High-Yield Orthopedic Board Exam MCQs: Joint Reconstruction, Trauma & Infection | Part 216

Key Takeaway
This page offers Part 216 of a comprehensive OITE/AAOS Orthopedic Board Review. It features 100 verified, high-yield MCQs on topics like arthroplasty, trauma, and hip, designed for orthopedic surgeons and residents. Use study or exam mode to prepare effectively for your certification.
About This Board Review Set
This is Part 216 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 216
This module focuses heavily on: Arthroplasty, Fracture, Hip, Infection, Knee, Revision, Tendon, Trauma.
Sample Questions from This Set
Sample Question 1: Ayear-oldmanundergoesremovalofaninfectedtotalhiparthroplasty(THA)andinsertionofanarticulatingantibiotic-loadedspacertotreatadeepperiprosthetichipinfection.Whileinanursinghome receivingintravenousantibiotics3weeksaftersurgery,thepatienttrips...
Sample Question 2: The injury seen in the CT scan shown in Figure 56 is related to or associated with injury to which of the following structures?...
Sample Question 3: Based on the findings seen in the radiograph in Figure 26, emergent management should consist of...
Sample Question 4: A 51-year-old plumber has a failed peroneus brevis tendon repair. He reports continued pain and swelling in the distal retrofibular area. MRI shows longitudinal tears of the peroneus longus and peroneus brevis. What is the surgical treatmen...
Sample Question 5: A 32-year-old man has posttraumatic arthritis after undergoing open reduction and internal fixation of a left acetabular fracture. A total hip arthroplasty is performed, and the radiograph is shown in Figure 18. What is the most common mode...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A year-old man undergoes removal of an infected total hip arthroplasty (THA) and insertion of an articulating antibiotic-loaded spacer to treat a deep periprosthetic hip infection. While in a nursing home receiving intravenous antibiotics 3 weeks after surgery, the patient trips and falls. Examination reveals swelling in the mid and distal thigh, intact skin and neurovascular structures, and severe pain with knee or hip movement. Radiographs of the femur are shown in 1 through What is the most appropriate treatment for the fracture below the implant?
Explanation
This patient has a type C periprosthetic femoral fracture. The articulating spacer is not involved in the fracture, which is well distal to the implant. The most appropriate treatment is open reduction and internal fixation of the fracture. Traction is not appropriate for this fracture because the injury can be treated surgically despite the history of previous hip infection. Traction would also be needed for at least 5 weeks and would delay the surgical treatment of the periprosthetic fracture until the time of second-stage revision THA. The fracture is fairly distal, and revision to a longer antibiotic-loaded implant or uncemented stem is not suitable for this fracture pattern, because it extends well past the isthmus. A femoral stem in the distal fragment would provide little stability for the fracture. Removal of the articulating spacer and reimplantation using a long-stem fluted uncemented hip replacement is not appropriate, because it would be premature to reimplant the man's hip while he is still receiving treatment for a deep hip infection.
Question 2
The injury seen in the CT scan shown in Figure 56 is related to or associated with injury to which of the following structures?
Explanation
REFERENCES: Ebraheim NA, Lu J, Yang H, et al: The fibular incisure of the tibia on CT scan: A cadaver study. Foot Ankle Int 1998;19:318-321.
Ebraheim NA, Lu J, Yang H, et al: Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: A cadaver study. Foot Ankle Int 1997;18:693-698.
Harper MC: Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int 2001;22:15-18.
Question 3
Based on the findings seen in the radiograph in Figure 26, emergent management should consist of
Explanation
REFERENCES: Isenberg J, Prokop A, Schellhammer F, et al: Palmar lunate dislocation. Unfallchirurg 2002;105:1133-1138.
Ruby LK: Fractures and dislocations of the carpus, in Browner BD, Jupiter JB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1367-1372.
Question 4
A 51-year-old plumber has a failed peroneus brevis tendon repair. He reports continued pain and swelling in the distal retrofibular area. MRI shows longitudinal tears of the peroneus longus and peroneus brevis. What is the surgical treatment of choice at this time?
Explanation
REFERENCES: Redfern D, Myerson M: The management of concomitant tears of the peroneus longus and brevis tendons. Foot Ankle Int 2004;25:695-707.
Borton DC, Lucas P, Jomha NM, et al: Operative reconstruction after transverse rupture of the tendons of both peroneus longus and brevis: Surgical reconstruction by transfer of the flexor digitorum longus tendon. J Bone Joint Surg Br 1998;80:781-784.
Question 5
A 32-year-old man has posttraumatic arthritis after undergoing open reduction and internal fixation of a left acetabular fracture. A total hip arthroplasty is performed, and the radiograph is shown in Figure 18. What is the most common mode of failure leading to revision in this group of patients?
Explanation
REFERENCES: Jimenez ML, Tile M, Schenk RS: Total hip replacement after acetabular fracture. Orthop Clin 1997;28:435-446.
Romness DW, Lewallen DG: Total hip arthroplasty after fracture of the acetabulum: Long-term results. J Bone Joint Surg Br 1990;72:761-764.
Question 6
Figures 3a and 3b show the current radiographs of a 59-year-old woman who has pain and deformity after undergoing bunion surgery 1 year ago. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Coughlin MJ, Mann RA: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby-Year Book, 2000, pp 150-269.
Skalley TC, Myerson MS: The operative treatment of acquired hallux varus. Clin Orthop 1994;306:183-191.
Question 7
During reconstruction of insertional gaps of a chronic Achilles tendon rupture, what tendon provides the most direct route of transfer?
Explanation
REFERENCES: Wilcox DK, Bohay DR, Anderson JG: Treatment of chronic achilles tendon disorders with flexor hallucis longus tendon transfer/augmentation. Foot Ankle Int 2000;21:1004-1010.
Wapner K, Pavlock GS, Hecht PJ, Naselli F, Walther R: Repair of chronic Achilles tendon rupture with flexor hallucis longus tendon transfer. Foot Ankle Int 1993;14:443-449.
Question 8
03 Which of the following findings is the best indication for the use of temporary external fixation of a femoral shaft fracture?

Explanation

These days, femoral shaft fractures at Tulane / Charity are commonly encountered by orthopaedic residents on the night-float team.
Despite the presence of a well-rested 4th year surgeon, definitive orthopaedic fixation is not always the correct answer for each trauma patient.

Tulane defines “Orthopaedic Tunnel Vision” as a condition commonly associated with a young MD at the Bulldog without a proper wing-man, trying to make advances on the wrong patron due to his relatively easy 80-hour work week schedule and a few too many refined hops.

Skeletal Trauma (p. 1967) describes “Orthopaedic Tunnel Vision” as looking at the orthopaedic injury without considering the patient’s injury in general. Femoral shaft fractures are typically high energy injuries which often do not occur in isolation. In these fractures, it is particularly important to not have tunnel vision.

Indications for temporary bridging external fixation includes hemodynamic instability
(ans. 2), acidosis, hypothermjia, hypoxemia, coagulopathy, sepsis or severely contaminated soft tissues that cannot be adequately debrided. Definitive fixation is performed after the general surgical and medical issues have resolved.

The other answer choices, including the type IIIA open fracture are not contraindications to definitive fixation in themselves (typically IM nailing—antegrade or retrograde).
Question 9
A college basketball player is struck in the eye by a player’s hand while driving to the basket. Fluorescein evaluation reveals the injury shown in Figure 18. Management should consist of
Explanation
REFERENCES: Brucker AJ, Kozart DM, Nichols CW, et al: Diagnosis and management of injuries to the eye and orbit, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby-Year Book, 1991, pp 650-670.
Zagelbaum BM: Treating corneal abrasions and lacerations. Phys Sports Med 1997;25:38-44.
Question 10
Figures below demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. A further work-up reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MRI with MARS. Revision THA is recommended. The most common complication following revision of a failed metal-on-metal hip arthroplasty is

Explanation
Question 11
Diagnostic work-up concluded that the patient has metastatic lymphoma. He has no neurologic deficit.Based on these findings, what is the most appropriate management for this spinal condition?
Explanation
Patients with no prior diagnosis of cancer may present with vertebral lesions. After obtaining initial radiographs, the next most appropriate step is to obtain an MRI with gadolinium. To determine the primary site of the disease, a CT of the chest, abdomen, and pelvis is the next step in establishing a diagnosis. Radiation therapy is the first line of treatment in spinal metastatic disease from lymphoma because it is a highly radiosensitive tumor.
Question 12
Figure 57 is the radiograph of a 58-year-old woman who is right-hand dominant and has fallen on her flexed right elbow and is seen in the emergency department reporting isolated episodes of right elbow pain. Examination reveals that the skin is contused but intact, and her distal neurovascular examination is normal. What is the most appropriate treatment? Review Topic

Explanation
construct is a commonly used technique but is reserved for simple fracture patterns without comminution. Excision and triceps advancement can be considered in elderly, low-demand patients that have small unreconstructable fracture patterns without associated elbow instability.
Question 13
An 18-year-old man has had an enlarging mass in his hand for the past 3 months. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 54a through 54d. What is the most likely diagnosis?
Explanation
REFERENCES: Abramovici L, Steiner GC: Bizarre parosteal osteochondromatous proliferation (Nora’s lesion): A retrospective study of 12 cases, 2 arising in long bones. Hum Pathol 2002;33:1205-1210.
Nora FE, Dahlin DC, Beabout JW: Bizarre parosteal osteochondromatous proliferations of the hands and feet. Am J Surg Pathol 1983;7:245-250.
Question 14
A 37-year-old man who works in a factory has isolated, lateral unicompartmental pain about his knee with activities. Nonsurgical management has failed to provide relief. The radiograph shown in Figure 45 reveals a tibiofemoral angle of approximately 15 degrees which is clinically correctable to neutral. What is the best surgical option in this patient?
Explanation
REFERENCES: Mathews J, Cobb AG, Richardson S, et al: Distal femoral osteotomy for lateral compartment osteoarthritis of the knee. Orthopedics 1998;21:437-440.
Cameron HU, Botsford DJ, Park YS: Prognostic factors in the outcome of supracondylar femoral osteotomy for lateral compartment osteoarthritis of the knee. Can J Surg 1997;40:114-118.
Question 15
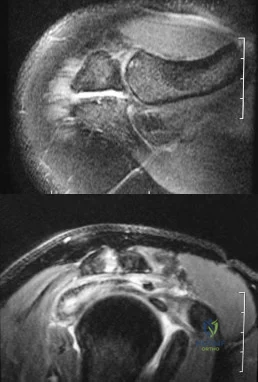
A 22-year-old professional baseball pitcher has had pain in the axillary region of his dominant shoulder for the past several weeks. While throwing a pitch during a game, he notes a sharp pulling sensation with a “pop” in his shoulder. Examination the following day reveals tenderness along the posterior axillary fold and pain and weakness with resisted extension of the shoulder. What is the most likely cause of his symptoms?
Explanation
REFERENCES: Schickendantz MS, Ho CP, Keppler L, et al: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains and related injuries.
Magn Reson Imaging Clin N Am 1999;7:39-49.
Livesey JP, Brownson P, Wallace WA: Traumatic latissimus dorsi: Tendon rupture. J Shoulder Elbow Surg 2002;11:642-644.
Question 16
A 41-year-old woman is brought to the emergency department after she was the unrestrained driver in a rollover motor vehicle accident. She was placed in a cervical collar and intubated at the scene. Her blood pressure is 80/40 and pulse is 140. She has obvious open fractures of the right forearm and left ankle. On exam, the lower extremities are externally rotated and the pubic symphysis is widened and unstable. Intravenous access is obtained and radiographs are pending. What is the most urgent next step in management?

Explanation
Question 17
The newborn foot deformity seen in Figures 64a and 64b should initially treated with
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American AcademAyL-oMfadOenrathCooppayedic Surgeons, 2006, pp 240-241.
Farsetti P, Weinstein SL, Ponseti IV: The Long-term functional and radiographic outcomes of untreated
and non-operatively treated metatarsus adductus. J Bone Joint Surg Am 1994;76:257-265. Question 65
A 4-year-old girl has been limping for the past 2 months. There is no history of trauma, previous injury, fever, or other systemic complaints. Examination reveals a moderate right knee effusio n with a 10-degree knee flexion contracture. What is the next most appropriate step in evaluation?
Arthroscopy
Antinuclear antibody
MRI
Bone scan
HLA-B27
DISCUSSION: The patient presents with juvenile idiopathic arthritis manifestations. The American College of Rheumatology defines this as one or more joints involved with swelling of 6 weeks or longer. A positive antinuclear antibody test would be diagnostic. Consideration should be made to have the patient see an ophthalmologist for evaluation of possible uveitis. Although the patient could have Lyme disease, that choice is not an option. The presence of an elevated antinuclear antibody by itself should not necessarily be used for diagnosing arthritis; however, the test does have clinical utility as a screening test. The frequency of a positive antinuclear antibody test is greatest in younger girls with oligoarticular disease and carries an increased risk for anterior uveitis. Arthroscopy might be indicated if this patient was presenting with a discoid meniscus, but there is no history of clicking, which is often one of the classic signs of discoid meniscus. MRI would not be used to diagnose juvenile idiopathic arthritis, but
MRI would be useful to help diagnose discoid meniscus. A bone scan would show increased uptake in the patient’s knee but again, this would not help diagnose her condition. HLA-B27 has no role in diagnosing juvenile idiopathic arthritis, especially in females.
REFERENCES: Iesaka K, Kubiak EN, Bong LR, et al: Orthopaedic surgical management of hip and knee involvement in patients with juvenile rheumatoid arthritis. Am J Orthop 2006;35:67-73.
Wright DA: Juvenile idiopathic arthritis, in Morrissey RT, Weinstein SL (eds): Love l and Winter’s Pediatric Orthopaedics, ed 6. Philadelphia PA, Lippincott Williams and Wilkins, 2006, pp 405-438. Question 66
An 18-month-old girl is brought in by her parents because of concerns about intoeing, bowlegs, and tripping and fa ling. Prenatal and birth history are otherwise unremarkable. The child’s growth and
development appear to be normal and she has a normal neurologic exam, a straight spine with no defects, and the hips are stable. Examination reveals hip internal rotation of 40 degrees and hip external rotation of 60 degrees. The thigh-foot angle is internal 30 degrees. Feet are straight and supple. Gait is characterized by intoeing with occasional tripping and falling. Based on these findings, what is the most appropriate action?
No treatment because internal tibial torsion slowly resolves on its own
Immediate treatment with a Denis-Browne bar
Distal tibial osteotomies
Proximal femoral derotational osteotomies
Treatment with twister cables PREFERRED RESPONSE: 1
DISCUSSION: The child has classic internal tibial torsion that is very commonly seen in younger children who are just beginning to walk. The normal outcome is for slow resolution of this problem and it seldom requires any treatment. Treatment with a Denis-Browne bar or with twister cables has not been proven to be effective. Surgical treatment at this point is premature and clearly not indicated.
REFERENCES: Lincoln TL, Suen PW: Common rotational variations in children. J Am Acad Orthop Surg 2003;11:312-320.
Staheli LT, Corbett M, Wyss C, et al: Lower-extremity rotational problems in children: Normal values to guide management. J Bone Joint Surg Am 1985;67:39-47.

Question 18
A 29-year-old woman reports dysesthesias and burning after undergoing bunion surgery that consisted of a proximal crescentic first metatarsal osteotomy 6 months ago. Examination reveals a positive Tinel’s sign at the proximal aspect of the healed incision. What injured nerve is responsible for her continued symptoms?
Explanation
REFERENCES: Kenzora JE: Sensory nerve neuromas: Leading to failed foot surgery. Foot Ankle 1986;7:110-117.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Question 19
An adult patient with a grade I isthmic spondylolisthesis at L5-S1 is most likely to have weakness of the
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 311-317.
Lauerman WC, Cain JE: Isthmic spondylolisthesis in the adult. J Am Acad Orthop Surg 1996;4:201-208.
Question 20
Epithelioid sarcoma most commonly occurs in which of the following anatomic locations?
Explanation
REFERENCES: Gupta TD, Chaudhuri P (eds): Tumors of the Soft Tissues, ed 2. Stamford, CT, Appleton and Lange, 1998, p 475.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St. Louis, MO, Mosby-Year Book, 1995, p 1074.
Question 21
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?
Explanation
REFERENCES: Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Lester B, Jeong GK, Weiland AJ, Wickiewicz TL: Quadrilateral space syndrome: Diagnosis, pathology, and treatment. Am J Orthop 1999;28:718-722.
Question 22
A 45-year-old man is seen in the emergency department after returning from a 2-hour airplane flight. He is reporting severe pain in his right leg but has no trouble moving his ankle, leg, or knee. Venous doppler testing reveals no evidence of deep venous thrombosis. He is placed on IV cephazolin but continues to worsen. On the third day in the hospital he has increased pain, some respiratory distress, and trouble maintaining his blood pressure. His leg takes on the appearance seen in Figure 15. An urgent MRI scan shows thickening of the subcutaneous tissues and superficial swelling in the leg but no evidence of an abscess. What is the next most appropriate step in management?
Explanation
after surgery.
REFERENCES: Fontes RA, Ogilvie CM, Miclau T: Necrotizing soft-tissue infections. J Am Acad Orthop Surg 2000;8:151-158.
Ozalay M, Ozkoc G, Akpinar S, et al: Necrotizing soft-tissue infection of a limb: Clinical presentation and factors related to mortality. Foot Ankle Int 2006;27:598-605.
Question 23
Figures below show the radiographs, and the CT obtained from a 58-year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when actively flexing her hip. She has trouble walking up stairs and getting out of her car. What is the most likely diagnosis?
Explanation
Groin pain after total hip replacement has a number of possible causes, and an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated, diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms or in any patient with a metal-on-metal bearing. This patient's symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning are indicated. Fluoroscope-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well positioned, then iliopsoas tenotomy should be considered.
Question 24
Figures 46a through 46d are the injury radiographs and postsurgical open treatment radiographs of a 13-year-old girl who fell while on a trampoline and sustained an injury to her right-dominant elbow. The skin is closed and she has normal vascular and neurologic examination findings. Which complication most likely could occur as a result of this injury and treatment?
Explanation
This girl sustained a fracture dislocation of the elbow with a severely displaced and rotated radial neck fracture. Required treatment was open reduction and internal fixation (ORIF). Less severely displaced radial neck fractures can be treated with closed reduction, percutaneous pinning, or flexible nail manipulation. In this scenario, interposed capsular tissue and rotation of the radial head were indications for ORIF. ORIF is associated with a higher risk for poor
outcomes. Complications following ORIF of radial neck fractures in children include posterior interosseous neuropraxia, valgus angulation, premature closure of the radial head physis, AVN of the radial head, nonunion, and elbow stiffness. Stiffness is most common. Compartment syndrome, infection, and anterior interosseous nerve palsy are less common complications.

CLINICAL SITUATION FOR QUESTIONS 47 THROUGH 50
A 6-year-old boy arrives at the emergency department with forearm pain. Today he was picking up his backpack when he felt a pop in his forearm that resulted in the current injury. His history is significant for 6 other fractures treated nonsurgically. His mother states that she had 15 fractures during childhood but is healthy now. Both the boy and his mother have blue sclera. Figures 47a and 47b are the radiographs of his injured forearm.
Question 25
Figures 34a and 34b show the axial and sagittal MRI scans of a 36-year-old man who reports the insidious onset of pain in the right shoulder. What is the most appropriate description of the acromial morphology? Review Topic
Explanation
Question 26
What is the most important consideration in the preoperative evaluation of a child with polyarticular or systemic juvenile rheumatoid arthritis (JRA)?
Explanation
this usually is not needed preoperatively. Uveitis and iritis are less likely in a child with systemic JRA.
Question 27
A 45-year-old woman has idiopathic scoliosis. Surgery is to include an anterior thoracic release through an open left thoracotomy. The thoracotomy will have what effect on the patient’s pulmonary function postoperatively? Review Topic
Explanation
function, compared to preoperative function, is rarely seen. This should be considered in planning surgical intervention in adults with scoliosis.
Question 28
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. Treatment should include

Explanation
Question 29
5cm. Recent radiographs are seen in Figures A and B. What is the most appropriate treatment plan?
Explanation
Subtrochanteric fractures can be treated with cephalomedullary nailing or fixed angle plates. Nailing of these fractures is technically challenging because the fracture must be reduced prior to nail passage. Failure to do so leads to varus and procurvatum malreduction.
Bellabarba et al. reviewed plating of femoral nonunions after intramedullary nailing. Of 23 nonunions, 21 healed at an average of 12 weeks. The remaining 2 cases required repeat plating (at 2 and 8 weeks) for hardware breakage because of noncompliance with weightbearing restrictions. They advocate plating because it allows for correction of malalignment and provides a biomechanically superior tension band construct.
Incorrect Answers:
OrthoCash 2020
A 38-year-old male was struck by a truck and sustained the injury seen in figure A. Treating this injury with an intramedullary nail with a larger radius of curvature can lead to what complication?

Posterior perforation of the distal femur
Varus malreduction
Comminution of the fracture site
Iatrogenic femoral neck fracture
Anterior perforation of the distal femur Corrent answer: 5
According to the study by Egol et al, the average femoral anterior radius of curvature was 120 cm (+/- 36 cm), and currently available femoral nails have a greater radius of curvature (i.e. more straight). This mismatch has been shown to lead to an increased risk of perforation of the anterior distal femur as the nail is impacted into the canal.
The referenced study by Tencer et al noted an increased risk of iatrogenic femoral fracture with anterior starting point >6mm from the anatomic axis.
They recommend starting in line with the femoral axis, or just a few millimeters anterior in order to minimize this risk.
Illustration A depicts anterior femoral cortex penetration secondary to nail/femur radius of curvature mismatch.

OrthoCash 2020
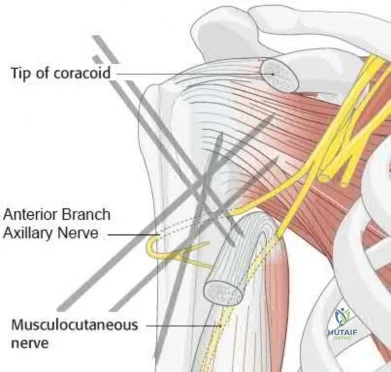
A 60-year-old woman is undergoing closed reduction and percutaneous pinning of a proximal humerus fracture. What structure is at greatest risk for injury from the pin marked by the red arrow in Figure A?
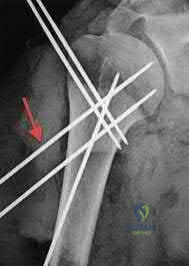
Anterior branch of the axillary nerve
Posterior humeral circumflex artery
Long head of the biceps tendon
Cephalic vein
Musculocutaneous nerve
Certain anatomic structures are at risk with percutaneous pinning of proximal humerus fractures. The red arrow in Figure A marks a proximal lateral pin that would place the anterior branch of the axillary nerve at risk.
Rowles and McGrory performed an anatomic study of the structures at risk with closed reduction and percuatneous pinning of the proximal humerus and found that proximal lateral pins were a mean of 3mm from the anterior branch of the axillary nerve. Pins placed through the anterior cortex and directed into the humeral head fragment were a mean of 2mm from the long head of the biceps tendon and greater tuberosity pins were found to be 8mm from the posterior humeral circumflex and 10mm from the main trunk of the axillary nerve as they penetrated the medial cortex of the humerus.
Jaberg et al retrospectively reviewed the clinical and radiographic results of 48 patients at an average of 3 years after undergoing closed reduction and percutaneous pinning of a proximal humerus fracture. 70% good to excellent results with their described technique, and the authors caution that radiographic malunion did not correlate with patient function.
Incorrect Answers
OrthoCash 2020
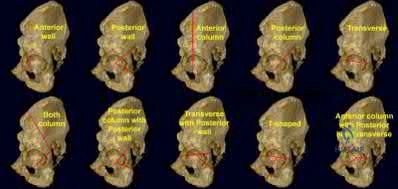
A 42-year-old female sustains the injury seen in the computed tomography images seen in Figures A and B. According to the Letournel classification, what is the injury pattern shown?

Posterior wall
Transverse
Anterior wall
Posterior column
Both column
The axial CT cut and Judet radiographic view shown reveals a transverse fracture pattern according to the Letournel classification system. This can be determined by the fact that the articular surface of the acetabulum is attached to the intact portion of the ilium, which is connected to the axial skeleton posteriorly through the sacroiliac joint. This differs from a both-column fracture, in which the articular surface of the acetabulum has no attachments to the axial skeleton due to fracture line(s). The axial CT scan also shows a vertical fracture line which is typical of a transverse fracture pattern.
Durkee et al review the classification schemes for these injuries, as well as comment on the importance of quality images (Judet views, CT, etc).
Figures A and B show a transverse acetabular fracture with mild displacement.
OrthoCash 2020
Which of the following is true regarding plating of humeral shaft fractures compared to intramedullary nailing?
worse functional results
higher need for subsequent surgeries
higher incidence of radial nerve injury
lower complication rates
decreased nonunion rates Corrent answer: 4
Controversy exists regarding nailing compared with plating of humeral shaft fractures, but the most recent and highest level evidence indicates decreased complication rates with open reduction and internal fixation of these injuries.
Lin et al found less blood loss with intramedullary nailing than plating, but nailing was also associated with increased shoulder surgery, likely due to disruption of the rotator cuff tendon during insertion.
Meekers et al found a higher union rate, better functional results and a lower reoperation rate after plate and screw fixation versus nailing. They concluded that plating was superior in most cases of humeral shaft fracture, however more recent studies have challenged these findings.
Heineman et al. (2012) have recently conducted an update on their meta-analysis to include more recent randomized studies. With the inclusion of newer studies the author found a statistically significant increase in total complication rate with the use of IM nailing compared with ORIF. The authors found no significant difference between the two treatment modalities for the secondary outcomes (nonunion, infection, nerve palsy, re-operation)
Incorrect Answers:
OrthoCash 2020
A 35-year-old male sustains the fracture seen in Figures A and B. Which of the following substances has been shown to result in the least radiographic subsidence when combined with open reduction and internal fixation?

Cancellous allograft bone chips
Autograft iliac crest
Femoral intramedullary reamings
Calcium phosphate cement
Calcium sulfate cement Corrent answer: 4
Figures A and B show a plateau fracture with a lateral split and depression of the articular surface. In treating tibial plateau fractures, calcium phosphate has been shown to have the least amount of articular subsidence on follow-up examinations due to its high compressive strength.
The study by Lobenhoffer et al noted improved radiographic outcomes and earlier weightbearing with usage of calcium phosphate cement. Welch and Zhang reproduced tibial plateau fractures in goats and compared cancellous autograft to calcium phosphate cement augmentation. At 24 hours, four of five specimens treated with autograft had subsidence of the fragment. Only two specimens from limbs treated with cement showed minimal subsidence; the remaining were congruent.
Yetkinler’s study compared cement to no cement treatment in a model of depressed plateau fractures. Calcium phosphate cement of high compressive
strength provided equivalent or better stability than conventional open reduction
and internal fixation with either auto/allograft bone which had both a lower compressive strength and reduced mechanical stability.
OrthoCash 2020
The modified Judet approach to the posterior scapula exploits the internervous interval between what two muscles?
Supraspinatus and infraspinatus
Supraspinatus and subscapularis
Infraspinatus and teres minor
Teres minor and teres major
Teres major and lattisimus Corrent answer: 3
The posterior or modified Judet approach to the scapula is typically used for internal fixation of scapular fractures. This approach utilizes a transverse incision over the scapular spine with detachment of the posterior deltoid. The interval between the infraspinatus (suprascapular n.) and teres minor (axillary n.) is identified and used to gain access to the posterior aspect of the scapula and glenoid.
The reference by Obremskey et al argues the approach "combines several important goals including: 1) exposure of all bony elements of the scapula which have adequate bone stock for internal fixation; 2) minimal trauma to the rotator cuff musculature; and 3) protection of the major neurologic structures (suprascapular nerve superiorly and axillary nerve laterally)." They believe "the main advantage of the exposure is limiting muscular dissection, which can potentially improve rehabilitation and limit morbidity of the operation."
OrthoCash 2020
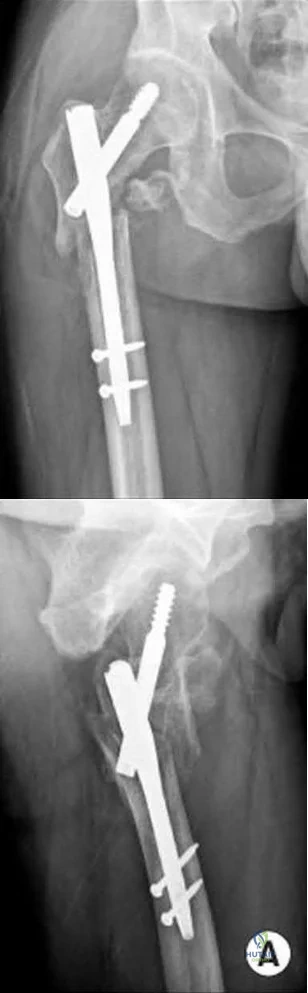
An 82-year-old female sustains an intertrochanteric hip fracture and is treated with a sliding hip screw. What is the most appropriate definitive step in treating the failure seen in figure A?

Non-weight bearing
Valgus proximal femoral osteotomy
Total hip arthroplasty
Revision open reduction and internal fixation
Proximal femoral resection Corrent answer: 3
Figure A shows superior cutout of the lag screw from the sliding hip screw as well as the superior cannulated screw used for an "antirotation" device.
In the referenced review article by Haidukewych and Berry, salvage of failed treatment of hip fractures in the elderly is limited by bone quality and comorbidities. They recommend total hip arthroplasty in this instance to restore function, decrease pain, and limit periods of immobilization. They mention that the major challenges for arthroplasty are: assessing the need for acetabular resurfacing, selecting the femoral implant, and managing the greater trochanter.
OrthoCash 2020
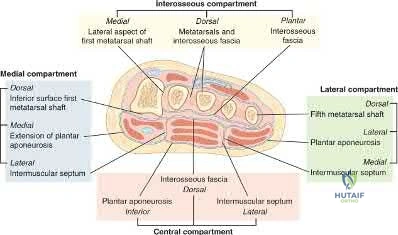
A 13-year-old boy falls out of a tree and sustains the injury seen in Figures A and B. He is taken to the OR for fixation of his fracture.
The next morning, the patient’s blood pressure is 185/105 mm Hg and pulse rate is 130. He complains of pain that is not improved with opiates. On physical exam, the foot is firm. The decision is made to obtain compartment pressures to rule out compartment syndrome of the foot. Which of the following paths in Figure C marks the
appropriate location to measure the central compartment, and what would be considered abnormal values?

Path A, absolute value of 30-45 mmHg or delta p > 30mmHg
Path B, absolute value of 30-45 mmHg or delta p > 30mmHg
Path B, absolute value of 30-45 mmHg or delta p < 30mmHg
Path C, absolute value of 30-45 mmHg or delta p > 30mmHg
Path C, absolute value of 30-45 mmHg or delta p < 30mmHg Corrent answer: 3
The correct approach to measure pressures in the central compartment of the foot is by directing the needle lateral and plantar through the abductor hallicus, just under the base of the first metatarsal. Abnormal values indicating the need for decompression are an absolute value of 30-45 mmHg or a Δp < 30mmHg (the difference between the patient's diastolic blood pressure and compartment pressures).
The most common symptom of compartment syndrome in the extremities is intense pain. However, compartment syndrome can be difficult to diagnose in children and patients who are comatose, nonverbal, and/or mentally compromised because they may not be able to properly express their level of pain. Additionally, in compartment syndrome of the foot, pain on passive extension of the toes may or may not be present, and swelling and absence of the dorsalis pedis pulse may be expected findings with extensive trauma to the foot, making the clinical diagnosis even more difficult. Thus, for patients with equivocal findings on physical exam, foot compartment pressures should be measured in order to confirm the diagnosis. There are 8 compartments in the foot: lateral, medial, central, and 4 interosseous. The lateral compartment
contains the abductor digiti minimi and flexor digiti minimi brevis, and is measured by directing the needle 1cm medial and plantar under the midshaft of the 5th metatarsal. The medial compartment contains the abductor hallicus and flexor hallicus brevis, and is measured by directing the needle lateral and plantar under the base of the first metatarsal. The central compartment contains the oblique head of the adductor hallucis, and is measured through the same approach as the medial compartment after advancing the needle more deeply. The 4 interosseous compartments entail the 2nd, 3rd, and 4th web spaces, and can be measured by directing the needle plantar into each respective dorsal webspace.
Ojika et al. performed a systematic review on foot compartment syndrome. They found that the most common cause of foot compartment syndrome was crush injury to the foot, and that diagnosis was mostly made through a combination of clinical findings and compartment pressure measurements.
Badhe et al. reported 4 cases where competent sensate patients developed compartment syndromes without any significant pain. They found that pain is not a reliable clinical indicator for underlying compartment syndrome, so in a competent sensate patient, the absence of pain does not exclude compartment syndrome. They concluded that a high index of clinical suspicion must prevail in association with either continuous compartment pressure monitoring or frequent repeated documented clinical examination with a low threshold for pressure measurement.
Flynn et al. looked at the diagnosis and outcome of acute traumatic compartment syndrome of the leg in children. They found that a delay in diagnosis may occur because acute traumatic compartment syndrome manifests itself more slowly in children or because the diagnosis is harder to establish in this age group. They state that the results of the present study should raise awareness of late presentation and the importance of vigilance for developing compartment syndrome in the early days after injury.
Figures A and B are lateral and Harris radiographs of the foot demonstrating a calcaneus fracture. Figure C is a cross-sectional image of the foot. Illustration A is an image depicting the compartments of the foot.
Incorrect Answers:
compartment. Additionally, a Δp < 30mmHg (not > 30mmHg) is considered abnormal.
OrthoCash 2020
A 35-year-old female presents to the emergency room after a motor vehicle collision where her leg was pinned under the car for over 30 minutes. A clinical photo and radiographs are shown. Which of the following is the most accurate way to diagnose compartment syndrome?

surgeon's palpation of the leg compartments
paresthesias in her foot
diastolic blood pressure minus intra-compartmental pressure is less than 30 mmHg
diastolic blood pressure minus intra-compartmental pressure is greater than 30 mmHg
intra-compartmental pressure measurement of 25 mmHg Corrent answer: 3
The clinical picture is consistent with compartment syndrome. The most accurate way to make the diagnosis is to measure the difference between the diastolic blood pressure and intracompartmental pressure (delta p).
In a prospective study of 116 patients with tibial diaphyseal fractures, McQueen et al found that the use of a differential pressure of 30 mmHg as a threshold for fasciotomy led to no missed cases of acute compartment syndrome. They recommended that a fasciotomy should be performed if the differential pressure level drops to under 30 mmHg.
The cited study by Kakar et al found the intraoperative DBP is significantly lower than the preoperative DBP in patient undergoing IM nailing for tibia shaft
fractures. Therefore, they emphasize that the surgeon should recognize that intraoperative DeltaP may be lower than DeltaP once the patient is awakened in deciding whether to perform a fasciotomy versus awaken the patient and perform serial examinations and or compartment pressure measurements.
An absolute intra-compartmental value greater than 30 to 45mmHg can also be used to make the diagnosis of compartment syndrome, but is more controversial than the delta p according to Kakar and Amendola.
OrthoCash 2020
What is the most common mode of failure of the lateral ulnar collateral ligament associated with an elbow dislocation?
ligament avulsion off the humeral origin
ligament avulsion off the ulnar insertion
midsubstance rupture
bony avulsion of the humeral origin
combined proximal and distal ligament avulsions Corrent answer: 1
The lateral ulnar collateral ligament (LUCL) is often injured with elbow dislocations, and is most commonly injured at the proximal origin.
McKee noted that in 62 consecutive operative elbow dislocations and fracture/dislocations, the LUCL was ruptured in all of the patients, proximally in 32, bony avulsion proximally in 5, midsubstance rupture in 18, ulnar detachment in 3, ulnar bony avulsion in only 1, and combined patterns in 3.
Pugh et al established a standard protocol to treat elbow fracture dislocations (terrible triad) which includes coronoid repair, radial head repair/replacement, LUCL repair, and MCL and/or external fixation as needed.
OrthoCash 2020
A 24-year-old male sustains the injury seen in Figure A after being thrown from a motorcycle at a high speed. Which of the following fixation methods has been shown to be the most stable fixation construct for this injury?

Posterior bridge plating and anterior ring external fixation
Percutaneous iliosacral screw and anterior ring external fixation
Percutaneous iliosacral screw and anterior ring internal fixation
Transiliac screw
Two percutaneous iliosacral screws Corrent answer: 3
Figure A shows an APC III injury, which is a rotationally and vertically unstable injury, with damage to the anterior ring, pelvic floor, and posterior ligamentous stabilizing structures.
The referenced study by Sagi et al found that biomechanically, a percutaneous iliosacral screw and anterior ring internal fixation was the most stable construct. In addition, he found no biomechanical support for addition of a second iliosacral screw.
OrthoCash 2020
A 33-year-old male patient presents with a comminuted open tibia fracture after involvement in a motor vehicle crash. He has a history of smoking but is otherwise healthy. He is given antibiotics, and taken immediately for irrigation and debridement, followed by an un-reamed stainless steel intramedullary nail. Due to bone loss there is a non-circumferential cortical defect measuring 12 mm at the fracture site. All of the following factors in this patient's history and presentation increase his risk for adverse outcome EXCEPT:
High-energy mechanism of injury
Use of un-reamed nail
Implant material
Fracture gap
History of smoking Corrent answer: 2
Of the factors listed only the use of an un-reamed intramedullary nail for an open tibia fracture has not been shown to increase the risk of adverse outcome or need for reoperation.
The treatment of open tibia fractures with intramedullary nailing can be complicated by many factors. High energy mechanism of injury, use of a stainless steel nail, residual fracture gap greater than 1 cm, and a history of smoking have all been shown to increase the risk of adverse outcome. The use of reamed and un-reamed nails for open tibia fractures have been studied, and no significant difference in outcome has been found.
Schemitsch et al. present data from a prospective randomized trial of tibia fractures treated with reamed or unreamed intrameduallry nails. They found no difference in risk of adverse outcome between reamed and un-reamed nails in open tibia fractures. They did, however, find an increased risk of adverse outcomes in high-energy mechanisms, use of stainless steel (versus titanium) rods, and a residual fracture gap of greater than 1 cm. They comment that their data did not show a significant increase in risk due to history of smoking, but cite other studies that have demonstrated such a relationship.
Bhandari et al. present data from a prospective randomized study of patients with tibia fractures randomized to reamed or un-reamed tibial nails. For closed fractures they found a lower rate of primary events (most commonly need for dynamization) in the reamed group. However, they found no difference in outcomes for either technique in open fractures.
Incorrect answers:
OrthoCash 2020
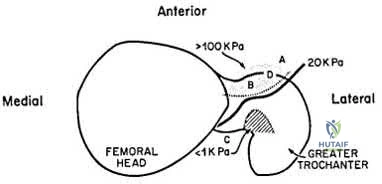
Following antegrade intramedullary nailing of a femoral shaft fracture, the complication shown in Figure A occurs. Which of the following errors most likely resulted in this complication?
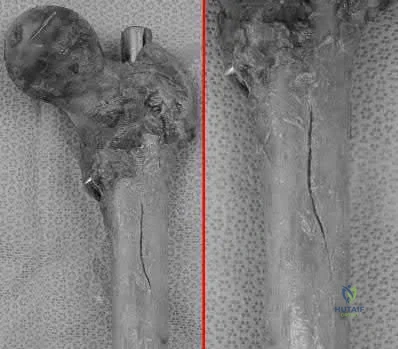
Applying external rotation torque on the proximal femur after placing proximal interlocking screws
Excessive interfragmentary compression of the fracture site prior to placing proximal interlocking screws
Using too anterior a starting point for a piriformis-entry point nail
Inserting a trochanteric-entry point nail through the piriformis fossa
Inserting a right femoral nail into the left femur Corrent answer: 3
Using a piriformis nail, a starting point that is too anterior will result in iatrogenic fracture ("bursting") of the proximal femur.
Antegrade nailing achieves fixation via 3-point fixation. In the sagittal plane, because of anterior sagittal bow, this is achieved at distal anterior cortex, middle posterior cortex (apex of curvature) and proximal anterior cortex. In the coronal plane, because of the lateral bow, this is achieved at the lateral distal femur, middle medial femur (apex of curvature), and proximal lateral femur (greater trochanter). Piriformis nails have a single sagittal bow.
Trochanteric nails are bowed in 2 planes, necessitating a twisting motion during insertion to negotiate both bows.
Papadakis et al. performed an experimental study on 18 cadaveric femora. Anterior bursting was found in 56% of nails placed too anteriorly. Bursting was not seen in nails placed through a more posterior entry point. They emphasize the location of the entry point when performing antegrade nailing.
Johnson et al. reviewed the biomechanical factors affecting fracture stability
and femoral bursting. They found that position of the starting hole was most important. Anterior displacement by >6mm led to high hoop stresses and bursting of the anterior cortex. This is important as an eccentrically reamed cortex may be difficult to recover from. They recommend either selecting a smaller diameter nail or overreaming by 1-2mm as a solution.
Figure A shows a fracture split of the proximal femur (left, without magnification; right, close-up). Illustration A shows anterior cortex pressures exceeding 100kPa for too-anterior entry points.
Incorrect Answers:
Wrong-side placement of a trochanteric entry nail would lead to varus malalignment at the fracture site, more so than placing a piriformis nail through the greater trochanter.
OrthoCash 2020
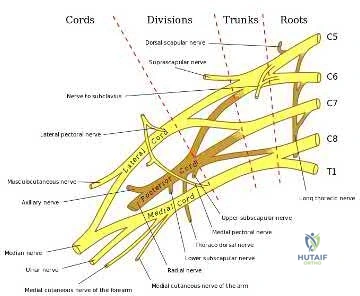
A 30-year-old male sustains a brachial plexus injury as the result of a motor vehicle collision. Palsy of which of the following muscles would not be expected with this injury if the injury was postganglionic in nature?
Rhomboid major
Extensor carpi radialis longus
Biceps brachii
Deltoid
Brachioradialis
A brachial plexus injury would involve all of the upper extremity muscles as well as most of the periscapular muscles. Complete plexus palsies are rare, and are often associated with scapulothoracic dissociation or other high-energy injuries.
Preganglionic injuries often involve the cervical paraspinal musculature as well as a complete plexus injury. EMG evidence of intact signals in the serratus anterior (long thoracic nerve) and rhomboids (dorsal scapular nerve) are suggestive of a postganglionic lesion/injury.
Tubbs et al. reported on the surgical anatomy of the dorsal scapular nerve in a cadaver study. They found that the nerve came off the C5 nerve root in 95%, ran 2.5cm medial to the spinal accessory nerve as it traveled on the anterior border of the trapezius muscle, and was intertwined with the dorsal scapular artery in all specimens.
Balakrishnan et al reported on the comparison of clinical exam and EMG in predicting site of lesions in brachial plexus injuries. The combination of EMG and exam localized the nerve injury in 80%, while the paraspinal EMG was the most sensitive solitary examination method (67%).
Illustration A shows a diagram of the brachial plexus. Incorrect Answers:
5: These muscles are all innervated by nerves that come from the brachial
plexus, and would be affected with a postganglionic injury.
OrthoCash 2020
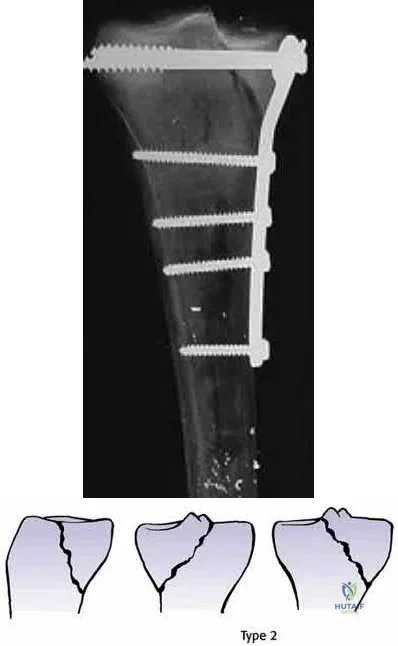
A 40-year-old male sustains a fall from a height. He sustains the isolated injury shown in the radiograph and CT images seen in Figures A through C. Surgery is planned. Which of the following constructs is the most appropriate definitive fixation for this injury?

Lateral locked plating
Medial bridge plating
Medial buttress plate
Medial lag screw with washers
External fixation
This patient has a medial tibial plateau fracture. Medial buttress plating (MBP) is indicated.
Medial tibial plateau fractures (Schatzker IV, Hohl and Moore II) may represent fracture dislocations of the knee. Neurovascular injuries must be excluded. In these instances, the medial fragment represents the stable fragment, and the rest of the tibia is the fractured fragment, with the entire leg acting as the lever arm.
Berkson et al. reviewed high energy tibial plateau fractures. Medial fractures may be treated with a medial plate or external fixation. Open reduction may be necessary because of fracture line obliquity and propensity of the medial plateau to shorten and rotate in the sagittal plane. Meniscal injuries should be repaired and avulsed cruciates fixed early. Collateral ligaments should be reconstructed after obtaining bone healing and range of motion.
Ratcliff et al. compared the stability of lateral locked plates and medial buttress plates in a cadaver model. They found that the medial buttress plate had greater fixation strength/failure force (4136N) compared with the lateral locking plate (2895N), although maximum cyclic displacement and residual displacement results were not different. They concluded that for vertically
orientated medial tibial plateau fractures, medial buttress plates were more stable.
Figure A is a radiograph showing a medial tibial plateau fracture extending across the tibial eminence. This is also classified as a Hohl and Moore Type II fracture. Figures B and C are coronal and axial CT scan images confirming the medial tibial plateau fracture and excluding a bicondylar fracture. Illustration A shows a medial tibial plateau fracture fixed with a medial buttress plate (cadaveric model with fibula removed). Illustration B shows the Hohl and Moore Type II fracture involving the entire condyle.
Incorrect Answers:
OrthoCash 2020
A 39-year-old female presents with the following motor vehicle crash with the injury seen in Figure A (immobilized in a pelvic binder). The iatrogenic neurologic injury most commonly caused by placement of the anterior construct for this injury, as shown in Figure B, would cause which of the following?
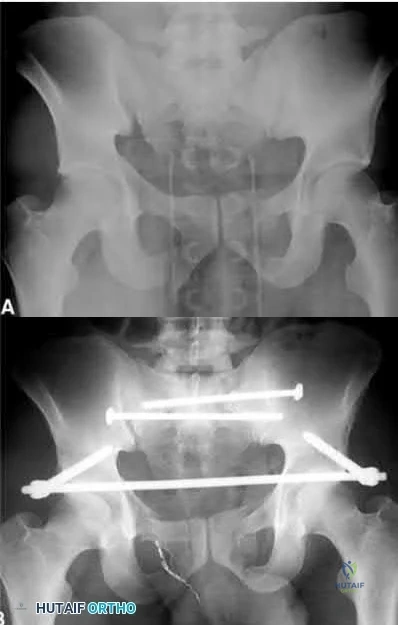
Weakness of hip flexion
Weakness of ankle dorsiflexion
Numbness of the medial thigh
Numbness of the lateral thigh
Numbness of the perineum Corrent answer: 4
This patient was treated with posterior stabilization, and an anterior subcutaneous internal fixator (ASIF). The most common neurologic injury seen following placement of the ASIF construct is irritation of the lateral femoral cutaneous nerve (LFCN), causing numbness and/or pain of the lateral thigh.
Unstable pelvic fractures can be treated in a multitude of ways. The ASIF construct is typically created by placing long pelvic screws or polyaxial pedicle screws in the supraacetabular region, similar to the supraacetabular pins for an
anterior external fixator. Then a curved bar is placed subcutaneously and connected to the supraacetabular screws. They are typically removed after 3-4 months when fracture healing is complete.
Vaidya et al. present a retrospective review of the use of ASIF as definitive treatment of unstable pelvic fractures. All patients in the study tolerated the construct well. LFCN irritation was seen in 30% of patients, and resolved in all but one patient.
Müller et al. present a retrospective review of the use of posterior stabilization and ASIF. They report an acceptably low complication rate, and good to excellent outcomes in 64.5% of patients.
Figure A is a radiograph demonstrating a right APC3 and left APC2 pelvic injury, imaged in a pelvic binder. Figure B is a postoperative radiograph following posterior stabilization and ASIF.
Incorrect answers:
OrthoCash 2020
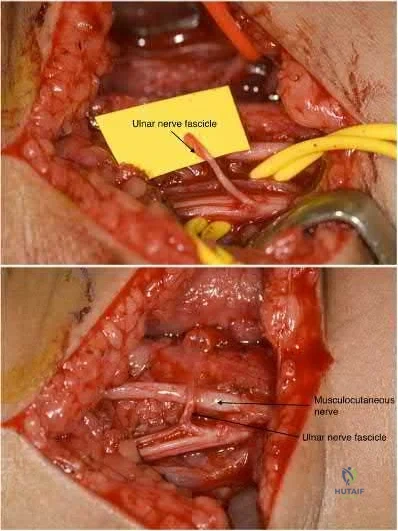
What would be the most appropriate surgical indication for transferring fascicles of the ulnar nerve to the motor nerve of the biceps and fascicles of the median nerve to the motor nerve of the brachialis?
C8 - T1 nerve root avulsion 3 months ago
C5 - C6 nerve root avulsion 2 months ago
Upper brachial plexus palsy 22 months ago
Medial and posterior cord injury from gunshot wound 2 months ago
C6 ASIA A spinal cord injury Corrent answer: 2
Transfer of fascicles from (1) ulnar nerve to the nerve to the biceps and (2) median nerve to the motor nerve of the brachialis would be appropriate in the
treatment of an acute (<3-6 months) upper brachial plexus palsy.
Upper trunk injury (C5, C6) often results from the avulsion of both the C5 and C6 nerve roots. Injuries of this nature usually result from a downward force on the shoulder with lateral bending of the cervical spine in the opposite direction. This results in what is commonly called an Erb-Duchenne palsy. Patients often present with a flail shoulder and loss of elbow flexion. Other common treatments for C5 and C6 root avulsion include neurotization of the musculocutaneous (MSC) nerve by the spinal accessory (SA) or intercostal nerve, and neurotization of the supra-scapular nerve by the SA.
Liverneaux et al. looked at short term results of (1) ulnar nerve fascicle transfer to the nerve to the biceps and (2) fascicle of the median nerve to the motor branch to the brachialis in 15 patients with acute C5 - C6 nerve root avulsion injuries. Grade 4 elbow flexion was restored in each of the 10 patients. There was no secondary deficit in grip strength or sensation.They concluded that this double nerve transfer technique will likely reduce the need for secondary procedures to augment elbow flexion.
Teboul et al. reviewed thirty-two patients with an upper nerve-root brachial plexus injury that underwent ulnar nerve fascicle transfer to the nerve of biceps to restore elbow flexion. After the nerve transfer, twenty-four patients achieved grade 3 elbow flexion strength or better. They note that this procedure will spare the C5 nerve root and other nerves for grafting or transfer elsewhere.
Illustration A shows harvesting of an ulnar nerve fascicle for transfer. Illustration B shows transfer of the fascicle of the ulnar nerve to the motor nerve of the biceps.
Incorrect Answers:
sensory quadriplegia. Nerve transfers using the ulnar nerve (C8-T1) would also be redundant as this nerve would be non-functional in this patient.
OrthoCash 2020
A 31-year-old female presents to the trauma bay following a motorcycle crash. Her blood pressure is 95/70 mmHg, heart rate is 115 bpm. Lactate measured in the trauma bay is 10 mmol/L. She has multiple rib fractures, pulmonary contusions, and a positive FAST exam requiring immediate exploratory laparotomy. After laparotomy her lacate remains unchanged. She has a closed right femur fracture and an open right tibia fracture as seen in Figures A and B. Besides antibiotics and thorough irrigation and debridement, which of the following would be an appropriate step in the immediate management of her fractures?

Reamed intramedullary nailing of the tibia and femur
Un-reamed intramedullary nailing of the tibia, and reamed intramedullary nailing of the femur
Reamed intramedullary nail of the tibia, and un-reamed intramedullary nail
of the femur
Posterior slab splint of the tibia, and 10 lbs skeletal traction of the femur
External fixation of the tibia and femur Corrent answer: 5
This patient is suffering from multiple injuries and has evidence of chest injury and incomplete resuscitation. The immediate treatment of her fractures should be external fixation for both the tibia and the femur.
For polytraumatized patients with multiple injuries including extremity fractures, damage control orthopaedics dictates that long bone fractures should be temporarily stabilized. Either inadequate stabilization, or early total care, such as a reamed or unreamed nails, can exacerbate the patient's condition and increase the risk of a second-hit phenomenon. For this patient with pulmonary contusions and continued elevation of lactate indicating end-organ hypoperfusion her extremities should have staged treatment according to damage control principles.
Morshed et al. present a retrospective review of polytraumatized patients with femur fractures and compared outcomes based on the time frame in which their fractures were definitively treated. They found delaying treatment at least 12 hours to allow appropriate resuscitation and treatment of other traumatic injuries led to a decrease in mortality of 50%. Patients with intra-abdominal injuries benefited most from staged treatment of the extremities.
Figure A is a radiograph showing a closed right femur fracture. Figure B is a radiograph of an open right tibia fracture.
Incorrect answers:
OrthoCash 2020
A 68-year-old woman undergoes a hemiarthroplasty for a proximal humerus fracture through a deltopectoral approach. What
range of motion exercise should not be utilized in the immediate postoperative period due to concerns about lesser tuberosity fixation?
Pendulums
Passive internal rotation of the shoulder to the plane of the body
Active forearm supination
Passive external rotation of the shoulder past 30 degrees
Passive forward flexin of the shoulder to 90 degrees Corrent answer: 4
Frankle et al found that passive external rotation of the shoulder placed the most stress on the lesser tuberosity fixation. The subscapularis tendon inserts on the lesser tuberosity and is the deforming force when placed under tension during external rotation. They also found that non-anatomic tuberosity reduction of 4-part proximal humerus fractures treated with hemiarthroplasty increased torque and impaired external rotation kinematics.
OrthoCash 2020
A 72-year-old female sustains a displaced intracapsular femoral neck fracture. Which of the following is TRUE regarding the long term differences between possible treatment options for this injury?
Patients undergoing total hip arthroplasty are more likely to experience persistent pain than those undergoing internal fixation
Patients undergoing total hip arthroplasty are less likely to require reoperation than those undergoing internal fixation
There is no difference in functional outcome scores between internal fixation and total hip arthroplasty
Patients undergoing internal fixation perform activities of daily living better than those undergoing total hip arthroplasty
Mortality rates are higher following total hip arthroplasty than internal fixation
Elderly patients with femoral neck fractures (FNF) undergoing total hip arthroplasty (THA) are less likely to require reoperation than those undergoing internal fixation.
Intracapsular FNF are common in elderly patients after a fall from standing height. Treatment depends on physiological age and displacement (Garden's classification). For displaced fractures, physiologically young patients are treated with internal fixation while physiologically old patients are treated with
either hemiarthroplasty (debilitated, less active patients) or THA (more active patients, those with acetabular disease or preexisting inflammatory arthritis).
Chammout et al. retrospectively compared the long term (17 years) results of THA (cemented both component) and ORIF (2 cannulated screws) in elderly patients (>65 years). They found no difference in mortality. But hip scores were higher and pain was better in the THA group, while reoperation rates were higher in the ORIF group. Walking speed was initially faster in the THA group, but later did not differ between groups. They recommend THA for elderly patients with displaced FNF.
Rogmark et al. prospectively compared closed reduction and internal fixation (CRIF) with arthroplasty (combining hemiarthroplasty and THA) at 2 years in elderly patients (>70 years). Failure rates were higher, pain was worse, and walking was more impaired after CRIF. They recommend arthroplasty for patients >70 with FNF.
Incorrect Answers:
OrthoCash 2020
A polytrauma patient underwent the following procedures: (1) statically locked intramedullary nailing for a right femoral shaft fracture; (2) open reduction with plate-and-screw fixation [ORIF] for a right simple distal fibula fracture; (3) ORIF right middle third radius and ulna fracture; and (4) ORIF left humeral shaft fracture. What is the appropriate weightbearing status for this patient?
Weight bearing as tolerated in all extremities
Early protected weight bearing right lower extremity in walking cast, weight bearing as tolerated left upper extremity, non-weight bearing right forearm
Weight bearing as tolerated in bilateral lower extremities and right upper extremity, non-weight bearing left upper extremity
Non-weight bearing bilateral upper extremities and right lower extremity
Non-weight bearing right upper and lower extremities, weight bearing as tolerated left upper and lower extremities without walking cast
The standard postoperative weightbearing for locked medullary nailing for femoral shaft fractures and humeral shaft fractures is weight bearing as tolerated (WBAT). Simple ORIF ankle fractures may be managed with early protected weight bearing. ORIF right middle third radius and ulna fracture should be managed with a period of non-weight bearing due to risk of secondary displacement of the fracture.
Tingstad et al. examined the effect of immediate weightbearing on plated fractures of the humeral shaft. They reported that immediate weightbearing on humeral shaft fractures, treated with plating and full weightbearing, did not have any negative effect on the union or malunion rates.
Brumback et al. evaluated the feasibility, safety and efficacy of immediate weightbearing after treatment of femoral shaft fractures with statically locked IM nail. Using biomechanical and clinical data, they showed that all fractures united with no loss of fixation or hardware failure.
Starkweather et al. retrospectively assessed the complications and loss of reduction in patients who bore weight in a short leg cast within 15 days after surgical repair of acute unilateral closed ankle fractures. Of the 81 ankle fracture radiographs, 80 (98.8%) showed no displacement in fracture reduction on the final follow-up examination. These results suggest early protected weightbearing may be safe.
Incorrect Answers:
OrthoCash 2020
A 22-year-old female falls off the back of a motorcycle and sustains the injury in Figure A. She is hemodynamically unstable and massive transfusion protocol is activated. What is the correct ratio of transfusion of packed red blood cells, platelets and plasma?

Question 30
Which of the following postoperative rehabilitation techniques causes minimal rotator cuff muscle activation? Review Topic
Explanation
Question 31
A 68-year-old male presents with gait instability, clumsiness of the hands, and the MRI images shown in Figure A. You decide to proceed with surgical decompression. When planning your surgical treatment, it is important to note that compared to a posterior approach, the anterior procedure has: Review Topic

Explanation
Cervical myelopathy has a progressive course and therefore if there is evidence of functional impairment surgical decompression is indicated. Either an anterior decompression or posterior decompression can be used depending on a variety of factors including number of levels involved and sagittal alignment of the cervical spine. In general, a posterior approach is used when three or more levels are involved and the spine is in neutral or lordotic alignment.
Fehlings et al. did a prospective study on the risks of complications associated with surgical treatment of cervical myelopathy. They found that combined anterior and posterior procedures had a significantly higher rate of complication than either anterior-only or posterior-only procedures. Posterior procedures had a higher rate of wound infections compared to anterior. They found no statistical difference in the over-all complication rate, incidence of C5 radiculopathy, or dysphagia between an anterior-only or posterior-only procedure.
Fehlings et al. did a prospective study on outcomes following surgical treatment of cervical myelopathy. At one year follow-up they found a significant improvement in mJOA score, Nurick grade, NDI score, and all SF-36v2 dimensions. With the exception of mJOA scores, these improvements were not statistically related to severity of disease.
Liu et al. performed a meta-analysis of outcomes following surgical decompression of cervical myelopathy. They found outcomes following anterior procedures were better than those for posterior procedures when there were less than 3 affected levels. With 3 or greater levels, no statistical difference in outcomes could be found between the two approaches. They note none of their reviewed publications represent high-quality prospective randomized trials.
Figure A is a sagittal MR image of the cervical spine showing multi-level degenerative disease with cord compression consistent with cervical myelopathy.
Incorrect Answers:
Question 32
Figures 39a and 39b show the radiographs of an otherwise healthy 10-year-old boy who has had thigh pain and a limp for the past 9 months. Examination reveals that the left lower extremity is 1 cm shorter, with reduced flexion, abduction, and internal rotation on the left side. The patient is at the 50th percentile for height and the 90th percentile for weight. Serum studies will most likely show
Explanation
REFERENCES: Loder RT, Hensinger RN: Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop 1997;17:205-211.
Loder RT, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Question 33
A 13-year-old girl has had increasing left hip pain for the past 4 months. A radiograph, bone scan, MRI scan, and photomicrograph are shown in Figures 1a through 1d. Which of the following immunohistochemistry results would confirm the most likely diagnosis?
Explanation
REFERENCES: Halliday BE, Slagel DD, Elsheikh TE, et al: Diagnostic utility of MIC-2 immunocytochemical staining in the differential diagnosis of small blue cell tumors. Diagn Cytopathol 1998;19:410-416.
Llombart-Bosch A, Navarro S: Immunohistochemical detection of EWS and FLI-1 proteins is Ewing sarcoma and primitive neuroectodermal tumors: Comparative analysis with CD99
(MIC-2) expression. Appl Immunohistochem Mol Morphol 2001;9:255-260.
Question 34
Pharmacoprophylaxis should be avoided in favor of a pneumatic compression device for a patient with
Explanation
For patients with known bleeding disorders, a pneumatic compression device alone is recommended over pharmacoprophylaxis to minimize risk for excessive bleeding and wound complications. Factor VIII deficiency (hemophilia) and active liver disease are the 2 conditions for which support is strongest to withhold anticoagulation. Protein C deficiency and protein S deficiency are associated with increased risk for thrombosis, as is the factor V Leiden mutation.
RESPONSES FOR QUESTIONS 159 THROUGH 162
Lateral femoral cutaneous
Superior gluteal
Inferior gluteal
Obturator
Sciatic
Which nerve listed above is at increased risk for injury when performing hip surgery through the following approaches?
Question 35
A 35-year-old man sustained a traumatic low ulnar nerve palsy 18 months ago. The extent of the clawing and intrinsic atrophy as well as the active radial deviation are seen in Figures 1 through 3. No hyperextensibility of any of the proximal interphalangeal (PIP) joints is observed. Preoperatively, the patient is not able to fully extend the PIP joints with the wrist in neutral position and the examiner holding the metacarpophalangeal (MCP) joints flexed. Figure 4 shows the intraoperative photograph obtained during the intrinsic reconstruction procedure that is performed. The tendon grafts were inserted distally into the

Explanation
Originally, Burkhalter and Strait recommended bony insertion into the proximal phalanx through a drill hole. This procedure does require more surgical dissection and flexes only the MCP joints; thus it cannot extend the PIP joints directly. It does improve clawing in the fingers if the PIPs can extend with preoperative MCP flexion. The ability to extend the PIP joints is evaluated preoperatively using the Bouvier test. With the wrist in neutral position, the examiner holds the MCPs flexed and looks for the ability in that position to actively extend the PIPs. If the patient is able to do so, then the test is considered positive, and this describes "simple" clawing. In such cases, procedures that flex only the MCPs are appropriate. The insertion sites for these procedures include the proximal phalanx, the first annular pulley, and the second annular pulley. If the Bouvier test is negative, then it is best to insert the tendon grafts distally into the lateral bands. This technique has a low chance of leading to hyperextension of the PIP joints, particularly when performed with a wrist extensor motor (which leaves the flexor digitorum superficialis undisturbed) and with no preoperative hyperextensibility of the PIPs.
Question 36
-The patient requests anatomic double-bundle ACL reconstruction. Compared with transtibial singlebundle ACL reconstruction, anatomic double-bundle ACL reconstruction is more likely to
Explanation
The radiograph shows a Segond fracture, an avulsion fracture involving the lateral capsular ligament.
This radiographic finding has been associated with ACL rupture in 75% to 100% of cases. Drilling the femoral tunnel through the anteromedial portal allows for independent access to the native femoral attachment. Fiber orientation is more oblique than with a transtibial technique and more closely resembles that of the native ligament. Double-bundle reconstruction attempts to duplicate native ACL anatomy.Biomechanical studies have shown that double-bundle reconstruction more
closely reproduces normal knee kinematics; however, this technique does not offer a clear advantage in terms of clinical outcomes.The iliotibial band inserts onto Gerdy’s tubercle. The popliteus tendon originates from the lateral femoral condyle. The lateral meniscus attaches near the intercondylar eminence at the anterior and posterior meniscal roots. Recent advances in ACL reconstruction focus on restoring the native ACL anatomy.Studies have determined that a knee flexion angle of 110 degrees is optimal to avoid blowout of the back wall and injury to the lateral structures while drilling.
Femoral tunnel length is typically shorter than with a transtibial approach and decreases with higher-flexion angles. Double-bundle reconstruction is associated with higher surgical costs because of the need for additional fixation and, in the case of allograft reconstruction, a second graft.
Question 37
Closed reduction and functional bracing would lead to significant upper extremity disability due to malunion.
Explanation
The referenced review article by Michelson covers rotational ankle fractures, with a review of the diagnosis, treatment options, and patient outcomes. He notes that unstable fractures (bimalleolar, bimalleolar equivalent, etc.) usually are managed with open reduction and internal fixation for optimal outcomes.
Incorrect answers:
Figure B shows a Weber C (high fibular) ankle fracture, PER, without any evidence of a medial malleolar fracture.
Figures C (SER IV), D (PER IV), and E (isloated medial malleolar fracture) all show fractures not suitable for screw fixation of the medial malleolus parallel to the joint since their fracture lines are not vertical.
OrthoCash 2020
Which of the following is an advantage of using blocking screws for tibial nailing?
Decrease risk of nail breakage
Eliminate use of interlocking screws
Allow for larger nail use
Enhance construct stiffness
Decrease torsional rigidity Corrent answer: 4
Blocking screws can be used to help obtain and maintain reductions, increase construct stiffness, and neutralize translational forces. There are no studies as of yet that find a blocking screw to decrease nail failure.
Krettek found that medial and lateral blocking screws can increase the primary stability of distal and proximal metaphyseal fractures after nailing and can be an effective tool for selected cases that exhibit malalignment and/or instability by decreasing mechanically measured deformation.
In a later clinical study, Krettek found that after using blocking screws, tibial healing was evident radiologically at a mean of 5.4 months with a decreased
rate of malunions.
Ricci also found that blocking screws are effective to help obtain and maintain alignment of fractures of the proximal third of the tibial shaft treated with intramedullary nails.
OrthoCash 2020
Following operative repair of lower extremity long bone and periarticular fractures, what is the time frame for patients to return to normal automobile braking time?
6 weeks after initiation of weight bearing
4 weeks postoperatively
8 weeks from the date of injury
Once full range of motion of the ankle and knee exist
At the time of bony union Corrent answer: 1
According to the first referenced study by Egol et al, appropriate braking time returns at a point 6 weeks after initiation of weightbearing after treatment of lower extremity long bone and periarticular fractures, as examined with a driving simulator. No differences were seen in return of braking time between periarticular fractures and long bone injuries.
The second reference by Egol studied only operatively treated ankle fractures and found that time to appropriate braking returns at 9 weeks postoperatively. Interestingly, no significant association was found between the functional scores and normalization of total braking time.
OrthoCash 2020
A 42-year-old male sustains the injury seen in figure A. What negative sequelae would occur with displacement of this fracture in the characteristic fashion?

Post-traumatic subtalar arthrosis
Stress fracture of the fibula
Reflex sympathetic dystrophy
Achilles tendon rupture
Posterior skin necrosis Corrent answer: 5
The radiograph shows a tongue-type calcaneus fracture, with major displacement of the posterior calcaneal body/tuberosity. The Achilles tendon insertion here causes characteristic proximal and posterior displacement, and with increasing displacement, posterior skin necrosis can be caused in a short period. Per the references, this should be treated urgently to prevent this sequelae. Lag screw fixation is appropriate for this fracture pattern, placed perpendicular to the fracture.
OrthoCash 2020
A 34-year-old male falls 10 feet from a balcony and is brought to the emergency room with the deformity seen in Figure A. Radiographs shown are shown in Figure B and C. Which of the following structures can block closed reduction of this injury pattern?

Flexor hallucis longus tendon
Extensor digitorum brevis muscle
Posterior tibial tendon
Tibialis anterior tendon
Plantar fascia
Figures A through C show a medial subtalar dislocation. Irreducible dislocations are typically the result of either inadequate sedation or interposed soft tissue structures.
In medial dislocations, the extensor digitorum brevis, the deep peroneal neurovascular bundle, or the joint capsule may block a closed reduction. In lateral dislocations, the most common structure implicated as a block to reduction is the posterior tibial tendon, although the flexor digitorum longs, posterior tibial neurovascular bundle or flexor hallucis may also block reduction.
Bibbo et al found that subtalar dislocations were irreducible 32% of the time and that 88% had ipsilateral foot and ankle injuries. At follow up, 89% of patients demonstrated radiographic changes of the subtalar joint, and had worse function on the side of the subtalar dislocation as demonstrated by lower
AOFAS scores.
Incorrect Answers:
OrthoCash 2020
Spontaneous rupture of the extensor pollicis longus tendon is most frequently associated with which of the following scenarios?
Non-displaced distal radius fracture
Non-displaced Rolando fracture
Second metacarpal base fracture
Boxer's fracture
Non-displaced radial styloid fracture Corrent answer: 1
Rupture of the extensor pollicis longus (EPL) tendon after non operative treatment for a distal radius fracture occurs with a 0.3-5% incidence. The causes of EPL rupture include mechanical irritation, attrition, and vascular impairment leading to delayed rupture. Synovitis of the extensor carpi radialis due to repetitive use may invade the EPL tendon and lead to rupture.
Recommended treatment in the pre-rupture setting includes a third dorsal compartment release with or without an extensor retinacular patch graft. Palmaris longus graft or a transfer from the extensor indicis proprius to the EPL tendon are reasonable treatment options. Results of all treatments seem to be clinically satisfactory.
The referenced article by Gelb is a review of the etiology and treatment of this injury. He reviews the above discussion and findings.
OrthoCash 2020
A 79-year-old cyclist is involved in an accident and sustains a displaced femoral neck fracture as seen in Figure A. What is the
optimal treatment?

Open reduction internal fixation
Bipolar hemiarthroplasty
Unipolar hemiarthroplasty
Total hip arthoplasty
Nonoperative treatment
An AP pelvis radiographs with a displaced femoral neck fracture is seen in Figure A. It important to note that degenerative changes are seen on this image. Both references suggest that elderly active individuals should be treated with a primary total hip after displaced femoral neck fractures.
In the first study by Blomfeldt et al, the group reviewed a series of patients who underwent either an acute primary total hip arthroplasty for a femoral neck fracture or a delayed primary hip after an attempt at ORIF. They found that the group treated with an acute primary total hip arthroplasty had better Harris hip and quality of life scores.
The second reference from Blomfeldt et al, studies a population of active elderly patients randomized to either a total hip arthroplasty or bipolar for femoral neck fractures. The group found no mortality or dislocation difference between the groups, but higher Harris hip scores at 1 year in patients treated with a total hip
arthroplasty.
OrthoCash 2020
A 53-year-old man sustains the injury seen in figure A and later undergoes open reduction and internal fixation. What variable will
most significantly increase his rate of degenerative arthritis in the long-term?

Postoperative joint stepoff
Alteration of limb mechanical axis
Fracture type
Male sex
Age greater than 50
Maintenance of mechanical axis correlates most with a satisfactory clinical outcome when managing an intra-articular fracture of the proximal tibia.
According to the study of plateau fractures with up to 27 year follow-up by Rademakers et al, malalignment of the limb by greater than 5 degrees tripled the rate of degenerative osteoarthritis (27% v. 9%). Age at time of injury had no effect on outcome; 31% had joint space narrowing but 64% of those knees were well tolerated.
Weigel and Marsh's study looked at high energy plateau fractures treated with staged external fixation followed by internal fixation, and noted a low rate of severe arthrosis even with mild to moderate joint incongruity.
Stevens et al noted a worse outcome with increasing age at presentation with these injuries; fracture type had a small influence and adequacy of reduction had no significant influence on outcome.
Figure A is a coronal CT image showing a lateral tibial plateau fracture with significant joint depression.
OrthoCash 2020
A 69-year-old male sustained a proximal humerus fracture that underwent open reduction and internal fixation nine months ago. He complains of constant pain and weakness; repeat radiographs are shown in Figures A and B. What is the most appropriate surgical treatment at this time?
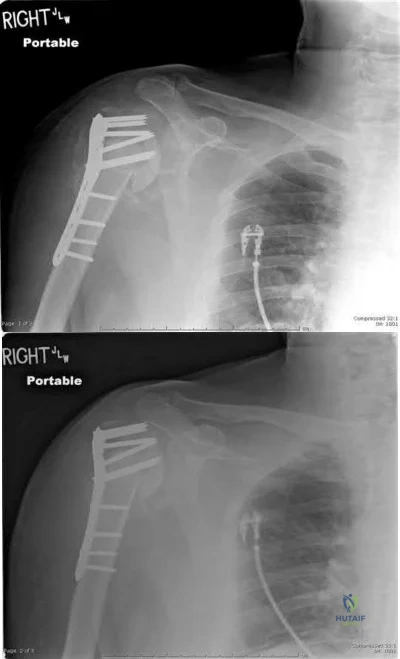
Revision open reduction and internal fixation
Valgus corrective osteotomy of proximal humerus
Shoulder arthroplasty
Shoulder arthrodesis
Humeral head resection Corrent answer: 3
Figures A and B show loss of fixation of a proximal humerus fracture. The most appropriate treatment for this scenario is a humeral arthroplasty, as the tenuous blood supply of the proximal humerus is likely chronically disrupted, leading to osteonecrosis and poor healing potential of the proximal humerus.
Traditionally, hemiarthroplasty was performed for these presentations, but reverse total shoulder arthroplasty has emerged as a potentially better
treatment method, especially if the rotator cuff function/status is unknown or poor.
According to the referenced article by Norris et al, delayed shoulder hemiarthroplasty decreased shoulder pain in 95% of patients but warned of technical difficulties and limited postoperative range of motion. A total shoulder arthroplasty is needed if glenoid erosion from the screw(s) or bone occurs.
OrthoCash 2020
During the ilioinguinal approach to the pelvis, the corona mortis artery must be identified and ligated if present. The corona mortis artery joins the external illiac artery with which other major artery?
Pudendal
Deep illiac circumflex
Hypogastric
Obturator
Testicular
The "corona mortis" (translated as “crown of death”) artery is a vascular variant that joins the external illiac and the obturator artery as it crosses the superior pubic ramus. Tornetta et al did a study where "fifty cadaver halves were dissected to determine the occurrence and location of the corona mortis. Anastomoses between the obturator and external iliac systems occurred in 84% of the specimens. Thirty-four percent had an arterial connection, 70% had a venous connection, and 20% had both. The distance from the symphysis to the anastomotic vessels averaged 6.2 cm (range, 3-9 cm)." The corona mortis can be injured in superior ramus fractures and iatrogenically while plating pelvic ring injuries using the ilioinguinal approach.
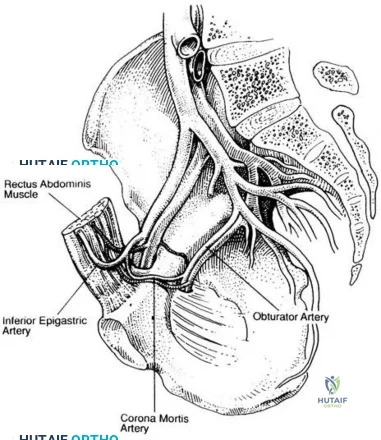
OrthoCash 2020
A 26-year-old male sustains a femoral shaft fracture treated with the implant shown in Figure A. Postoperatively, what muscular deficits can be expected at medium and long-term follow-up?

Weakness with hip abduction and knee flexion
Weakness with hip abduction and knee extension
Weakness with knee flexion and knee extension
Weakness with hip external rotation and hip abduction
Weakness with hip external rotation and hip flexion Corrent answer: 2
Figure A shows a femoral shaft fracture treated with an antegrade femoral nail. Long term deficits are weakness with knee extension (quadriceps) and hip abduction (glutei muscles).
The referenced study by Kapp et al noted long term quadriceps weakness as well as decreased bone mineral density in the femur (femoral neck by 9%, the lateral cortex by 20% and the medial cortex by 13%). It is unclear whether this is due to the injury, treatment, or a combination of both.
The second referenced study by Archdeacon et al also noted weakness in hip abduction, which showed time dependent improvement. He reports that increased early ipsilateral trunk lean is associated with worse recovery of abduction strength.
OrthoCash 2020
A 33-year-old male sustains the injury seen in Figure A as a result of a high-speed motor vehicle collision. Based on this image, what is the most likely acetabular fracture pattern?

Both column
Anterior column
Anterior column posterior hemitransverse
Transverse
T-type
The radiograph in Figure A shows a transverse acetabulum fracture. The iliopectineal (anterior column) and ilioischial lines (posterior column) are interrupted, revealing bicolumnar involvement; however, this is different than the both column fracture, as a transverse pattern has articular surface still in continuity with the axial skeleton via the sacroiliac joint.
The referenced article by Patel et al showed a wide variation of inter and intra-observer agreement in interpreting radiographs of acetabular fractures, with high agreement for basic radiographic classification and only slight to moderate agreement for other radiologic variables such as impaction.
The other referenced article by Letournel is a great review article regarding the initial classification of these fractures as well as a quick summary of his outcomes.
OrthoCash 2020
A 56-year-old carpenter sustains the closed injury seen in Figures A, B, and C. After temporary spanning external fixation is performed and soft tissue conditions improve, what strategy provides the optimal fixation for this fracture pattern?
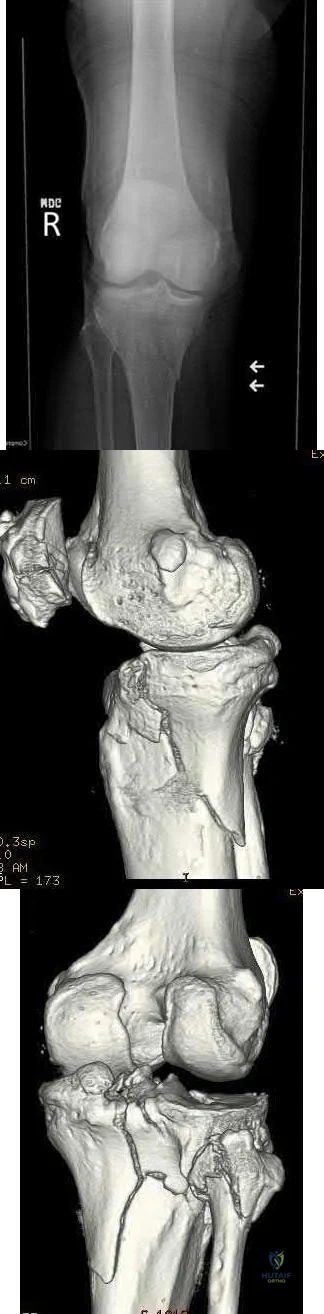
Anatomic lateral locking plate
Posteromedial and lateral plates
Anatomic medial locking plate
Conversion of the spanning external fixator to a hinged external fixator
Posterior buttress plate Corrent answer: 2
Figures A and B show a bicondylar tibial plateau fracture, with a typical appearing lateral fracture line and a posteromedial fracture line. The posteromedial sheared fracture piece is difficult, and/or sometimes impossible, to achieve appropriate stable fixation with a single lateral locking plate, as there will be limited screw purchase and fixation into the posteromedial fragment.
The referenced article by Georgiadis notes that a dual incision approach is safe and is associated with improved outcomes over their historical comparisons.
They describe the dual incisions and approaches in length, and review risks/issues with each approach.
The other referenced study by Bhattacharyya et al notes that these fractures have a typical appearance of the posteromedial fracture piece and that articular reduction quality is correlated with short-term results. They recommended buttress-type fixation of these fracture pieces.
OrthoCash 2020
A 31-year-old male sustains an irreducible ankle fracture-dislocation with the foot maintained in an externally rotated position. An AP and lateral radiograph are shown in figures A and B respectively. The attempted post reduction AP and lateral are shown in C and D. What structure is most likely preventing reduction?

Anterior-inferior tibiofibular ligament
Posterior-inferior tibiofibular ligament
Peroneus brevis tendon
Posterolateral ridge of the tibia
Flexor hallucis longus tendon Corrent answer: 4
As described by Hoblitzell et al, the so-called "Bosworth fracture-dislocation" is a rare fracture-dislocation of the ankle where the fibula becomes entrapped behind the tibia and becomes irreducible. It can cause compartment syndrome, as reported by Beekman and Watson.
Hoblitzell et al stress the importance and difficulty of recognizing these injuries. Standard radiographs are difficult to interpret due to the often severe external rotation of the foot. Prompt treatment, though can lead to good results in patients. The posterolateral ridge of the distal tibia hinders reduction and reduction often requires an open technique
Mayer and Evarts stated AP and mortise radiographs can be hard to interpret due to the external rotation posture of the foot. In their series a closed reduction consisting of traction and medial rotation applied to the foot while the fibular shaft is pushed laterally was successful in 3/4 patients.
OrthoCash 2020
A 37-year-old female sustains the injury seen in Figures A and B. At long-term follow up, degeneration of which of the following joints has been shown to have the highest rate of patient symptoms?

Tibiotalar joint
Talonavicular joint
Calcaneocuboid joint
Lisfranc joint
Subtalar joint
Figures A and B show a medial subtalar dislocation, which is more common than a lateral dislocation (65% vs. 35%).
The referenced article by Bibbo et al looked at long-term follow up of these patients, and noted that radiographic degeneration of the ankle and subtalar joints were 89%, although 31% of ankle joints were symptomatic and 68% of subtalar joints were symptomatic. Midfoot degeneration was seen radiographically in 72% (15% symptomatic).
OrthoCash 2020
In treating a lateral split-depression type tibial plateau fracture, which of the following adjuncts has been shown to have the least articular surface subsidence when used to fill the bony void?
Crushed cancellous allograft
Hydroxyapatite
Calcium phosphate cement
Autogenous iliac crest
Bisected diaphyseal humeral allograft Corrent answer: 3
In treating tibial plateau fractures, calcium phosphate has been shown to have the least amount of articular subsidence on follow-up examinations.
The referenced study by Russell et al noted a significantly increased rate of subsidence at 12 months with autograft as compared to calcium phosphate cement (in types I-VI).
The other referenced study by Lobenhoffer et al noted improved radiographic outcomes and earlier weightbearing with usage of calcium phosphate cement.
OrthoCash 2020
The pelvic spur sign on plain radiography is indicative of the following injuries?
Transtectal transverse acetabular fracture
Vertical shear pelvic ring injury
Displaced H-type sacral fracture
Both column acetabular fracture
Anterior-posterior type III pelvic ring injury Corrent answer: 4
The pelvic spur sign is indicative of a both column acetabular fracture. It is best seen on an AP or obturator oblique x-ray. The spur is the intact portion of the ilium, still attached to the axial skeleton and seen posterosuperior to the displaced acetabulum (typically medially displaced).
Illustration A shows the spur sign (arrows) on a CT image, while illustration B shows an obturator oblique of the pelvis and the spur sign is shown with the long tailed arrow (on the left of the image).
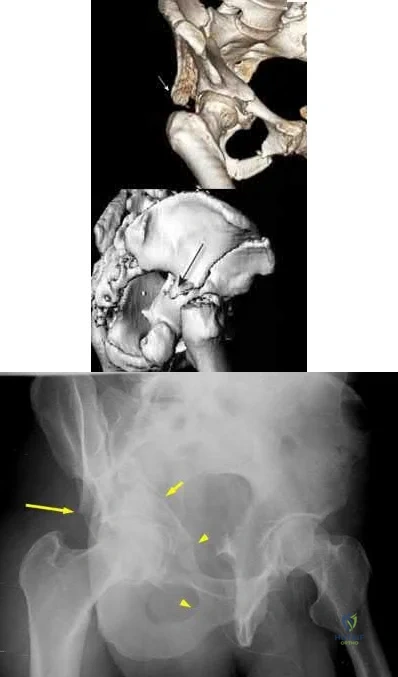
OrthoCash 2020
A 33-year-old male sustains a distal humerus fracture and is treated with open reduction and internal fixation of the distal humerus with olecranon osteotomy. A postoperative radiograph is shown in Figure A. A new deficit of the anterior interosseous nerve is now noted in the recovery room. What physical exam finding would be expected with this nerve injury?

Inability to flex radiocarpal joint
Loss of sensation over palmar aspect of thumb
Loss of sensation over dorsal hand first webspace
Inability to abduct index finger
Inability to flex thumb interphalangeal joint Corrent answer: 5
A deficit in the anterior interosseous nerve (AIN) would result in an inability to flex the interphalangeal joint (IPJ) of the thumb.
Injury to the AIN can be seen with K-wires that penetrate through the anterior cortex of the proximal ulna, such as mentioned above. The AIN is a branch of the median nerve that provides motor function to forearm/hand. It branches off from the median nerve 4 cm distal to the medial epicondyle, passes between the 2 heads of the pronator teres, travels through the forearm anterior to the interosseous membrane between the flexor pollicis longs (FPL) and flexor digitorum profundus (FDP), and then terminates in the pronator quadratus (PQ). The nerve gives of branches to the FDP, FPL, and PQ enabling for flexion of the distal phalangeal joint of the index and middle fingers, flexion of the IPJ of the thumb, and aids with pronation of the forearm, respectively.
Injury to the nerve will result in weakness in motor function to these muscles.
Mekail et al. reviewed the anterior approach to the proximal radius in order to describe and identify important neurovascular and musculoskeletal structures in the area. They were specifically aiming to determine the safest anatomic orientation for plate and screw fixation in regards to the posterior interosseous nerve. The authors, however, did discuss that medial plating was especially dangerous to the AIN, and significantly increased the risk of iatrogenic injury to the branch sent to the FPL.
Parker et al. reported a case report in a patient who experienced an AIN deficit postoperatively after tension banding of an olecranon fracture.
Intraoperatively, there were multiple passes of the K-wires in an attempt to find purchase in the anterior cortex of the ulna. The authors believed that during these passes, the nerve was injured and concluded that placing K-wires should not occur without radiologic visualization.
Figure A is a postoperative lateral radiograph after tension banding of the olecranon. Perforation of the anterior ulnar cortex can be seen by the K-wire which can cause damage to the AIN nerve. Illustration A is a schematic of the path of the AIN, its branches, and its function.
Incorrect Answers:
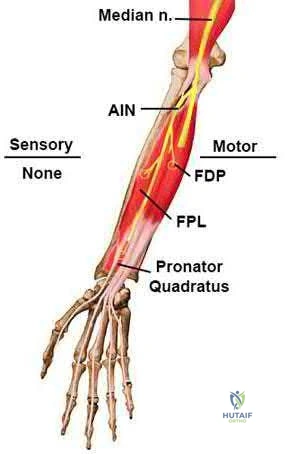
OrthoCash 2020
A computed tomography (CT) scan has been shown to be indicated for evaluation of all of the following aspects of acetabular fractures, EXCEPT:
Determination of surgical planning
Intra-articular loose bodies
Marginal impaction
Fracture piece size and position
Determination of pre-existing degenerative changes Corrent answer: 5
CT scanning is indicated in acetabular fractures for determination of surgical approach and techniques, evaluation of marginal impaction and presence of intra-articular loose bodies (especially after hip dislocation), and evaluation of fracture piece sizes and relative positions.
Kellam et al reviewed their initial experience with CT scanning and acetabular fractures, and noted a 25% change in surgical planning when CT was utilized versus plain radiographs; they also noted the ability to detect marginal impaction and fracture size/position was improved with CT.
OrthoCash 2020
A 69-year-old woman falls while getting out of her car and lands on her right shoulder sustaining a 4-part proximal humerus fracture. She subsequently undergoes surgery to treat the fracture, with immediate postoperative radiographs shown in Figure A. Six months following surgery, she denies shoulder pain, but she is unable to actively raise her hand above her shoulder. Which of the following is the most likely cause of this limitation?

Joint infection
Retroversion of the prosthesis
Glenoid arthritis
Axillary nerve injury
Greater tuberosity malunion Corrent answer: 5
The radiograph demonstrates a humeral hemiarthroplasty. Malunion of the greater tuberosity is a known complication of this procedure, and the most likely cause for loss of shoulder elevation.
Frankle et al in 2004 reported a 25% rate of greater tuberosity malunion. They discuss surgical techniques to improve fixation of the tuberosities following hemiarthroplasty for proximal humerus fractures.
Frankle et al in 2002 evaluated 5 different techniques to reattach the tuberosities following shoulder hemiarthroplasty in human cadavers. Findings suggested that a circumferential medial cerclage should be placed around the tuberosities to enhance the stability of the tuberosity repair.
Bosch et al reviewed 39 consecutive 3 or 4 part proximal humerus fractures that were treated with either primary hemiarthroplasty or secondary hemiarthroplasty following a primary ORIF. Patients who underwent primary
hemiarthroplasty reported better clinical outcomes. The authors concluded that elderly patients with 3 or 4 part humerus fractures are best treated with early arthroplasty.
OrthoCash 2020
An acetabular fracture with all segments of the articular surface detached from the intact posterior ilium is defined as what fracture pattern?
Transverse
Both column
Anterior column posterior hemitransverse
Posterior column with posterior wall
Anterior column with anterior wall Corrent answer: 2
A both column acetabular fracture is defined as an acetabular fracture with no articular surface in continuity with the remaining posterior ilium (and therefore, axial skeleton). The spur sign is a radiological sign seen with these fractures, and is the posterio-inferior aspect of the intact posterior ilium. The spur sign and other radiographic findings consistent with a both column acetabular fracture can be seen in Illustration A (AP), Illustration B (obturator oblique), and Illustration C (iliac oblique).
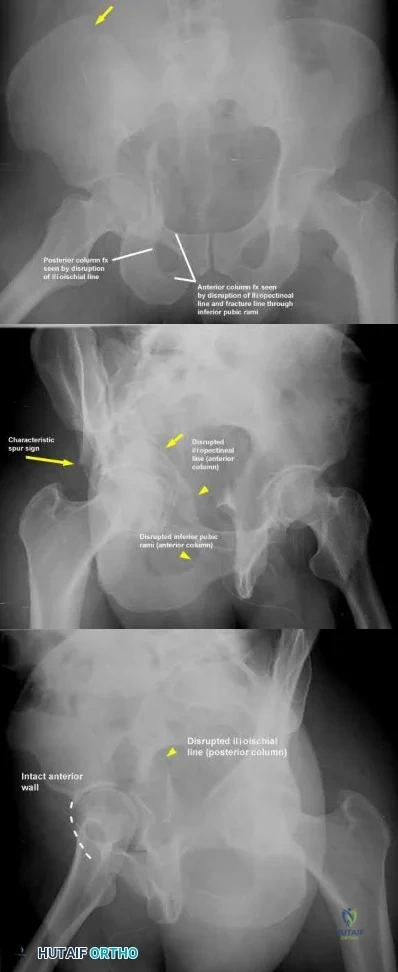
OrthoCash 2020
A large posteromedial tibial plateau fracture pattern, as seen with the bicondylar tibial plateau fracture shown in Figures A and B, is important to recognize because of which of the following factors?

Association with posteromedial corner of the knee injury
Association with anterior tibial artery injury
Possible need for dual plate fixation
Possible need for single extensile anterior approach to the knee
Increased risk of deep venous thrombosis Corrent answer: 3
Figures A and B show a bicondylar tibial plateau fracture with a large posteromedial fracture piece. This has clinical importance, as currently available plate/screw constructs often have poor fixation of this fracture segment, and this pattern often requires a second, posteromedial, approach and placement of a second plate/screw construct.
The referenced article by Barei et al notes a prevalence of posteromedial fracture pieces of nearly 33% of all bicondylar tibial plateau fractures. They also recommend supplementary or alternative fixation techniques when this pattern is recognized.
The referenced article by Higgins et al notes a 59% incidence of this fracture pattern (consisting of nearly 25% of the total joint surface) in bicondylar tibial plateau fractures, and recommends appropriate fixation to combat the vertical shear instability through a separate approach.
The last referenced study by Higgings et al notes a significantly increased rate of late fracture displacement in a biomechanical model with a single lateral locking plate as compared to a dual plate construct.
OrthoCash 2020
At the elbow, the anterior bundle of the medial collateral ligament inserts at which site?
Radial tuberosity
3mm distal to the tip of the coronoid
Anteromedial process of the coronoid
Medial border of the olecranon fossa
Radial side of ulna at origin of annular ligament Corrent answer: 3
The anterior bundle of the medial collateral ligament of the elbow inserts at the anteromedial process of the coronoid, also known as the sublime tubercle.
Fractures at this site have been shown to have worse results with nonoperative
treatment, due to increased rates of instability and post-traumatic arthrosis.
The referenced articles by Ring and Steinmann are great reviews of the topic of coronoid fractures. They review the diagnosis, treatment options, rehabilitation, and outcomes of these injuries. They focus on the importance of the coronoid in elbow stability, especially with base fractures, or ones that involve the sublime tubercle.
Illustration A depicts the anterior bundle of the MCL inserting at the sublime tubercle.
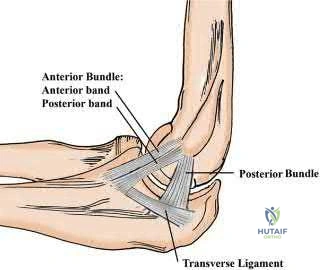
OrthoCash 2020
In the Lauge-Hansen classification system, a pronation-abduction ankle fracture has what characteristic fibular fracture pattern?
Transverse fracture below the level of the syndesmosis
Short oblique fracture running from anteroinferior to posteriosuperior
Short oblique fracture running from posteroinferior to anteriosuperior
Comminuted fracture at or above the level of the syndesmosis
Wagstaff fracture
In the Lauge-Hansen classification, the characteristic fibular fracture pattern in a pronation-abduction injury is a comminuted fibular fracture above the level of the syndesmosis. In the first stage of this injury pattern, the deltoid fails in tension, or an avulsion fracture of the medial malleolus occurs. In the second stage, the anterior inferior tibiofibular ligament ruptures, or a small bony avulsion of this ligament's insertion/origin occurs. The final stage includes the creation of a comminuted fibular fracture above the level of the syndesmosis.
The referenced article by Siegel et al noted that extraperiosteal bridge plating of these ankle injuries was safe and had excellent radiographic and clinical outcomes at final follow-up.
OrthoCash 2020
A 38-year-old male sustains the closed injury shown in Figures A and B. When treating this injury with an intramedullary nail, addition of blocking screws into which of the following positions can prevent the characteristic malunion deformity?
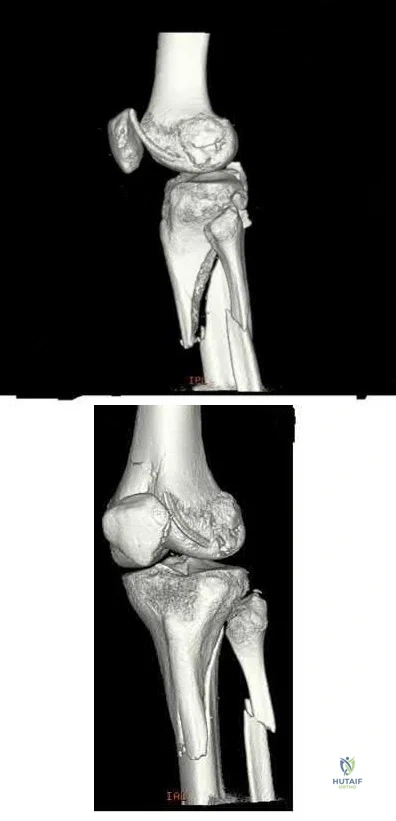
Anterior to the nail in the proximal segment; medial to the nail in the proximal segment
Anterior to the nail in the proximal segment; lateral to the nail in the proximal segment
Posterior to the nail in the proximal segment; lateral to the nail in the proximal segment
Anterior to the nail in the distal segment; lateral to the nail in the distal segment
Posterior to the nail in the distal segment; medial to the nail in the proximal segment
Figures A and B show a proximal tibia fracture, which is prone to malreduction/malunion into a characteristic valgus and procurvatum (apex anterior) deformity. Placement of screws in this instance posterior to the nail (medial to lateral) and lateral to the nail (anterior to posterior) in the proximal segment will prevent iatrogenic malalignment.
Intramedullary nails will not effect a reduction in metaphyseal proximal tibia fractures. Valgus and apex anterior deformities in these injuries may be caused by deforming muscular forces, limb positioning in hyper flexion, as well as iatrogenic deformity created by improper nail insertion technique. Blocking (Poller) screws are utilized to redirect intramedullary nails by creating an artificial cortex to guide the nail into appropriate position.
The referenced biomechanical study by Krettek et al noted that addition of blocking screws added increased stability to metaphyseal fractures.
Ricci et al noted no malalignment intraoperatively or at final follow-up of proximal tibia fractures treated with intramedullary nails if blocking screws were used.
OrthoCash 2020
In an uninjured proximal tibia which statement best describes the shape and position of the medial tibial plateau relative to the lateral tibial plateau?
More concave and more proximal
More convex and more proximal
More concave and more distal
More convex and more distal
Symetric in conture and more distal
The medial tibial plateau is more concave and more distal relative to the lateral tibial plateau.
Watson et al report "the medial tibial plateau has a more concave shape and is larger in both length and width than the lateral tibial plateau, which has a slightly convex shape. The lateral tibial plateau lies proximal to the medial plateau. The convexity of the lateral plateau helps differentiate it from the medial plateau on a lateral radiograph of the proximal tibia."
Illustration A shows the relative concavity of the medial and lateral proximal tibia.
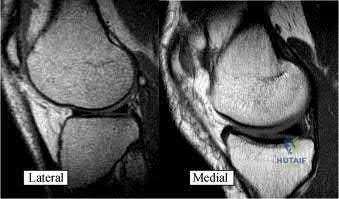
OrthoCash 2020
On average, the radial nerve travels from the posterior compartment of the arm and enters the anterior compartment at which of the following sites?
Spiral groove of the humerus
At the arcuate ligament of Osborne
10 cm distal to the lateral acromion
10 cm proximal to radiocapitellar joint
At the origin of the deep head of the triceps Corrent answer: 4
The radial nerve enters the anterior compartment through the intercompartmental fascia on average 10 cm proximal to the radiocapitellar joint. It has never been found to remain in the posterior compartment within
Question 38
A 25-year-old man undergoes surgical exploration for a laceration to his left palm, as shown in Figure 1. Injury to the structure indicated by the forceps leads to numbness of the
Explanation
A. arthrodesis of the DIP.
B. dorsal block pin fixation.
C. open reduction with screw fixation.
D. extension splint immobilization.
The patient sustained a mallet fracture with no evidence of joint subluxation. The risk of subluxation is increased if the size of the fragment is greater than one-third of the articular surface. Nonsurgical treatment is recommended in mallet fractures without subluxation and includes a mallet splint or cast immobilization holding the DIP joint in full extension for 6 weeks, followed by night splinting. A fusion is a salvage procedure and is not indicated for this injury.
59- What is the approximate ratio of the scaphoid distal (volar) blood supply to the proximal (dorsal) blood supply?
A. 20:80
B. 40:60
C. 60:40
D. 70:30
Gelberman and associates injected the radial and ulnar arteries of 15 cadavers with Ward's blue latex solution and cleared the specimens with full-strength bleach (sodium hypochlorite) and the Spalteholz technique, using formalin, formic acid, hydrogen peroxide, 95% ethanol, chloroform, and oil of wintergreen, in a process requiring about 3 weeks. This process produced a transparent bone, through which the stained vessels could be seen and photographed. The authors discovered that the radial and the anterior interosseous arteries supply the scaphoid. The volar supply enters through the volar tubercle and accounts
for 20% to 30% of the internal vascularity of the bone. 55
The authors found that the dorsal vessels entered through the dorsal ridge and, depending upon the vascular pattern encountered, they supplied between 70% and 85% of the scaphoid.
Morsy and associates recently used contrast micro-CT scanning and found that the average volume of the scaphoid supplied by the distal network was 16.9%, and that supplied by the proximal network was 83.1%. The authors determined that inserting the screw in the central axis had the lowest vascular impact, followed by dorsal insertion. The highest vascular impact was produced by the volar insertion axis.
60- Figures 1 and 2 display the AP and lateral radiographs of a 55-year-old laborer who has thumb metacarpophalangeal (MP) joint pain despite splint immobilization and medications. The most appropriate surgical treatment option for this patient is MP joint
A. arthroscopic debridement.
B. resection arthroplasty.
C. arthrodesis.
D. silicone replacement.
The patient has thumb MP osteoarthritis. The preferred surgical treatment option for thumb MP osteoarthritis is arthrodesis. The recommended position for thumb MP joint fusion is 5° to 15° of flexion and 15° of pronation. More recent studies have shown that fusion of the MP joint in a position of greater flexion may offload the trapeziometacarpal (TMC) joint
and shift the contact stress more dorsally on the TMC. Limited data exists regarding arthroscopic débridement, which has been reported for mild arthritis and synovitis. Resection arthroplasty is performed for TMC arthritis. Thumb MP arthroplasty is considered for extensive involvement of the TMC, MP, and IP joints to preserve MP joint motion; it would not be optimal for this laborer for whom stability is important.
61- What type of median-ulnar nerve interconnection carries only sensory fibers?
A. Martin-Gruber
B. Berrettini
C. Riche-Cannieu
D. Marinacci
Four interconnections of the median and ulnar nerves in the forearm, wrist, and hand have been described, and each has been further classified. The most common interconnection is the Berrettini. It is so common that it may be considered an anatomic normal rather than a variant. It contains sensory fibers and courses between the third common digital nerve of the median nerve to the fourth common digital nerve of the ulnar nerve. Because it is sensory only and involves a limited territory, no nerve conduction study evidence of this interconnection can be elicited.
The Martin-Gruber and Marinacci interconnections are found in the forearm and carry motor fibers. The Martin-Gruber interconnection travels from the median nerve or the anterior interosseous nerve proximally to the ulnar nerve distally. The Marinacci is the least common interconnection and runs from the proximal ulnar nerve to the distal median nerve. The Riche-Cannieu interconnection is a motor connection between the deep motor branch of the ulnar nerve and the recurrent motor branch of the median nerve in the hand.
62- Several pedicled dorsal distal radius bone grafts are available for the treatment of the prefragmentation stages of Kienböck disease. The arterial pedicle with the greatest arc of rotation is the
A. 1 + 2 intercompartmental supraretinacular.
B. 2 + 3 intercompartmental supraretinacular.
C. fourth extensor compartment.
D. 4 + 5 extensor compartment.
The 4 + 5 extensor compartment artery (ECA) pedicle has the greatest range of the listed pedicles. It is based on the posterior division of the anterior interosseous artery and can reach the proximal and distal carpal rows and the bases of the metacarpals in some instances. If the fourth ECA is not present, the 2 + 3 intercompartmental supraretinacular artery (ICSRA) graft can be used, because it also has a proximal connection to the fifth ECA. The 1 + 2 and the 2 + 3 ICSRA pedicles are available and useful in many situations, including scaphoid nonunion and the treatment of Kienböck disease, however their pedicles are much shorter than that of the 4 + 5 ECA.
Question 39
Figure 1 is an MRI scan of the right hip of a 19-year-old woman with a 6-month history of right groin pain. She was diagnosed with a stress fracture and was treated with 3 months of limited weight bearing. Figure 2 is a repeat MRI scan in which the edema pattern changed minimally but the pain worsened. Ibuprofen alleviates most of her pain. What is the best next step?

Explanation
cells, forms the nidus of the tumor, which is easily identified on CT scans.
Question 40
A 35-year-old woman reports worsening pain after undergoing a neurectomy in the third interspace for a Morton’s neuroma 12 months ago. She states that the pain is sharp and electrical, worse than before her surgery, and prevents her from participating in her usual work and exercise activities. Use of wider shoes and pads used before her surgery have failed to provide relief. Examination does not reveal any deformity or inflammation. Tenderness along with neuritic pain occurs with compression of the plantar aspect of the foot between the third and fourth metatarsal head area. To most reliably alleviate her pain, management should consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Johnson JE, Johnson KA, Unni KK: Persistent pain after excision of an interdigital neuroma: Results of reoperation. J Bone Joint Surg Am 1988;70:651-657.
Beskin JL, Baxter DE: Recurrent pain following interdigital neurectomy: A plantar approach. Foot Ankle 1988;9:34-39.
Amis JA, Siverhus SW, Liwnicz BH: An anatomic basis for recurrence after Morton’s neuroma excision. Foot Ankle 1992;13:153-156.
Question 41
Which of the following illustrations shown in Figures 21a through 21e correctly shows the projection of the sacroiliac joint on the outer table of the ilium?
Explanation
REFERENCES: Waldrop JT, Ebraheim NA, Yeasting RA, Jackson WT: The location of the sacroiliac joint on the outer table of the posterior ilium. J Orthop Trauma 1993;7:510-513.
Xu R, Ebraheim NA, Yeasting RA, Jackson WT: Anatomic considerations for posterior iliac bone harvesting. Spine 1996;21:1017-1020.
Question 42
Figure 1 shows the radiograph obtained from a 78-year-old woman who has a recent history of increasing thigh pain 12 years after undergoing total hip arthroplasty. Figure 2 depicts the radiograph obtained after she fell and was unable to ambulate. What is the most appropriate treatment?
Explanation
The surgical treatment of periprosthetic fractures of total hip replacement with a loose implant and progressive bone loss is associated with a high complication rate. The recent literature would favor the use of long "Wagner-type" stems, which have a long distal taper that may optimally engage the remaining femoral shaft isthmus. Plating options are problematic, because the intramedullary stem limits the ability to use screws with the plate. Using long distally fixed stems circumvents this problem by enhancing
fracture healing and creating a long-term prosthetic solution in these most difficult cases.
Question 43
A 13-year-old girl with adolescent idiopathic scoliosis is otherwise healthy with a normal neurologic examination and she began her menstrual cycle 3 months ago. Standing radiographs show a high left thoracic curve from T1-T6 that measures 29 degrees, a right thoracic curve from T7-L1 that measures 65 degrees, and a left lumbar curve from L1-L5 that measures 31 degrees, correcting to 12, 37, and 10 degrees, respectively, on bending films. Her Risser sign is 1. What is the most appropriate management? Review Topic
Explanation
Question 44
A 55-year-old woman develops posttraumatic arthritis in the elbow following a distal humerus fracture. What is the most likely mid-term (5-10 years after surgery) complication following semiconstrained total elbow arthroplasty (TEA)?
Explanation
intermediate-term follow-up.
Question 45
A 47-year-old, healthy, active patient presents with a sub-acute, full-thickness supraspinatus tear. His physical examination reveals significant weakness and pain with abduction. There was no glenohumeral instability. Radiographs demonstrate a type 1 acromion. An MRI scan shows a crescent shaped tear with 2-cm of tendinous retraction and no tendinous fatty changes. A subacromial corticosteroid injection 6 weeks ago provided him with 24 hours of pain relief but no improvement in strength. What would be the most appropriate treatment option? Review Topic QID:4501
Explanation
The primary purpose of rotator cuff repair is to restore muscle function. Secondary outcomes include reduction of pain and prevention of irreversible cuff changes, specifically muscular atrophy. Non-operative treatment (exercise, therapy and pain medications) are recommended for partial thickness tears. The indication of surgical repair includes, isolated supraspinatus weakness +/- pain that correlates with MRI imaging of a respective full thickness tear. Routine acrominoplasty is not recommended in conjunction with rotator cuff repair, especially with no previous symptoms of impingement.
Pedowitz et al. developed clinical practice guidelines for the treatment of rotator cuff pathology. The strongest supporting evidence in current literature was given a grade of 'moderate' with four treatment recommendations. These were,
Exercise and non-steroidal anti-inflammatory drugs can be used to manage partial thickness tears,
Routine acromioplasty is not required the time of cuff repair,
Non-cross-linked, porcine small intestine submucosal xenograft patches should not be used to manage cuff tears, and
Surgeons can advise patients that workers' compensation status correlates with a less favorable outcome after rotator cuff surgery.
Illustration A shows the different shapes of rotator cuff tears. Incorrect Answers:
Question 46
Figure 42 is a transverse MRI scan of the left shoulder. The arrow points to which of the following structures?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 234.
Question 47
-A 10-year-old boy sustained a displaced Salter-Harris type II supination/plantar flexion fracture of the left ankle. He underwent closed reduction under conscious sedation; however, postreduction radiographs showed continued 5-mm anterior widening of the tibial physis. What is the most likely cause of the widening?
Explanation
Question 48
A 42-year-old woman is brought to the emergency department following a motor vehicle accident. She has sustained multiple injuries, and she is intubated and pharmacologically paralyzed. Sagittal cervical CT scans through the right cervical facets, the left cervical facets, and the midline are shown in Figures 12a through 12c, respectively. Definitive management of her cervical injury should consist of
Explanation
REFERENCES: Jackson RS, Banit DM, Rhyne AL III, et al: Upper cervical spine injuries.
J Am Acad Orthop Surg 2002;10:271-280.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 49
What is the most likely cause of the lesion shown in Figures 35a and 35b?
Explanation
REFERENCES: Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.
Jarvinen TA, Jarvinen TL, Kaariainen M, et al: Muscle injuries: Biology and treatment. Am J Sports Med 2005;33:745-764.
Question 50
A 7-year-old girl who sustained a type III posteromedial extension supracondylar fracture underwent a closed reduction at the time of injury. Figure 27a shows the position of the fracture fragments prior to percutaneous medial and lateral pin fixation. Following surgery, healing was uneventful and the patient regained a full painless range of motion. Fifteen months after the injury, she now reports loss of elbow motion and moderate pain with activity. A current AP radiograph is shown in Figure 27b. What is the most likely cause of her symptoms?
Explanation
REFERENCES: Haraldsson S: The interosseous vasculature of the distal end of the humerus with special reference to the capitellum. Acta Orthop Scand 1957;27:81-93.
Morrissy RT, Wilkins KE: Deformities following distal humeral fracture in childhood. J Bone Joint Surg Am 1984;66:557-562.
Question 51
A 40-year-old female recreational basketball player notes pain deep within her shoulder that occurs with activity. Pain began insidiously 6 months previously. She has completed a physical therapy program, and an intra-articular corticosteroid injection provided excellent temporary relief. Physical examination shows symmetric range of motion of her shoulder. She has a positive O'Brien’s active compression test. There is no pain with cross-arm adduction or tenderness to palpation over the acromioclavicular joint. Resisted abduction is nonpainful and strong. MRI shows increased signal in the substance of the superior labrum, low-grade bursal surface fraying of the supraspinatus, and mild degenerative changes within the acromioclavicular joint. What is the best treatment option?
Explanation
Question 52
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. What is the most appropriate management of this condition?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross-sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 53
Figures below demonstrate the radiographs obtained from a 56-year-old man with a 3-year history of right groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?
Explanation
Chronic opioid consumption prior to total joint arthroplasty has been associated with increased pain after surgery, increased opioid requirements, a slower recovery and longer hospital stay, and higher 90-day postoperative complications compared with patients not on chronic opioids preoperatively. Based on this information, Nguyen and associates performed a study in three patient groups that included 1) chronic opioid users who underwent no preoperative intervention, 2) chronic opioid users who were weaned down to 50% of their prior opioid regimen, and 3) patients who were not chronic opioid users. The authors found that the reduction of preoperative opioid use improved postoperative function, pain, and recovery and that the weaned group performed more like the opioid naive group than the chronic opioid user
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to surgery.
Question 54
Figures 1 and 2 show the radiograph and CT obtained from a 78-year-old woman who underwent right total hip replacement in 1995. She initially did well with no pain. She was last seen 7 years ago and was having mild hip pain at that time. She was found to have a supra-acetabular cyst on radiographs. She has had severe right hip pain for the past 9 months while using a walker for ambulation. The initial blood work reveals an estimated erythrocyte sedimentation rate of 32 mm/hr, a C-reactive protein level of 0.5 mg/L, a serum cobalt level of 0.4 µg/L, and a serum chromium level of 0.6 µg/L. Right hip aspiration is performed, revealing a white blood cell count of 139, 52% neutrophils, and a negative leukocyte esterase test. What is the best next step?
Explanation
The hip replacement was performed in 1995, during the period when the previous generation of polyethylene was utilized. This polyethylene was subjected to irradiation in air, with subsequent oxidation and consequent osteolysis after implantation. The mechanism of osteolysis begins with the uptake of polyethylene particles by macrophages, which then initiate an inflammatory cascade and the release of osteolytic factors. This cycle continues, with eventual implant loosening and failure. The imaging shows significant osteolysis and raises concern for pelvic discontinuity and acetabular implant failure. The surgical treatment consists of acetabular reconstruction. In this patient, concern exists for discontinuity based on the substantial amount of bone loss and nonsupportive anterior and posterior columns. This scenario requires complex acetabular revision using a custom triflange device, distraction with a jumbo acetabular component, or placement of a porous metal cup/cage construct with augmentation. The laboratory values are not consistent with infection or failure due to metal debris.
Question 55
Spontaneous recovery of upper extremtiy motor function after a cerebrovascular accident occurs in which of the following predictable patterns?
Explanation
REFERENCE: Waters RL, Keenan ME: Surgical treatment of the upper extremity after stroke, in Chapman MW (ed): Operative Orthopedics. Philadelphia, PA, JB Lippincott, 1988, vol 2,
pp 1449-1450.
Question 56
During revision total knee arthroplasty (TKA), there is significant laxity in 90° of flexion and 10° short of full extension. Correcting the gap imbalance is best achieved by
Explanation
A. Nonoperative treatment with close radiographic follow-up
B. Revision THA with ceramic- on-polyethylene with abductor reconstruction
C. Removal of components and placement of spacer as stage 1 of 2-stage revision
D. Revision THA with metal-on- polyethylene and trochanteric slide
Question 57
A 38-year-old woman with diabetes mellitus reports a 6-week history of fever and pain localized to the right sternoclavicular joint. Local signs on examination include swelling about the joint, erythema, and increased warmth. Initial aspiration of the joint reveals Staphylococcus aureus. Radiographs reveal medial clavicular osteolysis. What is the most effective treatment at this time?
Explanation
REFERENCES: Wirth MA, Rockwood CA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 608-609.
Question 58
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of
Explanation
REFERENCES: Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
Howard FM, Dell PC: The unreduced carpal dislocation: A method of treatment. Clin Orthop 1986;202:112-116.
Question 59
A new composite material is being evaluated for potential use as a prosthetic ligament. In measuring the tensile strength of this material, why is it important to consider and accurately control the loading rate?
Explanation
Question 60
A 22-year-old male soccer player reports left hip and groin pain. He states that symptoms began before a preseason tournament but have worsened steadily for the past 2 weeks. He denies any recent fever or sickness and is otherwise healthy. Examination reveals tenderness over the symphysis pubis and pain with resisted rectus abdominus testing. Radiographs are negative. What is the next step in the proper management of this patient? Review Topic
Explanation
Question 61
What is the most common cause for late revision (> 2 years post op) total knee arthroplasty? i. Infection
Explanation
REFERENCE: Sharkey PF, Hozack WJ, Rothman RH, et al: Insall Award paper: Why are total knee arthroplasties failing today? Clin Orthop Relat Res 2002;404:7-13.
Figure 59a Figure 59b
Question 62
A previously healthy 20-year-old male wrestler is seen for evaluation and treatment of draining sores of the forearm. Empiric treatment for cellulitis was started with oral clindamycin with improvement. Culture of the drainage reveals methicillin-resistant staphylococcus aureus (MRSA). Sensitivities at 48 hours demonstrate additional resistance to erythromycin and a positive D-zone test. Definitive antibiotic treatment until resolution should consist of which of the following? Review Topic
Explanation
any signs of systemic illness, an oral antibiotic regimen is appropriate. When culture results reveal resistance to erythromycin, then a D-zone test should be performed to check for inducible clindamycin resistance. The D-zone test is performed by plating the sample on an agar and placing antibiotic disks made of clindamycin and erythromycin on the agar. A zone of inhibition in the shape of the letter D is seen with an inducible strain. If the D-zone test is positive, then clindamycin should not be used because the strain of MRSA can become resistant to the treatment. Therefore, because of the positive D-zone test, the antibiotic should be changed to oral doxycycline. IV antibiotics are not indicated for this infection. Oral rifampin should never be used as a single agent as resistance rapidly develops.
Question 63
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?
Explanation
REFERENCES: Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809.
Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Pape HC, Auf’m’Kolk M, Puffrath T, et al: Primary intramedullary femur fixation in multiple trauma patients with associated lung contusion: A cause of posttraumatic ARDS? J Trauma 1993;34:540-548.
Question 64
What is the most common complication associated with open reduction and internal fixation using a 90/90 plate configuration and olecranon osteotomy for an OTA type C2 distal humerus fracture?
Explanation
Question 65
Figure 45 shows the lateral radiograph of a 19-year-old swimmer who has had back pain for the past 2 months. What is the most likely diagnosis?
Explanation
REFERENCES: Papanicolaou N, Wilkinson RH, Emmans JB, Treves S, Micheli LJ: Bone scintigraphy and radiography in young athletes with low back pain. Am J Roentgenol 1985;145:1039-1044.
Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 291-302.
Question 66
An obese 4-year-old boy has infantile Blount’s disease. Radiographs reveal a metaphyseal-diaphyseal angle of 18 degrees and a depression of the medial proximal tibial physis. Management should consist of
Explanation
REFERENCES: Raney EM, Topoleski TA, Yaghoubian R, Guidera KJ, Marshall JG: Orthotic treatment of infantile tibia vara. J Pediatr Orthop 1998;18:670-674.
Loder RT, Johnston CE: Infantile tibia vara. J Pediatr Orthop 1987;7:639-646.
Question 67
A 12-year-old boy falls from a bicycle. A radiograph of his injured shoulder is shown in Figure 41. What is the optimal method of treatment?
Explanation
REFERENCES: Bishop JY, Flatow EL: Pediatric shoulder trauma. Clin Orthop Relat Res 2005;432:41-48.
Question 68
Which of the following complications is more likely with an inside-out repair technique compared to an all-inside techniques for a medial meniscus tear?
Explanation
REFERENCES: Farng E, Sherman O: Meniscal repair devices: A clinical and biomechanical literature review. Arthroscopy 2004;20:273-286.
Jones HP, Lemos MJ, Wilk RM, et al: Two-year follow-up of meniscal repair using a bioabsorbable arrow. Arthroscopy 2002;18:64-69.
Question 69
A 78-year-old woman underwent total hip arthroplasty 15 years ago. She reports a recent history of increasing thigh pain prior to a fall and is now unable to ambulate. Radiographs are shown in Figures 87a and 87b. What is the best treatment for this condition?
Explanation
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475503.
Kwong LM, Miller AJ, Lubinus P: A modular distal fixation option for proximal bone loss in revision total hip
arthroplasty: A 2- to 6-year follow-up study. J Arthroplasty 2003;18:94-97.
Question 70
An anterior approach to the sacroiliac joint is indicated with which of the following concomitant injuries?

Explanation
Question 71
A 21-year-old woman is struck by a car and sustains a Gustillo IIIB fracture of the tibia. The wound was debrided and immobilized with an external fixator. Radiographs are shown in Figure A. The soft tissue defect was covered with a free flap. Her recovery was complicated by wound infection with Klebsiella pneumoniae and Escherichia coli. One month after her injury, she underwent intramedullary nailing and placement of an antibiotic spacer measuring 15cm in length. Radiographs are shown in Figure B. At the next stage of surgery 6 weeks later, the surgeon should plan to do all of the following:

Explanation
The Masquelet staged technique of induced membranes is an option for filling large bone defects up to 25cm in length. This technique protects against autograft resorption, stimulates mesenchymal cell-to-osteoblast differentiation, maintains graft position, and prevents soft tissue interposition. Cement impregnation achieves high local antibiotic concentration without risk of systemic toxicity.
Ashman et al. discussed the techniques of addressing bone defects. Options include:
(1) acute limb shortening (up to 4cm in the tibia and humerus, and 7cm in the femur);
(2) distraction osteogenesis for defects up to 10cm long (at 1mm/day with consolidation period of 5days per mm, or total treatment time of up to 60days/cm), (3) autograft (up to 25cm of vascularized fibula, or 3cm of nonvascularized iliac crest),
and (4) Masquelet technique.
Taylor et al. reviewed the induced membranes technique. They found that the membrane is well vascularized and composed of type I collagen with fibroblasts with an inner epithelial cell layer. There is a high concentration of VEGF, RUNX2 (CBFA1), TGFß1, and BMP2. The membrane is sutured over bone graft to create a closed pouch. When a nail is present, they note a second internal membrane around the nail, potentially increasing local vascularity and osteoinductive factor concentration.
Figure A shows a Gustillo IIIB tibia fracture with a large bone defect held in a temporizing external fixator. Figure B shows the same defect following intramedullary nailing and with a cement spacer placed circumferentially around the nail in the defect.
Incorrect Answers
Question 72
A 3-year-old boy who was treated with Ponseti-method casting demonstrates supination of the affected foot during swing phase of gait. His ankle has 20 degrees of active and passive dorsiflexion and 45 degrees of plantar flexion. What is the most appropriate treatment? Review Topic
Explanation
Question 73
Which of the following is considered an inherent problem in using the distal oblique shortening (Weil) metatarsal osteotomy for dorsal metatarsophalangeal subluxation?
Explanation
REFERENCES: Trnka HJ, Nyska M, Parks BG, Myerson MS: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50.
Trnka HJ, Muhlbauer M, Zettl R, Myerson MS, Ritschl P: Comparison of the results of the Weil and Helal osteotomies for the treatment of metatarsalgia secondary to dislocation of the lesser metatarsophalangeal joints. Foot Ankle Int 1999;20:72-79.
Vandeputte G, Dereymaeker G, Steenwerckx A, Peeraer L: The Weil osteotomy of the lesser metatarsals: A clinical and pedobarographic follow-up study. Foot Ankle Int 2000;21:370-374.
Question 74
Which of the following statements best describes the typical early presentation of osteochondritis dissecans of the elbow? Review Topic
Explanation
Question 75
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the Review Topic
Explanation
Question 76
A 47-year-old woman underwent a distal chevron bunionectomy 2 months ago. Her postoperative recovery had been uneventful until 1 week ago. She now has new onset pain and dorsal swelling in the area of the third metatarsal. A radiograph is shown in Figure 27. What is the most likely diagnosis?
Explanation
REFERENCE: Boden BP, Osbahr DC: High risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Question 77
A 72-year-old man was involved in an automobile accident 4 weeks ago. Initially he noted pain about his nondominant left shoulder, which resolved within a few weeks after the accident. He now describes trouble with gripping and carrying items in his left hand. Radiographs are shown in Figures 20a through 20c. His signs and symptoms are the result of injury to which of the following ligaments?
Explanation
REFERENCES: Berger RA: The ligaments of the wrist: A current overview of anatomy with considerations of their potential functions. Hand Clin 1997;13:63-82.
Cohen MS, Taleisnik J: Direct ligamentous repair of scapholunate dissociation with capsulodesis augmentation. Tech Hand Up Extrem Surg 1998;2:18-24.
Question 78
A 75-year-old woman began a walking program 2 months after undergoing right total knee arthroplasty. She had to stop the program after 4 weeks because of hindfoot pain and ankle swelling. Radiographs are shown in Figures 42a and 42b. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA,
WB Saunders, 1995, p 2591.
Kearon C: Natural history of venous thromboembolism. Semin Vasc Med 2001;1:27-37.
Aldridge T: Diagnosing heel pain in adults. Am Fam Physician 2004;70;332-338.
Question 79
A 35-year-old man sustained a 10% compression fracture of the C5 vertebra in a diving accident. Radiographs show good alignment, and examination reveals no neurologic compromise. An MRI scan reveals no significant soft-tissue disruption posteriorly. Management should consist of
Explanation
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
Allen GL, Ferguson RL, Lehmann TR, O’Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
Question 80
A 27-year-old male competitive soccer player reports a 1-year history of pain in the adductor region that has prevented him from playing. Examination reveals tenderness about the adductor attachment to the pelvis, and pain at the same site with resisted contraction of the adductors. There is no tenderness over the hip joint and no signs of a sports hernia. Radiographs are normal. MRI does not show any evidence of enthesopathy. What is the next best step in management?
Explanation
REFERENCES: Schilders E, Bismil Q, Robinson P, et al: Adductor-related groin pain in competitive athletes: Role of adductor enthesis, magnetic resonance imaging, and entheseal pubic cleft injections. J Bone Joint Surg Am 2007;89:2173-2178.
Robinson P, Barron DA, Parsons W, et al: Adductor-related groin pain in athletes: Correlation of MR imaging with clinical findings. Skelet Radiol 2004;33:451-457.
Question 81
A funnel plot is used in meta-analyses to perform which of the following functions:
Explanation
Publication bias occurs because studies with a non-significant result, so-called
negative studies, have a higher likelihood of being rejected than positive studies, and are oftentimes not even submitted for publication. Funnel plots, which plot the effect size of a study against a measure of the study’s size are used to detect this bias. This method is based on the fact that larger studies have smaller variability, whereas small studies, which are more numerous, have larger variability. Thus the plot of a sample of studies without publication bias will produce a symmetrical, inverted-funnel shaped scatter, whereas a biased sample will result in a skewed plot.
Vavken et al. reviewed orthopaedic meta-analyses in order to determine whether publication bias was assessed and to evaluate its effect on the outcomes of these meta-analyses. They found that only 35% of all orthopaedic meta-analyses published between 1992 and 2008 in English and German assessed publication bias. Adjustment for publication bias did not produce significantly different results, but the magnitude of the pooled estimates in the affected meta-analyses changed by 29% on average.
Illustration A depicts a symmetrical funnel plot with no evidence for publication bias. Illustration B shows a skewed funnel plot suggesting publication bias, as it is missing studies in the lower left corner, i.e. ‘‘negative studies’’. Illustration C depicts a forest plot comparing the incidence of squeaking between ceramic-on-ceramic (COC) and ceramic-on-polyethylene (COP). Illustration D is an example of a ROC curve examining the probability of DVT.
Incorrect Answers:
Question 82
7 weeks from injury at a union rate of 94.5%. They concluded that functional bracing has many known benefits and remains a reliable treatment however certain parameters such as functional outcome, residual deformity, and loss of joint motion remain unclear and require further research.
Explanation
A patient presents with the injury shown in figures A and B. What has been associated with the technique depicted in figures C and D?
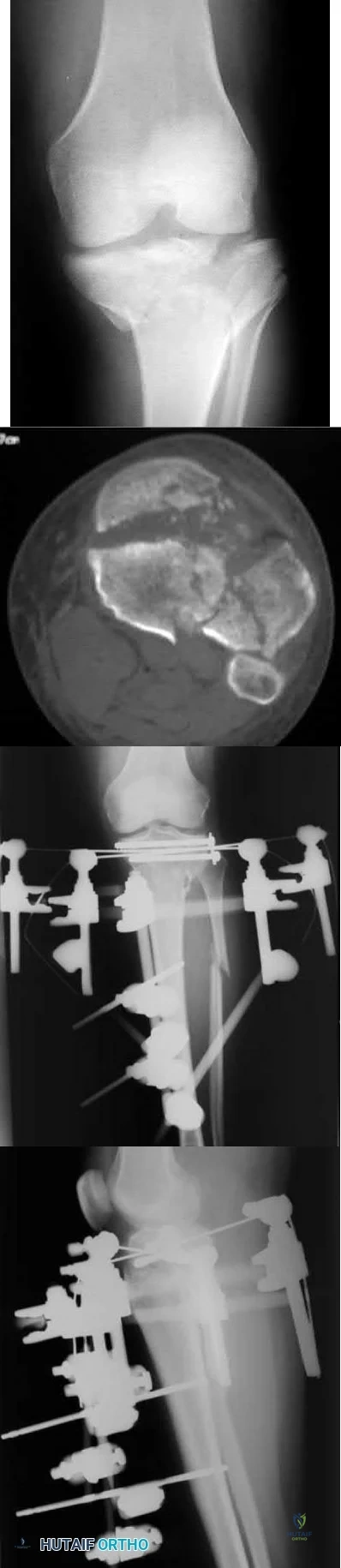
Longer operative times
Increased deep surgical infection rates
Unacceptably high malunion/nonunion rates
Slower early return to function
Longer hospital stays Corrent answer: 3
Treatment of Shatzker V and VI tibial plateau fractures with hybrid external fixation is associated with increased malunion and nonunion rates.
Hybrid external fixation for treating tibial plateau fractures involves the use of an external fixator to achieve reduction through ligamentotaxis. Additional fracture reduction is achieved through limited open incisions with fixation augmented through percutaneous cannulated screws. Definitive treatment with this technique avoids soft tissue complications that have been associated with traditional open reduction and internal fixation with bicondylar plating.
However, studies have reported high malunion and nonunion rates due to a lack of rigid fixation.
Bertrand et al. performed a prospective cohort study of patients undergoing either open reduction and internal fixation versus hybrid external fixation for Schatzker V and VI tibial plateau fractures. Hybrid external fixation was associated with significantly shorter operative times but insignificantly increased complication rates. They concluded that there were limited statistically differences between these techniques, but further studies are required before advising hybrid external fixation for higher Schatzker tibial plateau fractures.
Gross et al. performed a retrospective study of patients treated with hybrid external fixation for Shatzker V and VI tibial plateau fractures. The authors found there was an 80% union rate, a 70% satisfactory reduction rate, and a 52% rate of malunion. The development of osteoarthritis was associated with plateau widening, articular comminution, articular step-off, and incorrect mechanical alignment. The authors concluded that hybrid external fixation is an effective means for the treatment of tibial plateau fractures that minimizes tissue dissection, with decreased blood loss, and shorter operative times, but associated with a very high malunion rate.
Hall et al. performed a multicenter randomized controlled trial comparing the treatment of Schatzker V and VI fractures with open reduction and internal fixation with hybrid external fixation. Patients with hybrid external fixation had less intraoperative blood loss, fewer unanticipated secondary procedures, slightly faster return to pre-injury activity at 6 months and 1 year, and shorter
hospital stay. They concluded that both hybrid external fixation and open reduction and internal fixation provide effective means for fracture treatment, but hybrid external fixation avoids soft tissue complications with deleterious consequences.
Figure A is an AP radiograph of the right knee with a Schatzker VI tibial plateau fracture. Figure B is an axial CT slice of the articular surface of the tibia with extensive comminution. Figures C and D are the AP and lateral radiographs of the knee with a hybrid external fixation construct for a tibial plateau fracture
Incorrect answers:
OrthoCash 2020
An 89-year-old female sustained the injury shown in Figure A and underwent a hemiarthroplasty. Which of the following has been associated with increased rates of post-operative dislocation?

Posterior approach
Anterior approach
Anterolateral approach
Use of a bipolar implant
Use of a monopolar implant
The incidence of dislocation after hemiarthroplasty is highest when using a posterior approach.
Elderly femoral neck fractures are one of the most common fractures encountered by orthopaedists and will only become more common as the population continues to age. The displacement of the femoral head is associated with delayed union or nonunion, an increased risk of femoral head necrosis due to disrupted blood flow at the femoral neck, and failure of internal fixation devices. For this reason, displaced femoral neck fractures in older patients are often treated with hemiarthroplasty. Three approaches to hemiarthroplasty have been described: a lateral approach, a posterior approach, and an anterior approach. The posterior approach has been used more historically; however, its use has been called into question as it has been associated with increased dislocation rates.
Parker performed a trial on all patients with intracapsular femoral neck fractures being treated with hemiarthroplasty. Patients were randomized to surgery using either a lateral or posterior approach. They found that there were no statistically significant differences observed for any of the outcome measures including mortality, degree of residual pain and regain of walking ability. They concluded that both surgical approaches appear to produce comparable functional outcomes.
van der Sijp et al. performed a meta-analysis to compare the outcomes based on approaches for hemiarthroplasty in the treatment of proximal femur fractures. They found 21 studies and found that the posterior approach poses an increased risk of dislocation and reoperation compared to the lateral approach and anterior approaches. They conclude that there are no evident advantages of the posterior approach and its routine use for fracture-related hemiarthroplasty should be questioned.
Figure A is an AP pelvis radiograph demonstrating a displaced right femoral neck fracture.
Incorrect Answers:
OrthoCash 2020
A 50-year-old male sustained a humeral shaft fracture treated operatively 6 months ago. He denies medical problems but smokes 10 cigarettes per day. His current radiograph is shown in Figure A. He continues to have pain in his arm that is affecting his quality of life. On physical examination, there is motion at the fracture site. C-reactive protein and erythrocyte sedimentation rate are within normal limits. Which is the most appropriate definitive treatment for this fracture?

Exchange humeral nailing
Augmentative plating
Nail removal with open reduction compression plating
Smoking cessation and medical optimization
Nail removal with open reduction and compression plating with bone grafting
This patient has sustained an atrophic nonunion of a humeral shaft fracture treated with an intramedullary nail. The most appropriate definitive treatment is nail removal with open reduction and compression plating with bone grafting.
Most diaphyseal humeral fractures can be managed non-operatively with functional bracing. Operative treatment is indicated under a number of circumstances including open fractures, associated neurovascular injury, proximal and distal articular extension of the fracture, and in patients with other multiple injuries. Surgical stabilization can be accomplished with different implants and techniques. The two most common are plate and screw fixation and intramedullary nailing. Plate fixation has the advantages of potential absolute stability and sparing the rotator cuff from an incision. Intramedullary nailing has to be inserted proximally with potential damage to the rotator cuff. It, however, can be inserted with small incisions. If a nonunion develops after intramedullary nailing, nail removal and compression plating is the preferred treatment choice.
Heineman et al. performed a metanalysis on plate fixation or intramedullary nailing of humeral shaft fractures. They performed a literature search from 1967-2007 comparing nails and plates in patients with humeral shaft fractures that reported complications due to surgery. They found that the risk of a complication is lower when plating a fracture of the humeral shaft than when using an intramedullary nail.
Gerwin et al. performed an anatomical study to define the course of the radial nerve in the posterior aspect of the arm, with particular reference to its relationship to operative exposures of the posterior aspect of the humeral diaphysis. They found that the radial nerve crosses the posterior aspect of the humerus from an average of 20.7 +/- 1.2 centimeters proximal to the medial epicondyle to 14.2 +/- 0.6 centimeters proximal to the lateral epicondyle. They found the approach to permit the most visualization was the triceps reflecting approach.
Figure A is a lateral radiograph of an atrophic nonunion of a humeral shaft being stabilized with an intramedullary nail.
Incorrect Answers:
OrthoCash 2020
A 45-year-old man is struck while crossing a major highway and sustains the injury depicted in Figure A. Which of the following statements comparing the techniques in Figure B and C is most accurate?
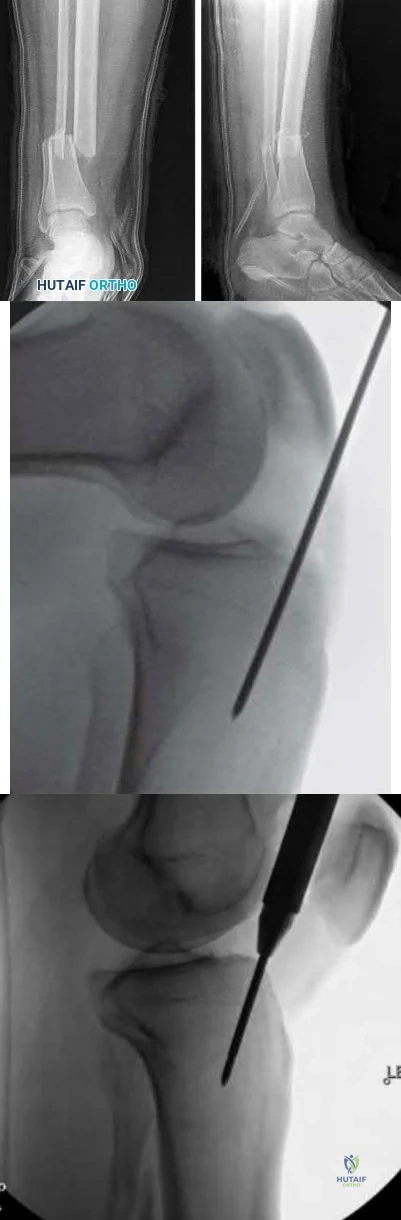
Technique depicted in Figure B is associated with an increased risk of septic arthritis
Technique depicted in Figure B is associated with increased rate of anterior knee pain
Technique depicted in Figure B is associated with improved postoperative fracture alignment
Technique depicted in Figure C is associated with an increased risk of septic arthritis
Technique depicted in Figure C is associated with improved postoperative fracture alignment
Compared to infrapatellar tibial nailing, suprapatellar tibial nailing is associated with improved postoperative fracture alignment.
While antegrade tibial nailing results in postoperative anterior knee pain in approximately 20% of patients, there is no significant difference in the incidence of anterior knee pain when the conventional infrapatellar approach is compared to suprapatellar approaches. In open tibial shaft fractures, no difference has been observed in the incidence of knee sepsis with either approach. However, several studies have demonstrated that intramedullary nail fixation through a suprapatellar approach is associated with a more accurate entry position and a more accurate fracture reduction when compared with an infrapatellar technique, particularly in more proximal and distal shaft
fractures, without evidence of a functional impact on the patellofemoral joint. Lastly, intraoperative radiography is generally less cumbersome with suprapatellar nailing.
Marecek et al. performed a multicenter comparison study of suprapatellar and infrapatellar approaches and the risk of knee sepsis after treatment of open tibia fractures. They reported no differences in the rates of infection, deep infection, or reoperation between suprapatellar and infrapatellar nailing groups. They concluded that the risk of knee sepsis after suprapatellar nailing of open fractures is low.
Avilucea et al. performed a retrospective cohort study comparing postoperative alignment after suprapatellar versus infrapatellar nailing for distal tibial shaft fractures. They reported a significantly increased rate of primary angular malalignment of greater than 5 degrees in the infrapatellar compared to the suprapatellar nailing cohort. They concluded that in the treatment of distal tibial fractures, suprapatellar nailing results in a significantly lower rate of malalignment compared with the infrapatellar nailing.
Jones et al. performed a study comparing the radiologic outcome and patient-reported function after suprapatellar and infrapatellar intramedullary nailing. They reported no difference in anterior knee pain, however, found a more accurate fracture reduction, both in terms of angulation and translation in the coronal plane, with the use of the suprapatellar technique. They concluded that when compared with infrapatellar nailing, the suprapatellar technique was not associated with more anterior knee pain, yet more accurate nail insertion and fracture reduction.
Figure A depicts a displaced distal third tibial shaft fracture. Figure B depicts the infrapatellar tibial nailing technique. Figure C depicts the suprapatellar tibial nailing technique.
Incorrect Answers:
OrthoCash 2020
A 56-year-old woman sustains the closed injury depicted in Figures A-B. On examination, her wrist is mildly swollen and she is unable to actively oppose her thumb. She also complains of some paresthesias in her thumb and index finger. The patient undergoes closed reduction and splinting; however, her paresthesias worsen significantly in the next 12 hours. What is the likely mechanism of her paresthesias and what is the most appropriate treatment?

Nerve compression; open reduction internal fixation with open carpal tunnel release
Nerve laceration; open reduction internal fixation with primary nerve repair or grafting
Decreased arterial inflow; fasciotomy with open reduction internal fixation
Reflex sympathetic dystrophy; vitamin C
Nerve compression; repeat closed reduction Corrent answer: 1
This patient is presenting with signs of acute carpal tunnel syndrome (CTS) in the setting of a displaced distal radial fracture. The pathogenesis of acute CTS is nerve compression, requiring urgent open carpal release with open reduction internal fixation (ORIF).
Acute CTS is a well-recognized phenomenon after distal radial fractures. Risk factors include ipsilateral upper extremity fractures, translation of the fracture fragments, and articular distal radius fractures (DRFs). Acute CTS can manifest with paresthesias in the median nerve distribution and opponens pollicis weakness. Acute CTS is an indication for urgent surgical decompression of the median nerve.
Odumala et al. performed a study to evaluate the role of carpal tunnel decompression in the prevention of median nerve dysfunction after buttress plating of DRFs. They reported that prophylactic decompression of the carpal tunnel results in twice the relative odds of developing median nerve dysfunction, which routinely self-resolved. They concluded that prophylactic median nerve decompression does not alter the course of median nerve dysfunction and may actually increase postoperative morbidity.
Medici et al. performed a case-control study to investigate whether carpal tunnel release (CTR) during fixation DRFs improves outcomes. They reported no statistically significant difference between the groups in VAS and Mayo Wrist Scores, however, an increased risk of subsequent CTR in the group who underwent ORIF with no CTR at the index procedure. They concluded that the release of the transverse carpal ligament during ORIF may reduce the incidence of postoperative median nerve dysfunction.
Niver et al. reviewed CTS after DRFs. They reported that acute CTS noted at the time of DRF warrants urgent surgical release of the carpal tunnel and fracture fixation, and that delayed CTS presenting after a distal radius fracture has healed may be managed in the standard fashion for CTR. They concluded that there is no role for prophylactic CTR at the time of distal radius fixation in a patient who is asymptomatic.
Figures A and B depict a displaced apex volar DRF and a mildly displaced ulnar styloid fracture.
Incorrect Answers:
OrthoCash 2020
Figures A and B depict the closed injury radiograph of a 79-year-old right-hand-dominant woman who fell on her left wrist. According to meta-analysis and systematic reviews, which of the following statements is most accurate regarding her injury?

Improved functional outcomes with open reduction internal fixation (ORIF) through FCR approach vs. closed treatment
No difference in radiographic outcomes after ORIF vs. closed treatment
No difference in functional outcomes after ORIF vs. closed treatment
Improved functional outcomes with closed treatment vs. ORIF
Improved functional outcomes with external fixation and K wire fixation vs. ORIF
This elderly patient has sustained a closed intra-articular and shortened distal radial fracture (DRF). Many studies have reported no difference in functional outcomes when patients aged 60 and over are treated in a closed manner versus operatively for unstable fractures.
The treatment of DRFs in the elderly population is controversial. A variety of nonoperative and operative treatments are available, including closed reduction and splinting/casting, K wire stabilization, external fixation, and ORIF. While conservative management of DRFs in the elderly is common,
recent systematic reviews and meta-analyses have demonstrated that despite worse radiographic outcomes after closed treatment of unstable fractures, functional outcomes were no different between patients treated closed versus surgically in patients over the age of 60 years.
Ju et al. published a systematic review and meta-analysis comparing treatment outcomes between nonsurgical and surgical treatment of unstable DRFs in the elderly. They reported no significant differences in DASH score, VAS pain score, grip strength, wrist extension, pronation, supination, and ulnar deviation between the groups. They concluded that operative and nonoperative treatments result in similar outcomes in the treatment of unstable DRFs in the elderly, with no impact on subjective function outcome and quality of life with closed treatment.
Diaz-Garcia et al. published a systematic review of the outcomes and complications after treating unstable DRFs in the elderly, comparing various treatment techniques. They reported significant differences in wrist motion, grip strength, DASH score, although these findings may not be clinically meaningful. They concluded that although the operatively treated group had improved radiographic outcomes, functional outcomes were no different when compared to the group treated in a closed manner.
Figure A depicts an unstable intra-articular and shortened DRF. Incorrect Answers:
no difference in functional outcomes between operative and closed treatment modalities for DRF.
OrthoCash 2020
An active 60-year-old woman falls from her attic and presents with the injury in Figure A. She undergoes successful closed reduction and sling immobilization. At follow up, she is unable to move her shoulder. New radiographs are depicted in Figures B and C. What is the next best step?
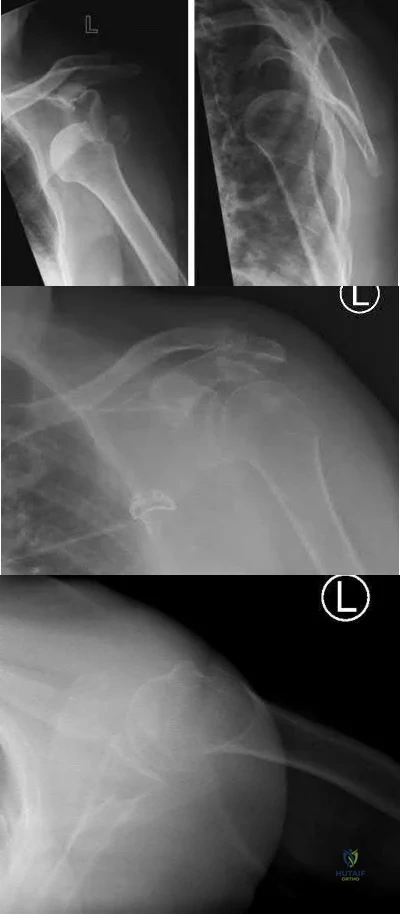
Continued sling immobilization
Closed reduction percutaneous pinning
Open reduction internal fixation
Hemiarthroplasty
Reverse total shoulder arthroplasty Corrent answer: 3
This active patient presents with a greater tuberosity fracture dislocation. Open reduction internal fixation (ORIF) is indicated, particularly when the greater tuberosity fragment is displaced greater than 5mm.
Many proximal humerus fractures are minimally displaced and respond acceptably to nonoperative management. Isolated greater tuberosity fractures or rotator cuff injuries are associated with shoulder dislocations in the elderly population. The greater tuberosity fragment undergoes deforming forces by the supraspinatus and infraspinatus muscles. In active patients, it is well-accepted that greater tuberosity fracture displacement greater than 5mm is an indication for ORIF to restore their ability to perform overhead activities and prevent impingement.
Schumaier et al. published a review article on the treatment of proximal humerus fractures in the elderly. They highlighted that while bone density was a predictor of reduction quality, social independence was a better predictor of outcome. They concluded that although the majority of minimally displaced fractures can be treated successfully with early physical therapy, treatment for displaced fractures should consider the patient's level of independence, bone quality, and surgical risk factors. They emphasized that there was no clear evidence-based treatment of choice, and the surgeon should consider their comfort level during their decision-making.
George et al. published a review article on greater tuberosity humerus fractures. They reported that these fractures may occur in the setting of anterior shoulder dislocations or impaction injuries against the acromion or superior glenoid, with surgical fixation recommended for fractures with greater than 5 mm of displacement in the general population or greater than 3 mm of displacement in active patients involved in frequent overhead activity. They recommended close followup and supervised rehabilitation to increase successful outcomes.
Figure A depicts a greater tuberosity fracture dislocation of the left shoulder. Figures B and C depict reduction of the glenohumeral joint with residual displacement of the greater tuberosity. Illustrations A and B depict radiographs after ORIF.
Incorrect Answers:

OrthoCash 2020
A 21-year-old football player is tackled as he falls onto an outstretched arm. He sustains the injury shown in Figure A. He undergoes successful operative treatment of his injury. In which order did his injury occur?

MCL > LCL > anterior capsule
MCL > anterior capsule > LCL
anterior capsule > MCL > LCL
LCL > anterior capsule > MCL
LCL > MCL > anterior capsule Corrent answer: 4
The patient sustained a terrible triad injury of the elbow, which progresses from the LCL to the anterior capsule and then the MCL.
Terrible triad injuries of the elbow are traumatic injuries that occur after a fall on an extended arm that results in a combination of valgus, axial, and posterolateral rotatory forces. The key features of a terrible triad injury include a radial head fracture, a coronoid fracture, and an elbow dislocation. Disruption of the structures in the elbow characteristically occurs from lateral to medial, affecting the LCL first, followed by the anterior capsule and MCL. Outcomes following terrible triad injuries have historically been poor; however, more recent literature has shown that good outcomes can be achieved with surgical stabilization of the elbow followed by an early rehabilitation protocol. Some authors use temporary immobilization, but range-of-motion exercises are typically initiated by 48 hours postoperatively. Active range of motion is particularly important, as it recruits muscles that act as dynamic stabilizers of the elbow. Depending on the injury, method of fixation, and stability that is achieved, the range of motion may be limited to 30° of extension during the early postoperative period but should allow full flexion.
Giannicola et al. (2013) performed a study to determine the critical time period for recovery of functional range of motion after surgical treatment of complex elbow instability (CEI). They found that the first 6 months after surgery represent the critical rehabilitation period to obtain a functional elbow and that elbow flexion recovered at a rate slower than that of the other elbow movements. They recommend that, following CEI surgical treatment, a rehabilitation program should be started promptly and should be continued for at least 6 months because a significant improvement of ROM occurs in this period.
Giannicola et al. (2015) performed a study analyzing the predictability of outcomes of terrible triad injuries (TTI) treated according to current diagnostic and surgical protocols. They found that the current diagnostic and therapeutic protocols allow for satisfactory clinical outcomes in a majority of cases but a high number of major and minor unpredictable complications still persist. Low compliance, obesity, and extensive soft elbow tissue damage caused by high-energy trauma represented negative prognostic factors unrelated to surgery.
McKee et al. performed a review on their standard surgical protocol for the treatment of elbow dislocations with radial head and coronoid fractures. Their surgical protocol included fixation or replacement of the radial head; fixation of the coronoid fracture, if possible; repair of associated capsular and lateral ligamentous injuries; and, in selected cases, repair of the medial collateral ligament and/or adjuvant-hinged external fixation. They found that their surgical protocol restored sufficient elbow stability to allow early motion postoperatively, enhancing the functional outcome. They recommend early operative repair with a standard protocol for these injuries.
Figure A is a lateral radiograph of the elbow demonstrating a terrible triad injury with a comminuted radial head/neck fracture, displaced coronoid fracture, and posterior elbow dislocation. Illustration A is a rendered image of the radiograph shown in Figure A with the components labeled.
Incorrect Answers:
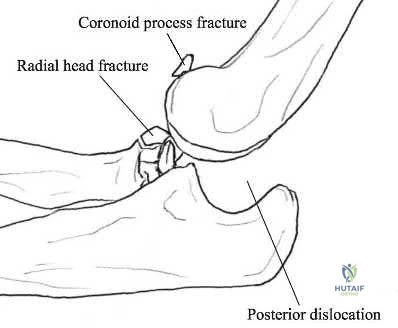
OrthoCash 2020
An 82-year-old female sustains the fracture shown in Figure A as the result of a ground level fall. Which of the following has been shown to be a reliable predictor of postoperative lateral wall fracture for this injury after treatment with a sliding hip screw?
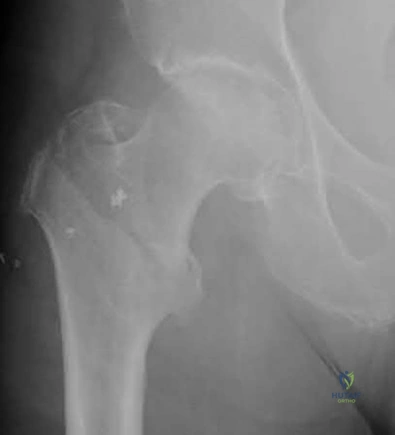
Reverse obliquity fracture pattern
Lateral wall thickness
Previous contralateral hip fracture
DEXA T-score <-2.0
Calcar comminution
Lateral wall thickness has been shown to be a predictor of postoperative lateral wall fracture. As the lateral wall thickness decreases, there is an increased chance of fracture.
Lateral wall fracture creates an unstable fracture pattern and increased screw sliding/collapse. This shortens the neck and abductors, leading to worse patient outcomes (radiographic and clinical). Recognition of a thin wall should lead toward the use of an intramedullary device or adjunct use of a trochanteric stabilizing plate with a sliding hip screw device.
Baumgaertner et al. reported that the failure of peritrochanteric fractures that have been treated with a fixed-angle sliding hip-screw device is frequently related to the position of the lag screw in the femoral head. They established the tip-apex distance as the sum of the distance from the tip of the lag screw to the apex of the femoral head on an anteroposterior radiograph and this distance on a lateral radiograph, after controlling for magnification. Upon reviewing their series, none of the 120 screws with a tip-apex distance of twenty-five millimeters or less cut out, but there was a very strong statistical relationship between an increasing tip-apex distance and the rate of cutout, regardless of all other variables related to the fracture.
Socci et al. performed a literature review of relevant papers and appropriate clinical databases and concluded that fixation of AO 31A1 fractures was best achieved with a sliding hip screw device and that all other types of intertrochanteric hip fractures be fixed with an intramedullary device.
Utrilla et al. reported no difference in outcome in stable fractures, but better mobility at one year following intramedullary fixation of unstable fractures.
Hsu et al. measured the thickness of the lateral wall of patients with AO/OTA 31-A1 and 31-A2 type intertrochanteric hip fractures. They found that the lateral wall thickness was a reliable predictor of postoperative lateral wall fracture for unstable AO Type A2 fractures and concluded that the lateral wall thickness threshold value for risk of developing a secondary lateral wall fracture was found to be 20.5 mm.
Figure A shows a standard obliquity intertrochanteric hip fracture.
Illustration A from the Hsu article demonstrates the measurement of the lateral wall thickness. The distance is measured along a 135-degree angle, between a point 3cm distal to the innominate tubercle of the greater trochanter and the fracture line (midway between the two cortical lines).
Incorrect Answers:
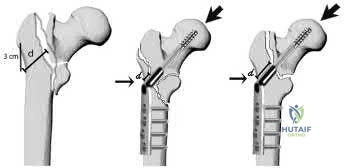
OrthoCash 2020
A 78-year-old patient presents with right hip pain and inability to bear weight after an unwitnessed fall at a nursing home. Figures A and B are the radiographs of the hip and pelvis. Which statement is true regarding the treatment of these injuries?

Smaller lateral wall thickness favors sliding hip screw constructs
Unstable fractures are best treated with sliding hip screw constructs
Avoiding distal locking screws in intramedullary implants protects against refracture
Stable fractures have no differences in outcomes between sliding hip screws and intramedullary implants
Implant stability has a greater impact on outcomes rather than reduction quality
Studies have shown that in stable intertrochanteric femur fractures there are no differences in outcomes between sliding hip screws and intramedullary implants.
Intertrochanteric femur fractures are one of the most common fractures in the geriatric population. Implant selection has been a great topic of research with most studies reporting minimal to no differences in outcomes between intramedullary and sliding hip screw constructs in stable fracture patterns.
Unstable fractures, however, are reportedly better treated with a distally locked intramedullary implant. The quality of fracture reduction has a greater impact on the overall outcome than implant selection.
Hsu et al. performed a retrospective study of risk factors for postoperative lateral wall fractures in patients treated with sliding hip screws for intertrochanteric femur fractures. They found that fracture classification and lateral wall thickness, which is measured from 3 cm distal from innominate tubercle and angled 135 degrees to the fracture line, were associated with postoperative lateral wall fracture. They recommended not treating intertrochanteric femur fractures with sliding hip screws if the lateral wall thickness is less than 20.5 mm.
Socci et al. reviewed the literature regarding the treatment of intertrochanteric femur fractures. Based on the literature, they recommend treatment of AO/OTA type 31A1 fractures with sliding hip screws, type 31A2 fractures with short intramedullary implants, and 31A3 fractures with long intramedullary implants. Simple basicervical fractures of the femoral neck can be treated with sliding hip constructs whereas comminuted fractures treated with intramedullary devices due to the inherent instability of the pattern. The most import aspect in fracture healing is the quality of the reduction rather than the choice of implant.
Lindvall et al. performed a retrospective study of refracture rates in patients treated with either long or short cephalomedullary nails. The authors found a 97% union rate with both implant types and refracture not associated with either long or short implants. Rather, refracture was associated with the lack of a distal locking screw. The authors recommended locking intramedullary implants to avoid refracture.
Utrilla et al. performed a randomized control trial of elderly patients treated
with compression hip screw or Trochanteric Gamma Nail for intertrochanteric femur fractures. They reported the only differences between the two implants were quicker operating time, less fluoroscopy use, and better walking with unstable fractures treated with intramedullary implants. The authors recommended either construct for stable fractures, but intramedullary implants for unstable fractures.
Figures A and B are the AP and lateral radiographs of the right hip radiographs demonstrating a simple and minimally displaced intertrochanteric femur fracture, classified as an AO/OTA 31A1 fracture. Illustration A depicts the AO/OTA classification system for proximal femur fractures.
Incorrect answers:
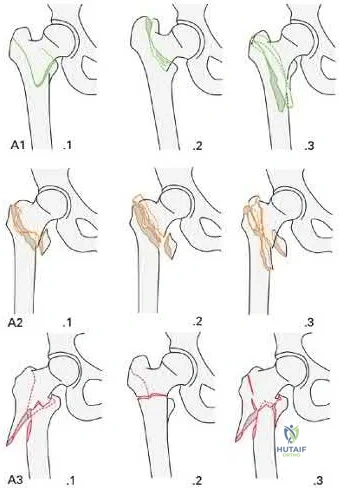
OrthoCash 2020
A 28-year-old male that sustained a closed left femoral shaft fracture 12 months ago and underwent intramedullary nailing presents with persistent pain in the right thigh. The patient walks with an antalgic gait. He denies any fevers or chills. His surgical sites are well healed and there are no signs of drainage. Serum ESR and CRP are 12 mm/hr (reference <20 mm/hr) and 0.9 mg/L (reference <2.5 mg/L), respectively. Figures A and B are the AP and lateral radiographs of the left femur. Which treatment option offers the highest chance of union and enables immediate weight-bearing?

Nail removal with compression plating and open bone grafting
Closed reamed exchange nailing
Nail dynamization
Nail retention with plate augmentation and bone grafting
Electrical bone stimulator Corrent answer: 4
The patient is presenting with a hypertrophic nonunion of the femur below the isthmus, which studies have shown to have a higher union rate when treated with plate augmentation. Retention of the nail allows for full weight-bearing postop.
Hypertrophic nonunion of the femur is the result of fracture site hypermobility with sufficient biology for healing. This is demonstrated with abundant callus formation without bridging trabeculae. Traditionally, this is treated with closed reamed exchange nailing which increased construct stiffness with a larger diameter nail, improved isthmic fit, and extrusion of reaming contents to the nonunion site. However, studies have demonstrated a higher union rate with open plate augmentation, bone grafting, and nail retention. This is due to the ability to correct nonunion site deformity, provide added compression at the nonunion site, and increase fracture site biology with bone graft.
Lynch et al. reviewed the literature regarding the treatment options for femoral nonunions. The literature suggests high union rates when hypertrophic nonunions are treated with exchanged reamed nailing. However, the use of augmentative plate fixation allows for further deformity correction. The proposed mechanism by which exchange reamed nailing is increased construct stiffness with a large diameter nail, usually by 1-2 mm, increased isthmic fit, and autogenous bone graft extrusion into the nonunion site.
Somford et al. performed a systematic review of the surgical treatment of femoral nonunions. Results demonstrate that exchange nailing provides a 73% union rate compared to plate augmentation of 96%. They speculated that there were increased indications for exchange nailing for oligotrophic nonunions in many of the included studies, which may have reduced the union rate. Further, plate augmentation does allow for deformity correction, which can further improve the union rate.
Figures A and B are the AP and lateral radiographs of the femur with hypertrophic nonunion as suggested with the abundant callus formation and broken distal interlock screws. Illustration A and B are the AP and lateral radiographs of the distal femur subsequent plate augmentation and fracture healing.
Incorrect Answers:

OrthoCash 2020
A 25-year-old male sustains the injury depicted in Figure A. He is splinted in the field, but on arrival to the emergency room, he complains of painful "tightness" around the leg and severe uncontrolled pain despite maximum dose narcotics. His pain is exacerbated when the toes and ankle are passively stretched in flexion and extension. What is the most appropriate next step in treatment?

External fixation with serial doppler examinations
Intramedullary nailing
Open reduction internal fixation using plates and screws
Immediate 2-compartment fasciotomies and external fixation
Immediate 4-compartment fasciotomies and external fixation Corrent answer: 5
This patient has clinical symptoms and signs of leg compartment syndrome and should undergo immediate fasciotomies of all 4 leg compartments, followed by external fixation for fracture stabilization.
Tibial fractures are among the most common reasons for compartment syndromes of the leg. A clinical assessment is key in the diagnosis of acute compartment syndrome. If there is uncertainty, intracompartmental pressure measurement has been advocated to help confirm the diagnosis. An absolute
compartment pressure >30 mm Hg or a difference in diastolic pressure and compartment pressure (delta p) <30 mmHg may help to confirm the necessity for fasciotomy.
McQueen et al. published a report of 25 patients with tibial diaphyseal fractures which had been complicated by an acute compartment syndrome. They reported significant differences in any sequelae of acute compartment syndrome between patients who underwent compartment pressure monitoring and those who had not. They recommended that all patients with tibial fractures should have continuous compartment monitoring to minimize the incidence of acute compartment syndrome.
Mawhinney et al. reported on three cases of tibial compartment syndrome after closed intramedullary nailing of the tibia. They reported that the only predisposing factors for the development of compartment syndrome were the surgery and the fracture itself. They concluded that tibial compartment syndrome is a relatively rare but significant complication of tibial nailing.
Figure A is an AP and lateral radiograph of the leg with displaced, comminuted middle third tibia and fibula fractures.
Incorrect Answers:
OrthoCash 2020
A 24-year-old male is brought to the ED after an MVC. He is found to have a closed comminuted segmental fibula fracture after a prolonged extraction from the vehicle. Several hours after arrival, the patient reports increasing pain and is noted to have an exacerbation of his pain with passive stretching of the ankle. He has a heart rate of 103 and a blood pressure of 141/87. Compartment pressures are obtained and are 27 mmHg in the anterior compartment, 47 mmHg in the lateral compartment, 28 mmHg in the superficial posterior compartment, and 27 mmHg in the deep posterior compartment. Which of the following correctly describes the initial pathophysiology of compartment syndrome and the neurologic deficit that would likely occur in this patient if left untreated?
Decreased arterial inflow; decreased sensation on the dorsum of his foot involving the first webspace
Decreased arterial inflow; decreased sensation on the dorsum of his foot involving the hallux, 3rd, and 4th toes
Decreased arterial inflow; inability to dorsiflex his ankle
Decreased venous outflow; decreased sensation on the dorsum of his foot involving the first webspace
Decreased venous outflow; decreased sensation on the dorsum of his foot involving the hallux, 3rd, and 4th toes
Compartment syndrome initially results from a decrease in venous outflow relative to arterial inflow. This patient has elevated pressures in the lateral compartment of the leg, which is where the superficial peroneal nerve runs to supply sensation to the dorsum of the foot including the hallux and 3rd and 4th toes.
Compartment syndrome results from compromised venous outflow from the leg relative to the arterial inflow. This venous congestion leads to elevated compartment pressures that ultimately lead to compromised arterial inflow without compartment release. There are 4 compartments in the leg: anterior, lateral, superficial posterior, and deep posterior. The anterior compartment contains the deep peroneal nerve, the lateral compartment of the leg contains the superficial peroneal nerve, and the deep posterior compartment contains the tibial nerve.
McQueen et al. performed a study to determine risk factors for acute compartment syndrome. They found that young patients, especially men, were most at risk of acute compartment syndrome after injury. They recommend that, when treating such injured patients, the diagnosis should be made early, utilizing measurements of tissue pressure.
Olson et al. published a review on acute compartment syndrome in lower extremity musculoskeletal trauma. They reported that acute compartment syndrome is a potentially devastating condition in which the pressure within an osseofascial compartment rises to a level that decreases the perfusion gradient across tissue capillary beds, leading to cellular anoxia, muscle ischemia, and death. They report that recognizing compartment syndromes requires having and maintaining a high index of suspicion, performing serial examinations in patients at risk, and carefully documenting changes over time.
Illustration A is a diagram depicting the compartments of the leg and its contents.
Incorrect Answers:

OrthoCash 2020
Which of the following amputations results in an approximate 40% increase in energy expenditure for ambulation?
Syme
Traumatic transtibial
Vascular transtibial
Traumatic transfemoral
Vascular transfemoral
The energy expenditure of a vascular transtibial amputation is approximately 40% greater.
The energy expenditure for ambulation increases with lower extremity amputation. Diabetics and vasculopathic patients who undergo amputation
have significantly increased energy requirements compared with nondiabetic patients undergoing amputations for trauma. The metabolic cost for a vascular transtibial amputation is 40% compared to a 25% increase in normal patients who sustain a traumatic amputation.
Huang et al. used a mobile instrument system to measure energy consumption by indirect calorimetry at rest and during ambulation in 25 unimpaired subjects, 6 unilateral below-knee (BK) amputee patients, 6 unilateral above-knee (AK) amputee patients and 4 bilateral AK amputee patients. They found that in comparison to unimpaired subjects, the mean oxygen consumption was 9% higher in unilateral BK amputee patients, 49% higher in unilateral AK amputee patients and 280% higher in bilateral AK amputee patients.
Pinzur et al. performed a study to measure cardiac function and oxygen consumption in 25 patients who underwent amputation for peripheral vascular disease (PVD), and in five similarly aged control patients without PVD. They found Normal walking speed and cadence decreased and oxygen consumption per meter walked increased with more proximal amputation. They conclude that peripheral vascular insufficiency amputees function at a level approaching their maximum functional capacity and more proximal amputation levels, the capacity to walk short or long distances is greatly impaired.
Incorrect Answers:
OrthoCash 2020
A 25-year-old man sustains the injury shown in Figures A-C. What is the primary advantage of using a trochanteric flip osteotomy (TFO) in treating this injury?

It may be performed in a minimally invasive manner
It involves minimal soft tissue stripping
It leads to higher union rates
It allows the surgeon to address all sites of injury through one approach
This patient has sustained a right hip fracture-dislocation with fractures of the femoral head and posterior wall. The TFO allows the surgeon to address all sites of injury through a single approach.
Femoral head fracture-dislocations are a result of high-energy trauma. Treatment ranges from closed reduction and conservative management to total hip arthroplasty. Intermediate options include open reduction and internal fixation or excision of fracture fragments. Complications of this injury include post-traumatic hip arthritis, avascular necrosis, and heterotopic ossification.
The injury is further complicated when a fracture of the acetabulum is concomitantly present. There has been no consensus treatment on this injury constellation as it presents quite rarely. The TFO is one approach that allows the surgeon to treat and stabilize both injuries concurrently. It should be noted that a surgical hip dislocation is performed in conjunction with the TFO to allow access to the femoral head.
Solberg et al. performed a retrospective study of patients sustaining Pipkin IV fracture/dislocations with a TFO. They had 12 patients over a 6 month period. They found that all patients healed radiologically and one patient developed osteonecrosis. 10 out of 12 patients had good to excellent outcomes. They concluded that using a surgical protocol with TFO rendered clinical results
comparable to previously reported outcomes in a series of isolated femoral head fractures.
Giannoudis et al. performed a systematic review to investigate data regarding femoral head fractures, particularly focusing on their management, complications and clinical results. They reported that fracture-dislocations were managed with emergent closed reduction, followed by definite treatment, aiming at an anatomic restoration of both fracture and joint incongruity. They concluded that neither the TFO nor an anterior approach seems to endanger femoral head blood supply compared to the posterior one, with the TFO possibly providing better long-term functional results and lower incidence of major complication rates.
Henle et al. reported on the result of 12 patients of femoral head fractures with associated posterior wall fractures treated with a TFO. They found good to excellent results in 10 patients. The two patients with poor outcome developed avascular necrosis of the femoral head and underwent total hip arthroplasty.
Heterotopic ossification was seen in five patients. They concluded that the TFO may lead to favorable outcomes in this injury constellation.
Figure A is an AP radiograph of the right hip demonstrating a femoral head fracture-dislocation. Figure B is an axial CT image demonstrating a posterior wall fracture. Figure C is an axial CT image demonstrating a femoral head fragment within the acetabulum. Illustration A is the Pipkin classification of femoral head fractures: Type I is below the fovea, Type II is above the fovea, Type III is associated with a femoral neck fracture, and Type IV is associated with an acetabular fracture.
Incorrect Answers:

OrthoCash 2020
A 30-year-old male is brought to your emergency department following a motor vehicle collision at high speed. He is intubated in the field for airway protection but is hemodynamically stable. Subsequent workup shows a displaced acetabular fracture, in addition to an intracranial bleed and liver laceration which do not require surgery. When placing an antegrade anterior column screw, what radiographic view should be used to avoid intra-pelvic screw penetration?
Iliac oblique view with hip and knee flexed
Iliac oblique inlet view
Obturator oblique view with hip and knee flexed
Obturator oblique outlet view
Obturator oblique inlet view Corrent answer: 2
The iliac oblique inlet view will best show the the anterior-posterior placement of an anterior column ramus screw.
Percutaneous and limited-open acetabular fixation is becoming increasingly common as it avoids the morbidity of extensile pelvic dissection and allows early mobilization. However, it relies heavily on a mastery of radiographic landmarks and ability to interpret these images to reduce fracture fragments without direct visualization. Slight deviations of the fluoroscopy beam and/or fracture displacement will distort the radiographic image. Without a facile ability to interpret these and make appropriate adjustments, percutaneous fixation will be extremely onerous.
Starr et al. described their early techniques for percutaneous and limited-open acetabular fixation. They first implemented this for minimally displaced fracture patterns but have expanded these to a wider range of pathology. They cite the benefit of earlier mobilization in the poly-traumatized patient as great use for this technique.
Mauffrey et al. reviewed radiograph utilization during acetabular fracture care. Though CT has added tremendously to demonstrating subtleties of acetabular fractures, they state the use of AP and orthogonal iliac and obturator oblique Judet views cannot be overlooked. Interpreting these radiographs allows the surgeon to recreate 2-dimensional images into a 3-dimensional fracture pattern and better understand the character of the injury.
Illustrations A and B demonstrate the iliac oblique inlet view and obturator oblique outlet views, respectively.
Illustration C demonstrates the relationship of the critical structures at risk of injury during anterior column screw placement. Illustrations D and E show the starting point with screw trajectory, and position of the hip during posterior column screw.
Incorrect Answers:
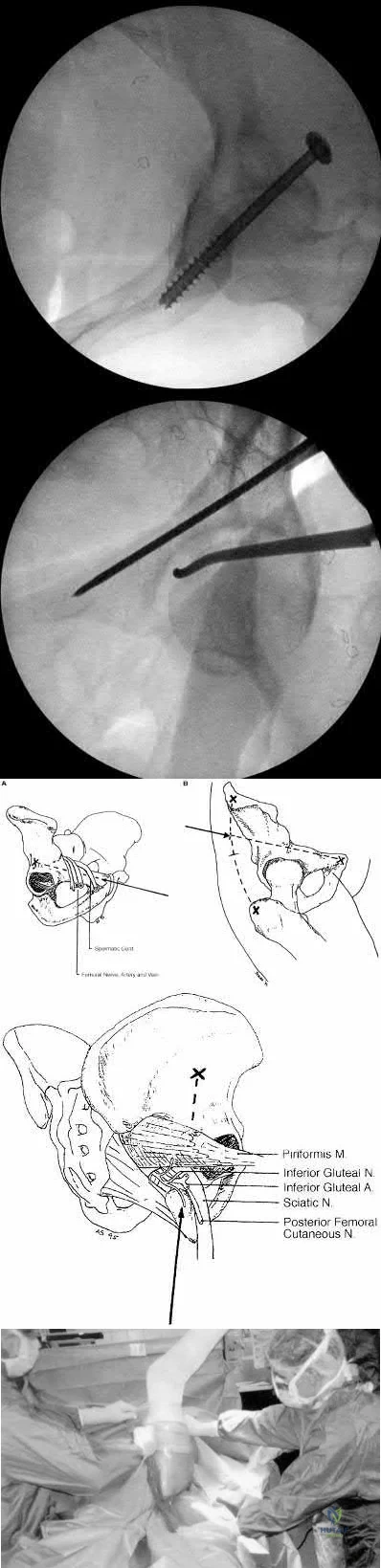
OrthoCash 2020
A 34-year-old male sustains the injury shown in Figures A and B. Which factor has been found to be elevated in the synovial fluid and contributes to post-traumatic arthritis?
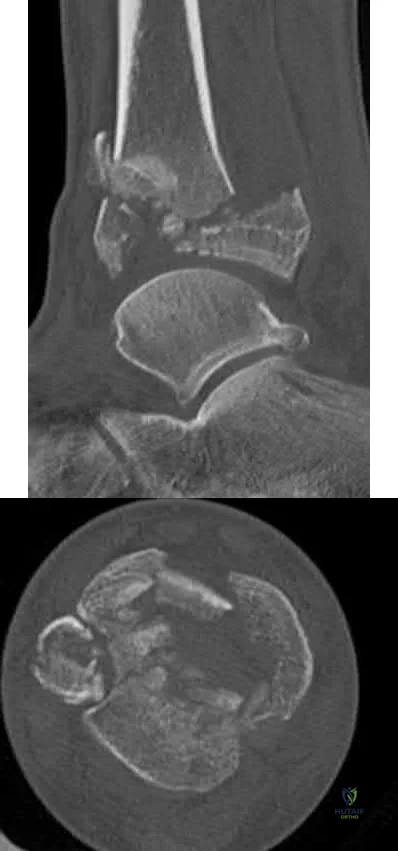
TGF-Beta
RANKL
IL-2
IL-6
cAMP
The patient has sustained a tibial plafond or pilon fracture as depicted in Figures A and B. IL-6 is one of many inflammatory molecules that has been found to be elevated in the synovial fluid following an intra-articular ankle fracture.
Post-traumatic arthritis following intra-articular fractures is a known complication. It commonly appears 1-2 years following injury and is related to chondrocyte death at the margins. There has not been shown to be any association between prolonged non-weight bearing, poor patient compliance with weight-bearing restrictions, and hardware reactions with the development of post-traumatic arthritis. However, literature has shown that the inflammatory molecules present in the synovial fluid can have a significant effect on the development of posttraumatic arthritis. Important inflammatory factors that have been found to be elevated include IL-6, IL-8, MMP-1, MMP-2, MMP-3, MMP-9 and MMP-10.
Adams et al. looked at the synovial fluid of 21 patients with an intra-articular ankle fracture and used the un-injured ankle as a control. They found the inflammatory molecules of GM-CSF, IL-10, IL-1 beta, IL-6, IL-8, IL-10, IL-12p70, TNF-alpha, MMP-1, MMP-2, MMP-3, MMP-9, MMP-10 were all elevated. They concluded that these inflammatory molecules may play a role in posttraumatic arthritis development.
Adams et al. looked at the synovial fluid of 7 patients from his previous 21 patients that had intra-articular ankle fractures. They found that IL-6, IL-8, MMP-1, MMP-2, and MMP-3 were significantly elevated in comparison to the uninjured ankle. They concluded that the sustained elevated intra-articular inflammatory environment is a potential contributor to post-traumatic arthritis.
Figures A and B are sagittal and axial CT slices, respectively, that depict a tibial plafond or pilon fracture.
Incorrect Answers:
immune system.
OrthoCash 2020
A 29-year-old female presents to the trauma bay from the scene of a high-speed motor vehicle accident. She is found to have a closed intraarticular distal radius fracture with a concomitant ulnar styloid base fracture. She subsequently undergoes ORIF of the distal radius fracture with a volar locking plate. The ulnar styloid fracture is not addressed. Which of the following, if present, is least likely to affect functional outcomes?
Ulnar styloid nonunion
DRUJ instability
Articular step-off >3mm
Radial shortening
Workers compensation claim Corrent answer: 1
Ulnar styloid non-unions do not affect the overall outcome of hand or wrist function following ORIF of distal radius fractures.
Ulnar styloid base fractures can be associated with DRUJ disruption and TFCC rupture. The DRUJ should be independently evaluated following ORIF of the distal radius. Without instability, unlar styloid fractures do not need to be addressed. If instability exists, the DRUJ should be treated as a separate entity, typically cross-pinned using k-wires. The result of ulnar styloid nonunions are inconsequential to the overall outcome of patients undergoing distal radius ORIF.
Daneshvar et al review the effects of ulnar styloid fractures on patients sustaining distal radius fractures. They report that patients with a concomitant ulnar styloid fracture had a slower recovery of wrist flexion and grip strength compared to those with an isolated distal radius fracture. They conclude, however, that even the presence of an ulnar styloid nonunion did not significantly affect outcomes.
Buijze et al review the clinical impact of united versus non-united fractures of the proximal half of the ulnar styloid following volar plate fixation of the distal radius. They report no difference in motion, strength or outcome scores
between the united and non-united groups at 6 months follow up. They conclude that nonunion of the ulnar styloid does not have an effect on the overall outcome of hand or wrist function.
Incorrect Answers:
OrthoCash 2020
Which of the following proximal humerus fractures has the highest likelihood of developing humeral head ischemia?

Posteromedial calcar length of the humeral head less than 8 mm and a loss of medial hinge are among the most reliable predictors of ischemia in the surgical management of humeral head fractures.
Proximal humerus fractures are classified based on the Neer classification, in which 4 parts are described: greater tuberosity, lesser tuberosity, articular surface, and the shaft. A fragment is considered a part if it is greater than 45 degrees angulated or displaced >1cm. The posterior humeral circumflex artery is the main blood supply to the humeral head. Following ORIF, humeral head ischemia may occur and is associated with the initial fracture pattern. Several factors including <8mm of calcar length attached to the articular segment, disruption of the medial hinge, displacement >10mm and angulation >45 degrees have been associated with a disruption of the vascular supply to the humeral head.
Campochiaro et al review Hertel’s criteria of calcar length and medial hinge integrity and its reliability in predicting humeral head necrosis. They reported a 3.7% incidence of ischemia across all 267 fractures evaluated. In those patients that developed AVN, 30% had all of the predictors described by Hertel, however, in the non-AVN group, only 4.7% had these same findings.
They concluded that while Hertel’s criteria are helpful, they may not be sufficient and the authors recommended 3-dimensional evaluation of any fracture involving the calcar.
Xu et al reviewed avascular necrosis in patients with proximal humerus fractures who were treated surgically. They reported on 291 patients throughout 7 studies in which there was no difference in the incidence of AVN for those treated surgically or nonoperatively. However, they concluded through subgroup analysis looking at different fixation constructs that, plate fixation specifically was associated with a higher risk of AVN than conservative management of proximal humerus fractures.
Figure A demonstrates a proximal humerus fracture with a medial calcar length of >8mm attached to the articular segment. Figure B is a proximal humerus fracture with a displaced greater tuberosity fragment. Figure C demonstrates a proximal humerus fracture with a medial calcar length of <8mm attached to the articular segment. Figure D is a displaced metadiaphyseal proximal humerus fracture in a skeletally immature patient. Figure E is a radiograph of a metadiaphyseal proximal humerus fracture in a skeletally mature patient with a medial calcar length >8mm.
Incorrect Answers:
OrthoCash 2020
A 34-year-old man presents with the closed injury depicted in Figure A after a high energy twisting injury. Which of the other injuries below is most commonly associated with his known injury?

Nondisplaced medial malleolus vertical shear fracture
Nondisplaced Volkmann's fragment
Nondisplaced Chaput's fragment
Nondisplaced lateral wall talar fracture
Posterior inferior tibiofibular ligament disruption Corrent answer: 2
This patient has sustained a distal third tibial shaft spiral fracture, which is commonly associated with nondisplaced posterior tibial plafond fractures, with the classic Volkmann's fragment.
Prior to operative management, distal third spiral tibial shaft fractures should always be evaluated for intra-articular extension. As this commonly associated injury can be missed on plain radiographs, an ankle CT is often recommended. This is especially important when intramedullary fixation is used for definitive management of the tibial shaft fracture, as nail insertion can displace a
previously nondisplaced intraarticular fracture. Anterior to posterior lag screw fixation prior to nailing may be useful in these cases.
Sobol et al. investigated the incidence of concomitant posterior malleolar fractures (PMFs) in operative distal third spiral tibial shaft fractures. They reported that spiral distal third tibial shaft fractures were identified with an ipsilateral posterior malleolus fracture in 92.3% of cases. They recommended a preoperative ankle CT in all cases with this specific fracture morphology to properly diagnose this commonly associated injury.
Hou et al. investigated the posterior malleolar fracture association with spiral tibial shaft fractures. They reported that plain radiography (both preoperative and intraoperative) resulted in rare identification of these associated injuries, which resulted in missed injuries. They concluded that a CT or MRI ankle may be a higher yield method to detect these injuries.
Figure A demonstrates a distal third spiral tibial shaft fracture. Illustration A is a schematic demonstrating the Volkmann, Chaput, and medial malleoli intraarticular fragments of the distal tibia.
Incorrect Answers:
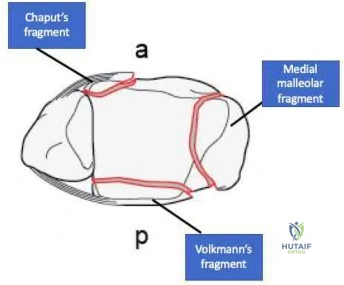
OrthoCash 2020
An 18-year-old male is admitted for a diaphyseal, open, tibial shaft fracture after falling off a motorcycle. He has a past medical history of nicotine dependence and obesity. He undergoes provisional splinting by the resident on call and is noted to be "neurovascularly intact" following splint placement. Throughout the evening, however, the patient has an increasing narcotic requirement and develops pain with passive stretch of his toes. What factor listed below is most associated with his progressive symptoms overnight?
Age < 20
Male gender
Body mass index >/ 30 kg/m^2
Open fracture
Nicotine use
The highest prevalence of compartment syndrome is found in patients aged 12-19 years, followed by 20-29 years.
One theory for the higher prevalence of compartment syndrome in younger patients is increased muscle mass in this cohort. If there is more muscle in a compartment, there is less room for swelling. On the flip side, elderly or deconditioned patients who have less muscle or fatty atrophy may be better able to accommodate muscle swelling. Additionally, a diaphyseal fracture location is associated with a higher risk of compartment syndrome. Again, this may be due to the fact that there is more muscle than tendon, and thus more swelling, in the proximal leg.
Shadgan et al. retrospectively reviewed 1,125 patients with diaphyseal tibia fractures to look for risk factors associated with the development of compartment syndrome. Compartment syndrome occurred in approximately 8% of patients with this injury. They concluded that younger patients were at a higher risk of developing compartment syndrome and that male gender, open fracture, and intramedullary nailing were not risk factors.
Beebe et al. set out to determine the correlation between the OTA/AO classification of tibia fractures and the development of compartment syndrome. they conducted a retrospective review of a prospectively collected database comprising 2,885 fractures. They concluded that age, sex, and the OTA/AO classification were highly predictive for the development of compartment syndrome in this cohort.
McQueen et al. similarly looked at predictors of compartment syndrome after tibial fractures in a retrospective cohort study. There were 1,388 patients in their study with ages ranging from 12-98; identical to the Shadgan study, 69% of patients were male. They concluded the strongest risk factor was age, with the highest prevalence in 12 to 19-year-olds.
Park et al. additionally analyzed 414 patients with tibia fractures in a retrospective cohort study. The main outcome measure of this study was the rate of clinically determined compartment syndromes requiring fasciotomy by anatomic region. The found that diaphyseal fractures were more frequently associated with the development of compartment syndrome than proximal (next most common site) and distal tibia fractures, specifically in younger patients.
Incorrect Answers:
OrthoCash 2020
Figure A is the radiograph of a 79-year-old female with elbow pain following a fall. Compared with a total elbow artrhoplasty, open reduction and internal fixation would most likely result in?

Greater Mayo Elbow Performance Score
Greater Disabilities of the Arm, Shoulder and Hand Score
Increased flexion-extension arc
Increased reoperation rate
Decreased complication rate Corrent answer: 4
This patient sustained a comminuted distal humerus fracture. Open reduction and internal fixation (ORIF) is found to have higher repoeration rates compared with total elbow arthroplasty (TEA) in the elderly: 27% versus 12%, respectively.
Distal humerus fractures account for approximately 30% of elbow fractures. There is often a low energy mechanism of injury in the elderly patient. While ORIF and TEA may be utilized in bicolumnar distal humerus fractures in the elderly patient, recent literature has demonstrated favorable outcomes with TEA in this aged cohort. TEA is indicated in the low demand osteoporotic patients with bicolumnar distal humerus fractures that are not amendable to ORIF. Utilization of TEA has demonstrated greater functional outcome scores, greater motion, less complications, and a lower revision rate.
Mckee et al. conducted a prospective, randomized, controlled trial comparing functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular, distal humeral fractures treated with ORIF or primary semiconstrained TEA. They reports that patients who underwent TEA had significantly better motion, performance and outcome scores, lower reoperation rates compared with the ORIF group. They concluded that TEA for the treatment of comminuted intra-articular distal humeral fractures resulted in more predictable and improved 2-year functional outcomes compared with ORIF and that TEA is a preferred alternative for ORIF in elderly patients with complex distal humeral fractures that are not amenable to stable fixation.
Githens et al. performed a systematic review and meta-analysis to analyze outcomes and complication rates in elderly patients with intra-articular distal humerus fractures being treated with either TEA or ORIF with locking plates. They report that TEA and ORIF for the treatment of geriatric distal humerus fractures produced similar functional outcome scores and range of motion.
However, they found a non-statistical trend toward a higher rate of major complications and reoperation after ORIF. They conclude that the quality of study methodology was generally weak and ongoing research including prospective trials and cost analysis is indicated.
Figure A is the AP radiograph of a comminuted bicolumnar distal humerus
fracture. Illustration A are the radiographs of a comminuted distal humerus fracture in an elderly patient treated with a TEA. Illustration B is the postoperative radiographs of a comminuted distal humerus fracture treated with ORIF.
Incorrect Answers:

OrthoCash 2020
Figure A is the postoperative radiograph of an 82-year-old female who was treated with a cephalomedually nail for a left intertrochanteric hip fracture. Which of the following is the most common complication following use of this device?

Anterior perforation of distal femur
Breakage of the screw
Implant cutout
Malunion
Nonunion
Intertrochanteric hip fractures are most commonly treated with a cephalomedullary nail. The most common complication following utilization of a cephalomedullary nail is implant failure and cutout.
Intertrochanteric hip fractures are extra-capsular injuries that are common in the elderly osteoporotic patient. These injuries carrry a 20-30% mortality rate in the first year following fracture. Femoral cephalomedullary nails are often used to treat these injuries. Often a helical blade or screw may be used to provide fixation within the femoral neck. Overall, the most common complication following use of this device is implant failure and cutout, which occurs most commonly within 3 months following surgery. A known risk factor of this complication is an increased tip-apex distance, with a 60% failure rate reported with a distance exceeding 45mm.
Gardner et al. reviewed the use of a helical blade device to stabilize
intertrochanteric hip fractures. They reported a mean telescoping in unstable and stable fractures of 4.3 mm and 2.6 mm, respectively. They also found that blade migration within the femoral head averaged 2.2 mm overall, with no difference between stable and unstable fractures. They concluded that position changes occurred within the first 6 weeks postoperatively, with no subsequent detectable migration or telescoping.
Haidukewych et al. reviewed patients with failed internal fixation of a hip fracture. They report that salvage options are dependent on the anatomic site of the nonunion, the quality of the remaining bone and articular surface, and patient factors such as age and activity level. They conclude that in younger patients with either a femoral neck or intertrochanteric fracture nonunion with a satisfactory hip joint, treatment typically involves revision internal fixation with or without osteotomy or bone grafting. Conversely, in older patients with poor remaining proximal bone stock or a badly damaged hip joint, conversion to hip arthroplasty is recommended.
Figure A is the AP radiograph of the right hip treated with a cephalomedullary nail. Illustration A demonstrates screw cutout.
Incorrect Answers:

OrthoCash 2020
Figure A is the radiograph of a 42-year-old female who presents to the trauma bay following a motor vehicle collision. She subsequently undergoes ORIF through a posterior approach. Iatrogenic injury to which nerve in Figure B is most likely with this approach?
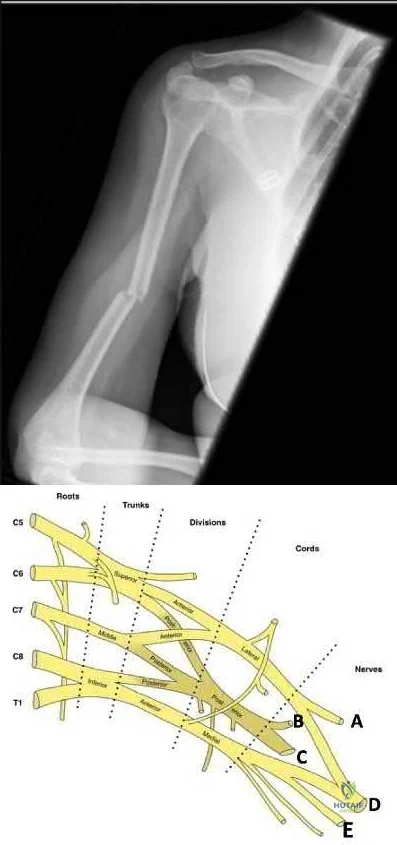
Question 83
Trabecular bone is remodeled through the formation of
Explanation
Question 84
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5° of angulation. When the MCP joint is flexed 30°, a radially directed stress produces 45° of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
REFERENCES: Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint.
J Am Acad Orthop Surg 1997;5:224-229.
Question 85
Sterilization of ultra-high molecular weight polyethylene by gamma irradiation in air will degrade its wear performance because of
Explanation
REFERENCES: Collier JP, Sutula LC, Currier BH, et al: Overview of polyethylene as a bearing material: Comparison of sterilization methods. Clin Orthop 1996;333:76-86.
McKellop H, Shen FW, Lu B, et al: Effect of sterilization method and other modifications on the wear resistance of acetabular cups made of ultra-high molecular weight polyethylene: A hip-simulator study. J Bone Joint Surg Am 2000;82:1708-1725.
Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.
Question 86
The arthroscopic views shown in Figures 31a and 31b reveal extensive synovitis in the anterolateral corner of the ankle overlying a band of tissue sometimes implicated in soft-tissue impingement of the ankle following a chronic sprain injury. This band is a portion of the
Explanation
REFERENCES: Bassett FH III, Gates HS III, Billys JB, et al: Talar impingement by the anteroinferior tibiofibular ligament: A cause of chronic pain in the ankle after inversion sprain.
J Bone Joint Surg Am 1990;72:55-59.
DiGiovanni BF, Fraga CJ, Cohen BE, et al: Associated injuries found in chronic lateral ankle instability. Foot Ankle Int 2000;21:809-815.
Question 87
A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time?
Explanation
REFERENCES: Findlay JM: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;39:210.
Dickman CA, Mamourian A, Sonntag VK, et al: Magnetic resonance imaging of the transverse atlantal ligament for the evaluation of atlantoaxial instability. J Neurosurgery 1991;75:221-227.
Question 88
A 45-year-old man falls from a skateboard and dislocates his elbow. After a closed reduction in the emergency department, his elbow is carefully examined. He has positive valgus stress, moving valgus stress, and milking maneuver tests. His elbow appears stable to varus stress and lateral pivot shift tests. What is the most appropriate manner of immobilizing the elbow for this patient?
Explanation
forearm should be splinted in full supination.
Question 89
- What is the most common nerve injury following a Monteggia fracture-dislocation of the forearm in adults?
Explanation
Question 90
What nerve is at greatest risk of harm from the portal shown in Figure 36?
Explanation
REFERENCES: Field LD, Altchek DW, Warren RF, O’Brien SJ, Skyhar MJ, Wickiewicz TL: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Papilion JD, Neff RS, Shall LM: Compression neuropathy of the radial nerve as a complication of elbow arthroscopy: A case report and review of the literature. Arthroscopy 1988;4:284-286.
Poehling GG, Whipple TL, Sisco L, Goldman B: Elbow arthroscopy: A new technique. Arthroscopy 1989;5:222-224.
Question 91
Figure 1 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop" and then needing help walking off the field. His knee is visibly swollen. The patient undergoes surgery to repair/reconstruct the damaged structure and has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they want to “get the therapy over with as fast as possible" to expedite his return to sports, and the surgeon and rehabilitation team consider their request. Compared with nonaccelerated rehabilitation, patients who follow an early accelerated rehabilitation protocol experience

Explanation
Question 92
The Cotton test evaluates which of the following structures?

Explanation
Question 93
- Gamma ray irradiation for sterilization of ultra-high molecular weight polyethylene in an oxygen environment can have what effect on the material?
Explanation
Question 94
A 69-year-old woman has rigid painful left pes planus that has become less symptomatic with casting. She has multiple comorbidities and is not a good surgical candidate. She has failed a trial of activity without any supports.
Explanation
Treatment for pes planus revolves around 2 clinical parameters: pain and rigidity. In the absence of pain, no intervention is warranted because there are no other symptoms that can reasonably be linked to the foot shape. Flexible pes planus (that corrects with heel rise) is usually normal and does not cause symptoms, but it can be associated with a symptomatic accessory navicular, in which case the patient may have pain over the medial navicular from either traction by the tibialis posterior or the act of rubbing against the medial shoe counter. Rigid pes planus is most frequently associated with a tarsal coalition, which classically presents in late adolescence but can become symptomatic for the first time in adults. The initial treatment for painful pes planus, whether flexible or rigid, is immobilization, usually in a walking cast. This often is sufficient to relieve symptoms on a permanent basis. Surgery should be contemplated only when this treatment fails. Adult-acquired flatfoot is most commonly attributable to tibialis posterior tendon dysfunction. In stage 3, the pes planus is rigid. If it is painful, surgical treatment, which consists of a triple arthrodesis, may be considered. However, if medical constraints or patient preference preclude surgery, an Arizona brace can provide sufficient support to reduce symptoms to an acceptable level to perform activities of daily living.
RECOMMENDED READINGS
Varner KE, Michelson JD. Tarsal coalition in adults. Foot Ankle Int. 2000 Aug;21(8):669-72. PubMed PMID: 10966365. View Abstract at PubMed
Lin JL, Balbas J, Richardson EG. Results of non-surgical treatment of stage II posterior tibial tendon dysfunction: a 7- to 10-year followup. Foot Ankle Int. 2008 Aug;29(8):781-6. doi: 10.3113/FAI.2008.0781. PubMed PMID: 18752775. View Abstract at PubMed
Chao W, Wapner KL, Lee TH, Adams J, Hecht PJ. Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int. 1996 Dec;17(12):736-41. PubMed PMID: 8973895. View Abstract at PubMed
Cha SM, Shin HD, Kim KC, Lee JK. Simple excision vs the Kidner procedure for type 2 accessory navicular associated with flatfoot in pediatric population. Foot Ankle Int. 2013 Feb;34(2):167-72. doi: 10.1177/1071100712467616. Epub 2013 Jan 15. PubMed PMID:
Question 95
A 17-year-old male soccer player sustains repeated lateral patellar dislocations refractory to physical therapy, bracing, and taping. After a workup including radiographs and MRI, the orthopaedic surgeon considers an isolated tibial tubercle osteotomy (TTO). He plans a 60-degree anteromedialization to address instability and to unload the patellofemoral joint. What is a relative contraindication to this procedure?
Explanation
TTO is a common treatment for patellofemoral instability. The angle of correction must be customized to each patient’s anatomy. For this patient, the orthopaedic surgeon plans an osteotomy that will both anteriorize and medialize the tubercle. This will consistently result in
a change of patellofemoral kinematics and contact pressures. Medialization decreases lateral and increases medial patellofemoral contact pressures, and anteriorization shifts contact pressures from distal to proximal. Significant anteriorization may not be desired in a patient with proximal patellar chondrosis unless a concomitant chondral procedure is performed as well. The patellar height (Caton-Deschamps ratio) is normal, precluding the need for distalization but not medialization. The TT-TG distance, at more than 20 mm, is a strong indication for osteotomy. The Q angle, although a less precise indicator of malalignment, is also elevated and would be considered an indication for osteotomy.

CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 41
A healthy, active 18-year-old man has acute-onset right knee pain and an inability to fully extend his knee following an attempt to stand from a seated position yesterday. He sustained a noncontact injury to his right knee while playing basketball 2 years ago and underwent primary anterior cruciate ligament (ACL) reconstruction with bone-patella-tendon-bone autograft and medial meniscus repair. He sustained another noncontact injury to the same knee 8 months later and underwent a revision ACL reconstruction using soft-tissue allograft and revision medial meniscus repair. He reports multiple episodes of “giving way” of his knee, but no pain prior to yesterday’s acute injury.
Question 96
During total hip arthroplasty, what characteristic of irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene should provide a more wear-resistant construct than traditional gamma- irradiated (2.5-4 Mrad)-in-air polyethylene mated with the same head?
Explanation
Highly cross-linked polyethylene makes material resistant to adhesive wear. Abrasive wear from third bodies does not decrease wear. The fatigue strength of such material is inferior to that of traditional polyethylene, and its resistance to creep is the same, if not lower, than that of traditional polyethylene.
Question 97
Posterior spinal fusion for scoliosis should be performed on a patient with Duchenne muscular dystrophy when
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 635-651.
Mubarak SJ, Morin WD, Leach J: Spinal fusion in Duchenne muscular dystrophy: Fixation and fusion to the sacropelvis? J Pediatr Orthop 1993;13:752-757.
Question 98
A follow-up examination of a patient 6 weeks after knee surgery reveals a range of motion from 5° to 55° of flexion. Which of the following statements best summarizes the role of manipulation under anesthesia for this patient?
Explanation
REFERENCE: Esler CN, Lock K, Harper WM, Gregg PJ: Manipulation of total knee replacements: Is the flexion gained retained? J Bone Joint Surg Br 1999;81:27-29.
Question 99
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
Explanation
REFERENCES: Waters PM, Mih AD: Fractures of the distal radius and ulna, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, p 361.
Paley D, McMurtry RY: Median nerve compression by volarly displaced fragments of the distal radius. Clin Orthop Relat Res 1987;215:139-147.
Question 100
A 73-year-old man stepped off a street curb and felt a crack in his left hip. He is now unable to bear weight. A radiograph is shown in Figure 54a. Biopsy specimens are shown in Figures 54b and 54c. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 269.
Mercuri M, Picci P, Campanacci L, et al: Dedifferentiated chondrosarcoma. Skeletal Radiol 1995;24:409-416.
