Orthopedic Board Review MCQs: Trauma, Shoulder & Foot | Part 200

Key Takeaway
This page offers Part 200 of a comprehensive OITE/AAOS Orthopedic Board Review. It features 100 high-yield, verified multiple-choice questions mirroring actual exam formats. Designed for orthopedic residents and surgeons, this quiz provides crucial practice and clinical explanations to ensure successful board certification.
About This Board Review Set
This is Part 200 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 200
This module focuses heavily on: Dislocation, Foot, Fracture, Shoulder, Trauma.
Sample Questions from This Set
Sample Question 1: A 23-year-old man reports a 6-year history of recurrent instability in the right dominant shoulder. He has not undergone surgery and has essentially stopped all of his sporting activities. On examination, he has instability and apprehension...
Sample Question 2: An orthopaedic surgeon in his first year of practice is negotiating with a private for-profit hospital to be their employed trauma specialist. The state of employment is known to have a high rate of malpractice claims because of a favorable...
Sample Question 3: Figures 41a and 41b show the radiographs of a 22-year-old woman who has a bunion on her left foot. She denies pain in the foot, but she reports increasing difficulty with shoe wear. Management should consist of...
Sample Question 4: A 40-year-old man is thrown off his motorcycle and sustains an open Type IIIA fracture shown in Figure A. He is taken to the operating room for debridement and reamed intramedullary nailing with a 10mm diameter nail. He returns at 10 months...
Sample Question 5: Of the following variables, which has the strongest influence on external fixator stiffness?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 23-year-old man reports a 6-year history of recurrent instability in the right dominant shoulder. He has not undergone surgery and has essentially stopped all of his sporting activities. On examination, he has instability and apprehension in the midrange of motion (abduction of 45 to 60 degrees with external rotation) and a palpable clunk representing a transient dislocation over the anterior glenoid rim. A three-dimensional CT scan is shown in Figure 31. What is the most appropriate surgical intervention to provide him with reliable stability postoperatively?
Explanation
A bony augmentation procedure such as the Lataijet has been well-described to provide a well functioning and stable shoulder joint. A hemiarthroplasty is not indicated in the absence of arthritis. Subscapularis
advancement will not address the bone loss.
REFERENCES: Hovelius L, Sandstrom B, Sundgren K, et al: One hundred eighteen Bristow-Latarjet repairs for recurrent anterior dislocation of the shoulder prospectively followed for fifteen years: Study I— clinical results. J Shoulder Elbow Surg 2004;13:509-516.
Schroder DT, Provencher MT, Mologne TS, et al: The modified Bristow procedure for anterior shoulder instability: 26-year outcomes in Naval Academy midshipmen. Am J Sports Med 2006;34:778-786.
Itoi E, Lee SB, Berglund LJ, et al: The effect of a glenoid defect on anteroinferior stability of the shoulder after Bankart repair: A cadaveric study. J Bone Joint Surg Am 2000;82:35-46.
Question 2
An orthopaedic surgeon in his first year of practice is negotiating with a private for-profit hospital to be their employed trauma specialist. The state of employment is known to have a high rate of malpractice claims because of a favorable plaintiff legal environment. During the course of negotiations, malpractice insurance is being discussed. The surgeon should ask the hospital to provide which type of malpractice insurance policy? Review Topic
Explanation
Question 3
Figures 41a and 41b show the radiographs of a 22-year-old woman who has a bunion on her left foot. She denies pain in the foot, but she reports increasing difficulty with shoe wear. Management should consist of
Explanation
REFERENCE: Mann RA, Coughlin MJ: Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 174.
Question 4
A 40-year-old man is thrown off his motorcycle and sustains an open Type IIIA fracture shown in Figure A. He is taken to the operating room for debridement and reamed intramedullary nailing with a 10mm diameter nail. He returns at 10 months with persistent pain at the fracture site with ambulation. Examination reveals healed wounds with no erythema, warmth or tenderness. Erythrocyte sedimentation rate and C-reactive protein levels are within normal limits. Radiographs taken at that time are shown in Figure B. What is the next best treatment step?

Explanation
Tibial delayed union can be defined as lack of union from 20-26 weeks post-injury, while nonunion is defined as lack of healing at >9mths post-injury, or absence of progressive signs of healing on radiographs for 3 consecutive months. Persistent pain is a symptom of nonunion. ESR and CRP are performed to rule out infection.
Bhandari et al. performed a blinded, multicenter trial on 622 reamed tibial nails and 604 unreamed tibial nails. In closed fractures, patients in the unreamed nail group were at greater risk of primary events than the reamed nail group. There was no difference in groups for open fractures. Primary events were defined as bone-grafting, implant exchange/removal, dynamization, and debridement.
Hak reviewed aseptic tibial nonunion. They discuss exchanged reamed nailing for diaphyseal nonunion, adjunctive plate fixation for metaphyseal nonunion, and nail removal and plating for metadiaphyseal nonunion, external fixation for infected nonunion and distraction osteogenesis of defects.
Figure A shows a mid-diaphyseal tibial fracture Figure B shows nonunion following
IM nailing of the fracture. Illustration A shows union following exchange nailing with a larger 12mm diameter nail.
Incorrect Answers:
Question 5
Of the following variables, which has the strongest influence on external fixator stiffness?
Explanation
Question 6
A 10-year-old child was referred for spinal curvature and a 2-year history of back pain. She has pain during the day and pain at night that wakes her from sleep and is temporarily relieved with nonsteroidal anti-inflammatory drugs. Examination shows very tight hamstrings and an irritative spinal curvature. Figures 71a through 7Id show radiographs, a bone scan, and a CT scan. What is the most appropriate treatment?
Explanation
REFERENCES: Frassica FJ, Waltrip RL, Sponseller PD, et al: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-
Question 7
An 11-year-old boy with bipolar disorder fell from a tree and sustained an open fracture dislocation of the right ankle with extensive abrasions of the leg. Immediate irrigation, debridement, reduction, and provisional fixation with Kirschner wires was performed. Twenty-four hours later, the patient’s blood pressure is 190/100 mm Hg and pulse rate is 120. He has required only 1 dose of an oral analgesic for pain control. His foot and ankle are markedly swollen, but there is no pain on passive extension of the toes. The dorsalis pedis pulse cannot be palpated. What is the most appropriate next treatment step? Review Topic
Explanation
(SBQ13PE.91) An 12-year-old girl presents with right hip pain. Bilateral frog laterals are shown in Figure A. Laboratory work-up reveals TSH 11 mIU/L (Ref range: 0.4-4.0 mIU/L) and Free T4 is 0.5 ng/dL (Ref range: 0.7-1.9 ng/dL). What is the most appropriate treatment recommendation? Review Topic

In situ pinning of right hip
Protected weight bearing and MRI of right hip
Immediate endocrine referral and treatment
Open biopsy right hip
In situ pinning bilateral hips PREFERRED RESPONSE 5
In patients with slipped capital femoral epiphysis (SCFE) and concomitant endocrinopathy, bilateral pinning is the recommended treatment.
This patient's laboratory values reveal hypothyroidism, which increases the risk of bilateral involvement. Thus, the most appropriate treatment recommendation is surgical fixation of both hips.
Wells et al. analyzed 131 SCFEs over a 30-year period. The authors noted that 100% of patients with associated endocrinopathy went onto contralateral slip and recommended not only prophylactic pinning, but in those with open triradiate cartilage, recommended preventative screening with TSH/Free T4 laboratory studies.
Riad et al. followed 90 patients and analyzed impact of age, gender and race on contralateral slip development. Girls under the age of 10 and boys under the age of 12 had a significantly increased risk of contralateral involvement. Therefore, the authors recommended contralateral pinning for girls and boys that met those age criteria, respectively.
Figure A exhibits a right SCFE on bilateral frog lateral views. Incorrect Answers:
Question 8
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?
Explanation
REFERENCES: Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Lester B, Jeong GK, Weiland AJ, Wickiewicz TL: Quadrilateral space syndrome: Diagnosis, pathology, and treatment. Am J Orthop 1999;28:718-722.
Question 9
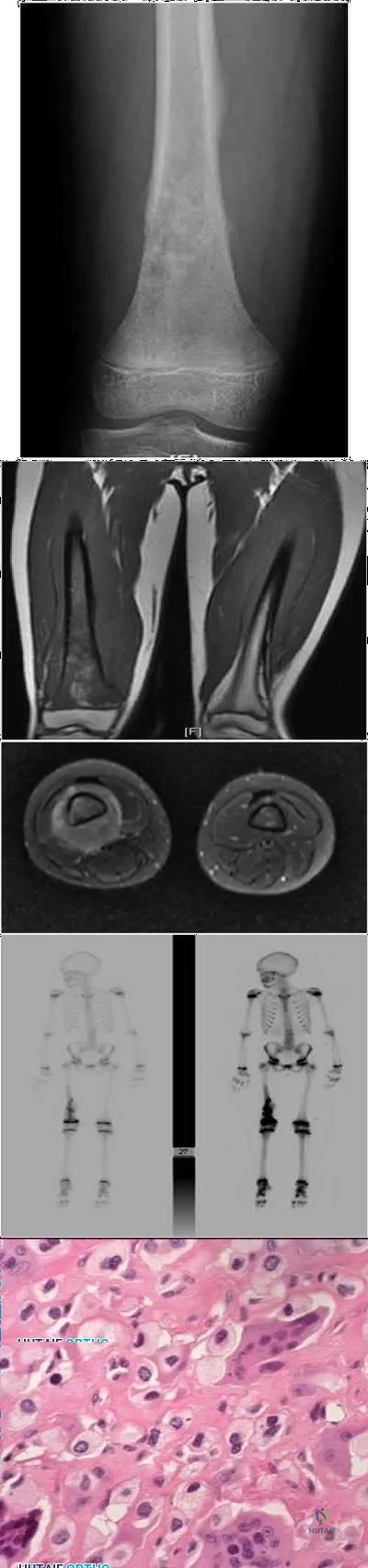
A 10-month-old boy has multiple skeletal lesions and a skin rash that he has had since he was a newborn. Based on the radiographs and biopsy specimens shown in Figures 79a through 79d, what is the most likely diagnosis?
Explanation
REFERENCES: Plasschaert F, Craig C, Bell R, et al: Eosinophilic granuloma: A different behaviour in children than in adults. J Bone Joint Surg Br 2002;84:870-872.
Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 857-876.
Question 10
A 60-year-old woman reports a painful hip arthroplasty after undergoing surgery 18 months ago. Radiographs show stable cementless implants without signs of ingrowth. Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h. Management should now consist of
Explanation
REFERENCES: Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
McAuley JP, Moreau G: Sepsis: Etiology, prophylaxis, and diagnosis, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 1295-1306.
Question 11
Which of the following surgical options after resection of a sarcoma about the knee would require a patient to expend the greatest amount of energy while walking?
Explanation
Question 12
A college athlete on a scholarship has a medical condition that you feel presents a life-threatening risk to him with participation in athletics. Because of the gravity of this decision and the potential effect it can have on the student/athlete's future, the college asks for your guidance. As the team physician for the college, what is your ethical obligation?
Explanation
Question 13
Figure 31 shows the radiograph of a 64-year-old woman who is seen in the emergency department following a motor vehicle accident. She has no voluntary motor function in her distal upper extremities or lower extremities. She does not have a bulbocavernosus reflex. She has a blood pressure of 80/50 mm Hg with a pulse of 50/min. Her hypotension does not improve with initial fluid resuscitation. Further treatment of her hypotension should consist of
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 179-187.
Nockels RP: Nonoperative management of acute spinal cord injury. Spine 2001;26:S31-S37.
Question 14
A previously healthy 20-year-old male wrestler is seen for evaluation and treatment of draining sores of the forearm. Empiric treatment for cellulitis was started with oral clindamycin with improvement. Culture of the drainage reveals methicillin-resistant staphylococcus aureus (MRSA). Sensitivities at 48 hours demonstrate additional resistance to erythromycin and a positive D-zone test. Definitive antibiotic treatment until resolution should consist of which of the following? Review Topic
Explanation
any signs of systemic illness, an oral antibiotic regimen is appropriate. When culture results reveal resistance to erythromycin, then a D-zone test should be performed to check for inducible clindamycin resistance. The D-zone test is performed by plating the sample on an agar and placing antibiotic disks made of clindamycin and erythromycin on the agar. A zone of inhibition in the shape of the letter D is seen with an inducible strain. If the D-zone test is positive, then clindamycin should not be used because the strain of MRSA can become resistant to the treatment. Therefore, because of the positive D-zone test, the antibiotic should be changed to oral doxycycline. IV antibiotics are not indicated for this infection. Oral rifampin should never be used as a single agent as resistance rapidly develops.
Question 15
The implant shown in Figures 47a and 47b is introduced submuscularly employing a minimally invasive technique. A percutaneous method of screw insertion is used distally. What nerve is most at risk?

Explanation
Question 16
Which of the following types of exercise used to increase flexibility is considered most beneficial in increasing joint range of motion?
Explanation
REFERENCES: Sady SP, Wortman M, Blanke D: Flexibility training: Ballistic, static or proprioceptive neuromuscular facilitation? Arch Phys Med Rehabil 1982;63:261-263.
Tanigawa MC: Comparison of the hold-relax procedure and passive mobilization on increasing muscle length. Phys Ther 1972;52:725-735.
Wallin D, Ekblom B, Grahn R, Nordenberg T: Improvement of muscle flexibility: A comparison between two techniques. Am J Sports Med 1985;13:263-268.
Question 17
There is a risk of impaired forearm rotation after tension band fixation of an olecranon fracture with which of the following?

Explanation
The referenced study by Candal-Couto et al is a cadaveric study that found that K-wire insertion in less than 30 degrees in an ulnar direction led to impingement of the K-wire on the radial head/neck, biceps or supinator. They recommend placing these wires away from this danger zone in order to minimize rotation blocks.
The referenced study by Matthews et al is a case series of two patients who had limited forearm rotation after K-wire fixation. The etiology of limited rotation was found to be from direct overpenetration of the K-wire, which led to a mechanical block.
Question 18
A 9-year-old child sustains a proximal tibial physeal fracture with a hyperextension mechanism. What structure is at most risk for serious injury?
Explanation
REFERENCE: Beaty JH, Kasser JR: Rockwood and Wilkins Fractures in Children. Philadelphia, PA, JB Lippincott, 2006, p 961.
Question 19
In what decade does the peak incidence of conventional osteosarcoma occur?
Explanation
REFERENCES: Simon MA, Springfield DS, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266.
Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989.
Wold L, et al: Osteogenic sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, p 14.
Question 20
When a structure like a long bone is under a bending load, its maximum stress is most dependent on what factor?
Explanation
REFERENCES: Hayes WC, Bouxsein ML: Biomechanics of cortical and trabecular bone: Implications for assessment of fracture risk, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 76-82.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 161-167.
Question 21
1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1% neutrophils. No growth of organisms is seen on routine culture. What is the best next step?
Explanation
This patient has a chronic quadriceps tendon rupture after total knee arthroplasty. Two previous primary repair attempts have failed, which is not surprising based on the poor results of primary repair reported in the literature. The patient also has an unstable knee and will require revision of some or all of the prosthesis to achieve a stable knee. Revision total knee arthroplasty with extensor mechanism allograft allows an allograft reconstruction of the ruptured quadriceps tendon. The other option is to utilize a synthetic mesh extensor mechanism reconstruction. These are likely to have the best result in this situation. Revision total knee arthroplasty with liner change and primary quadriceps repair is not the best form of management, because it involves a third attempt at primary tendon repair, which will likely fail again. Resection knee arthroplasty and arthrodesis with antegrade nail is a possible option but is not the best, because it would likely make driving and other daily activities difficult. Two-stage revision total
knee arthroplasty with extensor mechanism allograft is not the best option because the laboratory results
show no signs of infection, so a single-stage procedure is preferred.
Question 22
A 45-year-old previously healthy woman has experienced weakness and fatigability for 2 months. She states she feels best in the morning, but tires easily with exertion. If she sits and rests her strength improves, but she easily tires with each activity. When her fatigue is most severe, she has double vision. Physical examination is positive for ptosis with upward gaze after 20 seconds. When she holds her arms out straight she shows good initial strength, but rapidly decreasing strength with time. What is the pathologic cause of her muscle weakness? Review Topic
Explanation
Question 23
A 29-year-old obese patient is transferred from an outside facility for the management of a closed-head injury and the fracture shown in Figure A. He presents to the trauma bay as a transient responder to blood products, and undergoes urgent pre-surgical angiography embolization. Surgery is performed within 8 hours from the time of injury. The patient develops a deep wound infection 1 week post-operatively. Which of the following factors would be considered the MOST statistically significant predictor for post-operative infection in this patient.

Explanation
Question 24
A 23-year-old man reports pain on the superior aspect of his right shoulder with repetitive overhead activities and when lying on his right side. Figure 29 shows an axial MRI scan. What is the most likely diagnosis based on the MRI findings? Review Topic
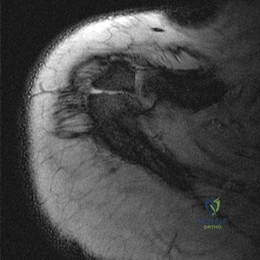
Explanation
Question 25
A young gymnast fell awkwardly onto an outstretched hand during a competition. At the time of impact, his forearm was positioned in supination. Axial and posterolateral forces were loaded along the forearm into the elbow and the elbow underwent a significant valgus thrust. What injury pattern is most likely to result from the combination of these forces at the elbow?
Explanation
The key features of a terrible triad injury include a radial head fracture, coronoid fracture, and dislocation of the elbow. Disruption of the lateral collateral ligament complex often concomitantly occurs. While restoration of the bony anatomy is important for static stability, the key primary stabilizer that needs to be addressed is the lateral collateral ligament complex. In acute injuries LCL repair may be possible. In chronic injury, LCL reconstruction would need to be considered.
O'Driscoll et al. 1991, examined 5 patients with recurrent posterolateral rotatory instability of the elbow. They showed that by applying supination of the forearm with a valgus moment and an axial compression force to the elbow while it is flexed from full extension, this can demonstrate posterolateral rotatory instability of the elbow. The elbow is reduced in full extension and must be subluxated as it is flexed in order to obtain a positive test result (a sudden reduction of the subluxation).
O'Driscoll et al. 1992 looked at a cadaveric study of the elbow. They showed that external rotation and valgus moments with axial forces resulted in posterior dislocations in 12 of the 13 specimens when the anterior medial collateral ligament (AMCL) remained intact. Clinically, it valgus stability in pronation is demonstrated, the AMCL can be assumed to be intact.
Illustration A and B shows radiographs of a terrible triad injury. There is posterolateral dislocation of the elbow with associated radial head fracture, coronoid fracture.
Incorrect Answers:
Question 26
Osteoclastic bone resorption is stimulated primarily by what molecular interaction?
Explanation
osteoclasts to enhance bone resorption. The pannus of rheumatoid arthritis and monosodium urate crystals of gouty tophi have been shown to trigger release of inflammatory cytokines such as IL-6, IL-8 and tumor necrosis factor alpha. The key to osteoclastic bone resorption of inflammatory arthropathy is regulated by the interaction of RANKL, expressed in osteoblasts and activated T cells, and RANK, expressed in osteoclast progenitors and mature osteoclasts. In inflammatory arthropathy, RANKL expression is increased and OPG is reduced, resulting in increased cortical and subchondral bone.
Question 27
A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause Review Topic
Explanation
Question 28
..Staging studies show no other lesions and surgical treatment is planned; when should a biopsy be performed?
Explanation
Figures 117a through 117c are the radiographs and MRI scan of a 16-year-old boy who has had a persistent fullness in his thigh since being kicked while playing soccer 4 weeks ago. He states that initially the area was painful, but now all symptoms other than the mass have resolved.

Question 29
On the morning of surgery the patient reports in the preop area that she has experienced skin breakdown over the second toe for 10 days. The extensor tendon is disrupted with an exposed proximal interphalangeal joint. She has been applying antibiotic ointment to the wound and denies fever or chills. What is the best plan of care?
Explanation
The clinical photograph shows a hallux valgus and a crossover toe deformity. The plantar plate must be damaged for a crossover toe deformity to develop. A moderately severe hallux valgus deformity without arthritic change is best treated with a bunionectomy with a proximal metatarsal osteotomy. The surgeon must assume that the open joint is at least colonized and at significant risk for postsurgical infection; consequently, it is best to cancel elective surgery, and surgical debridement of soft tissue and bone with deep cultures is recommended.
RECOMMENDED READINGS
Kaz AJ, Coughlin MJ. Crossover second toe: demographics, etiology, and radiographic assessment. Foot Ankle Int. 2007 Dec;28(12):1223-37. doi: 10.3113/FAI.2007.1223. PubMed PMID: 18173985. View Abstract at PubMed
Chalayon O, Chertman C, Guss AD, Saltzman CL, Nickisch F, Bachus KN. Role of plantar plate and surgical reconstruction techniques on static stability of lesser metatarsophalangeal joints: a biomechanical study. Foot Ankle Int. 2013 Oct;34(10):1436-42. doi: 10.1177/ 1071100713491728. Epub 2013 Jun 17. PubMed PMID: 23774466. View Abstract at PubMed
Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. View Abstract at PubMed
Question 30
- A 16-year-old girl who swims on her high school team reports pain in the shoulder after swimming. History reveals a glenohumeral dislocation at age 14 years while doing the backstroke. Examination shows a positive anterior apprehension sign. Treatment at this time should consist of
Explanation
p. 577: “A vigorous effort to stabilize the shoulder with exercises is particularly indicated in patients with multidirectional or posterior instability and in athletes requiring a completely normal or supranormal range of motion.”
p. 989: “If the [swimmer] has symptoms of subluxation, a conservative program that strengthens the external rotators is warranted. Surgery is seldom indicated.”
Question 31
Figures 1 through 6 reveal the radiographs and MR images of a 30-year-old man who has a 1-year history of atraumatic medial-sided left knee pain refractory to nonsurgical measures. What is the most appropriate treatment?

Explanation
Question 32
A patient who underwent a L4-L5 hemilaminotomy and partial diskectomy for radiculopathy 8 weeks ago now reports increasing low back pain without neurologic symptoms. A sagittal T2-weighted MRI scan is shown in Figure 13a, and a contrast enhanced T1-weighted MRI scan is shown in Figure 13b. What is the most appropriate management for the patient’s symptoms? Review Topic
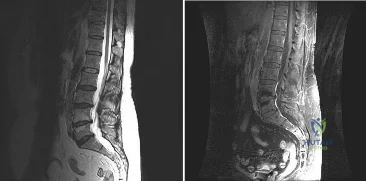
Explanation
pseudomeningocele is not present. A revision diskectomy is useful for recurrent radiculopathy but would not be helpful for degenerative low back pain.
(SBQ12SP.29) A 17-year-old female is undergoing posterior instrumented fusion from T5-T12 for adolescent idiopathic scoliosis. At the time of the correction maneuver, the neurophysiologist notifies you of a 60% decrease in somatosensory evoked potential (SSEP) amplitude throughout bilateral lower extremities. Which of the following is an acceptable approach to manage this finding? Review Topic
Immediate wake-up test with examination for clonus
Drop the mean arterial pressure (MAP) to ~60mmHg
Discontinue instrumentation and optimize MAP to 85mmHg or greater
Immediate infusion of intravenous corticosteroids
Modification of the anesthesia plan to include inhalational agents only followed by repeated SSEP testing
The patient has a significant drop in SSEP amplitudes at the completion of the corrective maneuver. The most appropriate response is to raise the MAP to 85 mmHg or greater, discontinue the instrumentation, re-evaluate the SSEPs, and if there is no improvement, to consider reversing the reduction of the deformity.
Intra-operative neurophysiologic monitoring is an effective method to monitor insults to the spinal cord and its exiting roots during spinal instrumentation. The common measurements include SSEPs, which monitor sensory potentials transmitted through the dorsal column system, and motor-evoked potentials (MEPs), which monitor motor response to a trans-cranial stimulus. Decreases in amplitude and latency of the circuits are recorded, however diminished signal amplitudes are more sensitive for neurologic injury, and decreases of of >50-60% being highly concerning. The wake-up test involves reversal of anesthesia so that an intra-operative neurologic examination can be performed.
Devlin et al. reviewed the basic science and practice of neurophysiologic monitoring in spine surgery. They proposed an algorithmic approach to managing intraoperative alerts which include discontinuation of inhalational anesthetics, increasing the MAP to >90 mmHg, discontinuing instrumentation, and performing a wake-up test if neurologic signals fail to normalize.
Herdmann et al. reviewed the practice of neurophysiologic monitoring and the effects of anesthesia upon signal transduction. They report that anesthesia affecting a neuron's intrinsic excitability can alter the results of monitoring. Inhalational anesthetics and decreased MAPs can be responsible for decreased amplitudes.
Vitale et. al. developed a consensus-based intraoperative checklist for management of lost neuromonitoring signals. In this checklist, the first steps across the surgical and anesthetic teams should include: stop the case and announce signal losses to the room, optimize the mean arterial pressure, discuss the status of anesthetic agents, and discuss reversible surgical actions just prior to signal loss.
Incorrect
Question 33
Figure 23 shows the postoperative radiograph of a patient who underwent an anterior cruciate ligament (ACL) reconstruction (with bone-patella tendon-bone autograft) that failed. He initially had loss of flexion postoperatively. What is the most likely cause of this failure?
Explanation
REFERENCES: Fu FH, Bennett CH, Latterman C, et al: Current trends in anterior cruciate ligament reconstruction: Part 1. Biology and biomechanics of reconstruction. Am J Sports Med 1999;27:821-830.
Fu FH, Bennett CH, Ma CB, et al: Current trends in anterior cruciate ligament reconstruction: Part II. Operative procedures and clinical correlations. Am J Sports Med 2000;28:124-130.
Question 34
A sagittal T1-weighted MRI scan of the knee joint is shown in Figure 23. What structure is identified by the arrow?
Explanation
REFERENCES: Gross ML, Grover JS, Bassett LW, Seeger LL, Finerman GA: Magnetic resonance imaging of the posterior cruciate ligament: Clinical use to improve diagnostic accuracy. Am J Sports Med 1992;20:732-737.
Sonin AH, Fitzgerald SW, Friedman H, Hoff FL, Hendrix RW, Rogers LF: Posterior cruciate ligament injury: MR imaging diagnosis and patterns of injury. Radiology 1994;190:455-458.
Question 35
-is the photograph of a 2-month-old infant with a left leg deformity. The mother’s pregnancy and delivery were unremarkable, and the infant is otherwise healthy. What is the most appropriate course of action?
Explanation


Question 36
In the Lauge-Hansen classification system, a pronation-abduction ankle fracture has what characteristic fibular fracture pattern?

Explanation
Question 37
Figure 28 shows the radiograph of a 6-year-old girl who has a right thoracic scoliosis that measures 60°. Examination shows multiple cafe-au-lait spots, and family history reveals that the child’s mother has the same disorder. The gene responsible for this disorder codes for
Explanation
REFERENCE: Beaty JH: Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 225-234.
Question 38
A 22-year-old ballet dancer undergoes hip arthroscopy for increasing hip pain and popping with activity. She experiences complete resolution of signs and symptoms post-operatively. Her pre- and post-operative magnetic resonance sagittal images shown in Figure A (left, pre-operative; right, post-operative). Which of the following pre-operative physical examination findings may have been positive? Review Topic
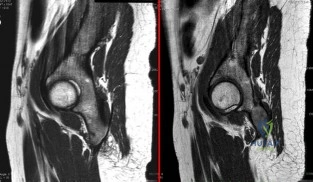
Explanation
Snapping hip exists in 3 forms: (1) external snapping hip, which is caused by the iliotibial band (ITB) sliding over the greater trochanter, (2) internal snapping hip, and
(3) intraarticular snapping hip, which is caused by loose bodies (traumatic, or from synovial chondromatoses) or labral tears. While painless snapping hip requires no treatment, painful snapping hip may be addressed with activity modification, physical therapy, steroid injections. Surgical release (ITB z-plasty or psoas tenotomy) is indicated if nonoperative management is unsuccessful.
Ilizaliturri et al. evaluated the results of endoscopic iliopsoas tendon release at the lesser trochanter (10 patients) vs endoscopic transcapsular psoas release from the peripheral compartment (9 patients). There were improvements in WOMAC scores in both groups, and no difference between groups. They conclude that both techniques are equally effective.
Marquez Arabia et al. evaluated if the psoas tendon regenerates after tenotomy in 27 patients. At 23 months, they found that tendon regeneration occurred in all patients, to
a mean circumference of 84% of the original. One patient had persistent pain, but all had 5/5 hip flexion strength. They hypothesize that the bulk of iliopsoas muscle fibers attaches directly to the proximal femoral shaft without a tendon, preventing retraction and allowing regeneration to occur easily.
Figure A shows pre- and post-operative arthroscopic psoas tenotomy magnetic resonance sagittal images. Illustration A shows the psoas tendon (white arrows) prior to transection. Illustration B shows the psoas tendon after transection (green arrows, proximal tendon segment; yellow arrows, distal segment). Illustration C and D are diagrams showing release at the level of the lesser trochanter and hip joint respectively.
Incorrect
90 degrees, but full external rotation. Answer 2: Decreased internal rotation and a positive impingement test (forced
flexion, adduction, femoroacetabular Answer 4: These
and internal
rotation) are classic findings
findings may
be found with intra-articular
for cam-type impingement loose bodies.
Question 39
A 24-year-old woman is thrown from her motorcycle and sustains the closed injury shown in Figures A through C. Open reduction and internal fixation is planned. What surgical technique will best allow visualization of the joint surface and allow early range of motion?

Explanation
Bicolumnar fixation of distal humerus fractures should follow the principles outlined by O'Driscoll: Distal fragments should be held by as many screws as possible; every screw in the distal fragments should pass through a plate; each screw should engage as many articular fragments as possible.
Galano et al. review treatment for bicolumnar distal humerus fractures. They note that the olecranon osteotomy, Alonso-Llames triceps sparing and Campbell triceps splitting approaches expose 57%, 46% and 35% of the articular surface, respectively. The OO and paratricipital (triceps sparing) approaches allow for early ROM. Protected motion is required for the O'Driscoll TRAP and Bryan-Morrey approaches for tendon-to-bone healing.
Coles et al. retrospectively reviewed the OO in fixation of 70 fractures. Osteotomy fixation was with an intramedullary screw and dorsal ulnar wiring, or with a plate.
The rate of OO increased with fracture difficulty (from AO type C1-C3). There was 1 delayed union but no nonunions.
Figures A and B show a AO/OTA type C2 intraarticular distal humerus fracture. Figure C is a coronal CT scan showing intraarticular comminution. Illustration A shows fixation of the fracture with bicolumnar plating through an olecranon osteotomy approach. Illustration B shows the various approaches to the distal humerus (left, Campbell triceps splitting; center left, O'Driscoll triceps reflecting anconeus pedicle; center right, Bryan-Morrey approach, leaving the triceps attached laterally to the fasciocutaneous flap, but elevating it off the ulna; right, olecranon osteotomy). Illustration C shows 3 methods of olecranon osteotomy (A and B, Intraarticular transverse; C-F, Extra-articular oblique; G, Intra-articular chevron).
Incorrect Answers:
(SBQ12TR.84) Figure A shows a radiograph of a 30-year-old male who underwent fixation of a left leg injury just over two years ago. He presents with persistent pain and drainage from the distal wound despite 4 months of oral antibiotics. He has no systemic symptoms. He has a past medical history of Grave's disease and Irritable Bowel Syndrome. What would be the best management at this stage? Review Topic

Chronic suppressive, culture-directed, antibiotic therapy
Above knee amputation
Endocrine consultation, irrigation and debridement, removal of hardware and negative-pressure wound therapy
Irrigation and debridement, removal of hardware, over-reaming medullary canal, external fixation and culture-directed antibiotics
Irrigation and debridement, retention of hardware, acute bone grafting and culture-directed antibiotics
This is a case of fracture nonunion in the setting of chronic osteomyelitis and infected hardware. The best treatment option available would be irrigation and debridement, removal of hardware, ring external fixator and culture directed antibiotics.
The management of infected nonunion in the setting of chronic osteomyelitis is technically demanding. The aims of treatment are to eradicate the infection and obtain bone union. Non-surgical options are largely unsuccessful in patients with draining chronic osteomyeltis in the setting of infected hardware and nonunion. Surgical options involve incision and debridement of necrotic tissue followed by reconstruction of bone and possible soft tissue (to provide healthy viable coverage). The most common techniques are ringed fixator/circular frames, staged intramedullary device with or without external fixator, free tissue transfer, or radical
debridement, bone grafting, and fixation.
Motsitsi et al. reviewed the management of infected nonunion of long bones. They suggest that the Ilizarov technique is regarded as a standard treatment in infected nonunion of the tibia. When there is bone defect after debridement, the bone can be shortened or treated with bone transport.
Egol et al look at a series of patients with chronic osteomyelitis. Limb salvage should be attempted in all patients. The presence of a chronic draining sinus requires surgical debridement and culture directed antibiotics. Infected hardware should be removed. A two-stage strategy is the best and well-proven treatment option.
Figure A shows a intramedullary nail in the left tibia. There is a moderate amount of bone loss at the fracture site with mixed sclerotic bone suggestive of osteomyelitis.
Incorrect Answers:
Question 40
During anatomic medial patellofemoral ligament (MPFL) reconstruction, the surgeon notes that the graft is becoming too tight with greater knee flexion. What is the most likely cause?
Explanation
Question 41
When using surgery extending to the pelvis to treat long spinal deformity in adults, the addition of anterior interbody structural support at the lumbosacral junction serves what biomechanical function?
Explanation
REFERENCES: Shufflebarger HL: Moss-Miami spinal instrumentation system: Methods of fixation of the spondylopelvic junction, in Margulies JI, Floman Y, Farcy JPC, et al (eds): Lumbosacral and Spinal Pelvic Fixation. Philadelphia, PA, Lippincott-Raven, 1996, pp 381-393.
Cunningham BW: A biomechanical approach to posterior spinal instrumentation: principles and applications, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 588-600.
Kostuik JP, Valdevit A, Chang HG, et al: Biomechanical testing of the lumbosacral spine. Spine 1998;23:1721-1728.
Question 42
A 13-year-old girl has had a firm mass and pain in her right shoulder for the past several weeks. She denies any history of trauma. A radiograph and MRI scan are shown in Figures 31a and 31b. Biopsy specimens are shown in Figures 31c and 31d. What is the most likely diagnosis?
Explanation
REFERENCES: Simon MA, Springfield DS, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266.
Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 43
When discussing treatment options with a 35 year-old healthy male with an isolated, closed tibial shaft fracture, the surgeon should inform him that in comparison to closed treatment, the advantages of intramedullary nail fixation include all of the following EXCCEPT?

Explanation
In a study of 94 tibial fractures, Finkemeier reported 10 (11%) had compartment syndromes. Three of the 10 patients developed the compartment syndrome postoperatively.
In comparing IM nailing to non-op, Bone et al showed that IM nailing had a shorter time to union (mean, 18 vs 26 weeks; p = 0.02), lower non-union rate (2% vs 10%), decresed incidence of shortening (2% vs 27%), and quicker return to work (mean, 4 vs 6.5 months), but no difference in compartment syndrome (0% in both groups).
The classic article cited by Sarmiento el al. reported that closed treatment with use of a prefabricated functional below-the-knee brace was effective in a study of 1000 closed diaphyseal fractures of the tibia with an incidence of nonunion of only 1.1%. However, those authors had very strict criteria for use of the fracture-brace (exclusion criteria included intact fibular, shortening >2cm).
Question 44
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?
Explanation
REFERENCE: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD,
Williams and Wilkins, 1998, pp 98-100.
Question 45
A 65-year-old woman has nausea, vomiting, and abdominal distention after undergoing total knee arthroplasty 48 hours ago. An abdominal radiograph is shown in Figure 14. Associated risk factors for this disorder include
Explanation
REFERENCES: Iorio R, Healy WL, Appleby D: The association of excessive warfarin anticoagulation and postoperative ileus after total joint replacement surgery. J Arthroplasty 2000;15:220-223.
Clarke HD, Berry DJ, Larson DR: Acute pseudo-obstruction of the colon as a postoperative complication of hip arthroplasty. J Bone Joint Surg Am 1997;79:1642-1647.
Question 46
An 18-year-old man underwent open reduction and internal fixation of a tibial spine avulsion and a posterolateral corner repair. Two years later, he underwent lateral collateral ligament (LCL) and posterolateral corner reconstruction because of instability. Examination reveals a pronounced lateral varus knee thrust when ambulating. Varus stress in 30 degrees of flexion produces a 10-mm opening that is eliminated in extension. The Lachman’s test is 2 mm with a firm end point, and the posterior drawer test is negative. Standing radiographs show widening of the lateral joint space and a 5-degree mechanical varus alignment. What is the most effective course of treatment?
Explanation
REFERENCES: Naudie DD, Amendola A, Fowler PJ: Opening wedge high tibial osteotomy for symptomatic hyperextension-varus thrust. Am J Sports Med 2004;32:60-70.
Covey DC: Injuries of the posterolateral corner of the knee. J Bone Joint Surg Am
2001;83:106-118.
Question 47
A 32-year-old woman has left second toe dactylitis (sausage toe). Radiographs show a “pencil in cup” distal interphalangeal joint deformity. Examination reveals that subtalar motion is markedly reduced. What is the most likely diagnosis?
Explanation
REFERENCES: Jahss MH: Disorders of the Foot and Ankle, ed 2. Philadelphia, PA,
WB Saunders, 1991, pp 1691-1693.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 172-173.
Question 48
A 22-year-old man who plays recreational soccer (Figure 41)
Explanation

Question 49
A 5-year-old boy sustained an elbow injury. Examination in the emergency department reveals that he is unable to flex the interphalangeal joint of his thumb and the distal interphalangeal joint of his index finger. The radial pulse is palpable at the wrist, and sensation is normal throughout the hand. Radiographs are shown in Figures 6a and 6b. In addition to reduction and pinning of the fracture, initial treatment should include
Explanation
REFERENCES: Cramer KE, Green NE, Devito DP: Incidence of anterior interosseous nerve palsy in supracondylar humerus fractures in children. J Pediatr Orthop 1993;13:502-505.
Sood MK, Burke FD: Anterior interosseous nerve palsy: A review of 16 cases. J Hand Surg Br 1997;22:64-68.
Question 50
For a patient with an unstable pelvic fracture, the amount of blood tranfusions required in the first 24 hours has shown to be most predictive for what variable?

Explanation
According to the referenced study by Smith et al, fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased ISS or RTS scores. Deaths were most commonly from exsanguination (<24 hours) or multiorgan failure (>24 hours).
Incorrect Answers: Choices 1-4 are not as predictive of mortality as choice 5.
Question 51
The nucleus pulposus of the intervertebral disk consists of chondrocyte-like cells that have a limited vascular supply and generate energy through which of the following?
Explanation
Question 52
An otherwise healthy 25-year-old man underwent a right anterior cruciate ligament reconstruction with a bone-patellar tendon-bone allograft. Routine preimplantation cultures of the allograft taken by the surgeon were positive for coagulase-negative Staphylococcus 5 days postoperatively. The patient has exhibited no evidence of clinical infection and his postoperative course has been uncomplicated during this time. What is the ideal management of this patient?
Explanation
implanted with a "contaminated" graft develop a clinical infection. The results of the current literature suggest that the treatment of low-virulence organisms is unnecessary if no evidence of clinical infection exists. Preimplantation cultures do not appear to correlate with clinical infection. Therefore, the routine culture of allograft tissue is not recommended.
Question 53
A 17-year-old woman seen in the emergency department reports right knee pain and swelling that has progressively worsened over the past several weeks. Radiographs are shown in Figures 31a and 31b. What is the most likely diagnosis?
Explanation
REFERENCES: Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Question 54
Arthrodesis
Explanation
with OA or RA. Certainly in patients who have glenoid bone deficiency precluding placement of a glenoid component…" as is apparent in this radiograph.
Question 55
A patient who underwent an L5-S1 hemilaminotomy and partial diskectomy for radiculopathy 3 weeks ago now reports increasing leg and back pain with radicular signs. An axial T2-weighted MRI scan is shown in Figure 97a, an axial T1-weighted MRI scan is shown in Figure 97b, and a contrast enhanced T1-weighted MRI scan is shown in Figure 97c. What is the most appropriate management for the patient's symptoms? Review Topic
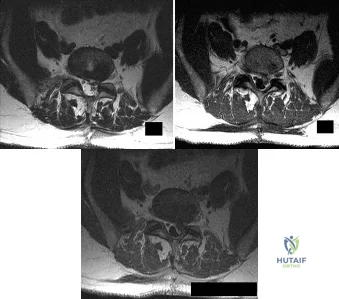
Explanation
Question 56
A collegiate rower reports the sudden onset of right chest pain while rowing. The athlete states that the pain is worse with deep inspiration and coughing. Examination reveals localized tenderness over the posterolateral corner of the eighth rib. What is the most likely diagnosis?
Explanation
REFERENCES: Karlson KA: Rib stress fractures in elite rowers. Am J Sports Med 1998;26:516-520.
Holden DL, Jackson DW: Stress fractures of the ribs in female rowers. Am J Sports Med 1985;13:342-348.
Question 57
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk?
Explanation
REFERENCES: Molnar GE, Gordon SU: Cerebral palsy: Predictive value of selected clinical signs for early prognostication of motor function. Arch Phys Med Rehabil 1976;57:153-158.
Wu YW, Day SM, Strauss DJ, et al: Prognosis for ambulation in cerebral palsy: A population-based study. Pediatrics 2004;114:1264-1271.
Question 58
A 78-year-old man with ankylosing spondylitis sustains a minor fall. Shortly afterward he experiences sudden worsening of his chronic back pain and is brought to the emergency department by his caregiver. Radiographs and a CT scan of the spine do not show a clear fracture. What is the most appropriate next step?
Explanation
Patients with ankylosing spondylitis are at high risk for occult fractures after low-energy injuries. Although radiographs and a CT scan do not demonstrate a spinal fracture in this patient, high risk for an unstable occult fracture necessitates further imaging with MRI to ensure that no fractures are missed. Although a CT scan is typically the primary imaging modality for workup of spine injuries in similar patients, CT and MRI complement each other and each detects fractures that are missed using the other modality. A CT myelogram might detect cord or root compression but would not aid in the diagnosis of an occult fracture. Nonsteroidal anti-inflammatory drugs are first-line treatment for idiopathic low-back pain. In a patient with ankylosing spondylitis at high risk for fracture, further workup is needed to rule out an occult fracture. Flexion and extension radiographs of the spine are inferior to MRI for evaluating occult fractures and ligamentous injuries. The primary concern for this patient remains an unstable spinal fracture, which necessitates an MRI of the spine before initiating a workup for other possible causes of his back pain.
RECOMMENDED READINGS
Duane TM, Cross J, Scarcella N, Wolfe LG, Mayglothling J, Aboutanos MB, Whelan JF, Malhotra AK, Ivatury RR. Flexion-extension cervical spine plain films compared with MRI in the diagnosis of ligamentous injury. Am Surg. 2010 Jun;76(6):595-8. PubMed PMID: 20583514. View Abstract at PubMed
Hitchon PW, From AM, Brenton MD, Glaser JA, Torner JC. Fractures of the thoracolumbar spine complicating ankylosing spondylitis. J Neurosurg. 2002 Sep;97(2 Suppl):218-22. PubMed PMID: 12296682. View Abstract at PubMed
Koivikko MP, Koskinen SK. MRI of cervical spine injuries complicating ankylosing spondylitis. Skeletal Radiol. 2008 Sep;37(9):813-9. doi: 10.1007/s00256-008-0484-x. Epub 2008 Apr
Question 59
Figure 51 shows the radiograph of a 42-year-old construction worker who has pain and limited motion in his dominant elbow. Management consisting of nonsteroidal anti-inflammatory drugs and cortisone has failed to provide relief. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Gramstad GD, Galatz LM: Management of elbow osteoarthritis. J Bone Joint Surg Am 2006;88:421-430.
Steinmann SP, King GJ, Savoie FH III, et al: Arthroscopic treatment of the arthritic elbow.
J Bone Joint Surg Am 2005;87:2114-2121.
Question 60
A toddler is brought in by his parents for evaluation of gait problems. Birth history and neurologic examination are unremarkable. After evaluating femoral torsion, tibial torsion, and foot contour, the diagnosis is excessive internal tibial torsion. The parents should be advised to expect which of the following outcomes? Review Topic
Explanation
Question 61
A 6-year-old sustains the injury shown in Figures A and B. The nerve most commonly affected by this fracture pattern innervates which of the following motor groups?

Explanation
The most common neurapraxia after pediatric extension-type supracondylar fractures involve the AIN. It supplies the FPL (thumb IP flexion), the pronator quadratus, and the FDP of the index/long fingers. Subsequently, patients are often unable to make an “a-ok” sign. Most of these neuropraxias resolve without complication. The ulnar nerve is most commonly implicated with flexion-type supracondylar fractures.
Abzug et al. review management of supracondylar fractures. They note that the AIN
is most commonly injured nerve in extension type supracondylar fractures. They note that nerve injuries often resolve within 6-12 weeks.
Babal et al. completed a meta-analysis to determine the risk of neurapraxia associated with pediatric supracondylar fractures. The rate of traumatic neurapraxia was 11.4% amongst 5000 patients. The AIN was affected 34.1% of the time. AIN neurapraxia was most common in extension type injuries.
Figures A and B show an AP and lateral radiographs of a displaced pediatric supracondylar fracture
Incorrect Answers
Question 62
Figures 52a and 52b show the plain radiographs of a 12-year-old girl who has right distal leg pain. She reports that symptoms are present with weight-bearing activities and improve with rest. Examination reveals diffuse tenderness over the distal tibial metaphysis and mild swelling. A photomicrograph of the biopsy specimen is shown in Figure 52c. What is the most likely diagnosis?
Explanation
REFERENCE: Picci P, Manfrini M, Zucchi Z, et al: Giant cell tumor of bone in skeletally immature patients. J Bone Joint Surg Am 1983;65:486-490.
Question 63
-What is the most likely mechanism of injury?
Explanation
The MRI scan shows a bone bruise of the lateral femoral condyle and lateral tibial plateau. This injury pattern is commonly associated with anterior cruciate ligament (ACL) rupture and an abnormal pivot shift test result. Treatment of an ACL tear in a high-demand athlete should consist of ligament reconstruction.In this patient, surgery should be delayed until she regains full range of motion to minimize risk for arthrofibrosis after surgery. Recent analysis has shown that the noncontact mechanism is more consistent with anterior translation, affecting both the medial and lateral compartments. The bone bruise in the lateral femoral condyle occurs more anterior than that of the medial femoral condyle, suggesting that internal rotation has occurred. The external rotation recurvatum test assesses for posterolateral corner injury, and a positive quadriceps active test is consistent with posterior cruciate ligament rupture. An abnormal patellar apprehension test result is suggestive of patellar instability. Nonsurgical treatment is unlikely to result in sufficient stability if this patient returns to sports at her preinjury level of activity.Primary ACL repair is associated with high failure rates. Although the precise mechanism of injury varies,injuries can be broadly classified into contact and noncontact injuries. Noncontact injuries occur with the knee in slight flexion, valgus, and internal rotation, and contact injuries typically involve a lateralside impact producing a valgus force to the knee. The valgus component of noncontact injuries has been thought to cause mainly lateral compartment bone bruising. Posterior translation is the most common mechanism of posterior cruciate ligament rupture, and hyperextension and varus is associated with posterolateral corner injury.
Question 64
During an open reduction internal fixation of a humerus fracture using the posterior approach, a surgeon can identify the posterior antebrachial cutaneous nerve and trace it proximally to which of the following nerves?

Explanation
Question 65
Figure 49 shows a histologic section of the lung in a patient who died during total hip arthroplasty. What unexpected finding is seen in the pulmonary capillaries?
Explanation
23 patients. Fat and marrow embolization during preparation of the femur or cementing of the femoral component was believed to be responsible for the cardiopulmonary collapse that occurred during arthroplasty. Although fat and marrow emboli were found in the pulmonary capillaries of most of the patients on autopsy, this histologic section shows two particles of cement in the pulmonary capillaries.
REFERENCES: Parvizi J, Holiday AD, Ereth MH, et al: The Frank Stinchfield Award. Sudden death during primary hip arthroplasty. Clin Orthop 1999;369:39-48.
Patterson BM, Healy JH, Cornell CN, et al: Cardiac arrest during hip arthroplasty with a cemented long-stem component: A report of seven cases. J Bone Joint Surg Am
1991;73:271-277.
Question 66
A 10-year-old boy has 2 months of right knee pain that started at summer camp. The patient denies constitutional symptoms. There is no lymphadenopathy present. CT of the chest shows no signs of metastatic disease. Imaging studies and biopsy results are shown in Figures A-E. What is the most likely diagnosis?
Explanation
Treatment for osteosarcoma includes neoadjuvant chemotherapy, wide resection, and adjuvant chemotherapy.
Question 67
A 59-year-old woman with a history of osteoporosis is involved in a high-speed motor vehicle accident, resulting in left hip pain and deformity. The initial radiograph from the trauma bay is shown in Figure 1. Postreduction CT is shown in Figures 2 through 4. What is the most appropriate definitive surgical treatment?
Explanation
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
Question 68
A patient reports pain in the hip with functional positioning. With the patient supine, pain in which of the following positions would be typical for femoral acetabular impingement? Review Topic
Explanation
(SBQ13PE.10) Which statement is true regarding discoid menisci? Review Topic
Most commonly involves the medial meniscus
Bilateral in >75% of cases
Asymptomatic discoid meniscus should undergo saucerization
Radiographs will commonly show a hyperplastic lateral intercondylar spine
Radiographs will commonly show squaring of affected condyle with cupping of tibial plateau
Radiographs of knees with discoid menisci will commonly show squaring of affected condyle (lateral>medial) with cupping of tibial plateau.
Discoid meniscus refers to the abnormal development of a hypertrophic and discoid shaped meniscus. It occurs in 3-5% of the population and it is considered the most common cause of a symptomatic clicking or clunking in a childs knee. The lateral meniscus is most commonly affected and it will occur bilaterally in 25% of affected
people. The Watanabe Classification describes the 3 types of discoid menisci. Type 1
= Incomplete, Type 2 = Complete, Type 3 = Wrisberg (lack of posterior meniscotibial attachment to tibia)
Kramer et al. looked at the presentation of pediatric knee pain. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the discoid meniscus.
Lee et al. retrospectively reviewed 36 patients aged less than 15 years who underwent arthroscopic procedures for torn discoid menisci. The mean patient age at the time of surgery was 9.5 years. They showed that partial meniscectomy yielded better radiologic results than subtotal/total meniscectomy for torn discoid menisci in this population.
Illustration A shows the 3 classifications of discoid menisus as originally described by Watanabe. Type 4 is a ring type discoid that was not originally described by Watanabe in his 1978 paper. Illustration B shows an AP and lateral radiograph of a discoid meniscus knee. Note squaring of affected lateral condyle in the presence of a lateral discoid meniscus. Illustration C shows 4 consecutive sagittal MRI images with meniscus continuity. It is important to note that the diagnosis of discoid menisci can be made when 3 or more 5mm sagittal images show meniscal continuity.
Incorrect Answers:
Question 69
A 27-year-old runner training for his first marathon reports lateral knee pain after an unusually long training run. He states that the most significant pain occurs while running downhill. Examination of the patient while he is laying on the unaffected side reveals increased pain when manual pressure is applied to the lateral femoral epicondylar area during knee range of motion of 30° to 45°. What is the most likely diagnosis?
Explanation
REFERENCES: Noble CA: The treatment of iliotibial band friction syndrome. Br J Sports Med 1979;13:51-54.
James SL: Running injuries to the knee. J Am Acad Orthop Surg 1995;3:309-318.
James SL, Jones DV: Biomechanical aspects of distance running, in Cavanagh PR (ed): Biomechanics of Distance Running. Champaign, IL, Human Kinetic Books, 1990, pp 249-269.
Question 70
When comparing gait parameters between a patient with an anterior cruciate ligament (ACL) deficiency to a patient with a normal knee, the patient with an ACL deficiency has which of the following? Review Topic
Explanation
Question 71
-The Coleman block test is used to test for
Explanation

Question 72
What is the best way to determine whether a radial head implant is too thick intraoperatively?
Explanation
Question 73
Which of the following is a long-term complication of ankle arthrodesis for posttraumatic arthritis?
Explanation
REFERENCES: Coester LM, Saltzman CL, Leupold J, Pontarelli W: Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am 2001;83:219-228.
Mazur JM, Schwartz E, Simon SR: Ankle arthrodesis: Long-term follow-up with gait analysis. J Bone Joint Surg Am 1979;61:964-975.
Question 74
A 12-year-old boy reports the acute onset of pain and a pop over the right side of his pelvis while swinging a baseball bat during a Little League game. Radiographs reveal an avulsion of the anterior superior iliac spine with 2 cm of displacement. Management should consist of Review Topic
Explanation
Question 75
The husband of a 22-year-old woman has hypophosphatemic rickets. The woman has no orthopaedic abnormalities, but she is concerned about her chances of having a child with the same disease. What should they be told regarding this disorder?
Explanation
REFERENCES: Herring JA: Metabolic and endocrine bone diseases, in Tachdjian’s Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743.
Sillence DO: Disorders of bone density, volume, and mineralization, in Rimoin DL, Conner JM, Pyerite RE, et al (eds): Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002.
Staheli LT: Practice of Pediatric Orthopedics. Philadelphia, PA, Lippincott Williams & Wilkins, 2001.
Question 76
A teenager had pain in the left buttock while running the hurdles. He was treated with 4 weeks of rest and crutch walking, and then started physical therapy for stretching and muscle strengthening. Nine months later he now reports pain with sitting and has not been able to resume running or sports activity. Figure 96 shows a radiograph of the pelvis. Treatment should consist of which of the following?
Explanation
REFERENCES: Fembach SK., Wilkinson RH: Avulsion injuries of the pelvis and proximal femur. AJR Am J Roentgenol 1981;137:581-584.
Watts HG: Fractures of the pelvis in children. Orthop Clin North Am 1976;7:615-624. Question 97
Congenital anomalies of the vertebral column are associated frequently with other organ system problems. In addition to radiographs of the spine, what other screening tests should be ordered?
Spinal MRI, coagulation panel
Liver enzymes, coagulation panel
Renal ultrasound, upper and lower GI
Cardiac evaluation/echocardiogram, upper and lower GI
Renal ultrasound, cardiac evaluation/echocardiogram, spinal MRI
DISCUSSION: Approximately 60% of patients with congenital anomalies of the spine have other associated findings. The spine develops around the same time as the cardiovascular system, the genitourinary system, and the musculoskeletal system. Around 20% of patients with congenital scoliosis have an associated urologic abnormality. Approximately 25% of patients with congenital scoliosis have an associated cardiac defect. Spinal cord abnormalities in one study occurred in approximately 37% of patients with congenital scoliosis.
REFERENCES: Basu PS, Elsebaie H, Noordeen MH: Congenital spinal deformity: A comprehensive assessment at presentation. Spine 2002;27:2255-2259.
Ferguson RL: Medical and congenital comorbidities associated with spinal deformities in the immature spine. J Bone Joint Surg Am 2007;89:34-41.
McMaster MJ, Ohtsuka K: The natural history of congenital scoliosis: A study of two hundred and fifty- one patients. J Bone Joint Surg Am 1982;64:1128-1147.
2010 Pediatric Orthopaedic Examination Answer Book • 81
Figure 98a Figure 98b
Question 77
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Explanation
REFERENCE: Daftari TK, Whitesides TE Jr, Heller JG, et al: Nicotine on the revascularization of bone graft: An experimental study in rabbits. Spine 1994;19:904-911.
Question 78
Which of the following findings helps to distinguish between stress fractures of the tibia and shin splints?
Explanation
After activity, pain persists longer with tibial stress fractures.
DISCUSSION: Anterior tibial pain can often be difficult to diagnose. A bone scan showing the tibial cortex in a diffuse, longitudinal orientation is consistent with shin splints compared to a more discreet, localized uptake more commonly seen with a stress fracture. Bone stress injuries are due to cyclical overuse of the bone. They are relatively common in athletes and military recruits but are also seem in otherwise healthy people who have recently started new or intensive physical activity. Diagnosis of bone stress injuries is based on the patient’s history of increased physical activity and on imaging findings.
The general symptom of a bone stress injury is stress-related pain. Bone stress injuries are difficult to diagnose based only on a clinical examination because the clinical symptoms may vary depending on the phase of the pathophysiological spectrum in the bone stress injury. Imaging studies are needed to ensure an early and exact diagnosis. If the diagnosis is made early, most bone stress injuries heal well without complications.
REFERENCES: Mubarak SJ, Gould RN, Lee YF, et al: The medial tibial stress syndrome: A cause of shin splints. Am J Sports Med 1982;10:201-205.
Knobloch K, Yoon U, Vogt PM: Acute and overuse injuries correlated to hours of training in master running athletes. Foot Ankle Int 2008:29:671-676.
Kiuru MJ, Pihlajamaki HK, Ahovuo JA: Bone stress injuries. Acta Radiol 2004;45:317-326.
Question 79
The arrow in the axial T 1 -weighted MRI scan shown in Figure 18 is pointing to which of the following structures?
Explanation
REFERENCES: Goss MS, Gelberman RH: The anatomy of the distal ulnar tunnel. Clin Orthop 1985;196:238-247.
Denman EE: The anatomy of the space of Guyon. Hand 1978;10:69-76.
Question 80
Six months later, the patient’s fracture has healed and a CT scan to further evaluate the physis is performed (Video 85). Based on these findings, how should you advise the family?
Explanation
The hypertrophic zone is the weakest biomechanical zone of the physis and is most likely to fracture. The deep peroneal nerve supplies motor innervation to the ankle and toe
dorsiflexors (anterior compartment) and the first web space, which, in this history, have deficits. The superficial peroneal nerve supplies sensation to the dorsum of the foot and motor to the lateral compartment peroneal musculature (ankle evertors), which also has deficits. The injury must involve both peroneal branches (the common peroneal nerve). Because sensation to the sole of the foot and toe/ankle plantar flexion is intact, the tibial nerve is intact.
Because the nerve was visualized intact, a neuropraxia is the most likely type of nerve injury. This should recover in time and does not necessitate urgent exploration. In pediatric patients, an advancing Tinel sign and partial nerve recovery by 3 months is expected and can be followed clinically. If there is no sign of nerve recovery, an electromyogram should be ordered with consideration for nerve exploration if there is no sign of reinnervation. There is no sign of compartment syndrome because the patient has an unchanged neurologic deficit, is comfortable, and has no pain with passive range of motion.
These injuries are associated with a very high rate of growth arrest (up to 80% in some studies). The CT scan shows an asymmetric growth arrest, which suggests angulation through the distal femur.
Question 81
A 14-year-old boy reports progressive right wrist pain. Radiographs are shown in Figure 3a, and a photomicrograph is shown in Figure 3b. What is the most likely diagnosis?
Explanation
REFERENCES: Lersundi A, Mankin HJ, Mourikis A, et al: Chondromyxoid fibroma: A rarely encountered and puzzling tumor. Clin Orthop Relat Res 2005;439:171-175.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 82
A 28-year-old man sustains the closed injury shown in Figures 3a through 3c after falling 8 feet while rock climbing. Management should consist of
Explanation
REFERENCES: Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp
1465-1518.
Grob D, Simpson LA, Weber BG, Bray T: Operative treatment of displaced talus fractures. Clin Orthop 1985;199:88-96.
Question 83
A 30-year-old patient has wrist pain. A radiograph and biopsy specimen are shown in Figures 34a and 34b. What is the most likely diagnosis?
Explanation
REFERENCES: Bieselker JL, Marcove RC, Huvos AG, Mike V: Aneurysmal bone cyst: A Clinico-pathologic study of 66 cases. Cancer 1973;26:615.
Martinez V, Sissons HA: A review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer 1988;61:2291.
Question 84
A 20-year-old man sustained an injury to his arm during a tug-of-war contest. An MRI scan is shown in Figure 18. What is the most likely diagnosis?
Explanation
REFERENCES: Heckman JD, Levine MI: Traumatic closed transection of the biceps brachii in the military parachutist. J Bone Joint Surg Am 1978;60:369-372.
Mellen PF: Parachute static line injury with vascular compromise. Mil Med 1989;154:364-365.
Question 85
Figure 38 shows the radiograph of a 75-year-old woman who has had right shoulder pain, difficulty sleeping on the affected arm, and difficulties performing activities of daily living for the past 6 weeks. Initial nonsurgical management includes analgesics, a subacromial cortisone injection, and gentle range-of-motion exercises. However, these modalities have failed to provide relief, and the patient reports that she is unable to elevate her arm. Her pain is worse and she would like the most reliable treatment method for pain relief and functional improvement. What is the best surgical treatment? Review Topic
Explanation
option, has long been the standard of care for rotator cuff tear arthropathy. However, careful examination of the literature reveals that the results have not been uniform.
Question 86
Figures 18a and 18b show the radiographs of a patient who has pain with walking. On careful questioning, it is determined that the discomfort occurs at push-off, or when the patient attempts to climb stairs. What nonsurgical option is most likely to ameliorate the symptoms?
Explanation
REFERENCES: Bono CM, Berberian WS: Orthotic devices: Degenerative disorders of the foot and ankle. Foot Ankle Clin 2001;6:329-340.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 58-63.
Question 87
A 56-year-old mechanic has had pain in the hypothenar region of his dominant right hand for the past 6 months. He reports weakness in his grip and pain is worse with activity. Which of the following examination findings is most suggestive of a cervical etiology? Review Topic
Explanation
Question 88
Which of the following is considered a limitation of the Short Form 36 (SF-36) general health status instrument when applied to musculoskeletal conditions?
Explanation
Multilingual validated translations have been produced in addition to international population data sets. The survey can be patient self-administered via office visit, mail, or telephone. A bias of lower over upper extremity function with regard to outcome measures employing the SF-36 has been demonstrated. Limits on the detection of certain changes in quality of life status may impose ceiling and floor effects on analysis and interpretation.
Question 89
- What is the treatment of choice for an adult who has an isolated fracture of the ulna at the junction of the distal and middle thirds, with 5 degrees apex dorsal angulation and 25% displacement?
Explanation
Question 90
-A 12-year-old boy who plays multiple sports has had insidious-onset heel pain while running for 4 months. On examination, he had ankle dorsiflexion of 5 degrees. The squeeze test result was positive and the Thompson test result was negative. He has no pain with forced ankle plantar flexion. What is the most likely diagnosis?
Explanation
A 15-year-old boy has had shoulder pain for 4 weeks during the middle of baseball season. The patient says his pain is “all over my shoulder.” Examination reveals tenderness to palpation over the anterolateral aspect of the shoulder. Internal and external rotation range of motion is restricted.
Radiographs show metaphyseal sclerosis.
Question 91
According to clinical and biomechanical studies, the most appropriate position for a headless scaphoid compression screw for repair of a scaphoid waist fracture is
Explanation
The position of a scaphoid screw for scaphoid fracture repair (Figure 1) is as critical as the position of a sliding hip screw for intertrochanteric fracture repair. Positioning the screw deep in the center of the densest portion of cancellous bone is beneficial for both of these fracture types.Trumble and associates have shown time to union for scaphoid nonunions to be decreased for centrally placed scaphoid screws. McCallister and associates documented improved biomechanical stability for scaphoid waist fractures repaired with a centrally placed screw vs an eccentrically placed screw. Dodds and associates

demonstrated significantly improved biomechanical stability with centrally placed long screws vs centrally placed short screws. The screw may be placed retrograde or antegrade. Although the screw position may be relatively parallel to the radial inclination as the shape of the scaphoid body follows the contour of the radial styloid, screw position should be assessed relative to the scaphoid’s own architecture. Placing the screw in a retrograde fashion can force the treating surgeon to start the screw eccentrically in an attempt to avoid the interference of the trapezium lying over the distal pole of the scaphoid. This may result in noncentral screw placement.
Question 92
What allograft has the highest antigenicity when used for ligament reconstruction about the knee?
Explanation
Question 93
In total knee arthroplasty, in vitro testing has shown that cross-linking can diminish the rate of polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
Explanation
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been shown to cause implant failure in the most recent clinical trials, but they remain the most important mechanical issues associated with current material processing methods.
Question 94
Figures 24a through 24c show the coronal T 1 -weighted, T 2 -weighted fat-saturated, and T 1 -weighted fat-saturated gadolinium MRI scans of the proximal thigh of a 52-year-old woman who reports a mass in the medial thigh and groin area. She notes that the fullness has grown in size over the course of many months. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCE: Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 95
A 42-year-old woman with a long-standing history of rheumatoid arthritis undergoes total shoulder arthroplasty for persistent pain that has failed to respond to nonsurgical management. Intraoperative radiographs reveal an oblique, minimally displaced fracture of the greater tuberosity. Based on these findings, what is the best course of action?
Explanation
REFERENCES: Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 215-225.
Frankle MA, Ondrovic LE, Markee BA, et al: Stability of tuberosity reattachment in proximal humeral hemiarthroplasty. J Shoulder Elbow Surg 2002;11:413-420.
Question 96
A patient who sustained injuries in a motorcycle accident 30 minutes ago has significant motor and sensory deficits corresponding to a C6 level of injury. A lateral radiograph obtained during the initial on-scene evaluation reveals bilateral jumped facets at C5-C6; this appears to be an isolated injury. The patient is awake and alert. The next step in management of the dislocation should consist of
Explanation
REFERENCES: Delamarter RB, Sherman J, Carr JB: Pathophysiology of spinal cord injury: Recovery after immediate and delayed decompression. J Bone Joint Surg Am
1995;77:1042-1049.
Star AM, Jones AA, Cotler JM, Balderston RA, Sinha R: Immediate closed reduction of cervical spine dislocations using traction. Spine 1990;15:1068-1072.
Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets: Case report. J Bone Joint Surg Am
1991;73:1555-1560.
Question 97
A 75-year-old man presents with worsening low back and bilateral leg pain. The pain worsens with ambulation and improves with sitting. On exam, he has strong DP and PT pulses. Straight leg raise is negative. A MRI of the lumbar spine is performed and is pictured in Figure A. On further questioning, which of the following is the patient also likely to report? Review Topic

Explanation
Lumbar spinal stenosis often results from degenerative changes of the intervertebral disc and facet joints which ultimately narrows the space available for the thecal sac and exiting nerve roots. Patients can present with neurogenic claudication, reported as worsening leg and/or back pain with ambulation and diminished walking capacity. MRI may demonstrate disc degeneration/bulging, hypertrophy of the ligamentum flavum and facet capsule, and narrowing of the central canal. Nonoperative management includes NSAIDs, PT and epidural steroid injections (ESI). Surgery is reserved for patients who have failed nonoperative measures and includes decompressive laminectomy with or without fusion depending on presence of instability.
Issack et al reviewed degenerative lumbar spinal stenosis. Unlike patients with vascular claudication, patients with neurogenic claudication are able to improve walking tolerance with postural changes, specifically with flexed-forward posture (such as leaning forward on a shopping cart). They are unable to improve their symptoms simply by cessation of walking. Patients with neurogenic claudication tend to lack the trophic changes of the skin on the legs/feet as well as diminished pulses characteristic of vascular disease.
Young et al reviewed the utilization of lumbar ESI for low back and leg pain. The authors concluded that lumbar ESI are a reasonable nonsurgical option to provide temporary symptomatic relief. Fluoroscopic guidance facilitates accurate placement of the injection into the epidural space, while its nonuse may lead to higher percentage of technical failures. Lastly, the transforaminal approach is more selective
than the interlaminar approach and can provide diagnostic information as well as symptom relief.
Figures A and B are T1 sagittal and T2 axial MR images, respectively, of the lumbar spine demonstrating significant central canal stenosis most notable at L4-L5 with broad disc protrusion, facet degeneration and infolding of the ligamentum flavum.
Incorrect
Responses:
Question 98
Figure 10 is an anteroposterior pelvis radiograph of an 82-year-old man who had right hip pain that began 2 weeks ago but has since resolved with use of over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs). Currently he has no pain. Examination of his hip shows decreased internal rotation and minimal pain at the extremes of motion. What is the most appropriate treatment at this point?

Explanation
The radiograph shown is consistent with Paget disease of the bone. It demonstrates classic findings of widened lamellae and disorganized sclerotic and lytic areas. The cause is not clearly defined, but may be linked to a viral infection and subsequent alterations of osteoblastic and osteoclastic activity. Most patients are asymptomatic, and Paget disease is often found incidentally on radiographs. In this case, the patient’s symptoms likely were caused by hip arthritis, but Paget disease can cause diffuse bone pain in some cases. Considering the patient’s mild and short-term symptoms, observation and NSAID use is most appropriate. An MRI scan or biopsy is indicated if sarcomatous transformation is suspected, but this condition is rare and is associated with a substantial, unrelenting increase in pain. SPEP and UPEP are tests for multiple myeloma, of which the radiographs show no signs.
RECOMMENDED READINGS
Ralston SH. Pathogenesis of Paget's disease of bone. Bone. 2008 Nov;43(5):819-25. doi: 10.1016/j.bone.2008.06.015. Epub 2008 Jul 11. Review. PubMed PMID: 18672105.View Abstract at PubMed
Bonenberger E, Einhorn T. Metabolic bone diseases. In: Callaghan JJ, Rosenberg
AG, Rubash HE, eds. The Adult Hip. 2nd ed. Philadelphia, PA: Lippincott Williams 14
& Wilkins; 2007:514-533.
Question 99
Which of the following methods best aids in diagnosis of an interdigital neuroma?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 145-147.
Bennett GL, Graham CE, Mauldin DM: Morton’s interdigital neuroma: A comprehensive treatment protocol. Foot Ankle Int 1995;16:760-763.
Question 100
When compared with patients having a body mass index (BMI) lower than 35, patients with a BMI above 40 who undergo primary total hip arthroplasty (THA) and total knee arthroplasty (TKA) are likely to have
Explanation
The obesity epidemic is increasing, and the number of patients with a BMI higher than 35 undergoing THA and TKA also is growing. Controversy exists over the optimal BMI cutoff and the ability to perform joint replacements safely in patients who are morbidly obese. Several clinical series and national database analyses have shown that morbidly obese patients undergoing THA or TKA are at increased risk for wound complications as well as 30-day and 90-day readmissions. These patients’ incisions are typically larger because of the size of the soft-tissue envelope. Although the clinical scores following successful THA or TKA often are lower than the scores of controls, the overall changes in clinical function and satisfaction are equivalent in nonobese and obese patients.
