OITE & ABOS Orthopedic Board Prep MCQs: Ankle, Elbow & Hip Arthroplasty | Part 172

Key Takeaway
This page offers Part 172 of a comprehensive OITE & AAOS Orthopedic Board Review quiz. Designed for orthopedic surgeons and residents, it features 100 high-yield, verified MCQs covering Ankle, Arthroplasty, Elbow, and Hip. Use study or exam modes to optimize your board certification preparation.
About This Board Review Set
This is Part 172 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 172
This module focuses heavily on: Ankle, Arthroplasty, Elbow, Hip.
Sample Questions from This Set
Sample Question 1: The patient has weakness with elbow flexion and has numbness down the anterior lateral aspect of the forearm....
Sample Question 2: In total hip arthroplasty, increasing the perpendicular distance from thecenterline of the femur to the center of rotation of the femoral head (femoral offset) results in...
Sample Question 3: Which of the following surgical devices employed for stabilization of the sternoclavicular joint is associated with the highest incidence of life-threatening complications?...
Sample Question 4: Figure 23 shows the radiograph of an elderly man who fell on his right arm. What is the most important determinate of a good outcome following this injury?...
Sample Question 5: Figures 42a through 42c show the clinical photographs and radiograph of a patient with diabetes mellitus who lives independently. The patient was admitted to the hospital late yesterday afternoon with clinical signs of sepsis. Parenteral an...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The patient has weakness with elbow flexion and has numbness down the anterior lateral aspect of the forearm.
Explanation
The Latarjet procedure was initially described in 1959 as a modification of the Bristow procedure. It has been used as a primary procedure to address instability, but is used more commonly for patients with instability and glenoid bone loss. In 2000, Burkhart and associates reported a 67% failure rate of the Bankart procedure in patients with an inverted pear-shaped glenoid (glenoid bone loss) or an engaging Hill-Sachs lesion, with a suggestion that a bone graft procedure would be optimal in this population. Complications following the Latarjet procedure have been reported as high as 25%, with the majority attributable to nerve injury, recurrent instability, and arthritis. Many of these complications are likely secondary to surgical technique. A coracoid graft that is placed too laterally or with prominent screws will overhang the glenoid and lead to early degenerative glenohumeral arthritis. A coracoid graft placed too medially can lead to recurrent instability secondary to an ineffective subscapularis sling and bone block. A coracoid graft placed inferiorly indicates dissection close to the axillary nerve, which can place tension on the axillary nerve or cause injury from direct trauma. After harvesting the coracoid graft, the surgeon must find the musculocutaneous nerve as it enters the conjoint tendon on the medial surface about 5 cm distal to the coracoid. Excessive dissection or retraction can lead to musculocutaneous nerve palsy.
Question 2
In total hip arthroplasty, increasing the perpendicular distance from the center line of the femur to the center of rotation of the femoral head (femoral offset) results in
Explanation
include an increased range of motion, better mechanical advantage for the abductors and decreased instability because of better soft tissue tension. According to Charnley,
increasing the femoral offset should improve the abductor lever arm which should decrease the abductor force required for walking, and therefore decrease the energy requirement for gait as well as the overall joint reactive force. The largest possible disadvantage of increasing the femoral offset is increasing the out of plane bending moment which puts stress on the prosthetic stem. Poly wear is a direct effect of surface area contact which is not changed with femoral Offset.
Question 3
Which of the following surgical devices employed for stabilization of the sternoclavicular joint is associated with the highest incidence of life-threatening complications?
Explanation
REFERENCES: Gilot GJ, Wirth MA, Rockwood CA: Injuries to the sternoclavicular joint, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott, Williams and Wilkins, 2006, vol 2, pp 1373-1374.
Lyons FA, Rockwood CA Jr: Migration of pins used in operations of the shoulder. J Bone Joint Surg Am 1990;72:1262-1267.
Question 4
Figure 23 shows the radiograph of an elderly man who fell on his right arm. What is the most important determinate of a good outcome following this injury?
Explanation
REFERENCES: Koval KJ, Gallagher MA, Marsicano JG, et al: Functional outcome after minimally displaced fractures of the proximal part of the humerus. J Bone Joint Surg Am 1997;79:203-207.
Hodgson SA, Mawson SJ, Stanley D: Rehabilitation after two-part fractures of the neck of the humerus. J Bone Joint Surg Br 2003;85:419-422.
Question 5
Figures 42a through 42c show the clinical photographs and radiograph of a patient with diabetes mellitus who lives independently. The patient was admitted to the hospital late yesterday afternoon with clinical signs of sepsis. Parenteral antibiotic therapy resolved the sepsis, and blood glucose levels are now well controlled. The patient has no palpable pulses. The ankle-brachial index is 0.70. Laboratory studies show a WBC count of 8,500/mm 3 , a serum albumin of 1.9 g/dL, and a total lymphocyte count of 1,500/mm 3 . What treatment has the best potential to optimize his survival and independence?
Explanation
REFERENCES: Pinzur MS, Stuck RR, Sage R, et al: Syme ankle disarticulation in patients with diabetes. J Bone Joint Surg Am 2003;85:1667-1672.
Pinzur MS, Smith D, Osterman H: Syme ankle disarticulation in peripheral vascular disease and diabetic foot infection: The one-stage versus two-stage procedure. Foot Ankle Int 1995;16:124-127.
Question 6
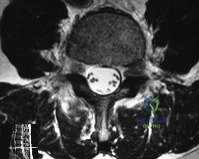
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?
Explanation
REFERENCES: Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
O’Hara LJ, Marshall RW: Far lateral lumbar disc herniation: The key to the intertransverse approach. J Bone Joint Surg Br 1997;79:943-947.
Question 7
A 22-year-old patient underwent successful reduction of a posterolateral elbow dislocation. Management should now consist of
Explanation
REFERENCES: Ross G, McDevitt ER, Chronister R, et al: Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med 1999;27:308-311.
O’Driscoll SW, Jupiter JB, King GJ, et al: The unstable elbow. J Bone Joint Surg Am 2000;82:724-738.
Question 8
What are the four most common soft-tissue sarcomas to spread via the lymph node system?
Explanation
REFERENCES: Riad S, Griffin AM, Liberman B, et al: Lymph node metastasis in soft-tissue sarcoma in an extremity. Clin Orthop Relat Res 2004;426:129-134.
Blazer DG III, Sabel MS, Sondak VK: Is there a role for sentinel lymph node biopsy in the management of sarcoma? Surg Oncol 2003;12:201-206.
Question 9
A 44-year-old man was involved in a low speed rear-end motor vehicle accident 4 weeks ago. He predominantly reports pain in the back of the neck, with occasional radiation into the trapezius region bilaterally. He denies any extremity pain. The pain has not changed in intensity, but is worse with neck range of motion. Cervical spine radiographs were negative for acute osseous trauma or instability. What is the next most appropriate step in management? Review Topic
Explanation
Question 10
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. If present, what is the most likely complication after surgical treatment in this scenario?
Explanation
and degenerative joint disease.
Question 11
- A 19-year-old man sustains a complete spinal cord injury at the C7 level as a result of diving into a lake. He has a blood pressure of 90/50 mm Hg, a pulse of 60/min, and respirations of 20/min. These values most likely signify
Explanation
Question 12
01 (left). What is the most appropriate next step?

Explanation
Knee dislocations are associated with popliteal artery injury in 18-45% of cases and range from intimal tears to complete transection. Amputation rates of 85% have been reported if revascularization is delayed greater than 6 to 8 hours. Neurologic injury occurs in 15-40% of cases and is most common after posterolateral dislocation. The peroneal nerve is more commonly injured.
Rihn et al. reviewed the acutely dislocated knee. They recommend a vascular consult if pulses are weak, or ABI is compromised. They warn that in arterial injury, pulses, temperature and capillary refill can be normal. If the limb remains ischemic, surgical exploration and revascularization is indicated.
Medina et al. systematically reviewed neurovascular injury after knee dislocation in 862 patients. Vascular injury rate was 18%, and nerve injury rate was 25%. Repair was performed in 80% of vascular injuries, and amputation in 12%. The most vascular injury was seen in KDIIIL injuries (32%) and posterior dislocation (25%).
Figure A is an AP radiograph of a posterior knee dislocation. Figure B is a lateral showing the same injury.
Incorrect Answers:
Question 13
CLINICAL SITUATION Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. Initial surgical management should consist of

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair,
but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 14
In recurrent posterior shoulder instability, what is the recommended approach to the posterior capsule?
Explanation
REFERENCES: Dreese J, D’Alessandro D: Posterior capsulorrhaphy through infraspinatus split for posterior instability. Tech Shoulder Elbow Surg 2005;6:199-207.
Shaffer BS, Conway J, Jobe FW, et al: Infraspinatus muscle-splitting incision in posterior shoulder surgery: An anatomic and electromyographic study. Am J Sports Med 1994;22:113-120.
Fuchs B, Jost B, Gerber C: Posterior-inferior capsular shift for the treatment of recurrent voluntary posterior subluxation of the shoulder. J Bone Joint Surg Am 2000;82:16-25.
Question 15
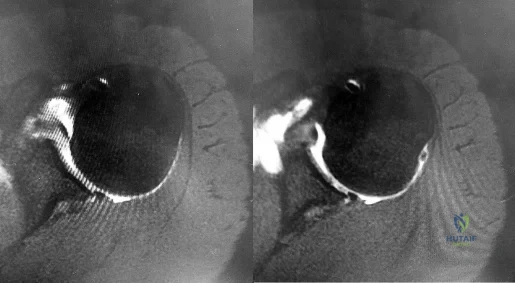
A college basketball player is struck in the eye by a player’s hand while driving to the basket. Fluorescein evaluation reveals the injury shown in Figure 18. Management should consist of
Explanation
REFERENCES: Brucker AJ, Kozart DM, Nichols CW, et al: Diagnosis and management of injuries to the eye and orbit, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby-Year Book, 1991, pp 650-670.
Zagelbaum BM: Treating corneal abrasions and lacerations. Phys Sports Med 1997;25:38-44.
Question 16
Figures 39a and 39b are the radiographs of a 45-year-old man with diabetes who fell 12 feet from a ladder and sustained an isolated closed injury to his left leg. Examination revealed that he was neurovascularly intact and compartments were soft. A damage control knee spanning external fixator was applied and after 2 weeks in the frame, his blisters have resolved and his skin now wrinkles. What is the most appropriate treatment?

Explanation
alignment while the soft-tissue injury recovers and to allow for surveillance and examination of the limb. The radiographs reveal a comminuted bicondylar pattern with significant depression of the lateral articular surface and a split fracture with condylar widening. This element of the fracture will require direct elevation of the joint surface and reduction/buttress of the lateral condyle. This is best achieved with a lateral plate with subchondral rafting screws. The medial articular surface is coronally split and the posteromedial fragment is displaced. This fragment requires direct reduction and buttress via a separate posteromedial approach which is frequently performed prior to the lateral approach and fixation. A lateral buttress plate or a lateral locking plate alone does not reliably capture or adequately support the displaced posteromedial fragment. A medial and lateral plate construct is less soft-tissue friendly, particularly if inserted through a single incision. A medial plate would also fail to give direct buttress to the posteromedial fragment.
Question 17
Osteonecrosis of the humeral head is a rare complication seen after dislocation of the glenohumeral joint in skeletally immature patients. When this complication is encountered, treatment should consist of Review Topic
Explanation
Question 18
The anterolateral (Watson-Jones) approach to the hip exploits the intermuscular interval between the
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 316-332.
Crenshaw AH (ed): Campbell’s Operative Orthopedics, ed 7. St Louis, MO, CV Mosby, 1987,
p 63.
Question 19
An otherwise healthy 33-year-old man who works in construction reports a 3-month history of knee pain. Radiographs are shown in Figures 9a and 9b. An axial T 1 -weighted MRI scan with contrast, an angiogram, and histologies are shown in Figures 9c through 9f. What is the most likely diagnosis?
Explanation
REFERENCES: Sheth DS, Yasko AW, Raymond AK, et al: Conventional and dedifferentiated parosteal osteosarcoma: Diagnosis, treatment, and outcome. Cancer 1996;78:2136-2145.
Lewis VO, Gebhardt MC, Springfield DS: Parosteal osteosarcoma of the posterior aspect of the distal part of the femur: Oncological and functional results following a new resection technique. J Bone Joint Surg Am 2000;82:1083-1088.
Question 20
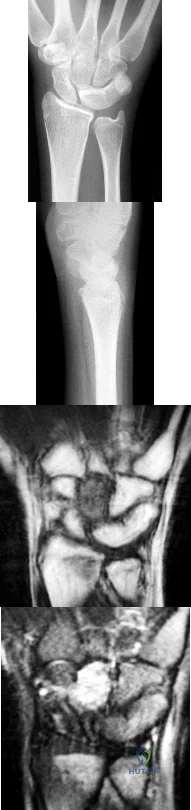
Figures 1 through 4 are the radiographs and MR images of a healthy 21-year-old woman who has had persistent dorsal wrist pain despite immobilization and no history of trauma. The surgical procedure associated with the best prognosis in this scenario is
Explanation
This patient has osteonecrosis of the capitate. The MR images show evidence of osteonecrosis with decreased signal on the T1-weighted image. The radiographs are unremarkable, with the exception of lunotriquetral coalition, which does not necessitate treatment. The etiology of osteonecrosis of the capitate may be related to trauma, abnormal Interosseous vascular supply, and hypermobility. Surgery is an option for patients with persistent symptoms despite immobilization. Vascularized bone graft should be considered in this scenario because there is no evidence of capitate collapse or arthritic change about the wrist. Free and local vascularized bone grafts have produced satisfactory results. Capitate excision with interposition arthroplasty is indicated for patients with proximal pole capitate collapse. Total wrist fusion is a salvage procedure and would be considered if there were evidence of collapse and arthritic change. PRC would leave the capitate articulating with the radius and is not indicated.
Question 21
Figure 35 is the radiograph of a 37-year-old woman who began having right forefoot pain about 4 weeks ago after increasing her daily running mileage. She denies any specific injury. Upon examination she has tenderness over the medial forefoot with mild swelling. In addition to her activity level, what is the primary etiology of the radiograph finding?

Explanation
Stress fractures are the result of physiological bone response to increased stress. Increased stress on bone triggers an increase in remodeling, which begins with resorption of bone at the site of stress. Ongoing stress can overwhelm bone strength, resulting in a fracture. In the foot this most commonly is seen in the second metatarsal at the junction of the middle and distal thirds. Contributing factors to increased loading of the second metatarsal include hallux valgus (decreased hallux loading transfers to the second metatarsal head), hallux rigidus (offloading of the hallux attributable to pain increases second metatarsal loading), and a long second metatarsal (increased duration of contact during push-off in the stance phase).
RECOMMENDED READINGS
Shindle MK, Endo Y, Warren RF, Lane JM, Helfet DL, Schwartz EN, Ellis SJ.
Stress fractures about the tibia, foot, and ankle. J Am Acad Orthop Surg. 2012 Mar;20(3):167-
Question 22
A 22-year-old javelin thrower reports that he has had increasing discomfort in his right elbow and loss of distance from his throws for the past 3 months. Examination reveals tenderness over the medial elbow. Application of valgus torque to the elbow through a passive range of motion elicits pain from 70 degrees to 120 degrees of flexion, with no pain at the limits of extension. What structure is primarily responsible for the patient's symptoms? Review Topic
Explanation
is a secondary stabilizer at 30 degrees of flexion, and not susceptible to valgus load when the anterior bundle is intact. The annular ligament and triceps insertion are not involved with medial instability of the elbow. Olecranon osteophytes likely cause pain in terminal extension of the elbow.
Question 23
Figure below shows the radiograph obtained from a 76-year-old woman who has sharp pain in her groin, thigh, and buttocks that worsens with activity. She has been dealing with this pain for more than a year but is otherwise healthy. Recently, she has begun to notice night pain. The pain no longer responds to NSAIDs. She would like to be able to dance at her daughter's wedding in 4 months and wonders how best to proceed. What is the best next step?
Explanation
The next best course of action is total hip arthroplasty. The patient is an otherwise healthy woman requesting pain relief and expresses a desire to be dancing in 4 months. She has had more than 6 months of symptoms that are classic hip osteoarthritis symptoms, with pain in the groin and thigh. Severe osteoarthritis is seen in the radiograph as well. NSAIDs are no longer working. Given the objective findings, the subjective reports, and the duration of symptoms, this patient merits surgery. Consideration for steroid injection is reasonable, but given her desire to be dancing in 4 months, an injection would increase her risk of infection if total hip arthroplasty were to be performed within 3 months of the
injection.
Question 24
If heel varus corrects with a Coleman block test, then the hindfoot deformity is flexible. This test proves that the varus is due to a
Explanation
REFERENCES: Younger AS, Hansen ST Jr: Adult cavovarus foot. J Am Acad Orthop Surg 2005;13:302-315.
Alexander IJ, Johnson KA: Assessment and management of pes cavus in Charcot-Marie-Tooth disease. Clin Orthop Relat Res 1989;246:273-281.
Question 25
In patients with suspected hepatitis C, which of the following tests is commonly used to confirm the diagnosis after a positive ELISA screening test?
Explanation
REFERENCES: de Medina M, Schiff ER: Hepatitis C: Diagnostic assays. Semin Liver Dis 1995;15:33-40.
McGrory BJ, Kilby AE: Hepatitis C virus infection: Review and implications for the orthopedic surgeon. Am J Orthop 2000;29:261-266.
Question 26
Which of the following structures are found in the anterior tarsal tunnel?
Explanation
REFERENCES: Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Sarrafian S: The Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 113-158.
Question 27
A researcher studies growth factors that have positive effects on cartilage healing. In vivo and in vitro experiments are performed with Growth Factor
Explanation
TGF-beta is the most thoroughly investigated member of the TGF-beta superfamily. This group includes TGF-beta1, BMP-2, and BMP-7. Besides the above activities, TGF-beta1 also stimulates chondrocyte synthetic activity and decreases the catabolic activity of IL-1.
Fortier et al. reviewed the role of growth factors in cartilage repair and modification
of osteoarthritis. They found that members of the TGF-beta superfamily, FGF family, IGF1, and PDGF have all been investigated as possible treatment augments in the management of chondral injuries and early arthritis. They concluded that more research was necessary before routine application.
Illustration A shows a summary of the different growth factors and their effects on cartilage.
Incorrect Answers:
Question 28
A 42-year-old woman reports neck stiffness, upper extremity pain, clumsiness, weakness, and instability of gait. Examination reveals 4+ of 5 strength in the upper extremities and 3+ biceps, brachioradialis, and patellar reflexes with a positive Hoffman sign bilaterally. MRI and CT scans are shown in Figures 10a and 10b. Based on the history and imaging findings, what is the most likely diagnosis? Review Topic

Explanation
Question 29
A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had increasing pain and elbow instability. There is no clinical evidence of infection, and radiographs show no new bony process. What is the best option for this patient?
Explanation
REFERENCES: Blaine TA, Adams R, Morrey BF: Total elbow arthroplasty after interposition arthroplasty for elbow arthritis. J Bone Joint Surg Am 2005;87;286-292.
Cheng SL, Morrey FB: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Question 30
A subtrochanteric femur fracture in which the lesser trochanter is intact is associated with what deformity?
Explanation
Question 31
A 50-year-old woman who underwent a joint replacement of the hallux metatarsophalangeal joint 6 months ago now has pain and swelling about the great toe. Radiographs are shown in Figures 39a and 39b. What is the next most appropriate step in management?
Explanation
REFERENCE: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 265-266.
Question 32
Which modality has the broadest application for reduction of postsurgical transfusion?
Explanation
TXA is easy to administer, inexpensive, and safe for virtually all patients. Multiple studies have demonstrated transfusion rates lower than 3% for total knee arthroplasty and lower than 10% for total hip arthroplasty. Regional and hypotensive anesthesia effectively reduce transfusion; however, they cannot be used in as wide a range of patients as TXA. A reduced transfusion trigger must be considered along with patient symptoms when determining the need for transfusion.
Question 33
Which of the following enzymes is used to resorb bone by mature osteoclasts?
Explanation
Question 34
Figures 4a through 4c show the radiographs of a 43-year-old woman who sustained a twisting injury to her right ankle. She has ankle pain and tenderness medially and laterally. To help determine the optimal treatment, an external rotation stress radiograph of the ankle is obtained. This test is designed to evaluate the integrity of what structure?
Explanation
REFERENCES: Egol KA, Amirtharajah M, Tejwani NC, et al: Ankle stress test for predicting the need for surgical fixation of isolated fibular fractures. J Bone Joint Surg Am 2004;86:2393-2398.
McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004;86:2171-2178.
Schock HJ, Pinzur M, Manion L, et al: The use of the gravity or manual-stress radiographs in the assessment of supination-external rotation fractures of the ankle. J Bone Joint Surg Br 2007;89:1055-1059.
Question 35
Thoracic disk herniations are most frequently found in what area of the spine?
Explanation
REFERENCES: Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864.
Bohlman HH, Zdeblick TA: Anterior excision of herniated thoracic discs. J Bone Joint Surg Am 1988;70:70-77.
Question 36
A 75-year-old woman who fell on her right knee now reports pain and is unable to bear weight. History reveals that she underwent total knee arthroplasty on the right knee 6 years ago. Radiographs are shown in Figure 5. Management should now consist of
Explanation
REFERENCES: Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209.
McLaren AC, DuPont JA, Schroeber DC: Open reduction internal fixation of supracondylar fractures above total knee arthroplasties using the intramedullary supracondylar rod. Clin Orthop 1994;302:194-198.
Figgie MP, Goldberg VM, Figgie HE III, et al: The results of treatment of supracondylar fracture above total knee arthroplasty. J Arthroplasty 1990;5:267-276.
Question 37
Figures below show the radiographs obtained from a 79-year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. No evidence of infection is seen. What is the most appropriate treatment?
Explanation
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis, as shown in Figures 3 and 4. They also assist in obtaining correct limb alignment. Short metaphyseal-engaging stems are associated with failure rates that range between 16% and 29%. Cemented stems may be shorter than press-fit stems, because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.
Question 38
A 56-year-old mechanic has had pain in the hypothenar region of his dominant right hand for the past 6 months. He reports weakness in his grip and pain is worse with activity. Which of the following examination findings is most suggestive of a cervical etiology? Review Topic
Explanation
Question 39
A 65-year-old female presents with the injury seen in Figures A and B after a motor vehicle collision. She is hemodynamically unstable and undergoes emergent pelvic supra-acetabular external fixation followed by laparotomy. She is now hemodynamically stable and cleared for surgery. She has no evidence of neurologic deficit on examination. Which of the following factors is a relative contraindication to open reduction and plating of her posterior pelvic injury from an anterior approach?

Explanation
Posterior pelvic ring injuries that are unable to be reduced by closed techniques may require open reduction via anterior or posterior approaches. Relative contraindications to anterior approach include comminuted sacral fractures, morbid obesity, iliac wing external fixation, and ipsilateral diverting colostomy. In the presence of a comminuted sacral fracture, aggressive medial dissection would be required and would place the L5 nerve root at risk.
Simpson et al describe their initial results with open reduction and internal fixation of the SI joint via an anterior exposure in a series of 16 patients. They note that sacral alar comminution is a contraindication to the anterior approach
Jones provides an overview of the operative treatment of posterior pelvic ring injuries. He demonstrates reduction and fixation techniques via both anterior and posterior exposures.
Incorrect Answers:
Question 40
Consider the theoretic articulation shown in Figure 11 as femoral and tibial components of a total knee prosthesis in which the components fit like a “roller in trough.” Which of the following best describes the articulation?
Explanation
REFERENCE: Alicea J: Scoring systems and their validation for the arthritic knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1507-1515.
Question 41
A 70-year-old man underwent primary total knee arthroplasty 3 months ago. Figures 7a and 7b show the radiograph and clinical photograph following incision and drainage of the wound 1 week ago. Aspiration of the joint reveals methicillin-sensitive Staphylococcus aureus. What is the next most appropriate step in management?
Explanation
REFERENCES: Harwin SF: The diagnosis and management of infected total knee replacement. Seminars Arthroplasty 2002;13:9-22.
Goldmann RT, Scuderi GR, Insall JN: 2-stage reimplantation for infected total knee replacement. Clin Orthop 1996;331:118-124.
Morrey BF, Westholm F, Schoifet S, Rand JA, Bryan RS: Long-term results of various treatment options for an infected total knee arthroplasty. Clin Orthop 1989;248:120-128.
Question 42
A 70-year-old woman has a preoperative anterior interscalene block prior to undergoing a total shoulder arthroplasty. After seating her in the beach chair position, she becomes acutely hypotensive. What is the most likely cause for the hypotension?
Explanation
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14:546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
Question 43
An injury to the axillary nerve would result in deltoid muscle weakness. 5 . An injury to the thoracodorsal nerve would result in latissimus dorsi weakness and would not cause scapular winging.

Explanation
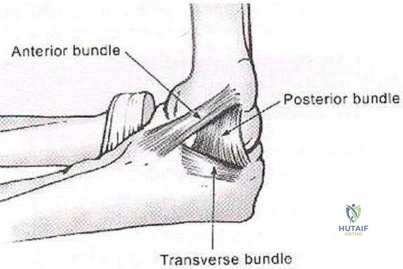
The medial ulnar collateral ligament, or medial collateral ligament of the elbow, is composed of three bundles: an anterior bundle, a posterior bundle, and a variable
transverse oblique bundle. During late cocking and early acceleration phases of the overhead throw, the medial UCL is subjected to the greatest amount of valgus stress to the elbow. During this phase, the forearm lags behind the upper arm and generates valgus stress while the elbow is primarily dependent on the anterior band of the UCL for stability. This puts the ligament at greatest risk of injury during this phase.
Fleisig et al. examined the kinetics of baseball pitching and the implications on injury mechanisms. They showed that the UCL contributes to 54% of the varus torque that is generated during the early acceleration of throwing. The position of greatest load occurred when the arm was flexed to 95 +/14 degrees with an applied valgus load.
Illustration A shows a diagram of the medial ulnar collateral ligament ligament bundles. Incorrect Answers:
A 14-year-old elite basketball player develops acute medial elbow pain after a fall. Physical examination reveals medial elbow tenderness over the submlime tubercle, but full range of motion. The provocative tests seen in Figure A exacerbate his elbow pain. Radiographs of the elbow are normal. What would be the next best step in treatment?
Supervised elbow stretching program Therapeutic elbow arthroscopy

Static elbow external fixation for 3 to 6 weeks, then MR arthrography if pain continues Activity avoidance for 6 weeks

Serial inflammatory markers and rheumatology referral
Figure A shows a moving valgus stress, which is a provocative test for ulnar collateral ligament (UCL) injury and elbow valgus instability. The initial treatment would be a short period of immobilization, rest and flexor pronator strengthening in this patient population.
Adolescent UCL injuries can be effectively treated with a short period of rest and NSAIDs to control pain. As the acute inflammation resolves, the patient can be started on a supervised therapy program. This should target flexor pronator muscles, as they are important secondary dynamic stabilizers of valgus stress. Once symptoms have improved and the athlete has regained full range of motion and strength, a mediated throwing program may be initiated. Throwing athletes should be educated to avoid provocative activities during this period.
Chen et al. wrote a JAAOS article on shoulder and elbow injuries in the skeletally immature athlete. They state that surgery is reserved for older athletes with persistent valgus instability despite > 6 months of non-surgical management.
Murthi et al. reviewed recurrent elbow instability. They state the anterior bundle of the medial ulnar collateral ligament complex is the primary valgus stabilizer of the elbow. The anterior band is taut for the first 60° of elbow flexion, and the posterior band is taut from 60° to 120° of flexion. The secondary valgus stabilizers of the elbow joint include the radial head, the anterior and posterior aspects of the capsule, and the muscular forces around the joint.
Figure A is showing a moving valgus stress. Illustration A shows provocative tests for valgus instability of the elbow. The image on the left shows a valgus stress test. This assesses the anterior bundle of the medial ulnar collateral ligament complex by flexing the elbow to 25-30 degrees and applying a valgus load across the elbow. The image on the right shows milking maneuver. This assesses the posterior bundle of the medial ulnar collateral ligament complex by pulling on the

beyond 90°. Incorrect Answers:
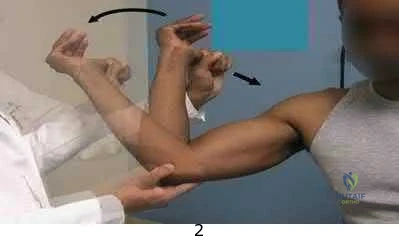
A young, healthy male undergoes a distal biceps repair and sustains an iatrogenic nerve injury during the procedure. Which of the following clinical findings are most likely to be seen in this circumstance? Inability to extend the thumb

Lateral volar forearm numbness Inability to flex the middle finger Medial volar forearm numbness Dorsal thumb numbness
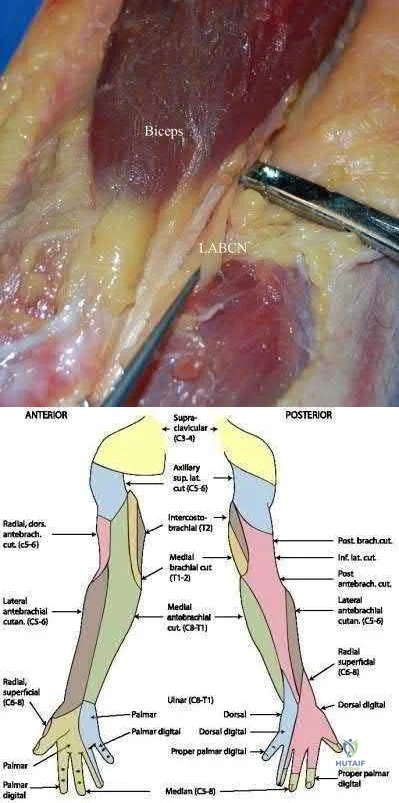
The most commonly injured nerve during a distal biceps repair is the lateral antebrachial cutaneous nerve (LABCN). Injury to this nerve would result in lateral volar forearm numbness.
Distal biceps avulsions can be partial or complete. Indications for surgical management include young, healthy patients who do not wish to sacrifice function, as well as partial biceps avulsions that do not respond to conservative management. Repair of a distal biceps avulsion can be approached through either an anterior one-incision technique or a two-incision technique (BoydAnderson). The one-incision technique uses the interval between the brachioradialis (radial nerve) and pronator teres (median nerve), while the two-incision technique uses this same interval in addition to a second posterolateral elbow incision. The lateral antebrachial cutaneous nerve is the most common nerve injured during either approach.
Kelly et al. retrospectively reviewed 74 distal biceps tendon repairs, and found five sensory nerve paresthesias. The lateral antebrachial cutaneous nerve was most commonly injured, followed by the superficial radial nerve.
Cain et al. retrospectively reviewed 198 distal biceps tendon repairs, and found a 36% complication rate. Lateral antebrachial cutaneous nerve paresthesias were found in 26%, while radial sensory nerve paresthesias were found in 6%, and posterior interosseous nerve (PIN) injury in 4%.
Illustration A shows the close relationship between the lateral antebrachial cutaneous nerve (LABCN) and the distal biceps. Illustration B shows the sensory nerves of the upper extremity and their respective areas of innervation.
Incorrect Answers:
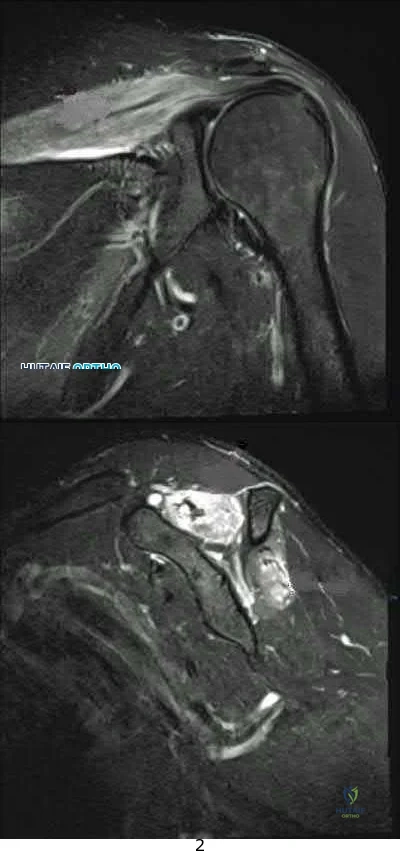
A 33-year-old female presents with left shoulder weakness. Two weeks prior to presentation, the patient experienced sudden-onset, left shoulder pain, which occurred a few days after receiving the influenza vaccine. The pain subsided over the next day, followed by gradual weakness of her shoulder and eventual general disuse of her left upper extremity. An initial visit to her primary care provider resulted in the recommendation of observation. On physical exam, there is weakness and gross atrophy of the shoulder girdle. Figures A & exhibit T2-weighted MRI images of her left shoulder. To further confirm her suspected diagnosis, she is sent for electromyography.
What is the expected result?
Normal results
Fibrillation potentials consistent with compression at the spinoglenoid notch 3 . Sharp waves and fibrillations potentials associated with the deltoid and biceps

Acute denervation of both peripheral nerve and nerve root distribution with sharp waves and fibrillation potentials

Early reinnervation with polyphasic motor unit potentials
This patient has Parsonage-Turner Syndrome, which, when tested on EMG during the first 3 weeks, exhibits acute denervation of both peripheral nerve and nerve root distributions with positive sharp waves and fibrillation potentials.
Parsonage-Turner Syndrome is an idiopathic disorder with an etiology that is still unknown. Typical antecedent events can involve a viral illness, recent immunization, or elective surgery. Clinical presentation is usually initiated by acute onset shoulder pain, which quickly subsides and is followed by gradual weakness. Early MRI exhibits edema in the effected muscles, and fatty infiltration in later stages. Treatment is typically non-operative, and resolution can be seen as early as 6 weeks from onset.
Tjoumakaris et al. provide a thorough review of the diagnosis and management of ParsonageTurner Syndrome. The authors report the usefulness of MRI, which exhibits early edema and later fatty infiltration in the affected muscles, and urge the use of EMG as a confirmatory diagnostic measure as well as a monitoring tool to track resolution. Early identification and diagnosis may be treated with a short course of steroids, which may help shorten symptoms.
Stutz et al. concisely summarize Parsonage-Turner Syndrome and provide typical presentation, diagnosis and management principles. The authors note the common association with viral illness and/or recent immunization along with the importance of obtaining a baseline chest radiograph to rule out a compressive Pancoast tumor. Management is typically supportive with eventual resolution.
Figures A, B, and C are T2-weighted coronal, sagittal, and axial cuts of the shoulder girdle with associated edema in the supraspinatus and infraspinatus typically seen in Parsonage-Turner Syndrome.
Incorrect answers:
A total shoulder arthroplasty (TSA) would be the most appropriate treatment in which of the following arthritic patients?
Question 44
What is the most common cause for late revision (> 2 years post op) total knee arthroplasty?
Explanation
REFERENCE: Sharkey PF, Hozack WJ, Rothman RH, et al: Insall Award paper: Why are total knee arthroplasties failing today? Clin Orthop Relat Res 2002;404:7-13.
Question 45
One of the serious potential complications of repair of distal biceps tendon ruptures is limited pronation and supination as a result of synostosis. What surgical approach and technique presents the highest risk for development of this complication?
Explanation
REFERENCE: Norris TR: Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, p 342.
Question 46
Figures 52a and 52b show the radiographs of a left proximal femoral lesion noted serendipitously following minor trauma to the left hip. The patient has no thigh pain and is fully active without limitation. What is the most likely diagnosis of this bony lesion?
Explanation
REFERENCE: Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 47
Figure 29a shows the clinical photograph of a 26-year-old woman who has had the leg deformity since birth. She reports difficulty with walking and weight bearing and notes increased discomfort and swelling when the leg is dependent. She denies any history of trauma or family history of a similar disorder. Examination reveals a fixed equinovarus deformity of the foot but no evidence of a limb-length discrepancy. No other cutaneous findings or soft-tissue masses are noted. Sagittal and axial T1- and T2-weighted MRI scans are shown in Figures 29b and 29c. What is the most likely diagnosis?
Explanation
REFERENCES: Berquist TH (ed): MRI of the Musculoskeletal System, ed 3. Philadelphia, PA, Lippincott Raven, 1997, p 771.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St. Louis, MO, Mosby Year Book, 1995, p 688.
Question 48
An 11-year-old girl is struck in the leg by a loaded sled while sledding and is seen in the emergency department; she is reporting severe knee pain. Radiographs are read as normal. Examination reveals that she is exquisitely tender over the proximal tibial physis. The neurovascular examination is normal. What is the next step in management? Review Topic
Explanation
Question 49
What is the most common fracture associated with a lateral subtalar dislocation?

Explanation
Post-reduction x-rays need to be scrutinized carefully for fractures of the tarsal bones as this is the most common injury associated with subtalar dislocations. Occult fractures of the lateral process of the talus are also associated with these injuries.
The referenced study by Wagner et al noted radiographic subtalar DJD in 2/3 of their patients, but noted no correlation between radiographic and clinical outcomes. The referenced study by Bibbo et al noted an 88% incidence of other concurrent injuries and an 89% rate of radiographic DJD at 5 year follow-up. The referenced article by Saltzman et al is a review of hindfoot dislocations.
Question 50
In performing an opening wedge high tibial osteotomy at the tibial tubercle, the osteotome extends 5 mm posteriorly and centrally out of the bone as shown in Figures 17a and 17b. What is the first structure it enters?
Explanation
REFERENCES: Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3.
Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 422.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, plate 480.
Question 51
-What is the most likely cause of an acute femur fracture in a 5-month-old child?
Explanation

Question 52
A 45-year-old right hand dominant female sustains a left shoulder injury after falling on ice 2 weeks ago. She is brought to the operating room for surgical intervention and positioned upright in a beach chair. Figures A and B are images taken from a posterior viewing portal with a 70 degree arthrosope. Figure C demonstrates the surgically repaired structure. Which of the following physical examination maneuvers would have been most likely abnormal in this patient PREOPERATIVELY? Review Topic

Explanation
Figure A as viewed from a posterior portal in the beach chair position of the left shoulder demonstrates a subscapularis tear with Figure B demonstrating medial instability of the long head of the biceps tendon. Figure C shows a repaired subscapularis to its footprint with double loaded screw-in anchors. A biceps tenodesis was concomitantly performed.
The key physical exam findings are positive Belly-press and Lift-off maneuvers, as well as weakness in internal rotation and increased passive external rotation. An MRI would confirm the diagnosis with discontinuity of the subscapularis and long-head of the biceps not located in the bicipital groove.
Faruqui et al present a Level 4 retrospective analysis of 52 patients. They found that the use of the belly press, lift-off, and bear hug tests had a collective sensitivity of 81%.
Yoon et al author a Level 2 prospective evaluation of 312 patients that underwent arthroscopic rotator cuff tear surgery. They investigated the sensitivity and specificity of the lift-off, internal rotation lag sign, belly-press, and bear-hug tests to evaluate subscapularis integrity. They found that a positive lift-off test was specific for the finding a full-thickness subscapularis tear. The lift-off, internal rotation lag sign, belly-press, and bear-hug tests show internal rotation strength deficit.
Figure A depicts an abnormal belly-press examination whereby the wrist flexes, and the elbow will fall posteriorly as the patient recruits the posterior deltoid to compensate for lack of the subscapularis. Illustration B demonstrates a normal belly-press examination. Illustration C shows a normal lift off test.
Incorrect Answers:
1: Jerk Test is positive if there is a 'clunk' or pain with the maneuver and is associated with posterior labral pathology. 2: Wright's test is where the shoulder is passively externally rotated and abducted while the patient turns their neck away from the tested extremity. It is a test for thoracic outlet syndrome. 4: Jobe's test is positive with supraspinatus weakness and or impingement. 5: Hornblower's test is positive if the arm falls into internal rotation. It may represent teres minor pathology.
Question 53
Figures 11a and 11b show the clinical photograph and radiograph of a newborn. Based on these findings, what is the best course of action?
Explanation
REFERENCES: Heyman CH, Herndon CH, Heiple KG: Congenital posterior angulation of the tibia with talipes calcaneus. J Bone Joint Surg Am 1959;41:476-488.
Hofmann A, Wenger DR: Posteromedial bowing of the tibia: Progression of discrepancy in leg lengths. J Bone Joint Surg Am 1981;63:384-388.
Question 54
A 34-year-old woman who is a professional skier (Figure 42)
Explanation

Question 55
Figure 1 shows the radiograph of a 71-year-old man who has had increasing pain and weakness in his shoulder for the past 3 years. Nonsurgical management has failed to provide relief. Examination shows 130 degrees of active forward flexion and intact external rotation strength. During surgery, a 1- x 1-cm rotator cuff tear involving the supraspinatus is encountered. Treatment should include
Explanation
REFERENCES: Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for treatment of defects in the rotator cuff and surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491.
Question 56
A diskectomy is performed in which the disk space is not aggressively debrided. When compared to techniques that involve aggressive debridement of the disk space, this results in
Explanation
This patient has disk herniation at the left L5-S1 level. This will generally affect the traversing S1 nerve. The S1 dermatome is on the lateral aspect and sole of the foot.
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183. View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
Question 57
A 14-year-old patient with an L3 myelomeningocele underwent anterior and posterior spinal fusion for a curve of 50°. Follow-up examination 1 week after the procedure now reveals persistent drainage from the posterior wound. Results of laboratory cultures show Streptococcus viridans, Staphylococcus aureus, and Enterococcus. In addition to IV antibiotics, surgical irrigation, and debridement, management should include
Explanation
REFERENCES: Lonstein JE: Complications of treatment, in Bradford DS, Lonstein JE, Moe JH, et al (eds): Moe’s Textbook of Scoliosis and Other Spinal Deformities, ed 2. Philadelphia, Pa, WB Saunders, 1987, p 476.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 713-721.
Question 58
An otherwise healthy 25-year-old man underwent a right anterior cruciate ligament reconstruction with a bone-patellar tendon-bone allograft. Routine preimplantation cultures of the allograft taken by the surgeon were positive for coagulase-negative Staphylococcus 5 days postoperatively. The patient has exhibited no evidence of clinical infection and his postoperative course has been uncomplicated during this time. What is the ideal management of this patient?
Explanation
implanted with a "contaminated" graft develop a clinical infection. The results of the current literature suggest that the treatment of low-virulence organisms is unnecessary if no evidence of clinical infection exists. Preimplantation cultures do not appear to correlate with clinical infection. Therefore, the routine culture of allograft tissue is not recommended.
Question 59
A 21-year-old man who underwent repair of a distal biceps tendon rupture using a two-incision approach 4 months ago now reports difficulty gaining rotation of his forearm. Figures 49a and 49b show the AP and lateral radiographs. What is the most likely cause of his problem?
Explanation
REFERENCES: Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed. 2. Philadelphia, PA, WB Saunders, 1993, pp 492-503.
Failla JM, Amadio PC, Morrey BF, Beckenbaugh RD: Proximal radioulnar synostosis after repair of distal biceps brachii rupture by the two-incision technique: Report of four cases. Clin Orthop 1990;253:133-136.
Question 60
A 10-year-old boy with an L1 myelomeningocele has a low-grade fever and a swollen thigh that is warm to touch and erythematous. AP and lateral radiographs are shown in Figures 24a and 24b. Management should consist of
Explanation
REFERENCES: Lock TR, Aronson DD: Fractures in patients who have myelomeningocele. J Bone Joint Surg Am 1989;71:1153-1157.
Kumar SJ, Cowell HR, Townsend P: Physeal, metaphyseal, and diaphyseal injuries of the lower extremities in children with myelomeningocele. J Pediatr Orthop 1984;4:25-27.
Question 61
below depict the radiographs obtained from a year-old woman who comes to the emergency department after experiencing a fall. She is an unassisted community ambulator with a history of right hip pain. What is the most appropriate surgical treatment for this fracture?
Explanation
This patient has pre-existing right hip osteoarthritis. The most correct option for the treatment of this active patient is a right total hip arthroplasty. Hemiarthroplasty would not address the patient's pain from osteoarthritis, and open reduction and internal fixation would not fix the femoral head issue or the
osteoarthritis.
Question 62
A 13-year-old girl sustained an isolated midshaft left femoral fracture in a motor vehicle accident. The fracture was treated with a rigid, antegrade intramedullary nail placed through the piriformis fossa. The fracture healed uneventfully, as shown in Figure 46a; however, at 12 months postoperatively she now reports left hip pain. A current AP radiograph and MRI scan are shown in Figures 46b and 46c. What complication occurred in this patient? Review Topic

Explanation
Question 63
Familial (Leiden) thrombophilia is of importance in joint arthroplasty because of an abnormality in the clotting cascade. Which of the following statements best describes the condition?
Explanation
Question 64
Which of the following lesions is best suited for autologous chondrocyte implantation?
Explanation
REFERENCES: Mandelbaum BR, Brown JE, Fu F, et al: Articular cartilage lesions of the knee. Am J Sports Med 1998;26:853-861.
Minas T, Nehrer S: Current concepts in the treatment of articular cartilage defects. Orthopedics 1997;20:525-538.
Brittberg M, Lindahl A, Nilsson A, Ohlsson C, Isaksson O, Peterson L: Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 1994;331:889-895.
Question 65
ofhat parameter is most commonly used to estimate the maximum tension a muscle can generating?
Explanation
The concept of physiologic cross section of a muscle from Weber and Fick, identifies the critical importance of the cross sectional area of all the fibers of a muscle as proportional to maximum tension. (Relationship between muscle size and muscle strength).
Question 66
An active, right-handed 71-year-old woman fell on her left shoulder and sustained the injury shown in the radiographs in 52a and 52b and the CT scan in 52c. Management should consist of
Explanation

Question 67
A 40-year-old man fell 10 feet from a tree and sustained the closed isolated injury shown in Figures 35a and 35b. Management consists of splinting. At his 2-week follow-up visit, he clinically passes the wrinkle test. He agrees to open reduction and internal fixation. What is the best surgical approach to obtain anatomic reduction and limit wound dehiscence?
Explanation
REFERENCES: Borrelli J Jr, Lashgari C: Vascularity of the lateral calcaneal flap: A cadaveric injection study. J Orthop Trauma 1999;13:73-77.
Freeman BJC, Duff S, Allen PE, et al: The extended lateral approach to the hindfoot: An anatomical basis and surgical implications. J Bone Joint Surg Br 1998;80:139-142.
Zwipp H, Tscherne H, Wulker N: Osteosynthesis of dislocated intra-articular calcaneus fractures. Unfallchirurg 1988;91:507-515.
Question 68
A 55-year-old male sustained the injury in Figure A. His injury was complicated by an acute compartment syndrome. He underwent external fixation of his extremity and four compartment fasciotomy. When should the treatment shown in Figure B be performed to minimize the risk of infection?

Explanation
Question 69
What is the most common cause of mechanical failure of an orthopaedic biomaterial during clinical use?
Explanation
REFERENCES: Lewis G: Fatigue testing and performance of acrylic bone-cement materials: State-of-the-art review. J Biomed Mater Res Br 2003;66:457-486.
Stolk J, Verdonschot N, Huiskes R: Stair climbing is more detrimental to the cement in hip replacement than walking. Clin Orthop 2002;405:294-305.
Wright TM, Maher SA: Biomaterials, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 70
A 25-year-old man is brought to the emergency department following a motor vehicle accident. Extrication time was 2 hours, and in the field he had a systolic blood pressure by palpation of 90 mm Hg. Intravenous therapy was started, and on arrival in the emergency department he has a systolic blood pressure of 90 mm Hg with a pulse rate of 130. Examination reveals a flail chest and a femoral diaphyseal fracture. Ultrasound of the abdomen is positive. The trauma surgeons take him to the operating room for an exploratory laparotomy. At the conclusion of the procedure, he has a systolic pressure of 100 mm Hg with a pulse rate of 110. Oxygen saturation is 90% on 100% oxygen, and he has a temperature of 95.0° F (35° C). What is the recommended treatment of the femoral fracture at this time?
Explanation
REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopaedic surgery. J Trauma 2002;53:452-461.
Bosse M, Kellam JF: Orthopaedic decision making in the multiple trauma patient, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 133-146.
Question 71
Figure 20 shows the MRI scan of a 20-year-old athlete who has a painful shoulder. This pathology is most commonly seen in
Explanation
REFERENCES: Misamore GW, Facibene WA: Posterior capsulorrhaphy for the treatment of traumatic recurrent posterior subluxations of the shoulder in athletes. J Shoulder Elbow Surg 2000;9:403-408.
Mair SD, Zarzour RH, Speer KP: Posterior labral injury in contact athletes. Am J Sports Med 1998;26:753-758.
Question 72
Figure 33 shows the MRI scan of a 55-year-old woman who has had a 6-week history of back and leg pain. Which of the following clinical scenarios is most consistent with the MRI scan findings at L4-L5? Review Topic
Explanation
Question 73
A 45-year-old woman awakens with the acute onset of burning left shoulder pain that radiates toward the axilla. She denies any history of trauma. On examination, she is unable to abduct her arm but has full passive shoulder motion. Her sensation is intact. Cervical spine examination reveals full range of motion and a negative Spurling’s test. Radiographs and MRI studies are normal for the cervical spine and shoulder. What is the most likely diagnosis?
Explanation
REFERENCES: Misamore GW, Lehman DE: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg Am 1996;78:1405-1408.
McCarty EC, Tsairis P, Warren RF: Brachial neuritis. Clin Orthop Relat Res 1999;368:37-43.
Question 74
A 16-year-old female dancer has persistent posterior ankle pain, particularly after a vigorous dancing schedule. Examination reveals tenderness both posteromedially and posterolaterally. MRI scans are seen in Figures 44a and 44b. What is the most likely diagnosis?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont IL, American Academy of Orthopaedic Surgeons, 1998, pp 315-332.
Hamilton WG, Hamilton LH: Foot and ankle injuries in dancers, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1225-1256.
Question 75
What is the advantage of percutaneous pedicle screw fixation over open instrumentation and fusion for a thoracolumbar burst fracture without neurologic deficit?
Explanation
A prospective randomized study on short-segment treatment of burst fractures with and without fusion demonstrated similar outcomes at 5 years with lower blood loss in the nonfusion group. There is by definition no fusion performed with percutaneous stabilization, so patients often develop hardware failure. Some surgeons routinely remove instrumentation following percutaneous stabilization, thus revision surgery is common. Clinical outcomes are not improved compared to open methods.
RECOMMENDED READINGS
Koreckij T, Park DK, Fischgrund J. Minimally invasive spine surgery in the treatment of thoracolumbar and lumbar spine trauma. Neurosurg Focus. 2014;37(1):E11. doi: 10.3171/2014.5.FOCUS1494. Review. PubMed PMID: 24981899. View Abstract at PubMed Jindal N, Sankhala SS, Bachhal V. The role of fusion in the management of burst fractures of the thoracolumbar spine treated by short segment pedicle screw fixation: a prospective randomised trial. J Bone Joint Surg Br. 2012 Aug;94(8):1101-6. doi: 10.1302/0301-620X.94B8.28311. PubMed PMID: 22844053. View Abstract at PubMed
Dai LY, Jiang LS, Jiang SD. Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures. a five to seven-year prospective randomized study. J Bone
Joint Surg Am. 2009 May;91(5):1033-41. doi: 10.2106/JBJS.H.00510. PubMed PMID:
Question 76
When comparing arthroscopic lavage and knee debridement with placebo in patients with chronic symptomatic osteoarthritis, what outcome has been demonstrated?
Explanation
Excluding a diagnosis of meniscal tear, loose body, or mechanical derangement, treating knee osteoarthritis of indeterminate cause with arthroscopic lavage and debridement has been found to provide no discernable benefit to offset the risk of surgery. The effects of arthroscopy have not been clinically significant in the vast majority of patient-oriented outcomes measures for pain and function at multiple
times between 1 week and 2 years after surgery.
Question 77
Figures 31a and 31b show the radiograph and MRI scan of an otherwise normal 3-month-old infant who has a spinal deformity. MRI reveals no intraspinal anomalies. What is the next step in management? Review Topic
Explanation
Question 78
A 7-year-old boy has had chronic left leg pain that is worse at night but is not activity related. Use of nonsteroidal anti-inflammatory drugs for the past 6 months has failed to provide relief. A CBC count with differential, erythrocyte sedimentation rate, and C-reactive protein are within normal limits. Radiographs and a CT scan are shown in Figures 31a through 31c. Management should consist of
Explanation
REFERENCES: Donahue F, Ahmad A, Mnaymneh W, Pevsner NH: Osteoid osteoma: Computed tomography guided percutaneous excision. Clin Orthop 1999;366:191-196.
Rosenthal DI, Hornicek FJ, Wolfe MW, et al: Percutaneous radiofrequency coagulation of osteoid osteoma compared with operative treatment. J Bone Joint Surg Am 1998;80:815-821.
Question 79
In a patient who has undergone fusion with instrumentation from T4 to the sacrum for adult scoliosis, at which site is a pseudarthrosis most likely to be discovered?
Explanation
REFERENCES: Saer EH III, Winter RB, Lonstein JE: Long scoliosis fusion to the sacrum in adults with nonparalytic scoliosis: An improved method. Spine 1990;15;650-653.
Kostuik JP, Hall BB: Spinal fusions to the sacrum in adults with scoliosis. Spine
1983;8:489-500.
Balderston RA, Winter RB, Moe JH, et al: Fusion to the sacrum for nonparalytic scoliosis in the adult. Spine 1986;11:824-829.
Question 80
The patient is given a blood transfusion. After starting the transfusion, nurses note that her temperature is 38.8°C and she has shaking and chills. What is the most likely cause of this problem?
Explanation
Blood management and venous thromboembolism prevention are important considerations in the perioperative management of THA. Recommendations now focus on presurgical optimization of hemoglobin, use of antifibrinolytics intrasurgically, and minimized use of transfusions. Current recommendations do not favor autologous blood donation for patients with hemoglobin levels higher than 13 g/dL. There is a move toward increased use of aspirin for venous thromboembolism prophylaxis, but this modality can cause GI bleeding that may necessitate blood transfusion. Transfusion reactions are rare, and the most common cause is administration of an incompatible unit because of clerical error.
Question 81
An elderly patient falls and sustains an extension injury to the neck that results in upper extremity weakness, spared perianal sensation, and lower extremity spasticity. These findings best describe what syndrome?
Explanation
motor function.
REFERENCES: Apple DF Jr: Spinal cord injury rehabilitation, in Rothman RH, Simeone FA (eds): The Spine, ed 3. Philadelphia, PA, WB Saunders, 1992, Chapter 31.
Leventhal MR: Fractures, dislocations and fracture-dislocations of spine, in Crenshaw AH (ed): Campbell’s Operative Orthopaedics, ed 8. St. Louis, MO, Mosby, 1992.
Question 82
The most favorable outcomes from release of the tarsal tunnel are in patients who have which of the following findings?
Explanation
REFERENCES: Beskin JL: Nerve entrapment syndromes of the foot and ankle. J Am Acad Orthop Surg 1997;5:261-269.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Question 83
From which artery does the princeps pollicis artery branch?
Explanation
The princeps pollicis artery can be located on the palmar aspect of the adductor pollicis and emerges into the subcutaneous tissue at the thumb metacarpophalangeal flexion crease. It branches from the radial artery just distal to the location of the deep palmar arch.
RECOMMENDED READINGS
Coleman SS, Anson B: Arterial patterns in the hand based on a study of 650 specimens. Surg Gynec Obstet 1961;4:409-424.
Ames EL, Bissonnette M, Acland R, Lister G, Firrell J. Arterial anatomy of the thumb. 78 J Hand Surg Br. 1993 Aug;18(4):427-36. PubMed PMID: 8409651. View Abstract at PubMed
Question 84
Flow cytometry of tumors measures the
Explanation
Question 85
A 17-year-old pitcher reports pain over the medial aspect of the elbow that occurs during the acceleration phase of throwing, and it prevents him from throwing at the velocity needed to be competitive. What structure is most likely injured in this patient? Review Topic
Explanation
Question 86
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals no other injuries. Radiographs are shown in Figures 35a and 35b. Initial management of this fracture should consist of
Explanation
REFERENCES: Meyers MH, McKeever FM: Fractures of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60
Janarv PM, Westblad P, Johansson C, Hirsch G: Long-term follow-up of anterior tibial spine fractures in children. J Pediatr Orthop 1995;15:63-68.
Kuhn JE, Sailer MJ, Sterett WI, Hawkins RJ: Arthroscopic technique for the treatment of tibial spine fractures in the skeletally immature patient. J Ortho Tech 1995;3:7-12.
Question 87
Excision of heterotopic bone about the forearm or elbow can be done with limited recurrence rates as early as which of the following after initial injury?

Explanation
The referenced study by McAuliffe et al is a retrospective review of heterotopic ossification (HO) about the elbow followed by 100 cGY (5 fractions over 1 week) of XRT as early as 3 months post-injury. They were able to achieve an average arc of motion > 100 degrees.
The other referenced study by Beingessner et al is a review of HO excision of the forearm. They found that excision and XRT, followed by 6 weeks of indomethacin, led to an increase of forearm motion from an average of 17 degrees to 136 degrees when the excision was done at 4 months post-injury.
Question 88
Thyroid hormone regulates skeletal growth at the physis by stimulation of
Explanation
REFERENCES: Ballock RT: Regulation of skeletal growth and maturation by thyroid hormone, in Buckwalter JA, Ehrlich MG, Sandell LJ, Trippel SB (eds): Skeletal Growth and Development: Clinical Issues and Basic Science Advances. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1998, pp 301-317.
Rosier RN, O’Keefe RJ, Reynolds PR, Hicks DG, Puzas JE: Expression and function of TGF-b= and PTHrP in the growth plate, in Buckwalter JA, Ehrlich MG, Sandell LJ, Trippel SB (eds): Skeletal Growth and Development: Clinical Issues and Basic Science Advances. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1998, pp 285-299.
Trippel SB: IGF-I and FGF-2 in growth plate regulation, in Buckwalter JA, Ehrlich MG, Sandell LJ, Trippel SB (eds): Skeletal Growth and Development: Clinical Issues and Basic Science Advances. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1998, pp 263-283.
Question 89
Figures 27a through 27c show the AP radiograph, MRI scan, and biopsy specimen of an otherwise healthy man who has a painful wrist. Serum chemistry studies are normal. What is the most likely diagnosis?
Explanation
REFERENCE: Vander Griend RA, Funderburk CH: The treatment of giant-cell tumors of the distal part of the radius. J Bone Joint Surg Am 1993;75:899-908.
Question 90
What mechanism of injury is most likely to cause a fracture of the anteromedial facet of the coronoid?
Explanation
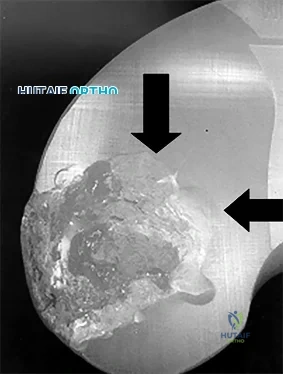
(SBQ12TR.86) Figure A shows intraoperative radiographs of a 45-year-old patient with a left elbow injury. What would be the next most appropriate step in this patients care?

Early range of motion
Hinged elbow brace for 4 weeks
Repair lateral collateral ligament
Remove and upsize implant
Remove and downsize implant
The intraoperative images are consistent with overstuffing of the ulnohumeral joint during a radial head replacement. The most appropriate next step would be removing and downsizing the implant.
Overstuffing the radiohumeral joint by >2.5 mm can significantly alter elbow kinematics. It has also shown to lead to pain and early joint disease. The most sensitive method to assess for overstuffing of the joint is by direct visualisation intraoperatively. This can be performed by visualising the lateral aspect of the ulnohumeral joint when the radial head is resected and comparing this to when the trial radial head is reduced in place. In comparison, radiographic asymmetry of the medial ulnohumeral joint has been shown to be less sensitive. Radiographic findings of incongruity of ulnohumeral joint only occurs when significant overlengthening of the radius occurs.
Frank et al. examined the effect of radial head thickness in seven cadaver specimens. They found that incongruity of the medial ulnohumeral joint would only become apparent radiographically after overlengthening of the radius by >or=6 mm.
Doornberg et al. examined seventeen computed tomography scans of the elbow to investigate the height of the radial head relative to the lateral edge and central ridge of the coronoid process. They found that the radial head was on average only 0.9 mm more proximal than the lateral edge of the coronoid process.
Figure A shows intraoperative radiographs of a patient that has undergone a radial head arthroplasty. There is significant widening of the medial ulnohumeral joint on an AP radiograph as well as widening of the ulnohumeral joint on the lateral radiograph,
Incorrect Answers:
Question 91
Giant cell tumors of bone can occur in many different areas throughout the body. All of the following are common locations for giant cell tumors of bone EXCEPT?
Explanation
Giant cell tumors are one of the more common tumors in young adults 22-40 years of age. There is much argument as to whether giant cell tumors arise in the metaphysis or the epiphysis, but most authors agree that giant cell tumors are very uncommon in the diaphysis. The most common sites of giant cell tumors in bone, which are the distal radius, sacrum, distal femur, proximal tibia and proximal humerus. Treatment typically involves intralesional curettage with adjuvant treatment (e.g., phenol, hydrogen peroxide, argon beam, etc).
Williams et al undertook a prospective study to evaulate the recurrence rate of giant cell tumors of the hand and they found that soft tissue extension of the tumor significantly increased the rate of local recurrence. This finding is significant because multiple previous studies have demonstrated similar higher recurrence rates for giant cell tumors with soft tissue extension in other areas like around the knee and the distal radius.
Illustration A are radiographs classic for a giant cell tumor showing a large lytic metaphseal-epiphyseal lesion in the distal femur. Illustration B is an axial CT of the distal femur showing the lytic giant cell tumor, abutting and fracturing the subchondral bone. Illustration C is histology classic for a giant cell tumor where the nuclei of the multi-nucleated giant cells look identical to the nuclei of the stromal cells.
Incorrect Answers:


What is the most appropriate treatment for a 65-year-old female with a 100-pack-year tobacco history who presents with a new painful lytic lesion in her femoral diaphysis?
Antegrade femoral nailing with reamings sent to pathology for analysis
Antegrade femoral nailing with adjuvant radiotherapy to the lesion 3
. Minimally invasive plating of the femur for stabilization and open cementation of the lesion
Referral to medical oncology for chemo-radiotherapy
Lesion biopsy with further treatment based on the results of the biopsy
New lesions which are not diagnosed by imaging and require surgical intervention need to have an appropriate biopsy with treatment dictated by the results of the biopsy. While this patient has a significant tobacco history, incorrect treatment of this lytic bone lesion could affect both her overall morbidity and mortality. As an example, a lytic high-grade chondrosarcoma may look exactly like a metastatic lesion but requires wide surgical excision, not just stabilization of an impending pathological fracture. Intramedullary nailing of a chondrosarcoma would spread the tumor the entire length of the bone and likely require a major amputation, not a limb salvage operation.
A 14-year-old child is referred to your office for evaluation of a tibia lesion found incidentally after a minor ankle injury. A radiograph of the child's ankle is shown in Figure A. What treatment do you suggest?

Endocrine consultation secondary to associated endocrine abnormalities
Surgical consultation secondary to associated gastrointestional cancers
Short leg cast and non-weight bearing for a minimum of 6 weeks
Open biopsy and tumor staging
Routine followup of tibial lesion
The radiograph is classic for a non-ossifying fibroma given the classic eccentric position, sclerotic margin, and benign appearance. Other than routine followup for the tibial lesion, this child requires no subsequent treatment. Marks and Bauer review the diagnosis, imaging, and treatment of many different fibrous tumors of bone and review the diagnostic imaging criteria specific to each subclass of bony fibrous tumors.
The chromosomal translocation t(X;18)is found in which of the following conditions?
Myxoid liposarcoma
Synovial Sarcoma
Osteosarcoma
Ewing's Sarcoma
Clear cell sarcoma
Synovial sarcoma is a rare soft tissue sarcoma with biphasic features of both spindle cell and epithelial differentiation. Synovial sarcoma is a rare high-grade tumor that spreads along fascial planes and, thus, can be much more widespread than apparent on initial evaluation. Males are more commonly affected than females with a ratio of 1.1:1. Synovial sarcoma is characterized by a specific chromosomal translocation t(X;18)(p11;q11) that is observed in more than 90% of cases. The t(X;18)(p11;q11) translocation fuses the SYT gene from chromosome 18 to either of 2 homologous genes at Xp11, either SSX1 or SSX2. The fusion proteins SYT-SSX1 and SYT-SSX2 function as aberrant transcriptional regulators, resulting in either activation of protooncogenes or inhibition of tumor suppressor genes.
Kawai et al found that SYT-SSX fusion transcripts are a defining diagnostic marker of synovial sarcomas. These fusion transcripts may yield important independent prognostic information and provide important information for different types of treatment.
Incorrect Answers
Question 92
A 44-year-old man sustains the injury shown in Figures 1 through 3. What is the most appropriate treatment?

Explanation
Reduction, either open or closed, with internal fixation (pinning) is the recommended treatment for the majority of these injuries. Closed reduction with pinning is most often performed for acute injuries. Open reduction with pinning is performed for those injuries that cannot be reduced by closed means or those with a delayed presentation. Four cases of successful closed reduction and splinting, all performed upon presentation in the emergency department, have been described by Storken and associates, but the authors note that their review of three prior reports uncovered cases of secondary dislocation, which required surgical stabilization. One of the dislocations occurred 4 months after the reduction. They assert that an indication for primary ORIF is a CMC dislocation associated with major fractures. Primary arthrodesis can be considered in cases with severe intra-articular comminution, but this procedure substantially limits the ability of the hand to increase and decrease the transverse metacarpal arch, which is an important functional movement. It can also lead to osteoarthritis of the triquetrohamate joint. Suspension arthroplasty has been described for old fracture-dislocations of the fifth CMC joint, using a partial slip of the extensor carpi ulnaris.








Question 93
Which of the following characteristics is seen in patients with osteochondritis dissecans of the elbow? Review Topic
Explanation
Question 94
CLINICAL SITUATION Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. This knee injury is best described as a

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair, but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 95
A 56-year-old woman underwent a total knee arthroplasty 2 years ago and now has pain and swelling. Radiographs of her knee are unremarkable. Her C-reactive protein (CRP) level is 3.0 (reference range [rr], 0.08–3.1 mg/L), and her erythrocyte sedimentation rate (ESR) is 18 mm/h (rr, 0-20 mm/h). Aspiration of the knee reveals a white blood cell (WBC) count of 1200/mm3 with a differential of 30% neutrophils and 70% monocytes. Cultures will not be available for several days, and the patient has not been taking antibiotics. Based on these findings, the most appropriate next step is
Explanation
ESR and CRP level are recommended as starting points in the workup for the diagnosis or exclusion of periprosthetic joint infection (PJI). When both the ESR and CRP findings are within defined limits, PJI is unlikely. When both test findings are positive, PJI must be considered and further investigation is warranted. Clinicians need to be aware of other inflammatory conditions such as rheumatoid arthritis that can lead to elevation of inflammatory markers.
A high likelihood of infection is noted when the knee aspirate contains more than 2500 WBCs per high-powered field (HPF) with a differential count exceeding 60% neutrophils. Using these criteria, Mason demonstrated a sensitivity of 98% and a specificity of 95% for infection diagnosis.
For this patient, the inflammatory markers are within normal limits. The aspiration result is below 2500 WBC/HPF with a low percentage of neutrophils. The likelihood of infection is remote, and further nonsurgical treatment should not include antibiotics. There is no indication for surgery based upon the information presented.

Question 96
Which examination finding points toward a brachial plexus injury rather than root avulsion?
Explanation
A brachial plexus injury distal to the root level should leave the rhomboid muscle with intact function. Root avulsions of C5-6 will cause weakness of the rhomboids. The branching of the dorsal scapular nerve is proximal and often spared with upper brachial plexus injuries. Winging and biceps weakness may occur
with either injury, and an ipsilateral fracture does not differentiate an avulsion from a brachial plexus injury.
Question 97
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk? Review Topic
Explanation
(SBQ13PE.27) A 15-year-old male patient presents requesting clearance to perform in the Special Olympics. He has had abnormal facies, has had mental developmental delay and cytogenetic analysis confirmed abnormalities on chromosome 21. Orthopaedically, he has been treated in the past for an elbow dislocation as well as bilateral patellar dislocation. He has already visited his cardiologist and endocrinologist and has been cleared. He has no complaints, denies any pain, difficulties with walking and reports that his training has been going well. What is the next best step? Review Topic
With a normal physical exam, patient can be cleared for participation
MRI bilateral knees and elbow to ensure no ligamentous injury
Referral to a neurologist for clearance
Lateral cervical spine flexion and extension radiographs
AP pelvis radiograph
Ruling-out C1-C2 instability with flexion/extension radiographs is necessary prior to any spine surgery or participation in sports in patients with Down's Syndrome.
Patients with Down's Syndrome typically present with generalized ligamentous laxity and decreased tone. Thus, dislocations (elbow or patella) along with asymptomatic instability in the cervical spine can commonly occur. Imaging analysis is necessary prior to sports participation.
McKay et al. performed a systematic review to summarize all congenital causes of cervical instability. They found in Down's patients, cervical instability due to ligamentous laxity is found mostly at C1-2. They recommend asymptomatic patients
with an ADI <4.5mm can resume unrestricted activities, while asymptomatic patients between 4.5-10mm should not participate in contact sports. With ADI >10mm OR symptoms/cord changes on MRI, surgery is recommended. Symptomatic patients with ADI between 4.5-10mm should be observed with activity restriction.
Dedlow et al. outlines the most recent 2011 update and guidelines for cervical instability in Down's syndrome patients. One of the major highlighted changes is the emphasis placed on radiographic re-examination, regardless of prior clearance. Re-examination should occur prior to participation in sports and/or the onset of new symptoms.
Illustrations A, B and C highlight the C1-2 instability on flexion-extension lateral radiographs. Careful attention can be placed on the relationship of the anterior arch of C1 and the dens (Illustration C). This allows for the measurements of ADI and the space available for the cord (SAC), which is highlighted in Illustration D.
Incorrect answers:
Question 98
A 24-year-old man is involved in a motor vehicle accident at 60 mph. He sustains multiple injuries including an intra-abdominal injury requiring a splenectomy and a closed right femoral shaft fracture. Which variable will best indicate the patient's resuscitation status when deciding whether to proceed with definitive care of the fracture at the conclusion of the laparotomy? Review Topic
Explanation
Question 99
A 38-year-old man reports right upper extremity pain that radiates from his neck to his anterior arm, dorsoradial forearm, and into the index finger. Examination reveals weakness of the biceps muscle group and loss of his brachioradialis reflex on that side. At which level is he most likely to have a right-sided cervical disk protrusion on an MRI scan? Review Topic 1 C4-C5 2 C5-C6 3 C6-C7
Explanation
Question 100
A 30-year-old patient has acetabular dysplasia and moderate secondary osteoarthrosis. Which of the following studies will best help predict the success of periacetabular osteotomy?
Explanation
REFERENCE: Murphy S, Deshmukh R: Periacetabular osteotomy: Preoperative radiographic predictors of outcome. Clin Orthop 2002;405:168-174.
