Full Question & Answer Text (for Search Engines)
Question 1:
A full-term newborn has webbing at the knees, rigid clubfeet, a Buddha-like posture of the lower extremities, and no voluntary or involuntary muscle action at and below the knees. Radiographs of the spine and pelvis reveal an absence of the lumbar spine and sacrum. What maternal condition is associated with this diagnosis?
Options:
- Alcoholism
- Drug abuse
- Down syndrome
- Diabetes mellitus
- Idiopathic scoliosis
Correct Answer: Diabetes mellitus
Explanation:
DISCUSSION: The history, physical examination, and radiographic findings are consistent with type IV sacral agenesis or caudal regression syndrome. These children are born with no lumbar spine or sacrum. The T12 vertebra is often prominent posteriorly. Popliteal webbing and knee flexion contractures are common with this diagnosis. There is a higher incidence of this diagnosis when the mother has diabetes mellitus. Maternal drug abuse and alcoholism can produce phenotypically unique children but without the findings described here. Maternal idiopathic scoliosis is not associated with caudal regression syndrome.
REFERENCES: Chan BW, Chan KS, Koide T, et al: Maternal diabetes increases the risk of caudal regression caused by retinoic acid. Diabetes 2002;51:2811-2816.
Zaw W, Stone DG: Caudal regression syndrome in twin pregnancy with type II diabetes.
J Perinatol 2002;22:171-174.
Question 2:
A 41-year-old man is involved in a high-speed motor vehicle crash and sustains a closed femoral midshaft fracture and a unilateral pulmonary contusion with a hemothorax, requiring placement of a chest tube. He has an initial blood pressure of 90/50 mm Hg. After receiving two liters of crystalloid, he has a blood pressure of 115/70 mm Hg and a heart rate of 90 bpm. He has normal mentation and does not require ventilator support. An arterial blood gas reveals that his delta base is
Options:
- Skeletal traction
- Temporizing external fixation
- Reamed intramedullary nailing
- Unreamed intramedullary nailing
- Open reduction and internal fixation
Correct Answer: Reamed intramedullary nailing
Explanation:
The patient responded to crystalloid resuscitation and hemodynamic parameters and the base deficit indicate that he is adequately resuscitated for definitive fracture care. In a resuscitated patient, a reamed nail is not detrimental in the setting of a pulmonary injury and is favorable for fracture union. An unreamed nail has a higher nonunion rate than a reamed nail for femoral fractures. In a skeletally mature patient with a midshaft fracture, an intramedullary nail is preferred to open reduction and internal fixation. In an adult patient, skeletal traction should be considered only as a temporary treatment prior to surgical fixation of the femoral fracture.
Question 3:
A 68-year-old man had a 3-year history of shoulder pain that failed to respond to nonsurgical management. Examination reveals forward elevation to 120 degrees and external rotation to 30 degrees. True AP and axillary radiographs and an axial CT scan are shown in Figures 1a through 1c. What management option would lead to the best long-term results? Review Topic
Options:
- Hemiarthroplasty
- Total shoulder arthroplasty
- Reverse total shoulder arthroplasty
- Arthroscopic debridement
- Glenoid osteotomy and interposition arthroplasty
Correct Answer: Total shoulder arthroplasty
Explanation:
The radiographs and CT scan reveal osteoarthritis with posterior subluxation and posterior bone loss. Total shoulder arthroplasty with reaming of the high side to neutralize the glenoid surface has been shown to yield better results than hemiarthroplasty. The amount of bone loss in this patient does not require posterior glenoid augmentation. Reverse total shoulder arthroplasty is indicated for rotator cuff tear arthropathy; therefore, it is not applicable. Arthroscopic debridement has yielded poor results with advanced osteoarthritis and posterior subluxation. Results from glenoid osteotomy have been variable and glenoid osteotomy is not indicated with associated osteoarthritis.
Question 4:
Figure 7 shows a sagittal T1-weighted MRI scan. What muscle/tendon is identified by the arrow? Review Topic
Options:
- Infraspinatus
- Teres minor
- Subscapularis
- Long head of triceps
- Latissimus dorsi
Correct Answer: Teres minor
Explanation:
The sagittal T1-weighted MRI scan is useful for interpreting the quality of muscle. The arrow is pointing to the teres minor.
Question 5:
A 25-year-old man is involved in a motor vehicle accident and brought to the emergency department at 4 am on Sunday morning. He has a closed distal third femoral shaft fracture. His leg is initially pulseless but after applying inline traction, a distal pulse can be palpated and the limb appears to be viable. The pulse in the injured limb “feels” different than the pulse in the uninjured limb. What is the next step in assessing the vascular status of this limb?
Options:
- Serial physical examinations
- Angiography
- Duplex ultrasound examination
- Ankle-brachial index (ABI)
- Measurement of compartment pressures
Correct Answer: Ankle-brachial index (ABI)
Explanation:
DISCUSSION: The patient initially has a distal third femoral fracture and a pulseless limb. The first step is to reduce the fracture and reassess the vascular status. Although the pulse returns, it feels different than the quality of the pulse in the contralateral uninjured extremity. There is a risk of a vascular injury with this fracture pattern due to tethering of the femoral vessels at the adductor hiatus; therefore, the vascular status needs further assessment since the pulses are not symmetrical. A physical examination is not very accurate in assessing whether a vascular injury is present; therefore, serial examinations are not appropriate. Angiography is very sensitive and specific but is time consuming and can cause complications secondary to the dye and the arterial puncture required to perform it. Duplex ultrasound is effective but is very operator-dependent and may not be available 24 hours a day. The ABI is easily performed and has been shown to be sensitive and specific. If the value is greater than 0.9, the negative predictive value is 99% and when the value is less than 0.9, it is 95% sensitive and 97% specific for a major arterial injury. It has been shown to be useful for blunt lower extremity injuries as well as knee dislocations.
REFERENCES: Levy BA, Zlowodzki MP, Graves M, et al: Screening for extremity arterial injury with the arterial pressure index. Am J Emerg Med 2005;23:689-695.
Abou-Sayed H, Berger DL: Blunt lower-extremity trauma and politeal artery injuries: Revisiting the case for selective arteriography. Arch Surg 2002;137:585-589.
Mills WJ, Barei DP, McNair P: The value of the ankle-brachial index for diagnosing arterial injury after knee dislocation: A prospective study. J Trauma 2004;56:1261-1265.
Question 6:
Which of the following diagnostic studies best distinguishes Ewing’s sarcoma from small cell osteosarcoma?
Options:
- Bone scan
- Cytogenetics
- DNA ploidy analysis
- Sentinel node biopsy
- L-lactate dehydrogenase (LDH)
Correct Answer: Cytogenetics
Explanation:
DISCUSSION: Cytogenetics best demonstrates the 11;22 translocation characteristic of Ewing’s sarcoma. The translocation also can be detected with polymerase chain reaction and fluorescent in situ hybridization. The Ewing antibody is used for immunostaining to check for cell membrane (surface) staining of a marker unrelated to the translocation; this could also help distinguish Ewing’s sarcoma from small cell osteosarcoma. A bone scan will show increased uptake with both types of tumors. Although most Ewing’s sarcoma tumors are diploid, some are polyploid as are most osteosarcomas. Flow cytometry is used to sort cells, sometimes based on antibody binding. LDH can be elevated in both Ewing’s sarcoma and osteosarcoma and is a poor prognostic indicator when elevated. Lymph node metastases are uncommon in both of these tumors.
REFERENCES: Perotti D, Corletto V, Giardini R, Parafioriti A, Fossati-Bellani F, Luksch R: Retrospective analysis of ploidy in primary osseous and extraosseous Ewing family tumors in children. Tumori 1998;84:493-498.
Riley RD, Burchill SA, Abrams KR, Heney D, Sutton AJ, Jones DR, et al: A systematic review of molecular and biological markers in tumours of the Ewing’s sarcoma family. Eur J Cancer 2003;39:19-30.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 11-20.
Question 7:
03 Which of the following findings is one of the diagnostic criteria for diffuse idiopathic skeletal hyperostosis?
Options:
- Flowing ossification along the anterolateral aspect of at least four contiguous vertebrae
- Disk space collapse in the involved vertebral segments
- Marginal syndesmophytes over four contiguous vertebrae
- Sacroiliac erosion or sclerosis
- Facet joint ankylosis Question 64.03
Correct Answer: Flowing ossification along the anterolateral aspect of at least four contiguous vertebrae
Explanation:
back answer
Diffuse idiopathic skeletal hyperostosis is a common disease, most prevalent in those over 50 years of age. The usual presentation is a middle-aged or older patient with chronic mild pain in the middle to lower back, spinal stiffness, and typical radiographic changes in the thoracic spine. Diffuse idiopathic skeletal hyperostosis is predominantly a radiographic diagnosis with 3 major diagnostic criteria. 1. Flowing ossification along the anterolateral aspect of at least four contiguous vertebrae. 2. Preservation of disk height in the involved vertebral segment; the relative absence of significant degenterative changes, such as marginal sclerosis in vertebral bodies or vacuum phenomenon. 3.
Absence of facet-joint ankylosis; absence of sacroiliac erosion, sclerosis, or intra-articular osseous fusion. Treatment is typically non-operative, with anti-inflammatories, activity modification and PT.
back to this question next question
Question 8:
A 58-year-old man has had increasing midback pain for 8 weeks. Radiographs reveal mild osteopenia and mild disk degeneration but no fractures or lesions. An MRI of the spine reveals diskitis with a small-intensity signal within the spinal canal that is consistent with an epidural abscess at T11-12. The patient is neurologically intact but in significant pain. CT-guided biopsy of the disk space is positive for methicillin-sensitive Staphylococcus aureus. What is the most appropriate treatment?
Options:
- Intravenous (IV) antibiotics for 6 weeks and clinical observation
- Observation and bracing alone
- Laminectomy and posterior spinal fusion with IV antibiotics
- Anterior spinal debridement and fusion with IV antibiotics
Correct Answer: Intravenous (IV) antibiotics for 6 weeks and clinical observation
Explanation:
DISCUSSION
The treatment of spinal infections is variable. A diskitis in a patient with a mechanically stable spine without neurologic compromise is typically treated with needle biopsy/culture and appropriate IV antibiotics. Epidural abscess often is considered one of the true orthopaedic emergencies that necessitates surgical intervention. However, there is growing evidence that medical management can be appropriate to treat epidural abscesses in certain cases. In cases involving neurologic deterioration, surgical decompression, drainage, and systemic IV antibiotics is the treatment of choice. Medical management of spinal abscesses can be considered when a patient refuses surgical decompression; surgery is contraindicated because of high risk, pain, or
infection; or paralysis lasting longer than 24 to 36 hours results in a likely inability to reverse the paralysis. Patients who are neurologically intact may also be treated with medical management alone if they are stable and have an identifiable microorganism that can be observed closely to assess for neurologic deterioration. If neurologic changes are noted, surgical decompression and debridement and continued IV antibiotic therapy are appropriate.
RECOMMENDED READINGS
Darouiche RO. Spinal epidural abscess. N Engl J Med. 2006 Nov 9;355(19):2012-20. Review. PubMed PMID: 17093252.
View Abstract at PubMed
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 9:
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior- stabilized TKA without evidence of component loosening. What is the most likely cause of this patient's pain?
Options:
- Patellar clunk syndrome
- Flexion gap instability
- Polyethylene wear
- Femoral component malrotation
Correct Answer: Patellar clunk syndrome
Explanation:
DISCUSSION:
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
Question 10:
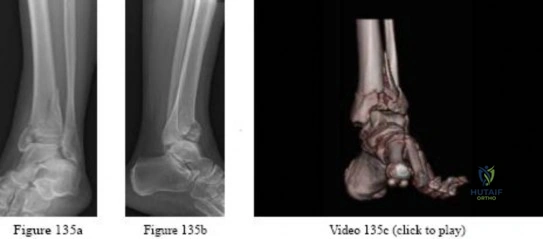
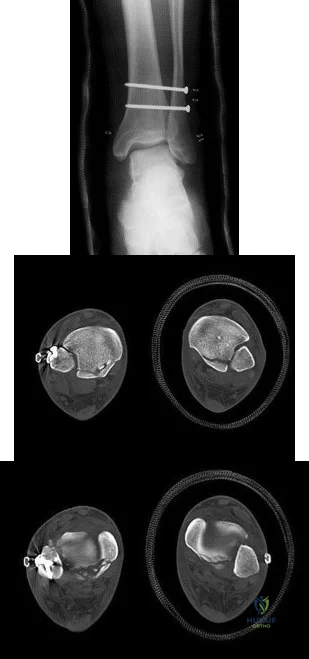
-A 45-year-old woman sustained a fall from height and has the injury shown in Figures 135a and 135b.A 3-dimensional reconstruction CT scan is shown in Figure 135c. Joint-spanning external fixation is applied on the day of injury. Ten days later, her skin is acceptable for definitive fixation. What is the most appropriate type of fixation for her fracture?
Options:
- Percutaneous screws and cast
- Conversion to a circular fixator
- Medial and anterolateral locked plates
- Medial and anterolateral nonlocked plates
- Lateral locked plate and medial malleolus screws
Correct Answer: Medial and anterolateral nonlocked plates
Question 11:
-What leads to muscle hypertrophy?
Options:
- Neural recruitment
- Active stretching
- Passive stretching
- Proprioceptive training
- Progressive overloading
Correct Answer: Progressive overloading
Question 12:
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of
Options:
- open reduction and internal fixation.
- a short leg weight-bearing cast.
- a short leg non-weight-bearing cast.
- first tarsometatarsal fusion.
- functional brace application and early range of motion.
Correct Answer: open reduction and internal fixation.
Explanation:
DISCUSSION: The dislocation is between the medial and middle cuneiform. Although the first and second tarsometatarsal joints are aligned, there is a gap between the cuneiforms. The radiograph shows a Lisfranc dislocation variant. In a healthy active individual, open reduction and internal fixation yields the best results. The reestablishment of the normal arch and medial column support with anatomic reduction is critical to obtaining the best possible outcome from these injuries.
REFERENCES: Teng AL, Pinzur MS, Lomasney L, et al: Functional outcome following anatomic restoration of the tarsal-metatarsal fracture dislocation. Foot Ankle Int
2002;23:922-926.
Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Question 13:
Which factor should most influence a patient's decision to have surgery for adult scoliosis if he or she is younger than age 50?
Options:
- Increasing coronal plane deformity
- Increasing pain
- Increasing sagittal balance
- Invasiveness of the surgical procedure
Correct Answer: Increasing coronal plane deformity
Explanation:
DISCUSSION
In a retrospective review of 137 patients treated surgically and 153 patients treated nonsurgically for adult scoliosis, Bess and associates found that surgical treatment for patients younger than 50 years of age was driven by increased coronal plane deformity, and surgical treatment for older patients was mandated by pain and disability. They also concluded that age, comorbidities, and sagittal balance did not influence treatment decisions.
RECOMMENDED READINGS
Bess S, Boachie-Adjei O, Burton D, Cunningham M, Shaffrey C, Shelokov A, Hostin R, Schwab F, Wood K, Akbarnia B; International Spine Study Group. Pain and disability determine treatment modality for older patients with adult scoliosis, while deformity guides treatment for younger patients. Spine (Phila Pa 1976). 2009 Sep 15;34(20):2186-90. PubMed PMID: 19752704.
View
Abstract at PubMed
Anderson DG, Albert T, Tannoury C. Adult scoliosis. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:331-338.
Question 14:
Which of the following pelvic injury types has the highest reported mortality rate?
Options:
- Anterior posterior compression (APC) III injury
- Lateral compression (LC) III injury
- Transverse-posterior wall acetabular fracture
- Vertical Shear
- Combined mechanical injury (CMI) Corrent answer: 1 Anterior posterior compression (APC) injuries have the highest mortality rates of the fracture patterns listed. APC injuries have high rates of concomitant thoracic and abdominal visceral injuries leading to the highest rates of mortality among pelvic fractures. Lateral compression (LC) fractures have particularly high incidences of associated brain and head injury with lower mortality than APC injuries. Overall, as the grade of pelvic ring injury increases the rates of associated injuries increases, regardless of exact mechanism of injury. The overall mortality rate for any pelvic trauma is roughly 15%, with APC III mortality around 37%, and overall APC mortality rates around 26%. LC of any grade has an estimated mortality around 13%. Vertical shear and CMI have estimated mortality of 25% and 17.1%, respectively. The lowest mortality rates are following acetabular fractures with estimates around 1.5%. Dalal et al retrospectively reviewed 340 trauma patients with pelvic injuries to analyze organ injury, resuscitative requirements, and outcomes. They found the highest mortality rates were in APC III and that more severe APC injuries had greater organ damage and mortality. They conclude that the mechanical force type and classification of injury are predictors of organ injury pattern, resuscitation needs, and mortality. Eastridge et al reviewed 1,014 injured pedestrians for pelvic injuries, associated injuries, and relationship of treatments to outcomes. They found the highest mortality rates were associated with APC III and LC III injuries patterns at 50%. They conclude that pelvic fractures are a sign of significant energy imparted on the body and severity of associated injuries lead to the high rates of morbidity and mortality. Illustration A and B show an APC III and LC III injury, respectively. Incorrect Answers:
Correct Answer: Lateral compression (LC) III injury
Explanation:
mechanism injuries all have lower mortality rates than APC injuries.
OrthoCash 2020
Question 15:
A patient with a history of chronic low back pain for several years reports decreased pain visual analog scores with the home use of a transcutaneous electrical neuromuscular stimulation (TENS) unit. This pain relief is most likely due to which of the following?
Options:
- Improved skeletal muscle strength and secondary spinal support
- Neuromodulation via presynaptic inhibition in the dorsal horn of the spinal cord
- Distraction sensory input
- Enhancement of muscle metabolic activity with improved lactic acid excretion
- Placebo effect
Correct Answer: Neuromodulation via presynaptic inhibition in the dorsal horn of the spinal cord
Explanation:
TENS units deliver superficial electrical stimulation. This electrical stimulation induces analgesia via inhibitory effects at the spinal cord level. The stimulation of small myelinated afferent fibers produces a presynaptic inhibition of the nociceptive transmission via unmyelinated C fibers, thus decreasing the transmission of pain stimuli. Additional benefit may come from the endogenous release of endorphins in the stimulated tissues.
Question 16:
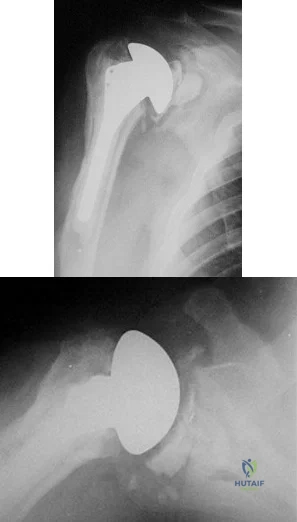
A 55-year-old man who underwent total shoulder arthroplasty 10 years ago recently reports an increase in shoulder pain. Laboratory studies consisting of a white blood cell count, erythrocyte sedimentation rate, and C-reactive protein are all negative, as is joint aspiration. Radiographs are shown in Figures 95a and 95b. If all intraoperative frozen sections are negative, what is the appropriate treatment during revision surgery to provide pain relief and improved function? Review Topic
Options:
- Placement of antibiotic spacer
- Removal of the glenoid, and possible bone grafting
- Conversion to reverse shoulder arthroplasty
- Referral to pain management
- Shoulder arthrodesis
Correct Answer: Removal of the glenoid, and possible bone grafting
Explanation:
The radiographs reveal a loose glenoid in the setting of no infection. Glenoid removal may give this patient the best chance of improved function and pain relief if sufficient bone stock remains. Bone grafting of defects may allow future glenoid implantation. Conversion to reverse shoulder arthroplasty would be a salvage procedure in this younger patient. Shoulder arthrodesis would be difficult and unpredictable after shoulder arthroplasty.
Question 17:
Evaluation of the percent of necrosis in the resected specimen after preoperative chemotherapy is of prognostic value for what type of sarcoma?
Options:
- Chondrosarcoma
- Soft-tissue sarcoma
- Rhabdomyosarcoma
- Parosteal osteosarcoma
- Osteosarcoma
Correct Answer: Osteosarcoma
Explanation:
DISCUSSION: To date, only the percent of necrosis after induction chemotherapy in high-grade osteosarcomas seems to be of prognostic value. The value in soft-tissue sarcoma and rhabdomyosarcoma is being evaluated but has not been substantiated. Chondrosarcomas and parosteal osteosarcomas are not treated with chemotherapy.
REFERENCES: Rosen G, Marcove RC, Caparros B, Nirenberg A, Kosloff C, Huvos AG: Primary osteogenic sarcoma: The rationale for pre-operative chemotherapy and delayed surgery. Cancer 1979,43:2163-2177.
Davis AM, Bell RS, Goodwin PJ: Prognostic factors in osteosarcoma: A critical review. J Clin Oncol 1994;12:423-431.
Wunder JS, Paulian G, Huvos AG, Heller G, Meyers PA, Healey JH: The histological response to chemotherapy as a predictor of the oncological outcome of operative treatment of Ewing sarcoma. J Bone Joint Surg Am 1998;80:1020-1033.
FOR ALL MCQS CLICK THE LINK ORTHO
MCQ BANK
Question 18:
A 10-year-old girl with a history of an obstetrical brachial plexus palsy has been referred for evaluation. Examination reveals a severe adduction internal rotation contracture of the shoulder and a mild flexion contracture of the elbow. Hand function is normal. Radiographs show mild glenohumeral joint incongruity. To achieve the best functional outcome, management should consist of
Options:
- physical therapy to stretch the tight structures.
- a humeral rotational osteotomy.
- anterior shoulder release and posterior muscle transfers.
- anterior shoulder release.
- shoulder fusion.
Correct Answer: a humeral rotational osteotomy.
Explanation:
DISCUSSION: The patient has an upper plexus palsy (Erb palsy) with severe shoulder contracture. While physical therapy for stretching is the treatment of choice to prevent contracture in the newborn, it is unlikely to be of benefit in the older child with an established contracture. Contracture release alone or in combination with muscle transfers can improve the cosmetic appearance, and in the case of a mild deformity, may also improve function. These procedures are less likely to help when there is deformity of the shoulder joint or when arthritic changes are present. The procedure of choice for an older child with joint deformity is rotational osteotomy of the proximal humerus because it can improve cosmesis and function, even in the face of joint deformity.
REFERENCES: Jahnke AH Jr, Bovill DF, McCarroll HR Jr, James P, Ashley RK: Persistent brachial plexus birth palsies. J Pediatr Orthop 1991;11:533-537.
Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L’Episcopo transfers in obstetrical palsy: A retrospective review of 20 cases. J Pediatr Orthop 1990;10:442-444.
Goddard NJ, Fixsen JA: Rotation osteotomy of the humerus for birth injuries of the brachial plexus. J Bone Joint Surg Br 1984;66:257-259.
Question 19:
Figures 1 and 2 are the MRI scans of a 57-year-old man who dislocated his left shoulder after a fall while playing tennis. On examination, he had full passive shoulder range of motion, but he was unable to actively elevate his injured shoulder. Sensation was intact to light touch over the lateral shoulder. What is the most likely etiology of his shoulder weakness?
Options:
- Axillary nerve injury
- Cervical radiculopathy involving the C6 nerve root
- Massive rotator cuff tear with loss of the transverse force couple
- Long head of the biceps tendon rupture with loss of superior stabilizing effect
Correct Answer: Massive rotator cuff tear with loss of the transverse force couple
Explanation:
This patient has a massive rotator cuff tear resulting in disruption of the transverse force couple between the subscapularis anteriorly and the infraspinatus and teres minor posteriorly. These muscles provide dynamic shoulder stability throughout active elevation, and loss of the force couple produces a pathologic increase in translation of the humeral head and decreased active abduction. Active shoulder elevation <90 degrees in the presence of full passive motion is termed pseudoparalysis. The most common neurologic deficit after shoulder dislocation is isolated injury to the axillary nerve. This patient's sensory examination suggests that the axillary nerve is intact. Cervical radiculopathy is less common after shoulder dislocation but has been reported. Conflicting evidence exists regarding the contribution of the long head of the biceps tendon to glenohumeral stability. One study reported minimal electromyographic activity in the biceps during ten basic shoulder motions.
Question 20:
below depict the AP and lateral radiographs obtained from a year-old man with long-standing right knee osteoarthritis and pain that is unresponsive to nonsurgical treatment. The patient undergoes navigated cruciate-retaining right total knee arthroplasty. After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office reporting continued pain 2 years after surgery. He describes instability, particularly when descending stairs. On examination, range of motion of 0° to 120° is observed, with no extensor lag. Slope of the tibial component is 7°. The knee is stable to varus and valgus stress in extension, but flexion instability is present in both the anterior-posterior direction and the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection work-up is negative. What is the most appropriate surgical intervention at this time?
Options:
- Tibial polyethylene exchange
- Revision of the femoral and tibial components and conversion to a posterior stabilized insert
- Revision of the femoral and tibial components to a constrained rotating hinge prosthesis
- Isolated femoral component revision and upsizing of the femoral implant with a new posterior cruciate ligament (PCL)-retaining polyethylene insert
Correct Answer: Revision of the femoral and tibial components and conversion to a posterior stabilized insert
Explanation:
DISCUSSION:
The patient’s symptoms at follow-up—pain, swelling, and difficulty descending stairs—suggest knee flexion instability. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant (depending on the condition of the ligaments) likely is needed to address his symptoms. The difference in extension stability and flexion stability makes polyethylene exchange a poor option. A constrained rotating hinge design is not necessary. Repeat use of a PCL-retaining insert is not recommended. Tibial and femoral revision both are required. Correction of excessive slope will be attained with tibial revision, femoral component revision is required to convert to a PCL-substituting design. There is also an opportunity to increase posterior condylar offset if needed.
Question 21:
It has been shown that bisphosphonate-based supportive therapy (pamidronate or zoledronate) reduces skeletal events (onset or progression of osteolytic lesions) both in patients with multiple myeloma and in cancer patients with bone metastasis. The use of biphosphonate therapy has been associated with
Options:
- increased medical complications of treatment.
- osteonecrosis of the jaw.
- improved long-term survival rates.
- anorexia.
- decreased quality of life measures.
Correct Answer: osteonecrosis of the jaw.
Explanation:
DISCUSSION: The use of bisphosphonates has been recently associated with the development of osteonecrosis of the jaw. Length of exposure seems to be the most important risk factor for this complication. The type of bisphosphonate may play a role and previous dental procedures may be a precipitating factor. Bisphosphonates are a class of therapeutic agents originally designed to treat loss of bone density (ie, alendronate). The primary mechanism of action of these drugs is inhibition of osteoclastic activity, and it has been shown that these drugs are useful in diseases with propensities toward osseous metastases. In particular, they are effective in diseases in which there is clear upregulation of osteoclastic or osteolytic activity, such as breast cancer and multiple myeloma, and have developed into a mainstay of treatment for individuals with these diseases. Although shown to reduce skeletal events, there has been no improvement in patient survival.
REFERENCES: Bamias A, Kastritis E, Bamia C, et al: Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: Incidence and risk factors. J Clin Oncol 2005;23:8580-8587.
Thakkar SG, Isada C, Smith J, et al: Jaw complications associated with bisphosphonate use in patients with plasma cell dyscrasias. Med Oncol 2006;23:51-56.
Van Poznak C: The phenomenon of osteonecrosis of the jaw in patients with metastatic breast cancer. Cancer Invest 2006;24:110-112.
Question 22:
A 24-year-old man has right forearm pain after sliding head first into home plate. Examination reveals that the arm is swollen, but there are no neurovascular deficits or skin lacerations. Radiographs reveal a both-bone forearm fracture. The ulna has an oblique fracture with a 30% butterfly fragment, and the radius is comminuted over 75% of its circumference. In addition to reduction and plate fixation of both bones, management should consist of
Options:
- bone grafting the radius only.
- bone grafting both the radius and ulna.
- bone graft substitute for both the radius and ulna.
- no additional grafting.
- no additional grafting but postoperative electrical stimulation.
Correct Answer: no additional grafting.
Explanation:
DISCUSSION: The patient has a both-bone fracture with a comminuted radial shaft. Open reduction and internal fixation of both bones is the treatment of choice. In the past, Chapman and associates recommended bone grafting radial shaft fractures with more than 30% comminution of the circumference. This has remained the recommendation in most textbooks. More recent studies, where modern biologic plating techniques were used, found that the addition of bone graft to comminuted fractures was not necessary because the union rate did not differ from that of nongrafted comminuted fractures.
REFERENCES: Anderson LD, Sisk TD, Tooms RE, Park WI III: Compression-plate fixation in acute diaphyseal fractures of the radius and ulna. J Bone Joint Surg Am 1975;57:287-297.
Chapman MW, Gordon JE, Zissimos AG: Compression-plate fixation of acute fractures of the diaphyses of the radius and ulna. J Bone Joint Surg Am 1989;71:159-169.
Wright RR, Schmeling GJ, Schwab JP: The necessity of acute bone grafting in diaphyseal forearm fractures: A retrospective review. J Orthop Trauma 1997;11:288-294.
Wei SY, Born CT, Abene A, Ong A, Hayda R, Delong WG Jr: Diaphyseal forearm fractures treated with and without bone graft. J Trauma 1999;46:1045-1048.
Question 23:
A 28-year-old man sustained a fracture-dislocation of T8 in a motor vehicle accident 1 week ago. The injury resulted in complete paraplegia. Management should consist of
Options:
- mobilization in a kinetic therapy bed for 8 weeks.
- initiation of a steroid protocol.
- immediate laminectomy of T7, T8, and T9.
- application of a total contact orthosis.
- open reduction and posterior segmental stabilization and grafting.
Correct Answer: open reduction and posterior segmental stabilization and grafting.
Explanation:
DISCUSSION: With a complete injury in the thoracic spinal cord, the likelihood of neurologic recovery is small. If possible, treatment should be planned to allow rapid mobilization and rehabilitation without the use of braces and their associated skin problems. The use of long segment fixation provides for rapid mobilization without having to use braces postoperatively. The use of steroid protocol is controversial and should be considered only if it can be started within 8 hours of the injury. Laminectomy is contraindicated because it will increase instability.
REFERENCE: Tasdemiroglu E, Tibbs PA: Long-term follow-up results of thoracolumbar fractures after posterior instrumentation. Spine 1995;20:1704-1708.
Question 24:
What is the main benefit of using metal-backed tibial components in total knee arthroplasty?
Options:
- Improve the conformity of the articular surfaces
- Reduce the maximum compressive stresses on the underlying cancellous bone
- Increase the tensile forces on the other condyle when one is loaded
- Decrease the thickness of the polyethylene tray
- Decrease the compressive forces on the polyethylene tray
Correct Answer: Reduce the maximum compressive stresses on the underlying cancellous bone
Explanation:
DISCUSSION: In a normal knee, the hard subchondral bone helps to distribute loads across the joint surface. A metal-backed tibial component in total knee arthroplasty decreases the compressive stresses on the underlying, softer cancellous bone by distributing the load over a larger surface area, particularly when one condyle is loaded. Although metallic base plates also increase the tensile forces on the other condyle when one is loaded and may decrease the thickness of the polyethylene tray, these are not benefits. Compressive forces on the polyethylene tray are increased with metal backing. The conformity of the articular surfaces is not affected by metal backing of the tibial component.
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
Question 25:
Figures 1 through 4 show the radiographs and MRI obtained from a 40-year-old man who has a 6-week history of ring finger pain, redness, and swelling after puncturing the finger with a toothpick. Purulent drainage from the puncture wound site grew Eikenella corrodens . The patient was initially treated with oral antibiotics for 10 days and then intravenous (IV) antibiotics for 3 weeks. What is the best next step in treatment?
Options:
- Continued IV antibiotics for 4 weeks
- Continued oral antibiotics for 6 weeks
- Bone scan, biopsy, and metastatic work-up
- Surgical débridement along with antibiotics
Correct Answer: Surgical débridement along with antibiotics
Explanation:
EXPLANATION:
This patient has a septic distal interphalangeal joint, which was treated with antibiotics alone. As a result, the patient developed osteomyelitis with bone destruction and abscess. The best way to treat this problem is to perform surgical débridement of bone and soft tissue, along with abscess drainage and an appropriate antibiotic regimen. Antibiotic treatment without surgery would not be successful in eliminating this particular infection. Bone scan with biopsy is not the correct option, because this problem is an infection
and not a tumor, and MRI already has provided enough diagnostic information.
Question 26:
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured? Review Topic
Options:
- Fourth cervical nerve root
- Upper trunk of the brachial plexus
- Middle trunk of the brachial plexus
- Lateral cord of the brachial plexus
- Axillary nerve
Correct Answer: Upper trunk of the brachial plexus
Explanation:
The athlete has symptoms referable to the axillary, musculocutaneous, and suprascapular nerves resulting from an injury to the upper trunk of the brachial plexus. This portion of the plexus is formed by contributions of the fourth through sixth cervical nerve roots. This area is often contused or stretched following a tackling maneuver that results in either depression of the shoulder from contact at Erb’s point or traction of the upper plexus from forced stretching of the neck to the contralateral side.
Question 27:
Figure 1 shows the radiograph of an 18-year-old patient who has severe knee pain. Treatment consisting of osteotomy should be perfomed
Options:
- above the tibial tubercle.
- at or just below the tibial tubercle.
- in the tibial diaphysis.
- on both the femur and tibia.
- on the femur alone.
Correct Answer: at or just below the tibial tubercle.
Explanation:
DISCUSSION: Very large corrections of tibial deformity can be achieved at or just below the tibial tubercle. This level of osteotomy maintains the relationship between the tubercle and the rest of the joint, does not alter patellofemoral mechanics, and avoids complicating possible future conversion to total knee arthroplasty. High tibial osteotomy is contraindicated for large corrections because of excessive elevation of the tibial tubercle and overhang of the lateral plateau. Correction in the tibial diaphysis creates a zig zag pattern in the tibia by correcting below the deformity and risks nonunion in cortical bone. There is no evidence that the femur is deformed; therefore, femoral osteotomy is not indicated.
REFERENCE: Murphy SB: Tibial osteotomy for genu varum: Indications, preoperative planning, and technique. Orthop Clin North Am 1994;25:477-482.
Question 28:
An orthopaedic surgeon in his first year of practice is negotiating with a private for-profit hospital to be their employed trauma specialist. The state of employment is known to have a high rate of malpractice claims because of a favorable plaintiff legal environment. During the course of negotiations, malpractice insurance is being discussed. The surgeon should ask the hospital to provide which type of malpractice insurance policy? Review Topic
Options:
- Claims made with "nose" coverage
- Claims made without tail coverage
- No policy because of employed status and sovereign immunity
- Occurrence coverage
- Occurrence coverage with "nose" coverage
Correct Answer: Occurrence coverage
Explanation:
An occurrence policy provides coverage for all claims made during employment irrespective of when it is filed (during or postemployment) and therefore is the best option. Claims made policy only covers suits for the time employed. A prepurchased "tail" is needed to provide coverage for cases that occurred during employment but filed postemployment. Nose coverage is applicable if the surgeon was previously employed and did not have tail coverage from previous employment, but this surgeon just emerged from training where it is not applicable. Claims made without tail coverage is unwise because the surgeon would be unprotected or have to purchase his own policy postemployment. Only in certain situations does sovereign immunity exist, and generally not in a for-profit system. Occurrence coverage with nose coverage is incorrect because it does not apply to this surgeon with no previous employment or claims policy lacking tail coverage.
Question 29:
A 19-year-old woman sustained a displaced talar neck fracture while cliff jumping. The fracture is managed with open reduction and internal fixation. Which of the following best describes the findings in the 2-months postoperative radiographs shown in Figures 67a and 67b, and subsequent treatment plan? Review Topic
Options:
- There is a positive Hawkins sign, indicating the patient is unlikely to develop osteonecrosis.
- There is a positive Hawkins sign, indicating the patient has developed osteonecrosis.
- Hawkins sign cannot be determined on radiographs; therefore, MRI is required.
- No Hawkins sign is visible, and therefore the patient is not likely to develop osteonecrosis.
- No Hawkins sign is visible; therefore, the patient should be kept non-weight-bearing until a Hawkins sign appears
Correct Answer: There is a positive Hawkins sign, indicating the patient is unlikely to develop osteonecrosis.
Explanation:
The radiographs reveal a positive Hawkins sign, a subchondral lucency in the talar dome best seen on a mortise radiograph indicating viability of the talar body. Once a Hawkins sign appears, it is unlikely that that the patient will develop osteonecrosis.
Osteonecrosis is best diagnosed with radiographs. Although MRI can be helpful in assessing the extent of osteonecrosis, it is unnecessary for purely diagnostic purposes. A Hawkins sign typically will appear at 6 to 8 weeks after fracture; however, the absence of a Hawkins sign at that time does not necessarily indicate osteonecrosis. Most authors agree that even in the absence of a Hawkins sign, weight bearing can commence at 10 to 12 weeks after surgery.
Question 30:
Osteolysis, after total knee arthroplasty performed without cement, most often occurs in the
Options:
- Patella
- Tibial stem
- Distal femoral interface
- Posterior femoral interface
- Sites of screw fixation for the tibia
Correct Answer: Sites of screw fixation for the tibia
Explanation:
As stated in the above article, the number one location for osteolysis is at the sites of screw fixation for the tibial component. Development of osteolysis on the tibial side of the implant may be influenced by three
factors. First gravity and weight bearing through the medial side of the knee tend to localize the debris particulate polyethylene on the tibial side. Second, on the femoral side if the osteolytic process is initiated along the implant-bone interface, the flanges of the femoral implant obscure a radiographic diagnosis. Finally, the addition of screws to the tibial implant provide avenues for the migration of debris into the bone. In the patients with osteolysis all had very large amounts of polythylene and metal particles less than one micrometer in size leading to intense histiolytic response.
Question 31:
Figure 21 shows the AP radiograph of a 41-year-old patient who sustained a closed bicolumnar fracture of the distal humerus that resulted in a painful nonunion. What is the best initial construct for rigid stabilization of this fracture pattern?
Options:
- Posterior “Y” plate fixation
- Dual one third tubular plate fixation with a hinged external fixator
- Dual one third tubular plate fixation
- Dual 3.5-mm reconstruction plate fixation
- Single lateral plate fixation with transcortical screw fixation
Correct Answer: Dual 3.5-mm reconstruction plate fixation
Explanation:
DISCUSSION: The dual plate fixation construct is significantly stronger than single plate or “Y” plate fixation. Two-plate constructs at right angles, the ulnar plate medially and the lateral plate posteriorly, would appear to be biomechanically optimal. This approach usually is feasible at the time of surgery. Clinically, dual 3.5-mm reconstruction or dynamic compression plates are superior to one third tubular plate fixation. Supplementary external fixation is not considered a better treatment option. Failure of fixation and nonunion are often the result of inadequate fixation and osteoporosis.
REFERENCES: Helfet DL, Hotchkiss RN: Internal fixation of the distal humerus: A biomechanical comparison of methods. J Orthop Trauma 1990;4:260-264.
Sodergard J, Sandelin J, Bostman O: Mechanical failures of internal fixation in T and Y fractures of the distal humerus. J Trauma 1992;33:687-690.
Question 32:
A patient who underwent open reduction and internal fixation of an olecranon fracture 2 months ago now reports painless limitation of motion. Examination reveals a well-healed incision and a flexion-extension arc from 40 degrees to 80 degrees. The patient has been performing home exercises. Radiographs are shown in Figures 26a and 26b. What is the most appropriate treatment?
Options:
- Continued observation and home therapy
- Radiation therapy, followed by aggressive range-of-motion exercises
- Formal physical therapy and static progressive splinting
- Revision open reduction and internal fixation and capsular release
- Manipulation under anesthesia
Correct Answer: Formal physical therapy and static progressive splinting
Explanation:
DISCUSSION: The radiographs do not show an articular malunion. Treatment is directed at the soft-tissue contracture and should begin with formal physical therapy and static progressive splinting. Radiation therapy is effective in the perioperative period and is indicated when ectopic bone formation is a concern.
REFERENCES: Morrey BF: The posttraumatic stiff elbow. Clin Orthop Relat Res
2005;431:26-35.
King GJ, Faber KJ: Posttraumatic elbow stiffness. Orthop Clin North Am 2000;31:129-143.
Question 33:
- In a patient with T10-level spinal cord injury, which of the following prognostic signs most likely suggests functional recovery in the lower extremities?
Options:
- T10 sensory pin-prick level
- Retained vibratory sensation at the ankles
- Presence of sacral sparing
- Retained spontaneous respiratory function
- Priapism
Correct Answer: Presence of sacral sparing
Explanation:
Sacral sparing is evidenced by perianal sensation, rectal motor function and great toe flexor activity. Presence of sacral sparing indicates an incomplete cord injury and the potential of more function after the resolution of spinal shock. If there is no evidence of spinal cord function below the level of the injury, including sacral sparing, and the bulbocavernosus reflex has not returned, no determination can be made regarding the completeness of the lesion.
Question 34:
A 25-year-old man injured his dominant shoulder after falling on his outstretched arm 4 months ago. Examination reveals that he cannot lift his arm above 90 degrees, and he has pronounced medial scapular winging. Management should consist of
Options:
- spinal accessory nerve exploration with repair.
- long thoracic nerve exploration with repair.
- a sling for comfort, followed by shoulder strengthening exercises.
- scapulothoracic arthrodesis.
- split pectoralis major transfer.
Correct Answer: a sling for comfort, followed by shoulder strengthening exercises.
Explanation:
DISCUSSION: Serratus anterior palsy or long thoracic nerve palsy is usually caused by traction injury to the nerve, blunt injury, or iatrogenic injury. The palsy results in winging of the scapula and medial rotation of the inferior pole of the scapula. A patient with this injury will usually recover in 12 to 18 months. Initial treatment should include observation and shoulder strengthening exercises. Nerve exploration with repair has not proven beneficial in changing the outcome. Many orthopaedic surgeons favor using a split pectoralis major transfer for symptomatic patients. Electrodiagnostic studies are helpful in confirming the diagnosis.
REFERENCES: Post M: Pectoralis major transfer for winging of the scapula. J Shoulder Elbow Surg 1995;4:1-9.
Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 35:
A 47-year-old man who works as a carpenter reports a 12-month history of painful mechanical locking of his dominant elbow in the mid range of movement. He also has progressive pain at terminal extension that has not responded to medication, rest, and intra-articular cortisone injection. Active range of movement is from 35 degrees to 130 degrees, and he has full pronation and supination. The ulnar nerve is stable, and he has no subjective or objective neurologic dysfunction in the hand. Radiographs are shown in Figures 22a and 22b. What is the most appropriate treatment? Review Topic
Options:
- Oral corticosteroid medication and changes in job activities
- Soft-tissue interposition arthroplasty
- Arthroscopic capsular release, loose body removal, and osteophyte decompression
- Radial head arthroplasty
- Total elbow arthroplasty
Correct Answer: Arthroscopic capsular release, loose body removal, and osteophyte decompression
Explanation:
The most appropriate treatment is arthroscopic capsular release, loose body removal, and osteophyte decompression. The patient has moderate osteoarthritis of the dominant elbow, with mechanical symptoms suggestive of loose osteochondral body formation. Because the patient has failed to respond to the typical nonsurgical therapeutic options, it is unlikely that further oral medication will be helpful, and job modification may not be practical at this stage. Soft-tissue arthroplasty may be reasonable to consider when less invasive methods, such as arthroscopy, fail. Isolated radial head arthroplasty would not sufficiently address the symptoms. Total elbow arthroplasty is indicated in cases of more advanced disease in older patients with lower physical demands.
Question 36:
What is the most appropriate treatment for a 17-year-old boy who sustained a gunshot wound to his forearm from a handgun with a muzzle-velocity of 1000 feet/second if he is neurovascularly intact and radiographs reveal no fracture?
Options:
- Irrigation and local wound care in the emergency department followed by 3 days of oral antibiotics
- Emergent irrigation and debridement in the operating room with vacuum-assisted wound closure
- Emergent irrigation and debridement in the operating room with 7 days of intravenous antibiotics
- Wound closure in the emergency department with follow-up wound check in 1 week
- Exploration and removal of all bullet fragments in the emergency department and 10 day course of oral antibiotics
Correct Answer: Irrigation and local wound care in the emergency department followed by 3 days of oral antibiotics
Explanation:
DISCUSSION: The question refers to appropriate management of a gunshot wound to the forearm. The first question that must be answered when evaluating gun shot injuries is whether the gunshot is low velocity or high velocity. Low-velocity wounds are less severe, are more common in the civilian population, and are typically attributed to bullets with muzzle velocities below 1,000 to 2,000 feet per second. Tissue damage is usually more substantial with higher-velocity (greater than 2,000 to 3,000 fps) military and hunting weapons. In this question, a muzzle velocity of 1,000 ft/sec is provided. Low velocity injuries with stable, non-operative fractures can be treated with local wound care and oral antibiotics.
The two referenced articles offer guidance for treating low-velocity gunshot injuries with stable, non-operative fracture patterns. The first article by Geissler et al is a retrospective study comparing 25 patients that prospectively received local irrigation and debridement, tetanus prophylaxis and a long acting cephalosporin intramuscularly to a random retrospective sample of 25 patients with similar ballistic-induced fractures and wounds managed by local debridement and 48h of intravenous antibiotics. One infection occurred in each group, requiring further therapy. It was concluded that patients with low-velocity gunshot induced fractures can be managed without the use of short-term intravenous antibiotics with no increased risk of infection.
In the second study, Dickey et al evaluated the efficacy of an outpatient management protocol for patients with a gunshot-induced fracture with a stable, non-operative configuration. 41 patients with a grade I or II open, nonoperative fracture secondary to a low-velocity bullet were treated with 1gm of cefazolin administered in the emergency room and a 7-day course of oral cephalexin. No patient developed a deep infection. Thus, local I&D, tetanus, and oral antibiotics for 2-3 days is adequate for low velocity gunshot wounds
Question 37:
Which of the following is an advantage of computer-assisted navigation used to place medullary nail interlocking screws compared to a freehand techinque?
Options:
- Reduced fluoroscopy time
- More reliable placement of interlocking screws through the nail
- Reduced procedure time
- Increased quality of fluoroscopic images
- Improved accuracy of screw length
Correct Answer: Reduced fluoroscopy time
Explanation:
DISCUSSION: Computer-assisted navigation has been shown to reduce radiation exposure for surgeons when performing interlocking of medullary nails compared to free-hand technique.
Ricci et al compared two fluoroscopic navigation tracking technologies, optical and electromagnetic versus standard freehand fluoroscopic targeting, in a standardized foam block model for placement of interlocking screws. They found that fluoroscopy time (seconds) and number of fluoroscopy images were significantly less when using the computer-guided systems than for freehand-unguided insertion. Average distance of pin placement from the target in the foam blocks was significantly greater for controls than for each of the navigated systems.
Suhm et al performed a prospective controlled clinical study to compare fluoroscopic guidance with fluoroscopy-based surgical navigation for distal locking of intramedullary implants. The surgical navigation group showed increased procedure time, but equivalent precision with reduced radiation exposure. There was no significant difference in the technical reliability between both groups.
Question 38:
In performing a posterior stabilized total knee arthroplasty (TKA), which component malpositioning is associated with the wear damage shown in this tibial component retrieval (Figure 172)?
Options:
- Excessive femoral component flexion
- Excessive anterior slope of the proximal tibia
- Excessive tibial component varus
- Excessive valgus resection of the distal femur
Correct Answer: Excessive femoral component flexion
Explanation:
DISCUSSION
The tibial polyethylene insert shows anterior post wear damage from anterior CAM-post impingement in a posterior stabilized knee. It is associated with excessive femoral component flexion and excessive posterior tibial slope in a TKA construct. It is not associated with coronal plane alignment.
Question 39:
Which of the following postoperative rehabilitation techniques causes minimal rotator cuff muscle activation? Review Topic
Options:
- Active forward flexion
- Passive forward flexion
- Active-assisted forward flexion
- Overhead pulley-assisted passive forward flexion
- Isometric strengthening
Correct Answer: Passive forward flexion
Explanation:
Electromyography (EMG) studies have shown that the rotator cuff is least active with passive range of motion and hence this is allowed early in most postoperative rotator cuff rehabilitation protocols. Active forward flexion, active-assisted motion, and isometric strengthening all cause activation of the rotator cuff muscles (as measured by EMG) and therefore should be introduced later in rehabilitation when the repair can withstand these forces. Whereas some authors have felt that pulley-assisted range of motion exercises are safe, EMG analysis has demonstrated that these exercises do cause activation of the rotator cuff musculature and probably should be avoided early in the rehabilitation protocol.
Question 40:
Degenerative spondylolisthesis of the cervical spine is most commonly seen at which of the following levels?
Options:
- C1-2
- C3-4
- C5-6
- C6-7
- C7-T1
Correct Answer: C3-4
Explanation:
DISCUSSION: Degenerative spondylolisthesis of the cervical spine is seen almost exclusively at C3-4 and C4-5; this is in contrast to degenerative changes, which are most commonly seen at C5-6 and C6-7.
REFERENCES: Tani T, Kawasaki M, Taniguchi S, et al: Functional importance of degenerative spondylolisthesis in cervical spondylotic myelopathy in the elderly. Spine 2003;28:1128-1134.
Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopedic Surgeons, 2002, pp 299-309.
Question 41:
A 56-year-old man sustained a nondisplaced extra-articular fracture of the proximal aspect of the third metatarsal after dropping a heavy object on his left foot. Management should consist of
Options:
- open reduction and internal fixation.
- external bone stimulation.
- percutaneous pin fixation.
- weight bearing in a walking boot or walking cast.
- open reduction and internal fixation and primary tarsometatarsal joint fusion.
Correct Answer: weight bearing in a walking boot or walking cast.
Explanation:
DISCUSSION: This injury pattern is one of a direct trauma to the mid aspect of the foot. Without additional forces involved, capsular ligamentous injury is not anticipated; therefore, the injury should be a stable pattern. Treatment should consist of protected weight bearing as tolerated in a walking boot or walking cast. Surgical intervention with open reduction and internal fixation, percutaneous pinning, or open reduction and internal fixation with primary tarsometatarsal joint fusion is not indicated with this pattern of injury. The use of external bone stimulation in this acute fracture setting is not indicated. With injuries to the midfoot area where the exact mechanism of injury is uncertain, there should be a high index of suspicion for an associated injury to the tarsometatarsal joint, and standing radiographs or stress radiographs should be obtained.
REFERENCES: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1265-1296.
Early JS: Fractures and dislocations of the midfoot and forefoot, in Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001,
pp 2181-2245.
Question 42:
Figures A and B are post-operative radiographs of a 54-year-old female. In the first 6 months after this procedure, what is the most likely factor for functional impairment in this patient?
Options:
- Osteonecrosis
- Anterior knee pain
- Re-fracture
- Hardware failure
- Non-union
Correct Answer: Osteonecrosis
Explanation:
A residual deficit in muscle performance and anterior knee pain are expected in the majority of patients at 6 months after surgical fixation of their patella fractures.
Anterior knee pain is reported to be a common symptom following treatment of patellar fractures. A likely contributing factor to the anterior knee pain is scarring and tightness of the structures surrounding the knee, as well as patella maltracking due to quadricep/hamstring weakness and/or poor muscle synchrony. Other factors for anterior knee pain may include symptomatic hardware, which may be treated with removal of fixation after union has been achieved.
Lazaro et al. looked at the outcome data on thirty patients with isolated unilateral patellar fractures. Anterior knee pain during activities of daily living was experienced by twenty-four (80%) of the patients. The knee extensor mechanism on the injured side had deficits in strength (-41%), power (-47%), and endurance (-34%) as compared with the uninjured side.
Lebrun et al. reviewed a series of 40 operatively treated patella fractures and found that at over 6 years postoperatively, significant symptomatic complaints and functional deficits persisted based on validated outcome measures as well as objective physical evaluations. Removal of symptomatic fixation was required in 52% of the patients treated with osteosynthesis, whereas 38% of those with retained fixation self-reported implant-related pain at least some of the time.
Figure A and B show AP and lateral radiographs of a comminuted patella fracture treated with a tension band repair construct. The articular surface looks well reduced.
Incorrect Answers:
Question 43:
Which of the following is the most sensitive parameter to detect the increased inflammatory response seen with both postoperative infection and the use of instrumentation in spinal surgery?
Options:
- Patient temperature
- WBC count
- Erythrocyte sedimentation rate
- C-reactive protein
- Rheumatoid Factor
Correct Answer: Patient temperature
Explanation:
CORRECT
DISCUSSION: The most sensitive parameter to detect inflammation elicited by implants and infection is the C-reactive protein (CRP).
CRP is an acute phase reactant that increases sharply immediately after surgery within 6 hours after tissue damage. CRP then peaks 2-3 days later and returns to normal levels 5-21 days after the inciting event. In contrast, ESR reaches its peak on days 4-11, then remains elevated for a prolonged period of time.
Takahashi et al performed a Level 3 study of patients who had undergone spinal surgery with and without instrumentation, with a primary outcome of infection. They concluded that renewed elevation of C-reactive protein, white blood cell count, and body temperature after postoperative days 4 to 7 may be a key indicator of postoperative infection.
Question 44:
Of the following factors, which is considered the most important prognostic indicator in soft-tissue sarcomas?
Options:
- Age of the patient
- Prior excisional biopsy
- Histologic subtype
- Superficial versus deep to the fascia location
- Size of the sarcoma
Correct Answer: Size of the sarcoma
Explanation:
DISCUSSION: Histologic grade, the presence or absence of metastatic disease, and tumor size are important prognostic factors. Of the available choices, however, the size of the sarcoma is the most important prognostic indicator. A tumor size of greater than 5 cm is a more important prognostic factor than tumor location. Patients with sarcomas that measure 5 cm or less have nearly identical 3-year survival rates regardless of whether the tumor is subcutaneous or deep. Histologic grade (high versus low) is an important factor. However, histologic subtype frequently is not as important a factor as tumor size.
REFERENCE: Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173.
Question 45:
-Figures 10a and 10b are the sagittal and coronal MRI scans of a 5-year-old boy who noticed “clicking” in his right knee. His family denied any trauma, but admitted that the child was active and fell frequently.Birth and developmental history were unremarkable, and specifically negative for other musculoskeletal conditions. On physical examination, there was no warmth, tenderness, or erythema, or effusion. The child had an audible and palpable clunk when the knee was taken from a position of extreme flexion to full extension. There was no anterior, posterior, medial, or lateral instability on examination or medial or lateral joint line tenderness. The child had not been systemically ill. Radiographs were unrevealing.What is the most likely diagnosis?
Options:
- Discoid lateral meniscus
- Congenital absence of the anterior cruciate ligament
- Torn medial meniscus
- Osteomyelitis of the distal femur DISCUSSION A discoid lateral meniscus is probably the most common cause of a symptomatic clicking or clunking in the knee in a young child. This is a congenital problem that can become symptomatic as soon as a child ambulates, or the condition may remain asymptomatic for several years. The meniscus develops from a cartilaginous anlage and at no point in its development is it discoid. The MRI scans reveal a band of meniscal tissue filling the joint’s lateral compartment on both sagittal and coronal images. A medial meniscal tear is usually accompanied by a history of injury and an effusion, which are not present in this child. There is also no joint line tenderness, which makes this diagnosis less likely. Congenital absence of the anterior cruciate ligament may be found in children born with congenital knee hyperextension, which is ruled out in this case by normal history and examination findings. Children with osteomyelitis are often systemically ill. On examination, they may have warmth and tenderness. MRI scans will often show an area of increased signal on T1-weighted images.
Correct Answer: Discoid lateral meniscus
Question 46:
EXT1
Options:
- This patient has multiple hereditary exostoses. Widening of the metaphysis is characteristic of multiple hereditary exostoses. Large sessile osteochondromas arise from the metaphysis and a large osteochondroma arises from the medial metaphysis with a characteristic cartilaginous cap. The computed tomography scan shows the widening and abnormal tubulation of the bone.
- No evidence of malignancy exists in this large osteochondroma. The cartilage cap is regular with no areas of bone destruction. One should also look for a soft tissue mass, which often shows areas of focal calcifications. No soft tissue masses are present in this patient.
- It is important to remember that this condition is autosomal dominant. The putative tumor suppressive gene mutation is EXT1, EXT2. The risk of low-grade chondrosarcoma occurring in this condition is approximately 10%.
Correct Answer: It is important to remember that this condition is autosomal dominant. The putative tumor suppressive gene mutation is EXT1, EXT2. The risk of low-grade chondrosarcoma occurring in this condition is approximately 10%.
Explanation:
slide 1 slide 2 slide 3
A patient presents with a hard leg mass and pain with activity. The anteroposterior and lateral radiographs are shown in Slide 1 and Slide 2. An axial computed tomography scan is shown in Slide 3. Which of the following would be the most appropriate treatment:
Question 47:
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of
Options:
- rigid open reduction and internal fixation of the os acromiale with autologous bone graft.
- arthroscopic repair of the rotator cuff and acromioplasty.
- arthroscopic excision of the os acromiale.
- arthroscopic decompression of the supraglenoid cyst.
- open distal clavicle excision (Mumford procedure).
Correct Answer: rigid open reduction and internal fixation of the os acromiale with autologous bone graft.
Explanation:
DISCUSSION: The MRI scans show a mesoacromion with tendonopathy of the supraspinatus. The history and physical findings indicate that the patient has a symptomatic os acromiale. Simple excision of the unstable os acromiale has not yielded consistently good results. Meticulous internal fixation using tension banding with cannulated screws and autologous bone grafting has shown good results for this problem.
REFERENCES: Hutchinson MR, Veenstra MA: Arthroscopic decompression of shoulder impingement secondary to os acromiale. Arthroscopy 1993;9:28-32.
Warner JJ, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Question 48:
A displaced pediatric supracondylar humerus fracture is treated with closed manipulation and placement of 2 Kirschner wires placed from the lateral side. What would be the effect of adding a third pin from the lateral side? Review Topic
Options:
- Increase risk for iatrogenic ulnar nerve injury
- Provide more construct stiffness than adding a medial pin
- Improve construct stiffness in the presence of medial column comminution
- Will not affect construct stiffness in the presence of residual distal fragment internal rotation
Correct Answer: Improve construct stiffness in the presence of medial column comminution
Explanation:
Multiple biomechanical studies have shown that the addition of a third pin from the lateral side improves construct stiffness in the presence of medial column loss or slight internal rotation of the distal fragment. The same studies show that addition of a medial pin (cross pinning) has essentially the same benefit. Placement of a medial pin increases risk for iatrogenic nerve injury.
Question 49:
Which of the following descriptions is true regarding APC-II (anterior-posterior compression) pelvic injuries as classified by Young and Burgess?
Options:
- Pubic symphysis diastasis, intact anterior sacroiliac ligaments, intact sacrotuberous ligament, intact posterior sacroiliac ligaments
- Pubic symphysis diastasis, torn anterior sacroiliac ligaments, intact sacrotuberous ligament intact posterior sacroiliac ligaments
- Pubic symphysis diastasis, intact anterior sacroiliac ligaments, torn sacrotuberous ligament, intact
- posterior sacroiliac ligaments
- Pubic symphysis diastasis, torn anterior sacroiliac ligaments, torn sacrotuberous ligament, intact posterior sacroiliac ligaments
- Pubic symphysis diastasis, intact anterior sacroiliac ligaments, torn sacrotuberous ligament, torn posterior sacroiliac ligaments
Correct Answer: Pubic symphysis diastasis, intact anterior sacroiliac ligaments, intact sacrotuberous ligament, intact posterior sacroiliac ligaments
Explanation:
DISCUSSION: APC II injuries are unstable injuries and occur as a result of high-energy trauma. Anatomic structures which are injured or torn include the pubic symphysis, anterior iliosacral ligaments, and the sacrotuberous ligaments. The posterior sacroiliac ligaments are spared in APC-II injuries, and differentiate an APC-II injury from an APC-III injury, in which the posterior ligaments are also torn.
Burgess et al review the classifications of pelvic ring disruptions and their association with mortality. They concluded that APC injuries required more blood replacement and were related to death more often than lateral compression, vertical shear, or combined mechanism pelvic injuries.
Tile studied the anatomy of anterior to posterior pelvic ring injuries. Although the anterior structures, the symphysis pubis and the pubic rami, contribute to 40% to the stiffness of the pelvis, clinical and biomechanical studies have shown that the posterior sacroiliac complex is more important to pelvic-ring stability. The posterior sacroiliac ligamentous complex is more important to pelvic-ring stability than the anterior structures and therefore, the classification of pelvic fractures is based on the stability of the posterior lesion.
Question 50:
In Dupuytren’s disease, the retrovascular cord typically displaces the radial proper digital nerve of the ring finger in what direction?
Options:
- Palmarly and radially
- Dorsally and ulnarly
- Palmarly and ulnarly
- Dorsally and radially
- Directly dorsal
Correct Answer: Palmarly and ulnarly
Explanation:
DISCUSSION: Retrovascular cords are common in Dupuytren’s disease and commonly require surgical treatment. Nerve injury in Dupuytren’s surgery is an infrequent complication that occurs partly because the digital nerves can be displaced from their normal anatomic relationships by retrovascular cords. The nerves are displaced superficially, toward the center of the digit (palmarly and ulnarly). This displacement is typically seen at the level of the metacarpophalangeal joint.
REFERENCE: Rayan GM: Palmar fascial complex anatomy and pathology in Dupuytren’s disease. Hand Clin 1999;15:73-86.
Question 51:
Which of the following is considered an important factor in improved cemented femoral stem survivorship?
Options:
- Precoated stem with methylmethacrylate
- Varus stem position
- 2 to 3 mm of circumferential cement mantle
- Dorr C or “stovepipe” femoral anatomy
- Sharp angled corners on the femoral stem
Correct Answer: 2 to 3 mm of circumferential cement mantle
Explanation:
DISCUSSION: Cement technique, relative stem to canal size and position, stem design, surgical technique, and femoral anatomy are important factors in cemented stem survivorship. Varus stem position, a wide diaphyseal to metaphyseal ratio (stovepipe femur), thin cement mantles (1 mm or less), and nonrounded femoral stem designs are negative prognostic factors for stem survivorship. Precoating with methylmethacrylate has not been shown to provide any increased survivorship over nonprecoated stems.
REFERENCES: Noble PC, Collier MB, Maltry JA, Kamaric E, Tullos HS: Pressurization and centalization enhance the quality and reproducibility of cement mantles. Clin Orthop 1998;355:77-89.
Crowninshield RD, Brand RA, Johnston RC, Milroy JC: The effect of femoral stem cross-sectional geometry on cement stresses in total hip reconstruction. Clin Orthop 1980;146:71-77.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 52:
..First-line treatment recommendations include
Options:
- synovectomy.
- arthrocentesis, compressive wrap, and rest.
- en bloc resection.
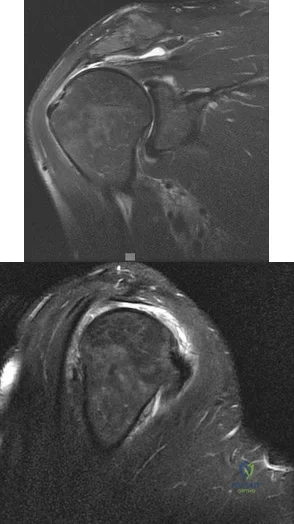
- intra-articular radioactive nucleotide injection. DISCUSSION… The MRI scans reveal classic findings of PVNS with low signal on proton density and T2 sequences and evidence of “blooming” on gradient echo sequences. A discrete mass suggestive of a sarcoma (which would typically appear dark on T1 and bright on T2, but heterogenous and enhancing) is not seen, and synovial sarcomas rarely arise in an intra-articular location. Cartilaginous nodules of synovial chondromatosis are not seen, and the abnormal synovial process indicates that this is more than just a posttraumatic hemarthrosis. Treatment is synovectomy; radiotherapy is reserved for select recurrent cases. Arthrocentesis would be used for a simple hemarthrosis, and resection used for a sarcoma.
Correct Answer: en bloc resection.
Explanation:
RESPONSES FOR QUESTIONS 47 THROUGH 52
Ultrasound
MRI scan of the thigh
Chest CT scan and whole-body bone scan
Positron emission tomography (PET) scan
Presurgical radiation therapy
Marginal resection
Radical resection and postsurgical radiation
Transverse incision centered over the mass
Incision centered over the mass in line with long axis of limb
Sentinel node biopsy
Core needle biopsy
For each soft-tissue mass clinical scenario or question below, match the most appropriate next evaluation or treatment step listed above.
Question 53:
Figure 17 is the radiograph of a 3-year-old girl who has shoulder pain after a fall. What is the best next step?
Options:
- 4 to 6 weeks of immobilization
- Incisional biopsy followed by curettage and bone grafting
- Irrigation and debridement and then antibiotics based on culture findings
- Radical excision
Correct Answer: 4 to 6 weeks of immobilization
Explanation:
DISCUSSION
Patients with a pathologic fracture of a unicameral bone cyst or simple bone cyst should first pursue nonsurgical treatment and 4 to 6 weeks of immobilization. Spontaneous healing occurs in fewer than 10% of patients, possibly due to cyst decompression. The most appropriate form of surgical treatment is controversial. Many substances have been injected with variable results. Injection with steroid, bone marrow, demineralized bone matrix, and calcium phosphate/calcium sulfate have been attempted. Curettage and bone grafting and
decompression have been attempted. Indications for treatment are based on cyst size, symptoms, and location. Unicameral bone cysts typically resolve as patients reach skeletal maturity.
CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 23
Figure 18 is the lateral radiograph of the lumbar spine of an 11-year-old boy who has had lower back pain for 2 months. There is no history of injury. He denies radiating pain to his legs, numbness, weakness, and bowel or bladder changes. His usual activities include soccer practices and games 3 to 5 times per week. He has used over-the-counter anti-inflammatory medications, but has had no other treatment.
Question 54:
An elite football player has sustained a left knee injury during play. A dynamic imaging analysis is performed on the affected knee, which shows anterior shift and internal rotation of the tibia at low flexion angles. There is also some mild medial translation of the tibia at greater flexion angles. What structure(s) have most likely been injury? Review Topic
Options:
- Anterior cruciate ligament
- Posterior cruciate ligament
- Posterior cruciate ligament and medial collateral ligament
- Medial collateral ligament
- Lateral collateral ligament, popliteal tendon and arcuate ligament
Correct Answer: Medial collateral ligament
Explanation:
This patient has sustained an anterior cruciate ligament (ACL) rupture.
The ACL is the primary restraint to anterior translation of the tibia relative to the femur. It also acts as secondary restraint to tibial rotation and varus/valgus rotation. ACL-deficient knees have been shown to have abnormal knee kinematics, which has been thought to contribute to the osteoarthritis that develops after injury.
DeFrate et al. examined the knee joint kinematics of 8 patients with unilateral anterior cruciate ligament rupture using in vivo imaging. They found significant anterior shift and internal rotation of the tibia at low flexion angles in ACL-deficient knees. They also noted some medial translation of the tibia between 15° and 90° of flexion.
Illustration A shows the effect of medial tibial translation on tibiofemoral contact in ACL-deficient knees. The medial translation of the tibia causes increased contact between the tibial spine and inner surface of the medial femoral condyle. This might be a contributing factor to the joint degeneration observed in ACL-deficient patients.
Incorrect Answers:
Question 55:
Sex-linked recessive Pseudohypoparathyroidism (AHO) - end-organ insensitivity; in AHO, germline mutation that leads to loss of function of Galpha S (GNAS1); causes end-organ resistance to PTH
Options:
- PHP - short stature, short metacarpals (4th and 5th), rounded facies
- Mental retardation, tetany
- Sex-linked dominant
- Laboratory features
- Hypocalcemia
- Hyperphopshatemia
- Normal PTH
Correct Answer: Sex-linked dominant
Explanation:
Which of the following is the defect in pseudohypoparathyroidism (Albright Hereditary Osteodystrophy [AHO]):
Question 56:
A 39-year-old man has had persistent right shoulder pain for the past 6 months. A formal physical therapy program has failed to provide relief, and an injection several months ago provided only short-term relief. Examination reveals a positive Neer and Hawkins test. There is no instability and the neurovascular
Options:
- Arthroscopic debridement alone of the partial rotator cuff tear
- Repair of the partial rotator cuff tear and subacromial decompression
- Arthroscopic debridement combined with subacromial decompression
- Arthroscopic subacromial decompression
- Biceps tenotomy
Correct Answer: Repair of the partial rotator cuff tear and subacromial decompression
Explanation:
Although arthroscopic debridement with or without subacromial decompression is a reasonable response, the patient has positive impingement signs. Several recent studies regarding the surgical treatment of partial rotator cuff tears have demonstrated good to excellent results after repair of tears involving more than 50% of the tendon thickness. This was shown specifically for bursal-sided tears and joint-side tears. Biceps tenotomy is not indicated in a young patient.
Question 57:
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. What is the underlying cause of the pathology noted in the figures?
Options:
- Genetic mutation
- Recurrent trauma
- Shallow intercondylar notch
- Congenital abnormality
Correct Answer: Congenital abnormality
Explanation:
The MR images show a tear through a discoid lateral meniscus. A discoid meniscus is caused by a failure of apoptosis during development in utero and is considered a congenital abnormality. Discoid menisci are prone to tearing and can be caused by minimal trauma. There is no known genetic cause for this condition. Radiographic findings that may be present in the setting of a discoid meniscus include lateral joint space widening, squaring of the lateral femoral condyle, and cupping of the lateral tibial plateau. Contralateral discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment
of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair.
Question 58:
Presence of diabetes-induced peripheral neuropathy has been shown to be an independent risk factor for postoperative complications of which of the following injuries?
Options:
- Distal radius fractures
- Patella fractures
- Metatarsal fractures
- Ankle fractures
- Distal femoral fractures
Correct Answer: Distal radius fractures
Explanation:
DISCUSSION: Presence of peripheral neuropathy has important implications in treating ankle fractures in diabetic patients. Increased immobilization periods, attention to tight glucose control, and adjunct/alternative operative techniques may be necessary for an optimal outcome. The first referenced article by Chaudry et al is an excellent review of diabetic ankle fractures. The second reference by Costigan et al noted that peripheral neuropathy is the most significant risk factor for postoperative complications, followed closely by lack of pedal pulses preoperatively. The last referenced article by Jones et al noted a significantly higher complication rate in diabetics with operative ankle fractures, and reported that neuroarthropathy is a significant risk factor for postoperative complications.
Question 59:
A 52-year-old woman with a 2-year history of a flexible (stage II) adult-acquired flatfoot deformity has failed to respond to nonsurgical management consisting of immobilization, custom orthotics, nonsteroidal anti-inflammatory drugs, and physical therapy. The patient is unable to perform a single limb heel rise. Weight-bearing radiographs are shown in Figures 30a through 30c. What is the most appropriate surgical correction?
Options:
- Tendon transfer, lateral column lengthening, and heel cord lengthening
- Triple arthrodesis and heel cord lengthening
- Tendon transfer, lateral column lengthening, medial column arthrodesis, and heel cord lengthening
- Tendon transfer, spring ligament repair, and heel cord lengthening
- Tendon repair, medial displacement calcaneal osteotomy, and heel cord lengthening
Correct Answer: Tendon transfer, lateral column lengthening, medial column arthrodesis, and heel cord lengthening
Explanation:
DISCUSSION: The patient has an atypical adult flatfoot deformity. The radiographs reveal forefoot abduction, mild loss of calcaneal pitch, and marked plantar flexion sag through the naviculocuneiform joint. The inability to perform a single limb heel rise indicates that the posterior tibial tendon is nonfunctional; however, the deformity remains flexible. In this patient, surgical treatment should include a tendon transfer, lateral column lengthening, medial column arthrodesis, and heel cord lengthening. Because a substantial portion of the deformity stems from the naviculocuneiform joint in this instance, tendon transfer and lateral column lengthening alone provide insufficient deformity correction. Triple arthrodesis and heel cord lengthening is best reserved for fixed flatfoot deformities. Soft-tissue procedures alone are associated with a high failure rate, as are attempted tendon repairs.
REFERENCES: Greisberg J, Assal M, Hansen ST Jr, et al: Isolated medial column stabilization improves alignment in adult-acquired flatfoot. Clin Orthop Relat Res 2005;435:197-202.
Greisberg J, Hansen ST Jr, Sangeorzan BJ: Deformity and degeneration in the hindfoot and midfoot joints of the adult acquired flatfoot. Foot Ankle Int 2003;24:530-534.
Question 60:
Wear of metal-on-metal articulations in total hip arthroplasty is characterized by which if the following findings?
Options:
- Fewer number of particles/wear volume compared with ceramic/ceramic bearings
- Increased incidence of cancer secondary to higher serum metal levels
- Rapidly declining levels of serum metal levels following hip arthroplasty
- back to this question next question
- Ionically charged wear particles
- Lower in vitro wear rates compared with ceramic/ceramic bearings
Correct Answer: Fewer number of particles/wear volume compared with ceramic/ceramic bearings
Explanation:
Poor reference for this question. You can arrive at the answer by strict process of elimination. A few things first. Keep in mind that ceramic/ceramic bearings have the lowest wear rates and thus produce fewer number of particles (1 and 5 out). Serum metal levels in metal-on-metal arthroplasties increase following surgery, as corrosion takes place (3 out). In the mid 90's there was a concern for malignancy in patients with metal-on-metal arthroplaties; however, studies have found gross variation in the incidence of cancer in patients with such arthroplasties, and no statistical significant difference. There is still no consensus concerning the long-term effects of metal-onmetal articulations (2 out).This leaves 4 as an attractive answer. We know that metals are subject to corrosion, which is a chemical reaction process that weakens the metal. All metals corrode; the severity of corrosion is determined by the chemical composition of the metal. There are three types of corrosion affecting implant materials: galvanic, crevice, and fatigue. Galvanic corrosion occurs when an electrical current is established between two metals that have different chemical compositions. To avoid catastrophic galvanic corrosion, stainless steel should never be used with either cobalt or titanium alloys. Crevice corrosion occurs when the fluid in contact with the metal becomes stagnant, which then becomes acidic secondary to oxygen depletion. Finally fatigue corrosion may occur if the passive oxide film on the implant surface has been scratched or cracked. Once fatigue corrosion begins, the implant weakens and may fail below the endurance limit of the material.
Orthopaedic Knowledge Update: Hip & Knee Reconstruction 2. Rosemont, IL, Americal Academy of Orthopaedic Surgeons, 2000, pp 25-34. Jazrawi L, Kummer FJ, Di Cesare PE: Alternative Bearing Surfaces for Total Joint Arthroplasty. J Am Acad Orthop Surg 1998;6:198-203
Which of the following findings is a predisposing factor for an acute lateral patellar dislocation?
Hypoplastic medial femoral condyle
Dysplastic vastus lateralis
Patella baja
Decreased Q angle
Excessive internal rotation of the femur
Most acute patellar dislocations occur during the second decade. Lateral dislocations are by far the most common direction of injury. Patients with abnormal patellofemoral mechanics sustain patellar dislocations with less trauma and soft tissue injury compared with normal subjects. Predisposing factors for dislocation include hypoplastic lateral femoral condyle, dysplastic vastus medialus obliqus (VMO), patella alta, contracted iliotibial band, tight lateral retinaculum, valgus knee deformity, increased Q angle, ligamentous laxity, lateral insertion of patellar tendon on tibia, excess internal rotation of the femur / external rotation of tibia, previous patellar dislocations and injury to medial patellofemoral ligament (MPFL). Some authors favor open exploration of the MPFL following arthroscopic examination for acute patella dislocations.
Braham S, Vrahas MS, Fu FH: Knee fractures in the athlete. Orthop Clin North Am 2002;33:566-574
Which of the following substances is labeled with technetium Tc 99m in a conventional bone scan?
calcium
phosphate
Alkaline phosphatase
Biphosphonate
Type I collagen
Item deleted 04.47
What is the preferred type of graft for skin loss of the palmar aspect of the hand?
Unmeshed split-thickness
Meshed split-thickness
Multiple pinch
Full-thickness
Full-thickness with attached subcutaneous fat
In general, soft tissue coverage in the hand should supply tissue that is thin, pliable, durable, and that allows for tendon gliding. The goal is to replace "like with like". Ideally, the reconstruction should allow for sensation, dynamic function, and restoration of form. Skin grafts are usually autografts and they are either splitthickness skin grafts (STSG) or full-thickness skin grafts (FTSG). Compared to STSG, full thickness grafts contract less, are more durable and flexible, and have better sensation. They are the preferred grafts for areas prone to shear and load such as fingertips, the palm, and areas over joints. STSG are better for dorsal hand wounds. STSG can be meshed or unmeshed. Meshed STSG have fewer problems with seromas, hematomas, and infections; therefore, they have better take. However, the appearance of unmeshed STSG is more aesthetically satisfying.
Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp470-492.
What ligament is attached to the displaced distal tibial articular fracture shown in Figures12a and 12b?
Anterior talofibular
Anterior tibiofibular
Posterior talofibular
Posterior tibiofibular
Calcaneofibular
Ankle (AP & lateral) x-rays show a non-displaced lateral malleolus fracture and a minimally displaced posterior malleolar fracture. Mortise is well preserved. No tibiotalar dislocation/subluxation. Medial malleolus seems intact. The injury to the posterior plafond component or
posterior malleolus is a posterolateral avulsion fracture resulting from the pull of the posterior-inferior tibiofibular ligament. If this fragment constitutes >25-30% of the plafond surface, and/or is displaced more than 2 mm, the fragment needs internal fixation. The origin of the posterior tibiofibular ligament is broad, covering most of the horizontal distal surface of the tibia. As the ligament fibers sweep laterally and distally to insert on the fibula they fit over the trochlea.
Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, Americal Academy of Orthopaedic Surgeons, 2000, pp 203-225
Michelson JD: Ankle fractures resulting from rotational injuries. J Am Acad Orthop Surg 2003;11:403-412
A 35-year-old man with ankylosing spondylitis has progressive sagittal plane imbalance, difficulty with horizontal gaze, and thigh fatigue with standing. Radiographs are shown in Figures 13a and 13b. Maximum correction of the sagittal decompensation can be accomplished at a single level by which of the following procedures?
Smith-Peterson osteotomy (posterior closing wedge hinging on the posterior longitudinal ligament)
Transpedicular wedge resection osteotomy
Combined anterior and posterior surgery
Anterior opening wedge osteotomy
Vertebral column resection
In the radiographs we have AP / lateral spinal xrays of a patient with known ankylosing spondylitis. Of note, there are bilateral total hip arthroplasties. There is marked thoracic kyphosis, and mild thoracolumbar scoliosis. No evidence of acute fx/ dislocations. Notice that the question specifically states… maximum correction of the sagittal decompensationcan be accomplished at a single levelby which of the following procedures? Surgical correction of the kyphosis deformity with osteotomy was first done in 1945. Since then, surgeons have tried several different approaches and techniques to correct the stiff kyphosis. The transpedicular wedge osteotomy was described by Thomasen (1985) for the correction of deformity secondary to ankylosing spondylitis. In this technique the spinous process of L2 and the upper part of L3 are removed; the laminae of the second and the upper part of the third lumbar vertebrae are also removed as well as the articular processes of L2-3 and the pedicles of L2. A wedge fracture is created on the posterior wall of the vertebral body of L2. Then, plates are fixed to the spinous processes of T12-L1 and L3-4. Thomasen osteotomy places the apex of correction anteriorly, serving to shorten the spine and avoid anterior column lengthening. Advantages include the prevention of neural compression by creation of a large, shared neural foramen through removal of the pedicles, limited stretch of anterior structures, and cancellous bone healing. This technique provides maximum correction of the deformity, and can be accomplished at a single level. You either know it, or you don’t.
Berven SH, Deriven V, Smith JA, Emami A, Hu SS, Bradford DS: Management of fixed sagittal plane deformity: Results of the transpedicular wedge osteotomy. Spine 2001;26:2036-2043.
Thomasen E: Vertebral osteotomy for correction of kyphosis in ankylosing spondylitis.
Clin Orthop 1985;194:142-152
Question 61:
Figure 82 is the MRI scan of a 15-year-old boy who has had knee pain with running for 5 months. Radiographs show an osteochondritis dissecans (OCD) lesion of the medial femoral condyle. What is the most appropriate treatment? Review Topic
Options:
- Arthroscopic or open reduction and internal fixation
- Arthroscopic loose body removal
- Activity restriction for up to 9 months
- Subchondral drilling
Correct Answer: Arthroscopic or open reduction and internal fixation
Explanation:
OCD is an acquired lesion of the subchondral bone. Patients with OCD initially report nonspecific pain and variable amounts of swelling. Initial radiographs help identify the lesion and establish the status of the physes. An MRI scan is useful for assessing the potential for the lesion to heal with nonsurgical treatment. Nonsurgical treatment is appropriate for small, stable lesions in patients with open physes and focuses on activity restriction for 3 to 9 months. Surgical treatment is necessary for unstable or detached lesions. Stable lesions with intact articular cartilage can be treated with subchondral drilling to stimulate vascular ingrowth, with radiographic healing at an average of 4.4 months. Fixation is indicated for unstable or hinged lesions, and stabilization of the fragment can be achieved using a variety of implants through an arthroscopic or open approach. The fragment should be salvaged and the normal articular surface restored whenever possible.
Question 62:
Which of the following is a significant risk factor for airway complications after anterior cervical surgery? Review Topic
Options:
- Smoking history
- Pulmonary disease
- Absence of drainage from surgical drains
- Surgical time of more than 5 hours
- Myelopathy
Correct Answer: Surgical time of more than 5 hours
Explanation:
In a study of 311 patients undergoing anterior cervical surgery only, a surgical time of more than 5 hours and exposure of four or more vertebral bodies involving C4 or higher were found to be risk factors for postoperative airway complications. Surprisingly, preoperative pulmonary status, smoking history, absence of drainage, and myelopathy were not associated with airway complications.
Question 63:
The best patient-related outcomes, following the surgical treatment of cauda equina syndrome secondary to a large L5-S1 disk herniation, are most closely related to which of the following?
Options:
- Extent of bowel and bladder dysfunction
- Extent of the motor deficit
- Extent of the perianal saddle anesthesia
- Timing of surgery
- Location of the herniation
Correct Answer: Timing of surgery
Explanation:
DISCUSSION: The most predictable positive outcome from spinal surgery due to a cauda equina syndrome is early surgical intervention before any significant neurologic deficit develops. Meta-analysis studies demonstrate that surgical intervention more than 48 hours after the onset of cauda equina syndrome show an increased risk for poor outcomes.
REFERENCES: Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522.
Kohles SS, Kohles JD, Karp AP, et al: Time-dependent surgical outcomes following cauda equina syndrome diagnosis: Comments on meta-analysis. Spine 2004;29:1281-1287.
Question 64:
Delayed-onset muscle soreness (DOMS) is initially evident at the muscle tendon junction and can spread throughout the entire muscle. It is primarily associated with what type of exercise? Review Topic
Options:
- Concentric
- Isometric
- Eccentric
- Plyometric
Correct Answer: Eccentric
Explanation:
DOMS is primarily associated with eccentric exercise because fiber lengthening occurs during muscle contraction. Muscle injury occurs very early during eccentric exercise, with structural disruption of the cytoskeleton. A significant increase in creatine kinase levels occurs 24 to 48 hours after exercise and may peak between 3 to 6 days after exercise. All other choices are not strongly associated with delayed muscle soreness.
Question 65:
An 85-year-old right hand dominant male sustains a fall onto his elbow while trying to get out of the car. His past medical history is significant for diabetes, congestive heart failure, and COPD. He lives in a nursing home, and is able to ambulate at baseline without and assistive devices. What would be the ideal definitive surgical treatment options in this patient? Review Topic
Options:
- ORIF through an olecranon osteotomy with 90-90 plating
- Total elbow arthroplasty through an anterolateral approach between the brachialis and biceps
- Acute elbow fusion
- ORIF through a tricep splitting approach with parallel plating
- Total elbow arthroplasty through a direct posterior tricep sparing approach
Correct Answer: Total elbow arthroplasty through an anterolateral approach between the brachialis and biceps
Explanation:
This elderly low-demand patient would most benefit from a total elbow arthroplasty (TEA) done through a direct posterior tricep sparing approach.
TEA is a preferred alternative for ORIF in elderly patients with complex distal humeral fractures that are not amenable to stable fixation. Elderly patients appear to accommodate to objective limitations in function with time, and suffer less complications with TEA than ORIF in select cases.
Sorensen et al evaluated short- to medium term outcome of total elbow arthroplasty (TEA) in complex fractures of the distal humerus by evaluating 24 consecutive cases. Twenty of the patients were followed for almost 2 years, and their MEPS were 15 excellent, 4 good and 1 fair result. They concluded that TEA in complex fractures of the distal humerus in elderly patients can result in acceptable short- to medium term outcome.
Mckee et al conducted a prospective, randomized, controlled trial to compare
functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular, distal humeral fractures treated with open reduction-internal fixation (ORIF) or primary total elbow arthroplasty (TEA). They randomized 42 patients and found that TEA for the treatment of comminuted intra-articular distal humeral fractures resulted in more predictable and improved 2-year functional outcomes compared with ORIF, based on the MEPS.
Illustration A shows radiographs of a TEA. Incorrect Answers:
Question 66:
An 18-year-old man who sustained a lumbar fracture-dislocation with an associated complete spinal cord injury 6 weeks ago underwent instrumented posterior thoracolumbar fusion a few days after the injury. While at a rehabilitation facility, routine postoperative surveillance radiographs are obtained (Figures 11a through 11d). What is the most appropriate next step in management? Review Topic
Options:
- Observation alone with continued rehabilitation of the spinal cord injury
- Thoracolumbosacral orthosis bracing for 3 months
- Revision and extension of the posterior instrumentation and fusion
- Anterior lumbar corpectomy and fusion
- Anterior/posterior lumbar decompression and fusion
Correct Answer: Revision and extension of the posterior instrumentation and fusion
Explanation:
The patient has sustained a traumatic spondylolisthesis at the level below the caudal instrumented level, likely not appreciated at the index surgery. Surveillance radiographs indicate that there is significant translation in the lumbar spine on sitting, indicating an unstable injury. The lack of significant bony involvement indicates that the injury is predominantly through the anterior and posterior ligamentous complexes, and thus is unlikely to stabilize with nonsurgical management. Because the patient reduces almost completely on lying supine, the most appropriate course of action is extension of the posterior fusion to include the level of the instability. Because the patient has a complete spinal cord injury below the level of the thoracic fracture, decompression is not indicated.
Question 67:
When reconstructing the anterior cruciate ligament (ACL) with autograft, what is the most common source of surgical failure?
Options:
- Graft choice
- Tunnel position
- Tibial fixation
- Femoral fixation
Correct Answer: Tunnel position
Explanation:
Technical failure is the most common reason for ACL reconstruction failure. Tunnel position is the most frequent cause for technical failure. Malpositioning of the tunnel affects the length of the graft, causing either decreased range of motion or increased graft laxity. Although graft choice is an important factor when planning an ACL reconstruction, overall outcomes with autograft tissues are fairly similar. Fixation of the graft at the femoral or tibial end is not as important as tunnel position.
Question 68:
A 19-year-old linebacker for a collegiate football team has had two episodes of bilateral arm tingling and weakness after tackling; the symptoms resolved after 30 minutes of rest. Three follow-up neurologic examinations have been normal. Cervical spine CT and MRI scans are shown in Figures 13a through 13c. What is the next best step in management?
Options:
- The addition of a neck roll to the helmet and continuation of play
- Electrodiagnostic studies
- A series of epidural steroid injections, followed by a return to play
- Methylprednisolone dose pack, followed by a return to play in 1 week
- No further participation in football
Correct Answer: No further participation in football
Explanation:
DISCUSSION: Cervical spinal stenosis is a contraindication to participation in collision and contact sports. Previously, the risks of permanent quadriparesis from cervical spinal stenosis were thought to be unclear and athletes with cervical spinal stenosis were often allowed to play contact sports. In 1996, Torg and associates reported that developmental narrowing of the cervical canal in a stable patient does not appear to predispose an individual to permanent catastrophic neurologic injury and therefore should not preclude an athlete from participation in contact sports. However, the current understanding is that the actual risks of permanent neurologic injury from cervical stenosis are significant. The Torg ratio was previously used for diagnosis but is more recently thought to be of low predictive value as reported by Cantu. Current methods for diagnosis of cervical spinal stenosis rely on MRI and CT. Current diagnosis is based on comparisons of measurements with normal values. A cervical canal of less than 13 mm is considered stenotic whereas a diameter of less than 10 mm is considered absolute stenosis as reported by Crowl and Kong. This patient has symptomatic stenosis and should not be cleared for contact sports. A neck roll will not prevent neurologic injury in the presence of cervical spinal stenosis. Electrodiagnostic studies are not likely to add any additional significant findings with central canal stenosis. Cervical traction is not of value in the long-term. Epidural steroid injections or a methylprednisolone dose pack are not of value in this situation.
REFERENCES: Torg JS, Naranja RJ Jr, Pavlov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Cantu RC: The cervical spinal stenosis controversy. Clin Sports Med 1998;17:121-126. Crowl AC, Kong JF: Cervical Spine, in Johnson DL, Mair SD (eds): Clinical Sports Medicine. Philadelphia, PA, Mosby Elsevier, 2006, pp 143-149.
Question 69:
Figure A is the radiograph of an 11-year-old boy who fell directly on his left shoulder while riding a bicycle. He complained of pain in his left shoulder. An MRI scan of the injury is likely to reveal what findings? Review Topic
Options:
- Disruption of the coracoclavicular ligaments
- Dislocation of the acromioclavicular joint
- Impingement of the inferior fragment on the brachial plexus
- Intact periosteal sleeve inferiorly
Correct Answer: Intact periosteal sleeve inferiorly
Explanation:
In children, fractures of the distal clavicle are almost always through the distal physis and adjacent metaphysis, and, consequently, the acromioclavicular joint is rarely dislocated. The coracoclavicular ligaments usually remain attached to the thick periosteum on the undersurface of the clavicle and are rarely damaged. Because of the thick periosteum and intact ligaments, these fractures are inherently stable and heal well with conservative treatment. In contrast, similar injuries in adults pose a higher risk for surgical intervention.
Question 70:
Intradiskal electrothermal therapy (IDET) uses an intradiskal catheter to deliver controlled thermal energy to the inner periphery of the annulus fibrosis of a chronically painful intervertebral disk. Lumbar diskography is used diagnostically to identify the presumed pain generator to be targeted with IDET. Based on the medical literature, what can be said about the current status of IDET?
Options:
- IDET has been proven to seal annular tears in the annulus fibrosis.
- IDET restores segmental stability by shrinking collagen fibrils in the disk.
- IDET has demonstrated no significant benefit over placebo in controlled trials.
- IDET is an unsafe procedure with significant risk of permanent complications.
- IDET has demonstrated poor clinical results in all reported series to date.
Correct Answer: IDET has demonstrated no significant benefit over placebo in controlled trials.
Explanation:
DISCUSSION: Intradiskal electrothermal therapy (IDET) initial clinical results were reported in 2000. The early case series were quite encouraging with reported therapeutic success rates of 60% to 80%. Early enthusiasm was high as IDET provided a nonsurgical treatment option for an otherwise complex and difficult clinical entity, chronic diskogenic low back pain. The actual mechanism of action was not well understood, and while the theoretic explanation made good sense, it did not hold up under laboratory testing. Soon clinical results from the field did not meet the high expectations set by the developers of the technique. Since those early case studies, a few level I evidence studies have been conducted, one by Freeman and associates and one by Pauza and associates. These randomized, placebo-controlled trials demonstrated no significant benefit of IDET over the placebo.
REFERENCES: Freeman BJ, Fraser RD, Cain CM, et al: A randomized, double-blind, controlled trial: Intradiscal electrothermal therapy versus placebo for the treatment of chronic discogenic low back pain. Spine 2005;30:2369-2377.
Pauza KJ, Howell S, Dreyfuss P, et al: A randomized, placebo-controlled trial of intradiscal electrothermal therapy for the treatment of discogenic low back pain. Spine J 2004;4:27-35.
Wetzel FT, McNally TA: Treatment of chronic discogenic low back pain with intradiskal electrothermal therapy. J Am Acad Orthop Surg 2003;11:6-11.
Question 71:
-A 16-year-old girl was seen after a motor vehicle collision. Imaging studies including plain radiographs,MRI scans, and CT scans confirm bilateral jumped facets at C5-6 without disk herniation. She is alert,oriented, and neurologically intact. What is the most appropriate next step?
Options:
- Awake closed reduction
- Application of a halo orthosis
- Placement of a cervical collar
- Open reduction under anesthesia
- Closed reduction under anesthesia
Correct Answer: Awake closed reduction
Question 72:
A healthy 64-year-old man just underwent an uncomplicated shoulder arthroplasty for severe glenohumeral osteoarthritis. Intraoperatively, 60 degrees of external rotation was obtained. Postoperatively, he starts on a range-of-motion program. What limitations are recommended? Review Topic
Options:
- No external rotation stretching for the first 6 weeks.
- No external rotation stretching for the first 3 weeks.
- Limit external rotation to the side to 60 degrees for the first 6 weeks.
- Limit external rotation to the side to 60 degrees for the first 3 weeks.
- No restrictions on external rotation stretching.
Correct Answer: Limit external rotation to the side to 60 degrees for the first 6 weeks.
Explanation:
The patient needs restrictions on his external rotation to allow healing of the subscapularis tendon repair. Limitation to 60 degrees is common if the tendon repair is robust and shows no evidence of tension on range-of-motion testing during the
surgery. Restriction from external rotation stretching for even 3 weeks would compromise his ultimate functional recovery.
Question 73:
In the arthroscopic photograph shown in Figure 5, the structure labeled “A” functions primarily as a restraint to translation of the humeral head in what direction?
Options:
- Inferiorly with the arm adducted to the side
- Anteriorly with the arm abducted to 45 degrees and at neutral rotation
- Anteriorly with the arm abducted to 45 degrees and maximally externally rotated
- Anteriorly with the arm abducted to 90 degrees and at neutral rotation
- Anteriorly with the arm abducted to 90 degrees and maximally externally rotated
Correct Answer: Inferiorly with the arm adducted to the side
Explanation:
DISCUSSION: The superior glenohumeral ligament identified as “A” in the figure functions primarily as a restraint to inferior glenohumeral translation of the adducted arm. The middle glenohumeral ligament is highly variable and pooly defined in up to 40% of the population and functions to restrain anterior translation of the externally rotated arm in the midrange of abduction. The anterior band of the inferior glenohumeral ligament is the primary restraint to anterior/inferior translation of the head with the shoulder abducted to 90 degrees and in maximum external rotation.
REFERENCES: Ticker JB, Bigliani LU, Soslowskiy LJ, et al: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
Owen MD, Kregel KC, Wall PT, Gisolfi CV: Effects of ingesting carbohydrate beverages during exercise in the heat. Med Sci Sports Exerc 1986;18:568-575.
Question 74:
During establishment of an anterior portal for hip arthroscopy, what structure is at greatest risk for injury? Review Topic
Options:
- Lateral femoral cutaneous nerve
- Femoral nerve
- Femoral artery
- Superior gluteal nerve
- Sciatic nerve
Correct Answer: Lateral femoral cutaneous nerve
Explanation:
The anterior portal for hip arthroscopy is approximately 6 cm distal to the anterior superior iliac spine, penetrating the muscle belly of the sartorius and the rectus femoris before entering through the anterior capsule. The lateral femoral cutaneous nerve is divided into three or more branches at the level of this portal and may be injured during portal placement. The femoral nerve and artery are more medial and at less risk. The superior gluteal and sciatic nerves are posterior and not at risk with an anterior portal.
Question 75:
Bridge plating of the olecranon is MOST appropriate in which of the following clinical scenarios?
Options:
- Fixation of an olecranon osteotomy used for distal humerus surgery in a 24-year-old male
- Simple transverse olecranon fracture in 33-year-old female
- Comminuted olecranon fracture in 45-year-old male
- Severely comminuted proximal olecranon fracture in an osteoporotic 91-year-old female
- Aphophyseal elbow fracture in 6-year-old male
Correct Answer: Fixation of an olecranon osteotomy used for distal humerus surgery in a 24-year-old male
Explanation:
DISCUSSION: Bridge plating is most appropriately used for fixation of comminuted fractures which are not able to be fixed anatomically. Of the choices listed above, this would be most appropriate in a comminuted fracture in a 45-year-old male. In contrast, literature shows that severely comminuted, osteoporotic low-demand elderly are best treated with olecranon fracture excision and triceps advancement when possible.
Bailey et al looked at the outcome of plate fixation of olecranon fractures. They concluded that plate fixation is effective for displaced olecranon fractures and leads to good functional outcome. There were low incidence of complications, although 20% did have removal of hardware due to irritation.
Hak et al reviewed the fixation options for olecranon fractures. In their review, they state that comminuted olecranon fractures can be treated by limited-contact dynamic-compression plates. They also supported the use of supplemental bone graft to support comminuted depressed articular fragments. Fragment excision and triceps advancement is appropriate in selected cases in which open reduction seems unlikely to be successful, such as in osteoporotic elderly patients with severely comminuted fractures.
Question 76:
What mechanism is most likely responsible for the initiation of mechanical failure seen at the midstem modular junction of modular revision hip stems?
Options:
- Fretting fatigue
- Etching
- Crevice corrosion
- Abrasive wear
Correct Answer: Fretting fatigue
Explanation:
The junction fracture is initiated in a fretting-fatigue mechanism and completed by a bending moment. Fretting fatigue occurs when contacting components experience cyclic loads while small oscillatory motion occurs between them. This increases tensile and shear stress, leading to small flaws that result in crack propagation. In the referenced study no evidence of corrosion was seen because there was no etching, pitting, corrosion products, or chloride formation. Etching is a finding seen in corrosion. Abrasive wear occurs when a rough surface glides against a softer surface. It is generally seen in polyethylene wear from bone or cement in third-body wear. Risk factors for stem breakage include high body mass index and lack of proximal bone support at the modular stem-junction area.
Question 77:
Figures below depict the radiographs obtained from a 76-year-old woman who comes to the emergency department after experiencing a fall. She is an unassisted community ambulator with a history of right hip pain. What is the most appropriate surgical treatment for this fracture?
Options:
- Cemented unipolar hemiarthroplasty
- Cemented bipolar hemiarthroplasty
- Total hip replacement
- Open reduction and internal fixation
Correct Answer: Total hip replacement
Explanation:
DISCUSSION:
This patient has pre-existing right hip osteoarthritis. The most correct option for the treatment of this active patient is a right total hip arthroplasty. Hemiarthroplasty would not address the patient's pain from osteoarthritis, and open reduction and internal fixation would not fix the femoral head issue or the osteoarthritis.
Question 78:
A 64-year-old man who underwent total shoulder arthroplasty 4 weeks ago is making satisfactory progress in physical therapy, but his therapist notes limitations in external rotation to neutral. A stretching program is started, and the patient suddenly gains 90 degrees of external rotation but now reports increased pain and weakness. What is the best course of action?
Options:
- Early surgical exploration and repair of the torn subscapularis tendon
- Observation and reassurance that the pain will resolve
- A slow progressive resistance program to restore strength
- CT to assess for component malrotation
- Electromyography to evaluate for possible nerve injury
Correct Answer: Early surgical exploration and repair of the torn subscapularis tendon
Explanation:
DISCUSSION: Nearly all approaches to shoulder arthroplasty require detachment of the subscapularis tendon from the humerus and subsequent repair. Healing of this tenotomy is one of the limiting factors in postoperative recovery. Failure of the tenotomy repair must be recognized and treated early with repeat repair or pectoralis muscle transfer for optimal results. Failure of the subscapularis is diagnosed clinically as excessive external rotation and weakness, especially in the lift-off or belly press position. Muscle testing can be difficult in the postoperative period and may not be possible to assess in those positions. Although MRI might be useful to confirm the diagnosis, studies may be limited by artifact. CT or electromyography would not be diagnostic.
REFERENCES: Wirth MA, Rockwood CA Jr: Complications of total shoulder-replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Miuer SL, Hazrati Y, Klepps S, et al: Loss of subscapularis function after shoulder replacement: A seldom recognized problem. J Shoulder Elbow Surg 2003;12:29-34.
Question 79:
The patient experiences little improvement with activity modification and more physical therapy. An intra-articular corticosteroid injection provides excellent relief, but relief only lasts for 1 month. The player requests further treatment for his hip and is counseled regarding surgical intervention. Hip arthroscopy is performed. Intrasurgically, a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. Which treatment is most appropriate considering these findings?
Options:
- Debridement of the labral tear plus bony resection of the pincer lesion
- Debridement of the labral tear and no bony resection of the pincer lesion
- Femoral neck osteoplasty plus labral repair using suture anchor
- Resection of the bony pincer lesion plus labral repair using suture anchor
Correct Answer: Resection of the bony pincer lesion plus labral repair using suture anchor
Explanation:
DISCUSSION
Video 67 for reference
This clinical scenario describes a patient with FAI attributable to pincer (acetabular) deformity. This form of FAI, which involves prominence of the anterosuperior acetabular lip, may be more common among women. Decreased range of motion and pain occur secondary to the abutment of the femoral head against the acetabular labrum and rim. Hip flexion, combined with adduction and internal rotation, recreates this contact and causes pain, but CAM or pincer etiology remains unknown.
The differential diagnosis of hip pain in a young athlete includes femoral neck stress reaction/fracture, sacroiliac arthritis, intra-articular loose body, trochanteric bursitis, osteitis pubis, and hernia. No information presented in this scenario suggests any of these causes. Diagnosis of FAI is best performed via MR imaging, with an arthrogram increasing the sensitivity and specificity for labral pathology. An ultrasound may be useful in the diagnosis of dysplasia or for dynamic assessment of a snapping hip, but ultrasound is not commonly used to diagnose labral pathology.
Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has important functions for hip stability and maintenance of the suction seal of the joint.
Question 80:
A 21-year-old professional ballet dancer reports a painful popping sensation over her right hip joint. Examination reveals that symptoms are reproduced with hip flexion and external rotation. Which of the following studies will best confirm the diagnosis?
Options:
- Radiographs
- Bone scan
- CT
- Ultrasonography
- MRI
Correct Answer: Ultrasonography
Explanation:
DISCUSSION: The patient has snapping hip syndrome of the internal type, which is more common in ballet dancers. It is caused by the iliopsoas tendon gliding over the iliopectineal line or the femoral head. The diagnosis usually can be made by the history and physical examination. Snapping is reproduced by hip flexion and extension or flexion with external rotation and abduction. Conventional and dynamic ultrasonography will confirm the snapping structure. Radiographs occasionally show calcifications near the lesser trochanter. MRI can be used to rule out other diagnoses that can simulate snapping hip.
REFERENCES: Gruen GS, Scioscia TN, Lowenstein JE: The surgical treatment of internal snapping hip. Am J Sports Med 2002;30:607-613.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 139-153.
Question 81:
Figure 20 shows the resting and stress radiographs of a patient who has had pain and feelings of instability after undergoing a total knee arthroplasty 1 year ago. Which of the following ligaments is not functional and is therefore responsible for the patient’s symptoms?
Options:
- Anterior cruciate
- Posterior cruciate
- Medial collateral
- Lateral collateral
- Patellar tendon/ligament
Correct Answer: Posterior cruciate
Explanation:
DISCUSSION: The radiographs show posterior instability caused by an absent posterior cruciate ligament. The tibia is significantly displaced posteriorly with respect to the femur. This can be demonstrated with a lateral radiograph obtained with the knee in flexion. The anterior cruciate ligament has been resected but is not responsible for the instability shown.
REFERENCE: Incavo SJ, Churchill DL: The role of the posterior cruciate ligament in total knee arthroplasty. Techniques Orthop 1999;14:267-273.
Question 82:
A 35-year-old man has profound deltoid weakness after sustaining a traumatic anterior shoulder dislocation 6 weeks ago. Electromyographic (EMG) studies confirm an axillary nerve injury. Follow-up examination at 3 months reveals no recovery of function. What is the best course of action?
Options:
- Surgical repair of the Bankart lesion
- Exploration of the axillary nerve
- MRI neurography
- Repeat EMG studies
- Continued observation and physical therapy
Correct Answer: Repeat EMG studies
Explanation:
DISCUSSION: Documenting the status of recovery at this time is appropriate; therefore, repeat EMG studies should be conducted to check for early signs of reinnervation. Timing of nerve exploration in this setting is debated, with authors suggesting exploration if there is no sign of recovery at 6 to 9 months.
REFERENCES: Perlmutter GS: Axillary nerve injury. Clin Orthop 1999;368:28-36.
Artico M, Salvati M, D’Andrea V, et al: Isolated lesions of the axillary nerves: Surgical treatment and outcome in twelve cases. Neurosurgery 1991;29:697-700.
Vissar CP, Coene LN, Brand R, et al: The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery: A prospective clinical and EMG study. J Bone Joint Surg Br 1999;81:679-685.
Pasila M, Jarma H, Kiviluoto O, et al: Early complications of primary shoulder dislocations. Acta Orthop Scand 1978;49:260-263.
Question 83:
A 12-year-old boy reports the acute onset of pain and a pop over the right side of his pelvis while swinging a baseball bat during a Little League game. Radiographs reveal an avulsion of the anterior superior iliac spine with 2 cm of displacement. Management should consist of
Options:
- open reduction and internal fixation of the fragment along with the rectus femoris.
- open reduction and internal fixation of the fragment along with the sartorius.
- open reduction and internal fixation of the fragment along with the iliopsoas.
- rest and protected weight bearing with crutches.
- excision of the fragment.
Correct Answer: rest and protected weight bearing with crutches.
Explanation:
DISCUSSION: Anterior superior iliac spine avulsion fractures are caused by sudden, forceful contractions of the sartorius and tensor fascia lata. These injuries occur in young athletes through the growth plate with the hip extended and the knee flexed, such as while sprinting or swinging a baseball bat. The athlete will often report a pop or snap at the time of injury. Displaced fractures usually can be seen on radiographs. CT or MRI can be obtained to confirm the diagnosis. In most patients, nonsurgical management consisting of rest and protected weight bearing yields satisfactory outcomes. Surgery is usually reserved for fractures with displacement of more than 3 cm and painful nonunions.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 139-153.
White KK, Williams SK, Mubarack SJ: Definition of two types of anterior superior iliac spine avulsion fractures. J Pediatr Orthop 2002;22:578-582.
Question 84:
The optimal method with which to diagnose component malrotation in total knee arthroplasty (TKA) is
Options:
- clinical assessment of foot position and patellar tracking.
- radiographic skyline view of the patella.
- CT scan with metal artifact suppression.
- MR imaging with metal artifact reduction sequences.
Correct Answer: CT scan with metal artifact suppression.
Explanation:
DISCUSSION
The epicondylar axis and tibial tubercle can be used as references on CT scans to quantitatively measure rotational alignment of the femoral and tibial components. This technique has been used to determine whether rotational malalignment is present and whether revision of 1 or both components may be indicated. Although clinical assessment is useful, malrotation can occur as a result of deformities unrelated to the arthroplasty. Similarly, an isolated radiographic skyline view of the patella may indicate a problem with patellar maltracking, but cannot quantitatively assess malrotation of the components. MR imaging proves useful for evaluating painful TKA, but it is dependent on the center’s quality and has not yet been shown to quantify component malrotation.
CLINICAL SITUATION FOR QUESTIONS 20 THROUGH 22
Figures 20a and 20b are the radiographs of an elderly woman who underwent total knee arthroplasty (TKA) several years ago. She now states that something is not right; her knee frequently swells and is diffusely painful, especially at the end of the day. She does not trust her knee, especially while going up and down stairs or getting up from a chair.
Question 85:
Figure 81 is the radiograph of a healthy 72-year-old man who has a 3-month history of medial knee pain. He denies any specific trauma. Until 3 months ago when the pain began, he had been an avid runner for many years. Initial treatment should be oral anti-inflammatory medication
Options:
- alone.
- with food.
- with a proton pump inhibitor.
- with glucosamine hydrochloride.
Correct Answer: with a proton pump inhibitor.
Explanation:
This patient has bone-on-bone end-stage arthritis that was asymptomatic until 3 months ago. Patients older than age 65 are at increased risk for adverse gastrointestinal effects when placed on nonsteroidal anti-inflammatory drugs, and they should be placed on a proton pump inhibitor prophylaxis at the same time. Use of glucosamine is controversial. Glucosamine hydrochloride has been shown in prospective studies to have no beneficial effect. However, glucosamine sulfate has been shown to have a positive effect on pain, but no effect on function.
Question 86:
A 26-year-old right hand-dominant man has had right shoulder pain for the past 6 months. History reveals that he was the starting pitcher for his high school team. Activity modification, physical therapy, cortisone injection, and anti-inflammatory drugs have failed to improve his symptoms. He has a positive O’Brien’s active compression test. What is the next most appropriate step in the diagnosis of this patient? Review Topic
Options:
- Diagnostic arthroscopy
- MRI-arthrography
- Stress radiographs
- CT
- Weighted radiographs of the arm
Correct Answer: MRI-arthrography
Explanation:
MRI-arthrography has been shown to be an accurate technique for assessing the glenoid labrum in patients with suspected labral tears. Often standard MRI technique will not identify labral lesions. The use of MRI-arthrography with an intra-articular injection of gadolinium provides improved visualization of labral lesions. Bencardino and associates demonstrated a sensitivity of 89%, a specificity of 91%, and an accuracy of 90% in detecting labral lesions. SLAP lesions can be visualized on coronal oblique sequences as a deep cleft between the superior labrum and the glenoid that extends well around and below the biceps anchor. Often, contrast will diffuse into the labral fragment, causing it to appear ragged or indistinct.
Question 87:
below show the radiographs, and the MRIs obtained from a year-old man with worsening left knee pain. A foot hip-to-ankle radiograph shows a degree varus knee deformity. The patient sustained a major left knee injury 5 years ago and a confirmed complete anterior cruciate ligament (ACL) tear. He managed this injury nonsurgically with a functional brace but experienced worsening pain. He was seen by an orthopaedic surgeon 18 months ago, and a medial meniscus tear was diagnosed; the tear was treated with an arthroscopic partial medial meniscectomy. Since then, his knee has been giving way more often, and he no longer feels safe working on a pitched roof. The patient received 6 months of formal physical therapy and was fitted for a new functional ACL brace, but he still has pain and instability. He believes he has exhausted his nonsurgical options and would like to undergo surgery. What is the most appropriate treatment at this time?
Options:
- ACL reconstruction and subsequent proximal tibial osteotomy
- ACL reconstruction alone
- Distal femoral osteotomy with simultaneous ACL reconstruction
- Proximal tibial osteotomy with subsequent ACL reconstruction
Correct Answer: Proximal tibial osteotomy with subsequent ACL reconstruction
Explanation:
DISCUSSION:
Proximal tibial osteotomy is the most appropriate intervention to correct varus malalignment and to reduce stress on the ACL. In some cases, proximal tibial osteotomy alone may address both pain and instability, but if instability persists, particularly in the setting in which instability can be dangerous, subsequent ACL reconstruction can further stabilize the knee with less stress on the graft after the correction of malalignment. Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should be performed only at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL
reconstruction alone is not indicated for this patient.
Question 88:
Figures A through C are the radiograph and CT scans of a 42-year-old man who sustained an injury to both of his ankles and underwent surgical repair 2 weeks prior to presentation to your office. One ankle is healing well. On the contralateral side, he reports pain and restricted ankle range of motion. Management should consist of
Options:
- the addition of more aggressive physiotherapy.
- observation and continued non-weight-bearing.
- addition of an anteriorly directed "syndesmosis screw."
- loosening the syndesmotic screws from an overtightened position.
- removal of screws, re-reduction of the syndesmosis, and revision fixation.
Correct Answer: removal of screws, re-reduction of the syndesmosis, and revision fixation.
Explanation:
This patient has a malreduced syndesmosis. The CT scans clearly show the fibula to be subluxated posteriorly relative to the incisura; therefore, surgical revision is warranted. Revision surgery should include either removal of the current screws with accurate reduction of the syndesmosis and new screw placement or repair of the posterior malleolar fragment, which will in turn reduce the syndesmosis. Addition of an anteriorly directed screw to the current construct will not change the malalignment. Loosening the syndesmotic screws or addition of aggressive physiotherapy will not correct the malrotation of the distal fibula within the incisura which is seen on the CT scan. Outcomes after these injuries are related to the reduction of the ankle mortise.
Question 89:
82 • American Academy of Orthopaedic Surgeons A 12-year-old girl is seen for left ankle pain. Radiographs reveal osteochondritis dissecans (OCD) involving the talus. What should the parents be told regarding management?
Options:
- No treatment is required because spontaneous healing is common.
- Nonsurgical management typically relieves pain and results in radiographic healing in less than 12 weeks.
- Nonsurgical management frequently relieves pain but often may not result in radiographic healing even 6 months after treatment.
- Hyperbaric oxygen treatment is helpful.
- Ankle fusion is frequently necessary.
Correct Answer: Nonsurgical management frequently relieves pain but often may not result in radiographic healing even 6 months after treatment.
Explanation:
DISCUSSION: Nonsurgical management of OCD of the talus in skeletally immature individuals frequently results in a fairly rapid decrease in symptoms, but radiographic abnormalities can frequently be found even 6 months after treatment. Spontaneous resolution of this condition is rare. Hyperbaric oxygen treatment has not been shown to be beneficial for this condition. Progression of the condition to the point of requiring ankle fusion is rare.
REFERENCES: Perumal V, Wall E, Babekir N: Juvenile osteochondritis dissecans of the talus. J Pediat Orthop 2007;27:821-825.
Letts M, Davidson D, Ahmer A: Osteochondritis dissecans of the talus in children. J Pediatr Orthop 2003;23:617-625.
Question 90:
The MRI scan shown in Figure 33 reveals the sequelae of an acute traumatic anteroinferior shoulder dislocation. The image reveals the typical separation of what two commonly injured structures? Review Topic
Options:
- Anteroinferior labrum from the bony glenoid
- Anteroinferior labrum from the cartilaginous surface of the glenoid
- Biceps tendon from its origin on the supraglenoid tubercle
- Anterior capsule from the proximal humerus
- Posteroinferior labrum from the bony glenoid
Correct Answer: Anteroinferior labrum from the bony glenoid
Explanation:
The MRI scan reveals the sequelae of an anteroinferior dislocation, specifically separation of the anteroinferior labrum from the bony glenoid. The separation does not classically occur only at the cartilage-labral junction, but extends to the bony surface of the medial glenoid neck. Separation of the biceps tendon from its origin on the supraglenoid tubercle (SLAP lesion) or separation of the anterior capsule with the proximal humerus (HAGL lesion) may occur but are not the most common sequelae and are not demonstrated in this MRI image. Anteroinferior shoulder dislocations normally do not affect the posterior labral structures. In their landmark study, Rowe and associates noted that this demonstrated lesion was the most common lesion, present in 85% of their series.
Question 91:
A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?
Options:
- Irrigation and debridement, external fixation of the ankle and foot, traction and pinning of the femur, open reduction and internal fixation of the forearm
- Irrigation and debridement, external fixation of the ankle, foot, and femur, splinting of the forearm
- Irrigation and debridement and open reduction and internal fixation of the ankle and foot, intramedullary nailing of the femur, open reduction and internal fixation of the forearm
- Irrigation and debridement and open reduction and internal fixation of the ankle and foot, intramedullary nailing of the femur, splinting of the forearm
- Irrigation and debridement, external fixation of the foot and ankle, intramedullary nailing of the femur, open reduction and internal fixation of the forearm
Correct Answer: Irrigation and debridement, external fixation of the ankle, foot, and femur, splinting of the forearm
Explanation:
DISCUSSION: The patient appears to be a borderline or unstable surgical patient following her initial trauma and spleenectomy (high base excess and low urine output). She needs continued resuscitation and minimal additional blood loss. This is best accomplished with irrigation and debridement of the ankle, external fixation of the ankle, foot, and femur, and splinting of the forearm. A traction pin for the femoral fracture will not control bleeding as well as an external fixator. Intramedullary nailing of the femur and open reduction and internal fixation of the forearm would be appropriate in patients that are euvolemic and stable.
REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
Taeger G, Ruchholtz S, Waydhas C, et al: Damage control orthopedics in patients with multiple injuries is effective, time saving, and safe. J Trauma 2005;59:409-416.
Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-452.
Renaldo N, Egol K: Damage-control orthopaedics: Evolution and practical applications.
Am J Orthop 2006;35:285-291.
Question 92:
A 37-year-old recreational athlete has osteoarthritis of the glenohumeral joint. He has failed nonsurgical measures and is interested in surgical intervention but would like to avoid arthroplasty. When performing shoulder arthroscopy for glenohumeral arthritis, which radiographic parameter is most predictive of clinical failure?
Options:
- Unipolar arthritis
- >3 mm of glenohumeral joint space
- Walch B2 glenoid morphology
- Small inferior humeral osteophyte
Correct Answer: Walch B2 glenoid morphology
Explanation:
Multiple studies have evaluated the utility of arthroscopy in the treatment of shoulder arthritis. Despite differing levels of success, a few common characteristics have been shown to lead to a higher probability of clinical failure. Mitchell and associates showed that shoulders with less joint space (1.3 mm vs 2.6 mm) and Walch type B2 and C glenoids were significantly more likely to fail than were Walch types A1, A2, and B1. Additionally, older patients (age >50 years) tended to have worse outcomes. Skelley and associates found that isolated capsular release and debridement had a high failure rate (conversion to total shoulder arthroplasty in 42% within 9 months) and postulated that patients undergoing concomitant procedures, such as biceps tenodesis, may fare better. Van Theil and associates found significant risk factors for failure included the presence of grade 4 bipolar disease, joint space <2 mm, and the presence of large osteophytes. They had a
22% conversion to total shoulder arthroplasty at 10.1 months.
Question 93:
What is the most common clinical presentation of a patient with a malignant bone tumor?
Options:
- Incidental finding
- Pain
- Pathologic fracture
- Deformity
- Presence of a mass
Correct Answer: Pain
Explanation:
DISCUSSION: The most common clinical presentation of a patient with a malignant bone tumor is pain. Malignant bone tumors rarely are diagnosed as an incidental finding or pathologic fracture. In patients who have a pathologic fracture on initial presentation, a history of increasing pain prior to the fracture is typical. While 90% of malignant bone tumors are associated with a soft-tissue mass, in many patients the soft-tissue component of the tumor is not clinically apparent.
REFERENCES: Buckwalter JA: Musculoskeletal neoplasms and disorders that resemble neoplasms, in Weinstein SL, Buckwalter JA (eds): Turek’s Orthopaedics: Principles and Their Application, ed 5. Philadelphia, PA, JB Lippincott, 1994, pp 290-295.
Mehlman CT, Crawford AH, McMath JA: Pediatric vertebral and spinal cord tumors: A retrospective study of musculoskeletal aspects of presentation, treatment, and complications. Orthopedics 1999;22:49-55.
Question 94:
A 22-year-old volleyball player has atrophy of the infraspinatus muscle. This deficit is the result of entrapment of what nerve?
Options:
- Axillary nerve in the posterolateral space
- Dorsal scapular nerve at the medial border of the scapula
- Suprascapular nerve in the scapular notch
- Suprascapular nerve in the spinoglenoid notch
- Subscapular nerve at the rotator interval
Correct Answer: Suprascapular nerve in the spinoglenoid notch
Explanation:
DISCUSSION: Suprascapular deficits, as the result of repetitive forceful internal rotation with overhead ball striking, occur in the spinoglenoid notch. Compression interferes with distal suprascapular nerve innervation to the infraspinatus, while allowing the supraspinatus to function normally. A scapular notch entrapment of this nerve would involve both the supraspinatus and the infraspinatus. The axillary, dorsal scapular, and subscapular nerves do not affect the infraspinatus.
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990;6:301-305.
Question 95:
- Which of the following medicolegal relationships between an attending surgeon and a resident assistant applies when a patient files a malpractice suit relating to surgical complications following a total knee arthroplasty?
Options:
- Respondeat superior
- Indemnity agreement
- Hold harmless agreement- attempt to shift liability from company to physician
- Comparative negligence-% of involvement
- Contributory negligence- resident contributed to the negligence
Correct Answer: Respondeat superior
Explanation:
“Let the master answer”. A resident has been authorized to act for or represent the supervising physician. As an agent for the supervisor, all acts of the resident are considered to be under the direction of the supervisor. This is the definition for respondeat superior. Hold harmless agreement attempts to shift liability from company to physician. Comparative negligence refers to the % of involvement. Contributory negligence is where the resident is accused of contributing to a negligent act.
Question 96:
Figures 57a and 57b are the MRI scans of a 61-year-old man who is unable to elevate his dominant arm following a golf injury 24 hours ago. He has moderate pain during attempted arm elevation. Examination reveals significant spinati atrophy and he is only able to elevate his arm fully overhead while supine. The neurologic examination is normal. What is the next most appropriate step in management? Review Topic
Options:
- Lidocaine injection test
- Supraspinatus strengthening
- Reverse shoulder arthroplasty
- Conventional total shoulder arthroplasty
- Arthroscopic rotator cuff repair/subacromial decompression
Correct Answer: Lidocaine injection test
Explanation:
The patient unknowingly has a chronic massive rotator cuff tear. Because of excellent compensation, he remained functional and was without symptoms. This is evidenced by the significant muscle atrophy. Following even trivial injury, the compensation process of arm elevation fails and the patient suddenly loses the ability to elevate the arm. At this time in management, it is critical to recognize that the rotator cuff had already been torn and that pain now prevents the patient from actively using the arm. To better ascertain a prognosis of return of function, injecting a local anesthetic (lidocaine) into the joint is important. If, with an anesthetized joint, the patient can now elevate the arm, a supine strengthening program will likely return the patient to his pre-injury state. If there is no improvement in the ability to elevate the arm after the injection, surgical considerations may become relevant. There is no role for arthroscopic repair in this chronic, massive rotator cuff tear and decompression would likely lead to superior escape. A reverse shoulder arthroplasty would be contraindicated in a very active 61-year-old patient who 2 days ago was functioning normally. Based on the MRI scan, there is no supraspinatus muscle remaining to strengthen. Total shoulder arthroplasty is contraindicated in patients with a deficient rotator cuff mechanism.
Question 97:
A healthy 52-year-old woman is seeking professional advice about management of osteoporosis. She has no risk factors for osteoporosis. What is the best recommendation for bone health for this patient?
Options:
- Bone mineral density testing performed semiannually
- No treatment
- A healthy diet high in calcium
- 1,000 to 1,500 mg calcium supplement plus 400 to 800 IU vitamin D per day
- Estrogen therapy
Correct Answer: 1,000 to 1,500 mg calcium supplement plus 400 to 800 IU vitamin D per day
Explanation:
DISCUSSION: Women older than age 50 years should receive daily supplementation with calcium and vitamin D to help preserve bone density. Bone mineral density testing is recommended for women age 65 years or older and postmenopausal women with at least one risk factor for osteoporotic fractures: prior fragility fracture, low estrogen levels, premature menopause, long-term secondary amenorrhea, glucocorticoid therapy, maternal history of hip fracture, or low body mass index. Hormone therapy is not approved for the treatment of osteoporosis.
REFERENCES: Gass M, Dawson-Hughes B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Lin JT, Lane JM: Osteoporosis: A review. Clin Orthop Relat Res 2004;425:126-134.
Question 98:
A newborn has an anterolateral bow of the tibia and a duplication of the great toe. Which of the following conditions will develop as the infant grows?
Options:
- Lisch nodules and axillary freckling
- Fracture of the tibia with pseudarthrosis
- Increased tibial bowing and varus deformity
- Decreased tibial bowing and limb-length discrepancy
- Progressive valgus of the ankle
Correct Answer: Decreased tibial bowing and limb-length discrepancy
Explanation:
DISCUSSION: Anterolateral bowing of the tibia is normally associated with congenital pseudarthrosis of the tibia. This, in turn, is associated with neurofibromatosis. Posterior bowing is more benign and usually corrects spontaneously. However, anterolateral bowing also corrects spontaneously, and the limb-length discrepancy may be the only remaining sequela when associated with duplication of the great toe. Lisch nodules and axillary freckling are pathognomonic findings in neurofibromatosis but would not be expected in this patient because this type of tibial deformity is not associated with neurofibromatosis.
REFERENCE: Weaver KM, Henry GW, Reinker KA: Unilateral duplication of the great toe with anterolateral tibial bowing. J Pediatr Orthop 1996;16:73-77.
Question 99:
A 56-year-old man with a history of chronic lower back pain from lumbar spondylosis reports a 2-day history of acute incapacitating back pain. He denies any history of acute trauma, although he reports the pain starting after a coughing spell. He also reports difficulty urinating and some fecal incontinence. Examination reveals generalized lower extremity weakness, saddle paresthesia, hyporeflexia in the lower extremities, and loss of rectal tone. What is the most appropriate management at this time?
Options:
- Immediate MRI of the lumbar spine
- General reassurance, anti-inflammatory drugs, and an early home exercise program
- Immediate radiographs of the lumbar spine and pain medications with 2 days of bed rest if the radiographs are normal
- Office caudal epidural steroid injection with follow-up in 1 week
- Outpatient MRI of the lumbar spine with follow-up in 1 week for test results
Correct Answer: Immediate MRI of the lumbar spine
Explanation:
DISCUSSION: Cauda equina syndrome is a medical emergency that must be quickly diagnosed and treated to avoid long-term complications. Cauda equina syndrome typically presents with low back pain, unilateral or usually bilateral sciatica, saddle sensory disturbances, bladder and bowel dysfunction, and variable lower extremity motor and sensory loss. Although a number of pathologies can cause cauda equina syndrome, in a patient with a history of chronic back pain, disk pathology is the most common cause of acute onset cauda equina syndrome. Whereas radiographs may be useful in a traumatic onset of symptoms, MRI is the most appropriate study. Cauda equina syndrome should be evaluated on an emergent basis and admission for work-up is appropriate.
REFERENCES: Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522.
Small SA, Perron AD, Brady WJ: Orthopedic pitfalls: Cauda equina syndrome. Am J Emerg Med 2005;23:159-163.
Question 100:
Figures 25a and 25b show the radiograph and MRI scan of a 7 1/2-year-old boy who has been limping for 1 year. His pain has worsened over the past 2 weeks, and his parents note swelling over the dorsum of the foot for the past 4 days. Examination reveals no fever, and laboratory studies show a WBC of 6,700/mm 3 , an erythrocyte sedimentation rate of 26 mm/h, and a normal C-reactive protein level. What is the most likely diagnosis?
Options:
- Acute hematogenous osteomyelitis
- Kohler’s disease
- Tarsal coalition
- Tuberculosis
- Lisfranc fracture-dislocation
Correct Answer: Tuberculosis
Explanation:
DISCUSSION: The diagnosis of tuberculous osteomyelitis in children is often delayed. In one series of 23 children, the average interval between the onset of symptoms and definite diagnosis was 4.3 months. In these patients, the presenting signs and symptoms were found to be mild, with the most common signs being localized swelling (69.6%) and a painful disability of the involved limbs (65.2%). A mild elevation of the erythrocyte sedimentation rate may be present, but the C-reactive protein level is usually normal. In patients who have osteoarticular tuberculosis, an MRI scan generally shows large intra-articular effusions, periarticular osteoporosis, and gross thickening of the synovial membrane. Differential diagnosis between tuberculosis and pyogenic arthritis is difficult, and an accurate diagnosis usually requires biopsy of synovial tissue. Aspiration of synovial fluid often results in insufficient information to make a diagnosis. Treatment generally consists of surgical debridement and combined antituberculous chemotherapy with isoniazid, ethambutol, and rifampin.
REFERENCES: Wang MN, Chen WM, Lee KS, Chin LS, Lo WH: Tuberculous osteomyelitis in young children. J Pediatr Orthop 1999;19:151-155.
Watts HG, Lifeso RM: Tuberculosis of the bones and joints. J Bone Joint Surg Am 1996;78:288-298.