Orthopedic Board Prep MCQs: Trauma, Arthroscopy & Lower Extremity Part 4

Key Takeaway
This page offers Part 4 of an OITE/AAOS Orthopedic Surgery Board Review. It features 100 high-yield, verified MCQs tailored for orthopedic residents and surgeons preparing for board certification. Utilize study and exam modes with detailed explanations covering Arthroscopy, Foot, Fracture, Hip, and Knee.
About This Board Review Set
This is Part 4 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 4
This module focuses heavily on: Arthroscopy, Foot, Fracture, Hip, Knee.
Sample Questions from This Set
Sample Question 1: A 23-year-old man is involved in a motor vehicle accident. An AP radiograph is shown in Figure 29a, and axial and sagittal CT scans are shown in Figures 29b and 29c. Neurologic examination shows 1/5 strength of his quadriceps and iliopsoas ...
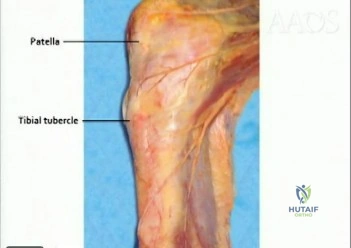
Sample Question 2: A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. Wh...
Sample Question 3: A 22-year-old ballet dancer undergoes hip arthroscopy for increasing hip pain and popping with activity. She experiences complete resolution of signs and symptoms post-operatively. Her pre- and post-operative magnetic resonance sagittal ima...
Sample Question 4: Locked lateral plate fixation of the proximal tibia is most appropriate for what Schatzker type fracture?...
Sample Question 5: A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a t...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 23-year-old man is involved in a motor vehicle accident. An AP radiograph is shown in Figure 29a, and axial and sagittal CT scans are shown in Figures 29b and 29c. Neurologic examination shows 1/5 strength of his quadriceps and iliopsoas on the right, with 1/5 quadriceps function on the left. Definitive treatment of his injury should consist of
Explanation
REFERENCES: Theiss SM: Thoracolumbar and lumbar spine trauma, in Stannard JP, Schmidt AH, Kregor PJ (eds): Surgical Treatment of Orthopaedic Trauma. New York, NY, Thieme, 2007, pp 179-207.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 2
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700.
Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Fischer SP, Fox JM, Del Pizzo W, Friedman MJ, Snyder SJ, Ferkel RD: Accuracy of diagnoses from magnetic imaging of the knee: A multi-center analysis of one thousand and fourteen patients. J Bone Joint Surg Am 1991;73:2-10.
Question 3
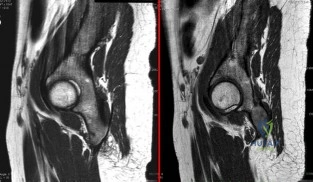
A 22-year-old ballet dancer undergoes hip arthroscopy for increasing hip pain and popping with activity. She experiences complete resolution of signs and symptoms post-operatively. Her pre- and post-operative magnetic resonance sagittal images shown in Figure A (left, pre-operative; right, post-operative). Which of the following pre-operative physical examination findings may have been positive? Review Topic
Explanation
Snapping hip exists in 3 forms: (1) external snapping hip, which is caused by the iliotibial band (ITB) sliding over the greater trochanter, (2) internal snapping hip, and
(3) intraarticular snapping hip, which is caused by loose bodies (traumatic, or from synovial chondromatoses) or labral tears. While painless snapping hip requires no treatment, painful snapping hip may be addressed with activity modification, physical therapy, steroid injections. Surgical release (ITB z-plasty or psoas tenotomy) is indicated if nonoperative management is unsuccessful.
Ilizaliturri et al. evaluated the results of endoscopic iliopsoas tendon release at the lesser trochanter (10 patients) vs endoscopic transcapsular psoas release from the peripheral compartment (9 patients). There were improvements in WOMAC scores in both groups, and no difference between groups. They conclude that both techniques are equally effective.
Marquez Arabia et al. evaluated if the psoas tendon regenerates after tenotomy in 27 patients. At 23 months, they found that tendon regeneration occurred in all patients, to
a mean circumference of 84% of the original. One patient had persistent pain, but all had 5/5 hip flexion strength. They hypothesize that the bulk of iliopsoas muscle fibers attaches directly to the proximal femoral shaft without a tendon, preventing retraction and allowing regeneration to occur easily.
Figure A shows pre- and post-operative arthroscopic psoas tenotomy magnetic resonance sagittal images. Illustration A shows the psoas tendon (white arrows) prior to transection. Illustration B shows the psoas tendon after transection (green arrows, proximal tendon segment; yellow arrows, distal segment). Illustration C and D are diagrams showing release at the level of the lesser trochanter and hip joint respectively.
Incorrect
90 degrees, but full external rotation. Answer 2: Decreased internal rotation and a positive impingement test (forced
flexion, adduction, femoroacetabular Answer 4: These
and internal
rotation) are classic findings
findings may
be found with intra-articular
for cam-type impingement loose bodies.
Question 4
Locked lateral plate fixation of the proximal tibia is most appropriate for what Schatzker type fracture?
Explanation
Question 5
A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 189-199.
Kwon BK, Vaccaro AR, Grauer JN, et al: Subaxial cervical spine trauma. J Am Acad Orthop Surg 2006;14:78-89.
Question 6
A biopsy of the involved physis in a patient with slipped capital femoral epiphysis (SCFE) would most likely reveal
Explanation
REFERENCES: Chung SM, Batterman SC, Brighton CT: Shear strength of the human femoral capital epiphyseal plate. J Bone Joint Surg Am 1976;58:94-103.
Raney EM, Ogden JA: Slipped capital femoral epiphysis. Current Ortho 1995;9:111-116.
Question 7
What is the most common nonanesthetic-related reversible cause of changes in intraoperative neurophysiologic monitoring data? Review Topic
Explanation
Question 8
A 40-year-old woman reports the atraumatic onset of severe knee pain and swelling after undergoing an uncomplicated elective cholecystectomy 1 week ago. She denies any history of diabetes mellitus or HIV but has had occasional episodes of mild knee pain and swelling that have always responded to nonsteroidal anti-inflammatory drugs. Radiographs are shown in Figures 5a and 5b. A knee aspiration yields a WBC count of 35,000/mm 3 . The aspirate should also yield which of the following findings?
Explanation
REFERENCES: Fisseler-Eckhoff A, Muller KM: Arthroscopy and chondrocalcinosis. Arthroscopy 1992;8:98-104.
Hough AJ Jr, Webber RJ: Pathology of the meniscus. Clin Orthop 1990;252:32-40.
Question 9
A 2-year-old child is being evaluated for limb-length and girth discrepancy. As a newborn, the patient was large for gestational age and had hypoglycemia. Current examination shows enlargement of the entire right side of the body, including the right lower extremity and foot. The skin shows no abnormal markings, and the neurologic examination is normal. The spine appears normal. Radiographs confirm a 2-cm discrepancy in the lengths of the lower extremities. Additional imaging studies should include
Explanation
REFERENCES: DeBaun MR, Tucker MA: Risk of cancer during the first four years of life in children from The Beckwith-Wiedemann Syndrome Registry. J Pediatr 1998;132:398-400.
Ballock RT, Wiesner GL, Myers MT, et al: Hemihypertrophy concepts and controversies.
J Bone Joint Surg Am 1997;79:1731-1738.
Carpenter CT, Lester EL: Skeletal age determination in young children: Analysis of three regions of the hand/wrist film. J Pediatr Orthop 1993;13:76-79.
Question 10
A 16-year-old competitive female swimmer has a 1-year history of left shoulder pain. She denies any specific injury to her shoulder. She reports that the pain is worse with swimming but also has pain with daily activities. She also notes similar occasional symptoms in her right shoulder. Examination reveals symmetric range of motion and rotator cuff strength. Examination of the left shoulder reveals 2+ anterior and posterior translation with pain in both directions and a 2-cm sulcus sign. The right shoulder also has 2+ anterior and posterior translation and a 2-cm sulcus sign with no pain. She also has hyperextension of the elbows and the ability to touch the radial border of her thumb to her forearm. What is the next step in management? Review Topic
Explanation
Question 11
Figure 46 shows the radiograph of a 65-year-old man who reports restricted range of motion and pain with sitting 18 months after undergoing right side revision total hip arthroplasty. What is the most appropriate management? L Intensive physiotherapy
Explanation
REFERENCES: Board TN, Karva A, Board RE, et al: The prophylaxis and treatment of heterotopic ossification following lower limb arthroplasty. J Bone Joint Surg Br 2007;89:434-440.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative
Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Question 12
The mangled extremity severity score (MESS) utilizes all of the following variables EXCEPT:

Explanation
The scoring system is as follows: 1. Skeletal / soft-tissue injury: Low energy = 1; Medium energy = 2; High energy = 3; very high energy = 4; 2. Limb ischemia: Pulse reduced or absent but perfusion normal = 1; Pulseless = 2; Cool, paralyzed, insensate = 3; 3. Shock: normotensive = 0; transient hypotension = 1; persistent hypotension = 2; 4. Age:
< 30 = 0; 30-50 = 1; >50 = 2. Limb category scores are doubled for ischemia > 6 hours. The system's original designers reported a cutoff of 7 as predicting amputation.
The referenced study by Ly et al found that the scoring system did not predict functional outcomes at 6 or 24 months. They also found that the Limb Salvage Index; the Predictive Salvage Index; the Nerve Injury, Ischemia, Soft-Tissue Injury, Skeletal Injury, Shock, and Age of Patient Score; and the Hannover Fracture Scale-98 all did not predict outcomes at 6 or 24 months.
Question 13
Which of the following design features of a femoral component used in a total knee arthroplasty best minimizes the patellar component contact stresses?
Explanation
REFERENCES: Petersilge WJ, Oishi CS, Kaufman KR, Irby SE, Colwell CW Jr: The effect of trochlear design on patellofemoral shear and compressive forces in total knee arthroplasty. Clin Orthop 1994;309:124-130.
Theiss SM, Kitziger KJ, Lotke PS, Lotke PA: Component design affecting patellofemoral complications after total knee arthroplasty. Clin Orthop 1996;326:183-187.
Healy WL, Wasliewski SA, Takei R, Oberlander M: Patellofemoral complications following total knee arthroplasty:. Correlation with implant design and patient risk factors. J Arthroplasty 1995;10:197-201.
Question 14
Risk for vascular injury during transtibial drilling for reconstruction of this injury is increased by
Explanation
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, 1 major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading.
In Question 12, the scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-
producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag.
Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used. Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
Question 15
Figure 26 shows the clinical photograph of a patient who has developed a residual limb ulcer following a traumatic transtibial amputation 2 years ago. What is the preferred treatment to resolve the ulcer?
Explanation
REFERENCES: Murnaghan JJ, Bowker JH: Musculoskeletal complications, in Smith DG, Michael JW, Bowker JH (eds): Atlas of Amputations and Limb Deficiencies, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 683-700.
Smith DG, Ferguson JR: Transtibial amputations. Clin Orthop Relat Res 1999;361:108-115.
Question 16
Which of the following best describes athletic pubalgia?
Explanation
REFERENCES: Meyers WC, Foley DP, Garrett WE, Lohnes JH, Mandlebaum BR: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Albers SL, Spritzer CE, Garrett WE Jr, Meyers WC: MR findings in athletes with pubalgia. Skeletal Radiol 2001;30:270-277.
Question 17
A 51-year-old butcher has an 18-month history of recalcitrant medial elbow pain, which is affecting his occupational demands. He describes the pain as mainly anterior and distal to the medial epicondyle. His symptoms are exacerbated with resisted wrist flexion and forearm pronation. On examination, he is also found to have a positive Tinel's sign at the elbow with weakness of intrinsic strength. He has attempted physical therapy, activity modification, bracing, and anti-inflammatory medication without any significant improvement. Presurgical counseling should include the understanding that
Explanation
of pathologic tissue, release of the flexor carpi radialis - pronator teres origin, and/or repair of the flexor carpi radialis - pronator teres origin. Several authors have raised concern of the impact of concomitant ulnar neuropathy on results following surgical treatment for medial epicondylitis. Kurvers and Verhaar and Gabel and Morrey, among others, have reported a statistically significant association between concomitant ulnar neuropathy and worse outcomes following surgery. Most patients can anticipate a return to prior activity levels after surgery without any consistently reported loss of flexor/pronator strength. Prior corticosteroid injections
have not been found to impact results.
Question 18
A 70-year-old former baseball catcher reports long-standing pain in the ring and little fingers. A gradient-echo MRI scan is shown in Figure 26. What is the most likely diagnosis?
Explanation
as indicated by the arrow. This technique suppresses the signal of the surrounding fat
and causes the stationary surrounding tissues to become intermediate in signal intensity.
The flowing blood is then easily identified with a bright signal because it does not absorb the radiofrequency pulse. Based on the findings, the diagnosis is an ulnar artery aneurysm, most likely caused by years of repetitive trauma as the result of catching baseballs. Neurolemmoma and giant cell tumor of the tendon sheath would be intermediately enhanced on this image sequence, and the continuity with the ulnar artery, demonstrated here, would not be expected. Lipomas are not enhanced using the gradient-echo technique. The chronic nature of the patient’s symptoms is not indicative of a hematoma, and the hematoma would be dark on this imaging sequence since it is stationary tissue.
REFERENCES: Koman LA, Ruch DS, Patterson Smith B, et al: Vascular disorders, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2, pp 2254-2302.
Holder LE, Merine DS, Yang A: Nuclear medicine, contrast angiography, and magnetic resonance imaging for evaluating vascular problems in the Hand: Vasospastic disorders. Hand Clin 1993;9:95-113.
Question 19
A 25-year-old lineman is referred to your office for a second opinion. 1 year ago, he underwent an arthroscopic procedure for shoulder instability. He complains of persistent sense of instability despite the surgery. Which of the following is a contraindication to revision arthroscopic labral repair for recurrent anterior glenohumeral instability? Review Topic
Explanation
Thermal capsulorrhaphy utilizes heat generated by radiofrequency or laser ablation to cause capsular shrinkage in an effort to treat shoulder instability. However, high recurrence rates have been found, especially around two to three weeks after the index procedure, when the capsular tissue is the weakest. In the setting of recurrence following thermal capsulorrhaphy, open revision is recommended.
Creighton et al. reported on a series of 18 patients undergoing revision arthroscopic stabilization. Of the 18, 3 failed with recurrent instability, all with previous thermal capsulorrhaphy.
Miniaci et al. reviewed the outcomes following thermal capsulorrhaphy noting high rates of recurrent instability, especially in the setting of initial treatment for multidirectional instability.
Park et al. reported on a series of 14 patients undergoing revision following thermal capsulorrhaphy. Ten out of 14 patients had signs of capsular thinning, insufficiency and attenuation.
Wong et al. surveyed 379 shoulder surgeons on the complications following thermal capsulorrhaphy. Capsular insufficiency and thinning were commonly associated with recurrent instability.
Hecht et al. performed thermal capsulorrhaphy and biomechanical analysis of the capsule in a sheep model. The authors found that the capsule was weakest at the 2-3 week post-operative timepoint, leading to the highest rate insufficiency, attenuation and mechanical failure at this time.
Incorrect answers:
Question 20
During a revision total knee arthroplasty (TKA), there is difficulty gaining exposure and a tibial tubercle osteotomy (TTO) is performed. The final components are stable and include a stemmed tibial component that bypasses the osteotomy site. The tibial tubercle is reattached to the osteotomy site with multiple cerclage wires. Following closure of the arthrotomy, the knee is flexed to 90 degrees, and there is no observed displacement of the TTO. What is the best next step in postsurgical rehabilitation?
Explanation
TTO is a recognized technique for improving exposure when performing TKA in a stiff knee. TTO has been reported to enhance surgical exposure and not adversely affect outcomes after TKA, but there is a 5% complication rate. The postsurgical routine following TTO
includes full weight-bearing activity and range of motion as tolerated. Caution should be exercised when manipulation is performed to improve knee flexion following a TTO.
Question 21
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior-stabilized TKA without evidence of component loosening. What is the most likely cause of this patient's pain?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
Question 22
Figure 2 shows the radiograph of a 72-year-old woman who reports pain after a fall. History includes several years of increasing thigh pain and limb shortening. Management consisting of an extensive work-up for infection reveals normal laboratory studies, a positive bone scan, and a negative hip aspiration. What is the most likely etiology of this complication?
Explanation
REFERENCES: Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242.
Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Kelley SS: Periprosthetic femoral fractures. J Am Acad Orthop Surg 1994;2:164-172.
Question 23
A 22-year-old volleyball player reports the insidious onset of superior and posterior shoulder pain. Radiographs are normal. An MRI scan is shown in Figure 25. What is the most specific physical examination finding?
Explanation
REFERENCES: Romeo AA, Rotenberg DD, Bach BR Jr: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
Question 24
In the anterior cruciate ligament-deficient knee, what structure provides an important secondary restraint to anterior tibial translation? Review Topic
Explanation
Question 25
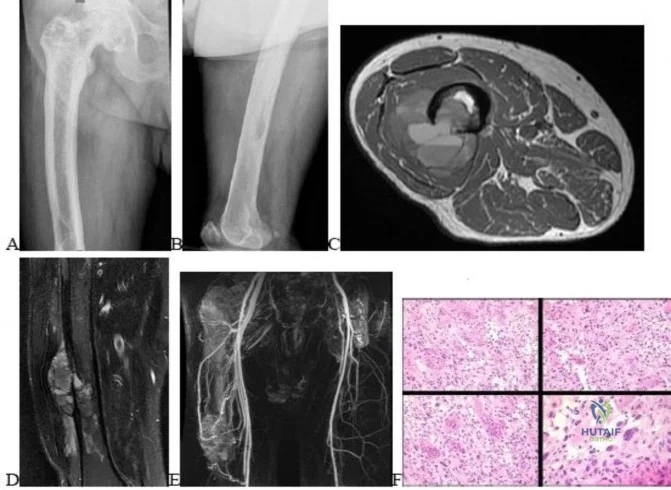
..Figures 112a and 112b are the anteroposterior and lateral radiographs of a 65-year-old man who has a significant history of tobacco abuse and a 6-week history of right thigh pain. Axial and sagittal MRI scans are seen in Figures 112c and 112d. His MR angiogram is shown in Figure 112e. A biopsy of a lesion is shown in Figure 112f. What is the most likely diagnosis?
Explanation
Figures 113a and 113b are the radiographs of a 68-year-old-man who has increasing pain in his left groin with weight-bearing activities and a Trendelenburg gait. Radiographs reveal a lytic lesion of the greater trochanter. An initial diagnosis of adenocarcinoma of the lung was made 1 year before this presentation. His lung cancer treatment consisted of partial lobectomy and postsurgical radiation therapy.


Question 26
An 82-year-old woman reports activity-related knee pain. History reveals that she underwent total knee arthroplasty 16 years ago. AP and lateral radiographs and a bone scan are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
well-defined borders. Joint space narrowing medially is consistent with polyethylene wear.
The most likely diagnosis is particle-mediated osteolysis. Metastatic tumors and primary sarcomas adjacent to an arthroplasty are extremely rare. In addition, malignant tumors and infection would more likely reveal a destructive lesion with poorly defined borders and increased uptake on a bone scan. Stress shielding with massive bone loss has not been described in knee arthroplasty literature, although this entity has been observed in fully porous-coated femoral implants in total hip arthroplasty.
REFERENCES: Robinson EJ, Mulliken BD, Bourne RB, et al: Catastrophic osteolysis in total knee replacement: A report of 17 cases. Clin Orthop Relat Res 1995;321:98-105.
Archibeck MJ, Jacobs JJ, Roebuck KA, et al: The basic science of periprosthetic osteolysis. Instr Course Lect 2001;50:185-195.
Bugbee WD, Culpepper WJ, Engh CA Jr, et al: Long-term clinical consequences of stress-shielding after total hip arthroplasty without cement. J Bone Joint Surg Am 1997;79:1007-1012.
Question 27
Figure 45 shows the radiograph of a 2-year-old patient who has progressive lumbar scoliosis as the result of hemivertebra. Examination reveals no associated cutaneous lesions, and an MRI scan shows no associated intraspinal anomalies. Treatment should consist of
Explanation
REFERENCE: Callahan BC, Georgopoulos G, Eilert RE: Hemivertebral excision for congenital scoliosis. J Pediatr Orthop 1997;17:96-99.
Question 28
78A B Figures 78a and 78b are the emergency department radiographs of an 83-year-old woman who tripped and braced herself against a wall; this was followed by shoulder pain. Which intervention would provide optimal treatment for this patient?

Explanation
Low-energy fractures in elderly patients typically are treated with nonsurgical care that involves early immobilization followed by early rehabilitation/therapy, especially when proximal humerus and distal humerus fractures are involved. Physical therapy should be initiated within the first 2 weeks. If surgery is needed ORIF is preferred for most fractures, but replacement may improve outcomes for unreconstructable fractures. The use of hemiarthroplasty vs reverse shoulder replacement is currently being debated.
For treatment of distal radius fractures in elderly patients, cast immobilization for about 6 weeks will allow for optimal fracture healing. This should be followed by aggressive therapy to improve range of motion and function. Moderately displaced fractures in elderly patients will result in satisfactory outcomes even though reduction may not be "anatomic."
RECOMMENDED READINGS
Arora R, Lutz M, Deml C, Krappinger D, Haug L, Gabl M. A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J Bone Joint Surg Am. 2011 Dec 7;93(23):2146-53. doi: 10.2106/JBJS.J.01597. PubMed PMID: 22159849. View Abstract
at PubMed
Tejwani NC, Liporace F, Walsh M, France MA, Zuckerman JD, Egol KA. Functional outcome following one-part proximal humeral fractures: a prospective study. J Shoulder Elbow Surg. 2008 Mar-Apr;17(2):216-9. doi: 10.1016/j.jse.2007.07.016. Epub 2008 Jan 22. PubMed
PMID: 18207430. View Abstract at PubMed
Solberg BD, Moon CN, Franco DP, Paiement GD. Locked plating of 3- and 4-part proximal humerus fractures in older patients: the effect of initial fracture pattern on outcome. J Orthop Trauma. 2009 Feb;23(2):113-9. doi: 10.1097/BOT.0b013e31819344bf. PubMed PMID:
Question 29
What factor induces myofibrillar muscle protein synthesis (MPS)? Review Topic
Explanation
Question 30
What are the most likely symptoms and examination findings related to the mass in zone 2 of Guyon’s canal seen in Figure 17?
Explanation
REFERENCES: Kuschner SH, Gelberman RH, Jennings C: Ulnar nerve compression at the wrist. J Hand Surg Am 1988;13:577-580.
Posner MA: Compressive neuropathies of the ulnar nerve at the elbow and wrist. Instr Course Lect 2000;49:305-317.
Question 31
A 20-year-old man involved in a motor vehicle accident is brought to the emergency department with a C6-7 unilateral facet dislocation. His neurologic examination reveals a focal left-sided C7 nerve root palsy. He is awake and cooperative with questioning and has no other obvious traumatic injuries. What is the most appropriate treatment at this time? Review Topic
Explanation
Question 32
Figure 1 is the MR image of a 55-year-old man who sustained an acute traumatic injury to his right shoulder with loss of active range of motion. He was initially evaluated by his primary care physician and treated with physical therapy without success. He was referred to an orthopaedist for surgical consultation 8 weeks after sustaining the injury. The orthopaedic surgeon performs a successful arthroscopic repair but notes poor tendon quality at the repair site. The treating surgeon keeps the patient in a sling full time for 6 weeks without formal therapy. One year after surgery, in comparison to early therapy, this rehabilitation program will likely result in
Explanation
A. better glenoid exposure than with stemmed prostheses.
B. reliable use in four-part proximal humerus fracture reconstruction.
C. use in proximal humeral malunion without the need for an osteotomy. D. improved long-term survivorship profile.
Question 33
Which Morton neuroma histology is most common?
Explanation
Morton neuroma is a compressive neuropathy of the interdigital nerves of the forefoot that most commonly is noted in the third web space. Perineural fibrosis is commonly noted on microscopic examination of resected tissue. This accounts for the relatively higher failure rate of neuroma decompression by transection of the intermetatarsal ligament as opposed to resection. Wallerian degeneration is seen following axonal transection in the distal part of the nerve. Distal axonopathy is degeneration of the axon and myelin and is associated with "stocking-glove" distribution neuropathy. Segmental demyelination is characterized by breakdown of myelin with an intact axon
and is associated with lead poisoning and hereditary sensory motor neuropathy.
RECOMMENDED READINGS
Akermark C, Crone H, Saartok T, Zuber Z. Plantar versus dorsal incision in the treatment of primary intermetatarsal Morton's neuroma. Foot Ankle Int. 2008 Feb;29(2):136-41. doi: 10.3113/FAI.2008.0136. PubMed PMID: 18315967.View Abstract at PubMed
Ha'Eri GB, Fornasier VL, Schatzker J. Morton's neuroma--pathogenesis and ultrastructure. Clin Orthop Relat Res. 1979 Jun;(141):256-9. PubMed PMID: 477115. View Abstract at PubMed
Graham CE, Graham DM. Morton's neuroma: a microscopic evaluation. Foot Ankle. 1984 Nov-Dec;5(3):150-3. PubMed PMID: 6519606. View Abstract at PubMed
Question 34
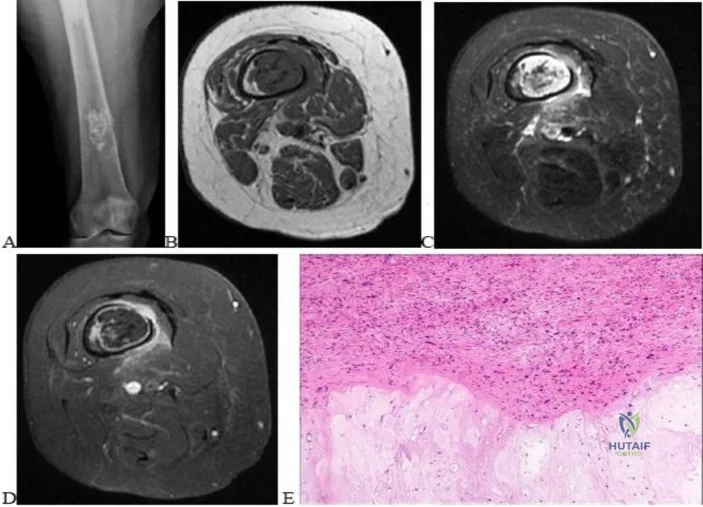
A 35-year-old patient has right hip pain. Figures 34a and 34b show the coronal MRI scan and the biopsy specimen. What is the most likely diagnosis?
Explanation
REFERENCES: Arlet J: Nontraumatic avascular necrosis of the femoral head: Past, present, and future. Clin Orthop 1992;277:12-21.
Stulberg BN, Bauer TW, Belhobek GH, Levine M, Davis A: A diagnostic algorithm for osteonecrosis of the femoral head. Clin Orthop 1989;249:176-182.
Question 35
A 17-year-old high school football player is seen for follow-up after sustaining an injury 3 days ago. He reports that he tackled a player, felt numbness throughout his body, and could not move for approximately 15 seconds. A spinal cord injury protocol was initiated on the field. Evaluation in the emergency department revealed a normal neurologic examination and full painless neck motion. He states that he has no history of a similar injury. An MRI scan of the cervical spine is normal. During counseling, the patient and his family should be informed that he has sustained
Explanation
REFERENCES: Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Odor JM, Watkins RG, Dillin WH, et al: Incidence of cervical spinal stenosis in professional and rookie football players. Am J Sports Med 1990;18:507-509.
Torg JS, Naranja RJ Jr, Palov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Vaccaro AR, Watkins B, Albert TJ, et al: Cervical spine injuries in athletes: Current return-to-play criteria. Orthopedics 2001;24:699-703.
Question 36
- A 32-year-old man has swelling of the knee as a result of falling with the knee flexed and his foot in plantar flexion. A Lachman’s test reveals an apparent increase in anterior translation. Passive external tibial rotation at 30 degrees and 90 degrees is equal to the contralateral side, and the quadriceps active test is positive on the affected side. The neurovascular examination is normal. Treatment should consist of
Explanation
Question 37
An obese 62-year-old man reports a 10-year history of progressive flatfoot deformity and a 3-month history of a painful callus along the plantar medial midfoot that has not improved with custom shoe wear, pedorthics, and callus care. There is no hindfoot motion, but functional ankle motion remains. He does not have diabetes mellitus. Radiographs are shown in Figures 27a and 27b. What is the best surgical option at this point?
Explanation
REFERENCES: Johnson JE, Yu JR: Arthrodesis techniques in the management of Stage II and III acquired adult flatfoot deformity. Instr Course Lect 2006;55:531-542.
Pinney SJ, Lin SS: Current concept review: Acquired adult flatfoot deformity. Foot Ankle Int 2006;27:66-75.
Question 38
What is the most common cause for late revision (> 2 years post op) total knee arthroplasty?
Explanation
REFERENCE: Sharkey PF, Hozack WJ, Rothman RH, et al: Insall Award paper: Why are total knee arthroplasties failing today? Clin Orthop Relat Res 2002;404:7-13.
Question 39
Among the options listed below, what is the best treatment for the complication shown in Figure 10c?
Explanation
Proximal femur fractures can be treated using a variety of implants including intramedullary nails, blade plates, and locking plates (now precontoured proximal femur plates). The comminution and lack of medial cortical support may predispose these fractures to nonunion.
The recent popularity of locking plates for proximal femur treatment has increased their use for this fracture; however, a disproportionately high rate of failure of these plates, including early implant failure with plate and screw breakage, cut out with varus collapse, and nonunion have been reported.?
Malreduction predisposes these fractures to failure. The initial postoperative radiographs do not reveal a varus malreduction because the tip of the greater trochanter is below the center of the femoral head.
Once failure occurs, the best fixation method among the options detailed is an intramedullary nail (second generation with screws into the femoral head) and restoration of alignment. THA is usually not recommended for treatment of subtrochanteric femur fractures in young patients.
RECOMMENDED READINGS
Wirtz C, Abbassi F, Evangelopoulos DS, Kohl S, Siebenrock KA, Krüger A. High failure rate of trochanteric fracture osteosynthesis with proximal femoral locking compression plate.
Injury. 2013 Jun;44(6):751-6. doi: 10.1016/j.injury.2013.02.020. Epub 2013 Mar 21. PubMed PMID: 23522837. View Abstract at PubMed
Floyd JC, O'Toole RV, Stall A, Forward DP, Nabili M, Shillingburg D, Hsieh A, Nascone JW. Biomechanical comparison of proximal locking plates and blade plates for the treatment of comminuted subtrochanteric femoral fractures. J Orthop Trauma. 2009 Oct;23(9):628-33. doi: 10.1097/BOT.0b013e3181b04835. PubMed PMID: 19897983. View Abstract at PubMed Glassner PJ, Tejwani NC. Failure of proximal femoral locking compression plate: a case series. J Orthop Trauma. 2011 Feb;25(2):76-83. doi: 10.1097/BOT.0b013e3181e31ccc.
PubMed PMID: 21245709. View Abstract at PubMed
Question 40
A 14-year-old girl has a painful hallux valgus deformity that has not responded to shoe modifications. Figure 21 shows a standing AP radiograph. What is the most appropriate surgical procedure?
Explanation
and a congruent metatarsophalangeal joint with an abnormal distal metatarsal articular
angle. Correction of both of these abnormalities requires a proximal and distal first
metatarsal osteotomy.
REFERENCES: Coughlin M: Juvenile bunions, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 297-339.
Peterson HA, Newman SR: Adolescent bunion treated with double osteotomy and longitudinal pin fixation of the first ray. J Pediatr Orthop 1993;13:80-84.
Question 41
The swelling pressure in cartilage is predominantly due to the association of exchangeable water with which of the following substances? Review Topic
Explanation
Question 42
A 2-year-old girl has had a swollen right knee for the past 7 weeks. There is no history of significant trauma, and she has not had a fever or been ill. Her parents report that she is stiff in the morning but otherwise does not report pain. A CBC count and erythrocyte sedimentation rate are normal. Treatment with naproxen at appropriate doses for the past 2 weeks has resulted in some improvement. Radiographs show only soft-tissue swelling. Examination reveals a healthy-appearing child with a warm and swollen right knee that is only slightly tender but lacks full extension by 20 degrees. What is the next most appropriate step in management?
Explanation
REFERENCES: Wolf MD, Lichter PR, Ragsdale CG: Prognostic factors in the uveitis of juvenile rheumatoid arthritis. Ophthalmology 1987;94:1242.
Cassidy JT, Petty RE: Textbook of Pediatric Rheumatology. Philadelphia, PA, WB Saunders, 2001, p 220.
Chalom ED, Goldsmith DP, Koehler MA, et al: Prevalence and outcome of uveitis in a regional cohort of patients with juvenile rheumatoid arthritis. J Rheumatol 1997;24:2031-2034.
Question 43
A 56-year-old male sustains a Type IIIB open, comminuted tibial shaft fracture distal to a well-fixed total knee arthroplasty that is definitively treated with a free flap and external fixation. Nine months after fixator removal, he presents with a painful oligotrophic nonunion. Laboratory workup for infection is negative. Passive knee range of motion is limited to 15 degrees. What is the most appropriate treatment for his nonunion?

Explanation
Wiss et al reported a series of fifty tibial non-unions with a similar clinical scenario. He reported that, with compression plating, 92% of the nonunions healed without further intervention. In their study, 39/50 patients, had autogenous bone grafting in addition to compression plating.
Question 44
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. If the patient chooses surgical reconstruction, he should be advised that, when compared with a transtibial technique, the tibial inlay technique has been shown to provide

Explanation
appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used. Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
Question 45
A 60-year-old woman reports a painful hip arthroplasty after undergoing surgery 18 months ago. Radiographs show stable cementless implants without signs of ingrowth. Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h. Management should now consist of
Explanation
REFERENCES: Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
McAuley JP, Moreau G: Sepsis: Etiology, prophylaxis, and diagnosis, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 1295-1306.
Question 46
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 123.
Question 47
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure A. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion? Review Topic

Explanation
Question 48
A patient reports persistent anterior shoulder pain following a forceful external rotation injury to the shoulder. An MRI scan is shown in Figure 4. The patient remains symptomatic despite 3 months of nonsurgical management. Treatment should now consist of Review Topic
Explanation
Question 49
Figures 7a and 7b show the radiographs of a 51-year-old woman who injured her left leg after falling off a stepladder. Surgical reconstruction is performed with a compression screw and side plate; the postoperative radiograph is shown in Figure 7c. Following gradual progression of weight bearing, she reports that she slipped again and placed full weight on the extremity. She now notes a new onset of increased pain in her left thigh and hip region. Follow-up radiographs are shown in Figures 7d and 7e. Reconstruction should consist of
Explanation
REFERENCES: Bridle SH, Patel AD, Bircher M, Calvert PT: Fixation of intertrochanteric fractures of the femur: A randomized prospective comparison of a gamma nail and dynamic hip screw. J Bone Joint Surg Br 1991;73:330-334.
DeLee JC: Fractures and dislocations of the hip, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1659-1825.
Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Sanders RW, Regazzoni P: Treatment of subtrochanteric femur fractures using the dynamic condylar screw. J Orthop Trauma 1989;3:206-213.
Question 50
After reduction and pinning, the radial pulse is absent by both palpation and Doppler. Capillary refill in the fingers appears normal. What is the most likely explanation?
Explanation
This is a classic extension-type supracondylar elbow fracture typically caused by a fall on an outstretched hand. The medial comminution of this fracture renders it predictably unstable and susceptible to varus malunion. Extra attention with fixation is required. In general, use of lateral-entry pins alone is effective for most supracondylar humeral fractures. The best technique for fixation with lateral-entry pins only involves maximization of pin separation at the fracture site, engaging sufficient bone in both the proximal segment and the distal fragment and using more than 2 lateral entry pins (if needed) for stability. In the presence of medial comminution, medial fixation also may be necessary.
Brachial artery spasm is the usual cause of absence of radial pulse if capillary refill is normal. Close postsurgical monitoring is warranted after reduction and pinning.
Question 51
Figure 12 shows the radiograph of a patient who has anterior knee pain. History reveals a femoral fracture at age 5 years. What is the most likely cause of the deformity?
Explanation
REFERENCES: Hresko MT, Kasser JR: Physeal arrest about the knee associated with non-physeal injuries of the lower extremity. J Bone Joint Surg Am 1989;71:698-703.
Bowler JR, Mubarak SJ, Wenger DR: Tibial physeal closure and genu recurvatum after femoral fracture: Occurrence without a tibial traction pin. J Pediatric Orthop 1990;10:653-657.
Question 52
A minimally invasive plate osteosynthesis is seen in Figure 15. The resultant fracture healing can best be attributed to a fixation construct that was

Explanation
Question 53
After making a tackle, a football player is found prone and unconscious without spontaneous respirations. Initial management should consist of
Explanation
REFERENCES: McSwain NE, Garnelli, RL: Helmet removal from injured patients. Bull of Am Coll Surg 1997;82:42-44.
Vegso JJ: Field evaluation and management of head and neck injuries. Post Grad Adv Sport Med 1987;10:2-10.
Question 54
A 12-year-old boy falls from a bicycle. A radiograph of his injured shoulder is shown in Figure 41. What is the optimal method of treatment?
Explanation
REFERENCES: Bishop JY, Flatow EL: Pediatric shoulder trauma. Clin Orthop Relat Res 2005;432:41-48.
Question 55
A 12-year-old girl who is 3 months postmenarchal undergoes full-time brace treatment for scoliosis. The posteroanterior radiograph (Figure A ) taken at that time reveals a right thoracic curve measures 28 degrees, and the left lumbar curve measures 23 degrees. At age 15, after 3 years of bracing, a repeat posteroanterior radiograph is obtained, now revealing a right thoracic curve measuring 11 degrees and the left lumbar curve measuring 19 degree, and Risser 4. Which statement best represents the indicated course of action in this patient? Review Topic

Explanation
Curves <25° can be treated with observation, while flexible curves from 25° to 45° in skeletally immature patients (Risser 0, 1, 2) should be treated with bracing. Bracing success is most commonly defined as <5° curve progression and failure is 6° or more curve progression at orthotic discontinuation (skeletal maturity), absolute progression to >45° either before or at skeletal maturity, or discontinuation in favor of surgery. Skeletal maturity is defined Risser sign 4, <1cm change in height over 2 visits 6 months apart, 2 years postmenarchal.
Richards et al. attempted to define parameters for future AIS bracing studies. Outcome measures should include patients with (1) <5° curve progression vs >6° progression at maturity, (2) curves exceeding 45° at maturity, or those who have had surgery recommendation/undergone.
Negrini et al. performed a Cochrane systematic review. Basing conclusions on 2
studies, they found that (1) a brace treated curve progression (74% success) better than observation (34% success) and electrical stimulation (33% success), and (2) a rigid brace is more successful than an elastic one (SpineCor) at curbing curve progression.
A
is
a
standing
PA
radiograph
showing.
Incorrect
Question 56
A 19-year-old man was struck by a car and is seen in the emergency department with a grade IIIC open distal tibia and fibula fracture. Examination reveals that the toes are cool and dusky with a sluggish capillary refill. Angiography reveals a lesion in the posterior tibial artery amenable to repair. There is no sensation on the plantar aspect of the foot, and he is unable to flex his toes. A clinical photograph and radiograph are shown in Figures 2a and 2b. What is the next most appropriate step in management?
Explanation
REFERENCES: Bosse MJ, McCarthy ML, Jones AL, et al: The insensate foot following severe lower extremity trauma: An indication for amputation? J Bone Joint Surg Am 2005;87:2601-2608.
Lange RH, Bach AW, Hansen ST Jr, et al: Open tibial fractures with associated vascular injuries: Prognosis for limb salvage. J Trauma 1985;25:203-208.
Mackenzie EJ, Bosse MJ, Kellam JF, et al: Factors influencing the decision to amputate or reconstruct after high-energy lower extremity trauma. J Trauma 2002;52:641-649.
Baumgaertner MR, Tornetta P III (eds): Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 65-74.
Question 57
Which nerve is most commonly injured after total knee arthroplasty?
Explanation
The tibial or peroneal nerves usually are not injured during total knee arthroplasty. Incidence of peroneal nerve damage is highest in knees with a valgus deformity and an associated flexion contracture attributable to nerve stretch. This nerve injury occurs in as many as 9% of patients undergoing knee arthroplasty. Tibial nerve injury is a rare occurrence and usually an iatrogenic transection injury. The infrapatellar branch of the saphenous nerve and its nerve plexus is commonly injured after the medial parapatellar approach, and altered sensation attributable to injury is reported in up to 70% of cases. Injury typically manifests as numbness inferior to the patella. The sartorial branch of the saphenous nerve provides sensation distal to the knee and is uncommonly injured with a medial parapatellar approach. These concepts are illustrated in video 57, “Selective Exposures in Orthopaedic Surgery: The Knee, 2nd Edition.”
RECOMMENDED READINGS
Clarke HD, Bush-Joseph CA, Wolf BR. Selective Exposures in Orthopaedic Surgery: The Knee, 2nd Edition [DVD]. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2012.
Hunter LY, Louis DS, Ricciardi JR, O'Connor GA. The saphenous nerve: its course and importance in medial arthrotomy. Am J Sports Med. 1979 Jul-Aug;7(4):227-30. PubMed PMID: 474860.View Abstract at PubMed
Mistry D, O'Meeghan C. Fate of the infrapatellar branch of the saphenous nerve post total knee arthroplasty. ANZ J Surg. 2005 Sep;75(9):822-4. PubMed PMID: 16174002.View Abstract at PubMed
Schinsky MF, Macaulay W, Parks ML, Kiernan H, Nercessian OA. Nerve injury after primary total knee arthroplasty. J Arthroplasty. 2001 Dec;16(8):1048-54. PubMed PMID: 11740762.View Abstract at PubMed
Question 58
A 58-year-old man with insulin-dependent diabetes mellitus underwent primary total knee arthroplasty (TKA). A full-thickness skin slough measuring 3 cm by 4 cm developed, with postsurgical exposure of the patellar tendon. No change is observed in the appearance of the wound after 2 weeks of wet-to-dry dressing changes. What is the best next treatment step for the soft-tissue defect?
Explanation
If wound healing does not occur and deep soft tissues such as the patellar tendon are exposed following TKA, local rotational flap is the procedure of choice. The procedure should be performed relatively early after the recognition of a soft-tissue wound-healing problem. In the setting of TKA, the gastrocnemius muscle is an excellent source of flaps for wound coverage of the proximal tibia.
Question 59
In an acute closed boutonniere injury, what is the most appropriate splinting technique for the proximal interphalangeal joint?
Explanation
REFERENCES: Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.
Lovet WL, McCalla MA: Management and rehabilitation of extensor tendon injuries. Orthop Clin North Am 1983;14:811-826.
Question 60
A 55-year-old woman undergoes an anterior cervical diskectomy and fusion at C5-C6 through a left-sided approach. One year later, she requires an anterior cervical diskectomy and fusion on another level. Which of the following is considered a contraindication to performing a right-sided approach for the revision procedure?
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 387-394.
Edwards CC II, Riew KD, Anderson PA, et al: Cervical myelopathy: Current diagnostic and treatment strategies. Spine J 2003;3:68-81.
Question 61
What is the most common complication requiring reoperation after dorsal plating for a distal radius fracture?
Explanation
REFERENCES: Rozental TD, Beredjiklian PK, Bozentka DJ: Functional outcome and complications following two types of dorsal plating for unstable fractures of the distal part of the radius. J Bone Joint Surg Am 2003;85:1956-1960.
Kambouroglou GK, Axelrod TS: Complications of the AO/ASIF titanium distal radius plate system (pi plate) in internal fixation of the distal radius: A brief report. J Hand Surg Am 1998;23:737-741.
Question 62
Which of the following findings is considered a contraindication for posterior decompression (with or without fusion) for myelopathy?
Explanation
REFERENCES: Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Malone DG, Benzel EC: Laminotomy and laminectomy for spinal stenosis causing radiculopathy or myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 817-823.
Question 63
Which of the following provocative tests would most likely be positive in a patient with medial epicondylitis? Review Topic
Explanation
Medial epicondylitis is an overuse syndrome of the flexor-pronator mass. The pronator teres (PT) and flexor carpi radialis (FCR) are thought to be most affected with this condition. It is most common in the dominant arm and occurs with activities that require repetitive wrist flexion/forearm pronation. Patients are most tender over the origin of PT and FCR at the medial epicondyle. Resisting a patient with their fist clenched, wrist flexed and pronated can cause worsening of their pain. This maneuver can be used as a provocative test for this condition.
Cain et al. reviewed elbow injuries in throwing athletes. They comment that the common flexor-pronator muscle origin provides dynamic support to valgus stress in the throwing elbow, especially during early arm acceleration and help produce wrist flexion during ball release.
Amin et al. reviewed the evaluation and management of medial epicondylitis. They report that medial epicondylitis typically occurs in the fourth through sixth decades of life, the peak working years, and equally affects men and women. Physical therapy and rehabilitation is the main aspect of recovery from medial epicondylitis, once acute symptoms have been alleviated.
Illustration A shows a video of this provocative test for medial epicondylitis. Incorrect Answers:
Question 64
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured?
Explanation
REFERENCES: Schenck CD: Anatomy of the innervation of the upper extremity, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face, ed 2. St Louis, MO, Mosby-Year Book, 1991.
Hershman EB: Brachial plexus injuries. Clin Sports Med 1990;9:311-329.
Question 65
A 17-year-old basketball player and pole vaulter who has had anterior knee pain for the past 18 months now reports a recent inability to jump. Based on the MRI scan shown in Figure 11, management should consist of
Explanation
REFERENCES: Al-Duri ZA, Aichroth PM: Surgical aspects of patella tendonitis: Techniques and results. Am J Knee Surg 2001;14:43-50.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 218-219.
Question 66
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Explanation
REFERENCE: Kelly MA: Nonprosthetic management of the arthritic knee, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 245-249.
Question 67
A B C Figures 30a through 30c are the radiograph and MR images of a 54-year-old woman who has severe leg pain with walking. Her treatment has included 12 weeks of physical therapy, anti-inflammatory medications, and narcotic pain relievers, and she is interested in surgery. Minimally invasive transforaminal lumbar interbody fusion (MIS TLIF) is recommended. When compared with open TLIF, MIS TLIF is associated with

Explanation
MIS TLIF involves a steep learning curve but is associated with similar longterm outcomes as open TLIF, arguably comparable or possibly lower complication rates, and equivalent fusion rates. The major distinguishing feature comparing open to minimally invasive surgery for this and other spinal diagnoses has been shorter hospital stays.
RECOMMENDED READINGS
Peng CW, Yue WM, Poh SY, Yeo W, Tan SB. Clinical and radiological outcomes of minimally invasive versus open transforaminal lumbar interbody fusion. Spine (Phila Pa 1976). 2009 Jun 1;34(13):1385-9. doi: 10.1097/BRS.0b013e3181a4e3be. PubMed PMID: 19478658. View
Abstract at PubMed
Lee KH, Yue WM, Yeo W, Soeharno H, Tan SB. Clinical and radiological outcomes of open versus minimally invasive transforaminal lumbar interbody fusion. Eur Spine J. 2012 Nov;21(11):2265-70. doi: 10.1007/s00586-012-2281-4. Epub 2012 Mar 28. PubMed PMID:
Question 68
A 28-year-old anesthesia resident has aching pain in his dominant right forearm after injuring it while playing basketball 1 week ago. He reports that he is unable to perform regional anesthesia that requires manipulation of a needle. Examination reveals that he is unable to flex the interphalangeal joint of the thumb, and flexion of the distal interphalangeal joint of the index finger is weak. Management should consist of
Explanation
REFERENCES: Miller-Breslow A, Terrono A, Millender LH: Nonoperative treatment of anterior interosseous nerve paralysis. J Hand Surg Am 1990;15:493-496.
Stern PJ, Fassler PR: Anterior interosseous nerve compression syndrome, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, 1991, vol 2, pp 983-1002.
Question 69
Figure 6 shows the lateral radiograph of a 22-year-old woman who has painful Scheuermanns’s kyphosis in the middle and lower thoracic spine. When planning surgical correction using instrumentation, the distal aspect of the instrumentation should ideally extend to the
Explanation
REFERENCES: Lowe TG: Scheuermann’s disease. Orthop Clin North Am 1999;30:475-487.
Lenke LG: Kyphosis of the thoracic and thoracolumbar spine in the pediatric patients: Prevention and treatment of surgical complications. Instr Course Lect 2004;53:501-510.
Question 70
A patient who underwent total knee arthroplasty 6 years ago now reports knee pain for the past 3 days following dental surgery. Cultures of the aspirate are positive for Staphylococcus epidermidis. Management should consist of
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 323-337.
Goldman RT, Scuderi GR, Insall JN: 2-stage reimplantation for infected total knee replacement. Clin Orthop 1996;331:118-124.
Question 71
..Figures 87a through 87e are the radiograph, MRI scans, and biopsy specimen of an 83-year-old woman who is experiencing pain in her distal thigh with activity and at night. She has undergone total hip arthroplasty for hip osteoarthritis. The most appropriate treatment is
Explanation
Figures 88a and 88b are the radiographs of a 70-year-old woman with a remote history of localized renal cell carcinoma. She has insidious onset of right shoulder pain that worsens with any activity and at night. She appears otherwise healthy.


Question 72
Kyphosis from a vertebral osteoporotic compression fracture often results in progressive kyphosis due to Review Topic
Explanation
Question 73
The MRI scan shown in Figure 33 reveals the sequelae of an acute traumatic anteroinferior shoulder dislocation. The image reveals the typical separation of what two commonly injured structures? Review Topic

Explanation
Question 74
A patient undergoes excision of a 3- x 3-cm soft-tissue sarcoma. The final histology results show tumor at the surgical margin. The surgical procedure performed is classified as
Explanation
REFERENCE: Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980;153:106-120.
Question 75
Which of the following is considered the most useful screening method for the evaluation of protective foot sensation in a patient with diabetes mellitus?
Explanation
REFERENCES: Pinzur MS, Shields N, Trepman E, Dawson P, Evans A: Current practice patterns in the treatment of Charcot foot. Foot Ankle Int 2000;21:916-920.
Smith KD, Emerzian GJ, Petrov O: A comparison of calibrated and non-calibrated 5.07 nylon monofilaments. Foot Ankle Int 2000;21:852-855.
Question 76
below depict the radiographs obtained from a year-old woman with a painful total knee arthroplasty. She describes an uneventful recovery with no wound-healing issues and was pain free for the first 10 years. Although reporting no trauma or inciting event, she now describes pain in the entire knee that is most severe with her first few steps. She has begun to notice night pain and, more recently, constant swelling. What is the most appropriate work-up at this time?
Explanation
An evaluation of the painful total knee must be supported by an understanding of the potential etiologies of pain. They may include, aseptic loosening, infection, osteolysis, gap imbalance, referred pain, stiffness, and complex regional pain syndrome. In this case, the patient demonstrates start-up pain and had no prior history of infections. Her radiographs show subsidence of the tibia, indicating a loose prosthesis. Knowing that the prosthesis is already loose precludes the need for a bone scan. It is, however, important to rule out infection in this case; therefore, CRP and ESR testing is essential. Aspiration is also recommended when going into knee arthroplasty, and infection is a concern.
Question 77
In the United States, groups at risk for community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) within the pediatric and adolescent populations include
Explanation
CA-MRSA is a growing problem in the United States. Groups at risk for CA-MRSA include athletes in contact sports and children in daycare. Tennis players, golfers, and runners are at lowest risk because their sports do not require close contact with teammates or competitors. Outbreaks have been noted in Alaskan native, Native American, and Pacific Islander minority populations.

CLINICAL SITUATION FOR QUESTIONS 64 THROUGH 68
Figures 64a through 64d are the radiographs of an 11-year-old boy with a prolonged history of activity-related ankle pain. An examination is notable for restricted subtalar motion and moderate pes planovalgus.
Question 78
What is the most common type of malalignment after intramedullary nailing of distal 1/3 tibia fractures?

Explanation
McKee et al randomized 85 patients undergoing intramedullary tibial nailing using manual traction with the leg draped free versus standard fracture table positioning and traction. They found that manual traction is an effective technique that can save a significant amount of time without sacrificing the quality of reduction or fixation of tibial shaft fractures.
Question 79
A 56-year-old man has a chief complaint of leg weakness and inability to walk. Examination reveals 5 out of 5 motor strength in all lower extremity muscle groups tested and normal sensation to light touch in both lower extremities. The patient is slow in getting up from a seated position and has an unsteady wide-based

Explanation
Question 80
A 24-year-old female soccer player has had lateral joint line pain and a recurrent effusion in the left knee after sustaining a twisting injury 6 weeks ago. She reports that symptoms worsen with athletic activities. MRI scans are shown in Figures 2a through 2c. What is the most likely diagnosis?
Explanation
REFERENCES: Jordan MR: Lateral meniscal variants: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:191-200.
Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 625-630.
Question 81
The addition of which of the following food supplements may lead to a decrease in neural tube defects?
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 111-122.
Lemke L, Dias L: Spina bifida, in Cramer KE, Scherl SA, Einhom TA (eds): Orthopaedic Surgery Essentials: Pediatrics. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 203-210.
Question 82
Which of the following is considered a risk factor for the development of low back pain?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 627-643.
Question 83
For patients undergoing a surgical procedure where the risk of requiring a transfusion is less than 10%, the International Committee of Effective Blood Usage suggests
Explanation
REFERENCES: Toy P, Beattie C, Gould S, et al: Transfusion alert: Use of autologous blood. National Heart, Lung, and Blood Institute Expert Panel on the use of autologous blood. Transfusion 1992;35:703-711.
Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 84
Figures 189a through 189d are the radiograph and MR images of the right hip of a 28-year-old woman who has had right hip pain for 3 years. The pain is felt in the groin area, is exacerbated by weight-bearing activities, and interferes with her activities of daily living. She has been seen several times and has attempted anti-inflammatory medications, physical therapy, and an intra-articular steroid injection with minimal relief. What is the most appropriate next step?
Explanation
Video 189 for reference
This patient has dysplasia with a lack of lateral femoral head coverage. The MR images do not demonstrate a labral tear. There is still preserved joint space and she is young, so it would be preferable to delay THA in her case. A Ganz periacetabular osteotomy can provide more adequate coverage of the femoral head and is a multiplanar correction of the dysplastic acetabulum. This osteotomy is an effective treatment for symptomatic dysplasia in prearthritic young adult hips. A femoral osteotomy is not likely to be effective in this scenario.
CLINICAL SITUATION FOR QUESTIONS 190 THROUGH 192
Eighteen years after undergoing right total hip arthroplasty (THA), a 79-year-old woman experiences several weeks of right groin pain. A hip examination reveals that she is walking with a mild limp with a walker. Hip radiographs reveal moderate polyethylene wear with well-fixed components and mild osteolysis in the greater trochanter. Analysis of a CT scan reveals that the acetabular component is osteointegrated in 49 degrees of abduction and 25 degrees of anteversion. Erythrocyte sedimentation rate and C-reactive protein findings are within defined limits.
Question 85
Diagnostic work-up concluded that the patient has metastatic lymphoma. He has no neurologic deficit.Based on these findings, what is the most appropriate management for this spinal condition?
Explanation
Patients with no prior diagnosis of cancer may present with vertebral lesions. After obtaining initial radiographs, the next most appropriate step is to obtain an MRI with gadolinium. To determine the primary site of the disease, a CT of the chest, abdomen, and pelvis is the next step in establishing a diagnosis. Radiation therapy is the first line of treatment in spinal metastatic disease from lymphoma because it is a highly radiosensitive tumor.
Question 86
Which of the following represents a contraindication for interspinous process decompression for the treatment of lumbar spinal stenosis? Review Topic
Explanation
Question 87
- A 25-yo man sustains the injury shown in Figures 29a and 29b as a result of high-speed trauma. Examination reveals diffuse weakness in the lower extremities that is slightly worse on the right side, and decreased rectal tone and sensation. A CT scan is shown in figures 29c and 29d. Definitive treatment of the injury to the spine is delayed because of a severe pulmonary contusion. At 15 days after the injury, the patient’s neurological status remains unchanged. Management should now consist of
Explanation
Question 88
Figures 52a and 52b show the radiographs of a left proximal femoral lesion noted serendipitously following minor trauma to the left hip. The patient has no thigh pain and is fully active without limitation. What is the most likely diagnosis of this bony lesion?
Explanation
REFERENCE: Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 89
A college basketball player is struck in the eye by a player’s hand while driving to the basket. Fluorescein evaluation reveals the injury shown in Figure 18. Management should consist of
Explanation
REFERENCES: Brucker AJ, Kozart DM, Nichols CW, et al: Diagnosis and management of injuries to the eye and orbit, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby-Year Book, 1991, pp 650-670.
Zagelbaum BM: Treating corneal abrasions and lacerations. Phys Sports Med 1997;25:38-44.
Question 90
A 12-year-old boy reports limping and chronic knee pain that is now inhibiting his ability to participate in sports. Clinical examination and radiographs of the knee are normal. Additional evaluation should include
Explanation
REFERENCES: Kocher MS, Bishop JA, Weed B, et al: Delay in diagnosis of slipped capital femoral epiphysis. Pediatrics 2004;113:322-325.
Matava MJ, Patton CM, Luhmann S, et al: Knee pain as the initial symptom of slipped capital femoral epiphysis: An analysis of initial presentation and treatment. J Pediatr Orthop 1999;19:455-460.
Question 91
A 17-year-old male lacrosse player sustains an ACL tear. Imaging reveals closed physes and you recommend a transphyseal ACL reconstruction. His mother asks whether a “cadaver tendon” can be used to reconstruct his ACL instead of using his own tendon. What is the most appropriate response regarding the use of allograft compared to autograft for ACL reconstruction in an active adolescent? Review Topic
Explanation
The incidence of anterior cruciate ligament (ACL) injuries in adolescent athletes has significantly increased over the recent years, now comprising 24.5% of all ligamentous knee injuries in high school athletes. In skeletally mature adolescents, transphyseal ACLR is often performed, similar to adult patients. Proposed advantages of allograft reconstruction in patients of all ages include lack of donor-site morbidity, absence of size limitation, preservation of knee flexor/extensor mechanism, less risk of postoperative knee stiffness/pain and cosmetic appearance. Benefits of autografts include strong structural and fixation properties as well as optimal biologic incorporation.
Kraeutler et al. performed a meta-analysis comparing bone-patellar tendon-bone (BPTB) autograft to allograft for ACLR. Patients who underwent ACLR with BPTB autograft demonstrated lower rates of graft rupture, lower levels of knee laxity, improved single-legged hop test results and were more satisfied postoperatively compared to ACLR with BPTB allograft. The authors therefore recommended BPTB
autograft
ACLR,
particularly
in
young
active
patients.
Engelman et al. performed a case-control study comparing ACLR in an adolescent cohort using autograft or allograft. Postoperative knee laxity and use of allograft were significantly related to graft failure and need for revision surgery. There was no difference in functional outcome scores, knee range of motion, infection or growth disturbance. There was no difference in graft survival between low-dose (<2 Mrad) gamma-irradiated allografts and nonirradiated allografts.
Pallis et al reported a prospective cohort study of 122 ACLR performed in cadets prior to matriculation at the United States Military Academy (USMA). Cadets who entered the USMA with an allograft ACLR were 7.7 times more likely to experience graft failure compared to BPTB and hamstring (HS) autograft groups. There was no significant difference in failure between the BPTB and HS autograft groups. The authors recommend autograft ACLR for young, active individuals.
Incorrect
Responses:
Question 92
- A 15-year-old girl has a thoracic kyphosis that causes mild pain. Examination reveals a sagittal curve measuring 55 degrees and wedging of the eighth through tenth vertebrae. The iliac apophyses are Risser 4. Management should include
Explanation
(2) with surgical fusion if >75o and Risser 3 or less, (3) with surgical fusion if >65o and Risser 4/5 if necessary or symptomatic. Posterior instrumentation, anterior release and interbody fusion is the treatment of choice for curves >75o, or those >55o on hyperextension. Other causes of kyphosis include trauma, infection, spondylitis, bone dysplasia, neoplasia, neurofibromatosis.
Question 93
A 23-year-old man sustained an injury to his left foot when a forklift rolled over it at work. Examination reveals marked swelling of the midfoot and forefoot, with tenderness to palpation over the medial hindfoot and dorsomedial forefoot. The distal dorsalis pedis pulse is audible on Doppler examination, and his sensation is intact to touch. Radiographs are shown in Figures 33a and 33b. Management should consist of
Explanation
REFERENCES: Resch S, Stenstrom A: The treatment of tarsometatarsal injuries. Foot Ankle 1990;11:117-123.
Schenck RC Jr, Heckman JD: Fractures and dislocations of the forefoot: Operative and nonoperative treatment. J Am Acad Orthop Surg 1995;3:70-78.
Kuo RS, Tejwani NC, Digiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Question 94
A 45-year-old man who underwent an ankle arthrodesis reports that for the first 6 years he had significant pain relief after the fusion healed. However, he now has increasing pain in the sinus tarsi. AP and lateral radiographs are shown in Figures 8a and 8b. What is the most likely cause of the patient’s symptoms?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 613-631.
Coester LM, Saltzman CL, Leupold J, Pontarelli W: Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am 2001;83:219-228.
Question 95
An 18-year-old man sustained closed humeral shaft and forearm fractures of his dominant arm in a motor vehicle accident. Neurovascular examination is intact, and his condition is stable. The best course of action for management of the injuries should be
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Bell MJ, Beachamp CG, Kellam JK, McMurtry RY: The results of plating humeral shaft fractures in patients with multiple injuries: The Sunnybrook experience. J Bone Joint Surg Br 1985;67:293-296.
Question 96
- What posterior pelvic ring injury is most commonly associated with neurologic compromise?
Explanation
associated with partial damage to the 5th lumbar root (5.9%). Zone 2-Sacral foramina region, outside of the sacral canal (i.e. distracters #3 and #4); associated with sciatica (28.4%) but rarely bladder dysfunction. Zone 3-Central sacral canal (AKA: Transverse Fx) (i.e. correct answer #2); associated with saddle anesthesia and loss of sphincter tone; neurologic damage (56.7%) and involvement of bowel, bladder, and sexual dysfunction (76.1%).
Question 97
A 61-year-old right-hand-dominant woman falls down the stairs, resulting in a left anteroinferior dislocation and noncomminuted greater tuberosity fracture. A closed glenohumeral reduction with intravenous sedation is performed in the emergency department. After reduction, the greater tuberosity fragment remains displaced by 2 mm. What is the most appropriate treatment?
Explanation
<3 mm in laborers and professional athletes can be treated successfully without surgery. Early passive range
of motion is important to avoid stiffness.
Question 98
Following its exit from the sciatic notch, the sciatic nerve passes between what two muscles?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 335-348.
Anderson JE (ed): Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Williams,
1978, Figure 4-34.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 99
-Video 3 shows the physical examination of the right hip of a 14-day-old full-term female infant. There is no history of breech presentation, she was born vaginally, and is the second child born to her mother. She is otherwise healthy and has been eating and gaining weight appropriately. What is the most appropriate course of action at this time?
Explanation
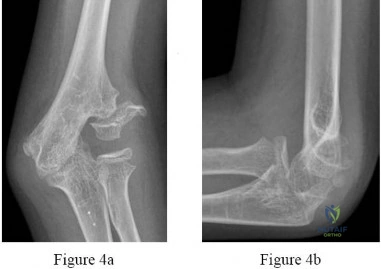
Question 100
An orthopaedic surgeon frequently uses hip and knee prostheses from a specific manufacturer. The surgeon becomes acquainted with the manufacturer’s representative who provides the support for these prostheses in the hospital. They develop a personal relationship outside of work through a common interest in sailing. Together they become interested in buying a sailboat. The manufacture’s representative suggests a partnership in a boat costing $200,000. The manufacture’s representative would purchase a 90% interest and the surgeon a 10% interest in the boat. There would be no restrictions on use of the boat by the surgeon. What should the orthopaedic surgeon do?
Explanation
partnership seems completely outside of the orthopaedic business relationship does not excuse it. Conflicts of interest should always be resolved and in the best interest of patient care, and in this case the best course clearly is to avoid the conflict of interest totally. An equal interest in the boat does not eliminate the conflict of interest.
