OITE & ABOS Ortho Board Prep: Trauma, Foot & Ankle, Elbow MCQs | Part 166
Key Takeaway
This page offers Part 166 of a comprehensive OITE & AAOS Orthopedic Surgery Board Review. Featuring 100 high-yield MCQs by Dr. Hutaif, it's designed for orthopedic residents and surgeons. Prepare for your AAOS and ABOS board certification exams with verified, exam-formatted questions covering key topics.
About This Board Review Set
This is Part 166 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 166
This module focuses heavily on: Ankle, Elbow, Foot, Fracture, Tendon, Trauma.
Sample Questions from This Set
Sample Question 1: A patient underwent an open reduction and internal fixation of a calcaneus fracture 6 months ago via an extensile lateral approach. He now reports burning pain on the lateral side of his ankle and foot. A local cortisone injection at the si...
Sample Question 2: Which of the following muscle tendons inserts just lateral to the long head of biceps tendon on the proximal humerus?...
Sample Question 3: A healthy, active, independent 74-year-old woman fell and sustained the elbow injury shown in Figures 41a and 41b. Management should consist of...
Sample Question 4: A 14-year-old boy reports pain in the distal thigh. He denies any history of trauma. Examination reveals tenderness and swelling of the distal thigh without effusion. A radiograph and CT scan are shown in Figures 10a and 10b. A biopsy speci...
Sample Question 5: Communication breakdown is the leading cause of which of the following?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A patient underwent an open reduction and internal fixation of a calcaneus fracture 6 months ago via an extensile lateral approach. He now reports burning pain on the lateral side of his ankle and foot. A local cortisone injection at the site of the tenderness, about 7 cm above the lateral heel, provided temporary relief of the pain. What is the recommended course of management for the persistent burning pain?
Explanation
Question 2
Which of the following muscle tendons inserts just lateral to the long head of biceps tendon on the proximal humerus?
Explanation
REFERENCE: Bal GK, Basamania CJ: Pectoralis major tendon ruptures: Diagnosis and treatment. Tech Shoulder Elbow Surg 2005;6:128-134.
Question 3
A healthy, active, independent 74-year-old woman fell and sustained the elbow injury shown in Figures 41a and 41b. Management should consist of
Explanation
REFERENCES: Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intra-articular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480.
Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humerus fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
Obremskey WT, Bhandari M, Dirschl DR, et al: Internal fixation versus arthroplasty of comminuted fractures of the distal humerus. J Orthop Trauma 2003;17:463-465.
Question 4
A 14-year-old boy reports pain in the distal thigh. He denies any history of trauma. Examination reveals tenderness and swelling of the distal thigh without effusion. A radiograph and CT scan are shown in Figures 10a and 10b. A biopsy specimen is shown in Figure 10c. Management should consist of
Explanation
REFERENCES: Simon MA, Springfield DS, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-200.
Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, p 232.
Question 5
Communication breakdown is the leading cause of which of the following?
Explanation
Poor communication sets up environments in which medical errors can take place. Per the Joint Commission, medical errors may be the among the top 10 causes of death in the United States. Establishing open lines of communication is critical to reduce the risk of error and enhance patient safety.
Gandhi et al. designed a framework to study missed or delayed diagnoses and their causes. The most significant factors contributing to errors were poor handoffs, failures in judgment, failures in memory and failures in knowledge.
O’Daniel et al. review the importance of professional communication and collaborative team efforts. They note that patient safety is at risk when poor communication is in place. The leading cause for medication errors, treatment delays and wrong-site surgeries is communication failure.
Illustration A shows the leading causes of death in the United States. This includes “preventable errors” as a cause.
Incorrect Answers:
Question 6
A 40-year-old man who is an avid weight lifter has had chronic pain in the proximal anterior shoulder for the past year. He denies any history of trauma. Examination reveals tenderness at the intertubercular groove, a positive speed test, and a positive Neer impingement sign. Nonsurgical management has failed to provide relief, and he is now considering surgery. Arthroscopic findings in the glenohumeral joint are shown in Figure 31. Based on these findings, treatment should consist of
Explanation
REFERENCES: Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310.
Burkhead WZ, Arcand MA, Zeman C, et al: The biceps tendon, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1996.
Question 7
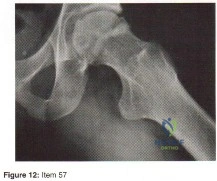
A 25-year-old male sustains the isolated injury shown in Figure A. Antegrade intramedullary nailing is planned for definite fixation within the next 12 hours. After obtaining lateral radiographs of the injury site, what would be the next best step in management of this patient?

Explanation
Femoral neck fractures are seen less than 10% of the time with femoral shaft fractures, but they are frequently missed on initial evaluation. The neck fracture line is almost vertical and nondisplaced, or minimally displaced. Therefore fine (2-mm) cut CT scan through the femoral neck should be ordered in the preoperative workup of these patients.
Tornetta et al. reported that they reduced the delay in diagnosis of concomitant femoral neck fractures by 91% by instituting a protocol that included: dedicated AP internal rotation plain radiograph, a fine (2-mm) cut CT scan through the femoral neck, an intraoperative fluoroscopic lateral radiograph prior to fixation, as well as postoperative AP and lateral radiographs of the hip in the operating room prior to awakening the patient.
Figure A shows a trauma view lower extremity radiograph with an isolated left midshaft femur fracture.
Incorrect Answers:
setting of fracture. Answer 5: The age, injury and fracture pattern are not consistent with a pathologic femur fracture.
Question 8
Figure 53 shows a thoracolumbar specimen as viewed from posterior to anterior following removal of all posterior elements. Which of the following structures does the red string pass under?
Explanation
REFERENCE: Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 2, p 1465.
Question 9
A 19-year-old football player who sustained three traumatic anterior shoulder dislocations underwent surgery to repair a Bankart lesion. Nine months after surgery, examination reveals stability, elevation to 150 degrees, external rotation to 0 degrees with the elbow at his side and to 50 degrees at 90 degrees of abduction, and internal rotation to T12. If his range of motion does not improve, he is at most risk for
Explanation
REFERENCES: Hawkins RJ, Angelo RL: Glenohumeral osteoarthrosis: A late complication of the Putti-Platt repair. J Bone Joint Surg Am 1990;72:1193-1197.
Norns TR: Complications following anterior instability repairs, in Bigliani LU (ed): Complication of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993, pp 98-116.
Question 10
- While under a physician’s care, a 45-year-old man verbally abuses the staff and nurses who are attempting to carry out orders. A decision to discharge the patient is best carried out by
Explanation
Question 11
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk?
Explanation
REFERENCES: Molnar GE, Gordon SU: Cerebral palsy: Predictive value of selected clinical signs for early prognostication of motor function. Arch Phys Med Rehabil 1976;57:153-158.
Wu YW, Day SM, Strauss DJ, et al: Prognosis for ambulation in cerebral palsy: A population-based study. Pediatrics 2004;114:1264-1271.
Question 12
A 16-year-old boy falls while playing soccer. He reports that his knee buckled when he planted his leg to kick a ball. He noticed an obvious deformity of his knee, which spontaneously resolved with a “clunk.” He could not finish the game but was able to bear weight with a limp. He has had two similar episodes but has never sought medical attention. An initial examination demonstrated an effusion, tenderness at the proximal medial collateral region and medial patellofemoral retinaculum, decreased range of motion, and patella apprehension. A lateral patellar glide performed at 30° of flexion was 3+. He was otherwise ligamentously stable, and there were no other noteworthy findings.Figures 3 and 4 are this patient's proton density fat-saturated MR images. His tibial tubercle-trochlear groove (TT-TG) distance is 12 mm, and he has normal limb-alignment film findings. Treatment at this stage should include

Explanation
Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed. Normal TT-TG values, an increased lateral patellar glide, and a history of recurrent patellar dislocations after trauma suggest MPFL incompetence and the need for reconstruction.
Question 13
A 63-year-old male, with history of myocardial infarction, presents with buttock and leg pain. He states the pain is worse when climbing stairs, and is absent when walking down a hill. He reports when walking on a flat surface the pain begins after roughly 50 meters, but if he stops walking and remains standing upright, the pain resolves after a few minutes. He denies any leg pain when sitting and driving a car. These symptoms are most consistent with: Review Topic
Explanation
Vascular claudication refers to the pain, aching or fatigue of the muscles of the buttocks, thigh and/or calf that occurs with exertion, and is related to a failure to meet muscular oxygen requirements, usually caused by peripheral vascular disease impeding blood flow to the peripheral muscles.
Neurogenic claudication is the classic symptom caused by lumbar spinal stenosis. Neurogenic claudication classically presents with bilateral buttock pain with upright activities, but seems to improve by postural changes that flex the lumbar spine. These posture changes are thought to increase the cross sectional area of the central canal, which relieves pressure on the affected area.
Issack et al. reviewed degenerative lumbar spinal stenosis. They state that patients with vascular claudication will have similar symptoms of leg cramping, whether ambulating or riding a stationary bicycle. In comparison, patients with neurogenic
claudication have diminished symptoms of claudication while positioned seated.
Young et al. reviewed the use of lumbar epidural/transforaminal steroids for managing spinal disease. They report that two thirds of acute low back pain episodes resolve within 7 weeks, so the utility and practice patterns regarding the timing and number of epidural/transforaminal steroid injections is usually based on expert opinion, rather than high level research evidence.
Illustration A shows an angiogram of a patients with normal (left) vs abnormal (right) arterial vasculature. Illustration B shows the typical MRI of a patient with spinal stenosis.
Incorrect
Question 14
A 12-year-old boy has had left thigh pain for the past 4 months. Examination shows lack of internal rotation and abduction, and external rotation with hip flexion. A radiograph is shown in Figure 87. What is the most appropriate treatment? Review Topic

Explanation
Question 15
Figures 31a and 31b are the radiographs of a 5-year-old boy with an elbow injury.
Explanation
Figure 26 shows lucent areas of both femoral condyles. This may represent a variation of ossification, in which case this boy’s knee pain is coincidental. Another possibility is atypical osteochondritis dissecans. An MRI will distinguish between the 2 entities and will guide treatment.
Figures 27a and 27b show healing rib and distal tibia fractures. These fractures likely are attributable to child abuse. A plain radiographic skeletal survey is sufficient for orthopaedic needs.
A triplane fracture of the distal tibia is revealed in Figure 28. A CT scan will quantify displacement and identify fracture fragments for planning of screw trajectories if open reduction and internal fixation is indicated (displacement > 2 mm).
In Figure 29, the linear lucency of the capitellum indicates an early osteochondritis dissecans. An MRI will allow staging of the lesion.
Figure 30 shows that the left radius and ulna do not align with the humerus; this is the likely result of a transphyseal fracture of the distal humerus. An arthrogram will outline the unossified distal humerus and allow for reduction. For an unstable neonate, this likely can be performed in the NICU.
Figures 31a and 31b reveal a widely displaced lateral condyle fracture for which open reduction and internal fixation is required. No advanced imaging is necessary.

Question 16
Which of the following complications may occur subsequent to resurfacing hip arthroplasty for osteonecrosis of the hip but not after total hip arthroplasty?
Explanation
REFERENCES: Gabriel JL, Trousdale RT: Stem fracture after hemiresurfacing for femoral head osteonecrosis. J Arthroplasty 2003;18:96-99.
Amstutz HC, Campbell PA, Le Duff MJ: Fracture of the neck of the femur after surface arthroplasty of the hip. J Bone Joint Surg Am 2004;86:1874-1877.
Question 17
- Which of the following methods of treatment of a displaced Lisfranc fracture-dislocation will most reliably lead to good functional results?
Explanation
Question 18
A 35-year-old man is brought to the emergency department following a motorcycle accident. He is breathing spontaneously and has a systolic blood pressure of 80 mm Hg, a pulse rate of 120/min, and a temperature of 98.6° F (37° C). Examination suggests an unstable pelvic fracture; AP radiographs confirm an open book injury with vertical displacement on the left side. Ultrasound evaluation of the abdomen is negative. Despite administration of 4 L of normal saline solution, he still has a systolic pressure of 90 mm Hg and a pulse rate of 110. Urine output has been about 20 mL since arrival 35 minutes ago. What is the next best course of action?
Explanation
REFERENCE: Mayo K, Kellam JK: Pelvic ring disruptions, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1052-1108.
Question 19
A patient who underwent open reduction and internal fixation of an olecranon fracture 2 months ago now reports painless limitation of motion. Examination reveals a well-healed incision and a flexion-extension arc from 40 degrees to 80 degrees. The patient has been performing home exercises. Radiographs are shown in Figures 26a and 26b. What is the most appropriate treatment?
Explanation
REFERENCES: Morrey BF: The posttraumatic stiff elbow. Clin Orthop Relat Res
2005;431:26-35.
King GJ, Faber KJ: Posttraumatic elbow stiffness. Orthop Clin North Am 2000;31:129-143.
Question 20
Surgical treatment for this patient should include
Explanation

Video 22 for reference
This patient has an unstable cruciate-retaining TKA. The tibial cut appears to be substantial, necessitating a very thick polyethylene liner. In addition, the femoral component may be slightly more proximally located. Tests for flexion-extension gap balancing would indicate flexion instability. However, the possibility of infection remains, so screening blood tests are appropriate. The surgical treatment for this unstable knee is revision TKA to a more constrained implant, ensuring flexion-extension gap balancing. No evidence indicates that the knee is infected. A thicker polyethylene insert will not adequately balance the knee.

Question 21
A 65-year-old woman with type II diabetes mellitus (most recent Hgb A1C was 8.2) has had 3 days of left knee pain. Physical examination of the left knee reveals erythema, warmth and a large effusion. Range of motion is painful and limited to 30 degrees of flexion. She is found to be hypotensive and not responding to volume resuscitation. She requires phenylephrine to maintain Mean Arterial Pressure (MAP) of 70. ESR and CRP are elevated and Lactate is 3.1 mmol/L. What is the next best intervention for this patient’s treatment?
Explanation
Question 22
Figures 38a and 38b show the AP and lateral radiographs of a 12-year-old baseball pitcher who has pain in his right dominant elbow. Management should consist of
Explanation
REFERENCES: Cabanela ME, Morrey BF: Fractures of the olecranon, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 2000, pp 365-379.
Nuber GW, Diment MT: Olecranon stress fractures in throwers: A report of two cases and a review of the literature. Clin Orthop 1992;278:58-61.
Question 23
Following a fall from a height of 5 feet, a patient reports pain along the lateral border of the foot. The CT scan shown in Figure 54 indicates what pathology?
Explanation
REFERENCE: Robbins MI, Wilson MG, Sella EJ: MR imaging of anterosuperior calcaneal process fractures. Am J Roentgenol 1999;172:475-479.
Question 24
A 51-year-old woman has had progressively increasing right knee pain for the past 6 months. She has a history of metastatic renal cell carcinoma to the lung and the skeletal system. Radiographs are seen in Figures 18a and 18b. The next step in management of the right distal femur lesion should consist of
Explanation
REFERENCES: Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Sim FH: Metastatic bone disease of the pelvis and femur. Instr Course Lect 1992;41:317-327.
Question 25
Eosinophilic granuloma frequently occurs as a solitary lesion in the tubular long bones. After biopsy, what is the best course of action?
Explanation
REFERENCE: Simon M, Springfield D, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 200.
Question 26
Which characteristic of complex regional pain syndrome (CRPS) type 2 differentiates it from CRPS 1?
Explanation
CRPS 2 develops after nerve injury, whereas CRPS 1 occurs without nerve injury. The diagnostic criteria are otherwise the same for the 2 conditions. A 3-phase bone scan can be helpful; a pattern of increased uptake in all 3 phases, and particularly diffuse periarticular uptake in and around the joints of the affected extremity during the delayed phase, is considered typical of CRPS, especially during the first 6 months; however, it is not specific enough to be used as a diagnostic criteria. Unfortunately, the pathophysiological mechanisms underlying CRPS remain unclear, and, as such, no standard diagnostic test for CRPS exists. There are 3 major sets of diagnostic criteria for CRPS: the International Association for the Study of Pain (IASP) criteria, the Budapest Research Criteria, and the Veldman criteria. According to IASP, CRPS type
1 involves an initiating noxious event or a cause of immobilization; continuing pain/allodynia/hyperalgesia for which the pain is disproportionate to any known inciting event; evidence of edema, changes in skin blood flow, or abnormal pseudomotor activity in the region of pain; and exclusion of the diagnosis by the existence of other conditions that would otherwise account for the degree of pain and dysfunction. CRPS type 2 is a syndrome that develops after nerve injury, contends IASP. Spontaneous pain or allodynia/hyperalgesia occurs and is not necessarily limited to the territory of the injured nerve; there is or has been evidence of edema, a skin blood flow abnormality, or abnormal sudomotor activity in the region of pain since the inciting event; and the diagnosis is excluded by the existence of conditions that would otherwise account for the degree of pain and dysfunction.
Question 27
What is the most common donor site complication following a free vascularized fibular graft for osteonecrosis of the femoral head?
Explanation
REFERENCE: Urbaniak J, Harvey E: Revascularization of the femoral head in osteonecrosis. J Am Acad Orthop Surg 1998;6:44-54.
Question 28
A patient reports pain in the hip with functional positioning. With the patient supine, pain in which of the following positions would be typical for femoral acetabular impingement?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 411-424.
Beck M, Leunig M, Parvizi J, et al: Anterior femoroacetabular impingement: Part II. Midterm results of surgical treatment. Clin Orthop 2004;418:67-73.
McCarthy JC, Noble PC, Schuck MR, et al: The role of labral lesions to development of early degenerative hip disease. Clin Orthop 2001;393:25-37.
Question 29
In infantile idiopathic scoliosis, which of the following factors suggests progression?
Explanation
REFERENCES: Mehta MH: The rib-vertebra angle in the early diagnosis between resolving and progressive infantile scoliosis. J Bone Joint Surg Br 1972;54:230-243.
Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, p 697.
Question 30
Figure 33 shows the radiograph of a 28-year-old avid golfer who has chronic right wrist pain. Management should consist of
Explanation
REFERENCES: Geissler WB: Carpal fractures in athletes. Clin Sports Med 2001;20:167-188.
Rettig ME, Dassa GL, Raskin KB, Melone CP Jr: Wrist fractures in the athlete: Distal radius and carpal fractures. Clin Sports Med 1988;17:469-489.
Question 31
A 15-year-old male jumps off a 6 foot ramp and lands awkwardly. His knee swells up immediately and he is taken to the emergency room. Figures A is a sagittal CT scan image. In the next 3 hours, he complains of increasing leg pain. This is likely because of injury to which of the following structures? Review Topic

Explanation
Tibial tubercle fractures usually occur during aggressive quadriceps contraction during sports. The Ogden classification classifies this by site of fracture (Type I, through the tubercle; Type II, at the level of the tibial physis; Type III, extending through the anterior tibial epiphysis). Other complications include extensive soft tissue damage, periosteal stripping, vascular compromise and intra-articular damage.
Pandya et al. reviewed 41 tibial tubercle fractures. They found compartment syndrome or vascular compromise in nearly 10%. They found that the degree of injury was underestimated 50% of the time when classified using lateral radiographs alone. They recommend CT scan or MRI as an adjunct. If intra-articular involvement is seen, arthroscopy or open arthrotomy should be performed.
Pape et al. describe 2 case reports of anterior compartment syndrome after tibial tubercle fracture. The compartment syndrome occurs as a result of proximity of the tibial tubercle physis to the anterior tibial recurrent artery.
Figure A shows the sagittal reconstruction CT image showing intraarticular involvement. Illustrations A and B are axial and coronal CT images in the subchondral region showing the fracture line traversing the zone between fused and unfused physis (see Illustration C for physeal closure pattern). Illustration C shows the direction of closure of the proximal tibial physis. In the sagittal plane, the proximal tibial physis closes from posterior to anterior, then to the tubercle apophysis which closes from proximal to distal also. In the coronal plane, the physis closes from medial to lateral. In the axial plane, the physis closes from posteromedial to anterolateral. Illustration D shows the anterior tibial recurrent artery.
Incorrect Answers:
Question 32
Figure 41a shows the AP radiograph of a 15-year-old boy who reports lateral knee pain. Figures 41b and 41c show a radiograph of the distal femur that was obtained 5 years ago and a current CT scan. The indication for surgery in this patient would be
Explanation
REFERENCES: Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 1626-1659.
Simon MA, Springfield DS, et al: Common Benign Bone Tumors and Usual Treatment: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 181-205.
Question 33
below show the radiographs obtained from a year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. No evidence of infection is seen. What is the most appropriate treatment?
Explanation
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis, as shown in Figures 3 and 4. They also assist in obtaining correct limb alignment. Short metaphyseal-engaging stems are associated with failure rates that range between 16% and 29%. Cemented stems may be shorter than press-fit stems, because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.
Question 34
A 21-year-old female college athlete sustained a stress fracture of the fifth metatarsal 1 year ago which was treated successfully with surgical stabilization and she returned to normal activities. She now has a tension-sided femoral neck fracture. Along with surgical fixation of the fracture, what is the next step in management? Review Topic
Explanation
Question 35
A 72-year-old man with diabetic neuropathy and 5 degrees of valgus talar tilt; he has pursued nonsurgical treatment for 30 years and now has unrelenting pain
Explanation
Arthritis of the ankle and hindfoot can pose challenges. Depending upon patient age, comorbidities, and alignment, a variety of surgical interventions may be offered. A total ankle replacement may be considered for patients older than 60 years of age who have minimal misalignment and low-demand lifestyles. In all other cases, ankle fusion must be considered. The nonsurgical care of ankle arthritis includes anti-inflammatory medication, intra-articular steroid injections, bracing with customized products such as the Arizona brace, or a molded foot and ankle orthosis.
Patients with diabetes and Charcot arthropathy may be treated nonsurgically with total-contact casting during acute and active or "hot" phases and accommodative shoes during consolidation and stable or "cool" phases. When the patient has recurrent ulcers or major anatomy changes, surgical intervention must be considered. Tibiotalocalcaneal fusion helps to realign the foot and ankle and make it more braceable in the setting of ankle and hindfoot Charcot disease.
RECOMMENDED READINGS
Queen RM, Adams SB Jr, Viens NA, Friend JK, Easley ME, Deorio JK, Nunley JA. Differences in outcomes following total ankle replacement in patients with neutral alignment compared with tibiotalar joint malalignment. J Bone Joint Surg Am. 2013 Nov 6;95(21):1927-34. doi: 10.2106/JBJS.L.00404. PubMed PMID: 24196462. View Abstract at PubMed
Nunley JA, Caputo AM, Easley ME, Cook C. Intermediate to long-term outcomes of the STAR Total Ankle Replacement: the patient perspective. J Bone Joint Surg Am. 2012 Jan 4;94(1):43-8. doi: 10.2106/JBJS.J.01613. PubMed PMID: 22218381. View Abstract t PubMed
Saltzman CL, Mann RA, Ahrens JE, Amendola A, Anderson RB, Berlet GC, Brodsky JW, Chou LB, Clanton TO, Deland JT, Deorio JK, Horton GA, Lee TH, Mann JA, Nunley JA, Thordarson DB, Walling AK, Wapner KL, Coughlin MJ. Prospective controlled trial of STAR total ankle replacement versus ankle fusion: initial results. Foot Ankle Int. 2009 Jul;30(7):579-96. doi: 10.3113/FAI.2009.0579. PubMed PMID: 19589303. View Abstract at PubMed
Faraj AA, Loveday DT. Functional outcome following an ankle or subtalar arthrodesis in adults. Acta Orthop Belg. 2014 Jun;80(2):276-9. PubMed PMID: 25090803. View Abstract at PubMed Grear BJ, Rabinovich A, Brodsky JW. Charcot arthropathy of the foot and ankle associated with rheumatoid arthritis. Foot Ankle Int. 2013 Nov;34(11):1541-7. doi: 10.1177/1071100713500490. Epub 2013 Jul 30. PubMed PMID: 23900228. View Abstract at PubMed
Question 36
What is the most frequent location of entrapment of the deep peroneal nerve?
Explanation
REFERENCES: Kopell HP, Thompson WA: Peripheral entrapment neuropathies of the lower extremity. N Engl J Med 1960;262:56-60.
Schon LC, Mann RA: Diseases of the nerves, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 1, pp 675-677.
Question 37
Which of the following have been found to affect the rate of perioperative infections or wound complication rates in foot and ankle surgery?
Explanation
REFERENCES: Bibbo C, Anderson RB, Davis WH, et al: The influence of rheumatoid chemotherapy, age, and presence of rheumatoid nodules on postoperative complications in rheumatoid foot and ankle surgery: Analysis of 725 procedures in 104 patients. Foot Ankle Int 2003;24:40-44.
Bibbo C, Goldberg JW: Infections and healing complications after elective orthopaedic foot and ankle surgery during tumor necrosis factor-alpha inhibition therapy. Foot Ankle Int
2004;25:331-335.
Sorensen LT, Karlsmark T, Gottrup F: Abstinence from smoking reduces incisional wound infection: A randomized controlled trial. Ann Surg 2003;238:1-5.
Question 38
An elderly woman with radiographic evidence of spinal stenosis reports difficulty walking and calf pain that is relieved by rest and a change of position. The most likely cause of pain is ischemia of the
Explanation
Question 39
Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?

Explanation
Bae et al reviewed thirty-six cases of compartment syndrome in 33 pediatric patients. Approximately 75% of these patients developed compartment syndrome in the setting of fracture. "They found pain, pallor, paresthesia, paralysis, and pulselessness were relatively unreliable signs and symptoms of compartment syndrome in these children. An increasing analgesia requirement in combination with other clinical signs, was a more sensitive indicator of compartment syndrome."
Whitesides et al summarizes the diagnosis and treatment of acute compartment syndrome. They emphasize the need for early diagnosis, as "muscles tolerate 4 hours of ischemia well, but by 6 hours the result is uncertain; after 8 hours, the damage is irreversible." They recommend fasciotomy be performed when tissue pressure rises past 20 mm Hg below diastolic pressure.
Question 40
A 27-year-old man has recurrent anterior shoulder instability following an arthroscopic Bankart repair 4 years ago. Current CT scans are shown in Figures 19a and 19b. Deficiency of what mechanism is most likely to contribute to the current joint instability? Review Topic

Explanation
Question 41
A 60-year-old right hand-dominant women fell on her outstretched arm and sustained an anterior shoulder dislocation. The shoulder is reduced in the emergency department and she is seen for follow-up 1 week later wearing a sling. Examination reveals that she has significant difficulty raising her arm in forward elevation and has excessive external rotation compared to the contralateral shoulder. What is the next most appropriate step in management?
Explanation
REFERENCES: Stayner LR, Cumming J, Andersen J, et al: Shoulder dislocations in patients older than 40 years of age. Orthop Clin North Am 2000;31:231-239.
Neviaser RJ, Neviaser TJ, Neviaser JS: Concurrent rupture of the rotator cuff and anterior dislocation of the shoulder in the older patient. J Bone Joint Surg Am 1988;70:1308-1311.
Question 42
Figure 94 is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal. After injury to the structure as indicated by the asterisks, which examination test most likely will demonstrate an abnormal finding?
Explanation
The structure shown is the PL bundle of the anterior cruciate ligament (ACL), which is tight near terminal knee extension. Biomechanical analysis suggests the PL bundle provides a greater degree of rotational stability than the anteromedial bundle. The pivot-shift test evaluates for rotational instability of the ACL, while the Lachman test assesses anterior-posterior stability. The posterior drawer and PL drawer test findings are positive after a posterior cruciate ligament tear and PL corner injury, respectively.
RESPONSES FOR QUESTIONS 95 THROUGH 98
Axillary nerve injury
Musculocutaneous nerve injury
Radial nerve injury
Glenoid fracture
Loss of reduction
Deltoid detachment
Chondrolysis
Recurrent instability
Propionibacterium acnes (P. acnes) infection
Staphylococcus epidermidis
Staphylococcus aureus
Select the complication listed above that is most commonly associated with the shoulder arthroscopy scenarios described below.
Question 43
Figure 1 is the MRI scan of a 15-year-old boy who has had knee pain with running for 5 months. What is the most appropriate treatment?
Explanation
outcomes? 16
A. Decreased American Orthopaedic Foot and Ankle Society (AOFAS) scores at 2- year follow-up
B. Slower return to work
C. Increased rate of hardware removal
D. Decreased rate of syndesmotic malreduction
The clinical vignette demonstrates an unstable left ankle syndesmotic injury, also known as a “high ankle sprain”. The distal tibiofibular syndesmosis comprises five structures: the anteroinferior tibiofibular ligament, posteroinferior tibiofibular ligament, the interosseous membrane, the interosseous ligament, and the inferior transverse ligament.
This injury commonly occurs secondary to a forced external rotation motion of the foot. Stable grade 1 strains without diastasis on stress radiographs can be treated with a period of non-weight bearing followed by physical therapy. Unstable injuries, grade 2 and 3, which demonstrate diastasis on external rotation stress radiographs, are commonly treated operatively. Fixation constructs commonly include screw fixation, suture button fixation, or a hybrid combination technique. Naqvi and associates demonstrated more accurate syndesmotic reduction with suture button fixation versus screw fixation. Syndesmotic malreduction has been shown to be an important independent predictor of decreased clinical outcomes. Andersen and associates demonstrated higher AOFAS scores and diminished syndesmotic widening at radiographic follow-up at 2 years with suture button fixation. In a systematic review, Zhang and associates demonstrated higher AOFAS scores, diminished need for implant removal (3.7% vs 40.2%), diminished implant failure, and lower rates of malreduction (1% vs 12%). Thornes and associates demonstrated a faster return to work following suture button fixation versus screw fixation.
21- A 26-year-old weightlifter has increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication, corticosteroid injections, and rest fails to alleviate his symptoms. He undergoes an arthroscopic distal clavicle resection with excision of the distal 8 mm of clavicle (Mumford procedure). Three months after surgery, he reports mild pain and popping by his clavicle. His clavicle demonstrates mild posterior instability on examination without any obvious deformity on his radiographs. What structures were
compromised during his excision? 17
A. Anterior and superior acromioclavicular joint ligaments
B. Posterior and superior acromioclavicular joint ligaments
C. Conoid ligament
D. Trapezoid ligament
The posterior and superior acromioclavicular ligaments provide the most restraint to posterior translation of the acromioclavicular joint and must be preserved during a Mumford procedure. Anterior and superior acromioclavicular joint ligaments are the opposite of the preferred response and prevent anterior translation of the clavicle. Injuries to the conoid and trapezoid ligaments are more pronounced with grade III or higher acromioclavicular separations, with superior migration of the clavicle relative to the acromion.
22- Figures 1 and 2 are the T2-weighted MRI scans of a 54-year-old woman with medial knee pain and catching of 6 months’ duration. What treatment option is most likely to be associated with a favorable outcome?
A. Physical therapy
B. Meniscal repair
C. Meniscectomy
D. Reconstruction
The MRI scans reveal a posterior horn root tear of the medial meniscus. LaPrade and associates found that outcomes after posterior meniscal root 18
repair significantly improved postoperatively and patient satisfaction was high, regardless of age or meniscal laterality. Patients aged <50 years had outcomes similar to those of patients ≥50 years, as did patients who underwent medial versus lateral root repair. In patients undergoing pullout fixation for posterior medial meniscus root tear, Chung and associates (in “Pullout Fixation of Posterior Medial Meniscus Root Tears”) found that patients with decreased meniscus extrusion at postoperative 1 year have more favorable clinical scores and radiographic findings at midterm follow-up than those with increased extrusion at 1 year. Krych and associates found that nonoperative treatment of medial meniscus posterior horn root tears is associated with poor clinical outcome, worsening arthritis, and a relatively high rate of arthroplasty at 5-year follow-up. Reconstruction would have no role in the setting of a reparable meniscal root tear.
22- A 24-year-old semiprofessional baseball player has noted increasing medial elbow pain for the past 2 months. This has been associated with a concomitant loss in velocity and control. He denies pain, numbness, or tingling in the hand or digits. Examination demonstrates medial elbow tenderness and swelling. Elbow range of motion is full. There is pain with milking maneuver and valgus stress test. Tinel’s sign is negative over the cubital tunnel, and there is no ulnar nerve subluxation. His MRI scan is shown in Figure 1. After thorough discussion, the player elects to undergo surgical intervention. What surgical variable has been associated with inferior outcomes?
A. Use of palmaris autograft
B. Ulnar nerve transposition
C. Muscle-splitting approach
D. Use of a docking technique
The information and image provided describe a throwing athlete with a complete tear of his ulnar collateral ligament (UCL) of the elbow. Numerous techniques have been described for UCL reconstruction, and at this time, optimal graft choice and fixation methods have not been established. Most studies show no.
major differences in outcome between gracilis autograft palmaris autograft, and allograft. Similarly, no clear advantage has been established when comparing use of bone tunnels with interference screws, tunnels with a docking technique, modified docking techniques, and combination
Question 44
A 32-year-old male hockey player who is right-hand dominant was checked from behind and landed with full force into the boards. In the emergency department he reports shortness of breath. Figure 113 shows a 2-D CT scan. What is the best initial treatment for this injury?
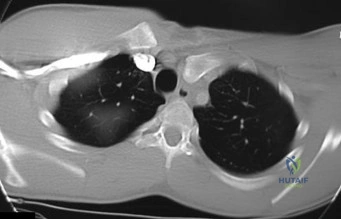
Explanation
Question 45
Which of the following is the preferred treatment for symptomatic localized pigmented villonodular synovitis (PVNS) of the knee?
Explanation
REFERENCES: Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis.
J Am Acad Orthop Surg 2006;14:376-385.
Kim SJ, Shin SJ, Choi NH, et al: Arthroscopic treatment for localized pigmented villonodular synovitis of the knee. Clin Orthop Relat Res 2000;379:224-230.
Question 46
Figures 3a and 3b show the inversion stress radiographs of a patient’s ankle. What is the most likely ligament injury pattern?
Explanation
REFERENCES: Harper MC: Stress radiographs in the diagnosis of lateral instability of the ankle and hindfoot. Foot Ankle 1992;13:435-438.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 39-54.
Question 47
An otherwise healthy 25-year-old man sustained a wound with a 1-cm by 1.5-cm soft-tissue loss over the volar aspect of the middle phalanx of his middle finger. After appropriate debridement and irrigation, the flexor digitorum profundus tendon and neurovascular bundles are visible. The wound should be treated with a
Explanation
flap is ideal for small wounds on the volar aspect of digits. A thenar flap is suitable for tip injuries. A lateral arm flap will not reach the fingers. A Moberg flap is limited to distal injuries of the thumb.
REFERENCES: Kappel DA, Burech JG: The cross-finger flap: An established reconstructive procedure. Hand Clin 1985;1:677-683.
Lister GD: Skin flaps, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1741.
Question 48
A 60-year-old woman has activity-related hip pain after undergoing arthroplasty 5 years ago. She has severe Parkinsonism and denies fevers or chills. Radiographs are shown in Figures 45a and 45b. What is the most likely cause of her pain?
Explanation
REFERENCES: Harris WH, McCarthy JC, O’Neill DA: Femoral component loosening using contemporary techniques of femoral cement fixation. J Bone Joint Surg Am 1982;64:1063-1067.
Callaghan JJ, Rosenberg AG, Rubash H (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 960, 1228-1229.
Maloney WJ, Schmalzreid T, Harris WH: Analysis of long-term cemented total hip arthroplasty retrievals. Clin Orthop Relat Res 2002;405:70-78.
Question 49
A 35-year-old man sustained a 10% compression fracture of the C5 vertebra in a diving accident. Radiographs show good alignment, and examination reveals no neurologic compromise. An MRI scan reveals no significant soft-tissue disruption posteriorly. Management should consist of
Explanation
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
Allen GL, Ferguson RL, Lehmann TR, O’Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
Question 50
If a percutaneous iliosacral screw is placed too anteriorly, and the screw exits anterior to the sacral ala before re-entering the sacral body, what will be the most likely finding postoperatively?

Explanation
Question 51
The cortical injury to the posterolateral distal fibula shown in Figure 25 indicates involvement of which of the following structures?
Explanation
REFERENCES: Murr S: Dislocation of the peroneal tendons with marginal fracture of the lateral malleolus. J Bone Joint Surg Br 1961;43:563-565.
Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1090-1209.
Question 52
The direct anterior (Smith-Peterson) approach to hip arthroplasty is most commonly associated with injury to what nerve?
Explanation
Some authors have reported the incidence of lateral femoral cutaneous nerve neuropraxia following hip arthroplasty with the direct anterior approach to be near 80%, but resolution of the sensory deficits has been observed in most patients over time. Femoral nerve palsy has been reported to occur in .64% to 2.3% direct lateral (Hardinge) and anterolateral (Watson-Jones) approaches, and the superior gluteal nerve may be injured with proximal extension of the abductor muscular dissection. The posterior approach has been reported to be associated with sciatic nerve injury, especially in cases of dysplasia. Pudendal nerve injury has not been reported with the anterior, anterolateral, direct lateral, or posterior approaches to hip
arthroplasty. It has been reported following hip arthroscopy and the use of a traction table, however.
Question 53
A 16-year-old girl sustains the closed injury shown in Figure 1. On physical examination, she is found to have a complete radial nerve palsy. Her fracture is treated nonsurgically, and her nerve palsy is followed clinically for improvement. What muscle is most likely to improve last as her nerve recovers?
Explanation
Question 54
A surgeon prepares a medial gastrocnemius rotational flap to cover a medial proximal tibia defect at the time of revision knee replacement surgery. To optimize coverage, the surgeon must optimally mobilize which artery?
Explanation
The medial sural arteries vascularize the gastrocnemius, plantaris, and soleus muscles proximally. These arteries arise from the popliteal artery. If this artery is not adequately mobilized, a gastrocnemius soleus flap can be devascularized.
Question 55
A 69-year-old man sustains a traumatic amputation to the distal phalanx of his little finger while working with power tools. Radiographs are shown in Figures 27a and 27b. The patient was instructed how to perform wet-to-dry dressing changes in the emergency department. Clinical pictures taken in the office are shown in Figures 27c through 27e. What is the most appropriate management of this soft-tissue wound?
Explanation
REFERENCES: Jebson PL, Louis DS: Amputations, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 1947.
Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Question 56
Figures below demonstrate the radiographs obtained from a 56-year-old man with a 3-year history of right groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?
Explanation
Chronic opioid consumption prior to total joint arthroplasty has been associated with increased pain after surgery, increased opioid requirements, a slower recovery and longer hospital stay, and higher 90-day postoperative complications compared with patients not on chronic opioids preoperatively. Based on this information, Nguyen and associates performed a study in three patient groups that included 1) chronic opioid users who underwent no preoperative intervention, 2) chronic opioid users who were weaned down to 50% of their prior opioid regimen, and 3) patients who were not chronic opioid users. The authors found that the reduction of preoperative opioid use improved postoperative function, pain, and recovery and that the weaned group performed more like the opioid naive group than the chronic opioid user
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to
surgery.
Question 57
Figures 43a and 43b show the T 1 - and T 2 -weighted MRI scans of a 78-year-old woman who reports the sudden atraumatic onset of well-localized medial knee pain. Pain is worse at night and also occurs with weight-bearing activity. What is the most likely diagnosis?
Explanation
REFERENCES: Soucacos PN, Berris AE, Xenakis TH, et al: Knee osteonecrosis: Distinguishing features in differential diagnosis, in Urbanik JR, Jones JD (eds): Osteonecrosis. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 413-424.
Ecker ML, Lotke PA: Osteonecrosis of the medial part of the tibial plateau. J Bone Joint Surg Am 1995;77:596-601.
Question 58
What is the most common nonanesthetic-related reversible cause of changes in intraoperative neurophysiologic monitoring data? Review Topic
Explanation
Question 59
A 40-year-old man has a palpable mass over the dorsum of the ankle. He reports no history of direct trauma but notes that he sustained a laceration to the middle of his leg 6 weeks ago. Examination reveals a 4-cm x 1-cm mass. T 1 - and T 2 -weighted MRI scans are shown in Figures 12a and 12b. An intraoperative photograph and biopsy specimen are shown in Figures 12c and 12d. What is the most likely diagnosis?
Explanation
REFERENCES: Otte S, Klinger HM, Loreaz F, Haerer T: Operative treatment in case of closed rupture of the anterior tibial tendon. Arch Orthop Traum Surg 2002;122:188-190.
Kausch T, Rutt J: Subcutaneous rupture of the tibialis anterior tendon: Review of the literature and case report. Arch Orthop Traum Surg 1998;117:290-293.
Question 60
Figure 40 shows the radiograph of a 30-year-old woman who has a painful elbow. Examination reveals a deformed skull, multiple cafe-au-lait spots, and bone deformities. What is the most likely diagnosis?
Explanation
REFERENCES: Albright F, Butler AM, Hampton AO, et al: Syndrome characterized by osteitis fibrosa disseminata, areas of pigmentation and endocrine dysfunction with precocious puberty in females. N Engl J Med 1937;216:727-746.
Danon M, Robboy SJ, Kim S, Scully R, Crawford JD: Cushing syndrome, sexual precocity, and polyostotic fibrous dysplasia (Albright syndrome) in infancy. J Pediatr 1975;87:917-921.
Grabias SL, Campbell CJ: Fibrous dysplasia. Orthop Clin North Am 1977;8:771-783.
Question 61
Figure 6a shows the radiograph of a 50-year-old man who sustained an anterior dislocation of the shoulder. He undergoes closed reduction, and the postreduction radiograph is shown in Figure 6b. Management should now consist of
Explanation
REFERENCES: Neer CS II: Displaced proximal humeral fractures: II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
Flatow EL, Cuomo F, Maday MG, et al: Open reduction and internal fixation of two-part displaced fractures of the greater tuberosity of the proximal part of the humerus. J Bone Joint Surg Am 1991;73:1213-1218.
Question 62
Revision of failed hip resurfacing arthroplasty should involve
Explanation
Hip resurfacing offers several potential advantages over conventional total hip arthroplasty, particularly for patients younger than 75 years of age. This intervention can be
relatively bone conserving and is appropriate in settings involving proximal femoral deformity, precluding the use of a traditional femoral component. The use of hip resurfacing in osteonecrosis has been controversial, however. Although there are several reports of successful use of these implants to address osteonecrosis, concerns remain about extensive femoral head involvement (exceeding 40%) and ability to support the femoral head cap. Consequently, hip resurfacing is not recommended for patients with large femoral head lesions.
Evaluation of painful hip resurfacings requires a systematic approach. Radiographs can help surgeons assess implant position, loosening, or fractures. Serological studies including ESR, CRP, and serum cobalt and chromium levels can give clues as to whether infection, metallosis, or both are the underlying cause(s) of failure. Hip aspiration in the setting of metal-on-metal bearings necessitates a manual cell count and differential to avoid falsely elevated automated cell counts.
Revision of failed hip resurfacings should involve revisions of both the femoral and acetabular components. Although successful retention of the acetabular shell has been described, concerns remain regarding cup circumference mismatch, which can lead to suboptimal clearance between the new bearing surfaces.

Question 63
-Postsurgically, the patient recovers well and is fully rehabilitated. He demonstrates full motion with no instability or pain and is cleared to return to play 12 months after the surgery. He asks for your advice regarding use of a functional brace for playing basketball following his reconstruction. What is the most appropriate recommendation?
Explanation
The athlete most likely suffered an acute ACL rupture however the presence of a lipohemarthrosis is concerning for the possibility of an intraarticular fracture. Because of this, the patient should not be allowed full weight bearing until a fracture is ruled out with radiographs. Given the athlete’s inability to perform a straight leg raise, the extensor mechanism is not functioning and a telescoping knee brace locked in extension should be utilized. A neoprene knee sleeve does not have a role in the
treatment of this acute injury.The radiographs reveal a lateral avulsion fracture off of the proximal tibial epiphysis which is known as a Segond fracture. It is indicative of an ACL injury and the fracture fragment seen is the consequence of the lateral capsule injury sustained during the pivot-shift mechanism. There is no radiographic evidence of a medial tibial plateau fracture. A radiographic sign of a chronic MCL injury is known as a Pellegrini-Stieda lesion and this is seen as calcification of the femoral origin of the MCL. A radiographic sign of an acute LCL rupture would be an avulsion fracture of the tip of the fibula.The MRI shows kissing contusions of the posterolateral tibial plateau and the midpoint of the lateral femoral condyle. These “kissing lesions” are seen as a result of a pivot shift mechanism of injury and are diagnostic for an ACL rupture. The most common associated injury in an acute ACL rupture is a lateral meniscus tear. Medial meniscus tears are more common in chronic ACL injuries. PCL rupture and PLC injury are all associated injuries seen in acute ACL rupture; however, these are much less common than meniscal tears. The team physician has a role in encouraging, but
not demanding, the athlete to report the injury andtreatment to the scholarship school’s coaching staff. What the athlete decides to do is his decision; the physician would be violating the athlete’s HIPAA rights as well as their confidence by reporting it directly to the scholarship school. Clearly the physician should not discourage the athlete from reporting the injury. The athlete is 18 years old and, as such, the physician would need the athlete’s permission to discuss any medical issues with the family in keeping with HIPAA.
The athlete’s exam demonstrates incompetence of both bundles of the ACL as demonstrated by the loss of stability with anterior translation of the tibia (Lachman test) as well as with rotation (pivot shift). The external rotation stress with the knee in 30 degrees of flexion tests the competence of the posterolateral corner while rotation at 90 degrees of flexion tests the PCL. Since the athlete’s knee is stable to posterior drawer testing demonstrating an intact PCL and the external rotation at 30 degrees is equivalent to that at 90 degrees, the posterolateral corner in intact.
The ACL has two separate and distinct bundles, the AM and PL. Each bundle takes on tension at varying degrees of knee flexion and therefore each bundle is thought to have a varying contribution to the stability of the knee. The AM bundle takes on tension with the knee in flexion and the PL bundle is tight in extension. Neither bundle is isometric during knee range of motion. Both bundles have contributions to rotational stability of the knee throughout the range of motion.
The success of traditional trans-tibial single-bundle ACL reconstruction has recently been called into question given the demonstration of persistent rotational instability following reconstruction. The persistence of rotational instability in trans-tibial single bundle ACL reconstruction has been attributed to the location of the graft in a vertically malpositioned femoral tunnel. The goal of double-bundle ACL reconstruction is to more accurately reproduce the native ACL and provide grafts that contribute to anteroposterior stability as well as rotational stability by placing the grafts in more anatomic locations not central in the knee axis. There is an increased cost and surgical time associated with double-bundle reconstruction.
The use of functional braces following ACL reconstruction is a surgeon’s preference because there is no difference in retear rate with or without a brace. Some authors recommend brace use for one to two years following ACL reconstruction for all athletic activities, but this is not supported by the literature. No literature exists showing a higher rate of reinjury with a functional brace and off-the shelf and custom braces have been found to be equivalent leading those who advocate for braces to recommend off-theshelf braces given their significantly lower cost.
Question 64
A 35-year-old construction worker continues to have weakness with lifting overhead 2 years after he was treated with physical therapy for a "chest muscle" tear. An obvious deformity noted in his axilla worsens with resisted extension and adduction. A clinical photograph and MRI scan are shown in Figures 119a and 119b. What is the most appropriate treatment? Review Topic
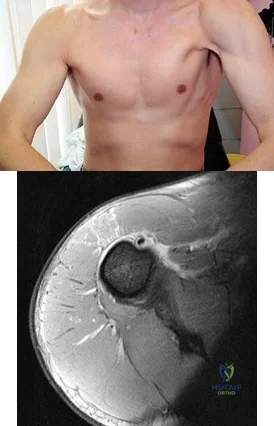
Explanation
Question 65
A 60-year-old patient had the procedure shown in Figure 7 performed 5 years ago. When converting this patient to a total knee arthroplasty (TKA), what patellar problem is commonly encountered intraoperatively?
Explanation
REFERENCES: Yoshino N, Shinro T: Total knee arthroplasty after failed high tibial osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA,
JB Lippincott, 2003, vol 2, pp 1265-1271.
Meding JB, Keating EM, Ritter MA, et al: Total knee arthroplasty after high tibial osteotomy:
A comparison study in patients who had bilateral total knee replacement. J Bone Joint Surg Am 2000;82:1252-1259.
Question 66
Which sterilization method is expected to produce the most degradation of an allograft used for anterior cruciate ligament reconstruction?
Explanation
A biomechanical study compared unprocessed, irradiated (2.0 Mrad-2.8 Mrad), and supercritical CO2-treated soft-tissue allografts and demonstrated a 27% to 36% decrease in stiffness of the supercritical CO2-treated grafts. No significant difference was found between the irradiated and untreated soft-tissue allografts. Low-dose (1.0 Mrad-1.2 Mrad) gamma irradiation of bone-patellar-tendon-allograft has been shown to produce a 20% decrease in graft stiffness. Deep freezing or cleansing with 4% chlorhexidine gluconate does not appear to adversely affect the biomechanical properties of the allograft tissue.

CLINICAL SITUATION FOR QUESTIONS 43 THROUGH 46
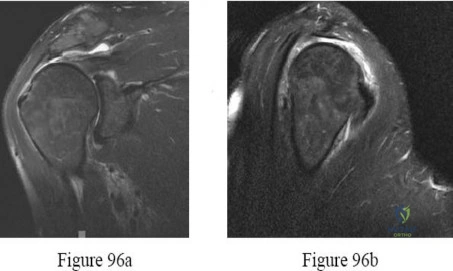
Figures 43a and 43b are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable.
Question 67
Following spinal cord injury (SCI), methylprednisolone (a bolus of 30 mg/kg plus 5.4 mg/kg per hour over 24 hours) initiated within 8 hours of injury has been associated with which of the following MRI findings? Review Topic
Explanation
Question 68
A healthy 27 year-old-male is brought into the emergency department after a fall from height. He has a suspected left C8-T1 nerve injury. Which of the following findings would most suggest a root avulsion injury rather than a brachial plexus injury at this level?
Explanation
Brachial plexus injuries are often classified as preganglionic vs. postganglionic injuries. Preganglionic injuries are typically avulsion injuries proximal to the dorsal root ganglion. Clinical features suggestive of lower root avulsion injury include a person falling from height clutching on object to save himself, Horner’s syndrome (drooping of the eyelid (ptosis), pupillary constriction (miosis) and anhidrosis), absence of a Tinel sign or tenderness to percussion in the neck, and a normal histamine test (C8-T1 sympathetic ganglion - intact triple response (redness, wheal, flare)).
Caporrino et al. reviewed 102 patients to assess the best modality (e.g. physical examination, MRI and nerve conduction studies [NCSs]) for diagnosing and localizing brachial plexus injuries. They found the best diagnostic performance with physical examination (sensitivity = 97.8%; specificity = 30.8%) and NCSs (sensitivity
= 98.9%; specificity = 23.1%). MRI had inferior performance for all measurements. They conclude that NCSs exhibited superior performance to MRI, and should be considered a more reliable supporting tool after detailed physical examination.
Incorrect Answers:
Question 69
- Figure 12 shows the frog-lateral radiograph of a 45-year-old man who has a painful left hip. What is the most likely diagnosis?
Explanation
Question 70
The load versus deformation curve of the functional spinal unit (FSU) is made up of the neutral zone, the elastic zone, and the plastic zone. What is the plastic zone of the curve believed to represent?
Explanation
REFERENCES: Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 15-23.
Panjabi MM, White AA: Physical properties and functional biomechanics of the spine, in White AA, Panjabi MM: Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 1-83.
Question 71
Venous thromboembolism may occur after total joint arthroplasty. The risk of this complication is elevated in patients with
Explanation
Obesity, a prior history of venous thromboembolism, and metabolic syndrome have all been associated with an increased risk of thromboembolism. A recent meta-analysis showed that diabetes had no significant relationship with venous thromboembolism following hip or knee arthroplasty. Tranexamic acid is an antifibrinolytic agent that has been shown to reduce blood loss substantially following hip and knee arthroplasty. It has also been shown to be safe in patients with severe medial comorbidities and a prior history of venous thromboembolism.
Question 72
Which of the following lesions most closely resembles Ewing’s sarcoma histologically?
Explanation
REFERENCE: Wold LE, McLeod RA, Sim FH, Unni KK: Atlas of Orthop Pathology. Philadelphia, PA, WB Saunders, 1990.
Question 73
A 79-year-old woman reports a history of left leg pain with walking. Her pain is exacerbated with walking and stair climbing, and her symptoms are improved by standing after she stops walking. Lumbar flexion does not provide any significant improvement of the symptoms and sitting does not significantly change symptoms. Her leg pain is worse at night and she obtains relief by hanging her leg over the side of the bed. The neurologic examination is essentially normal. Examination of the lower extremities demonstrates mild early trophic changes, and her pulses distally are palpable but are diminished bilaterally. Radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management?
Explanation
REFERENCES: Aufderheide TP: Peripheral arteriovascular disease, in Rosen P, Barkin R (eds): Emergency Medicine: Concepts and Clinical Practice, ed 4. St Louis, MO, Mosby, 1998,
pp 1826-1844.
Mirkovic S, Garfin SR: Spinal stenosis: History and physical examination. Instr Course Lect 1994;43:435-440.
Question 74
After closed reduction of the dislocation shown in Figure 42, it is essential to avoid placing the upper extremity in what position for the first 4 to 6 weeks?
Explanation
REFERENCES: Burkhead WZ Jr, Rockwood CA Jr: Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 1986;68:724-731.
Pollock RG, Bigliani LU: Recurrent posterior shoulder instability: Diagnosis and treatment.
Clin Orthop 1993;291:85-96.
Question 75
-Figures 55a and 55b are the radiograph and CT scan of a 61-year-old woman who has had neck pain after being involved in a high-speed motor vehicle collision. Examination reveals normal strength and sensation in both upper and lower extremities, normal rectal tone, and no other injuries. The C1-C2 lateral mass overhang measures 8.5 mm. What is the most appropriate treatment option?
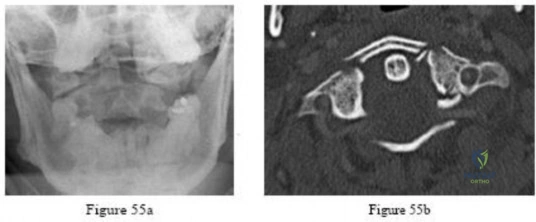
Explanation

Question 76
Recent randomized controlled trials comparing early passive range of motion to 6 weeks of immobilization after successful arthroscopic rotator cuff repair concluded that, compared to immobilization, early passive range of motion resulted in: Review Topic
Explanation
Traditionally, most surgeons recommended early post-operative range of motion exercises for their patients in order to prevent adhesions and ultimately stiffness. However, recent evidence has found that there is no difference in the healing rate, range of motion or functional outcome between patients who undergo early versus delayed (i.e. initial 6 weeks of immobilization) passive range of motion exercises after arthroscopic rotator cuff repair.
Kim et al. conducted a randomized controlled trial comparing early passive range of motion vs. immobilization in 106 patients who underwent arthroscopic repair for full-thickness rotator cuff tears. They found that there was no clinically or statistically significant difference between the two groups in pain, healing or function.
Keener et al. also conducted a randomized controlled trial of 124 patients who were undergoing arthroscopic repair of a full-thickness rotator cuff tear and found no difference between early and delayed range of motion in healing and functional outcome.
Cuff & Pupello also compared early vs. delayed range of motion during the postoperative rehabilitation phase in a randomized controlled trial of 68 individuals undergoing arthroscopic rotator cuff repair and found no significant difference in range of motion or healing.
Incorrect Answers:
Question 77
A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion, but there is very little pain at rest. She has no pertinent medical history and does not smoke. Figures 23a and 23b show current radiographs. What is the most appropriate surgical option?

Explanation
Question 78
-Figures 14a through 14d are the radiographs and sagittal T1- and T2-weighted MRI scans of an otherwise healthy 10-year-old girl who has experienced 3 weeks of worsening pain with weight bearing and is now refusing to bear weight to either of her lower extremities. She denies any history of injury or trauma.She has not had any fevers or recent illnesses. She denies any numbness or parasthesias. She has had no bowel or bladder incontinence. In the emergency department she is afebrile and tender to palpation over the midlumbar spine. She has pain with hyperextension and flexion of her back. Her white blood cell count is 11.4 (reference range, 4.5-11.0 x109/L), erythrocyte sedimentation rate is 40 mm/h (reference range, 0-20 mm/h), and C-reactive protein is 2.6 mg/L (reference range, 0.08-3.1 mg/L). What is the most appropriate course of action at this time?

Explanation

Question 79
A 16-year-old boy with osteochondritis dissecans of the capitellum has intermittent symptoms of catching and locking. Examination is unremarkable. Radiographs reveal a loose body anteriorly with a diameter of 10 mm. To remove the loose body, elbow arthroscopy is being considered. Which of the following procedures would minimize the risk of neurovascular complication during the procedure?
Explanation
REFERENCES: Lynch GJ, Meyers JF, Whipple TL, Caspari RB: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
O’Driscoll S: Loose bodies and synovial conditions, in Green D, Hotchkiss R, Pederson W (eds): Green’s Operative Hand Surgery. New York, NY, Churchill Livingstone, 1999, pp 235-249.
Question 80
What vessel is marked with an asterisk in Figure 44?
Explanation
REFERENCES: Agur AM, Dalley AF (eds): Grant’s Atlas of Anatomy, ed 12. Philadelphia, PA, Lippincott Williams and Wilkins, 2008.
Uflacker R: Atlas of Vascular Anatomy: An Angiographic Approach, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006.
Question 81
What is the most common reason an individual with a malignant soft-tissue tumor in the extremities seeks medical attention?
Explanation
REFERENCES: Brouns F, Stas M, De Wever I: Delay in diagnosis of soft tissue sarcomas. Eur J Surg Oncol 2003;29:440-445.
Rougraff B: The diagnosis and management of soft tissue sarcomas of the extremities in the adult. Curr Probl Cancer 1999;23:1-50.
Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 82
A 45-year-old man reports a history of a popping sensation and pain in the right shoulder while lifting boxes 6 months ago. The pain has persisted with loss of motion of the shoulder. Radiographs and MRI scans are shown in Figures 47a through 47d. Which of the following studies is likely to produce a significant positive result? Review Topic

Explanation
Question 83
A 22-year-old woman injured her ankle when she fell off a ladder. Radiographs reveal a displaced large posterior malleolus fracture of about 45% of the joint. What is the best definitive treatment?
Explanation
optimal function can be achieved. Open reduction and internal fixation allows this achievement. In cases where comminution exists, absolute stability may have to be sacrificed so as to not strip small comminuted bone fragments. Therefore, a bridging technique is worthwhile. External fixation can be used as a temporary technique until the soft tissues are more amenable to definitive fixation. Cast treatment is not indicated in adult forearm fractures. Locking nails for forearm use are not reamed. With regards to articular fractures, anatomic reduction and rigid stabilization are required to achieve the best results and allow for fracture healing. This environment also allows for the best chance of the cartilage repair process to form "hyaline-like" cartilage. Open reduction and internal fixation with absolute stability is the mainstay of treatment for partial articular fractures such as split depression tibial plateau fractures and posterior malleolus fractures involving greater than about 25% to 30% of the joint. The gold standard for the treatment of a closed femur fracture is a reamed intramedullary locked nail. Results are uniformly excellent. This can be done without stripping of the soft tissues such as in open reduction and internal fixation. External fixation can be used as a temporary device in patients in extremis for damage control reasons.Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr. Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am. 1986 Sep;68(7):1008-17. http://www.ncbi.nlm.nih.gov/pubmed/3745238')">View Abstract at PubMedJones DB Jr, Kakar S. Adult diaphyseal forearm fractures: intramedullary nail versus plate fixation. J Hand Surg Am. 2011 Jul;36(7):1216-9. Epub 2011 May
Question 84
- A 10-year-old boy twisted his ankle while skateboarding and has pain and swelling around the lateral ankle just distal to the fibula. Radiographs are obtained and a lesion is identified in the distal tibia as seen in Figures 273a and 273b. Two weeks later he has no pain to palpation in the region and denies antecedent pain. What is the most appropriate treatment for this lesion?

Explanation

Question.1 .A 49-year-old weekend athlete has a 4-week history of pain in his unilateral plantar heel that is most severe for the first 20 steps upon arising in the morning. He has an area of maximal tenderness on the plantar medial aspect of the heel pad at the origin of the plantar fascia. He has only improved 30% after a 3-week course of physical therapy with toe intrinsic muscle strengthening and arch- and tendo-Achilles stretching. What is the best next treatment step?
Release the plantar fascia.
Inject the plantar fascia with platelet-rich plasma.
Prescribe a night splint and continue physical therapy.
Administer extracorporeal shockwave therapy to the heel.
Perform a series of 3 steroid injections into the plantar fascia.

Question.2 .Figures 16a and 16b are the radiographs of a 38-year-old carpenter with progressively worsening ankle pain; 14 years ago, he was involved in an all-terrain vehicle collision. Anti-inflammatory medication,corticosteroid injections, and bracing no longer effectively control his pain. The pain now interferes with his work and family responsibilities. Examination reveals an antalgic limp, varus deformity, limited ankle motion, limited eversion, and normal strength. Treatment should now consist of

ankle arthrodesis.
total ankle arthroplasty.
distal tibia osteotomy.
lateral ligament repair.
deltoid ligament release.
Question. 3 .A 48-year-old woman had total knee arthroplasty. She is unable to “lift her toes or ankle to her nose.”After 2 months of physical therapy, she has a slapping gait. What is the best next treatment step?
Ankle fusion
Ankle-foot orthosis
Sural nerve graft
Medial heel post
Laminectomy of L4/5
Question. 4 .Figures 46a through 46c are the CT scans of an 18-year-old who sustained an injury 3 weeks ago and now has ankle pain. Examination reveals an ankle effusion and painful range of motion. Recommended treatment should consist of
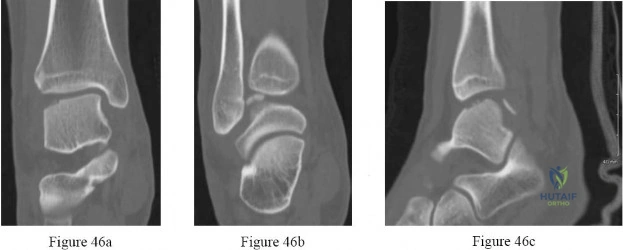
transtalar drilling.
fixation of the fragment.
osteochondral autograft.
weight bearing in a boot with early range of motion.
cast immobilization and nonweight-bearing activity for 6 weeks.
Question. 5 .A 47-year-old woman has a closed, displaced, Weber C bimalleolar ankle fracture. Past medical history includes diabetes mellitus for 7 years controlled with diet and an oral hypoglycemic agent. Semmes-Weinstein sensory testing reveals absence of sensation to the 5.07/10-gm monofilament on the plantar aspect of both feet. The skin is intact with 2+ pedal pulses. Treatment should include
open reduction with limited internal fixation.
closed reduction and application of an external fixator.
closed reduction and total contact cast immobilization.
retrograde intramedullary rod fixation with ankle fusion.
internal fixation and an extended period of immobilization.

Question. 6 .Figures 68a and 68b are the clinical photographs of a 55-year-old woman who had a right hindfoot fusion 3 years ago for a pes planovalgus deformity. Since the surgery, she has had lateral hindfoot pain and places most of the weight-bearing load on the lateral border of her foot when walking. What is the most likely cause of her symptoms?

Deltoid insufficiency
Excessive forefoot abduction
Residual heel valgus
Residual Achilles tendon contracture
Malposition of the transverse tarsal joint
Question 85
Induction coupling stimulates bone growth through all of the following direct effects EXCEPT:
Explanation
In basic science studies, electrical stimulation (i.e. induction coupling), has been shown to promote bone healing via release of growth factors that induce osteoblast differentiation/proliferation. Electrical current can be placed around bone in various ways, creating a current to stimulate growth factor release and subsequent osteoblast proliferation.
Aaron et al. summarized, in a systematic review, the effects of various types of electrical stimulation on bone and bone healing. Regardless of type (i.e. inductive coupling, capacitive coupling, direct current), they report electricity and/or electromagnetic fields promote gene expression of growth factors that promote an osteogenic environment.
Illustration A depicts a cathode placed directly to allograft with a subcutaneously placed electrical stimulator. Illustration B depicts cathodes placed anteriorly and posteriorly around the hip, connected to an outside power source to create the necessary current. Illustration C depicts an inductive coil placed laterally on the skin in order to create an electrical current.
Incorrect answers:
Question 86
A teenager is undergoing a correction of deformity and lengthening of the femur. Distractions are proceeding as expected; however, during his 6-week follow-up examination, the patient reports that the distraction motors have become harder to turn over for the past 2 to 3 days. Figures 37a and 37b show current radiographs. What is the most likely complication being encountered?
Explanation
REFERENCES: Paley D: Problems, obstacles and complications of limb lengthening, in Maiocchi AB, Aronson J (eds): Operative Principles of Ilizarov. Baltimore, MD, Williams & Wilkins, 1991, p 360.
Herring JA: Limb length discrepancy, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics,
ed 3. Philadelphia, PA, WB Saunders, 2002, p 1088.
Question 87
An obtunded 80-year-old man was found alone in his apartment after an apparent fall. A CT scan performed in the emergency department shows that he has an extensile injury of an ankylosed cervical spine. The fracture extends across the ossified C5-C6 disk space and into the lamina of C5. There is 1.5 cm of widening between the C5 and C6 vertebrae anteriorly. The patient's family asks you about the long-term impact of the fracture on his functional capacity and survival. You advise them that patients with fractures of the cervical spine with ankylosing conditions have
Explanation
Several studies have found that rates of neurologic deficit and mortality are higher for patients with ankylosing spondylitis and a spinal fracture than for age-matched controls. The 2011 work of Schoenfeld and associates, which directly compared patients with cervical fractures in ankylosed spines to age-and sex-matched controls who also had cervical fractures but no ankylosing condition, demonstrated that those with ankylosing spondylitis were at elevated risk for mortality for up to 2 years after sustaining a fracture. In a study by Westerveld and associates, the rate of neurologic deficit among patients with ankylosing spondylitis and a spinal fracture was 57.1% compared to 12.6% among controls.
RECOMMENDED READINGS
Westerveld LA, van Bemmel JC, Dhert WJ, Oner FC, Verlaan JJ. Clinical outcome after traumatic spinal fractures in patients with ankylosing spinal disorders compared with control patients. Spine J. 2014 May 1;14(5):729-40. doi: 10.1016/j.spinee.2013.06.038. Epub 2013 Aug 27. PubMed PMID: 23992936. View Abstract at PubMed
Schoenfeld AJ, Harris MB, McGuire KJ, Warholic N, Wood KB, Bono CM. Mortality in elderly patients with hyperostotic disease of the cervical spine after fracture: an age- and sex-matched study. Spine J. 2011 Apr;11(4):257-64. doi: 10.1016/j.spinee.2011.01.018. Epub 2011 Mar 5. PubMed PMID: 21377938. View Abstract at PubMed
Question 88
Figures 25a and 25b show the radiographs of a 66-year-old man who has had a long history of bilateral painful flatfoot deformities. Examination reveals that his foot is partially correctable passively, albeit with discomfort, and he has an Achilles tendon contracture. An ankle-foot orthosis has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004,
pp 115-120.
Walling AK: Symposium: Adult acquired flatfoot. Clin Orthop 1999;365:2-99.
Question 89
A 53-year-old woman reports a 4-month history of gradual onset diffuse shoulder pain and limited function. She has had no prior treatment, and her medical history is unremarkable. Examination reveals globally painful active range of motion to 120 degrees forward elevation, 25 degrees external rotation with the arm at the side, and internal rotation to the sacrum. Passive range of motion is also limited in comparison with the contralateral shoulder. Radiographs are shown in Figures 31a through 31c. What is the most appropriate management? Review Topic

Explanation
Question 90
Which of the following is a recognized predictor of mortality after hip fracture?

Explanation
The study by Richmond et al looked at 836 patients treated for a hip fracture and found that this injury is not associated with significant excess mortality amongst patients older than age 85. However, in younger patients, those with ASA classifications of 3 or 4 have significant excess mortality following hip fracture that persists up to 2 years after injury.
Question 91
A 53-year-old woman has severe neck and left shoulder pain after a rollover motor vehicle accident. Radiographs and a CT scan of the cervical spine are shown in Figures 34a through 34c. Management should consist of
Explanation
REFERENCES: Levine AM, Mazel C, Roy-Camille R: Management of fracture separations of the articular mass using posterior cervical plating. Spine 1992;17:S447-S454.
Levine AM: Facet fractures and dislocations, in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 360-362.
Whitehill R, Richman JA, Glaser JA: Failure of immobilization of the cervical spine by the halo vest: A report of five cases. J Bone Joint Surg Am 1986;68:326-332.
Garvey TA, Eismont FJ, Roberti LJ: Anterior decompression, structural bone grafting, and Caspar plate stabilization for unstable cervical spine fractures and/or dislocations. Spine 1992;17:S431-S435.
Question 92
A 42-year-old man sustained a burst fracture at L2 in a motor vehicle accident. Examination reveals that he is neurologically intact. Figure 18 shows a cross-sectional CT scan through the fracture. If the fracture is managed nonsurgically for the next 2 years, the retained fragments can be expected to
Explanation
REFERENCES: Mumford J, Weinstein JN, Spratt KF, et al: Thoracolumbar burst fractures: The clinical efficacy and outcome of nonoperative management. Spine 1993;18:955-970.
Wood KB, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurologic deficit: A prospective, randomized study. J Bone Joint Surg Am 2003;85:773-781.
Question 93
The posterior horn of the medial meniscus receives its primary blood supply from what artery?
Explanation
REFERENCES: Insall J, Scott WN: Anatomy, in Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, pp 64-70.
Scapinelli R: Vascular anatomy of the human cruciate ligaments and surrounding structures. Clin Anat 1997;10:151-162.
Question 94
What tendon is closest to an appropriately placed anterolateral portal for ankle arthroscopy?
Explanation
REFERENCE: Ogut T, Akgun I, Kesmezacar H, et al: Navigation for ankle arthroscopy: Anatomical study of the anterolateral portal with reference to the superficial peroneal nerve. Surg Radiol Anat 2004;26:268-274.
Question 95
What factor is associated with a high risk of developing pseudotumors after metal-on-metal hip resurfacing?
Explanation
Question 96
Which of the following is considered an advantage of arthroscopic distal clavicle excision compared with open distal clavicle excision?
Explanation
in 20 patients who underwent open distal clavicle excision that resulted in failure, 15 of those patients had a superior labral anterior posterior (SLAP) lesion. Of these 15 patients who had the lesion treated surgically, 9 went on to a good to excellent result after the surgery was performed arthroscopically. Fewer complications, lower infection rate, and decreased surgical time have not been documented in the literature. Arthroscopic technique sacrifices the inferior acromioclavicular ligament and preserves the superior acromioclavicular ligament.
REFERENCES: Berg EE, Ciullo JV: The SLAP lesion: A cause of failure after distal clavicle resection. Arthroscopy 1997;13:85-89.
Lemos MJ, Tolo ET: Complications of the treatment of acromioclavicular and sternoclavicular joint injuries, including instability. Clin Sports Med 2003;22:371-385.
Question 97
MRI results are shown in Figure 1 for a 22-year-old, right-hand dominant collegiate athlete who reports a 6-month history of progressive weakness in his right arm. He denies any specific traumatic event. He has altered his weight-lifting activities and tried over-the-counter ibuprofen without benefit. No appreciable deformity or atrophy is found on examination of the upper extremities. He demonstrates full active shoulder range of motion, and there is no weakness with abduction in the plane of the scapula. Belly press test findings are normal, but weakness is seen in external rotation with the arm in adduction. He does not demonstrate anterior apprehension, and there is no instability with load and shift testing. Radiographs are unremarkable. What is the best surgical option?
Explanation
A. Pain with elbow extension in forearm pronation
B. Mechanical symptoms when rising from a chair
C. Valgus instability
D. Tenderness over the medial collateral ligament (MCL)
Excessive resection of the common extensor origin posterior to the equator of the radiocapitellar joint may lead to iatrogenic lateral collateral ligament (LCL) injury, causing posterior lateral rotatory instability (PLRI). Patients may present with lateral elbow pain, a positive lateral pivot shift test, or mechanical symptoms/subjective instability when pushing up from a chair (positive chair rise test). PLRI is often provoked with combined elbow extension and forearm supination, as the posterior support for the radiocapitellar joint has been lost. Therefore, placing the forearm in pronation during elbow extension places the radiocapitellar joint in a more stable position and is less likely to induce pain or mechanical symptoms. Valgus instability and MCL tenderness would be associated with an MCL injury.
56- A 75-year-old man presents with complaints of shoulder pain, bruising, and weakness following a fall onto his outstretched hand. He underwent an uncomplicated anatomic total shoulder arthroplasty 5 years prior with good range of motion and strength. His current radiographs are shown in Figures 1 and 2. What is the most appropriate next step to restore this patient’s function?
Question 98
A 38-year-old woman has a lesion on her left foot that has increased in size over the past 6 months. The clinical photograph is shown in Figure 17a, and a photomicrograph of the biopsy specimen is shown in Figure 17b. What is the most likely diagnosis?
Explanation
REFERENCES: Hughes LE, Horgan K, Taylor BA, Laidler P: Malignant melanoma of the hand and foot: Diagnosis and management. Br J Surg 1985;72:811-815.
Fortin PT, Freiberg AA: Malignant melanoma of the foot and ankle. J Bone Joint Surg Am 1995;77:1396-1403.
Question 99
-are the radiographs of a 7-year-old girl who was evaluated for a visible elbow deformity by a foster parent. She thought the child fell, but her history was vague. On physical examination, a large prominence was seen over the posterolateral elbow, and the girl lacks the terminal 20 degrees of elbow extension. She has 75 degrees of elbow pronation and supination. She was nontender on examination. What is the most appropriate next treatment step?
Explanation

Question 100
A 38-year-old man reports a 6-week history of shoulder pain and stiffness after falling on the stairs and landing onto the affected side. Radiographs are shown in Figures 54a and 54b. What is the most appropriate treatment? Review Topic

Explanation
