Orthopedic Surgery Board Review MCQs: Spine, Arthroplasty & Trauma | Part 187

Key Takeaway
This page offers Part 187 of a professional interactive MCQ set for orthopedic surgeons and residents. It provides 100 high-yield, OITE-formatted questions with detailed explanations for AAOS/ABOS board exam preparation. Enhance clinical knowledge and ensure readiness for certification.
About This Board Review Set
This is Part 187 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 187
This module focuses heavily on: Arthroplasty, Fracture, Knee, Nerve, Spine.
Sample Questions from This Set
Sample Question 1: Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy? Review Topic...
Sample Question 2: A 65-year-old woman has nausea, vomiting, and abdominal distention after undergoing total knee arthroplasty 48 hours ago. An abdominal radiograph is shown in Figure 14. Associated risk factors for this disorder include...
Sample Question 3: To prevent injury to the posterior interosseous nerve during the approach for reduction and fixation of a fracture of the radial head, anterior retraction should be performed with the forearm...
Sample Question 4: From which artery does the princeps pollicis artery branch?...
Sample Question 5: Vertebral fractures are common in the thoracolumbar spine. What is the most important factor that determines the strength of the cancellous bone in the vertebral body?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy? Review Topic
Explanation
Question 2
A 65-year-old woman has nausea, vomiting, and abdominal distention after undergoing total knee arthroplasty 48 hours ago. An abdominal radiograph is shown in Figure 14. Associated risk factors for this disorder include
Explanation
REFERENCES: Iorio R, Healy WL, Appleby D: The association of excessive warfarin anticoagulation and postoperative ileus after total joint replacement surgery. J Arthroplasty 2000;15:220-223.
Clarke HD, Berry DJ, Larson DR: Acute pseudo-obstruction of the colon as a postoperative complication of hip arthroplasty. J Bone Joint Surg Am 1997;79:1642-1647.
Question 3
To prevent injury to the posterior interosseous nerve during the approach for reduction and fixation of a fracture of the radial head, anterior retraction should be performed with the forearm
Explanation
Deep surgical dissection-Fully pronate the forearm to move the posterior interosseous nerve away from the operative field. Incise the capsule of the elbow joint longitudinally to reveal the underlying capitulum, the radial head, and the annular ligament. Do not incise the capsule too far anteriorly; the radial nerve runs over the front of the anterolateral portion of the elbow capsule. Do not continue their dissection below the annular ligament or retract vigorously, distally, or anteriorly, because the posterior interosseous nerve lies within the substance of the supinator muscle and is vunerable to injury.
Dangers: Nerves-The posterior interosseous nerve is in no danger as long as the dissection remains proximal to the annular ligament. Pronation of the forearm keeps the nerve as far from the operative field as it possible can be. To ensure the safety of the nerve, take great care to place the retractors directly on the bone and be careful in their placement. Because the posterior interosseous nerve actually may touch the bone of the radial neck, directly opposite the bicipital tuberosity, placing retractors behind it poses a risk.
Question 4
From which artery does the princeps pollicis artery branch?
Explanation
The princeps pollicis artery can be located on the palmar aspect of the adductor pollicis and emerges into the subcutaneous tissue at the thumb metacarpophalangeal flexion crease. It branches from the radial artery just distal to the location of the deep palmar arch.
RECOMMENDED READINGS
Coleman SS, Anson B: Arterial patterns in the hand based on a study of 650 specimens. Surg Gynec Obstet 1961;4:409-424.
Ames EL, Bissonnette M, Acland R, Lister G, Firrell J. Arterial anatomy of the thumb. 78 J Hand Surg Br. 1993 Aug;18(4):427-36. PubMed PMID: 8409651. View Abstract at PubMed
Question 5
Vertebral fractures are common in the thoracolumbar spine. What is the most important factor that determines the strength of the cancellous bone in the vertebral body?
Explanation
REFERENCES: Carter DR, Hayes WC: The compressive behavior of bone as a two-phase porous structure. J Bone Joint Surg Am 1977;59:954-962.
Keaveny TM: Strength of trabecular bone, in Cowin SC (ed): Bone Mechanics Handbook. Boca Raton, FL, CRC Press, 2001, pp 16-1-16-8.
Question 6
What joint always remains uninvolved in all stages of scapholunate advanced collapse (SLAC) deformity of the wrist?
Explanation
REFERENCES: Wyrick JD: Proximal row carpectomy and intercarpal arthrodesis for the management of arthritis. J Am Acad Orthop Surg 2003;11:277-281.
Watson HK, Ballett FL: The SLAC wrist: Scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg Am 1984;9:358-365.
Watson HK, Ryu J: Evolution of arthritis of the wrist. Clin Orthop 1986;202:57-67.
Question 7
A 55-year-old woman with type I diabetes mellitus has a chronic ulcer over the dorsum of her right foot and reports forefoot pain. Examination reveals 1- x 2-cm nondraining ulcer over the dorsum of the foot. The patient has 1-2+ pain with compression of the foot and ankle. She has a weakly palpable posterior tibial pulse and an absent dorsalis pedis pulse. There is no erythema, cellulitis, or drainage. Radiographs are normal. Which of the following diagnostic studies should be obtained?
Explanation
REFERENCES: Wagner FW Jr: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981;2:64-122.
Apelqvist J, Castenfors J, Larson J, Stenstrom A, Agardh CD: Prognostic value of systolic ankle and toe blood pressure levels in outcome of diabetic foot ulcer. Diabetes Care 1989;12:373-378.
Question 8
Based on the radiographic findings shown in Figure 41, which of the following wrist ligaments is most likely disrupted?
Explanation
REFERENCES: Linscheid RL, Dobyns JH, Beabout JW, et al: Traumatic instability of the wrist: Diagnosis, classification, and pathomechanics. J Bone Joint Surg Am 1972;54:1612-1632.
Mayfield JK, Johnson RP, Kilcoyne RK: Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-241.
Berger RA: Ligament anatomy, in Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist, Diagnosis and Operative Management. St Louis, MO, Mosby, 1998, pp 73-105.
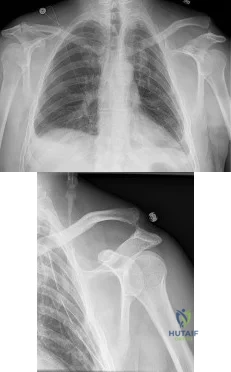
Question 9
-What is the etiology of this patient’s problem?
Explanation
Little leaguer’s shoulder is an overuse condition of the proximal humeral physis. Patients report diffuse pain that is worse with throwing. Factors that contribute to the condition include excessive throwing,improper throwing mechanics, and muscle-tendon imbalance. Radiographs usually show widening of the proximal humeral physis, and, in more severe cases, metaphyseal demineralization or fragmentation. Surgical fixation is not required for healing. Treatment involves rest until symptoms resolve, followed by initiation of an interval throwing program. Pitching coaches should evaluate throwing mechanics and maintain pitch counts. The dominant shoulders of throwing athletes undergo adaptive changes, resulting in increased external rotation and decreased internal rotation. These changes occur secondary to softtissue and bony adaptations, including increased humeral retroversion. Ischemia has been implicated as a potential cause of osteochondritis dissecans lesions. Rotator cuff tendonitis presents with anterolateral shoulder pain that is worse with activity. Pain is reproduced with resisted supraspinatus testing, and radiograph findings are typically normal.
Adolescent shoulder injuries are often caused by subtle, atraumatic instability most often sustained in sports with overhead movements, including baseball. These symptoms are more likely to occur in athletes with evidence of increased soft-tissue laxity.
Question 10
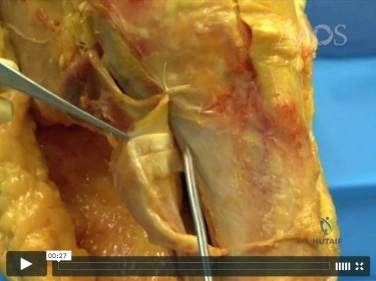
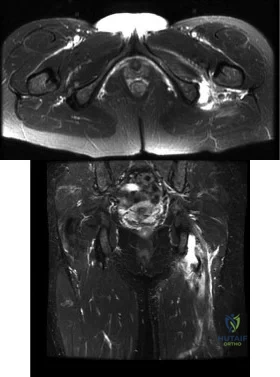
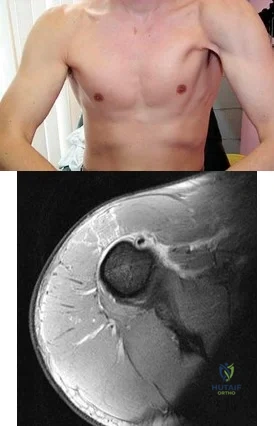
Figures A and B are axial and coronal MRI images of a 21-year-old male athlete. He injured his left leg during a hurdling race approximately 1 week ago. What would be the next best step in the management of this injury? Review Topic
Explanation
Athletes participating in sports that require sprinting, jumping, acceleration and deceleration are at increased risk of sustaining a proximal hamstring tendon avulsion. The greatest predictor of this injury is prior hamstring injury. Other risk factors include increasing age, high training demand, increased body mass index and tight hip flexor muscles. MRI is the gold standard imaging to identify these images. Open hamstring tendon repair is recommended in athletes when all of the hamstring tendons have avulsed off their origin or 2 tendons have avulsed and retracted more than 2 cm.
Cohen et al. wrote a JAAOS article on acute proximal hamstring rupture. They point out that testing the peroneal branch of the sciatic nerve function is important in the physical examination, as injury to this branch will cause weakness of the short head of the biceps femoris and may slow potential postoperative rehabilitation.
Lefevre et al. reviewed the return to sports after surgical repair of acute proximal hamstring ruptures. They performed a prospective observational study that included 34 patients. Patients returned to sports within a mean 5.7 ± 1.6 months, at the same level in 27 patients (79.4 %) and at a lower level in 7 patients (20.6 %). They conclude that surgical repair of acute proximal hamstring ruptures has the potential to significantly improve the functional prognosis of patients with these injuries.
Figures A and B shows a significant amount of swelling and hematoma around the hamstring tendon. The whole ischial tuberosity is denuded of tendon, which is consistent with a complete rupture. Illustration A shows a large posterior thigh ecchymosis commonly seen with this injury. The ecchymosis presents approximately 1 week following injury, which is know as latent ecchymosis. Illustration B shows a
schematic and intraoperative image of the open tendon repair of an acute injury.
Incorrect
Question 11
A 45-year-old man who sustains a medial subtalar dislocation while playing basketball undergoes immediate closed reduction. No fractures or osteochondral defects are noted on postreduction radiographs. The next most appropriate step in management should consist of
Explanation
REFERENCE: Saltzman C, Marsh JL: Hindfoot dislocations: When are they not benign? J Am Acad Orthop Surg 1997;5:192-198.
Question 12
A 29-year-old man reports severe knee instability and popliteal pain. History reveals that he had polio of the left lower extremity as a child and has been brace-free his entire life. Examination reveals that he walks with 40° of knee hyperextension and has a fixed ankle equinus deformity of 30° . He has no active motors about the knee or ankle. Which of the following methods will provide knee stability and pain relief?
Explanation
REFERENCE: Michael JW: Lower limb orthoses, in Goldberg B, Hsu JD (eds): Atlas of Orthoses and Assistive Devices. St Louis, MO, Mosby, 1997, pp 209-224.
Question 13
A 17-year-old football player is tackled with an opposing player's helmet hitting him hard in the abdomen. He is knocked backwards and suffers a diaphyseal femur fracture. He denies any loss of consciousness. Vital signs reveal a heart rate of 118, mean arterial pressure (MAP) of 68, and a respiration rate of 32 per minute. A FAST ultrasound study shows trace free fluid in the perisplenic space. A CBC taken prior to bolus IV fluids reveals a hematocrit of 48%, and a blood gas shows a lactate level of 1.8 and a base excess of -2.0. Which of the follow statements regarding the patient's hemodynamic status is correct?
Explanation
Hypovolemic shock leads to poor tissue perfusion due to inadequate flow or oxygenation. If a patient is in compensated shock (i.e. normal vital signs), there may be ongoing inadequate perfusion of some end-organs. Elevated lactate or a base deficit are markers of poor end-organ perfusion, thus when normalized indicate appropriate end-organ perfusion even if vital sign derangements persist.
Rossaint et al. wrote a comprehensive review article in 2006 in which they discuss principles of fluid management, coagulopathy, hypothermia and tissue oxygenation in hypovolemic shock. In addition to prolonged elevated lactate levels correlating to mortality, lactate levels (or base deficits) can be used to evaluate for compensated shock in the setting of normal hemodynamic status.
Illustration A shows the classification of hypovolemic shock. Note the percent of blood loss required for vital sign abnormalities.
Incorrect Answers:
setting of massive blood loss. The hematocrit only changes once the patient has physiologic or iatrogenic fluid shifts in response to the blood loss. Answer 3: Vital sign derangements indicate uncompensated shock, but do not directly measure tissue perfusion or end-organ damage Answer 5: Though uncommon, bleeding from isolated femur fractures can lead to Class II shock (blood loss 15-30%)
Question 14
As a diaphyseal fracture heals, peripheral callus forms about the shaft axis, creating a structure with a substantially larger diameter than the original diaphyseal shaft. What biomechanical properties does this callus impart to the healing fracture site?
Explanation
The biomechanical role of the peripheral callus is to provide initial stability to the fracture and to act as a scaffold for gradual mineralization. Because the bending stiffness of a structure is proportional to the 4th power of the diameter, a peripherally located callus provides substantial stability to the fracture, despite the relatively low stiffness and strength of callus. For example, doubling the diameter of the callus increases the resistance to bending by a factor of 16. As mineralization progresses, the bending stiffness and strength of the healed fracture eventually may be substantially greater than that of the original, intact bone.
Augat et al. review the mechanical and biological aspects of fracture healing. They report that increased diameter of periosteal callus formation benefits healing by enlarging the cross-sectional area of area of the bridging tissue and reducing interfragmentary motion. Patients with osteoporosis are known to have decreased callus mineralization and biomechanical properties.
Incorrect Answers:
Question 15
Figures 1 and 2 are the MRI scans of a 35-year-old right-hand dominant man who has right elbow pain after trying to lift a large television at home. An examination reveals ecchymosis, an abnormal hook test, and altered biceps muscle contour. What treatment is most likely to result in a satisfactory and predictable outcome?
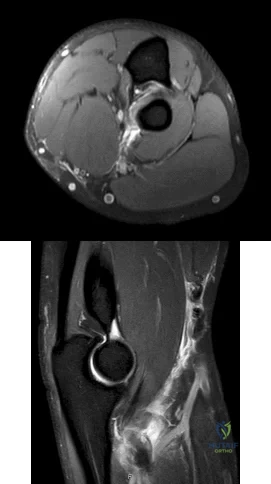
Explanation
Question 16
..One week after closed reduction of a primary anterior shoulder dislocation, a 25-year-old athlete should be counseled that
Explanation
A 65-year-old man experienced 6 years of worsening shoulder pain. Examination demonstrates stiffness and crepitus with range of motion, but full rotator cuff strength in all planes. Radiographs show advanced shoulder osteoarthritis, and an MRI scan ordered by the patient's primary care physician shows an intact rotator cuff.
Question 17
Figure 13 shows the radiographs of a 56-year-old woman who has pain and varus knee deformity after undergoing total knee arthroplasty 8 years ago. Aspiration and studies for infection are negative. During revision surgery, management of the tibial bone loss is best achieved by
Explanation
REFERENCES: Mow CS, Wiedel JD: Structural allografting in revision total knee arthroplasty. J Arthroplasty 1996;11:235-241.
Engh GA, Herzwurm PJ, Parks NL: Treatment of major defects of bone with bulk allografts and stemmed components during total knee arthroplasty. J Bone Joint Surg Am 1997;79:1030-1039.
Clatworthy MG, Ballance J, Brick GW, Chandler HP, Gross AE: The use of structural allograft for uncontained defects in revision total knee arthroplasty: A minimum five-year review. J Bone Joint Surg Am 2001;83:404-411.
Question 18
The spinal cord terminates as the conus medullaris at what vertebral level in adults? Review Topic 1 T12
Explanation
Question 19
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms? Review Topic
Explanation
Question 20
Figures 1 through 3 demonstrate the radiographs obtained from a 25-year-old man who injured his right, by punching a wall 3 weeks earlier. He notes pain and deformity about the ulnar aspect of his hand. The best treatment option is

Explanation
The initial radiographs reveal a fourth and fifth carpometacarpal (CMC) joint fracture dislocation. The injury is associated with a shear fracture of the dorsal rim of the hamate. Further assessment with CT might be helpful in fully evaluating the extent of injury. Extensor carpi ulnaris is a deforming force at the base of the fifth metacarpal. This unstable fracture dislocation could be treated with closed reduction and pinning if the patient presented within a few days of injury. However, because he presented in a delayed fashion (3 weeks after injury), open reduction with internal fixation was required (Figures 4 and 5). In the series by Zhang and associates, patients with fourth and fifth CMC fracture dislocations presenting in a delayed fashion and treated nonsurgically had suboptimal results. Therefore, closed reduction and casting are not appropriate. An arthrodesis and resection arthroplasty are salvage procedures considered for a painful arthritic joint and would less likely should not be considered for this acute injury.



Question 21
A 28-year-old woman who is training for the New York Marathon reports pain in the posteromedial aspect of her right ankle. Examination reveals tenderness just posterior to the medial malleolus. Radiographs are normal. An MRI scan is shown in Figure 3. What is the most likely diagnosis?
Explanation
REFERENCES: Boden BP, Osbahr DC: High risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Lee JK, Yao L: Stress fractures: MR imaging. Radiology 1988;169:217-220.
Question 22
Which of the following statements regarding conus medullaris syndrome is most accurate?
Explanation
REFERENCES: Haher TR, Felmly WT, O’Brien M: Thoracic and lumbar fractures: Diagnosis and management, in Bridwell KH, Dewald RL, Hammerberg KW, et al (eds): The Textbook of Spinal Surgery, ed 2. New York, NY, Lippincott Williams & Wilkins, 1977, pp 1773-1778.
Reitman CA (ed): Management of Thoracolumbar Fractures. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 35-45.
Question 23
A complication unique to computer navigation of total knee arthroplasty (TKA) is
Explanation
Threaded pins are frequently inserted into the femoral shaft and tibial shafts or proximal tibia to attach arrays for tracking devices. There have been case reports of fractures propagating through the pin tracks, which is a complication unique to computer navigation. Intercondylar fractures can occur following posterior stabilized TKA. Vascular injury, ligament disruption, and nerve palsy are rare complications following TKA performed with or without computer navigation.

CLINICAL SITUATION FOR QUESTIONS 111 THROUGH 113
Figure 111 is the anteroposterior radiograph of a 79-year-old woman with a presurgical diagnosis of osteonecrosis who sustained a periprosthetic tibia fracture following her total knee arthroplasty (TKA).
Question 24
A 69-year-old man reports pain over his bunion while wearing shoes and pain in the joint with push-off when barefoot. Nonsurgical management has failed to provide relief. Radiographs are shown in Figures 8a and 8b. What is the surgical procedure of choice?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 3-15.
Tourne Y, Saragaglia D, Zattara A, et al: Hallux valgus in the elderly: Metatarsophalangeal arthrodesis of the first ray. Foot Ankle Int 1997;18:195-198.
Question 25
Which of the following forms of nonsurgical management is considered best for acute low back pain without radiculopathy?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
Helfgott SM: Sensible approach to low back pain. Bull Rheum Dis 2001;3:50.
Question 26
Which gene mutation or polymorphism has been shown to most increase the risk for venous thromboembolic disease after elective total joint arthroplasty?
Explanation
Simultaneous bilateral TKA accounts for approximately 6% of the TKAs performed in the United States and is more frequently performed for women. The incidence of pulmonary embolism in this group was between 0.57 and 1.14, according to a 1999 to 2008 registry-based study in the United States. There was not a significant change in incidence during that period. Hypoxemia alone is not an indication for advanced testing for pulmonary embolism. Winters and associates demonstrated that to avoid unnecessary testing, the use of a hypoxia algorithm is a reasonable first step. The use of pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism in patients undergoing elective hip or knee arthroplasty and who are not at elevated risk beyond that of the surgery itself for venous thromboembolism or bleeding was given a Moderate grade of recommendation in the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty. Various genetic factors are associated with increased risk for venous thromboembolic disease after TKA. A recent meta-analysis evaluated the genetic and polymorphism profiles associated with venous thromboembolism after arthroplasty. The mutation MTHFR/C677T/TT carried the highest risk (OR 2.36; 95% CI, 1.03-5.42, P = 0.04) for the gene mutations and polymorphisms studied. With the increased use of TXA as a blood-conservation strategy for total joint arthroplasty, there is a theoretical concern about an increased risk for venous thromboembolic disease. A recent study by Duncan and associates included 13,262 elective total joint arthroplasty procedures and demonstrated that TXA does not increase the risk of venous thromboembolism.

Question 27
Denosumab, a monoclonal antibody used to treat osteoporosis, works through inhibition of
Explanation
Question 28
Which of the following is true regarding plating of humeral shaft fractures compared to intramedullary nailing?

Explanation
Question 29
A sagittal T1-weighted MRI scan of the knee joint is shown in Figure 23. What structure is identified by the arrow?
Explanation
REFERENCES: Gross ML, Grover JS, Bassett LW, Seeger LL, Finerman GA: Magnetic resonance imaging of the posterior cruciate ligament: Clinical use to improve diagnostic accuracy. Am J Sports Med 1992;20:732-737.
Sonin AH, Fitzgerald SW, Friedman H, Hoff FL, Hendrix RW, Rogers LF: Posterior cruciate ligament injury: MR imaging diagnosis and patterns of injury. Radiology 1994;190:455-458.
Question 30
..Figure 93 is the radiograph of a 72-year-old woman. Treatment includes fixation of the ulna. What options are recommended for the radius?
Explanation

Figure 94 is the anteroposterior radiograph of a 75-year-old woman who has a 5-year history of progressive pain, crepitus, and loss of motion in her shoulder. She had a rotator cuff repair 10 years ago. Examination reveals 60 degrees of active forward elevation and 20 degrees of external rotation with her arm at her side. Passively she can be brought to 160 degrees of forward elevation and 90 degrees of external rotation with her arm at her side. A glenohumeral joint injection with local anesthetic eliminated pain, but there is no observed change in active motion.
Question 31
What is the most common physical finding in a patient with femoroacetabular impingement (FAI)? Review Topic
Explanation
Question 32
A year-old woman underwent a left total knee arthroplasty 6 years ago. She initially did well after surgery but sustained a fall 2 months ago while at work. She now describes left knee pain and instability and an inability to straighten her knee since the fall. She has been using a hinged knee brace, which provides partial support. On examination, she has passive range of motion of 0° to 115° and active range of motion of 80° to -115°. Her radiographs are shown in below. What is the best option for the restoration of her function?
Explanation
The patient has an extensor mechanism disruption with patellar tendon rupture. This injury is treated with extensor mechanism reconstruction in the setting of previous total knee arthroplasty. There is a reported high failure rate with attempted repair. Revision to hinge knee arthroplasty would provide implant stability but would not restore the extensor mechanism. The patient is relatively young and is working, so reconstruction would offer better long-term function than a drop lock brace, which can be better used in low-functioning patients with this type of injury. Extensor mechanism reconstruction historically has been accomplished with allograft material, but a novel technique using synthetic mesh also has proved successful in treating this difficult problem.
Question 33
A 28-year-old woman who is an avid runner reports pain about the left hip with activities. Nonsurgical management has failed to provide relief. An MRI arthrogram is shown in Figure 47. What is the most likely diagnosis?
Explanation
REFERENCES: Guanche CA, Sikka RS: Acetabular labral tears with underlying chondralmalacia: A possible association with high-level running. Arthroscopy 2005;21:580-585.
McCarthy JC: The diagnosis and treatment of labral and chondral injuries. Instr Course Lect 2004;53:573-577.
Question 34
Figures 13a and 13b show the MRI scans of a 70-year-old patient who has a posterior calf mass. Examination reveals that the mass extends to the midcalf level. A biopsy specimen reveals a high-grade soft-tissue sarcoma. Metastatic work-up shows no lesions. Management should consist of
Explanation
REFERENCES: Lindberg RD, Martin RG, Romsdahl MM, et al: Conservative surgery and post-operative radiotherapy in 300 adults with soft tissue sarcoma. Cancer 1981;47:2391-2397.
Sim FT, Frassica FS, Frassica DA: Soft tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Rosenberg SA, Tepper J, Glatstein E, et al: The treatment of soft-tissue sarcomas of the extremities: Prospective randomized evaluations of (1) limb sparing surgery plus radiation therapy compared with amputation and (2) The roll of adjuvant chemotherapy. Am Surg 1982;196:305-315.
Question 35
Which of the following positions of immobilization has been shown to best approximate the anterior labrum against the glenoid rim following anterior dislocation of the shoulder?
Explanation
REFERENCE: Itoi E, Sashi R, Minagawa H, et al: Position of immobilization after dislocation of the glenohumeral joint: A study with use of magnetic resonance imaging. J Bone Joint Surg Am 2002;84:873-874.
Question 36
Figures 4a through 4c show the radiographs of a 43-year-old woman who sustained a twisting injury to her right ankle. She has ankle pain and tenderness medially and laterally. To help determine the optimal treatment, an external rotation stress radiograph of the ankle is obtained. This test is designed to evaluate the integrity of what structure?
Explanation
REFERENCES: Egol KA, Amirtharajah M, Tejwani NC, et al: Ankle stress test for predicting the need for surgical fixation of isolated fibular fractures. J Bone Joint Surg Am 2004;86:2393-2398.
McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004;86:2171-2178.
Schock HJ, Pinzur M, Manion L, et al: The use of the gravity or manual-stress radiographs in the assessment of supination-external rotation fractures of the ankle. J Bone Joint Surg Br 2007;89:1055-1059.
Question 37
What complication is frequently associated with the Weil lesser metatarsal osteotomy (distal, oblique) in the treatment of claw toe deformities?
Explanation
REFERENCES: Trnka HJ, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int
2001;22:47-50.
Trnka HJ, Muhlbauer M, Zettl R, et al: Comparison of the results of the Weil and Helal osteotomies for the treatment of metatarsalgia secondary to dislocation of the lesser metatarsophalangeal joints. Foot Ankle Int 1999;20:72-79.
Question 38
A 20-year-old football player sustains a dorsiflexion external rotation injury to his right ankle. During sideline evaluation, which of the following findings best indicates a syndesmosis ankle sprain without diastasis?
Explanation
REFERENCES: Nussbaum ED, Hosea TM, et al: Prospective evaluation of syndesmosis ankle sprains without diastasis. Am J Sports Med 2001;29:31-35.
Miller CD, Shelton WR, Barrett GR, et al: Deltoid and syndesmosis ligament injury of the ankle without fracture. Am J Sports Med 1985;23:746-750.
Amendola A: Controversies in diagnosis and management of syndesmosis injuries of the ankle. Foot Ankle 1992;13:44-50.
Question 39
What is the most important consideration in the preoperative evaluation of a child with polyarticular or systemic juvenile rheumatoid arthritis (JRA)?
Explanation
this usually is not needed preoperatively. Uveitis and iritis are less likely in a child with systemic JRA.
Question 40
In long-term follow-up studies of cemented total knee arthroplasty (TKA), the lowest rates of osteolysis have been associated with which design feature?
Explanation
The lowest reported rates of osteolysis involving cemented TKAs are associated with monolithic tibial components. Modular components and cemented metal-backed patella components are associated with a high prevalence of backside tibial insert wear and osteolysis.
Question 41
Figure 36a shows the current radiograph of a 65-year-old woman who slipped and fell. History reveals that prior to the fall she was actively functioning without pain. Figure 36b shows a radiograph obtained 1 year ago. Based on the fracture pattern, the failure is most likely related to
Explanation
REFERENCES: Johansson JE, McBroom R, Barrington TW, Hunter GA: Fracture of the ipsilateral femur in patients with total hip replacement. J Bone Joint Surg Am 1981;63:1435-1442.
Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242.
Question 42
A 15-year-old girl sustained the injury shown in Figures 70a and 70b when she jumped from the back of a moving truck. She is seen in the emergency department 2 hours after her injury. She has no other injuries. Her foot is warm and she has a normal motor and sensory examination. Pulses are only evident on Doppler. What is the most appropriate management? Review Topic

Explanation
Question 43
A 74-year-old woman has had acute medial right knee pain for the past 3 months. She denies any history of trauma or previous problems. Coronal and sagittal MRI scans are shown in Figures 11a and 11b. What is the most likely diagnosis? Review Topic
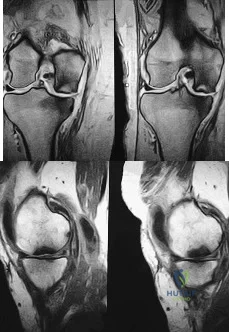
Explanation
Question 44
A 45-year-old woman with a long-standing history of diabetes mellitus has a large draining plantar ulcer of the right foot. Examination reveals some local cellulitis and erythema surrounding the ulcer. A clinical photograph is shown in Figure 7. Based on these findings, what is the most appropriate antibiotic?
Explanation
REFERENCES: Pinzur MS, Slovenkai MD, Trepman E: Guidelines for diabetic foot care. Foot Ankle Int 1999;20:695-702.
Eckman MH, Greenfield S, Mackey WC, et al: Foot infections in diabetic patients: Decision and cost-effectiveness analyses. JAMA 1995;273:712-720.
Question 45
Figures 8a and 8b show the current radiographs of a 10-year-old boy with a hip disorder who was treated with an abduction orthosis 3 years ago. If no further remodeling occurs, what is the most likely prognosis?
Explanation
REFERENCES: Stulberg SD, Cooperman DR, Wallenstein R: The natural history of Legg-Calve-Perthes disease. J Bone Joint Surg Am 1984;66:479-489.
McAndrew MP, Weinstein SL: A long-term follow-up of Legg-Calve-Perthes disease. J Bone Joint Surg Am 1984;66:860-869.
Question 46
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
REFERENCES: Apple DF: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 1130-1131.
Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 544-545.
Question 47
Emergent management of acute tooth displacement (luxation) includes
Explanation
REFERENCES: Flores MT, Andreasen JO, Bakland LK, et al: Guidelines for the evaluation and management of traumatic dental injuries. Dent Traumatol 2001; 17:97-102.
Ranalli DN, Demas PN: Orofacial injuries from sport preventive measures for sports medicine. Sports Med
2002;2:409-418.
Question 48
A 65-year-old man undergoes L4-L5 laminectomy and instrumented fusion for lumbar spinal stenosis. Post procedure radiograph is shown in figure A. Postoperatively, he develops numbness and tingling along the lateral aspect of his thigh with no associated foot symptoms or weakness. Which of the following is the most likely cause of this finding? Review Topic

Explanation
Careful patient position during orthopaedic surgery is of the utmost importance to prevent nerve injury. When patients are placed lateral for hip procedures, adequate positioning and padding of bony prominences and nerves is necessary to prevent complications. During prone position for spine surgery, the lateral femoral cutaneous nerve can be compressed under the iliac crest padded rest leading to meralgia parasthetica (MP). Numbness and tingling over the lateral thigh are usually temporary. The ulnar nerve at the elbow can also be at risk due to pressure from the positioning of the arms and the brachial plexus can be compromised by possible stretch.
Cho et al. review the literature regarding development of paresthesia due to compression of the LFCN after prone positioning for spinal surgery. They reported up to 24% incidence of after surgery. Surgery longer than 3.5 hours and shorter distance between the pelvic posts were implicated in development of MP. They recommened the patient should be positioned symmetrically, with smaller bolsters under the ASIS and adequate distance between the two pelvic posts.
Labrom et al. examined the use of SSEPs during scoliosis surgery to evaluate positional-related brachial plexopathy. They found that 27 of 434 patients had 30 percent or greater loss of SSEP during surgery. There was a significant association with prone versus supine positioning (p<0.01).
Schwartz et al. used neurological monitoring to identify the incidence and location of position-induced nerve injury in anterior cervical spine surgery. 1.8% of 3806 patients showed evidence of impending neurological injury. The majority of these cases were
at the brachial plexus during shoulder taping and application of counter traction.
Figure A is an AP lumbar spine radiograph showing intact hardware from L4-L5 laminectomy and fusion.
Incorrect
Question 49
A 65-year-old woman with type II diabetes mellitus (most recent Hgb A1C was 8.2) has had 3 days of left knee pain. Physical examination of the left knee reveals erythema, warmth and a large effusion. Range of motion is painful and limited to 30 degrees of flexion. She is found to be hypotensive and not responding to volume resuscitation. She requires phenylephrine to maintain Mean Arterial Pressure (MAP) of 70. ESR and CRP are elevated and Lactate is 3.1 mmol/L. What is the next best intervention for this patient’s treatment?
Explanation
Question 50
What preoperative factor correlates best with the outcome of rotator cuff repair?
Explanation
REFERENCES: Iannotti JP: Full-thickness rotator cuff tears: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
Iannotti JP, Bernot MP, Kuhlman JR, Kelley MJ, Williams GR: Postoperative assessment of shoulder function: A prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996;5:449-457.
Question 51
Porous hydroxyapatite is placed into a bone defect. Incorporation of this bone graft substitute is expected to follow which of the following patterns?
Explanation
Question 52
Which of the following situations is most likely to decrease sentinel event errors?
Explanation
Research has shown that 70% of sentinel event errors are caused by improper communication. Specific ways to improve communication include effective clinical handover between shifts and breaking down the "hierarchy" so that all members of the team can discuss their expectations and concerns. Barriers to effective communication include distractions, cultural differences, power distance relationships, time pressures, and lack of organization.
Leonard et al. describe specific clinical experiences in the application of surgical briefings, properties of high reliability perinatal care, the value of critical event training and simulation, and benefits of a standardised communication process in the care of patients transferred from hospitals to skilled nursing facilities. They recommend embedding standardized tools and behaviors to bridge differences in communications styles between clinicians.
Incorrect Answers:
Question 53
Figure 24 shows the radiograph of a 47-year-old woman who has severe right hip pain and a limp. Management should consist of
Explanation
REFERENCE: Jaroszynski G, Woodgate IG, Saleh KJ, Gross AE: Total hip replacement for the dislocated hip. Instr Course Lect 2001;50:307-316.
Question 54
A 70-year-old woman is brought to the emergency department with a two-part greater tuberosity fracture with an anterior subcoracoid dislocation. One day after successful closed reduction, examination reveals marked swelling of the involved arm, forearm, and hand, as well as large amounts of “weeping” serous fluid but no obvious lacerations. The fingers are warm and pink, and the pulses are normal distally with good refill. Edema is present. There is no pain with passive and active motion of the elbow, wrist, and fingers. What is the next most appropriate step in management?
Explanation
REFERENCE: Killewich LA, Bedford GR, Black KW, et al: Diagnosis of deep venous thrombosis: A prospective study comparing duplex scanning to contrast venography.
Circulation 1989;79:810.
Question 55
What is the most appropriate treatment?
Explanation
A common postsurgical problem after TKA is a sudden increase of pain that typically occurs about 2 to 3 weeks after surgery. ESR findings are not reliable during the acute postsurgical period. A CRP level exceeding 100 mg/L during the acute postsurgical period is a joint aspiration indication. If the patient does not have sepsis, there is no emergency. This pain is likely attributable to too much activity during physical therapy. Observation is recommended for this patient.
Question 56
An 80-year-old man has had increasing shoulder pain for the past 4 months. He reports that it began with soreness and stiffness after chopping some wood. A coronal MRI scan is shown in Figure 16. Initial management should consist of
Explanation
REFERENCES: Rockwood CA Jr, Williams GR Jr, Burkhead WZ Jr: Debridement of degenerative, irreparable lesions of the rotator cuff. J Bone Joint Surg Am 1995;77:857-866.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 299-312.
Question 57
A 50-year-old man fell from a ladder onto his left shoulder and sustained the injury shown in the radiographs in Figures 71a and 71b. He underwent surgery with repair of the coracoclavicular ligaments and deltotrapezial fascia with coracoclavicular screw placement. Which of the following statements regarding postoperative complications is most accurate? Review Topic
Explanation
Question 58
When using the direct lateral (or Hardinge) approach for hip arthroplasty, three muscles are detached from the femur. In addition to the vastus lateralis, they include the
Explanation
REFERENCES: Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 333-335.
Hardinge K: The direct lateral approach to the hip. J Bone Joint Surg Br 1982;64:17-19.
Question 59
Figure 56 is the radiograph of an otherwise healthy 3-year-old boy who fell and sustained the isolated injury shown. What is the best treatment modality?
Explanation
At 3 years of age, children do well with nonsurgical treatment with early spica casting and early mobilization. There is no indication to perform surgical stabilization in such a closed isolated injury. The fracture is not shortened unacceptably according to clinical practice guidelines, and traction for this fracture is unnecessary. Traction also may be problematic for the family and healthcare system.
RESPONSES FOR QUESTIONS 57 THROUGH 62
Cortical thickening in the region of the lesion
Erosive metaphyseal lesion with loss of cortical integrity
Normal bony anatomy on radiographs
Diffuse articular erosion with loss of joint space
Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
Eccentric well-circumscribed metaphyseal lesion with a scalloped border
Match the orthopaedic condition described below with the expected radiographic finding listed above.
Question 60
Glenohumeral inferior stability in the adducted shoulder position is primarily a function of the
Explanation
REFERENCES: Warner JJ, Deng XH, Warren RF, Torzilli PA: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
Harryman DT II, Sidles JA, Harris SL, Matsen FA III: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
Question 61
A 68-year-old man presents with severe right shoulder pain. He had a prolonged course of physical therapy and received several cortisone injections for his pain without improvement. Examination reveals pseudoparalysis of the right shoulder with a 20-degree external rotation lag with the shoulder adducted. With the shoulder placed in 90 degrees of abduction, he can actively externally rotate his shoulder. The patient was treated with a medialized reverse prosthesis shown in Figure A. Which of the following statement is true regarding this treatment option? Review Topic

Explanation
RTSA is most commonly indicated for rotator cuff arthropathy. However, indications for use now include shoulder pseudoparalysis, anterosuperior escape of the humeral head, acute 3 or 4-part proximal humerus fractures, and greater tuberosity fracture nonunions. Contraindications to RTSA included deltoid dysfunction, insufficient glenoid bone stock, and bony deficiency of the acromion.
Edwards et al. prospectively evaluated the risk of shoulder dislocation after reverse TSA. They found a significantly increased risk of dislocation (p=0.012) in patients with an irreparable subscapularis at time of surgery. There were no dislocations in the reparable group. Dislocations were more likely in patients with proximal humeral nonunions and failed prior arthroplasty.
Mulieri et al. looked at the use of reverse TSA in patients with irreparable massive rotator cuff tears without evidence of glenohumeral arthritis. All outcomes were improved postoperatively, and they advocate for reverse TSA in this subset of patients. Survivorship was over 90% at more than 4 years average follow up.
Boileau et al. evaluated the clinical outcomes of isolated biceps tenotomy/tenodesis in patients with massive rotator cuff tears and a biceps lesion. They found that the procedure can effectively treat pain and improve function in these patients. There was no difference in patients undergoing tenotomy versus tenodesis.
Figure A is a right shoulder radiograph status post RTSA with components in adequate position.
Incorrect Answers:
Question 62
What role does quorum sensing play in the development of a bacterial biofilm?
Explanation
Question 63
Figure 24 shows the radiograph of a 4-year-old girl with spina bifida. Examination reveals an L3 motor level, excellent sitting and standing balance, and satisfactory range of motion at the hips. Management should consist of
Explanation
REFERENCE: Heeg M, Broughton NS, Menelaus MB: Bilateral dislocation of the hip in spina bifida: A long-term follow-up study. J Pediatr Orthop 1998;18:434-436.
Question 64
Figures below show the clinical photograph and radiograph obtained from a 62-year-old man who has deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?

Explanation
Figure 1 reveals an external rotation deformity of the right lower extremity. This deformity can have numerous causes, including extra-articular deformity. Figure 2 reveals a loose, subsided femoral component. Femoral stems typically subside into retroversion due to proximal femoral biomechanics, which cause a compensatory external rotation deformity. The combined findings from both images suggest an external rotation deformity most likely related to subsidence into retroversion.
Question 65
An 81-year-old man with severe low back pain reports right extensor hallucis longus and anterior tibialis weakness and difficulty urinating over the past 24 hours. He has a temperature of 101 degrees F (38.3 degrees C). MRI scans are shown in Figures 31a and 31b. Management should consist of
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 257-271.
Reihsaus E, Waldbaur H, Seeling W: Spinal epidural abscess: A meta-analysis of 915 patients. Neurosurg Rev 2000;23:175-204.
Question 66
A 45-year-old woman has severe anterior knee pain. Her radiographs indicate end-stage patellofemoral compartment osteoarthritis. The tibiofemoral compartments are preserved. Extensive nonsurgical treatment has failed to provide relief, and she is offered patellofemoral arthroplasty (PFA). What is the most common long-term mode of failure for PFA using an implant with an onlay prosthesis design?
Explanation
Contemporary onlay-design trochlear prostheses in PFA replace the entire anterior trochlear surface. Previous inlay designs were inset within the native trochlea and carried a higher risk of catching and patellar instability, particularly in patients with trochlear dysplasia; they also generally have higher failure rates. The current most common mode of failure is progression of arthritis throughout the knee, in some series as high as 25% at 15 years. Aseptic loosening, particularly of cemented implants, is less common. Infection is an uncommon long-term complication. Patients considering PFA should be advised of the risk of arthritis progression. Many authors routinely obtain a preoperative MRI to assess the status of the tibiofemoral compartments.
Question 67
Reverse total shoulder arthroplasty improves kinematics in the rotator cuff deficient joint by what directional change to the center of rotation? Review Topic
Explanation
Question 68
- Figure 67 shows the AP radiograph of both knees of a 26-year-old woman. A review of the patient’s medical record will most likely reveal a history of
Explanation
Question 69
A 2-year-old child is brought in by his parents for evaluation of intoeing. The child has a normal neuromuscular examination, but the heel bisector line is in the fourth web space, indicating a severe flexible metatarsus adductus deformity. The remainder of the lower extremity examination is unremarkable. What is the most appropriate treatment?
Explanation
REFERENCES: Beaty J: Congenital anomalies of the lower extremity, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. Philadelphia PA, Mosby, 2003, pp 983-988.
Katz K, David R, Soudry M: Below-knee plaster cast for the treatment of metatarsus adductus.
J Pediatr Orthop 1999;19:49-50.
Weinstein SL: Bristol-Myers Squibb/Zimmer award for distinguished achievement in orthopaedic research. Long-term follow-up of pediatric orthopaedic conditions: Natural history and outcomes
of treatment. J Bone Joint Surg Am 2000;82:980-990.
Question 70
- What is the primary mechanism of wear of polyethylene acetabular components?
Explanation
Question 71
Which of the following patients requires preoperative noninvasive cardiac testing?
Explanation
REFERENCES: Bushnell BD, Horton JK, McDonald MF, et al: Perioperative medical comorbidities in the orthopaedic patient. J Am Acad Orthop Surg 2008;16:216-227.
Auerback A, Goldman L: Assessing and reducing the cardiac risk of noncardiac surgery. Circulation 2006;113:1361-1376.
Fischgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 105-113.

Question 72
A 26-year-old man sustains a displaced bimalleolar fracture by sliding into second base while playing baseball. Following initial closed reduction and splinting of the fracture, moderate swelling is noted. What is the safest time to perform surgery?
Explanation
REFERENCES: Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119.
Hahn DM, Colton CL, Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
Question 73
A 35-year-old man sustained a 10% compression fracture of the C5 vertebra in a diving accident. Radiographs show good alignment, and examination reveals no neurologic compromise. An MRI scan reveals no significant soft-tissue disruption posteriorly. Management should consist of
Explanation
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
Allen GL, Ferguson RL, Lehmann TR, O’Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
Question 74
Figure 11a shows the clinical photograph of a 46-year old woman who reports a 3-week history of pain and a “lump” at the base of her neck. She is otherwise in good health and denies any trauma. A 3-D reconstruction CT is shown in Figure 11b. What is the most likely diagnosis?
Explanation
REFERENCES: Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 1078-1079.
Rockwood CA, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Question 75
Persistent symptoms and decreased function following distal clavicle resection, coracoacromial ligament transfer, and augmentation (modified Weaver-Dunn) are most likely related to Review Topic
Explanation
Question 76
The incidence of ipsilateral phrenic nerve blockade after an interscalene block approaches
Explanation
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14;546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
Question 77
Progressive paralysis is most likely to be seen in association with what type of congenital vertebral abnormality?
Explanation
REFERENCES: McMaster MJ, Singh H: Natural history of congenital kyphosis and kyphoscoliosis: A study of one hundred and twelve patients. J Bone Joint Surg Am 1999;81:1367-1383.
Dubousset J: Congenital kyphosis and lordosis, in Weinstein SL (ed): The Pediatric Spine: Principles and Practice, ed 1. New York, NY, Raven Press, 1994, pp 245-258.
Question 78
The diagnosis of an infection after total knee arthroplasty is most reliably proven based on what single study?
Explanation
REFERENCES: Windsor RE, Bono JV: Infected total knee replacements. J Am Acad Orthop Surg 1994;2:44-53.
Windsor RE, Insall JN, Urs WK, et al: Two-stage reimplantation for the salvage of total knee arthroplasty complicated by infection: Further follow-up and refinement of indications. J Bone Joint Surg Am 1990;72:272-278.
Question 79
A 60-year-old woman has a mass in the right scapula. Figures 25a and 25b show a CT scan and a biopsy specimen. The cells are lymphocyte common antigen positive, Ewing’s specific antigen (CD99) negative, and keratin negative. What is the next step in management?
Explanation
REFERENCES: Finiewicz K, van Biesen K: Non-Hodgkins lymphoma, in Golomb H, Vokes E (eds): Oncologic Therapies, ed 2. Berlin, Germany, Springer, 2003, pp 295-318.
Lems P, Primus G, Anastas J, Doherty D, Montag AG, Peabody TD, Simon MA: Oncologic outcomes of primary lymphoma of bone in adults. Clin Orthop 2003;415:90-97.
Question 80
Figures 1 through 3 are the radiographs of a 27-year-old man who has had wrist pain since falling 1 day ago. Which treatment offers the best prognosis for prevention of carpal collapse and progressive arthritis?

Explanation
Although this patient’s history includes a recent fall, the radiographs show evidence of a scaphoid nonunion with carpal collapse but no arthritis. Obtaining union of the scaphoid is important to prevent progressive carpal collapse and arthritic changes. ORIF with bone graft is most appropriate to obtain union and correct the collapse deformity. Screw fixation with volar wedge graft often is performed to realign a scaphoid humpback deformity, although cancellous bone graft also is a reasonable option. Vascularized bone graft is considered for a nonunion of long duration, avascular necrosis of the proximal pole, and failed prior surgery. Cast immobilization will not lead to union of the scaphoid. Percutaneous screw fixation is not indicated for the treatment of a displaced nonunion. A proximal
row carpectomy is a salvage procedure and is not indicated for this patient because there are no arthritic changes.
Question 81
A 73-year-old man sustains the fracture shown in Figure 62. Which of the following factors or combination of factors puts this patient at highest risk for nonunion if nonsurgical management is used?

Explanation
Question 82
A collegiate football player who sustained a blow to the head during the first quarter of a game is confused for several minutes after the hit but does not lose consciousness. He had two similar episodes in games earlier in the season. When should he be allowed to return to play?
Explanation
REFERENCES: Guskiewwicz KM, Barth JT: Head injuries, in Schenk RC Jr (ed): Athletic Training and Sports Medicine. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 143-167.
Kelly JP, Rosenberg JH: Diagnosis and management of concussion in sports. Neurology 1997;48:575-580.
Question 83
The sublime tubercle of the elbow serves as the insertion site of the Review Topic
Explanation
Question 84
An 11-year-old boy sustained an injury to his arm in gym class. He denies prior pain in the arm. Radiographs are shown in Figures 48a and 48b. What is the next most appropriate step in the management of this lesion?
Explanation
REFERENCES: Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Deyoe L, Woodbury DF: Unicameral bone cyst with fracture. Orthopedics 1985;8:529-531.
Question 85
A 35-year-old construction worker continues to have weakness with lifting overhead 2 years after he was treated with physical therapy for a "chest muscle" tear. An obvious deformity noted in his axilla worsens with resisted extension and adduction. A clinical photograph and MRI scan are shown in Figures 119a and 119b. What is the most appropriate treatment? Review Topic
Explanation
Question 86
Figures below depict the radiographs obtained from a 76-year-old woman with a painful total knee arthroplasty. She describes an uneventful recovery with no wound-healing issues and was pain free for the first 10 years. Although reporting no trauma or inciting event, she now describes pain in the entire knee that is most severe with her first few steps. She has begun to notice night pain and, more recently, constant swelling. What is the most appropriate work-up at this time?
Explanation
An evaluation of the painful total knee must be supported by an understanding of the potential etiologies of pain. They may include, aseptic loosening, infection, osteolysis, gap imbalance, referred pain, stiffness, and complex regional pain syndrome. In this case, the patient demonstrates start-up pain and had no prior history of infections. Her radiographs show subsidence of the tibia, indicating a loose prosthesis. Knowing that the prosthesis is already loose precludes the need for a bone scan. It is, however, important to rule out infection in this case; therefore, CRP and ESR testing is essential. Aspiration is also recommended when going into knee arthroplasty, and infection is a concern.
Question 87
Which of the following is associated with the use of bisphosphonates in the setting of metastatic breast cancer to the spine?
Explanation
REFERENCE: Body JJ: Breast cancer: Bisphosphonate therapy for metastatic bone disease. Clin Cancer Res 2006;12:6258s-6263s.
Question 88
The usual presentation of traumatic subscapularis tears is most often seen after forced
Explanation
REFERENCES: Kreuz PC, Remiger A, Erggelet C, et al: Isolated and combined tears of the subscapularis tendon. Am J Sports Med 2005;33:1831-1837.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 89
A year-old man who underwent right total knee replacement surgery 2 and a half years ago has had knee pain since surgery. The pain is diffuse, constant, and made worse with activity. He notes warmth and swelling in his knee. Examination shows a well-healed incision, no erythema, moderate warmth, synovitis, and an effusion. The knee is stable, and has an arc of flexion between 3° and 120°. Radiographs show well-fixed and well-aligned implants. What is the most appropriate initial treatment?
Explanation
This patient's history and physical findings are concerning for deep infection. Inflammatory markers, including ESR and CRP, should be obtained first. If the levels are elevated, knee aspiration should be performed for the synovial cell count and culture. A bone scan is not indicated in an initial investigation for deep infection; it is rarely helpful and is not cost effective. CT to assess implant rotation is an appropriate investigation for knee pain when the clinical scenario is not suspicious for a deep infection
and when infection has been excluded.
Question 90
Why is tendon considered an anisotropic material?
Explanation
REFERENCES: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180.
Lu L, Kaufman KR, Yaszemski MJ: Biomechanics, in Einhorn TA, O’Keefe RJ,
Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 91
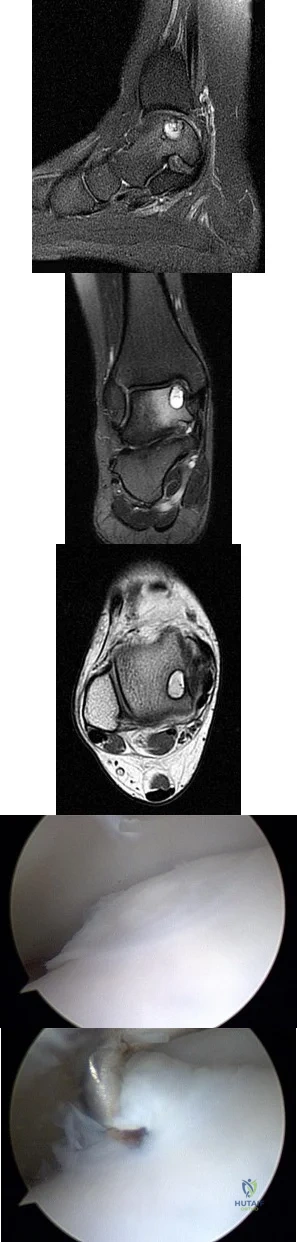
A B C D E Figures 45a through 45c are the MR images of a 22-year-old woman who has had 6 months of ankle pain related to activities of daily living. She recently completed a course of cast immobilization and protected weight bearing without symptom resolution. Figures 45d and 45e are the intraoperative arthroscopy images after minimal probing. What is the most appropriate treatment?
Explanation
The MR images reveal a large cystic medial talar dome osteochondral lesion (OCL) in a patient who has failed nonsurgical treatment. Ankle fusion is inappropriate because the patient has an otherwise normal ankle. Arthroscopic debridement and drilling are appropriate for smaller (< 1.5 cm sq) noncystic lesions. Retrograde drilling and bone grafting is an option in the treatment of cystic OCL if the cartilage surface is intact; however, intraoperative arthroscopy images show that this patient's cartilage surface is unstable. Osteochondral allografts and autografts are effective in the treatment of large cystic talar dome OCLs but are not appropriate for the initial surgical treatment of smaller lesions like this one.
RECOMMENDED READINGS
Hannon CP, Smyth NA, Murawski CD, Savage-Elliott I, Deyer TW, Calder JD, Kennedy JG. Osteochondral lesions of the talus: aspects of current management. Bone Joint J. 2014 Feb;96-B(2):164-71. doi: 10.1302/0301-620X.96B2.31637. Review. PubMed PMID:
Question 92
A 29-year-old ultramarathoner, who is halfway into a 50-mile race, is sweating profusely. He suddenly collapses, is unresponsive, and has violent muscle contractions. Prior to these symptoms, he had been drinking water at every water stop (every 1 mile). What is the most likely diagnosis?
Explanation
REFERENCES: Griffin LY: Emergency preparedness: Things to consider before the game starts. J Bone Joint Surg Am 2005;87:894-902.
Rehrer NJ: Fluid and electrolyte balance in ultra-endurance sport. Sports Med 2001;31:701-715.
Question 93
A 21-year-old woman with Marfan syndrome is seeking evaluation of her scoliosis. She reports no back or leg pain, and the neurologic examination is normal. Lateral and bending radiographs are shown in Figures 7a through 7e. Management should consist of
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 161-171.
Turi M, Johnston CE II, Richards BS: Anterior correction of idiopathic scoliosis using TSRH instrumentation. Spine 1993;18:417-422.
Moskowitz A, Trommanhauser S: Surgical and clinical results of scoliosis surgery using Zielke instrumentation. Spine 1993;18:2444-2451.
Question 94
A 7-year-old girl with a known diagnosis of neurofibromatosis has neck pain and deformity. She has been wearing a soft cervical collar for the past 2 months with mild relief of her symptoms. An MRI scan shows several small neurofibromas on the left side of the cervical spine near the foramina at C6 and 7. A lateral cervical spine radiograph is shown in Figure 34. What is the most appropriate management?
Explanation
REFERENCES: Crawford AH, Schorry EK: Neurofibromatosis update. J Pediatr Orthop 2006;26:4I3- 423. MehJman CT, Al-Sayyad MJ, Crawford AH: Effectiveness of spinal release and halo-femoral traction in the management of severe spinal deformity. J Pediatr Orthop 2004;24:667-673.
Question 95
A 16-year-old high school football player who sustained an acute forceful dorsiflexion ankle injury reported that he felt a pop and then noted immediate swelling over the lateral malleolus. Examination 24 hours later reveals moderate swelling and tenderness along the lateral malleolus. The external rotation, squeeze, anterior drawer, and talar tilt tests are negative. Subluxation of the peroneal tendons is palpable over the peroneal groove of the fibula. Radiographs reveal a small cortical avulsion off the distal rim of the fibula. The stress views show no instability. Initial management for this injury should include
Explanation
REFERENCES: Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Marti R: Dislocation of the peroneal tendons. Am J Sports Med 1977;5:19-22.
Question 96
When comparing the overall outcomes of surgical versus nonsurgical treatment of stable thoracolumbar burst fractures in patients without neurologic injury, 5 years following injury, the principle differences lie in Review Topic
Explanation
Question 97
A 75-year-old patient returns for follow-up after undergoing bilateral total hip arthroplasty (THA). The right hip is a hybrid THA performed 12 years ago, whereas the left hip is a cementless THA performed 10 years ago. Both acetabular components are the same type, same size, and from the same manufacturer. Both femoral heads are 28-mm cobalt-chromium components. What is the most likely explanation for the advanced polyethylene wear in one hip?
Explanation
5 years of shelf life, polyethylene oxidized rather slowly. However, polyethylene components with a shelf life of more than 5 years would be expected to have minimal mechanical toughness and would likely fail rapidly if implanted. Bohl and associates evaluated 135 patients who had undergone total knee arthroplasty. Survivorship at 5 years was 100% for components with a shelf life of less than 4 years, 89% for components with a shelf life of 4 to 8 years, and 79% for components with a shelf life of more than 8 years. Sychterz and associates reported no correlation between shelf life and true wear rates for components with a shelf life of less
than 3 years. In summary, both in vivo and in vitro data suggest that shelf life in excess of
3 to 5 years has a direct effect on wear of polyethylene.
REFERENCES: Currier BH, Currier JH, Collier JP, et al: Shelf life and in vivo duration: Impacts on performance of tibial bearings. Clin Orthop 1997;342:111-122.
Bohl JR, Bohl WR, Postak PD, et al: The Coventry Award: The effects of shelf life on clinical outcome for gamma sterilized polyethylene tibial components. Clin Orthop 1999;367:28-38.
Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.
Question 98
After performing a total hip arthroplasty through a posterolateral approach, an orthopaedic surgeon is unable to adequately externally rotate the leg and subsequently exposes the anterior capsule. When releasing the inferior aspect of the anterior capsule, pulsatile bleeding is encountered. A branch of which artery is most likely lacerated?
Explanation
Branches of the lateral femoral circumflex artery arise from the inferior aspect of the anterior hip capsule. They can be injured when removing the anterior capsule from any approach. The inferior gluteal artery supplies the gluteus maximus. The medial femoral circumflex artery enters the hip joint along the path of the obturator externus tendon. The femoral artery crosses the anterior hip joint in the superior-to-inferior direction and is located just medial to the hip joint.

Question 99
A 12-year-old boy falls from a bicycle. A radiograph of his injured shoulder is shown in Figure 41. What is the optimal method of treatment?
Explanation
REFERENCES: Bishop JY, Flatow EL: Pediatric shoulder trauma. Clin Orthop Relat Res 2005;432:41-48.
Question 100
A 59-year-old man reports moderate shoulder pain and very restricted range of motion after undergoing humeral arthroplasty for osteoarthritis 1 year ago. An AP radiograph is shown in Figure 32. Management should now consist of
Explanation
REFERENCES: Neer CS II, Kirby RM: Revision of humeral head and total shoulder arthroplasties. Clin Orthop 1982;170:189-195.
Petersen SA, Hawkins RJ: Revision of failed total shoulder arthroplasty. Orthop Clin North Am 1998;29:519-533.
