Orthopedic Surgery Board Review MCQs: Shoulder, Spine, Foot & Ankle | Part 167

Key Takeaway
This page presents Part 167 of a comprehensive Orthopedic Surgery Board Review series. It features 100 high-yield MCQs, mirroring OITE/AAOS exam format, designed for orthopedic surgeons and residents preparing for certification. Questions cover Deformity and Shoulder, offering interactive study and exam modes with detailed explanations.
About This Board Review Set
This is Part 167 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 167
This module focuses heavily on: Deformity, Shoulder.
Sample Questions from This Set
Sample Question 1: A 42-year-old woman who has had an 18-month history of severe low back pain is referred to your office for surgical evaluation. She reports that the pain initially began with right lower extremity pain and management consisted of oral analg...
Sample Question 2: Figures 1 and 2 display the radiographs obtained from a woman who had volar plating of the distal radius 8 months earlier. Two days ago, she noticed she could not actively extend her thumb. What is the most appropriate treatment that would ...
Sample Question 3: Figures 18a through 18c show the clinical photograph, radiograph, and CT scan of a 21-year-old man who reports persistent pain after injuring his right shoulder 4 months ago. What is the most likely factor associated with this patient’s dia...
Sample Question 4: The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports, and the surgeon and reha...
Sample Question 5: Figures 9a and 9b are the radiographs of a 19-year-old woman with a painful juvenile bunion. The pathologic findings associated with this deformityinclude a...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 42-year-old woman who has had an 18-month history of severe low back pain is referred to your office for surgical evaluation. She reports that the pain initially began with right lower extremity pain and management consisted of oral analgesics, nonsteroidal anti-inflammatory drugs, and muscle relaxants. She has seen a chiropractor as well as a pain management specialist and she is status-post epidural steroid injections. She has also completed exhaustive physical therapy, as she is a certified athletic trainer and runs a health fitness program at a community hospital. Currently, she denies lower extremity pain and her pain is isolated to her low back and is subjectively graded as 8/10, with 10 being the worst pain she has ever experienced. The pain is interfering with her activities of daily living and she is seeking definitive treatment. Figures 32a through 32c show current MRI scans. Based on the current available medical literature, what is the most appropriate treatment?
Explanation
REFERENCES: Gibson JN, Waddell G: Surgery for degenerative lumbar spondylosis: Updated Cochrane Review. Spine 2005;30:2312-2320.
Fritzell P, Hagg O, Wessberg P, et al: 2001 Volvo Award Winner in Clinical Studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: A multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine 2001;26:2521-2532.
Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Question 2
Figures 1 and 2 display the radiographs obtained from a woman who had volar plating of the distal radius 8 months earlier. Two days ago, she noticed she could not actively extend her thumb. What is the most appropriate treatment that would restore active thumb extension?
Explanation
Although the fracture is aligned in anatomic position, prominence of a least one of the distal screws is evident on the lateral radiographic view. The prominent screw is the most likely cause of the EPL tendon rupture. If the patient chooses surgical treatment, the best option would be removal of the offending hardware combined with extensor indicis proprius to EPL tendon transfer. Intercalary grafting would also be an acceptable option. If the tendon transfer were to be performed alone, the prominent screw(s) could rupture the transferred tendon as well. Also, it is rarely possible to repair the EPL tendon primarily in such cases, because this rupture is an attrition type. Casting would obviously not provide any benefit in this situation, and IP arthrodesis would not be the first surgical treatment option. This problem can be avoided by using shorter screws or not placing screws in plate holes that direct screws into the third dorsal extensor compartment. Intraoperative fluoroscopy and special views, such as the carpal shoot-through view, are useful for avoiding this complication.
Question 3
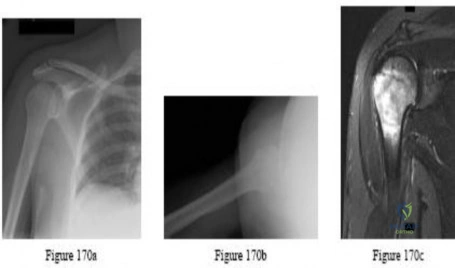
Figures 18a through 18c show the clinical photograph, radiograph, and CT scan of a 21-year-old man who reports persistent pain after injuring his right shoulder 4 months ago. What is the most likely factor associated with this patient’s diagnosis?
Explanation
REFERENCES: Lazarus MD, Seon C: Fractures of the clavicle, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, vol 2, pp 1241-1242.
White RR, Anson PS, Kristiansen T, et al: Adult clavicle fractures: Relationship between mechanism of injury and healing. Orthop Trans 1989;13:514-515.
Question 4
The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports, and the surgeon and rehabilitation team consider their request. Compared to nonaccelerated rehabilitation, patients who follow an early accelerated rehabilitation protocol experience
Explanation
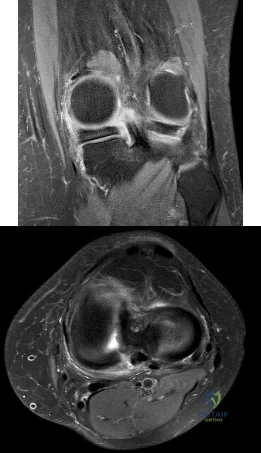
The MR image shows bone bruises (“kissing contusions”) consistent with an ACL tear. During the ACL subluxation event, the posterolateral tibia plateau subluxes anteriorly, making contact with the mid portion of the lateral femoral condyle and resulting in this characteristic bone bruise pattern on MRI. Randomized clinical trials comparing early accelerated vs nonaccelerated rehabilitation programs have demonstrated no significant differences in longterm results with regard to function, reinjury, and successful return to play. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
Question 5
Figures 9a and 9b are the radiographs of a 19-year-old woman with a painful juvenile bunion. The pathologic findings associated with this deformity include a

Explanation
The radiographs show a hallux valgus deformity with a laterally deviated distal metatarsal articular surface, a large intermetatarsal angle with medial deviation at the first metatarsocuneiform joint, an elongated medial collateral ligament, and a contracted lateral collateral ligament. There is no distal 1-2 transverse intermetatarsal ligament. The distal transverse ligament in the first interspace extends from the second metatarsal to the lateral (fibular) sesamoid, remains intact, and keeps the sesamoids in a lateral position as the first metatarsal head migrates medially.
RECOMMENDED READINGS
Coughlin MJ. Roger A. Mann Award. Juvenile hallux valgus: etiology and treatment. Foot Ankle Int. 1995 Nov;16(11):682-97. PubMed PMID: 8589807.
View Abstract at PubMed
Coughlin MJ, Mann RA. Hallux valgus. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:183-226.
Question 6
Which of the following is considered the best method for the prevention of wrong-site surgery?
Explanation
REFERENCES: DeGiovanni CW, Kang L, Manuel J: Patient compliance in avoiding wrong site surgery. J Bone Joint Surg Am 2003;85:815-819.
American Academy of Orthopaedic Surgeons. Advisory Statement: Wrong-site Surgery. Document 1015, 2002 Sept. www.aaos.org/wordhtml/papers/advismt/wrong.htm.
Question 7
A 35-year-old man presents one week after an acute right shoulder posterior dislocation after being electrocuted. He is evaluated in the emergency department and undergoes closed reduction. The patient reports global right shoulder pain and limited active and passive range of motion. He has mild anterior and lateral bruising. He is distally neurovascularly intact. Current radiographs and an MRI scan are shown in Figures 1 through 3. What is the best next step?
Explanation
Question 8
- Figure 16 shoes the AP radiograph of a 32-year-old man with a fracture cephalad to the fovea of the femoral head. A CT scan shows a single head fragment. After closed reduction of the hip, there is 5 mm of residual articular incongruity. Management should now include
Explanation
Question 9
Which of the following findings is seen in the chest radiograph shown in Figure 13?
Explanation
REFERENCE: Bone LB: Emergency treatment of the injured patient, in Browner BD, Jupiter JB, Levine AM, Trafton PG (eds): Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 133-138.
Question 10
A 7-year-old boy with spastic diplegia is a limited community ambulator. He has a moderately severe crouched gait. The parents request a treatment that will result in a permanent decrease in lower extremity muscle tone. This is best accomplished with
Explanation
REFERENCES: Arens LJ, Peacock WJ, Peter J: Selective posterior rhizotomy: A long-term follow-up study. Childs Nerv Syst 1989;5:148-152.
Koman LA, Paterson Smith B, Balkrishnan R: Spasticity associated with cerebral palsy in children: Guidelines for the use of botulinum-A toxin. Paediatr Drugs 2003;5:11-23.
Johnson MB, Goldstein L, Thomas SS, et al: Spinal deformity after selective dorsal rhizotomy in ambulator patients with cerebral palsy. J Pediatr Orthop 2004;24:529-536.
Question 11
What is the most common behavioral effect of anabolic steroid use in athletes?
Explanation
REFERENCES: Hartgens F, Kuipers H: Effects of androgenic-anabolic steroids in athletes. Sports Med 2004;34:513-554.
Blue JG, Lombardo JA: Steroids and steroid-like compounds. Clin Sports Med
1999;19:667-689.
Question 12
Radiographs of a 15-year-old girl with knee pain reveal a radiopaque lesion of the distal femoral metaphysis and epiphysis with a small associated soft-tissue mass. A biopsy specimen shows osteoid and pleomorphic cells with multiple mitotic figures. Staging studies show no other sites of disease. Treatment should consist of
Explanation
REFERENCE: Simon MA, Springfield DS, et al: Common Malignant Bone Tumors: Osteosarcoma. Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 265-274.
Question 13
- The familial occurrence of Legg-Calve-Perthes disease may, in some cases, be attributed to
Explanation
Question 14
A 61-year-old woman has increasing pain in her left great toe. She states that she has had discomfort for years but now has pain with all shoe wear. A radiograph is shown in Figure 35. To provide the most predictable pain-free result, treatment should consist of
Explanation
REFERENCES: Mann RA: Disorders of the first metatarsophalangeal joint. J Am Acad Orthop Surg 1995;3:34-43.
Coughlin MJ, Abdo RV: Arthrodesis of the first metatarsophalangeal joint with Vitallium plate fixation. Foot Ankle Int 1994;15:18-28.
Question 15
An 18-year-old girl with quadriplegic cerebral palsy underwent posterior spinal fusion from T2 to the pelvis 3 weeks ago. She now has a low-grade fever and mild midline erythema in a 1-cm area from which there is slight clear yellowish drainage. What is the next most appropriate step in management?
Explanation
REFERENCES: Theiss SM, Lonstein JE, Winter RB: Wound infections in reconstructive spine surgery. Orthop Clin North Am 1996;27:105-110.
Richards BS: Delayed infections following posterior spinal instrumentation for the treatment of idiopathic scoliosis. J Bone Joint Surg Am 1995;77:524-529.
Question 16
During revision total knee arthroplasty (TKA), there is significant laxity in 90° of flexion and 10° short of full extension. Correcting the gap imbalance is best achieved by
Explanation
A. Nonoperative treatment with close radiographic follow-up
B. Revision THA with ceramic- on-polyethylene with abductor reconstruction
C. Removal of components and placement of spacer as stage 1 of 2-stage revision
D. Revision THA with metal-on- polyethylene and trochanteric slide
Question 17
What is the primary problem in rickets osteomalacia?
Explanation
Question 18
Figures 74a through 74c are the postsurgical radiographs of a 74-year-old man who has stiffness in his right knee 8 weeks after undergoing elective right total knee arthroplasty (TKA). The surgery was performed for primary varus osteoarthritis and was uncomplicated. His range of motion is 5 to 80 degrees. What is the most appropriate next treatment step?
Explanation
Stiffness following TKA is a disabling complication. One option involves MUA, a valuable technique with which to increase range of motion after TKA for patients with stiff knees. A systematic review of the literature was performed to identify studies that reported the clinical outcomes and measured range of motion for patients undergoing MUA. Fourteen studies (913 patients) reported range of motion results following MUA at up to 10-year followup. The review demonstrated that MUA for a stiff primary TKA is an efficacious procedure to restore range of motion, and it carries a low complication rate. Early gains in motion were
reported to be maintained in the long term. A second review systematically evaluated the outcomes of 4 treatments for arthrofibrosis that develops subsequent to TKA (MUA, arthroscopic debridement, open surgical release, and revision TKA). This study showed that there were no significant differences in the Knee Society Score of the 4 treatment modalities. Although open surgical release resulted in the greatest increase in range of motion, there were methodological study limitations because the majority of the papers were case series, which decreased the quality of the evidence. Response 1 is correct because the TKA appears appropriately sized and is well aligned. Responses 2 and 3 are incorrect, considering the early time frame (8 weeks) from initial surgery. Although the patella is unresurfaced in the radiographs, there is no indication for revision TKA (even secondary patellar resurfacing) at this early juncture.
Question 19
83A B year-old with the injury pattern seen on the left lower extremity in CT images in Figures 83a and 83b

Explanation
In Figures 79a through 79c, CT images show a Schatzker IV medial tibial plateau fracture. This fracture is best treated with a medial incision and posteromedial plate, which will function as an antiglide or buttress plate. Percutaneous screw fixation is insufficient for this injury. Lateral fixation is not needed, and in many instances will not capture the medial fragment even with locking fixation. ?
In Figures 80a and 80b, the patient has a fairly well-aligned bicondylar tibial plateau fracture. The lateral joint is significantly depressed, necessitating open reduction and elevation with stabilization. The posteromedial fragment is often missed with single lateral locked plating and is best treated with a posteromedial plate. Percutaneous fixation does not address the joint depression.
In Figure 81, the patient has a classic split depression lateral tibial plateau fracture (Schatzker II). The joint must be reduced from a lateral approach and then supported and stabilized. Definitive ORIF with a lateral plate can be performed when appropriate.
In Figures 82a and 82b, the radiographs show a Schatzker I nondisplaced tibial plateau fracture that is amenable to percutaneous screw fixation if surgical intervention is required. The fracture pattern can be treated surgically, although, considering the comminution at the inferior aspect, late displacement could occur. The other surgical approaches mentioned are not required for this injury.
In Figures 83a and 83b, a lateral split depression tibial plateau fracture is noted (similar to the fracture seen in Figure 81). The same logic applies.
RECOMMENDED READINGS
Higgins TF, Kemper D, Klatt J. Incidence and morphology of the posteromedial fragment in bicondylar tibial plateau fractures. J Orthop Trauma. 2009 Jan;23(1):45-51. doi: 10.1097/BOT.0b013e31818f8dc1. PubMed PMID: 19104303. View Abstract at PubMed Berkson EM, Virkus WW. High-energy tibial plateau fractures. J Am Acad Orthop Surg. 2006 Jan;14(1):20-31. Review. PubMed PMID: 16394164. View Abstract at PubMed
Barei DP, O'Mara TJ, Taitsman LA, Dunbar RP, Nork SE. Frequency and fracture morphology of the posteromedial fragment in bicondylar tibial plateau fracture patterns. J Orthop Trauma. 2008 Mar;22(3):176-82. doi: 10.1097/BOT.0b013e318169ef08. PubMed PMID: 18317051.
View Abstract at PubMed
Lowe JA, Tejwani N, Yoo B, Wolinsky P. Surgical techniques for complex proximal tibial fractures. J Bone Joint Surg Am. 2011 Aug 17;93(16):1548-59. PubMed PMID: 22204013. View Abstract at PubMed
Weil YA, Gardner MJ, Boraiah S, Helfet DL, Lorich DG. Posteromedial supine approach for reduction and fixation of medial and bicondylar tibial plateau fractures. J Orthop Trauma. 2008 May-Jun;22(5):357-62. doi: 10.1097/BOT.0b013e318168c72e. PubMed PMID:
Question 20
A 6-year-old boy with spastic diplegic cerebral palsy has a crouched gait. Examination reveals hip flexion contractures of 15 degrees and popliteal angles of 70 degrees. Equinus contractures measure 10 degrees with the knees extended. Which of the following surgical procedures, if performed alone, will worsen the crouching?
Explanation
REFERENCES: Gage JR: Distal hamstring lengthening/release and rectus femoris transfer, in Sussman MD (ed): The Diplegic Child. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1992, pp 324-326.
Bleck EE: Orthopaedic Management of Cerebral Palsy, in Saunders Monographs in Clinical Orthopaedics. Philadelphia, PA, WB Saunders, vol 2, 1979.
Question 21
Which is the best initial study for the diagnostic evaluation of diskogenic low back pain?
Explanation
REFERENCE: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 319-329.
Question 22
An orthopaedic surgeon in his first year of practice is negotiating with a private for-profit hospital to be their employed trauma specialist. The state of employment is known to have a high rate of malpractice claims because of a favorable plaintiff legal environment. During the course of negotiations, malpractice insurance is being discussed. The surgeon should ask the hospital to provide which type of malpractice insurance policy? Review Topic
Explanation
Question 23
Which examination finding points toward a brachial plexus injury rather than root avulsion?
Explanation
A brachial plexus injury distal to the root level should leave the rhomboid muscle with intact function. Root avulsions of C5-6 will cause weakness of the rhomboids. The branching of the dorsal scapular nerve is proximal and often spared with upper brachial plexus injuries. Winging and biceps weakness may occur
with either injury, and an ipsilateral fracture does not differentiate an avulsion from a brachial plexus injury.
Question 24
A 67-year-old retired steelworker was involved in a motor vehicle accident and sustained a midcervical spinal cord injury. Radiographs and MRI scans reveal severe cervical stenosis and spondylosis without fractures or dislocations. Neurologic examination reveals an ASIA C spinal cord impairment with greater motor involvement of the upper extremities than the lower extremities. What is the probability that the patient eventually will become ambulatory?
Explanation
(ASIA C and D) ultimately walked. The poorest prognosis, however, was in ASIA C patients older than age 50, in which only 40% walked.
REFERENCES: Penrod LE, Hegde SK, Ditunno JF Jr: Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990;71:963-968.
Northrup BE: Acute injuries to the spine and spinal cord: Evaluation and early treatment, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, p 735.
Question 25
A 42-year-old man who is right-hand dominant injured his right shoulder when he fell from a ladder onto his outstretched arm 1 hour ago. Radiographs reveal a two-part greater tuberosity anterior fracture-dislocation. Initial management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Flatow EL, Cuomo F, Maday MG, Miller SR, McIlveen SJ, Bigliani LU: Open reduction and internal fixation of two-part displaced fractures of the greater tuberosity of the proximal part of the humerus. J Bone Joint Surg Am 1991;73:1213-1218.
Question 26
Figure 36a shows the current radiograph of a 65-year-old woman who slipped and fell. History reveals that prior to the fall she was actively functioning without pain. Figure 36b shows a radiograph obtained 1 year ago. Based on the fracture pattern, the failure is most likely related to
Explanation
REFERENCES: Johansson JE, McBroom R, Barrington TW, Hunter GA: Fracture of the ipsilateral femur in patients with total hip replacement. J Bone Joint Surg Am 1981;63:1435-1442.
Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242.
Question 27
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of
Explanation
REFERENCES: Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
Howard FM, Dell PC: The unreduced carpal dislocation: A method of treatment. Clin Orthop 1986;202:112-116.
Question 28
A 15-year-old boy reports a 2-day history of progressive left buttock pain and severe limping. He denies any history of trauma or radiation of the pain. He has an oral temperature of 100.4 degrees F (38 degrees C). Examination reveals that the lumbar spine and left hip have unguarded motion. The abdomen is nontender. There is moderate tenderness of the left sacroiliac region with no palpable swelling. Pain is elicited when the left lower extremity is placed in the figure-4 position (FABER test). Laboratory studies show a peripheral WBC count of 11,500/mm P 3 P (normal to 10,500/mm P 3 P ) and an erythrocyte sedimentation rate of 38 mm/h (normal up to 20 mm/h). Radiographs of the pelvis, hips, and lumbar spine are normal. A nucleotide bone scan (posterior view) is shown in Figure 44. Initial management should consist of
Explanation
Tc 99m bone scan will localize the problem in 90% of patients but may occasionally give a
false-negative result in early cases. If suspicion is high, a gallium scan or MRI scan may help confirm the diagnosis of sacroiliitis. Needle aspiration of the sacroiliac joint is difficult; therefore, antibiotic selection is usually empiric or based on blood cultures. Sacroiliitis that is the result of connective tissue inflammatory disease is usually bilateral and without fever or leukocytosis. The lack of hip irritability, spinal rigidity, and abdominal tenderness helps to rule out other causes of limping with fever, such as psoas abscess, diskitis, and septic hip.
REFERENCES: Aprin H, Turen C: Pyogenic sacroiliitis in children. Clin Orthop
1993;287:98-106.
Osman AA, Govender S: Septic sacroiliitis. Clin Orthop 1995;313:214-219.
Question 29
A 7-year-old girl with spinal muscular atrophy (SMA) type II has popping of the left hip. Examination reveals painless subluxation of the joint in adduction with palpable reduction in abduction. Radiographs show coxa valga, subluxation of the left hip, and pelvic obliquity with elevation of the left hemipelvis. Treatment should consist of
Explanation
REFERENCES: Sporer SM, Smith BG: Hip dislocation in patients with spinal muscular atrophy. J Pediatr Orthop 2003;23:10-14.
Thompson CE, Larsen LJ: Recurrent hip dislocation in intermediate spinal atrophy.
J Pediatr Orthop 1990;10:638-641.
Question 30
A patient has a humeral shaft fracture and is scheduled to undergo open reduction and internal fixation with a plate. What surgical approach will provide the greatest amount of exposure?
Explanation
REFERENCES: DeFranco MJ, Lawton JN: Radial nerve injuries associated with humeral fractures. J Hand Surg Am 2006;31:655-663.
Gerwin M, Hotchkiss RN, Weiland AJ: Alternative operative exposure of the posterior aspect of the humeral diaphysis with reference to the radial nerve. J Bone Joint Surg Am 1996;78:1690-1695.
Question 31
- A clinical trial is being conducted on a new orthopaedic device that is different from existing devices that are moderately successful, but have frequent complications when used to treat fractures in the elderly. To comply with international standards for clinical trials, the investigator must include in the study design
Explanation
Question 32
What is the primary limiting membrane and mechanical support for the periphery of the physis?
Explanation
REFERENCES: Netter FH: Growth plate, in Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 166-167.
Asher MA (ed): Orthopaedic Knowledge Update 1. Chicago, IL, American Academy of Orthopaedic Surgeons, 1984, pp 15-28.
Question 33
A corset-type brace may help reduce symptoms during an episode of acute low back pain as the result of
Explanation
REFERENCES: Nachemson A, Morris JM: In vivo measurements of intradiscal pressure: Discometry, a method for determination of pressure in the low lumbar disc. J Bone Joint Surg Am 1964;46:1077-1092.
Axelsson P, Johnsson R, Stromqvist B: Effect of lumbar orthosis on intervertebral mobility: A roentgen stereophotogrammetric analysis. Spine 1992;17:678-681.
Question 34
03 An 18 month old child has bilateral “corner fractures” of the distal femoral metaphyses of unknown origin. Following a skeletal survey, the first step in management should consist of
Explanation
back to this question next question
Question 35
A 40-year-old man reports an enlarging soft-tissue mass in his right shoulder. Based on the MRI scan and biopsy specimens shown in Figures 40a through 40c, what is the most likely diagnosis?
Explanation
are arranged in short, irregular bundles and fascicles and are adjacent to collagen and reticulin. The lesions can appear to be more myxoid or more fibrotic in nature and this correlates to the duration of symptoms. The lesions with a short duration of symptoms have a more myxoid appearance in contrast to those of longer duration characterized by hyaline fibrosis.
REFERENCES: Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 250-266.
Wang XL, De Schepper AM, Vanhoenacker F, et al: Nodular fasciitis: Correlation of MRI findings and histopathology. Skeletal Radiol 2002;31;155-161.
Question 36
..A 75-year-old woman sustained a 4-part fracture dislocation of the proximal humerus with a comminuted humeral head. You decide to perform a reverse total shoulder replacement because of her age and activity level. This will be your first reverse total shoulder replacement. It is common practice in your hospital for an industry representative to be present when new implants are brought into the operating room. What information are you required to disclose?
Explanation
Arthroscopic or open debridement and capsular release
Interposition arthroplasty
Ulnohumeral arthrodesis
Linked total elbow arthroplasty (TEA)
Unlinked TEA
What surgical procedure listed above is most associated with the conditions defined below?
Question 37
Posterior inferior tibiofibular ligament (PITFL) The syndesmosis between the tibia and fibula at the ankle consists of five defined structures ( Slide ):
Explanation
Question 38
A 30-year-old man landed on his shoulder in a fall off his mountain bike. An AP radiograph and CT scan are shown in Figures 34a and 34b. Management should consist of
Explanation
REFERENCES: Jakob RP, Miniaci A, Anson PS, et al: Four-part valgus impacted fractures of the proximal humerus. J Bone Joint Surg Br 1991;73:295-298.
Resch H, Povacz P, Frohlich R, et al: Percutaneous fixation of three- and four-part fractures of the proximal humerus. J Bone Joint Surg Br 1997;79:295-300.
Question 39
With the arm abducted 90 degrees and fully externally rotated, which of the following glenohumeral ligaments resists anterior translation of the humerus? Review Topic
Explanation
Question 40
Figures 28a through 28c show the MRI scans of a 30-year-old woman who weighs 290 lb and has low back and left leg pain. She also reports frequent urinary dribbling, which her gynecologist has advised her may be related to obesity. Examination will most likely reveal
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Appleton, WI, Century-Crofts, 1976.
Hollinshead WH (ed): Anatomy for Surgeons: The Back and the Limbs, ed 3. Philadelphia, PA, Harper & Rowe, 1982.
Question 41
Figure 7 shows the MRI scan of a 23-year-old competitive rugby player who has anterior ankle pain and swelling. He states that he has been playing for many years and has sprained his ankle several times. Examination will reveal what specific hallmark feature?
Explanation
REFERENCES: Ogilvie-Harris DJ, Mahomed N, Demaziere A: Anterior impingement of the ankle of the ankle treated by arthroscopic removal of bony spurs. J Bone Joint Surg Br 1993;75:437-440.
Cannon LB, Hackney RG: Anterior tibiotalar impingement associated with chronic ankle instability. J Foot Ankle Surg 2000;39:383-386.
Question 42
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits.The patient undergoes successful primary THA with a metal-on-metal bearing. At 1-year follow-up, she reports no pain and is highly satisfied with the procedure. However, 3 years after the index procedure, she reports atraumatic right hip pain that worsens with activities. Radiographs reveal the implants in good position with no sign of loosening or lysis. An initial laboratory evaluation reveals a normal sedimentation rate and C-reactive protein (CRP) level. The most appropriate next diagnostic step is
Explanation
THA has proven to be durable and reliable for pain relief and improvement of function in patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A
metal-on-metal articulation is associated with excellent wear rates in vitro. Because it offers a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions—including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis after the possible transfer of metal ions across the placental barrier—make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.The work-up of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including the erythrocyte sedimentation rate, C-reactive protein (CRP) level, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging, including MRI with MARS, should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following a revision of failed metal-on-metal hip replacements.
Question 43
Figures 33a and 33b show the standing posteroanterior and lateral radiographs of a 59-year-old woman with adult idiopathic scoliosis. She underwent a prior decompressive laminectomy and fusion at L4-S1 to address lumbar stenosis. She now reports progressive lower back pain and a feeling of being shifted to the right. If surgical intervention is considered, what is the most important goal in improving her health-related quality of life (HRQL) outcomes? Review Topic

Explanation
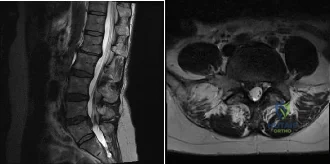
(SBQ12SP.24) A 39-year-old man presents to clinic with a 3-week history of low back pain that radiates to the right lower extremity. On examination, he has mildly decreased sensation over the dorsum of the foot and positive straight leg raise on the right side. MRI images are shown in Figure A and B. Which of the following is true regarding this patient's condition? Review Topic
Nonoperative management with NSAIDS and physical therapy is effective for 50% of patients
Surgical treatment is indicated in patients with diminished sensation
Surgical treatment is equivalent to nonoperative management in terms of pain and function
Good surgical outcome is associated with mainly back complaints
Size of disc herniations typically decrease over time without surgical intervention
The patient is presenting with a lumbar disc herniation at the L4-L5 level. The size of disc herniations decrease in most patients over time without surgical intervention.
Lumbar disc herniations are the result of recurrent torsional strain, which leads to small tears of the annulus fibrosus, ultimately allowing herniation of the nucleus pulposis. First line treatment consists of NSAIDS, muscle relaxants and physical therapy and is effective in 90% of patients. Second line treatment typically involves epidural and selective nerve root corticosteroid injections. Microdiscectomy is reserved for patients with more than 6 weeks of disabling pain that has failed nonoperative management, progressive weakness, or cauda equina syndrome.
In the Spine Patient Outcomes Research Trial (SPORT), Weinstein et al. investigated patient outcomes and satisfaction after operative and nonoperative management of lumbar disc herniations. While the randomized arm of the study did show statistically significant differences in the intent-to-treat analysis due to significant crossover of patients, the observational cohort revealed a significant improvement in pain, function, and disability for patients treated with surgery versus nonoperative measures.
Benson et al. looked at the natural history of massive herniated discs in 37 patients with 7-year follow up. They found a more than 60% reduction in disc size over this time period. Reduction in disc size did not correlate with clinical improvement.
Figure A and B are sagittal and axial T2 MRI images, respectively, showing a right sided lumbar disc herniation at the L4-L5 level.
Incorrect Answers:
Question 44
What is the most common clinical presentation of a patient with a malignant bone tumor?
Explanation
REFERENCES: Buckwalter JA: Musculoskeletal neoplasms and disorders that resemble neoplasms, in Weinstein SL, Buckwalter JA (eds): Turek’s Orthopaedics: Principles and Their Application, ed 5. Philadelphia, PA, JB Lippincott, 1994, pp 290-295.
Mehlman CT, Crawford AH, McMath JA: Pediatric vertebral and spinal cord tumors: A retrospective study of musculoskeletal aspects of presentation, treatment, and complications. Orthopedics 1999;22:49-55.
Question 45
Figure 40 shows the AP radiograph of a 55-year-old man who reports left knee pain. Which of the following conditions is least likely to produce this radiographic presentation?
Explanation
REFERENCES: Klippel JH (ed): Primer on the Rheumatic Diseases, ed 11. Atlanta, GA, Arthritis Foundation, 1997, pp 226-229 and 328-331.
Resnick D, Wayama G: Diagnosis of Bone and Joint Disorders, ed 2. Philadelphia, PA, WB Saunders, 1988, pp 1675, 1779.
Question 46
After trial placement of components in a primary total knee arthroplasty, the knee is unable to come to full extension, but the flexion gap is appropriately balanced. After adequate soft-tissue releases have been performed, what is the next most appropriate action to balance the reconstruction?
Explanation
REFERENCES: Ayers DC, Dennis DA, Johanson NA, et al: Common complications of total knee arthroplasty. J Bone Joint Surg Am 1997;79:278-311.
Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 281-286.
Question 47
An adult patient has a closed humeral fracture that was treated nonsurgically and a concomitant radial nerve injury. Six weeks after injury, electromyography shows no evidence of recovery. Management should now consist of
Explanation
REFERENCES: Pollock FH, Drake D, Bovill EG, et al: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Mohler LR, Hanel DP: Closed fractures complicated by peripheral nerve injury. J Am Acad Orthop Surg 2006;14:32-37.
Question 48
An obese 10-year-old boy has had left groin pain and a limp for the past 2 months. Examination reveals decreased abduction and internal rotation. Laboratory studies show normal renal function and an elevated thyroid-stimulating hormone (TSH) level. AP and frog lateral radiographs of the pelvis are shown in Figures 30a and 30b. What is the best course of action?
Explanation
REFERENCES: Loder RT, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Wells D, King JD, Roe TF, Kaufman FR: Review of slipped capital femoral epiphysis associated with endocrine disease. J Pediatr Orthop 1993;13:610-614.
Question 49
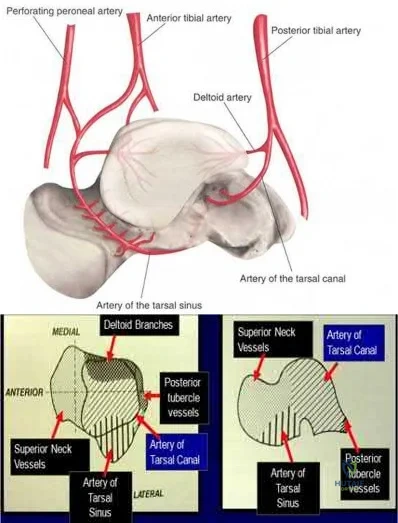
A 29-year-old male sustains the isolated lower extremity injury shown in Figure A. During open reduction, what structure must be kept intact in order to protect the remaining blood supply to the talar body?

Explanation
The review article by Fortin et al discusses talar blood supply, injury mechanisms and classifications, and treatment options. They state that the main artery to the body of the talus is the artery of the tarsal canal, which is a branch of the posterior tibial artery. The peroneal and anterior tibial artery also contribute branches to the talus.
Illustration A and B show the arterial network of the talus.
OrthoCash 2020
Question 50
A further workup reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MARS MR imaging. Revision THA is recommended. The most common complication following revision of a failed metal-on-metal hip arthroplasty is
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on-metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.
The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts.
The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 51
A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 189-199.
Kwon BK, Vaccaro AR, Grauer JN, et al: Subaxial cervical spine trauma. J Am Acad Orthop Surg 2006;14:78-89.
Question 52
- A patient sustained a joint depression-type fracture of the calcaneus that healed despite lack of treatment. The loss of dorsiflexion the patient is now experiencing is most likely the result of
Explanation
Question 53
A displaced pediatric supracondylar humerus fracture is treated with closed manipulation and placement of 2 Kirschner wires placed from the lateral side. What would be the effect of adding a third pin from the lateral side? Review Topic
Explanation
Question 54
-A 42-year-old patient with a right distal radius fracture underwent open reduction and internal fixation. To reduce the likelihood of complex regional pain syndrome, the most appropriate medication is
Explanation

Question 55
Figure 30 shows an axial T1-weighted MRI scan of a patient’s right shoulder. The arrows are pointing to what normal structure?
Explanation
REFERENCES: Connell DA, Potter HG, Sherman MF, et al: Injuries of the pectoralis major muscle: Evaluation with MR imaging. Radiology 1999;210:785-791.
Carrino JA, Chandnanni VP, Mitchell DB, et al: Pectoralis major muscle and tendon tears: Diagnosis and grading using magnetic resonance imaging. Skeletal Radiol 2000;29:305-313.
Ohashi K, El-Khoury GY, Albright JP, et al: MRI of complete rupture of the pectoralis major muscle. Skeletal Radiol 1996;25:625-628.
Question 56
Which structure(s) is/are most at risk with surgical treatment of displaced clavicle fractures with ORIF?
Explanation
Complications associated with nonsurgical treatment of displaced midshaft clavicle fractures are uncommon. Although intrathoracic and local vascular complications have been reported with clavicle fracture, subclavian artery aneurysm and pneumothorax are rare. Malunion to some degree is inevitable with nonsurgical treatment of displaced clavicle fractures, but only about 9% of patients develop symptomatic malunion. Nonunion occurs in about 15% of patients.
Previously identified risk factors for nonunion of clavicle fractures include female gender, displacement exceeding 100%, comminution, and advanced age. Research demonstrates the strongest risk factors are smoking, comminution, and fracture displacement. Rate of nonunion in 1 study was approximately 13%. Murray and associates showed that by estimating the risk of nonunion using their model and operating only on fractures with at least a 40% chance of nonunion, they would only need to operate on 1.7 patients to prevent 1 nonunion (decreased from 7.5 procedures per nonunion if operating on all displaced midshaft fractures). This data could potentially be used to limit unnecessary procedures and decrease costs associated with treatment of clavicle fractures.
Hardware removal is the most common reason for revision surgery. Symptomatic malunion and supraclavicular nerve entrapment are rare after surgery. Nonunion is uncommon (in fewer than 2% of cases). The main reason for revision surgery is hardware removal to address local irritation/prominent hardware or infection.
An anatomical study demonstrated that in 97% of clavicles, 2 to 3 branches of the supraclavicular nerve were crossing the clavicle with wide location variability in the zone in which most clavicle fractures occur and surgery would take place. The subclavian vein and artery and brachial are rarely injured,
although there are case reports of injury to all either by the displaced fracture fragments or errant hardware.
RECOMMENDED READINGS
McKee RC, Whelan DB, Schemitsch EH, McKee MD. Operative versus nonoperative care of displaced midshaft clavicular fractures: a meta-analysis of randomized clinical trials. J Bone Joint Surg Am. 2012 Apr 18;94(8):675-84. doi: 10.2106/JBJS.J.01364. Review. PubMed PMID: 22419410.View Abstract at PubMed
Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am. 2004 Jul;86-A(7):1359-65. PubMed PMID: 15252081.View Abstract at PubMed
Murray IR, Foster CJ, Eros A, Robinson CM. Risk factors for nonunion after nonoperative treatment of displaced midshaft fractures of the clavicle. J Bone Joint Surg Am. 2013 Jul 3;95(13):1153-8. doi: 10.2106/JBJS.K.01275. PubMed PMID: 23824382.View Abstract at
PubMed
Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. J Bone Joint Surg Am. 2007 Jan;89(1):1-10. PubMed PMID: 17200303.View Abstract at PubMed
Nathe T, Tseng S, Yoo B. The anatomy of the supraclavicular nerve during surgical approach to the clavicular shaft. Clin Orthop Relat Res. 2011 Mar;469(3):890-4. doi: 10.1007/s11999-010-1608-x. Epub 2010 Oct 9. PubMed PMID: 20936387.View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 26 AND 27

A

B

C

D
Figures 26a through 26c are the radiographs of a 50-year-old athlete who sustained an injury to his right foot; the foot was plantar flexed and another player landed on the posterior aspect of his heel. After sustaining the injury he was unable to bear weight, and 3 days later he was seen in the emergency department because of persistent pain and tenderness over his midfoot.
Question 57
Which of the follow scenarios is most likely to be amenable to a complete repair of a massive rotator cuff tear? Review Topic
Explanation
Question 58
An inverted radial reflex is associated with
Explanation
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 762.
Vaccaro AR, Betz RR, Zeidman SM (eds): Principles and Practice of Spine Surgery. St Louis, MO, Mosby, 2002, p 323.
Question 59
Figure 25 shows the clinical photograph of a 48-year-old man who has had a forefoot ulcer for the past 4 months. History reveals that he has had type II diabetes mellitus for the past 10 years. Examination reveals sensory and motor neuropathy, with weak ankle dorsiflexion. The ankle cannot be passively dorsiflexed past a neutral position. Initial management should consist of
Explanation
REFERENCES: Lin SS, Lee TH, Wapner KL: Plantar forefoot ulceration with equinus deformity of the ankle in diabetic patients: The effect of tendo-Achilles lengthening and total contact casting. Orthopedics 1996;19:465-475.
Armstrong DG, Stacpoole-Shea S, Nguyen H, Harkless LB: Lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot. J Bone Joint Surg Am 1999;81:535-538.
Question 60
The vessel seen in the clinical photographs shown in Figures 50a and 50b (1,2 intercompartmental supraretinacular artery) is being dissected to be used as a source of vascularized bone graft for a patient who is scheduled to undergo internal fixation of a scaphoid nonunion. This vessel is a branch of what artery?
Explanation
REFERENCES: Sheetz KK, Bishop AT, Berger RA: The arterial blood supply of the distal radius and ulna and its potential use in vascularized pedicled bone grafts. J Hand Surg 1995;20:902-914.
Steinmann SP, Bishop AT, Berger RA: Use of the 1,2 intercompartmental supraretinacular artery as a vascularized pedicle bone graft for difficult scaphoid nonunion. J Hand Surg
2002;27:391-401.
Question 61
If a laminectomy for spinal stenosis is performed, which of the following is an indication for concomitant arthrodesis at that level?
Explanation
REFERENCES: Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-807.
Garfin SR, Rauschning W: Spinal stenosis. Instr Course Lect 2001;50:145-152.
Question 62
Which intervention most effectively prevents surgical-site infections following spine surgery?
Explanation
The use of IV antibiotics for prophylaxis of surgical-site infection is supported by Level 1 evidence in spine surgery. It has been given a "B" recommendation by the North American Spine Society. The use of specific bathing solutions the day of surgery may be beneficial, but the evidence in spine surgery is lacking. Similarly, evidence for use of vancomycin (either topically or IV) is not supported by high-level studies, although retrospective and basic science studies support topical vancomycin use.
RECOMMENDED READINGS
Brown MD, Brookfield KF. A randomized study of closed wound suction drainage for extensive lumbar spine surgery. Spine (Phila Pa 1976). 2004 May 15;29(10):1066-8. PubMed PMID: 15131430. View Abstract at PubMed
Diab M, Smucny M, Dormans JP, Erickson MA, Ibrahim K, Lenke LG, Sucato DJ, Sanders JO. Use and outcomes of wound drain in spinal fusion for adolescent idiopathic scoliosis. Spine (Phila Pa 1976). 2012 May 15;37(11):966-73. doi: 10.1097/BRS.0b013e31823bbf0b.
PubMed PMID: 22037527. View Abstract at PubMed
Evaniew N, Khan M, Drew B, Peterson D, Bhandari M, Ghert M. Intrawound vancomycin to prevent infections after spine surgery: a systematic review and meta-analysis. Eur Spine J. 2014 May 18. [Epub ahead of print] PubMed PMID: 24838506. View Abstract at PubMed Rubinstein E, Findler G, Amit P, Shaked I. Perioperative prophylactic cephazolin in spinal surgery. A double-blind placebo-controlled trial. J Bone Joint Surg Br. 1994 Jan;76(1):99-
Question 63
A year-old active woman undergoes elective total hip replacement in which a posterior approach is used. She has minimal pain and is discharged to home 2 days after surgery. Four weeks later, she dislocates her hip while shaving her legs. She undergoes a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Explanation
First-time early dislocations are often treated successfully without revision surgery, especially when no component malalignment is present. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful but is usually reserved for patients with recurrent dislocations.
Question 64
An open biopsy specimen of a radiodense distal clavicle lesion in a 12-year-old girl shows chronic polyclonal inflammatory cells without granuloma formation. Laboratory studies show that bacterial, fungal, and acid-fast bacillus cultures are negative. Subsequently, a similar lesion is noted in the fibula. The next most appropriate step in management should consist of
Explanation
REFERENCE: Carr AJ, Cole WG, Roberton DM, Chow CW: Chronic multifocal osteomyelitis. J Bone Joint Surg Br 1993;75:582-591.
Question 65
Figure 81 is a lateral thoracic spine radiograph of a 76-year-old man with a history of ankylosing spondylitis who falls and strikes his back. He has moderate thoracic discomfort. An initial examination does not reveal neurologic deficits. He is discharged home that day, but returns 3 days later with profound weakness in his legs. Which imaging study should have been obtained at his initial presentation?
Explanation
Patients with ankylosing spondylitis are at high risk for occult vertebral fractures that are not readily detectable on radiographs. The treating surgeon must have a high suspicion for fractures in these patients and pursue further imaging of the spine with CT and (often) MRI. Even among patients who are neurologically intact, fracture displacement and neurologic deterioration can occur if fractures are not recognized early and appropriately stabilized. Fractures in patients with ankylosing spondylitis are extremely unstable and are associated with high risk for delayed neurological deterioration. Although plain film imaging of the entire spine should be considered, occult fractures can easily be missed. Imaging of the sacroiliac joints can be helpful to establish the diagnosis of ankylosing spondylitis but would not identify an occult fracture of the vertebra in this patient.
RECOMMENDED READINGS
Finkelstein JA, Chapman JR, Mirza S. Occult vertebral fractures in ankylosing spondylitis. Spinal Cord. 1999 Jun;37(6):444-7. PubMed PMID: 10432265. View Abstract at PubMed Harrop JS, Sharan A, Anderson G, Hillibrand AS, Albert TJ, Flanders A, Vaccaro AR. Failure of standard imaging to detect a cervical fracture in a patient with ankylosing spondylitis. Spine (Phila Pa 1976). 2005 Jul 15;30(14):E417-9. PubMed PMID: 16025019. View Abstract at PubMed
Westerveld LA, Verlaan JJ, Oner FC. Spinal fractures in patients with ankylosing spinal disorders: a systematic review of the literature on treatment, neurological status and
complications. Eur Spine J. 2009 Feb;18(2):145-56. doi: 10.1007/s00586-008-0764-0. Epub 2008 Sep 13. Review. PubMed PMID: 18791749. View Abstract at PubMed
Question 66
Which of the following is considered the treatment of choice for a 3-cm chondroblastoma of the distal femoral epiphysis with no intra-articular extension?
Explanation
REFERENCES: Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748.
Simon M, Springfield D, et al: Chrondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 67
In Gustilo type III open tibial diaphyseal fractures, which of the following factors is associated with an increased risk of a poor functional outcome?
Explanation
(3 days or less from injury as compared to more than 3 days), and the timing of bone grafting after injury (within or after 3 months) did not impact the infection or union rates and had no effect on functional outcome. The LEAP study has shown at 7-year follow-up that patients who are definitively treated with external fixation have a significantly longer time to union, poorer functional outcomes, longer time to achieve full weight bearing, and more time in the hospital.
REFERENCES: Webb LX, Bosse MJ, Castillo RC, et al: Analysis of surgeon-controlled variables in the treatment of limb-threatening type-III open tibial diaphyseal fractures. J Bone Joint Surg Am 2007;89:923-928.
Question 68
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?
Explanation
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Omer GE Jr: Osteotomy of the clavicle in surgical reduction of anterior sternoclavicular dislocation. J Trauma 1967;7:584-590.
Question 69
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
Explanation
REFERENCES: Schulman AM, Claridge JA, Carr G, et al: Predictors of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:795-800.
Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: Endpoints of resuscitation. J Trauma 2004;57:898-912.
Question 70
Figures 54a and 54b show the radiograph and MRI scan of a 7-year-old boy who has a painful right thoracic scoliosis that measures 35°. Neurologic examination is normal. Management should consist of
Explanation
REFERENCES: Zadeh HG, Sakka SA, Powell MP, Mehta MH: Absent superficial abdominal reflexes in children with scoliosis: An early indicator of syringomyelia. J Bone Joint Surg Br 1995;77:762-767.
Schwend RM, Hennrikus W, Hall JE, Emans JB: Childhood scoliosis: Clinical indications for magnetic resonance imaging. J Bone Joint Surg Am 1995;77:46-53.
Farley FA, Song KM, Birch JG, Browne R: Syringomyelia and scoliosis in children. J Pediatr Orthop 1995;15:187-192.
Question 71
A 62-year-old man has a severe pes planus and pain in the hindfoot. Radiographs show advanced degenerative changes at the talonavicular and subtalar joints with good preservation of the ankle joint. What is the most appropriate surgical procedure to alleviate his pain?
Explanation
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 269-282.
Graves SC, Stephenson K: The use of subtalar and triple arthrodesis in the treatment of posterior tibial tendon dysfunction. Foot Ankle Clin 1997;2:319.
Question 72
Which method of flexor tendon repair that necessitates excursion through the A2 pulley allows for the most thorough assessment of tendon gliding?
Explanation
Wide-awake repair under only local anesthesia, regardless of the technique, allows direct inspection of the tendon repair and active excursion. Regional anesthesia and Bier block anesthesia do not allow active motion (Bier block necessitates continued use of a tourniquet, which limits muscle function). The A2
pulley should be preserved, especially the distal 50%, to maintain tendon function. All of the listed techniques for suture repair are acceptable options.
Question 73
Which 2 tendons are identified in the dissection shown in Video 92?
Explanation
RECOMMENDED READINGS
Babb JR, Detterline AJ, Noyes FR. AAOS Orthopaedic Video Theater. The Key to the Knee: A Layer-by-Layer Video Demonstration of Medial and Anterior Anatomy. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2009.
Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:493-568.
Question 74
A 45-year-old man is seeking evaluation of an injury sustained in a motor vehicle accident 10 weeks ago. Current radiographs are shown in Figures 2a and 2b. Based on the radiographic findings, what is the most likely diagnosis?
Explanation
REFERENCES: Elgafy H, Ebraheim NA, Tile M, Stephen D, Kase J: Fractures of the talus: Experience of two level 1 trauma centers. Foot Ankle Int 2000;21:1023-1029.
Berlet GC, Lee TH, Massa EG: Talar neck fractures. Orthop Clin North Am 2001;32:53-64.
Question 75
A 7-year-old girl is hit by a motor vehicle and sustains the isolated ipsilateral injuries shown in Figures 16a and 16b. What is the optimal definitive method of treatment?
Explanation
REFERENCES: Poolman RW, Kocher MS, Bhandari M: Pediatric femoral fractures:
A systematic review of 2422 cases. J Orthop Trauma 2006;20:648-654.
Anglen JO, Choi L: Treatment options in pediatric femoral shaft fractures. J Orthop Trauma 2005;19:724-733.
Beaty JH: Operative treatment of femoral shaft fractures in children and adolescents. Clin Orthop Relat Res 2005;434:114-122.
Question 76
An extended head hemiarthroplasty (rotator cuff tear arthropathy head) has what theoretic advantage when compared to a standard hemiarthroplasty?
Explanation
REFERENCES: Visotsky JL, Basamania C, Seebauer L, et al: Cuff tear arthropathy: Pathogenesis, classification, and algorithm for treatment. J Bone Joint Surg Am 2004;86:35-40.
Zuckerman JD, Scott AJ, Gallagher MA: Hemiarthroplasty for cuff tear arthropathy. J Shoulder Elbow Surg 2000;9:169-172.
Question 77
Figures 1 and 2 are the T2-weighted MR images of a 54-year-old woman with medial knee pain and catching of 6 months’ duration. Which treatment option is most likely to be associated with a favorable outcome?
Explanation
Question 78
Which of the following is considered the most appropriate shoe modification following transmetatarsal amputation?
Explanation
REFERENCES: Philbin TM, Leyes M, Sferra JJ, Donley BG: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Marks RM: Mid-foot/mid-tarsus amputations. Foot Ankle Clin 1999;4:1-16.
Question 79
Myodesis of which muscle group is most important for optimal outcome after transfemoral amputation?

Explanation
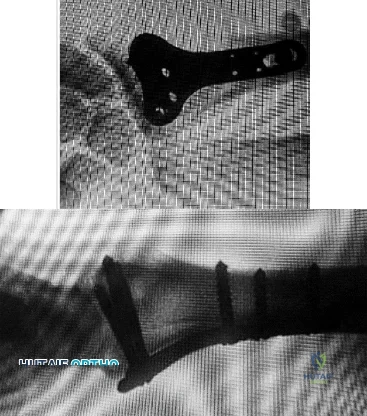
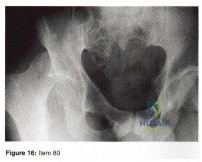
Question 80
Figures below show the radiographs, and the CT obtained from a 58-year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when actively flexing her hip. She has trouble walking up stairs and getting out of her car. What is the most likely diagnosis?

Explanation
Groin pain after total hip replacement has a number of possible causes, and an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated, diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms or in any patient with a metal-on-metal bearing. This patient's symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning are indicated. Fluoroscope-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well positioned, then iliopsoas tenotomy should be considered.
Question 81
1 and 2 show the radiographs obtained from a year-old morbidly obese man who underwent left total hip replacement 7 years ago and did well, with no symptoms prior to the current presentation. He recently rose from a seated position and felt a pop in the hip, with immediate pain and inability to bear weight. Any pressure on the left foot now produces a painful, grinding sensation with loss of left hip stability. What is the best next step?
Explanation
The modular femoral stem has fractured. Changing the liner to a constrained design is not warranted at this time based on the information provided. Revision of the acetabular implant is appropriate because of the potential for damage to the existing cup from metal debris and femoral implant contact and to convert from a metal-on-metal articulation. Nonsurgical management would not provide pain relief or improvement; revision of the total hip arthroplasty is recommended. The implant failed in a short time, and retention of the femoral stem is not recommended because of the concern for failure with only a neck exchange. A dual-mobility bearing may be a good option if the surgeon plans to retain the acetabular component. Extended trochanteric osteotomy is a useful technique for the removal of a well-fixed femoral implant. In this patient, femoral stem removal without
osteotomy would be difficult due to the fracture of the implant’s femoral neck and the
inability to gain purchase for extraction.
Question 82
Which of the following indicates resolution of a postoperative wound infection? Review Topic
Explanation
Question 83
What is the most common pediatric soft-tissue sarcoma?
Explanation
REFERENCE: Wexler LH, Helman LJ: Pediatric soft tissue sarcomas. CA Cancer J Clin 1994;44:211-247.
Question 84
- A 76-year-old woman who underwent primary total knee arthroplasty 9 months ago falls and sustains a transverse fracture of the proximal third of the patella that is displaced 5 mm. Although the knee is painful, she is able to ambulate and has a 5-degree extension lag. The component appears to be well fixed. Treatment should now include
Explanation
Question 85
A 43-year-old man who works as a plumber has a painful stiff elbow in his dominant arm. He notes that while he recalls no single event of injury, he thinks the many years of pulling wrenches and soldering pipes have resulted in his problem. He reports that he has pain with any motion in bending his arm and can no longer straighten his elbow. Examination reveals generalized swelling of the elbow, both medial and lateral with a range of motion that lacks 45 degrees of extension and flexes only to 110 degrees. Pronation and supination are also limited to 45 degrees. Audible crepitus is perceived but there is no instability. Radiographs reveal advanced osteoarthritis at the radiocapitellar and ulnohumeral joints with complete loss of articular cartilage. What is the most appropriate initial treatment option? Review Topic
Explanation
must respect the physical demands of the patient while trying to preserve joint motion and function with tolerable symptoms. Osteophyte resection and capsular release have offered many patients significant improvement in their symptoms while allowing them to return to most activities. The osteophyte resection and releases can be done effectively by an open or arthroscopic approach. Whereas total elbow arthroplasty would likely result in better and more thorough pain relief, it would not tolerate the occupational demands of this individual. There is no role for physical therapy initially in the face of advanced, painful arthritis associated with long-standing fixed joint contractures. Elbow fusion results in severe loss of function and its indication is rare and usually considered in the face of unmanageable sepsis. Radial head resection may improve symptoms related to the radial capitellar arthritis but would not improve range of motion or end range impingement pain. Also, radial head resection should be avoided in heavy laborers with elbow arthritis because it would lead to increased loads across the arthritic ulnohumeral joint.
Question 86
Figures 155a and 155b are the plain radiographs of a 17-year-old boy who recently noted painless swelling in his distal thigh. Examination reveals a firm, fixed, deep distal thigh mass. There is no associated tenderness. What is the best next treatment step?

Explanation
Question 87
Figure 31 shows the radiograph of an 8-year-old boy who has a swollen forearm after falling out of a tree. Examination reveals that all three nerves are functionally intact, and there is no evidence of circulatory embarrassment. Management should consist of
Explanation
REFERENCES: Gibson WK, Timperlake RW: Operative treatment of a type IV Monteggia fracture-dislocation in a child. J Bone Joint Surg Br 1992;74:780-781.
Stanley EA, DeLaGarza JF: Part IV: Monteggia fracture. Dislocations in children, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 576-577.
Question 88
An 85-year-old right hand dominant male sustains a fall onto his elbow while trying to get out of the car. His past medical history is significant for diabetes, congestive heart failure, and COPD. He lives in a nursing home, and is able to ambulate at baseline without and assistive devices. What would be the ideal definitive surgical treatment options in this patient? Review Topic

Explanation
TEA is a preferred alternative for ORIF in elderly patients with complex distal humeral fractures that are not amenable to stable fixation. Elderly patients appear to accommodate to objective limitations in function with time, and suffer less complications with TEA than ORIF in select cases.
Sorensen et al evaluated short- to medium term outcome of total elbow arthroplasty (TEA) in complex fractures of the distal humerus by evaluating 24 consecutive cases. Twenty of the patients were followed for almost 2 years, and their MEPS were 15 excellent, 4 good and 1 fair result. They concluded that TEA in complex fractures of the distal humerus in elderly patients can result in acceptable short- to medium term outcome.
Mckee et al conducted a prospective, randomized, controlled trial to compare
functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular, distal humeral fractures treated with open reduction-internal fixation (ORIF) or primary total elbow arthroplasty (TEA). They randomized 42 patients and found that TEA for the treatment of comminuted intra-articular distal humeral fractures resulted in more predictable and improved 2-year functional outcomes compared with ORIF, based on the MEPS.
Illustration A shows radiographs of a TEA. Incorrect Answers:
Question 89
Which of the following provocative tests would most likely be positive in a patient with medial epicondylitis? Review Topic
Explanation
Medial epicondylitis is an overuse syndrome of the flexor-pronator mass. The pronator teres (PT) and flexor carpi radialis (FCR) are thought to be most affected with this condition. It is most common in the dominant arm and occurs with activities that require repetitive wrist flexion/forearm pronation. Patients are most tender over the origin of PT and FCR at the medial epicondyle. Resisting a patient with their fist clenched, wrist flexed and pronated can cause worsening of their pain. This maneuver can be used as a provocative test for this condition.
Cain et al. reviewed elbow injuries in throwing athletes. They comment that the common flexor-pronator muscle origin provides dynamic support to valgus stress in the throwing elbow, especially during early arm acceleration and help produce wrist flexion during ball release.
Amin et al. reviewed the evaluation and management of medial epicondylitis. They report that medial epicondylitis typically occurs in the fourth through sixth decades of life, the peak working years, and equally affects men and women. Physical therapy and rehabilitation is the main aspect of recovery from medial epicondylitis, once acute symptoms have been alleviated.
Illustration A shows a video of this provocative test for medial epicondylitis. Incorrect Answers:
Question 90
An 18-year-old woman sustains a twisting injury of the knee while skiing. Figures 7a and 7b show the radiograph and coronal MRI scan of the knee. In addition to the injury shown, what is the most likely associated injury?
Explanation
REFERENCES: Goldman AB, Pavlov H, Rubenstein D: The Segond fracture of the proximal tibia: A small avulsion that reflects major ligamentous damage. Am J Roentgenol 1988;151:1163-1167.
Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 91
Bisphosphonates are indicated in the treatment of osteoporosis in patients who have a DEXA T-score of
Explanation
REFERENCE: Gass M, Dawson-Hughs B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Question 92
The most important radiographic predictor of a good clinical outcome following adult spinal deformity surgery is correction of Review Topic
Explanation
Question 93
Osteolysis after total knee arthroplasty can be minimized through prosthetic design features such as
Explanation
REFERENCE: O’Rourke M, Callaghan J, Goetz D, Sullivan P, Johnson R: Osteolysis associated with a cemented modular posterior cruciate substituting total knee design. J Bone Joint Surgery Am 2002;84:1362-1371.
Question 94
A 26-year-old man is brought to the emergency department unresponsive and intubated after being found lying on the side of the road. He has a Glasgow Coma Scale score of 6. A chest tube has been inserted on the right side of the chest for a pneumothorax. An abdominal CT scan reveals a small liver laceration and minimal intraperitoneal hematoma. A pneumatic antishock garment (PASG) is on but not inflated. He has bilateral tibia fractures. A pelvic CT scan shows an anterior minimally displaced left sacral ala fracture and left superior and inferior rami fractures. He has received 2 L of saline solution and 4 units of blood but remains hemodynamically unstable. What is the next most appropriate step in management?
Explanation
REFERENCES: Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: Effective classification system and treatment protocols. J Trauma 1990;30:848-856.
Evers BM, Cryer HM, Miller FB: Pelvic fracture hemorrhage: Priorities in management. Arch Surg 1989;124:422-424.
Flint L, Babikian G, Anders M, Rodriguez J, Steinberg S: Definitive control of mortality from severe pelvic fracture. Ann Surg 1990;211:703-707.
Question 95
Which of the following benign bone lesions can develop lung metastases?
Explanation
REFERENCES: Roberts PF, Taylor JG: Multifocal benign chondroblastomas: Report of a case. Hum Pathol 1980;11:296-298.
Bloem JL, Mulder JD: Chondroblastoma: A clinical and radiological study of 104 cases. Skeletal Radiol 1985;14:1-9.
Question 96
A 40-year-old woman reports the atraumatic onset of severe knee pain and swelling after undergoing an uncomplicated elective cholecystectomy 1 week ago. She denies any history of diabetes mellitus or HIV but has had occasional episodes of mild knee pain and swelling that have always responded to nonsteroidal anti-inflammatory drugs. Radiographs are shown in Figures 5a and 5b. A knee aspiration yields a WBC count of 35,000/mm 3 . The aspirate should also yield which of the following findings?
Explanation
REFERENCES: Fisseler-Eckhoff A, Muller KM: Arthroscopy and chondrocalcinosis. Arthroscopy 1992;8:98-104.
Hough AJ Jr, Webber RJ: Pathology of the meniscus. Clin Orthop 1990;252:32-40.
Question 97
An otherwise healthy 25-year-old man with an isolated closed mid-diaphyseal femoral fracture undergoes intramedullary nailing. Compared with nonreamed nailing, reamed femoral nailing is associated with a higher rate of Review Topic
Explanation
Question 98
What neurovascular structure is most at risk when performing an inside-out repair of the posterior horn of the medial meniscus?
Explanation
REFERENCES: Cannon WD Jr, Morgan CD: Meniscal repair: Arthroscopic repair techniques. Instr Course Lect 1994;43:77-96.
Scott GA, Jolly BL, Henning CE: Combined posterior incision and arthroscopic intra-articular repair of the meniscus: An examination of factors affecting healing. J Bone Joint Surg Am 1986;68:847-861.
Question 99
Figures below depict the AP and lateral radiographs obtained from a 64-year-old man with long-standing right knee osteoarthritis and pain that is unresponsive to nonsurgical treatment. The patient undergoes navigated cruciate-retaining right total knee arthroplasty. After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office reporting continued pain 2 years after surgery. He describes instability, particularly when descending stairs. On examination, range of motion of 0° to 120° is observed, with no extensor lag. Slope of the tibial component is 7°. The knee is stable to varus and valgus stress in extension, but flexion instability is present in both the anterior-posterior direction and the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection work-up is negative. What is the most appropriate surgical intervention at this time?

Explanation
The patient’s symptoms at follow-up—pain, swelling, and difficulty descending stairs—suggest knee flexion instability. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant (depending on the condition of the ligaments) likely is needed to address his symptoms. The difference in extension stability and flexion stability makes polyethylene exchange a poor option. A constrained rotating hinge design is not necessary. Repeat use of a PCL-retaining insert is not recommended. Tibial and femoral revision both are required. Correction of excessive slope will be attained with tibial revision, femoral component revision is required to convert to a PCL-substituting design. There is also an opportunity to increase posterior condylar offset if needed.
Question 100
8 degrees respectively. Isolated LCL repair neutralized varus laxity, suggesting that repair of this structure was more important thatn radial head replacement for gross stability of the elbow.
Explanation

OrthoCash 2020
A 36-year-old woman presents with a grade 3 open midshaft femoral shaft fracture as the result of a high-speed motor vehicle collision. Concomitant injuries include a high-grade splenic laceration requiring splenectomy as well as a subdural hematoma that requires monitoring and maintenance of cerebral perfusion pressure. After irrigation and debridement of the open fracture, which of the following is the most appropriate management of the femoral shaft fracture at this time?
Placement of antibiotic beads, wound closure and immobilization
Reamed antegrade intramedullary nailing
Unreamed antegrade intramedullary nailing
Wound closure and Hare traction splint placement
Placement of an external fixator Corrent answer: 5
The clinical scenario is consistent with a femoral shaft fracture in a patient that is not stable from a neurosurgical perspective. Therefore, the most appropriate treatment at this time is placement of an external fixator.
When evaluating polytrauma patients with long bone fractures, timing of surgery must be approached considering all clinical conditions. One factor most likely to adversely affect long term outcome in polytrauma patients with severe brain injury is intra-operative hypotension; therefore, whenever a patient has a subdural hematoma that requires close observation, definitive surgery of long bone fractures should be delayed.
Flierl et al. review the immunopathophysiology of traumatic brain injury and the role of the orthopaedic surgeon in avoiding a "second hit" injury to the brain by appropriately timing the fixation of femoral shaft fractures. They recommend a multidisciplinary approach, taking individual patient-specific factors into consideration and in general, DCO principles for severe head-injured patients (GCS 3-13) and "early total care" principles for patients with mild head injury (GCS 14-15).
Illustration A is a visual representation of the treatment algorithm recommended in the article.
Incorrect Answers:
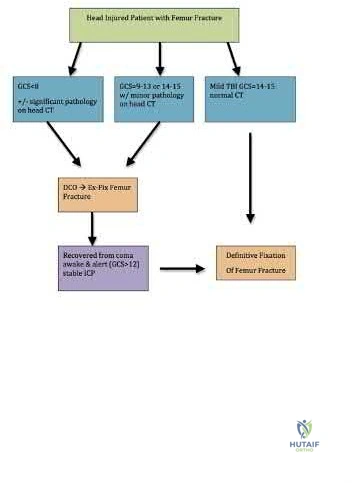
OrthoCash 2020
A 23-year-old healthy male was involved in a motor vehicle collision and sustained the injury seen in Figure A. Physical examination after ORIF of the plateau fracture revealed a Grade 3 Lachman, varus laxity at both 0 and 30 degrees of knee flexion, and 15 degrees of external rotation asymmetry at 30 degrees of knee flexion. Which of the following structures (indicated with asterisk*) must be surgically repaired to restore stability to the knee?

This patient sustained a high-energy injury to the left knee, including a tibial plateau fracture as well as both anterior cruciate ligament (ACL) and posterolateral corner (PLC) injuries as indicated on the physical examination findings. In addition to ORIF of the plateau fracture, the surgical plan should include ACL reconstruction as well as posterolateral corner (PLC) reconstruction, specifically with lateral meniscal repair and allograft reconstruction of the lateral collateral ligament (LCL,asterisk in Figure C) and popliteofibular ligaments.
The PLC consists of static (LCL, popliteus tendon, popliteofibular ligament, lateral capsule) and dynamic (biceps femoris, popliteus muscle, IT band, lateral head of the gastrocnemius) structures. Failure to identify a PLC injury associated with an ACL injury often leads to failure of ACL repair.
Stannard et al. reported on the clinical outcomes of 22 patients with PLC injuries (7 isolated) who underwent modified 2-tailed reconstruction of the popliteofibular ligament and LCL utilizing transtibial and transfibular bone tunnels. At an average 29.5 months post-operatively, the authors noted excellent results with restoration of range of motion and stability in both the isolated and multiligamentous injured groups.
Stannard et al. reported on a separate cohort of 56 patients with PLC injuries either undergoing direct repair or modified 2-tailed reconstruction. The authors noted significantly inferior results in the repair group (37% failures) compared to the reconstruction group (9%) failures, and concluded that reconstruction is the procedure of choice for the majority of patients who sustain high-energy PLC injuries.
Levy et al. reported on 28 patients with multiligament knee injuries undergoing either direct PLC repair with staged cruciate ligament reconstruction or delayed single-stage multiligament reconstruction. The authors noted a significantly higher rate of failure in the repair/staged group compared to the delayed reconstruction group, and deemed reconstruction to be a more reliable option than repair alone in the multiligamentously injured knee.
Figure A includes AP and lateral radiographs of the left tibia demonstrating a
comminuted lateral tibia plateau fracture. Figure C demonstrates a gross dissection of the posterolateral corner (left knee), with the asterisk on the lateral collateral ligament (LCL)
Incorrect answers:
OrthoCash 2020
A 25-year-old, training for a marathon, presents with persistent heel pain over the past several weeks. He has difficulty with ambulation and has an antalgic gait. A squeeze test of the heel is positive. A lateral foot radiograph is shown Figure A. Of the options listed below, what is the most appropriate next step in management?

EMG/NCV study
Heel pad cortisone injection
Physical therapy with Graston techniques to plantar fascia
MRI of the foot
Non-weight bearing cast for 4-6 months Corrent answer: 4
Based on the clinical findings and imaging shown, one should be suspicious for a calcaneal stress fracture. This can be confirmed by obtaining an MRI.
Calcaneal stress fractures are often associated with increases in training intensity. They may be seen in patients with the female athletic triad. An MRI is used to help delineate the diagnosis when it is not clear from the history and physical exam.
Neufeld et al. review the diagnosis and management of plantar fasciitis. They note that there are many causes of inferior heel pain, including nerve compression, FHL tendinitis and calcaneal stress fractures. The latter commonly presents with diffuse swelling and pain with medial to lateral compression of the heel.
Figure A shows a lateral radiograph of the foot with no obvious osseous abnormality of the calcaneus.
Illustration A shows a T1 weighted sagittal reconstruction of an MRI that is demonstrative of a dark line; this is consistent with a stress fracture.
Incorrect Answers

OrthoCash 2020
A 28 year-old-male presents with the injury pattern seen in Figure A. Which of the following is a risk factor for wound complications following operative treatment?

Open injury
Workers' Compensation involvement
Adjunct use of allograft
Contralateral calcaneus fracture
Male sex
According to the referenced study by Folk et al, the risk of early wound complications is highest in open injuries, diabetics, and smokers.
No significant differences were seen in complication rates in terms of: age, sex, other pre-existing medical conditions, social history, mechanism of injury, time from injury to surgical stabilization, the type of incision used, use of preoperative antibiotics, or type of wound closure.
Notably, 25% of the patients had some sort of early wound complication, and 21% of the patients required surgical treatment due to their wound complication.
Their conclusion: "Smoking, diabetes, and open fractures all increase the risk of wound complication after surgical stabilization of calcaneus fractures.
Cumulative risk factors increase the likelihood of wound complications."
OrthoCash 2020
A 86-year-old man slips on the ice and falls sustaining the injury shown in Figure A. He has Type 2 diabetes mellitus, atrial fibrillation, coronary artery disease, end-stage renal disease on dialysis and chronic obstructive lung disease. All of the following variables are associated with increased mortality at one year after injury EXCEPT?

Intertrochanteric fracture
Two or more pre-existing medical conditions
Age of eighty-five years or more
Male gender
Operative fixation within 48 hours
Operative fixation within 48 hours is not associated with increased mortality. However, operative delay of 3 or more days results in increased mortality.
Medical optimization and surgery for hip fractures in elderly patients should be performed as soon as possible following admission to hospital. Surgical intervention in elderly hip fracture patients reduces morbidity and mortality.
Postoperatively, weightbearing as tolerated decreases the risk for poor outcomes and decreases complications e.g. muscle atrophy, pressure sores, pneumonia, urinary retention.
Zuckerman et al. reviewed mortality associated with operative delay in older patients with hip fractures. They found that operative delay of 3 or more calendar days results in greater 1-year mortality. Other predictors of mortality include age >85yrs, male sex, presence of 2 or more pre-existing medical conditions, ASA grade III or IV, and inter-trochanteric fracture.
Switzer et al. reviewed perioperative considerations in the geriatric patient. They showed that hip fracture repair after 2 days results in decrease in independent living, pressure sores and longer hospital stay. They found with early surgery, pain, length of hospital stay and 1-month mortality was reduced.
Figure A shows unstable intertrochanteric fracture. Incorrect Answers:
mortality.
OrthoCash 2020
Which of the following processes relies on an exopolysaccharide glycocalyx?
Osteoclast differentiation
Biofilm creation
Metastatic bone disease
Endochondral bone formation
Intramembranous bone formation Corrent answer: 2
Exopolysaccharide glycocalyx allows bacteria to adhere to orthopaedic implants and elude antimicrobial therapies through the creation of biofilms.
Biofilms are defined as a structured community of bacterial cells enclosed in a self-produced polymeric matrix and adherent to an inert or living surface.
Biofilm production usually occurs within 4 weeks, and is extraordinarily hard to eradicate with antibiotic therapy alone. In the setting of a chronic infection of an orthopaedic implant (>4 weeks), explantation of the implant followed by antimicrobial therapy is the most reliable method of curing the infection.
Nguyen et al. reviewed 21 patients who underwent revision arthroplasty with negative intraoperative cultures. After standard cultures were obtained (all negative), the implants underwent an ultrasound protocol to theoretically disrupt the biofilm. 1 of the 21 implants grew coag-negative Staph after the bath.
Fux et al. reviewed biofilms with respect to orthopaedic and non-orthopaedic conditions. They discussed how aspirations are often falsely negative possibly because the microorganisms persist only within a biofilm on the synovia but not in planktonic form.
Illustration A and the video provided show the process of biofilm formation. Incorrect Answers:
pathway.
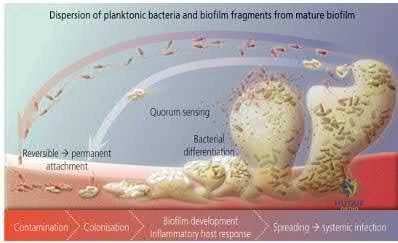
OrthoCash 2020
A ballistics expert examines the effects of bullets on tissues. He defines a "penetrating missile" as one that delivers an entrance wound but no exit wound, and a "perforating missile" as one that possesses both entrance and exit wounds. He also defines bullet "yaw" as the tumble of a bullet or its tendency to turn sideways in flight. A diagram of bullet yaw is seen in Figure A. Which of the following scenarios leads to the greatest transfer of kinetic energy to tissues?
Penetrating missile with mass "2m", velocity "v", yaw of 90 degrees at the point of impact
Perforating missile with mass "m", velocity "2v", yaw of 0 degrees at the point of impact
Penetrating missile with mass "m", velocity "2v", yaw of 90 degrees at the point of impact
Perforating missile with mass "m", velocity "2v", yaw of 90 degrees at the point of impact
Penetrating missile with mass "2m", velocity "v", yaw of 0 degrees at the point of impact
A penetrating (but not perforating) missile with highest velocity (2v) and largest yaw (90 degrees, or sideways travel) leads to greatest transfer of
kinetic energy.
The kinetic energy (E) of a bullet is proportional to its mass (m), and velocity
(v) squared. A bullet of mass m traveling at 2v will have greater E than one of mass 2m traveling at v. Maximum energy transfer is achieved with yaw of 90 degrees (sideways). Yaw is decreased with longer distances of bullet travel, allowing a bullet to strike its target nose-on. Penetrating (non-exiting) missiles deliver all their contained kinetic energy, while perforating (exiting) missiles transfer significantly less energy to tissues
Bartlett et al. reviewed ballistics and gunshot injuries. They state that energy transfer depends on 6 factors including: (1) amount of kinetic energy at impact, (2) stability and entrance profile (yaw), (3) caliber, construction and configuration of the bullet, (4) distance and path traveled within the body (penetrating vs perforating), (5) biological characteristics of tissues impacted, and (6) mechanism of tissue disruption (stretching, tearing, crushing).
Figure A illustrates the concept of bullet yaw. Illustration A shows blocks of gelatin perforated by similar caliber missiles at different velocities (A, 1,000fps; B, 2,800 fps), with arrows indicating missile tracks.
Incorrect Answers:

OrthoCash 2020
A 35-year-old man is thrown from his vehicle and sustains a left proximal femoral shaft fracture and right distal femoral shaft fracture. The surgeon elects to treat both fractures with reamed intramedullary nailing. Which of the following is true regarding the risk of malrotation?
The left femur (proximal fracture) is at increased risk of internal malrotation and the right femur (distal fracture) is at increased risk of external malrotation.
The left femur (proximal fracture) is at increased risk of external malrotation and the right femur (distal fracture) is at increased risk of internal malrotation.
Malrotation does not depend on fracture location, but whether the nail is placed antegrade or retrograde.
Both femora are at increased risk of internal malrotation.
Malrotation does not depend on fracture location, but whether the nail uses a piriformis entry point or a trochanteric entry point.
In proximal femoral fractures, the distal fragment (femoral shaft) will be relatively internally rotated. In distal femoral fractures, the distal fragment will be relatively externally rotated.
The direction of femoral malrotation depends on the pull of attached muscles. In PROXIMAL fractures, the proximal fragment is externally rotated by the iliopsoas, short external rotators and abductors. This leads to relative internal rotation of the distal fragment (femoral shaft), leading to INTERNAL malrotation. In DISTAL fractures, the proximal fragment (femoral shaft) is pulled medially by the adductors, while the distal fragment is pulled into external rotation by the lateral gastrocnemius and plantaris, leading to EXTERNAL malrotation.
Lindsey et al. reviewed malrotation following femoral shaft nailing and found that malrotation was present in up to 27.6% of all femoral shaft fractures managed this way. Risk was highest with pure transverse fractures (OTA 32-A3), and Winquist III and IV fractures (OTA 32-C). Using a fracture table increases risk of internal malrotation, and supine positioning with a bump (without fracture table) increases risk of external malrotation.
Ricci et al. reviewed nailing of femoral shaft fractures. They recommend the following to obtain correct rotation: (1) using alignment of the anterior superior iliac spine, patella and second toe, (2) fluoroscopic evaluation of cortical widths, key fragments or femoral anteversion, (3) checking both legs for symmetry before leaving the operating room. They also state that "The direction of femoral malrotation is based on which attached muscles are
involved. For example, proximal femur fractures tend toward net internal rotation of the femoral shaft secondary to the pull of the iliopsoas muscle, short external rotators, and glutei on the proximal femur. The relative external rotation of the proximal femur results in internal rotation of the distal segment. Conversely, external malrotation can occur in distal femoral fractures secondary to the pull of the adductor muscles on the proximal fragment and the pull of the plantaris and lateral gastrocnemius muscles on the distal fragment."
Illustration A shows how muscle attachments affect fracture deformity and predispose to malrotation.
Incorrect Answers
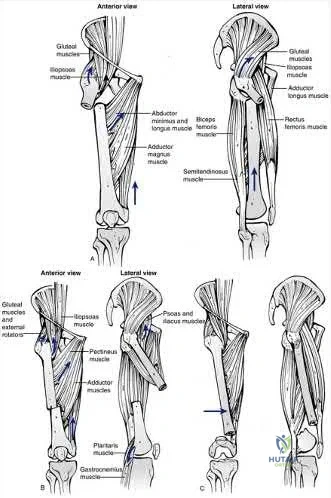
OrthoCash 2020
A 30-year-old man is brought to your level 1 trauma center with a closed left diaphyseal humerus fracture, a closed left midshaft femur fracture, right sided rib fractures, and multiple facial fractures following a motorcycle accident. He is neurovascularly intact in his left arm and leg. Figure A shows a radiograph of his left humerus. What would be the most appropriate definitive treatment?

Non-operative management of the humerus and plating of the femur
Plating of the humerus and intramedullary nailing of the femur
Non-operative management of the humerus and intramedullary nailing of the femur
Plating of both the humerus and femur
Intramedullary nailing of the humerus and plating of the femur Corrent answer: 2
The clinical scenario involves a polytrauma patient with ipsilateral humerus and femur fractures. The humerus should be plated to facilitate early weight bearing, allowing for mobilization with crutches.
Humeral shaft fractures account for 3-5% of all fractures and follow a bimodal distribution. Most humerus fractures can be treated non-operatively with a coaptation splint, followed by functional bracing. However, a strong relative indication for surgical management is a polytrauma patient. Plating of humerus fractures has high union rates and facilitates early weight bearing, which is necessary for rehabilitation with a concomitant lower extremity injury.
Bell et al. retrospectively reviewed the outcomes of polytrauma patients treated with plate fixation for humeral shaft fractures. All but one of the fractures united, and patients had excellent function following surgery, allowing early weight-bearing through the injured extremity.
Heineman et al. recently updated their systematic review of randomized controlled trials comparing plating with intramedullary nailing for humeral shaft fractures. They conclude that current literature supports a reduction in complication rates when plating humeral shaft fractures compared to intramedullary nailing.
Tingstad et al. performed a retrospective study evaluating immediate weightbearing with plated humeral shaft fractures. They demonstrated that ORIF of humeral shaft fractures followed by early weight-bearing was safe and efficacious.
Figure A is an AP x-ray of a left humeral shaft fracture. Illustration A shows the diaphyseal humerus fracture from Figure A following ORIF with a plate.
Incorrect Answers:

OrthoCash 2020
Risk of postoperative fixation failure for a complete sacral fracture has been associated with what variable?
Anterior pelvic ring fixation method
Vertical nature of sacral fracture
Iliosacral screw length
Number of iliosacral screws
Age > 50
Illustration A, a coronal CT image, shows a vertical sacral fracture, which creates a vertically unstable pelvic ring. Percutaneous iliosacral screw fixation is a useful technique in the management of vertically unstable pelvic fractures, but a vertical sacral fracture should make the surgeon more wary of fixation failure and loss of reduction.
According to the referenced study by Griffin et al, fixation failure of iliosacral screws was significantly associated with vertical sacral fractures and not with any of the other answers listed above. All cases of hardware failure occured within the first 3 weeks; a lesser relationship between hardware failure and sacroiliac joint injury was noted.

OrthoCash 2020
Which muscle shown in Figure A-E derives its innervation from the posterior cord of the brachial plexus?

Figure D shows the subscapularis. It is innervated by the upper and lower subscapular nerves derived from the posterior cord of the brachial plexus.
While the subscapularis is innervated by the upper and lower subscapular nerves, it may also be innervated by a middle subscapular nerve. The upper subscapular nerve consistently originates from the posterior cord (C5-C6) and usually innervates the bulk of the muscle, but the lower subscapular nerve often shows variation. The most common variation of the lower subscapular nerve is as a branch of the axillary nerve, yet this has not been shown to place the nerve at greater risk during surgery.
Lyons et al. review subscapularis tears, including diagnosis and management. While they recommend repair of acute tears, they state that repair of chronic tears is often impossible and may require tendon or muscle transfers.
Kasper et al. dissected 20 cadavers to detail the innervation of the subscapularis muscle. They found a highly variable pattern of innervation, with 25% of cadavers having a lower subscapular nerve arising from the axillary nerve.
Illustration A shows a picture of the brachial plexus. Incorrect Answers:
musculocutaneous nerve derived from the lateral cord.
lateral pectoral nerves derived from the medial and lateral cords, respectively. Answer 3: Image shows the rhomboid major, innervated by the dorsal scapular nerve derived from the C5 nerve root.
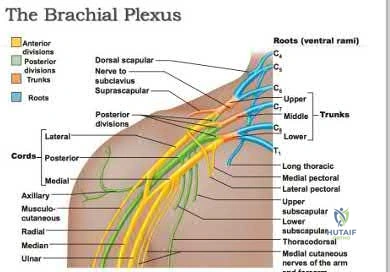
OrthoCash 2020
A 19-year-old male sustains the injury shown in Figure A while skiing. Injury to what structure should be evaluated intraoperatively during fixation of the fibula?

Deltoid ligament
Syndesmosis
Proximal fibula
Calcaneofibular ligament
Posterior tibial tendon Corrent answer: 2
According to the referenced study by Jenkinson et al, up to 37% of operatively treated ankle fractures can have undetected syndesmotic instability when examined intraoperatively. This is important due to the negative effects of a displaced mortise and the abnormal loading forces seen on the talus with even a 2mm lateral shift. Also, fibular fractures >4.5cm proximal to the mortise are more likely to be associated with syndesmotic instability, especially when deltoid ligament tears are present. When fixing the syndesmosis, Tornetta et al's referenced study has shown that the syndesmotic compression has no negative effects on ankle range of motion.
OrthoCash 2020
An 19-year-old male presents to the emergency room following an motor vehicle accident as an unrestrained driver. Examination reveals unilateral jugular vein engorgement. Chest and special view
radiographs are seen in Figures A and B respectively. Following CT scan of the chest, the next step in management is

Nonsurgical management and follow-up CT scan in 6 weeks
Closed reduction in the emergency room under sedation
Closed reduction in the operating room under general anesthesia with thoracic surgery on standby, followed by immobilization for 4 weeks
Closed reduction in the operating room under general anesthesia with thoracic surgery on standby, followed by compression plating
Open reduction in the operating room under general anesthesia, followed by transarticular pinning with K-wires
This patient has a right posterior sternoclavicular (SC) dislocation. Management involves closed reduction and bracing. Closed reduction should be performed with a thoracic surgeon available in the event of mediastinal involvement.
The SC joint can dislocate anteriorly or posteriorly. Posterior dislocations are first treated with closed reduction. If closed reduction fails, open reduction is indicated. Early complications of posterior SC dislocation include pneumothorax, laceration/erosion/occlusion of great vessels, esophageal rupture and brachial plexus compression. Late complications include tracheoesophageal fistula, stridor and dysphagia.
Groh et al. reviewed traumatic SC injuries. Reduction maneuvers in posterior SC dislocation include: (1) traction on the arm and slowly bringing it into extension, (2) traction with the arm in adduction and posterior pressure applied to the shoulder, and (3) pulling anteriorly on a towel clip encircling the medial clavicle. Chronic instability after posterior SC dislocations can be managed with figure-of-8 semitendinosus graft or medial clavicle resection and reattachment of the clavicle to the first rib with dacron tape.
Glass et al. performed a systematic review on SC dislocations. They found mediastinal compression occurred 30% of the time with posterior dislocations.
Figures A and B are radiographs demonstrating asymmetry of the SC joints, characteristic of a right posterior SC dislocation (Figure B is not a serendipity view). Illustration A demonstrates how in POSTERIOR dislocation, the clavicle appears INFERIOR, and in ANTERIOR dislocation, the clavicle appears SUPERIOR on a serendipity view radiograph respectively. Illustration B shows the imaging technique for a serendipity view radiograph. Illustration C is a reconstructed CT image of the patient showing left posterior SC dislocation.
Incorrect Answers:
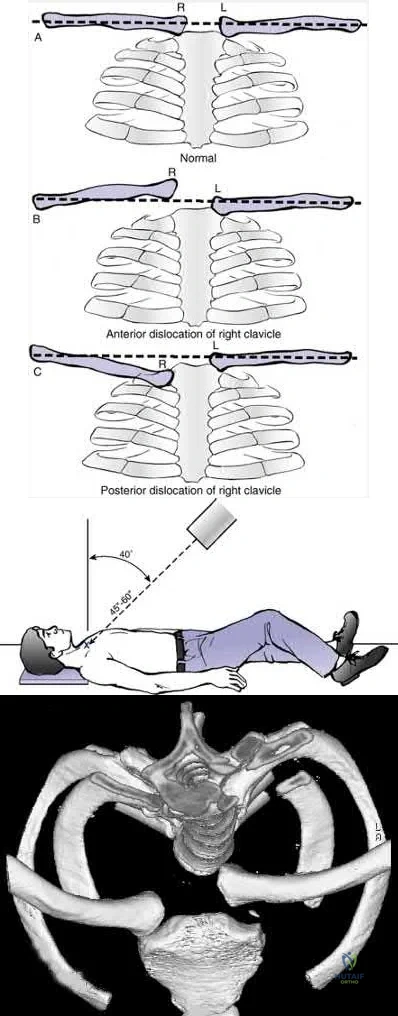
OrthoCash 2020
Figure A shows an isolated left ankle injury in an active 48-year-old recreational hockey player. Past medical history includes insulin dependent diabetes mellitus for 35 years. On physical examination the patient is unable to feel a 5.07 gm monofilament on the plantar aspect of his foot. His pedal pulses are palpable. Of the following options, what would be the recommended treatment?

Closed reduction and casting for 6 weeks
Closed reduction and casting for 12 weeks
Open reduction and internal fixation with restricted weight bearing for 2 weeks
Open reduction and internal fixation with restricted weight bearing for 6
weeks
Open reduction and internal fixation with restricted weight bearing for 12 weeks
Figure A shows an unstable, ankle fracture-dislocation in a otherwise healthy 48-year-old diabetic patient. The most appropriate management would be open reduction and internal fixation with an extended period of restricted weight-bearing.
Surgical treatment of unstable ankle fractures in diabetic patients is associated with a high complication rates. Diabetic patients are inherently poor healers due to the alterations in their microvascular system. Over-fixation of the fracture and extended immobilization has been shown to reduce wound and bone healing complications associated with diabetes. Surgical techniques typically call for multiple syndesmotic screws, stronger plates (vs 1/3 tubular plates) and prolonged periods of immobilization.
Jani et al. retrospectively examined a cohort of 15 patients with diabetes mellitus who sustained unstable ankle fractures. The combination of transarticular fixation (Retrograde transcalcaneal-talar-tibial fixation using large Steinmann pins or screws) and prolonged (>12 weeks), protected weightbearing provided 13 of 15 patients with a stable ankle for weight bearing.
Wukich et al. compared the complication rates of ankle fracture fixation in 46 patients with complicated diabetes and 59 patients with uncomplicated diabetes. They found that patients with complicated diabetes had 3.4 times increased risk of a non-infectious complications (eg. malunion, nonunion or Charcot arthropathy) and 5 times higher likelihood of needing revision surgery/arthrodesis.
Figure A shows AP and lat radiographs of SER4 ankle fracture-dislocation. Incorrect Answers:
fractures. Again, these need to be treated with an extended period of immobilization.
OrthoCash 2020
Fixed-angle implants are often used for fixation of distal femur fractures. Three commonly used implants (Implants A, B and C) are shown in Figures A, B and C respectively. Which of the following statements is true reagarding these implants?
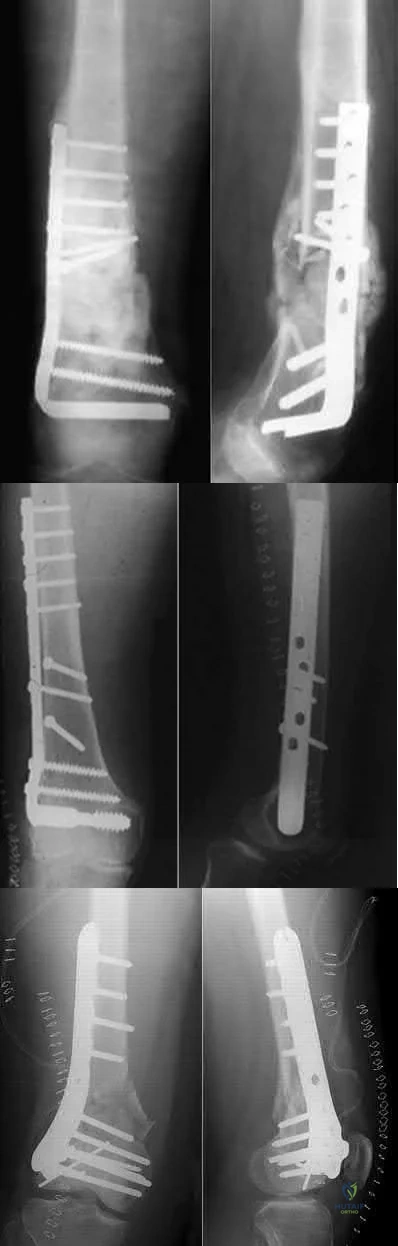
Implant B is better able to control fractures with a small distal segment than Implants A and C.
Implant C is better able to control coronal plane fractures than Implants A and B.
During insertion, Implant C results in removal of a larger amount of bone, compared with Implants A and B.
Implant A demonstrates less subsidence and greater load to failure compared with Implant C.
Implant A demonstrates lower fixation strength in torsional loading compared with Implant C
Implant C (locking compression plate, LCP) affords better control of coronal plane fractures than Implant A (95-degree angled blade plate, ABP) and Implant B (dynamic condylar screw, DCS).
The LCP allows for better control of coronal plane and multi-fragmented fractures because the multiple locking screws at the distal end secure the plate at multiple points and allow capture of fracture fragments in different planes.
Newer polyaxial locking plates have even greater versatility in screw positioning.
Vallier et al. reviewed their experience with the ABP and LCP in distal femur fixation. They note that complications and secondary procedures (treatment of infection, nonunion, malunion, prominent implant removal) were more frequent in LCP than ABP patients.
Gwathmey et al. reviewed the fixation of distal femoral fractures. They state that the LCP is biomechanically superior to the ABP in cyclic loading and ultimate strength. However, the LCP has less fixation strength in torsional loading.
Figure A shows a 95-degree angled blade plate. Figure B shows a dynamic condylar screw. Figure C shows a locking compression plate. Illustration A shows a coronal plane fracture (Hoffa fracture, OTA 33-B3).
Incorrect Answers:
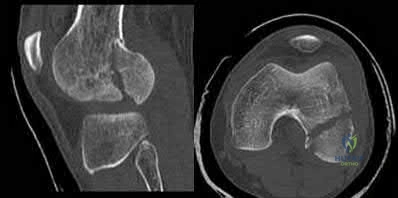
OrthoCash 2020
A 34-year-old man is involved in a motor vehicle accident and sustains an open tibia fracture and is treated with intramedullary nailing. For the next 4 years, he continues to have pain and persistent discharge from a sinus over his shin. He ambulates with crutches and refrains from putting weight on the extremity. The clinical appearance and radiographs are seen in Figures A and B. Wound culture reveals methicillin-resistant Staphylococcus aureus (MRSA). What is the next step in treatment?

Retention of tibial nail, lifelong intravenous antibiotic suppression
Debridement and lavage, exchange nailing using a larger diameter nail, intravenous antibiotics for 6 weeks.
Debridement and lavage, excision of sinus tract, implant removal, intravenous antibiotics for 6 weeks.
Debridement and lavage, addition of ring fixator, intravenous antibiotics for 6 weeks.
Debridement and lavage, excision of sinus tract, exchange nailing using antibiotic impregnated-cement nail, intravenous antibiotics for 6 weeks.
The patient has chronic osteomyelitis and an infected nonunion complicating previous IM nailing of an open tibia fracture. Successful treatment requires debridement, removal of the existing tibial nail, placement of an antibiotic-impregnated rod and IV antibiotics. Sinus tract excision and biopsy is important to exclude malignant transformation (Marjolin's ulcer).
Intramedullary infection is a recognized complication of IM nailing, especially in the setting of an open fracture. When the fracture fails to unite prior to deep infection treatment options include: nail removal and antibiotic exchange nailing, nail removal, intramedullary debridement and uniplanar external
fixation, or nail removal and resection of the infected segment with circular frame application and bone transport.
Paley et al. first described the treatment of intramedullary infection with antibiotic-impregnated cement nails in 6 femora, 2 tibiae and 1 humerus. There was no recurrence of infection. The antibiotic-impregnated cement nail fills the canal dead space while locally eluting high concentrations of antibiotics (for up to 36 wk), and is easy to remove.
Qiang et al. described antibiotic-cement rod placement in 19 patients (5 femora, 14 tibiae). There was no recurrence of infection. 11 cases went on to union, 6 cases achieved partial union, 1 case had nonunion and 1 went on to amputation.
Riel et al. described the method of creating a PMMA-coated nail. They advocate this method because it provides limited axial and bending stability (but no rotational stability).
McGrory et al. described 53 patients with malignancy complicating chronic osteomyelitis. 50 patients had squamous cell carcinoma. Most had mixed infections, predominantly Staph and Strep.
Figure A shows a poor soft tissue envelope with a draining sinus consistent with chronic osteomyelitis. Figure B is an AP radiograph showing fluffy callus formation, lack of bony bridging and interlocking screw back out. Combined with the clinical picture this would be consistent with deep infection.
Illustration A shows the steps of making an antibiotic-impregnated cement rod using a 3 mm guidewire, chest tube and cement gun. Illustration B is a lateral radiograph of a cement rod in the tibia.
Incorrect Answers:

OrthoCash 2020
A 45-year-old construction worker sustains a fall and presents with an isolated injury to his upper extremity. Radiographs of the affected wrist are shown in Figure A. After soft tissue swelling subsides, open reduction and internal fixation of the distal radius is performed. Following fixation, a "shuck" test is performed and shows persistent instability of the distal radioulnar joint. Incompetence of which of the following anatomic structures is the most likely etiology of this finding?

Radioulnar ligaments of the TFCC
Ulnar collateral ligament
Fracture fixation
Ulnolunate ligament of the TFCC
Ulnotriquetral ligament of the TFCC Corrent answer: 1
The patient has sustained a distal radius fracture and concomitant ulnar styloid fracture. The shuck test is performed after fixation of the distal radius to assess the status of the DRUJ, namely the radioulnar ligaments.
Injuries to the DRUJ often occur with distal radius fractures. The presence of an ulnar styloid fracture may signify injury to the DRUJ. After the distal radius has been fixed, the shuck test is performed. This test is completed with the elbow at 90 degrees of flexion, the forearm in neutral rotation, followed by pronation and supination. The examiner attempts to translate the ulnar in the sagittal plane. Excessive sagittal plane ulnar translation signifies DRUJ injury.
Kim et al. review the effect of ulnar styloid nonunion on functional outcome after distal radius ORIF. Of the 91 patients treated with distal radius ORIF, 22% were found to have a nonunion of the ulnar styloid. There was no
difference in wrist functional outcomes, ulnar sided wrist pain, or DRUJ stability.
Sammer et al. reviewed 144 patients undergoing ORIF of the distal radius. The DRUJ was stable in all patients after internal fixation. An ulnar styloid fracture was found in 88 patients. Functional outcome scores were not affected by the presence of an ulnar styloid fracture. Additionally, the size of the fracture, extent of displacement, or healing status did not affect the outcome.
Figure A shows a PA radiograph of the wrist demonstrating a comminuted distal radius fracture with a concomitant ulnar styloid fracture. Illustration A shows an example of the shuck test used to test the DRUJ.
Incorrect Answers:
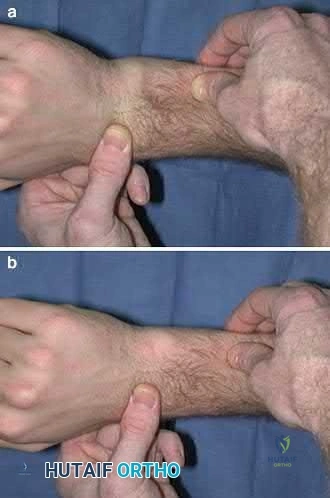
OrthoCash 2020
Which of the following deformities is most common after the amputation shown in Figure A?

Pes cavus
Pes planus
Hindfoot valgus
Equinovarus
Calcaneovalgus
The most common deformity after a midfoot amputation as shown in Figure A is an equinuovarus deformity due to the pull of the Achilles and plantarflexors in face of loss of the common extensors and distal insertion of the tibialis anterior.
Ng et al. review foot and ankle amputations, and review the issues inherent with each amputation level, including prosthesis fitting and use. They also mention that careful repair of all released or transected tendons is needed to maintain a plantigrade foot.
Early reviews the importance of soft tissue balancing with midfoot amputations. They note that the attachment of the resected tendons into the more proximal retained bones is critical for success in restoration of foot position and ambulation capabilities.
Figure A shows a midfoot amputation as the result of trauma. Illustration A shows the lateral view of the amputation, with an obvious equinus deformity.
Incorrect Answers:

OrthoCash 2020
A 68-year-old patient undergoes total knee arthroplasty for end-stage degenerative joint disease. Two years later, she trips and falls at home and sustains a fracture seen in Figures A and B. Before her fall, she was a community ambulator and had no knee pain. The component is determined to be stable and the surgeon decides to treat this fracture with closed reduction and retrograde intramedullary fixation with a supracondylar nail. Which of the following statements is true?

The starting point tends to be more posterior than usual, resulting in hyperextension at the fracture site.
An arthrotomy is not necessary
A high-speed carbide burr is usually necessary to enlarge the box for nail entry.
The backup plan should include devices that allow multiple points of fixation in the distal segment, such as dynamic condylar screw and fixed angle blade plate.
The backup plan should include devices that resist varus collapse, such as condylar buttress plates.
The patient has a cruciate-retaining (CR) prosthesis. The starting point for nail entry is more posterior than normal because of the femoral component. This leads to hyperextension at the fracture site.
Periprosthetic femur fractures above total knee implants occur in 2% of patients. It is important to note: (1) pre-injury function, to determine if the prosthesis was loose, (2) the type of implant (CR vs posterior stabilized, PS) as a PS implant with a closed box would make retrograde intramedullary nailing more difficult (the surgeon has to consider the size of the box vs size of the
nail, and if the box is smaller than the nail, must be prepared to enlarge the box with a metal-cutting burr, which has inherent problems of introducing wear debris into the joint), (3) pre-fracture radiographs help determine the position of the implants (flexion-extension, varus-valgus). These fractures can be treated with non-locking condylar buttress plates (not recommended today), fixed angle devices and intramedullary nailing.
McLaren et al. describe 7 osteopenic patients (mean age, 61yrs, range 47-84yrs) treated with retrograde supracondylar nailing. They suggest not reaming, and placing 2-3 screws in the distal fragment. This may require leaving the nail protruding by 1cm. They then suggest removing the protruding segment with a burr at the end of the procedure.
Haidukewych et al. debate plating vs nailing in a 80yr old osteopenic patient. It may be difficult to introduce retrograde intramedullary nails through the same incision if dense scar tissue is present. On the other hand, most plates require extensive dissection and do not respect the soft tissues and fracture biology, except for LISS plates and nails.
Figures A and B show a displaced Lewis and Rorabeck type II periprosthetic fracture. Illustration A shows the technique of retrograde supracondylar nailing. With the knee flexed, the fracture is reduced and the entry point is in the intercondylar notch. Illustration B shows a comparison between PS and CR implants. Note the "box" in the PS implant. This is absent in the CR implant.
Illustration C shows the Lewis and Rorabeck classification.
Incorrect Answers:

OrthoCash 2020
A 34-year-old female is involved in a high-speed motor vehicle collision and sustains a traumatic proximal forearm amputation. She successfully undergoes debridement and closure, and six weeks later, is fitted with her temporary prosthesis. In order to optimize her
outcomes upon returning to work as a secretary, which of the following is recommended?
Obtaining formal functional capacity testing
Waiting for final prosthesis fitting prior to full release
Minimize use of her prosthetic while at work
Allowing return to work when full elbow range of motion is seen
Offer outpatient psychological counseling Corrent answer: 5
Upper extremity trauma has serious, acute psychological effects that can linger long after the physical injury. These effects may negatively affect patient-reported outcomes, and may also be associated with worsening pain complaints. Coping and stress management techniques can be reviewed with formal psychological counseling, and should be offered to all patients who have underwent an amputation.
Richards et al surveyed 34 patients who had emergency upper extremity surgery and found high levels of psychological distress in patients, including 29% with high levels of both depression and post-traumatic stress disorder (PTSD). They also found that disability was strongly related to pain, depression, and PTSD symptoms.
Mallette et al assessed the attitudes of hand surgery patients and hand surgeons regarding psychologic influences on illness and compared their attitudes with those of the general population. They found that surgeons underestimated the openness of patients to discuss psychological issues and that patients believed in the strong effect of psychologic factors on healing and pain.
Illustration A shows a myoelectric prosthesis in a military veteran. Incorrect Answers:
Workers' Compensation is involved or formal disability proceedings occur. Answer 2: Final prosthetic fitting is not necessary for full release.

OrthoCash 2020
A 40-year-old male patient sustains a bimalleolar ankle fracture and undergoes open reduction and internal fixation. Four months later, he returns for follow-up with mild ankle discomfort, and a radiograph is shown in Figure A. What is the most appropriate next step in treatment?

Syndesmosis sagittal plane reduction and fixation
Syndesmosis coronal plane reduction and fixation
Osteotomy and revision of the fibula and syndesmosis
Retrieval of osteochondral fragment
Revision plating of the fibula and syndesmosis reduction and fixation.
This patient has undergone ORIF of the lateral malleolus with shortening of the lateral malleolus and lateral tibiotalar tilt. Revision surgery would entail bone grafting and re-plating of the fibula.
Malunion of the fibula component of ankle fractures lead to tibiotalar instability and post-traumatic ankle arthritis. The distal fragment is usually shortened and externally rotated. The osteotomy can restore length and correct rotation.
Markers for potential instability include: (1) asymmetry of the medial-lateral clear spaces, (2) talar tilt >2mm, (3) talar subluxation, (4) abnormal talocrural angle (normal, 75-86deg).
Chu et al. opined that reconstruction for distal fibula malunions should include:
(1) osteotomy, (2) +/- syndesmotic fixation and (3) autologous bone graft. They recommend: (1) low oblique osteotomy for fractures below the
syndesmosis, (2) transverse osteotomy above the syndesmosis for high fractures (PER4) and low fractures with tibiofibular instability, (3) inspection of the tibiofibular joint through an anterolateral window to ensure anatomic reduction.
Weber et al. described a method of corrective lengthening osteotomy of the fibula in 23 cases. They described 3 criteria for assessing normal fibular length. Seventeen patients had good-excellent results, and 6 had fair-poor results (1 of these 6 needed ankle fusion).
Figure A is an AP radiograph of a distal fibula fracture fixed in a shortened position with lateral talar tilt and degenerative changes at the anterolateral tibiotalar joint. Illustration A is an anteroposterior radiograph after fibular osteotomy and correction with medial distal tibial autograft to correct talar tilt and restore anatomic fibular length. Illustration B shows the normal talocrural angle. Illustration C shows the Weber-Simpson method of fibula lengthening used in Illustration A.
Incorrect Answers:
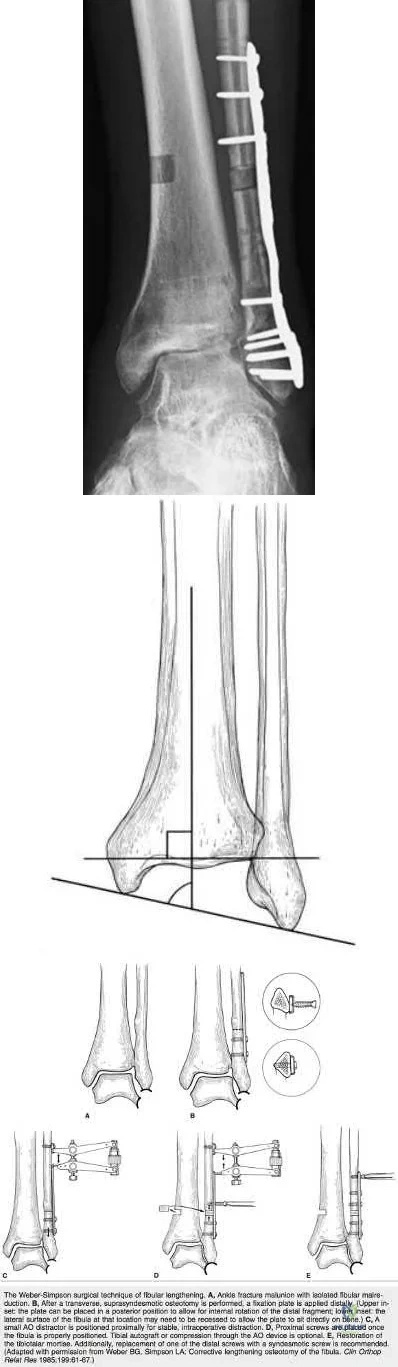
OrthoCash 2020
A 38-year-old concert violinist presents after falling onto a pronated, outstretched hand this morning. She complains of lateral elbow pain. Examination reveals lateral elbow tenderness, and an 80 degree arc of flexion-extension and 60 degree arc of prono-supination, with extremes of motion limited by pain. There is no bony block to motion. Radiographs of her injury are seen in Figures A through D. The most appropriate treatment plan that would allow her to return to her occupation would be

Sling immobilization for 2 days, followed by active mobilization.
Long-arm cast immobilization for 1 week, followed by active mobilization.
Long-arm cast immobilization for 1 week, followed by passive mobilization.
Long-arm cast immobilization for 2 weeks
Open reduction and internal fixation Corrent answer: 1
This patient has a Mason Type I radial head fracture (minimally displaced, no mechanical block, intra-articular displacement <2mm). Non-operative treatment is recommended. Sling immobilization for 2 days followed by active mobilization is recommended.
Radial head fractures occur after axial loading/fall onto a pronated, outstretched hand as the most force is transmitted from the wrist to the radial head in this position. For Type II and III fractures, open reduction and internal fixation is indicated. For Type III fractures with more than 3 fragments, radial head replacement is advocated. Radial head excision in the acute setting is generally not recommended to prevent late proximal radial migration and ulnocarpal impingement, as an easily missed Essex-Lopresti injury is possible; any patient with a painful DRUJ or mid forearm in the face of a radial head fracture should not undergo excision.
Paschos et al. compared (1) immediate active mobilization vs (2) sling immobilization for 2 days, followed by active mobilization vs (3) immobilization in a cast for 7 days followed by active mobilization. Early mobilization (Groups 1 and 2) had better ROM and less pain at 4 wks. Group 2 had better pain relief than Group 1 in the first 3 days, and the best functional scores at 12wks. They recommend early mobilization after a delay of 48 hours.
Tejwani et al. reviewed current management of radial head and neck fractures. Most fractures can be managed nonoperatively with early motion if there is no instability or block to elbow motion. Complex fractures require ORIF or arthroplasty (fragment >1/3 of the radial head, ORIF not possible).
Figures A through D are radiographs showing an undisplaced simple (AO/OTA 21-B2.1) radial head fracture.
Incorrect Answers:
OrthoCash 2020
What is the primary advantage of two incisions compared to one for open reduction internal fixation of a both bones forearm fracture?
lower risk of synostosis
lower risk of wound complications
lower rate of radial neuritis
less pronator teres denervation
lower malunion rate Corrent answer: 1
Post-osteosynthetic synostosis is a known complication in both bone forearm fractures. The risk is increased in fractures of the proximal 1/3 of the ulna and radius. Other risk factors include severity of injury, head trauma, polytrauma. Vince et al found synostosis was often associated with bone fragments or hardware in the interosseous space. Bauer et al found 1/65 cases treated utilizing the two-incision approach developed synostosis, while 5/12 cases in which the fractures were stabilized using a single incision developed synostoses. They recommended a two incision approach to both bones ORIF.
OrthoCash 2020
A 25-year-old female presents to the emergency room for the fourth time in the last week. She has vague complaints of extremity pain. Physical examination by a male ER resident has been limited each visit because she is terrified of the pain that the clinician may cause. On physical examination, she is withdrawn and frightened.
Regions of ecchymosis are noted throughout chest and abdomen. She has requested multiple radiographs, MRI and CT scans. Today's imaging (radiographs, MRI, CT scan) has been unrevealing. What is the most likely diagnosis?
Malingering
Complex regional pain syndrome
Anxiety disorder
Intimate partner violence
Fibromyalgia
Based on the history and clinical presentation, the most likely diagnosis is intimate partner violence.
Domestic violence or intimate partner violence can be in the form of mental or physical abuse, neglect or abandonment. Close to 25% of women will experience domestic violence. Risk factors include young age (19-29 years of age), females, pregnancy and lower socioeconomic status. Affected patients will have repeated visits to the emergency room, find reasons to stay in a treatment facility for an extended period of time and constantly seek approval
of their partner.
Shields et al. reviewed factors influence outcome in treatment of patients affected by domestic violence. They found that positive outcomes were associated with interdisciplinary approaches to management. This included better history assessment, providing written documentation regarding intervention and better access to information on community resources.
Illustration A is a chart documenting the frequency of female domestic violence throughout the world as of 2012.
Incorrect Answers

OrthoCash 2020
Which of the following injuries is most likely associated with the fracture seen in Figure A?

Medial meniscal tear
Lateral meniscal tear
Lateral collateral ligament rupture
Medial collateral ligament rupture
Posterior cruciate ligament rupture Corrent answer: 2
Lateral meniscal tears are most commonly associated with Schatzker II tibial plateau fractures (split/depressed).
Soft tissue pathology is common in tibial plateau fractures. In general, fractures that are largely displaced and/or a result of high energy trauma are more likely to have associated soft tissue pathology. A majority of meniscal injuries that occur in the setting of tibial plateau fractures are meniscocapsular detachments. This has important implications for healing (more reliable healing in the vascular zone). Additionally, the meniscus usually remains in close contact with the femoral condyle, while the tibial plateau widens around it. It is generally agreed upon that meniscal tears should be repaired, if possible, at the time of internal fixation to decrease the likelihood of postraumatic arthritis.
Gardner et al. review 62 patients with Schatzker II tibial plateau fractures that had an MRI preoperatively. For displaced fractures, the incidence of lateral meniscal tears was 83%, while the incidence of lateral collateral and posterior cruciate ligament injuries was 30%.
Ringus et al. attempted to determine if the degree of lateral tibial plateau fracture depression on computed tomography (CT) images predicted the presence of lateral meniscus tears. Fractures with > 9mm depression had an eight-fold increase in lateral meniscal tears, and those younger than 48 years-old had a four-fold increase in lateral meniscal tears.
Illustration A shows an MRI of a Schatzker II tibial plateau fracture with a lateral meniscal detachment and a medial meniscal tear. Illustration B shows the Schatzker Classification, I-VI.
Incorrect Answers:
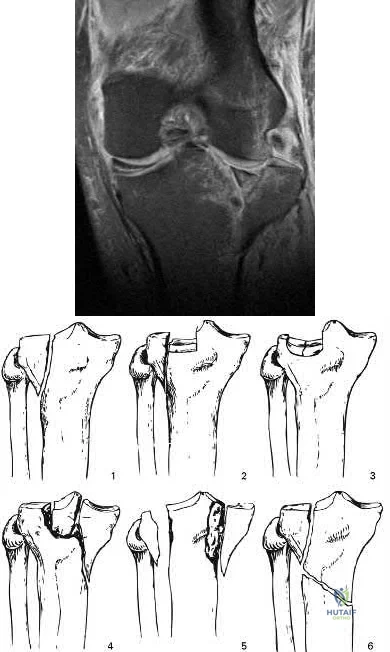
OrthoCash 2020
A 26-year-old male sustains a traction injury to his left arm after a motorcycle crash with resulting weakness in this left upper extremity. An electromyography (EMG) done shows normal cervical paraspinal muscle activity. Which of the following statements is true regarding this injury?
The injury has likely resulted in the avulsion of several nerve roots
Physical exam would likely reveal drooping of his left eyelid and anhidrosis
Intact paraspinal musculature on EMG is suggestive of a post-ganglionic lesion
Immediate surgical intervention with neurotization would eliminate weakness and restore function
The patient would show a normal histamine test Corrent answer: 3
Normal cervical paraspinal muscle activity on EMG is characteristic of a postganglionic injury.
Determining whether a brachial plexus injury is pre- or post-ganglionic has important treatment and prognostic implications. Findings that suggest a preganglionic lesion include Horner syndrome (ptosis, miosis, anhidrosis), a medially winged scapula, loss of paraspinal musculature activity on EMG, and a normal histamine test. These injuries tend to have a worse prognosis than post-ganglionic lesions, which show an abnormal histamine test and intact cervical paraspinal activity on EMG.
Moran et al. review brachial plexus injuries. They recommend a baseline EMG for non-operative injuries at 3-4 weeks time after Wallerian degeneration has occurred.
Shin et al. also review brachial plexus injuries. While an MRI can visualize much of the brachial plexus and may be able to demonstrate neuromas, a CT myelogram still remains the primary mode of radiographic evaluation for nerve root avulsion in the acute setting.
Illustration A shows the difference between a pre- and post-ganglionic lesion. Illustration B shows the brachial plexus for reference.
Incorrect Answers:
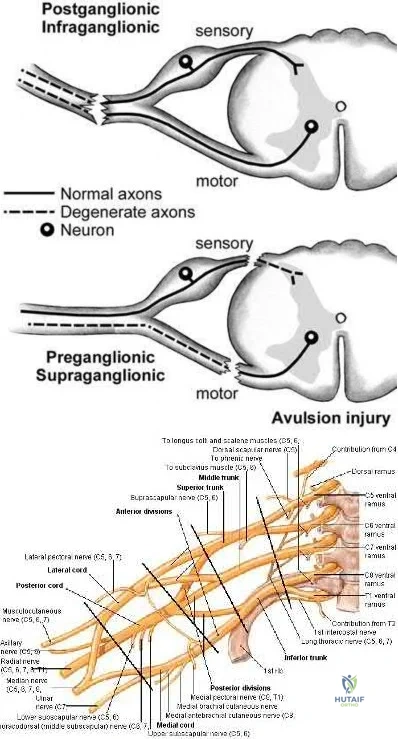
OrthoCash 2020
A 25-year-old male pedestrian sustained a Type II open tibia fracture after being struck by a car at 10:00PM. He was transported to a Level I trauma hospital where he was given intravenous antibiotics
and tetanus at 10:45PM. He underwent irrigation and debridement of the wound with 9L of saline solution and was treated with reamed intramedullary nail fixation at 11:45PM. A vacuum assisted dressing was placed over a 5x3cm skin deficit. What part of his overall treatment has shown to reduce the risk of infection THE MOST at the site of injury?
Early tetanus administration
Early intravenous antibiotic administration
Reamed intramedullary nail fixation
Irrigation and debridement of the open fracture with 9L of solution
Vacuum assisted dressings over skin deficit Corrent answer: 2
The most important factor shown to reduce the risk of infection at the site of an open fracture is early intravenous antibiotic administration.
Infection risk after Gustilo Type II open fractures ranges from 10-20% in large studies. Antibiotic treatment initiated within 3 hours from the time of injury has shown to significantly reduce the rate of infection. Antibiotic coverage for Type II open fractures should cover gram positive bacteria. Soil-contaminated wounds should include anaerobic coverage. The dose of antibiotic given must be within a therapeutic range and titrated to the patient's weight (e.g. Ancef 2 g IV for >70 kg). Duration of antibiotic therapy has been suggested to be between 1 and 3 days, although there is no agreement on a firm end point.
Pollak et al. reviewed a large cohort of open fractures treated at Level I trauma centers. They demonstrated a significant decrease in infection rate with either early direct admission (<2 hours) or transfer (<11 hours) for ONLY type III open tibia fractures. They did not not discuss timing of antibiotic treatment because this was not prospectively collected. Although they did not collect data on antibiotic treatment, the authors theorize that early transfer potentially resulted in earlier administration of antibiotics.
Patzakis et al. examined a series of 1104 open fractures to determine the factors contributing to infection. They showed the most important factor in reducing the infection rate was the early administration of antibiotics.
Illustration A is table showing the Gustilo classification of open fractures. Incorrect Answers
in open fractures, however, the most important factor has been shown to be
early antibiotic therapy.
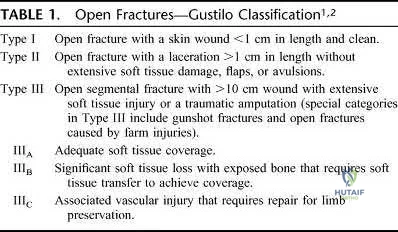
OrthoCash 2020
A 65-year-old female sustained the injury seen in Figure A after a slip and fall getting out of the shower. She is an avid golfer and walks the course on most days. Her past medical history includes borderline hypertension and migraine headaches. Which treatment option has shown to have the lowest re-operation rate and best clinical outcomes scores in this patient population?

Closed reduction with cannulated screw fixation
Open reduction with cannulated screw fixation
Closed reduction and short intramedullary nail fixation
Hemiarthroplasty
Total hip arthroplasty
Figure A shows a displaced right femoral neck fracture in an active, healthy elderly patient. Treatment of her hip fracture with total hip arthroplasty (THA) has shown to have the lowest re-operation rates and best functional outcome scores when compared to internal fixation devices and hemiarthroplasty.
Large studies have shown the incidence of femoral head AVN to be approximately 30-45% with displaced femoral neck fractures (Garden III-IV). For this reason, treatment of these injuries in elderly patients have supported arthroplasty over ORIF. Treatment of patients with THA vs. hemiarthroplasty have also been investigated. Studies have shown that THA has lower reoperation rates and improved functional outcome scores in younger, active elderly patients compared to hemiarthroplasty.
Avery et al. prospectively followed a cohort of 81 patients treated with THA vs. hemiarthroplasty in high functioning elderly patients with displaced femoral neck fractures. They showed a lower mortality rate (p = 0.013) and trend towards superior function in patients treated with THA. Advantages with THA vs hemiarthroplasty must be traded off against a slightly higher risk of dislocations.
Hedbeck et al. performed a randomized controlled trial involving 120 elderly patients with acutely displaced femoral neck fractures that were treated with either bipolar hemiarthroplasty or THA. They showed Harris hip scores and EQ-5D scores in favour of THA. They suggested treatment with THA in elderly, lucid patients with displaced femoral neck fractures.
Figure A is a AP pelvic radiograph. The most obvious finding is a displaced femoral neck fracture.
Incorrect Answers:
OrthoCash 2020
A 30-year-old man is the front seat passenger in a motor vehicle accident. He presents with deformity in his knee seen in Figures A and
B. Radiographs are seen in Figures C and D. Examination reveals weak foot pulses. After unsuccessful attempts at closed reduction, it is noted that the pulses are no longer palpable and the foot is cool. What is the next step in treatment?

Open reduction through an anteromedial approach, spanning external fixation. If pulses do not return, perform popliteal artery exploration.
Closed reduction in the operating room using a femoral distractor. If pulses do not return, perform on-table angiogram.
Manual in-line skeletal traction using a calcaneal pin in the emergency room, provisional long-leg splinting. If pulses do not return, perform computed tomography angiography in the radiology suite.
Manual in-line skeletal traction using a proximal tibial pin in the emergency room, provisional long-leg splinting. If pulses do not return, perform standard angiography in the angiography suite.
Open reduction through a posterior approach, spanning external fixation. If pulses do not return, perform popliteal artery exploration.
This patient has a posterolateral knee dislocation with a avascular limb. Urgent surgical intervention is warranted. The medial femoral condyle (MFC) has button-holed through the medial capsuloligamentous structures, leaving skin and medial subcutaneous tissues entrapped between the MFC and the joint cavity producing a ‘pucker sign’. An anteromedial approach is necessary.
Stabilization is then best achieved with an external fixator. Persistent ischemia (absence of pulses after reduction) is an indication for popliteal artery exploration.
Posterolateral dislocations are caused by a posterior-directed and rotational force, and are often irreducible. Vascular injury arises because of proximal tethering (fibrous adductor hiatus tunnel) and distal tethering (fibrous soleus hiatus tunnel) at the popliteal fossa.
Rihn et al. outlined the treatment algorithm for acutely dislocated knees. If pulses return after reduction, radiographs and evaluation of ABI are indicated. If ABI<0.9, CT angiography or formal angiography is indicated. If ABI >0.9, a period of in-hospital observation is indicated. If pulses remain absent and the limb remains ischemic following reduction, emergent surgical exploration and revascularization in the operating room is necessary. The spanning external fixator supplies enough rigidity to maintain reduction and allows access for serial neurovascular examinations.
Patterson et al. examined knee dislocations with vascular injury in the Lower Extremity Assessment Project (LEAP) study. Of the 18 patients in this group, all required popliteal arterial repair. Overall, 14 patients were treated with limb salvage and 4 patients were treated with an amputation. Patients with salvaged limbs had moderate to high level of disability 2 years after injury.
Figures A and B show the clinical appearance of posterolateral knee dislocation with a ‘pucker sign’. Figures C and D are radiographs showing posterolateral knee dislocation. These radiographs classically show 1 view of the tibia, but another view of the femur. Thus, the AP XR shows an AP of the tibia, but an oblique of the femur. Similarly, the lateral XR shows a lateral of the tibia, and an oblique of the femur. This is because XR technologist determines the AP/lateral projection based on the position of the foot (which follows the tibia).
Incorrect Answers:
OrthoCash 2020
An ankle-brachial index is most commonly indicated after sustaining which of the following fracture patterns, seen in Figures A-E?

Figure C shows a Schatzker IV tibial plateau fracture, or medial fracture-dislocation of the knee. Of the fracture patterns shown, Schatzker IV tibial plateau fractures have the highest incidence of vascular injury and most often require measurement of an ankle-brachial index (ABI) to rule-out associated vascular injury.
Schatzker IV tibial plateau fractures (fracture of the medial plateau) are rare and are most commonly associated with high-energy trauma after a varus/axial load. At the time of initial injury, the fracture pattern produces a temporary dislocation of the knee, placing tension on the peroneal nerve and popliteal artery. Because of the likelihood of associated popliteal artery injury, ankle-brachial indices, frequent neurovascular checks, and arteriography are commonly performed following injury.
Berkson et al. review high-energy tibial plateau fractures. They state that Schatzker IV fractures are usually the result of high-energy trauma, and have a high incidence of popliteal artery and peroneal nerve injury. In contrast, Schatzker V and VI are more commonly associated with compartment syndrome.
Gardner et al. review 103 tibial plateau fractures. 77% of fractures had an associated rupture of either cruciate or collateral ligaments. 86% of Schatzker IV fractures had an associated medial meniscus tear.
Illustration A is a worksheet for calculating the ankle brachial index. An ABI less than 0.90 has been shown to have a sensitivity exceeding 87% and a specificity exceeding 97% for identifying lower-extremity arterial injury.
Incorrect Answers:
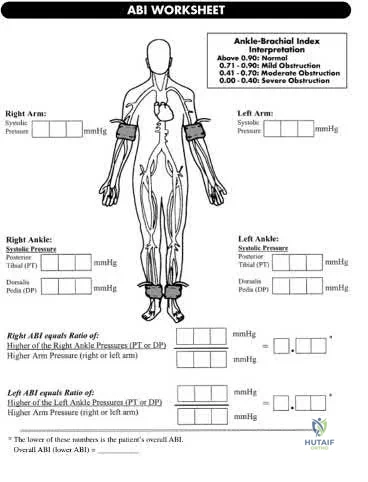
OrthoCash 2020
A 34-old-male was involved in a high speed MVC. He sustained an injury to his right leg as seen in Figures A and B. He was treated initially with external fixation for 11 days before his soft-tissues would permit definitive open internal fixation. After removing the external fixator and plating the fibula, what would be next step in the operative plan for reduction and fixation of this injury?

Application of an anterolateral pre-contoured plate with distal locking screws to the tibia
Anatomical reduction and stabilization of the tibial articular surface
Application of a medial pre-contoured plate with distal non-locking screws to the tibia
Anatomical reduction and stabilization of the tibial metaphyseal segment
Proximal screw insertion with non-locking screws to distract the metaphyseal fracture comminution
Figures A and B show an AO/OTA Type C Pilon fracture with metaphyseal comminution and intra-articular involvement of the tibia. There is an associated fibula fracture. The next step in the operative treatment of this injury, after removal of external fixation, would be anatomical reduction and stabilization of the articular surface.
The first step in the treatment of pilon fractures involves anatomical reduction and stabilization of the articular surface. This can be accomplished with pointed reduction clamps, K-wires, lag screws, or any combination of these. Plate fixation and reduction of the metaphyseal comminution should occur after the joint surface has been re-established. Simple fibular fractures can be plated before fixation of the tibia. Comminuted fibular fractures are usually better reconstructed after the tibia has been repaired, so that the tibia and talus can be used as a guide for positioning of the lateral malleolus.
Sirkin et al. reviewed the protocol for treatment of complex pilon fractures. They showed that the severity of soft-tissue injury will dictate the timing of fixation and choice of implant. To avoid wound healing problems, it is generally accepted that two or more stages of repair should be used.
Figure A, B and C show a high energy fracture to the distal tibia. Incorrect Answers:
reduction and stabilization of the articular fracture fragments. The use of medial and anterolateral locking plates are appropriate for fixation of this fracture. Longer implants improve load distribution and stability.
securing the proximal end of the plate to the tibial shaft. A kick-stand screw can be placed in the most proximal hole to increase the working length of the plate. This can be placed percutaneously if desired.
OrthoCash 2020
Which of the following ankle fractures seen in Figures A-E most likely occurred as a result of abduction of the foot relative to the tibia?

