Orthopedic Board Exam MCQs: Arthroplasty, Sports Medicine & Trauma | Part 192

Key Takeaway
This page presents Part 192 of a comprehensive orthopedic board review series by Dr. Mohammed Hutaif. It features 100 verified, high-yield MCQs in OITE/AAOS exam format, covering Arthroplasty and Trauma. Designed for orthopedic residents and surgeons, it provides interactive study and exam modes to master your board certification.
About This Board Review Set
This is Part 192 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 192
This module focuses heavily on: Arthroplasty, Elbow, Knee, Ligament, Nerve, Revision, Trauma.
Sample Questions from This Set
Sample Question 1: The knee arthroplasty type associated with the highest 5-year revision rate is...
Sample Question 2: CLINICAL SITUATIONFigures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled bli...
Sample Question 3: A professional pitcher reports pain localized to the medial aspect of his throwing elbow. History reveals that he was pitching in a playoff game and heard and felt a pop in his elbow. MRI reveals a complete ulnar-sided avulsion of the media...
Sample Question 4: A 10-year-old boy tripped as he was running down a hill, felt a painful pop in his right knee, and was unable to bear weight on the involved lower extremity. Examination reveals a tense effusion and an extensor lag of the right knee. Figure...
Sample Question 5: A 16-year-old boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals a large, deeply fixed, soft-tissue mass in the thigh. Laboratory results show an elevated erythrocyte sedimentation rate ...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The knee arthroplasty type associated with the highest 5-year revision rate is
Explanation
Revision rates for UKA at 10 years are lower than 5% at specialty centers. However, the 10-year revision rate associated with UKA in registries such as the National Joint Registry for England and Wales is 2 to 3 times that of TKA. Among partial knee replacements, patellofemoral arthroplasty is associated with the highest revision rate at every time interval.

CLINICAL SITUATION QUESTIONS 167 THROUGH 169
Figures 167a and 167b are the radiographs of a middle-age man. He is a noncompliant patient who has severe insulin-dependent diabetes and a below-knee amputation on the right side. He is usually in a wheelchair, does not use a prosthesis, transfers using a walker, and resides in an institution. He had an infection in the left leg years ago, which was treated successfully with intravenous antibiotics (the details are unknown). His left knee is mildly painful, swollen but not warm, has limited range of motion (40-140 degrees), and is grossly unstable.
Question 2
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. Initial surgical management should consist of

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but
typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Question 3
A professional pitcher reports pain localized to the medial aspect of his throwing elbow. History reveals that he was pitching in a playoff game and heard and felt a pop in his elbow. MRI reveals a complete ulnar-sided avulsion of the medial collateral ligament (MCL). Examination reveals valgus instability and ulnar nerve involvement. What recommendations should be made based on the patient’s desire to return to sport?
Explanation
REFERENCES: Miller MD, Cooper DE, Warner JJP (eds): Review of Sports Medicine and Arthroscopy. Philadelphia, PA, WB Saunders, 1995, p 230.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, p 227.
Altchek DW, Andrews JR (eds): The Athlete’s Elbow. Philadelphia, PA, Lippincott Williams
& Wilkins, 2001, p 91.
Question 4
A 10-year-old boy tripped as he was running down a hill, felt a painful pop in his right knee, and was unable to bear weight on the involved lower extremity. Examination reveals a tense effusion and an extensor lag of the right knee. Figures 36a and 36b show AP and lateral radiographs. Management should consist of
Explanation
The distal fragment can be much larger than it appears on the radiographs because it consists largely of cartilage.
REFERENCES: Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Grogan DP, Carey TP, Leffers D, et al: Avulsion fractures of the patella. J Pediatr Orthop 1990; 10:721 - 730. Question 37
When addressing a proximal intertrochanteric or subtrochanteric fracture in a juvenile with open growth plates, the arterial supply from what artery at the neck must be preserved?
Lateral femoral circumflex
Medial femoral circumflex
Superior gluteal
Inferior gluteal
Obturator
DISCUSSION: The medial femoral circumflex artery supplies blood to the femoral head. Its position along the posterior-superior femoral neck places this structure at risk with intramedullary nailing of the femur. Therefore, lateral entry through the greater trochanter is preferred when intramedullary fixation is performed.
REFERENCES: Gordon JE, Swenning TA, Burd TA, et al: Proximal femoral radiographic changes after lateral transtrochanteric intramedullary nail placement in children. J Bone Joint Surg Am 2003;85:1295- 1301.
Green NE, Swiontkowski MF: Skeletal Trauma in Children, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 419-424.
Question 5
A 16-year-old boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals a large, deeply fixed, soft-tissue mass in the thigh. Laboratory results show an elevated erythrocyte sedimentation rate (ESR) and leukocytosis. A plain radiograph and MRI scan are shown in Figures 1a and 1b. Biopsy specimens are shown in Figures 1c and 1d. What is the most likely diagnosis?
Explanation
REFERENCE: Simon MA, Springfield DS, et al: Ewing’s Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 287-297.
Question 6
A 22-year-old right hand-dominant man who fell off his motorcycle onto the tip of his right shoulder 2 weeks ago now reports pain and difficulty raising his right arm. Examination reveals tenderness and gross movement over the lateral scapular spine and severe weakness during resisted abduction. A radiograph and 3D-CT scan are shown in Figures 24a and 24b. What is the next most appropriate step in management?
Explanation
REFERENCES: Ogawa K, Naniwa T: Fractures of the acromion and the lateral scapular spine.
J Shoulder Elbow Surg 1997;6:544-548.
Ada Jr, Miller ME: Scapular fractures: Analysis of 113 cases. Clin Orthop Relat Res 1991;269:174-180.
Question 7
A 10-year-old girl sustained a Gartland type III supracondylar fracture after falling off a trampoline 1 hour ago. She has a well perfused hand but no palpable pulses. The remainder of her examination is otherwise normal. What is the next step in treatment? Review Topic
Explanation
If there is evidence of vascular compromise, the fracture should be reduced and pinned urgently and the limb reevaluated.
Question 8
Figure 31 shows the radiograph of an 8-year-old boy who has a swollen forearm after falling out of a tree. Examination reveals that all three nerves are functionally intact, and there is no evidence of circulatory embarrassment. Management should consist of
Explanation
REFERENCES: Gibson WK, Timperlake RW: Operative treatment of a type IV Monteggia fracture-dislocation in a child. J Bone Joint Surg Br 1992;74:780-781.
Stanley EA, DeLaGarza JF: Part IV: Monteggia fracture. Dislocations in children, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 576-577.
Question 9
A 72-year-old man undergoes an uncomplicated cementless total hip arthroplasty for advanced osteoarthritis. At his 6-week postoperative follow-up, he has minimal pain and is progressing well with his mobility. Radiographs show early formation of Brooker grade III heterotopic bone around his hip. What is the best treatment of the heterotopic bone at this time?
Explanation
REFERENCES: Balboni TA, Gobezie R, Mamon HJ: Heterotopic ossification: Pathophysiology, clinical features, and the role of radiotherapy for prophylaxis. Int J Radiat Oncol Biol Phys 2006;65:1289-1299. Fransen M, Neal B: Non-steroidal anti-inflammatory drugs for preventing heterotopic bone formation after hip arthroplasty. Cochrane Database Syst Rev 2004;3:CD001160.
Neal BC, Rodgers A, Clark T, et al: A systematic survey of 13 randomized trials of non-steroidal antiinflammatory

drugs for the prevention of heterotopic bone formation after major hip surgery. Acta Orthop Scand 2000;71:122-128.
Question 10
8 (Normal ratio = 0.8 - 1.2). The most common symptoms associated with patella baja include anterior impingement, knee pain, and knee stiffness.
Explanation

OrthoCash 2020
A 88-year-old female fell onto her right hip sustaining the fracture shown in Figure A. Past medical history is significant for mild dementia and moderate coronary artery disease. At baseline, she ambulates with a walker. There are concerns about her ability to maintain weight-bearing precautions following surgery. Which of the following is most appropriate for management of the femoral side?

Revision total hip replacement with a proximally coated femoral stem
Open reduction, internal fixation with plate and cerclage wires
Proximal femoral replacement with megaprosthesis
Impaction bone grafting
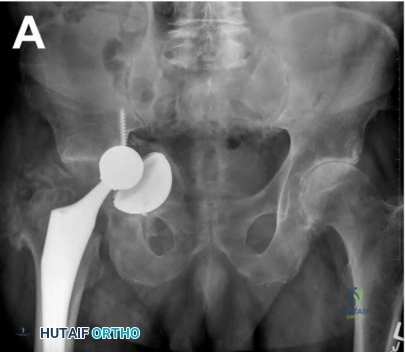
Cortical strut allograft with cerclage wiring Corrent answer: 3
The radiograph shows a Vancouver B3 periprosthetic fracture with poor proximal femoral bone stock. Given her age, co-morbidities, and dementia, the appropriate management of her condition would be a proximal femoral replacement with megaprosthesis. This can allow for immediate weightbearing in the post-operative period.
Vancouver B3 periprosthetic fractures are fractures around or just below the tip of a loose stem with poor proximal femoral bone stock. Options for management of this fracture include a fully coated stem, a fluted tapered stem, a proximal femoral replacement with megaprosthesis, allograft-prosthesis composite, and impaction bone grafting. In elderly patients with comorbidities and an inability to maintain the strict weight-bearing precautions that impaction bone grafting and allograft prosthetic replacements require, proximal femoral replacement with a megaprosthesis is the best option.
Duncan et al. were the originators of the Vancouver classification system for
periprosthetic fractures. Type A fractures are peritrochanteric, type B fracture are around the stem tip, and type C fractures are well below the stem tip.
Parvizi et al. review the indications for proximal femoral replacements with megaprostheses. They conclude it is a reasonable option for elderly patients with massive proximal femoral bone loss. The most frequent complications are aseptic loosening and dislocation.
Klein et al. identified 23 patients who underwent proximal femoral replacement for a Vancouver type-B3 periprosthetic fracture. At a follow-up of 3 years, 22 of 23 patients were walking with minimal pain. The most frequent complications were persistent drainage (2), dislocation (2), refracture (1) and acetabular cage failure (1).
Figure A shows a Vancouver B3 periprosthetic fracture with loose stem and poor proximal bone stock. Illustration A shows an example of a proximal femoral replacement. Illustration B shows a radiograph of a proximal femoral replacement used for a failed total hip replacement with massive bone loss. Illustration C shows the Vancouver classification (A, B1, B2, B3, C)
Incorrect Answers:

OrthoCash 2020
A minimal-incision technique with an incision no more than 10 centimeters has which of the following advantages compared to a standard incision for a total hip replacement?
lower post-operative visual analogue pain score
less transfusion requirement
shorter length of stay
better cosmetic result
less pain medication requirement Corrent answer: 4
Ogonda et al randomized patients to standard (16cm) versus MIS incision (<10 cm). They found no significant difference with respect to postoperative hematocrit, blood transfusion requirements, pain scores, or analgesic use.
There were also no differences in early walking ability or length of hospital stay and no differences in component alignment.
OrthoCash 2020
What is an advantage of utilizing a 36-mm instead of a 28-mm femoral head in the setting of a revision total hip arthroplasty?
Compensating for abductor deficiency
Decreasing volumetric wear
Decreasing trunion stress
Delaying neck-socket impingement
Compensating for vertical cup placement Corrent answer: 4
Increasing femoral head size delays neck-socket impingement, enhancing stability by increasing the excursion distance prior to dislocation.
The optimal bearing in total hip arthroplasty (THA) should allow for the best stability and function while preserving implant longevity. Greater motion, stability, and patient satisfaction have been correlated with larger femoral head sizes. Stability is associated with an increased displacement distance in larger diameter heads prior to a dislocation event (increased jump distance) combined with a greater impingement-free range of motion. Although larger femoral head sizes are associated with greater volumetric wear and trunion stress (and possible taper corrosion), newer bearings such as ceramic-on-ceramic may help mitigate these factors.
Kung et al. examined the effect of femoral head size and abductor integrity on dislocation events after revision THA. They separated 230 patients who underwent revision THA into 4 groups: (1) intact abductors mechanism + 28-mm femoral head, (2) absent abductor mechanism + 28-mm femoral head,
(3) intact abductor mechanism + 36-mm femoral head, and (4) absent abductor mechanism + 36-mm femoral head. They found that in patients with intact abductor mechanisms, the 36-mm femoral head was associated with a lower dislocation rate with 6-month minimum follow-up; femoral head size did not reduce dislocation events in patients with deficient abductor mechanisms.
Burroughs et al. performed an in-vitro study evaluating the range of motion and stability in THA with 28-44-mm femoral head sizes. They found that
femoral heads >32-mm provided for greater ROM and decreased component impingement. For these reasons, the authors conclude that large femoral heads may be beneficial in revision THA.
Illustration 1 demonstrates the increased jump distance when utilizing a larger diameter femoral head. Illustration 2 demonstrates a greater impingement-free range of motion with a larger femoral head.
Incorrect Answers:
OrthoCash 2020
A 65-year-old male is now 6 weeks status post an uncomplicated total knee arthroplasty. Figures A and B represent his x-rays at today's visit. His primary complaint is knee stiffness. His current passive range of motion is 0-80 degrees, compared to 120 degrees
preoperatively, and he has failed to improve with physical therapy. He is otherwise afebrile, has no incisional erythema or pain, and CRP is within normal limits. Manipulation under anesthesia (MUA) will provide the largest improvement in flexion if performed before which of the following:

Before 6 weeks
Before 12 weeks
Before 26 weeks
Before 34 weeks
Outcomes after MUA are equivalent if performed within 1 year of surgery Corrent answer: 2
Manipulation under anesthesia (MUA) yields the greatest gain in flexion and improvement in overall range of motion if performed within 12 weeks postoperatively.
Post-operative knee stiffness (flexion < 90 degrees) occurs in 1.3%-12% of patients who undergo TKA. The preoperative risk factors for stiffness include decreased preoperative range of motion, age, diabetes mellitus, and socioeconomic status. Surgical factors can also contribute, including
overstuffing the patellofemoral joint, tight flexion/extension gaps, and excessive tightening of the extensor mechanism. If left untreated, loss of flexion negatively impacts functional outcomes, patient satisfaction, and ability to perform activities of daily living. MUA is considered the initial management for patients with flexion less than 90 degrees.
Issa et al. studied the optimal timing of MUA. They found that patients undergoing MUA before 12 weeks had a significantly higher mean gain in flexion (36.5° versus 17°), higher final range of motion (119° versus 95°), and higher Knee Society objective (89 versus 84 points) and function scores (88 versus 83 points) than those who had late manipulation under anesthesia (after 12 weeks). There was no statistically significant difference between MUA before 6 weeks vs MUA before 12 weeks.
Desai et al. similarly demonstrated that maximum flexion gains were achieved when MUA was performed between 12-14 weeks post-operatively. They also demonstrated that there is no benefit to multiple manipulations, with no observed flexion gain after the initial intervention.
Incorrect Answers:
OrthoCash 2020
A 51-year-old male presents with worsening left hip pain over the past 8 months. The patient reports hip surgery 5 years prior as seen in Figures A and B. His CRP level is within normal limits, ESR is at the upper limit of normal, and automated cell count following a hip aspiration yields a WBC of 15,000/µL (rr, 4500-11000µL) and 85% PMNs. Metal ion testing reveals elevated serum cobalt and chromium levels. What is the next best step?

Manual cell count of synovial fluid
stage revision arthroplasty
Acetabular cup revision with bone grafting
Femoral revision with cerclage wire placement
Hip arthrodesis
The patient has had a metal-on-metal (MoM) hip resurfacing with osteolysis. It is likely his WBC count is falsely elevated secondary to metal debris and corrosion. The next best step is a manual cell count to evaluate for metal debris, clots, fragmented cells, or other defects preventing accurate automated cell count.
Diagnosis of infection in the setting of MoM bearing surface can be difficult given very similar presentations. Typical workup includes CRP, ESR, synovial fluid WBC, and differential. Metal debris and corrosion reactions can confound the synovial fluid analysis leading to falsely elevated WBC counts in cases of aseptic failure. Prosthetic joint infection (PJI) and metallosis can occur concurrently so aggressive diagnostic testing is important for surgical decision making. Manual cell count of synovial fluid samples can identify metal debris and avoid false positives from automated cell testing. Supplementary tests, such as MARS MRI, metal ion levels, manual cell count, and repeat aspiration, can help guide appropriate management in these scenarios.
Yi et al. investigated ESR, CRP, synovial WBC and differential in diagnosing PJI in the setting of MoM hips or non-MoM hips undergoing revision for corrosion
or full thickness wear. They found that synovial fluid WBC count can be confounded by inaccurate automated cell counts secondary to foreign material and degenerating cells. They conclude that diagnosis of PJI in the setting of failed MoM bearings or corrosion is difficult due to falsely positive synovial fluid WBC.
Carrothers et al. evaluated the prevalence of complications of hip resurfacing arthroplasty. They found the most common complication was fracture of the femoral neck, followed by loosening of the acetabular component, femoral head collapse, loosening of a femoral component, infection, aseptic lymphocyte-dominated vasculitis-associated lesion (ALVAL), loosening of both components, and malposition of the acetabular component. They conclude that knowledge of complications following hip resurfacing is important to help select patients and counsel them on risks prior to surgery.
Figures A and B show a metal-on-metal hip resurfacing with supra-acetabular osteolysis.
Incorrect Answers:
OrthoCash 2020
An 87-year-old female presents with longstanding knee pain. The structures identified in Figure A are formed through the pathologic activation of endochrondral ossification. The pathway involved in this process involves which of the following signaling molecules?

Indian hedgehog (Ihh)
Peroxisome proliferator-activated receptor gamma (PPARG)
Receptor activator of nuclear factor kappa-ligand (RANKL)
Osteoprotegerin (OPG)
Sclerostin
Osteoarthritis and formation of osteophytes are felt to be mediated by the differentiation of quiescent chondrocytes through the Indian hedgehog signaling pathway.
Indian hedgehog (Ihh) is an important mediator of chondrocyte and osteoblast differentiation in prenatal endochondral bone formation. Adult articular cartilage without osteoarthritis does not have active Ihh signaling. However, Ihh and its downstream signaling proteins have been found to be unregulated in osteoarthritic joints. Ihh may play an important role in activating endochondral ossification leading to some of the clinical features of osteoarthritis (osteophytes and subchondral cysts). Modulation of Ihh has therapeutic potential in the treatment of osteoarthritis.
Maeda et al. studied mice with Ihh genes ablated from postnatal chondrocytes.
They found a loss of columnar structure, premature vascular invasion, and formation of ectopic hypertrophic chondrocytes in the growth plate. They concluded that Ihh is essential for maintained trabecular bone, skeletal growth, and articular cartilage.
Wang et al. reviewed the molecular mechanisms associated with cartilage degeneration in osteoarthritis. The study found that upregulation of the Ihh signaling molecules leads to the development of osteoarthritis, similar to that found in injury-induced controls. Additionally, they found that inhibiting the Ihh pathway reduces the severity of injury-induced osteoarthritis in mouse models.
Figure A shows a knee with varus deformity and severe medial sided arthritis with femoral and tibial sided osteophytes(red arrows).
Incorrect Answers:
OrthoCash 2020
Figure 1 is the AP pelvis radiograph of a 55-year-old male with known hip dysplasia and chronic right hip pain. He has no prior surgical history and is otherwise healthy. Your initial plan is to reconstruct his hip center at the site of his true acetabulum. Your preoperative template demonstrates that your acetabular component will have 40° of abduction, 15° of anteversion. However, there will be 25% uncoverage at the superolateral margin. What is the most appropriate next step to ensure adequate cup fixation?

Increase the abduction angle to 60 degrees for better coverage
Medialize the acetabular component beyond the medial wall for improved coverage
Elevate the hip center in search of better bone stock
Accept 25% uncoverage and proceed with total hip arthroplasty as templated
Use cement augments to improve superolateral coverage of the acetabular component
The most appropriate next step is to proceed with total hip arthroplasty (THA) as templated. Less than 30% of uncoverage is acceptable and has not been associated with increased rates of aseptic loosening.
Dysplasia of the hip broadly refers to abnormal development of the hip that leads to poor acetabular coverage of the femoral head. The characteristic pelvic deformities of dysplasia include a retroverted acetabulum with bone loss at the superolateral margin. As a result, there is often insufficient bone stock to provide complete coverage of the acetabular component when placed at the true hip center. Insufficient coverage (<60-70%) can lead to a lack of initial stability and early failure. If the pre-operative template suggests extreme superolateral bone loss, the surgeon must then consider alternative methods of achieving satisfactory fixation, including downsizing the acetabular component size, medializing or elevating the hip center, or use of trabecular metal augments or cement augmentation for better coverage.
Haddad et al. discuss pre-operative considerations when performing primary total hip arthroplasty on dysplastic hips. The literature review suggests that
less than 30% uncoverage does not increase the risk of aseptic loosening.
Paavilainen et al. studied the short-term outcomes on 100 cementless total hip replacements in severely dysplastic hips. They describe the importance of exposing the proximal aspect of the pubic and ischial bones since the pelvic wall is usually hypoplastic, and the use of augmentation when the superolateral rim was deficient. Overall, their outcomes with cementless total hip replacements were equivalent to cemented prostheses.
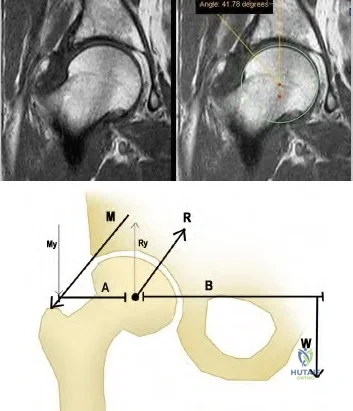
Figure A is an AP pelvis radiograph demonstrating a dysplastic right hip. Illustration A is a T1-weighted coronal MRI of a hip. Hip dysplasia can be assessed using the center-edge angle, the angle formed between a vertical line through the center of the femoral head and a line connecting the center of the femoral head with the lateral edge of the acetabulum. Less than 20° is one marker of hip dysplasia. Illustration B demonstrates the concept of joint reactive forces. Joint reactive force is minimized when the moment arm of body weight and abductor tensioning are balanced. Anatomic changes that reduce abductor tension such as elevating the hip center, decreasing femoral head size, and increased valgus neck angle increase the joint reactive force.
Incorrect Answers:
OrthoCash 2020
A 65-year-old man presents to your clinic with chronic, progressive knee pain. Figure A is an x-ray of his right knee. He would like to pursue non-surgical treatment options. The AAOS clinical practice guidelines on the treatment of symptomatic knee arthritis support which of the following with "strong evidence"?

NSAIDs; tramadol
Weight loss; arthroscopic debridement
Weight loss; intra-articular steroid injections
Valgus-offloading brace; glucosamine chondroitin injections
Tramadol; acupuncture
The AAOS clinical practice guidelines (CPG) summary "strongly" recommends tramadol or NSAIDs for the treatment of symptomatic knee osteoarthritis.
Symptomatic knee osteoarthritis is widespread, with an incidence of 240 people per 100,000. Symptoms are often progressive, though addressing the modifiable risk factors of muscle weakness, large BMI, and repetitive loading can help with pain control. Definitive management is total knee arthroplasty, however, non-operative interventions are often successful in delaying surgery, particularly in younger patients.
The AAOS Clinical Practice Guideline Summary performed a systematic review of the available literature to propose evidence-based guidelines for the management of symptomatic knee osteoarthritis. The current guidelines show strong support for the engagement in physical activity (such as guided physical therapy), non-steroidal anti-inflammatory drugs, and Tramadol for the management of symptomatic osteoarthritis. The Clinical Guidelines provided “strong” evidence against acupuncture, glucosamine and chondroitin, hyaluronic acid, and arthroscopy with lavage or debridement.
Fishman et al. performed a double-blind, randomized study of 552 patients studying the efficacy of Tramadol vs placebo in the management of arthritic knee pain. Tramadol demonstrated a statistically significant improvement in knee pain over placebo as reported by the Patient Global Rating of Pain Relief Scale.
Incorrect Answers:
OrthoCash 2020
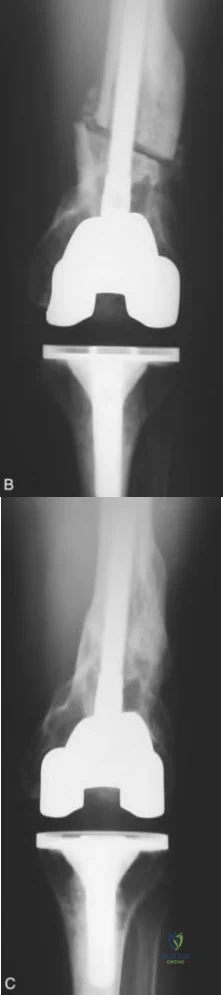
An 82-year-old healthy male presents to the ED with right leg pain and inability to bear weight after a fall from standing. He has a history
of revision right total knee arthroplasty performed 5 years ago and was doing well until his fall this morning. On exam, he is able to actively extend his knee, though limited by pain, and is neurovascularly intact. Figures A-B are radiographs of his distal femur. What is the most appropriate treatment?

Retrograde intramedullary nail
Revision total knee arthroplasty with a stemmed femoral component
Nonoperative management with application of a long leg cast
Open reduction and internal fixation with a lateral plate
Antegrade intramedullary nail Corrent answer: 4
Open reduction and internal fixation with a lateral plate is the most appropriate treatment for this supracondylar periprosthetic femur fracture above a well-fixed total knee arthroplasty (TKA).
Supracondylar periprosthetic femur fractures are defined as fractures within 15cm of the joint line or within 5cm of the proximal end of the implant in the case of a stemmed component. Risk factors include rheumatoid arthritis, neurologic disorders, steroid use, anterior cortical notching of the femoral
component and revision TKA. Nonoperative management usually requires long-term immobilization, which can result in significant loss of knee range of motion (ROM). Therefore, surgical treatment is often preferred. An acceptable outcome is > 90° of knee ROM, fracture shortening < 2cm, varus/valgus malalignment < 5°, and flexion/extension malalignment < 10°.
Su et al. performed a literature review of the management of periprosthetic femur fractures above a TKA. First, it is crucial to determine the stability of the femoral component. An unstable femoral component requires either revision TKA or distal femoral replacement, depending on the quality of the distal femoral bone stock. A fracture with a stable femoral component can be well fixed with a buttress plate or retrograde intramedullary nail. In a series of 12 patients undergoing fracture fixation with lateral plate, all patients healed and returned to pre-fracture ambulatory status.
Zehntner et al. studied the surgical outcomes of buttress plating in 6 supracondylar femur fractures above TKA. There was no nonunion, loss of fixation or infection. Knee ROM averaged 97°, and all patients were ambulating postoperatively.
Figures A and B represent AP and lateral radiographs of a supracondylar periprosthetic femur fracture above a stemmed TKA. Illustrations C and D represent AP and lateral radiographs of a supracondylar periprosthetic femur fracture above a stemmed TKA status post repair with lateral plate.
Incorrect Answers:

OrthoCash 2020
A 60-year-old woman presents for follow-up two weeks after right total knee arthroplasty. She complains of significant anterior knee pain after fall from standing onto a flexed knee. On physical exam, her passive range of motion is 0-120 degrees and she is stable to varus and valgus stress. She is able to achieve full extension with active range of motion, though she is experiencing severe pain. Lateral radiograph of the knee is provided in Figure A. What is the most appropriate next step?

Non-operative management with long leg cast
Closed treatment with immediate active range of motion
Removal of patellar component with early active range of motion
Open reduction and internal fixation of patella with wire or screw fixation
Extensor mechanism repair with Achilles allograft and revision of the patella Corrent answer: 1
The appropriate treatment for a transverse periprosthetic patella fracture with an intact extensor mechanism is closed treatment and immobilization in a long leg cast.
Periprosthetic patella fracture after total knee arthroplasty is rare (incidence of 0.68%-5.2%) and is overwhelmingly secondary to a traumatic mechanism.
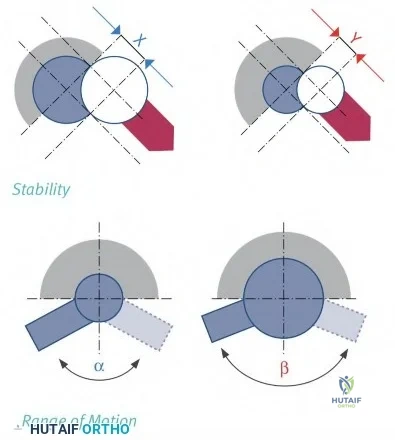
Risk factors include excessive patella resection, use of cementless components, and elevated BMI. Broadly, the treatment algorithm for periprosthetic patella fracture depends on the stability of the implant and the involvement of the extensor mechanism. Ortiquerra and Berry classified periprosthetic patella fractures as intact extensor mechanism with well a fixed implant (Type I), extensor mechanism disruption with either a loose or stable implant (Type II), or intact extensor mechanism with a loose implant (Type III). Generally, fractures associated with component loosening or extensor mechanism injuries (Type II & Type III) require revision surgery and often yield poor results. Type I fractures are successfully managed non-operatively.
Nam et al. reviewed the management of extensor mechanism complications in
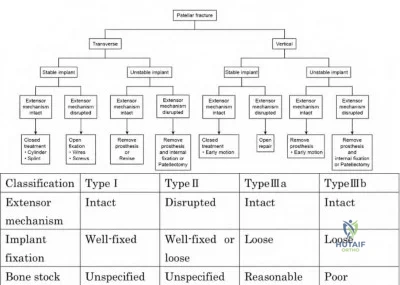
total knee arthroplasty. They report excellent results in Type I peri-prosthetic patella fractures managed non-operatively, with only 1 failure in 37 patients. They propose a treatment algorithm based upon fracture pattern (transverse vs vertical), component fixation, and extensor mechanism integrity. Type I injuries with transverse fractures should be immobilized in long leg casts, whereas Type I injuries with vertical fractures are more stable and can benefit from early active range of motion.
Cottino el al. similarly review the outcomes of peri-prosthetic patella fractures. They report a 50% complication rate and a 20-40% re-operation rate for type II and type III injuries, even with anatomic reductions.
Figure A is a lateral radiograph of the knee that demonstrates a transverse peri-prosthetic patella fracture without component loosening. There is no obvious extensor mechanism injury and the prompt indicates extension is intact. Illustration A represents the peri-prosthetic patella fracture treatment algorithm as proposed by Nam et al. Illustration B represents the Ortiquerra and Berry peri-prosthetic patella fracture classification.
Incorrect Answers:
OrthoCash 2020
A 68-year-old healthy male with a history of a right total hip arthroplasty 8 years prior presents with one year of right hip pain and several months of inability to bear weight. An AP pelvis radiograph is shown in Figure A. ESR is 8 mm/hr and CRP is 1 mg/L. What is the best treatment option?
Cemented acetabular cup with morselized bone graft
Two stage revision with antibiotic spacer
Cup-cage construct with or without morselized bone graft
Definitive removal of hardware/Girdlestone procedure
Anterior and posterior column plates with hemispherical uncemented cup Corrent answer: 3
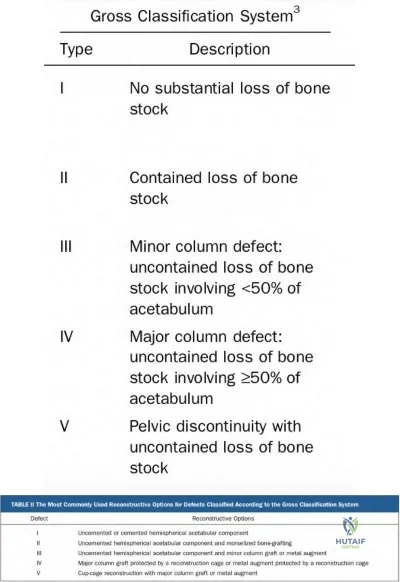
Cup-cage constructs have demonstrated excellent outcomes in patients with pelvic discontinuity and Gross type V acetabular defects.
When treating chronic pelvic discontinuities, four general principles need to be addressed: 1) restoration of the acetabulum by reconnecting the ischium to the ilium, 2) optimizing contact of bleeding bone to component surfaces with ingrowth potential, 3) grafting osseous deficiencies, 4) obtaining a mechanically stable reconstruction to protect components until ingrowth is achieved. There are several different classifications of acetabular bone loss, though the Gross classification is unique in that it not only grades the degree of bone loss but also provides reconstructive options that may be considered (Illustration A & B). Due to the segmental bone loss associated with Gross
Types IV and V defects, cup-cage constructs are used to bridge segmental defects or areas of discontinuity.
DeBoer et al. studied the long-term outcomes of 28 patients with pelvic discontinuity treated with custom triflange acetabular prostheses. They reported no instances of broken screws, implant migration, or component revision at 10 years. Complications included one partial sciatic nerve palsy and five patients with dislocation.
Makinen et al. reviewed the role of cages in revision arthroplasty. In Gross Type V defects, cages provide mechanical stability to protect the acetabular cup until ingrowth is achieved. They report two case series following cup-cage reconstructions for pelvic discontinuity, demonstrating 88% survival at 44.6 months and 87.2% survival at 82 months. The survivorship of cage only constructs was 49.9% at seven years.
Figure A demonstrates a failed right total hip arthroplasty with associated chronic pelvic discontinuity. Illustration A demonstrates the Gross classification for acetabular bone defects. Illustration B demonstrates the suggested reconstructive options for defects classified according to the Gross classification system.
Incorrect Answers:
OrthoCash 2020
A 60-year-old male presents with significant left knee pain and end-stage osteoarthritis. He failed non-operative management and is requesting a total knee arthroplasty (TKA). His past medical history is significant for a left distal femur fracture that occurred when he was struck by a car 30 years prior. A standing, full-length radiograph of his left lower extremity is shown in Figure A. His femoral coronal plane deformity measures 28 degrees. When proceeding with a TKA, what must be done to address this patient's coronal deformity?

Soft tissue balancing and intra-articular bone cuts
Distal femoral medial closing-wedge osteotomy
Distal femoral lateral closing-wedge osteotomy
High tibial osteotomy
Hinged TKA
Coronal plane deformities of the femur >20 degrees require an extra-articular femoral osteotomy to achieve proper mechanical alignment when performing a TKA.
Coronal and sagittal plane deformities of the femur less than 20 degrees can usually be addressed with intra-articular bone cuts and soft tissue balancing. Attempting to correct deformities greater than this without an extra-articular osteotomy can compromise ligamentous stability. This highlights the importance of careful pre-operative templating/planning and obtaining full-length, standing radiographs when clinically warranted. Although correcting severe deformities with staged or concomitant extra-articular osteotomies can be challenging, they are often successful when properly executed.
Lonner et al. provided a retrospective case series and review article addressing
severe extra-articular deformities with simultaneous femoral osteotomy and TKA in patients with osteoarthritis. In their 10-patient series, they were successful in restoring coronal alignment within two degrees of anatomic in all patients. They suggest securing the femoral osteotomy site with a plate or locked intramedullary nail, depending on the osteotomy site.
Rajgopal et al. presented a case series of TKA in 36 knees in the setting of extra-articular deformities. In this series, they treated all patients with intraarticular bone resection and soft-tissue balancing to address their deformities. Femoral-coronal, sagittal, and tibial-coronal deformities successfully treated included 11-18 degrees, 0-15 degrees, and 12-24 degrees, respectively.
Figure A is a standing, full-length radiograph of the left lower extremity demonstrating a significant coronal plane deformity resulting from a previous distal femur fracture malunion. Illustration A is a left knee radiograph demonstrating an extra-articular distal femoral osteotomy with placement of a fluted, press-fit stem. Illustration B is the same patient at 3-year follow-up demonstrating a fully healed osteotomy and maintained hardware alignment.
Incorrect Answers:
OrthoCash 2020
A 76-year-old female presents with right hip pain 6 years after total hip arthroplasty. She denies constitutional symptoms at this time. On physical examination, her incision is well healed. Current radiographs are shown in Figures A and B. In addition to a complete blood count (CBC), C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR), an alpha-defensin immunoassay is ordered. What does the alpha-defensin immunoassay test for?

The presence of an intra-articular, antimicrobial peptide
The presence of an antimicrobial peptide within serum
The presence of an intra-articular, pro-inflammatory marker
The presence of an intra-articular, pro-inflammatory cytokine
The presence of intra-articular leukocytosis Corrent answer: 1
A synovial alpha-defensin immunoassay tests for the presence of an intraarticular, antimicrobial peptide.
When there is suspicion of a periprosthetic infection, laboratory workup should
include CRP and ESR. If suspicion remains after laboratory examination, an aspiration of the joint should be performed for cell count and culture. A fairly recent test developed to aid in the diagnosis of PJI is the synovial alpha-defensin immunoassay. Defensins are antimicrobial peptides that are active against many bacteria, fungi, and enveloped viruses. Alpha-defensin is an antimicrobial peptide which is abundant in neutrophils and macrophages. It is present in the natural local tissue response to infection. In the setting periprosthetic joint infection (PJI) the levels of intra-articular alpha-defensin increase substantially and may reach levels that can be detected by an immunoassay. Alpha-defensin may be more prone to false positive results in adverse local tissue reaction caused by a metal-on-metal arthroplasty.
Bonanzinga et al. performed a prospective study to determine the reliability of the alpha-defensin immunoassay for diagnosing PJI. They aspirated hips and knees in all patients presenting with pain in both primary and revision arthroplasties. They found the sensitivity of the alpha-defensin immunoassay was 97%, the specificity was 97%, the positive predictive value was 88%, and the negative predictive value was 99% (95% CI, 96%–99%). They conclude that alpha-defensin appears to be a reliable test.
Shinsky et al. performed a study to evaluate the utility of commonly available tests for determining the presence of PJI in patients undergoing revision total hip arthroplasty. 235 consecutive total hip arthroplasties undergoing revision were evaluated. They found that no hip in a patient with a preoperative ESR of
<30 mm/hr and a CRP of <10 mg/dL was infected. They also conclude that a synovial fluid cell count of >3000 white blood cells/mL was the most predictive perioperative testing modality when ESR and CRP were elevated as well.
Figures A and B are AP and lateral radiographs of the right hip, respectively, demonstrating a region of periarticular erosions around the proximal femoral stem.
Incorrect Answers:
OrthoCash 2020
A 72-year-old male presents to your clinic with a 6-month history of left groin pain without preceding trauma. He previously underwent an uneventful left total hip arthroplasty 15-years prior at an outside institution. He has been ambulating with a cane for the last month due to pain. A left hip radiograph is obtained and presented in Figure A. Less than 4 centimeters of intact diaphyseal bone remains distal to the isthmus. An infection work-up is negative. Of the choices provided, what is the most appropriate management option at this time?

Continued observation
Placement of a femoral cortical strut allograft and cerclage wires
Femoral revision with impaction grafting and a cementless femoral stem
Femoral revision with a metaphyseal-engaging tapered stem
Femoral revision with a modular fluted tapered stem Corrent answer: 5
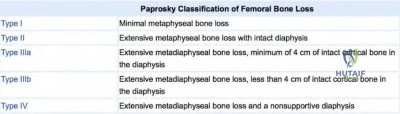
This patient has a Paprosky type-IIIB femoral defect (less than 4cm diaphyseal bone available for distal fixation) that can be revised with a modular fluted tapered stem
Femoral revision with a modular fluted tapered stem is the preferred method
in the treatment of Paprosky type-IIIB femoral defects. Proximal femoral replacement, allograft prosthetic composite, resection arthroplasty, and impaction grafting may also be considered in the treatment of Paprosky type-IIIB and IV femoral defects. Impaction grafting involves creating a neomedullary canal by impacting cancellous bone chips into the femoral canal followed by cementation of the final femoral component.
Valle et al. present a review article describing the Paprosky classification of femoral defects as well as treatment options. They differentiate a type-IIIA and IIIB defect as having >4 and <4 centimeters of intact diaphyseal bone available for distal fixation, respectively.
Hartman et al. describe management strategies for femoral fixation in the setting of revision total hip arthroplasty. They review classification systems of femoral bone loss and provide an overview of various treatment options. The authors feel that type-II and IIIA defects can be effectively treated with cylindrical, extensively porous-coated implants, whereas IIIB defects can usually be treated with a modular fluted tapered stem.
Figure A show a total hip arthroplasty with less than 4cm of diaphyseal bone available for distal fixation with extensive metaphyseal and diaphyseal bone loss. Illustration A shows a diagram of the Paprosky classification for femoral bone loss.
Incorrect Answers:
OrthoCash 2020
An 85-year-old woman sustains a ground level fall. Her THA was done 25 years ago. She was previously ambulatory but with a significant limp. With regard to the femur specifically, what is the Vancouver classification and preferred treatment option?

Vancouver C, revision to proximal femoral replacement
Vancouver B1, ORIF with impaction grafting
Vancouver AG, ORIF
Vancouver B3, revision to proximal femoral replacement
Vancouver B2, ORIF with femoral strut allograft augmentation Corrent answer: 4
The periprosthetic femoral fracture should be classified as Vancouver B3 given the location around the femoral stem with very poor proximal femoral bone stock, thus making reconstruction of this bone unrealistic. The best treatment options for a B3 fracture would be revision of the stem to a proximal femoral replacement or proximal femoral allograft composite.
The Vancouver periprosthetic classification system is one of the most useful classifications in orthopaedics as it can reliably guide treatment. Vancouver B1 or C type fractures confer a well-fixed stem and so ORIF would be the
treatment of choice. B2 and B3 fractures signify a loose femoral stem and so revision is necessary while B3 fractures have very poor proximal bone quality making any reliance on metaphyseal proximal bone for fixation or reconstruction futile.
Klein et al. retrospectively reviewed 21 patients (mean age 79) with Vancouver B3 fractures treated with a proximal femoral replacement. At most recent follow-up, 20/21 patients were ambulatory with no or minimal pain.
They note a relatively high complication rate (2 recurrent dislocators, 1 repeat fracture, 1 acetabular complication, 2 infections treated with I&D). However, given the circumstances and morbidity of non-operative management, they still recommend a proximal femoral replacement for this complicated patient group.
Savvidou et al. offer a good review of proximal femoral replacement both for periprosthetic fracture and also revision THA with significant proximal bone loss. They emphasize the complications such as dislocation and aseptic loosening and offer recommendations for minimizing them such as a large femoral head, soft tissue repair, and preservation/repair of abductors.
Figure A demonstrates a cemented total hip arthroplasty with significant osteolytic changes about both the femoral and acetabular components with multiple fractures around the grossly loose femoral stem. Taken from Klein et. al.
Illustration A demonstrates an example of a proximal femoral replacement. Taken from Savvidou et al.
Incorrect Answers:

OrthoCash 2020
Which of the following liner types have been associated with early acetabular component loosening?
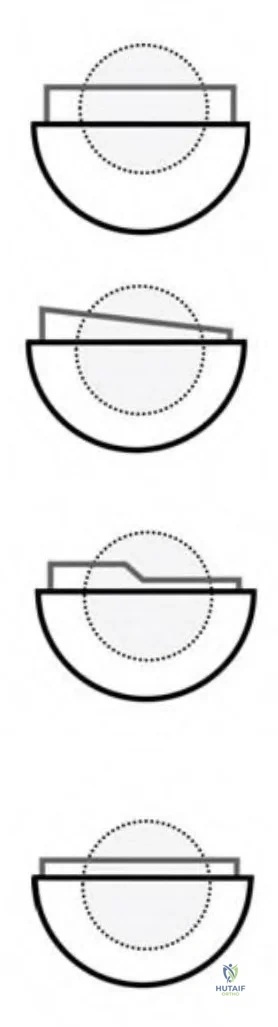
Figures B and C Corrent answer: 1
Figure A is an illustration of a lateralized or offset acetabular liner which has been shown to have a higher rate of loosening with primary and revision total hip arthroplasty (THA).
Extended offset polyethylene liners allow restoration of soft tissue tension by adding 4 to 10 mm of additional offset to the acetabular side. They translate the center of hip rotation laterally which will increase offset in the horizontal plane and add a few millimeters of additional limb lengthening in the vertical plane. The lateral translation of the center of rotation has been found to increase joint reaction forces and polyethylene wear. Additionally, this results
in an eccentric loading pattern and leads to increased torsional forces at the liner-shell interface and the bone-implant interface. This may cause motion at the interface resulting in failure of ingrowth and early loosening.
Glori performed a study to determine if torsion on an offset acetabular component may increase the risk of fixation failure. He found that a 70 kg person walking normally on a well-positioned 10-mm offset component will produce more torsion compared to a 4-mm offset component. Vertical cup placement was also found to increase torsion. He concludes that these torsional moments are comparable to moments shown to cause failure of the initial interference fit of cementless acetabular components in vitro. He suggests that after using an offset cementless acetabular component, one should initially limit weight bearing to minimize the risk of failure.
Archibeck et. al reviewed 1919 patients with primary THA and 346 with revision THA to evaluate acetabular component loosening. A 7-mm offset acetabular liner was used in 120 of the primary and 100 of the revision THAs. The aseptic loosening rate in the primary THA group was 0.12% in the standard offset and 4.2% in the extended offset groups at a minimum of 2 years follow-up. The aseptic loosening rate in the revision group was 1.7% in the standard and 7% in the extended offset groups at a mean of 4 years follow-up. They conclude that offset acetabular liners have a high failure rate in primary and revision THA.
Figure A is an illustration depicting an offset acetabular component. Figure B is an illustration depicting an oblique acetabular component or a face-changing liner. Figure C is an illustration depicting an elevated rim acetabular component or a lipped liner. Figure D is an illustration depicting a standard offset component.
Incorrect Answers:
OrthoCash 2020
During a revision hip surgery, which of the following muscles labeled in Figure 1 can be transferred in the setting of an abductor deficiency?
Question 11
An 82-year-old osteoporotic woman undergoes total hip arthroplasty for osteoarthritis. During implant trialing, a crack is heard. Intraoperative fluoroscopy reveals a long, spiral fracture of the distal femur. The fracture is reduced and fixed with an anatomic locking plate. The rest of the total hip arthroplasty proceeds uneventfully. Following surgery the surgeon has a meeting with the family and apologizes and provides full disclosure, accepts responsibility, provides a detailed explanation as to what happened, and gives reassurance that steps will be taken to prevent recurrences. This communication approach will most likely
Explanation
In the event of a medical error or adverse event, effective communication with the patient and family is necessary. Effective communication should comprise: an apology, full disclosure (an explanation of what happened), accepting responsibility, and corrective steps that will be taken to prevent recurrence.While accepting responsibility is integral to the explanation process, it is different from accepting blame.
Mazor et al. found patients would more likely change physicians and seek legal advice in situations with a life-threatening outcome where physicians chose nondisclosure. They recommend full disclosure, acceptance of responsibility, an apology, detailed explanations, and assurances that steps will be taken to prevent recurrences will result in positive outcomes in terms of patient satisfaction, trust, and emotional response.
MacDonald et al. addressed medical errors in an editorial. Besides full disclosure, they feel that an apology is necessary. This includes an acknowledgement of the event and one’s role in the event, and a genuine expression of regret. Apology laws exist to to reduce concerns about legal implications of disclosure and apology.
Incorrect Answers:
Question 12
A 9-year-old child has right groin pain after falling from a tree. Examination reveals that the right leg is held in external rotation, and there is significant pain with attempts at passive range of motion. Radiographs are shown in Figures 43a and 43b. Management should consist of
Explanation
REFERENCES: Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
Hughes LO, Beaty JH: Fractures of the head and neck of the femur in children. J Bone Joint Surg Am 1994;76:283-292.
Question 13
An orthopaedic surgeon frequently uses hip and knee prostheses from a specific manufacturer. The surgeon becomes acquainted with the manufacturer's representative who provides the support for these prostheses in the hospital. They develop a personal relationship outside of work through a common interest in sailing. Together they become interested in buying a sailboat. The manufacturer's representative suggests a partnership in a boat costing $200,000. The manufacturer's representative would purchase a 90% interest and the surgeon a 10% interest in the boat. There would be no restrictions on use of the boat by the surgeon. What should the orthopaedic surgeon do?
Explanation
Question 14
A 56-year-old man with poorly controlled diabetes mellitus has rapidly developing and advancing erythema, warmth and swelling with bullae formation on the left lower extremity. These findings appear to be advancing proximally several millimeters per hour. Culture results are most likely to reveal
Explanation
the diagnosis is confirmed and an extensive debridement should be performed. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score can be utilized to risk stratify people who have signs of cellulitis and determine the likelihood of necrotizing fasciitis being present. It uses six serologic measures, including C-reactive protein, total white blood cell count, hemoglobin, sodium, creatinine and glucose.
Polymicrobial synergistic infection was the most common cause of necrotizing fasciitis (48 patients; 53.9%) with streptococci and enterobacteriaceae being the most common isolates. Group-A streptococcus was the most common cause of monomicrobial necrotizing fasciitis. The most common associated comorbidity was diabetes mellitus (63 patients; 70.8%).
Question 15
A 26-year-old man was thrown from a car and sustained the injury seen in Figures 44a and 44b. Nonsurgical management of this injury is recommended. Which of the following factors increases the risk of nonunion?
Explanation
REFERENCES: Hill JM, McGuire MH, Crosby LA: Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br 1997;79:537-539.
Wick M, Muller EJ, Kollig E: Midshaft fractures of the clavicle with a shortening of more than
2 cm predispose to nonunion. Arch Orthop Trauma Surg 2001;121:207-211.
Robinson CM, Court-Brown CM, McQueen MM, et al: Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am
2004;86:1359-1365.
Question 16
A 20-year-old college pitcher reports medial elbow pain after 3 innings of hard throwing. He recalls no injury and reports no pain with light throwing. The examination shown in the clinical photograph in Figure 48 reproduces the elbow pain. What is the most likely diagnosis? Review Topic

Explanation
Question 17
A newborn has been referred for evaluation of a deformed foot. Prenatal and birth history are unremarkable. Examination reveals a rocker bottom appearance to the foot, and a longitudinal arch cannot be created. A palpable lump is appreciated on the plantar medial surface. What is the best course of action?
Explanation
REFERENCES: Napiontek M: Congenital vertical talus: A retrospective and critical review of 32 feet operated on by peritalar reduction. J Pediatr Orthop 1995;4:179-187.
Oppenheim W, Smith C, Christie W: Congenital vertical talus. Foot Ankle 1985;5:198-204.
Question 18
When performing the exposure for an anterior approach to the cervical spine, the surgical dissection should not enter the plane between the trachea and the esophagus and excessive retraction should be avoided to prevent injury to the
Explanation
REFERENCES: Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Patel CK, Fischgrund JS: Complications of anterior cervical spine surgery. Instr Course Lect 2003;52:465-469.
Question 19
In patients with suspected hepatitis C, which of the following tests is commonly used to confirm the diagnosis after a positive ELISA screening test?
Explanation
REFERENCES: de Medina M, Schiff ER: Hepatitis C: Diagnostic assays. Semin Liver Dis 1995;15:33-40.
McGrory BJ, Kilby AE: Hepatitis C virus infection: Review and implications for the orthopedic surgeon. Am J Orthop 2000;29:261-266.
Question 20
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?
Explanation
REFERENCES: Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
O’Hara LJ, Marshall RW: Far lateral lumbar disc herniation: The key to the intertransverse approach. J Bone Joint Surg Br 1997;79:943-947.
Question 21
- A 40-year old man has limited, painful motion in dorsiflexion at the metatarsophalangeal (MTP) joint of the right great toe, despite nonsurgical treatment. Radiographs show dorsal and medial osteophytes and minimal narrowing of the articular space. Treatment should consist of
Explanation
Question 22
A 40-year-old man with an acetabular chondrosarcoma has a small soft-tissue mass. Treatment should consist of
Explanation
REFERENCES: Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM: Chondrosarcoma of the pelvis: Prognostic factors for 67 patients treated with definitive surgery. Cancer 1996;78:745-750.
Question 23
A 10-day-old girl has decreased active motion of the left upper extremity. The mother reports a difficult vaginal delivery with presumed shoulder dystocia. Examination shows full passive range of motion of the shoulder, elbow, and wrist but only active flexion of the fingers and wrist. Factors predictive of a good outcome include which of the following?
Explanation
Question 24
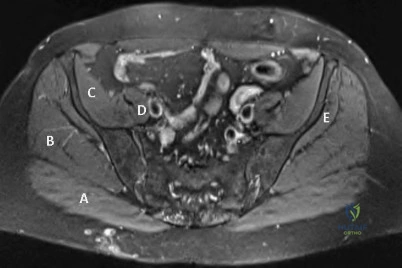
The patient undergoes hip arthroscopy and the image of the right hip is shown in Figure 39. Repair of the injured structure would be expected to improve
Explanation
The radiographic studies reveal both acetabular dysplasia and cam-type femoroacetabular impingement. The MR image shows an acetabular labral tear. Structural abnormalities of the hip, including femoroacetabular impingement, have commonly been identified in association with labral tears. Disruption of the ligamentum teres is not associated with impingement conditions in the absence of trauma.
The patient has acetabular dysplasia with a decreased lateral center-edge angle and also has visible cam-type femoroacetabular impingement. The common pathway for joint degeneration in hips with cam-type femoral head anatomy includes the development of cartilage damage in the anterior or superolateral aspects of the acetabular cartilage. Paralabral cysts may be seen more commonly in association with acetabular dysplasia, although the patient’s radiographs did not demonstrate substantial cystic changes. Osteochondral loose bodies and ligamentum teres ruptures can be seen at arthroscopy in a small number of cases.
There are several proposed roles of the acetabular labrum. It can increase the depth of the acetabular socket by as much as 21% to 28%. Roles of the acetabular labrum include joint lubrication, shock absorption, and pressure distribution. Recent studies assessing the effects of loading on joint stability for both normal and dysplastic hips did not demonstrate a substantial role of the labrum in differences in loading. Although joint stability might be improved following surgical repair, acetabular dysplasia is not likely to be resolved with acetabular labral repair alone.
RECOMMENDED READINGS
Tibor LM, Leunig M. The pathoanatomy and arthroscopic management of femoroacetabular impingement. Bone Joint Res. 2012 Oct 1;1(10):245-57. doi: 10.1302/2046-3758.110.2000105.PubMed: 23610655. View Abstract at PubMed
Peelle MW, Della Rocca GJ, Maloney WJ, Curry MC, Clohisy JC. Acetabular and femoral radiographic abnormalities associated with labral tears. Clin Orthop Relat Res. 2005 Dec;441:327-33. PubMed PMID: 16331022. View Abstract at PubMed
Ross JR, Zaltz I, Nepple JJ, Schoenecker PL, Clohisy JC. Arthroscopic disease classification and interventions as an adjunct in the treatment of acetabular dysplasia. Am J Sports Med. 2011 Jul;39 Suppl:72S-8S. doi: 10.1177/0363546511412320.
PubMed PMID: 21709035. View Abstract at PubMed
James SL, Ali K, Malara F, Young D, O'Donnell J, Connell DA. MRI findings of 37
femoroacetabular impingement. AJR Am J Roentgenol. 2006 Dec;187(6):1412-9. PubMed PMID: 17114529. View Abstract at PubMed
Groh MM, Herrera J. A comprehensive review of hip labral tears. Curr Rev Musculoskelet Med. 2009 Jun;2(2):105-17. doi: 10.1007/s12178-009-9052-9. Epub 2009 Apr 7. PubMed PMID: 19468871. View Abstract at PubMed
Henak CR, Ellis BJ, Harris MD, Anderson AE, Peters CL, Weiss JA. Role of the acetabular labrum in load support across the hip joint. J Biomech. 2011 Aug 11;44(12):2201-6. doi: 10.1016/j.jbiomech.2011.06.011. Epub 2011 Jul 14. PubMed PMID: 21757198. View Abstract at PubMed
Question 25
- A 14-year-old girl has idiopathic scoliosis with a 52-degree right thoracic curve and a 36-degree left lumbar curve. The rotation of the apical vertebra appears greater in the thoracic curve. A sagittal view radiograph shows the spine to be virtually straight. The iliac apophyses are Risser 2. Treatment should consist of
Explanation
Question 26
What structure is located immediately posterior to the capsule at the posterior cruciate ligament tibial insertion?
Explanation
tibial insertion, separated only by the posterior capsule of the knee. When performing
a posterior cruciate ligament reconstruction, this artery is at risk for injury during creation
of the tibial tunnel.
REFERENCES: Jackson DW, Proctor CS, Simon TM: Arthroscopic assisted PCL reconstruction: A technical note on potential neurovascular injury related to drill bit configuration. J Arthroscopy 1993;9:224-227.
Malek MM, Fanelli GC: Technique of arthroscopically assisted PCL reconstruction. Orthopedics 1993;16:961-966.
Question 27
..A lateral radiograph (Figure 131a), sagittal short tau inversion recovery MRI scan (Figure 131b), and an axial T1 contrast MRI scan (Figure 131c) were performed on a 15-year-old boy who has injured his right knee twice during the last 5 months. He has a reduced range of motion of the knee and posterior thigh tenderness. A biopsy showed bland spindle cells, giant cells, and blood-filled spaces without endothelial lining. What is the most appropriate treatment?

Explanation

Figure 132 is the bone scan of a 73-year-old man who is referred from his family doctor with diffuse bone pain, fatigue, and right knee pain. Examination is notable for pain with motion about the right knee and mild hyporeflexia.
Question 28
Which of the following anatomic structures are in contact with internal impingement in the throwing athlete? Review Topic
Explanation
Question 29
A 38-year-old man caught his index finger in a volleyball net. He noted an angular deformity of the finger that was reduced when a teammate pulled on his finger. Three weeks later, he now reports trouble extending his finger. A clinical photograph is shown in Figure 55. What anatomic structure is most likely injured?
Explanation
REFERENCES: Peimer CA, Sullivan DJ, Wild DR: Palmar dislocation of the proximal interphalangeal joint. J Hand Surg Am 1984;9:39-48.
Glickel SZ, Barron OA, Catalano LW: Dislocation and ligament injuries in the digits, in
Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 355.
Question 30
A 75-year-old man who is right-hand dominant has had a painful right shoulder for the past 6 months, with no improvement with nonsurgical management. Examination reveals an active motion of 60 degrees of forward flexion and abduction, with severe crepitus and pain. Radiographs reveal a high-riding humeral head with severe glenohumeral arthritic changes. What is the most appropriate treatment? Review Topic
Explanation
Question 31
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
Explanation
REFERENCES: Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273.
Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Kim WY, Hearn TC, Seleem O, et al: Effect of pin location on stability of pelvic external fixation. Clin Orthop Relat Res 1999;361:237-244.
Question 32
Patients who have osteonecrosis of the humeral head and who have the best prognosis are those with which of the following conditions?
Explanation
REFERENCES: Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head.
J Shoulder Elbow Surg 2002;11:281-298.
Mansat P, Huser L, Mansat M, et al: Shoulder arthroplasty for atraumatic avascular necrosis of the humeral head: Nineteen shoulders followed up for a mean of seven years. J Shoulder Elbow Surg 2005;14:114-120.
Question 33
A 46-year-old man sustains a calcaneal fracture in a fall off a scaffold. During surgical reconstruction using an extended lateral incision, the fracture is reduced and fixed with a plate and screws. One of the posterior facet screws is found to be 5 mm out of the bone on the Harris view. What structure is most likely at risk because of this finding?
Explanation
REFERENCES: Hollinshead WH: Anatomy for Surgeons, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 802-852.
Rosenberg AS, Cheung Y: Diagnostic imaging of the ankle and foot, in Jahss MH (ed): Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991, pp 109-154.
Waggoner AM, Smith JW: Internal fixation of calcaneus fractures: An anatomical study of structures at risk. J Orthop Trauma 1995;9:107-112.
Question 34
Which of the following changes is seen with age and degeneration in the intervertebral disk? Review Topic
Explanation
Question 35
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. Further workup confirms an anterosuperior tear of the acetabular labrum and prominence of the acetabulum. What is the most likely location of a chondral injury associated with these findings?

Explanation
Question 36
Figures 1 through 4 are the radiographs and MR images of a healthy 21-year-old woman who has had persistent dorsal wrist pain despite immobilization and no history of trauma. The surgical procedure associated with the best prognosis in this scenario is
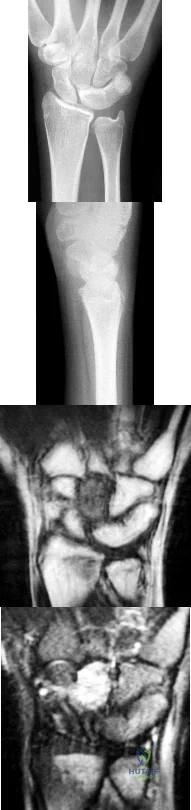
Explanation
This patient has osteonecrosis of the capitate. The MR images show evidence of osteonecrosis with decreased signal on the T1-weighted image. The radiographs are unremarkable, with the exception of lunotriquetral coalition, which does not necessitate treatment. The etiology of osteonecrosis of the capitate may be related to trauma, abnormal Interosseous vascular supply, and hypermobility. Surgery is an option for patients with persistent symptoms despite immobilization. Vascularized bone graft should be considered in this scenario because there is no evidence of capitate collapse or arthritic change about the wrist. Free and local vascularized bone grafts have produced satisfactory results. Capitate excision with interposition arthroplasty is indicated for patients with proximal pole capitate collapse. Total wrist fusion is a salvage procedure and would be considered if there were evidence of collapse and arthritic change. PRC would leave the capitate articulating with the radius and is not indicated.
Question 37
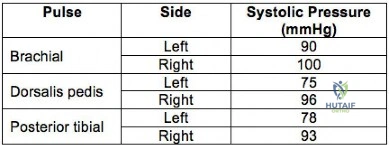
A 32-year-old professional skydiver lands awkwardly during a jump. He presents to the emergency room with bilateral knee injuries. Following successful closed reduction of both extremities, both feet are warm and pulses are present. Bedside doppler assessment is performed and the results are seen in Figure A. What would be the most appropriate next step in treatment?
Explanation
Injury to the popliteal artery is present in 10-40% of knee dislocations (KD). ABI
<0.9 has sensitivity of 87% and specificity of 97% for the diagnosis of arterial disruption. Delayed recognition of an occlusive injury (>8 hours) is likely to result in above knee amputation.
Stannard et al. examined the role of selective arteriography based on serial physical examination. They found arterial injury in 7% (9 out of 134 knees), and abnormal physical findings in 10 patients, with only 1 false positive. They recommend arteriography for patients with decreased pulses, color or temperature, expanding knee hematoma, or an abnormal physical examination prior to presentation in the emergency department.
Mills et al. reviewed the value of ABI for diagnosing arterial injury after knee dislocation. They found that of the 29% with ABI <0.9, all required surgery for arterial injury. Of the remaining patients with ABI >0.9, none had vascular injury. They concluded ABI >0.9 has negative predictive value of 100%.
Nicandri et al. reviewed an algorithm for selective angiography. They recommend the following: (1) Intact pulses and ABI >0.9, observation for 24 hours. (2) Asymmetric pulses or ABI <0.9, arteriogram. (3) Hard signs of vascular injury (absent distal pulses, distal ischemia, active hemorrhage, expanding pulsatile hematoma), surgical exploration.
Figure A is a table showing systolic pressure readings at different sites. To calculate the ABI, the highest measured arterial pressure in the ankle or foot is divided by the higher brachial arterial pressure from both upper extremities.
Incorrect Answers:
Question 38
An AP radiograph of the pelvis is shown in Figure 4. What muscle attaches to the avulsed fragment of bone identified by the arrow?
Explanation
REFERENCES: Woodburne RT (ed): Essentials of Human Anatomy. New York, NY, Oxford University Press, 1978, pp 542-545.
Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Question 39
Which of the following lesions is best suited for autologous chondrocyte implantation?
Explanation
REFERENCES: Mandelbaum BR, Brown JE, Fu F, et al: Articular cartilage lesions of the knee. Am J Sports Med 1998;26:853-861.
Minas T, Nehrer S: Current concepts in the treatment of articular cartilage defects. Orthopedics 1997;20:525-538.
Brittberg M, Lindahl A, Nilsson A, Ohlsson C, Isaksson O, Peterson L: Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 1994;331:889-895.
Question 40
0 sustained a subcapital fracture of her hip. She is an avid tennis player, and history reveals no previous fractures. What is the most appropriate follow-up care? Review Topic
Explanation
Question 41
What is a known risk factor for wound infection after spinal fusion for neuromuscular scoliosis? Review Topic
Explanation
<1500 cells/µL (reference range, 1000-4800/µL) has been associated with increased postoperative wound infections.
Question 42
A 22-year-old woman injured her ankle when she fell off a ladder. Radiographs reveal a displaced large posterior malleolus fracture of about 45% of the joint. What is the best definitive treatment?
Explanation
optimal function can be achieved. Open reduction and internal fixation allows this achievement. In cases where comminution exists, absolute stability may have to be sacrificed so as to not strip small comminuted bone fragments. Therefore, a bridging technique is worthwhile. External fixation can be used as a temporary technique until the soft tissues are more amenable to definitive fixation. Cast treatment is not indicated in adult forearm fractures. Locking nails for forearm use are not reamed. With regards to articular fractures, anatomic reduction and rigid stabilization are required to achieve the best results and allow for fracture healing. This environment also allows for the best chance of the cartilage repair process to form "hyaline-like" cartilage. Open reduction and internal fixation with absolute stability is the mainstay of treatment for partial articular fractures such as split depression tibial plateau fractures and posterior malleolus fractures involving greater than about 25% to 30% of the joint. The gold standard for the treatment of a closed femur fracture is a reamed intramedullary locked nail. Results are uniformly excellent. This can be done without stripping of the soft tissues such as in open reduction and internal fixation. External fixation can be used as a temporary device in patients in extremis for damage control reasons.Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr. Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am. 1986 Sep;68(7):1008-17. http://www.ncbi.nlm.nih.gov/pubmed/3745238')">View Abstract at PubMedJones DB Jr, Kakar S. Adult diaphyseal forearm fractures: intramedullary nail versus plate fixation. J Hand Surg Am. 2011 Jul;36(7):1216-9. Epub 2011 May
Question 43
In which scenario is application of NPWT contraindicated?
Explanation
The most common complication associated with NPWT is a rash on the skin resulting from contact with a suction sponge. In a 2001 study by Webb and Schmidt, 2.2% of patients treated with NPWT had a rash that resolved within 48 hours. To minimize risk for this rash, care should be taken to avoid overlap of the sponge onto intact skin. If skin overlap is unavoidable, a lower-pressure setting should be used.
Acute bacterial infection is possible in this scenario, but there would likely be additional findings such as purulence in the wound itself. Similarly, an acute allergic reaction could be found within the wound and not just at the skin edge. Skin irritation from excessive adhesive plastic tension can result in blistering or shearing avulsion but not skin-edge erythema. Skin necrosis from the original trauma would result in skin-edge duskiness instead of erythema.
A study by Timmers and associates showed a statistically significant increase in microvascular blood flow to the skin under a sponge at subatmospheric pressures. Angiogenesis occurs in the area of the wound vacuum from the negative pressure and increased blood flow, not from the sponge material itself. There has been no indication that antibiotic concentration is increased in the setting of negative pressure therapy because antibiotics would be evacuated along with the fluid. NPWT does not result in increased temperatures that would kill pathogens.
NPWT is contraindicated in the setting of neoplasm because its effect on tumors is unknown. There is potential for increased angiogenesis in residual tumor cells, which could lead to recurrence or even metastasis. NPWT has been used safely and effectively for coverage of open fractures between initial debridement and definitive coverage. Fasciotomy wounds are frequently covered with NPWT dressings on a temporary basis with excellent results.
NPWT has been used to temporize wounds with exposed bone before flap coverage. Wounds with excessive tension frequently can be closed after short-term coverage with NPWT dressings.
RECOMMENDED READINGS
Webb LX, Schmidt U. [Wound management with vacuum therapy]. Unfallchirurg. 2001 Oct;104(10):918-26. German. PubMed PMID: 11699301.View Abstract at PubMed
Webb LX. New techniques in wound management: vacuum-assisted wound closure. J Am Acad Orthop Surg. 2002 Sep-Oct;10(5):303-11. PubMed PMID: 12374481. View Abstract at PubMed
Timmers MS, Le Cessie S, Banwell P, Jukema GN. The effects of varying degrees of pressure delivered bynegative-pressure wound therapy on skin perfusion. Ann Plast Surg. 2005 Dec;55(6):665-71. PubMed PMID: 16327472. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 68 AND 69

Figure 68 is the radiograph of a 17-year-old girl who is treated with closed reduction and percutaneous screw fixation for her displaced femoral neck fracture. Capsulotomy of the hip is not performed. After surgery, the patient is instructed to maintain touch-down weight-bearing status for 3 months.
Question 44
Which of the following studies is considered most sensitive in monitoring a therapeutic response in acute hematogenous osteomyelitis?
Explanation
REFERENCE: Unidia-Kallio L, et al: Serum c-reactive protein, ESR and WBC in acute hematogenous osteomyelitis in children. Pediatrics 1994;93:59-62.
Question 45
below show the radiographs obtained from a year-old woman with a year history of progressive hip pain in the left groin with activity, which is unresponsive to activity modification and physical therapy. Examination reveals normal range of motion, with pain on anterior impingement testing. What treatment is associated with the best long-term results?
Explanation
This patient has symptomatic femoroacetabular impingement as well as clinical and radiographic signs of acetabular retroversion, including a cross-over sign, ischial spine sign, and posterior wall sign bilaterally. Good midterm to long-term outcomes have been reported with reverse (anteverting) Bernese periacetabular osteotomy (PAO). In patients with less retroversion, open or arthroscopic rim trimming with labral refixation have shown good short-term results, but longer-term results have yet to be fully delineated. Isolated hip arthroscopy and labral repair would not be indicated without addressing the retroversion deformity. Femoral varus rotational osteotomy plays no role in the treatment of this pathology. Open surgical dislocation with rim trimming could be considered in patients with less deformity, but some studies have shown inferior long-term results compared with reverse PAO.
Question 46
Which of the following patients has the highest risk of developing recurrent instability after an arthroscopic Bankart procedure for anterior shoulder instability? Review Topic
Explanation
The surgical management of anterior shoulder instability consists of both arthroscopic and open approaches. The guiding principles for treatment are the restoration of the normal glenoid labrum anatomy and retensioning of the inferior glenohumeral ligament which is achieved via soft-tissue reconstructions (repair of any labral detachment +/- capsular shift) or bony procedures (such as transfer of the coracoid process).
Ahmed et al. reviewed 302 patients who had undergone arthroscopic Bankart repair and capsular shift for the treatment of recurrent anterior glenohumeral instability. The prevalence of patient and injury-related risk factors for recurrence was assessed. The rate of recurrent glenohumeral instability after arthroscopic Bankart repair and capsular shift was 13.2%. The risk of recurrence was independently predicted by the patient’s age at surgery, the severity of glenoid bone loss, and the presence of an engaging Hill-Sachs lesion.
Balg et al. identified risk factors for recurrent instability after arthroscopic Bankart procedure in 131 consecutive patients. Age under 20 years at the time of surgery; involvement in competitive or contact sports or those involving forced overhead activity; shoulder hyperlaxity; a Hill-Sachs lesion present on an AP radiograph of the shoulder in external rotation and/or loss of the sclerotic inferior glenoid contour were all identified as risk factors. These factors were integrated into a 10-point preoperative instability severity index score (ISIS). Patients with a score over 6 points had an unacceptable recurrence risk of 70%.
Illustration A summarizes the components of the ISIS as developed by Balg and Boileau.
Incorrect Answers:
Question 47
A patient is scheduled to undergo total knee arthroplasty (TKA) following failure of nonsurgical management. History reveals that she underwent a patellectomy as a teenager as the result of a motor vehicle accident. Examination reveals normal ligamentous stability. For the most predictable outcome, which of the following implants should be used?
Explanation
ligament-sparing knee (P < 0.01). The patella functions to increase the lever arm of the extensor mechanism and to position the quadriceps tendon and the patellar ligament roughly parallel to the anterior cruciate ligament and posterior cruciate ligament, respectively. The patellar ligament thereby provides a strong reinforcing structure that functions to prevent excessive anterior translation of the femur during flexion of the knee. The absence of the patella results in the patellar ligament and the quadriceps tendon being relatively in line with one another. After a patellectomy, the resultant quadriceps force is no longer parallel to the posterior cruciate ligament. This results in loss of the reinforcing function of the patellar ligament. The authors believe this loss of reinforcing function may place increased stresses on the posterior cruciate ligament and posterior aspect of the capsule, which may result in stretching of these structures over time. They found a high rate of anteroposterior instability, a high prevalence of recurvatum, and a high rate of loss of full active extension compared with passive extension in the posterior cruciate ligament-sparing group, which supports their theory.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
Paletta GA Jr, Laskins RS: Total knee arthroplasty after a previous patellectomy. J Bone Joint Surg Am 1995;77:1708-1712.
Question 48
Scapular notching following reverse shoulder arthroplasty may be minimized by what technical modification? Review Topic
Explanation
Question 49
Figures 1a through 1c show the radiograph and MRI scans of a 16-year-old patient who has a painful hip. Examination reveals a significant limp, limited abduction and internal rotation, and severe pain with internal rotation and adduction. A biopsy specimen is shown in Figure 1d. What is the deposited pigment observed in this condition?
Explanation
REFERENCES: Bhimani MA, Wenz JF, Frassica FJ: Pigmented villonodular synovitis: Keys to early diagnosis. Clin Orthop 2001;386:197-202.
Cotten A, Flipo RM, Chastanet P, et al: Pigmented villonodular synovitis of the hip: Review of radiographic features in 58 patients. Skeletal Radiol 1995;24:1-6.
Question 50
Increasing articular conformity of the tibial polyethylene insert of a fixed-bearing total knee arthroplasty (TKA) prosthesis will have which of the following biomechanical effects?
Explanation
REFERENCES: D’Lima DD, Chen PC, Colwell CW Jr: Polyethylene contact stresses, articular congruity, and knee alignment. Clin Orthop 2001;392:232-238.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 265-274.
Question 51
A 35-year-old woman states that she stepped on a piece of glass 6 months ago and reports numbness and shooting pain along the plantar lateral forefoot. She had previously received steroid injections in the 3 to 4 webspace. Examination reveals mild tenderness along the plantar fascia; no Tinel’s sign is noted plantar medially and no Mulder’s click is noted distally. An MRI scan is shown in Figure 7. What is the most likely cause of the numbness?
Explanation
REFERENCES: Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop Relat Res 1992;279:229-236.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional. Philadelphia, PA, JB Lippincott, 1983.
Question 52
An 8-year-old boy is diagnosed with acute onset cauda equina syndrome. A radiograph, MRI scans, and a biopsy specimen are shown in Figures 57a through 57d. What is the most appropriate treatment?
Explanation
REFERENCES: Mankin HJ, Hornicek FJ, Ortiz-Cruz E, et al: Aneurysmal bone cyst: A review of 150 patients. J Clin Oncol 2005;23:6756-6762.
Garg S, Mehta S, Dormans JP: Modern surgical treatment of primary aneurysmal bone cyst of the spine in children and adolescents. J Ped Orthop 2005;25:387-392.
Question 53
Which of the following describes the correct proximal to distal progression of the annular and cruciform pulleys of the digits?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 176-186.
Strickland J: Flexor tendon-acute injuries, in Green D, Hotchkiss R, Pederson W (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1853-1855.
Question 54
Patient-specific instrumentation (PSI) reliably demonstrates which benefit over conventional intramedullary guidance systems?
Explanation
Cost is usually increased with PSI because the theoretical decreased number of surgical trays and shortened surgical time do not offset cost of presurgical imaging and extra cost associated with the necessary jigs. Studies do not demonstrate a reliable improvement in functional outcomes or coronal alignment when PSI is compared to standard instrumentation. Evidence reveals that PSI necessitates fewer trays than standard instrumentation.
Question 55
Which factor should most influence a patient's decision to have surgery for adult scoliosis if he or she is younger than age 50?
Explanation
In a retrospective review of 137 patients treated surgically and 153 patients treated nonsurgically for adult scoliosis, Bess and associates found that surgical treatment for patients younger than 50 years of age was driven by increased coronal plane deformity, and surgical treatment for older patients was mandated by pain and disability. They also concluded that age, comorbidities, and sagittal balance did not influence treatment decisions.
RECOMMENDED READINGS
Bess S, Boachie-Adjei O, Burton D, Cunningham M, Shaffrey C, Shelokov A, Hostin R, Schwab F, Wood K, Akbarnia B; International Spine Study Group. Pain and disability determine treatment modality for older patients with adult scoliosis, while deformity guides treatment for younger patients. Spine (Phila Pa 1976). 2009 Sep 15;34(20):2186-90. PubMed PMID: 19752704.View Abstract at PubMed
Anderson DG, Albert T, Tannoury C. Adult scoliosis. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:331-338.
Question 56
- The radiographs shown in Figures 71a through 71c, and the CT scan shown in Figure 71d reveal an acetabular fracture that should be classified as
Explanation
Note the classic “Spur Sign” seen in these radiographs. This is pathognomonic of a both-column fracture of the acetabulum.
The other defining feature of the both column fx (as evident by these films) is that there is no intact acetabulum connected to the bone fragment which is connected to the ipsilateral SI joint.
Question 57
Which of the following nonunions is appropriately treated with exchange reamed nailing without bone graft augmentation?

Explanation
Question 58
A 22-year-old female collegiate javelin thrower has shoulder pain. She notes that her pain is primarily located in the posterior aspect of her shoulder, is exacerbated with throwing, and she experiences maximal tenderness in the extreme cocking phase of the throwing cycle. On examination, she reports deep posterior shoulder pain when the arm is abducted 90 degrees and maximally externally rotated to 110 degrees. This reproduces her symptoms precisely. Shoulder radiographs are normal. What is the most likely diagnosis? Review Topic
Explanation
Question 59
Figures 23a and 23b show the MRI scans of a 50-year-old woman who has increasing gait disturbance. She reports three falls in the past week. Examination reveals hyperreflexia, motor weakness in the biceps and triceps, and a positive Hoffman’s sign. What is the most appropriate treatment plan? Review Topic

Explanation
(SBQ12SP.77) A 68-year-old is undergoing lateral lumbar interbody fusion using the tranpsoas approach. Which of the following statements is true regarding the safe approach zone for this procedure as you move cranial to caudal in the lumbar spine? Review Topic
Safe approach zone increases due to vessels moving more ventral
Safe approach zone increases due to lumbar plexus moving more dorsal
Safe approach zone decreases due to vessels moving more dorsal
Safe approach zone decreases due to lumbar plexus moving more ventral
Safe approach zone remains the same throughout the lumbar spine
As you move cranial to caudal in the lumbar spine, the safe approach zone for the lateral transpsoas approach decreases due to the more ventral position of the lumbar plexus.
Lateral lumbar interbody fusion has become more common for degenerative spine disorders and adjacent segment degeneration. This transpsoas approach is typically useful for pathology from L1-L2 disc space to the L4-L5 disc space and places the lumbar plexus at risk. Working at the more caudal disc spaces is especially difficult given the more ventral position of the plexus, but the use of triggered EMG retractors and probes can help prevent nerve injuries. Surgical approach can be especially difficult in patients with rotational deformities.
Benglis et al. did a cadaver study with specimens placed lateral to trace the course of the lumbar plexus. They found that the plexus move more ventral with respect to the disc space moving more caudal in the lumbar spine.
Park et al. used 10 cadaver specimens to measure the distance of the lumbar nerve roots from the center of the disc space in the lateral approach. While disc space access was generally safe, there was less distance to the nerve root for more caudal disc levels.
Regev et al. did a MRI study to evaluate the safe working corridor for the lateral approach. The safe zone narrows considerably in the L4-L5 disc space due to more
ventral position of the nerve roots, and they recommend careful monitoring when addressing this level.
Incorrect
Question 60
A 10-year-old boy who plays baseball reports acute pain after throwing a softball from the outfield to second base. A radiograph is shown in Figure 26. Management should consist of
Explanation
REFERENCE: Yandow SM, Lundeen GA, Scott SM, Coffin C: Autogenic bone marrow injections as a treatment for simple bone cyst. J Pediatr Orthop 1998;18:616-620.
Question 61
When harvesting iliac crest bone graft during a posterior spinal decompression and fusion, injury to which of the following nerves may result in painful neuromas or numbness over the skin of the buttocks?
Explanation
REFERENCES: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD,
Williams and Wilkins, 1998, pp 770-773.
Kurz LT, Garfin SR, Booth RE: Harvesting autogenous iliac bone grafts: A review of complications and techniques. Spine 1989;14:1324-1331.
Question 62
During the first 2 years of life, which of the following actions is most responsible for increasing structural stability of the physis?
Explanation
REFERENCES: Burkus J, Ogden J: Development of the distal femoral epiphysis: A microscopic morphological investigation of the zone of Ranvier. J Pediatr Orthop 1984;4:661-668.
Shapiro F, Holtrop ME, Glimcher MJ: Organization and cellular biology of the perichondrial ossification groove of Ranvier: A morphological study in rabbits. J Bone Joint Surg Am 1977;59:703-723.
Question 63
What is the most common reason an individual with a malignant soft-tissue tumor in the extremities seeks medical attention?
Explanation
REFERENCES: Brouns F, Stas M, De Wever I: Delay in diagnosis of soft tissue sarcomas. Eur J Surg Oncol 2003;29:440-445.
Rougraff B: The diagnosis and management of soft tissue sarcomas of the extremities in the adult. Curr Probl Cancer 1999;23:1-50.
Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 64
Tension force in the anterior cruciate ligament during passive range of motion is highest at
Explanation
REFERENCES: Markolf KL, Burchfield DM, Shapiro MM, et al: Biomechanical consequences of replacement of the anterior cruciate ligament with a patellar ligament allograft. Part II: Forces in the graft compared with forces in the intact ligament. J Bone Joint Surg Am 1996;78:1728-1734.
Beynnon BD, Johnson RJ, Fleming BC, et al: The measurement of elongation of anterior cruciate-ligament grafts in vivo. J Bone Joint Surg Am 1994;76:520-531.
Question 65
Type I collagen fibers in peripheral nerves are primarily responsible for which of the following?
Explanation
The COL1A1 gene produces a component of type I collagen, called the pro-alpha1(I) chain. This chain combines with another pro-alpha1(I) chain and also with a pro-alpha2(I) chain (produced by the COL1A2 gene) to make a molecule of type I procollagen. These triple-stranded, rope-like procollagen molecules must be processed by enzymes outside the cell. Once these molecules are processed, they arrange themselves into long, thin fibrils that cross-link to one another in the spaces around cells. The cross-links result in the formation of very strong mature type I collagen fibers.
Wong et al. provide a review of the basic science behind nerve healing and the recovery after nerve repair. They note the importance of minimizing additional surgical insult and careful handling of nerve tissue during repair to optimize outcomes.
Pertici et al. noted that autologous nerve implantation to bridge a long nerve gap presents the greatest regenerative performance in spite of substantial drawbacks. They were able to show improved nerve guided regrowth with a type I collagen matrix conduit as compared to a conduit made of a mix of type I and type III collagen.
Illustration A shows a diagram of type I collagen, showing the rope-like characteristics behind the tensile strength.
Incorrect Answers:
Question 66
A toddler is brought in by his parents for evaluation of gait problems. Birth history and neurologic examination are unremarkable. After evaluating femoral torsion, tibial torsion, and foot contour, the diagnosis is excessive internal tibial torsion. The parents should be advised to expect which of the following outcomes? Review Topic
Explanation
Question 67
repair of the rotator cuff
Explanation
Question 68
A 38-year-old woman has a lesion on her left foot that has increased in size over the past 6 months. The clinical photograph is shown in Figure 17a, and a photomicrograph of the biopsy specimen is shown in Figure 17b. What is the most likely diagnosis?
Explanation
REFERENCES: Hughes LE, Horgan K, Taylor BA, Laidler P: Malignant melanoma of the hand and foot: Diagnosis and management. Br J Surg 1985;72:811-815.
Fortin PT, Freiberg AA: Malignant melanoma of the foot and ankle. J Bone Joint Surg Am 1995;77:1396-1403.
Question 69
A 25-year-old construction worker lands on his outstretched hand in a fall. The position of his wrist at the time of impact causes a force that leads to hyperextension, ulnar deviation, and intercarpal supination. Radiographs are shown in Figures 48a and 48b. What type of injury pattern is shown?
Explanation
REFERENCES: Mayfield JK, Johnson RP, Kilcoyne RK: Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-241.
Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J: Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-779.
Question 70
In patients with Crowe types III and IV developmental dysplasia of the hip with high hip centers, acetabular reconstruction often requires lowering the acetabular component into the native acetabulum. In doing so, considerable risk for limb lengthening beyond 4 cm exists, making the hip difficult to reduce and raising the risk for nerve injury. Which technique is used to overcome this problem?
Explanation
When substantial lengthening of a dysplastic hip will occur because a high dislocation is relocated into a considerably lower acetabulum, a femoral shortening may be necessary to reduce the hip and avoid a stretch injury to the sciatic nerve. No other choice specifically addresses the need for femoral shortening, and high offset stems and lateralized liners may exacerbate the problem if used alone and without femoral shortening.
Question 71
What is the heaviest weight that can be safely applied to the adult cervical spine via Gardner-Wells tong traction?
Explanation
REFERENCES: Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Anderson DG, Vacccaro AR, Gavin K: Cervical orthoses and cranioskeletal traction, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005,
pp 110-121.
Question 72
A 42-year-old athletic trainer has a persistent popping sensation about the lateral ankle associated with weakness and pain following a remote injury. Deficiency in what structure directly leads to this pathology?
Explanation
the condition.
REFERENCE: Maffuli N, Ferran NA, Oliva F, et al: Recurrent subluxation of the peroneal tendons. Am J Sports Med 2006;34:986-992.
Question 73
A 34-year-old male presents with elbow pain after sustaining a ground level fall 2 weeks ago. An injury radiograph is shown in Figure
Explanation

OrthoCash 2020
Question 74
Which of the following statements regarding conus medullaris syndrome is most accurate?
Explanation
REFERENCES: Haher TR, Felmly WT, O’Brien M: Thoracic and lumbar fractures: Diagnosis and management, in Bridwell KH, Dewald RL, Hammerberg KW, et al (eds): The Textbook of Spinal Surgery, ed 2. New York, NY, Lippincott Williams & Wilkins, 1977, pp 1773-1778.
Reitman CA (ed): Management of Thoracolumbar Fractures. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 35-45.
Question 75
Which of the following is considered the preferred approach to resect a lesion in the posterior one third of the proximal humerus?
Explanation
REFERENCE: Berger RA, Buckwalter JA: A posterior surgical approach to the proximal part of the humerus. J Bone Joint Surg Am 1989;71:407-410.
Question 76
A 65-year-old woman with type II diabetes mellitus (most recent Hgb A1C was 8.2) has had 3 days of left knee pain. Physical examination of the left knee reveals erythema, warmth and a large effusion. Range of motion is painful and limited to 30 degrees of flexion. She is found to be hypotensive and not responding to volume resuscitation. She requires phenylephrine to maintain Mean Arterial Pressure (MAP) of 70. ESR and CRP are elevated and Lactate is 3.1 mmol/L. What is the next best intervention for this patient’s treatment?
Explanation
Question 77
Figures 45a and 45b show the radiographs of a 46-year-old man who reports the acute onset of right knee pain and is unable to bear weight on the extremity. His medical history is unremarkable. The next most appropriate step in management should consist of
Explanation
REFERENCE: Rougraff BT, Kneisl JS, Simon MA: Skeletal metastases of unknown origin: A prospective study of a diagnostic strategy. J Bone Joint Surg Am 1993;75:1276-1281.
Question 78
A 77-year-old woman who underwent total knee arthroplasty 16 years ago now reports pain, swelling, and notable crepitation with range of motion. AP, lateral, and Merchant radiographs are shown in Figures 54a through 54c. What is the most likely diagnosis?
Explanation
REFERENCES: Poss R (ed): Orthopaedic Knowledge Update 3. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, pp 590-593.
Leopold SS, Berger RA, Patterson L, et al: Serum titanium level for diagnosis of a failed metal-backed patellar component. J Arthroplasty 2000;15:938-943.
Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1993, pp 613-614.
Question 79
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following?
Explanation
REFERENCES: Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10.
Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Edwards TB, Walch G, Sirveaux F, et al: Repair of tears of the subscapularis. J Bone Joint Surg Am 2005;87:725-730.
Question 80
A 28-year-old cowgirl was injured while herding cattle 1 week ago. A radiograph and CT scans are shown in Figures 13a through 13c. What is the most appropriate management for this injury?
Explanation
REFERENCES: Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96.
Templeman DC, Schmidt AH, Sems SA, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.
Tile M: Management, in Tile M: Fractures of the Pelvis and Acetabulum, ed 2. Philadelphia, PA, Williams and Wilkins, 1995, pp 108-134.
Question 81
Figures 5a and 5b show the radiographs of a 21 -year-old wrestler who reports that his leg was rolled over while wrestling. The patient has decreased sensation and function in the distribution of the peroneal nerve, and he has absent pulses. What is the most appropriate initial management at this time?
Explanation
intervention of the artery, but documentation with studies would be appropriate. Delayed reconstruction of injured structures is appropriate.
REFERENCES: Fanelli GC, Orcutt DR, Edson CJ: The multiple- ligament injured knee: Evaluation, treatment, and results. Arthroscopy 2005;21:471 -486.
McDonough EB Jr, Wojtys EM: Multiligamentous injuries of the knee and associated vascular injuries.
Am J Sports Med 2009;37:156-159.
Wascher DC: High-velocity knee dislocation with vascular injury: Treatment principles. Clin Sports Med 2000;19:457-477.
Question 82
An 11-year-old basketball player reports that he felt a painful pop in the left knee when he stumbled while running. He is unable to bear weight on the extremity and cannot actively extend the knee against gravity. Examination reveals a large knee effusion. A lateral radiograph is shown in Figure 7. Management should consist of
Explanation
REFERENCES: Maguire JK, Canale ST: Fractures of the patella in children and adolescents.
J Pediatr Orthop 1993;13:567-571.
Grogan DP, Carey TP, Leffers D, et al: Avulsion fractures of the patella. J Pediatr Orthop 1990;10:721-730.
Question 83
A 35-year-old woman dislocated her right shoulder in a fall from a step stool several months ago. She now reports several painful recurrences. Examination reveals anterior and inferior apprehension that reproduces her symptoms. An MRI scan is shown in Figure 17. Management should consist of
Explanation
REFERENCES: Wolf EM, Cheng JC, Dickson K: Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Bokor DJ. Conboy VB. Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br
1999;81:93-96.
Coates MH, Breidahl W: Humeral avulsion of the anterior band of the inferior glenohumeral ligament with associated subscapularis bony avulsion in skeletally immature patients. Skeletal Radiol 2001;30:661-666.
Question 84
Spontaneous entrapment of the posterior interosseous nerve most commonly occurs in which of the following locations?
Explanation
REFERENCE: Spinner RJ, Spinner M: Nerve entrapment syndromes, in Morrey BF: The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 839-862.
Question 85
A patient undergoes an arthroscopic debridement for lateral epicondylitis. Postoperatively she reports pain and a sense of clicking of the elbow. Examination reveals apprehension to supination, load, and extension. What structure has been injured resulting in the clinical presentation?
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 318.
O’ Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Question 86
What is the most common complication following metatarsal osteotomy for a bunion deformity in an adolescent?
Explanation
Physeal arrest of the first metatarsal-“While an open epiphysis cannot be considered an absolute contraindication to an osteotomy in either the proximal phalanx, or proximal first metatarsal, it is
important at surgery to determine the exact location of the metaphyseal epiphysis to avoid injury.” Pg. 307 Mann, Surgery of Foot and Ankle.
In studies performed by Blais et. Al. A females full foot growth is usually achieved by 14 years and at 12 years an average less than 1 cm of total foot growth remains with less than 50% of this growth at the proximal epiphysis. Males’ terminal growth expected at 16 years of age with 3cm left at 12 years and approximately 1.5 cm of metatarsal growth.
Most studies show recurrence of Hallux Valgus deformity after surgical correction in the juvenile as inordinately high.
Question 87
A 61-year-old man reports right hip pain and limited motion after undergoing total hip arthroplasty for posttraumatic arthritis 1 year ago. Figure 6 shows an AP radiograph of the pelvis. To improve motion and relieve pain, management should consist of
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Iorio R, Healy WL: Heterotopic ossification after total hip and total knee arthroplasty: Risk factors, prevention, and treatment. J Am Acad Orthop Surg 2002;10:409-416.
Question 88
A 34-year-old woman reports constant midlateral arm pain after sustaining minimal trauma to the shoulder. Radiographs and a biopsy specimen are shown in Figures 29a and 29b. What is the most likely diagnosis?
Explanation
REFERENCES: Campanacci M, Baldini N, Boriani S, et al: Giant cell tumor of bone. J Bone Joint Surg Am 1987;69:106-114.
Goldenberg RR, Campbell CJ, Bonfiglio M: Giant cell tumor of bone: An analysis of two hundred and eighteen cases. J Bone Joint Surg Am 1970;52:619-664.
Question 89
In infantile idiopathic scoliosis, which of the following factors suggests progression? Review Topic
Explanation
Question 90
below demonstrate the radiographs obtained from a year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. A further work-up reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MRI with MARS. Revision THA is recommended. The most common complication following revision of a failed metal-on- metal hip arthroplasty is
Explanation
Question 91
Figures 71a and 71b/ are the MR images of a 65-year-old man who dislocated his shoulder. What is his most likely chief symptom?
Explanation
This patient has a massive rotator cuff tear resulting in disruption of the transverse force couple between the subscapularis anteriorly and the infraspinatus and teres minor posteriorly. These muscles provide dynamic shoulder stability throughout active elevation. Loss of the force couple produces a pathologic increase in translation of the humeral head and decreased active abduction and external rotation, which results in difficulty raising an arm. The most common neurologic deficit after shoulder dislocation is isolated injury to the axillary nerve that supplies sensation to the lateral aspect of the shoulder, not the anterior aspect. Recurrent instability is uncommon unless there is a labral tear or massive subscapularis tear. The biceps muscle is not viewed in the MR images, and a complete proximal biceps tendon rupture would be uncommon in the setting of an anterior shoulder dislocation.

CLINICAL SITUATION FOR QUESTIONS 72 THROUGH 75
Figures 72a through 72e are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0 degrees
to 90 degrees and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted.
Question 92
A 16-year-old girl has had pain and swelling along the medial arch of her left foot for the past 3 months. She also reports pain from shoe wear and while running. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 40a through 40c. What is the next most appropriate step in management?
Explanation
REFERENCES: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, p 655.
Bennett GL, Weiner DS, Leighley B: Surgical treatment of symptomatic accessory tarsal navicular. J Pediatr Orthop 1990;10:445-449.
Question 93
A 6-year-old boy with severe spastic quadriplegic cerebral palsy is nonambulatory. Examination reveals 10° of hip abduction on the left and 30° on the right with the hips and knees extended. The Thomas test shows 20° of flexion bilaterally, and Ely test results are 3+/4 bilaterally. Radiographs show a center edge angle of 0° on the left and -10° on the right. The neck shaft angles are 170° bilaterally. Which of the following procedures would offer the best results?
Explanation
REFERENCES: Tylkowski CM, Rosenthal RK, Simon SR: Proximal femoral osteotomy in cerebral palsy. Clin Orthop 1980;151:183-192.
Brunner R, Baumann JU: Long-term effects of intertrochanteric varus-derotation osteotomy on femur and acetabulum in spastic cerebral palsy: An 11- to 18-year follow-up study. J Pediatr Orthop 1997;17:585-591.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 94
Figures 1 through 4 are the CT scans and intraoperative image of a 17-year-old boy who sustained a gunshot wound to his knee. What is the most appropriate definitive surgical management for his articular cartilage defect?
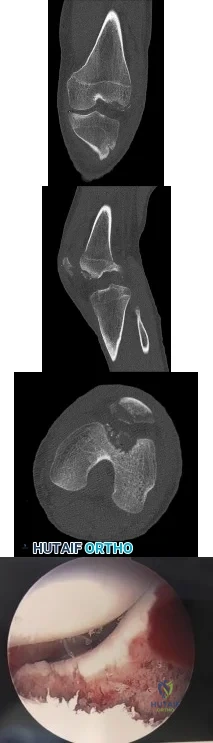
Explanation
Question 95
A 46-year-old man has acute tenderness along the ulnar aspect of the wrist after falling on his outstretched hand while playing basketball. Examination reveals tenderness and mild swelling along the volar ulnar aspect of the wrist. Radiogaphs are shown in Figures 14a through 14c. Management should consist of
Explanation
REFERENCES: Failla JM, Amadio PC: Recognition and treatment of uncommon carpal fractures. Hand Clin 1988;4:469-476.
Botte MJ, Gelberman RH: Fractures of the carpus, excluding the scaphoid. Hand Clin 1987;3:149-161.
Question 96
- What factor is most commonly associated with malignant transformation of a giant cell tumor?
Explanation
Question 97
A 29-year-old man sustained an injury when he was playing basketball, landing on his left knee while jumping for a rebound. He had vague pain in the anterior aspect of the knee for several weeks. The initial radiographs were negative with the exception of a large traumatic effusion. Examination reveals no apparent ligament instability but a significant extension lag of 30 degrees. There was a palpable defect above the superior pole of the patella. What is the most appropriate management? Review Topic
Explanation
Question 98
What is the typical MRI signal intensity of bone marrow affected by acute osteomyelitis?
Explanation
REFERENCES: Unger E, Moldofsky P, Gatenby R, et al: Diagnosis of osteomyelitis by MR imaging. Am J Roentgenol 1988;150:605-610.
Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 150-163.
Question 99
A 62-year-old woman with soft-tissue calcifications and telangiectasia has severe pain in the left index, middle, ring, and little fingers. History reveals that she does not smoke. The clinical history and arteriogram shown in Figure 6 are consistent with which of the following conditions?
Explanation
REFERENCES: Koman LA, Ruch DS, Patterson Smith B, et al: Vascular disorders, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2, pp 2254-2302.
Miller LM, Morgan RF: Vasospastic disorders: Etiology, recognition, and treatment. Hand Clin 1993;9:171-187.
Question 100
A 41-year-old right-hand-dominant man has been treated nonsurgically for right elbow arthritis. His radiographs reveal end-stage ulnohumeral arthritis with complete loss of the joint space. He reports pain during the mid-arc of elbow flexion and extension. During the last 8 years, he has attempted activity modification, medication, physical therapy, and multiple cortisone injections. His symptoms have progressed, resulting in constant pain, loss of a functional range of motion, and an inability to perform many activities of daily living. Secondary to his age and activity demands, he undergoes a soft-tissue interposition arthroplasty of his elbow with an Achilles allograft. Which presurgical finding correlates with elevated risk for postsurgical complications?
Explanation
restrictions for patients after surgery and remains a reasonable salvage procedure. Larson and Morrey published their findings on 38 patients with a mean age of 39 years following soft-tissue interposition arthroplasty for posttraumatic and inflammatory end-stage elbow arthritis. These investigators reported a significant improvement in Mayo Elbow Performance Score in addition to improvement in the flexion- extension arc from 51° to 97° after surgery. They reported worse results and elevated incidence of complications for patients with presurgical elbow instability upon examination; retained hardware from prior
surgery was not deemed a contraindication.
