Orthopedic Board Prep MCQs: Arthroplasty, Infection & Nerve | Part 170

Key Takeaway
This page presents Part 170 of a comprehensive orthopedic board review quiz, specifically designed for orthopedic residents and surgeons. It offers 100 verified, high-yield MCQs, formatted like OITE and AAOS exams, crucial for board certification preparation with detailed explanations.
About This Board Review Set
This is Part 170 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 170
This module focuses heavily on: Arthroplasty, Hip, Infection, Knee, Nerve.
Sample Questions from This Set
Sample Question 1: Which laboratory findings would most support a diagnosis of prosthetic joint infection (PJI) in a hip or knee arthroplasty performed 3 weeks ago?...
Sample Question 2: What is an example of cognitive rest after concussion? Review Topic...
Sample Question 3: Which of the following structures is predominantly composed of Type 1 collagen? Review Topic...
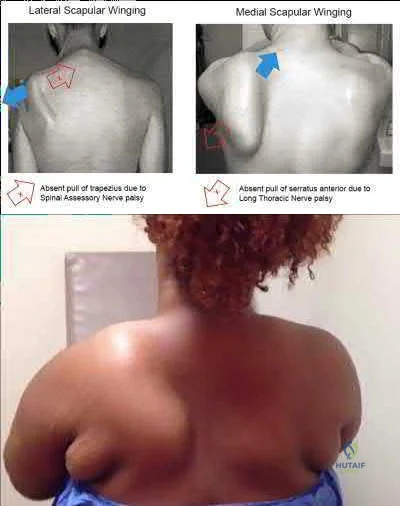
Sample Question 4: An injury to the axillary nerve would result in deltoid muscle weakness. 5 . An injury to the thoracodorsal nerve would result in latissimus dorsi weakness and would not cause scapular winging....
Sample Question 5: A B...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which laboratory findings would most support a diagnosis of prosthetic joint infection (PJI) in a hip or knee arthroplasty performed 3 weeks ago?
Explanation
The diagnosis of acute PJI is associated with different criteria than the diagnosis of a chronic PJI. There is no agreed-upon threshold for ESR during the acute period (6 weeks) following total joint arthroplasty. The CRP threshold is higher during the acute period (100 mg/L vs 10 mg/L for a chronic infection). The threshold for synovial fluid analysis for an acute PJI is 10000 cells/µL and more than 90% PMN neutrophils vs 3000 cells/µL and more than 80% PMN neutrophils for a chronic infection.

Question 2
What is an example of cognitive rest after concussion? Review Topic
Explanation
Question 3
Which of the following structures is predominantly composed of Type 1 collagen? Review Topic
Explanation
Type 1 collagen accounts for more than 90% of the total collagen content in the body. Type 1 collagen is found in bone, ligament, tendon, meniscus, annulus of intervertebral discs, skin, healed cartilage, scar tissue, and nerves.
Duthon et al present a review of the ACL and its histologic and mechanical properties. The ACL has a mean length of 32 mm and a width of 7-12 mm. They state that the ACL has a microstructure of collagen bundles of multiple types (mostly type I) and a matrix made of a network of proteins, glycoproteins, elastic systems, and glycosaminoglycans with multiple functional interactions.
Incorrect
1: Epithelial
2: L4 disc
Basement
Membrane is made up of Type
nucleus pulposus is composed of mostly Type
4 collagen.
2 collagen
4: Medial femoral condyle articular cartilage is comprised mostly of Type 2 collagen. 5: Dupuytren's contracture tissue is mostly Type 3 collagen.
Question 4
An injury to the axillary nerve would result in deltoid muscle weakness. 5 . An injury to the thoracodorsal nerve would result in latissimus dorsi weakness and would not cause scapular winging.
Explanation
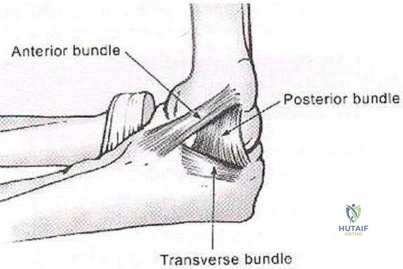
The medial ulnar collateral ligament, or medial collateral ligament of the elbow, is composed of three bundles: an anterior bundle, a posterior bundle, and a variable
transverse oblique bundle. During late cocking and early acceleration phases of the overhead throw, the medial UCL is subjected to the greatest amount of valgus stress to the elbow. During this phase, the forearm lags behind the upper arm and generates valgus stress while the elbow is primarily dependent on the anterior band of the UCL for stability. This puts the ligament at greatest risk of injury during this phase.
Fleisig et al. examined the kinetics of baseball pitching and the implications on injury mechanisms. They showed that the UCL contributes to 54% of the varus torque that is generated during the early acceleration of throwing. The position of greatest load occurred when the arm was flexed to 95 +/14 degrees with an applied valgus load.
Illustration A shows a diagram of the medial ulnar collateral ligament ligament bundles. Incorrect Answers:
A 14-year-old elite basketball player develops acute medial elbow pain after a fall. Physical examination reveals medial elbow tenderness over the submlime tubercle, but full range of motion. The provocative tests seen in Figure A exacerbate his elbow pain. Radiographs of the elbow are normal. What would be the next best step in treatment?
Supervised elbow stretching program Therapeutic elbow arthroscopy

Static elbow external fixation for 3 to 6 weeks, then MR arthrography if pain continues Activity avoidance for 6 weeks

Serial inflammatory markers and rheumatology referral
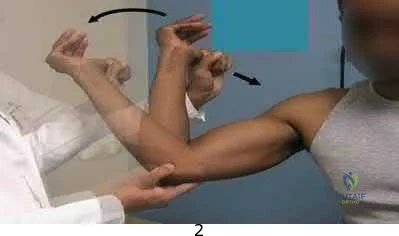
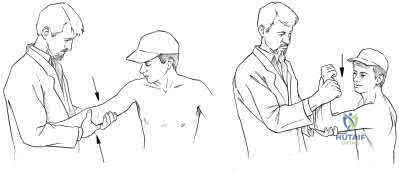
Figure A shows a moving valgus stress, which is a provocative test for ulnar collateral ligament (UCL) injury and elbow valgus instability. The initial treatment would be a short period of immobilization, rest and flexor pronator strengthening in this patient population.
Adolescent UCL injuries can be effectively treated with a short period of rest and NSAIDs to control pain. As the acute inflammation resolves, the patient can be started on a supervised therapy program. This should target flexor pronator muscles, as they are important secondary dynamic stabilizers of valgus stress. Once symptoms have improved and the athlete has regained full range of motion and strength, a mediated throwing program may be initiated. Throwing athletes should be educated to avoid provocative activities during this period.
Chen et al. wrote a JAAOS article on shoulder and elbow injuries in the skeletally immature athlete. They state that surgery is reserved for older athletes with persistent valgus instability despite > 6 months of non-surgical management.
Murthi et al. reviewed recurrent elbow instability. They state the anterior bundle of the medial ulnar collateral ligament complex is the primary valgus stabilizer of the elbow. The anterior band is taut for the first 60° of elbow flexion, and the posterior band is taut from 60° to 120° of flexion. The secondary valgus stabilizers of the elbow joint include the radial head, the anterior and posterior aspects of the capsule, and the muscular forces around the joint.
Figure A is showing a moving valgus stress. Illustration A shows provocative tests for valgus instability of the elbow. The image on the left shows a valgus stress test. This assesses the anterior bundle of the medial ulnar collateral ligament complex by flexing the elbow to 25-30 degrees and applying a valgus load across the elbow. The image on the right shows milking maneuver. This assesses the posterior bundle of the medial ulnar collateral ligament complex by pulling on the

beyond 90°. Incorrect Answers:
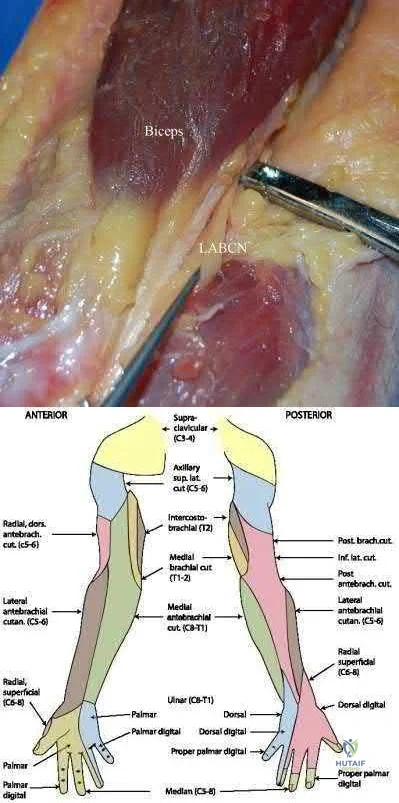
A young, healthy male undergoes a distal biceps repair and sustains an iatrogenic nerve injury during the procedure. Which of the following clinical findings are most likely to be seen in this circumstance? Inability to extend the thumb

Lateral volar forearm numbness Inability to flex the middle finger Medial volar forearm numbness Dorsal thumb numbness
The most commonly injured nerve during a distal biceps repair is the lateral antebrachial cutaneous nerve (LABCN). Injury to this nerve would result in lateral volar forearm numbness.
Distal biceps avulsions can be partial or complete. Indications for surgical management include young, healthy patients who do not wish to sacrifice function, as well as partial biceps avulsions that do not respond to conservative management. Repair of a distal biceps avulsion can be approached through either an anterior one-incision technique or a two-incision technique (BoydAnderson). The one-incision technique uses the interval between the brachioradialis (radial nerve) and pronator teres (median nerve), while the two-incision technique uses this same interval in addition to a second posterolateral elbow incision. The lateral antebrachial cutaneous nerve is the most common nerve injured during either approach.
Kelly et al. retrospectively reviewed 74 distal biceps tendon repairs, and found five sensory nerve paresthesias. The lateral antebrachial cutaneous nerve was most commonly injured, followed by the superficial radial nerve.
Cain et al. retrospectively reviewed 198 distal biceps tendon repairs, and found a 36% complication rate. Lateral antebrachial cutaneous nerve paresthesias were found in 26%, while radial sensory nerve paresthesias were found in 6%, and posterior interosseous nerve (PIN) injury in 4%.
Illustration A shows the close relationship between the lateral antebrachial cutaneous nerve (LABCN) and the distal biceps. Illustration B shows the sensory nerves of the upper extremity and their respective areas of innervation.
Incorrect Answers:
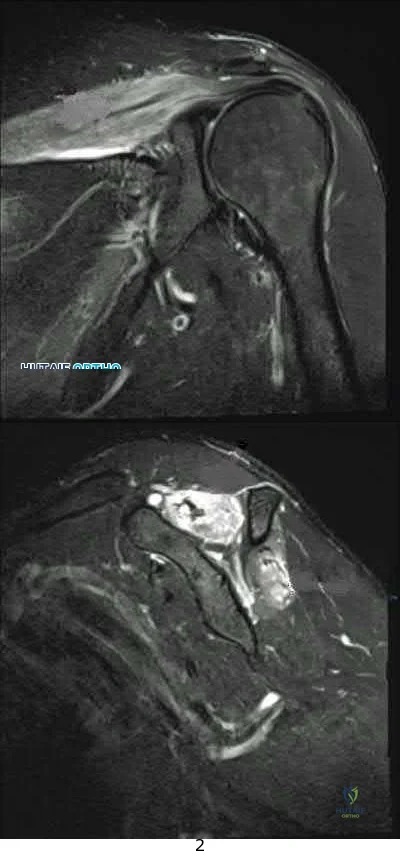
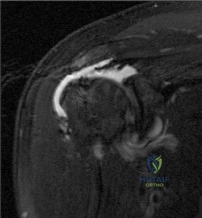
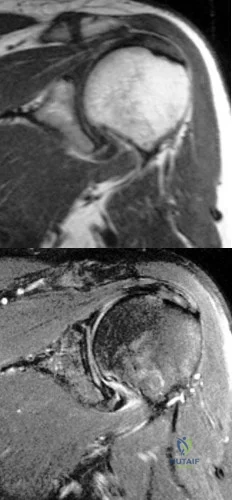
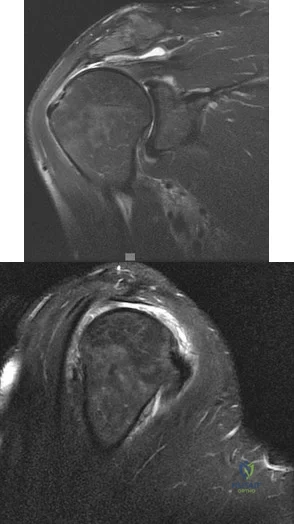
A 33-year-old female presents with left shoulder weakness. Two weeks prior to presentation, the patient experienced sudden-onset, left shoulder pain, which occurred a few days after receiving the influenza vaccine. The pain subsided over the next day, followed by gradual weakness of her shoulder and eventual general disuse of her left upper extremity. An initial visit to her primary care provider resulted in the recommendation of observation. On physical exam, there is weakness and gross atrophy of the shoulder girdle. Figures A & exhibit T2-weighted MRI images of her left shoulder. To further confirm her suspected diagnosis, she is sent for electromyography.
What is the expected result?
Normal results
Fibrillation potentials consistent with compression at the spinoglenoid notch 3 . Sharp waves and fibrillations potentials associated with the deltoid and biceps

Acute denervation of both peripheral nerve and nerve root distribution with sharp waves and fibrillation potentials

Early reinnervation with polyphasic motor unit potentials
This patient has Parsonage-Turner Syndrome, which, when tested on EMG during the first 3 weeks, exhibits acute denervation of both peripheral nerve and nerve root distributions with positive sharp waves and fibrillation potentials.
Parsonage-Turner Syndrome is an idiopathic disorder with an etiology that is still unknown. Typical antecedent events can involve a viral illness, recent immunization, or elective surgery. Clinical presentation is usually initiated by acute onset shoulder pain, which quickly subsides and is followed by gradual weakness. Early MRI exhibits edema in the effected muscles, and fatty infiltration in later stages. Treatment is typically non-operative, and resolution can be seen as early as 6 weeks from onset.
Tjoumakaris et al. provide a thorough review of the diagnosis and management of ParsonageTurner Syndrome. The authors report the usefulness of MRI, which exhibits early edema and later fatty infiltration in the affected muscles, and urge the use of EMG as a confirmatory diagnostic measure as well as a monitoring tool to track resolution. Early identification and diagnosis may be treated with a short course of steroids, which may help shorten symptoms.
Stutz et al. concisely summarize Parsonage-Turner Syndrome and provide typical presentation, diagnosis and management principles. The authors note the common association with viral illness and/or recent immunization along with the importance of obtaining a baseline chest radiograph to rule out a compressive Pancoast tumor. Management is typically supportive with eventual resolution.
Figures A, B, and C are T2-weighted coronal, sagittal, and axial cuts of the shoulder girdle with associated edema in the supraspinatus and infraspinatus typically seen in Parsonage-Turner Syndrome.
Incorrect answers:
A total shoulder arthroplasty (TSA) would be the most appropriate treatment in which of the following arthritic patients?
Question 5
A B
Explanation
The radiographs reveal a tibial pilon fracture with an extruded and rotated anterior tibial fragment that lies deep to the anterior compartment neurovascular bundle, which contains the deep peroneal nerve. This nerve innervates the anterior compartment muscles and the extensor digitorum brevis and extensor hallucis brevis muscles and provides sensation to the dorsal aspect of the first interspace. An injury to the deep peroneal nerve at this level will only affect the innervation to the extensor digitorum brevis and extensor hallucis brevis muscles and the innervation of the first interspace. The superficial peroneal nerve innervates
the lateral compartment muscles above the level of this injury and innervates the dorsum of the foot. The medial forefoot is innervated by the saphenous nerve and the posterior tibial nerve innervates the posterior compartment muscles above the level of the injury. The sural nerve innervates the lateral foot and has no motor component, and the superficial peroneal nerve innervates the peroneus longus, which plantar flexes the first metatarsal above the level of the injury.
RECOMMENDED READINGS
Agur AM, Dalley AF, eds. Grant’s Atlas of Anatomy. 13th ed. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 2013:362-370.
Hoppenfeld S, de Boer P, Buckley R, eds. Surgical Exposures in Orthopaedics: The Anatomic Approach. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:625-673.
Question 6
A 69-year-old patient with diabetes has had acute-onset back pain and difficulty with ambulation for several hours. Evaluation reveals a temperature of 38.3°C, a white blood cell (WBC) count of 14000/µL (reference range [rr], 4500-11000/µL), C-reactive protein (CRP) level of 120 mg/L (rr, 0.08-3.1 mg/L), erythrocyte sedimentation rate of 130 mm/h (rr, 0-20 mm/h), normal rectal examination findings, and normal sensation to light touch. Motor function testing of the lower extremities reveals 3/5 ankle dorsiflexion and 4/5 plantar flexion strength bilaterally. An MR image reveals a large epidural abscess from L1-5. What is the most appropriate treatment at this time?
Explanation
Epidural abscess is a serious and potentially disastrous condition. Although medical management is effective in some situations, surgical decompression is considered urgent with the presence of a neurological deficit. Medical management can be considered in the case of a neurologically intact patient, particularly when the microorganism has been identified. If medical management is chosen, careful observation and serial examination for neurologic deterioration is required. Surgical decompression is indicated if a patient's neurologic status worsens or if medical management failure is noted. Additionally, diabetes, a CRP level higher than 115 mg/L, WBC higher than 12500/µL , and bacteremia have proven predictive of medical treatment failure. This patient would be a better candidate for urgent surgical decompression and subsequent IV antibiotics than for medical management.
RECOMMENDED READINGS
Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.View Abstract at PubMed
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 7
.A 22-year-old collegiate baseball pitcher has had posterior shoulder pain with decreased throwing velocity and accuracy over the past several months. Examination of the abducted shoulder in the supine position reveals 120 degrees of external rotation, 40 degrees of internal rotation on the throwing side, 100 degrees of external rotation, and 70 degrees of internal rotation on the nonthrowing side. The remainder of the clinical examination is unremarkable. An MRI scan shows a small partial articular-sided infraspinatus tear. Initial treatment should consist of
Explanation

Question 8
When performing a long fusion to the sacrum in an osteopenic patient in whom optimal sagittal balance is restored, which of the following is a benefit of extending the distal fixation to the pelvis, rather than the sacrum alone?
Explanation
REFERENCE: Hu SS, Berven SH, Bradford DS: Adult spinal deformity, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 465-477.
Question 9
A transverse humeral shaft fracture that occurs between a stiff arthritic shoulder joint; a stiff, arthritic elbow joint is treated nonsurgically in a hanging-arm cast
Explanation
In 1977, Perren and Cordey penned a German manuscript that first described an interpretation of mechanical influences on tissue differentiation. This became known as the Strain Theory of Perren. In 1980, a second manuscript by the same authors was published in English. Within this manuscript, Perren wrote, "These thoughts about the mechanical influences on tissue differentiation are not intended as conclusive evidence since precise data are still not available, but we hope that they will stimulate thought and provide a basis for discussion." More than 30 years later, these thoughts continue to stimulate discussion and research on cell mechanotransduction. This theory is still being manipulated in surgical theatres all around the world in an attempt to more consistently achieve fracture healing. Strain is a magnitude of deformation. As typically defined, it is the change in dimension of a deformed object during loading divided by its original dimension. This is difficult to work with intraoperatively. The fraction below illustrates a simpler way to regard this concept:
Strain = Magnitude of displacement between fragments during loading / Total resting distance between fragments after stabilization
By remembering that low strain generally leads to bone formation and healing, it is possible to manipulate this fraction intraoperatively to achieve success. When a simple fracture pattern is anatomically reduced and compressed, then the total resting distance between fragments after stabilization approaches 0. This means the numerator must be near 0 to achieve a low-strain environment. This is what occurs in absolute stability (no motion between fracture fragments under physiologic load) and primary bone healing occurs. When a multifragmentary fracture pattern is treated with bridge plating, the total resting distance between fragments after stabilization is a larger number (consider the additive distance between the different fragments). In this case, the numerator can be larger to achieve a low-strain environment. This is what happens in relative stability (controlled motion between fracture fragments under physiologic load). Secondary bone healing occurs. Now consider the third scenario: a simple fracture pattern that is fixed with a small gap. The total resting distance is still a small number. Based on the theory, eliminating motion by creating a stiff construct should lead to healing, but it does not. Creating absolute stability with a gap means that primary bone healing cannot occur (because cutting cones cannot cross the gap) and secondary bone healing cannot occur (because there is not enough motion to induce callus formation). This is where the strain theory breaks down and how many nonunions occur. In the fourth scenario, a high-strain environment is present and commonly leads to a nonunion (as predicted by the theory). The simple fracture pattern is too mobile, and nonfunctional callus often occurs.
RECOMMENDED READINGS
Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br. 2002 Nov;84(8):1093-110. Review. PubMed PMID: 12463652. View Abstract at PubMed
Epari DR, Duda GN, Thompson MS. Mechanobiology of bone healing and regeneration: in vivo models. Proc Inst Mech Eng H. 2010 Dec;224(12):1543-53. Review. PubMed PMID: 21287837.View Abstract at PubMed
Question 10
- A high school distance runner reports a 3-week history of heel pain while running. Examination elicits no pain with dorsiflexion or with palpitation of the plantar fascia; however, pain is evident with palpitation over the muscular origin of the abductor hallucis. What is the most likely etiology of the pain?
Explanation
Question 11
A 67-year-old female presents with shoulder pain for 3 months after falling down stairs. Imaging demonstrates a large rotator cuff tear involving multiple tendons. You perform an arthroscopic rotator cuff repair and biceps tenodesis. At her 2 month follow up, she reports worsening shoulder pain and decreased range of motion. Examination reveals active forward flexion to 80°. Passive range of motion is full. There is a positive external rotation lag sign. An MRI is performed and is pictured in Figure A. Which is the best treatment for this patient? Review Topic
Explanation
Failed rotator cuff repair is multifactorial. Structural failure of repair is the result of both intrinsic and extrinsic factors. Intrinsic factors include advancing patient age, increasing tear size, poor tendon and muscle quality, systemic disease and smoking history. Extrinsic factors include inadequate biomechanical construct or repair configuration and overaggressive postoperative rehabilitation.
Denard et al authored a review article on revision rotator cuff repair. Indications for revision repair are persistent symptoms despite nonoperative management in whom infection and advanced degenerative changes have been ruled out. Satisfactory results have been reported following revision repair of recurrent rotator cuff tears, particularly with arthroscopic techniques. Female sex and preoperative forward flexion < 135° is associated with poorer outcomes.
Lambers Heerspink et al found that increasing age, larger tear size and additional biceps or acromioclavicular (AC) joint procedures have a negative influence on cuff integrity at follow up. Smoking, duration of symptoms, obesity and medical comorbidities were not found to influence cuff integrity in this study. Only AC procedures and workers’ compensation status were associated with worse functional outcomes.
Figure A is a coronal T2 MRI demonstrating a failed rotator cuff repair with retear. Incorrect Responses:
Question 12
A 42-year-old woman who has had an 18-month history of severe low back pain is referred to your office for surgical evaluation. She reports that the pain initially began with right lower extremity pain and management consisted of oral analgesics, nonsteroidal anti-inflammatory drugs, and muscle relaxants. She has seen a chiropractor as well as a pain management specialist and she is status-post epidural steroid injections. She has also completed exhaustive physical therapy, as she is a certified athletic trainer and runs a health fitness program at a community hospital. Currently, she denies lower extremity pain and her pain is isolated to her low back and is subjectively graded as 8/10, with 10 being the worst pain she has ever experienced. The pain is interfering with her activities of daily living and she is seeking definitive treatment. Figures 32a through 32c show current MRI scans. Based on the current available medical literature, what is the most appropriate treatment?
Explanation
REFERENCES: Gibson JN, Waddell G: Surgery for degenerative lumbar spondylosis: Updated Cochrane Review. Spine 2005;30:2312-2320.
Fritzell P, Hagg O, Wessberg P, et al: 2001 Volvo Award Winner in Clinical Studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: A multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine 2001;26:2521-2532.
Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Question 13
A 20-year-old man is brought to the emergency department after a high-speed motor vehicle accident. His initial blood pressure is 70/40 mm Hg. He is currently receiving intravenous fluids as well as blood. His Focused Assessment with Sonography for Trauma examination did not show any free fluid in his abdomen and his chest radiograph is unremarkable. An AP pelvis radiograph is shown in Figure 15. What is the next most appropriate step in the management of his pelvic injury? Review Topic

Explanation
Question 14
An otherwise healthy 57-year-old woman has limited range of motion and moderate effusion after undergoing total knee arthroplasty 6 months ago. One of two cultures of joint aspirate reveals methicillin-resistant Staphylococcus epidermidis. Management should now consist of
Explanation
REFERENCES: Drancourt M, Stein A, Argenson JN, et al: Oral rifampin plus ofloxacin for treatment of staphylococcus-infected orthopedic implants. Antimicrob Agents Chemother 1993;37:1214-1218.
Duncan CP, Beauchamp C: A temporary antibiotic-loaded joint replacement system for the management of complex infections involving the hip. Orthop Clin North Am 1993;24:751-759.
Oyen WJ, Claessens RA, van Horn JR, et al: Scintiographic detection of bone and joint infections with indium-111-labeled nonspecifonal human immunoglobulin G. J Nucl Med 1990;31:403-412.
Question 15
In a patient with a C5-6 herniation, the most likely sensory deficit will be in the
Explanation
REFERENCE: Hoppenfeld S: Evaluation of nerve root lesions involving the upper extremity, in Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-23.
Question 16
A 35-year-old rock climber sustains an L1 burst fracture from a 30-foot fall while climbing. He sustained no other fractures or serious injuries. He is neurologically intact and has minimal posterior tenderness without increased spinous process separation on examination. Radiographs reveal kyphosis of 20 degrees between T12 and L2 with 30% vertebral height loss. A CT scan shows 55% canal compromise. What is the most appropriate management? Review Topic
Explanation
Question 17
Figure 51 shows an arthroscopic view of the patellofemoral joint from an inferolateral portal. The arrow points to which of the following structures? Review Topic

Explanation
Question 18
Two weeks after undergoing total knee arthroplasty, a 68-year-old woman experiences moderate, yet worsening, knee pain. Upon examination, she can walk with a cane but she has swelling with mild reactive erythema. She has a well-healed incision with no drainage. A review of her medications reveals the she has been taking warfarin and has an international normalized ratio (INR) of 4.0. Her erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level are slightly elevated, and radiographs are unremarkable other than for effusion. What is the most likely diagnosis?
Explanation
This patient likely has a hemarthrosis related to INR elevation. The slight elevations in ESR and CRP are likely attributable to the nature of the surgery itself rather than an infection, and the mild reactive erythema is likely attributable to the hemarthrosis.
Question 19
Acute redislocation of the glenohumeral joint is a complication that occurs following a first-time dislocation. This is most often seen with
Explanation
REFERENCES: Robinson CM, Kelly M, Wakefield AE: Redislocation of the shoulder during the first six weeks after a primary anterior dislocation: Risk factors and results of treatment.
J Bone Joint Surg Am 2002;84:1552-1559.
Bigliani LU, Newton PM, Steinmann SP, et al: Glenoid rim lesions associated with recurrent anterior dislocation of the shoulder. J Sports Med 1998;26:41-45.
Question 20
Which of the following pharmacologic agents is most likely to adversely affect the success rate of bony union after lumbar arthrodesis?
Explanation
REFERENCES: Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Dimar JR II, Ante WA, Zhang YP, et al: The effects of nonsteroidal anti-inflammatory drugs on posterior spinal fusions in the rat. Spine 1996;21:1870-1876.
Question 21
A 45-year-old woman with grade II adult-acquired flatfoot deformity has pain on the lateral side of her foot just distal to the tip of the fibula. Which component of a comprehensive flatfoot reconstruction most likely will address the deformity responsible for this pain?
Explanation
Patients develop lateral ankle pain with progression of adult-acquired flatfoot deformity. This is associated with increased hindfoot valgus deformity. Calcaneal fibular impingement has been considered the primary cause of this pain. Studies demonstrate that arthrosis of the posterior facet of the subtalar joint strongly correlates with lateral pain in adult-acquired flatfoot deformity. Both conditions are related to hindfoot valgus deformity. Although lateral column lengthening is a powerful tool for correction of flatfoot deformity, its effect on hindfoot deformity is less defined. Lateral column lengthening provides better correction of the longitudinal arch of the midfoot and realignment of the medial column than other osteotomies. A medializing calcaneal osteotomy has a significant linear effect on hindfoot valgus alignment. Spring ligament reconstruction and medial cuneiform opening-wedge osteotomies have less effect on hindfoot alignment than the medial calcaneal slide.
RECOMMENDED READINGS
Ellis SJ, Deyer T, Williams BR, Yu JC, Lehto S, Maderazo A, Pavlov H, Deland JT. Assessment of lateral hindfoot pain in acquired flatfoot deformity using weightbearing multiplanar imaging. Foot Ankle Int. 2010 May;31(5):361-71. doi: 10.3113/FAI.2010.0361. PubMed PMID:
Question 22
A 30-month-old boy underwent open reduction of his right hip to address developmental hip dysplasia. The reduction was performed through an anterior approach, and a shortening femoral osteotomy was not performed. Four months after surgery, hip radiographs reveal absence of ossification of the femoral epiphysis and fragmentation of the ossific nucleus. What is the likely cause of this complication?
Explanation
The incidence of pediatric hip dysplasia is approximately 1 per 100 live births, with hip dislocation present in 1 in 1000 births. Two surgical approaches primarily are used for surgical reduction in the dislocated pediatric hip: the modified medial approach as described by Weinstein and the
anterior Smith-Peterson approach. The Weinstein modification of the Ludloff approach exploits the interval between the pectineus muscle and the femoral neurovascular bundles rather than the interval between the pectineus and the adductor longus and brevis. The modified “bikini” anterior Smith-Peterson approach passes between the sartorius and tensor fascia lata superficially and between the rectus and gluteus medius during deep dissection.
When using the medial approach, the neurovascular bundle is particularly at risk, including the medial circumflex femoral vessels that supply blood to the femoral head ossific nucleus. Damage to this structure increases risk for osteonecrosis of the femoral head. Unlike the anterior approach, the medial approach does not allow for the performance of a capsulorrhaphy, poses higher risk for postprocedure redislocation, and is less useful in children of walking age. Identification of the ligamentum teres during deep dissection assists in localization of the true bony acetabulum.
The anatomic structure primarily at risk during the anterior approach is the lateral femoral cutaneous nerve. Excessive traction or transection of this structure will result in numbness in the proximal lateral thigh. This surgical approach allows for identifying and addressing all potential impediments to reduction: the redundant capsule, hypertrophic labrum, hypertrophic ligamentum teres, pulvinar, iliopsoas tendon, and transverse acetabular ligament. In older children who undergo open reduction with periacetabular osteotomy without a concomitant proximal femoral shortening osteotomy, reduction may be accompanied by increased pressure on the femoral head which, in turn, may result in secondary osteonecrosis of the femoral head.
RECOMMENDED READINGS
Karol LA. Developmental dysplasia of the hip. In: Song KM, ed. Orthopaedic Knowledge Update: Pediatrics 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2011:159-167.
Vitale MG, Skaggs DL. Developmental dysplasia of the hip from six months to four years of age. J Am Acad Orthop Surg. 2001 Nov-Dec;9(6):401-11. Review. PubMed PMID: 11730331. View Abstract at PubMed
Weinstein SL, Ponseti IV. Congenital dislocation of the hip. J Bone Joint Surg Am. 1979 Jan;61(1):119-
Question 23
What structure is most at risk for injury from a retractor against the tracheoesophageal junction during an anterior approach to the cervical spine?
Explanation
REFERENCES: Ebraheim NA, Lu J, Skie M, et al: Vulnerability of the recurrent laryngeal nerve in the anterior approach to the lower cervical spine. Spine 1997;22:2664-2667.
Kilburg C, Sullivan HG, Mathiason MA: Effect of approach side during anterior cervical discectomy and fusion on the incidence of recurrent laryngeal nerve injury. J Neurosurg Spine 2006;4:273-277.
Question 24
The standard Bankart lesion involves detachment of the labrum along with which of the following capsular ligaments? Review Topic
Explanation
Question 25
A 29-year-old male sustained a mid-shaft femur fracture in a motor cycle accident. Even if asymptomatic, what additional radiographs must be obtained either preoperatively or intraoperatively before performing intramedullary nailing of the femoral shaft fracture?

Explanation
Question 26
During the revision surgical procedure, thoracic pedicle screws are placed. Following placement, triggered electromyography (EMG) is performed by stimulating the pedicle screw heads. During testing the right T2 pedicle screw head returns a threshold of 2 mA. What does this reading indicate?
Explanation
This patient has developed a proximal junctional kyphosis following a long posterior fusion performed for treatment of degenerative lumbar scoliosis. Risk factors for proximal junctional kyphosis in the setting of instrumented fusions performed for degenerative scoliosis include advanced age, 360-
degree fusions, extension of fusion constructs to the sacrum, and upper instrumented vertebrae at the level of T1-3. The patient's junctional kyphosis is attributable to failure of the disk and ligamentous structures at T2-3 and would be graded as type I using the classification system of Yagi and associates. Most symptomatic proximal junctional kyphoses are treated with posterior extension of the fusion construct to a more proximal level spanning the kyphosed region. The use of orthoses or simple removal of instrumentation is unlikely to substantively impact symptoms or address the proximal kyphosis. Diabetes and obesity are known factors that increase risk for postsurgical infection following a spine fusion procedure. The most frequent complication following revision surgery for proximal junctional kyphosis, however, is the need for further surgery. In the study by Yagi and associates, 48% of patients who underwent revision surgery for proximal kyphosis developed further adjacent segment degeneration. In the proximal thoracic spine, where the pedicle may be narrow, triggered EMG testing of inserted pedicle screws may be used to assess for violation of the pedicle wall during insertion. In the setting of triggered EMG, thresholds exceeding 10 mA indicate a well-placed pedicle screw. Thresholds lower than 4 mA to 6 mA indicate that a screw is directly contacting a neural structure. Thresholds between 9 mA and 10 mA suggest that a breach of the pedicle may be present, but the screw is not contacting a neural structure.
RECOMMENDED READINGS
Yagi M, Rahm M, Gaines R, Maziad A, Ross T, Kim HJ, Kebaish K, Boachie-Adjei O; Complex Spine Study Group. Characterization and surgical outcomes of proximal junctional failure in surgically treated patients with adult spinal deformity.Spine (Phila Pa 1976). 2014 May 1;39(10):E607-14. doi: 10.1097/BRS.0000000000000266. PubMed PMID: 24525992. View
Abstract at PubMed
Cammarata M, Aubin CÉ, Wang X, Mac-Thiong JM. Biomechanical risk factors for proximal junctional kyphosis: a detailed numerical analysis of surgical instrumentation variables. Spine (Phila Pa 1976). 2014 Apr 15;39(8):E500-7. doi: 10.1097/BRS.0000000000000222. PubMed
PMID: 24480964. View Abstract at PubMed
Kim HJ, Lenke LG, Shaffrey CI, Van Alstyne EM, Skelly AC. Proximal junctional kyphosis as a distinct form of adjacent segment pathology after spinal deformity surgery: a systematic review. Spine (Phila Pa 1976). 2012 Oct 15;37(22 Suppl):S144-64. doi: 10.1097/BRS.0b013e31826d611b. PubMed PMID: 22885829. View Abstract at PubMed Schoenfeld AJ, Carey PA, Cleveland AW 3rd, Bader JO, Bono CM. Patient factors, comorbidities, and surgical characteristics that increase mortality and complication risk after spinal arthrodesis: a prognostic study based on 5,887 patients. Spine J. 2013 Oct;13(10):1171-9. doi: 10.1016/j.spinee.2013.02.071. Epub 2013 Apr 9. PubMed PMID:
Question 27
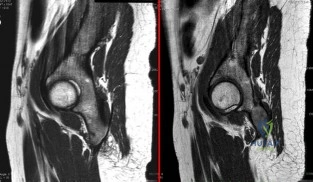
A 22-year-old ballet dancer undergoes hip arthroscopy for increasing hip pain and popping with activity. She experiences complete resolution of signs and symptoms post-operatively. Her pre- and post-operative magnetic resonance sagittal images shown in Figure A (left, pre-operative; right, post-operative). Which of the following pre-operative physical examination findings may have been positive? Review Topic
Explanation
Snapping hip exists in 3 forms: (1) external snapping hip, which is caused by the iliotibial band (ITB) sliding over the greater trochanter, (2) internal snapping hip, and
(3) intraarticular snapping hip, which is caused by loose bodies (traumatic, or from synovial chondromatoses) or labral tears. While painless snapping hip requires no treatment, painful snapping hip may be addressed with activity modification, physical therapy, steroid injections. Surgical release (ITB z-plasty or psoas tenotomy) is indicated if nonoperative management is unsuccessful.
Ilizaliturri et al. evaluated the results of endoscopic iliopsoas tendon release at the lesser trochanter (10 patients) vs endoscopic transcapsular psoas release from the peripheral compartment (9 patients). There were improvements in WOMAC scores in both groups, and no difference between groups. They conclude that both techniques are equally effective.
Marquez Arabia et al. evaluated if the psoas tendon regenerates after tenotomy in 27 patients. At 23 months, they found that tendon regeneration occurred in all patients, to
a mean circumference of 84% of the original. One patient had persistent pain, but all had 5/5 hip flexion strength. They hypothesize that the bulk of iliopsoas muscle fibers attaches directly to the proximal femoral shaft without a tendon, preventing retraction and allowing regeneration to occur easily.
Figure A shows pre- and post-operative arthroscopic psoas tenotomy magnetic resonance sagittal images. Illustration A shows the psoas tendon (white arrows) prior to transection. Illustration B shows the psoas tendon after transection (green arrows, proximal tendon segment; yellow arrows, distal segment). Illustration C and D are diagrams showing release at the level of the lesser trochanter and hip joint respectively.
Incorrect
90 degrees, but full external rotation. Answer 2: Decreased internal rotation and a positive impingement test (forced
flexion, adduction, femoroacetabular Answer 4: These
and internal
rotation) are classic findings
findings may
be found with intra-articular
for cam-type impingement loose bodies.
Question 28
An active 49-year-old woman who sustained a diaphyseal fracture of the clavicle 8 months ago now reports persistent shoulder pain with daily activities. An AP radiograph is shown in Figure 8. Management should consist of
Explanation
shown some healing response with callus formation, but these techniques are not successful
in an atrophic nonunion. The preferred technique for achieving union is open reduction and internal fixation with bone graft. Percutaneous fixation has no role in treatment of nonunions
of the clavicle.
REFERENCES: Boyer MI, Axelrod TS: Atrophic nonunion of the clavicle: Treatment by compression plating, lag-screw fixation and bone graft. J Bone Joint Surg Br 1997;79:301-303.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
Question 29
What is the most common adverse postoperative complication of laminoplasty for multilevel cervical spondylotic myelopathy?
Explanation
REFERENCES: Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Edwards CC II, Riew KD, Anderson PA, et al: Cervical myelopathy: Current diagnostic and treatment strategies. Spine J 2003;3:68-81.
Question 30
Figure 3 shows the AP radiograph of a patient with diabetes mellitus who has knee pain. A semiconstrained knee prosthesis was used in this patient to prevent which of the following complications?
Explanation
REFERENCES: Parvizi J, Marrs J, Morrey BF: Total knee arthroplasty for neuropathic (Charcot) joints. Clin Orthop 2003;416:145-150.
Kim YH, Kim JS, Oh SW: Total knee arthroplasty in neuropathic arthropathy. J Bone Joint
Surg Br 2002;84:216-219.
Question 31
A 63-year-old man with type I diabetes mellitus who underwent open forefoot amputation now has a high fever, and an elevated WBC count and blood glucose levels. Repeat laboratory studies the day after surgery show a WBC count of 9,500/mm 3 , a serum albumin level of 1.9 g/dL, and a total lymphocyte count of 1,900/mm 3 . Examination reveals that he is afebrile, and his blood glucose level is now normal. An ultrasound Doppler of the dorsalis pedis artery shows an ankle-brachial index of 0.6. A transcutaneous partial pressure measurement of oxygen at the ankle joint shows a level of 38 mm Hg. What is the best course of action?
Explanation
REFERENCE: Pinzur MS, Stuck RM, Sage R, et al: Syme ankle disarticulation in patients with diabetes. J Bone Joint Surg Am 2003;85:1667-1672.
Question 32
A 35-year-old man sustained a traumatic low ulnar nerve palsy 18 months ago. The extent of the clawing and intrinsic atrophy as well as the active radial deviation are seen in Figures 1 through 3. No hyperextensibility of any of the proximal interphalangeal (PIP) joints is observed. Preoperatively, the patient is not able to fully extend the PIP joints with the wrist in neutral position and the examiner holding the metacarpophalangeal (MCP) joints flexed. Figure 4 shows the intraoperative photograph obtained during the intrinsic reconstruction procedure that is performed. The tendon grafts were inserted distally into the

Explanation
Originally, Burkhalter and Strait recommended bony insertion into the proximal phalanx through a drill hole. This procedure does require more surgical dissection and flexes only the MCP joints; thus it cannot extend the PIP joints directly. It does improve clawing in the fingers if the PIPs can extend with preoperative MCP flexion. The ability to extend the PIP joints is evaluated preoperatively using the Bouvier test. With the wrist in neutral position, the examiner holds the MCPs flexed and looks for the ability in that position to actively extend the PIPs. If the patient is able to do so, then the test is considered positive, and this describes "simple" clawing. In such cases, procedures that flex only the MCPs are appropriate. The insertion sites for these procedures include the proximal phalanx, the first annular pulley, and the second annular pulley. If the Bouvier test is negative, then it is best to insert the tendon grafts distally into the lateral bands. This technique has a low chance of leading to hyperextension of the PIP joints, particularly when performed with a wrist extensor motor (which leaves the flexor digitorum superficialis undisturbed) and with no preoperative hyperextensibility of the PIPs.
Question 33
An 11-year-old child has Ewing’s sarcoma of the femoral diaphysis with a small soft-tissue mass. Staging studies show no evidence of metastases. Treatment should consist of
Explanation
REFERENCES: Toni A, Neff JR, Sudanese A, et al: The role of surgical therapy in patients with non-metastatic Ewing’s sarcoma of the limbs. Clin Orthop 1991;286:225.
Picci P, Rougraff BT, Bacci G, et al: Prognostic significance of histopathologic response to chemotherapy in non-metastatic Ewing’s sarcoma of the extremities. J Clin Oncol 1993;11:1763.
Gibbs CP Jr, Weber K, Scarborough MT: Malignant Bone Tumors. Instr Course Lect 2002;51:413-428.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 34
Which of the following is considered the lowest level that a standard thoracolumbosacral orthosis (TLSO) can immobilize?
Explanation
REFERENCES: White AA, Panjabi MM: Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 475-509.
Norton PL, Brown T: The immobilizing efficiency of back braces. J Bone Joint Surg Am 1957;39:111-139.
Question 35
Figure 242 is the anteroposterior radiograph of a 28-year-old man who underwent resection and reconstruction for an Ewing sarcoma. What is the most common functional deficit encountered during rehabilitation?
Explanation

Question 36
A collegiate division I football player ruptures his anterior cruciate ligament (ACL). After counseling him, you agree to perform a double-bundle ACL reconstruction. Which of the following is a correct statement for this technique? Review Topic
Explanation
Question 37
What form of fixation is associated with the highest incidence of osseous union when using segmental allograft reconstruction following tumor resection?
Explanation
REFERENCE: Vander Griend RA: The effect of internal fixation on the healing of large allografts. J Bone Joint Surg Am 1994;76:657-663.
Question 38
Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?
Explanation
REFERENCES: Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, Pa, Lippincott-Raven, 1998, pp 789-802.
Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
MacDonald SJ, Hersche O, Ganz R: Periacetabular osteotomy in the treatment of neurogenic acetabular dysplasia. J Bone Joint Surg Br 1999;81:975-978.
Question 39
Which of the following results cannot be achieved with an in-shoe orthosis?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 55-64.
Bono CM, Berberian WS: Orthotic devices: Degenerative disorders of the foot and ankle. Foot Ankle Clin 2001;6:329-340.
Buonomo LJ, Klein JS, Keiper TL: Orthotic devices: Custom-made, prefabricated, and material selection. Foot Ankle Clin 2001;6:249-252.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 40
Figures 1 through 3 show the radiographs obtained from a 40-year-old woman who injured her right index finger in a bicycle collision. Failure to restore sagittal plane alignment would likely result in

Explanation
The radiographs reveal an extra-articular proximal phalanx fracture of the index finger. The fracture is comminuted with dorsal angulation of the distal fragment. The question specifically asks about the restoration of sagittal alignment. The fracture is comminuted with dorsal angulation of the distal fragment. The other options are incorrect, because overlapping of the digits occurs with rotational malalignment, the development of arthritis may occur with intra-articular fractures, and hyperextension would not occur with this type of deformity.
Question 41
At a minimum 2-year follow-up and compared with the metacarpophalangeal (MCP) joint, pyrolytic carbon resurfacing arthroplasties of the proximal interphalangeal (PIP) joint
Explanation
Wall and Stern published a report on MCP joint pyrolytic carbon arthroplasty for osteoarthritis and another on PIP joint pyrolytic carbon resurfacing arthroplasty for osteoarthritis. They found different outcomes, and MCP joint implants outperformed PIP joint implants. Of eleven MCP joint arthroplasties, two produced asymptomatic squeaking and clicking, whereas eleven of 31 PIP joint implants produced this problem. No dislocations were reported among the MCP joint implants, but five PIP joint dislocations were observed. Outcomes were measured by the Michigan Hand Outcomes Questionnaire in both studies and were satisfactory for the MCP joint implants, with an average score of 80. The PIP implants did not fare as well, showing a higher degree of pain along with an average score of 53. The authors noted that, in the 15 patients in the PIP study who had unilateral surgery, the uninvolved, nonsurgical hand motion was actually statistically significantly (P<0.01) better than the surgical hand. MCP joint motion increased from 62º before surgery to 76º after surgery, whereas PIP joint motion got worse after surgery, with the average motion decreasing from 57º to 31º.
Question 42
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. The patient participates in physical therapy for 8 weeks with his team's trainer but notes little improvement. What is the most appropriate next diagnostic step to determine the cause of his pain?

Explanation
used to diagnose labral pathology. Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result in a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has important functions for hip stability and maintenance of the suction seal of the joint.
Question 43
A 10-year-old boy reports a gradual onset of weakness; however, he is fully ambulatory. History reveals that he has a 17-year-old brother who has just stopped walking because of a similar condition. Laboratory studies show a creatine kinase level of 5,480 IU/L (normal 25 to 232 IU/L), and examination shows a slightly positive Gower sign. What is the most likely diagnosis?
Explanation
REFERENCES: Matsuo M: From molecular diagnosis to gene therapy. Brain Dev 1996;18:167-172.
Darras BT: Molecular genetics of Duchenne and Becker muscular dystrophy. J Pediatr 1990;117:1-15.
Gutmann DH, Fischbeck KH: Molecular biology of Duchenne and Becker’s muscular dystrophy: Clinical applications. Ann Neurol 1989;26:189-194.
Question 44
Figure 45 shows the radiograph of a 2-year-old patient who has progressive lumbar scoliosis as the result of hemivertebra. Examination reveals no associated cutaneous lesions, and an MRI scan shows no associated intraspinal anomalies. Treatment should consist of
Explanation
REFERENCE: Callahan BC, Georgopoulos G, Eilert RE: Hemivertebral excision for congenital scoliosis. J Pediatr Orthop 1997;17:96-99.
Question 45
A 62-year-old man has had worsening pain in the left shoulder for the past 6 weeks without trauma. He participated in physical therapy to "strengthen" his shoulder; however, it failed to provide relief. On examination, his right shoulder motion is 180, 60, and T8 (forward flexion, external rotation, and internal rotation). His left shoulder motion, both active and passive, is 150, 40, and L1. T1- and T2-weighted MRI scans are shown in Figures 106a and 106b with an official diagnosis of partial supraspinatus tendon tear. What is the appropriate treatment? Review Topic
Explanation
Question 46
Which of the following provocative tests would most likely be positive in a patient with medial epicondylitis? Review Topic
Explanation
Medial epicondylitis is an overuse syndrome of the flexor-pronator mass. The pronator teres (PT) and flexor carpi radialis (FCR) are thought to be most affected with this condition. It is most common in the dominant arm and occurs with activities that require repetitive wrist flexion/forearm pronation. Patients are most tender over the origin of PT and FCR at the medial epicondyle. Resisting a patient with their fist clenched, wrist flexed and pronated can cause worsening of their pain. This maneuver can be used as a provocative test for this condition.
Cain et al. reviewed elbow injuries in throwing athletes. They comment that the common flexor-pronator muscle origin provides dynamic support to valgus stress in the throwing elbow, especially during early arm acceleration and help produce wrist flexion during ball release.
Amin et al. reviewed the evaluation and management of medial epicondylitis. They report that medial epicondylitis typically occurs in the fourth through sixth decades of life, the peak working years, and equally affects men and women. Physical therapy and rehabilitation is the main aspect of recovery from medial epicondylitis, once acute symptoms have been alleviated.
Illustration A shows a video of this provocative test for medial epicondylitis. Incorrect Answers:
Question 47
If a surgeon inadvertently burrs through the midlateral wall of C5 during a anterior corpectomy, what structure is at greatest risk for injury?
Explanation
REFERENCES: Pfeifer BA, Freidberg SR, Jewell ER: Repair of injured vertebral artery in anterior cervical procedures. Spine 1994;19:1471-1474.
Gerszten PC, Welch WC, King JT: Quality of life assessment in patients undergoing nucleoplasty-based percutaneous discectomy. J Neurosurg Spine 2006;4:36-42.
Question 48
Figures 1 and 2 are the MRI scans of a 57-year-old man who dislocated his left shoulder after a fall while playing tennis. On examination, he had full passive shoulder range of motion, but he was unable to actively elevate his injured shoulder. Sensation was intact to light touch over the lateral shoulder. What is the most likely etiology of his shoulder weakness?
Explanation
Question 49
A sagittal T1-weighted MRI scan of the knee joint is shown in Figure 23. What structure is identified by the arrow?
Explanation
REFERENCES: Gross ML, Grover JS, Bassett LW, Seeger LL, Finerman GA: Magnetic resonance imaging of the posterior cruciate ligament: Clinical use to improve diagnostic accuracy. Am J Sports Med 1992;20:732-737.
Sonin AH, Fitzgerald SW, Friedman H, Hoff FL, Hendrix RW, Rogers LF: Posterior cruciate ligament injury: MR imaging diagnosis and patterns of injury. Radiology 1994;190:455-458.
Question 50
Duchenne’s muscular dystrophy is a genetic disorder that is transmitted by which of the following modes of inheritance?
Explanation
REFERENCES: Fitzgerald RH, Kaufer H, Malkani AL: Orthopaedics. St Louis, MO, Mosby Year Book, 2002, pp 1573-1583.
Smith SA, Swaiman HF: Muscular dystrophies, in Swaiman KF, Ashwall S (eds): Pediatric Neurology Principles and Practice, ed 3. St Louis, MO, Mosby, 1999, pp 1235-1237.
Question 51
Figure 14 shows the AP radiograph of a patient who underwent prosthetic arthroplasty 8 years ago and has now become symptomatic again over the past 18 months. A WBC count and erythrocyte sedimentation rate are within normal limits, and aspiration of the glenohumeral joint yields a negative Gram stain and cultures. Which of the following procedures will most likely provide the best pain relief and function?
Explanation
REFERENCES: Antuna SA, Sperling JW, Cofield RH, et al: Glenoid revision surgery after total shoulder arthroplasty. J Shoulder Elbow Surg 2001;10:217-224.
Rodosky MW, Bigliani LU: Surgical treatment of non-constrained glenoid component failure. Oper Tech Orth 1994;4:226-236.
Question 52
Which of the following statements most accurately describes the risk of ileus following total joint arthroplasty?
Explanation
REFERENCE: Parvizi J, Han SB, Tarity TD, et al: Postoperative ileus after total joint arthroplasty. J Arthroplasty 2008;23:360-365.
Question 53
In the evaluation of Lisfranc injuries, which radiographic studies should routinely be obtained?
Explanation
It is estimated that as many as 20% of Lisfranc injuries are missed on initial radiographic examination. Weight-bearing bilateral radiographs should be performed routinely. CT scan, MRI, and stress radiographs performed under anesthesia may be needed in select cases. The Lisfranc ligament stabilizes the midfoot and consists of the dorsal and plantar oblique ligaments and the strong interosseous ligaments. All 3 extend from the base of the second metatarsal to the medial cuneiform. The “fleck sign" is a small avulsion fracture at the medial base of the second metatarsal, representing an avulsion of the Lisfranc ligament. The current treatment recommendation for displaced Lisfranc subluxations and dislocations is to perform ORIF with rigid fixation using either screws or plates and screws. Kirschner wire fixation may lead to recurrence after pin removal. Closed reduction and casting alone cannot permanently reduce the dislocation.
RECOMMENDED READINGS
Clanton TO, Waldrop III NE. Athletic injuries to the soft tissues of the foot and ankle. In: Coughlin MJ, Saltzman CL, Anderson RB, eds. Mann's Surgery of the Foot and Ankle. Vol 2. 9th ed. Philadelphia, PA: Elsevier-Saunders; 2014:1531-1687.
Karges DB. Foot trauma. In: Cannada LK, ed. Orthopaedic Knowledge Update 11. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:631-643.
CLINICAL SITUATION FOR QUESTIONS 5 THROUGH 8
A

B

Figures 5a and 5b are the clinical photograph and AP radiograph of a 55-year-old woman who has a painful right forefoot deformity. There is no history of antecedent trauma. The 1-2 intermetatarsal angle is 17 degrees, and the hallux valgus angle is 35 degrees.
Question 54
A 30-year-old man caught his dominant little finger on the straps of his windsurfing board 10 days ago. He reports swelling about the distal phalanx and has difficulty completely extending the distal interphalangeal joint. A radiograph is shown in Figure 47. What is the most appropriate treatment for this injury?
Explanation
REFERENCES: Baratz ME, Schmidt CC, Hughes TB: Extensor tendon injuries, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 192.
Bendre AA, Hartigan BJ, Kalainov DM: Mallet finger. J Am Acad Orthop Surg 2005;13:336-344.
Question 55
An increase in advanced glycation end-products (AGEs) is characteristic of which of the following clinical conditions and results in which pathologic process?
Explanation
AGEs are produced from spontaneous nonenzymatic glycation of proteins when sugars (glucose, fructose, ribose) react with lysine or arginine residues. Because of the low turnover, cartilage is susceptible to AGEs accumulation. The accumulation of AGEs has been thought to play a role in the development of OA of the knee and ankle.
Li et al. reviewed age-related changes in cartilage. They state that with aging, there is excessive collagen cross-linking increases cartilage stiffness, while shortening/degradation of aggrecan leads to loss of sugar side chains and water-binding ability, while increased levels of AGEs are associated with a decline in anabolic activity. There is also increased chondrocyte death and/or apoptosis.
Anderson et al. reviewed the relationship between osteoarthritis and aging. They state that knee cartilage thins with aging (especially on the femoral and patellar sides, suggesting a gradual loss of cartilage matrix. AGEs formation leads to modification of type II collagen by cross-linking of collagen molecules, increasing stiffness and brittleness and increasing susceptibility to fatigue failure.
Incorrect Answers:
Question 56
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
REFERENCES: Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Gerber C, Sebesta A: Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: A preliminary report. J Shoulder Elbow Surg 2000;9:483-490.
Question 57
What part of the glenoid labrum has the least vascularity?
Explanation
REFERENCE: Cooper DE, Arnoczky SP, O’Brien SJ, et al: Anatomy, histology and vascularity of the glenoid labrum: An anatomical study. J Bone Joint Surg Am 1992;74:46-52.
Question 58
.What is the most appropriate treatment if instability is present at the time of evaluation?
Explanation

Question 59
An otherwise healthy 37-year-old man fell off the flatbed of a delivery truck and landed directly on his dominant left hand. Surgical stabilization of a distal radius fracture is performed. An intraoperative radiograph is shown in Figure 22. What is the next most appropriate step in management?
Explanation
REFERENCES: Smith DW, Henry MK: Comprehensive management of soft-tissue injuries associated with distal radius fractures. J ASSH 2002;3:153-164.
Fernandez DL, Wolfe SW: Distal radius fractures, in Green DP, Hotchkiss RN, Pederson WC,
et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 693.
Question 60
Halo treatment for preadolescent children typically requires the use of which of the following? Review Topic
Explanation
Question 61
The posterior approach to the proximal radius uses what intermuscular interval?
Explanation
REFERENCES: Spinner M: Injuries to the Major Branches of Peripheral Nerves of the Forearm, ed 2. Philadelphia, PA, WB Saunders, 1978, pp 66-77.
Henry AK: Extensile Exposure, ed 3. New York, NY, Churchill Livingstone, 1995.
Question 62
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. The patient fails an extensive course of physical therapy and is unable to return to baseball. He and his orthopaedic surgeon elect to proceed with surgery. During a repeat evaluation, he has negative sulcus and Beighton sign findings, and radiographs show 5° of glenoid retroversion. What is the most appropriate surgical plan?

Explanation
and degenerative joint disease.
Question 63
A 45-year-old man falls from a skateboard and dislocates his elbow. After a closed reduction in the emergency department, his elbow is carefully examined. He has positive valgus stress, moving valgus stress, and milking maneuver tests. His elbow appears stable to varus stress and lateral pivot shift tests. What is the most appropriate manner of immobilizing the elbow for this patient?
Explanation
forearm should be splinted in full supination.
Question 64
Which of the following tissues has the highest maximum load to failure?
Explanation
REFERENCES: Woo SL, Hollis JM, Adams DJ, et al: Tensile properties of the human femur-anterior cruciate ligament-tibia complex: The effects of specimen age and orientation. Am J Sports Med 1991;19:217-225.
Staubli HU, Schatzmann L, Brunner P, et al: Quadriceps tendon and patellar ligament cryosectional anatomy and structural properties in young adults. Knee Surg Sports Traumatol Arthrosc 1996;4:100-110.
Wilson TW, Zafuta MP, Zobitz M: A biomechanical analysis of matched bone-patellar tendon-bone and doubled looped semitendinosus and gracilis tendon grafts. Am J Sports Med 1999;27:202-207.
Question 65
When an adult hip is surgically dislocated for relief of femoro-acetabular impingment, what is the risk of postoperative iatrogenic osteonecrosis?
Explanation
REFERENCE: Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U: Surgical dislocation of the adult hip: A technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124.
Question 66
Cortical bone demonstrates viscoelastic behavior as its mechanical properties are sensitive to strain rate and duration of applied load. Regarding longitudinal strain in cortical bone, which of the following statements regarding this characteristic is true?
Explanation
For LOW strain rates typical of normal activity (physiological strain rates of <0.1/s), bone is ELASTIC and DUCTILE (increasing ultimate strain with increasing strain rate). There is a ductile-to-brittle transition with increasing strain rate from normal to
supranormal rates. For EXTREMELY HIGH supranormal strain rates (>0.1/s, high impact trauma), bone is VISCOELASTIC and BRITTLE (low ultimate strain with increasing strain rate). Bone also becomes stronger and stiffer (higher modulus, steeper slope of stress-strain plot) as strain rate increases. This viscoelastic property helps in damping muscle contracture.
Natali and Meroi reviewed studies examining mechanical properties of bone. Mechanical properties are correlated with moisture, deformation rate, density and region of bone. Mechanical adaptation of bone is affected by strain rate (rate at which bone is deformed), strain mode (tension, compression, shear), strain direction (direction of strain relative to bone surface), strain frequency (cycles/second), stimulus duration (period over which deformation cycles are applied), strain distribution (pattern of strain magnitude across bone section) and strain energy (energy stored during deformation).
Illustration A shows the mechanical properties of bone with increasing strain rates. Incorrect Answers:
increase. During normal activity, as strain rate increases, bone is more ductile. With high impact trauma, bone is more brittle.
Question 67
A 7-year-old girl with a known diagnosis of neurofibromatosis has neck pain and deformity. She has been wearing a soft cervical collar for the past 2 months with mild relief of her symptoms. An MRI scan shows several small neurofibromas on the left side of the cervical spine near the foramina at C6 and 7. A lateral cervical spine radiograph is shown in Figure 34. What is the most appropriate management? Review Topic

Explanation
Question 68
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms? Review Topic
Explanation
Question 69
A 47-year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the aspiration and proceed to a revision TKA with possible augments on standby.
Question 70
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with
Explanation
REFERENCES: Bokor DJ, Conboy VB, Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br 1999;81:93-96.
Wolf EM, Cheng JC, Dickson K: Humeral avulsion of the inferior glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Question 71
Figures 39a and 39b show the current radiographs of an 8-year-old girl who has had pain in the left thigh for the past 3 months. She was recently diagnosed with hypothyroidism and started treatment 1 week ago. Examination reveals a mild abductor deficiency limp on the left side. She lacks 30 degrees internal rotation on the left hip compared with the right hip. Management should consist of
Explanation
“pre-slip.” Muscle strengthening, hip spica casting, and closed reduction have no place in the primary treatment of a stable slipped capital femoral epiphysis.
REFERENCES: Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Loder R, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Aronson DD, Carlson WE: Slipped capital femoral epiphysis: A prospective study of fixation with a single screw. J Bone Joint Surg Am 1992;74:810-819.
Question 72
A 30-year-old man who participates in recreational sports reports the spontaneous onset of intermittent pain and swelling about the right knee. Examination reveals a 3+ effusion, with a range of motion of 10° to 60°. He has mild diffuse tenderness but no instability. MRI scans and an arthroscopic view are shown in Figures 39a through 39c. Management should consist of
Explanation
REFERENCES: Coolican MR, Dandy DJ: Arthroscopic management of synovial chondromatosis of the knee: findings and results in 18 cases. J Bone Joint Surg Br
1989;71:498-500.
Ogilvie-Harris DJ, Saleh K: Generalized synovial chondromatosis of the knee: A comparison
of removal of the loose bodies alone with arthroscopic synovectomy. Arthroscopy
1994;10:166-170.
Question 73
Figure 1 shows the radiograph of an 18-year-old patient who has severe knee pain. Treatment consisting of osteotomy should be perfomed
Explanation
REFERENCE: Murphy SB: Tibial osteotomy for genu varum: Indications, preoperative planning, and technique. Orthop Clin North Am 1994;25:477-482.
Question 74
A 46-year-old man reports occasional squeaking of his hip 2 years after undergoing an uneventful total hip arthroplasty. History reveals no pain, physical examination cannot reproduce audible squeaking, and radiographs show appropriate implant position. What is the most appropriate management?
Explanation
Hopefully, with a better understanding of acoustic phenomena following ceramic total hip arthroplasty, this complication can be minimized.
REFERENCES: Yang CC, Kim RH, Dennis DA: The squeaking hip: A cause for concem-disagrees. Orthopedics
2007;30:739-742.
Walter WL, O’Toole GC, Walter WK, et al: Squeaking in ceramic-on-ceramic hips: The importance of acetabular component orientation. J Arthroplasty 2007;22:496-503.

Figure 80a Figure 80b
Question 75
A 27-year-old male competitive soccer player reports a 1-year history of pain in the adductor region that has prevented him from playing. Examination reveals tenderness about the adductor attachment to the pelvis, and pain at the same site with resisted contraction of the adductors. There is no tenderness over the hip joint and no signs of a sports hernia. Radiographs are normal. MRI does not show any evidence of enthesopathy. What is the next best step in management?
Explanation
REFERENCES: Schilders E, Bismil Q, Robinson P, et al: Adductor-related groin pain in competitive athletes: Role of adductor enthesis, magnetic resonance imaging, and entheseal pubic cleft injections. J Bone Joint Surg Am 2007;89:2173-2178.
Robinson P, Barron DA, Parsons W, et al: Adductor-related groin pain in athletes: Correlation of MR imaging with clinical findings. Skelet Radiol 2004;33:451-457.
Question 76
What is the standard interval for placement of an anterolateral portal in ankle arthroscopy?
Explanation
Question 77
Figure 1 is the MRI scan of a 35-year-old female soccer player who injured her knee during a game. Given the findings of the scan, physical examination is most likely to reveal
Explanation
Question 78
- Radiographs of the cervical spine of a 73-year-old man who fell down stairs reveal cervical spondylosis without evidence of fracture or dislocation. MRI and CT scans are consistent with the plain radiographs. After 72 hours, neurologic evaluation reveals intact sensation; however, weakness of the upper extremities is greater than that of the lower extremities. What is the most likely diagnosis?
Explanation
extremity deep pressure and proprioceptive preserved. 3-Posterior cord syndrome is rare with loss of deep pressure, deep pain, and proprioception. 4-Brown-Sequard syndrome-Uncommon-Ipsilateral motor deficit, contralateral pain and temperature deficit. 5-Cervical nerve root injury- functional impairment of the cervical spine. Symptoms are often acute and severe, dependent on the level of the lesion. An infraforaminal protrusion may compress only the spinal root ganglion resulting in severe brachialgia with paresthesia and numbness but with little or no motor involvement.
Question 79
An 18-year-old high school football player sustains a thigh injury that results in the findings shown in Figure 1. Initial management should consist of
Explanation
REFERENCES: Anderson JE (ed): Grant’s Atlas of Anatomy. Baltimore, MD, Williams & Wilkins, 1978, pp 4.39-4.49.
Brumet ME, Hontas RB: The thigh, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Antao NA: Myositis of the hip in a professional soccer player: A case report. Am J Sports Med 1988;16:82-83.
Jackson DW, Feagin JA: Quadriceps contusions in young athletes: Relation of severity of injury to treatment and prognosis. J Bone Joint Surg Am 1973;55:95-105.
Question 80
A 74-year-old patient is seen for follow-up 6 weeks after undergoing a total shoulder arthroplasty for glenohumeral osteoarthritis. The patient missed the 2-week follow-up appointment and is currently wearing a sling. The incision is well healed with no signs of breakdown. Examination reveals that passive range of motion is forward elevation of 90 degrees, external rotation at the side 0 degrees, and internal rotation up the back is to the level of the greater trochanter. A radiograph shows no signs of fracture or dislocation. What is the next most appropriate management for this patient? Review Topic
Explanation
Question 81
When compared with patients having a body mass index (BMI) lower than 35, patients with a BMI above 40 who undergo primary total hip arthroplasty (THA) and total knee arthroplasty (TKA) are likely to have
Explanation
The obesity epidemic is increasing, and the number of patients with a BMI higher than 35 undergoing THA and TKA also is growing. Controversy exists over the optimal BMI cutoff and the ability to perform joint replacements safely in patients who are morbidly obese. Several clinical series and national database analyses have shown that morbidly obese patients undergoing THA or TKA are at increased risk for wound complications as well as 30-day and 90-day readmissions. These patients’ incisions are typically larger because of the size of the soft-tissue envelope. Although the clinical scores following successful THA or TKA often are lower than the scores of controls, the overall changes in clinical function and satisfaction are equivalent in nonobese and obese patients.
Question 82
Figures 111a and 111b show axial MRI scans of a 24-year-old man who injured his right shoulder several years ago and now reports continued difficulty with the shoulder and has pain with activity. He reports that when the injury occurred, he felt that his shoulder "popped" but he never required closed reduction. He wore a
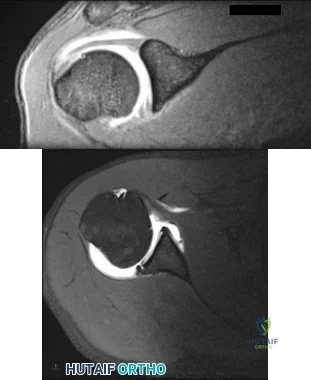
Explanation
Question 83
What is the best indication for prosthetic radial head arthroplasty following fracture?
Explanation
Question 84
A 22-year-old man sustained a stable pelvic fracture, bilateral femur fractures, and a left closed humeral shaft fracture in a motor vehicle accident. Examination 24 hours after injury reveals that the patient is confused and has shortness of breath. A clinical photograph of his conjunctiva is shown in Figure 44. He has a temperature of 101 degrees F (38.3 degrees C) and a pulse rate of 120/min. Laboratory studies show a hemoglobin level of 8 g/dL, a platelet count of 50,000/mm3, and a PaO2 of 57 mm Hg on 2L of oxygen. What is the most likely diagnosis?
Explanation
REFERENCE: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 308-316.
Question 85
A 9-year-old boy has lateral right knee pain. An MRI scan shows a discoid lateral meniscus with a partial tear in its central portion. Treatment should consist of Review Topic
Explanation
Question 86
Which of the following is not considered to be a part of the constellation of the clinical entities known as the female athlete triad? Review Topic
Explanation
The female athlete triad was coined in 1992 by the American College of Sports Medicine as a complex disorder more prevalent in the adolescent and young female
athlete population including decreased bone mineral density (BMD), menstrual dysfunction, and low energy availability with or without a concomitant eating disorder. Treatment should involve a multidisciplinary approach, including psychological and nutritional counseling for eating behaviors and dietary management, reduction of training intensity to decrease risk of stress fractures, and initiating calcium and vitamin D supplements for osteoporosis.
Nazem et al performed a systematic review of articles containing the female athlete triad, reviewing diagnosis via screening during physical examinations as well as laboratory and imaging evaluation for menstrual dysfunction, low energy availability, and low bone mineral density. They state that potential complications including possible infertility, decreased immune function, cardiovascular disease, and irreversible loss of bone mineral density. They concluded that prevention, early recognition, and a multidisciplinary treatment team with a focus on proper nutrition and natural return of menses is vital.
Nattiv et al review the position of the American College of Sports Medicine regarding the female athlete triad, including screening for the triad at the pre-participation physical, discouragement of unhealthy weight loss practices. Essential members of the multidisciplinary treatment team include a health-care professional, a registered dietitian, and a mental health practitioner. They endorse that the first aim of treatment for any triad component is to increase energy availability by increasing energy intake and reducing exercise energy expenditure.
Question 87
Figures 1 and 2 are the radiographs of a 17-year-old man who injured his wrist 6 months ago. He is experiencing pain and limited motion. What is the most effective treatment option?
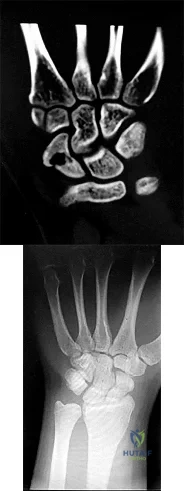
Explanation
Figures 1 and 2 show a scaphoid nonunion with substantial bone resorption at the nonunion site. Cast immobilization and bracing with bone stimulator use would not be successful treatments at this point because the fracture is 6 months old and there is considerable bone resorption at the fracture site. Scaphoid excision with intercarpal fusion is an option to use only after bone-grafting procedures have failed or arthritis is present. Bone-grafting procedures using both vascularized and nonvascularized graft sources are associated with a high success rate that decreases with avascular necrosis of the proximal pole. If left untreated, scaphoid nonunions can progress to carpal collapse and degenerative arthritis.
Question 88
During excision of a Baker cyst, the base or stalk is usually found between the
Explanation
REFERENCES: Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA,
WB Saunders, 1995, p 379.
Justis EJ Jr: Nontraumatic disorders, in Crenshaw AH (ed): Campbell’s Operative Orthopaedics, ed 7. Philadelphia, PA, Lippincott, 1987, vol 3, p 2257.
Question 89
- Figures 3a and 3b show the finger deformity that a 13-year-old girl has had since birth. What is the most likely diagnosis?
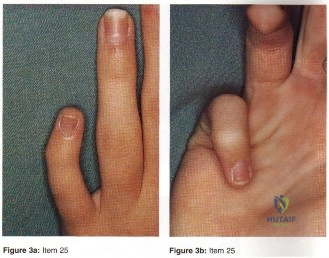
Explanation
definitions of the other distracters are self-explanatory (Staheli, Fundamental of Pediatric Orthopedics, 1998): Camptodactyly: non-painful flexion deformity of the PIP joint (i.e. AP Plane); abnormality of the insertions of the intrinsics and extrinsics flexor tendons; both hereditary and non-hereditary forms. Symbrachydactyly: digital absence in the form of transverse efficiency; teratogenic etiology resulting in absence distal metacarpals with finger nubbins. Kirner’s deformity: rare progressive deformity of the terminal phalanx of the small fingers with fingernails a curved and clubbed appearance; usually bilateral and appears during adolescence. Digiti minimi adductus: no such deformity found mention in the literature.
Question 90
A 12-month-old boy has right congenital fibular intercalary hemimelia with a normal contralateral limb. A radiograph of the lower extremities shows a limb-length discrepancy of 2 cm. All of the shortening is in the right tibia. Assuming that no treatment is rendered prior to skeletal maturity, the limb-length discrepancy will most likely
Explanation
REFERENCES: Paley D, Bhave A, Herzenberg JE, et al: Multiplier method for predicting
limb-length discrepancy. J Bone Joint Surg Am 2000;82:1432-1446.
Moseley CF: A straight-line graph for leg length discrepancies. Clin Orthop 1978;136:33-40.
Question 91
In recurrent posterior shoulder instability, what is the recommended approach to the posterior capsule?
Explanation
REFERENCES: Dreese J, D’Alessandro D: Posterior capsulorrhaphy through infraspinatus split for posterior instability. Tech Shoulder Elbow Surg 2005;6:199-207.
Shaffer BS, Conway J, Jobe FW, et al: Infraspinatus muscle-splitting incision in posterior shoulder surgery: An anatomic and electromyographic study. Am J Sports Med 1994;22:113-120.
Fuchs B, Jost B, Gerber C: Posterior-inferior capsular shift for the treatment of recurrent voluntary posterior subluxation of the shoulder. J Bone Joint Surg Am 2000;82:16-25.
Question 92
A 25-year-old woman has lower leg pain during exercise without numbness, tingling, or weakness. The symptoms resolve by the following day. Compartment pressure measurements obtained 1 minute after exercise are shown in Figure 19a (Table 1). She undergoes anterior compartment fasciotomy with complete resolution of symptoms. Two years later, she has recurrent pain and tightness with exercise. Radiographs, a technetium bone scan, and noninvasive vascular study findings are normal. Compartment pressure measurements obtained 1 minute after exercise are shown in Figure 19b (Table 2). What is the most likely etiology for her recurrent symptoms?
Explanation
Exertional compartment syndrome involves an increase in compartment pressure caused by exercise or sports activity that restricts blood flow in the compartment, resulting in pain with continued activity. Compartment pressures of at least 15 mm Hg measured at rest, at least 30 mm Hg measured 1 minute after exercise, and at least 20 mm Hg measured 5 minutes after exercise are diagnostic. Surgical fasciotomy for exertional compartment syndrome is successful for the majority of patients, but recurrence rates as high as 20% have been reported. Scar formation within the fascial defect can result in recurrent symptoms and/or nerve entrapment, and recurrence is typically observed after an initial symptom-free period. In a series of 18 patients, recurrent symptoms occurred at a mean of 23.5 months after the index procedure. Other potential causes of recurrence include inadequate fascial release, failure to recognize involvement of other compartments, nerve compression, and misdiagnosis. Surgical complications after fasciotomy include hemorrhage leading to excessive fibrosis, neurovascular injury, and hematoma or seroma formation.
Question 93
In the normal adult, the distance between the basion and the tip of the dens with the head in neutral position is how many millimeters?
Explanation
REFERENCES: Wiesel SW, Rothman RH: Occipitoatlantal hypermobility. Spine 1979;4:187-191.
Wholey MH, Browner AJ, Baker HL Jr: The lateral roentgenogram of the neck: With comments on the atlanto odontoid-basion relationship. Radiol 1958;71:350-356.
Question 94
A 36-year-old woman with familial neurofibromatosis has an enlarging mass in the posterior thigh. The lesion has slowly increased in size and is now constantly painful. Pressure on the mass causes dysesthesias in the foot. Figures 44a through 44c show T 1 -weighted, STIR, and T 1 -weighted fat-saturated gadolinium scans, respectively. Figure 44d shows a PET scan. What does this lesion most likely represent?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 225-230.
Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 4218-4235.
Question 95
Figures below depict the radiographs obtained from a 60-year-old man with instability and pain 1 year after primary right total knee arthroplasty. He states that he had surgery on two occasions for a tendon rupture that was repaired with sutures but that his knee popped again, and now the leg is unable to hold his weight. On examination, he is in no acute distress. His height is 6'3", and he weighs 240 pounds. He is ambulatory with crutches. Range of motion of the right knee is 50° to 120° actively and 0° to 120° passively. More than 10° of varus/valgus laxity and more than 5 mm of anteroposterior drawer are present. A palpable defect is observed in the tissue just proximal to the patella. The incision is well healed. The erythrocyte sedimentation rate is 46 mm/h (reference range 0 to 20 mm/h) and the C-reactive protein level is 2.04 mg/L (reference range 0.08 to 3.1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1% neutrophils. No growth of organisms is seen on routine culture. What is the best next step?

Explanation
This patient has a chronic quadriceps tendon rupture after total knee arthroplasty. Two previous primary repair attempts have failed, which is not surprising based on the poor results of primary repair reported in the literature. The patient also has an unstable knee and will require revision of some or all of the prosthesis to achieve a stable knee. Revision total knee arthroplasty with extensor mechanism allograft allows an allograft reconstruction of the ruptured quadriceps tendon. The other option is to utilize a synthetic mesh extensor mechanism reconstruction. These are likely to have the best result in this situation. Revision total knee arthroplasty with liner change and primary quadriceps repair is not the best form of management, because it involves a third attempt at primary tendon repair, which will likely fail again. Resection knee arthroplasty and arthrodesis with antegrade nail is a possible option but is not the best, because it would likely make driving and other daily activities difficult. Two-stage revision total
knee arthroplasty with extensor mechanism allograft is not the best option because the laboratory results show no signs of infection, so a single-stage procedure is preferred.
Question 96
-A 45-year-old woman sustained a fall from height and has the injury shown in Figures 135a and 135b.A 3-dimensional reconstruction CT scan is shown in Figure 135c. Joint-spanning external fixation is applied on the day of injury. Ten days later, her skin is acceptable for definitive fixation. What is the most appropriate type of fixation for her fracture?
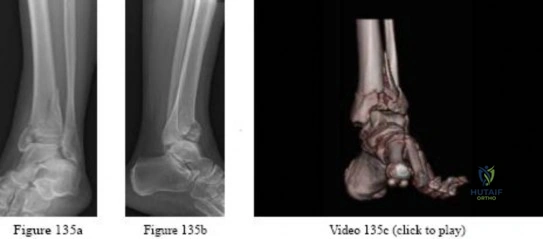
Explanation

Question 97
A 17-year-old high school football player is seen for follow-up after sustaining an injury 3 days ago. He reports that he tackled a player, felt numbness throughout his body, and could not move for approximately 15 seconds. A spinal cord injury protocol was initiated on the field. Evaluation in the emergency department revealed a normal neurologic examination and full painless neck motion. He states that he has no history of a similar injury. An MRI scan of the cervical spine is normal. During counseling, the patient and his family should be informed that he has sustained
Explanation
REFERENCES: Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Odor JM, Watkins RG, Dillin WH, et al: Incidence of cervical spinal stenosis in professional and rookie football players. Am J Sports Med 1990;18:507-509.
Torg JS, Naranja RJ Jr, Palov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Vaccaro AR, Watkins B, Albert TJ, et al: Cervical spine injuries in athletes: Current return-to-play criteria. Orthopedics 2001;24:699-703.
Question 98
Immediately after undergoing lumbar instrumentation, a patient reports severe right leg pain and has 4+/5 weakness. Figure 24 shows an axial CT scan of L5. Exploratory surgery will most likely reveal
Explanation
REFERENCES: Esses SI, Sachs BL, Dreyzin V: Complications associated with the technique of pedicle screw fixation: A selected survey of ABS members. Spine 1993;18:2231-2238.
Laine T, Lund T, Ylikoski M, et al: Accuracy of pedicle screw insertion with and without computer assistance: A randomised controlled clinical study in 100 consecutive patients. Eur Spine J 2000;9:235-240.
Lonstein JE, Denis F, Perra JH, et al: Complications associated with pedicle screws. J Bone Joint Surg Am 1999;81:1519-1528.
Question 99
A 51-year-old woman is seen for evaluation of chronic supraspinatus and infraspinatus tendon tears. Three years ago, in an attempted repair the surgeon was unable to repair the supraspinatus and infraspinatus tendon tears. Currently she has a marked amount of pain, reduced range of motion, and weakness. Examination reveals anterosuperior escape. Radiographs show no signs of arthritic changes. You are considering a latissimus dorsi tendon transfer. During the discussion, you mention that
Explanation
REFERENCES: Gerber C, Maquieira G, Espinosa N: Latissimus dorsi transfer for the treatment of irreparable rotator cuff tears: Factors affecting outcome. J Bone Joint Surg Am
2006;88:113-120.
Iannotti JP, Hennigan S, Herzog R, et al: Latissimus dorsi tendon transfer for irreparable posterosuperior rotator cuff tears. J Bone Joint Surg Am 2006;88:342-348.
Question 100
Intraoperative frozen section analysis reveals 10 neutrophils per high-power field and a positive gram stain result. What is the best next step?
Explanation
The radiograph reveals a rotator cuff dysfunction secondary to malpositioning of the humeral stem and a nonanatomic humeral head. Glenohumeral kinematics have been altered, resulting in damage to the rotator cuff, which in turn has led to impingement with the coracoacromial arch. This single radiograph reveals excessive humeral head height, “overstuffing” of the joint, and severe narrowing of the acromiohumeral interval. Osteolysis and implant loosening are not radiographically apparent. An orthogonal view (axillary lateral) would be necessary to evaluate for shoulder instability. A CT arthrogram is the most appropriate advanced imaging test in the setting of a retained shoulder arthroplasty to evaluate the integrity of the rotator cuff. An MRI evaluation would be obfuscated by artifact. Three-phase and indium-tagged white blood cell scans may be appropriate in the setting of an occult infection evaluation, but not as a test to evaluate rotator cuff injury.
In the absence of infection with rotator cuff compromise, the most appropriate procedure(s) during revision would involve humeral component explantation and conversion to rTSA Revision anatomic hemiarthroplasty may provide pain relief, but function may not appreciably change because of the unbalanced forced couples of the rotator cuff complex. Placement of a glenoid component in the setting of an irreparable rotator cuff tear is contraindicated because rapid glenoid loosening will occur due to eccentric loading during active shoulder motion. Resection arthroplasty should be reserved for recalcitrant cases of infection because this procedure does not provide functional improvement.
In the event that frozen section analysis and positive gram stain results indicate an infection, the treating surgeon should remove all components, perform a thorough debridement and irrigation of suspect tissue, implant an antibiotic spacer, and perform a second-stage reconstruction when deemed appropriate (in light of laboratory studies, repeat shoulder aspiration, frozen section analysis, and arthroscopic soft-tissue biopsy findings). Irrigation and debridement with primary exchange/conversion of components remains inferior to 2-stage reconstruction for infection eradication. Resection arthroplasty remains a salvage procedure for resistant cases that preclude reimplantation and generally is performed for symptom control and sepsis prevention.
RECOMMENDED READINGS
Bohsali KI, Wirth MA, Rockwood CA Jr. Complications of total shoulder arthroplasty. J Bone Joint Surg Am. 2006 Oct;88(10):2279-92. Review. PubMed PMID: 17015609. View Abstract at PubMed
Florschütz AV, Lane PD, Crosby LA. Infection after primary anatomic versus primary reverse total shoulder arthroplasty. J Shoulder Elbow Surg. 2015 Aug;24(8):1296-301. doi: 10.1016/j.jse.2014.12.036. Epub 2015 Feb 19. PubMed PMID: 25704211. View Abstract at PubMed
Padegimas EM, Maltenfort M, Ramsey ML, Williams GR, Parvizi J, Namdari S. Periprosthetic shoulder infection in the United States: incidence and economic burden. J Shoulder Elbow Surg. 2015 May;24(5):741-6. doi: 10.1016/j.jse.2014.11.044. Epub 2015 Jan 13. View Abstract at PubMed
Leung B, Horodyski M, Struk AM, Wright TW. Functional outcome of hemiarthroplasty compared with reverse total shoulder arthroplasty in the treatment of rotator cuff tear arthropathy. J Shoulder Elbow Surg. 2012 Mar;21(3):319-23. doi: 10.1016/j.jse.2011.05.023. Epub 2011 Aug 26. PubMed PMID: 21872496. View Abstract at PubMed
Iannotti JP, Spencer EE, Winter U, Deffenbaugh D, Williams G. Prosthetic positioning in total shoulder arthroplasty. J Shoulder Elbow Surg. 2005 Jan-Feb;14(1 Suppl S):111S-121S. PubMed PMID: 15726070. View Abstract at PubMed
Iannotti JP, Gabriel JP, Schneck SL, Evans BG, Misra S. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am. 1992 Apr;74(4):491-500. PubMed PMID: 1583043.View Abstract at PubMed
Grosso MJ, Frangiamore SJ, Ricchetti ET, Bauer TW, Iannotti JP. Sensitivity of frozen section histology for identifying Propionibacterium acnes infections in revision shoulder arthroplasty. J Bone Joint Surg Am. 2014 Mar 19;96(6):442-7. doi: 10.2106/JBJS.M.00258. View Abstract at PubMed
