Orthopedic Surgery Board Review MCQs: Hip, Shoulder & Arthroplasty | Part 179

Key Takeaway
This page offers Part 179 of a comprehensive Orthopedic Surgery Board Review MCQ set for orthopedic surgeons and residents preparing for OITE and AAOS exams. It features 100 high-yield, verified multiple-choice questions focusing on Arthroplasty, Hip, and Shoulder, designed to mirror official exam formats for effective preparation.
About This Board Review Set
This is Part 179 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 179
This module focuses heavily on: Arthroplasty, Hip, Shoulder.
Sample Questions from This Set
Sample Question 1: An 18-year-old boxer sustained a blow to his right eye in a boxing match. Examination on the sideline reveals hyphema, reduced visual acuity and color vision, and a visual field cut. What is the next step in management? Review Topic...
Sample Question 2: An 18-year-old man has had an enlarging mass in his hand for the past 3 months. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 54a through 54d. What is the most likely diagnosis?...
Sample Question 3: A 71-year-old man has worsening left hip pain and is indicated for a left total hip arthroplasty (THA). Figure 1 shows a preoperative plan for the patient. The patient is scheduled for a left THA using a direct anterior approach with the pi...
Sample Question 4: A unilateral "piano key" sign, indicates...
Sample Question 5: A 19-year-old college pitcher reports posterior shoulder discomfort that started recently with pitching. He is able to throw with normal velocity and control, but his pain in the early acceleration phase of throwing is getting worse. Examin...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
An 18-year-old boxer sustained a blow to his right eye in a boxing match. Examination on the sideline reveals hyphema, reduced visual acuity and color vision, and a visual field cut. What is the next step in management? Review Topic
Explanation
Question 2
An 18-year-old man has had an enlarging mass in his hand for the past 3 months. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 54a through 54d. What is the most likely diagnosis?
Explanation
REFERENCES: Abramovici L, Steiner GC: Bizarre parosteal osteochondromatous proliferation (Nora’s lesion): A retrospective study of 12 cases, 2 arising in long bones. Hum Pathol 2002;33:1205-1210.
Nora FE, Dahlin DC, Beabout JW: Bizarre parosteal osteochondromatous proliferations of the hands and feet. Am J Surg Pathol 1983;7:245-250.
Question 3
A 71-year-old man has worsening left hip pain and is indicated for a left total hip arthroplasty (THA). Figure 1 shows a preoperative plan for the patient. The patient is scheduled for a left THA using a direct anterior approach with the pictured implants. If this plan is followed as pictured, what is the likely outcome for this patient? Figure could not be loaded
Explanation
A. spinal fusion.
B. BMI and implant size.
C. mismatch between the metaphysis and diaphysis.
D. modular neck prosthesis.
Question 4
A unilateral "piano key" sign, indicates
Explanation
The piano key sign is a demonstration of instability at the DRUJ, typically seen after healing from a distal radius fracture with an associated ulnar styloid fracture (as in this case) or other wrist injury. The hand is pushed down against a table top, and the distal radius translates dorsally (with the distal ulna apparently moving volarly). In fact, the distal radius is the mobile segment, while the distal ulna is fixed in space. Treatment involves repair or reconstruction of the foveal insertion of the triangular fibrocartilage complex (TFCC) and distal radioulnar ligaments. This type of instability is also common in malunions of the distal radius or distal one-third of the radial shaft (Galeazzi-type fractures). In malunions, DRUJ instability can be treated with a corrective osteotomy of the distal radius to restore the anatomic relationship between the distal ulna and the distal radius at the DRUJ. Radiocarpal and midcarpal instability do not involve the DRUJ. Disruption of the interosseous membrane (in isolation, with intact distal radioulnar ligaments and an intact TFCC) does not lead to translational instability of the DRUJ. Although hypermobility syndrome may lead to ligamentous laxity, it does not lead to unilateral DRUJ instability.
Question 5
A 19-year-old college pitcher reports posterior shoulder discomfort that started recently with pitching. He is able to throw with normal velocity and control, but his pain in the early acceleration phase of throwing is getting worse. Examination reveals symmetric rotator cuff strength and no increased anterior or posterior translation of either shoulder. He has some discomfort with his shoulder in abduction and external rotation. Supine range of motion of the right shoulder in 90 degrees of abduction reveals external rotation to 100 degrees and internal rotation to 25 degrees. His left shoulder has 95 degrees of external rotation and 45 degrees of internal rotation. He is not playing the next 2 weeks and requests some exercises that he can do on his own. Which of the following exercises will most likely improve his shoulder symptoms? Review Topic
Explanation
protraction, such as punches, and scapular retraction, such as row exercises, can all be helpful for the disabled throwing shoulder, but they will not restore the decreased internal rotation.
Question 6
Following total elbow arthroplasty, patients should be instructed to Review Topic
Explanation
Question 7
- In a fatigue test, the maximum stress under which the material will not fail, regardless of how many loading cycles are applied, is defined as
Explanation
Question 8
A defect in the gene coding for fibrillin-1 would lead to which diagnosis? Review Topic
Explanation
Marfan Syndrome is a genetic disorder of connective tissue typically caused by a mutation in the gene coding for the fibrillin-1 protein. Affected patients are typically very tall with long limbs and thin fingers and toes. Marfan Syndrome patients have many common features including ectopic lens, aortic root dilation, scoliosis, protrusio acetabuli, and ligamentous laxity.
Shirley et al. present a review of Marfan Syndrome with emphasis on the musculoskeletal manifestations including ligamentous laxity, protrusio acetabuli, and scoliosis. They note that scoliosis in these patients, when compared to those with idiopathic scoliosis, commonly progresses faster, is more resistant to bracing, and has a higher association with dural ectasia.
Dean presents a review of Marfan Syndrome and its underlying genetic cause of a mutation in fibrillin. They state that diagnosis can be made using the Ghent nosology (see Illustration A) which can diagnose or rule out the condition in 86% of patients. They caution using these criteria in young children as some features of Marfan Syndrome may not present until later ages.
Illustration A is a summary of the 2010 Revised Ghent nosology for diagnosing Marfan Syndrome.
Incorrect Answers:
Question 9
-Assuming that the lesion can be covered appropriately and there is no drainage from the lesion, when should the patient be allowed to safely return to wrestling?
Explanation
This patient has cellulitis, which is typically caused by group A Streptococcus or Staphylococcus. The patient’s lack of improvement with first-line antibiotics is concerning for methicillin-resistant Staphylococcus aureus (MRSA) infection. MRSA cellulitis is becoming more prevalent in young athletes,and a high index of suspicion is required to provide appropriate intervention during this
aggressive disease process. The diagnosis is typically made clinically without the use of cultures. Oral trimethoprimsulfamethoxazole (a sulfonamide-class drug) double strength twice daily for 10 to 14 days or doxycycline (a tetracycline-class drug) 100 mg twice daily for 10 to 14 days are recommended for first-line treatment of suspected MRSA cellulitis. There is no indication to proceed with irrigation and debridement; however, if the patient develops a soft-tissue abscess or the underlying joint becomes involved, this would be an appropriate intervention. Switching the athlete to an IV cephalosporin (cefazolin) is not likely to be effective against the presumed resistant bacteria.
Ciprofloxacin (a fluoroquinolone-class drug) is effective against many bacteria, but not MRSA. The current recommendation for wrestlers with cellulitis is that return to competition be allowed after 72 hours of antibiotic treatment if there has been no extension of the cellulitis for 48 hours, the lesion can be covered, and there is no drainage from the lesion. The other responses are not current recommendations for return to competition.
Question 10
Figure 21 is the radiograph of a 45-year-old woman who was severely injured in a motorcycle crash. Her injuries include a traumatic subarachnoid hemorrhage, bilateral pneumothoraces with pulmonary contusions and flail chest, fracture-dislocation of the left hip, and open fractures of the right distal femur and proximal tibia. Antibiotics and tetanus are administered in the emergency department. The patient is intubated and bilateral chest tubes are placed. A closed reduction is performed on the left hip. After appropriate resuscitation, what is the most appropriate initial management of the right knee injury?

Explanation
Question 11
What is the most anatomic location for placement of the femoral tunnel in anterior cruciate ligament reconstruction?
Explanation
REFERENCES: Johnson RJ, Beynnon BD, Nichols CE, Renstrom PA: The treatment of injuries of the anterior cruciate ligament. J Bone Joint Surg Am 1992;74:140-151.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
Question 12
Compared with wear rates of metal-on-standard polyethylene bearings (75 to 250 m m/y), the wear rate of metal-on-metal bearings for hip arthroplasty is approximately how many micrometers per year?
Explanation
REFERENCES: McKellop H, Park SH, Chiesa R, et al: In vivo wear of three types of metal on metal hip prostheses during two decades of use. Clin Orthop 1996;329:S128-S140.
Schmalzried TP, Callaghan JJ: Wear in total hip and knee replacements. J Bone Joint Surg Am 1999;81:115-136.
Question 13
Second impact syndrome (SIS) after head injury is characterized by which of the following? Review Topic
Explanation
Question 14
A 62-year-old man has cervical myelopathy with no evidence of cervical radiculopathy. MRI reveals stenosis at C4-5 and C5-6 with severe cord compression. Examination will most likely reveal which of the following findings?
Explanation
REFERENCES: Sachs BL: Differential diagnosis of neck pain, arm pain and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 741-742.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 673-680.
Question 15
- Which of the following events is most likely to occur following a complete transection of a peripheral nerve?
Explanation
Question 16
- Figures 42a and 42b show the sagittal and axial MRI scans of a 24-year-old patient who has sciatia. Which of the following combinations of physical findings is most consistent wit the MRI studies?
Explanation
Question 17
Myositis ossificans is a recognized complication of contusion to the quadriceps muscle. During early rehabilitation, this condition is most likely to be exacerbated by
Explanation
REFERENCES: Brunet ME, Hontas RB: The thigh, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Cushner FD, Morwessel RM: Myositis ossificans traumatica. Orthop Rev 1992;21:1319-1326.
Question 18
- Which of the following conditions is associated é the highest mortality in patients é a pelvic fracture?
Explanation
Question 19
A 72-year-old man was scheduled for left total knee replacement. He has a history of hypertension and deep venous thrombosis (DVT) in his right lower extremity after an ankle fracture 2 years ago that was treated nonsurgically. The patient asked about the recommended types of DVT prophylaxis or investigations. Based on the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty , what is an acceptable option?
Explanation
Question 20
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. Left untreated, injury to this structure most likely will lead to degenerative changes in

Explanation
Dial test finding. A valgus-producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used. Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
Question 21
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 22
What risk factor is most associated with progression of idiopathic scoliosis to a curve requiring surgery?
Explanation
30 degrees at this time are likely to reach surgical range.
REFERENCES: Little DG, Song KM, Katz D, et al: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am 2000;82:685-693.
Sanders JO, Moreland M, Bassett G: Idiopathic scoliosis: Prevalence and natural history, in DeWald R (ed): Spinal Deformities: The Comprehensive Text. New York, NY, Thieme Medical Publishers, 2003.
Question 23
An 18-year-old collegiate basketball player has had a 3-month history of activity-related back pain. She describes isolated low back pain without radiation that increases with training and playing basketball. Her pain resolves with rest. Physical therapy for 6 weeks has failed to provide relief. An axial CT scan is shown in Figure 17a, and Figures 17b and 17c show sagittal CT reconstructions through the right and left lumbar facets, respectively. Further management should consist of which of the following?
Explanation
REFERENCES: Debnath UK, Freeman BJ, Grevitt MP, et al: Clinical outcome of symptomatic unilateral stress injuries of the lumbar pars interarticularis. Spine 2007;32:995-1000.
Bono CM: Low-back pain in athletes. J Bone Joint Surg Am 2004;86:382-396.
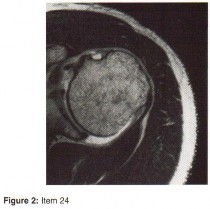
Question 24
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior-stabilized TKA without evidence of component loosening. What is the recommended treatment for this patient?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor
mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful total knee arthroplasty.
Question 25
Which of the following have been found to affect the rate of perioperative infections or wound complication rates in foot and ankle surgery?
Explanation
REFERENCES: Bibbo C, Anderson RB, Davis WH, et al: The influence of rheumatoid chemotherapy, age, and presence of rheumatoid nodules on postoperative complications in rheumatoid foot and ankle surgery: Analysis of 725 procedures in 104 patients. Foot Ankle Int 2003;24:40-44.
Bibbo C, Goldberg JW: Infections and healing complications after elective orthopaedic foot and ankle surgery during tumor necrosis factor-alpha inhibition therapy. Foot Ankle Int
2004;25:331-335.
Sorensen LT, Karlsmark T, Gottrup F: Abstinence from smoking reduces incisional wound infection: A randomized controlled trial. Ann Surg 2003;238:1-5.
Question 26
A 43-year-old woman is referred after excisional biopsy of a cutaneous soft-tissue mass from her left shoulder. Based on the biopsy specimens shown in Figures 44a and 44b, what is the best course of action?
Explanation
REFERENCES: Lindner NJ, Scarborough MT, Powell GJ, et al: Revision surgery in dermatofibrosarcoma protuberans of the trunk and extremities. Eur J Surg Oncol
1999;25:392-397.
Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 491-505.
Question 27
below show the radiographs, MRI, and MR arthrogram obtained from a year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy.When counseling patients who have a cam deformity, the orthopaedic surgeon should note that
Explanation
Question 28
During placement of an external fixator for a distal radius fracture, the most commonly injured nerve is a branch of which of the following nerves? Review Topic
Explanation
(SBQ12TR.106) A 67-year-old female sustains the injury shown in Figure A after a trip and fall. When discussing the outcomes of surgery with the patient, which of the following statements is true?

Post-surgical mortality rates are significantly lower after total hip arthroplasty compared to hemiarthroplasty
Internal fixation shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to arthroplasty
Bipolar hemiarthroplasty shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to unipolar hemiarthroplasty
A delay in surgery greater than 48 hours is recommended if the patient has multiple medical comorbiditiesm which are not fully optimized
Dislocation rates are equivalent between total hip arthroplasty and hemiarthroplasty
Moderate evidence supports that hip fracture surgery within 48 hours of admission is associated with better outcomes. However, patients with significant medical comorbidity should be fully optimized before surgery.
Although several studies have shown a benefit to surgery within 48 hours, no definitive time frame has been elucidated. The majority of literature has shown improved outcomes in regards to pain, complications, and length of stay with early surgery. Patients with significant medical comorbidities have been shown to have the highest mortality rates.
Moran et al. aimed to determine whether a delay in surgery for hip fractures had an affect on postoperative mortality among elderly patients. In an observational study of 2660 patients, they showed that mortality following hip fracture surgery was 9% at 30-days, 19% at 90-days, and 30% at 12-months. Patients with medical comorbidities had 2.5 times the risk of death within 30-days of surgery. In addition, individuals who had surgery delayed beyond 4 days had increased mortality at 90-days and 12-months.
Papakostidis et al. examined the timing of internal fixation of intracapsular fractures of the neck of femur on the development of late complications, particularly osteonecrosis of femoral head (ONFH) and non-union. They showed no benefit of
early surgery on incidence of AVN. However, delay of internal fixation of more than
24 hours showed increased rates of non-union.
Figure A shows a displaced right femoral neck fracture. Incorrect Answers:
Question 29
Figures 142a and 142b are the current radiographs of an 89-year-old woman who had open reduction and internal fixation (ORIF) of a distal periprosthetic femur fracture 4 months ago. An examination reveals well-healed incisions, a painful range of motion from 15 to 85 degrees, and normal neurovascular function. An infection workup, including an erythrocyte sedimentation rate and C-reactive protein level, is negative. The most appropriate treatment option is
Explanation
Current periprosthetic fracture treatments after TKA include ORIF via plating, retrograde nailing, or revision using standard revision TKA components or a distal femoral arthroplasty. Locked plating has demonstrated a trend toward increased nonunion rates when compared to retrograde nailing, as evidenced in this patient. The advanced age of the patient, the presence of failed fixation, and the significant amount of bone loss preclude a trial of further nonsurgical treatment or revision ORIF. A review of 3 methods for treatment of comminuted distal periprosthetic femur fractures in patients older than age 70 demonstrated that distal femur arthroplasty should be considered in patients with advanced age and poor bone quality who require early mobilization. As a result, treatment of this patient with a revision TKA using a distal femoral arthroplasty would be the preferred response because of the bone quality and fracture pattern. Above-knee amputation is a salvage procedure and is not indicated at this time.
Question 30
Total hip arthroplasty is most appropriate for the injury shown in Figure A for which of the following patients?

Explanation
Displaced femoral neck fractures can present a challenge to treat. In younger patients with good bone stock a closed vs. open reduction and internal fixation should be attempted. For active older patients a total hip arthroplasty is the best option, especially if there is pre-existing arthritis in the injured hip. THA provides the best function with the least pain and less need for repeat surgery (compared to hemiarthroplasty). For low-demand or debilitated patients, for patients older than age 80, or for those who can not reliably follow hip precautions a hemiarthroplasty provides the lowest risk of dislocation, and thus would be the treatment of choice.
Macaulay et al. present a prospective randomized trial of patients with femoral neck fractures treated with THA vs hemiarthroplasty. They found that functional outcomes and patient satisfaction were higher in the THA group without significant increased risk of complications. Inclusion criteria required patients to be over age 50, be a community ambulator, and were excluded for presence of dementia.
Abboud et al. retrospectively reviewed patients treated with THA for osteoarthritis and compared them to patients treated with THA for a femoral neck fracture. They found no significant difference between the two groups for outcomes or complications.
Figure A is an AP radiograph demonstrating a displaced femoral neck fracture.
Incorrect Answers:
Question 31
Which of the following statements best describes the outcome of the routine use of continuous passive motion (CPM) machines after total knee arthroplasty (TKA)?
Explanation
REFERENCES: Pellicci PM, Tria AJ, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 287-293.
McInnes J, Larson MG, Daltroy LH, et al: A controlled evaluation of continuous passive motion in patients undergoing total knee arthroplasty. JAMA 1992;268:1423-1428.
Kumar PJ, McPherson EJ, Dorr LD, et al: Rehabilitation after total knee arthroplasty: A comparison of 2 rehabilitation techniques. Clin Orthop 1996;331:93-101.
Question 32
The essential lesion in recurrent or posterior instability following simple dislocation of the elbow typically involves which of the following structures?
Explanation
Question 33
He is intubated and being resuscitated. The calf is very swollen with compartment pressures: anterior 25 mm Hg, lateral 24 mm Hg, deep posterior 21 mm Hg, and
Explanation
Question 34
below show the clinical photograph and radiograph obtained from a year-old man who has deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?
Explanation
Figure 1 reveals an external rotation deformity of the right lower extremity. This deformity can have numerous causes, including extra-articular deformity. Figure 2 reveals a loose, subsided femoral component. Femoral stems typically subside into retroversion due to proximal femoral biomechanics, which cause a compensatory external rotation deformity. The combined findings from both images suggest an external rotation deformity most likely related to subsidence into retroversion.
Question 35
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads? Review Topic
Explanation
Question 36
A full-term newborn has webbing at the knees, rigid clubfeet, a Buddha-like posture of the lower extremities, and no voluntary or involuntary muscle action at and below the knees. Radiographs of the spine and pelvis reveal an absence of the lumbar spine and sacrum. What maternal condition is associated with this diagnosis?
Explanation
REFERENCES: Chan BW, Chan KS, Koide T, et al: Maternal diabetes increases the risk of caudal regression caused by retinoic acid. Diabetes 2002;51:2811-2816.
Zaw W, Stone DG: Caudal regression syndrome in twin pregnancy with type II diabetes.
J Perinatol 2002;22:171-174.
Question 37
In the setting of a proximal tibial plateau fracture and its repair, which of the following materials is an isotropic material?
Explanation
REFERENCE: Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 58-59.
Question 38
In the most common condition causing a winged scapula, which of the following nerves is affected? Review Topic
Explanation
Question 39
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured?
Explanation
REFERENCES: Schenck CD: Anatomy of the innervation of the upper extremity, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face, ed 2. St Louis, MO, Mosby-Year Book, 1991.
Hershman EB: Brachial plexus injuries. Clin Sports Med 1990;9:311-329.
Question 40
Familial (Leiden) thrombophilia is of importance in joint arthroplasty because of an abnormality in the clotting cascade. Which of the following statements best describes the condition?
Explanation
Question 41
An active 36-year-old woman with rheumatoid arthritis has continued forefoot discomfort despite the use of orthotics and shoe wear modifications. A radiograph and a clinical photograph are shown in Figures 26a and 26b. Treatment at this point should consist of
Explanation
REFERENCES: Ouzounian T: Rheumatoid arthritis of the foot & ankle, in Myerson MS (ed): Foot & Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 2, pp 1189-1204.
Mann RA, Thompson FM: Arthrodesis of the first metatarsophalangeal joint for hallux valgus in rheumatoid arthritis. J Bone Joint Surg Am 1984;66:687-692.
Coughlin MJ: Rheumatoid forefoot reconstruction: A long-term followup study. J Bone Joint Surg Am 2000;82:322-341.
Question 42
Deep venous thromboses are primarily composed of red blood cells and fibrin. What is fibrin?
Explanation
Question 43
What is the most reproducible landmark for the accurate anatomic placement of the tibial tunnel for an anterior cruciate ligament (ACL) reconstruction?
Explanation
REFERENCES: Hutchinson MR, Bae TS: Reproducibility of anatomic tibial landmarks for anterior cruciate ligament reconstructions. Am J Sports Med 2001;29:777-780.
McGuire DA, Hendricks SD, Sanders HM: The relationship between anterior cruciate ligament reconstruction tibial tunnel location and the anterior aspect of the posterior cruciate ligament insertion. Arthroscopy 1997;13:465-473.
Question 44
A lO'/z-year-old boy sustained the injury shown in Figure 72 when he fell out of a tree. This is a closed, neurologically intact injury and the patient has no head injury or loss of consciousness. He weighs 115 pounds and is otherwise healthy. What is the optimal treatment option for this injury?
Explanation
REFERENCES: Flynn JM, Schwend RM: Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg 2004;12:347-359.
Gordon JE, Swenning TA, Burd TA, et al: Proximal femoral radiographic changes after lateral transtrochanteric intramedullary nail placement in children. J Bone Joint Surg Am 2003;85:1295-1301.
Figure 73a Figure 73b
Question 45
You have been waiting to enroll a patient into your recent institutional review board (IRB)-approved clinical research protocol. A patient is admitted who, upon initial screening, meets all inclusion criteria. However, he has late-stage dementia, and you are told by your research coordinator that this condition is an exclusionary criterion. This scenario demonstrates the need for which aspect of proper informed consent?
Explanation
Question 46
Which of the following is accurate regarding low-molecular-weight heparin used for deep venous thrombosis (DVT) prophylaxis in total joint arthroplasty?
Explanation
to 18 hours. This is greater than the 1 hour half-life of unfractionated heparin.
Low-molecular-weight heparin offers an advantage over unfractionated heparin by selectively targeting Factor Xa while having a lesser effect on circulating thrombin (Factor IIa). Circulating thrombin Factor IIa is needed for local hemostasis at the site of the surgical wound. Clinical studies have shown a reduction by one third in the incidence of thrombocytopenia with the use of low-molecular-weight heparin. Low-molecular-weight heparin has been shown to demonstrate similar clinical results compared to warfarin with respect to preventing thromboembolic disease after total hip arthroplasty and complications such as bleeding.
REFERENCES: Zimlich RH, Fulbright BM, Friedman RJ: Current status of anticoagulation therapy after total hip and total knee arthroplasty. J Am Acad Orthop Surg 1996;4:54-62.
Colwell CW Jr, Spiro TE, Trowbridge AA, et al: Use of enoxaparin, a low-molecular-weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14.
Torholm C, Broeng L, Jorgensen PS, et al: Thromboprophylaxis by low-molecular-weight heparin in elective hip surgery: A placebo controlled study. J Bone Joint Surg Br 1991;73:434-438.
Question 47
They found statistically significant decreases in need for secondary intervention, hardware failure, and infection as well as faster wound healing and faster time to fracture union.
Explanation
A 76-year old patient underwent partial foot amputation through the talonavicular and calcaneocuboid joints. Besides Achilles tendon lengthening, what additional procedure(s) may be required to prevent the most common post-operative deformity?
Posterior capsule release
Anterior tibialis transfer to the talar neck
Anterior tibialis transfer to cuboid
Flexor hallucis longus transfer to calcaneus
Peroneus brevis transfer to calcaneus Corrent answer: 2
Achilles tendon lengthening AND anterior tibialis transfer to the talar neck would be required to prevent equinovarus deformity.
Partial foot amputation through the talonavicular and calcaneocuboid joints is also known as the Chopart amputation. Chopart amputation alone is known to result in significant equinovarus deformity. This deformity results in excessive pressure on the anterior wound during gait, causing pain and wound complications. Transfer of the tibialis anterior tendon to talar neck will provide force, and muscle tone, that promotes ankle dorsiflexion. Lengthening of the Achilles tendon will also reduce the equinus moment force across the ankle joint.
Dillion et al. examined the gait patterns of partial foot amputees. They found that amputations proximal to the metatarsal heads compromised the normal propulsive function of the foot and ankle. The ideal level of amputation to maintain normal propulsive function was distal to the metatarsal heads (i.e., disarticulating the metatarsophalangeal (MTP) joint).
Illustration A is a lateral radiograph showing a Chopart amputation. Incorrect Answers:
prevent the equinovarus deformity.

OrthoCash 2020
A 32-year-old male is involved in a motor vehicle collision and sustains the injury seen in Figure A. What is the most common urological injury associated with this injury pattern?

Testicular torsion
Posterior urethral tear
Bladder denervation
Testicular rupture
Renal hematoma
The figure shows an anteroposterior pelvic ring injury. The most common urological injury with pelvic ring injuries remains the posterior urethral tear, followed by bladder rupture.
Watnik et al notes lower urinary tract (bladder to end of urethra) injuries in up to 25% of patients with this injury. He reports that when contaminated urine communicates with the anterior arch, the possibility of infection exists, and early repair of bladder disruptions with simultaneous anterior arch plating minimizes this risk.
Routt et al notes that even with simultaneous treatment of these injuries, complications are common (late stricture in 44%, impotence in 16%, delayed incontinence in 20% of females, anterior deep pelvic infection in 4%). Despite this, they report that early urological repairs are easily performed at the time of anterior pelvic open reduction and internal fixation.
OrthoCash 2020
A 26-year-old women, 31-weeks pregnant, presents to the emergency department with the injury shown in Figure A. She states the injury occurred while lifting a heavy vacuum five days ago. She suffers from chronic headaches and sleep disturbances. On inspection, there are multiple dorsal and volar bruising over her wrist and upper arm. She is neurologically intact. After closed reduction and immobilizing the arm, what would be the next best step in management of this patient?

Diagnostic wrist arthroscopy
Urgent MRI wrist
Skeletal survey radiographs
Request a consultation with social worker in the hospital
Urgent open reduction internal fixation Corrent answer: 4
This patient presents with classic features of domestic violence. The most appropriate next step would be consultation with a social worker at the hospital, assess for child and patient safety, and encouraging the patient to seek self-protection.
Factors suggestive of domestic violence in the patient include pregnancy, delayed presentation after injury, inconsistent history, multiple bruises and complaints of chronic headache/sleep disturbances. Victims frequently miss days of work and as a result are at risk for losing their jobs. Victims are also more likely to engage in high-risk behavior with sex, drugs, alcohol, smoking, and eating.
The AAOS published a document outlining the Orthopaedic Surgeon’s responsibilities in domestic and family violence. Musculoskeletal injuries that should raise a suspicion of a problem include (1) Multiple injuries/fractures; (2) Unusual patterns of injury/fracture; (3) Injuries/fractures of varying ages; (4)
Injuries/fractures inconsistent with or disproportional to the history; (5) Multiple injuries treated in different hospital emergency departments or by different providers.
Incorrect Answers:
OrthoCash 2020
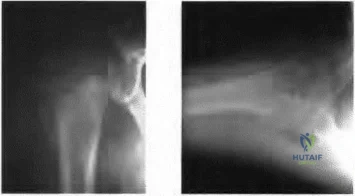
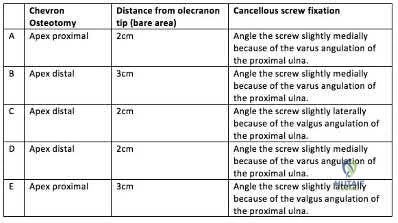
A 45-year-old man undergoes open reduction and internal fixation for a comminuted intra-articular humerus fracture . An olecranon osteotomy is performed and subsequently fixed with an intramedullary cancellous screw. Which of the following options in the table shown in Figure A best describes the characteristics of this osteotomy?
Question 48
The findings in Brown-Sequard syndrome include loss of which of the following? Review Topic
Explanation
Question 49
Which of the following is a function of siRNA (small interfering RNA)?
Explanation
siRNA are short (usually 20 to 24-bp) double-stranded RNA (dsRNA) sequences with phosphorylated 5' ends and hydroxylated 3' ends. Because of their ability to block a gene of interest, they have been generating interest in the treatment of disease processes that involve gene expression.
Noh et al. study the affects of PD98059, an extracellular signal-regulated kinase 1/2 (ERK1/2) inhibitor, on osteosarcoma. They found that blocking the ERK1/2 pathway with PD98059 induces osteosarcoma cell death by inhibiting a potential drug-resistance mechanism.
Illustration A shows how siRNA works to block translation of mRNA. Incorrect Answers:
Question 50
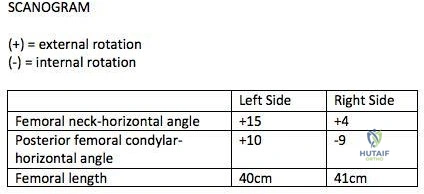
A 26-year-old male underwent statically locked intramedullary nail fixation for a comminuted left femur fracture. An early post-operative computed tomography (CT) scanogram was taken to check rotational alignment, as shown in Figure A. What would be the next best step in the management of this patient?
Explanation
>15 degrees and symptomatic. Therefore, the most appropriate next step would be to continue with postoperative observation and close follow-up.
The primary purpose of CT scanogram is to measure the angle of rotation of the femoral neck relative to the femoral condyle. To do this, the right and left femurs must be scanned together using a 5mm helical slice scanner at the hip and knee. The first slice should reveal the alignment of the femoral neck, so as to allow for measurement of the femoral neck-to-horizontal (FNH) angle. The second slice should reveal the alignment of the posterior femoral condyles. This allows measurement of the posterior condyle-to-horizontal (PCH) angle. Finally, to calculate the rotational alignment (RA), the FNH angle and PCH angles are subtracted (e.g., RA = FNH -PCH). Normal RA is usually +5 to +20 degrees, which is also referred to as 5 to 20 degrees of femoral anteversion.
Lindsey et al. reviewed femoral malrotation following intramedullary nail fixation. They showed the incidence of rotational malalignment was ~28%. Normal femoral neck anteversion (angle of the femoral neck relative to the transverse axis through the femoral condyles) is ~11-13°. However, they noted that some patients have up to 15° difference in rotation in native limbs. Therefore <15 degrees of rotational difference after fixation is considered acceptable.
Gugala et al. examined the long-term functional implications for patients with iatrogenic femoral malrotation following femoral intramedullary nail fixation. They
showed that patients can compensate for even significant femoral malrotation (up to 30 degrees) and tolerate it well. However, external femoral malrotation (more common) appears to be better compensated/tolerated than internal malrotation.
Figure A shows that the left femoral neck is externally rotated (ER) by 15° to the horizontal (ER15). The right femoral neck is externally rotated (ER) by 4° to the horizontal (ER4). The left distal fragment is ER10. The right distal fragment is internally rotated (IR) by 9°. Thus, left femur has a total (ER15)-(ER10)= (+15)-(+10)=(+5), and right femur has (ER4)-(IR9)= (+4)-(-9)=(+13) to the horizontal. Therefore, the difference is 8 degrees.
Incorrect Answers:
>15 degrees and symptomatic.
Question 51
Figure 199 is the clinical photograph of a 68-year-old man with a history of atrial fibrillation who was treated with warfarin. Nine days after undergoing elective total hip arthroplasty, he has a swollen left thigh. His wound remains dry and he is afebrile. His erythrocyte sedimentation rate (ESR) is 25 mm/h (reference range [rr], 0-20 mm/h) and C-reactive protein (CRP) level is 6.1 mg/L (rr, 0.08-3.1 mg/L). Aspiration reveals 3246 white blood cells (WBCs)/µL with 47% polymorphonucleocytes. Treatment at this time should consist of
Explanation
This patient has a large postsurgical hematoma. Although his ESR and CRP level are elevated, they are not considered elevated given his recent surgery. Additionally, the hip aspiration reveals a synovial cell count lower than 10000 WBC/µL along with a low percentage of polymorphonucleocytes. Treatment at this time should consist of observation. The hematoma is likely attributable to postsurgical anticoagulation, considering his history of atrial fibrillation.
Question 52
A 15-year-old girl reports popping and clicking at the sternoclavicular joint and an intermittent asymmetrical prominence of the medial head of the clavicle. She denies any history of trauma or other symptoms. Management should consist of
Explanation
REFERENCES: Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998,
p 583.
Question 53
During the approach to the lumbar spine for an L4-L5 anterior lumbar interbody fusion, which structure generally is found overlying the anterior surface of the L4 vertebra?
Explanation
During an anterior approach to the L4-L5 disk space for anterior lumbar interbody fusion, meticulous exposure is paramount to allow for safe preparation of the disk space and subsequent arthrodesis. Although all of these structures can come into play during the exposure, the aorta lies anterior to the L4 vertebral body and bifurcates at this level. The vena cava bifurcates just distal to this. The ureters lie to both sides of the anterior spine. The right common iliac artery and the left common iliac vein originate after the bifurcation of the great vessels and lie caudal to the L4 vertebra.
RECOMMENDED READINGS
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:226-235.
Agur AMR, Lee MJ, eds. Grant's Atlas of Anatomy. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1999:89.
Question 54
- The Injury Severity Score (ISS), using point scores from five different body systems, is a method that aids in predicting the chances of mortality in a patient with multiple injuries by
Explanation
Question 55
Following spinal cord injury (SCI), methylprednisolone (a bolus of 30 mg/kg plus 5.4 mg/kg per hour over 24 hours) initiated within 8 hours of injury has been associated with which of the following MRI findings? Review Topic
Explanation
Question 56
Figure 12 shows the lumbar CT scan of a 24-year-old man who was injured in a snowmobile accident. What is the mechanism of injury?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Spivak JM, Vaccaro AR, Cotler JM: Thoracolumbar spine trauma: Principles of management. J Am Acad Orthop Surg 1995;3:353-360.
Question 57
A 28-year-old woman has left shoulder pain and a tender soft-tissue mass. Based on the MRI scan and biopsy specimens shown in Figures 74a through 74c, what is the most likely diagnosis?
Explanation
REFERENCES: Damron TA, Sim FH: Soft-tissue tumors about the knee. J Am Acad Orthop Surg 1997;5:141-152.
Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 1146-1167.
Question 58
Which of the following findings helps to distinguish between stress fractures of the tibia and shin splints? Review Topic
Explanation
The general symptom of a bone stress injury is stress-related pain. Bone stress injuries are difficult to diagnose based only on a clinical examination because the clinical symptoms may vary depending on the phase of the pathophysiological spectrum in the bone stress injury. Imaging studies are needed to ensure an early and exact diagnosis. If the diagnosis is made early, most bone stress injuries heal well without complications.
Question 59
A 21-year-old college student fell from a balcony and landed on his outstretched right hand. He is seen in the emergency department 4 hours later and reports wrist pain and diffuse hand numbness. The volar forearm compartment is soft and there is no pain with passive finger extension. Radiographs are shown in Figures 25a and 25b. Definitive treatment should consist of
Explanation
REFERENCES: Herzberg G, Forissier D: Acute dorsal trans-scaphoid perilunate fracture-dislocations: Medium-term results. J Hand Surg Br 2002;27:498-502.
Melone CP Jr, Murphy MS, Raskin KB: Perilunate injuries: Repair by dual dorsal and volar approaches. Hand Clin 2000;16:439-448.
Herzberg G, Comtet JJ, Linscheid RL, et al: Perilunate dislocations and fracture-dislocations:
A multicenter study. J Hand Surg Am 1993;18:768-779.
Question 60
A 47-year-old man has acute right shoulder pain after falling off a ladder. The MRI scan shown in Figure 9 reveals
Explanation
REFERENCES: Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Iannotti JP, Zlatkin MB, Esterhai JL, et al: Magnetic resonance imaging of the shoulder: Sensitivity, specificity, and predictive value. J Bone Joint Surg Am 1991;73:17-29.
Question 61
A 20-year-old elite college football player has ecchymosis, swelling, and pain on the lateral side of his foot after a game. Radiographs are shown in Figures 31a through 31c. Management should consist of
Explanation
REFERENCES: Glasgow MT, Naranja RJ Jr, Glasgow SG, et al: Analysis of failed surgical management of fractures of the base of the fifth metatarsal distal to the tuberosity: The Jones fracture. Foot Ankle Int 1996;17:449-457.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-252.
Question 62
Figure 40 shows the radiographs of a 2-year-old boy who has a deformed leg. The patient is ambulatory and has no pain. What is the most appropriate management?
Explanation
REFERENCES: Murray HH, Lovell WW: Congenital pseudarthrosis of the tibia: A long-term follow-up study. Clin Orthop 1982;166:14-20.
Crossett LS, Beaty JH, Betz RR, et al: Congenital pseudarthrosis of the tibia: Long-term
follow-up study. Clin Orthop 1989;245:16-18.
Question 63
Which of the following anatomic structures is labeled 6 in Figure 27?
Explanation
REFERENCES: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, p 467.
Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 309.
Question 64
Figure 13 is the photograph of 18-month-old triplets with a lower-limb condition. What is the best initial treatment? Review Topic

Explanation
(SBQ13PE.56) A 22-month-old female is hospitalized with a fever and malaise. She is found to be bacteremic, and blood cultures grow methicillin-sensitive Staphylococcus aureus (MSSA). During her hospitalization, the pediatrician notices her arm is slightly swollen and appears painful to use. MRI is obtained and demonstrated in figure A. Which feature of the MRI suggests the need for surgical management? Review Topic

Brodie's Abscess
Osteomyelitis of the humeral metaphysis
Subperiosteal abscess of the humerus
Presence of subcutaneous air
High risk of proximal humeral growth arrest
This patient has osteomyelitis of the humerus with a large subperiosteal abscess. The presence of subperiosteal abscess necessitates surgical intervention for irrigation and debridement (I&D).
The diagnosis of acute osteomyelitis in children is made based upon a constellation of findings including pain, systemic signs of infection, elevated serum inflammatory markers, and imaging studies demonstrative of osseous infection. It is most commonly hematogenously spread to the metaphysis of immature bone, which is highly vascular prior to skeletal maturity. Treatment involves obtaining specimen for culture, empiric antibiotic treatment, and surgical irrigation and debridement of known abscesses. The end-point of treatment is return of pain-free functionality and the resolution of local/systemic signs of infection.
Conrad reviewed the management of acute hematogenous osteomyelitis and emphasized that surgical intervention in the presence of abscess can be both therapeutic and diagnostic: I&D can obtain culture and narrow the antibiotic plan.
Jones et. al. reviewed chronic pediatric osteomyelitis and report that surgery is the mainstay of treatment because removal of dead bone is essential for resolution of infection. This may be performed with sequestrectomy and curettage, with an emphasis on prevention of pathologic fracture, growth disturbances, bone loss, joint involvement, and permanent loss of function.
Figure A is a coronal STIR MRI image of the humerus demonstrating osteomyelitis
with extensive subperiosteal abscess.
Incorrect Answers:
Brodie's abscess is a type of subacute osteomyelitis which remains indolent and creates a focal intra-osseous abscess. This is not demonstrated in the clinical image.
The patient does have osteomyelitis of the humeral metaphysis, but this alone is not the indication for surgery. Uncomplicated osteomyelitis may be treated effectively with antibiotics alone.
Presence of subcutaneous air is suggestive of necrotizing fasciitis, which is a surgical emergency. The MRI however does not demonstrate this finding.
The infection and its surgical management both increase risk of injury to the proximal humeral physis and has the potential for growth arrest or angular deformity.
(SBQ13PE.3) Figure A demonstrates a physical examination maneuver in a 1 month old infant. What is this maneuver? Review Topic

Ortolani Test
Barlow Test
Galeazzi Sign
Patrick test
Teratologic Sign
Figure A shows a schematic image of the Ortalani test.
The Ortolani test, or Ortolani maneuver, is part of the physical examination for developmental dysplasia of the hip. It is used alongside the Barlow test to detect subluxated hips that are either reducible or irreducible. A positive sign is a distinctive 'clunk' which can be heard and felt as the femoral head relocates anteriorly into the acetabulum.
Guille et al. showed that the use of Pavlik harness has become the mainstay of initial treatment for the infant who has not yet begun to stand. If concentric reduction of the hip cannot be obtained, surgical reduction of the dislocated hip is the next step before they are able to stand.
Video V is a lecture discussing the hip examination of the infant. Incorrect Answers:
pressure on the knee, directing the force the femoral head posteriorly. A positive Barlow test would result in posterior subluxation/dislocation of the hip. Answer 3: Galeazzi test is performed by flexing an infant's knees in the supine position so that the ankles touch the buttocks. If the knees are not level then the test is positive, which indicates a potential congenital hip issue (e.g. DDH). Answer 4: Patrick or Faber test (flexion, abduction, external rotation) has been described both for stressing the SI joint and for isolating symptoms to the hip Answer 5: Teratologic dislocation of the hip is a term used to imply that the hip joint did not develop normally in utero, thus the hip is in a fixed dislocated position at birth.
Question 65
A patient who underwent a total knee arthroplasty for osteoarthritis 18 months ago now reports the sudden development of pain in the ipsilateral knee. Radiographs and examination of the knee are unremarkable. Aspiration of the synovial fluid 3 days later reveals a WBC count of 1,500/mm 3 . The cells consist of 30% neutrophils and 70% monocytes. Culture results will not be available for several days. The patient has not been on antibiotics prior to this point. Based on these findings, what is the most appropriate management?
Explanation
REFERENCES: Trampuz A, Hanssen AD, Osmon DR, et al: Synovial fluid leukocyte count and differential for the diagnosis of prosthetic knee infection. Am J Med 2004;117:556-562.
Mason JB, Fehring TK, Odum SM, et al: The value of white blood cell counts before revision total knee arthroplasty. J Arthroplasty 2003;18:1038-1043.
Kersey R, Benjamin J, Mason B: White blood cell counts and differential in synovial fluid of aseptically failed total knee arthroplasty. J Arthroplasty 2000;15:301-304.
Question 66
Which of the following tissues used for anterior cruciate ligament (ACL) reconstruction has the highest maximum load to failure?
Explanation
REFERENCES: Hamner DL, Brown CH Jr, Steiner ME, Hecker AT, Hayes WC: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Cooper DE, Deng XH, Burstein AL, Warren RF: The strength of the central third patellar tendon graft: A biomechanical study. Am J Sports Med 1993;21:8l8-823.
Brown CH Jr, Steiner ME, Carson EW: The use of hamstring tendons for anterior cruciate ligament reconstruction: Technique and results. Clin Sports Med 1993;12:723-756.
Engebretsen L, Lewis JL: Graft selection and biomechanical considerations in ACL reconstruction. Sports Med Arthroscopy Rev 1996;4:336-341.
Question 67
A diskectomy is performed in which the disk space is not aggressively debrided. When compared to techniques that involve aggressive debridement of the disk space, this results in
Explanation
This patient has disk herniation at the left L5-S1 level. This will generally affect the traversing S1 nerve. The S1 dermatome is on the lateral aspect and sole of the foot.
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183. View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
Question 68
A 17-year-old high school football player reports wrist pain after being tackled. Radiographs are shown in Figures 22a through 22c. What is the recommended intervention?
Explanation
REFERENCES: Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
Raskin KB, Parisi D, Baker J, et al: Dorsal open repair of proximal pole scaphoid fractures. Hand Clin 2001;17:601-610.
Question 69
A 25-year-old motorcyclist has a knee dislocation that is reduced by the trauma surgeon in the emergency department. Radiographs show no fracture and a reduced knee joint. What is the most appropriate initial step for evaluation of a potential arterial injury?
Explanation
Question 70
What method of spinal fixation requires the largest force to disrupt the bone-implant interface?
Explanation
Question 71
A 44-year-old man sustains the injury shown in Figures 1 through 3. What is the most appropriate treatment?

Explanation
Reduction, either open or closed, with internal fixation (pinning) is the recommended treatment for the majority of these injuries. Closed reduction with pinning is most often performed for acute injuries. Open reduction with pinning is performed for those injuries that cannot be reduced by closed means or those with a delayed presentation. Four cases of successful closed reduction and splinting, all performed upon presentation in the emergency department, have been described by Storken and associates, but the authors note that their review of three prior reports uncovered cases of secondary dislocation, which required surgical stabilization. One of the dislocations occurred 4 months after the reduction. They assert that an indication for primary ORIF is a CMC dislocation associated with major fractures. Primary arthrodesis can be considered in cases with severe intra-articular comminution, but this procedure substantially limits the ability of the hand to increase and decrease the transverse metacarpal arch, which is an important functional movement. It can also lead to osteoarthritis of the triquetrohamate joint. Suspension arthroplasty has been described for old fracture-dislocations of the fifth CMC joint, using a partial slip of the extensor carpi ulnaris.








Question 72
Hip pain of month duration has developed in a year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. The patient has a final culture that reveals methicillin-resistant Staphylococcus aureus (MRSA). If the attending physician recommends the two-stage protocol, including the use of an antibiotic-cement spacer, what is the most likely prognosis for this patient?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin- resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was
21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California
Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 73
Figures 34a and 34b show the axial and sagittal MRI scans of a 36-year-old man who reports the insidious onset of pain in the right shoulder. What is the most appropriate description of the acromial morphology?
Explanation
REFERENCES: Sher JS: Anatomy, biomechanics, and pathophysiology of rotator cuff disease, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, p 23.
Sammarco VJ: Os acromiale: Frequency, anatomy, and clinical implications. J Bone Joint Surg Am 2000;82:394-400.
Question 74
A 68-year-old woman undergoes hemiarthroplasty for a proximal humerus fracture. What post-operative motion should be limited as it puts the most stress on the lesser tuberosity fragment fixation?

Explanation
Question 75
A 60-year-old man who underwent left partial knee arthroplasty 6 months earlier was doing well until he experienced left knee pain and swelling for 4 weeks following a dental procedure. The left knee aspirate was bloody, with a white blood cell count of 8,000 and 70% neutrophils. Culture grew group B Streptococcus ( Granulicatella adiacens ), and serologies were elevated, with an erythrocyte sedimentation rate of 55 mm/h (reference range: 0 to 20 mm/h) and a C-reactive protein level of 24 mg/L (reference range: 0.08 to 3.1 mg/L). What is the best next step?
Explanation
This complication is best addressed with either a single-stage or two-stage total knee arthroplasty. A recent report suggests that a single-stage arthroplasty can be effective, although many surgeons would perform a two-stage procedure with an articulating or static spacer. Arthroscopic would be non-effective, especially given 4 weeks of symptoms. Resection arthroplasty without a spacer would leave an unstable and poorly functioning extremity. Knee fusion should be used as a salvage procedure.
Question 76
Figure 1 is the MRI scan of a 19-year-old man who has an acute anterior shoulder dislocation. The bony fragment occupies 10% of the glenoid articular surface. What is the most appropriate treatment?
Explanation
Question 77
A 58-year-old woman with rheumatoid arthritis and a severe hindfoot valgus deformity now reports recurrent lateral ankle pain. Examination reveals pain over the fibula and sinus tarsi, with a valgus hindfoot that is passively correctable. Despite the use of an ankle-foot orthosis, this is the second time this problem has occurred. Radiographs and a clinical photograph are shown in Figures 28a through 28c. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Stephens HM, Walling AK, Solmen JD, Tankson CJ: Subtalar repositional arthrodesis for adult acquired flatfoot. Clin Orthop 1999;365:69-73
Easley ME, Trnka HJ, Schon LC, Myerson MS: Isolated subtalar arthrodesis. J Bone Joint Surg Am 2000;82:613-624.
Question 78
What is the most common diagnosis in a patient older than age 40 years with a destructive bony lesion?
Explanation
REFERENCE: CA, January/February 2000, vol 50, no. 1 (Cancer Statistics).
Question 79
A player on a professional football team sustains a knee injury and is diagnosed with an anterior cruciate ligament rupture. When employed as the team physician, your ethical obligation is to inform
Explanation
Question 80
5 mm of change in the atlanto-dens interval (ADI) between flexion and extension views
Explanation
With the introductions of disease-modifying antirheumatic agents (DMARDs), the incidence of RA patients undergoing cervical spine surgery has decreased significantly. Basilar invagination, atlantoaxial instability, and subaxial subluxation are the three most common manifestations of cervical disease. Multiple studies in RA patients with untreated or poorly controlled disease have led to the development of a set of measurements that identify patients who require surgical intervention and predict outcome after surgery. Additionally, progressive neurological compromise and
refractory
pain
are
indications
for
intervention.
Kim and Hilibrand reviewed management of the rheumatoid cervical spine and outline parameters for surgical intervention. These include a PADI < 14 mm, cervicomedullary angle <135 degrees, progressive neurological deficit, refractory pain, atlantoaxial impaction as determined by migration >5 mm rostral to McGregor's line, and subaxial canal diameter < 14 mm.
Boden et al. analyzed 73 patients followed for rheumatoid cervical spine disease with an average follow up of 7 years. They found that the PADI correlated with paralysis. Patients with PADI less than 10 mm had no recovery, and all patients with PADI greater than 14 mm had full recovery.
Illustration A demonstrates the measurement of the ADI and PADI. Illustration B demonstrates how to measure the cervicomedullary angle (as marked by A), which is typically determined on MRI
Incorrect
Question 81
A 34-year-old woman has had painful snapping and popping in the elbow since falling while in-line skating 6 months ago. The popping also occurs when she pushes off with her hands to rise from a seated position. Initial radiographs were normal, and she was told that she had sprained her elbow. Examination reveals few findings except that she is very apprehensive when the forearm is forcefully supinated with the elbow extended or partially flexed. A radiograph taken in that position is shown in Figure 24. Treatment should consist of
Explanation
REFERENCES: O’Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Burgess RC, Sprague HH: Post-traumatic posterior radial head subluxation: Two case reports. Clin Orthop 1984;186:192-194.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Question 82
Figure below shows the standing AP radiograph obtained from a 55-year-old man who has a 5-year history of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. What is the UKA survivorship for a 55-year-old patient, compared with the survivorship for total knee arthroplasty?
Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact anterior cruciate ligament (ACL). The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph aids the orthopaedic surgeon in determining the correction of the varus deformity and assessing the lateral compartment. An inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared with other age groups, but survivorship is lower for UKA than for TKA. No studies to date have shown any differences in survivorship between fixed-bearing and mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, which occurs in less than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA are low. Arthritis may progress faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
Question 83
When elevating the arm, the ratio of scapulothoracic to glenohumeral motion over the total range of motion is best described as
Explanation
REFERENCES: Inman VT, Saunders JR, Abbott LC: Observations of the function of the shoulder joint. Clin Orthop 1996;330:3-12.
Freedman L, Munro RH: Abduction of the arm in the scapular plane: Scapular and glenohumeral movements. J Bone Joint Surg Am 1966;18:1503.
Question 84
Figures 20a and 20b show the radiographs of a 14-year-old boy who sustained a twisting injury to his ankle. If attempted closed reduction is unsuccessful, what is the primary reason to proceed with surgical treatment?
Explanation
REFERENCES: Vaccaro A (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 757-765.
Kling TF Jr, Bright RW, Hensinger RN: Distal tibial physeal fractures in children that may require open reduction. J Bone Joint Surg Am 1984;66:647-657.
Spiegel PG, Mast JW, Cooperman DR, et al: Triplane fractures of the distal tibial epiphysis.
Clin Orthop Relat Res 1984;188:74-89.
Question 85
A 26-year-old woman who noted right-sided lumbosacral pain 10 days ago while vacuuming now reports that the pain has intensified. She denies any history of back problems. No radicular component is present, and her neurologic examination is normal. The next most appropriate step in management should consist of
Explanation
REFERENCES: Bigos S, Boyer O, Braen GR, et al: Acute low back pain in adults: Clinical practice guideline No. 14. AHCPR Publication No. 95-0642. Rockville, MD, Agency for Health Care Policy and Research, Public Health Service, US Department of Health and Human Services, December, 1994.
Deyo RA: Conservative therapy for low back pain: Distinguishing useful from useless therapy. JAMA 1983;250:1057-1062.
Question 86
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?
Explanation
REFERENCE: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD,
Williams and Wilkins, 1998, pp 98-100.
Question 87
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function. A pathognomonic radiographic feature of this injury is a

Explanation
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Question 88
Figure 1 shows the radiograph obtained from a 67-year-old man recently diagnosed with osteoarthritis, 8 years after receiving a left metal-on-metal total hip arthroplasty (THA). The acetabular component has a modular cobalt alloy acetabular liner. The patient states that he did very well postoperatively, but for the last 6 months has noted worsening pain and swelling in his left hip. Serum metal ion testing reveals a chromium level of 12.4 ng/mL, compared with a normal level of less than 0.3 ng/mL, and a cobalt level of 11.8 ng/mL, compared with a normal level less than 0.7 ng/mL. An MRI with metal artefact reduction sequence (MARS) was performed and is shown in Figure 2. What is the most appropriate management at this time?

Explanation
Metal-on-metal THA was initially introduced in the 1990s, with the proposed advantages of decreased wear and improved stability. However, catastrophic adverse local tissue reactions associated with their use has raised numerous concerns. The work-up of a patient with a prior metal-on-metal total hip arthroplasty involves a thorough history and physical examination; blood analysis, including the erythrocyte sedimentation rate, C-reactive protein, and metal ion levels; and secondary imaging, including ultrasonography, CT, and MRI. In a patient with clinical symptoms, elevated metal ion levels, and a large fluid collection seen on MRI, the most appropriate treatment would be removal of the metal-on-metal bearing. Given the presence of an adverse reaction involving cobalt and chromium, a revision ceramic head may be most appropriate to avoid the potential of trunnion-associated corrosion.
Question 89
A patient with a transverse femur fracture undergoes statically locked antegrade intramedullary nailing. Postoperatively, the patient appears to have a
Explanation
Question 90
A 15-year-old girl sustained the injury shown in Figures 70a and 70b when she jumped from the back of a moving truck. She is seen in the emergency department 2 hours after her injury. She has no other injuries. Her foot is warm and she has a normal motor and sensory examination. Pulses are only evident on Doppler. What is the most appropriate management? Review Topic

Explanation
Question 91
Spondyloepiphyseal dysplasia congenita and tarda, precocious osteoarthropathy, and Stickler syndrome are caused by a mutation in the gene coding for
Explanation
Question 92
Figure 9 shows a cross-sectional view of the spinal cord at the lower cervical level. Injury to the structure indicated by the black arrow will lead to what neurologic deficit?
Explanation
REFERENCES: Bohlman H, Ducker T, Levine A: Spine trauma in adults, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 911.
Northrup B: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, p 545.
Question 93
The fracture seen in Figure 1 is most likely associated with injury to what ligamentous structure?
Explanation
A. Methicillin-resistant Staphylococcus aureus (MRSA)
B. Cutibacterium acnes
C. Enterococcus species
D. Staphylococcus epidermidis
C acnes is the most common organism recovered in prosthetic shoulder infections (33%), Coagulase-negative Staphylococcus is second (21%), Methicillin-sensitive S aureus (13%), and S epidermidis (10%). MRSA accounts for 5% and Enterococcus species, 1.5%.
Question 94
Figures 80a and 80b are the radiographs of a 21-year-old football player who underwent anterior cruciate ligament (ACL) reconstruction with patellar tendon autograft 1 year ago. He reports mild stiffness in his knee. Upon examination, he has a negative Lachman test result, trace effusion, and range of motion from 0 to 85 degrees of knee flexion. Which factor is most contributory to his examination findings?
Explanation
Technical failure is the most common reason for ACL reconstruction failure. Tunnel position is the most frequent cause of technical failure. Malpositioning of the tunnel affects the length of the graft, causing either decreased range of motion or increased graft laxity. This patient has anterior and vertical placement of his femoral tunnel, which has been shown to cause stiffness in knee flexion. Although graft choice is an important factor when planning ACL reconstruction, overall outcomes with autograft tissues are fairly similar. Fixation of the graft at the femoral or tibial end is not as important as tunnel position. Fixing the graft in flexion can cause extension loss when isometry is not achieved, but this condition is not touched upon in this scenario.
CLINICAL SITUATION FOR QUESTIONS 81 THROUGH 84
Figures 81a through 81d are the MR images of a 25-year-old man with left knee pain after a motorcycle collision. He has palpable pedal pulses with an ankle-brachial index of 0.95. Neurologic examination findings of the injured extremity are normal.
Question 95
A year-old woman had a primary total hip arthroplasty 7 years ago that included a proximally coated titanium stem, a cobalt alloy femoral head, a titanium hemispherical acetabular component, and a polyethylene liner. She did well for 4 years but has now had two dislocations and reports pain and weakness around the left hip. She denies any fevers, chills, or constitutional symptoms. On examination, the patient walks well without any signs of an antalgic or Trendelenburg gait. Her abductor mechanism demonstrates good strength. Her erythrocyte sedimentation rate and C-reactive protein level are normal. On radiographs, all components appear well fixed and in good alignment. What is the most appropriate treatment at this time?
Explanation
Trunnionosis is a recently recognized complication following total hip arthroplasty and can occur when a cobalt alloy femoral head is used on a titanium alloy or cobalt alloy femoral stem. Patients often present with pain or swelling around the hip but at times can present with instability. Certain femoral stem designs have been associated with increased reports of trunnionosis. In a patient with a cobalt alloy femoral head who presents with instability, swelling, and weakness around the hip, the potential for trunnionosis and
an adverse local tissue reaction should be considered.
Question 96
What is the primary mechanism of injury for the fracture shown in Figures 33a and 33b?
Explanation
REFERENCES: Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 267-272.
Dias LS, Giegerich CR: Fractures of the distal tibial epiphysis in adolescence. J Bone Joint Surg Am 1983;65:438-444.
Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Question 97
-Figures 55a and 55b are the radiograph and CT scan of a 61-year-old woman who has had neck pain after being involved in a high-speed motor vehicle collision. Examination reveals normal strength and sensation in both upper and lower extremities, normal rectal tone, and no other injuries. The C1-C2 lateral mass overhang measures 8.5 mm. What is the most appropriate treatment option?
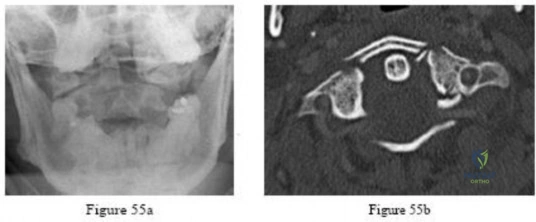
Explanation

Question 98
-What do the T2-weighted, fat-saturated MRI scans shown in Figures 76a through 76d reveal?
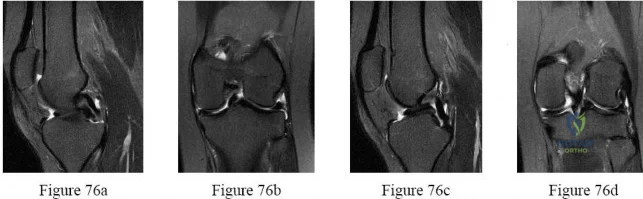
Explanation
Question 99
A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman test with a soft endpoint, varus laxity at 30°, and a positive dial test at 30° that dissipates at 90° of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome?
Explanation
Question 100
A 30-year-old man undergoes arthroscopic Bankart repair for recurrent anterior dislocation. He continues to experience instability postoperatively. Examination reveals a positive apprehension test. Radiographs of both shoulders are seen in Figure A. CT scan of his left shoulder is seen in Figure B. What is the best treatment option? Review Topic
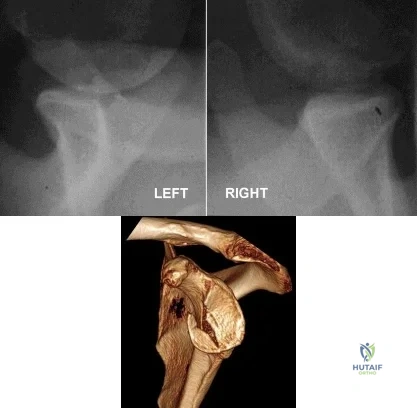
Explanation
Patients with glenoid bone defects >20-30% have a high recurrence rate (>60%) after Bankart repair alone. Bone grafting is necessary to offer containment. Autograft options include coracoid transfer (such as the Latarjet procedure which extends the articular arc and creates a conjoined tendon sling) and iliac crest bone grafting.
Burkhart et al. addressed glenohumeral bone defects. They advise that significant bone deficits cannot be adequately addressed via arthroscopic Bankart repair alone. The Latarjet transfer creates an extra-articular platform to extend the articular arc of the glenoid.
Hantes et al. assessed Latarjet repairs using CT. They found that there is almost
complete repair of a 25% to 30% glenoid defect when using the Latarjet procedure.
Figure A comprises comparison Bernageau view glenoid profile radiographs of both shoulders. Figure B is a 3D reconstruction CT with showing glenoid bone deficiency (inverted pear deformity) with a large bony Bankart lesion. Illustration A shows the method of obtaining a Bernageau glenoid profile view. Illustration B shows the "cliff sign" of anterior glenoid bone loss. Illustration C depicts the Latarjet procedure. Illustration D depicts reduction in the articular arc with anterior glenoid loss.
Incorrect Answers:
