Orthopedic Board Prep MCQs: Adult Reconstruction & Foot | Part 174

Key Takeaway
This page offers Part 174 of a comprehensive OITE and AAOS Orthopedic Board Review MCQ series by Dr. Mohammed Hutaif. It features 100 high-yield, verified multiple-choice questions, mirroring OITE and AAOS exam formats. Designed for orthopedic residents and surgeons, it provides essential practice for board certification preparation.
About This Board Review Set
This is Part 174 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 174
This module focuses heavily on: Arthroplasty, Foot, Hip, Knee.
Sample Questions from This Set
Sample Question 1: Ayear-oldwomanisscheduledtoundergorighttotalhiparthroplasty.Herpreoperativeradiographisshowninbelow.Toavoidincreasingthispatient’scombinedoffsetwhilemaintainingherleglength, what is the most appropriate surgical plan?...
Sample Question 2: ..First-line treatment recommendations include...
Sample Question 3: An 18-year-old man sustains a twisting injury to the left knee while playing football. An MRI scan is shown in Figure 48. What is the most likely diagnosis? Review Topic...
Sample Question 4: Figure 19 shows the radiograph of a 6-month-old infant who has limited hip motion. History reveals no complications during pregnancy or delivery. Examination reveals that hip abduction is 45 degrees in flexion bilaterally. The neurologic ex...
Sample Question 5: -The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports,and the surgeon and reha...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A year-old woman is scheduled to undergo right total hip arthroplasty. Her preoperative radiograph is shown in below. To avoid increasing this patient’s combined offset while maintaining her leg length, what is the most appropriate surgical plan?
Explanation
The management of patients with proximal femoral deformity can be difficult. Appropriate implant selection and preoperative templating are critical. In this patient, it would be difficult to avoid increasing the combined offset by too much, which could contribute to the overtensioning of the soft tissues and trochanteric pain. By medializing the acetabular component (decreasing the combined offset), using a low offset femoral component or a cemented component placed more valgus (decreasing the combined offset), and making a longer neck cut (to avoid shortening of the lower extremity), restoration of the patient’s native offset and leg length can be achieved.
Question 2
..First-line treatment recommendations include
Explanation
Ultrasound
MRI scan of the thigh
Chest CT scan and whole-body bone scan
Positron emission tomography (PET) scan
Presurgical radiation therapy
Marginal resection
Radical resection and postsurgical radiation
Transverse incision centered over the mass
Incision centered over the mass in line with long axis of limb
Sentinel node biopsy
Core needle biopsy
For each soft-tissue mass clinical scenario or question below, match the most appropriate next evaluation or treatment step listed above.
Question 3
An 18-year-old man sustains a twisting injury to the left knee while playing football. An MRI scan is shown in Figure 48. What is the most likely diagnosis? Review Topic

Explanation
Question 4
Figure 19 shows the radiograph of a 6-month-old infant who has limited hip motion. History reveals no complications during pregnancy or delivery. Examination reveals that hip abduction is 45 degrees in flexion bilaterally. The neurologic examination is normal. What is the best course of action?
Explanation
REFERENCE: Castelein RM, Korte J: Limited hip abduction in the infant. J Pediatr Orthop 2001;21:668-670.
Question 5
-The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports,and the surgeon and rehabilitation team consider their request. Compared to nonaccelerated rehabilitation,patients who follow an early accelerated rehabilitation protocol experience
Explanation
The Lachman test is the most sensitive examination for acute ACL injuries. ACL injury rates are higher in women than in men. This likely is attributable to anatomic differences (smaller notches, smaller ligaments, and different landing biomechanics). Lateral meniscal tears are more common than medial tears. The anterior drawer test is accentuated with 30 degrees of external rotation of the tibia. The MRI scan shows bone bruises consistent with an ACL tear. It is also always necessary to examine other structures of the knee in patients with ACL tears. All ligaments of the affected knee should be assessed.Lateral meniscal tears are frequently associated with ACL tears. Medial meniscal tears and posterolateral corner deficiency are also possible. Randomized clinical trials comparing an early accelerated vs nonaccelerated rehabilitation have demonstrated no significant differences in long-term results. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
Question 6
A 20-year-old woman with spastic hemiplegia is evaluated for function and hygiene issues with her right wrist. Her wrist has a resting posture of 90° of flexion and can be passively extended to 65° of flexion. Her fingers are flexed into her palm but can be passively extended with the wrist at 95°. What treatment is likely to provide the most durable result for improved hygiene, function, and cosmesis?
Explanation
The patient has a static deformity of the wrist with a fixed flexion deformity of more than 45°. Soft-tissue procedures such as those referenced in options A and B would not be sufficient to address the degree of contracture. Additionally, Botulinum toxin injections would not provide relief for capsular contractures. Wrist arthrodesis combined with a proximal row carpectomy has been shown to provide a functional and cosmetic alternative for patients with severe wrist flexion contractures.
Question 7
By which mechanism can a true aneurysm of the ulnar artery result?
Explanation
Question 8
The patient has weakness with elbow flexion and has numbness down the anterior lateral aspect of the forearm.
Explanation
The Latarjet procedure was initially described in 1959 as a modification of the Bristow procedure. It has been used as a primary procedure to address instability, but is used more commonly for patients with instability and glenoid bone loss. In 2000, Burkhart and associates reported a 67% failure rate of the Bankart procedure in patients with an inverted pear-shaped glenoid (glenoid bone loss) or an engaging Hill-Sachs lesion, with a suggestion that a bone graft procedure would be optimal in this population. Complications following the Latarjet procedure have been reported as high as 25%, with the majority attributable to nerve injury, recurrent instability, and arthritis. Many of these complications are likely secondary to surgical technique. A coracoid graft that is placed too laterally or with prominent screws will overhang the glenoid and lead to early degenerative glenohumeral arthritis. A coracoid graft placed too medially can lead to recurrent instability secondary to an ineffective subscapularis sling and bone block. A coracoid graft placed inferiorly indicates dissection close to the axillary nerve, which can place tension on the axillary nerve or cause injury from direct trauma. After harvesting the coracoid graft, the surgeon must find the musculocutaneous nerve as it enters the conjoint tendon on the medial surface about 5 cm distal to the coracoid. Excessive dissection or retraction can lead to musculocutaneous nerve palsy.
Question 9
A 13-year-old boy sustains a valgus stress injury to the knee while playing football, and he is unable to bear weight after the injury. Examination reveals tenderness medially superior to the joint line. The knee is held in flexion, and he has a large effusion and localized medial swelling. Plain radiographs show no obvious fracture. What is the next diagnostic step?
Explanation
REFERENCES: Smith L: Concealed injury to the knee. J Bone Joint Surg Am 1962;44:1659-1660.
Beaty JH, Kumar A: Fractures about the knee in children. J Bone Joint Surg Am 1994;76:1870-1880.
Question 10
A decrease in alkaline phosphatase would most likely be manifest in which metabolic disorder?
Explanation
TNSALP is found in osteoblasts and hydrolyzes inorganic phosphates, leading to an increase in serum phosphate levels, which helps to maintain physiologic levels. A decrease in this process impairs bone mineralization leading to rickets. In the perinatal period, hypophosphatasia and decreased mineralization leads to caput membraneceum, shortened limbs and respiratory failure. Childhood hypophosphatasia is marked by premature loss of deciduous teeth and rachitic deformities. Adult hypophosphatasia I is characterized by teeth and chest wall deformities (similar to adolescent hypophosphatasia) as well as recurrent metatarsal and femoral stress fractures.
Mornet reviewed hypophosphatasia and the alkaline phosphatase mutations. Screening for the 65 distinct mutation can aid in diagnosis and family counseling in severe forms.
Illustration A shows abnormal dentition found in hypophosphatasia. Illustration B shows widespread rachitic changes characteristic of hypophosphatasia.
Incorrect Answers:
Question 11
A previously healthy 13-year-old girl has had thigh pain for the past 3 weeks. The radiograph shown in Figure 47a reveals a lesion in the right femur. A bone scan and CT scan of the chest show no evidence of other lesions. A biopsy specimen is shown in Figure 47b. What is the most likely diagnosis?
Explanation
REFERENCES: Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby, 1988.
Mirra, JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989.
Question 12
Figure 62 shows the radiograph of a 46-year-old man who has had increasing shoulder pain and diminishing motion over the last 10 years. Because his difficulties are severely impacting his quality of life, he is seeking advice and treatment options. Twenty five years ago, he underwent a shoulder stabilization procedure for recurrent shoulder dislocations. Examination reveals he can only elevate his arm to less than shoulder level and his external rotation is no more than 10 degrees. Management consisting of nonsteroidal anti-inflammatory drugs and intra-articular steroid injections has failed to provide relief. What is the most appropriate treatment recommendation? Review Topic

Explanation
arthritis of dislocation is 45 years old. Despite the young age of these patients, total shoulder arthroplasty offers the most predictable improvement in pain and function. However, the patient must be made aware of the need to protect the arm from excessive loads to protect the glenoid implant. Because there is complete loss of articular cartilage and incongruent joint surfaces, there is no role for arthroscopic debridement and capsular release. Injections offer little, if any, chance of improvement with the prior history of nonresponse. Physical therapy predictably makes patients worse because loading the arthritic joint generates more pain. Reverse shoulder arthroplasty is reserved for elderly patients with severe rotator cuff deficiency. A humeral head arthroplasty, while potentially more ideal than a total shoulder arthroplasty because of glenoid concerns, would likely not offer pain relief in the face of the significant glenoid involvement and incongruity.
Question 13
Which of the following is the strongest contraindication to unicompartmental knee arthroplasty (UKA)?
Explanation
REFERENCES: Lotke PA (ed): Knee Arthroplasty: Master Techniques in Orthopaedic Surgery. New York, NY, Raven Press, 1995, pp 275-293.
Insall JN, Windsor RE, Scott WN, et al (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 805-814.
Tabor OB Jr, Tabor OB: Unicompartmental arthroplasty: A long-term follow-up study.
J Arthroplasty 1998;13:373-379.
Question 14
An 81-year-old man with severe low back pain reports right extensor hallucis longus and anterior tibialis weakness and difficulty urinating over the past 24 hours. He has a temperature of 101 degrees F (38.3 degrees C). MRI scans are shown in Figures 31a and 31b. Management should consist of
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 257-271.
Reihsaus E, Waldbaur H, Seeling W: Spinal epidural abscess: A meta-analysis of 915 patients. Neurosurg Rev 2000;23:175-204.
Question 15
Familial (Leiden) thrombophilia is of importance in joint arthroplasty because of an abnormality in the clotting cascade. Which of the following statements best describes the condition?
Explanation
Question 16
In patients with suspected hepatitis C, which of the following tests is commonly used to confirm the diagnosis after a positive ELISA screening test?
Explanation
REFERENCES: de Medina M, Schiff ER: Hepatitis C: Diagnostic assays. Semin Liver Dis 1995;15:33-40.
McGrory BJ, Kilby AE: Hepatitis C virus infection: Review and implications for the orthopedic surgeon. Am J Orthop 2000;29:261-266.
Question 17
What muscles are responsible for the most common deformity after antegrade intramedullary nailing for a subtrochanteric femur fracture?

Explanation
The reference by French et al is a review on 45 patients with subtrochanteric fractures treated with cephalomedullary interlocked nailing. Based on femoral neck-shaft angle, 61% of the fractures were reduced in at least 5º varus. The authors attributed this malalignment to failure to counteract muscle forces acting on the proximal fragment, combined with the adducted position of the distal femur during portal creation.
The reference by Ricci et al is a report of 403 femoral shaft fractures treated with intramedullary nailing. Patients with proximal femoral shaft fractures were found to have the highest incidence of malalignment. The most common deformity in this group was varus, followed by procurvatum (or flexion).
Question 18
Poor pre-injury cognitive function has been proven to increase mortality for which of the following injuries?

Explanation
Question 19
Which of the following radiographic views best depicts a Hill-Sachs defect?
Explanation
REFERENCE: Rockwood CA, et al: X-ray evaluation of shoulder problems, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 1, pp 178-207.
Question 20
A 32-year-old volleyball player has dull posterior shoulder pain. An examination reveals moderate external rotation weakness with his arm at his side, but normal strength on supraspinatus isolation. Deltoid and supraspinatus bulk appear normal, although there appears to be mild infraspinatus atrophy. Sensation is normal throughout the shoulder and shoulder girdle. What is the most likely diagnosis?
Explanation
This clinical scenario describes a patient with an isolated injury affecting the infraspinatus muscle. The anatomic location of such a lesion would be at the spinoglenoid notch, at which the suprascapular nerve may be compressed distal to its innervation of the supraspinatus but proximal to the infraspinatus innervation. A calcified transverse scapular ligament would also affect the suprascapular nerve but is proximal to the innervation of both muscles. Quadrilateral space syndrome would affect innervation of the deltoid (and teres minor). Parsonage-Turner syndrome is a more diffuse, and often severely painful, brachial plexus neuropathy.
Question 21
A 17-year-old high school soccer player sustains an anterior cruciate ligament (ACL) tear at the beginning of the season. An MRI scan confirms a complete ACL tear with no meniscal injuries. The patient plans an early return to play and would like to avoid surgery. Therefore, the patient and family should be advised that nonsurgical management consisting of rehabilitative exercises and the use of a functional knee brace will most likely result in
Explanation
REFERENCES: Shelton WR, Barrett GR, Dukes A: Early season anterior cruciate ligament tears: A treatment dilemma. Am J Sports Med 1997;25:656-658.
Snyder-Mackler L, Fitzgerald GK, Bartolozzi AR III, Ciccotti MG: The relationship between passive joint laxity and functional outcome after anterior cruciate ligament injury. Am J Sports Med 1997;25:191-195.
Question 22
A 35-year-old rock climber sustains an L1 burst fracture from a 30-foot fall while climbing. He sustained no other fractures or serious injuries. He is neurologically intact and has minimal posterior tenderness without increased spinous process separation on examination. Radiographs reveal kyphosis of 20 degrees between T12 and L2 with 30% vertebral height loss. A CT scan shows 55% canal compromise. What is the most appropriate management? Review Topic
Explanation
Question 23
A 17-year-old javelin thrower reports medial-sided elbow pain and diminished grip strength while throwing. He has decreased sensation in the little and ring fingers of his throwing hand only while throwing. The sensory deficits resolve at rest. Examination of the elbow reveals no instability and full motion. He has a positive Tinel’s sign over the cubital tunnel and a positive elbow flexion test. Radiographs are normal. What is the next most appropriate step in management?
Explanation
REFERENCES: Posner MA: Compressive neuropathies of the ulnar nerve at the elbow and wrist. Instr Course Lect 2000;49:305-317.
Omer GE, Spinner M, Van Beek AL (eds): Management of Peripheral Nerve Problems, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 65-69.
Question 24
Figures 31a and 31b show the radiograph and MRI scan of an otherwise normal 3-month-old infant who has a spinal deformity. MRI reveals no intraspinal anomalies. What is the next step in management?
Explanation
REFERENCES: Basu PS, Elsebaie H, Noordeen MH: Congenital spinal deformity:
A comprehensive assessment at presentation. Spine 2002;27:2255-2259.
Hedequist D, Emans J: Congenital scoliosis. J Am Acad Orthop Surg 2004;12:266-275.
Question 25
In recurrent posterior shoulder instability, what is the recommended approach to the posterior capsule?
Explanation
REFERENCES: Dreese J, D’Alessandro D: Posterior capsulorrhaphy through infraspinatus split for posterior instability. Tech Shoulder Elbow Surg 2005;6:199-207.
Shaffer BS, Conway J, Jobe FW, et al: Infraspinatus muscle-splitting incision in posterior shoulder surgery: An anatomic and electromyographic study. Am J Sports Med 1994;22:113-120.
Fuchs B, Jost B, Gerber C: Posterior-inferior capsular shift for the treatment of recurrent voluntary posterior subluxation of the shoulder. J Bone Joint Surg Am 2000;82:16-25.
Question 26
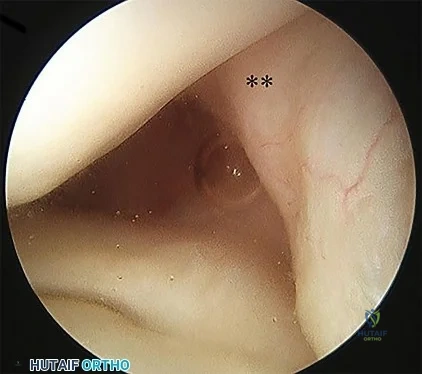
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior-stabilized TKA without evidence of component loosening. What is the most likely cause of this patient's pain?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
Question 27
A 10-month-old boy has an untreated developmental hip dislocation.
Explanation
Early radiographic findings of avascular necrosis (AVN) of the hip include sclerosis and a subchondral lucency. A common presentation of Legg-Calve-Perthes disease (idiopathic pediatric hip AVN) is intermittent pain in the thigh, groin, or knee with an examination localizing to the hip; a Trendelenburg gait or sign; and painful, restricted passive hip range of motion. AVN also may be observed in association with a slipped capital femoral epiphysis (SCFE). AVN risk is highest in the setting of an unstable SCFE (10%-60%); risk is 0% to 1.4% when the SCFE is stable. A multicenter review of the modified Dunn procedure for treatment of unstable SCFE noted an AVN rate of 26%.
The most common deformity associated with SCFE is proximal femoral varus, flexion, and external rotation leading to an abnormal femoral head-neck junction offset. This causes a loss of passive hip flexion and internal rotation and the phenomenon of obligate external
rotation with flexion. The residual deformity frequently results in femoroacetabular impingement. Labral tears also are associated with cam impingement secondary to underlying osseous abnormalities including abnormal femoral head-neck junction offset.
Endocrinopathies potentially are associated with SCFE because of hormone-related physeal changes and subsequent mechanical insufficiency of the proximal femoral physis. With renal osteodystrophy, the physeal widening results from secondary hyperparathyroidism and progressive proximal femoral deformity may develop. Optimal medical management of hyperparathyroidism is essential. Surgical stabilization via in situ fixation of the proximal femur is indicated when SCFE is diagnosed.
The proximal femoral epiphysis secondary ossification center commonly appears between the ages of 4 and 7 months. In the setting of developmental hip dislocation, the appearance of the secondary ossification center is commonly delayed. After closed or open reduction of developmental dysplasia of the hip, failure of the femoral head ossific nucleus to appear within 12 months following the reduction is a sign of proximal femoral growth disturbance and AVN.

Question 28
Figures 9a and 9b show the radiographs of a 75-year-old man who underwent a revision total knee arthroplasty with a long-stemmed tibial component. In rehabilitation, he reports fullness and tenderness in the proximal medial leg (at the knee). The strategy that would best limit this postoperative problem is use of
Explanation
REFERENCE: Gustke K: Cemented tibial stems are not requisite in revision. Orthopedics 2004;27:991-992.
Question 29
A 34-year- woman has pain at the base of the thumb that worsens é pinching activities. Nonsurgical treatment has failed to provide relief. Examination reveals that the basilar joint is hypermobile, tender and painful when stressed. A radiograph of the trapeziometacarpal joint shows normal contour with widening when compared with the opposite side. Management should consist of
Explanation
Question 30
A neurologic injury at T11-L2 with loss of bowel and bladder control is best described as what syndrome?
Explanation
REFERENCES: Apple DF Jr: Spinal cord injury rehabilitation, in Rothman RH, Simeone FA (eds): The Spine, ed 3. Philadelphia, PA, WB Saunders, 1992, Chapter 31.
Weisberg LA: Neurologic localization: Lesions below foramen magnum, in Weisberg LA, Strub RL, Garcia CA (eds): Adult Neurology, ed 2. St. Louis, MO, Mosby, 1993.
Question 31
- Which of the following conditions is most likely inherited as an autosomal dominant trait?
Explanation
Question 32
Figures 1 and 2 are the radiographs of a 55-year-old man who has a 3-year history of right shoulder pain. He has maximized nonoperative management and is interested in operative treatment. He had an open Bankart repair 20 years ago and did well until a few years ago. What is most important to know when deciding on the best surgical treatment for this patient?
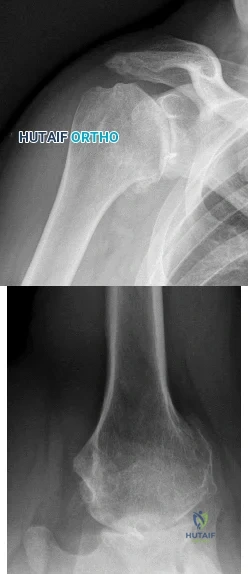
Explanation
Although the radiographs do not reveal any obvious signs of rotator cuff failure, the patient had had an open Bankart 20 years ago. The integrity of the subscapularis tendon following a previous open shoulder procedure is crucial in deciding which type of arthroplasty to consider. Range of motion and infraspinatus strength do not affect the decision-making process, assuming the rotator cuff is intact. Activity level can be important when deciding whether to proceed with an arthroplasty, but it is not as important as the rotator cuff integrity when choosing which
arthroplasty to use.
Question 33
What is the most common maxillofacial/dental injury in ice hockey?
Explanation
displacement of the tooth from aleveolar support. A crown fracture is an incomplete loss or fracture of the tooth enamel without loss of the tooth. The other injuries (mandible fracture, lip laceration, tooth
avulsion, and temporomandibular contusion) occur but are not nearly as common.
REFERENCES: Lahti H, Sane J, Ylipaavalniemi P: Dental injuries in ice hockey games and training. Med Sci Sports Exerc 2002;34:400-402.
Minkoff J, Stecker S, Varlotta GP, et al: Ice hockey, in Fu FH, Stone DA (eds): Sports Injuries, ed 2.
Philadelphia, PA, 2001, pp 516-517.
Question 34
Figure 35 is the radiograph of a 37-year-old woman who began having right forefoot pain about 4 weeks ago after increasing her daily running mileage. She denies any specific injury. Upon examination she has tenderness over the medial forefoot with mild swelling. In addition to her activity level, what is the primary etiology of the radiograph finding?

Explanation
Stress fractures are the result of physiological bone response to increased stress. Increased stress on bone triggers an increase in remodeling, which begins with resorption of bone at the site of stress. Ongoing stress can overwhelm bone strength, resulting in a fracture. In the foot this most commonly is seen in the second metatarsal at the junction of the middle and distal thirds. Contributing factors to increased loading of the second metatarsal include hallux valgus (decreased hallux loading transfers to the second metatarsal head), hallux rigidus (offloading of the hallux attributable to pain increases second metatarsal loading), and a long second metatarsal (increased duration of contact during push-off in the stance phase).
RECOMMENDED READINGS
Shindle MK, Endo Y, Warren RF, Lane JM, Helfet DL, Schwartz EN, Ellis SJ.
Stress fractures about the tibia, foot, and ankle. J Am Acad Orthop Surg. 2012 Mar;20(3):167-
Question 35
A 17-year-old African American high school football player is in the afternoon session of an August “2-a-day” practice. He tells his trainer he is experiencing weakness, dizziness, and nausea. The ambient temperature is 31°C with a relative humidity of 70%. An examination by the team trainer reveals a body temperature of 39°C and headache, chills, confusion, and disorientation. What is the most likely diagnosis?
Explanation
Heat exhaustion and heatstroke are both forms of heat illness during which the body is unable to self-regulate internal temperature. The hallmarks of heatstroke are altered mental status and/or core temperature higher than 40°C. Heat exhaustion may be marked by nausea, vomiting, headache, dizziness, chills, and excessive sweating, but there are no mental status
changes. In heatstroke, sweating can often slow or cease as dysregulation worsens. Simple dehydration would not result in mental status changes or elevated core temperature. Sickle-cell crisis is marked by extreme pain, with location depending on the site of crisis. Four main patterns are common: bone, chest, abdominal, or joint crises. Sickle-cell crisis can be precipitated by dehydration, although it also can occur as a result of cold exposure.
Question 36
Compared with surgically treated patients, patients with extra-articular distal third humeral shaft fractures that are treated nonsurgically with functional bracing can be expected to show which of the following findings?
Explanation
Question 37
Which of the following muscles has dual innervation?
Explanation
REFERENCE: Mahakkanukrauh P, Somsarp V: Dual innervation of the brachialis muscle.
Clin Anat 2002;15:206-209.
Question 38
Which of the following postoperative rehabilitation techniques causes minimal rotator cuff muscle activation? Review Topic
Explanation
Question 39
- What is the usual mechanism of injury for the fracture shown in Figures 49a and 49b?

Explanation
Question 40
A 50-year-old man fell from a ladder onto his left shoulder and sustained the injury shown in the radiographs in Figures 71a and 71b. He underwent surgery with repair of the coracoclavicular ligaments and deltotrapezial fascia with coracoclavicular screw placement. Which of the following statements regarding postoperative complications is most accurate? Review Topic
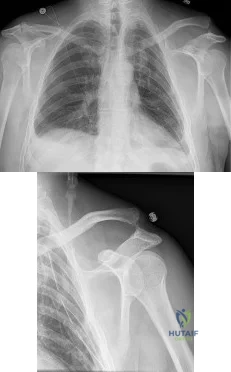
Explanation
Question 41
Figure 1 shows the radiograph obtained from a 67-year-old woman who has progressive wrist pain. She undergoes a salvage motion-sparing surgery that relies on the intact cartilage of the capitate head. It is necessary to preserve what structure during this procedure?
Explanation
The radioscaphocapitate ligament must be preserved in cases of proximal row carpectomy or scaphoidectomy with four-corner fusion. Failure to do so can result in ulnar translocation of the carpus. The attachment of the long radiolunate ligament to the lunate is compromised in proximal row carpectomy, although it is left intact in scaphoidectomy with four-corner fusion. Preservation of the dorsal radiocarpal ligament through a limited arthrotomy is advocated by Ozyurekoglu and Turker as a method of preserving the blood and nerve supply of the carpus, but this technique has not been proven to be required. The authors did cut through the dorsal intercarpal ligament in their exposure.
Question 42
Radiographs of a 15-year-old girl with knee pain reveal a radiopaque lesion of the distal femoral metaphysis and epiphysis with a small associated soft-tissue mass. A biopsy specimen shows osteoid and pleomorphic cells with multiple mitotic figures. Staging studies show no other sites of disease. Treatment should consist of
Explanation
REFERENCE: Simon MA, Springfield DS, et al: Common Malignant Bone Tumors: Osteosarcoma. Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 265-274.
Question 43
A year-old man reports symptomatic medial knee pain that has become progressively worse during the past year. MRI reveals a complex, posterior horn medial meniscus tear with associated medial lateral and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable relief of symptoms?
Explanation
Total knee replacement is a well-established surgery for diffuse, symptomatic osteoarthritis of the knee joint, and its efficacy has been shown in many studies. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee, arthroscopy in the setting of existing osteoarthritis is efficacious for relieving the signs and symptoms of a torn meniscus but not for osteoarthritis. Likewise, in young and active patients, clinical outcomes show improvement after realignment osteotomy for single- compartment osteoarthritis. Unicondylar knee replacement is not indicated for tricompartmental disease
of the knee.
Question 44
A 45-year-old distance runner has a hyaluronic acid injection to his knee because of degenerative arthritis. He immediately develops a severe rash and a systemic hypersensitivity reaction. This patient most likely is also allergic to which of the following?
Explanation
REFERENCES: Gloyscen DN, Gillespie MJ, Schenek RC: The effects of medication in sports injuries, in DeLee JC, Drez D Jr, Miller MD (eds): Orthopedic Sports Medicine: Principles and Practice, ed 2.
Philadelphia, PA, WB Saunders, 2003, vol 1, pp 121-124.
Schenck RC Jr: New approaches to the treatment of osteoarthritis: Oral glucosamine and chondroitin sulfate. Instr Course Lect 2000;49:491-494.
Question 45
Which factor increases the success rate associated with all-inside lateral meniscal repair?
Explanation
Decreased patient age, neutral alignment, and a concomitant ACL tear are associated with improved success rates of meniscal repair. Meniscus tears on the contralateral side of the knee and articular cartilage defects are not associated with improved healing rates.
RESPONSES FOR QUESTIONS 5 THROUGH 6
Physical therapy and a home exercise program
Corticosteroid injection
Arthroscopic debridement
Microfracture
Osteochondral autograft transplantation (OAT)
Match the treatment above with the clinical scenario below
Question 46
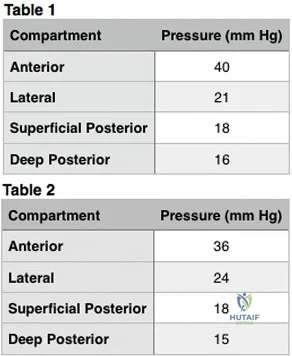
Figure 91 is the radiograph of a 20-year-old man who kicked a door while intoxicated. At the emergency department, his leg is placed into a long-leg cast. After 2 hours, he reports increasing pain, numbness, and tingling in his toes. What is the most appropriate initial treatment?

Explanation
(SBQ12TR.88) When evaluating a fracture dislocation of the elbow, a varus and posteromedial rotation mechanism of injury typically results in what injury pattern?
A fracture of the radial head requiring ORIF
A highly comminuted radial head fracture requiring radial head arthroplasty or resection
An MCL injury requiring repair
A type I avulsion fracture of the coronoid
An anteromedial coronoid fracture
A varus and posteromedial rotation mechanism of injury typically results in a fracture of the anteromedial facet of the coronoid which frequently requires reduction and fixation to restore stability.
A varus and posteromedial mechanism of injury about the elbow presents with an injury pattern distinctly different from other injury patterns. A key part of treating this injury pattern is recognizing a fracture of the anteromedial facet of the coronoid, which often requires reduction and fixation to restore stability about the elbow. It is important to recognize this during preoperative planning since this injury typically requires a medial approach.
Steinman presents a review article describing coronoid fracture patterns and their mechanisms of injury.
Doornberg and Ring present a level 4 review showing that coronoid fracture patterns and their required treatments are predictable based on mechanism of injury. Varus and posteromedial mechanisms were found to reliably create a fracture of the anteromedial facet of the coronoid, and were associated with sparing of the MCL and radial head.
Doornberg and Ring also presented a Level 3 review of anteromedial facet cornoid fractures. They found that they could not be adequately visualized and treated from a lateral approach, and that they typically required reduction and fixation to restore adequate stability to the elbow. This stresses the importance of recognizing this injury pattern during preoperative planning.
Illustrations A and B are AP and lateral radiographs of an elbow following a varus/posteromedial injury with an anteromedial coronoid facet fracture. Illustration C is a diagram demonstrating fracture lines that create an anteromedial facet fracture fragment. This fracture can be subclassified into three subtypes [anteromedial rim (a), rim plus tip (b), and rim and tip plus the sublime tubercle (c)]
Incorrect answers:
(SBQ12TR.78) A 67-year-old female patient presents with increasing right hip/thigh pain over the past three months, which is now recalcitrant to anti-inflammatories. There is no history of trauma or constitutional symptoms. Her past medical history consists of hypertension, coronary artery disease, osteoporosis and gastric reflux. Physical examination reveals mild pain at the extremes of range of motion of the hip and a painful right sided limp. A radiograph of the right hip is seen in Figure A. What would be the most appropriate treatment for this patient at this time? Review Topic
Observation only
Referral to physiotherapy
MRI spine and hip
Total hip arthroplasty
Intramedullary femoral nail
This osteoporotic female patient is presenting with subtrochanteric lateral cortical thickening and hip pain. This is consistent with an insufficiency fracture of the femur secondary to use of bisphosphonate medication for treatment of osteoporosis. The most appropriate treatment would be intramedullary femoral nail fixation.
Bisphosphonate medications have been shown to be associated with atypical (subtrochanteric) femur fractures. These patients often have prodromal hip pain and lateral cortical thickening on radiographs prior to fracture. In addition, there has shown to be a significantly increased risk of fracture in the presence of the “dreaded black line” that occurs at the site of thickening.
Lenart et al. examined a case series of patients using bisphosphonates for the treatment of osteoporosis. They identified 15 postmenopausal women who had been receiving alendronate for a mean (±SD) of 5.4±2.7 years and who presented with atypical low-energy fractures. Cortical thickening was present in the contralateral femur in all the patients with this pattern.
Goh et al. retrospectively reviewed patients who had presented with a low-energy subtrochanteric fractures. They identified 13 women of whom nine were on long-term alendronate therapy. Five of these nine patients had prodromal pain in the affected hip in the months preceding the fall, and three demonstrated a stress reaction in the cortex in the contralateral femur.
Figure A shows a right hip radiograph with subtrochanteric lateral cortical thickening. There is mild arthritic changes in the hip. Illustration A shows a bone scan and radiographs of subtrochanteric lateral cortical thickening that resulted in fracture.
Incorrect Answers
Question 47
What artery provides the only direct vascularizaton to both the intraneural and extraneural blood supply of the ulnar nerve just proximal to the cubital tunnel?
Explanation
REFERENCE: Yamaguchi K, Sweet FA, Bindra R, et al: The extraneural and intraneural arterial anatomy of the ulnar nerve at the elbow. J Shoulder Elbow Surg 1999;8:17-21.
Question 48
Which of the following best describes the relationship of the anterior tibial artery and dorsalis pedis artery to the extensor hallucis longus (EHL) tendon as they progress from the level of the ankle to the dorsum of the foot?
Explanation
REFERENCES: Resch S: Functional anatomy and topography of the foot and ankle, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 1, pp 25-49.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Question 49
What is the most common physical finding in myelopathic patients? Review Topic
Explanation
Question 50
When treating a proximal tibia fracture, the surgeon decides to (1) use blocking screws in the proximal fragment, and (2) pick the intramedullary nail based on the location of the Herzog curve. Which of the following combinations will best prevent the classic deformity associated with this fracture?
Explanation
Up to 58% of proximal tibial fractures are malaligned. Malalignment arises because the nail fits loosely in the wide metaphyses and cannot control alignment. Without close fit of the nail at the fracture site, the nail will not align the fracture independent of a stable reduction and careful nail path. Blocking screws serve to reduce the size of the proximal metaphyseal canal and guide final nail passage.
Stinner et al. discuss strategies in proximal tibial fracture nailing. They describe an accurate starting point (using the twin peaks AP view or fibular bisector AP view, and flat plateau lateral view). They emphasize fracture reduction prior to reaming and implant placement.
Hiesterman reviewed nailing of extra-articular proximal tibial fractures. Techniques described include blocking screws, unicortical plating, using a universal distractor, nailing in flexion/locking in extension, semiextended nailing (including percutaneous suprapatellar quads-splitting approaches), multiple proximal interlocking screws (>=3).
Illustration A shows placement of a coronal blocking screw. Illustration B shows placement of a sagittal blocking screw. Illustration C shows the effect of the Herzog curve. A more distal Herzog curve leads to a "wedge" effect and fracture displacement whereas a proximal Herzog curve contains the fracture. The "wedge" effect occurs as the nail is seated and impinges on the posterior cortex of the distal segment accentuating an apex anterior deformity because of the effective widening of the nail above the bend and posterior force on the distal segment to match the nail shape.
Incorrect Answers:
Question 51
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on
Explanation
REFERENCE: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 325-335.
Question 52
A “p value” of 4% (p=0.04) indicates that the
Explanation
The p value is the probability that the chance selection of patients might suggest a difference in treatment that was not real. Only with a small p value are we willing to believe that the observed difference in treatment is very likely real and not simply due to chance.
The confidence interval provides a measure of the magnitude of the possible difference between two groups of patients, regardless of whether or not the p value was small. This makes the confidence interval more informative than the p value when different treatments are compared. This is much beyond the scope of this review.
Question 53
Which of the following statements best describes the instantaneous axis of rotation (IAR) for the functional spinal unit? Review Topic
Explanation
Question 54
Figure 131 is the abdominal radiograph of a 70-year-old man who experiences nausea and abdominal tightness 48 hours after undergoing left total knee arthroplasty. An examination reveals severe abdominal distension and markedly decreased bowel sounds. Insertion of a nasogastric tube does not relieve abdominal tightness. What is the best next step?
Explanation
The abdominal radiograph reveals an acute colonic pseudo-obstruction. It is associated with parenteral narcotic use and hypokalemia. Initial treatment is insertion of a nasograstric tube, discontinuation of parenteral narcotics, and correction of electrolyte imbalances. If a pseudo-obstruction is not relieved, colonoscopy should be performed.
Question 55
What type of cementless femoral fixation results in the highest rate of distal femoral osteolysis?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Emerson RH Jr, Sanders SB, Head WC, Higgins L: Effect of circumferential plasma-spray porous coating on the rate of femoral osteolysis after total hip arthroplasty. J Bone Joint Surg Am 1999;81:1291-1298.
Question 56
A 47-year-old man has an acute swollen, red, painful first metatarsophalangeal joint. He denies any history of similar symptoms. What is the first step in evaluation?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 172-173.
Jahss MH: Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991,
pp 1712-1718.
Question 57
A 22-year-old man who sustained a Gustilo-Anderson grade IIIC open fracture of the right tibia and fibula was treated with an immediate open transtibial amputation. After two serial debridements, he underwent wound closure with a posterior myocutaneous soft-tissue flap. What is the preferred method of early rehabilitation?
Explanation
REFERENCES: Burgess EM, Romano RL, Zettl JH: The Management of Lower Extremity Amputations. Washington, DC, US Government Printing Office, 1969, also at: www.prs-research.org.
Smith DG, McFarland LV, Sangeorzan BJ, et al: Postoperative dressing and management strategies for transtibial amputations: A critical review. J Rehabil Res Dev 2003;40:213-224.
Question 58
Figure 37 shows a coronal T2-weighted MRI scan. What is the name of the labeled torn structure?
Explanation
are intact.
REFERENCES: Potter HG, Weiland AJ, Schatz JA, et al: Posterolateral rotatory instability of the elbow: Usefulness of MR imaging in diagnosis. Radiology 1997;204:185-189.
King JC, Spencer EE: Lateral ligamentous instability: Techniques of repair and reconstruction. Techniques in Orthopaedics 2000;8:93-104.
Question 59
A 23-year-old woman has had vague left knee pain for the past 6 months. A radiograph and CT scan are shown in Figures 50a and 50b. What is the most likely diagnosis?
Explanation
REFERENCES: Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 185-196.
Okada K, Frassica FJ, Sim FH, Beabout JW, Bond JR, Unni KK: Parosteal osteosarcoma. A clinicopathological study. J Bone Joint Surg Am 1994;76:366-378.
Question 60
A construction worker sustained a comminuted calcaneus fracture 2 years ago. He now reports progressive hindfoot pain with the recent onset of anterior ankle pain. A lateral hindfoot radiograph is shown in Figure 31. Treatment should consist of
Explanation
REFERENCES: Carr JB, Hansen ST, Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Myerson M, Quill GE Jr: Late complications of fractures of the calcaneus. J Bone Joint Surg Am 1993;75:331.
Question 61
A 5-month-old girl with arthrogryposis has a limb-length discrepancy. Examination and radiographs reveal unilateral hip dislocation. Management should consist of
Explanation
REFERENCES: Staheli LT, Chew DE, Elliot JS, Mosca VS: Management of hip dislocations in children with arthrogryposis. J Pediatr Orthop 1987;7:681-685.
Szoke G, Staheli LT, Jaffe K, Hall JG: Medial-approach open reduction of hip dislocation in amyoplasia-type arthrogryposis. J Pediatr Orthop 1996;16:127-130.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996.
Question 62
What factor is associated with a high risk of developing pseudotumors after metal-on-metal hip resurfacing?
Explanation
Question 63
A sentinel event is defined as an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. What is the most common sentinel event related to spine surgery?
Explanation
REFERENCES: Wong DA, Watters WC III: To err is human: Quality and safety issues in spine care. Spine 2007;32:S2-S8.
Wong DA: Spinal surgery and patient safety: A systems approach. J Am Acad Orthop Surg 2006;14:226-232.
Question 64
The parents of a 3-year-old girl who has had pain and swelling in the right ankle for the past 3 months now report that she has a limp and that the right knee and both ankles are painful and swollen. The limp and difficulty walking are most severe in the morning when the child first gets out of bed and are also more severe after extended walking. The parents deny fever, chills, weight loss, or night pain. Examination shows mild swelling and slightly restricted motion of the right knee and both ankles but is otherwise normal. In addition to initiation of treatment, the child should be referred to which of the following specialists?
Explanation
REFERENCES: Carey TP: Inflammatory arthritides: Juvenile rheumatoid arthritis, seronegative spondyloarthropathies, transient synovitis, hemophilic arthropathy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1315-1321.
Wright D: Juvenile idiopathic arthritis, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001,
pp 427-458.
Question 65
A 42-year-old female with chronic discogenic back pain undergoes lumbar spine surgery via retroperitoneal approach. Figure A is the postoperative radiograph of her lumbar spine. Six weeks after the surgery the patient develops worsening low back pain. You obtain a radiograph of her lumbar spine, pictured in Figure B. What is the next best step in management? Review Topic

Explanation
Management of failed TDR is dictated by (1) patient symptoms and (2) radiographic implant position. Asymptomatic patients with implant subsidence without extrusion can be managed with close observation. Patients with persistent symptomatic back pain relating to facet joint or implant microinstability in the setting of an otherwise well-positioned TDR can be treated with posterior stabilization alone. Symptomatic patients with unacceptable implant position (i.e. complete dislodgement, fracture) require either revision arthroplasty or conversion to arthrodesis (anterior +/-
posterior).
Harrison et al. authored a report detailing a case of failed L5-S1 TDR with anterior dislocation of the polyethylene inlay and bilateral L5 pars fractures noted 2 weeks postoperatively. It is unclear whether the pars defect was missed following previous microdiscectomy, acquired during instrumentation, or acquired postoperatively due to abnormal endplate forces during rehabilitation. The patient underwent removal of TDR components and revision to anterior arthrodesis followed by percutaneous fixation of the bilateral L5 pars fractures.
Patel et al. published a review of the literature regarding revision lumbar TDR. Retroperitoneal revision procedures are complicated by higher risk of injury to vascular structures (16.7% versus 3.6% at primary surgery) and urogenital structures due to adhesions. Revision surgery should only be performed by surgeons familiar with the retroperitoneal approach to the spine. Alternative surgical approaches, such as the far lateral approach, should be considered to access the anterior spine at L4-L5 and above.
Madigan et al. reviewed the management of lumbar degenerative disc disease (DDD). They state that TDR is a motion-sparing surgical option designed to temper the problem of adjacent-segment disease. They report that long-term studies are limited, but point out that several short-term comparisons between TDR and ALIF show equivalent improvement in pain and function, equal complication rate, shorter hospitalization and lower rate of reoperation in the TDR group.
Figure A is a lateral radiograph of the lumbar spine showing L5-S1 total disc replacement. Figure B is a lateral radiograph of the lumbar spine showing L5-S1 total disc replacement with anterior dislocation of the polyethylene inlay.
Incorrect Responses:
Question 66
Which of the following vertebrae has the smallest pedicle isthmic width in a nondeformity patient?
Explanation
REFERENCE: Ofiram E, Polly DW, Gilbert TJ Jr, et al: Is it safe to place pedicle screws in the lower thoracic spine than in the upper lumbar spine? Spine 2007;32:49-54.
Question 67
A 47-year-old woman underwent a distal chevron bunionectomy 2 months ago. Her postoperative recovery had been uneventful until 1 week ago. She now has new onset pain and dorsal swelling in the area of the third metatarsal. A radiograph is shown in Figure 27. What is the most likely diagnosis?
Explanation
REFERENCE: Boden BP, Osbahr DC: High risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Question 68
A patient has had a locked posterior dislocation of the shoulder for the past 6 months. After undergoing total shoulder arthroplasty that includes adequate anterior releases and posterior capsulorrhaphy, the patient still exhibits posterior instability intraoperatively. The postoperative rehabilitation regimen should include
Explanation
REFERENCES: Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Loebenberg MI, Cuomo F: The treatment of chronic anterior and posterior dislocations of the glenohumeral joint and associated articular surface defects. Orthop Clin North Am 2000;31:23-24.
Question 69
Where is the watershed zone for tarsal navicular vascularity?
Explanation
REFERENCES: Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004,
pp 239-242.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983,
pp 299-302.
Question 70
A 62-year-old patient is seen for routine follow-up after undergoing cementless total hip arthroplasty 2 years ago. The patient reports limited range of motion that severely affects daily activities. A radiograph is shown in Figure 51. Management should now consist of
Explanation
REFERENCES: Ayers DC, Evarts CM, Parkinson JR: The prevention of heterotopic ossification in high-risk patients by low-dose radiation therapy after total hip arthroplasty. J Bone Joint Surg Am 1986;68:1423-1430.
Healy WL, Lo TC, DeSimone AA, et al: Single-dose irradiation for the prevention of heterotopic ossification after total hip arthroplasty: A comparison of doses of five hundred and fifty and seven hundred centigray. J Bone Joint Surg Am 1995;77:590-595.
Question 71
Figure 4 shows the MRI scan of a patient who has had bilateral leg pain, weakness, diffuse numbness, and urinary retention for the past week. Examination reveals that motor strength is diffusely decreased, although it may be secondary to pain. The patient is numb throughout both legs, and reflexes in the lower extremities are absent. Rectal examination shows decreased tone, but voluntary tightening is present. Management should consist of
Explanation
REFERENCES: Kostuik JP, Harrington I, Alexander D, Rand W, Evans D: Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am 1986;68:386-391.
Wisneski RJ, Garfin SR, Rothman RH, Lutz GE: Lumbar disk disease, in Herkowitz HN, Garfin SR, Balderston RA, et al (eds): The Spine, ed 4. Philadelphia, PA,WB Saunders, 1992, vol 1,
pp 613-679.
Question 72
A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause Review Topic
Explanation
Question 73
Which of the following is considered the most appropriate indication for conversion of a hip fusion to total hip arthroplasty?
Explanation
REFERENCES: Santore RF: Hip reconstruction: Nonarthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 109-115.
Callaghan JJ, Brand RA, Pedersen DR: Hip arthrodesis: A long-term follow-up. J Bone Joint Surg Am 1985;67:1328-1335.
Question 74
Bridge plating of the olecranon is MOST appropriate in which of the following clinical scenarios?

Explanation
Bailey et al looked at the outcome of plate fixation of olecranon fractures. They concluded that plate fixation is effective for displaced olecranon fractures and leads to good functional outcome. There were low incidence of complications, although 20% did have removal of hardware due to irritation.
Hak et al reviewed the fixation options for olecranon fractures. In their review, they state that comminuted olecranon fractures can be treated by limited-contact dynamic-compression plates. They also supported the use of supplemental bone graft to support comminuted depressed articular fragments. Fragment excision and triceps advancement is appropriate in selected cases in which open reduction seems unlikely to be successful, such as in osteoporotic elderly patients with severely comminuted fractures.
Question 75
Which of the following classes of antibiotics works by binding to the 30S-ribosomal subunit?
Explanation
Aminoglycosides are among the oldest classes of antibiotics. They are act by binding to the 30S ribosomal subunit and are considered bactericidal. Due to their effectiveness on Gram-negative bacteria they are often used in conjunction with cephalosporins for treatment of open fractures. Care must be taken when using aminoglycosides due to their potential nephrotoxicity and ototoxicity.
Mader et al. present an instructional course lecture reviewing common antibiotics and their mechanisms of action. For aminoglycosides, they comment that their primary use is for aerobic Gram-negative organisms, particularly enterobacter species and P. aeruginosa. Aminoglycosides have realtively poor activity against Gram-positive organisms and should not be used for staph or strep species.
Illustration A is a diagram showing the mechanism of action of different antibiotics. Incorrect Answers:
Question 76
The posterior cord of the brachial plexus terminates into what two main branches?
Explanation
REFERENCE: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 228-236.
Question 77
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior- stabilized TKA without evidence of component loosening. What is the most likely cause of this patient's pain?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
Question 78
What is the most significant benefit of percutaneous transforaminal lumbar interbody fusion (TLIF) vs open posterior lumbar interbody fusion (PLIF)?
Explanation
Humphreys and associates in a retrospective review of TLIF vs PLIF found fusion rates, surgical time, and length of hospital stay were similar with both procedures. The only benefits associated with TLIF were less blood loss and preservation of the paraspinal muscle sleeve. Manos and associates in a cadaver study found no difference in the volume of disk material evacuated or the area of endplate exposed in either procedure.
RECOMMENDED READINGS
Humphreys SC, Hodges SD, Patwardhan AG, Eck JC, Murphy RB, Covington LA. Comparison of posterior and transforaminal approaches to lumbar interbody fusion. Spine (Phila Pa 1976). 2001 Mar 1;26(5):567-71. PubMed PMID: 11242386. View Abstract at PubMed
Manos R, Sukovich W, Weistroffer J: Transforaminal lumbar interbody fusion: Minimally invasive versus open disc excision and endplate preparation. Presented at the 12th International Meeting of Advanced Spine Techniques, Banff, Alberta, Canada, July 7-9, 2005.
Question 79
Following irrigation and debridement, what is the preferred method of fixation for a displaced open tibia fracture with a 16-cm clean wound?
Explanation
Question 80
Benign Ethnic Neutropenia is more common in males.
Explanation
Access to pediatric orthopaedic management has been well investigated. Numerous Level 4 studies have shown that orthopaedic offices in urban and rural areas prefer treating patients with private insurance over patients with Medicaid.
Iobst et al. telephoned 100 urban and rural orthopaedic outpatient offices to schedule an appointment for a 10-year-old patient with a forearm fracture. They showed that 8/100 offices would schedule an appointment within 1 week to the child with Medicaid insurance, as compared to 36/100 that gave an appointment to a child with private insurance.
Pierce et al. contacted 42 orthopaedic practices to schedule an appointment for a 14- year-old patient with an ACL injury. They showed that 38/42 offices scheduled an appointment for the child within 2 weeks with private insurance. This compared to 6/42 that scheduled an appointment for a similar child with Medicaid.
Incorrect Answers:
The perioperative use of which medication has been shown to increase the risk of post-operative infection following orthopaedic procedures in patients with rheumatoid arthritis (RA)?
Naproxen
Leflunomide
Sulfasalazine
Etanercept
Aspirin
Of the medications listed, only etanercept has been shown to increase the risk of post- operative infection following orthopaedic procedures in patients with RA.
Etanercept is a TNF-alpha antagonist with a short half-life that is administered once or twice weekly in patients with RA. Since TNF-alpha plays a central role in the pathogenesis of RA and is instrumental in causing joint destruction, the inhibition of this molecule has shown excellent results in controlling disease. The most powered study on TNF-alpha inhibitor use in the perioperative period following an orthopaedic procedures demonstrated a significant increase in
post-operative infection.
Howe et al. review the medical management of patients with RA who underwent orthopaedic procedures. They state that while there is conflicting information regarding TNF-alpha antagonists, they recommend holding them prior to major orthopaedic interventions.
Giles et al. review 91 patients with rheumatoid arthritis who underwent an orthopaedic procedure. They found TNF-alpha inhibitor therapy to be significantly associated with the development of a serious postoperative infection (p=.041)
Perhala et al. review 61 patients with RA who were treated with methotrexate during the perioperative period surrounding a total joint arthroplasty. They
failed to find a significant increase in complications in this patient group, stating the perioperative use of methotrexate does not affect wound healing or increase the likelihood of periprosthetic infection.
Illustration A shows the site of action of TNA-alpha inhibitors in the RA pathway.
Incorrect Answers:
Communication breakdown is the leading cause of which of the following?
Delayed diagnoses
Medication errors
Surgical site infections
1 and 2
All of the above
Communication failures are the leading cause of wrong side surgeries, medication errors and diagnostic delays.
Poor communication sets up environments in which medical errors can take place. Per the Joint Commission, medical errors may be the among the top 10 causes of death in the United States. Establishing open lines of communication is critical to reduce the risk of error and enhance patient safety.
Gandhi et al. designed a framework to study missed or delayed diagnoses and their causes. The most significant factors contributing to errors were poor handoffs, failures in judgment, failures in memory and failures in knowledge.
O’Daniel et al. review the importance of professional communication and collaborative team efforts. They note that patient safety is at risk when poor communication is in place. The leading cause for medication errors, treatment delays and wrong-site surgeries is communication failure.
Illustration A shows the leading causes of death in the United States. This includes “preventable errors” as a cause.
Incorrect Answers:
treatment, medication errors and wrong side surgery
Which of the following is true regarding osteoprotegerin (OPG)?
It is secreted by osteoclasts
It increases bone resorption
Binds to prostoglandin E2 before stimulating osteoclasts
Osteoprotegerin knock-out mice develop osteopetrosis
Binds to and sequesters RANKL
Osteoprotegerin is a decoy receptor for RANKL. Binding to RANKL causes decreased production of osteoclasts by inhibiting the differentiation of osteoclast precursors.
Bone resporption/remodeling is a complex process regulated by a large variety of molecules. Molecules that have shown to inhibit osteoclasts include OPG, calcitonin, estrogen, TGF-B, and IL-10. Corticosteroids have been shown to decrease production of OPG, thereby enhancing osteoclast formation and longevity. Prolia, or denosumab, is a newly approved drug used to treat osteoporosis and has a mechanism of action similar to osteoprotegerin
(inhibits binding of RANKL to RANK).
Boyle et al. review osteoclast differentiation and activation. The authors state that targeted disruption of OPG causes increased osteoclastogenesis and/or activation resulting in osteopenia.
Illustration A shows how OPG binds to RANKL inhibiting the stimulation of osteoclasts.
Incorrect Answers:
A 55-year-old woman has T-score -2.0 at the femoral neck. According to the World Health Organization Fracture Risk Assessment Tool (FRAX), she has a ten- year probability of sustaining a hip fracture of 1.5% and a ten-year probability of sustaining a major osteoporotic fracture of 8.9%. Which of the following statements is true regarding her antiresorptive therapy management?
Antiresorptive therapy should be started based on her T-score
Antiresorptive therapy should be started based on her risk of hip fracture alone
Antiresorptive therapy should be started based on her risk of major osteoporotic fracture alone
Antiresorptive therapy should not be started
Antiresorptive therapy should be started based on her risks of both hip fracture and major osteoporotic fracture
This patient has osteopenia. Assessment by FRAX shows that ten-year risk of hip fracture is less than 3% and her ten-year risk of major osteoporosis- related fracture is less than 20%. Therefore, antiresorptive therapy is not indicated at this time.
According to the 2008 National Osteoporosis Foundation guidelines, pharmacologic treatment for osteoporosis should be considered if patients are
postmenopausal women or men greater than 50 years old AND meet one of the following criteria: (1) they have a prior hip or vertebral fracture, (2) they have a T score -2.5 or less at the femoral neck or spine, (3) they have a T score between -1.0 and -2.5 at the femoral neck or spine AND a 10-year risk of hip fracture greater than 3% or 10-year risk of major osteoporosis-related fracture greater than 20%.
FRAX (World Health Organization Fracture Risk Assessment Tool) calculates
year risk of fracture based on the following variables: age, sex, race, height, weight, BMI, history of fragility fracture, parental history of hip fracture, use of oral glucocorticoids, secondary osteoporosis and alcohol use to calculate 10-year risk of fracture.
Unnanuntana et al. reviewed the assessment of fracture risk. Besides FRAX score and T-score, they discussed biochemical markers of bone formation and resorption, which are useful for monitoring the efficacy of antiresorptive / anabolic therapy, and may help identify patients at high risk for fracture.
Ekman et al. reviewed the role of the orthopaedic surgeon in minimizing mortality and morbidity associated with fragility fractures. The surgeon should consider prescribing appropriate medications, physical therapy, assessing fall risk and preventing falls and changing lifestyle factors (exercise, smoking and alcohol).
Illustration A shows the FRAX online tool (http://www.shef.ac.uk/FRAX/tool.aspx?country= =9).Illustration B shows the clinical risk factors considered in FRAX calculation.
Incorrect Answers:
A 32-year-old runner sustains a trimalleolar left ankle fracture. She undergoes open reduction and internal fixation and is kept non- weightbearing after surgery. At 2 months, what changes will occur in the articular cartilage of both her knees as a result of her current weightbearing regimen?
Cartilage thickening in the left (ipsilateral) knee and no change in cartilage thickness in the right (contralateral) knee
Cartilage thinning in both knees
Cartilage thinning in the left (ipsilateral) knee and no change in cartilage thickness in the right (contralateral) knee
Cartilage thinning in the left (ipsilateral) knee and increased cartilage thickness in the right (contralateral) knee
Increased cartilage thickness in both knees
After a period of off-loading, the off-loaded limb will experience cartilage thinning. The contralateral limb will not demonstrate any cartilage changes.
Physiologic loading of cartilage increases proteoglycan synthesis and cell proliferation and is chondroprotective. Joint immobilization leads to cartilage thinning, tissue softening, and reduced proteoglycan content, leading to cartilage erosion. Joint overuse leads to cartilage damage (in vitro only).
Hinterwimmer et al. examined cartilage atrophy after partial load bearing
using quantitative MRI. They found cartilage thinning in all knee compartments (greatest thinning, medial tibia; least thinning, patella). There was no change in cartilage morphology in the contralateral knee.
Sun reviewed the relationship between mechanical loading and cartilage degeneration. In OA, cartilage breakdown occurs at the articular surface, and is then fueled by synovial proteases and cytokines. In RA, synovial cells and macrophages are the source of degradative enzymes and incite cartilage destruction.
Milward-Sadler et al. examined mRNA levels following mechanical stimulation in normal and osteoarthritic chondrocytes. Normal chondrocytes showed increased aggrecan mRNA and decreased matrix metalloproteinase 3 (MMP-3) mRNA after stimulation. This
chondroprotective response was absent in osteoarthritic chondrocytes.
Illustration A shows pro- and anti-inflammatory mechanisms of mechanical loading on chondrocytes. Underloading and overloading induce cartilage damage through pathways involving the upregulation of MMPs and ADAMTSs (ADAMTS, a disintegrin and metalloproteinase with thrombospondin motifs, or aggrecanase). Physiological loading blocks these increases.
Incorrect Answers:
A morbidly obese 40-year-old man is scheduled to undergo hemilaminectomy for resection of an painful osteoid osteoma of the T6 lamina. He is positioned prone on a Jackson table and localization is performed with intraoperative fluoroscopy prior to the start of the case. At close to the end of the case, intraoperative frozen section reveals only normal bone fragment from the resected lamina. A probe is placed and a cross-table lateral radiograph reveals that the T7 lamina was resected instead of T6. At this point, the surgeon should
do all of the following EXCEPT
Complete the surgery
Abort the case and obtain further imaging
Apologize to the patient and family
Formally document the error in the operative report
Inform the patient and family immediately after the operation
Fluoroscopic localization of the correct thoracic vertebra can be difficult in the obese
patient. Upon detection of wrong level surgery, he should not abort the case. Rather, he should perform the desired procedure at the correct site, and advise the patient and family upon completion.
Adverse events are inevitable. The correct action following wrong-site surgery is to perform the desired procedure at the correct site followed by frank and honest communication with the patient/family. Open, honest communication favorably affects patient behavior, health outcomes, patient satisfaction, and often reduces the incidence of medical professional liability actions. The
discussion should include a disclosure of known facts and an explanation as to the likely cause, as well as ongoing treatment, follow up care, and prognosis.
The AAOS Information Statement about Wrong Site Surgery identifies 3 treatment steps following discovery of an error during surgery under general anesthesia: Return the patient to his preoperative condition, perform the correct procedure at the correct site, and advise the patient and family of what occurred and the likely consequences, if any, of the wrong- site surgery.
The AAOS Information Statement on Communicating Adverse Events states that the surgeon has an ethical and professional obligation to disclose the error to the patient and/or family. Disclosure should include what happened, why it happened, health implications, and what measures are being instituted to prevent recurrences.
Incorrect Answers:
All of the following are Standards of Professionalism relating to interactions with industry for practicing orthopaedic surgeons EXCEPT:
Decline gifts from industry with a market value over $100 (unless they are medical textbooks or patient educational materials)
Disclose to the patient any financial arrangements with industry that relates to the patient's treatment
Accept no direct financial inducements from industry for utilizing a particular implant
Disclose any relationship with industry to colleagues who may be influenced by your work
Decline to participate in industry sponsored non-CME courses or
conferences
The AAOS has adopted the Standards of Professionalism (SOP). These SOP’s establish mandatory, minimum levels of acceptable conduct for fellows and members of the AAOS to engage in relationships with industry. There are 17 standards with relation to industry. Answer choice 5 is not a SOP as surgeons are allowed to participate in or consult in meetings that are conducive to the effective exchange of information. The SOP also stipulate that tuition, travel, and modest hospitality (including meals and receptions) are allowed to attend an industry-sponsored non-CME course.
A prospective randomized trial is conducted to test the efficacy of Vitamin C versus placebo in treating patients who develop chronic regional pain syndrome (CRPS) after distal radius fractures. At first follow-up, the rates of CRPS are 1% and 9% in the study and placebo group, respectively. Which statistical test is most appropriate to determine significance?
Single factor analysis of variance
Chi-square test
Student t-test
Mann-Whitney rank sum test
Wilcoxon rank sum test
In the study provided, we need to determine whether distributions of categorical variables differ from one another. The appropriate study is the chi- square test.
Data can be classified as numerical (continuous) or categorical (proportional). Responses to such questions as "What is your major?" or Do you own a car?" are categorical because they yield data such as "biology" or "no." In contrast, responses to such questions as "How tall are you?" or "What is your G.P.A.?" are numerical. When comparing two independent means from numeric data, a t-test is performed. However, if categorical data is being compared, the chi- square test will determine if the proportions are really different.
Kocher et al. review basic clinical epidemiology and biostatistics relevant to orthopaedic surgery. Amongst other things, they describe that data can be summarized in terms of measures of central tendency, such as mean, median, and mode, and in terms of measures of dispersion, such as range, standard deviation, and percentiles.
Illustration A shows an algorithm for determining which test to use for varying data. Incorrect Answers:
distributed.
A 35-year-old patient is involved in a motor vehicle accident and sustains multiple fractures including a closed comminuted proximal meta-diaphyseal tibia fracture. The surgeon is considering bridge plating the fracture using a minimally invasive approach. Which of the following is true regarding bridge plating?
A locked plate construct (locked screws) or hybrid construct (locked and non- locked screws) is necessary.
Periosteal stripping is performed through two incisions proximal and distal to the fracture.
Bridge plating is performed following direct reduction of the fracture.
AO Type A diaphyseal fractures are best treated with this technique.
Bridge plating with a long working length creates a flexible, axially stable construct.
In bridged plating, only the most proximal and distal screw holes are filled. This creates a flexible, axially stable construct.
Bridge plating is applicable to all long-bone fractures with complex fragmentation and where intramedullary nailing or conventional plate fixation is not suitable. The construct preserves the blood supply to the fracture fragments as the fracture site is undisturbed during the operative procedure. It provides RELATIVE stability, allowing for some motion at the fracture site, leading to callus formation and secondary bone healing. The construct is FLEXIBLE because of increased distance between the 2 screws closest to the fracture (long working length), allowing for stress distribution and permitting more motion at the fracture site. The construct is also AXIALLY STABLE because the plate acts as an extramedullary splint and resists axial compression.
Livani et al. advocate using an anterior or antero-lateral approach for minimally invasive plating of the humerus. They recommend that distal access is obtained first, allowing identification of the lateral antebrachial cutaneous nerve. For distal fractures, they recommend extending the plate down to the lateral column.
Apivatthakakul et al. defined minimally-invasive plate osteosynthesis (MIPO) danger zones from the lateral epicondyle. They found the musculocutaneous nerve averaged 18- 43% of the humeral length, the danger zone for the radial nerve averaged 36-59% of the humeral length, and the most dangerous screws that penetrated or touched the radial nerve lay 47-53% of the humeral length.
Illustration A shows a distal tibia fracture. Illustration B shows radiographs 5 months after bridge plating of this fracture. There is callus formation, characteristic of indirect bone healing.
periosteal blood supply is critical.
Which of the following components of bone is most responsible for compressive strength?
Type I collagen
Osteocalcin
Proteoglycans
Osteonectin
Osteopontin
Proteoglycans, in addition to calcium hydroxyapatite [Ca10(PO4)6(OH)2], are most responsible for providing compressive strength.
Bone is composed of both organic and inorganic components. Inorganic components include calcium hydroxyapatite and osteocalcium phosphate. Organic components include collagen, proteoglycans, matrix proteins, cytokines and growth factors. While Type I collagen is responsible for providing the tensile strength of bone, proteoglycans and calcium hydroxyapatite [Ca10(PO4)6(OH)2] are most responsible for providing compressive strength. Proteoglycans contain a core protein with various
numbers of covalently attached side chains of glycosaminoglycans. In addition to providing compressive strength, they are also responsible for binding growth factors and inhibiting mineralization.
Knothe et al. review the osteocyte. They discuss that osteocytes are the most abundant
cells in bone, are actively involved in maintaining the bony matrix, and may act as mechanosensors.
Illustration A shows a proteoglycan aggregate, which can form when individual molecules link onto a chain of hyaluronic acid.
Incorrect Answers:
A prospective, randomized controlled trial of 150 patients undergoing total hip arthroplasty is performed to test whether repair of the capsule during a posterior approach reduces post-operative dislocations in the first three months. The study found no difference in dislocation rate if the capsule was repaired versus not repaired (p =
.34). Subsequently, a multicenter follow-up study of 2000 patients showed that repairing the capsule led to a decreased dislocation rate
in the first three months (p = .03). Assuming the second study reflects reality, which of the following errors occurred in the first study?
Observer bias
Type-II error
Alpha error
Type-I error
Confounding error
In this situation, the null hypothesis was accepted when it should have been rejected.
This is a type-II error.
A study can have two types of errors. Type-I errors, or alpha errors, occur when the null hypothesis is rejected when it should have been accepted. The alpha level refers to the probability of a type-I error. By convention, the alpha level of significance is set at 0.05, which means that we accept the finding of a significant association if there is less than a one in twenty chance that the observed association was due to chance alone. Type-II errors, or beta errors, occur when the null hypothesis is accepted when it should be rejected. This
often occurs when studies are underpowered. In the example above, the null hypothesis is that repair of the capsule does not reduce dislocations within the first three months. Since the first study did not show a statistically significant difference, the null hypothesis was accepted. Since a more powered study showed that repair of the capsule does reduce dislocations, the null hypothesis should have been rejected in the initial study (if it was adequately powered).
Fosgate et al. review the importance of sample size calculations when performing research. They state that sample size ensures statistical significance if the subsequent data collection is perfectly consistent with the assumptions made for the sample size calculation (assuming power was set as
50% or greater).
Illustration A shows the difference between type-I and type-II errors. Video V is a lecture discussing statistical definition review of PPV, NPV, sensitivity and specificity.
Incorrect Answers:
that properly constructed studies attempt to avoid.
Which of the following is a potential cause of fretting corrosion?
The micromotion at the femoral head-neck junction in a modular total hip replacement
A stainless-steel cerclage wire is in contact with a titanium-alloy femoral stem
Friction between polyethylene liner and femoral head leading to osteolysis
The formation of pits within a stainless-steel plate and the subsequent release of metal ions
The formation of an adherent oxide coating on titanium implants
Micromotion at the femoral head-neck junction can lead to fretting corrosion, one of the most common causes of failure of a modular implant.
Modular components give surgeons excellent intraoperative flexibility, but are susceptible to various types of corrosion. While titanium and cobalt-chrome contain a protective surface oxide layer, continued micromotion at the modular junction may disrupt the protective layer leading to fretting corrosion, defined as micromotion at contact sites under load. This may eventually lead to a painful synovitis that necessitates a revision procedure.
Srinivasan et al. review modularity in total hip arthroplasty. Amongst other things, they discuss the modularity of the femoral head/neck junction, describing the morse taper interlocking system that provides both axial and rotational stability.
Illustration A shows an example of corrosion at the head/neck junction of a total hip arthroplasty.
Incorrect Answers:
Which of the following situations is most likely to decrease sentinel event errors?
Physician and nurse training is lengthened by 20%
Resident hours are decreased to 55 hours per week
An environment is created where all members of the healthcare team feel empowered to express their concerns and beliefs
Holding individuals responsible for errors in clinical judgement
Physicians and nurses are assigned to a smaller number of patients
Creating an environment where all members of the healthcare team feel empowered to express their beliefs increases communication, the key element in decreasing sentinel events.
Research has shown that 70% of sentinel event errors are caused by improper communication. Specific ways to improve communication include effective clinical handover between shifts and breaking down the "hierarchy" so that all members of the team can discuss their expectations and concerns. Barriers to effective communication include distractions, cultural differences, power distance relationships, time pressures, and lack of organization.
Leonard et al. describe specific clinical experiences in the application of surgical briefings, properties of high reliability perinatal care, the value of critical event training and simulation, and benefits of a standardised communication process in the care of patients transferred from hospitals to skilled nursing facilities. They recommend embedding standardized tools and behaviors to bridge differences in communications styles between clinicians.
Incorrect Answers:
Which of the following side effects is most strongly associated with the use of NSAIDs?
Hepatic dysfunction
Renal impairment
Prolonged QTc
Seizures
Hematuria
All NSAIDs have the potential to cause serious renal impairment.
NSAIDs work by inhibiting the cyclooxygenase pathway (COX), which is comprised of the COX-1 and COX-2 pathways. The COX-1 pathway is involved in prostaglandin E2– mediated gastric mucosal protection and thromboxane effects on coagulation, while the COX-2 pathway is mainly involved with the modulation of pain and fever without effect on platelet function. While selective COX-2 inhibitors have a decreased side effect profile, all NSAIDS
have the potential to cause renal impairment and their use should be limited in patients with underlying renal disease.
Horlocker et al. review multimodal pain management in the perioperative setting of a total joint arthroplasty. Specifically, they note that NSAIDs should be used cautiously in patients with underlying renal dysfunction who are to undergo a procedure with major blood loss.
Griffin et al. reviewed 1,799 patients hospitalized for acute renal failure. They found that NSAIDs increased the risk of renal failure by 58% and that NSAID use resulted in 25 excess hospital admissions per 10,000 years of use.
Illustration A shows the COX pathways and their inhibition by NSAIDs. Incorrect Answers:
It is recommended that invasive dental work be completed prior to the initiation of which of the following medications?
Glucosamine
Cholecalciferol
Levothyroxine
Teriparatide
Bisphosphonates
Bisphosphonate therapy combined with invasive dental work increases the risk for development osteonecrosis of the jaw.
Bisphosphonates are a class of drugs that prevent bone mass loss by inhibiting osteoclast resorption. They are used in the treatment of vertebral compression fractures, non- vertebral fragility fractures, osteogenesis imperfecta, multiple myeloma, and avascular necrosis. Because bisphosphonates have been associated with osteonecrosis of the jaw, it is suggested that all invasive
dental work be completed prior to initiation of treatment.
Pazianas et al. (2011) review the safety profile of bisphosphonates. Specifically, they cite gastrointestinal discomfort, atypical femur fractures, osteonecrosis of the jaw, ocular inflammation, and musculoskeletal pain as common side effects. They state there is limited evidence surrounding
bisphosphonate's association with esophageal cancer and atrial fibrillation.
Pazianas et al. (2007) reviewed 11 publications that reported 26 cases of osteonecrosis of the jaw following initiation of bisphosphonate treatment. Age
>60 years, female sex, and previous invasive dental treatment were the most common characteristics of those who developed ONJ.
Illustration A shows the various bisphosphonates and their mechanisms of action. Illustration B shows an example of osteonecrosis of the jaw, a side effect that has been linked to bisphonphonate treatment.
Incorrect Answers:
Figures A and B show radiographs of a 24-year-old female with a soccer injury. A physical examination reveals an isolated, closed injury with no clinical features of neurovascular injury or compartment syndrome. She has been consented to be treated with intramedullary nail fixation. A pre-operative note by the anaesthesiology team makes reference to the patients fair skin and natural red-hair color. How will this information affect the post-operative management of this patient?
Longer duration of anticoagulation due to increased risk of DVT
Avoiding anticoagulation medications due to increased risk of bleeding
Require higher dosages of post-operative analgesia
Longer period of non-weight bearing on surgical limb
Avoiding opioids due to higher risk of unrecognized allergies
Female patients with natural red-hair may require higher dosages of post- operative analgesia compared to other hair types.
Melanocortin-1-receptor (MC1R) is one of the key proteins involved in hair color and skin tone. Mutations of the MC1R alleles can render this protein non- functional, which results in a phenotype of red-hair and fair skin. Mutations of the MC1R have shown to modulate the pain response and opioid efficacy in these patients. Women are more commonly affected and often require more anaesthetic and higher dosages of opioid to achieve comparable MAC level and pain-relief, respectively, as women with other hair types.
Liem et al. showed that a greater concentration of induction and maintenance agents (sevoflurane and desflurane, respectively) were required to sustain comparable MAC levels in red-haired patients as dark haired patients.
Fillingim et al. reviewed the affect of gender, sex and pain. They concluded there is a biopsychosocial element of pain that is perceived differently by men and women. In terms of postoperative and procedural pain, the outcome might be more severe in women than men.
Delaney et al. looked at the involvement of the melanocortin-1 receptor in acute pain in mice. They found that while the MC1R is better known as a gene involved in mammalian hair colour, it was shown to be involved in the pain pathway of inflammatory but not neuropathic origin. Mutations of MC1R showed increased tolerance to noxious pain stimulus in mice.
Figures A and B are AP and lateral radiographs of a left tibia. There is a low energy, distal third shaft fracture with no cortical apposition on the AP view.
Incorrect Answers:
Which of the following medications used for thromboprophylaxis following orthoapedic surgery is a direct inhibitor of factor Xa?
Dextran
Rivaroxaban (Xarelto)
Coumadin
Fondaparinux (Arixtra)
Aspirin
Rivaroxaban (Xarelto), an oral anticoagulant, is a direct inhibitor of factor Xa.
Rivaroxaban (Xarelto) is a member of a new class of oral, direct (antithrombin- independent) factor Xa inhibitors, which restrict thrombin generation both in vitro and in vivo. Inhibition of Factor Xa interrupts the intrinsic and extrinsic pathway of the blood coagulation cascade, inhibiting both thrombin formation and development of thrombi.
Eriksson et al. compare rivaroxaban to enoxaparin for the prevention of symptomatic venous embolism following total hip arthroplasty. Major venous thromboembolism occurred in 4 of 1686 patients (0.2%) in the rivaroxaban group and in 33 of 1678 patients (2.0%) in the enoxaparin group. Additionally, major bleeding events were similar between the two groups.
Illustration A shows the mechanisms of action of various agents used for thromboprophylaxis.
Incorrect Answers:
as Protein C and Protein S.
The origin of bovine derived grafts is particularly important to which of the following religious groups?
Christianity
Islam
Hinduism
Buddhism
Judaism
The origin of bovine-derived surgical implants should be discussed in further detail with patients ascribing to Hinduism.
Patients come from a variety of religious backgrounds. Depending on a patient’s religion, the origin of surgical implants may have implications for their use. In Hinduism, bovine animals are considered sacred. Use of cow by- products is considered purifying in nature. Subsequently, the origin of bovine derived implants should be discussed with patients ascribing to Hinduism.
Easterbrook et al. evaluated the utility of porcine and bovine surgical implants amongst those of Jewish, Muslim and Hindu faiths. Hindu religious leaders, who were surveyed, did not approve of the use of bovine surgical implants.
Enoch et al. evaluated the acceptability of biological products amongst various religious groups. The Hindu religious leaders were found to not have an objection to the use of biological implants derived from cows.
Illustration A shows a clinical photo of a fetal bovine derived dermal substitute. Incorrect Answers:
Immunological testing of anti-cyclic citrullinated peptide antibodies (anti- CCP) is most commonly used for the diagnosis and prognosis of which immunological condition?
Ankylosis spondylitis
Rheumatoid arthritis
Psoriatic arthritis
Systemic lupus erythematosus
Reiter's syndrome
Anti-cyclic citrullinated peptide antibodies (anti-CCP) are commonly used as a marker for the diagnosis and prognosis of rheumatoid arthritis (RA).
Immunological studies are commonly performed to investigate cases of suspected rheumatoid arthritis. Rheumatoid factor has historically been used as a primary marker for RA. However, in more recent years, the use of anti- CCP antibodies has shown to be as sensitive as, and more specific than, rheumatoid factor (RF) in early and fully established disease. In general, anti-
CCP assays equate to a sensitivity of 50-75% and a specificity of 90-95%. High levels of anti-CCP have been shown to be indicative of a more erosive disease process and may be detected before the onset of arthritis.
Gardner and Kadel reviewed the laboratory studies most commonly used in rhuematologic diseases. Standard ordering for clinically suspected RA include Rf, anti- CCP, ESR/CRP as well as other markers of autoimmune diseases such as antinuclear antibodies, anticardiolipin antibodies and lupus anticoagulant, HLA-B27, and uric acid levels.
Illustration A shows the sensitivity and specificity of anti-CCP vs. RF in a variety of autoimmune diseases.
Incorrect Answers:
Vitamin C has been shown to decrease the likelihood of which of the following complications following surgery on the foot and ankle in non-diabetic patients?
Nonunion
Complex Regional Pain Syndrome, type II
Malunion
Complex Regional Pain Syndrome, type I
Wound infection
Vitamin C has been shown to decrease the likelihood of developing complex regional pain syndrome (CRPS), type 1, when given post-operatively to patients undergoing foot and ankle and wrist surgery.
CRPS is a frequent post-operative complication, with rates varying from 10-
37%. Type I CRPS does not have an identifiable nerve lesion, while type II has an identifiable nerve lesion. Multiple studies have shown that vitamin C decreases rates of CRPS following distal radius fractures, and more recently, the same has been shown following foot and ankle surgery. While the exact mechanism of CRPS is unknown, vitamin C has been shown to reduce lipid peroxidation, scavenge hydroxyl radicals, protect the capillary endothelium, and inhibit vascular permeability. All of these characteristics of vitamin C may play a role in modulating the pain pathway.
Zollinger et al. perform a double-blind, prospective, multicenter trial where
416 patients with 427 wrist fractures were randomly allocated to treatment with placebo or treatment with 200, 500, or 1500 mg of vitamin C daily for fifty days. The prevalence of complex regional pain syndrome was 2.4% in the vitamin C group and 10.1% in the placebo group.
Besse et al. compare two groups of patients undergoing surgery on the foot and ankle to determine the effect of vitamin C on the development of CRPS, type I. CRPS type I occurred in 18 cases (9.6%) in the group not given vitamin C, and 4 cases (1.7%) in the group given vitamin C.
Illustration A shows an example of a limb affected by CRPS. Note the increased swelling, a common physical exam finding in patients afflicted with the disease.
Incorrect Answers:
A 25-year-old Spanish speaking male presents to the emergency department 6 hours after sustaining the injury seen in Figure A. He is grossly intoxicated and screaming in pain. Physical examination reveals a closed injury with overlying muscular compartments that are extremely firm to palpation. After sedating the patient, measurements of the intracompartmental pressures were all found to be
>75mmHg. His wife is Spanish speaking and expected to arrive to the hospital in 2-3 hours with a relative to help with translation. No medical translator is
available. You attempt to outline the risk and benefits of surgery to the patient, but the he repeatedly interrupts you and yells out ,"No surgery!". An English-Spanish speaking friend is with the patient and says that he has known the patient for over 2 years and will help with any decision making. What would be the next most appropriate step in the management of this patient?
Delay surgery to monitor the patient for impending compartment syndrome
Proceed with surgery with urgent fasciotomy after documenting the necessity of treatment without consent
Delay the surgery until the wife arrives and able to give informed consent with the aid of a translator
Proceed with surgery for urgent fasciotomy after obtaining informed consent from the patients friend
Respect the patients autonomy and reassess the patient in the morning when he demonstrates capacity to accurately comprehend the proposed treatment
This patient is presenting with compartment syndrome of the right tibia. In a situation of required surgery for limb threatening injury without available legal consent the surgeon should confirm and document the necessity of care with a fellow colleague.
Physicians are responsible for whether a patient is able to reasonably understand their medical condition and the nature of any proposed medical procedure, including the risks, benefits, and available alternatives. If the patient lacks this capacity, disclosure imposed by the doctrine of informed
consent are excused because irreparable harm that may result from the physician’s hesitation to provide treatment. Detailed documentation is also important. In addition, the attending physician should contact the Risk Management Dept at the hospital for support prior to surgical intervention or have a medical translator involved to ensure information is being translated properly.
Katz et al. reviewed the medical decision making process of Hispanic people. They showed that Hispanic people are more likely to permit their physician to take the predominant role in making health decisions compared to Non- Hispanic people.
Figure A shows a comminuted tibia and fibula fracture. Incorrect Answers
A Spanish speaking child sustained the injury seen in Figure A after a fall at school. He was casted in the emergency department without the assistance of an interpreter and advised to return to see an orthopaedic surgeon in 1 week. However, the family returns to the emergency department with the child 3 months later, still in the cast. What is the most likely reason the child did not attend the recommended orthopaedic follow-up visit.?
The child is a victim of neglect
The child had no symptoms of pain
He was allowed to return to school wearing the cast
Concerns of cost
Follow-up instructions were not effectively communicated
The most likely reason the child did not attend the recommended orthopaedic follow-up visit was a language barrier preventing effective communication of the intended follow-up instructions.
Communication skills and cultural competence is a key element in good orthopaedic care. Poor communication can often lead to devastating outcomes. In this example, poor communication resulted in this patient being lost to
follow-up. Language barriers must be accommodated and alternative methods of communication must be utilized.
Levinson et al. examined how patients present their medical issues in clinical encounters and how physicians respond to these clues in routine primary care and surgical settings. They showed that good communication relies mostly on the physicians ability to identify patient clues within the clinical encounter.
Poor communication between the physician tended to delay clinical visits, poor follow-up and unsatisfactory outcomes.
Figure A is an AP radiograph of the elbow in a skeletally immature patient. Figure B is a lateral radiograph of the elbow with a posterior fat pad sign, suggestive of an occult fracture.
Incorrect Answers:
A 25-year-old female presents to the emergency room within increasing left shoulder pain after walking into a door 5 months ago. She previously sustained a femoral fracture 2 years ago after tripping on a rug. Relevant skeletal survey radiographs and tissue biopsy results are shown in Figures A through D. Laboratory investigations show normal glomerular filtration rate and creatinine clearance. Dual energy x-ray absorptiometry (DEXA) scan shows T-score of -1.4 and
-1.2 at the hip and lumbar spine, respectively. Which of the following laboratory values in Figure E most likely reflects this patient's condition?
A
B
C
D
E
This patient has primary hyperparathyroidism. Laboratory investigations are likely to show elevated serum intact parathyroid hormone (PTH), alkaline phosphatase (ALP) and ionized serum calcium, and low serum phosphate.
Primary hyperparathyroidism is most commonly caused by a single adenoma (80-90%). Besides the signs and symptoms of hypercalcemia, patients present
with calcification of menisci and articular cartilage, erosions in hand bones, "salt and pepper skull", and brown tumors (osteoclastomas), which appear as lytic regions expanding the cortex and causing pathological fractures, so named because of hemosiderin deposition.
Singhal et al. reviewed primary hyperparathyroidism. They advocate routine serum calcium levels for patients with pathologic fractures. If this is elevated, total and ionized calcium and intact PTH levels should be obtained. They feel that surgery for orthopaedic stabilization and parathyroidectomy should be performed simultaneously for better outcome.
Mankin et al. reviewed metabolic bone disease. They suggest that patients with mild disease with normal calcium levels do not require treatment. For patients with high calcium levels, treatment should include maintenance of fluid balance, localization and removal of the adenoma, bony stabilization, and medications (calcitonin, estrogen, bisphosphonates, and calcimimetics such as cinacalcet).
Figure A is an AP radiograph showing a lytic expansile lesion with pathological fracture in metadiaphyseal region of left humerus with similar lesion in the
fifth posterior rib. Figure B is an AP radiograph showing a lytic expansile lesion in the third metacarpal of the right hand and the fifth metacarpal of the left hand. Figure C is a low power micrograph of a brown tumor demonstrating a central zone of bone resorption, and filling with fibroblastic tissue, with a peripheral rim of osteoid production. Figure D is a high power micrograph of a brown tumor. In areas of bone resorption, there are numerous osteoclast-like giant cells amidst a fibrous stroma. This is unlike a true giant cell tumor, which lacks a fibrogenic stroma.
Incorrect Answers:
and impaired 1,25-dihydroxyvitamin D production by the diseased kidneys. This patient has normal renal function. Answer 3: Elevated PTH, ALP, serum calcium and phosphate occur in tertiary hyperparathyroidism. This again occurs in chronic renal disease after prolonged chronic secondary hyperparathyroidism or after renal transplantation, where the parathyroid glands become autonomous and PTH levels do not normalize. This patient has normal renal function.
elevated.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 81
Figures below show the radiographs, and the MRIs obtained from a 32-year-old man with worsening left knee pain. A 3-foot hip-to-ankle radiograph shows a 13-degree varus knee deformity. The patient sustained a major left knee injury 5 years ago and a confirmed complete anterior cruciate ligament (ACL) tear. He managed this injury nonsurgically with a functional brace but experienced worsening pain. He was seen by an orthopaedic surgeon 18 months ago, and a medial meniscus tear was diagnosed; the tear was treated with an arthroscopic partial medial meniscectomy. Since then, his knee has been giving way more often, and he no longer feels safe working on a pitched roof. The patient received 6 months of formal physical therapy and was fitted for a new functional ACL brace, but he still has pain and instability. He believes he has exhausted his nonsurgical options and would like to undergo surgery. What is the most appropriate treatment at this time?

Explanation
Proximal tibial osteotomy is the most appropriate intervention to correct varus malalignment and to reduce stress on the ACL. In some cases, proximal tibial osteotomy alone may address both pain and instability, but if instability persists, particularly in the setting in which instability can be dangerous, subsequent ACL reconstruction can further stabilize the knee with less stress on the graft after the correction of malalignment. Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should be performed only at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL reconstruction alone is not indicated for this patient.
Question 82
A 43-year-old man sustained a closed, intra-articular pilon fracture. It has now been 1 year since he underwent open reduction and internal fixation. Which of the following statements most accurately describes his perceived outcome? Review Topic
Explanation
Question 83
Two years after undergoing a total shoulder arthroplasty, a patient reports increasing pain, stiffness, and swelling, and has an increased white blood cell count. Radiographs show lucencies around the glenoid and humeral components. You suspect infection. Which of the following is the most likely responsible organism? Review Topic
Explanation
Question 84
A 42-year-old patient has had painful inferior subluxation of the glenohumeral joint following a recent cerebrovascular accident (CVA). Figure 34 shows the AP radiograph of the shoulder. Management should consist of
Explanation
REFERENCES: Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
McCollough NC III: Orthopaedic evaluation and treatment of the stroke patient. Instr Course Lect 1975;24:45-55.
Question 85
The patient returns 1 year later to report curling of her toes and numbness on the plantar surface of her foot. What is the most likely cause of this condition?
Explanation
Radiographs reveal a Lisfranc fracture dislocation with fractures of the first and second metatarsals. Tenting of skin that is over a bony prominence is an orthopaedic emergency. The fracture dislocation should be reduced without delay. There is no evidence of compartment syndrome of the foot, but this may develop and monitoring is necessary. Toe deformity may develop on a delayed basis because of the subclinical presentation. Nerve irritation is not uncommon with dorsal midfoot surgical incisions. A positive Tinel test result over the midfoot in the distribution of the superficial common peroneal nerve is consistent with a stretch injury to this nerve. CRPS is usually associated with multiple nerve distributions and autonomic nerve findings such as cold hypersensitivity and hyperhidrosis.
RECOMMENDED READINGS
Benirschke SK, Meinberg EG, Anderson SA, Jones CB, Cole PA. Fractures and dislocations of the midfoot: Lisfranc and Chopart injuries. Instr Course Lect. 2013;62:79-91. PubMed PMID: 23395016. View Abstract at PubMed
Schepers T, Oprel PP, Van Lieshout EM. Influence of approach and implant on reduction accuracy and stability in lisfranc fracture-dislocation at the tarsometatarsal joint. Foot Ankle Int. 2013 May;34(5):705-10. doi: 10.1177/1071100712468581. Epub 2013 Jan 14. PubMed
PMID: 23637239. View Abstract at PubMed
Question 86
- A patient sustains a closed dorsal dislocation of the proximal interphalangeal joint of the middle finger without an associated fracture. Closed treatment results in a cocentric stable reduction. The finger is not immobilized. Which of the following conditions may appear 1 year later?
Explanation

Examination of a 3-year-old boy who slammed his finger in a door 3 months ago reveals 0 to 40 degrees of proximal interphalangeal joint motion. Radiographs are shown in Figures 47a and 47b. Management should consist of
Volar osteotomy
Observation only
Flexor tenolysis
Volar plate arthoplasty
A hinged distraction external fixator
Subcondylar fractures of the proximal and middle phalynx occur at the neck of the phalynx, usually as a result of a crush injury, and almost exclusively in the pediatric age group. The distal fragment rotates dorsally and the degree of displacement may be misjudged if a true lateral is not obtained. If malunion occurs there is block to flexion. Subcondylar fossa reconstruction by removal of bone through a palmar approach removes this boney block.
Question 87
What is the most frequent late complication of cementless fixation in total knee arthroplasty?
Explanation
REFERENCES: Peters PC, Engh GA, Dwyer KA, Vinh TN: Osteolysis after total knee arthroplasty without cement. J Bone Joint Surg Am 1992;74:864-876.
Parks NL, Engh GA, Topoleski LDT, Emperado J: Modular tibial insert micromotion: A concern with contemporary knee implants. Clin Orthop 1998;356:10-15.
Question 88
Based on the Young and Burgess classification of pelvic ring injuries, an anterior-posterior compression type II injury does not result in disruption of which of the following?

Explanation
well as sacrotuberous and sacrospinous ligaments. An APC III also involves disrupted posterior SI ligaments, causing complete SI joint disruption with potential translational and rotational displacement.
The reference by Young et al is a classic article that describes the Young and Burgess classification of pelvic ring injuries. They retrospectively analyzed pelvic ring radiographs and discussed four patterns of injury: anteroposterior compression, lateral compression, vertical shear, and a complex/combined pattern.
The reference by Burgess et al is a validation of the aforementioned classification and study, as they reviewed 210 consecutive patients who sustained a pelvic ring injury. They validated the classification scheme and found that overall blood replacement averaged: lateral compression, 3.6 units; anteroposterior compression, 14.8 units; vertical shear, 9.2 units; combined mechanical, 8.5 units. Overall mortality was: lateral compression, 7.0%; anteroposterior, 20.0%, vertical shear, 0%; combined mechanical, 18.0%.
Incorrect answers:
1,2,4,5: An APC - 2 pelvic ring injury involves injury to all of these structures.
Question 89
A 35-year-old patient is involved in a motor vehicle accident and sustains multiple fractures including a closed comminuted proximal meta-diaphyseal tibia fracture. The surgeon is considering bridge plating the fracture using a minimally invasive approach. Which of the following is true regarding bridge plating? Review Topic
Explanation
Bridge plating is applicable to all long-bone fractures with complex fragmentation and where intramedullary nailing or conventional plate fixation is not suitable. The construct preserves the blood supply to the fracture fragments as the fracture site is undisturbed during the operative procedure. It provides RELATIVE stability, allowing for some motion at the fracture site, leading to callus formation and secondary bone healing. The construct is FLEXIBLE because of increased distance between the 2 screws closest to the fracture (long working length), allowing for stress distribution and permitting more motion at the fracture site. The construct is also
AXIALLY STABLE because the plate acts as an extramedullary splint and resists axial compression.
Livani et al. advocate using an anterior or antero-lateral approach for minimally invasive plating of the humerus. They recommend that distal access is obtained first, allowing identification of the lateral antebrachial cutaneous nerve. For distal fractures, they recommend extending the plate down to the lateral column.
Apivatthakakul et al. defined minimally-invasive plate osteosynthesis (MIPO) danger zones from the lateral epicondyle. They found the musculocutaneous nerve averaged 18-43% of the humeral length, the danger zone for the radial nerve averaged 36-59% of the humeral length, and the most dangerous screws that penetrated or touched the radial nerve lay 47-53% of the humeral length.
Illustration A shows a distal tibia fracture. Illustration B shows radiographs 5 months after bridge plating of this fracture. There is callus formation, characteristic of indirect bone healing.
Question 90
A 50-year-old woman who underwent a joint replacement of the hallux metatarsophalangeal joint 6 months ago now has pain and swelling about the great toe. Radiographs are shown in Figures 39a and 39b. What is the next most appropriate step in management?
Explanation
REFERENCE: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 265-266.
Question 91
A 53-year-old man has a 4- x 5-cm high-grade soft-tissue sarcoma in the midthigh. As part of the staging evaluation, regional nodes should be assessed by
Explanation
REFERENCE: Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 92
-This boy’s parents are eager to get him back on the field as soon as possible. What is the most appropriate treatment option?
Explanation
Although a recent increase in the number of pitches may have contributed to this patient’s development of little leaguer’s shoulder, the most significant overall factor is age. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress, and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Genetic factors and gender have not been studied in association with little leaguer’s shoulder. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms.Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to baseline pitching is implemented until the patient is back to baseline. This protocol has a long-term success rate exceeding 90%.

Question 93
What structure (arrow) is shown in Figure 24?
Explanation
REFERENCES: Onibokun A, Khoo LT, Holly L: Anterior retroperitoneal approach to the lumbar spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 101-105.
Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.
Question 94
A 48-year-old male is involved in a motorycycle accident and arrives in the trauma bay in hypovolemic shock. He receives 6 units of packed red blood cells during his resuscitation. Which of the following viral microbes is he most at risk of exposure from the transfusions?

Explanation
Question 95
A 42-year-old man sustained a burst fracture at L2 in a motor vehicle accident. Examination reveals that he is neurologically intact. Figure 18 shows a cross-sectional CT scan through the fracture. If the fracture is managed nonsurgically for the next 2 years, the retained fragments can be expected to
Explanation
REFERENCES: Mumford J, Weinstein JN, Spratt KF, et al: Thoracolumbar burst fractures: The clinical efficacy and outcome of nonoperative management. Spine 1993;18:955-970.
Wood KB, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurologic deficit: A prospective, randomized study. J Bone Joint Surg Am 2003;85:773-781.
Question 96
Which wear mechanism is most likely responsible for the wear damage on the modular tibial insert retrieval shown in Figure 82?
Explanation
The figure shows the top side of a retrieved tibial liner. Pitting and delamination, which are associated with fatigue wear, are noted. Creep is deformation without wear. Adhesive and abrasive wear is associated with removal of material on the back side of modular tibial components.
CLINICAL SITUATION FOR QUESTIONS 83 THROUGH 87
A bilateral cemented total knee arthroplasty (TKA) was performed on an otherwise healthy 63-year-old woman. The surgery and immediate postsurgical course were uneventful. Two days after surgery, while in physical therapy at the hospital, the patient’s oxygen saturation is noted at 92%.
Question 97
A 20-year-old college soccer player comes for an evaluation 6 months after an injury during which he landed awkwardly from a jump. Although physical therapy, ice, and activity modification have helped him return to baseline motion, strength, and swelling, he continues to have lateral knee pain. He also notes a popping sensation on the lateral side of his knee with activity. A Lachman test, anterior and posterior drawer tests, a pivot shift test, and McMurray test findings are all negative. MR images reveal a 12-mm x 15-mm osteochondral defect in the lateral femoral condyle with full-thickness cartilage loss and approximately 4 mm of subchondral bone loss.
Explanation
Patellofemoral pain in a young athlete without patellar instability or a chondral or osteochondral defect often can be managed with nonsurgical treatment such as physical therapy and a home exercise program. Microfracture surgery is associated with good short-term results for younger athletes. Patients with no history of prior surgery, primary chondral rather than osteochondral lesions, and lesions smaller than 2 cm have experienced the best results. Microfracture surgery performed for chondral lesions of the central aspect of the medial femoral condyle is associated with worse results. Decreased activity levels over time of patients who undergo microfracture surgery are a concern. OAT provides good outcomes and return-to-sports rates for athletic people who are younger and have lesions smaller than 2 cm. Patients with lesions on the lateral femoral condyle have better success rates. Both microfracture surgery and OAT provide better results for chondral defects than osteochondral defects. OAT is associated with better results than microfracture for medium-sized lesions between 2 cm and 4 cm, while autologous chondrocyte implantation yields better improvement for patients with defects larger than 4 cm. All of the surgical techniques listed for articular cartilage repair are associated with better outcomes for patients younger than age 30.
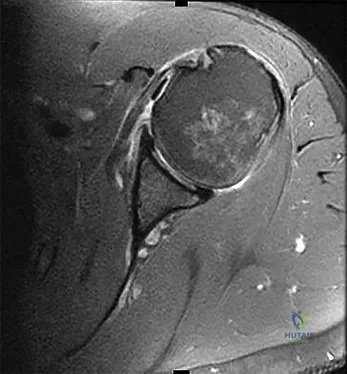
Question 98
ACL rehabilitation often includes exercises with the distal end of the extremity fixed in place with axial loading and co-contracture of muscle groups to help stabilize the joint. This type of exercise is more commonly referred to as: Review Topic
Explanation
Closed chain exercises are preferred for any rehabilitation protocol that wants to minimize stress across a potentially unstable joint. After ACL reconstruction it is important to begin motion and strengthening but not stress the reconstructed ligament which may lead to loss of stability or failure.
An example of a closed chain exercise of the quadriceps is a squat or leg press in which the foot is fixed against the floor/plate and both the quadriceps and hamstrings can contract together keeping the knee joint stable and preventing excess stress across the reconstructed ACL. An example of an open chain exercise of the quadriceps is a seated leg extension in which the foot is not fixed and the quadriceps contract in isolation. This creates a strong anterior pull on the tibia which can lead to excess stress on the ACL graft.
Beynnon et al. present a review on the behavior of ACL grafts during rehabilitation. They found that exercises that produce the least amount of stress across an ACL graft are either dominated by hamstring muscle contraction, involve quadriceps muscle activity with the knee flexed at 60° or greater, or involve active knee motion between
35°
and
90°
of
flexion.
Illustration A is an example of a squat, which is a closed chain exercise. Notice the feet are fixed in place against the floor. Illustration B is an example of a seated leg extension, which is an open chain exercise. Notice the feet are not fixed in place and no axial loading or co-contracture can occur.
Incorrect
Question 99
The spinal cord terminates as the conus medullaris at what vertebral level in adults? Review Topic 1 T12
Explanation
Question 100
A 2-year-old girl has the fracture shown in Figures 5a and 5b. This fracture is most commonly associated with which of the following entities? Review Topic
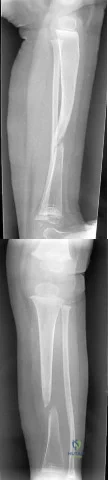
Explanation
