Orthopedic Board Prep MCQs: Trauma, Knee & Foot Surgery | Part 180
Key Takeaway
This page offers Part 180 of a comprehensive OITE/AAOS Orthopedic Surgery Board Review. Featuring 100 verified, high-yield MCQs, it's designed for orthopedic residents and surgeons preparing for board certification exams. Utilize interactive study or exam modes with clinical explanations to master crucial topics like Elbow, Foot, and Trauma.
About This Board Review Set
This is Part 180 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 180
This module focuses heavily on: Elbow, Foot, Fracture, Knee, Tendon, Trauma.
Sample Questions from This Set
Sample Question 1: What is the best option for treatment of the fracture shown in Figure 55?...
Sample Question 2: Figure 38a shows the radiograph of a 12-year-old boy who underwent a reamed intramedullary nailing for a closed femoral shaft fracture. One year after rod removal, he reports groin pain. A current radiograph is shown in Figure 38b. The find...
Sample Question 3: Figures 100a and 100b are the MRI scans of a 45-year-old man who has had elbow and proximal forearm pain for the past 8 months. He can recall no specific trauma and symptoms have not lessened despite his adopting job modifications that limi...
Sample Question 4: Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of...
Sample Question 5: Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal L...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What is the best option for treatment of the fracture shown in Figure 55?

Explanation
Question 2
Figure 38a shows the radiograph of a 12-year-old boy who underwent a reamed intramedullary nailing for a closed femoral shaft fracture. One year after rod removal, he reports groin pain. A current radiograph is shown in Figure 38b. The findings are most likely the result of
Explanation
REFERENCES: Letts M, Jarvis J, Lawton L, et al: Complications of rigid intramedullary rodding of femoral shaft fractures in children. J Trauma 2002;52:504-516.
Stans AA, Morrissy RT, Renwick SE: Femoral shaft fracture treatment in patients age 6 to 16 years. J Pediatr Orthop 1999;19:222-228.
Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop 1997;338:60-73.
Beaty JH, Austin SM, Warner WC, et al: Interlocking intramedullary nailing of femoral-shaft fractures in adolescents: Preliminary results and complications. J Pediatr Orthop
1994;14:178-183.
Question 3
Figures 100a and 100b are the MRI scans of a 45-year-old man who has had elbow and proximal forearm pain for the past 8 months. He can recall no specific trauma and symptoms have not lessened despite his adopting job modifications that limit lifting. He has discomfort with resisted elbow extension and pronation. The biceps tendon can be easily palpated. Treatment should consist of which of the following? Review Topic
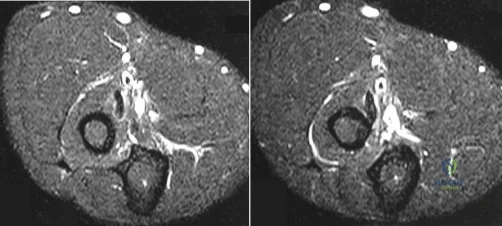
Explanation
physical therapy, and modality, surgical treatment is indicated. Exploration, debridement, and reattachment with one of a variety of techniques are the standards of care. No lipomatous mass is seen on the MRI scan. There is no weakness in finger extension to suggest posterior interosseous nerve palsy. Transfer of the biceps would result in loss of supination strength. Endoscopic biceps tendon surgery is reserved for long-head pathology.
Question 4
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of
Explanation
REFERENCES: Teng AL, Pinzur MS, Lomasney L, et al: Functional outcome following anatomic restoration of the tarsal-metatarsal fracture dislocation. Foot Ankle Int
2002;23:922-926.
Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Question 5
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. Left untreated, injury to this structure most likely will lead to degenerative changes in

Explanation
Dial test finding. A valgus-producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used. Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
Question 6
Which of the following nerves is susceptible to entrapment near the calcaneal attachment site of the plantar fascia and can mimic or co-exist with plantar fasciitis?
Explanation
REFERENCES: Bordelon RL: Heel pain, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 837-857.
Mann RA, Baxter DE: Diseases of the nerves, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 543-574.
Baxter DE: The heel in sport. Clin Sports Med 1994;13:683-693.
Question 7
A 16-year-old boy sustains a twisting injury to the left knee while wrestling. MRI scans are shown in Figures 22a through 22c. What is the most likely diagnosis? Review Topic

Explanation
Question 8
Which of the following complications is more likely with an inside-out repair technique compared to an all-inside techniques for a medial meniscus tear?
Explanation
REFERENCES: Farng E, Sherman O: Meniscal repair devices: A clinical and biomechanical literature review. Arthroscopy 2004;20:273-286.
Jones HP, Lemos MJ, Wilk RM, et al: Two-year follow-up of meniscal repair using a bioabsorbable arrow. Arthroscopy 2002;18:64-69.
Question 9
A 7-year-old boy has had low back pain for the past 3 weeks. Radiographs reveal apparent disk space narrowing at L4-5. The patient is afebrile. Laboratory studies show a WBC count of 9,000/mm P 3 P and a C-reactive protein level of 10 mg/L. A lumbar MRI scan confirms the loss of disk height at L4-5 and reveals a small perivertebral abscess at that level. To achieve the most rapid improvement and to lessen the chances of recurrence, management should consist of
Explanation
REFERENCES: Ring D, Johnston CE II, Wenger DR: Pyogenic infectious spondylitis in children: The convergence of discitis and vertebral osteomyelitis. J Pediatr Orthop
1995;15:652-660.
Crawford AH, Kucharzyk DW, Ruda R, et al: Diskitis in children. Clin Orthop 1991;266:70-79.
Question 10
Kinematic testing of patellofemoral motion demonstrates that malalignment that produces increased Q angle causes a shift of the patella laterally in the trochlear groove and is most pronounced during what phase of the flexion arc? Review Topic
Explanation
Question 11
A 55-year-old man who underwent total shoulder arthroplasty 10 years ago recently reports an increase in shoulder pain. Laboratory studies consisting of a white blood cell count, erythrocyte sedimentation rate, and C-reactive protein are all negative, as is joint aspiration. Radiographs are shown in Figures 95a and 95b. If all intraoperative frozen sections are negative, what is the appropriate treatment during revision surgery to provide pain relief and improved function? Review Topic
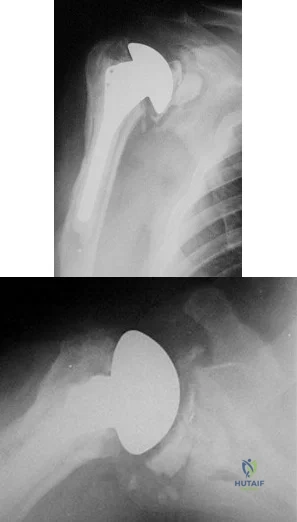
Explanation
Question 12
Examination of an obese 3-year-old girl reveals 30 degrees of unilateral genu varum. A radiograph of the involved leg with the patella forward is shown in Figure 10. Management should consist of
Explanation
REFERENCES: Johnston CE II: Infantile tibia vara. Clin Orthop 1990;255:13-23.
Richards BS, Katz DE, Sims JB: Effectiveness of brace treatment in early infantile Blount’s disease. J Pediatr Orthop 1998;18:374-380.
Question 13
A 13-year-old pitcher reports the immediate onset of medial elbow pain after throwing a pitch. Upon examination, the patient is tender to palpation at the medial epicondyle and has pain and instability with valgus testing of the elbow. What would be the most appropriate initial diagnostic test for this patient?
Explanation
injury and/or bony injury.
Question 14
When discussing treatment options with a 35 year-old healthy male with an isolated, closed tibial shaft fracture, the surgeon should inform him that in comparison to closed treatment, the advantages of intramedullary nail fixation include all of the following EXCCEPT?

Explanation
In a study of 94 tibial fractures, Finkemeier reported 10 (11%) had compartment syndromes. Three of the 10 patients developed the compartment syndrome postoperatively.
In comparing IM nailing to non-op, Bone et al showed that IM nailing had a shorter time to union (mean, 18 vs 26 weeks; p = 0.02), lower non-union rate (2% vs 10%), decresed incidence of shortening (2% vs 27%), and quicker return to work (mean, 4 vs 6.5 months), but no difference in compartment syndrome (0% in both groups).
The classic article cited by Sarmiento el al. reported that closed treatment with use of a prefabricated functional below-the-knee brace was effective in a study of 1000 closed diaphyseal fractures of the tibia with an incidence of nonunion of only 1.1%. However, those authors had very strict criteria for use of the fracture-brace (exclusion criteria included intact fibular, shortening >2cm).
Question 15
A decrease in alkaline phosphatase would most likely be manifest in which metabolic disorder?
Explanation
TNSALP is found in osteoblasts and hydrolyzes inorganic phosphates, leading to an increase in serum phosphate levels, which helps to maintain physiologic levels. A decrease in this process impairs bone mineralization leading to rickets. In the perinatal period, hypophosphatasia and decreased mineralization leads to caput membraneceum, shortened limbs and respiratory failure. Childhood hypophosphatasia is marked by premature loss of deciduous teeth and rachitic deformities. Adult hypophosphatasia I is characterized by teeth and chest wall deformities (similar to adolescent hypophosphatasia) as well as recurrent metatarsal and femoral stress fractures.
Mornet reviewed hypophosphatasia and the alkaline phosphatase mutations. Screening for the 65 distinct mutation can aid in diagnosis and family counseling in severe forms.
Illustration A shows abnormal dentition found in hypophosphatasia. Illustration B shows widespread rachitic changes characteristic of hypophosphatasia.
Incorrect Answers:
Question 16
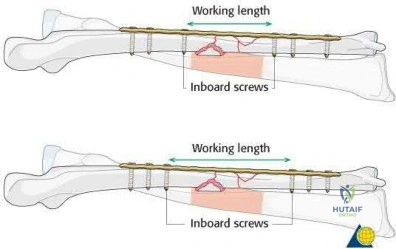
What is a known risk factor for lateral distal femoral locking plate failure when used for the fixation of comminuted extra-articular fractures?
Explanation
Implant failure is common in distal femur fractures stabilized with plate fixation. Contributors to failure include a short working length of the construct, plate-screw density more than 0.5 and short plate lengths. This will lead to failure as it causes increased strain on the plate over a short segment, and
does not allow enough motion at the fracture site to form bone for healing by secondary intention.
Ricci et al. reviewed 355 cases of distal femur plate fixation. 64 patients (19%) required reoperation to promote union, including 30 that had a planned staged bone grafting. Risk factors for proximal implant failure included open fracture, smoking, increased body mass index, and shorter plate length.
Kregor et al. reviewed 119 patients with distal femoral plate fixation. They found that 93% fractures healed without acute bone grafting. Complications included 5 losses of proximal fixation, 2 nonunions, and 3 acute infections.
Illustration A is an AP of the distal femur demonstrating a comminuted distal femur fracture which has failed fixation with a laterally based distal femur locking plate. It has undergone varus collapse which is a common mechanism of failure for these injuries. Illustration B is a series of AP radiographs of the distal femur of the same patient that was revised to an intramedullary retrograde nail. Illustration C and D show the concepts of plate length, plate-to-screw density and the working length of the plate.
Incorrect Answers:

OrthoCash 2020
Question 17
A 42-year-old man sustained a fracture of the distal radius with subsequent stiffness in the ipsilateral shoulder. Despite a 6-month program of range-of-motion exercises, external rotation at the side is limited to 10 degrees. Attempts at closed manipulation are unsuccessful. Treatment should now consist of
Explanation
REFERENCE: Harryman DT II, Matsen FA III, Sidles JA: Arthroscopic management of refractory shoulder stiffness. Arthroscopy 1997;13:133-147.
Question 18
A 12-year-old girl who is 3 months postmenarchal undergoes full-time brace treatment for scoliosis. The posteroanterior radiograph (Figure A ) taken at that time reveals a right thoracic curve measures 28 degrees, and the left lumbar curve measures 23 degrees. At age 15, after 3 years of bracing, a repeat posteroanterior radiograph is obtained, now revealing a right thoracic curve measuring 11 degrees and the left lumbar curve measuring 19 degree, and Risser 4. Which statement best represents the indicated course of action in this patient? Review Topic

Explanation
Curves <25° can be treated with observation, while flexible curves from 25° to 45° in skeletally immature patients (Risser 0, 1, 2) should be treated with bracing. Bracing success is most commonly defined as <5° curve progression and failure is 6° or more curve progression at orthotic discontinuation (skeletal maturity), absolute progression to >45° either before or at skeletal maturity, or discontinuation in favor of surgery. Skeletal maturity is defined Risser sign 4, <1cm change in height over 2 visits 6 months apart, 2 years postmenarchal.
Richards et al. attempted to define parameters for future AIS bracing studies. Outcome measures should include patients with (1) <5° curve progression vs >6° progression at maturity, (2) curves exceeding 45° at maturity, or those who have had surgery recommendation/undergone.
Negrini et al. performed a Cochrane systematic review. Basing conclusions on 2
studies, they found that (1) a brace treated curve progression (74% success) better than observation (34% success) and electrical stimulation (33% success), and (2) a rigid brace is more successful than an elastic one (SpineCor) at curbing curve progression.
A
is
a
standing
PA
radiograph
showing.
Incorrect
Question 19
5 units PRBCs. The estimated blood loss was 1276cc and not affected by the fracture pattern or high/low energy pattern. They concluded that preoperative hemorrhage contributed to transfusion needs more than intraoperative blood loss.
Explanation
Lateral malleolus fractures can be treated with a variety of techniques, including posterior antiglide plating or lateral neutralization plating. What is an advantage of using lateral neutralization plating instead of posterior antiglide plating?
Decreased joint penetration of distal screws
Increased rigidity
Decreased need for delayed hardware removal
Decreased peroneal irritation
Improved distal fixation Corrent answer: 4
Posterior antiglide plating is a technique that involves placement of a plate on the posterior aspect of the distal fibula, using the plate as a reduction tool and direct buttress against distal fracture fragment displacement.
Schaffer et al showed from a biomechanical standpoint that posterior antiglide plating was superior to lateral neutralization plating for distal fibula fracture fixation.
Weber et al reported a (30/70) 43% rate of plate removal secondary to peroneal discomfort. In addition, peroneal tendon lesions were found in 9 of the 30 patients.
OrthoCash 2020
A 24-year-old female sustains a surgical neck proximal humerus fracture in a motor-vehicle collision. She undergoes open reduction and internal fixation but heals in 45 degrees of varus and has significant limitation of shoulder range of motion despite 9 months of conservative treatments. What is the most appropriate treatment at this time?
Manipulation under anesthesia
Humeral head resurfacing
Shoulder hemiarthroplasty
Revision open reduction internal fixation with osteotomy
Reverse total shoulder arthroplasty Corrent answer: 4
Malunions of the proximal humerus typically result in significant restrictions in range of motion. This young patient has sustained a proximal humeral malunion, and treatment should include a corrective osteotomy for improved outcomes, as she has failed conservative treatment.
The cited reference by Williams et al as well as the referenced article by Siegel et al explain various techniques in management of proximal humerus malunions. They state that the two primary indications for surgical management of proximal humerus malunion include 1) pain and 2) diminished function resulting from limited range of motion. Because this patient is young, you would attempt revision ORIF/osteotomy as opposed to humeral head arthroplasty.
OrthoCash 2020
A 6-year-old boy with progressive bilateral genu varum undergoes the surgeries shown in Figure A. On postoperative rounds later that day, the patient appears sedated after several doses of pain medication. His toes are pink with brisk capillary refill however, passive motion of his toes causes pain. Among the answer choices listed, what is the best management strategy for this child?

Elevate his legs and reevaluate on morning rounds
Adjust his pain medication to accommodate for his increasing pain
Administer a muscle relaxant for leg spasms
Cast removal and measurement of compartment pressures with a standard device
Examine the cast for areas of constriction and reevaluate in the morning Corrent answer: 4
Intracompartmental pressure measurements should be performed when pain with passive motion of the toes is found in young patients with insufficient clinical data to establish a definitive diagnosis of compartment syndrome. The child in this clinical vignette has Blount’s disease which was treated with bilateral tibial osteotomies, a procedure commonly associated with compartment syndrome.
Pain with passive stretch is the most sensitive clinical sign of elevated compartment pressures prior to the onset of ischemia in compartment syndrome. Pain is difficult to assess in children at baseline, therefore, a high level of suspicion should exist and compartment pressure monitoring should be performed in unreliable patients.
Mubarak et al. reported on a series of 27 patients subjected to intracompartmental pressure monitoring for a clinical suspicion of acute compartment syndrome. The wick catheter technique was employed not only to aid in the diagnosis of compartment syndrome at an early stage but also to indicate the effectiveness of the decompressions when used intraoperatively during fasciotomies.
Matsen et al. reported on 24 children with compartment syndrome following injuries and surgery. The most common etiologies identified were fractures, vascular injuries, and tibial osteotomies. Compartment pressure measurements were helpful in establishing the diagnosis of compartment syndrome in young patients and in those with neurologic or vascular injuries with ambiguous clinical findings.
Figure A reveals an AP radiograph of bilateral knees status post valgus-producing tibial osteotomies and epiphysiolyses of the medial tibial physes in a 6-year-old male with Blount’s disease.
Incorrect Answers:
OrthoCash 2020
A 16-year-old male was struck by an automobile while riding his bicycle. He sustained the injuries in Figure A. Which of the following orthopedic injuries is MOST associated with this injury?

Brachial plexus injury
Ipsilateral clavicle fracture
Pelvic ring injury
Rib fracture
Spine fracture
Figure A demonstrates a scapula body fracture. Rib fractures are the most common orthopedic injury associated with these high-energy fractures, with a 52% incidence.
Scapula fractures are associated with high-energy trauma and have a reported mortality rate of 2-5%. Approximately 50% of high-energy scapular fractures involve the body and spine. Most scapular fractures may be treated conservatively with sling immobilization followed by early motion with no expected functional deficits. Indications for operative management of scapular fractures include glenohumeral instability with >25% of glenoid involvement or
>5mm of articular step-off, excessive medialization of the glenoid, displaced scapular neck or coracoid fractures, and open fractures.
Baldwin et al. retrospectively reviewed 9,543 scapular fractures utilizing the US National Trauma Database. They reported that the most commonly associated fractures were rib fractures (52.9%), followed by fractures of the spine (29.2%), clavicle (25.2%), and pelvis (15.3%). They concluded that lung and head injuries occurred in 47.1% and 39.1% of the cases, respectively.
Brown et al. retrospectively reviewed the association between scapular fractures (SF) and blunt thoracic aortic injury (BTAI). They found that in 35,541 blunt trauma admissions, SF and BTAI occurred in 1.1% and 0.6% of patients, respectively. They noted that most of the patients with SF had associated injuries (99%), but only four patients with SF had BTAI. The most common injuries associated with SF were rib (43%), lower extremity (36%), and upper extremity (33%) fractures. They concluded that SF is uncommon after blunt trauma, but patients with SF almost always have significant associated injuries and indicates a high amount of energy.
Figure A demonstrates a high-energy scapular body fracture which may benefit from surgical intervention
Incorrect Answers:
OrthoCash 2020
Which of the following amputations will lead to the greatest oxygen requirement per meter walked following prosthesis fitting?
Above-knee-amputation (transfemoral)
Below-knee-amputation (transtibial)
Through Knee
Syme
Midfoot
The general trend is increasing energy requirement for more proximal amputations. Amputation should be performed at the lowest possible level in order to preserve the most function.
Pinzur compared 5 patients with amputations at midfoot, Syme’s, BKA, through knee, and AKA with five controls. Walking speed and cadence decreased while oxygen consumption per meter walked increased with each more proximal amputation.
The only exception is the Syme which was the most energy efficient even though it is more proximal to the midfoot amputation.
OrthoCash 2020
An otherwise healthy 30-year-old male sustains a left forearm injury as a result of a fall from a ladder. Initial examination in the emergency room reveals a clean 2 centimeter laceration over the volar forearm associated with the radiographs shown in Figures A and B. Treatment should consist of irrigation and debridement of the wound followed by which of the following?

Closed reduction and casting of left radius and ulna
Temporary external fixation of the left radius and ulna
Definitive external fixation of the left radius and ulna
Open reduction and internal fixation of the left radius and ulna with delayed skin closure
Open reduction and internal fixation of the left radius and ulna with immediate skin closure
The clinical scenario is consistent with an open fractures of the distal radial and ulnar shafts. Literature shows that definitive plating of an open forearm fracture followed by primary closure of the wound is acceptable treatment at the time of injury.
Chapman et al performed a retrospective review of 50 patients with immediate internal plate fixation of an open diaphyseal fracture of the forearm. The functional results were excellent or good in 85%.
The review by Levin is a comprehensive review of the literature on early versus delayed closure of open fractures, and covers the change in thought from previous literature, including change in technology, surgical techniques, and a more critical review of previous literature.
OrthoCash 2020
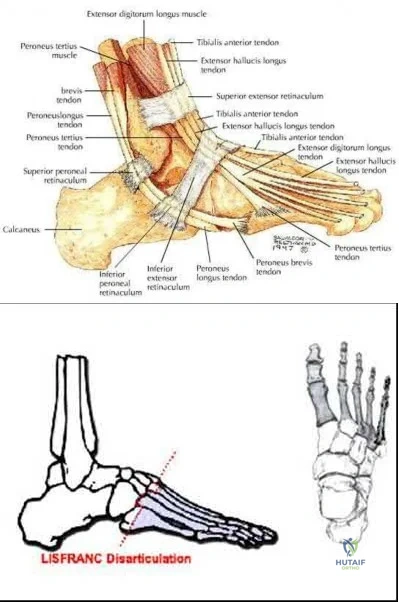
During a Lisfranc (tarsometatarsal) amputation of the foot, which of the following is crucial to prevent the patient from having a supinated foot during gait.
Releasing the posterior tibialis tendon
Preserving the soft-tissue envelope (peroneus brevis, tertius and plantar fascia) around the fifth metatarsal base
Myodesis of the anterior tibialis to the medial and middle cuneiforms
Lengthening of the gastrocsoleus (achilles tendon)
Osteotomy through 1st metatarsal Corrent answer: 2
A Lisfranc amputation is through the tarsometatarsal joints, except the 2nd metatarsal, which is osteotomized to preserve the stability of the medial cuneiform. To prevent the patient from supinating the foot following this amputation, the evertors on the foot must be maintained. The principal evertors are the peroneus brevis and longus (Illustration A). Therefore, the function of the peroneus brevis must be preserved. Technically this is done preserving the soft-tissue envelope (peroneus brevis, tertius and plantar fascia) around the fifth metatarsal base.
Illustration B depicts the level of a Lisfranc amputation of the foot. Incorrect Answers:
The posterior tibialis is the primary supinator of the foot, and releasing it
would lead to an eversion deformity. The tibialis posterior tendon attachment to the bases of the second and third metatarsals will actually be released with this amputation, but the main attachment to the navicular preserved.
The anterior tibialis dorsiflexes and inverts the foot, but transferring it to the medial and middle cuneiforms would mimick its native function to dorsiflex and invert the foot.
A lengthened Achilles would lead to increased dorsiflexion, not supination.
Osteotomy of 2nd MT is crucial to preserve the medial cuneiform and midfoot stable.
OrthoCash 2020
A 39-year-old male is thrown from his motorcycle into a fast-food restaurant and sustains a closed pelvic ring injury. During placement of percutaneous iliosacral screws, the outlet radiograph in Figure A is obtained. What purpose does this view serve?
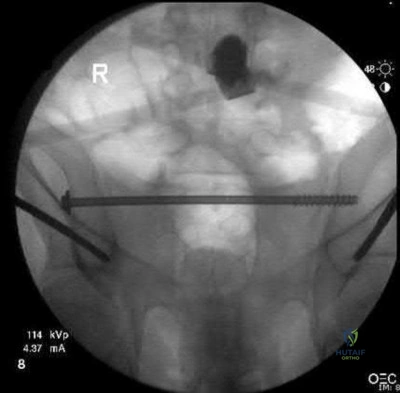
Evaluation of possible injury to L5 nerve root
Evaluation of anterior-posterior position of screw(s)
Best visualization of sagittal curvature of sacral ala
Best visualization of spinal canal
Best visualization of sacral neural foramina Corrent answer: 5
Figure A shows an intraoperative outlet view, which provides the best visualization of the neural foramina (and possible screw placement into these foramina). This view provides information regarding cephalad-caudad placement of the screw, whereas the inlet view provides information regarding the anterior-posterior position of the screw. The lateral sacral view provides information regarding the sagittal curvature of the sacral ala and gives information regarding possible iatrogenic L5 nerve injury as it goes over the sacral ala.
The referenced article by Routt et al is a review article regarding the safety and techniques of percutaneous pelvic ring fixation.
OrthoCash 2020
A 35-year-old male sustains a closed Schatzker VI tibial plateau fracture. Two weeks following external fixation, examination reveals intact sensation, palpable pulses and no soft tissue compromise. An axial CT image is shown in Figure A. What is the optimal surgical plan?
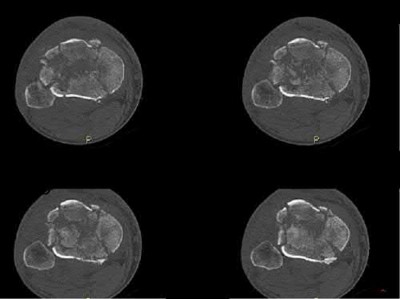
Medial and lateral plate fixation through two approaches
Medial and lateral plate fixation through a single anterior approach
Lateral locking plate fixation
Continued external fixation until union
Multiplanar transarticular external fixator Corrent answer: 1
The Figure shows a bicondylar tibial plateau fracture. The goals that need to be met when treating tibial plateau fractures are the following: restoration of mechanical axis alignment, restoration of condylar width, articular reduction, and restoration of knee stability. Since the soft tissue envelope is favorable, open reduction internal fixation with dual incisions and dual plates will provide the best probablity of achieving those goals.
Gosling et al did a biomechanical evaluation in cadavers comparing lateral locked plating with a combined medial and lateral plate and found no difference in resistance to vertical subsidence even with loads exceeding the average body weight. However, this was a cadaveric study with no mention and capability of analyzing articular reduction. Lateral locked plating only allows for indirect reduction of the medial plateau.
Barei et al in a retrospective review found that comminuted bicondylar tibial plateau fractures can be successfully treated with open reduction and medial and lateral plate fixation using 2 incisions, and postulate that the use of 2 incisions may contribute to a lower wound complication rate. A two incision approach allows not necessarily for a stronger construct as some studies are controversial, but for a more accurate reduction and restoration of alignment.
OrthoCash 2020
Which of the following is true regarding the use of the saline injection load test to diagnose traumatic knee arthrotomies?
Addition of methylene blue to the saline load test increases the sensitivity of the test
Injection of 110ml of saline will diagnose 95% of knee arthrotomies
Injection of 175ml of saline will diagnose 99% of knee arthrotomies
A superomedial injection location requires significantly less fluid than a inferoeromedial injection location
A history and physical exam by an orthopaedic surgeon has equivalent sensitivity to saline load test at detecting a traumatic arthrotomy
Injection of 175ml of saline will diagnose 99% of knee arthrotomies.
Clinical evaluation alone to determine if a periarticular laceration has penetrated the joint can often be incorrect. A Saline Load Test (SLT) is an effective methods to detect intraarticular penetration. New studies have shown addition of methylene blue does not improve the diagnostic value of the saline load test. The use of a CT scan can be helpful, especially in the presence of intra-articular air.
Voit et al. investigated the sensitivity of the clinical exam and a saline load test in 50 consecutive patients with periarticular lacerations suggestive of joint penetration. In 14 there was leakage of fluid on saline load test. In six of these patients, the clinician had judged there was no traumatic arthrotomy based on physical exam and clinical history. They therefore concluded performing a saline load test is important adjunct and the clinical exam alone can not be relied on to detect traumatic arthrotomies.
Nord et al. found that the volumes of saline that were needed in order to effectively diagnose 75%, 90%, 95%, and 99% of the knee arthrotomies were
110, 145, 155, and 175 mL, respectively. They also found that an inferomedial injection location required significantly less fluid than a superomedial injection location did.
Metzger et al. studied 58 patients that underwent saline load test with about 100ml of saline injected (methylene blue 29, normal saline 29). They found that the false-negative rate was 67% (methylene blue 69%, normal saline 66%). They concluded the addition of methylene blue does not improve the diagnostic value of the saline load test.
Konda et al. performed a study evaluationg the role of CT scan versus saline load test. They found that the sensitivity and specificity of the CT scan to detect traumatic arthrotomy was 100%. In a subgroup of 37 patients that received both a CT scan and the conventional saline load test, the sensitivity and specificity of the CT scan was 100% compared to 92% for the saline load test (p<0.001).
Incorrect Answers:
OrthoCash 2020
A 36-year-old rancher is involved in a tractor roll-over accident and sustains the injury shown in Figure A to his dominant right arm. After undergoing rigid anatomic fixation of the fracture, the distal radio-ulnar joint (DRUJ) remains incongruent. What is the next step in management?

Revision plating of the fracture
Revision reduction and intramedullary fixation
Reduction of interposed extensor carpi ulnaris tendon
Reduction of interposed pronator quadratus tendon
Reduction of interposed flexor carpi ulnaris tendon Corrent answer: 3
The most likely cause of persistent DRUJ incongruity after anatomic reduction and fixation of the radial shaft fracture of the answers above is interposition of the extensor carpi ulnaris (ECU) tendon. The tendon must be extricated from the joint to permit DRUJ reduction.
Gaeleazzi fracture-dislocations, such as that seen in Figure A, are typically stable once the radial shaft fracture is anatomically reduced. After fixation, the DRUJ is translated in pronation, supination, and in a neutral position to test for stability. A “clunk” during passive motion of the DRUJ is further evidence of gross instability. Gross laxity can be treated by splinting in supination or by pinning the DRUJ. However, ECU tendon interposition has been reported as a possible cause of a persistently irreducible DRUJ. Radiographic findings typically demonstrate a dorsally displaced ulnar head and a widened DRUJ. The interposed tendon must be removed from the joint, often through a separate dorsal approach to permit DRUJ reduction.
Bruckner et al. review the evaluation and management of complex dislocations of the DRUJ. The authors note that these injuries are associated with frequent irreducibility, recurrent subluxation, or soft reduction of the DRUJ secondary to interposed tissue. In their institutional series, four of the 11 cases of Galeazzi fractures were associated with complex DRUJ dislocations, most commonly due to displacement of the ECU tendon volar to the ulna, necessitating open reduction. They cautioned that unobtainable or unconvincing reductions should warrant surgical exploration.
Paley et al. reported two cases of an irreducible DRUJ after radial shaft fracture fixation. The authors describe an empty ECU tendon sulcus on the dorsum of the wrist in both cases. One case was noted and addressed intraoperatively.
However, the second case was not identified and this patient went on to endure persistent subluxation and diastasis of the DRUJ, ultimately experiencing a poor result. The authors advocate a separate dorsal exposure to reduce the ECU.
Hanel and Scheid reported a case of entrapment of the ECU in the DRUJ in a skeletal immature 12 year old boy. They noted that intraoperative radiographic analysis was significant for a widened DRUJ and dorsally displaced ulnar head. These authors too advocated a separate dorsal exposure to approach and extricate the ECU tendon.
Incorrect answers
OrthoCash 2020
A 58-year-old right-hand-dominant computer programmer trips and falls onto his right arm. He reports right arm pain and that his elbow felt "sloppy". His initial lateral radiograph is shown in Figure A. The orthopedic junior resident counsels him that he will likely need a radial head arthroplasty, ligament repair, and possible fixation of the ulna. What factor would most significantly affect the decision to surgically address the ulna fracture?

Degree of radial head comminution
The deforming force acting on the avulsed fracture fragment
Size of fragment and elbow stability after radial head replacement
The degree of fracture displacement
Patient age and bone quality Corrent answer: 3
The size of the fragment and degree of elbow instability following radial head fixation or replacement most often determines the intraoperative decision on coronoid fragment fixation.
The radial head is a secondary restraint to posterolateral rotatory instability (PLRI) of the elbow, while the coronoid provides an anterior and varus buttress to the ulnohumeral joint, resisting posterior dislocation. The medial ulnar collateral ligament attaches to the anteromedial facet of the coronoid, so large medial facet fractures may displace and cause varus posteromedial instability (PMRI). However, in terrible triad injuries (causing PLRI), small coronoid tip fractures are more common. These are typically left as they most often do not contribute to elbow instability. Therefore in most cases, radial head replacement and lateral ligamentous repair are sufficient to restore stability.
However larger coronoid base fractures may require fixation in order to stabilize the elbow. In these cases, the coronoid fracture may be addressed through the lateral window after radial head resection and before the trial implant is assessed. The anterior capsule can be tied down to the ulna or if the fracture is large enough, it may sometimes tolerate internal fixation.
Conversely, a buttress plate for the coronoid may be applied via a medial approach in the setting of a large coronoid base fracture as in PMRI.
Ring et al. reviewed 11 terrible triad injuries including 7 of which had the radial head surgically addressed and 4 of which had undergone radial head excision. The authors found that all four patients who underwent radial head excision dislocated after surgery. Only four patients had a satisfactory result, and all of these had fixation of the radial head, two requiring concomitant repair of the lateral ulnar collateral ligament (LUCL). The authors concluded that terrible triad injuries were unstable, prone to redislocation and that radiocapitellar contact is critical for ulnohumeral stability.
Pugh et al. reviewed 36 cases of terrible triad injuries in which all coronoid fractures were addressed, either with screw fixation or suture repair of the anterior capsule. The authors reported that the average arc of motion postoperatively was 112 degrees, Mayo score was 88, and concentric stability was restored in 34/36. There were 8 complications requiring re-operation. They concluded that coronoid fixation with radial head fixation or replacement yields a stable elbow suitable for early motion.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They found that radial head excision even in the setting of an intact LUCL lead to posterolateral laxity. Furthermore, if 30% of the coronoid tip was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement. However, if 50% of the coronoid was
excised, even with a radial head replacement dislocation occurred. They concluded that so long as the radial head is replaced, small coronoid fractures may not need to be repaired.
Figure A demonstrates a comminuted radial head fracture, a small coronoid fracture, and subluxation of the ulnohumeral joint.
Incorrect answers:
OrthoCash 2020
What is the most appropriate plating technique utilized for the medial malleolus fracture typically seen in a displaced supination-adduction ankle fracture?
Tension band plating
Antiglide plating
Bridge plating
Neutralization plating
Submuscular plating
A supination-adduction ankle fracture leads to a vertical fracture of the medial malleolus. Traditional fixation of the medial malleolus with oblique screws from the tip of the malleolus directed proximally will ineffectively protect against shear forces at the fracture site; these also are directed quite obliquely to the vertical fracture line, and therefore have poor biomechanical resistance to failure. An antiglide plate is used medially to prevent displacement of the fracture segment due to shear forces.
According to the referenced article by Toolan et al, placement of two horizontal (perpendicular to the fracture line) lag screws from medial to lateral are
biomechanically the most important aspect of the construct whether a plate is used or not.
OrthoCash 2020
A 25-year-old Norwegian amateur curler slips on the ice, falling onto an outstretched right elbow. He is taken to the local teaching hospital and radiographs demonstrate a significantly comminuted radial head fracture and coronoid base fracture. His elbow is reduced and splinted. To restore stability and allow early range of motion, which of the following will most likely need to be performed in most cases?
Radial head fixation or replacement
Radial head fixation or replacement and coronoid fixation
Radial head fixation or replacement, coronoid fixation, and lateral ulnar collateral ligament (LUCL) repair
Radial head fixation or replacement, coronoid fixation, LUCL and medial ulnar collateral ligament (MUCL) repair
Radial head fixation or replacement, coronoid fixation, LUCL and MUCL repair, and application of a hinged fixator
The patient has sustained a "terrible triad" injury, classically involving a radial head fracture, coronoid fracture, and elbow dislocation. These often involve LUCL injuries and a traumatic injury in the radiocapitellar joint. Stability is achieved with radial head replacement (or fixation), coronoid fixation (in cases with a large coronoid fracture), and lateral soft tissue repair.
Posterolateral rotatory instability (PLRI) following a terrible triad injury is usually caused by a fall on an extended arm that produces a valgus, axial, and rotatory force. The mechanism of injury begins laterally and moves medially.
Hence, the LUCL fails first, followed by the anterior capsule (or coronoid), and lastly the MUCL. Even following fixation, patients often lose some degree of their flexion-extension arc, may develop post-traumatic arthritis, or most commonly may have persistent instability. The radial head is a primary restraint to PLRI and must be either replaced with a prosthesis or fixed in the setting of a terrible triad injury. Replacement is typically chosen when the radial head is in more than 3 fragments. Coronoid fractures should be fixed when they involve >30-50% of the coronoid base. However, the best way to determine if coronoid fixation is necessary is with an intraoperative fluoroscopic examination.
Forthman et al. reviewed outcomes following the management of 34 elbow fracture-dislocations. In all cases, the radial head was replaced or underwent fixation. The MUCL was not repaired in any case. The authors noted only 2 cases of post-operative instability, one terrible triad, and one combined capitellum and trochlea fracture. The authors noted that both cases were related to non-compliance. The remaining 32 averaged 120 degrees of flexion-extension and 74% had good-excellent outcomes. The authors concluded that MUCL repair is not required for elbow dislocations so long as the radial head, large coronoid fractures, and LUCL are addressed.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They found that radial head excision even in the setting of an intact LCL leads to posterolateral laxity. If 30% of the coronoid was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement. However, if 50% of the coronoid was excised, even with a radial head replacement, dislocation occurred. This led the authors to conclude that long as the radial head was replaced, small coronoid fractures may not need to be repaired.
Papatheodorou et al. reviewed 14 terrible triad injuries (all of which had Regan-Morrey type 1 or 2 coronoid fractures) that underwent surgical fixation or replacement of the radial head combined with LUCL repair. The authors noted that intraoperative stability was confirmed in all cases without coronoid fixation, MCL repair, or an external fixator. The authors concluded that coronoid fixation is not required in fractures up to 50% the height of the coronoid and that MCL repair is not necessary.
Incorrect answers:
OrthoCash 2020
A 32-year-old female sustains the injury shown in Video A. The right-sided pelvic injury is best classified as which of the following?
Lateral compression 1
Lateral compression 2
Vertical shear
Anterior-posterior compression 2
Anterior-posterior compression 3
The injury shown in Video V reveals a right sided posterior ilium fracture, which is known as a crescent fracture. The presence of a crescent fracture is consistent with a lateral compression type 2 injury; this differentiates this from a type I injury. The ipsilateral anterior sacrum has a small impaction injury anteriorly while the contralateral SI joint has a minor amount of anterior sacral impaction indicative of a lateral compression type I injury.
The reference by Burgess et al is the primary source of the mechanism classification of pelvic ring injuries. Overall blood replacement averaged 5.9 units (lateral compression, 3.6 units; anteroposterior compression, 14.8 units; vertical shear, 9.2 units; combined mechanical, 8.5 units). Overall mortality was 8.6% (lateral compression, 7.0%; anteroposterior, 20.0%, vertical shear,
0%; combined mechanical, 18.0%).
Incorrect answers:
1: The presence of a crescent fracture means this is at least a LC-2 injury. The left-sided fracture pattern is consistent with an LC-1 pattern.
3: A vertical shear fracture pattern would exhibit some vertical displacement and does not typically exhibit the crescent fragment.
4: The fracture pattern does not match an anterior-posterior compression pattern.
5: The fracture pattern does not match an anterior-posterior compression pattern.
OrthoCash 2020
A 35-year-old zookeeper fell 10 feet while preparing an exhibit for a grand reopening, landing on his left arm. The patient is then evaluated by a keen orthopedic resident in the emergency room who describes the zookeeper's injuries to his chief. He describes a comminuted radial head fracture and posterolateral ulnohumeral dislocation. The chief resident orders a CT scan which demonstrates a coronoid fracture involving 50% the height with no involvement of the anteromedial facet. During surgery, the trauma surgeon replaces the radial head and repairs the lateral collateral ligament complex. The
elbow is splinted in elbow flexion and pronation. The patient begins range of motion exercises with her occupational therapist 3 days after surgery, and her elbow dislocates. What is the most likely reason for her instability?
Length of immobilization
Position of immobilization
Lack of coronoid fixation with medial buttress plate
Lack of coronoid fixation from lateral approach
Lack of medial collateral ligament repair Corrent answer: 4
The zookeeper sustained a "terrible triad" injury with resulting posterolateral rotatory instability (PLRI). To prevent post-operative instability, large coronoid fractures should be fixed, and this would be performed through a lateral approach given that the radial head will be replaced.
The coronoid serves as an anterior and varus buttress to the ulnohumeral joint, resisting posterior dislocation. Though the coronoid tip has no soft tissue attachments, the medial ulnar collateral ligament attaches to the anteromedial facet of the coronoid. A coronoid fracture through the anteromedial facet, such as in the setting of posteroMEDIAL rotatory instability, would require a medial buttress plate to restore varus stability. In a coronoid base fracture involving 50% of the coronoid, fixation is required even when a radial head arthroplasty is performed. This can be done with suture fixation via a bone tunnel through the ulna or with screws from dorsal to volar. Failure to fix a large coronoid base fracture would result in persistent instability, as with the patient in this vignette.
Ring et al. reviewed 11 terrible triad injuries - including 7 of which had the radial head surgically addressed and 4 of which underwent radial head excision. They noted that all four patients who underwent radial head excision dislocated after surgery. Moreover, only four patients had a satisfactory result, and all of these had fixation of the radial head, with two requiring concomitant repair of the lateral ulnar collateral ligament (LUCL). The authors concluded that terrible triad injuries are unstable, prone to redislocation and that radiocapitellar contact is critical for ulnohumeral stability.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They showed that radial head excision even with an intact LUCL resulted in persistent posterolateral laxity. If 30% of the coronoid was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement alone. If 50% of the coronoid was excised, even with
a radial head replacement, dislocation occurred. The authors concluded that so long as the radial head was replaced, small coronoid fractures may not need to be repaired, but large fractures involving 50% or more would require fixation even if the radial head and LUCL were addressed.
Moro et al. treated 25 unreconstructible radial head fractures with a metal radial head arthroplasty. The authors reported a DASH score of 17, PRWE of 17, and Mayo elbow score of 80. Poor outcomes were seen in those with psychiatric disorders or those involved in a worker's compensation claim. The authors reported that radial head arthroplasty resulted in stable elbows with mild-moderate physical impairment.
Ring, Quintero, and Jupiter reviewed 56 patients with radial head fractures who underwent surgical fixation. Of the comminuted Mason type-3 fractures that underwent ORIF, they found that 13/14 had a poor result. The authors recommend that fractures with 3 or fewer fragments are amenable to fixation while those with 4 or more articular fragments are not.
Incorrect answers:
OrthoCash 2020
Which of the following injuries would require plating of the radius along with closed reduction and evaluation of the distal radioulnar joint (DRUJ)?
Nightstick fracture
Galeazzi fracture
Monteggia fracture
Rolando fracture
Smith fracture
A Galeazzi fracture is a fracture of the distal third of the radius with dislocation of the distal radioulnar joint. It commonly results from a fall onto an outstretched hand with the forearm in pronation.
A Galeazzi fracture is an injury that requires surgical treatment in an adult. The algorithm includes anatomic reduction and fixation of the radial shaft, and closed reduction of the DRUJ with assessment of stability. If the DRUJ remains unstable, supination of the wrist may reduce the DRUJ. Otherwise, either open or closed reduction with pinning can be undertaken to stabilize the joint. The closer the radius fracture is to the DRUJ, the more likely it is to be unstable.
Acute intervention results in improved outcomes as compared to delayed reconstruction.
Rettig et al. retrospectively analyzed 40 patients with Galeazzi fracture-dislocations that were treated with open reduction and internal fixation of the radial shaft fracture. They noted that a radial shaft fracture located within
Question 20
A 28-year-old woman has had pain in her hand and mild swelling of the little finger for the past 2 months. A radiograph is shown in Figure 41a, and the biopsy specimen is shown in Figures 41b and 41c. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 225.
McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 227.
Question 21
What are the four most common soft-tissue sarcomas to spread via the lymph node system?
Explanation
REFERENCES: Riad S, Griffin AM, Liberman B, et al: Lymph node metastasis in soft-tissue sarcoma in an extremity. Clin Orthop Relat Res 2004;426:129-134.
Blazer DG III, Sabel MS, Sondak VK: Is there a role for sentinel lymph node biopsy in the management of sarcoma? Surg Oncol 2003;12:201-206.
Question 22
A 42-year-old woman is brought to the emergency department following a motor vehicle accident. She has sustained multiple injuries, and she is intubated and pharmacologically paralyzed. Sagittal cervical CT scans through the right cervical facets, the left cervical facets, and the midline are shown in Figures 12a through 12c, respectively. Definitive management of her cervical injury should consist of
Explanation
REFERENCES: Jackson RS, Banit DM, Rhyne AL III, et al: Upper cervical spine injuries.
J Am Acad Orthop Surg 2002;10:271-280.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 23
Figure below depicts the radiograph obtained from a 30-year-old woman who began having more right than left hip pain during a recent pregnancy. Physical examination reveals increased range of motion with positive flexion abduction and external rotation and flexion adduction and internal rotation as well as pain with external logroll. Assessment of Figure below reveals
Explanation
Studies have demonstrated that pelvic inclination can dramatically affect the interpretation of radiographs in the dysplastic hip, with 9° of increased pelvic inclination leading to the presence of crossover signs and posterior wall signs. A distance of 30 mm to 50 mm from the sacrococcygeal junction to the pubis is often used to assess the adequacy of pelvic inclination on radiographs, although Siebenrock and associates determined the mean difference to be 32 mm in men and 47 mm in women. In this patient, the pelvic inclination is dramatically increased, leading to overestimation of acetabular retroversion.
Question 24
A 13-year-old girl with adolescent idiopathic scoliosis is otherwise healthy with a normal neurologic examination and she began her menstrual cycle 3 months ago. Standing radiographs show a high left thoracic curve from T1-T6 that measures 29 degrees, a right thoracic curve from T7-L1 that measures 65 degrees, and a left lumbar curve from L1-L5 that measures 31 degrees, correcting to 12, 37, and 10 degrees, respectively, on bending films. Her Risser sign is 1. What is the most appropriate management? Review Topic
Explanation
Question 25
A 17-year-old high school football player injures his right ankle during a game. Examination reveals swelling and a closed ankle deformity, with normal foot circulation and sensation. Radiographs are shown in Figures 10a and 10b. In addition to closed reduction, management should include
Explanation
REFERENCES: Browner BD, Jupiter JB, Levine AM, Trafton PG: Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 1887-1957.
Stiehl JB: Ankle fractures with diastasis. Instr Course Lect 1990;39:95-103.
Question 26
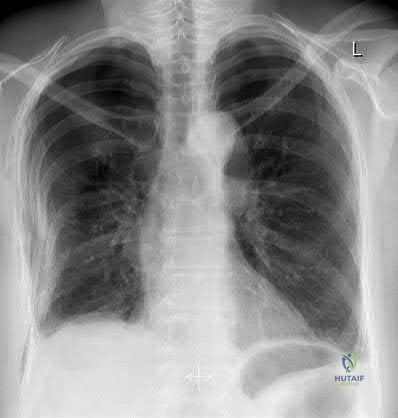
Figure 17 shows the radiograph of an 82-year-old right-hand dominant woman who fell while weeding her garden. She has severe right shoulder pain. She is neurovascularly intact. What is the most appropriate treatment? Review Topic

Explanation
Question 27
Figures 10a through 10c show the radiographs of an 85-year-old man who underwent a revision total knee arthroplasty for loosening of the tibial component 6 months ago. He now reports a mildly uncomfortable mass on the anterior part of the knee joint. Examination reveals 95 degrees of motion and good quadriceps strength, and he can ambulate with minimal pain with a walker. History reveals chronic lymphocytic leukemia for which he is taking antineoplastic medication. Culture of the mass aspirate grew Candida albicans on two separate occasions. The patient and the family strongly prefer nonsurgical management. If long-term suppression is chosen as treatment, what advice should be given to the patient and family?
Explanation
REFERENCE: Mulvey TJ, Thornhill TS: Infected total knee arthroplasty, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2,
pp 1857-1890.
Question 28
Which of the following changes is seen with age and degeneration in the intervertebral disk? Review Topic
Explanation
Question 29
.What is the most appropriate treatment if instability is present at the time of evaluation?
Explanation

Question 30
-Where is the physis with the highest growth rate (in mm per year) located?
Explanation

Question 31
A 22-year-old man reports anterior knee pain, swelling, and is unable to perform a straight leg raise after undergoing endoscopic anterior cruciate ligament (ACL) reconstruction with a bone-patellar tendon-bone autograft 1 week ago. He is afebrile. Examination reveals a clean incision, moderate effusion, a weak isometric quadriceps contraction, active knee range of motion of 5 degrees to 45 degrees, and the patella is ballottable. Knee radiographs show postoperative changes with good femoral and tibial tunnel placements, and normal patellar height. What is the next most appropriate step in management?
Explanation
REFERENCES: Kennedy JC, Alexander IJ, Hayes KC: Nerve supply of the human knee and its functional importance. Am J Sports Med 1982;10:329-335.
Fahrer H, Rentsch HU, Gerber NJ, et al: Knee effusion and reflex inhibition of the quadriceps: A bar to effective retraining. J Bone Joint Surg Br 1988;70:635-638.
Question 32
A 12-year-old boy is emergently transported to the emergency department following a motor vehicle accident. He was restrained in the back seat with a lap belt. On a physical exam bruising is noted across his abdomen as shown in Figure A. Lateral radiographs are shown in Figure B. Which of the following injuries are most frequently associated with this injury pattern? Review Topic

Explanation
A Chance fracture injury is a flexion-distraction injury of the spine. The anterior column (vertebral body) collapses under compression and the posterior elements fail under tension (rupture of the interspinous ligaments or avulsion fracture of the spinous process). A common mechanism is a MVA where the child is wearing a seatbelt, leading to a "seatbelt sign". In the presence of a "seatbelt" sign, on should have a high suspicion for a bowel injury.
Reid et al. reported seven cases of pediatric patients with Chance fractures. All had associated intraabdominal bowel injury.
Holland et al. retrospectively reviewed 28 pediatric patients with Chance fractures, 71% sustained following road trauma. Eleven percent had associated small bowel injury, but all patients had abnormal abdominal CT scans.
Figure A is a clinical photo of a 'seatbelt sign' following a motor vehicle accident. Figure B exhibits a "bony" Chance fracture where the spinous process has been avulsed. Illustration A depict the failure of the anterior column under compression and failure of the posterior column under tension.
Incorrect answers:
(SBQ12SP.32) A 48-year-old man is involved in a motor vehicle accident and is taken to an outside hospital where he undergoes CT imaging, displayed in Figures A-B. Approximately 36 hours later he is transferred to your hospital for further evaluation and management. On exam, he has tenderness over his upper cervical spine and is neurologically intact with no myelopathic signs. What is the most appropriate treatment method for this patient and why? Review Topic

Soft cervical orthosis because his gender puts him at a low risk of nonunion.
Halo vest immobilization because the degree of fracture displacement puts him at a low risk of nonunion.
Anterior screw fixation because his delayed time to treatment puts him at an high risk of nonunion.
Posterior C1-C2 fusion with rigid instrumentation because his age puts him at a high risk of nonunion.
Posterior C1-C2 fusion with sublaminar wiring because the degree of fracture angulation puts him at a high risk of nonunion.
The patient has a type II odontoid fracture and should be managed with halo vest immobilization as he has minimal fracture displacement (< 5mm) and no other risk factors for nonunion.
Type II odontoid fractures comprise 35% of all C2 fractures and have the highest nonunion rate. Commonly cited risk factors for nonunion include posterior displacement, posterior angulation, delayed initiation of treatment, fracture comminution and advanced age. Patients without these risk factors can often be successfully managed with halo vest immobilization. Elderly patients are frequently unable to tolerate halo vest immobilization and can be placed in a rigid cervical orthosis. Patients at high risk for nonunion are generally managed surgically with either anterior screw fixation, posterior rigid fixation (C1-C2 transarticular screw construct versus C1 lateral mass screw + C2 pedicle screw construct), or posterior C1-C2 sublaminar wiring.
Greene et al found that type II odonotoid fractures that were displaced >/= 6mm had a nonunion rate of 86% compared to 18% in patients with < 6mm displacement. This was statistically significant regardless of direction of displacement. Age was not significantly associated with nonunion.
Koivikko et al performed a retrospective review of conservatively treated type II odontoid fractures and identified risk factors for nonunion. Fracture gap > 1mm, posterior displacement > 5mm, posterior angulation > 20°, delayed start of treatment
> 4 days and posterior redisplacement > 2mm were all correlated with nonunion. In this study, anterior displacement, gender and age were unrelated to nonunion.
Figures A and B are coronal and sagittal CT scans of the cervical spine, respectively, demonstrating a noncomminuted type II odontoid fracture with minimal posterior displacement and angulation.
Incorrect
Responses:
Question 33
Figures 18a and 18b show the radiographs of a 13-year-old baseball player who sustained a patellar dislocation with an associated lateral femoral condyle fracture. What ligament is attached to this fragment?
Explanation
REFERENCES: Jobe CM, Wright M: Anatomy of the knee, in Fu FH, Harner CD, Vince KG (eds): Knee Surgery. Baltimore, MD, Williams & Wilkins, 1994, pp 1-54.
Moore KL, Dalley AF: Lower limb, in Moore KL, Dalley AF (eds): Clinically Oriented Anatomy, ed 4. Philadelphia, PA, Lippincott, Williams & Wilkins, 1999, pp 503-664.
Question 34
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome?
Explanation
REFERENCES: Lalonde F, Letts M, Yang JP, et al: An analysis of burst fractures of the spine in adolescents. Am J Orthop 2001;30:115-120.
Clark P, Letts M: Trauma to the thoracic and lumbar spine in the adolescent. Can J Surg 2001;44:337-345.
Been HD, Bouma GJ: Comparison of two types of surgery for thoraco-lumbar burst fractures: Combined anterior and posterior stabilization vs posterior instrumentation only. Acta Neurochir (Wien) 1999;141:349-357.
Question 35
A patient who underwent open reduction and internal fixation of an olecranon fracture 2 months ago now reports painless limitation of motion. Examination reveals a well-healed incision and a flexion-extension arc from 40 degrees to 80 degrees. The patient has been performing home exercises. Radiographs are shown in Figures 26a and 26b. What is the most appropriate treatment?
Explanation
REFERENCES: Morrey BF: The posttraumatic stiff elbow. Clin Orthop Relat Res
2005;431:26-35.
King GJ, Faber KJ: Posttraumatic elbow stiffness. Orthop Clin North Am 2000;31:129-143.
Question 36
A 45-year-old man has persistent hindfoot pain that is aggravated by weight-bearing activities. History reveals that he sustained a calcaneus fracture 2 years ago, and he underwent a subtalar fusion 1 year ago. Examination reveals tenderness in the sinus tarsi and across the transverse tarsal joint. A plain radiograph and a CT scan are shown in Figures 24a and 24b. A technetium Tc 99m bone scan reveals uptake at the subtalar joint and at the transverse tarsal joints. Management should now consist of
Explanation
REFERENCES: Graves SC, Mann RA, Graves KO: Triple arthrodesis in older adults: Results after long-term follow-up. J Bone Joint Surg Am 1993;75:355-362.
Haddad SL, Myerson MS, Pell RF IV, Schon LC: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Sangeorzan BJ, Smith D, Veith R, Hansen ST Jr: Triple arthrodesis using internal fixation in treatment of adult foot disorders. Clin Orthop 1993;294:299-307.
Sangeorzan BJ: Salvage procedures for calcaneus fractures. Instr Course Lect 1997;46:339-346.
Wapner KL: Triple arthrodesis in adults. J Am Acad Orthop Surg 1998;6:188-196.
Question 37
The arrow in Figure 11 points toward a finding consistent with which of the following?
Explanation
REFERENCES: McLain R, Weinstein J (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 1173.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 674.
Question 38
Figure 9 shows the radiograph of a 75-year-old woman who reports the sudden onset of disabling medial knee pain. What is the most likely diagnosis?
Explanation
REFERENCES: Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 413-418.
Insall JN, Windsor RE, Scott WN, Kelly MA, Aglietti P (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 609-634.
Question 39
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 40
A 51-year-old butcher has an 18-month history of recalcitrant medial elbow pain, which is affecting his occupational demands. He describes the pain as mainly anterior and distal to the medial epicondyle. His symptoms are exacerbated with resisted wrist flexion and forearm pronation. On examination, he is also found to have a positive Tinel’s sign at the elbow with weakness of intrinsic strength. He has attempted physical therapy, activity modification, bracing, and anti-inflammatory medication without any significant improvement. Presurgical counseling should include the understanding that
Explanation
of pathologic tissue, release of the flexor carpi radialis - pronator teres origin, and/or repair of the flexor carpi radialis - pronator teres origin. Several authors have raised concern of the impact of concomitant ulnar neuropathy on results following surgical treatment for medial epicondylitis. Kurvers and Verhaar and Gabel and Morrey, among others, have reported a statistically significant association between concomitant ulnar neuropathy and worse outcomes following surgery. Most patients can anticipate a return to prior activity levels after surgery without any consistently reported loss of flexor/pronator strength. Prior corticosteroid injections
have not been found to impact results.
Question 41
Which of the following changes occur in articular cartilage with age?
Explanation
Question 42
A patient who was involved in a motor vehicle accident 2 weeks ago now reports neck pain. Work-up reveals no evidence of nerve root involvement or acute radiographic abnormality. The patient appears to have a hyperextension soft-tissue injury of the neck (whiplash). What is the best course of treatment at this time?
Explanation
REFERENCES: Borchgrevink GE, Kaasa A, McDonagh D, Stiles TC, Haraldseth O, Lereim I: Acute treatment of whiplash neck injuries: A randomized trial during the first 14 days after a car accident. Spine 1998;23:25-31.
Mealy K, Brennan H, Fenelon GC: Early mobilization of acute whiplash injuries. Br Med J 1986;292:656-657.
Question 43
What is one of the principle concerns when a fracture such as the one seen in Figure 18 is encountered?
Explanation
REFERENCES: Ludwig S, Zarro CM: Complications encountered in the management of patients with ankylosing spondylitis, in Vaccaro AR, Regan JJ, Crawford AH, et al (eds): Complications of Pediatric and Adult Spine Surgery. New York, NY, Marcel Dekker, 2004,
pp 279-290.
Wu CT, Lee ST: Spinal epidural hematoma and ankylosing spondylitis: Case report and review of the literature. J Trauma 1998;44:558-561.
Question 44
A study is conducted to measure the difference in bone mineral density between postmenopausal women taking a drug treatment versus those taking a placebo. What is the most important result to be reported from this study?
Explanation
(ie, the means and standard deviations).
REFERENCE: Ebramzadeh E, McKellop H, Dorey F, et al: Challenging the validity of conclusions based on P-values alone: A critique of contemporary clinical research design and methods. Instr Course Lect 1994;43:587-600.
Question 45
In total knee arthroplasty, in vitro testing has shown that cross-linking can diminish the rate of polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
Explanation
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been shown to cause implant failure in the most recent clinical trials, but they remain the most important mechanical issues associated with current material processing methods.
Question 46
A 35-year-old laborer who sustained a forefoot injury 10 years ago has returned to work but reports a progressively painful deformity of the hallux and continued midfoot pain that is aggravated by weight-bearing activities. Shoe wear modifications have failed to provide relief. Direct palpation reveals no pain at the first metatarsocuneiform joint. A radiograph is shown in Figure 11. What is the next most appropriate step in management?
Explanation
REFERENCES: Kitaoka HB, Patzer GL: Arthrodesis versus resection arthroplasty for failed hallux valgus operations. Clin Orthop 1998;347:208-214.
McGarvey WC, Braly WG: Bone graft in hindfoot arthrodesis: Allograft vs autograft. Orthopedics 1996;19:389-394.
Ouzounian TJ: Metatarsophalangeal arthrodesis for salvage of failed hallux valgus surgery. Foot Ankle Clin 1997;2:741-752.
Question 47
A 58-year-old man has had a 3-year history of recurrent ulcerations of the left ankle and instability despite multiple attempts at custom bracing, contact casting, and surgical debridement. He has an ankle-brachial index of 0.76. A clinical photograph and radiographs are shown in Figures 16a through 16c. Treatment should now consist of
Explanation
REFERENCES: Pinzur MS, Kelikian A: Charcot ankle fusion with a retrograde locked intramedullary nail. Foot Ankle Int 1997;18:699-704.
Herbst SA: External fixation of Charcot arthropathy. Foot Ankle Clin 2004;9:595-609.
Question 48
A patient underwent an anterior cervical diskectomy and interbody fusion for a C5-6 herniated nucleus pulposus and left C6 radiculopathy 8 months ago. He now reports new onset of severe neck pain and left C6 radicular pain, with wrist extension weakness. The radiograph and CT scan shown in Figures 26a and 26b reveal pseudarthrosis at C5-6. The next step in management should consist of
Explanation
REFERENCES: Brodsky AE, Khalil MA, Sassard WR, Neuman BP: Repair of symptomatic pseudarthrosis of anterior cervical fusion: Posterior versus anterior repair. Spine
1992;17:1137-1143.
Tribus CB, Corteen DP, Zdeblick TA: The efficacy of anterior cervical plating in the management of symptomatic pseudarthrosis of the cervical spine. Spine 1999;24:860-864.
Farey ID, McAfee PC, Davis RF, Long DM: Pseudarthrosis of the cervical spine after anterior arthrodesis: Treatment by posterior nerve root decompression, stabilization, and arthrodesis.
J Bone Joint Surgery Am 1990;72:1171-1177.
Question 49
The need for postoperative allogeneic blood transfusions after total hip arthroplasty has been shown to be reduced when using
Explanation
(p < 0.001) after surgery.
REFERENCES: Waddell JP: Evidence-based orthopedics. J Bone Joint Surg Am 2001;83:788.
Feagan BG, Wang CJ, Kirkley A, et al: Erythropoietin with iron supplementation to prevent allogeneic blood transfusion in total hip joint arthroplasty: A randomized, controlled, trial. Ann Intern Med 2000;133:845-854.
Question 50
During the early swing phase of the normal gait cycle, what lower extremity muscle is primarily contracting?
Explanation
REFERENCES: Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Wootten ME, Kadaba MP, Cochran GV: Dynamic electromyography II: Normal patterns during gait. J Orthop Res 1990;8:259-265.
Question 51
What measure of physiologic status best evaluates whether an injured patient is fully resuscitated and best predicts that perioperative complications will be minimized following definitive stabilization of long bone fractures?
Explanation
REFERENCES: Blow O, Magliore L, Claridge JA, et al: The golden hour and silver day: Detection and correction of occult hypoperfusion within 24 hours improves outcomes from major trauma. J Trauma 1999;47:964-977.
Crowl A, Young JS, Kahler DM, et al: Occult hypoperfusion is associated with increased morbidity in patients undergoing early femur fracture fixation. J Trauma 2000;48:260-267.
Shulman AM: Prediction of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:725-800.
Question 52
The mother of a 2-year-old boy reports that he had pain in the right hip all night and refuses to walk on the leg this morning. He is afebrile. Examination reveals pain on hip extension and adduction, but he is able to internally and externally rotate the hip approximately 20 degrees in each direction without pain. Laboratory studies reveal a WBC count of 7,400/mm 3 , with 62% polymorphonuclear neutrophil leukocytes. The AP radiograph shown in Figure 15 reveals a left teardrop distance of 8 mm, while the right side measures 10 mm. Which of the following diagnostic studies will best help confirm the diagnosis?
Explanation
REFERENCE: Tachdjian MO: Pediatric Orthopedics, ed 2. Philadelphia, PA, WB Saunders, 1990, pp 1415-1435.
Question 53
An MRI arthrogram of the elbow is shown in Figure 6. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: Carrino JA, Morrison WB, Zou KH, et al: Noncontrast MR imaging and MR arthrography of the ulnar collateral ligament of the elbow: Prospective evaluation of two-dimensional pulse sequences for detection of complete tears. Skeletal Radiol 2001;30:625-632.
Munshi M, Pretterklieber ML, Chung CB, et al: Anterior bundle of ulnar collateral ligament: Evaluation of anatomic relationships by using MR imaging, MR arthrography, and gross anatomic and histologic analysis. Radiology 2004;231:797-803.
Question 54
An otherwise healthy 25-year-old man with an isolated closed mid-diaphyseal femoral fracture undergoes intramedullary nailing. Compared with nonreamed nailing, reamed femoral nailing is associated with a higher rate of Review Topic
Explanation
Question 55
An 11-year-old boy sustained an injury to his arm in gym class. He denies prior pain in the arm. Radiographs are shown in Figures 48a and 48b. What is the next most appropriate step in the management of this lesion?
Explanation
REFERENCES: Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Deyoe L, Woodbury DF: Unicameral bone cyst with fracture. Orthopedics 1985;8:529-531.
Question 56
A 25-year-old tennis player has shoulder pain and weakness to external rotation. MRI scans are shown in Figures 16a and 16b. What is the most likely cause of his weakness?
Explanation
REFERENCES: Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Inokuchi W, Ogawa K, Horiuchi Y: Magnetic resonance imaging of suprascapular nerve palsy.
J Shoulder Elbow Surg 1998;7;223-227.
Question 57
A 34-year- woman has pain at the base of the thumb that worsens é pinching activities. Nonsurgical treatment has failed to provide relief. Examination reveals that the basilar joint is hypermobile, tender and painful when stressed. A radiograph of the trapeziometacarpal joint shows normal contour with widening when compared with the opposite side. Management should consist of
Explanation
Question 58
- Which of the following laws describes the mechanical effects believed to play a role in the etiology of adolescent tibia vara?
Explanation
Question 59
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
Explanation
REFERENCES: Schulman AM, Claridge JA, Carr G, et al: Predictors of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:795-800.
Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: Endpoints of resuscitation. J Trauma 2004;57:898-912.
Question 60
An 8-year-old girl injures her elbow playing soccer. After attempted reduction in the emergency department, radiographs of the elbow are shown in Figures 35a through 35c. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop
2000;20:7-14.
Hashemi-Nejad A, Goddard NJ: Radial head fractures. Br J Hosp Med 1994;51:223-226.
Rodriguez Merchan EC: Displaced fractures of the head and neck of the radius in children: Open reduction and temporary transarticular internal fixation. Orthopedics 1991;14:697-700.
Question 61
A surgeon prepares a medial gastrocnemius rotational flap to cover a medial proximal tibia defect at the time of revision knee replacement surgery. To optimize coverage, the surgeon must optimally mobilize which artery?
Explanation
The medial sural arteries vascularize the gastrocnemius, plantaris, and soleus muscles proximally. These arteries arise from the popliteal artery. If this artery is not adequately mobilized, a gastrocnemius soleus flap can be devascularized.
Question 62
- A physician who is currently in a fellowship program receives notification of a pending malpractice suit that refers to an incident that occurred 2 years ago when the physician was a resident. The physician would be insured if the residency program provided what type of insurance coverage?
Explanation
Question 63
A medial plate is best used to treat tibial plateau fractures when there is
Explanation
The patient's plain radiographs demonstrate a bicondylar tibial plateau fracture with complete separation of the diaphysis from the epiphysis, making this a Schatzker VI injury. Clinically, the patient is neurovascularly intact with symmetric palpable pulses, and ankle brachial indices are not necessary.
There is significant lateral tibial plateau displacement with the lateral femoral condyle down into the plateau defect. Considering the swelling, abrasions, and severity of the injury, a bridging external fixator is warranted followed by CT imaging.
The ligamentotaxis will provide better definition of the injury and joint fragments and allow for soft-tissue rest and subsidence of the swelling for eventual surgical intervention. Oblique views will not add as much information as CT imaging, which will show the bicondylar nature of the injury and the proximal tibia essentially split centrally with the tubercle as a separate fragment. A midline incision with medial and lateral plating has fallen out of
favor secondary to wound-healing complications. Comminution of the metaphysis or the lateral side is not an absolute indication for a medial plate. Open lateral fractures can still be managed with a laterally based plate depending on the soft-tissue injury.
RECOMMENDED READINGS
Higgins TF, Kemper D, Klatt J. Incidence and morphology of the posteromedial fragment in bicondylar tibial plateau fractures. J Orthop Trauma. 2009 Jan;23(1):45-51. doi: 10.1097/BOT.0b013e31818f8dc1. PubMed PMID: 19104303. View Abstract at PubMed Higgins TF, Klatt J, Bachus KN. Biomechanical analysis of bicondylar tibial plateau fixation: how does lateral locking plate fixation compare to dual plate fixation? J Orthop Trauma. 2007 May;21(5):301-6. PubMed PMID: 17485994. View Abstract at PubMed
Berkson EM, Virkus WW. High-energy tibial plateau fractures. J Am Acad Orthop Surg. 2006 Jan;14(1):20-31. Review. PubMed PMID: 16394164. View Abstract at PubMed
Barei DP, O'Mara TJ, Taitsman LA, Dunbar RP, Nork SE. Frequency and fracture morphology of the posteromedial fragment in bicondylar tibial plateau fracture patterns. J Orthop Trauma. 2008 Mar;22(3):176-82. doi:10.1097/BOT.0b013e318169ef08. PubMed PMID: 18317051.
View Abstract at PubMed
Barei DP, Nork SE, Mills WJ, Coles CP, Henley MB, Benirschke SK. Functional outcomes of severe bicondylar tibial plateau fractures treated with dual incisions and medial and lateral plates. J Bone Joint Surg Am. 2006 Aug;88(8):1713-21. PubMed PMID: 16882892. View Abstract at PubMed
Hall JA, Beuerlein MJ, McKee MD; Canadian Orthopaedic Trauma Society. Open reduction and internal fixation compared with circular fixator application for bicondylar tibial plateau fractures. Surgical technique. J Bone Joint Surg Am. 2009 Mar 1;91 Suppl 2 Pt 1:74-88. doi: 10.2106/JBJS.G.01165. PubMed PMID: 19255201. View Abstract at PubMed
Lowe JA, Tejwani N, Yoo B, Wolinsky P. Surgical techniques for complex proximal tibial fractures. J Bone Joint Surg Am. 2011 Aug 17;93(16):1548-59. PubMed PMID: 22204013. View Abstract at PubMed
Weil YA, Gardner MJ, Boraiah S, Helfet DL, Lorich DG. Posteromedial supine approach for reduction and fixation of medial and bicondylar tibial plateau fractures. J Orthop Trauma. 2008 May-Jun;22(5):357-62. doi: 10.1097/BOT.0b013e318168c72e. PubMed PMID:
Question 64
A 45-year-old man reports a history of a popping sensation and pain in the right shoulder while lifting boxes 6 months ago. The pain has persisted with loss of motion of the shoulder. Radiographs and MRI scans are shown in Figures 47a through 47d. Which of the following studies is likely to produce a significant positive result? Review Topic

Explanation
Question 65
- Figures 3a and 3b show the finger deformity that a 13-year-old girl has had since birth. What is the most likely diagnosis?
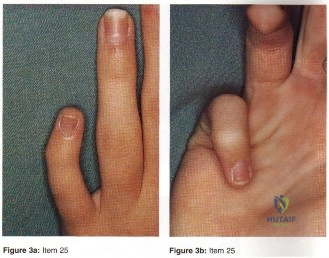
Explanation
definitions of the other distracters are self-explanatory (Staheli, Fundamental of Pediatric Orthopedics, 1998): Camptodactyly: non-painful flexion deformity of the PIP joint (i.e. AP Plane); abnormality of the insertions of the intrinsics and extrinsics flexor tendons; both hereditary and non-hereditary forms. Symbrachydactyly: digital absence in the form of transverse efficiency; teratogenic etiology resulting in absence distal metacarpals with finger nubbins. Kirner’s deformity: rare progressive deformity of the terminal phalanx of the small fingers with fingernails a curved and clubbed appearance; usually bilateral and appears during adolescence. Digiti minimi adductus: no such deformity found mention in the literature.
Question 66
What is the most common arthroscopic finding of internal impingement in an overhead athlete?
Explanation
REFERENCES: Jobe CM: Posterior superior impingement of the rotator cuff on the glenoid rim as a cause of shoulder pain in the overhead athlete. Arthroscopy 1993;9:697-699.
McFarland EG, Hsu C, Neir C, O’Neil O: Internal impingement of the shoulder: A clinical and arthroscopic analysis. J Shoulder Elbow Surg 1999;8:458-460.
Question 67
CLINICAL SITUATION Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities. What is the best next step in the patient’s evaluation?

Explanation
but she has not had any issues since the flap. She has abundant callus formation but the fracture line is still visible and unchanged on 2 sets of radiographs. The patient has persistent pain. The best initial evaluation is to ensure that there is no underlying infection with laboratory studies, including a complete blood count (CBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Nuclear medicine studies have questionable utility, but may be helpful if the inflammatory markers from laboratory studies come back elevated. A CT scan is not warranted because the sequential radiographs show persistent fracture lines and no changes. The patient has a hypertrophic nonunion. Originally, she had appropriate treatment and has shown the ability to make callus, thus her biologic capacity appears to be intact and bone grafting is not needed. The hypertrophic nature of her fracture nonunion indicates that she needs more stability. The best treatment for a hypertrophic nonunion of the tibia is exchange nailing. Based on successive radiographs and the lack of healing, observation is probably just delaying the inevitable. Plating with retention of the nail can be useful in recalcitrant long bone non-union, especially in the femur.
Question 68
A 57-year-old man with type II diabetes mellitus was successfully treated for a first occurrence forefoot full-thickness (Wagner II) diabetic foot ulcer underlying the third metatarsal head with associated hammertoe with a series of weight-bearing total contact casts. There was no evidence of osteomyelitis. The ulcer is now fully healed. He is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. What is the next most appropriate step in management?
Explanation
REFERENCES: Pinzur MS, Slovenkai MP, Trepman E, et al: Guidelines for diabetic foot care: Recommendations endorsed by the Diabetes Committee of the American Orthopaedic Foot and Ankle Society. Foot Ankle Int 2005;26:113-119.
Pinzur MS, Dart HC: Pedorthic management of the diabetic foot. Foot Ankle Clin 2001;6:205-214.
Question 69
Figure 41a shows the AP radiograph of a 15-year-old boy who reports lateral knee pain. Figures 41b and 41c show a radiograph of the distal femur that was obtained 5 years ago and a current CT scan. The indication for surgery in this patient would be
Explanation
REFERENCES: Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 1626-1659.
Simon MA, Springfield DS, et al: Common Benign Bone Tumors and Usual Treatment: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 181-205.
Question 70
A 60-year-old man reports increasing pain in his right foot with limited ankle dorsiflexion and anterior ankle pain after sustaining a fracture of the calcaneus in a fall several years ago. Bracing, nonsteroidal anti-inflammatory drugs, and cortisone injections have failed to provide significant relief. Radiographs are shown in Figures 19a and 19b. What is the next most appropriate step in management?
Explanation
REFERENCE: Robinson TF, Murphy GA: Arthrodesis as salvage for calcaneal avulsions. Foot Ankle Clin 2002;7:107-120.
Question 71
Which of the following substances does not have androgenic effects?
Explanation
REFERENCES: Silver M: Use of ergogenic aids by athletes. J Am Acad Orthop Surg 2001;9:61-70.
Blue JG, Lombardo JA: Steroids and steroid-like compounds. Clin Sports Med 1999;18:667-689.
Question 72
6 grams each per 40 mg PMMA
Explanation
Vancomycin and tobramycin do not produce systemic toxicity in doses as high as 10.5 grams of vancomycin and 12.5 grams of tobramycin per 40 mg of PMMA.
RECOMMENDED READINGS
Hake ME, Young H, Hak DJ, Stahel PF, Hammerberg EM, Mauffrey C. Local antibiotic therapy strategies in orthopaedic trauma: Practical tips and tricks and review of the literature. Injury. 2015 Aug;46(8):1447-56. doi: 10.1016/j.injury.2015.05.008. Epub 2015 May 14. Review. PubMed PMID: 26007616. View Abstract at PubMed
Springer BD, Lee GC, Osmon D, Haidukewych GJ, Hanssen AD, Jacofsky DJ. Systemic safety of high-dose antibiotic-loaded cement spacers after resection of an infected total knee arthroplasty. Clin Orthop Relat Res. 2004 Oct;(427):47-51. PubMed PMID: 15552135. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 84 THROUGH 86
Figure 84 is the noncontrast MR image obtained at 2 weeks postinjury for a 52-year-old man who was injured after falling from a ladder. His arm is caught in an abducted, externally rotated
position. There is no sense of dislocation. Initial radiograph findings are normal. The radiologic review reads “Probable superior labral anterior to posterior (SLAP) tear.”
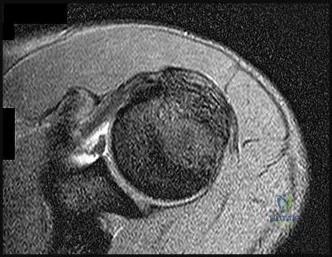
Question 73
An year-old African American woman who lives in a large city is scheduled for total hip arthroplasty to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
Explanation
Demographic factors are associated with increased risk for MRSA colonization, so it is important to identify vulnerable patients. Female gender and advanced age reduce the risk for colonization, whereas African American race increases this risk. Urban environments do not influence MRSA colonization.
Question 74
A 13-year-old gymnast has had recurrent right elbow pain for the past year. She denies any history of trauma. Rest and anti-inflammatory drugs have failed to provide relief. Examination reveals no localized tenderness and only slight loss of both flexion and extension (10 degrees). What is the most likely diagnosis?
Explanation
REFERENCES: Krijnen MR, Lim L, Willems WJ: Arthoscopic treatment of osteochondritis dissecans of the capitellum: Report of 5 female athletes. Arthroscopy 2003;19:210-214.
Schenck RC, Goodnight JM: Osteochondritis dissecans. J Bone Joint Surg Am 1996;3:439-456.
Question 75
What is the most common physical examination finding in a patient with chronic painful spondylolysis? Review Topic
Explanation
Question 76
-The patient requests anatomic double-bundle ACL reconstruction. Compared with transtibial singlebundle ACL reconstruction, anatomic double-bundle ACL reconstruction is more likely to
Explanation
The radiograph shows a Segond fracture, an avulsion fracture involving the lateral capsular ligament.
This radiographic finding has been associated with ACL rupture in 75% to 100% of cases. Drilling the femoral tunnel through the anteromedial portal allows for independent access to the native femoral attachment. Fiber orientation is more oblique than with a transtibial technique and more closely resembles that of the native ligament. Double-bundle reconstruction attempts to duplicate native ACL anatomy.Biomechanical studies have shown that double-bundle reconstruction more
closely reproduces normal knee kinematics; however, this technique does not offer a clear advantage in terms of clinical outcomes.The iliotibial band inserts onto Gerdy’s tubercle. The popliteus tendon originates from the lateral femoral condyle. The lateral meniscus attaches near the intercondylar eminence at the anterior and posterior meniscal roots. Recent advances in ACL reconstruction focus on restoring the native ACL anatomy.Studies have determined that a knee flexion angle of 110 degrees is optimal to avoid blowout of the back wall and injury to the lateral structures while drilling.
Femoral tunnel length is typically shorter than with a transtibial approach and decreases with higher-flexion angles. Double-bundle reconstruction is associated with higher surgical costs because of the need for additional fixation and, in the case of allograft reconstruction, a second graft.
Question 77
Which of the following tissues has the highest maximum load to failure?
Explanation
REFERENCES: Woo SL, Hollis JM, Adams DJ, et al: Tensile properties of the human femur-anterior cruciate ligament-tibia complex: The effects of specimen age and orientation. Am J Sports Med 1991;19:217-225.
Staubli HU, Schatzmann L, Brunner P, et al: Quadriceps tendon and patellar ligament cryosectional anatomy and structural properties in young adults. Knee Surg Sports Traumatol Arthrosc 1996;4:100-110.
Wilson TW, Zafuta MP, Zobitz M: A biomechanical analysis of matched bone-patellar tendon-bone and doubled looped semitendinosus and gracilis tendon grafts. Am J Sports Med 1999;27:202-207.
Question 78
A funnel plot is used in meta-analyses to perform which of the following functions:
Explanation
Publication bias occurs because studies with a non-significant result, so-called
negative studies, have a higher likelihood of being rejected than positive studies, and are oftentimes not even submitted for publication. Funnel plots, which plot the effect size of a study against a measure of the study’s size are used to detect this bias. This method is based on the fact that larger studies have smaller variability, whereas small studies, which are more numerous, have larger variability. Thus the plot of a sample of studies without publication bias will produce a symmetrical, inverted-funnel shaped scatter, whereas a biased sample will result in a skewed plot.
Vavken et al. reviewed orthopaedic meta-analyses in order to determine whether publication bias was assessed and to evaluate its effect on the outcomes of these meta-analyses. They found that only 35% of all orthopaedic meta-analyses published between 1992 and 2008 in English and German assessed publication bias. Adjustment for publication bias did not produce significantly different results, but the magnitude of the pooled estimates in the affected meta-analyses changed by 29% on average.
Illustration A depicts a symmetrical funnel plot with no evidence for publication bias. Illustration B shows a skewed funnel plot suggesting publication bias, as it is missing studies in the lower left corner, i.e. ‘‘negative studies’’. Illustration C depicts a forest plot comparing the incidence of squeaking between ceramic-on-ceramic (COC) and ceramic-on-polyethylene (COP). Illustration D is an example of a ROC curve examining the probability of DVT.
Incorrect Answers:
Question 79
A 12-year-old gymnast has had elbow pain for 4 weeks. She denies any specific trauma to the elbow. Examination reveals lateral pain and no instability on testing. Range of motion is as follows: 15 degrees, loss of elbow extension, normal flexion, and normal pronation and supination. Radiographs reveal a 3- x 7-mm radiolucency of the capitellum. A T1-weighted MRI scan reveals a single solitary lesion, and T2-weighted images show no signal around the lesion. There are no intra-articular loose bodies. Appropriate management should include which of the following? Review Topic
Explanation
Question 80
When performing elbow arthroscopy, it is often necessary to evaluate the posterior compartment. When entering the posterior compartment of the elbow, what are the two safest and most commonly used portals? Review Topic
Explanation
Question 81
A 38-year-old man caught his index finger in a volleyball net. He noted an angular deformity of the finger that was reduced when a teammate pulled on his finger. Three weeks later, he now reports trouble extending his finger. A clinical photograph is shown in Figure 55. What anatomic structure is most likely injured?
Explanation
REFERENCES: Peimer CA, Sullivan DJ, Wild DR: Palmar dislocation of the proximal interphalangeal joint. J Hand Surg Am 1984;9:39-48.
Glickel SZ, Barron OA, Catalano LW: Dislocation and ligament injuries in the digits, in
Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 355.
Question 82
When conducted at near physiologic strain rates, tensile studies of the inferior glenohumeral ligament (IGHL) have shown that the
Explanation
REFERENCES: Bigliani LU, Pollock RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Ticker JB, Bigliani LU, Soslowsky LJ, Pawluk RJ, Flatow EL, Mow VC: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
Question 83
Which of the following postoperative rehabilitation techniques causes minimal rotator cuff muscle activation? Review Topic
Explanation
Question 84
Results of a study demonstrating no difference between treatments when a difference truly exists is an example of which of the following?
Explanation
fragile p-values is that small sample sizes may result in wide variability of p-values with only one change in a data point for a given group. This singular change could be a chance occurrence, but it still can affect the statisticalsignificance of the outcomes analysis. Fragility of p-values is limited by increasing sample sizes. Negative predictive value is the proportion of patients with negative test results who are correctly diagnosed.
Question 85
Figure 7 shows a sagittal T1-weighted MRI scan. What muscle/tendon is identified by the arrow? Review Topic

Explanation
Question 86
Figure 35 is the radiograph of a 37-year-old woman who began having right forefoot pain about 4 weeks ago after increasing her daily running mileage. She denies any specific injury. Upon examination she has tenderness over the medial forefoot with mild swelling. In addition to her activity level, what is the primary etiology of the radiograph finding?

Explanation
Stress fractures are the result of physiological bone response to increased stress. Increased stress on bone triggers an increase in remodeling, which begins with resorption of bone at the site of stress. Ongoing stress can overwhelm bone strength, resulting in a fracture. In the foot this most commonly is seen in the second metatarsal at the junction of the middle and distal thirds. Contributing factors to increased loading of the second metatarsal include hallux valgus (decreased hallux loading transfers to the second metatarsal head), hallux rigidus (offloading of the hallux attributable to pain increases second metatarsal loading), and a long second metatarsal (increased duration of contact during push-off in the stance phase).
RECOMMENDED READINGS
Shindle MK, Endo Y, Warren RF, Lane JM, Helfet DL, Schwartz EN, Ellis SJ.
Stress fractures about the tibia, foot, and ankle. J Am Acad Orthop Surg. 2012 Mar;20(3):167-
Question 87
A 7-year-old sustains the isolated injury shown in Figures A and B. On physical examination there is no evidence of soft tissue compromise and he is able to make an okay sign, give a thumbs up sign and cross his fingers. Which treatment will minimize complications? Review Topic

Explanation
Supracondylar fractures are common pediatric elbow injuries. Extension type injuries account for 95-98% of all cases. Non-displaced injuries may be treated conservatively. Displaced fractures are treated with closed reduction and percutaneous pinning. Use of laterally divergent pin constructs avoids risk of ulnar nerve injury, while maintaining satisfactory fracture alignment.
Slobogean et al. retrospectively reviewed pediatric supracondylar fractures to identify if there was an increased risk of ulnar nerve injury with crossed pin configurations. They found a higher incidence of ulnar nerve injury with crossed pinning constructs. For every 28 crossed pin constructs, there was one ulnar nerve injury identified.
Woratanarat et al. retrospectively reviewed supracondylar fractures to identify differences in the outcomes between lateral pinning versus crossed pinning constructs. No difference was found for loss of fixation or development of late deformity between the two groups. Crossed pin constructs were associated with a 4.3 times higher risk of iatrogenic ulnar nerve injury.
Omid et al. review pediatric supracondaylar humerus fractures. They note that lateral pinning is as stable as crossed pinning when appropriately spread-out at the fracture line. This also avoids the risk of ulnar nerve injury.
Figures A and B show AP and lateral radiographs of a pediatric supracondylar fracture. This would be classified as a Gartland Type 3.
Incorrect Answers:
Question 88
Integrins function in which of the following ways?
Explanation
Integrins are a large family of heteromeric cell surface receptors composed of non-covalently bound alpha and beta subunits which interact with extracellular matrix molecules, serum constituents and various adhesion molecules. Specifically, aVß3 is a type of integrin found on osteoclasts that attaches to bone by coupling with vitronectin.
Bikle reviews the cause of bone loss during periods of unloading. They state the during periods of rest, integrin expression is decreased, leading to disuse osteoporosis. They argue that drugs that selectively regulate the integrin signaling pathway may
reverse bone loss during periods of disuse.
Illustration A shows an example of an osteoclast attaching to bone via the integrin aVß3.
Incorrect
1:
This
is
the
function
of osteocytes.
2:
This
is
the
function
of osteoblasts.
3:
This
is
the
function
of
osteoprogenitor cells.
Question 89
In a retroperitoneal approach to the lumbar spine, what nerve is commonly found on the psoas muscle?
Explanation
REFERENCES: Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer-Verlag, 1983, p 107.
Johnson R, Murphy M, Southwick W: Surgical approaches to the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1559.
Gray’s Anatomy. New York, NY, Bounty Books, 1977, pp 1226-1227.
Question 90
Which of the following types of nonunions is most likely to achieve union following a reamed exchange intramedullary nailing only?

Explanation
Question 91
The rate of complications after in situ pinning of a chronic slipped capital femoral epiphysis is highest with placement of the screw in what quadrant of the femoral head?
Explanation
REFERENCES: Raney EM, Ogden JA: Slipped capital femoral epiphysis. Current Ortho 1995;9:111-116.
Stambough JL, Davidson RS, Ellis RD, et al: Slipped capital femoral epiphysis: An analysis of 80 patients as to pin placement and number. J Pediatr Orthop 1986;6:265-273
Question 92
A 78-year-old man is seen in the emergency room 3 hours after a fall from a standing position. The patient sustained a mild scalp laceration and the injury shown in Figure 90. He reports severe neck pain and is unable to move his hands and legs. Examination reveals absent motor function in the wrist flexors, triceps, and fingers. He cannot move his lower extremities during motor testing. The patient has some sensation in the lower extremities. Bulbocavernosus reflex is absent. Based on examination findings and the imaging findings, what is the most definitive treatment option? Review Topic
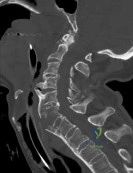
Explanation
(SBQ13PE.22) A 11-year-old male is referred for evaluation of scoliosis by his primary care physician. He has a normal birth and development history and denies any neurologic deficits or pain. On physical examination, he is neurologically intact with normal reflexes and tone. A PA radiograph is shown in Figure A. What is the next best step? Review Topic

Custom orthosis prescription to initiate bracing
Physical therapy referral and observation
Bending and lumbar oblique radiographs
Total spine CT
Total spine MRI
A left thoracic curve is an abnormal finding and warrants further work-up with a total axis MRI in order to rule out concomitant neurologic abnormalities such as a spinal cord cyst and/or syrinx.
In adolescent idiopathic scoliosis (AIS), the most commonly occurring curve is a right thoracic curve. Left thoracic curves are not as common, and warrants total axis MRI in order to rule out concomitant central axis abnormalities. This is imperative not only during initial work-up, but most importantly for operative planning.
Spiegel et al. performed a a retrospective radiographic review on 41 patients with scoliosis associated with a Chiari I malformation and/or syringomyelia. Approximately 50% of patients had an "atypical" pattern (left thoracic, double thoracic, triple, long right thoracic). The authors recommend that MRI should be considered in these patients.
Gillingham et al. provides a thorough review of early onset scoliosis and notes the relatively high incidence of concurrent central axis abnormalities, even in patients with normal neurologic exams. Rates have been reported upwards of 21.7%, with malformations including Chiari Type 1, dural ectasias, syrinx, and spinal cord cysts.
Figure A exhibits a left thoracic curve. Further imaging in this patient revealed a syrinx which required decompression.
Incorrect answers:
thoracic
curve.
Question 93
A 12-year-old boy has had progressive pain and flatfeet for the past year. Pain is increased with weight-bearing activities. Examination reveals that subtalar motion is absent. On standing, the patient has obvious hindfoot valgus and loss of the normal arch bilaterally. Plain radiographs are shown in Figures 43a through 43c, and a CT scan is shown in Figure 43d. What is the most likely diagnosis?
Explanation
REFERENCES: Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 583-595.
Question 94
Venous thromboembolism may occur after total joint arthroplasty. The risk of this complication is elevated in patients with
Explanation
Obesity, a prior history of venous thromboembolism, and metabolic syndrome have all been associated with an increased risk of thromboembolism. A recent meta-analysis showed that diabetes had no significant relationship with venous thromboembolism following hip or knee arthroplasty. Tranexamic acid is an antifibrinolytic agent that has been shown to reduce blood loss substantially following hip and knee arthroplasty. It has also been shown to be safe in patients with severe medial comorbidities and a prior history of venous thromboembolism.
Question 95
Figure 92 is the radiograph of a 45-year-old man who was thrown from his horse and now reports groin pain. Which of the following is the most common long-term sequelae of this injury?

Explanation
Question 96
A 14-year-old boy with a history of cerebral palsy has a clawed hallux, cavus foot deformity, and associated pain. Examination reveals pain under the first metatarsal head and a rigid first tarsometatarsal joint. Treatment should consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 79-100.
Tynan MC, Klenerman L: The modified Robert Jones tendon transfer in cases of pes cavus and clawed hallux. Foot Ankle Int 1994;15:68-71.
Question 97
A patient with a bone mineral density (BMD) T-score of -2.6 would be considered to have
Explanation
Question 98
A 66-year-old woman who requires a cane for ambulation now notes increasing difficulty in using the cane after undergoing total elbow arthroplasty 3 months ago. AP and lateral radiographs are shown in Figures 15a and 15b. What is the most likely diagnosis?
Explanation
REFERENCES: Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orhthopaedic Surgeons, 2002, pp 323-327.
Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000,
pp 598-601.
Question 99
A 16-year-old boy with osteochondritis dissecans of the capitellum has intermittent symptoms of catching and locking. Examination is unremarkable. Radiographs reveal a loose body anteriorly with a diameter of 10 mm. To remove the loose body, elbow arthroscopy is being considered. Which of the following procedures would minimize the risk of neurovascular complication during the procedure?
Explanation
REFERENCES: Lynch GJ, Meyers JF, Whipple TL, Caspari RB: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
O’Driscoll S: Loose bodies and synovial conditions, in Green D, Hotchkiss R, Pederson W (eds): Green’s Operative Hand Surgery. New York, NY, Churchill Livingstone, 1999, pp 235-249.
Question 100
A B C D Figures 75a through 75d show the radiographs of an 85-year-old woman who fell from a step and sustained a right proximal femur fracture. Six months after surgery she has knee pain. What is the most likely cause of her pain?

Explanation
Three cases of anterior distal femoral cortex penetration during intramedullary nailing for subtrochanteric fractures were documented by Ostrum and Levy in a 2005 study. Case 1 involved a Zimmer (Warsaw, Indiana) M/DN antegrade femoral nail, Case 2 involved a Stryker (Mahwah, New Jersey) long-stem Gamma nail, and Case 3 a DePuy Synthes (West Chester, Pennsylvania) titanium femoral nail with spiral blade locking. The anterior Zimmer nail penetration resulted in a displaced supracondylar fracture, which subsequently required revision. The Gamma nail as well as the DePuy Synthes nail were left impaled through the distal femoral cortex, and the subtrochanteric fractures went on to union. The anteroposterior radius of curvature for the Zimmer, long Gamma, and DePuy Synthes nails is 257 cm, 300 cm, and 150 cm, respectively. It is estimated that the radius of curvature of the femoral diaphyseal canal is 114 to 120 cm. It appears that the difference in femoral anteroposterior bow between the bone and the implant is a contributing factor to distal femoral anterior cortex penetration in intramedullary nailing of subtrochanteric fractures. There is no evidence of osteoarthrosis on the radiographs. Although nonunion is possible, based on the radiographic findings it is more likely that this patient's pain is attributable to the curvature of the nail. The lateral image of the hip reveals an appropriate starting point for the device.
RECOMMENDED READINGS
Ostrum RF, Levy MS. Penetration of the distal femoral anterior cortex during intramedullary nailing for subtrochanteric fractures: a report of three cases. J Orthop Trauma. 2005 Oct;19(9):656-60. PubMed PMID: 16247312.View Abstract at PubMed
Egol KA, Chang EY, Cvitkovic J, Kummer FJ, Koval KJ. Mismatch of current intramedullary nails with the anterior bow of the femur. J Orthop Trauma. 2004 Aug;18(7):410-5. PubMed PMID: 15289685. View Abstract at PubMed
RESPONSES FOR QUESTIONS 76 THROUGH 78
- Nonsurgical treatment with closed reduction and immobilization
- Early mobilization with physical therapy initiated within 2 weeks
- Open reduction and internal fixation (ORIF) with locked implants
- Use of supplemental bone graft or substitutes
- Arthroplasty
- Workup for osteoporosis and counseling
Which intervention listed is most appropriate to address each scenario described?

76A B
