Full Question & Answer Text (for Search Engines)
Question 1:
What factor is associated with a high risk of developing pseudotumors after metal-on-metal hip resurfacing?
Options:
- Large-diameter components
- Age 40 or older for men
- Age 40 or younger for women
- Diagnosis of primary osteoarthritis
Correct Answer: Age 40 or younger for women
Explanation:
The recent experience of a large clinical cohort revealed the most likely risk factors as being female gender, age younger than 40, small components, and a diagnosis of hip dysplasia causing osteoarthritis. Failure was least likely among men and after procedures involving larger components. These data have prompted some authors to caution against using metal-on-metal hip resurfacing in women and to primarily target candidates who are men younger than age 50. Small components may be more prone to failure because of malpositioning and edge loading, which have been noted to be more common in dysplasia cases.
Question 2:
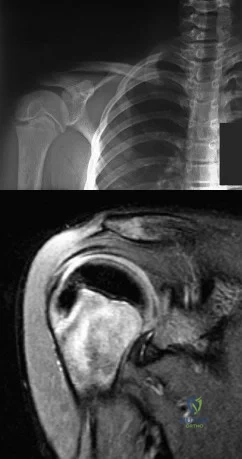
A 35-year-old man presents one week after an acute right shoulder posterior dislocation after being electrocuted. He is evaluated in the emergency department and undergoes closed reduction. The patient reports global right shoulder pain and limited active and passive range of motion. He has mild anterior and lateral bruising. He is distally neurovascularly intact. Current radiographs and an MRI scan are shown in Figures 1 through 3. What is the best next step?
Options:
- Open reduction internal fixation (ORIF)
- Sling immobilization in external rotation
- Bristow-Latarjet
- Shoulder hemiarthroplasty The patient has sustained a displaced lesser tuberosity fracture with medial displacement following a posterior shoulder dislocation. Nonoperative management would risk long-term loss of normal subscapularis function, as well as anterior shoulder instability. An ORIF of lesser tuberosity is recommended. The current radiographs do not demonstrate any obvious compromise of glenoid bone stock that would necessitate a coracoid transfer. The humeral head is not compromised; therefore, a hemiarthroplasty is not indicated. Correct answer : A 57 76- A 51-year-old man sustains the injury shown in the MRI scan in Figures 1 and 2 following a fall. After a thorough discussion regarding risks and benefits, he elects to proceed with surgery. What is the most appropriate surgical treatment for his fracture?
- Open reduction internal fixation with locking plate
- Intramedullary (IM) nail
- Hemiarthroplasty
- Closed reduction and percutaneous pinning The patient has sustained a complex proximal humerus fracture with head split component and multiple articular fragments. When the articular surface is significantly compromised, arthroplasty procedures are favored. The only procedure listed that addresses the damaged humeral head is hemiarthroplasty, making it the correct response. Although a possible option, ORIF would be difficult due to the fragmented humeral head, and there would be a high risk for fracture collapse or avascular necrosis. IM nailing will not provide enough control of the fracture pieces, nor will it replace the damaged articular surface. Closed reduction is not an option given the complex nature of the fracture.
Correct Answer: Bristow-Latarjet
Explanation:
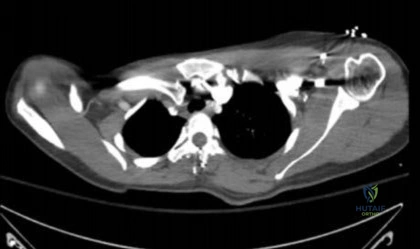
A 68-year-old man presents with chronic progressive right shoulder pain and loss of motion. He has active shoulder elevation of 120° and 5-/5 shoulder forward flexion strength limited by pain. He has exhausted nonsurgical management over the past year and is now interested in surgical intervention. Figure 1 is the preoperative axial CT scan of his shoulder. During surgical reconstruction, the surgeon should anticipate the location of maximal glenoid erosion to be
Question 3:
A year-old man undergoes removal of an infected total hip arthroplasty (THA) and insertion of an articulating antibiotic-loaded spacer to treat a deep periprosthetic hip infection. While in a nursing home receiving intravenous antibiotics 3 weeks after surgery, the patient trips and falls. Examination reveals swelling in the mid and distal thigh, intact skin and neurovascular structures, and severe pain with knee or hip movement. Radiographs of the femur are shown in 1 through What is the most appropriate treatment for the fracture below the implant?
Options:
- Balanced traction to address concern for persistent infection with reoperation
- Open reduction and internal fixation of the fracture with a lateral plate and screws
- Removal of the articulating spacer and revision to a longer-stem antibiotic-loaded articulating spacer
- Removal of the articulating spacer and reimplantation using a long-stem fluted uncemented hip replacement
Correct Answer: Open reduction and internal fixation of the fracture with a lateral plate and screws
Explanation:
DISCUSSION:
This patient has a type C periprosthetic femoral fracture. The articulating spacer is not involved in the fracture, which is well distal to the implant. The most appropriate treatment is open reduction and internal fixation of the fracture. Traction is not appropriate for this fracture because the injury can be treated surgically despite the history of previous hip infection. Traction would also be needed for at least 5 weeks and would delay the surgical treatment of the periprosthetic fracture until the time of second-stage revision THA. The fracture is fairly distal, and revision to a longer antibiotic-loaded implant or uncemented stem is not suitable for this fracture pattern, because it extends well past the isthmus. A femoral stem in the distal fragment would provide little stability for the fracture. Removal of the articulating spacer and reimplantation using a long-stem fluted uncemented hip replacement is not appropriate, because it would be premature to reimplant the man's hip while he is still receiving treatment for a deep hip infection.
Question 4:
Which of the following statements best describes labral tears in the hip?
Options:
- They are unrelated to degenerative joint disease.
- They lead to increased movement of the femur relative to the acetabulum.
- They usually result from lesions of the ligamentum teres.
- They only occur with abnormal bone morphology.
- They commonly occur in the posteroinferior quadrant of the hip.
Correct Answer: They lead to increased movement of the femur relative to the acetabulum.
Explanation:
DISCUSSION: Labral and chondral lesions are observed within the anterosuperior quadrant of the acetabulum. Tearing of the labrum markedly reduces resistance to joint motion, leading to instability.
The most common associated lesions are chondral injuries. They can occur with or without abnormal bone morphology. The etiology for labral tears can be from traumatic and degenerative causes, structural abnormalities from femoroacetabular impingement, developmental abnormalities, and hip instability.
REFERENCES: Beck M, Kalhor M, Leunig M, et al: Hip morphology influences the pattern of damage to the acetabular cartilage: Femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br 2005;87:1012-1018.
Ito K, Leunig M, Ganz R: Histopathologic features of the acetabular labrum in femoroacetabular impingement. Clin Orthop Relat Res 2004;429:262-271.
Crawford MJ, Dy CJ, Alexander JW, et al: The 2007 Frank Stinchfield Award. The biomechanics of the hip labrum and the stability of the hip. Clin Orthop Relat Res 2007;465:16-22.
Question 5:
A 58-year-old woman underwent a left total knee arthroplasty 6 years ago. She initially did well after surgery but sustained a fall 2 months ago while at work. She now describes left knee pain and instability and an inability to straighten her knee since the fall. She has been using a hinged knee brace, which provides partial support. On examination, she has passive range of motion of 0° to 115° and active range of motion of 80° to -115°. Her radiographs are shown in Figures below. What is the best option for the restoration of her function?
Options:
- Revision total knee arthroplasty with placement of a hinge constrained device
- Patellar tendon repair with nonabsorbable suture and patellar resurfacing
- Hinged knee brace with drop lock design to restore stability during ambulation
- Extensor mechanism reconstruction using synthetic mesh or allograft
Correct Answer: Extensor mechanism reconstruction using synthetic mesh or allograft
Explanation:
DISCUSSION:
The patient has an extensor mechanism disruption with patellar tendon rupture. This injury is treated with extensor mechanism reconstruction in the setting of previous total knee arthroplasty. There is a reported high failure rate with attempted repair. Revision to hinge knee arthroplasty would provide implant stability but would not restore the extensor mechanism. The patient is relatively young and is working, so reconstruction would offer better long-term function than a drop lock brace, which can be better used in low-functioning patients with this type of injury. Extensor mechanism reconstruction historically has been accomplished with allograft material, but a novel technique using synthetic mesh also has proved successful in treating this difficult problem.
Question 6:
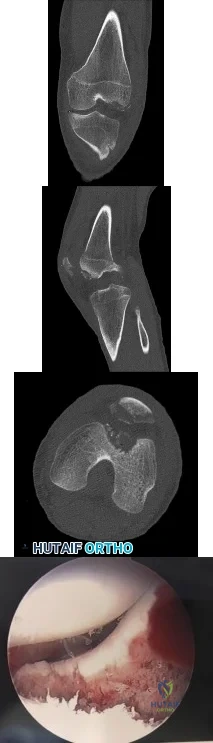
A 10-year-old boy tripped as he was running down a hill, felt a painful pop in his right knee, and was unable to bear weight on the involved lower extremity. Examination reveals a tense effusion and an extensor lag of the right knee. Figures 36a and 36b show AP and lateral radiographs. Management should consist of
Options:
- long leg casting in 30 degrees of flexion for 6 weeks.
- a long leg cast in full extension for 6 weeks.
- knee arthroscopy to rule out internal derangement.
- physical therapy for range of motion and quadriceps strengthening.
- open reduction and internal fixation.
Correct Answer: a long leg cast in full extension for 6 weeks.
Explanation:
DISCUSSION: The examination and radiographs are consistent with a sleeve fracture of the patella, which is an avulsion fracture of the distal pole of the patella with a disruption of the extensor mechanism. Treatment is open reduction and internal fixation of the patella, and repair of the extensor mechanism.
The distal fragment can be much larger than it appears on the radiographs because it consists largely of cartilage.
REFERENCES: Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Grogan DP, Carey TP, Leffers D, et al: Avulsion fractures of the patella. J Pediatr Orthop 1990; 10:721 - 730. Question 37
When addressing a proximal intertrochanteric or subtrochanteric fracture in a juvenile with open growth plates, the arterial supply from what artery at the neck must be preserved?
Lateral femoral circumflex
Medial femoral circumflex
Superior gluteal
Inferior gluteal
Obturator
DISCUSSION: The medial femoral circumflex artery supplies blood to the femoral head. Its position along the posterior-superior femoral neck places this structure at risk with intramedullary nailing of the femur. Therefore, lateral entry through the greater trochanter is preferred when intramedullary fixation is performed.
REFERENCES: Gordon JE, Swenning TA, Burd TA, et al: Proximal femoral radiographic changes after lateral transtrochanteric intramedullary nail placement in children. J Bone Joint Surg Am 2003;85:1295- 1301.
Green NE, Swiontkowski MF: Skeletal Trauma in Children, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 419-424.
Question 7:
A 28-year-old man has left knee pain after a snow skiing accident. The MRI scan shown in Figure 47 reveals which of the following?
Options:
- Osteosarcoma
- Bucket-handle medial meniscal tear
- Lateral collateral ligament tear
- Bone bruise
- Tibial spine avulsion
Correct Answer: Bone bruise
Explanation:
DISCUSSION: Bone bruises are often noted on MRI after anterior cruciate and medial collateral ligament injuries. The significance of these injuries awaits long-term follow-up studies. The areas of increased signal on T
2
-weighted images represent areas of acute hemorrhage and are secondary to microfractures of the adjacent medullary trabeculae.
REFERENCES: Wright RW, Phaneuf MA, Limbird TJ, et al: Clinical outcome of isolated subcortical trabecular fractures (bone bruise) detected on magnetic resonance imaging in knees. Am J Sports Med 2000;28:663-667.
Faber KJ, Dill JR, Amendola A, et al: Occult osteochondral lesions after anterior cruciate ligament rupture: Six-year magnetic resonance imaging follow-up study. Am J Sports Med 1999;27:489-494.
Question 8:
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?
Options:
- Adhesive capsulitis
- Calcific tendinitis
- Anterior shoulder dislocation
- Posterior shoulder dislocation
- Glenohumeral osteoarthritis
Correct Answer: Posterior shoulder dislocation
Explanation:
DISCUSSION: The patient has a posterior shoulder dislocation. The AP radiograph shows overlapping of the humeral head on the glenoid. The scapular Y view shows his humeral articular surface posterior to the glenoid. The posterior shoulder dislocation is frequently missed because the patient is comfortable in the "sling" position with the arm adducted and internally rotated across the abdomen. The marked restriction in external rotation on examination raises the suspicion of a posterior dislocation, adhesive capsulitis, or glenohumeral osteoarthritis. The posterior dislocation is diagnosed based on the radiographic findings. An axillary view or CT is recommended to better evaluate the dislocation.
REFERENCES: Robinson CM, Aderinto J: Posterior shoulder dislocations and
fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.
Cicak N: Posterior dislocation of the shoulder. J Bone Joint Surg Br 2004;86:324-332.
Question 9:
Titanium and its alloys are unsuitable candidates for which of the following implant applications?
Options:
- Fracture plates
- Femoral heads in a hip prosthesis
- Bone screws
- Intramedullary nails
- Porous coatings for bone ingrowth
Correct Answer: Femoral heads in a hip prosthesis
Explanation:
DISCUSSION: Titanium alloy is highly biocompatible, has higher strength than stainless steel, and is highly resistant to corrosion. It is particularly suited for use in fracture plates, bone screws, and intramedullary nails because of its low modulus of elasticity (low stiffness), which can reduce stress shielding. It is also widely used for porous-ingrowth coatings. However, clinical experience has shown that titanium alloy bearing surfaces such as a femoral ball are highly susceptible to severe metallic wear, particularly in the presence of third-body abrasive particles (PMMA fragments, bone chips, metal debris, etc).
REFERENCES: McKellop HA, Sarmiento A, Schwinn CP, et al: In vivo wear of titanium-alloy hip prostheses. J Bone Joint Surg Am 1990;72:512-517.
Salvati EA, Betts F, Doty SB: Particulate metallic debris in cemented total hip arthroplasty. Clin Orthop 1993;293:160-173.
Evans BG, Salvati EA, Huo MH, et al: The rationale for cemented total hip arthroplasty. Orthop Clin North Am 1993;24:599-610.
Question 10:
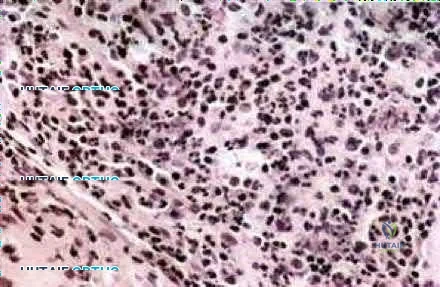
03 advancement at age 6 years. What is the most likely diagnosis?
Options:
- Osteomyelitis
- Lymphoma
- Eosinophilic granuloma
- Tuberculosis
- Ewing’s sarcoma back answer
Correct Answer: Osteomyelitis
Explanation:
Figure 15a shows areas of permeative lucency and sclerosis in the proximal femur as well as evidence of a screw (from the previous trochanteric advancement). Figure 15b shows the CT scan of the femur with possible thickening of the cortex and a moth eaten appearance of the bone. Figure 15c shows the biopsy specimen with mixed inflammatory cells. These are all indicative of osteomyelitis. The first radiographic sign of osteomyelitis tends to be an ill-defined area of lucency, followed by areas of sclerosis and periosteal new bone formation as the bone reacts to the infection. Biopsy specimens should show mixed inflammatory cells.
back to this question next question
Question 11:
Ceramic bone substitutes have which of the following properties?
Options:
- There is vascular ingrowth and subsequent graft resorption with host bone ingrowth.
- Their interconnectivity is similar to that of cancellous bone.
- They are brittle with significant tensile strength.
- They are resorbed at a fairly constant rate.
- Due to their strength, rigid stabilization of the surrounding bone is not necessary.
Correct Answer: There is vascular ingrowth and subsequent graft resorption with host bone ingrowth.
Explanation:
DISCUSSION: Ceramics have the following properties: They are resorbed at varying rates, and the chemical composition of the ceramic significantly affects the rate of resorption. For example, tricalcium phosphate (TCP) undergoes biologic resorption 10 to 20 times faster than hydroxyapatite. The partial conversion of TCP to hydroxyapatite once it is in the body significantly reduces the rate of resorption. Some segments of hydroxyapatite can remain in place in the body for 7 to 10 years. In clinical trials, TCP more readily remodels because of its porosity, but it is weaker. The success of converted corals as a bone graft substitute relies on a complex sequence of events of vascular ingrowth, differentiation of osteoprogenitor cells, bone remodeling, and graft resorption occurring together with host bone ingrowth into and on the porous coralline microstructure or voids left behind during resorption.
REFERENCES: Lane JM, Bostrom MP: Bone grafting and new composite biosynthetic graft materials. Instr Course Lect 1998;47:525-534.
Walsh WR, Chapman-Sheath PJ, Cain S, et al: A resorbable porous ceramic composite bone graft substitute in a rabbit metaphyseal defect model. J Orthop Res 2003;21:655-661.
Wright TM, Maher SA: Biomaterials, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 12:
Figure 13 shows the clinical photograph of a 66-year-old man who has had an increasingly painful right foot deformity for the past 3 years. Examination reveals that the subtalar joint is fixed in 15° of valgus, and forefoot supination can be corrected to 10° from neutral. Nonsurgical management has failed to provide relief. Treatment should now consist of
Options:
- medial sliding calcaneal osteotomy with flexor digitorum longus (FDL) transfer.
- isolated subtalar arthrodesis.
- isolated talonavicular arthrodesis.
- triple arthrodesis.
- subtalar arthroereisis.
Correct Answer: triple arthrodesis.
Explanation:
DISCUSSION: The most important determining factor for correction of an adult flatfoot without an arthrodesis is the flexibility of the subtalar and transverse tarsal joints. Rigid deformities cannot be corrected with a medial sliding calcaneal osteotomy with FDL transfer or a subtalar arthroereisis. Isolated subtalar or talonavicular arthrodesis does not correct the deformities entirely. If the patient has forefoot supination that can be corrected to less than 7°, an isolated subtalar fusion is a possible alternative.
REFERENCE: Mann RA: Flatfoot in adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 757-784.
Question 13:
A 13-year-old boy has had pain and swelling in his ankle for the past several months. Based on the radiograph, MRI scan, and biopsy specimen shown in Figures 77a through 77c, what is the best course of action?
Options:
- Observation
- Curettage and bone grafting
- Radiofrequency ablation
- Radiation therapy
- Wide resection
Correct Answer: Curettage and bone grafting
Explanation:
DISCUSSION: Chondroblastomas are benign cartilage lesions frequently seen in adolescents or young adults. They are found in the epiphyseal or apophyseal regions of bones. The radiograph shows a radiolucent lesion with mineralization and a well-marginated rim of reactive bone. The lesion is composed of sheets of immature chondroblasts (polygonal cells with a clear, bluish cytoplasm and a small round central nucleus). In some regions, classic “chicken-wire” matrix calcifications and a “cobblestone” pattern of cell arrangement may be seen. Treatment consists of curettage and bone grafting.
REFERENCES: Campanacci M: Bone and Soft Tissue Tumors, ed 2.
New York, NY, Springer-Verlag, 1999, pp 247-264.
Lin PP, Thenappan A, Deavers MT, et al: Treatment and prognosis of chondroblastoma. Clin Orthop Relat Res 2005;438:103-109.
Question 14:
A concern when choosing irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene rather than lower dose–irradiated (4 Mrad) polyethylene is related to its inferior resistance to
Options:
- adhesive wear.
- abrasive wear.
- fatigue wear.
- creep.
Correct Answer: fatigue wear.
Explanation:
DISCUSSION
The higher the dose of radiation to the polyethylene, the higher the amount of cross-linking. Adhesive and abrasive wear resistance increases with an increase in cross-linking. However, fatigue properties of the material are decreased when polyethylene is melted (to remove free radicals) during the cross-linking process. Creep (deformation without wear) is also slightly increased with cross-linking of polyethylene.
Question 15:
A 6-year-old child has a fixed flexion deformity of the interphalangeal (IP) joint of the right thumb. The thumb is morphologically normal, with a nontender palpable nodule at the base of the metacarpophalangeal joint. Clinical photographs are shown in Figures 42a and 42b. Based on these findings, what is the treatment of choice?
Options:
- Complete release of the proximal annular pulley of the flexor sheath
- Removal of the nodule in the flexor pollicis longus
- Fractional lengthening of the flexor pollicis longus tendon at the musculotendinous junction
- Steroid injection into the palpable nodule
- No treatment because this condition normally spontaneously resolves
Correct Answer: Complete release of the proximal annular pulley of the flexor sheath
Explanation:
DISCUSSION: The child has a trigger thumb deformity. A trigger thumb is a developmental mechanical problem rather than a congenital deformity. The anomaly generally is not noted at birth. A fixed flexion deformity of the IP joint of the thumb most commonly occurs in children in the first 2 years of life. A stretching and splinting program may correct the deformity in the first year of life, but nonsurgical management after age 3 years results in a success rate of only 50%. Release of the proximal annular pulley of the flexor sheath is recommended at this age.
REFERENCES: Tan AH, Lam KS, Lee EH: The treatment outcome of trigger thumb in children. J Pediatric Orthop B 2002;11:256-259.
Slakey JB, Hennrikus WL: Acquired thumb flexion contracture in children: Congenital trigger thumb. J Bone Joint Surg Br 1996;78:481-483.
Herring JA: Disorders of the upper extremity: Thumb dysplasia, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, p 445.
Question 16:
Six weeks after open reduction internal fixation of a closed tibial pilon fracture, a patient has a draining wound with surrounding erythema and swelling. Radiographs show lucency around screws. What is the most appropriate treatment sequence?
Options:
- Start IV antibiotics, obtain wound swab for culture, perform irrigation and debridement and retain hardware
- Start IV antibiotics, obtain deep soft tissue and bone cultures in OR, perform irrigation and debridement and remove hardware
- Obtain wound swab for culture, start IV antibiotics, perform irrigation and debridement and remove hardware
- Obtain deep bone and soft tissue cultures in OR, start IV antibiotics, perform irrigation and debridement and remove hardware
Correct Answer: Obtain deep bone and soft tissue cultures in OR, start IV antibiotics, perform irrigation and debridement and remove hardware
Explanation:
Discussion: Management of acutely infected wounds is primarily surgical. Osteomyelitis frequently involves Orthopaedic hardware, which would ideally be removed or replaced given biofilm involvement. Multiple operative cultures of fluid collections, soft tissues and bone should routinely be obtained. Culture yield is highest if cultures are obtained before empiric antibiotic treatment is started. Tissue samples are greatly preferred to swabs, which are notoriously inaccurate.
Question 17:
A 6-year-old boy has had increasing pain and a mass in the suprapatellar region of the right femur for the past week. Examination of the mass reveals it may be firm, immobile, and tender to palpitation. The patient has no systemic symptoms. Laboratory studies show a WBC of 7000 per cubic millimeter, a hematocrit of 40%, and an erythrocyte sedimentation rate of 10 mm/hr. radiographs are normal. Figures 64a and 64b show saggital and axial T1-weighted MRI scans. Figure 64c shows frozen section pathology of the biopsy specimen. What is the most likely diagnosis?
Options:
- Synovial sarcoma
- Soft-tissue abcess
- Rhabdomyosarcoma
- Eosinophilic granuloma
- Nodular pigmented villonodular synovitis
Correct Answer: Soft-tissue abcess
Explanation:
Multiple hints in this history, MRI and pathology section leads to the diagnosis of soft tissue abscess. The sarcomas are slow growing and mostly are asymptomatic. The mass is tender and enlarging over the past week. PVNS would give the patient a painful boggy joint and this mass is supracondyler. Esinophilic granuloma would give a punched-out lesion in the long bones on the plain radiographs. The best clue is the slide given which shows inflammatory cells. PVNS would show hemosiderin stained giant cells, synovial sarcoma would reveal a biphasic pattern of spindle cells, E.G. would show eosinophils and histiocytes, and rhabdomyosarcoma would have cross striation within the tumor cells.
Question 18:
Survival rates for children with soft-tissue sarcoma other than rhabdomyosarcoma are best correlated with
Options:
- size of the tumor.
- histologic grade.
- histologic subtype.
- use of adjuvant chemotherapy.
- age of the patient.
Correct Answer: histologic grade.
Explanation:
DISCUSSION: In review of 154 patients with nonrhabdomyosarcoma, Rao reported that histologic grade, tumor invasiveness, and adequate surgical margin were the most important prognostic factors. Histologic subtype, use of adjuvant chemotherapy, and patient age were not as important. Size related to degree of invasiveness was not statistically significant.
REFERENCES: Rao BN: Nonrhabdomyosarcoma in children: Prognostic factors influencing survival. Semin Surg Oncol 1993;9:524-531.
Andrassy R, et al: Non-rhabdomyosarcoma Soft-Tissue Sarcomas: Pediatric Surgical Oncology. Philadelphia, PA, WB Saunders, p 221.
Question 19:
Which of the following factors has NOT been found to be a significant independent predictor of moderate or severe pain 6 months after musculoskeletal injury?
Options:
- Failure to complete high school
- Self-reported preinjury pain-related disability
- Disability compensation
- Male gender
- Moderate or severe pain at discharge from the acute hospital
Correct Answer: Failure to complete high school
Explanation:
Age and gender have not been found to be significant independent predictors of moderate or severe pain 6 months after musculoskeletal injury.
Williamson et al. performed a prospective cohort study of 1290 trauma patients in 2 Australian hospitals using a self-rated pain scale and a SF-12. They found that the prevalence of moderate or severe pain was 48% at discharge and 30% at 6 months post-injury. Failure to complete high school, self-reported preinjury pain-related disability, eligibility for compensation (payment for medical treatment, rehabilitation services, disability services, and income assistance), and moderate or severe pain at discharge from the acute hospital were found to be independent predictors of moderate or severe pain at 6 months post-injury.
Vranceanu et al. published a Level 5 review reporting that psychosocial factors are important and treatable correlates of disabling musculoskeletal pain. They encourage orthopaedic surgeons to diminish pain intensity and pain-related disability by teaming up with psychologists and other health-care providers in multidisciplinary teams to address cognitive, affective, behavioral, and social aspects of pain.
Incorrect Answers:
Question 20:
extensor tendons, 3) flexor tendons, 4) arteries, 5) nerves, 6) veins (can be done prior to nerve repair) , 7) skin.
Options:
- Sabapathy et al. review replantation surgery in the upper extremity. They discuss that a “functional extremity” could be reconstructed at the upper-arm level in 22% to 34%, at the proximal forearm level in 30% to 41%, and at the distal forearm level in 56% to 80% of cases.
- Hanel et al. review wrist level and proximal amputations in the upper extremity. Among other things, they state that wrist-proximal amputations should be performed before 12 hours of cold ischemia time or 6 hours of warm ischemia time have elapsed.
- Figure A shows a sharp transcarpal amputation. Incorrect Answers:
Correct Answer: Sabapathy et al. review replantation surgery in the upper extremity. They discuss that a “functional extremity” could be reconstructed at the upper-arm level in 22% to 34%, at the proximal forearm level in 30% to 41%, and at the distal forearm level in 56% to 80% of cases.
Explanation:
outcomes than above the elbow replantations.
A 45-year-old carpenter sustained a table saw injury to his right hand while at work earlier today. Evaluation in the Emergency Department reveals the defect depicted in Figure A. An island volar advancement flap was selected for wound closure. What is the largest defect that could be covered with this technique?
less than 1 cm
1.5 cm
Question 21:
.Figures 41a through 41c are the radiograph and MRI scans of a 76-year-old woman who has intractable left shoulder pain. She was given 2 cortisone injections and oral pain medication without experiencing lasting relief. Examination reveals 60 degrees of active forward elevation (120 degrees passively), 30 degrees of external rotation lag, and a positive Hornblower sign. Pain relief and improved functionality will most likely be achieved with
Options:
- continued nonsurgical treatment.
- hemiarthroplasty with partial rotator cuff repair.
- reverse total shoulder arthroplasty with latissimus dorsi transfer.
- rotator cuff repair without acromioplasty, preserving the coracoacromial ligament.
- limited-goals debridement of the rotator cuff and glenohumeral joint without rotator cuff repair.
Correct Answer: reverse total shoulder arthroplasty with latissimus dorsi transfer.
Question 22:
Which of the following types of ultra-high molecular weight polyethylene has been associated with the poorest clinical performance?
Options:
- Compression molded
- Heat pressed
- Ram extruded
- Gamma irradiated
- Ethylene oxide sterilized
Correct Answer: Heat pressed
Explanation:
DISCUSSION: Numerous studies have documented the poor performance of heat-pressed ultra-high molecular weight polyethylene used in the porous-coated anatomic tibial inserts of both total knee and unicompartmental arthroplasty. The other processing and sterilization methods have not been associated with significantly high failure rates.
REFERENCES: Wright TM, Rimnac CM, Stulberg SD, et al: Wear of polyethylene in total joint replacements: Observations from retrieved PCA knee implants. Clin Orthop 1992;276:126-134.
Landy MM, Walker PS: Wear of ultra-high molecular-weight polyethylene components of 90 retrieved knee prostheses. J Arthroplasty 1988;3:S73-S85.
Skyrme AD, Mencia MM, Skinner PW: Early failure of the porous-coated anatomic cemented unicompartmental knee arthroplasty: . A 5- to 9-year follow-up study. J Arthroplasty 2002;17:201-205.
Question 23:
A 5-year-old boy is seen in the emergency department with a 2-day history of refusing to walk. Examination shows that he has a temperature of 102.2 degrees F (39 degrees C) and limited range ot motion of the right hip. The AP pelvic radiograph is normal. The WBC count is normal but the C-reactive protein and erythrocyte sedimentation rate (ESR) are elevated. What is the next step in management?
Options:
- IV antibiotics
- Oral antibiotics
- Ibuprofen
- Observation and repeat evaluation in 2 weeks
- Aspiration of the right hip
Correct Answer: Aspiration of the right hip
Explanation:
DISCUSSION: The history, physical examination, and laboratory studies suggest a septic hip. Recent studies indicate that a child with elevated ESR, a WBC count of greater than 12,000/mm3, a temperature of greater than 38.5 degrees, and unwillingness to walk is very likely to have septic arthritis of the hip versus toxic synovitis. The best way to confirm the diagnosis is by hip aspiration. No medications should be started until a diagnosis is made. Toxic synovitis is common, but significantly less likely if three of the above criteria are present. This condition usually responds well to ibuprofen, but requires close observation. Septic hips are considered urgent conditions and therefore a repeat evaluation in 2 weeks is inappropriate.
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2109-2113.
Abel MF (ed): Orthopaedic Knowlede Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 62-65.
Kocher MS, Mandiga R, Murphy JM, et al: A clinical practice guideline for treatment of septic arthritis
in children: Efficacy in improving process of care and effect on outcome of septic arthritis of the hip. J Bone Joint Surg Am 2003;85:994-999.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinica l prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 24:
Which of the following patients is considered the most appropriate candidate for selective dorsal rhizotomy?
Options:
- Nonambulatory 2-year-old with spastic diplegia
- Nonambulatory 2-year-old with spastic quadriplegia
- Nonambulatory 12-year-old with spastic quadriplegia
- Ambulatory 4-year-old with spastic diplegia
- Ambulatory 9-year-old with hemiplegia and athetosis
Correct Answer: Ambulatory 4-year-old with spastic diplegia
Explanation:
DISCUSSION: While other surgical and nonsurgical options exist for management of spasticity, the criteria originally laid out by Peacock and associates describe the most appropriate candidate for rhizotomy as a patient with spastic diplegia who is between the ages of 4 to 8 years and has a stable gait pattern that is limited by lower extremity spasticity. Rhizotomy is not recommended in patients with athetosis because of unpredictable results. In addition, rhizotomy should be avoided in nonambulatory patients with spastic quadriplegia because it is associated with significant spinal deformities.
REFERENCES: Peacock WJ, Arens LJ, Berman B: Cerebral palsy spasticity: Selective posterior rhizotomy. Pediatr Neurosci 1987;13:61-66.
Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29.
Mooney JF III, Millis MB: Spinal deformity after selective dorsal rhizotomy in patients with cerebral palsy. Clin Orthop 1999;364:48-52.
Question 25:
Examination of an 18-year-old professional soccer player who was forcefully kicked across the shin while attempting a slide tackle reveals a marked effusion and limited motion of the knee. The tibia translates 12 mm posterior to the femoral condyles when the knee is held in 90 degrees of flexion. There is no posteromedial or posterolateral instability. Management should consist of
Options:
- early reconstruction of all injured structures.
- knee immobilization in 30 degrees of flexion for 2 to 4 weeks.
- knee immobilization in full extension for 2 to 4 weeks.
- protected weight bearing and intense hamstring strengthening.
- no weight bearing, followed by a gradual return to sports.
Correct Answer: knee immobilization in full extension for 2 to 4 weeks.
Explanation:
DISCUSSION: The patient has an acute grade III posterior cruciate ligament injury. The majority of grade I and II injuries can be treated with protected weight bearing and quadriceps rehabilitation, and most patients can return to sports within 2 to 4 weeks. In contrast, grade III injuries require immobilization in full extension for 2 to 4 weeks to protect the posterior cruciate ligament and the other posterolateral structures presumed to be damaged. The mainstay of postinjury rehabilitation for all posterior cruciate ligament injuries is quadriceps strengthening exercises, which have been shown to counteract posterior tibial subluxation.
REFERENCES: Miller MD, Bergfeld JA, Fowler PJ, Harner CD, Noyes FR: The posterior cruciate ligament injured knee: Principles of evaluation and treatment. Instr Course Lect 1999;48:199-207.
Posterior Cruciate Ligament Injuries in Principles and Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott, Williams and Wilkins, 2000.
Question 26:
For this patient, which TKA design is most appropriate?
Options:
- Bicruciate-retaining TKA
- Unicompartmental arthroplasty
- Hinged TKA
- Posterior substitution TKA
Correct Answer: Posterior substitution TKA
Explanation:
DISCUSSION
TKA in the setting of valgus deformities poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when used as a rotational reference point, can lead to internal rotation of the femoral component if not recognized. This malrotation will in turn lead to patellofemoral maltracking or instability, which is a common complication associated with primary TKA. The deformity is too severe to consider a bicruciate-retaining TKA or unicompartmental arthroplasty and does not necessitate a hinged TKA.
Question 27:
Figure 25 shows the CT scan of an adult patient who has neck pain following a motor vehicle accident. What is the most likely diagnosis?
Options:
- Jefferson’s fracture
- C1-C2 rotational instability
- Transverse ligament rupture
- Normal finding
- Basilar invagination
Correct Answer: Transverse ligament rupture
Explanation:
DISCUSSION: If the atlanto-dens interval is greater than 3 mm in an adult, a transverse ligament rupture usually is suspected. The atlanto-dens interval can be seen with CT or in lateral radiographs of the upper cervical spine. Transverse ligament rupture can occur as an isolated entity or in association with an odontoid or a Jefferson’s fracture. Patients with this type of injury usually require fusion.
REFERENCES: Dickman CA, Greene KA, Sonntag VK: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;38:44-50.
Clark CR: The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 362-363.
Question 28:
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management? Review Topic
Options:
- Immobilization in a sling and swathe
- Open capsular shift
- Arthroscopic capsular plication
- Thermal capsulorrhaphy
- Physical therapy and home exercises
Correct Answer: Physical therapy and home exercises
Explanation:
Multidirectional instability of the shoulder is defined as symptomatic instability in two or more directions (anterior, posterior) but must include a component of inferior instability. Initial treatment should always include physical therapy and instruction in a home exercise program that emphasizes periscapular and rotator cuff strengthening to improve the dynamic stability of the glenohumeral joint. Immobilization has not been shown to be effective. Open capsular shift and arthroscopic capsular plication remain the surgical options when appropriate nonsurgical management fails (typically a minimum of 6 months of dedicated therapy and home program). Thermal capsulorrhaphy remains controversial but is not recommended by many clinicians because of reported complications including recurrent instability, axillary nerve injury, chondrolysis, and capsular injury.
Question 29:
Figures 1 through 4 are the CT scans and intraoperative image of a 17-year-old boy who sustained a gunshot wound to his knee. What is the most appropriate definitive surgical management for his articular cartilage defect?
Options:
- Microfracture
- Autologous chondrocyte implantation
- Osteochondral allograft transfer
- Dejour trochleoplasty
Correct Answer: Osteochondral allograft transfer
Explanation:
The images show a full-thickness cartilage defect with significant bony involvement >4 cm
2
. Microfracture should be considered for lesions <2 cm
2
without an underlying osseous defect. Autologous chondrocyte implantation, although used for lesions between 1 and 10 cm
2
, should be restricted for defects with minimal (<8 mm depth) bone loss. Osteochondral allograft transfer with the mosaicplasty technique (transfer of multiple plugs) would be well-suited for this large defect with significant osseous involvement. Dejour trochleoplasty is performed for patellar instability to correct trochlear dysplasia and
would not be indicated in this case.
Question 30:
A 12-year-old boy who pitches on two “select” baseball teams has had pain in his dominant right shoulder for the past 6 weeks. The pain is present only with throwing and is associated with decreased throwing velocity and control. He has no radiation of pain or paraesthesias of the upper extremity. An AP radiograph and MRI scan are shown in Figures 19a and 19b, respectively. Management should consist of Review Topic
Options:
- rest from throwing activities.
- a subacromial corticosteroid injection.
- open reduction and internal fixation.
- arthroscopic labral repair.
- biopsy of the proximal humerus.
Correct Answer: rest from throwing activities.
Explanation:
The imaging study demonstrates characteristics of Little Leaguer’s shoulder, including physeal widening. This condition is secondary to overuse (typically throwing) and responds well to rest from the inciting activity. There is no evidence from the patient’s history or examination that he has an impingement syndrome, nor is there any indication of labral pathology on the MRI scan. The changes in the proximal humerus are classic for this condition and are not suggestive of a neoplastic process requiring biopsy for definitive diagnosis.
Question 31:
Patients with tarsal tunnel syndrome are most likely to obtain a favorable outcome from decompression of the posterior tibial nerve if which of the following conditions is present?
Options:
- A space-occupying lesion is compressing the tarsal tunnel.
- Nerve conduction velocity studies reveal slowing across the medial malleolus.
- The posterior tibial tendon is ruptured.
- The integrity of the posterior tibial tendon is compromised.
- The spring ligament is ruptured, resulting in the development of a dynamic flatfoot.
Correct Answer: A space-occupying lesion is compressing the tarsal tunnel.
Explanation:
DISCUSSION: In one series, only 44% of patients demonstrated good results from tarsal tunnel decompression if they did not have a mass in the tarsal tunnel. Conditions that produce a traction neuropathy of the posterior tibial nerve are unlikely to respond to neurolysis. The most favorable condition associated with a good response to decompression is when a compressing anatomic structure can be removed from the tarsal tunnel.
REFERENCES: Frey C, Kerr R: Magnetic resonance imaging and the evaluation of tarsal tunnel syndrome. Foot Ankle 1993;14:159-164.
Garrett AL: Poliomyelitis, in Nickel VL (ed): Orthopaedic Rehabilitation. New York, NY, Churchill Livingston, 1982, pp 449-458.
Pfeiffer WH, Cracchiolo A III: Clinical results after tarsal tunnel decompression. J Bone Joint Surg Am 1994;76:1222-1230.
Question 32:
Which method of flexor tendon repair that necessitates excursion through the A2 pulley allows for the most thorough assessment of tendon gliding?
Options:
- strand repair with 6-0 epitendinous suture with Bier block anesthesia
- strand repair with 6-0 epitendinous suture under local anesthesia only
- strand repair with regional anesthesia
- Repair of the flexor tendon with incision of the remaining A2 pulley
Correct Answer: strand repair with 6-0 epitendinous suture under local anesthesia only
Explanation:
EXPLANATION:
Wide-awake repair under only local anesthesia, regardless of the technique, allows direct inspection of the tendon repair and active excursion. Regional anesthesia and Bier block anesthesia do not allow active motion (Bier block necessitates continued use of a tourniquet, which limits muscle function). The A2
pulley should be preserved, especially the distal 50%, to maintain tendon function. All of the listed techniques for suture repair are acceptable options.
Question 33:
A 20-year-old college pitcher reports medial elbow pain after 3 innings of hard throwing. He recalls no injury and reports no pain with light throwing. The examination shown in the clinical photograph in Figure 48 reproduces the elbow pain. What is the most likely diagnosis? Review Topic
Options:
- Flexor-pronator avulsion
- Ulnar nerve subluxation
- Medial collateral ligament injury
- Lateral ulnar collateral ligament rupture
- Triceps tendon subluxation
Correct Answer: Medial collateral ligament injury
Explanation:
The milking test, as seen in the photograph, elicits pain when a tear is present in the medial collateral ligament. Complete rupture is possible but unlikely when there is no history of trauma and the patient is able to throw pain-free for several innings. Subluxation of the ulnar nerve and triceps tendon subluxation present as a painful snapping over the medial aspect of the elbow.
Question 34:
A 32-year-old man notes increasing back pain and progressive paraparesis over the past few weeks. He is febrile, and laboratory studies show a WBC of 12,500/mm3. MRI scans are shown in Figures 6a and 6b. Management should consist of
Options:
- CT-guided needle aspiration and organism-appropriate antibiotics.
- laminectomy and postoperative bracing.
- posterior fusion with instrumentation and IV antibiotics.
- anterior debridement and strut graft, with possible posterior instrumentation.
- posterior extracavitary decompression alone.
Correct Answer: anterior debridement and strut graft, with possible posterior instrumentation.
Explanation:
DISCUSSION: Indications for surgery in spinal infections include progressive destruction despite antibiotic treatment, an abscess requiring drainage, neurologic deficit, need for diagnosis, and/or instability. This patient has a progressive neurologic deficit. Debridement performed at the site of the abscess should effect canal decompression. Once the debridement is complete back to viable bone, the defect can be reconstructed with a strut graft. Additional posterior stabilization is used as deemed necessary by the degree of anterior destruction. CT-guided needle aspiration, while occasionally useful in the earliest phases of an infection, produces frequent false-negative results and would provide little useful information in the management of this patient.
REFERENCES: Emery SE, Chan DP, Woodward HR: Treatment of hematogenous pyogenic vertebral osteomyelitis with anterior debridement and primary bone grafting. Spine 1989;14:284-291.
Lifeso RM: Pyogenic spinal sepsis in adults. Spine 1990;15:1265-1271.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 713-721.
Question 35:
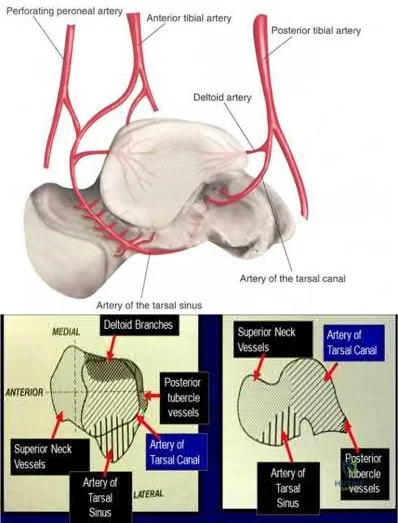
A 29-year-old male sustains the isolated lower extremity injury shown in Figure A. During open reduction, what structure must be kept intact in order to protect the remaining blood supply to the talar body?
Options:
- Medial malleolus
- Deltoid ligament
- Anterior talofibular ligament
- Lateral malleolus
- Calcaneonavicular ligament
Correct Answer: Deltoid ligament
Explanation:
Figure A represents a type 3 Hawkins talar neck fracture. A type 3 injury is defined as a displaced fracture of the talar neck with dislocation of body of talus from both the subtalar joint and the tibiotalar joint. In these injuries, the talar body fragment typically rotates around intact deltoid ligament fibers to lie in soft tissues with the fracture surface pointing laterally and cephalad. Often, the deltoid branch of the posterior tibial artery, which lies between the leaves of the deltoid ligament and supplies up to 1/2 of the medial talar body, is the only remaining blood supply. Therefore, the deltoid ligament must be preserved to lower the risk of avascular necrosis. When performing a medial malleolar osteotomy, the deltoid ligament must remain in continuity with the malleolus to prevent disruption of the blood supply.
The review article by Fortin et al discusses talar blood supply, injury mechanisms and classifications, and treatment options. They state that the main artery to the body of the talus is the artery of the tarsal canal, which is a branch of the posterior tibial artery. The peroneal and anterior tibial artery also contribute branches to the talus.
Illustration A and B show the arterial network of the talus.
OrthoCash 2020
Question 36:
Which of the following is considered the most effective means of identifying an evolving motor tract injury during cervical spine surgery? Review Topic
Options:
- Mean arterial blood pressure monitoring
- SSEP monitoring
- Free-run electromyography
- Transcranial motor monitoring (tceMEP)
- Wake-up test
Correct Answer: Transcranial motor monitoring (tceMEP)
Explanation:
In a study of 427 patients undergoing cervical spine surgery, 12 patients demonstrated substantial or complete loss of amplitude of the tceMEPs. Ten of those patients had complete reversal of the loss following prompt intraoperative intervention. SSEP monitoring failed to identify any changes in one of the two patients that awoke with a new motor deficit. SSEP changes lagged behind the tceMEP changes in patients in
which major changes were detected by both modalities. TceMEP monitoring was 100% sensitive and 100% specific. SSEP monitoring was only 25% sensitive and 100% specific.
Question 37:
Figure 28 is the lateral radiograph of a patient who sustained an intraarticular fracture of the calcaneus. The structure (*) depicted by the arrows most likely represents which osseous component of the calcaneus?
Options:
- Middle facet
- Sustentaculum tali
- Extruded lateral wall
- Medial portion of the posterior facet
- Lateral portion of the posterior facet
Correct Answer: Lateral portion of the posterior facet
Explanation:
Fractures of the calcaneus occur as a result of shear and compression forces. Foot position at the time of impact, the force of the impact, and bone quality all dictate the degree of comminution and fracture line orientation. Two primary fracture lines are consistently observed, one of which divides the calcaneus into medial and lateral portions. An essential feature of this fracture line is that it creates a fragment (sustentaculum tali) that remains attached to the talus by the interosseous ligament. This medial portion (constant fragment) of the posterior facet retains its normal anatomic position beneath the posterior talus. Its corresponding lateral component (labeled with an * in the figure), however, can be found displaced inferiorly within the body of the calcaneus. It is often rotated 90 degrees (as depicted in Figure 28) in relation to the remainder of the subtalar joint. This gives the appearance of what has been described as the "double-density" sign. The middle facet is more anterior and less commonly displaced. The lateral wall is nonarticular.
Question 38:
A 62-year-old active man returns for routine follow-up 16 years after hip replacement. He has no hip pain. Radiographs reveal a well-circumscribed osteolytic lesion around a single acetabular screw. All hip components are perfectly positioned. Comparison radiographs obtained 6 months later show an increase in the size of the osteolytic lesion. CT depicts a well-described lesion that is 3 cm at its largest diameter and is localized around one screw hole with an eccentric femoral head. What treatment is appropriate, assuming that well-fixed cementless total hip components are in place?
Options:
- Revision of the polyethylene liner, removal of the screw, and debridement of the osteolytic lesion with or without bone grafting
- Revision of the acetabular component to a newer design without screws
- Removal of the screw, revision of the polyethylene liner, and stem cell injection into the lytic lesion
- Removal of the offending screw from the metal socket and placement of a new polyethylene liner in the existing socket
Correct Answer: Revision of the polyethylene liner, removal of the screw, and debridement of the osteolytic lesion with or without bone grafting
Explanation:
DISCUSSION:
Given a well-fixed acetabular metal shell and a localized osteolytic lesion, good outcomes can be expected from liner revision in this clinical scenario with retention of the metal socket, assuming no damage to the components or other unexpected findings arise during revision surgery. Here, complete cup revision is not warranted, considering the appropriate implant position. Beaulé and associates reviewed 83 consecutive patients (90 hips) in whom a well-fixed acetabular component was retained in a clinical scenario such as the one described. No hip showed recurrence or expansion of periacetabular osteolytic lesions. If the metal cup is unstable, acetabular component revision may be indicated.
Question 39:
The husband of a 22-year-old woman has hypophosphatemic rickets. The woman has no orthopaedic abnormalities, but she is concerned about her chances of having a child with the same disease. What should they be told regarding this disorder?
Options:
- Their sons will have a 50% chance of having this X-linked dominant disorder.
- All of their daughters will be carriers or will have this disorder.
- They should be advised to not have any children as the risk of having boys with the disorder and girls who will be carriers is too hard for any parent.
- As long as the woman does not carry the trait, the children will not be affected because the husband has the disease and this is an X-linked dominant disorder.
- Their sons or daughters may be born with this disorder, but males are more severely affected.
Correct Answer: All of their daughters will be carriers or will have this disorder.
Explanation:
DISCUSSION: Hypophosphatemia is a rare genetic disease usually inherited as an X-linked dominant trait. The fact that the woman has no skeletal manifestations would indicate that the husband has the X-linked mutation. The disease is more severe in boys than it is in girls. The husband will not transmit the disease to his sons. However, all of their daughters will be affected either with the disease or as carriers. If the woman has the disease or the trait, there is a 50% chance that her sons will inherit the disease and a 50% chance that her daughters will be carriers or have a milder form of the disease. Parents should be advised to have genetic counseling so they can be informed when deciding whether to have children.
REFERENCES: Herring JA: Metabolic and endocrine bone diseases, in Tachdjian’s Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743.
Sillence DO: Disorders of bone density, volume, and mineralization, in Rimoin DL, Conner JM, Pyerite RE, et al (eds): Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002.
Staheli LT: Practice of Pediatric Orthopedics. Philadelphia, PA, Lippincott Williams & Wilkins, 2001.
Question 40:
Thyroid hormone regulates skeletal growth at the physis by stimulation of
Options:
- proteoglycan and aggrecan synthesis in the zone of proliferation.
- fibroblast growth factor (FGF) activity.
- transforming growth factor type beta (TGF- b =) and parathyroid hormone-related protein (PTHrP) activity.
- chondrocyte proliferation.
- chondrocyte hypertrophy, type X collagen synthesis, and alkaline phosphatase activity.
Correct Answer: chondrocyte hypertrophy, type X collagen synthesis, and alkaline phosphatase activity.
Explanation:
DISCUSSION: Children with hypothyroidism have delayed bone age, reduced thickness of the physis, disorganization of the cartilage columns of the physis, and impaired differentiation of proliferating chondrocytes into hypertrophic cells. As a result, these children have severe growth retardation, and slipped capital femoral epiphysis may develop because of mechanical weakening of the physis. Thyroid hormone regulates terminal differentiation of the growth plate chondrocytes, with a resultant increase in type X collagen and alkaline phosphatase. These substances are important factors in matrix mineralization. Insulin-like growth factors and FGF-2 appear to act synergistically to stimulate mitotic activity of the growth plate chondrocytes. TGF-
b
= and PTHrP stimulate proteoglycan synthesis and mitotic activity of the chondrocytes and inhibit type X collagen and alkaline phosphatase activity.
REFERENCES: Ballock RT: Regulation of skeletal growth and maturation by thyroid hormone, in Buckwalter JA, Ehrlich MG, Sandell LJ, Trippel SB (eds): Skeletal Growth and Development: Clinical Issues and Basic Science Advances. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1998, pp 301-317.
Rosier RN, O’Keefe RJ, Reynolds PR, Hicks DG, Puzas JE: Expression and function of TGF-
b
= and PTHrP in the growth plate, in Buckwalter JA, Ehrlich MG, Sandell LJ, Trippel SB (eds): Skeletal Growth and Development: Clinical Issues and Basic Science Advances. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1998, pp 285-299.
Trippel SB: IGF-I and FGF-2 in growth plate regulation, in Buckwalter JA, Ehrlich MG, Sandell LJ, Trippel SB (eds): Skeletal Growth and Development: Clinical Issues and Basic Science Advances. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1998, pp 263-283.
Question 41:
Following total knee arthroplasty, a patient is noted to have asymmetrical absent pulses and poor capillary refill. What is the next most appropriate step in management?
Options:
- Observation of the limb for 4 hours to see if the arterial spasm resolves
- Measurement of lower leg compartment pressures
- Magnetic resonance angiogram
- Emergent return to the operating room for wound exploration while the patient anesthesia
- Return to the operating room, obtain a vascular surgery consultation, and intraoperative arteriogram
Correct Answer: Return to the operating room, obtain a vascular surgery consultation, and intraoperative arteriogram
Explanation:
is still under
perform an
DISCUSSION: An assessment of the location of the vascular compromise is necessary prior to surgical exploration. Vascular repair will most likely require a separate surgical exposure. Vascular reperfusion may be accomplished at the time of an arteriogram with the use of a stent in certain situations. Return to the operating room with vascular surgical consultation and intraoperative arteriogram is appropriate.
An immediate postoperative compartment syndrome is unlikely. Magnetic resonance angiogram is not appropriate because of the potential for a delay in diagnosis.
REFERENCE: Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001 ;9;253-257.
Question 42:
Figure 36 shows the AP pelvic radiograph of a 26-month-old boy who has a limp. He has no significant medical history and no pain. What is the most appropriate treatment plan? Review Topic
Options:
- Physical therapy
- Application of a Pavlik harness
- Arthrogram and closed reduction with spica casting under anesthesia
- Femoral lengthening with a unilateral fixator
- Open reduction with femoral shortening, capsulorrhaphy, and a spica cast
Correct Answer: Open reduction with femoral shortening, capsulorrhaphy, and a spica cast
Explanation:
The radiograph reveals a complete hip dislocation. A Pavlik harness is an accepted method of treatment for a dislocated hip up until 6 months of age. Closed reduction and spica casting with an arthrogram is often successful in young children up to 1-1/2 years to 2 years of age. Open reduction, capsulorrhaphy, and a spica cast is commonly recommended for younger children when attempts at closed reduction have failed or when the child is older than 2 years of age. A femoral shortening is also generally recommended in children older than 2 years of age in an attempt to reduce the muscle/compressive forces on the reduced hip.
(SBQ13PE.38) Pavlik harness treatment is appropriate for which of the following?:
Review Topic
4 year old with a diaphyseal femur fracture and a neuromuscular disorder with lower extremity spasticity
2 month old with a displaced spiral mid-diaphyseal femur fracture
9 month old with a diaphyseal femur fracture with <2cm shortening
9 month old with a diaphyseal femur fracture with >2cm shortening
4 year old with a diaphyseal femur fracture, closed head injury and chest trauma
Treatment with Pavlik harness or spica cast are options for patients <6 months of age with diaphyseal femur fractures. Pavlik harness provides adequate pain control for the short time required for healing in this age group. Significant remodeling potential can be expected.
Because of the significant remodeling and quick healing, treatment of diaphyseal femur fractures in children younger than 6 months focuses on providing comfort and avoiding complications. Spica casting likewise results in stable union without longterm sequelae but minor skin complications are more common and some favor Pavlik treatment in this age group.
Kocher et al. provide the AAOS Clinical Practice Guideline for the treatment of pediatric diaphyseal femur fractures. Their recommendation for diaphyseal femur fractures in children less than 6 months is Grade C, based on Level IV evidence (one retrospective comparative study and one case series). They recommend that Pavlik and spica casting are both acceptable treatment options in this age group.
Flynn et al. review the management of pediatric femoral shaft fractures. They recommend Pavlik treatment for children 6 months of age or less in preference to a spica cast, sometimes supplemented with a simple splint. This avoids the skin complications of spica casting.
Incorrect answers:
Question 43:
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. What is the most appropriate management of this condition?
Options:
- Continue to observe with repeat radiographs in 6 months B. Fluoroscopic-guided iliopsoas tendon cortisone injection C. Hip aspiration
- Serum cobalt and chromium levels and metal-reduction MRI scan
Correct Answer: Continue to observe with repeat radiographs in 6 months B. Fluoroscopic-guided iliopsoas tendon cortisone injection C. Hip aspiration
Explanation:
DISCUSSION:
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross- sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 44:
A 32-year-old woman has an isolated left posterior wall acetabular fracture in which about 25% of the wall surface is involved. Which of the following criteria would indicate the need for surgical reduction and fixation?
Options:
- Fracture comminution
- Displacement of 1 mm at the fracture site
- Involvement of the ischial facet
- Femoral head subluxation during fluoroscopic examination
- Presence of a bilateral pneumothorax
Correct Answer: Femoral head subluxation during fluoroscopic examination
Explanation:
DISCUSSION: Fractures with a posterior wall fragment that makes up less than one third of the surface generally are stable. Conversely, fractures with a fragment making up more than 50% of the surface are unstable. Patients with an intermediate fracture fragment should undergo a fluoroscopic examination under sedation or anesthesia to determine if the fragment is truly stable. If so, the patient can be treated nonoperatively and safely mobilized.
REFERENCES: Tornetta P III: Non-operative management of acetabular fractures: The use of dynamic stress views. J Bone Joint Surg Br 1999;81:67-70.
Keith JE Jr, Brashear HR Jr, Guilford WB: Stability of posterior fracture-dislocations of the hip: Quantitative assessment using computed tomography. J Bone Joint Surg Am 1988;70:711-714.
Question 45:
A 58-year-old woman is seen in the emergency department after falling at home. History reveals that she underwent right total knee arthroplasty 2 years ago. Radiographs are shown in Figures 56a and 56b. What is the most appropriate treatment?
Options:
- Closed reduction and casting
- Bed rest and skeletal traction
- Open reduction and internal fixation
- Retrograde intramedullary nailing
- Revision of the femoral component with a stemmed component
Correct Answer: Open reduction and internal fixation
Explanation:
DISCUSSION: The radiographs show an oblique periprosthetic distal femoral fracture. Of the options listed, open reduction and internal fixation is the most appropriate surgical option because a well-fixed, posterior stabilized closed box femoral component is present. Nonsurgical methods are not favored because of the highly displaced, unstable fracture pattern and prolonged immobility. Revision with a stemmed component is an option but would sacrifice more bone stock in this younger patient.
REFERENCES: Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209.
Raab GE, Davis CM III: Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty 2005;20:984-989.
Tharani R, Nakasone C, Vince KG: Periprosthetic fractures after total knee arhtroplasty.
J Arthroplasty 2005;20:27-32.
Question 46:
Which of the following is considered the most common complication of the impaction grafting technique for femoral revision surgery?
Options:
- Loss of fixation
- Osteolysis
- Bone graft resorption
- Early stem subsidence
- Infection
Correct Answer: Early stem subsidence
Explanation:
DISCUSSION: Impaction grafting technique for femoral revision surgery has become increasingly popular over the past decade. This technique is designed to address cavitary deficiencies of the femur. The femoral stem is inserted with cement fixation. Its clinical efficacy has not been shown to be superior to extensively porous-coated stems. Early subsidence of the stem has been reported in more than 50% of the patients. However, loss of fixation has occurred infrequently (5%) in reported series conducted by experienced surgeons. It has not been shown to have a higher infection rate.
REFERENCES: Gie GA, Linder L, Ling RS, Simon JP, Slooff TH, Timperley AJ: Impacted cancellous allografts and cement for revision total hip arthroplasty. J Bone Joint Surg Br 1993;75:14-21.
Meding JB, Ritter MA, Keating ME, Faris PM: Impaction bone-grafting before insertion of a femoral stem with cement in revision total hip arthroplasty: A minimum two-year follow-up study. J Bone Joint Surg Am 1998;79:1834-1841.
Question 47:
A 4-year-old boy sustains the injury shown in Figures 10a and 10b as a result of being hit and dragged by a car. Wound closure is best accomplished by
Options:
- Sural artery island flap.
- Free rectus abdominis flap.
- Extensor digitorum brevis flap.
- Staged cross leg flap.
- Split-thickness skin graft.
Correct Answer: Free rectus abdominis flap.
Explanation:
The indications for a free flap coverage for the foot and ankle include loss of skin and subcutaneous tissue with exposed bone, tendon, and neurovascular structures and, on occasion, surgical hardware; local options are not available or feasible and coverage is necessary to provide
healing and survival of the underlying structures, prevent infection, and provide a durable and/or flexible cover. Furthermore, the standard cross-leg flap no longer is used because of significant problems with positioning and joint stiffness, and because it provides inadequate coverage material. For the various surfaces of the ankle and dorsum of the foot, very few local tissues are available to provide coverage when free skin grafting is insufficient. Thus, out of the possible answers, free rectus abdominis flap is the preferred response.
Question 48:
-What is the most likely mechanism of injury?
Options:
- External rotation
- Posterior translation
- Hyperextension and varus
- Anterior translation and internal rotation
Correct Answer: Anterior translation and internal rotation
Explanation:
DISCUSSION FOR QUESTIONS 56 THROUGH 58
The MRI scan shows a bone bruise of the lateral femoral condyle and lateral tibial plateau. This injury pattern is commonly associated with anterior cruciate ligament (ACL) rupture and an abnormal pivot shift test result. Treatment of an ACL tear in a high-demand athlete should consist of ligament reconstruction.In this patient, surgery should be delayed until she regains full range of motion to minimize risk for arthrofibrosis after surgery. Recent analysis has shown that the noncontact mechanism is more consistent with anterior translation, affecting both the medial and lateral compartments. The bone bruise in the lateral femoral condyle occurs more anterior than that of the medial femoral condyle, suggesting that internal rotation has occurred. The external rotation recurvatum test assesses for posterolateral corner injury, and a positive quadriceps active test is consistent with posterior cruciate ligament rupture. An abnormal patellar apprehension test result is suggestive of patellar instability. Nonsurgical treatment is unlikely to result in sufficient stability if this patient returns to sports at her preinjury level of activity.Primary ACL repair is associated with high failure rates. Although the precise mechanism of injury varies,injuries can be broadly classified into contact and noncontact injuries. Noncontact injuries occur with the knee in slight flexion, valgus, and internal rotation, and contact injuries typically involve a lateralside impact producing a valgus force to the knee. The valgus component of noncontact injuries has been thought to cause mainly lateral compartment bone bruising. Posterior translation is the most common mechanism of posterior cruciate ligament rupture, and hyperextension and varus is associated with posterolateral corner injury.
Question 49:
A cortisone injection in the subacromial space will most likely result in
Options:
- elevated blood glucose levels in patients with diabetes.
- increased instability in multidirectional patients.
- accelerated rupture of the long head of the biceps.
- accelerated osteoporosis of the tuberosity.
- altered proprioception of the glenohumeral joint.
Correct Answer: elevated blood glucose levels in patients with diabetes.
Explanation:
DISCUSSION: A cortisone injection in the subacromial space will most likely result in elevated blood glucose levels in patients with type I diabetes mellitus. Patients should be warned of this potential complication. Cortisone does not have an effect on instability or proprioception, and a single injection would not affect osteoporosis. Repetitive injections or injection into the tendon itself could accelerate rupture of the biceps tendon.
REFERENCES: Matsen FA III, Arntz CT: Subacromial impingement, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 623-646.
Koehler BE, Urowitz MB, Killinger DW: The systemic effects of intra-articular corticosteroid. J Rheumatol 1974;1:117-125.
Question 50:
Which of the following is considered an advantage of metal femoral heads compared with ceramic heads?
Options:
- Superior lubrication properties
- Smoother surface
- Less susceptible to third body wear
- More inert material
- Greater neck-length options
Correct Answer: Greater neck-length options
Explanation:
DISCUSSION: Ceramic-on-ceramic bearing surfaces have superior tribological properties and show lower linear wear than metal-on-metal implants. However, because of their lower strength and vulnerability to fracture, design considerations constrain the neck-length options available to ensure optimal taper fit.
REFERENCE: Cook SD: Materials consideration in total joint replacement, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 27-33.
Question 51:
A 56-year-old male sustains a Type IIIB open, comminuted tibial shaft fracture distal to a well-fixed total knee arthroplasty that is definitively treated with a free flap and external fixation. Nine months after fixator removal, he presents with a painful oligotrophic nonunion. Laboratory workup for infection is negative. Passive knee range of motion is limited to 15 degrees. What is the most appropriate treatment for his nonunion?
Options:
- Knee manipulation under anesthesia
- Cast immobilization and use of a bone stimulator
- Unilateral external fixation
- Intramedullary nailing
- Compression plating
Correct Answer: Knee manipulation under anesthesia
Explanation:
DISCUSSION: At 9 months, observation is no longer an option, as the fracture is not healing and is adjacent to a arthrofibrotic joint. Plate osteosynthesis has been shown to be an effective method of treatment for patients who have had an open fracture of the tibia that has failed to unite after external fixation and/or immobilization in a cast.
Wiss et al reported a series of fifty tibial non-unions with a similar clinical scenario. He reported that, with compression plating, 92% of the nonunions healed without further intervention. In their study, 39/50 patients, had autogenous bone grafting in addition to compression plating.
Question 52:
A 42-year-old patient undergoes resection of the medial clavicle for painful sternoclavicular degenerative joint disease. The postoperative course is complicated by an increase in symptoms, a medial bump, and subjective tingling in the digits. A clinical photograph and radiograph are shown in Figures 20a and 20b. What is the most appropriate procedure at this time?
Options:
- Semitendinosis figure-of-eight graft
- Subclavius tendon transfer
- Medial clavicular osteotomy
- Medial clavicular resection
- Sternoclavicular arthrodesis
Correct Answer: Semitendinosis figure-of-eight graft
Explanation:
DISCUSSION: Improved peak-to-load failure data have been demonstrated by reconstruction of the sternoclavicular joint using a semitendinosis graft in a figure-of-eight pattern through the clavicle and manubrium. Resection of the medial clavicle, which compromises the integrity of the costoclavicular ligament, results in medial clavicular instability.
REFERENCES: Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 608-609.
Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Question 53:
Which of the following is a recognized consequence of hip fusion?
Options:
- Low back pain
- Contralateral knee laxity
- Difficulty delivering children
- Meralgia paresthetica
- Contralateral abductor weakness
Correct Answer: Low back pain
Explanation:
DISCUSSION: Low back pain is an expected long-term complication of fusion; ipsilateral knee laxity is frequently encountered, as is degeneration of the contralateral hip. Hip fusion is equally valuable for both men and women, with both genders reporting satisfactory sexual function. Female patients often deliver by elective Cesarean section, although vaginal deliveries are reported.
REFERENCES: Liechti R (ed): Hip Arthrodesis and Associated Problems. Berlin, Germany, Springer-Verlag, 1978, pp 109-117.
Sponseller PD, McBeath AA, Perpich M: Hip arthrodesis in young patients: A long-term follow-up study. J Bone Joint Surg Am 1984;66:853-859.
Question 54:
A 56-year-old mechanic has had pain in the hypothenar region of his dominant right hand for the past 6 months. He reports weakness in his grip and pain is worse with activity. Which of the following examination findings is most suggestive of a cervical etiology?
Options:
- Relief of symptoms with shoulder abduction (placing hand over the head)
- Hypothenar atrophy
- Reproduction of pain with hyperflexion and contralateral rotation of the head
- Positive Tinel’s sign at the levator scapulae
- Subluxable ulnar nerve at the cubital tunnel
Correct Answer: Relief of symptoms with shoulder abduction (placing hand over the head)
Explanation:
DISCUSSION: Hypothenar atrophy is a nonspecific sign that can be seen in ulnar neuropathy, C8 radiculopathy, or even cervical myelopathy; however, the atrophy usually is not unilateral and includes other muscle groups. The Spurling test is an excellent method of eliciting cervical radicular pain but involves hyperextension and ipsilateral rotation of the cervical spine, resulting in nerve root compression by reducing the cross-sectional area of the ipsilateral neuroforamen. Tinel’s sign at the levator scapulae, if present, is indicative of an upper cervical (C3 or C4) radiculopathy. A subluxable ulnar nerve at the cubital tunnel, while often asymptomatic, points toward cubital tunnel syndrome as an etiology for this patient’s pain. The shoulder abduction relief (SAR) sign (relief of upper extremity pain with shoulder abduction) is virtually pathognomic of cervical radiculopathy because this maneuver results in relaxation of a compressed and/or inflamed cervical nerve root. The SAR sign is the converse analog of the straight leg raising sign in the lumbar examination for lumbar radiculopathy, as it relieves tension in the nerve root, thereby relieving symptoms.
REFERENCES: Ducker TB, Zeidman SM: Neurologic and functional evaluation, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 143-161.
An HS: Clinical presentation of discogenic neck pain, radiculopathy, and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 755-764.
Hoppenfeld S: Physical examination of the cervical spine and temporomandibular joint, in Physical Examination of the Spine and Extremities. New York, NY, Appleton-Century-Crofts, 1976, pp 105-132.
Question 55:
Which modality has the broadest application for reduction of postsurgical transfusion?
Options:
- Regional anesthesia
- Tranexamic (TXA) acid administration
- Reduced transfusion trigger
- Hypotensive anesthesia
Correct Answer: Tranexamic (TXA) acid administration
Explanation:
DISCUSSION
TXA is easy to administer, inexpensive, and safe for virtually all patients. Multiple studies have demonstrated transfusion rates lower than 3% for total knee arthroplasty and lower than 10% for total hip arthroplasty. Regional and hypotensive anesthesia effectively reduce transfusion; however, they cannot be used in as wide a range of patients as TXA. A reduced transfusion trigger must be considered along with patient symptoms when determining the need for transfusion.
Question 56:
A 14-year-old girl has had progressive heel pain for the past several months. Based on the radiograph, MRI scan, and biopsy specimens shown in Figures 37a through 37d, treatment should include
Options:
- observation.
- wide resection.
- radiation therapy.
- extended curettage.
- chemotherapy.
Correct Answer: extended curettage.
Explanation:
DISCUSSION: An aneurysmal bone cyst is a benign, locally destructive lesion of bone. Most are seen in patients in the second decade of life. The clinical presentation varies, but most patients have pain, tenderness, swelling, and/or pathologic fracture. Radiographs show a radiolucent lesion sometimes with expansile remodeling of the cortex. MRI best detects the commonly seen fluid-fluid levels associated with this lesion. Histologic findings include
blood-filled spaces with bland fibrous connective tissue septa. The stroma has histiocytes, fibroblasts, scattered giant cells, hemosiderin, and occasional inflammatory cells. Treatment of these lesions consists of extended curettage, plus or minus the use of adjuvants (liquid nitrogen, phenol, argon beam coagulation), and finally filling the bone void (allograft or other bone substitute).
REFERENCES: Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
Ramirez AR, Stanton RP: Aneurysmal bone cyst in 29 children. J Pediatr Orthop 2002;22:533-539.
Question 57:
Figures 6a and 6b are the radiographs of an injury for which a closed reduction procedure was unsuccessful. A dorsal approach to the metacarpophalangeal (MP) joint is chosen for open reduction. What is the most likely structure to impede the reduction?
Options:
- Flexor tendon
- Adductor aponeurosis
- Dorsal capsule
- Palmar plate
Correct Answer: Palmar plate
Explanation:
DISCUSSION
The radiograph shows the proximal phalanx nearly parallel with the metacarpal, where the simple dorsal dislocation of the phalanx is nearly perpendicular to the joint. A simple dislocation can be converted into a complex dislocation with attempts at closed reduction. The palmar plate, which is entrapped within the MP joint, should be incised longitudinally through its midline, allowing the metacarpal head to be reduced. For reduction of a simple dislocation, the wrist should be flexed to allow relaxation of the flexor tendons, and distal traction as well as volar-directed pressure to the base of the proximal phalanx can be successful in reducing a simple dislocation. Surgical reduction can be approached either dorsally or volarly. The volar approach jeopardizes the digital nerve. With a dorsal approach, the extensor hood and dorsal capsule should be incised longitudinally.
RECOMMENDED READINGS
Becton JL, Christian JD Jr, Goodwin HN, Jackson JG 3rd. A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am. 1975 Jul;57(5):698-700.
Green DP, Terry GC. Complex dislocation of the metacarpophalangeal joint. Correlative pathological anatomy. J Bone Joint Surg Am. 1973 Oct;55(7):1480-6.
Question 58:
A unilateral "piano key" sign, indicates
Options:
- distal radioulnar joint (DRUJ) instability.
- interosseous membrane disruption.
- midcarpal instability.
- physiologic motion of hypermobility syndrome.
Correct Answer: distal radioulnar joint (DRUJ) instability.
Explanation:
EXPLANATION:
The piano key sign is a demonstration of instability at the DRUJ, typically seen after healing from a distal radius fracture with an associated ulnar styloid fracture (as in this case) or other wrist injury. The hand is pushed down against a table top, and the distal radius translates dorsally (with the distal ulna apparently moving volarly). In fact, the distal radius is the mobile segment, while the distal ulna is fixed in space. Treatment involves repair or reconstruction of the foveal insertion of the triangular fibrocartilage complex (TFCC) and distal radioulnar ligaments. This type of instability is also common in malunions of the distal radius or distal one-third of the radial shaft (Galeazzi-type fractures). In malunions, DRUJ instability can be treated with a corrective osteotomy of the distal radius to restore the anatomic relationship between the distal ulna and the distal radius at the DRUJ. Radiocarpal and midcarpal instability do not involve the DRUJ. Disruption of the interosseous membrane (in isolation, with intact distal radioulnar ligaments and an intact TFCC) does not lead to translational instability of the DRUJ. Although hypermobility syndrome may lead to ligamentous laxity, it does not lead to unilateral DRUJ instability.
Question 59:
An elite football player has sustained a left knee injury during play. A dynamic imaging analysis is performed on the affected knee, which shows anterior shift and internal rotation of the tibia at low flexion angles. There is also some mild medial translation of the tibia at greater flexion angles. What structure(s) have most likely been injury? Review Topic
Options:
- Anterior cruciate ligament
- Posterior cruciate ligament
- Posterior cruciate ligament and medial collateral ligament
- Medial collateral ligament
- Lateral collateral ligament, popliteal tendon and arcuate ligament
Correct Answer: Medial collateral ligament
Explanation:
This patient has sustained an anterior cruciate ligament (ACL) rupture.
The ACL is the primary restraint to anterior translation of the tibia relative to the femur. It also acts as secondary restraint to tibial rotation and varus/valgus rotation. ACL-deficient knees have been shown to have abnormal knee kinematics, which has been thought to contribute to the osteoarthritis that develops after injury.
DeFrate et al. examined the knee joint kinematics of 8 patients with unilateral anterior cruciate ligament rupture using in vivo imaging. They found significant anterior shift and internal rotation of the tibia at low flexion angles in ACL-deficient knees. They also noted some medial translation of the tibia between 15° and 90° of flexion.
Illustration A shows the effect of medial tibial translation on tibiofemoral contact in ACL-deficient knees. The medial translation of the tibia causes increased contact between the tibial spine and inner surface of the medial femoral condyle. This might be a contributing factor to the joint degeneration observed in ACL-deficient patients.
Incorrect Answers:
Question 60:
A 2-year-old child is brought in by his parents for evaluation of intoeing. The child has a normal neuromuscular examination, but the heel bisector line is in the fourth web space, indicating a severe flexible metatarsus adductus deformity. The remainder of the lower extremity examination is unremarkable. What is the most appropriate treatment?
Options:
- Observation as the deformity should resolve in time
- Wearing of straight last shoes
- Serial stretching and casting for the next 6 to 12 weeks
- Heyman, Herndon, and Strong capsular release at the tarsometatarsal and intermetatarsal joints
- Berman and Gartland dome-shaped osteotomies of the metatarsal bases
Correct Answer: Serial stretching and casting for the next 6 to 12 weeks
Explanation:
DISCUSSION: Weinstein reported on 31 patients (45 feet) with congenital metatarsus adductus followed for an average of 33 years. Twenty-nine feet had moderate to severe deformities treated with manipulation and casting with a 90% success rate. In a young child, surgery is not indicated until nonsurgical management has failed. In patients 2 to 4 years of age, tarsometatarsal capsulotomies are indicated, whereas multiple metatarsal osteotomies are reserved for recalcitrant deformities in children older than 4 years of age. Mild or moderate metatarsus adductus that is passively correctable will resolve without treatment.
REFERENCES: Beaty J: Congenital anomalies of the lower extremity, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. Philadelphia PA, Mosby, 2003, pp 983-988.
Katz K, David R, Soudry M: Below-knee plaster cast for the treatment of metatarsus adductus.
J Pediatr Orthop 1999;19:49-50.
Weinstein SL: Bristol-Myers Squibb/Zimmer award for distinguished achievement in orthopaedic research. Long-term follow-up of pediatric orthopaedic conditions: Natural history and outcomes
of treatment. J Bone Joint Surg Am 2000;82:980-990.
Question 61:
Figures 50a and 50b show the standing clinical photographs of a 12-year-old boy who has had increasing pain in the left foot for the past 9 months. He reports that the pain is activity related, aching in nature, and localized to the medial aspect of the midfoot and hindfoot. History reveals that he sustained a puncture wound located superior and posterior to the medial malleolus from a plate glass window 18 months ago. Examination reveals no restriction of ankle or subtalar motion, normal neurovascular status, no masses, and a well-healed 1.5-cm laceration posterior to the superior aspect of the medial malleolus. Inversion strength of the foot is decreased to grade 3/5. Radiographs of the foot show no bony abnormalities. Treatment should consist of
Options:
- application of a UCBL orthoses.
- application of an ankle-foot orthosis.
- transfer of the flexor digitorum longus to the posterior tibialis tendon.
- a lengthening osteotomy of the calcaneus.
- talocalcaneal arthrodesis.
Correct Answer: transfer of the flexor digitorum longus to the posterior tibialis tendon.
Explanation:
DISCUSSION: The photographs show a planovalgus posture of the foot. The foot deformity and decreased inversion strength are secondary to laceration of the posterior tibial tendon 18 months ago. If the injury had been recognized acutely, optimal treatment would have consisted of repair of the tendon; however, contracture now precludes that possibility. Therefore, transfer of the flexor digitorum longus or flexor hallucis longus is the preferred treatment. In adults with posterior tibial dysfunction, the entire tendon is typically degenerated and the transfer must be anchored through a drill hole in the navicular. In this patient, the distal end of the posterior tibial tendon is a satisfactory insertion site. Lengthening osteotomy of the calcaneus could be combined with the tendon transfer if the patient had a fixed deformity of the foot. UCBL orthoses and an ankle-foot orthosis are not considered good long-term solutions for a 12-year-old patient.
REFERENCES: Mosca VS: Flexible flatfoot and skewfoot, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 355-376.
Myerson MS: Adult acquired flatfoot deformity: Treatment of dysfunction of the posterior tibial tendon, in Springfield DS (ed): Instructional Course Lectures 46. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1997, pp 393-405.
Question 62:
The patient returns 1 year later to report curling of her toes and numbness on the plantar surface of her foot. What is the most likely cause of this condition?
Options:
- CRPS
- Plantar fasciitis
- Plantar fibromatosis
- Subclinical compartment syndrome
Correct Answer: Subclinical compartment syndrome
Explanation:
DISCUSSION
Radiographs reveal a Lisfranc fracture dislocation with fractures of the first and second metatarsals. Tenting of skin that is over a bony prominence is an orthopaedic emergency. The fracture dislocation should be reduced without delay. There is no evidence of compartment syndrome of the foot, but this may develop and monitoring is necessary. Toe deformity may develop on a delayed basis because of the subclinical presentation. Nerve irritation is not uncommon with dorsal midfoot surgical incisions. A positive Tinel test result over the midfoot in the distribution of the superficial common peroneal nerve is consistent with a stretch injury to this nerve. CRPS is usually associated with multiple nerve distributions and autonomic nerve findings such as cold hypersensitivity and hyperhidrosis.
RECOMMENDED READINGS
Benirschke SK, Meinberg EG, Anderson SA, Jones CB, Cole PA. Fractures and dislocations of the midfoot: Lisfranc and Chopart injuries. Instr Course Lect. 2013;62:79-91. PubMed PMID: 23395016.
View Abstract at PubMed
Schepers T, Oprel PP, Van Lieshout EM. Influence of approach and implant on reduction accuracy and stability in lisfranc fracture-dislocation at the tarsometatarsal joint. Foot Ankle Int. 2013 May;34(5):705-10. doi: 10.1177/1071100712468581. Epub 2013 Jan 14. PubMed
PMID: 23637239.
View Abstract at PubMed
Question 63:
CLINICAL SITUATION Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities. Assuming her workup is negative for any other causes, what is the best treatment option?
Options:
- Observation for a month
- Plate the tibia after removing the nail
- Autogenous bone graft to the tibia
- Exchange nailing of the tibia
Correct Answer: Exchange nailing of the tibia
Explanation:
Discussion: The patient had an open fracture that was initially treated with what appears to be appropriate irrigation and debridement and intramedullary nail placement. The post-operative infection and need for rotational flap is worrisome, but she has not had any issues since the flap. She has abundant callus formation but the fracture line is still visible and unchanged on 2 sets of radiographs. The patient has persistent pain. The best initial evaluation is to ensure that there is no underlying infection with laboratory studies, including a complete blood count (CBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Nuclear medicine studies have questionable utility, but may be helpful if the inflammatory markers from laboratory studies come back elevated. A CT scan is not warranted because the sequential radiographs show persistent fracture lines and no changes. The patient has a hypertrophic nonunion. Originally, she had appropriate treatment and has shown the ability to make callus, thus her biologic capacity appears to be intact and bone grafting is not needed. The hypertrophic nature of her fracture nonunion indicates that she needs more stability. The best treatment for a hypertrophic nonunion of the tibia is exchange nailing. Based on successive radiographs and the lack of healing, observation is probably just delaying the inevitable. Plating with retention of the nail can be useful in recalcitrant long bone non-unions, especially in the femur.
Question 64:
What percent of adult patients with rheumatoid arthritis test positive for rheumatoid factor?
Options:
- Less than 20%
- 20% to 40%
- 50%
- 80% to 90%
- More than 95%
Correct Answer: 80% to 90%
Explanation:
Rheumatoid factor is present in 80% to 90% of adult patients with rheumatoid arthritis. Although rheumatoid factor is very sensitive, it is not very specific. Antinuclear antibodies (ANA) can be detected in 30% to 40% of patients with rheumatoid arthritis.
Question 65:
Figures below show the radiograph and the MRI scan obtained from a 37-year-old woman with a 2-month history of left hip pain. Which presurgical factor is most commonly associated with a poor outcome after a hip joint salvage procedure?
Options:
- Age older than 40 years
- Body mass index higher than 30
- Tönnis grade of 2 or higher
- Outer bridge grade of III or IV
Correct Answer: Tönnis grade of 2 or higher
Explanation:
DISCUSSION:
MRI reveals an anterior labral tear, and the radiograph shows minimal arthritis with possible dysplasia. The most common location of pain in patients with a labral tear is the groin, and the most common physical finding is a positive impingement test result. Pain during sitting, clicking, and buttock pain are frequently described by patients with a labral tear, but these symptoms are less common than groin pain. A positive posterior impingement test finding is more common in patients with a posterior labral tear. Although age over 40 years and a body mass index higher than 30 can adversely affect clinical outcomes after joint preservation procedures such as PAO, hip arthroscopy, and femoral acetabular impingement surgery, the presence of hip arthritis on presurgical radiographs is the most commonly mentioned cause of failed hip joint preservation surgery. Tönnis grade is a radiographic measure of hip arthritis. A higher Outerbridge score is associated with more frequent poor outcomes after hip arthroscopy; however, the
Outerbridge cartilage score is determined by direct visualization at the time of surgery. The Outerbridge score cannot be determined presurgically.
Question 66:
The artery of Adamkiewicz (arteria radicularis, arteria magna) is most commonly found on the
Options:
- right side between T5 and T7.
- right side between T9 and T11.
- left side between T5 and T7.
- left side between T9 and T11.
- left side between L1 and L3.
Correct Answer: left side between T9 and T11.
Explanation:
DISCUSSION: Approximately 75% of people have the artery on the left side between T9 and T11. Its relevance to iatrogenic spinal cord problems is still uncertain.
REFERENCES: Stambaugh J, Simeone F: Vascular complication in spine surgery, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1715.
Lazorthes G: Arterial vascularization of the spinal cord. J Neurosurg 1971;35:253-262.
Question 67:
In the anterior cruciate ligament-deficient knee, what structure provides an important secondary restraint to anterior tibial translation? Review Topic
Options:
- Anterior horn of the lateral meniscus
- Posterior cruciate ligament
- Posterior horn of the medial meniscus
- Popliteus tendon
- Quadriceps muscle
Correct Answer: Posterior horn of the medial meniscus
Explanation:
Cadaveric studies have demonstrated the important role of the posterior horn of the medial meniscus in stabilizing the anterior cruciate ligament-deficient knee with significantly greater resultant force in the medial meniscus when subjected to anterior tibial loads. The posterior horn of the medial meniscus is thought to limit anterior tibial translation by acting as a buttress by wedging against the posterior aspect of the medial femoral condyle. The other soft tissues mentioned do not play any significant role in prevention of anterior tibial translation in the anterior cruciate ligament-deficient knee.
Question 68:
A 9-year-old boy has lateral right knee pain. An MRI scan shows a discoid lateral meniscus with a partial tear in its central portion. Treatment should consist of Review Topic
Options:
- arthroscopic saucerization of the meniscus.
- lateral total menisectomy.
- meniscal transplant.
- arthroscopy and repair of the central tear.
- casting for 6 weeks followed by physical therapy.
Correct Answer: arthroscopic saucerization of the meniscus.
Explanation:
A tear of the mid portion of a stable discoid lateral meniscus should be treated with a partial menisectomy with saucerization. Lateral total menisectomy is contraindicated because of the poor long-term results following this procedure. Meniscal transplant and casting do not have a role in this scenario, although meniscal repairs may be needed for peripheral meniscal instability.
Question 69:
A 22-year-old right hand-dominant man who fell off his motorcycle onto the tip of his right shoulder 2 weeks ago now reports pain and difficulty raising his right arm. Examination reveals tenderness and gross movement over the lateral scapular spine and severe weakness during resisted abduction. A radiograph and 3D-CT scan are shown in Figures 24a and 24b. What is the next most appropriate step in management?
Options:
- Open reduction and internal fixation
- External bone stimulator
- Ninety-degree abduction splint
- Arthroscopic acromioplasty
- Fragment excision
Correct Answer: Open reduction and internal fixation
Explanation:
DISCUSSION: The patient has a displaced scapular spine fracture that has resulted in shoulder weakness from a poor deltoid lever arm. The downward tilt may lead to subacromial impingement and rotator cuff dysfunction. Open reduction and internal fixation would best allow normal deltoid and shoulder function. Bone stimulators and abduction bracing may lead to healing but in a malunited position. Arthroscopic acromioplasty and fragment excision should be avoided.
REFERENCES: Ogawa K, Naniwa T: Fractures of the acromion and the lateral scapular spine.
J Shoulder Elbow Surg 1997;6:544-548.
Ada Jr, Miller ME: Scapular fractures: Analysis of 113 cases. Clin Orthop Relat Res 1991;269:174-180.
Question 70:
A 22-year-old man sustained a shoulder dislocation while playing collegiate football at age 18. Since that time, he has dislocated the shoulder three more times despite physical therapy. His last dislocation occurred 4 weeks ago while sleeping. What is the most appropriate management for this patient? Review Topic
Options:
- Corticosteroid injection
- Changing the physical therapist to an athletic trainer
- A 1-month trial of nonsteroidal anti-inflammatory drugs (NSAIDs)
- Shoulder immobilization for 6 weeks
- A discussion regarding surgical stabilization procedures
Correct Answer: A discussion regarding surgical stabilization procedures
Explanation:
The patient sustained a traumatic shoulder dislocation at age 18 that has subsequently failed to respond to nonsurgical management. Discussion of surgical stabilization procedures is warranted at this time. A corticosteroid injection or a trial of NSAIDs will not provide any stabilizing effect. Further immobilization in this patient population has not been shown to improve stability.
Question 71:
A 22-year-old woman underwent closed reduction and percutaneous pinning with casting of a displaced extra-articular distal radius fracture. The surgery was completed with a supraclavicular regional anesthesia. After the block wears off, she reports new onset dense numbness in the palmar aspect of the thumb, index, and middle fingers as well as severe pain in the hand. What is the next step in management?
Options:
- Bivalve the cast and follow up in 1 week
- Return to the operating room for open carpal tunnel release
- Compartment pressure monitoring of the hand
- Emergent nerve conduction velocity studies
- Exploration of the supraclavicular brachial plexus
Correct Answer: Return to the operating room for open carpal tunnel release
Explanation:
The injury represents a somewhat uncommon problem after surgical treatment of distal radius fractures; however, vigilance is required to detect the acute presentation of a carpal tunnel syndrome. In this case, urgent release of the tunnel is recommended. Bivaling the cast alone is indicated when the pain is less severe, and only when the numbness is very minimal and more generalized. Compartment syndrome of the hand is almost unheard of in the setting of a distal radius fracture; rather it is more commonly associated with a crush injury to the hand. There is no role for emergent nerve conduction velocity studies or brachial plexus exploration.
Question 72:
The majority of severe cervical spine injuries occurring in contact sports evolve during axial loading and flexion of the cervical spine. At what minimum degree of flexion does axial loading place the cervical spine at risk during contact sports?
Options:
- 15 degrees
- 30 degrees
- 45 degrees
- 60 degrees
- 75 degrees
Correct Answer: 30 degrees
Explanation:
DISCUSSION: The paravertebral musculature, the intervertebral disks, and the normal lordotic curvature of the cervical spine can absorb much of the imparted energy of collision. However, when the neck is flexed approximately 30 degrees, the normal lordotic curvature is flattened and the forces applied to the vertex of the head are directed at a straight segmented column. In this situation, the cervical spine is less able to absorb the applied force. With mounting axial load, compressive deformation occurs within the intervertebral disks, causing angular deformation and buckling. The spine will fail in flexion, with resultant fracture, subluxation, or dislocation. A rotatory component added to axial compression can cause concomitant extension, rotation, and shear injury patterns. The National Football Head and Neck Injury Registry has made two recommendations to the NCAA Football Rules Committee to minimize the risk of such injuries: (1) No player should intentionally strike an opponent with the crown or top of the helmet; and (2) No player should deliberately use his helmet to butt or ram an opponent.
REFERENCES: Thomas BE, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
Torg JS, Truex R Jr, Quedenfeld TC, Burstein A, Spealman A, Nichols C III: The National Football Head and Neck Injury Registry: Report and conclusions 1978. JAMA 1979;241:1477-1479.
Question 73:
What is the most likely complication following treatment of the humeral shaft fracture shown in Figure 6?
Options:
- Nonunion
- Shoulder pain
- Infection
- Elbow injury
- Radial nerve injury
Correct Answer: Shoulder pain
Explanation:
DISCUSSION: The humerus was treated with an intramedullary nail. Findings from two prospective randomized studies of intramedullary nailing or compression plating of acute humeral fractures have shown approximately a 30% incidence of shoulder pain with antegrade humeral nailing. This is the most common complication in both of these series. Nonunions are present in approximately 5% to 10% of humeral fractures treated with an intramedullary nail. Infection has an incidence of approximately 1%. Elbow injury is unlikely unless the nail is excessively long. Rarely, injury to the radial nerve is possible if it is trapped in the intramedullary canal.
REFERENCES: Chapman JR, Henley MB, Agel J, et al: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
McCormack RG, Brien D, Buckley RE, et al: Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail: A prospective, randomised trial. J Bone Joint Surg Br 2000;82:336-339.
Question 74:
- Which of the following laws describes the mechanical effects believed to play a role in the etiology of adolescent tibia vara?
Options:
- Wolff’s
- Hooke’s
- Hilton’s
- Muller-Haeckel
- Heuter-Volkmann
Correct Answer: Heuter-Volkmann
Explanation:
This is one of those OITE questions that there is no way to make an educated guess. You either knew this or simply picked the best sounding answer. Wolff’s Law, which we are all familiar with, states that the bone builds structural development most suited for the stresses applied. I could not find Hooke’s and Hilston’s Laws in any orthopaedic or medical text and therefore, believe these were simply “fillers” to make five selections. Muller-Haeckel Law is from the Biogenetics principal that living matter always arises from pre-existing living matter (very profound). Finally, the Heuter-Volkmann Law is one that applies to many mechanisms in orthopaedics, but this question is specifically regarding tibia vara. This law states that increased pressure/strain across the epiphyseal plate on the medial aspect of the knee will inhibit its longitudinal growth. Conversely, Depelch’s Law not mentioned in the question, but certain to show up in future OITE’s states that distraction at the level of the physeal plate will cause increases longitudinal growth.
Question 75:
Figures 1 and 2 are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg. What is the most likely diagnosis for the source of this patient's pain?
Options:
- Cam-type femoroacetabular impingement
- Pincer-type femoroacetabular impingement
- Hip flexor strain
- Athletic pubalgia
Correct Answer: Cam-type femoroacetabular impingement
Explanation:
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement. Surgical treatment for cam impingement can be effective for symptomatic patients. Even among high-level athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable with those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment. Byrd and Jones described five patients who developed transient neurapraxias that resolved uneventfully. The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a
periacetabular osteotomy can develop a more retroverted acetabulum as well.
Question 76:
What nerve is most likely to be injured during the anterior exposure of C2-3?
Options:
- Facial
- Superior laryngeal
- Vagus
- Hypoglossal
- Phrenic
Correct Answer: Hypoglossal
Explanation:
DISCUSSION: The hypoglossal nerve exits from the ansa cervicalis at approximately the C2-3 level and can be injured during retraction up to the C2 level. The superior laryngeal nerve lies at about C4-5. The facial nerve is much higher. The vagus nerve runs with the internal jugular and carotid much more laterally. The phrenic nerve exits posteriorly.
REFERENCES: Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-54.
Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.
Question 77:
A 43-year-old woman is referred after excisional biopsy of a cutaneous soft-tissue mass from her left shoulder. Based on the biopsy specimens shown in Figures 44a and 44b, what is the best course of action?
Options:
- Marginal resection
- Observation
- Wide tumor bed resection
- Radiation therapy
- Chemotherapy
Correct Answer: Wide tumor bed resection
Explanation:
DISCUSSION: Dermatofibrosarcoma protuberans (DFSP) is a rare superficial sarcoma that is frequently misdiagnosed at presentation. It is frequently excised prior to suspecting that the lesion is a sarcoma and if not appropriately treated with tumor bed resection to obtain wide margins, these lesions have a high incidence of local recurrence. It is recommended that the wide excision include the deep fascia and a 2.5- to 3-cm cuff of normal-appearing skin. Distant disease spread is rare and usually occurs in the face of a multiply recurrent lesion. Despite the apparent gross circumscription of these lesions, the tumor diffusely infiltrates the dermis and subcutaneous tissues. A characteristic histologic finding can be seen in the deep margins of the tumor where it intricately interdigitates with normal fat.
REFERENCES: Lindner NJ, Scarborough MT, Powell GJ, et al: Revision surgery in dermatofibrosarcoma protuberans of the trunk and extremities. Eur J Surg Oncol
1999;25:392-397.
Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 491-505.
Question 78:
A patient with diabetic peripheral neuropathy undergoes a partial first ray amputation for a chronic ulcer beneath the first metatarsal head. The insertion of the anterior tibialis is preserved. The patient has 10 degrees of passive dorsiflexion at the ankle and no other foot deformities or ulcers. Which of the following is considered appropriate shoe wear for this patient?
Options:
- Snug fitting shoe to block side-to-side motion that is common after this procedure
- Leather sole shoe to prevent catching the shoe on carpet which is common with crepe-soled shoes
- Lateral wedge on the shoe to offset the external rotation during the toe-off phase of gait commonly seen after this procedure
- Steel shank to extend the foot lever and prevent deformity at the toe break
- Custom-made shoe to provide the best possible fit and function
Correct Answer: Steel shank to extend the foot lever and prevent deformity at the toe break
Explanation:
DISCUSSION: The steel shank is a flat 1-inch steel strip placed between layers of the shoe to extend the foot lever and prevent deformity at the toe break seen following a partial first ray amputation. A rocker sole may be added as well to facilitate transition from foot flat to the toe-off phase of gait. Proper shoe fit is important, but “snug” fitting shoes in a patient with peripheral neuropathy and likely fluctuations in volume from intermittent swelling are to be avoided. A custom shoe is an unnecessary expense. The patient has at least 10 degrees of dorsiflexion at the ankle with an intact anterior tibialis muscle; therefore, catching the sole on carpeting should not be a problem.
REFERENCES: Philbin TM, Leyes M, Sferra JJ, et al: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Pinzur MS, Dart HC: Pedorthic management of the diabetic foot. Foot Ankle Clin 2001;6:205-214.
Question 79:
Which of the following nerves is susceptible to entrapment near the calcaneal attachment site of the plantar fascia and can mimic or co-exist with plantar fasciitis?
Options:
- First branch of the lateral plantar nerve
- Dorsal cutaneous branch of the superficial peroneal nerve
- Medial calcaneal branch of the posterior tibial nerve
- Lateral branch of the medial plantar nerve
- Communicating branch of the fourth common digital nerve
Correct Answer: First branch of the lateral plantar nerve
Explanation:
DISCUSSION: The first branch of the lateral plantar nerve is susceptible to entrapment beneath the deep fascia of the adductor hallucis muscle adjacent to the calcaneal attachment of the plantar fascia. This can be a cause of chronic heel pain. Additionally, the nerve is vulnerable to injury by a blind dissection in releasing the plantar fascia. The dorsal cutaneous branch of the superficial peroneal nerve supplies sensation to the dorsum of the foot. The medial calcaneal branch of the posterior tibial nerve lies in the subcutaneous tissues and innervates the skin of the heel. It is vulnerable to injury from skin incisions on the medial side of the heel. The lateral branch of the medial plantar nerve forms the second and third common digital nerves. Entrapment of the proper medial plantar nerve can occur at the master knot of Henry. This is well distal to the calcaneal attachment of the plantar fascia, and the pain usually radiates more distally in the arch, separate from heel pain. The communicating branch of the fourth common digital nerve crosses to the third common digital nerve. Therefore, the third common digital nerve receives supply from both the lateral and medial plantar nerves. This dual supply has been implicated in the increased incidence of digital neuroma of the third common digital nerve.
REFERENCES: Bordelon RL: Heel pain, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 837-857.
Mann RA, Baxter DE: Diseases of the nerves, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 543-574.
Baxter DE: The heel in sport. Clin Sports Med 1994;13:683-693.
Question 80:
Which of the following growth factors binds and activates the lipoprotein receptor-related protein 5/6 (LRP5/6) during bone development? Review Topic
Options:
- Transforming growth factor-beta
- Platelet-derived growth factor
- Parathyroid hormone
- Bone morphogenetic protein
- Wnt protein
Correct Answer: Wnt protein
Explanation:
Wnt and Hedgehog (Hh) signaling pathways are key regulators of bone formation. Mutations in the Wnt and Hh pathways result in skeletal malformations as well as osteoarthritis. Wnts are a large family of secreted proteins (19 different members in the human genome) that transduce their signal through several pathways. The most studied of these pathways is the Wnt/beta-catenin pathway, in which Wnt protein binds to the LRP5/6 receptor at the cell surface and activates an intracellular cascade. This cascade leads to translocation of beta-catenin into the nucleus to activate transcription of genes that control osteoblast differentiation. Agents that stimulate this pathway are under investigation for treatment of osteoporosis.
Question 81:
Preventing "missed" femoral neck fractures associated with ipsilateral femoral shaft fractures is best achieved with
Options:
- - an examination.
- - dedicated anteroposterior and lateral hip radiographs.
- - thin-cut pelvic CT images with coronal and sagittal reconstructions.
- - MRI.
Correct Answer: - thin-cut pelvic CT images with coronal and sagittal reconstructions.
Explanation:
DISCUSSION
Ipsilateral femoral neck and shaft fractures occur in up to 6% of femur fractures. A femoral neck fracture is often vertical and nondisplaced. A high degree of suspicion is necessary to avoid "missed" femoral neck fractures in patients with this condition. Although an examination and dedicated hip radiographs help to avoid missed injuries, a significant decrease in missed
injuries has been described with the use of thin-cut pelvic CT images. In patients who undergo trauma, a pelvic CT scan is often performed to assess for associated injuries and is easily reviewed to examine the femoral neck. Although MRI is advocated to identify isolated occult femoral neck fractures, CT has been described as the method of choice with which to identify ipsilateral femoral neck and shaft fractures in the trauma population. Currently, no literature supports the use of MRI in this population.
RECOMMENDED READINGS
Tornetta P 3rd, Kain MS, Creevy WR. Diagnosis of femoral neck fractures in patients with a femoral shaft fracture. Improvement with a standard protocol. J Bone Joint Surg Am. 2007 Jan;89(1):39-43. PubMed PMID: 17200308.
View Abstract at PubMed
Kuhn KM, Agarwal A. Femoral fractures. In: Cannada LK, ed. Orthopaedic Knowledge Update
Question 82:
Which component is most common to both simple and complex elbow dislocations?
Options:
- radial head fracture
- radial neck fracture
- loss of terminal extension
- coronoid tip fracture
- coronoid base fracture
Correct Answer: radial head fracture
Explanation:
DISCUSSION: Elbow dislocations are classified as either simple (no associated fracture) or complex (associated fracture). The goal of treatment is a stable joint that tolerates early motion. The initial range of motion is the stable arc found on postreduction examination. Studies have demonstrated a better outcome when simple elbow dislocations are treated non-surgically rather than with surgical repair. Simple elbow dislocations usually have an excellent outcome (return of functional range of motion with normal strength). A loss of terminal extension is the most common sequelae.
Question 83:
Compared with wear rates of metal-on-standard polyethylene bearings (75 to 250 m m/y), the wear rate of metal-on-metal bearings for hip arthroplasty is approximately how many micrometers per year?
Options:
- Less than 0.5
- 2 to 5
- 5 to 20
- 20 to 50
- 50 to 150
Correct Answer: 2 to 5
Explanation:
DISCUSSION: Studies on older systems, as well as newer designs, have confirmed that metal-on-metal bearing surfaces undergo linear wear of 2 to 5
m
m per year. Ceramic bearing surfaces produced with recent technology perform even better, with a wear rate of 0.5 to 2.5
m
m per year. Clinical wear rates of metal-on-crosslinked polyethylene have not yet been determined.
REFERENCES: McKellop H, Park SH, Chiesa R, et al: In vivo wear of three types of metal on metal hip prostheses during two decades of use. Clin Orthop 1996;329:S128-S140.
Schmalzried TP, Callaghan JJ: Wear in total hip and knee replacements. J Bone Joint Surg Am 1999;81:115-136.
Question 84:
Which of the following structures are found in the anterior tarsal tunnel?
Options:
- Extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, deep peroneal nerve
- Extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, superficial peroneal nerve
- Extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, deep peroneal nerve, superficial peroneal nerve
- Extensor hallucis brevis, extensor hallucis longus, extensor digitorum longus, dorsalis pedis artery, deep peroneal nerve
- Dorsalis pedis artery, deep peroneal nerve, superficial peroneal nerve
Correct Answer: Extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, deep peroneal nerve
Explanation:
DISCUSSION: The contents of the anterior tarsal tunnel are the extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, and the deep peroneal nerve. The term “anterior tarsal tunnel syndrome” is used to specifically describe the compression of the deep peroneal nerve under the inferior extensor retinaculum. With nerve compression, patients report a burning sensation across the dorsum of the foot with paresthesias in the first web space. There also may be wasting and weakness of the extensor digitorum brevis.
REFERENCES: Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Sarrafian S: The Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 113-158.
Question 85:
Examination of a 12-year-old girl with a painful flatfoot deformity reveals tenderness in the region of the sinus tarsi and no appreciable subtalar motion. Radiographs are shown in Figures 48a through 48c. Two attempts to relieve her symptoms by cast immobilization fail to relieve the pain. Management should now consist of
Options:
- triple arthrodesis.
- manipulation of the foot under general anesthesia.
- continued nonsurgical management until the synchondrosis ossifies.
- resection of the coalition and interposition with the extensor digitorum brevis.
- a medial closing wedge osteotomy of the calcaneus.
Correct Answer: resection of the coalition and interposition with the extensor digitorum brevis.
Explanation:
DISCUSSION: Surgical treatment is indicated for a symptomatic tarsal coalition that has failed to respond to nonsurgical management. In this patient, the radiographs reveal a calcaneonavicular coalition and no degenerative changes. The patient is symptomatic, and two attempts at use of a short leg walking cast have failed to provide relief. For calcaneonavicular coalitions, good results have been reported following resection and interposition of the extensor digitorum brevis. A retrospective study of this procedure achieved good to excellent results in 58 of 75 feet (77%). Degenerative arthritis or persistent pain following resection of a coalition is a reasonable indication for a triple arthodesis. A medial closing wedge osteotomy of the calcaneus may be indicated for a rigid flatfoot with severe valgus deformity. There are no studies documenting the long-term effectiveness of a manipulation under general anesthesia for this condition.
REFERENCES: Gonzalez P, Kumar SJ: Calcaneonavicular coalition treated by resection and interpostion of the extensor digitorum brevis muscle. J Bone Joint Surg Am 1990;72:71-77.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 211-218.
Question 86:
Which of the following definitions best describes Batson’s vertebral vein system?
Options:
- A system of valves that allows retrograde embolism
- A vascular system that bypasses organs such as the breast, prostate, lung, kidney, and thyroid
- A system of veins within the thoracoabdominal cavity that are not subject to compression or collapse by increases in intra-abdominal pressure
- A series of valveless veins that allow tumor cell extravasation
- A longitudinal vein system with a segmental distribution to the vertebra that extends from the dural venous sinuses of the skull to the sacrum
Correct Answer: A series of valveless veins that allow tumor cell extravasation
Explanation:
DISCUSSION: The venous plexus was described by Batson and helps to explain the common distribution of metastatic cells to the vertebrae, skull, ribs, and proximal long bones. Batson studied the vertebral vein system extensively by using contrast agents in human cadavers and live monkeys. Batson’s plexus is a valveless system that allows retrograde embolism from the major organs such as the breast, prostate, lung, kidney, and thyroid. It is located within the thoracoabdominal cavity and has connections to the proximal long bones and an intercommunicating network of thin-walled veins with a low intraluminal pressure.
REFERENCES: Batson OV: Function of vertebral veins and their role in spread of metastases. Ann Surg 1940;112:138-149.
Coman DR, de Long RP: Role of vertebral venous system in metastasis of cancer to spinal column: Experiments with tumor-cell suspensions in rats and rabbits. Cancer 1951;4:610-618.
Question 87:
Where is the underlying defect in a rhizomelic dwarf with the findings shown in Figure 5?
Options:
- Type I collagen
- Type II collagen
- Collagen oligomeric protein (COMP)
- Sulfate transport
- Fibroblast growth factor receptor 3
Correct Answer: Fibroblast growth factor receptor 3
Explanation:
DISCUSSION: The radiograph shows the typical findings of achondroplasia. The defect is in fibroblast growth factor receptor 3. The pedicles narrow distally in the lumbar spine. The pelvis is low and broad with narrow sciatic notches and ping-pong paddle-shaped iliac wings. This is often called a champagne glass pelvis. Type I collagen abnormalities are typically found in osteogenesis imperfecta, and type II collagen defects are found in spondyloepiphyseal dysplasia and Kneist syndrome. COMP is defective in multiple epiphyseal dysplasia. Sulfate transport defects are seen in diastrophic dysplasia.
REFERENCES: Johnson TR, Steinbach LS: Essentials of Musculoskeletal Imaging. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 809-812.
Caffey J: Achondroplasia of the pelvis and lumbosacral spine: Some roentgenographic features. Am J Roentgenol 1958;80:449.
Question 88:
Figure 23 shows the radiograph of a 7 year-old girl with a low thoracic-level myelomeningocele. She has a history of skin ulcers over the apex of the deformity, but her current skin condition is good. Management of the spinal deformity should consist of
Options:
- physical therapy for hip stretching exercises.
- kyphectomy and posterior fusion with instrumentation.
- anterior release and fusion using a rib strut graft.
- anterior release and strut grafting and posterior fusion with instrumentation.
- bracing.
Correct Answer: kyphectomy and posterior fusion with instrumentation.
Explanation:
DISCUSSION: This form of severe kyphosis results in intractable difficulties with sitting position, compression of internal organs, and chronic skin breakdown. Kyphectomy and posterior fusion with instrumentation, while associated with a high rate of complications, provides one of the best solutions to this clinical dilemma. The other choices are either completely ineffective or inadequate in managing this degree of deformity.
REFERENCES: Lindseth RE: Spine deformity in myelomeningocele. Instr Course Lect 1991;40:273-279.
Sharrard J, Drennan JC: Osteotomy excision of the spine for lumbar kyphosis in older children with myelomeningocele. J Bone Joint Surg Br 1972;54:50-60.
Question 89:
A 34-year-old man sustains an extra-articular fracture of the proximal phalanx of his right index finger in a fall. Examination reveals that the fracture is closed and oblique in orientation. Closed reduction and splinting fail to maintain the reduction. Management should now consist of
Options:
- repeat closed reduction and buddy taping.
- closed reduction and percutaneous pin fixation, followed by casting.
- open reduction and plate fixation, followed by casting.
- open reduction and screw fixation, followed by splinting and early motion.
- open reduction and intramedullary fixation with absorbable implants.
Correct Answer: closed reduction and percutaneous pin fixation, followed by casting.
Explanation:
DISCUSSION: The patient has an unstable oblique fracture of the proximal phalanx that is easily reducible but unstable; therefore, the treatment of choice is closed reduction and percutaneous pin fixation, followed by casting. Closed reduction and percutaneous pin fixation offers a better functional result than open reduction and plate fixation. Repeat closed reduction and buddy taping is inadequate because of the inherently unstable fracture pattern. Buddy taping will allow the dislocation to recur. The other options represent more aggressive surgical techniques than are necessary to treat this fracture.
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Green DP, Anderson JR: Closed reduction and percutaneous pin fixation of fractured phalanges. J Bone Joint Surg Am 1973;55:1651-1653.
Question 90:
Which of the following is a significant risk factor for airway complications after anterior cervical surgery? Review Topic
Options:
- Smoking history
- Pulmonary disease
- Absence of drainage from surgical drains
- Surgical time of more than 5 hours
- Myelopathy
Correct Answer: Surgical time of more than 5 hours
Explanation:
In a study of 311 patients undergoing anterior cervical surgery only, a surgical time of more than 5 hours and exposure of four or more vertebral bodies involving C4 or higher were found to be risk factors for postoperative airway complications. Surprisingly, preoperative pulmonary status, smoking history, absence of drainage, and myelopathy were not associated with airway complications.
Question 91:
A 38-year-old female with a grade IIIB open tibia fracture is scheduled to undergo definitive fixation and subsequent flap coverage with the orthopaedic and plastic surgery teams. She is met in the pre-operative area by the surgical intern and paperwork is completed per institutional protocol. She is then brought back to the operating room. Which of the following is true regarding the pre-surgical timeout?
Options:
- The surgical intern must be present because he brought the patient to the operating room
- The timeout cannot begin without the implant representative
- If both the orthopaedic and plastic surgical teams are present, a single timeout is sufficient for the entire procedure
- The timeout may be completed as long as the attending is in an adjacent operating room
- The pre-surgical timeout has not been shown to decrease complication rates
Correct Answer: The surgical intern must be present because he brought the patient to the operating room
Explanation:
If both teams are present, a single timeout is sufficient for the entire procedure. If one team is absent, a second timeout needs to be completed prior to start of the second part of the procedure.
The WHO pre-surgical safety checklist involves assessment at three points during an operative procedure: before induction of anesthesia, before skin incision, and before the patient leaves the operating room. Some components of the checklist include
confirming IV access and allergies, administration of antibiotic prophylaxis, and surgical site verification. The surgeon has been shown to be the most effective team member at reducing complications when using the checklist.
Haynes et al. evaluated the effects of the WHO pre-surgical checklist on perioperative complication rates at eight international sites. They found a significant reduction in rates of complications and death in patients over the age of 16 undergoing noncardiac procedures after implementation of the checklist.
Illustration A shows the WHO pre-surgical checklist Incorrect Answers:
present for the timeout. Answer 2: The implant representative is not necessary for the timeout. Answer 4: The attending surgeon needs to be present in the same OR for the timeout. Answer 5: The timeout has been shown to decrease rates of complication and death.
Question 92:
Figures 5a and 5b show the radiographs of a 45-year-old patient. What is the most likely diagnosis?
Options:
- Glenoid dysplasia
- Rheumatoid arthritis with centralization
- Osteoarthritis with posterior glenoid wear
- Posterior scapular fracture deformity
- Traumatic posterior subluxation of the shoulder
Correct Answer: Glenoid dysplasia
Explanation:
DISCUSSION: Glenoid dysplasia is an uncommon anomaly that usually has a benign course but may result in shoulder pain, arthritis, or multidirectional instability. Shoulder pain and instability often improve with shoulder strengthening exercises.
REFERENCES: Wirth MA, Lyons FR, Rockwood CA Jr: Hypoplasia of the glenoid: A review of sixteen patients. J Bone Joint Surg Am 1993;75:1175-1184.
Resnick D, Walter RD, Crudale AS: Bilateral dysplasia of the scapular neck. Am J Roentgenol 1982;139:387-390.
Question 93:
In a pilon fracture, the Chaput fragment typically maintains soft tissue attachment via which of the following structures?
Options:
- Interosseous ligament
- Anterior inferior tibiofibular ligament
- Posterior inferior tibiofibular ligament
- Deltoid ligament
- Tibiotalar ligament
Correct Answer: Interosseous ligament
Explanation:
DISCUSSION: The Chaput fragment, highlighted by the arrow in Illustration A, is the anterolateral fragment of the distal tibia. This section of bone attaches to the anterior inferior tibiofibular ligament and is often hinged off this structure due to the fracture. A pilon fracture is often split into three main fragments at the joint level (Illustration B): Chaput fragment (anterolateral), Volkmann fragment (posterolateral), and a medial fragment. The Volkmann fragment is the attachment site of the posterior inferior tibiofibular ligament. The Wagstaff fragment is the fibular corollary to the Chaput fragment, and serves as the other attachment of the anterior inferior tibiofibular ligament
Question 94:
A 13-year-old pitcher reports the immediate onset of medial elbow pain after throwing a pitch. Upon examination, the patient is tender to palpation at the medial epicondyle and has pain and instability with valgus testing of the elbow. If the patient were a college pitcher with a similar clinical presentation and physical examination, what anatomic structure would most likely be injured?
Options:
- Ulnar collateral ligament (UCL)
- Pronator teres
- Ligament of Struthers
- Lateral collateral ligament
Correct Answer: Ulnar collateral ligament (UCL)
Explanation:
The patient has an acute avulsion fracture of the medial epicondyle, which can occur in response to the valgus load placed on the elbow while throwing. Diagnosis is confirmed by radiograph, with comparison views of the uninjured elbow to evaluate for physeal closure versus injury. In older pitchers, the UCL fails rather than the bone of the medial epicondyle. Advanced imaging may be necessary to confirm the diagnosis of an UCL
injury and/or bony injury.
Question 95:
A 25 year-old-male presents with the injury seen in Figure A. Which of the following would be a contraindication to closed management with a functional brace?
Options:
- Radial nerve injury
- 1 cm shortening
- 20 degree varus deformity
- Brachial plexus injury
- Comminuted fracture pattern
Correct Answer: Radial nerve injury
Explanation:
Closed treatment of humeral shaft fractures with functional bracing is indicated in the vast majority of isolated injuries. An ipsilateral brachial plexus injury, however, is a contraindication to nonoperative management in a functional brace.
Indications for operative management of humeral shaft fractures are limited given the high rates of union and ability of adjacent joints to compensate for deformity. Intact muscular tone is necessary to effect bony apposition in closed treatment with a functional brace. The absence of neurologic and muscle function in patients with a flail extremity leads to increased rates of nonunion and malunion.
Rutgers and Ring conducted a retrospective review of patients managed with functional bracing of humeral shaft fractures at a single institution. The authors found a 90% overall union rate, with maintenance of shoulder and elbow motion. They caution though, that 29% of their proximal third fractures went on to nonunion.
Figure A demonstrates an AP radiograph of a comminuted humeral shaft fracture with varus alignment.
Incorrect Answers:
Question 96:
Anterior subluxation in a throwing athlete is most commonly the result of
Options:
- avulsion of the inferior glenohumeral ligament from the glenoid.
- avulsion of the inferior glenohumeral ligament from the humerus.
- fracture of the anterior glenoid rim.
- excessive capsular laxity from microtrauma.
- a large Hill-Sachs lesion.
Correct Answer: excessive capsular laxity from microtrauma.
Explanation:
DISCUSSION: Subtle anterior subluxation in the throwing athlete most frequently results from excessive capsular laxity because of repetitive microtrauma. Avulsion of the inferior glenohumeral ligament from the glenoid, or more rarely from the humerus, occurs with macrotrauma. A large Hill-Sachs lesion and a glenoid rim fracture also may result from a traumatic anterior dislocation.
REFERENCES: Kvitne RS, Jobe FW: The diagnosis and treatment of anterior instability in the throwing athlete. Clin Orthop 1993;291:107-123.
Jobe FW, Tibone JE, Jobe CM, Kvitne RS: The shoulder in sports, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1999, pp 961-990.
Question 97:
A 59-year-old woman underwent open reduction and internal fixation (ORIF) of her ankle 6 months ago, with subsequent hardware removal 3 months later. She now reports persistent, diffuse ankle pain, swelling, and limited range of motion. Figure 48 shows an oblique radiograph of the ankle. What is the next most appropriate step in management?
Options:
- Physical therapy
- Hardware removal
- Repeat placement of a syndesmotic screw
- Deltoid ligament reconstruction
- Revision ORIF with exploration of the syndesmosis and medial ankle
Correct Answer: Revision ORIF with exploration of the syndesmosis and medial ankle
Explanation:
DISCUSSION: The radiographs demonstrate persistent widening of the medial clear space with an ossicle. This represents soft-tissue interposition-scar tissue, the deltoid ligament, or the posterior tibialis tendon. Physical therapy will not improve the symptomatic malalignment. Hardware removal would be indicated for pain localized to the lateral fibula. Repeat syndesmotic screw fixation alone will not reduce the malalignment. Deltoid ligament repair may be necessary but will need to be combined with debridement of the medial ankle and syndesmosis, as well as repeat placement of one or more syndesmotic screws to maintain the reduction.
REFERENCES: Weening B, Bhandari M: Predictors of functional outcome following transsyndesmotic screw fixation of ankle fractures. J Orthop Trauma 2005;19:102-108.
Harper MC: Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int 2001;22:15-18.
Question 98:
Which of the following pieces of equipment currently offers the greatest opportunity for lowering the number of equestrian injuries? Review Topic
Options:
- Knee pads
- Wrist guards
- Boots
- Helmets
- Quick release stirrups
Correct Answer: Helmets
Explanation:
Ball and associates reported that "horseback riding was more dangerous than motorcycle riding." In a 10-year study of major traumatic injuries, they reported that 151 (2%) of 7,941 trauma patients had major equestrian injuries (injury severity score
> or = 12). Injuries included the chest (54%), head (48%), abdomen (22%), and extremities (17%). Only 9% of riders wore helmets, and 64% believed the accident was preventable. The authors noted that "helmet and vest use will be targeted in future injury prevention strategies." In another study, Frankel and associates noted that helmet use was only documented in 34% of riders. Although orthopaedic injuries are common, knee pads, wrist guards, boots, and quick release stirrups would most likely have less impact on injury prevention.
Question 99:
An 8-year-old girl was treated for a Salter-Harris type I fracture of the right distal femur 2 years ago. She has symmetric knee flexion, extension, and frontal alignment to her contralateral knee. She has a 1-cm limb-length discrepancy of the femur. She has always been in the 50th percentile for height and her skeletal age matches her chronologic age. She has a complete physeal closure of the right distal femur. What is the expected limb-length discrepancy at maturity?
Options:
- 3 cm
- 6 cm
- 10 cm
- 14 cm
- 18 cm
Correct Answer: 6 cm
Explanation:
DISCUSSION: The child has a near complete central physeal arrest of the distal femur. She will develop worsening limb-length discrepancy. She is growing at the average rate for the population. The distal femoral physis grows roughly at a rate of 9 mm/year. Girls finish their growth roughly at 14 years. Thus, at maturity, the uninjured side will be 6.4 cm longer than the injured side. Since she has not developed an angular deformity at this point and her arrest is central, she is unlikely to develop angular deformity in any plane.
REFERENCES: Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphysiodesis. J Pediatr Orthop 1996;16:173-179.
Moseley CF: Assessment and prediction in leg-length discrepancy. Instr Course Lect 1989;38:325-330.
AL-Madena Copy
Question 100:
-During preparticipation physicals for college football, an athlete tests positive for the sickle-cell trait.With regard to clearance to play, his team physician should
Options:
- counsel the athlete about his personal risk for bone infarcts.
- recommend a prophylactic splenectomy prior to participation.
- bar the athlete from participating in National Collegiate Athletic Association-sanctioned events.
- assure the athlete that he can participate in football without concern.
- ensure that the athlete is given adequate recovery time and remains hydrated.
Correct Answer: ensure that the athlete is given adequate recovery time and remains hydrated.