Orthopedic Board Review MCQs: Trauma, Foot & Ankle, Arthroplasty | Part 195

Key Takeaway
This page offers Part 195 of an Orthopedic Surgery Board Review series, featuring 100 verified, high-yield MCQs. Designed for orthopedic surgeons and residents, it mirrors AAOS/OITE exam formats, providing crucial practice on topics like Ankle, Foot, and Trauma for certification success.
About This Board Review Set
This is Part 195 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 195
This module focuses heavily on: Ankle, Arthroplasty, Deformity, Foot, Trauma, Wrist.
Sample Questions from This Set
Sample Question 1: An 18-year-old high school football player exits the field after making a tackle on the opening kickoff. He reports “feeling out of it” and states that he has a headache. He does not recall any loss of consciousness and has no amnesia. He i...
Sample Question 2: What is the primary indication for performing a total wrist arthroplasty in a patient with painful rheumatoid arthritis?...
Sample Question 3: -A form of renal osteodystrophy that is characterized by pure osteomalacia is caused by...
Sample Question 4: A 14-year-old boy has medial ankle pain, progressive unilateral flatfoot deformity, and pain with most activities of daily living. He denies any recent injury. His parents recall that at age 7 years he sustained an injury that was treated a...
Sample Question 5: When balancing gaps in the coronal plane, what structure preferentially impacts the flexion space more than the extension space?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
An 18-year-old high school football player exits the field after making a tackle on the opening kickoff. He reports “feeling out of it” and states that he has a headache. He does not recall any loss of consciousness and has no amnesia. He is unable to list the months of the year in reverse order on questioning. He does not return to the game and feels normal at the completion of the game. What is the most sensitive test in assessing deficits after mild traumatic brain injury?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 37-38.
62 • American Academy of Orthopaedic Surgeons
Maroon JC, Lovell MR, Norwig J, et al: Cerebral concussion in athletics: Evaluation and neuropsychological testing. Neurosurgery 2000;47:659-672.
Question 2
What is the primary indication for performing a total wrist arthroplasty in a patient with painful rheumatoid arthritis?
Explanation
Question 3
- A form of renal osteodystrophy that is characterized by pure osteomalacia is caused by
Explanation
Question 4
A 14-year-old boy has medial ankle pain, progressive unilateral flatfoot deformity, and pain with most activities of daily living. He denies any recent injury. His parents recall that at age 7 years he sustained an injury that was treated as a sprain. Examination reveals valgus deformity with painless, unrestricted passive motion of the ankle. He has grossly equal limb lengths. A radiograph of the affected ankle is shown in Figure 48a, and the contralateral ankle is shown in Figure 48b. Management should consist of
Explanation
REFERENCES: Thompson DM, Calhoun JH: Advanced techniques in foot and ankle reconstruction. Foot Ankle Clin 2000;5:417-442.
Ting AJ, Tarr RR, Sarmiento A, Wagner K, Resnick C: The role of subtalar motion and ankle contact pressure changes from angular deformities of the tibia. Foot Ankle 1987;7:290-299.
Tarr RR, Resnick CT, Wagner KS, Sarmiento A: Changes in tibiotalar joint contact areas following experimentally induced tibial angular deformities. Clin Orthop 1985;199:72-80.
Question 5
When balancing gaps in the coronal plane, what structure preferentially impacts the flexion space more than the extension space?
Explanation
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point,
can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
Question 6
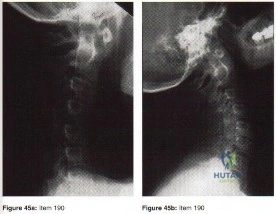
A 33-year-old woman sustains a C6 burst fracture diving into a swimming pool, resulting in a complete spinal cord injury. The canal compromise is shown in Figures 8a and 8b. Functional recovery would be maximized with
Explanation
REFERENCES: Bohlman HH, Anderson PA: Anterior decompression and arthrodesis of the cervical spine: Long-term motor improvement. Part I: Improvement in incomplete traumatic quadriparesis. J Bone Joint Surg Am 1992;74:671-682.
Benz R, Abitbol JJ, Ozanne S, Garfin SR: Cervical burst fractures, in Levine AM, Eismont FJ, Garfin SR, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 300-330.
Question 7
A 52-year-old woman who is right hand-dominant sustains an injury to her elbow in a fall. A radiograph is shown in Figure 60. The preferred treatment of this injury pattern should include
Explanation
REFERENCES: Egol KA, Tejwani NC, Bazzi J, et al: Does a Monteggia variant lesion result in a poor functional outcome? A retrospective study. Clin Orthop Relat Res 2005;438:233-238.
Jupiter JB, Leibovic SJ, Ribbans W, et al: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
Konrad GG, Kundel K, Kreuz PC, et al: Monteggia fractures in adults: Long-term results and prognostic factors. J Bone Joint Surg Br 2007;89:354-360.
Question 8
A 50-year-old patient underwent multiple debridements for an open radial shaft fracture with bone loss. The bed currently shows no evidence of infection but has a 14-cm diaphyseal bone defect. The most appropriate treatment includes open reduction and internal fixation along with
Explanation
A. clinical examination.
B. invasive pressure measurement.
C. arterial Doppler study.
D. MRI.
Compartment syndrome of the hand can result from a variety of factors, including a traumatic event such as crush injury, fracture, vascular insult, a high-pressure injection injury, or an insect or spider bite. The treatment involves decompressive fasciotomy of the involved compartments. The diagnosis of hand compartment syndrome is determined by history, examination, and objective testing. Patients experience pain out of proportion to the injury, along with swelling and tense skin. Pain may occur with passive motion of the metacarpophalangeal joints as the intrinsic muscles are stretched. Invasive intracompartmental pressures can be measured in the compartments of the hand but not in the fingers. Arterial Doppler studies assess arterial blood flow,
and an abnormality would be a late finding. 41
MRI would show edema of the hand and fingers, but the decision to perform surgical release is less likely made from the findings. The most appropriate method of determining the need for finger fasciotomy is the history and physical examination.
45- Figures 1 and 2 show the MRI studies of a 35-year-old manual laborer with persistent wrist pain despite immobilization. At the time of surgery, collapse of the capitate and arthritic changes of the midcarpal joint are noted. What is the most appropriate procedure for this condition?
A. Local vascularized bone graft
B. Proximal row carpectomy
C. Midcarpal fusion
D. Total wrist arthroplasty
The T1-weighted MRI reveals decreased signal that is consistent with avascular necrosis (AVN) of the capitate. Figure 2 demonstrates increased signal of the capitate consistent with edema. The etiology of AVN of the capitate may be related to trauma, abnormal interosseous vascular supply, and hypermobility. Surgical treatment is considered for patients who have had persistent symptoms despite immobilization. At the time of surgery, collapse of the capitate and arthritic changes would be treated most appropriately with a salvage procedure. A midcarpal fusion is a motion-preserving salvage procedure and is the most appropriate option given to address the pain associated with the midcarpal arthritic changes. The alternative options are not appropriate for this patient. Local vascularized bone grafts are considered for situations in which no evidence of capitate collapse or arthritis is observed.
Question 9
A healthy, active year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in A radiograph taken after the fall is shown in He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?
Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 10
The superior glenohumeral ligament primarily restrains
Explanation
REFERENCES: Warner JJ, Deng XH, Warren RF, et al: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy Orthopaedic Surgeons, 1994, pp 165-177.
Question 11
A 19-year-old girl has had pain and swelling in the right ankle for the past 4 months. She denies any history of trauma. Examination reveals a small soft-tissue mass over the anterior aspect of the ankle and slight pain with range of motion of the ankle joint. The examination is otherwise unremarkable. A radiograph and MRI scan are shown in Figures 45a and 45b, and biopsy specimens are shown in Figures 45c and 45d. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 198-199.
Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 200-202.
Question 12
A 43-year-old man sustained a closed, intra-articular pilon fracture. It has now been 1 year since he underwent open reduction and internal fixation. Which of the following statements most accurately describes his perceived outcome? Review Topic
Explanation
Question 13
A football player sustains a traumatic anterior inferior dislocation of the shoulder in the last game of the season. It is reduced 20 minutes later in the locker room. The patient is neurologically intact and has regained motion. If the patient undergoes arthroscopic evaluation, what finding is seen most consistently?
Explanation
REFERENCES: Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.
Bottoni CR, Wilckens JH, DeBerardino TM, et al: A prospective, randomized evaluation of arthroscopic stabilization versus nonoperative treatment in patients with acute, traumatic,
first-time shoulder dislocations. Am J Sports Med 2002;30:576-580.
Question 14
A 67-year-old retired steelworker was involved in a motor vehicle accident and sustained a midcervical spinal cord injury. Radiographs and MRI scans reveal severe cervical stenosis and spondylosis without fractures or dislocations. Neurologic examination reveals an ASIA C spinal cord impairment with greater motor involvement of the upper extremities than the lower extremities. What is the probability that the patient eventually will become ambulatory?
Explanation
(ASIA C and D) ultimately walked. The poorest prognosis, however, was in ASIA C patients older than age 50, in which only 40% walked.
REFERENCES: Penrod LE, Hegde SK, Ditunno JF Jr: Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990;71:963-968.
Northrup BE: Acute injuries to the spine and spinal cord: Evaluation and early treatment, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, p 735.
Question 15
Which of the following radiographic parameters is most predictive of a poor result following multilevel fusion surgery for adult degenerative scoliosis? Review Topic
Explanation
Question 16
Which of the following hip fracture patterns is at increased risk of proximal fragment flexion malreduction with dynamic hip screw fixation?

Explanation
Mohan et al conducted a study to assess the effect of clockwise rotational torque onto the fracture configuration in unstable and stable intertrochanteric fractures fixed with a dynamic hip screw construct. They found that 11 out of 30 unstable fractures showed an anterior spike (flexion malreduction) in left-sided fixations due to clockwise torque. This malreduction was not present in right-sided or stable fractures.
Question 17
The radiograph seen in Figure 67 reveals an ankle fracture in a 65-year-old woman who slipped on the ice. She has a history of diabetes mellitus for the past 7 years and reports that she maintains fair control of her diabetes; her last HgbA1c was 8%. The patient is a community ambulatory who lives independently. Examination reveals she has absent sensation with the 5.07 monofilament. When determining management, the physician must consider which of the following?

Explanation
Question 18
A 35-year-old woman began to train for a half marathon. After 8 weeks of increasing her mileage, what changes can you expect in her Achilles tendon?
Explanation
Question 19
What is the most common neurologic complication following an anterior cervical diskectomy and fusion?
Explanation
REFERENCES: Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Apfelbaum RI, Kriskovich MD, Haller JR: On the incidence, cause, and prevention of recurrent laryngeal nerve palsies during anterior cervical spine surgery. Spine 2000;25:2906-2912.
Question 20
A 72-year-old man with a history of Parkinson’s disease, stable coronary artery disease, and mild renal insufficiency is seen for hip arthroplasty. Which of the following is considered the most appropriate bearing of choice?
Explanation
REFERENCES: Bragdon CR, Greene ME, Freiberg AA, et al: Radiostereometric analysis comparison of wear of highly cross-linked polyethylene against 36- vs 28-mm femoral heads. J Arthroplasty 2007;22:125-129.
MacDonald SJ: Metal-on-metal total hip arthroplasty: The concerns. Clin Orthop Relat Res 2004;429:86- 93.
Question 21
A 21-year-old man has had posterior neck discomfort for the past 6 months. A whole-body bone scan and a cervical single-photon emission CT reveal increased activity at the C7 spinous process. MRI reveals multifocal involvement of the spinous process lamina and facet of C7. A CT-directed needle biopsy reveals osteoblastoma. What is the best course of action?
Explanation
REFERENCES: Bridwell KH, Ogilvie JW: Primary tumors of the spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery. Philadelphia, PA, JB Lippincott, 1991, vol 2, pp 1143-1174.
Ozaki T, Liljenquist U, Hillmann A, et al: Osteoid osteoma and osteoblastoma of the spine: Experience with 22 patients. Clin Orthop 2002;397:394-402.
Question 22
A year-old active woman undergoes elective total hip replacement in which a posterior approach is used. She has minimal pain and is discharged to home 2 days after surgery. Four weeks later, she dislocates her hip while shaving her legs. She undergoes a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Explanation
First-time early dislocations are often treated successfully without revision surgery, especially when no component malalignment is present. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful but is usually reserved for patients with recurrent dislocations.
Question 23
A radiograph, MRI scans, and a biopsy specimen of a 9-year-old boy with thigh pain are shown in Figures 37a through 37d. Management should consist of
Explanation
REFERENCES: Sailer SL: The role of radiation therapy in localized Ewing’ sarcoma. Semin Radiat Oncol 1997;7:225-235.
Shankar AG, Pinkerton CR, Atra A, Ashley S, Lewis I, Spooner D, et al: Local therapy and other factors influencing site of relapse in patients with localised Ewing’s sarcoma. United Kingdom Children’s Cancer Study Group (UKCCSG). Eur J Cancer 1999;35:1698-1704.
Carrie C, Mascard E, Gomez F, Habrand JL, Alapetite C, Oberlin O, et al: Nonmetastatic pelvic Ewing sarcoma: Report of the French society of pediatric oncology. Med Pediatr Oncol 1999;33:444-449.
Terek RM, Brien EW, Marcove RC, Meyers PA, Lane JM, Healey JH: Treatment of femoral Ewing’s sarcoma. Cancer 1996;78:70-78.
Question 24
Which of the following illustrations shown in Figures 21a through 21e correctly shows the projection of the sacroiliac joint on the outer table of the ilium?
Explanation
REFERENCES: Waldrop JT, Ebraheim NA, Yeasting RA, Jackson WT: The location of the sacroiliac joint on the outer table of the posterior ilium. J Orthop Trauma 1993;7:510-513.
Xu R, Ebraheim NA, Yeasting RA, Jackson WT: Anatomic considerations for posterior iliac bone harvesting. Spine 1996;21:1017-1020.
Question 25
below show the radiographs obtained from a year old man with progressively worsening right side hip pain over the last 8 months. He is 6 feet tall, with a BMI of 51 kg/m 2 and reports that his index total hip arthroplasty was performed 8 years ago. The preoperative work-up includes negative infectious laboratory results. What is the most appropriate surgical plan for revision of the femoral component in this patient?
Explanation
Submit Answer
The patient’s radiographs demonstrate varus femoral remodeling around a broken cylindrical, distally fixed femoral stem. Proximal femoral remodeling around loose or fractured stems occurs in 21% to 42% of femoral revisions, based on the definitions outlined by Foran and associates. In definition 1, varus femoral remodeling occurs when the template falls within 2 mm of the endosteal cortex of the metaphysis on templating with a diaphyseal engaging stem. In definition 2, varus femoral remodeling = when the template crosses the lateral femoral cortex proximally. Based on the templating or drawing a line from the isthmus proximally along the lateral cortex, implantation of a straight stem would perforate the cortex proximally, indicating varus femoral remodeling. An extended trochanteric osteotomy would aid in the removal of the well-fixed distal segment and enable the safe insertion of the new femoral component. The approach is not the concern in this case, because extended trochanteric osteotomies have been described from the posterior and direct lateral approaches with excellent outcomes and union rates. The key is that the extended osteotomy is necessary and not a trochanteric slide or standard (shorter or incomplete trochanteric) osteotomy. These types would not provide access to the well-fixed distal stem, nor would they afford a straight tube in which to insert a new femoral component.
Question 26
Figures 34a through 34c show an axial proton density (spin echo long TR, short TE) image, a sagittal inversion recovery (STIR) image, and a sagittal T1-weighted (short TR, short TE) image of the left thigh. What is the most likely diagnosis?
Explanation
REFERENCE: El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 123.
Question 27
The afferent pain innervation of the L3-L4 facet joint arises from the medial branch nerve of
Explanation
REFERENCES: Nade SL, Bell E, Wyke BD: The innervation of the lumbar spinal joint and its significance. J Bone Joint Surg Br 1980;62:255-261
Kornick C, Kramarich SS, Lamer TJ, et al: Complications of lumbar facet radiofrequency denervation. Spine 2004;29:1352-1354.
Question 28
Explanation
In the context of viewing a lateral cervical spine to evaluate cranial setting, multiple lines can be used to assess anatomic relationships (i.e. McRae’s Chamberlin’s, or McGregor’s) McRae’s and Chamberlin’s use the foramen magnum as one land mark. Commonly, however, the margins of the foramen magnum are difficult to precisely identify. McGregor’s line connects the posterior margin of the hard palate to the most caudal point of the occiput and is easier to use. The tip of the odontoid should not project more than 4.5 mm above this line.
Anterior subluxation of more than 10-12 mm implies destruction of the entire ligamentous complex.
An atlantoaxial distance greater than 3.5mm is considered abnormal in an adult. The subaxial cervical spine is affected through involvement of the facets, interspinous ligaments, and intervertebral discs (spondylodiscitis). The initial site of destruction has been postulated to be through synovitis of the neurocentral joints with erosion of the adjacent disc and bone causing subluxation, or through primary facetal arthritis and ligamentous laxity causing secondary chronic discovertebraltrauma and destructive hypermobile segmentsis associated with disc destruction and toward the C2-C3 and C3-C4 segments, typically lack osteophytes, and often are at multiple levels, giving a stepladder appearance.
Question 29
A healthy, active, independent 74-year-old woman fell and sustained the elbow injury shown in Figures 41a and 41b. Management should consist of
Explanation
REFERENCES: Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intra-articular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480.
Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humerus fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
Obremskey WT, Bhandari M, Dirschl DR, et al: Internal fixation versus arthroplasty of comminuted fractures of the distal humerus. J Orthop Trauma 2003;17:463-465.
Question 30
A 70-year-old man undergoes removal of an infected total hip arthroplasty (THA) and insertion of an articulating antibiotic-loaded spacer to treat a deep periprosthetic hip infection. While in a nursing home receiving intravenous antibiotics 3 weeks after surgery, the patient trips and falls. Examination reveals swelling in the mid and distal thigh, intact skin and neurovascular structures, and severe pain with knee or hip movement. Radiographs of the femur are shown in Figures 1 through 4. What is the most appropriate treatment for the fracture below the implant?

Explanation
This patient has a type C periprosthetic femoral fracture. The articulating spacer is not involved in the fracture, which is well distal to the implant. The most appropriate treatment is open reduction and internal fixation of the fracture. Traction is not appropriate for this fracture because the injury can be treated surgically despite the history of previous hip infection. Traction would also be needed for at least 5 weeks and would delay the surgical treatment of the periprosthetic fracture until the time of second-stage revision THA. The fracture is fairly distal, and revision to a longer antibiotic-loaded implant or uncemented stem is not suitable for this fracture pattern, because it extends well past the isthmus. A femoral stem in the distal fragment would provide little stability for the fracture. Removal of the articulating spacer and reimplantation using a long-stem fluted uncemented hip replacement is not appropriate, because it would be premature to reimplant the man's hip while he is still receiving treatment for a deep hip infection.
Question 31
In the treatment of thoracic disk herniations, what approach is associated with the highest risk of iatrogenic paraplegia?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 87-96.
Stillerman CB, Chen TC, Couldwell WT, Zhang W, Weiss MH: Experience in the surgical mangement of 82 symptomatic herniated thoracic discs and review of the literature. J Neurosurg 1998;88:623-633.
Question 32
What is the typical axial plane transverse angulation of the thoracic pedicles? Review Topic
Explanation
Question 33
With comparison to a below the knee amputation, each of the following are disadvantages of a through the knee amputation EXCEPT:

Explanation
The cohort study by MacKenzie et al prospectively followed 161 patients that were part of the Lower Extremity Assessment Project (LEAP). These patients underwent an above-the-ankle amputation at a trauma center within 3 months following the injury and followed for 2 years. This study revealed that through-the-knee amputations had significantly worse scores for the objective performance measures of self-selected walking speed, independence in transfers, walking, and stair-climbing. Through-the-knee amputees also had worse SIP scores than AKA and BKA patients. Physicians were also less satisfied with both the clinical and the cosmetic recovery of the patients with a through-the-knee amputation. It should be noted that patients with a BKA had a faster walking speed than those with an AKA. Despite the worse SIP scores for through-the-knee amputations, patients actually reported less pain than those with an AKA or BKA, though this wasn't statistically significant.
(SBQ06.2) A 21-year-old male presents to the emergency department after sustaining a gun shot wound to his back. Subsequent radiographs reveal a bullet in the L2 vertebral body. Physical exam shows no neurologic deficits. He undergoes emergent laparotomy and is found to have a small bowel laceration. What would be the preferred treatment following his exploratory laparotomy and small bowel repair?

Intravenous antibiotic coverage for Gram negative bacteria for 7 days

Surgical decompression and bullet fragment removal

Observation

Broad-spectrum oral antibiotic coverage for 7 days
Broad-spectrum intravenous antibiotic coverage for 7 days
DISCUSSION: The clinical presentation is consistent with a GSW with bowel perforation and a retained bullet in the vertebral body. Because the patient is neurologically intact broad-spectrum intravenous antibiotic coverage for 7 days is the most appropriate treatment.
Gunshot wounds to the spine present relatively little risk of infection in most cases. When there has been an injury to the small bowel, the risk of infection can be minimized with a 7-day course of broad-spectrum antibiotics. Indications for surgery include when a neurological deficit is present that correlates with imaging findings of neurological compression by the missile, or when the missile is in contact with the CSF posing a risk for metal toxicity.
Roffi et al performed a Level 4 study of 42 patients that sustained a gunshot wound that perforated the stomach or bowel and then entered the spinal column. They found that an extended regimen of broad spectrum antibiotics combined with bedrest appeared to significantly reduce the risk of spinal or paraspinal infection, whereas early bullet removal did not significantly prevent the occurrence of infection.
Velmahoos et al performed a Level 4 study including 24 patients that sustained a gunshot wound to the spine with associated colonic injury. They found that the incidence of sepsis was 8.4% (compared to 5% in non-bowel injuries) and concluded that retainment of the bullet did not increase the rate of sepsis.
Incorrect Answers:
Question 34
When performing the exposure for an anterior approach to the cervical spine, the surgical dissection should not enter the plane between the trachea and the esophagus and excessive retraction should be avoided to prevent injury to the
Explanation
REFERENCES: Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Patel CK, Fischgrund JS: Complications of anterior cervical spine surgery. Instr Course Lect 2003;52:465-469.
Question 35
What factor highly correlates with poor outcomes after surgery for femoroacetabular impingement?
Explanation
Question 36
What is the most common foot and ankle deformity in patients with arthrogryposis?
Explanation
REFERENCES: Guidera KJ, Drennan JC: Foot and ankle deformities in arthrogryposis multiplex congenita. Clin Orthop 1985;194:93-98.
Handelsman JE, Badalamente MA: Neuromuscular studies in clubfoot. J Pediatr Orthop 1981;1:23-32.
Dias LS, Stern LS: Talectomy in the treatment of resistant talipes equinovarus deformity in myelomeningocele and arthrogryposis. J Pediatr Orthop 1987;7:39-41.
Question 37
Patients with patellar clunk syndrome are best managed by which of the following methods?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 329.
Diduch DR, Scuderi GR, Scott WN, et al: The efficacy of arthroscopy following total knee replacement. Arthroscopy 1997;13:166-171.
Lucas TS, DeLuca PF, Nazarian DG, et al: Arthroscopic treatment of patellar clunk. Clin Orthop 1999;367:226-229.
Question 38
During primary total knee arthroplasty, what is the maximum distance the joint line can be raised or lowered before poor motion, joint instability, and increased chance of revision occur?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 339-365.
Question 39
What is the most likely diagnosis based on the MRI findings shown in Figures 87a and 87b? Review Topic

Explanation
Question 40
Figure 19 shows the radiograph of a 12-year-old boy who sustained an injury to his hand when another child fell on him. Management should consist of
Explanation
REFERENCES: Carey TP: Fracture and dislocations of the phalanges, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 435-436.
Ogden JA: Skeletal Injury in the Child. New York, NY, Springer-Verlag, 2000, p 668.
Question 41
What is the most likely late complication associated with cementless total knee replacement?
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
Question 42
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for
Explanation
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Song KM, Sloboda JF: Acute hematogenous osteomyelitis in children. J Am Acad Orthop Surg 2001;9:166-175.
Question 43
All of the following are considered contraindications to the use of functional bracing of a humeral shaft fracture EXCEPT:

Explanation
Commonly accepted parameters for closed treatment include less than 30 degrees of varus angulation, 20 degrees of anterior/posterior angulation, and 3 cm of shortening. Operative indications are: associated vascular injuries, bilateral humeral shaft fractures, polytrauma patient (including paraplegia), segmental fractures, injury to the brachial plexus, pathological fractures, floating elbow, and floating shoulder.
The article by Rutgers and Ring found that proximal one-third oblique humeral shaft fractures had an unacceptably high 29% rate of nonunion treated with a functional brace.
The article by Sarmiento et al found a 97% rate of union, a radial nerve palsy incidence of 11%, and no contraindication to the use of functional braces in humeral shaft fractures associated with radial nerve palsy.
The review article by Defranco and Lawton states that 70% of these radial nerve injuries recover spontaneously. They note that it "seems reasonable, however, to consider surgical intervention (radial nerve exploration) between 4 and 6 months based on the patient’s clinical course."
Question 44
Rickets can be best characterized by which of the following radiographic changes in children?
Explanation
Question 45
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?
Explanation
REFERENCES: Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809.
Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Pape HC, Auf’m’Kolk M, Puffrath T, et al: Primary intramedullary femur fixation in multiple trauma patients with associated lung contusion: A cause of posttraumatic ARDS? J Trauma 1993;34:540-548.
Question 46
Figure 10 shows the MRI scan of a 56-year-old woman with metastatic breast cancer who now reports progressive paraparesis. Her general health remains good. Treatment should consist of
Explanation
REFERENCE: Fardin DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 123-133.
Question 47
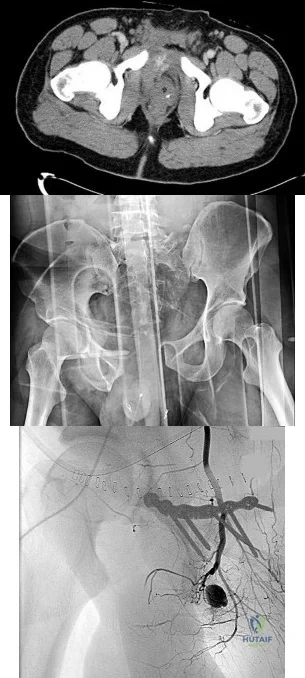
4A 4B 4C A 30-year-old man was involved in a high-speed motorcycle collision and sustained the injury shown in Figure 4a. Hypotension ensued shortly after arrival in the emergency department. Figure 4b is the initial contrast pelvic CT image with an unrecognized blush consistent with arterial bleeding. During surgical repair, the patient was noted to have active bleeding and an angiogram was obtained (Figure 4c). Which structure is the likely cause of his bleeding?
Explanation
Pelvic bleeding occurs predominantly from disruption of the posterior venous plexus and bleeding from the fractured bone. Occasionally arterial bleeding is seen, with injury to the superior gluteal artery most common. Anterior pelvic bleeding occurs from injury to the obturator artery (commonly from a pubic bone fracture laceration) and less frequently from the pudendal artery near the symphysis. The location of the bleeding on CT and angiography images does not correspond to the superior gluteal, external iliac, or femoral arteries.
RECOMMENDED READINGS
Suzuki T, Smith WR, Moore EE. Pelvic packing or angiography: competitive or complementary? Injury. 2009 Apr;40(4):343-53. Epub 2009 Mar 17. Review.PubMed PMID: 19278678. View Abstract at PubMed
Loffroy R, Yeguiayan JM, Guiu B, Cercueil JP, Krausé D. Stable fracture of the pubic rami: a rare cause of life-threatening bleeding from the inferior epigastric artery managed with transcatheter embolization. CJEM. 2008 Jul;10(4):392-5. PubMed PMID: 18652733. View Abstract at PubMed
White CE, Hsu JR, Holcomb JB. Haemodynamically unstable pelvic fractures.Injury. 2009 Oct;40(10):1023-30. Epub 2009 Apr 16. Review. PubMed PMID:19371871. View Abstract at PubMed
RESPONSES FOR QUESTIONS 5 THROUGH 8

5A

5B
- Avascular necrosis, head collapse, and screw penetration
- Fixation failure and varus collapse
- Humeral stem loosening
- Glenoid component loosening
- Hardware failure (breakage of plate or screws)
- Shoulder dislocation
Please choose from the responses to identify the most likely complication in each scenario.
Question 48
During a dual incision fasciotomy of the leg, the soleus is elevated from the tibia to allow access to which of the following compartments?

Explanation
Question 49
What is the most significant prognostic factor in nontraumatic osteonecrosis of the humeral head?
Explanation
REFERENCES: Cruess RL: Osteonecrosis of bone: Current concepts as to etiology and pathogenesis. Clin Orthop 1986;208:30-39.
Cruess RL: Steroid-induced avascular necrosis of the humeral head: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
Rutherford CS, Cofield RH: Osteonecrosis of the shoulder. Orthop Trans 1987;11:239.
Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Relationship of disease stage, extent, and cause to natural history. J Shoulder Elbow Surg 1999;8:559-564.
Question 50
A collegiate rower reports the sudden onset of right chest pain while rowing. The athlete states that the pain is worse with deep inspiration and coughing. Examination reveals localized tenderness over the posterolateral corner of the eighth rib. What is the most likely diagnosis?
Explanation
REFERENCES: Karlson KA: Rib stress fractures in elite rowers. Am J Sports Med 1998;26:516-520.
Holden DL, Jackson DW: Stress fractures of the ribs in female rowers. Am J Sports Med 1985;13:342-348.
Question 51
Assuming that the fracture shown in this radiograph (Figure 1) is aligned on the anteroposterior radiograph and heals in this position, secondary to fracture malalignment, there will be loss of active

Explanation
This is a transverse proximal phalanx fracture with apex volar angulation. The fracture displaces into an apex volar angulated position under the pull of the central slip on the distal fragment and the interossei insertions at the base of proximal phalanx. Although it is possible to lose motion in flexion or extension of the MP or PIP joints, the biomechanics will not allow full extension of the PIP joint. If allowed to heal in apex palmar malunion, the predicted corresponding extensor lags are for a 10-degree lag at 16 degrees of angular deformity, a 24-degree lag at 27 degrees of deformity, and a 66-degree lag at 46 degrees of deformity. These fractures usually can be treated with closed reduction with or without percutaneous pinning. With surgical treatment, there may be loss of motion both at the MP and PIP joints.
Question 52
Denosumab, a monoclonal antibody used to treat osteoporosis, works through inhibition of
Explanation
Question 53
A B C Figures 89a through 89c are the radiographs of a 35-year-old woman who has had 7 years of progressive ankle pain. She experiences stiffness and pain despite the use of an ankle-foot orthosis. Examination reveals pain along the anterior tibiotalar joint without tenderness to the subtalar or talonavicular joints. What is the most appropriate surgical intervention?

Explanation
This patient has isolated posttraumatic ankle arthritis with significantly decreased ankle range of motion that is best treated with an isolated ankle arthrodesis to eliminate pain. Because this patient is younger than 50 years of age and has limited presurgical range of motion, she is not a candidate for ankle arthroplasty. Additionally, TAA outcomes among patients who have a posttraumatic etiology are worse than for those with osteoarthritis. Tibiotalocalcaneal arthrodesis is suited for patients with associated subtalar
arthritis or rigid hindfoot deformity that necessitates correction. Anterior tibial exostectomy will not resolve the underlying arthritic pain and is not indicated.
RECOMMENDED READINGS
Easley ME, Adams SB Jr, Hembree WC, DeOrio JK. Results of total ankle arthroplasty. J Bone Joint Surg Am. 2011 Aug 3;93(15):1455-68. doi: 10.2106/JBJS.J.00126. Review. PubMed PMID: 21915552. View Abstract at PubMed
Spirt AA, Assal M, Hansen ST Jr. Complications and failure after total ankle arthroplasty. J Bone Joint Surg Am. 2004 Jun;86-A(6):1172-8. PubMed PMID: 15173289. View Abstract at PubMed
Ajis A, Henriquez H, Myerson M. Postoperative range of motion trends following total ankle arthroplasty. Foot Ankle Int. 2013 May;34(5):645-56. doi: 10.1177/1071100713481433. Epub 2013 Mar 11. PubMed PMID: 23478890. View Abstract at PubMed
Thomas R, Daniels TR, Parker K. Gait analysis and functional outcomes following ankle arthrodesis for isolated ankle arthritis. J Bone Joint Surg Am. 2006 Mar;88(3):526-35. PubMed PMID: 16510818. View Abstract at PubMed
Coester LM, Saltzman CL, Leupold J, Pontarelli W. Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am. 2001 Feb;83-A(2):219-28. PubMed PMID: 11216683. View Abstract at PubMed
Question 54
A B C Figures 30a through 30c are the radiograph and MR images of a 54-year-old woman who has severe leg pain with walking. Her treatment has included 12 weeks of physical therapy, anti-inflammatory medications, and narcotic pain relievers, and she is interested in surgery. Minimally invasive transforaminal lumbar interbody fusion (MIS TLIF) is recommended. When compared with open TLIF, MIS TLIF is associated with

Explanation
MIS TLIF involves a steep learning curve but is associated with similar longterm outcomes as open TLIF, arguably comparable or possibly lower complication rates, and equivalent fusion rates. The major distinguishing feature comparing open to minimally invasive surgery for this and other spinal diagnoses has been shorter hospital stays.
RECOMMENDED READINGS
Peng CW, Yue WM, Poh SY, Yeo W, Tan SB. Clinical and radiological outcomes of minimally invasive versus open transforaminal lumbar interbody fusion. Spine (Phila Pa 1976). 2009 Jun 1;34(13):1385-9. doi: 10.1097/BRS.0b013e3181a4e3be. PubMed PMID: 19478658. View
Abstract at PubMed
Lee KH, Yue WM, Yeo W, Soeharno H, Tan SB. Clinical and radiological outcomes of open versus minimally invasive transforaminal lumbar interbody fusion. Eur Spine J. 2012 Nov;21(11):2265-70. doi: 10.1007/s00586-012-2281-4. Epub 2012 Mar 28. PubMed PMID:
Question 55
What muscle is most often encountered during surgical approaches to C5-6?
Explanation
REFERENCES: Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-56.
Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.
Question 56
- A 23 year old man has a minimally comminuted midshaft fracture of the femur with 2cm entrance and exit wounds as a result of a low-velocity gunshot. Definitive management should be
Explanation
Question 57
Figure A is an AP radiograph of a 68-year-old man who presents to clinic with shoulder pain and dysfunction. On examination of his shoulder, he has pseudoparalysis with attempt at forward elevation and a positive hornblower's sign while demonstrating normal belly press test. Treatment should consist of: Review Topic

Explanation
RTSA can improve pain and function in shoulders with forward elevation pseudoparalysis secondary to rotator cuff tear arthropathy. Following arthroplasty, the deltoid alone can restore overhead elevation but it does not address active external rotation deficit. LDT is a well described procedure for treatment of irreparable posterosuperior rotator cuff tear. Combining RTSA and LDT can address both deficits and in select patients yields significant pain relief and restoration of function.
Walch et al found that hornblower's sign had 100% sensitivity and 93% specificity for irreparable degeneration of teres minor.
Puskas et al present clinical outcomes of RTSA combined with LDT for treatment of chronic combined pseudoparesis of elevation and external rotation of the shoulder in 40 patients. At a mean follow-up of 53 months, the author report excellent clinical outcomes.
Figure A demonstrates a proximal migration of the humerus resulting in femoralization of the humeral head and acetabularization of the acromion from a massive rotator cuff tear.
Incorrect answers:
Question 58
An acute posterolateral disk herniation at the L4-5 level will most likely affect what nerve root? Review Topic
Explanation
Question 59
An otherwise healthy 35-year-old woman reports dorsal wrist pain and has trouble extending her thumb after sustaining a minimally displaced fracture of the distal radius 3 months ago. What is the next most appropriate step in management?
Explanation
REFERENCES: Christophe K: Rupture of the extensor pollicis longus tendon following Colles fracture. J Bone Joint Surg Am 1953;35:1003-1005.
Hove LM: Delayed rupture of the thumb extensor tendon: A 5-year study of 18 consecutive cases. Acta Orthop Scand 1994;65:199-203.
Question 60
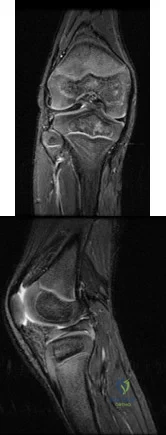
Figures 10a and 10b are the sagittal and coronal MRI scans of a 5-year-old boy who noticed “clicking” in his right knee. His family denied any trauma, but admitted that the child was active and fell frequently. Birth and developmental history were unremarkable, and specifically negative for other musculoskeletal conditions. On physical examination, there was no warmth, tenderness, or erythema, or effusion. The child had an audible and palpable clunk when the knee was taken from a position of extreme flexion to full extension. There was no anterior, posterior, medial, or lateral instability on examination or medial or lateral joint line tenderness. The child had not been systemically ill. Radiographs were unrevealing. What is the most likely diagnosis? Review Topic
Explanation
Question 61
After making a tackle, a football player is found prone and unconscious without spontaneous respirations. Initial management should consist of
Explanation
REFERENCES: McSwain NE, Garnelli, RL: Helmet removal from injured patients. Bull of Am Coll Surg 1997;82:42-44.
Vegso JJ: Field evaluation and management of head and neck injuries. Post Grad Adv Sport Med 1987;10:2-10.
Question 62
Figure 26 shows the radiograph of an otherwise healthy Caucasian 5-year-old boy who has a painless limp. What is the best treatment option?
Explanation
REFERENCES: Herring JA, Kim HT, Browne R: Legg-Calve-Perthes disease: Prospective multicenter study of the effect of treatment on outcome. J Bone Joint Surg Am 2004;86:2121-2134.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 691-704.
Question 63
Figure 42 is a transverse MRI scan of the left shoulder. The arrow points to which of the following structures?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 234.
Question 64
A 44-year-old man reports persistent left leg pain following a L5-S1 hemilaminotomy and partial diskectomy. Examination shows a grade 4 weakness of the left extensor hallucis longus and a positive left straight leg raise. A radiograph is shown in Figure 1a, and sagittal and axial MRI scans are shown in Figures 1b and 1c. Nonsurgical management consisting of medication, physical therapy, and injections has failed to provide relief. Surgical management should consist of Review Topic
Explanation
Question 65
Figure 26 is the radiograph of a 33-year-old woman who was involved in a high-speed motor vehicle crash. Her initial blood pressure is 80/50 mm Hg and she has a pulse rate of 120 bpm. After hemodynamic stabilization and temporizing measures have been performed, the patient is cleared for surgery. What is the most appropriate method of definitive fixation?

Explanation
Question 66
New computer scanning technology for socket design has achieved which of the following improvements in amputee care?
Explanation
Question 67
Which of the following are considered appropriate nonsurgical bracing/orthotic options for a supple adult-acquired flatfoot deformity with forefoot abduction, secondary to posterior tibial tendon insufficiency?
Explanation
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Imhauser CW, Abidi NA, Frankel DZ, et al: Biomechanical evaluation of the efficacy of external stabilizers in conservative treatment of acquired flat foot deformity. Foot Ankle Int 2002;23:727-737.
Question 68
A 16-year-old girl has had anterior leg pain and a mass for the past 8 months. Figures 2a and 2b show a radiograph and an H & E histologic specimen. Which of the following disorders is believed to be a precursor of this lesion?
Explanation
REFERENCE: Springfield DS, Rosenberg AE, Mankin HJ, et al: Relationship between osteofibrous dysplasia and adamantinoma. Clin Orthop 1994;309:234-244.
Question 69
Figure 1 shows a patient with an open tibia fracture who presents to the emergency department after a propeller injury in brackish water (river water and sea water). What is the most appropriate antibiotic coverage for this patient?

Explanation
soil-borne pathogens (clostridial species). Vancomycin is not indicated for coverage in marine environments, rather it is more commonly used for populations with a high prevalence of nosocomial infections. Sulfamethoxazole-trimethoprim is not used for open fracture coverage.
Question 70
A 38-year-old man sustains a complete avulsion with retraction of the ischial attachment of the hamstring muscles in a fall while water skiing. He indicates that he is an aggressive athlete who participates regularly in multiple running and cutting-type sports, and he strongly desires to continue his athletic competition. Management should consist of
Explanation
REFERENCES: Orava S, Kujala UM: Rupture of the ischial origin of the hamstring muscles. Am J Sports Med 1995;23:702-705.
Clanton TO, Coupe KJ: Hamstring strains in the athlete: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:237-248.
Question 71
Sciatic nerve
Explanation
The principal thrombogenic stimulus leading to the production of venous thromboembolic disease during total hip arthroplasty occurs at which time:
Question 72
Which of the following medications inhibits release of neurotransmitters by binding to presynaptic calcium channels?
Explanation
Gabapentin (also known as Neurontin) is a medication that is commonly used to treat neuropathic pain. It acts by binding the alpha2delta subunit of voltage-dependent calcium channels on the presynaptic membrane. This serves to increase GABA synthesis, as well as inhibit the release of excitatory neurotransmitters. These neurotransmitters are believed to be part of the pathway leading to neuropathic pain.
Bennett et al. provide a review of the pharmacology of gabapentin for the use of neuropathic pain. They note effective antihyperalgesic and antiallodynic properties of gabapentin but not significant anti-nociceptive action. Among patients with neuropathic pain they found an average pain score reduction of 2.05 points on an 11 point Likert scale, which compared favorably to placebo.
Mehta et al. explored outcomes of gabapentin and pregabalin (Lyrica) for use in patients with spinal cord injury. Both agents were found to decrease pain and secondary conditions such as sleep disturbance. They did not directly compare these agents to other analgesic medications.
Guy et al. present a meta-analysis of the use of anticonvulsants (such as gabapentin) to treat pain in patients with spinal cord injury. Large effect size was seen in 4 of 6 studies looking at the effectiveness of gabapentin.
Illustration A show the mechanism of currently available antiepileptic drugs (AEDs) that target several molecules at the excitatory synapse. Gabapentin and pregabalin bind to the a2d subunit of voltage-gated Ca2+ channels, which is thought to be associated with a decrease in neurotransmitter release.
Incorrect Answers
Question 73
Figure 36a shows the current radiograph of a 65-year-old woman who slipped and fell. History reveals that prior to the fall she was actively functioning without pain. Figure 36b shows a radiograph obtained 1 year ago. Based on the fracture pattern, the failure is most likely related to
Explanation
REFERENCES: Johansson JE, McBroom R, Barrington TW, Hunter GA: Fracture of the ipsilateral femur in patients with total hip replacement. J Bone Joint Surg Am 1981;63:1435-1442.
Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242.
Question 74
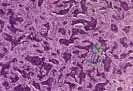
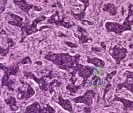
Chondrosarcoma The plain radiographs show a purely lytic destructive lesion that is poorly marginated. The technetium bone scan does not show any major uptake. The computerized tomography scan shows purely lytic bone destruction with breakthrough of the cortical bone. Complete destruction of the cortical bone is suggestive of a malignancy. The magnetic resonance image shows a lesion that is homogenously low on T1-weighted images and high on T2-weighted images. Surgeons cannot make a definitive diagnosis based upon the radiographic features. The most common malignancies in this age group are:
Explanation
Slide 5 Slide 6
A 50-year-old woman has had severe hip pain for 4 months. Her plain radiographs (Slide 1), technetium bone scan (Slide 2), computerized tomography scan (Slide 3), and coronal T1- and T2-weighted magnetic resonance images (Slide 4) are presented. A needle biopsy is also performed (Slides 5 and 6). Which of the following treatment regimens would be the most appropriate:
Question 75
Figure 3a is the initial radiograph of a 19-year-old man who sustained a closed clavicle fracture. Figures 3b and 3c show postoperative radiographs. If the patient had been treated nonsurgically, which of the following would most likely occur?
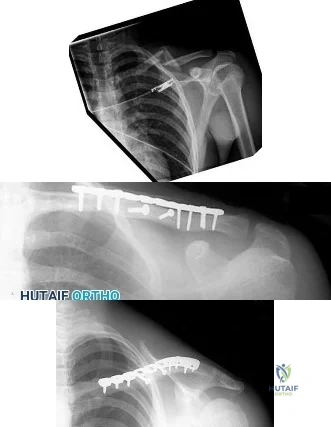
Explanation
Question 76
A 70-year-old woman with a body mass index (BMI) of 34 and a history of hypercholesterolemia has elected to undergo total hip arthroplasty. Her son recently learned he has factor V Leiden following an episode of pulmonary embolism. What are this patient's risk factors for thromboembolic disease?
Explanation
Risk stratification is one of the most critical clinical evaluations to undertake before performing total joint arthroplasty. Many factors have been identified that increase the risk for venous thromboembolism (VTE) The major factors include previous VTE, obesity, type of surgery (such as total joint arthroplasty), hypercoagulable states, myocardial infarction, congestive heart failure, family history of VTE, and hormone replacement therapy. Hypercholesterolemia is not a risk factor for thromboembolic disease.
Question 77
A high school football player asks you about an oral supplement that increases body mass and improves sprint times. He would like to use it to improve performance. What is the most likely agent? Review Topic
Explanation
Question 78
A radiologist's report of a lateral knee radiograph comments that the height of the patella is 4 cm, and the length of the patellar tendon is 3 cm. Which of the following may lead to this measurement? Review Topic
Explanation
The measurements described allow you measure an Insall-Salvati Index (ISI). The ISI is the ratio of the patellar tendon length to the patellar height (distance from the superior pole to the inferior pole). These measurements give a ratio of 0.75 which indicates the presence of patella baja. Normal values range from 0.8 to 1.2. A lower ratio is diagnostic of patella baja, while a higher ratio is diagnostic of patella alta. The ISI as well as some other measures of the patella's position within the trochlea are important when evaluating conditions such as patellar instability or patellofemoral
pain.
Insall and Salvati present their original paper describing the anatomy of the knee with respect to patellar positioning. They note that previous methods of determining patellar positioning was either too complicated, or too subjective. They found the length of the patellar tendon and the height of the patella to be approximately equal, and saw no variations greater than 20%. Thus they proposed the ISI with "normal" values ranging from 0.8 to 1.2.
Shabshin et al. present a study making similar calculations as the ISI but done on sagittal MRI rather than lateral radiographs. They found a slightly higher degree of variation, and defined "normal" as ranging from 0.79 to 1.52. They also noted females tended to have higher ratios on average compared to males.
Aglietti et al. compared various measurements of the patellofemoral joint in a group of asymptomatic knees compared to knees with recurrent patellar subluxation. The normal knees were found to have an ISI of about 1, average congruence angle of -8, and an average Q angle of 15°. The subluxating knees had higher ISIs (average 1.23), higher congruence angles (average +16), and a higher Q angles (average 20°).
Illustration A shows how to measure and calculate the ISI. Illustration B shows measurements of the patellofemoral joint that may help identify presence of trochlear dysplasia and patellar maltracking.
Incorrect Answers:
Question 79
A patient undergoes excision of a 3- x 3-cm soft-tissue sarcoma. The final histology results show tumor at the surgical margin. The surgical procedure performed is classified as
Explanation
REFERENCE: Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980;153:106-120.
Question 80
A 5-year-old boy reports intermittent left elbow pain. History reveals that he injured his elbow 4 months ago, but had no treatment. He is now using his arm normally but reports pain almost daily. Examination reveals tenderness over the lateral epicondyle and a prominence is evident. Range of motion is from -5 degrees to 120 degrees. Radiographs are shown in Figure 67. Management should include
Explanation
REFERENCES: Wattenbarger JM, Gerardi J, Johnson CE: Late open reduction internal fixation of lateral condyle fractures. J Pediatr Orthop 2002;223:94-398.
Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Question 81
A 72-year-old woman is scheduled to undergo right total hip arthroplasty. Her preoperative radiograph is shown in Figure below. To avoid increasing this patient’s combined offset while maintaining her leg length, what is the most appropriate surgical plan?

Explanation
The management of patients with proximal femoral deformity can be difficult. Appropriate implant selection and preoperative templating are critical. In this patient, it would be difficult to avoid increasing the combined offset by too much, which could contribute to the overtensioning of the soft tissues and trochanteric pain. By medializing the acetabular component (decreasing the combined offset), using a low offset femoral component or a cemented component placed more valgus (decreasing the combined offset), and making a longer neck cut (to avoid shortening of the lower extremity), restoration of the patient’s native offset and leg length can be achieved.
Question 82
An active, right-handed 71-year-old woman fell on her left shoulder and sustained the injury shown in the radiographs in 52a and 52b and the CT scan in 52c. Management should consist of
Explanation

Question 83
A 55-year-old woman with type I diabetes mellitus has a chronic ulcer over the dorsum of her right foot and reports forefoot pain. Examination reveals 1- x 2-cm nondraining ulcer over the dorsum of the foot. The patient has 1-2+ pain with compression of the foot and ankle. She has a weakly palpable posterior tibial pulse and an absent dorsalis pedis pulse. There is no erythema, cellulitis, or drainage. Radiographs are normal. Which of the following diagnostic studies should be obtained?
Explanation
REFERENCES: Wagner FW Jr: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981;2:64-122.
Apelqvist J, Castenfors J, Larson J, Stenstrom A, Agardh CD: Prognostic value of systolic ankle and toe blood pressure levels in outcome of diabetic foot ulcer. Diabetes Care 1989;12:373-378.
Question 84
Following application of topical lidocaine, copious arterial bleeding is noted from the region of 1 neurovascular bundle, and the digit remains cool and pale. What is the best next step?
Explanation
DISCUSSION
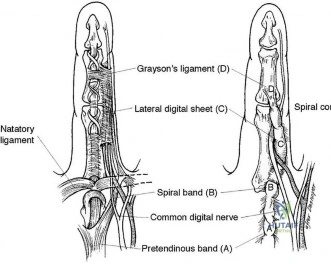
Used with permission from Benson LS, Williams CS, Kahle M. Dupuytren’s contracture. J Am Acad Surg. 1998
Jan-Feb;6(1):24-35. Review
The spiral cord seen in Dupuytren disease arises from the confluence of abnormal fascial thickening of the spiral bands, lateral digital sheet, and Grayson’s ligament. The orientation of these contributing structures results in a continuous band of fibrous tissue spiraling around the neurovascular bundle. As the developing spiral cord contractures from distal to proximal, the cord itself becomes increasingly linear and shorter, causing displacement of the neurovascular bundle both centrally and superficially. This displacement of the neurovascular bundle brings it closer to the skin and midline, making it more vulnerable to surgical trauma.
Studies have demonstrated a high association between a PIP joint flexion contracture and a spiral cord (Figure 52). Spiral cords are also seen in association with a soft, fleshy mass between the proximal digital flexion crease and distal palmar crease in the interdigital space referred to as an interdigital soft-tissue mass. This represents displacement of normal subcutaneous tissues by contracture of the diseased fascia associated with the spiral cord. Dupuytren diathesis, MCP joint contracture, and the presence of knuckle pads are not indicative of a spiral cord.
A complication following surgical treatment of Dupuytren contracture is trauma to the neurovascular bundle. This can be a consequence of blunt or sharp trauma. In the case of traumatic stretch injury from retraction, vasospasm may develop. The treatment of vasospasm includes flexion, warming the digit, and application of topical medication to treat vasospasm. Allowing the newly extended digit to flex is an important first step, particularly in the case of chronic and severe PIP joint contractures. In these cases, the vessel may have shortened over time, and full extension may cause intimal trauma and secondary vasospasm. Cold is also a stimulus for reactive vasospasm, so warming the digit with warm saline irrigation can be helpful. Finally, topically applied lidocaine (without vasoconstrictive additives) can help diminish vasospasm and lead to digital reperfusion. Phentolamine is useful in cases of prolonged vasospasm secondary to administration of anesthetics containing epinephrine. Streptokinase is a thrombolytic agent that may be useful in treatment of embolic or thrombotic vascular disease. Systemic heparin is useful for digital vessel repair but should not be necessary to treat simple vasospasm.
Copious bleeding in the region of the neurovascular bundle following palmar fasciectomy is an indication of potential arterial trauma. In the setting of arterial laceration, direct repair is necessary, particularly when the digit is dysvascular. This means that both digital vessels are involved or that the intact vessel is insufficient to adequately perfuse the digit. During surgery, the vessels can be directly visualized, and arteriography is unlikely to add additional information of value. Streptokinase is not indicated in this situation because it is useful for thrombolysis rather than vascular repair. Ligation of a traumatized digital artery might be appropriate for a digit that is otherwise well perfused; however, this is not appropriate in the setting of a dysvascular digit. Direct suture of the arterial laceration or segmental grafting necessary to restore adequate digital perfusion in this scenario.
RECOMMENDED READINGS
Rayan GM. Dupuytren disease: Anatomy, pathology, presentation, and treatment. J Bone Joint Surg Am. 2007 Jan;89(1):189-98. Review. PubMed PMID: 17256226. View Abstract at PubMed
Watson HK, Paul H Jr. Pathologic anatomy. Hand Clin. 1991 Nov;7(4):661-8. Review. PubMed PMID: 1769988. View Abstract at PubMed
Jones NF, Huang JI. Emergency microsurgical revascularization for critical ischemia during surgery for Dupuytren's contracture: a case report. J Hand Surg Am. 2001 Nov;26(6):1125-8. PubMed PMID: 11721263. View Abstract at PubMed
Question 85
A 23-year-old woman falls from a bicycle and sustains a right knee injury. Figures 12a through 12d show radiographs and MRI scans of the knee. What is the most likely diagnosis?
Explanation
REFERENCES: Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
Wiss DA, Watson JT: Fractures of the tibial plateau, in Rockwood CA, Green DP, Bucholz RW, et al (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott-Raven, 1996, pp 1920-1953.
Lubowitz JH, Elson WS, Guttmann D: Arthroscopic treatment of tibial plateau fractures: Intercondylar eminence avulsion fractures. Arthroscopy 2005;21:86-92.
Question 86
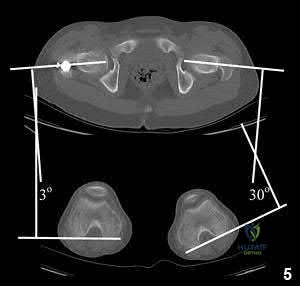
A 55-year-old male is involved in a motorcycle crash and sustains a closed, right-sided, midshaft femur fracture. This is an isolated injury. He is treated with retrograde femoral nailing, and postoperatively is noted to have 30 degrees of internal rotation of the operative extremity, when compared with his nonsurgical side. Which of the following is the most likely cause of this malrotation deformity?
Explanation
Postsurgical internal malrotation after treatment for a diaphyseal femur fracture typically occurs either via internal rotation of the distal segment relative to the proximal or external rotation of the proximal segment relative to the distal. These clinical findings are consistent with an iatrogenic increase in femoral anteversion.
Dimitriou et al. performed a study to quantify the side-to-side anatomic variation in the proximal femur and the implications for preoperative planning and leg length discrepancy following hip arthroplasty. CT-based 3D femoral models were reconstructed for 122 paired femurs in 61 young healthy subjects with no history of hip pathology. Significant side-to-side differences were found in femoral anteversion, horizontal offset, and femoral head center location.
They concluded that relying on the anatomic landmarks of the contralateral femur during hip arthroplasty may not necessarily result in restoration of native anatomy and leg-length.
Karaman et al. conducted a study which saught to clarify the influence of a femoral rotational malalignment of ≥10° after intramedullary nailing on daily activities. They evaluated twenty-four femoral shaft fracture patients treated with closed antegrade IMN, and determined the presence of malrotation with post-operative CT scans. Ten of the 24 patients had a CT-detected true rotational malalignment of ≥10° compared with the unaffected side, and were noted to have significantly worse functional outcome scores compared with normally rotated femoral shaft patients.
Espinoza et al. present a technique using intraoperative fluoroscopy and the anteversion inherent to the IM nail for obtaining appropriate femoral rotational alignment during surgery. The authors state that their technique reliably sets the femoral anteversion within a normal physiologic range with minimal additional intraoperative steps and without preoperative measurements.
Illustration A shows a CT evaluation of femoral malrotation. The angle on the uninjured side measures 30°, while the malrotated fractured side measures only 3°, indicating a 27° external rotation deformity.
Incorrect Answers:
OrthoCash 2020
Question 87
04 A pt wishes to return to driving after undergoing surgery for a displaced fibular fracture of the right ankle. A return to nml braking
Explanation
A computerized driving simulator was developed andtested. Eleven healthy volunteers were tested once to establishnormal mean values (Group I), and a group of thirty-one volunteerswith a fracture of the right ankle were tested at six, nine,and twelve weeks following operative repair (Group II). Thesubjects were tested with a series of driving scenarios (city,suburban, and highway). Scores on the Short Form MusculoskeletalAssessment were recorded at six, nine, and twelve weeks andwere compared with the results of the driving test. The effect of the time of the visit and of the testing conditionon the braking times was investigated.
Conclusion: By nine weeks, the total braking time of patientswho have undergone fixation of a displaced right ankle fracturereturns to the normal, baseline value
Question 88
In the preoperative planning of revision acetabular reconstruction, the surgeon should identify significant posterior column deficiency by noting which of the following radiographic features?
Explanation
REFERENCES: Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Campbell DG, Masri BA, Garbuz DS, Duncan CP: Acetabular bone loss during revision total hip replacement: Preoperative investigation and planning, in Zuckerman J (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 43-56.
Question 89
Which of the following statements best describes labral tears in the hip? Review Topic
Explanation
Question 90
When harvesting iliac crest bone graft during a posterior spinal decompression and fusion, injury to what structure can result in painful neuromas or numbness over the skin of the buttocks?
Explanation
REFERENCES: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and Wilkins 1998, pp 770-773.
Kurz LT, Garfin SR, Booth RE Jr: Harvesting autogenous iliac bone grafts: A review of complications and techniques. Spine 1989;14:1324-1331.
Mrazik J, Amato C, Leban S, et al: The ilium as a source of autogenous bone grafting: Clinical considerations. J Oral Surg 1980;38:29-32.
Question 91
A 22-year-old patient has had severe groin pain for many months and is unable to engage in any physical activity. The AP radiograph of the pelvis shows minimal arthritis. The lateral radiograph of the hip is shown in Figure 33a. An MR-arthrogram is shown in Figure 33b. What is the most appropriate treatment at this stage? Review Topic

Explanation
Question 92
A 68-year-old woman underwent an uncemented medial/lateral tapered femoral placement during a total hip arthroplasty. The orthopaedic surgeon noticed a nondisplaced vertical fracture in the calcar region of the femoral neck during final implant insertion. What is the most appropriate treatment?
Explanation
The recognized treatment for a proximal periprosthetic fracture is to first identify the extent and then optimize the correction of the fracture. Several studies indicate that proximal cerclage wiring is adequate to create "barrel hoop" stability of the proximal femur. Braided cables offer superior stability compared with twisted wires or Luque wires. Finally, the appropriate postoperative treatment is protected
weight bearing for 6 weeks, with periodic radiographs taken at 2-week intervals. Other options such as
cementing the femoral stem and using a revision arthroplasty device are indicated for unstable fractures.
Question 93
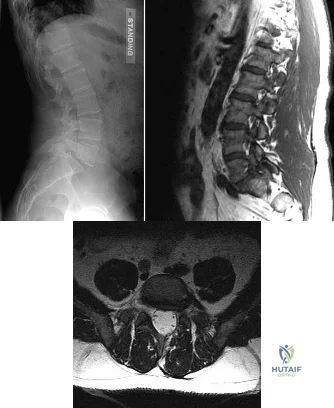
Figures 42a through 42c show the MRI scans of a 56-year-old woman with progressively worsening low back and bilateral lower extremity pain. Based on these images, what muscle or muscle group would be expected to be weak on physical examination? Review Topic

Explanation
with L5-S1 spondylolisthesis. Many patients with spondylolisthesis report hamstring tightness; however, these structures are not usually weak. Quadriceps and tibialis anterior weakness is seen with L4 nerve root irritation. The gastrocnemius is generally weak in S1 nerve root syndromes.
Question 94
The implant shown in Figures 47a and 47b is introduced submuscularly employing a minimally invasive technique. A percutaneous method of screw insertion is used distally. What nerve is most at risk?

Explanation
Question 95
A 58-year-old woman is seen in the emergency department after falling at home. History reveals that she underwent right total knee arthroplasty 2 years ago. Radiographs are shown in Figures 56a and 56b. What is the most appropriate treatment?
Explanation
REFERENCES: Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209.
Raab GE, Davis CM III: Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty 2005;20:984-989.
Tharani R, Nakasone C, Vince KG: Periprosthetic fractures after total knee arhtroplasty.
J Arthroplasty 2005;20:27-32.
Question 96
Mirror therapy is indicated for which of the following clinical conditions?
Explanation
Under mirror therapy, a patient is allowed to feel the imaginary movement of the removed body part behaving as normal body movement through a mirror. The mirror
image of the normal body part helps reorganize and integrate the mismatch between proprioception and visual feedback of the amputated segment.
Tilak et al. performed a randomized controlled trial of 26 patients with phantom limb pain, and found that mirror therapy as well as transcutaneous electrical nerve stimulation both significantly improved pain scores, but no difference was seen between the two groups. They recommend use of both modalities in treatment of phantom limb pain, as they are noninvasive and inexpensive.
Chan et al. reviewed 22 patients utilizing mirror therapy for amputation related phantom limb pain, and found that patients reported a significant decrease in pain when utilizing this treatment modality as compared to covered mirror therapy or mental imagery therapy.
Illustration A shows a patient with an upper extremity amputation using a mirror to perform movements during a mirror therapy session.
Incorrect Answers:
Question 97
A 66-year-old woman was a restrained passenger in an automobile accident. She sustained a direct blow to her nondominant left hand as the airbag in her automobile deployed and she now reports pain, swelling, and difficulty moving her fingers. Radiographs are shown in Figures 58a and 58b. Appropriate definitive treatment should consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 286.
Faraj AA, Davis TR: Percutaneous intramedullary fixation of metacarpal shaft fractures. J Hand Surg Br 1999;24:76-79.
Question 98
-What is the most common impediment to successful closed reduction of the injury seen in Figures 9aand 9b?

Explanation

Question 99
Endurance training stimulates which of the following physiologic adaptations in the athlete? Review Topic
Explanation
Question 100
Which of the following is most associated with local recurrence of the lesion seen in the radiograph and MRI scan shown in Figures 27a and 27b?
Explanation
REFERENCES: Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
Vergel De Dios AM, Bond JR, Shives TC, et al: Aneurysmal bone cyst: A clinicopathologic study of 238 cases. Cancer 1992;69:2921-2931.
