Orthopedic Board Review MCQs: Foot & Ankle, Hip, Trauma & Sports Medicine | Part 219

Key Takeaway
This interactive quiz offers Part 219 of a comprehensive Orthopedic Surgery board review. It features 100 high-yield, OITE/AAOS-modelled MCQs for orthopedic residents and surgeons preparing for AAOS/ABOS certification. The content helps master exam topics via interactive study and exam modes.
About This Board Review Set
This is Part 219 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 219
This module focuses heavily on: Foot, Fracture, Hip, Ligament.
Sample Questions from This Set
Sample Question 1: What complication is more likely following excessive medial retraction of the anterior covering structures during the anterolateral (Watson-Jones) approach to the hip?...
Sample Question 2: In the treatment of intra-articular calcaneal fractures, surgical reduction and fixation has been shown to have improved outcomes over nonoperative treatment in all of the following patient groups EXCEPT:...
Sample Question 3: 04 Which of the following laboratory studies is predictive of wound healing prior to performing a lower extremity amputation?...
Sample Question 4: Figure 16 shows the lateral radiograph of a patient who is scheduled to undergo an anterior cruciate ligament (ACL) reconstruction. If the graft is tensioned at 20° of flexion and the femoral tunnel is created by passing a reamer over the g...
Sample Question 5: Which of the following imaging modalities is most accurate in locating a toothpick in the plantar arch of the foot?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What complication is more likely following excessive medial retraction of the anterior covering structures during the anterolateral (Watson-Jones) approach to the hip?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 325.
Anderson JE: Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-17, 4-18.
Question 2
In the treatment of intra-articular calcaneal fractures, surgical reduction and fixation has been shown to have improved outcomes over nonoperative treatment in all of the following patient groups EXCEPT:

Explanation
Question 3
04 Which of the following laboratory studies is predictive of wound healing prior to performing a lower extremity amputation?
Explanation
(eliminates false positive predictions with using area under the Doppler waveform). Pressures less than 20 mm Hg are predictive of poor healing. Miller 505-6
back to this question next question
Question 4
Figure 16 shows the lateral radiograph of a patient who is scheduled to undergo an anterior cruciate ligament (ACL) reconstruction. If the graft is tensioned at 20° of flexion and the femoral tunnel is created by passing a reamer over the guide wire marked “A,” the resulting ligament reconstruction will excessively
Explanation
REFERENCES: Daniel DM, Fritschy D: Anterior cruciate ligament injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 1994, pp 1313-1360.
Larson RL, Tailon M: Anterior cruciate ligament insufficiency: Principles of treatment. J Am Acad Orthop Surg 1994;2:26-35.
Question 5
Which of the following imaging modalities is most accurate in locating a toothpick in the plantar arch of the foot?
Explanation
REFERENCES: Mizel MS, Steinmetz ND, Trepman E: Detection of wooden foreign bodies in muscle tissue: Experimental comparison of computed tomography, magnetic resonance imaging, and ultrasonography. Foot Ankle Int 1994;15:437-443.
Jacobson JA, Powell A, Craig JG, et al: Wooden foreign bodies in soft tissue: Detection at US. Radiology 1998;206:45-48.
Question 6
A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
Explanation
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
Question 7
Compared to metal-on-polyethylene total hip bearing surfaces, the debris particles generated by metal-on-metal articulations are
Explanation
metal-on-metal articulations in total hip arthroplasty are several orders of magnitude smaller
and may be up to 100 times more numerous than those found with metal-on-polyethylene articulations.
REFERENCES: Davies AP, Willert HG, Campbell PA, et al: An unusual lymphocytic perivascular infiltration in tissues around contemporary metal-on-metal joint replacements.
J Bone Joint Surg Am 2005;87:18-27.
Firkins PJ, Tipper JL, Saadatzadeh MR, et al: Quantitative analysis of wear and wear debris from metal-on-metal hip prostheses tested in a physiological hip joint simulator. Biomed Mater Eng 2001;11:143-157.
Question 8
A 45-year-old man has severe pain in both feet after his boots become wet while hunting. Examination 3 hours after the onset of symptoms reveals that his feet are cold to touch and the skin appears blanched. Management should consist of
Explanation
REFERENCES: Pinzur MS: Frostbite: Prevention and treatment. Biomechanics 1997;4:14-21.
Fritz RL, Perrin DH: Cold exposure injuries: Prevention and treatment. Clin Sports Med 1989;8:111-128.
Question 9
A 23-year-old man who was the restrained driver in a car involved in a high-speed motor vehicle accident sustained the closed injury shown in Figures 32a through 32c. Which of the following factors has the greatest impact on the risk of osteonecrosis?
Explanation
REFERENCES: Lindvall E, Haidukewych G, Dipasquale T, et al: Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am 2004;86:2229-2234.
Vallier HA, Nork SE, Barei DP, et al: Talar neck fractures: Results and outcomes. J Bone Joint Surg Am 2004;86:1616-1624.
Question 10
Which of the following factors is associated with improved outcomes following surgery for hip fractures?
Explanation
Question 11
The patient is given a blood transfusion. After starting the transfusion, nurses note that her temperature is 38.8°C and she has shaking and chills. What is the most likely cause of this problem?
Explanation
Blood management and venous thromboembolism prevention are important considerations in the perioperative management of THA. Recommendations now focus on presurgical optimization of hemoglobin, use of antifibrinolytics intrasurgically, and minimized use of transfusions. Current recommendations do not favor autologous blood donation for patients with hemoglobin levels higher than 13 g/dL. There is a move toward increased use of aspirin for venous thromboembolism prophylaxis, but this modality can cause GI bleeding that may necessitate blood transfusion. Transfusion reactions are rare, and the most common cause is administration of an incompatible unit because of clerical error.
Question 12
Which of the following aids in correction of patellar tracking after total knee arthroplasty (TKA)?
Explanation
REFERENCES: Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 1245-1258.
Merkow RL, Soudry M, Insall JN: Patellar dislocation following total knee replacement. J Bone Joint Surg Am 1985;67:1321-1327.
Question 13
A 20-year-old collegiate pitcher sustains a medial collateral ligament (MCL) rupture of his throwing elbow for which surgical reconstruction is necessary. The goal of surgery is anatomic restoration of the MCL. Which statement best describes the kinematics of the native MCL?
Explanation
full extension and full flexion. True lateral radiographs reveal that the flexion-extension axis, or center of rotation, of the elbow lies in the center of the trochlea and capitellum. The origin of the anterior bundle of the MCL lies slightly posterior to the rotational center of the elbow. The anterior bundle is further divided into an anterior band and a posterior band. The eccentric origin of these anterior bundle components in relation to the rotational center through the trochlea creates a CAM effect during flexion and extension. The anterior band tightens during extension, and the posterior band tightens during flexion. This reciprocal tightening of the two functional components of the anterior bundle allows the ligament to remain taut throughout the full range of flexion. Cadaver dissection studies have identified the origin and insertion of both the medial and lateral stabilizing elbow ligaments. The anterior bundle of the MCL is isometric throughout the flexion/extension arc of motion, making Response C incorrect. The posterior bundle of the MCL elongates with elbow flexion, so Responses B and D are incorrect. The posterior bundle of the MCL also demonstrates the most change in
length from extension to flexion of all the elbow ligaments.
Question 14
A 26-year-old man is brought to the emergency department unresponsive and intubated after being found lying on the side of the road. He has a Glasgow Coma Scale score of 6. A chest tube has been inserted on the right side of the chest for a pneumothorax. An abdominal CT scan reveals a small liver laceration and minimal intraperitoneal hematoma. A pneumatic antishock garment (PASG) is on but not inflated. He has bilateral tibia fractures. A pelvic CT scan shows an anterior minimally displaced left sacral ala fracture and left superior and inferior rami fractures. He has received 2 L of saline solution and 4 units of blood but remains hemodynamically unstable. What is the next most appropriate step in management?
Explanation
REFERENCES: Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: Effective classification system and treatment protocols. J Trauma 1990;30:848-856.
Evers BM, Cryer HM, Miller FB: Pelvic fracture hemorrhage: Priorities in management. Arch Surg 1989;124:422-424.
Flint L, Babikian G, Anders M, Rodriguez J, Steinberg S: Definitive control of mortality from severe pelvic fracture. Ann Surg 1990;211:703-707.
Question 15
A 3-year-old child sustains a T2/T3 fracture-dislocation with complete paraplegia secondary to a car accident in which the child was an unrestrained passenger. What is the likelihood that this child will develop subsequent spinal deformity in the future?
Explanation
REFERENCES: Mayfield JK, Erkkila JC, Winter RB: Spine deformity subsequent to acquired childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-1411.
Dearolf WW III, Betz RR. Vogl LC, et al: Scoliosis in pediatric spinal cord-injured patients. J Pediatr Orthop 1990;10:214-218.
Mehta S, Betz RR. Mulcahey MJ, et al: Effect of bracing on paralytic scoliosis secondary to spinal cord injury. J Spinal Cord Med 2004;27:S88-S92.
Question 16
Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease that is characterized by
Explanation
Question 17
A 30-year-old man reports pain and weakness in his right arm. Examination reveals grade 4 strength in wrist flexion and elbow extension, decreased sensation over the middle finger, and decreased triceps reflex. These symptoms are most compatible with impingement on what spinal nerve root?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Upper Saddle River, NJ, Prentice Hall, 1976, p 125.
Lauerman WC, Goldsmith ME: Spine, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 353-378.
Question 18
A healthy 16-year-old boy has had increasing pain in the right knee for the past 3 months. Examination reveals warmth and swelling around the distal femur. Radiographs and an MRI scan are shown in Figures 51a through 51c, and a biopsy specimen is shown in Figure 51d. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 205.
Question 19
A 20-year-old college pitcher reports medial elbow pain after 3 innings of hard throwing. He recalls no injury and reports no pain with light throwing. The examination shown in the clinical photograph in Figure 48 reproduces the elbow pain. What is the most likely diagnosis?
Explanation
REFERENCES: Williams RJ III, Urquhart ER, Altchek DW: Medial collateral ligament tears in the throwing athlete. Instr Course Lect 2004;53:579-586.
Cain EL Jr, Dugas JR, Wolf RS, et al: Elbow injuries in throwing athletes: A current concepts review. Am J Sports Med 2003;31:621-635.
Question 20
The patient does well initially but returns for the 4-month postsurgical evaluation with ongoing stiffness and pain despite going to physical therapy twice weekly and working on motion at home. She is unable to bear weight comfortably. What is the best next step?
Explanation
In a skeletally immature patient with OCD and minor symptoms, the lesion can be observed and healing obtained with activity limitations if the cartilage is stable (but this cannot be determined radiographically or clinically). Activity restriction and serial follow-up are appropriate if an MRI reveals a stable lesion. MRI is indicated when there is concern that a lesion may be unstable. Surgical treatment depends on MRI findings.
Observation is recommended for OCD lesions in growing patients for 6 months because healing has been observed. Early surgical procedures, although they may be needed in the future, are not appropriate for patients with well-controlled symptoms.
If symptoms continue for longer than 6 months, arthroscopic drilling is not indicated for unstable OCD. The appropriate treatment is OCD fixation. Debridement is not appropriate with a stable lesion.
Evaluation of the fixation and stability of the lesion with advanced imaging after weight bearing and therapy initiation is the most appropriate option. Manipulating the knee without determining whether the stiffness is attributable to subsidence of the fixation or mechanical block is not appropriate. After 4 months, aspiration of a hematoma (if still present) would not yield much benefit. More therapy is not likely to be useful when a patient is attending therapy regularly and working on a home program.

Question 21
A 68-year-old man reports a 4-week history of progressive left-sided lower back and hip pain. The pain is in the posterior buttock region with radiation to the groin and to the left anterior knee region. The pain is aggravated with walking and improves with rest. There is no history of previous trauma. Radiographs are seen in Figures 14a and 14b, and MRI scans are seen in Figures 14c through 14e. What is the most appropriate treatment option at this time?
Explanation
REFERENCES: Wong DA, Transfeldt E: Macnab’s Backache, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2007, pp 339-361.
Spivak JM, Connolly PJ (ed): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 43-56.
Question 22
A 13-year-old gymnast has had recurrent right elbow pain for the past year. She denies any history of trauma. Rest and anti-inflammatory drugs have failed to provide relief. Examination reveals no localized tenderness and only slight loss of both flexion and extension (10 degrees). What is the most likely diagnosis?
Explanation
REFERENCES: Krijnen MR, Lim L, Willems WJ: Arthoscopic treatment of osteochondritis dissecans of the capitellum: Report of 5 female athletes. Arthroscopy 2003;19:210-214.
Schenck RC, Goodnight JM: Osteochondritis dissecans. J Bone Joint Surg Am 1996;3:439-456.
Question 23
A 22-year-old man sustained a cervical fracture-dislocation of the C5-6 level in a motor vehicle accident along with an associated spinal cord injury. Six months after his injury, he has 4 out of 5 biceps on the left, with 5 out of 5 biceps on the right. Deltoid is graded at 5 out of 5 bilaterally. There is 0 strength in the triceps, wrist flexors, wrist extensors, and digital extensors. He has neurogenic bowel and bladder with absent perianal sensation and no voluntary motor in the lower extremities. The patient's neurologic deficit is best categorized as which of the following? Review Topic
Explanation
Question 24
A 70-year-old man reports symptomatic medial knee pain that has become progressively worse during the past year. MRI reveals a complex, posterior horn medial meniscus tear with associated medial lateral and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable relief of symptoms?
Explanation
Total knee replacement is a well-established surgery for diffuse, symptomatic osteoarthritis of the knee joint, and its efficacy has been shown in many studies. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee, arthroscopy in the setting of existing osteoarthritis is efficacious for relieving the signs and symptoms of a torn meniscus but not for osteoarthritis. Likewise, in young and active patients, clinical outcomes show improvement after realignment osteotomy for single-compartment osteoarthritis. Unicondylar knee replacement is not indicated for tricompartmental disease of the knee.
Question 25
Figure 1 shows a radiograph obtained from an active 30-year-old man who sustained an injury to his ring finger 1 week earlier. The most appropriate treatment is

Explanation

Figure 1 reveals evidence of an intra-articular distal phalanx fracture with a distal interphalangeal (DIP) joint dorsal subluxation. This injury is unstable and requires surgical management for an active individual. Volar distal phalanx fractures are often associated with flexor digitorum profundus avulsion injuries, which are addressed concomitantly. This injury was treated with ORIF of the intra-articular fracture, pinning of the DIP joint, and repair of an avulsed flexor digitorum profundus tendon with a button on the dorsal nail plate, as shown in Figure 2. Splint immobilization would not maintain a reduction of this unstable injury. The terminal tendon is not injured in this patient but is often injured in a dorsal distal phalanx fracture with a volar dislocation. Arthrodesis of the DIP is a salvage procedure and would not be considered acutely.
Question 26
Which of the following is a function of siRNA (small interfering RNA)?
Explanation
siRNA are short (usually 20 to 24-bp) double-stranded RNA (dsRNA) sequences with phosphorylated 5' ends and hydroxylated 3' ends. Because of their ability to block a gene of interest, they have been generating interest in the treatment of disease processes that involve gene expression.
Noh et al. study the affects of PD98059, an extracellular signal-regulated kinase 1/2 (ERK1/2) inhibitor, on osteosarcoma. They found that blocking the ERK1/2 pathway with PD98059 induces osteosarcoma cell death by inhibiting a potential drug-resistance mechanism.
Illustration A shows how siRNA works to block translation of mRNA. Incorrect Answers:
Question 27
Figure 46 shows the radiograph of an obese 12-year-old boy who has had left hip pain for the past 3 months. What is the best course of action?
Explanation
REFERENCES: Loder RT, Aronsson DD, Greenfield ML: The epidemiology of bilateral slipped capital femoral epiphysis: A study of children in Michigan. J Bone Joint Surg Am 1993;75:1141-1147.
Aronsson DD, Karol LA: Stable slipped capital femoral epiphysis: Evaluation and management. J Am Acad Orthop Surg 1996;4:173-181.
Hurley JM, Betz RR, Loder RT, Davidson RS, Alburger PD, Steel HH: Slipped capital femoral epiphysis: The prevalence of late contralateral slip. J Bone Joint Surg Am 1996;78:226-230.
Loder RT, Aronson DD, Dobbs MB, Weinstein SL: Slipped capital femoral epiphysis. J Bone Joint Surg Am 2000;82:1170-1188.
Question 28
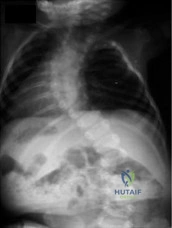
Figures 82a through 82c show the radiograph and 3-dimensional (3-D) CT scans of a 2-year-old boy whose scoliosis has progressed 15 degrees during the past year. The child is clinically healthy. He has been walking since 11 months of age. An MRI scan of the entire spine revealed no other anomalies. What additional study is indicated? Review Topic
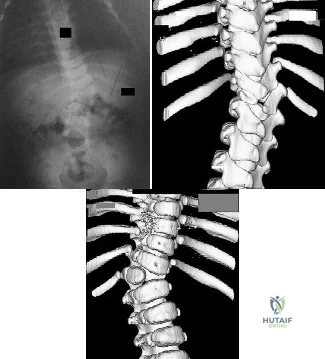
Explanation
Question 29
A 47-year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the
aspiration and proceed to a revision TKA with possible augments on standby.
Question 30
Bacterial resistance to antibiotics in biofilm is an example of Review Topic
Explanation
known as quorum sensing. Once the bacteria produce a mature biofilm, they enter a greatly reduced or stationary phase of growth. Lastly, high-shear environments seem to stimulate biofilm production.
Question 31
- A right-handed 35-year old man who underwent a Putti-Platt repair for recurrent anterior instability 20 years ago now has increasing shoulder pain and stiffness. Examination of the shoulder reveals internal rotation to the posterior superior iliac spine and external rotation to 10 degrees with the shoulder adducted. The supraspinatus and infraspinatus are moderately atrophied. What is the most likely diagnosis?
Explanation
Question 32
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. What is the most appropriate management of this condition?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross-sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 33
Figures below show the radiographs obtained from a 75-year-old woman who underwent right total hip arthroplasty in 2009. She did well until last month, when a right posterior hip dislocation occurred after she fell from her bed to the floor. Successful closed reduction was performed. She sustained two more posterior dislocations requiring closed reduction under anesthesia. The surgical report from the index arthroplasty notes a 54-mm monoblock acetabular component with a 28-mm inner diameter compression molded polyethylene and a high offset neck cementless stem with a +8-mm length, 28-mm head. What is the best next step?

Explanation
This patient has demonstrated recurrent instability, and her current implants lack the modularity to upsize and improve the head-neck ratio and range to impingement. Given the monoblock acetabular component and a +7-mm neck length, the best option is revision to a large-diameter femoral head or dual-mobility component. Placement of a hip spica cast and resection arthroplasty are unreasonable. Revision to a longer ball length likely would not solve this recurrent instability pattern.
Question 34
In obstetrical brachial plexus palsy, which of the following signs is associated with the poorest prognosis for recovery in a 2-month-old infant?
Explanation
REFERENCES: Clarke HM, Curtis CG: An approach to obstetrical brachial plexus injuries. Hand Clin 1995;11:563-581.
Narakas AO: Injuries to the brachial plexus, in Bora FW (ed): The Pediatric Upper Extremity: Diagnosis and Management. Philadelphia, PA, WB Saunders, 1986, p 247.
Question 35
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. Treatment should include

Explanation
Question 36
below show the radiographs obtained from a year old man with progressively worsening right side hip pain over the last 8 months. He is 6 feet tall, with a BMI of 51 kg/m 2 and reports that his index total hip arthroplasty was performed 8 years ago. The preoperative work-up includes negative infectious laboratory results. What is the most appropriate surgical plan for revision of the femoral component in this patient?
Explanation
Submit Answer
The patient’s radiographs demonstrate varus femoral remodeling around a broken cylindrical, distally fixed femoral stem. Proximal femoral remodeling around loose or fractured stems occurs in 21% to 42% of femoral revisions, based on the definitions outlined by Foran and associates. In definition 1, varus femoral remodeling occurs when the template falls within 2 mm of the endosteal cortex of the metaphysis on templating with a diaphyseal engaging stem. In definition 2, varus femoral remodeling = when the template crosses the lateral femoral cortex proximally. Based on the templating or drawing a line from the isthmus proximally along the lateral cortex, implantation of a straight stem would perforate the cortex proximally, indicating varus femoral remodeling. An extended trochanteric osteotomy would aid in the removal of the well-fixed distal segment and enable the safe insertion of the new femoral component. The approach is not the concern in this case, because extended trochanteric osteotomies have been described from the posterior and direct lateral approaches with excellent outcomes and union rates. The key is that the extended osteotomy is necessary and not a trochanteric slide or standard (shorter or incomplete trochanteric) osteotomy. These types would not provide access to the well-fixed distal stem, nor would they afford a straight tube in which to insert a new femoral component.
Question 37
Which of the following is considered a physiologic effect of anemia?
Explanation
REFERENCE: Carson JL, Duff A, Poses RM, et al: Effect of anemia and cardiovascular disease on surgical mortality and morbidity. Lancet 1996;348:1055-1060.
Question 38
Figure 1 is the MR image of a high school soccer player who sustained a right knee injury during a game while making a cut toward the ball. He felt a pop and his leg gave way. During physical examination, as the knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a "clunk" within the knee. What is the most likely biomechanical basis for the "clunk"?

Explanation
Question 39
A 48-year-old man undergoes arthroscopy to repair a rotator cuff tear. During the arthroscopy, the tear is characterized and found to involve the entire supraspinatus and a majority of the infraspinatus tendons. After mobilization, the posterior rotator cuff can reach the greater tuberosity. However, the supraspinatus tendon cannot reach its insertion point at the greater tuberosity. What is the most appropriate treatment? Review Topic
Explanation
release, reverse acromioplasty, and tenotomy of the biceps tendon may improve shoulder pain. If these procedures fail, then a muscle transfer procedure can also be considered in select patients. If, however, a portion of the rotator cuff can be repaired, even partial repair can balance the coronal and axial forces about the shoulder to restore the kinematics of the joint. Reverse total shoulder arthroplasty is not appropriate for this relatively young patient.
Question 40
When standing, dorsiflexion of the great toe will accentuate
Explanation
REFERENCES: Mann RA: Biomechanics of the foot and ankle, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 1-44.
Hicks JH: The mechanics of the foot: II. The plantar aponeurosis and the arch. J Anat 1954;88:25.
Question 41
A 35-year-old man who has had a 6-month history of low back pain and tenderness now reports worsening pain and stiffness in the hips and entire back. An AP radiograph of the pelvis demonstrates fusion of the sacroiliac joints bilaterally. What is the next most appropriate step in management? Review Topic
Explanation
disease, further work-up in a patient with potential ankylosing spondylitis is not warranted. Sacroiliac joint anesthetic injections and sacroiliac fusion are not recommended treatments for early ankylosing spondylitis. Aspiration of the sacroiliac joints can be done if sacroiliac joint infection is suspected; however, in the absence of fever or other constitutional symptoms, infection is unlikely.
Question 42
A 68-year-old man with no significant medical history underwent a total knee arthroplasty 4 years ago. A radiograph is shown in Figure 55. He reports that he had no problems with the knee until 6 weeks ago when he noted the gradual onset of pain following a colonoscopy. Examination reveals a painful, swollen knee. Knee aspiration reveals a WBC count of 40,000/mm 3 . Management should consist of
Explanation
REFERENCES: Swanson KC, Windsor RE: Diagnosis of infection after total knee arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1485-1491.
Hanssen AD, Rand JA, Osmon DR: Management of the infected total knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 1070-1089.
Question 43
The force generated by a muscle is most highly dependent on its
Explanation
Question 44
An otherwise healthy 54-year-old man who underwent a successful multilevel lumbar decompression and fusion 4 years ago now reports increasingly severe bilateral thigh claudication with paresthesia and severe back pain for the past 12 months. Physical therapy, bracing, and epidural steroids have failed to provide relief. A radiograph and MRI scans are shown in Figures 15a through 15c. He is afebrile, and laboratory studies show an erythrocyte sedimentation rate of 5 mm/h and a normal WBC count. What is the best course of action?
Explanation
kyphosis and stenosis. Because he is healthy, has responded well to previous surgery,
|and has a potentially correctable lesion, he is not a good candidate for an end-stage failed
back procedure such as a morphine pump. The stenosis is exacerbated by the deformity; therefore, a simple decompression will contribute to instability. Because of the kyphosis and the patient’s relatively young age, the treatment of choice is restoration of sagittal alignment and posterior decompression.
REFERENCE: Eck JC, Humphreys SC, Hodges SD: Adjacent-segment degeneration after lumbar fusion: A review of clinical, biomechanical, and radiographic studies. Am J Orthop 1999;28:336-340.
Question 45
An 18-year-old collegiate football player injures his right shoulder during a tackle. He reports pain and numbness in the shoulder and numbness radiating to his fingers. His symptoms improve within 15 minutes and he has no residual symptoms. This condition is best known as Review Topic
Explanation
Question 46
What is the most common non-anesthetic-related reversible cause of sustained changes in intraoperative neurophysiologic monitoring signals during spinal surgery? Review Topic
Explanation
Question 47
The natural history of cervical spondylolytic myelopathy is best described as
Explanation
REFERENCES: Emery SF: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Lees F, Turner JA: The natural history and prognosis of cervical spondylosis. Brit Med J 1963;2:1607-1610.
Clarke E, Robinson PK: Cervical myelopathy: A complication of cervical spondylosis. Brain 1956;79:486-510.
Question 48
Figures 12a and 12b show the radiographs of a 56-year-old man with diabetes mellitus who has had left foot swelling with no pain for the past several weeks. He denies any history of trauma. Examination reveals warmth, moderate swelling, no tenderness, and mild pes planus with standing. Pulses are palpable, and his sensory examination is grossly intact to light touch. Standing radiographs are shown in Figures 12c and 12d. What is the most likely diagnosis?
Explanation
REFERENCES: Brodsky JW: The diabetic foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 895-969.
Myerson MS: Diabetic neuroarthropathy, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 439-465.
Question 49
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured? Review Topic
Explanation
Question 50
Which of the following factors is associated with decreases in active periprosthetic osteolysis in total hip arthroplasty?
Explanation
REFERENCES: Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in ultra-high molecular weight components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051.
Fisher J, Hailey JL, Chan KL, et al: The effect of aging following irradiation on the wear of UHMWPE. Trans Orthop Res Soc 1995;20:12.
Archibeck MJ: The basic science of periprosthetic osteolysis. Instr Course Lect
2001;50:185-195.
Question 51
Denosumab, a monoclonal antibody used to treat osteoporosis, works through inhibition of
Explanation
Question 52
A 16-year-old girl has had pain in the left groin for the past 4 months. She notes that the pain is worse at night; however, she denies any history of trauma and has no constitutional symptoms. There is no history of steroid or alcohol use. Examination reveals pain in the left groin with rotation of the hip. There is no associated soft-tissue mass. A radiograph and MRI scan are shown in Figures 32a and 32b, and biopsy specimens are shown in Figures 32c and 32d. What is the most likely diagnosis?
Explanation
REFERENCES: Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Simon M, Springfield D, et al: Chrondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990,
pp 62-67.
Question 53
A 55-year-old woman is referred for evaluation of a painful knee replacement. She underwent total knee arthroplasty (TKA) more than 1 year ago without perioperative complications but has had consistent pain since the surgery. The patient’s preoperative radiographs and postoperative radiographs are shown in Figures below. Examination reveals medial laxity during valgus stress testing and range of motion of 0° to 70°. Her erythrocyte sedimentation rate and C-reactive protein level are normal. What is the best next step?
Explanation
The radiographs show substantial valgus malalignment of the femoral component, with lateral mechanical axis deviation. Clinically, by examination she displays instability and stiffness as a result. Revision knee replacement is appropriate and should consist of total revision to stemmed femoral and tibial components with a varus-valgus constrained insert, given the likely attenuation of the medial collateral ligament. Open debridement with ligament balancing and polyethylene exchange do not address the underlying cause and are inappropriate. Distal femoral osteotomy is not useful in the setting of previous total knee replacement.
Nonsurgical treatment with an unloader brace would be ineffective in correcting the alignment.
Question 54
A child presents with the radiograph shown in Figure A. Which of the following conditions is LEAST likely to be associated with this disorder? Review Topic
Explanation
Congenital scoliosis is associated with other anomalies 60% of the time. These anomalies can appear independently, or as part of the VACTERL syndrome (vertebral anomalies, anorectal atresia, tracheoesophageal fistula, and renal and vascular anomalies). Other associated orthopedic conditions include clubfoot, developmental dysplasia of the hip, limb hypoplasia, Sprengel’s deformity, Klippel-Feil syndrome, foot asymmetry, vertical tali, leg atrophy and pes cavus.
Hedequist et al. (2004) reviewed congenital scoliosis. They recommend surgery in young children, severe deformities, or deformities that tend to progress rapidly, truncal imbalance, and anomalies at the cervicothoracic and lumbosacral junction (because of imbalance in the shoulders/neck and lumbar region respectively). Surgical options include in situ fusion, convex hemiepiphysiodesis, hemivertebra excision, correction and instrumented fusion, osteotomies with fusion, growing rods and expandable ribs.
Hedequist et al. (2007) reviewed congenital scoliosis. They state that fully segmented hemivertebra with definable disks above and below are more likely to cause curvature compared with an unsegmented hemivertebra fused to the vertebra above and below. Also, anomalies at the cervicothoracic and lumbosacral junctions produce more visible deformities than that at other areas.
Figure A shows a spine with multiple hemivertebrae, examples of failure of formation in congenital scoliosis.
Incorrect Answers:
Question 55
Limited weight bearing usually is recommended following open reduction and internal fixation of intra-articular lower extremity fractures. A bone graft, or bone graft substitute is often placed in the metaphyseal void beneath the reduced articular fragments. Which of the following bone grafts or bone graft substitutes will most likely permit earlier weight bearing without subsidence of the articular reduction?
Explanation
Question 56
Figures below show the radiographs obtained from an 86-year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 57
A 21-year-old man has mild but persistent aching pain in his left proximal thigh during impact loading activities. He denies pain at rest and has no other symptoms. Figures 34a through 34e show the radiographs and T1-weighted, T2-weighted, and gadolinium MRI scans of the left hip. What is the most likely diagnosis?
Explanation
REFERENCES: Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
May DA, Good RB, Smith DK, et al: MR imaging of musculoskeletal tumors and tumor mimickers with intravenous gadolinium: Experience with 242 patients. Skeletal Radiol 1997;26:2-15.
Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 4023-4034.
Question 58
A 27-year-old man has had pain in the right index finger for the past 9 months. The pain is completely relieved with ibuprofen. An AP radiograph and CT scan are shown in Figures 80a and 80b. What is the most likely diagnosis?
Explanation
radiolucent nidus. A small area of calcification may be present within the center of the nidus. The radiolucent nidus is surrounded by a thick rim of sclerotic bone. These diagnostic
features are frequently better seen on CT. An increase in cyclooxygenase activity has been demonstrated within osteoid osteomas, which may explain why aspirin and other nonsteroidal anti-inflammatory drugs classically relieve the pain associated with these lesions.
REFERENCES: Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 121-130.
Question 59
A 45-year-old woman has had intense pain in her foot for the last 3 days. She also reports a mild fever and difficulty with shoe wear. Examination reveals a swollen, slightly erythematous warm foot with tenderness at the great toe metatarsophalangeal joint and pain with passive motion of the joint. An AP radiograph is shown in Figure 13. Which of the following will best aid in determining a definitive diagnosis?

Explanation
REFERENCES: Wise CM, Agudelo CA: Diagnosis and management of complicated gout. Bull Rheum Dis 1998;47:2-5.
Harris MD, Siegel LB, Alloway JA: Gout and hyperuricemia. Am Fam Physician 1999;59:925-934.
Question 60
Figure 35 shows the radiograph of a 35-year-old weightlifter who has had pain with overhead lifts for the past 7 months. Cortisone injections in the acromioclavicular joint provided only temporary relief. A bone scan reveals increased activity of the acromioclavicular joint. Treatment should now consist of
Explanation
REFERENCES: Flatow EL, Cordasco FA, McCluskey GM, Bigliani LU: Arthroscopic resection of the distal clavicle via a superior portal: A critical quantitative radiographic assessment of bone removal. Arthroscopy 1990;6:153-154.
Lyons FR, Rockwood CA: Osteolysis of the clavicle, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 541-546.
Question 61
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management?
Explanation
REFERENCES: Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
D’Alessandro DF, Bradley JP, Fleischli JE, et al: Prospective evaluation of thermal capsulorrhaphy for shoulder instability: Indications and results, two- to five-year follow-up.
Am J Sports Med 2004;32:21-33.
Levine WN, Clark AM Jr, D’Alessandro DF, et al: Chondrolysis following arthroscopic thermal capsulorrhaphy to treat shoulder instability: A report of two cases. J Bone Joint Surg Am 2005;87:616-621.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 278-279.
Question 62
A homebound 75-year-old woman with diabetes mellitus has had progressive left knee pain and swelling for the past 6 weeks. She is febrile with a temperature of 103 degrees F (39.5 degrees C). History reveals that she underwent arthroplasty 5 years ago. Examination shows passive range of motion of 0 to 100 degrees with no active extension. Knee aspiration reveals purulent fluid with a Gram stain showing gram-negative rods. A radiograph is shown in Figure 27. In addition to IV antibiotics, which of the following management options offers the best chance of a successful outcome?
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgery, 2002, pp 513-536.
Hanssen AD, Rand JA: Evaluation and treatment of infection at the site of a total hip or knee arthroplasty. Instr Course Lect 1999;48:111-122.
Question 63
A cartilage water content increase is the hallmark of which osteoarthritis stage?
Explanation
Question 64
Nutritional rickets is associated with which of the following changes in chemical blood level?
Explanation
and low to normal serologic levels of calcium. To boost serum calcium levels, there is a compensatory increase in PTH and bone resorption, leading to increased alkaline
phosphatase levels.
REFERENCES: Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94.
Pettifor J: Nutritional and drug-induced rickets and osteomalacia, in Farrus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 399-466.
Einhorn TA: Metabolic bone disease, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 65
Patients who sustain bilateral femoral shaft fractures when compared to unilateral femur fractures have higher rates of the following EXCEPT:

Explanation
Question 66
Figures below show the radiographs, MRI, and MR arthrogram obtained from a 25-year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy.When counseling patients who have a cam deformity, the orthopaedic surgeon should note that
Explanation
Question 67
Figures below show the radiographs, and the CT obtained from a 58-year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when actively flexing her hip. She has trouble walking up stairs and getting out of her car. What is the most likely diagnosis?

Explanation
Groin pain after total hip replacement has a number of possible causes, and an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated, diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms or in any patient with a metal-on-metal bearing. This patient's symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning are indicated. Fluoroscope-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well positioned, then iliopsoas tenotomy should be considered.
Question 68
A healthy 65-year-old woman undergoes anatomic total shoulder arthroplasty to address osteoarthritis (OA). The surgery is uncomplicated. What is the most common indication for future revision?
Explanation
inflammatory arthritis. Infections, periprosthetic fractures, and rotator cuff tears are uncommon. In the population-based study by Matsen and associates, 10% of the revisions were performed for loosening versus
7% for infection and 7% for rotator cuff tearing.
Question 69
A previously healthy 65-year-old woman has a closed fracture of the right clavicle after falling down the basement stairs. Examination reveals good capillary refill in the digits of her right hand. Radial and ulnar pulses are 1+ at the right wrist compared with 2+ on the opposite side. In the arteriogram shown in Figure 36, the arrow is pointing at which of the following arteries?
Explanation
REFERENCE: Radke HM: Arterial circulation of the upper extremity, in Strandness DE Jr (ed): Collateral Circulation in Clinical Surgery. Philadelphia, PA, WB Saunders, 1969, pp 294-307.
Question 70
A comparison of dural tears repaired with suture alone and those treated by suture with fibrin glue supplementation will reveal which of the following findings?
Explanation
REFERENCES: Cain JE Jr, Rosenthal HG, Broom MJ, Jauch EC, Borek DA, Jacobs RR: Quantification of leakage pressures after durotomy repairs in the canine. Spine 1990;15:969-970.
Cain JE Jr, Dryer RF, Barton BR: Evaluation of dural closure techniques: Suture methods, fibrin adhesive sealant, and cyanoacrylate polymer. Spine 1988;13:720-725.
Question 71
A 14-year-old boy has failed physical therapy management for Scheuermann kyphosis, and an extension thoracolumbosacral orthosis brace is recommended. The boy and his parents are told that the brace will force his thoracic spine into normal sagittal alignment and put the anterior vertebral bodies of the thoracic segment into tension, which will induce bone growth and normalization of wedge-shaped vertebrae. What name is associated with this process?
Explanation
remodels in response to mechanical stress, with the correlate that increased stress causes increased growth, and decreased stress leads to bone loss.
Question 72
-Figures 52c and 52d show the proton density fat-saturated MRI scans. Treatment at this stage includes arthroscopy and
Explanation
This patient’s examination indicates a patellar or peripatellar knee injury. Initial evaluation with radiographs will assess for fracture, subluxation, or osteochondral injury. Examination findings did not demonstrate a need for emergent surgery, an MRI scan, or an ultrasound, so radiographs are the initial diagnostic imaging choice. Radiographs show an osseous or osteochondral loose fragment.
There is no evidence of obvious nondisplaced fracture or physeal changes. In suspected patella dislocation or subluxation with loose fragment seen on radiographs, an MRI scan is indicated. Lateral release alone is seldom indicated in a knee that was normal before injury. Acute proximal realignment has not been shown to alter long-term outcomes for first-time dislocators. The examination and MRI scan did not indicate a need for MCL repair. Closed reduction of the osteochondral fragment would not be indicated or appropriate for this injury. Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed.
Question 73
Etanercept is a recombinant genetically engineered fusion protein used to treat rheumatoid arthritis. What is its mode of action?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowlegde Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 193-199.
Question 74
A year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the
aspiration and proceed to a revision TKA with possible augments on standby.
Question 75
A 62-year-old active man returns for routine follow-up 16 years after hip replacement. He has no hip pain. Radiographs reveal a well-circumscribed osteolytic lesion around a single acetabular screw. All hip components are perfectly positioned. Comparison radiographs obtained 6 months later show an increase in the size of the osteolytic lesion. CT depicts a well-described lesion that is 3 cm at its largest diameter and is localized around one screw hole with an eccentric femoral head. What treatment is appropriate, assuming that well-fixed cementless total hip components are in place?
Explanation
Given a well-fixed acetabular metal shell and a localized osteolytic lesion, good outcomes can be expected from liner revision in this clinical scenario with retention of the metal socket, assuming no damage to the components or other unexpected findings arise during revision surgery. Here, complete cup revision is not warranted, considering the appropriate implant position. Beaulé and associates reviewed 83 consecutive patients (90 hips) in whom a well-fixed acetabular component was retained in a clinical scenario such as the one described. No hip showed recurrence or expansion of periacetabular osteolytic lesions. If the metal cup is unstable, acetabular component revision may be indicated.
Question 76
Which structure is shown in Video 27? 27

Explanation
Video 27 shows the medial patellofemoral ligament running from the medial epicondyle of the femur to the medial portion of the patella. The posterior oblique ligament and the superficial medial collateral ligament run from medial epicondyle to the tibia.
RECOMMENDED READINGS
Babb JR, Detterline AJ, Noyes FR. AAOS Orthopaedic Video Theater. The Key to the Knee: A Layer-by-Layer Video Demonstration of Medial and Anterior Aatomy. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2009.
Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:493-568.
Question 77
What is the most anatomic location for placement of the femoral tunnel in anterior cruciate ligament reconstruction?
Explanation
REFERENCES: Johnson RJ, Beynnon BD, Nichols CE, Renstrom PA: The treatment of injuries of the anterior cruciate ligament. J Bone Joint Surg Am 1992;74:140-151.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
Question 78
Based on the Young and Burgess classification of pelvic ring injuries, an anterior-posterior compression type II injury does not result in disruption of which of the following?

Explanation
well as sacrotuberous and sacrospinous ligaments. An APC III also involves disrupted posterior SI ligaments, causing complete SI joint disruption with potential translational and rotational displacement.
The reference by Young et al is a classic article that describes the Young and Burgess classification of pelvic ring injuries. They retrospectively analyzed pelvic ring radiographs and discussed four patterns of injury: anteroposterior compression, lateral compression, vertical shear, and a complex/combined pattern.
The reference by Burgess et al is a validation of the aforementioned classification and study, as they reviewed 210 consecutive patients who sustained a pelvic ring injury. They validated the classification scheme and found that overall blood replacement averaged: lateral compression, 3.6 units; anteroposterior compression, 14.8 units; vertical shear, 9.2 units; combined mechanical, 8.5 units. Overall mortality was: lateral compression, 7.0%; anteroposterior, 20.0%, vertical shear, 0%; combined mechanical, 18.0%.
Incorrect answers:
1,2,4,5: An APC - 2 pelvic ring injury involves injury to all of these structures.
Question 79
An active 66-year-old man who underwent total shoulder arthroplasty 3 years ago now reports pain. Laboratory studies reveal an elevated erythrocyte sedimentation rate and C-reactive protein. Intraoperative frozen section reveals greater than 10 white blood cells per high power field on two slides and the Gram stain reveals gram-positive cocci in clusters. What is the most appropriate surgical treatment to eradicate the infection and maintain function? Review Topic
Explanation
Question 80
Which of the following methods is effective in correcting recurrent dislocation following total hip arthroplasty?
Explanation
REFERENCES: Woo RY, Morrey BF: Dislocations after total hip arthroplasty. J Bone Joint Surg Am 1982;64:1295-1306.
Goetz DD, Capello WN, Callaghan JJ, Brown TD, Johnston RC: Salvage of a recurrently dislocating total hip prosthesis with use of a constrained acetabular component: A retrospective analysis of fifty-six cases. J Bone Joint Surg Am 1998;80:502-509.
Question 81
What is the most common physical examination finding in a patient with chronic painful spondylolysis? Review Topic
Explanation
Question 82
Figures 22a and 22b show the radiographs of a patient who reports stiffness of the hip and associated pain. Management should consist of
Explanation
REFERENCES: Pellegrini VD Jr, Koniski AA, Gastel JA, Rubin P, Evarts CM: Prevention of heterotopic ossification with irradiation after total hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
Warren SB, Brooker AF Jr: Excision of heterotopic bone followed by irradiation after total hip arthroplasty. J Bone Joint Surg Am 1992;74:201-210.
Question 83
A 14-year-old boy sustains a right leg injury after being thrown from his motorcycle while racing. He reports diffuse right leg pain starting at his knee and proceeding distally to include his foot. After the injury the patient’s mother reports the tibia moving posteriorly then anteriorly while she was supporting the leg. In the emergency department 4 hours after injury, examination reveals a large knee effusion, firm compartments of the leg, a palpable posterior tibialis pulse with a warm, pink foot, and capillary refill of 2 seconds at the toes. His blood pressure is 100/50 mm Hg. Motor examination is intact, but there is decreased sensation in the dorsal first interspace and plantar aspect of the foot. Compartment pressure measurement reveals all four compartments with pressures of 33, 36, 33, and 38 mm Hg respectively. Radiographs are shown in Figure 59a and 59b. The remainder of the skeletal examination is normal. What is the optimal management for this injury?
Explanation
REFERENCE: Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, pp 1057-1061.
Question 84
The illustration shown in Figure 19 shows a Chamberlain line. What is the most likely diagnosis?
Explanation
REFERENCES: Wiesel SW, Rothman RH: Occipito-atlantal hypermobility.
Spine 1979;4:187-191.
Clark CR: The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 50-51.
Question 85
Figure 44 shows the radiograph of an 11-year-old girl who has hip pain. Further diagnostic workup should include
Explanation
REFERENCES: Steel HH: Protrusio acetabuli: Its occurrence in the completely expressed Marfan syndrome and its musculoskeletal component and a procedure to arrest the course of protrusion in the growing pelvis. J Pediatr Orthop 1996;16:704-718.
Wenger DR, Ditkoff TJ, Herring JA, Mauldin DM: Protrusio acetabuli in Marfan’s syndrome. Clin Orthop 1980;147:134-138.
Question 86
When examining a patient with marked hyperreflexia, which of the following findings best suggests that the condition is not caused by a cerivcal spine pathology?
Explanation
REFERENCES: Montgomery DM, Brower RS: Cervical spondylotic myelopathy: Clinical syndrome and natural history. Orthop Clin North Am 1992;23:487-493.
Ono K, Ebara S, Fuji T, Yonenobu K, Fujiwara K, Yamashita K: Myelopathy hand: New clinical signs of cervical cord damage. J Bone Joint Surg Br 1987;69:215-219.
An HS, Simpson JM: Surgery of the Cervical Spine. Baltimore, MD, Williams and
Wilkins, 1994.
Question 87
During total knee arthroplasty, the patella is noted to subluxate laterally despite a lateral retinacular release. Which of the following methods is most likely to improve patellar stability?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 207, 323-337
Pagnano MW, Trousdale RT, Stuart MJ, et al: Rotating platform knees did not improve patellar tracking: A prospective, randomized study of 240 primary total knee arthroplasties. Clin Orthop 2004;428:221-227.
Lotke PA, Garino JP (eds): Revision Total Knee Arthroplasty. Philadelphia PA, Lippincott-Raven, 1999, pp 427-435.
Question 88
A 63-year-old man with type I diabetes mellitus who underwent open forefoot amputation now has a high fever, and an elevated WBC count and blood glucose levels. Repeat laboratory studies the day after surgery show a WBC count of 9,500/mm 3 , a serum albumin level of 1.9 g/dL, and a total lymphocyte count of 1,900/mm 3 . Examination reveals that he is afebrile, and his blood glucose level is now normal. An ultrasound Doppler of the dorsalis pedis artery shows an ankle-brachial index of 0.6. A transcutaneous partial pressure measurement of oxygen at the ankle joint shows a level of 38 mm Hg. What is the best course of action?
Explanation
REFERENCE: Pinzur MS, Stuck RM, Sage R, et al: Syme ankle disarticulation in patients with diabetes. J Bone Joint Surg Am 2003;85:1667-1672.
Question 89
- Which of the following acetabular/femoral head components would be expected to show an optimal combination of linear and volumetric wear?
Explanation
Question 90
-The patient experienced little improvement with activity modification and physical therapy. An intraarticular corticosteroid injection provides excellent but short-lived pain control. She requests surgical treatment for her hip and she is counseled regarding arthroscopy and consent is obtained. Intraoperatively,a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. What treatment is most appropriate considering these findings?
Explanation
The clinical scenario, examination, and MRI scans are consistent with a pincer-type FAI. The decreased range of motion is secondary to the pain produced by the continued abutment of the femoral head against the anterosuperior acetabulum. Flexing the hip while internally rotating and adducting the leg recreates this contact and is typically painful. No clinical signs suggest sacroiliac joint arthritis, an intra-articular loose body, or trochanteric bursitis, although these are all diagnoses that should be considered in a patient with a painful hip. The most sensitive and specific study to detect an acetabular labral tear is an MRI arthrogram of the hip. This study should be obtained in this patient to evaluate the labrum as well as the status of the articular cartilage. An MRI scan without intra-articular contrast is not as sensitive as an arthrogram. An ultrasound can provide a dynamic assessment of the hip and help in the setting of a snapping hip; however, this study is not reliable to determine the presence of a labral tear. In the setting of pincer FAI, the forced leverage of the anterosuperior femoral head upon the anterior acetabulum results in abnormal forces against the posteroinferior acetabulum. This continued force can lead to a chondral lesion in this location know as a “counter-coup” injury. Chondral lesions of the femoral head are rare in the setting of pincer FAI. The posterosuperior quadrant does not experience increased force and rarely sustains chondral injuries. The patient is a young, active individual with no pre-existing degenerative changes, so repair of the tear with bony resection of the pincer lesion is the most appropriate treatment.A capsulolabral detachment should be repaired because these tears can heal and the labrum functions as a seal, preventing egress of synovial fluid from the joint space. If the pincer lesion is not resected, the patient will continue to experience abnormal contact and the repair will likely fail. There is no evidence that the patient has a cam impingement, and recontouring of the femoral head/neck junction is not appropriate. Simple debridement should be reserved for intrasubstance tears of the labrum, which would not be expected to heal with repair.
CLINICAL SITUATION FOR QUESTIONS 30 THROUGH 32
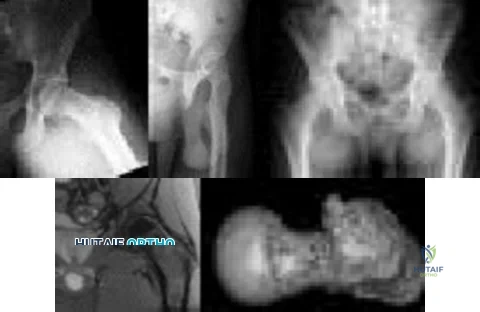
Figures 30a and 30b are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he
believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg.


Question 91
A 30-year-old man has had intermittent swelling of his right ankle for the past 6 months. He denies any history of trauma. Radiographs reveal osteolytic changes on both sides of the joint. An axial CT scan and a T 2 -weighted MRI scan are shown in Figures 40a and 40b. He undergoes surgical excision. An intraoperative photograph and a biopsy specimen are shown in Figures 40c and 40d. What is the most likely diagnosis?
Explanation
REFERENCES: Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Simon M, Springfield D: Surgery for the Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 36.
Question 92
A 43-year-old bus driver sustains a hyperextension injury to her arm and shoulder 4 months after undergoing an open Bankart repair. Examination reveals increased external rotation, anterior shoulder pain, and internal rotation weakness. Her examination also reveals the findings shown in Figure 44. What is the most likely diagnosis?
Explanation
REFERENCES: Hertel R, Ballmer FT, Lombert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313.
Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 93
When do most symptomatic thromboembolic events occur after total joint arthroplasty?
Explanation
Most clinical venous thromboembolism events occur between the second and sixth weeks after surgery. It is estimated that 10% of patients are readmitted to the hospital within the first 3 months after total hip or knee arthroplasties. Most pulmonary events on the day of surgery are related to fat embolism or cardiac events.
Question 94
Which of the following tumors is most likely to present with a pathologic fracture in a child?
Explanation
REFERENCES: Wilkins RM: Unicameral bone cysts. J Am Acad Orthop Surg 2000;8:217-224.
Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Hecht AC, Gebhardt MC: Diagnosis and treatment of unicameral and aneurysmal bone cysts in children. Curr Opin Pediatr 1998;10:87-94.
Question 95
A skeletally mature 15-year-old girl who was thrown from the car in a rollover accident sustained the injuries shown in Figures 23a through 23d. Examination reveals no neurologic deficit, but the patient has moderate posterior spinal tenderness at the level of the injury. What is the most appropriate treatment?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Chow GH, Nelson BJ, Gebhard JS, Brugman JL, Brown CW, Donaldson DH: Functional outcome of thoracolumbar burst fractures managed with hyperextension casting or bracing and early mobilization. Spine 1996;21:2170-2175.
Question 96
Which of the following complications is more likely with an inside-out repair technique compared to an all-inside techniques for a medial meniscus tear? Review Topic
Explanation
Question 97
It has been shown that bisphosphonate-based supportive therapy (pamidronate or zoledronate) reduces skeletal events (onset or progression of osteolytic lesions) both in patients with multiple myeloma and in cancer patients with bone metastasis. The use of biphosphonate therapy has been associated with
Explanation
REFERENCES: Bamias A, Kastritis E, Bamia C, et al: Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: Incidence and risk factors. J Clin Oncol 2005;23:8580-8587.
Thakkar SG, Isada C, Smith J, et al: Jaw complications associated with bisphosphonate use in patients with plasma cell dyscrasias. Med Oncol 2006;23:51-56.
Van Poznak C: The phenomenon of osteonecrosis of the jaw in patients with metastatic breast cancer. Cancer Invest 2006;24:110-112.
Question 98
Figure 7 shows the radiograph of a 64-year-old man who has neck pain and weakness of the upper and lower extremities following a motor vehicle accident. Examination reveals 3/5 quadriceps and 4/5 hip flexors but no ankle dorsiflexion or plantar flexion. His intrinsics are 1/5, with finger flexors of 3/5. He is awake, alert, and cooperative. Management should consist of
Explanation
open reduction.
REFERENCES: Star AM, Jones AA, Cotler JM, et al: Immediate closed reduction of cervical spine dislocations using traction. Spine 1990;15:1068-1072.
Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocations using traction weight up to 140 pounds. Spine 1993;18:386-390.
Question 99
-Figure 162 is the CT scan of a 74-year-old woman who struck her head during a ground-level fall and has severe neck pain. Examination reveals normal strength and sensation in her upper and lower extremities.What is the most appropriate treatment option?

Explanation

Question 100
An 18-year-old man sustained a traumatic laceration of the common peroneal nerve when glass fell on the outer part of his leg 1 year ago. He has used a molded foot and ankle orthosis for the past 10 months, but would now like surgical intervention. Electromyography shows no function in the anterior or lateral compartments. He has 5/5 muscle strength of the superficial and deep posterior compartments. What is the most appropriate treatment?
Explanation
hallucis longus tendon transfer would not take the deforming force and make it a corrective force.
