Orthopedic Board Exam MCQs: Arthroplasty & Wrist Surgery | Part 60

Key Takeaway
This page offers Part 60 of a comprehensive OITE/AAOS Orthopedic Surgery Board Review. It features 100 high-yield, verified MCQs tailored for orthopedic residents and surgeons. This interactive quiz focuses on Arthroplasty and Wrist, providing vital practice to prepare for board certification exams.
About This Board Review Set
This is Part 60 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 60
This module focuses heavily on: Arthroplasty, Wrist.
Sample Questions from This Set
Sample Question 1: Figure 33 shows the radiograph of a 28-year-old avid golfer who has chronic right wrist pain. Management should consist of...
Sample Question 2: Which of the following is accurate regarding low-molecular-weight heparin used for deep venous thrombosis (DVT) prophylaxis in total joint arthroplasty?...
Sample Question 3: Figures 1 and 2 are the radiographs of an 18-year-old man who had surgery 6 months ago at an outside institution. He is being referred now because he has persistent pain. He is tender over the scaphoid at the snuffbox. What is the most appr...
Sample Question 4: A 26-year-old man falls off a motorcycle and injures his left wrist. There are no open wounds and the neurovascular examination is normal. Radiographs are shown in Figures 10a and 10b. Definitive management should consist of...
Sample Question 5: A 19-year-old college student reports a 1-week history of wrist pain following an intramural rugby match. A PA radiograph is shown in Figure 6. He denies any prior wrist injury. What is the best course of action?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 33 shows the radiograph of a 28-year-old avid golfer who has chronic right wrist pain. Management should consist of
Explanation
REFERENCES: Geissler WB: Carpal fractures in athletes. Clin Sports Med 2001;20:167-188.
Rettig ME, Dassa GL, Raskin KB, Melone CP Jr: Wrist fractures in the athlete: Distal radius and carpal fractures. Clin Sports Med 1988;17:469-489.
Question 2
Which of the following is accurate regarding low-molecular-weight heparin used for deep venous thrombosis (DVT) prophylaxis in total joint arthroplasty?
Explanation
to 18 hours. This is greater than the 1 hour half-life of unfractionated heparin.
Low-molecular-weight heparin offers an advantage over unfractionated heparin by selectively targeting Factor Xa while having a lesser effect on circulating thrombin (Factor IIa). Circulating thrombin Factor IIa is needed for local hemostasis at the site of the surgical wound. Clinical studies have shown a reduction by one third in the incidence of thrombocytopenia with the use of low-molecular-weight heparin. Low-molecular-weight heparin has been shown to demonstrate similar clinical results compared to warfarin with respect to preventing thromboembolic disease after total hip arthroplasty and complications such as bleeding.
REFERENCES: Zimlich RH, Fulbright BM, Friedman RJ: Current status of anticoagulation therapy after total hip and total knee arthroplasty. J Am Acad Orthop Surg 1996;4:54-62.
Colwell CW Jr, Spiro TE, Trowbridge AA, et al: Use of enoxaparin, a low-molecular-weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14.
Torholm C, Broeng L, Jorgensen PS, et al: Thromboprophylaxis by low-molecular-weight heparin in elective hip surgery: A placebo controlled study. J Bone Joint Surg Br 1991;73:434-438.
Question 3
Figures 1 and 2 are the radiographs of an 18-year-old man who had surgery 6 months ago at an outside institution. He is being referred now because he has persistent pain. He is tender over the scaphoid at the snuffbox. What is the most appropriate next imaging step in his pain workup?

Explanation
Scaphoid nonunions are difficult to diagnose on plain radiographs, which offer poor reliability when attempting to determine if there is bridging trabeculae crossing the fractures site. CT scans are more useful for diagnosing scaphoid nonunion. When scanned using conventional axial cuts, the slices mayskip through the fracture nonunion site, thereby missing the defect, even with reformats. MR imaging is useful in diagnosing acute scaphoid fractures and has a high sensitivity and diagnostic value for excluding scaphoid fractures as well. Contrast does not enhance the utility of MR imaging in fracture diagnosis.
Question 4
A 26-year-old man falls off a motorcycle and injures his left wrist. There are no open wounds and the neurovascular examination is normal. Radiographs are shown in Figures 10a and 10b. Definitive management should consist of
Explanation
REFERENCES: May MM, Lawton JN, Blazar PE: Ulnar styloid fractures associated with distal radius fractures: Incidence and implications for distal radioulnar joint instability. J Hand Surg Am 2002;27:965-971.
Nana AD, Joshi A, Lichtman DM: Plating of the distal radius. J Am Acad Orthop Surg 2005;13:159-171.
Question 5
A 19-year-old college student reports a 1-week history of wrist pain following an intramural rugby match. A PA radiograph is shown in Figure 6. He denies any prior wrist injury. What is the best course of action?
Explanation
REFERENCES: Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
Chan KW, McAdams TR: Central screw placement in percutaneous screw scaphoid fixation: A cadaveric comparison of proximal and distal techniques. J Hand Surg Am 2004;29:74-79.
Bedi A, Jebson PJ, Hayden RJ, et al: Internal fixation of acute non-displaced scaphoid waist fractures via a limited dorsal approach: An assessment or radiographic and functional outcomes. J Hand Surg Am 2007;32:326-333.
McCallister WV, Knight J, Kaliappan R, et al: Central placement of the screw in simulated fractures of the scaphoid waist: A biomechanical study. J Bone Joint Surg Am 2003;85:72-77.
Question 6
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. What test should be performed to aid in this diagnosis?
Explanation
Question 7
A 13-year-old girl who competes in gymnastics reports the insidious onset of lateral left elbow pain over the past 6 months. She also notes occasional catching episodes in the elbow; however, she denies any history of trauma. Examination reveals tenderness over the lateral epicondyle and extensor muscle origin. The elbow is stable and has full flexion, but lacks 10° of full extension. An AP plain radiograph and an MRI scan are shown in Figures 17a and 17b. Management of the elbow should consist of
Explanation
REFERENCES: Baumgarten TE, Andrews JR, Satterwhite YE: The arthroscopic classification and treatment of osteochondritis dissecans of the capitellum. Am J Sports Med
1998;26:520-530.
Jackson DW, Silvino N, Reiman P: Osteochondritis in the female gymnast’s elbow. Arthroscopy 1989;5:129-136.
Ruch DS, Cory JW, Poehling GG: The arthroscopic management of osteochondritis dissecans of the adolescent elbow. Arthroscopy 1998;14:797-803.
Question 8
A 25-year-old construction worker lands on his outstretched hand in a fall. The position of his wrist at the time of impact causes a force that leads to hyperextension, ulnar deviation, and intercarpal supination. Radiographs are shown in Figures 48a and 48b. Management should consist of
Explanation
REFERENCES: Kozin SH: Perilunate injuries: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:114-120.
Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J: Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-779.
Sotereanos DG, Mitsionis GJ, Ginnakopoulos PN, Tomaino MM, Herndon JH: Perilunate dislocation and fracture dislocation: A critical analysis of the volar-dorsal approach. J Hand Surg Am 1997;22:49-56.
Question 9
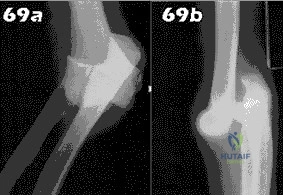
- Following closed reduction for the injury shown in Figures 69a and 69b, treatment should consist of
Explanation
Repair or reconstruction of the medial and lateral collateral ligaments-Acute dislocations can be reduced in supination and tested for valgus stability in pronation. Treatment is determined by the stability following reduction. When there are fractures, the principle is to fix the bones so that the only limitation is the ligaments and then to repair them if the elbow is not stable enough to permit early motion.
Immobilization for 14 days-The longer the immobilization had been, the larger the flexion contracture (p less than 0.001) and the more severe the symptoms of pain were. The results indicate that early active motion is the key factor in rehabilitation of the elbow after a dislocation. Simple dislocation of the elbow in the adult. Results after
closed treatment. Immobilization for 25 days- See above.
Question 10
Which of the following treatments of polyethylene results in the highest amount of oxidative degradation?
Explanation
REFERENCES: Sanford WM, Saum KA: Accelerated oxidative aging testing of UHMWPE. Trans Orthop Res Soc 1995;20:119.
Sun DC, Schmidig G. Stark C, et al: On the origins of a subsurface oxidation maximum and its relationship to the performance of UHMWPE implants. Trans Soc Biomater 1995;18:362.
Callaghan JJ, Dennis DA, Paprosky WA, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 35-41.
McKellup HA: Bearing surfaces in total hip replacement: State of the art and future developments. Instr Course Lect 2001;50:165-179.
Question 11
What fibers of the anterior cruciate ligament tighten with extension of the knee? Review Topic
Explanation
Question 12
-The use of a soft cervical orthosis is most supported for which injury?
Explanation

Question 13
Which of the following best characterizes bone mineralization?
Explanation
REFERENCES: Lian JB, Stein GS, Canalis E, et al: Bone formation: Osteoblast lineage cells, growth factors, matrix proteins, and the mineralization process, in Favus MJ (ed): Primer on Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 14-29.
Gehron RP, Boskey AL: The biochemistry of bone, in Marcus R, Feldman D, Kelsey J (eds): Osteoporosis. San Diego, CA, Academic Press, 1996, pp 95-184.
Question 14
A 40-year-old male patient sustains a bimalleolar ankle fracture and undergoes open reduction and internal fixation. Four months later, he returns for follow-up with mild ankle discomfort, and a radiograph is shown in Figure A. What is the most appropriate next step in treatment?

Explanation
Malunion of the fibula component of ankle fractures lead to tibiotalar instability and post-traumatic ankle arthritis. The distal fragment is usually shortened and externally rotated. The osteotomy can restore length and correct rotation. Markers for potential instability include: (1) asymmetry of the medial-lateral clear spaces, (2) talar tilt
>2mm, (3) talar subluxation, (4) abnormal talocrural angle (normal, 75-86deg).
Chu et al. opined that reconstruction for distal fibula malunions should include: (1) osteotomy, (2) +/- syndesmotic fixation and (3) autologous bone graft. They recommend: (1) low oblique osteotomy for fractures below the syndesmosis, (2) transverse osteotomy above the syndesmosis for high fractures (PER4) and low fractures with tibiofibular instability, (3) inspection of the tibiofibular joint through an anterolateral window to ensure anatomic reduction.
Weber et al. described a method of corrective lengthening osteotomy of the fibula in 23 cases. They described 3 criteria for assessing normal fibular length. Seventeen patients had good-excellent results, and 6 had fair-poor results (1 of these 6 needed ankle fusion).
Figure A is an AP radiograph of a distal fibula fracture fixed in a shortened position with lateral talar tilt and degenerative changes at the anterolateral tibiotalar joint. Illustration A is an anteroposterior radiograph after fibular osteotomy and correction
with medial distal tibial autograft to correct talar tilt and restore anatomic fibular length. Illustration B shows the normal talocrural angle. Illustration C shows the Weber-Simpson method of fibula lengthening used in Illustration A.
Incorrect Answers:
Question 15
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms?
Explanation
A traumatic blow to the outstretched arm results in posterior glenohumeral forces. Labral detachment at the glenoid rim is common. Patients report slipping or pain with posteriorly directed pressure. Rarely do these patients have true dislocations that require reduction; however, recurrent episodes of subluxation or pain are not uncommon. Posterior repair has
been shown to be successful in the treatment of traumatic instability.
REFERENCES: Bottoni CR, Franks BR, Moore JH, et al: Operative stabilization of posterior shoulder instability. Am J Sports Med 2005;33:996-1002.
Williams RJ III, Strickland S, Cohen M, et al: Arthroscopic repair for traumatic posterior shoulder instability. Am J Sports Med 2003;31:203-209.
Kim SH, Ha KI, Park JH, et al: Arthroscopic posterior labral repair and capsular shift for traumatic unidirectional recurrent posterior subluxation of the shoulder. J Bone Joint Surg Am 2003;85:1479-1487.
Question 16
Figure 26 shows the radiograph of an otherwise healthy Caucasian 5-year-old boy who has a painless limp. What is the best treatment option?
Explanation
REFERENCES: Herring JA, Kim HT, Browne R: Legg-Calve-Perthes disease: Prospective multicenter study of the effect of treatment on outcome. J Bone Joint Surg Am 2004;86:2121-2134.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 691-704.
Question 17
Figure 4a shows the radiograph of a 20-year-old man who has an injury to the right shoulder. Figure 4b shows an arthroscopic view (posterior portal). The arrow points to a Review Topic
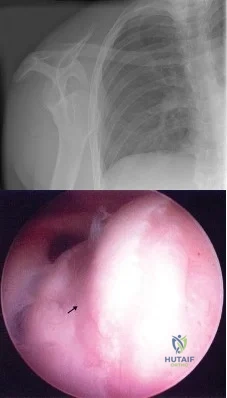
Explanation
Question 18
Figure 53a shows the AP radiograph of a 70-year-old patient who is scheduled to undergo unicompartmental knee arthroplasty. Figure 53b shows the immediate postoperative radiograph, and the radiograph shown in Figure 53c, obtained 6 months after surgery, shows a medial tibial plateau fracture. The etiology of the fracture is best related to
Explanation
REFERENCES: Brumby SA, Carrington R, Zayontz S, et al: Tibial plateau stress fracture: A complication of unicompartmental knee arthroplasty using 4 guide pinholes. J Arthroplasty 2003;18:809-812.
Yang KY, Yeo SJ, Lo NN: Stress fracture of the medial tibial plateau after minimally invasive unicompartmental knee arthroplasty: A report of 2 cases. J Arthroplasty 2003;18:801-803.
Vince KG, Cyran LT: Unicompartmental knee arthroplasty: New indications, more complications? J Arthroplasty 2004;19:9-16.
Question 19
Figure 20 shows the resting and stress radiographs of a patient who has had pain and feelings of instability after undergoing a total knee arthroplasty 1 year ago. Which of the following ligaments is not functional and is therefore responsible for the patient’s symptoms?
Explanation
REFERENCE: Incavo SJ, Churchill DL: The role of the posterior cruciate ligament in total knee arthroplasty. Techniques Orthop 1999;14:267-273.
Question 20
Figures 1 and 2 are the radiographs of a 36-year-old right-hand-dominant man who has had persistent wrist pain for 6 months after a motor vehicle collision. The initial treatment was splint immobilization. What is the best next step?

Explanation
This patient has a chronic untreated volar lunate dislocation. Lunate dislocations are usually the result of a high-energy injury. Recommended treatment for an acute lunate dislocation is ORIF with repair of injured structures (ligament and bone). If the patient has paresthesias in a median nerve distribution, carpal tunnel release is recommended in the same setting as ORIF. Six months after injury, the prognosis for successful ORIF is poor and proximal row carpectomy is recommended. Among perilunate/lunate dislocations, 25% are initially missed. If a patient arrives for treatment and there is evidence of radiocarpal and midcarpal arthrosis, wrist arthrodesis is recommended.
Question 21
Citrate dextrose - anticoagulant used with whole blood during the process of preparation of the PRP before centrifugation. 3,4,5) TGF-beta, IL-8, and PDGF are all proteins released by the platelets upon activation.
Explanation
Arrington et al reviewed 414 consecutive iliac crest harvest procedures and reported a 10% rate of minor complications and 5.8% of major complications (deep infection, nerve injuries, herniation, fractures, hematomas). They note that with proper surgical technique, the incidence of the complications can be minimized.
Ahlmann et al compared the morbidity related to the harvest of anterior iliac crest bone graft with that related to the harvest of posterior iliac crest bone graft and to determine differences in functional outcome. The rates of both minor complications (p = 0.006) and all complications (p = 0.004) were significantly higher after the anterior harvest procedures than they were after the posterior procedures. The postoperative pain at the donor site was significantly more severe (p = 0.0016) and of significantly greater duration (p
= 0.0017) after the anterior harvests.
Which of the following statements is inaccurate in describing the origin and purpose of the Institutional Review Boards (IRB)?
Began with the Nuremberg Code of Medical Ethics, which was developed by the Nuremberg Military Tribunal after the investigation of Nazi physicians
Fetuses, pregnant women, and children are considered vulnerable populations but prisoners are not
Emphasizes dignity and autonomy, and encompasses informed consent (quid vide)
The process for obtaining informed consent for patients included in clinical trials is mandated by the Institutional Review Board (IRB).
Requires fair selection of subjects and equal distribution of the benefits and burdens of research
Fetuses, pregnant women, prisoners, and children are all considered vulnerable populations by Institutional Review Boards (IRB). The process for obtaining informed consent for patients included in clinical trials is mandated by the IRB.
The article by Fisher is a commentary that reviews the clinical trials industry. She urges researchers to communicate the larger details of the research enterprise to patients and to compensate for asymmetrical power relations in society as a whole. Without these things, she believes, it will be impossible to protect against misunderstandings and therapeutic misconceptions.
Which of the following best describes a Bonferroni correction?
An analysis that starts with a particular probability of an event (the prior probability) and incorporates new information to generate a revised probability (a posterior probability)
Human behavior that is changed when participants are aware that their behavior is being observed.
Used to assess the relationship between two normally distributed continuous variables
A post-hoc statistical correction made to P values when several dependent
or independent statistical tests are being performed simultaneously on a single data set
The ability of a study to detect the difference between two interventions if one in fact exists
A Bonferroni correction is a post-hoc statistical correction made to P values when several dependent or independent statistical tests are being performed simultaneously on a single data set.
To perform a Bonferroni correction, divide the critical P value (alpha level) by the number of comparisons being made. For example, if 10 hypotheses are being tested, the new critical P value would be (alpha level)/10. The statistical power of the study is then calculated based on this modified P value.
Guyatt et al. discusses hypothesis testing and the role of alpha levels and P values. They report that the Bonferroni correction is derived from testing a dependent or independent hypotheses on a set of data and finding that the probability of a type I error is offset by testing each hypothesis at a statistical significance level divided by the number of times what it would be if only one hypothesis were tested.
Incorrect Answers:
A 10-year-old child falls from a standing height and sustains the injury shown in Figure A. Her medical history includes hearing defects and the facial appearance shown in Figure B. In addition to operative fixation of her fracture she is scheduled to receive cyclical intravenous
pamidronate administration as a treatment after the fracture is healed. Which of the following is associated with this form of treatment?
No change in bone pain
No change in future fracture incidence
An increase in osteoblast density
An increased risk of secondary osteosarcoma
An increase in bone density
The history and images are consistent with osteogenesis imperfecta (OI). Olecranon avulsion fractures are often seen in patients with OI and children presenting with these should be evaluated for OI. The clinical image of blue sclera can also be a characteristic finding in patients with OI. The Bisphosphonates have been shown to decrease fracture incidence and bone pain while improving bone density and overall function in OI patients.
Zeitlin et al performed a Level 5 review of OI. They state that Sillence Types I through IV are a mutation in the COL1A1 and COL1A2 genes that encode type I collagen. They report that cyclical intravenous pamidronate administration reduces bone pain and fracture incidence, and increases bone density and
level of ambulation.
Burnei et al also performed a Level 5 review of OI. They report that the use of bone marrow transplantation to increase osteoblast density in OI patients is currently being
researched as a potential treatment of OI.
A 35-year-old male presents with pain and limited range of motion 3 months after arthroscopic Bankart repair of his right shoulder. His postoperative course included a continuous intra- articular infusion pump for 3 days, use of a sling for 4 weeks, and initiation of passive range of motion below the level of the shoulder. At 4 weeks postoperatively he started active range of motion exercises, and started an isotonic strengthening program at the 9 week interval. Which of the following options is the MOST appropriate step in his management?
Reassurance and appropriate followup
Focused physical therapy on aggressive ROM exercises and modalities
Intra-articular injection of corticosteroids to decrease post-operative inflammation
Shoulder radiograph series to assess for chondrolysis
Arthroscopic vs open Bankart revision surgery for failed repair
The above patient was issued an intra-articular infusion of lidocaine for pain control after his surgery and may have developed shoulder chondrolysis. This complication after the use of intra-articular pumps has recently become more well known. The U.S. Federal drug and Administration (FDA) has issued a warning on the adminstration of continuous intra-articular infusion of local anesthestics for pain control.
The FDA has reviewed 35 cases of patients developing chondrolysis after intra- articular infusions, some being as early as 2 months after their surgery. The average time of diagnosis in these cases with chondrolysis were at an average of 8.5 months after the infusion. The majority of the reported cases occurred following shoulder surgeries. Joint pain, stiffness, and loss of motion were the most common physical complaints. As a result of their findings, the FDA issued
a warning for surgeons to be aware and monitor for signs and symptoms of chondrolysis.
Illustration A shows a radiograph consistent with chondrolysis in a patient status post arthroscopic Bankart repair. This image shows the loss of joint height in the glenohumeral joint due to chondrolysis. Also, 2 suture anchors are visible as well in the glenoid from the Bankart repair. Illustration B shows an arthroscopic image of chondrolysis and Illustrations C and D demonstrate chondrolyis viewed from an open approach.
Regarding bone densitometry, a T-score of -3.5 is defined as which of the following?
Normal bone
Osteopenia
Age appropriate bone loss
Osteoporosis
None. One cannot make this diagnosis without further information.
A T-score of -3.5 is defined as osteoporosis, regardless of the other clinical factors.
As described in the review by Kanis et al., the World Health Organization (WHO) has defined the following categories based on bone density in white women:
Normal bone: T-score greater than -1 Osteopenia: T-score between -1 and -2.5 Osteoporosis: T-score less than -2.5
The WHO committee did not have enough data to create definitions for men or other ethnic groups. T-score is a comparison of a patient's BMD to that of a healthy thirty-year- old of the same sex and ethnicity. Z-score is the number of standard deviations a patient's BMD differs from the average BMD of their age, sex, and ethnicity.
A 67-year-old female presented 2 months ago to her primary care physician with left sided thigh pain. A radiograph was taken at that time and is shown in Figure A. She was diagnosed at that time with a quadriceps strain and given a prescription for ibuprofen and physical therapy. She is now in the emergency room with severe left thigh pain and inability to bear weight on the left lower extremity after bending down to tie her shoes. She denies any constitutional symptoms. A current radiograph from the emergency room is shown in Figure B. Which of the following most likely explains this patient's fracture?
Long-term corticosteroid use
Secondary malignancy arising from Paget disease
Long-term alendronate use
Long-term ergocalciferol use
Short-term teraparatide use
Subtrochanteric stress reaction (Figure A) and low-energy transverse fracture (Figure B) is a complication of long-term bisphosphonate use documented in the literature. Of note, a healed right sided subtrochanteric femur fracture is also visualized in Figure A.
Neviaser et al conducted a Level 4 study of 70 patients with low energy femur fractures. They found that a simple, transverse pattern and hypertrophy of the diaphyseal cortex are associated with alendronate use with 98% specificity. They report that the average alendronate usage time was 6.9 years in patients exhibiting this pattern of fracture.
Capeci et al performed a Level 4 review of alendronate therapy and its association with unilateral low-energy subtrochanteric and diaphyseal femur fractures. They recommended consideration of discontinuing alendronate with the consultation of an endocrinologist if a fracture occurs. They also recommend routine contralateral leg surveillance after to rule out contralateral stress fracture. If contralateral stress fracture is found, it it is recommended that it is treated with prophylactic intramedullary fixation.
Imaging typically shows lateral cortical thickening in the subtrochanteric femur as demonstrating on the coronal and axial CT scans shown in Illustration A and B, respectively.
In the study by Moseley et al published in the New England Journal of Medicine, 180 patients with knee osteoarthritis were randomly assigned via sealed envelope to receive arthroscopic débridement, arthroscopic lavage, or placebo surgery. Outcomes were assessed by blinded evaluators at several points over a 2 year period
with the use of five self-reported pain and function scores. There was a greater than 90% follow-up in the study. This study is best described as having which level of evidence?
Therapeutic study, evidence level I
Therapeutic study, evidence level II
Diagnostic study, evidence level I
Diagnostic study, evidence level II
Prognostic study, evidence level I
Therapeutic studies investigate the results of treatment. Level 1 evidence includes randomized controlled trial with statistically significant difference or no statistically significant difference but narrow confidence interval.
A level II therapeutic study would include a lesser-quality randomized controlled trial (eg,
<80% follow-up, no blinding, or improper randomization). A non-randomized prospective cohort study that compares the results of treatment or systematic reviews of level II studies or level I studies with heterogenous results would also be considered a level II study.
Prognostic studies investigate the effect of a patient characteristic on the outcome of disease. Diagnostic studies investigate the efficacy of a diagnostic test. Illustration A is a table detailing the levels of evidence.
A clinical trial is underway for patients with wrist extensor tendinitis. One group of 100 patients are treated with short arm casting. Another group of 100 patients are treated with physical therapy. During analysis of the results, it becomes apparent that 30 patients in the physical therapy group did not complete the full course of physical therapy. Despite not completing a full course of physical therapy, these 30 patients were included in the physical therapy group for analysis. This analysis is an example of which of the following?
Per-protocol
Crossover analysis
Intent-to-treat
Bayesian analysis
Effect size
The following is an example of intent-to-treat analysis.
The intent-to-treat approach aims to keep similar groups similar by not
allowing for patient selection based on post-randomization outcomes (including failure to comply with the protocol). This type of analysis ensures the power of randomization so that important unknown variables that impact outcome are likely to be dispersed equally in each comparison group. Conversely, a per- protocol comparison in a clinical trial excludes patients who were not compliant with the protocol guidelines.
Berger et al., in a Level 5 review, discuss many of the principles beyond randomization that are critical for preserving the comparability of the different groups. They report that masking, allocation concealment, restrictions on the randomization, adjustment for prognostic variables, and the intent-to-treat approach to data analysis are important features of designing a good clinical trial.
Incorrect Answers:
guidelines
A 32-year-old male is being seen in your office for evaluation of a possible rotator cuff tear. He has been seen in your office by one of
your partners previously after surgical treatment of a femoral shaft fracture. How much time has to pass since last evaluation or treatment in your group for this patient to revert to a new patient under CPT guidelines?
6 months
1 year
18 months
2 years
3 years
By CPT definition, a new patient is “one who has not received any professional services from the physician, or another physician of the same specialty who belongs to the same group practice, within the past three years.” By contrast, an established patient has received professional services from the physician or another physician in the same group and the same specialty within the prior three years.
The referenced study by Shalowitz reviewed 500 Medicare claims and found an overall coding error rate of 32.4%, with high levels of consultation coding errors. He reports that changing ambulatory consultation codes to those for new patient visits would save Medicare $534.5 million per year.
As a result of this study, as well as others, Medicare does not recognize consultation codes.
A 55-year-old healthy female presents for a routine physical exam. When discussing bone health and osteoporosis prevention, what dose of calcium and vitamin D should be recommended for daily consumption?
1,500mg of calcium and 1,000 IUs of vitamin D
2,200mg of calcium and 1,000 IUs of vitamin D
750mg of calcium and 5,000 IUs of vitamin D
750mg of calcium and 10,000 IUs of vitamin D
2,200mg of calcium and 5,000 IUs of vitamin D
The National Osteoporosis Foundation recommends a daily intake of 1,200- 1500mg of calcium 800-1,000 IUs of vitamin D for adults over the age of 50.
The review article by Gehrig et al discusses the factors surrounding osteoporosis that can be modified to optimize fracture risk reduction. They report that non-prescription interventions such as calcium and vitamin D supplementation, fall prevention, hip protectors, and balance and exercise programs are treatment options.
What is the function of the core binding factor alpha-1 (Cbfa1/Runx2)?
Phosphorylation and intracellular activation of signal transducers and activators of transcription (STATs)
Chemotaxis of mesenchymal stem cells to sites of skeletal fractures
Tumor-induced osteolysis
Osteoclastic apoptosis
Osteoblastic differentiation
As described by Ducy et al., Cbfa1/Runx2 is a key transcription factor associated with osteoblast differentiation, skeletal morphogenesis, and acts as a scaffold for nucleic acids and regulatory factors involved in skeletal gene expression. A stop codon mutation in the Cbfa 1 gene causes cleidocranial dysplasia. Stem cell chemotaxis (moving to various sites in the body) is accomplished through a variety of cytokines, one of which is platelet derived growth factor. Tumor-induced osteolysis occurs secondary to tumor-produced cytokine activation of osteoclasts. Osteoclastic apoptosis occurs secondary to bisphosphonates.
Ballock and O'Keefe review the development, growth, and complex cytokine interaction required for normal growth plate function.
A 20-year-old male is involved in motor vehicle collision and sustains a depressed tibial plateau fracture. When performing surgery, if calcium sulfate is used as the primary bone substitute void filler, an increase in which of the following outcomes may be expected as compared to autograft?
Increased complications due to serous drainage
Improved clinical outcomes as shown by more rapid time to healing
Improved clinical outcomes as shown by SF-36 scores
Increased complications due to autoimmune reactions and graft rejection
Equivalent complication rates and clinical outcomes
Calcium sulfate bone graft substitute has demonstrated an increased rate of serous drainage at the surgical site. Evidence examining the use of calcium sulfate in the treatment of bone nonunions revealed a significant failure rate, suggesting that this material, used in isolation, is not optimal to promote union in that setting.
Beuerlein and Mckee reviewed the literature, showing that calcium sulfate is
an effective void filler in metaphyseal defects after impacted fracture reduction (calcaneus, tibial plateau) or simple bone cysts. However, they report that calcium sulfate is associated with serous wound drainage especially when used at subcutaneous sites and in amounts greater than 20ml.
Ziran et al present a series of 41 patients undergoing bone grafting for atrophic/avascular nonunions with adjunctive calcium sulfate-demineralized bone matrix (Allomatrix). Of the 41 patients, 13 (32%) had drainage that necessitated surgical procedures and 14 (34%) developed a deep infection.
A 46-year-old female begins to have personality changes, cognitive decline, and chorea. Her father began having similar but less severe symptoms at age 55 before passing away 6 years later. One of her 2 older siblings has also begun to show deterioration. Which of the following describes the hereditary pattern of this disease?
Autosomal dominant with variable penetrance
Autosomal recessive with variable penetrance
X-linked recessive
Autosomal dominant with anticipation
Autosomal dominant with imprinting
This clinical vignette describes a patient with Huntington's disease. Huntington's disease has an autosomal dominant hereditary pattern with anticipation.
Anticipation is a term used to describe trinucleotide repeat
disorders that if passed on, will present earlier and more severely in affected subjects than in their affected parent. In Huntington's disease, it is due to a "CAG" trinucleotide repeat on chromosome 4. Subjects with an affected parent have a 50% chance of inheriting the disease from them, and if present will have more severe disease.
Deighton et al provide a review on the genetics of musculoskeletal disease including the hereditary pattern of anticipation.
All of the following are indications for locked plating technology EXCEPT:
Periarticular fracture with metaphyseal comminution
Fracture in osteoporotic bone
Bridge plating for severely comminuted fractures
Compression plating of transverse fracture
Plating of fractures where anatomical constraints prevent plating on the tension side of the bone
Locked plates are indicated for indirect fracture reduction, diaphyseal/metaphyseal fractures in osteoporotic bone, bridging severely comminuted fractures, and the plating of fractures where anatomical constraints prevent plating on the tension side of the bone.
Locked plates and conventional plates rely on completely different mechanical principles to provide fracture fixation and in so doing they provide different biological environments for healing. Approaches to internal fixation have become more biologic. Greater emphasis is placed on vascularity and soft tissue integrity. Locked plates, analogous to rigid internal fixators, can provide relative stability favorable to secondary fracture healing. If applied appropriately, they can
avoid soft tissue compromise. The key to this new generation of plates is the locking mechanism of the screw to the plate, which provides angular stability and avoids compression of the plate to the periosteum. Favorable biomechanical and clinical results continue to expand the number of appropriate indications for use of locked plating devices, although exact indications for their use have yet to be precisely defined.
The referenced articles by Haidukewych and Egol et al are reviews of the biomechanical characteristics of locked plating technology.
Which of the following lists these materials in order of increasing modulus of elasticity?:
Cortical bone; Titanium; Cobalt-chrome; Stainless steel; Ceramic
Titanium; Cortical bone; Ceramic; Cobalt-chrome; Stainless steel
Cortical bone; Titanium; Stainless steel; Cobalt-chrome; Ceramic
Stainless steel; Titanium; Cortical bone; Ceramic; Cobalt Chrome
Cortical bone; Stainless steel; Titanium; Cobalt-chrome; Ceramic
Cortical bone has the lowest modulus of elasticity of the materials listed, followed by titanium, stainless steel, cobalt-chrome alloy, then ceramic.
Young's modulus of elasticity is the ratio of stress to strain, and represents the stiffness of a material and its ability to resist deformation when placed under tension. Of the materials listed, titanium has the stiffness closest to cortical bone. Ceramic has the highest modulus of elasticity, making it the most stiff of the materials listed.
Illustration A (from Miller's Review) shows the relative stiffnesses of various orthopaedically relevant materials. Young's modulus is the slope of the lines shown. Illustration B (Google images) charts their Young's Modulus.
Incorrect answers:
Which of the following substances increases the chondrogenic phenotype of intervertebral disk cells and matrix synthesis?
Osteoprotegrin
Osteonectin
Hyperosmotic saline
Corticosteroids
Bone morphogenic proteins
Bone morphogenic proteins have been shown to increase chondrogenic phenotype expression and increase matrix synthesis of the intervertebral disc in animal studies.
Bone morphogenetic protein-2, bone morphogenetic protein-7, and
transforming growth factor-beta are morphogens that have been shown to alter the phenotype of target cells without increasing cellular proliferation. Within the intervertebral disk, these factors have the potential to increase the chondrogenic phenotype among disk cells, and this results in the increased production of the disk matrix. Mitogenic molecules, such as insulin-like growth factor-1 and fibroblast growth factor, function to increase cellular proliferation.
Miyamoto et al. evaluated rabbits that underwent annulus fibrosus (AF) injury where they either injected a control or BMP into the nucleus pulposus. The BMP injection significantly restored disc height and improved the modulus as compared to control injections. They concluded the biochemical data suggested that the OP-1-induced restoration of the disc space was a consequence of the increased activity of anabolic pathways that resulted in biochemical changes in the IVD.
Kim et al. evaluated mRNA levels of BMP-2, BMP-7, and TGF-beta in a rabbit model of intervertebral discs. Compared to young rabbits, old rabbits generally had higher levels of mRNA expression of these three cytokines in both the annulus fibrosus and nucleus pulposus. The similar patterns of up-regulation in gene expression with age shown by these 3 anabolic cytokines suggest a common pathway in terms of regulation and transcription in the early stage of disc degeneration.
Incorrect Answers:
A colleague is struggling to obtain a perfect lateral radiograph for distal locking screw placement. Other than good technique, how might the surgeon best reduce the amount of radiation exposure to the patient and personnel when using fluoroscopy?
The use of continuous fluoroscopy while manipulating the leg
Standing directly behind the cathode ray tube
Advising the technician to position the fluoroscopy beam on command
Placement of the image intensifier receptor as close to the patient as possible
Placement of the cathode ray tube as close to the patient as possible
Placing the image intensifier as close as clinically possible to the patient, scatter radiation exposure to the personnel is minimized.
Numerous steps have been described to decrease radiation in the operating room. They include:
Decrease time of exposure
Decrease dose of exposure
Beam collimation
The use of mini C arm
Inverting the C arm (shortens distance between body part and collection surface)
Surgeon’s control of the C arm
Use of protective equipment (glasses, thyroid shields, aprons)
Increase the distance from the X ray source
Maniscalco et al. compared the amount radiation exposure during open lumbar microdiscectomy and minimally invasive microdiscectomy. MIS lumbar microdiscectomy cases expose the surgeon to significantly more radiation than open microdiscectomy.
Interestingly, standing in a substerile room during x- ray localization in open cases is not fully protective.
Illustration A shows an image of radiation scatter with fluoroscopy. Radiation hits the patient’s tissue, interacts and then changes direction. The greatest dose received is directly perpendicular to the fluoroscopy and next to the patient.
Incorrect Answers:
A 72-year-old active man presents with chronic right-sided pelvic pain for the last 2 years. His radiographs are depicted in Figure A. He has tried multiple courses of activity modification and anti- inflammatory medications to no avail. His orthopedic oncologist performs a biopsy (depicted in Figure B) and elects to initiate Zoledronate. Which of the following is a known complication
associated with this treatment if rendered long-term?
Malignant degeneration to osteosarcoma
Malignant degeneration to chondrosarcoma
Malignant degeneration to fibrosarcoma
Atypical distal femur transverse fractures
Osteonecrosis of mandible
This patient's pelvic radiograph reveals cortical thickening, coarse trabeculae, and sclerosis, which is characteristic of Paget's disease, depicted in the histological section in Figure B. Bisphosphonate treatment is an appropriate treatment for Paget's disease. However, long-term administration of intravenous (IV) bisphosphonates (i.e.
Zoledronate) may result in osteonecrosis of the jaw.
Osseous lesions from Paget's disease have increased osteoclastic bone resorption, marrow fibrosis, increased bone vascularity, and increased disorganized bone formation, resulting in a mosaic (woven and lamellar bone) appearance on histology. Asymptomatic patients may be treated with
observation and symptomatic management reserved as first-line management. When recalcitrant to symptomatic management, bisphosphonate therapy helps control osteoclast lytic activity and reduces pain. However, when administered long-term, side-effects may include atypical subtrochanteric femur fractures and jaw osteonecrosis (especially when given IV). Administration of Teriparatide (Forteo) is contraindicated in these patients due to the increased risk of Pagetoid malignant transformation. Malignant transformation to Paget's sarcoma occurs in 1% of patients.
Langston et al. performed a randomized trial of intensive bisphosphonate treatment versus symptomatic management in Paget's disease of bone. They reported that while serum alkaline phosphatase (ALP) levels were significantly lower in the intensive treatment group than in with the symptomatic treatment group, there was no difference in the quality of life, pain scores, hearing loss, or rates of surgical intervention in the two cohorts. They concluded that
striving to maintain normal ALP levels with intensive bisphosphonate therapy confers no clinical advantage over symptom-driven management in patients with Paget's disease of bone.
Figure A demonstrates Paget's disease of the right hemipelvis. Figure B demonstrates the
histology of Paget's disease of bone (woven bone and irregular broad trabeculae with disorganized cement lines in a mosaic pattern). Illustration A and B demonstrate osteonecrosis of the jaw and atypical subtrochanteric femur stress fracture, respectively, after long-term bisphosphonate use.
Incorrect Answers:
A long oblique diaphyseal fracture is internally fixed with 2 lag screws. There is 2 mm of residual fracture fragment gap following screw fixation. This construct has which of the following compared to a comminuted diaphyseal fracture
internally fixed with a long bridge plating technique?
Greater interfragmental strain
Greater ductility
Greater primary Haversian remodeling
Greater union rate
Greater callus volume formation
A long oblique diaphyseal fracture with 2 mm of residual displacement after being internally fixed with lag screws has greater interfragmental strain than comminuted fractures treated with bridge plating or fractures that are anatomically reduced and internally fixed.
Perrens’ theory of strain states that there is a relationship between decreasing strain and increasing the potential for osteogenesis across a fracture or fusion site. The strain theory states that for two given fracture segments, the healing interface will possess a force- generated motion potential that is contingent on the stability of the original fixation construct. Mathematically, the strain for
any given force is equal to the change in the interface length divided by the original interface length. Therefore, with an unstable construct, the healing gap may undergo excessive motion with resultant increasing strain. It has been shown that strain of less than 2% will yield absolute stability and subsequent primary bone healing. Comminuted fractures have multiple fracture lines therefore the force is dissipated over multiple fracture lines and interfragmentary strain is decreased.
A 75-year-old woman presents with acute severe back pain after sustaining a mechanical fall while walking out of her yard. She denies pain in her buttocks or legs. On physical exam she has point tenderness over the L1 spinous process. Figure A depicts her current radiograph. Which of the following statements is true regarding here underlying metabolic condition and associated pathology?
Kyphoplasty is indicated within the first week if the pain is severe enough to warrant narcotic medication.
Her underlying metabolic bone condition leads to decreased bone quantity with normal bone quality.
A DEXA T-score of -2.1 in this individual would confirm the diagnosis of osteoporosis according to the WHO.
A 25-hydroxy Vitamin D level of 16ng/mL in this individual would confirm the diagnosis of osteoporosis according to the WHO.
The fracture pattern in Figure A is the third most common fragility fracture in the United States
This clinical presentation is consistent with an L1 osteoporotic compression fracture due to underlying osteoporosis. Osteoporosis is characterized by decreased bone quantity with normal bone quality.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Vertebral compression fractures are the most common type of fragility fracture in patients with osteoporosis. Management should begin with a proper evaluation to identify the etiology of the fracture and appropriate intervention to rectify the underlying pathology.
Evaluation includes bone densitometry, lab testing of Vitamin D and calcium. The World Health Organization (WHO)
classifies bone density in postmenopausal women based on T-scores, with classification based on the lowest T-score of the spine, femoral neck, trochanter, or total hip. Osteoporosis is defined by T-scores 2.5 or greater standard deviations below the peak bone mass of a 25-year-old individual.
Gehrig et al. published an Instructional Course Lecture on the management and treatment strategies for orthopaedic surgeons. They reported that osteoporosis may be present in patients with and without fracture and that the ultimate goal in managing and treating osteoporosis is to optimize fracture risk reduction. They recommended non-pharmacologic interventions including calcium, vitamin D supplementation, fall prevention, hip protectors, and balance and exercise programs to minimize fracture risk.
The United States Preventive Services Task Force published clinical guidelines on osteoporosis screening. They recommended screening for osteoporosis in women aged 65 years or older and in younger women whose fracture risk is equal to or greater than that of a 65-year-old white woman who has no additional risk factors. They concluded that the current evidence is insufficient to assess the balance of risks and benefits of screening for osteoporosis in men.
Figure A depicts an L1 vertebral compression fracture. Incorrect Answers:
year-old woman with long standing rheumatoid arthritis presents with worsening bilateral foot pain. She sees a podiatrist for shaving of her plantar forefoot calluses. She has tried orthotics and custom shoes but notes worsening foot pain that is limiting her daily activities. Plain radiographs of her feet are pictured in Figure A. Which
of the following images depicts the surgical treatment that would result in the best functional outcome for this patient?
This patient has a classic rheumatoid arthritis (RA) forefoot deformity and would benefit most from first metatarsophalangeal (MTP) joint fusion, hammertoe correction and lesser metatarsal (MT) head resections, pictured in Figure E.
Nearly 90% of patients with chronic RA develop forefoot deformities, most commonly hallux valgus, fixed hammering of the lesser toes and subluxation/dislocation of the lesser MTP joints. Nonoperative management includes orthotic use and shoewear modification. The gold standard surgical treatment involves stabilization of the first ray with a first MTP joint fusion, hammertoe correction and resection of the lesser MT heads (Hoffman-Clayton procedure).
Coughlin et al highlighted that achievement of stable realignment of the first ray is the key factor in reconstruction of a RA forefoot. Stable fusion of the first MTP joint increases weight-bearing along the medial column, minimizes stress on the lesser MTP joints and protects the relocated plantar fat pad. Patients who underwent first MTP fusion, lesser MT head resections and open hammertoe correction had a high level of satisfaction postoperatively.
Mann et al performed a retrospective review of 20 patients with severe RA forefoot deformities who underwent first MTP joint fusion. These patients demonstrated an increase in weight-bearing of the hallux and resultant decrease in metatarsalgia and plantar callosities compared to patients who underwent a first MTP resection arthroplasty
(Keller arthroplasty). The patients in this study noted significant functional improvement postoperatively and no patients required custom shoes or orthotics.
Figure A is an AP radiograph of bilateral feet demonstrating the classic RA forefoot deformity with severe hallux valgus, dislocation of the lesser MTP joints and erosive changes of the MT heads. Figure B shows a hallux valgus realignment procedure with a distal osteotomy and hammertoe correction with a 2nd MT shortening osteotomy (Weil osteotomy), proximal interphalangeal (PIP) joint resection and K wire fixation. Figure C displays a first tarsometatarsal (TMT) joint fusion (Lapidus procedure) and Weil osteotomies
of the 2nd through 4th MTs. Figure D demonstrates a first MTP joint fusion and Weil osteotomies of the 2nd through 4th MTs. Figure E shows a first MTP joint fusion, resection of the 2nd through 5th MT heads and hammertoe correction with PIP joint resection and K wire fixation. Figure F displays a resection of the
first MTP joint proximal phalanx base (Keller arthroplasty) and hammertoe correction with PIP joint resection and K wire fixation.
Incorrect Responses:
What type of fracture healing occurs in a femoral shaft fracture treated with an intramedullary nail?
Primary fracture healing
Secondary fracture healing
Extramembranous ossification
Haversian remodelling
"Cutting cone" remodelling
Intramedullary nails function as internal splints that allow for secondary fracture healing.
Secondary bone healing involves responses in the periosteum and external soft tissues. Here both committed osteoprogenitor cells and uncommitted undifferentiated mesenchymal cells contribute to the process of fracture healing by recapitulation of embryonic intramembranous ossification and endochondral bone formation. The response from the periosteum is a fundamental reaction to bone injury and is enhanced by motion and inhibited by rigid fixation.
Bong et al. reviewed the biomechanics and biology of long bone fracture healing with Intrameduallary nailing. They showed that reaming and the insertion of intramedullary nails can have early deleterious effects on
endosteal and cortical blood flow initially. However, the canal reaming appears to have an overall positive effect at the fracture site as it increases extra
osseous circulation and applies bone graft to the fracture site.
Illustration A shows a series of radiographs of a fracture healed by secondary intention with an IM nail.
Incorrect Answers:
healing of bone.
A 67-year-old woman sustained the injury shown in Figure A approximately 14 months ago, which was managed with closed reduction and casting. She presents with new symptoms of hyperalgesia, allodynia, and hyperhidrosis of her wrist. She denies any recent fevers or chills. Her current radiographs reveal a well-healed fracture without any significant malunion. What is the
pathophysiology likely attributable to her current symptoms?
Pre-ganglion brachial plexopathy
Aberrant inflammatory and vasomotor response
Exaggerated vasoconstriction of the wrist and digital arteries
Incomplete glycosaminoglycan breakdown products causing dysfunction
Connective tissue disorder
The patient is presenting with complex regional pain syndrome (CRPS) after a healed distal radial fracture. The pathophysiology of CRPS is that of aberrant inflammatory and vasomotor response in a region of prior trauma resulting in pain out of proportion, skin discoloration, and vasomotor disturbances.
Patients who develop CRPS often have a history of trauma, but the condition may also occur after surgery. Common symptoms of CRPS include hyperalgesia, often described as burning, throbbing, shooting, or aching. Patients may also experience hyperalgesia, allodynia, and hyperpathia. More objective signs of CRPS may include motor dysfunction (tremors, dystonia, loss of strength), skin, hair, and other trophic changes about the affected extremity, as are symptoms of autonomic dysfunction. CRPS is often sub- classified into 2 types. Type 1 is more common and does not involve specific nerve damage, whereas type 2 involves damage to a specific nerve.
Hogan et al. reviewed the evaluation and treatment of complex regional pain syndrome. They report that although there are many divergent and often conflicting theories, the cause of the severe pain, alterations in regional blood flow, and edema noted in CRPS is unknown. They concluded that CRPS is a challenging diagnosis and as such should be managed by a multidisciplinary team, including chronic pain management specialists,
physical therapists, and orthopedic surgeons.
Shah et al. reviewed the diagnosis and treatment of CRPS. They reported that sweat quantification testing, skin thermography, and electromyography may
be useful in the diagnosis of CRPS, but these tests are often unreliable given is a lack of diagnostic sensitivity. They concluded that the treatment of CRPS remains controversial, and includes medications (antiepileptics, antidepressants, NSAIDS, bisphosphonates, free radical scavengers, vitamin C, and topical anesthetics), physical therapy, regional anesthesia, and neuro- modulation.
Figure A depicts an extra-articular distal radius fracture. Illustration A depicts an example of a wrist affected by CRPS, with notably increased swelling, which is a common finding in patients afflicted with the disease.
Incorrect Answers:
After application of a unilateral tibial external fixator, it is observed that the frame does not provide sufficient rigidity across the fracture site. Altering the external fixator in which of the following ways will have the greatest impact on frame stiffness?
Increasing the distance between pins in each fragment
Increasing the pin diameter
Reducing the distance between bone and connecting bar
Increasing the connecting bar diameter
Adding one stacked connecting bar
While all of the aforementioned factors will increase frame stiffness, pin diameter has the greatest influence on stability of unilateral frames.
Unilateral frames are distinguished from circular frames in that they are positioned on one side of the limb. The overall stability of the frame can be varied by altering the number of pins, the distance between pins, pin diameter, connecting rod diameter, number of connecting rods, distance between bone and connecting rods, and use of multiplanar fixation. The pin diameter has the biggest contribution, as the stiffness of the pin is correlated to the fourth power of its radius.
Fragomen et al. looked at the mechanics of external fixation. They state that the diameter of the half Schantz pin should be less than one-third of the bone diameter to minimize the risk of fracture at the pin site. Unicortical half pins also increase the risk of fracture.
Therefore, pins should be bicortical.
Tencer et al. examined the mechanical properties of external fixation. They showed that frame rigidity could be maximized by increasing the pin separation distance in each fracture fragment, increasing the number of pins and decreasing the sidebar offset distance from bone.
Illustration A shows a schematic of the factors contributing to frame stability. Incorrect Answers:
Locking plate technology is least indicated for which of the following Figures?
Of the fracture patterns listed, all have some indication for locking plate fixation except answer 2. Transverse midshaft both bone forearm fractures are typically treated with non- locked compression plating techniques.
The use of locking plate fixation is an evolving topic in orthopaedics, and exact uses may vary. Well accepted indications for locking plate fixation include indirect fracture reduction, diaphyseal/metaphyseal fractures in osteoporotic bone, bridging of severely comminuted fractures, and plating of fractures where anatomical constraints prevent plating on the tension side of the bone (e.g. short segment fixation).
Anglen et al. performed a level-IV meta-analysis of 33 papers reviewing the use and outcomes of locking plate fixation. They found no standard indications for use, and due to heterogeneity of the studies reviewed had no specific
recommendations for use.
Cantu et al. presented a level-V review of the use of locking plate fixation. They cite 5 indications for use: metaphyseal or intra-articular fractures, highly comminuted fractures particularly involving diaphyseal and metaphyseal bone, osteoporotic bone, proximal tibia and distal femur fractures, and periprosthetic fractures. They also cite 4 relative contraindications: fractures best served
with a construct other than a plate, severe soft tissue injury precluding placement of a plate, simple fracture patterns that can be adequately treated with non-locking constructs, and fractures that would require bending the plate.
Figure A is a comminuted Schatzker VI tibial plateau fracture. Figure B is a transverse both bone forearm fracture. Figure C is an intra-articular pilon fracture. Figure D is a comminuted distal humerus fracture. Figure E Vancouver B1 periprosthetic hip fracture.
Incorrect Answers:
All of the following are true regarding osteocalcin EXCEPT which of the
following?
It is the most prevalent non-collagenous protein in bone
It is expressed by mature osteoblasts
It is considered a marker for osteoblast differentiation
It is a glycoprotein that binds calcium
Higher levels are correlated with increases in bone mineral density during osteoporosis treatment
Pure fact question from basic science. “Osteocalcin is the most prevalent noncollagenous protein in bone” (from Miller's Review). It is expressed by mature osteoblasts and is a marker of osteoblast differentiation. Osteocalcin is the most specific marker of the osteoblast phenotype and is expressed only in mature osteoblasts. During osteoporosis treatment, serum levels correlate
with increases in bone mineral density. Osteonectin, not osteocalcin, is a glycoprotein that binds calcium.
An otherwise healthy young male sustains a significantly comminuted fracture of the 2nd metacarpal shaft and undergoes external fixation as definitive management. The type of bony healing obtained with this treatment is similar to the bony healing for the appropriate treatment of all the following injuries EXCEPT?
The patient has undergone external fixation for his 2nd metacarpal shaft fracture which is an example of enchondral healing (secondary bone healing) which occurs with non- rigid fixation, such as bracing, casting, external fixation, bridge plating, and intramedullary nailing. Of the images shown, Figure D is an example of a patient with an unstable Weber B ankle fracture
with a simple oblique pattern that would preferentially be treated with primary bone healing with ORIF (anatomic stability).
Bone healing occurs via primary healing (intramembranous healing, absolute stability) or secondary healing (enchondral healing, relative stability) depending on the method of fixation. Fractures that require primary bone healing are ones in which anatomic reduction without callus formation is preferred (peri-articular fractures, both bone forearm fractures, non- comminuted ankle fractures with disruption of the ankle syndesmosis).
Primary healing leads to healing via cutting cones and occurs without the production of any callus (which may impede rotation in both bone forearm fractures and cause articular malalignment in peri-articular and peri- syndesmotic fractures). Fractures that may be treated with secondary bone healing and callus formation, do not require anatomic stability and may have fracture site micromotion during the healing process. Intramedullary nailing, external fixation and closed treatment with bracing/splinting/casting all allow motion at the fracture site and lead to secondary bone healing.
Perren reviews the biological and mechanical properties of bone remodeling and the complex interplay of patient, injury and surgical factors that influence healing. The use of relative stability fixation techniques allows the bone to overcome the initial excess strain at a fracture site and build a scaffold that brings the strain to more reasonable levels. The author stresses the importance of understanding bone biology to select optimal implant and methods of surgical fixation.
Bong et al. reviewed the biomechanics and biology of long bone fracture healing with Intramedullary nailing. They showed that reaming and the insertion of intramedullary nails can have early deleterious effects on
endosteal and cortical blood flow initially. However, the canal reaming appears to have an overall positive effect at the fracture site as it increases extraosseous circulation and applies bone graft to the fracture site.
Figure A shows the AP and lateral radiographs of a segmental oblique midshaft tibia fracture. Figure B is an AP radiograph of an unstable intertrochanteric femur fracture with disruption of the calcar. Figure C shows the AP and lateral radiographs of a midshaft transverse femur fracture. Figure D shows the AP and lateral radiographs of a simple oblique weber B ankle fracture with medial clear space widening. Figure E shows a displaced 5th metacarpal neck fracture with dorsal angulation.
Illustration A is the injury in Figure A treated with intramedullary nailing with resulted callus formation. Illustration B is the injury in Figure B treated with cephallomedullary nailing with resulting callus formation. Illustration C is the injury in Figure C treated with intramedullary nailing with resulting callus formation. Illustration D is the injury in Figure D treated with a lag screw and neutralization plating (anatomic stability). Illustration E is the injury in Figure
E treated with closed reduction and casting with subsequent healing with callus formation.
Incorrect Answers:
This is an example of secondary bone healing.
A 7-year-old recent immigrant presents with pain and tenderness over the legs. Physical exam shows the gums have a bluish-purple hue with areas of hemorrhages. A radiograph is shown in Figure A. In Figure B, what region of the growth plate is most affected in this condition?
A
B
C
D
E
The clinical presentation and radiographs are consistent with scurvy. The radiographs show a dense band (White line of Frankl) at the growing metaphyseal end which is characteristic of scurvy. Scurvy is a disease resulting from a deficiency of vitamin C (ascorbic acid), which is required for the synthesis of collagen in humans. Impaired collagen synthesis in scurvy leads to fragile capillaries, resulting in abnormal bleeding, and altered bone formation at the growth plate. More specifically, scurvy affects the spongiosa
the most (but not exclusively) in the metaphysis, which is depicted by region E in the illustration.
It is considered optimal to obtain written informed consent for an elective surgical procedure in which of the following clinical settings?
By the hospital risk manager upon admission
By the nurse in pre-op holding
By the surgeon in pre-op holding
By the surgeon's scheduler greater than 7 days prior
By the surgeon in the office within 7 days prior
The reference by Bhattacharyya et al notes that the location where the informed consent was obtained is important. When informed consent was obtained by the operating surgeon in the office, there was a decreased risk of indemnity payment (p < 0.004). This finding is likely due to the effect of communication on malpractice claims. Poor communication has been established as the critical factor linked to malpractice claims. It seems logical that the physician-patient communication that occurs in the office is more interactive and substantive than discussions that occur on the hospital floor or in the preoperative holding area. A closed claims analysis conducted in Florida, which included 127 mothers of infants who had experienced permanent perinatal injuries and who subsequently sued their physicians, showed that nearly all complained that their physicians would not talk, answer questions,
or listen. Clearly, the office is the best setting for quality discussions on informed consent to occur.
A 45 year-old woman who has not reached menopause yet falls from a standing height and sustains a distal radius fracture. A DEXA scan reveals a T- score of -2.2. Which of the following treatments is indicated in this patient?
1,700 mg of calcium
1,200 mg of calcium
1,700 mg of vitamin D
1,200 mg of iron
1,700 mg of PTH
The current recommendations for further prevention of any fragility fracture include 1200- 1500mg of elemental calcium intake per day and 400-800 IU of vitamin D per day. Of note, these doses are indicated only for prevention and not sufficient for active treatment of osteoporosis (T score less than -2.5).
Medications that are approved by the FDA for active treatment of osteoporosis: alendronate, risedronate, raloxifene, estrogen, calcitonin. These medications and preventative measures help to reduce fragility fractures by as much as 50%.
Freedman et al. performed a retrospective study that looked at a cohort of patients with fragility fractures and then looked at the type and frequency of osteoporosis related interventions. They found that only 60% of patients actually were either prescribed a
medication, given a referral, or ordered additional workup (DEXA scan).
Schulman et al. reviewed a series of 80 female patients regarding osteoporosis and bone health, and found that the outpatient sports medicine office setting was an excellent opportunity to educate patients on these topics. The patients' post-education test scores increased significantly after a brief counseling session, and increases in daily calcium intake and exercise levels were also seen.
Hypophosphatasia is associated with which of the following laboratory findings?
Hyperbilirubinemia
Decreased urinary phosphoethanolamine
Decreased urinary inorganic pyrophosphate
Decreased serum phosphate
Decreased serum alkaline phosphatase
Alkaline phosphatase is a marker of bone formation and is elevated when bone formation is increased. Hypophosphatasia is an autosomal recessive disorder caused by an inborn error in the production of alkaline phosphatase (tissue- nonspecific isoenzyme of alkaline phosphatase: TNSALP), leading to low alkaline phosphatase levels. Increased urinary phosphoethanolamine is also diagnostic.
Which of the following statements regarding COX-2 is FALSE?
It causes mesenchymal stem cells to differentiate into osteoblasts
COX-2 knockout mice heal fractures more quickly than control mice
COX-2 is an enzyme which converts arachidonic acid to prostaglandin endoperoxide H2
Most NSAIDS non-specifically inhibit both COX-1 and COX-2 enzymes
The expression of COX-2 is upregulated in several human cancers
Cycloxygenase-2 (COX-2,aka prostaglandin-endoperoxide synthase 2) is an enzyme which converts arachidonic acid to prostaglandin endoperoxide H2. COX-2 is not expressed under normal conditions, but elevated levels are found during general states of inflammation. Zhang et al and Simon et al have both studied the role of COX-2 with regard to fracture healing. Zhang et al created
a COX-2 knockout mouse (one which does not express the COX-2 gene). This COX-2 knockout mouse has been shown to heal fractures more slowly than COX-1 knockout
mice or normal controls, thus identifying the role of COX-2 in general inflammation and bone repair. Zhang et al hypothesize that COX-2 causes mesenchymal progenitor cells to differentiate into osteoblasts, thus promoting new bone formation. Simon et al showed the delayed effects of fracture healing when animals were treated with COX-2 inhibitors.
Gerstenfeld et al. studied the reversibility of COX-2 inhibition on the short term bone healing in an animal model. They found that COX-2 inhibitors block fracture healing more than NSAIDS and the magnitude of this effect is related to the duration of treatment.
While specific inhibitors of COX-2 exist, traditional
NSAIDs non-specifically inhibit both COX-1 and COX-2 enzymes. In addition to its role in inflammation, COX-2 has been shown to be upregulated in many human cancers such as gallbladder carcinoma.
A 60-year-old man has had intermittent pain in his right great toe for the past 2 years. What is the most likely cause for the lesions shown in Figure A?
Monosodium urate crystal deposition
Calcium pyrophosphate deposition
Renal osteodystrophy
Tuberculosis
Sarcoidosis
Gout is a disorder of nucleic acid metabolism that leads to monosodium urate crystal deposition in the joints. The most common area of the body to be affected by gout is the first toe. The radiograph in Figure A demonstrates joint space narrowing of the 1st
metarsalphalangeal joint and the arrows show medial soft tissue swelling at the 1st MTP with soft tissue radio-densities and some erosive changes consistent with gout.
Weinfeld et al report their experience over a 7 year period with hallux MTP arthritis in 439 patients they treated. Surgical indications included pain, shoewear problems, and failure of non-operative management.
Reber et al describe a rare case of tophaceous gout in the medial sesamoid of the hallux and review the diagnosis, pathophysiology, and suggested management.
Eggebeen reports "gout is caused by monosodium urate crystal deposition in tissues leading to arthritis, soft tissue masses (i.e., tophi), nephrolithiasis, and urate nephropathy. The biologic precursor to gout is elevated serum uric acid levels (i.e., hyperuricemia). The diagnosis is confirmed if monosodium urate crystals are present in synovial fluid."
Incorrect Answers:
Which of the following pharmacologic agents is associated with the highest risk of bleeding and thrombocytopenia?
Coumadin
Enoxaparin
Unfractionated heparin
Dalteparin
Protamine sulfate
Of the options listed unfractionated heparin is associated with the highest rate of bleeding and thrombocytopenia. This may occur as part of a syndrome called Heparin Induced Thrombocytopenia (HIT).
Unfractionated heparin works in the coagulation cascade by binding and enhancing the ability of antithrombin III to inhibit factors IIa, III, Xa. A known complication of unfractionated heparin use is Heparin Induced Thrombocytopenia (HIT). Heparin Induced Thrombocytopenia (HIT) is caused by the formation of abnormal antibodies that activate platelets leading to abnormal formation of blood clots inside a blood vessel, leading to
bleeding and thrombocytopenia.
Dorr et al. reviewed multimodal thromboprophylaxis for total hip and knee arthroplasty based on risk assessment in 1179 patients. They recommend careful use and monitoring of thromboprophylaxis after arthroplasty procedures to protect patients from thromboembolic events while also limiting adverse clinical outcomes secondary to thromboembolic, vascular, and bleeding complications.
Mont et al. performed a study on preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty. They recommended all patients do early mobilization and receive pharmacologic prophylaxis and mechanical compressive devices for the prevention of thromboembolic disease. The group did not recommend any specific pharmacologic agents and/or mechanical devices.
Illustration A shows a figure of the coagulation cascade and the target molecule of both unfractionated heparin and low molecular weight heparin.
Incorrect Answers:
Which of the following series of lab values is most consistent with a diagnosis of high turnover renal osteodystrophy?
Decreased calcium, increased serum phosphate, increased alkaline phosphatase, increased parathyroid hormone
Decreased calcium, decreased serum phosphate, increased alkaline phosphatase, increased parathyroid hormone
Increased calcium, normal serum phosphate, increased alkaline
phosphatase, normal parathyroid hormone
Decreased calcium, increased serum phosphate, normal alkaline phosphatase, decreased parathyroid hormone
Increased calcium, normal serum phosphate, normal or high alkaline phosphatase, increased parathyroid hormone
Decreased calcium, increased serum phosphate, increased alkaline phosphatase, and increased parathyroid hormone are all characteristic of renal osteodystrophy.
Renal osteodystrophy represents a spectrum of disease seen in patients with chronic renal disease. It is characterized by bone mineralization deficiency due to electrolyte and endocrine abnormalities. High turnover renal osteodystrophy is classically associated with significantly increased phosphate and parathyroid hormone (PTH) levels. Chronic renal disease leads to a decrease in renal phosphorus excretion, which leads to phosphate retention and a significant increase in PTH levels. This ultimately can lead to tertiary hyperparathyroidism.
Tejwani et al present a review article on renal osteodystrophy. They state that in high- turnover renal osteodystrophy PTH secretion is increased and, in the absence of medical intervention, leads to parathyroid gland hyperplasia. This hyperplasia is associated with loss of feedback inhibition in normal regulation of PTH secretion; consequently, even after correction of the renal disease, the parathyroid gland continues to secrete excessive levels of PTH.
Illustration A shows a pathologic fracture secondary to renal osteodystrophy. Incorrect Answers:
This series of lab values is consistent with a diagnosis of nutritional rickets due to vitamin D deficiency.
This series of lab values is consistent with a diagnosis of low-turnover renal osteodystrophy. This is classically caused by excess deposition of aluminum into bone which impairs PTH release from the parathyroid gland and disrupts the mineralization process.
This series of lab values is consistent with a diagnosis of hypoparathroidism. 5-This series of lab values is consisten with a diagnosis of primary hyperparathryoidism.
A 28-year-old African-American male with a history of Sickle Cell Disease complains of progressive left hip pain for the past two years. He denies any causative injuries. His images are shown in Figures A and B. Which of the following mechanisms is most likely responsible for his symptoms?
Blood disorder due to abnormal hemoglobin S alleles
Progressive slippage of physis though the hypertrophic zone
Osteomyelitis most likely due to Salmonella species
Accumulation of glycosaminoglycan breakdown products
COL5A1 or COL5A2 mutation
The clinical presentation and images are most consistent with left hip osteonecrosis as a result of coagulation and vascular occlusion caused by sickle cell anemia.
Sickle cell disease is a genetic disorder of hemoglobin synthesis characterized by 2 abnormal hemoglobin S alleles. Under low oxygen conditions the affected blood cells become "sickle shaped" and unable to pass through vessels. This results in vascular occlusion that may have a variety of clinical consequences depending on the body part affected.
Hernigou et al. review the natural history of symptomatic osteonecrosis in adults with sickle cell disease. Once symptomatic , osteonecrosis of the hip in sickle cell disease has a high likelihood of progressing and leading to femoral head collapse. Deterioration can be rapid and in most patients operative intervention is necessary to prevent further collapse or alleviate intractable pain.
Mont et al. performed a literature review on the natural history of untreated asymptomatic osteonecrosis of the femoral head. Their findings supported that asymptomatic osteonecrosis had a high prevalence of progression to symptomatic femoral head collapse. Small, medially located lesions had a low rate of progression, while medium to large sized osteonecrotic lesions did progress in a substantial number of patients. They recommended
consideration of joint-preserving surgical treatment in asymptomatic patients with a medium-sized or large, laterally located lesion.
Figure A shows an AP pelvis with left hip osteonecrosis. Figure B shows a T2 coronal MRI with left hip osteonecrosis. Illustration A shows an example of a hemoglobin molecule which has become "sickle shaped," and as a result is unable to pass through vessels efficiently.
Incorrect Answers:
slipped capital femoral epiphysis.
What mechanism allows Staphylococcus epidermidis to adhere to surfaces and resist phagocytosis?
Creation of active efflux pumps
Methylation of 23s rRNA
Biofilm production
Alteration of cell wall permeability
Beta-lactamase production
Staphylococcus epidermidis is a gram-positive bacteria that utilizes a glycocalyx/biofilm to adhere to orthopedic implants and other surfaces and resist phagocytosis.
The biofilm creates a well-protected environment where bacteria can proliferate and thrive essentially undetected by the host immune system. This leads to chronic infections of orthopedic implants that can go undetected for years.
Arciola et al note that S. epidermidis can colonize surfaces in a self-generated viscous biofilm composed of polysaccharides and that the ica genes found in
56% of S. epidermidis isolates were associated with their ability to produce biofilm.
Olson et al discuss the importance of polysaccharide intercellular adhesin (PIA), a
substance produced by 50-60% of S. epidermidis strains, in the adherence of S. epidermidis to biomaterials through biofilm creation. PIA plays a critical role in initial adherence of S. epidermidis to biomaterials, biofilm
maturation and aggregation.
Illustration A shows microscopy of Staphylococcus epidermidis, which is a gram- positive, coagulase-negative cocci. Illustration B is an overview of the different classes of organisms in microbiology.
Incorrect Answers:
Compared to cold-forged cobalt chrome, titanium alloys have which property?
Increased fatigue strength
Increased yield strength
Increased endurance limit
Decreased ductility
Decreased tensile strength
Titanium implants have decreased tensile (ultimate) strength when compared to cobalt chrome.
Ultimate strength, or tensile strength, is the maximum stress a material can withstand before undergoing breakage or failure. The ranking of ultimate strength, from highest to lowest is: 1) cobalt chrome, 2)titanium, 3)stainless steel, and 4) cortical bone.
Young's modulus of elasticity is defined as the measure of stiffness of a material in the elastic zone. A higher Young's modulus indicates a stiffer material. While titanium is highly biocompatible with a low modulus of elasticity (Young's modulus), it has poor wear characteristics making it non- suitable for femoral heads in total hip arthroplasty.
Long et al. present a review on titanium implants with a focus on bio- mechanical properties. Their study supports previous data which showed high rates of ultra-high molecular weight polyethylene wear due to accelerated breakdown when in contact with a titanium surface.
Incorrect Answers:
Peak bone mass attainment in both men and women is most dependent on which sex-steroid?
Testosterone
Progesterone
Growth Hormone
Estrogen
Cortisol
Estrogen has been shown to be important for both men and women in attaining peak bone mass.
Risk factors for osteoporosis are: increasing age, female sex, early menopause, fair-skinned, family history of hip fracture, low body weight, smoking, glucocorticoid use, excessive alcohol, low protein intake, and anticonvulsant or antidepressant use.
Which of the following contributes most to the ability of hyaline cartilage to attract water?
Aggrecan
Biglycan
Decorin
Fibromodulin
Osteocalcin
Aggrecan molecules bind to hyaluronic acid molecules via link proteins to form a macromolecule complex, known as a proteoglycan aggregate, which attracts water.
Proteoglycans are composed of subunits known as glycosaminoglycans. Glycosaminoglycans include two subtypes: chondroitin sulfate and keratin sulfate. These glycosaminoglycans link to a protein core by sugar bonds to form an aggrecan molecule. Link proteins then stabilize many of these aggrecan molecules to hyaluronic acid to form the proteoglycan aggregate. Cartilage also contains ancillary proteoglycans that are much smaller than the aggregating proteoglycans. These small proteoglycans include decorin, biglycan, and fibromodulin. They bind to other molecules (eg, type II collagen) and assist in matrix stabilization.
Ulrich-Vinther et al. authored a Level 5 review on cartilage structure. The negative charge present within the hyaline cartilage extracellular matrix attracts cations and results in an increase in tissue osmolality. This then attracts water, which decreases the osmolality. Thus, articular cartilage has a high tissue pressure, but the presence of type II collagen matrix prevents it from swelling.
Nap et al. present a basic science review article on aggrecans. They discus that the main function of aggrecan in cartilage is to resist compressive forces.
They note that the negative charge of the aggrecan molecule disaccharides create the high osmotic swelling pressure of cartilage.
Illustration A depicts the molecular organization of an aggregated proteoglycan molecule. Incorrect Answers:
What effect do bisphosphonate medications have on spinal fusion surgery when taken in the postoperative period?
Any effect can be counteracted by taking calcium supplements
No effect
Increased risk of wound infection
Smaller fusion mass
Decreased fusion rate
Bisphosphonates (e.g. alendronate) are used to treat osteoporosis. The mechanism of action is inhibiting the formation of the ruffled border of osteoclasts, resulting in decreasing bone turnover.
Huang et al performed a rat study comparing alendronate to placebo and found that fusion rates were lower in those treated with alendronate. However,
the fusion masses were larger in the alendronate treated rats despite lower fusion rates (why #4 is incorrect).
Lehman et al in another placebo controlled rate study found that the fusion rates for placebo (76%) were greater than the alendronate group (45%). Alendronate works on osteoclasts and does not affect calcium directly. Taking calcium should have no effect on alendronate (why #1 is incorrect). At this time there are no formal recommendations of when to stop bisphosphonate medication prior to spinal fusion surgery.
A therapeutic study presents a systematic review of 15 high- quality randomized controlled trials with homogeneous results. What level of evidence is this considered?
I
II
III
IV
V
A systematic review of high-quality clinical trials is considered a Level I study.
A systematic review is a powerful tool used to identify, evaluate and appraise all high- quality research related to a specific question. Systematic reviews, in contrast to most narrative review articles, adhere to strict scientific design by following eight steps; 1) defining a question and developing inclusion criteria,
Question 22
An 18-month-old child was involved in a motor vehicle accident and sustained an isolated injury to the left upper extremity. A radiograph is shown in Figure 33. What is the most appropriate management for this injury?

Explanation
Question 23
A 50-year-old patient who plays tennis sustained the deformity shown in Figure 27 following a high volley. Further diagnostic work-up should include
Explanation
REFERENCES: Neer CS II, Bigliani LU, Hawkins RJ: Rupture of the long head of the biceps related to the subacromial impingement. Orthop Trans 1977;1:114.
Hawkins RJ, Murnaghan JP: The shoulder, in Gruess RL, Ronnie WRJ (eds): Adult Orthopaedics. New York, NY, Churchill Livingstone, 1984, pp 945-1054.
Question 24
When performing a Kocher approach to the radial head for open reduction internal fixation the forearm is held in pronation. What structure is this maneuver attempting to protect?

Explanation
Question 25
The radiographs and CT scan seen in Figures 28a through 28d reveal what type of acetabular fracture pattern?
Explanation
REFERENCES: Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 26
-The patient experienced little improvement with activity modification and physical therapy. An intraarticular corticosteroid injection provides excellent but short-lived pain control. She requests surgical treatment for her hip and she is counseled regarding arthroscopy and consent is obtained. Intraoperatively,a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. What treatment is most appropriate considering these findings?
Explanation
The clinical scenario, examination, and MRI scans are consistent with a pincer-type FAI. The decreased range of motion is secondary to the pain produced by the continued abutment of the femoral head against the anterosuperior acetabulum. Flexing the hip while internally rotating and adducting the leg recreates this contact and is typically painful. No clinical signs suggest sacroiliac joint arthritis, an intra-articular loose body, or trochanteric bursitis, although these are all diagnoses that should be considered in a patient with a painful hip. The most sensitive and specific study to detect an acetabular labral tear is an MRI arthrogram of the hip. This study should be obtained in this patient to evaluate the labrum as well as the status of the articular cartilage. An MRI scan without intra-articular contrast is not as sensitive as an arthrogram. An ultrasound can provide a dynamic assessment of the hip and help in the setting of a snapping hip; however, this study is not reliable to determine the presence of a labral tear. In the setting of pincer FAI, the forced leverage of the anterosuperior femoral head upon the anterior acetabulum results in abnormal forces against the posteroinferior acetabulum. This continued force can lead to a chondral lesion in this location know as a “counter-coup” injury. Chondral lesions of the femoral head are rare in the setting of pincer FAI. The posterosuperior quadrant does not experience increased force and rarely sustains chondral injuries. The patient is a young, active individual with no pre-existing degenerative changes, so repair of the tear with bony resection of the pincer lesion is the most appropriate treatment.A capsulolabral detachment should be repaired because these tears can heal and the labrum functions as a seal, preventing egress of synovial fluid from the joint space. If the pincer lesion is not resected, the patient will continue to experience abnormal contact and the repair will likely fail. There is no evidence that the patient has a cam impingement, and recontouring of the femoral head/neck junction is not appropriate. Simple debridement should be reserved for intrasubstance tears of the labrum, which would not be expected to heal with repair.
CLINICAL SITUATION FOR QUESTIONS 30 THROUGH 32
Figures 30a and 30b are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he
believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg.


Question 27
A 63-year-old woman with osteopenia is struck by a motor vehicle and sustains a Schatzker 2 (AO/OTA Type B) fracture of the lateral tibial plateau. She has 1.5 cm of joint depression and 7 mm of condylar widening. What is the most appropriate surgical fixation for this injury?
Explanation
Illustration A shows a tibial plateau fracture. Incorrect Answers:
2: Screws alone are unlikely to be adequately stable in this patient.
3: External fixation is not enough to reduce and hold the joint reduced. 4: Locking plates do not provide buttress effect when used in pure locking mode. In addition, locking plates add significant incremental cost to the procedure. 5: A unicondylar injury does not require dual plating.
Question 28
Clinical staging of osteomyelitis using the Cierney-Mader classification system takes into account which of the following factors?
Explanation
Question 29
03 The sagittal oblique MRI scan shown in Figure 70 reveals a lesion in the shoulder that typically affects what neurologic structure?
Explanation
The cysts form either because of a lesion of the capsulolabral complex at the superior/posterosuperior glenoid in the shoulder or because of myxoid degeneration of the capsule.
back to this question next question
Question 30
Figure 1 shows the radiograph of a 68-year-old man who underwent revision hip arthroplasty with impaction grafting of the femur and cementing of a tapered component into the graft 2 years ago. The patient remains symptom-free. Which of the following best describes the most likely histologic appearance of the proximal femur if a biopsy was performed?
Explanation
REFERENCES: Nelissen RG, Bauer TW, Weidenhielm LR, LeGolvan DP, Mikhail WE: Revision hip arthroplasty with the use of cement and impaction grafting: Histological analysis of four cases. J Bone Joint Surg Am 1995;77:412-422.
Gie GA, Linder L, Ling RS, Simon JP, Slooff TJ, Timperley AJ: Impacted cancellous allografts and cement for revision total hip arthroplasty. J Bone Joint Surg Br 1993;75:14-21.
Question 31
Radiating pain associated with a posterolateral thoracic disk herniation typically follows what pattern? Review Topic
Explanation
Question 32
A 6-year-old boy had a 4-day history of worsening atraumatic right thigh and knee pain. He was seen in the emergency department, where he had a temperature of 39.1°C. Laboratory studies reveal a white blood cell count of 15000 /µL (reference range, 4500-11000 /µL). He had a small knee effusion with range of motion 0 to 90 degrees and a swollen, painful, hot distal thigh. The knee effusion was aspirated, revealing a white blood cell (WBC) count of 2000 with negative gram stain (reference range < 2000 WBC/mL). The boy was admitted to the pediatric medical service and intravenous (IV) antibiotics were initiated. The next day, MR imaging was obtained and orthopaedics was consulted. Based on Figures 8a and 8b, what is the most appropriate description of his condition?
Explanation
The MRI scans show an advanced distal femur osteomyelitis with a substantial subperiosteal abscess. This necessitates open drainage; by definition, an abscess is avascular, so antibiotics cannot be delivered to the area without drainage.

CLINICAL SITUATION FOR QUESTIONS 9 THROUGH 12
Figures 9a and 9b are the radiographs of a 9-year-old boy who fell from the monkey bars and sustained a closed fracture of the elbow.
Question 33
A 19-year-old linebacker for a collegiate football team has had two episodes of bilateral arm tingling and weakness after tackling; the symptoms resolved after 30 minutes of rest. Three follow-up neurologic examinations have been normal. Cervical spine CT and MRI scans are shown in Figures 13a through 13c. What is the next best step in management?
Explanation
REFERENCES: Torg JS, Naranja RJ Jr, Pavlov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Cantu RC: The cervical spinal stenosis controversy. Clin Sports Med 1998;17:121-126. Crowl AC, Kong JF: Cervical Spine, in Johnson DL, Mair SD (eds): Clinical Sports Medicine. Philadelphia, PA, Mosby Elsevier, 2006, pp 143-149.
Question 34
- The lateral fragment of bone (Segond fracture) associated with an injury of the anterior cruciate ligament is the result of an avulsion of the
Explanation
Question 35
Figure 18 shows the radiograph of a patient with a total hip arthroplasty dislocation. During revision, increasing the diameter of the femoral head while maintaining the ratio of head-to-neck diameter constant has the effect of
Explanation
Scifert and associates used a three-dimensional finite element model to study various combinations of femoral head size and neck ratios. They found that increasing the diameter of the femoral head while maintaining a constant head-to-neck diameter had the effect of significantly increasing the resisting moment necessary to induce a dislocation. The higher the head-to-neck ratio, the greater the range of motion until impingement and the greater the range of motion to dislocation.
REFERENCE: Scifert CF, Brown TD, Pedersen DR, Callaghan JJ: A finite element analysis of factors influencing total hip dislocation. Clin Orthop 1998;355:152-162.
Question 36
Which of the following conditions routinely requires early surgical intervention in patients with Marfan syndrome? Review Topic
Explanation
Question 37
A 46-year-old male construction worker has right hip pain that has failed to respond to nonsurgical management. His body mass index (BMI) is 32, he is 6’2” tall, and he has no other medical comorbidities. AP and lateral radiographs of the right hip are shown in Figures 23a and 23b. The patient inquires about his suitability for metal-on-metal hip resurfacing. The patient should be educated that he is at higher risk for failure secondary to which of the following?
Explanation
The results of hip resurfacing arthroplasty have been reported to be best in young, male patients who are younger than 55 years of age with a diagnosis of osteoarthritis. Although some authors advocate metal- on-metal hip resurfacing as an option for patients with osteonecrosis of the femoral head, in this particular patient, given the size of the necrotic segment, he would be at higher risk for failure and a conventional total hip arthroplasty would be a more conservative option. As the acetabulum is resurfaced in metal- on-metal hip resurfacing, the secondary changes of the acetabulum are not an issue and his BMI is in an acceptable range for the procedure.
REFERENCES: Mont MA, Ragland PS, Etienne G, et al: Hip resurfacing arthroplasty. J Am Acad Orthop Surg 2006;14:454-463.
Revell MP, McBryde CW, Bhatnagar S, et al: Metal-on-metal hip resurfacing in osteonecrosis of the femoral head. J Bone Joint Surg Am 2006;88:98-103.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65. Question 24
A 31-year-old woman had disabling right knee pain. An arthroscopic assessment reveals chondromalacia of both the lateral femoral condyle and tibial plateau. The standing femorotibial axis measures 10 degrees of valgus. The
optimum treatment of this condition should include
distal femoral varus osteotomy.
osteoarticular transplant to the lateral femoral condyle.
unicondylar arthroplasty.
high tibial osteotomy.
Fulkerson tibial tubercle transfer. PREFERRED RESPONSE: 1
DISCUSSION: The long-term outcome of a distal femoral varus osteotomy has been quite favorable and should remain the primary choice for this young active woman. Sharma and associates have shown that a 5-degree valgus malalignment has a five-fold chance of progressing at least one grade within 18 months, making a corrective osteotomy the most important surgical maneuver.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and function decline in knee osteoarthritis. JAMA 2001 ;286:188-195.
Murray PB, Rand JA: Symptomatic valgus knee: The surgical options. J Am Acad Orthop Surg 1993; 1:19.
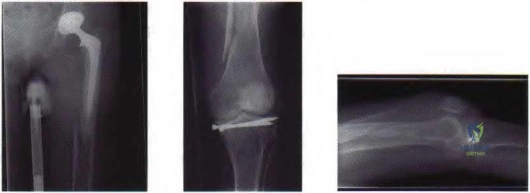
Figure 25a Figure 25b Figure 25c
Question 38
- A 14-year-old patient who has homocystinuria and is Risser 3 is referred for surgical treatment of scoliosis. In addition to the usual risks associated with posterior spinal fusion, the family should be advised that the patient ‘s underlying condition significantly increases the perioperative risk of
Explanation
1 and 2 are concerns during spinal fusion but are not specific to this disease. 4 may occur with homocystinuria but is not related to spinal fusion. 5 occurs with PSF in the younger population because of the growth potential remaining.
Question 39
Up to what time frame are the risks minimized in anterior revision disk replacement surgery? Review Topic
Explanation
Question 40
What pathology is most likely to result in failure of an arthroscopic Bankart repair?
Explanation
REFERENCES: Burkhart SS, De Beer JF: Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 2000;16:677-694.
Cole BJ, Romeo AA: Arthroscopic shoulder stabilization with suture anchors: Technique, technology, and pitfalls. Clin Orthop 2001;390:17-30.
Question 41
Thyroid hormone regulates skeletal growth at the physis by stimulation of
Explanation
REFERENCES: Ballock RT: Regulation of skeletal growth and maturation by thyroid hormone, in Buckwalter JA, Ehrlich MG, Sandell LJ, Trippel SB (eds): Skeletal Growth and Development: Clinical Issues and Basic Science Advances. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1998, pp 301-317.
Rosier RN, O’Keefe RJ, Reynolds PR, Hicks DG, Puzas JE: Expression and function of TGF-b= and PTHrP in the growth plate, in Buckwalter JA, Ehrlich MG, Sandell LJ, Trippel SB (eds): Skeletal Growth and Development: Clinical Issues and Basic Science Advances. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1998, pp 285-299.
Trippel SB: IGF-I and FGF-2 in growth plate regulation, in Buckwalter JA, Ehrlich MG, Sandell LJ, Trippel SB (eds): Skeletal Growth and Development: Clinical Issues and Basic Science Advances. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1998, pp 263-283.
Question 42
An investigation studying whether physical therapy or subacromial injection can be successfully used to treat shoulder pain is conducted. Two groups are identified. One group is prescribed physical therapy, while the other receives a subacromial injection. The groups have similar baseline demographics and shoulder pathologies. Ten patients are randomized in each group and findings show that there is no significant difference in any patient-reported outcome measure. An increase in sample size would reduce the risk of what parameter?
Explanation
Question 43
A 35-year-old construction worker sustained a midshaft clavicle fracture that developed a hypertrophic nonunion. One year after the injury, it was internally fixed without bone graft. Four months after the surgery he was asymptomatic and he was released to full activity. Five months following surgery, the patient was digging a ditch and he felt pain in the clavicle. The 4-month and 5-month postoperative radiographs are shown in Figures 117a and 117b. What is the most likely cause of this failure? Review Topic
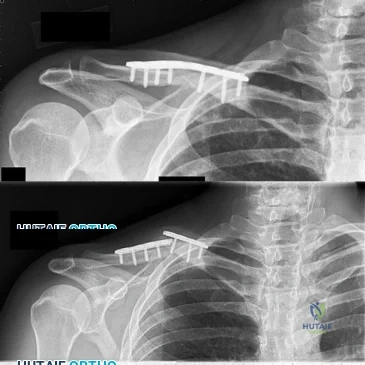
Explanation
Question 44
A patient who is an observant Jehovah’s Witness requires major surgery for scoliosis that will likely result in significant blood loss. Which of the following might the patient consider allowing the surgical team to use?
Explanation
REFERENCES: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
www.watchtower.org. Official Web Site of Jehovah’s Witnesses. Link verified as active as of August 8, 2008.
Question 45
During surgical hip dislocation for the management of femoral acetabular impingement, preservation of what structure is paramount to maintaining vascularity to the femoral head?
Explanation
REFERENCES: Gautier E, Ganz K, Krugel N, et al: Anatomy of the medial femoral circumflex artery and its surgical implications. J Bone Joint Surg Br 2000;82:679-683.
Ganz R, Gill TJ, Gautier E, et al: Surgical dislocation of the adult hip: A technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001; 83:11191124.
Question 46
A 56-year-old male sustains a Type IIIB open, comminuted tibial shaft fracture distal to a well-fixed total knee arthroplasty that is definitively treated with a free flap and external fixation. Nine months after fixator removal, he presents with a painful oligotrophic nonunion. Laboratory workup for infection is negative. Passive knee range of motion is limited to 15 degrees. What is the most appropriate treatment for his nonunion?

Explanation
Wiss et al reported a series of fifty tibial non-unions with a similar clinical scenario. He reported that, with compression plating, 92% of the nonunions healed without further intervention. In their study, 39/50 patients, had autogenous bone grafting in addition to compression plating.
Question 47
A 17-year-old high school football player injures his right ankle during a game. Examination reveals swelling and a closed ankle deformity, with normal foot circulation and sensation. Radiographs are shown in Figures 10a and 10b. In addition to closed reduction, management should include
Explanation
REFERENCES: Browner BD, Jupiter JB, Levine AM, Trafton PG: Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 1887-1957.
Stiehl JB: Ankle fractures with diastasis. Instr Course Lect 1990;39:95-103.
Question 48
Which of the following statements best describes results that have been reported with roentgen stereophotogrammetric analysis (RSA)?
Explanation
varus-coronal plane and retroversion-transverse plane, or both) has been associated with a higher risk of loosening of the component.
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 100.
Question 49
Five weeks after the patient completes a 6-week course of antibiotics, his ESR is 24 mm/h and CRP level is 10 mg/L, which is similar to the levels at 6 weeks. What is the most appropriate treatment at this time?
Explanation
This patient has both serologic and synovial fluid findings that are concerning for indolent infection. He was taking antibiotics at the time of aspiration. The AAOS clinical practice guideline, The Diagnosis of Periprosthetic Joint Infections of the Hip and Knee, suggests that patients discontinue antibiotics for a minimum of 2 weeks and that a repeat aspiration should be performed in cases of contradictory findings. In this situation, the cell count is elevated
along with an elevated ESR and CRP level. As a result, the appropriate treatment at this time is to reaspirate his hip.
This patient has a periprosthetic joint infection with a draining sinus tract. He has had symptoms for several months and, as a result, irrigation and debridement are not indicated. A single-stage surgery may be performed in some centers for healthy patients with susceptible organisms. However, single-stage reconstructions are generally performed with cemented implants in patients without a draining sinus tract. A 2-stage procedure with an antibiotic spacer is the surgical treatment modality most likely to eradicate this infection.
Serologic findings have significantly improved since the time of the prior surgical procedure. Surgical intervention does not need to be delayed until these values have completely normalized.
Question 50
Figure 51 shows an arthroscopic view of the patellofemoral joint from an inferolateral portal. The arrow points to which of the following structures? Review Topic

Explanation
Question 51
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the
Explanation
REFERENCES: Miller DB Jr: Arthroscopic meniscus repair. Am J Sports Med 1988;16:315-320.
Nawab A, Hester PW, Caborn DN: Arthroscopic meniscus repair, in Miller MD, Cole BJ (eds): Textbook of Arthroscopy. Philadelphia, PA, WB Saunders, 2004, pp 517-537.
Question 52
What is the most serious complication that may occur with a ceramic-on-ceramic bearing in a total hip prosthesis?
Explanation
Question 53
Split posterior tibial tendon transfer is used in the treatment of children with cerebral palsy. Which of the following patients is considered the most appropriate candidate for this procedure?
Explanation
REFERENCES: Green NE, Griffin PP, Shiavi R: Split posterior tibial-tendon transfer in spastic cerebral palsy. J Bone Joint Surg Am 1983;65:748-754.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 2, pp 1142-1152.
Question 54
A 72-year-old patient fell 3 weeks after undergoing a total hip arthroplasty using cementless fixation of the femoral component. She sustained a comminuted Vancouver type B-2 fracture with displacement of the calcar fragment. What is the best treatment option?
Explanation
The patient has an acute postoperative fracture of the proximal femur with subsidence. It is also common that the stem retroverts relative to the femur. It is most often seen in proximally porous coated stems within 90 days of surgery, one paper found it to occur 0.7% of the time in modern implants. There is always a debate whether this is a missed intraoperative fracture, or a new fracture that has resulted from an event of increased hoop stresses. Removal of the primary stem, placement of a diaphyseal engaging stem (most frequently a tapered-fluted stem), and cabling of the fracture is the most successful treatment.
Question 55
A 42-year-old woman has persistent thumb pain that she notes is worse with opening jars and turning her car key. Opponens splinting provides some relief, but she is poorly tolerant of the splint. Finkelstein’s test is negative, and a carpometacarpal grind test is positive. The radiographs shown in Figures 48a and 48b reveal minimal degenerative changes at the first carpometacarpal joint. What is the best course of action?
Explanation
REFERENCES: Tomaino MM: Treatment of Eaton stage I trapeziometacarpal disease with thumb metacarpal extension osteotomy. J Hand Surg Am 2000;25:1100-1106.
Pellegrini VD Jr, Parentis M, Judkins A, et al: Extension metacarpal osteotomy in the treatment of trapeziometacarpal osteoarthritis: A biomechanical study. J Hand Surg Am 1996;21:16-23.
Tomaino MM, Pellegrini VD, Burton RI: Arthroplasty of the basal joint of the thumb: Long-term follow-up after ligament reconstruction with tendon interposition. J Bone Joint Surg Am 1995;77:346-355.
Question 56
What is the primary indication for performing an arthroscopic synovectomy on a patient with hemophilia that is the result of factor VIII deficiency? Review Topic
Explanation
Question 57
Which of the following is considered the preferred approach to resect a lesion in the posterior one third of the proximal humerus?
Explanation
REFERENCE: Berger RA, Buckwalter JA: A posterior surgical approach to the proximal part of the humerus. J Bone Joint Surg Am 1989;71:407-410.
Question 58
Among patients with adolescent idiopathic scoliosis, a thoracolumbosacral orthosis is most effective for which type of curve?
Explanation
A thoracolumbosacral orthosis is most effective for bracing of curves when the apex is at T7 or below. Bracing is used for patients who are skeletally immature (Risser stage 0, 1, or 2), and it is recommended that the brace be worn 16 to 23 hours per day and continued until skeletal maturity or until the curve progresses to beyond 45 degrees, at which point bracing is no longer considered effective.
RECOMMENDED READINGS
Luhmann SJ, Skaggs DL: Pediatric spine conditions, in Lieberman JR (ed): AAOS Comprehensive Orthopaedic Review. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2009, pp 245-265.
Shaughnessy WJ. Advances in scoliosis brace treatment for adolescent idiopathic scoliosis. Orthop Clin North Am. 2007 Oct;38(4):469-75, v. Review. PubMed PMID: 17945126. View Abstract at PubMed
Question 59
-What is the most likely cause of an acute femur fracture in a 5-month-old child?
Explanation

Question 60
-A 51-year-old man has a slowly expanding upper-extremity mass. Examination reveals a firm 3-cm mass in his midvolar forearm. Radiographs are normal. You suspect a soft-tissue sarcoma. The best imaging study would be
Explanation

Question 61
A 16-year-old boy has abdominal and back pain after being involved in a high-velocity head-on motor vehicle accident. He was restrained in the rear of the automobile by a lap belt only. A radiograph and CT scan are shown in Figure 47. The patient has no other injuries. Optimal management should include
Explanation
REFERENCES: Greenwald TA, Mann DC: Pediatric seatbelt injuries: Diagnosis and treatment of lumbar flexion-distraction injuries. Paraplegia 1994;32:743-751.
Glassman SD, Johnson JR, Holt RT: Seatbelt injuries in children. J Trauma 1992;33:882-886.
Raney EM, Bennett JT: Pediatric Chance fracture. Spine 1992;17:1522-1524.
Question 62
- A 45-year-old man sustains the shoulder injury shown in the radiographs in Figure 55a and 55b and the CT scan in Figures 55c and 55d. Management should consist of
Explanation
Question 63
Venous thrombolembolism is a common complication following total hip and total knee arthroplasty; therefore, prophylaxis is deemed efficacious. Several studies on low-molecular-weight heparin (LMWH) have shown which of the following findings?
Explanation
REFERENCES: Colwell CW Jr, Collis DK, Paulson R, et al: Comparison of enoxaparin and warfarin for the prevention of venous thromboembolic disease after total hip arthroplasty:. Evaluation during hospitalization and three months after discharge. J Bone Joint Surg Am 1999;81:932-940.
Salvati EA, Pelligrini VD Jr, Sharrock NE, et al: Recent advances in venous thromboembolic prophylaxis during and after total hip replacement. J Bone Joint Surg Am 2000;82:252-270.
Question 64
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of Review Topic
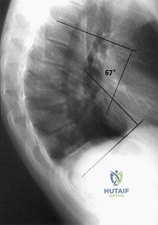
Explanation
Question 65
A 32-year-old volleyball player has dull posterior shoulder pain. An examination reveals moderate external rotation weakness with his arm at his side, but normal strength on supraspinatus isolation. Deltoid and supraspinatus bulk appear normal, although there appears to be mild infraspinatus atrophy. Sensation is normal throughout the shoulder and shoulder girdle. What is the most likely diagnosis?
Explanation
This clinical scenario describes a patient with an isolated injury affecting the infraspinatus muscle. The anatomic location of such a lesion would be at the spinoglenoid notch, at which the suprascapular nerve may be compressed distal to its innervation of the supraspinatus but proximal to the infraspinatus innervation. A calcified transverse scapular ligament would also affect the suprascapular nerve but is proximal to the innervation of both muscles. Quadrilateral space syndrome would affect innervation of the deltoid (and teres minor). Parsonage-Turner syndrome is a more diffuse, and often severely painful, brachial plexus neuropathy.
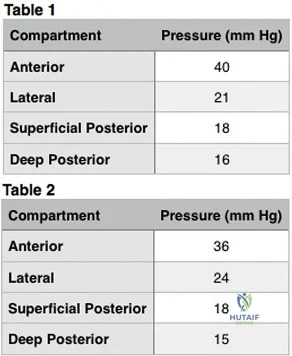
Question 66
-Figure 39 is the anteroposterior radiograph of a marathon runner who has left groin pain that prevents her from running. She recently got back into her usual running routine after an ankle injury preventedbher from running for several months. She now has pain with any weight bearing. What is the most appropriate treatment option?
Explanation

Question 67
A 14-year-old football player has had right knee pain for the past 2 months; however, he denies any history of trauma. Examination shows an abductor lurch and increased external rotation of the right lower extremity. The best course of action should be to
Explanation
REFERENCES: Boyer DW, Mickelson MR, Ponseti IV: Slipped capital femoral epiphysis: Long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am 1981;63:85-95.
Stasikelis PJ, Sullivan CM, Philips WA, Polard JA: Slipped capital femoral epiphysis: Prediction of contralateral involvement. J Bone Joint Surg Am 1996;78:1149-1155.
Question 68
Spontaneous recovery of upper extremtiy motor function after a cerebrovascular accident occurs in which of the following predictable patterns?
Explanation
REFERENCE: Waters RL, Keenan ME: Surgical treatment of the upper extremity after stroke, in Chapman MW (ed): Operative Orthopedics. Philadelphia, PA, JB Lippincott, 1988, vol 2,
pp 1449-1450.
Question 69
Treatment of an atrophic nonunion of the radial diaphysis should include which of the following?

Explanation
Question 70
A 57-year-old man with type I diabetes mellitus has had a tender, erythematous right sternoclavicular joint for the past 2 weeks. Radiographs reveal mild osteolysis without arthritic changes, within normal limits. Management should consist of
Explanation
REFERENCES: Bremner RA: Monarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, p 488.
Question 71
An 80-year-old man who was involved in a fall from ground height is evaluated in the emergency department for head lacerations and mild neck pain. Examination reveals only mild tenderness of the posterior neck region with some limitation of motion. Neurologic examination is normal. Radiographs of the cervical spine are shown in Figures 58a and 58b. What is the next most appropriate step in management for this patient? Review Topic

Explanation
Question 72
A 35-year-old woman who is training for a triathlon has had a 2-month history of heel pain with weight bearing and is unable to run. History reveals that she is amenorrheic. Examination reveals that she is thin and has pain over the heel that is exacerbated with medial and lateral compression. Range of motion and motor and sensory function are normal. Radiographs are normal. What is the most likely diagnosis?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 179-191.
Question 73
A 52-year-old woman has a 60-degree extensor lag following a right total knee arthroplasty performed 16 months ago. Since the time of her primary total knee arthroplasty she has undergone primary repair of a patellar tendon rupture that occurred after a fall 8 months ago. A lateral radiograph of the knee is shown in Figure 52. A CT scan obtained to determine component rotation showed that the femoral component is internally rotated 9 degrees and the tibial component is internally rotated 12 degrees. Appropriate management at this time should include
Explanation
Attempts at secondary repair have been associated with high failure rates whereas the use of an extensor mechanism allograft has been shown to more effectively restore active extension in a substantial percentage of patients. Important aspects of the technique include fully tensioning the graft in full extension and immobilization of the extremity for 6 to 8 weeks postoperatively to allow for graft healing. Nonsurgical management will not result in an acceptable outcome for a young patient, and attempted secondary repair is associated with a high rate of failure, even when augmented with local tissues. This patient has gross rotational
malalignment of the components and the surgeon faced with this problem should consider obtaining a CT scan to determine component rotation preoperatively.
REFERENCES: Burnett RS, Berger RA, Paprosky WG, et al: Extensor mechanism allograft reconstruction after total knee arthroplasty: A comparison of two techniques. J Bone Joint Surg Am 2004;86:2694-2699.
Nazarian DG, Booth RE: Extensor mechanism allografts in total knee arthroplasty. Clin Orthop Relat Res
1999;367-123-129. , „. H
AL-Madena Copy ^Lj-^M) <UjJlU

Question 74
A 7-year-old boy has a limp with pain and tenderness over the distal right femur. Radiographs are shown in Figures 5a and 5b. Based on these findings, what is the best course of action?
Explanation
REFERENCES: Dormans, JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Easley ME, Kneisl JS: Pathologic fractures through nonossifying fibromas: Is prophylactic treatment warranted? J Pediatr Orthop 1997;17:808-813.
Question 75
A 10-year-boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals no soft-tissue mass, and mild tenderness. Figures 33a and 33b show the plain radiograph and MRI scan, and the biopsy specimens are shown in Figures 33c and 33d. What is the most likely diagnosis?
Explanation
REFERENCE: Simon MA, Springfield DS, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-200.
Question 76
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include
Explanation
REFERENCES: Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
Question 77
Figure 34 shows the standing AP radiograph of a 2-year-old girl who has a left bowleg deformity. Her mother states that she first noticed the problem when the child began walking at age 10 months, and the deformity has worsened over the past 6 months. Examination reveals a definite lateral thrust of the knee during the stance phase of gait. Management should consist of
Explanation
REFERENCES: Zionts LE, Shean CJ: Brace treatment of early infantile tibia vara. J Pediatr Orthop 1998;18:102-109.
Richards BS, Katz DE, Sims JB: Effectiveness of brace treatment in early infantile Blount’s disease. J Pediatr Orthop 1998;18:374-380.
Raney EM, Topoleski TA, Yaghoubian R, Guidera KJ, Marshall JG: Orthotic treatment of infantile tibia vara. J Pediatr Orthop 1998;18:670-674.
Question 78
Which of the following diagnostic studies best distinguishes Ewing’s sarcoma from small cell osteosarcoma?
Explanation
REFERENCES: Perotti D, Corletto V, Giardini R, Parafioriti A, Fossati-Bellani F, Luksch R: Retrospective analysis of ploidy in primary osseous and extraosseous Ewing family tumors in children. Tumori 1998;84:493-498.
Riley RD, Burchill SA, Abrams KR, Heney D, Sutton AJ, Jones DR, et al: A systematic review of molecular and biological markers in tumours of the Ewing’s sarcoma family. Eur J Cancer 2003;39:19-30.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 11-20.
Question 79
A 23-year-old baseball pitcher reports pain in the posterior aspect of his dominant shoulder during the late cocking phase of throwing. With the dominant shoulder positioned in 90 degrees of abduction from the body and with the scapula stabilized, examination reveals 135 degrees of external rotation and 20 degrees of internal rotation. Examination of the opposite shoulder reveals 100 degrees of external rotation and 75 degrees of internal rotation. Both shoulders are stable on examination. Radiographs and MRI scans are unremarkable. What is the primary cause of his pain?
Explanation
REFERENCES: Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Meister K: Injuries to the shoulder in the throwing athlete. Part one: Biomechanics, pathophysiology, classification of injury. Am J Sports Med 2000;28:265-275.
Question 80
Figure 57 is the radiograph of a 58-year-old woman who is right-hand dominant and has fallen on her flexed right elbow and is seen in the emergency department reporting isolated episodes of right elbow pain. Examination reveals that the skin is contused but intact, and her distal neurovascular examination is normal. What is the most appropriate treatment? Review Topic

Explanation
construct is a commonly used technique but is reserved for simple fracture patterns without comminution. Excision and triceps advancement can be considered in elderly, low-demand patients that have small unreconstructable fracture patterns without associated elbow instability.
Question 81
An 80-year-old woman notes a painless mass posterior to her left knee. MRI scans are shown in Figures 31a and 31b. What is the best course of action?
Explanation
REFERENCES: Dlabach JA: Nontraumatic soft tissue disorders, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. Philidelphia, PA, Mosby, 2003, vol 1, pp 885-969.
Fritschy D, Fasel J, Imbert JC, et al: The popliteal cyst. Knee Surg Sports Traumatol Arthrosc 2006;14:623-628.
Question 82
A 77-year-old woman who underwent a cemented total hip arthroplasty 10 years ago now reports groin pain. Examination reveals a loosened acetabular component and a well-fixed femoral component. Treatment should consist of revision of
Explanation
REFERENCES: Peters CL, Kull L, Jacobs JJ, Rosenberg AG, Galante JO: The fate of well fixed cemented femoral components left in place at the time of revision of the acetabular component. J Bone Joint Surg Am 1997;79:701-706.
Poon ED, Lachiewicz PF: Results of isolated acetabular revisions: The fate of the unrevised femoral component. J Arthroplasty 1998;13:42-49.
Moskal JT, Shen FH, Brown TE: The fate of stable femoral components retained during isolated acetabular revision: A six- to twelve-year follow-up study. J Bone Joint Surg Am
2002;84:250-255.
Templeton JE, Callaghan JJ, Goetz DD, Sullivan PM, Johnston RC: Revision of a cemented acetabular component to a cementless acetabular component. A ten- to fourteen-year follow-up study. J Bone Joint Surg Am 2001;83:1706-1711.
Question 83
Which of the following can be seen in the heart of a well-conditioned athlete? Review Topic
Explanation
Question 84
What is the most likely late complication associated with cementless total knee replacement?
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
Question 85
A 72-year-old woman with diabetes mellitus has right hand numbness. Provocative test findings are consistent with carpal tunnel syndrome, and electrodiagnostic study (EDS) findings show prolonged median motor and sensory distal latencies with low-amplitude thenar compound muscle action potential. Poor prognosis is most associated with which factor?
Explanation
Although carpal tunnel syndrome remains a clinical diagnosis, EDS findings have become important tools. Moderate disease is defined as abnormal median sensory distal latency and prolonged median motor distal latency. Severe disease is defined as prolonged median motor and sensory distal latencies witheither absent sensory nerve action potential or mixed nerve action potential or low-amplitude or absent thenar compound muscle action potential. Although female gender and diabetes are considered risk factors, there is little association with postsurgical outcome. Severe disease as confirmed by EDS is the factor most strongly associated with poor recovery after surgery.
Question 86
A study is proposed in which 2 groups of patients are randomized to treatment with bisphosphonates or placebo. This is an example of what study type?
Explanation
Question 87
Figure 43 shows an arthroscopic view of a right shoulder through a lateral portal in the beach chair position. The arrow is pointing to what structure?
Explanation
REFERENCES: Mazzocca AD, Noerdlinger M, Cole B, et al: Arthroscopy of the shoulder: Indications and general principles of techniques, in McGinty JB (ed): Operative Arthroscopy,
ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 412-427.
Burkhart, SS: Arthroscopic management of rotator cuff tears, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 508-546.
Question 88
Which of the following substances is least likely to affect the success of bone union after lumbar arthrodesis?
Explanation
REFERENCES: Glassman SD, Rose SM, Dimar JR, Puno RM, Campbell MJ, Johnson JR: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Deguchi M, Rapoff AJ, Zdeblick TA: Posterolateral fusion for isthmic spondylolisthesis in adults: Analysis of fusion rate and clinical results. J Spinal Disord 1998;11:459-464.
Dimar JR II, Ante WA, Zhang YP, Glassman SD: The effect of nonsteroidal anti-inflammatory drugs on posterior spinal fusions in the rat. Spine 1996;21:1870-1876.
Question 89
A 10-year-old boy has activity-related knee pain that is poorly localized. He denies locking, swelling, or giving way. Examination shows mild tenderness at the medial femoral condyle and painless full range of motion without ligamentous instability. Radiographs are shown in Figures 2a through 2c. What is the best course of action?
Explanation
REFERENCES: Linden B: Osteochondritis dissecans of the femoral condyles: A long term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
Cahill BR: Osteochondritis dissecans of the knee: Treatment of juvenile and adult forms. J Am Acad Orthop Surg 1995;3:237-247.
Cahill BR, Navarro R: The results of conservative management of juvenile osteochondritis dissecans using joint scintigraphy: A prospective study. Am J Sports Med 1989;17:601-606.
Question 90
Figure 17 shows the AP radiograph of a 75-year-old man with right hip pain. The femoral component is loose. The mechanism of loosening is most likely secondary to
Explanation
REFERENCES: Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 217-238.
Peter CL, Rivero DP, Kull LR, et al: Revision total hip arthroplasty without cement: Subsidence of proximally porous-coated femoral components. J Bone Joint Surg Am 1995;77:1217-1226.
Question 91
A 56-year-old woman sustained the fracture shown in Figures 30a and 30b in a motor vehicle accident. What mechanism is most likely responsible for the injury? Review Topic
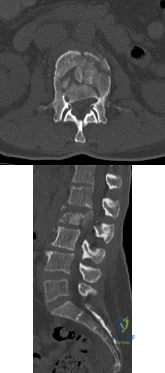
Explanation
Question 92
A 7-year-old patient has had a painless limp for several months. Examination reveals pain and spasm with internal rotation, and abduction is limited to 10° on the involved side. Management consists of 1 week of bed rest and traction, followed by an arthrogram. A maximum abduction/internal rotation view is shown in Figure 40a, and abduction and adduction views are shown in Figures 40b and 40c. The studies are most consistent with
Explanation
REFERENCE: Reinker KA: Early diagnosis and treatment of hinge abduction in Legg-Perthes disease. J Pediatr Orthop 1996;16:3-9.
Question 93
Figures 21a through 21c show the radiographs of a 70-year-old woman who has persistent pain with activity after undergoing hip revision 6 months ago. Treatment should now consist of
Explanation
REFERENCES: Gill TJ, Sledge JB, Muller ME: The Burch-Schneider anti-protrusio cage in revision total hip arthroplasty: Indications, principles, and long-term results. J Bone Joint Surg Br 1998;80:946-953.
Sharkey PF, Hozack WJ, Callaghan JJ, et al: Acetabular fracture associated with cementless acetabular component insertion: A report of 13 cases. J Arthroplasty 1999;14:426-431.
Question 94
-Ten or more years after severe polytrauma, premenopausal women, compared to men
Explanation
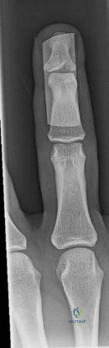
Question 95
A young man sustains a lumbar strain in an on-the-job motor vehicle accident. Both he and his treating physician feel that he is capable of limited duty with appropriate restrictions shortly after the injury. What term best describes his work status?
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 131-137.
Question 96
A 14-year-old boy who is right handed reports right shoulder pain. Radiographs show a lucent lesion of the proximal humeral epiphysis with a narrow zone of transition. Results of an open biopsy confirm the presence of a chondroblastoma. Based on these findings, the next most appropriate step in management should consist of
Explanation
is not indicated in the initial treatment of an intraosseous chondroblastoma.
REFERENCES: Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 589-623.
Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Question 97
What clinical scenario is most consistent with the MR image of the L4-L5 disk level shown in Figure 14? Review Topic
Explanation
Question 98
Figure 9 is the clinical photograph of a 68-year-old woman 10 days after undergoing primary total knee replacement. She is experiencing hemarthrosis, discoloration, and bruising of the soft tissue about the knee; her history includes persistent serous drainage. This clinical appearance likely is associated with
Explanation
Certain anticoagulants are associated with an increased risk for wound complications. Two studies showed an increase in postsurgical bleeding and wound drainage following use of LMWH. Other investigators have associated use of anticoagulants such as LMWH with an increased incidence of persistent wound drainage and subsequent infection. Current evidence does not support a significant difference in complication rates with and without the use of wound drains or a tourniquet. Regional anesthesia has been associated with less blood loss than general anesthesia and is not associated with a difference in wound complication incidence.

Question 99
A 62-year-old man with diabetes mellitus has had a persistent 2-cm ulcer under the third metatarsal head for the past 4 months. He reports that he has had similar ulcers twice before, and both healed with nonsurgical management. He has used multiple types of commercial walking braces, shoes, and commercial dressings without resolution. He is insensate to the Semmes-Weinstein 5.07 monofilament. When the wound is probed with culture swab, there is no communication with the metatarsal head. Radiographs, bone scans, and laboratory studies reveal no evidence of osteomyelitis. What is the most predictable method of accomplishing wound healing without recurrence?
Explanation
REFERENCES: Robertson DD, Mueller MJ, Smith KE, et al: Structural changes in the forefoot of individuals with diabetes and a prior plantar ulcer. J Bone Joint Surg Am 2002;84:1395-1404.
Mueller MJ, Sinacore DR, Hastings MK, et al: Effect of Achilles tendon lengthening on neuropathic plantar ulcers. J Bone Joint Surg Am 2003;85:1436-1445.
Question 100
A 2-year-old boy has complete absence of the sacrum and lower lumbar spine. What is the most likely long-term outcome if no spinal pelvic stabilization is performed?
Explanation
REFERENCES: Tachdjian MO: The spine: Congenital absence of the sacrum and lumbosacral vertebrae (lumbosacral agenesis), in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 3, p 2228.
Renshaw TS: Sacral agenesis: A classification and review of twenty-three cases. J Bone Joint Surg Am 1978;60:373-383.
