Full Question & Answer Text (for Search Engines)
Question 1:
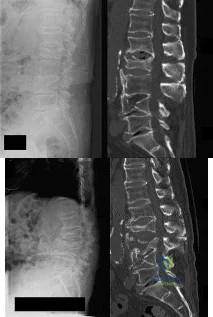
When using surgery extending to the pelvis to treat long spinal deformity in adults, the addition of anterior interbody structural support at the lumbosacral junction serves what biomechanical function?
Options:
- Improves the bone mineral density of the vertebral bodies
- Reduces the strain at the adjacent intervertebral disk
- Reduces the stiffness of the posterior instrumentation
- Reduces the strain on posterior instrumentation
- Increases the strength of the posterior instrumentation
Correct Answer: Reduces the strain on posterior instrumentation
Explanation:
DISCUSSION: Shufflebarger and others have reported that the placement of anterior interbody structural support at the lumbosacral junction increases the overall construct stiffness and reduces the strain on posterior instrumentation, thereby reducing the risk of screw pull-out or fracture. The stiffness of the posterior instrumentation actually increases, whereas the actual strength of the instrumentation remains the same. Actual strain measured at an adjacent intervertebral disk to a fusion construct is expected to increase.
REFERENCES: Shufflebarger HL: Moss-Miami spinal instrumentation system: Methods of fixation of the spondylopelvic junction, in Margulies JI, Floman Y, Farcy JPC, et al (eds): Lumbosacral and Spinal Pelvic Fixation. Philadelphia, PA, Lippincott-Raven, 1996, pp 381-393.
Cunningham BW: A biomechanical approach to posterior spinal instrumentation: principles and applications, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 588-600.
Kostuik JP, Valdevit A, Chang HG, et al: Biomechanical testing of the lumbosacral spine. Spine 1998;23:1721-1728.
Question 2:
A 42-year-old man sustained the periprosthetic fracture shown in Figures 19a and 19b. The femoral component is well fixed. What is the next most appropriate step in management?
Options:
- Closed reduction and bracing
- Retrograde femoral intramedullary nailing
- Open reduction and internal fixation of the fracture, leaving the femoral stem in place
- Open reduction and internal fixation of the fracture and insertion of a proximally porous-coated stem
- Open reduction and internal fixation of fracture fragments and insertion of a fully porous-coated femoral stem with diaphyseal fixation distal to the fracture
Correct Answer: Open reduction and internal fixation of the fracture, leaving the femoral stem in place
Explanation:
DISCUSSION: The patient has a periprosthetic fracture below the femoral stem. The component is porous coated and well fixed. Open reduction and internal fixation, leaving the stem in place, can be performed when bone quality is good. Plating with or without allograft struts and supplemental cerclage fixation generally is acceptable. If the component is loose, revision to a longer device is recommended with appropriate stabilization of the fracture using the aforementioned methods. If bone loss has occurred, allograft supplementation or a tumor prosthesis may be indicated. Fractures located well below the stem tip can be treated without regard for the prosthesis. Closed reduction and bracing is not associated with good results for periprosthetic femoral fractures. Retrograde intramedullary nailing is not appropriate for this fracture.
REFERENCES: Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.
Bono JV, McCarthy JC, Thornhill TS, Bierbaum BE, Turner RH (eds): Revision Total Hip Arthroplasty. New York, NY, Springer Verlag, 1999, pp 530-592.
Question 3:
What is the function of the rotator cuff during throwing?
Options:
- Limits humeral head translation in the transverse plane but not in the sagittal plane
- Limits superior migration but not anterior and posterior translation
- Limits superior migration and anterior and posterior translation
- Provides little control of superior anterior and posterior translation
- Creates inferior migration with maximal contraction during acceleration
Correct Answer: Limits superior migration and anterior and posterior translation
Explanation:
DISCUSSION: The coupled action of the rotator cuff prevents superior migration and controls anterior and posterior translation by depressing the humeral head.
REFERENCES: Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
Abrams JS: Special shoulder problems in the throwing athlete: Pathology, diagnosis, and nonoperative management. Clin Sports Med 1991;10:839-861.
Question 4:
Bone morphogenetic proteins transduce intracellular signal through what class of cell surface receptor?
Options:
- Mitogen-activated protein kinase
- Tyrosine kinase
- Serine-threonine kinase
- Aurora kinase
- Glycogen synthase kinase 3
Correct Answer: Serine-threonine kinase
Explanation:
Bone morphogenetic proteins (BMPs) are extracellular proteins belonging to the TGF-beta superfamily of molecules. Members of this family include BMPs, growth and differentiation factors (GDFs), anti-mnllerian hormone (AMH), activin, Nodal, and TGF-beta. These proteins exert their action by binding to cell surface receptors of the serine-threonine kinase class to activate intracellular signaling pathways. The other kinase participate in various cell signaling functions, but are not associated with BMP.
Question 5:
A 72-year-old man who underwent total shoulder arthroplasty 2 years ago slipped on ice and fell on his shoulder 3 weeks ago. Immediately after falling he was unable to elevate his arm. Motor examination reveals deltoid 5-/5, subscapularis 5-/5, external rotation 4-/5, and supraspinatus 2/5. Radiographs are shown in Figures 8a and 8b. What is the most likely diagnosis? Review Topic
Options:
- Anterior shoulder dislocation
- Humeral component loosening
- Glenoid component loosening
- Glenoid component catastrophic fracture
- Rotator cuff tear
Correct Answer: Rotator cuff tear
Explanation:
The patient has a traumatic rotator cuff tear. The history of the fall, the weakness on examination, and normal radiographic findings make a traumatic rotator cuff tear the most likely diagnosis. An MRI scan can be obtained to further evaluate the integrity of the rotator cuff. The axillary radiograph shows a reduced, nondislocated total shoulder arthroplasty. His radiographs show a well-seated humeral stem and no signs of loosening. The glenoid is a cemented all-polyethylene component with no evidence of radiolucent lines surrounding the cemented pegs. The polyethylene glenoid component is radiolucent; however, the space between the metallic humeral head and the glenoid bone is the thickness of the polyethylene glenoid component. If the humeral head were directly against the glenoid bone, then catastrophic fracture of the glenoid would be the working diagnosis.
Question 6:
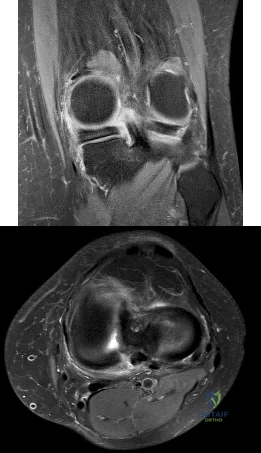
The MRI scan shown in Figure 33 reveals the sequelae of an acute traumatic anteroinferior shoulder dislocation. The image reveals the typical separation of what two commonly injured structures? Review Topic
Options:
- Anteroinferior labrum from the bony glenoid
- Anteroinferior labrum from the cartilaginous surface of the glenoid
- Biceps tendon from its origin on the supraglenoid tubercle
- Anterior capsule from the proximal humerus
- Posteroinferior labrum from the bony glenoid
Correct Answer: Anteroinferior labrum from the bony glenoid
Explanation:
The MRI scan reveals the sequelae of an anteroinferior dislocation, specifically separation of the anteroinferior labrum from the bony glenoid. The separation does not classically occur only at the cartilage-labral junction, but extends to the bony surface of the medial glenoid neck. Separation of the biceps tendon from its origin on the supraglenoid tubercle (SLAP lesion) or separation of the anterior capsule with the proximal humerus (HAGL lesion) may occur but are not the most common sequelae and are not demonstrated in this MRI image. Anteroinferior shoulder dislocations normally do not affect the posterior labral structures. In their landmark study, Rowe and associates noted that this demonstrated lesion was the most common lesion, present in 85% of their series.
Question 7:
What is the most important sign of impending modulation with rapid progression of a spinal deformity in neurofibromatosis?
Options:
- Apical curve rotation
- Anterior vertebral body erosions
- Cervical spine involvement
- Penciling of three or more ribs
- Curve magnitude of more than 50 degrees
Correct Answer: Penciling of three or more ribs
Explanation:
DISCUSSION: Rib penciling is the only singular factor; 87% of the curves progressed significantly in patients with three or more penciled ribs. Modulation in neurofibromatosis scoliosis implies the change from an idiopathic type to a dysplastic type of curve with rapid progression and the need for aggressive stabilization by fusion.
REFERENCES: Crawford AH, Schorry EK: Neurofibromatosis in children: The role of the orthopaedist. J Am Acad Orthop Surg 1999;7:217-230.
Durrani AA, Crawford AH, Chouhdry SN, et al: Modulation of spinal deformities in patients with neurofibromatosis type 1. Spine 2000;25:69-75.
Question 8:
Figure 53 shows the radiograph of a 48-year-old man who has a left side periprosthetic femoral fracture around the femoral stem of a previous revision hip arthroplasty. What is the most appropriate treatment?
Options:
- Open reduction and internal fixation with a plate
- Open reduction and internal fixation with a cable
- Revision with a short stem and plate fixation
- Revision with allograft prosthesis composite
- Removal of the proximal femoral bone and replacement with a cemented segmental prosthesis
Correct Answer: Revision with allograft prosthesis composite
Explanation:
DISCUSSION: In type B3 fractures, the proximal femur is so deficient that it cannot be treated with open reduction and internal fixation or support a new femoral component. In younger patients, the femur can be reconstructed with allograft prosthesis composite to restore bone stock. Removal of the distal stem with trephines would compromise fixation with cement. Elderly and low-demand patients can be treated more simply with a cemented segmental replacement prosthesis, such as that used for tumor reconstruction.
REFERENCES: Parvizi J, Tarity TD, Slenker N, et al: Proximal femoral replacement in patients with non-neoplastic conditions. J Bone Joint Surg Am 2007;89:1036-1043.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Lee SR, Bostrom MP: Periprosthetic fractures of the femur after total hip arthroplasty. Instr Course Lect 2004;53:111-118.
Question 9:
A 12-year-old girl has had progressive left knee pain for the past 4 months. She reports that the pain is unrelated to activity, and she has no history of fever or recent infections. Examination reveals full range of motion of the knee but tenderness along the medial joint line. Plain radiographs and MRI scans are shown in Figures 39a through 39d. A biopsy specimen of the lesion is shown in Figure 39e. Treatment should include
Options:
- curettage.
- systemic antibiotics.
- observation and protected weight bearing.
- chemotherapy.
- radiation therapy.
Correct Answer: curettage.
Explanation:
DISCUSSION: The lesion is a chondroblastoma. The plain radiographs show a well-defined radiolucent lesion in the distal femoral epiphysis of a skeletally immature patient. The margins are well defined, suggesting a benign growth. The epiphysis is an unusual location for bone tumors, except for chondroblastomas. Of all chondroblastomas, 95% are located within the epiphysis. The MRI scans show a punctate appearance that is commonly seen in cartilage lesions. The biopsy specimen shows a chondroid lesion with polygonal chondrocytes. These findings are consistent with a chondroblastoma. The natural history of chondroblastomas is for continued growth and bone destruction if left untreated. Treatment should consist of curettage, with or without the use of physical or chemical adjuvants, and bone grafting.
REFERENCE: Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Question 10:
A 35-year-old active woman with rheumatoid arthritis experiences right shoulder pain following an extended course of corticosteroids (Figures 96a and 96b).
Options:
- Humeral head resurfacing/shoulder hemiarthroplasty
- Anatomic total shoulder arthroplasty (TSA)
- Reverse total shoulder arthroplasty (rTSA)
- Rotator cuff repair
- Open reduction and internal fixation (ORIF)
Correct Answer: Humeral head resurfacing/shoulder hemiarthroplasty
Explanation:
DISCUSSION
The indication for anatomic TSA is end-stage glenohumeral arthritis with an intact rotator cuff. For the 62-year-old man, his radiographs reveal osteoarthritis, and his MR image shows an intact rotator cuff. Although humeral head replacement has historically been employed for this disorder, pain relief is not as reliable as with TSA, and the revision rate is higher. rTSA is generally reserved for patients with a nonfunctional rotator cuff.
For this 58-year-old patient with a full-thickness rotator cuff tear, preserved motion, and weakness in forward elevation, a rotator cuff repair is the most appropriate treatment. In the absence of degenerative changes, shoulder hemiarthroplasty or anatomic TSA is not indicated. Although indications for rTSA continue to evolve, well-compensated range of motion and a medium-sized rotator cuff tear in a younger patient are not among them.
rTSA is an emerging treatment for comminuted proximal humerus fractures in elderly patients. Although hemiarthroplasty has been a traditional treatment, current evidence suggests rTSA more reliably restores range of motion, and this 78-year-old patient's CT scan shows a small and comminuted greater tuberosity fragment that is unlikely to heal. ORIF is another option, but the CT scan also shows a small humeral head fragment that suggests osteopenia, making fixation more tenuous and likely less reliable.
A common problem associated with hemiarthroplasty for glenohumeral osteoarthritis is symptomatic glenoid degeneration that necessitates revision. This 55-year-old patient’s images reveal this is the case, although his infection workup is negative. His examination findings suggest an intact subscapularis repair. With a functioning rotator cuff and symptomatic glenoid arthritis, a conversion to anatomic TSA is indicated. In the absence of a functioning rotator cuff in an older patient, an rTSA is a better option.
This 72-year-old patient has classic symptoms and radiographs of cuff tear arthropathy. For patients with massive rotator cuff tear and glenohumeral arthritis, neither anatomic TSA nor rotator cuff repair is indicated. Hemiarthroplasty has historically been indicated for cuff tear arthropathy, but rTSA outcomes for this disorder have been superior and are now the preferred option.
Comminuted proximal humerus fractures in young, active patients are treated primarily with ORIF. The absence of glenohumeral arthritis removes anatomic TSA as a possibility, and concerns about implant longevity in younger, active patients such as this 40-year-old laborer contraindicate rTSA. Hemiarthroplasty is still employed in 3- and 4-part fractures but is generally reserved for subacute presentations or dislocations in which the humeral head is dysvascular and unlikely to survive. In this acute setting, a fixation procedure is preferred.
The 71-year-old patient who has had 2 failed rotator cuff repairs has an MR image that reveals another recurrent tear that is retracted to the glenoid. Her examination findings reveal classic signs
of a decompensated rotator cuff tear with pseudoparalysis and weakness in forward elevation. Although infection is a concern in the setting of multiply failed rotator cuff repair, the workup is negative in this scenario. Because this patient has a dysfunctional rotator cuff and has failed previous attempts at repair, a conversion to rTSA is the better option. In the absence of degenerative changes, hemiarthroplasty and anatomic TSA are not indicated.
The indications for hemiarthroplasty continue to narrow, but it is still a consideration for young patients with unipolar shoulder degeneration. In this 35-year-old patient, her MR image shows avascular necrosis in the humeral head, and her arthroscopy suggests arthritic change only on the humeral side with an uncompromised glenoid. To best treat young and active patients, a hemiarthroplasty that articulates with healthy glenoid cartilage can provide good pain relief and functional outcomes. Anatomic TSA is also reasonable but not an optimal option considering the normal glenoid condition. rTSA is not a consideration when a young patient’s MR images reveal an intact rotator cuff.
RECOMMENDED READINGS
Torchia ME, Cofield RH, Settergren CR. Total shoulder arthroplasty with the Neer prosthesis: longterm results. J Shoulder Elbow Surg. 1997 Nov-Dec;6(6):495-505. PubMed PMID: 9437598.
View
Abstract at PubMed
Chalmers PN, Slikker W 3rd, Mall NA, Gupta AK, Rahman Z, Enriquez D, Nicholson GP. Reverse total shoulder arthroplasty for acute proximal humeral fracture: comparison to open reduction-internal fixation and hemiarthroplasty. J Shoulder Elbow Surg. 2014 Feb;23(2):197-204. doi: 10.1016/j.jse.2013.07.044. Epub 2013 Sep 27. PubMed PMID: 24076000.
View Abstract at PubMed
Groh GI, Wirth MA. Results of revision from hemiarthroplasty to total shoulder arthroplasty utilizing modular component systems. J Shoulder Elbow Surg. 2011 Jul;20(5):778-82. doi: 10.1016/j.jse.2010.09.014. Epub 2011 Jan 13. PubMed PMID: 21232989.
View Abstract at PubMed
Orfaly RM, Rockwood CA Jr, Esenyel CZ, Wirth MA. Shoulder arthroplasty in cases with avascular necrosis of the humeral head. J Shoulder Elbow Surg. 2007 May-Jun;16(3 Suppl):S27-32. Epub 2006 Nov 16. PubMed PMID: 17113317.
View Abstract at PubMed
Sershon RA, Van Thiel GS, Lin EC, McGill KC, Cole BJ, Verma NN, Romeo AA, Nicholson GP. Clinical outcomes of reverse total shoulder arthroplasty in patients aged younger than 60 years. J Shoulder Elbow Surg. 2014 Mar;23(3):395-400. doi: 10.1016/j.jse.2013.07.047. Epub 2013 Oct 12. PubMed PMID: 24129052.
View Abstract at PubMed
Question 11:
-are the anteroposterior (AP) and lateral radiographs of the right elbow of a 7-yearold boy who fell off the monkey bars onto his outstretched right hand. Immediate pain and swelling were noted around his elbow; there were no other injuries. His hand was neurovascularly intact. What is the best treatment for this fracture?
Options:
- Closed reduction and casting in the emergency department
- Closed reduction and percutaneous pinning of the fracture
- Open reduction and plate fixation of the fracture in the operating room with early mobilization and no cast
- Cast immobilization in the emergency department with the expectation that this injury will heal and remodel uneventfully DISCUSSION-Displaced supracondylar fractures are best treated with surgical closed reduction and pin fixation followed by casting for 3 weeks. Closed reduction alone requires hyperflexion to hold the reduction and poses higher risk for compartment syndrome and Volkmann ischemia. Plate fixation in this age group is unnecessary considering robust periosteum and rapid healing with pin fixation. Casting the fracture without reduction will lead to a malunion that does not usually remodel. The radiographs reveal that the anterior humeral line does not intersect the capitellum in the lateral view, and the Baumann angle is disrupted in the AP view.
Correct Answer: Closed reduction and percutaneous pinning of the fracture
Question 12:
An 18-year-old boy reports increasing pain with weight bearing on his right leg and at night. Examination reveals swelling around the right midcalf. Radiographs and an MRI scan are shown in Figures 13a through 13c, and a biopsy specimen is shown in Figure 13d. What is the preferred treatment?
Options:
- Chemotherapy and surgical resection
- Debridement and IV antibiotics
- Chemotherapy alone
- Radiation therapy alone
- Surgical resection alone
Correct Answer: Chemotherapy and surgical resection
Explanation:
DISCUSSION: The findings are consistent with Ewing’s sarcoma. The radiographs reveal a lytic lesion in the diaphysis of the right fibula. There is elevation of the periosteum and evidence of a surrounding soft-tissue mass. The biopsy specimen shows diffuse small round blue cells surrounding the lamellar bone. It is the second most common malignant bone tumor in children. The most common treatment regimen consists of chemotherapy followed by surgical resection and/or radiation therapy. Surgical resection is employed when the lesion can be removed with wide margins and causes less morbidity than radiation therapy.
REFERENCES: McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 258.
Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 13:
Figure 6 shows an object being held in an outstretched hand. To offset the moment created by the object (ignoring the weight of the forearm), the biceps must generate a force of
Options:
- 5 N.
- 15 N.
- 30 N.
- 75 N.
- 150 N.
Correct Answer: 75 N.
Explanation:
DISCUSSION: Answering this question requires understanding of two important biomechanics concepts. First, because neither the object being held in the hand nor the body is moving and, hence, their accelerations are zero, the problem is one of static equilibrium in which the sum of the moments acting on the body is zero. Second, a moment is the action of a force that causes an object to rotate about any point away from its line of action. The magnitude of the moment is the magnitude of the force multiplied by the perpendicular distance between the line of action and the point (often called the moment arm or lever arm). In this problem, two forces are causing moments about the elbow. The magnitude of the moment caused by the object in the hand is 5 N times 30 cm or 150 N-cm. To maintain equilibrium, the moment caused by the biceps force must also have a magnitude of 150 N-cm. Its moment arm is 2 cm, so the magnitude of the biceps force is 150 N-cm divided by 2 cm, which equals 75 N. In general, functional loads such as the object are always at a mechanical advantage (ie, have a longer moment arm) over the muscle. Therefore, muscles must generate large forces to overcome the moments caused by even small functional loads.
REFERENCES: An KN, Chao ES, Kaufman KR: Analysis of muscle and joint loads, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 1-14.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-143.
Question 14:
- A 40-year old man has limited, painful motion in dorsiflexion at the metatarsophalangeal (MTP) joint of the right great toe, despite nonsurgical treatment. Radiographs show dorsal and medial osteophytes and minimal narrowing of the articular space. Treatment should consist of
Options:
- Arthrodesis of the MTP joint
- A Silastic implant of the MTP joint
- Resection arthroplasty of the MTP joint
- Cheilctomy of the MTP joint
- Osteotomy of the base of the proximal phalanx
Correct Answer: Cheilctomy of the MTP joint
Explanation:
Cheilectomy, the excision of an irregular osseous rim that interferes with motion of a joint was performed on the distal part of the metatarsal of patients who had hallux rigidus. In this study by Mann, published in JBJS 1988, they were able to conclude that cheilectomy is a better method of treatment for hallux rigidus than arthrodesis, resection arthroplasty, or arthroplasty with the use of a flexible implant. In older adults who present late, with more severe X-Ray changes, Keller procedure is indicated.
Question 15:
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has
Options:
- UCL repair and nighttime elbow extension splinting
- UCL repair with ulnar nerve decompression in situ
- Allograft UCL reconstruction with interference screws
- Autograft UCL reconstruction with ulnar nerve transposition
- Autograft UCL reconstruction using a docking technique
Correct Answer: Autograft UCL reconstruction with ulnar nerve transposition
Explanation:
High-level pitchers with symptomatic UCL tears require reconstruction, with autograft being the best studied graft selection. With concomitant ulnar nerve symptoms, a simultaneous ulnar nerve transposition provides good results. Ligament “repairs” and allograft reconstructions have not shown good long-term results.
Question 16:
What is the most common surgical cause of the foot deformity shown in Figure 9?
Options:
- Medial tibial sesamoid subluxation
- Overcorrection of the intermetatarsal angle
- Excessive postoperative dressing application
- Excessive medial eminence resection
- Excessive lateral soft-tissue release and lateral sesamoidectomy
Correct Answer: Excessive lateral soft-tissue release and lateral sesamoidectomy
Explanation:
DISCUSSION: The radiograph shows a hallux varus deformity. Iatrogenically acquired hallux varus is most often the result of excessive lateral soft-tissue release, sesamoidectomy, or both. It also can be caused by a medial tibial sesamoid subluxation in conjunction with excessive postoperative dressing application, overcorrection of the intermetatarsal angle, or excessive medial eminence resection.
REFERENCES: Donley BG: Acquired hallux varus. Foot Ankle Int 1997;18:586-592.
Myerson MS, Komenda GA: Results of hallux varus correction using an extensor brevis tenodesis. Foot Ankle Int 1996;17:21-27.
Question 17:
Which of the following is not considered to be a part of the constellation of the clinical entities known as the female athlete triad? Review Topic
Options:
- Decreased bone mineral density
- Menstrual dysfunction
- Low energy availability with an eating disorder
- Low energy availability without an eating disorder
- Thyroid dysfunction
Correct Answer: Decreased bone mineral density
Explanation:
Thyroid dysfunction is not one of the clinical entities included in the female athlete triad.
The female athlete triad was coined in 1992 by the American College of Sports Medicine as a complex disorder more prevalent in the adolescent and young female
athlete population including decreased bone mineral density (BMD), menstrual dysfunction, and low energy availability with or without a concomitant eating disorder. Treatment should involve a multidisciplinary approach, including psychological and nutritional counseling for eating behaviors and dietary management, reduction of training intensity to decrease risk of stress fractures, and initiating calcium and vitamin D supplements for osteoporosis.
Nazem et al performed a systematic review of articles containing the female athlete triad, reviewing diagnosis via screening during physical examinations as well as laboratory and imaging evaluation for menstrual dysfunction, low energy availability, and low bone mineral density. They state that potential complications including possible infertility, decreased immune function, cardiovascular disease, and irreversible loss of bone mineral density. They concluded that prevention, early recognition, and a multidisciplinary treatment team with a focus on proper nutrition and natural return of menses is vital.
Nattiv et al review the position of the American College of Sports Medicine regarding the female athlete triad, including screening for the triad at the pre-participation physical, discouragement of unhealthy weight loss practices. Essential members of the multidisciplinary treatment team include a health-care professional, a registered dietitian, and a mental health practitioner. They endorse that the first aim of treatment for any triad component is to increase energy availability by increasing energy intake and reducing exercise energy expenditure.
Question 18:
Figures below show the radiographs, MRI, and MR arthrogram obtained from a 25-year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy.When counseling patients who have a cam deformity, the orthopaedic surgeon should note that
Options:
- osteoarthritis of the hip is likely to occur later in life.
- correction prevents later development of osteoarthritis.
- most acetabular tears are symptomatic, and surgical treatment will be necessary.
- this is an inherited deformity.
Correct Answer: osteoarthritis of the hip is likely to occur later in life.
Explanation:
Multiple studies have confirmed that cam or pincer anatomy is commonly present in asymptomatic hips. According to a large systematic review, cam deformities are present in approximately one-third of asymptomatic hips in young adults, and the proportion is higher than 50% in the subgroup of athletes. Ganz and associates proposed that femoral acetabular impingement is the root cause of osteoarthritis in most nontraumatic, nondysplastic hips, and functional improvement with surgical correction of the deformity has been demonstrated. Despite the link between cam deformity and hip osteoarthritis, a corresponding link between the correction of the deformity and prevention of osteoarthritis has never been proven. The results of cam deformity correction, typically including repair of the degenerative labral tear, are much poorer when substantial joint space loss is present. A typical joint space cutoff of 2 mm or less is used to recommend against hip preservation surgery.
Question 19:
Figures 87a and 87b are the radiographs of an 18-year-old pedestrian who was struck by a car. During intramedullary nailing, it is difficult to maintain proper alignment. Poller blocking screws placed in the proximal fragment at which position(s) relative to the nail can help prevent the typical deformity?
Options:
- Anterior only
- Anterior and medial
- Anterior and lateral
- Posterior and medial
- Posterior and lateral
Correct Answer: Posterior and lateral
Explanation:
This is a proximal one third tibial shaft fracture. Typically nailing of this fracture creates a valgus and procurvatum malalignment that must be addressed. This can be difficult when using an intramedullary nail in the wide metaphyseal bone of the proximal tibia. To help direct and center the nail in the metaphysis, blocking screws can be used. Blocking screws should be placed where the nail should not travel. If the nail was passed with the proximal fragment in this position, it would occupy the lateral and posterior aspects of the metaphyseal fragment. To prevent this, blocking screws should be placed in the lateral and posterior aspects of the proximal fragment.
Question 20:
Bisphosphonates are indicated in the treatment of osteoporosis in patients who have a DEXA T-score of
Options:
- between 0 and 1.
- between 0 and -1.
- -3.5 and are already on teriparatide.
- within one standard deviation from the mean.
- less than -1.
Correct Answer: less than -1.
Explanation:
DISCUSSION: Bisphosphonates are indicated in the treatment of osteoporosis. They have been shown to reduce the incidence of vertebral and extremity fractures in patients with a T-score of less than -1.
REFERENCE: Gass M, Dawson-Hughs B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Question 21:
An AP radiograph of the pelvis is shown in Figure 4. What muscle attaches to the avulsed fragment of bone identified by the arrow?
Options:
- Short head of the biceps femoris
- Adductor longus
- Pectineus
- Piriformis
- Semitendinosus
Correct Answer: Semitendinosus
Explanation:
DISCUSSION: The radiograph reveals an avulsion of the ischial apophysis, most likely the result of violent contraction of the attached hamstring tendons (semimembranosus, semitendinosus, and long head of the biceps femoris). The short head of the biceps femoris arises from the linea aspera on the posterior femur. The pectineus and adductor longus attach to the pubic portion of the pelvis. The piriformis runs from the sacrum to the femur.
REFERENCES: Woodburne RT (ed): Essentials of Human Anatomy. New York, NY, Oxford University Press, 1978, pp 542-545.
Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Question 22:
A 10-year-old girl who is Risser stage 0 has back deformity associated with neurofibromatosis type 1 (NF1). She has no back pain. Examination shows multiple cafe-au-lait nevi with normal lower extremity neurologic function and reflexes. Standing radiographs of the spine show a short 50-degree right thoracic scoliosis with a kyphotic deformity of 55 degrees (apex T8). A 10-degree progression in scoliosis has occurred during the past 1 year. There is no cervical deformity. MRI shows mild dural ectasia, primarily in the upper lumbar region. Management should consist of Review Topic
Options:
- observation with repeat radiographs in 6 months.
- a thoracolumbosacral orthosis (TLSO).
- in situ posterior spinal fusion without instrumentation, followed by full-time TLSO bracing.
- anterior spinal convex hemiepiphysiodesis.
- combined anterior and posterior spinal arthrodesis with instrumentation.
Correct Answer: combined anterior and posterior spinal arthrodesis with instrumentation.
Explanation:
Scoliotic deformities in patients with NF1 are often dysplastic with short, angular curves. Posterior arthrodesis is made more difficult by the presence of kyphosis and of weak posterior elements caused by dural ectasia. Combined anterior and posterior spinal arthrodesis is generally preferred for progressive dysplastic curves to maximize deformity correction and to decrease the risk of pseudarthrosis. Anterior fusion may also prevent crankshaft phenomenon in young children. Brace treatment is not effective for large, rigid, or dysplastic curves.
Question 23:
During a percutaneous plating of a proximal tibia fracture requiring a 13-hole minimally invasive locking plate system, the placement of the distal most screws should be done through a small open incision to avoid injury to what structure?
Options:
- Superficial peroneal nerve
- Saphenous nerve
- Posterior tibial artery
- Peroneal artery
- Peroneal tendons
Correct Answer: Superficial peroneal nerve
Explanation:
The superficial and deep peroneal nerves are consistently at risk near the distal holes of long locking proximal tibia plates but can be avoided with a small open incision for those screws. The peroneal tendons are more posterior at that level. The saphenous nerve is medial. The peroneal artery runs behind the fibula and is not at risk. The posterior tibial artery is posterior to the tibia.
Question 24:
Which of the following provocative tests would most likely be positive in a patient with medial epicondylitis? Review Topic
Options:
- Resisted forearm pronation and wrist flexion with a clenched fist
- Resisted forearm supination and wrist extension with a clenched fist
- Dynamic valgus stress test
- Milking maneuver
- Pinch grip test
Correct Answer: Milking maneuver
Explanation:
A provocative test for medial epicondylitis can be elicited by applying resistance to a patient with their fist clenched, wrist flexed and pronated.
Medial epicondylitis is an overuse syndrome of the flexor-pronator mass. The pronator teres (PT) and flexor carpi radialis (FCR) are thought to be most affected with this condition. It is most common in the dominant arm and occurs with activities that require repetitive wrist flexion/forearm pronation. Patients are most tender over the origin of PT and FCR at the medial epicondyle. Resisting a patient with their fist clenched, wrist flexed and pronated can cause worsening of their pain. This maneuver can be used as a provocative test for this condition.
Cain et al. reviewed elbow injuries in throwing athletes. They comment that the common flexor-pronator muscle origin provides dynamic support to valgus stress in the throwing elbow, especially during early arm acceleration and help produce wrist flexion during ball release.
Amin et al. reviewed the evaluation and management of medial epicondylitis. They report that medial epicondylitis typically occurs in the fourth through sixth decades of life, the peak working years, and equally affects men and women. Physical therapy and rehabilitation is the main aspect of recovery from medial epicondylitis, once acute symptoms have been alleviated.
Illustration A shows a video of this provocative test for medial epicondylitis. Incorrect Answers:
Question 25:
Figures 32a and 32b show the radiographs of an active 13-year-old boy who has persistent left thigh pain and a limp despite a trial of protected weight bearing. Management should consist of
Options:
- curettage and bone grafting.
- systemic chemotherapy.
- an intralesional steroid injection.
- en block resection with autograft reconstruction.
- low-dose radiation therapy.
Correct Answer: curettage and bone grafting.
Explanation:
DISCUSSION: The plain radiographs show an eccentric metaphyseal lesion involving a long bone in a skeletally immature patient. The lesion is longer than it is wide, with distinctly lobular outer edges that are sclerotic. These findings are characteristic of a nonossifying fibroma. Small asymptomatic lesions may be followed clinically. Larger lesions that occupy greater than two thirds of the width of the shaft and are located in areas of high mechanical stress such as the femur are more prone to fracture than smaller lesions. Pain is often a sign of impending fracture or the presence of a small fracture that may not be apparent on radiographs. The natural history of the lesion is to resolve over a period of years. The procedure that would allow the patient to return to contact sports is curettage and bone grafting. Intralesional steroid injection has been advocated in the treatment of unicameral bone cysts and eosinophilic granuloma but not nonossifying fibromas. En block resection is not indicated for a benign lesion. Low-dose radiation therapy has been used for eosinophilic granuloma but not for nonossifying fibromas.
REFERENCES: Walker RN, Green NE, Spindler KP: Stress fractures in skeletally immature patients. J Pediatr Orthop 1996;16:578-584.
Arata MA, Peterson HA, Dahlin DC: Pathological fractures through non-ossifying fibromas: Review of the Mayo Clinic experience. J Bone Joint Surg Am 1981;63:980-988.
Question 26:
A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?
Options:
- Asymmetric joint space narrowing
- Sacroiliac joint ankylosis
- Progressive superior and lateral migration of the femoral head
- Periarticular osteopenia
- Hip synovitis
Correct Answer: Periarticular osteopenia
Explanation:
DISCUSSION: Radiographic findings in patients with rheumatoid arthritis include symmetric joint space narrowing, periacetabular and femoral head erosions, and diffuse periarticular osteopenia. In advanced stages, protrusio acetabuli is a common finding. Ranawat and associates have shown a rate of superior femoral head migration of 4.5 mm per year and medial (axial) migration of 2.5 mm per year. Asymmetric joint space narrowing is a classic radiographic finding of degenerative arthrosis. Sacroiliac joint ankylosis commonly occurs in ankylosing spondylitis. Hip synovitis is a pathologic diagnosis, not a radiographic finding.
REFERENCES: Lachiewicz PF: Rheumatoid arthritis of the hip. J Am Acad Orthop Surg 1997;5:332-338.
Stuchin SA, Johanson NA, Lachiewicz PF, Mont MA: Surgical management of inflammatory arthritis of the adult hip and knee, in Zuckerman JS (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-109.
Question 27:
Figures 150a through 150d are the radiographs and MR images of a 37-year-old woman who has a 3-month history of severe right hip pain. She does not recall any trauma prior to the pain onset and denies any past steroid exposure. She has 3 children and is not currently pregnant. The pain is located in her groin and the onset was sudden. The pain is refractory to anti-inflammatory medications. What is the most appropriate treatment?
Options:
- Toe-touch weight-bearing activity and supportive care
- Core decompression and femoral head grafting
- Periacetabular osteotomy
- Hemiarthroplasty
Correct Answer: Toe-touch weight-bearing activity and supportive care
Explanation:
DISCUSSION
The patient’s MR images are consistent with transient hip osteoporosis. No signs suggest avascular necrosis. She has no joint narrowing. Transient osteoporosis of the hip is characterized by bone marrow edema in the femoral head and neck. This condition affects more men than women and is sometimes seen in the third trimester of pregnancy but can be seen in women who are not pregnant as well. This is a self-limiting condition, and the treatment is limited weight-bearing activity until the symptoms resolve. Core decompression is rarely used in these cases. There is no indication for arthroplasty or osteotomy in this scenario.
Question 28:
A 23-year-old woman sustains an injury to her right hand after falling off her snowboard. Examination reveals that she has difficulty moving her fingers. A radiograph and a clinical photograph are shown in Figures 8a and Figure 8b. Management should consist of
Options:
- closed reduction and buddy taping.
- in situ pinning.
- open reduction and internal fixation.
- casting for 6 weeks.
- dynamic extension splinting.
Correct Answer: open reduction and internal fixation.
Explanation:
DISCUSSION: The radiograph reveals oblique fractures of the third and fourth metacarpals. The rotational component of the fracture displacement is well visualized on the clinical photograph, which shows scissoring of the middle finger over the ring finger. The fracture obliquity results in rotational deformity that cannot be adequately maintained and held by closed treatment. The treatment of choice is open reduction and internal fixation.
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
Freeland AE, Benoist LA, Melancon KP: Parallel miniature screw fixation of spiral and long oblique hand phalangeal fractures. Orthopedics 1994;17:199-200.
Freeland AE, Geissler WB: Plate fixation of metacarpal shaft fractures, in Blair WF (ed): Techniques in Hand Surgery. Baltimore, MD, Williams and Wilkins, 1996, pp 255-264.
Question 29:
The most important radiographic predictor of a good clinical outcome following adult spinal deformity surgery is correction of Review Topic
Options:
- pelvic incidence.
- listhesis.
- rotational deformity.
- sagittal balance.
- coronal deformity.
Correct Answer: sagittal balance.
Explanation:
Surgery for adult deformity, such as degenerative scoliosis and kyphosis, has gained popularity in recent years. Improved fixation techniques, such as pedicle screws, and increased familiarity and comfort with anterior surgery have resulted in greater curve correction. Multiple studies have demonstrated that correction of sagittal balance is the most important radiographic predictor of a good clinical outcome. While correction of coronal deformity is often a surgical goal, it does not appear to be as important in improving patient outcomes. Correction of listhesis, particularly in the surgical treatment of adult spondylolisthesis, is controversial because its impact on clinical outcomes has not been clearly established. Rotational deformities, though often present with adult scoliosis, are difficult to correct. Pelvic incidence is a fixed parameter that is unchanged with surgery.
Question 30:
What type of medial collateral ligament tear heals the most reliably? Review Topic
Options:
- Proximal
- Midsubstance
- Distal
- Associated with an anterior cruciate ligament tear
- Associated with a posterior cruciate ligament tear
Correct Answer: Proximal
Explanation:
Proximal medial collateral ligament (MCL) injuries adjacent to the medial epicondyle heal robustly. These proximal injuries are more prone to calcification, characterized clinically with temporarily increased pain and stiffness. The distal MCL, despite its long attachment site on the proximal tibia, heals less well. MCL injuries associated with other ligament injuries heal less reliably.
Question 31:
Which of the following best describes the mechanical response of the inferior glenohumeral ligament to repetitive subfailure strains?
Options:
- Decreased peak load response and length decreases
- Decreased peak load response and recoverable length increases
- Decreased peak load response and unrecoverable length increases
- Increased peak load response and recoverable length increases
- Increased peak load response and unrecoverable length increases
Correct Answer: Decreased peak load response and unrecoverable length increases
Explanation:
DISCUSSION: Repetitive subfailure strains have been shown to affect the mechanical behavior of the inferior glenohumeral ligament, producing dramatic declines in the peak load response and length increases that are largely unrecoverable. In another study, anteroinferior subluxation was found to result in nonrecoverable strain in the anteroinferior capsule, varying from 3% to 7% through a range of joint subluxation.
REFERENCES: Pollock RG, Wang VM, Bucchieri JS, et al: Effects of repetitive subfailure strains on the mechanical behavior of the inferior glenohumeral ligament. J Shoulder Elbow Surg 2000;9:427-435.
Malicky DM, Kuhn JE, Frisancho JC, et al: Nonrecoverable strain fields of the anteroinferior glenohumeral capsule under subluxation. J Shoulder Elbow Surg 2002;11:529-540.
Question 32:
A 16-year-old girl has had painless swelling in her posterior left arm for the past 4 months. A radiograph, MRI scans, and an incisional biopsy specimen are shown in Figures 43a through 43d. What is the cytogenetic translocation most commonly associated with this tumor?
Options:
- (X; 18) (p11; q11)
- (11; 22) (q24; q12)
- (12; 22) (q13; q12)
- (2; 13) (q35; q14)
- (12; 16) (q13; p11)
Correct Answer: (X; 18) (p11; q11)
Explanation:
DISCUSSION: This is a case of synovial sarcoma. The radiograph shows some soft-tissue swelling in the upper arm. The MRI scans show a lesion that has increased signal on T
2
-weighted images and low signal on T
1
-weighted images. There is a suggestion of a large cystic component to this lesion. The pathology shows a biphasic population of cells, a spindle cell component, and an epithelioid component. Up to 20% of synovial cell sarcomas have areas of cyst formation. The most common cytogenetic translocation with synovial cell sarcoma is X; 18. The 11; 22 translocation is most commonly associated with Ewing’s sarcomas; the 12; 22 translocation is most commonly associated with clear cell sarcomas; the 2; 13 translocation is most commonly associated with alveolar rhabdomyosarcomas, and the 12; 16 translocation is most commonly associated with myxoid liposarcomas.
REFERENCES: Kawai A, Woodruff J, Healey JH, et al: SYT-SSX gene fusion as a determinant of morphology and prognosis in synovial sarcoma. New Engl J Med 1998;338:153-160.
Sandberg AA: Cytogenetics and molecular genetics of bone and soft tissue tumors. Am J Med Genet 2002;115:189-193.
Question 33:
Examination of a 45-year-old man with Charcot-Marie-Tooth disease reveals a cavus foot, a tight Achilles tendon, and forefoot callus formation. Radiographs reveal advanced degenerative changes in the hindfoot. Shoe wear modifications have failed to provide relief. Treatment should now consist of
Options:
- triple arthrodesis.
- Achilles tendon lengthening and Steindler stripping.
- calcaneal osteotomy.
- multiple metatarsal osteotomies.
- midfoot osteotomy.
Correct Answer: triple arthrodesis.
Explanation:
DISCUSSION: The patient has the typical end stage residuals from long-standing Charcot-Marie-Tooth disease. Initial management consisting of shoe wear modifications and orthotic devices is preferred, but these are not successful when the disease process has progressed. Surgical correction with calcaneal osteotomy or Achilles tendon lengthening and Steindler stripping is not indicated in the presence of significant hindfoot arthritis. Because this patient has findings consistent with hindfoot arthritis, a triple arthrodesis with correction of the cavus deformity is the preferred treatment.
REFERENCES: Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth disease. J Bone Joint Surg Br 1989;71:17-20.
Wetmore RS, Drennan JC: Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 1989;71:417-422.
Question 34:
A 38-year-old marathon runner has had Achilles tendon pain for the past 2 months. Examination reveals that the tendon is thickened and tender proximal to the calcaneal insertion. The tendon sheath is not thickened or tender. The pathophysiology of the tendon is best described as
Options:
- acute inflammation.
- chronic inflammation.
- partial tendon rupture.
- anaerobic degeneration.
- impaired collagen cross-linking.
Correct Answer: anaerobic degeneration.
Explanation:
DISCUSSION: Atraumatic Achilles tendon disease can be differentiated into Achilles tendinosis and peritendinitis. Thickening and tenderness of the Achilles tendon are present in both, but thickening and tenderness of the tendon sheath indicates peritendinitis. Histologic examination of Achilles tendinosis reveals an absence of acute and chronic inflammatory cells. Radiologists often diagnose partial tendon rupture by MRI and there may be microscopic longitudinal tears present, but there is no mechanical compromise as would be implied by a partial rupture. The thickening typically occurs in the portion of the tendon with the poorest blood supply, and biochemical analysis detects high levels of lactate and other products of anaerobic glycolysis.
REFERENCES: Astrom M, Rausing A: Chronic Achilles tendinopathy: A survey of surgical and histopathologic findings. Clin Orthop 1995;316:151-164.
Ohberg L, Lorentzon R, Alfredson H: Neovascularisation in Achilles tendons with painful tendinosis but not in normal tendons: An ultrasonographic investigation. Knee Surg Sports Traumatol Arthrosc 2001;9:233-238.
Alfredson H, Bjur D, Thorsen K, et al: High intratendinous lactate levels in painful chronic Achilles tendinosis: An investigation using microdialysis technique. J Orthop Res
2002;20:934-938.
Question 35:
When performing a bunionectomy with a release of the lateral soft-tissue structures, the surgeon is cautioned against releasing the conjoined tendon that inserts along the lateral base of the proximal phalanx of the great toe. This conjoined tendon is made up of what two muscles?
Options:
- Flexor hallucis longus and flexor hallucis brevis
- Flexor hallucis longus and adductor hallucis
- Flexor hallucis brevis and adductor hallucis
- Flexor hallucis longus and abductor hallucis
- Flexor hallucis brevis and abductor hallucis
Correct Answer: Flexor hallucis brevis and adductor hallucis
Explanation:
DISCUSSION: Owens and Thordardson cautioned surgeons not to release the conjoined tendon from the base of the proximal phalanx of the great toe because of an increased risk of iatrogenic hallux varus. Release of the transverse and oblique heads of the adductor hallucis is largely accomplished by releasing the soft tissue adjacent to the lateral sesamoid, without releasing tissue from the base of the proximal phalanx. The conjoined tendon is made up of the flexor hallucis brevis and the adductor hallucis.
REFERENCES: Owens S, Thordardson DB: The adductor hallucis revisited. Foot Ankle Int 2001;22:186-191.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983, chapter 5.
Question 36:
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include
Options:
- close observation with frequent neurovascular checks.
- emergency angiography.
- emergency exploration of the brachial artery.
- removal of pin fixation and exploration of the brachial artery.
- thrombectomy.
Correct Answer: close observation with frequent neurovascular checks.
Explanation:
DISCUSSION: In a study of over 400 patients with displaced supracondylar fractures, 3.2% of the fractures were associated with the absence of the radial pulse with an otherwise well-perfused hand. Based on this study, a period of close observation with frequent neurovascular checks should be completed before attempting invasive correction of the problem. Because of the satisfactory results with expectant management, angiography, exploration, removal of fixation and exploration, and thrombectomy are contraindicated.
REFERENCE: Sabharwal S, Tredwell SJ, Beauchamp RD, Mackenzie WG, Jakubec DM, Cairns R: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 37:
The main arterial supply to the humeral head is provided by which of the following arteries?
Options:
- Anterior humeral circumflex
- Posterior humeral circumflex
- Thoracoacromial
- Subscapular
- Deep (profunda) brachial
Correct Answer: Anterior humeral circumflex
Explanation:
DISCUSSION: The main arterial supply to the humeral head is provided by the ascending branch of the anterior humeral circumflex artery and its intraosseous continuation, the arcuate artery. There are significant intraosseous anastomoses between the arcuate artery, the posterior humeral circumflex artery through vessels entering the posteromedial aspect of the proximal humerus, the metaphyseal vessels, and the vessels of the greater and lesser tuberosities. Four-part fractures and dissection during exposure affect perfusion of the humeral head.
REFERENCES: Brooks CH, Revell WJ, Heatley FW: Vascularity of the humeral head after proximal humeral fractures: An anatomical cadaver study. J Bone Joint Surg Br 1993;75:132-136.
Gerber C, Schneeberger AG, Vinh TS: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 38:
A 57-year-old man has right knee osteoarthritis and is indicated for a total knee arthroplasty (TKA). The patient has questions regarding the use of preoperative 3-dimensional imaging to develop custom cutting guides. Current data have been shown to support what proposed benefits with the use of custom cutting guides versus conventional instrumentation?
Options:
- Improved coronal component alignment
- Improved clinical outcomes
- Decreased instrument trays
- Improved axial component alignment Custom cutting guides were developed and introduced with numerous proposed benefits. including improved component coronal and axial alignment, clinical outcomes, and cost-efficiency. Unfortunately, numerous studies have failed to demonstrate these benefits. Overall coronal and implant component alignment have been shown to be similar with the use of conventional instrumentation versus custom cutting guides, and there has been no improvement in clinical outcomes. Furthermore, the costs associated with preoperative imaging and guide fabrication often offset the intraoperative savings associated with decreased instrument trays, sterilization procedures, and operating time. The use of custom cutting guides does decrease the number of instrument trays needed to perform a TKA, as long as recuts are not performed.
Correct Answer: Decreased instrument trays
Explanation:
Figures 1 through 5 are the radiographs and CT scans of a 67-year-old man who has had intermittent anterior and medial pain since his left total knee arthroplasty (TKA) 12 years ago. Examination reveals full range of motion and positive posterior drawer. His pain has been recalcitrant to physical therapy, nonsteroidal anti-inflammatory drugs, and brace treatment. What is the most appropriate treatment?
Question 39:
Figures 1 and 2 are the T2-weighted MR images of a 54-year-old woman with medial knee pain and catching of 6 months’ duration. Which treatment option is most likely to be associated with a favorable outcome?
Options:
- Physical therapy
- Meniscal repair
- Menisectomy
- Reconstruction
Correct Answer: Menisectomy
Explanation:
MR images reveal a posterior horn root tear of the medial meniscus. LaPrade and associates found that outcomes after posterior meniscal root repair significantly improved postoperatively and patient satisfaction was high, regardless of age or meniscal laterality. Patients aged <50 years had outcomes similar to those of patients ≥50 years, as did patients who underwent medial versus lateral root repair. In patients undergoing pullout fixation for posterior medial meniscus root tear, Chung and associates (in “Pullout Fixation of Posterior Medial Meniscus Root Tears”) found that patients with decreased meniscus extrusion at postoperative 1 year have more favorable clinical scores and radiographic findings at midterm follow-up than those with increased extrusion at 1 year. Krych and associates found that nonoperative treatment of medial meniscus posterior horn root tears is associated with poor clinical outcome, worsening arthritis, and a relatively high rate of arthroplasty at 5-year follow-up. Reconstruction would have no role
in the setting of a reparable meniscal root tear.
Question 40:
…Giant-cell tumor of bone usually involves the epiphysis of long bones. What is the next most common type of tumor involving this anatomical location?
Options:
- Conventional chondrosarcoma
- Aneurysmal bone cyst
- Chondroblastoma
- Osteoblastoma DISCUSSION.. Giant-cell tumor is the most common lesion involving the epiphysis, although its epicenter is usually in the metaphysis, and in the rare case of giant-cell tumor occurring in a skeletally immature patient, giant-cell tumor is located in the metaphysis. It also can involve the flat bone of the pelvis and sacrum. Chondroblastoma exclusively occurs in the epiphysis of skeletally immature patients. It is more common than the other responses. Although conventional chondrosarcoma does not involve the epiphysis, clear-cell chondrosarcoma involves the epiphysis as well; however, it is rare and less common than chondroblastoma. Aneurysmal bone may occur in the epiphysis; however, it is often seen with other benign tumors such as chondroblastoma or giant-cell tumor. It is less common in this location than chondroblastoma. Osteoblastoma does not classically appear at the epiphysis. It is more commonly seen in the spine or the diaphysis of long bones.
Correct Answer: Chondroblastoma
Explanation:
CLINICAL SITUATION FOR QUESTIONS 71 THROUGH 73
Figures 71a through 71e are the radiographs, MRI scan, and CT scans of a 14-year-old-boy who has cyclical pain in his thigh. His symptoms began approximately 6 months ago. He complains of increased pain when he runs and also of pain that wakes him at night. This pain is relieved by nonsteroidal anti-inflammatory drugs (NSAIDs).
Question 41:
A 26-year-old man is involved in a high-speed motorcycle accident. He sustains a grade IIIB open tibia fracture. Examination reveals a large soft-tissue defect and an insensate foot. What is the expected outcome in this scenario? Review Topic
Options:
- Equal functional outcome when limb salvage is compared with amputation
- Worse functional outcome with limb salvage than with primary amputation
- Better functional outcome when amputation is compared with limb salvage
- Amputation within 6 months of injury
- Permanent loss of plantar sensation
Correct Answer: Equal functional outcome when limb salvage is compared with amputation
Explanation:
The Lower Extremity Assessment Project data have shown that absent plantar sensation is not an indication for primary amputation. When looking at a comparison between an insensate salvage group and a sensate salvage group at 2 years follow-up, both groups had an equal proportion (55%) of normal plantar sensation and functionally both groups were equivalent. Absent plantar sensation at initial evaluation is not prognostic for long-term plantar sensory status or functional outcome.
Question 42:
A 35-year-old man has profound deltoid weakness after sustaining a traumatic anterior shoulder dislocation 6 weeks ago. Electromyographic (EMG) studies confirm an axillary nerve injury. Follow-up examination at 3 months reveals no recovery of function. What is the best course of action?
Options:
- Surgical repair of the Bankart lesion
- Exploration of the axillary nerve
- MRI neurography
- Repeat EMG studies
- Continued observation and physical therapy
Correct Answer: Repeat EMG studies
Explanation:
DISCUSSION: Documenting the status of recovery at this time is appropriate; therefore, repeat EMG studies should be conducted to check for early signs of reinnervation. Timing of nerve exploration in this setting is debated, with authors suggesting exploration if there is no sign of recovery at 6 to 9 months.
REFERENCES: Perlmutter GS: Axillary nerve injury. Clin Orthop 1999;368:28-36.
Artico M, Salvati M, D’Andrea V, et al: Isolated lesions of the axillary nerves: Surgical treatment and outcome in twelve cases. Neurosurgery 1991;29:697-700.
Vissar CP, Coene LN, Brand R, et al: The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery: A prospective clinical and EMG study. J Bone Joint Surg Br 1999;81:679-685.
Pasila M, Jarma H, Kiviluoto O, et al: Early complications of primary shoulder dislocations. Acta Orthop Scand 1978;49:260-263.
Question 43:
Figures 36a and 36b show the radiographs of a 3-year old child who has a congenital upper extremity deformity. Which of the following features would be a major contraindication to a centralization procedure?
Options:
- Complete absence of the thumb
- Thrombocytopenia
- Patient age of less than 5 years
- Lack of elbow motion
- Absence of the radial artery
Correct Answer: Lack of elbow motion
Explanation:
DISCUSSION: The patient has bilateral absent radii or radial clubhand. Patients who lack elbow flexion take advantage of the hand position to reach their mouths, and a centralization procedure would take away that ability. This procedure can be performed on patients with partial to complete absence of the radius. A hypoplastic thumb can be addressed at a staged procedure; it does not represent a contraindication to centralization. Complete thumb absence can be addressed by pollicizing the index ray.
REFERENCES: Green DP: Operative Hand Surgery, ed 2. New York, NY, Churchill Livingstone, 1988, pp 269-271.
Goldberg MJ, Meyn M: The radial clubhand. Orthop Clin North Am 1976;7:341-359.
Question 44:
- To maximally resist apex anterior angulation in the tibia, the pins of a unilateral external fixator should be oriented in which of the following planes?
Options:
- Coronal
- Sagittal
- Anteromedial, midway between the sagittal and the coronal
- Proximal pins sagittal, distal pins coronal
- Proximal pins coronal, distal pins sagittal
Correct Answer: Sagittal
Explanation:
The structural and geometric fixator properties that best neutralize the prevailing anteroposterior and transverse bending moments at a tibial fracture site were analyzed in anatomic specimens. Clinically and mechanically, anterior unilateral frames were most effective, particularly when applied with relatively stiff components with a maximal spread between the pins in each main bony fragment and with placement of the longitudinal rod.
Question 45:
What factor is considered one of the early changes in osteoarthritic cartilage?
Options:
- Decreased water content
- Increased proteoglycan content
- Decreased loading of the solid matrix
- Increased cartilage tissue permeability
Correct Answer: Increased cartilage tissue permeability
Explanation:
DISCUSSION:
The normal regulation of a cartilage surface is a delicate balance of degradation and synthesis. When this normal regulation of the cartilage is disturbed, a proinflammatory state tips the cellular pathway in the direction of degradation. The proinflammatory state upregulates the production of cytokines and proteolytic enzymes, specifically matrix metalloproteinases. These enzymes attack the proteoglycan content of the cartilage, leading to an overall reduction in the proteoglycan content. This reduction in content leads to increased permeability of the cartilage substrate. With increased permeability, water is able to move into the cartilage itself, thereby increasing the overall water content within the cartilage in an arthritic state. Finally, because of the increased permeability and increased water content, the overall load or pressure placed on the underlying solid matrix is increased. Increased water content, decreased proteoglycan content, and an increased load on the solid matrix are typical of an osteoarthritic process within normal cartilage. Therefore, the only correct option is that the cartilage has an increased amount of permeability in osteoarthritis.
Question 46:
A 38-year-old man has winging of the ipsilateral scapula after undergoing a transaxillary resection of the first rib 3 weeks ago. What is the most likely cause of this finding?
Options:
- Persistent thoracic outlet syndrome
- Injury to the upper trunk of the brachial plexus
- Injury to the long thoracic nerve
- Injury to the lower trunk of the brachial plexus
- Injury to the spinal accessory nerve
Correct Answer: Injury to the long thoracic nerve
Explanation:
DISCUSSION: During transaxillary resection of the first rib, the long thoracic nerve is at risk as it passes either through or posterior to the middle scalene muscle. Injury to this nerve may occur as the result of overly aggressive retraction of the middle scalene during the procedure.
REFERENCES: Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Todd TW: The descent of the shoulder after birth: Its significance in the production of pressure-symptoms on the lowest brachial trunk. Anat Anz 1912;41:385-397.
Question 47:
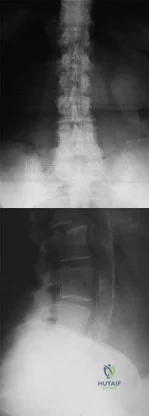
A 66-year-old man reports a 2-week history of worsening low back and leg pain. He reports that his pain is aggravated by lying down and relieved by standing and walking. He notes that he has been losing weight recently and that his pain has been awakening him during the night. His medical history is significant for hypertension, coronary artery disease, and prostate cancer. His physical examination is essentially unremarkable. Lumbar radiographs are within normal limits. What is the most appropriate management for this patient?
Options:
- MRI of chest
- Laboratory studies, including a complete blood cell (CBC) count, erythrocyte sedimentation rate (ESR), and urinalysis, PSA, CEA
- Activity alterations to avoid undue back irritation
- Comfort measures, including medications
- Spinal manipulative therapy within the first 6 weeks
Correct Answer: Laboratory studies, including a complete blood cell (CBC) count, erythrocyte sedimentation rate (ESR), and urinalysis, PSA, CEA
Explanation:
DISCUSSION: In the initial assessment of acute low back pain in adults, no diagnostic testing is indicated during the first 4 weeks in the absence of “red flags” for a serious underlying condition. The purpose of the initial assessment of acute low back pain in adults is to rule out serious underlying conditions presenting as low back pain. The Agency for Healthcare Policy and Research, in its 1994 clinical practice guideline, identified four serious conditions that may present with low back pain, including fracture, tumor, infection, and cauda equina syndrome. This patient has five “red flags” for a spinal tumor as a possible etiology of his low back pain, including age of older than 50 years, constitutional symptoms (recent weight loss), pain worse when supine, severe nighttime pain, and a history of cancer. Of these, his history of cancer is most significant, as greater than 90% of spinal tumors are metastatic. In order of frequency, breast, prostate, lung, and kidney make up approximately 80% of all secondary spread to the spine. In the presence of “red flags” for tumor or infection, it is recommended that the clinician obtain a CBC count, ESR, and a urinalysis. If these are within normal limits and suspicions still remain, consider consultation or seek further evidence with a bone scan, radiographs, or additional laboratory studies. Negative radiographs alone are insufficient to rule out disease. If radiographs are positive, the anatomy can be better defined with MRI.
REFERENCES: Agency for Health Care Policy and Research, Bigos SJ (ed): Acute Low Back Problems in Adults. Rockville, MD, US Department of Health and Human Services, AHCPR Publication 95-0642, Clinical Practice Guideline #14, 1994.
Gertzbein SD: Metastatic spine tumors, in Herkowitz HN, Dvorak J, Bell G, et al (eds): The Lumbar Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 792-802.
Question 48:
Figures 51a and 51b show the AP and lateral radiographs of the elbow of a 26-year-old man who fell. Closed reduction was performed in the emergency department, and management consisted of immobilization for 3 weeks prior to the initiation of motion. At 12 weeks after injury, he reports continued feelings of instability and catching in his elbow when using his arms to rise from a chair. Which of the following procedures needs to be performed, at a minimum, to reestablish stability of the elbow? Review Topic
Options:
- Medial collateral ligament repair
- Medial collateral ligament reconstruction
- Hinged external fixation
- Lateral collateral ligament repair
- Lateral collateral ligament reconstruction
Correct Answer: Lateral collateral ligament reconstruction
Explanation:
The patient has chronic posterolateral instability of the elbow following dislocation. The lateral collateral ligament complex is responsible for maintaining stability of the elbow. Because of the chronicity of the injury, the ligamentous tissues are frequently attenuated and not amenable to simple repair; while the native ligament can be imbricated, reconstruction with allograft or autograft is recommended. Medial collateral ligament reconstruction or hinged external fixation is needed only if restoration of the lateral ligamentous complex does not restore elbow stability; however, these procedures are rarely required. Lateral elbow pain when rising from a chair is equivalent to a positive pivot shift test.
Question 49:
A 2-year-old girl has had a swollen right knee for the past 7 weeks. There is no history of significant trauma, and she has not had a fever or been ill. Her parents report that she is stiff in the morning but otherwise does not report pain. A CBC count and erythrocyte sedimentation rate are normal. Treatment with naproxen at appropriate doses for the past 2 weeks has resulted in some improvement. Radiographs show only soft-tissue swelling. Examination reveals a healthy-appearing child with a warm and swollen right knee that is only slightly tender but lacks full extension by 20 degrees. What is the next most appropriate step in management?
Options:
- MRI
- Arthrocentesis for synovial fluid cell count and bacterial culture
- Ophthalmology consultation
- Angiotensin converting enzyme (ACE) level
- Technetium radioisotope bone scan
Correct Answer: Ophthalmology consultation
Explanation:
DISCUSSION: Up to 30% of children with juvenile rheumatoid arthritis (increasingly known now as juvenile idiopathic arthritis or JIA) already have potentially damaging uveitis at the time of diagnosis. This patient has typical oligoarticular JRA (JIA) and therefore is at significant risk for uveitis. MRI, radioisotope scanning, or an ACE level most likely would not provide additional useful diagnostic information because intra-articular derangement, osteomyelitis, or sarcoidosis are all unlikely. Arthrocentesis and triamcinolone hexacetonide joint injection might be indicated if continued use of nonsteroidal medication does not result in improvement, but should be held off for at least an additional 4 to 6 weeks to see if continued use of naproxen results in control of the arthritis.
REFERENCES: Wolf MD, Lichter PR, Ragsdale CG: Prognostic factors in the uveitis of juvenile rheumatoid arthritis. Ophthalmology 1987;94:1242.
Cassidy JT, Petty RE: Textbook of Pediatric Rheumatology. Philadelphia, PA, WB Saunders, 2001, p 220.
Chalom ED, Goldsmith DP, Koehler MA, et al: Prevalence and outcome of uveitis in a regional cohort of patients with juvenile rheumatoid arthritis. J Rheumatol 1997;24:2031-2034.
Question 50:
When performing knee arthroplasty, which of the following procedures provides the most consistent fixation for the tibial component?
Options:
- Cementless fixation of the tibial component
- Augmenting cementless fixation of the tibial component with pegs or screws
- Cementing the metaphyseal portion and press fitting the keel of the tibial component
- Cementing the metaphyseal and keel portions of the tibial component
- Cemented fixation of the tibial component with screws
Correct Answer: Cementing the metaphyseal and keel portions of the tibial component
Explanation:
DISCUSSION: All of the options, except cementing the metaphyseal portion and press fitting the keel of the tibial component, have been shown to create strong and long-lasting constructs; however, cementing of both the platform and the keel offers the most predictable solution. Cementing the platform and not the keel has been shown to have a higher loosening rate than the more traditional methods of fully cementing or using screws to augment fixation.
REFERENCE: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 457-468.
Question 51:
A patient presents to the emergency department with the injury seen in Figure A. Which of the following is true about radial nerve palsies associated with isolated humeral shaft fractures after low velocity gunshot wounds?
Options:
- The initial treatment involves debridement, irrigation, nerve exploration, and osteosynthesis.
- The radial nerve palsy is often a result of neurotmesis.
- Initial treatment involves splinting and observation for return of neurologic function.
- Electrophysiologic testing for radial nerve palsies is indicated after 2-3 weeks without improvement.
- The radial nerve palsy will not resolve regardless of attempted interventions.
Correct Answer: The radial nerve palsy will not resolve regardless of attempted interventions.
Explanation:
When a patient sustains an isolated humeral shaft fracture and radial nerve palsy from a GSW, the initial treatment involves splinting with observation.
The majority of humeral shaft fractures are treated initially with a coaptation splint and then transitioned to a functional brace. Absolute surgical indications for operative management include: open fracture, brachial plexus injury, compartment syndrome, floating elbow, or vascular injury. A radial nerve palsy is not an indication for surgical management of an isolated humeral shaft fracture. Radial nerve injury from a low-velocity GSW is similar to that of blunt force trauma and thus, immediate exploration is not necessary. Instead, nerve function should be observed. Seventy percent of these nerve injuries will resolve spontaneously. Additionally, the patient should receive a short course of antibiotics as any low velocity GSW would be treated.
Guo et al retrospectively reviewed the electrophysiologic data for 40 radial nerve palsies caused by GSWs and blunt trauma. After characterizing the palsies by level of injury, completeness of nerve injury, and other associated nerves injured, they found there to be no difference in any of these variables between GSW induced radial nerve palsies and blunt trauma induced palsies.
Vaidya et al retrospectively reviewed the outcomes of 54 patients with humeral shaft fractures resulting from low velocity GSWs comparing operative and non-operative treatments. They found that patients receiving non-operative management did well and that 70% of radial nerve palsies in the non-operative treatment group resolved on
their own. They recommended non-operative treatment for the majority of isolated humeral shaft fractures resulting from civilian gunshot wounds.
Figure A is a radiograph of a humeral shaft fracture after a GSW. Illustration A is a radiograph of a humeral shaft fracture with a coaptation in place. Illustration B is an example of a functional brace.
Incorrect answers:
Question 52:
Currently, what is the most common clinical study type in the orthopaedic literature?
Options:
- Level 1 (prospective, randomized trial)
- Level 2 (cohort trial)
- Level 3 (retrospective case control)
- Level 4 (retrospective case series)
- Level 5 (expert opinion)
Correct Answer: Level 4 (retrospective case series)
Explanation:
Although a recent push for prospective, randomized trials has been advocated by multiple orthopaedic journals, many studies published continue to be of Level 4 evidence (retrospective case series). Case series represented 64% of all studies reviewed by Freedman and associates in 2001 from the British and American volumes of Journal of Bone and Joint Surgery and from Clinical Orthopaedics and Related Research. Obremskey and associates published that 58.1% of all studies from nine orthopaedic journals were Level 4 evidence. Further investigation of more current trends is likely warranted with the current emphasis on publishing higher level-of-evidence studies in orthopaedic journals.
Question 53:
Radiographs of a 7-year-old child show mid-diaphyseal fractures of the radius and ulna. Closed reduction with sedation in the emergency department is performed. Postreduction radiographs demonstrate 18 degrees angulation, 30% translation, and what appears to be 20 degrees of rotational malalignment. Based on these findings, what is the next most appropriate step in management? Review Topic
Options:
- Another attempt at closed reduction in the operating room
- Open reduction with plating of the radius only
- Open reduction with plating of the ulna only
- Open reduction with plating of both the radius and ulna
- Close monitoring with follow-up radiographs in 1 week
Correct Answer: Open reduction with plating of both the radius and ulna
Explanation:
In children younger than 8 years of age, acceptable reduction parameters for fractures of the forearm are less than 20 degrees of angulation, 100% translation, and less than 45 degrees of malrotation. Weekly monitoring for loss of reduction and unstable fractures requiring further intervention is needed. When acceptable alignment can be maintained, good outcomes can be expected in this age group. In patients older than 10 years, angulation of less than 10 degrees, full translation, and malrotation of 30 degrees can be accepted. When surgical treatment is indicated, plating of one or both bones is acceptable. However, in this patient, the reduction is acceptable so a repeat closed reduction attempt and surgical treatment are not needed.
(SBQ13PE.17) A 14 year-old girl falls from the monkey bars, sustaining the injury shown in Figures A and B. This is a closed injury and she is neurovascularly intact. When deciding on optimal treatment, what are the acceptable parameters for angulation, malrotation, and bayonet apposition, respectively, in this patient?
Review
Topic
10 degrees, 30 degrees, Yes, allowed
10 degrees, 0 degrees, Yes, allowed
0 degrees, 0 degrees, None
0 degrees, 10 degress, None
10 degrees, 15 degrees, None
Both bone fractures that occur in adolescents, especially in patients close to skeletal maturity, have very little potential for remodeling, and therefore, require anatomic restoration of the deformity.
As patients get older and closer to skeletal maturity, closed reduction alone typically is not sufficient to obtain and maintain anatomic reduction. Often, operative intervention is required via either intramedullary nailing (IMN) or plating.
Hertel et al. retrospectively reviewed diaphyseal plating of over 160 both bone forearm fractures in a wide age range of patients, which included adolescent patients (16 years old). The authors reported over a 96% union rate, low overall complication rate, and near zero refracture rate following subsequent hardware removal. The authors determined internal fixation with 3.5mm low contact dynamic compression plates sufficient for optimal results.
Baldwin et al, in this systematic review and meta-analysis compared the use of IMN and plate osteosynthesis for the treatment of pediatric both bone fractures. A total of 12 studies were included for analysis. The authors noted excellent union and outcome results for both treatment modalities, although although there was a significantly higher rate of hardware removal (94% vs. 49%) in IMNs. While there was a slight trend toward increased rates of non-union with IMN, it was not statistically significant.
Figures A and B show AP and lateral radiographs of a both bones forearm fracture in a near skeletally mature individual. Despite minimal angulation on the lateral, the deformity present in the coronal plane is unacceptable. Illustration A depicts the recommended parameters suggested by Baldwin et al. JOT 2014 for angulation, malrotation and bayonet apposition.
Incorrect answers:
Question 54:
What are the five most common tumors that metastasize to bone?
Options:
- Breast, cervical, ovarian, thyroid, lung
- Breast, prostate, lung, renal, thyroid
- Renal, thyroid, prostate, breast, gastrointestinal
- Prostate, lung, breast, renal, laryngeal
- Prostate, breast, lung, thyroid, gastrointestinal
Correct Answer: Breast, prostate, lung, renal, thyroid
Explanation:
DISCUSSION: The five most common primary carcinomas that metastasize to bone are breast, prostate, lung, renal, and thyroid in decreasing order of incidence.
REFERENCES: Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
CA, January/February 2000, vol 50, no. 1 (Cancer Statistics).
Question 55:
03 Which of the following findings is the best indication for the use of temporary external fixation of a femoral shaft fracture?
Options:
- Type IIIA open fracture
- back to this question next question
- Hemodynamic instability
- Segmental fracture
- Distal one third fracture
- Ipsilateral tibial shaft fracture 33.03
Correct Answer: back to this question next question
Explanation:
These days, femoral shaft fractures at Tulane / Charity are commonly encountered by orthopaedic residents on the night-float team.
Despite the presence of a well-rested 4th year surgeon, definitive orthopaedic fixation is not always the correct answer for each trauma patient.
Tulane defines “Orthopaedic Tunnel Vision” as a condition commonly associated with a young MD at the Bulldog without a proper
wing-man, trying to make advances on the wrong patron due to his relatively easy 80-hour work week schedule and a few too many refined hops.
Skeletal Trauma (p. 1967) describes “Orthopaedic Tunnel Vision” as looking at the orthopaedic injury without considering the
patient’s injury in general. Femoral shaft fractures are typically high energy injuries which often do not occur in isolation. In these fractures, it is particularly important to not have tunnel vision.
Indications for temporary bridging external fixation includes hemodynamic instability
(ans. 2), acidosis, hypothermjia, hypoxemia, coagulopathy, sepsis or severely contaminated soft tissues that cannot be adequately debrided. Definitive fixation is performed after the general surgical and medical issues have resolved.
The other answer choices, including the type IIIA open fracture are not contraindications to definitive fixation in themselves (typically IM nailing—antegrade or retrograde).
Question 56:
All of the following are factors associated with transfer of patients to Level 1 trauma centers EXCEPT:
Options:
- Male
- Medicaid insurance
- Injury severity score of 36
- Caucasian race
- One or more comorbidity
Correct Answer: Male
Explanation:
DISCUSSION: Caucasian race has not been found to be a predictor for transfer to a Level 1 trauma center. The retrospective case-control study by Koval et al found that African-American race, presence of medical comorbidity, medicaid insurance, and male gender are predictors for transfer of patients to a trauma center that have ISS scores less than 9. The article by Nathens et al found that lack of insurance was an independent predictor for transfer to a trauma center after adjusting for differences in injury severity. An injury severity score of 36 represents a patient that has sustained life-threatening polytrauma and should be transferred to a Level 1 trauma center.
Question 57:
Figures 14a and 14b show the initial radiographs of an 18-year-old man who fell while snowboarding. Figures 14c and 14d show the radiographs obtained following closed reduction. Examination reveals that the elbow is stable with range of motion. Management should now consist of
Options:
- immediate return to unrestricted activity.
- a posterior long arm splint for 7 to 10 days, followed by elbow range-of-motion exercises.
- a long arm cast for 4 weeks.
- immediate surgical repair of the collateral ligaments.
- immediate surgical repair of the collateral ligaments and placement of a hinged external fixator.
Correct Answer: a posterior long arm splint for 7 to 10 days, followed by elbow range-of-motion exercises.
Explanation:
DISCUSSION: The initial radiographs reveal a simple elbow dislocation without associated fractures. After successful closed reduction, the range of stability should be assessed. If the elbow is stable, nonsurgical management should consist of a short period of immobilization followed by range-of-motion exercises. Immobilization for more than 3 weeks results in significant elbow stiffness. Surgical repair is indicated for dislocations that are irreducible, have associated fractures, or where stability cannot be maintained with closed treatment.
REFERENCES: Cohen MS, Hastings H II: Acute elbow dislocations: Evaluation and management. J Am Acad Orthop Surg 1998;6:15-23.
O’Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 409-420.
Question 58:
A 33-year-old male suffers a gunshot to the right forearm as seen in figure A. There is a 2 cm radial-sided wound with exposed bone. What is the most appropriate treatment?
Options:
- Irrigation and debridement with open reduction and internal fixation of the radius and ulna with 3.5-mm LC-DCP bridge plate
- Closed reduction and sugartong splint with ORIF within 2 weeks
- Irrigation and debridement with open reduction and internal fixation of the radius and ulna with 4.5-mm LC-DCP compression plate
- Irrigation and debridement with open reduction and internal fixation of the radius and ulna with 4.5-mm LC-DCP bridge plate
- Irrigation and debridement definitive external fixation Corrent answer: 1 The patient has a comminuted, relatively high-energy open fracture of the right radius and ulna, which is best treated with irrigation and debridement of the gunshot wounds followed by early internal fixation if possible using a 3.5 mm LC-DCP plate placed with a bridging technique. Diaphyseal forearm fractures are best treated with open reduction and internal fixation to restore anatomic alignment and absolute stability. Typically this is achieved by the use of 3.5 mm plates, placed in such a manner to produce interfragmentary compression. Due to the comminution in this case, bridge plating will provide a superior outcome as it will minimize interfragmentary strain and preserve the local bone biology. Multiple studies have demonstrated that open reduction and internal fixation at the initial encounter is appropriate, even if there is comminution, bone loss, or an open injury requiring multiple debridements. Anderson et al. performed a retrospective study of 87 patients with 129 diaphyseal forearm fractures treated with dynamic compression plates. Open fractures were fixed primarily and the overall union rate was 98%. Refracture occurred in 2 patients after removal of 4.5 mm plates, whereas there were no refractures after removal of the 3.5 mm plates. Moed et al. reviewed 57 patients that underwent immediate internal fixation of a diaphyseal forearm fracture. Functional results were good to excellent in 85% of patients and there were 2 deep infections and 6 non-unions overall. The authors conclude immediate plate fixation is an appropriate treatment method for open diaphyseal forearm fractures and recommend autogenous grafting at the time of wound closure. Jones et al. analyzed a retrospective case series of 18 patients with grade 3 open diaphyseal forearm fractures treated with irrigation and debridement and immediate open reduction and internal fixation followed by aggressive soft tissue management over the following weeks. Their treatment protocol provided good to excellent results in 66% of patients, indicating immediate reduction and fixation may be an acceptable treatment for some patients. Figure A demonstrates comminuted radius and ulna shaft fractures with retained bullet fragments. Incorrect answers:
Correct Answer: Irrigation and debridement definitive external fixation Corrent answer: 1 The patient has a comminuted, relatively high-energy open fracture of the right radius and ulna, which is best treated with irrigation and debridement of the gunshot wounds followed by early internal fixation if possible using a 3.5 mm LC-DCP plate placed with a bridging technique. Diaphyseal forearm fractures are best treated with open reduction and internal fixation to restore anatomic alignment and absolute stability. Typically this is achieved by the use of 3.5 mm plates, placed in such a manner to produce interfragmentary compression. Due to the comminution in this case, bridge plating will provide a superior outcome as it will minimize interfragmentary strain and preserve the local bone biology. Multiple studies have demonstrated that open reduction and internal fixation at the initial encounter is appropriate, even if there is comminution, bone loss, or an open injury requiring multiple debridements. Anderson et al. performed a retrospective study of 87 patients with 129 diaphyseal forearm fractures treated with dynamic compression plates. Open fractures were fixed primarily and the overall union rate was 98%. Refracture occurred in 2 patients after removal of 4.5 mm plates, whereas there were no refractures after removal of the 3.5 mm plates. Moed et al. reviewed 57 patients that underwent immediate internal fixation of a diaphyseal forearm fracture. Functional results were good to excellent in 85% of patients and there were 2 deep infections and 6 non-unions overall. The authors conclude immediate plate fixation is an appropriate treatment method for open diaphyseal forearm fractures and recommend autogenous grafting at the time of wound closure. Jones et al. analyzed a retrospective case series of 18 patients with grade 3 open diaphyseal forearm fractures treated with irrigation and debridement and immediate open reduction and internal fixation followed by aggressive soft tissue management over the following weeks. Their treatment protocol provided good to excellent results in 66% of patients, indicating immediate reduction and fixation may be an acceptable treatment for some patients. Figure A demonstrates comminuted radius and ulna shaft fractures with retained bullet fragments. Incorrect answers:
Explanation:
Question 59:
A 65-year-old woman has significant neck pain after falling and striking her head. A radiograph and sagittal CT scan are shown in Figures 23a and 23b. What is the most likely diagnosis?
Options:
- Degenerative spondylolisthesis
- Superior facet fracture
- Inferior facet fracture
- Perched unilateral facet dislocation
- Bilateral facet dislocation
Correct Answer: Perched unilateral facet dislocation
Explanation:
DISCUSSION: The radiograph shows a displacement of C5 on C6 of approximately 25%. The CT scan shows a perched facet at C5-6. There is no evidence of a facet fracture. A bilateral facet dislocation would show a displacement of more than 50%.
REFERENCES: Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, pp 927-937.
Vaccaro AR, Betz RR, Zeidman SM (eds): Principles and Practice of Spine Surgery. St Louis, MO, Mosby, 2003, pp 455-458.
Question 60:
When performing a right proximal humeral hemiarthroplasty, the relative placements of the lesser tuberosity relative to the biceps tendon is best depicted, in Figure 175, by the Review Topic
Options:
- lesser tuberosity at A, biceps at B.
- lesser tuberosity at B, biceps at C.
- lesser tuberosity at C, biceps at B.
- lesser tuberosity at A, biceps at C.
- lesser tuberosity at C, biceps at D.
Correct Answer: lesser tuberosity at A, biceps at B.
Explanation:
The lesser tuberosity should be placed at position A, and the biceps tendon at position
B. One of the most common errors during proximal humeral arthroplasty is the use of the lateral keel of the prosthesis as the landmark, around which the tuberosities are reconstructed. If this is done, the anterior soft tissue/bone element is stretched, while the posterior soft tissue/bone element is lax, with a resultant loss of external rotation of the arm. The biceps should be used as the proper landmark for tuberosity reconstruction and in its absence, the anterior aspect of the prosthesis, where the bicipital groove would have been, should be used as the central juncture of tuberosity reconstruction. The upper border of the pectoralis is best used to gauge appropriate height but knowing that the biceps tendon runs directly underneath the tendon insertion can also aid in estimating the proper location.
Question 61:
Figure 56 is the radiograph of an otherwise healthy 3-year-old boy who fell and sustained the isolated injury shown. What is the best treatment modality?
Options:
- Elastic intramedullary nailing
- Submuscular plating
- Early hip spica casting
- Traction as definitive treatment
Correct Answer: Early hip spica casting
Explanation:
DISCUSSION
At 3 years of age, children do well with nonsurgical treatment with early spica casting and early mobilization. There is no indication to perform surgical stabilization in such a closed isolated injury. The fracture is not shortened unacceptably according to clinical practice guidelines, and traction for this fracture is unnecessary. Traction also may be problematic for the family and healthcare system.
RESPONSES FOR QUESTIONS 57 THROUGH 62
Cortical thickening in the region of the lesion
Erosive metaphyseal lesion with loss of cortical integrity
Normal bony anatomy on radiographs
Diffuse articular erosion with loss of joint space
Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
Eccentric well-circumscribed metaphyseal lesion with a scalloped border
Match the orthopaedic condition described below with the expected radiographic finding listed above.
Question 62:
Staphylococcus aureus develops methicillin resistance through production of which of the following agents?
Options:
- Beta-lactam
- Catalase
- Oxidase
- Penicillin-binding protein 2a
- Glycocalix
Correct Answer: Penicillin-binding protein 2a
Explanation:
DISCUSSION: Organisms may develop resistance to antibiotics by production of specific enzymes. S aureus develops methicillin resistance by production of penicillin-binding protein 2a (PBP2a). The strains of S aureus that have acquired the mecA gene for PBP2a are designated as methicillin-resistant S aureus (MRSA). The enzyme manifests resistance to covalent modification by beta-lactam antibiotics at the active-site serine residue in two ways. First, the microscopic rate constant for acylation (k2) is attenuated by three to four orders of magnitude over the corresponding determinations for penicillin-sensitive PBPs. Second, the enzyme shows elevated dissociation constants (Kd) for the noncovalent preacylation complexes with the antibiotics, the formation of which ultimately would lead to enzyme acylation. The two factors working in concert effectively prevent enzyme acylation by the antibiotics in vivo, giving rise to drug resistance. Catalase and oxidase are enzymes produced by some bacteria that confer virulence to the organism but do not make the organisms methicillin resistant. Glycocalix is the pericellular layer produced by bacteria that serves many functions including attachment to surfaces. Beta-lactam describes a class of antibiotics.
REFERENCES: Fuda C, Suvorov M, Vakulenko SB, et al: The basis for resistance to beta-lactam antibiotics by penicillin-binding protein 2a (PBP2a) of methicillin-resistant staphylococcus aureus. J Biol Chem 2004;279:40802-40806.
Lim D, Strynadka NC: Structural basis for the beta lactam resistance of PBP2a from methicillin-resistant Staphylococcus aureus. Nat Struct Biol 2002;9:870-876.
Schwarz EM: Infections in orthopaedics, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 63:
- Resurfacing the patella during a total knee replacement is strongly indicated when the diagnosis is
Options:
- Rheumatoid arthritis
- Posttraumatic arthritis
- Degenerative osteoarthritis
- Osteonecrosis of the tibial plateau
- Osteonecrosis of the medial femoral condyle
Correct Answer: Rheumatoid arthritis
Explanation:
A study by Boyd, et. al. was performed to determine patellar complications after TKA, with the use of an unconstrained prosthesis, with and without resurfacing of the patella. “Chronic pain (post-operative, peripatellar pain) in the group that had not had resurfacing was noted in 40 (13 percent) of the 300 knees that were affected by inflammatory arthritis (rheumatoid arthritis [RA], juvenile RA and miscellaneous subcategories), and in 11 (6 percent) of the 195 knees affected by degenerative osteoarthrosis…A revision to resurface the patella was performed in all 51 knees that caused chronic pain and had not had resurfacing of the patella.
Hence, chronic pain after TKA without resurfacing the patella was more common in knees affected by rheumatoid arthritis than in those affected by degenerative osteoarthritis. The authors of the study recommend that the patella be resurfaced when an unconstrained prosthesis is used in patients with a diagnosis of inflammatory arthritis and to a lesser degree osteoarthrosis.
Question 64:
You are interested in learning a new technique for minimally invasive total knee arthroplasty. The Keyhole Genuflex system seems appealing to you because the instrumentation comes with wireless controls. What is an acceptable arrangement to learn more about this system?
Options:
- You and your spouse attend dinner at a local restaurant with the local representative to discuss the Keyhole Genuflex knee.
- Keyhole pays your tuition to attend a CME course sponsored by the American Association of Hip & Knee Surgeons where both the Genuflex and the competing Styph total knee are discussed and demonstrated.
- Keyhole will pay your expenses to attend a workshop at their company headquarters, to learn how to implant the Genuflex knee and to see how the implant is manufactured and tested.
- Keyhole will pay you $500 for each knee that you implant if you switch from your current total knee system.
- After you have implanted 25 Genuflex knees, Keyhole will list you on their website as a consultant, pay you a consulting fee of $5,000 per year, and invite you to a golf tournament for their consultants at a resort.
Correct Answer: Keyhole will pay your expenses to attend a workshop at their company headquarters, to learn how to implant the Genuflex knee and to see how the implant is manufactured and tested.
Explanation:
Both the American Academy of Orthopaedic Surgeons (AAOS) and AdvaMed, the medical device manufacturer's trade organization, have written guidelines that address potential conflicts of interest regarding interactions between physicians and manufacturer's representatives when it comes to patients' best interest. The AAOS feels that the orthopaedic profession exists for the primary purpose of caring for the patient and that the physician-patient relationship is the central focus of all ethical concerns. When an orthopaedic surgeon receives anything of significant value from industry, a potential conflict of interest exists. The AAOS believes that it is acceptable for industry to provide financial and other support to orthopaedic surgeons if such support has significant educational value and has the purpose of improving patient care. All dealings between orthopaedic surgeons and industry should benefit the patient and be able to withstand public scrutiny. A gift of any kind from industry should in no way influence the orthopaedic surgeon in determining the most appropriate treatment for his or her patient. Orthopaedic surgeons should not accept gifts or other financial support with conditions attached. Subsidies by industry to underwrite the costs of educational events where CME credits are provided can contribute to the improvement of patient care and are acceptable. A corporate subsidy received by the conference's sponsor is acceptable; however, direct industry reimbursement for an orthopaedic surgeon to attend a CME educational event is not appropriate. Special circumstances may arise in which orthopaedic surgeons may be required to learn new surgical techniques demonstrated by an expert or to review new implants or other devices on-site. In these circumstances, reimbursement for expenses may be appropriate.
Question 65:
Figure 28 shows the radiograph of a 6-year-old girl who has a right thoracic scoliosis that measures 60°. Examination shows multiple cafe-au-lait spots, and family history reveals that the child’s mother has the same disorder. The gene responsible for this disorder codes for
Options:
- dystrophin.
- frataxin.
- neurofibromin.
- peripheral myelin protein.
- sulfate transport protein.
Correct Answer: neurofibromin.
Explanation:
DISCUSSION: The patient has the dystrophic type of scoliosis seen in patients with neurofibromatosis type I (NF-1). The NF-1 gene is located on chromosome 17 and codes for neurofibromin, believed to be a tumor-suppresser gene. Abnormalities in the dystrophin gene are seen in Duchenne muscular dystrophy and Becker muscular dystrophy. A mutation in the frataxin gene is responsible for Friedreich ataxia. The most common type of hereditary motor and sensory neuropathy (Charcot-Marie-Tooth), HMSN type IA is caused by a complete duplication of the peripheral myelin protein gene. A defect in the cellular sulfate transport protein results in undersulfation of proteoglycans seen in diastrophic dysplasia.
REFERENCE: Beaty JH: Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 225-234.
Question 66:
Figure 1 depicts an intraoperative photograph obtained following proximal row carpectomy. The black dot denotes the capitate. The top of the figure is radial and the bottom of the figure is ulnar. Surgical disruption of the structure identified by the forceps would result in
Options:
- loss of active thumb interphalangeal (IP) flexion.
- distal radioulnar joint instability.
- avascular necrosis of the capitate.
- ulnar carpal translocation.
Correct Answer: ulnar carpal translocation.
Explanation:
EXPLANATION:
The structure identified by the forceps is the radioscaphocapitate ligament. During a proximal row carpectomy, it is very important to identify and protect this ligament. Compromise of the ligament would result in ulnar translocation of the carpus and early failure of the proximal row carpectomy procedure. If the ligament is injured during surgery, immediate repair should be performed. Green and associates discuss the importance of the radioscaphocapitate ligament in stabilizing the carpus after this procedure is performed. Nakamura and associates compared 3-mm, 6-mm, and 10-mm radial styloidectomies, and only the 3-mm styloidectomy subsequently preserved carpal stability. Compromise of the radioscaphocapitate ligament occurred when larger portions of the radial styloid were excised. Distal radioulnar joint instability would result only from the disruption of the distal radioulnar joint stabilizers. Avascular necrosis would not occur, because the capitate receives its blood supply mainly from the palmar vessels. Finally, loss of active thumb IP flexion would not occur, because the flexor pollicis longus tendon would remain intact even if ligament compromise were to occur.
Question 67:
A professional pitcher reports pain localized to the medial aspect of his throwing elbow. History reveals that he was pitching in a playoff game and heard and felt a pop in his elbow. MRI reveals a complete ulnar-sided avulsion of the medial collateral ligament (MCL). Examination reveals valgus instability and ulnar nerve involvement. What recommendations should be made based on the patient’s desire to return to sport?
Options:
- Surgical reconstruction
- Rest, followed by physical therapy
- Splinting in 15 degrees of flexion
- Primary repair
- Arthroscopic debridement, followed by bracing in full extension for 4 weeks
Correct Answer: Surgical reconstruction
Explanation:
DISCUSSION: Injuries to the MCL usually result from repetitive high valgus stress on the medial aspect of the elbow joint due to overhead throwing or racquet sports. Excessive stresses during the late cocking and acceleration phase of throwing can injure the anterior band of the MCL. Clinically, the injuries may present as chronic or acute, and a pop may be noted in the latter. Associated ulnar nerve involvement is common. Valgus instability is present in about 25% of patients. Patients typically are athletes who participate in throwing and have localized medial elbow pain and tenderness along the course of a ligament that extends from the medial epicondyle of the distal humerus to the sublime tubercle of the ulna. Surgical reconstruction is the procedure of choice in an athlete desiring a return to a high level of throwing.
REFERENCES: Miller MD, Cooper DE, Warner JJP (eds): Review of Sports Medicine and Arthroscopy. Philadelphia, PA, WB Saunders, 1995, p 230.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, p 227.
Altchek DW, Andrews JR (eds): The Athlete’s Elbow. Philadelphia, PA, Lippincott Williams
& Wilkins, 2001, p 91.
Question 68:
A 44-year-old man was involved in a low speed rear-end motor vehicle accident 4 weeks ago. He predominantly reports pain in the back of the neck, with occasional radiation into the trapezius region bilaterally. He denies any extremity pain. The pain has not changed in intensity, but is worse with neck range of motion. Cervical spine radiographs were negative for acute osseous trauma or instability. What is the next most appropriate step in management? Review Topic
Options:
- Continued observation
- Cervical epidural injections
- Nonsteroidal anti-inflammatory drugs (NSAIDs), activity modification, and physical therapy
- Cervical facet blocks
- Cervical MRI
Correct Answer: Nonsteroidal anti-inflammatory drugs (NSAIDs), activity modification, and physical therapy
Explanation:
The patient was involved in a low speed rear-end collision and sustained a whiplash-type injury, with management most often being nonsurgical. After 4 weeks of persistent pain, continued observation is not reasonable. Studies have shown that treatment including NSAIDs, activity modification and a brief duration of physical therapy allows for improved outcomes after whiplash-type injuries when compared with observation alone. An MRI scan of the cervical spine is not indicated at this time and represents an unnecessary expense. Cervical epidural and facet injections are not indicated in the treatment of patients with whiplash injuries.
Question 69:
A 79-year-old woman reports a history of left leg pain with walking. Her pain is exacerbated with walking and stair climbing, and her symptoms are improved by standing after she stops walking. Lumbar flexion does not provide any significant improvement of the symptoms and sitting does not significantly change symptoms. Her leg pain is worse at night and she obtains relief by hanging her leg over the side of the bed. The neurologic examination is essentially normal.
Options:
- Decompression and posterior fusion at L4-L5
- Epidural steroid injection at L4-5
- Nonsteroidal medications and physical therapy for 6 weeks
- Measurement of the ankle-brachial index
- CT myelogram
Correct Answer: Measurement of the ankle-brachial index
Explanation:
The patient has symptoms that are more consistent with vascular claudication than with the pseudoclaudication anticipated from lumbar spinal stenosis. Therefore, the patient is a candidate for further vascular work-up. The radiographs reveal early spinal stenosis and spondylolisthesis at L4-5 but also show significant calcification of the iliac arteries, suggestive of peripheral vascular disease. Vascular claudication is a manifestation of peripheral vascular disease and presents with crampy leg pain that is exacerbated by physical exertion. The pain is easily relieved by standing still or sitting. Unlike pseudoclaudication, a forward-flexed posture and/or sitting does not improve the symptoms. Night pain is common in vascular claudication due to the elevation of the extremities and patients often report pain improvement by hanging their extremities in a dependent position. In evaluation of a patient with suspected vascular claudication, the five “P’s” of vascular insufficiency should be monitored, including pulselessness, paralysis, paresthesia, pallor, and pain. While pain and paresthesias can be common in both vascular claudication and pseudoclaudication, the presence of any of the remaining symptoms is suggestive of vascular disease.
Question 70:
A 45-year-old man reports severe discomfort following a twisting injury to his right ankle and foot. Plain radiographs are negative; however, the CT scans shown in Figures 39a and 39b reveal a fracture. Management should consist of
Options:
- open reduction and internal fixation.
- percutaneous pin fixation.
- excision of the fracture fragment.
- primary calcaneocuboid joint arthrodesis.
- a walking cast or removable cast boot.
Correct Answer: a walking cast or removable cast boot.
Explanation:
DISCUSSION: The CT scans show a fracture of the anterior process of the calcaneus that involves less than 25% of the joint surface with minimal to no displacement. The preferred treatment is external immobilization in either a walking cast or, more typically, a removable cast boot. For larger fractures that involve more than 25% of the articular surface with joint incongruity, open reduction and internal fixation may be indicated. Primary calcaneocuboid joint arthrodesis is not warranted because symptoms are rare in most patients. Delayed excision of the fragment is a late reconstructive option if painful nonunion develops. Percutaneous pin fixation is not indicated beceause there tends to be inherent stability in this fracture.
REFERENCES: Heckman JD: Fractures and dislocations in the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2267-2405.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Question 71:
A 22-year-old male soccer player reports left hip and groin pain. He states that symptoms began before a preseason tournament but have worsened steadily for the past 2 weeks. He denies any recent fever or sickness and is otherwise healthy. Examination reveals tenderness over the symphysis pubis and pain with resisted rectus abdominus testing. Radiographs are negative. What is the next step in the proper management of this patient? Review Topic
Options:
- Rest, nonsteroidal anti-inflammatory drugs, rehabilitation, and gradual return to play
- Aspiration of the symphysis pubis followed by an appropriate course of antibiotics
- Referral to a general surgeon for hernia evaluation
- Rigid plating across the symphysis to address instability
- MRI evaluation of the symphysis
Correct Answer: Rest, nonsteroidal anti-inflammatory drugs, rehabilitation, and gradual return to play
Explanation:
Appropriate management of osteitis pubis includes rest, nonsteroidal anti-inflammatory drugs, directed rehabilitation, and gradual return to sports. Lack of fever or chills excludes osteomyelitis as a source of pain. Examination with tenderness over the symphysis pubis and pain with resisted rectus abdominus testing is consistent with osteitis pubis as opposed to a sports hernia, where a patient would be tender in the abdomen, not the pubis. There is no symphyseal instability that would require symphyseal plating.
Question 72:
-Figures a and b are the anteroposterior and lateral plain radiographs of a 45-year-old woman who had severe bilateral leg pain for 6 months. Figures 5c and 5d are her sagittal and axial T2-weighted MRI scans. After attempting nonsurgical treatment including physical therapy and epidural injections, she continued to experience persistent pain. What is the most appropriate treatment?
Options:
- Open biopsy
- Incision and debridement
- Decompression
- Decompression and instrumented fusion
- Decompression and uninstrumented fusion
Correct Answer: Decompression and instrumented fusion
Question 73:
A 4-year-old child sustains a spiral fracture to the tibia in an unwitnessed fall. History reveals three other fractures to long bones, and the parents are vague about the etiology of each. There is no family history of bone disease. The parents ask if the child has osteogenesis imperfecta (OI); however, there are no clinical or radiographic indications of this diagnosis. In addition to fracture care, management should include
Options:
- notification of child protective services and hospital admission.
- a punch biopsy of skin for collagen analysis.
- DNA testing for OI.
- calcium, phosphate, and alkaline phosphatase studies.
- placement of intramedullary rods to prevent further fractures.
Correct Answer: notification of child protective services and hospital admission.
Explanation:
DISCUSSION: Child abuse and OI are frequently both in the differential diagnosis of a child with multiple fractures. If OI is suspected, testing is appropriate to confirm this diagnosis. This may include skull radiographs to look for wormian bones and/or fibroblast culturing and collagen analysis of a punch biopsy. Unfortunately, because of the large number of mutations that can yield the disease, DNA testing is not commercially available for OI. In this patient, however, the physician suspects nonaccidental trauma and is legally obligated in most states to notify child protective services. Because the child may be at considerable risk of further injury, hospitalization is indicated to protect the child until child protective services can complete a home investigation and assess the degree of risk. Work-up for both OI and child abuse can be done during the hospitalization.
REFERENCES: Rockwood CA, Wilkins KE, King RE (eds): Fractures in Children. Philadelphia, PA, JB Lippincott, 1984, vol 3, pp 173-175.
Kempe CH, Silverman FN, Stelle BF, Droegemueller W, Silver HK: The battered-child syndrome. JAMA 1962;181:17-24.
Akbarnia BA, Akbarnia NO: The role of the orthopedist in child abuse and neglect. Orthop Clin North Am 1976;7:733-742.
Question 74:
The nucleus pulposus of the intervertebral disk consists of chondrocyte-like cells that have a limited vascular supply and generate energy through which of the following?
Options:
- Anaerobic glycolysis
- Kreb's cycle
- Ketosis
- Gluconeogenesis
- Lipogenesis
Correct Answer: Anaerobic glycolysis
Explanation:
The intervertebral disk is an avascular structure in the adult. Nucleus pulposus cells have a critical need for glucose because they obtain their energy primarily by glycolysis, even in the absence of oxygen. Disk cells do not require oxygen to remain alive but they die at low glucose levels or acidic pH. Nutrients are supplied from the blood vessels at the margins of the disk and have to traverse the cartilaginous end plate to reach the disk cells. The loss of the nutrient supply through the vertebral body will starve the cells in the disk center and may be a major factor in disk degeneration.
Question 75:
03 A 28-year-old man who sustained the injury shown in Figure 31 is hemodynamically unstable. In addition to fluid resuscitation, the next most appropriate step in management should include
Options:
- angiography and embolization.
- an emergent exploratory laparotomy.
- external pelvic stabilization.
- open reduction and internal fixation.
- closed reduction and percutaneous screw fixation. backanswer Question 112.03
Correct Answer: external pelvic stabilization.
Explanation:
The radiograph shows us a pelvic inlet view of an APC II or III pelvic ring injury with syndesmotic disruption greater than 5cm, and a right SI joint disruption as well. APC (and some VS) injuries are associated with increases in pelvic volume allowing occult blood loss. All of the responses are viable options, but on a spectrum of timing. ORIF and CRPSF are both more elective options that require appropriate pre-operative planning and a stable patient, not to be undertaken in a hemodynamically unstable patient. The article referenced from JBJS 2002 reviewed 150 patients with pelvis fractures and the use of angiography for the management of “haemorrhage.” They concluded/recommended skeletal stabilization as the first line of treatment, followed by possible laparotomy and packing of pelvic retroperitoneum as a second line of treatment, with pelvic angiography and embolization only in those patients that were unresponsive to both previous interventions. They based their recommendations also on anatomical studies that suggested that the surfaces of the fracture and veins, rather than arteries, were the major sources of bleeding in these patients. External pelvic stabilization in their study included external fixators, pneumatic anti-shock garments, and pelvic clamps.
Cook RE, Keating JF, Gillespie I: The role of angiography in the management of haemorrhage from major fractures of the pelvis. J Bone Joint Surg Br 2002;84:178-182.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp395-405.
back to this question next question
Question 76:
An 18-year-old male soccer player sustains a knee injury during a game. Examination is notable for a positive pivot shift test. What other physical examination finding is most likely to be present? Review Topic
Options:
- Medial joint line tenderness
- Lateral joint line tenderness
- Positive dial test at 30° of knee flexion
- Varus laxity at 30° of knee flexion
- Positive posterior drawer test
Correct Answer: Positive posterior drawer test
Explanation:
The patient has sustained a tear of his anterior cruciate ligament (ACL), as demonstrated by the positive pivot shift test; therefore, he would most likely exhibit lateral joint line tenderness indicative of a lateral meniscus tear, the most common intraarticular injury associated with an ACL tear.
ACL tears usually occur as a result of a non-contact pivoting injury. Abnormal anterior translation results in bone contusions of mid-lateral femoral condyle and posterolateral tibia, which can be seen on MRI. Other concomitant intraarticular injuries include meniscal tears (lateral > medial), chondral damage and other ligamentous injury (MCL, LCL, PLC) usually found in cases of higher energy trauma such as a knee dislocation.
Piasecki et al prospectively analyzed intraarticular injuries associated with ACL tears in high school athletes by gender and sport. There was no significant difference in mechanism of injury between sexes. Female basketball and soccer players had fewer intraarticular injuries (medial femoral condyle lesions, medial and lateral meniscus tears) compared to male athletes. The authors hypothesized that women may therefore enjoy a better prognosis following reconstruction.
Spindler et al performed a prospective cohort study investigating concomitant intraarticular injuries in patients who underwent ACL reconstruction. Eighty percent of patients had a bone bruise on MRI, 68% involving the lateral condyle. At time of arthroscopic reconstruction, meniscal tears were identified in 56% of lateral menisci and 37% of medial menisci.
Incorrect Responses:
Question 77:
Which of the following would be associated with the spinal deformity shown in Figures 79a and 79b? Review Topic
Options:
- Improved gait
- Deformity progression
- Delayed satiety
- No further risk of fracture
- Improved lung function
Correct Answer: Deformity progression
Explanation:
The images delineate progressive osteoporotic collapse. As outlined by Kado and associates, Schlaich and associates, and Gold and associates, the progression of spinal deformity and the functional consequences of vertebral compression fractures are persistent even in those patients who are pain free. Vertebral compression fractures are associated with deteriorating gait, early satiety, further future fracture risk, and deteriorating lung function.
Question 78:
A 3-year-old child has bilateral genu varum and short stature. Radiographs show physeal widening and generalized osteopenia. The femora and tibiae show anterolateral bowing. Laboratory studies show low normal serum calcium values, significantly decreased serum phosphate levels, and normal parathyroid hormone (PTH), alkaline phosphatase, and vitamin-D levels. These findings are consistent with
Options:
- nutritional rickets.
- renal osteodystrophy.
- primary hyperparathyroidism.
- hypophosphatasia.
- vitamin D-resistant rickets.
Correct Answer: vitamin D-resistant rickets.
Explanation:
DISCUSSION: Children with vitamin D-resistant rickets are short in stature and have genu varum, physeal widening, and generalized osteopenia. The abnormality in inherited vitamin
D-resistant rickets is the renal tubule’s inability to resorb phosphate leading to hypophosphatemia. Laboratory findings in the condition are normal or near normal serum calcium values, significantly decreased serum phosphate levels, elevated alkaline phosphatase levels, and normal PTH and vitamin-D levels. The most common form is inherited as an
X-linked dominant trait. Nutritional rickets has a normal or low serum phosphate levels, normal or low serum calcium values, and decreased levels of 25(OH) vitamin D and
1,25-dihydroxyvitamin D. Hypophosphatasia is a rare condition characterized by a deficiency of alkaline phosphatase in the serum and tissues, leading to generalized abnormal mineralization of bone. Primary hyperparathyroidism usually is caused by a parathyroid adenoma, and the child generally has abdominal problems and hypercalcemic crisis. Laboratory findings include elevated serum calcium values, alkaline phosphatase levels, and PTH levels, and decreased serum phosphate levels. Children with renal osteodystrophy tend to have genu valgum, and laboratory findings include elevated serum phosphate, alkaline phosphatase, and PTH levels, and low serum calcium values. Findings of renal disease include elevated BUN and creatinine.
REFERENCES: Herring JA: Metabolic and endocrine bone diseases, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, pp 1686-1710.
Zaleske DJ: Metabolic and endocrine abnormalities, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 181-203.
Question 79:
Which of the following has been associated with a decreased rate of glenoid component radiolucent lines?
Options:
- A curve-backed pegged cemented polyethylene glenoid component
- A curve-backed keeled cemented polyethylene glenoid component design
- A flat-backed keeled cemented polyethylene glenoid component
- An oversized pegged cemented glenoid component
- A superiorly placed pegged glenoid component
Correct Answer: A curve-backed pegged cemented polyethylene glenoid component
Explanation:
DISCUSSION: According to a recent study, cemented pegged glenoid components had fewer radiolucent lines initially and at 2-year follow-up when compared to a cemented keeled design. Curve-backed designs have also shown fewer radiolucent lines when compared to flat-backed designs. Oversizing the glenoid can lead to impaired rotator cuff function and decreased range of motion. An off-centered glenoid can lead to early loosening.
REFERENCES: Gartsman GM, Elkousy HA, Warnock KM, et al: Radiographic comparison of pegged and keeled glenoid components. J Shoulder Elbow Surg 2005;14:252-257.
Szabo I, Buscayret F, Edwards TB, et al: Radiographic comparison of flat-back and convex-back glenoid components in total shoulder arthroplasty. J Shoulder Elbow Surg 2005;14:636-642.
Mileti J, Boardman ND III, Sperling JW, et al: Radiographic analysis of polyethylene glenoid components using modern cementing techniques. J Shoulder Elbow Surg 2004;13:492-498.
Question 80:
Chemotherapy for this condition is
Options:
- contraindicated when pathology is benign.
- associated with a high risk for subsequent myelodysplastic syndrome.
- provides dramatic survival benefits.
- provides modest survival benefits.
Correct Answer: provides modest survival benefits.
Explanation:
DISCUSSION
This patient has a dedifferentiated liposarcoma within a preexisting atypical lipomatous tumor. The imaging demonstrates a large fatty mass with increased internal septations proximally (the atypical lipomatous tumor) and a solid enhancing mass distally (the dedifferentiated portion). A biopsy reveals a high-grade liposarcoma. The other diagnostic responses do not reflect sarcomatous transformation of the lesion.
Surgical treatment of a high-grade sarcoma involves wide surgical resection. Radiation decreases local recurrence but does not clearly influence overall survival. The role of chemotherapy in high-grade soft-tissue sarcomas remains investigational; there is a modest (8%-15%) associated improvement in overall survival.
Intramuscular lipomas and atypical lipomatous tumors are treated with marginal resection alone. Radiation therapy for soft-tissue sarcomas may be given before or after surgery. When administered before surgery, patients have a higher wound complication rate but better long-term function attributable to lower rates of lymphedema, fibrosis, and contractures.
RECOMMENDED READINGS
Schlieman M, Smith R, Kraybill WG. Adjuvant therapy for extremity sarcomas. Curr Treat Options Oncol. 2006 Nov;7(6):456-63. Review. PubMed PMID: 17032558.
View Abstract at PubMed
Yang JC, Chang AE, Baker AR, Sindelar WF, Danforth DN, Topalian SL, DeLaney T, Glatstein E, Steinberg SM, Merino MJ, Rosenberg SA. Randomized prospective study of the benefit of adjuvant radiation therapy in the treatment of soft tissue sarcomas of the extremity. J Clin Oncol. 1998 Jan;16(1):197-203. PubMed PMID: 9440743.
View Abstract at PubMed
Soft tissue tumors. In: Damron TA, ed.
Orthopaedic Surgery Essentials: Oncology and Basic Science
. Philadelphia, PA: Lippincott Williams and Wilkins; 2008:87-92
Question 81:
The 5-year outcome for patients with sciatica secondary to lumbar disk herniation shows which of the following results?
Options:
- Patients have the same likelihood of receiving disability whether treated with or without surgery.
- Sixty percent of surgically treated patients undergo at least one more operation within 5 years.
- Only 20% of patients treated with surgery report improved symptoms of back and/or leg pain.
- A smaller portion of surgical patients, compared to nonsurgically treated patients, report improvement.
- Fifty percent of patients treated nonsurgically seek surgery within 5 years.
Correct Answer: Patients have the same likelihood of receiving disability whether treated with or without surgery.
Explanation:
DISCUSSION: Atlas and associates, in the Maine Lumbar Spine Study, reported that overall, patients treated initially with surgery reported better outcomes. By 5 years, 19% of surgical patients had undergone at least one additional lumbar spine operation, and 16% of nonsurgical patients had opted for at least one lumbar spine operation. At the 5-year follow-up, 70% of patients initially treated surgically reported improvement in their predominant symptom (back or leg pain) versus 56% of those initially treated nonsurgically. They also noted that there was no difference in the proportion of patients receiving disability compensation at the 5-year follow-up.
REFERENCE: Atlas SJ, Keller RB, Chang Y, et al: Surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: Five-year outcomes from the Maine Lumbar Spine Study. Spine 2001;26:1179-1187.
Question 82:
At the first postoperative visit after mini-open carpal tunnel release, a patient reports hand weakness. Poor index finger interphalangeal joint extension and metacarpophalangeal joint flexion are present. This finding is most consistent with
Options:
- unrecognized injury to the recurrent motor branch.
- neuropraxia of the proper palmar digital nerve.
- new-onset stenosing flexor tenosynovitis.
- injury to the flexor digitorum profundus to the index finger.
Correct Answer: neuropraxia of the proper palmar digital nerve.
Explanation:
EXPLANATION:
Complications after carpal tunnel release are relatively uncommon. The clinical picture described above is most consistent with lumbrical muscle weakness secondary to neuropraxia of the proper palmar digital nerve to the index finger supplying motor innervation to that muscle. The recurrent motor branch of the median nerve innervates the thenar musculature and would not present as index finger weakness. A new onset of trigger finger may result from a loss of the pulley effect of the transverse carpal ligament, postoperative tendon inflammation, or previously unrecognized flexor tendon triggering. Flexor digitorum profundus to the index finger lies deep within the carpal tunnel, making its injury unlikely. If
it were injured, the result would not be weakness of interphalangeal joint extension.
Question 83:
A 77-year-old woman who underwent total knee arthroplasty 16 years ago now reports pain, swelling, and notable crepitation with range of motion. AP, lateral, and Merchant radiographs are shown in Figures 54a through 54c. What is the most likely diagnosis?
Options:
- Failure of patellar polyethylene
- Loosening of the femoral component
- Loosening of the tibial component
- Loosening of the patellar component
- Wear-induced osteolysis
Correct Answer: Failure of patellar polyethylene
Explanation:
DISCUSSION: The Merchant radiograph shows a lateral patellar shift with total polyethylene failure, resulting in a metal-on-metal bearing. This problem is associated with metal-backed patellar components. Component fixation appears solid, and no osteolysis is evident.
REFERENCES: Poss R (ed): Orthopaedic Knowledge Update 3. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, pp 590-593.
Leopold SS, Berger RA, Patterson L, et al: Serum titanium level for diagnosis of a failed metal-backed patellar component. J Arthroplasty 2000;15:938-943.
Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1993, pp 613-614.
Question 84:
A 10-year-old boy with a history of retinoblastoma now reports right knee pain. AP and lateral radiographs are shown in Figures 3a and 3b. What is the most likely diagnosis?
Options:
- Ewing’s sarcoma
- Primitive neuroectodermal tumor
- Osteosarcoma
- Osteonecrosis
- Osteomyelitis
Correct Answer: Osteosarcoma
Explanation:
DISCUSSION: The radiographs show a bone-producing lesion in the femoral diaphysis. The radiographic appearance of small round cell tumors is more permeative with an elevated periosteum and no matrix production. The appearance of this lesion is most consistent with osteosarcoma. Patients who carry the Rb gene are predisposed to osteosarcoma. However, Ewing’s sarcoma, primitive neuroectodermal tumor, and osteomyelitis can all occur in this location.
REFERENCES: Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
Chauveinc L, Mosseri V, Quintana E, Desjardins L, Schlienger P, Doz F, Dutrillaux B: Osteosarcoma following retinoblastoma: Age at onset and latency period. Ophthalmic Genet 2001;22:77-88.
Question 85:
Where does the median nerve pass in the proximal forearm?
Options:
- Through the pronator teres and deep to the flexor digitorum superficialis
- Deep to the pronator teres and superficial to the flexor digitorum superficialis
- Deep to the pronator teres and deep to the flexor digitorum superficialis
- Adjacent to the ulnar artery
- Superficial to the pronator teres and flexor digitorum superficialis
Correct Answer: Through the pronator teres and deep to the flexor digitorum superficialis
Explanation:
DISCUSSION: The median nerve passes through the pronator teres and deep to the flexor digitorum superficialis. The ulnar artery passes deep to both.
REFERENCES: Anderson JE (ed): Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Williams and Wilkins, 1978, pp 6-55.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 120.
Question 86:
A 45-year-old right-hand dominant woman falls onto an outstretched left hand. Imaging shows a complex elbow dislocation. The postreduction CT scan demonstrates a reduced joint, comminuted radial head fracture, and type I coronoid fracture. Surgical intervention is recommended to address the involved structures. Which component of the intervention adds the most rotational stability?
Options:
- ixation of the coronoid fragment
- Radial head arthroplasty
- Repair or reconstruction of the lateral collateral ligament (LCL) complex
- Repair or reconstruction of the medial collateral ligament (MCL) This represents a terrible triad injury, with elbow dislocation, radial head fracture, and coronoid fracture. The LCL complex is typically disrupted in this injury pattern. Repair or reconstruction of this structure provides the greatest increase in rotational stability of the elbow.
Correct Answer: Repair or reconstruction of the lateral collateral ligament (LCL) complex
Explanation:
A 68-year-old right-hand dominant woman has experienced progressive right elbow pain and loss of motion for several years. She has failed nonsurgical treatment and elects to undergo a total elbow arthroplasty (TEA). In comparison to a linked prosthesis, an unlinked prosthesis has which reported distinction with extended follow-up?
A. Improved longevity in comparison to the linked prosthesis
B. A significantly larger flexion-extension arc
C. A higher incidence of postsurgical instability
D. Lower frequency of ulnar nerve dysfunction
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
Question 87:
A 47-year-old woman has had left medial clavicle pain for the past 6 months. History is remarkable for mediastinal non-Hodgkin’s lymphoma, treated with mantel radiation 22 years ago. A radiograph, CT scan, MRI scan, and a biopsy specimen are shown in Figures 68a through 68d. What is the most likely diagnosis?
Options:
- Radiation-associated sarcoma
- Radiation-associated osteonecrosis
- Clavicular osteomyelitis
- Sternoclavicular septic arthritis
- Sternoclavicular degenerative joint disease
Correct Answer: Radiation-associated sarcoma
Explanation:
DISCUSSION: Radiation-associated sarcomas typically occur at least 5 years following radiation therapy, in the radiation therapy field, and with different histology than the original disease. The radiograph shows a lytic destructive lesion of the medial clavicle. The radiographic differential could include any of the above etiologies. The CT and MRI scans show this same reaction with extension into the adjacent soft tissue and periosteal reaction. These findings eliminate a degenerative process or radiation-induced osteonecrosis but do not distinguish between a neoplastic and infectious process. A PET scan showed marked uptake in the distal clavicle, which is more consistent with a malignant neoplastic process than a reactive process, like that of an infection. These findings, combined with the cellular atypia and bone formation on the biopsy specimen, confirm the diagnosis of radiation-associated sarcoma. In this older patient, radiation-associated sarcoma appears in an unusual location secondary to her previous radiation treatment in that region, which can occur 3 to 50 years after previous radiation therapy.
REFERENCES: Shaheen M, Deheshi BM, Riad S, et al: Prognosis of radiation-induced bone sarcoma is similar to primary osteosarcoma. Clin Orthop Relat Res 2006;450:76-81.
Tabone MD, Terrier P, Pacquement H, et al: Outcome of radiation-related osteosarcoma after treatment of childhood and adolescent cancer: A study of 23 cases. J Clin Oncol 1999;17:2789-2795.
Question 88:
An 18-year-old lacrosse player sustained a hamstring pull during a game. Examination the next day reveals ecchymosis through the posterior thigh and a palpable defect in the hamstring musculature in the middle third of the thigh. What is the most likely site of anatomic injury?
Options:
- Rupture of the biceps femoris at the myotendinous junction
- Rupture of the biceps femoris muscle belly
- Avulsion of the common hamstring origin from the ischium
- Complete rupture of the semimembranosus muscle belly
- Complete tear of all hamstring muscles
Correct Answer: Rupture of the biceps femoris at the myotendinous junction
Explanation:
DISCUSSION: Hamstring strains are common in athletes. Basic science research and clinical data indicate that the majority of these injuries occur at the myotendinous junction, not within the muscle belly. Avulsion of hamstring origin from the ischial tuberosity does occur but is less common. Complete tearing of all hamstring muscles is unlikely to occur.
REFERENCES: Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 17-33.
Clanton TO, Coupe KJ: Hamstring strains in athletes: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:237-248.
Question 89:
Figures 23a and 23b show the radiographs of a 75-year-old woman who sustained an injury to her nondominant hand. Initial treatment should consist of
Options:
- closed reduction and splinting.
- open reduction and internal fixation through a volar approach.
- external fixation and Kirschner wire fixation.
- intrafocal pinning and casting.
- acceptance of alignment and bracing.
Correct Answer: closed reduction and splinting.
Explanation:
DISCUSSION: Definitive treatment decisions for displaced distal radius fractures in the elderly are based on a number of factors related to the fracture pattern and patient demographics. The first step in any treatment algorithm is a closed reduction and splinting with reassessment of alignment parameters. This is an extra-articular fracture with dorsal angulation. Low-demand elderly patients can be treated well with accepted minor malreduction.
REFERENCES: Handoll HH, Madhok R: Conservative interventions for treating distal radial fractures in adults. Cochrane Database Syst Rev 2003;2:CD000314.
Young CF, Nanu AM, Checketts RG: Seven-year outcome following Colles’ type distal radial fracture: A comparison of two treatment methods. J Hand Surg Br 2003;28:422-426.
Question 90:
What is the most common complication associated with scalene regional anesthesia for shoulder procedures?
Options:
- Cardiovascular collapse
- Block failure
- Seizure secondary to intravascular injection
- Phrenic nerve injury
- Laryngeal nerve injury
Correct Answer: Block failure
Explanation:
DISCUSSION: Failure of the scalene block, necessitating general anesthesia or the immediate administration of narcotic medications, is the most common complication, occurring in 3% to 18% of patients. Cardiac arrest or cardiovascular collapse has been reported in anecdotal occurrences. Seizure that is the result of intravascular injection of local anesthetic is a rare complication, with an incidence reported of 0% to 6%. Neurologic complications, including laryngeal and phrenic nerve injuries, are rare although parathesias lasting up to 2 weeks have been reported in up to 3% of patients.
REFERENCES: Weber SC, Jain R: Scalene regional anesthesia for shoulder surgery in a community setting: An assessment of risk. J Bone Joint Surg Am 2002;84:775-779.
Conn RA, Colfield RH, Byer DE, Lindstromberg JW: Interscalene block anesthesia for shoulder surgery. Clin Orthop 1987;216:94-98.
Question 91:
An active, right-handed 71-year-old woman fell on her left shoulder and sustained the injury shown in the radiographs in 52a and 52b and the CT scan in 52c. Management should consist of
Options:
- hemiarthroplasty
- open reduction and internal fixation
- closed reduction and percutaneous pinning
- a sling and early pedulum exercises
- a sling and swathe for 6 weeks, followed by shoulder rehabilitation
Correct Answer: hemiarthroplasty
Explanation:
Prosthetic hemiarthroplasty is the accepted form of treatment for badly displaced fractures and fracture dislocations, including 4-part fractures, head splitting fractures and fractures with impression defects involving more than 45 % of the humeral head. Displacement is classified as >1cm or angulated > 45 degrees. About 15% of all shoulder fx’s are considered displaced.
Question 92:
What is the most common nonanesthetic-related reversible cause of changes in intraoperative neurophysiologic monitoring data? Review Topic
Options:
- Pedicle screw misplacement
- Patient positioning
- Spinal cord ischemia
- Retractor placement
- Hypotension
Correct Answer: Patient positioning
Explanation:
Patient positioning that results in local nerve compression, plexus traction, or improper neck alignment is the most common nonanesthetic-related cause of changes in intraoperative neurophysiologic monitoring data during spinal surgery.
Question 93:
Which of the following statements is true regarding the posterior oblique portion of the medial collateral ligament of the elbow? Review Topic
Options:
- Can be released to gain flexion in patients with post-traumatic contracture
- Has the highest tensile strength of any elbow ligament
- Is reconstructed in the Tommy John procedure
- Is the primary ligamentous restraint to valgus force during throwing
- Is responsible for the pivot shift of the elbow
Correct Answer: Is responsible for the pivot shift of the elbow
Explanation:
Addressing flexion in a post-traumatic contracture of the elbow requires releasing the posterior oblique ligament (or band) of the medial ulnar collateral complex.
The medial ulnar collateral ligament is one of the primary static stabilizers of the elbow and is composed of three parts: anterior, posterior and transverse. The MCL provides resistance to valgus and distractive stresses. The anterior oblique fibers (of the anterior bundle) are the most important against valgus stresses. The posterior bundle is involved elbow contractures and releasing it can yield significant flexion gains, without creating valgus instability.
Morrey et al. performed a pilot study on 4 specimens and found the valgus stability is equally divided among the medial collateral ligament complex, anterior capsule, and bony articulation in full extension; whereas, at 90 degrees of flexion the contribution of the anterior capsule is assumed by the medial collateral ligament which provides approximately 55% of the stabilizing contribution to valgus stress.
Regan et al. was a subsequent study by the same group that found the posterior medial collateral ligament (PMCL) was taut only when the elbow was in a flexed position. Among the collateral ligaments, the anterior (AMCL) was the strongest and stiffest. (Of note, using present terminology these would be referred to as posterior oblique and anterior oblique portions of the medial ulnar collateral complex).
Wada et al. reported a series of open medial releases for post-traumatic elbow contracture and found scarring on the posterior oblique bundle in all cases. Large increases in flexion were achieved by releasing this structure and the capsule without the need for a lateral incision in most cases.
Illustrations A and B show the posterior oblique portion of the medial collateral ligament. Illustration C shows the most recent terminology and identifies the area to be resected for stiffness.
Incorrect Answers:
Question 94:
Figures 31a and 31b show the T1- and T2-weighted MRI scans of a patient’s knee joint. What is the most likely diagnosis?
Options:
- Torn anterior cruciate ligament
- Torn medial meniscus
- Staphylococcus infection
- Rheumatoid arthritis
- Tibial plateau fracture
Correct Answer: Tibial plateau fracture
Explanation:
DISCUSSION: The scans show a lipohemarthrosis. There is the characteristic layering of a superior zone containing fat (high signal intensity), a central zone containing serum (low signal intensity), and an inferior zone that contains red blood cells (low signal intensity). The most common cause of a lipohemarthrosis is an intra-articular fracture with leakage of marrow fat into the joint.
REFERENCES: Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
Kier R, McCarthy SM: Lipohemarthrosis of the knee: MR imaging. J Comput Assist Tomogr 1990;14:395-396.
Question 95:
What is the most common complication of using structural bulk allograft to reconstruct segmental defects of the acetabulum?
Options:
- Infection
- Early loss of cup fixation
- Graft resorption and collapse
- Limb-length discrepancy
- Dislocation
Correct Answer: Graft resorption and collapse
Explanation:
DISCUSSION: Both autograft and allograft have been used for complex acetabular reconstructions. They have been shown to be successful in the short term. However, graft resorption with collapse and subsequent cup loosening have occurred at high rates for both types of grafts, especially if reinforcement rings or cages are not used.
REFERENCES: Jasty M, Harris WH: Salvage total hip reconstruction in patients with major acetabular bone deficiency using structural femoral head allografts. J Bone Joint Surg Br 1990;72:63-67.
Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Kwong LM, Jasty M, Harris WH: High failure rate of bulk femoral head allografts in total hip acetabular reconstructions at 10 years. J Arthroplasty 1993;8:341-346.
Question 96:
A 35-year-old man has had a mass on the bottom of his foot for the past 6 months. He reports that initially the mass was exquisitely painful but now is minimally tender. Examination reveals a 2.5- x 2.0-cm firm, noncompressible, nonmobile mass contiguous with the plantar fascia in the distal arch. The mass is particularly prominent with passive dorsiflexion of the ankle and toes. What is the best course of action?
Options:
- Observation
- Incisional biopsy
- Excisional biopsy
- MRI
- Ultrasound
Correct Answer: Observation
Explanation:
DISCUSSION: The history is most consistent with a plantar fibroma. The nodules typically are located within the substance of the plantar aponeurosis. The clinical appearance is usually diagnostic without the need for advanced imaging studies. While the lesion may be prominent and painful to direct palpation, the anatomic location is usually off of the weight-bearing surface. Observation with or without an accommodative orthotic is the treatment of choice. Recurrence is common following attempted excision.
REFERENCES: Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Durr HR, Krodel A, Trouillier H, Lienemann A, Refior HJ: Fibromatosis of the plantar fascia: Diagnosis and indications for surgical treatment. Foot Ankle Int 1999;20:13-17.
Question 97:
Figures 38a and 38b show the CT scans of a 64-year-old woman. What is the most likely diagnosis?
Options:
- Calcaneal fibular abutment
- Symmetrical narrowing of the subtalar joint consistent with an inflammatory arthropathy
- Cystic lesion of the tibia consistent with enchondroma
- Stress fracture of the talus
- A lateral malleolar fracture
Correct Answer: Calcaneal fibular abutment
Explanation:
DISCUSSION: The CT scans show large cystic lesions in the talus and calcaneus with complete subluxation of the subtalar joint, allowing the calcaneus to slide laterally until it becomes blocked by the fibula. The cause of this subluxation is severe posterior tibial tendon dysfunction. Although no fibular fracture has yet appeared, it can occur with continued stress from the calcaneus. There is, however, a pathologic fracture in the medial calcaneus through a medial degenerative cyst. The joint space is irregular and not symmetrical as would be seen in an inflammatory arthropathy. Cystic lesions are not present in the tibia. No stress fracture is seen in the talus.
REFERENCES: Coughlin MJ: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 437-499.
Anderson RB, Davis WH: Management of the adult flatfoot deformity, in Myerson M (ed):
Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1017-1039.
Question 98:
Figures 47a through 47f show the AP radiograph, bone scan, CT scan, MRI scan, and biopsy specimens of a 30-year-old woman who has had vague left shoulder pain for 1 year. Management should consist of
Options:
- curettage.
- radiation therapy.
- radiation therapy and chemotherapy.
- antibiotics.
- wide resection.
Correct Answer: curettage.
Explanation:
DISCUSSION: The histology shows eosinophils with a background of larger cells (Langerhans’ cells). This is consistent with eosinophilic granuloma. Localized sites are best treated with curettage, steroid injection, or observation. Chemotherapy is used only if there is systemic involvement.
REFERENCES: Mirra JM: Eosinophilic granuloma, in Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. London, England, Lea and Febiger, 1989, pp 1023-1060.
Sessa S, Sommelet D, Lascombes P, Prevot J: Treatment of Langerhans-cell histiocytosis in children: Experience at the Children’s Hospital of Nancy. J Bone Joint Surg Am 1994;76:1513-1525.
Mickelson MR, Bonfiglio M: Eosinophilic granuloma and its variations. Orthop Clin North Am 1977;8:933-945.
Question 99:
Osteoporotic vertebral compression fractures are associated with Review Topic
Options:
- neurologic deterioration in 33% of patients.
- osteomalacia in 50% of patients.
- a further fracture risk rate of 20%.
- chronic pain in 75% of patients.
- a 2-year mortality rate that is less than that associated with hip fractures.
Correct Answer: a further fracture risk rate of 20%.
Explanation:
Osteoporotic vertebral compression fractures are associated with neurologic complications in less than 1% of patients. After the initial fracture however, patients have a 20% risk of further fractures. The mortality rate of patients with vertebral fractures exceeds that of patients with hip fractures when they are followed beyond 6 months.
Question 100:
Figure 17 shows the clinical photograph of a 45-year-old female tennis player who has right arm pain and weakness with elevation after undergoing a cervical biopsy several months ago. The cause of her shoulder weakness is damage to the
Options:
- spinal accessory nerve, causing shoulder elevation with the scapula translated and the inferior angle rotated medially.
- spinal accessory nerve, causing shoulder depression with the scapula translated laterally and the inferior angle rotated laterally.
- long thoracic nerve, causing shoulder elevation with the scapula translated medially and the inferior angle rotated medially.
- long thoracic nerve, causing shoulder depression with the scapula translated laterally and the inferior angle rotated laterally.
- thoracodorsal nerve, causing shoulder depression with the scapula translated laterally and the inferior angle rotated laterally.
Correct Answer: spinal accessory nerve, causing shoulder depression with the scapula translated laterally and the inferior angle rotated laterally.
Explanation:
DISCUSSION: The patient has primary scapulotrapezius winging caused by surgical damage to the spinal accessory nerve during a lymph node biopsy. Other causes include blunt trauma, traction, and penetrating injuries. With spinal accessory palsy, the shoulder appears depressed and laterally translated because of unopposed serratus anterior muscle function. With primary serratus anterior winging that is the result of long thoracic nerve palsy, the scapula assumes a position of elevation and medial translation with the inferior angle rotated medially. The thoracodorsal nerve innervates the latissimus dorsi and is not associated with scapular winging.
REFERENCES: Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Wright TA: Accessory spinal nerve injury. Clin Orthop 1975;109:15-18.