinoglenoid notch, as well as extrinsic compression by soft-tissue masses.
Figures A is a coronal MRI showing a large hyperintense mass medial to the glenoid articulation. Figure B shows an axial MRI of the lesion posterior to the glenoid. Illustration A shows a diagram of the posterior right shoulder. The suprascapular nerve can be seen traveling through the spinoglenoid notch. Incorrect Answers:
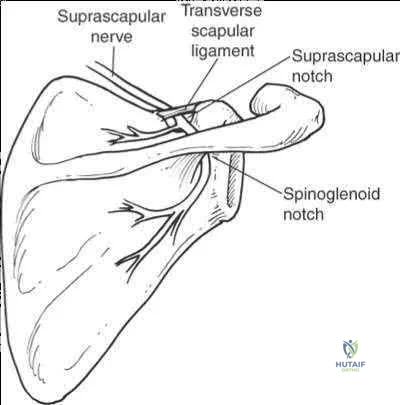
A 12-year-old right-hand-dominant pitcher presents with progressive right shoulder pain. He is now unable to pitch. He is tender to palpation over the lateral shoulder and has pain with rotation. An AP radiograph of the affected shoulder is shown in Figures A and a contralateral radiograph is shown in Figure B. What is the most likely diagnosis?
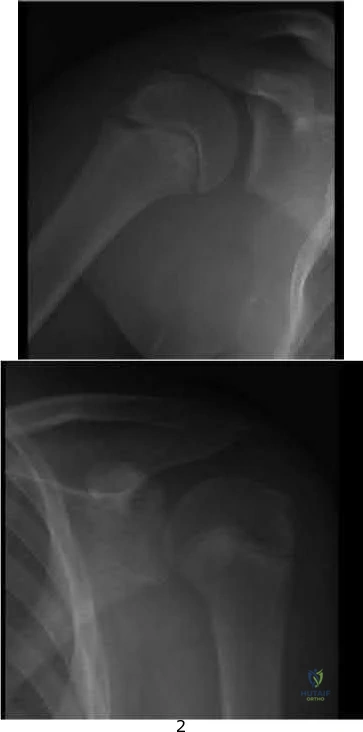
Septic arthritis of the shoulder SLAP tear
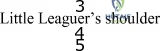
External impingement Internal impingement

proximal humerus. Patients may report a recent increase in pitching regimen. On examination, there is focal tenderness at the level of the physis. Treatment focuses on rest, physical therapy and a progressive throwing program. Pitching is often stopped for 2-3 months during rehabilitation.
Chen et al. review shoulder and elbow injuries in the young athlete. Little
Leaguer's shoulder results from epiphyseal lysis secondary to microtrauma. Pain over the anterolateral shoulder may be elicited on examination. The mainstay of treatment is 2-3 months of rest and return to pitching via a progressive throwing program.

Mcfarland et al. review techniques to prevent injuries in the throwing athletes. They note that overuse injures can be avoided when appropriate throwing mechanics are enforced and pitch counts are li
physeal widening noted especially when compared to the contralateral normal pediatric shoulder view seen in Figure B.
Incorrect Answers:
A 35-year-old carpenter has pain in the antecubital fossa that is worse with turning a screwdriver. He has undergone non-operative treatment for 6 months without relief. On physical examination his hook test is normal and there is pain and weakness with resisted supination. Radiographs are shown in Figures A-C. A MRI of the right elbow is shown in Figure D. The next most appropriate treatment is?

Exploration of the radial tunnel Superficial radial neurectomy

Detachment and repair of the biceps tendon Transfer of the biceps to the brachialis EMG with nerve conduction study
While complete trauamtic rupture of the distal biceps is more common, partial tears have been reported in the literature. The most common presentation is pain in the antecubital fossa worse with resisted supination.
Conservative management consists of NS

Transfer to the brachialis improves flexion strength but not supination.
Ramsey et al present a review article on distal biceps tendon injuries. They state that the most successful management of partial distal biceps tears that have failed conservative management is to surgically treat it like a complete rupture with release and surgical reattachment of the distal biceps to the radial tuberosity.
Figures A-C are normal radiographs of the elbow. Figure D is a crossreferenced axial and coronal T2 MRI that demonstrates increased signal and partial distal biceps tendon tearing. Illustration C shows the resected region of distal biceps tendon in the same patient and had an excellent functional outcome following distal biceps release and surgical reattachment with 2 double-loaded suture anchors.
Video V demonstrates The hook test for detecting complete distal biceps tendon avulsions.

A 49-year-old man sustains a dislocation of his left elbow that is successfully reduced and splinted. He misses his scheduled follow-up appointments and returns 6 weeks later. He is immediately enrolled in a course of vigorous physical therapy. At a repeat visit at 6 months, examination reveals that he lacks 40 degrees of elbow extension, and has flexion to 80 degrees. He is taken to the operating room for surgical release. Figures A and B are diagrams depicting the ligamentous attachments about the elbow. To restore elbow flexion, in addition to releasing the articular capsule, which ligament should be released?
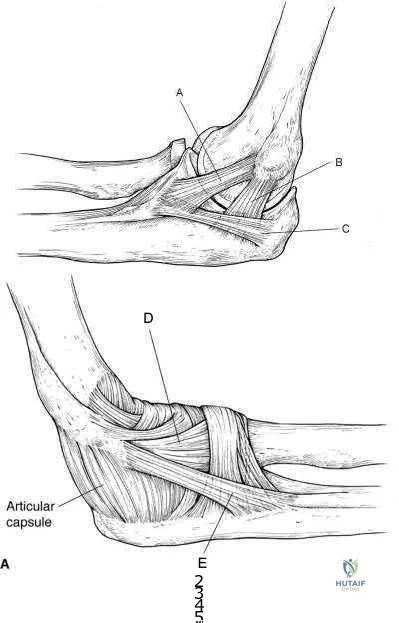
Ligament A Ligament B Ligament C Ligament D Ligament E
In addition to capsular release, the posterior band of the medial collateral ligament (MCL) should be released.
The posterior band of the MCL is attached dorsal to the axis of rotation and has greater variation in length. It increases in length by 9 mm between 60° and 120° of flexion. Posterior band contracture leads to loss of elbow flexion. In contrast, the anterior band of the MCL (AMCL) maintains a constant length ( isometric) throughout the entire arc of movement. Anterior capsule contracture leads to loss of extension.
Wada et al. treated 14 elbows with post traumatic contracture. Through a medial incision, the ulnar nerve was freed and the posterior band and posteromedial joint capsule were excised. Mean flexion increased from 89° preop to 127° postop. Anterior capsulectomy was performed for limited extension.
Morrey et al. studied structures providing stability about the elbow. They found that the anterior capsule stabilizes the elbow to varus-valgus stress in extension, not in flexion. The anterior band of the MCL is a primary stabilizer, especially in flexion.
Figures A and B are medial and lateral illustrations of the elbow, respectively, depicting the ligamentous attachments. Illustrations A and B are radiographs are 3D CT reconstruction images of the left elbow, respectively, showing heterotopic ossification around the posterior band of the MCL.
Incorrect Answers:

A 23-year-old male sustains a dislocation of his elbow that was successfully closed reduced in the emergency room. 3 months later, the patient presents with pain and a catching sensation in his elbow. On physical exam, he is noted to have a positive lateral pivot-shift test. Incompetence of which of the following ligaments in Figure A is most commonly associated with his condition?
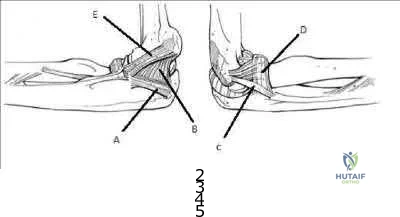
A B C D E
The patient is presenting with symptoms and physical exam consistent with posterolateral rotatory instability. Injury to the lateral ulnar collateral ligament
( LUCL), labeled C in Figure A, allows an abnormal external rotation
( supination) of the ulna on the humerus. This results in posterolateral rotatory instability. Posterolateral rotatory instability often presents as pain and recurrent clicking, snapping, clunking, or locking of the elbow. It should be noted that frank dislocations are not the most common presenting symptom. The physical exam is usually benign except for a positive lateral pivot-shift test or posterolateral rotatory drawer test. While injury to the LUCL is thought to be the primary pathology, other ligamentous stabilizers of the elbow may play a role.
Mehta et al. review posterolateral rotatory instability of the elbow. They state the instability usually results from an elbow dislocation with subsequent failure to heal of the ligamentous structures.
Patients with recurrent instability often require surgical intervention, as bracing is typically cumbersome and ineffective.
The video provided shows how to perform the lateral pivot-shift test. The patient is placed in the supine postion with forearm overhead and elbow extended. The elbow is then supinated with force and flexed to >40° while a valgus load applied. A positive result is palpable / visible clunk as the ulna and radius reduce suddenly. Illustration A shows the posterolateral rotatory drawer test.
External rotation and posterior forces are applied to the forearm attempting to sublux the radius posterior to the capitellum.
Incorrect Answers:
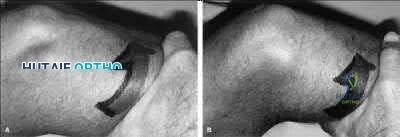
Figure A is the MR image of the left shoulder of an active 47year-old painter who has been experiencing shoulder pain for 9 months. In addition to the finding shown in Figure A, MRI examination of the intra-articular portion of the biceps tendon shows fraying greater than 50%. He has not obtained relief from an 8 month course of non-operative management including non-steroidal antiinflammatory medications, physical therapy and corticosteroid injection. What is the best next step in treatment?

New course of physical therapy

Activity shutdown with 6 weeks sling immobilization

Arthroscopic superior labrum anterior to posterior (SLAP) tear repair Arthroscopic debridement and possible biceps tenotomy versus tenodesis

Arthroscopic rotator cuff repair and acromioplasty
This patient has a Type II SLAP lesion. These should only rarely be repaired in patients older than 40 years of age. If a source of pain refractory to nonoperative management, biceps tenotomy or tenodesis should be considered.
SLAP repair for Type II SLAP lesions is a procedure that has enjoyed a high success rate in young patients. These are generally not indicated for repair in patients greater than 40 years of age due to high rate of stiffness postoperatively. A subset of patients continue to do poorly after SLAP repair. Poor range of motion and the development of post-surgical adhesive capsulitis is often an etiology for poor results. Arthrofibrosis recalcitrant to diligent therapy over many months can be treated with arthroscopic capsular release. This is predicated on failure of a dedicated course of physical therapy as part of a non-operative management course lasting greater than six months. As the propensity for stiffness increases with age, consideration should be treated with SLAP tear debridement and biceps tenotomy or tenodesis in patients greater than 40 years old. Tenotomy or tenodesis, however, can be effective at providing pain relief in the presence of proximal biceps tendon pathology.
Katz et al. reviewed 34 patients who presented to their group for management of failed SLAP repair. 50% were Worker's Compensation cases. The mean age at the time of initial SLAP repair was 43 years. They treated these patients conservatively initially followed by revision surgery in 21 cases. All completed a course of physical therapy initially. They concluded that once a patient has failed SLAP repair, there is a high chance of further conservative treatment failing. Although revision surgery improves outcomes, 32% will continue to have a "suboptimal" result. Holloway et al. reviewed 50 patients who underwent arthroscopic capsular release for adhesive capsulitis, comparing three groups: (1) post-surgical; (2) post-fracture; and (3) idiopathic adhesive capsulitis. All patients had completed supervised physical therapy and a home exercise program for at least one year. They concluded that arthroscopic capsular release improved range of motion equally for all three groups but patients in the post-surgical group had poorer subjective pain, function and satisfaction scores.
Figure A is an MRI showing a Type II SLAP tear. Illustration A shows the classification of SLAP lesions.
Incorrect Answers:
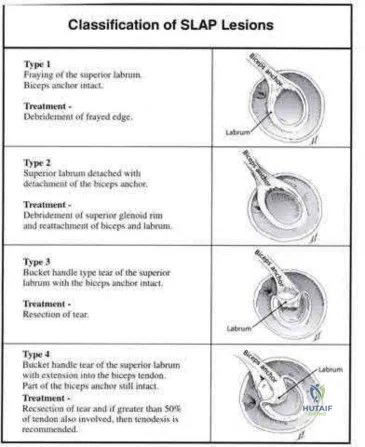
A 30-year-old man undergoes arthroscopic Bankart repair for recurrent anterior dislocation. He continues to experience instability postoperatively. Examination reveals a positive apprehension test. Radiographs of both shoulders are seen in Figure A. CT scan of his left shoulder is seen in Figure B. What is the best treatment option?
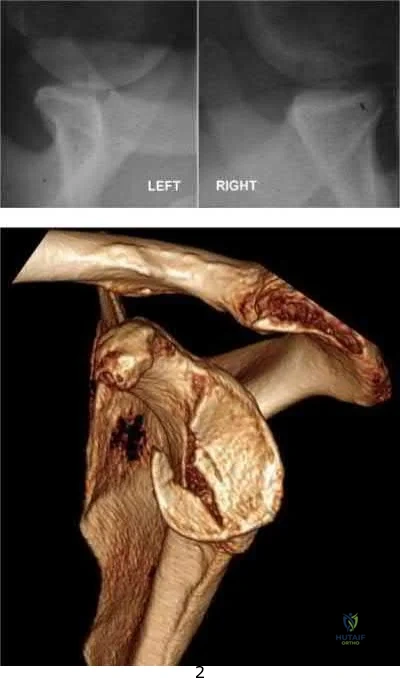
Bankart repair

Humeral head bone augmentation Remplissage

Coracoid autograft Connolly procedure
This patient has anterior glenoid bone deficiency (inverted pear glenoid) from a large bony Bankart lesion that was not adequately addressed in the index procedure. This is best treated with bony augmentation using the Latarjet vascularized coracoid transfer.
Patients with glenoid bone defects >20-30% have a high recurrence rate
(>60%) after Bankart repair alone. Bone grafting is necessary to offer containment. Autograft options include coracoid transfer (such as the Latarjet procedure which extends the articular arc and creates a conjoined tendon sling) and iliac crest bone grafting.
Burkhart et al. addressed glenohumeral bone defects. They advise that significant bone deficits cannot be adequately addressed via arthroscopic Bankart repair alone. The Latarjet transfer creates an extra-articular platform to extend the articular arc of the glenoid.
Hantes et al. assessed Latarjet repairs using CT. They found that there is almost complete repair of a 25% to 30% glenoid defect when using the Latarjet procedure.
Figure A comprises comparison Bernageau view glenoid profile radiographs of both shoulders.
Figure B is a 3D reconstruction CT with showing glenoid bone deficiency (inverted pear deformity) with a large bony Bankart lesion. Illustration A shows the method of obtaining a Bernageau glenoid profile view. Illustration B shows the "cliff sign" of anterior glenoid bone loss.
Illustration C depicts the Latarjet procedure. Illustration D depicts reduction in the articular arc with anterior glenoid loss.
Incorrect Answers:
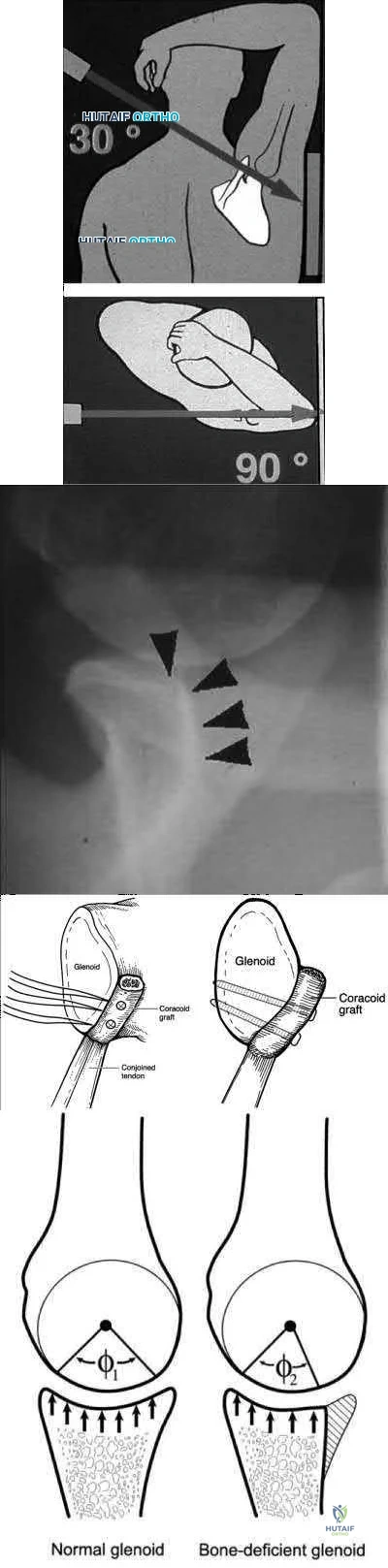
Figure A shows an arthroscopic picture of a 62-year-old male undergoing repair of a torn subscapularis tendon. In the image shown, G represents the glenoid, H represents the humeral head, and the dotted line represents the superolateral border of the subscapularis tendon. Which two ligaments form the structure marked with the asterisk?

Inferior and middle glenohumeral ligaments Middle and superior glenohumeral ligaments Coracohumeral and coracoacromial ligaments

Coracohumeral and superior glenohumeral ligaments Superior and inferior glenohumeral ligaments
The coracohumeral and superior glenohumeral ligaments form a complex that marks the superolateral margin of the subscapularis tendon.
In chronic or degenerative tears, the subscapularis will often retract medially and become scarred to the deltoid fascia. This makes identification difficult during arthroscopic repair. The coracohumeral and superior glenohumeral ligaments form a complex that inserts on the superolateral margin of the subscapularis. This "comma sign" can usually be identified during arthroscopic repair making identification of the subscapularis tendon an easier task.
Burkhart and Brady present surgical pearls for arthroscopic repairs of the subscapularis. Amongst other things, they state the subscapularis is almost always repairable with proper mobilization, but an Achilles tendon allograft or a subcoracoid pectoralis major transfer may be used for a severely degenerated subscapularis.
Lo and Burkhart describe the comma sign for repair of chronic subscapularis tears. They describe how the superior glenohumeral ligament/coracohumeral ligament complex and subscapularis tendon are intimately associated, and often tear off the humerus while remaining attached to each other. This complex, when torn, forms a "comma sign," that marks the superior and lateral margins of the subscapularis tendon.
Illustration A shows why the convergence of the superior glenohumeral and coracohumeral ligaments on the superolateral border of the subscapularis is referred to as the "comma sign." Incorrect Answers:
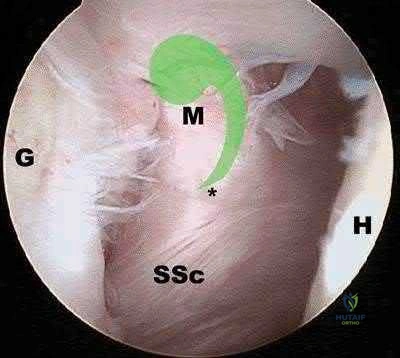
A 52-year-old man sustained the left elbow injury shown in Figure A while playing basketball 2.5 months ago. He underwent the procedure shown in Figure B. Post-operatively he was mobilized in a hinged brace. On examination today, his arc of elbow flexion is 75 degrees with loss of 45 degrees of full extension. His Disabilities of the Arm, Shoulder and Hand (DASH) Outcome Measure score is 45 points. What initial treatment option will likely provide the greatest improvement in this patients DASH score and functional range of motion?

Self-directed exercise therapy Supervised exercise therapy

Supervised exercise therapy with static progressive elbow splinting Continuous passive motion device

Closed manipulation under anesthesia
The clinical presentation is consistent with post-traumatic elbow stiffness following an elbow fracture-dislocation. Supervised exercise therapy with static elbow splinting over a 6 month period
has shown to have a significant improvement on DASH scores and functional range of motion (ROM) in patients with post-traumatic elbow stiffness.
Post-traumatic elbow stiffness is often difficult to manage. The ultimate goal of treatment is to restore a functional range of elbow motion (30° to 130°). Nonoperative modalities are considered the first-line of treatment. Aggressive physical therapy has traditionally been advocated. However, the use of static progressive elbow splinting with a turnbuckle, alongside aggressive physical therapy, has shown to provide better functional outcomes. Treatment is usually maintained over a period of 6-12 months. Surgery is considered when nonoperative therapy fails.
Doornberg et al. looked at a retrospective case series of 29 patients with posttraumatic elbow stiffness. They showed that static progressive splinting can help gain additional motion when standard exercises fail to produce additional improvements.
Lindenhovius et al. randomized sixty-six patients with post-traumatic elbow stiffness into static progressive elbow splint therapy or dynamic elbow splinting over a 12 month period. There was no significant difference in outcomes between treatment modalities. ROM increased by 40° vs. 39° at six months, respectively. DASH scores improved from 50 vs 45 at enrollment to 32 vs. 25 at six months, respectively.
Figure A shows a posterior elbow dislocation with an associated medial epicondyle fracture. Figure B shows ORIF of the fracture seen in Figure A. Illustration A shows a static progressive turnbuckle elbow splint used for posttraumatic elbow stiffness.
Incorrect Answers:
tissues, causing hemarthrosis and additional fibrosis in the joint.

A 25-year-old right-hand baseball pitcher presents with persistent shoulder pain for the past several months in his dominant throwing arm. On physical examination, he is found to have full arc of motion with the exception of an internal rotation deficit of 30 degrees compared to his contralateral side. He is asked to complete the exercise shown in the video in Figure V. This form of rehabilitation is meant to address pathology in which anatomic structure?

Superior glenohumeral ligament Middle glenohumeral ligament

Anterior band of the inferior glenohumeral ligament Superior band of the inferior glenohumeral ligament

Posterior band of the inferior glenohumeral ligament

tissues in patients demonstrating symptoms of internal impingement. The sleeper stretch helps to address posterior tightness and the only posterior structure listed in the responses is the posterior band of the inferior glenohumeral ligament (posterior IGHL).
Internal impingement is a significant cause of pain in throwing athletes. It results from impingement of the articular undersurface of the posterior supraspinatus against the posteriorsuperior glenoid.
This is thought to be secondary to tightness in the posterior soft tissues including the capsule and posterior band of the IGHL. The mainstay of non-operative management is posterior capsular stretching with the sleeper stretches and cross-body adduction stretches. Heyworth et al. review the etiology, diagnosis and management of internal impingement of the shoulder. They note that repetitive contact between greater tuberosity and glenoid rim posterosuperiorly lead to impingement of the posterior rotator cuff and labrum. This occurs when the arm is externally rotated and abducted.
Tyler et al. reviewed the effects of posterior capsular stretching on alleviating symptoms in patients with internal impingement. Twenty-

Figure V is a video that demonstrates the sleeper stretch to address tightness of the posterior soft tissues. The arm is forward flexed 90 degrees and the patient lies on his side in order to stabilize the scapula while the arm is internally rotated. Illustration A depicts the sleeper stretch.
Incorrect Answers:
not the focus of the sleeper stretch.
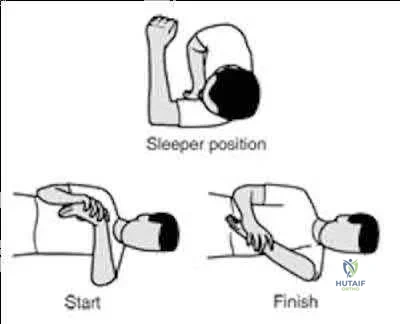
A 28-year-old professional baseball pitcher sustains a complete rupture of his ulnar collateral ligament. He is neurovascularly intact on exam. Which of the following surgical reconstruction techniques has been shown to result in the lowest complication rate and best patient outcome?

Splitting of flexor-pronator mass, figure-of-8 graft fixation. Splitting of flexor-pronator mass, docking graft fixation.

Splitting of flexor-pronator mass, docking graft fixation, ulnar nerve transposition. Detachment of flexor-pronator mass, figure-of-8 graft fixation, ulnar nerve transposition.

Detachment of flexor-pronator mass, docking graft fixation, ulnar nerve transposition.
Ulnar collateral ligament (UCL) reconstruction using a flexor-pronator musclesplitting approach and a docking graft fixation technique are associated with the lowest complication rate and best patient outcomes.
Vitale et al. performed a systematic review of retrospective cohort studies evaluating UCL reconstruction techniques in overhead athletes. They demonstrated that the flexor-pronator musclesplitting approach was associated with better outcomes than detachment of the flexorpronator mass, had a lower rate of postoperative ulnar neuropathy, and a lower overal complication rate. They also found fixation of the graft utilizing the docking technique was associated with better outcomes than the figure-of-8 technique. Abandoning the obligatory ulnar nerve transposition was associated with improved patient outcomes (89% vs. 75%) and a lower rate of postoperative ulnar neuropathy (4% vs. 9%).
Rettig et al performed a case series review of 31 overhead throwing athletes with ulnar collateral ligament injuries managed nonoperatively with 3 months rest followed by rehabilitation exercises. They concluded that 42% of athletes were able to return to their previous level of competition at an average of 6 months from diagnosis (earlier than reconstruction). The authors were unable to identify any patient-specific factors (duration of symptoms, age, acuity of onset) that would predict the success of nonoperative treatment.
Illustration A shows the figure-of-8 (Jobe) graft fixation technique. It is performed by passing the tendon graft through two bone tunnels in the medial epicondyle of the humerus and through one tunnel in the ulnar sublime tubercle. The graft is then sutured to itself in a figure-of-8 configuration. Illustration B shows the docking graft fixation technique. The graft is placed in a triangular configuration through a single humeral tunnel. The suture limbs are then brought out through two separate bone holes and tied over a bony bridge on the superior aspect of the medial epicondyle.
Incorrect Answers:

The right shoulder exercise seen in Figure A will put the LEAST amount of stretch on which structure?
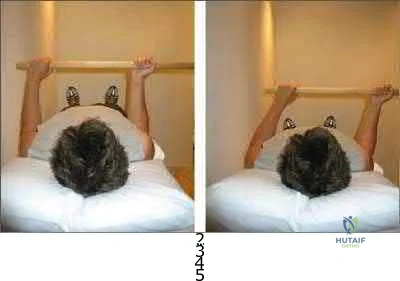
Inferior glenohumeral ligament Coracohumeral ligament Anterior-superior capsule Superior glenohumeral ligament Posterior capsule
Shoulder wand exercises, as shown in Figure A, are used to increase external range of motion of the shoulder. With the arm adducted and the elbow flexed, this exercise will put the LEAST amount of stretch on the posterior capsule.
External rotation shoulder wand exercises are commonly used for the treatment of adhesive capsulitis. Adhesive capsulitis is most commonly caused by contracture of the rotator interval. The rotator interval includes the anterior-superior capsule, superior glenohumeral ligament, coracohumeral ligament and long head biceps tendon. The structure most commonly contracted is the anterior-superior capsule, which limits external rotation when the arm is adducted. Kuhn et al. showed that in the neutral position, each ligament except the posterior capsule significantly affected the torque required for external rotation. The greatest effect on resisting external rotation at 0 degrees of abduction was the entire inferior glenohumeral ligament > coracohumeral ligament
> anterior band of the inferior glenohumeral ligament > superior and middle glenohumeral ligament.
Harryman et al. looked at the role of the rotator interval capsule in passive motion and stability of the shoulder. They found operative alteration of this capsular interval was found to affect flexion, extension, external rotation, and adduction of the humerus with respect to the scapula. Limitation of external motion was increased by operative imbrication of the rotator interval and decreased by sectioning of the rotator interval capsule.
Kim et al. reviewed shoulder MRIs to determine if abnormalities of the rotator interval were correlated with chronic shoulder instability. They found a significantly larger rotator interval height, rotator interval area, and rotator interval index in patients with chronic anterior shoulder instability compared to patients without instability.
Figure A shows a patient performing an exercise to increase right shoulder external rotation with a wand/stick. The right arm is fully adducted by her side, and her elbow flexed at 90 degrees.
Incorrect Answers:
) A 55-year-old male returns for followup 3 months after reverse shoulder arthroplasty. He reports limited function of his right shoulder but no antecedent trauma. A radiograph of his shoulder is shown in Figure A. All of the following variables are associated with this complication EXCEPT:

History of malunited proximal humerus fracture Proximal humeral bone loss

Failed primary arthroplasty Rheumatoid arthritis

Fixed preoperative glenohumeral dislocation
Rheumatoid arthritis is not associated with reverse shoulder arthroplasty (RSA) dislocation. RSA dislocation is a known complication of RSA. Risks include proximal humeral bone loss, chronic fracture sequelae with malunited/ununited tuberosities, failed previous arthroplasty, and fixed glenohumeral dislocation preoperatively. An irreparable subscapularis tears may be less of an issue with newer implant designs.
Trappey et al. studied instability and infection rates after RSA. They found that the rate of instability was similar in primary and revision surgery, but the rate of infection was higher in revision surgery. Instability was highest in the fracture sequelae group because of malunited tuberosities, contractures and proximal humeral bone loss.
Favre et al. examined the effect of component positioning on RSA stability.
They found that humeral version was more important than glenoid version. Stability is improved with the humerus in neutral or slight anterversion. They recommend avoiding retroversion >10deg. Edwards et al. examined subscapularis insufficiency and the risk of RSA dislocation. They found that of 138 RSA, all 7 dislocations occurred in patients with an irreparable subscapularis.
Dislocation was also more likely in patients with complex diagnoses, including proximal humeral nonunion, fixed dislocation, and failed prior arthroplasty.
Figure A shows reverse shoulder arthroplasty dislocation. Incorrect Answers:
) A 45-year-old man complains of chronic right shoulder pain. He has a history of chronic steroid use because of asthma. He recently completed a course of physical therapy
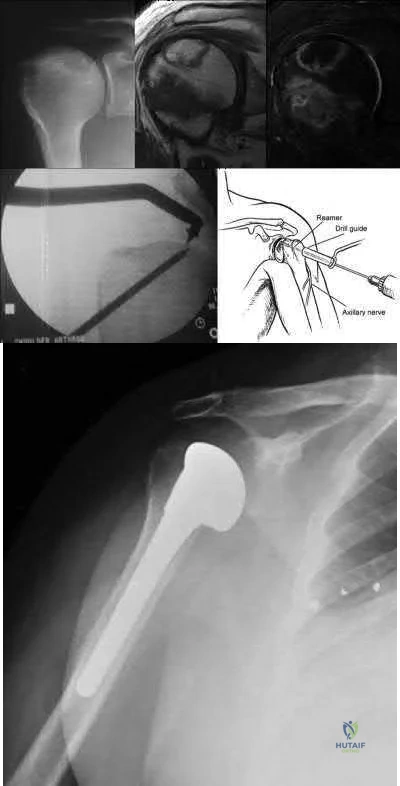
and has given up his job as a laborer in favor of a desk job. Examination reveals diminished shoulder abduction strength. A radiograph of his shoulder is shown in Figure A. Which of the following surgical treatment options (Figures B through F) is the most appropriate?

Figure B Figure C Figure D Figure E Figure F
This patient has early stage avascular necrosis (AVN) of the humeral head without subchondral collapse/flattening, likely related to chonic steroid use.
Core decompression is indicated.
Treatment of humeral head AVN is dependent on Cruess Stage. Precollapse stages (Stage I and II) may be treated by core decompression and joint preservation. Hemiarthroplasty is used for Stage III-IV disease. Total shoulder arthroplasty is used for Stage V disease. Resurfacing may be used for Stage III disease with focal chondral defects and sufficient remaining epiphyseal bone stock for fixation.
Harreld et al. reviewed humeral head AVN. They advocate attempting core decompression and arthroscopy for Stage III disease, and then tailoring resurfacing or replacement depending on defect size.
Smith et al. reviewed 31 hemiarthroplasties for steroid-related AVN (6 Stage III, 16 Stage IV, 5 Stage V). Unsatisfactory results were found in 45%. This was associated with glenoid cartilage wear over time. However, they still believed hemiarthroplasty was appropriate for younger active patients with stage III or stage IV disease.
LaPorte et al. performed core decompression for various stages of AVN.
Results were successful in 94%, 88%, 70% and 14% of Ficat-Arlet Stages I, II, III and IV humeral head AVN respectively, and more successful for nonsteroid related cases compared with steroidrelated cases. They recommend this treatment for Stages I-III.
Figure A comprises a radiograph showing Cruess Stage II disease ("snowcap" sign indicating sclerosis, preservation of the head contour and absence of subchondral collapse, left), a T1weighted
MRI (center) and T2-weighted fat saturated MRI (right) showing a variegated pattern of osteonecrosis, but with preservation of normal head contour. Figure B shows core decompression. Figure C shows hemiarthroplasty. Figure D shows reverse shoulder arthroplasty. Figure E shows resurfacing. Figure F shows total shoulder arthroplasty. Illustration A depicts the Cruess staging system. Illustration B shows a possible algorithm for management where they use the Ficat stages adapted from the hip.
Incorrect Answers:
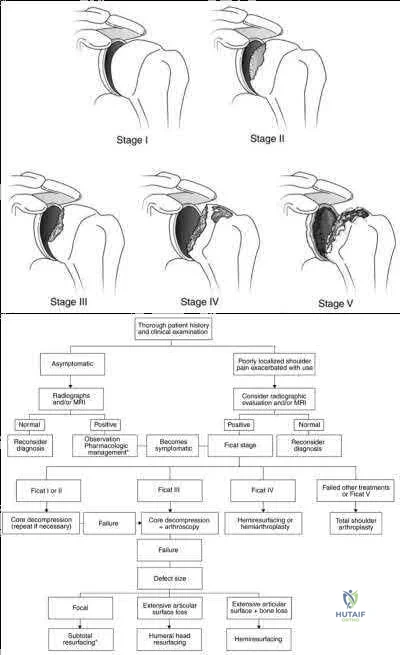
A 56-year-old otherwise healthy woman undergoes uncomplicated arthroscopic repair of a full-thickness rotator cuff tear. Prior to the procedure, the patient had attempted a long,
protracted course of physical therapy in an attempt to regain function without surgery. At her 10 day post-operative visit, she tearfully informs you that she cannot see her physical therapist because she has used up her 24-visit allotment for the year. She has 4 more weeks
until her insurance year turns over, and she does not have the financial means to pay out of pocket. What is the best next course of action?
Request a peer-to-peer review for authorization of additional visits or else the patient is likely to have a poor result

Provide a brief explanation and sheet of exercises for periscapular and cuff strengthening exercises using a resistance band

Test her range of motion and strength, and if limited, have her return weekly to your clinic for a guided home rehabilitation program

Explain to her that seeing a physical therapist during the first 6 weeks following cuff repair will not affect her range of motion one year removed from surgery

Give her a prophylactic corticosteroid injection to avoid early post-operative adhesive capsulitis
Early motion following rotator cuff repair has not been shown to impact range of motion and stiffness at one year post-operative clinical examinations.
Stiffness is a complication of protecting rotator cuff repairs from early re-tear with sling immobilization. However, with sling immobilization of up to 6 weeks, there is evidence of no increase in long-term stiffness. Accordingly, supervised physical therapy is not required in the first 6 weeks following arthroscopic rotator cuff repairs in order to obtain a good result.
Parsons et al. retrospectively reviewed 43 patients with full-thickness cuff tears who underwent a conservative early-postoperative protocol involving sling immobilization for 6 weeks with no formal therapy during that time. 10 /43 patient were characterized as stiff at their 6-week postoperative visit. At one year, there was no difference in the range of motion of the early stiff group compared to the non-stiff group.
Trenerry et al. collected prospective data on 209 consecutive patients undergoing primary rotator cuff repair. They found that patients in the stiffest quartile of range of motion testing at 6 weeks progressively regained range of motion by a post-operative visit at 72 weeks. The predictor of slowest recovery of early post-operative stiffness was found to be an internal rotation deficit with the patient reaching behind his or her back.
Incorrect Answers:
1: Early supervised physical therapy has not been shown to be essential to obtaining good motion post-operatively.
2 and 3: Strength testing and home strengthening programs in the early postoperative period would put the repair at risk for early failure.
5: Prophylactic corticosteroids are not indicated for prevention of postoperative stiffness, and furthermore, could theoretically interfere with healing.
A 62-year-old woman presents with chronic shoulder pain. On physical exam, she has anterior shoulder pain and her symptoms are reproduced with provocative testing of the biceps including supination against resistance and forward flexion of the shoulder against resistance. Internal and external rotation are painful, but her range of motion is intact. Shoulder radiograph and MRI images are shown in Figures A-E. Which of the following statements is true regarding the patient's condition?
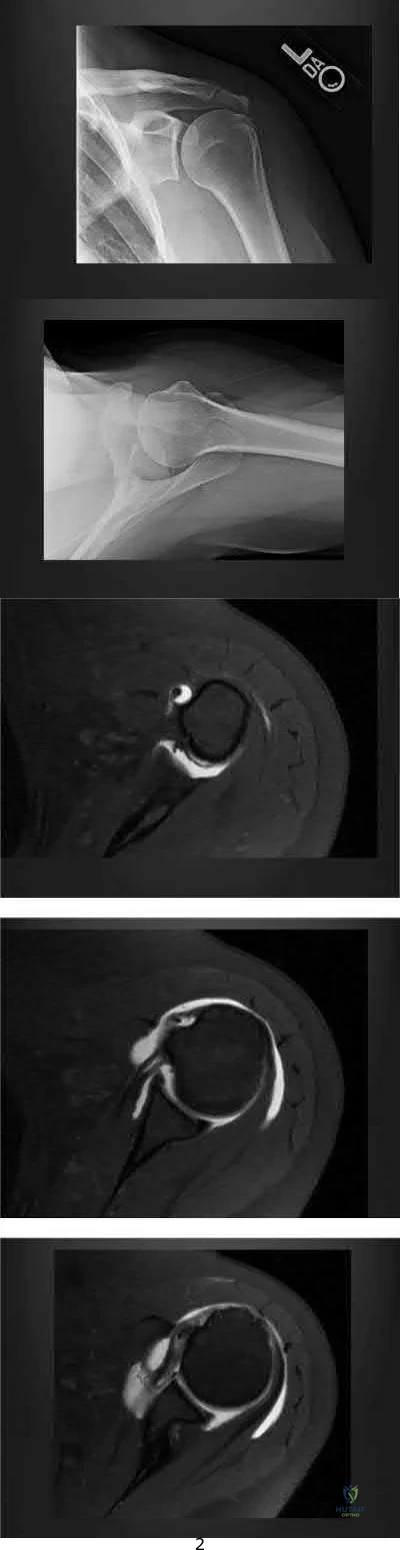
Her clinical examination is most consistent with a SLAP tear, which should be repaired. Her biceps pathology is due to her partial tearing of her subscapularis

She has isolated degenerative biceps tendonosis and an injection may cure her symptoms

She has end-stage rotator cuff arthropathy and should consider a reverse total shoulder arthroplasty

Her subacromial impingement is causing her biceps tendon sheath to be inflamed
The subscapularis tendon is the most important medial restraint to subluxation or dislocation of the long head of the biceps tendon (LHBT).
Anterior shoulder pain and positive provocative biceps clinical examination tests are common in patients with concomitant rotator cuff pathology. A consequence of subscapularis tendon tears -even partial tears - is that the LHBT can subluxate medially out of the intertubercular groove, as the subscapularis tendon is the most important restraint to medial instability of the LHBT. This instability can cause both pain and inflammation around the biceps tendon, leading to pain with resisted supination (Yergason's test) or resisted forward flexion (Speeds' test).
Walch et al. wrote a case series on 71 cases of biceps tendon instability. They found that dislocated LHBTs were associated with partial or complete subscapularis tears in 96% of cases.
Maier et al. published clinical results of treating acute traumatic medial LHBT instability with open repair of the subscapularis tendon and stabilization of the LHBT. They showed equivalent functional clinical outcomes to biceps tenotomy or tenodesis, with improved cosmesis and decreased muscle cramping.
Figures A and B show Grashey and axillary lateral views of the patient and demonstrate an os acromiale. Figures C, D, and E are axillary T2 MRI images. Figure C shows the tendon of the long head of the biceps in the distal aspect of the biceps grove. Moving proximally, Figure D shows the tendon subluxated onto the lesser tubercle and Figure E shows it fully dislocated medially.
Incorrect Answers:
A 78-year-old male presents to clinic 4 weeks after left total shoulder arthroplasty. He has not been wearing his sling and reports that he developed increased pain after slipping in the shower. He used the arm to catch himself from falling. On examination, he can flex the shoulder to 70 degrees, limited by pain. Active external rotation with arm at the side is 50 degrees and active internal rotation is 5 degrees. Passive external rotation is to 80 degrees. A radiograph of the left shoulder is shown below in Figure A. What other complaint is the patient most likely to have?

Pain with palpation of the bicipital groove Pain with palpation over the subdeltoid bursa Sensory loss over the lateral shoulder

Sensation of shoulder instability with external rotation Sensation of shoulder instability with internal rotation
The clinical presentation is consistent with a tear of the subscapularis, which is a well-described complication after total shoulder arthroplasty. The most likely additional complaint this patient will have is anterior shoulder instability, noticeable with external rotation of the shoulder.
Total shoulder arthroplasty is the preferred treatment for glenohumeral arthritis in patients with intact rotator cuff and good glenoid bone stock. The surgical approach involves detaching the subscapularis and capsule from the anterior humerus and dislocating the humeral head anteriorly. Post operatively, external rotation is limited to protect the subscapularis repair. If there is suspicion of a postoperative subscapularis tear, and ultrasound can be performed to confirm the diagnosis.
Miller et al. reported 7 cases of subscapularis tendon rupture after total shoulder arthroplasty, all of which were subsequently repaired. Decreased functional outcomes were observed in these patients, with lengthening techniques to address internal rotation contractures and prior surgery involving the subscapularis tendon as risk factors for rupture
Westoff et al. performed static and dynamic ultrasounds on 22 patients after total shoulder arthroplasty evaluating for numerous periarticular pathologies. The authors concluded that sonography is a useful tool for evaluation of periimplant tissues after TSA.
Figure A shows an intact left total shoulder arthroplasty without evidence of fracture, dislocation, or hardware loosening. Illustration A shows the incision for the subscapularis tendon during TSA. Incorrect Answers:
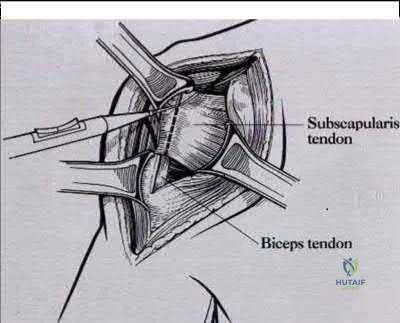
A 25-year-old lineman is referred to your office for a second opinion. 1 year ago, he underwent an arthroscopic procedure for shoulder instability. He complains of persistent sense of instability despite the surgery. Which of the following is a contraindication to revision arthroscopic labral repair for recurrent anterior glenohumeral instability?
Glenoid bone loss of 10%

Capsular attenuation from prior thermal capsulorraphy Anterior labral periosteal sleeve avulsion (ALSPA ) lesion Glenoid labral articular defect (GLAD) lesion

Combined Superior Labrum from Anterior to Posterior tear (SLAP) and recurrent Bankart lesion
Capsular attenuation or postthermal capsular necrosis from prior thermal capsulorraphy is a contraindicated to arthroscopic repair.
Thermal capsulorrhaphy utilizes heat generated by radiofrequency or laser ablation to cause capsular shrinkage in an effort to treat shoulder instability. However, high recurrence rates have been found, especially around two to three weeks after the index procedure, when the capsular tissue is the weakest. In the setting of recurrence following thermal capsulorrhaphy, open revision is recommended.
Creighton et al. reported on a series of 18 patients undergoing revision arthroscopic stabilization. Of the 18, 3 failed with recurrent instability, all with previous thermal capsulorrhaphy. Miniaci et al. reviewed the outcomes following thermal capsulorrhaphy noting high rates of recurrent instability, especially in the setting of initial treatment for multidirectional instability. Park et
al. reported on a series of 14 patients undergoing revision following thermal capsulorrhaphy. Ten out of 14 patients had signs of capsular thinning, insufficiency and attenuation.
Wong et al. surveyed 379 shoulder surgeons on the complications following thermal capsulorrhaphy. Capsular insufficiency and thinning were commonly associated with recurrent instability.
Hecht et al. performed thermal capsulorrhaphy and biomechanical analysis of the capsule in a sheep model. The authors found that the capsule was weakest at the 2-3 week post-operative timepoint, leading to the highest rate insufficiency, attenuation and mechanical failure at this time.
Incorrect answers:
A 47-year-old landscaper presents with worsening left shoulder pain and weakness. Three years ago, he injured the left shoulder in a fall and elected for nonoperative
management to minimize time off from work. Physical therapy was effective until 6 months ago when his shoulder function worsened to the point that he is now unable to work.

Examination of his active range of motion reveals forward elevation 120° with pain, abduction 100°, IR at neutral to T8 and ER at neutral 5°. He has a positive ER lag sign and Hornblower's sign. Belly press and lift-off tests are normal. A recent radiograph is shown in Figures A. MRI images are shown in Figures B and C. Which of the following is the best treatment option?
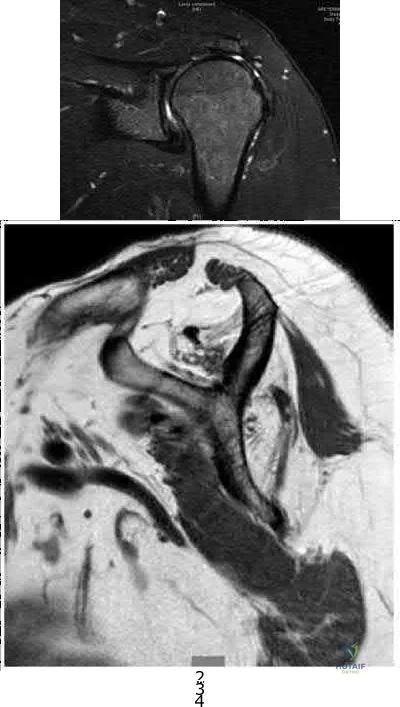
Continue physical therapy Latissimus dorsi transfer Arthroscopic rotator cuff repair Pectoralis major transfer

Reverse total shoulder arthroplasty
This patient has a chronic massive posterosuperior rotator cuff tear with marked atrophy, tendon retraction and loss of external rotation strength that is impacting his daily life. The best treatment option for this middle-aged laborer with an irreparable posterosuperior rotator cuff tear is a latissimus dorsi transfer to restore external rotation strength and motion.
Irreparable rotator cuff tears are marked by: (1) Superior displacement of the humeral head (AHI < 5-7mm), (2) Fatty infiltration of the rotator cuff muscles ( Goutallier stage 3-4), (3) Increased duration of the tendon tear and (4) Profound external rotation weakness. These findings are predictive of poorquality tissue and stiffness of the muscle-tendon unit, not amenable to primary repair. In this setting, a latissimus dorsi transfer can be utilized to restore shoulder strength, function and improve pain. Relative contraindications include subscapularis deficiency, deltoid deficiency, pseudoparalysis of the shoulder and advanced glenohumeral arthritis.
Gerber et al. performed a case series analysis of 67 patients with irreparable rotator cuff tears managed with latissimus dorsi transfer. Patients with an intact subscapularis demonstrated improvement in pain, range of motion and strength postoperatively, while no improvement was noted in patients with subscapularis deficiency. The authors conclude that latissimus dorsi transfer should not be performed in the setting of poor subscapularis function.
Iannotti et al. found that better clinical results following latissimus dorsi transfer were associated with: preserved active shoulder range of motion and strength (specifically forward elevation > 90° and external rotation > 20°), synchronous firing of the transferred latissimus dorsi muscle and male gender.
Figure A is an AP radiograph of the left shoulder with superior migration of the humeral head (AHI
< 5mm) and no evidence of glenohumeral arthritis. Figures B and C show a retracted posterosuperior rotator cuff tear and Goutallier stage 4 atrophy (more fat than muscle) of the supraspinatus, infraspinatus and teres minor, rendering this tear irreparable. Illustration A shows a latissimus dorsi transfer. The latissimus dorsi tendon is positioned over the top of the humeral head, covering most of the rotator cuff defect. The tendon is then secured to the subscapularis tendon edge and lesser tuberosity anteriorly, the remnant supraspinatus and infraspinatus tendons medially, and the greater tuberosity laterally.
Incorrect Answers:
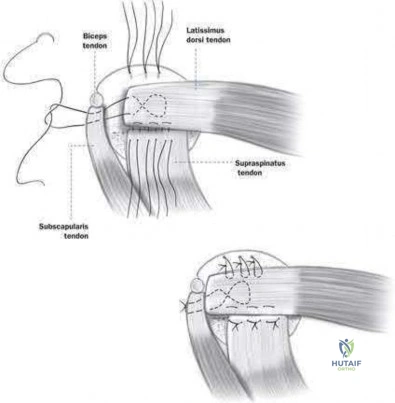
A collegiate swimmer develops medial winging of the scapula. If the EMG and nerve conduction studies are abnormal, the most likely nerve roots to be involved are?

C7, C8, T 1 C6, C7, C 8 C5, C6, C 7 C4, C5, C 6 C3, C4, C 5
Classic medial winging of the scapula is due to paralysis of the serratus anterior muscle which is supplied by the long thoracic nerve which holds the scapula to the chest wall and prevents the inferior angle of the scapula from migrating medially. It is innervated by the long thoracic nerve (C5, 6, 7).
Surgical treatment may include partial pec major transfer. Lateral winging may be caused by spinal accessory nerve palsy (CN XI, also ventral ramus C2,3,4). The nerve may be injured during neck surgery. This causes trapezius weakness, allowing the inferior pole of the scapula to migrate laterally. The modified Eden-Lange procedure may be used for this type of winging.
Gregg et al. describes paralysis of the serratus muscle in young athletes which they felt was due to repetitive traction. Full recovery usually occurs in an average of 9 months, and they recommend that surgical methods of treatment should be reserved for patients in whom function fails to return after a twoyear period.
Foo et al. describes a larger cohort of 20 patients again treated expectantly with observation and physical therapy. They reported consistent recovery but that it can take up to 2 years.
Illustration A shows a clinical photo of medial scapular winging. Illustration V is an instructional video of scapular winging. It begins with a clinical video of the condition.
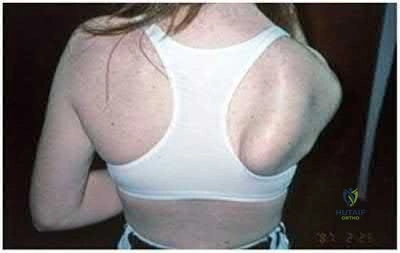
A 62-year-old man complains of shoulder pain for 2 years. He has had 1 course of intra articular sodium hyaluronate and 6 weeks of physical therapy with little relief. Examination reveals diminished arm flexion and abduction secondary to pain. Radiographs of his shoulder are shown in Figures A and B. According to the American Academy of Orthopaedic Surgeons Clinical Practice Guidelines, what is the next best step?

Humeral head replacement arthroplasty Hemiarthroplasty and ream-and-run glenoid procedure

Cuff tear arthropathy (CTA) prosthesis

Total shoulder arthroplasty with a metal-backed cemented glenoid component Total shoulder arthroplasty with an all-polyethylene cemented glenoid component
This patient has end-stage glenohumeral osteoarthritis (GH OA). According to the AAOS CPG, total shoulder arthroplasty (TSA) is recommended using an allpolyethylene cemented glenoid component.
TSA is indicated for cases of end-stage GH OA. It is preferred to hemiarthroplasty. It is contraindicated in cases with insufficient glenoid bone stock (glenoid wear to the level of the coracoid), rotator cuff arthropathy or irreparable cuff tears and deltoid dysfunction. It provides good pain relief and has good survival at 10 years (>90%).
Radnay et al. performed a systematic review involving 1952 patients comparing TSA with humeral head replacement (HHR). They found that TSR provided greater pain relief, range of motion, patient satisfaction, and had lower revision rates. They recommend TSA over HHR for GH OA. Izquierdo et al. described the AAOS Clinical Practice Guidelines (CPG) regarding treatment of GH OA. This is summarized in Illustration A.
Figures A and B show end-stage GH OA with large osteophytes and subchondral sclerosis. There is significant glenoid wear and posterior subluxation (Walch B glenoid deformity). Illustration A is a table summarizing the AAOS CPG on treatment of GH OA. Illustration B shows a CTA humeral component. It is not paired with a glenoid component.
Incorrect Answers:
Metal-backed glenoids have higher rates of revision than all-polyethylene glenoids.
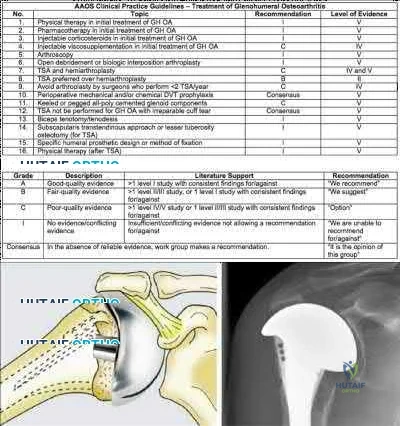
Posterior glenohumeral dislocations are as common as anterior dislocations in which of the following patient groups?
Football players

Marfan's syndrome patients Renal failure patients Epilepsy patients

Women
Millett et al and Robinson et al provide review articles on posterior shoulder dislocations, which are rare clinical entities that occur during seizures and electrocution (due to tetanic muscle contraction) or as a result of high energy trauma. Robinson et al noted that poor prognostic factors associated with posterior shoulder dislocation include late diagnosis, large bony defect of humeral head, associated proximal humerus fracture, and need for arthroplasty. In Gerber's series, posterior dislocations occurred with equal frequency to anterior in a cohort of epilepsy patients.
What nerve is injured most commonly during the superficial dissection when repairing a distal biceps rupture through a single incision anterior approach?

Medial antebrachial cutaneous nerve Lateral antebrachial cutaneous nerve Superficial radial nerve

Ulnar nerve

Posterior interosseous nerve
The lateral antebrachial cutaneous nerve (LABCN) is at risk during the superficial dissection when repairing a distal biceps rupture through a single incision anterior approach.
The LABCN is the terminal cutaneous branch of the musculocutaneous nerve, which supplies sensation to the volar-lateral aspect of the forearm. The LABCN pierces the deep fascia of the arm lateral to the musculotendinous junction of the distal biceps tendon after lying on top or piercing through the brachialis muscle. It exits the arm and lies in the subcutaneous tissues of the antecubital fossa. It is important to retract this nerve laterally during the approach to the distal biceps tendon.
Cohen describes the importance of identifying the LABCN during the superficial dissection as injury to this nerve is not uncommon (5-7%). Injury to the PIN (5 %) is devastating and occurs with retractor placement during the deep dissection and the use of suspensory fixation on the posterior cortex of the radius.
The review article by Ramsey et al covers the surgical anatomy and complications of biceps surgery, including injury to the LABCN.
Illustration A shows the LABCN relative to the anterolateral approach to the elbow which is commonly used to repair distal biceps avulsions. Illustration B shows the close proximity of the LABCN to the distal biceps in a human specimen.
Incorrect Responses:
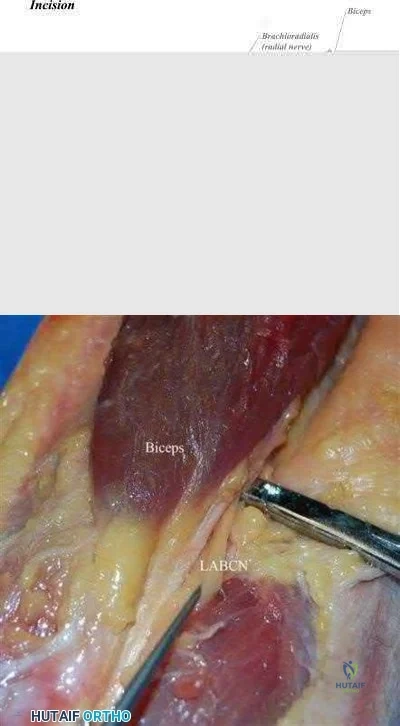
An MRI of the shoulder in a patient with chronic quadrilateral space syndrome is most likely to show which of the following?

Increased intra-capsular volume Loss of intra-capsular volume Fatty atrophy of the infraspinatus Fatty atrophy of the teres minor

Fatty atrophy of the latissimus dorsi
Quadrilateral space syndrome involves dysfunction of the axillary nerve, perhaps by entrapment or compression, resulting in the functional denervation of the teres minor.
The quadrilateral space is a potential space formed by the long head of the triceps medially, the humerus laterally, the teres minor above, and the teres major below. The axillary nerve and posterior circumflex humeral artery travel through this space.
The Sanders article describes the MRI appearance, which is that the muscle appears streaked with white on MRI and atrophied (See illustration A) consistent with fatty atrophy. Sanders group report this finding in 3% of shoulder MRIs. The posterior circumflex humeral artery also travels with the axillary nerve as it travels through this space. Loss of capsular volume on an arthrogram study is suggestive of adhesive capsulitis.
Illustration B is a diagram which shows the borders of the quadrilateral (or quadrangular) space.
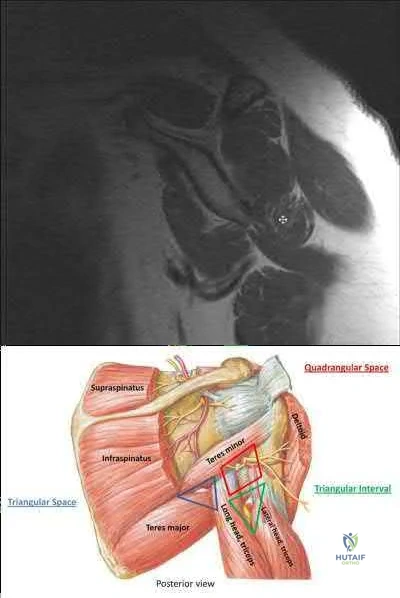
A 21-year-old collegiate volleyball player is noted to have weakness in external rotation and isolated atrophy of the infraspinatus on physical examination as seen in Figure A. An axial MRI image is shown in Figure B. This clinical condition is most likely caused by compression of the:
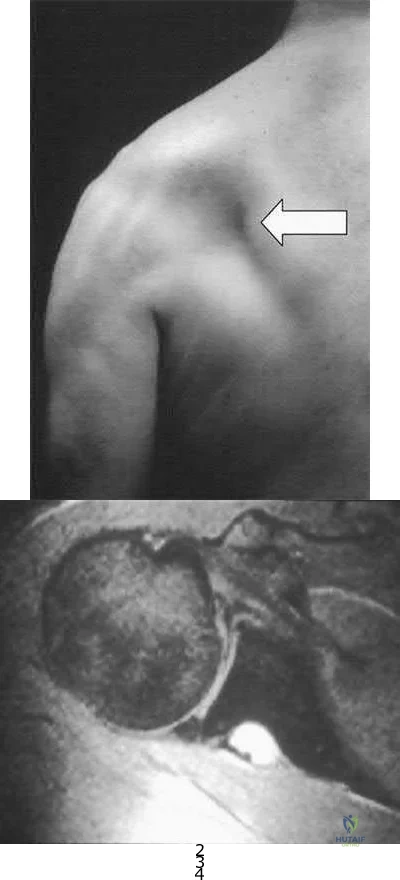
Axillary nerve at the triangular space Suprascapular nerve in the suprascapular notch Axillary nerve in the quadrangular space Suprascapular nerve in the spinoglenoid notch

Long thoracic nerve anterior to the scalenus and the first rib and posterior to the clavicle
The clinical presentation is consistent for a suprascapular neuropathy caused by compression of the suprascapular nerve by a cyst in the spinoglenoid notch.
The suprascapular nerve arises from the upper trunk of the brachial plexus with contributions from C5-6. It travels through the suprascapular notch of the scapula where it gives motor branches to the supraspinatus then around the spinoglenoid notch where it innervates the infraspinatus.
Compression of the nerve at the suprascapular notch will cause denervation and atrophy of both the supraspinatus and infraspinatus while compression at the spinoglenoid notch affects the infraspinatus in isolation. This is commonly seen in overhead athletes who sustain a SLAP tear and resultant spinoglenoid notch cyst as seen in the MRI. This will cause weakness and atrophy of the infraspinatus and can be noted both clinically and radiographically. Appropriate operative management is still not clear in the literature with some authors reporting a need for labral repair + cyst decompression and others reporting good outcomes with labral repair alone. Other cases have been treated with needle aspiration.
The cited reference by Cummins et al reviews the various causes, diagnosis, and treatment of suprascapular neuropathy.
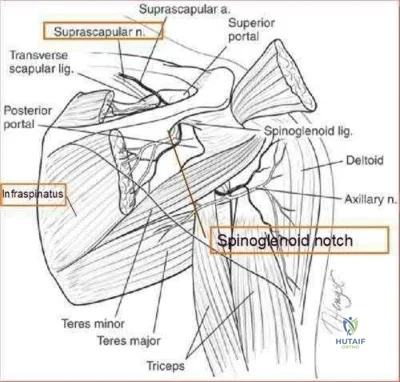
The reference by Martin et al is a retrospective study of the results of nonoperative treatment of suprascapular neuropathy in which 5 had excellent results and 7 had good results.
Which of the following provocative tests would most likely be positive in a patient with medial epicondylitis?

Resisted forearm pronation and wrist flexion with a clenched fist Resisted forearm supination and wrist extension with a clenched fist Dynamic valgus stress test

Milking maneuver Pinch grip test
A provocative test for medial epicondylitis can be elicited by applying resistance to a patient with their fist clenched, wrist flexed and pronated.
Medial epicondylitis is an overuse syndrome of the flexor-pronator mass. The pronator teres (PT) and flexor carpi radialis (FCR) are thought to be most affected with this condition. It is most common in the dominant arm and occurs with activities that require repetitive wrist flexion/forearm pronation. Patients are most tender over the origin of PT and FCR at the medial epicondyle.
Resisting a patient with their fist clenched, wrist flexed and pronated can cause worsening of their pain. This maneuver can be used as a provocative test for this condition.
Cain et al. reviewed elbow injuries in throwing athletes. They comment that the common flexorpronator muscle origin provides dynamic support to valgus stress in the throwing elbow, especially during early arm acceleration and help produce wrist flexion during ball release.
Amin et al. reviewed the evaluation and management of medial epicondylitis. They report that medial epicondylitis typically occurs in the fourth through sixth decades of life, the peak working years, and equally affects men and women. Physical therapy and rehabilitation is the main aspect of recovery from medial epicondylitis, once acute symptoms have been alleviated.
Illustration A shows a video of this provocative test for medial epicondylitis. Incorrect Answers:

A 72-year-old woman presents for follow-up after elbow surgery. Her radiographs are shown in Figures A and B. Which of the following pre-operative diagnoses is a relative contraindication to the use of this prosthesis design?

Acute intra-articular distal humerus fracture Malunited intra-articular distal humerus fracture Late-stage rheumatoid arthritis

Post-traumatic bony ankylosis Osteoarthritis
This patient has had an unconstrained total elbow arthroplasty (TEA).
Unconstrained TEA is least preferred for late-stage rheumatoid arthritis where there is significant capsuloligamentous instability and bony erosion.
Unconstrained (unlinked or resurfacing prosthesis) TEA depend on intact bony and ligamentous constraints for stability. These are appropriate for humeroulnar conditions with intact collateral ligaments and radiocapitellar articulation e.g. osteoarthritis, post-traumatic arthritis, intra-articular distal humerus fracture, and malunion of the distal humerus. Conditions with increased risk of

instability (ligamentous injury, rheumatoid arthritis) will benefit from a linked or semiconstrained prosthesis.
Mansat et al. reviewed the Coonrad-Morrey linked (semi-constrained) TEA implant in 70 patients after 5 years. They found that patients with inflammatory arthritis had higher function than those with traumatic conditions
( fractures, nonunions and post-traumatic arthritis). Survival rate was 98% and 91 % at 5 and 10 years, respectively. They concluded that this implant provided satisfactory treatment for different indications although radiolucent lines and bushing wear were a concern.
Hildebrand et al. reviewed the functional outcome of the Coonrad-Moorey prosthesis in 51 elbows after 50 months. The inflammatory arthritis group had higher performance scores than the traumatic/post-traumatic conditions group. Isometric extensor torque was found to be less than the nonoperated side. Radiolucency was noted in 11 elbows.
Figures A and B show an unconstrained TEA with radial head replacement. Illustration A shows more examples of unconstrained TEA. Illustration B shows a semiconstrained TEA. The arrow points to the anterior flange. Illustration C shows radiolucent lines around the stems. Illustration D shows severe bushing wear leading to locking mechanism failure. Illustration E is a table comparing linked and unlinked implants.
Incorrect Answers:

A professional baseball team has several pitchers with complaints of velocity loss with their pitches and shoulder pain of their dominant shoulders during spring training. Pitch counts are properly monitored. The average glenohumeral internal rotation deficit on the pitching staff is 45 degrees. The best intervention would be:
Pitchers throwing less fastballs and more changeups

Evaluate the pitchers elbows for ulnar collateral ligament acute ruptures. Increasing the weight training for the deltoid and latissimus dorsi muscles Focused stretches and therapies that address posterior capsular tightness Firing the general manager for finding pitchers that "lose their stuff"
Glenohumeral Internal Rotation Deficit (GIRD) is a phenomenon that occurs in baseball pitchers and is due to posterior capsular tightness. Treatment should begin with a therapy program addressing the pathologic posterior capsule.
GIRD is a phenomenon that is frequently found in high-level overhead throwing athletes, predominantly baseball pitchers. It is defined as the measured difference in internal rotation between the non-dominant arm and dominant arm. Worsening range of motion deficits are seen with increased repetitions, both over a single season and a career. GIRD > 25º is associated with development of shoulder pathologies or pain requiring periods of inactivity. Cessation of overhead throwing activities and initiation of a stretching program to address posterior capsular contractures is largely effective (90% in some series).
Burkhart et al. reviewed the conditions associated with high-level overhead throwing athletes shoulders, culminating in a theory of pathologic progression to "dead arm syndrome" (loss of velocity and effective pitching). Their theory attributes adaptive hyperexternal rotation (occurs during late-cocking / early acceleration phases of pitching) to lead to posterior-inferior capsular contracture and GIRD. Subsequent injuries to anterior structures - including SLAP lesions - would then occur.
Illustration A is a cartoon depiction of how to perform the sleeper stretch. This is a common component of a pitcher's maintenance stretching program.
Incorrect Answers:
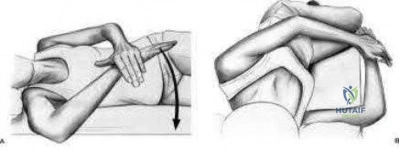
A 68-year-old man presents with severe right shoulder pain. He had a prolonged course of physical therapy and received several cortisone injections for his pain without improvement. Examination reveals pseudoparalysis of the right shoulder with a 20-degree external rotation lag with the shoulder adducted. With the shoulder placed in 90 degrees of abduction, he can actively externally rotate his shoulder. The patient was treated with a medialized reverse prosthesis shown in Figure A. Which of the following statement is true regarding this treatment option?

It is contraindicated in patients with shoulder pseudoparalysis

It can be used in patients with deltoid dysfunction when combined with latissimus dorsi transfer It shifts the center of rotation of the shoulder superior and lateral

The risk of scapular notching is increased with inferior placement of the glenoid component The risk of instability is increased with an irreparable subscapularis
The clinical presentation is consistent with a patient with pseudoparalysis that was treated with a reverse total shoulder arthroplasty (RTSA). The risk of postoperative instability is increased in patients with an irrepairable subscapularis when a medialized reverse prosthesis is used. Answers 1-4 are false statements.
RTSA is most commonly indicated for rotator cuff arthropathy. However, indications for use now include shoulder pseudoparalysis, anterosuperior escape of the humeral head, acute 3 or 4-part proximal humerus fractures, and greater tuberosity fracture nonunions. Contraindications to RTSA included deltoid dysfunction, insufficient glenoid bone stock, and bony deficiency of the acromion. Edwards et al. prospectively evaluated the risk of shoulder dislocation after reverse TSA. They found a significantly increased risk of dislocation (p=0.012) in patients with an irreparable subscapularis at time of surgery. There were no dislocations in the reparable group. Dislocations were more likely in patients with proximal humeral nonunions and failed prior arthroplasty. Mulieri et al. looked at the use of reverse TSA in patients with irreparable massive rotator cuff tears without evidence of glenohumeral arthritis. All outcomes were improved postoperatively, and they advocate
for reverse TSA in this subset of patients. Survivorship was over 90% at more than 4 years average follow up.
Boileau et al. evaluated the clinical outcomes of isolated biceps tenotomy/tenodesis in patients with massive rotator cuff tears and a biceps lesion. They found that the procedure can effectively treat pain and improve function in these patients. There was no difference in patients undergoing tenotomy versus tenodesis.
Figure A is a right shoulder radiograph status post RTSA with components in adequate position. Incorrect Answers:
Figure A shows immediate post-operative radiographs of a 75year-old patient with primary osteoarthritis. She presents 3 years later with increasing pain and weakness in the shoulder despite home physical therapy. Examination reveals limited active range of motion, with forward elevation of 80 degrees and external rotation of 50 degrees. Her deltoid function is intact. Repeat radiographs are seen in Figure B. Which treatment option would provide the best functional outcome for this patient?
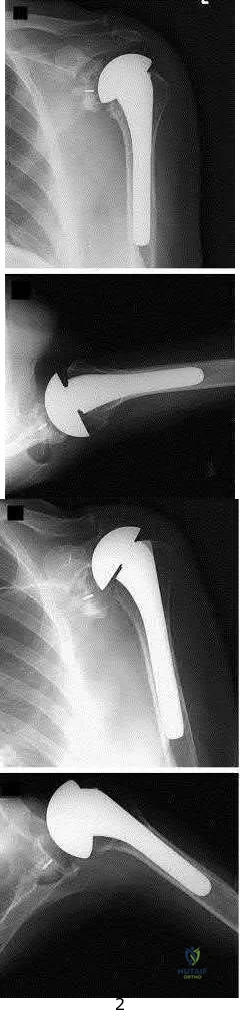
Open tendon transfer
Corticosteriod injection and supervised physical therapy

Open rotator cuff repair, subacromial decompression and distal clavical excision Revision to reverse shoulder arthroplasty

Revision to cuff arthropathy hemiarthroplasty
This patient presents with failed total shoulder arthroplasty. The best treatment option for functional outcome would be revision to reverse shoulder arthroplasty (rTSA).
RTSA is considered a viable treatment option for patients with failed shoulder arthroplasty. It allows for improved arm elevation and abduction in the setting of nonfunctional rotator cuff muscles, as seen in this example. Despite the expanding indications for rTSA, there are high complication rates in the revision setting. Complication rates for rTSA after failed shoulder arthroplasty have been reported to be between 11-36%. This procedure should, therefore, be performed by surgeons with extensive training in reconstructive shoulder arthroplasty.
Patel et al. retrospectively reviewed 31 patients (mean age, 68.7 years) who underwent rTSA for treatment of a failed shoulder arthroplasty. They found the greatest improvement with active forward elevation from 44° preoperatively to 108 ° postoperatively (P < .001). Complications occurred in 3 patients with periprosthetic fracture.
Hattrup et al. reviewed a series of 19 patients that underwent open rotator cuff repair after shoulder arthroplasty. Out of the 19 patients only 4 shoulders were successfully repaired. They concluded that successful rotator cuff repair after shoulder arthroplasty is possible but failure is more common. Figure A shows a left total shoulder arthroplasty that is well reduced in the glenoid. Figure B shows antero-superior escape of the prosthesis, indicative of a massive rotator cuff tear.
Incorrect Answers:
A 35-year-old man awoke following a night of heavy drinking with severe right shoulder pain and inability to raise his arm above his head. A radiograph from the emergency room is provided in Figure A. He was treated with a sling for a diagnosis of rotator cuff tear. Six weeks later, he complains of continued pain and difficulty using the arm. Which of the following is the next best step in management?

Physical therapy for range of motion followed by rotator cuff and deltoid strengthening exercises

Axillary radiograph of the shoulder

EMG to evaluate the suprascapular and axillary nerves Arthroscopic rotator cuff repair

Open subacromial decompression and latissimus dorsi transfer for massive cuff tear
The radiograph demonstrates overlap of the humeral head and glenoid suggesting shoulder dislocation. An Axillary radiograph is necessary to evaluate concentric reduction vs. dislocation of the shoulder. An example is provided in illustration A. Posterior shoulder dislocations can be easily be missed without the proper orthogonal views of the shoulder. Perron reviews the proper identification and emergency room care of posterior shoulder dislocation. Richardson found axillary radiographs to be more sensitive than trans-scapular radiographs for identifying posterior shoulder dislocations.

Recent randomized controlled trials comparing early passive range of motion to 6 weeks of immobilization after successful arthroscopic rotator cuff repair concluded that, compared to immobilization, early passive range of motion resulted in:
Higher Constant scores at 12 months

Increased rates of re-rupture as determined by ultrasound Equivalent functional outcomes

Less pain at 6 months

Inceased range of motion at 12 months
A series of high-quality RCTs have demonstrated that early passive range of motion has equivalent functional outcomes when compared to 6 weeks of immobilization after arthroscopic rotator cuff surgery.
Traditionally, most surgeons recommended early post-operative range of motion exercises for their patients in order to prevent adhesions and ultimately stiffness. However, recent evidence has found that there is no difference in the healing rate, range of motion or functional outcome between patients who undergo early versus delayed (i.e. initial 6 weeks of immobilization) passive range of motion exercises after arthroscopic rotator cuff repair.
Kim et al. conducted a randomized controlled trial comparing early passive range of motion vs. immobilization in 106 patients who underwent arthroscopic repair for full-thickness rotator cuff tears. They found that there was no clinically or statistically significant difference between the two groups in pain, healing or function.
Keener et al. also conducted a randomized controlled trial of 124 patients who were undergoing arthroscopic repair of a full-thickness rotator cuff tear and found no difference between early and delayed range of motion in healing and functional outcome.
Cuff & Pupello also compared early vs. delayed range of motion during the post-operative rehabilitation phase in a randomized controlled trial of 68 individuals undergoing arthroscopic rotator cuff repair and found no significant difference in range of motion or healing.
Incorrect Answers:
A 49-year-old male presents with right shoulder pain and weakness after undergoing open cervical lymph node biopsy approximately one year ago. A pertinent finding from the physical exam is seen in Figure A, with the patients arms by his side. Physical exam finding with the arms in a position of 90 degrees of forward elevation and 10 degrees of external rotation are shown in Figure B.
What nerve is most likely injured?

Long thoracic Suprascapular Spinal accessory Axillary Thoracodorsal
The patient is presenting with LATERAL scapular winging which is a result of injury to the spinal accessory nerve and resultant trapezius muscle palsy.
The spinal accessory nerve is fundamental to scapulothoracic function and essential for scapulohumeral rhythm. This nerve is vulnerable along its superficial course. The majority of injuries to the spinal accessory nerve are iatrogenic and occur secondary to head and neck surgery. There is often a marked delay in recognition and initiating treatment. Surgical treatment with the Eden-Lange transfer lateralizes the levator scapulae and rhomboids (transfer from medial border to lateral border)
Camp et al. reviewed the results of 111 patients who underwent operative management of a lesion to the spinal accessory nerve. They found that the majority (~80%) of injuries were sustained iatrogenically and that diagnosis was delayed for approximately 12 months.
Pikkarainen et al. reviewed the natural history of isolated serratus palsy. They found that symptoms mostly recover in 2 years, but at least one-fourth of the patients will have long-lasting symptoms, especially pain.
Figure A depicts a patient with lateral scapular winging. Figure B demonstrates physical exam of this patient with their arms in a position of 90 degrees of forward elevation and 10 degrees of external rotation. Illustration A highlights the difference between medial and lateral scapular winging. Illustration B depicts another example of a patient with lateral scapular winging.
Incorrect Answers:
An injury to the long thoracic nerve would result in serratus anterior palsy which would lead to MEDIAL scapular winging.

An injury to the suprascapular nerve would result in weakness and wasting of the supraspinatus and/or infraspinatus.
Question 100
Figure 28 is the radiograph of a 25-year-old soccer player who twisted her left ankle 1 week ago. She has pain and swelling over the anterolateral ankle and there is ecchymosis over the lateral ankle. She has these muscle group findings: anterior tibial tendon-right 5/5, left 5/5; posterior tibial tendon-right 5/5, left 5/5; peroneals-right 5/5, left 4/5; Achilles-right 5/5, left 5/5. What is the best next diagnostic or treatment step?

Explanation
Thousands of ankle sprains occur in the United States every day. Most affected patients do not have serious sequelae associated with their injury. In this case, a young athlete sprained her ankle. Her only area of tenderness is isolated to the anterior talofibular ligament. She also has associated weakness. The radiograph shows an os subfibulare; this is an entity that she likely was born with. There is no indication of bony pain, and it is too soon to test for instability; consequently, no further imaging is required. Considering the nature of the sprain and her weakness, physical therapy with proprioceptive training and peroneal strengthening would be most beneficial.
RECOMMENDED READINGS
Lephart SM, Pincivero DM, Giraldo JL, Fu FH. The role of proprioception in the management and rehabilitation of athletic injuries. Am J Sports Med. 1997 Jan-Feb;25(1):130-7. PubMed PMID: 9006708. View Abstract at PubMed
McGuine TA, Keene JS. The effect of a balance training program on the risk of ankle sprains in high school athletes. Am J Sports Med. 2006 Jul;34(7):1103-11. Epub 2006 Feb 13. PubMed PMID: 16476915. View Abstract at PubMed
Chun TH, Park YS, Sung KS. The effect of ossicle resection in the lateral ligament repair for treatment of chronic lateral ankle instability. Foot Ankle Int. 2013 Aug;34(8):1128-33. doi: 10.1177/1071100713481457. Epub 2013 Mar 7. PubMed PMID: 23471672.View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 29 THROUGH 33
Figures 29a and 29b are the weight-bearing radiographs of a 49-year-old woman who has had several months of increasing pain and deformity in her left foot. She points to her plantar medial arch as her area of greatest pain; however, she also has pain just distal to the tip of the distal fibula. Her pain worsens with walking or navigating stairs. Upon examination she has a flexible unilateral pes planus deformity with increased heel valgus and forefoot abduction. She is unable to perform a single heel raise.

29A

B
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding orthopedic-board-review-oite-aaos-part-255