Full Question & Answer Text (for Search Engines)
Question 1:
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure A. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion? Review Topic
Options:
- Total elbow arthroplasty
- Open reduction and internal fixation
- Radial head arthroplasty
- Sling and swathe
- Bone stimulator
Correct Answer: Total elbow arthroplasty
Explanation:
Total elbow arthroplasty has become the treatment of choice for complex, comminuted distal humeral fractures in patients older than age 70 years. It yields a faster recovery with more predictable functional outcomes, although limitations of lifting weight of more than 5 pounds must be followed to avoid loosening.
Question 2:
A soccer player who sustained a twisting injury to the right ankle while making a cut is unable to bear weight and has diffuse tenderness over the anterior and lateral aspects of the ankle. Examination also shows a positive squeeze test. Plain radiographs and a stress radiograph are shown in Figures 26a through 26c. Radiographs of the leg and knee are normal. What is the most appropriate management?
Options:
- Short leg non-weight-bearing cast for 6 weeks
- Air-stirrup splint and limited activity in 3 to 6 weeks
- Air-stirrup splint and resumption of activities as tolerated
- Immediate repair of the peroneal retinaculum
- Immediate reduction and placement of a syndesmotic screw
Correct Answer: Immediate reduction and placement of a syndesmotic screw
Explanation:
DISCUSSION: The mechanism of injury, physical examination, and radiographs indicate a “high” ankle sprain with disruption of the distal tibiofibular ligaments and interosseous membrane. These injuries typically involve pronation and external rotation forces. In addition, recovery is significantly delayed, often requiring 6 to 8 weeks to heal. Radiographs obtained months after recovery often show calcification within the distal syndesmosis, which is not typically symptomatic. This patient has gross instability, resulting in a high incidence of chronic diastasis and subluxation leading to impaired function. Treatment should consist of reduction and stabilization with a transsyndesmotic screw because this injury demonstrates a widened syndesmosis.
REFERENCES: Boytim MJ, Fisher DA, Neumann L: Syndesmotic ankle sprains. Am J Sports Med 1991;19:294-298.
Miller CD, Shelton WR, Barrett GR, et al: Deltoid and syndesmosis ligament injury of the ankle without fracture. Am J Sports Med 1995;23:746-750.
Question 3:
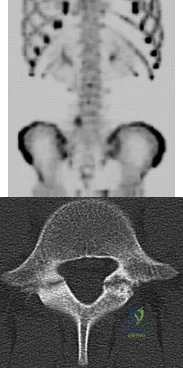
In a patient with vertebral tuberculosis, which of the following characteristics is most predictive of progression of the kyphosis?
Options:
- Involvement of the vertebral body and posterior elements
- Involvement of the thoracic vertebrae
- Involvement of the lumbar vertebrae
- Age of the patient
- Pretreatment degree of kyphosis
Correct Answer: Involvement of the vertebral body and posterior elements
Explanation:
DISCUSSION: In patients with vertebral tuberculosis, involvement of the anterior and posterior elements creates an instability and severe kyphotic collapse can occur. This characteristic has been shown to have a stronger association than level of involvement, age, or pretreatment degree of deformity. In the absence of instability, anterior growth can resume after treatment, leading to a decrease in the deformity.
REFERENCES: Rajasekaran S: The natural history of post-tubercular kyphosis in children: Radiological signs which predict late increase in deformity. J Bone Joint Surg Br
2001;83:954-962.
Rajasekaran S, Shanmagasundaram TK, Prabhakar R, Dheenadhayalan J, Shetty AP, Shetty DK: Tuberculous lesions of the lumbosacral region: A 15-year follow-up of patients treated by ambulant chemotherapy. Spine 1998;23:1163-1167.
Question 4:
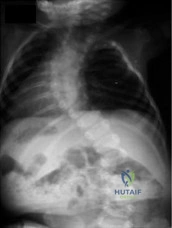
Figure below shows the radiograph obtained from a 68-year-old man who fell 3 weeks after undergoing a successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?
Options:
- Open reduction and internal fixation (ORIF) of the fracture
- Removal of the current stem, femur ORIF, and insertion of a longer revision stem
- Femur ORIF with cables and strut graft, leaving the current stem in situ
- Femur ORIF combined with reimplantation of the primary component
Correct Answer: Removal of the current stem, femur ORIF, and insertion of a longer revision stem
Explanation:
DISCUSSION:
The fracture has occurred around the stem, representing a Vancouver type B fracture, and the stem is clearly loose, making it a type B2 fracture. The appropriate treatment is removal of the loose in situ stem; ORIF of the femur using cerclage wires, cables, or a plate; and insertion of a longer revision stem such as a tapered fluted modular titanium or fully porous coated cylindrical stem to bypass the fracture. All of the other options are incorrect, because they represent inappropriate treatment options for a Vancouver type B2 fracture.
Question 5:
- Which of the following shoulder girdle muscles is most active during forward flexion?
Options:
- Biceps
- Trapezius
- Infraspinatus
- Pectoralis major
- Serratus anterior
Correct Answer: Serratus anterior
Explanation:
The percentage of recorded EMG activity indicates the level of activity of a given muscle but does not indicate the force generated. During forward elevation, the upper portion of the trapezius, levator scapulae, and serratus anterior contract to produce a scapular rotating force upward, increasing the stability of the glenohumeral joint. The essential muscles for forward elevation are the deltoid, the supraspinatus, the trapezius and the serratus anterior. EMG reveals the serratus to be most active.
Question 6:
What muscle is most often encountered during surgical approaches to C5-6?
Options:
- Omohyoid
- Cricohyoid
- Splenius capitus
- Thyrohyoid
- Posterior digastric
Correct Answer: Omohyoid
Explanation:
DISCUSSION: The omohyoid muscle crosses the surgical field from inferior lateral to anterior superior traveling from the scapula to the hyoid bone and may need to be transected. The posterior digastric crosses the field as well but higher near C3-4. The other muscles run longitudinally.
REFERENCES: Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-56.
Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.
Question 7:
- A 6-year-old boy sustained a fracture of the medial malleolus as a result of twisting his ankle. The fracture line extends from the joint surface proximally and medially to include a small fragment of the metaphysis, with a displacement of 3 mm. Management should consist of
Options:
- Acceptance of the current position of the ankle
- Open reduction and fixation in the epiphysis only
- ORIF with a small-fragment T-plate from the malleolus up to the metaphysis
- Closed reduction by eversion of the ankle and application of a bivalved long leg cast
- CRUGA and fixation with a malleolar screw from the malleolus into the metaphysis
Correct Answer: Open reduction and fixation in the epiphysis only
Explanation:
Salter-Harris III and IV fractures of the medial aspect of the distal tibia commonly cause growth disturbances, such as shortening and varus angulation, unless an anatomical reduction of the physis is obtained. The authors of the reference (Drs Kling, Bright, and Hensinger) felt that these fractures needed to be “perfectly reduced” to minimize any gap, primarily to prevent a bone bridge from forming. According to Spiegel, any of these fractures with 2 mm or more should be openly reduced.
The authors felt that “anatomical reduction” must include closure of the physeal gap and restoration of rotational alignment of the fracture fragment. They recommended that these fractures be treated with ORIF, consisting of small, smooth Kirschner wires from one epiphyseal fragment to the other. The pins should diverge or converge to prevent any slippage or rotation. They do not recommend crossing the physis with fixation devices, for this may lead to further injury.
Question 8:
When performing a revision total knee arthroplasty, trial components are inserted and the knee is stable in extension and loose in flexion. Which step should be taken to create a stable construct?
Options:
- Insert a constrained tibial insert
- Insert a thicker tibial component
- Insert a larger femoral component
- Augment the distal portion of the femoral component
Correct Answer: Insert a larger femoral component
Explanation:
DISCUSSION
The surgeon is facing a common scenario that occurs in revision knee surgery: a loose flexion gap with an appropriate extension gap. A flexion gap can be tightened by translating the femoral component more posteriorly and using an oversized femoral component. Insertion of a thicker tibial component changes both the flexion and extension gap. Augmentation of the distal femur tightens only the extension gap. A constrained insert would only be indicated if oversizing of the femoral component did not adequately tension the flexion gap.
Question 9:
Figure 61 shows the radiograph of a 28-year-old professional football player who sustained a hyperextension injury to the great toe. He continued to play with pain and loss of push-off strength. What is the most likely diagnosis?
Options:
- Hallux rigidus
- Fracture of the sesamoid
- Disruption of the plantar plate
- Osteonecrosis of the metatarsal head
- Rupture of the flexor hallucis longus
Correct Answer: Disruption of the plantar plate
Explanation:
Upon review of the radiograph give, there is no evidence of fracture or osteonecrosis. Upon review of the article above the most likely diagnosis is “Turf-Toe” or the disruption of the plantar plate. The patient has mechanism of injury, hyperextension and sequelae, decreased push-off strength, which is consistent with this diagnosis. Rupture of the FHL would most likely result in inability to continue playing while hallux rigidus is a potential chronic sequelae with associated dorsal osteophyte formation.
Question 10:
Radiographs of a 12-year-old boy who has knee pain show a 2-cm osteochondral lesion of the lateral aspect of the medial femoral condyle. The fragments are not detached from the femur. Initial management should consist of
Options:
- casting in flexion.
- observation.
- arthroscopic drilling and pinning of the lesion.
- removal and reattachment of the osteochondral lesion.
- allograft transplantation for the lesion.
Correct Answer: casting in flexion.
Explanation:
DISCUSSION: For a pediatric patient without mechanical symptoms, initial management of an osteochondral defect lesion that is not detached should consist of casting in flexion. Failure to respond to several weeks or months of nonsurgical management may warrant surgical treatment.
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 505-520.
Question 11:
Figures 2a and 2b show the clinical photograph and radiograph of a 16-year-old cheerleader who fell on her left lower extremity while performing a pyramid. Following adequate sedation, closed reduction is performed, but an incomplete reduction is noted. What structure is most likely preventing a reduction?
Options:
- Extensor digitorum brevis
- Anterior talofibular
- Posterior tibial tendon
- Anterior tibial tendon
- Peroneus brevis tendon
Correct Answer: Peroneus brevis tendon
Explanation:
DISCUSSION: The stretched peroneus brevis muscle and tendon follow anterior to the fibula and are most likely incarcerated with reduction. The anterior talofibular ligament is too small to prevent reduction of the ankle joint itself. The extensor digitorum brevis originates from the talus; therefore, it is not involved in the tibiotalar joint. The posterior tibial tendon lies medially and would not be interposed into the ankle joint. Similarly, the anterior tibialis tendon also would not be involved.
REFERENCES: Pehlivan O, Akmaz I, Solakoglu C, et al: Medial peritalar dislocation. Arch Orthop Trauma Surg 2002;122:541-543.
Rivera F, Bertone C, De Martino M, et al: Pure dislocation of the ankle: Three case reports and literature review. Clin Orthop 2001;382:179-184.
Question 12:
Treatment consisting of halo vest immobilization is most likely to fail with which of the following cervical injuries? Review Topic
Options:
- C1 lateral mass fracture
- C2 pars fracture
- C4 burst fracture
- C5 burst fracture
- C6-C7 facet fracture-dislocation
Correct Answer: C6-C7 facet fracture-dislocation
Explanation:
Facet joint fracture or dislocation is associated with an increased risk of loss of alignment with halo vest immobilization. The recently published study by van Middendorp and associates confirms the findings of prior studies that facet fracture-subluxations or dislocations are difficult to immobilize with a halo vest due to a limited ability to maintain reduction and alignment. C2 pars fractures, burst fractures, and C1 lateral mass fractures can be managed with halo vest immobilization.
Question 13:
A 46-year-old woman fell from her bicycle and sustained the injury shown in Figure 24. Which of the following ligaments has been disrupted?
Options:
- Acromioclavicular
- Acromioclavicular and coracoclavicular
- Coracoclavicular
- Coracoacromial and sternoclavicular
- Sternoclavicular
Correct Answer: Acromioclavicular and coracoclavicular
Explanation:
DISCUSSION: The radiograph shows a type V acromioclavicular joint injury. Type V injuries involve disruption of the acromioclavicular and coracoclavicular ligaments. Type I injuries involve a sprain of the acromioclavicular joint ligaments. Type II injuries involve disruption of the acromioclavicular joint ligaments; the coracoclavicular ligaments are partially injured. Sternoclavicular ligaments stabilize the medial clavicle and the sternum; they are not damaged with acromioclavicular joint dislocations.
REFERENCES: Fukuda K, Craig EV, An KN, et al: Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Joint Surg Am 1986;68:434-439.
Bosworth B: Complete acromioclavicular dislocation. N Engl J Med 1949;241:221-225.
Question 14:
An 8-year-old boy reports progressive difficulty with walking. Examination reveals muscle weakness, with proximal groups more affected than distal muscles. Deep tendon reflexes are within normal limits. Laboratory studies show a creatine kinase level of 7,200 IU. Based on these findings, what is the most likely diagnosis?
Options:
- Becker muscular dystrophy
- Spinal muscular atrophy, type III
- Emery-Dreifuss dystrophy
- Limb girdle dystrophy
- Guillain-Barre syndrome
Correct Answer: Becker muscular dystrophy
Explanation:
DISCUSSION: Patients with Becker muscular dystrophy have an abnormality in dystrophin, but unlike patients with Duchenne muscular dystrophy, some dystrophin is present. As a result, the progression of muscle weakness is slower, with the diagnosis typically made after age 8 years. Similar to patients with Duchenne muscular dystrophy, patients with Becker muscular dystrophy have pseudohypertrophy of the calves, markedly increased creatine kinase levels, and X-linked transmission of the condition. In addition, these patients are more prone to cardiomyopathy; a condition that should be carefully evaluated if any surgery is required. Patients with spinal muscular atrophy also have proximal muscle weakness, but the onset of weakness occurs earlier in childhood. These patients also have absent deep tendon reflexes and fasciculations, but pseudohypertrophy is absent and creatine kinase levels are normal. Patients with Emery-Dreifuss dystrophy may have a similar clinical picture to Becker’s muscular dystrophy, but pseudohypertrophy is absent and creatine kinase levels are only mildly elevated. In addition, neck extension, elbow flexion, and ankle equinus contractures develop at an early age. Limb girdle dystrophy is a group of progressive muscular dystrophies that is not associated with pseudohypertrophy or a significant elevation of creatine kinase levels. Guillain-Barre syndrome is a condition associated with results from postinfectious demyelination of the peripheral nerve. These patients have the acute onset of weakness, hypotonia, and areflexia; creatine kinase levels are normal.
REFERENCES: Sussman MD: Muscular dystrophy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1573-1583.
Thompson GH, Berenson FR: Other neuromuscular disorders, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, vol 1, pp 633-676.
Question 15:
- A healed fracture of the tibia that demonstrates 25 degrees apex posterior angulation and 28 degrees varus angulation on AP and lateral radiographs is most accurately described as a
Options:
- Complex deformity with an angulation in two planes
- Single deformity less than 20 degrees, apex posterolateral
- Single deformity greater than 30 degrees, apex posterolateral
- Single deformity less than 20 degrees, apex posteromedial
- Single deformity greater than 30 degrees, apex posteromedial
Correct Answer: Single deformity greater than 30 degrees, apex posterolateral
Explanation:
Deformities that are seen simultaneously on the AP and lateral roentgenograms of the same bone are actually shadows of the true deformity. If, for example, angulation is seen at the site of a fracture on both of the standard roentgenograms, then the true plane of angulation is somewhere between the coronal and sagittal planes, and the actual amount of angulation is greater than that visualized on either roentgenogram. Because the standard roentgenograms are orthogonal (at right angles) to each other, it is possible to calculate the actual plane and angle of deformity on the basis of dimensions measured from the roentgenograms.
Question 16:
Figures 32a and 32b show the radiographs of a 13-year-old boy who sustained a fracture while playing football 1 week ago. Management at the time of injury included application of a cast and the use of crutches. A follow-up office visit reveals a normal neurologic examination, and the patient reports no discomfort with the cast and crutches. Management should now include
Options:
- cast wedging in the outpatient clinic.
- closed reduction under anesthesia and application of a new long leg cast.
- reduction and placement of an intramedullary rod.
- anatomic open reduction and compression plating with interfragmentary screws.
- pins and plaster to maintain the reduction.
Correct Answer: cast wedging in the outpatient clinic.
Explanation:
DISCUSSION: Stable fractures and minimally displaced fractures in children can and should be treated by closed methods. Because loss of reduction is common, alignment of tibia fractures must be monitored closely for the first 3 weeks after cast application. This is most easily handled in a cooperative patient by cast wedging. Some children require application of a second cast under general anesthesia 2 to 3 weeks after injury, particularly if the subsidence of swelling has caused the cast to loosen. Surgical indications include the presence of soft-tissue injuries, unstable fracture patterns, fractures associated with compartment syndrome, and the child with multiple injuries. Surgical options in children include percutaneous pins, external fixation, plates and screws, and intramedullary nails.
REFERENCES: Heinrich SD: Fractures of the shaft of the tibia and fibula, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1340-1346.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 583-595.
Question 17:
Which of the following best describes carbohydrate loading?
Options:
- A method of improving the performance of nonendurance athletes
- A technique to improve athletic performance without any deleterious side effects
- Tapering caloric intake along with training the week before an endurance event
- The practice of decreasing training and increasing carbohydrate intake the week before an endurance event
- Dietary manipulation to improve glycogen stores by increasing athletic activity and decreasing carbohydrate intake
Correct Answer: The practice of decreasing training and increasing carbohydrate intake the week before an endurance event
Explanation:
DISCUSSION: Carbohydrate loading is the practice of maximizing glycogen stores by decreasing training and increasing carbohydrate intake the week before an endurance event. Nonendurance athletes do not benefit from this because glycogen depletion is not the limiting factor during a normal competition. Potential side effects of carbohydrate loading are water retention, muscle stiffness, and weight gain.
REFERENCES: Coyle EF, Hagberg JM, Hurley BF, et al: Carbohydrate feeding during prolonged strenuous exercise can delay fatigue. J Appl Physiol 1983;55:230-235.
Costill DL, Sherman WM, Fink WJ, et al: The role of dietary carbohydrates in muscle glycogen resynthesis after strenuous running. Am J Clin Nutr 1981;34:1831-1836.
Sherman WM, Doyle JA, Lamb DR, et al: Dietary carbohydrate, muscle glycogen, and exercise performance during 7 d of training. Am J Clin Nutr 1993;57:27-31.
Question 18:
A 45 year-old woman who has not reached menopause yet falls from a standing height and sustains a distal radius fracture. A DEXA scan reveals a T-score of -2.2. Which of the following treatments is indicated in this patient?
Options:
- 1,700 mg of calcium
- 1,200 mg of calcium
- 1,700 mg of vitamin D
- 1,200 mg of iron
- 1,700 mg of PTH
Correct Answer: 1,200 mg of calcium
Explanation:
The current recommendations for further prevention of any fragility fracture include 1200-1500mg of elemental calcium intake per day and 400-800 IU of vitamin D per day. Of note, these doses are indicated only for prevention and not sufficient for active treatment of osteoporosis (T score less than -2.5).
Medications that are approved by the FDA for active treatment of osteoporosis: alendronate, risedronate, raloxifene, estrogen, calcitonin. These medications and preventative measures help to reduce fragility fractures by as much as 50%.
Freedman et al. performed a retrospective study that looked at a cohort of patients with fragility fractures and then looked at the type and frequency of osteoporosis related interventions. They found that only 60% of patients actually were either prescribed a medication, given a referral, or ordered additional workup (DEXA scan).
Schulman et al. reviewed a series of 80 female patients regarding osteoporosis and bone health, and found that the outpatient sports medicine office setting was an excellent opportunity to educate patients on these topics. The patients' post-education test scores increased significantly after a brief counseling session, and increases in daily calcium intake and exercise levels were also seen.
Question 19:
What type of brace is shown in Figures 22a and 22b?
Options:
- Charcot restraining orthotic walker (CROW)
- University of California Biomechanics Laboratory (UCBL) orthosis
- Double upright ankle-foot orthosis
- Chopart’s prosthesis
- Below-knee prosthesis
Correct Answer: Charcot restraining orthotic walker (CROW)
Explanation:
DISCUSSION: The figures show a Charcot restraining orthotic walker (CROW). This brace has been used as a customized total contact fit removable brace to maintain foot alignment as the patient evolves from Eichenholz stage 1 to Eichenholz stage 3 Charcot arthropathy.
REFERENCES: Mehta JA, Brown C, Sargeant N: Charcot restraint orthotic walker. Foot Ankle Int 1998;19:619-623.
Morgan JM, Biehl WC III, Wagner FW Jr: Management of neuropathic arthropathy with the Charcot restraint orthotic walker. Clin Orthop 1993;296:58-63.
Question 20:
Figure 7 shows a sagittal T1-weighted MRI scan. What muscle/tendon is identified by the arrow? Review Topic
Options:
- Infraspinatus
- Teres minor
- Subscapularis
- Long head of triceps
- Latissimus dorsi
Correct Answer: Teres minor
Explanation:
The sagittal T1-weighted MRI scan is useful for interpreting the quality of muscle. The arrow is pointing to the teres minor.
Question 21:
A 71-year-old woman who reports long-term use of oral steroids for asthma is referred for treatment of a distal humerus fracture. Radiographs reveal diffuse osteopenia and a severely comminuted intra-articular fracture. What is the most appropriate treatment?
Options:
- Long arm cast immobilization
- Total elbow arthroplasty
- Open reduction and internal fixation
- Osteoarticular allograft
- Resection arthroplasty
Correct Answer: Total elbow arthroplasty
Explanation:
DISCUSSION: Several studies have documented the satisfactory outcomes of total elbow arthroplasty when osteosynthesis is not feasible for fixation of a distal humerus fracture, particularly in the physiologically older patient with low functional demands. Total elbow arthroplasty should be considered when a comminuted intra-articular distal humerus fracture occurs in a woman older than age 65 years, particularly with such associated comorbidities as systemic steroid use, osteoporosis, or rheumatoid arthritis.
REFERENCES: Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947.
Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intraarticular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480.
Garcia JA, Mykula R, Stanley D: Complex fractures of the distal humerus in the elderly: The role of total elbow replacement as primary treatment. J Bone Joint Surg Br 2002;84:812-816.
Question 22:
A child presents with the radiograph shown in Figure A. Which of the following conditions is LEAST likely to be associated with this disorder? Review Topic
Options:
- Unilateral absent kidney
- Sever's disease
- Ventricular septal defect
- Tethered cord
- Thumb hypoplasia
Correct Answer: Unilateral absent kidney
Explanation:
Sever's disease (calcaneal apophysitis) is not associated with congenital scoliosis.
Congenital scoliosis is associated with other anomalies 60% of the time. These anomalies can appear independently, or as part of the VACTERL syndrome (vertebral anomalies, anorectal atresia, tracheoesophageal fistula, and renal and vascular anomalies). Other associated orthopedic conditions include clubfoot, developmental dysplasia of the hip, limb hypoplasia, Sprengel’s deformity, Klippel-Feil syndrome, foot asymmetry, vertical tali, leg atrophy and pes cavus.
Hedequist et al. (2004) reviewed congenital scoliosis. They recommend surgery in young children, severe deformities, or deformities that tend to progress rapidly, truncal imbalance, and anomalies at the cervicothoracic and lumbosacral junction (because of imbalance in the shoulders/neck and lumbar region respectively). Surgical options include in situ fusion, convex hemiepiphysiodesis, hemivertebra excision, correction and instrumented fusion, osteotomies with fusion, growing rods and expandable ribs.
Hedequist et al. (2007) reviewed congenital scoliosis. They state that fully segmented hemivertebra with definable disks above and below are more likely to cause curvature compared with an unsegmented hemivertebra fused to the vertebra above and below. Also, anomalies at the cervicothoracic and lumbosacral junctions produce more visible deformities than that at other areas.
Figure A shows a spine with multiple hemivertebrae, examples of failure of formation in congenital scoliosis.
Incorrect Answers:
Question 23:
What is the most common cause of errors that harm patients? Review Topic
Options:
- Communication breakdown
- Equipment breakdown
- Nursing competence
- Patient noncompliance
- Physician competence
Correct Answer: Communication breakdown
Explanation:
The AMA report identified communication breakdown as the most common cause of errors that harm patients. It is extremely important to learn to communicate effectively with your patients. Understanding cultural and language differences helps avoid communication errors.
Question 24:
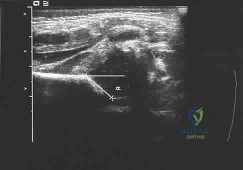
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management? Review Topic
Options:
- Reposition the harness to hold the hips in 70 degrees of abduction
- Closed reduction and arthrography under anesthesia
- Open reduction and a spica cast
- Continued harness treatment in the current position
- Spica cast
Correct Answer: Continued harness treatment in the current position
Explanation:
The infant has a well-positioned hip in the Pavlik harness and treatment should be continued in the current position. The success rate is over 90% with the use of this device for a dislocatable hip. Ultrasound is a useful tool to confirm appropriate positioning of the cartilaginous femoral head during treatment. If the femoral head is
not reduced after 2 to 3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness.
Question 25:
Which of the following illustrations shown in Figures 21a through 21e correctly shows the projection of the sacroiliac joint on the outer table of the ilium?
Options:
Correct Answer: 21c
Explanation:
DISCUSSION: The projection of the sacroiliac joint on the outer surface of the ilium should be well understood to avoid violation of the joint during bone graft harvesting and to help in insertion of the screw across the joint. The sacroiliac joint has superior and inferior limbs. The average lengths of the superior and inferior limbs are 4.4 cm and 5.6 cm, respectively. The average width of each limb is 2.0 cm. The average distance from the longitudinal axis of the superior limb to the posterior superior iliac spine is 5.5 cm. The average longitudinal axis of the inferior limb is 1.2 cm superior to the inferior margin of the posterior inferior iliac spine. The average angle between the two axes is 93 degrees. Figure 21c most closely shows the projection of the sacroiliac joint on the outer table of the ilium.
REFERENCES: Waldrop JT, Ebraheim NA, Yeasting RA, Jackson WT: The location of the sacroiliac joint on the outer table of the posterior ilium. J Orthop Trauma 1993;7:510-513.
Xu R, Ebraheim NA, Yeasting RA, Jackson WT: Anatomic considerations for posterior iliac bone harvesting. Spine 1996;21:1017-1020.
Question 26:
Nutritional rickets in the US occurs more frequently in infants older than 6 months of age who do not receive vitamin D supplementation and are Review Topic
Options:
- Caucasian and formula fed.
- Caucasian and breast fed.
- African American and formula fed.
- African American and breast fed.
- Asian and formula fed.
Correct Answer: African American and breast fed.
Explanation:
Numerous reports suggest an increased frequency of nutritional rickets in the US in children with dark skin pigmentation who are breast fed past 6 months of age without vitamin D supplementation. Nutritional rickets is rare in light-skinned children or those who are formula fed.
Question 27:
A 24-year-old man sustains an injury to his right elbow after falling 10 feet. Radiographs are shown in Figures 41a and 41b. Treatment should consist of
Options:
- open reduction and internal fixation, followed by casting.
- open reduction and internal fixation, followed by early range of motion.
- open reduction and internal fixation, medial collateral ligament repair, and early range of motion.
- open reduction and internal fixation of the ulna, application of a hinged external fixator, and early range of motion.
- closed reduction and splinting, followed by early range of motion.
Correct Answer: open reduction and internal fixation, followed by early range of motion.
Explanation:
DISCUSSION: Transolecranon fracture-dislocations are most effectively managed with open reduction and internal fixation, followed by early aggressive range of motion. Concomitant injury to the collateral ligament is rare, and stability is achieved by anatomic reconstruction of the olecranon fracture with rigid fixation. The need for collateral ligament repair or a hinged external fixator is uncommon in this fracture pattern.
REFERENCE: Ring D, Jupiter JB, Sanders RW, et al: Transolecranon fracture-dislocation of the elbow. J Orthop Trauma 1997;11:545-550.
Question 28:
Which of the following growth factors binds and activates the lipoprotein receptor-related protein 5/6 (LRP5/6) during bone development? Review Topic
Options:
- Transforming growth factor-beta
- Platelet-derived growth factor
- Parathyroid hormone
- Bone morphogenetic protein
- Wnt protein
Correct Answer: Wnt protein
Explanation:
Wnt and Hedgehog (Hh) signaling pathways are key regulators of bone formation. Mutations in the Wnt and Hh pathways result in skeletal malformations as well as osteoarthritis. Wnts are a large family of secreted proteins (19 different members in the human genome) that transduce their signal through several pathways. The most studied of these pathways is the Wnt/beta-catenin pathway, in which Wnt protein binds to the LRP5/6 receptor at the cell surface and activates an intracellular cascade. This cascade leads to translocation of beta-catenin into the nucleus to activate transcription of genes that control osteoblast differentiation. Agents that stimulate this pathway are under investigation for treatment of osteoporosis.
Question 29:
A 30-year-old man caught his dominant little finger on the straps of his windsurfing board 10 days ago. He reports swelling about the distal phalanx and has difficulty completely extending the distal interphalangeal joint. A radiograph is shown in Figure 47. What is the most appropriate treatment for this injury?
Options:
- Extension splinting of the proximal interphalangeal and distal interphalangeal joints
- Extension splinting of the distal interphalangeal joint
- Transarticular pinning of the distal interphalangeal joint
- Extension block pinning of the distal interphalangeal joint
- Open reduction and internal fixation of the distal phalanx
Correct Answer: Extension splinting of the distal interphalangeal joint
Explanation:
DISCUSSION: The radiograph reveals a “bony mallet injury.” As the distal phalanx is not volarly subluxated, extension splinting, similar to a classic mallet injury without bony involvement, is appropriate. If there is volar subluxation associated with a large bony fragment, surgical intervention is appropriate.
REFERENCES: Baratz ME, Schmidt CC, Hughes TB: Extensor tendon injuries, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 192.
Bendre AA, Hartigan BJ, Kalainov DM: Mallet finger. J Am Acad Orthop Surg 2005;13:336-344.
Question 30:
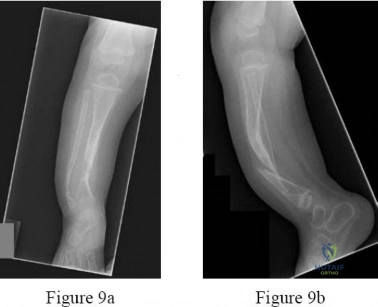
The mother of an otherwise healthy 1-month-old infant reports that he is not moving his left leg after falling from his high chair 2 days ago. He has a temperature of 99.5°F (37.5°C). Examination reveals that the left thigh is moderately tender to palpation. Because the infant is apprehensive, range of motion is difficult to quantify, but appears to be normal at the hips and ankles. Range of motion of the left knee is approximately 25° to 90°. A radiograph of the leg is shown in Figure 27. Management should consist of
Options:
- application of a long leg splint and admission to the hospital for further evaluation and consultation.
- application of a long leg cast, with follow-up radiographs in 3 days.
- immediate application of a spica cast under general anesthesia.
- a CBC, an erythrocyte sedimentation rate, blood cultures, aspiration of the distal femur for culture, and hospital admission with administration of IV antibiotics if required.
- a CBC, an erythrocyte sedimentation rate, a technetium bone scan, and consultation for bone marrow aspiration.
Correct Answer: application of a long leg splint and admission to the hospital for further evaluation and consultation.
Explanation:
DISCUSSION: The patient has a bucket-handle fracture of the distal femur with bilateral corner fractures of the distal femur and a transverse fracture of the proximal tibia. These fractures are virtually pathognomonic of child abuse. The infant should be admitted to the hospital, and child protection services should be notified for investigation of possible abuse. A skeletal survey should be obtained, along with laboratory studies that include a CBC, a platelet count, a prothrombin time, a partial thromboplastin time, and a bleeding time.
REFERENCES: Akbarnia BA: The role of the orthopaedic surgeon in child abuse, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1315-1334.
Black GB: Child abuse fractures, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 931-944.
Question 31:
-What is the most appropriate next treatment step?
Options:
- Open biopsy
- Extension casting
- CT scan of the chest
- Blood culture and image-guided needle biopsy or aspiration
Correct Answer: Blood culture and image-guided needle biopsy or aspiration
Explanation:
DISCUSSION FOR QUESTIONS 7 AND 8
Based on the patient’s signs and symptoms, the most likely diagnosis is osteomyelitis of the spine. The imaging studies do not reveal a herniated disk, which would be unusual in someone of this age. Aneurysmal bone cysts would involve the posterior elements with a more expansive lesion of bone, whereas this lesion involves primarily the body and anterior column. Hemangioma would likely not be present with systemic signs or symptoms and has a more characteristic coarse trabecular pattern on radiographs and scans. Given the likelihood that this patient has osteomyelitis of the spine, blood cultures may yield an organism about 50% of the time. If cultures are negative, an image-guided biopsy is warranted. A diagnosis needs to be established before treatment such as extension casting or bracing is rendered. Open biopsy may still be needed if needle biopsy is not diagnostic, but this is not the first treatment option. A chest CT scan is not appropriate as a first step when a tumor is presumed and a diagnosis has not been established.
Question 32:
A 12-year-old girl is seen for left ankle pain. Radiographs reveal osteochondritis dissecans (OCD) involving the talus. What should the parents be told regarding management? Review Topic
Options:
- No treatment is required because spontaneous healing is common.
- Nonsurgical management typically relieves pain and results in radiographic healing in less than 12 weeks.
- Nonsurgical management frequently relieves pain but often may not result in radiographic healing even 6 months after treatment.
- Hyperbaric oxygen treatment is helpful.
- Ankle fusion is frequently necessary.
Correct Answer: Nonsurgical management frequently relieves pain but often may not result in radiographic healing even 6 months after treatment.
Explanation:
Nonsurgical management of OCD of the talus in skeletally immature individuals frequently results in a fairly rapid decrease in symptoms, but radiographic abnormalities can frequently be found even 6 months after treatment. Spontaneous resolution of this condition is rare. Hyperbaric oxygen treatment has not been shown to be beneficial for this condition. Progression of the condition to the point of requiring ankle fusion is rare.
Question 33:
Figure 1 is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal. What is the main function of the structure delineated by the black asterisks?
Options:
- Resist anterior translation during knee flexion
- Resist posterior translation during knee flexion
- Resist rotatory loads during knee flexion
- Resist rotatory loads during knee extension
Correct Answer: Resist rotatory loads during knee extension
Explanation:
The structure shown is the posterolateral bundle of the anterior cruciate ligament (ACL). This bundle is optimally positioned in the knee to resist rotatory forces during terminal knee extension. "Resist anterior translation during knee flexion" best describes the anteromedial bundle. "Resist rotatory loads during knee flexion" is unlikely because the posterolateral bundle is tightest during knee extension. The posterior cruciate ligament, not the ACL, functions to resist posterior translation.
Question 34:
A 70-year-old woman has a 3-year history of gradually increasing diffuse and global right knee pain. Her main issues are difficulty with stairs, stiffness with prolonged sitting, and swelling. She has taken NSAIDs and has received intra-articular steroid injections, all with decreasing efficacy. Her right knee examination reveals a range of motion of 15° to 80° with a fixed deformity to varus and valgus stress. Her symptoms are no longer manageable nonsurgically. Radiographs reveal a 30-degree mechanical axis deformity. When using the measured resection technique during total knee arthroplasty (TKA), the best way to avoid femoral malrotation is to reference the
Options:
- anteroposterior axis.
- tibial intramedullary axis.
- posterior condylar axis.
- femoral intramedullary axis.
Correct Answer: anteroposterior axis.
Explanation:
DISCUSSION:
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point, can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking
or instability, which is a common complication associated with primary TKA.
Question 35:
As reflected by the SF-36 scores, patients with which of the following conditions demonstrate the most disability in physical function?
Options:
- AIDS
- Polytrauma
- Pelvic fracture
- Pilon fracture
- Acute myocardial infarction (AMI)
Correct Answer: Pilon fracture
Explanation:
DISCUSSION: Pollak and associates found that the average SF-36 score for patients who sustained a pilon fracture was significantly lower than patients with diabetes mellitus, AIDS, hypertension, asthma, migraines, pelvic fracture, polytrauma, and AMI. Moreover, patients having undergone pilon fixation scored lower on all but three of the SF-36 scales (vitality, mental health, and emotional health).
REFERENCE: Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 36:
Figures 28a through 28d show the radiographs and MRI scans of a 20-year-old basketball player who sustained an inversion injury to his right ankle. Management should consist of
Options:
- open reduction and internal fixation.
- a short leg cast for 6 weeks.
- ankle arthroscopy, removal of the fragment, and drilling of the base of the lesion.
- ankle arthroscopy and internal fixation.
- functional ankle rehabilitation that emphasizes range of motion, peroneal strengthening, and proprioceptive training.
Correct Answer: ankle arthroscopy, removal of the fragment, and drilling of the base of the lesion.
Explanation:
DISCUSSION: Osteochondral fractures involving the talar dome have been classified based on radiographic and MRI findings. A nondisplaced and incomplete fracture may be treated effectively with a short leg cast and no weight bearing for 6 weeks. This patient has a complete, separated, and displaced osteochondral fragment involving the midlateral talar dome that will most likely cause pain, mechanical symptoms, and effusion if treated nonsurgically. In addition, there is very little bone remaining on the fragment, making the likelihood of healing with open reduction and internal fixation problematic. The treatment of choice includes arthroscopy, removal of the loose fragment, curettage or drilling of the base, and a rehabilitation program that emphasizes peroneal strengthening, range of motion, and proprioceptive training.
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
Baker CL, Morales RW: Arthroscopic treatment of tranchondral talar dome fractures: A long-term follow-up study. Arthroscopy 1999;15:197-202.
Question 37:
A 20-year-old collegiate football player sustains an injury to his left foot 3 weeks before the start of the fall season. Examination reveals localized tenderness over the lateral midfoot and normal foot alignment. Radiographs are shown in Figures 28a through 28c. What is the treatment of choice?
Options:
- Intramedullary screw fixation
- Onlay bone graft
- Application of a walking boot with weight bearing as tolerated
- Application of a short leg cast with weight bearing as tolerated
- Application of a short leg cast and non-weight-bearing
Correct Answer: Intramedullary screw fixation
Explanation:
DISCUSSION: Due to the relatively high incidence of delayed union and nonunion associated with this mildly displaced Jones-type fracture, and the temporal proximity to his playing season, intramedullary screw fixation is the treatment of choice in this collegiate athlete to best ensure healing and expedite his return to football. If nonsurgical management were elected, application of a non-weight-bearing short leg cast would be appropriate since a higher likelihood of healing is expected with it versus a short leg walking cast. The risk of recurrent fracture of fractures that heal with nonsurgical management has reportedly been high (approximately 30%).
REFERENCES: Quill GE: Fractures of the proximal fifth metatarsal. Orthop Clin North Am 1995;26:353-361.
Torg JS, Balduini FC, Zelko RR, et al: Fractures of the base of the fifth metatarsal distal to the tuberosity: Classification and guidelines for nonsurgical and surgical management. J Bone Joint Surg Am 1984;66:209-214.
Dameron TB Jr: Fractures of the proximal fifth metatarsal: Selecting the best treatment option.
J Am Acad Orthop Surg 1995;3:110-114.
Question 38:
A 1-year-old infant has the hand deformities shown in Figure 40. What pathologic process is the most likely cause of these deformities?
Options:
- Genetic mutation
- Teratogen exposure
- Amniotic rupture
- Iatrogenic influences
- Developmental field disruption
Correct Answer: Amniotic rupture
Explanation:
DISCUSSION: Streeter’s dysplasia is clearly related to rupture of the amnion in utero and is now most commonly referred to as premature amnion rupture sequence. The deformities arise from amniotic bands that wrap about protruding parts and from uterine packing because of the accompanying oligohydramnios. Clubfoot can develop as a result of the latter mechanism. Three limb involvement is most commonly seen, along with syndactyly. Treatment involves resection of bands and Z-plasty of skin. The disease is not genetic and has not been related to teratogen exposure or to iatrogenic influences such as amniocentesis. Developmental field disruption is not seen in this disease, and the growth potential of the involved parts is normal unless neurovascular disruption has arisen from band formation.
REFERENCE: Foulkes GD, Reinker K: Congenital constriction band syndrome: A seventy-year experience. J Pediatr Orthop 1994;14:242-248.
Question 39:
A baseball pitcher has intractable posterior and superior shoulder pain. The arthroscopic view seen in Figure 25 shows no Bankart or Hill-Sachs lesion and a negative drive-through sign. There are no signs of ligamentous laxity, but active compression and anterior slide tests are positive. Treatment should consist of
Options:
- open fixation of the SLAP lesion with a screw that can be removed later.
- arthroscopic repair of the SLAP lesion with suture anchors.
- arthroscopic repair of the SLAP lesion with suture anchors with a thermal capsular shift.
- arthroscopic repair of the SLAP lesion with suture anchors and a rotator cuff interval closure.
- arthroscopic repair of the SLAP lesion with suture anchors and an arthroscopic capsular placation.
Correct Answer: arthroscopic repair of the SLAP lesion with suture anchors.
Explanation:
DISCUSSION: According to Morgan and associates, a type II SLAP lesion can create or is associated with a superior instability pattern. They suggest that this can exist without a co-existing anteroinferior instability pattern. They reported that repair of the SLAP lesion alone resulted in satisfactory outcomes in 90% of patients and a return to throwing in more than 90% of pitchers. The arthroscopic findings in this patient do not support a diagnosis of anteroinferior laxity or instability; therefore, thermal capsular shift or capsular placation is not necessary.
REFERENCES: Morgan CD, Burkhart SS, Palmeri M, et al: Type II SLAP lesions: Three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy 1998;14:553-565.
Mileski RA, Snyder RJ: Superior labral lesions in the shoulder: Pathoanatomy and surgical management. J Am Acad Orthop Surg 1998;6:121-131.
Levitz CL, Dugas J, Andrews JR: The use of arthroscopic thermal capsulorrhaphy to treat internal impingement in baseball players. Arthroscopy 2001;17:573-577.
Question 40:
When comparing mobile-bearing total knee arthroplasty (TKA) to fixed-bearing total condylar arthroplasty, the mobile-bearing procedure provides
Options:
- no improvement in survivorship.
- approximately 15 degrees greater flexion.
- appreciable reduction in wear rates.
- a faster recovery profile.
- better quadriceps strength.
Correct Answer: no improvement in survivorship.
Explanation:
DISCUSSION: Survivorship is similar in the two groups. In a recent study, mobile-bearing TKAs showed a slightly higher maximum flexion than the total condylar fixed-bearing-type designs (112 degrees versus 108 degrees with no difference in recovery rate). Using a fixed-bearing or a mobile-bearing design did not seem to influence the recovery rate in early results after knee arthroplasty. Mobile-bearing arthroplasties are suggested, in theory, to offer a reduction in polyethylene wear; however, clinical studies have not yet proven this. Recovery rates have yet to be statistically seen as improved with either method. Differences in strength have not been shown.
REFERENCES: Aglietti P, Baldini A, Buzzi R, et al: Comparison of mobile-bearing and fixed-bearing total knee arthroplasty: A prospective randomized study. J Arthroplasty 2005;20:145-153.
Sorrells RB: The rotating platform mobile bearing TKA. Orthopedics 1996;19:793-796.
Dennis DA, Komistek RD: Kinematics of mobile-bearing total knee arthroplasty. Instr Course Lect 2005;54:207-220.
Question 41:
A full-term newborn has webbing at the knees, rigid clubfeet, a Buddha-like posture of the lower extremities, and no voluntary or involuntary muscle action at and below the knees. Radiographs of the spine and pelvis reveal an absence of the lumbar spine and sacrum. What maternal condition is associated with this diagnosis?
Options:
- Alcoholism
- Drug abuse
- Down syndrome
- Diabetes mellitus
- Idiopathic scoliosis
Correct Answer: Diabetes mellitus
Explanation:
DISCUSSION: The history, physical examination, and radiographic findings are consistent with type IV sacral agenesis or caudal regression syndrome. These children are born with no lumbar spine or sacrum. The T12 vertebra is often prominent posteriorly. Popliteal webbing and knee flexion contractures are common with this diagnosis. There is a higher incidence of this diagnosis when the mother has diabetes mellitus. Maternal drug abuse and alcoholism can produce phenotypically unique children but without the findings described here. Maternal idiopathic scoliosis is not associated with caudal regression syndrome.
REFERENCES: Chan BW, Chan KS, Koide T, et al: Maternal diabetes increases the risk of caudal regression caused by retinoic acid. Diabetes 2002;51:2811-2816.
Zaw W, Stone DG: Caudal regression syndrome in twin pregnancy with type II diabetes.
J Perinatol 2002;22:171-174.
Question 42:
The radiographic feature seen in Figure 37 that best indicates a slow-growing process is the
Options:
- deformity of the fibula.
- wide base of the lesion.
- lack of joint deformity.
- medullary canal extending into the lesion.
- lack of periosteal reaction.
Correct Answer: deformity of the fibula.
Explanation:
DISCUSSION: For the fibula (or any bone) to bow, a long-standing process needs to be present. Pressure from a rapid process would cause erosion, not allowing the bone to remodel. The other features are helpful confirmatory findings but also may be associated with aggressive processes. In this patient, the fibular deformity is caused by a sessile osteochondroma of the tibia.
REFERENCES: Lodwick GS, Wilson AJ, Farrell C, Virtama P, Dittrich F: Determining growth rates of focal lesions of bone from radiographs. Radiology 1980;134:577-583.
Moser RP Jr, Madewell JE: An approach to primary bone tumors. Radiol Clin North Am 1987;25:1049-1093.
Question 43:
A 17-year-old boy is shot in the left side of the neck at the C5-6 level and sustains an incomplete spinal cord injury that is called a Brown-Sequard syndrome. Which of the following best describes the expected deficits? Review Topic
Options:
- Profound bilateral wrist extensor, finger flexor, and intrinsic weakness with good preservation of lower extremity motor function
- Severe bilateral upper and lower extremity weakness, pain and temperature sensory deficit but preservation of deep pressure and proprioception
- Weakness of the right upper and lower extremity with diminished pain and temperature sensation on the left side of the body
- Left wrist extensor weakness and numbness along the radial border of the left forearm extending into the thumb and index finger
- Weakness of the left upper and lower extremity with diminished pain and temperature sensation on the right side of the body
Correct Answer: Weakness of the left upper and lower extremity with diminished pain and temperature sensation on the right side of the body
Explanation:
Brown-Sequard syndrome is an incomplete spinal cord injury that involves damage unilaterally to the cord, most commonly from penetrating trauma. The motors fibers of the cord decussate within the brainstem so the motor deficit is ipsilateral to the injury; whereas, the pain and temperature fibers cross midline immediately on entering the cord so that the sensory deficit is contralateral to the injury. This patient was shot in the left side, thus he would have weakness of the left upper and lower extremity with diminished pain and temperature sensation on the right side of the body. Response 3 describes opposite symptoms that would result from a right-sided injury. Response 1 describes a central syndrome with greater upper than lower extremity involvement. Response 2 is an anterior cord syndrome with only preservation of the posterior columns of the cord. Response 4 describes a C6 root injury.
Question 44:
Figure 7 shows the AP radiograph of a 60-year-old man who has had pain in the thigh for past 6 months. History reveals that he underwent hip replacement 1 year ago. The radiographic changes are most likely the result of what process?
Options:
- Microtrauma
- Mechanical loosening
- Septic loosening
- Neoplasia
- Congenital anomaly
Correct Answer: Septic loosening
Explanation:
DISCUSSION: The arrows in the radiograph point to circumferential radiolucencies that strongly support the diagnosis of septic loosening. Radiolucent lines that occur in such a short time are also typical of an infection.
REFERENCES: Garvin KL, Hanssen AD: Infection after total hip arthroplasty: Past, present, and future. J Bone Joint Surg Am 1995;77:1576-1588.
Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
Question 45:
A 6-year-old girl has a painless spinal deformity. Examination reveals 2+ and equal knee jerks and ankle jerks, negative clonus, and a negative Babinski. The straight leg raising test is negative. Abdominal reflexes are asymmetrical. PA and lateral radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management? Review Topic
Options:
- MRI of the spinal axis
- Physical therapy
- A brace for scoliosis
- Observation, with reevaluation in 6 to 12 months
- Posterior spinal fusion from T6 to T12
Correct Answer: MRI of the spinal axis
Explanation:
The patient has an abnormal neurologic exam as shown by the abnormal abdominal reflexes. Furthermore, she has a significant curve and is younger than age 10 years. These findings are not consistent with idiopathic scoliosis. MRI will best rule out syringomyelia or an intraspinal tumor. Bracing and surgery are not indicated for this small curvature prior to obtaining an MRI scan.
Question 46:
Figure 8 shows the radiograph of a 72-year-old man who has had severe pain in the left hip for the past 3 weeks. History reveals alcohol abuse. The next most appropriate step should consist of
Options:
- hip aspiration.
- Doppler ultrasound.
- AP tomograms.
- a CT scan.
- a technetium Tc 99m bone scan.
Correct Answer: hip aspiration.
Explanation:
DISCUSSION: The radiograph reveals destruction of the femoral head with loss of the articular cartilage. These findings are consistent with an infected hip, and aspiration will confirm the diagnosis. Although the patient could have advanced osteonecrosis, typically the cartilage interval is maintained and such destruction is rarely associated with osteonecrosis.
REFERENCE: Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 157-161.
Question 47:
Figures 1 and 2 show the radiographs obtained from a 68-year-old morbidly obese man who underwent left total hip replacement 7 years ago and did well, with no symptoms prior to the current presentation. He recently rose from a seated position and felt a pop in the hip, with immediate pain and inability to bear weight. Any pressure on the left foot now produces a painful, grinding sensation with loss of left hip stability. What is the best next step?
Options:
- Revision of the acetabular implant to a constrained bearing with modular exchange of the femoral head and neck
- Revision of the acetabular and femoral implants
- Retention of the acetabular implant with modular exchange of the femoral head and neck
- Revision of the femoral component alone with a new ceramic head
Correct Answer: Revision of the acetabular and femoral implants
Explanation:
DISCUSSION:
The modular femoral stem has fractured. Changing the liner to a constrained design is not warranted at this time based on the information provided. Revision of the acetabular implant is appropriate because of the potential for damage to the existing cup from metal debris and femoral implant contact and to convert from a metal-on-metal articulation. Nonsurgical management would not provide pain relief or improvement; revision of the total hip arthroplasty is recommended. The implant failed in a short time, and retention of the femoral stem is not recommended because of the concern for failure with only a neck exchange. A dual-mobility bearing may be a good option if the surgeon plans to retain the acetabular component. Extended trochanteric osteotomy is a useful technique for the removal of a well-fixed femoral implant. In this patient, femoral stem removal without
osteotomy would be difficult due to the fracture of the implant’s femoral neck and the inability to gain purchase for extraction.
Question 48:
Bone morphogenetic proteins transduce intracellular signal through what class of cell surface receptor?
Options:
- Mitogen-activated protein kinase
- Tyrosine kinase
- Serine-threonine kinase
- Aurora kinase
- Glycogen synthase kinase 3
Correct Answer: Serine-threonine kinase
Explanation:
Bone morphogenetic proteins (BMPs) are extracellular proteins belonging to the TGF-beta superfamily of molecules. Members of this family include BMPs, growth and differentiation factors (GDFs), anti-mnllerian hormone (AMH), activin, Nodal, and TGF-beta. These proteins exert their action by binding to cell surface receptors of the serine-threonine kinase class to activate intracellular signaling pathways. The other kinase participate in various cell signaling functions, but are not associated with BMP.
Question 49:
Which of the following is considered the most accurate test to determine the amount of limb-length discrepancy in a patient with a knee flexion contracture of 35°?
Options:
- Standing block test
- Standing AP radiograph of the pelvis with blocks under the foot of the short leg
- CT scanogram
- Scanogram
- Measurement from the anterior superior iliac spine to the medial malleolus
Correct Answer: CT scanogram
Explanation:
DISCUSSION: Flexion contractures and angular deformities of a limb cause inaccurate limb-length measurement results with most clinical methods. A CT scanogram is more accurate than standard scanograms for determining limb length in patients with knee flexion contractures of 30° or more. The cost and time necessary to complete the examinations are comparable, but the CT scanogram delivers only 20% of the radiation needed for standard scanograms.
REFERENCES: Aaron A, Weinstein D, Thickman D, Eilert R: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
Tachdjian MO: Pediatric Orthopedics. Philadelphia, Pa, WB Saunders, 1990, pp 2867-2870.
Question 50:
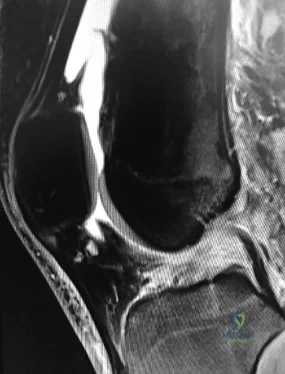
Figure 11 shows the lateral radiograph of a 16-year-old boy who has been unable to participate in sports activities because of pain in the anterior aspect of the knee. He states that the pain is aching in nature and is located in the region of the tibial tuberosity. He denies having joint effusion or symptoms of instability. Management should consist of
Options:
- phonophoresis treatment and a program of quadriceps stretching.
- application of a hinge, post, and shell design functional knee brace.
- application of a hinge, post, and strap design functional knee brace.
- an MRI scan of the knee, a CT scan of the chest, a technetium Tc 99m bone scan, liver function tests, and a biopsy of the proximal tibia.
- excision of the ossicle and prominence of the tibial tuberosity.
Correct Answer: excision of the ossicle and prominence of the tibial tuberosity.
Explanation:
DISCUSSION: The prognosis for most patients with Osgood-Schlatter disease is good. When the secondary ossification center unites with the main body of the tibial tubercle, the patellar tendon has a more rigid anchor, and heterotopic ossification and its associated reaction often become quiescent. However, even after closure of the growth plates, some patients have persistent symptoms. Excision of the ossicle and prominence of the tibial tuberosity decompresses the patellar tendon and allows most patients to resume sports activities. Nonsurgical modalities are ineffective. Better results have been reported after excision than after drilling of the tubercle. Excision of the ossicle is not indicated prior to skeletal maturity because symptoms will resolve in most patients when the secondary ossification center unites.
REFERENCES: Flowers MJ, Bhadreshwar DR: Tibial tuberosity excision for symptomatic Osgood-Schlatter disease. J Pediatr Orthop 1995;15:292-297.
Greene WB: Osteochondrosis and tibia vara, in Canale ST, Beaty JH (eds): Operative Pediatric Orthopaedics, ed 2. Philadelphia, Pa, Mosby, 1995, pp 804-854.
Question 51:
03 Which of the following is considered a normal age-related change in the intervertebral disk in the elderly?
Options:
- increased proteoglycan concentration
- increased biosynthetic function
- increased viable cell concentration in the central region
- decreased water content 5) decreased stiffness back answer Question 40.03
Correct Answer: decreased water content 5) decreased stiffness back answer Question 40.03
Explanation:
Remember 2 things Dr. Brinker has said about collagen:
“collagen dehydrates when it gets older” “water follows the proteoglycans”
We all know that as we get older our collagen is less pliable and, specifically, our disks shrink, bulge, and are stiffer. They’re smaller and stiffer because there’s less water. There’s less water because there’s less proteoglycans. There’s less proteoglycans because there’s less biosynthetic function. There’s less biosynthetic function because there are fewer viable cells. Why are there fewer viable cells? I don’t know. Neither do the authors of the Academy Basic Science Textbook. Presumably one day we’ll find the gene(s) / protein(s) / cue(s) that are responsible for the overall slow, programmed decline of our bodies that we call “aging.”
[1]
back to this question next question
[1]
Orthopaedic Basic Science 2nd ed. Pg 558
Question 52:
A 56-year-old man with poorly controlled diabetes mellitus has rapidly developing and advancing erythema, warmth and swelling with bullae formation on the left lower extremity. These findings appear to be advancing proximally several millimeters per hour. Culture results are most likely to reveal
Options:
- group A Streptococcus.
- Methicillin-resistant staphylococcus aureus.
- Clostridium.
- polymicrobial infection.
Correct Answer: polymicrobial infection.
Explanation:
Discussion: Necrotizing fasciitis (NF) results in the death of the body's soft tissue. It is a severe disease of sudden onset that spreads rapidly. Symptoms include red or purple skin in the affected area, with severe pain, fever, and vomiting. The most commonly affected areas are the limbs and perineum. Early diagnosis is difficult as the disease often looks like a simple superficial skin infection in the early stages. While a number of laboratory and imaging modalities can raise the suspicion for necrotizing fasciitis, the gold standard for diagnosis is a surgical exploration in the setting of high suspicion. When in doubt, a small "keyhole" incision can be made into the affected tissue. If a finger easily separates the tissue along the fascial plane,
the diagnosis is confirmed and an extensive debridement should be performed. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score can be utilized to risk stratify people who have signs of cellulitis and determine the likelihood of necrotizing fasciitis being present. It uses six serologic measures, including C-reactive protein, total white blood cell count, hemoglobin, sodium, creatinine and glucose.
Polymicrobial synergistic infection was the most common cause of necrotizing fasciitis (48 patients; 53.9%) with streptococci and enterobacteriaceae being the most common isolates. Group-A streptococcus was the most common cause of monomicrobial necrotizing fasciitis. The most common associated comorbidity was diabetes mellitus (63 patients; 70.8%).
Question 53:
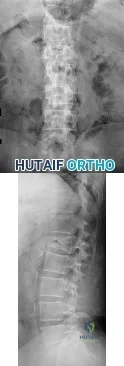
A 75-year-old woman reports persistent severe low back pain after lifting a bag of groceries 8 weeks ago. She denies the presence of any lower extremity pain, weakness, or other symptoms. AP and lateral lumbar spine radiographs are shown in Figures 47a and 47b. For further evaluation, what imaging study should be obtained next? Review Topic
Options:
- Lumbar spine flexion and extension radiographs
- Lumbar spine CT
- Lumbar spine MRI
- Whole body bone scan
- Tagged white blood cell scan
Correct Answer: Lumbar spine MRI
Explanation:
The radiographs show a L1 vertebral compression fracture. MRI scans of the lumbar spine are indicated to help determine the age of the fracture via evaluation of the fat-suppressed T2-weighted images. If those images show edema (bright signal) within the fracture, it can be assumed to be an acute or subacute fracture. Also, MRI scans may help further characterize the fracture as a benign osteoporosis-related fracture versus a pathologic fracture. Lastly, MRI scans allow for evaluation of the absence, presence, and degree of spinal stenosis. Although a lumbar spine CT scan is also a good option as a next step, given that the patient has a known fracture as seen on the radiographs, MRI scans will likely provide more relevant information in this case. A CT scan may assist in the evaluation of the posterior vertebral body wall and posterior elements in patients with burst fractures. A three-phase bone scan is a good alternative for the evaluation of the acuity of vertebral compression fractures in patients who have a contraindication to MRI scans. Flexion-extension radiographs are most commonly used to evaluate for instability and will not help determine the age of this fracture. Tagged white blood cell scans are performed to evaluate for infection, which is highly unlikely in this patient.
Question 54:
In an effort to reduce costs, a limited MRI sequence is planned to detect a possible occult hip fracture. What is the anticipated fracture signal?
Options:
- Bright on T 1 and T 2
- Dark on T 1 and T 2
- Dark on T 1 , bright on T 2
- Bright on T 1 , dark on T 2
- Enhancement by gadolinium
Correct Answer: Dark on T 1 , bright on T 2
Explanation:
DISCUSSION: At present, radiologists perform multiple MRI images to rule out all possible diagnoses. The ability to specify the anticipated changes on MRI should become more important as a means of reducing costs. MRI is sensitive to changes in free water (or hemorrhage) and thus this will appear dark on T
1
and bright on T
2
.
REFERENCES: Miller MD: Review of Orthopaedics, ed 3. Philadelphia PA, WB Saunders, 2000, p 116.
Guanche CA, Kozin SH, Levy AS, et al: The use of MRI in the diagnosis of occult hip fractures in the elderly: A preliminary review. Orthopedics 1994;17:327-330.
Question 55:
The inheritance of the deformity shown in Figure 1 is most commonly
Options:
- autosomal-recessive.
- autosomal-dominant.
- x-linked dominant.
- mitochondrial.
- sporadic.
Correct Answer: autosomal-dominant.
Explanation:
DISCUSSION: Cleft hand and cleft foot malformations are commonly inherited as autosomal-dominant traits and are associated with a number of syndromes. An autosomal-recessive and an x-linked inheritance pattern have also been described, but these are much less common and are usually atypical. In the common autosomal-dominant condition, nearly one third of the known carriers of the gene show no hand or foot abnormalities. This is known as reduced penetrance. The disorder may be variably expressed; affected family members often exhibit a range from mild abnormalities in one limb only to severe anomalies in four limbs. Variable expressivity and reduced penetrance can cause difficulty in counseling families regarding future offspring in an affected family. Many patients have a cleft hand that may be caused by the split-hand, split-foot gene (SHFM1) localized on chromosome 7q21.
REFERENCE: Kay SPJ: Cleft hand, in Green DP (ed): Green’s Operative Hand Surgery. Philadelphia, Pa, Churchill Livingston, 1999, pp 402-414.
Question 56:
-
Options:
- Surgery is being considered for a 30-month-old child who has the deformity shown in Figure 21. Which of the following studies should be ordered before proceeding with surgery?
- Liver profile
- Myleogram
- Platelet count
- CT scan of the head
- Angiogram of the extremity
Correct Answer: Myleogram
Explanation:
Discussion: Radial deficiency is associated with other abnormalities. 40% of patients with unilateral and 77% of bilateral involvement will have associated malformations:
Holt-Oram syndrome – Radial deficiency and cardial septal defect.
Fanconi syndrome – Severe aplastic anemia
TAR syndrome
Trisomy 17
VATER syndrome
Because of the association with severe aplastic anemia, a platelet count should be done before any surgical intervention
.
Question 57:
ACL rehabilitation often includes exercises with the distal end of the extremity fixed in place with axial loading and co-contracture of muscle groups to help stabilize the joint. This type of exercise is more commonly referred to as: Review Topic
Options:
- Eccentric contraction
- Closed chain exercise
- Open chain exercise
- Proprioceptive neuromuscular facilitation
- Isometric contraction
Correct Answer: Open chain exercise
Explanation:
A "closed chain exercise" is one in which the distal end of the extremity is fixed, allowing axial loading of the extremity with co-contracture of muscles decreasing stress across that joint.
Closed chain exercises are preferred for any rehabilitation protocol that wants to minimize stress across a potentially unstable joint. After ACL reconstruction it is important to begin motion and strengthening but not stress the reconstructed ligament which may lead to loss of stability or failure.
An example of a closed chain exercise of the quadriceps is a squat or leg press in which the foot is fixed against the floor/plate and both the quadriceps and hamstrings can contract together keeping the knee joint stable and preventing excess stress across the reconstructed ACL. An example of an open chain exercise of the quadriceps is a seated leg extension in which the foot is not fixed and the quadriceps contract in isolation. This creates a strong anterior pull on the tibia which can lead to excess stress on the ACL graft.
Beynnon et al. present a review on the behavior of ACL grafts during rehabilitation. They found that exercises that produce the least amount of stress across an ACL graft are either dominated by hamstring muscle contraction, involve quadriceps muscle activity with the knee flexed at 60° or greater, or involve active knee motion between
35°
and
90°
of
flexion.
Illustration A is an example of a squat, which is a closed chain exercise. Notice the feet are fixed in place against the floor. Illustration B is an example of a seated leg extension, which is an open chain exercise. Notice the feet are not fixed in place and no axial loading or co-contracture can occur.
Incorrect
Question 58:
Storage of musculoskeletal allografts by cryopreservation is achieved by
Options:
- replacing water in the tissue with alcohol to a moisture level of 5% and then using a vacuum process to remove the alcohol from the tissue.
- maintaining maximum cellular viability of fresh tissue without long-term storage.
- using chemicals to remove cellular water and controlled rate freezing to prevent ice crystal formation.
- freezing the graft twice and packaging the tissue without solution at minus 80 degrees C.
- freezing the graft in water without an antibiotic solution soak during quarantine, with final storage in liquid nitrogen.
Correct Answer: using chemicals to remove cellular water and controlled rate freezing to prevent ice crystal formation.
Explanation:
DISCUSSION: Cryopreservation uses chemicals to remove cellular water and controlled rate freezing to prevent ice crystal formation. The tissue is procured, cooled to wet ice temperature for quarantine, and then stored in a container with cryoprotectant solution of dimethyl
sulfoxide or glycerol which displaces the cellular water. The controlled rate freezing is then done to prevent ice crystal formation. Fresh allografts are not frozen in order to maintain maximum cellular viability, and this process limits the shelf life of osteochondral allografts. Freeze-drying involves replacement of water in the tissue with alcohol to a moisture level of
5% and then uses a vacuum process to remove the alcohol from the tissue. Preparation of fresh frozen grafts involves freezing the graft twice and packaging the tissue without solution at
minus 80 degrees C.
REFERENCES: American Association of Tissue Banks: Standards for Tissue Banking. MacLean, VA, American Association of Tissue Banks, 1999.
Vangsness CT Jr, Triffon MJ, Joyce MJ, et al: Soft tissue allograft reconstruction of the human knee: A survey of the American Association of Tissue Banks. Am J Sports Med 1996;24:230-234.
Brautigan BE, Johnson DL, Caborn DM, et al: Allograft tissues, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 2003, pp 205-213.
Question 59:
A 45-year-old right-hand dominant woman falls onto an outstretched left hand. Imaging shows a complex elbow dislocation. The postreduction CT scan demonstrates a reduced joint, comminuted radial head fracture, and type I coronoid fracture. Surgical intervention is recommended to address the involved structures. Which component of the intervention adds the most rotational stability?
Options:
- ixation of the coronoid fragment
- Radial head arthroplasty
- Repair or reconstruction of the lateral collateral ligament (LCL) complex
- Repair or reconstruction of the medial collateral ligament (MCL) This represents a terrible triad injury, with elbow dislocation, radial head fracture, and coronoid fracture. The LCL complex is typically disrupted in this injury pattern. Repair or reconstruction of this structure provides the greatest increase in rotational stability of the elbow.
Correct Answer: Repair or reconstruction of the lateral collateral ligament (LCL) complex
Explanation:
A 68-year-old right-hand dominant woman has experienced progressive right elbow pain and loss of motion for several years. She has failed nonsurgical treatment and elects to undergo a total elbow arthroplasty (TEA). In comparison to a linked prosthesis, an unlinked prosthesis has which reported distinction with extended follow-up?
A. Improved longevity in comparison to the linked prosthesis
B. A significantly larger flexion-extension arc
C. A higher incidence of postsurgical instability
D. Lower frequency of ulnar nerve dysfunction
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
Question 60:
During reconstruction of insertional gaps of a chronic Achilles tendon rupture, what tendon provides the most direct route of transfer?
Options:
- Flexor hallucis longus
- Flexor digitorum longus
- Peroneus longus
- Posterior tibial
- Quadratus planti
Correct Answer: Flexor hallucis longus
Explanation:
DISCUSSION: The flexor hallucis longus tendon provides the best, most direct route of transfer for filling Achilles tendon gaps. The tendon lies lateral to the neurovascular structures, making it safe for harvest and providing a direct route for transfer into the calcaneus without crossing these important structures. The flexor hallucis longus tendon also has muscle belly that extends distal on the tendon itself, often beyond the actual tibiotalar joint. When the tendon is transferred, this muscle belly brings excellent blood supply to the anterior portion of the reconstruction.
REFERENCES: Wilcox DK, Bohay DR, Anderson JG: Treatment of chronic achilles tendon disorders with flexor hallucis longus tendon transfer/augmentation. Foot Ankle Int 2000;21:1004-1010.
Wapner K, Pavlock GS, Hecht PJ, Naselli F, Walther R: Repair of chronic Achilles tendon rupture with flexor hallucis longus tendon transfer. Foot Ankle Int 1993;14:443-449.
Question 61:
The afferent pain innervation of the L3-L4 facet joint arises from the medial branch nerve of
Options:
- L2.
- L3.
- L4.
- L2 and L3.
- L3 and L4.
Correct Answer: L2 and L3.
Explanation:
DISCUSSION: Afferent pain fibers to the lumbar facet joints arise from the medial branch nerves originating from the next two cephalad levels. Therefore, innervation of the L3-L4 facet joint arises from the L2 and L3 medial branch nerves. This effect should be taken into account when considering a medial branch block or facet denervation. The medial branch nerve arises from the dorsal ramus of the exiting nerve root.
REFERENCES: Nade SL, Bell E, Wyke BD: The innervation of the lumbar spinal joint and its significance. J Bone Joint Surg Br 1980;62:255-261
Kornick C, Kramarich SS, Lamer TJ, et al: Complications of lumbar facet radiofrequency denervation. Spine 2004;29:1352-1354.
Question 62:
A patient who underwent intramedullary nailing of a femoral shaft fracture 2 weeks ago now reports groin pain. What is the next most appropriate step in management?
Options:
- Obtain a radiograph of the hip
- Obtain radiographs of the lumbar spine
- Obtain an MRI scan of the lumbar spine
- Review the radiographic report from the time of injury
- Reassure the patient that the pain will improve and order physical therapy
Correct Answer: Obtain a radiograph of the hip
Explanation:
Whereas ipsilateral fractures of the femoral neck and shaft are uncommon, it is critical to recognize a femoral neck fracture that may occur in conjunction with a femoral shaft fracture. The combined injury is seen in 2% to 9% of femoral shaft fractures and may initially be missed in as many as one third of the cases. Preoperative examination of a thin cut CT scan and dedicated AP internal rotation views of the femoral neck can help identify this injury. In addition, the intraoperative AP and lateral hip fluoroscopic view should be examined, and a dedicated radiograph of the hip obtained at the conclusion of the surgery. At follow-up, Tornetta and associates has recommended
obtaining a dedicated AP radiograph of the hip with the leg internally rotated 15 to 20 degrees. Because the femoral neck is anteverted, 15 to 20 degrees of internal rotation of the hip offers the best view of the femoral neck. Whereas associated lumbar spine pathology may cause groin pain, the presence of a missed femoral neck fracture must first be ruled out prior to investigating other sources of pain.
Question 63:
What factor is associated with the highest risk for in-hospital complications for patients undergoing a lumbar fusion for degenerative spondylolisthesis? Review Topic
Options:
- Hospital size
- Gender
- Race
- Age
- One comorbidity
Correct Answer: Age
Explanation:
Age and having three or more comorbidities is associated with a higher rate of complications in patients undergoing a lumbar fusion for lumbar degenerative spondylolisthesis. Race, gender, and hospital size have not been found to be associated with higher complication rates.
Question 64:
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function?
Options:
- Resurfacing hemiarthroplasty
- Resurfacing hemiarthroplasty with fascial glenoid resurfacing
- Resurfacing hemiarthroplasty with cemented glenoid component
- Stemmed hemiarthroplasty
- Stemmed total shoulder arthroplasty
Correct Answer: Stemmed hemiarthroplasty
Explanation:
DISCUSSION: The radiograph and intraoperative photograph show osteonecrosis with near complete head loss/collapse. A stemmed implant is more appropriate in this patient because there is very little bone to support a resurfacing implant. In a younger patient, a glenoid implant should be delayed as long as possible because of the eventual need for revision secondary to glenoid loosening and wear, especially in a young active male. The hemiarthroplasty may be converted to a total shoulder arthroplasty in the future.
REFERENCES: Levy O, Copeland SA: Cementless surface replacement arthroplasty of the shoulder: 5- to 10-year results with the Copeland mark-2 prosthesis. J Bone Joint Surg Br 2001;83:213-221.
Burroughs PL, Gearen PF, Petty WR, et al: Shoulder arthroplasty in the young patient.
J Arthroplasty 2003;18:792-798.
Question 65:
A 26-year-old weightlifter has increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication, corticosteroid injections, and rest fails to alleviate his symptoms. He undergoes an arthroscopic distal clavicle resection with excision of the distal 8 mm of clavicle (Mumford procedure). Three months after surgery, he reports mild pain and popping by his clavicle. His clavicle demonstrates mild posterior instability on examination without any obvious deformity on his radiographs. What structures were compromised during his excision?
Options:
- Anterior and superior acromioclavicular joint ligaments
- Posterior and superior acromioclavicular joint ligaments
- Conoid ligament
- Trapezoid ligament
Correct Answer: Posterior and superior acromioclavicular joint ligaments
Explanation:
The posterior and superior acromioclavicular ligaments provide the most restraint to posterior translation of the acromioclavicular joint and must be preserved during a Mumford procedure. Anterior and superior acromioclavicular joint ligaments are the opposite of the preferred response and prevent anterior translation of the clavicle. Injuries to the conoid and trapezoid ligaments are more pronounced with grade III or higher acromioclavicular separations, with superior migration of the clavicle relative to the acromion.
Question 66:
In performing an opening wedge high tibial osteotomy at the tibial tubercle, the osteotome extends 5 mm posteriorly and centrally out of the bone as shown in Figures 17a and 17b. What is the first structure it enters?
Options:
- Popliteal artery
- Popliteal vein
- Tibial nerve
- Popliteus muscle
- Soleus muscle
Correct Answer: Popliteus muscle
Explanation:
DISCUSSION: The major risk of performing a high tibial osteotomy is neurovascular injury. The new version of the high tibial osteotomy makes a transverse osteotomy at the level of the tibial tubercle. The osteotome is protected by the oblique belly of the popliteus muscle. The popliteal artery and vein and tibial nerve all lie posterior to the muscle. The soleus muscle originates below this level.
REFERENCES: Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3.
Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 422.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, plate 480.
Question 67:
Talar compression syndrome in ballet dancers typically involves injury to which of the following structures?
Options:
- Sustentaculum tali
- Lateral process of the talus
- Posterior process of the calcaneus
- Os tibialis externum
- Os trigonum
Correct Answer: Os trigonum
Explanation:
DISCUSSION: Talar compression syndrome is also known as os trigonum syndrome or posterior ankle impingement syndrome and occurs in activities involving extreme ankle plantar flexion. It involves pinching of the posterior talus (os trigonum or posterior process of the talus) between the calcaneus and tibia. The flexor hallucis longus also may be impinged. The other structures are not commonly injured in this syndrome.
REFERENCES: Brodsky AE, Khalil MA: Talar compression syndrome. Am J Sports Med 1986;14:472-476.
Wredmark T, Carlstedt CA, Bauer H, Saartok T: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
Marotta JJ, Micheli LJ: Os trigonum impingement in dancers. Am J Sports Med 1992;20:533-536.
Question 68:
A 13-year-old girl presents with back pain for 6 months. Figures A and B are SPECT scan and CT images taken at the time of presentation. What is the most likely diagnosis? Review Topic
Options:
- Osteoid osteoma
- Bone island
- Spondylolysis
- Osteoblastic metastases
- Aneurysmal bone cyst
Correct Answer: Osteoid osteoma
Explanation:
This
patient
has
spondylolysis.
Spondylolysis is a common cause of back pain in children/adolescents. It is common in sports with repetitive hyperextension (gymnasts, weightlifters, football linemen). It is best seen on lateral and oblique radiographs, CT (best study to diagnose and delineate anatomy), and SPECT.
Saifuddin et al. reviewed the orientation of the pars fracture. They found that only 32% of defects were oriented within 15° of the 45° lateral oblique plane and would be
visible on oblique radiographs. They thus recommend CT scans for spondylolysis.
Cheung et al. reviewed spondylolysis and spondylolisthesis. They advocate pars repair for symptomatic spondylolysis and low-grade, mobile spondylolisthesis with pars defects cephalad to L5 and for those with multiple-level defects.
Figure A is a 99mTc-MDP SPECT scan showing increased uptake at the right L5 pars interarticularis. Figure B is an axial helical CT image showing bilateral spondylolysis at L5. Illustration A is a corresponding sagittal reconstruction image demonstrating right pars fracture into the right L5 superior facet. Illustration B shows the appearance of osteoblastic metastasis (green arrow). Illustration C shows the options for pars repair.
Incorrect
Question 69:
In the absence of developmental dysplasia of the hip, what is the most common cause of osteoarthritis? Review Topic
Options:
- Legg-Calve-Perthes disease
- Traumatic labral tear
- Repetitive high-impact activity such as football
- Femoroacetabular impingement
- Hip injury resulting from a direct impact such as a knee hitting a dashboard
Correct Answer: Femoroacetabular impingement
Explanation:
Femoroacetabular impingement is a mechanism for the development of early osteoarthritis for most nondysplastic hips. Early surgical intervention for treatment of femoroacetabular impingement, besides providing relief of symptoms, may decelerate the progression of the degenerative process for this group of young patients. There are two general types of femoroacetabular impingement. In cam impingement, the femoral deformity is usually a bump on the head-and-neck junction that impinges on the acetabular rim. The pincer type of impingement is caused by deformity on the acetabular side such as a deep socket or acetabular overcoverage due to retroversion. Both mechanisms create an obstacle for flexion and internal rotation.
Question 70:
An 18-year-old boy has had pain in the right knee for the past 6 months. Examination reveals some fullness behind the knee but no significant palpable soft-tissue mass. There is no effusion, and he has full knee range of motion. The remainder of the examination is unremarkable. A radiograph and MRI scans are shown in Figures 33a through 33c, and biopsy specimens are shown in Figures 33d and 33e. What is the most likely diagnosis?
Options:
- Parosteal osteosarcoma
- Classic osteogenic sarcoma
- Ewing’s sarcoma
- Osteochondroma
- Chondrosarcoma
Correct Answer: Parosteal osteosarcoma
Explanation:
DISCUSSION: The patient has parosteal osteosarcoma. The posterior aspect of the distal femur is the typical location for this variant of osteogenic sarcoma. The imaging studies indicate a surface lesion with no involvement of the adjacent intramedullary canal. The histologic appearance is that of a low-grade fibroblastic osteosarcoma, consisting of relatively mature bone and a bland fibroblastic stroma lacking cytologic atypia and mitotic activity. A cartilaginous component is also frequently seen. Classic osteosarcoma typically has a more aggressive radiologic and histologic appearance. Sessile osteochondromas, while common behind the knee, have a presence of hematopoietic marrow and fat. The cartilage found in the associated cartilaginous cap is oriented. Chondrosarcomas are more typical in an older age group and have a histologic pattern consisting of malignant chondroid.
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 20-21.
Unni KK, Dahlin DC, Beabout JW, Ivins JC: Parosteal osteogenic sarcoma. Cancer 1976;37:2466-2475.
Question 71:
What artery provides the only direct vascularizaton to both the intraneural and extraneural blood supply of the ulnar nerve just proximal to the cubital tunnel?
Options:
- Superior ulnar collateral
- Inferior ulnar collateral
- Posterior ulnar recurrent
- Brachial
- Ulnar
Correct Answer: Inferior ulnar collateral
Explanation:
DISCUSSION: The superior ulnar collateral, inferior ulnar collateral, and posterior ulnar recurrent arteries provide consistent vascular supply to the ulnar nerve. This supply is segmental in nature. No identifiable direct anastomosis is seen between the superior ulnar collateral and the posterior ulnar recurrent arteries. The inferior ulnar collateral artery provides the only direct vascularization to the nerve and is located in the region just proximal to the cubital tunnel. The segmental nature of the blood supply to the ulnar nerve underscores the importance of its preservation during transposition.
REFERENCE: Yamaguchi K, Sweet FA, Bindra R, et al: The extraneural and intraneural arterial anatomy of the ulnar nerve at the elbow. J Shoulder Elbow Surg 1999;8:17-21.
Question 72:
What percent of patients initially diagnosed with classic, high-grade osteosarcoma of the extremity have visible evidence of pulmonary metastasis on CT of the chest?
Options:
- 5% to 10%
- 10% to 20%
- 40% to 50%
- 60% to 80%
- 80% to 90%
Correct Answer: 10% to 20%
Explanation:
DISCUSSION: CT studies show that approximately 10% to 20% of patients with high-grade osteosarcoma have pulmonary metastases at diagnosis. Although not visible on current staging studies, it is believed that up to 80% of patients have micrometastatic disease that requires systemic chemotherapy. Because it is not possible to identify those patients who do not have disseminated micrometastatic disease, most patients are treated presumptively with chemotherapy.
REFERENCES: Kaste SC, Pratt CB, Cain AM, et al: Metastases detected at the time of diagnosis of primary pediatric extremity osteosarcoma at diagnosis: Imaging features. Cancer 1999;86:1602-1608.
Link MP, Goorin AM, Miser AW, et al: The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600-1606.
Question 73:
Figures 11a and 11b show the radiographs of a 50-year-old man who was struck by a car. Treatment should consist of
Options:
- cemented bipolar hemiarthroplasty.
- cementless bipolar hemiarthroplasty.
- hybrid total hip arthroplasty.
- cementless total hip arthroplasty.
- open reduction and internal fixation.
Correct Answer: open reduction and internal fixation.
Explanation:
DISCUSSION: The patient has a displaced femoral neck fracture. Although the treatment remains controversial, most clinicians advocate either a closed or open reduction in younger active patients. Achieving an anatomic reduction is necessary to avoid loss of reduction, nonunion, or osteonecrosis. An acceptable reduction may have up to 15° of valgus angulation and 10° of posterior angulation. Parallel multiple screws or pins are the most common method of internal fixation. Prosthetic replacement is generally reserved for older and less active individuals.
REFERENCES: Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 97-108.
Asnis SE, Wanek-Sgaglione L: Intracapsular fractures of the femoral neck: Results of cannulated screw fixation. J Bone Joint Surg 1994;76A:1793-1803.
Question 74:
Baseball pitchers who have internal impingement will most likely demonstrate what changes in range of motion?
Options:
- Increase in internal rotation, decrease in external rotation
- Increase in internal rotation, increase in external rotation
- Decrease in internal rotation, decrease in external rotation
- Decrease in internal rotation, increase in external rotation
- Decrease in forward flexion, increase in external rotation
Correct Answer: Decrease in internal rotation, increase in external rotation
Explanation:
DISCUSSION: Pitchers tend to have a decrease in internal rotation and an increase in external rotation. The increase in external rotation is felt to be multifactorial. An increase in humeral retroversion occurs from repeated throwing. This results in increased soft-tissue stretching and results in a posterior capsular contracture.
REFERENCES: Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.
Crockett HC, Gross LB, Wilk KE, et al: Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. Am J Sports Med 2002;30:20-26.
Question 75:
The diagnosis of an infection after total knee arthroplasty is most reliably proven based on what single study?
Options:
- Leukocyte count and C-reactive protein
- Radiographs
- Technetium Tc 99m and gallium bone scans
- Aspiration of joint fluid
- MRI
Correct Answer: Aspiration of joint fluid
Explanation:
DISCUSSION: In a study of 52 patients with infected total knee arthroplasties, Windsor and associates showed that the average leukocyte count was 8,300/mm
3
and that aspirated knee fluid was positive in all patients except one. Knee radiographs can be unclear in showing infection, which may be present without radiographic signs of loosening. Technetium Tc 99m and gallium bone scans may not conclusively show the presence of infection, particularly in the first 3 years after knee arthroplasty.
REFERENCES: Windsor RE, Bono JV: Infected total knee replacements. J Am Acad Orthop Surg 1994;2:44-53.
Windsor RE, Insall JN, Urs WK, et al: Two-stage reimplantation for the salvage of total knee arthroplasty complicated by infection: Further follow-up and refinement of indications. J Bone Joint Surg Am 1990;72:272-278.
Question 76:
An otherwise healthy 50-year-old man who is a smoker undergoes a posterior spine fusion with instrumentation for spondylolisthesis. What can the patient do to minimize his risk for pseudarthrosis?
Options:
- Increase calcium and vitamin D intake
- Avoid all nonsteroidal anti-inflammatory drugs (NSAIDs)
- Maintain smoking cessation
- Engage in early physical therapy to strengthen the trunk musculature
Correct Answer: Maintain smoking cessation
Explanation:
Smoking is the biggest risk factor for nonunion and should be strictly avoided. NSAIDs interfere with bone healing, but not as strongly as smoking. Early mobilization would potentially stress the construct, inducing movement that leads to nonunion. Without history of calcium and vitamin D deficiency, increasing intake would not decrease the risk of nonunion.
Question 77:
Figures below show the radiographs obtained from a 90-year-old woman who is seen in the emergency department after a fall from a height. She has right hip and thigh pain and is unable to bear weight. Based on this patient's history and imaging, what is the best next step?
Options:
- Hip revision and implantation of a proximal femoral replacement
- Hip revision and implantation of a tapered fluted stem
- Open reduction and internal fixation with a locked plate and allograft struts
- Erythrocyte sedimentation rate and C-reactive protein laboratory studies
Correct Answer: Erythrocyte sedimentation rate and C-reactive protein laboratory studies
Explanation:
DISCUSSION:
Periprosthetic fracture is the third most common reason (after loosening and infection) for revision surgery after total hip arthroplasty (THA). Late periprosthetic fracture risk is 0.4% to 1.1% after primary
THA and 2.1% to 4% after revision THA. Risk factors for periprosthetic fracture include age over 70 years, decreasing bone mass, and loosening of implants and osteolysis. The risk of concomitant infection in the presence of a periprosthetic fracture is 11%, according to Chevillotte and associates. Obtaining presurgical aspiration or intrasurgical tissue for culture is recommended if concomitant infection is suspected.
Question 78:
Figure 1 is the radiograph of an otherwise healthy 68-year-old man with a 4-year history of increasing global left knee pain. He has noticed stiffness, and despite physical therapy, bracing and nonsteroidal anti-inflammatory drugs, he has continued to develop worsening symptoms and progression in his deformity. Physical examination demonstrates 80°of flexion and a 10° flexion contracture. What is the best next step?
Options:
- Manipulation under anesthesia
- Left total knee arthroplasty (TKA)
- Stem cell injection
- Unicompartmental knee arthroplasty in the lateral compartment The patient has a valgus deformity and has developed stiffness in both flexion and extension. Given the progressive loss of motion, progression to TKA is indicated. Manipulation under anesthesia would not be efficacious to prevent the progressive loss of motion without correcting the underlying mechanical issues. The patient has global pain; and therefore, unicompartmental knee arthroplasty is not ideal. Stem cell injection in this setting has not been proven.
Correct Answer: Left total knee arthroplasty (TKA)
Explanation:
Figures 1 and 2 are the radiographs of a 70-year-old man who underwent knee explantation with antibiotic spacer placement. At the time of second- stage surgery for reimplantation of a total knee arthroplasty, a medial parapatellar arthrotomy is used to access the knee. An extensive synovectomy is performed and the gutters are recreated. Medial and lateral joint line releases are done, and scar tissue is removed from around the patella. The cement spacer is removed and the nail is cut and extracted. However, despite this, the knee only flexes 45° and lateral exposure is compromised. What is the best next step?
Question 79:
Figure 24 shows an axial MRI scan of the ankle. The arrowhead is pointing to what structure?
Options:
- Tibial nerve
- Flexor hallucis longus
- Tibialis posterior
- Peroneus longus
- Peroneus brevis
Correct Answer: Peroneus brevis
Explanation:
DISCUSSION: The peroneus brevis is easily identified by its location behind the fibula and its distal muscle belly. Axial MRI images provide a reliable guide even when one of the peroneals is completely ruptured, subluxated out of the peroneal groove, or absent.
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. New York, NY, Lippincott, 1993, pp 234-235.
Sammarco GJ: Peroneus longus tendon tears: Acute and chronic. Foot Ankle Int
1995;16:245-253.
Question 80:
Compared to similar patients who do not donate autologous blood, patients with normal baseline hemoglobin who donate autologous blood prior to undergoing primary total hip arthroplasty are likely to
Options:
- receive an allogeneic transfusion.
- experience cardiac complications perioperatively.
- have a greater likelihood of receiving a transfusion perioperatively.
- have a higher hemoglobin at the time of discharge.
- have deep venous thrombosis postoperatively.
Correct Answer: have a greater likelihood of receiving a transfusion perioperatively.
Explanation:
DISCUSSION: Billote and associates compared patients with normal baseline hemoglobin levels who did and did not donate autologous blood prior to total hip arthroplasty. No patients received allogeneic blood perioperatively, and the autologous donors had significantly lower hemoglobin levels at the time of surgery and in the recovery room. Of the autologous donors, 69% received an autologous transfusion. The authors concluded that autologous donation was unnecessary in patients undergoing primary total hip arthroplasty who had a normal hemoglobin.
REFERENCES: Billote D, Glisson SN, Green D, Wixson RL: A prospective, randomized study of preoperative autologous donation for hip replacement surgery. J Bone Joint Surg Am 2002;84:1299-1304.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 47-53.
Question 81:
A 19-year-old linebacker for a collegiate football team has had two episodes of bilateral arm tingling and weakness after tackling; the symptoms resolved after 30 minutes of rest. Three follow-up neurologic examinations have been normal. Cervical spine CT and MRI scans are shown in Figures 13a through 13c. What is the next best step in management? Review Topic
Options:
- The addition of a neck roll to the helmet and continuation of play
- Electrodiagnostic studies
- A series of epidural steroid injections, followed by a return to play
- Methylprednisolone dose pack, followed by a return to play in 1 week
- No further participation in football
Correct Answer: No further participation in football
Explanation:
Cervical spinal stenosis is a contraindication to participation in collision and contact sports. Previously, the risks of permanent quadriparesis from cervical spinal stenosis were thought to be unclear and athletes with cervical spinal stenosis were often allowed to play contact sports. In 1996, Torg and associates reported that developmental narrowing of the cervical canal in a stable patient does not appear to predispose an individual to permanent catastrophic neurologic injury and therefore should not preclude an athlete from participation in contact sports. However, the current understanding is that the actual risks of permanent neurologic injury from cervical stenosis are significant. The Torg ratio was previously used for diagnosis but is more recently thought to be of low predictive value as reported by Cantu. Current methods for diagnosis of cervical spinal stenosis rely on MRI and CT. Current diagnosis is based on comparisons of measurements with normal values. A cervical canal of less than 13 mm is considered stenotic whereas a diameter of less than 10 mm is considered absolute stenosis as reported by Crowl and Kong. This patient has symptomatic stenosis and should not be cleared for contact sports. A neck roll will not prevent neurologic injury in the presence of cervical spinal stenosis. Electrodiagnostic studies are not likely to add any additional significant findings with central canal stenosis. Cervical traction is not of value in the long-term. Epidural steroid injections or a methylprednisolone dose pack are not of value in this situation.
Question 82:
An 11-year-old girl is struck in the leg by a loaded sled while sledding and is seen in the emergency department; she is reporting severe knee pain. Radiographs are read as normal. Examination reveals that she is exquisitely tender over the proximal tibial physis. The neurovascular examination is normal. What is the next step in management?
Options:
- Splinting, admission, and frequent neurovascular checks
- Cylinder cast and discharge
- Four-compartment calf fasciotomy
- Non-weight-bearing, a knee immobilizer, and follow- up in 1 week
Correct Answer: Splinting, admission, and frequent neurovascular checks
Explanation:
DISCUSSION: The anatomic lesion in this patient is not exactly defined, but she has most likely sustained an injury about the knee. A Salter-Harris type I proximal tibial physeal fracture is likely. The normal radiograph reading can be misleading because these injuries may displace and spontaneously reduce. The child is at risk of compartment syndrome although she is currently not displaying signs of it. Thus, even though this injury may seem trivial by radiographic findings, it should be treated like a knee dislocation with a risk of late developing compartment syndrome. MRI or CT may be necessary to define the injury. She does not require emergent treatment, but merits close observation for possible compartment syndrome. Any of the possible injuries about the knee can be unstable and require internal fixation after reduction.
REFERENCES: McGuigan JA, O’Reilly MJ, Nixon JR: Popliteal arterial thrombosis resulting from disruption of the upper tibial epiphysis. Injury 1984;16:49-50.
Burkhart SS, Peterson HA: Fractures of the proximal tibial epiphysis. J Bone Joint Surg Am
1979;61:996-
1002
.
Question 83:
A follow-up examination of a patient 6 weeks after knee surgery reveals a range of motion from 5° to 55° of flexion. Which of the following statements best summarizes the role of manipulation under anesthesia for this patient?
Options:
- Manipulation under anesthesia offers the best chance of improving and maintaining the patient’s range of motion.
- The gains from manipulation under anesthesia are only temporary and rarely last more than 6 months.
- Increasing the frequency and intensity of physical therapy over the next 2 months will have the same effect as manipulation under anesthesia.
- The risks of fracture are so great from manipulating a knee that the patient should be advised to live with a limited range of motion.
- The patient’s final result will be poor with or without manipulation.
Correct Answer: Manipulation under anesthesia offers the best chance of improving and maintaining the patient’s range of motion.
Explanation:
DISCUSSION: Esler and associates evaluated the use of manipulation under anesthesia in 47 knees. Manipulation was considered when intensive physical therapy failed to increase flexion to more than 80°. The mean time from arthroplasty to manipulation was 11.3 weeks, and the mean active flexion before manipulation was 62°. One year later, the mean gain was 33°. Definite sustained gains in flexion were achieved even when manipulation was performed 4 or more months after arthroplasty. An additional 21 patients who met the criteria for manipulation declined the procedure, and despite continued physical therapy, they showed no significant increase in knee flexion.
REFERENCE: Esler CN, Lock K, Harper WM, Gregg PJ: Manipulation of total knee replacements: Is the flexion gained retained? J Bone Joint Surg Br 1999;81:27-29.
Question 84:
A 65-year-old woman has had chronic aching discomfort involving her elbow for the past 6 months. Radiographs and a biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?
Options:
- Metastatic carcinoma (thyroid)
- Multiple myeloma
- Lymphoma
- Synovial cell sarcoma
- Osteomyelitis
Correct Answer: Multiple myeloma
Explanation:
DISCUSSION: The histologic features of multiple myeloma are distinctive for this lesion. The plasma cells are round or oval and have an eccentric nucleus and prominent nucleolus. These characteristics and a clear area next to the eccentric nucleus representing the prominent Golgi center are pathognomonic for plasma cells. Lymphoma is in the differential diagnosis; the most frequent types that occur in bone are large cell or mixed small and large cell types. The histologic appearance of the specimen is not consistent with the other choices.
REFERENCE: Dorfman HD, Bodgan C: Immunohematopoietic tumors, in Dorfman HD, Bogdan C (eds): Bone Tumors. St Louis, MO, Mosby, 1998, Chapter 12.
Question 85:
Following its exit from the sciatic notch, the sciatic nerve passes between what two muscles?
Options:
- Piriformis and superior gemellus
- Superior gemellus and obturator internus
- Inferior gemellus and quadratus femoris
- Gluteus medius and minimus
- Quadratus femoris and gluteus maximus
Correct Answer: Piriformis and superior gemellus
Explanation:
DISCUSSION: Though anatomic variations exist, both divisions of the sciatic nerve most commonly pass between the piriformis and superior gemellus. This anatomic consideration is relevant during the posterior approach to the hip, where careful retraction of the rotators avoids sciatic nerve injury.
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 335-348.
Anderson JE (ed): Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Williams,
1978, Figure 4-34.
FOR ALL MCQS CLICK THE LINK ORTHO
MCQ BANK
Question 86:
A 55-year-old male sustained the injury in Figure A. His injury was complicated by an acute compartment syndrome. He underwent external fixation of his extremity and four compartment fasciotomy. When should the treatment shown in Figure B be performed to minimize the risk of infection?
Options:
- Before fasciotomy closure
- At fasciotomy closure
- After fasciotomy closure
- After 24 hours of antibiotic treatment
- Timing of definitive fixation does not alter infection risk Corrent answer: 5 The timing of definitive fixation of tibial plateau fractures in patients with fasciotomies has no impact on infection risk. The incidence of compartment syndrome is high in tibial plateau fractures. In the presence of tense anterior and lateral tibial compartments, combined with pain with passive stretch of involved muscles or unrelenting pain, compartment pressures should be measured and fasciotomies performed when necessary. Schatzker type V and VI fractures are more likely to have this potential complication. Examination of leg compartments should be repeated at regular intervals because compartment syndrome may occur 24 hours or more after injury. Zura et al. performed a study to analyze whether there is an association between infection and the timing of definitive fracture fixation in relation to fasciotomy closure or coverage. They found that no statistical difference in the rate of infection when tibial plateau fractures with four-compartment fasciotomies were treated with open reduction and internal fixation before fasciotomy closure, at fasciotomy closure, or after fasciotomy closure. They conclude that timing of definitive fracture treatment can be determined by the medical condition of the patient. Shah et al. performed a retrospective chart review of all bicondylar tibial plateau fractures that had fixation with two incisions. They reported an infection rate of 13.8% which is lower than historical reports. They concluded that the lower infection rate was due to their treatment algorithm that requires recovery of the soft tissue envelope prior to definitive fixation. Figure A demonstrates a bicondylar tibial plateau fracture. Figure B demonstrates fixation of a tibial plateau fracture through a dual plating technique. Incorrect Answers:
Correct Answer: Before fasciotomy closure
Explanation:
Question 87:
Closed chain kinetic exercises are differentiated from open chain exercises by which of the following? Review Topic
Options:
- Increased joint shear
- Maximally rehabilitate individual muscles
- Achieve normal motion in all the joints of the kinetic chain
- Maximize joint distraction
- The compressive nature of applied loads
Correct Answer: The compressive nature of applied loads
Explanation:
Closed chain kinetic exercises confer a margin of safety and are protective of healing or repaired tissues by the compressive nature of the applied forces. Closed chain kinetic exercise is associated with decreased shear, translation, and distraction of the joints within the chain. Because of patterns of motion with closed chain kinetic exercises, individual muscles may not be maximally strengthened or all joint motion returned to normal. Closed chain kinetic exercises may be used earlier in the rehabilitation process.
Question 88:
The postoperative neurologic prognosis of a patient who has a tumor that is compressing the spinal cord and causing a neurologic deficit depends primarily on the
Options:
- pretreatment neurologic status.
- extent of spinal cord compression.
- extent of bony deformity.
- MRI findings.
- dimension of the spinal canal.
Correct Answer: pretreatment neurologic status.
Explanation:
DISCUSSION: The tumor biology, location, and pretreatment neurologic status are the best predictors of a patient’s postoperative neurologic prognosis. Between 60% to 90% of patients who are ambulatory at the time of diagnosis will retain this ability after treatment. Location is important in that less space is available for the cord in the thoracic spine. Lesions located in vascular watershed regions may disrupt the vascular supply of the cord.
REFERENCES: Weinstein JN: Differential diagnosis and surgical treatment of primary benign and malignant neoplasms, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 1, pp 829-860.
Siegal T, Siegal T: Current considerations in the management of neoplastic spinal cord compression. Spine 1989;14:223-228.
Question 89:
Figure 54 shows the preoperative radiograph of a 45-year-old woman who is considering total hip arthroplasty with her orthopaedic surgeon. What femoral characteristic is a typical concern in this patient?
Options:
- Osteopenia
- Excessive anteversion
- Excessive varus
- Excessive bowing
- Stove-pipe femur
Correct Answer: Excessive anteversion
Explanation:
DISCUSSION: Developmental dysplasia of the hip (DDH) leads to early arthritis of the hip as seen in this patient. Although DDH is believed to mostly affect the acetabulum, most patients with DDH also have anatomic aberrations of the femur. Using three-dimensional computer models generated by reconstruction of CT scans, dysplastic femurs were shown to have shorter necks and smaller, straighter canals than the controls. The shape of the canal became more abnormal with increasing subluxation. The studies also have shown that the primary deformity of the dysplastic femur is rotational, with an increase in anteversion of 5 degrees to 16 degrees, depending on the degree of subluxation of the hip. The rotational deformity of the dysplastic femur arises within the diaphysis between the lesser trochanter and the isthmus and is not attributable to a torsional deformity of the metaphysis. Osteopenia is not a concern in a patient with an excellent cortical index (thick cortices and narrow canal). Femoral varus or bowing of the femur is not a typical finding in patients with DDH.
REFERENCES: Noble PC, Kamaric E, Sugano N, et al: Three-dimensional shape of the dysplastic femur: Implications for THR. Clin Orthop 2003;417:27-40.
Sugano N, Noble PC, Kamaric E, et al: The morphology of the femur in developmental dysplasia of the hip. J Bone Joint Surg Br 1998;80:711-719.
Question 90:
Which of the following is most predictive of a medial side ankle injury in the presence of a fibula fracture above the level of the joint?
Options:
- Severe medial ankle tenderness
- Severe medial ankle ecchymosis
- Stress radiographs showing the medial clear space measuring 6 mm and the superior joint space measuring 3 mm
- Inability to ambulate
- Medial ankle swelling
Correct Answer: Stress radiographs showing the medial clear space measuring 6 mm and the superior joint space measuring 3 mm
Explanation:
DISCUSSION: Isolated Lauge-Hansen supination-external rotation-type ankle fractures comprise 20% to 40% of ankle fractures and nonsurgical management is effective for managing SER-2 ankle fractures. Tornetta and associates recently showed that medial ankle tenderness, ecchymosis, and swelling are not reliable findings when trying to determine deltoid competence. Stress radiographs showing a medial clear space of greater than 4 mm or one that is also 1 mm greater than the superior joint space, or any lateral talar subluxation are indicative of deltoid incompetence and indicative of a SER-4 ankle fracture.
REFERENCES: McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004:86;2171-2178.
Kristensen KD, Hansen T: Closed treatment of ankle fractures: Stage II supination-eversion fractures followed for 20 years. Acta Orthop Scand 1985;56:107-109.
Michelson JD: Fractures about the ankle. J Bone Joint Surg Am 1995;77:142-152.
Question 91:
A 13-year-old boy hyperextends his knee while playing basketball and reports a pop that is followed by a rapid effusion. A lateral radiograph is shown in Figure 4. Initial management consists of attempted reduction with extension, with no change in position of the fragment. What is the next most appropriate step in management?
Options:
- A long leg cast in 90° of knee flexion for 6 weeks
- Open reduction and internal fixation with a transphyseal 6.5-mm screw and washer
- Arthroscopic anterior cruciate ligament reconstruction with hamstring tendons
- Arthroscopic debridement and staged anterior cruciate ligament reconstruction when skeletally mature
- Open reduction and internal fixation with suture or intra-epiphyseal screw placement
Correct Answer: Open reduction and internal fixation with suture or intra-epiphyseal screw placement
Explanation:
DISCUSSION: Avulsion fractures of the tibial spine are rare injuries that result from rapid deceleration or hyperextension of the knee in skeletally immature individuals. This injury is the equivalent of ruptures of the anterior cruciate ligament in adults. These fractures are classified as types 1 through 3. Type 1 is a minimally displaced fracture, type 2 fractures have an intact posterior hinge, and type 3 fractures have complete separation. The radiograph demonstrates a completely displaced, or type III, tibial spine avulsion. Surgical reduction is indicated in type 2 fractures that fail to reduce with knee extension and in all type 3 fractures. Reduction may be arthroscopic or open, with fixation of the bony fragment using a method that maintains physeal integrity and prevents later growth arrest. Preferred techniques would be with suture or an intra-epiphyseal screw
REFERENCES: Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60.
Mulhall KJ, Dowdall J, Grannell M, et al: Tibial spine fractures: An analysis of outcome in surgically treated type III injuries. Injury 1999;30:289-292.
Owens BD, Crane GK, Plante T, et al: Treatment of type III tibial intercondylar eminence fractures in skeletally immature athletes. Am J Orthop 2003;32:103-105.
Vocke
AK, Vocke AR: Cartilaginous avulsion fracture of the tibial spine. Orthopedics 2002;25:1293-1294.
Question 92:
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?
Options:
- Suprascapular nerve entrapment
- Supraspinatus and infraspinatus tendon tear
- Muscular dystrophy
- Thoracic outlet syndrome
- Spinal accessory nerve disruption
Correct Answer: Suprascapular nerve entrapment
Explanation:
DISCUSSION: The sagittal image reveals increased signal and decreased size of the supraspinatus and infraspinatus muscles, indicating muscle atrophy. The rotator cuff tendon signal is normal. The subscapularis and teres minor muscles are unaffected. Muscular dystrophy and thoracic outlet syndrome would be expected to have a more global effect. Although muscular atrophy can occur in the setting of a rotator cuff tear, the coronal image shows an intact supraspinatus. The suprascapular nerve supplies the supraspinatus and infraspinatus muscles. Therefore, suprascapular nerve entrapment would result in atrophy of these muscles with sparing of the surrounding musculature. Any lesion within the suprascapular notch, including neoplastic disease, a venous varix, or neuroma, can place pressure on the suprascapular nerve. Suprascapular nerve entrapment most commonly results from extension of a paralabral cyst or ganglion, often with associated labral pathology. Spinal accessory nerve disruption would show trapezius muscle atrophy.
REFERENCES: Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 123.
Question 93:
The patient shown in Figure 44 reports that her toes hurt when she walks. Management should consist of
Options:
- shoe modifications for comfort.
- fourth metatarsal lengthening.
- fourth metatarsophalangeal fusion.
- fourth ray resection.
- soft-tissue releases and muscle balancing.
Correct Answer: shoe modifications for comfort.
Explanation:
DISCUSSION: Brachymetatarsia is a congenital hypoplasia of one or more metatarsals. Shortening of the fourth metatarsal is the most common form of brachymetatarsia and is often bilateral. Taping and manipulative reduction attempts are ineffective, and extensor tenotomy and capsulotomy are not likely to sufficiently correct the deformity. Fusion or metatarsal lengthening result in complications and generally are not indicated. Shoe modifications, such as extra-depth or extra-wide shoes, generally will improve symptoms. If pressure and trauma persist in the older child, metatarsal lengthening or amputation may be indicated.
REFERENCES: Stevens PM: Toe deformities, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, p 195.
Tachdjian MO: Pediatric Orthopedics, ed 2. Philadelphia, PA, WB Saunders, 1990,
pp 2633-2637.
Question 94:
A 27-year-old woman reports the acute atraumatic onset of burning pain in her right shoulder followed a week later by significant weakness and the inability to abduct her shoulder. One week prior to this incident she had recovered from a flu-like syndrome. Examination reveals full passive motion of the shoulder and the inability to actively raise the arm. Sensation in the right upper extremity is normal. Cervical spine examination is normal. Radiographs of the shoulder and cervical spine are normal. What is the most likely diagnosis?
Options:
- Calcific tendinitis
- Poliomyelitis
- Diskogenic cervical spine disease
- Impingement
- Brachial neuritis
Correct Answer: Brachial neuritis
Explanation:
DISCUSSION: The patient has symptoms and examination findings of acute brachial neuritis which is often a diagnosis of exclusion. The recent viral flu-like symptoms have shown a correlation with the development of this disorder. The acute, severe shoulder weakness excludes calcific tendinitis, impingement, and poliomyelitis. A normal cervical spine examination makes cervical disk disease unlikely.
REFERENCES: Turner JW, Parsonage MJ: Neuralgic amyotrophy (paralytic brachial neuritis). Lancet 1957;2:209-212.
Omer GE, Spinner M, Van Beek AL (eds): Management of Peripheral Nerve Problems, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 101-104.
Question 95:
In long-term follow-up studies of cemented total knee arthroplasty (TKA), the lowest rates of osteolysis have been associated with which design feature?
Options:
- Metal-backed patellar components
- Modular cruciate-retaining tibial inserts
- Modular cruciate-substituting tibial inserts
- Monolithic tibial trays
Correct Answer: Monolithic tibial trays
Explanation:
DISCUSSION
The lowest reported rates of osteolysis involving cemented TKAs are associated with monolithic tibial components. Modular components and cemented metal-backed patella components are associated with a high prevalence of backside tibial insert wear and osteolysis.
Question 96:
A year-old man undergoes removal of an infected total hip arthroplasty (THA) and insertion of an articulating antibiotic-loaded spacer to treat a deep periprosthetic hip infection. While in a nursing home receiving intravenous antibiotics 3 weeks after surgery, the patient trips and falls. Examination reveals swelling in the mid and distal thigh, intact skin and neurovascular structures, and severe pain with knee or hip movement. Radiographs of the femur are shown in 1 through What is the most appropriate treatment for the fracture below the implant?
Options:
- Balanced traction to address concern for persistent infection with reoperation
- Open reduction and internal fixation of the fracture with a lateral plate and screws
- Removal of the articulating spacer and revision to a longer-stem antibiotic-loaded articulating spacer
- Removal of the articulating spacer and reimplantation using a long-stem fluted uncemented hip replacement
Correct Answer: Open reduction and internal fixation of the fracture with a lateral plate and screws
Explanation:
DISCUSSION:
This patient has a type C periprosthetic femoral fracture. The articulating spacer is not involved in the fracture, which is well distal to the implant. The most appropriate treatment is open reduction and internal fixation of the fracture. Traction is not appropriate for this fracture because the injury can be treated surgically despite the history of previous hip infection. Traction would also be needed for at least 5 weeks and would delay the surgical treatment of the periprosthetic fracture until the time of second-stage revision THA. The fracture is fairly distal, and revision to a longer antibiotic-loaded implant or uncemented stem is not suitable for this fracture pattern, because it extends well past the isthmus. A femoral stem in the distal fragment would provide little stability for the fracture. Removal of the articulating spacer and reimplantation using a long-stem fluted uncemented hip replacement is not appropriate, because it would be premature to reimplant the man's hip while he is still receiving treatment for a deep hip infection.
Question 97:
After performing an open distal clavicle excision and resecting 15 mm of distal clavicle, which potential concern for shoulder function could result?
Options:
- Persistent pain attributable to inadequate resection
- Complex regional pain syndrome
- Fracture
- AC joint instability
Correct Answer: AC joint instability
Explanation:
DISCUSSION
AC joint arthritis often is marked by pain along the anterior and superior aspects of the shoulder. It can occasionally radiate into the trapezius and the anterolateral neck region. A patient may have tenderness to palpation directly at the AC joint or pain with the cross-body adduction stress test and the O'Brien active compression test. During the cross-body adduction test, this patient has pain when the examiner lifts his arm in 90 degrees of forward flexion and maximally adducts it across his body. Although the cross-body adduction test is the most sensitive provocative test for AC joint osteoarthritis at 77%, the O’Brien active compression test has been shown to be most specific at 95%.
Physical therapy, rest, activity modification, and other nonsurgical treatments might not reverse osteoarthritis changes at the AC joint, but these interventions can often help improve pain, range of motion, and function. A corticosteroid injection into the AC joint may be an option if nonsurgical treatments do not work, although Wasserman and associates demonstrated that only 44% of AC joint injections accurately entered the joint.
Persistent pain is the most common complication following distal clavicle excision. Although the exact amount of distal clavicle that should be resected is a topic of debate, resection of 10 mm or more of the distal clavicle may lead to instability of the AC joint, especially if the AC capsule is sectioned.
Question 98:
Figure 81 is the radiograph of a healthy 72-year-old man who has a 3-month history of medial knee pain. He denies any specific trauma. Until 3 months ago when the pain began, he had been an avid runner for many years. Initial treatment should be oral anti-inflammatory medication
Options:
- alone.
- with food.
- with a proton pump inhibitor.
- with glucosamine hydrochloride.
Correct Answer: with a proton pump inhibitor.
Explanation:
This patient has bone-on-bone end-stage arthritis that was asymptomatic until 3 months ago. Patients older than age 65 are at increased risk for adverse gastrointestinal effects when placed on nonsteroidal anti-inflammatory drugs, and they should be placed on a proton pump inhibitor prophylaxis at the same time. Use of glucosamine is controversial. Glucosamine hydrochloride has been shown in prospective studies to have no beneficial effect. However, glucosamine sulfate has been shown to have a positive effect on pain, but no effect on function.
Question 99:
9A 9B 9C 9D Figures 9a through 9d are the radiographs of a 21-year-old woman who is involved in a high-speed motor vehicle collision and sustains an isolated right closed-foot injury. Before surgery, the patient is advised about the relatively poor long-term outcomes associated with this injury. What is the most common reason for functional limitations after surgical treatment in this scenario?
Options:
- - Subtalar arthritis
- - Osteonecrosis
- - Nonunion
- - Varus malunion
Correct Answer: - Subtalar arthritis
Explanation:
DISCUSSION
When a displaced talar neck fracture occurs, the rate of osteonecrosis is high; however, many revascularize the talus without collapse. A nonunion can occur but is less common than osteonecrosis and arthritis. A varus malunion can be debilitating and lead to subtalar arthritis. In a fracture with the talar body dislocated posteromedially (such as in this example) neurologic deficits in the tibial nerve distribution are common but typically improve with urgent
reduction. Studies show that posttraumatic subtalar arthritis is common after this injury and is the most likely cause of long-term functional impairment.
RECOMMENDED READINGS
Vallier HA, Nork SE, Barei DP, Benirschke SK, Sangeorzan BJ. Talar neck fractures: results and outcomes. J Bone Joint Surg Am. 2004 Aug;86-A(8):1616-24. PubMed PMID: 15292407.
View Abstract at PubMed
Lindvall E, Haidukewych G, DiPasquale T, Herscovici D Jr, Sanders R. Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am. 2004 Oct;86-A(10):2229-34. PubMed PMID: 15466732.
View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 10 THROUGH 12
10A
10B
10C
Figure 10a is the radiograph of a 30-year-old man who sustained an injury in a motor vehicle collision.
Question 100:
Figures below show the radiographs obtained from a 79-year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. No evidence of infection is seen. What is the most appropriate treatment?
Options:
- Retain the components, and implant a tibial strut allograft.
- Revise the tibial component with a metaphyseal cone and metaphyseal uncemented stem.
- Revise the tibial component with a metaphyseal cone and a press-fit diaphyseal-engaging stem.
- Revise the tibial component with a long cemented diaphyseal-engaging stem.
Correct Answer: Revise the tibial component with a metaphyseal cone and a press-fit diaphyseal-engaging stem.
Explanation:
DISCUSSION:
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis, as shown in Figures 3 and 4. They also assist in obtaining correct limb alignment. Short metaphyseal-engaging stems are associated with failure rates that range between 16% and 29%. Cemented stems may be shorter than press-fit stems, because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.