OITE & ABOS Board Review: Trauma, Hip, Knee, & Wrist MCQs | Part 188

Key Takeaway
This page presents Part 188 of an OITE and ABOS orthopedic board review quiz. It features 100 high-yield, verified MCQs covering Arthroscopy, Hip, Knee, Trauma, and Wrist. Authored by Dr. Hutaif, this resource is vital for orthopedic surgeons and residents preparing for their board certification exams.
About This Board Review Set
This is Part 188 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 188
This module focuses heavily on: Arthroscopy, Hip, Knee, Ligament, Trauma, Wrist.
Sample Questions from This Set
Sample Question 1: A 10-year-old boy has had wrist pain for the past 3 months. He denies any history of trauma. He reports mild tenderness associated with a palpable mass. A radiograph and biopsy specimens are shown in Figures 52a through 52c. What is the mos...
Sample Question 2: What percent of adult patients with rheumatoid arthritis test positive for rheumatoid factor?...
Sample Question 3: Nonossifying fibroma...
Sample Question 4: A 29-year-old woman who underwent an anterior cruciate ligament (ACL) reconstruction 6 months ago now reports difficulty achieving full knee extension, and physical therapy fails to provide relief. The knee is stable on ligament testing. Fi...
Sample Question 5: A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 1. A r...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 10-year-old boy has had wrist pain for the past 3 months. He denies any history of trauma. He reports mild tenderness associated with a palpable mass. A radiograph and biopsy specimens are shown in Figures 52a through 52c. What is the most likely diagnosis?
Explanation
REFERENCES: Schajowicz F: Tumors and Tumorlike Lesions of Bone: Pathology, Radiology, and Treatment, ed 2. Berlin, Springer-Verlag, 1994, pp 147-151.
Weiner SD: Enchondroma and chondrosarcoma of bone: Clinical, radiologic, and histologic differentiation. Instr Course Lect 2004;53:645-649.
Question 2
What percent of adult patients with rheumatoid arthritis test positive for rheumatoid factor?
Explanation
Question 3
Nonossifying fibroma
Explanation
Early osteomyelitis and septic arthritis appear as normal bony anatomy on radiographs, with perhaps only soft-tissue swelling seen. Radiographic changes with metaphyseal erosion appear in a delayed fashion, often after 7 or more days in indolent infections, but may present earlier in association with virulent infections such as methicillin-resistant Staphylococcus aureus. Osteoid osteoma has a radiolucent small nidus that may be difficult to see on radiograph; however, chronic cases cause marked cortical hypertrophy. Unicameral bone cysts are expansile metaphyseal lesions that are never wider than the physis. They are symmetric, well circumscribed, and can have cortical thinning. When fractures through the cyst are
present, the fallen leaf sign is visible as cortical fragments fall to the bottom of the cyst. Nonossifying fibromas are eccentric metaphyseal lesions with scalloped borders.
Question 4
A 29-year-old woman who underwent an anterior cruciate ligament (ACL) reconstruction 6 months ago now reports difficulty achieving full knee extension, and physical therapy fails to provide relief. The knee is stable on ligament testing. Figure 3 shows the findings at a repeat arthroscopy. Treatment should now include
Explanation
REFERENCES: Delince P, Krallis P, Descamps PY, et al: Different aspects of the cyclops lesion following anterior cruciate ligament reconstruction: A multifactorial etiopathogenesis. Arthroscopy 1998;14:869-876.
Fisher SE, Shelbourne KD: Arthroscopic treatment of symptomatic extension block complicating anterior cruciate ligament reconstruction. Am J Sports Med 1993;4:558-564.
Question 5
A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 1. A radiograph taken after the fall is shown in Figure 2. He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?

Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 6
A 10-year-old child was referred for spinal curvature and a 2-year history of back pain. She has pain during the day and pain at night that wakes her from sleep and is temporarily relieved with nonsteroidal anti-inflammatory drugs. Examination shows very tight hamstrings and an irritative spinal curvature. Figures 71a through 7Id show radiographs, a bone scan, and a CT scan. What is the most appropriate treatment?
Explanation
REFERENCES: Frassica FJ, Waltrip RL, Sponseller PD, et al: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-
Question 7
All of the following techniques can help to prevent apex-anterior angulation during intramedullary nailing of proximal one-third tibia fractures EXCEPT:

Explanation
Question 8
Compared with percutaneous pinning with Kirschner wires (K-wires), the treatment of metacarpal neck fractures with cannulated intramedullary screws is associated with
Explanation
In a biomechanical study, headless compression screws showed superior load to failure, higher three-point bending strength, and greater strength in axial loading compared with percutaneous K-wire fixation for metacarpal neck fractures. Headless compression screws provide greater initial stability to allow earlier motion in the postoperative period. No data comparing infection rates between the two methods of fixation are available; however, it is assumed that K-wires placed outside of the skin would have increased rates of infection. Neither fixation method would increase the time to healing.
Question 9
What is the most specific physical examination finding? Review Topic

Explanation
Question 10
Which of the following represents a contraindication for interspinous process decompression for the treatment of lumbar spinal stenosis? Review Topic
Explanation
Question 11
…What is the etiology of the pain associated with this lesion?
Explanation

Question 12
What range of motion parameters are required for a patient with posttraumatic elbow stiffness to accomplish all the normal activities of daily living?
Explanation
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Morrey BF, Askew LJ, Chao EY: A biomechanical study of normal functional elbow motion. J Bone Joint Surg Am 1981;63:872-877.
Question 13
Figure 1 shows the radiograph of a 71-year-old man who has had increasing pain and weakness in his shoulder for the past 3 years. Nonsurgical management has failed to provide relief. Examination shows 130 degrees of active forward flexion and intact external rotation strength. During surgery, a 1- x 1-cm rotator cuff tear involving the supraspinatus is encountered. Treatment should include
Explanation
REFERENCES: Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for treatment of defects in the rotator cuff and surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491.
Question 14
A 23-year-old college basketball player reports persistent lateral ankle pain after sustaining an inversion injury 6 months ago. Examination reveals pain over the anterolateral ankle, absence of swelling, and no clinical instability. Management consisting of vigorous physical therapy fails to provide relief, and a intra-articular corticosteroid injection provides only temporary relief. Radiographs obtained at the time of injury and subsequent AP and varus stress views are normal. A recent MRI scan fails to show any abnormalities. Management should now include
Explanation
REFERENCES: Ferkel RD, Fasulo GJ: Arthroscopic treatment of ankle injuries. Orthop Clin North Am 1994;25:17-32.
Ferkel RD, Karzel RP, Del Pizzo W, Friedman MJ, Fischer SP: Arthroscopic treatment of anterolateral impingement of the ankle. Am J Sports Med 1991;19:440-446.
Question 15
When evaluating a patient with hallux rigidus, what is the most important clinical factor indicating the need for an arthrodesis as opposed to a cheilectomy?
Explanation
REFERENCES: Coughlin MJ, Shurnas PS: Hallux rigidus: Grading and long-term results of operative treatment. J Bone Joint Surg Am 2003;85:2072-2088.
Easley ME, Davis WH, Anderson RB: Intermediate to long-term follow-up of medial-approach dorsal cheilectomy for hallux rigidus. Foot Ankle Int 1999;20:147-152.
Question 16
A 35-year-old construction worker has developed isolated lateral compartment arthritis. He has lost 50 pounds, now has a body mass index of 30, and still has pain that limits his activities of daily living and work despite receiving a 4-month course of nonsteroidal anti-inflammatory medications and 2 intra-articular cortisone injections. His range of motion is 5 to 110 degrees, and his mechanical axis is 18 degrees of valgus. What is the most appropriate surgical treatment for this patient?
Explanation
Knee arthritis in a young laborer is challenging to address. A surgeon could perform an arthroplasty, but there is concern for early failure and the subsequent need for multiple revisions during this patient’s lifespan. Indications for distal femoral varus osteotomy include at least a 12- to 15-degree valgus mechanical axis and range of motion of at least 15 to 90 degrees. Contraindications for this procedure include inflammatory arthritis and restricted knee motion.
RESPONSES FOR QUESTIONS 138 THROUGH 141
Acute periprosthetic infection
Chronic periprosthetic infection
Joint dislocation
Periprosthetic fracture
Pseudotumor
Femoral nerve palsy
Sciatic nerve palsy
Aseptic prosthetic loosening
Select the total hip arthroplasty (THA) complication listed above that most commonly is associated with the clinical scenario described below.
Question 17
A 32-year-old construction worker reports a persistent burning, tingling sensation on the dorsum of his right foot and significant sensitivity on the plantar surface after a 500-lb steel beam dropped on it 8 weeks ago. Initial radiographs revealed no fractures, and the skin remained intact at the time of injury. Physical therapy, anti-inflammatory drugs, and a serotonin reuptake inhibitor have failed to provide relief. What is the next most appropriate step in management?
Explanation
REFERENCES: Cepeda MS, Lau J, Carr DB: Defining the therapeutic role of local anesthetic sympathetic blockade in complex regional pain syndrome: A narrative and systematic review. Clin J Pain 2002;18:216-233.
Perez RS, Kwakkel G, Zuurmond WW, et al: Treatment of reflex sympathetic dystrophy (CRPS type 1): A research synthesis of 21 randomized clinical trials. J Pain Symptom Manage 2001;21:511-526.
Tran KM, Frank SM, Raja SN, et al: Lumbar sympathetic block for sympathetically maintained pain changes in cutaneous temperatures and pain perception. Anesth Analg 2000;90:1396-1401.
Stanton-Hicks M, Baron R, Boas R, et al: Complex regional pain syndromes: Guidelines for therapy. Clin J Pain 1998;14:155-166.
Question 18
Figures 56a through 56c show the radiograph, CT scan, and biopsy specimen of a 44-year-old man who underwent chemotherapy and radiation therapy for lymphoma of the distal femur 20 years ago. His current problem is most likely related to
Explanation
REFERENCES: Mirra J (ed): Bone Tumors: Clinical, Radiologic and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, p 353.
Huvos A, Woodard H, Cahan W, et al: Postradiation osteogenic sarcoma of bone and soft tissue. A clinical pathologic study of 66 Patients. Cancer 1985;55:1244.
Question 19
A 35-year-old woman began to train for a half marathon. After 8 weeks of increasing her mileage, what changes can you expect in her Achilles tendon?
Explanation
Question 20
Figure 37 shows the radiograph of a 23-year-old football player who sustained a blow to the anterior aspect of his shoulder. Examination reveals pain and limited rotation. He is unable to flex the arm above the shoulder. Management should include which of the following studies?
Explanation
REFERENCES: Bloom MH, Obata WG: Diagnosis of posterior dislocation of the shoulder with the use of Velpeau axillary and angle-up roentgenographic views. J Bone Joint Surg Am 1967;49:943-949.
Rockwood CA: Subluxations and dislocations about the shoulder, in Rockwood CA, Green DP (eds): Fractures in Adults, ed 2. Philadelphia, PA, JB Lippincott, 1984, vol 1, pp 806-856.
Question 21
A 12-year-old girl with juvenile rheumatoid arthritis (JRA) has had chronic pain and synovitis about the knee that is now well-controlled medically. Examination reveals 20° of valgus at the knee. Knee range of motion shows 10° to 90° of flexion. Treatment should consist of
Explanation
REFERENCE: Rydholm U, Brattstrom H, Bylander B, Lidgren L: Stapling of the knee in juvenile chronic arthritis. J Pediatr Orthop 1987;7:63-68.
Question 22
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management?
Explanation
REFERENCES: Miller P, Kendrick D, Bentley E, et al: Cost effectiveness of lumbar spine radiographs in primary care patients with low back pain. Spine 2002;27:2291-2297.
Wong DA, Transfeldt E: Macnab’s Backache, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins 2007, pp 298-338.
Question 23
What pharmacologic agents are preferred for the treatment of symptomatic active Paget’s disease?
Explanation
REFERENCE: Delman PD, Meunier PJ: The management of Paget’s disease. N Eng J Med 1997;336:558-566.
Question 24
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and Review Topic
Explanation
Question 25
A 9-year-old girl has pain over the fifth toe that is aggravated by shoe wear. Clinical photographs are shown in Figures 28a and 28b. Treatment of this deformity should consist of
Explanation
REFERENCES: Black GB, Grogan DP, Bobechko WP: Butler arthroplasty for correction of adducted fifth toe: A retrospective study of 36 operations between 1968 and 1982. J Pediatr Orthop 1985;5:439-441.
Paton RW: V-Y plasty for correction of varus fifth toe. J Pediatr Orthop 1990;10:248-249.
Coughlin MJ, Mann RA: Lesser toe deformities, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 5. St Louis, MO, Mosby, 1986, pp 132-157.
Question 26
Kinematic testing of patellofemoral motion demonstrates that malalignment that produces increased Q angle causes a shift of the patella laterally in the trochlear groove and is most pronounced during what phase of the flexion arc?
Explanation
REFERENCES: Ramappa AJ, Apreleva M, Harrold FR, et al: The effects of medialization and anteromedialization of the tibial tubercle on patellofemoral mechanics and kinematics. Am J Sports Med 2006;34:749-756.
Huberti HH, Hayes WC: Patellofemoral contact pressure: The influence of q-angle and tendofemoral contact. J Bone Joint Surg Am 1984;66:715-724.
Question 27
What bilateral surgical intervention is considered inappropriate based on the findings shown in the radiograph in Figure 52?
Explanation
REFERENCES: Mont MA, Jones LC, Sotereanos DG, et al: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 28
A 25-year-old male is involved in an high-speed motor vehicle collision and sustains a closed femoral shaft fracture. During further evaluation, a CT scan of the chest/abdomen/pelvis reveals a non-displaced ipsilateral femoral neck fracture. Which of the following treatment options will most likely achieve anatomic healing of both fractures, mobilize the patient, and minimize the risk of complications?

Explanation
Question 29
A 12-year-old boy who pitches on two “select” baseball teams has had pain in his dominant right shoulder for the past 6 weeks. The pain is present only with throwing and is associated with decreased throwing velocity and control. He has no radiation of pain or paraesthesias of the upper extremity. An AP radiograph and MRI scan are shown in Figures 19a and 19b, respectively. Management should consist of Review Topic
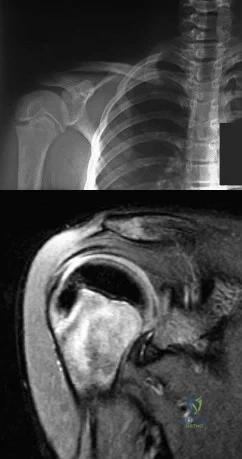
Explanation
Question 30
Which of the following aids in correction of patellar tracking after total knee arthroplasty (TKA)?
Explanation
REFERENCES: Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 1245-1258.
Merkow RL, Soudry M, Insall JN: Patellar dislocation following total knee replacement. J Bone Joint Surg Am 1985;67:1321-1327.
Question 31
What cardiac condition causes most upper extremity emboli?
Explanation
Atrial fibrillation is responsible for approximately 80% of all upper extremity emboli. All other cardiac conditions listed can cause upper extremity emboli; however, atrial fibrillation is the most common cause. Patients with an upper extremity embolic event should undergo prompt evaluation, with a careful history and physical examination as well as focused laboratory tests for hypercoagulability. Arterial Doppler studies or angiography is/are warranted. Electrocardiogram and echocardiogram are also used to evaluate for potential cardiac abnormalities. Consultation with vascular, radiology, and cardiology personnel is often necessary when patients present with upper extremity emboli. Treatment usually involves anticoagulation, embolectomy if necessary, and treatment for any recognized cardiac abnormality.
Question 32
An anatomic reduction is obtained at the femoral neck. The most likely reason for development of avascular necrosis (AVN) in this scenario would be
Explanation
A damage-control approach is indicated for this patient. Debridement of the open fracture wound and rapid stabilization without an extensive surgical
approach are indicated. Rapid percutaneous fixation of the femoral neck would compromise long-term outcomes for this displaced fracture because obtaining a quality reduction and fixation construct is critical for the long-term outcome. This patient likely would not tolerate cephalomedullary nailing or open approaches very well at this time.
A vertically oriented (Pauwels 3) femoral neck fracture is more common in younger patients who sustain high-energy injuries. Because of the mechanism of injury, many of these patients have associated injuries. This is a biomechanically challenging fracture because the fracture is subject to shear forces rather than compression, making it inherently unstable. This type of fracture often necessitates different fixation strategies to counter shearing forces, such as use of a transversely oriented (Pauwels) screw to compress the fracture or a fixed-angle device.
The femoral neck fracture should be prioritized in this scenario. This does not necessarily mean that the femoral neck should be repaired first, but the strategy should emphasize optimal fixation of the femoral neck. It has been demonstrated that this is less successful when using a single implant to repair both fractures. It is possible to place femoral neck fixation around an antegrade femoral nail; however, it is much more likely that optimal fixation will be achieved with shaft fixation that does not obstruct placement of fixation for the femoral neck.
AVN is more common among physiologically young patients after femoral neck fractures. The higher energy of injury is a likely contributor. Closed reduction has not been shown to increase the risk for AVN when an anatomic reduction is obtained. A surgical delay of 24 hours does not cause AVN. Patients with associated femoral shaft fractures are not at increased risk for AVN; in fact, some studies have shown a relatively lower rate of AVN when a femoral neck fracture is associated with a femoral shaft fracture.
RECOMMENDED READINGS
Liporace F, Gaines R, Collinge C, Haidukewych GJ. Results of internal fixation of Pauwels type-
3 vertical femoral neck fractures. J Bone Joint Surg Am. 2008 Aug;90(8):1654-9. doi: 10.2106/JBJS.G.01353. PubMed PMID: 18676894. View Abstract at PubMed
Bedi A, Karunakar MA, Caron T, Sanders RW, Haidukewych GJ. Accuracy of reduction of ipsilateral femoral neck and shaft fractures--an analysis of various internal fixation strategies. J Orthop Trauma. 2009 Apr;23(4):249-53. doi: 10.1097/BOT.0b013e3181a03675. PubMed PMID: 19318867. View Abstract at PubMed
Haidukewych GJ, Rothwell WS, Jacofsky DJ, Torchia ME, Berry DJ. Operative treatment of femoral neck fractures in patients between the ages of fifteen and fifty years. J Bone Joint Surg Am. 2004 Aug;86-A(8):1711-6. PubMed PMID: 15292419. View Abstract at PubMed Peljovich AE, Patterson BM. Ipsilateral femoral neck and shaft fractures. J Am Acad Orthop Surg. 1998 Mar-Apr;6(2):106-13. PubMed PMID: 9682073. View Abstract at PubMed
Upadhyay A, Jain P, Mishra P, Maini L, Gautum VK, Dhaon BK. Delayed internal fixation of fractures of the neck of the femur in young adults. A prospective, randomised study comparing closed and open reduction. J Bone Joint Surg Br. 2004 Sep;86(7):1035-40. PubMed PMID: 15446534. View Abstract at PubMed
RESPONSES FOR QUESTIONS 96 THROUGH 99
- Warfarin (Coumadin)
- Dabigatran (Pradaxa)
- Rivaroxaban (Xarelto)
- Apixaban (Eliquis)
Match the appropriate oral anticoagulant listed with the description.
This medication is a vitamin K antagonist and can be reversed.
- Warfarin (Coumadin)
- Dabigatran (Pradaxa)
- Rivaroxaban (Xarelto)
- Apixaban (Eliquis)
Question 33
Figure 19 shows an arthroscopic view from the anterior lateral portal of the knee looking into the suprapatella pouch. The use of an electrothermal device during this procedure most commonly causes significant postoperative complications by damaging which of the following structures?
Explanation
REFERENCES: Cash JD, Hughston JC: Treatment of acute patella dislocation. Am J Sports Med 1988;16:244-249.
Henry R, Goletz B, Williamson C: Lateral release in patello-femoral subluxation. Am J Sports Med 1986;14:121.
Question 34
- A 23 year old man has a minimally comminuted midshaft fracture of the femur with 2cm entrance and exit wounds as a result of a low-velocity gunshot. Definitive management should be
Explanation
Question 35
A 25-year-old athletic woman has a 16-week history of left lower-extremity radiating pain in an S1 distribution. MR images obtained by her family physician reveal a large L5-S1 paracentral disk herniation impinging on the left S1 nerve root. You suggest a left-sided L5-S1 microdiskectomy and tell her that when comparing tubular diskectomy and open procedures
Explanation
Several comparative studies have reported no difference in functional outcomes between tubular diskectomy and microsurgical lumbar diskectomy. A recent systematic review by Kamper and associates in which conventional microdiskectomy and minimally invasive approaches were compared revealed that there was no difference between the procedures in terms of clinical outcomes, complication risk, or rate of revision surgery.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis. Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183.View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
Question 36
A 67-year-old man who underwent humeral head arthroplasty for a four-part fracture 6 months ago reports that he is still unable to actively elevate his arm. Rehabilitation after surgery consisted of a sling with passive range-of-motion exercises for 2 weeks and then progressed to active-assisted and strengthening exercises at 3 weeks. Radiographs are shown in Figures 28a and 28b. What is the primary cause of his inability to elevate the arm?
Explanation
REFERENCES: Hartsock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humeral fractures. Orthop Clin North Am 1998;29:467-475.
Hughes M, Neer CS: Glenohumeral joint replacement and postoperative rehabilitation.
Phys Ther 1975;55:850-858.
Compito CA, Self EB, Bigliani LU: Arthroplasty and acute shoulder trauma. Clin Orthop 1994;307:27-36.
Question 37
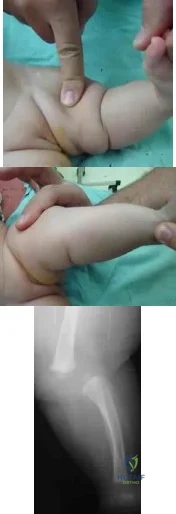
A mother brings in her 6-month-old infant with a knee deformity. The child had previously been treated with serial casting in flexion for 3 month at an outside facility. Examination reveals passive hyperextension to 25° and passive flexion to 15° as shown in Figures A and B respectively. A lateral radiograph of the knee is shown in Figure C. What is the most appropriate next step in treatment? Review Topic
Explanation
Congenital knee dislocation is rare. The etiology is thought to be quadriceps contracture. It is associated with developmental dysplasia of the hip (DDH) and clubfoot (CTEV). In newborn infant, casting or bracing with the knee in flexion
should be performed. If this fails, percutaneous or open VY quadricepsplasty, followed by above-knee casting, is indicated.
Abdelaziz et al. proposed a new grading system (Tarek CDK grading system-see Illustrations A and B) and treatment protocol as follows: (1) Serial casting for Grade 1 regardless of age and in neonates with grade 2 <1mth. If flexion to >90° is achieved within 4 weeks, then serial casting is continued; if range remains <90°, percutaneous quadriceps recession (PQR) is performed. (2) PQR is performed in Grade 2 CDK in infants >1 month of age upon presentation. (3) VY quadricepsplasty is indicated in patients with Grade 3 CDK or in recurrent cases.
Klingele et al. describe ACL shortening and reinforcement in 2 patients with congenital knee dislocation who developed ACL incompetence due to elongation. They conclude that stabilizing and reinforcing the ACL may prevent long-term anterior instability, hyperextension and recurrent deformity.
Figures A and B show the range of motion of the knee (25deg hyperextension to 15deg flexion). Figure C is a lateral radiograph showing congenital dislocation of the knee. Illustrations A and B show the Tarek grading system. Illustration C shows the different techniques of quadricepsplasty (upper row, structures divided and skin incisions used; lower row, how lengthening of the quadriceps mechanism is achieved). The most common PQR is the Roy-Crawford technique. The most common VYQ is the Curtis-Fisher technique.
Incorrect Answers:
Question 38
A 17-year-old boy who fell on a pitchfork in a barn 1 day ago now has a painful, swollen forearm. Examination reveals erythema, exquisite tenderness, and crepitus to palpation of the forearm. He has a pulse rate of 110/min and a blood pressure of 80/60 mm Hg. Radiographs show subcutaneous air and no fractures. Gram stain of wound drainage reveals a gram-positive bacillus. The next most appropriate step in management should consist of
Explanation
REFERENCES: Pellegrini VD, Evarts CM: Complications, in Rockwood CA Jr, Green DP (eds): Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, pp 365-370.
Gerding DN, Peterson LR: Infections caused by anaerobic bacteria, in Shulman ST, Phair JP, Peterson LR, Warren JR (eds): Infectious Diseases, ed 5. Philadelphia, PA, WB Saunders, 1997, pp 416-417.
Stephens DC: Myositis and fascitis, in Root RK (ed): Clinical Infectious Diseases, ed 1. Oxford, England, Oxford Press University, 1999, pp 769-770.
Question 39
Flexion-distraction injuries of the thoracolumbar spine are most frequently associated with injury to what organ system?
Explanation
REFERENCES: Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 351-360.
Inaba K, Kirkpatrick AW, Finkelstein J, et al: Blunt abdominal aortic trauma in association with thoracolumbar spine fractures. Injury 2001;32:201-207.
Question 40
A 46-year-old woman sustains an extra-articular fracture of the distal radius and undergoes open reduction and internal fixation with a volar plate and screw construct. During postoperative recovery from this injury, what benefit does formal physical therapy have as compared to a patient-guided home exercise program?

Explanation
The reference by Wakefield and McQueen is a randomized controlled trial of 96 patients, comparing formal hand physiotherapy to a home exercise regimen. There was no difference in grip strength, pronation/supination, radial/ulnar deviation, or hand function. The authors concluded that there were no significant benefits to formal physiotherapy.
The study by Souer et al is a level I study evaluating formal therapy and patient-guided exercise program for patients who underwent ORIF of a distal radius fracture with a volar plate and screw construct. This study showed a significant decrease in wrist ROM and grip strength with formal therapy. There were no differences in arm-specific disability (DASH score) at any time point.
Question 41
A 30-year-old man has had a 3-day history of severe, incapacitating lower back pain without radiation. He reports improvement with rest. He denies any history of trauma, has no constitutional symptoms, and his neurologic examination is normal. What is the best course of action?
Explanation
REFERENCE: Deyo RA, Diehl AK, Rosenthal M: How many days of bed rest for acute low back pain? A randomized clinical trial. N Engl J Med 1986;315:1064-1070.
Question 42
A healthy 64-year-old man just underwent an uncomplicated shoulder arthroplasty for severe glenohumeral osteoarthritis. Intraoperatively, 60 degrees of external rotation was obtained. Postoperatively, he starts on a range-of-motion program. What limitations are recommended? Review Topic
Explanation
surgery. Restriction from external rotation stretching for even 3 weeks would compromise his ultimate functional recovery.
Question 43
An 80-year-old African American woman who lives in a large city is scheduled for total hip arthroplasty to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
Explanation
Demographic factors are associated with increased risk for MRSA colonization, so it is important to identify vulnerable patients. Female gender and advanced age reduce the risk for colonization, whereas African American race increases this risk. Urban environments do not influence MRSA colonization.
Question 44
An 18-year-old collegiate football player injures his right shoulder during a tackle. He reports pain and numbness in the shoulder and numbness radiating to his fingers. His symptoms improve within 15 minutes and he has no residual symptoms. This condition is best known as
Explanation
REFERENCES: Safran MR: Nerve injury about the shoulder in athletes. Part 2: Long thoracic nerve, spinal accessory nerve, burners/stingers, thoracic outlet syndrome. Am J Sports Med 2004;32:1063-1076. Aval SM, Durand P Jr, Shankwiler JA: Neurovascular injuries to the athlete’s shoulder: Part I. J Am Acad Orthop Surg 2007;15:249-256.
Question 45
A 19-year-old man has had back pain with activity, especially running in soccer and baseball, for the past 4 months. He denies any history of trauma. Examination reveals no motor weakness or sensory changes in the lower extremities. Range of motion shows increased pain with extension and mild limitation with flexion. A sitting straight leg raising test is limited at approximately 60 degrees bilaterally by back and buttocks pain. Plain radiographs are normal. MRI scans are shown in Figures 13a through 13e. What is the most likely diagnosis?
Explanation
REFERENCES: Wiltse LL, Rothman SL: Spondylolisthesis: Classification, diagnosis and natural history. Sem Spine Surg 1993;5:264-280.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 129-137.
Question 46
In the evaluation of somatosensory-evoked potential waveforms for intraoperative neuromonitoring for spinal surgery, the minimum criteria for determining potentially significant changes include Review Topic
Explanation
Question 47
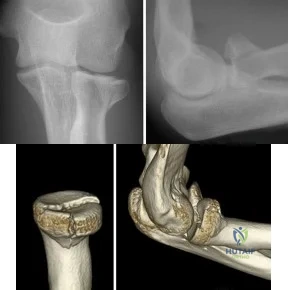
A 25-year-old woman sustains a fall on an outstretched hand. She complains of elbow pain. Examination reveals tenderness over the lateral elbow and pain on elbow motion. Injury radiographs and CT scans are shown in Figures A and B, respectively. What is the next best step?
Explanation
Non-/minimally displaced radial head fractures without a block to rotation can be managed nonoperatively. Complete articular fractures with >=3 fragments do better with radial head replacement. Indications for ORIF include large articular surface fragments, > 2 mm of displacement, mechanical block to forearm rotation, or associated fractures or ligament injuries requiring surgery.
Pike et al. retrospectively compared patients undergoing ORIF for isolated radial head fractures with radial fractures associated with other fractures/dislocations. They found no differences in pain/disability and complications or secondary capsular release between groups.
Yoon et al. retrospectively compared isolated partial articular displaced (2-5mm) radial head fractures treated nonoperatively vs ORIF. They found no clinical benefit with ORIF compared to non-operative management. The ORIF group had more complications. Younger patient age and larger fracture displacement favored operative intervention. Younger patients fared worse.
Figures A and B are radiographs and 3D reformatted CT images showing a displaced partial articular radial head fracture.
Incorrect Answers:
>= 3 fragments.
Question 48
Which factor is a contraindication to surgical treatment of a symptomatic CAM deformity?
Explanation
Multiple studies have confirmed that CAM or pincer anatomy is commonly present in asymptomatic hips. According to a large systematic review, CAM deformities are present in approximately one-third of asymptomatic hips in young adults, and the proportion was higher than 50% in the subgroup of athletes.
Ganz and associates proposed that femoral acetabular impingement is the root cause of osteoarthritis in the majority of nontraumatic, nondysplastic hips, and functional improvement with surgical correction of the deformity has been demonstrated. Despite the link between CAM deformity and hip osteoarthritis, a corresponding link between correction of the deformity and prevention of osteoarthritis has never been proven.
Results of CAM deformity correction, typically including repair of the degenerative labral tear, are much poorer when there is significant joint space loss. A typical joint space cutoff of 2 mm or less is used to recommend against hip preservation surgery.
Question 49
Alpha fetoprotein (AFP) can be seen in many cancers, but is most commonly seen in hepatocellular carcinomas.
Explanation
aspirated from the inflamed joint. Patients with gout may also have tophaceous deposits within the skin or bursae of the extremities. Elevated urine pH, serum uric acid, and serum phosphate can all be associated with numerous conditions and are not specific to gout. Calcium pyrophosphate crystals are associated with chondrocalcinosis (pseudogout).
A 72-year-old woman is evaluated for sacrococcygeal pain sustained after a twisting injury. Radiographic and MRI evaluation confirms the presence of a nondisplaced fracture at the sacrococcygeal junction. Over a 3-week period, the pain has gotten significantly better. No additional lesions or injuries are noted.
Laboratory studies show a serum calcium level of 8.8 mg/dL (normal 8.6-10.3 mg/dL) and a 25-OH Vitamin D level of 14 ng/mL (normal
80 ng/mL). What is the most appropriate treatment for this patient?
Expectant observation
Calcium supplementation
High dose vitamin D supplementation
Bisphosphonate therapy
Surgical fixation of the sacrococcygeal fracture
Chronic Vitamin D deficiency leads to problems with bone health and has been shown to increase the risk of falls in the elderly. Appropriate supplementation of Vitamin D has been shown to decrease this risk. Conversion in the skin decreases with age and may be nearly nonexistent in darkly pigmented individuals. Vitamin D3 is the preferred form for supplementation, but D2 is the form most available by prescription in the US. Hypervitaminosis D is rare and very high doses can be tolerated without significant concern for toxicity. Because the patient has sustained one insufficiency fracture, she is at risk for insufficiency fractures in other skeletal locations, rendering expectant observation insufficient. Her serum calcium is normal, and with a low Vitamin
D level, calcium utilization in her system would be inadequate. Bisphosphonate therapy in addition to calcium and vitamin D supplementation may provide a good long-term solution, but should not be instituted until the bone mineral imbalance has been adequately corrected. Surgical fixation of this fracture is not indicated, particularly in lieu of improving symptoms.
Figures 70a and 70b show the radiograph and MRI scan of a 66- year-old man who has fatigue, weight loss, and muscle weakness. Examination reveals marked pain and discomfort in the left mid leg. Biopsy specimens are shown in Figures 70c and 70d. What is the most likely diagnosis?
Mastocytosis
Multiple myeloma
Hyperparathyroidism
Metastatic carcinoma
Multicentric giant cell tumor
The signs and symptoms of hyperparathyroidism are similar to those in patients with diffuse skeletal metastases. Serum markers are very helpful in making the diagnosis. In this patient, the radiograph shows multiple lesions in the tibia and proximal fibula that have a variable appearance. For example the mid-tibial lesion is radiolucent and slightly expansile whereas the more proximal tibial lesions are radiodense. The proximal fibula lesion is mixed (radiolucent/radiodense). These findings would be very uncommon in patients with myeloma, metastatic disease, or multicentric giant cell tumor. The histopathology shows a bland fibrous stroma with multiple multinucleated
giant cells. On higher power, the stromal cells are spindled and the giant cells are relatively small in contrast to giant cell tumor where the giant cells are larger and the stromal cells are more rounded with nuclei that closely resemble those in the giant cells.
There is blood extravasation (stromal
hemorrhage) and hemosiderin deposition. The constellation of findings is most consistent with brown tumors due to hyperparathyroidism (secondary to a parathyroid adenoma in this patient).
A 68-year-old woman has had progressive pain in the right thigh for the past several months. She has a history of hypertension, treated with hydrochlorothiazide and osteoporosis treated with alendronate
for 10 years. At this point, she is virtually wheelchair bound.
Radiographs are shown in Figures 78a and 78b. Additional studies show no signs of systemic disease. What is the most likely etiology of her condition?
Prolonged use of bisphosphonates
Use of calcium-wasting diuretics
Occult metastatic cancer
Vitamin D-resistant rickets
Disuse osteopenia
The patient has been on alendronate for 10 years and has evidence of a proximal diaphyseal fatigue fracture. These have been associated with long- term use of bisphosphonates. Staging studies have failed to show systemic disease, and while metastasis with an unidentifiable primary does occur, it would be unlikely to present with this radiographic appearance, now recognized to be classic for stress fractures associated with chronic bisphosphonate usage. Hydrochlorothiazide does not cause calcium wasting. Vitamin D-resistant rickets would be a long-standing event and would present much earlier in life, often with pronounced deformities. Whereas the patient's progression to intolerance of weight bearing likely has led to some degree of disuse osteopenia, the underlying problem is the long-term bisphosphonate exposure.
A surgeon recommends an interscalene regional block to a patient undergoing shoulder arthroscopy. When asked about potential complications, which of the following is most likely to occur?
Persistent motor neuropathy
Sensory neuropathy
Complex regional pain syndrome
Pneumothorax
Cardiac arrythmia and arrest
Sensory neuropathy is the most common complication seen with interscalene regional block.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Bishop et al. retrospectively reviewed 478 patients who had shoulder surgery under interscalene regional block. A total of 462 patients (97%) had a successful block. While all of the answers have been described, in this study no patient had a seizure, pneumothorax, cardiac event, or other major complication. Twelve (2.3%) of the 512 patients who had a block had minor complications, which included sensory neuropathy in eleven patients and a complex regional pain syndrome that resolved at three months in one patient. For ten of the eleven patients, the neuropathy had resolved by six months.
Cathepsin K is an enzyme produced by osteoclasts. What is the function of cathepsin K?
Reduction of disulfide bonds in the extracellular matrix
Bone resorption
Activation of RANK (Receptor activator of nuclear factor kappa-B)
Antagonize the action of RANK
Absorb water in the extracellular matrix
Cathepsin K is an enzyme produced and released by osteoclasts at the ruffled border that functions to resorb bone. Cathepsin K inhibitors are being clinically evaluated as potential anti-resorptive drugs for use in osteoporosis treatment. Other proteins associated with osteoclasts include tartrate-resistant acid phosphatase (TRAP) and calcitonin receptor.
Illustration A is a drawing that depicts the action of cathepsin k within osteoclasts.
What is the primary problem in rickets osteomalacia?
Defect in the zone of proliferation within the physis
Defect in type I collagen
Defect in the ext-1 gene
Low level of calcium
Production of dysplastic fibrous bone
Rickets is a disorder of bones in children that results from decreased calcium available in the blood resulting in poor mineralization of bone that can lead to fractures and deformity. The most common cause of rickets is from vitamin D deficiency but it can also be caused by poor nutrition or gastrointestinal
disease that results in poor calcium absorption such as celiac disease or severe diarrhea from other causes. Rickets is not primarily a physeal disorder. Osteogenesis imperfecta is caused by a defect in type I collagen. A defect in
the ext-1 gene is often seen in patients with multiple hereditary exostoses. Fibrous dysplasia also can result in bone deformity and fractures due to production of dysplastic fibrous bone but is not caused by calcium or vitamin D deficiency.
If an orthopaedic surgeon receives royalties from a company for his or her participation in the design and development of a product, and uses that same product for the care of his or her patients, what is the orthopaedic surgeon's obligation?
Obligated to disclose only the fact that he or she was involved in the design and development
Obligated to disclose only the company relationship if there is a state law requiring it
Obligated to disclose his or her full relationship with the company, including the fact that he or she receives royalties
No obligation to disclose this private matter to the patient
Avoid this situation because it should not exist since he or she cannot use such a product
The AAOS has a specific code of ethics and professionalism that addresses this issue: "When an orthopaedic surgeon receives anything of value, including royalties, from a manufacturer, the orthopaedic surgeon must disclose this fact to the patient." It is derived from a broader document developed by the American Medical Association, and is applicable to all physicians. At present, this is an ethical issue receiving greater federal scrutiny. This issue has had a greater effect on the public's perception of the integrity of the orthopaedic profession.
A minimally invasive plate osteosynthesis is seen in Figure 15. The resultant fracture healing can best be attributed to a fixation construct that was
stiff and stable.
flexible and stable.
facilitating direct osteonal healing.
inhibitory to endochondral ossification.
stimulatory to intramembranous ossification.
Locked plating constructs with long-working lengths provide flexible but stable constructs that promote (not inhibit) endochondral ossification. Because of the longer working length they are not stiff, and these fractures do not heal with intramembranous ossification which occurs in bones like the calvarium. Direct osteonal healing is usually seen with constructs
where absolute stability is achieved through interfragmentary compression, unlike in this case.
An orthopaedic surgeon makes an incision on a right knee and realizes that the patient was supposed to have a left total knee arthroplasty. The surgeon should do which of the following?
Leave the wound open and talk to the family immediately.
Close the wound, abort the surgery, and talk to the patient and family when the patient is awake.
Close the wound, complete the left knee arthroplasty, and talk to the family after the surgery is complete.
Complete the surgery and talk directly to the patient the following day on rounds.
Discuss the problem in the office the next week in a calm reassuring manner.
The AAOS recommendation is to complete the correct surgery, repair the incorrect surgery to as close to normal as possible, and then discuss it openly with the family after the surgery is complete. Prompt informing is necessary. Aborting the surgery then results in the patient requiring a second anesthesia and surgical time needlessly.
Spindled cells that are surrounded in mature osteoid that
connect to other similar cells via canaliculi are best described as which of the following?
Osteoblasts
Osteoclasts
Osteocytes
Histiocytes
Megakaryocytes
Osteocyte cell processes travel through canaliculi to interconnect with other osteocytes and cells on the bone surfaces. Osteoblasts are cells that produce bone matrix and are seen rimming immature bone. Osteoclasts are large multinucleated cells that resorb bone and are found in Howship's lacunae. Megakaryocytes and histiocytes are found in marrow but not mature bone cortex.
A 48-year-old woman has an open subtrochanteric femur fracture. No other injuries are reported. After thorough evaluation, it is determined that she will need emergent surgical fixation. The patient and family indicate that they are practicing Jehovah's witnesses and desire adherence to the religious standards with respect to blood product usage. The patient signs a valid advanced directive confirming these wishes. Which of the following would be considered acceptable treatment?
Whole blood
Platelets
Plasma
Starch product (ie, Hetastarch, Hespan)
Donor-directed blood from a family member who is a practicing Jehovah's witness
Jehovah's witnesses beliefs regarding blood products stems from direct interpretation of passages from the bible. The use of crystalloid, starch products such as Hetastarch and colloids are accepted. Typically Jehovah's witnesses will accept most medical treatment but refrain from the use of blood products including whole blood, packed red cells, platelets, white cells, or plasma. Any autologous transfusion, whether from the patient themself or donor directed, is forbidden. The use of cell-saver type processes is a matter of individual choice by the patient. The use of hemoglobin-based oxygen carriers are now accepted by many patients but it is important to respect the wishes of each individual patient. It is very important to discuss preoperatively with the patient and family their wishes and thoughts on what is acceptable to use. Many facilities have adopted
bloodless-surgery protocols and committees that definitively outline the measures that can be used and take into consideration the many ethical issues involved in taking care of these patients.
In a diagnostic test, the proportion of individuals who are truly free of a designated disorder identified by the test is known as
specificity.
sensitivity.
accuracy.
positive predictive value.
negative predictive value.
Specificity refers to the proportion of individuals who are truly free of the designated disorder who are so identified by the test. Sensitivity refers to the proportion of individuals who truly have the disorder who are so identified by the test. Positive predictive value refers to the proportion of individuals with a positive test who have the disorder. Negative predictive value refers to the proportion of individuals with a negative test who are free of the disorder.
Accuracy is the overall ability to identify patients with the disorder (true positives) and without the disorder (true negatives) in the study population.
An orthopaedic surgeon in his first year of practice is negotiating with a private for-profit hospital to be their employed trauma specialist. The state of employment is known to have a high rate of malpractice claims because of a favorable plaintiff legal environment. During the course of negotiations, malpractice insurance is being discussed. The surgeon should ask the hospital to provide which type of malpractice insurance policy?
Claims made with "nose" coverage
Claims made without tail coverage
No policy because of employed status and sovereign immunity
Occurrence coverage
Occurrence coverage with "nose" coverage
An occurrence policy provides coverage for all claims made during employment irrespective of when it is filed (during or postemployment) and therefore is the best option. Claims made policy only covers suits for the time employed. A prepurchased "tail" is needed to provide coverage for cases that occurred during employment but filed postemployment. Nose coverage is applicable if the surgeon was previously employed and did not have tail coverage from previous employment, but this surgeon just emerged from training where it is not applicable. Claims made without tail coverage is unwise because the surgeon would be unprotected or have to purchase his own policy postemployment.
Only in certain situations does sovereign immunity exist, and generally not in a for-profit system. Occurrence coverage with nose coverage
is incorrect because it does not apply to this surgeon with no previous employment or claims policy lacking tail coverage.
Results of a study demonstrating no difference between treatments when a difference truly exists is an example of which of the following?
Statistical insignificance
Type I error
Type II error
Fragile p-values
Negative predictive value
A type II error (also known as a beta error) occurs when results demonstrate that two groups are similar when, in reality, they are different (with regard to the statistic being measured). Type I errors show that a difference exists when, in reality, no difference exists. A statistically insignificant result may lead an investigator to conclude that no difference exists between two groups; this may be correct (and therefore not a type II error). The concept of
fragile p-values is that small sample sizes may result in wide variability of p- values with only one change in a data point for a given group. This singular change could be a chance occurrence, but it still can affect the statistical significance of the outcomes analysis.Fragility of p-values is limited by increasing sample sizes. Negative predictive value is the
proportion of patients with negative test results who are correctly diagnosed.
A patient with a transverse femur fracture undergoes statically locked antegrade intramedullary nailing. Postoperatively, the patient appears to have a rotational deformity of greater than 25 degrees. The surgeon informs the patient, who chooses to undergo corrective treatment with removal of distal interlocking screws, rotational correction, and relocking of the screws. The patient goes on to heal
but has persistent hip pain and a limp that does not improve completely after extensive rehabilitation. There is complete healing, no evidence of infection, no hardware issues, no ectopic bone, and rotational studies indicate less than 2 degrees of malrotation. Functional capacity testing reveals the affected abductor and quadriceps function to be about 85% of the uninjured side and the patient returns to work and most of his recreational activities except rock climbing. Two days before the statute of limitations, the patient
files a malpractice suit alleging negligence of surgery, loss of function, consortium, and pain and suffering due to the surgeon's efforts. What action should the surgeon and the defense team take?
Settle the case because the surgeon made an error that resulted in unnecessary surgery, and thus the case is indefensible.
Settle the case because they are likely to lose the case, and it would be cheaper to settle than to defend.
Defend the case alleging that there was no error, and no damages, and that the patient is malingering.
Defend the case because despite there being an error, the error was corrected and there were little or no damages compared with expected outcomes.
Contact the patient directly to discuss why he is suing and attempt an amicable resolution.
To establish negligence, certain criteria must be met. 1) A duty was owed by the surgeon (in this case, yes, a relationship was established). 2) The duty was breached, where the provider failed to meet the standard of care (there
was a technical error, but it was corrected). 3) The breach caused an injury. In this case, the patient had an outcome that was very acceptable, as
documented with outcome studies, for femur fractures. Also, the rotational error and locking distally would have had little impact on the hip, whereas antegrade nailing itself is expected to result in some objective impairment of the hip in some patients. 4) Damages were incurred as a result. In this case, the patient returned to work and could not rock climb which could be reasonably expected with a femur fracture in some patients, and cannot be causally linked to the corrective surgery. For all practical purposes, the patient had a very acceptable outcome. Thus, settling the case for an error would be rather permissive and the important issue is that the surgeon recognized the problem, addressed it, and fulfilled his or her postoperative responsibility. The case is very defendable, and thus it is unlikely to be lost. Defending the case and alleging no error is incorrect because there was an error. The surgeon should never function outside of his or her legal counsel once a suit is filed.
You design a research study in which you ask patients who have a nonunion of the tibia to fill out a questionnaire in which they report on a variety of medical conditions and social/behavioral practices. You compare these findings to a similar group who did not develop a nonunion in order to identify medical and/or social conditions that might be risk factors for the development of tibial nonunions. This would be an example of what type of study?
Case series
Meta-analysis
Case control study
Retrospective cohort study
Prospective cohort study
A case control series starts with the occurrence of a specific disease or observation, and then compares data on those individuals to a similar group without the disease (control group) in order to identify potential risk factors for the development of the disorder. A case series is an observational study in which an investigator follows a series of patients who received a specific treatment, recording the results and outcomes of that treatment. A meta- analysis is the combination of several separate studies that look at similar hypotheses in an effort to create a larger patient population for analysis. A cohort study looks for the incidence of a specific outcome in two groups (cohorts) of patients who are similar with the exception of a particular
research variable (risk factor).
Which gene or protein is the most specific marker of mature osteoblasts but is not expressed by immature, proliferating osteoblasts?
Osteocalcin
TGF-B
COLIIA1
cFOS
IL-1
Osteocalcin is the most specific marker of the osteoblast phenotype and is expressed only in mature osteoblasts. TGF-B is a growth factor involved in the differentiation of multiple cell lines. For bone, TGF-B plays a role in stem cell differentiation into mesenchymal stem cells along osteoblast pathways. COLIIA1 is the gene for Type II Collagen and is involved in chondrocyte differentiation. cFOS is involved in osteoclast differentiation. In regards to
bone metabolism, IL-1 stimualtes osteoclastic bone resorption.
A workers' compensation carrier for a local manufacturing company requests a second opinion on a 59-year-old man who sustained a crush injury to his foot and leg at work 6 months ago. His leg and foot were pinned between a forklift and a wall when an employee he was supervising lost control of the forklift. The employer
suspects that the injured worker is malingering because the treating physician released him to work, but he has not returned to work. Which of the following elements of your history will best help you determine that the injured worker does not want to return to work out of fear of a confrontation with the employee he was supervising?
Formality
Empathy
Yes-no questions
Taking copious notes
Sitting leaning back in a chair
Empathy during the interview demonstrates compassion and earns the patient's trust; which, in turn, enables the patient to discuss any agenda or concerns he or she may otherwise feel uncomfortable revealing. It is also important to engage the patient to establish a trusting relationship and thus understand all the factors impacting the patient. A formal attitude toward the patient makes it difficult to engage the patient to be "drawn in." An engaged patient is more comfortable, reliable, and thorough when providing a history. Closed-end, yes-no questions do not allow the patient to detail all of the subtle nuances of their condition and its effect on their life. Taking copious notes likewise prevents engagement of the patient and the distraction of taking
notes may cause the physician to miss an important detail. It is better to lean forward in a chair when interviewing a patient because this suggests the physician is genuinely interested, whereas leaning back in a chair suggests the physician is simply waiting for the patient to finish talking. Avoid interrupting the patient when talking.
When a Workers' Compensation patient recovers after an injury to a point that further restoration of function is no longer anticipated, he or she is said to have reached which of the following?
Functional capacity
Maximum medical improvement
Permanent disability
Impairment rating
Predesignation
This is the definition of maximum medical improvement (MMI). The patient has essentially reached the plateau of his improvement.
Functional capacity evaluations (FCE) are based upon a theoretical model of comparing job demands to worker capabilities. The results of FCEs are often used to determine musculoskeletal capacity to return to work.
Strong et al. reported on the use of FCE in the Workers' Compensation system, and note how these FCE results are required by employers to determine the level of return to work of their employees. They also mention that the reports are frequently perceived with a negative tone. The employees reported a wider range of restrictions in their varied life roles than did the FCE reports, which deal more narrowly with work roles.
Pransky et al. reported that although FCE's are relied upon for determination of ability to perform physical work, several scientific, legal, and practical concerns persist. They note that test criteria often do not accurately reflect real-life job requirements or performance, and subjective evaluation remains common. They conclude that more research into predictive linking of FCE outcomes with occupational outcomes is necessary to determine their role in the Workers' Compensation system.
Incorrect Answers:
1: A functional capacity evaluation (FCE) is set of tests, practices and observations that are combined to determine the ability of the evaluated to function in a variety of circumstances (most often employment) in an objective manner.
3: Permanent disability is any lasting disability that results in a reduced earning capacity after maximum medical improvement is reached; this implies that MMI must be reached before this is determined.
4: Impairment rating is an objective data point obtained by a physician reviewing the patient's overall condition during a functional capacity evaluation.
5: This is the process a patient uses to tell their employer they want a personal physician to treat them for a work injury.
A physician receives a summons that he is being sued. The first step should be to
call the patient and apologize.
notify the medical liability carrier.
contact an attorney with whom the physician is familiar with and have the attorney review the records.
be sure to discard any handwritten phone messages because they are not discoverable.
find a colleague with a similar subspecialty and have the colleague review the record before doing anything.
The most appropriate first step is to notify the medical liability carrier. The medical liability carrier will assign an attorney who is likely to be more appropriate. A review by a colleague may be requested by the defense attorney but that should be at their discretion. Patient apology is appropriate early on when and if you discover an error.
Records should be reviewed, but never altered.
Currently, what is the most common clinical study type in the orthopaedic literature?
Level 1 (prospective, randomized trial)
Level 2 (cohort trial)
Level 3 (retrospective case control)
Level 4 (retrospective case series)
Level 5 (expert opinion)
Although a recent push for prospective, randomized trials has been advocated by multiple orthopaedic journals, many studies published continue to be of Level 4 evidence (retrospective case series). Case series represented 64% of all studies reviewed by Freedman and associates in 2001 from the British and American volumes of Journal of Bone and Joint Surgery and from Clinical Orthopaedics and Related Research.
Obremskey and associates published that
Question 50
A 57-year-old man has had a 2-week history of neck pain. He has no history of radiating symptoms, and has no complaints of numbness or paresthesias. There was no trauma associated with the onset of the pain. Figure 26 shows the MRI scan initially obtained by his family physician. What should the patient be told regarding the prevalence of the MRI findings in his age group? Review Topic

Explanation
Question 51
Preoperative chemotherapy and wide excision Tumoral calcinosis is a heritable condition that is characterized by periarticular metastatic calcification. Most patients are black, and the inheritance is usually autosomal recessive. Metastatic calcifications occur around joints and in the skin, marrow, teeth, and blood vessels. The periarticular masses may grow quite large and are attached to the fascia, but they are extra-articular. The masses may occur at the shoulder, hip, and elbow. Radiographically: The masses are composed of heavy, amorphous calcification in nodules. Laboratory:
Explanation
A 20-year-old woman has a large mass over the right hip. An anteroposterior and oblique radiographs are shown in Slides 1 and
Question 52
below depict the radiographs obtained from a year-old woman with a painful total knee arthroplasty. She describes an uneventful recovery with no wound-healing issues and was pain free for the first 10 years. Although reporting no trauma or inciting event, she now describes pain in the entire knee that is most severe with her first few steps. She has begun to notice night pain and, more recently, constant swelling. What is the most appropriate work-up at this time?
Explanation
An evaluation of the painful total knee must be supported by an understanding of the potential etiologies of pain. They may include, aseptic loosening, infection, osteolysis, gap imbalance, referred pain, stiffness, and complex regional pain syndrome. In this case, the patient demonstrates start-up pain and had no prior history of infections. Her radiographs show subsidence of the tibia, indicating a loose prosthesis. Knowing that the prosthesis is already loose precludes the need for a bone scan. It is, however, important to rule out infection in this case; therefore, CRP and ESR testing is essential. Aspiration is also recommended when going into knee arthroplasty, and infection is a concern.
Question 53
A 12-year-old boy sustained a grade III open tibial fracture 1 week ago and underwent multiple debridements and fracture fixation. He now has a soft-tissue defect that measures 6 cm × 6 cm, with an area of exposed bone and muscle on the distal medial leg that is a few centimeters proximal to the ankle. Management of the soft-tissue defect should now consist of
Explanation
A free flap and skin graft would be required for closure. VAC is very effective in soft-tissue defects such as this one. Healthy granulation tissues form quickly. VAC can be the definitive treatment, or it can be used before skin grafting. Wet-to-dry dressings could promote granulation, but the process is hastened substantially by VAC. Amputation is not a consideration because there are no signs of infection or fracture healing problems at this time.
REFERENCES: Mooney JF III, Argenta LC, Marks MW, et al: Treatment of soft tissue defects in pediatric patients using the V.A.C. system. Clin Orthop 2000;376:26-31.
Caniano DA, Ruth B, Teich S: Wound management with vacuum-assisted closure: Experience in 51 pediatric patients. J Pediatr Surg 2005;40:128-132.
Question 54
In a statement put forth by AAOS, the role of the orthopaedic surgeon in the face of domestic and family abuse includes all of the following EXCEPT: Review Topic
Explanation
The statement put forth by the AAOS implores the orthopaedic surgeon to be aware of the integral components to identify, document, and care for minors, elders, and/or partners who are victims of domestic abuse.
Zilmer et al. in a JAAOS review and the basis for the AAOS statement emphasizes the ability to identify abuse, which includes, but is not limited to frequent/multiple injuries, temporal abnormalities in multiple injuries, frequent visits/utilization of the emergency department, and/or unusual injuries/fracture patterns not consistent with the clinical picture. Meticulous documentation is of paramount importance, in addition to communicating your concerns to the appropriate emergency department personnel.
Incorrect answers:
Question 55
-An athletic 30-year-old sustained multiple injuries in a high-speed motor vehicle collision that resulted in a loss of approximately 30% of blood volume. On arrival to the emergency department, the heart rate is100 and blood pressure is 104/62. The best means with which to evaluate true hemodynamic status is
Explanation
Question 56
An otherwise healthy 45-year-old woman reports the onset of severe right leg pain. Figure 20a shows an axial MRI scan of the L4-5 level, and Figure 20b shows a sagittal view with the arrow at the L4-5 level. What nerve root is the most likely source of her pain?
Explanation
REFERENCES: McCulloch JA: Microdiscectomy, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 2, pp 1765-1783.
Hodges SD, Humphreys SC, Eck JC, Covington LA: The surgical treatment of far lateral L3-L4 and L4-L5 disc herniations: A modified technique and outcomes analysis of 25 patients. Spine 1999;24:1243-1246.
Question 57
They used three outcome tools, SF-36, WOMAC, and Modified Boston Children's Hospital Grading System to evaluate the the two groups at a minimum of 2 years from injury. The foot injury group, including all types of foot fractures, had a poor outcome when using any of these measures. Turchin concludes that “Foot injuries cause significant disability to multiply injured patients. More attention should be given to these injuries, and more
Explanation
Excessive bleeding into joints and muscles is a common manifestation of hemophilia. The iliacus muscle is a frequent site of hemorrhage in patients with severe or moderate hemophilia. Intramuscular hematoma of the iliacus muscle is likely to occur following play or sporting events that include forceful contraction of the hip flexor muscles. As the hematoma expands, it may
compress the adjacent femoral nerve, potentially resulting in complete femoral nerve palsy. Femoral nerve compression typically includes paresthesias in the distribution of the terminal saphenous nerve branch.
Gilbert et al. review the complex relationship between recurrent bleeding, synovitis, and the development of arthritis in the patient with hemophilia. They discuss both conservative and surgical treatment modalities in these patients and recommend arthroscopic synovectomy for the knee and ankle joints. They conclude that the greatest risk to these procedures is a decreased range of motion.
Kuo et al. reports on a fourteen-year-old healthy boy with an 11-day history of pain and weakness in the right lower limb following a fall. They report pain in the right lower extremity, numbness of the anterior aspect of the right thigh and medial border of the right leg and foot, inability to ambulate and
weakened quadriceps muscle strength. MRI revealed an iliacus hematoma with a complete femoral nerve palsy. He underwent CT-guided percutaneous drainage for decompression with complete resolution of the palsy.
Illustration A is a diagram of dermatomal distribution. Illustration B shows the lumbar plexus demonstrating the intimate relationship of the femoral nerve to the iliacus muscle.
Incorrect Answers:
A 45-year-old male trauma patient presents with multiple extremity injuries including the foot injury shown in Figure A. The foot fracture is treated surgically, and heals without any initial complications. At a minimum of 12 months, this patient will be expected to have which of the following scores compared to a
Patients with pauciarticular juvenile rheumatoid arthritis (JRA), specifically the subgroup with elevated antinuclear antibody (ANA) titers, are associated with the highest incidence (~75%) of anterior uveitis. As a result, referral for an ophthalmology consultation is recommended.
Pauciarticular JRA is the most common subgroup of JRA and typically presents between the ages of 2 to 4 years with mild swelling of one to four joints. The diagnosis is typically one of exclusion as laboratory studies, including erythrocyte sedimentation rate and rheumatoid factor, are usually within normal limits. In JRA, iridocyclitis, a type of anterior uveitis typically occurs following the onset of synovitis but may precede the joint symptoms. This iridocyclitis is frequently indolent but requires immediate ophthalmologic consultation for a slit-lamp examination because if left untreated, anterior uveitis may progress to loss of vision.
Foeldavri et al. review JRA anterior uveitis. They report an overall incidence of
10%, but this is dependent on the JRA subtype. They noted that a large proportion of children with JRA develop uveitis in the first year of disease and
90% after 4 years. They state that early age of JRA onset, oligoarticular subtype, and ANA reactivity are the main risk factors for the development of uveitis. They conclude that JRA-associated uveitis is important to recognize and treat early to prevent any visual damage.
Hawkins et al. review bilateral chronic anterior uveitis in JRA. They report that female gender, oligoarthritis, and presence of antinuclear antibodies are risk factors.
They report on treatment options, including the use of biologics. They conclude that stepwise immunomodulatory therapy is indicated, with new biologic drugs being used in cases of refractory uveitis.
Incorrect Answers:
Anterior 4: Pompe disease is a glycogen storage disease which may lead to ptosis (drooping of the upper eyelid), not anterior uveitis
A 9-year-old male with hemophilia A presents with severe groin pain, parasthesias over the medial aspect of the distal tibia, and difficulty ambulating several hours after a soccer game. He is believed to have an intramuscular hematoma surrounding the iliacus muscle. Which nerve is MOST likely to be compressed?
Which of the following conditions places the patient at highest risk for anterior uveitis and necessitates referral to an ophthalmologist?
Salmonella is a classic cause of osteomyelitis in patients with sickle cell disease.
Sickle cell disease is a genetic disorder of hemoglobin synthesis. The disease occurs in two phenotypes: sickle cell anemia (most severe) and sickle cell trait (most common). The two most common causes of osteomyelitis in children with sickle cell disease are
Staphylococcus aureus and Salmonella. Although S. aureus is the most common cause of osteomyelitis in the general population, the literature varies on which is the most common in patients with sickle cell disease. The increased risk in these patients may be associated with gastrointestinal microinfarcts, poor circulation of blood in bone, and splenic infarcts that predispose patients to infection by encapsulated bacteria (i.e., Salmonella).
Piehl et al. analyzed records of seven hundred seventeen patients with sickle cell disease treated over a thirteen-year period. They identified and retrospectively reviewed sixteen cases of osteomyelitis in fifteen patients. The authors found Salmonella to be the causative organism in thirteen cases with Proteus mirabilis, Escherichia coli, and Staphylococcus aureus all affecting one patient each. The authors report the annual incidence of osteomyelitis in their series as 0.36%.
Givner et al. reviewed sixty-eight cases of osteomyelitis in children with sickle cell disease and positive cultures over a ten year period. Of the sixty-eight, 50 (75%) yielded Salmonella and Staphylococci was isolated 7 (10%). In
addition, the authors report non-speciated gram-positive cocci were isolated in
11 (16%), non-speciated gram-negative rods in 5 (7%), and non-specified bacteria in 2 (3%). The authors conclude Salmonella is the most common pathogen causing osteomyelitis in patients with major sickle hemoglobinopathies.
Epps et al. reviewed fifteen patients with sickle cell disease and osteomyelitis. Staphylococcus aureus was isolated in eight cases (53%), Salmonella in six (40%), and Proteus mirabilis in one (7%). The authors conclude S. aureus, not Salmonella, may be the most common cause of osteomyelitis associated in patients with sickle-cell disease.
Figure A demonstrates an osteolytic lesion of the distal tibia and Figure F demonstrates sickle-shaped erythrocytes.
Incorrect Answers
Low toughness is a disadvantage of ceramic bearings in total hip arthroplasty.
Ceramic is a non-metal that demonstrates excellent wear characteristics when used with polyethylene in total hip arthroplasty. Although it has a high Young's modulus, it has a low fracture toughness. Subsequently, ceramic is poorly resistant to crack formation. In contrast, UHMWPE has a high fracture toughness because of the presence of very long hydrocarbon chains.
Santavirta et al. review alternative bearing materials to improve wear in total hip arthroplasty. Alumina ceramics are noted to be biostable and bioinert. The best wear properties are noted with ceramic-on-ceramic bearings. For current ceramic constructs, fracture risk is less than 1 per 1000.
Lang et al. review the use of ceramics in total hip replacement. The authors note that ceramic has high compressive strength and high wettability. Low fracture toughness and linear elastic behavior increase the risk of breakage of ceramic components under stress. Processing improvements, enhanced head- neck interfaces and liner modifications have lead to a decrease in the rate of ceramic fracture.
Illustration A shows a compromised ceramic head as a manifestation of the low fracture toughness of the material.
Incorrect Answers:
An 8-year-old African American female presents with lower extremity pain and subjective fever. On exam there is tenderness about the distal tibia. Further workup reveals elevated inflammatory markers and a lytic lesion (Figure A). An aspirate is obtained and cultures grow Salmonella. Additional investigation is most likely to reveal which of the following findings (Figure B-F)?
An ideal fluid film lubrication regime minimizes friction. A larger head size results in a greater development of full-film lubrication due to the increased relative sliding velocity of the larger bearing surfaces. Increased surface roughness inhibits the formation of the film lubrication. The most important factor influencing the predicted lubrication film thickness
has been found to be the radial clearance between the ball and the socket.
Jin et al report that slight clearance, not complete congruence, is optimal for formation of the optimal fluid film lubrication. They note that full fluid film lubrication may be achieved in these hard/hard bearings provided that the surface finish of the bearing surface and the radial clearance are chosen correctly and maintained.
Dumbleton reviewed the literature of metal-on-metal THA and concluded that the current literature does not show any clinical benefit of metal-on-metal compared to metal on poly. Metal-on-metal has been shown to have higher metal ion level in blood, and measurement of these levels is recommended to help identify those at risk of adverse effects from metal on metal prostheses.
Low toughness is a disadvantage of which of the following bearing surfaces used in total hip arthroplasty?
This attending did not fully disclose that the resident would be performing the cementing portions of the case unsupervised. This represents an ethically unsound scenario as the patient was misled regarding involvement of the resident in their surgery.
The informed consent process is grounded in the ethical principle of autonomy. Informed consent represents a shared decision making process where a
patient understands all the risks and benefits of a surgery fully and makes an informed decision. However, the patient's choice of surgeon is felt to be critical
to the informed consent process and any variation from that surgeon performing the surgery should be discussed explicitly. A surgeon who performs surgery or part of surgery on the patient without prior consent may be held liable for battery.
Kocher presents three cases demonstrating the spectrum of "ghost surgery". They state the substitution of an authorized surgeon with an unauthorized surgeon or allowing surgical trainees to operate without appropriate guidance constitutes "ghost surgery".
Deviation from what is explicitly discussed has been justified in an emergency scenario or if the treatment is aimed at an overall condition.
Bhattacharyya et al reviewed malpractice claims for factors that positively correlated with successful defense. They found that those who performed informed consent in the office had lower risk of malpractice payment. They conclude surgeons can decrease their risk of malpractice claims by performing informed consent in the office and documenting the discussion.
Incorrect Answers:
Which of the following features of metal-on-metal total hip arthroplasty does not allow for improved fluid film lubrication between the components?
The patient sustained a fragility fracture with lab work consistent with primary hyperparathyroidism.
Hyperparathyroidism is commonly caused by increased activity of the parathyroid glands resulting in high levels of PTH. Increased circulating levels of PTH leads to calcium being "sucked" out of bone and into the serum. This
alteration in calcium hemostasis leads to low-density bone and a predisposition to fragility type fractures. When present, lab values are much different from standard age-related osteoporosis. Furthermore, referral to medical and surgical endocrinology specialists for directed treatments may improve overall bone quality and prevent further fragility fractures.
Fraser summarizes primary and secondary hyperparathyroidism. He describes the normal physiologic response to low calcium of an increase in PTH. Increased PTH has three downstream effects of increased tubular resorption of calcium by the kidneys, increased osteoclast activity to harvest calcium from bone, and increased active vitamin D levels leading to increased bowel absorption of calcium.
Singhal et al. reviewed hyperparathyroidism and what the orthopedic surgeon should know. They state when a patient presents with a pathologic fracture and elevated serum calcium levels, an appropriate lab workup for hyperparathyroidism should be done. They stated when surgery is needed for hyperparathyroidism and fracture, surgery can safely be performed simultaneously as demonstrated by 3 case examples.
Figure A exhibits a left femoral neck fracture, which is a fragility fracture associated with poor bone density. Illustration A is a figure from Fraser's article exhibiting the
feedback loop from the hypothalamus, pituitary, adrenal/glandular axis.
Incorrect answers:
Prior to undergoing a total knee arthroplasty at an academic medical center a patient is told during informed consent by the attending surgeon that resident involvement in the case will be limited to retracting. During the case the attending is present up to trialing of the selected components. The surgeon leaves prior to cementing to start trialing components in another case while the chief resident remains alone in the room for the completion of the case. Which of the following is true regarding the ethics of this practice?
Patients in factorial randomized control trials (RCT) are assigned to groups that receive a specific combination of interventions and non-interventions.
In factorial RCTs, patients are randomized to groups receiving treatment A and B, treatment A or control, treatment B or control, or no treatment. This study design is useful because two interventions can be assessed with the same
study population and any interaction between the treatments can be determined (for example, does treatment A work differentially when combined with treatment B). Other randomized control trial designs include parallel, cluster, and crossover. Parallel studies are performed by having two or more groups that exclusively have one intervention without group overlap.
Crossover studies have each group receive each intervention in a random sequence. Cluster design studies have pre-existing groups of participants
(such as schools, or cities) that are randomly selected to receive or not receive an intervention.
Karlsson and the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine published an exhaustive guide to research for evidence-based medicine in a step-wise fashion. They cover levels of evidence, design for randomized control trials and the CONSORT checklist. They also describe proper study design of cohort, case- control, case series, systematic review, meta-analysis studies. The second half of the guide discusses appropriate outcome measures, statistical analyses, and data interpretation, reporting complications, and concludes with steps to writing a scientific article.
Incorrect Answers:
A 66-year-old woman falls from standing and sustains the injury shown in Figure A. Her most recent T score was -1.9, 3 months prior to presentation. Preoperative lab work reveals elevated serum calcium, elevated alkaline phosphatase, decreased serum phosphorus, and elevated parathyroid hormone (PTH). Which of the following correctly describes the underlying etiology of her osteopenia?
The most recent update of the CDC guidelines for the prevention of SSI issues a category IA strong recommendation stating that "in clean and clean- contaminated procedures, do not administer additional antimicrobial prophylaxis doses after the surgical incision is closed in the operating room, even in the presence of a drain."
The previous 2002 CDC guidelines for the prevention of SSI focused on three performance parameters: (1) initiation of parenteral antibiotics within 1 hour of the surgical incision, (2) selection of an appropriate antibiotic, and (3) discontinuation of antibiotics within 24 hours. The most recent updated 2017
CDC guidelines for the prevention of SSI has several notable changes with an emphasis that additional doses of antibiotics after initial prophylaxis are no longer recommended.
Berrios-Torres et al. review the 2017 updates to the CDC guidelines for prophylaxis against SSI. Strong recommendations include that in clean and clean-contaminated cases, additional antimicrobial prophylaxis should not be administered after the surgical incision is closed in the operating room, even in the presence of a drain. Furthermore, the authors discuss that there is no evidence that re-dosing intraoperative antibiotics or continuation of antibiotics until surgical drains have been removed provides any additional protection against surgical site infection.
O'Hara et al. highlights the key updates in the most recent CDC guidelines for prevention of SSI. The authors present specific suggestions for translating these recommendations into evidence-based policies and practices. They conclude that the implementation of new and existing guidelines in SSI prevention requires thoughtful and careful collaboration with several inter- professional and interdisciplinary teams.
Incorrect Answers:
Which of the following study designs describes a randomized controlled trial in which two interventions are applied separately or in combination to study groups?
The patient has an allergy to cephalosporins and a history of an MRSA infection. Of the choices listed, vancomycin is the best preoperative antibiotic for this patient.
The choice of preoperative antibiotics is of great interest given the large
medical and economic cost of periprosthetic infections. Standard preoperative prophylaxis in patients undergoing total joint arthroplasty consists of cefazolin or cefuroxime. In patients with beta-lactam allergies, the treatment options include clindamycin or vancomycin. Vancomycin is often the antibiotic of choice given it's higher efficacy with regard to MRSA prevention. In those patients who are considered at risk for MRSA infection and a beta-lactam allergy, vancomycin can be supplemented with an aminoglycoside (gentamicin) or aztreonam.
Bratzler et al. review antimicrobial prophylaxis for surgery and state for orthopedic joint replacement procedures cefazolin or cefuroxime is the recommended antibiotic. For patients with a confirmed beta-lactam allergy, they recommend vancomycin or clindamycin. They also state antibiotics should be stopped within 24hrs after surgery.
Dellinger et al. review antibiotics for surgical prophylaxis. They state the standard antibiotics for orthopedic procedures are cefazolin or cefuroxime. They state if there is also a concern for MRSA infection vancomycin can be added in addition to the above antibiotics.
Incorrect Answers:
Which of the following is STRONGLY recommended by the most recent (2017) Centers for Disease Control and Prevention (CDC) Guidelines with regard to antimicrobial prophylaxis for the prevention of surgical site infection (SSI)?
Clindamycin is a bacterial protein synthesis inhibitor by inhibiting ribosomal translocation at the 50S subunit.
Clindamycin is primarily bacteriostatic but may be bactericidal at higher concentrations.
Side effects of clindamycin may include a hypersensitivity reaction and pseudomembranous colitis. Resistance to clindamycin is conferred by a plasmid that alters the 50s ribosome binding site for clindamycin. The D- zone test is used to determine whether an organism has inducible resistance
to clindamycin.
Marcotte and Trzeciak published a review on community-acquired methicillin- resistant Staphylococcus aureus (CA-MRSA). They reported that CA-MRSA
does not have predictable susceptibility to clindamycin. They conclude that clindamycin also presents a risk for the development of Clostridium difficile colitis and inducible clindamycin resistance for which a D-zone test should be performed when culture results reveal erythromycin resistance.
Steward et al. performed a lab study to determine the efficacy of testing for induced clindamycin resistance in erythromycin-resistant Staphylococcus aureus. They reported that resistance to erythromycin and clindamycin can occur through methylation of their ribosomal target site (50s), which is mediated by erm genes. They conclude that disk diffusion is the preferred method for testing S. aureus isolates for inducible clindamycin resistance.
Incorrect Answers:
A 68-year-old man is scheduled to undergo total hip arthroplasty. He states he had an anaphylactic reaction after taking cefazolin for an MRSA hand infection 10 years ago. Which of the following best describes the preoperative antibiotic that should be administered for this patient?
Advanced glycation end-products (AGEs) cause excessive cross-linking of collagen in aging articular cartilage. As a result, the stiffness is increased.
AGEs are produced by spontaneous nonenzymatic glycation of proteins when sugars (glucose, fructose, ribose) react with lysine or arginine residues. The most abundant matrix protein in cartilage is Type II collagen. AGEs cause changes to the aging cartilage matrix and the aging chondrocyte. The increased cross-linking of Type II collagen results in an increase in cartilage stiffness (i.e. increase in the modulus of elasticity) and an increase in brittleness (i.e. less strain needed to go from the yield point to the fracture point on the stress-strain curve). As a result of the change in the aging cartilage’s biomechanical properties, it's susceptible to fatigue failure. Additionally, AGEs decrease the anabolic response of chondrocytes from autocrine signaling via TGF-beta, IGF-1, BMP-7, and OP-1. These two initial mechanisms contribute to aging cartilage to eventually lead to the development of osteoarthritis.
Li et al. reviewed age-related changes in cartilage and seek to define the different
mechanisms between aging cartilage and osteoarthritis. They state that with AGEs, there is excessive collagen cross-linking increases cartilage stiffness, while shortening/degradation of aggrecan leads to loss of sugar side chains and water-binding ability. Additionally, increased levels of AGEs are associated with a decline in anabolic activity. They state that these changes to cartilage make it more vulnerable to damage and therefore the onset of osteoarthritis. This is contrast to the initial steps in the mechanism of osteoarthritis which is characterized by cell proliferation, formation of chondrocyte clusters, increased synthesis of irregular cartilage matrix, and eventually a pro-catabolic and pro-inflammatory state that results in an imbalance in cartilage homeostasis and cartilage matrix breakdown.
Anderson et al. reviewed the relationship between osteoarthritis and aging.
They state that knee cartilage thins with aging, especially on the femoral and patellar sides, suggesting a gradual loss of cartilage matrix. AGEs formation leads to modification of type II collagen by cross-linking of collagen molecules, increasing stiffness and brittleness and increasing susceptibility to fatigue failure. Furthermore, describe the senescent phenotype of the chondrocyte
and its similarities with osteoarthritic chondrocyte phenotype.
Incorrect Answers:
Which of the following antibiotics works by binding to the 50S ribosomal subunit?
The patient has clinical signs and symptoms of gout. Figure D would correspond to this diagnosis as it shows negatively birefringent needle-shaped monosodium urate crystals.
Gout is an idiopathic disorder of nucleic acid metabolism that leads to hyperuricemia and deposition of monosodium urate crystals, most commonly in the joints of the lower limb (knee, ankle, and classically the 1st metatarsophalangeal joint). Diagnosis can be confirmed with joint arthrocentesis revealing negatively birefringent needle-shaped crystals. Treatment of acute gout flares is generally comprised of NSAIDs and colchicine, and chronic gout is treated with allopurinol to prevent the build-up
of uric acid.
Shmerling et al. prospectively analyzed the synovial fluid test results of 100 consecutive patients undergoing diagnostic arthrocentesis. They noted that synovial fluid white blood cell count (WBC) and the percentage of polymorphonuclear cells performed well as discriminators between inflammatory and noninflammatory diseases. Given the diagnostic value of synovial WBCs, the authors concluded that ordering of chemistry studies of synovial fluid should be discouraged because they are likely to provide misleading or redundant information.
Chiodo et al. review the use of intra-articular aspiration and injections for both diagnosis and treatment of disorders of the lower extremity such as infectious arthritis, gout, pigmented villonodular synovitis (PVNS), rheumatoid arthritis, and hemophilia. The authors discuss the importance of knowledge of regional anatomy, procedural indications, and appropriate techniques for successful aspiration/injection. The authors review safe and effective aspiration and injection techniques for the lower extremity, including the hip, knee, foot, and ankle.
Figure A reveals hemosiderin stained multinucleated giant cells consistent with PVNS. Figure B is a gram stain revealing gram-positive cocci in clusters consistent with Staphylococcus aureus. Figure C reveals rhomboid-shaped, positively birefrigerant crystal consistent with calcium pyrophosphate/pseudogout. Figure D reveals negatively birefringent needle- shaped crystals of monosodium urate/gout. Figure E reveals a collection of histiocytes and inflammatory cells around prominent intimal hyperplasia.
Incorrect Answers
An increase in advanced glycation end-products (AGEs) is characteristic of which of the following clinical conditions and results in which pathologic process?
Regardless of the number of level I studies included in a systematic review, having one study with <80% follow-up decreases the level of evidence for this review from level I to level II.
After classifying the type of study (e.g. therapeutic study, prognostic study, diagnostic study, economic analysis, or decision analysis) the “level of evidence” is then determined. The level of evidence (on a scale of I through V) for medical research is determined. It is important to consider the characteristics of a study’s design. This would include the percent follow-up, utilization of a control group, presence of blinding, heterogeneity of results, and process of randomization. Specific to meta-analyses and systematic reviews, it is important to know that the lowest quality study used in the review determines the level of evidence. In evidence-based medicine, higher levels of evidence have a larger impact on clinical recommendations.
Bhandari et al. analyzed the interobserver agreement among reviewers in categorizing the type of study, level of evidence, and subclassification for different clinical studies. The authors had 6 different surgeons with different levels of training in epidemiology analyzed 51 separate papers published in JBJS. The results demonstrated that the interobserver absolute agreement for the type of study and the level evidence was 82% and 67%, respectively. The epidemiology-trained reviewers had nearly perfect agreement in categorizing the type of study, level of evidence, and subclassification.
Wright et al. published an editorial introducing the different types of study designs and defined the different levels of evidence. Illustration A is a figure from this editorial.
Incorrect Answers:
A 55-year-old male, alcoholic, presents to the ER with acute right knee swelling and pain x 3 days. He admits to prior episodes of this pain that resolve after a few days. Serum labs reveal an ESR of 40 mm/hr and CRP of 5 mg/dl. He undergoes right knee aspiration and based on the results, he is discharged home on colchicine with the presumed diagnosis of gout. Which of the following images of the aspiration results are consistent with this diagnosis?
conclude that the patient populations and outcomes measure are homogenous and you do not have any concerns with randomization. You notice one of
the studies included had 70% follow-up, yet the remaining studies had
>80% follow-up. Knowing this, you appropriately assign what level of evidence to the systematic review?
The correct sequence of events should be the surgeon reads the surgical information on the consent to the patient, then the surgeon marks the surgical site with the patient’s assistance, then allows the anesthesia team to perform their procedure, and then performs a final Time-Out with the surgical team immediately prior to the surgical incision.
Orthopedic surgical patients are at risk of surgical errors due the number of procedures that can be performed on the bilateral extremities. The responsibility to identify the correct surgical procedure at the correct location has expanded beyond only the surgeon. The entire surgical team is
responsible for confirming the patient, surgical site, and surgical procedure. All members on the surgical team should be valued and emboldened to “speak up’ and actively participate. To help improve communication and reduce complications, surgical safety checklists have become common. In a statement
published by the AAOS is 2015, they support the use of standardized surgical systems, including the use checklists, as it is critically important to keep patients safe. In 1998, the AAOS introduced the “Sign Your Site” safety program to reduce wrong-site surgeries through improved site identification. Permanent ink should be used to mark the site(s) with the patient's assistance prior to surgery, and the site(s) should be confirmed by the surgical team during the Time-Out immediately before the start of the surgical procedure.
Singer et al. performed a study to evaluate the association between surgical teamwork and surgery safety checklist performance. Their results emphasized the importance of surgeon buy-in and clinical leadership to initiating and maintaining surgical safety checklists. In addition to surgeon buy-in and clinical leadership, factors that help maintain high-quality and consistent surgical teamwork were communication, coordination, respect, and assertiveness.
Incorrect Answers:
You are reviewing a systematic review on the 90-day complication rate and outcome for same day total joint arthroplasty for publication. After you analyze the methodology of the 6 randomized controlled trials included in the review, you
preoperative paperwork outside the room. The patient is taken to surgery and receives an interscalene block on the left shoulder after sedation. At the final Time- Out, the surgeon realizes a discrepancy with the laterality when the consent is read aloud. The surgeon aborts the case and wakes the patient. What is the correct sequence of events that should have happened to prevent this error? A: The surgeon begins
the surgery B: The surgical team performs a Time-Out C: The surgeon marks the surgical site D: The surgeon reads the surgical information on the consent to the patient E: The anesthesia team administers a local extremity block
Enchondral ossification occurs with relative stability constructs, which is represented by the bridge plate in figure C.
Fracture healing is a complex process that occurs in several key steps. The type of healing that occurs is dependent on the stability and strain of the fracture environment. In constructs with very little strain, also referred to as absolute stability, there is primary bone healing through Haversian remodeling. This produces very little callus and does not rely on a cartilage precursor. Relative stability constructs with higher strains produce a cartilage precursor, which subsequently ossifies in later stages of healing, also referred to as enchondral ossification.
Perren reviewed the biological mechanisms of fracture healing. The author discussed the importance of skeletal stiffness for limb function in addition to the healing process that utilizes soft tissue compensatory mechanisms to aid
in fracture healing. The author concluded that the goal of fracture healing is to obtain a functional limb to allow for daily mobility and activity.
Gerstenfeld et al. investigated the effect of non-selective and COX-2 selective NSAIDs effects on bone healing in a rat model. They reported a significantly higher nonunion rate in valdecoxib treated rats compared to the ketorolac group. They also noted that withdrawal of either drug at six days resulted in prostaglandin E2 levels returning to normal levels after 14 days. The authors concluded that COX-2 specific NSAIDs inhibited bone healing greater than nonspecific NSAIDs with the magnitude of the effect dependent on the duration of treatment, but the effects on prostaglandin E2 levels appear reversible with discontinuation of the drug.
Figure A is the AP radiograph of the left distal tibia with three lag screws through a spiral fracture. Figure B is the lateral radiograph of the right elbow with an olecranon plate.
Figure C is the AP radiograph of the right distal femur with a lateral bridge plate. Figure D is an AP radiograph of the left ankle with a lag screw and neutralization plate on the distal fibula. Figure E is the lateral radiograph of the forearm with a compression plate on the radius.
Incorrect Answers:
A 31-year-old man is scheduled to undergo a right shoulder arthroscopic labral repair. The surgeon is running behind and hurries to the preoperative holding area. The surgeon greets the patient and verbally confirms the operative site with the patient. The surgeon leaves the patient’s room and completes the appropriate
The yield point is the transition point between elastic and plastic deformation. The yield strength is defined as the amount of stress necessary to produce a specific amount of permanent deformation.
Stress is the amount of force applied to a material and strain is the deformation resulting
from that stress. This is graphically depicted as a stress- strain curve, where the X-axis represents strain and the Y-axis represents stress. The elastic modulus of a material is the linear region of the graph (rise over run/stress on strain). Remember, an elastic material is one that resists a change in shape (less strain or deformation under increasing stress). Non- linear regions include the toe region for some materials (tendons/ligaments) and the plastic zone, which occurs after the yield point.
Mantripragada et al. provide a review of recent advances in designing orthopaedic implants. Of note, they discuss modifications to metallic implants to reduce unwanted effects, such as nickel-free stainless steel. They also go over newer alloys with desirable mechanical and biological properties, such as tantalum, niobium, zirconium, and magnesium.
Kennedy et al. provide a classic in-vitro tension study of the human knee ligaments. They used an Instron Tension Analyzer to test the ultimate failure of the medial collateral, lateral collateral, anterior cruciate, and posterior cruciate ligaments at different loading rates. They found that the posterior cruciate ligament was the strongest (the other ligaments were all of
comparable strength) and that microscopic failure occurred before macroscopic failure. Illustration A represents a stress-strain curve.
Incorrect Answers:
is a phenomenon especially associated with a ductile material; the diameter of the material is diminished prior to fracture.
material can absorb before fracture and is the area under the stress-strain curve. Answer 5: The toe region is seen in materials such as ligaments and tendons and represents the straightening of the crimped ligament fibers.
Which of the following fixation constructs would achieve fracture healing through enchondral ossification?
The preosteoclast (precursor to the osteoclast) is the only cell of myeloid origin. The remainder of the cells involved in bone formation, remodeling, and metabolism are of mesenchymal origin.
Osteoclast signaling, function, and biology have grown increasingly well understood over the past few decades. Osteoclast activity is regulated by
osteoblasts, thereby coupling bone formation and resorption. Osteoclast differentiation from myeloid precursor cells is stimulated by key molecules including RANK, PU-1, and CSF-1. An understanding of these molecular pathways is essential to developing effective directed anti-resorptive therapies.
Zaidi et al. present a comprehensive review of proliferation, differentiation, and hormonal regulation of cells of the bone. The authors specifically discuss the unique origin of the osteoclast from the myeloid lineage and conversely the mesenchymal origin of the osteoblast. Furthermore, they highlight the
most recent understanding of the molecular mechanisms involved in osteoclast formation
and signaling, including M-CSF and RANKL.
Caterson et al. discusses mesenchymal differentiation in the context of musculoskeletal regeneration. The authors review the growth factors and bioactive signaling molecules involved in directed differentiation itno the various mesodermal lineages including bone, cartilage, muscle, tendon, marrow, and adipose. They emphasize the importance of understanding these pathways to regenerative medicine.
Illustration A is a diagram illustrating the difference between mesenchymal and myeloid lineages.
Incorrect answers:
The point on a stress-strain curve that separates the plastic and elastic regions is defined as which of the following:
Due to the risk of inducible clindamycin resistance in erythromycin-resistant MRSA, a D-test should be performed.
Isolates of MRSA that are resistant to erythromycin have been shown to become resistant to clindamycin through a process called inducible resistance, which is conferred by a plasmid that alters the 50S ribosome binding site for both clindamycin and erythromycin. Thus, when culture results reveal erythromycin-resistant MRSA, a D-zone test should be performed to check for inducible clindamycin resistance. The D-zone test is performed by
placing an erythromycin disk in proximity to a clindamycin disk on an agar plate inoculated with methicillin-resistant S aureus (MRSA). A zone of inhibition in the shape of the letter "D" is seen with an inducible strain and is considered a positive test. If the D- zone test is positive, then clindamycin should not be used because the strain of MRSA can become resistant to the treatment.
Marcotte et al. published a review on community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA). They reported that clindamycin has activity against Streptococcus species, but it is not as predictable against CA- MRSA. Clindamycin also presents a risk for the development of Clostridium difficile colitis and inducible clindamycin resistance. for which a D-zone test should be performed when culture results reveal erythromycin resistance.
Steward et al. performed a study to determine the efficacy of testing for induced clindamycin resistance in erythromycin-resistant Staphylococcus aureus. They reported that resistance to erythromycin and clindamycin can occur through methylation of their ribosomal target site (25), which is typically mediated by erm genes. They found that disk diffusion is the preferred method for testing S. aureus isolates for inducible clindamycin resistance.
Illustration A is an image of a positive D-zone test, which indicates inducible clindamycin resistance.
Incorrect Answers:
Which of the following cells involved in bone metabolism derives from a myeloid origin?
Enoxaparin primarily exerts its effects by inhibiting Factor Xa, which is labeled C in Figure A.
Enoxaparin is a low molecular weight heparin (LMWH) that primarily exerts its effects by inhibiting Factor Xa. It achieves this by binding to antithrombin to form a complex that irreversibly inactivates clotting factor Xa. Enoxaparin has the advantage of not requiring laboratory monitoring and can be reversed with protamine sulfate. However, it is important to note that protamine sulfate is less effective in reversing enoxaparin compared to unfractionated heparin (UFH).
Hyers published a review on the past, present, and future management of venous thromboembolism. He found that, for the most part, LMWH and other newer anticoagulants have been shown to be superior to UFH in terms of the venographic endpoint. He also reports that several meta-analyses have demonstrated that LMWH offers superior benefit to UFH for VTE prevention in hip and knee surgery patients.
Tørholm et al. performed a study to determine outcomes of thromboprophylaxis using LMWH compared to placebo in elective hip surgery. They found that 9 (16%) patients in the treatment group and 19 (35%) in the placebo group developed deep venous thrombosis. The risk of thrombosis in the placebo group was increased with prolonged surgery and occurred more frequently during the first 4 postoperative days. They concluded that LMWH offers safe and easily administered thromboprophylaxis in total hip replacement.
Figure A is an image of the coagulation cascade. Illustration A is an image of the
coagulation cascade with the sites of action of the various anticoagulants labeled.
Incorrect Answers:
A 42-year-old IV drug user presents to the emergency department with a large abscess on his forearm. A bedside I&D is performed and he is started on broad-spectrum IV antibiotics. Initial results from his cultures demonstrate methicillin-resistant Staphlycoccus aureus (MRSA) that is also resistant to erythromycin. The team would like to transition him to oral clindamycin. Prior to transitioning him to clindamycin, which additional laboratory test should be performed?
Teriparatide promotes bone formation in patients at high risk of fractures due to severe osteoporosis that is refractory to multiple treatments, including bisphosphonates and cement augmentation. Teriparatide is a human recombinant N-terminal parathyroid hormone.
Teriparatide administered in daily injections results in bony formation, whereas continuous infusion results in bony resorption. In rat models, teriparatide caused an increase in the incidence of osteosarcoma, and thus should only be prescribed for patients for whom the potential benefits outweigh the potential risk. It can be administered in isolation or as an adjunct treatment during bisphosphonate therapy. However, in patients on long-term bisphosphonate therapy, discontinuation of bisphosphonates are advised to reduce potential complications of atypical femur fractures and jaw osteonecrosis.
Watts et al. published a review article on postmenopausal osteoporosis. They reported that bisphosphonates can accumulate in bone, thus after a period of treatment, lower- risk patients should be offered a drug holiday. Denosumab, on the other hand, is not sustained when treatment is discontinued, so no drug holiday is warranted. They concluded that, although there are safety
concerns regarding atypical femoral fracture and osteonecrosis of the jaw with long term use, the benefit of hip fracture risk reduction far outweighs the risk of these relatively uncommon side effects.
Song et al. performed a meta-analysis to investigate the effect of teriparatide monotherapy and the additive effect of teriparatide on antiresorptive agents in postmenopausal women with osteoporosis. They reported that teriparatide monotherapy significantly improved bone mineral density (BMD) in the lumbar spine, total hip, and femoral neck compared with placebo; the additive effect
of teriparatide over hormone replacement therapy (HRT) and denosumab agents was evident in all 3 skeletal sites; however, teriparatide plus alendronate did not demonstrate additive effect in total hip and femoral neck. They concluded that, for patients with osteoporosis who were at high risk for fracture, BMD increased more in patients receiving teriparatide than in those receiving alendronate.
Saag et al. compared the use of teriparatide or alendronate in the management of glucocorticoid-induced osteoporosis. They reported that BMD had increased more in the teriparatide group than in the alendronate group in the lumbar spine and total hip at 6 and 12 months, respectively. They also reported significantly fewer new vertebral fractures in the teriparatide group compared to the alendronate group. They concluded that in severely osteoporotic patients at high risk for fracture, BMD increased more in patients receiving teriparatide than in those receiving alendronate.
Figure A depicts multiple vertebral insufficiency fractures in the setting of a prior cement augmentation procedure.
Incorrect Answers:
Where in the coagulation cascade shown in Figure A does enoxaparin primarily exert its effects?
This patient is presenting with signs of a septic nonunion after open reduction and internal fixation (ORIF) of a radial shaft fracture. Of the choices listed, C- reactive protein (CRP) is the best predictor of infection in the setting of nonunion.
Nonunions after fracture fixation may occur from infection. The most sensitive and readily-available laboratory marker to detect infection is the CRP. CRP is an acute phase reactant that significantly rises within 6 hours after tissue damage or onset of clinical infection. CRP then peaks 2-3 days later and returns to normal levels 5-21 days after the inciting event if it is treated (e.g. antibiotics for cellulitis). In septic nonunions, the chance of fracture healing is low if the infection is not properly treated, and chronic infection can lead to substantially elevated CRP values.
Wang et al. evaluated the effectiveness of laboratory tests in the diagnosis of
infected nonunion. They reported that the sensitivity and specificity of CRP for detection of infected nonunions are both higher than those of IL-6. They concluded that the diagnostic utility of CRP was superior to IL-6, which is contrary to similar studies comparing these markers in prosthetic joint infection patients.
Stucken et al. performed a study to investigate the utility of a standardized protocol to rule out infection in high-risk patients and to evaluate the efficacy of each component of the protocol. They reported that the ESR and the CRP levels were both independently accurate predictors of infection. They
concluded that their protocol can help surgeons to risk-stratify patients prior to the surgical treatment of a nonunion, allowing them to counsel patients more appropriately.
Figure A depicts a nonunion of a radial shaft fracture after ORIF. Incorrect Answers:
An 85-year-old woman presents with severe back pain and the CT shown in Figure A. Her history is notable for prior vertebral compression fractures for which she underwent a cement augmentation procedure. She has been on bisphosphonates for the last 5 years, without improvement of her osteoporosis. She has no history of malignancy. What is the mechanism of action of the medication that should be prescribed for her refractory osteoporosis?
A receiver operating characteristic (ROC) curve is used to determine responsiveness.
Responsiveness is a measure of the diagnostic ability of different tests. It can be determined by calculating the C-statistic, which represents the area under a
Receiver Operating Characteristic (ROC) curve. On a ROC curve, the false positive rate (1 - specificity) is plotted on the x-axis, while the true positive rate (sensitivity) is plotted on the y-axis. The higher the area under the curve, the more responsive the outcome measure. A value of 0.5 indicates a random chance and a therefore useless test, while values above 0.75 usually are considered to be adequately responsive.
Kocher et al. published a review on clinical epidemiology and biostatistics for orthopaedic surgeons. They reported that the relationship between the sensitivity and specificity of a diagnostic test can be portrayed with use of a receiver operating characteristic (ROC) curve. A ROC graph shows the relationship between the true- positive rate (sensitivity) on the y-axis and the false-positive rate (1 − specificity) on the x-axis plotted at each possible cutoff. Overall diagnostic performance can be evaluated on the basis of the area under the ROC curve.
Hanley et al. published a review on the meaning and use of the area under a receiver operating characteristic (ROC) curve. They reported that it represents the probability that a randomly chosen diseased subject is (correctly) rated or ranked with greater suspicion than a randomly chosen non-diseased subject.
Illustration A is an example of a ROC curve. Illustration B is an example of a funnel plot. Illustration C is an example of a Kaplan-Meier curve. Illustration D is a table outlining the interpretation of the Cronbach alpha coefficient. Illustration E is an example of a forest plot.
Incorrect Answers:
A 32-year-old man underwent open reduction and internal fixation for an open radial shaft fracture 6 months ago. He is now experiencing fevers and chills at night and pain and swelling over the surgical site. A current radiograph is depicted in Figure A. What is the most accurate laboratory test for assessing his most likely diagnosis?
The Patient-Reported Outcomes Measurement Information System (PROMIS) has been shown to have reduced floor and ceiling effects compared to other assessment tools.
The PROMIS system was developed to produce a highly reliable, precise, and versatile assessment of outcomes. When administered in a computerized adaptive mode, each question that is answered is followed with a customized follow-up question based on the previous response, which allows for reduced testing items and time. Further, the results of the assessment are reported in T-scores with 50 being the population norm and with a standard deviation of
Question 58
Figures 11a and 11b show the T2-weighted MRI scans of the lumbar spine of a 53-year-old woman who has low back and right lower extremity pain. What structure is the arrow pointing to in Figure 11a? Review Topic
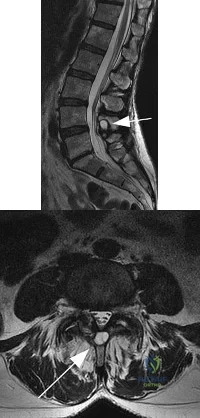
Explanation
Question 59
A 17-year-old girl is involved in a motor vehicle collision and sustains the injury shown in Figures 46a through 46c. She is neurologically intact in her bilateral lower extremities. Definitive treatment should consist of A B C

Explanation
The figures reveal a fracture-dislocation at L1-2. Proper treatment consists of posterior reduction, stabilization, and fusion 2 levels above and below the level of injury. Short-segment stabilization schemes do not stabilize the injury properly, and longer-segment constructs are not necessary. Anterior treatment is not indicated in fracture-dislocations.
RECOMMENDED READINGS
Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004 Nov-Dec;12(6):424-35. Review. PubMed PMID: 15615508. View Abstract at PubMed
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
Question 60
Which of the following is a relative contraindication to performing laminoplasty in a patient with cervical myelopathy? Review Topic
Explanation
Question 61
A 45-year-old man undergoes an anterior cervical diskectomy and fusion at C5-6 and C6-7 with instrumentation. During the first postoperative visit at 1 week, the patient reports difficulty swallowing and mild anterior cervical tightness. The anterior wound is benign and the patient denies any dyspnea or shortness of breath. A postoperative radiograph is seen in Figure 25. What is the most appropriate management at this time?
Explanation
6 months with nonsurgical management. A minority of patients experience moderate or severe symptoms by 6 months after the procedure. Female gender and multiple surgical levels have been identified as risk factors for the development of postoperative dysphagia.
REFERENCES: Lee MJ, Bazaz R, Furey CG, et al: Risk factors for dysphagia after anterior cervical spine surgery: A two-year prospective cohort study. Spine J 2007;7:141-147.
Bazaz R, Lee MJ, Yoo JU: Incidence of dysphagia after anterior cervical spine surgery:
A prospective study. Spine 2002;27:2453-2458.
Question 62
Figures 30a through 30c show the CT scans and standing lateral radiograph of a 30-year-old woman who was injured in a fall while snowboarding. She is neurologically intact in the lower extremities and has normal rectal tone and sensation. She has tenderness at the thoracolumbar junction but no ecchymosis or palpable defect. Mobilization in a thoracolumbosacral orthosis for this patient has been proven to result in which of the following clinical outcomes? Review Topic

Explanation
Question 63
A 27-year-old woman sustained a bilateral C5-6 facet subluxation in a motor vehicle accident. Neurologic evaluation reveals normal motor, sensory, and reflex functions. She is awake, alert, and cooperative. Initial management should consist of
Explanation
REFERENCE: Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets: Case reports. J Bone Joint Surg Am 1991;73:1555-1560.
Question 64
A 34-year-old man underwent a transtibial amputation as the result of a work-related injury. The amputation was performed at the inferior level of the tibial tubercle. The residual limb has a soft-tissue envelope composed of gastrocnemius muscle that is used as soft-tissue cushioning for the distal tibia. Despite undergoing several prosthetic fittings, he continues to report pain and instability. Examination reveals that the prosthesis appears to fit well with no apparent pressure points or areas of skin breakdown. He is not willing to have any further surgery. Which of the following modifications will most likely provide relief?
Explanation
REFERENCES: Bowker JH, Goldberg B, Poonekar PD: Transtibial amputation: Surgical procedures and postsurgical management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 429-452.
Kapp S, Cummings D: Transtibial amputation: Prosthetic management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 453-478.
Question 65
Figure 1 is the radiograph of an otherwise healthy 68-year-old man with a 4-year history of increasing global left knee pain. He has noticed stiffness, and despite physical therapy, bracing and nonsteroidal anti-inflammatory drugs, he has continued to develop worsening symptoms and progression in his deformity. Physical examination demonstrates 80°of flexion and a 10° flexion contracture. What is the best next step?
Explanation
Question 66
Which of the following findings helps to distinguish between stress fractures of the tibia and shin splints? Review Topic
Explanation
The general symptom of a bone stress injury is stress-related pain. Bone stress injuries are difficult to diagnose based only on a clinical examination because the clinical symptoms may vary depending on the phase of the pathophysiological spectrum in the bone stress injury. Imaging studies are needed to ensure an early and exact diagnosis. If the diagnosis is made early, most bone stress injuries heal well without complications.
Question 67
Figure 40 shows the plain radiograph of a 30-year-old woman who has had a long history of standing bilateral anterior knee pain and a sense of patellar instability without frank dislocation. Nonsurgical management consisting of anti-inflammatory drugs and physical therapy has failed to provide relief. Examination reveals full range of motion of both knees, with moderate patellofemoral crepitance. Patellar apprehension and patellar grind tests are positive. The Q-angle measures 20°. Management should now consist of
Explanation
REFERENCES: Boden BP, Pearsall AW, Garrett We Jr, et al: Patellofemoral instability: Evaluation and management. J Am Acad Orthop Surg 1997;5:47-57.
Fulkerson JP: Patellofemoral pain disorders: Evaluation and management. J Am Acad Orthop Surg 1994;2:124-132.
Question 68
The World Health Organization (WHO) developed specific criteria for osteoporosis in 1994 based on the T-score obtained by dual-energy absorptiometry (DEXA). The T-score represents the number of standard deviations that the individual's bone mineral density differs from the normal peak bone mass in young adults. Osteoporosis is defined as a T-score of 1 +2.5 or below. 2 -1.0 to -2.0.
Explanation
Question 69
A teenager is undergoing a correction of deformity and lengthening of the femur. Distractions are proceeding as expected; however, during his 6-week follow-up examination, the patient reports that the distraction motors have become harder to turn over for the past 2 to 3 days. Figures 37a and 37b show current radiographs. What is the most likely complication being encountered?
Explanation
REFERENCES: Paley D: Problems, obstacles and complications of limb lengthening, in Maiocchi AB, Aronson J (eds): Operative Principles of Ilizarov. Baltimore, MD, Williams & Wilkins, 1991, p 360.
Herring JA: Limb length discrepancy, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics,
ed 3. Philadelphia, PA, WB Saunders, 2002, p 1088.
Question 70
Which of the following best describes the use of epidural morphine and steroid paste after laminectomy?
Explanation
REFERENCES: Kramer MH, Mangram AJ, Pearson ML, et al: Surgical-site complications associated with a morphine nerve paste used for postoperative pain control after laminectomy. Infect Control Hosp Epidemiol 1999;20:183-186.
Lowell TD, Errico TJ, Eskenazi MS: Use of steroids after discectomy may predispose to infection. Spine 2000;25:516-519.
Question 71
- A 39-year-old woman jammed her long finger playing softball 24 hours ago. She is unable to actively extend the proximal interphalangeal joint; however, when the joint is brought passively into full extension, she is able to maintain that position. Management should consist of
Explanation
Question 72
Which of the following factors is associated with the worst prognosis in soft-tissue sarcomas?
Explanation
REFERENCES: Collin C, Goobold J, Hadju SI, Brennan MF: Localized extremity soft tissue sarcoma: An analysis of factors affecting survival. J Clin Oncol 1987;5:601-612.
Eilber FC, Rosen G, Nelson SE, et al: High-grade extremity soft tissue sarcomas: Factors predictive of local recurrence and its effect on morbidity and mortality.
Ann Surg 2003;237:218-226.
Question 73
A 25-year-old farm worker sustained a grade III open fracture of the midshaft of the left tibia after falling from a ladder. Which of the following antibiotic regimens is best for this patient?
Explanation
REFERENCES: Holton PD, Mader J, Nelson CL, Osmon DR, Patzakis MJ: Antibiotics for the practicing orthopaedic surgeon. Instr Course Lect 2000;341:36-42.
Wilkins J, Patzakis M: Choice and duration of antibiotics in open fractures. Orthop Clin North Am 1991;22:433-437.
Question 74
Figure 11a shows the AP pelvis radiograph of a 25-year-old man who sustained a spinal cord injury 10 years ago. A bone scan and a CT scan are shown in Figures 11b and 11c. To prevent recurrence after resection, management should consist of
Explanation
REFERENCES: Moore K, Goss K, Anglen J: Indomethacin versus radiation therapy for prophylaxis against heterotopic ossification in acetabular fracture. J Bone Joint Surg Br 1998;80:259.
Stover S, Niemann K, Tullos J: Experience with surgical resection of heterotopic bone in spinal cord injury patients. Clin Orthop 1991;263:71-77.
Question 75
A 32-year-old male hockey player who is right-hand dominant was checked from behind and landed with full force into the boards. In the emergency department he reports shortness of breath. Figure 113 shows a 2-D CT scan. What is the best initial treatment for this injury?
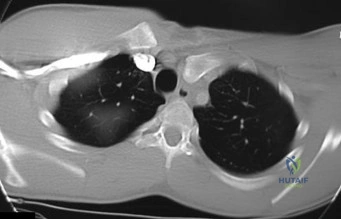
Explanation
Question 76
What is the most common cause of early failure for patellofemoral arthroplasty?
Explanation
REFERENCES: Lonner JH: Patellofemoral arthroplasty. J Am Acad Orthop Surg 2007;15:495-506. Argenson JN, Flecher X, Parratte S, et al: Patellofemoral arthroplasty: An update. Clin Orthop Relat Res 2005;440:50-53.

Question 77
A 16-year-old boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals a large, deeply fixed, soft-tissue mass in the thigh. Laboratory results show an elevated erythrocyte sedimentation rate (ESR) and leukocytosis. A plain radiograph and MRI scan are shown in Figures 1a and 1b. Biopsy specimens are shown in Figures 1c and 1d. What is the most likely diagnosis?
Explanation
REFERENCE: Simon MA, Springfield DS, et al: Ewing’s Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 287-297.
Question 78
Figure 27 shows the radiograph of a 68-year-old woman with a history of rheumatoid arthritis who was injured in a fall. History reveals that she has been asymptomatic since undergoing a left total knee arthroplasty 9 years ago. Management should consist of
Explanation
REFERENCE: Ayers DC: Supracondylar fracture of the distal femur proximal to a total knee replacement, in Springfield DS (ed): Instructional Course Lectures 46. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-203.
Question 79
A 35-year-old construction worker continues to have weakness with lifting overhead 2 years after he was treated with physical therapy for a "chest muscle" tear. An obvious deformity noted in his axilla worsens with resisted extension and adduction. A clinical photograph and MRI scan are shown in Figures 119a and 119b. What is the most appropriate treatment? Review Topic
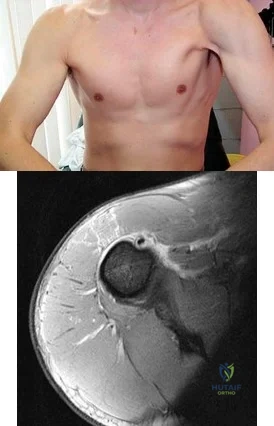
Explanation
Question 80
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity. Postoperative radiographs are shown in Figures 3 and 4. How does the plate function?

Explanation
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
Question 81
Figures 15a and 15b are intrasurgical photographs from the posterolateral viewing portal that were taken at the beginning and end of a right shoulder arthroscopic procedure performed on a 54-year-old man. This technique demonstrates superior results compared to traditional arthroscopic techniques when evaluating which outcome?
Explanation
The images reveal a medium-sized tear of the rotator cuff. As more clinical studies are published comparing double-row with single-row rotator cuff repair, it has become clear that the retear rate is lower with a double-row construct for small and medium-sized tears. This may be attributable to the stronger time-zero repair construct that double-row repair provides. No study to date has demonstrated a significant difference in clinical outcomes (functional and pain scores at any time) or time to healing between the 2 techniques.

CLINICAL SITUATION FOR QUESTIONS 16 THROUGH 17
Figure 16 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop," and then he needed help walking off the field. His knee is visibly swollen.
Question 82
The authors found that all 9 patients went on to both clinical and radiographic union. They concluded that the Masquelet technique was successful in effectively reconstructing traumatic and posttraumatic bony defects in the forearm with a low incidence of complications.
Explanation
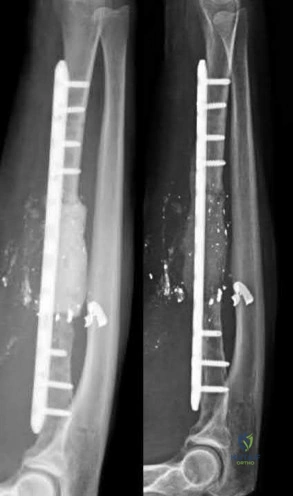
A 25-year-old male runs into a tree while going 45 mph on his motorcycle. He presents to your level 1 trauma hospital with the injuries shown in figures A through C. After closed reduction, which of the following is true with respect to treatment for this patient?

Heterotopic ossification is uncommon
Minifragment screws are sufficient for fracture fixation
Kocher-Langenbeck is the optimal surgical approach for this injury
Fragment excision leads to improved outcomes compared to open reduction and internal fixation
A 2 mm fragment step-off is considered the cut-off for non-surgical management
This patient has sustained a Pipkin II femoral head fracture with associated anterior hip dislocation. An open reduction with internal fixation of the femoral head fragments with direct visualization is indicated to restore stability and congruity of the hip joint. These fractures can be treated with mini-fragment screws with excellent reduction and purchase without risks of extensive chondral injury or screw prominence.
Femoral head fractures are uncommon injuries usually associated with hip dislocations. They are classified using the Pipkin Classification (Illustration B). While resection of small femoral head fracture fragments can be considered (Pipkin I) as sufficient and satisfactory treatment, this fragment is large and displaced and thus should be treated with ORIF for optimal results. Regarding the surgical approach, advocates for the direct anterior approach state direct access to the anterior portion of the femoral head with decreased overall complication rates. Other approaches, including surgical hip dislocation and Kocher-Langenbeck, are also useful depending on associated injuries (acetabulum fractures, etc.) and location of the head fragment. ORIF of these fractures can be performed with the use of countersunk mini-fragment screws, headless screws and even bioabsorbable pins to avoid prominence or extensive chondral injury.
Marecek et al. authored a review article on femoral head fractures. They described these injuries as being generally associated with hip dislocations and require prompt reduction. They noted that the surgical fixation of the femoral head is generally done through the direct anterior approach or via a surgical hip dislocation depending on associated injuries. The authors also discussed the importance of using mini-frag screws to avoid hardware prominence. They also noted that while heterotopic ossification is a common finding after the anterior approach for these injuries, it is rarely proven to be symptomatic.
Giannoudis et al. reviewed femoral head fractures focusing on management, complications and clinical results. They reported on 453 femoral head fractures in 450 patients. Regarding Pipkin Is, they noted that fragment excision gave better results compared to ORIF (p=0.07), while Pipkin IIs showed improved outcomes with ORIF. Regarding complications, they noted the following rates: wound infection (3%), sciatic nerve palsy (4%), AVN (11.9%), post-traumatic OA (20%) and HO (16.8%). They also noted the anterior approach was associated with promising long-term functional results and a lower incidence of major complication rates.
Figure A is an AP pelvis radiograph revealing a left hip dislocation with a large femoral head fracture extending into the weight-bearing zone of hip joint
(Pipkin II). Figures B and C are CT scan images revealing an anteriorly dislocated hip with a large femoral head fracture without associated acetabulum fractures. Illustration A is the post-op fluoroscopy showing ORIF of femoral head with multiple 2.7 cortical screws. Illustration B demonstrates the Pipkin classification for femoral head fractures.
Incorrect Answers:

Which of the following describes the most common organism cultured from septic olecranon bursitis?
Gram positive cocci in chains
Gram positive bacilli in branches
Gram positive cocci in pairs and clusters
Gram negative diplococci
Gram negative bacilli with thin rods Correct answer: 3
The most common cultured organism in the setting of septic olecranon bursitis is Staphylococcus aureus (S. aureus), appearing as gram positive cocci in pairs and clusters.
S. aureus is responsible organism in approximately 80% of cases of septic olecranon and prepatellar bursitis. Mixed flora is also common. Patient demographics in both conditions are similar, more commonly involving middle-aged males. Direct inoculation is presumed to be the primary culprit as opposed to hematogenous seeding, as blood supply to the bursal tissue is poor. Differentiating infectious from non-infectious bursitis can be challenging.
Aaron et al. provide a review article on the four most common types of bursitis: olecranon, prepatellar, trochanteric, and retrocalcaneal. They note that olecranon bursitis is the most common superficial bursitis, and that a careful history and physical exam can help differentiate infectious from noninfectious olecranon bursitis. The authors discuss one series of 46 patients demonstrating that a skin temperature overlying the affected bursa ≥2.2°C than the contralateral, unaffected bursa had a 100% sensitivity and 94% specificity in diagnosing a septic process.
Illustration A shows a patient with olecranon bursitis. Illustration B shows the classic gram stain for S. aureus (gram positive cocci in pairs and clusters).
Incorrect Answers:

During a trauma conference, a hand surgeon presents a case of a 25-year-old male who injured his elbow while roller skating. While describing the patient's radiographs, he reports that this injury is associated with valgus posterolateral rotatory instability. Which of the following images is most likely the patient's radiograph?

Posterolateral rotatory instability (PLRI) can result from a "terrible triad" fracture-dislocation pattern (seen in Figure E), classically involving a radial head fracture, coronoid tip or base fracture, and an elbow dislocation.
Terrible triad injuries typically occur with axial loading, supination, and a valgus directed force through the elbow. In comparison to PLRI which results from a terrible triad injury, posteromedial rotatory instability (PMRI) commonly results from an anteromedial coronoid facet fracture following a varus-directed force. These injuries also very frequently also have a lateral collateral ligament complex injury but often have no radial head fracture. PLRI is far more common than PMRI. Generally with a PLRI pattern, the lateral collateral ligament complex fails first, followed by injury to the anterior capsule or coronoid, and lastly the medial collateral ligament complex is affected. Nonoperative management is possible, but only indicated in small, non-displaced radial head fractures with small coronoid tip fractures. Typically, terrible triad injuries are addressed surgically with radial head fixation or arthroplasty, lateral collateral ligament repair, and, less commonly, coronoid fracture fixation or anterior capsule repair.
Ring et al. reviewed 56 patients who had been treated with an ORIF of the radial head at 48 months after injury. They found unsatisfactory outcomes for patients who had an ORIF of radial head fractures with greater than 3 articular fragments. The authors recommended ORIF of radial head fractures with 3 or few fragments.
Steinmann performed a review of coronoid process fractures. The author reports that with an anteromedial coronoid fracture, the anteroposterior (AP) radiograph of the elbow will demonstrate progressive narrowing of the joint space from lateral to medial. Dr. Steinmann concludes that an important determinant of stability is the involvement of the sublime tubercle (insertion point of the MCL), and that medial instability is likely with involvement of the sublime tubercle.
Mathew et al. review the anatomic, biomechanical, and operative principles of terrible triad injuries. The authors discuss that the primary goal of fixation is to stabilize the elbow and allow early range of motion. They underscore technical improvements and implant developments which have improved outcomes.
Figure A demonstrates a capitellum fracture. Figure B demonstrates an olecranon fracture.
Figure C demonstrates a displaced radial head fracture.
Figure D demonstrates an anteromedial facet coronoid fracture.
Figure E demonstrates a terrible triad injury with a radial head fracture,
coronoid tip fracture, and elbow subluxation.
Incorrect Answers:
A 32-year-old soccer player presents with severe right ankle pain and inability to bear weight after sustaining a slide-tackle injury during a game. Radiographs are shown in Figures A and B. Given the nature of his injury, he is taken for surgical reduction and fixation. Following medial malleolar fixation, the syndesmosis is addressed. All of the following are true regarding the most appropriate intraoperative technique for anatomic syndesmotic reduction EXCEPT:

The axis of the reduction clamp should parallel the anatomic trans-syndesmotic angle
The lateral tine of the clamp should be seated just posterior to the lateral malleolar ridge
The medial tine should be placed on the anterior third of the tibia on a true lateral fluoroscopic view of the ankle
The reduction clamp should be placed 1-2cm proximal to the tibial plafond
The surgeon should apply judicious compression under fluoroscopic visualization to avoid over-compression of the syndesmosis
When placing a clamp across the syndesmosis to facilitate reduction, the lateral tine should be placed directly on the lateral malleolar ridge. Placing the lateral tine either more anteriorly or posteriorly has been shown to result in sagittal malreduction from fibular translation.
Syndesmotic reduction has proven to be technically challenging, with reportedly greater than 50% of cases resulting in malreduction. Provisional reduction is most often attained via a pointed reduction clamp. Placement of the lateral tine is outlined above. The medial tine should be placed at the anatomic midportion of the medial tibia, which can be confirmed
fluoroscopically as the anterior third of the tibia on a true lateral view of the ankle. It is important to maintain the axis of the clamp parallel to the joint line and to the anatomic syndesmotic angle. The clamp should furthermore be maintained 1-2cm proximal to the mortise, at the level of the incisura, to avoid deformation or undue translation of the fibula. Lastly, over-compression of the syndesmosis has been demonstrated, though the clinical implications remain controversial.
Putnam et al. performed a radiographic analysis of the ideal orientation for placement of a syndesmotic reduction clamp. Based on the CT scans of uninjured adult ankles, the authors showed that the trans-syndesmotic axis could be most reliably paralleled by a reduction clamp by placing the lateral tine on the lateral malleolar ridge and the medial tine radiographically within the anterior third of the tibia, anatomically half-way between the anterior and posterior cortices. They further specified that the ideal location was within the central one-third of the distance from the anterior tibial cortex to the anterior fibular cortex.
Cosgrove et al. prospectively evaluated the effect of medial clamp tine positioning on the incidence of syndesmotic malreduction. The authors found that malreduction most often resulted from deviation of the clamp axis from the syndesmotic axis. With the clamp at 1-2cm proximal to the mortise and the lateral tine on the lateral malleolar ridge, the ideal position of the medial tine was within the anterior third of the tibia. The rate of sagittal malreduction increased substantially with increasingly posterior placement of the medial tine. The medial clamp position did not affect coronal plane malreduction.
Gardner et al. review the technical considerations in reduction and fixation of syndesmotic injuries. The authors stress careful positioning of the reduction clamp, advocating that the clamp should be placed from the lateral malleolar ridge to the center of the anteroposterior width of the medial tibia.
Additionally, they note that placement too proximal or distal results in coronal plane deformity of the fibula, and that over-compression of the syndesmosis is certainly possible.
Figure A is the AP radiograph of the left ankle demonstrating a displaced medial malleolar fracture and syndesmotic widening. Figure B is the lateral radiograph of the ipsilateral knee showing an associated proximal fibular fracture.
Illustration A shows the syndesmotic angle and anatomic trans-syndesmotic axis as compared to the AP and lateral fluoroscopic axes. Illustration B shows the ideal positioning of the medial tine within the anterior third of the tibia on a true lateral view of the ankle.
Incorrect answers:
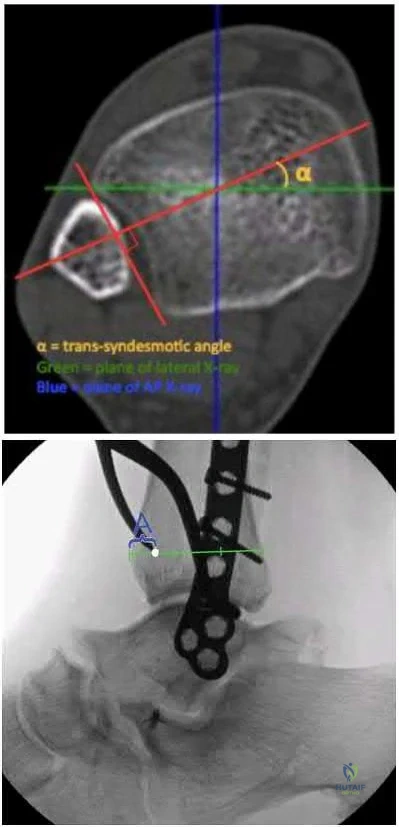
A 45-year-old male injures his wrist during Live Action Role Play in Chicago two weeks ago. He underwent operative fixation by and presents to your clinic for his 2 week follow-up visit. You review his operative note in which the surgeon reports having to apply a volar
locking plate in a distal position to secure the difficult intra-articular fracture. The patient shows you the lateral film in Figure A. You remove his splint, he has no difficulty moving any fingers, very minimal pain, and is not taking any narcotic medication. How do you counsel him about his post-operative period?

The plate may need to removed once the fracture is healed to reduce the chance of flexor pollicis longus injury
The plate may need to removed once the fracture is healed to reduce the chance of flexor carpi radialis injury
The plate may need to removed once the fracture is healed to reduce the chance of flexor digitorum superficialis – index finger injury
The patient should undergo revision fixation as soon as possible
The plate is in appropriate position and will likely never need to be removed Correct answer: 1
This patient’s volar locking plate (VLP) is distal to the "watershed line", extending volarly beyond the most volar aspect of the distal radius. He is at greatest risk for an attritional rupture of the FPL.
A VLP placed this distal and volar is more likely to cause flexor tendon injury.
Up to 12% of all patients undergoing volar plate fixation will experience flexor tendon injury, and the FPL is the most common tendon associated with the VLP (57% of total flexor tendon ruptures). The average time from fixation to flexor tendon rupture has been cited at 9 months. To judge if a plate is volar to the watershed line, a plum line can be made in the proximal direction from the most volar edge of the distal radius. If a plate is volar to this (Soong) line, the patient is thought to be at a higher risk for flexor tendon injury. As a result, this patient should be followed closely and if pain with thumb flexion is present after 3 months, the surgeon should consider plate removal so long as the fracture is healed to reduce the chance of FPL rupture. Ruptured tendons require repair, grafting, or transfer with hardware removal.
Griffin and Chhabra comprehensively reviewed the risk factors and adverse events following VLP fixation of distal radius fractures, including flexor tendonitis and rupture. They found that risk factors for flexor tendon rupture following VLP fixation included plate placement distal to the watershed line and that PQ repair does not seem to affect flexor tendonitis.
Agnew et al. analyzed wrist MRIs to determine the relationship between the flexor tendons and the watershed line. They found that at 3mm proximal to the watershed line, the FPL and FDP to the index finger were 2.6 and 2.2mm anterior to the volar rim of the distal radius. The authors suggested that distally placed plates are incredibly close to the flexor tendons.
Chilelli et al. described 24 of 48 wrists which had VLP following distal radius fracture and went on to experiences loss of FPL flexion post-operatively. They found that FPL ROM generally returned after 52 days, however with an associated average loss of 11° in thumb IPJ ROM. The authors attribute this to stripping of FPL from the bone during the volar approach.
Soong et al. divided patients who underwent VLP fixation for distal radius fractures into three groups according to position of plate relative to a plum line extending proximally from the most volar and distal aspect of the distal radius: those with a VLP dorsal to the Soong line (grade 0), those with the VLP volar to the Soong line but proximal to the rim (grade 1), and those with a VLP volar to the Soong line and at or distal to rim (grade 2). Of the 73 cases reviewed, the authors reported three flexor tendon ruptures, two of which were grade 2 position. The authors concluded that both position of plate and type of plate were contributors to flexor tendon injury following VLP fixation.
Figure A is a lateral radiograph of the wrist demonstrating appropriate reduction and fixation but with the VLP volar to the "watershed" or Soong line.
Illustration A is a lateral radiograph with Soong's line drawn to show that this plate is too volar.
Incorrect Answers:

A 42-year-old construction worker sustains a crush injury to the hand at a job site. He has immediate pain and significant swelling, and is taken to the local emergency department for evaluation. Radiographs do not demonstrate any fracture or dislocation. On exam,
he experiences severe pain with passive motion at the metacarpal phalangeal joints and when the wrist is flexed and extended.
Otherwise he has intact sensation and appropriate capillary refill. What is the next best step in diagnosis or treatment?
Advanced imaging
Arterial Doppler
Admission for overnight observation
Surgical intervention
Pain control
This patient presents with compartment syndrome of the hand. A history and clinical exam are the best tools to identify the diagnosis, and the treatment consists of emergent fasciotomies.
Compartment syndrome of the hand may be secondary to trauma, burn, IV drug use, extravasation of IV fluids, or major limb revascularization. The diagnosis is usually made with pain out of proportion to exam, particularly with passive stretch of the digits. It is possible to have compartment syndrome without neurovascular changes (paresthesia, pallor, pulselessness), particularly earlier in the presentation. Compartment measurements may be obtained and are considered diagnostic with an absolute value greater than 30mmHg or when the compartment pressure is within 30mmHg of the patient's diastolic blood pressure. However pressure testing is not necessary in most cases, but may be particularly important in the patient who is obtunded, intubated, or who had a block, as the physical exam will be confounded. There are ten hand compartments: hypothenar, thenar, adductor pollicis, four dorsal interosseous, and three palmar interosseous; and emergent surgical release of all ten compartments is indicated.
Codding et al. comprehensively reviewed hand compartment syndrome. The authors identify the history and physical exam as the most critical aspect of the diagnosis. More specifically, they noted that pain with passive stretch of the MCPJ is the most sensitive clinical sign on physical exam. The authors conclude the short comings of the research on hand compartment syndrome, but note the potential morbidity of a missed diagnosis is so great that the threshold for surgical intervention should be very low.
Lipschitz et al. reviewed the measurement of compartment pressures in the hand. The authors discussed technical pearls including leveling the monitor at the level of the heart, using local analgesia on the skin only, inserting the needle perpendicular to the skin, and measuring all 10 hand compartments.
They noted that any measurement greater than 30mmHg or within 30mmHg of the diastolic blood pressure may be considered diagnostic.
Illustration A shows the standard incisions utilized to release all ten hand compartments. Incisions are generally placed directly overlaying the thenar musculature, hypothenar musculature, the carpal tunnel, and dorsally over the metacarpals. The radial and ulnar border of each metacarpal are incised through the dorsal incisions to release the interossei compartments.
Incorrect Answers:

A 60-year-old woman with a history of well-controlled diabetes and hypertension sustained a fall into a ditch yesterday and presents with persistent left ankle pain and deformity. The injury is closed, and the patient is neurovascularly intact. Injury films are shown in Figures A and B. An unsuccessful attempt at reduction in the emergency department with sedation was made. What is the cause of failure of closed reduction?

Subacute nature of fracture
Incarceration of the deltoid ligament
Incarceration of the fibula behind the posterolateral ridge of tibia
Entrapment of the flexor hallucis longus (FHL) tendon
Entrapment of the extensor digitorum brevis (EDB) Correct answer: 3
The patient has sustained a Bosworth fracture-dislocation, which is a fixed dislocation of the fractured fibula behind the posterolateral tibial ridge. These fractures are generally irreducible via a closed means and require open reduction.
The initial radiographs in this vignette reveal posterior subluxation of the talus and fibula without significant coronal plane deformity. This deformity should raise the suspicion of a Bosworth fracture-dislocation, especially if closed reduction is unsuccessful. Bosworth fracture-dislocations can often be associated with posterior malleolar fractures, specifically of the posterolateral rim of the distal tibia. These injuries often fail closed reduction, given the engagement of the fibula behind the posterolateral tibial ridge, and frequently require open reduction. In this situation, the most effective method to reduce the fracture is through a posterolateral approach. This is the same approach that can then be utilized for the fixation of the posterolateral fragment and fibula.
Delasotta et al. discussed a case presentation of a 24-year-old male with a Bosworth fracture-dislocation in which the anterior compartment musculature was interposed within the fracture site, impairing both closed and eventual open reduction of the injury. The authors go on to discuss how 3D CT reconstruction of the bone and soft tissues can aid in both the diagnosis and preoperative planning of such injuries. They also note that these injuries should be admitted for compartment and neurovascular checks and undergo urgent surgical treatment.
Gardner et al. performed a cadaveric study directly comparing fixation of posterior malleolar fractures to syndesmotic stabilization in a simulated stage IV pronation-external rotation injury. Compared with the intact specimens, the authors found that fixation of the posterior malleolus restored 70% of the native stiffness, but syndesmosis stabilization only restored 40%. The authors concluded that given the likely integrity of the posterior inferior tibiofibular ligament in the setting of posterior malleolar fractures, anatomic reduction and fixation may be more appropriate than syndesmotic stabilization and better suited to restore stability.
Switaj et al. retrospectively evaluated the incidence of posterior malleolar fractures and posterior pilon variants in a 270 patients with operatively treated ankle fractures. The authors noted a relative frequency of posterior malleolar fractures of 50% and that of the posterior pilon variants of 20% within the entire cohort. While they found no significant difference in frequency of posterior malleolar or posterior pilon variants with regard to either AO/OTA or Lauge-Hansen classification, patients with posterior pilon variants were significantly older.
Figure A and B show the AP and lateral views of an ankle revealing a lateral malleolar fracture with tibiotalar subluxation and posterior dislocation of the fibula with respect to the posterolateral ridge of the tibia, consistent with a
Bosworth fracture-dislocation.
Incorrect answers:
A 42-year-old male who works as a professional clown presents with severe ankle pain and gross deformity after tripping and falling over his props at a children’s birthday party. His radiograph is shown in Figure A. Following fixation of the medial and lateral malleolar fractures, the syndesmosis is assessed and is found to be persistently unstable. All of the following are true regarding posterior malleolar fixation EXCEPT:

Fixation of the posterior malleolus obviates the need for syndesmotic fixation in most cases
Fixation of the posterior malleolus remains biomechanically inferior to trans-articular syndesmotic fixation
Functional and radiographic outcomes following posterior malleolar fixation are at least equivalent if not superior to those following syndesmotic fixation
Non-anatomic fixation of the posterior malleolus will compromise syndesmotic fixation
The syndesmosis is often incompletely injured in the setting of a posterior malleolar fracture
Fixation of the posterior malleolus has been shown to be biomechanically superior to single-screw trans-articular syndesmotic fixation. Anatomic reduction and fixation will most often obviate the need for syndesmotic fixation, as the posterior inferior tibiofibular ligament (PITFL) is typically intact and attached to the fragment.
Posterior malleolar integrity is essential to ankle function and stability. The posterior malleolus not only contains the talus posteriorly but adds to articular congruity for tibiotalar load transfer and contributes to rotatory ankle stability through the PITFL. As a result, posterior malleolar fractures compromise these critical functions. Operative management is therefore aimed at containment of
the talus, restoration of articular congruity, reduction of the incisura, and restoring integrity to the syndesmosis. Functional and radiographic outcomes following posterior malleolar fixation have been shown to be at least equivalent to those following syndesmotic fixation.
Miller et al. compared the need for syndesmotic fixation in bi- and tri-malleolar ankle fractures following anatomic reduction and fixation in the prone position versus initial conservative management in the supine position. The authors found that fixation of the posterior malleolus obviated the need for syndesmotic fixation in 97.9% of cases, while nearly 25% of patients with no initial fixation required stabilization. They concluded that prone positioning and anatomic fixation of the posterior malleolus should be performed as this adequately restored syndesmotic stability in almost all cases.
Gardner et al. performed a radiographic evaluation of syndesmotic integrity in the setting of pronation-external rotation stage 4 ankle fractures with associated posterior malleolar fractures. Based on radiographs and MRI, no complete tears of the posterior-inferior tibiofibular ligament were evident. The fracture pattern was then simulated in cadavers, and posterior malleolar fixation restored 70% of the native stability while syndesmotic fixation alone restored only 40% of the native stability. The authors advocated for posterior malleolar fixation over syndesmotic stabilization.
Miller et al. prospectively compared the outcomes following posterior malleolar and syndesmotic fixation for unstable ankle fractures with partial syndesmotic injury. At a minimum one-year follow-up, the authors found that patients who had undergone open reduction with fixation of posterior malleolar fractures had no difference in outcomes as compared to those who underwent syndesmotic fixation. They concluded that not only was syndesmotic reduction maintained at final follow-up following posterior malleolar fixation, but that functional outcomes were at least equivalent to syndesmotic fixation.
Fitzpatrick et al. evaluated the impact of posterior malleolar fixation toward restoring syndesmotic stability in a cadaveric supination-external rotation stage 4 fracture model. The authors found that failure to fix or anatomically reduce posterior malleolar fragments resulted in non-anatomic translation of the fibula and ultimately in syndesmotic malreduction. They advocated for anatomic reduction and fixation of larger posterior malleolar fractures.
Figure A is an AP radiograph of the right ankle demonstrating a displaced trimalleolar ankle fracture with maintained relationship between the distal fibula and posterior malleolar fragment.
Incorrect Answers:
A 35-year-old morbidly obese female presents with global right ankle pain and significant swelling after a misstep over one of her cats on the stairs. She is unable to bear weight, but the skin is intact. Injury films are shown in Figures A through D. What is the internervous plane through which direct anatomic reduction and fixation of both fractures could best be achieved?



Question 83
A 25-year-old man is brought to the emergency department following a motor vehicle accident. Extrication time was 2 hours, and in the field he had a systolic blood pressure by palpation of 90 mm Hg. Intravenous therapy was started, and on arrival in the emergency department he has a systolic blood pressure of 90 mm Hg with a pulse rate of 130. Examination reveals a flail chest and a femoral diaphyseal fracture. Ultrasound of the abdomen is positive. The trauma surgeons take him to the operating room for an exploratory laparotomy. At the conclusion of the procedure, he has a systolic pressure of 100 mm Hg with a pulse rate of 110. Oxygen saturation is 90% on 100% oxygen, and he has a temperature of 95.0° F (35° C). What is the recommended treatment of the femoral fracture at this time?
Explanation
REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopaedic surgery. J Trauma 2002;53:452-461.
Bosse M, Kellam JF: Orthopaedic decision making in the multiple trauma patient, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 133-146.
Question 84
Figure 1 points to the "tear drop" of the wrist. This radiographic landmark represents which anatomic portion of the wrist?
Explanation
Question 85
A 45-year-old man sustained the injury seen in Figure 130a 6 weeks ago. He denies any prior injury to his shoulder. After treatment of the injury in the emergency department, he was noted to have significant weakness with empty can testing and external rotation at the side. He has full passive range of motion with forward flexion, abduction, and internal and external rotation, but has difficulty initiating abduction with his arm at his side. He has negative apprehension and relocation signs. A detailed neurologic examination shows no deficits. A coronal image from a follow-up MRI scan is seen in Figure 130b. Follow-up radiographs reveal no fractures. What is the most appropriate next step in his treatment? Review Topic
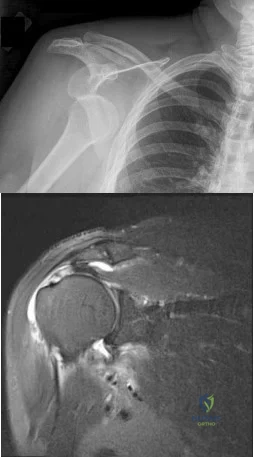
Explanation
Question 86
- A branch of what nerve is at risk for injury when vigorous superior/medial retraction is applied to the interval between the teres minor and the infraspinatus during a posterior approach to the shoulder?
Explanation
Question 87
A 38-year-old man who is an avid runner reports a several month history of right hip pain. Based on the radiograph and cross-sectional CT scan shown in Figures 33a and 33b, what is the most likely diagnosis for the lesions seen on the femoral neck?
Explanation
REFERENCES: Pitt MJ, Graham AR, Shipman JH, et al: Herniation pit of the femoral neck. Am J Roentgenol 1982;138:1115-1121.
Daenen B, Preidler KW, Padmanabhan S, et al: Symptomatic herniation pits of the femoral neck: Anatomic and clinical study. Am J Roentgenol 1997;168:149-153.
Question 88
A 21-year-old soccer player reports pain and is unable to straighten his knee following an acute injury during a game. He is unable to continue to play. An MRI scan is shown in Figure 3. What is the next most appropriate step in management?
Explanation
REFERENCES: Critchley IJ, Bracey DJ: The acutely locked knee: Is manipulation worthwhile? Injury 1985;16:281-283.
Bansal P, Deehan DJ, Gregory RJ: Diagnosing the acutely locked knee. Injury 2002;33:495-498.
Question 89
A toddler is brought in by his parents for evaluation of gait problems. Birth history and neurologic examination are unremarkable. After evaluating femoral torsion, tibial torsion, and foot contour, the diagnosis is excessive internal tibial torsion. The parents should be advised to expect which of the following outcomes? Review Topic
Explanation
Question 90
Figures 1 through 6 reveal the radiographs and MR images of a 30-year-old man who has a 1-year history of atraumatic medial-sided left knee pain refractory to nonsurgical measures. What is the most appropriate treatment?

Explanation
Question 91
A 6-year-old boy is being treated for acute hematogeneous osteomyelitis of the distal femur with intravenous antibiotics. The best method to determine the success or failure of initial treatment is by serial evaluations of which of the following studies?
Explanation
REFERENCES: Unkila-Kallio L. Kallio MJ, Eskola J, et al: Serum C-reactive protein, erythrocyte sedimentation rate, and white blood cell count in acute hematogenous osteomyelitis of children. Pediatrics 1994;93:59-62.
Herring JA(ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia. PA. WB Saunders, 2008, pp 2090-2100.
AL-Madena Copy
Question 92
The peroneus tertius is a commonly used landmark for arthroscopic portal placement. What is the function of this tendon?
Explanation
REFERENCES: Joshi SD, Joshi SS, Athavale SA: Morphology of the peroneus tertius muscle.
Clin Anat 2006;19:611-614.
Williams PL, Bannister LH, Berry MM, et al (eds): Gray’s Anatomy, ed 38. London, Churchill Livingston, 1995, p 883.
Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 21.
Question 93
A 17-year-old woman seen in the emergency department reports right knee pain and swelling that has progressively worsened over the past several weeks. Radiographs are shown in Figures 31a and 31b. What is the most likely diagnosis?
Explanation
REFERENCES: Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Question 94
A 67-year-old woman is seen in the emergency department after falling at home. Radiographs before and after treatment are shown in Figures 49a and 49b, respectively. Which of the following best explains the 8-week postinjury clinical findings seen in Figure 49c?
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 273-284.
Neviaser RJ, Neviaser TJ, Neviaser JS: Anterior dislocation of the shoulder and rotator cuff rupture. Clin Orthop Relat Res 1993;291:103-106.
Question 95
The MRI scans reveal a root tear of the medial meniscus. Studies demonstrate that this tear pattern greatly increases the tibiofemoral contact forces. These forces, and meniscal extrusion, worsen with increasing flexion. Correct answer : B 69- A 45-year-old postmenopausal smoker with a body mass index (BMI) of 22 has had severe knee pain for the past year. The pain has been progressing and the patient is now only able to perform activities of daily living. Knee radiographs reveal medial compartment osteoarthritis without any involvement of the patellofemoral joint or the lateral compartment. What is the contraindication for a high tibial osteotomy (HTO) in this patient?
Explanation
A. Healed one-level anterior cervical fusion
B. Congenital atlanto-occipital fusion
C. Cervical disk herniation previously treated nonoperatively
D. Spina bifida occulta
The one overriding principle regarding the return to any collision sport, as Torg and associates has described, is that the athlete be "neurologically intact, asymptomatic, and pain-free and have full strength and full cervical range of motion". Forces exerted on the cervical spine can be absorbed by the "elasticity of the intervertebral disk, the mobility of the spine itself, and the impact of absorbing capabilities of the cervical paravertebral musculature". The C1 and C2 levels (atlanto-occipital level) control movement of the skull and articulate the large motion movements. Specifically, partial or complete 56
congenital fusion of the atlas to the base of the occiput results in progressive cord compression by the posterior lip of the foramen magnum. It can result in sudden death.
A cervical disk herniation that was previously treated nonsurgically and is not causing cord compression in the currently asymptomatic patient is not a contraindication to return to collision sports. Spina bifida occulta is common (10-20% of healthy individuals). It is typically an incidental finding and does not result in neurologic problems. If individuals have a healed anterior, lateral or posterior disk herniation that is treated nonsurgically and they are currently asymptomatic, then there is no contraindication to participation in contact sports. If they require a diskectomy and fusion and they have a solid/healed fusion, are asymptomatic and neurologically intact with full and pain-free range of motion, then there is no contraindication to return to collision sports. An acute disk herniation, a disk herniation with associated pain or neurologic symptoms, or the presence of cord compression or loss of normal lordosis are all contraindications.
71- Based on the injury shown on the axial MRI scan of the shoulder in Figure 1, what other pathology should be closely examined for during surgery?
A. Subscapularis tear
B. Supraspinatus tear
C. Superior labral anterior- posterior (SLAP) tear
D. Bankart tear
The axial MRI scan reveals a subluxated biceps tendon. In the study by Koh and associates, 85% of patients with a biceps subluxation on MRI were found to have a subscapularis tear at the time of arthroscopy. These are not always obvious on the MRI, and close inspection of the leading edge/upper border of the subscapularis tendon at the time of arthroscopy is necessary. Although supraspinatus tears, SLAP tears, and Bankart tears can all occur in conjunction with a biceps subluxation, none have been shown to be strongly correlated with this pathology, nor as specific to this pathology.
73- Figures 1 through 4 are the MRI scans of a 24-year-old former collegiate basketball player who injured his left knee while playing recreational basketball 10 days prior to presentation. He landed from a jump awkwardly and reported that his knee gave out. He heard a pop at the time of injury and was unable to continue playing. He complains of medial and lateral knee pain and difficulty with weight bearing. On physical examination, he has a moderate effusion and his range of motion is from 10° to 80°. Ligament examination reveals a 2B Lachman, negative posterior drawer as well as negative varus and valgus stress testing. What is the diagnosis?
A. Meniscus tear
B. Anterior cruciate ligament (ACL) tear
C. ACL tear and posterior cruciate ligament (PCL) tear
D. ACL tear and medial meniscus tear
Question 96
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. A large intra-articular and intrapelvic pseudotumor has developed. What predominant histological feature(s) is/are present in such a lesion?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross-sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 97
Which of the following is true regarding plating of humeral shaft fractures compared to intramedullary nailing?

Explanation
Question 98
A 27-year-old woman has a bilateral C5-C6 facet dislocation and quadriparesis after being involved in a motor vehicle accident. Initial management consisted of reduction with traction, but she remains a Frankel A quadriplegic. To facilitate rehabilitation, surgical stabilization and fusion is planned. From a biomechanical point of view, which of the following techniques is the LEAST stable method of fixation?
Explanation
REFERENCES: Sutterlin CE III, McAfee PC, Warden KE, et al: A biomechanical evaluation of cervical spine stabilization methods in a bovine model: Static and cyclical loading. Spine 1988;13:795-802.
Coe JD, Warden KE, Sutterlin CE III, et al: Biomechanical evaluation of cervical spine stabilization methods in a human cadaveric model. Spine 1989;14:1122-1131.
Question 99
..Figure 76 is the radiograph of a 77-year-old patient with a history of myeloma who has had severe arm pain after opening a jar. Pain was present for 3 months prior to injury. The most biomechanically stable construct for this fracture is
Explanation
Figures 77a through 77c are the radiograph and MRI scans of a 45-year-old woman who enjoys dancing and has had left ankle pain for approximately 1 month with minimal trauma. She has slightly limited ankle dorsiflexion with a mechanical block with pain.

Question 100
Figures 10a and 10b show the radiographs of an athletic 9-year-old boy who has activity-related anterior knee pain with intact active knee extension. Examination reveals tenderness to palpation over the inferior pole of the patella. There is no effusion or ligamentous instability. Initial management should consist of
Explanation
REFERENCES: Stanitski CL: Anterior knee pain syndromes in the adolescent. J Bone Joint Surg Am 1993;75:1407-1416.
Stanitski CL: Anterior knee pain syndromes in the adolescent, in Schafer M (ed): Instructional Course Lectures 43. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1994, pp 211-220.
