Orthopedic Board Review MCQs: Trauma, Arthroplasty & Foot/Ankle | Part 56

Key Takeaway
This page presents Part 56 of an OITE and AAOS orthopedic surgery board review. It offers 100 high-yield, verified MCQs for orthopedic residents and surgeons. This interactive quiz aids rigorous board exam preparation with detailed clinical explanations and dual study modes.
About This Board Review Set
This is Part 56 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 56
This module focuses heavily on: Ankle, Arthroplasty, Deformity, Foot, Fracture, Hip, Infection, Knee, Shoulder, Trauma.
Sample Questions from This Set
Sample Question 1: A 38-year-old female with a grade IIIB open tibia fracture is scheduled to undergo definitive fixation and subsequent flap coverage with the orthopaedic and plastic surgery teams. She is met in the pre-operative area by the surgical intern ...
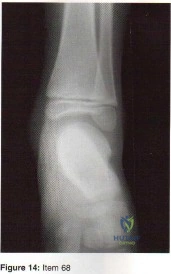
Sample Question 2: Which of the following conditions is typically associated with the ankle deformity shown in figure 14?...
Sample Question 3: Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following afootball injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusio...
Sample Question 4: A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvo...
Sample Question 5: Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stagedebilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplas...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 38-year-old female with a grade IIIB open tibia fracture is scheduled to undergo definitive fixation and subsequent flap coverage with the orthopaedic and plastic surgery teams. She is met in the pre-operative area by the surgical intern and paperwork is completed per institutional protocol. She is then brought back to the operating room. Which of the following is true regarding the pre-surgical timeout?
Explanation
The WHO pre-surgical safety checklist involves assessment at three points during an operative procedure: before induction of anesthesia, before skin incision, and before the patient leaves the operating room. Some components of the checklist include
confirming IV access and allergies, administration of antibiotic prophylaxis, and surgical site verification. The surgeon has been shown to be the most effective team member at reducing complications when using the checklist.
Haynes et al. evaluated the effects of the WHO pre-surgical checklist on perioperative complication rates at eight international sites. They found a significant reduction in rates of complications and death in patients over the age of 16 undergoing noncardiac procedures after implementation of the checklist.
Illustration A shows the WHO pre-surgical checklist Incorrect Answers:
present for the timeout. Answer 2: The implant representative is not necessary for the timeout. Answer 4: The attending surgeon needs to be present in the same OR for the timeout. Answer 5: The timeout has been shown to decrease rates of complication and death.
Question 2
Which of the following conditions is typically associated with the ankle deformity shown in figure 14?
Explanation
Question 3
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. What is the underlying cause of the pathology noted in the figures?

Explanation
Question 4
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of
Explanation
REFERENCES: Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 5
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits.The patient undergoes successful primary THA with a metal-on-metal bearing. At 1-year follow-up, she reports no pain and is highly satisfied with the procedure. However, 3 years after the index procedure, she reports atraumatic right hip pain that worsens with activities. Radiographs reveal the implants in good position with no sign of loosening or lysis. An initial laboratory evaluation reveals a normal sedimentation rate and C-reactive protein (CRP) level. The most appropriate next diagnostic step is
Explanation
THA has proven to be durable and reliable for pain relief and improvement of function in patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A
metal-on-metal articulation is associated with excellent wear rates in vitro. Because it offers a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions—including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis after the possible transfer of metal ions across the placental barrier—make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.The work-up of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including the erythrocyte sedimentation rate, C-reactive protein (CRP) level, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging, including MRI with MARS, should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following a revision of failed metal-on-metal hip replacements.
Question 6
Which of the following factors is considered most important when assessing an ankle fracture for surgical treatment?
Explanation
REFERENCES: Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119.
Hahn DM, Colton CL: Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
Question 7
A 16-year-old girl has had pain and swelling along the medial arch of her left foot for the past 3 months. She also reports pain from shoe wear and while running. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 40a through 40c. What is the next most appropriate step in management?
Explanation
REFERENCES: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, p 655.
Bennett GL, Weiner DS, Leighley B: Surgical treatment of symptomatic accessory tarsal navicular. J Pediatr Orthop 1990;10:445-449.
Question 8
What nerve is most at risk during placement of the anterolateral portal in elbow arthroscopy?
Explanation
REFERENCES: O’Driscoll SW, Morrey BF: Elbow arthroscopy, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 21-34.
Field LD, Altchek DW, Warren RF, O’Brien SJ, Skyhar MJ, Wickiewicz TL: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Question 9
-Figures 56a and 56b are the MRI scans of a 2-year-old girl who has a fever of 39°C and inability to move her left arm. She has not had any recent injury and is otherwise healthy. Radiograph findings of her left upper extremity are normal. What is the most appropriate treatment?
Explanation

Question 10
A young male patient underwent intramedullary nail fixation for a diaphyseal femur fracture. A post-operative CT scanogram is performed to assess rotational alignment between the surgical and non-surgical femur. Which of the following measurement(s) are considered acceptable differences in regards to femoral rotational malreduction after intramedullary nail fixation as compared to the uninjured femur?
Explanation
The maximum acceptable difference in rotational malreduction between the surgical and contralateral legs for femoral version is 15°. Therefore, answers 1 and 2 are correct.
Normal femoral neck anteversion is approximately 11-13°, with a normal range between 5-20°. The variation within the same patients can also be up to 15° difference between limbs. Current literature has shown that this 15° difference is well tolerated by patients, including when this has occured as a result of rotational malreduction following intramedullary nail fixation for a diaphyseal femur fracture.
Ayalon et al. aimed to compare the difference in femoral version (DFV) after intramedullary nailing performed by a trauma-trained and non-trauma trained surgeon. The mean post-operative DFV was 8.7° in these patients, compared to 10.7° in those treated by surgeons of other subspecialties. Post-operative version or percentage of DFV >15° did not significantly differ between these two groups.
Omar et al. studied the utility of pre-operative 'virtual reduction' of bilateral femoral fractures that were initially stabilized with external fixation. After external fixation, the mean rotational difference between both legs was 15.0°
± 10.2°. Following virtual reduction, the mean rotational difference between both legs was 2.1° ± 1.2°, after intramedullary nailing, compared to 6.1° ±
Question 11
The diagnosis of an infection after total knee arthroplasty is most reliably proven based on what single study?
Explanation
REFERENCES: Windsor RE, Bono JV: Infected total knee replacements. J Am Acad Orthop Surg 1994;2:44-53.
Windsor RE, Insall JN, Urs WK, et al: Two-stage reimplantation for the salvage of total knee arthroplasty complicated by infection: Further follow-up and refinement of indications. J Bone Joint Surg Am 1990;72:272-278.
Question 12
What percentage of bone weight is collagen?
Explanation
Question 13
Which of the following factors has the greatest effect on the pull-out strength of a lumbar pedicle screw?
Explanation
REFERENCES: Wittenberg RH, Shea M, Swartz DE, et al: Importance of bone mineral density in instrumented spine fusions. Spine 1991;16:647-652.
Zindrick MR, Wiltse LL, Widell EH, et al: A biomechanical study of intrapeduncular screw fixation in the lumbosacral spine. Clin Orthop 1986;203:99-112.
Question 14
A polytrauma patient sustains a right bicondylar tibial plateau fracture and a right humeral shaft fracture both treated with open reduction, internal fixation. He also underwent statically locked intramedullary nailing of a left femoral shaft fracture. What is the appropriate weightbearing status?

Explanation
Question 15
Figure 7 shows the radiograph of a 64-year-old man who has neck pain and weakness of the upper and lower extremities following a motor vehicle accident. Examination reveals 3/5 quadriceps and 4/5 hip flexors but no ankle dorsiflexion or plantar flexion. His intrinsics are 1/5, with finger flexors of 3/5. He is awake, alert, and cooperative. Management should consist of
Explanation
open reduction.
REFERENCES: Star AM, Jones AA, Cotler JM, et al: Immediate closed reduction of cervical spine dislocations using traction. Spine 1990;15:1068-1072.
Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocations using traction weight up to 140 pounds. Spine 1993;18:386-390.
Question 16
Following spinal cord injury (SCI), methylprednisolone (a bolus of 30 mg/kg plus 5.4 mg/kg per hour over 24 hours) initiated within 8 hours of injury has been associated with which of the following MRI findings? Review Topic
Explanation
Question 17
A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman with a soft endpoint, varus laxity at 30 degrees, and a positive dial test at 30 degrees that dissipates at 90 degrees of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome? Review Topic
Explanation
(SBQ12SP.35) A 16-year-old male football player is tackled into the ground during a game. He comes to the sideline with unilateral upper extremity pain, burning dysesthesias, and muscle weakness. Several minutes later, his symptoms resolve. In this scenario, what muscles are most likely to be affected? Review Topic
Deltoid and biceps
Triceps
Wrist flexors
Finger flexors
Interossei
This patient presents with a 'burner' or 'stinger,' a transient unilateral neurapraxia that most commonly involves the biceps, deltoid and rotator cuff muscles.
Hypotheses for the mechanism of neurapraxia in stingers include nerve root compression in the neural foramen as a result of extension and compression, traction on the brachial plexus or a direct blow to the plexus. C5-C6 is the most commonly involved level, indicating root injury or upper trunk brachial plexus injury. Unilateral and transient symptoms are required for diagnosis. Bilateral 'stinger' symptoms of numbness, tingling, and weakness are consistent with cervical spinal cord neurapraxia. Return to play in contact sports is contraindicated with bilateral symptoms prior to MRI evaluation of the cervical spine.
Shannon et al. review burner syndrome in athletes. They emphasize that criteria for return to play are based on a complete and thorough neurologic and physical exam. Normal strength and sensation in both upper extremities as well as a normal cervical spine exam (including range of motion, compression, Spurling's, Adson's, and resistive head pressures) are required for return to play. Any positive findings mandate withdrawal of the player from competition.
Illustration A shows hypothesized areas of involvement by mechanism according to
Shannon et al. A, Extension-ipsilateral compression. B, Flexion-contralateral flexion (traction) or direct trauma.
Incorrect Answer Answer Answer
2:
3:
4:
Wrist Finger
Triceps
flexors flexors
C7 C7 C8
Question 18
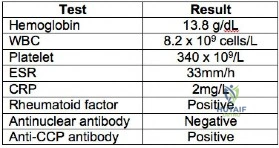
A 38-year-old man is being considered for medial meniscus transplantation following an arthroscopic subtotal meniscectomy performed at the time of ACL reconstruction. His body mass index (BMI) is 28kg/m2. Laboratory tests are shown in Figure A. Standing long-leg radiographs reveal a 4 degree valgus deformity compared with the contralateral side, with the weightbearing line running through the lateral tibial spine. His arthroscopic photos also revealed a 1.7cm wide Outerbridge II chondral lesion over the lateral femoral condyle and synovitis. What factor in this patient is an absolute contraindication to meniscal transplantation? Review Topic
Explanation
Besides inflammatory arthritis, other absolute contraindications include diffuse arthritis, Outerbridge grade IV changes, untreated tibiofemoral subluxation, synovial disease, previous joint infection, skeletal immaturity, or marked obesity.
Lee et al. reviewed meniscal transplantation. They recommend meniscal transplantation only after nonoperative measures (unloading braces, weight loss, activity modification, analgesia) have failed. Indications include young patients (<50yo) with symptoms referable to a meniscus-deficient tibiofemoral compartment, with a stable knee with normal alignment, with intact articular surfaces (grade I or II).
Figure A is a table showing this patient's lab results. He has positive RF and anti-CCP antibody. In addition, he has synovial changes on arthroscopy. These findings are significant for active RA.
Incorrect Answers:
Meniscus transplantation can be attempted if cruciate ligament deficiency was addressed, or there are plans for concurrent or staged reconstruction. Answer 3: Varus/valgus malalignment is not an absolute contraindication although concurrent/staged treatment is necessary to correct alignment. Answer 4: Outerbridge Grade I and II chondral defects are not contraindications. Knees with Outerbridge III lesions may still be considered if defects are focal and concomitant treatment is performed. Answer 5: Marked obesity is a contraindication. This is not present in this individual.
Question 19
Eosinophilic granuloma frequently occurs as a solitary lesion in the tubular long bones. After biopsy, what is the best course of action?
Explanation
REFERENCE: Simon M, Springfield D, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 200.
Question 20
A radiograph of a 12-year-old boy who has had an insidious onset of pain in the right hip for the past 6 weeks shows diffuse narrowing of the joint space. Examination reveals that he is afrebile, and the range of motion of the hip is less than 50% of normal in all planes. Laboratory studies show an erythrocyte sedimentation rate of 21 mm/hr and a WBC of 11,000/mm3. What is the most likely diagnosis?
Explanation
This patient has no history of hemophilia given. Hemophilic arthropathy begins with a hemarthrosis.
In osteoid osteoma the pain is typically unrelenting, sharp, boring, worse at night, and relieved with aspirin. It is not associated with joint space narrowing.
The most common age for Legg-Calve-Perthes disease is 4-8 years. It causes AVN of the femoral head and widening of the medial joint space is an early radiographic finding.
In Bleck’s report on Idiopathic Chondrolysis JBJS 1983 nine cases were seen at the reporting institution between 1973 and 1978. The average age was 11.5 years. All the patients were otherwise healthy and had no history of systemic illness of previous trauma. All the patients reported the insidious onset of pain in the anterior part of the hip. All had a decreased passive ROM. Radiographic examination showed regional osteoporosis, premature closure of the femoral capital physis, narrowing of the joint space, and lateral overgrowth of the femoral head on the neck. All laboratory examinations were negative for evidence of infection or rheumatoid arthritis. Treatment consists of administration of aspirin, active non-loading exercise of the hip, and protected weight-bearing with crutches.
Question 21
- Which of the following types of sarcoma of the bone is most sensitive to external beam radiation?
Explanation
Question 22
Figure 13 shows the clinical photograph of a 66-year-old man who has had an increasingly painful right foot deformity for the past 3 years. Examination reveals that the subtalar joint is fixed in 15° of valgus, and forefoot supination can be corrected to 10° from neutral. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
REFERENCE: Mann RA: Flatfoot in adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 757-784.
Question 23
A 56-year-old man has had a 2-year history of slowly progressive neck pain and bilateral arm aching. Over the past year, he has noticed intermittent, diffuse numbness in both hands, with decreased grip strength and mild hand clumsiness. He denies any problems with balance. Examination shows a wide-based gait, intrinsic wasting, and a postive Hoffman's sign bilaterally. An MRI scan of the cervical spine is shown in Figure 16. What is the most appropriate treatment? Review Topic

Explanation
Question 24
A 25 year-old-male presents with the injury seen in Figure A. Which of the following would be a contraindication to closed management with a functional brace?

Explanation
Indications for operative management of humeral shaft fractures are limited given the high rates of union and ability of adjacent joints to compensate for deformity. Intact muscular tone is necessary to effect bony apposition in closed treatment with a functional brace. The absence of neurologic and muscle function in patients with a flail extremity leads to increased rates of nonunion and malunion.
Rutgers and Ring conducted a retrospective review of patients managed with functional bracing of humeral shaft fractures at a single institution. The authors found a 90% overall union rate, with maintenance of shoulder and elbow motion. They caution though, that 29% of their proximal third fractures went on to nonunion.
Figure A demonstrates an AP radiograph of a comminuted humeral shaft fracture with varus alignment.
Incorrect Answers:
Question 25
Revision of failed hip resurfacing arthroplasty should involve
Explanation
Hip resurfacing offers several potential advantages over conventional total hip arthroplasty, particularly for patients younger than 75 years of age. This intervention can be
relatively bone conserving and is appropriate in settings involving proximal femoral deformity, precluding the use of a traditional femoral component. The use of hip resurfacing in osteonecrosis has been controversial, however. Although there are several reports of successful use of these implants to address osteonecrosis, concerns remain about extensive femoral head involvement (exceeding 40%) and ability to support the femoral head cap. Consequently, hip resurfacing is not recommended for patients with large femoral head lesions.
Evaluation of painful hip resurfacings requires a systematic approach. Radiographs can help surgeons assess implant position, loosening, or fractures. Serological studies including ESR, CRP, and serum cobalt and chromium levels can give clues as to whether infection, metallosis, or both are the underlying cause(s) of failure. Hip aspiration in the setting of metal-on-metal bearings necessitates a manual cell count and differential to avoid falsely elevated automated cell counts.
Revision of failed hip resurfacings should involve revisions of both the femoral and acetabular components. Although successful retention of the acetabular shell has been described, concerns remain regarding cup circumference mismatch, which can lead to suboptimal clearance between the new bearing surfaces.

Question 26
The term anorexia athletica refers to a problem whose criteria include all of the following, EXCEPT Review Topic
Explanation
Question 27
Diagnostic work-up concluded that the patient has metastatic lymphoma. He has no neurologic deficit.Based on these findings, what is the most appropriate management for this spinal condition?
Explanation
Patients with no prior diagnosis of cancer may present with vertebral lesions. After obtaining initial radiographs, the next most appropriate step is to obtain an MRI with gadolinium. To determine the primary site of the disease, a CT of the chest, abdomen, and pelvis is the next step in establishing a diagnosis. Radiation therapy is the first line of treatment in spinal metastatic disease from lymphoma because it is a highly radiosensitive tumor.
Question 28
Figures 1 and 2 are the radiographs of an 18-year-old man who had surgery 6 months ago at an outside institution. He is being referred now because he has persistent pain. He is tender over the scaphoid at the snuffbox. What is the most appropriate next imaging step in his pain workup?

Explanation
Scaphoid nonunions are difficult to diagnose on plain radiographs, which offer poor reliability when attempting to determine if there is bridging trabeculae crossing the fractures site. CT scans are more useful for diagnosing scaphoid nonunion. When scanned using conventional axial cuts, the slices mayskip through the fracture nonunion site, thereby missing the defect, even with reformats. MR imaging is useful in diagnosing acute scaphoid fractures and has a high sensitivity and diagnostic value for excluding scaphoid fractures as well. Contrast does not enhance the utility of MR imaging in fracture diagnosis.
Question 29
Epithelioid sarcoma most commonly occurs in which of the following anatomic locations?
Explanation
REFERENCES: Gupta TD, Chaudhuri P (eds): Tumors of the Soft Tissues, ed 2. Stamford, CT, Appleton and Lange, 1998, p 475.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St. Louis, MO, Mosby-Year Book, 1995, p 1074.
Question 30
A 67-year-old woman has had pain in the area of the metatarsal heads and toes bilaterally for the past 18 months. She describes a diffuse discomfort and a constant burning sensation. She notes that the area feels swollen. Examination reveals that her pulses are normal, and there is no frank swelling or focal tenderness. What is the most likely diagnosis?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-121.
Gorson KC, Ropper AH: Idiopathic distal small fiber neuropathy. Acta Neurol Scand 1995;92:376-382.
Question 31
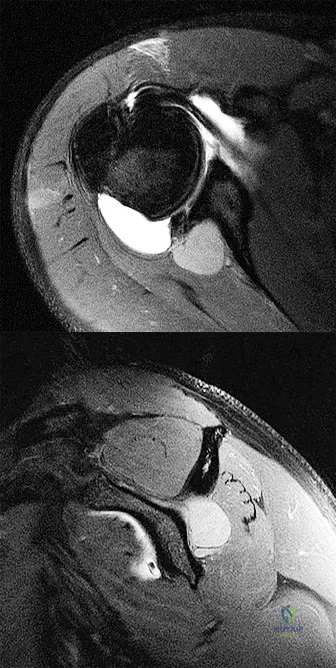
Rupture of the structure shown in the axial cross and the sagittal sections in Figures 100a and 100b causes weakness in

Explanation
The structure identified is the distal biceps tendon. Rupture of this tendon causes weakness in both flexion and supination. The biceps tendon does not affect extension or pronation.
RECOMMENDED READINGS
Baker BE, Bierwagen D. Rupture of the distal tendon of the biceps brachii. Operative versus non-operative treatment. J Bone Joint Surg Am. 1985 Mar;67(3):414-7. PubMed PMID: 3972865. View Abstract at PubMed
Mazzocca AD, Spang JT, Arciero RA. Distal biceps rupture. Orthop Clin North Am. 2008 Apr;39(2):237-49, vii. doi: 10.1016/j.ocl.2008.01.001. Review. PubMed PMID: 18374814. View Abstract at PubMed
Question 32
- A 13-year-old quarterback feels a “pop” in his knee while being tackled. Radiographs of the knee and results of a Lachman’s test are normal. Examination reveals tenderness over the distal femoral physis. To help confirm the diagnosis, management should first include
Explanation
Question 33
A 43-year-old soccer player who had knee pain following a twisting injury underwent an arthroscopic meniscectomy 6 months ago. He continues to report posterior knee pain. Examination reveals soft-tissue fullness and tenderness just above the popliteal fossa, trace knee effusion, full range of knee motion, no instability, and negative meniscal signs. Radiographs show some mild medial joint space narrowing but no other bony changes. What is the next most appropriate step in management?
Explanation
11 patients. The authors noted that oncologic surgical treatment was affected in 15 of the
25 patients. The most frequent causes of erroneous diagnosis were initial poor quality radiographs and an unquestioned original diagnosis despite persistent symptoms. Persistent symptoms warrant further diagnostic studies, not additional treatment such as physical therapy, corticosteroid injection, or an unloader brace. Although a bone scan may be helpful in this case and confirm arthrosis of the medial compartment, the suspicion of a soft-tissue mass makes MRI the imaging modality of choice.
REFERENCES: Muscolo DL, Ayerza MA, Makino A, et al: Tumors about the knee misdiagnosed as athletic injuries. J Bone Joint Surg Am 2003;85:1209-1214.
Lewis MM, Reilly JF: Sports tumors. Am J Sports Med 1987;15:362-365.
Question 34
A 35-year-old woman undergoes an L4-5 anterior fusion via a left retroperitoneal approach. Postoperative examination reveals that her right foot is cool and pale. Her neurologic examination is normal, and her pedal pulses are asymmetric. What is the most likely reason for the right foot finding?
Explanation
REFERENCES: Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, p1550.
Benzel EC (ed): Spine Surgery Techniques, Complication Avoidance and Management. New York, NY, Churchill Livingstone, 1999, p 190.
Question 35
What is the most frequent late complication of cementless fixation in total knee arthroplasty?
Explanation
REFERENCES: Peters PC, Engh GA, Dwyer KA, Vinh TN: Osteolysis after total knee arthroplasty without cement. J Bone Joint Surg Am 1992;74:864-876.
Parks NL, Engh GA, Topoleski LDT, Emperado J: Modular tibial insert micromotion: A concern with contemporary knee implants. Clin Orthop 1998;356:10-15.
Question 36
Anterior penetration of an iliosacral screw through the sacral ala would most likely lead to weakness of which of the following movements?

Explanation
The referenced study by Routt et al reviewed 177 patients with pelvic ring injuries treated with these screws and found that quality triplanar imaging decreased intraoperative and postoperative complications. They also recommend supplemental fixation of iliosacral screws with posterior plating in noncompliant patients.
Question 37
The injury shown in Figure 24 was most likely caused by what mechanism of injury?
Explanation
REFERENCE: Kellam JF, Mayo K: Pelvic ring disruptions, in Browner BD, Jupiter JB,
Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1,
pp 1052-1108.
Question 38
Osteolysis after total knee arthroplasty can be minimized through prosthetic design features such as
Explanation
REFERENCE: O’Rourke M, Callaghan J, Goetz D, Sullivan P, Johnson R: Osteolysis associated with a cemented modular posterior cruciate substituting total knee design. J Bone Joint Surgery Am 2002;84:1362-1371.
Question 39
A patient with degenerative osteoarthritis of the sternoclavicular (SC) joint reports constant pain, discomfort, and marked prominence and instability of the SC joint following medial clavicle resection. Which of the following procedures is most likely to produce these signs and symptoms?
Explanation
REFERENCES: Bremner RA: Nonarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 583-586.
Question 40
A 25-year-old woman has significant pain and swelling in her left ankle after falling off her bicycle. Examination reveals that she is neurovascularly intact. Radiographs are shown in Figures 33a through 33c. What is the next most appropriate step in management?
Explanation
REFERENCES: Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Harper MC: Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int 2001;22:15-18.
Question 41
What is the recommended insertion torque for halo pins in adults?
Explanation
REFERENCES: Botte MJ, Byrne TP, Garfin SR: Application of the halo device for immobilization of the cervical spine utilizing an increased torque pressure. J Bone Joint Surg Am 1987;69:750-752.
Garfin SR, Lee TO, Roux RD, et al: Structural behavior of the halo orthosis pin-bone interface: Biomechanical evaluation of standard and newly designed stainless steel halo fixation pins. Spine 1986;11:977-981.
Vaccaro AR, Botte MD, Bengt IL, et al: Cervical orthotics including traction and halo devices, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 113-140.
Question 42
A 45-year-old man seen in the emergency department reports a 1-week history of worsening low back pain and a progressive neurologic deficit in the S1 distribution. Examination reveals 2/5 strength in the gastrocnemius. Laboratory studies show a WBC count of 13,500/mm 3 and an erythrocyte sedimentation rate of 74 mm/h. Radiographs of the lumbosacral spine show narrowing of the L5-S1 disk space, with irregularity of the end plates. A sagittal T 2 -weighted MRI scan is shown in Figure 8. Definitive management should consist of
Explanation
REFERENCES: Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 165-189.
Modic MT, Feiglin DH, Piraino DW, et al: Vertebral osteomyelitis: Assessment using MR. Radiology 1985;157;157-166.
Question 43
A 40-year-old female recreational basketball player notes pain deep within her shoulder that occurs with activity. Pain began insidiously 6 months previously. She has completed a physical therapy program, and an intra-articular corticosteroid injection provided excellent temporary relief. Physical examination shows symmetric range of motion of her shoulder. She has a positive O'Brien’s active compression test. There is no pain with cross-arm adduction or tenderness to palpation over the acromioclavicular joint. Resisted abduction is nonpainful and strong. MRI shows increased signal in the substance of the superior labrum, low-grade bursal surface fraying of the supraspinatus, and mild degenerative changes within the acromioclavicular joint. What is the best treatment option?
Explanation
Question 44
What muscles are responsible for the most common deformity after antegrade intramedullary nailing for a subtrochanteric femur fracture?

Explanation
The reference by French et al is a review on 45 patients with subtrochanteric fractures treated with cephalomedullary interlocked nailing. Based on femoral neck-shaft angle, 61% of the fractures were reduced in at least 5º varus. The authors attributed this malalignment to failure to counteract muscle forces acting on the proximal fragment, combined with the adducted position of the distal femur during portal creation.
The reference by Ricci et al is a report of 403 femoral shaft fractures treated with intramedullary nailing. Patients with proximal femoral shaft fractures were found to have the highest incidence of malalignment. The most common deformity in this group was varus, followed by procurvatum (or flexion).
Question 45
-Where is the physis with the highest growth rate (in mm per year) located?
Explanation

Question 46
A 40-year-old woman has local back pain and intense burning pain in her perianal region after being shot twice in the back. Motor and sensory examination of her lower extremities reveals no apparent deficit. She has present but decreased sensation in her perianal region, an intact anal wink, good rectal tone, and an intact bulbocavernosus reflex. Radiographs and CT scans are shown in Figures 3a through 3d. What is the next most appropriate step in management?
Explanation
REFERENCES: Bracken MB, Shepard MJ, Holford TR: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury. JAMA 1997;277:1597-1604.
Waters RL, Adkins RH: The effects of removal of bullet fragments retained in the spinal canal: A collaborative study by the National Spinal Cord Injury Model Systems. Spine
1991;16:934-939.
Stauffer ES, Wood RW, Kelly EG: Gunshot wounds of the spine: The effects of laminectomy.
J Bone Joint Surg Am 1979;61:389-392.
Question 47
A 35-year-old woman began to train for a half marathon. After 8 weeks of increasing her mileage, what changes can you expect in her Achilles tendon?
Explanation
Question 48
Figure 32 shows the radiograph of a laborer who jammed his thumb in a fall. Examination reveals pain at the base of the thumb and proximal thenar eminence region. Management should consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
Howard FM: Fracture of the basal joint of the thumb. Clin Orthop 1987;220:46-51.
Question 49
A 54-year man has left shoulder pain and weakness after falling while skiing 4 months ago. Examination reveals full range of motion passively, but he has a positive abdominal compression test and weakness with the lift-off test. External rotation strength with the arm at the side and strength with the arm abducted and internally rotated are normal. MRI scans are shown in Figures 1a and 1b. Treatment should consist of
Explanation
REFERENCES: Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 31-56.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon: Results of operative treatment. J Bone Joint Surg Am 1996;78:1015-1023.
Question 50
A 22-year-old competitive volleyball player has shoulder pain, and rest and a cortisone injection have failed to provide relief. Examination reveals atrophy along the posterior scapula, but an MRI scan does not reveal a rotator cuff tear or labral cyst. What is the most likely cause for the shoulder weakness?
Explanation
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990;6:301-305.
Question 51
A 43-year-old man sustained a closed, intra-articular pilon fracture. It has now been 1 year since he underwent open reduction and internal fixation. Which of the following statements most accurately describes his perceived outcome? Review Topic
Explanation
Question 52
A 44-year-old man sustains the injury shown in Figures 1 through 3. What is the most appropriate treatment?

Explanation
Reduction, either open or closed, with internal fixation (pinning) is the recommended treatment for the majority of these injuries. Closed reduction with pinning is most often performed for acute injuries. Open reduction with pinning is performed for those injuries that cannot be reduced by closed means or those with a delayed presentation. Four cases of successful closed reduction and splinting, all performed upon presentation in the emergency department, have been described by Storken and associates, but the authors note that their review of three prior reports uncovered cases of secondary dislocation, which required surgical stabilization. One of the dislocations occurred 4 months after the reduction. They assert that an indication for primary ORIF is a CMC dislocation associated with major fractures. Primary arthrodesis can be considered in cases with severe intra-articular comminution, but this procedure substantially limits the ability of the hand to increase and decrease the transverse metacarpal arch, which is an important functional movement. It can also lead to osteoarthritis of the triquetrohamate joint. Suspension arthroplasty has been described for old fracture-dislocations of the fifth CMC joint, using a partial slip of the extensor carpi ulnaris.








Question 53
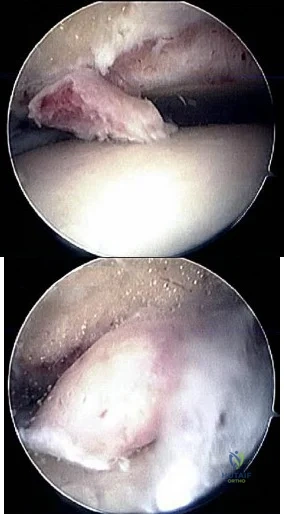
40A B Figures 40a and 40b are this patient's intraoperative arthroscopic images. The abnormality seen here illustrates which of the patient's clinical findings?
Explanation
Ankle sprains are the most common musculoskeletal injury; however, most of these sprains do not progress to chronic instability. Initial injuries are treated with RICE (rest, ice, compression, elevation), range of motion, weight bearing
as tolerated, and proprioceptive therapy. Lace-up ankle braces are most effective during the subacute period after a sprain. Structured physical therapy focused on proprioception is recommended for 6 weeks. Examination findings for ankle ligament instability are unreliable because of associated subtalar joint motion. Casting is not as effective as functional rehabilitation. Stress radiographs are recommended, but a clear pathologic range of measurements is not defined. Generalized ligament laxity can result in false-positive findings of instability; therefore, contralateral stress radiographs are often necessary for comparison. The difference in anterior drawer measurement between both ankles should not exceed 5mm. Likewise, the difference in talar tilt measurement between both ankles should be 5 or fewer degrees. Patients with mechanical symptoms, a joint effusion, or continued pain may have an intra-articular pathology such as a loose body or osteochondral lesion. Ankle instability can exist without ligamentous laxity. Symptoms of chronic instability can result from osteochondral lesions of talus, peroneal tendon pathology, loose bodies, anterior ankle impingement, and fracture nonunions. Although there is not sufficient evidence to recommend arthroscopy prior to all ligament reconstructions, arthroscopy is recommended when other pathology is suspected.
RECOMMENDED READINGS
Colville MR. Surgical treatment of the unstable ankle. J Am Acad Orthop Surg. 1998 Nov-Dec;6(6):368-77. Review. PubMed PMID: 9826420. View Abstract at PubMed
DiGiovanni CW, Brodsky A. Current concepts: lateral ankle instability. Foot Ankle Int. 2006 Oct;27(10):854-66. Review. PubMed PMID: 17054892. View Abstract at PubMed
Maffulli N, Ferran NA. Management of acute and chronic ankle instability. J Am Acad Orthop Surg. 2008 Oct;16(10):608-15. Review. PubMed PMID: 18832604. View Abstract at PubMed
Question 54
A 47-year-old woman has had a 1-month history of left hip and medial thigh pain that is exacerbated by sitting. Laboratory studies show a total protein level of 8.2 g/dL (normal 6.0 to 8.0) and an immunoglobulin G (IGG) level of 2,130 mg/dL (normal 562 to 1,835). A radiograph, CT scan, and biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 16.
Question 55
When performing surgery on a patient with insertional Achilles tendinitis and a Haglund’s deformity, how much of the Achilles tendon insertion can be safely detached without having to consider reattachment with bone anchors?
Explanation
REFERENCES: Kolodziej P, Glisson RR, Nunley JA: Risk of avulsion of the Achilles tendon after partial excision for treatment of insertional tendinitis and Haglund’s deformity: A biomechanical study. Foot Ankle Int 1999;20:433-437.
Sammarco GJ, Taylor AL: Operative management of Haglund’s deformity in the nonathlete: A retrospective study. Foot Ankle Int 1998;19:724-729.
Question 56
A 48-year-old ski instructor dislocates his nondominant shoulder in a fall. Management consisting of application of a sling for 1 week results in improvement in his pain. Follow-up examination 6 weeks after the injury reveals that the patient continues to have difficulty with shoulder elevation. Management should now include
Explanation
REFERENCES: Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Matsen FA III, Thomas SC, Rockwood CA: Anterior glenohumeral instability, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 526-622.
Question 57
- A patient undergoes an acute repair of a laceration of the median nerve in the antecubital fossa. A lack of functional recovery 6 months later is most likely due to
Explanation
Functional recovery is generally complete after a crush injury because the basement membrane and endoneurium are left intact, and the damaged axons can regenerate within their original endoneurial tubes and reinnervate their original target organ. After a complete lesion to the nerve, however, functional recovery of movement is often quite poor. The loss of functional recovery probably is related to the failure of the axons to regenerate and the misdirection of regenerating axons, which leads to inappropriate innervation of denervated muscles. Inappropriate innervation is thought to result in a loss in the ability to accurately recruit individual muscles and motor units within a muscle, resulting in the loss of motor control.
Question 58
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement?
Explanation
REFERENCES: Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Werner CM, Steinmann PA, Gilbart M, et al: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 59
A 13-year-old baseball pitcher presents with worsening medial-sided elbow pain. He pitches 7 months out of the year, throws 85 pitches per game and plays in two games per week. His fastball speed is approximately 75mph. He regularly plays outfield once he has been relieved of pitching. Which of the following is most likely contributing to his elbow pain? Review Topic
Explanation
Little League elbow is a medial-sided overuse injury that occurs in the skeletally immature athlete. During execution of the baseball pitch, tremendous valgus and extension stresses occur at the elbow. Repetitive microtrauma can ultimately injure the medial epicondyle apophysis, ulnar collateral ligament or the flexor-pronator muscle mass. Limiting the number of pitches and innings played per game, as well as the number of months of competitive pitching per year, has been recommended to prevent these overuse injuries in the young athlete.
Olsen et al performed a case control study to determine risk factors associated with the development of shoulder and elbow injuries in adolescent baseball pitchers. Greater than 8 months of competitive pitching per year, more than 80 pitches per game and a fastball speed of greater than 85mph were all associated with increased risk of injury. Continued pitching despite arm fatigue and pain, being a starting pitcher, greater number of warm-up pitches, participating in showcases and regular use of NSAIDs were also associated with injury. The type of pitch (fastball, changeups and breaking balls) and continued play in a different position once being relieved was not associated with increased risk of injury.
Andrews et al authored a review article on ulnar collateral ligament injuries in throwing athletes. According to the USA Baseball Medical/Safety Advisory Committee, young baseball pitchers should avoid breaking pitches, such as curveballs and sliders, and avoid year-round baseball. A minimum of 3 months of complete rest from pitching per year is vital. Youth pitching coaches should be educated to ensure proper pitching mechanics are being reinforced.
Illustration A is a table depicting the recommended maximum number of pitches by age group.
Incorrect Answers:
Question 60
Figure 28 shows the postoperative radiograph of a 36-year-old patient. The cerclage cable was placed for a minimal medial calcar fracture seen during femoral preparation. In the immediate postoperative period, what is the highest level of activity that would be safely permitted?
Explanation
REFERENCES: Berend KR, Lombardi AV Jr, Mallory TH, et al: Cerclage wires or cables for the management of intraoperative fracture associated with a cementless, tapered femoral prosthesis: Results at 2 to 16 years. J Arthroplasty 2004;19:17-21.
Schmidt AH, Kyle RF: Periprosthetic fractures of the femur. Orthop Clin North Am 2002;33:143-152.
Greidanus NV, Mitchell PA, Masri BA, et al: Principles of management and results of treating the fractured femur during and after total hip arthroplasty. Instr Course Lect 2003;52:309-322.
Question 61
A transverse humeral shaft fracture that occurs between a stiff arthritic shoulder joint; a stiff, arthritic elbow joint is treated nonsurgically in a hanging-arm cast
Explanation
In 1977, Perren and Cordey penned a German manuscript that first described an interpretation of mechanical influences on tissue differentiation. This became known as the Strain Theory of Perren. In 1980, a second manuscript by the same authors was published in English. Within this manuscript, Perren wrote, "These thoughts about the mechanical influences on tissue differentiation are not intended as conclusive evidence since precise data are still not available, but we hope that they will stimulate thought and provide a basis for discussion." More than 30 years later, these thoughts continue to stimulate discussion and research on cell mechanotransduction. This theory is still being manipulated in surgical theatres all around the world in an attempt to more consistently achieve fracture healing. Strain is a magnitude of deformation. As typically defined, it is the change in dimension of a deformed object during loading divided by its original dimension. This is difficult to work with intraoperatively. The fraction below illustrates a simpler way to regard this concept:
Strain = Magnitude of displacement between fragments during loading / Total resting distance between fragments after stabilization
By remembering that low strain generally leads to bone formation and healing, it is possible to manipulate this fraction intraoperatively to achieve success. When a simple fracture pattern is anatomically reduced and compressed, then the total resting distance between fragments after stabilization approaches 0. This means the numerator must be near 0 to achieve a low-strain environment. This is what occurs in absolute stability (no motion between fracture fragments under physiologic load) and primary bone healing occurs. When a multifragmentary fracture pattern is treated with bridge plating, the total resting distance between fragments after stabilization is a larger number (consider the additive distance between the different fragments). In this case, the numerator can be larger to achieve a low-strain environment. This is what happens in relative stability (controlled motion between fracture fragments under physiologic load). Secondary bone healing occurs. Now consider the third scenario: a simple fracture pattern that is fixed with a small gap. The total resting distance is still a small number. Based on the theory, eliminating motion by creating a stiff construct should lead to healing, but it does not. Creating absolute stability with a gap means that primary bone healing cannot occur (because cutting cones cannot cross the gap) and secondary bone healing cannot occur (because there is not enough motion to induce callus formation). This is where the strain theory breaks down and how many nonunions occur. In the fourth scenario, a high-strain environment is present and commonly leads to a nonunion (as predicted by the theory). The simple fracture pattern is too mobile, and nonfunctional callus often occurs.
RECOMMENDED READINGS
Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br. 2002 Nov;84(8):1093-110. Review. PubMed PMID: 12463652. View Abstract at PubMed
Epari DR, Duda GN, Thompson MS. Mechanobiology of bone healing and regeneration: in vivo models. Proc Inst Mech Eng H. 2010 Dec;224(12):1543-53. Review. PubMed PMID: 21287837.View Abstract at PubMed
Question 62
Which of the following is the strongest contraindication to unicompartmental knee arthroplasty (UKA)?
Explanation
REFERENCES: Lotke PA (ed): Knee Arthroplasty: Master Techniques in Orthopaedic Surgery. New York, NY, Raven Press, 1995, pp 275-293.
Insall JN, Windsor RE, Scott WN, et al (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 805-814.
Tabor OB Jr, Tabor OB: Unicompartmental arthroplasty: A long-term follow-up study.
J Arthroplasty 1998;13:373-379.
Question 63
..Approximately what percentage of the time does an unknown primary cancer get identified as part of a full metastatic work-up that includes radiographs; blood tests; a CT scan of the chest, abdomen and pelvis; whole-body bone scan; and biopsy of the metastatic focus?
Explanation
Figures 20a and 20b are the radiographs of an 83-year-old active, independent, and healthy woman who has experienced 2 months of right lower thigh and knee pain. Her pain increased progressively over the course of several weeks. While exiting a car she “bumped” her knee against the door, felt a “crack,” and developed excruciating pain. She could no longer ambulate and was brought to the hospital.
Question 64
Tendons should have what ratio of matrix protein?
Explanation
Question 65
Figures 1 and 2 are the radiographs of a 35-year-old right-hand-dominant man who has had progressive right wrist pain for 1 year. There is no history of trauma, and he has had no treatment to date. He reports some pain at rest with limited motion and substantial pain with use. He is currently out of work on short-term disability because of this wrist problem. An examination reveals mild dorsal wrist swelling, decrease wrist range of motion, and decreased grip strength. Contralateral wrist examination findings are normal. What is the most appropriate course of treatment?

Explanation
This patient has late-stage Kienböck disease. According to the Lichtman classification for Kienböck disease, this would represent stage IIIB, with lunate collapse/fragmentation, loss of carpal height secondary to proximal capitate migration, and a flexed scaphoid. The lateral radiograph reveals a radioscaphoid angle exceeding 60 degrees, so disease stage is IIIB. According to Condit and associates, when the presurgical radioscaphoid angle exceeds 60 degrees, results are poor when an attempt to maintain the lunate is made. As a result, the procedure with the most predictable outcome is a proximal row carpectomy. A radial-shortening osteotomy could be performed because the ulnar variance is negative. Considering the marked lunate fragmentation and collapse, a vascularized bone graft likely is contraindicated and associated with less predictable results than a proximal row carpectomy. There is no role for supervised hand therapy and splinting in the setting of advanced Kienböck disease. Similarly, there is no role for maintenance of the lunate in the setting of advanced collapse and fragmentation.
Question 66
Figures A and B are radiographic images of an 85-year-old woman with isolated left hip pain. She describes a non-syncopal fall from standing 4 hours ago. Physical examination reveals pain with log-rolling the left thigh and the inability to bear weight on the affected leg. The radiologist reports no fracture in the left hip. What would be the next best step? Review Topic

Explanation
Moderate evidence supports MRI as the advanced imaging of choice for diagnosis of presumed hip fracture not apparent on initial radiographs. MRI has been shown to be able to detect occult fractures earlier than bone scan, with better spatial resolution. Usually the MRI should be obtained in less than 24 hours from the time of injury. For situations in which MRI is not immediately available, bone scan can be considered after 72 hours form the time of injury. However, this may compromise patient care and put the patient at risk of fracture displacement.
Cannon et al. reviewed the imaging of choice in occult hip fracture. They showed that physical examination yields a poor sensitivity identifying occult hip fractures, with log-rolling and straight-leg raise as 50% and 70%, respectively. The most sensitive modality for occult fracture identification was MRI.
Iwata et al. retrospectively reviewed a cohort of 35 patients with clinically suspected fractures of the hip that underwent MRI. All radiographs were negative. In 26 of these patients, a T1-weighted coronal MRI showed a hip fracture with 100% sensitivity.
Roberts et al. reviewed the 2015 AAOS Clinical Practice Guideline: Management of Hip Fractures in the Elderly. They report moderate evidence that supports MRI as the advanced imaging of choice for diagnosis of presumed hip fractures not apparent on initial radiographs.
Figure A is a AP radiograph of the left hip and pelvis. Apart from a healed fracture of the ischiopubic rami and generalized osteopenia, there is no obvious hip fracture. Figure B is a coronal CT image that does not demonstrate evidence of an acute hip fracture. Illustration A is a T1 weighted MR image that shows a non displaced fracture (white arrow) through the intertrochanteric region of the left proximal femur.
Incorrect Answers:
(SBQ12TR.32) A 20-year-old male is taken to the emergency department following a motorcycle collision with the injury seen in Figures A and B. He undergoes serial debridements with placement of an antibiotic bead pouch, followed by intramedullary nailing and free tissue transfer. His preoperative examination is notable for absent plantar sensation. Which of the following is predictive of a worse long term outcome in this patient?

Absent plantar sensation at presentation
Depression at 3 months post-injury
Use of an intramedullary nail
Free tissue transfer instead of rotational flap
Need for multiple debridements
The presence of depression at the 3 months post-injury is a significant predictor of worse long term outcome as well as lower return to work rates in patients that present with limb threatening lower extremity trauma.
The findings of the Lower Extremity Assessment Project (LEAP study) has challenged many of the long-held beliefs of lower extremity trauma surgery, including the concept that patients with absent plantar sensation should undergo immediate amputation . The LEAP study has also brought to light the importance of socioeconomic and psychosocial factors in patient outcomes following these injuries.
Bosse et al analyzed a subgroup of 55 patients from the LEAP study with absent plantar sensation at presentation. Those patients that underwent limb salvage despite absent sensation (n=26) had no significant difference in functional outcome when compared with either insensate patients who underwent amputation or a matched control group of sensate patients with similar injuries. All but one patient in the salvage group had return of some sensation at 2-year follow up and the authors concluded that an insensate plantar foot at presentation should not be included in the algorithm for amputation.
Mackenzie and Bosse reviewed the results of the LEAP study with particular emphasis on the social and economic variables that influence outcomes in severe lower extremity. The authors note that 19% of patients screened positive for severe depression. The presence of anxiety, pain and depression at 3 months post-injury were significant predictors of poor outcome
Incorrect Answers:
tissue for type IIIB tibia fractures. Answer 5: The number of debridements has not been shown to influence outcome.
Question 67
A 68-year-old woman with metastatic breast carcinoma is seen in the emergency department. She appears lethargic, and she reports abdominal pain, nausea, and constipation. An EKG reveals a shortened QT interval. The only physical finding on examination is diffuse hyporeflexia. What is the most appropriate step in management?
Explanation
REFERENCE: Stewart AF: Clinical practice: Hypercalcemia associated with cancer. N Engl J of Med 2005;352:373-379.
Question 68
A patient with a previously pain-free knee replacement now reports a sudden inability to ambulate. Radiographs of the knee are shown in Figures 33a and 33b. Management should consist of
Explanation
REFERENCES: Insall J, Salvati E: Patella position in the normal knee joint. Radiology 1971;101:101-104.
Lynch AF, Rorabeck CH, Bourne RB: Extensor mechanism complications following total knee arthroplasty. J Arthroplasty 1987;2:135-140.
Rand JA, Morrey BF, Bryan RS: Patellar tendon rupture after total knee arthroplasty. Clin Orthop 1989;244:233-238.
Question 69
Figure 31 shows the radiograph of a 64-year-old woman who is seen in the emergency department following a motor vehicle accident. She has no voluntary motor function in her distal upper extremities or lower extremities. She does not have a bulbocavernosus reflex. She has a blood pressure of 80/50 mm Hg with a pulse of 50/min. Her hypotension does not improve with initial fluid resuscitation. Further treatment of her hypotension should consist of
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 179-187.
Nockels RP: Nonoperative management of acute spinal cord injury. Spine 2001;26:S31-S37.
Question 70
A 14-year-old boy reports a 4-month history of increasing backache with difficulty walking long distances. His parents state that he walks with his knees slightly flexed and is unable to bend forward and get his hands to his knees. He denies numbness, tingling, and weakness in his legs and denies loss of bladder and bowel control. A lateral radiograph of the lumbosacral spine is shown in Figure 18. What is the best surgical management for this condition?
Explanation
L5 to S1 usually is not successful for a slip that is greater than 50%. Isolated anterior spinal fusion has not been successful, and direct repair of the pars defect is only useful for spondylolysis without spondylolisthesis.
REFERENCES: Lenke LG, Bridwell KH: Evaluation and surgical treatment of high-grade isthmic dysplastic spondylolisthesis. Instr Course Lect 2003;52:525-532.
Ginsburg GM, Bassett GS: Back pain in children and adolescents: Evaluation and differential diagnosis. J Am Acad Orthop Surg 1997:5:67-78.
Question 71
A right-handed 24-year-old professional baseball player injured his left shoulder 6 weeks ago when he dove forward and landed hard with the arm extended. He reports that the shoulder “slipped out” and “went back in.” The shoulder did not need to be reduced. He now reports deep pain in the front of the shoulder when batting on either side and is hesitant to raise his left arm up over his head to catch a ball. Examination reveals no obvious deformities of the shoulder and a somewhat guarded, limited range of motion in all planes. Provocative tests for the rotator cuff and labrum are equivocal. MRI scans are shown in Figures 16a and 16b. What is the best course of action?
Explanation
REFERENCES: Abrams JS, Savoie FH III, Tauro JC, et al: Recent advances in the evaluation and treatment of shoulder instability: Anterior, posterior and multidirectional. Arthroscopy 2002;18:1-13.
DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.
Question 72
Figures 1 through 5 show the radiographs obtained from a 37-year-old man who has a 10-year history of right, ulnar-sided wrist pain and a volar ulnar prominence with wrist supination. Approximately 20 years ago, he had a forearm injury that was definitively treated in a long arm cast. What surgical treatment option is most likely to improve his symptoms and maintain pronosupination?

Explanation
The patient sustained a radial shaft fracture with subsequent apex volar malunion. As a result, his distal ulna subluxates volarly with wrist supination. Radiographs of the wrist reveal minimal arthritic changes. The most appropriate treatment option is to surgically correct his radial shaft malunion, which would indirectly address his DRUJ instability. A DRUJ ligament reconstruction or triangular fibrocartilage complex repair could be used to augment DRUJ stability; however, they might be unnecessary after correction of the radial shaft malunion. A DRUJ ligament reconstruction alone would not achieve stability of the DRUJ joint and maintain full wrist pronosupination. An ulnar head implant arthroplasty would not be reliable in eliminating the instability or the pain. Similarly, a one-bone forearm procedure might
improve the patient's pain and instability but at the cost of abnormal wrist and forearm mechanics and kinematics.
Question 73
The parents of a previously healthy 3-year-old child report that she refused to walk on awakening. Examination later in the day reveals that the patient can walk but with a noticeable limp. She has a temperature of 99.5 degrees F (37.5 degrees C). Range of motion measurements are shown in Figure 50. An AP pelvis radiograph is normal. Laboratory studies show a WBC count of 9,000/mm 3 and an erythrocyte sedimentation rate of 10 mm/h. Management should consist of
Explanation
REFERENCES: Del Beccaro MA, Champoux AN, Bockers T, Mendelman PM: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Annals Emerg Med 1992;21:1418-1422.
Kehl DK: Developmental coxa vara, transient synovitis, and idiopathic chondrolysis of the hip, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1035-1058.
Question 74
A patient reports changes in vocal quality after undergoing a right-sided anterior cervical approach to C6. Which of the following nerves has most likely been injured?
Explanation
Question 75
A 47-year-old man who is an avid tennis player and laborer has had one year of shoulder pain and weakness. His pain occurs at night and radiates to the deltoid laterally. The patient denies any anterior based pain. He reports no prior surgeries and has been managed with steroid injections and physical therapy. On examination, he has full passive motion with significant weakness with external rotation. His neurologic examination is unremarkable. MRI evaluation reveals a posterior-superior rotator cuff tear with Goutallier grade 4 fatty infiltrate in the supraspinatus and infraspinatus with retraction beyond the glenoid. He is concerned about the lack of rotation of his arm and reports that this disability creates significant disability with his occupation as a mason. What is the best next step?
Explanation
Question 76
A 16-year-old girl has had hip pain for 1 year. Approximately 2 months ago she noted the development of a hard mass in the right buttock that has steadily increased in size. She now reports severe pain in the right buttock, with radiation down the leg and numbness involving the right foot and toes. A radiograph is shown in Figure 70a and an axial postcontrast T 1 -weighted MRI scan is shown in Figure 70b. A biopsy specimen is shown in Figure 70c. The chest CT shows multiple lung metastases. Treatment of this lesion should consist of
Explanation
REFERENCES: Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Thacker MM, Temple HT, Scully SP: Current treatment for Ewing’s sarcoma. Expert Rev Anticancer Ther 2005;5:319-331.
Weber KL: Current concepts in the treatment of Ewing’s sarcoma. Expert Rev Anticancer Ther 2002;2:687-694.
Question 77
2010 Pediatric Orthopaedic Examination Answer Book • 9 A 9-year-old girl has had bilateral knee and leg pain for the past 2 years. The family has noted increasing deformity in both lower extremities. She is less than the fifth percentile for height. Examination reveals bilateral femoral bowing, mild medial-lateral laxity of the knees, and the deformities shown in the radiograph seen in Figure 3. What is the most likely diagnosis?
Explanation
There is an asymmetry of the deformities that makes diastrophic dysplasia less likely.
REFERENCES: Goldberg MJ, Yassir W, Sadeghi-Nejad A: Clinical analysis of short stature. J Pediatr Orthop 2002;22:690-696.
Parmar VS, Stanitski DF, Stanitski CL: Interpretation of radiographs in a pediatric limb deformity practice: Do
radiologists contribute? J Pediatr Orthop 1999;19:732-734. Question 4
Patients with slipped capital femoral epiphysis are more likely to experience a delay in definitive diagnosis if they initially present to a physician reporting which of the following problems?
L Limp
Hip pain
Knee pain
Proximal thigh pain
Buttock pain
DISCUSSION: A delay in diagnosis of slipped capital femoral epiphysis (SCFE) can lead to significant worsening of the deformity or even progression from a stable to an unstable SCFE. Those patients that report knee pain as their primary complaint are most likely to experience significant delay. Other variables associated with this delay include Medicaid insurance and stable SCFE.
REFERENCES: Kocher MS, Bishop JA, Weed B, et al: Delay in diagnosis of slipped capital femoral epiphysis.
AL-Madena Copy
10 • American Academy of Orthopaedic Surgeons
Pediatrics 2004;113:e322-e325.
Rahme D, Comley A, Foster B, et al: Consequences of diagnostic delays in slipped capital femoral epiphysis. J Pediatr Orthop B 2006;15:93-97.
Question 78
All of the following are advantages of supine over lateral positioning during intramedullary nailing of subtrochanteric femur fractures EXCEPT:

Explanation
Advantages of the supine position include: may help protect a potentially unstable spine, facilitates access to sites other than the injured femur, shorter setup time, rotational and angulatory deformities may be more easily appreciated. Disadvantages of the supine position include: starting point localization may be more difficult.
Question 79
Figures 1 and 2 are the AP and lateral radiographs of a 32-year-old man 10 years after anterior cruciate ligament (ACL) reconstruction. The patient now has worsening medial knee pain and a failed ACL with instability. What is the best surgical option?

Explanation
Question 80
Figures 100a and 100b are the MRI scans of a 45-year-old man who has had elbow and proximal forearm pain for the past 8 months. He can recall no specific trauma and symptoms have not lessened despite his adopting job modifications that limit lifting. He has discomfort with resisted elbow extension and pronation. The biceps tendon can be easily palpated. Treatment should consist of which of the following? Review Topic
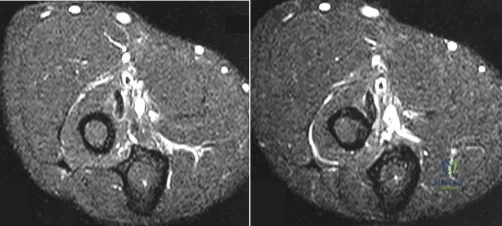
Explanation
physical therapy, and modality, surgical treatment is indicated. Exploration, debridement, and reattachment with one of a variety of techniques are the standards of care. No lipomatous mass is seen on the MRI scan. There is no weakness in finger extension to suggest posterior interosseous nerve palsy. Transfer of the biceps would result in loss of supination strength. Endoscopic biceps tendon surgery is reserved for long-head pathology.
Question 81
What is the most important feature in choosing an outcome instrument to assess shoulder disorders?
Explanation
REFERENCES: Leggin BG, Iannotti JP: Shoulder outcome measurement, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, p 1027.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 47-55.
Question 82
Deep posterior compartment
Explanation
The structures at risk are the anterior tibial artery and deep peroneal nerve in the anterior compartment, superficial peroneal nerve in the lateral compartment, sural nerve in the superficial posterior compartment, and posterior tibial nerve and posterior tibial and peroneal arteries and veins in the deep posterior compartment.
Question 83
What is the most common complication of halo vest immobilization in adults?
Explanation
REFERENCES: Baum JA, Hanley EN Jr, Pullekines J: Comparison of halo complications in adults and children. Spine 1989;14:251-252.
Garfin SR, Botte MJ, Waters RL, Nickel VL: Complications in the use of the halo fixation device. J Bone Joint Surg Am 1986;68:320-325.
Nemeth JA, Mattingly LG: Six-pin halo fixation and the resulting prevalence of pin-site complications. J Bone Joint Surg Am 2001;83:377-382.
Question 84
A 17-year-old male football player is seen 1 week after developing symptoms of infectious mononucleosis in the middle of the season. Examination reveals evidence of splenomegaly. He and his parents want to know if he can play in a game the following day. What is the most appropriate recommendation? Review Topic
Explanation
Question 85
Which of the following is most frequently associated with heterotopic ossification about the shoulder?
Explanation
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, p 291.
Neer CS: Displaced proximal humerus fractures: Part II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
Question 86
- A 15-year-old girl has a thoracic kyphosis that causes mild pain. Examination reveals a sagittal curve measuring 55 degrees and wedging of the eighth through tenth vertebrae. The iliac apophyses are Risser 4. Management should include
Explanation
(2) with surgical fusion if >75o and Risser 3 or less, (3) with surgical fusion if >65o and Risser 4/5 if necessary or symptomatic. Posterior instrumentation, anterior release and interbody fusion is the treatment of choice for curves >75o, or those >55o on hyperextension. Other causes of kyphosis include trauma, infection, spondylitis, bone dysplasia, neoplasia, neurofibromatosis.
Question 87
Hip pain of 1-month duration has developed in a 72-year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. What is this patient's prognosis for infection resolution?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin- resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was
21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 88
repair of the rotator cuff
Explanation
Question 89
Figure 29 shows the radiograph of a 25-year-old woman who has had a 3-month history of ankle pain after sustaining an inversion injury to the ankle. She reports occasional catching, but no sense of instability. Examination reveals ligament stability. Management should consist of
Explanation
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
Pettine KA, Morrey BF: Osteochondral fractures of the talus: A long-term follow-up. J Bone Joint Surg Br 1987;69:89-92.
Question 90
-In the shoulder position of 90-degree forward flexion and internal rotation, what is the most important static stabilizer of the glenohumeral joint?
Explanation
A 17-year-old high school wrestler sustains an abrasion over the posterior aspect of his right elbow during a match. During the next few days the abrasion becomes erythematous and he is placed on oral cephalexin 500 mg four times per day. The erythema extends proximally despite the antibiotic regimen. The patient is afebrile, there is no fluid collection associated with the lesion, and his elbow joint is not involved.
Question 91
Figure 21 is the radiograph of a 45-year-old woman who was severely injured in a motorcycle crash. Her injuries include a traumatic subarachnoid hemorrhage, bilateral pneumothoraces with pulmonary contusions and flail chest, fracture-dislocation of the left hip, and open fractures of the right distal femur and proximal tibia. Antibiotics and tetanus are administered in the emergency department. The patient is intubated and bilateral chest tubes are placed. A closed reduction is performed on the left hip. After appropriate resuscitation, what is the most appropriate initial management of the right knee injury?

Explanation
Question 92
- A 10-year-old boy twisted his ankle while skateboarding and has pain and swelling around the lateral ankle just distal to the fibula. Radiographs are obtained and a lesion is identified in the distal tibia as seen in Figures 273a and 273b. Two weeks later he has no pain to palpation in the region and denies antecedent pain. What is the most appropriate treatment for this lesion?

Explanation

Question.1 .A 49-year-old weekend athlete has a 4-week history of pain in his unilateral plantar heel that is most severe for the first 20 steps upon arising in the morning. He has an area of maximal tenderness on the plantar medial aspect of the heel pad at the origin of the plantar fascia. He has only improved 30% after a 3-week course of physical therapy with toe intrinsic muscle strengthening and arch- and tendo-Achilles stretching. What is the best next treatment step?
Release the plantar fascia.
Inject the plantar fascia with platelet-rich plasma.
Prescribe a night splint and continue physical therapy.
Administer extracorporeal shockwave therapy to the heel.
Perform a series of 3 steroid injections into the plantar fascia.

Question.2 .Figures 16a and 16b are the radiographs of a 38-year-old carpenter with progressively worsening ankle pain; 14 years ago, he was involved in an all-terrain vehicle collision. Anti-inflammatory medication,corticosteroid injections, and bracing no longer effectively control his pain. The pain now interferes with his work and family responsibilities. Examination reveals an antalgic limp, varus deformity, limited ankle motion, limited eversion, and normal strength. Treatment should now consist of

ankle arthrodesis.
total ankle arthroplasty.
distal tibia osteotomy.
lateral ligament repair.
deltoid ligament release.
Question. 3 .A 48-year-old woman had total knee arthroplasty. She is unable to “lift her toes or ankle to her nose.”After 2 months of physical therapy, she has a slapping gait. What is the best next treatment step?
Ankle fusion
Ankle-foot orthosis
Sural nerve graft
Medial heel post
Laminectomy of L4/5
Question. 4 .Figures 46a through 46c are the CT scans of an 18-year-old who sustained an injury 3 weeks ago and now has ankle pain. Examination reveals an ankle effusion and painful range of motion. Recommended treatment should consist of
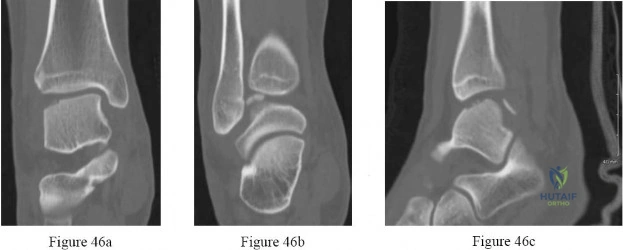
transtalar drilling.
fixation of the fragment.
osteochondral autograft.
weight bearing in a boot with early range of motion.
cast immobilization and nonweight-bearing activity for 6 weeks.
Question. 5 .A 47-year-old woman has a closed, displaced, Weber C bimalleolar ankle fracture. Past medical history includes diabetes mellitus for 7 years controlled with diet and an oral hypoglycemic agent. Semmes-Weinstein sensory testing reveals absence of sensation to the 5.07/10-gm monofilament on the plantar aspect of both feet. The skin is intact with 2+ pedal pulses. Treatment should include
open reduction with limited internal fixation.
closed reduction and application of an external fixator.
closed reduction and total contact cast immobilization.
retrograde intramedullary rod fixation with ankle fusion.
internal fixation and an extended period of immobilization.

Question. 6 .Figures 68a and 68b are the clinical photographs of a 55-year-old woman who had a right hindfoot fusion 3 years ago for a pes planovalgus deformity. Since the surgery, she has had lateral hindfoot pain and places most of the weight-bearing load on the lateral border of her foot when walking. What is the most likely cause of her symptoms?

Deltoid insufficiency
Excessive forefoot abduction
Residual heel valgus
Residual Achilles tendon contracture
Malposition of the transverse tarsal joint
Question 93
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
Explanation
REFERENCES: Waters PM, Mih AD: Fractures of the distal radius and ulna, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, p 361.
Paley D, McMurtry RY: Median nerve compression by volarly displaced fragments of the distal radius. Clin Orthop Relat Res 1987;215:139-147.
Question 94
A 27-year-old man has had pain in the right index finger for the past 9 months. The pain is completely relieved with ibuprofen. An AP radiograph and CT scan are shown in Figures 80a and 80b. What is the most likely diagnosis?
Explanation
radiolucent nidus. A small area of calcification may be present within the center of the nidus. The radiolucent nidus is surrounded by a thick rim of sclerotic bone. These diagnostic
features are frequently better seen on CT. An increase in cyclooxygenase activity has been demonstrated within osteoid osteomas, which may explain why aspirin and other nonsteroidal anti-inflammatory drugs classically relieve the pain associated with these lesions.
REFERENCES: Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 121-130.
Question 95
A 23-year-old man reports pain on the superior aspect of his right shoulder with repetitive overhead activities and when lying on his right side. Figure 29 shows an axial MRI scan. What is the most likely diagnosis based on the MRI findings? Review Topic
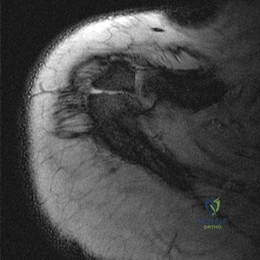
Explanation
Question 96
A patient with a grade 2 L5-S1 isthmic spondylolisthesis reports low back pain and bilateral lower extremity pain. Nonsurgical management has failed to provide relief, and the patient is now a candidate for surgical intervention. The
Explanation
Question 97
Figure 41 shows the MRI scan of a 38-year-old weightlifter. What does the arrow on the MRI scan indicate? Review Topic
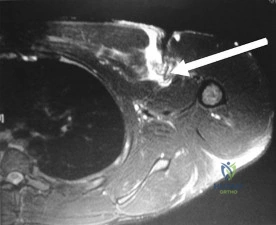
Explanation
Question 98
A 37-year-old racquet player had dominant shoulder pain for 1 year, and cortisone injections provided only temporary relief. Because MRI findings did not reveal a rotator cuff tear, he underwent arthroscopic treatment including subacromial decompression and spur removal below the distal clavicle. Three years following surgery, he now reports that the pain has returned. What is the most likely cause of his pain?
Explanation
REFERENCES: Fischer BW, Gross RM, McCarthy JA: Incidence of acromioclavicular joint complications after arthroscopic subacromial decompression. Arthroscopy 1999;15:241-248.
Hazel RM, Tasto JP, Klassen J: Arthroscopic subacromial decompression: A 9-year follow-up. Arthroscopy 1998;14:419.
Barber FA: Coplaning of the acromioclavicular joint. Arthroscopy 2001;17:913-917.
Question 99
-Which gene mutation is associated with the condition shown in Figures a and b?

Explanation

Question 100
Figure 24 shows the radiograph of a 10-year-old boy who sustained a valgus injury to the knee. Examination reveals grade III medial laxity. Initial management should consist of
Explanation
REFERENCES: DeLee JC: Ligamentous injury of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994,
vol 3, pp 406-432.
Clanton TO, DeLee JC, Sanders B, Neidre A: Knee ligament injuries in children. J Bone Joint Surg Am 1979;61:1195-1201.
Torg JS, Pavlov H, Morris VB: Salter-Harris type III fracture of the medial femoral condyle occurring in the adolescent athlete. J Bone Joint Surg Am 1981;63:586-591.
