OITE & ABOS Orthopedic MCQs: Hip, Arthroplasty & Trauma Part 242

Key Takeaway
This page offers Part 242 of a comprehensive OITE & AAOS Orthopedic Surgery Board Review. Featuring 100 high-yield, verified MCQs tailored for surgeons preparing for ABOS/AAOS certification. It includes interactive study/exam modes, focusing on topics like Arthroplasty and Hip, crucial for effective board exam preparation.
About This Board Review Set
This is Part 242 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 242
This module focuses heavily on: Arthroplasty, Dislocation, Fracture, Hip, Revision.
Sample Questions from This Set
Sample Question 1: Two years ago, a 63-year-old man underwent right total hip arthroplasty (THA) with a modular femoral head-neck and neck-stem prosthesis (a photograph of the removed implantis shown in Figure 181). He now has increasing hip pain. Radiographs...
Sample Question 2: Bioabsorbable polymers are used in a wide range of orthopaedic devices, including anchors, staples, pins, plates, and screws. What is the primary drawback for bioabsorbable implants?...
Sample Question 3: In revision total hip arthroplasty, an acetabular reconstruction cage is best indicated for which of the following patterns of bone loss?...
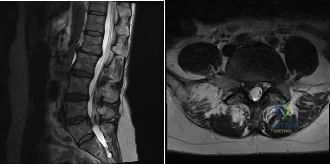
Sample Question 4: In an effort to reduce costs, a limited MRI sequence is planned to detect a possible occult hip fracture. What is the anticipated fracture signal?...
Sample Question 5: What type of injury is considered the major mechanism of cervical fracture, dislocation, and quadriplegia in contact sports and diving?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Two years ago, a 63-year-old man underwent right total hip arthroplasty (THA) with a modular femoral head-neck and neck-stem prosthesis (a photograph of the removed implant is shown in Figure 181). He now has increasing hip pain. Radiographs reveal a stable hip arthroplasty and elevated serum cobalt and chromium levels. MR imaging is obtained, and, based on these findings, the patient’s hip is revised. Which corrosion type likely is responsible for this THA failure?
Explanation
Micromotion at the femoral head-neck or stem-neck junction can lead to fretting corrosion. Fretting corrosion is among the most common causes of failure in modular components. Modularity gives surgeons additional intraoperative flexibility but has resulted in corrosion-related failure and an implant recall. Although titanium and cobalt-chrome contain a protective surface oxide layer, continued micromotion at the modular junction may disrupt the protective layer, resulting in fretting corrosion. This may eventually lead to excessive metal ion formation and painful synovitis that necessitates a revision procedure. Galvanic corrosion is attributable to a mismatch in electrochemical gradients between dissimilar metals. Crevice or pitting corrosion occurs in fatigue cracks because of differences in oxygen tension.
Question 2
Bioabsorbable polymers are used in a wide range of orthopaedic devices, including anchors, staples, pins, plates, and screws. What is the primary drawback for bioabsorbable implants?
Explanation
REFERENCES: Ambrose CG, Clanton TO: Bioabsorbable implants: Review of clinical experience in orthopedic surgery. Ann Biomed Eng 2004;32:171-177.
Bergsma JE, de Bruijn WC, Rozema FR, et al: Late degradation tissue response to poly
(L-lactide) bone plates and screws. Biomaterials 1995;16:25-31.
Question 3
In revision total hip arthroplasty, an acetabular reconstruction cage is best indicated for which of the following patterns of bone loss?
Explanation
REFERENCES: Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
Berry DJ, Muller ME: Revision arthroplasty using an anti-protrusio cage for massive acetabular bone deficiency. J Bone Joint Surg Br 1992;74:711-715.
Question 4
In an effort to reduce costs, a limited MRI sequence is planned to detect a possible occult hip fracture. What is the anticipated fracture signal?
Explanation
REFERENCES: Miller MD: Review of Orthopaedics, ed 3. Philadelphia PA, WB Saunders, 2000, p 116.
Guanche CA, Kozin SH, Levy AS, et al: The use of MRI in the diagnosis of occult hip fractures in the elderly: A preliminary review. Orthopedics 1994;17:327-330.
Question 5
What type of injury is considered the major mechanism of cervical fracture, dislocation, and quadriplegia in contact sports and diving?
Explanation
REFERENCES: Cantu RC: Head and spine injuries in youth sports. Clin Sports Med 1995;14:517-532.
Proctor MR, Cantu RC: Head and neck injuries in young athletes. Clin Sports Med 2000;19:693-715.
Torg JS: Epidemiology, pathomechanics, and prevention of athletic injuries to the cervical spine. Med Sci Sports Exerc 1985;17:295-303.
Question 6
- A 14-year-old patient who has homocystinuria and is Risser 3 is referred for surgical treatment of scoliosis. In addition to the usual risks associated with posterior spinal fusion, the family should be advised that the patient ‘s underlying condition significantly increases the perioperative risk of
Explanation
1 and 2 are concerns during spinal fusion but are not specific to this disease. 4 may occur with homocystinuria but is not related to spinal fusion. 5 occurs with PSF in the younger population because of the growth potential remaining.
Question 7
A 68-year-old woman underwent a successful total right hip arthroplasty with a metal-on-metal articulation and cementless porous-coated components. Three months later, she underwent identical surgery on the left hip. Three months after surgery on the left hip, she reports groin pain on ambulation. Examination reveals significant groin discomfort with passive hip motion, particularly at the extremes of motion. Radiographs are shown in Figures 21a and 21b. Laboratory studies show an erythrocyte sedimentation rate of 35 mm/h and a C-reactive protein of 0.9. Aspiration yields scant growth of Staphylococcus epidermidis in the broth only, with no evidence of loosening on arthrography. A second aspiration yields scant growth of Staphylococcus epidermidis in the broth only. What is the most likely cause of the patient’s pain?
Explanation
REFERENCES: White RE: Evaluation of the painful total hip arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998,
vol 2, pp 1377-1385.
Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
Question 8
A 65 year-old female presents to your clinic with a chief complaint of difficulty walking. She states that she has had low back pain and balance difficulties for the last 2 years, but over the last few months new bilateral posterior thigh and buttock pain has prevented her from walking more than 100 feet. She states the only place she can walk comfortably is in the grocery store. On physical exam she is unable to preform a tandem gait, and she has 5/5 strength with hip flexion, knee flexion/extension, ankle dorsiflexion/plantar flexion and great toe extension. Her sensation is intact in L2-S2, and she has equal and symmetric 3+ achilles and patellar reflexes. She has 8 beats of clonus, and a down-going Babinski reflex bilaterally.

Explanation
While 79% of patients with cervical myelopathy will have at least one sign on physical exam, the absence of a one or more signs such as a Babinski reflex or a Hoffman's sign does not rule out the diagnosis of myelopathy. Tandem cervical and lumbar stenosis occurs in between 5 and 25% of patients with lumbar stenosis, and because of the stepwise progressive nature of myelopathy, it is critical not to miss this diagnosis.
Rhee et al. found that the sensitivity and specificity of specific physical exam findings varies in patients with myelopathy. Overall 79% of patients will have at least one physical exam sign of myelopathy, with biceps hyperreflexia (62%) and the Hoffman sign (59%) being the most sensitive. Classic upper motor neuron findings in the lower extremity such as an upward Babinski reflex (13%) and clonus (13%) are not sensitive.
Lee et al. performed a cadaveric study of 440 specimens to identify the overall prevalence of stenosis in the population. They found 5.4% of the specimens had cervical stenosis and 5.9% had lumbar stenosis. A total of 0.9% had both cervical and lumbar stenosis.
Bajwa et al. evaluated over 1,000 skeletal remains to determine if tandem stenosis (concomitant lumbar and cervical stenosis) is due to an increased risk of disc degeneration or a congenitally small vertebral canal, and they concluded that tandem stenosis is likely due to a congenitally small vertebral canal in both the cervical and lumbar spine.
Figure A and B demonstrate an AP and lateral radiograph of the lumbar spine respectively. A degenerative L4/5 spondylolisthesis is present.
Incorrect answers:
Question 9
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of
Explanation
REFERENCES: Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
Moor TJ: Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma 1993;7:11-14.
Question 10
Figure 36 shows the radiograph of a patient who has hip pain and is unable to ambulate. What is the most appropriate management for this patient?
Explanation
REFERENCES: Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.
Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.
Question 11
Figures 2a and 2b show the radiographs of a 72-year-old man with aseptic loosening of the tibial component of his total knee arthroplasty. Optimal management should include
Explanation
The insertions of the lateral ligaments are absent, thereby rendering the lateral side of the knee predictably unstable. Also, the large valgus deformity compromises the medial collateral ligament. The posterior cruciate ligament is also likely to be deficient with this much tibial bone destruction. The patient requires a posterior stabilized femoral component at the minimum, and possibly a constrained femoral component. Retention of the femoral component, even though it may be well-fixed, jeopardizes the outcome.
REFERENCES: Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 137-250.
Insall JN, Windsor RE, Scott WN, et al: (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 935-957.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 339-365.
Question 12
A 14-year-old girl has had progressive heel pain for the past several months. Based on the radiograph, MRI scan, and biopsy specimens shown in Figures 37a through 37d, treatment should include
Explanation
blood-filled spaces with bland fibrous connective tissue septa. The stroma has histiocytes, fibroblasts, scattered giant cells, hemosiderin, and occasional inflammatory cells. Treatment of these lesions consists of extended curettage, plus or minus the use of adjuvants (liquid nitrogen, phenol, argon beam coagulation), and finally filling the bone void (allograft or other bone substitute).
REFERENCES: Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
Ramirez AR, Stanton RP: Aneurysmal bone cyst in 29 children. J Pediatr Orthop 2002;22:533-539.
Question 13
A 21-year-old woman with Marfan syndrome is seeking evaluation of her scoliosis. She reports no back or leg pain, and the neurologic examination is normal. Lateral and bending radiographs are shown in Figures 7a through 7e. Management should consist of
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 161-171.
Turi M, Johnston CE II, Richards BS: Anterior correction of idiopathic scoliosis using TSRH instrumentation. Spine 1993;18:417-422.
Moskowitz A, Trommanhauser S: Surgical and clinical results of scoliosis surgery using Zielke instrumentation. Spine 1993;18:2444-2451.
Question 14
Which lower extremity muscle is first weakened in Charcot-Marie-Tooth (CMT) disease?
Explanation
Although many of the lower extremity muscles may be affected in CMT, those innervated by the longest axons have been shown to be affected first. In the lower extremity the muscles innervated by the longest axons are the intrinsic foot muscles. The tibialis anterior and the peroneus brevis may be severely affected but not before the foot intrinsics. The peroneus longus typically is spared, resulting in the cavus.
RECOMMENDED READINGS
Pareyson D, Marchesi C. Diagnosis, natural history, and management of Charcot-Marie-Tooth disease. Lancet Neurol. 2009 Jul;8(7):654-67. Review. PubMed PMID: 19539237. View Abstract at PubMed
Wenz W, Dreher T. Charcot-Marie-Tooth disease and the cavovarus foot. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:291-306.
CLINICAL SITUATION FOR QUESTIONS 60 THROUGH 63
Figure 60 is the standing radiograph of a 27-year-old man who played football throughout his teen years. During those years, he noted that he had less mobility of his left foot and ankle. He twisted his left foot and ankle 8 months ago and has tried over-the-counter nonsteroidal anti-inflammatory drugs and a brace. He now has pain and edema in the left sinus tarsi area. Upon examination the following arcs of motion are identified: ankle dorsiflexion-right, 5 degrees/left, 5 degrees; ankle plantar flexion-right, 30 degrees/left 30 degrees; foot inversion-right, 10 degrees/left, 5 degrees; foot eversion-right, 10 degrees/left 5 degrees.

Question 15
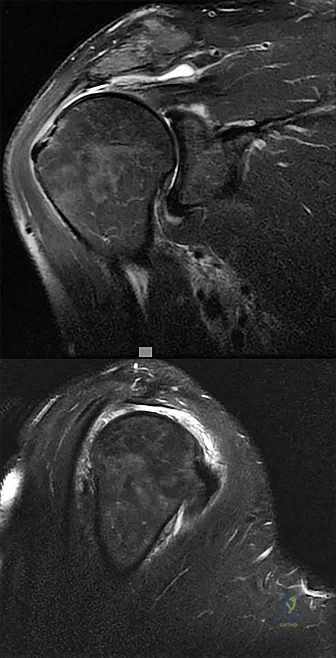
A 32-year-old woman has had pain and a visibly growing mass in the shoulder for 3 years but denies any history of trauma. Examination reveals a swollen, boggy shoulder mass. The AP radiograph and MRI scan are shown in Figures 20a and 20b. Figures 20c through 20e show a portion of the excised mass and the photomicrographs of the biopsy specimen. What is the most likely diagnosis?
Explanation
REFERENCES: Murphy FP, Dahlin DC, Sullivan CR: Articular synovial chondromatosis. J Bone Joint Surg Am 1982;44:77-86.
Milgram JW: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801.
Question 16
During a posterior cruciate ligament (PCL)-retaining total knee arthroplasty, a critical principle to remember is to
Explanation
Maintenance of the joint line and accurately tensioning the PCL are critical in the proper execution of a PCL-retaining total knee arthroplasty. Appropriate tension helps ensure femoral rollback and avoid stiffness or instability. Raising the joint line to help ensure full extension should be avoided in cruciate-retaining knees, because doing so creates an unfavorable kinematic environment. The three important principles of surgical technique needed to maintain appropriate tensioning of the PCL include 1) choosing the proper femur size to reproduce the native femoral anterior/posterior dimension, 2) reproducing the joint line by resecting as much tibia from the healthy side as will be replaced by the smallest thickness of the tibial component and, 3) ensuring that full extension is achieved by soft-tissue releases and not by taking additional distal femur, as may be done in a posterior stabilized approach. Another important principle is to re-create the natural degree of the patient’s posterior tibial slope to avoid tightness in flexion.
Question 17
Treatment of this fracture should consist of
Explanation
Varus posteromedial rotatory instability is a complex injury pattern that starts with varus stress resulting in a fracture of the anteromedial coronoid. The anterior MCL attaches to the sublime tubercle, which is part of the anteromedial coronoid facet. The posterior MCL attaches to the posterior medial aspect of the ulna. The radial collateral and lateral ulnar collateral attach to the ulna at the crista supinatoris. The bony landmark is the sublime tubercle; as noted above, the crista supinatoris is lateral on the ulna. The radial notch is also lateral and is the articulation between the proximal ulna and proximal radius. The anteromedial coronoid facet is part of the coronoid, which extends more lateral and anterior than the anteromedial facet. The anteromedial facet represents the critical weight-bearing portion of the ulnohumeral joint. Damage to this structure causes posteromedial subluxation that often results in severe progressive arthritis. The coronoid is the larger structure of which the anteromedial coronoid facet is a portion. The posteromedial coronoid facet does not appear to be critical in weight bearing. The radial notch is not associated with increased stress with weight bearing. The treatment of displaced fractures of this structure is open reduction and internal fixation utilizing buttress plating. Closed treatment is acceptable only for nondisplaced fractures with appropriate radiographic follow-up. Suture fixation is not advocated because of inadequate strength.
RECOMMENDED READINGS
Pollock JW, Brownhill J, Ferreira L, McDonald CP, Johnson J, King G. The effect of anteromedial facet fractures of the coronoid and lateral collateral ligament injury on elbow stability and kinematics. J Bone Joint Surg Am. 2009 Jun;91(6):1448-58. doi: 10.2106/JBJS.H.00222.
Sanchez-Sotelo J, O'Driscoll SW, Morrey BF. Anteromedial fracture of the coronoid process of the ulna. J Shoulder Elbow Surg. 2006 Sep-Oct;15(5):e5-8. Epub 2006 Jul 26. Erratum in: J Shoulder Elbow Surg. 2007 Jan-Feb;16(1):127. PubMed PMID: 16979044.
Question 18
Which of the following methods is effective in correcting recurrent dislocation following total hip arthroplasty?
Explanation
REFERENCES: Woo RY, Morrey BF: Dislocations after total hip arthroplasty. J Bone Joint Surg Am 1982;64:1295-1306.
Goetz DD, Capello WN, Callaghan JJ, Brown TD, Johnston RC: Salvage of a recurrently dislocating total hip prosthesis with use of a constrained acetabular component: A retrospective analysis of fifty-six cases. J Bone Joint Surg Am 1998;80:502-509.
Question 19
A 9-year-old girl has pain over the fifth toe that is aggravated by shoe wear. Clinical photographs are shown in Figures 28a and 28b. Treatment of this deformity should consist of
Explanation
REFERENCES: Black GB, Grogan DP, Bobechko WP: Butler arthroplasty for correction of adducted fifth toe: A retrospective study of 36 operations between 1968 and 1982. J Pediatr Orthop 1985;5:439-441.
Paton RW: V-Y plasty for correction of varus fifth toe. J Pediatr Orthop 1990;10:248-249.
Coughlin MJ, Mann RA: Lesser toe deformities, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 5. St Louis, MO, Mosby, 1986, pp 132-157.
Question 20
A 64-year-old woman sustains a fracture to her distal femur 5 years after undergoing total knee arthroplasty. When choosing between locked femoral plating and retrograde femoral nailing, which factor is important to consider based on this patient’s surgical record?
Explanation
Treatment of periprosthetic supracondylar femoral fractures is complex and may involve the use of a retrograde intramedullary femoral nail or locked or unlocked femoral plate. Knowledge of certain measurements specific to the model of the implant, specifically to the minimal intercondylar distance and the position of the notch on the femoral component in relation to the intramedullary canal, is crucial when choosing a retrograde nail over a locked femoral plate. Although the surgical approach, presence of an anterior femoral notch, and previous tourniquet time are interesting to consider, none of these factors would preclude the ability to proceed with femoral intramedullary nailing.

CLINICAL SITUATION FOR QUESTIONS 128 THROUGH 130
Figure 128 is the radiograph of a 78-year-old nursing home resident who has hypertension and peripheral vascular disease. He has developed acute severe hip pain 20 years after undergoing a cementless total hip arthroplasty (THA) and subsequent revision for instability. He was previously ambulatory with a walker and now can no longer ambulate. His erythrocyte sedimentation rate is 8 mm/h (reference range [rr], 0-20 mm/h) and C-reactive protein level is
Question 21
Suprapatellar intramedullary nailing for tibia fractures when compared to infrapatellar nailing is associated with
Explanation
Question 22
Radiographs of a pediatric patient reveal a suspected osteosarcoma of the distal femur. Additional staging studies should consist of
Explanation
REFERENCE: O’Reilly R, Link M, Fletcher B, et al: NCCN pediatric osteosarcoma practice guidelines: The National Comprehensive Cancer Network. Oncology (Huntingt) 1996;10:1799-1806, 1812.
Question 23
Staged open reduction and internal fixation with free flap soft tissue reconstruction is the most appropriate definitive treatment method for which of the following tibial injuries?

Explanation
Typically, treatment of Type IIIB tibial shaft fractures should be staged. Initially tetanus prophylaxis, antibiotics with gram negative and positive coverage, and application of an external fixator with repeat I&D’s are employed for immediate fracture care. Plating is usually required in the presence of significant intra-articular fracture involvement.
Incorrect Answers: Typically, proximal third tibia fractures requiring soft tissue coverage can be treated with a gastrocnemius rotation flap and middle third tibia fractures with soft tissue defects can be reliably covered with a soleus rotation flap. Therefore, a free flap is rarely indicated in the proximal and middle tibia.
Question 24
A 55-year-old woman with a history of untreated idiopathic scoliosis has had neurogenic claudication for the past several months. MRI reveals spinal stenosis at L2-L3, L3-L4, and L4-L5. Radiographs show a 45° lumbar curve from T10 to L4, with a degenerative spondylolisthesis at L4-L5. Laminectomy at the stenotic levels and stabilization of the deformity are planned. Which of the following is NOT considered an absolute indication for extending the fusion to the sacrum, rather than stopping at L5?
Explanation
REFERENCES: Bradford DS, Tay BK, Hu SS: Adult scoliosis: Surgical indications, operative management, complications, and outcomes. Spine 1999;24:2617-2629.
Bridwell KH: Where to stop the fusion distally in adult scoliosis: L4, L5, or the sacrum? Instr Course Lect 1996;45:101-107.
Edwards CC II, Bridwell KH, Patel A, et al: Long adult deformity fusions to L5 and the sacrum: A matched cohort analysis. Spine 2004;29:1996-2005.
Question 25
When performing a gastrocnemius recession, what structure should be protected?
Explanation
REFERENCES: Pinney SJ, Sangeorzan BJ, Hanen ST Jr: Surgical anatomy of the gastrocnemius resection (Strayer procedure). Foot Ankle Int 2004;25:247-250.
Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 415-417.
Question 26
Figures 33a and 33b show the standing posteroanterior and lateral radiographs of a 59-year-old woman with adult idiopathic scoliosis. She underwent a prior decompressive laminectomy and fusion at L4-S1 to address lumbar stenosis. She now reports progressive lower back pain and a feeling of being shifted to the right. If surgical intervention is considered, what is the most important goal in improving her health-related quality of life (HRQL) outcomes? Review Topic

Explanation
(SBQ12SP.24) A 39-year-old man presents to clinic with a 3-week history of low back pain that radiates to the right lower extremity. On examination, he has mildly decreased sensation over the dorsum of the foot and positive straight leg raise on the right side. MRI images are shown in Figure A and B. Which of the following is true regarding this patient's condition? Review Topic
Nonoperative management with NSAIDS and physical therapy is effective for 50% of patients
Surgical treatment is indicated in patients with diminished sensation
Surgical treatment is equivalent to nonoperative management in terms of pain and function
Good surgical outcome is associated with mainly back complaints
Size of disc herniations typically decrease over time without surgical intervention
The patient is presenting with a lumbar disc herniation at the L4-L5 level. The size of disc herniations decrease in most patients over time without surgical intervention.
Lumbar disc herniations are the result of recurrent torsional strain, which leads to small tears of the annulus fibrosus, ultimately allowing herniation of the nucleus pulposis. First line treatment consists of NSAIDS, muscle relaxants and physical therapy and is effective in 90% of patients. Second line treatment typically involves epidural and selective nerve root corticosteroid injections. Microdiscectomy is reserved for patients with more than 6 weeks of disabling pain that has failed nonoperative management, progressive weakness, or cauda equina syndrome.
In the Spine Patient Outcomes Research Trial (SPORT), Weinstein et al. investigated patient outcomes and satisfaction after operative and nonoperative management of lumbar disc herniations. While the randomized arm of the study did show statistically significant differences in the intent-to-treat analysis due to significant crossover of patients, the observational cohort revealed a significant improvement in pain, function, and disability for patients treated with surgery versus nonoperative measures.
Benson et al. looked at the natural history of massive herniated discs in 37 patients with 7-year follow up. They found a more than 60% reduction in disc size over this time period. Reduction in disc size did not correlate with clinical improvement.
Figure A and B are sagittal and axial T2 MRI images, respectively, showing a right sided lumbar disc herniation at the L4-L5 level.
Incorrect Answers:
Question 27
A 22-year-old college football player reports shortness of breath and dyspnea after a tackle. Examination reveals tachypnea, tachycardia, the trachea is shifted to the right, and there are decreased breath sounds on the left lung fields. The first line of treatment on the field should be
Explanation
REFERENCES: Amaral JF: Thoracoabdominal injuries in the athlete. Clin Sports Med 1997;16:739-753.
Perron AD: Chest pain in athletes. Clin Sports Med 2003;22:37-50.
Question 28
Regarding the role of the orthopaedic surgeon in addressing domestic and family violence, all of the following statements are true EXCEPT:

Explanation
state. The AAOS Advisory statement gives information to assist in meeting the ethical and legal obligations on Domestic and Family Violence and Abuse.
Domestic and family violence affects over 10% of the US population (approximately 32 million Americans). Child abuse and neglect contributed to 1,400 fatalities in 2002 and there was 565,747 reports of suspected elder abuse.
Reporting of suspected child abuse is required in all states. The orthopaedic surgeon should hospitalize elderly victims who are in immediate danger and help develop a plan to insure their safety.
Question 29
A 50-year-old competitive tennis player sustained a shoulder dislocation after falling on his outstretched arm 3 weeks ago. He now reports that he has regained motion but continues to have painful elevation and weakness in external rotation. A subacromial cortisone injection provided 3 weeks of relief, but the pain has returned. Which of the following studies will best aid in diagnosis?
Explanation
REFERENCES: Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Matsen FA III, Thomas SC, Rockwood CA: Anterior glenohumeral instability, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 526-622.
Question 30
The fracture shown in Figure 32 is strongly indicative of what diagnosis?
Explanation
REFERENCES: Kocher MS, Kasser JR: Orthopaedic aspects of child abuse. J Am Acad Orthop Surg 2000;8:10-20.
Kleinman PK, Marks SC, Blackbourne B: The metaphyseal lesion in abused infants: A radiologic-histopathologic study. Am J Roentgenol 1986;146:895-905.
Question 31
A 6-year-old boy has leg pain. A radiograph, MRI, CT, and bone scans, and a biopsy specimen are shown in Figures 14a through 14e. What is the most likely diagnosis?
Explanation
REFERENCES: Fletcher BD, Hanna SL: Pediatric musculoskeletal lesions simulating neoplasms. Magn Reson Imaging Clin N Am 1996;4:721-747.
Hanna SL, Fletcher BD, Kaste SC, Fairclough DL, Parham DM: Increased confidence of diagnosis of Ewing sarcoma using T2-weighted MR images. Magn Reson Imaging 1994;12:559-568.
Question 32
A patient who has had neck pain radiating down the arm for the past 4 weeks reports that the pain was excruciating during the first week. Management consisting of anti-inflammatory drugs and physical therapy has decreased the neck and arm symptoms from 10/10 to 3/10. He remains neurologically intact. MRI and CT scans are shown in Figures 5a and 5b. The best course of action should be
Explanation
REFERENCES: Saal JS, Saal JA, Yurth EF: Nonoperative management of herniated cervical intervertebral disc with radiculopathy. Spine 1996;21:1877-1883.
Komori H, Shinomiya K, Nakai O, Yamaura I, Takeda S, Furuya K: The natural history of herniated nucleus pulposus with radiculopathy. Spine 1996;21:225-229.
Question 33
Figure 56 is the MR image of a 20-year-old Division I baseball pitcher who has a 1-month history of medial elbow pain in his throwing arm. He also notes a decrease in both control and pitching velocity. An examination reveals tenderness at the medial epicondyle that is exacerbated with valgus elbow stress. The strongest indication for ulnar collateral ligament (UCL) reconstruction is
Explanation
All responses represent findings that may be associated with chronic UCL insufficiency. Responses 1 and 3 reflect injury to the UCL itself. In most patients, particularly young patients, UCL reconstruction should not be considered until an appropriate trial of nonsurgical measures has failed. This trial should include, at a minimum, 6 weeks of throwing abstinence followed by rehabilitation to address pitching mechanics and shoulder motion deficits and core strengthening. Although the decision to enter the MLB draft may influence surgical decision making, a pitcher with a 1-month history of elbow symptoms should attempt nonsurgical therapy before making a surgical decision that is not based on clinical data.
Question 34
A full-term newborn has webbing at the knees, rigid clubfeet, a Buddha-like posture of the lower extremities, and no voluntary or involuntary muscle action at and below the knees. Radiographs of the spine and pelvis reveal an absence of the lumbar spine and sacrum. What maternal condition is associated with this diagnosis?
Explanation
REFERENCES: Chan BW, Chan KS, Koide T, et al: Maternal diabetes increases the risk of caudal regression caused by retinoic acid. Diabetes 2002;51:2811-2816.
Zaw W, Stone DG: Caudal regression syndrome in twin pregnancy with type II diabetes.
J Perinatol 2002;22:171-174.
Question 35
Based on the MRI scan shown in Figure 6, the abnormal signal is seen in what carpal bone?
Explanation
REFERENCES: Cooney WP, Linscheid RL, Dobyns JH: The Wrist: Diagnosis and Operative Treatment. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 278-282.
Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2238-2240.
Question 36
A 36-year-old nurse has had redness, pain, and small vesicles on the pulp of her middle finger for the past 3 days. Management should consist of
Explanation
REFERENCES: Fowler JR: Viral Infections. Hand Clin 1989;5:613-627.
Jebsen PL: Infections of the fingertip: Paronychias and felons. Hand Clin 1998;14:547-555.
Question 37
During the early swing phase of the normal gait cycle, what lower extremity muscle is primarily contracting?
Explanation
REFERENCES: Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Wootten ME, Kadaba MP, Cochran GV: Dynamic electromyography II: Normal patterns during gait. J Orthop Res 1990;8:259-265.
Question 38
What is the most common donor site complication following a free vascularized fibular graft for osteonecrosis of the femoral head?
Explanation
REFERENCE: Urbaniak J, Harvey E: Revascularization of the femoral head in osteonecrosis. J Am Acad Orthop Surg 1998;6:44-54.
Question 39
A 45-year-old man who is a smoker has a significant hemothorax and bilateral closed femoral fractures. On insertion of a chest tube, 1,100 mL of blood was returned. He has had 75 mL of chest tube output over the last 2 hours while being resuscitated in the ICU. His base deficit is now 2 and his urine output has been 3 mL/kg over the last hour. What is the next most appropriate step in management?
Explanation
REFERENCES: Nork SE, Agel J, Russell GV, et al: Mortality after reamed intramedullary nailing of bilateral femur fractures. Clin Orthop Relat Res 2003;415:272-278.
Pape HC, Zelle BA, Hildebrand F, et al: Reamed femoral nailing in sheep: Does irrigation and aspiration of intramedullary contents alter the systemic response? J Bone Joint Surg Am 2005;87:2515-2522.
Question 40
A 35-year-old man has profound deltoid weakness after sustaining a traumatic anterior shoulder dislocation 6 weeks ago. Electromyographic (EMG) studies confirm an axillary nerve injury. Follow-up examination at 3 months reveals no recovery of function. What is the best course of action?
Explanation
REFERENCES: Perlmutter GS: Axillary nerve injury. Clin Orthop 1999;368:28-36.
Artico M, Salvati M, D’Andrea V, et al: Isolated lesions of the axillary nerves: Surgical treatment and outcome in twelve cases. Neurosurgery 1991;29:697-700.
Vissar CP, Coene LN, Brand R, et al: The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery: A prospective clinical and EMG study. J Bone Joint Surg Br 1999;81:679-685.
Pasila M, Jarma H, Kiviluoto O, et al: Early complications of primary shoulder dislocations. Acta Orthop Scand 1978;49:260-263.
Question 41
A 13-year-old baseball pitcher presents with worsening medial-sided elbow pain. He pitches 7 months out of the year, throws 85 pitches per game and plays in two games per week. His fastball speed is approximately 75mph. He regularly plays outfield once he has been relieved of pitching. Which of the following is most likely contributing to his elbow pain? Review Topic
Explanation
Little League elbow is a medial-sided overuse injury that occurs in the skeletally immature athlete. During execution of the baseball pitch, tremendous valgus and extension stresses occur at the elbow. Repetitive microtrauma can ultimately injure the medial epicondyle apophysis, ulnar collateral ligament or the flexor-pronator muscle mass. Limiting the number of pitches and innings played per game, as well as the number of months of competitive pitching per year, has been recommended to prevent these overuse injuries in the young athlete.
Olsen et al performed a case control study to determine risk factors associated with the development of shoulder and elbow injuries in adolescent baseball pitchers. Greater than 8 months of competitive pitching per year, more than 80 pitches per game and a fastball speed of greater than 85mph were all associated with increased risk of injury. Continued pitching despite arm fatigue and pain, being a starting pitcher, greater number of warm-up pitches, participating in showcases and regular use of NSAIDs were also associated with injury. The type of pitch (fastball, changeups and breaking balls) and continued play in a different position once being relieved was not associated with increased risk of injury.
Andrews et al authored a review article on ulnar collateral ligament injuries in throwing athletes. According to the USA Baseball Medical/Safety Advisory Committee, young baseball pitchers should avoid breaking pitches, such as curveballs and sliders, and avoid year-round baseball. A minimum of 3 months of complete rest from pitching per year is vital. Youth pitching coaches should be educated to ensure proper pitching mechanics are being reinforced.
Illustration A is a table depicting the recommended maximum number of pitches by age group.
Incorrect Answers:
Question 42
Figures 9a and 9b show the radiographs of a 75-year-old man who underwent a revision total knee arthroplasty with a long-stemmed tibial component. In rehabilitation, he reports fullness and tenderness in the proximal medial leg (at the knee). The strategy that would best limit this postoperative problem is use of
Explanation
REFERENCE: Gustke K: Cemented tibial stems are not requisite in revision. Orthopedics 2004;27:991-992.
Question 43
An otherwise healthy 16-year-old dancer reports a 1-month history of leg pain. AP and lateral radiographs of the distal femur are shown in Figures 67a and 67b. What is the next most appropriate step in management?
Explanation
REFERENCES: Gebhardt MC, Ready JE, Mankin HJ: Tumors about the knee in children. Clin Orthop Relat Res 1990;255:86-110.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Question 44
A 30-year-old man sustains a head injury as well as a femur and pelvis fractures as the result of a rollover motor vehicle accident. He is initially comatosed, but recovers cognitive function after 10 days in the hospital. Soon after awakening he complains of wrist pain and an x-ray demonstrates a distal radius fracture. What is the most likely explanation for this delayed diagnosis?

Explanation
Question 45
A 60-year-old woman with a history of osteoporosis fell from a standing height and sustained a supracondylar distal humerus fracture with an intercondylar extension. Which of the following plate constructs yields the highest stiffness for fixation of the fracture?
Explanation
Question 46
A 5-year-old boy has a deformity of his right arm after falling from a jungle gym. A radiograph is shown in Figure 37. Management should consist of
Explanation
REFERENCES: Wilkins KE: Changes in the management of Monteggia fractures. J Pediatr Orthop 2002;22:548-554.
Kay RM, Skaggs DL: The pediatric Monteggia fracture. Am J Orthop 1998;27:606-609.
Ring D, Jupiter JB, Waters PM: Monteggia fractures in children and adults. J Am Acad Orthop Surg 1998;6:215-224.
Question 47
Figure 70 is the radiograph of a 14-year-old girl with increasing posterior ankle pain, especially during pointe technique exercises. Nonsurgical measures such as modification, stretching, and injection have been unsuccessful. Which nerve is most vulnerable to injury during endoscopic excision of this lesion?
Explanation
The pathology is that of posterior ankle impingement, which is secondary to a symptomatic os trigonum. Endoscopic excision necessitates posteromedial and posterolateral ankle portals. Although plantar numbness has been described as a relatively common postsurgical complication, the neurovascular structure most commonly injured is the sural nerve.
Question 48
Figures 36a and 36b are the radiographs of a 79-year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. There is no evidence of infection. What is the most appropriate treatment?
Explanation
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis (Figures 36c and 36d). They also assist in obtaining correct limb alignment. Short metaphyseal-engaging stems are associated with failure rates between
16% and 29%. Cemented stems may be shorter than press-fit stems because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.
RESPONSES FOR QUESTIONS 37 THROUGH 40
Lateral femoral cutaneous nerve
Lateral femoral circumflex artery
Superior gluteal nerve
Superior gluteal artery
Sciatic nerve
Femoral artery
Femoral vein
Femoral nerve
Saphenous branch of the femoral nerve
Profunda femoris artery
Inferior gluteal nerve
Match each description below with the anatomic structure listed above.
Question 49
- Which of the following neurovascular structures is at greatest risk during the introduction of acetabular component fixation screws during total hip replacement?
Explanation
system they found that the posterior superior and posterior inferior quadrants of the acetabulum are the safest locations for screw placement because of better bone stock as well as less neurovascular structures as compared to the anterior quadrants.
Question 50
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
Explanation
REFERENCES: Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273.
Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Kim WY, Hearn TC, Seleem O, et al: Effect of pin location on stability of pelvic external fixation. Clin Orthop Relat Res 1999;361:237-244.
Question 51
Central cord syndrome would most likely be seen in which of the following patients? Review Topic
Explanation
Central cord syndrome is most commonly caused by cervical hyperextension in older patients with underlying cervical spondylosis. It is thought to be due to compression between anterior osteophytes and posterior infolded ligamentum flavum during hyperextension. This preferentially affects the motor tracks closest to midline, and thus motor function is impaired greater than sensation, and upper extremities more affected than lower extremities (remember upper motor tracks are more central in the lateral corticospinal tract)
Nowak et al. present a review article on central cord syndrome. They cite the most common cause of central cord syndrome as a hyperextension mechanism in an elderly patient with preexisting spondylosis.
Gupta et al. present a review article on the management of spinal cord injuries. They discuss advances and ongoing study in acute management, surgical techniques, pharmacoptherapies, and cellular transplantation. They recommend a multidisciplinary approach to treating spinal cord injuries.
Dvorak et al. present results of long term follow-up after traumatic central cord syndrome. They found average improvement of ASIA motor scores (AMS) from 58.7 to 92.3. Bowel and bladder control returned in 81% and independent ambulation returned in 86%. Variables correlated with final AMS were AMS at injury, formal education, and presence of spasticity during follow-up.
Illustration A shows the blood supply to the spinal cord. Illustration B shows the area affected by central cord syndrome to help explain why it produces the described deficits.
Incorrect answers:
may be seen in the presence of congenital cervical stenosis. However, this is not the most common cause. Answer 4: Aortic aneurysm repair would more commonly lead to anterior cord syndrome.
Question 52
A 17-year-old girl who initially presented as a child with multiple skeletal lesions, café-au-lait spots, and precocious puberty now has bone pain. A recent bone scan reveals multiple areas of increased scintigraphic uptake, including bilateral proximal femurs. A radiograph is shown in Figure 19. Besides activity modification, what is the next best line of treatment for decreasing her pain?
Explanation
REFERENCES: DiCaprio MR, Enneking WF: Fibrous dysplasia: Pathophysiology, evaluation and treatment. J Bone Joint Surg Am 2005;87:1848-1864.
Zacharin M, O’Sullivan M: Intravenous pamidronate treatment of polyostotic fibrous dysplasia associated with McCune Albright syndrome. J Pediatr 2000;137:403-409.
Question 53
What is the most frequent location of entrapment of the deep peroneal nerve?
Explanation
REFERENCES: Kopell HP, Thompson WA: Peripheral entrapment neuropathies of the lower extremity. N Engl J Med 1960;262:56-60.
Schon LC, Mann RA: Diseases of the nerves, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 1, pp 675-677.
Question 54
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of Review Topic
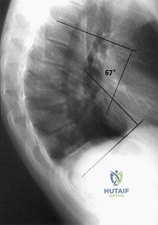
Explanation
Question 55
Which of the following nerves is most commonly injured during arthroscopy of the ankle?
Explanation
Question 56
Figures 10a and 10b show the radiographs of an athletic 9-year-old boy who has activity-related anterior knee pain with intact active knee extension. Examination reveals tenderness to palpation over the inferior pole of the patella. There is no effusion or ligamentous instability. Initial management should consist of
Explanation
REFERENCES: Stanitski CL: Anterior knee pain syndromes in the adolescent. J Bone Joint Surg Am 1993;75:1407-1416.
Stanitski CL: Anterior knee pain syndromes in the adolescent, in Schafer M (ed): Instructional Course Lectures 43. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1994, pp 211-220.
Question 57
Storage of musculoskeletal allografts by cryopreservation is achieved by
Explanation
sulfoxide or glycerol which displaces the cellular water. The controlled rate freezing is then done to prevent ice crystal formation. Fresh allografts are not frozen in order to maintain maximum cellular viability, and this process limits the shelf life of osteochondral allografts. Freeze-drying involves replacement of water in the tissue with alcohol to a moisture level of
5% and then uses a vacuum process to remove the alcohol from the tissue. Preparation of fresh frozen grafts involves freezing the graft twice and packaging the tissue without solution at
minus 80 degrees C.
REFERENCES: American Association of Tissue Banks: Standards for Tissue Banking. MacLean, VA, American Association of Tissue Banks, 1999.
Vangsness CT Jr, Triffon MJ, Joyce MJ, et al: Soft tissue allograft reconstruction of the human knee: A survey of the American Association of Tissue Banks. Am J Sports Med 1996;24:230-234.
Brautigan BE, Johnson DL, Caborn DM, et al: Allograft tissues, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 2003, pp 205-213.
Question 58
A 23-year-old male college quarterback presents with acute left shoulder pain after being tackled. A radiograph of the injury is shown in figure A. After successful closed reduction, what shoulder position should be avoided in order to minimize the risk of a repeat injury? Review Topic

Explanation
Shoulder stability is achieved through the both dynamic and static stabilizers. The static stabilizers include the bony morphology of the joint, glenoid labrum, capsule, and glenohumeral ligaments. The contributions of the glenohumeral ligaments to shoulder stability are dependent upon the position of the humerus relative to the glenoid. Posterior stability is afforded to the joint by the superior glenohumeral ligament (SGHL) and the posterior band of the inferior glenohumeral ligament (IGHL). The SGHL specifically is taught and provides posterior stability with the shoulder in flexion, adduction, and internal rotation.
Kim et. al. reviewed their experience treating 27 athletes diagnosed with traumatic posterior shoulder instability and treated with arthroscopic posterior labral repair and capsular shift. Most patients were found to have an incompletely stripped posterior capsulolabral complex. After arthroscopic repair and shift, all 26 of the 27 patients treated had improved shoulder function and objective scores, a stable shoulder, and were able to return to sport.
Millett et. al. reviewed posterior shoulder instability. They describe the static restraints of the posterior shoulder as the SGHL, posterior band of IGHL, and the coraohumeral ligament (CHL). The SGHL and CHL are both taught in the position of flexion, adduction, and internal rotation, whereas the posterior band of the IGHL is taught in abduction. They describe posterior instability occuring secondary to overhead sports due to repetitive microtrauma causing gradual capsular failure.
Figure A is an axillary radiograph of the left shoulder demonstrating a posterior dislocation and an engaging reverse Hill-Sachs lesion.
Incorrect Answers:
Question 59
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management? Review Topic
Explanation
Question 60
A 70-year-old man is experiencing neck pain, progressive weakness, and numbness in his arms and legs without bowel or bladder dysfunction or dysphagia. Upon examination, he has atrophy of his upper extremities but normal muscle bulk in his legs. Strength is diffusely 4/5 throughout. Cervical spine radiographs show spondylosis. Electromyography (EMG) reveals fibrillations with increased amplitude in the extensor carpi radialis and pronator teres. Nerve conduction studies demonstrate slowing conduction diffusely in the sural, peroneal, and ulnar nerves, and severe slowing in the median nerve. Testing of the tongue and thoracic paraspinal muscles does not show fibrillations or positive short waves. What is the most likely diagnosis? Review Topic
Explanation
Question 61
An 18-year-old football player reports acute pain and swelling after a direct injury to his plantar flexed foot. Examination reveals midfoot swelling and tenderness. Nonstanding radiographs are normal. What is the next most appropriate step in management?
Explanation
to activity.
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 39-54.
Chiodo CP, Myerson MS: Developments and advances in the diagnosis and treatment of injuries with the transmetatarsal joint. Orthop Clin North Am 2001;32:11-20.
Question 62
A 13-year-old girl has had a firm mass and pain in her right shoulder for the past several weeks. She denies any history of trauma. A radiograph and MRI scan are shown in Figures 31a and 31b. Biopsy specimens are shown in Figures 31c and 31d. What is the most likely diagnosis?
Explanation
REFERENCES: Simon MA, Springfield DS, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266.
Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 63
-A 42-year-old woman has had right wrist pain for 2 years. She tried splint wear and naproxen and has had 3 steroid injections, each time experiencing less relief.
Explanation

Question 64
An 18-year-old collegiate football player injures his right shoulder during a tackle. He reports pain and numbness in the shoulder and numbness radiating to his fingers. His symptoms improve within 15 minutes and he has no residual symptoms. This condition is best known as
Explanation
REFERENCES: Safran MR: Nerve injury about the shoulder in athletes. Part 2: Long thoracic nerve, spinal accessory nerve, burners/stingers, thoracic outlet syndrome. Am J Sports Med 2004;32:1063-1076. Aval SM, Durand P Jr, Shankwiler JA: Neurovascular injuries to the athlete’s shoulder: Part I. J Am Acad Orthop Surg 2007;15:249-256.
Question 65
A 35-year-old man with a history of spine surgery 5 years ago reports the recent development of frequent low back pain radiating to the legs. The patient blames a low-energy fall that occurred 9 months ago for the recent symptoms. Radiographs reveal previous interbody fusions of L4-L5 and L5-S1, with hardware present. The vertebrae appear well-fused and stable. What is the most likely cause of the low back pain? Review Topic
Explanation
Question 66
Figure 53 shows the arteriogram of a 45-year-old man who has severe vasculitis. What do the findings show?
Explanation
REFERENCE: Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadephia, PA, Mosby-Year Book, 1998, p 110.
Question 67
Which stress fracture location is reported most frequently among ballet dancers?
Explanation
Stress fractures are a frequent overuse injury among professional ballet dancers. The most common location is at the proximal metaphyseal-diaphyseal junction of the second metatarsal. Repetitive stress injuries and fractures of the tibial sesamoid, tarsal navicular, and base of the fifth metatarsal occur among other athletes.
RECOMMENDED READINGS
O'Malley MJ, Hamilton WG, Munyak J, DeFranco MJ. Stress fractures at the base of the second metatarsal in ballet dancers. Foot Ankle Int. 1996 Feb;17(2):89-94. PubMed PMID: 8919407. View Abstract at PubMed
Micheli LJ, Sohn RS, Solomon R. Stress fractures of the second metatarsal involving Lisfranc's joint in ballet dancers. A new overuse injury of the foot. J Bone Joint Surg Am. 1985 Dec;67(9):1372-5. PubMed PMID: 4077907. View Abstract at PubMed
Gehrmann RM, Renard RL. Current concepts review: Stress fractures of the foot. Foot Ankle Int. 2006 Sep;27(9):750-7. Review. PubMed PMID: 17038292. View Abstract at PubMed
Question 68
During what phase of the throwing motion is the highest torque measured across the glenohumeral joint?
Explanation
REFERENCES: Jobe FW, Moynes DR, Tibone JE, Perry J: An EMG analysis of the shoulder in pitching: A second report. Am J Sports Med 1984;12:218-220.
Pappas AM, Zawacki RM, Sulliva TJ: Biomechanics of baseball pitching: A preliminary report. Am J Sports Med 1985;13:216-222.
Altcheck DW, Dines DM: Shoulder injuries in the throwing athlete. J Am Acad Orthop Surg 1995;3:159-165.
Question 69
A 37-year-old man who works in a factory has isolated, lateral unicompartmental pain about his knee with activities. Nonsurgical management has failed to provide relief. The radiograph shown in Figure 45 reveals a tibiofemoral angle of approximately 15 degrees which is clinically correctable to neutral. What is the best surgical option in this patient?
Explanation
REFERENCES: Mathews J, Cobb AG, Richardson S, et al: Distal femoral osteotomy for lateral compartment osteoarthritis of the knee. Orthopedics 1998;21:437-440.
Cameron HU, Botsford DJ, Park YS: Prognostic factors in the outcome of supracondylar femoral osteotomy for lateral compartment osteoarthritis of the knee. Can J Surg 1997;40:114-118.
Question 70
A 20-year-old man with fascioscapulohumeral dystrophy has severe scapular winging of both shoulders. He can no longer abduct above 80 degrees, and it affects his activities of daily living. A clinical photograph is shown in Figure 26. Definitive management should consist of
Explanation
REFERENCES: Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Bunch WH, Siegel IM: Scapulothoracic arthrodesis in fascioscapulohumeral muscular dystrophy: Review of seventeen procedures with three to twenty-one-year follow-up. J Bone Joint Surg Am 1993;75:372-376.
Question 71
During right knee anterior cruciate ligament (ACL) reconstruction, after drilling an appropriately positioned and referenced tibial tunnel, the surgeon finds that the transtibial guide is placing the femoral tunnel at 11:30 within the intercondylar notch. Which of the following choices will best enable appropriate graft placement in this clinical scenario? Review Topic
Explanation
minimize errant tunnel placement, demonstrated in the literature as the most common cause of ACL failure and need for revision. In this not uncommon clinical scenario, simply converting to a two-incision ACL technique or drilling through the anteromedial portal with the knee hyperflexed will permit accurate femoral tunnel placement and increase the likelihood of an optimal clinical outcome. Femoral tunnel accuracy with these techniques is enhanced by a lower starting point in the intercondylar notch. Familiarity with these techniques is valuable for surgeons performing ACL reconstruction. Revising the tibial tunnel in this scenario would likely lead to bone compromise of the proximal tibia and may interfere with graft fixation and incorporation. Converting to a double-bundle ACL with a transtibial technique would not correct the vertical femoral tunnel. Hyperflexion of the knee may improve femoral tunnel placement to some extent, but is unlikely to allow anatomic placement of a femoral tunnel when the transtibial guide lies in a clearly excessive vertical position.
Question 72
What is the most appropriate treatment at this time?
Explanation
Prompt diagnosis and treatment of patients with spinal epidural abscess is crucial to maintain and/or improve neurologic function. This clinical scenario stresses the importance of advanced imaging studies. It is also important to recognize the imaging features of spinal epidural abscess. T1-weighted gadolinium-enhanced images show ring enhancement with a central nonenhancing, low-signal area. In such a case, urgent decompression is indicated. Because of the location of the abscess, which is anterior to the spinal cord, an anterior decompression and reconstruction (ie, fusion) is probably the best treatment plan. Steroids are contraindicated in the presence of an epidural abscess. IV antibiotics alone will not adequately treat a patient with a neurological deficit. A posterior laminectomy and fusion will not safely allow access to the abscess.
RECOMMENDED READINGS
Bluman EM, Palumbo MA, Lucas PR. Spinal epidural abscess in adults. J Am Acad Orthop Surg. 2004 May-Jun;12(3):155-63. Review. PubMed PMID: 15161168. View Abstract at PubMed Ghobrial GM, Beygi S, Viereck MJ, Maulucci CM, Sharan A, Heller J, Jallo J, Prasad S, Harrop JS. Timing in the surgical evacuation of spinal epidural abscesses. Neurosurg Focus. 2014 Aug;37(2):E1. doi: 10.3171/2014.6.FOCUS14120. PubMed PMID: 25081958. View Abstract
at PubMed
This is the last question of the exam.




Question 73
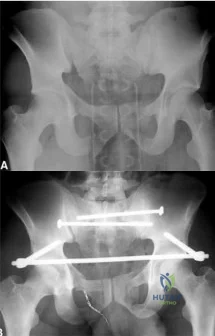
A 39-year-old female presents with the following motor vehicle crash with the injury seen in Figure A (immobilized in a pelvic binder). The iatrogenic neurologic injury most commonly caused by placement of the anterior construct for this injury, as shown in Figure B, would cause which of the following?
Explanation
Unstable pelvic fractures can be treated in a multitude of ways. The ASIF construct is typically created by placing long pelvic screws or polyaxial pedicle screws in the supraacetabular region, similar to the supraacetabular pins for an anterior external fixator. Then a curved bar is placed subcutaneously and connected to the supraacetabular screws. They are typically removed after 3-4 months when fracture healing is complete.
Vaidya et al. present a retrospective review of the use of ASIF as definitive treatment of unstable pelvic fractures. All patients in the study tolerated the construct well. LFCN irritation was seen in 30% of patients, and resolved in all but one patient.
Müller et al. present a retrospective review of the use of posterior stabilization and ASIF. They report an acceptably low complication rate, and good to excellent outcomes in 64.5% of patients.
Figure A is a radiograph demonstrating a right APC3 and left APC2 pelvic injury, imaged in a pelvic binder. Figure B is a postoperative radiograph following posterior stabilization and ASIF.
Incorrect answers:
Question 74
A 55-year-old man reports increasing weakness in his arms that has progressed to his lower limbs, resulting in frequent tripping and falling. Examination reveals weakness in shoulder abduction and external and internal rotation bilaterally. Fasciculation is noted. He also has weakness in elbow flexion and extension bilaterally, and his grip strength is diminished. An electromyogram and nerve conduction velocity studies show decreased amplitude of compound motor action potential, slightly slowed motor conduction velocity, and denervation signs with decreased recruitment in all extremities. The sensory study is normal. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: de Carvalho M, Johnsen B, Fuglsang-Frederiksen A: Medical technology assessment: Electrodiagnosis in motor neuron diseases and amyotrophic lateral sclerosis. Neurophysiol Clin 2001;31:341-348.
Daube JR: Electrodiagnostic studies in amyotrophic lateral sclerosis and other motor neuron disorders. Muscle Nerve 2000;23:1488-1502.
Troger M, Dengler R: The role of electromyography (EMG) in the diagnosis of ALS. Amyotroph Lateral Scler Other Motor Neuron Disord 2000;1:S33-S40.
Question 75
A 20-year-old woman with a history of subtotal meniscectomy has a painful knee. What associated condition is a contraindication to proceeding with a meniscal allograft?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 499.
Question 76
In the evaluation of somatosensory-evoked potential waveforms for intraoperative neuromonitoring for spinal surgery, the minimum criteria for determining potentially significant changes include Review Topic
Explanation
Question 77
Which of the following is true regarding plating of humeral shaft fractures compared to intramedullary nailing?

Explanation
Question 78
Which of the following complications is uniquely associated with an anterior approach to the lumbosacral junction?
Explanation
REFERENCES: Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.
Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer-Verlag, 1983, p 107.
An HS, Riley LH III: An Atlas of Surgery of the Spine. New York, NY, Lippincott Raven, 1998, p 263.
Question 79
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 80
An adult patient has an 8- x 4- x 10-cm soft-tissue mass located within the adductor compartment of the thigh. Staging studies should consist of
Explanation
REFERENCES: Demetri GD, Pollock R, Baker L, et al: NCCN sarcoma practice guidelines: National Comprehensive Cancer Network. Oncology (Huntingt) 1998;12:183-218.
Pollock R, Brennan M, Lawrence W Jr: Society of Surgical Oncology practice guidelines: Soft-tissue sarcoma surgical practice guidelines. Oncology (Huntingt) 1997;11:1327-1332.
Question 81
A 24-year-old man has had pain in the left knee for the past several months. He reports that initially the pain was associated with weight-bearing activities, but it has now become more constant. He denies any swelling but reports a lateral fullness at the tibial plateau. Figures 23a through 23e show radiographs, a bone scan, and T1- and T2-weighted MRI scans. What is the most likely diagnosis?
Explanation
REFERENCES: Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H,
Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 3939-3962.
Question 82
A 27-year-old man has recurrent right shoulder instability. He first dislocated his shoulder in college while playing rugby and was treated nonsurgically. Since then, he has sustained nearly 1 dozen dislocations and says that his shoulder always feels “loose.” The shoulder recently dislocated in his sleep and while he was putting on clothes. Which factor is a contraindication to an arthroscopic soft-tissue repair?
Explanation
There is much debate in the literature regarding optimal techniques for treatment of shoulder instability. Although some studies suggest that open stabilization may result in lower recurrence rates in contact athletes, this approach is now under scrutiny. Extensive labral involvement (posterior labral involvement in this scenario) is likely more accessible via arthroscopic methods. Although HAGL lesions may be more easily accessible via an open approach (particularly for inexperienced arthroscopists), numerous authors describe successful repair via arthroscopic techniques. Among these responses, the strongest indication for an open approach, including possible bony transfer, is high-grade glenoid bone loss. Although the critical amount of bone loss is a topic of debate, most surgeons and authors suggest a cutoff of 20% to 25%.

CLINICAL SITUATION FOR QUESTIONS 90 THROUGH 92
Figure 90 is the radiograph of a 14-year-old pitcher who plays in a year-round baseball program and has vague pain in his dominant shoulder. The pain occurs with throwing, and it has been worsening for 2 months. Pain typically occurs during the late cocking phase of throwing. He has no tenderness of the rotator cuff and 5/5 rotator cuff strength. His arc of motion is symmetric between his dominant and nondominant arms. The sulcus sign is negative.
Question 83
Reverse total shoulder arthroplasty improves kinematics in the rotator cuff deficient joint by what directional change to the center of rotation? Review Topic
Explanation
Question 84
Avascular necrosis
Explanation
A 9-year-old girl sustains an injury (Slide) as a result of a fall. What is her risk of avascular necrosis:
Question 85
A 39-year-old male falls off his bicycle and complains of neck pain and tingling in his fingers. Trauma series radiographs are seen in Figures A and B. Which of the following is likely to be true? Review Topic

Explanation
Cervical spine fractures are not uncommon in ankylosing spondylitis because of osteoporosis and the long lever arm from fused vertebrae. They commonly occur because of hyperextension of the cervical spine (usually C5-7) and have a high rate of neurologic injury. AS fractures have a higher rate of neurologic injury than DISH fractures. Posterior decompression and stabilization with long constructs is necessary
Whang et al. reviewed spine injuries in 12 patients with AS and 18 patients with DISH. Most injuries involved C5-C7. Patients with AS were more likely to have severe neurologic injury (41% ASIA A) than DISH (44% ASIA E). There was 81% good-excellent outcome and 4 deaths related to halo vest use.
Caron et al. reviewed spine fractures in patients with ankylosing spine disorders (AS and DISH). AS patients were younger than DISH patients. Spinal cord injury was present in 58%. Surgery was performed on 67% and comprised instrumentation 3 levels above/below the injury. Mortality correlated with age. Mortality was 32%.
Westerveld et al. performed a systematic review on spine injuries in ankylosing spinal disorders. Most patients had sustained low energy trauma (fall from sitting/standing). In DISH, most fractures were through the vertebral body. In AS, vertebral body fractures equaled those through the disc. Surgery was performed for neurological deterioration, unstable fracture and the presence of an epidural hematoma.
Figure A shows a hyperextension injury at C6-7 (Type I, disc or Type IV,anterior disc, posterior body) cervical spine fracture in ankylosis spondylitis. Visible radiographic characteristics include osteopenia, bamboo spine, marginal syndesmophytes and ossfication of the disc space. Figure B is a chest radiograph showing thoracic syndesmophytes consistent with ankylosing spondylitis. Figure C shows bilateral sacroilitis and hip joint space narrowing typical of ankylosing spondylitis. Illustration A shows the Caron classification of spine fractures in ankylosing spondylitis (Type A, disc injury; Type B, body injury; Type C, anterior body, posterior disc injury; Type D, anterior disc, posterior body injury). Illustration B shows the difference between the marginal osteophytes of AS and nonmarginal osteophytes of DISH in the cervical spine. If you have osteophytes that are building up, and project out anterior to the anterior cortex of the vertebral bodies, like "flowing wax" it is DISH.
Incorrect Answers:
1:
This
is
characteristic
of
Klippel-Feil
syndrome
Question 86
An 18-year-old woman sustains a twisting injury of the knee while skiing. Figures 7a and 7b show the radiograph and coronal MRI scan of the knee. In addition to the injury shown, what is the most likely associated injury?
Explanation
REFERENCES: Goldman AB, Pavlov H, Rubenstein D: The Segond fracture of the proximal tibia: A small avulsion that reflects major ligamentous damage. Am J Roentgenol 1988;151:1163-1167.
Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 87
A patient with deficient anteroinferior bone stock undergoes a Latarjet procedure that transfers a portion of the coracoid to the glenoid rim and secures it with two screws. After surgery, the patient reports numbness on the anterolateral forearm. To verify the diagnosis, what muscle should be tested for strength?
Explanation
REFERENCES: Ho E, Cofield RH, Balm MR, Hattrup SJ, Rowland CM: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270.
Boardman ND 3rd, Cofield RH: Neurologic complications of shoulder surgery. Clin Orthop 1999;368:44-53.
Allain J, Goutallier D, Glorion C: Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder. J Bone Joint Surg Am 1998;80:841-852.
Question 88
Which of the following factors has been shown to increase mortality in poly-trauma patients with severe head injuries?

Explanation
Chesnut et al demonstrated that hypotension (SBP <90mmHg) was profoundly detrimental, occurring in 35% of these patients and associated with 150% increase in mortality.
Pietropaoli et al reviewed 53 patients with severe head injuries and required early surgical intervention (surgery within 72 hours of injury). All patients were initially normotensive on arrival. There were 17 patients (32%) who developed intra-operative hypotension and 36 (68%) who remained normotensive throughout surgery. The mortality rate was 82% in the IH group and 25% in the normotensive group.
Question 89
What is the preferred treatment of displaced distal clavicle fractures in children less than eight years old?

Explanation
Question 90
Which of the following is a true statement regarding thoracic disk herniations? Review Topic
Explanation
common in the lower third near the thoracolumbar region. Posterior laminectomy and disk excision has the highest rate of neurologic deterioration and is not recommended. Multiple studies have shown that herniated thoracic disks can be found at one or more levels in 40% of asymptomatic individuals.
Question 91
Figures 21a and 21b show the radiographs of a 12-year-old patient with an L4-level myelomeningocele who has scoliosis that has been slowly progressing for the past several years. There has been no loss of motor function. An MRI scan shows no syringomyelia or increased hydrocephalus. Management should consist of
Explanation
REFERENCES: Ward WT, Wenger DR, Roach JW: Surgical correction of myelomeningocele scoliosis: A critical appraisal of various spinal instrumentation systems. J Pediatr Orthop 1989;9:262-268.
Muller EB, Nordwall A: Brace treatment of scoliosis in children with myelomeningocele. Spine 1994;19:151-155.
Question 92
A 35-year-old man reports a 2-year history of right groin pain. The pain is made worse with hip flexion, prolonged sitting, and cycling. A radiograph and MRI scan are shown in Figures 16a and 16b. Nonsurgical management has failed to provide relief. What is the best surgical option?
Explanation
REFERENCES: Espinosa N, Rothenfluh DA, Beck M, et al: Treatment of femoro-acetabular impingement: Preliminary results of labral refixation. J Bone Joint Surg Am 2006;88:925-935.
Parvizi J, Leunig M, Ganz R: Femoroacetabular impingement. J Am Acad Orthop Surg 2007;15:561-570. Trousdale RT: Acetabular osteotomy: Indications and results. Clin Orthop Relat Res 2004;429:182-187.
Question 93
-A 37-year-old woman has a 2-month history of weakness in thumb and finger extension, but has normal radial deviation during extension of the wrist. An MRI scan of her forearm shows no abnormality. She does not recall any traumatic event. Needle electromyography findings show fibrillations and reduced
Explanation

Question 94
A 13-year-old pitcher is hit in the left intercostal space by a line drive ball. He collapses, is apneic and unresponsive, and his radial pulse is absent. What is the next step in management? Review Topic
Explanation
Question 95
-What is the most appropriate initial treatment?
Explanation
Based upon the history and description of the wound, this patient has sustained a frostbite injury to the anterior skin without evidence of infection. Frostbite, a thermal injury to local tissues, can be classified into first-, second-, third-, and fourth-degree injuries. First-degree injuries are characterized by a central whitish area surrounded by erythema. Second- and third-degree injuries are characterized by blisters that appear within the first 24 hours. Second-degree blisters are clear or cloudy, while third-degree blisters are hemorrhagic. Fourth-degree injuries are characterized by tissue necrosis. Treatment of a frostbite injury should begin as soon as it is identified, even if severity has not been determined. Treatment includes protection against mechanical irritation and keeping the injured area away from heat. The limb should be elevated and clear blisters debrided; dark blisters should be drained but not debrided. Topical treatment includes aloe application every 6 hours (silver sulfadiazine for open wounds). Nonsteroidal anti-inflammatory drugs can be given along with PCN G (500,000 U) or clindamycin (600 mg) IV every 6hours for 48 to 72 hours as prophylaxis against infection.Multiple skin incisions on the front of the knee place the skin at healing risk after surgery.
Skin oxygenation is further compromised by a lateral release, which disrupts the superior lateral geniculate artery in the peripatellar vascular anastomosis. When addressing compromised perfusion to the skin, the orthopaedic surgeon may consider not performing a lateral release, using the medial parapatellar incision,and/or not using a tourniquet during surgery. In this patient, the use of cold therapy further compromised perfusion to the skin. This patient’s wound does not reflect infection, but rather frostbite from the compromised skin perfusion and the application of cold therapy.

The physiologic responses to the effects of freezing temperatures on limbs have been categorized into 4 phases. Phase I, cooling and freezing, is characterized by vasoconstriction and vasospasm. The freezing results in mechanical destruction of cell membranes in endothelial cells in small capillaries. Phase II,rewarming, initiates as heat absorbed by the limb begins an exothermic reaction as extracellular and intracellular crystals melt. Intracellular swelling occurs and small capillaries become highly permeable,resulting in extravasation of fluid and causing edema and blisters. Phase III is characterized by progressive tissue injury resulting from inflammation, vascular stasis, and thrombosis leading to ischemia.Phase IV is recovery that can progress along 3 potential pathways: complete healing, healing with later sequelae, or early tissue necrosis leading to gangrene.
CLINICAL SITUATION FOR QUESTIONS 85 THROUGH 87
Figure 85 is the radiograph of a 13-year-old right-handed baseball player who has experienced 2 months of right-dominant shoulder pain. As a pitcher, he says he cannot “throw hard” without pain, and he develops a dull ache if he throws more than 15 pitches.
Question 96
The CT scan reveals a nondisplaced greater trochanteric fracture. The patient is now experiencing severe pain. What is the most appropriate treatment at this time?
Explanation
This patient presents with significant polyethylene wear, which can lead to both osteolysis and synovitis. However, synovitis usually manifests as a mild to moderate chronic ache, which should explain the discomfort. Although infection should always be ruled out with new-onset pain, no clinical parameters suggest acute hematogenous infection. Similarly, without any mention of back pain or neuropathy, radicular pain from the spine is unlikely. If this patient has a nondisplaced greater trochanteric fracture noted on MR imaging, the optimal immediate mode of treatment is to not rush into surgery despite the mild osteolysis. The patient’s severe pain is likely attributable to the nondisplaced greater trochanteric fracture rather than wear-induced synovitis, which typically presents as a mild to moderate ache. It is recommended to
allow the fracture to heal to avoid fracture displacement. Once the fracture is healed, a revision surgery with liner exchange can be recommended. Based on this clinical scenario, the acetabular component is within what is largely considered the “safe-zone” in THA. Despite this patient’s dislocations, the preferred treatment modality is to revise to a constrained liner. This patient had a well-functioning hip for longer than 15 years. Therefore, conversion to a constrained liner is the best treatment.
Question 97
A 73-year-old man who underwent repair of the left rotator cuff 6 years ago reports good pain relief but notes residual weakness of the left shoulder, especially with overhead tasks. He denies having pain at night and has minimal discomfort with activities of daily living but is dissatisfied with his shoulder strength. Radiographs show an acromiohumeral interval of 2 mm. Appropriate management should consist of
Explanation
REFERENCES: Bigliani LU, Cordasco FA, McIlveen SJ, Musso ES: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515.
DeOrio JK, Cofield RH: Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am 1984;66:563-567.
Gerber C, Vinh TS, Hertel R, Hess CW: Latissimus dorsi transfer for the treatment of massive tears of the rotator cuff: A preliminary report. Clin Orthop 1988;232:51-61.
Question 98
Histologically, synovial chondromatosis is characterized by
Explanation
REFERENCES: Milgram JM: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;l59:792-801.
Murphy FP, Dahlin DC, Sullivan CR: Articular synovial chondromatosis. J Bone Joint Surg Am 1962;44:77.
Question 99
A year-old man with insulin-dependent diabetes mellitus underwent primary total knee arthroplasty (TKA). A full-thickness skin slough measuring 3 cm by 4 cm developed, with postsurgical exposure of the patellar tendon. No change is observed in the appearance of the wound after 2 weeks of wet-to-dry dressing changes. What is the best next treatment step for the soft-tissue defect?
Explanation
If wound healing does not occur and deep soft tissues such as the patellar tendon are exposed following TKA, local rotational flap is the procedure of choice. The procedure should be performed relatively early after the recognition of a soft-tissue wound-healing problem. In the setting of TKA, the gastrocnemius muscle is an excellent source of flaps for wound coverage of the proximal tibia.
Question 100
The main advantage of surgical repair of an acute Achilles tendon rupture, when compared with nonsurgical management, is reduced
Explanation
REFERENCES: Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036.
Cetti R, Christensen SE, Ejsted R, Jensen NM, Jorgensen U: Operative versus nonoperative treatment of Achilles tendon rupture: A prospective randomized study and review of the literature. Am J Sports Med 1993;21:791-799.
Nistor L: Surgical and non-surgical treatment of Achilles tendon rupture. J Bone Joint Surg Am 1981;63:394-399.
