Orthopedic Surgery Board Review MCQs: Ligament, Nerve & Spine | Part 239

Key Takeaway
This page offers Part 239 of a comprehensive OITE/AAOS Orthopedic Surgery Board Review series for residents and surgeons. It features 100 high-yield, verified MCQs by Dr. Mohammed Hutaif, specifically covering Ligament and Nerve topics. Utilize study and exam modes to rigorously prepare for your board certification.
About This Board Review Set
This is Part 239 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 239
This module focuses heavily on: Ligament, Nerve.
Sample Questions from This Set
Sample Question 1: The findings in Brown-Sequard syndrome include loss of which of the following? Review Topic...
Sample Question 2: preservation of the radioscaphocapitate ligament, the most radial of the palmar extrinsic ligaments, which prevents ulnar subluxation after proximal row carpectomy....
Sample Question 3: Which of the following structures is most vulnerable during a medial sesamoidectomy of the hallux?...
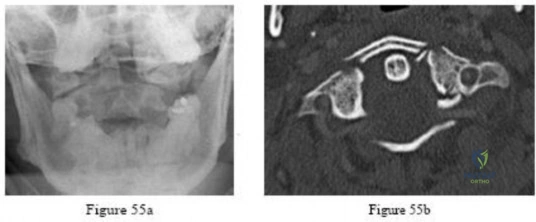
Sample Question 4: -Figures 55a and 55b are the radiograph and CT scan of a 61-year-old woman who has had neck pain after being involved in a high-speed motor vehicle collision.Examination reveals normal strength and sensation in both upper and lower extremit...
Sample Question 5: What spinal nerves in the cauda equina are primarily responsible for innervation of the bladder?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The findings in Brown-Sequard syndrome include loss of which of the following? Review Topic
Explanation
Question 2
preservation of the radioscaphocapitate ligament, the most radial of the palmar extrinsic ligaments, which prevents ulnar subluxation after proximal row carpectomy.
Explanation
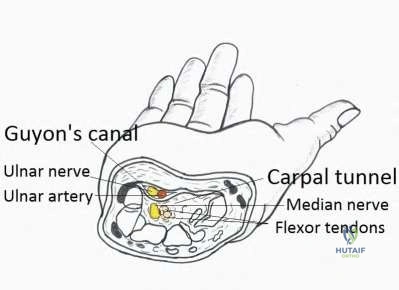
A 37-year-old patient with type I diabetes mellitus has a flexor tenosynovitis of the thumb flexor tendon sheath following a kitchen knife puncture wound to the volar aspect of the thumb. Left unattended, this infection will likely first spread proximally creating an abscess in which of the following spaces of the palm?
Central space
Hypothenar space
Carpal tunnel
Posterior adductor space
Thenar space CORRECT ANSWER: 5
Flexor tenosynovitis of the thumb flexor tendon sheath can spread proximally and form an abscess within the thenar space of the palm. The flexor pollicis longus tendon does not pass through the central space of the palm or the hypothenar space of the palm. The flexor pollicis longus tendon does pass through the carpal tunnel, but this is not a palmar space. The three palmar spaces include the hypothenar space, the thenar space, and the central space. The posterior adductor space would likely only be involved secondarily after spread from a thenar space infection.
New painful paresthesias near the site of the incision after an ulnar nerve transposition is the result of injury to what nerve?
Medial antebrachial cutaneous
Lateral antebrachial cutaneous
Posterior antebrachial cutaneous
Medial brachial cutaneous
Dorsal antebrachial cutaneous
Branches of the medial antebrachial cutaneous nerve can often be identified during routine ulnar nerve surgery crossing the medial aspect of the elbow. It should be preserved to avoid development of painful paresthesias.
A 21-year-old man who was injured in a snowboarding accident 18 months ago now reports wrist pain. An MRI scan is shown in Figure
Question 3
Which of the following structures is most vulnerable during a medial sesamoidectomy of the hallux?
Explanation
REFERENCE: Sarrafian SK: Anatomy of the Foot and Ankle, Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, p 377.
Question 4
-Figures 55a and 55b are the radiograph and CT scan of a 61-year-old woman who has had neck pain after being involved in a high-speed motor vehicle collision. Examination reveals normal strength and sensation in both upper and lower extremities, normal rectal tone, and no other injuries. The C1-C2 lateral mass overhang measures 8.5 mm. What is the most appropriate treatment option?
Explanation

Question 5
What spinal nerves in the cauda equina are primarily responsible for innervation of the bladder?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton-Century-Crofts, 1976, p 254.
Pick TP, Howden R (edS): Gray’s Anatomy. New York, NY, Bounty Books, 1977, p 1004.
Question 6
03 A 23 year old sustains an isolated right knee dislocation in an MVA. A closed reduction is performed and confirmed with radiographs. What is the next appropriate study?
Explanation
OKU Truama 2 says “the use of ABI with the blood pressure cuff and Doppler evaluation of the distal circulation has been proposed as effective in determining any occult vascular injury. A ratio > 0.9indicates a normal study.”[1] The referenced article confirms this. “Confirmation of the safety and accuracy of physical exam in the evaluation of knee dislocation for injury of the popliteal artery.” J. Trauma2002; 52: 247-252
back to this question next question
[1] OKU Trauma 2 pg 151-153
Question 7
Figure below depicts the radiograph obtained from a 52-year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?
Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 8
During total knee arthroplasty using a posterior cruciate-retaining design, excessive tightness in flexion is noted, while the extension gap is felt to be balanced. Which of the following actions will effectively balance the knee?
Explanation
REFERENCE: Ayers DC, Dennis DA, Johanson NA, Pelligrini VD: Common complications of total knee arthroplasty. J Bone Joint Surg Am 1997;79:278-311.
Question 9
Which repair technique for an osteochondral lesion of the medial talus shoulder produces hyaline cartilage that is similar to native cartilage and will not degrade over time?
Explanation
Autologous osteochondral transplantation (typically involving tubular grafts harvested from the knee) has been shown to replace a talar defect with viable hyaline cartilage. The results over the medium term show good clinical outcomes, and MRI studies reveal cartilage repair similar to native cartilage. Chondroplasty and arthroscopic bone-marrow stimulation are both associated with good clinical results for smaller lesions, but these techniques develop fibrocartilaginous repair tissue composed of type I collagen instead of hyaline cartilage. Osteochondral transplantation of fresh allografts performed less than 14 days after harvest contains high chondrocyte viability. Few clinical studies report long-term results, but radiographic studies demonstrate high rates of collapse and resorption. Joint space narrowing has been noted in 60% of ankles treated with bulk grafts after an average of 44 months. Autologous chondrocyte implantation (both periosteum-covered and matrix-associated techniques) has been shown to create hyaline cartilage in some studies, but fibrocartilage creation has been reported in others.
RECOMMENDED READINGS
Schachter AK, Chen AL, Reddy PD, Tejwani NC. Osteochondral lesions of the talus. J Am Acad Orthop Surg. 2005 May-Jun;13(3):152-8. Review. PubMed PMID: 15938604. View Abstract at PubMed
Mitchell ME, Giza E, Sullivan MR. Cartilage transplantation techniques for talar cartilage lesions. J Am Acad Orthop Surg. 2009 Jul;17(7):407-14. Review. PubMed PMID: 19571296. View Abstract at PubMed
Murawski CD, Kennedy JG. Operative treatment of osteochondral lesions of the talus. J Bone Joint Surg Am. 2013 Jun 5;95(11):1045-54. doi: 10.2106/JBJS.L.00773. Review. PubMed PMID: 23780543. View Abstract at PubMed
Question 10
What is the most common cause of rotator cuff injury in high school athletes?
Explanation
REFERENCES: Wilkins KE: Shoulder injuries: Epidemiology, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 175-182.
Sher JS: Anatomy, biomechanics, and pathophysiology of rotator cuff disease, in Iannnotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 3-30.
Question 11
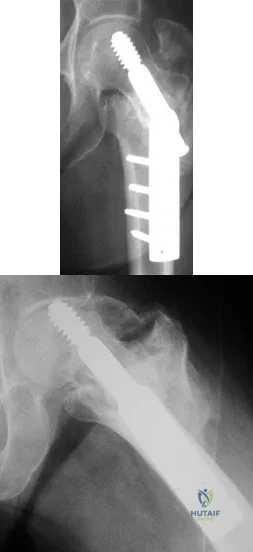
Figures A and B show the six-month follow-up radiographs of a 62-year-old woman who sustained a hip fracture in a fall. Prior to the fall, the patient was active and had no difficulty with ambulation. The patient underwent open reduction and internal fixation with a sliding hip screw device. She has difficulty with ambulation, continues to walk with a walker, and reports startup pain. What is the most appropriate management at this time? Review Topic
Explanation
Question 12
Figures 42a and 42b shows the radiographs of a 20-year-old man who sustained a hyperextension injury to his little finger. Multiple attempts at closed reduction have been unsuccessful. Management should now consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Becton JL, Christian JD Jr, Goodwin HN, Jackson JG III: A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am 1975;57:698-700.
Green DP, Terry GC: Complex dislocation of the metacarpophalangeal joint: Correlative pathological anatomy. J Bone Joint Surg Am 1973;55:1480-1486.
Question 13
During surgical treatment of the most common variation of distal femoral "Hoffa" fractures, which of the following orientations for screw fixation should be used?

Explanation
Hoffa fractures are coronally oriented fractures of the femoral condyles, with most occurring in the lateral condyle. They are commonly associated with high-energy fractures of the distal femur and can often be overlooked during the assessment and treatment of distal femur fractures. Hoffa fractures are best evaluated using CT scans.
Nork et al. studied the association of supracondylar-intercondylar distal femoral fractures and coronal plane fractures. Of 202 supracondylar-intercondylar distal femoral fractures, they found coronal plane fractures were diagnosed in 38%. A coronal fracture of the lateral femoral condyle was involved more frequently than the medial condyle. Eighty-five percent of these coronal fractures involved a single lateral femoral condyle.
Holmes et al. looked at five cases of coronal fractures of the femoral condyle. All cases received open reduction and internal fixation with lag screws through a formal parapatellar approach. They reported good results with all fractures healing within 12 weeks without complications with final range of motion at least 0 degrees to 115 degrees.
Question 14
Figures 10a and 10b show the clinical photograph and MRI scan of a plantar foot lesion. If excisional biopsy is performed, what is the most likely complication?
Explanation
If surgery is indicated, wide local excision with excision of the entire plantar fascia is usually indicated. The main problem with simple excision of the lesion is the high chance of recurrence. The other listed complications are those that are a result of the wide local excision.
REFERENCES: Aluisio FV, Mair SD, Hall RL: Plantar fibromatosis: Treatment of primary and recurrent lesions and factors associated with recurrence. Foot Ankle Int 1996;17:672-678.
Bos GD, Esther RJ, Woll TS: Foot tumors: Diagnosis and treatment. J Am Acad Orthop Surg 2002;10:259-270.
Question 15
An 11-year-old boy with bipolar disorder fell from a tree and sustained an open fracture dislocation of the right ankle with extensive abrasions of the leg. Immediate irrigation, debridement, reduction, and provisional fixation with Kirschner wires was performed. Twenty-four hours later, the patient’s blood pressure is 190/100 mm Hg and pulse rate is 120. He has required only 1 dose of an oral analgesic for pain control. His foot and ankle are markedly swollen, but there is no pain on passive extension of the toes. The dorsalis pedis pulse cannot be palpated. What is the most appropriate next treatment step? Review Topic
Explanation
(SBQ13PE.91) An 12-year-old girl presents with right hip pain. Bilateral frog laterals are shown in Figure A. Laboratory work-up reveals TSH 11 mIU/L (Ref range: 0.4-4.0 mIU/L) and Free T4 is 0.5 ng/dL (Ref range: 0.7-1.9 ng/dL). What is the most appropriate treatment recommendation? Review Topic

In situ pinning of right hip
Protected weight bearing and MRI of right hip
Immediate endocrine referral and treatment
Open biopsy right hip
In situ pinning bilateral hips PREFERRED RESPONSE 5
In patients with slipped capital femoral epiphysis (SCFE) and concomitant endocrinopathy, bilateral pinning is the recommended treatment.
This patient's laboratory values reveal hypothyroidism, which increases the risk of bilateral involvement. Thus, the most appropriate treatment recommendation is surgical fixation of both hips.
Wells et al. analyzed 131 SCFEs over a 30-year period. The authors noted that 100% of patients with associated endocrinopathy went onto contralateral slip and recommended not only prophylactic pinning, but in those with open triradiate cartilage, recommended preventative screening with TSH/Free T4 laboratory studies.
Riad et al. followed 90 patients and analyzed impact of age, gender and race on contralateral slip development. Girls under the age of 10 and boys under the age of 12 had a significantly increased risk of contralateral involvement. Therefore, the authors recommended contralateral pinning for girls and boys that met those age criteria, respectively.
Figure A exhibits a right SCFE on bilateral frog lateral views. Incorrect Answers:
Question 16
During the revision surgical procedure, thoracic pedicle screws are placed. Following placement, triggered electromyography (EMG) is performed by stimulating the pedicle screw heads. During testing the right T2 pedicle screw head returns a threshold of 2 mA. What does this reading indicate?
Explanation
This patient has developed a proximal junctional kyphosis following a long posterior fusion performed for treatment of degenerative lumbar scoliosis. Risk factors for proximal junctional kyphosis in the setting of instrumented fusions performed for degenerative scoliosis include advanced age, 360-
degree fusions, extension of fusion constructs to the sacrum, and upper instrumented vertebrae at the level of T1-3. The patient's junctional kyphosis is attributable to failure of the disk and ligamentous structures at T2-3 and would be graded as type I using the classification system of Yagi and associates. Most symptomatic proximal junctional kyphoses are treated with posterior extension of the fusion construct to a more proximal level spanning the kyphosed region. The use of orthoses or simple removal of instrumentation is unlikely to substantively impact symptoms or address the proximal kyphosis. Diabetes and obesity are known factors that increase risk for postsurgical infection following a spine fusion procedure. The most frequent complication following revision surgery for proximal junctional kyphosis, however, is the need for further surgery. In the study by Yagi and associates, 48% of patients who underwent revision surgery for proximal kyphosis developed further adjacent segment degeneration. In the proximal thoracic spine, where the pedicle may be narrow, triggered EMG testing of inserted pedicle screws may be used to assess for violation of the pedicle wall during insertion. In the setting of triggered EMG, thresholds exceeding 10 mA indicate a well-placed pedicle screw. Thresholds lower than 4 mA to 6 mA indicate that a screw is directly contacting a neural structure. Thresholds between 9 mA and 10 mA suggest that a breach of the pedicle may be present, but the screw is not contacting a neural structure.
RECOMMENDED READINGS
Yagi M, Rahm M, Gaines R, Maziad A, Ross T, Kim HJ, Kebaish K, Boachie-Adjei O; Complex Spine Study Group. Characterization and surgical outcomes of proximal junctional failure in surgically treated patients with adult spinal deformity.Spine (Phila Pa 1976). 2014 May 1;39(10):E607-14. doi: 10.1097/BRS.0000000000000266. PubMed PMID: 24525992. View
Abstract at PubMed
Cammarata M, Aubin CÉ, Wang X, Mac-Thiong JM. Biomechanical risk factors for proximal junctional kyphosis: a detailed numerical analysis of surgical instrumentation variables. Spine (Phila Pa 1976). 2014 Apr 15;39(8):E500-7. doi: 10.1097/BRS.0000000000000222. PubMed
PMID: 24480964. View Abstract at PubMed
Kim HJ, Lenke LG, Shaffrey CI, Van Alstyne EM, Skelly AC. Proximal junctional kyphosis as a distinct form of adjacent segment pathology after spinal deformity surgery: a systematic review. Spine (Phila Pa 1976). 2012 Oct 15;37(22 Suppl):S144-64. doi: 10.1097/BRS.0b013e31826d611b. PubMed PMID: 22885829. View Abstract at PubMed Schoenfeld AJ, Carey PA, Cleveland AW 3rd, Bader JO, Bono CM. Patient factors, comorbidities, and surgical characteristics that increase mortality and complication risk after spinal arthrodesis: a prognostic study based on 5,887 patients. Spine J. 2013 Oct;13(10):1171-9. doi: 10.1016/j.spinee.2013.02.071. Epub 2013 Apr 9. PubMed PMID:
Question 17
What measure of physiologic status best evaluates whether an injured patient is fully resuscitated and best predicts that perioperative complications will be minimized following definitive stabilization of long bone fractures?
Explanation
REFERENCES: Blow O, Magliore L, Claridge JA, et al: The golden hour and silver day: Detection and correction of occult hypoperfusion within 24 hours improves outcomes from major trauma. J Trauma 1999;47:964-977.
Crowl A, Young JS, Kahler DM, et al: Occult hypoperfusion is associated with increased morbidity in patients undergoing early femur fracture fixation. J Trauma 2000;48:260-267.
Shulman AM: Prediction of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:725-800.
Question 18
Which of the following areas of the vertebral segment has the highest ratio of cortical to cancellous bone? Review Topic
Explanation
Question 19
Figures 45a and 45b show the radiographs of a 40-year-old woman with rheumatoid arthritis who is unable to straighten her ring and little fingers. Examination reveals that the fingers can be passively corrected, but she is unable to actively maintain the fingers in extension. Management should consist of
Explanation
REFERENCES: Feldon P, Terrono AL, Nalebuff EA, et al: Rheumatoid arthritis and other connective tissue diseases: Tendon ruptures, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999,
pp 1669-1684.
Moore JR, Weiland AJ, Valdata L: Tendon ruptures in the rheumatoid hand: Analysis of treatment and functional results in 60 patients. J Hand Surg Am 1987;12:9-14.
Leslie BM: Rheumatoid extensor tendon ruptures. Hand Clin 1989;5:191-202.
Question 20
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. The patient fails an extensive course of physical therapy and is unable to return to baseball. He and his orthopaedic surgeon elect to proceed with surgery. During a repeat evaluation, he has negative sulcus and Beighton sign findings, and radiographs show 5° of glenoid retroversion. What is the most appropriate surgical plan?
Explanation
and degenerative joint disease.
Question 21
Osteopenia is defined by the World Health Organization (WHO) as a bone mineral density (BMD) that is
Explanation
The T-score represents a comparison to young normals or optimum peak density. The Z-score represents a comparison of BMD to age-matched normals. Measurements of bone mineral density (BMD) at various skeletal sites help in predicting fracture risk. Hip BMD best predicts fracture of the hip, as well as fractures at other sites.
REFERENCE: Kanis JA, Johnell O, Oden A, et al: Risk of hip fracture according to the World Health Organization criteria for osteopenia and osteoporosis. Bone 2000;27:585-590.
Question 22
A 59-year-old woman with a history of osteoporosis is involved in a high-speed motor vehicle accident, resulting in left hip pain and deformity. The initial radiograph from the trauma bay is shown in Figure 1. Postreduction CT is shown in Figures 2 through 4. What is the most appropriate definitive surgical treatment?
Explanation
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
Question 23
Examination of a 12-year-old girl with a painful flatfoot deformity reveals tenderness in the region of the sinus tarsi and no appreciable subtalar motion. Radiographs are shown in Figures 48a through 48c. Two attempts to relieve her symptoms by cast immobilization fail to relieve the pain. Management should now consist of
Explanation
REFERENCES: Gonzalez P, Kumar SJ: Calcaneonavicular coalition treated by resection and interpostion of the extensor digitorum brevis muscle. J Bone Joint Surg Am 1990;72:71-77.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 211-218.
Question 24
A positive straight leg raising sign is when pain radiates distal to the knee when the affected leg is passively elevated. The increased tension generally occurs between Review Topic
Explanation
Question 25
A 5-year-old girl sustains an isolated injury to the right shoulder area after falling off the monkey bars. Examination reveals intact neurovascular function in the extremity distally, but she is quite uncomfortable. An AP radiograph of the proximal humerus is shown in Figure 24. Her parents state that she is a very talented gymnast. Considering her age and potential athletic career, management should consist of
Explanation
REFERENCES: Martin RF: Fractures of the proximal humerus and humeral shaft, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994,
pp 144-148.
Sanders JO, Rockwood CA Jr, Curtis RJ: Fractures and dislocation of the humeral shaft and shoulder, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 937-939.
Question 26
Compared to postoperative radiation therapy, preoperative radiation therapy has a higher rate of what complication?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Davis AM, O’Sullivan B, Turcotte R, et al: Late radiation morbidity following randomization to preoperative versus postoperative radiotherapy in extremity soft tissue sarcoma. Radiother Oncol 2005;75:48-53.
Question 27
Figure 74 shows the radiograph of an 84-year-old woman who reports severe right knee pain. At the time of total knee arthroplasty, she is found to have gross insufficiency and attenuation of the medial collateral ligament (MCL) complex. Optimal management should consist of
Explanation
REFERENCES: Lachiewicz PF, Soileau ES: Ten-year survival and clinical results of constrained components in primary total knee arthroplasty. J Arthroplasty 2006;21:803-808.
Anderson JA, Baldini A, MacDonald JH, et al: Primary constrained condylar knee arthroplasty without stem extensions for the valgus knee. Clin Orthop Relat Res 2006;442:199-203.

Question 28
An 82-year-old osteoporotic woman undergoes total hip arthroplasty for osteoarthritis. During implant trialing, a crack is heard. Intraoperative fluoroscopy reveals a long, spiral fracture of the distal femur. The fracture is reduced and fixed with an anatomic locking plate. The rest of the total hip arthroplasty proceeds uneventfully. Following surgery the surgeon has a meeting with the family and apologizes and provides full disclosure, accepts responsibility, provides a detailed explanation as to what happened, and gives reassurance that steps will be taken to prevent recurrences. This communication approach will most likely
Explanation
In the event of a medical error or adverse event, effective communication with the patient and family is necessary. Effective communication should comprise: an apology, full disclosure (an explanation of what happened), accepting responsibility, and corrective steps that will be taken to prevent recurrence.While accepting responsibility is integral to the explanation process, it is different from accepting blame.
Mazor et al. found patients would more likely change physicians and seek legal advice in situations with a life-threatening outcome where physicians chose nondisclosure. They recommend full disclosure, acceptance of responsibility, an apology, detailed explanations, and assurances that steps will be taken to prevent recurrences will result in positive outcomes in terms of patient satisfaction, trust, and emotional response.
MacDonald et al. addressed medical errors in an editorial. Besides full disclosure, they feel that an apology is necessary. This includes an acknowledgement of the event and one’s role in the event, and a genuine expression of regret. Apology laws exist to to reduce concerns about legal implications of disclosure and apology.
Incorrect Answers:
Question 29
A 20-year-old athlete sustains a 2- x 3-cm grade IV chondral injury to the right knee. After failure of nonsurgical management, which of the following procedures would ensure the highest percentage of hyaline-like cartilage?
Explanation
REFERENCES: Brittberg M, Lindahl A, Nilsson A, et al: Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 1994;331:889-895.
Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 787-804.
Question 30
A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
Explanation
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
Question 31
A 47-year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the
aspiration and proceed to a revision TKA with possible augments on standby.
Question 32
A 19-year-old college football player reports persistent weakness, tingling, and numbness of both upper extremities at half time. He states that these symptoms initially occurred after tackling an opposing player with his head early in the game. History reveals that he has had “burners” in the past that typically resolved within 15 to 30 minutes. Examination reveals pain-free cervical motion, weakness to shoulder abduction testing bilaterally, normal upper extremity reflexes, and decreased sensation over both shoulders and the upper arms. Appropriate initial management should consist of
Explanation
REFERENCES: Torg JS, Sennett B, Pavlov H, et al: Spear tackler’s spine: An entity precluding participation in tackle football and collision activities that expose the cervical spine to axial energy inputs. Am J Sports Med 1993;21:640-649.
Torg JS: Cervical spinal stenosis with cord neurapraxia and transient quadriplegia. Sports Med 1995;20:429-434.
Torg JS, Guille JT, Jaffe S: Injuries to the cervical spine in American football players. J Bone Joint Surg Am 2002;84:112-122.
Question 33
A 26-year-old professional rodeo bull rider sustained a grade III midshaft femoral fracture after being thrown from his bull. He underwent closed interlocking intermedullary nailing with a titanium rod, and his recovery was uneventful. Prior to returning to competition, the patient must
Explanation
least 1 year.
REFERENCES: Brumback RJ, Ellison TS: Intermedullary nailing of femoral stress fractures. J Bone Joint Surg Am 1992;74:106-112.
Bucholz RW, Jones A: Fractures of the shaft of the femur. J Bone Joint Surg Am
1991;73:1561-1566.
Butler MS, Brumback RJ: Interlocking nailing for ipsilateral fractures of the femur, femoral shaft, and distal part of the femur. J Bone Joint Surg Am 1991;73:1492-1502.
Question 34
Risk for vascular injury during transtibial drilling for reconstruction of this injury is increased by
Explanation
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, 1 major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading.
In Question 12, the scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-
producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag.
Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used. Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
Question 35
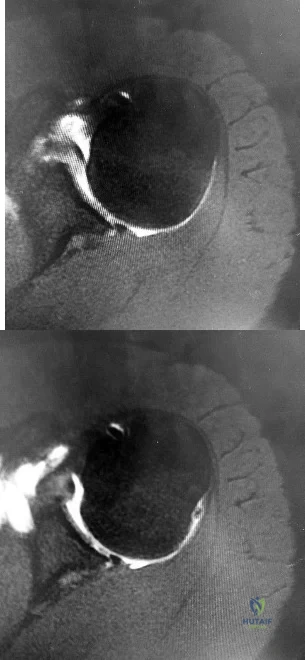
- Figures 38a & 38b show radiographs of a 40 year old man who underwent a Putti-Platt repair for recurrent dislocations at age 22. He reports increasing pain in the shoulder and limited motion for five years. Examination reveals 130 degrees of elevation and 15 degrees of external rotation. Non-surgical treatment has failed. Treatment should now consist of what?
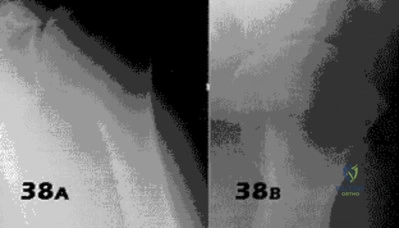
Explanation
Late onset of pain (average 13 years) was noted following this procedure in a small number of patients. The pain is attributed to excessive G-H compressive forces due to limited external rotation. NSAIDS and PT are first line treatments. If these fail, the authors demonstrated good results with release of the anterior structures. Choices 3 & 4 would probably be reserved for patients older than 50 with more advanced signs of degenerative disease.
Question 36
A 7-year-old boy has a limp with pain and tenderness over the distal right femur. Radiographs are shown in Figures 5a and 5b. Based on these findings, what is the best course of action?
Explanation
REFERENCES: Dormans, JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Easley ME, Kneisl JS: Pathologic fractures through nonossifying fibromas: Is prophylactic treatment warranted? J Pediatr Orthop 1997;17:808-813.
Question 37
A 35-year-old laborer who sustained a forefoot injury 10 years ago has returned to work but reports a progressively painful deformity of the hallux and continued midfoot pain that is aggravated by weight-bearing activities. Shoe wear modifications have failed to provide relief. Direct palpation reveals no pain at the first metatarsocuneiform joint. A radiograph is shown in Figure 11. What is the next most appropriate step in management?
Explanation
REFERENCES: Kitaoka HB, Patzer GL: Arthrodesis versus resection arthroplasty for failed hallux valgus operations. Clin Orthop 1998;347:208-214.
McGarvey WC, Braly WG: Bone graft in hindfoot arthrodesis: Allograft vs autograft. Orthopedics 1996;19:389-394.
Ouzounian TJ: Metatarsophalangeal arthrodesis for salvage of failed hallux valgus surgery. Foot Ankle Clin 1997;2:741-752.
Question 38
A 13-year-old baseball pitcher presents with worsening medial-sided elbow pain. He pitches 7 months out of the year, throws 85 pitches per game and plays in two games per week. His fastball speed is approximately 75mph. He regularly plays outfield once he has been relieved of pitching. Which of the following is most likely contributing to his elbow pain? Review Topic
Explanation
Little League elbow is a medial-sided overuse injury that occurs in the skeletally immature athlete. During execution of the baseball pitch, tremendous valgus and extension stresses occur at the elbow. Repetitive microtrauma can ultimately injure the medial epicondyle apophysis, ulnar collateral ligament or the flexor-pronator muscle mass. Limiting the number of pitches and innings played per game, as well as the number of months of competitive pitching per year, has been recommended to prevent these overuse injuries in the young athlete.
Olsen et al performed a case control study to determine risk factors associated with the development of shoulder and elbow injuries in adolescent baseball pitchers. Greater than 8 months of competitive pitching per year, more than 80 pitches per game and a fastball speed of greater than 85mph were all associated with increased risk of injury. Continued pitching despite arm fatigue and pain, being a starting pitcher, greater number of warm-up pitches, participating in showcases and regular use of NSAIDs were also associated with injury. The type of pitch (fastball, changeups and breaking balls) and continued play in a different position once being relieved was not associated with increased risk of injury.
Andrews et al authored a review article on ulnar collateral ligament injuries in throwing athletes. According to the USA Baseball Medical/Safety Advisory Committee, young baseball pitchers should avoid breaking pitches, such as curveballs and sliders, and avoid year-round baseball. A minimum of 3 months of complete rest from pitching per year is vital. Youth pitching coaches should be educated to ensure proper pitching mechanics are being reinforced.
Illustration A is a table depicting the recommended maximum number of pitches by age group.
Incorrect Answers:
Question 39
Persistent symptoms and decreased function following distal clavicle resection, coracoacromial ligament transfer, and augmentation (modified Weaver-Dunn) are most likely related to Review Topic
Explanation
Question 40
During right knee anterior cruciate ligament (ACL) reconstruction, after drilling an appropriately positioned and referenced tibial tunnel, the surgeon finds that the transtibial guide is placing the femoral tunnel at 11:30 within the intercondylar notch. Which of the following choices will best enable appropriate graft placement in this clinical scenario? Review Topic
Explanation
minimize errant tunnel placement, demonstrated in the literature as the most common cause of ACL failure and need for revision. In this not uncommon clinical scenario, simply converting to a two-incision ACL technique or drilling through the anteromedial portal with the knee hyperflexed will permit accurate femoral tunnel placement and increase the likelihood of an optimal clinical outcome. Femoral tunnel accuracy with these techniques is enhanced by a lower starting point in the intercondylar notch. Familiarity with these techniques is valuable for surgeons performing ACL reconstruction. Revising the tibial tunnel in this scenario would likely lead to bone compromise of the proximal tibia and may interfere with graft fixation and incorporation. Converting to a double-bundle ACL with a transtibial technique would not correct the vertical femoral tunnel. Hyperflexion of the knee may improve femoral tunnel placement to some extent, but is unlikely to allow anatomic placement of a femoral tunnel when the transtibial guide lies in a clearly excessive vertical position.
Question 41
The pathophysiology of a claw toe deformity includes muscular imbalance caused by which of the following relatively strong structures?
Explanation
REFERENCES: Mizel MS, Yodlowski ML: Disorders of the lesser metatarsophalangeal Joints.
J Am Acad Orthop Surg 1995;3:166-173.
Coughlin MJ, Mann RA: Surgery of the Foot and Ankle, ed. 7. St Louis, MO, Mosby, 1999,
pp 325-328.
Question 42
What procedure can eliminate a sulcus sign? Review Topic
Explanation
Question 43
A 10-year-old girl is treated for a tibia/fibula fracture with a long leg cast. The on-call resident is called to evaluate the patient for increasing pain medicine requirements and tingling in her foot. Examination of the cast reveals that the ankle has been immobilized in 10 degrees of dorsiflexion. What ankle position results in the safest compartment pressures in a casted lower leg?

Explanation
Weiner et al measured intramuscular compartment pressure in the anterior and deep posterior compartments of the leg in seven healthy adults who had long leg casts placed. They found that in a casted leg the intramuscular pressure in the anterior compartment was lowest with the ankle in neutral, and the deep posterior compartments was lowest when the ankle joint was in the resting position to approximately 37 degrees of plantar flexion. Based on this, they concluded that the safest ankle casting position regarding compartment pressure is between 0 and 37 degrees of plantar flexion. After the cast was bivalved, they noted a significant decrease in intramuscular pressure of 47 per cent in the anterior compartment and of 33 per cent in the deep posterior compartment. Constrictive casts and abberant ankle positioning can exacerbate pain/symptoms. Loosening of the cast by bivalving, spreading, and cutting underlying stockinette/softroll should always be the first step in management of possible compartment syndrome.
Question 44
The oblique radiograph of the foot and the CT scan shown in Figures 10a and 10b show a patient whose symptoms have failed to respond to rest and non-steroidal anti-inflammatory drugs. What is the best course of action?
Explanation
REFERENCES: Haddad SL: Disorders of tendons: Peroneal tendon dysfunction, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999,
pp 812-817.
MacDonald BD, Wertheimer SJ: Bilateral os peroneum fractures: Comparison of conservative and surgical treatment and outcomes. J Foot Ankle Surg 1997;36:220-225.
Question 45
Which of the following design features of a femoral component used in a total knee arthroplasty best minimizes the patellar component contact stresses?
Explanation
REFERENCES: Petersilge WJ, Oishi CS, Kaufman KR, Irby SE, Colwell CW Jr: The effect of trochlear design on patellofemoral shear and compressive forces in total knee arthroplasty. Clin Orthop 1994;309:124-130.
Theiss SM, Kitziger KJ, Lotke PS, Lotke PA: Component design affecting patellofemoral complications after total knee arthroplasty. Clin Orthop 1996;326:183-187.
Healy WL, Wasliewski SA, Takei R, Oberlander M: Patellofemoral complications following total knee arthroplasty:. Correlation with implant design and patient risk factors. J Arthroplasty 1995;10:197-201.
Question 46
A 20-year-old college soccer player comes for an evaluation 6 months after an injury during which he landed awkwardly from a jump. Although physical therapy, ice, and activity modification have helped him return to baseline motion, strength, and swelling, he continues to have lateral knee pain. He also notes a popping sensation on the lateral side of his knee with activity. A Lachman test, anterior and posterior drawer tests, a pivot shift test, and McMurray test findings are all negative. MR images reveal a 12-mm x 15-mm osteochondral defect in the lateral femoral condyle with full-thickness cartilage loss and approximately 4 mm of subchondral bone loss.
Explanation
Patellofemoral pain in a young athlete without patellar instability or a chondral or osteochondral defect often can be managed with nonsurgical treatment such as physical therapy and a home exercise program. Microfracture surgery is associated with good short-term results for younger athletes. Patients with no history of prior surgery, primary chondral rather than osteochondral lesions, and lesions smaller than 2 cm have experienced the best results. Microfracture surgery performed for chondral lesions of the central aspect of the medial femoral condyle is associated with worse results. Decreased activity levels over time of patients who undergo microfracture surgery are a concern. OAT provides good outcomes and return-to-sports rates for athletic people who are younger and have lesions smaller than 2 cm. Patients with lesions on the lateral femoral condyle have better success rates. Both microfracture surgery and OAT provide better results for chondral defects than osteochondral defects. OAT is associated with better results than microfracture for medium-sized lesions between 2 cm and 4 cm, while autologous chondrocyte implantation yields better improvement for patients with defects larger than 4 cm. All of the surgical techniques listed for articular cartilage repair are associated with better outcomes for patients younger than age 30.
Question 47
A 10-year-old boy has 2 months of right knee pain that started at summer camp. The patient denies constitutional symptoms. There is no lymphadenopathy present. CT of the chest shows no signs of metastatic disease. Imaging studies and biopsy results are shown in Figures A-E. What is the most likely diagnosis?
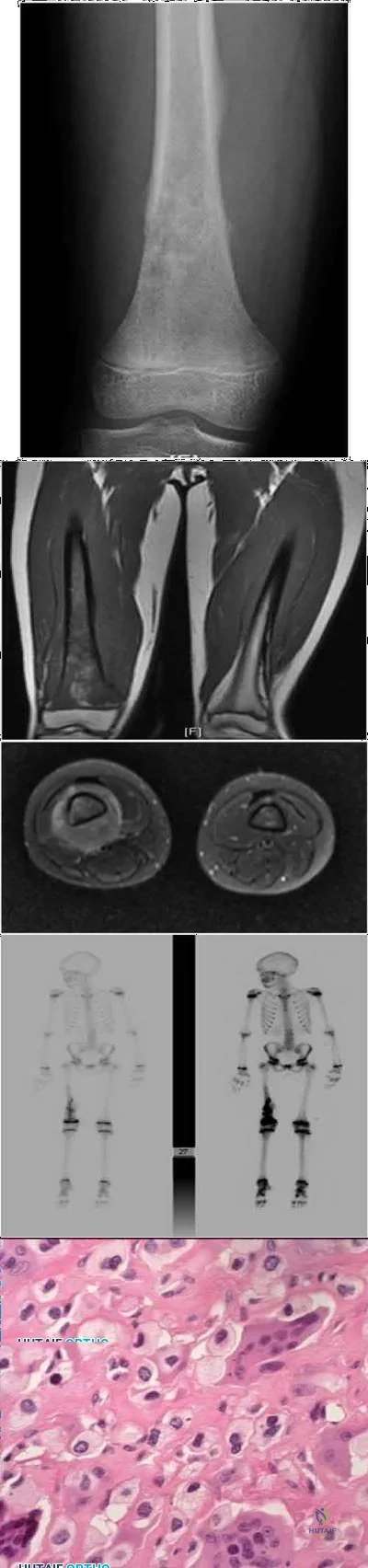
Explanation
Treatment for osteosarcoma includes neoadjuvant chemotherapy, wide resection, and adjuvant chemotherapy.
Question 48
A 17-year-old girl is involved in a motor vehicle collision and sustains the injury shown in Figures 46a through 46c. She is neurologically intact in her bilateral lower extremities. Definitive treatment should consist of A B C

Explanation
The figures reveal a fracture-dislocation at L1-2. Proper treatment consists of posterior reduction, stabilization, and fusion 2 levels above and below the level of injury. Short-segment stabilization schemes do not stabilize the injury properly, and longer-segment constructs are not necessary. Anterior treatment is not indicated in fracture-dislocations.
RECOMMENDED READINGS
Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004 Nov-Dec;12(6):424-35. Review. PubMed PMID: 15615508. View Abstract at PubMed
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
Question 49
Gaucher’s disease is manifested by reticuloendothelial system macrophage accumulation of
Explanation
REFERENCES: Beatty JH: Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 247-252.
Goldblatt J, Sacks S, Beighton P: The orthopedic aspects of Gaucher disease. Clin Orthop 1978;137:208-214.
Beutler E: Gaucher’s disease. N Engl J Med 1991;325:1354-1360.
Question 50
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. Based on the pathology noted, which finding may be found on plain knee radiographs?

Explanation
Question 51
Well-differentiated liposarcomas never have chromosomal abnormalities. Liposarcomas account for approximately 10% to 15% of sarcomas. Some general statements about liposarcomas are listed below:
Explanation
Question 52
A 16-year-old ice hockey player is struck on the chest by the puck. He skates a few strides and then collapses. What is the most likely diagnosis?
Explanation
REFERENCES: Maron BJ, Strasburger JF, Kugler JD, Bell BM, Brodkey FD, Poliac LC: Survival following blunt chest impact-induced cardiac arrest during sports activities in young athletes. Am J Cardiol 1997;79:840-841.
Link MS, Maron BJ, Estes NAM III: Commotio cordis, in Estes NAM III, Salem DN, Wang PJ (eds): Sudden Cardiac Death in the Athlete. Armonk, NY, Futura, 1998, pp 515-528.
Question 53
Vertebral fractures are common in the thoracolumbar spine. What is the most important factor that determines the strength of the cancellous bone in the vertebral body?
Explanation
REFERENCES: Carter DR, Hayes WC: The compressive behavior of bone as a two-phase porous structure. J Bone Joint Surg Am 1977;59:954-962.
Keaveny TM: Strength of trabecular bone, in Cowin SC (ed): Bone Mechanics Handbook. Boca Raton, FL, CRC Press, 2001, pp 16-1-16-8.
Question 54
Figure 53 shows the arteriogram of a 45-year-old man who has severe vasculitis. What do the findings show?
Explanation
REFERENCE: Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadephia, PA, Mosby-Year Book, 1998, p 110.
Question 55
A 30-year-old woman injured her ankle playing soccer 3 months ago. She now reports popping and pain over the lateral side of her ankle. An MRI scan is shown in Figure 33. What structure needs to be repaired to alleviate the popping?
Explanation
REFERENCES: Jones DC: Tendon disorders of the foot and ankle. J Am Acad Orthop Surg 1993;1:87-94.
Timins ME: MR imaging of the foot and ankle. Foot Ankle Clin 2000;5:83-101.
Question 56
A 12-year-old girl who plays softball has chronic lateral hindfoot aching pain that is aggravated by weight-bearing activity. She reports that the pain has recurred after initial improvement with cast immobilization, and it continues to limit her overall level of activity. Radiographs are seen in Figures 40a through 40c. What is the most appropriate surgical treatment?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 757-765.
Lemley F, Berlet G, Hill K, et al: Current concepts review: Tarsal coalition. Foot Ankle Int 2006;27:1163-1169.
Question 57
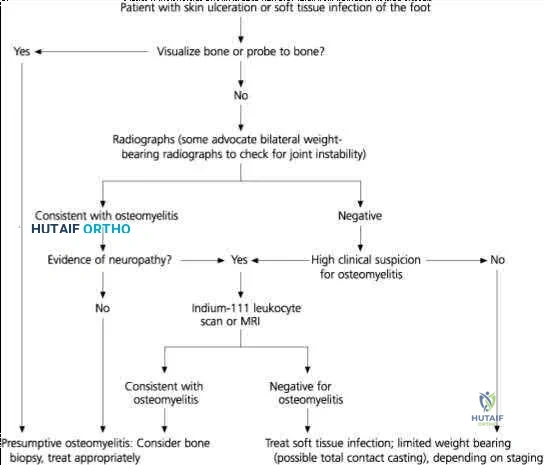
A 55-year-old woman with type I diabetes mellitus has a chronic ulcer over the dorsum of her right foot and reports forefoot pain. Examination reveals 1- x 2-cm nondraining ulcer over the dorsum of the foot. The patient has 1-2+ pain with compression of the foot and ankle. She has a weakly palpable posterior tibial pulse and an absent dorsalis pedis pulse. There is no erythema, cellulitis, or drainage. Radiographs are normal. Which of the following diagnostic studies should be obtained?
Explanation
REFERENCES: Wagner FW Jr: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981;2:64-122.
Apelqvist J, Castenfors J, Larson J, Stenstrom A, Agardh CD: Prognostic value of systolic ankle and toe blood pressure levels in outcome of diabetic foot ulcer. Diabetes Care 1989;12:373-378.
Question 58
Two weeks after undergoing total knee arthroplasty, a 68-year-old woman experiences moderate, yet worsening, knee pain. Upon examination, she can walk with a cane but she has swelling with mild reactive erythema. She has a well-healed incision with no drainage. A review of her medications reveals the she has been taking warfarin and has an international normalized ratio (INR) of 4.0. Her erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level are slightly elevated, and radiographs are unremarkable other than for effusion. What is the most likely diagnosis?
Explanation
This patient likely has a hemarthrosis related to INR elevation. The slight elevations in ESR and CRP are likely attributable to the nature of the surgery itself rather than an infection, and the mild reactive erythema is likely attributable to the hemarthrosis.
Question 59
A 25-year-old woman has significant pain and swelling in her left ankle after falling off her bicycle. Examination reveals that she is neurovascularly intact. Radiographs are shown in Figures 33a through 33c. What is the next most appropriate step in management?
Explanation
REFERENCES: Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Harper MC: Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int 2001;22:15-18.
Question 60
-A 51-year-old man has a slowly expanding upper-extremity mass. Examination reveals a firm 3-cm mass in his midvolar forearm. Radiographs are normal. You suspect a soft-tissue sarcoma. The best imaging study would be
Explanation

Question 61
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?
Explanation
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Omer GE Jr: Osteotomy of the clavicle in surgical reduction of anterior sternoclavicular dislocation. J Trauma 1967;7:584-590.
Question 62
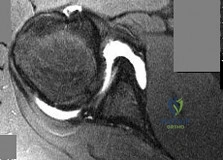
A 39-year-old man presents with back pain radiating to the left lower extremity for the past 6 weeks. Magnetic resonance images of the pathology are
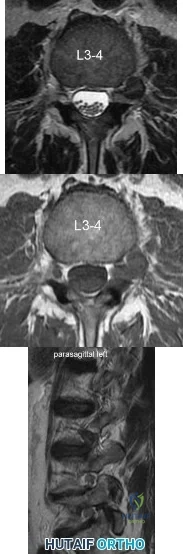
Explanation
Far lateral disc herniations constitute approximately 5-10 percent of disc hernations in the lumbar spine. Given the more vertical anatomy of lumbar nerve roots, at a given disc level, a central or paracentral herniation will affect the traversing nerve root (e.g. nerve root of level below) and a far lateral herniation will affect the exiting nerve root (e.g. nerve root of the level above). Similar to the more common central and paracentral herniations, approximately 90% of patients will improve without surgical intervention. When surgical intervention is needed, the paraspinal approach of Wiltse is utilized.
Marquadt et al. reported long term outcomes of surgical management of far lateral disc herniations. At an average of 146 months follow up, 56.3% of patients had complete relief of symptoms and 27.6% had permanent residual symptoms. Over 75% of patients subjectively rated their outcomes as excellent.
Figure A and B are T2 and T1 axial MRI images, respectively, showing the L3-L4 disc space with a left far lateral disc herniation. Figure C is a left parasagittal T2 MRI image showing impingement on the L3 nerve root. Structures are labeled in illustration A. Illustration B shows the dermatomes of the lower extremity.
Incorrect Answers:
Question 63
The optimal method with which to diagnose component malrotation in total knee arthroplasty (TKA) is
Explanation
The epicondylar axis and tibial tubercle can be used as references on CT scans to quantitatively measure rotational alignment of the femoral and tibial components. This technique has been used to determine whether rotational malalignment is present and whether revision of 1 or both components may be indicated. Although clinical assessment is useful, malrotation can occur as a result of deformities unrelated to the arthroplasty. Similarly, an isolated radiographic skyline view of the patella may indicate a problem with patellar maltracking, but cannot quantitatively assess malrotation of the components. MR imaging proves useful for evaluating painful TKA, but it is dependent on the center’s quality and has not yet been shown to quantify component malrotation.

CLINICAL SITUATION FOR QUESTIONS 20 THROUGH 22
Figures 20a and 20b are the radiographs of an elderly woman who underwent total knee arthroplasty (TKA) several years ago. She now states that something is not right; her knee frequently swells and is diffusely painful, especially at the end of the day. She does not trust her knee, especially while going up and down stairs or getting up from a chair.
Question 64
What proteinaceous compound binds to hyaluronic acid to function as an effective boundary molecular layer in articular cartilage?
Explanation
Question 65
The first branch of the lateral plantar nerve innervates the
Explanation
REFERENCES: Pansky B, House EH: Review of Gross Anatomy, ed 3. New York, NY, Macmillan, 1975, pp 464-476.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983,
pp 325-328.
Question 66
Which of the following has been associated with a decreased rate of glenoid component radiolucent lines?
Explanation
REFERENCES: Gartsman GM, Elkousy HA, Warnock KM, et al: Radiographic comparison of pegged and keeled glenoid components. J Shoulder Elbow Surg 2005;14:252-257.
Szabo I, Buscayret F, Edwards TB, et al: Radiographic comparison of flat-back and convex-back glenoid components in total shoulder arthroplasty. J Shoulder Elbow Surg 2005;14:636-642.
Mileti J, Boardman ND III, Sperling JW, et al: Radiographic analysis of polyethylene glenoid components using modern cementing techniques. J Shoulder Elbow Surg 2004;13:492-498.
Question 67
ofhat parameter is most commonly used to estimate the maximum tension a muscle can generating?
Explanation
The concept of physiologic cross section of a muscle from Weber and Fick, identifies the critical importance of the cross sectional area of all the fibers of a muscle as proportional to maximum tension. (Relationship between muscle size and muscle strength).
Question 68
The skeletal muscle length-tension relationship for voluntary force generation is observed with which of the following biomechanical paradigms? Review Topic
Explanation
Question 69
A 42-year-old athletic trainer has a persistent popping sensation about the lateral ankle associated with weakness and pain following a remote injury. Deficiency in what structure directly leads to this pathology?
Explanation
the condition.
REFERENCE: Maffuli N, Ferran NA, Oliva F, et al: Recurrent subluxation of the peroneal tendons. Am J Sports Med 2006;34:986-992.
Question 70
Osteochondritis dissecans of the capitellum is a source of elbow pain and most commonly occurs in what patient population?
Explanation
REFERENCES: Baumgarten TE, Andrews JR, Satterwhite YE: The arthroscopic classification and treatment of osteochondritis dissecans of the capitellum. Am J Sports Med 1998;26:520-523.
Takahara M, Ogino T, Fukushima S, et al: Nonoperative treatment of osteochondritis dissecans of the humeral capitellum. Am J Sports Med 1999;27:728-732.
Question 71
An 11-year-old basketball player reports that he felt a painful pop in the left knee when he stumbled while running. He is unable to bear weight on the extremity and cannot actively extend the knee against gravity. Examination reveals a large knee effusion. A lateral radiograph is shown in Figure 7. Management should consist of Review Topic

Explanation
Question 72
Figures 132a and 132b are the lateral and anteroposterior radiographs of a 15-year-old boy with a 6-month history of recurrent, activity-related posterior elbow pain when pitching. Two separate 6-week periods of rest have failed to provide relief. What is the next best step to enable him to return to play? Review Topic

Explanation
cessation from throwing followed by appropriate physiotherapy, surgical management with cannulated screw fixation is appropriate and has been demonstrated to have favorable success rates. Hinged-elbow bracing will not facilitate healing or return to play. Long-arm casting is likely to result in stiffness and would not be unreasonable for a short duration at the onset of symptoms, but is less likely to be helpful at this point. Plate fixation is not indicated for treatment of this injury.
Question 73
A 25-year-old man is brought to the emergency department following a motor vehicle accident. Extrication time was 2 hours, and in the field he had a systolic blood pressure by palpation of 90 mm Hg. Intravenous therapy was started, and on arrival in the emergency department he has a systolic blood pressure of 90 mm Hg with a pulse rate of 130. Examination reveals a flail chest and a femoral diaphyseal fracture. Ultrasound of the abdomen is positive. The trauma surgeons take him to the operating room for an exploratory laparotomy. At the conclusion of the procedure, he has a systolic pressure of 100 mm Hg with a pulse rate of 110. Oxygen saturation is 90% on 100% oxygen, and he has a temperature of 95.0° F (35° C). What is the recommended treatment of the femoral fracture at this time?
Explanation
REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopaedic surgery. J Trauma 2002;53:452-461.
Bosse M, Kellam JF: Orthopaedic decision making in the multiple trauma patient, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 133-146.
Question 74
Which of the following conditions is considered a relative contraindication to interscalene nerve block for patients scheduled to undergo shoulder surgery?
Explanation
REFERENCES: Chelly JE: Indications for upper extremity blocks, in Chelly JE (ed): Peripheral Nerve Blocks, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 19-27.
Misamore GW, Sallay PI: A prospective analysis of the safety and efficacy of interscalene brachial plexus block anesthesia for shoulder surgery. J Shoulder Elbow Surg 2007;16:e39.
Question 75
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm P 3 P , an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
REFERENCES: Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Kocher MS, Zurakowski D, Kasser JR: Differentiating between septic arthritis and transient synovitis of the hip in children: An evidence-based clinical prediction algorithm. J Bone Joint Surg Am 1999;81:1662-1670.
Question 76
A positive Froment sign indicates weakness of which of the following muscles?
Explanation
REFERENCE: Burton RI: The Hand: Examination and Diagnosis. Chicago, IL, American Society for Surgery of the Hand, 1978, pp 26-27.
Question 77
A 3-year-old child sustains a T2/T3 fracture-dislocation with complete paraplegia secondary to a car accident in which the child was an unrestrained passenger. What is the likelihood that this child will develop subsequent spinal deformity in the future? Review Topic
Explanation
Question 78
A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman test with a soft endpoint, varus laxity at 30°, and a positive dial test at 30° that dissipates at 90° of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome?
Explanation
Question 79
A 37-year-old man with a history of congenital flatfoot reports worsening pain on the medial aspect of his ankle for the past year. The pain is worse with weight bearing and is better with rest and the use of an ankle brace. What findings are shown on the MRI scans shown in Figures 18a through 18c?
Explanation
REFERENCES: Slovenkai MP: Clinical and radiographic evaluation (Adult flatfoot: Posterior tibial tendon dysfunction). Foot Ankle Clin 1997;2:241-260.
Conti S, Michelson J, Jahss M: Clinical significance of magnetic resonance imaging in preoperative planning for reconstruction of posterior tibial tendon ruptures. Foot Ankle 1992;13:208-214.
Question 80
A 24-year-old man has bilateral hip pain. An examination and imaging studies (plain radiographs and MR imaging) confirm evidence of femoroacetabular impingement (FAI) with a CAM deformity in both hips. The patient mentions that he has a 19-year-old brother who has occasional hip pain. With respect to his brother’s pain, how should you counsel the patient?
Explanation
Evidence suggests that FAI is more common in siblings of patients with FAI, particularly those with a CAM deformity. It is unlikely this patient has well-established osteoarthritis, even in the presence of FAI.

CLINICAL SITUATION FOR QUESTIONS 145 THROUGH 147
Figures 145a and 145b are the radiographs of a 56-year-old man who has had persistent pain in his right groin since undergoing primary total hip surgery 11 months ago. His erythrocyte sedimentation rate (ESR) is 38 mm/h (reference range [rr], 0-20 mm/h) and C-reactive protein (CRP) level is 28 mg/L (rr, 0.08-3.1 mg/L). A hip aspiration performed while the patient was taking antibiotics demonstrated 3200 white blood cells/µL with no growth. Treatment should consist of
Question 81
An 11-year-old girl is struck in the leg by a loaded sled while sledding and is seen in the emergency department; she is reporting severe knee pain. Radiographs are read as normal. Examination reveals that she is exquisitely tender over the proximal tibial physis. The neurovascular examination is normal. What is the next step in management?
Explanation
REFERENCES: McGuigan JA, O’Reilly MJ, Nixon JR: Popliteal arterial thrombosis resulting from disruption of the upper tibial epiphysis. Injury 1984;16:49-50.
Burkhart SS, Peterson HA: Fractures of the proximal tibial epiphysis. J Bone Joint Surg Am
1979;61:996- 1002.
Question 82
A patient sustained a puncture wound to the plantar aspect of his foot. He was wearing shoes and socks at the time of the injury. Systemic antibiotic administration with specific coverage for which bacterial species (in addition to Staphylococcus aureus) should be instituted?
Explanation
Puncture wounds sustained through a shoe and sock increase risk for Pseudomonas infection. Clostridium are associated with soil-contaminated wounds. Mycobacterium marinum is associated with injuries sustained within water.
RECOMMENDED READINGS
DeCoster TA, Miller RA. Management of Traumatic Foot Wounds. J Am Acad Orthop Surg. 1994 Jul;2(4):226-230. PubMed PMID: 10709013. View Abstract at PubMed
Raikin SM. Common infections of the foot. In: Richardson EG, ed. Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2004:199-205.
Question 83
A 19-year-old woman reports persistent neck pain for 2 years. Pain is relieved with aspirin. A bone scan shows intense uptake in the superior, posterior portion of the C3 vertebral body. A sagittal CT reconstruction is shown in Figure 5. Treatment should consist of
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 351-366.
Hadjipavlou AG, Lander PH, Marchesi D, et al: Minimally invasive surgery for ablation of osteoid osteoma of the spine. Spine 2003;28:E472-E477.
Question 84
A 77-year-old man who underwent right total knee replacement surgery 2 and a half years ago has had knee pain since surgery. The pain is diffuse, constant, and made worse with activity. He notes warmth and swelling in his knee. Examination shows a well-healed incision, no erythema, moderate warmth, synovitis, and an effusion. The knee is stable, and has an arc of flexion between 3° and 120°. Radiographs show well-fixed and well-aligned implants. What is the most appropriate initial treatment?
Explanation
This patient's history and physical findings are concerning for deep infection. Inflammatory markers, including ESR and CRP, should be obtained first. If the levels are elevated, knee aspiration should be performed for the synovial cell count and culture. A bone scan is not indicated in an initial investigation for deep infection; it is rarely helpful and is not cost effective. CT to assess implant rotation is an appropriate investigation for knee pain when the clinical scenario is not suspicious for a deep infection and when infection has been excluded.
Question 85
- Which of the following factors is used to determine torsional rigidity of a long bone fracture under internal or external fixation?
Explanation
quantity having a magnitude and direction. Torsion involves shear and tensile stresses that cause deformation. Thus torsional rigidity is related to bone rotation and the torque applied to it.
Question 86
The cervical disk herniation shown in the MRI scans in Figures 30a and 30b will most likely create which of the following constellations of symptoms?
Explanation
REFERENCES: Klein JD, Garfin SR: Clinical evaluation of patients with suspected spine problems, in Frymoyer JW (ed): Adult Spine: Principles and Practice, ed 2. Philadephia, PA, Lippincott-Raven, 1997, pp 319-330.
Hoppenfeld S: Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-49.
Question 87
A 37-year-old recreational tennis player undergoes surgery for tennis elbow. Following surgery, she describes clicking and popping on the lateral aspect of the elbow. A lateral pivot shift test is positive. What is the most likely cause of her symptoms?
Explanation
REFERENCES: O’Driscoll SW, Morrey BF: Surgical reconstruction of the lateral collateral ligament, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 169-182.
O’Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Question 88
Figure 1 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain?
Explanation
Question 89
Figures 31a and 31b show the radiograph and MRI scan of an otherwise normal 3-month-old infant who has a spinal deformity. MRI reveals no intraspinal anomalies. What is the next step in management?
Explanation
REFERENCES: Basu PS, Elsebaie H, Noordeen MH: Congenital spinal deformity:
A comprehensive assessment at presentation. Spine 2002;27:2255-2259.
Hedequist D, Emans J: Congenital scoliosis. J Am Acad Orthop Surg 2004;12:266-275.
Question 90
Based on the findings seen in the radiograph in Figure 26, emergent management should consist of
Explanation
REFERENCES: Isenberg J, Prokop A, Schellhammer F, et al: Palmar lunate dislocation. Unfallchirurg 2002;105:1133-1138.
Ruby LK: Fractures and dislocations of the carpus, in Browner BD, Jupiter JB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1367-1372.
Question 91
Histologically, synovial chondromatosis is characterized by
Explanation
REFERENCES: Milgram JM: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;l59:792-801.
Murphy FP, Dahlin DC, Sullivan CR: Articular synovial chondromatosis. J Bone Joint Surg Am 1962;44:77.
Question 92
Figure 10 shows the radiograph of an 18-year-old woman who sustained a spinal cord injury in a motor vehicle accident. Based on the radiographic findings, her injury is best described as
Explanation
REFERENCE: Allen BL Jr, Ferguson RL, Lehmann TR, O’Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
Question 93
A 43-year-old woman has an enlarging mass in the left groin. A radiograph, CT scan, and a biopsy specimen are shown in Figures 42a through 42c. Treatment should consist of
Explanation
REFERENCES: Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM: Chondrosarcoma of the pelvis: Prognostic factors for 67 patients treated with definitive surgery. Cancer 1996;78:745-750.
Enneking WF, Dunham WK: Resection and reconstruction for primary neoplasms involving the innominate bone. J Bone Joint Surg Am 1978;60:731-746.
Question 94
Antibiotic-loaded bone cement prostheses, such as that shown in Figure 8, are best created by using which of the following methods?
Explanation
High-dose antibiotic-loaded bone cements are described as those containing greater than 1.0 g of antibiotic per 40 g of cement. Effective elution levels have been documented with 3.6 g tobramycin and 1.0 g vancomycin per 40 g of bone cement. This was documented by Penner and associates. Furthermore, it was shown that the combination of the two antibiotics in the bone cement improved the elution of both antibiotics.
REFERENCES: Hanssen AD, Spangehl MJ: Practical applications of antibiotic-loaded bone cement for treatment of infected joint replacements. Clin Orthop 2004;427:79-85.
Penner MJ, Masri BA, Duncan CP: Elution characteristics of vancomycin and tobramycin combined in acrylic bone-cement. J Arthroplasty 1996;11:939-944.
Question 95
An operating room intervention that should be undertaken by anesthesia staff during the cementing of a femoral stem is to
Explanation
Young age is a risk factor for early failure of cementless femoral components. Surgeons could consider cementing for patients older than 80 years of age. The Dorr classification has been shown to favor a cemented femoral stem in Dorr type C bone. Dorr type B bone can potentially sustain a proximally porous ingrowth stem. Osteoporosis is a risk factor for early failure of cementless femoral components.
Earlier designs for cemented femoral stems used microtexture to interlock the stem into the cement mantle. If these stems became loose, they would abrade the cement and loosen the stem further. Successful cemented femoral components are polished and have smooth edges with tapered bodies. Collars do not add to the design of femoral stems.
Patients are at risk for hypotension during the femoral pressurization process. With that in mind, the surgeon should make sure the anesthesiologist is ready to respond to hypotension. The FiO2 should be increased. The IV fluid rate also should be increased, and the anesthesiologist should be prepared with phenylephrine to support the patient’s blood pressure if he or she becomes hypotensive.

Question 96
Figure 18 shows the radiograph of a patient with a total hip arthroplasty dislocation. During revision, increasing the diameter of the femoral head while maintaining the ratio of head-to-neck diameter constant has the effect of
Explanation
Scifert and associates used a three-dimensional finite element model to study various combinations of femoral head size and neck ratios. They found that increasing the diameter of the femoral head while maintaining a constant head-to-neck diameter had the effect of significantly increasing the resisting moment necessary to induce a dislocation. The higher the head-to-neck ratio, the greater the range of motion until impingement and the greater the range of motion to dislocation.
REFERENCE: Scifert CF, Brown TD, Pedersen DR, Callaghan JJ: A finite element analysis of factors influencing total hip dislocation. Clin Orthop 1998;355:152-162.
Question 97
A patient undergoes a simple excision of a 3-cm superficial mass in the thigh at another institution. The final pathology reveals a leiomyosarcoma, without reference to the margins. What is the recommendation for definitive treatment?
Explanation
a reexcision of the tumor bed is recommended.
REFERENCE: Noria S, Davis A, Kandel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 98
Figure 23 shows the postoperative radiograph of a patient who underwent an anterior cruciate ligament (ACL) reconstruction (with bone-patella tendon-bone autograft) that failed. He initially had loss of flexion postoperatively. What is the most likely cause of this failure?
Explanation
REFERENCES: Fu FH, Bennett CH, Latterman C, et al: Current trends in anterior cruciate ligament reconstruction: Part 1. Biology and biomechanics of reconstruction. Am J Sports Med 1999;27:821-830.
Fu FH, Bennett CH, Ma CB, et al: Current trends in anterior cruciate ligament reconstruction: Part II. Operative procedures and clinical correlations. Am J Sports Med 2000;28:124-130.
Question 99
A 25-year-old man injures his shoulder while skiing. Examination reveals increased passive external rotation, pain in the cocked position, and a positive lift-off test. What is the most likely diagnosis?
Explanation
REFERENCES: Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Hawkins RJ, Bokor DJ: Clinical evaluation of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 149-177.
Question 100
A 12-year-old boy has had progressive pain and flatfeet for the past year. Pain is increased with weight-bearing activities. Examination reveals that subtalar motion is absent. On standing, the patient has obvious hindfoot valgus and loss of the normal arch bilaterally. Plain radiographs are shown in Figures 43a through 43c, and a CT scan is shown in Figure 43d. What is the most likely diagnosis?
Explanation
REFERENCES: Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 583-595.
