Orthopedic Board Review MCQs: Trauma & Foot Surgery | Part 205

Key Takeaway
This page offers Part 205 of a comprehensive orthopedic board review. It features 100 verified, high-yield MCQs formatted like OITE and AAOS exams. Designed for orthopedic surgeons and residents, it provides essential practice through interactive Study and Exam modes, focusing on dislocation, foot, fracture, and trauma for board certification.
About This Board Review Set
This is Part 205 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 205
This module focuses heavily on: Dislocation, Foot, Fracture, Trauma.
Sample Questions from This Set
Sample Question 1: A 35-year-old runner has pain beneath the second metatarsophalangeal joint. He reports that he has significantly decreased his running distance since the onset of the pain. He denies any history of trauma or injury to the foot. A radiograph...
Sample Question 2: Which of the following is indicative of a patient who has been successfully resuscitated following a trauma?...
Sample Question 3: A man sustained the injury shown in Figures 51a and 51b. He underwent closed reduction of the radial head dislocation and open reduction and internal fixation of the ulnar fracture. What is the most common cause of persistent radial head su...
Sample Question 4: Anabolic steroid use has which of the following effects on serum lipoprotein levels?...
Sample Question 5: A 34-year-old male arrives intubated with a closed head injury to the trauma bay after a motor vehicle accident. After initial hospital workup and resuscitation, he is transferred to the intensive care unit. In addition to multiple systemic...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 35-year-old runner has pain beneath the second metatarsophalangeal joint. He reports that he has significantly decreased his running distance since the onset of the pain. He denies any history of trauma or injury to the foot. A radiograph is shown in Figure 14. Initial management should consist of
Explanation
REFERENCES: Trepman E, Yeo SJ: Nonoperative treatment of metatarsophalangeal joint synovitis. Foot Ankle Int 1995;16:771-777.
Mizel MS, Michelson JD: Nonsurgical treatment of monarticular nontraumatic synovitis of the second metatarsophalangeal joint. Foot Ankle Int 1997;18:424-426.
Question 2
Which of the following is indicative of a patient who has been successfully resuscitated following a trauma?

Explanation
Question 3
A man sustained the injury shown in Figures 51a and 51b. He underwent closed reduction of the radial head dislocation and open reduction and internal fixation of the ulnar fracture. What is the most common cause of persistent radial head subluxation?
Explanation
REFERENCES: Jupiter JB, Kellam JF: Diaphyseal fractures of the forearm, in Browner B, Jupiter J, Levine A, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1992, pp 1421-1454.
Ring D, Jupiter JB, Simpson NS: Monteggia fractures in adults. J Bone Joint Surg Am 1998;80:1733-1744.
Question 4
Anabolic steroid use has which of the following effects on serum lipoprotein levels?
Explanation
REFERENCES: Hartgens F, Rietjens G, Keizer HA, et al: Effects of androgenic-anabolic steroids on apolipoproteins and lipoprotein (a). Br J Sports Med 2004;38:253-259.
Blue JG, Lombardo JA: Steroids and steroid-like compounds. Clin Sports Med
1999;18:667-689.
Question 5
A 34-year-old male arrives intubated with a closed head injury to the trauma bay after a motor vehicle accident. After initial hospital workup and resuscitation, he is transferred to the intensive care unit. In addition to multiple systemic injuries, he sustained the closed injury shown in Figure A. Intracompartmental pressure monitoring of the limb measure in a range from 28-30 mm Hg. Which of the following sustained blood pressure measurements would support the treatment of limb fasciotomy? Review Topic 1 110/60 mmHg 2 115/55 mmHg 3 92/64 mmHg

Explanation
Given the poor outcomes associated with missed compartment syndromes, it is important to obtain both clinical and objective data when determining if a patient needs fasciotomies. A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam - especially with intubated patients. An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) <30 mm Hg may help to confirm the necessity for fasciotomy.
McQueen et al. prospectively reviewed 116 patients with tibia fractures that had continuous monitoring of their anterior compartment for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of
30 mmHg is a more reliable indicator of compartment syndrome.
Olson et al. provide a review of compartment syndrome for the lower extremity. They discuss a variety of injuries and medical conditions that may initiate acute compartment syndrome, including fractures, bleeding disorders, and other trauma. Although the diagnosis is primarily a clinical one, they also recommend supplementation with compartment pressure measurements in equivocal cases.
Figure A shows a closed comminuted tibial shaft fracture. Incorrect Answers:
Question 6
A 40-year-old right hand-dominant construction worker has had a 6-month history of aching left shoulder pain that is worse after working a long day. Examination reveals limited range of motion and good strength when compared to his asymptomatic right arm. He has not had any orthopaedic intervention to date. Radiographs are shown in Figures 43a and 43b. What is the most appropriate treatment?
Explanation
REFERENCES: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.
Skedros JG, O’Rourke PJ, Zimmerman JM, et al: Alternatives to replacement arthroplasty for glenohumeral arthritis, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 485-499.
Question 7
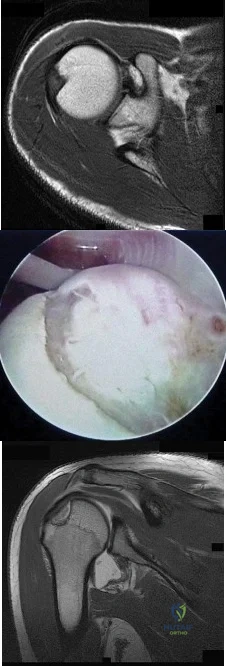
A 72-year-old female presents to your office with a 24-month old painful nonunion of a 3-part fracture of the proximal humerus. She has been treated conservatively with range of motion exercises but continues to complain of debilitating pain and dysfunction. Operative management should include:

Explanation
The referenced article by Cheung et al reviews treatment options for proximal humeral nonunions and reports successful use of arthroplasty in treating elderly osteoporotic proximal humeral nonunions as a pain relieving procedure.
Dines reported a case series of 20 chronic post-traumatic proximal humerus fractures including nonunions that were treated with shoulder arthroplasty achieving fair to excellent results in 90% at mid-term follow-up
Question 8
A 19-year-old man has had back pain with activity, especially running in soccer and baseball, for the past 4 months. He denies any history of trauma. Examination reveals no motor weakness or sensory changes in the lower extremities. Range of motion shows increased pain with extension and mild limitation with flexion. A sitting straight leg raising test is limited at approximately 60 degrees bilaterally by back and buttocks pain. Plain radiographs are normal. MRI scans are shown in Figures 13a through 13e. What is the most likely diagnosis?
Explanation
REFERENCES: Wiltse LL, Rothman SL: Spondylolisthesis: Classification, diagnosis and natural history. Sem Spine Surg 1993;5:264-280.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 129-137.
Question 9
A 42-year-old man reports the recent onset of right hip pain. A radiograph and MRI scan are shown in Figures 38a and 38b. A WBC count, erythrocyte sedimentation rate, and hip aspiration are within normal limits. Management should now consist of
Explanation
REFERENCES: Potter H, Moran M, Scheider R, et al: Magnetic resonance imaging in diagnosis of transient osteoporosis of the hip. Clin Orthop 1992;280:223-229.
Bijl M, van Leeuwen MA, van Rijswijk MH: Transient osteoporosis of the hip: Presentation of typical cases for review of the literature. Clin Exp Rheumatol 1999;17:601-604.
Montella BJ; Nunley JA, Urbaniak JR: Osteonecrosis of the femoral head associated with pregnancy: A preliminary report. J Bone Joint Surg Am 1999;81:790-798.
Question 10
- A clinical trial is being conducted on a new orthopaedic device that is different from existing devices that are moderately successful, but have frequent complications when used to treat fractures in the elderly. To comply with international standards for clinical trials, the investigator must include in the study design
Explanation
Question 11
An active 45-year-old man sustained an acute traumatic anteroinferior dislocation. MRI scans and an arthroscopic view are shown in Figures 36a through
Explanation
Question 12
Figure 42 shows the radiograph of a patient with spinal muscular atrophy. Examination reveals good upper extremity function, and she can tie her shoes and propel a manual wheelchair. Posterior instrumentation and fusion may result in
Explanation
REFERENCES: Bentley G, Haddad F, Bull TM, Seingry D: The treatment of scoliosis in muscular dystrophy using modified Luque and Harrington-Luque instrumentation. J Bone Joint Surg Br 2001;83:22-28.
Furumasu J, Swank SM, Brown JC, Gilgoff I, Warath S, Zeller J: Functional activities in spinal muscular atrophy patients after spinal fusion. Spine 1989;14:771-775.
Granata C, Cervellati S, Ballestrazzi A, Corbascio M, Merlini L: Spine surgery in spinal muscular atrophy: Long-term results. Neuromuscul Disord 1993;3:207-215.
Question 13
A patient with myelopathy underwent a one-level corpectomy 1 day ago and is now home. In the middle of the night he calls to report markedly increased difficulty in swallowing, diaphoresis, a change in his voice, and difficulty lying flat. What is the best course of action?
Explanation
REFERENCES: Emery SE, Smith MD, Bohlman HH: Upper-airway obstruction after multilevel cervical corpectomy for myelopathy. J Bone Joint Surg Am 1991;73:544-551.
McAfee PC, Bohlman HH, Riley LH Jr, Robinson RA, Southwick WO, Nachlas NE: The anterior retropharyngeal approach to the upper part of the cervical spine. J Bone Joint Surg Am 1987;69:1371-1383.
Question 14
A patient who underwent intramedullary nailing of a femoral shaft fracture 2 weeks ago now reports groin pain. What is the next most appropriate step in management?
Explanation
obtaining a dedicated AP radiograph of the hip with the leg internally rotated 15 to 20 degrees. Because the femoral neck is anteverted, 15 to 20 degrees of internal rotation of the hip offers the best view of the femoral neck. Whereas associated lumbar spine pathology may cause groin pain, the presence of a missed femoral neck fracture must first be ruled out prior to investigating other sources of pain.
Question 15
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms?
Explanation
A traumatic blow to the outstretched arm results in posterior glenohumeral forces. Labral detachment at the glenoid rim is common. Patients report slipping or pain with posteriorly directed pressure. Rarely do these patients have true dislocations that require reduction; however, recurrent episodes of subluxation or pain are not uncommon. Posterior repair has
been shown to be successful in the treatment of traumatic instability.
REFERENCES: Bottoni CR, Franks BR, Moore JH, et al: Operative stabilization of posterior shoulder instability. Am J Sports Med 2005;33:996-1002.
Williams RJ III, Strickland S, Cohen M, et al: Arthroscopic repair for traumatic posterior shoulder instability. Am J Sports Med 2003;31:203-209.
Kim SH, Ha KI, Park JH, et al: Arthroscopic posterior labral repair and capsular shift for traumatic unidirectional recurrent posterior subluxation of the shoulder. J Bone Joint Surg Am 2003;85:1479-1487.
Question 16
Examination of a 28-year-old woman reveals a moderate hallux valgus deformity and a prominence of the medial eminence. She reports that she can participate in all activities, wear 3-inch heels with minimal discomfort, and walk in a 1-inch heel with no pain. However, she is concerned that the deformity will get worse and requests recommendations regarding surgical correction. What is the best course of action?
Explanation
REFERENCES: Donley BG, Tisdel CL, Sferra JJ, Hall JO: Diagnosing and treating hallux valgus: A conservative approach for a common problem. Cleve Clin J Med 1997;64:469-474.
Teitz CC, Hu SS, Arendt EA: The female athlete: Evaluation and treatment of sports-related problems. J Am Acad Orthop Surg 1997;5:87-96.
Question 17
- A 12-year-old Little League pitcher has had pain in the dominant shoulder for the past week that prevents him from pitching. Examination reveals normal strength, full range of motion, normal stability, and mild tenderness about the proximal humerus. Radiographs with comparison views of the opposite shoulder show widening of the proximal humerus physis. Management should include
Explanation
Treatment requires cessation of repetitive physeal stress. There is no long-term sequelae. The athlete can return to same sports in the following season with emphasis on preseason conditioning.
Question 18
The view from an anterosuperior portal of the right shoulder shown in Figure 12 reveals which of the following findings?
Explanation
REFERENCES: Wolf EM, Cheng JC, Dickson K: Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Bigliani LU, Pollack RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Warner JJ, Beim GM: Combined Bankart and HAGL lesion associated with anterior shoulder instability. Arthroscopy 1997;13:749-752.
Question 19
A 68-year-old woman with a history of rheumatoid arthritis has had neck pain and weakness in all four extremities that has become worse in the past 6 months. She has gone from a community to a household ambulator and uses a wheelchair outside of the home. Examination of the extremities reveals poor coordination, diffuse weakness, hyperactive reflexes, and bilateral sustained clonus. She has a broad-based and unsteady gait. The posterior atlanto-dens interval is 12 mm. Based on these findings and the radiograph and MRI scan shown in Figures 13a and 13b, the treatment of choice is surgical decompression and stabilization. However, the patient inquires about the prognosis with surgery compared to nonsurgical management. Assuming there are no complications from surgery, the patient should be informed that, with surgery, she will most likely
Explanation
REFERENCES: Matsunaga S, Sakou T, Onishi T, et al: Prognosis of patients with upper cervical lesions caused by rheumatoid arthritis: Comparison of occipitocervical fusion between C1 laminectomy and nonsurgical management. Spine 2003;28:1581-1587.
Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am
1993;75:1282-1297.
Question 20
Among the ankle arthroscopy portals described below, which portal is at highest risk for serious complications?
Explanation
All of the portals listed pose risk for some structures. Because they have been shown to be the safest, the most common anterior portals are the anteromedial and the anterolateral. The safest posterior portal is the posterolateral portal. Because of the location of the posterior medial tendons and the neurovascular bundle, the posteromedial portal is at highest risk for serious complications.
RECOMMENDED READINGS
Golanó P, Vega J, Pérez-Carro L, Götzens V. Ankle anatomy for the arthroscopist. Part I: The portals. Foot Ankle Clin. 2006 Jun;11(2):253-73, v. Review. PubMed PMID: 16798511.View Abstract at PubMed
Ferkel RD, Hommen JP. Arthroscopy of the ankle and foot. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 2. 8th ed. Philadelphia, PA: Mosby; 2007:1641-1726.
Figure 90 is an intraoperative image showing the medial approach to the elbow. The arm is proximal and to the right, and the forearm is distal and to the left. The blue arrow points to the medial epicondyle. A black arrow points to a piece of glass in a nervous structure. This injury most likely would affect which distal muscular structure?

Extensor digiti minimi
Flexor digitorum superficialis (FDS) to the index finger 77
Abductor pollicis brevis
First dorsal interossei
DISCUSSION
The intraoperative image shows a piece of glass splitting the ulnar nerve in the cubital tunnel. The extensor digiti minimi is innervated by the radial nerve. The FDS to the index finger and the abductor pollicis brevis are innervated by the median nerve. The first dorsal interossei is the last muscle innervated by the ulnar nerve.
RECOMMENDED READINGS
Miller MD. Review of Orthopaedics. 3rd ed. New York, NY: Saunders; 2000.
Anderson JE. Grant’s Atlas of Anatomy. 8th ed. Baltimore, MD: Williams & Wilkins; 1983.
Question 21
A 32-year-old man sustained a fracture of his upper arm in a motor vehicle accident. Radiographs are shown in Figure 32. Because of other associated injuries, surgical stabilization is chosen. What technique will result in the least complications and the best outcome?
Explanation
REFERENCES: Schemitsch EH, Bhandari M: Fractures of the humeral shaft, in Browner BD: Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1481-1511.
Chapman JR, Henley MB, Agel J: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
Question 22
A 65-year-old woman has had chronic aching discomfort involving her elbow for the past 6 months. Radiographs and a biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
REFERENCE: Dorfman HD, Bodgan C: Immunohematopoietic tumors, in Dorfman HD, Bogdan C (eds): Bone Tumors. St Louis, MO, Mosby, 1998, Chapter 12.
Question 23
An 18-year-old man has acute respiratory distress after sustaining injuries in a motorcycle accident. He has a blood pressure of 80/60 mm Hg and a pulse rate of 110/min. Examination reveals chest tympany to percussion, distended neck veins, and deviation of the trachea away from his right hemithorax where the breath sounds are diminished. Heart sounds are regular and normal on auscultation. Initial management should consist of
Explanation
REFERENCE: Mattox KL, Feliciano DV, Moore EE (eds): Management of Shock, ed 4. New York, NY, McGraw Hill, 2000, p 215.
Question 24
The management of a complex multifragmentary diaphyseal fracture of either the tibia or femur has changed during the last decade. Which of the following principles of treatment is now considered less important?
Explanation
REFERENCES: Perren SM, Claes L: Biology and mechanics of fracture management, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000,
pp 7-32.
deBoer P: Diaphyseal fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 93-104.
Mast J, Jakob R, Ganz R: Planning and Reduction Techniques in Fracture Surgery. Berlin, Springer-Verlag, 1989.
Question 25
A 38-year-old man who is an avid tennis player has had persistent pain over the medial aspect of his knee for the past 6 years. He notes that the pain occurs on a daily basis with any significant activity. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 22a and 22b. What is the best course of action?
Explanation
REFERENCES: Nagel A, Insall JN, Scuderi GR: Proximal tibial osteotomy: A subjective outcome study. J Bone Joint Surg Am 1996;78:1353-1358.
Rinonapoli E, Mancini GB, Corvaglia A, et al: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Manifold SG, Kelly MA, Richardson L, et al: Osteotomies about the knee, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 947-961.
Question 26
The sartorius muscle is innervated by which of the following nerves?
Explanation
REFERENCES: Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, p 404.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 139.
Question 27
Figures 29a and 29b show the AP and lateral radiographs of a 30-year-old man who has increasingly worse back pain and stiffness. Examination shows painful, limited spinal range of motion. There is no neurologic deficit. What laboratory study would be most helpful in confirming the diagnosis?
Explanation
REFERENCES: Calin A: Ankylosing spondylitis. Clin Rheum Dis 1985;11:41-60.
Booth R, Simpson J, Herkowitz H: Arthritis of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 431.
van der Linden S, Valkenburg H, Cats A: The risk of developing ankylosing spondylitis in HLA-B27 positive individuals: A family and population study. Br J Rheumatol 1983;22:18-19.
Question 28
Figure 21 shows the AP radiograph of a 41-year-old patient who sustained a closed bicolumnar fracture of the distal humerus that resulted in a painful nonunion. What is the best initial construct for rigid stabilization of this fracture pattern?
Explanation
REFERENCES: Helfet DL, Hotchkiss RN: Internal fixation of the distal humerus: A biomechanical comparison of methods. J Orthop Trauma 1990;4:260-264.
Sodergard J, Sandelin J, Bostman O: Mechanical failures of internal fixation in T and Y fractures of the distal humerus. J Trauma 1992;33:687-690.
Question 29
A patient has a C6 spinal cord injury. Following stabilization of the spine, the patient should be advised that their expected maximum level of function
Explanation
Question 30
A 20-year-old basketball player reports a 6-month history of right groin pain that radiates into his testicles with activities of daily living. He denies any history of trauma. Examination reveals tenderness about the groin, and he has full hip range of motion. The abdomen is soft. Radiographs are normal. Nonsurgical management has consisted of rest and physical therapy, but he continues to have pain. What is the next step in management?
Explanation
REFERENCES: Kluin J, den Hoed PT, van Linschoten R, et al: Endoscopic evaluation and treatment of groin pain in the athlete. Am J Sports Med 2004;32:944-949.
Genitsaris M, Goulimaris I, Sikas N: Laparoscopic repair of groin pain in athletes. Am J Sports Med 2004;32:1238-1242.
Meyers WC, Foley DP, Garrett WE, et al: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Question 31
A patient wakes up with a foot drop following open reduction internal fixation of a posterior wall/posterior column acetabular fracture. What position of the leg causes the highest intraneural pressure in the sciatic nerve?

Explanation
Question 32
What is the most common cause of the new onset of amenorrhea in a female endurance athlete who is not sexually active?
Explanation
REFERENCES: Constantini NW: Clinical consequences of amenorrhea. Sports Med 1994;17:213-223.
Bennell KL, Malcolm SA, Thomas SA, et al: Risk factors for stress fractures in track and field athletes: A twelve-month prospective study. Am J Sports Med 1996;24:810-818.
Question 33
A 65-year-old man with ankylosing spondylitis has neck pain after falling back over his lawnmower, striking his thoracic spine, and forcing his neck into extension. Examination reveals subtle weakness of the intrinsics and finger flexors at approximately 4+/5. Initial management consists of immobilization in a rigid collar, and placing his head in the anatomic position. Radiographs reveal a subtle extension fracture of the lower cervical spine. Approximately 6 hours after the injury, he reports increasing paresthesias in his upper and lower extremities, and examination now shows his intrinsics are 2/5, finger flexors are 3/5, and his triceps are now weak at 4/5 on manual motor testing. In addition, his lower extremities now show weakness in both dorsal and plantar flexion of the ankle in the range of 4/5. Repeat radiographs appear unchanged. An MRI scan is shown in Figure 2. Management should now consist of
Explanation
REFERENCES: Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142.
Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Question 34
Figure 1 is the MR image of a 43-year-old man who has left shoulder pain and weakness after a fall. An examination reveals active forward elevation at 120° and positive Yergason and lift-off test examination findings. Arthroscopy reveals that the articular surfaces of the glenohumeral joint have a normal appearance without significant degenerative changes. What is the most appropriate treatment at this time?

Explanation
Question 35
A 16-year-old high school football player sustains an injury to the left hip. The avulsed fragment identified by the arrow in Figure 34 represents the origin of which of the following structures?
Explanation
REFERENCES: Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Mader TJ: Avulsion of the rectus femoris tendon: An unusual type of pelvic fracture. Pediatr Emerg Care 1990;6:198-199.
Question 36
During a transperitoneal approach to the L5-S1 interspace, care must be taken to protect the superior hypogastric plexus from injury. Which of the following techniques reduces the risk of neurologic injury?
Explanation
REFERENCE: Transperitoneal midline approach to L4-S1, in Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer Verlag, 1983, pp 123-129.
Question 37
Which of the following types of osteosarcoma is associated with the best prognosis & long survival?
Explanation
p. 163 (in Paget’s disease): “Although long-term survival is rare for patients with this type of sarcoma, four patients have survived more than 10 years.”
p. 164 (in irradiated bone): “The location of these tumors in unresectable locations such as the skull, clavicle, scapula, and spine explains the traditionally poor prognosis.”
Question 38
- A 32-year-old has diffuse pain, weakness, and limited overhead motion in the shoulder as a result of falling on his outstretched arm 2 months ago. Examination reveals medial scapular winging, and an electromyogram shows denervation of the long thoracic nerve. Management should consist of
Explanation
Question 39
A 37-year-old man with a history of congenital flatfoot reports worsening pain on the medial aspect of his ankle for the past year. The pain is worse with weight bearing and is better with rest and the use of an ankle brace. What findings are shown on the MRI scans shown in Figures 18a through 18c?
Explanation
REFERENCES: Slovenkai MP: Clinical and radiographic evaluation (Adult flatfoot: Posterior tibial tendon dysfunction). Foot Ankle Clin 1997;2:241-260.
Conti S, Michelson J, Jahss M: Clinical significance of magnetic resonance imaging in preoperative planning for reconstruction of posterior tibial tendon ruptures. Foot Ankle 1992;13:208-214.
Question 40
Figures 177a and 177b are the radiographs of a 7-year-old boy with spastic cerebral palsy. He has quadriparetic involvement and is unable to ambulate. He has very limited abduction, 30 degrees of flexion contractures, and pain on abduction. Bilateral varus osteotomies are scheduled with acetabular procedures to improve stability. Which type of acetabular osteotomy should be performed?
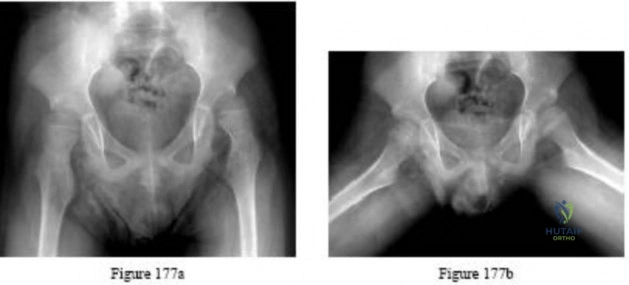
Explanation

Question 41
During surgical treatment of the most common variation of distal femoral "Hoffa" fractures, which of the following orientations for screw fixation should be used?

Explanation
Hoffa fractures are coronally oriented fractures of the femoral condyles, with most occurring in the lateral condyle. They are commonly associated with high-energy fractures of the distal femur and can often be overlooked during the assessment and treatment of distal femur fractures. Hoffa fractures are best evaluated using CT scans.
Nork et al. studied the association of supracondylar-intercondylar distal femoral fractures and coronal plane fractures. Of 202 supracondylar-intercondylar distal femoral fractures, they found coronal plane fractures were diagnosed in 38%. A coronal fracture of the lateral femoral condyle was involved more frequently than the medial condyle. Eighty-five percent of these coronal fractures involved a single lateral femoral condyle.
Holmes et al. looked at five cases of coronal fractures of the femoral condyle. All cases received open reduction and internal fixation with lag screws through a formal parapatellar approach. They reported good results with all fractures healing within 12 weeks without complications with final range of motion at least 0 degrees to 115 degrees.
Question 42
Pharmacoprophylaxis should be avoided in favor of a pneumatic compression device for a patient with
Explanation
For patients with known bleeding disorders, a pneumatic compression device alone is recommended over pharmacoprophylaxis to minimize risk for excessive bleeding and wound complications. Factor VIII deficiency (hemophilia) and active liver disease are the 2 conditions for which support is strongest to withhold anticoagulation. Protein C deficiency and protein S deficiency are associated with increased risk for thrombosis, as is the factor V Leiden mutation.
RESPONSES FOR QUESTIONS 159 THROUGH 162
Lateral femoral cutaneous
Superior gluteal
Inferior gluteal
Obturator
Sciatic
Which nerve listed above is at increased risk for injury when performing hip surgery through the following approaches?
Question 43
Which nerve root contributes to both the sciatic and femoral nerves?
Explanation
The lumbosacral plexus is formed from the lumbar and sacral roots that are redistributed into the obturator, femoral, and sciatic nerves. The obturator nerve is composed of the L1, L2, and L3 roots. The femoral nerve has contributions from the L3 and L4 roots. The sciatic nerve contains the L4, L5, S1, and lower sacral roots. Therefore, only the L4 root contributes to the femoral and sciatic (via the lumbosacral trunk) nerves, which allows it to innervate the quadriceps and the anterior tibialis muscles.
RECOMMENDED READINGS
Question 44
A 32-year-old man sustained an injury to the right thumb metacarpophalangeal (MP) joint ulnar collateral ligament (UCL) and is undergoing surgical repair (Figure 1). What structure in the clinical photograph is blocking reduction of the ulnar collateral ligament?

Explanation
When the thumb MP UCL is torn from the proximal phalanx, the distal stump can be displaced superficial to the adductor aponeurosis, known as a Stener lesion. The adductor aponeurosis effectively blocks reduction of the ligament to the normal attachment site. The EPB and EPL tendons are dorsal to the UCL, and the ulnar sesamoid bone/volar plate are in a volar position in relation to the UCL. The dorsal capsule would also not block reduction of the UCL due to it's anatomic location. The other responses do not block the UCL with this type of injury.
Question 45
The biopsy specimens seen in Figures 55a and 55b are from a lytic lesion in the sacrum of a 58-year-old man. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 372.
Fuchs B, Dickey ID, Yaszemski MJ, et al: Operative management of sacral chordoma. J Bone Joint Surg Am 2005;87:2211-2216.
Fourney DR, Rhines LD, Hentschel SJ, et al: En bloc resection of primary sacral tumors: Classification of surgical approaches and outcome. J Neurosurg Spine 2005;3:111-122.
Question 46
- In revision hip arthroplasty, which of the following is the 5- to 10-year reported graft failure rate when using structural acetabular allografts in the repair of acetabular deficiencies?
Explanation
Question 47
Passage of a sodium ion through a voltage-gated channel leads to which of the following?
Explanation
Voltage-gated channel are shut when the membrane potential is near the resting potential of the cell, but they rapidly begin to open if the membrane potential increases to a precisely defined threshold value. When the channels open (in response to depolarization in transmembrane voltage), they allow an inward flow of sodium ions, which changes the electrochemical gradient, which in turn produces a further rise in the membrane potential. This then causes more channels to open, producing a greater electric current across the cell membrane, and so on.
Lee et al. present a review article on nerve conduction and needle electromyography studies. They note that the three types of nerve conduction study are motor, sensory,
and mixed, of which motor is the least sensitive. In addition, they report that peripheral nerve entrapment initially results in focal demyelination; thus, nerve conduction velocity slows across the site. However, with radiculopathy and nerve root compression, the nerve conduction study may be normal.
Catterall presents a review article covering an overview of structural models of voltage-dependent activation, sodium selectivity and conductance, drug block and both fast and slow inactivation. He notes that voltage-gated sodium channels initiate action potentials in nerve, muscle and other excitable cells.
Illustration A is a diagram that shows the electrical recordings of an action potential, along with labels of each section of the process.
Question 48
A healthy 72-year-old woman is seen 14 days after cemented total knee arthroplasty. She reports increasing pain and swelling for the last 4 days accompanied by 4 days of wound drainage. Examination reveals that she is afebrile, and has erythema and moderate serosanguinous drainage from the wound. The knee is moderately swollen. Aspiration of the knee reveals no organisms on Gram stain. Culture results are expected back in 48 hours. Optimal management should consist of
Explanation
8 • American Academy of Orthopaedic Surgeons
DISCUSSION: Increased pain, swelling, erythema, and drainage 2 weeks removed from the primary arthroplasty are all signs of a probable infection. Erythrocyte sedimentation rate and C-reactive protein may not be helpful as they are elevated postoperatively even in the absence of infection. Even in the absence of infection, persistent wound drainage is an indication for surgical debridement to prevent subsequent infection. When a postoperative infection is easily recognized by clinical examination, there is no need to wait for a positive culture before proceeding with debridement.
REFERENCES: Weiss AP, Krackow KA: Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993;8:285-289.
Jaberi FM, Parvizi J, Haytmanek CT, et al: Procrastination of wound drainage and malnutrition affect the outcome of joint arthroplasty. Clin Orthop Relat Res 2008;466:1368-1371.
Insall JN, Windsor RE, Scott, WN: Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 959-964.
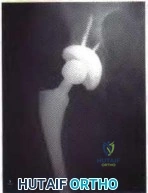
Figure 3a Figure 3b
Question 49
Based on the MR arthrogram of the elbow shown in Figure 8, which of the following structures is torn?
Explanation
MR arthrography provides improved sensitivity compared to conventional MRI, without contrast, for the detection of UCL pathology, particularly in the subacute or chronic setting. After the soft-tissue edema and joint fluid associated with the injury have resolved, the torn end of the ligament may lie in contact with its adjacent attachment and create a false-negative appearance. In this patient, a noncontrasted MR arthrogram showed no tear, yet the tear is apparent with intra-articular contrast and distention. MR arthrography of the elbow also may be useful in detecting intra-articular bodies or in evaluation for loose osteochondral fragments or flaps.
REFERENCES: Morrey BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128.
Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 200-210.
Question 50
The first branch of the lateral plantar nerve innervates the
Explanation
REFERENCES: Pansky B, House EH: Review of Gross Anatomy, ed 3. New York, NY, Macmillan, 1975, pp 464-476.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983,
pp 325-328.
Question 51
Figures 1 through 4 are the CT scans and intraoperative image of a 17-year-old boy who sustained a gunshot wound to his knee. What is the most appropriate definitive surgical management for his articular cartilage defect?
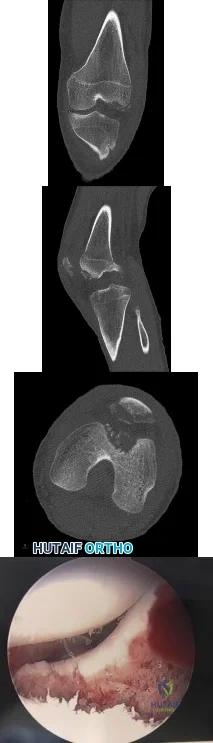
Explanation
Question 52
A 16-year-old girl has a painful foot mass. A radiograph, MRI scan, and biopsy specimens are shown in Figures 35a through 35d. What is the most likely diagnosis?
Explanation
REFERENCES: Ghert MA, Scully SP, Harrelson JM: Pigmented villonodular synovitis of the foot and ankle: A review of six cases. Foot Ankle Int 1999;20:326-330.
Jones BC, Sundaram M, Kransdorf MJ: Synovial sarcoma: MR imaging findings in 34 patients. Am J Roentgenol 1993;161:827-830.
Sartoris DJ, Resnick D: Magnetic resonance imaging of pediatric foot and ankle disorders. J Foot Surg 1990;29:489-494.
Scully SP, Temple HT, Harrelson JM: Synovial sarcoma of the foot and ankle. Clin Orthop 1999;364:220-226.
Question 53
Biofilm is believed to play a major role in the pathogenesis of periprosthetic joint infection. Biofilm allows for the bacterial population to evade the effects of antimicrobial therapy primarily through
Explanation
The intrinsic risk for colonization and subsequent infection associated with implants is exacerbated by implants’ tendency to become coated in host proteins such as fibrinogen and fibronectin shortly after implantation. Following initial adherence and colonization, bacteria are thought to form a complex matrix of an extracellular polymetric substance, serving as a protective scaffold in which they can survive despite the competence of the host’s immune system or the presence of antimicrobial agents. There is no evidence that biofilm directly inhibits antibiotics.
CLINICAL SITUATION FOR QUESTIONS 117 THROUGH 119
A 79-year-old woman is experiencing chronic right hip pain. All of her pain is in her right groin, and it worsens with activity. She has failed nonsurgical treatment with nonsteroidal anti-inflammatory drugs, activity modification, and occasional corticosteroid injections. She would like to proceed with surgical treatment.
Question 54
A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate Review Topic

Explanation
Question 55
A 7-year-old girl reports foot pain and has difficulty ambulating. History reveals that she fell off a scooter 1 week ago, and there is possible exposure to a tick bite. A radiograph is shown in Figure 29. What is the best course of action?
Explanation
REFERENCES: Borges JL, Guille JT, Bowen JR: Kohler’s bone disease of the tarsal navicular. J Pediatr Orthop 1995;15:596-598.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 65-78.
Question 56
Figure 46 shows the radiograph of an obese 12-year-old boy who has had left hip pain for the past 3 months. What is the best course of action?
Explanation
REFERENCES: Loder RT, Aronsson DD, Greenfield ML: The epidemiology of bilateral slipped capital femoral epiphysis: A study of children in Michigan. J Bone Joint Surg Am 1993;75:1141-1147.
Aronsson DD, Karol LA: Stable slipped capital femoral epiphysis: Evaluation and management. J Am Acad Orthop Surg 1996;4:173-181.
Hurley JM, Betz RR, Loder RT, Davidson RS, Alburger PD, Steel HH: Slipped capital femoral epiphysis: The prevalence of late contralateral slip. J Bone Joint Surg Am 1996;78:226-230.
Loder RT, Aronson DD, Dobbs MB, Weinstein SL: Slipped capital femoral epiphysis. J Bone Joint Surg Am 2000;82:1170-1188.
Question 57
An otherwise healthy 57-year-old man has persistent, severe hip pain after undergoing total hip arthroplasty 3 months ago. What is the next most appropriate step in management?
Explanation
REFERENCES: Drancourt M, Stein A, Argenson JN, et al: Oral rifampin plus ofloxacin for treatment of staphylococcus-infected orthopedic implants. Antimicrob Agents Chemother 1993;37:1214-1218.
Duncan CP, Beauchamp C: A temporary antibiotic-loaded joint replacement system for the management of complex infections involving the hip. Orthop Clin North Am 1993; 24: 751-759.
Oyen WJ, Claessens RA, van Horn JR, et al: Scintiographic detection of bone and joint infections with indium-111-labeled nonspecifonal human immunoglobulin G. J Nucl Med 1990;31:403-412.
Question 58
The findings in Brown-Sequard syndrome include loss of which of the following? Review Topic
Explanation
Question 59
Nonsurgical management of pectoralis major tears is likely to result in weakness of glenohumeral Review Topic
Explanation
Question 60
A 15-year-old girl has had a painful mass on the medial aspect of her left thigh for the past 5 years. The pain is present only when she is performing athletic activities and is completely relieved with rest. A radiograph and MRI scan are shown in Figures 29a and 29b. The patient and her parents would like to have the mass removed. What further diagnostic studies are required prior to considering surgical resection?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Murphey MD, Choi JJ, Kransdorf, MJ, et al: Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-1434.
Question 61
Figure A is an AP radiograph of a 68-year-old man who presents to clinic with shoulder pain and dysfunction. On examination of his shoulder, he has pseudoparalysis with attempt at forward elevation and a positive hornblower's sign while demonstrating normal belly press test. Treatment should consist of: Review Topic

Explanation
RTSA can improve pain and function in shoulders with forward elevation pseudoparalysis secondary to rotator cuff tear arthropathy. Following arthroplasty, the deltoid alone can restore overhead elevation but it does not address active external rotation deficit. LDT is a well described procedure for treatment of irreparable posterosuperior rotator cuff tear. Combining RTSA and LDT can address both deficits and in select patients yields significant pain relief and restoration of function.
Walch et al found that hornblower's sign had 100% sensitivity and 93% specificity for irreparable degeneration of teres minor.
Puskas et al present clinical outcomes of RTSA combined with LDT for treatment of chronic combined pseudoparesis of elevation and external rotation of the shoulder in 40 patients. At a mean follow-up of 53 months, the author report excellent clinical outcomes.
Figure A demonstrates a proximal migration of the humerus resulting in femoralization of the humeral head and acetabularization of the acromion from a massive rotator cuff tear.
Incorrect answers:
Question 62
What percentage of bone weight is collagen?
Explanation
Question 63
Which of the following best describes the recommended treatment for a 13-year-old pitcher with a painful chronic stress injury to the proximal humeral physis as confirmed on an MRI scan? Review Topic
Explanation
Question 64
Which specific legislative Act in the United States was created to require reporting of annual monetary gifts or compensation of more than $10 by orthopaedic implant companies to physicians?
Explanation
Under this Act, all manufacturers of drugs and devices covered under Medicare, Medicaid, and SCHIP are obliged to federally report payments beyond $10 annually to physicians and academic centers. The Act was first introduced in 2007, enacted in 2010, and in 2014 the first data (from 2012) was reported publicly online in the Open Payment Program of the Centers for Medicare and Medicaid Services website.
Samuel et al analyze orthopedic surgeons available data from the Sunshine Act regarding industry payments and find over 110 million USD paid to approximately 15,000 orthopedic surgeons over the 5-month study period. No long term data exists to determine if these payments have any affect in healthcare.
Incorrect Answers:
Question 65
In the normal adult, the distance between the basion and the tip of the dens with the head in neutral position is how many millimeters?
Explanation
REFERENCES: Wiesel SW, Rothman RH: Occipitoatlantal hypermobility. Spine 1979;4:187-191.
Wholey MH, Browner AJ, Baker HL Jr: The lateral roentgenogram of the neck: With comments on the atlanto odontoid-basion relationship. Radiol 1958;71:350-356.
Question 66
-What is the mechanism of action of tranexamic acid in controlling traumatic hemorrhage?
Explanation

Question 67
A patient has a vertically and rotationally unstable hemipelvis following a motor vehicle accident. An indication for application of an anterior resuscitative pelvic external fixator is made. Two options with regard to pin insertion location are considered as seen in Figure 20. When compared to pins in position A, the pins in position B may be more advantageous because
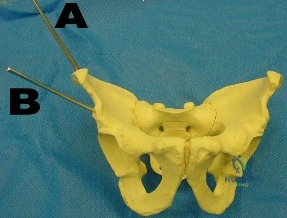
Explanation
Question 68
Figures 76a and 76b are the sagittal T1-weighted MRI scans of an active 27-year-old man who has had left dominant extremity shoulder pain and weakness for the past 5 months. He denies any history of a precipitating event but recalls that the pain began around the time he started lifting weights after a year off from lifting. Examination reveals full range of active and passive motion, negative Hawkins and Neer impingement signs, 5/5 abduction strength, 5/5 external rotation strength with arm adducted at his side, and a negative belly press, Gerber lift-off, and O'Brien's test. He does have weakness with resisted external rotation with the arm abducted to 90 degrees. Radiographs are unremarkable. An MRI arthrogram shows no rotator cuff tear or labral tears. What is the most likely diagnosis? Review Topic

Explanation
Question 69
A 5-year-old boy reports intermittent left elbow pain. History reveals that he injured his elbow 4 months ago, but had no treatment. He is now using his arm normally but reports pain almost daily. Examination reveals tenderness over the lateral epicondyle and a prominence is evident. Range of motion is from -5 2010 Pediatric Orthopaedic Examination Answer Book • 55 degrees to 120 degrees. Radiographs are shown in Figure 67. Management should include
Explanation
REFERENCES: Wattenbarger JM, Gerardi J, Johnson CE: Late open reduction internal fixation of lateral condyle fractures. J Pediatr Orthop 2002;223:94-398.
Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Question 70
A 10-month-old boy has an untreated developmental hip dislocation.
Explanation
Early radiographic findings of avascular necrosis (AVN) of the hip include sclerosis and a subchondral lucency. A common presentation of Legg-Calve-Perthes disease (idiopathic pediatric hip AVN) is intermittent pain in the thigh, groin, or knee with an examination localizing to the hip; a Trendelenburg gait or sign; and painful, restricted passive hip range of motion. AVN also may be observed in association with a slipped capital femoral epiphysis (SCFE). AVN risk is highest in the setting of an unstable SCFE (10%-60%); risk is 0% to 1.4% when the SCFE is stable. A multicenter review of the modified Dunn procedure for treatment of unstable SCFE noted an AVN rate of 26%.
The most common deformity associated with SCFE is proximal femoral varus, flexion, and external rotation leading to an abnormal femoral head-neck junction offset. This causes a loss of passive hip flexion and internal rotation and the phenomenon of obligate external
rotation with flexion. The residual deformity frequently results in femoroacetabular impingement. Labral tears also are associated with cam impingement secondary to underlying osseous abnormalities including abnormal femoral head-neck junction offset.
Endocrinopathies potentially are associated with SCFE because of hormone-related physeal changes and subsequent mechanical insufficiency of the proximal femoral physis. With renal osteodystrophy, the physeal widening results from secondary hyperparathyroidism and progressive proximal femoral deformity may develop. Optimal medical management of hyperparathyroidism is essential. Surgical stabilization via in situ fixation of the proximal femur is indicated when SCFE is diagnosed.
The proximal femoral epiphysis secondary ossification center commonly appears between the ages of 4 and 7 months. In the setting of developmental hip dislocation, the appearance of the secondary ossification center is commonly delayed. After closed or open reduction of developmental dysplasia of the hip, failure of the femoral head ossific nucleus to appear within 12 months following the reduction is a sign of proximal femoral growth disturbance and AVN.

Question 71
A 50-year-old woman reports a burning sensation on the plantar aspect of her left forefoot, distal to the metatarsal heads between her third and fourth digits. Palpation of the third web space recreates her symptoms. Which of the following will most accurately aid in confirming a diagnosis?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 145-151.
Quinn TJ, Jacobson JA, Craig JG, et al: Sonography of Morton’s neuromas. Am J Roentgenol 2000;174:1723-1728.
Question 72
A 16-year-old boy falls while playing soccer. He reports that his knee buckled when he planted his leg to kick a ball. He noticed an obvious deformity of his knee, which spontaneously resolved with a “clunk.” He could not finish the game but was able to bear weight with a limp. He has had two similar episodes but has never sought medical attention. An initial examination demonstrated an effusion, tenderness at the proximal medial collateral region and medial patellofemoral retinaculum, decreased range of motion, and patella apprehension. A lateral patellar glide performed at 30° of flexion was 3+. He was otherwise ligamentously stable, and there were no other noteworthy findings. What do Figures 1 and 2 reveal?
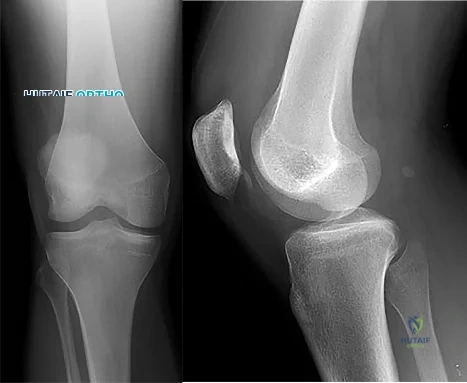
Explanation
Question 73
A 58-year-old man has a painful right hip 3 years after undergoing a large head metal-on-metal total hip arthroplasty (THA) in which the components are well positioned. MR imaging confirms a cystic mass around the hip and metal ion levels show a marked increase in cobalt compared to chromium levels. The erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level are within defined limits. What is the most likely cause for his discomfort?
Explanation
This patient presents with a pseudotumor likely attributable to local tissue reaction resulting from either articular metal wear debris and/or corrosion and fretting of the trunnion. The trunnion is a more likely source of the problem for a number of reasons: good position of metal articulation, increased trunnion corrosion and fretting associated with large-head THA, and markedly increased cobalt levels compared to chromium levels. Infection is very unlikely
in the setting of normal ESR and CRP findings. MR imaging findings are consistent with pseudotumor and not iliopsoas tendonitis or trochanteric bursitis.

CLINICAL SITUATION FOR QUESTIONS 42 THROUGH 45
Figures 42a through 42e are the radiographs, MR image, and MR arthrogram of a 25-year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has either competed or practiced 5 to 6 times per week since the age of
Question 74
ofhat parameter is most commonly used to estimate the maximum tension a muscle can generating?
Explanation
The concept of physiologic cross section of a muscle from Weber and Fick, identifies the critical importance of the cross sectional area of all the fibers of a muscle as proportional to maximum tension. (Relationship between muscle size and muscle strength).
Question 75
A 47-year-old woman falls and sustains a direct blow to her middle finger. She notes pain and swelling and is unable to move the proximal interphalangeal (PIP) or distal interphalangeal (DIP) joints. Radiographs are shown in Figures 8a through 8c. Proper management should consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Kozin SH, Thoder JJ, Lieberman G: Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg 2000;8:111-121.
Question 76
The arrow in Figure 39 is pointing to which of the following ligaments?
Explanation
REFERENCES: Berger RA: Ligament anatomy, in Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist, Diagnosis and Operative Management. St Louis, MO, Mosby, 1998,
pp 73-105.
Adams BD, Divelbiss BJ: Anatomy of the wrist ligaments, in Trumble TE (ed): Carpal Fracture-Dislocatons. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 1-5.
Question 77
A young active patient with a complete isolated posterior cruciate ligament (PCL) tear undergoes a double bundle PCL reconstruction. The tensioning pattern of the anterolateral (AL) and posteromedial (PM) bundles most likely to reproduce the most normal knee kinematics would be to tension
Explanation
REFERENCES: Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin T, Woo SL: Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med 2000;28:144-151.
Mannor DA, Shearn JT, Grood ES, Noyes FR, Levy MS: Two-bundle posterior cruciate ligament reconstruction: An in vitro analysis of graft placement and tension. Am J Sports Med 2000;28:833-845.
Question 78
Which of the following is considered a risk factor for the development of low back pain?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 627-643.
Question 79
What procedure can eliminate a sulcus sign? Review Topic
Explanation
Question 80
At the level of the midcalf, the plantaris tendon is found at which of the following locations?
Explanation
REFERENCES: Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3.
Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 475.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, plate 491.
Question 81
Receptor activator of nuclear factor kappa b (RANKL) and macrophage colony stimulating factor (MCSF) signaling pathways are necessary for the formation of multinucleated osteoclasts that resorb bone. Which of the following cells are known to produce RANKL?
Explanation
Question 82
A 78-year-old male presents to clinic 4 weeks after left total shoulder arthroplasty. He has not been wearing his sling and reports that he developed increased pain after slipping in the shower. He used the arm to catch himself from falling. On examination, he can flex the shoulder to 70 degrees, limited by pain. Active external rotation with arm at the side is 50 degrees and active internal rotation is 5 degrees. Passive external rotation is to 80 degrees. A radiograph of the left shoulder is shown below in Figure A. What other complaint is the patient most likely to have? Review Topic

Explanation
Total shoulder arthroplasty is the preferred treatment for glenohumeral arthritis in patients with intact rotator cuff and good glenoid bone stock. The surgical approach involves detaching the subscapularis and capsule from the anterior humerus and dislocating the humeral head anteriorly. Post operatively, external rotation is limited to protect the subscapularis repair. If there is suspicion of a postoperative subscapularis tear, and ultrasound can be performed to confirm the diagnosis.
Miller et al. reported 7 cases of subscapularis tendon rupture after total shoulder arthroplasty, all of which were subsequently repaired. Decreased functional outcomes were observed in these patients, with lengthening techniques to address internal rotation contractures and prior surgery involving the subscapularis tendon as risk factors for rupture
Westoff et al. performed static and dynamic ultrasounds on 22 patients after total shoulder arthroplasty evaluating for numerous periarticular pathologies. The authors concluded that sonography is a useful tool for evaluation of peri-implant tissues after TSA.
Figure A shows an intact left total shoulder arthroplasty without evidence of fracture, dislocation, or hardware loosening. Illustration A shows the incision for the subscapularis tendon during TSA.
Incorrect Answers:
Question 83
A 10-year-boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals no soft-tissue mass, and mild tenderness. Figures 33a and 33b show the plain radiograph and MRI scan, and the biopsy specimens are shown in Figures 33c and 33d. What is the most likely diagnosis?
Explanation
REFERENCE: Simon MA, Springfield DS, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-200.
Question 84
An 18-year-old collegiate basketball player has had a 3-month history of activity-related back pain. She describes isolated low back pain without radiation that increases with training and playing basketball. Her pain resolves with rest. Physical therapy for 6 weeks has failed to provide relief. An axial CT scan is shown in Figure 17a, and Figures 17b and 17c show sagittal CT reconstructions through the right and left lumbar facets, respectively. Further management should consist of which of the following?
Explanation
REFERENCES: Debnath UK, Freeman BJ, Grevitt MP, et al: Clinical outcome of symptomatic unilateral stress injuries of the lumbar pars interarticularis. Spine 2007;32:995-1000.
Bono CM: Low-back pain in athletes. J Bone Joint Surg Am 2004;86:382-396.
Question 85
Talar compression syndrome in ballet dancers typically involves injury to which of the following structures?
Explanation
REFERENCES: Brodsky AE, Khalil MA: Talar compression syndrome. Am J Sports Med 1986;14:472-476.
Wredmark T, Carlstedt CA, Bauer H, Saartok T: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
Marotta JJ, Micheli LJ: Os trigonum impingement in dancers. Am J Sports Med 1992;20:533-536.
Question 86
A 9-month-old nonambulatory girl is seen in the emergency department with a fracture of her right forearm. The mother says she fell from the changing table yesterday and continues to cry and not use her right arm. Radiographs are shown in Figure 31. Treatment should consist of which of the following? Review Topic

Explanation
efficient way to evaluate for other fractures. A MRI of the brain is not indicated unless fundoscopic examination reveals an abnormality.
Question 87
An ulnar nerve palsy at the level of the wrist is typically associated with deficits in the palmaris brevis, the hypothenar muscles, and what other groups of muscles?
Explanation
median nerve.
REFERENCES: Goldfarb CA, Stern PJ: Low ulnar nerve palsy. JASSH 2003;3:14-26.
Omer G: Ulnar nerve palsy, in Green DP, Hotchkiss R, Pederson W (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, pp 1526-1541.
Question 88
A 21-year-old man sustains multiple gunshot wounds to his right upper extremity. He can not extend his digits or his thumb but can extend and radially deviate his wrist. An injury to the radial nerve or one of its branches has most likely occurred at which of the following locations?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 53.
Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 428-429.
Question 89
A 2-year-old child is brought in by his parents for evaluation of intoeing. The child has a normal neuromuscular examination, but the heel bisector line is in the fourth web space, indicating a severe flexible metatarsus adductus deformity. The remainder of the lower extremity examination is unremarkable. What is the most appropriate treatment?
Explanation
REFERENCES: Beaty J: Congenital anomalies of the lower extremity, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. Philadelphia PA, Mosby, 2003, pp 983-988.
Katz K, David R, Soudry M: Below-knee plaster cast for the treatment of metatarsus adductus.
J Pediatr Orthop 1999;19:49-50.
Weinstein SL: Bristol-Myers Squibb/Zimmer award for distinguished achievement in orthopaedic research. Long-term follow-up of pediatric orthopaedic conditions: Natural history and outcomes
of treatment. J Bone Joint Surg Am 2000;82:980-990.
Question 90
- A 31-year-old man who is a recent immigrant from Guatemala has had pain in his back and thighs for the past 12 months. History notes a recent diagnosis of gout, and the patient reports falling a distance of 3 feet on his buttocks immediately before the pain began. Examination reveals that he is neurologically intact. Plain radiographs are shown in Figures 44a and 44b, and T2-weighted MRI scans are shown in Figures 44c and 44d. The most likely cause of the pathologic fracture is
Explanation
The MR demonstrates involvement of L1 and adjacent disc spaces. With peri-vertebral edema and mass involving the posterior aspect of the vertebral body, placing pressure on the spinal cord. There is also involvement of the L2-3 disc with early signal changes.
The slow clinical course of the patients symptoms, being from a third world country and the findings on imaging studies, with an anterior wedge compression fracture. The level most commonly involved with TB is lower thoracic and upper lumbar. The anterior wedging results in the classic “Gibbus”.
Some of the MR findings are also consistent with metastatic disease, but with the localized mass, peri-vertebral abscess make this choice more unlikely.
The usual findings on MR found with TB are: Confluently decreased signal intensity of the vertebral bodies associated interspace with poor distinction between these on short TR/short TE images: Abnormal increased signal of the disk on long TR/long TE images with an abnormal configuration (i.e., absent intranuclear cleft): Increased signal of the vertebral endplates at the abnormal disk level on long TR/long TE images.
Question 91
Hip pain of month duration has developed in a year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. What is this patient's prognosis for infection resolution?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin- resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was
21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 92
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
Explanation
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
Question 93
A 72-year-old woman who sustained a cerebrovascular accident 9 months ago now has a fixed elbow flexion contracture of 80 degrees. Management should consist of
Explanation
REFERENCE: Waters RL, Keenan ME: Surgical treatment of the upper extremity after stroke, in Chapman MW (ed): Operative Orthopedics. Philadelphia, PA, JB Lippincott, 1988, vol 2,
pp 1449-1450.
Question 94
A 65-year-old woman with a history of diabetes mellitus and plantar ulcers has an erythematous and swollen right foot and ankle. Despite IV antibiotics, the erythema spreads to her lower calf within 24 hours. She has a systolic blood pressure of 80/55 mm Hg and a pulse rate of 120. Laboratory studies show a creatinine level of 1.5 mg. Initial management should consist of
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 199-205.
Fontes RA Jr, Ogilvie CM, Miclau T: Necrotizing soft-tissue infections. J Am Acad Orthop Surg 2000;8:151-158.
Question 95
Figures 38a and 38b
Explanation
Inversion of the ankle can cause various injuries about the foot and ankle, all via the same mechanism. Fifth metatarsal base avulsion (Figure 35) fractures can be treated with use of a walking boot until pain subsides. Jones fractures (Figure 36) can be treated with surgical or nonsurgical treatment, although young, active patients are perhaps better treated with ORIF, which can decrease disability time. Treatment of an anterior process calcaneus fracture (Figure 37) is similar to that for a fifth metatarsal base avulsion fracture. Figures 38a and 38b show a calcaneal fracture-dislocation, which necessitates ORIF.
RECOMMENDED READINGS
Schepers T, Backes M, Schep NW, Carel Goslings J, Luitse JS. Functional outcome following a locked fracture-dislocation of the calcaneus. Int Orthop. 2013 Sep;37(9):1833-8. PubMed PMID: 23959223. View Abstract at PubMed
Polzer H, Polzer S, Mutschler W, Prall WC. Acute fractures to the proximal fifth metatarsal bone: development of classification and treatment recommendations based on the current evidence. Injury. 2012 Oct;43(10):1626-32. doi: 10.1016/j.injury.2012.03.010. Epub 2012 Mar 30. Review. PubMed PMID: 22465516. View Abstract at PubMed
Roche AJ, Calder JD. Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2013 Jun;21(6):1307-15. doi: 10.1007/s00167-012-2138-8. Epub 2012 Sep 6. Review. PubMed PMID: 22956165. View Abstract at PubMed
Berkowitz MJ, Kim DH. Process and tubercle fractures of the hindfoot. J Am Acad Orthop Surg. 2005 Dec;13(8):492-502. Review. PubMed PMID: 16330511. View Abstract at PubMed
Question 96
Which of the following methods accurately describes the measurement of tip-apex-distance as it relates to placement of a lag screw in the femoral head?

Explanation
TAD is a useful intraoperative indicator of deep and central placement of the lag screw in the femoral head, regardless of whether a nail or a plate is chosen to fix a fracture. A TAD of <25mm has been shown to minimize the risk of fixation cut-out in stable and unstable intertrochanteric hip fractures.
Baumgaertner et al examined factors leading to the failure of sliding hip screws (SHS) in the treatment of 198 intertrochanteric fractures. They determined that the tip-apex distance (TAD) is a reproducible, standard measurement to predict SHS failure. The average TAD for successful fractures was 24mm while the average TAD for failures was 38mm. No screw with a TAD <25mm failed. Calculation of the TAD is shown in Illustration B.
Kyle et al reviewed 622 intertrochanteric fractures. For unstable patterns, a SHS was superior to a fixed angle nail. Early ambulation and weight bearing contributed to improved results
Question 97
In obstetrical brachial plexus palsy, which of the following signs is associated with the poorest prognosis for recovery in a 2-month-old infant?
Explanation
REFERENCES: Clarke HM, Curtis CG: An approach to obstetrical brachial plexus injuries. Hand Clin 1995;11:563-581.
Narakas AO: Injuries to the brachial plexus, in Bora FW (ed): The Pediatric Upper Extremity: Diagnosis and Management. Philadelphia, PA, WB Saunders, 1986, p 247.
Question 98
A 12-year-old boy reports the acute onset of pain and a pop over the right side of his pelvis while swinging a baseball bat during a Little League game. Radiographs reveal an avulsion of the anterior superior iliac spine with 2 cm of displacement. Management should consist of
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 139-153.
White KK, Williams SK, Mubarack SJ: Definition of two types of anterior superior iliac spine avulsion fractures. J Pediatr Orthop 2002;22:578-582.
Question 99
All of the following are advantages of supine over lateral positioning during intramedullary nailing of subtrochanteric femur fractures EXCEPT:

Explanation
Advantages of the supine position include: may help protect a potentially unstable spine, facilitates access to sites other than the injured femur, shorter setup time, rotational and angulatory deformities may be more easily appreciated. Disadvantages of the supine position include: starting point localization may be more difficult.
Question 100
A still active 86-year-old pastry chef falls in her kitchen and notes pain and deformity of her little finger. There are no open wounds. Radiographs are shown in Figures 49a and 49b. What is the most appropriate management?
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Kozin SH, Thoder JJ, Lieberman G: Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg 2000;8:111-121.
