Orthopedic Board Review MCQs: Arthroplasty, Trauma & Spine | Part 15

Key Takeaway
This Orthopedic Surgery Board Review quiz offers 100 high-yield MCQs for orthopedic surgeons preparing for AAOS & OITE board exams. It features verified questions, actual exam format simulation, and interactive study/exam modes to master critical topics for certification.
About This Board Review Set
This is Part 15 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 15
This module focuses heavily on: Arthroplasty, Fracture, Hip, Tendon.
Sample Questions from This Set
Sample Question 1: What is the most appropriate initial diagnostic imaging study for a patient with presumed diskogenic low-back pain?...
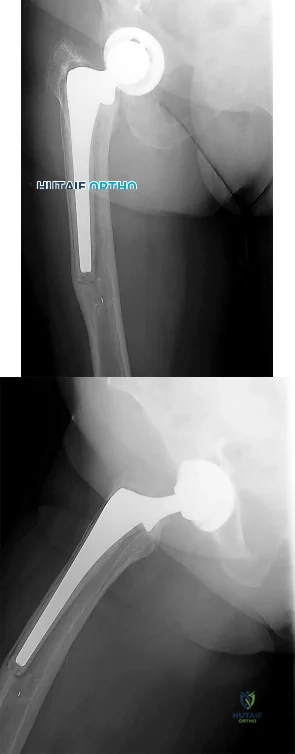
Sample Question 2: Which of the following complications may occur subsequent to resurfacing hip arthroplasty for osteonecrosis of the hip but not after total hip arthroplasty?...
Sample Question 3: -Figures 3a and 3b are the clinical photographs of a 35-year-old man seen 3 months after repair of an acute Achilles tendon rupture. He has no constitutional symptoms and is unable to perform a single heelrise test. The most appropriate tre...
Sample Question 4: When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the Review Topic...
Sample Question 5: Which of the following is considered a contraindication to cement injection techniques, such as kyphoplasty or vertebroplasty, in the treatment of osteoporotic compression fractures?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What is the most appropriate initial diagnostic imaging study for a patient with presumed diskogenic low-back pain?
Explanation
Radiography is the best initial study. Vacuum phenomenon may be found within the disk space. Other possible sources for back pain such as osteoporotic collapse, osteolytic collapse, and deformity also can be evaluated. The other tests may be beneficial and are more appropriate as later imaging options.
RECOMMENDED READINGS
Yu WD, Williams SL. Spinal imaging: Radiographs, computed tomography, and magnetic resonance imaging. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine
Question 2
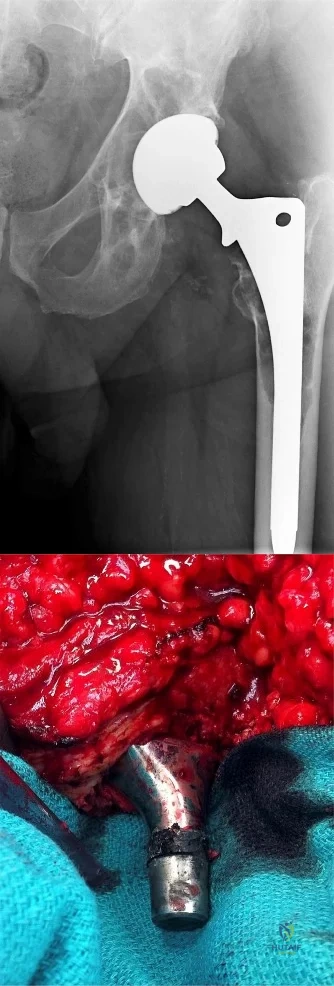
Which of the following complications may occur subsequent to resurfacing hip arthroplasty for osteonecrosis of the hip but not after total hip arthroplasty?
Explanation
REFERENCES: Gabriel JL, Trousdale RT: Stem fracture after hemiresurfacing for femoral head osteonecrosis. J Arthroplasty 2003;18:96-99.
Amstutz HC, Campbell PA, Le Duff MJ: Fracture of the neck of the femur after surface arthroplasty of the hip. J Bone Joint Surg Am 2004;86:1874-1877.
Question 3
-Figures 3a and 3b are the clinical photographs of a 35-year-old man seen 3 months after repair of an acute Achilles tendon rupture. He has no constitutional symptoms and is unable to perform a single heelrise test. The most appropriate treatment is

Explanation
Question 4
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the Review Topic
Explanation
Question 5
Which of the following is considered a contraindication to cement injection techniques, such as kyphoplasty or vertebroplasty, in the treatment of osteoporotic compression fractures?
Explanation
REFERENCES: Phillips FM, Pfeifer BA, Leiberman IH, et al: Minimally invasive treatment of osteoporotic vertebral compression fractures: Vertebroplasty and kyphoplasty. Instr Course Lect 2003;52:559-567.
Truumees E, Hilibrand A, Vaccaro AR: Percutaneous vertebral augmentation. Spine J 2004;4:218-229.
Rao RD, Singrakhia MD: Painful osteoporotic vertebral fracture: Pathogenesis, evaluation, and roles of vertebroplasty and kyphoplasty in its management. J Bone Joint Surg Am 2003;85:2010-2022.
Question 6
Which lower extremity muscle is first weakened in Charcot-Marie-Tooth (CMT) disease?
Explanation
Although many of the lower extremity muscles may be affected in CMT, those innervated by the longest axons have been shown to be affected first. In the lower extremity the muscles innervated by the longest axons are the intrinsic foot muscles. The tibialis anterior and the peroneus brevis may be severely affected but not before the foot intrinsics. The peroneus longus typically is spared, resulting in the cavus.
RECOMMENDED READINGS
Pareyson D, Marchesi C. Diagnosis, natural history, and management of Charcot-Marie-Tooth disease. Lancet Neurol. 2009 Jul;8(7):654-67. Review. PubMed PMID: 19539237. View Abstract at PubMed
Wenz W, Dreher T. Charcot-Marie-Tooth disease and the cavovarus foot. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:291-306.
CLINICAL SITUATION FOR QUESTIONS 60 THROUGH 63
Figure 60 is the standing radiograph of a 27-year-old man who played football throughout his teen years. During those years, he noted that he had less mobility of his left foot and ankle. He twisted his left foot and ankle 8 months ago and has tried over-the-counter nonsteroidal anti-inflammatory drugs and a brace. He now has pain and edema in the left sinus tarsi area. Upon examination the following arcs of motion are identified: ankle dorsiflexion-right, 5 degrees/left, 5 degrees; ankle plantar flexion-right, 30 degrees/left 30 degrees; foot inversion-right, 10 degrees/left, 5 degrees; foot eversion-right, 10 degrees/left 5 degrees.

Question 7
A 15-year-old boy who participates in track reports acute pain along the left iliac crest during a sprint. Examination reveals that the anterior superior iliac spine is nontender. The most likely diagnosis is an injury to the
Explanation
REFERENCES: Clancy WG Jr, Foltz AS: Iliac apophysitis and stress fractures in adolescent runners. Am J Sports Med 1976;4:214-218.
Waters PM, Millis MB: Hip and pelvic injuries in the young athlete, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 279-293.
Lombardo SJ, Retting AC, Kerlan RK: Radiographic abnormalities of the iliac apophysis in adolescent athletes. J Bone Joint Surg Am 1983;65:444-446.
Paletta GA Jr, Andrish JT: Injuries about the hip and pelvis in the young athlete. Clin Sports Med 1995;14:591-628.
Question 8
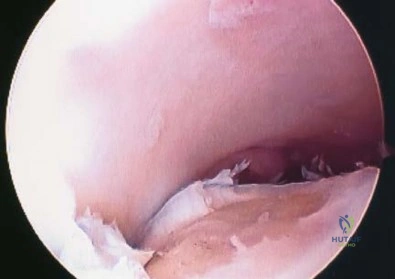
At the time of arthroscopy, a 9-year-old boy was found to have a Watanabe type II discoid lateral meniscus. What is the most appropriate treatment? Review Topic
Explanation
Question 9
One year after undergoing a primary total knee arthroplasty, a 65-year-old man has a 1-week history of new onset anterior knee pain. He can perform a straight-leg raise with no extension lag. Radiographs reveal a transverse patella fracture with 8 mm of displacement and an intact patellar component. The best course of treatment is
Explanation
This patient has a displaced periprosthetic patella fracture with an intact extensor mechanism. Surgical treatment for this condition has been associated with relatively poor clinical results because the fracture occurs late (attributable to patella osteonecrosis). The optimal initial treatment is to treat the fracture nonsurgically with immobilization of the knee in extension either with a long-leg cast or knee immobilizer.
Question 10
A 14-year-old Little League pitcher who plays in 2 leagues concurrently has pain in his throwing shoulder while pitching but not at rest.
Explanation
Multidirectional shoulder instability can be diagnosed by demonstrating instability in at least 2 planes. The sulcus sign is often present with a prominent depression below the acromion when traction is applied to the arm. The mechanism of anterior shoulder dislocation or subluxation is most commonly a combination of abduction, external rotation, and a posteriorly directed force applied to the arm. Among baseball players, the lead shoulder is susceptible to posterior capsulolabral lesions termed “batter’s shoulder.” SLAP tears are common among overhead
athletes and can cause symptoms similar to impingement as well as a glenohumeral internal rotation deficit, which may predispose players to labral tears. Little League shoulder is an overuse injury typically seen in baseball pitchers who are around 14 years of age. It is an osteochondrosis of the proximal humeral epiphysis attributable to overuse from throwing.
RECOMMENDED READINGS
Kang RW, Mahony GT, Harris TC, Dines JS. Posterior instability caused by batter's shoulder. Clin Sports Med. 2013 Oct;32(4):797-802. doi: 10.1016/j.csm.2013.07.012. Epub 2013 Aug 22. Review. PubMed PMID: 24079435. View Abstract at PubMed
Carson WG Jr, Gasser SI. Little Leaguer's shoulder. A report of 23 cases. Am J Sports Med. 1998 Jul-Aug;26(4):575-80. PubMed PMID: 9689382. View Abstract at PubMed
Ren H, Bicknell RT. From the unstable painful shoulder to multidirectional instability in the young athlete. Clin Sports Med. 2013 Oct;32(4):815-23. doi: 10.1016/j.csm.2013.07.014. Review. PubMed PMID: 24079437. View Abstract at PubMed
Werner BC, Brockmeier SF, Miller MD. Etiology, Diagnosis, and Management of Failed SLAP Repair. J Am Acad Orthop Surg. 2014 Sep;22(9):554-565. Review. View Abstract at PubMed
Question 11
A 15-year-old boy with a type I hereditary sensory motor neuropathy (Charcot-Marie-Tooth disease) reports recurrent ankle sprains and significant pain in the hindfoot and midfoot despite orthotic management. Examination reveals that he walks with a drop foot and has dynamic clawing of the toes. Clinical photographs of the left foot are shown in Figure 7. Management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 235-245.
Coleman SS: Complex Foot Deformities in Children. Philadelphia, Pa, Lea & Febiger, 1983, pp 147-165.
Thometz JG, Gould JS: Cavus deformity, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 12
Which of the following types of iliac osteotomy provides the greatest potential for increased coverage?
Explanation
REFERENCES: Millis MB, Poss R, Murphy SB: Osteotomies of the hip in the prevention and treatment of osteoarthritis, in Eilert RE (ed): Instructional Course Lectures XLI. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1992, pp 145-154.
Weinstein SL: Developmental hip dysplasia and dislocation, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 903-950.
Question 13
Figure 1 is the ultrasound of a 23-year-old patient who has had a volar radial 1.5-cm tender and painful wrist mass for 6 months. The additional workup prior to surgery should consist of

Explanation
The ultrasound shows a homogeneous anechoic mass consistent with a ganglion cyst. As a benign lesion, no further workup or biopsy is required prior to a marginal surgical excision other than age-appropriate laboratory studies. An MRI study with contrast would provide no diagnostic benefit.
Question 14
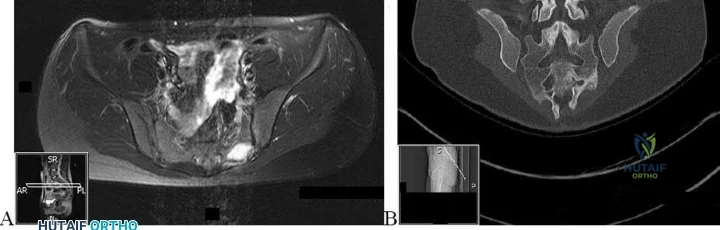
A 43-year-old man is currently taking medication for the disease condition shown in Figure A. His wife is taking the same medication. Her radiograph is shown in Figure B. What is the medication? Review Topic

Explanation
TNF-a inhibitors are biological agents approved for 2nd-line treatment of AS. These include etanercept, infliximab, adalimumab, golimumab, and certolizumab pegol, which are all approved for treatment of RA and psoriatic arthritis as well. Additional biological agents unique to RA are IL1 antagonists (e.g. anakinra), B cell inhibitors (rituximab), T cell inhibitors (abatacept), IL6 receptor inhibitors (tocilizumab) and Janus kinase (JAK) pathway inhibitors (tofacitinib).
Kubiak et al. reviewed the orthopaedic management of AS. They support using anti–TNFa medications when there is: (1) definitive diagnosis of AS, (2) disease lasting > 4 weeks, (3) refractory disease, (4) failure of corticosteroid sacroiliac joint injections,
(5) failure of sulfasalazine for peripheral disease, and (6) no medical contraindications to the initiation of treatment.
Khalessi et al. reviewed the medical management of AS. They discuss physical therapy, education, and medications and radiation therapy. Non-biological medications include NSAIDs, coxibs, corticosteroids and DMARDS (sulfasalazine and methotrexate). They note that both sulfasalazine and methotrexate do not improve pain or function from AS spinal disease.
Figure A shows bilateral sacroiliitis and bilateral hip arthritis, which in a young male patient, is highly suggestive of AS. Figure B shows ulnar drift of the digits and MCPJ subluxation characteristic of RA.
Incorrect Answers:
is a tyrosine-kinase inhibitor used
to treat Philadelphia
(Ph+)
chronic
myelogenous
leukemia
(CML).
Question 15
An 85-year-old obese woman has left knee pain. She had surgery 5 years ago for a patellar nonunion after total knee arthroplasty that was complicated by infection, which was treated with implant removal and patellectomy. She has not been ambulatory since then. She states she is no longer on antibiotics. She has moderate pain, but her primary problem is instability of the knee. She has a 40° extensor lag. Darkening of the skin is present distal to the incision consistent with venous stasis changes. The erythrocyte sedimentation rate is 12 mm/h (reference range 0 to 20 mm/h) and her C-reactive protein level is 1.0 mg/L (reference range 0.08 to 3.1 mg/L). Left knee aspiration shows a white blood cell count of 800 and 20% neutrophils. What is the best next step?
Explanation
This patient is elderly, obese, and nonambulatory and has a chronic quadriceps tendon rupture after infected total knee arthroplasty. Her potential for ambulation after revision total knee arthroplasty is very low. Primary repair of the tendon is unlikely to be successful, even with augmentation, so revision total knee arthroplasty with primary quadriceps tendon repair and two-stage revision knee arthroplasty and quadricep repair with Achilles allograft are not the best management techniques. Extensor mechanism allograft could be done but would have a high failure rate in a patient of this size. No sign of infection is seen, based on laboratory studies, so a two-stage procedure is not necessary. The best management although not optimal, would be treatment in a drop-lock brace. Arthrodesis is also an option, but would have a high complication rate, and in a patient that is nonambulatory, a fused knee would be increasingly difficult with activities of daily living and mobility.
Question 16
The addition of which of the following food supplements may lead to a decrease in neural tube defects?
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 111-122.
Lemke L, Dias L: Spina bifida, in Cramer KE, Scherl SA, Einhom TA (eds): Orthopaedic Surgery Essentials: Pediatrics. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 203-210.
Question 17
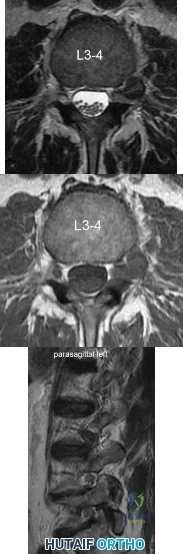
A 39-year-old man presents with back pain radiating to the left lower extremity for the past 6 weeks. Magnetic resonance images of the pathology are
Explanation
Far lateral disc herniations constitute approximately 5-10 percent of disc hernations in the lumbar spine. Given the more vertical anatomy of lumbar nerve roots, at a given disc level, a central or paracentral herniation will affect the traversing nerve root (e.g. nerve root of level below) and a far lateral herniation will affect the exiting nerve root (e.g. nerve root of the level above). Similar to the more common central and paracentral herniations, approximately 90% of patients will improve without surgical intervention. When surgical intervention is needed, the paraspinal approach of Wiltse is utilized.
Marquadt et al. reported long term outcomes of surgical management of far lateral disc herniations. At an average of 146 months follow up, 56.3% of patients had complete relief of symptoms and 27.6% had permanent residual symptoms. Over 75% of patients subjectively rated their outcomes as excellent.
Figure A and B are T2 and T1 axial MRI images, respectively, showing the L3-L4 disc space with a left far lateral disc herniation. Figure C is a left parasagittal T2 MRI image showing impingement on the L3 nerve root. Structures are labeled in illustration A. Illustration B shows the dermatomes of the lower extremity.
Incorrect Answers:
Question 18
Which of the following properties apply to the human meniscus when compared with articular cartilage?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 3-23.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, AAOS, 1999, pp 349-354.
Question 19
A 28-year-old construction worker sustains the closed injury shown in Figures A and B after a fall from a height. He is taken to the operating room. What is the next best step?

Explanation
In the distal tibial metaphysis, there is no snug endosteal fit for an IM nail. Center-center nail placement in both proximal and distal fragments is necessary to maintain alignment. There is also increased stress on distal locking bolts to maintain fracture alignment. Assuming static medial-lateral distal locking screws, accurate coronal plane and rotational alignment is achieved by fibular plating as a first step. This also
prevents late loss of alignment because of distal locking screw toggle. Reamed nailing allows a stiffer, larger nail to be placed, and allows redistribution of endosteal osteogenic material to the fracture site. Although there is endosteal vascular compromise, this does not affect fracture healing because of intact periosteal supply.
Bhandari et al. conducted a prospective, randomized, blinded comparison of 622 patients who had reamed nailing, and 604 who had unreamed nailing. For closed fractures, a significantly greater number in the unreamed group required bone grafting, implant exchange and dynamization. There was no difference in groups for open fracture nailing.
Egol et al. retrospectively reviewed distal metaphyseal tibia-fibula fractures treated with IM nailing with (25 cases) and without (47 cases) adjunctive plating. They found that plating was associated with maintenance of reduction (significant) as was the use of 2 medial-lateral distal locking bolts (not significant). They recommend fibular plating when IM nailing for distal tibia fractures.
Figures A and B show an extraarticular distal tibia fracture with distal fibula fracture. Incorrect Answers
Question 20
A 53-year-old man with a history of severe left hip pain has a significant limp that is the result of a 5-cm limb-length discrepancy. An AP radiograph is shown in Figure 48. The underlying etiology is most likely related to a history of
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 3-23.
Question 21
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?
Explanation
REFERENCE: Cohen M, McMurtry RY, Jupiter JB: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1328-1335.
Question 22
An acetabular reinforcement cage is most often indicated for which of the following conditions?
Explanation
REFERENCES: Berry DJ, Lewallen DG, Hanssen A, Cabanela ME: Pelvic discontinuity in revision total hip arthroplasty. J Bone Joint Surg Am 1999;81:1692-1702.
Whaley AL, Berry DJ: Extra-large uncemented hemisphere acetabular components for revision THA. J Bone Joint Surg Am 2001;83:1352-1357.
Question 23
Which of the following patient factors is associated with recurrent radicular pain following lumbar diskectomy for sciatica?
Explanation
REFERENCES: Carragee EJ, Han MY, Suen PW, et al: Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment type and anular competence. J Bone Joint Surg Am 2003;85:102-108.
Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Question 24
What is the most common diagnosis in a patient older than age 40 years with a destructive bony lesion?
Explanation
REFERENCE: CA, January/February 2000, vol 50, no. 1 (Cancer Statistics).
Question 25
Which of the following medications may have a negative effect on bone healing following fracture?
Explanation
REFERENCES: Gerstenfeld LC, Thiede M, Seibert K, et al: Differential inhibition of fracture healing by non-selective and cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs. J Orthop Res 2003;21:670-675.
Harder AT, An YH: The mechanisms of the inhibitory effects of nonsteroidal anti-inflammatory drugs on bone healing: A concise review. J Clin Pharmacol 2003;43:807-815.
Question 26
A 50-year-old competitive tennis player sustained a shoulder dislocation after falling on his outstretched arm 3 weeks ago. He now reports that he has regained motion but continues to have painful elevation and weakness in external rotation. A subacromial cortisone injection provided 3 weeks of relief, but the pain has returned. Which of the following studies will best aid in diagnosis?
Explanation
REFERENCES: Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Matsen FA III, Thomas SC, Rockwood CA: Anterior glenohumeral instability, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 526-622.
Question 27
What is the minimum hours per day of wear that has been correlated with the effectiveness of bracing on curve progression in idiopathic scoliosis? Review Topic
Explanation
Question 28
….Figures 83a through 83c are the radiograph and MRI scans of a 16-year-old girl who had posterior knee pain after a dance recital 3 weeks ago; the pain resolved 1 week ago with ibuprofen use. What is the appropriate treatment for this patient?
Explanation
Figures 84a and 84b are the CT and MRI scans of a 17-year-old girl with a painful lumbosacral scoliosis that has been present for 12 months. Examination is notable only for pain over the left sacral region and a postural scoliosis leaning away from this side.
Question 29
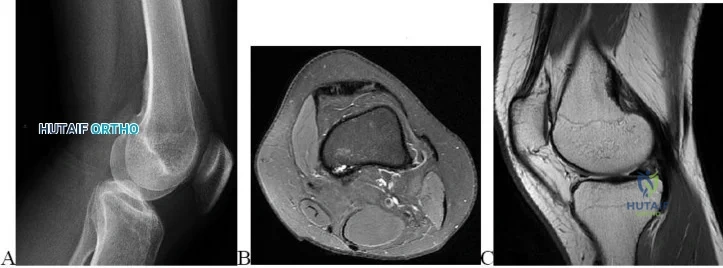
-What is the most likely mechanism of injury?
Explanation
The MRI scan shows a bone bruise of the lateral femoral condyle and lateral tibial plateau. This injury pattern is commonly associated with anterior cruciate ligament (ACL) rupture and an abnormal pivot shift test result. Treatment of an ACL tear in a high-demand athlete should consist of ligament reconstruction.In this patient, surgery should be delayed until she regains full range of motion to minimize risk for arthrofibrosis after surgery. Recent analysis has shown that the noncontact mechanism is more consistent with anterior translation, affecting both the medial and lateral compartments. The bone bruise in the lateral femoral condyle occurs more anterior than that of the medial femoral condyle, suggesting that internal rotation has occurred. The external rotation recurvatum test assesses for posterolateral corner injury, and a positive quadriceps active test is consistent with posterior cruciate ligament rupture. An abnormal patellar apprehension test result is suggestive of patellar instability. Nonsurgical treatment is unlikely to result in sufficient stability if this patient returns to sports at her preinjury level of activity.Primary ACL repair is associated with high failure rates. Although the precise mechanism of injury varies,injuries can be broadly classified into contact and noncontact injuries. Noncontact injuries occur with the knee in slight flexion, valgus, and internal rotation, and contact injuries typically involve a lateralside impact producing a valgus force to the knee. The valgus component of noncontact injuries has been thought to cause mainly lateral compartment bone bruising. Posterior translation is the most common mechanism of posterior cruciate ligament rupture, and hyperextension and varus is associated with posterolateral corner injury.
Question 30
Which of the following is considered the treatment of choice for a chondroblastoma of the proximal tibial epiphysis without intra-articular extension?
Explanation
REFERENCES: Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Simon MA, Springfield DS, et al: Chondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 31
A 22-year-old man sustained a stable pelvic fracture, bilateral femur fractures, and a left closed humeral shaft fracture in a motor vehicle accident. Examination 24 hours after injury reveals that the patient is confused and has shortness of breath. A clinical photograph of his conjunctiva is shown in Figure 44. He has a temperature of 101 degrees F (38.3 degrees C) and a pulse rate of 120/min. Laboratory studies show a hemoglobin level of 8 g/dL, a platelet count of 50,000/mm3, and a PaO2 of 57 mm Hg on 2L of oxygen. What is the most likely diagnosis?
Explanation
REFERENCE: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 308-316.
Question 32
What type of exercise is used early in the rehabilitation process to safely stimulate co-contraction of the scapular and rotator cuff muscles?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 129-136.
Kibler WB: Shoulder rehabilitation: Principles and practice. Med Sci Sports Exerc
1998;30:S40-50.
Question 33
A 34-year-old woman who is a professional skier (Figure 42)
Explanation

Question 34
In either a ceramic-on-highly-cross-linked polyethylene (HXPE) or metal-on-HXPE component, increasing the ball head size leads to
Explanation
Increasing the size of the ball head increases the primary arc of motion prior to impingement and the jump distance prior to dislocation, assuming an acetabular component abduction of less than 90 degrees. Although HXPE has demonstrated decreases in linear wear rates even with ball head sizes larger than 28 mm, volumetric wear remains a concern. A larger ball head size does not significantly change offset, and larger metal ball heads are not associated with decreased risk for corrosion.
Question 35
- To maximally resist apex anterior angulation in the tibia, the pins of a unilateral external fixator should be oriented in which of the following planes?
Explanation
Question 36
Your 25-year-old patient complains of anterior knee pain after retrograde femoral nailing for a diaphyseal fracture and asks you why you didn’t perform antegrade nailing as he has seen on the internet. You tell him that retrograde nailing is your preferred technique over antergrade nailing for diaphyseal femoral fractures because it has been shown to have?

Explanation
Question 37
A 22-year-old woman reports a 4-year history of worsening low back and left lower extremity pain following a motor vehicle accident. Management consisting of physical therapy, chiropractic manipulation, and interventional pain management, including sacroiliac joint injections and epidural steroid injections, has failed to provide relief. A sagittal T 2 -weighted MRI scan is shown in Figure 8. No nerve root compression is seen on axial images. She is currently working and lives with her fiancé. She smokes half a pack of cigarettes per day and reports depression on her health history. She is being maintained on narcotic analgesics and is having increasing difficulty performing her activities of daily living secondary to pain. What is the most appropriate management at this time?
Explanation
REFERENCES: Carragee EJ, Paragioudakis SJ, Khurana S: 2000 Volvo Award winner in clinical studies: Lumbar high-intensity zone and discography in subjects without low back problems. Spine 2000;25:2987-2992.
Pneumaticos SG, Reitman CA, Lindsey RW: Diskography in the evaluation of low back pain.
J Am Acad Orthop Surg 2006;14:46-55.
Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Carragee EJ: Clinical practice: Persistent low back pain. N Engl J Med 2005;352:1891-1898.
Question 38
A 38-year-old man sustains a terrible triad injury consisting of an elbow dislocation, comminuted and displaced radial head fracture, and a type I coronoid fracture. Intraoperative findings after radial head replacement and lateral collateral ligament complex repair reveal persistent instability consisting of medial opening on valgus stress and posteromedial subluxation of the ulnohumeral and radiocapitellar joints. What is the best next step?
Explanation
normally correct the medial instability. Articulated versus static external fixation can be considered if
restoration of the ligamentous constraint of the medial side of the elbow cannot be accomplished surgically.
Question 39
A 31-year-old woman has increasing pain and tightness in her right knee, with occasional stiffness and recurrent hemorrhagic effusions. MRI scans are shown in Figures 2a and 2b. What is the most likely diagnosis?
Explanation
REFERENCES: De Ponti A, Sansone V, Malchere M: Result of arthroscopic treatment of pigmented villonodular synovitis of the knee. Arthroscopy 2003;19:602-607.
Chin KR, Barr SJ, Winalski C, et al: Treatment of advanced primary and recurrent diffuse pigmented villonodular synovitis of the knee. J Bone Joint Surg Am 2002;84:2192-2202.
Bhimani MA, Wenz JF, Frassica FJ: Pigmented villonodular synovitis: Keys to early diagnosis. Clin Orthop 2001;386:197-202.
Question 40
A 46-year-old competitive cyclist falls while racing and suffers an isolated fracture as seen in Figure A. He is positioned on a fracture table and a closed reduction maneuver is attempted, unsuccessfully. Which of the following treatment plans is most appropriate?

Explanation
Displaced femoral neck fractures in young patients have created many treatment controversies that are ongoing in the literature due to devastating consequences of poor outcomes, including nonunion and osteonecrosis of the femoral head. Although poorly defined, the quality of reduction is associated with rates of both nonunion and osteonecrosis. A closed reduction that is malangulated (>10 degrees varus/valgus or anteversion/retroversion) or has significant displacement (5 mm or more in ANY view) is unacceptable, and an open reduction should be performed. Of course, this can be very difficult to assess in the operating room, where uncalibrated fluoroscopy with difficult to obtain tangential imaging is heavily relied upon to make this assessment. Accordingly, when the quality of closed reduction is questionable, the best treatment plan is to obtain a better reduction with direct visualization of the femoral neck prior to fixation.
A systematic review of the literature by Pauyo, et al. cites numerous studies showing a higher incidence of osteonecrosis of the femoral head in patients with displaced femoral neck fractures treated with unsatisfactory reductions. Furthermore, performing multiple closed reduction attempts is also associated with a higher risk of osteonecrosis.
Upadhyay et al. performed a randomized controlled trial of 102 patients with femoral neck fractures treated with closed or open reductions, which were randomized. The groups had similar rates of nonunions and osteonecrosis of the femoral head; however, subanalysis revealed a "poor" reduction was the highest predictor of poor outcome, whether the reduction was attempted open or closed. Interestingly, the quality of reduction was more important than the implant used or the timing of surgery (including surgeries performed > 48h after injury).
Figure A shows a pre-operative AP x-ray of the patient's high-energy femoral neck fracture. Illustrations A and B are intraoperative fluoroscopic and post-operative CT scans of this same patient, highlighting that fluoroscopy may "hide" the degree of residual displacement.
Incorrect Answers:
While intriguing, this is not currently the standard of practice; additionally, the stem already states that the reduction is "unsuccessful"
Repeated closed reduction maneuvers may further propagate comminution and damage the blood supply to the femoral head, in theory
Any stepoff of 5 mm seen on x-ray is a marker of worse outcomes. Remember, tangential imaging of the femoral neck is difficult to obtain, and if 7 mm is seen, in actuality it may be a larger amount of displacement. Think of the femoral neck as a complex cylindrical tube of bone with asymmetric cortices (e.g. the calcar) - to obtain the perfect fluoroscopic image for measuring maximal displacement, a perfect perpendicular view to this displacement is required, which is very difficult to do before provisional fixation is placed.
Question 41
A 72-year-old female sustains a displaced intracapsular femoral neck fracture. Which of the following is TRUE regarding the long term differences between possible treatment options for this injury?
Explanation
Intracapsular FNF are common in elderly patients after a fall from standing height. Treatment depends on physiological age and displacement (Garden's classification). For displaced fractures, physiologically young patients are treated with internal fixation while physiologically old patients are treated with either hemiarthroplasty (debilitated, less active patients) or THA (more active patients, those with acetabular
disease or preexisting inflammatory arthritis).
Chammout et al. retrospectively compared the long term (17 years) results of THA (cemented both component) and ORIF (2 cannulated screws) in elderly patients (>65 years). They found no difference in mortality. But hip scores were higher and pain was better in the THA group, while reoperation rates were higher in the ORIF group. Walking speed was initially faster in the THA group, but later did not differ between groups. They recommend THA for elderly patients with displaced FNF.
Rogmark et al. prospectively compared closed reduction and internal fixation (CRIF) with arthroplasty (combining hemiarthroplasty and THA) at 2 years in elderly patients (>70 years). Failure rates were higher, pain was worse, and walking was more impaired after CRIF. They recommend arthroplasty for patients >70 with FNF.
Question 42
Baseball pitchers who have internal impingement will most likely demonstrate what changes in range of motion?
Explanation
REFERENCES: Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.
Crockett HC, Gross LB, Wilk KE, et al: Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. Am J Sports Med 2002;30:20-26.
Question 43
A 30-year-old man reports pain and weakness in his right arm. Examination reveals grade 4 strength in wrist flexion and elbow extension, decreased sensation over the middle finger, and decreased triceps reflex. These symptoms are most compatible with impingement on what spinal nerve root?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Upper Saddle River, NJ, Prentice Hall, 1976, p 125.
Lauerman WC, Goldsmith ME: Spine, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 353-378.
Question 44
A 16-year-old female with adolescent idiopathic scoliosis undergoes posterior spinal fusion with instrumentation. The thoracic pedicle screws were placed using a tap 1 mm smaller than the screw diameter and a straightforward trajectory that runs parallel to the superior endplate. This techniques allows for which of the following: Review Topic
Explanation
Contemporary segmental pedicle screw placement used in the treatment of scoliosis deformity offer significantly higher screw pullout and deformity correction than prior hook and wire constructs. Additionally, screw insertional torque has been found in numerous studies to correlate with resistance to screw pullout. Several factors have been found to increase maximum screw insertional torque, including tapping 1mm smaller than the screw diameter and using the straightforward trajectory. It is important to note that while undertapping makes for a stronger screw, there are some studies that suggest not tapping at all makes for an even stronger screw.
Lehman et al. performed a biomechanical study evaluating maximum insertional torque when tapping line to line, undertapping by 0.5mm, and undertapping by 1mm in 34 fresh frozen cadavers. They found undertapping the thoracic pedicle by 1mm increased maximum insertional torque by 47% when compared to undertapping by 0.5mm and by 93% when compared to line to line tapping.
Kuklo et al. performed a biomechanical study on thirty cadavers using the straightforward technique (sagittal trajectory of the screws parallels the superior endplate of the vertebral body) versus anatomic trajectory (22 degrees in the cephalo-caudad direction in the sagittal plane). They found maximum insertional torque to be
Question 45
A 66-year-old male sustains an open crush injury to his right lower leg with significant skin loss. His history is significant for COPD, diabetes controlled with an insluin pump, and testicular cancer treated with bleomycin twenty years ago. A radiograph of the chest shows a pneumothorax which is treated with a thoracostomy tube. Which of the following is not a contraindication to hyperbaric oxygen treatment for this patient?

Explanation
Hyperbaric oxygen therapy potentially can provide enhanced oxygen delivery to peripheral tissues affected by vascular disruption, cytogenic and vasogenic edema, and cellular hypoxia caused by extremity trauma. The idea behind HBO is to provide enhanced oxygen delivery to peripheral tissues affected by vascular disruption, cytogenic and vasogenic edema, and cellular hypoxia caused by extremity trauma.
Greensmith et al provide a review of HBO therapy and discuss the relative and absolute contraindications and indications for this treatment. They report in patients with crush injury or early compartment syndrome, hyperbaric oxygen therapy may reduce the penumbra of cells at risk for delayed necrosis and secondary ischemia. They report that both animal studies and prospective human clinical trials suggest the benefits of such therapy.
Buettner et al found that based on clinical evidence and cost analysis, medical institutions that treat open fractures and crush injuries are justified in incorporating HBO theray as a standard of care.
Illustration A shows an example of a hyperbaric oxygen(HBO) chamber. Incorrect Answers:
Question 46
1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1% neutrophils. No growth of organisms is seen on routine culture. What is the best next step?
Explanation
This patient has a chronic quadriceps tendon rupture after total knee arthroplasty. Two previous primary repair attempts have failed, which is not surprising based on the poor results of primary repair reported in the literature. The patient also has an unstable knee and will require revision of some or all of the prosthesis to achieve a stable knee. Revision total knee arthroplasty with extensor mechanism allograft allows an allograft reconstruction of the ruptured quadriceps tendon. The other option is to utilize a synthetic mesh extensor mechanism reconstruction. These are likely to have the best result in this situation. Revision total knee arthroplasty with liner change and primary quadriceps repair is not the best form of management, because it involves a third attempt at primary tendon repair, which will likely fail again. Resection knee arthroplasty and arthrodesis with antegrade nail is a possible option but is not the best, because it would likely make driving and other daily activities difficult. Two-stage revision total
knee arthroplasty with extensor mechanism allograft is not the best option because the laboratory results
show no signs of infection, so a single-stage procedure is preferred.
Question 47
When performing a flexor tendon repair of a digit other than the thumb, what structures of the flexor tendon sheath should be preserved?
Explanation
REFERENCES: Doyle JR: Anatomy of the finger flexor tendon sheath and pulley system.
J Hand Surg Am 1988;13:473-484.
Strickland JW: Flexor tendon injuries: I. Foundations of treatment. J Am Acad Orthop Surg 1995;3:44-54.
Question 48
To adequately expose the volar plate of the proximal interphalangeal joint of the finger, which of following pulleys is typically incised?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 176-186.
Strickland J: Flexor tendon-acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2,
pp 1853-1855.
Lin GT, Amadio PC, An KN, et al: Functional anatomy of the human digital flexor pulley system. J Hand Surg Am 1989;14:949-956.
Question 49
A 40-year-old right hand-dominant construction worker has had a 6-month history of aching left shoulder pain that is worse after working a long day. Examination reveals limited range of motion and good strength when compared to his asymptomatic right arm. He has not had any orthopaedic intervention to date. Radiographs are shown in Figures 43a and 43b. What is the most appropriate treatment?
Explanation
REFERENCES: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.
Skedros JG, O’Rourke PJ, Zimmerman JM, et al: Alternatives to replacement arthroplasty for glenohumeral arthritis, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 485-499.
Question 50
A 3-year-old boy has a rigid 40-degree lumbar scoliosis that is the result of a fully segmented L5 hemivertebra. All other examination findings are normal. Management should consist of
Explanation
REFERENCES: Bradford DS, Boachie-Adjei O: One-stage anterior and posterior hemivertibral resection and arthrodesis for congenital scoliosis. J Bone Joint Surg Am 1990;72:536-540.
Lazar RD, Hall JE: Simultaneous anterior and posterior hemivertebra excision. Clin Orthop 1999;364:76-84.
Question 51
A 35-year-old man falls off of a roof and sustains an extra-articular supracondylar elbow fracture. He had normal sensation in all fingers after the injury and before undergoing surgery to repair the fracture. The ulnar nerve was not transposed but was inspected prior to wound closure. Ten days after surgery, the patient has numbness in his small finger and is unable to cross his fingers. His elbow range of motion is 40° to 100°. What is the next appropriate step in management?
Explanation
Question 52
A 5-year-old boy reports intermittent left elbow pain. History reveals that he injured his elbow 4 months ago, but had no treatment. He is now using his arm normally but reports pain almost daily. Examination reveals tenderness over the lateral epicondyle and a prominence is evident. Range of motion is from -5 degrees to

Explanation
(SBQ13PE.40) Immediate spica casting is most appropriate for which of the following?: Review Topic
2-month-old girl with a displaced spiral mid-diaphyseal femur fracture
A 26-month-old boy with a displaced spiral mid-diaphyseal femur fracture with <2 centimeters of shortening
3-day-old with teratologic right hip dislocation
9-year-old boy with a displaced spiral mid-diaphyseal femur fracture
12-year-old girl weighing 90 pounds with a displaced spiral mid-diaphyseal femur fracture
Children older than 6 months and up to 6 years with diaphyseal femur fractures may be treated with spica casting.
Children younger than 6 months may only require a Pavlik harness. Immediate spica casting is indicated in children 6 months to 6 years with less than 2 cm of shortening. Each additional cm of shortening at presentation doubles the risk of loss of reduction (1 cm: 12%, 2 cm: 24%, 3 cm; 50%).
Kocher et al. provide the AAOS Clinical Practice Guideline for the treatment of pediatric diaphyseal femur fractures. Their recommendation for diaphyseal femur fractures with <2 cm shortening in children 6 months to 5 years is Grade B, based on Level II evidence (two level II and one level I study). They recommend early spica or traction with delayed spica. They suggest early spica, as this is more convenient than traction.
In an earlier article, Flynn et al. review the management of pediatric femoral shaft fractures. They recommend early spica casting for the child between 1 and 6 years in
low-energy femoral fractures with up to 2 cm shortening. Illustration A shows several styles of lower extremity spica casts.
Incorrect answers:
Question 53
Figures 1 and 2 are the most recent radiographs of an 18-year-old high school student who sustains an anterior shoulder dislocation playing recreational football. He has a low Beighton score on physical examination. He was closed reduced and underwent a course of physical therapy but had a second dislocation playing recreational basketball. What is the most appropriate course of treatment, with the lowest complication rate, to prevent further dislocation?

Explanation
injury and hardware problems, exceeds that of arthroscopic Bankart repair.
Question 54
Pelvic packing for a hemodynamically unstable patient with a pelvic ring fracture is best described by which of the following techniques?
Explanation
Question 55
A 19-year-old linebacker for a collegiate football team has had two episodes of bilateral arm tingling and weakness after tackling; the symptoms resolved after 30 minutes of rest. Three follow-up neurologic examinations have been normal. Cervical spine CT and MRI scans are shown in Figures 13a through 13c. What is the next best step in management?
Explanation
REFERENCES: Torg JS, Naranja RJ Jr, Pavlov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Cantu RC: The cervical spinal stenosis controversy. Clin Sports Med 1998;17:121-126. Crowl AC, Kong JF: Cervical Spine, in Johnson DL, Mair SD (eds): Clinical Sports Medicine. Philadelphia, PA, Mosby Elsevier, 2006, pp 143-149.
Question 56
Figures 21a and 21b show the clinical photograph and radiograph of a 15-year-old girl who has a deformity of her feet. Her parents are concerned because there is a family history of Charcot-Marie-Tooth disease. The patient reports some mild instability of the ankle and has noticed mild early callosities; however, she is not having any significant pain. Coleman block testing reveals a forefoot valgus and supple hindfoot. She has weakness to eversion and dorsiflexion. Initial management should consist of
Explanation
REFERENCES: Pinzur MS: Charcot’s foot. Foot Ankle Clin 2000;5:897-912.
Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 57
Figures 5a and 5b show the radiographs of an 11-year-old boy who felt a pop and immediate pain in his right knee as he was driving off his right leg to jam a basketball. Examination reveals that the knee is flexed, and the patient is unable to actively extend it or bear weight on that side. There is also a large effusion. Management should include
Explanation
REFERENCES: Heckman JD, Alkire CC: Distal patellar pole fractures: A proposed common mechanism of injury. Am J Sports Med 1984;12:424-428.
Tolo VT: Fractures and dislocations around the knee, in Green NE, Swiontkowski MF (eds): Skeletal Trauma in Children. Philadelphia, Pa, WB Saunders, 1994, vol 3, pp 380-382.
Question 58
Disadvantages of anterior-inferior plate fixation for acute clavicular fractures relative to superior plating include
Explanation
Question 59
A 20-year-old man has a large soft-tissue mass behind his knee. MRI scans are shown in Figures 10a through 10c. Figure 10d shows a clinical photograph of his chest. The patient’s condition is most likely a result of a defect in what gene?
Explanation
REFERENCES: Theos A, Korf BR, American College of Physicians, et al: Pathophysiology of neurofibromatosis Type 1. Ann Intern Med 2006;144:842-849.
Menendez LR: Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002.
Question 60
When a structure like a long bone is under a bending load, its maximum stress is most dependent on what factor?
Explanation
REFERENCES: Hayes WC, Bouxsein ML: Biomechanics of cortical and trabecular bone: Implications for assessment of fracture risk, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 76-82.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 161-167.
Question 61
A 77-year-old woman who underwent a cemented total hip arthroplasty 10 years ago now reports groin pain. Examination reveals a loosened acetabular component and a well-fixed femoral component. Treatment should consist of revision of
Explanation
REFERENCES: Peters CL, Kull L, Jacobs JJ, Rosenberg AG, Galante JO: The fate of well fixed cemented femoral components left in place at the time of revision of the acetabular component. J Bone Joint Surg Am 1997;79:701-706.
Poon ED, Lachiewicz PF: Results of isolated acetabular revisions: The fate of the unrevised femoral component. J Arthroplasty 1998;13:42-49.
Moskal JT, Shen FH, Brown TE: The fate of stable femoral components retained during isolated acetabular revision: A six- to twelve-year follow-up study. J Bone Joint Surg Am
2002;84:250-255.
Templeton JE, Callaghan JJ, Goetz DD, Sullivan PM, Johnston RC: Revision of a cemented acetabular component to a cementless acetabular component. A ten- to fourteen-year follow-up study. J Bone Joint Surg Am 2001;83:1706-1711.
Question 62
Figure 9 is the radiograph of a 24-year-old amateur marathon runner who has ankle pain. She previously sustained a metatarsal stress fracture. In addition to asking about her training routine and the type of footwear she uses, the orthopaedic surgeon should inquire about this patient's history of nutrition and

Explanation
Several studies have reported an increased incidence of stress fractures in female athletes, including fractures of the foot and ankle in runners. The
female athlete triad describes a condition involving decreased bone density, anorexia, and amenorrhea. In addition to asking about this woman's exercise routine, the orthopaedic surgeon should obtain a comprehensive menstrual and dietary history in the context of multiple stress fractures. A review of genetics, rheumatology, and cardiovascular disorders is less likely to generate an etiology.
RECOMMENDED READINGS
Kasser JR, ed. Orthopaedic Knowledge Update 5: Home Study Syllabus. Rosemont, IL: American Academy of Orthopaedic Surgeons; 1996:96-99.
Arendt EA. Osteoporosis in the athletic female: Amenorrhea and amenorrheic osteoporosis. In: Pearl AJ, ed. AOSSM: The Athletic Female. Champaign, IL: Human Kinetics; 1993:41-59. Brukner PD, Khan KM. Clinical Sports Medicine. Sydney: McGraw-Hill; 1991:17.
RESPONSES FOR QUESTIONS 10 THROUGH 13
Ankle replacement
Ankle fusion
Tibiotalocalcaneal fusion
Total contact cast
Intra-articular steroid injection
Match the appropriate treatment listed above with the patient scenario described below.
Question 63
A patient with no history of patellar instability sustains a traumatic lateral patellar dislocation. What structure most likely has been torn?
Explanation
REFERENCES: Desio SM, Burks RT, Bachus KN: Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med 1998;26:59-65.
Conlan T, Garth WP Jr, Lemons JE: Evaluation of the medial soft-tissue restraints of the extensor mechanism of the knee. J Bone Joint Surg Am 1993;75:682-693.
Warren LF, Marshall JL: The supporting structures and layers on the medial compartment of the knee: An anatomical analysis. J Bone Joint Surg Am 1979;61:56-62.
Question 64
A 31-year-old male sustains an ipsilateral displaced transverse acetabular fracture, pubic rami fractures, and a sacroiliac joint dislocation. What structure should be reduced and stabilized first?

Explanation
The referenced article by Matta reviewed 259 patients with acetabular fractures treated within 21 days of injury and found that the hip joint can be preserved and post-traumatic osteoarthrosis can be avoided if an anatomical reduction is achieved.
Question 65
Figure 109 is the radiograph of an 11-year-old boy who felt a snap in his right hip while jumping hurdles during track practice yesterday. He complains of pain to his right groin region and is walking with a limp. What physical examination test will cause the patient to experience the most discomfort?

Explanation
Question 66
A patient undergoes a simple excision of a 3-cm superficial mass in the thigh at another institution. The final pathology reveals a leiomyosarcoma, without reference to the margins. What is the recommendation for definitive treatment?
Explanation
a reexcision of the tumor bed is recommended.
REFERENCE: Noria S, Davis A, Kandel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 67
Figures below depict the radiographs obtained from a 76-year-old woman who comes to the emergency department after experiencing a fall. She is an unassisted community ambulator with a history of right hip pain. What is the most appropriate surgical treatment for this fracture?
Explanation
This patient has pre-existing right hip osteoarthritis. The most correct option for the treatment of this active patient is a right total hip arthroplasty. Hemiarthroplasty would not address the patient's pain from osteoarthritis, and open reduction and internal fixation would not fix the femoral head issue or the
osteoarthritis.
Question 68
Figures below demonstrate the radiographs obtained from a 56-year-old man with a 3-year history of right groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?
Explanation
Chronic opioid consumption prior to total joint arthroplasty has been associated with increased pain after surgery, increased opioid requirements, a slower recovery and longer hospital stay, and higher 90-day postoperative complications compared with patients not on chronic opioids preoperatively. Based on this information, Nguyen and associates performed a study in three patient groups that included 1) chronic opioid users who underwent no preoperative intervention, 2) chronic opioid users who were weaned down to 50% of their prior opioid regimen, and 3) patients who were not chronic opioid users. The authors found that the reduction of preoperative opioid use improved postoperative function, pain, and recovery and that the weaned group performed more like the opioid naive group than the chronic opioid user
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to
surgery.
Question 69
Standard guidelines necessitate the use of intraoperative neurophysiological monitoring for patients undergoing surgery for which condition?
Explanation
There are currently no official guidelines on the appropriate use of neuromonitoring in spine surgery. In general, use of neuromonitoring is at surgeon discretion and often is based on the surgeon's perceived risk for neurologic injury during surgery and medicolegal concerns. In most reports,
neuromonitoring is considered useful in cases of deformity correction, spinal cord decompression, instrumentation placement, and revision surgery. However, even for some of these cases, studies have shown limited benefits of neuromonitoring and substantial associated costs.
RECOMMENDED READINGS
Lall RR, Lall RR, Hauptman JS, Munoz C, Cybulski GR, Koski T, Ganju A, Fessler RG, Smith ZA. Intraoperative neurophysiological monitoring in spine surgery: indications, efficacy, and role of the preoperative checklist. Neurosurg Focus. 2012 Nov;33(5):E10. doi: 10.3171/2012.9.FOCUS12235. Review. PubMed PMID: 23116090. View Abstract at PubMed Peeling L, Hentschel S, Fox R, Hall H, Fourney DR. Intraoperative spinal cord and nerve root monitoring: a survey of Canadian spine surgeons. Can J Surg. 2010 Oct;53(5):324-8. PubMed PMID: 20858377. View Abstract at PubMed
Garces J, Berry JF, Valle-Giler EP, Sulaiman WA. Intraoperative neurophysiological monitoring for minimally invasive 1- and 2-level transforaminal lumbar interbody fusion: does it improve patient outcome? Ochsner J. 2014 Spring;14(1):57-61. PubMed PMID: 24688334. View Abstract at PubMed
Question 70
Figures 191a and 191b are the radiographs of an 18-year-old man who had an ankle fracture requiring open reduction and internal fixation 2 years ago. He has a progressive symptomatic ankle deformity.Surgical intervention should consist of

Explanation

Question 71
A 6-year-old African-American boy with sickle cell disease has had pain and limited use of his right arm for the past 3 days. History reveals that he sustained a humeral fracture approximately 3 years ago. A lateral radiograph is shown in Figure 25. Based on these findings, a presumptive diagnosis of chronic osteomyelitis is made. What are the two most likely organisms?
Explanation
REFERENCES: Piehl FC, David RJ, Prugh SI: Osteomyelitis in sickle cell disease. J Pediatr Orthop 1993;13:225-227.
Givner LB, Luddy RE, Schwartz AD: Etiology of osteomyelitis in patients with major sickle hemoglobinopathies. J Pediatr 1981;99:411-413.
Epps CH Jr, Bryant DD III, Coles MJ, Castro O: Osteomyelitis in patients who have sickle-cell disease: Diagnosis and management. J Bone Joint Surg Am 1991;73:1281-1294.
Lovell and Winter’s Pediatric Orthopaedics, ed 4, 1996.
Question 72
A 32-year-old runner has pain in the medial arch that radiates into the medial three toes. He reports the presence of pain only when running. Examination reveals normal hindfoot alignment. There is a weakly positive Tinel’s sign over the posterior tibial nerve. Tenderness is noted with palpation over the plantar medial area in the vicinity of the navicular tuberosity. What is the most likely diagnosis?
Explanation
REFERENCES: Rask MR: Medial plantar neurapraxia (jogger’s foot): Report of three cases. Clin Orthop 1978;134:193-195.
Murphy PC, Baxter DE: Nerve entrapment of the foot and ankle in runners. Clin Sports Med 1985;4:753-763.
Lutter LD: Surgical decisions in athletes’ subcalcaneal pain. Am J Sports Med 1986;14:481-485.
Question 73
A 44-year-old farmer involved in a rollover accident on his tractor sustained an L1 burst fracture with a 20% loss of anterior vertebral body height, 30% canal compromise, and 15 degrees of kyphosis. He remains neurologically intact. The preferred initial course of action should consist of
Explanation
REFERENCES: Hartman MB, Chrin AM, Rechtine GR: Nonoperative treatment of thoracolumbar fractures. Paraplegia 1995;33:73-76.
Chow GH, Nelson BJ, Gebhard JS, Brugman JL, Brown CW, Donaldson DH: Functional outcome of thoracolumbar burst fractures managed with hyperextension casting or bracing and early mobilization. Spine 1996;21:2170-2175.
Kraemer WJ, Schemitsch EH, Lever J, McBroom RJ, McKee MD, Waddel JP: Functional outcome of thoracolumbar burst fractures without neurological deficit. J Orthop Trauma 1996;10:541-544.
Question 74
A 9-year-old child sustained a fracture-dislocation of C-5 and C-6 with a complete spinal cord injury. What is the likelihood that scoliosis will develop during the remaining years of his growth?
Explanation
REFERENCES: Brown JC, Swank SM, Matta J, et al: Late spinal deformity in quadriplegic children and adolescents. J Pediatr Orthop 1984;4:456-461.
Lancourt JE, Dickson JH, Carter RE: Paralytic spinal deformity following traumatic spinal-cord injury in children and adolescents. J Bone Joint Surg Am 1981;63:47-53.
Dearolf WW III, Betz RR, Vogel LC, et al: Scoliosis in pediatric spinal cord-injured patients.
J Pediatr Orthop 1990;10:214-218.
Question 75
A 25-year-old man has chronic back pain that has been slowly worsening. He has no constitutional symptoms, and he denies any previous medical problems. Examination shows a tall lean build with no objective neurologic findings or skin lesions. Figure 32 shows a T2-weighted sagittal MRI scan. What is the most likely diagnosis?
Explanation
REFERENCES: Ahn NU, Sponseller PD, Ahn UM, Nallamshetty L, Kuszyk BS, Zinreich SJ: Dural ectasia is associated with back pain in Marfan’ syndrome. Spine 2000;25:1562-1568.
Villeirs GM, Van Tongerloo AJ, Verstraete KL, Kunnen MF, De Paepe AM: Widening of the spinal canal and dural ectasia in Marfan’s syndrome: Assessment by CT. Neuroradiology 1999;41:850-854.
Question 76
03 Early failure of a unicompartmental knee arthroplasty that is the result of polyethylene wear is primarily caused by
Explanation
back to this question next question
Question 77
A 47-year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the aspiration and proceed to a revision TKA with possible augments on standby.
Question 78
A 71-year-old man has worsening left hip pain and is indicated for a left total hip arthroplasty (THA). Figure 1 shows a preoperative plan for the patient. The patient is scheduled for a left THA using a direct anterior approach with the pictured implants. If this plan is followed as pictured, what is the likely outcome for this patient? Figure could not be loaded
Explanation
A. spinal fusion.
B. BMI and implant size.
C. mismatch between the metaphysis and diaphysis.
D. modular neck prosthesis.
Question 79
A 53-year-old man reports a 5-week history of worsening low back pain accompanied by bilateral knee and ankle pain and swelling. He also reports a lesser degree of neck and left elbow pain. He denies any history of trauma or provocative episodes. His medical history is significant for Reiter’s syndrome more than 25 years ago, with no subsequent exacerbations. Furthermore, he has recently returned from a vacation in Costa Rica and noted the development of infectious gastroenteritis with diarrhea within 1 week of his return. This was treated with a 10-day course of oral antibiotics and has since resolved. He denies any significant bowel or urinary symptoms at this time. His neurologic examination is essentially within normal limits, but is somewhat limited by his low back and leg pain. What further investigation is most appropriate at this time?
Explanation
REFERENCES: Gardner GC, Kadel NJ: Ordering and interpreting rheumatologic laboratory tests. J Am Acad Orthop Surg 2003;11:60-67.
Shojania K: Rheumatology: 2. What laboratory tests are needed? CMAJ 2000;162:1157-1163.
Question 80
A 14-year-old girl has had mild pain and nail deformity of the great toe for the past 4 months. A radiograph is shown in Figure 50. What is the most likely etiology of the lesion?
Explanation
REFERENCES: Lokiec F, Ezra E, Krasin E, Keret D, Wientraub S: A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop 2001;21:76-79.
Letts M, Davidson D, Nizalik E: Subungual exostosis: Diagnosis and treatment in children. J Trauma 1998;44:346-349.
Davis DA, Cohen PR: Subungual exostosis: Case report and review of the literature. Pediatr Dermatol 1996;13:212-218.
Question 81
A 51-year-old woman is seen for evaluation of chronic supraspinatus and infraspinatus tendon tears. Three years ago, in an attempted repair the surgeon was unable to repair the supraspinatus and infraspinatus tendon tears. Currently she has a marked amount of pain, reduced range of motion, and weakness. Examination reveals anterosuperior escape. Radiographs show no signs of arthritic changes. You are considering a latissimus dorsi tendon transfer. During the discussion, you mention that
Explanation
REFERENCES: Gerber C, Maquieira G, Espinosa N: Latissimus dorsi transfer for the treatment of irreparable rotator cuff tears: Factors affecting outcome. J Bone Joint Surg Am
2006;88:113-120.
Iannotti JP, Hennigan S, Herzog R, et al: Latissimus dorsi tendon transfer for irreparable posterosuperior rotator cuff tears. J Bone Joint Surg Am 2006;88:342-348.
Question 82
A 14-year-old male soccer player was seen initially in the emergency room 1 week ago after an acute right hip injury during a soccer tournament. The patient reports that the hip pain has improved, but still requires crutches for long distance ambulation. His radiograph is seen in Figure A. What would be the next most appropriate step in management? Review Topic

Explanation
The diagnosis of an avulsion fracture of the anterior superior iliac spine is made on the basis of: 1. History (sudden contraction of the sartorial and tensor fasciae latae muscle), 2. Physical findings (tenderness over the anterior superior iliac spine [ASIS] and pain with straight-leg raise), 3. Patient's age (most commonly in adolescents or young adults), and 4. Radiographs (confirmed fracture on standard views of the pelvis). Treatment of these injuries is almost always conservative with crutches and progressive weight-bearing activities as tolerated. The relative indications for operative treatment include displacement of the fracture fragment > 3 cm or painful non-union.
White et al. defined two types of anterior superior iliac spine avulsion fractures. A sartorius avulsion fracture (Type 1) usually occurs when sprinting. The fracture fragment is usually small and displaced anteriorly. The tensor avulsion fracture (Type 2) usually occurs when twisting the trunk (e.g. swinging a bat). This fragment is usually larger than Type 1 fractures and more likely to be displaced laterally.
Holden et al. reviewed pediatric pelvic fractures. They state that avulsion fractures of the anterior superior iliac spine are usually low-energy injures, and are not associated with other life-threatening injuries. They do not require an extensive workup (e.g. CT scanning)
Figure A is an antero-posterior view of the pelvis with a small right-sided avulsion fracture of the anterior superior iliac spine.
Incorrect Answers:
Question 83
-A 16-year-old girl was seen after a motor vehicle collision. Imaging studies including plain radiographs,MRI scans, and CT scans confirm bilateral jumped facets at C5-6 without disk herniation. She is alert,oriented, and neurologically intact. What is the most appropriate next step?
Explanation
Question 84
Which of the following orthotic features best reduces pain in patients with hallux rigidus?
Explanation
REFERENCES: Beskin JL: Hallux rigidus. Foot Ankle Clin 1999;4:335-353.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 17-25.
Question 85
A 56-year-old man has a chief complaint of leg weakness and inability to walk. Examination reveals 5 out of 5 motor strength in all lower extremity muscle groups tested and normal sensation to light touch in both lower extremities. The patient is slow in getting up from a seated position and has an unsteady wide-based

Explanation
Question 86
A 25-year-old carpenter falls on his outstretched arm. What physical finding best correlates with the lesion seen on the MRI scan shown in Figure 3?
Explanation
REFERENCES: Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Greis PE, Kuhn JE, Schultheis J, et al: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Question 87
A transverse humeral shaft fracture that occurs between a stiff arthritic shoulder joint; a stiff, arthritic elbow joint is treated nonsurgically in a hanging-arm cast
Explanation
In 1977, Perren and Cordey penned a German manuscript that first described an interpretation of mechanical influences on tissue differentiation. This became known as the Strain Theory of Perren. In 1980, a second manuscript by the same authors was published in English. Within this manuscript, Perren wrote, "These thoughts about the mechanical influences on tissue differentiation are not intended as conclusive evidence since precise data are still not available, but we hope that they will stimulate thought and provide a basis for discussion." More than 30 years later, these thoughts continue to stimulate discussion and research on cell mechanotransduction. This theory is still being manipulated in surgical theatres all around the world in an attempt to more consistently achieve fracture healing. Strain is a magnitude of deformation. As typically defined, it is the change in dimension of a deformed object during loading divided by its original dimension. This is difficult to work with intraoperatively. The fraction below illustrates a simpler way to regard this concept:
Strain = Magnitude of displacement between fragments during loading / Total resting distance between fragments after stabilization
By remembering that low strain generally leads to bone formation and healing, it is possible to manipulate this fraction intraoperatively to achieve success. When a simple fracture pattern is anatomically reduced and compressed, then the total resting distance between fragments after stabilization approaches 0. This means the numerator must be near 0 to achieve a low-strain environment. This is what occurs in absolute stability (no motion between fracture fragments under physiologic load) and primary bone healing occurs. When a multifragmentary fracture pattern is treated with bridge plating, the total resting distance between fragments after stabilization is a larger number (consider the additive distance between the different fragments). In this case, the numerator can be larger to achieve a low-strain environment. This is what happens in relative stability (controlled motion between fracture fragments under physiologic load). Secondary bone healing occurs. Now consider the third scenario: a simple fracture pattern that is fixed with a small gap. The total resting distance is still a small number. Based on the theory, eliminating motion by creating a stiff construct should lead to healing, but it does not. Creating absolute stability with a gap means that primary bone healing cannot occur (because cutting cones cannot cross the gap) and secondary bone healing cannot occur (because there is not enough motion to induce callus formation). This is where the strain theory breaks down and how many nonunions occur. In the fourth scenario, a high-strain environment is present and commonly leads to a nonunion (as predicted by the theory). The simple fracture pattern is too mobile, and nonfunctional callus often occurs.
RECOMMENDED READINGS
Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br. 2002 Nov;84(8):1093-110. Review. PubMed PMID: 12463652. View Abstract at PubMed
Epari DR, Duda GN, Thompson MS. Mechanobiology of bone healing and regeneration: in vivo models. Proc Inst Mech Eng H. 2010 Dec;224(12):1543-53. Review. PubMed PMID: 21287837.View Abstract at PubMed
Question 88
In an isolated ankle syndesmotic injury, the fibula is unstable in the incisura fibularis of the tibia. In what direction is the fibula most unstable?

Explanation
The first referenced article by Xenos et al found that stress lateral radiographs have more interobserver reliability than stress AP/mortise radiographs and that two syndesmotic screws are stronger than one.
The referenced article by Candal-Couto et al is a biomechanical study that found more anterior-posterior instability in a syndesmosis injury model, and more ankle instability is noted with syndesmosis injury and a concomitant deltoid injury. The referenced article by Zalavras et al is an excellent review article on ankle syndesmosis injuries.
Question 89
A 45-year-old man who has had recurrent pain and swelling of the left Achilles tendon insertion for the past 10 years reports that physical therapy and activity modification have provided relief in the past. He now has continued pain despite these efforts. He also reports occasional bouts of dysuria that he attributes to a history of prostatitis. He also notes recent eye irritation that he attributes to allergies. A lateral heel radiograph is shown in Figure 33. Which of the following laboratory studies would best aid in diagnosis?
Explanation
REFERENCE: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 560-650.
Question 90
A 61-year-old right-hand-dominant woman falls down the stairs, resulting in a left anteroinferior dislocation and noncomminuted greater tuberosity fracture. A closed glenohumeral reduction with intravenous sedation is performed in the emergency department. After reduction, the greater tuberosity fragment remains displaced by 2 mm. What is the most appropriate treatment?
Explanation
<3 mm in laborers and professional athletes can be treated successfully without surgery. Early passive range
of motion is important to avoid stiffness.
Question 91
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?
Explanation
REFERENCES: Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
McFarland EG, Hsu CY, Neira C, O’Neil O: Internal impingement of the shoulder: A clinical and arthroscopic analysis. J Shoulder Elbow Surg 1999;8:458-460.
Question 92
A 32-year-old man sustains a forceful inversion injury while playing soccer. Examination reveals tenderness in the lateral hindfoot and midfoot region with associated ecchymosis and swelling. Radiographs show proximal migration of the os peroneum. Active eversion is still present. These findings indicate disruption of the
Explanation
REFERENCES: Thompson FM, Patterson AH: Rupture of the peroneus longus tendon: Report of three cases. J Bone Joint Surg Am 1989;71:293-295.
Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1090-1209.
Question 93
-A 51-year-old man has a slowly expanding upper-extremity mass. Examination reveals a firm 3-cm mass in his midvolar forearm. Radiographs are normal. You suspect a soft-tissue sarcoma. The best imaging study would be
Explanation

Question 94
Examination of a 5-year-old boy with amyoplasia shows a flexion contracture of 70° of the right knee. The active arc of motion is from 70° to 90°, and the opposite knee has a flexion contracture of 10°. Both hips are dislocated with flexion contractures of 10°, passive hip motion is from 10° to 90° of flexion, and the feet are plantigrade and easily braceable. Despite a daily stretching program, the parents and physical therapists note that it is increasingly difficult for him to walk because of the flexion contracture of the right knee. Management of the knee flexion contracture should now include
Explanation
REFERENCES: Sarwark JF, MacEwen GD, Scott CI Jr: Amyoplasia (a common form of arthrogryposis). J Bone Joint Surg Am 1990;72:465-469.
DelBello DA, Watts HG: Distal femoral extension osteotomy for knee flexion contracture in patients with arthrogryposis. J Pediatr Orthop 1996;16:122-126.
Sells JM, Jaffe KM, Hall JG: Amyoplasia, the most common type of arthrogryposis: The potential for good outcome. Pediatrics 1996;97:225-231.
Question 95
Ulnar collateral ligament (UCL) reconstruction using a modified Jobe technique
Explanation
Certain complications are more strongly associated with the approach and surgical procedure for elbow pathology. With a 2-incision distal biceps repair, heterotopic ossification
with a radial-ulnar synostosis is a concern. This complication can be minimized through irrigation of bone debris and care to avoid dissection between the radius and ulna. With a single-incision distal biceps repair, the lateral antebrachial cutaneous nerve is retracted during the procedure. Numbness on the lateral side of the forearm is common, although often temporary. During arthroscopic debridement for lateral epicondylitis, injury to the radial UCL can occur, leading to posterolateral rotatory instability of the elbow. The modified Jobe technique for UCL reconstruction typically involves an ulnar nerve transposition during the procedure. Numbness and tingling in the fourth and fifth digits are concerns when this procedure is performed.
Question 96
A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient’s history is significant for smoking. The most immediate appropriate postoperative management for this patient should include
Explanation
REFERENCES: Sagi HC, Beutler W, Carroll E, et al: Airway complications associated with surgery on the anterior cervical spine. Spine 2002;27:949-953.
Epstein NE, Hollingsworth R, Nardi D, et al: Can airway complications following multilevel anterior cervical surgery be avoided? J Neurosurg 2001;94:185-188.
Emery SE, Smith MD, Bohlman HH: Upper-airway obstruction after multi-level cervical corpectomy for myelopathy. J Bone Joint Surg Am 1991;73:544-551.
Question 97
An 8-year-old boy with severe hemophilia A (factor VIII) and no inhibitor is averaging eight transfusions per month for bleeding into the right ankle. Examination shows synovial hypertrophy; range of motion consists of 0° of dorsiflexion and 20° of plantar flexion. The patient’s knees, elbows, and left ankle have no restriction of motion. Standing radiographs of the right ankle are shown in Figure 18. Management should consist of
Explanation
REFERENCES: Greene WB: Synovectomy of the ankle for hemophilic arthropathy. J Bone Joint Surg Am 1994;76:812-819.
Greene WB: Chronic inflammatory arthridities and diseases related to the hematopoietic system, in Drennan JC (ed): The Child’s Foot and Ankle, New York, NY, Raven Press, 1992, pp 461-482.
Question 98
Myositis ossificans is a recognized complication of contusion to the quadriceps muscle. During early rehabilitation, this condition is most likely to be exacerbated by
Explanation
REFERENCES: Brunet ME, Hontas RB: The thigh, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Cushner FD, Morwessel RM: Myositis ossificans traumatica. Orthop Rev 1992;21:1319-1326.
Question 99
An 11-year-old girl has had pain in the medial arch of her foot for the past 3 months. She reports that pain is present even with daily activities such as walking to class at school, and ibuprofen provides some relief. She denies any history of trauma. Examination reveals a flexible pes planus with focal tenderness over a prominent tarsal navicular tuberosity. Radiographs show a prominent accessory navicular. Management should consist of
Explanation
REFERENCE: Bordelon RL: Flatfoot in children and young adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 717-756.
Question 100
What is the most common site of metastases from a soft-tissue sarcoma?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 255-259.
