Orthopedic Board Review MCQs: Knee, Nerve, Revision & Shoulder Surgery | Part 189

Key Takeaway
This page offers Part 189 of a comprehensive, interactive MCQ bank for orthopedic surgeons. Featuring 100 verified, high-yield questions in OITE/AAOS format, it's designed for rigorous board exam preparation. Access two learning modes—Study and Exam—with detailed clinical explanations to master crucial orthopedic topics.
About This Board Review Set
This is Part 189 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 189
This module focuses heavily on: Knee, Nerve, Revision, Shoulder.
Sample Questions from This Set
Sample Question 1: At the time of acetabular revision, retention of well-fixed femoral components inserted with first-generation cementing technique is most commonly associated with which of the following factors?...
Sample Question 2: A 48-year-old man who is scheduled to undergo total knee replacement has an X-linked clotting disorder that leads to abnormal bleeding and recurrent, spontaneous hemarthrosis. Before undergoing surgery, he should have replacement therapy of...
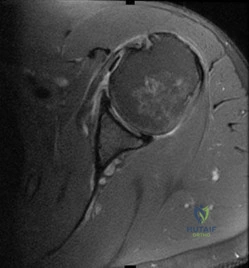
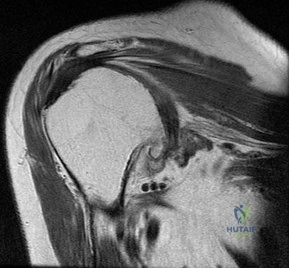
Sample Question 3: Figure 72 is the MRI scan of a 61-year-old man who had left shoulder pain with a massive rotator cuff tear. Active forward elevation was 120 degrees. Arthroscopic examination revealed that the rotator cuff tear was irreparable. The articula...
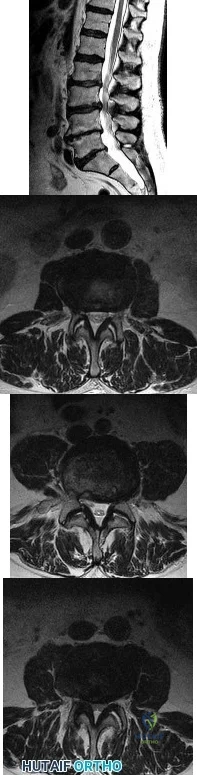
Sample Question 4: A 25-year-old athletic woman has a 16-week history of left lower-extremity radiating pain in an S1 distribution. MR images obtained by her family physician reveal a large L5-S1 paracentral disk herniation impinging on the left S1 nerve root...
Sample Question 5: Figures 1 and 2 depict the postoperative radiographs obtained from a 22-year-old man who was involved in a motor vehicle accident. The most likely limitation in motion arising from this treatment is...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
At the time of acetabular revision, retention of well-fixed femoral components inserted with first-generation cementing technique is most commonly associated with which of the following factors?
Explanation
Question 2
A 48-year-old man who is scheduled to undergo total knee replacement has an X-linked clotting disorder that leads to abnormal bleeding and recurrent, spontaneous hemarthrosis. Before undergoing surgery, he should have replacement therapy of
Explanation
Question 3
Figure 72 is the MRI scan of a 61-year-old man who had left shoulder pain with a massive rotator cuff tear. Active forward elevation was 120 degrees. Arthroscopic examination revealed that the rotator cuff tear was irreparable. The articular surfaces of the glenohumeral joint have a normal appearance without significant degenerative changes. What is the most appropriate treatment option? Review Topic
Explanation
Question 4
A 25-year-old athletic woman has a 16-week history of left lower-extremity radiating pain in an S1 distribution. MR images obtained by her family physician reveal a large L5-S1 paracentral disk herniation impinging on the left S1 nerve root. You suggest a left-sided L5-S1 microdiskectomy and tell her that when comparing tubular diskectomy and open procedures
Explanation
Several comparative studies have reported no difference in functional outcomes between tubular diskectomy and microsurgical lumbar diskectomy. A recent systematic review by Kamper and associates in which conventional microdiskectomy and minimally invasive approaches were compared revealed that there was no difference between the procedures in terms of clinical outcomes, complication risk, or rate of revision surgery.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis. Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183.View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
Question 5
Figures 1 and 2 depict the postoperative radiographs obtained from a 22-year-old man who was involved in a motor vehicle accident. The most likely limitation in motion arising from this treatment is

Explanation
This patient sustained fractures of his radius and ulna; both were treated with plate and screw fixation. The plate used on the radius was straight, resulting in loss of the radial bow, which is critical for enabling the radius to curve around the ulna during pronation. This patient is unable to pronate beyond 20°. Schemitsch and Richards correlated a good functional outcome, defined as more than 80% of normal rotation of the forearm, with restoration of the normal amount and location of the radial bow. Additionally, they related the restoration of grip strength with appropriate restoration of the radial bow. Matthews and associates reported little significant loss of rotation with 10° of angulation; however, 20° of angulation resulted in a statistically and clinically significant loss of forearm rotation.
Question 6
A 4-year-old boy sustained a nondisplaced, but complete, fracture of the left proximal tibial metaphysis 1 year ago. The fracture healed uneventfully in an anatomic position. Examination of the injured extremity now reveals 18° of valgus compared with 3° of valgus on the opposite side. Management should now include
Explanation
REFERENCES: Zionts LE, MacEwen GD: Spontaneous improvement of posttraumatic tibia valga. J Bone Joint Surg Am 1986;68:680-687.
Beaty JH, Kumar A: Fractures about the knee in children. J Bone Joint Surg Am 1994;76:1870-1880.
Question 7
Which of the following cardiac conditions is considered an absolute contraindication to vigorous exercise?
Explanation
sudden death in young athletes. HCM phenotype becomes evident by age 13 to 14 years. Those at higher risk include individuals with cardiac symptoms, a family history of inherited cardiac disease, and those with a family history of premature sudden death. Echocardiography is useful for detecting structural heart disease, including the cardiomyopathies and valvular abnormalities. Trained adolescent athletes demonstrated greater absolute left ventricular wall thickness (LVWT) compared to controls. HCM should be considered in any trained adolescent male athlete with a LVWT of more than 12 mm (female of more than 11 mm) and a nondilated ventricle. Adolescent and adult athletes differ with respect to the range of LVWT measurements, as a manifestation of left ventricular hypertrophy (LVH). Differentiating LVH (“athlete’s heart”) from HCM involves looking at additional echocardiographic features. Sharma and associates reported that adolescents with HCM had a small or normal-sized left ventricle (less than 48 mm) chamber size, while those with LVH had a chamber size at the upper limits of normal (52 mm to 60 mm).
REFERENCES: Sharma S, Maron BJ, Whyte G, et al: Physiologic limits of left ventricular hypertrophy in elite junior athletes: Relevance to differential diagnosis of athlete’s heart and hypertrophic cardiomyopathy. J Am College Cardiol 2002;40:1431-1436.
Maron BJ, Spirito P, Wesley Y, et al: Development and progression of left ventricular hypertrophy in children with hypertrophic cardiomyopathy. N Engl J Med 1986;315:610-614.
Pelliccia A, Culasso F, Di Paolo FM, et al: Physiologic left ventricular cavity dilatation in elite athletes. Ann Intern Med 1999;130:23-31.
Question 8
In addition to pain, which of the following factors are considered most predictive of the risk of pathologic fracture?
Explanation
REFERENCES: Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 9
Which of the following occurs frequently after nonsurgical management of displaced intra-articular fractures of the calcaneus?
Explanation
Question 10
In surgically treating hand and finger infections in patients with diabetes mellitus, what factor is associated with higher amputation rates?
Explanation
REFERENCES: Gonzalez MH, Bochar S, Novotny J, et al: Upper extremity infections in patients with diabetes mellitus. J Hand Surg Am 1999;24:682-686.
Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Kour AK, Looi KP, Phone MH, et al: Hand infections in patients with diabetes. Clin Orthop Relat Res 1996;331:238-244.
Question 11
Arthritic change in cartilage is characterized by which of the following findings?
Explanation
Question 12
A 78-year-old man has a history of worsening bilateral calf pain with activity. MRI scans are shown in Figures 31a through 31d. His symptoms are not improved with forward flexion of the lumbar spine. His lower extremity pain is relieved when he sits or ceases activity. Which of the following tests would be most helpful in establishing a diagnosis? Review Topic
Explanation
Decreased range of motion and hip joint pain, especially in internal rotation and abduction, are common findings in patients with degenerative arthritis of the hip. While post-myelography CT has been found superior to MRI as a single study for the preoperative planning of decompression for lumbar spinal stenosis, it will not assist in differentiating vascular from neurogenic claudication.
Question 13
Integrins function in which of the following ways?
Explanation
Integrins are a large family of heteromeric cell surface receptors composed of non-covalently bound alpha and beta subunits which interact with extracellular matrix molecules, serum constituents and various adhesion molecules. Specifically, aVß3 is a type of integrin found on osteoclasts that attaches to bone by coupling with vitronectin.
Bikle reviews the cause of bone loss during periods of unloading. They state the during periods of rest, integrin expression is decreased, leading to disuse osteoporosis. They argue that drugs that selectively regulate the integrin signaling pathway may
reverse bone loss during periods of disuse.
Illustration A shows an example of an osteoclast attaching to bone via the integrin aVß3.
Incorrect
1:
This
is
the
function
of osteocytes.
2:
This
is
the
function
of osteoblasts.
3:
This
is
the
function
of
osteoprogenitor cells.
Question 14
A child with an idiopathic clubfoot is successfully treated by the Ponseti method. The risk of recurrence of the deformity is most dependent on which of the following factors? Review Topic
Explanation
Question 15
A patient with Paget disease who is intolerant of bisphosphonates is given calcitonin. What is the mechanism of action of calcitonin?
Explanation
Question 16
Figures 5a and 5b show the clinical photograph and radiograph of a patient who has difficulty wearing shoes and has persistent symptoms medially and laterally at the first and fifth metatarsophalangeal joints. Because shoe modifications have failed to provide relief, management should now consist of
Explanation
REFERENCES: Mann RA, Coughlin MJ: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 415-435.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 163-173.
Question 17
A 55-year-old man falls from a ladder and dislocates his nondominant shoulder. He undergoes an uncomplicated closed reduction under sedation in the emergency department. Postreduction radiographs reveal a small Hill-Sachs lesion and no other bony abnormalities. Six weeks after the dislocation, the patient has persistent pain at rest and forward elevation and external rotation weakness, but the remaining motor function in the extremity and sensation are intact. What is the best next step?
Explanation
modalities do not adequately address the concern over his potential for having sustained a rotator cuff tear.
Question 18
A B C D Figures 75a through 75d show the radiographs of an 85-year-old woman who fell from a step and sustained a right proximal femur fracture. Six months after surgery she has knee pain. What is the most likely cause of her pain?

Explanation
Three cases of anterior distal femoral cortex penetration during intramedullary nailing for subtrochanteric fractures were documented by Ostrum and Levy in a 2005 study. Case 1 involved a Zimmer (Warsaw, Indiana) M/DN antegrade femoral nail, Case 2 involved a Stryker (Mahwah, New Jersey) long-stem Gamma nail, and Case 3 a DePuy Synthes (West Chester, Pennsylvania) titanium femoral nail with spiral blade locking. The anterior Zimmer nail penetration resulted in a displaced supracondylar fracture, which subsequently required revision. The Gamma nail as well as the DePuy Synthes nail were left impaled through the distal femoral cortex, and the subtrochanteric fractures went on to union. The anteroposterior radius of curvature for the Zimmer, long Gamma, and DePuy Synthes nails is 257 cm, 300 cm, and 150 cm, respectively. It is estimated that the radius of curvature of the femoral diaphyseal canal is 114 to 120 cm. It appears that the difference in femoral anteroposterior bow between the bone and the implant is a contributing factor to distal femoral anterior cortex penetration in intramedullary nailing of subtrochanteric fractures. There is no evidence of osteoarthrosis on the radiographs. Although nonunion is possible, based on the radiographic findings it is more likely that this patient's pain is attributable to the curvature of the nail. The lateral image of the hip reveals an appropriate starting point for the device.
RECOMMENDED READINGS
Ostrum RF, Levy MS. Penetration of the distal femoral anterior cortex during intramedullary nailing for subtrochanteric fractures: a report of three cases. J Orthop Trauma. 2005 Oct;19(9):656-60. PubMed PMID: 16247312.View Abstract at PubMed
Egol KA, Chang EY, Cvitkovic J, Kummer FJ, Koval KJ. Mismatch of current intramedullary nails with the anterior bow of the femur. J Orthop Trauma. 2004 Aug;18(7):410-5. PubMed PMID: 15289685. View Abstract at PubMed
RESPONSES FOR QUESTIONS 76 THROUGH 78
- Nonsurgical treatment with closed reduction and immobilization
- Early mobilization with physical therapy initiated within 2 weeks
- Open reduction and internal fixation (ORIF) with locked implants
- Use of supplemental bone graft or substitutes
- Arthroplasty
- Workup for osteoporosis and counseling
Which intervention listed is most appropriate to address each scenario described?

76A B
Question 19
A 10-month-old infant has no flexion at the elbows, mild flexion contractures at the wrist, a rigid clubfoot deformity on the left foot, and a rigid rocker bottom deformity on the right foot. Examination of the patient's hips reveals limited
Explanation
Question 20
A 17-year-old high school football linebacker sustains an injury while making a tackle. His initial symptoms are right shoulder pain, bilateral biceps weakness, and right arm numbness. The symptoms only last a few minutes, and he continues to play in the game. He tells his parents after the game, and they bring him to your office for evaluation the next day. He no longer has any symptoms, and his examination findings and cervical spine radiographs are normal. What is the best next step?
Explanation
Question 21
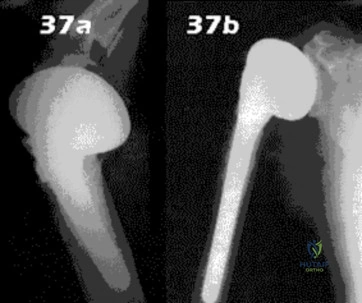
- Figures 37a & 37b show radiographs of a right handed, 78 year old man who had painful G-H arthritis, moderate limitation of motion, and good strength prior to replacement of the humeral head 2 years ago. At the time of treatment, the rotator cuff was intact. He now has limited motion, weakness, and persistent pain in the shoulder. What is the most likely diagnosis?
Explanation
The referenced text states that the most frequent complications in shoulder hemiarthroplasty are due to rotator cuff and tuberosity problems or postoperative instability. Return of motion is expected to be two-thirds to three fourths of pre-operative. 80-90% of patients undergoing hemiarthroplasty experience pain relief. Of the 10-20% who fail to get relief, conversion to total shoulder arthroplasty should be considered. The referenced article discusses the excellent results of TSA and not the reasons for hemi failure. The point strongly emphasized in the article was that for those patients requiring conversion to TSA, strongly suspect infection.
Question 22
A 35-year-old woman with type 1 diabetes mellitus has been treated for the past 2 years at a wound care center for persistent bilateral fifth metatarsal head ulcers. Management has consisted of shoe wear modifications, treatment with multiple enzymatic ointments, and a fifth metatarsal head resection on the left side. Physical examination reveals intact pulses, minimal ankle dorsiflexion, neutral hindfoot, and a persistent ulcer under the fifth metatarsal heads. What treatment will best help heal the ulcers?
Explanation
REFERENCES: Laughlin RT, Calhoun JH, Mader JT: The diabetic foot. J Am Acad Orthop Surg 1995;3:218-225.
Aronow MS, Diaz-Doran V, Sullivan RJ, et al: The effect of triceps surae contracture force on plantar foot pressure distribution. Foot Ankle Int 2006;27:43-52.
Question 23
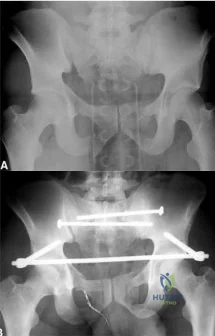
A 39-year-old female presents with the following motor vehicle crash with the injury seen in Figure A (immobilized in a pelvic binder). The iatrogenic neurologic injury most commonly caused by placement of the anterior construct for this injury, as shown in Figure B, would cause which of the following?
Explanation
Unstable pelvic fractures can be treated in a multitude of ways. The ASIF construct is typically created by placing long pelvic screws or polyaxial pedicle screws in the supraacetabular region, similar to the supraacetabular pins for an anterior external fixator. Then a curved bar is placed subcutaneously and connected to the supraacetabular screws. They are typically removed after 3-4 months when fracture healing is complete.
Vaidya et al. present a retrospective review of the use of ASIF as definitive treatment of unstable pelvic fractures. All patients in the study tolerated the construct well. LFCN irritation was seen in 30% of patients, and resolved in all but one patient.
Müller et al. present a retrospective review of the use of posterior stabilization and ASIF. They report an acceptably low complication rate, and good to excellent outcomes in 64.5% of patients.
Figure A is a radiograph demonstrating a right APC3 and left APC2 pelvic injury, imaged in a pelvic binder. Figure B is a postoperative radiograph following posterior stabilization and ASIF.
Incorrect answers:
Question 24
A patient who underwent a L4-L5 hemilaminotomy and partial diskectomy for radiculopathy 8 weeks ago now reports increasing low back pain without neurologic symptoms. A sagittal T2-weighted MRI scan is shown in Figure 13a, and a contrast enhanced T1-weighted MRI scan is shown in Figure 13b. What is the most appropriate management for the patient’s symptoms? Review Topic

Explanation
pseudomeningocele is not present. A revision diskectomy is useful for recurrent radiculopathy but would not be helpful for degenerative low back pain.
(SBQ12SP.29) A 17-year-old female is undergoing posterior instrumented fusion from T5-T12 for adolescent idiopathic scoliosis. At the time of the correction maneuver, the neurophysiologist notifies you of a 60% decrease in somatosensory evoked potential (SSEP) amplitude throughout bilateral lower extremities. Which of the following is an acceptable approach to manage this finding? Review Topic
Immediate wake-up test with examination for clonus
Drop the mean arterial pressure (MAP) to ~60mmHg
Discontinue instrumentation and optimize MAP to 85mmHg or greater
Immediate infusion of intravenous corticosteroids
Modification of the anesthesia plan to include inhalational agents only followed by repeated SSEP testing
The patient has a significant drop in SSEP amplitudes at the completion of the corrective maneuver. The most appropriate response is to raise the MAP to 85 mmHg or greater, discontinue the instrumentation, re-evaluate the SSEPs, and if there is no improvement, to consider reversing the reduction of the deformity.
Intra-operative neurophysiologic monitoring is an effective method to monitor insults to the spinal cord and its exiting roots during spinal instrumentation. The common measurements include SSEPs, which monitor sensory potentials transmitted through the dorsal column system, and motor-evoked potentials (MEPs), which monitor motor response to a trans-cranial stimulus. Decreases in amplitude and latency of the circuits are recorded, however diminished signal amplitudes are more sensitive for neurologic injury, and decreases of of >50-60% being highly concerning. The wake-up test involves reversal of anesthesia so that an intra-operative neurologic examination can be performed.
Devlin et al. reviewed the basic science and practice of neurophysiologic monitoring in spine surgery. They proposed an algorithmic approach to managing intraoperative alerts which include discontinuation of inhalational anesthetics, increasing the MAP to >90 mmHg, discontinuing instrumentation, and performing a wake-up test if neurologic signals fail to normalize.
Herdmann et al. reviewed the practice of neurophysiologic monitoring and the effects of anesthesia upon signal transduction. They report that anesthesia affecting a neuron's intrinsic excitability can alter the results of monitoring. Inhalational anesthetics and decreased MAPs can be responsible for decreased amplitudes.
Vitale et. al. developed a consensus-based intraoperative checklist for management of lost neuromonitoring signals. In this checklist, the first steps across the surgical and anesthetic teams should include: stop the case and announce signal losses to the room, optimize the mean arterial pressure, discuss the status of anesthetic agents, and discuss reversible surgical actions just prior to signal loss.
Incorrect
Question 25
Which of the following is helpful on physical examination to diagnose a fixed posterior shoulder dislocation? Review Topic
Explanation
Question 26
A 56-year-old woman undergoes an arthroscopic rotator cuff repair for a two-tendon retracted tear (supraspinatus and infraspinatus), requiring the use of four suture anchors placed in a double row technique. At her 1 month follow-up visit, what is the appropriate recommendation for her continued rehabilitation program? Review Topic
Explanation
Question 27
Which of the following illustrations shown in Figures 21a through 21e correctly shows the projection of the sacroiliac joint on the outer table of the ilium?
Explanation
REFERENCES: Waldrop JT, Ebraheim NA, Yeasting RA, Jackson WT: The location of the sacroiliac joint on the outer table of the posterior ilium. J Orthop Trauma 1993;7:510-513.
Xu R, Ebraheim NA, Yeasting RA, Jackson WT: Anatomic considerations for posterior iliac bone harvesting. Spine 1996;21:1017-1020.
Question 28
The usual presentation of traumatic subscapularis tears is most often seen after forced
Explanation
REFERENCES: Kreuz PC, Remiger A, Erggelet C, et al: Isolated and combined tears of the subscapularis tendon. Am J Sports Med 2005;33:1831-1837.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 29
During anterior surgery on the cervical spine, at what level would the lateral dissection of the longus coli muscle most likely cause Horner’s syndrome?
Explanation
REFERENCE: Ebraheim NA, Lu J, Yang H, Heck BE, Yeasting RA: Vulnerability of the sympathetic trunk during the anterior approach to the lower cervical spine.
Spine 2000;25:1603-1606.
Question 30
What is the most common complication of using structural bulk allograft to reconstruct segmental defects of the acetabulum?
Explanation
REFERENCES: Jasty M, Harris WH: Salvage total hip reconstruction in patients with major acetabular bone deficiency using structural femoral head allografts. J Bone Joint Surg Br 1990;72:63-67.
Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Kwong LM, Jasty M, Harris WH: High failure rate of bulk femoral head allografts in total hip acetabular reconstructions at 10 years. J Arthroplasty 1993;8:341-346.
Question 31
…The patient underwent an uneventful arthroscopic repair and did well until 1 year later when she crashed during a race. She tore her anterior cruciate ligament (ACL) and underwent reconstruction. Followup after her successful ACL reconstruction reveals complaints of new shoulder pain and posterior instability from using crutches after her ACL surgery. A new MRI scan is shown in Figure 24. What factors are most likely associated with this patient’s recurrence?
Explanation
Question 32
A 31-year-old woman underwent a left Kidner procedure 3 months ago. She now has pain overlying the medial column of the foot. She withdraws the foot when touching of the medial foot is attempted. Examination reveals allodynia, pain, hyperalgesia, and edema of the medial foot. What is the most likely diagnosis?
Explanation
Question 33
Based on the findings seen in the radiograph in Figure 26, emergent management should consist of
Explanation
REFERENCES: Isenberg J, Prokop A, Schellhammer F, et al: Palmar lunate dislocation. Unfallchirurg 2002;105:1133-1138.
Ruby LK: Fractures and dislocations of the carpus, in Browner BD, Jupiter JB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1367-1372.
Question 34
After trial placement of components in a primary total knee arthroplasty, the knee is unable to come to full extension, but the flexion gap is appropriately balanced. After adequate soft-tissue releases have been performed, what is the next most appropriate action to balance the reconstruction?
Explanation
REFERENCES: Ayers DC, Dennis DA, Johanson NA, et al: Common complications of total knee arthroplasty. J Bone Joint Surg Am 1997;79:278-311.
Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 281-286.
Question 35
This medication, a factor Xa inhibitor, currently is not approved for venous thromboembolism (VTE) prophylaxis.
Explanation
Warfarin has a long clinical track record and is well known among most physicians. It is a vitamin K antagonist that can be monitored with prothrombin time (INR) testing and reversed with vitamin K and fresh frozen plasma if needed. Newer oral anticoagulants are becoming more common and offer the advantage of being rapidly active without a need for monitoring. These oral anticoagulants are not reversible, which can complicate the treatment of patients who present with bleeding or require surgery. Dabigatran (Pradaxa) is a direct thrombin inhibitor that is approved for stroke prevention in atrial fibrillation. It is not reversible, and a surgical delay of 24 to 48 hours is recommended for all but emergent surgeries. A longer delay is recommended with renal insufficiency. Rivaroxaban (Xarelto) is an oral factor Xa inhibitor that is approved for atrial fibrillation and the treatment of VTE and deep vein thrombosis prophylaxis. It offers the advantage of daily dosing. It
is not reversible and a surgical delay of 36 to 48 hours is recommended. Apixaban (Eliquis) is another factor Xa inhibitor for which twice-daily dosing is required. It is currently approved for stroke prevention in atrial fibrillation, and a surgical delay of 36 to 48 hours is recommended.
RECOMMENDED READINGS
Gonsalves WI, Pruthi RK, Patnaik MM. The new oral anticoagulants in clinical practice. Mayo Clin Proc. 2013 May;88(5):495-511. doi: 10.1016/j.mayocp.2013.03.006. Review. Erratum in: Mayo Clin Proc. 2013 Jul;88(7):777. PubMed PMID: 23639500. View Abstract at PubMed Alquwaizani M, Buckley L, Adams C, Fanikos J. Anticoagulants: A Review of the Pharmacology, Dosing, and Complications. Curr Emerg Hosp Med Rep. 2013 Apr 21;1(2):83-97. Print 2013 Jun. PubMed PMID: 23687625. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 100 AND 101
A 55-year-old woman slipped on ice while getting out of her car and sustained the injury shown in Figure 100.

Question 36
Which of the following conditions precludes performing a tendon transfer?
Explanation
REFERENCES: Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. St Louis, MO, Mosby, 2003, pp 1283-1287.
Coughlin MJ, Mann RA: Disorders of tendons, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 786-861.
Question 37
An 18-month-old child was involved in a motor vehicle accident and sustained an isolated injury to the left upper extremity. A radiograph is shown in Figure 33. What is the most appropriate management for this injury?

Explanation
Question 38
A 15-year-old boy has hindfoot pain and very limited subtalar motion. A CT scan reveals a talocalcaneal coalition involving 40% of the middle facet. He has no degeneration of the posterior subtalar facet. Following failure of nonsurgical management, treatment should consist of
Explanation
REFERENCES: Sullivan JA: The child’s foot, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 2, pp 1077-1135.
Scranton PE Jr: Treatment of symptomatic talocalcaneal coalition. J Bone Joint Surg Am 1987;69:533-539.
Question 39
A 13-year-old gymnast presents with ongoing knee pain for the past few months. She tried conservative measures including kinesiotaping, physical therapy and rest. On physical exam, she has normal valgus alignment, negative patellar tilt and discomfort with resisted open chain knee extension. A representative radiographs are shown in Figure A-C. What is the most likely clinical diagnosis? Review Topic

Explanation
Evaluation of a patient with patellofemoral pain requires a physical examination and plain radiographs. Appropriate examination of all structures around the knee is critical to rule out other diagnoses. An MRI is useful for evaluating intra-articular or intra-osseous lesions, if clinical suspicion is suggestive of this. Treatment is predominantly conservative, with focus on low impact exercises that maximize aerobic conditioning.
Earl et al. review the epidemiology, etiology and management of patellofemoral syndrome. They note that there is no clear cause of this issue, although issues related to the quadriceps and dynamic malalignment may be contributory.
Outerbridge et al. describe overuse injuries in the young athletic patient. They provide an overview of diagnosis and management specific to this patient population.
Figures A, B and C show AP, lateral and merchant radiographs of a normal knee in a skeletally immature individual. No osseous abnormalities are identified.
Incorrect
Question 40
A 52-year-old, right hand dominant man comes for evaluation of right shoulder pain that has been intermittently bothering him for three months. The pain is worse with overhead activities. He denies any history of trauma. His range of forward elevation in the plane of the scapula is painful and is limited to 145 degrees, compared to 170 degrees on his unaffected side. A radiograph is shown in Figure A. He saw another orthopedist a month ago, who ordered an MRI, which showed a small, partial thickness supraspinatus tendon tear. He received a subacromial injection of lidocaine at that time which temporarily relieved 90 percent of the pain he felt with passive forward elevation of his shoulder past 90 degrees. Today he is requesting a subacromial injection of platelet rich plasma (PRP). You tell him that with regard to pain, function and range of motion, subacromial injection of PRP: Review Topic

Explanation
PRP injection.
Platelet rich plasma has been used for the treatment of chronic tendinopathy in different areas with mixed results. No benefit to patients with symptoms of subacromial impingement has been demonstrated for subacromial injection of PRP, when added to a standard therapy program.
Kesikburun et al. conducted a randomized controlled trial in which patients with rotator cuff tendinopathy or partial rotator cuff tears were randomized to receive ultrasound-guided subacromial injection of either PRP or lidocaine, followed by a standard six-week therapy program. The authors found no difference in pain, range of motion or validated outcome scores at one year follow up.
Hall et al. reviewed sports medicine applications for PRP. At that time (2009), with regard to PRP, they concluded that there was "little clinical evidence for its use."
Ketola et al. sought to determine the effectiveness of subacromial decompression for the treatment of subacromial impingement syndrome. They randomized 140 patients to a supervised exercise program or arthroscopic subacromial decompression followed by a supervised exercise program. They found no clinically important differences between the two groups at 24 months follow up.
Figure A shows a right shoulder radiograph without osseous pathology. Incorrect answers:
Question 41
- What is the most common nerve injury following a Monteggia fracture-dislocation of the forearm in adults?
Explanation
Question 42
Up to what time frame are the risks minimized in anterior revision disk replacement surgery? Review Topic
Explanation
Question 43
Based on the findings shown in Figures 22a and 22b, corrective surgery to obtain maximal safe correction and optimal instrumentation fixation should be performed at which of the following locations?
Explanation
REFERENCES: Shufflebarger HL, Clark CE: Thoracolumbar osteotomy for postsurgical sagittal imbalance. Spine 1992;17:S287-S290.
Murrey DB, Brigham CD, Kiebzak GM, et al: Transpedicular decompression and pedicle subtraction osteotomy (eggshell procedure): A retrospective review of 59 patients. Spine 2002;27:2338-2345.
Question 44
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management? Review Topic
Explanation
Question 45
Early postoperative infections following primary total hip arthroplasty are most likely caused by which organism?
Explanation
S aureus is the most common organism cultured in early (fewer than 4 weeks postoperative) periprosthetic infections. Methicillin-resistant S aureus is becoming a more common pathogen in certain patient populations. B hemolytic Streptococcus and some gram-negative infections can also be found in early postoperative infections. S epidermidis, S viridans, and P acnes are more commonly found in late (more
than 4 weeks postoperative) infections.
Question 46
A 19-year-old girl has had pain and swelling in the right ankle for the past 4 months. She denies any history of trauma. Examination reveals a small soft-tissue mass over the anterior aspect of the ankle and slight pain with range of motion of the ankle joint. The examination is otherwise unremarkable. A radiograph and MRI scan are shown in Figures 45a and 45b, and biopsy specimens are shown in Figures 45c and 45d. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 198-199.
Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 200-202.
Question 47
- A consecutive series of 50 patients is randomized to receive either treatment A or treatment B. At a 10-year follow up, patient satisfaction with treatment is measured. Which of the following statistical calculations will provide the most information regarding the magnitude of possible differences between the two groups of patients?
Explanation
Question 48
A 32-year-old man sustains a pilon fracture which is treated initially with a spanning external fixator, as shown in figure A. He is now 3 weeks from injury and skin swelling has subsided significantly. What is the most appropriate definitive treatment?

Explanation
OrthoCash 2020
Question 49
An otherwise healthy 25-year-old man underwent a right anterior cruciate ligament reconstruction with a bone-patellar tendon-bone allograft. Routine preimplantation cultures of the allograft taken by the surgeon were positive for coagulase-negative Staphylococcus 5 days postoperatively. The patient has exhibited no evidence of clinical infection and his postoperative course has been uncomplicated during this time. What is the ideal management of this patient?
Explanation
implanted with a "contaminated" graft develop a clinical infection. The results of the current literature suggest that the treatment of low-virulence organisms is unnecessary if no evidence of clinical infection exists. Preimplantation cultures do not appear to correlate with clinical infection. Therefore, the routine culture of allograft tissue is not recommended.
Question 50
A 14-year-old female has anal hemorrhoids. The General Surgical team has asked for a consultation in regards to her history of hand, wrist, and ankle joint pain and swelling over the past 3 years. Her physical examination reveals a swollen left wrist, right knee and left ankle. Lab work shows low hemoglobin, low albumin, elevated erythrocyte sedimentation rate (ESR), elevated antinuclear antibody (ANA) count, and a negative rheumatoid factor. Radiography of the affected joints are normal. What additional work up is required prior to her rectal surgery? Review Topic
Explanation
JIA is a persistent autoimmune inflammatory arthritis lasting more than 6 weeks in a patient younger than 16 years of age. Serologic testing for this condition will usually show elevated ESR/CRP, low hemoglobin, low albumin and an elevated anti-nuclear antibody (ANA) count, as well as negative rheumatoid factor and positive HLA-B27. Radiographs of the c-spine should be considered in patients undergoing intubation as cervical kyphosis, facet ankylosis, and atlantoaxial subluxation is associated with this condition.
Punaro et al. reviewed rheumatologic conditions in children. The typical patient with
oligoarticular JIA is a white female (5:1, F:M), with a peak onset between ages 1 and 3 years. Nearly half of patients have monoarticular involvement, with the knee and ankle being most commonly involved. Uveitis is typically chronic, bilateral, and asymptomatic.
Borchers et al. reviewed juvenile idiopathic arthritis (JIA). They state that no laboratory test can conclusively establish a rheumatic diagnosis. They state that laboratory tests will be negative for systemic inflammation and antinuclear antibody (ANA) test has no use in screening for JIA, as it has a high false positive rate.
Incorrect Answers:
Question 51
A 19-year-old man has had intermittent progressive knee pain with ambulation and pain at night following a rodeo accident 4 weeks ago. Figures 4a through 4e show the radiographs, a bone scan, CT scan, and T2-weighted MRI scan. What is the most likely diagnosis?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 3800-3833.
Question 52
Figure 10 is an anteroposterior pelvis radiograph of an 82-year-old man who had right hip pain that began 2 weeks ago but has since resolved with use of over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs). Currently he has no pain. Examination of his hip shows decreased internal rotation and minimal pain at the extremes of motion. What is the most appropriate treatment at this point?

Explanation
The radiograph shown is consistent with Paget disease of the bone. It demonstrates classic findings of widened lamellae and disorganized sclerotic and lytic areas. The cause is not clearly defined, but may be linked to a viral infection and subsequent alterations of osteoblastic and osteoclastic activity. Most patients are asymptomatic, and Paget disease is often found incidentally on radiographs. In this case, the patient’s symptoms likely were caused by hip arthritis, but Paget disease can cause diffuse bone pain in some cases. Considering the patient’s mild and short-term symptoms, observation and NSAID use is most appropriate. An MRI scan or biopsy is indicated if sarcomatous transformation is suspected, but this condition is rare and is associated with a substantial, unrelenting increase in pain. SPEP and UPEP are tests for multiple myeloma, of which the radiographs show no signs.
RECOMMENDED READINGS
Ralston SH. Pathogenesis of Paget's disease of bone. Bone. 2008 Nov;43(5):819-25. doi: 10.1016/j.bone.2008.06.015. Epub 2008 Jul 11. Review. PubMed PMID: 18672105.View Abstract at PubMed
Bonenberger E, Einhorn T. Metabolic bone diseases. In: Callaghan JJ, Rosenberg
AG, Rubash HE, eds. The Adult Hip. 2nd ed. Philadelphia, PA: Lippincott Williams 14
& Wilkins; 2007:514-533.
Question 53
A 2-year-old girl has had a swollen right knee for the past 7 weeks. There is no history of significant trauma, and she has not had a fever or been ill. Her parents report that she is stiff in the morning but otherwise does not report pain. A CBC count and erythrocyte sedimentation rate are normal. Treatment with naproxen at appropriate doses for the past 2 weeks has resulted in some improvement. Radiographs show only soft-tissue swelling. Examination reveals a healthy-appearing child with a warm and swollen right knee that is only slightly tender but lacks full extension by 20 degrees. What is the next most appropriate step in management?
Explanation
REFERENCES: Wolf MD, Lichter PR, Ragsdale CG: Prognostic factors in the uveitis of juvenile rheumatoid arthritis. Ophthalmology 1987;94:1242.
Cassidy JT, Petty RE: Textbook of Pediatric Rheumatology. Philadelphia, PA, WB Saunders, 2001, p 220.
Chalom ED, Goldsmith DP, Koehler MA, et al: Prevalence and outcome of uveitis in a regional cohort of patients with juvenile rheumatoid arthritis. J Rheumatol 1997;24:2031-2034.
Question 54
What is the most common primary malignant tumor of bone in childhood?
Explanation
REFERENCES: Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 226.
Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 55
A 40-year-old patient who has a type II odontoid fracture is placed in a halo vest for 12 weeks; however, current radiographs show no evidence of healing. The next most appropriate step in management should consist of
Explanation
REFERENCES: Montesano PX: Anterior and posterior screw and plate techniques used in the cervical spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1996, vol 2, pp 1743-1761.
Bohler J: Anterior stabilization for acute fractures and non-unions of the dens. J Bone Joint Surg Am 1982;64:18-27.
Anderson PA, Steinmann JC: Internal fixation of the cervical spine, in Frymoyer JW (ed): The Adult Spine, Principles and Practice, ed 2. Philadelphia, PA, Lippincott Raven, 1997, pp 1119-1147.
Question 56
A 19-year-old collegiate lacrosse player has bilateral lower extremity pain during training runs and practice sessions. She says her pain is only associated with activity, always begins 4 to 5 minutes into an activity, and resolves within 10 minutes after activity cessation. She reports a feeling of numbness and tingling in her first- and second-toe web space with continued activity. She has no pain while at rest and has tried nonsteroidal anti-inflammatory drugs, ice baths, and rehabilitation techniques with her athletic trainers without experiencing noticeable changes. Which test has the highest specificity and sensitivity for the pathology suspected?
Explanation
Chronic exertional compartment syndrome (CECS) is an uncommon cause of pain that is most often encountered in athletes or military populations. The diagnosis is suggested by pain after the start of the activity with resolution of symptoms when the activity stops. Traditionally, the diagnosis was established by measuring intracompartment pressures at 1 and 5 minutes of
activity. Roscoe and associates have shown that using continuous pressure monitoring during the activity until pain forces subjects to stop provides higher sensitivity and specificity than the traditional diagnostic technique. Palpating the leg is not as sensitive or specific as direct pressure monitoring. Although certain changes can be seen on MRI in CECS, this is not the diagnostic study of choice.
Question 57
Figures 18a and 18b show the radiographs of a patient who has pain with walking. On careful questioning, it is determined that the discomfort occurs at push-off, or when the patient attempts to climb stairs. What nonsurgical option is most likely to ameliorate the symptoms?
Explanation
REFERENCES: Bono CM, Berberian WS: Orthotic devices: Degenerative disorders of the foot and ankle. Foot Ankle Clin 2001;6:329-340.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 58-63.
Question 58
When considering a flexor digitorum longus tendon transfer as part of the surgical treatment in patients with symptomatic flatfoot deformity caused by posterior tibial tendon insufficiency, which of the following patients is the most appropriate candidate?
Explanation
REFERENCES: Pedowitz WJ, Kovatis P: Flatfoot in the adult. J Am Acad Orthop Surg 1995;3:293-302.
Mann RA: Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 167-296.
Question 59
A 37-year-old recreational tennis player undergoes surgery for tennis elbow. Following surgery, she describes clicking and popping on the lateral aspect of the elbow. A lateral pivot shift test is positive. What is the most likely cause of her symptoms?
Explanation
REFERENCES: O’Driscoll SW, Morrey BF: Surgical reconstruction of the lateral collateral ligament, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 169-182.
O’Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Question 60
Avascular necrosis
Explanation
A 9-year-old girl sustains an injury (Slide) as a result of a fall. What is her risk of avascular necrosis:
Question 61
The safest surgical approach to the insertion of the tibial posterior cruciate ligament uses the interval between which of the following muscles?
Explanation
inlay reconstruction.
REFERENCES: Berg EE: Posterior cruciate ligament tibial inlay reconstruction. Arthroscopy 1995;8:95-99.
Burks RT, Schaffer JJ: A simplified approach to the tibial attachment of the posterior cruciate ligament. Clin Orthop 1990;254:216-219.
Question 62
-A 42-year-old patient with a right distal radius fracture underwent open reduction and internal fixation. To reduce the likelihood of complex regional pain syndrome, the most appropriate medication is
Explanation

Question 63
A 14-year-old girl reports hip pain that is exacerbated by weight bearing. A radiograph and biopsy specimen are shown in Figures 16a and 16b. The best course of management should be
Explanation
REFERENCES: Azouz EM, Karamitsos C, Reed MH, Baker L, Kozlowski K, Hoeffel JC: Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-420.
Hecht AC, Gebhardt MC: Diagnosis and treatment of unicameral and aneurysmal bone cysts in children. Curr Opin Pediatr 1998;10:87-94.
Question 64
What role does quorum sensing play in the development of a bacterial biofilm?
Explanation
Question 65
The Chi-square test is most appropriate for which of the following?
Explanation
When considering which statistical test to use the investigator must consider how many groups are being compared, and if the data collected is numerical or categorical, and parametric or non-parametric. When the study is comparing proportions of categorical data the appropriate test will be either a Chi-square test, or a Fisher exact test. The Fisher exact test is preferred when there is less than 5 data points in any group being compared.
Illustration A is a flow chart demonstrating how to determine which statistical test is most appropriate.
Incorrect answers:
with the Mann-Whitney U test Answer 3: Comparing means of parametric data between 3 or more groups is best done with Analysis of variance (ANOVA) Answer 5: Comparing proportions of categorical data between groups when at least one group has less than 5 samples or data points is best done with the Fisher exact test
Question 66
Within the menisci, the majority of the large collagen fiber bundles are oriented in what configuration?
Explanation
REFERENCES: Mow VC, et al: Structure and function relationships of the menisci of the knee, in Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, pp 37-57.
DeHaven KE, Arnoczky SP: Meniscus repair: Basic science, indications for repair, and open repair. Instr Course Lect 1994;43:65-76.
Question 67
An 76-year-old woman falls from standing and sustains the injury shown in Figure A. Her most recent T score was -1.9, 3 months prior to presentation. If labwork were performed, which values would be consistent with her bone density score?

Explanation
In the setting of osteopenia/osteoporosis, there is a positive feedback to increase PTH in response to low serum calcium levels. In response, there is a corresponding increase in alkaline phosphatase and decrease in phosphorous and circulating vitamin D levels.
Fraser writes a concise, yet thorough synopsis on primary and secondary hyperparathyroidism. In the article, the summary regarding osteopenia/osteoporosis (typically a state of hypovitamin D) begins by stating an initial state of decreased ionised calcium, which increases PTH, results in 3 primary effects: an attempt to increase gut absorption of Ca, mobilize Ca from the bone via osteoclasts and activate vitamin D at the kidney (1,25-vitamin D).
Figure A exhibits a left femoral neck fracture, which is a fragility fracture associated with poor bone density. Illustration A is a figure from Fraser's article exhibiting the feedback loop from the hypothalamus, pituitary, adrenal/glandular axis.
Incorrect answers:
Question 68
The great medullary artery, also known as the Adamkiewicz artery, originates from which of the following arteries?
Explanation
REFERENCES: Lu J, Ebraheim NA, Biyani A, Brown JA, Yeasting RA: Vulnerability of great medullary artery. Spine 1996;21:1852-1855.
Rogers FB, Osler TM, Shackford SR, Wald SL: Isolated stab wound to the artery of Adamkiewicz: Case report and review of the literature. J Trauma 1997;43:549-551.
Question 69
A 14-year-old girl has had progressive heel pain for the past several months. Based on the radiograph, MRI scan, and biopsy specimens shown in Figures 37a through 37d, treatment should include
Explanation
blood-filled spaces with bland fibrous connective tissue septa. The stroma has histiocytes, fibroblasts, scattered giant cells, hemosiderin, and occasional inflammatory cells. Treatment of these lesions consists of extended curettage, plus or minus the use of adjuvants (liquid nitrogen, phenol, argon beam coagulation), and finally filling the bone void (allograft or other bone substitute).
REFERENCES: Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
Ramirez AR, Stanton RP: Aneurysmal bone cyst in 29 children. J Pediatr Orthop 2002;22:533-539.
Question 70
A 74-year-old woman with rheumatoid arthritis reports shoulder pain that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 23a and 23b. Examination reveals active forward elevation to 120 degrees and external rotation to 30 degrees. What treatment option results in the most predictable pain relief and function? Review Topic

Explanation
Question 71
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
Explanation
REFERENCES: Waters PM, Mih AD: Fractures of the distal radius and ulna, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, p 361.
Paley D, McMurtry RY: Median nerve compression by volarly displaced fragments of the distal radius. Clin Orthop Relat Res 1987;215:139-147.
Question 72
When discussing treatment options with a 35 year-old healthy male with an isolated, closed tibial shaft fracture, the surgeon should inform him that in comparison to closed treatment, the advantages of intramedullary nail fixation include all of the following EXCCEPT?

Explanation
In a study of 94 tibial fractures, Finkemeier reported 10 (11%) had compartment syndromes. Three of the 10 patients developed the compartment syndrome postoperatively.
In comparing IM nailing to non-op, Bone et al showed that IM nailing had a shorter time to union (mean, 18 vs 26 weeks; p = 0.02), lower non-union rate (2% vs 10%), decresed incidence of shortening (2% vs 27%), and quicker return to work (mean, 4 vs 6.5 months), but no difference in compartment syndrome (0% in both groups).
The classic article cited by Sarmiento el al. reported that closed treatment with use of a prefabricated functional below-the-knee brace was effective in a study of 1000 closed diaphyseal fractures of the tibia with an incidence of nonunion of only 1.1%. However, those authors had very strict criteria for use of the fracture-brace (exclusion criteria included intact fibular, shortening >2cm).
Question 73
A 48-year-old man is brought in by emergency services after falling down a flight of stairs. He complains of weakness in both hands. Examination reveals weak grip bilaterally. Injury CT scans are shown in Figure A. What is the most appropriate treatment option? Review Topic
Explanation
The C-spine is the most common site of fracture in AS and is most susceptible to hyperextension injuries. When surgical intervention is required, multiple points of fixation both above and below the fracture are necessary. This is due to co-existing osteoporosis and abnormally increased forces from long lever arms of the ankylosed spine, both of which make the construct susceptible to failure and screw pullout.
Kubiak et al. reviewed the orthopaedic management of AS. They report bone scan, MRI or fine-cut CT is necessary because fractures are often missed on plain x-rays because of distortion of anatomy or difficulty with positioning.
Whang et al. reviewed spinal injuries in 12 patients with AS and 18 patients with DISH. Most injuries involved C5-C7. Patients with AS were more likley to have severe neurologic injury (41% ASIA A) than DISH (44% ASIA E). There was 81% good-excellent outcome and 4 deaths related to halo vest use.
Figure A is a sagittal CT reconstructed image showing a nondisplaced shear fracture through the C6 vertebral body and C5 posterior elements. Illustrations A and B are postop AP and lateral radiographs showing posterior decompression and C3-T2 fusion with lateral mass fixation in the cervical spine and pedicle screw fixation in the upper thoracic spine.
Incorrect Answers:
performed through a posterior approach. If there is significant osteoporosis and the risk of construct failure is high, a 360-approach may be necessary.
Question 74
You are evaluating a patient with recurrent patellar instability who has failed conservative management. MRI demonstrates articular cartilage loss in the patella. In addition to a cartilage restoration procedure, you recommend the procedure depicted in Figures A and B. Which of the following imaging findings best supports your decision? Review Topic

Explanation
Recurrent patellar instability is often associated with chondral lesions of the patellofemoral joint. In addition to managing the cartilage injury, the underlying etiology of the instability must also be addressed to ensure a successful outcome. Patellar instability may arise from coronal or rotational malalignment, patella alta, trochlear dysplasia or damage to soft tissue restraints including the medial patellofemoral ligament (MPFL). Rotational malalignment, defined by a TT-TG distance > 20mm, can be addressed by AMZ. Medialization of the tubercle restores a normal TT-TG distance while anteriorization of the tubercle unloads patellofemoral contact forces.
Beck et al performed a cadaveric study measuring patellofemoral contact pressures on the trochlear surface following AMZ. They found that anteromedialization decreased the mean contact pressures and shifted contact pressures to the medial trochlea. The authors concluded that while this procedure successfully unloads the lateral trochlea, it likely has minimal benefit for central chondral defects and may be detrimental for medial chondral defects where contact pressures are increased.
Strauss et al authored a review article detailing the surgical treatment options for patellofemoral cartilage lesions, including concomitant realignment/unloading procedures. AMZ is designed to correct rotational malalignment while unloading the patellofemoral compartment in the setting of cartilage restoration surgery. While AMZ has demonstrated good outcomes for lesions located in the lateral facet or distal
pole of the patella, poor outcomes have been seen with medial facet or central trochlear lesions.
Figures A and B are the AP and lateral radiographs, respectively, of a knee s/p AMZ, also know as a Fulkerson procedure. Illustration A is an algorithm detailing the approach to recurrent patellar instability in both skeletally immature and mature patients. Illustration B demonstrates how to measure the TT-TG distance, the distance between two lines drawn perpendicular to the posterior condylar axis to the tibial tubercle and deepest portion of the trochlear groove (normal 8-10mm). Illustration C depicts the measurement of the femoral trochlear angle or sulcus angle (normal 137°
+/- 8°). Illustration D shows how to measure lateral patellar tilt (normal < 5°). Illustration E is a postoperative radiograph after AMZ. A long (> 5cm) and thick (> 0.75cm) osteotomy cut is required to allow adequate fixation with two screws.
Incorrect Responses:
Question 75
A 36-year-old woman has neck pain in the upper cervical region and occipital discomfort after being involved in a motor vehicle accident. Examination reveals no forehead or scalp lacerations. The neurologic examination is normal. A CT scan shows no evidence of bony injury. Figures 39a and 39b show a lateral radiograph and an MRI scan. Management should consist of
Explanation
REFERENCES: Kurz LT: Transverse atlantal ligament insufficiency, in Clark CR (ed):
The Cervical Spine. Philadelphia, PA, Lippincott-Raven, 1998, pp 401-407.
Fielding JW, Cochran GB, Lansing JF III, et al: Tears of the transverse ligament of the atlas:
A clinical and biomechanical study. J Bone Joint Surg Am 1974;56:1683-1691.
Question 76
An adult with a distal humeral fracture underwent open reduction and internal fixation. What is the most common postoperative complication?
Explanation
REFERENCES: Webb LX: Distal humerus fractures in adults. J Am Acad Orthop Surg 1996;4:336-344.
McKee MD, Wilson TL, Winston L, et al: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Question 77
What structure is marked Q in the diagram of the brachial plexus shown in Figure 22?
Explanation
REFERENCES: Anderson JE (ed): Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Williams and Wilkins, 1978, pp 6-24.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 63.
Question 78
A 26-year-old man is brought to the emergency department unresponsive and intubated after being found lying on the side of the road. He has a Glasgow Coma Scale score of 6. A chest tube has been inserted on the right side of the chest for a pneumothorax. An abdominal CT scan reveals a small liver laceration and minimal intraperitoneal hematoma. A pneumatic antishock garment (PASG) is on but not inflated. He has bilateral tibia fractures. A pelvic CT scan shows an anterior minimally displaced left sacral ala fracture and left superior and inferior rami fractures. He has received 2 L of saline solution and 4 units of blood but remains hemodynamically unstable. What is the next most appropriate step in management?
Explanation
REFERENCES: Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: Effective classification system and treatment protocols. J Trauma 1990;30:848-856.
Evers BM, Cryer HM, Miller FB: Pelvic fracture hemorrhage: Priorities in management. Arch Surg 1989;124:422-424.
Flint L, Babikian G, Anders M, Rodriguez J, Steinberg S: Definitive control of mortality from severe pelvic fracture. Ann Surg 1990;211:703-707.
Question 79
A 47-year-old woman has had a 1-month history of left hip and medial thigh pain that is exacerbated by sitting. Laboratory studies show a total protein level of 8.2 g/dL (normal 6.0 to 8.0) and an immunoglobulin G (IGG) level of 2,130 mg/dL (normal 562 to 1,835). A radiograph, CT scan, and biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 16.
Question 80
Following a partial muscle laceration, keeping the affected extremity immobilized for 2 weeks before starting an exercise program will likely lead to: Review Topic
Explanation
Healing a muscle injury involves two competing processes: regeneration of muscle fibers and formation of granulation tissue. Starting motion too soon after injury may increase the area of fibrous scar, and limit the ability of new muscle fibers to penetrate this area. Prolonged immobilization limits scar production but penetrating muscle fibers will lack appropriate orientation, and the muscle as whole begins to atrophy. Three to 5 days of immobilization has been shown to limit scar tissue production
while the early motion helps generate appropriately organized muscle fibers and maintain strength and range of motion.
Järvinen et al. present a review of muscle injury and healing. They found that immediate mobilization led to a large area of dense scar tissue that regenerating muscle fibers could not adequately penetrate. Prolonged immobilization allowed muscle fibers to regenerate but they lacked appropriate morphology. Following 3-5 days of immobilization they found less scar tissue, better penetration of regenerated muscle fibers, and the regenerated fibers were more well aligned with the uninjured fibers surrounding them.
Menetrey et al. present a mouse model of muscle laceration comparing a short period of immobilization (5 days) to suture repair of the muscle. They found quicker healing and greater strength in the suture repair group. Tetanus strength at one month after injury was (compared to an uninjured control) 81% for sutured muscle, 35% for the early mobilization only group, and 18% for the prolonged immobilization group.
Illustration A is a histology section of lacerated muscle after 7 days of immobilization. The area is infiltrated with granulation tissue and few regenerating myofibers. Illustration B is a histology section of lacerated muscle after 14 days of immobilization. Further infiltration with granulation tissue and mononuclear cells can be seen with regenerating myofibers only at the periphery.
Incorrect answers:
Question 81
What is the most common reason for reoperation in total knee arthroplasty?
Explanation
REFERENCES: Blasier RB, Matthews LS: Complications of prosthetic knee arthroplasty, in Epps CH (ed): Complications in Orthopaedic Surgery. Philadelphia, PA, JP Lippincott, 1994, pp 1066-1069.
Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620.
Wilson MG, Kelley K, Thornhill TS : Infection as a complication of total knee-replacement arthroplasty: Risk factors and treatment in sixty-seven cases. J Bone Joint Surg Am 1990;72:878-883.
Question 82
Figures 45a through 45c show the radiograph, CT scan, and MRI scan of a 15-year-old boy who has lateral ankle pain. What is the most likely diagnosis?
Explanation
REFERENCES: Richardson EG: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 702-732.
Oestreich AE, Mize WA, Crawford AH, et al: The “anteater nose”: A direct sign of calcaneonavicular coalition on the lateral radiograph. J Pediatr Orthop 1987;7:709-711.
Question 83
Which of the following is most commonly inherited as a X-linked recessive disorder? Review Topic
Explanation
Duchenne's muscular dystrophy is caused by a mutation in the dystrophin gene. X-linked recessive inheritance is a mode of inheritance in which a mutation in a gene on the X chromosome causes the phenotype to be expressed (1) in males (who are necessarily hemizygous for the gene mutation because they have only one X chromosome) and (2) in females who are homozygous for the gene mutation (i.e., they have a copy of the gene mutation on each of their two X chromosomes).
Zane reviewed paediatric neuromuscular disorders. Duchenne's muscular dystrophy patients will show markedly elevated CPK levels (10-200x normal). Muscle biopsy will show connective tissue infiltration, foci of necrosis and absent dystrophin with staining.
Illustration A shows an illustration of Gowers sign. This indicates weakness of the proximal muscles. It is characteristic of patients with Duchenne's muscular dystrophy.
Incorrect Answers:
Question 84
Which of the following represents a contraindication for interspinous process decompression for the treatment of lumbar spinal stenosis? Review Topic
Explanation
Question 85
A 4-year-old boy sustains the injury shown in Figures 10a and 10b as a result of being hit and dragged by a car. Wound closure is best accomplished by
Explanation
healing and survival of the underlying structures, prevent infection, and provide a durable and/or flexible cover. Furthermore, the standard cross-leg flap no longer is used because of significant problems with positioning and joint stiffness, and because it provides inadequate coverage material. For the various surfaces of the ankle and dorsum of the foot, very few local tissues are available to provide coverage when free skin grafting is insufficient. Thus, out of the possible answers, free rectus abdominis flap is the preferred response.
Question 86
A 30-year-old accountant and recreational softball player, who is seen at the end of his baseball season, reports a several month history of pain along the medial side of his dominant elbow. He cannot identify a specific injury and notes it only hurts when he throws the ball in from the outfield. Besides the pain, he remarks that his speed and distance while throwing have diminished considerably. Examination reveals tenderness along the medial elbow but no weakness or gross instability is found. Radiographs are normal. Based on the history, what is the most likely diagnosis? Review Topic
Explanation
the forearm during resisted forearm pronation and is not associated with the throwing motion in particular. Valgus extension overload may mimic medial collateral ligament injury, not varus extension injuries. Medial epicondylitis may be confused with ligament insufficiency but the examination and a history of pain only while throwing make this an unlikely diagnosis.
Question 87
- Figure 67 shows the AP radiograph of both knees of a 26-year-old woman. A review of the patient’s medical record will most likely reveal a history of
Explanation
Question 88
Which of the following best describes the course of the median nerve at the elbow?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8,
pp 46-47.
Question 89
Osteoporotic vertebral compression fractures are associated with Review Topic
Explanation
Question 90
A further workup reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MARS MR imaging. Revision THA is recommended. The most common complication following revision of a failed metal-on-metal hip arthroplasty is
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on-metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.
The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts.
The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 91
- A 14-year-old patient who has homocystinuria and is Risser 3 is referred for surgical treatment of scoliosis. In addition to the usual risks associated with posterior spinal fusion, the family should be advised that the patient ‘s underlying condition significantly increases the perioperative risk of
Explanation
1 and 2 are concerns during spinal fusion but are not specific to this disease. 4 may occur with homocystinuria but is not related to spinal fusion. 5 occurs with PSF in the younger population because of the growth potential remaining.
Question 92
Figures 9a and 9b show the spinal radiographs of a 3-year-old child with short limb dwarfism. The lateral radiograph is obtained with maximal lumbar extension. Management should consist of
Explanation
REFERENCE: Pauli RM, Breed A, Horton VK, Glinski LP, Reiser CA: Prevention of fixed angular kyphosis in achondroplasia. J Pediatr Orthop 1997;17:726-733.
Question 93
Which of the following best describes the recommended treatment for a 13-year-old pitcher with a painful chronic stress injury to the proximal humeral physis as confirmed on an MRI scan? Review Topic
Explanation
Question 94
When performing a cruciate-retaining total knee arthroplasty, trial components are inserted. The knee comes to full extension but is tight in flexion. The surgeon should consider
Explanation
In this scenario, the flexion gap needs to be increased. Increase in flexion gap can be accomplished by downsizing the femoral component and increasing posterior tibial slope. In posterior cruciate-retaining TKA procedures, recession or release of the posterior cruciate ligament can loosen the flexion gap, allowing for an increase in flexion. Flexing the femoral
component tightens the flexion gap, and downsizing the tibial insert thickness decreases flexion and extension gaps, while resection of the distal femur only increases the extension gap.

CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 55
Figure 52 is the standing anteroposterior radiograph of a 55-year-old man who has a 5-year history of daily left knee pain with weight-bearing activities. He denies night pain or symptoms of instability. Upon examination his range of motion is 0 to 140 degrees. He has a mild, fully correctable varus deformity and a negative Lachman test result. He has failed nonsurgical treatment.
Question 95
A teenage female is referred to you for evaluation of curvature in her back that was discovered on routine school screening. She is diagnosed with adolescent idiopathic scoliosis. In which of the following scenarios is a bracing program the most appropriate treatment? Review Topic

Explanation
The treatment of adolescent idiopathic scoliosis (AIS) depends on the magnitude and location of curve as well skeletal maturity of the patient. For curves less than 20 degrees, observation is appropriate until skeletal maturity, with closer intervals during
times of peak growth. Curves between 20-25 and 45 degrees in patients who are Risser stage 0,1 or 2 are best treated with bracing to stop progression. Curves with an apex at T7 or below are typically treated with a Boston brace. Curves over 50 degrees generally warrant a discussion about surgery to prevent progression past maturity.
In a landmark study, Weinstein et al. evaluated both a randomized and preference based cohort of bracing versus observation. The trial was stopped early due to efficacy of bracing. The rate of treatment success was 72% after bracing and 48% after observation. Treatment success was strongly correlated to time of brace wear.
Schlenzka et al. reviewed indications, treatment, and complications associated with brace treatment of AIS. They state that further evidence is necessary to evaluate the efficacy of bracing in AIS.
Figure 1, 2, and 3 are radiographs depicting Risser stage 0, 1, and 4 respectively. Illustration B shows radiographs of all Risser stages. Illustration C is the Lenke classification system for idiopathic scoliosis.
Incorrect Answers:
Question 96
A 17-year-old male football player is seen 1 week after developing symptoms of infectious mononucleosis in the middle of the season. Examination reveals evidence of splenomegaly. He and his parents want to know if he can play in a game the following day. What is the most appropriate recommendation? Review Topic
Explanation
Question 97
It is recommended that invasive dental work be completed prior to the initiation of which of the following medications?
Explanation
Bisphosphonates are a class of drugs that prevent bone mass loss by inhibiting osteoclast resorption. They are used in the treatment of vertebral compression fractures, non-vertebral fragility fractures, osteogenesis imperfecta, multiple myeloma, and avascular necrosis. Because bisphosphonates have been associated with osteonecrosis of the jaw, it is suggested that all invasive dental work be completed prior to initiation of treatment.
Pazianas et al. (2011) review the safety profile of bisphosphonates. Specifically, they cite gastrointestinal discomfort, atypical femur fractures, osteonecrosis of the jaw, ocular inflammation, and musculoskeletal pain as common side effects. They state there is limited evidence surrounding bisphosphonate's association with esophageal cancer and atrial fibrillation.
Pazianas et al. (2007) reviewed 11 publications that reported 26 cases of osteonecrosis of the jaw following initiation of bisphosphonate treatment. Age >60 years, female sex, and previous invasive dental treatment were the most common characteristics of those who developed ONJ.
Illustration A shows the various bisphosphonates and their mechanisms of action. Illustration B shows an example of osteonecrosis of the jaw, a side effect that has been linked to bisphonphonate treatment.
Incorrect Answers:
Question 98
A 65-year-old woman has nausea, vomiting, and abdominal distention after undergoing total knee arthroplasty 48 hours ago. An abdominal radiograph is shown in Figure 14. Associated risk factors for this disorder include
Explanation
REFERENCES: Iorio R, Healy WL, Appleby D: The association of excessive warfarin anticoagulation and postoperative ileus after total joint replacement surgery. J Arthroplasty 2000;15:220-223.
Clarke HD, Berry DJ, Larson DR: Acute pseudo-obstruction of the colon as a postoperative complication of hip arthroplasty. J Bone Joint Surg Am 1997;79:1642-1647.
Question 99
A middle-aged man sustains traumatic loss of the second, third, and fourth toes in a lawnmower accident. The wound is grossly contaminated with soil. Penicillin is added to his antibiotic regimen for coverage of what bacteria? Review Topic
Explanation
Question 100
Refers to the effectiveness of various antibiotics against a particular microorganism.
Explanation
Knowledge of the basic nomenclature of antibiotic use is important to effectively treat patients and communicate with colleagues. The effectiveness of an antimicrobial against an infecting organism is measured by the MIC, which refers to the concentration needed to prevent growth of a microorganism on culture medium, and MBC, which is the smallest concentration of the antibiotic necessary to kill the microorganism in culture. Typically, an antibiotic is considered bactericidal if the MBC is no more than 4 times the MIC. The spectrum of antimicrobial coverage refers to an agent’s effectiveness against a range of bacteria. An antibiogram refers to the tabulation of prevalence of different bacteria in a specific setting or specific patient population. Antibiotic susceptibility and resistance refers to the bacteria’s ability to be affected or unaffected by a given antibiotic.

