OITE & ABOS Orthopedic Board Prep MCQs: Knee, Shoulder & Tumor Part 8
Key Takeaway
This page offers Part 8 of a high-yield MCQ bank for orthopedic surgeons and residents preparing for OITE/AAOS board certification. Featuring 100 verified questions covering Arthroplasty, Knee, Shoulder, and Tumor, it provides interactive study and exam modes with detailed explanations for comprehensive review.
About This Board Review Set
This is Part 8 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 8
This module focuses heavily on: Arthroplasty, Knee, Shoulder, Tumor.
Sample Questions from This Set
Sample Question 1: When 6 weeks of noninvasive nonsurgical management fails to provide relief for a lumbar disk herniation, a trial of epidural steroid injections is likely to yield which of the following results?...
Sample Question 2: A 47-year-old man undergoes a posterior cervical procedure for a benign tumor. Postoperatively, severe dysfunction with decreased forward elevation and abduction develops and he has lateral winging of the scapula. What is the recommended tr...
Sample Question 3: A patient sustained a sharp laceration to the base of his left, nondominant thumb 4 months ago. Examination reveals no active flexion but full passive motion of the interphalangeal joint. What is the best treatment option?...
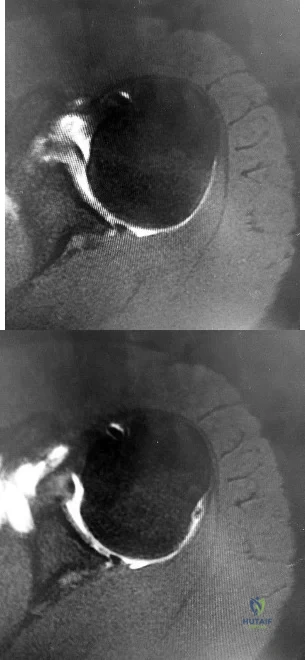
Sample Question 4: A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with...
Sample Question 5: In long-term follow-up studies of cemented total knee arthroplasty (TKA), the lowest rates of osteolysis have been associated with which design feature?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
When 6 weeks of noninvasive nonsurgical management fails to provide relief for a lumbar disk herniation, a trial of epidural steroid injections is likely to yield which of the following results?
Explanation
REFERENCES: Butterman GR: Treatment of lumbar disc herniation: Epidural steroid injection compares with discectomy: A prospective, randomized study. J Bone Joint Surg Am 2004;86:670-679.
Butterman GR: Lumbar disc herniation regression after successful epidural steroid injection.
J Spinal Disord Tech 2002;15:469-476.
Question 2
A 47-year-old man undergoes a posterior cervical procedure for a benign tumor. Postoperatively, severe dysfunction with decreased forward elevation and abduction develops and he has lateral winging of the scapula. What is the recommended treatment to best restore motion and function? Review Topic
Explanation
Question 3
A patient sustained a sharp laceration to the base of his left, nondominant thumb 4 months ago. Examination reveals no active flexion but full passive motion of the interphalangeal joint. What is the best treatment option?
Explanation
REFERENCES: Schneider LH, Wiltshire D: Restoration of flexor pollicis longus function by flexor digitorum superficialis transfer. J Hand Surg Am 1983;8:98-101.
Posner MA: Flexor superficialis tendon transfers to the thumb: An alternative to the free tendon graft for treatment of chronic injuries within the digital sheath. J Hand Surg Am 1983;8:876-881.
Question 4
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with
Explanation
REFERENCES: Bokor DJ, Conboy VB, Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br 1999;81:93-96.
Wolf EM, Cheng JC, Dickson K: Humeral avulsion of the inferior glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Question 5
In long-term follow-up studies of cemented total knee arthroplasty (TKA), the lowest rates of osteolysis have been associated with which design feature?
Explanation
The lowest reported rates of osteolysis involving cemented TKAs are associated with monolithic tibial components. Modular components and cemented metal-backed patella components are associated with a high prevalence of backside tibial insert wear and osteolysis.
Question 6
A 24-year-old collegiate pitcher has had increasing pain over his medial elbow for 3 months. He has point tenderness over his medial epicondyle and reproduction of his symptoms with a valgus stress test. What phase of the throwing cycle most likely will reproduce his symptoms? Review Topic
Explanation
Question 7
An otherwise healthy 16-year-old boy who has had thoracolumbar pain with an increasingly worse deformity for the past 2 years now reports that the pain is worse at night. He responded well to nonsteroidal anti-inflammatory drugs initially, but they have become less effective. He denies any neurologic or constitutional symptoms. Examination is consistent with a mild thoracolumbar scoliosis and is otherwise normal. Laboratory studies show a normal CBC, erythrocyte sedimentation rate, and C-reactive protein. Standing radiographs show a 20 degrees left thoracolumbar scoliosis, and he has a Risser stage of 4. A bone scan shows increased uptake at L2; a CT scan through this level is shown in Figure 18. Management should now consist of
Explanation
REFERENCES: Cove JA, Taminiau AH, Obermann WR, Vanderschueren GM: Osteoid osteoma of the spine treated with percutaneous computed tomography-guided thermocoagulation. Spine 2000;25:1283-1286.
Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Pettine KA, Klassen RA: Osteoid-osteoma and osteoblastoma of the spine. J Bone Joint Surg Am 1986;68:354-361.
Question 8
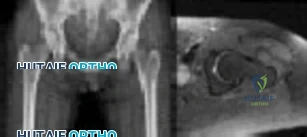
Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with a 2-month history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?

Explanation
Question 9
Figure 63 shows the radiographs of a 23-year-old man who sustained a twisting injury at work. Swelling, tenderness, and ecchymosis are noted about the entire midfoot. What associated injury is most likely to be problematic?
Explanation
REFERENCE: Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.
Question 10
During the anterior approach for repair of a distal biceps tendon rupture, what structure, shown under the scissors in Figure 6, is at risk for injury?
Explanation
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Ramsey ML: Distal biceps tendon injuries: Diagnosis and management. J Am Acad Orthop Surg 1999;7:199-207.
Question 11
A 52-year-old man has pain in the sternal area after landing on his right shoulder in a fall from his bicycle. In addition, he reports that he had difficulty swallowing and breathing immediately after the fall, but the symptoms resolved. A CT scan reveals a posterior sternoclavicular dislocation. Initial management should include
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont IL, American Academy of Orthopaedic Surgeons, 1999, pp 287-297.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 1010-1017.
Question 12
For the athlete performing heavy exercise, the magnitude of core temperature and heart rate increase is most proportional to
Explanation
REFERENCES: Latzka WA, Montain SJ: Water and electrolyte requirements for exercise. Clin Sports Med 1999;18:513-524.
Montain SJ, Sawka MN, Latzka WA, et al: Thermal and cardiovascular strain from hypohydration: Influence of exercise intensity. Int J Sports Med 1998;19:87-91.
Sawka MN, Young AJ, Francesconi RP, et al: Thermoregulatory and blood responses during exercise at graded hypohydration levels. J Appl Physiol 1985;59:1394-1401.
Question 13
A young man sustains a lumbar strain in an on-the-job motor vehicle accident. Both he and his treating physician feel that he is capable of limited duty with appropriate restrictions shortly after the injury. What term best describes his work status?
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 131-137.
Question 14
A 40-year-old woman has had sciatic pain on the left side for the past 8 weeks. She reports that the pain radiates to her posterior thigh, lateral calf, and into the dorsum of her left foot. Neurologic examination shows weakness of the left extensor hallucis longus. Axial T 2 -weighted MRI scans through L4-L5 are shown in Figure 14. Management should consist of
Explanation
REFERENCES: Epstein NE: Lumbar laminectomy for the resection of synovial cysts and coexisting lumbar spinal stenosis or degenerative spondylolisthesis: An outcome study. Spine 2004;29:1049-1055.
Shah RV, Lutz GE: Lumbar intraspinal synovial cysts: Conservative management and review of the world’s literature. Spine J 2003;3:479-488.
Question 15
A 26-year-old female twists her knee while playing soccer and sustains the injury shown in Figure A. She undergoes a reconstructive surgery and is started on an accelerated rehabilitation program. Which of the following is true regarding this type of rehabilitation protocol? Review Topic

Explanation
Rehabilitation after ACL reconstruction is necessary for a successful surgical outcome and remains an important topic of research interest. Accelerated programs allow for earlier weightbearing and certain strengthening exercises, rather than waiting several weeks before performing certain activities which put strain on the graft. Despite initial concerns that accelerated rehabilitation programs may lead to worse outcomes, many studies have demonstrated comparable outcomes between accelerated and nonaccelerated rehabilitation programs. No significant long-term differences have been reported regarding ACL laxity, range of motion, strength, or return to sports. Use of an accelerated program does not imply earlier return to sports. The optimal time to return to sports has not yet been elucidated.
Beynnon et al. performed a randomized controlled trial of patients who underwent ACL reconstruction with bone-patellar tendon-bone autograft comparing rehabilitiaton with either accelerated (19 week) or nonaccelerated (32 week) programs. At final evaluation, patients in both programs had the same increase in the envelope of knee laxity, clinical assessment, functional performance, proprioception,
and
thigh
muscle
strength.
Kruse et al. presented a systematic review evaluating studies on rehabilitation following ACL reconstruction. The authors found that accelerated rehabilitation does not appear to be harmful. It is likely safe for patients to begin immediate postoperative weight bearing, range of motion from 0-90 degrees of flexion, and perform closed-chain exercises. Bracing following ACL reconstruction is neither necessary nor beneficial and often adds to the cost of the procedure.
Figure A is a sagittal MRI demonstrating a complete ACL tear.
Incorrect
Question 16
A 3-year old child from an isolated mountain area is evaluated for multiple medical problems, including vomiting, loss of appetite, polyuria, and failure to thrive. History reveals the child was normal at birth. The parents, who appear healthy, are second cousins and have two other children who are normal. The parents state that they know of another family member who died at age 6 years after a similar medical history. Radiographs of the lower extremities show bowing of the long bones with cupping and widening of the physes. What is the most likely diagnosis?
Explanation
hemolytic anemia, rhabdomyolysis, and hepatocellular injury that began during refeeding and resolved with treatment. The signs and symptoms, pathophysiology, and treatment of refeeding hypophosphatemia are reviewed.
Renal Osteodystrophy-Musculoskeletal complications in patients with chronic renal failure are common and may be related to the disease itself or to treatment. The altered metabolism in patients with chronic renal failure leads to renal osteodystrophy, which consists of osteomalacia and secondary hyperparathyroidism [1]. Erosive changes attributable to secondary hyperparathyroidism may be easily confused with rheumatoid arthritis, seronegative spondyloarthropathies, infection, or even malignancy.
Primary Hyperparathyroidism-Preferential involvement of cortical bone with apparent preservation of cancellous bone in primary hyperparathyroidism was confirmed by percutaneous bone biopsy. Over 80% of patients had a mean cortical width below the expected mean, whereas cancellous bone volume in over 80% of patients was above the expected mean.
Skeletal disease in primary hyperparathyroidism J Bone Miner Res 1989 Jun; 4(3):283-91
Nutritional vitamin D deficiency-Rickets, osteomalacia, and renal osteodystrophy are disorders of the mineralization of bone that result from a lack of available calcium, phosphorus, or both. The diseases that result from numerous mechanisms present with a symptom-sign-radiographic complex with such a high degree of stereotypy that laboratory investigation is often required to distinguish one form from another. The disorders in children, known as rickets, produce bowing and other deformities of the long bones and dwarfism. These disorders are principally related to the profound effect of the deficiency states on the epiphyseal plate; whereas the same disorders in adults produce an often severe osteopenia and pathologic fractures. Because of newer developments in our understanding of the factors affecting calcium-phosphorus
hemostasis and vitamin D metabolism, many of the children and Rickets, osteomalacia, and renal osteodystrophy.
Question 17
Which of the following is considered a potential advantage in prophylaxis for the prevention of deep venous thrombosis associated with the use of low-molecular weight heparin (LMWH) as compared with fixed-dose unfractionated heparin?
Explanation
REFERENCES: Colwell CW Jr, Spiro TE, Trowbridge AA: Use of enoxaparin, a low-molecular weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14.
Bara L, Billaud E, Kher A, Samama M: Increased anti-Xa bioavailability for a low-molecular weight heparin (PK 10169) compared with unfractionated heparin. Semin Thromb and Hemost 1985;11:316-317.
Paiement GD: Prevention and treatment of venous thromboembolic disease complications in primary hip arthroplasty patients, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 331-335.
Question 18
Figures 42a and 42b shows the radiographs of a 20-year-old man who sustained a hyperextension injury to his little finger. Multiple attempts at closed reduction have been unsuccessful. Management should now consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Becton JL, Christian JD Jr, Goodwin HN, Jackson JG III: A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am 1975;57:698-700.
Green DP, Terry GC: Complex dislocation of the metacarpophalangeal joint: Correlative pathological anatomy. J Bone Joint Surg Am 1973;55:1480-1486.
Question 19
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management?
Explanation
REFERENCES: Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
D’Alessandro DF, Bradley JP, Fleischli JE, et al: Prospective evaluation of thermal capsulorrhaphy for shoulder instability: Indications and results, two- to five-year follow-up.
Am J Sports Med 2004;32:21-33.
Levine WN, Clark AM Jr, D’Alessandro DF, et al: Chondrolysis following arthroscopic thermal capsulorrhaphy to treat shoulder instability: A report of two cases. J Bone Joint Surg Am 2005;87:616-621.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 278-279.
Question 20
A healthy 70-year-old man has a swollen knee after undergoing a knee replacement 10 years ago. Aspiration of the knee reveals cloudy, viscous synovial fluid. Laboratory studies show an erythrocyte sedimentation rate of 10 mm/h and a C-reactive protein level of less than 0.5. What is the most likely diagnosis?
Explanation
REFERENCE: Barrack RL, Jennings RW, Wolfe MW, Bertot AJ: The value of preoperative aspiration before total knee revision. Clin Orthop 1997;345:8-16.
Question 21
What is the most significant factor affecting long-term survival for a patient with bone sarcoma?
Explanation
REFERENCES: Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res 1980;153:106-120.
Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 22
- Which of the following nerves lying between the gluteus medius and minimus is at risk for injury in a lateral approach to the hip?
Explanation
The direct lateral approach (Transgluteal approach). No true intervenous plane (“split the fibers” of the gluteus medius “distal to the point where the superior gluteal nerve supplies the muscle”). “Do not (split) more than 3 cm above the upper boarder of the trochanter.”
Question 23
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. The patient fails an extensive course of physical therapy and is unable to return to baseball. He and his orthopaedic surgeon elect to proceed with surgery. During a repeat evaluation, he has negative sulcus and Beighton sign findings, and radiographs show 5° of glenoid retroversion. What is the most appropriate surgical plan?
Explanation
and degenerative joint disease.
Question 24
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include
Explanation
REFERENCES: Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
Question 25
A 5-year-old boy reports intermittent left elbow pain. History reveals that he injured his elbow 4 months ago, but had no treatment. He is now using his arm normally but reports pain almost daily. Examination reveals tenderness over the lateral epicondyle and a prominence is evident. Range of motion is from -5 degrees to

Explanation
(SBQ13PE.40) Immediate spica casting is most appropriate for which of the following?: Review Topic
2-month-old girl with a displaced spiral mid-diaphyseal femur fracture
A 26-month-old boy with a displaced spiral mid-diaphyseal femur fracture with <2 centimeters of shortening
3-day-old with teratologic right hip dislocation
9-year-old boy with a displaced spiral mid-diaphyseal femur fracture
12-year-old girl weighing 90 pounds with a displaced spiral mid-diaphyseal femur fracture
Children older than 6 months and up to 6 years with diaphyseal femur fractures may be treated with spica casting.
Children younger than 6 months may only require a Pavlik harness. Immediate spica casting is indicated in children 6 months to 6 years with less than 2 cm of shortening. Each additional cm of shortening at presentation doubles the risk of loss of reduction (1 cm: 12%, 2 cm: 24%, 3 cm; 50%).
Kocher et al. provide the AAOS Clinical Practice Guideline for the treatment of pediatric diaphyseal femur fractures. Their recommendation for diaphyseal femur fractures with <2 cm shortening in children 6 months to 5 years is Grade B, based on Level II evidence (two level II and one level I study). They recommend early spica or traction with delayed spica. They suggest early spica, as this is more convenient than traction.
In an earlier article, Flynn et al. review the management of pediatric femoral shaft fractures. They recommend early spica casting for the child between 1 and 6 years in
low-energy femoral fractures with up to 2 cm shortening. Illustration A shows several styles of lower extremity spica casts.
Incorrect answers:
Question 26
Figures 28a through 28d show the radiographs and MRI scans of a 20-year-old basketball player who sustained an inversion injury to his right ankle. Management should consist of
Explanation
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
Baker CL, Morales RW: Arthroscopic treatment of tranchondral talar dome fractures: A long-term follow-up study. Arthroscopy 1999;15:197-202.
Question 27
The patient develops an inability to dorsiflex her foot 2 days after surgical intervention while she is sitting in a chair after physical therapy. Initial treatment should consist of
Explanation
Gamma irradiation produces free radicals. Although these free radicals can form cross-links with other polyethylene chains, the free radicals can also form a bond with oxygen, resulting in early oxidation. Gamma irradiation in air produces the highest risk for oxidized polyethylene, resulting in the highest risk for wear, delamination, and subsequent osteolysis.
This patient demonstrates severe periarticular osteolysis. When she is asymptomatic, this suggests the acetabular and femoral components remain well fixed to the bone. Consequently, she can be treated by removing the wear generator (polyethylene exchange), along with bone grafting of the osteolytic defect. Considering the extensive amount of osteolysis, observation for 1 year would not be appropriate.
The psoas is the anatomic structure that runs anterior to the acetabulum. The femoral neurovascular structures are at risk if the retractor is placed anterior and inferior to the psoas tendon.
The patient develops a foot drop 2 days after surgery. As a result, it can be assumed that the nerve was not injured directly during the surgical procedure. Although MR imaging or a CT scan may be indicated to identify an evolving hematoma, the immediate concern is to minimize pressure on the sciatic nerve. Tension on the nerve can be decreased by flexing the surgical knee and positioning the bed flat.
Question 28
- Which of the following procedures is associated with the highest risk of osteonecrosis of the metatarsal head?
Explanation
Question 29
A 69-year-old woman has just undergone an uncomplicated total shoulder arthroplasty for glenohumeral osteoarthritis. A press-fit humeral stem and a cemented all-polyethylene glenoid component were placed. At this point, what is the postoperative rehabilitation plan? Review Topic
Explanation
Question 30
Figures 24a through 24c show the coronal T 1 -weighted, T 2 -weighted fat-saturated, and T 1 -weighted fat-saturated gadolinium MRI scans of the proximal thigh of a 52-year-old woman who reports a mass in the medial thigh and groin area. She notes that the fullness has grown in size over the course of many months. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCE: Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 31
Figure 40 shows the AP radiograph of a 55-year-old man who reports left knee pain. Which of the following conditions is least likely to produce this radiographic presentation?
Explanation
REFERENCES: Klippel JH (ed): Primer on the Rheumatic Diseases, ed 11. Atlanta, GA, Arthritis Foundation, 1997, pp 226-229 and 328-331.
Resnick D, Wayama G: Diagnosis of Bone and Joint Disorders, ed 2. Philadelphia, PA, WB Saunders, 1988, pp 1675, 1779.
Question 32
What is the most common physical finding in myelopathic patients? Review Topic
Explanation
Question 33
A 16-year-old snowboarder has significant pain and is still unable to bear weight after sustaining a lateral ankle injury in a fall 1 week ago. Examination reveals swelling and tenderness in the sinus tarsi. AP, lateral, and mortise radiographs of the ankle are unremarkable. Management should consist of
Explanation
REFERENCES: Kirkpatrick DP, Hunter RE, Janes PC, Mastrangelo J, Nicholas RA: The snowboarder’s foot and ankle. Am J Sports Med 1998;26:271-277.
Ebraheim NA, Skie MC, Podeszwa DA, Jackson WT: Evaluation of process fractures of the talus using computed tomography. J Orthop Trauma 1994;8:332-337.
Question 34
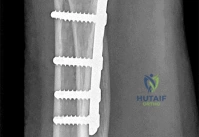
Figures 1 through 3 are the radiographs of a 55-year-old woman who underwent a volar plating of an extra-articular distal radius fracture 2 weeks ago. She is experiencing weakness with flexion of the interphalangeal (IP) thumb joint. IP joint flexion was normal before surgery. What is the best next step?

Explanation
Prevalence of flexor tendon rupture after distal radius fracture is between 2% and 12%. The FPL tendon is the most common flexor tendon rupture associated with volar plating. It is usually seen with plates that are distal to the watershed line (W) and with plates extending volar to the critical line (C) (Figure below). The watershed line (W) is the location of the origin of the volar carpal ligaments and the bone prominence

at which flexor tendons are most closely opposed to the distal radius (Figure 4). In this scenario, the lateral radiograph shows that the plate is not distal to the watershed line (W) and is between the critical line (C) and the line parallel to the volar cortex of the radius (R). This is the optimal position for the plate. Placement of a volar locking plate distal to the watershed line of the distal radius and excessive plate prominence has been associated with FPL tendon rupture. This patient is only 2 weeks past surgery and there is some FPL function. FPL weakness after volar distal radius plating is common and has been seen in as many as 50% of patients. This usually recovers spontaneously by 2 months, and no treatment is needed. A nerve conduction study would be indicated if an anterior interosseous nerve compression were considered, but it is too early for this test. A CT scan could be obtained to judge the alignment of the fracture fragment and position of the screws, but it is not indicated in this case. Exploration could be performed if an FPL rupture were considered, but, because it is only 2 weeks after surgery, there is some FPL function, the plate is proximal to the watershed line, and immediate exploration is not indicated. If this does not improve after 2 to 3 months, further investigation with ultrasound or MRI would be indicated.
Question 35
Which of the following findings can cause a dorsal bunion in a patient with neuromuscular disease?
Explanation
REFERENCES: Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 289-302.
Tachdjian MO: Pediatric Orthopedics ed 2. Philadelphia, PA, WB Saunders, 1990,
pp 1937-1946.
Question 36
A 37-year-old laborer falls 12 feet and sustains a comminuted tibial plafond fracture. Three years after treatment using standard techniques, what will be the most likely outcome?
Explanation
REFERENCES: Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Marsh JL, Weigel DP, Dirschl DR: Tibial plafond fractures: How do these ankles function over time? J Bone Joint Surg Am 2003;85:287-295.
Question 37
Figure below shows the standing AP radiograph obtained from a 55-year-old man who has a 5-year history of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. What is the UKA survivorship for a 55- year-old patient, compared with the survivorship for total knee arthroplasty?
Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact anterior cruciate ligament (ACL). The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph aids the orthopaedic surgeon in determining the correction of the varus deformity and assessing the lateral compartment. An inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared with other age groups, but survivorship is lower for UKA than for TKA. No studies to date have shown any differences in survivorship between fixed-bearing and mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, which occurs in less than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA are low. Arthritis may progress
faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
Question 38
Figures 28a and 28b show the sagittal and axial lumbar MRI scans of a 72-year-old man who reports dull aching back pain that spreads to his legs, calves, and buttocks. He has had the pain for several years and it is precipitated by standing and walking and relieved by sitting. His symptoms have been worsening over the past year and he notes that he is leaning forward while walking to help relieve his symptoms. He has had no treatment to date. What is his prognosis if he chooses to pursue nonsurgical management for this condition?
Explanation
REFERENCES: Amundsen T, Weber H, Nordal HJ, et al: Lumbar spinal stenosis: Conservative or surgical management? A prospective 10-year study. Spine 2000;25:1424-1435.
Hilibrand AS, Rand N: Degenerative lumbar stenosis: Diagnosis and management. J Am Acad Orthop Surg 1999;7:239-249.
Tadokoro K, Miyamoto H, Sumi M, et al: The prognosis of conservative treatments for lumbar spinal stenosis: Analysis of patients over 70 years of age. Spine 2005;30:2458-2463.
Question 39
In patients with displaced radial neck fractures treated with open reduction and internal fixation with a plate and screws, the plate must be limited to what surface of the radius to avoid impingement on the proximal ulna?
Explanation
REFERENCES: Smith GR, Hotchkiss RN: Radial head and neck fractures: Anatomic guidelines for proper placement of internal fixation. J Shoulder Elbow Surg 1996;5:113-117.
Caputo AE, Mazzocca AD, Santoro VM: The nonarticulating portion of the radial head: Anatomic and clinical correlations for internal fixation. J Hand Surg Am 1998;23:1082-1090.
Question 40
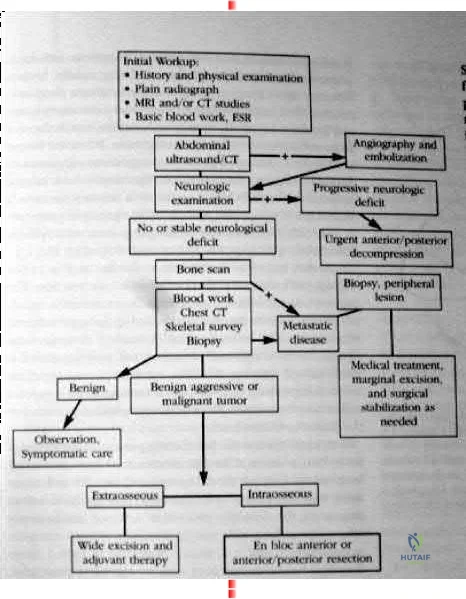
maximize physical capacity and 4) obtain local control of the disease. Other trivia from the references include: After the lung and liver the skeletal system is the third most common site of metastasis. The spine is the most common site of skeletal metastasis. 60% of all skeletal lesions and 36% are asymptomatic. Breast, prostate, lung and renal carcinoma comprise 80% of the carcinomatous skeletal metastasis. 70% metastasis occur in the thoracic and thoracolumbar regions. 21% had involvement of the lumbar and sacral regions. 8% involved the cervical and cervicothoracic regions together. As many as 90% of patients who die of cancer may have Spinal metastasis at autopsy, and only half of patients who die from cancer will have symptoms from spinal mets. Fewer than 10% with spinal mets are treated surgically. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont IL., American academy of orthopaedic surgeons, 2002, pp 723-736. back to this question next question 03 What is the most frequently encountered complication following juvenile hallux valgus correction?
Explanation

Coglin’s referenced paper is a study out of Idaho. 11 year retrospective study of 45 patients (60 feet). A multiprocedural approach was used to surgically correct the deformity. There were 6 recurrences of the deformities and eight
complications (6 cases of hallux varus, one case of wire breakage and one case of undercorrection.) So according to their reference this question has two correct answers.

Postoperative complications have been frequently reported following juvenile hallux valgus corrections. Recurrence following surgery is probably the most frequently reported complication and is likely due to the high rate of congruency associated with a juvenile hallux valgus deformity.

OKU Foot and Ankle 2 Rosemont IL., American academy of orthopaedic surgeons, pp135-150.
back to this question next question
Question 41
What is the most common cause of errors that harm patients? Review Topic
Explanation
Question 42
The anatomy of the sciatic nerve as it exits the pelvis is best described as exiting through the
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 347.
Anderson JE: Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-34, 4-36.
Hollingshead WH: Anatomy for Surgeons: The Back and Limbs, ed 2. Hagerstown, MD, Harper & Row, 1969, pp 607-609.
Question 43
Figure A shows intraoperative images of a right knee in an 8-year-old boy after he sustained an injury. Which of the following is the most common indication for performing this procedure? Review Topic

Explanation
Arthroscopic treatment of lateral discoid meniscus injuries has the advantages of reducing trauma, precise resection or repair of the meniscus and saucerization of the remaining discoid meniscus. Operative treatment is usually limited to patients with pain and mechanical symptoms that are undergoing partial meniscectomy or repair. Asymptomatic discoid meniscus without tears are not considered a surgical indication for routine saucerization.
Kramer et al. reviewed the diagnosis and treatment of traumatic discoid meniscal tears in children. They report that knee shape, size and skeletal maturity must be considered when determining the optimal method of repair. However, all symptomatic torn discoid menisci are best treated with saucerization and repair.
Good et al. looked at the arthroscopic techniques of discoid meniscus repair. Arthroscopic saucerization was successful in 28 of 30 knees and meniscal repair in 23 of 30 knees. At final follow-up, all patients exhibited full knee flexion beyond 135 degrees. In 3 of 30 patients there was residual knee pain, and four reported intermittent mechanical symptoms.
Figure A shows a series of arthroscopic images of the right knee lateral compartment. There is a sequential saucerization of the discoid meniscus.
Incorrect Answers:
(SBQ13PE.83) 8-year-old boy complains of intermittent painless clicking in his knee. His physical examination is normal. His family doctor orders an MRI, which reveals an incomplete lateral discoid meniscus without evidence of tear. What is the most appropriate treatment? Review Topic
Observation only
Diagnostic arthroscopy
Saucerization of meniscus
Saucerization of meniscus and microfracture
Saucerization and stabilization of the mensicus
The clinical presentation is consistent with a asymptomatic discoid meniscus. The most appropriate treatment at this time would be observation only.
MRI scans of the knee are very sensitive for identifying discoid menisci. Diagnosis is usually made when there are 3 or more 5mm sagittal MRI images showing meniscal continuity. Treatment is mostly focused on conservative modalities. Asymptomatic tears are usually treated with observation only. Saucerization is indicated for recurrent locking, swelling, persistent pain, or radiographic evidence of a meniscal tear.
Watanabe et al. described three types of discoid lateral menisci based on arthroscopic appearance. In this classification, discoid menisci with normal peripheral attachments are either type I (complete) or type II (incomplete). Type III discoid menisci, the so-called Wrisberg ligament type, are lacking posterior capsular attachments with the exception of the posterior meniscofemoral ligament.
Kramer et al. looked at the presentation of pediatric knee pain and discoid meniscus. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the meniscus.
Illustration A shows the cross-section of normal meniscus. Illustration B shows the Watanabe classification.
Incorrect Answers:
Question 44
-The use of a soft cervical orthosis is most supported for which injury?
Explanation

Question 45
Figure 11 shows the radiograph of an 18-year-old soccer player who reports recurrent lateral foot pain after sustaining an inversion injury. History reveals that 6 months ago he had been treated in a non-weight-bearing cast for a fifth metatarsal fracture. Management should consist of
Explanation
REFERENCES: Torg JS, Balduini FC, Zelko RR, Pavlov H, Peff TC, Das M: Fractures of the base of the fifth metatarsal distal to the tuberosity: Classification and guidelines for nonsurgical and surgical management. J Bone Joint Surg Am 1984;66:209-214.
DeLee JC: Fractures and dislocations of the foot, in Mann R, Coughlin M (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 1465-1503.
Question 46
An 84-year-old female community ambulator with a history of hypertension undergoes a right hip hemiarthroplasty for a femoral neck fracture. When performed in the post-operative period, the timed up and go (TUG) test may be used to predict which patient outcome?
Explanation
Hip fractures are a cause of significant functional decline for elderly patients. Many outcome tests have been developed to prediction function after hip fracture to manage patient expectations and to assist in rehabilitation planning. The TUG test objectively measures functional mobility and dynamic balance. The test is performed by timing the amount of seconds it requires for a patient to stand up from a chair, walk 10ft (3.05m), return to the chair, and sit.
Laflamme et al performed a prospective study evaluating the utility of the TUG test to predict functional outcomes in patients undergoing hip hemiarthroplasty for femoral neck fracture. The TUG scores were significantly higher at 4-days and 3-weeks postoperatively in patients requiring a walking aid compared with patients walking independently at two-years. Patients who performed the test in >58s at 4-days postoperatively had an eightfold greater risk of requiring an assistive device.
Springer et al prospectively analyzed the unipedal stance test (UPST) with eyes open and closed in healthy subjects to establish normative values for the test across age and gender groups. Performance on the test was found to be age-specific and not related to gender. The UPST is a method of quantifying static balance ability.
Kristensen et al studied the relative and absolute inter tester reliability of TUG in patients with hip fractures. The authors found that the TUG has a high interobserver reliability and an improvement by 6.2 seconds for a patient with a baseline of 20s indicates a change in functional mobility.
Video A shows the timed up and go test.
Incorrect Answers:
Question 47
A 30-year-old man landed on his shoulder in a fall off his mountain bike. An AP radiograph and CT scan are shown in Figures 34a and 34b. Management should consist of
Explanation
REFERENCES: Jakob RP, Miniaci A, Anson PS, et al: Four-part valgus impacted fractures of the proximal humerus. J Bone Joint Surg Br 1991;73:295-298.
Resch H, Povacz P, Frohlich R, et al: Percutaneous fixation of three- and four-part fractures of the proximal humerus. J Bone Joint Surg Br 1997;79:295-300.
Question 48
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function?
Explanation
REFERENCES: Levy O, Copeland SA: Cementless surface replacement arthroplasty of the shoulder: 5- to 10-year results with the Copeland mark-2 prosthesis. J Bone Joint Surg Br 2001;83:213-221.
Burroughs PL, Gearen PF, Petty WR, et al: Shoulder arthroplasty in the young patient.
J Arthroplasty 2003;18:792-798.
Question 49
A 13-year-old boy has pain and a firm mass in his left knee. A radiograph and MRI scan are shown in Figures 2a and 2b, and a biopsy specimen is shown in Figure 2c. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: Simon M, Springfield D, et al: Osteogenic sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 267.
Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990,
pp 14-15.
Question 50
Patient outcomes can be improved and early post-injury management errors decreased by adhering to the Advanced Trauma Life Support (ATLS) protocol. This protocol includes criteria for inter-hospital transfer when the patient's needs exceed the resources available. Which of the following would it be acceptable to manage without interfacility transfer to a trauma center?
Explanation
While most patients can receive all their definitive care at any hospital to which they present, early recognition of those that require transfer to a trauma center is essential to maximizing outcomes. Inherent in such identification is physician's' assessment of their own and their institutions' abilities and the limits thereof.
Van Olden et al. prospectively studied severely injured patients consecutively presenting to two community hospitals in the Netherlands. Comparison was made between patients treated prior to and after introduction of ATLS training to physicians at the studied hospitals. There was no difference in overall mortality between the two groups. however, there was a significant reduction in mortality in the first 60 minutes after admission, from 24.2% pre-ATLS to 0.0% post-ATLS.
Ali et al. studied trauma outcomes and mortality in patients presenting to the largest hospital in Trinidad and Tobago for the four years prior to and after introduction of ATLS training for physicians in the emergency department. Trauma mortality decreased to 33.5% from 67.5% after introduction of ATLS. Post-injury functional outcomes were also improved.
Illustration A shows the ATLS guidelines for interfacility transfer in table format. Incorrect answers:
Question 51
A 28-year-old male sustains a fall on icy ground and fractures his ankle. An intraoperative fluoroscopy image is shown in Figure A. This fixation suggests that the mechanism of injury was one of

Explanation
A vertical fracture of the medial malleolus is characteristic of a Lauge-Hansen SA fracture. Bimalleolar SA fractures will also demonstrate a distal fibular avulsion. Another characteristic is impaction of anteromedial distal tibia by the talar dome. An anteromedial surgical approach allows visualization of this region, elevation of impaction, and bone grafting of the defect if necessary.
Dumigan et al. analyzed 4 different methods of treating vertical shear fractures with polyurethane models. They found that fixation with a 4 hole 1/3 tubular plate with 2 screws in the distal fragment was stiffer than fixation with the same plate with 1 screw in the distal fragment (3 in the proximal), fixation with two 3.5mm cortical screws with washers, and fixation with two 4mm cortical screws with washers. They recommend plating over screw-alone constructs.
McConnell et al. reported 8 cases of anteromedial marginal impaction in SA fractures. They note that 44 fractures were SA type. Following reduction and fixation, all 8 patients had excellent outcome and no arthritis. They recommend an anteromedial approach to the medial malleolus for visualization.
Figure A is a lateral radiograph showing fixation of both malleoli with reconstruction plates. Illustration A is an postoperative AP fluoroscopy image. Illustration B is an injury film demonstrating the same SA ankle fracture. Illustration C shows articular impaction at the medial shoulder of the ankle joint typical of SA injuries. Illustration D shows marginal impaction in SA fractures.
Incorrect Answers
(SBQ12TR.76) A 24-year-old male sustains the fracture dislocation shown in Figure
A. How is this fracture pattern best classified?

Moore I
Moore II
Schatzker III
Schatzker V
OTA type 41B3
Figure A shows a Moore Type II fracture. Moore type II fractures consist of fractures involving the entire tibial condyle, where the fracture line begins in the opposite compartment and extends across the tibial eminence.
A number of classification systems are used to describe tibial plateau fractures. The main classification systems that are widely used include Schatzker, AO/OTA, Hohl and Moore. The Moore classification describes high energy fracture-subluxation injuries of the knee. This is thought to have clinical implications as the type of fracture pattern can indicate an associated soft-tissue injury.
Moore retrospectively reviewed over a 1000 proximal tibia fractures to devise a classification systems based on the characteristic of five types of tibia plateau fracture patterns. He believed this system helped to better understand knee instability and concomitant soft-tissue injury. For example, Moore Type III fractures (rim avulsion) are associated with a high rate of neurovascular injury.
Figure A shows a fracture involving the entire tibial condyle. Illustration A shows a schematic diagram of the Moore classification (I - V). Illustration B shows a table that
describes the Moore classification (I - V).
Incorrect Answers:
Question 52
A 74-year-old woman with rheumatoid arthritis has pain in the shoulder that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 24a and 24b. Active forward elevation is 120 degrees and external rotation is 30 degrees. At the time of surgery, a 1-cm rotator cuff tear is found, which is repairable. Which of the following treatment options will result in the most predictable pain relief and function? Review Topic

Explanation
Question 53
A 34-year-old man underwent a transtibial amputation as the result of a work-related injury. The amputation was performed at the inferior level of the tibial tubercle. The residual limb has a soft-tissue envelope composed of gastrocnemius muscle that is used as soft-tissue cushioning for the distal tibia. Despite undergoing several prosthetic fittings, he continues to report pain and instability. Examination reveals that the prosthesis appears to fit well with no apparent pressure points or areas of skin breakdown. He is not willing to have any further surgery. Which of the following modifications will most likely provide relief?
Explanation
REFERENCES: Bowker JH, Goldberg B, Poonekar PD: Transtibial amputation: Surgical procedures and postsurgical management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 429-452.
Kapp S, Cummings D: Transtibial amputation: Prosthetic management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 453-478.
Question 54
A 56-year-old woman sustains a type IIIB open tibial shaft fracture. She undergoes irrigation and debridement and intramedullary nailing with flap coverage 24 hours later. Cultures are taken pre-debridement and post-debridement. She develops a surgical site infection at 6 weeks, which requires removing the hardware and placing show Commented [1]: an external fixator. Deep cultures are most likely to pathogens found in
Explanation
In another study, before any interventions were performed, initial aerobic and anaerobic cultures of the wounds of 117 consecutive open extremity fractures grades I through III were obtained. The results of these cultures were correlated with the development of a wound infection. If an infection occurred, the organism grown from the infected wound was compared with any organism grown from the primary wound cultures. Of the initial cultures, 76% (89/117) did not demonstrate any growth, while the other 24% (28/117) only grew skin flora. There were only 7 (6%) wound infections, and 71% (5/7) initially did not grow any organisms. Of the isolates that grew from the initial cultures, none were the organisms that eventually led to
Question 55
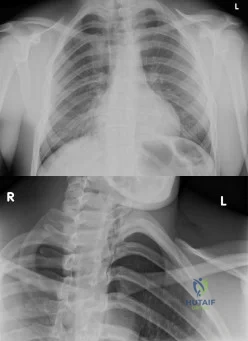
An 19-year-old male presents to the emergency room following an motor vehicle accident as an unrestrained driver. Examination reveals unilateral jugular vein engorgement. Chest and special view radiographs are seen in Figures A and B respectively. Following CT scan of the chest, the next step in management is Review Topic
Explanation
The SC joint can dislocate anteriorly or posteriorly. Posterior dislocations are first treated with closed reduction. If closed reduction fails, open reduction is indicated. Early complications of posterior SC dislocation include pneumothorax, laceration/erosion/occlusion of great vessels, esophageal rupture and brachial plexus compression. Late complications include tracheoesophageal fistula, stridor and dysphagia.
Groh et al. reviewed traumatic SC injuries. Reduction maneuvers in posterior SC dislocation include: (1) traction on the arm and slowly bringing it into extension, (2) traction with the arm in adduction and posterior pressure applied to the shoulder, and
(3) pulling anteriorly on a towel clip encircling the medial clavicle. Chronic instability after posterior SC dislocations can be managed with figure-of-8 semitendinosus graft or medial clavicle resection and reattachment of the clavicle to the first rib with dacron tape.
Glass et al. performed a systematic review on SC dislocations. They found mediastinal compression occurred 30% of the time with posterior dislocations.
Figures A and B are radiographs demonstrating asymmetry of the SC joints, characteristic of a right posterior SC dislocation (Figure B is not a serendipity view). Illustration A demonstrates how in POSTERIOR dislocation, the clavicle appears INFERIOR, and in ANTERIOR dislocation, the clavicle appears SUPERIOR on a serendipity view radiograph respectively. Illustration B shows the imaging technique for a serendipity view radiograph. Illustration C is a reconstructed CT image of the patient showing left posterior SC dislocation.
Incorrect Answers:
Question 56
In a patient with a soft-tissue sarcoma treated by wide excision and radiation therapy, the risk of subsequent fracture is probably most influenced by
Explanation
REFERENCES: Bell RS, O’Sullivan B, Nguyen C, et al: Fractures following limb-salvage surgery and adjuvant irradation for soft-tissue sarcoma. Clin Orthop 1991;271:265-271.
Lin PP, Boland PJ, Healey JH: Treatment of femoral fractures after irradiation. Clin Orthop 1998;352:168-178.
Question 57
A 45-year-old man undergoes an anterior cervical diskectomy and fusion at C5-6 and C6-7 with instrumentation. During the first postoperative visit at 1 week, the patient reports difficulty swallowing and mild anterior cervical tightness. The anterior wound is benign and the patient denies any dyspnea or shortness of breath. A postoperative radiograph is seen in Figure 25. What is the most appropriate management at this time?
Explanation
6 months with nonsurgical management. A minority of patients experience moderate or severe symptoms by 6 months after the procedure. Female gender and multiple surgical levels have been identified as risk factors for the development of postoperative dysphagia.
REFERENCES: Lee MJ, Bazaz R, Furey CG, et al: Risk factors for dysphagia after anterior cervical spine surgery: A two-year prospective cohort study. Spine J 2007;7:141-147.
Bazaz R, Lee MJ, Yoo JU: Incidence of dysphagia after anterior cervical spine surgery:
A prospective study. Spine 2002;27:2453-2458.
Question 58
A patient notes pain under the first metatarsophalangeal joint following a soccer injury. The MRI scans shown in Figures 27a and 27b reveal what pathologic finding?
Explanation
REFERENCES: Watson TS, Anderson RB, Davis WH: Periarticular injuries to the hallux metatarsophalangeal joint in athletes. Foot Ankle Clin 2000;5:687-713.
Tewes DP, Fischer DA, Fritts HM, et al: MRI findings of acute turf toe: A case report and review of anatomy. Clin Orthop 1994;304:200-203.
Question 59
Figure 8 shows the AP radiograph of a 33-year-old woman who sustained a midshaft clavicle fracture from a motorcycle accident 15 months ago. She continues to have significant pain with activities of daily living. Management should consist of
Explanation
REFERENCES: Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
Question 60
A 43-year-old man who works as a plumber has a painful stiff elbow in his dominant arm. He notes that while he recalls no single event of injury, he thinks the many years of pulling wrenches and soldering pipes have resulted in his problem. He reports that he has pain with any motion in bending his arm and can no longer straighten his elbow. Examination reveals generalized swelling of the elbow, both medial and lateral with a range of motion that lacks 45 degrees of extension and flexes only to 110 degrees. Pronation and supination are also limited to 45 degrees. Audible crepitus is perceived but there is no instability. Radiographs reveal advanced osteoarthritis at the radiocapitellar and ulnohumeral joints with complete loss of articular cartilage. What is the most appropriate initial treatment option? Review Topic
Explanation
must respect the physical demands of the patient while trying to preserve joint motion and function with tolerable symptoms. Osteophyte resection and capsular release have offered many patients significant improvement in their symptoms while allowing them to return to most activities. The osteophyte resection and releases can be done effectively by an open or arthroscopic approach. Whereas total elbow arthroplasty would likely result in better and more thorough pain relief, it would not tolerate the occupational demands of this individual. There is no role for physical therapy initially in the face of advanced, painful arthritis associated with long-standing fixed joint contractures. Elbow fusion results in severe loss of function and its indication is rare and usually considered in the face of unmanageable sepsis. Radial head resection may improve symptoms related to the radial capitellar arthritis but would not improve range of motion or end range impingement pain. Also, radial head resection should be avoided in heavy laborers with elbow arthritis because it would lead to increased loads across the arthritic ulnohumeral joint.
Question 61
A 13-year-old boy who has a history of a pituitary adenoma has an unstable unilateral slipped capital femoral epiphysis. What is the indication for prophylactic pinning of the contralateral, unslipped side? Review Topic
Explanation
Question 62
What structure has been described as having a risk of injury with retractor placement on the sacrum during combined acetabular-pelvic ring surgery using the Stoppa approach with a lateral window?

Explanation
Question 63
A 14-year-old boy reports a 4-month history of increasing backache with difficulty walking long distances. His parents state that he walks with his knees slightly flexed and is unable to bend forward and get his hands to his knees. He denies numbness, tingling, and weakness in his legs and denies loss of bladder and bowel control. A lateral radiograph of the lumbosacral spine is shown in Figure 18. What is the best surgical management for this condition?
Explanation
L5 to S1 usually is not successful for a slip that is greater than 50%. Isolated anterior spinal fusion has not been successful, and direct repair of the pars defect is only useful for spondylolysis without spondylolisthesis.
REFERENCES: Lenke LG, Bridwell KH: Evaluation and surgical treatment of high-grade isthmic dysplastic spondylolisthesis. Instr Course Lect 2003;52:525-532.
Ginsburg GM, Bassett GS: Back pain in children and adolescents: Evaluation and differential diagnosis. J Am Acad Orthop Surg 1997:5:67-78.
Question 64
Use of long-term (at least 5 years) bisphosphonate medications for osteoporosis is associated with
Explanation
Fragility or osteoporotic fractures are common in postmenopausal women and older men and include fractures of the proximal humerus and distal radius and hip and vertebral compression fractures. The most reliable predictor of a fragility fracture is a past fragility fracture; consequently, it is important to elicit history. Assessment of vitamin D and calcium levels is important when treating these patients because many of them have low levels.
Use of bisphosphonates for treatment of osteoporosis results in atypical femur fractures and a decrease in risk for fragility fractures (including hip fractures). There also are reports of osteonecrosis of the mandible with prolonged use of these drugs. Current medical literature suggests stopping these drugs after 3 to 5 years to allow bone remodeling.
RECOMMENDED READINGS
Shane E, Burr D, Ebeling PR, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster D, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Koval K, Lane JM, McKiernan F, McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Sen HT, van der Meulen MC, Weinstein RS, Whyte M; American Society for Bone and Mineral Research. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2010 Nov;25(11):2267-94. doi: 10.1002/jbmr.253. Erratum in: J Bone Miner Res. 2011 Aug;26(8):1987. PubMed PMID: 20842676. View Abstract at PubMed
Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster DW, Ebeling PR, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Lane JM, McKiernan F,McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Howe TS, van der Meulen MC, Weinstein RS, Whyte MP. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American society for bone and mineral research. J Bone
Miner Res. 2014 Jan;29(1):1-23. doi:10.1002/jbmr.1998. Epub 2013 Oct 1. PubMed PMID: 23712442. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 92 THROUGH 95
A 23-year-old man is involved in a motorcycle collision and sustains a displaced transcervical femoral neck fracture with an associated open comminuted femoral shaft fracture.
Question 65
In the normal adult, the distance between the basion and the tip of the dens with the head in neutral position is how many millimeters?
Explanation
REFERENCES: Wiesel SW, Rothman RH: Occipitoatlantal hypermobility. Spine 1979;4:187-191.
Wholey MH, Browner AJ, Baker HL Jr: The lateral roentgenogram of the neck: With comments on the atlanto odontoid-basion relationship. Radiol 1958;71:350-356.
Question 66
Figures below show the radiograph and the MRI scan obtained from a 37-year-old woman with a 2-month history of left hip pain. Which presurgical factor is most commonly associated with a poor outcome after a hip joint salvage procedure?
Explanation
MRI reveals an anterior labral tear, and the radiograph shows minimal arthritis with possible dysplasia. The most common location of pain in patients with a labral tear is the groin, and the most common physical finding is a positive impingement test result. Pain during sitting, clicking, and buttock pain are frequently described by patients with a labral tear, but these symptoms are less common than groin pain. A positive posterior impingement test finding is more common in patients with a posterior labral tear. Although age over 40 years and a body mass index higher than 30 can adversely affect clinical outcomes after joint preservation procedures such as PAO, hip arthroscopy, and femoral acetabular impingement surgery, the presence of hip arthritis on presurgical radiographs is the most commonly mentioned cause of failed hip joint preservation surgery. Tönnis grade is a radiographic measure of hip arthritis. A higher Outerbridge score is associated with more frequent poor outcomes after hip arthroscopy; however, the
Outerbridge cartilage score is determined by direct visualization at the time of surgery. The Outerbridge score cannot be determined presurgically.
Question 67
What is the most important feature in choosing an outcome instrument to assess shoulder disorders?
Explanation
REFERENCES: Leggin BG, Iannotti JP: Shoulder outcome measurement, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, p 1027.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 47-55.
Question 68
A 15-year-old high school soccer player collides with an opponent and is unconscious when the trainer arrives on the field. He is conscious within 15 seconds, breathing appropriately, and denies any headache, neck pain, or nausea. It is his first head injury. Provided that the athlete is free of symptoms, when should he be allowed to return to athletic activity?
Explanation
week period out of sport. The last week prior to return must be symptom-free and the athlete should not have symptoms in practice.
REFERENCES: Cantu RC: Return to play guidelines after a head injury. Clin Sports Med 1998;17:45-60.
Stevenson KL, Adelson PD: Pediatric sports-related head injuries, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 781.
Question 69
-Postsurgically, the patient recovers well and is fully rehabilitated. He demonstrates full motion with no instability or pain and is cleared to return to play 12 months after the surgery. He asks for your advice regarding use of a functional brace for playing basketball following his reconstruction. What is the most appropriate recommendation?
Explanation
The athlete most likely suffered an acute ACL rupture however the presence of a lipohemarthrosis is concerning for the possibility of an intraarticular fracture. Because of this, the patient should not be allowed full weight bearing until a fracture is ruled out with radiographs. Given the athlete’s inability to perform a straight leg raise, the extensor mechanism is not functioning and a telescoping knee brace locked in extension should be utilized. A neoprene knee sleeve does not have a role in the
treatment of this acute injury.The radiographs reveal a lateral avulsion fracture off of the proximal tibial epiphysis which is known as a Segond fracture. It is indicative of an ACL injury and the fracture fragment seen is the consequence of the lateral capsule injury sustained during the pivot-shift mechanism. There is no radiographic evidence of a medial tibial plateau fracture. A radiographic sign of a chronic MCL injury is known as a Pellegrini-Stieda lesion and this is seen as calcification of the femoral origin of the MCL. A radiographic sign of an acute LCL rupture would be an avulsion fracture of the tip of the fibula.The MRI shows kissing contusions of the posterolateral tibial plateau and the midpoint of the lateral femoral condyle. These “kissing lesions” are seen as a result of a pivot shift mechanism of injury and are diagnostic for an ACL rupture. The most common associated injury in an acute ACL rupture is a lateral meniscus tear. Medial meniscus tears are more common in chronic ACL injuries. PCL rupture and PLC injury are all associated injuries seen in acute ACL rupture; however, these are much less common than meniscal tears. The team physician has a role in encouraging, but
not demanding, the athlete to report the injury andtreatment to the scholarship school’s coaching staff. What the athlete decides to do is his decision; the physician would be violating the athlete’s HIPAA rights as well as their confidence by reporting it directly to the scholarship school. Clearly the physician should not discourage the athlete from reporting the injury. The athlete is 18 years old and, as such, the physician would need the athlete’s permission to discuss any medical issues with the family in keeping with HIPAA.
The athlete’s exam demonstrates incompetence of both bundles of the ACL as demonstrated by the loss of stability with anterior translation of the tibia (Lachman test) as well as with rotation (pivot shift). The external rotation stress with the knee in 30 degrees of flexion tests the competence of the posterolateral corner while rotation at 90 degrees of flexion tests the PCL. Since the athlete’s knee is stable to posterior drawer testing demonstrating an intact PCL and the external rotation at 30 degrees is equivalent to that at 90 degrees, the posterolateral corner in intact.
The ACL has two separate and distinct bundles, the AM and PL. Each bundle takes on tension at varying degrees of knee flexion and therefore each bundle is thought to have a varying contribution to the stability of the knee. The AM bundle takes on tension with the knee in flexion and the PL bundle is tight in extension. Neither bundle is isometric during knee range of motion. Both bundles have contributions to rotational stability of the knee throughout the range of motion.
The success of traditional trans-tibial single-bundle ACL reconstruction has recently been called into question given the demonstration of persistent rotational instability following reconstruction. The persistence of rotational instability in trans-tibial single bundle ACL reconstruction has been attributed to the location of the graft in a vertically malpositioned femoral tunnel. The goal of double-bundle ACL reconstruction is to more accurately reproduce the native ACL and provide grafts that contribute to anteroposterior stability as well as rotational stability by placing the grafts in more anatomic locations not central in the knee axis. There is an increased cost and surgical time associated with double-bundle reconstruction.
The use of functional braces following ACL reconstruction is a surgeon’s preference because there is no difference in retear rate with or without a brace. Some authors recommend brace use for one to two years following ACL reconstruction for all athletic activities, but this is not supported by the literature. No literature exists showing a higher rate of reinjury with a functional brace and off-the shelf and custom braces have been found to be equivalent leading those who advocate for braces to recommend off-theshelf braces given their significantly lower cost.
Question 70
Figure 76 is the MR image of a 16-year-old high school football player who sustained a traumatic dominant shoulder dislocation during a game. On-field reduction was unsuccessful. The shoulder is reduced in the emergency department, and the player and his family followup in clinic. Which factor is most associated with failure of surgical treatment in this scenario?
Explanation
The MR image reveals a Bankart lesion. Arthroscopic Bankart repair failure likelihood is increased by numerous factors. Age, number of recurrences, and bony defects are most associated with failure of arthroscopic repair. Shoulder dominance, amount of periosteal
stripping, and difficulty of reduction do not correlate with increased recurrence risk following surgery.
CLINICAL SITUATION FOR QUESTIONS 77 THROUGH 79
A 17-year-old volleyball player has a 3-month history of gradually worsening right shoulder pain. She describes a vague sensation of her shoulder “popping out of place” and weakness associated with overhead activities. She has intermittent generalized paresthesias in her right upper extremity, and she has discontinued participation in sports as a result of her symptoms. Glenohumeral range of motion is symmetric bilaterally. Empty can test findings are negative with full strength of the supraspinatus. An active compression test is negative, and sulcus sign findings are positive. An anterior apprehension test produces pain that is unrelieved with a relocation test. A cervical spine examination is unremarkable.
Question 71
A healthy 16-year-old boy has had increasing pain in the right knee for the past 3 months. Examination reveals warmth and swelling around the distal femur. Radiographs and an MRI scan are shown in Figures 51a through 51c, and a biopsy specimen is shown in Figure 51d. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 205.
Question 72
Figures 23a and 23b show the radiograph and clinical photograph of a patient who reports a reduced ability to flex the interphalangeal joint of her great toe after undergoing a Chevron-Akin bunionectomy. What is the most likely cause?
Explanation
REFERENCES: Tollison ME, Baxter DE: Combination chevron plus Akin osteotomy for hallux valgus: Should age be a limiting factor? Foot Ankle Int 1997;18:477-481.
Scaduto AA, Cracchiolo A III: Lacerations and ruptures of the flexor or extensor hallucis longus tendons. Foot Ankle Clin 2000;5:725-736.
Question 73
Which of the following tendons is found in the same dorsal compartment of the wrist as the posterior interosseous nerve?
Explanation
1st Compartment: Abductor pollicis longus, extensor pollis brevis
2nd Compartment: Extensor carpi radialis brevis, extensor carpi radialis longus
3rd Compartment: Extensor pollicis longus
4th Compartment: Extensor digitorum comminus, extensor indicus proprius, posterior interosseous nerve
5th Compartment: Extensor digiti minimi
6th Compartment: Extensor carpi ulnaris
The extensor indicis proprius is also contained in the fourth dorsal compartment. The extensor digiti minimi is located in the fifth dorsal compartment. The extensor carpi radialis brevis is located in the second dorsal compartment. The extensor pollicis longus is located in the third dorsal compartment, and the abductor pollicis longus is located in the first dorsal compartment.
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 150-151.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 60.
Question 74
A 9-year-old child has right groin pain after falling from a tree. Examination reveals that the right leg is held in external rotation, and there is significant pain with attempts at passive range of motion. Radiographs are shown in Figures 43a and 43b. Management should consist of
Explanation
REFERENCES: Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
Hughes LO, Beaty JH: Fractures of the head and neck of the femur in children. J Bone Joint Surg Am 1994;76:283-292.
Question 75
A 51-year-old female sustained a comminuted radial head fracture with 4 fragments and an associated elbow dislocation. She was initially closed reduced and splinted with the elbow joint in a reduced position and presents to the orthopedists office 10 days later. In response to the patient's question of what treatment offers the best chance for a good outcome, the surgeon should recommend?

Explanation
Question 76
- A 47-year-old woman who reports mild, aching pain in her knee has no history of trauma. Examination of the knee is normal. Figure 23a shows the AP radiograph. A bone scan shows increased uptake at this site only. Figure 23b shows the CT scan, and Figure 23c shows the histology from the CT scan-guided needle biopsy. Treatment should include
Explanation
The modern technique for the removal of a giant cell tumor involves wide decortication of all the bone overlying the area of the tumor. The cavity is filled with methylmethacrylate bone cement and covered with demineralized bone matrix to stimulate the restoration of strong cortical
boundaries. The other procedures are much more invasive and not necessary to treat a low-grade neo-plastic lesion such as a giant cell tumor. Fewer complications and better functional results have been found after intralesional excision and insertion of methylmethacrylate than other techniques.
Question 77
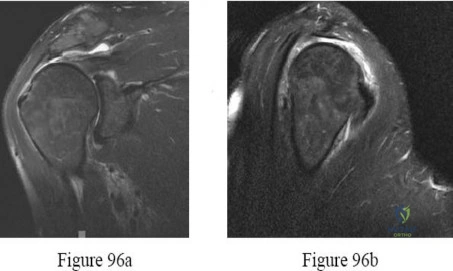
If the structure marked by the tip of the probe in Figure 94 is repaired to the bony glenoid with suture anchors during an arthroscopic stabilization procedure, what is the most likely result? Review Topic

Explanation
Question 78
Osteoarthritic cartilage is characterized by decreased
Explanation
Chondrocytes in OA are much more metabolically active than those of normal cartilage. Studies reveal measuring the levels of utilization on sulfate and H-glucosamine informing components of cartilage matrix. The amount of DNA also rises in OA cartilage most noticeable at the articular chondrocyte.
The synthesis of hyaluronate increases. Recent data suggests 1) hyaluronate that is synthesized is abnormal and, hence, does not allow aggregation; or 2) The excess synthesis is a response to a rapid degradation of synthesized product. This is in light of the fact that synthesis increases, yet concentration of hyaluronate decreases.
The correct answer is that proteoglycan content decreases. The synthesis of proteoglycan increases in OA, but due to the increased rate of breakdown of proteoglycan there is a net result of lowered proteoglycan content.
Question 79
An 18-year-old woman injures her left knee playing soccer. At the time of anterior cruciate ligament (ACL) reconstruction, she was noted to have an irreparable posterior horn medial meniscus tear. Partial meniscectomy will have what primary effect? Review Topic
Explanation
Question 80
Figures 1 and 2 are the radiographs of a 55-year-old man who has a 3-year history of right shoulder pain. He has maximized nonoperative management and is interested in operative treatment. He had an open Bankart repair 20 years ago and did well until a few years ago. What is most important to know when deciding on the best surgical treatment for this patient?
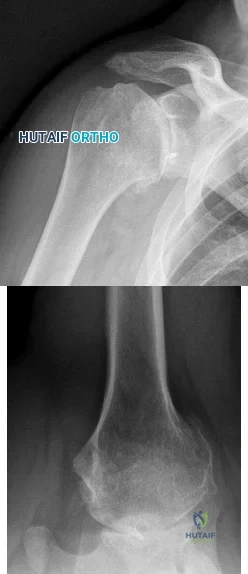
Explanation
Although the radiographs do not reveal any obvious signs of rotator cuff failure, the patient had had an open Bankart 20 years ago. The integrity of the subscapularis tendon following a previous open shoulder procedure is crucial in deciding which type of arthroplasty to consider. Range of motion and infraspinatus strength do not affect the decision-making process, assuming the rotator cuff is intact. Activity level can be important when deciding whether to proceed with an arthroplasty, but it is not as important as the rotator cuff integrity when choosing which
arthroplasty to use.
Question 81
When treating a stable 2-part intertrochanteric hip fracture with a sliding hip screw construct, what is the minimum amount of screw holes that are needed in the side plate for successful fixation?

Explanation
The referenced article by Bolhofner et al reviews a series of 69 patients with a sliding hip screw and two hole side plate and notes that they did not have any failure of the side plate construct.
The referenced article by McLoughlin et al is a biomechanical evaluation of 2 versus 4 hole plates and found that peak load in the failure test was not found to be statistically different between the two-hole and four-hole designs. In cyclic testing, the two-hole configuration exhibited statistically smaller fragment migration in both shear and distraction than the four-hole design.
Question 82
Which of the following genetic disorders has an X-linked recessive inheritance pattern?
Explanation
linked recessive disorders occur when a mutation occurs on the X chromosome that causes the phenotype to be expressed in males and in females who are homozygous for the gene mutation. These disorders are much more common in males since they only have one X chromosome. Other X-linked recessive disorders include: Duchenne muscular dystrophy, Becker's muscular dystrophy, Hunter's syndrome, and spondyloepiphyseal dysplasia (SED) tarda.
Vanderhave et al. reviewed the orthopaedic consideration in patients with hemophilia. Amongst other things, they discuss arthroplasty in patients with this condition. While they are at higher risk for stiffness and acute hemarthrosis following total knee arthroplasty, ~90-95% of patients have good or excellent results.
Illustration A shows how hemophilia is inherited through a punnett square. Illustration B shows how a weak clotting mechanism causes increased bleeding in patients with hemophilia.
Incorrect Answers:
Question 83
Following a partial muscle laceration, keeping the affected extremity immobilized for 2 weeks before starting an exercise program will likely lead to: Review Topic
Explanation
Healing a muscle injury involves two competing processes: regeneration of muscle fibers and formation of granulation tissue. Starting motion too soon after injury may increase the area of fibrous scar, and limit the ability of new muscle fibers to penetrate this area. Prolonged immobilization limits scar production but penetrating muscle fibers will lack appropriate orientation, and the muscle as whole begins to atrophy. Three to 5 days of immobilization has been shown to limit scar tissue production
while the early motion helps generate appropriately organized muscle fibers and maintain strength and range of motion.
Järvinen et al. present a review of muscle injury and healing. They found that immediate mobilization led to a large area of dense scar tissue that regenerating muscle fibers could not adequately penetrate. Prolonged immobilization allowed muscle fibers to regenerate but they lacked appropriate morphology. Following 3-5 days of immobilization they found less scar tissue, better penetration of regenerated muscle fibers, and the regenerated fibers were more well aligned with the uninjured fibers surrounding them.
Menetrey et al. present a mouse model of muscle laceration comparing a short period of immobilization (5 days) to suture repair of the muscle. They found quicker healing and greater strength in the suture repair group. Tetanus strength at one month after injury was (compared to an uninjured control) 81% for sutured muscle, 35% for the early mobilization only group, and 18% for the prolonged immobilization group.
Illustration A is a histology section of lacerated muscle after 7 days of immobilization. The area is infiltrated with granulation tissue and few regenerating myofibers. Illustration B is a histology section of lacerated muscle after 14 days of immobilization. Further infiltration with granulation tissue and mononuclear cells can be seen with regenerating myofibers only at the periphery.
Incorrect answers:
Question 84
A 25 year-old-male presents with the injury seen in Figure A. Which of the following would be a contraindication to closed management with a functional brace?

Explanation
Indications for operative management of humeral shaft fractures are limited given the high rates of union and ability of adjacent joints to compensate for deformity. Intact muscular tone is necessary to effect bony apposition in closed treatment with a functional brace. The absence of neurologic and muscle function in patients with a flail extremity leads to increased rates of nonunion and malunion.
Rutgers and Ring conducted a retrospective review of patients managed with functional bracing of humeral shaft fractures at a single institution. The authors found a 90% overall union rate, with maintenance of shoulder and elbow motion. They caution though, that 29% of their proximal third fractures went on to nonunion.
Figure A demonstrates an AP radiograph of a comminuted humeral shaft fracture with varus alignment.
Incorrect Answers:
Question 85
A 35-year-old man is seen in the emergency department with a bullet wound to the foot that occurred 2 hours ago. Examination reveals a 0.5-cm entrance wound on the dorsum of the foot and a 1.5-cm exit wound on the plantar aspect. Exploration of the plantar wound in the emergency department reveals bone and metal fragments. Radiographs reveal a comminuted, unstable fracture of the base of the first metatarsal and cuneiform. Management should consist of tetanus toxoid, and
Explanation
REFERENCES: Holmes GB Jr: Gunshot wounds of the foot. Clin Orthop Relat Res
2003;408:86-91.
Bartlett CS, Helfet DL, Hausman MR, et al: Ballistics and gunshot wounds: Effects on musculoskeletal tissues. J Am Acad Orthop Surg 2000;8:21-36.
Question 86
A B Figures 90a and 90b are MR images of a 34-year-old man who is referred to your office by his primary care physician after failing 4 months of nonsurgical treatment that included epidural steroids for severe right arm pain occurring in a C6 distribution. He also has associated paresthesias in this region. The patient is weak in elbow flexion and wrist extension. What are his likely outcomes if he is treated with a posterior foraminotomy instead of anterior cervical diskectomy and fusion (ACDF)?

Explanation
This patient has a right-sided C5-C6 disk herniation causing C6 radicular symptoms in the right upper extremity. Studies have shown that both ACDF and posterior foraminotomy confer similar results in terms of pain relief and functional outcome. Patients treated with posterior foraminotomy are at higher risk for neck pain and recurrence of radiculopathy at the same level. Those who receive ACDF are at higher risk for occurrence of radiculopathy at an adjacent level.
RECOMMENDED READINGS
Rao RD, Currier BL, Albert TJ, Bono CM, Marawar SV, Poelstra KA, Eck JC. Degenerative cervical spondylosis: clinical syndromes, pathogenesis, and management. J Bone Joint Surg Am. 2007 Jun;89(6):1360-78. Review. PubMed PMID: 17575617. View Abstract at PubMed Bolesta MJ, Gill K. Acute neck pain and cervical disk herniation. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:227-234.
Question 87
Figures below show the radiographs, MRI, and MR arthrogram obtained from a 25-year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy. What is the primary cause of a cam deformity?
Explanation
Question 88
When planning revision of a total hip arthroplasty where an acetabular reconstruction will be required, what prerequisite is important to ensure long-term success of a cementless component?
Explanation
REFERENCE: Gross AE, Allan DG, Catre M, et al: Bone grafts in hip replacement surgery: The pelvic side. Orthop Clin North Am 1993;24:679-695.
Question 89
A 4-month-old infant is unable to flex her elbow as a result of an obstetrical brachial plexus palsy. This most likely illustrates a predominate injury to what structure? Review Topic
Explanation
Question 90
The use of multiagent adjuvant chemotherapy is associated with a clear survival benefit in which of the following diseases?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 53.
Link M, Goorin A, Miser A, et al: The effect of adjuvant chemotherapy and relapse free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600-1606.
Question 91
Figure 36 shows the AP pelvic radiograph of a 26-month-old boy who has a limp. He has no significant medical history and no pain. What is the most appropriate treatment plan? Review Topic

Explanation
(SBQ13PE.38) Pavlik harness treatment is appropriate for which of the following?: Review Topic
4 year old with a diaphyseal femur fracture and a neuromuscular disorder with lower extremity spasticity
2 month old with a displaced spiral mid-diaphyseal femur fracture
9 month old with a diaphyseal femur fracture with <2cm shortening
9 month old with a diaphyseal femur fracture with >2cm shortening
4 year old with a diaphyseal femur fracture, closed head injury and chest trauma
Treatment with Pavlik harness or spica cast are options for patients <6 months of age with diaphyseal femur fractures. Pavlik harness provides adequate pain control for the short time required for healing in this age group. Significant remodeling potential can be expected.
Because of the significant remodeling and quick healing, treatment of diaphyseal femur fractures in children younger than 6 months focuses on providing comfort and avoiding complications. Spica casting likewise results in stable union without longterm sequelae but minor skin complications are more common and some favor Pavlik treatment in this age group.
Kocher et al. provide the AAOS Clinical Practice Guideline for the treatment of pediatric diaphyseal femur fractures. Their recommendation for diaphyseal femur fractures in children less than 6 months is Grade C, based on Level IV evidence (one retrospective comparative study and one case series). They recommend that Pavlik and spica casting are both acceptable treatment options in this age group.
Flynn et al. review the management of pediatric femoral shaft fractures. They recommend Pavlik treatment for children 6 months of age or less in preference to a spica cast, sometimes supplemented with a simple splint. This avoids the skin complications of spica casting.
Incorrect answers:
Question 92
A 16-year-old high school student undergoes a routine preparticipation physical examination at the beginning of the school year. Examination reveals marked laxity of both shoulders but only mild generalized laxity in other joints. The load and shift test allows for anterior humeral translation to the glenoid rim and posterior humeral translation beyond the glenoid rim. The sulcus sign is present. What is the next most appropriate step in management?
Explanation
REFERENCES: Harryman DT, Sidles JA, Harris SL, Matsen FA III: Laxity of the normal glenohumeral joint: A quantitative in vivo assessment. J Shoulder Elbow Surg 1992;1:66-76.
Hawkins RJ, Bokor RJ: Clinical evaluation of shoulder problems, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, p 186.
McFarland EG, Campbell G, McDowell J: Posterior shoulder laxity in asymptomatic athletes. Am J Sports Med 1996;24:468-471.
Linter SA, Levy A, Kenter K, Speer KP: Glenohumeral translation in the asymptomatic athlete’s shoulder and its relationship to clinically measurable anthropometric variables. Am J Sports Med 1996;24:716-720.
Question 93
1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1% neutrophils. No growth of organisms is seen on routine culture. What is the best next step?
Explanation
This patient has a chronic quadriceps tendon rupture after total knee arthroplasty. Two previous primary repair attempts have failed, which is not surprising based on the poor results of primary repair reported in the literature. The patient also has an unstable knee and will require revision of some or all of the prosthesis to achieve a stable knee. Revision total knee arthroplasty with extensor mechanism allograft allows an allograft reconstruction of the ruptured quadriceps tendon. The other option is to utilize a synthetic mesh extensor mechanism reconstruction. These are likely to have the best result in this situation. Revision total knee arthroplasty with liner change and primary quadriceps repair is not the best form of management, because it involves a third attempt at primary tendon repair, which will likely fail again. Resection knee arthroplasty and arthrodesis with antegrade nail is a possible option but is not the best, because it would likely make driving and other daily activities difficult. Two-stage revision total
knee arthroplasty with extensor mechanism allograft is not the best option because the laboratory results
show no signs of infection, so a single-stage procedure is preferred.
Question 94
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms? Review Topic
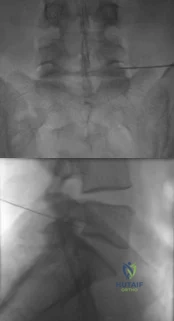
Explanation
Question 95
Which of the following represents a contraindication for interspinous process decompression for the treatment of lumbar spinal stenosis? Review Topic
Explanation
Question 96
A 59-year-old man reports moderate shoulder pain and very restricted range of motion after undergoing humeral arthroplasty for osteoarthritis 1 year ago. An AP radiograph is shown in Figure 32. Management should now consist of
Explanation
REFERENCES: Neer CS II, Kirby RM: Revision of humeral head and total shoulder arthroplasties. Clin Orthop 1982;170:189-195.
Petersen SA, Hawkins RJ: Revision of failed total shoulder arthroplasty. Orthop Clin North Am 1998;29:519-533.
Question 97
A 29-year-old woman reports shoulder pain after sustaining a minor fall 6 weeks ago. She has a history of celiac sprue. Radiographs of the forearm and shoulder are shown in Figures 53a and 53b. Which of the following serum abnormalities would be expected?
Explanation
REFERENCES: Potts JT: Parathyroid hormone: Past and present. J Endocrinol 2005;187:311-325.
Corazza GR, Di Stefano M, Maurino E, et al: Bones in coeliac disease: Diagnosis and treatment. Best Pract Res Clin Gastroenterol 2005;19:453-465.
Mankin HJ, Mankin CJ: Metabolic bone disease: An update. Instr Course Lect 2003;52:769-784.
Question 98
What is a common clinical finding in patients with severe hypercalcemia secondary to bony metastasis?
Explanation
REFERENCE: Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 99
A 40-year-old woman with history of intravenous drug abuse and ongoing Staphylococcus aureus septicemia is referred for intractable neck pain with radiation down her arm. She also complains of progressive hand weakness. Examination reveals long tract signs in the lower extremities. Her MRI scan is shown in Figure A. Besides intravenous antibiotics, what is the most appropriate next step in treatment? Review Topic
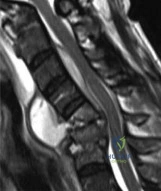
Explanation
Spinal epidural abscesses are more common in immunodeficient patients and IV drug abusers. They result in verebral body destruction and instability. In addition to draining the abscess and necrotic bone, the instability has to be addressed by instrumentation and fusion, even in the face of infection. Structural support can include cages with morselized bone graft, or structural allograft fixation of anterior and middle column and/or pedicle screw instrumentation of the posterior column.
Shousha et al. reviewed the treatment of cervical spondylodiscitis in 30 patients. They found an epidural abscess in 80% of patients, and noncontiguous discitis in 47% of cases. Thus, they recommend MRI of the entire spine in all cases, and surgery for intractable neck pain, septicemia, epidural abscess, neurological compromise, gross
kyphotic deformity with extensive destruction, and failure of conservative treatment.
Heyde et al. reviewed cervical spondylodiscitis in 20 patients. All cases had postoperative antibiotic therapy for 8–12 weeks. At 37 months (range 24–63), all cases went on to union and there were no recurrences of infection. There was improvement in preoperative neurological status in all cases, leading them to recommend early surgical intervention.
Figure A is an MRI scan showing spondylodiscitis C5–C7 with partial destruction of the vertebral bodies and epidural abscess formation. Illustration A shows the lateral xray (left) and MRI (right) of the same patient 9 months postoperatively after corpectomy C5 and C6 and posterior instrumentation.
Incorrect
Question 100
- Which of the following radiographic findings would be characteristic of the knee joints of a patient with neuropathic osteoarthropathy of the knee?
Explanation
The loss of sensation to the joint is followed by severe degenerative changes, osteophyte formation, articular and subchondral fractures, and often calcification of surrounding soft tissues. In the knee, this is a tricompartmental disease and will not selectively affect one compartment over another.
