OITE & ABOS Orthopedic Board Prep MCQs: Trauma, Sports Medicine & Hand | Part 6

Key Takeaway
This page offers Part 6 of a comprehensive OITE & AAOS Orthopedic Surgery Board Review series by Dr. Mohammed Hutaif. It features 100 high-yield MCQs, formatted like real exams, for orthopedic surgeons and residents. Practice in study or exam modes with explanations and references to master topics like Hip, Knee, and Wrist.
About This Board Review Set
This is Part 6 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 6
This module focuses heavily on: Deformity, Fracture, Hip, Knee, Ligament, Wrist.
Sample Questions from This Set
Sample Question 1: What allograft has the highest antigenicity when used for ligament reconstruction about the knee?...
Sample Question 2: A patient has a displaced complex intra-articular distal humeral fracture. What factor is considered most important when deciding on what surgical approach to use?...
Sample Question 3: A 75-year-old man has persistent radial sided hand and wrist pain. Radiographs demonstrate severe scaphotrapezial trapezoidal arthritis. His basal joint is unaffected. His pain has failed to improve with bracing, activity modification, and ...
Sample Question 4: What clinical finding is associated with the least favorable prognosis in an adolescent patient who has been diagnosed with a high-grade osteosarcoma of the distal femur?...
Sample Question 5: A 2-year-old child has refused to bear weight on his leg for the past 2 days. His parents report that he will crawl, has no fever, and has painless full range of motion of his hip and knee. Examination reveals no deformity or bruising, but ...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What allograft has the highest antigenicity when used for ligament reconstruction about the knee?
Explanation
Question 2
A patient has a displaced complex intra-articular distal humeral fracture. What factor is considered most important when deciding on what surgical approach to use?
Explanation
REFERENCES: McKee MD, Mehne DK, Jupiter JP: Fractures of the distal humerus: Part II, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1483-1522
McKee MD, Wilson TL, Winston L, Schemitsch EH, Richards RR: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Patterson SD, Bain GI, Mehta JA: Surgical approaches to the elbow. Clin Orthop
2000;370:19-33.
Bryan RS, Morrey BF: Extensive posterior exposure of the elbow: A triceps-sparing approach. Clin Orthop 1982;166:188-192.
Question 3
A 75-year-old man has persistent radial sided hand and wrist pain. Radiographs demonstrate severe scaphotrapezial trapezoidal arthritis. His basal joint is unaffected. His pain has failed to improve with bracing, activity modification, and image-guided corticosteroid injection. He has elected surgical treatment. What longterm complication can arise from a distal scaphoid resection?
Explanation
Resection of the distal pole of the scaphoid eliminates the arthritic contact at the scaphotrapeziotrapezoid joint; however, it functionally shortens the scaphoid. Theoretically, the lunate is at equilibrium between the extension moment of the capitate and the triquetrum and the flexion moment of the scaphoid. Shortening the scaphoid allows the extension moment of the triquetrum to predominate, pulling the lunate into extension and creating a DISI deformity. Concomitant capsulodesis or interposition is recommended by some authors to prevent this complication.
Question 4
What clinical finding is associated with the least favorable prognosis in an adolescent patient who has been diagnosed with a high-grade osteosarcoma of the distal femur?
Explanation
REFERENCE: Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlation. Philadelphia, PA, Lea and Febiger, 1989, pp 344-350.
Question 5
A 2-year-old child has refused to bear weight on his leg for the past 2 days. His parents report that he will crawl, has no fever, and has painless full range of motion of his hip and knee. Examination reveals no deformity or bruising, but there is mild swelling and tenderness over the anterior tibia. C-reactive protein, WBC count, and erythrocyte sedimentation rate studies are normal. Radiographs are negative. What is the best course of action?
Explanation
REFERENCES: Halsey MF, Finzel KC, Carrion WV, Haralabatos SS, et al: Toddler’s fracture: Presumptive diagnosis and treatment. J Pediatr Orthop 2001;21:152-156.
Oudjihane K, Newman B, Oh KS, et al: Occult fractures in preschool children. Trauma 1988;28:858-860.
Question 6
below show the radiographs, and the MRIs obtained from a year-old man with worsening left knee pain. A foot hip-to-ankle radiograph shows a degree varus knee deformity. The patient sustained a major left knee injury 5 years ago and a confirmed complete anterior cruciate ligament (ACL) tear. He managed this injury nonsurgically with a functional brace but experienced worsening pain. He was seen by an orthopaedic surgeon 18 months ago, and a medial meniscus tear was diagnosed; the tear was treated with an arthroscopic partial medial meniscectomy. Since then, his knee has been giving way more often, and he no longer feels safe working on a pitched roof. The patient received 6 months of formal physical therapy and was fitted for a new functional ACL brace, but he still has pain and instability. He believes he has exhausted his nonsurgical options and would like to undergo surgery. What is the most appropriate treatment at this time?
Explanation
Proximal tibial osteotomy is the most appropriate intervention to correct varus malalignment and to reduce stress on the ACL. In some cases, proximal tibial osteotomy alone may address both pain and instability, but if instability persists, particularly in the setting in which instability can be dangerous, subsequent ACL reconstruction can further stabilize the knee with less stress on the graft after the correction of malalignment. Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should be performed only at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL
reconstruction alone is not indicated for this patient.
Question 7
A 13-year-old boy who has a history of a pituitary adenoma has an unstable unilateral slipped capital femoral epiphysis. What is the indication for prophylactic pinning of the contralateral, unslipped side? Review Topic
Explanation
Question 8
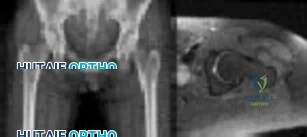
Figures below show the radiograph and the MRI scan obtained from a 37-year-old woman with a 2-month history of left hip pain. Which presurgical factor is most commonly associated with a poor outcome after a hip joint salvage procedure?
Explanation
MRI reveals an anterior labral tear, and the radiograph shows minimal arthritis with possible dysplasia. The most common location of pain in patients with a labral tear is the groin, and the most common physical finding is a positive impingement test result. Pain during sitting, clicking, and buttock pain are frequently described by patients with a labral tear, but these symptoms are less common than groin pain. A positive posterior impingement test finding is more common in patients with a posterior labral tear. Although age over 40 years and a body mass index higher than 30 can adversely affect clinical outcomes after joint preservation procedures such as PAO, hip arthroscopy, and femoral acetabular impingement surgery, the presence of hip arthritis on presurgical radiographs is the most commonly mentioned cause of failed hip joint preservation surgery. Tönnis grade is a radiographic measure of hip arthritis. A higher Outerbridge score is associated with more frequent poor outcomes after hip arthroscopy; however, the
Outerbridge cartilage score is determined by direct visualization at the time of surgery. The Outerbridge score cannot be determined presurgically.
Question 9
What is the plasma half-life of warfarin?
Explanation
Question 10
The blood supply to the anterior cruciate ligament is primarily derived from what artery?
Explanation
REFERENCES: Arnoczky SP: Blood supply to the anterior cruciate ligament and supporting structures. Orthop Clin North Am 1985;16:15-28.
Arnoczky SP, Rubin RM, Marshall JL: Microvasculature of the cruciate ligaments and its response to injury. J Bone Joint Surg Am 1979;61:1221-1229.
Question 11
A 68-year-old woman underwent an uncemented medial/lateral tapered femoral placement during a total hip arthroplasty. The orthopaedic surgeon noticed a nondisplaced vertical fracture in the calcar region of the femoral neck during final implant insertion. What is the most appropriate treatment?
Explanation
The recognized treatment for a proximal periprosthetic fracture is to first identify the extent and then optimize the correction of the fracture. Several studies indicate that proximal cerclage wiring is adequate to create "barrel hoop" stability of the proximal femur. Braided cables offer superior stability compared with twisted wires or Luque wires. Finally, the appropriate postoperative treatment is protected
weight bearing for 6 weeks, with periodic radiographs taken at 2-week intervals. Other options such as cementing the femoral stem and using a revision arthroplasty device are indicated for unstable fractures.
Question 12
An adult with a distal humeral fracture underwent open reduction and internal fixation. What is the most common postoperative complication?
Explanation
REFERENCES: Webb LX: Distal humerus fractures in adults. J Am Acad Orthop Surg 1996;4:336-344.
McKee MD, Wilson TL, Winston L, et al: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Question 13
When compared to patients with a body mass index (BMI) lower than 35, patients with a BMI above 40 who undergo primary total hip arthroplasty (THA) and total knee arthroplasty (TKA) are likely to have
Explanation
The obesity epidemic is increasing, and the number of patients with a BMI higher than 35 undergoing THA and TKA is increasing. Controversy exists regarding the optimal BMI cutoff and the ability to perform joint replacements safely in patients who are morbidly obese. Several clinical series as well as national database analyses have shown that morbidly obese patients undergoing THA/TKA are at increased risk for wound complications and 30- and 90-day readmissions. These patients’ incisions are typically larger because of the size of the soft-tissue envelope; although their clinical scores following successful THA/TKA often are lower than scores for controls, the overall change in clinical function and satisfaction is equivalent among nonobese and obese patients.

CLINICAL SITUATION FOR QUESTIONS 96 THROUGH 99
Figures 96a through 96c are the anteroposterior and lateral radiographs of a 64-year-old man with long-standing right knee osteoarthritis and pain unresponsive to nonsurgical treatment. This patient is scheduled for navigated cruciate-retaining right total knee arthroplasty. His range of motion is 20 to 120 degrees before surgery. Following bone resections and release of the posterolateral capsule and iliotibial band the knee is stable and extends fully, but during knee flexion there is lift-off of the anterior portion of the trial insert. Alignment is neutral to the mechanical axis. A distal femoral medial resection involved 9 mm of bone with a 9-mm-thick implant. An appropriate tibial resection was perpendicular to the long axis, and the posterior tibial slope was 7 degrees.
Question 14
Which radiographic abnormality most accurately serves as a predictor of ankle syndesmosis disruption?
Explanation
Normal syndesmotic relationships include a tibiofibular clear space smaller than 6 mm on both AP and mortise views. In a 1989 cadaveric study by Harper and Keller, a tibiofibular clear space exceeding 6 mm on both the AP and mortise views was the most reliable predictor of early syndesmotic widening. Tibiofibular overlap is measured 1 cm proximal to the plafond. Normal values exceed 6 mm or 42% of the width of the fibula on the AP view, or 1 mm on the mortise view. Proximal fibula fracture can occur in isolation without syndesmotic injury, frequently after direct trauma. The medial clear space is the distance between the lateral border of the medial malleolus and the medial border of the talus and is measured at the level of the talar dome. In the mortise view with the ankle in neutral dorsiflexion, the medial clear space should be equal to or smaller than the superior clear space between the talar dome and the tibial plafond. ?A normal medial clear space may be present with syndesmotic injury and consequently lacks sensitivity and specificity.
RECOMMENDED READINGS
Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. View Abstract at PubMed
Wuest TK. Injuries to the Distal Lower Extremity Syndesmosis. J Am Acad Orthop Surg. 1997 May;5(3):172-181. PubMed PMID: 10797219. View Abstract at PubMed
Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 40
A 41-year-old man sustained a twisting injury while running up stairs 4 weeks ago. He was treated in an ankle brace and has been bearing weight since the injury occurred. He has no history of ankle problems, but he now has ankle pain, swelling, and instability. The pain is aggravated by stairs, and the instability is worse on unlevel ground. Radiographs do not show a fracture.
Question 15
A 17-year-old high school soccer player sustains an anterior cruciate ligament (ACL) tear at the beginning of the season. An MRI scan confirms a complete ACL tear with no meniscal injuries. The patient plans an early return to play and would like to avoid surgery. Therefore, the patient and family should be advised that nonsurgical management consisting of rehabilitative exercises and the use of a functional knee brace will most likely result in
Explanation
REFERENCES: Shelton WR, Barrett GR, Dukes A: Early season anterior cruciate ligament tears: A treatment dilemma. Am J Sports Med 1997;25:656-658.
Snyder-Mackler L, Fitzgerald GK, Bartolozzi AR III, Ciccotti MG: The relationship between passive joint laxity and functional outcome after anterior cruciate ligament injury. Am J Sports Med 1997;25:191-195.
Question 16
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
REFERENCES: Apple DF: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 1130-1131.
Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 544-545.
Question 17
9A 9B 9C 9D Figures 9a through 9d are the radiographs of a 21-year-old woman who is involved in a high-speed motor vehicle collision and sustains an isolated right closed-foot injury. Before surgery, the patient is advised about the relatively poor long-term outcomes associated with this injury. What is the most common reason for functional limitations after surgical treatment in this scenario?

Explanation
When a displaced talar neck fracture occurs, the rate of osteonecrosis is high; however, many revascularize the talus without collapse. A nonunion can occur but is less common than osteonecrosis and arthritis. A varus malunion can be debilitating and lead to subtalar arthritis. In a fracture with the talar body dislocated posteromedially (such as in this example) neurologic deficits in the tibial nerve distribution are common but typically improve with urgent
reduction. Studies show that posttraumatic subtalar arthritis is common after this injury and is the most likely cause of long-term functional impairment.
RECOMMENDED READINGS
Vallier HA, Nork SE, Barei DP, Benirschke SK, Sangeorzan BJ. Talar neck fractures: results and outcomes. J Bone Joint Surg Am. 2004 Aug;86-A(8):1616-24. PubMed PMID: 15292407. View Abstract at PubMed
Lindvall E, Haidukewych G, DiPasquale T, Herscovici D Jr, Sanders R. Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am. 2004 Oct;86-A(10):2229-34. PubMed PMID: 15466732. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 10 THROUGH 12

10A

10B

10C
Figure 10a is the radiograph of a 30-year-old man who sustained an injury in a motor vehicle collision.
Question 18
A 20-year-old man is brought to the emergency department after a high-speed motor vehicle accident. His initial blood pressure is 70/40 mm Hg. He is currently receiving intravenous fluids as well as blood. His Focused Assessment with Sonography for Trauma examination did not show any free fluid in his abdomen and his chest radiograph is unremarkable. An AP pelvis radiograph is shown in Figure 15. What is the next most appropriate step in the management of his pelvic injury? Review Topic
Explanation
Question 19
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. What is the most appropriate management of this condition?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross- sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 20
A 23-year-old male is involved in a motor vehicle accident and sustains a left open femur fracture, right open humeral shaft fracture, and an LC-II pelvic ring injury. Which of the following best describes the radiographic findings associated with this pelvic injury pattern using the Young-Burgess Classification system?

Explanation
Burgess et al discuss the effectiveness of a treatment protocol as determined by their pelvic injury classification and hemodynamic status. The injury classification system was based on lateral compression, anteroposterior compression, vertical shear, and combined mechanical injury types. They found that their classification-based treatment protocols reduce the morbidity and mortality related to pelvic ring disruption.
Tile discusses acute pelvic trauma and his classification system for pelvic injuries (ie. Types A, B, and C). He states that any classification system must be seen only as a general guide to treatment, and that the management of each patient requires careful, individualized decision making.
Incorrect
2:
This
describes
an
APC-II
injury
3:
This
describes
an
APC-III
injury
4:
This
describes
and
LC-I
injury
Question 21
A distal radius fracture in an elderly man is strongly predictive for what subsequent injury?
Explanation
REFERENCE: Haentjens P, Autier P, Collins J, et al: Colles fracture, spine fracture, and subsequent risk of hip fracture in men and women: A meta-analysis. J Bone Joint Surg Am 2003;85:1936-1943.
Question 22
A 45-year-old man has severe pain in both feet after his boots become wet while hunting. Examination 3 hours after the onset of symptoms reveals that his feet are cold to touch and the skin appears blanched. Management should consist of
Explanation
REFERENCES: Pinzur MS: Frostbite: Prevention and treatment. Biomechanics 1997;4:14-21.
Fritz RL, Perrin DH: Cold exposure injuries: Prevention and treatment. Clin Sports Med 1989;8:111-128.
Question 23
Which of the following methods of meniscal repair has the highest load to failure strength?
Explanation
REFERENCES: DeHaven KE: Meniscus repair. Am J Sports Med 1999;27:242-250.
Dervin GF, Downing KJ, Keene GC, McBride DG: Failure strengths of suture versus biodegradable arrow for meniscal repair: An in vitro study. Arthroscopy 1997;13:296-300.
Barber FA: Endoscopic meniscal repair: The T-fix technique. Sports Med Arthroscopy Rev 1999;7:28-33.
Question 24
A surgeon decides to report outcomes for a new surgical procedure that he has performed on 10 patients who have a rare type of arthritis. He provides data on the functional and subjective patient outcomes. This type of study design is best described as a
Explanation
Question 25
Examination of a 25-year-old man who was injured in a motor vehicle accident reveals a fracture-dislocation of C5-6 with a Frankel B spinal cord injury. He also has a closed right femoral shaft fracture and a grade II open ipsilateral midshaft tibial fracture. Assessment of his vital signs reveals a pulse rate of 45/min, a blood pressure of 80/45 mm Hg, and respirations of 25/min. A general surgeon has assessed the abdomen, and a peritoneal lavage is negative. His clinical presentation is most consistent with what type of shock?
Explanation
REFERENCE: Sutton DC, Siveri CP, Cotler JM: Initial evaluation and management of the spinal injured patient, in Cotler JM, Simpson JM, An HS, et al (eds): Surgery of Spinal Trauma. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 113-126.
Question 26
During a posterior cruciate ligament (PCL)-retaining total knee arthroplasty, a critical principle to remember is to
Explanation
Maintenance of the joint line and accurately tensioning the PCL are critical in the proper execution of a PCL-retaining total knee arthroplasty. Appropriate tension helps ensure femoral rollback and avoid stiffness or instability. Raising the joint line to help ensure full extension should be avoided in cruciate- retaining knees, because doing so creates an unfavorable kinematic environment. The three important principles of surgical technique needed to maintain appropriate tensioning of the PCL include 1) choosing the proper femur size to reproduce the native femoral anterior/posterior dimension, 2) reproducing the joint line by resecting as much tibia from the healthy side as will be replaced by the smallest thickness of the tibial component and, 3) ensuring that full extension is achieved by soft-tissue releases and not by taking additional distal femur, as may be done in a posterior stabilized approach. Another important principle is to re-create the natural degree of the patient’s posterior tibial slope to avoid tightness in
flexion.
Question 27
A 19-year-old collegiate middistance runner has a 4-year history of bilateral leg pain. Pain begins within 10 minutes after starting to run and is described as a “tightness and cramping in the front of the legs.” Symptoms resolve within 15 to 20 minutes of running cessation. A presumptive diagnosis of exercise-induced compartment syndrome (EICS) is made, and the patient elects to undergo compartmental pressure testing. What is the strongest indication for elective fasciotomy of the anterior compartment?
Explanation
This clinical scenario describes a patient with EICS, marked by a nonphysiologic rise in muscle compartment pressure during exercise. Pressure testing is the best currently accepted method of diagnosis. Most physicians use the following criteria for diagnosis: resting pressure higher than 15 mm Hg, 1-minute postexercise pressure higher than 30 mm Hg, or 5-minute postexercise pressure higher than 20 mm Hg. Only 1-minute postexercise anterior compartment pressure of 42 mm Hg meets these criteria. Neurologic symptoms in the plantar foot would imply involvement of the posterior compartments and would not support the diagnosis of anterior compartment involvement.
Question 28
With respect to femoral component design, stress relief osteopenia in the proximal femur following noncemented total hip arthroplasty appears to be most strongly influenced by the
Explanation
Question 29
In patient selection for meniscal allograft transplantation, which of the following variables has the greatest influence on outcome?
Explanation
REFERENCES: Carter TR: Meniscal allograft transplantation. Sports Med Arthroscopy Rev 1999;7:51-63.
Garrett JC: Meniscal transplantation: A review of 43 cases with two- to seven-year follow-up. Sports Med Arthroscopy Rev 1993;2:164-167.
van Arkel ER, de Boer HH: Human meniscal transplantation: Preliminary results at 2- to 5-year follow-up. J Bone Joint Surg Br 1995;77:589-595.
Question 30
Thoracic disk herniations are most frequently found in what area of the spine?
Explanation
REFERENCES: Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864.
Bohlman HH, Zdeblick TA: Anterior excision of herniated thoracic discs. J Bone Joint Surg Am 1988;70:70-77.
Question 31
A 29-year-old woman who underwent an anterior cruciate ligament (ACL) reconstruction 6 months ago now reports difficulty achieving full knee extension, and physical therapy fails to provide relief. The knee is stable on ligament testing. Figure 3 shows the findings at a repeat arthroscopy. Treatment should now include
Explanation
REFERENCES: Delince P, Krallis P, Descamps PY, et al: Different aspects of the cyclops lesion following anterior cruciate ligament reconstruction: A multifactorial etiopathogenesis. Arthroscopy 1998;14:869-876.
Fisher SE, Shelbourne KD: Arthroscopic treatment of symptomatic extension block complicating anterior cruciate ligament reconstruction. Am J Sports Med 1993;4:558-564.
Question 32
The axial stability of a 4-pin uniplanar external fixator used to treat a patient who has a transverse midthird fracture of the tibia with a 5-mm fracture gap can be most greatly increased by
Explanation
Bone contact allows load sharing between bone and fixator for compressive, torsional, and certain bending loads. Without bone contact, the external fixator must support the full load. It is also possible to apply compression across a fracture gap using an external fixator. With transverse fractures, application of compression across the fracture site can greatly increase the stiffness of the framebone system.

Question 33
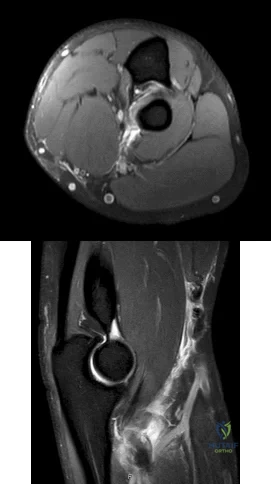
Figures 1 and 2 are the MRI scans of a 35-year-old right-hand dominant man who has right elbow pain after trying to lift a large television at home. An examination reveals ecchymosis, an abnormal hook test, and altered biceps muscle contour. What treatment is most likely to result in a satisfactory and predictable outcome?
Explanation
Question 34
Figure 23 shows the radiograph of a 55-year-old man who underwent a total hip arthroplasty 5 years ago. Management should now consist of
Explanation
REFERENCES: Lewallen DG, Berry DJ: Periprosthetic fracture of the femur after total hip arthroplasty: Treatment and results to date, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-249.
Bethea JS, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Question 35
- Chronic flatfoot deformity is most commonly associated with a contracture of the
Explanation
Deltoid ligament, plantar fascia, or intrinsic tendon contracture would not cause this deformity.
Question 36
04 Which of the following laboratory studies is predictive of wound healing prior to performing a lower extremity amputation?
Explanation
(eliminates false positive predictions with using area under the Doppler waveform). Pressures less than 20 mm Hg are predictive of poor healing. Miller 505-6
back to this question next question
Question 37
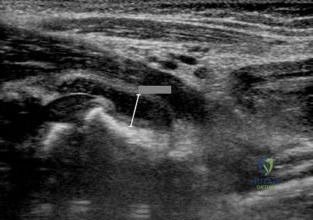
What is the most common associated pathology in patients who have suprascapular nerve entrapment secondary to ganglion cysts?
Explanation
REFERENCES: Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
Iannotti JP, Ramesey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Moore TP, Fritts HM, Quick DC, Buss DD: Suprascapular nerve entrapment caused by supraglenoid cyst compression. J Shoulder Elbow Surg 1997;6:455-462.
Question 38
A 25-year-old male sustains the isolated injury shown in Figure A. Antegrade intramedullary nailing is planned for definite fixation within the next 12 hours. After obtaining lateral radiographs of the injury site, what would be the next best step in management of this patient?

Explanation
Femoral neck fractures are seen less than 10% of the time with femoral shaft fractures, but they are frequently missed on initial evaluation. The neck fracture line is almost vertical and nondisplaced, or minimally displaced. Therefore fine (2-mm) cut CT scan through the femoral neck should be ordered in the preoperative workup of these patients.
Tornetta et al. reported that they reduced the delay in diagnosis of concomitant femoral neck fractures by 91% by instituting a protocol that included: dedicated AP internal rotation plain radiograph, a fine (2-mm) cut CT scan through the femoral neck, an intraoperative fluoroscopic lateral radiograph prior to fixation, as well as postoperative AP and lateral radiographs of the hip in the operating room prior to awakening the patient.
Figure A shows a trauma view lower extremity radiograph with an isolated left midshaft femur fracture.
Incorrect Answers:
setting of fracture. Answer 5: The age, injury and fracture pattern are not consistent with a pathologic femur fracture.
Question 39
The major blood supply to the cruciate ligaments arises from which of the following structures?
Explanation
REFERENCES: Arnoczky SP: Anatomy of the anterior cruciate ligament. Clin Orthop 1983;172:19-25.
Arnoczsky SP: Blood supply to the anterior cruciate ligament and supporting structures. Orthop Clin North Am 1985;16:15-28.
Question 40
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure A. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion? Review Topic

Explanation
Question 41
A 35-year-old man has had a mass on the bottom of his foot for the past 6 months. He reports that initially the mass was exquisitely painful but now is minimally tender. Examination reveals a 2.5- x 2.0-cm firm, noncompressible, nonmobile mass contiguous with the plantar fascia in the distal arch. The mass is particularly prominent with passive dorsiflexion of the ankle and toes. What is the best course of action?
Explanation
REFERENCES: Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Durr HR, Krodel A, Trouillier H, Lienemann A, Refior HJ: Fibromatosis of the plantar fascia: Diagnosis and indications for surgical treatment. Foot Ankle Int 1999;20:13-17.
Question 42
- Demyelination diseases as multiple sclerosis and Guillain-Barre $ create neurologic symptoms by
Explanation
Question 43
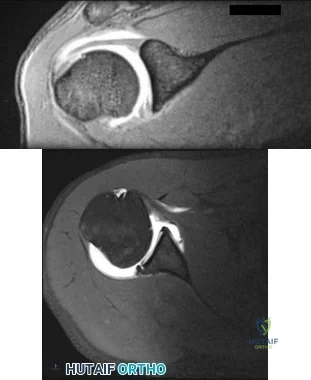
Based on the injury shown on the axial MRI scan of the shoulder in Figure 1, what other pathology should be closely examined for during surgery?
Explanation
specific to this pathology.
Question 44
The best candidate for a reverse total shoulder arthroplasty is a patient with rotator cuff tear arthropathy with Review Topic
Explanation
Question 45
Figure 23 shows the radiograph of an elderly man who fell on his right arm. What is the most important determinate of a good outcome following this injury?
Explanation
REFERENCES: Koval KJ, Gallagher MA, Marsicano JG, et al: Functional outcome after minimally displaced fractures of the proximal part of the humerus. J Bone Joint Surg Am 1997;79:203-207.
Hodgson SA, Mawson SJ, Stanley D: Rehabilitation after two-part fractures of the neck of the humerus. J Bone Joint Surg Br 2003;85:419-422.
Question 46
A complication unique to computer navigation of total knee arthroplasty (TKA) is
Explanation
Threaded pins are frequently inserted into the femoral shaft and tibial shafts or proximal tibia to attach arrays for tracking devices. There have been case reports of fractures propagating through the pin tracks, which is a complication unique to computer navigation. Intercondylar fractures can occur following posterior stabilized TKA. Vascular injury, ligament disruption, and nerve palsy are rare complications following TKA performed with or without computer navigation.

CLINICAL SITUATION FOR QUESTIONS 111 THROUGH 113
Figure 111 is the anteroposterior radiograph of a 79-year-old woman with a presurgical diagnosis of osteonecrosis who sustained a periprosthetic tibia fracture following her total knee arthroplasty (TKA).
Question 47
A patient has had a locked posterior dislocation of the shoulder for the past 6 months. After undergoing total shoulder arthroplasty that includes adequate anterior releases and posterior capsulorrhaphy, the patient still exhibits posterior instability intraoperatively. The postoperative rehabilitation regimen should include
Explanation
REFERENCES: Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Loebenberg MI, Cuomo F: The treatment of chronic anterior and posterior dislocations of the glenohumeral joint and associated articular surface defects. Orthop Clin North Am 2000;31:23-24.
Question 48
At what age does the lateral epicondyle normally ossify in males?
Explanation
Question 49
The biopsy specimens seen in Figures 55a and 55b are from a lytic lesion in the sacrum of a 58-year-old man. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 372.
Fuchs B, Dickey ID, Yaszemski MJ, et al: Operative management of sacral chordoma. J Bone Joint Surg Am 2005;87:2211-2216.
Fourney DR, Rhines LD, Hentschel SJ, et al: En bloc resection of primary sacral tumors: Classification of surgical approaches and outcome. J Neurosurg Spine 2005;3:111-122.
Question 50
Which of the following best characterizes the antigenicity of allograft bone?
Explanation
REFERENCES: Crawford MJ, Swenson CL, Arnoczky SP, et al: Lyophilization does not inactivate infectious retrovirus in systemically infected bone and tendon allografts. Am J Sports Med 2004;32:580-586.
Stevenson S, Li XQ, Davy DT, et al: Critical biological determinants of incorporation of non-vascularized cortical bone grafts: Quantification of a complex process and structure. J Bone Joint Surg Am 1997;79:1-16.
Simon SR (eds): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 277-320.
Question 51
A previously healthy 13-year-old girl has had thigh pain for the past 3 weeks. The radiograph shown in Figure 47a reveals a lesion in the right femur. A bone scan and CT scan of the chest show no evidence of other lesions. A biopsy specimen is shown in Figure 47b. What is the most likely diagnosis?
Explanation
REFERENCES: Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby, 1988.
Mirra, JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989.
Question 52
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include
Explanation
REFERENCE: Sabharwal S, Tredwell SJ, Beauchamp RD, Mackenzie WG, Jakubec DM, Cairns R: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 53
The natural history of cervical spondylolytic myelopathy is best described as
Explanation
REFERENCES: Emery SF: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Lees F, Turner JA: The natural history and prognosis of cervical spondylosis. Brit Med J 1963;2:1607-1610.
Clarke E, Robinson PK: Cervical myelopathy: A complication of cervical spondylosis. Brain 1956;79:486-510.
Question 54
Arthrodesis
Explanation
with OA or RA. Certainly in patients who have glenoid bone deficiency precluding placement of a glenoid component…" as is apparent in this radiograph.
Question 55
What structure has been described as having a risk of injury with retractor placement on the sacrum during combined acetabular-pelvic ring surgery using the Stoppa approach with a lateral window?

Explanation
Question 56
-An infant was born with complex syndactyly involving all 4 fingers of both hands, short and deformed thumbs, and similar syndactyly involving both feet. In addition, an altered facial appearance was noted with protruding eyes, a towered cranium, and midface hypoplasia. This appearance is characteristic of which syndrome?
Explanation
Question 57
A 2-year-old child is brought in by his parents for evaluation of intoeing. The child has a normal neuromuscular examination, but the heel bisector line is in the fourth web space, indicating a severe flexible metatarsus adductus deformity. The remainder of the lower extremity examination is unremarkable. What is the most appropriate treatment?
Explanation
REFERENCES: Beaty J: Congenital anomalies of the lower extremity, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. Philadelphia PA, Mosby, 2003, pp 983-988.
Katz K, David R, Soudry M: Below-knee plaster cast for the treatment of metatarsus adductus.
J Pediatr Orthop 1999;19:49-50.
Weinstein SL: Bristol-Myers Squibb/Zimmer award for distinguished achievement in orthopaedic research. Long-term follow-up of pediatric orthopaedic conditions: Natural history and outcomes
of treatment. J Bone Joint Surg Am 2000;82:980-990.
Question 58
What is the most important preoperative factor predicting conversion to total hip arthroplasty after arthroscopic surgery of the hip?
Explanation
The authors cited in the references examined large databases to determine the risk factors for conversion to total hip arthroplasty after arthroscopic surgery of the hip. In the study by Kester and associates, obesity had an odds ratio (OR) of 5.6 for conversion to hip arthroplasty, whereas age over 60 years had an OR of
Question 59
Two major pharmacologic classes of bisphosphonates exist: nitrogen-containing and non-nitrogen-containing compounds. The nitrogen-containing compounds work by which of the following actions?
Explanation
Question 60
A 66-year-old woman who requires a cane for ambulation now notes increasing difficulty in using the cane after undergoing total elbow arthroplasty 3 months ago. AP and lateral radiographs are shown in Figures 15a and 15b. What is the most likely diagnosis?
Explanation
REFERENCES: Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orhthopaedic Surgeons, 2002, pp 323-327.
Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000,
pp 598-601.
Question 61
Figure below depicts the radiograph obtained from a 30-year-old woman who began having more right than left hip pain during a recent pregnancy. Physical examination reveals increased range of motion with positive flexion abduction and external rotation and flexion adduction and internal rotation as well as pain with external logroll. Assessment of Figure below reveals

Explanation
Studies have demonstrated that pelvic inclination can dramatically affect the interpretation of radiographs in the dysplastic hip, with 9° of increased pelvic inclination leading to the presence of crossover signs and posterior wall signs. A distance of 30 mm to 50 mm from the sacrococcygeal junction to the pubis is often used to assess the adequacy of pelvic inclination on radiographs, although Siebenrock and associates determined the mean difference to be 32 mm in men and 47 mm in women. In this patient, the pelvic inclination is dramatically increased, leading to overestimation of acetabular retroversion.
Question 62
Which of the following is considered the best method to measure limb-length discrepancy in a patient with a knee flexion contracture?
Explanation
REFERENCES: Aaron A, Weinstein D, Thickman D, et al: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
Tachdjian MO: Clinical Pediatric Orthopaedics: The Art of Diagnosis and Principles of Management. Stamford, CT, Appleton and Lange, 1997, pp 237-240.
Question 63
Which of the following factors is most critical to the success of a meniscal allograft transplantation?
Explanation
cryopreservation of the graft to ensure cell viability is not necessary. There is a limited immune response to musculoskeletal allografts; therefore, immunosuppression, as is required for visceral organ transplantation, is not indicated.
Question 64
A 20-year-old collegiate pitcher sustains a medial collateral ligament (MCL) rupture of his throwing elbow for which surgical reconstruction is necessary. The goal of surgery is anatomic restoration of the MCL. Which statement best describes the kinematics of the native MCL?
Explanation
full extension and full flexion. True lateral radiographs reveal that the flexion-extension axis, or center of rotation, of the elbow lies in the center of the trochlea and capitellum. The origin of the anterior bundle of the MCL lies slightly posterior to the rotational center of the elbow. The anterior bundle is further divided into an anterior band and a posterior band. The eccentric origin of these anterior bundle components in relation to the rotational center through the trochlea creates a CAM effect during flexion and extension. The anterior band tightens during extension, and the posterior band tightens during flexion. This reciprocal tightening of the two functional components of the anterior bundle allows the ligament to remain taut throughout the full range of flexion. Cadaver dissection studies have identified the origin and insertion of both the medial and lateral stabilizing elbow ligaments. The anterior bundle of the MCL is isometric throughout the flexion/extension arc of motion, making Response C incorrect. The posterior bundle of the MCL elongates with elbow flexion, so Responses B and D are incorrect. The posterior bundle of the MCL also demonstrates the most change in
length from extension to flexion of all the elbow ligaments.
Question 65
Figure 3 is the clinical photograph of a 20-year-old college soccer player who has a 7-day history of worsening left ankle pain and swelling after being slide-tackled in a game. Radiograph findings of his ankle and foot are normal. He complains of malaise. His history includes a severe ankle sprain 3 months ago. The sprain caused him to miss half the season, but he was able to play in the last 2 games. What is the most appropriate treatment? Review Topic

Explanation
Question 66
A 35-year-old carpenter sustained an injury to his dominant shoulder in a fall. He reports that he felt a sharp tearing sensation as he held on to a scaffold to keep from falling. Examination reveals swelling and ecchymosis down the upper arm, weakness to internal rotation, and deformity of the anterior axilla. He has good strength in external rotation and no apprehension with instability testing. Radiographs are normal. Management should consist of
Explanation
REFERENCES: Hanna CM, Glenny AB, Stanley SN, et al: Pectoralis major tears: Comparison of surgical and conservative treatment. Br J Sports Med 2001;35:202-206.
Connell DA, Potter HG, Sherman MF, et al: Injuries of the pectoralis major muscle: Evaluation with MR imaging. Radiology 1999;210:785-791.
Question 67
extensor tendons, 3) flexor tendons, 4) arteries, 5) nerves, 6) veins (can be done prior to nerve repair) , 7) skin.
Explanation
A 45-year-old carpenter sustained a table saw injury to his right hand while at work earlier today. Evaluation in the Emergency Department reveals the defect depicted in Figure A. An island volar advancement flap was selected for wound closure. What is the largest defect that could be covered with this technique?

less than 1 cm
1.5 cm
Question 68
What is the primary indication for performing a total wrist arthroplasty in a patient with painful rheumatoid arthritis?
Explanation
Question 69
-A 15-year-old boy with mild type I osteogenesis imperfecta (OI) has a midshaft radius/ulna fracture that is in bayonet apposition with loss of the radial bow and 40-degree apex volar and ulnar angulation. Closed reduction improves the angulation to 20 degrees; the bayonet apposition and loss of radial bow remains.His contralateral forearm has a normal appearance upon examination. What is the best treatment for this fracture?
Explanation

Question 70
When polyethylene is exposed to radiation and subsequently heated, certain chemical changes occur in the material. Which of the following statements best describes these changes?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 32-33.
Question 71
- Which of the following provides the most stable fixation for comminuted fractures of the posterior acetabular wall?
Explanation
According to Rockwood & Green and Browner & Jupiter the key to fixing these fractures is to re-establish a congruent articular surface. The other four distracters (i.e. cable, methylmethacrylate, multiple lag screws, and multiple K-wires) may achieve initial stability, but reduction will not be maintained. In addition, further studies show a higher incidence of mortality and complications with the use of lag screws and K-wires alone (Browner & Jupiter, Skeletal trauma, 1998)
Question 72
What is the most common bacteria cultured from dog and cat bites to the upper extremity?
Explanation
REFERENCE: Talan DA, Citron DM, Abrahamian FM, et al: Bacteriologic analysis of infected dog and cat bites. Emergency Medicine Animal Bite Infection Study Group. N Engl J Med 1999;340:85-92.
Question 73
Figure 10 is an anteroposterior pelvis radiograph of an 82-year-old man who had right hip pain that began 2 weeks ago but has since resolved with use of over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs). Currently he has no pain. Examination of his hip shows decreased internal rotation and minimal pain at the extremes of motion. What is the most appropriate treatment at this point?

Explanation
The radiograph shown is consistent with Paget disease of the bone. It demonstrates classic findings of widened lamellae and disorganized sclerotic and lytic areas. The cause is not clearly defined, but may be linked to a viral infection and subsequent alterations of osteoblastic and osteoclastic activity. Most patients are asymptomatic, and Paget disease is often found incidentally on radiographs. In this case, the patient’s symptoms likely were caused by hip arthritis, but Paget disease can cause diffuse bone pain in some cases. Considering the patient’s mild and short-term symptoms, observation and NSAID use is most appropriate. An MRI scan or biopsy is indicated if sarcomatous transformation is suspected, but this condition is rare and is associated with a substantial, unrelenting increase in pain. SPEP and UPEP are tests for multiple myeloma, of which the radiographs show no signs.
RECOMMENDED READINGS
Ralston SH. Pathogenesis of Paget's disease of bone. Bone. 2008 Nov;43(5):819-25. doi: 10.1016/j.bone.2008.06.015. Epub 2008 Jul 11. Review. PubMed PMID: 18672105.View Abstract at PubMed
Bonenberger E, Einhorn T. Metabolic bone diseases. In: Callaghan JJ, Rosenberg
AG, Rubash HE, eds. The Adult Hip. 2nd ed. Philadelphia, PA: Lippincott Williams 14
& Wilkins; 2007:514-533.
Question 74
Osteopenia is defined by the World Health Organization (WHO) as a bone mineral density (BMD) that is
Explanation
The T-score represents a comparison to young normals or optimum peak density. The Z-score represents a comparison of BMD to age-matched normals. Measurements of bone mineral density (BMD) at various skeletal sites help in predicting fracture risk. Hip BMD best predicts fracture of the hip, as well as fractures at other sites.
REFERENCE: Kanis JA, Johnell O, Oden A, et al: Risk of hip fracture according to the World Health Organization criteria for osteopenia and osteoporosis. Bone 2000;27:585-590.
Question 75
A 55-year-old woman undergoes an anterior cervical diskectomy and fusion at C5-C6 through a left-sided approach. One year later, she requires an anterior cervical diskectomy and fusion on another level. Which of the following is considered a contraindication to performing a right-sided approach for the revision procedure?
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 387-394.
Edwards CC II, Riew KD, Anderson PA, et al: Cervical myelopathy: Current diagnostic and treatment strategies. Spine J 2003;3:68-81.
Question 76
A 58-year-old man with insulin-dependent diabetes mellitus underwent primary total knee arthroplasty (TKA). A full-thickness skin slough measuring 3 cm by 4 cm developed, with postsurgical exposure of the patellar tendon. No change is observed in the appearance of the wound after 2 weeks of wet-to-dry dressing changes. What is the best next treatment step for the soft-tissue defect?
Explanation
If wound healing does not occur and deep soft tissues such as the patellar tendon are exposed following TKA, local rotational flap is the procedure of choice. The procedure should be performed relatively early after the recognition of a soft-tissue wound-healing problem. In the setting of TKA, the gastrocnemius muscle is an excellent source of flaps for wound coverage of the proximal tibia.
Question 77
An 8-year-old girl was treated for a Salter-Harris type I fracture of the right distal femur 2 years ago. Examination reveals symmetric knee flexion, extension, and frontal alignment compared to the contralateral knee. She has 1-cm of shortening of the right femur. History reveals that she has always been in the 50th percentile for height, and her skeletal age matches her chronologic age. Radiographs are shown in Figure 9. What is the expected consequence at maturity?
Explanation
REFERENCES: Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphysiodesis. J Pediatr Orthop 1996;16:173-179.
Moseley CF: Assessment and prediction in leg-length discrepancy. Instr Course Lect 1989;38:325-330.
Question 78
A 12-year-old boy is emergently transported to the emergency department following a motor vehicle accident. He was restrained in the back seat with a lap belt. On a physical exam bruising is noted across his abdomen as shown in Figure A. Lateral radiographs are shown in Figure B. Which of the following injuries are most frequently associated with this injury pattern? Review Topic

Explanation
A Chance fracture injury is a flexion-distraction injury of the spine. The anterior column (vertebral body) collapses under compression and the posterior elements fail under tension (rupture of the interspinous ligaments or avulsion fracture of the spinous process). A common mechanism is a MVA where the child is wearing a seatbelt, leading to a "seatbelt sign". In the presence of a "seatbelt" sign, on should have a high suspicion for a bowel injury.
Reid et al. reported seven cases of pediatric patients with Chance fractures. All had associated intraabdominal bowel injury.
Holland et al. retrospectively reviewed 28 pediatric patients with Chance fractures, 71% sustained following road trauma. Eleven percent had associated small bowel injury, but all patients had abnormal abdominal CT scans.
Figure A is a clinical photo of a 'seatbelt sign' following a motor vehicle accident. Figure B exhibits a "bony" Chance fracture where the spinous process has been avulsed. Illustration A depict the failure of the anterior column under compression and failure of the posterior column under tension.
Incorrect answers:
(SBQ12SP.32) A 48-year-old man is involved in a motor vehicle accident and is taken to an outside hospital where he undergoes CT imaging, displayed in Figures A-B. Approximately 36 hours later he is transferred to your hospital for further evaluation and management. On exam, he has tenderness over his upper cervical spine and is neurologically intact with no myelopathic signs. What is the most appropriate treatment method for this patient and why? Review Topic

Soft cervical orthosis because his gender puts him at a low risk of nonunion.
Halo vest immobilization because the degree of fracture displacement puts him at a low risk of nonunion.
Anterior screw fixation because his delayed time to treatment puts him at an high risk of nonunion.
Posterior C1-C2 fusion with rigid instrumentation because his age puts him at a high risk of nonunion.
Posterior C1-C2 fusion with sublaminar wiring because the degree of fracture angulation puts him at a high risk of nonunion.
The patient has a type II odontoid fracture and should be managed with halo vest immobilization as he has minimal fracture displacement (< 5mm) and no other risk factors for nonunion.
Type II odontoid fractures comprise 35% of all C2 fractures and have the highest nonunion rate. Commonly cited risk factors for nonunion include posterior displacement, posterior angulation, delayed initiation of treatment, fracture comminution and advanced age. Patients without these risk factors can often be successfully managed with halo vest immobilization. Elderly patients are frequently unable to tolerate halo vest immobilization and can be placed in a rigid cervical orthosis. Patients at high risk for nonunion are generally managed surgically with either anterior screw fixation, posterior rigid fixation (C1-C2 transarticular screw construct versus C1 lateral mass screw + C2 pedicle screw construct), or posterior C1-C2 sublaminar wiring.
Greene et al found that type II odonotoid fractures that were displaced >/= 6mm had a nonunion rate of 86% compared to 18% in patients with < 6mm displacement. This was statistically significant regardless of direction of displacement. Age was not significantly associated with nonunion.
Koivikko et al performed a retrospective review of conservatively treated type II odontoid fractures and identified risk factors for nonunion. Fracture gap > 1mm, posterior displacement > 5mm, posterior angulation > 20°, delayed start of treatment
> 4 days and posterior redisplacement > 2mm were all correlated with nonunion. In this study, anterior displacement, gender and age were unrelated to nonunion.
Figures A and B are coronal and sagittal CT scans of the cervical spine, respectively, demonstrating a noncomminuted type II odontoid fracture with minimal posterior displacement and angulation.
Incorrect
Responses:
Question 79
A 35-year-old active woman with rheumatoid arthritis experiences right shoulder pain following an extended course of corticosteroids (Figures 96a and 96b).

Explanation
The indication for anatomic TSA is end-stage glenohumeral arthritis with an intact rotator cuff. For the 62-year-old man, his radiographs reveal osteoarthritis, and his MR image shows an intact rotator cuff. Although humeral head replacement has historically been employed for this disorder, pain relief is not as reliable as with TSA, and the revision rate is higher. rTSA is generally reserved for patients with a nonfunctional rotator cuff.
For this 58-year-old patient with a full-thickness rotator cuff tear, preserved motion, and weakness in forward elevation, a rotator cuff repair is the most appropriate treatment. In the absence of degenerative changes, shoulder hemiarthroplasty or anatomic TSA is not indicated. Although indications for rTSA continue to evolve, well-compensated range of motion and a medium-sized rotator cuff tear in a younger patient are not among them.
rTSA is an emerging treatment for comminuted proximal humerus fractures in elderly patients. Although hemiarthroplasty has been a traditional treatment, current evidence suggests rTSA more reliably restores range of motion, and this 78-year-old patient's CT scan shows a small and comminuted greater tuberosity fragment that is unlikely to heal. ORIF is another option, but the CT scan also shows a small humeral head fragment that suggests osteopenia, making fixation more tenuous and likely less reliable.
A common problem associated with hemiarthroplasty for glenohumeral osteoarthritis is symptomatic glenoid degeneration that necessitates revision. This 55-year-old patient’s images reveal this is the case, although his infection workup is negative. His examination findings suggest an intact subscapularis repair. With a functioning rotator cuff and symptomatic glenoid arthritis, a conversion to anatomic TSA is indicated. In the absence of a functioning rotator cuff in an older patient, an rTSA is a better option.
This 72-year-old patient has classic symptoms and radiographs of cuff tear arthropathy. For patients with massive rotator cuff tear and glenohumeral arthritis, neither anatomic TSA nor rotator cuff repair is indicated. Hemiarthroplasty has historically been indicated for cuff tear arthropathy, but rTSA outcomes for this disorder have been superior and are now the preferred option.
Comminuted proximal humerus fractures in young, active patients are treated primarily with ORIF. The absence of glenohumeral arthritis removes anatomic TSA as a possibility, and concerns about implant longevity in younger, active patients such as this 40-year-old laborer contraindicate rTSA. Hemiarthroplasty is still employed in 3- and 4-part fractures but is generally reserved for subacute presentations or dislocations in which the humeral head is dysvascular and unlikely to survive. In this acute setting, a fixation procedure is preferred.
The 71-year-old patient who has had 2 failed rotator cuff repairs has an MR image that reveals another recurrent tear that is retracted to the glenoid. Her examination findings reveal classic signs
of a decompensated rotator cuff tear with pseudoparalysis and weakness in forward elevation. Although infection is a concern in the setting of multiply failed rotator cuff repair, the workup is negative in this scenario. Because this patient has a dysfunctional rotator cuff and has failed previous attempts at repair, a conversion to rTSA is the better option. In the absence of degenerative changes, hemiarthroplasty and anatomic TSA are not indicated.
The indications for hemiarthroplasty continue to narrow, but it is still a consideration for young patients with unipolar shoulder degeneration. In this 35-year-old patient, her MR image shows avascular necrosis in the humeral head, and her arthroscopy suggests arthritic change only on the humeral side with an uncompromised glenoid. To best treat young and active patients, a hemiarthroplasty that articulates with healthy glenoid cartilage can provide good pain relief and functional outcomes. Anatomic TSA is also reasonable but not an optimal option considering the normal glenoid condition. rTSA is not a consideration when a young patient’s MR images reveal an intact rotator cuff.
RECOMMENDED READINGS
Torchia ME, Cofield RH, Settergren CR. Total shoulder arthroplasty with the Neer prosthesis: longterm results. J Shoulder Elbow Surg. 1997 Nov-Dec;6(6):495-505. PubMed PMID: 9437598. View Abstract at PubMed
Chalmers PN, Slikker W 3rd, Mall NA, Gupta AK, Rahman Z, Enriquez D, Nicholson GP. Reverse total shoulder arthroplasty for acute proximal humeral fracture: comparison to open reduction-internal fixation and hemiarthroplasty. J Shoulder Elbow Surg. 2014 Feb;23(2):197-204. doi: 10.1016/j.jse.2013.07.044. Epub 2013 Sep 27. PubMed PMID: 24076000. View Abstract at PubMed
Groh GI, Wirth MA. Results of revision from hemiarthroplasty to total shoulder arthroplasty utilizing modular component systems. J Shoulder Elbow Surg. 2011 Jul;20(5):778-82. doi: 10.1016/j.jse.2010.09.014. Epub 2011 Jan 13. PubMed PMID: 21232989. View Abstract at PubMed
Orfaly RM, Rockwood CA Jr, Esenyel CZ, Wirth MA. Shoulder arthroplasty in cases with avascular necrosis of the humeral head. J Shoulder Elbow Surg. 2007 May-Jun;16(3 Suppl):S27-32. Epub 2006 Nov 16. PubMed PMID: 17113317. View Abstract at PubMed
Sershon RA, Van Thiel GS, Lin EC, McGill KC, Cole BJ, Verma NN, Romeo AA, Nicholson GP. Clinical outcomes of reverse total shoulder arthroplasty in patients aged younger than 60 years. J Shoulder Elbow Surg. 2014 Mar;23(3):395-400. doi: 10.1016/j.jse.2013.07.047. Epub 2013 Oct 12. PubMed PMID: 24129052. View Abstract at PubMed
Question 80
All of the following techniques can help to prevent valgus angulation during intramedullary nailing of proximal one-third tibia fractures EXCEPT:

Explanation
A final technical trick is the usage of blocking (Poller) screws - the referenced article by Ricci et al had 100% correction and maintenance of reduction with usage of blocking screws without other adjunct techniques. These should be placed in the lateral aspect of the proximal and distal fragments when needed.
The referenced study by Krettek et al is a biomechanical evaluation of blocking screws in a tibial model that showed significantly increased strength when they were utilized.
Question 81
What three structures are considered the primary constraints necessary for elbow stability?
Explanation
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Question 82
A patient who underwent primary total hip arthroplasty 7 years ago that resulted in excellent pain relief and a normal gait now reports pain and a limp. Postoperative and current AP radiographs are shown in Figures 2a and 2b. What is the most likely cause of the pathology seen?
Explanation
REFERENCES: Claus MC, Hopper RH, Engh CA: Fractures of the greater trochanter induced by osteolysis with the anatomic medullary locking prosthesis. J Arthroplasty 2002;17:706-712.
Heekin RD, Engh CA, Herzwurm MF: Fractures through cystic lesions of the greater trochanter: A cause of late pain after cementless total hip arthroplasty. J Arthroplasty 1996;11:757-760.
Question 83
Which of the following is the most relevant clinical factor in the maturation assessment of an adolescent female athlete contemplating anterior cruciate ligament (ACL) reconstruction?
Explanation
REFERENCES: Micheli LJ, Foster TE: Acute knee injuries in the immature athlete. Instr Course Lect 1993;42:473-481.
Stanitski CL: Anterior cruciate ligament injury in the skeletally immature patient: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:146-158.
Fowler PJ: Anterior cruciate ligament injuries in the child, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2067-2074.
Question 84
1 and 2 show the radiograph and CT obtained from a year-old woman who underwent right total hip replacement in She initially did well with no pain. She was last seen 7 years ago and was having mild hip pain at that time. She was found to have a supra-acetabular cyst on radiographs. She has had severe right hip pain for the past 9 months while using a walker for ambulation. The initial blood work reveals an estimated erythrocyte sedimentation rate of 32 mm/hr, a C-reactive protein level of 5 mg/L, a serum cobalt level of 4 µg/L, and a serum chromium level of 6 µg/L. Right hip aspiration is performed, revealing a white blood cell count of 139, 52% neutrophils, and a negative leukocyte esterase test. What is the best next step?
Explanation
The hip replacement was performed in 1995, during the period when the previous generation of polyethylene was utilized. This polyethylene was subjected to irradiation in air, with subsequent oxidation and consequent osteolysis after implantation. The mechanism of osteolysis begins with the uptake of polyethylene particles by macrophages, which then initiate an inflammatory cascade and the release of osteolytic factors. This cycle continues, with eventual implant loosening and failure. The imaging shows significant osteolysis and raises concern for pelvic discontinuity and acetabular implant failure. The surgical treatment consists of acetabular reconstruction. In this patient, concern exists for discontinuity based on the substantial amount of bone loss and nonsupportive anterior and posterior columns. This scenario requires complex acetabular revision using a custom triflange device, distraction with a jumbo acetabular component, or placement of a porous metal cup/cage construct with augmentation. The laboratory values are not consistent with infection or failure due to metal debris.
Question 85
During an anterior retroperitoneal approach to the low lumbar spine, the iliac vessels are mobilized along the lateral side, allowing them to be retracted toward the midline. To gain adequate mobility of the common iliac vein for exposure of L5, it is important to identify which of the following structures?
Explanation
REFERENCE: Gray H: Anatomy of the Human Body. Philadelphia, PA, Lea & Febiger,
1918, 2000.
Question 86
When comparing the failure load of an evenly tensioned four-stranded hamstring tendon anterior cruciate ligament autograft to a 10-mm bone-patellar tendon-bone autograft, the hamstring graft will fail at a tension
Explanation
REFERENCES: Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA: Arthroscopic reconstruction of the anterior cruciate ligament: A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 1999;27:448-454.
Hamner DL, Brown CH Jr, Steiner ME, et al: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Noyes FR, Butler DL, Grood ES, et al: Biomechanical analysis of human ligament grafts used in knee-ligament repairs and reconstructions. J Bone Joint Surg Am 1984;66:344-352.
Question 87
What term best describes the process involved when a growth factor produced by an osteoblast stimulates the differentiation of an adjacent undifferentiated mesenchymal cell during fracture repair?
Explanation
REFERENCES: Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044.
Zuscik MJ, Drissi MH, Reynolds PR, et al: Molecular and cell biology in orthopaedics, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006,
in press.
Question 88
Figure 53 shows the radiograph of a 48-year-old man who has a left side periprosthetic femoral fracture around the femoral stem of a previous revision hip arthroplasty. What is the most appropriate treatment?
Explanation
REFERENCES: Parvizi J, Tarity TD, Slenker N, et al: Proximal femoral replacement in patients with non-neoplastic conditions. J Bone Joint Surg Am 2007;89:1036-1043.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.

Lee SR, Bostrom MP: Periprosthetic fractures of the femur after total hip arthroplasty. Instr Course Lect 2004;53:111-118.
Question 89
When planning scoliosis surgery for a patient with a 50-degree thoracolumbar curve and spinal muscular atrophy, it is most important to include
Explanation
REFERENCES: Daher YH, Lonstein JE, Winter RB, Bradford DS: Spinal surgery in spinal muscular atrophy. J Pediatr Orthop 1985;5:391-395.
Aprin H, Bowen JR, MacEwen GD, et al: Spinal arthrodesis in patients with spinal muscle atrophy. J Bone Joint Surg Am 1982;64:1179-1187.
Question 90
What are the proposed biomechanical advantages of the Grammont reverse total shoulder arthroplasty when compared to a standard shoulder arthroplasty?
Explanation
REFERENCES: Werner CM, Steinmann PA, Gilbert M: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Rittmeister M, Kerschbaumer M: Grammont reverse total shoulder arthroplasty in patients with rheumatoid arthritis and nonreconstructible rotator cuff lesions. J Shoulder Elbow Surg 2001;10:17-22.
Question 91
The third plantar intrinsic muscle layer of the foot consists of which of the following structures?
Explanation
REFERENCE: Resch S: Functional anatomy and topography of the foot and ankle, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 32-33.
Question 92
Figures 111a and 111b show axial MRI scans of a 24-year-old man who injured his right shoulder several years ago and now reports continued difficulty with the shoulder and has pain with activity. He reports that when the injury occurred, he felt that his shoulder "popped" but he never required closed reduction. He wore a
Explanation
Question 93
An 18-year-old gymnast has had a 1-year history of foot pain. Examination reveals medial midfoot tenderness without swelling. Non-weight-bearing in a cast for 6 weeks has failed to provide relief. An axial CT scan of the midfoot is shown in Figure 20. What is the optimal treatment for this condition?
Explanation
REFERENCES: Quirk RM: Stress fractures of the navicular. Foot Ankle Int 1998;19:494-496.
Saxena A, Fullem B, Hannaford D: Results of treatment of 22 navicular stress fractures and a new proposed radiographic classification system. J Foot Ankle Surg 2000;39:96-103.
Question 94
A 74-year-old woman with rheumatoid arthritis has pain in the shoulder that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 24a and 24b. Active forward elevation is 120 degrees and external rotation is 30 degrees. At the time of surgery, a 1-cm rotator cuff tear is found, which is repairable. Which of the following treatment options will result in the most predictable pain relief and function? Review Topic

Explanation
Question 95
A 23-year-old baseball pitcher reports pain in the posterior aspect of his dominant shoulder during the late cocking phase of throwing. With the dominant shoulder positioned in 90 degrees of abduction from the body and with the scapula stabilized, examination reveals 135 degrees of external rotation and 20 degrees of internal rotation. Examination of the opposite shoulder reveals 100 degrees of external rotation and 75 degrees of internal rotation. Both shoulders are stable on examination. Radiographs and MRI scans are unremarkable. What is the primary cause of his pain?
Explanation
REFERENCES: Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Meister K: Injuries to the shoulder in the throwing athlete. Part one: Biomechanics, pathophysiology, classification of injury. Am J Sports Med 2000;28:265-275.
Question 96
The vessel seen in the clinical photographs shown in Figures 50a and 50b (1,2 intercompartmental supraretinacular artery) is being dissected to be used as a source of vascularized bone graft for a patient who is scheduled to undergo internal fixation of a scaphoid nonunion. This vessel is a branch of what artery?
Explanation
REFERENCES: Sheetz KK, Bishop AT, Berger RA: The arterial blood supply of the distal radius and ulna and its potential use in vascularized pedicled bone grafts. J Hand Surg 1995;20:902-914.
Steinmann SP, Bishop AT, Berger RA: Use of the 1,2 intercompartmental supraretinacular artery as a vascularized pedicle bone graft for difficult scaphoid nonunion. J Hand Surg
2002;27:391-401.
Question 97
A 65-year-old man has a painful mass of the middle finger. A clinical photograph, lateral radiograph, coronal MRI scan, and biopsy specimen are seen in Figures 20a through 20d. What is the most likely diagnosis?
Explanation
REFERENCES: Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 181-193.
Question 98
Figure 10 shows the radiograph of a 9-year-old girl who injured her left lower leg after being thrown from a horse. Examination reveals no other injuries. Which of the following forms of management will provide the lowest rate of complications and the earliest return to function?
Explanation
REFERENCES: Ligier JN, Metaizeau JP, Prevot J, Lascombes P: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Heinrich SD, Drvaric D, Darr K, MacEwen GD: Stabilization of pediatric diaphyseal femoral fractures with flexible intramedullary nails (a technique paper). J Orthop Trauma 1992;6:452-459.
Question 99
Figure 3 shows the radiograph of an asymptomatic 10-year-old boy. Management should consist of
Explanation
REFERENCES: Pizzutillo PD, Hummer CD III: Nonoperative treatment for painful adolescent spondylolysis or spondylolisthesis. J Pediatr Orthop 1989;9:538-540.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 129-137.
Question 100
Figures 1 and 2 are the radiographs of a 24-year-old male wrestler who underwent surgery for recurrent shoulder dislocations using coracoid autograft. At his first postoperative visit, the patient complains of decreased sensation on the lateral aspect of his forearm. The patient’s symptoms are most likely due to injury of the
Explanation
