Orthopedic Surgery Board Review MCQs: Trauma, Sports Medicine & Nerve | Part 57

Key Takeaway
This page offers Part 57 of a comprehensive OITE and AAOS Orthopedic Surgery Board Review series. It provides 100 high-yield, verified multiple-choice questions (MCQs) for orthopedic surgeons and residents preparing for their board certification exams. Utilize interactive study and exam modes to enhance your clinical knowledge and test readiness.
About This Board Review Set
This is Part 57 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 57
This module focuses heavily on: Ankle, Elbow, Fracture, Ligament, Nerve.
Sample Questions from This Set
Sample Question 1: A professional pitcher reports pain localized to the medial aspect of his throwing elbow. History reveals that he was pitching in a playoff game and heard and felt a pop in his elbow. MRI reveals a complete ulnar-sided avulsion of the media...
Sample Question 2: -The lateral fragment of bone (Segond fracture) associated with an injury of the anterior cruciate ligament is the result of an avulsion of the...
Sample Question 3: Figures 20a and 20b are the radiographs of a 19-year-old woman who was involved in a motor vehicle accident. What mechanism of injury is most consistent with the injury?...
Sample Question 4: A 16-year-old female dancer has persistent posterior ankle pain, particularly after a vigorous dancing schedule. Examination reveals tenderness both posteromedially and posterolaterally. MRI scans are seen in Figures 44a and 44b. What is th...
Sample Question 5: A patient reports hyperesthesia over the base of the thenar eminence following volar locked plating of a distal radius fracture. A standard volar approach of Henry was used. What is the most likely cause of the hyperesthesia?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A professional pitcher reports pain localized to the medial aspect of his throwing elbow. History reveals that he was pitching in a playoff game and heard and felt a pop in his elbow. MRI reveals a complete ulnar-sided avulsion of the medial collateral ligament (MCL). Examination reveals valgus instability and ulnar nerve involvement. What recommendations should be made based on the patient’s desire to return to sport?
Explanation
REFERENCES: Miller MD, Cooper DE, Warner JJP (eds): Review of Sports Medicine and Arthroscopy. Philadelphia, PA, WB Saunders, 1995, p 230.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, p 227.
Altchek DW, Andrews JR (eds): The Athlete’s Elbow. Philadelphia, PA, Lippincott Williams
& Wilkins, 2001, p 91.
Question 2
- The lateral fragment of bone (Segond fracture) associated with an injury of the anterior cruciate ligament is the result of an avulsion of the
Explanation
Question 3
Figures 20a and 20b are the radiographs of a 19-year-old woman who was involved in a motor vehicle accident. What mechanism of injury is most consistent with the injury?

Explanation
Question 4
A 16-year-old female dancer has persistent posterior ankle pain, particularly after a vigorous dancing schedule. Examination reveals tenderness both posteromedially and posterolaterally. MRI scans are seen in Figures 44a and 44b. What is the most likely diagnosis?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont IL, American Academy of Orthopaedic Surgeons, 1998, pp 315-332.
Hamilton WG, Hamilton LH: Foot and ankle injuries in dancers, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1225-1256.
Question 5
A patient reports hyperesthesia over the base of the thenar eminence following volar locked plating of a distal radius fracture. A standard volar approach of Henry was used. What is the most likely cause of the hyperesthesia?
Explanation
REFERENCES: Jupiter JB, Fernandez DL, Toh CL, et al: Operative treatment of volar intra-articular fractures of the distal end of the radius. J Bone Joint Surg Am 1996;78:1817-1828.
Hoppenfield S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, JB Lippincott, 1994, pp 156-176.
Question 6
A 36-year-old skier sustains a grade III posterior cruciate ligament (PCL) tear. Where will increased contact pressures develop over time?
Explanation
REFERENCE: Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 767.
Question 7
What approach should be chosen for the injury seen in Figure 67? Review Topic

Explanation
Innervates the medial aspect of the proximal thigh
Originates from the dorsal roots of L4-L5
Course runs medial to the femoral artery
Courses along the medial border of the psoas muscle
Courses under the inguinal ligament PREFERRED RESPONSE 5
Question 8
A 20-year-old college athlete is seen for follow-up after sustaining an injury at football practice 2 days ago. He reports that he tackled a player and felt neck pain and numbness in both arms. The numbness resolved within seconds, but his neck remains painful and stiff. He denies any history of neck pain or injury. Examination reveals limited neck motion. The neurologic examination and radiographs are normal. MRI scans of the cervical spine are shown in Figure 34. During counseling, the patient, his family, and his coach should be informed that he has an acute cervical disk herniation and cannot play
Explanation
REFERENCES: Morganti C, Sweeney CA, Albanese SA, Burak C, Hosea T, Connolly PJ: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Vaccaro AR, Watkins B, Albert TJ, Pfaff WL, Klein GR, Silber JS: Cervical spine injuries in athletes: Current return-to-play criteria. Orthopedics 2001;24:699-705.
Question 9
Which factor increases the success rate associated with all-inside lateral meniscal repair?
Explanation
Decreased patient age, neutral alignment, and a concomitant ACL tear are associated with improved success rates of meniscal repair. Meniscus tears on the contralateral side of the knee and articular cartilage defects are not associated with improved healing rates.
RESPONSES FOR QUESTIONS 5 THROUGH 6
Physical therapy and a home exercise program
Corticosteroid injection
Arthroscopic debridement
Microfracture
Osteochondral autograft transplantation (OAT)
Match the treatment above with the clinical scenario below
Question 10
A 56-year-old man has a chief complaint of leg weakness and inability to walk. Examination reveals 5 out of 5 motor strength in all lower extremity muscle groups tested and normal sensation to light touch in both lower extremities. The patient is slow in getting up from a seated position and has an unsteady wide-based

Explanation
Question 11
According to clinical and biomechanical studies, the most appropriate position for a headless scaphoid compression screw for repair of a scaphoid waist fracture is
Explanation
The position of a scaphoid screw for scaphoid fracture repair (Figure 1) is as critical as the position of a sliding hip screw for intertrochanteric fracture repair. Positioning the screw deep in the center of the densest portion of cancellous bone is beneficial for both of these fracture types.Trumble and associates have shown time to union for scaphoid nonunions to be decreased for centrally placed scaphoid screws. McCallister and associates documented improved biomechanical stability for scaphoid waist fractures repaired with a centrally placed screw vs an eccentrically placed screw. Dodds and associates

demonstrated significantly improved biomechanical stability with centrally placed long screws vs centrally placed short screws. The screw may be placed retrograde or antegrade. Although the screw position may be relatively parallel to the radial inclination as the shape of the scaphoid body follows the contour of the radial styloid, screw position should be assessed relative to the scaphoid’s own architecture. Placing the screw in a retrograde fashion can force the treating surgeon to start the screw eccentrically in an attempt to avoid the interference of the trapezium lying over the distal pole of the scaphoid. This may result in noncentral screw placement.
Question 12
A 45-year-old man falls from a skateboard and dislocates his elbow. After a closed reduction in the emergency department, his elbow is carefully examined. He has positive valgus stress, moving valgus stress, and milking maneuver tests. His elbow appears stable to varus stress and lateral pivot shift tests. What is the most appropriate manner of immobilizing the elbow for this patient?
Explanation
forearm should be splinted in full supination.
Question 13
-The patient requests anatomic double-bundle ACL reconstruction. Compared with transtibial singlebundle ACL reconstruction, anatomic double-bundle ACL reconstruction is more likely to
Explanation
The radiograph shows a Segond fracture, an avulsion fracture involving the lateral capsular ligament.
This radiographic finding has been associated with ACL rupture in 75% to 100% of cases. Drilling the femoral tunnel through the anteromedial portal allows for independent access to the native femoral attachment. Fiber orientation is more oblique than with a transtibial technique and more closely resembles that of the native ligament. Double-bundle reconstruction attempts to duplicate native ACL anatomy.Biomechanical studies have shown that double-bundle reconstruction more
closely reproduces normal knee kinematics; however, this technique does not offer a clear advantage in terms of clinical outcomes.The iliotibial band inserts onto Gerdy’s tubercle. The popliteus tendon originates from the lateral femoral condyle. The lateral meniscus attaches near the intercondylar eminence at the anterior and posterior meniscal roots. Recent advances in ACL reconstruction focus on restoring the native ACL anatomy.Studies have determined that a knee flexion angle of 110 degrees is optimal to avoid blowout of the back wall and injury to the lateral structures while drilling.
Femoral tunnel length is typically shorter than with a transtibial approach and decreases with higher-flexion angles. Double-bundle reconstruction is associated with higher surgical costs because of the need for additional fixation and, in the case of allograft reconstruction, a second graft.
Question 14
A 35-year-old woman began to train for a half marathon. After 8 weeks of increasing her mileage, what changes can you expect in her Achilles tendon?
Explanation
Question 15
A 19-year-old linebacker for a collegiate football team has had two episodes of bilateral arm tingling and weakness after tackling; the symptoms resolved after 30 minutes of rest. Three follow-up neurologic examinations have been normal. Cervical spine CT and MRI scans are shown in Figures 13a through 13c. What is the next best step in management?
Explanation
REFERENCES: Torg JS, Naranja RJ Jr, Pavlov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Cantu RC: The cervical spinal stenosis controversy. Clin Sports Med 1998;17:121-126. Crowl AC, Kong JF: Cervical Spine, in Johnson DL, Mair SD (eds): Clinical Sports Medicine. Philadelphia, PA, Mosby Elsevier, 2006, pp 143-149.
Question 16
A 13-year-old boy injured his knee playing basketball and is now unable to bear weight. Examination reveals tenderness and swelling at the proximal anterior tibia, with a normal neurologic examination. AP and lateral radiographs are shown in Figures 1a and 1b. Management should consist of
Explanation
REFERENCES: McKoy BE, Stanitski CL: Acute tibial tubercle avulsion fractures. Orthop Clin North Am 2003;34:397-403.
Zionts LE: Fractures around the knee in children. J Am Acad Orthop Surg 2002;10:345-355.
Question 17
-Images from an MRI scan of this patient’s left hip are shown in Figure 30c through 30e. What is the most likely cause of his acute pain?
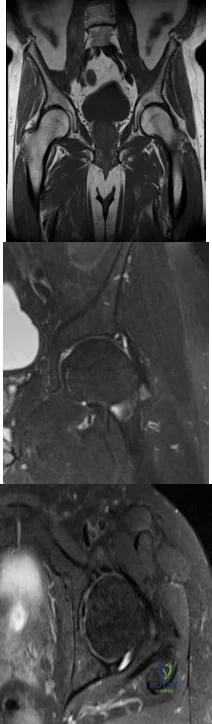
Explanation
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement.Surgical treatment for cam impingement can be effective for symptomatic patients. Even among highlevel athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable to those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment.Byrd and Jones described 5 patients who developed transient neurapraxias that resolved uneventfully.The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a periacetabular osteotomy can develop a more retroverted acetabulum as well.
Question 18
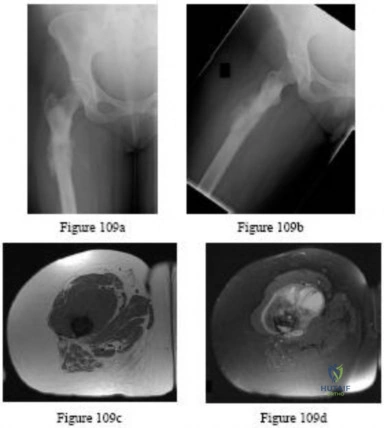
A 43-year-old man has had right groin pain for the past 3 months. A radiograph, CT scan, and biopsy specimen are shown in Figures 18a through 18c. What is the most likely diagnosis?
Explanation
REFERENCES: Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 71-92.
Question 19
A 35-year-old active woman with rheumatoid arthritis experiences right shoulder pain following an extended course of corticosteroids (Figures 96a and 96b).

Explanation
The indication for anatomic TSA is end-stage glenohumeral arthritis with an intact rotator cuff. For the 62-year-old man, his radiographs reveal osteoarthritis, and his MR image shows an intact rotator cuff. Although humeral head replacement has historically been employed for this disorder, pain relief is not as reliable as with TSA, and the revision rate is higher. rTSA is generally reserved for patients with a nonfunctional rotator cuff.
For this 58-year-old patient with a full-thickness rotator cuff tear, preserved motion, and weakness in forward elevation, a rotator cuff repair is the most appropriate treatment. In the absence of degenerative changes, shoulder hemiarthroplasty or anatomic TSA is not indicated. Although indications for rTSA continue to evolve, well-compensated range of motion and a medium-sized rotator cuff tear in a younger patient are not among them.
rTSA is an emerging treatment for comminuted proximal humerus fractures in elderly patients. Although hemiarthroplasty has been a traditional treatment, current evidence suggests rTSA more reliably restores range of motion, and this 78-year-old patient's CT scan shows a small and comminuted greater tuberosity fragment that is unlikely to heal. ORIF is another option, but the CT scan also shows a small humeral head fragment that suggests osteopenia, making fixation more tenuous and likely less reliable.
A common problem associated with hemiarthroplasty for glenohumeral osteoarthritis is symptomatic glenoid degeneration that necessitates revision. This 55-year-old patient’s images reveal this is the case, although his infection workup is negative. His examination findings suggest an intact subscapularis repair. With a functioning rotator cuff and symptomatic glenoid arthritis, a conversion to anatomic TSA is indicated. In the absence of a functioning rotator cuff in an older patient, an rTSA is a better option.
This 72-year-old patient has classic symptoms and radiographs of cuff tear arthropathy. For patients with massive rotator cuff tear and glenohumeral arthritis, neither anatomic TSA nor rotator cuff repair is indicated. Hemiarthroplasty has historically been indicated for cuff tear arthropathy, but rTSA outcomes for this disorder have been superior and are now the preferred option.
Comminuted proximal humerus fractures in young, active patients are treated primarily with ORIF. The absence of glenohumeral arthritis removes anatomic TSA as a possibility, and concerns about implant longevity in younger, active patients such as this 40-year-old laborer contraindicate rTSA. Hemiarthroplasty is still employed in 3- and 4-part fractures but is generally reserved for subacute presentations or dislocations in which the humeral head is dysvascular and unlikely to survive. In this acute setting, a fixation procedure is preferred.
The 71-year-old patient who has had 2 failed rotator cuff repairs has an MR image that reveals another recurrent tear that is retracted to the glenoid. Her examination findings reveal classic signs
of a decompensated rotator cuff tear with pseudoparalysis and weakness in forward elevation. Although infection is a concern in the setting of multiply failed rotator cuff repair, the workup is negative in this scenario. Because this patient has a dysfunctional rotator cuff and has failed previous attempts at repair, a conversion to rTSA is the better option. In the absence of degenerative changes, hemiarthroplasty and anatomic TSA are not indicated.
The indications for hemiarthroplasty continue to narrow, but it is still a consideration for young patients with unipolar shoulder degeneration. In this 35-year-old patient, her MR image shows avascular necrosis in the humeral head, and her arthroscopy suggests arthritic change only on the humeral side with an uncompromised glenoid. To best treat young and active patients, a hemiarthroplasty that articulates with healthy glenoid cartilage can provide good pain relief and functional outcomes. Anatomic TSA is also reasonable but not an optimal option considering the normal glenoid condition. rTSA is not a consideration when a young patient’s MR images reveal an intact rotator cuff.
RECOMMENDED READINGS
Torchia ME, Cofield RH, Settergren CR. Total shoulder arthroplasty with the Neer prosthesis: longterm results. J Shoulder Elbow Surg. 1997 Nov-Dec;6(6):495-505. PubMed PMID: 9437598. View Abstract at PubMed
Chalmers PN, Slikker W 3rd, Mall NA, Gupta AK, Rahman Z, Enriquez D, Nicholson GP. Reverse total shoulder arthroplasty for acute proximal humeral fracture: comparison to open reduction-internal fixation and hemiarthroplasty. J Shoulder Elbow Surg. 2014 Feb;23(2):197-204. doi: 10.1016/j.jse.2013.07.044. Epub 2013 Sep 27. PubMed PMID: 24076000. View Abstract at PubMed
Groh GI, Wirth MA. Results of revision from hemiarthroplasty to total shoulder arthroplasty utilizing modular component systems. J Shoulder Elbow Surg. 2011 Jul;20(5):778-82. doi: 10.1016/j.jse.2010.09.014. Epub 2011 Jan 13. PubMed PMID: 21232989. View Abstract at PubMed
Orfaly RM, Rockwood CA Jr, Esenyel CZ, Wirth MA. Shoulder arthroplasty in cases with avascular necrosis of the humeral head. J Shoulder Elbow Surg. 2007 May-Jun;16(3 Suppl):S27-32. Epub 2006 Nov 16. PubMed PMID: 17113317. View Abstract at PubMed
Sershon RA, Van Thiel GS, Lin EC, McGill KC, Cole BJ, Verma NN, Romeo AA, Nicholson GP. Clinical outcomes of reverse total shoulder arthroplasty in patients aged younger than 60 years. J Shoulder Elbow Surg. 2014 Mar;23(3):395-400. doi: 10.1016/j.jse.2013.07.047. Epub 2013 Oct 12. PubMed PMID: 24129052. View Abstract at PubMed
Question 20
Figure 10 shows the MRI scan of a 56-year-old woman with metastatic breast cancer who now reports progressive paraparesis. Her general health remains good. Treatment should consist of
Explanation
REFERENCE: Fardin DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 123-133.
Question 21
During spinal deformity surgery, which of the following is the most specific early indicator of an intraoperative injury to the spinal cord? Review Topic
Explanation
Question 22
An increase in advanced glycation end-products (AGEs) is characteristic of which of the following clinical conditions and results in which pathologic process?
Explanation
AGEs are produced from spontaneous nonenzymatic glycation of proteins when sugars (glucose, fructose, ribose) react with lysine or arginine residues. Because of the low turnover, cartilage is susceptible to AGEs accumulation. The accumulation of AGEs has been thought to play a role in the development of OA of the knee and ankle.
Li et al. reviewed age-related changes in cartilage. They state that with aging, there is excessive collagen cross-linking increases cartilage stiffness, while shortening/degradation of aggrecan leads to loss of sugar side chains and water-binding ability, while increased levels of AGEs are associated with a decline in anabolic activity. There is also increased chondrocyte death and/or apoptosis.
Anderson et al. reviewed the relationship between osteoarthritis and aging. They state that knee cartilage thins with aging (especially on the femoral and patellar sides, suggesting a gradual loss of cartilage matrix. AGEs formation leads to modification of type II collagen by cross-linking of collagen molecules, increasing stiffness and brittleness and increasing susceptibility to fatigue failure.
Incorrect Answers:
Question 23
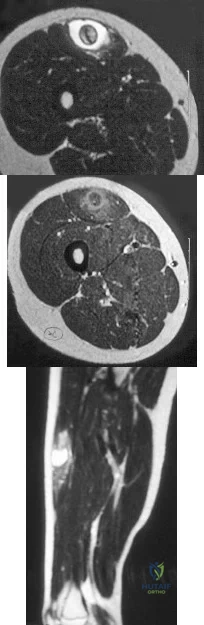
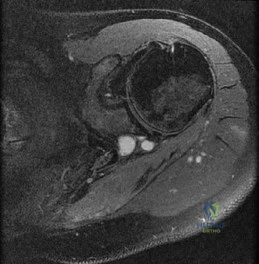
Figures 24a through 24c show the coronal T 1 -weighted, T 2 -weighted fat-saturated, and T 1 -weighted fat-saturated gadolinium MRI scans of the proximal thigh of a 52-year-old woman who reports a mass in the medial thigh and groin area. She notes that the fullness has grown in size over the course of many months. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCE: Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 24
Lipohemarthrosis of the knee is most likely secondary to which of the following?

Explanation
Question 25
Embolic material generated during total knee arthroplasty (TKA) shown in Figure 29 is composed of which of the following substances?
Explanation
REFERENCES: Markel DC, Femino JE, Farkas P, et al: Analysis of lower extremity embolic material after total knee arthroplasty in a canine model. J Arthroplasty 1999;14:227-232.
Pell AC, Christie J, Keating JF, et al: The detection of fat embolism by transoesophageal echocardiography during reamed intramedullary nailing: A study of 24 patients with femoral and tibial fractures. J Bone Joint Surg Br 1993;75:921-925.
McGrath BJ, Hsia J, Boyd A, et al: Venous embolization after deflation of lower extremity tourniquets. Anesth Analg 1994;78:349-353.
Question 26
A patient has multidirectional instability of the shoulder that has not responded to nonsurgical management. Successful surgical treatment will most likely include which of the following? Review Topic
Explanation
instability treated surgically following failure to respond to nonsurgical management has been shown to be associated with classic Bankart lesions, Hill-Sachs defects, glenoid chondral lesions, and even SLAP lesions (Werner). However, these lesions were seen in a lower percentage than that found for unidirectional anterior dislocations. Likewise, these lesions do not appear to be significant in influencing treatment in the majority of patients.
Question 27
A 72-year-old female sustains a displaced intracapsular femoral neck fracture. Which of the following is TRUE regarding the long term differences between possible treatment options for this injury?
Explanation
Intracapsular FNF are common in elderly patients after a fall from standing height. Treatment depends on physiological age and displacement (Garden's classification). For displaced fractures, physiologically young patients are treated with internal fixation while physiologically old patients are treated with either hemiarthroplasty (debilitated, less active patients) or THA (more active patients, those with acetabular
disease or preexisting inflammatory arthritis).
Chammout et al. retrospectively compared the long term (17 years) results of THA (cemented both component) and ORIF (2 cannulated screws) in elderly patients (>65 years). They found no difference in mortality. But hip scores were higher and pain was better in the THA group, while reoperation rates were higher in the ORIF group. Walking speed was initially faster in the THA group, but later did not differ between groups. They recommend THA for elderly patients with displaced FNF.
Rogmark et al. prospectively compared closed reduction and internal fixation (CRIF) with arthroplasty (combining hemiarthroplasty and THA) at 2 years in elderly patients (>70 years). Failure rates were higher, pain was worse, and walking was more impaired after CRIF. They recommend arthroplasty for patients >70 with FNF.
Question 28
Up to what time frame are the risks minimized in anterior revision disk replacement surgery? Review Topic
Explanation
Question 29
A 31-year-old man sustained a closed injury to his arm in a motor vehicle accident 16 months ago. Treatment of the fracture consisted of intramedullary nailing of the humerus. He now reports pain with minimal activities. Clinical examination and laboratory studies suggest no signs of infection. Radiographs are seen in Figures 12a through 12c. Treatment should now consist of
Explanation
REFERENCES: Zuckerman J, Giordanno C, Rosen H: Treatment of humeral shaft non-unions, in Bigliani L (ed): Complications of shoulder surgery. Baltimore, MD, William & Wilkins, 1993, pp 173-190.
Jupiter JB: Complex non-union of the humeral diaphysis: Treatment with a medial approach,
an anterior plate, and a vascularized fibular graft. J Bone Joint Surg Am 1990;72:701-707.
Question 30
A 12-year-old male sustains a ulnar fracture with an associated posterior-lateral radial head dislocation. After undergoing closed reduction, the radiocapitellar joint is noted to remain non-concentric. What is the most likely finding?

Explanation
Question 31
Examination of a 6-year-old boy who sustained a displaced Salter-Harris type II fracture of the distal radius reveals 35 degrees of volar angulation. A satisfactory reduction is obtained with the aid of a hematoma block. At the 10-day follow-up examination, radiographs show loss of reduction and 35 degrees of volar angulation. Management should now consist of
Explanation
be damaged.
REFERENCES: Dimeglio A: Growth in pediatric orthopaedics, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 33-62.
Waters PM: Forearm and wrist fractures, in Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 251-258.
Question 32
A 69-year-old man sustains a traumatic amputation to the distal phalanx of his little finger while working with power tools. Radiographs are shown in Figures 27a and 27b. The patient was instructed how to perform wet-to-dry dressing changes in the emergency department. Clinical pictures taken in the office are shown in Figures 27c through 27e. What is the most appropriate management of this soft-tissue wound?
Explanation
REFERENCES: Jebson PL, Louis DS: Amputations, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 1947.
Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Question 33
Osteonecrosis of the femoral head after intramedullary nailing in children is thought to be the result of injury to the
Explanation
REFERENCES: Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop 1997;338:60-73.
Rockwood CA, Wilkins KE, Beaty JH: Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, p 1214.
Question 34
Figures below show the radiographs obtained from a 19-year-old woman with a 3-year history of progressive hip pain in the left groin with activity, which is unresponsive to activity modification and physical therapy. Examination reveals normal range of motion, with pain on anterior impingement testing. What treatment is associated with the best long-term results?

Explanation
This patient has symptomatic femoroacetabular impingement as well as clinical and radiographic signs of acetabular retroversion, including a cross-over sign, ischial spine sign, and posterior wall sign bilaterally. Good midterm to long-term outcomes have been reported with reverse (anteverting) Bernese periacetabular osteotomy (PAO). In patients with less retroversion, open or arthroscopic rim trimming with labral refixation have shown good short-term results, but longer-term results have yet to be fully delineated. Isolated hip arthroscopy and labral repair would not be indicated without addressing the retroversion deformity. Femoral varus rotational osteotomy plays no role in the treatment of this pathology. Open surgical dislocation with rim trimming could be considered in patients with less deformity, but some studies have shown inferior long-term results compared with reverse PAO.
Question 35
A 32-year-old motorcycle rider is involved in a motor vehicle accident and radiographs show a burst fracture at L2 with 20 degrees of kyphosis. The neurologic examination is consistent with unilateral motor and sensory involvement of the L5, S1, S2, S3, and S4 nerve roots. He has no other injuries. CT demonstrates 20% anterior canal compromise with displaced laminar fractures at the level of injury. What is the best option for management of this patient? Review Topic
Explanation
Question 36
Patients with which of the following primary carcinomas have the shortest overall survival rate after a solitary metastasis to bone?
Explanation
REFERENCE: CA, January/February 2000, vol 50, no. 1 (Cancer Statistics).
Question 37
A 56-year-old man who underwent a left total hip arthroplasty 8 years ago is seen following a fall from a standing height. A radiograph obtained at 2 years postoperatively is shown in Figure 55a and a current radiograph obtained in the emergency department is shown in Figure 55b. On further questioning, he reports pain in this thigh for the past 3 years that has been increasing in intensity. Appropriate management at this time includes which of the following?
Explanation
REFERENCES: Masri BA, Meek RM, Duncan CP: Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res 2004;420:80-95.
Springer BD, Berry DJ, Lewallen DB: Treatment of periprosthetic femoral fractures following total hip
arthroplasty with femoral component revision. J Bone Joint Surg Am 2003;85:2156-2162. Question 56
A 62-year-old woman who underwent a primary total knee arthroplasty under a combined spinal-epidural anesthetic presents 5 hours postoperatively with severe pain in the extremity that is unresponsive to narcotic pain medication. A tourniquet was used during the procedure. On examination, the patient is unable to dorsiflex or plantar flex the foot and the pulses appear to be asymmetric. What is the next most appropriate step in management?
Discontinuation of the epidural and serial neurologic exams
Loosening of the surgical bandages and elevation of the extremity
MRI of the spine to evaluate for an epidural hematoma
Return to the operating room for angiography and vascular bypass
Return to the operating room for angiography, vascular bypass, and four-compartment fasciotomy PREFERRED RESPONSE: 5
DISCUSSION: The patient has clinical evidence of vascular injury and compartment syndrome. An emergent
vascular consult and a return to the operating room for an angiogram and revascularization are needed. In these situations, thrombectomy alone is often not sufficient and a bypass is typically required. A four-compartment fasciotomy should be done following revascularization of the extremity.
REFERENCES: Calligaro KD, Dougherty MJ, Ryan S, et al: Acute arterial complications associated with total hip and knee arthroplasty. J Vase Surg 2003;38:1170-1177.
Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001;9:253-257.
Ninomiya JT, Dean JC, Goldberg VM: Injury to the popliteal artery and its anatomic location in total knee
arthroplasty. J Arthroplasty 1999;14:803-809.
Question 38
A 42-year-old college professor reports persistent pain at the hypothenar eminence 9 months after falling from his bicycle. Initial radiographs were reportedly normal. Use of a wrist splint for the last 2 months has failed to provide relief. A radiograph obtained by his primary care physician prior to referral is seen in Figure 31. What is the most appropriate treatment?
Explanation
REFERENCE: Fleege MA, Jebson PJ, Renfrew DL, et al: Pisiform fractures. Skeletal Radiol 1991;20:169-172.
Question 39
- Which of the following conditions associated with a closed fracture of the clavicle indicates the need for open reduction and internal fixation?
Explanation
Question 40
A 32-year-old man sustains a forceful inversion injury while playing soccer. Examination reveals tenderness in the lateral hindfoot and midfoot region with associated ecchymosis and swelling. Radiographs show proximal migration of the os peroneum. Active eversion is still present. These findings indicate disruption of the
Explanation
REFERENCES: Thompson FM, Patterson AH: Rupture of the peroneus longus tendon: Report of three cases. J Bone Joint Surg Am 1989;71:293-295.
Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1090-1209.
Question 41
An eversion mechanism of injury is associated with which of the following ankle conditions?
Explanation
REFERENCES: Casillas MM: Ligament injuries of the foot and ankle in the athlete, in DeLee JC, Drez D, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2323-2357.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 233-245.
Question 42
A baseball player has had diffuse scapular soreness for the past 8 weeks. He reports that it began insidiously over several days and gradually has become worse. He denies any history of trauma. Examination reveals drooping of the shoulder, with lateral winging of the scapula at rest. He is otherwise neurologically intact. What is the best course of action?
Explanation
REFERENCES: Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop 1999;368:5-16.
Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop 1999;368:17-27.
Mariani PP, Santoriello P, Maresca G: Spontaneous accessory nerve palsy. J Shoulder Elbow Surg 1998;7:545-546.
Porter P, Fernandez GN: Stretch-induced spinal accessory nerve palsy: A case report. J Shoulder Elbow Surg 2001;10:92-94.
Cohn BT, Brahms MA, Cohn M: Injury to the eleventh cranial nerve in a high school wrestler. Orthop Rev 1986;15:59-64.
Question 43
78A B Figures 78a and 78b are the emergency department radiographs of an 83-year-old woman who tripped and braced herself against a wall; this was followed by shoulder pain. Which intervention would provide optimal treatment for this patient?

Explanation
Low-energy fractures in elderly patients typically are treated with nonsurgical care that involves early immobilization followed by early rehabilitation/therapy, especially when proximal humerus and distal humerus fractures are involved. Physical therapy should be initiated within the first 2 weeks. If surgery is needed ORIF is preferred for most fractures, but replacement may improve outcomes for unreconstructable fractures. The use of hemiarthroplasty vs reverse shoulder replacement is currently being debated.
For treatment of distal radius fractures in elderly patients, cast immobilization for about 6 weeks will allow for optimal fracture healing. This should be followed by aggressive therapy to improve range of motion and function. Moderately displaced fractures in elderly patients will result in satisfactory outcomes even though reduction may not be "anatomic."
RECOMMENDED READINGS
Arora R, Lutz M, Deml C, Krappinger D, Haug L, Gabl M. A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J Bone Joint Surg Am. 2011 Dec 7;93(23):2146-53. doi: 10.2106/JBJS.J.01597. PubMed PMID: 22159849. View Abstract
at PubMed
Tejwani NC, Liporace F, Walsh M, France MA, Zuckerman JD, Egol KA. Functional outcome following one-part proximal humeral fractures: a prospective study. J Shoulder Elbow Surg. 2008 Mar-Apr;17(2):216-9. doi: 10.1016/j.jse.2007.07.016. Epub 2008 Jan 22. PubMed
PMID: 18207430. View Abstract at PubMed
Solberg BD, Moon CN, Franco DP, Paiement GD. Locked plating of 3- and 4-part proximal humerus fractures in older patients: the effect of initial fracture pattern on outcome. J Orthop Trauma. 2009 Feb;23(2):113-9. doi: 10.1097/BOT.0b013e31819344bf. PubMed PMID:
Question 44
What is the primary benefit of using rhBMP-2 instead of autogenous bone graft inside an anterior spinal fusion cage?
Explanation
REFERENCE: Burkus JK, Gornet MF, Dickman CA, et al: Anterior lumbar interbody fusion using rhBMP-2 with tapered interbody cages. J Spinal Disord Tech 2002;15:337-349.
Question 45
Which of the following pelvic injury types has the highest reported mortality rate?
Explanation

OrthoCash 2020
Question 46
Which of the following conditions routinely requires early surgical intervention in patients with Marfan syndrome? Review Topic
Explanation
Question 47
.A 22-year-old collegiate baseball pitcher has had posterior shoulder pain with decreased throwing velocity and accuracy over the past several months. Examination of the abducted shoulder in the supine position reveals 120 degrees of external rotation, 40 degrees of internal rotation on the throwing side, 100 degrees of external rotation, and 70 degrees of internal rotation on the nonthrowing side. The remainder of the clinical examination is unremarkable. An MRI scan shows a small partial articular-sided infraspinatus tear. Initial treatment should consist of
Explanation

Question 48
What is the most common surgical cause of the foot deformity shown in Figure 9?
Explanation
REFERENCES: Donley BG: Acquired hallux varus. Foot Ankle Int 1997;18:586-592.
Myerson MS, Komenda GA: Results of hallux varus correction using an extensor brevis tenodesis. Foot Ankle Int 1996;17:21-27.
Question 49
A 14-year-old girl reports a 3-week history of anterior thigh pain and a palpable mass after sustaining a soccer-related injury. Examination reveals a tender, firm mass in the midportion of the rectus femoris. MRI scans are shown in Figures 39a through 39c. What is the most appropriate management? Review Topic
Explanation
Question 50
Figure 6 shows the radiograph of a 14-year-old baseball player who felt a pop and had an immediate onset of pain in his elbow after a hard throw from the outfield. The best course of action should be to
Explanation
REFERENCES: Case SL, Hennrikus WL: Surgical treatment of displaced medial epicondyle fractures in adolescent athletes. Am J Sports Med 1997;25:682-686.
Woods GW, Tullos HS: Elbow instability and medial epicondyle fractures. Am J Sports Med 1977;5:23-30.
Question 51
Figures below depict the radiographs obtained from a 76-year-old woman who comes to the emergency department after experiencing a fall. She is an unassisted community ambulator with a history of right hip pain. What is the most appropriate surgical treatment for this fracture?
Explanation
This patient has pre-existing right hip osteoarthritis. The most correct option for the treatment of this active patient is a right total hip arthroplasty. Hemiarthroplasty would not address the patient's pain from osteoarthritis, and open reduction and internal fixation would not fix the femoral head issue or the
osteoarthritis.
Question 52
below depict the AP and lateral radiographs obtained from a year-old man with long-standing right knee osteoarthritis and pain that is unresponsive to nonsurgical treatment. The patient undergoes navigated cruciate-retaining right total knee arthroplasty. After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office reporting continued pain 2 years after surgery. He describes instability, particularly when descending stairs. On examination, range of motion of 0° to 120° is observed, with no extensor lag. Slope of the tibial component is 7°. The knee is stable to varus and valgus stress in extension, but flexion instability is present in both the anterior-posterior direction and the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection work-up is negative. What is the most appropriate surgical intervention at this time?
Explanation
The patient’s symptoms at follow-up—pain, swelling, and difficulty descending stairs—suggest knee flexion instability. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant (depending on the condition of the ligaments) likely is needed to address his symptoms. The difference in extension stability and flexion stability makes polyethylene exchange a poor option. A constrained rotating hinge design is not necessary. Repeat use of a PCL-retaining insert is not recommended. Tibial and femoral revision both are required. Correction of excessive slope will be attained with tibial revision, femoral component revision is required to convert to a PCL-substituting design. There is also an opportunity to increase posterior condylar offset if needed.
Question 53
A 38-year-old man has an enlarging left paraspinal soft-tissue mass. Based on the MRI scans and biopsy specimens shown in Figures 32a through 32e, what is the most likely diagnosis?
Explanation
of surgical resection, radiation therapy, chemotherapeutic protocols, hormone modulation, and/or anti-inflammatory medications.
REFERENCES: Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 309-337.
Spear MA, Jennings LC, Mankin HJ, et al: Individualizing management of aggressive fibromatoses. Int J Radiat Oncol Biol Phys 1998;40:637-645.
Question 54
In patient selection for meniscal allograft transplantation, which of the following variables has the greatest influence on outcome?
Explanation
REFERENCES: Carter TR: Meniscal allograft transplantation. Sports Med Arthroscopy Rev 1999;7:51-63.
Garrett JC: Meniscal transplantation: A review of 43 cases with two- to seven-year follow-up. Sports Med Arthroscopy Rev 1993;2:164-167.
van Arkel ER, de Boer HH: Human meniscal transplantation: Preliminary results at 2- to 5-year follow-up. J Bone Joint Surg Br 1995;77:589-595.
Question 55
Examination of a hand with compartment syndrome is most likely to reveal which of the following?
Explanation
REFERENCES: Oullette EA, Kelly R: Compartment syndromes of the hand. J Bone Joint Surg Am 1996;78:1515-1522.
Dellaero DT, Levin LS: Compartment syndrome of the hand: Etiology, diagnosis, and treatment. Am J Orthop 1996;25:404-408.
Question 56
Figure 1 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop" and then needing help walking off the field. His knee is visibly swollen. The patient undergoes surgery to repair/reconstruct the damaged structure and has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they want to “get the therapy over with as fast as possible" to expedite his return to sports, and the surgeon and rehabilitation team consider their request. Compared with nonaccelerated rehabilitation, patients who follow an early accelerated rehabilitation protocol experience

Explanation
Question 57
A 25-year-old tennis player has shoulder pain and weakness to external rotation. MRI scans are shown in Figures 16a and 16b. What is the most likely cause of his weakness?
Explanation
REFERENCES: Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Inokuchi W, Ogawa K, Horiuchi Y: Magnetic resonance imaging of suprascapular nerve palsy.
J Shoulder Elbow Surg 1998;7;223-227.
Question 58
A 61-year-old right-hand-dominant woman falls down the stairs, resulting in a left anteroinferior dislocation and noncomminuted greater tuberosity fracture. A closed glenohumeral reduction with intravenous sedation is performed in the emergency department. After reduction, the greater tuberosity fragment remains displaced by 2 mm. What is the most appropriate treatment?
Explanation
<3 mm in laborers and professional athletes can be treated successfully without surgery. Early passive range
of motion is important to avoid stiffness.
Question 59
Thoracic disk herniations are most frequently found in what area of the spine?
Explanation
REFERENCES: Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864.
Bohlman HH, Zdeblick TA: Anterior excision of herniated thoracic discs. J Bone Joint Surg Am 1988;70:70-77.
Question 60
The majority of severe cervical spine injuries occurring in contact sports evolve during axial loading and flexion of the cervical spine. At what minimum degree of flexion does axial loading place the cervical spine at risk during contact sports?
Explanation
REFERENCES: Thomas BE, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
Torg JS, Truex R Jr, Quedenfeld TC, Burstein A, Spealman A, Nichols C III: The National Football Head and Neck Injury Registry: Report and conclusions 1978. JAMA 1979;241:1477-1479.
Question 61
A 10‘/2-year-old boy sustained the injury shown in Figure 72 when he fell out of a tree. This is a closed, neurologically intact injury and the patient has no head injury or loss of consciousness. He weighs 115 pounds and is otherwise healthy. What is the optimal treatment option for this injury?
Explanation
REFERENCES: Flynn JM, Schwend RM: Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg 2004;12:347-359.
Gordon JE, Swenning TA, Burd TA, et al: Proximal femoral radiographic changes after lateral transtrochanteric intramedullary nail placement in children. J Bone Joint Surg Am 2003;85:1295-1301.
Figure 71a Figure 71b Figure 71c Figure 71d
Question 62
- A form of renal osteodystrophy that is characterized by pure osteomalacia is caused by
Explanation
Question 63
-Figures a through c are the MRI scans of a 21-year-old woman with recurrent shoulder instability and pain after an open anterior stabilization procedure. Positive belly-press test findings were positive.At surgery she was found to have an irreparable tear of the tendon injury identified preoperatively. The procedure to address the dynamic stabilizer deficit places which nerve at most risk?
Explanation
Question 64
A 26-year-old man has had a 2-year history of pain and stiffness after sustaining a comminuted olecranon fracture. Treatment at the time of injury consisted of open reduction and internal fixation with tension band wiring. Examination reveals motion of 45 degrees to 110 degrees and pain throughout the arc of motion. Resisted flexion and extension are painful. Forearm rotation is normal. Radiographs are shown in Figure 51. Treatment should consist of
Explanation
REFERENCES: Morrey BF: Distraction arthroplasty: Clinical applications. Clin Orthop 1993;293:46-54.
O’Driscoll SW: Elbow arthritis: Treatment options. J Am Acad Orthop Surg 1993;1:106-116.
Question 65
Figure below shows the radiograph obtained from a 73-year-old woman who returns status post total hip arthroplasty 14 years earlier. She denies pain and has no discomfort on examination. She then undergoes revision total hip arthroplasty with head and liner exchange and bone grafting. After a physical therapy session two days after surgical intervention, she develops inability to dorsiflex the foot while she is sitting in a chair. The initial treatment should consist of

Explanation
Gamma irradiation produces free radicals. Although these free radicals can form cross-links with other polyethylene chains, the free radicals can also form a bond with oxygen, resulting in early oxidation. Gamma irradiation in air produces the highest risk for oxidized polyethylene, resulting in the highest risk for wear, delamination, and subsequent osteolysis. This patient demonstrates severe periarticular osteolysis. When she is asymptomatic, this suggests the acetabular and femoral components remain well fixed to the bone. Consequently, she can be treated by removing the wear generator (polyethylene exchange), along with bone grafting of the osteolytic defect. Considering the extensive amount of osteolysis indefinite observation would not be appropriate. A foot drop develops 2 days after surgery. As a result, it can be assumed that the nerve was not injured directly during the surgical procedure. Although MRI or CT may be indicated to identify an evolving hematoma, the immediate concern is to minimize pressure on the sciatic nerve. Tension on the nerve can be reduced by flexing the surgical knee and positioning the bed flat.
Question 66
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with a prognosis if this patient is having a reaction to metal debris?
Explanation
Question 67
A year-old woman with a history of osteoporosis is involved in a high-speed motor vehicle accident, resulting in left hip pain and deformity. The initial radiograph from the trauma bay is shown in Postreduction CT is shown in 2 through What is the most appropriate definitive surgical treatment?
Explanation
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
Question 68
A 57-year-old man has had a 2-week history of neck pain. He has no history of radiating symptoms, and has no complaints of numbness or paresthesias. There was no trauma associated with the onset of the pain. Figure 26 shows the MRI scan initially obtained by his family physician. What should the patient be told regarding the prevalence of the MRI findings in his age group? Review Topic

Explanation
Question 69
Figure 12 shows the radiograph of a 15-year-old boy with cerebral palsy who has pain at the first metatarsophalangeal joints. He is a community ambulator. Management consisting of accommodative shoes has failed to provide relief. What is the treatment of choice?
Explanation
REFERENCES: Davids JR, Mason TA, Danko A, et al: Surgical management of hallux valgus deformity in children with cerebral palsy. J Pediatr Orthop 2001;21:89-94.
Jenter M, Lipton GE, Miller F: Operative treatment for hallux valgus in children with cerebral palsy. Foot Ankle Int 1998;19:830-835.
Question 70
What is the dominant component of articular cartilage extracellular matrix by weight?
Explanation
REFERENCES: Buckwalter JA, Mankin HJ: Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Inst Course Lect 1998;47:487-504.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 3-18.
Question 71
Which of the following lesions most closely resembles Ewing’s sarcoma histologically?
Explanation
REFERENCE: Wold LE, McLeod RA, Sim FH, Unni KK: Atlas of Orthop Pathology. Philadelphia, PA, WB Saunders, 1990.
Question 72
A 9-month-old nonambulatory girl is seen in the emergency department with a fracture of her right forearm. The mother says she fell from the changing table yesterday and continues to cry and not use her right arm. Radiographs are shown in Figure 31. Treatment should consist of which of the following? Review Topic

Explanation
efficient way to evaluate for other fractures. A MRI of the brain is not indicated unless fundoscopic examination reveals an abnormality.
Question 73
Rickets can be best characterized by which of the following radiographic changes in children?
Explanation
Question 74
Which of the following muscle tendons inserts just lateral to the long head of biceps tendon on the proximal humerus?
Explanation
REFERENCE: Bal GK, Basamania CJ: Pectoralis major tendon ruptures: Diagnosis and treatment. Tech Shoulder Elbow Surg 2005;6:128-134.
Question 75
Figure 1 is the MRI scan of a 15-year-old boy who has had knee pain with running for 5 months. What is the most appropriate treatment?
Explanation
outcomes? 16
A. Decreased American Orthopaedic Foot and Ankle Society (AOFAS) scores at 2- year follow-up
B. Slower return to work
C. Increased rate of hardware removal
D. Decreased rate of syndesmotic malreduction
The clinical vignette demonstrates an unstable left ankle syndesmotic injury, also known as a “high ankle sprain”. The distal tibiofibular syndesmosis comprises five structures: the anteroinferior tibiofibular ligament, posteroinferior tibiofibular ligament, the interosseous membrane, the interosseous ligament, and the inferior transverse ligament.
This injury commonly occurs secondary to a forced external rotation motion of the foot. Stable grade 1 strains without diastasis on stress radiographs can be treated with a period of non-weight bearing followed by physical therapy. Unstable injuries, grade 2 and 3, which demonstrate diastasis on external rotation stress radiographs, are commonly treated operatively. Fixation constructs commonly include screw fixation, suture button fixation, or a hybrid combination technique. Naqvi and associates demonstrated more accurate syndesmotic reduction with suture button fixation versus screw fixation. Syndesmotic malreduction has been shown to be an important independent predictor of decreased clinical outcomes. Andersen and associates demonstrated higher AOFAS scores and diminished syndesmotic widening at radiographic follow-up at 2 years with suture button fixation. In a systematic review, Zhang and associates demonstrated higher AOFAS scores, diminished need for implant removal (3.7% vs 40.2%), diminished implant failure, and lower rates of malreduction (1% vs 12%). Thornes and associates demonstrated a faster return to work following suture button fixation versus screw fixation.
21- A 26-year-old weightlifter has increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication, corticosteroid injections, and rest fails to alleviate his symptoms. He undergoes an arthroscopic distal clavicle resection with excision of the distal 8 mm of clavicle (Mumford procedure). Three months after surgery, he reports mild pain and popping by his clavicle. His clavicle demonstrates mild posterior instability on examination without any obvious deformity on his radiographs. What structures were
compromised during his excision? 17
A. Anterior and superior acromioclavicular joint ligaments
B. Posterior and superior acromioclavicular joint ligaments
C. Conoid ligament
D. Trapezoid ligament
The posterior and superior acromioclavicular ligaments provide the most restraint to posterior translation of the acromioclavicular joint and must be preserved during a Mumford procedure. Anterior and superior acromioclavicular joint ligaments are the opposite of the preferred response and prevent anterior translation of the clavicle. Injuries to the conoid and trapezoid ligaments are more pronounced with grade III or higher acromioclavicular separations, with superior migration of the clavicle relative to the acromion.
22- Figures 1 and 2 are the T2-weighted MRI scans of a 54-year-old woman with medial knee pain and catching of 6 months’ duration. What treatment option is most likely to be associated with a favorable outcome?
A. Physical therapy
B. Meniscal repair
C. Meniscectomy
D. Reconstruction
The MRI scans reveal a posterior horn root tear of the medial meniscus. LaPrade and associates found that outcomes after posterior meniscal root 18
repair significantly improved postoperatively and patient satisfaction was high, regardless of age or meniscal laterality. Patients aged <50 years had outcomes similar to those of patients ≥50 years, as did patients who underwent medial versus lateral root repair. In patients undergoing pullout fixation for posterior medial meniscus root tear, Chung and associates (in “Pullout Fixation of Posterior Medial Meniscus Root Tears”) found that patients with decreased meniscus extrusion at postoperative 1 year have more favorable clinical scores and radiographic findings at midterm follow-up than those with increased extrusion at 1 year. Krych and associates found that nonoperative treatment of medial meniscus posterior horn root tears is associated with poor clinical outcome, worsening arthritis, and a relatively high rate of arthroplasty at 5-year follow-up. Reconstruction would have no role in the setting of a reparable meniscal root tear.
22- A 24-year-old semiprofessional baseball player has noted increasing medial elbow pain for the past 2 months. This has been associated with a concomitant loss in velocity and control. He denies pain, numbness, or tingling in the hand or digits. Examination demonstrates medial elbow tenderness and swelling. Elbow range of motion is full. There is pain with milking maneuver and valgus stress test. Tinel’s sign is negative over the cubital tunnel, and there is no ulnar nerve subluxation. His MRI scan is shown in Figure 1. After thorough discussion, the player elects to undergo surgical intervention. What surgical variable has been associated with inferior outcomes?
A. Use of palmaris autograft
B. Ulnar nerve transposition
C. Muscle-splitting approach
D. Use of a docking technique
The information and image provided describe a throwing athlete with a complete tear of his ulnar collateral ligament (UCL) of the elbow. Numerous techniques have been described for UCL reconstruction, and at this time, optimal graft choice and fixation methods have not been established. Most studies show no.
major differences in outcome between gracilis autograft palmaris autograft, and allograft. Similarly, no clear advantage has been established when comparing use of bone tunnels with interference screws, tunnels with a docking technique, modified docking techniques, and combination
Question 76
Figures 86a through 86c are the radiographs and biopsy specimen of a 14-year-old boy who has had left knee pain for 4 weeks. What is the most likely diagnosis?
Explanation
Question 77
A 37-year-old man with a history of congenital flatfoot reports worsening pain on the medial aspect of his ankle for the past year. The pain is worse with weight bearing and is better with rest and the use of an ankle brace. What findings are shown on the MRI scans shown in Figures 18a through 18c?
Explanation
REFERENCES: Slovenkai MP: Clinical and radiographic evaluation (Adult flatfoot: Posterior tibial tendon dysfunction). Foot Ankle Clin 1997;2:241-260.
Conti S, Michelson J, Jahss M: Clinical significance of magnetic resonance imaging in preoperative planning for reconstruction of posterior tibial tendon ruptures. Foot Ankle 1992;13:208-214.
Question 78
Figure 1 shows a radiograph obtained from an active 30-year-old man who sustained an injury to his ring finger 1 week earlier. The most appropriate treatment is

Explanation

Figure 1 reveals evidence of an intra-articular distal phalanx fracture with a distal interphalangeal (DIP) joint dorsal subluxation. This injury is unstable and requires surgical management for an active individual. Volar distal phalanx fractures are often associated with flexor digitorum profundus avulsion injuries, which are addressed concomitantly. This injury was treated with ORIF of the intra-articular fracture, pinning of the DIP joint, and repair of an avulsed flexor digitorum profundus tendon with a button on the dorsal nail plate, as shown in Figure 2. Splint immobilization would not maintain a reduction of this unstable injury. The terminal tendon is not injured in this patient but is often injured in a dorsal distal phalanx fracture with a volar dislocation. Arthrodesis of the DIP is a salvage procedure and would not be considered acutely.
Question 79
Which of the following radiographic views best assesses anterior coverage of the dysplastic hip?
Explanation
REFERENCES: Klaue K, Wallin A, Ganz R: CT evaluation of coverage and congruency of the hip prior to osteotomy. Clin Orthop 1988;232:15-25.
Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 80
A 25-year-old left hand-dominant man has severe left shoulder pain after being involved in a high-speed motor vehicle accident. Examination reveals that he is unable to move the left shoulder. His neurovascular status is intact in the entire left upper extremity. A radiograph is shown in Figure 19. What is the most appropriate surgical management of this injury?
Explanation
REFERENCES: Ko JY, Yamamoto R: Surgical treatment of complex fractures of the proximal humerus. Clin Orthop Relat Res 1996;327:225-237.
Aschauer E, Resch H: Four-part proximal humeral fractures: ORIF, in Warner JP, Iannotti JP, Flatow EL (eds): Complex and Revision Problems in Shoulder Surgery, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 289-309.
Question 81
A 21-year-old professional ballet dancer reports a painful popping sensation over her right hip joint. Examination reveals that symptoms are reproduced with hip flexion and external rotation. Which of the following studies will best confirm the diagnosis? Review Topic
Explanation
Question 82
A football player injures his knee when he is tackled and falls awkwardly. He does not note any discreet “pop,” but pain prevents him from returning to the game. An effusion is noted the following day and an MRI scan is ordered. Selected images are shown in Figures 1 through 3. Based on these images, physical examination findings likely include

Explanation
Question 83
Long-term alendronate (Fosamax) use for osteoporosis has been associated with which of the following?
Explanation
fractures of the femur. Osteonecrosis of the jaw has been described but not in other anatomic locations. Scurvy occurs because of a lack of vitamin C and use of bisphosphonates is not associated with uterine cancer or a detached retina.
Question 84
.Figures 75a through 75d are the radiograph, CT scan, bone scan, and biopsy of a 45-year-old man who has had a several-month history of progressive pain in his right hip and groin region. Based on these images and histology, what is the most appropriate treatment?
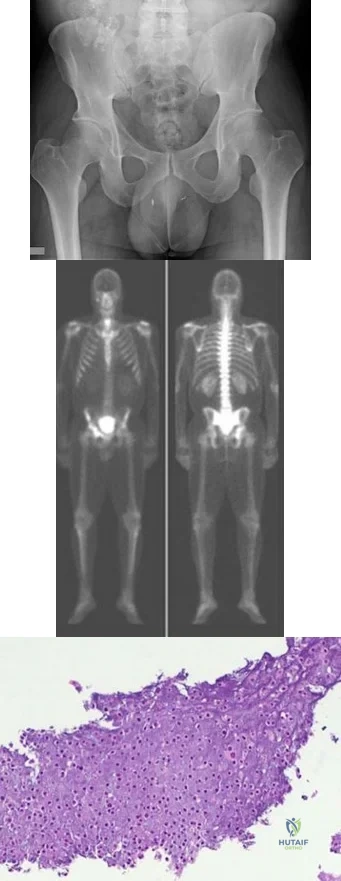
Explanation

Question 85
A 75-year-old woman notes a slowly enlarging mass in the right anterior thigh. Her medical history is significant only for hypertension. An MRI scan of her thigh is shown in Figures 60a through 60d. Which of the following surgical margins is the most appropriate for removal of this lesion?
Explanation
REFERENCES: Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
Rozental TD, Khoury LD, Donthineni-Rao R, et al: Atypical lipomatous masses of the extremities: Outcome of surgical treatment. Clin Orthop Relat Res 2002;398:203-211.
Question 86
Figures 40a and 40b show the pre- and postoperative radiographs of an 82-year-old woman with bilateral hip pain who has had staged total hip arthroplasties. To minimize potential injury to the sciatic nerve at the time of surgery, the surgeon should
Explanation
limb lengthening.
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 430-431.
Sanchez-Sotelo J, Berry DJ, Trousdale RT, et al: Surgical treatment of developmental dysplasia of the hip in adults: II. Arthroplasty options. J Am Acad Orthop Surg 2002;10:334-344.
Question 87
A 23-year-old soccer player sustains a grade III complete posterior cruciate ligament (PCL) tear after colliding with another player. In reconstructing the PCL, it is optimal to reconstruct the
Explanation
REFERENCES: Harner CD, Xerogeanes JW, Livesay GA, et al: The human posterior cruciate ligament complex: An interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-745.
Burns WC II, Draganich LF, Pyevich M, Reider B: The effect of femoral tunnel position and graft tensioning technique on posterior laxity of the posterior cruciate ligament-reconstructed knee. Am J Sports Med 1995;23:424-430.
Question 88
Figures 25a and 25b are the radiographs of a 63-year-old man who had right total hip arthroplasty (THA) 4 months ago. Progressive stiffness began 2 months after surgery, and he now reports pain only after prolonged physical activity. His examination reveals normal gait and painless range of motion with flexion of 70 degrees, extension of 0 degrees, internal rotation of 20 degrees, external rotation of 20 degrees, abduction of 10 degrees, and adduction of 10 degrees. His erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels are within defined limits. Physical therapy has produced no benefit. What is the most appropriate next step?
Explanation
This patient presents with HO 4 months after undergoing THA. Symptomatic HO may complicate nearly 7% of primary THA cases. Improvement in pain is expected within 6 months, and most patients will not need surgical treatment. Surgical excision may be warranted for symptomatic patients after full maturation of the HO, usually 6 to 18 months after the surgery. Patients can be followed with repeated serum alkaline phosphatase levels, which are elevated initially and should return to normal upon maturation of HO. Alternatively, a bone scan can show decreased activity once the HO has matured. Twenty-five milligrams of indomethacin 3 times daily for 6 weeks or 1 dose of irradiation at 700 to 800 Gy is effective in the prevention of HO, not for the treatment of established HO.
RESPONSES FOR QUESTIONS 26 THROUGH 29
Minimum inhibitory concentration (MIC)
Minimum bactericidal concentration (MBC)
Antiobiotic susceptibility
Antibiograms
Antimicrobial resistance
Spectrum of coverage
Match the description below with the appropriate response above.
Question 89
Which group experiences the highest rate of anterior cruciate ligament (ACL) tears?
Explanation
ACL tears are several times more common among women than men. Women who land from jumps in increased valgus and external rotation are at particularly increased risk for ACL tears. Women have smaller notch widths and a smaller ACL cross-sectional area than men, but these factors have not been proven to increase risk for ACL tears.

CLINICAL SITUATION FOR QUESTIONS 64 THROUGH 67
Figure 64 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain.
Question 90
A 20-year-old man involved in a motor vehicle accident is brought to the emergency department with a C6-7 unilateral facet dislocation. His neurologic examination reveals a focal left-sided C7 nerve root palsy. He is awake and cooperative with questioning and has no other obvious traumatic injuries. What is the most appropriate treatment at this time? Review Topic
Explanation
Question 91
Figures 1 through 3 show the clinical photographs obtained from a 45-year-old woman who is right-hand dominant. She has pain in the left ring proximal interphalangeal (PIP) joint that gets worse during lifting or gripping activities. On examination, she has PIP range of motion of 15° to 50° with laxity of the radial collateral ligament and tenderness around the joint. The flexor and extensor tendons are intact. She has rotational malalignment when making a composite fist. Radiographs reveal end-stage arthritis at the PIP joint. She elects to move forward with surgery and undergoes arthroplasty. What component of the examination is essential to determine which implant arthroplasty—silicone or surface replacement—is best?
Explanation
This patient has end-stage arthritis in conjunction with ligament insufficiency. The treatment for arthritis is arthroplasty or fusion. Given that her ring finger is affected, arthroplasty is recommended to preserve motion and grip. Two types of arthroplasties are available: silicone and surface replacement. The prerequisites are the same for both and include good bone stock, good sensibility of the joint, adequate soft-tissue coverage, and normally functioning tendons. Adequate collateral ligaments are required for surface replacement arthroplasty. This patient has a deficiency of the radial collateral ligament, evidenced by her clinical examination. Thus, silicone arthroplasty is the recommended option for joint replacement in this patient.
Question 92
The use of bisphosphonates in children with osteogenesis imperfecta is becoming more widely accepted as treatment to improve quality of life and to decrease the risks of fracture. What is the mechanism by which bisphosphonates work?
Explanation
Question 93
An 18-year-old lacrosse player is diagnosed with infectious mononucleosis. What is the recommendation for return to play?
Explanation
REFERENCES: Auwaerter PG: Infectious mononucleosis: Return to play. Clin Sports Med 2004;23:485-497.
Kinderknecht JJ: Infectious mononucleosis and the spleen. Curr Sports Med Rep
2002;1:116-120.
Question 94
The primary purpose of obtaining the radiograph shown in Figure 9 is to assess
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Lequesne M, deSez S: Le faux profil du bassin: Nouvelle incidence radiographique pour l’etude de la hance. Son utilite dans les dysplasies et les differentes coxopathies. Rev Rhum Mal Osteoartic 1961;28:643.
Question 95
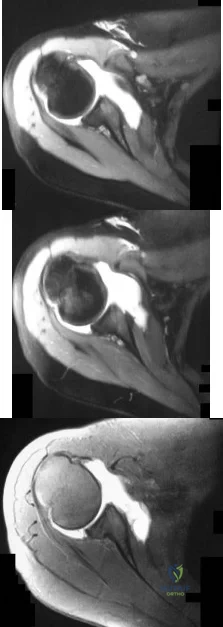
Figure 7 is the MR image of a 43-year-old man who has left shoulder pain with a traumatic rotator cuff tear after a fall. An examination reveals active forward elevation at 120 degrees and positive Yergason and lift-off test results. Arthroscopy reveals that the articular surfaces of the glenohumeral joint have a normal appearance without significant degenerative changes. What is the most appropriate treatment at this time?
Explanation
Video 7 for reference
The MR image shows medial subluxation of the biceps tendon, which can be confused with an articular loose body. In the clinical scenario of biceps instability/subluxation, the rationale regarding tenodesis is to address the painful dislocation and subluxation of the biceps tendon from the bicipital groove.
The MR image does not show a loose body or Bankart lesion. Patients with irreparable rotator cuff tears with a severe external rotation deficit and a deficient teres minor may experience a better functional result with latissimus dorsi transfer.
Question 96
Figures 52a and 52b show the radiographs of a left proximal femoral lesion noted serendipitously following minor trauma to the left hip. The patient has no thigh pain and is fully active without limitation. What is the most likely diagnosis of this bony lesion?
Explanation
REFERENCE: Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 97
Which of the following is associated with increased fetal morbidity and mortality in acetabular fractures during pregnancy?
Explanation
Question 98
Figures 19a through 19c show radiographs of the cervical spine of an asymptomatic patient with Down syndrome who wants to participate in a Special Olympics running event. The neurologic examination is normal. Management should consist of
Explanation
REFERENCES: American Academy of Pediatrics Committee of Sports Medicine and Fitness: Atlantoaxial instability in Down syndrome. Pediatrics 1995;96:151-154.
Copley LA, Dormans JP: Cervical spine disorders in infants and children. J Am Acad Orthop Surg 1998;6:204-214.
Tredwell SJ, Newman DE, Lockitch G: Instability of the upper cervical spine in Down syndrome. J Pediatr Orthop 1990;10:602-606.
Question 99
Which component is most common to both simple and complex elbow dislocations?

Explanation
Question 100
Which factor should most influence a patient's decision to have surgery for adult scoliosis if he or she is younger than age 50?
Explanation
In a retrospective review of 137 patients treated surgically and 153 patients treated nonsurgically for adult scoliosis, Bess and associates found that surgical treatment for patients younger than 50 years of age was driven by increased coronal plane deformity, and surgical treatment for older patients was mandated by pain and disability. They also concluded that age, comorbidities, and sagittal balance did not influence treatment decisions.
RECOMMENDED READINGS
Bess S, Boachie-Adjei O, Burton D, Cunningham M, Shaffrey C, Shelokov A, Hostin R, Schwab F, Wood K, Akbarnia B; International Spine Study Group. Pain and disability determine treatment modality for older patients with adult scoliosis, while deformity guides treatment for younger patients. Spine (Phila Pa 1976). 2009 Sep 15;34(20):2186-90. PubMed PMID: 19752704.View Abstract at PubMed
Anderson DG, Albert T, Tannoury C. Adult scoliosis. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:331-338.
