Orthopedic Board Prep MCQs: Elbow, Fracture & Nerve | OITE & ABOS Part 218

Key Takeaway
This page offers a professional medical board review quiz, Part 218, for orthopedic surgeons preparing for AAOS and ABOS board certification exams. It contains 100 high-yield, verified MCQs in OITE/AAOS format, focusing on Elbow, Fracture, and Nerve topics. Designed to simulate the real exam for optimal preparation.
About This Board Review Set
This is Part 218 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 218
This module focuses heavily on: Elbow, Fracture, Nerve.
Sample Questions from This Set
Sample Question 1: A 72-year-old female presents to the office 5 weeks after distal radius fracture surgery with the findings seen in Figure A. She performed daily cleansingwith soap and water and dry dressings. Which of the following has been shown to decrea...
Sample Question 2: An acute posterolateral disk herniation at the L4-5 level will most likely affect what nerve root? Review Topic...
Sample Question 3: Failure of high tibial osteotomy (HTO) is most closely associated with which of the following factors?...
Sample Question 4: Closed chain kinetic exercises are differentiated from open chain exercises by which of the following? Review Topic...
Sample Question 5: View Abstract at PubMedFigures 87a and 87b are sagittal and coronal MR images of the affected elbow of a 36-year-old man who has a history of painful mechanical symptoms in his dominant arm when extending his elbow in full supination. What ...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 72-year-old female presents to the office 5 weeks after distal radius fracture surgery with the findings seen in Figure A. She performed daily cleansing with soap and water and dry dressings. Which of the following has been shown to decrease the risk of developing this complication?

Explanation
The risks of external fixation include cellulitis, pin-track drainage, osteomyelitis and pin loosening. The rate of complications is about 20%. Chlorhexidine gluconate has broad spectrum activity against gram-positive and negative bacteria by disrupting cell membranes. It is not affected by blood and has low skin irritancy. Studies show that simple pin-site care (showers, dry dressings) maintains a low infection rate.
Egol et al. performed a randomized trial examining external fixation pin tracts about the wrist. They compared (1) weekly dry dressings, (2) daily pin care with half normal saline (NS) and hydrogen peroxide (H2O2) and (3) chlorhexidine discs with weekly changes. They found pin-site complications in 19%, with no difference between the 3 groups. They do not recommend additional wound care beyond sterile dressings.
Stinner et al. performed a survey on the use of half-pins by the limb lengthening and reconstruction society. They found that most respondents preferred hydroxyapatite coating (81%) because of improved fixation and decreased loosening (less radiographic pin-tract rarefaction and greater extraction torque, which may lead to
lower infection rates). Most encouraged shower (60%) and washing solution (67%)(soap and water, peroxide or saline) for pin site care.
Figure A shows an external fixator around the wrist with cellulitis around the proximal half-pins.
Incorrect Answers
Question 2
An acute posterolateral disk herniation at the L4-5 level will most likely affect what nerve root? Review Topic
Explanation
Question 3
Failure of high tibial osteotomy (HTO) is most closely associated with which of the following factors?
Explanation
with HTO.
REFERENCES: Naudie D, Borne RB, Rorabeck CH, Bourne TJ: Survivorship of the high tibial valgus osteotomy: A 10- to 22-year followup study. Clin Orthop 1999;367:18-27.
Rinonapoli E, Mancini GB, Corvaglia A, Musiello S: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Coventry MB, Ilstrup DM, Wallrichs SL: Proximal tibial osteotomy: A critical long-term study of eighty-seven cases. J Bone Joint Surg Am 1993;75:196-201.
Question 4
Closed chain kinetic exercises are differentiated from open chain exercises by which of the following? Review Topic
Explanation
Question 5
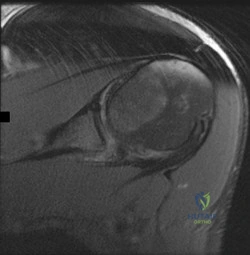
View Abstract at PubMed Figures 87a and 87b are sagittal and coronal MR images of the affected elbow of a 36-year-old man who has a history of painful mechanical symptoms in his dominant arm when extending his elbow in full supination. What is the most likely cause of his painful snapping? A B

Explanation
The MRI studies show a radiocapitellar plica. This anomalous structure has been associated with symptomatic snapping. Lacertus fibrosis contracture will not cause painful snapping. An intra-articular pathology such as loose bodies is not present on these imaging studies. Olecranon fossa impingement causes posterior pain in extension and is not shown in the images.
RECOMMENDED READINGS
Antuna SA, O'Driscoll SW. Snapping plicae associated with radiocapitellar chondromalacia. Arthroscopy. 2001 May;17(5):491-5. PubMed 11337715. View Abstract at PubMed
Ruch DS, Papadonikolakis A, Campolattaro RM. The posterolateral plica: a cause of refractory lateral elbow pain. J Shoulder Elbow Surg. 2006 May-Jun;15(3):367-70. PubMed PMID: 16679240. View Abstract at PubMed
Question 6
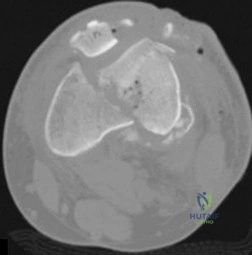
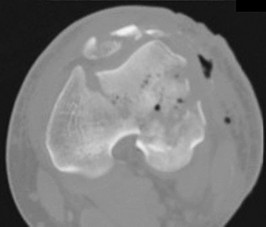
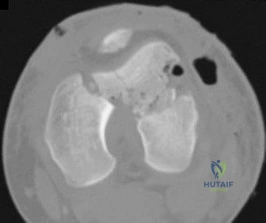
A 21-year-old man has mild but persistent aching pain in his left proximal thigh during impact loading activities. He denies pain at rest and has no other symptoms. Figures 34a through 34e show the radiographs and T1-weighted, T2-weighted, and gadolinium MRI scans of the left hip. What is the most likely diagnosis?
Explanation
REFERENCES: Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
May DA, Good RB, Smith DK, et al: MR imaging of musculoskeletal tumors and tumor mimickers with intravenous gadolinium: Experience with 242 patients. Skeletal Radiol 1997;26:2-15.
Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 4023-4034.
Question 7
This condition is most prevalent in people of which ancestry?
Explanation
The radiograph of the lateral lumbosacral spine reveals an isthmic spondylolysis with a Meyerding grade 1 spondylolisthesis. The incidence of spondylolysis in the general population is around 5%, and grade 1 or 2 slips are present in the majority of children with a spondylolysis. Many cases of spondylolysis are painless and discovered incidentally, but, when painful, hyperextension of the lumbar spine may stress the area of the pars defect and exacerbate a patient’s symptoms. A diagnosis can usually be determined with a lateral radiograph of the lumbar spine. Although oblique lumbar radiographs are frequently ordered, several studies have shown that they do not increase diagnostic or prognostic accuracy. Progression of an isthmic spondylolysis, with or without a grade 1 or 2 listhesis, to a serious slip that might
necessitate surgical intervention is rare and occurs in fewer than 5% of patients. Chance for progression diminishes with age, with patients at highest risk prior to the adolescent growth spurt. Spondylolysis may have a genetic component; an increased prevalence has been found in some families and in some ethnic groups, especially among the Native American population.

Question 8
A 12-year-old boy has a head-on head collision while playing soccer. He had no loss of consciousness but has persistent headaches for 2 weeks. The patient is now back to school and has no headaches. What is the best next step?
Explanation
Question 9
Figure 242 is the anteroposterior radiograph of a 28-year-old man who underwent resection and reconstruction for an Ewing sarcoma. What is the most common functional deficit encountered during rehabilitation?
Explanation

Question 10
Ewing’s sarcoma of bone most commonly occurs in which of the following locations?
Explanation
REFERENCES: Simon M, Springfield D, et al: Ewing’s Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 287.
Wold LA, et al: Ewing’s Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 210-211.
Question 11
Figures 1 through 3 demonstrate the radiographs obtained from a 45-year-old construction worker who has wrist pain, loss of motion, and loss of strength. Nonsurgical measures have failed, and the patient requests surgery. What is the best surgical option for this patient?

Explanation
This patient has a physically demanding occupation. His radiographs show a long-standing nonunion with avascular necrosis and collapse of the proximal pole. This condition is referred to as a scaphoid nonunion advanced collapse wrist (SNAC). He has advanced arthritis of the capitolunate joint, but the radiolunate joint is preserved. The best option for him would be scaphoid excision with four-corner fusion. Proximal row carpectomy, would be incorrect because of the advanced arthritis of the capitolunate joint. This procedure relies on normal cartilage/joint articulation of the capitate as well as of the lunate fossa of the distal radius. Proximal pole scaphoid excision alone would not address the advanced arthritis of the capitolunate joint. Scaphoid fixation with bone grafting would not address the midcarpal arthritis and advanced proximal pole collapse.
Question 12
The use of knee arthroscopy following total knee arthroplasty is most effective in treating which of the following conditions?
Explanation
REFERENCES: Lucas TS, DeLuca PF, Nazarian DG, et al: Arthroscopic treatment of patellar clunk. Clin Orthop 1999;367:226-229.
Takahashi M, Miyamoto S, Nagano A: Arthroscopic treatment of soft-tissue impingement under the patella after total knee arthroplasty. Arthroscopy 2002;18:E20.
Question 13
What is the heaviest weight that can be safely applied to the adult cervical spine via Gardner-Wells tong traction?
Explanation
REFERENCES: Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Anderson DG, Vacccaro AR, Gavin K: Cervical orthoses and cranioskeletal traction, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005,
pp 110-121.
Question 14
What pharmacologic agents are preferred for the treatment of symptomatic active Paget’s disease?
Explanation
REFERENCE: Delman PD, Meunier PJ: The management of Paget’s disease. N Eng J Med 1997;336:558-566.
Question 15
A 4-year-old boy sustained a nondisplaced, but complete, fracture of the left proximal tibial metaphysis 1 year ago. The fracture healed uneventfully in an anatomic position. Examination of the injured extremity now reveals 18° of valgus compared with 3° of valgus on the opposite side. Management should now include
Explanation
REFERENCES: Zionts LE, MacEwen GD: Spontaneous improvement of posttraumatic tibia valga. J Bone Joint Surg Am 1986;68:680-687.
Beaty JH, Kumar A: Fractures about the knee in children. J Bone Joint Surg Am 1994;76:1870-1880.
Question 16
A 46-year-old man reports occasional squeaking of his hip 2 years after undergoing an uneventful total hip arthroplasty. History reveals no pain, physical examination cannot reproduce audible squeaking, and radiographs show appropriate implant position. What is the most appropriate management?
Explanation
Hopefully, with a better understanding of acoustic phenomena following ceramic total hip arthroplasty, this complication can be minimized.
REFERENCES: Yang CC, Kim RH, Dennis DA: The squeaking hip: A cause for concem-disagrees. Orthopedics
2007;30:739-742.
Walter WL, O’Toole GC, Walter WK, et al: Squeaking in ceramic-on-ceramic hips: The importance of acetabular component orientation. J Arthroplasty 2007;22:496-503.

Figure 80a Figure 80b
Question 17
A year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. A large intra-articular and intrapelvic pseudotumor has developed. What predominant histological feature(s) is/are present in such a lesion?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross- sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic
feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 18
A 28-year-old professional dancer reports a 3-month history of progressive pain in the posterior aspect of the left ankle. Her symptoms are worse when she assumes the en pointe position. Examination reveals tenderness to palpation at the posterolateral aspect of the ankle posterior to the peroneal tendons which is made worse with passive plantar flexion. There is no nodularity, fluctuance, or tenderness of the Achilles tendon. The neurovascular examination is unremarkable. A lateral radiograph and MRI scan are shown in Figures 16a and 16b, respectively. Management should consist of
Explanation
REFERENCES: Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057.
Mouhsine E, Crevoisier X, Leyvraz P, et al: Post-traumatic overload or acute syndrome of the os trigonum: A possible cause of posterior ankle impingement. Knee Surg Sports Traumatol Arthrosc 2004;12:250-253.
Wredmark T, Carlstedt CA, Bauer H, et al: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
Question 19
Which of the following represents the most appropriate treatment at this time?
Explanation
This is a classic presentation of a giant cell tumor. It is a benign aggressive bone tumor consisting of distinct undifferentiated mononuclear cells. Most occur in patients 30 years to 50 years of age (90% are older than age 20 years) and affect woman more than men. Pain and swelling for 2 to 3 months is classic.The most common location is the distal femur. The biopsy specimen shows multinucleated giant cells amid a background of mononuclear cells. This benign tumor may rarely metastasize to the lung (less than 2% of the time). A CT scan of the chest is required to rule out any further lesions. Curettage, with local adjuvants, such as phenol, cryotherapy, or argon beam, and cementation represents the best treatment option at this time.
CLINICAL SITUATION FOR QUESTIONS 107 THROUGH 109
An otherwise healthy 65-year-old man reports progressive and unrelenting back pain for the last 6 weeks that is nonmechanical in nature. He denies leg pain, weakness, bowel or bladder symptoms, and any significant past medical history. His pain is increased at night. Examination reveals pain with percussion throughout his thoracic spine. He is neurologically intact. AP and lateral radiographs of the thoracic and lumbar areas show diffuse osteopenia with no fractures.
Question 20
An 8-year-old girl injures her elbow playing soccer. After attempted reduction in the emergency department, radiographs of the elbow are shown in Figures 35a through 35c. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop
2000;20:7-14.
Hashemi-Nejad A, Goddard NJ: Radial head fractures. Br J Hosp Med 1994;51:223-226.
Rodriguez Merchan EC: Displaced fractures of the head and neck of the radius in children: Open reduction and temporary transarticular internal fixation. Orthopedics 1991;14:697-700.
Question 21
An axillary nerve lesion may cause weakness in the deltoid and the
Explanation
REFERENCE: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs. New York, NY, Harper & Row, 1969.
Question 22
Figure 1 is the MRI scan of a 19-year-old man who has an acute anterior shoulder dislocation. The bony fragment occupies 10% of the glenoid articular surface. What is the most appropriate treatment? Review Topic
Explanation
Question 23
A professional baseball player has had intermittent, mild shoulder pain for the past 2 years. Nonsurgical management has consisted of anti-inflammatory drugs. Examination reveals atrophy of the infraspinatus muscle but not the supraspinatus. There is weakness in external rotation with the arm at his side but not at 90 degrees of abduction. He has no weakness or pain with resisted abduction. Electromyography confirms an isolated lesion of the suprascapular nerve branch to the infraspinatus. He is otherwise neurologically intact. An MRI scan of the shoulder shows no cysts but confirms atrophy of the infraspinatus muscle. What is the next most appropriate step in management?
Explanation
REFERENCES: Cummins CA, Bowen M, Anderson K, et al: Suprascapular nerve entrapment at the spinoglenoid notch in a professional baseball pitcher. Am J Sports Med 1999;27:810-812.
Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
Ferretti A, De Carli A, Fontana M: Injury of the suprascapular nerve at the spinoglenoid notch: The natural history of infraspinatus atrophy in volleyball players. Am J Sports Med 1998;26:759-763.
Question 24
Figure below depicts the radiograph obtained from a 52-year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?
Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 25
A 25-year-old tennis player has shoulder pain and weakness to external rotation. MRI scans are shown in Figures 16a and 16b. What is the most likely cause of his weakness?
Explanation
REFERENCES: Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Inokuchi W, Ogawa K, Horiuchi Y: Magnetic resonance imaging of suprascapular nerve palsy.
J Shoulder Elbow Surg 1998;7;223-227.
Question 26
A 40-year-old man is thrown off his motorcycle and sustains an open Type IIIA fracture shown in Figure A. He is taken to the operating room for debridement and reamed intramedullary nailing with a 10mm diameter nail. He returns at 10 months with persistent pain at the fracture site with ambulation. Examination reveals healed wounds with no erythema, warmth or tenderness. Erythrocyte sedimentation rate and C-reactive protein levels are within normal limits. Radiographs taken at that time are shown in Figure B. What is the next best treatment step?

Explanation
Tibial delayed union can be defined as lack of union from 20-26 weeks post-injury, while nonunion is defined as lack of healing at >9mths post-injury, or absence of progressive signs of healing on radiographs for 3 consecutive months. Persistent pain is a symptom of nonunion. ESR and CRP are performed to rule out infection.
Bhandari et al. performed a blinded, multicenter trial on 622 reamed tibial nails and 604 unreamed tibial nails. In closed fractures, patients in the unreamed nail group were at greater risk of primary events than the reamed nail group. There was no difference in groups for open fractures. Primary events were defined as bone-grafting, implant exchange/removal, dynamization, and debridement.
Hak reviewed aseptic tibial nonunion. They discuss exchanged reamed nailing for diaphyseal nonunion, adjunctive plate fixation for metaphyseal nonunion, and nail removal and plating for metadiaphyseal nonunion, external fixation for infected nonunion and distraction osteogenesis of defects.
Figure A shows a mid-diaphyseal tibial fracture Figure B shows nonunion following
IM nailing of the fracture. Illustration A shows union following exchange nailing with a larger 12mm diameter nail.
Incorrect Answers:
Question 27
A 30-year-old farmer undergoes replantation of an above-the-elbow amputation. What form of management is most important following this surgery?
Explanation
REFERENCES: Wood MB: Replantations about the elbow, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1985, pp 472-480.
Goldner RD, Nunley JA: Replantation proximal to the wrist, in Wood MD (ed) Hand Clinics: Microsurgery. Philadelphia, PA, WB Saunders, 1992, pp 413-425.
Question 28
A 75-year-old woman who sustained a fall now reports neck pain and upper extremity weakness. Examination reveals 4 of 5 strength in the upper extremities and 5 of 5 strength in the lower extremities. Radiographs show multilevel degenerative disk disease. An MRI scan is shown in Figure 96. Her clinical presentation is most compatible with which of the following? Review Topic

Explanation
Question 29
Figures 1 and 2 are the most recent radiographs of an 18-year-old high school student who sustains an anterior shoulder dislocation playing recreational football. He has a low Beighton score on physical examination. He was closed reduced and underwent a course of physical therapy but had a second dislocation playing recreational basketball. What is the most appropriate course of treatment, with the lowest complication rate, to prevent further dislocation?

Explanation
injury and hardware problems, exceeds that of arthroscopic Bankart repair.
Question 30
Poor pre-injury cognitive function has been proven to increase mortality for which of the following injuries?

Explanation
Question 31
In total knee arthroplasty, in vitro testing has shown that cross-linking can diminish the rate of polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
Explanation
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been shown to cause implant failure in the most recent clinical trials, but they remain the most important mechanical issues associated with current material processing methods.
Question 32
A 20-year-old basketball player sustains a knee injury during a game and is seen in the orthopaedic clinic 3 days after injury. Examination reveals a positive Lachman, pivot shift, joint line tenderness, and moderate effusion. Which of the following tissue injuries is most likely causing the jointline tenderness?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, p 201.
Greis PE, Bardana DD, Holmstrom MC, et al: Meniscal injury: I. Basic science and evaluation. J Am Acad Orthop Surg 2002;10:168-176.
Duncan JB, Hunter R, Purnell M, et al: Meniscal injuries associated with acute anterior cruciate ligament tears in alpine skiers. Am J Sports Med 1995;23:170-172.
Question 33
With respect to the structure identified by the arrow in Figure 22b, the meniscofemoral 25 ligaments are
Explanation
The stress radiographs demonstrate posterior instability of the right knee in flexion. The MR images demonstrate injury to both the anterior and posterior cruciate ligament (PCL), with the stump identified with the arrow on the MR image (Figure 22b). The PCL has 2 functional bands. The anterolateral bundle originates from the roof of the intercondylar notch. It runs in a posterolateral direction onto the tibial crest between the posterior attachment of the medial and lateral menisci. During a double-bundled posterior ligament reconstruction, the
anterolateral bundle is tensioned with the knee in a position of mid flexion. The posteromedial bundle has a variable pattern of tension both in extension and in high flexion. Tensioning of the posteromedial bundle in extension may contribute to resistance against knee hyperextension.
The meniscofemoral ligaments are variably present. Although 93% of knees have been reported to have at least 1 meniscofemoral ligament present, both ligaments are simultaneously present in approximately 50% of knees. The ligament of Humphrey (anterior meniscofemoral ligament) and ligament of Wrisberg (posterior meniscofemoral ligament) are delineated by their anatomic relationship to the posterior cruciate.
RECOMMENDED READINGS
Amis AA, Bull AM, Gupte CM, Hijazi I, Race A, Robinson JR. Biomechanics of the PCL and related structures: posterolateral, posteromedial and meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2003 Sep;11(5):271-81. Epub 2003 Sep 5. Review. PubMed PMID: 12961064.View Abstract at PubMed
Amis AA, Gupte CM, Bull AM, Edwards A. Anatomy of the posterior cruciate ligament and the meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):257-63. Epub 2005 Oct 14. Review. PubMed PMID: 16228178.
View Abstract at PubMed . 26
Question 34
At what age does the lateral epicondyle normally ossify in males?
Explanation
Question 35
Figure 16 shows the radiograph of an otherwise healthy 62-year-old woman who fell. Management should consist of
Explanation
REFERENCES: Springer BD, Berry DJ, Lewallen DG: Treatment of periprosthetic fractures following total hip arthroplasty with femoral component revision. J Bone Joint Surg Am 2003;85:2156-2162.
Duwelius PJ, Schmidt AH, Kyle RF, et al: A prospective, modernized treatment protocol for periprosthetic femur fractures. Orthop Clin North Am 2004;35:485-492.
Question 36
below shows the abdominal radiograph obtained from a year-old woman who experiences nausea and abdominal tightness 48 hours following left total knee arthroplasty performed under general anesthesia. She received 24 hours of cefazolin antibiotic prophylaxis and a patient-controlled analgesia narcotic pump for pain management. She has been receiving warfarin for thromboembolic prophylaxis. Her severe abdominal distension and markedly decreased bowel sounds are most likely secondary to the administration of
Explanation
The radiograph reveals severe intestinal dilatation, which has occurred as the result of acute colonic pseudo-obstruction and is associated with excessive narcotic administration following total joint arthroplasty. Anesthetic type, antibiotic administration, and warfarin have not been associated with this obstruction. Electrolyte imbalances such as hypokalemia have been associated with postsurgical acute colonic pseudo-obstruction.
Question 37
A 36-year-old man was injured in a motorcycle collision and sustained the injury shown in Figure 70. He has a blood pressure (BP) of 70/40 mm Hg, pulse of 148 beats per minute (bpm), and Glasgow Coma Scale score of 6 (scores lower than 8 indicate severe brain injury), and there is negligible urine output. His airway is secure and intravenous (IV) access is obtained. Two liters of warm crystalloid solution are given; repeated vital signs reveal the same BP and a pulse of 142 bpm. What is the best next step?

Explanation
This patient has an anteroposterior compression pelvic fracture associated with shock. In patients with closed pelvic fractures and hypotension, mortality rises to approximately 1 in 4 (10%-42%) and hemorrhage is the major reversible contributing factor. Initial management of a major pelvic disruption associated with hemorrhage requires hemorrhage control and rapid fluid resuscitation. A pelvic binder should be placed to reduce pelvic volume. The patient has signs and symptoms of class IV hemorrhage, which include marked tachycardia exceeding 140, a significant decrease in BP, and a very narrow pulse pressure. Urinary output is negligible, and mental status is markedly depressed. The skin is cold and pale. The degree of exsanguination with class IV hemorrhage is immediately life threatening, and rapid transfusion and immediate surgical intervention are necessary. Nonresponse to fluid administration indicates persistent blood loss. Blood preparation should be emergency blood release. Type and cross-match of blood can be used for additional resuscitation in transient responders.
RECOMMENDED READINGS
Olson SA, Reilly MC, eds. Acetabular and Pelvic Fractures. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2007:15-42.
Advanced Trauma Life Support for Doctors, ed 8. Chicago, IL, American College of Surgeons, 2008.
RESPONSES FOR QUESTIONS 71 THROUGH 74
- Retrograde intramedullary (IM) nailing
- Open reduction and internal fixation (ORIF) with screws alone
- Locking condylar plate
- Circular external fixation
- Lateral and medial plates
Which treatment option listed is best for each patient described?
71A

B
C
D
A 54-year-old healthy man with the condition seen in Figures 71a through 71d
- Retrograde intramedullary (IM) nailing
- Open reduction and internal fixation (ORIF) with screws alone
- Locking condylar plate
- Circular external fixation
- Lateral and medial plates
Question 38
Regarding bone erosion in rheumatoid arthritis, which of the following statements is true?
Explanation
Cytokines TNF, IL-1 and IL-6 are key players in RA. TNF stimulates migration of osteoclast precursors from the bone marrow into the periphery, and stimulates expression of surface receptors to facilitate differentiation. In the joint, M-CSF and RANKL stimulate differentiation towards osteoclasts. Final differentiation into bone-resorbing osteoclasts is achieved following contact with the bone surface.
Schett et al. reviewed bone erosions in RA. They state that the main triggers of bone erosion are synovitis, RANKL, and anti-citrullinated protein antibodies. In RA, there is an abundance of osteoclasts in bone erosions, but a paucity of mature osteoblasts, suggesting the presence of molecules that block osteoblast differentiation.
Ideguchi et al. investigated whether repair of erosions occurs in patients with rheumatoid arthritis (RA) treated with conventional disease-modifying anti-rheumatic drugs (DMARDs). They detected repair of erosions in 10.7% of RA patients treated with DMARDs. They recommend the use of DMARDs to reduce disease activity and thus reduce erosions.
Illustration A shows the action of antirheumatic drugs on osteoclast differentiation and bone erosion.
Question 39
What neurologic structure is most at risk when performing intramedullary screw fixation of a fifth metatarsal base fracture?
Explanation
REFERENCES: Donley BG, McCollum MJ, Murphy GA, Richardson EG: Risk of sural nerve injury with intramedullary screw fixation of fifth metatarsal fractures: A cadaver study. Foot Ankle Int 1999;20:182-184.
Lawrence SJ, Botte MJ: The sural nerve in the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
Question 40
Figure 53 shows the MRI scan of a 53-year-old carnival worker who has pain and swelling in the left shoulder as a result of attempting to stop a roller coaster car with his arm. Examination reveals decreased ROM, apprehension, and inability to move the dorsum of his hand away from his back. Treatment should consist of
Explanation
Question 41
Figure 2 shows the lateral radiograph of an 8-year-old boy who sustained an acute injury to the elbow after falling down the stairs. Management should consist of
Explanation
REFERENCES: Murphy DF, Greene WB, Gilbert JA, Dameron TB Jr: Displaced olecranon fractures in adults: Biomechanical analysis of fixation methods. Clin Orthop 1987;224:210-214.
Chambers HG, Wilkins KE: Part IV: Fractures of the proximal radius and ulna, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 629-630.
Question 42
A 72-year-old man has had persistent pain after undergoing a hemiarthroplasty 18 months ago. Radiographs are shown in Figures 50a and 50b. What is the most likely cause of his problem?
Explanation
REFERENCES: Haidukewych GJ, Israel TA, Berry DJ: Long-term survivorship of cemented bipolar hemiarthroplasty for fracture of the femoral neck. Clin Orthop Relat Res 2002;403:118-126.
Lestrange NR: Bipolar hemiarthroplasty for 496 hip fractures. Clin Orthop Relat Res 1990;251:7-19.
Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, p 158.
Question 43
Corticosteroids inhibit the formation of effectors of the inflammatory pathway via inhibition of
Explanation
Question 44
Figures 21a and 21b show the clinical photograph and radiograph of a 15-year-old girl who has a deformity of her feet. Her parents are concerned because there is a family history of Charcot-Marie-Tooth disease. The patient reports some mild instability of the ankle and has noticed mild early callosities; however, she is not having any significant pain. Coleman block testing reveals a forefoot valgus and supple hindfoot. She has weakness to eversion and dorsiflexion. Initial management should consist of
Explanation
REFERENCES: Pinzur MS: Charcot’s foot. Foot Ankle Clin 2000;5:897-912.
Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 45
A 17-year-old boy underwent open reduction and internal fixation of a navicular fracture 5 days ago. A follow-up examination now reveals a tensely swollen foot with erythema and multiple skin bullae. The patient is febrile and has marked pain with palpation of the entire forefoot and hindfoot. What is the next step in management?
Explanation
REFERENCES: Ault MJ, Geiderman J, Sokolov R: Rapid identification of group A streptococcus as the cause of necrotizing fasciitis. Ann Emerg Med 1996;28:227-230.
McHenry CR, Piotrowski JJ, Pentrinic D, Malangoni MA: Determinants of mortality for necrotizing soft-tissue infections. Ann Surg 1995;221:558-563.
Question 46
Based on the findings shown in Figures 22a and 22b, corrective surgery to obtain maximal safe correction and optimal instrumentation fixation should be performed at which of the following locations?
Explanation
REFERENCES: Shufflebarger HL, Clark CE: Thoracolumbar osteotomy for postsurgical sagittal imbalance. Spine 1992;17:S287-S290.
Murrey DB, Brigham CD, Kiebzak GM, et al: Transpedicular decompression and pedicle subtraction osteotomy (eggshell procedure): A retrospective review of 59 patients. Spine 2002;27:2338-2345.
Question 47
15% to 2.5%. Acute Charcot arthropathy almost always appears with signs of inflammation. Profound unilateral swelling, an increase in local skin temperature (generally, an increase of 3° to 7° above the nonaffected foot's skin temperature), erythema, joint effusion, and bone resorption in an insensate foot are present. These characteristics, in the presence of intact skin and a loss of protective sensation, are often pathognomonic of acute Charcot arthropathy. Cellulitis is an infection of the skin. Examination would reveal erythema, edema, and pain. Osteomyelitis is an infection of the bone. Examination may reveal edema, drainage, and pain.
Explanation
Which of the following clinical scenarios represents the strongest indication for locked plating technique in a 70-year-old woman?
Segmentally comminuted ulnar fracture
Simple diaphyseal fracture of the humerus
Transverse midshaft displaced clavicle fracture
Periprosthetic femur fracture distal to a well-fixed total hip arthroplasty
Schatzker 2 fracture of the tibia with severe joint depression and comminution
Locking screw fixation is a relatively new option in the armamentarium of orthopaedic surgeons treating fractures. The understanding of the biomechanics, implications to healing, and optimal indications and surgical techniques is still in evolution. A periprosthetic proximal femur fracture with a stable prosthesis is best treated with open reduction and internal fixation with locking proximal fixation with or without cerclage cables. Diaphyseal fractures treated with compression plating or bridge plating can be treated well with conventional implants unless osteoporosis is severe. An AO/OTA B-type partial articular fracture is also better suited to standard buttress plating with periarticular rafting lag screws. Locking fixation is not always required for a transverse displaced midshaft clavicle fracture.
What is the post-amplification product of reverse transcription polymerase chain reaction (RT-PCR)?
RNA
DNA
Protein
Mitochondria
Immunoglobulins
Reverse transcription polymerase chain reaction (RT-PCR) is a variant of polymerase chain reaction (PCR) used in molecular biology to generate many copies of a DNA sequence from fragments of RNA. The RNA strand is first reverse transcribed into its DNA complement, followed by amplification of the resulting DNA using polymerase chain reaction. Polymerase chain reaction amplifies short segments of DNA by using the temperature stable DNA polymerase enzyme.
A 63-year-old woman falls from standing and lands on her right hand. She complains of deformity and wrist pain. Radiographs are provided in Figure A. Following closed reduction, the patient inquires whether she has osteoporosis and if she is likely to have another fracture. In counselling the patient, which of the following is the strongest predictor for a future fracture from low energy trauma?
Bone mineral density T-score < -2.5
Low vitamin D levels
Family history of osteoporosis
History of a prior fragility fracture
Ten year history of oral prednisone use
Each of the answer choices is a risk factor for subsequent fragility fracture, but patient history of a prior fragility fracture is the strongest predictor.
Bouxsein et al reviews the proper care, diagnosis, and prevention of fragility fractures. History of a fragility fracture is the greatest predictor of a future fracture from low energy trauma. Appropriate care includes not only treatment of the fracture itself, but also proper evaluation to identify the etiology of the fracture and appropriate intervention to rectify the underlying pathology. Evaluation includes bone densitometry, lab testing of Vitamin D and calcium.
A T-score compares your bone density to the optimal peak bone density for your gender. It is reported as number of standard deviations below the average. A T-score of -1 to -2.5 is considered osteopenia, and a risk for developing osteoporosis. A T- score of less than -2.5 is diagnostic of osteoporosis.
Long-term alendronate (Fosamax) use for osteoporosis has been associated
with which of the following?
Scurvy
Detached retina
Uterine carcinoma
Osteonecrosis of the femoral head
Diaphyseal femoral insufficiency fractures
Alendronate is a bisphosphonate that inhibits the ruffled border of the osteoclast. When used long term, this class of medication prevents the normal bone remodeling process. Long-term use has recently been shown to be associated with insufficiency fractures of the femur. Osteonecrosis of the jaw has been described but not in other anatomic locations. Scurvy occurs because of a lack of vitamin C and use of bisphosphonates is not associated with
uterine cancer or a detached retina.
Implants composed of polylactic acid are excreted by what system after they are absorbed?
Hepatic
Renal
Respiratory
Gastrointestinal
Polylactic acid suture and suture anchors are popular bioabsorbable orthopaedic implants. This material undergoes hydrolysis of the ester background in vivo. Resulting lactic acid enters the tricarboxylic acid (Krebs)
cycle and is excreted as carbon dioxide by the lungs. Polyglycolic acid and poly(p- dioxanone) may also be excreted by the kidneys.
A patient sustains a grade III medial collateral ligament injury. One year later, when compared to collagen in an uninjured ligament, an increase is likely in the
gross number of fibers.
proportion of type III fibers.
cross-linking.
mass and diameter of fibers.
Studies on animal models have shown that there is a change in collagen fiber type and distribution early in the healing process. There is a higher portion of type III fibers than in
normal ligament initially, but this ratio returns to normal about 1 year after the injury occurs. Healing ligaments show an increased number of collagen fibers, but the number of mature collagen cross-links is
45% of predicted value after 1 year. There is also a decrease in the mass and diameter of the collagen fibers.
Sclerostin and dickkopf-1 (Dkk-1) are direct inhibitors of what pathway related to bone and/or cartilage regulation?
Bone morphogenetic protein (BMP)/SMAD pathway
Receptor activator of nuclear factor kappa beta (RANK)/RANK ligand (RANKL) pathway
Wnt/Beta-catenin (ß-catenin) pathway
Parathyroid hormone (PTH) pathway
Dkk-1 and sclerostin are proteins that inhibit the binding of the Wnt molecule to receptors LRP5/6. In the absence of sclerostin and Dkk-1, Wnt binds to its receptor, which in turn inhibits phosphorylation of the ß-catenin. The unphosphorylated ß-catenin then builds up in the cytoplasm of the cell, allowing it to be transported to the nucleus of the cell. Once in the nucleus, ß- catenin will lead to upregulation of a series of proteins involved in osteoblast formation differentiation. Knocking out or inhibiting sclerostin or Dkk-1 results in increased bone mass secondary to constitutive activation of the Wnt/ß- catenin pathway. The other responses are not directly affected by Dkk-1 or sclerostin. RANKL and RANK are expressed on osteoblasts and osteoclasts, respectively, and are involved in osteoblast-mediated osteoclast activation. BMPs work through SMADs to cause osteoblastic differentiation, and there is reported crosstalk between the Wnt and BMP pathways (but this is an indirect link). Finally, PTH at physiologic levels binds to osteoblasts, causing a series of events that lead to osteoblast-mediated osteoclast activation and subsequent increased bone resorption.
During endochondral ossification of the growth plate, the process that most contributes to the longitudinal growth of long bones is
chondrocyte apoptosis.
chondrocyte hypertrophy.
chondrocyte proliferation.
growth plate matrix synthesis.
The growth plate is divided into 5 distinct zones: reserve, proliferative, maturation, hypertrophy, and vascular invasion. During growth-plate chondrocyte hypertrophy, intracellular volume and an increase in chondrocyte height are responsible for most growth of long bones. Other factors that contribute to bone growth are chondrocyte proliferation and matrix synthesis, but to a lesser degree than chondrocyte hypertrophy. Growth plate chondrocytes undergo programmed cell death (apoptosis) after hypertrophy
takes place.
Bacterial resistance to tetracycline is confirmed by ribosome protection, tetracycline modification, and
altered RNA polymerase.
altered membrane binding protein.
increased drug efflux.
DNA gyrase mutation.
Mutations of bacterial DNA gyrase can decrease the effectiveness of quinolones. Altered membrane-binding protein is observed with resistance to ?
-lactam antibiotics. Tetracyclines are antibiotics that inhibit bacterial growth by stopping protein synthesis. Three specific mechanisms of tetracycline
resistance have been identified: increased tetracycline efflux, ribosome protection, and tetracycline modification. Alteration of RNA polymerase is found in resistance to rifampin.
A 14-year-old boy has failed physical therapy management for Scheuermann kyphosis, and an extension thoracolumbosacral orthosis brace is recommended. The boy and his parents are told that the brace will force his thoracic spine into normal sagittal alignment and put the anterior vertebral bodies of the thoracic segment into tension, which will induce bone growth and normalization of wedge- shaped
vertebrae. What name is associated with this process?
Hooke's law
Kirchhoff's law
Wolff's law
Heuter-Volkmann principle
The Heuter-Volkmann principle shows that bone placed in longitudinal tension will tend to stimulate longitudinal growth, and that compressive longitudinal forces inhibit longitudinal growth, making this response the best choice. Hooke's law relates to stress being proportional to strain and is not directly related to bone growth. Kirchhoff's laws apply to electrical circuit design. Wolff's law states that bone remodels in response to mechanical stress, with the correlate that increased stress causes increased growth, and decreased stress leads to bone loss.
A tendon repair is thought to be weakest during which phase of tendon healing?
Inflammatory
Proliferation
Maturation
Remodeling
Healing after a tendon repair or rupture has the following stages: inflammatory, cellular proliferation, and remodeling. During the inflammatory phase, neutrophils and macrophages migrate into the injury site and release chemotactic factors that recruit fibroblasts. A tendon is thought to be weakest
5 to 21 days after repair, which coincides with the inflammatory phase. During the proliferative phase, inflammatory cells secrete cytokines and growth
factors (platelet-derived growth factor, insulin-like growth factor, bone morphogenetic protein (BMP)-12 and BMP 13, and transforming growth factor- beta) that promote differentiation of fibroblasts. Fibrosis and decreased cellularity are the hallmarks of the remodeling stage.
A 4-year-old boy has bilateral genu varum and is in the fifth percentile for height for his age. A younger sister has less severe genu varum. Radiographs reveal physeal cupping and widening on both the distal femur and proximal tibia. Laboratory studies show sodium 145 mEq/L (reference range, 136-142 mEq/L), potassium 4.0 mEq/L (reference range, 3.5-5.0 mEq/L), calcium 9.0 mg/dL (reference range, 8.2-10.2 mg/dL), phosphorous 2 mg/dL (reference range, 4-
Question 48
Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Agins HJ, Alcock NW, Bansal M, et al: Metallic wear in failed titanium-alloy total hip replacements: A histological and quantitative analysis. J Bone Joint Surg Am 1988;70:347-356.
Robinson RP, Lovell TP, Green TM, Bailey GA: Early femoral component loosening in DF-80 total hip arthroplasty. J Arthroplasty 1989;4:55-64.
Question 49
What changes in muscle physiology would be expected in an athlete who begins a rigorous aerobic program for an upcoming marathon?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 89-125.
Thayer R, Collins J, Noble EG, et al: A decade of aerobic endurance training: Histological evidence for fibre type transformation. J Sports Med Phys Fitness 2000;40:284-289.
Question 50
A 30-year-old woman injured the ring finger of her nondominant hand while playing baseball 5 weeks ago. She now reports pain and limited motion of the proximal interphalangeal (PIP) joint. A lateral fluoroscopy image is shown in Figure 36. Treatment of the PIP joint should consist of
Explanation
REFERENCES: Dionysian E, Eaton RG: The long-term outcome of volar plate arthroplasty of the proximal interphalangeal joint. J Hand Surg Am 2000;25:429-437.
Eaton RG, Malerich MM: Volar plate arthroplasty of the proximal interphalangeal joint: A review of ten years’ experience. J Hand Surg Am 1980;5:260-268.
Deitch MA, Kiefhaber TR, Comisar BR, et al: Dorsal fracture dislocations of the proximal interphalangeal joint: Surgical complications and long-term results. J Hand Surg Am 1999;24:914-923.
Question 51
While performing long fusion with osteotomies for a patient with adult scoliosis and sagittal plane deformity, the neurophysiologist reports a change in motor-evoked potentials in the lower extremities. What is the most appropriate next step?
Explanation
The use of intraoperative neuromonitoring is expanding, especially in the setting of deformity surgery. Changes in monitoring are concerning for the possibility of a neurologic injury; however, several other factors can alter signals. These include hypotension, changes in anesthesia depth and medications, the use of paralytic agents, and technical issues such as leads falling out or becoming disconnected. If a change in neuromonitoring signals is noted, these factors should be checked first to rule out false-positive findings. If this does not correct the problem, the wound should be explored to ensure there is no compression on the neural elements. Finally, if the deformity has been corrected, some of the correction can be released in an attempt to improve the signals. A wake-up test is difficult to perform and does not provide specific information regarding the location of the problem or how to correct it. Steroids may be used depending on surgeon preference, but should not be used until neurologic injury is ruled out. Any neuromonitoring changes always necessitate immediate investigation.
RECOMMENDED READINGS
Ziewacz JE, Berven SH, Mummaneni VP, Tu TH, Akinbo OC, Lyon R, Mummaneni PV. The design, development, and implementation of a checklist for intraoperative neuromonitoring changes. Neurosurg Focus. 2012 Nov;33(5):E11. doi: 10.3171/2012.9.FOCUS12263. PubMed PMID: 23116091. View Abstract at PubMed
Malhotra NR, Shaffrey CI. Intraoperative electrophysiological monitoring in spine surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2167-79. doi: 10.1097/BRS.0b013e3181f6f0d0.
Review. PubMed PMID: 21102290. View Abstract at PubMed
Question 52
A 17-year-old high school gymnast who has peripatellar knee pain has been unable to practice on a consistent basis for the past 3 years. She denies any specific injury events. Physical therapy for modalities, quadriceps strengthening, and hamstring stretching provide temporary relief. A trial of patellar taping significantly reduces her pain. Examination reveals an 15-degree Q angle, moderate lateral facet tenderness, negative patellar apprehension, and the inability to evert the patella. Radiographs show a moderate lateral patellar tilt. Treatment should now consist of
Explanation
REFERENCES: Gambardella RA: Techical pitfalls of patellofemoral surgery. Clin Sports Med 1999;18:897-903.
Post WR: Clinical evaluation of patients with patellofemoral disorders. Arthroscopy 1999;15:841-851.
Question 53
- Which of the following acetabular/femoral head components would be expected to show an optimal combination of linear and volumetric wear?
Explanation
Question 54
A patient who underwent an L5-S1 hemilaminotomy and partial diskectomy for radiculopathy 3 weeks ago now reports increasing leg and back pain with radicular signs. An axial T2-weighted MRI scan is shown in Figure 97a, an axial T1-weighted MRI scan is shown in Figure 97b, and a contrast enhanced T1-weighted MRI scan is shown in Figure 97c. What is the most appropriate management for the patient's symptoms? Review Topic
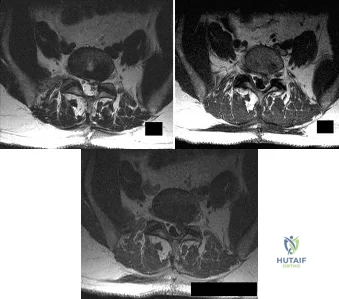
Explanation
Question 55
A 17-year-old high school football player sustains a traumatic anterior shoulder dislocation, resulting in a small bony Bankart lesion and small Hill-Sachs lesion. The patient undergoes an arthroscopic Bankart repair with incorporation of the bone fragment and returns to play football the following year. He has a recurrent dislocation at football practice but decides to finish the football season before considering additional treatment. He sustains nine additional dislocations, with the last dislocation occurring while sleeping.What diagnostic test is most appropriate when planning revision surgery?
Explanation
more likely to have pain after surgery. Age and activity level are lesser influences on satisfaction.
Question 56
Figures 1 through 4 are the CT scans and intraoperative image of a 17-year-old boy who sustained a gunshot wound to his knee. What is the most appropriate definitive surgical management for his articular cartilage defect?
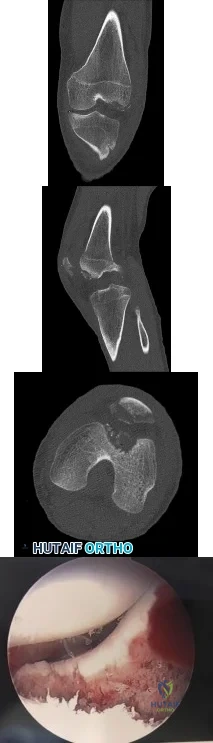
Explanation
Question 57
A 15-year-old girl reports a 6-month history of activity-related knee pain and swelling. A radiograph, MRI scan, and biopsy specimen are shown in Figures 21a through 21c. What is the most likely diagnosis?
Explanation
REFERENCES: Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 295-313.
Lin PP, Thenappan A, Deavers MT, et al: Treatment and prognosis of chondroblastoma. Clin Orthop Relat Res 2005;438:103-109.
Question 58
A 22-year-old woman sustains the injury seen in Figure 12 as a result of a motor vehicle crash. What factor is most closely associated with development of osteonecrosis?

Explanation
(SBQ12TR.90) A 40-year-old male sustained the injury seen in Figure A, and subsequently underwent the procedure shown in Figure B. One hour post-operatively he starts to complain of pain in the operative leg, and the pain is unchanged with active or passive stretch. The external dressing is released with little resolution of symptoms. His blood pressure is 115/78 mm Hg with compartment pressures in the leg measuring 31 to 35 mm Hg. His ABI index is 1.1 in the leg. What would be the next step in management? Review Topic

MRI angiography of leg
Four-compartment fasciotomy
Follow-up examination the following day
Continued monitoring and serial examinations
EMG study
The patient is at risk for developing compartment syndrome of the leg. The next most appropriate step would be to support his systemic blood pressure and monitor compartment pressures.
A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam.
An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) <30 mm Hg may help to confirm the necessity for fasciotomy. However, the treatment of early compartment syndrome should be to initially improve the limbs perfusion pressure gradient. This can be done by treating underlying factors such as hypotension, coagulopathy, or vascular compromise due to either a true vascular injury or artificially by external compression. Frequent reassessment is then critical to effectively manage these patients. If clinical diagnosis persists despite these efforts, urgent fasciotomy would be considered.
McQueen looked at 116 patients with tibial diaphyseal fractures who had continuous monitoring of anterior compartment pressure for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of 30 mmHg is a more reliable indicator of compartment syndrome.
White et al. looked at 101 patients with tibial fractures with satisfactory Delta P measurements. THey found that patients with elevated intramuscular pressures >30 mm Hg after tibial fracture do not have a greater incidence of complications than those with low pressures, so long that Delta P <30 mm Hg.
Figure A shows a Shatzker V tibial plateau fracture. Figure B shows fixation of fracture seen in Figure A.
Incorrect Answers:
30 mm Hg or persistently elevated absolute compartment pressures.. Answer 3: It would not be appropriate to leave this patient with impending compartment syndrome.
(SBQ12TR.57) A 56-year-old right hand dominant attorney falls from standing and sustains the closed injury shown in Figure A. The treating surgeon elects to fix her fracture using a plate and screw construct. Based on the available imaging, which of the following fracture characteristics best justifies this fixation choice?

Fracture displacement
Intra-articular fracture extension
The fracture extends distal to the coronoid
Oblique fracture line
Fracture comminution
This patient has a displaced, intra-articular, comminuted olecranon fracture. Comminution is an indication for plate fixation.
Most displaced olecranon fractures are treated operatively. Options include tension band constructs, intramedullary screws, plate and screw fixation or fragment excision with triceps advancement. Any construct relying on inter-fragmentary compression (tension band, intramedullary screws) requires a non-comminuted fracture pattern. Plate fixation is indicated in the setting of comminution, extension past the coronoid, or in the setting of associated instability.
Bailey et al. retrospectively reviewed 25 patients who underwent plate fixation of displaced olecranon fractures. Twenty-two of 25 patients had good or excellent outcomes. Five of 25 patients (20%) of patients required plate removal for symptomatic hardware. The authors concluded that plate fixation was an effective treatment for displaced olecranon fractures, with good functional outcomes.
Figure A shows a displaced, comminuted olecranon fracture without evidence of propagation past the coronoid.
Incorrect answers:
congruity but does not dictate implant selection. Answer 3. Extension distal to the coronoid is an indication for plate fixation but there is no evidence of such extension on the radiograph shown Answer 4. This fracture is comminuted, without a distinct fracture line.
Question 59
Figures 34a and 34b show the radiographs of a 28-year-old man who fell on his outstretched arm with significant force while mountain biking. The nerve deficit most likely to occur would result in weakness of
Explanation
REFERENCES: Bado JL: The Monteggia lesion. Clin Orthop 1967;50:71-86.
Jupiter JB, Leibovic SJ, Ribbans W, Wilk RM: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
Question 60
A 22-year-old man who sustained a Gustilo-Anderson grade IIIC open fracture of the right tibia and fibula was treated with an immediate open transtibial amputation. After two serial debridements, he underwent wound closure with a posterior myocutaneous soft-tissue flap. What is the preferred method of early rehabilitation?
Explanation
REFERENCES: Burgess EM, Romano RL, Zettl JH: The Management of Lower Extremity Amputations. Washington, DC, US Government Printing Office, 1969, also at: www.prs-research.org.
Smith DG, McFarland LV, Sangeorzan BJ, et al: Postoperative dressing and management strategies for transtibial amputations: A critical review. J Rehabil Res Dev 2003;40:213-224.
Question 61
Figures 17a and 17b show the AP and lateral radiographs of a 75-year-old woman who reports giving way and shifting of the knee, particularly when she is descending stairs or ambulating on level surfaces. History reveals a total knee replacement 5 years ago. Treatment should consist of
Explanation
REFERENCE: Pagnano MW, Cushner FD, Scott WN: Role of the posterior cruciate ligament in total knee arthroplasty. J Am Acad Orthop Surg 1998;6:176-187.
Question 62
Which of the following statements best describes the process of articular cartilage degeneration in osteoarthritis?
Explanation
REFERENCE: Buckwalter JA, Mankin HJ, Grodzinsky AJ: Articular cartilage and osteoarthritis. Instr Course Lect 2005;54:465-480.
Question 63
Figures 15a and 15b show the radiographs of an 18-year-old mountain biker who came off of a 15-foot ramp and sustained an injury to his ankle. Because the local rural hospital had no orthopaedic surgeon available, he was transported to a Level 1 emergency department 10 hours after his initial injury. Examination reveals that the injury remains closed. Management should consist of
Explanation
REFERENCES: Tornetta P III, Weiner L, Bergman M, et al: Pilon fractures: Treatment with combined internal and external fixation. J Orthop Trauma 1993;7:489-496.
Sirkin M, Sanders R, DiPasquale T, Herscovici D Jr: A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 1999;13:78-84.
Question 64
An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes
Explanation
REFERENCE: Rettig ME, Raskin KB: Galeazzi fracture-dislocation: A new treatment-oriented classification. J Hand Surg Am 2001;26:228-235.
Question 65
Figures 11a and 11b show the radiographs of a 50-year-old man who was struck by a car. Treatment should consist of
Explanation
REFERENCES: Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 97-108.
Asnis SE, Wanek-Sgaglione L: Intracapsular fractures of the femoral neck: Results of cannulated screw fixation. J Bone Joint Surg 1994;76A:1793-1803.
Question 66
Figures 1 and 2 are the CT and MRI scans of a patient with shoulder instability. Contrasting these two imaging techniques for decision making in shoulder instability would suggest
Explanation
A. Inability to flex the distal interphalangeal joint of the index finger
B. Positive Froment’s sign
C. Weakness with wrist extension
D. Decreased capillary refill
Question 67
A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time? Review Topic

Explanation
(SBQ13PE.82) A renal ultrasound should be obtained in a patient with which of the following diagnoses? Review Topic
Congenital pseudoarthrosis of the clavicle
Accessory navicular
Congenital scoliosis
Charcot-Marie-Tooth Disease
Congenital curly toe
A renal ultrasound should be obtained in a patient with congenital scoliosis.
Congenitial scoliosis has a prevalence that is estimated at 1% to 4% in general population. It is associated with systemic anomalies in up to 61% of cases. The most common anomalies are cardiac defects, genitourinary defects and spinal cord malformations. As such, additional imaging of these systems should be considered in the initial work-up of these patients.
Ruf et al. retrospectively investigated 56 consecutive operative cases of congenital scoliosis. The average age at surgery was 9.9 years (1.5–17 years). There was one wound complication, 2 hardware failures, 1 revision and no neurological complications. They concluded that one-stage posterior hemivertebra resection and instrumentation was safe in this population.
Xu et al. examined the efficacy of selective partial hemivertebra excision via posterior-only approach in 17 adolescent patients with congenital kyphoscoliosis. There were no postoperative infections and no neurological complications. They concluded that this approach may be most successful in patients aged 9 to 14 years old, with the Risser sign grades from 0–3 and Cobb angles <60°.
Illustration A from Erol et al (UPOJ, Vol 15, 2002;37-42) shows a diagram of 'types' of congenital scoliosis based on the morphology of the vertebrae.
Incorrect Answers:
Question 68
Halo treatment for preadolescent children typically requires the use of which of the following? Review Topic
Explanation
Question 69
When performing a cruciate-retaining total knee arthroplasty, trial components are inserted. The knee comes to full extension but is tight in flexion. The surgeon should consider
Explanation
In this scenario, the flexion gap needs to be increased. Increase in flexion gap can be accomplished by downsizing the femoral component and increasing posterior tibial slope. In posterior cruciate-retaining TKA procedures, recession or release of the posterior cruciate ligament can loosen the flexion gap, allowing for an increase in flexion. Flexing the femoral
component tightens the flexion gap, and downsizing the tibial insert thickness decreases flexion and extension gaps, while resection of the distal femur only increases the extension gap.

CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 55
Figure 52 is the standing anteroposterior radiograph of a 55-year-old man who has a 5-year history of daily left knee pain with weight-bearing activities. He denies night pain or symptoms of instability. Upon examination his range of motion is 0 to 140 degrees. He has a mild, fully correctable varus deformity and a negative Lachman test result. He has failed nonsurgical treatment.
Question 70
What neurovascular structure is at greatest risk when creating a proximal anterolateral elbow arthroscopy portal? Review Topic
Explanation
Question 71
A 60-year-old woman has a mass in the right scapula. Figures 25a and 25b show a CT scan and a biopsy specimen. The cells are lymphocyte common antigen positive, Ewing’s specific antigen (CD99) negative, and keratin negative. What is the next step in management?
Explanation
REFERENCES: Finiewicz K, van Biesen K: Non-Hodgkins lymphoma, in Golomb H, Vokes E (eds): Oncologic Therapies, ed 2. Berlin, Germany, Springer, 2003, pp 295-318.
Lems P, Primus G, Anastas J, Doherty D, Montag AG, Peabody TD, Simon MA: Oncologic outcomes of primary lymphoma of bone in adults. Clin Orthop 2003;415:90-97.
Question 72
A patient has a large T11-T12 disk herniation that is causing substantial compression of the spinal cord. The patient reports walking imbalance over the past few weeks. Examination of the patient's reflexes is likely to show Review Topic
Explanation
Question 73
During impaction of a cementless acetabular component, the posterior column was fractured and found to be displaced. Which of the following is considered the most appropriate surgical option?
Explanation
REFERENCES: Berry DJ: Antiprotrusio cages for acetabular revision. Clin Orthop 2004;420:106-112.
Peterson CA, Lewallen DG: Periprosthetic fracture of the acetabulum after total hip arthroplasty. J Bone Joint Surg Am 1996;78:1206-1213.
Question 74
A 42-year-old woman complains of ankle pain with weightbearing for the last 2 years. She recalls spraining her ankle more than 10 years ago. She plays tennis and regularly walks 5 miles a day for exercise, but has had to give up these activities over the last few months because of pain. Examination reveals limitation in ankle dorsi- and plantar flexion. A course of non-operative management has been unsuccessful. Which of the following options will most likely provide pain relief and allow her to return to her previous activity level?

Explanation
Supramalleolar osteotomy may be performed for varus (medial opening wedge or lateral closing wedge) or valgus (lateral opening wedge or medial closing wedge) ankles. They are suited for near-normal ROM minimal talar-tilt or varus heel alignment, asymmetric ankle arthritis (confined to medial or lateral compartment; corresponding to Takakura Stage II or IIIA for medial ankle arthritis).
Pagenstert et al. looked at realignment surgery for posttraumatic arthritis in 35 patients. For valgus ankles, they performed 18 medial closing wedge and 1 lateral opening wedge osteotomies. For varus ankles, they performed 7 medial opening wedge and 4 lateral closing wedge osteotomies. There was improvement in pain (7/10 to 3/10), ROM (33° to 38°) and Takakura score (2.3 to 1.3).
Lee et al. described supramalleolar osteotomy for medial arthritis in 16 patients. There was improvement in AOFAS score (62 to 82), Takakura stage (2.9 to 2.3), tibial-anterior surface angle (85 to 100°). Patients with low postoperative talar tilt (TT) had better clinical and radiographic results than those with high TT. Greater postoperative heel valgus predicted for postoperative subfibular pain.
Figure A shows valgus alignment at the ankle. Illustration A shows the same ankle following medial closing wedge supramalleolar osteotomy. Illustration B is a table showing the Takakura classification. Illustration C demonstrates correction of the tibial-anterior surface angle (TAS) following supramalleolar osteotomy.
Incorrect Answers:
Question 75
A 28-year-old man has had a 2-week history of right posterior leg pain, with numbness and tingling in the same distribution. He denies any problems with bowel or bladder function. Examination shows intact motor strength in his bilateral lower extremities, with numbness to light touch in the lateral border of his right foot. Over the past 2 weeks, his leg pain has improved significantly. MRI scans are shown in Figures 57a and 57b. What is the most appropriate course of management? Review Topic

Explanation
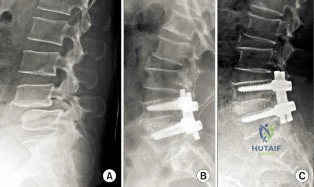
(SBQ12SP.9) A 62-year-old male underwent posterior spinal instrumented fusion for degenerative lumbar spondylolithesis one year ago. He presents to office complaining of persistent lower back pain. The pain initially improved but over the last 6 months he has had recurring pain at the site of the surgery primarily with activity. He denies back pain at rest or night pain. Physical examination reveals a well healed wound and no physical abnormalities. He has no tenderness to palpation to the thoracic or lumbar spine. He has no neurological deficits. His laboratory results show an erythrocyte sedimentation rate (ESR) = 8 mm/h and C-reactive protein (CRP) = 3 mg/L at the last visit which are both within normal limits. Figure A shows a series of radiographs from his pre-operative, 3 month post-operative and 1 year post-operative clinic visits, respectively. Which of the following investigations would best confirm the suspected underlying diagnosis? Review Topic
MRI of lumbar spine
Repeat ESR/CRP and whole body bone scan
CT of lumbar spine
Dynamic flexion/extension plain film radiographs
Dynamic lateral bending plain film radiographs
This patient has clinical and radiographic features of failed spinal arthrodesis. CT scan have been shown to be the most relable method for assessing spinal fusion postoperatively.
Reported rates of nonunion following posterior spinal fusion range from 0-70%. Rates are variable due to the various operative techniques, underlying diagnoses as well as asymptomatic patients. Non-union may lead to changes in alignment, spinal instability and potential neurological injury. Static radiographs have long been used as a practical method of fusion assessment, but these tend to significantly overestimate the presence of a solid fusion. Lack of movement at a fused segment, on dynamic views, does not confirm fusion. CT offers excellent bony resolution and are less affected by metal artifact compared to MRI.
Patel et al. showed that tobacco use, malnutrition, oral anti-inflammatory use, multilevel fusion, prior spine surgery, and sagittal imbalance are all risk factors for spinal nonunion.
Mok et al. looked at erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels after spinal surgery and compared their usefulness as predictors of infectious complications in the early postoperative period. They found that CRP is more applicable, predictable, and responsive in the early postoperative period compared with ESR. Using a second rise or failure to decrease as expected for CRP is sensitive for infection.
Shelby et al. reviewed the radiological assessment of spinal fusion. They comment that fine-cut imaging, multiplanar reconstruction, and metal artifact reduction have increased the ability to assess fusion on CT.
Figure A shows a series of lateral radiographs of the lumbar spine with posterior spinal instrumentation. Illustration A shows a lateral CT scan image of multi-level pseudoarthrosis after posterior spinal instrumented fusion. Illustration B shows an
intra-operative
view
of
spinal
pseudoarthrosis
(white
arrow).
Incorrect
(SBQ12SP.19) A 41-year-old male presents with acute onset of low back pain that started when he was trying to lift a heavy box while helping his brother move apartments two days ago. The pain has been severe enough to cause him to miss work yesterday. He has no neurologic deficits. What are the chances he will return to work within 6 weeks? Review Topic
1 80 to 90%
2 70 to 80%
3 60 to 70%
4 50 to 60%
5 40 to 50%
Most adults (up to 80%) will experience an episode of low back pain in their lifetime. In those whose pain is severe enough to cause them to miss work, 60 to 70% will return by 6 weeks, and 80 to 90% will return by 12 weeks.
Low back pain is common in adults. Most patients experience resolution of symptoms quickly and have no lasting loss of function. However, 5 to 10% develop chronic pain. Recurrence of pain is common, and is part of the natural history, occurring in 20 to 72% of patients. After 12 weeks, return to work rates are slow.
Shen et al. review the nonoperative management of acute and chronic low back pain. The authors note that none of the available interventions has been proven by high quality large randomized controlled trials. The authors believe that low dose oral
steroids are safe in the short term and that injection therapy should not be used without a reasonable presumptive diagnosis.
Madigan et al. review the management of lumbar degenerative disease. The authors emphasize that the majority of patients improve within 6 weeks with or without treatment. For patients that do not, the authors do not recommend epidural injection, as there are no good studies to support their use in the treatment of discogenic back pain. When surgical treatment is indicated they state that arthrodesis is the gold standard, although the long term results of total disk arthroplasty are being elucidated.
Illustration A shows a table of available non-operative treatment modalities for back pain. Illustration B shows a list of possible diagnoses associated with acute low back pain, with those associated with neurogenic pain italicized. Illustration C shows a list of 'red flag' symptoms indicating serious/emergent causes of low back pain.
Incorrect
2:
Longer
to than
90%
Question 76
A football player sustains a traumatic anterior inferior dislocation of the shoulder in the last game of the season. It is reduced 20 minutes later in the locker room. The patient is neurologically intact and has regained motion. If the patient undergoes arthroscopic evaluation, what finding is seen most consistently?
Explanation
REFERENCES: Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.
Bottoni CR, Wilckens JH, DeBerardino TM, et al: A prospective, randomized evaluation of arthroscopic stabilization versus nonoperative treatment in patients with acute, traumatic,
first-time shoulder dislocations. Am J Sports Med 2002;30:576-580.
Question 77
Figure 29a shows the clinical photograph of a 26-year-old woman who has had the leg deformity since birth. She reports difficulty with walking and weight bearing and notes increased discomfort and swelling when the leg is dependent. She denies any history of trauma or family history of a similar disorder. Examination reveals a fixed equinovarus deformity of the foot but no evidence of a limb-length discrepancy. No other cutaneous findings or soft-tissue masses are noted. Sagittal and axial T1- and T2-weighted MRI scans are shown in Figures 29b and 29c. What is the most likely diagnosis?
Explanation
REFERENCES: Berquist TH (ed): MRI of the Musculoskeletal System, ed 3. Philadelphia, PA, Lippincott Raven, 1997, p 771.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St. Louis, MO, Mosby Year Book, 1995, p 688.
Question 78
A 45-year-old woman sustains an injury to her lower leg. Examination reveals that there is a deformity with no neurologic or vascular problems. The skin is intact. Radiographs are shown in Figures 46a and 46b. Which of the following factors would make closed management the least appropriate choice for this injury?
Explanation
REFERENCES: Trafton PG: Tibial shaft fractures, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 2153-2169.
Martinez A, Sarmiento A, Latta LL: Closed fractures of the proximal tibia treated with a functional brace. Clin Orthop 2003;417:293-302.
Question 79
Figures below show the radiographs obtained from a 68-year old man with progressively worsening right side hip pain over the last 8 months. He is 6 feet tall, with a BMI of 51 kg/m2 and reports that his index total hip arthroplasty was performed 8 years ago. The preoperative work-up includes negative infectious laboratory results. What is the most appropriate surgical plan for revision of the femoral component in this patient?
Explanation
Submit Answer
The patient’s radiographs demonstrate varus femoral remodeling around a broken cylindrical, distally fixed femoral stem. Proximal femoral remodeling around loose or fractured stems occurs in 21% to 42% of femoral revisions, based on the definitions outlined by Foran and associates. In definition 1, varus femoral remodeling occurs when the template falls within 2 mm of the endosteal cortex of the metaphysis on templating with a diaphyseal engaging stem. In definition 2, varus femoral remodeling = when the template crosses the lateral femoral cortex proximally. Based on the templating or drawing a line from the isthmus proximally along the lateral cortex, implantation of a straight stem would perforate the cortex proximally, indicating varus femoral remodeling. An extended trochanteric osteotomy would aid in the removal of the well-fixed distal segment and enable the safe insertion of the new femoral component. The approach is not the concern in this case, because extended trochanteric osteotomies have been described from the posterior and direct lateral approaches with excellent outcomes and union rates. The key is that the extended osteotomy is necessary and not a trochanteric slide or standard (shorter or incomplete trochanteric) osteotomy. These types would not provide access to the well-fixed distal stem, nor would they afford a straight tube in which to insert a new femoral component.
Question 80
-Sideline examination of this patient showed no cervical pain or tenderness; motor and sensory function were normal; and his pupils were equal, round, and reactive. He was alert and oriented to the score of game, time on the clock, and current quarter of play. His iliac crest had mild tenderness but no swelling or crepitus. The player states that he has a slight headache and is no longer dizzy. What is the most appropriate treatment?
Explanation
Although this player limps off the field, the fact that he felt dizzy, had a headache, and did not initially recognize that he was playing in the third quarter indicates that he sustained a concussion. The player should be kept out of the game until a cognitive examination and repeat physical assessment is completed.Even if his physical symptoms have resolved, a certain period of time has expired, or he states that he is“ready,” he should not be returned to play prior to this assessment. Sending the patient to an emergency department should be considered only after this assessment and appropriate initial sideline treatment is initiated. The Consensus Statement on Concussion in Sport recommends that no athlete with concussion symptoms be returned to same-day play. This patient still has a slight headache, but even if this resolved he should not return to the game. Adolescents and high school athletes may have neurophysiological deficits that may not be evident on the sideline, or they may have a delayed onset of symptoms. A graduated return to play for future games is recommended.
CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29
A 32-year-old woman has a 2-year history of progressively worsening right groin pain that is exacerbated by activity. She reports no traumatic injury and an extensive work-up by her gynecologist has ruled out an intrapelvic source of her pain. The patient is a recreational athlete and exercises regularly in the gym.The pain is preventing her from performing these activities. She reports no catching or locking symptoms.Her examination reveals a physically fit female (BMI of 20) with limited right hip range of motion. She has no tenderness to palpation around the hip. While lying supine and bringing her hip into progressive flexion with internal rotation and adduction, her groin pain is reproduced. She has normal limb lengths and demonstrates weakness secondary to pain with hip flexion on the affected side.
Question 81
Figures 35a and 35b show the radiographs of a patient who underwent debridement of a chronically infected, fully constrained knee prosthesis and now reports pain and instability despite bracing. History reveals that the patient has had no drainage since undergoing the last debridement 6 months ago. A C-reactive protein level and aspiration are negative for infection. Treatment should now consist of
Explanation
REFERENCES: Rand JA: Alternatives to reimplantation for salvage of the total knee arthroplasty complicated by infection. J Bone Joint Surg Am 1993;75:282-289.
Lai KA, Shen WJ, Yang CY: Arthrodesis with a short Huckstep nail as a salvage procedure for failed total knee arthroplasty. J Bone Joint Surg Am 1998;80:380-388.
Damron TA, McBeath AA: Arthrodesis following failed total knee arthroplasty: Comprehensive review and meta-analysis of recent literature. Orthopedics 1995;18:361-368.
Question 82
Which of the following clinical scenarios represents an appropriate indication for convex hemiepiphysiodesis/hemiarthrodesis in the treatment of a child with a congenital spinal deformity?
Explanation
REFERENCE: Winter RB, Lonstein JE, Denis F, Sta-Ana de la Rosa H: Convex growth arrest for progressive congenital scoliosis due to hemivertebrae. J Pediatr Orthop 1988;8:633-638.
Question 83
What clinical scenario is most consistent with the MR image of the L4-L5 disk level shown in Figure 14? Review Topic
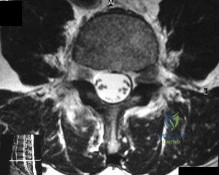
Explanation
Question 84
A 19-year-old male collegiate rower has a 3-month history of right shoulder pain. There was no inciting trauma prior to the onset of his pain. He also complains of weakness, particularly in abduction and overhead activity. Examination reveals no range-of-motion deficits. Strength testing of the right shoulder demonstrates 4/5 motor strength in forward elevation and abduction. His Beighton hypermobility score is 3/9. Figure 1 shows his scapular position during a wall pushup maneuver. An EMG would likely reveal damage to what nerve?

Explanation
Question 85
The patient undergoes further testing and it is discovered that the lesion encompasses 70% of the joint. What is the best next treatment option?
Explanation
A tarsal coalition is an abnormal connection of 2 or more bones in the foot. Although tarsal coalitions are present at birth, children and adults typically do not show signs of the disorder until early adolescence or later. The exact incidence of the disorder is hard to determine; however, it is caused by a gene mutation that affects cells that produce the tarsal bones. The 2 most common locations for tarsal coalitions are between the calcaneus and the navicular or between the talus and the calcaneus. It is estimated that 1 out of every 100 people may have a tarsal coalition. In 50% of cases, both feet are affected. Tarsal coalitions are rarely discovered until symptoms arise. Symptoms may include stiff and painful feet, a rigid flatfoot, or increased pain or a limp with high-level activities. Upon examination, symptoms may include tenderness in the area of the coalition, loss of motion, rigid flat feet, and arthritic changes of the joint. Imaging studies begin with radiographs. A CT scan can provide bony detail for imaging tarsal coalitions and determining the extent of the coalition and any accompanying degenerative change. MRI can provide details of the soft tissues. Treatment includes nonsurgical care including rest, orthotics, a temporary boot or cast, and injections. Surgical options include resection with interposition of muscle or fatty tissue from another area of the body or fusions when large (exceeding 50% of the joint), more severe coalitions are encountered.
RECOMMENDED READINGS
Lemley F, Berlet G, Hill K, Philbin T, Isaac B, Lee T. Current concepts review: Tarsal coalition. Foot Ankle Int. 2006 Dec;27(12):1163-9. Review. PubMed PMID: 17207452. View Abstract at PubMed
Badgley CE. Coalition of the calcaneus and the navicular. Arch Surg. 1927;15:75-88. Conway JJ, Cowell HR. Tarsal coalition: clinical significance and roentgenographic demonstration. Radiology. 1969 Mar;92(4):799-811. PubMed PMID: 5767760. View Abstract at PubMed
Herzenberg JE, Goldner JL, Martinez S, Silverman PM. Computerized tomography of talocalcaneal tarsal coalition: a clinical and anatomic study. Foot Ankle. 1986 Jun;6(6):273-
Question 86
Based on the MR arthrogram of the elbow shown in Figure 8, which of the following structures is torn?
Explanation
MR arthrography provides improved sensitivity compared to conventional MRI, without contrast, for the detection of UCL pathology, particularly in the subacute or chronic setting. After the soft-tissue edema and joint fluid associated with the injury have resolved, the torn end of the ligament may lie in contact with its adjacent attachment and create a false-negative appearance. In this patient, a noncontrasted MR arthrogram showed no tear, yet the tear is apparent with intra-articular contrast and distention. MR arthrography of the elbow also may be useful in detecting intra-articular bodies or in evaluation for loose osteochondral fragments or flaps.
REFERENCES: Morrey BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128.
Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 200-210.
Question 87
Which of the following is considered a contraindication to functional bracing for the treatment of humeral shaft fractures?
Explanation
1) massive soft-tissue or bone loss; 2) an unreliable or noncompliant patient; and 3) an inability to maintain acceptable fracture alignment of up to 20 degrees of anterior or posterior angulation, 30 degrees of varus or valgus angulation, and greater than 3 cm of shortening.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Pollock FH, Drake D, Bovill EG, Day L, Trafton PG: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Sarmiento A. Zagorski JB, Zych GA, et al: Functional bracing for the treatment of fractures of the humeral diaphysis. J Bone Joint Surg Am 2000;82:478-486.
Question 88
A 45-year-old recreational tennis player underwent arthroscopic decompression and mini-open repair of a small supraspinatus tendon tear 3 weeks ago after nonsurgical management failed to provide relief. He now has pain, swelling about the wound, erythema, and purulent drainage. The patient is returned to the operating room for irrigation, debridement, and cultures. What is the most common organism causing this infection?
Explanation
REFERENCES: Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Settecerri JJ, Pitner MA, Rock MG, et al: Infection after rotator cuff repair. J Shoulder Elbow Surg 1999;8:1-5.
Question 89
Figures 15a and 15b are the radiographs of a 28-year-old man who fell from a height and sustained an isolated closed diaphyseal femur fracture that was treated with reamed antegrade femoral nailing 8 months ago. He now reports persistent pain during ambulation. He smokes one pack of cigarettes per day but is otherwise healthy. He denies any infectious history or symptoms, and laboratory studies show a normal WBC count, erythrocyte sedimentation rate, and C-reactive protein. What is the most appropriate treatment?

Explanation
Question 90
What is the most significant prognostic factor in nontraumatic osteonecrosis of the humeral head?
Explanation
REFERENCES: Cruess RL: Osteonecrosis of bone: Current concepts as to etiology and pathogenesis. Clin Orthop 1986;208:30-39.
Cruess RL: Steroid-induced avascular necrosis of the humeral head: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
Rutherford CS, Cofield RH: Osteonecrosis of the shoulder. Orthop Trans 1987;11:239.
Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Relationship of disease stage, extent, and cause to natural history. J Shoulder Elbow Surg 1999;8:559-564.
Question 91
A 70-year-old woman with a body mass index (BMI) of 34 and a history of hypercholesterolemia has elected to undergo total hip arthroplasty. Her son recently learned he has factor V Leiden following an episode of pulmonary embolism. What are this patient's risk factors for thromboembolic disease?
Explanation
Risk stratification is one of the most critical clinical evaluations to undertake before performing total joint arthroplasty. Many factors have been identified that increase the risk for venous thromboembolism (VTE) The major factors include previous VTE, obesity, type of surgery (such as total joint arthroplasty), hypercoagulable states, myocardial infarction, congestive heart failure, family history of VTE, and hormone replacement therapy. Hypercholesterolemia is not a risk factor for thromboembolic disease.
Question 92
A 15-year-old male jumps off a 6 foot ramp and lands awkwardly. His knee swells up immediately and he is taken to the emergency room. Figures A is a sagittal CT scan image. In the next 3 hours, he complains of increasing leg pain. This is likely because of injury to which of the following structures? Review Topic

Explanation
Tibial tubercle fractures usually occur during aggressive quadriceps contraction during sports. The Ogden classification classifies this by site of fracture (Type I, through the tubercle; Type II, at the level of the tibial physis; Type III, extending through the anterior tibial epiphysis). Other complications include extensive soft tissue damage, periosteal stripping, vascular compromise and intra-articular damage.
Pandya et al. reviewed 41 tibial tubercle fractures. They found compartment syndrome or vascular compromise in nearly 10%. They found that the degree of injury was underestimated 50% of the time when classified using lateral radiographs alone. They recommend CT scan or MRI as an adjunct. If intra-articular involvement is seen, arthroscopy or open arthrotomy should be performed.
Pape et al. describe 2 case reports of anterior compartment syndrome after tibial tubercle fracture. The compartment syndrome occurs as a result of proximity of the tibial tubercle physis to the anterior tibial recurrent artery.
Figure A shows the sagittal reconstruction CT image showing intraarticular involvement. Illustrations A and B are axial and coronal CT images in the subchondral region showing the fracture line traversing the zone between fused and unfused physis (see Illustration C for physeal closure pattern). Illustration C shows the direction of closure of the proximal tibial physis. In the sagittal plane, the proximal tibial physis closes from posterior to anterior, then to the tubercle apophysis which closes from proximal to distal also. In the coronal plane, the physis closes from medial to lateral. In the axial plane, the physis closes from posteromedial to anterolateral. Illustration D shows the anterior tibial recurrent artery.
Incorrect Answers:
Question 93
A 68-year-old male presents with gait instability, clumsiness of the hands, and the MRI images shown in Figure A. You decide to proceed with surgical decompression. When planning your surgical treatment, it is important to note that compared to a posterior approach, the anterior procedure has: Review Topic

Explanation
Cervical myelopathy has a progressive course and therefore if there is evidence of functional impairment surgical decompression is indicated. Either an anterior decompression or posterior decompression can be used depending on a variety of factors including number of levels involved and sagittal alignment of the cervical spine. In general, a posterior approach is used when three or more levels are involved and the spine is in neutral or lordotic alignment.
Fehlings et al. did a prospective study on the risks of complications associated with surgical treatment of cervical myelopathy. They found that combined anterior and posterior procedures had a significantly higher rate of complication than either anterior-only or posterior-only procedures. Posterior procedures had a higher rate of wound infections compared to anterior. They found no statistical difference in the over-all complication rate, incidence of C5 radiculopathy, or dysphagia between an anterior-only or posterior-only procedure.
Fehlings et al. did a prospective study on outcomes following surgical treatment of cervical myelopathy. At one year follow-up they found a significant improvement in mJOA score, Nurick grade, NDI score, and all SF-36v2 dimensions. With the exception of mJOA scores, these improvements were not statistically related to severity of disease.
Liu et al. performed a meta-analysis of outcomes following surgical decompression of cervical myelopathy. They found outcomes following anterior procedures were better than those for posterior procedures when there were less than 3 affected levels. With 3 or greater levels, no statistical difference in outcomes could be found between the two approaches. They note none of their reviewed publications represent high-quality prospective randomized trials.
Figure A is a sagittal MR image of the cervical spine showing multi-level degenerative disease with cord compression consistent with cervical myelopathy.
Incorrect Answers:
Question 94
During surgical treatment of the most common variation of distal femoral "Hoffa" fractures, which of the following orientations for screw fixation should be used?

Explanation
Hoffa fractures are coronally oriented fractures of the femoral condyles, with most occurring in the lateral condyle. They are commonly associated with high-energy fractures of the distal femur and can often be overlooked during the assessment and treatment of distal femur fractures. Hoffa fractures are best evaluated using CT scans.
Nork et al. studied the association of supracondylar-intercondylar distal femoral fractures and coronal plane fractures. Of 202 supracondylar-intercondylar distal femoral fractures, they found coronal plane fractures were diagnosed in 38%. A coronal fracture of the lateral femoral condyle was involved more frequently than the medial condyle. Eighty-five percent of these coronal fractures involved a single lateral femoral condyle.
Holmes et al. looked at five cases of coronal fractures of the femoral condyle. All cases received open reduction and internal fixation with lag screws through a formal parapatellar approach. They reported good results with all fractures healing within 12 weeks without complications with final range of motion at least 0 degrees to 115 degrees.
Question 95
- To maximally resist apex anterior angulation in the tibia, the pins of a unilateral external fixator should be oriented in which of the following planes?
Explanation
Question 96
Figure 7 shows the MRI scan of a 23-year-old competitive rugby player who has anterior ankle pain and swelling. He states that he has been playing for many years and has sprained his ankle several times. Examination will reveal what specific hallmark feature?
Explanation
REFERENCES: Ogilvie-Harris DJ, Mahomed N, Demaziere A: Anterior impingement of the ankle of the ankle treated by arthroscopic removal of bony spurs. J Bone Joint Surg Br 1993;75:437-440.
Cannon LB, Hackney RG: Anterior tibiotalar impingement associated with chronic ankle instability. J Foot Ankle Surg 2000;39:383-386.
Question 97
Figure 36a shows the current radiograph of a 65-year-old woman who slipped and fell. History reveals that prior to the fall she was actively functioning without pain. Figure 36b shows a radiograph obtained 1 year ago. Based on the fracture pattern, the failure is most likely related to
Explanation
REFERENCES: Johansson JE, McBroom R, Barrington TW, Hunter GA: Fracture of the ipsilateral femur in patients with total hip replacement. J Bone Joint Surg Am 1981;63:1435-1442.
Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242.
Question 98
A 77-year-old man with diabetes mellitus has had a nonhealing Wagner grade I ulcer under the medial sesamoid for the past 3 months. He smokes tobacco regularly. He has undergone several debridements and total contact casting. Examination reveals no palpable pulses. He has no erythema or purulence, and he is afebrile. Radiographs reveal no abnormalities. What is the best initial diagnostic test to help determine why the ulcer has failed to heal?
Explanation
REFERENCE: Brodsky JW: Evaluation of the diabetic foot. Instr Course Lect 1999;48:289-303.
Question 99
Which one of the following lower extremity amputations requires a soft-tissue balancing procedure to prevent deformity following amputation? Review Topic
Explanation
Question 100
The posterior horn of the medial meniscus receives its primary blood supply from what artery?
Explanation
REFERENCES: Insall J, Scott WN: Anatomy, in Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, pp 64-70.
Scapinelli R: Vascular anatomy of the human cruciate ligaments and surrounding structures. Clin Anat 1997;10:151-162.
