Orthopedic Surgery Board Review MCQs: Spine, Trauma, & Knee | Part 233

Key Takeaway
This page provides 100 high-yield, verified multiple-choice questions (MCQs) for orthopedic surgeons and residents. Designed in OITE/AAOS format, it's an essential tool for board certification exam preparation, offering study and exam modes with detailed clinical explanations and references.
About This Board Review Set
This is Part 233 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 233
This module focuses heavily on: Cartilage, Foot, Fracture, Infection, Knee, Spine.
Sample Questions from This Set
Sample Question 1: Which of the following results cannot be achieved with an in-shoe orthosis?...
Sample Question 2: A 35-year-old rock climber sustains an L1 burst fracture from a 30-foot fall while climbing. He sustained no other fractures or serious injuries. He is neurologically intact and has minimal posterior tenderness without increased spinous pro...
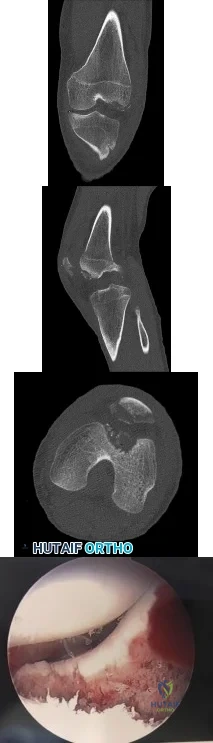
Sample Question 3: Figures 1 through 4 are the CT scans and intraoperative image of a 17-year-old boy who sustained a gunshot wound to his knee. What is the most appropriate definitive surgical management for his articular cartilage defect?...
Sample Question 4: The risk for postoperative wound infection after lumbar spine surgery is reduced most by the use of...
Sample Question 5: When comparing arthroscopic lavage and knee debridement with placebo in patients with chronic symptomatic osteoarthritis, what outcome has been demonstrated?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following results cannot be achieved with an in-shoe orthosis?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 55-64.
Bono CM, Berberian WS: Orthotic devices: Degenerative disorders of the foot and ankle. Foot Ankle Clin 2001;6:329-340.
Buonomo LJ, Klein JS, Keiper TL: Orthotic devices: Custom-made, prefabricated, and material selection. Foot Ankle Clin 2001;6:249-252.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 2
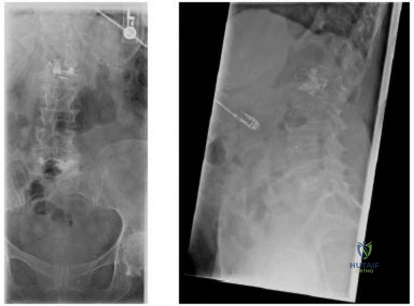
A 35-year-old rock climber sustains an L1 burst fracture from a 30-foot fall while climbing. He sustained no other fractures or serious injuries. He is neurologically intact and has minimal posterior tenderness without increased spinous process separation on examination. Radiographs reveal kyphosis of 20 degrees between T12 and L2 with 30% vertebral height loss. A CT scan shows 55% canal compromise. What is the most appropriate management? Review Topic
Explanation
Question 3
Figures 1 through 4 are the CT scans and intraoperative image of a 17-year-old boy who sustained a gunshot wound to his knee. What is the most appropriate definitive surgical management for his articular cartilage defect?
Explanation
Question 4
The risk for postoperative wound infection after lumbar spine surgery is reduced most by the use of
Explanation
Question 5
When comparing arthroscopic lavage and knee debridement with placebo in patients with chronic symptomatic osteoarthritis, what outcome has been demonstrated?
Explanation
Excluding a diagnosis of meniscal tear, loose body, or mechanical derangement, treating knee osteoarthritis of indeterminate cause with arthroscopic lavage and debridement has been found to provide no discernable benefit to offset the risk of surgery. The effects of arthroscopy have not been clinically significant in the vast majority of patient-oriented outcomes measures for pain and function at multiple times between 1 week and 2 years after surgery.
Question 6
Figure 26 is the radiograph of a 33-year-old woman who was involved in a high-speed motor vehicle crash. Her initial blood pressure is 80/50 mm Hg and she has a pulse rate of 120 bpm. After hemodynamic stabilization and temporizing measures have been performed, the patient is cleared for surgery. What is the most appropriate method of definitive fixation?

Explanation
Question 7
What term best describes the process involved when a growth factor produced by an osteoblast stimulates the differentiation of an adjacent undifferentiated mesenchymal cell during fracture repair?
Explanation
REFERENCES: Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044.
Zuscik MJ, Drissi MH, Reynolds PR, et al: Molecular and cell biology in orthopaedics, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006,
in press.
Question 8
Which of the following types of intra-articular pathology is associated with lateral meniscal cysts? Review Topic
Explanation
Question 9
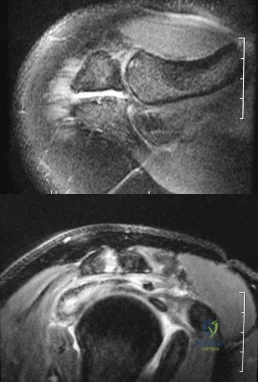
A 12-year-old pitcher has had a 2-month history of pain in his right dominant shoulder after throwing. He reports that the pain has gradually progressed to the point where he cannot throw without pain. He also notes that the pain now awakens him at night if he has been active. Anti-inflammatory drugs have failed to provide relief. Examination reveals no abnormalities except for some localized tenderness over the proximal humerus. Figures 32a and 32b show radiographs of both shoulders. What is the most likely diagnosis?
Explanation
REFERENCES: Albert MJ, Drvaric DM: Little League shoulder: Case report. Orthopedics 1990;13:779-781.
Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 10
What is the most common nonanesthetic-related reversible cause of changes in intraoperative neurophysiologic monitoring data?
Explanation
REFERENCES: Jones SC, Fernau R, Woeltjen BL: Use of somatosensory evoked potentials to detect peripheral ischemia and potential injury resulting from positioning of the surgical patient: Case reports and discussion. Spine J 2004;4:360-362.
Schwartz DM, Sestokas AK, Hilibrand AS, et al: Neurophysiological identification of position-induced neurologic injury during anterior cervical spine surgery. J Clin Monit Comput 2006;20:437-444.
Question 11
The infection work-up is negative. What is the best next step?

Explanation
The cross-table lateral radiograph shows that the patient has decreased acetabular anteversion. She is likely impinging on her cup in flexion and levering the femoral component posteriorly. Given a well-fixed and well-aligned femoral component and a negative infection work-up, the preferred treatment is to revise the acetabulum with a goal of increasing acetabular anteversion to avoid prosthetic impingement. Conversion to a constrained or elevated rim liner is suboptimal in this setting, because the problem is impingement. Indications for a constrained liner are neuromuscular compromise, abductor deficiency, or instability despite well-fixed and well-placed components. Given her 5 of 5 abductor strength, gluteus medius repair is not indicated.
Question 12
Anterior perforation of the distal femur from antegrade femoral nailing has been attributed to what factor?

Explanation
The radius of curvature is generally smaller (114-120 cm) than many earlier generation femoral nails (up to 300 cm), and the referenced article by Ostrum et al describes a case series of 3 such patients with subtrochanteric fractures. He noted that the difference in femoral anteroposterior bow between the bone and the implant is a contributing factor to distal femoral anterior cortex penetration in intramedullary nailing of subtrochanteric fractures.
Illustration A shows an example of a nail penetrating the anterior femoral cortex.
Question 13
According to Musculoskeletal Infection Society (MSIS) guidelines, which set of patient laboratory study results fits the definition of chronic prosthetic joint infection?
Explanation
The MSIS definition of periprosthetic joint infection was updated in 2014 with two major and six minor criteria. The presence of one major criterion or three minor criteria is diagnostic for infection. The major criteria are two positive cultures with the same organism or a draining sinus tract. The current MSIS minor criteria are 1) an elevated ESR (more than 30 mm/hr) and CRP level (more than 10 mg/L), 2) an elevated synovial WBC count (more than 3,000 cells per/microliter), 3) an elevated synovial fluid polymorphonuclear count (more than 80%), 4) a positive histological analysis of periprosthetic tissue, and 5) a single positive culture.
Question 14
A 69-year-old woman has just undergone an uncomplicated total shoulder arthroplasty for glenohumeral osteoarthritis. A press-fit humeral stem and a cemented all-polyethylene glenoid component were placed. At this point, what is the postoperative rehabilitation plan? Review Topic
Explanation
Question 15
A 45-year-old tennis player undergoes surgery for chronic lateral epicondylitis. After returning to play, he notes increasing lateral elbow pain with mechanical catching and locking. Examination shows positive supine posterolateral rotatory instability. What ligament has been injured? Review Topic
Explanation
Question 16
The use of multiagent adjuvant chemotherapy is associated with a clear survival benefit in which of the following diseases?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 53.
Link M, Goorin A, Miser A, et al: The effect of adjuvant chemotherapy and relapse free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600-1606.
Question 17
A 30-year-old man has pain in the left arm after a motor vehicle accident. His neurovascular examination is intact, and radiographs are shown in Figures 25a and 25b. What is the best course of management?
Explanation
REFERENCES: Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Yokoyama K, Itoman M, Kobayashi A, et al: Functional outcomes of “floating elbow” injuries in adult patients. J Orthop Trauma 1998;12:284-290.
Question 18
A 12-year-old girl who plays softball has chronic lateral hindfoot aching pain that is aggravated by weight-bearing activity. She reports that the pain has recurred after initial improvement with cast immobilization, and it continues to limit her overall level of activity. Radiographs are seen in Figures 40a through 40c. What is the most appropriate surgical treatment? Review Topic

Explanation
appears to be helpful. A hindfoot arthrodesis (usually triple) would be reserved if coalition resection proves to be unsuccessful. Achilles tendon lengthening and orthotic support, as well as debridement of the sinus tarsi, are not expected to result in a satisfactory outcome. The patient does not have a flatfoot deformity.
(SBQ13PE.64) A 5-year-old boy presents to clinic for evaluation of bilateral foot deformities shown in Figure 1. He is fully active and has no pain. The feet appear normal when he is sitting on the examination table, and there is supple passive motion at the subtalar joint. Passive ankle dorsiflexion is to neutral with knee in extension and 15 degrees with knee in flexion. What is the most appropriate next step? Review Topic

Spine MRI
Standing radiographs of the bilateral feet
Gastrocnemius stretching and nightime use of ankle foot orthosis
Gastrocnemius stretching and use of UCBL orthotic when ambulating
Gastrocnemius stretching
The patient is presenting with bilateral flexible pes planovalgus (or flexbile flatfoot). The most appropriate treatment in patients with a tight heel cord and no pain is gastrocnemius stretching
A flexible flatfoot in a child typically resolves spontaneously. Radiographs are typically indicated when there is pain to rule out other conditions. Treatment for patients without pain includes observation and gastrocnemius stretching. If there is pain, soft arch support or a more rigid UCBL can be used, but orthotics do not change the natural history. In patients with continued tightness in the heel cord despite aggressive stretching, gastrocnemius lengthening may be necessary.
Mosca reviews the management of flexible flatfeet in children and adolescents. He reports that there is no compelling evidence that an arch can be created with use of
orthotics. He proposes the following algorithm: patients with asymptomatic flatfeet are observed; symptomatic flatfeet with tight heel cords undergoing stretching until they become asymptomatic; symptomatic flatfeet with tight heel cords that do not respond to stretching (rare cases) are considered for surgery.
Figure A shows a young a patient with bilateral flatfeet when standing. Incorrect Answers:
abnormalities can seen in patients with cavovarus deformity Answer 2: Radiographs are indicated when there is pain to rule out other conditions. Answer 3: Ankle foot orthoses are not used for pes planovalgus Answer 4: UCBL would be indicated if the patient was having pain.
(SBQ13PE.42) Submuscular bridge plating is appropriate treatment for which of the following? Review Topic
A 2-month-old female with displaced, spiral, mid-diaphyseal femur fracture
A 26-month-old boy with a displaced spiral mid-diaphyseal femur fracture with
<2cm shortening
A 7-year old boy with a transverse, non-comminuted mid-diaphyseal femur fracture
A 7-year-old boy with a highly comminuted mid-diaphyseal femur fracture
A 15-year-old girl with a displaced butterfly fragmented mid-diaphyseal femur fracture
Submuscular bridge plating is appropriate for length-unstable femur fractures in skeletally immature patients ages 6 years and older.
Traditional plating of diaphyseal femur fractures in children has been abandoned due to the large incision and significant periosteal stripping involved. Submuscular plating with limited incisions and percutaneously applied fixation is a more biologically friendly way to achieve rigid internal fixation in length-unstable fracture patterns. External fixation is another acceptable option for these fractures. Locked plating, on the other hand, provides an 'internal external fixator,' avoids pin site issues and allows rapid mobilization while providing a biologically favorable environment for healing.
Kocher et al. provide the AAOS Clinical Practice Guideline for the treatment of pediatric diaphyseal femur fractures. They concluded that there was insufficient evidence regarding submuscular bridge plating to include it in the guideline.
Flynn et al. review the management of pediatric femoral shaft fractures. The note that
the narrow indications for plating of pediatric femoral fractures are open fractures, multiple trauma, head injury or compartment syndrome in patients less than 12 years old. Plating allows rigid fixation with readily available equipment and allows for rapid mobilization.
Hedequist et al. present a Technical Tricks paper in which they detail their surgical technique for submuscular bridge plating. They recommend this fixation strategy for patients between age 6 and skeletal maturity with comminuted diaphyseal femur fractures that are not easily treated by other methods.
Illustration A shows a preoperative and postoperative radiograph of a comminuted pediatric femur fracture treated with submuscular plating.
Incorrect answers:
(SBQ13PE.88) A 12-month-old boy attends a government regulated childcare center. His parents are called after a fall. Non-accidental trauma has been ruled out. On physical examination the right elbow is swollen and tender. He is unwilling to allow you to move the arm. Radiographs of the elbow are shown in Figure A. What is the orthopaedic management of this injury? Review Topic

Observation only
Elbow sling for 3 to 4 weeks
Rigid elbow immobilisation for 4 to 5 weeks
Admit for 24-48 hours for continuous intracompartmental pressure measurements
Operative fixation with percutaneous pinning PREFERRED RESPONSE 5
This patient presents with a distal humeral physeal separation. The most appropriate treatment would be closed reduction with internal fixation with percutaneous pins.
Displaced distal humerus physeal separation is typically seen in children under the age of 3 and has a high association with child abuse. The diagnosis can be a difficult as radiographs of a distal humeral physeal separation may be subtle. Often, radiographs show no obvious fracture, but can appear like an elbow dislocation since the secondary ossification centers have not yet developed. MRI or arthrogram can be used to aid in diagnosis.
Shrader et al. reviewed pediatric supracondylar fractures and pediatric physeal elbow fractures. They state the key to diagnosis of distal humerus physeal separation is the assessment is the radial head–capitellum relationship. These injuries should be fixed with closed reduction and smooth wire pinning. An elbow arthrogram may be considered intraoperatively for these patients because of the difficulty visualizing the distal humeral anatomy in children so young.
Skaggs et al. reviewed the diagnosis and management of pediatric elbow fractures. He states that child abuse should be suspected in all cases of elbow fracture when the child is less than 3 years of age and/or the injury pattern occur from a shearing mechanism. The displacement of physeal elbow fractures is almost always posteromedial.
Figure A shows AP and lateral radiographs with posteromedial displacement of the radial and ulnar shafts relative to the distal humerus. This is consistent with distal humeral physeal separation.
Incorrect Answers:
Question 19
A 57-year-old man with type I diabetes mellitus has had a tender, erythematous right sternoclavicular joint for the past 2 weeks. Radiographs reveal mild osteolysis without arthritic changes, within normal limits. Management should consist of
Explanation
REFERENCES: Bremner RA: Monarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, p 488.
Question 20
A 35-year-old man has had a mass on the bottom of his foot for the past 6 months. He reports that initially the mass was exquisitely painful but now is minimally tender. Examination reveals a 2.5- x 2.0-cm firm, noncompressible, nonmobile mass contiguous with the plantar fascia in the distal arch. The mass is particularly prominent with passive dorsiflexion of the ankle and toes. What is the best course of action?
Explanation
REFERENCES: Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Durr HR, Krodel A, Trouillier H, Lienemann A, Refior HJ: Fibromatosis of the plantar fascia: Diagnosis and indications for surgical treatment. Foot Ankle Int 1999;20:13-17.
Question 21
Sterilization of ultra-high molecular weight polyethylene by gamma irradiation in air will degrade its wear performance because of
Explanation
REFERENCES: Collier JP, Sutula LC, Currier BH, et al: Overview of polyethylene as a bearing material: Comparison of sterilization methods. Clin Orthop 1996;333:76-86.
McKellop H, Shen FW, Lu B, et al: Effect of sterilization method and other modifications on the wear resistance of acetabular cups made of ultra-high molecular weight polyethylene: A hip-simulator study. J Bone Joint Surg Am 2000;82:1708-1725.
Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.
Question 22
A 51-year-old plumber has a failed peroneus brevis tendon repair. He reports continued pain and swelling in the distal retrofibular area. MRI shows longitudinal tears of the peroneus longus and peroneus brevis. What is the surgical treatment of choice at this time?
Explanation
REFERENCES: Redfern D, Myerson M: The management of concomitant tears of the peroneus longus and brevis tendons. Foot Ankle Int 2004;25:695-707.
Borton DC, Lucas P, Jomha NM, et al: Operative reconstruction after transverse rupture of the tendons of both peroneus longus and brevis: Surgical reconstruction by transfer of the flexor digitorum longus tendon. J Bone Joint Surg Br 1998;80:781-784.
Question 23
A 45-year-old distance runner has a hyaluronic acid injection to his knee because of degenerative arthritis. He immediately develops a severe rash and a systemic hypersensitivity reaction. This patient most likely is also allergic to which of the following?
Explanation
REFERENCES: Gloyscen DN, Gillespie MJ, Schenek RC: The effects of medication in sports injuries, in DeLee JC, Drez D Jr, Miller MD (eds): Orthopedic Sports Medicine: Principles and Practice, ed 2.
Philadelphia, PA, WB Saunders, 2003, vol 1, pp 121-124.
Schenck RC Jr: New approaches to the treatment of osteoarthritis: Oral glucosamine and chondroitin sulfate. Instr Course Lect 2000;49:491-494.
Question 24
A 35-year-old man who has had a 6-month history of low back pain and tenderness now reports worsening pain and stiffness in the hips and entire back. An AP radiograph of the pelvis demonstrates fusion of the sacroiliac joints bilaterally. What is the next most appropriate step in management? Review Topic
Explanation
disease, further work-up in a patient with potential ankylosing spondylitis is not warranted. Sacroiliac joint anesthetic injections and sacroiliac fusion are not recommended treatments for early ankylosing spondylitis. Aspiration of the sacroiliac joints can be done if sacroiliac joint infection is suspected; however, in the absence of fever or other constitutional symptoms, infection is unlikely.
Question 25
A 65-year-old right–hand-dominant woman has been experiencing thenar and wrist pain for 18 months. She has no history of trauma. The pain worsens during the opening of jars, grasping, writing, and repetitive thumb use. Examination reveals tenderness to palpation over the volar thenar eminence, just distal to the scaphoid tubercle, and along the flexor carpi radialis sheath. A Watson scaphoid shift test produces pain but no instability or clunk. Radiographs reveal isolated scaphotrapeziotrapezoidal (STT) arthritis with mild dorsal intercalated segment instability (DISI) deformity. She has worn a splint on and off for the past year, has had multiple cortisone injections, and has modified her activity, all of which helped initially. She wants to move forward with surgical intervention. STT arthrodesis is chosen over distal pole scaphoid excision. What factor in her evaluation indicates that arthrodesis would be preferred over distal pole excision?
Explanation
Isolated STT arthritis is common and can cause substantial patient disability and pain. After nonsurgical treatment has failed, surgical intervention is warranted. Surgical options include distal pole scaphoid excision, STT arthrodesis, or carpometacarpal (CMC) arthroplasty, if concomitant thumb CMC degenerative changes are present. Distal pole scaphoid excision is less commonly employed for the treatment of STT arthritis, because of the potential development of intercalated segmental instability. However, distal pole scaphoid excision is less technically demanding, engenders fewer surgical complications, and promotes a faster return to previous activity levels. In any patient with preoperative carpal malalignment, removing the distal pole of the scaphoid would exacerbate that deformity and could lead to symptoms from the DISI deformity. Thus, in this patient with mild DISI deformity seen on preoperative radiographs, STT arthrodesis is the most appropriate treatment option.
Question 26
A 45-year-old IV drug abuser has sternoclavicular (SC) joint pain for the past 2 weeks. He is afebrile and physical exam findings include point tenderness and swelling. He most likely has septic arthritis of the sternoclavicular joint. If so, what is the most likely infecting organism?

Explanation
According to the reference by Ross et al, Staphylococcus aureus accounts for 49% of infections. SC joint arthritis accounts for 1% of septic arthritis in the general population but 17% in the IV drug abuse population. Symptoms include spontaneous swelling with the appearance of joint subluxation and localized pain. These patients are not uncommonly afebrile.
Question 27
A 16-year-old boy has had knee pain for the past 6 months, and activity restrictions have not provided relief. An MRI scan reveals a stable 1.5 cm by 1 cm osteochondritis dissecans on the weight-bearing surface of the lateral femoral condyle. What is the best course of treatment? Review Topic
Explanation
Question 28
In hybrid arthroplasty, the use of a polymethylmethacrylate (PMMA) precoated femoral component has been shown to result in
Explanation
REFERENCES: Sporer SM, Callaghan JJ, Olejniczak JP, Goetz DD, Johnston RC: The effects of surface roughness and polymethylmethacrylate precoating on the radiographic and clinical results of the Iowa hip prosthesis: A study of patients less than fifty years old. J Bone Joint Surg Am 1999;81:481-492.
Schulte KR, Callaghan JJ, Kelley SS, Johnston RC: The outcome of Charnley total hip arthroplasty with cement after a minimum twenty-year follow-up: The results of one surgeon. J Bone Joint Surg Am 1993;75:961-975.
Question 29
Figure 44 shows the radiograph of an 11-year-old girl who has hip pain. Further diagnostic workup should include
Explanation
REFERENCES: Steel HH: Protrusio acetabuli: Its occurrence in the completely expressed Marfan syndrome and its musculoskeletal component and a procedure to arrest the course of protrusion in the growing pelvis. J Pediatr Orthop 1996;16:704-718.
Wenger DR, Ditkoff TJ, Herring JA, Mauldin DM: Protrusio acetabuli in Marfan’s syndrome. Clin Orthop 1980;147:134-138.
Question 30
Longitudinal radioulnar dissociation, including Essex Lopresti fractures, requires disruption of the interosseous membrane (IOM). The interosseous membrane (IOM) consists of all of the following ligaments EXCEPT?

Explanation
The IOM bridges the radius and ulna and acts as a hinge for rotation of radius about ulna. The central portion is thickened, and forms the central band which is the most important ligament for IOM load distribution characteristics.
Noda et al, in a cadaver study, identified the precise anatomical insertions and attachment points of each of the 5 IOM components. They found the most distal and proximal ends of the radial origin of the central band were 53% and 64% of total radial length from the tip of the radial styloid, whereas those of the ulnar insertion were 29% and 44% of total ulnar length from the ulnar head.
Pfaeffle et al also performed a cadaveric biomechanical study applying compressive loads to specimens with IOMs that are intact, cut, or cut/reconstructed with flexor carpi radialis allografts. They found that reconstruction of the IOM can restore the normal load transfer chararcteristics and that the central band of the IOM is the most important portion of the IOM to be reconstructed.
Question 31
What is the most common indication for revision following unconstrained elbow arthroplasty?
Explanation
REFERENCES: King GJ, Itoi E, Niebur GL, et al: Motion and laxity of the capitellocondylar total elbow prosthesis. J Bone Joint Surg Am 1994;76:1000-1008.
Ring D, Koris M, Jupiter JB: Instability after total elbow arthroplasty. Orthop Clin North Am 2001;32:671-677.
Question 32
The peroneus tertius is a commonly used landmark for arthroscopic portal placement. What is the function of this tendon?
Explanation
REFERENCES: Joshi SD, Joshi SS, Athavale SA: Morphology of the peroneus tertius muscle.
Clin Anat 2006;19:611-614.
Williams PL, Bannister LH, Berry MM, et al (eds): Gray’s Anatomy, ed 38. London, Churchill Livingston, 1995, p 883.
Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 21.
Question 33
A 68-year-old woman has been progressing slowly after undergoing humeral head replacement for a four-part fracture 3 months ago. She has not regained active elevation, she feels an audible clunk on attempting elevation, and she reports pain and weakness. She used a sling for 2 weeks in the immediate postoperative period. Radiographs are shown in Figure 37a through 37c. Management should consist of
Explanation
REFERENCES: Brown TD, Bigliani LU: Complications with humeral head replacement. Orthop Clin North Am 2000;31:77-90.
Muldoon MP, Cofield RH: Complications of humeral head replacement for proximal humeral fractures. Instr Course Lect 1997;46:15-24.
Question 34
A skeletally mature 15-year-old girl who was thrown from the car in a rollover accident sustained the injuries shown in Figures 23a through 23d. Examination reveals no neurologic deficit, but the patient has moderate posterior spinal tenderness at the level of the injury. What is the most appropriate treatment?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Chow GH, Nelson BJ, Gebhard JS, Brugman JL, Brown CW, Donaldson DH: Functional outcome of thoracolumbar burst fractures managed with hyperextension casting or bracing and early mobilization. Spine 1996;21:2170-2175.
Question 35
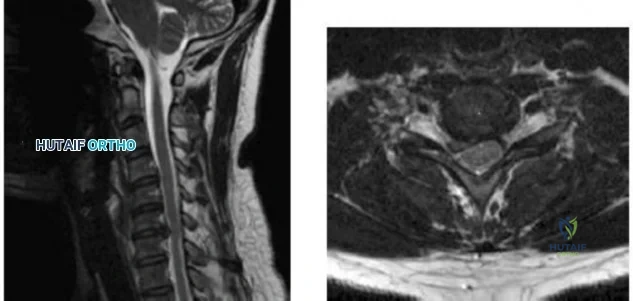
-Figures a and b are the MRI scans of the cervical spine without contrast of a 38-year-old man with neck pain radiating into the right upper extremity for the past 4 weeks. He denies numbness or weakness.Examination was significant for reproduction of pain going down the right arm with neck extension and right lateral rotation. What is the next treatment step?
Explanation
Question 36
Figures 3a and 3b show the MRI scans of a patient with neck pain. What is the most likely diagnosis?
Explanation
REFERENCES: Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Funasaki H, Winter RB, Lonstein JB, et al: Pathophysiology of spinal deformities in neurofibromatosis: An analysis of seventy-one patients who had curves associated with dystrophic changes. J Bone Joint Surg Am 1994;76:692-700.
Question 37
A total knee arthroplasty is recommended to a mentally competent 68-year-old woman who has disabling knee pain caused by degenerative arthritis. Her son has researched the procedure on the internet and prefers the Acme Female Knee for his mother. You have designed the Axis Woman's Knee, for which you receive royalties, and use it exclusively. Which of the following ethical principles takes precedence in guiding her treatment?
Explanation
Question 38
What mechanism of injury is most likely to cause a fracture of the anteromedial facet of the coronoid?
Explanation
(SBQ12TR.86) Figure A shows intraoperative radiographs of a 45-year-old patient with a left elbow injury. What would be the next most appropriate step in this patients care?
Early range of motion
Hinged elbow brace for 4 weeks
Repair lateral collateral ligament
Remove and upsize implant
Remove and downsize implant
The intraoperative images are consistent with overstuffing of the ulnohumeral joint during a radial head replacement. The most appropriate next step would be removing and downsizing the implant.
Overstuffing the radiohumeral joint by >2.5 mm can significantly alter elbow kinematics. It has also shown to lead to pain and early joint disease. The most sensitive method to assess for overstuffing of the joint is by direct visualisation intraoperatively. This can be performed by visualising the lateral aspect of the ulnohumeral joint when the radial head is resected and comparing this to when the trial radial head is reduced in place. In comparison, radiographic asymmetry of the medial ulnohumeral joint has been shown to be less sensitive. Radiographic findings of incongruity of ulnohumeral joint only occurs when significant overlengthening of the radius occurs.
Frank et al. examined the effect of radial head thickness in seven cadaver specimens. They found that incongruity of the medial ulnohumeral joint would only become apparent radiographically after overlengthening of the radius by >or=6 mm.
Doornberg et al. examined seventeen computed tomography scans of the elbow to investigate the height of the radial head relative to the lateral edge and central ridge of the coronoid process. They found that the radial head was on average only 0.9 mm more proximal than the lateral edge of the coronoid process.
Figure A shows intraoperative radiographs of a patient that has undergone a radial head arthroplasty. There is significant widening of the medial ulnohumeral joint on an AP radiograph as well as widening of the ulnohumeral joint on the lateral radiograph,
Incorrect Answers:
Question 39
A 26-year-old weightlifter had increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication,
Explanation
Question 40
In long-term follow-up studies of cemented total knee arthroplasty (TKA), the lowest rates of osteolysis have been associated with which design feature?
Explanation
The lowest reported rates of osteolysis involving cemented TKAs are associated with monolithic tibial components. Modular components and cemented metal-backed patella components are associated with a high prevalence of backside tibial insert wear and osteolysis.
Question 41
A 4-month-old infant is unable to flex her elbow as a result of an obstetrical brachial plexus palsy. This most likely illustrates a predominate injury to what structure? Review Topic
Explanation
Question 42
An 18-year-old lacrosse player sustained a hamstring pull during a game. Examination the next day reveals ecchymosis through the posterior thigh and a palpable defect in the hamstring musculature in the middle third of the thigh. What is the most likely site of anatomic injury?
Explanation
REFERENCES: Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 17-33.
Clanton TO, Coupe KJ: Hamstring strains in athletes: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:237-248.
Question 43
Figure 24 shows the radiograph of an otherwise healthy 56-year-old patient who reports hip pain after undergoing a primary cementless hip replacement 4 months ago. The next most appropriate step should consist of
Explanation
REFERENCE: Fitzgerald RH Jr: Infected total hip arthroplasty: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:249-262.
Question 44
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?
Explanation
REFERENCES: Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Morgan WJ, Slowman LS: Acute hand and wrist injuries in athletes: Evaluation and management. J Am Acad Orthop Surg 2001;9:389-400.
Question 45
A 38-year-old man sustained a complete thoracic spinal cord injury at age 14. An MRI scan of his shoulder, when compared with studies from uninjured controls, is more likely to show which of the following? Review Topic
Explanation
Question 46
A 30-year-old woman injured her ankle playing soccer 3 months ago. She now reports popping and pain over the lateral side of her ankle. An MRI scan is shown in Figure 33. What structure needs to be repaired to alleviate the popping?
Explanation
REFERENCES: Jones DC: Tendon disorders of the foot and ankle. J Am Acad Orthop Surg 1993;1:87-94.
Timins ME: MR imaging of the foot and ankle. Foot Ankle Clin 2000;5:83-101.
Question 47
Figures below demonstrate the radiographs obtained from a 56-year-old man with a 3-year history of right groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?
Explanation
Chronic opioid consumption prior to total joint arthroplasty has been associated with increased pain after surgery, increased opioid requirements, a slower recovery and longer hospital stay, and higher 90-day postoperative complications compared with patients not on chronic opioids preoperatively. Based on this information, Nguyen and associates performed a study in three patient groups that included 1) chronic opioid users who underwent no preoperative intervention, 2) chronic opioid users who were weaned down to 50% of their prior opioid regimen, and 3) patients who were not chronic opioid users. The authors found that the reduction of preoperative opioid use improved postoperative function, pain, and recovery and that the weaned group performed more like the opioid naive group than the chronic opioid user
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to surgery.
Question 48
Figures below show the radiographs obtained from a 75-year-old woman who underwent right total hip arthroplasty in 2009. She did well until last month, when a right posterior hip dislocation occurred after she fell from her bed to the floor. Successful closed reduction was performed. She sustained two more posterior dislocations requiring closed reduction under anesthesia. The surgical report from the index arthroplasty notes a 54-mm monoblock acetabular component with a 28-mm inner diameter compression molded polyethylene and a high offset neck cementless stem with a +8-mm length, 28-mm head. What is the best next step?

Explanation
This patient has demonstrated recurrent instability, and her current implants lack the modularity to upsize and improve the head-neck ratio and range to impingement. Given the monoblock acetabular component and a +7-mm neck length, the best option is revision to a large-diameter femoral head or dual-mobility component. Placement of a hip spica cast and resection arthroplasty are unreasonable. Revision to a longer ball length likely would not solve this recurrent instability pattern.
Question 49
A 55-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing left shoulder pain for the past 2 years despite nonsurgical management. No focal weakness is noted during examination of the shoulder. AP and axillary radiographs are shown in Figures 47a and 47b. Treatment should consist of
Explanation
REFERENCES: Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Kelly IG, Foster RS, Fisher WD: Neer total shoulder replacement in rheumatoid arthritis. J Bone Joint Surg Br 1987;69:723-726.
Question 50
Figure 26 shows the radiograph of an otherwise healthy Caucasian 5-year-old boy who has a painless limp. What is the best treatment option?
Explanation
REFERENCES: Herring JA, Kim HT, Browne R: Legg-Calve-Perthes disease: Prospective multicenter study of the effect of treatment on outcome. J Bone Joint Surg Am 2004;86:2121-2134.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 691-704.
Question 51
Figures 34a and 34b show the axial and sagittal MRI scans of a 36-year-old man who reports the insidious onset of pain in the right shoulder. What is the most appropriate description of the acromial morphology? Review Topic
Explanation
Question 52
A patient underwent an open reduction and internal fixation of a calcaneus fracture 6 months ago via an extensile lateral approach. He now reports burning pain on the lateral side of his ankle and foot. A local cortisone injection at the site of the tenderness, about 7 cm above the lateral heel, provided temporary relief of the pain. What is the recommended course of management for the persistent burning pain?
Explanation
Question 53
Pedicle subtraction osteotomies (PSO) are commonly performed in the lumbar spine to treat sagittal imbalance. What is the most common complication following a PSO in the lumbar spine? Review Topic
Explanation
Question 54
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management?
Explanation
REFERENCES: Miller P, Kendrick D, Bentley E, et al: Cost effectiveness of lumbar spine radiographs in primary care patients with low back pain. Spine 2002;27:2291-2297.
Wong DA, Transfeldt E: Macnab’s Backache, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins 2007, pp 298-338.
Question 55
Which of the following conditions routinely requires early surgical intervention in patients with Marfan syndrome? Review Topic
Explanation
Question 56
Following an acute dislocation of the patella, the risk of a recurrent dislocation is greater if the patient has which of the following findings?
Explanation
REFERENCES: Cash JD, Hughston JC: Treatment of acute patellar dislocation. Am J Sports Med 1988;16:244-249.
Larsen E, Lauridsen F: Conservative treatment of patellar dislocations: Influence of evident factors on the tendency to redislocation and the theraputic result. Clin Orthop
1982;171:131-136.
Question 57
Pharmacoprophylaxis should be avoided in favor of a pneumatic compression device for a patient with
Explanation
For patients with known bleeding disorders, a pneumatic compression device alone is recommended over pharmacoprophylaxis to minimize risk for excessive bleeding and wound complications. Factor VIII deficiency (hemophilia) and active liver disease are the 2 conditions for which support is strongest to withhold anticoagulation. Protein C deficiency and protein S deficiency are associated with increased risk for thrombosis, as is the factor V Leiden mutation.
RESPONSES FOR QUESTIONS 159 THROUGH 162
Lateral femoral cutaneous
Superior gluteal
Inferior gluteal
Obturator
Sciatic
Which nerve listed above is at increased risk for injury when performing hip surgery through the following approaches?
Question 58
Figures 1 and 2 are the MR arthrogram images of a 20-year-old right-hand dominant collegiate basketball player who sustained an initial shoulder dislocation 1 year ago. In the month prior to presentation, he dislocated his shoulder two more times. Each time it occurred when going up for a rebound and an opponent grabbed the ball from behind him, hyperextending his shoulder. Physical examination demonstrates full range of motion, absence of atrophy, a positive apprehension sign and relocation test, and a positive Kim test. What is the best next step?
Explanation
physical examination and advanced imaging in these patients are crucial in directing appropriate treatment.
Question 59
-Which treatment approach for acetabular fractures carries the highest risk for heterotopic ossification?
Explanation
Question 60
Figures 233a through 233c are the radiographs and biopsy specimen of a 32-year-old woman who has had progressive ankle pain for 6 months. What is the most appropriate treatment option?

Explanation

Question 61
Staged open reduction and internal fixation with free flap soft tissue reconstruction is the most appropriate definitive treatment method for which of the following tibial injuries?

Explanation
Typically, treatment of Type IIIB tibial shaft fractures should be staged. Initially tetanus prophylaxis, antibiotics with gram negative and positive coverage, and application of an external fixator with repeat I&D’s are employed for immediate fracture care. Plating is usually required in the presence of significant intra-articular fracture involvement.
Incorrect Answers: Typically, proximal third tibia fractures requiring soft tissue coverage can be treated with a gastrocnemius rotation flap and middle third tibia fractures with soft tissue defects can be reliably covered with a soleus rotation flap. Therefore, a free flap is rarely indicated in the proximal and middle tibia.
Question 62
A cartilage water content increase is the hallmark of which osteoarthritis stage?
Explanation
Question 63
Figure 18a shows the clinical photograph of a 2-year old boy who has a deformity of the right leg. Examination reveals eight cutaneous markings similar to those shown in Figure 18b. Radiographs are shown in Figure 18c. Management should consist of
Explanation
REFERENCES: Crawford AH Jr, Bagamery N: Osseous manifestations of neurofibromatosis in childhood. J Pediatr Orthop 1986;6:72-88.
Schoenecker PL, Rich MM: The lower extremity, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, vol 2, pp 1059-1104.
Question 64
A patient reports a sudden recurrence of sciatica on her left side after undergoing a successful left L4-L5 diskectomy 15 months ago. Which of the following imaging modalities is most accurate in differentiating recurrence of the disk herniation from postoperative epidural scar tissue?
Explanation
cause of the encroachment. Answer #2 makes no sense. Answers #3 and #4 are incorrect because the MRI is now the standard imaging modality.
Question 65
You are evaluating a patient with recurrent patellar instability who has failed conservative management. MRI demonstrates articular cartilage loss in the patella. In addition to a cartilage restoration procedure, you recommend the procedure depicted in Figures A and B. Which of the following imaging findings best supports your decision? Review Topic

Explanation
Recurrent patellar instability is often associated with chondral lesions of the patellofemoral joint. In addition to managing the cartilage injury, the underlying etiology of the instability must also be addressed to ensure a successful outcome. Patellar instability may arise from coronal or rotational malalignment, patella alta, trochlear dysplasia or damage to soft tissue restraints including the medial patellofemoral ligament (MPFL). Rotational malalignment, defined by a TT-TG distance > 20mm, can be addressed by AMZ. Medialization of the tubercle restores a normal TT-TG distance while anteriorization of the tubercle unloads patellofemoral contact forces.
Beck et al performed a cadaveric study measuring patellofemoral contact pressures on the trochlear surface following AMZ. They found that anteromedialization decreased the mean contact pressures and shifted contact pressures to the medial trochlea. The authors concluded that while this procedure successfully unloads the lateral trochlea, it likely has minimal benefit for central chondral defects and may be detrimental for medial chondral defects where contact pressures are increased.
Strauss et al authored a review article detailing the surgical treatment options for patellofemoral cartilage lesions, including concomitant realignment/unloading procedures. AMZ is designed to correct rotational malalignment while unloading the patellofemoral compartment in the setting of cartilage restoration surgery. While AMZ has demonstrated good outcomes for lesions located in the lateral facet or distal
pole of the patella, poor outcomes have been seen with medial facet or central trochlear lesions.
Figures A and B are the AP and lateral radiographs, respectively, of a knee s/p AMZ, also know as a Fulkerson procedure. Illustration A is an algorithm detailing the approach to recurrent patellar instability in both skeletally immature and mature patients. Illustration B demonstrates how to measure the TT-TG distance, the distance between two lines drawn perpendicular to the posterior condylar axis to the tibial tubercle and deepest portion of the trochlear groove (normal 8-10mm). Illustration C depicts the measurement of the femoral trochlear angle or sulcus angle (normal 137°
+/- 8°). Illustration D shows how to measure lateral patellar tilt (normal < 5°). Illustration E is a postoperative radiograph after AMZ. A long (> 5cm) and thick (> 0.75cm) osteotomy cut is required to allow adequate fixation with two screws.
Incorrect Responses:
Question 66
Which of the following conditions is typically associated with the ankle deformity shown in figure 14?
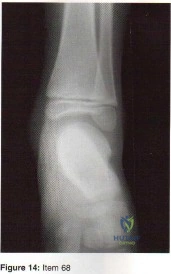
Explanation
Question 67
A 63-year-old man has had increasing left leg pain over the last several months. History reveals that he has had recurring cyclic pain in the leg for the past several years. Radiographs show an enlarged, sclerotic tibia, with thickened coarse trabeculae and varus bowing. What is the most appropriate management for this patient? Review Topic
Explanation
Question 68
A patient undergoes hip arthroscopy, and the pathology is seen in Figure 18. What is the most likely diagnosis?
Explanation
REFERENCE: Byrd JWT: Operative Hip Arthroscopy. New York, NY, Thieme Medical Publishers, 1998, pp 93-104.
Question 69
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads? Review Topic
Explanation
Question 70
An orthopaedic surgeon frequently uses hip and knee prostheses from a specific manufacturer. The surgeon becomes acquainted with the manufacturer’s representative who provides the support for these prostheses in the hospital. They develop a personal relationship outside of work through a common interest in sailing. Together they become interested in buying a sailboat. The manufacture’s representative suggests a partnership in a boat costing $200,000. The manufacture’s representative would purchase a 90% interest and the surgeon a 10% interest in the boat. There would be no restrictions on use of the boat by the surgeon. What should the orthopaedic surgeon do?
Explanation
partnership seems completely outside of the orthopaedic business relationship does not excuse it. Conflicts of interest should always be resolved and in the best interest of patient care, and in this case the best course clearly is to avoid the conflict of interest totally. An equal interest in the boat does not eliminate the conflict of interest.
Question 71
Figure 22 shows the MRI scan of a 20-year-old female basketball player who has pain over the anterior knee that interferes with her performance. Examination reveals phase III Blazina patellar tendinosis. Management should consist of
Explanation
REFERENCES: Blazina ME, et al: Jumper’s knee. Orthop Clin North Am 1973;4:665.
Kelly DW, Carter VS, Jobe FW, Kerlan RK: Patellar and quadriceps tendon ruptures: Jumper’s knee. Am J Sports Med 1984;12:375-380.
Krums PE, Ryder B: Operative treatment of patella tendon disorders. Operative Techniques Sports Med 1994;2:303.
Rows J, et al: Patella tendinitis (jumper’s knees). Am J Sports Med 1978;6:362.
Question 72
A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
Explanation
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
Question 73
The best candidate for a reverse total shoulder arthroplasty is a patient with rotator cuff tear arthropathy with Review Topic
Explanation
Question 74
A patient reports pain in the hip with functional positioning. With the patient supine, pain in which of the following positions would be typical for femoral acetabular impingement? Review Topic
Explanation
(SBQ13PE.10) Which statement is true regarding discoid menisci? Review Topic
Most commonly involves the medial meniscus
Bilateral in >75% of cases
Asymptomatic discoid meniscus should undergo saucerization
Radiographs will commonly show a hyperplastic lateral intercondylar spine
Radiographs will commonly show squaring of affected condyle with cupping of tibial plateau
Radiographs of knees with discoid menisci will commonly show squaring of affected condyle (lateral>medial) with cupping of tibial plateau.
Discoid meniscus refers to the abnormal development of a hypertrophic and discoid shaped meniscus. It occurs in 3-5% of the population and it is considered the most common cause of a symptomatic clicking or clunking in a childs knee. The lateral meniscus is most commonly affected and it will occur bilaterally in 25% of affected
people. The Watanabe Classification describes the 3 types of discoid menisci. Type 1
= Incomplete, Type 2 = Complete, Type 3 = Wrisberg (lack of posterior meniscotibial attachment to tibia)
Kramer et al. looked at the presentation of pediatric knee pain. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the discoid meniscus.
Lee et al. retrospectively reviewed 36 patients aged less than 15 years who underwent arthroscopic procedures for torn discoid menisci. The mean patient age at the time of surgery was 9.5 years. They showed that partial meniscectomy yielded better radiologic results than subtotal/total meniscectomy for torn discoid menisci in this population.
Illustration A shows the 3 classifications of discoid menisus as originally described by Watanabe. Type 4 is a ring type discoid that was not originally described by Watanabe in his 1978 paper. Illustration B shows an AP and lateral radiograph of a discoid meniscus knee. Note squaring of affected lateral condyle in the presence of a lateral discoid meniscus. Illustration C shows 4 consecutive sagittal MRI images with meniscus continuity. It is important to note that the diagnosis of discoid menisci can be made when 3 or more 5mm sagittal images show meniscal continuity.
Incorrect Answers:
Question 75
Figures 21a and 21b show the radiograph and CT scan of a 14-year-old patient with thigh pain. The next most appropriate step in management should consist of
Explanation
REFERENCES: Frassica FJ, Waltrip RL, Sponseller PD, Ma LD, McCarthy EF Jr: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-574.
Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid osteoma. J Bone Joint Surg Am 1992;74:179-185.
Rosenthal DI, Hornicek FJ, Wolfe MW, Jennings LC, Gebhardt MC, Mankin HJ: Percutaneous radiofrequency coagulation of osteoid osteoma compared with operative treatment. J Bone Joint Surg Am 1998;80:815-821.
Question 76
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has failed to provide relief. He has concomitant cubital tunnel symptoms that worsen while throwing. What is his best surgical option?
Explanation
REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Ciccotti MG, Jobe FW: Medial collateral ligament instability and ulnar neuritis in the athlete’s elbow. Instr Course Lect 1999;48:383-391.
Question 77
A 21-year-old professional ballet dancer reports a painful popping sensation over her right hip joint. Examination reveals that symptoms are reproduced with hip flexion and external rotation. Which of the following studies will best confirm the diagnosis? Review Topic
Explanation
Question 78
Which of the following plain radiographic views of the shoulder best reveals a Hill-Sachs lesion of the humeral head?
Explanation

Question 79
What assay most directly assesses gene expression at the posttranslational level?
Explanation
REFERENCES: Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 19-76.
Question 80
The risk of local recurrence after surgical resection of a soft-tissue sarcoma is most closely related to
Explanation
REFERENCES: Lewis JJ, Leung D, Heslin M, Woodruff JM, Brennan MF: Association of local recurrence with subsequent survival in extremity soft tissue sarcoma. J Clin Oncol 1997;15:646-652.
Meterissian SH, Reilly JA Jr, Murphy A, Romsdahl MM, Pollock RE: Soft-tissue sarcomas of the shoulder girdle: Factors influencing local recurrence. Distant metastases and survival. Ann Surg Oncol 1995;2:530-536.
Question 81
You design a research study in which you ask patients who have a nonunion of the tibia to fill out a questionnaire in which they report on a variety of medical conditions and social/behavioral practices. You compare these findings to a similar group who did not develop a nonunion in order to identify medical and/or social conditions that might be risk factors for the development of tibial nonunions. This would be an example of what type of study?
Explanation
Question 82
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
Explanation
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Question 83
Which of the following best describes the course of the median nerve at the elbow?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8,
pp 46-47.
Question 84
All of the following indicators of resuscitation may be within normal limits for a trauma patient that is in "compensated" shock EXCEPT:

Explanation
Question 85
A 22-year-old professional baseball catcher has posterior shoulder pain and severe external rotation weakness with the arm in adduction. Radiographs are normal. MRI scans are shown in Figures 15a through 15c. Management should consist of
Explanation
REFERENCES: Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment.
J Bone Joint Surg Am 2000;82:415-424.
Martin SD, Warren RF, Martin TL, et al: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
Question 86
Epithelioid sarcoma most commonly occurs in which of the following anatomic locations?
Explanation
REFERENCES: Gupta TD, Chaudhuri P (eds): Tumors of the Soft Tissues, ed 2. Stamford, CT, Appleton and Lange, 1998, p 475.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St. Louis, MO, Mosby-Year Book, 1995, p 1074.
Question 87
- In a fatigue test, the maximum stress under which the material will not fail, regardless of how many loading cycles are applied, is defined as
Explanation
Question 88
Figures 1a and 1b are the recent radiographs of an 82-year-old man with rheumatoid arthritis who underwent total knee arthroplasty (TKA) 18 years ago. These radiographs reveal osteolysis with loosening of the tibial component. Aspiration and laboratory study findings for infection are negative. During the revision TKA, treatment of tibial bone loss should consist of
Explanation

Video 1 for reference
For severe tibial defects (Anderson Orthopaedic Research Institute [AORI] types 2 and 3), metaphyseal fixation is necessary to achieve construct fixation during revision TKA. Metaphyseal fixation may be achieved with cement, structural allograft, or conical metallic implants. The major concerns regarding structural allograft are graft resorption and mechanical failure and technical issues related to fashioning the graft and obtaining a good host-allograft interface. In a systematic review, porous metal cones were associated with a decreased loosening rate in AORI 2 and 3 defects compared to structural allografts. Metallic trabecular metal cones and metaphyseal porous coated sleeves provide a stable construct with which to support the tibial component during revision TKA. Clinical results with these devices include good metaphyseal fixation for severe tibial bone defects.
Question 89
In the treatment of thoracic disk herniations, what approach is associated with the highest risk of iatrogenic paraplegia?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 87-96.
Stillerman CB, Chen TC, Couldwell WT, Zhang W, Weiss MH: Experience in the surgical mangement of 82 symptomatic herniated thoracic discs and review of the literature. J Neurosurg 1998;88:623-633.
Question 90
Figures 48a and 48b show the radiographs of a 26-year-old woman who fell down two steps and twisted her foot and ankle. What is the most appropriate treatment for this injury?
Explanation
REFERENCES: Vorlat P, Achtergael W, Haentjens P: Predictors of outcome of non-displaced fractures of the base of the fifth metatarsal. Int Orthop 2007;31:5-10.
Wiener BD, Linder JF, Giattini JF: Treatment of fractures of the fifth metatarsal: A prospective study. Foot Ankle Int 1997;18:267-269.
Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.
Question 91
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads?
Explanation
REFERENCE: Rhee JM, Schaufele M, Abdu WA: Radiculopathy and the herniated lumbar disc: Controversies regarding pathophysiology and management. J Bone Joint Surg Am 2006;88:2070-2080.
Question 92
Figure 37 shows the standing lateral radiograph of a 62-year-old woman who reports lower back pain and the inability to stand upright. What permanent anatomic pelvic parameter should be measured and considered when determining the amount of lumbar lordosis correction that will be necessary to obtain sagittal balance? Review Topic
Explanation
permanent pelvic parameter that is unaffected by pelvic rotation. Acetabular and femoral version have not been found to be associated with lumbar lordosis.
Question 93
A 52-year-old man who weighs 325 lb is wheelchair-bound from severe degenerative arthritis of the left hip. Twenty-four hours after cementless total hip arthroplasty, he develops shortness of breath and evaluation shows a saddle pulmonary embolus. The patient is started on enoxaparin sodium at 150 mg every 12 hours. Two days later, the patient’s hematocrit is 20% despite four units of transfused packed cells, and he now has developed a complete sciatic nerve palsy. What is the best course of action?
Explanation
REFERENCES: Della Valle CJ, Steiger DJ, Di Cesare PE: Thromboembolism after hip and knee arthroplasty: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:327-336.
Weil Y, Mattan Y, Goldman V, et al: Sciatic nerve palsy due to hematoma after thrombolysis therapy for acute pulmonary embolism after total hip arthroplasty. J Arthroplasty 2006;21:456-459.
American Academy of Orthopaedic Surgeons Guideline on the Prevention of Symptomatic Pulmonary Embolism in Patients Undergoing Total Hip or Knee Arthroplasty, www.aaos.org/research/guidelines/ PEguide.asp
Question 94
In a retroperitoneal approach to the lumbar spine, what structure runs along the medial aspect of the psoas and along the lateral border of the spine?
Explanation
REFERENCES: Watkins RG (ed): Surgical Approaches to the Spine. New York, NY, Springer-Verlag, 1983, p 107.
Johnson R, Murphy M, Sourthwick W: Surgical approaches to the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1559.
Question 95
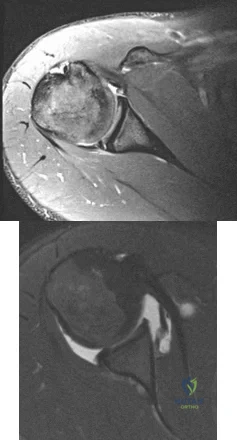
Figure 1 is the radiograph of an 11-year-old baseball pitcher who has had right shoulder pain for the past 3 months. He has full range of motion and normal strength in both external rotation and abduction, although all tests cause him discomfort over the lateral and anterior shoulder. What is the most likely basis for his injury?

Explanation
throws should be avoided at certain ages.
Question 96
A 32-year-old man presents to the emergency department with a humeral shaft fracture. He has wrist drop as well as impaired finger and thumb extension. Which motor function would be expected to recover last?

Explanation
Abrams et al detailed the order of innervation of the radial nerve and found the following order (proximal to distal): brachioradialis, extensor carpi radialis longus, supinator, extensor carpi radialis brevis, extensor digitorum communis, extensor carpi ulnaris, extensor digiti quinti, abductor policis longus, extensor policis longus, extensor policis brevis, and extensor indicis proprius.
Branovacki et al found a slightly different pattern: brachioradialis, extensor carpi radialis longus, superficial sensory, extensor carpi radialis brevis, supinator, extensor digitorum/extensor carpi ulnaris, extensor digiti minimi, abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus and extensor indicis proprius.
While both extensor digitorum and extensor indicis proprius extend the index finger MCP joint, only extensor indicis proprius hyperextends the index finger past neutral
Question 97
Which of the following ligaments is most commonly involved in posterolateral rotatory instability of the elbow?
Explanation
REFERENCES: Morrey BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128.
O’Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Question 98
A deficiency of which of the following is associated with an increased risk of venous thromboembolism?
Explanation
Question 99
Figure 1 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop" and then needing help walking off the field. His knee is visibly swollen. The patient undergoes surgery to repair/reconstruct the damaged structure and has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they want to “get the therapy over with as fast as possible" to expedite his return to sports, and the surgeon and rehabilitation team consider their request. Compared with nonaccelerated rehabilitation, patients who follow an early accelerated rehabilitation protocol experience

Explanation
Question 100
A 70-year-old man has worn through his metal-backed patellar component and sustained damage to the femoral component. Following removal of the components and debridement of the metal-stained synovium, the surgeon finds that the thickness of the remaining patella is 10 mm. Treatment should now include
Explanation
REFERENCES: Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620.
Pagnano MW, Scuderi GR, Insall JN: Patellar component resection in revision and reimplantation total knee arthroplasty. Clin Orthop 1998;356:134-138.
Barrack RL, Matzkin E, Ingraham R, Engh G, Rorabeck C: Revision knee arthroplasty with patella replacement versus bony shell. Clin Orthop 1998;356:139-143.
