Orthopedic Surgery Board Review MCQs: Sports Medicine & Arthroplasty | Part 181

Key Takeaway
This page provides Part 181 of a comprehensive Orthopedic Surgery Board Review. It features 100 verified, high-yield MCQs for orthopedic surgeons and residents preparing for AAOS and OITE board certification exams. Utilize Study or Exam Mode with full explanations to master topics like Arthroplasty, Knee, and Shoulder for optimal exam readiness.
About This Board Review Set
This is Part 181 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 181
This module focuses heavily on: Arthroplasty, Deformity, Dislocation, Knee, Ligament, Shoulder.
Sample Questions from This Set
Sample Question 1: What are the proposed biomechanical advantages of the Grammont reverse total shoulder arthroplasty when compared to a standard shoulder arthroplasty?...
Sample Question 2: A patient with an acromioclavicular dislocation has a very prominent distal clavicle. Examination reveals that the deformity increases rather than reduces with an isometric shoulder shrug. Which of the following structures is most likely in...
Sample Question 3: A 17-year-old high school soccer player sustains an anterior cruciate ligament (ACL) tear at the beginning of the season. An MRI scan confirms a complete ACL tear with no meniscal injuries. The patient plans an early return to play and woul...
Sample Question 4: An acetabular reinforcement cage is most often indicated for which of the following conditions?...
Sample Question 5: What would be the advantage of surgery for the patient described in this scenario?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What are the proposed biomechanical advantages of the Grammont reverse total shoulder arthroplasty when compared to a standard shoulder arthroplasty?
Explanation
REFERENCES: Werner CM, Steinmann PA, Gilbert M: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Rittmeister M, Kerschbaumer M: Grammont reverse total shoulder arthroplasty in patients with rheumatoid arthritis and nonreconstructible rotator cuff lesions. J Shoulder Elbow Surg 2001;10:17-22.
Question 2
A patient with an acromioclavicular dislocation has a very prominent distal clavicle. Examination reveals that the deformity increases rather than reduces with an isometric shoulder shrug. Which of the following structures is most likely intact?
Explanation
REFERENCE: Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocations. Am J Sports Med 1995;23:324-331.
Question 3
A 17-year-old high school soccer player sustains an anterior cruciate ligament (ACL) tear at the beginning of the season. An MRI scan confirms a complete ACL tear with no meniscal injuries. The patient plans an early return to play and would like to avoid surgery. Therefore, the patient and family should be advised that nonsurgical management consisting of rehabilitative exercises and the use of a functional knee brace will most likely result in
Explanation
REFERENCES: Shelton WR, Barrett GR, Dukes A: Early season anterior cruciate ligament tears: A treatment dilemma. Am J Sports Med 1997;25:656-658.
Snyder-Mackler L, Fitzgerald GK, Bartolozzi AR III, Ciccotti MG: The relationship between passive joint laxity and functional outcome after anterior cruciate ligament injury. Am J Sports Med 1997;25:191-195.
Question 4
An acetabular reinforcement cage is most often indicated for which of the following conditions?
Explanation
REFERENCES: Berry DJ, Lewallen DG, Hanssen A, Cabanela ME: Pelvic discontinuity in revision total hip arthroplasty. J Bone Joint Surg Am 1999;81:1692-1702.
Whaley AL, Berry DJ: Extra-large uncemented hemisphere acetabular components for revision THA. J Bone Joint Surg Am 2001;83:1352-1357.
Question 5
What would be the advantage of surgery for the patient described in this scenario?
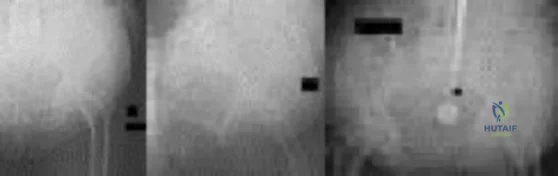
Explanation
The MR image of the lumbar spine postgadolinium contrast shows a ring-enhancing fluid collection. Ring-enhancing lesions within the spinal canal on postgadolinium MR images are indicative of epidural abscess. It is important to obtain a culture-specific diagnosis to inform the choice of antibiotics and educate patients regarding the likelihood of failure for standalone antibiotic therapy. Infection with MSSA, age younger than 65 years, the absence of neurologic deficit, and lumbar abscess location are all factors that point toward a patient being a reasonable candidate for a trial of culture-specific IV antibiotics. In this case, nafcillin is a suitable treatment for MSSA. The antibiotic should be initiated and closely observed with serial labs (WBC, ESR, CRP, repeat blood cultures) to ensure that the patient responds appropriately to therapy and that neurologic deficits do not develop. In the setting of epidural abscess, surgery is performed to evacuate the abscess and reverse or prevent neurologic deterioration. In the current scenario in which sepsis is not an issue, scant high-quality evidence shows that surgical intervention influences risk for mortality or chronic pain following epidural abscess.
RECOMMENDED READINGS
Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.View Abstract at PubMed
Adogwa O, Karikari IO, Carr KR, Krucoff M, Ajay D, Fatemi P, Perez EL, Cheng JS, Bagley CA, Isaacs RE. Spontaneous spinal epidural abscess in patients 50 years of age and older: a 15-year institutional perspective and review of the literature: clinical article. J Neurosurg Spine. 2014 Mar;20(3):344-9. doi: 10.3171/2013.11.SPINE13527. Epub 2013 Dec 20. Review.
PubMed PMID: 24359002.View Abstract at PubMed
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014
Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 6
A 53-year-old woman reports a 4-month history of gradual onset diffuse shoulder pain and limited function. She has had no prior treatment, and her medical history is unremarkable. Examination reveals globally painful active range of motion to 120 degrees forward elevation, 25 degrees external rotation with the arm at the side, and internal rotation to the sacrum. Passive range of motion is also limited in comparison with the contralateral shoulder. Radiographs are shown in Figures 31a through 31c. What is the most appropriate management? Review Topic

Explanation
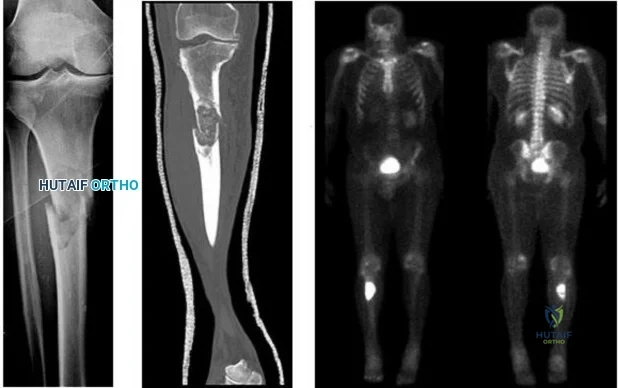
Question 7
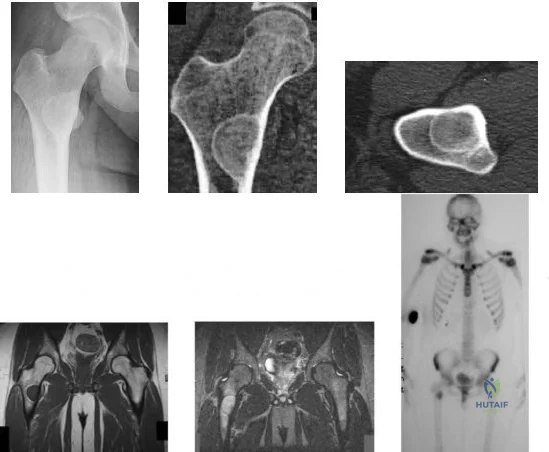
A 15-year-old boy reports leg pain after being tackled during football practice. Radiographs and a CT scan are shown in Figures 46a through 46c. The patient has a pathologic fracture through what underlying lesion?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 69-75.
Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 8
A 35-year-old man who is an avid weight lifter competing in local tournaments reports new onset pain and loss of motion in his dominant right shoulder. Examination reveals joint line tenderness, active elevation to 100 degrees, and external rotation to 10 degrees. His contralateral shoulder reveals 170 degrees forward elevation and 50 degrees external rotation. Radiographs are shown in Figures 46a and 46b. What is the next most appropriate step in management? Review Topic

Explanation
Question 9
A 40-year-old man with an acetabular chondrosarcoma has a small soft-tissue mass. Treatment should consist of
Explanation
REFERENCES: Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM: Chondrosarcoma of the pelvis: Prognostic factors for 67 patients treated with definitive surgery. Cancer 1996;78:745-750.
Question 10
A 65-year-old woman has nausea, vomiting, and abdominal distention after undergoing total knee arthroplasty 48 hours ago. An abdominal radiograph is shown in Figure 14. Associated risk factors for this disorder include
Explanation
REFERENCES: Iorio R, Healy WL, Appleby D: The association of excessive warfarin anticoagulation and postoperative ileus after total joint replacement surgery. J Arthroplasty 2000;15:220-223.
Clarke HD, Berry DJ, Larson DR: Acute pseudo-obstruction of the colon as a postoperative complication of hip arthroplasty. J Bone Joint Surg Am 1997;79:1642-1647.
Question 11
What is the most consistent finding regarding glenohumeral kinematics in patients with symptomatic tears of the rotator cuff?
Explanation
REFERENCES: Yamaguchi K, Sher JS, Anderson WK, et al: Glenohumeral motion in patients with rotator cuff tears: A comparison of asymptomatic and symptomatic shoulders. J Shoulder Elbow Surg 2000;9:6-11.
Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
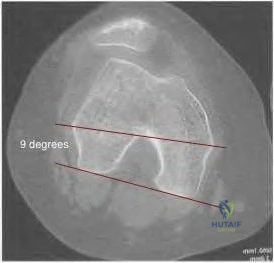
Question 12
98 degrees (range, 0 degrees to 9 degrees). In knees with varus joint lines
Explanation
Question 13
A new composite material is being evaluated for potential use as a prosthetic ligament. In measuring the tensile strength of this material, why is it important to consider and accurately control the loading rate?
Explanation
Question 14
A 24-year-old man sustains the injury shown in Figures 19a through 19e in a paragliding accident. He is neurologically intact. He also sustained fractures of his left femur and right distal radius. Which of the following represents the best option for management of the spinal injury?
Explanation
REFERENCES: McLain RF, Benson DR: Urgent surgical stabilization of spinal fractures in polytrauma patients. Spine 1999;24:1646-1654.
Wood K, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: A prospective, randomized study.
J Bone Joint Surg Am 2003;85:773-781.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 15
A “p value” of 4% (p=0.04) indicates that the
Explanation
The p value is the probability that the chance selection of patients might suggest a difference in treatment that was not real. Only with a small p value are we willing to believe that the observed difference in treatment is very likely real and not simply due to chance.
The confidence interval provides a measure of the magnitude of the possible difference between two groups of patients, regardless of whether or not the p value was small. This makes the confidence interval more informative than the p value when different treatments are compared. This is much beyond the scope of this review.
Question 16
What is the mechanism of action of bisphosphonates?
Explanation
REFERENCES: Gass M, Dawson-Hughes B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 226-227.
Question 17
A 25-year-old man is brought to the emergency department following a motor vehicle accident. Extrication time was 2 hours, and in the field he had a systolic blood pressure by palpation of 90 mm Hg. Intravenous therapy was started, and on arrival in the emergency department he has a systolic blood pressure of 90 mm Hg with a pulse rate of 130. Examination reveals a flail chest and a femoral diaphyseal fracture. Ultrasound of the abdomen is positive. The trauma surgeons take him to the operating room for an exploratory laparotomy. At the conclusion of the procedure, he has a systolic pressure of 100 mm Hg with a pulse rate of 110. Oxygen saturation is 90% on 100% oxygen, and he has a temperature of 95.0° F (35° C). What is the recommended treatment of the femoral fracture at this time?
Explanation
REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopaedic surgery. J Trauma 2002;53:452-461.
Bosse M, Kellam JF: Orthopaedic decision making in the multiple trauma patient, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 133-146.
Question 18
Figure 8 shows the radiograph of a 72-year-old man who has had severe pain in the left hip for the past 3 weeks. History reveals alcohol abuse. The next most appropriate step should consist of
Explanation
REFERENCE: Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 157-161.
Question 19
Figures 23a and 23b show the AP and lateral radiographs of a 67-year-old woman who has severe left knee pain when ambulating. History reveals that she underwent primary total knee arthroplasty 7 years ago. The patient reports increasing deformity over the past several years and uses a knee brace and a cane. Examination reveals that she walks with a varus thrust and has an uncorrectable varus deformity with valgus force. What is the primary reason for implant failure?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 275-279.
Question 20
The patient does well initially but returns for the 4-month postsurgical evaluation with ongoing stiffness and pain despite going to physical therapy twice weekly and working on motion at home. She is unable to bear weight comfortably. What is the best next step?
Explanation
In a skeletally immature patient with OCD and minor symptoms, the lesion can be observed and healing obtained with activity limitations if the cartilage is stable (but this cannot be determined radiographically or clinically). Activity restriction and serial follow-up are appropriate if an MRI reveals a stable lesion. MRI is indicated when there is concern that a lesion may be unstable. Surgical treatment depends on MRI findings.
Observation is recommended for OCD lesions in growing patients for 6 months because healing has been observed. Early surgical procedures, although they may be needed in the future, are not appropriate for patients with well-controlled symptoms.
If symptoms continue for longer than 6 months, arthroscopic drilling is not indicated for unstable OCD. The appropriate treatment is OCD fixation. Debridement is not appropriate with a stable lesion.
Evaluation of the fixation and stability of the lesion with advanced imaging after weight bearing and therapy initiation is the most appropriate option. Manipulating the knee without determining whether the stiffness is attributable to subsidence of the fixation or mechanical block is not appropriate. After 4 months, aspiration of a hematoma (if still present) would not yield much benefit. More therapy is not likely to be useful when a patient is attending therapy regularly and working on a home program.

Question 21
During cemented total hip arthroplasty, peak pulmonary embolization of marrow contents occurs when the
Explanation
REFERENCES: Lewallen DG, Parvizi J, Ereth MH: Perioperative mortality associated with hip and knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 119-127.
Ereth MH, Weber JG, Abel MD, et al: Cemented versus noncemented total hip arthroplasty: Embolism, hemodynamics, and intrapulmonary shunting. Mayo Clin Proc 1992;67:1066-1074.
Question 22
In the treatment of acetabular dysplasia, what type of pelvic osteotomy leaves the “teardrop” in its original position and redirects the acetabulum?
Explanation
REFERENCES: Lack W, Windhager R, Kutschera HP, Engel A: Chiari pelvic osteotomy for osteoarthritis secondary to hip dysplasia: Indications and long-term results. J Bone Joint Surg Br 1991;73:229-234.
Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Ninomija S, Tagwa H: Rotational acetabular osteotomy for the dysplastic hip. J Bone Joint Surg Am 1984;66:430.
Question 23
..Figures 107a through 107c are the radiograph, CT, and bone scan of a 68-year-old man. While walking, he collapsed and was unable to ambulate because of pain and deformity in his right leg. What is the most appropriate next step?
Explanation
Glomus tumor
Diffuse pigmented villonodular synovitis (PVNS)
Extra-abdominal fibromatosis
Schwannoma
Hemangioma
Please match the characteristics below to the condition listed above.
Question 24
Following surgery for an ankle fracture, which of the following is considered the most important factor in achieving a satisfactory outcome? Review Topic
Explanation
Question 25
What inflammatory mediator has been most closely associated with the magnitude of the systemic inflammatory response to trauma and with the development of multiple organ dysfunction syndrome (MODS)?
Explanation
REFERENCES: Patrick DA, Moore FA, Moore EE, et al: Jack A. Barney Resident Research Award winner: The inflammatory profile of interleukin-6, interleukin-8, and soluble intercellular adhesion molecule-1 in postinjury multiple organ failure. Am J Surg 1996;172:425-429.
Pape HC, van Griesven M, Rice J, et al: Major secondary surgery in blunt trauma patients and perioperative cytokine liberation: Determination of the clinical relevance of biochemical markers. J Trauma 2001;50:989-1000.
Giannoudis PV: When is the safest time to undertake secondary definitive fracture stabilization procedures in multiply injured patients who were initially managed using a strategy of primary temporary skeletal fixation. J Trauma 2002;52:811-812.
Question 26
An 18-year-old girl with quadriplegic cerebral palsy underwent posterior spinal fusion from T2 to the pelvis 3 weeks ago. She now has a low-grade fever and mild midline erythema in a 1-cm area from which there is slight clear yellowish drainage. What is the next most appropriate step in management?
Explanation
REFERENCES: Theiss SM, Lonstein JE, Winter RB: Wound infections in reconstructive spine surgery. Orthop Clin North Am 1996;27:105-110.
Richards BS: Delayed infections following posterior spinal instrumentation for the treatment of idiopathic scoliosis. J Bone Joint Surg Am 1995;77:524-529.
Question 27
A 41-year-old right-hand-dominant man has been treated nonsurgically for right elbow arthritis. His radiographs reveal end-stage ulnohumeral arthritis with complete loss of the joint space. He reports pain during the mid-arc of elbow flexion and extension. During the last 8 years, he has attempted activity modification, medication, physical therapy, and multiple cortisone injections. His symptoms have progressed, resulting in constant pain, loss of a functional range of motion, and an inability to perform many activities of daily living. Secondary to his age and activity demands, he undergoes a soft-tissue interposition arthroplasty of his elbow with an Achilles allograft. Which presurgical finding correlates with elevated risk for postsurgical complications?
Explanation
restrictions for patients after surgery and remains a reasonable salvage procedure. Larson and Morrey published their findings on 38 patients with a mean age of 39 years following soft-tissue interposition arthroplasty for posttraumatic and inflammatory end-stage elbow arthritis. These investigators reported a significant improvement in Mayo Elbow Performance Score in addition to improvement in the flexion- extension arc from 51° to 97° after surgery. They reported worse results and elevated incidence of complications for patients with presurgical elbow instability upon examination; retained hardware from prior
surgery was not deemed a contraindication.
Question 28
Four weeks after undergoing elective THA, an 80-year-old man is in the emergency department with sudden-onset right hip pain and an inability to bear weight after bending over in his garden.
Explanation
In Question 138, pain and swelling following a metal-on-metal large-head THA represent a classic presentation for a pseudotumor from metallosis secondary to either articular metal wear or trunnionosis. For this patient, infection should be ruled out with laboratory studies (erythrocyte sedimentation rate and C-reactive protein) and joint aspiration. Metal ion levels and metal artifact reduction sequence MR imaging or ultrasound would be helpful to confirm the diagnosis of pseudotumor. In Question 139, chronic hip pain following elective THA with an antecedent postsurgical wound constitutes a typical presentation for chronic periprosthetic infection. Aseptic loosening could be considered although the timeline is short; bloodwork and joint aspiration would be appropriate investigations. In Question 140, giving way of the knee suggests quadriceps muscle dysfunction likely related to prolonged pressure on the femoral nerve from retractors during a long revision case. The pattern of weakness does not fit a sciatic nerve palsy. In Question 141, the presentation is typical of a prosthetic dislocation, most of which occur during the early postsurgical period following THA.

Question 29
Botulinum toxin is used to treat vasospastic disorders of the hand such as the Raynaud phenomenon to improve digital perfusion and reduce pain. Botulinum toxin enables which transmitter to be unopposed, resulting in vasodilation?
Explanation
Nitric oxide is the only transmitter listed that is not inhibited by botulinum toxin. Substance P and glutamate are inhibited by botulinum toxin from release by pain nociceptors, thus reducing pain. Fonseca and associates have postulated that botulinum toxin inhibits the RhoA kinase pathway by blocking reactive oxygen species, which in turn does not allow actin/myosin to activate, thus preventing vasoconstriction of smooth muscle. Blocking the RhoA kinase pathway allows the action of nitric oxide to be unopposed, causing vasodilation. Nitric oxide is a potent vasodilator. Thus, botulinum toxin promotes nitric oxide activity to increase vasodilation.
Question 30
A 7-year-old girl has pain and swelling of the right elbow after falling off her bicycle. Radiographs are shown in Figure 31. What is the most appropriate initial step in management?
Explanation
REFERENCES: Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425.
Attarian DE: Lateral condyle fractures: Missed diagnoses in pediatric elbow injuries. Mil Med 1990;155:433-434.
Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Badelon O, Bensahel H, Mazda K, et al: Lateral humeral condylar fractures in children: A report of 47 cases. J Pediatr Orthop 1988;8:31-34.
Question 31
During a revision total knee arthroplasty (TKA), there is difficulty gaining exposure and a tibial tubercle osteotomy (TTO) is performed. The final components are stable and include a stemmed tibial component that bypasses the osteotomy site. The tibial tubercle is reattached to the osteotomy site with multiple cerclage wires. Following closure of the arthrotomy, the knee is flexed to 90 degrees, and there is no observed displacement of the TTO. What is the best next step in postsurgical rehabilitation?
Explanation
TTO is a recognized technique for improving exposure when performing TKA in a stiff knee. TTO has been reported to enhance surgical exposure and not adversely affect outcomes after TKA, but there is a 5% complication rate. The postsurgical routine following TTO
includes full weight-bearing activity and range of motion as tolerated. Caution should be exercised when manipulation is performed to improve knee flexion following a TTO.
Question 32
A surgeon prepares a medial gastrocnemius rotational flap to cover a medial proximal tibia defect at the time of revision knee replacement surgery. To optimize coverage, the surgeon must optimally mobilize which artery?
Explanation
The medial sural arteries vascularize the gastrocnemius, plantaris, and soleus muscles proximally. These arteries arise from the popliteal artery. If this artery is not adequately mobilized, a gastrocnemius soleus flap can be devascularized.
Question 33
Corticosteroids inhibit the formation of effectors of the inflammatory pathway via inhibition of
Explanation
Question 34
All of the following are considered contraindications to the use of functional bracing of a humeral shaft fracture EXCEPT:

Explanation
Commonly accepted parameters for closed treatment include less than 30 degrees of varus angulation, 20 degrees of anterior/posterior angulation, and 3 cm of shortening. Operative indications are: associated vascular injuries, bilateral humeral shaft fractures, polytrauma patient (including paraplegia), segmental fractures, injury to the brachial plexus, pathological fractures, floating elbow, and floating shoulder.
The article by Rutgers and Ring found that proximal one-third oblique humeral shaft fractures had an unacceptably high 29% rate of nonunion treated with a functional brace.
The article by Sarmiento et al found a 97% rate of union, a radial nerve palsy incidence of 11%, and no contraindication to the use of functional braces in humeral shaft fractures associated with radial nerve palsy.
The review article by Defranco and Lawton states that 70% of these radial nerve injuries recover spontaneously. They note that it "seems reasonable, however, to consider surgical intervention (radial nerve exploration) between 4 and 6 months based on the patient’s clinical course."
Question 35
Figure 40 shows the plain radiograph of a 30-year-old woman who has had a long history of standing bilateral anterior knee pain and a sense of patellar instability without frank dislocation. Nonsurgical management consisting of anti-inflammatory drugs and physical therapy has failed to provide relief. Examination reveals full range of motion of both knees, with moderate patellofemoral crepitance. Patellar apprehension and patellar grind tests are positive. The Q-angle measures 20°. Management should now consist of
Explanation
REFERENCES: Boden BP, Pearsall AW, Garrett We Jr, et al: Patellofemoral instability: Evaluation and management. J Am Acad Orthop Surg 1997;5:47-57.
Fulkerson JP: Patellofemoral pain disorders: Evaluation and management. J Am Acad Orthop Surg 1994;2:124-132.
Question 36
Which of the following is not considered to be a part of the constellation of the clinical entities known as the female athlete triad? Review Topic
Explanation
The female athlete triad was coined in 1992 by the American College of Sports Medicine as a complex disorder more prevalent in the adolescent and young female
athlete population including decreased bone mineral density (BMD), menstrual dysfunction, and low energy availability with or without a concomitant eating disorder. Treatment should involve a multidisciplinary approach, including psychological and nutritional counseling for eating behaviors and dietary management, reduction of training intensity to decrease risk of stress fractures, and initiating calcium and vitamin D supplements for osteoporosis.
Nazem et al performed a systematic review of articles containing the female athlete triad, reviewing diagnosis via screening during physical examinations as well as laboratory and imaging evaluation for menstrual dysfunction, low energy availability, and low bone mineral density. They state that potential complications including possible infertility, decreased immune function, cardiovascular disease, and irreversible loss of bone mineral density. They concluded that prevention, early recognition, and a multidisciplinary treatment team with a focus on proper nutrition and natural return of menses is vital.
Nattiv et al review the position of the American College of Sports Medicine regarding the female athlete triad, including screening for the triad at the pre-participation physical, discouragement of unhealthy weight loss practices. Essential members of the multidisciplinary treatment team include a health-care professional, a registered dietitian, and a mental health practitioner. They endorse that the first aim of treatment for any triad component is to increase energy availability by increasing energy intake and reducing exercise energy expenditure.
Question 37
What acetabular procedure for developmental dysplasia of the hip does not require a concentric reduction of the femoral head in the acetabulum?
Explanation
REFERENCES: Staheli LT, Chew DE: Slotted acetabular augmentation in childhood adolescence. J Pediatr Orthop 1992;12:569-580.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 618-650.
Question 38
Which 2 tendons are identified in the dissection shown in Video 92?
Explanation
RECOMMENDED READINGS
Babb JR, Detterline AJ, Noyes FR. AAOS Orthopaedic Video Theater. The Key to the Knee: A Layer-by-Layer Video Demonstration of Medial and Anterior Anatomy. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2009.
Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:493-568.
Question 39
A 13-year-old girl injures her ankle playing soccer. Radiographs reveal a displaced Tillaux fracture. CT scans are shown in Figure 25. What is the most important consideration for appropriate management?
Explanation
REFERENCES: Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment.
J Am Acad Orthop Surg 2001;9:268-278.
Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Duchesneau S, Fallat LM: The Tillaux fracture. J Foot Ankle Surg 1996;35:127-133.
Question 40
The third plantar intrinsic muscle layer of the foot consists of which of the following structures?
Explanation
REFERENCE: Resch S: Functional anatomy and topography of the foot and ankle, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 32-33.
Question 41
In girls with idiopathic scoliosis, peak height velocity (PHV) typically occurs at what point?
Explanation
require surgery.
REFERENCES: Little DG, Song KM, Katz D, Herring JA: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am
2000;82:685-693.
Anderson M, Hwang SC, Green WT: Growth of the normal trunk in boys and girls during the second decade of life; related to age, maturity, and ossification of the iliac epiphyses. J Bone Joint Surg Am 1965;47:1554-1564.
Question 42
Which of the following is most associated with local recurrence of the lesion seen in the radiograph and MRI scan shown in Figures 27a and 27b?
Explanation
REFERENCES: Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
Vergel De Dios AM, Bond JR, Shives TC, et al: Aneurysmal bone cyst: A clinicopathologic study of 238 cases. Cancer 1992;69:2921-2931.
Question 43
High periosteal signal; normal marrow T1 signal; high marrow T2 signal
Explanation
Which of the following treatment methods is used for the majority of patients with a stress fracture:
Question 44
A 52-year-old woman has bicompartmental osteoarthritis following patellectomy. Treatment should consist of
Explanation
REFERENCES: Martin SD, Haas SB, Insall JN: Primary total knee arthroplasty after patellectomy. J Bone Joint Surg Am 1995;77:1323-1330.
Pagnano MW, Cushner FD, Scott WN: Role of the posterior cruciate ligament in total knee arthroplasty. J Am Acad Orthop Surg 1998;6:176-187.
Question 45
Which component is most common to both simple and complex elbow dislocations?

Explanation
Question 46
Which of the following is considered the most appropriate shoe modification following transmetatarsal amputation?
Explanation
REFERENCES: Philbin TM, Leyes M, Sferra JJ, Donley BG: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Marks RM: Mid-foot/mid-tarsus amputations. Foot Ankle Clin 1999;4:1-16.
Question 47
Figures 45a and 45b show the radiographs of a 14-year-old boy who sustained a distal radius fracture while playing hockey. After 1 year the patient is asymptomatic. Follow-up and comparison radiographs and an MRI scan are shown in Figures 45c and 45d. What is the next most appropriate step in management?
Explanation
REFERENCES: Vanheest A: Wrist deformities after fracture. Hand Clin 2006;22:113-120.
Bae DS, Waters PM: Pediatric distal radius fractures and triangular fibrocartilage complex injuries. Hand Clin 2006;22:43-53.
Question 48
What role does quorum sensing play in the development of a bacterial biofilm?
Explanation
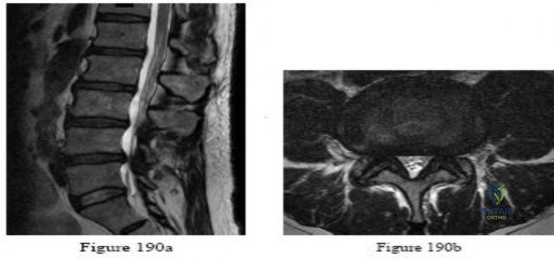
Question 49
-Figures 190a and 190b are the sagittal and axial T2-weighted MRI scans of a 75-year-old man who is experiencing progressively worsening bilateral lower-extremity pain and difficulty walking distances. In another 4 years, nonsurgical treatment of his condition--compared to surgical treatment--is expected to result in
Explanation

Question 50
A 32-year-old recreational basketball player underwent a successful anterior cruciate ligament (ACL) reconstruction using hamstring autograft approximately 15 months ago. His chart notes that he has good functional knee outcome scores as tested by his physical therapist. However, he has not returned to play despite being cleared by his physician 3 months ago. After successful ACL reconstruction, which of the following factors has shown to contribute the greatest influence on a player's decision to return to sport? Review Topic
Explanation
The return to their preinjury level of sport is frequently expected within 1 year after anterior cruciate ligament (ACL) reconstruction, yet many athletes do not achieve this milestone. Having a previous ACL reconstruction to either knee, poorer hop-test symmetry and subjective knee function, and more negative psychological responses were associated with not returning to the preinjury level sport. Fear of reinjury is considered one of the most common reasons cited for a postoperative reduction in or
cessation of sports participation.
Tjong et al. conducted a qualitative study of 31 patients, aged 18 to 40 years, to understand the factors influencing a patient's decision to return to his or her preinjury level of sport after ACL reconstruction. They found 3 overarching factors what largely influenced their decision to return to the preinjury sport: fear, lifestyle changes, and innate personality traits. This highlighted the importance of recognizing and addressing the psychological factors and lifestyle changes that significantly contribute to a patient's postoperative decision to return to sport.
Ardern et al. investigated the return-to-sport rates at 2 years after ACL reconstruction in athletes. At 2 years after surgery, 66% were playing sport, with 41% playing their preinjury level of sport and 25% playing a lower level of sport. Demographics, physical function, and psychological factors were supported as the most important influencing factors for the return to their preinjury level of sport.
Incorrect Answers:
Question 51
A 20-year-old collegiate football player who sustained blunt head trauma during the first half of a game is emotional and confused. During the halftime intermission, his affect, memory, and disorientation are totally resolved and have returned to preinjury baseline. The only residual finding is a very mild headache. He wants to play the second half. What is the most appropriate course of action?
Explanation
REFERENCES: Garrick J (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 29-48.
Guskiewicz KM, McCrea, Marshall SW, et al: Cumulative effects associated with recurrent concussion in collegiate football players: The NCAA Concussion Study. JAMA
2003;290:2549-2555.
Question 52
Figures below show the radiographs obtained from an 86-year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 53
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
corrective osteotomy.
REFERENCES: O’Driscoll SW, Spinner RJ, McKee MD, et al: Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-1369.
Gurkan I, Bayrakci K, Tasbas B, et al: Posterior instability of the shoulder after supracondylar fractures recovered with cubitus varus deformity. J Pediatr Orthop 2002;22:198-202.
Spinner RJ, O’Driscoll SW, Davids JR, et al: Cubitus varus associated with dislocation of both the medial portion of the triceps and the ulnar nerve. J Hand Surg 1999;24:718-726.
Question 54
A 40-year-old man has had hip pain with increased activity over the past year. Examination reveals restriction of motion and tenderness with combined hip flexion, adduction, and internal rotation. An AP radiograph is shown in Figure 34. What is the most likely diagnosis?
Explanation
REFERENCES: Beall DP, Sweet CF, Martin HD, et al: Imaging findings of femoraoacetabular impingement syndrome. Skeletal Radiol 2005;34:691-701.
Mardones RM, Gonzalez C, Chen Q, et al: Surgical treatment of femoroacetabular impingement: Evaluation of the effect of the size of the resection. J Bone Joint Surg Am 2006;88:84-91.
Question 55
A 79-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing right shoulder pain for the past year, and nonsurgical management has failed to provide relief. Her neurologic examination is entirely normal, but she is unable to elevate her arm against gravity. An AP radiograph is shown in Figure 13. Treatment should consist of
Explanation
REFERENCES: Neer CS II, Watson KC, Stanton FJ: Recent experience in total shoulder replacement. J Bone Joint Surg Am 1982;64:319-337.
Neer CS II: Glenohumeral arthroplasty, in Neer CS II (ed): Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 143-271.
Pollock RG, Deliz ED, McIlveen ST, et al: Prosthetic replacement in rotator cuff deficient shoulders. J Shoulder Elbow Surg 1992;1:173-186.
Sneppen O, Fruensgaard S, Johannsen HV, Olsen BS, Sojbjerg JO, Anderson NH: Total shoulder replacement in rheumatoid arthritis: Proximal migration and loosening. J Shoulder Elbow Surg 1996;5:47-52.
Question 56
A 13-year-old boy sustains a valgus stress injury to the knee while playing football, and he is unable to bear weight after the injury. Examination reveals tenderness medially superior to the joint line. The knee is held in flexion, and he has a large effusion and localized medial swelling. Plain radiographs show no obvious fracture. What is the next diagnostic step?
Explanation
REFERENCES: Smith L: Concealed injury to the knee. J Bone Joint Surg Am 1962;44:1659-1660.
Beaty JH, Kumar A: Fractures about the knee in children. J Bone Joint Surg Am 1994;76:1870-1880.
Question 57
When using the direct lateral (or Hardinge) approach for hip arthroplasty, three muscles are detached from the femur. In addition to the vastus lateralis, they include the
Explanation
REFERENCES: Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 333-335.
Hardinge K: The direct lateral approach to the hip. J Bone Joint Surg Br 1982;64:17-19.
Question 58
A 26-year-old weightlifter had increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication,
Explanation
Question 59
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and
Explanation
REFERENCES: Botte MJ, Byrne TP, Abrams RA, et al: Halo skeletal fixation: Techniques of application and prevention of complications. J Am Acad Orthop Surg 1996;4:44-53.
Garfin SR, Botte MJ, Nickel VL: Complications in the use of the halo fixation device. J Bone Joint Surg Am 1987;69:954.
Question 60
When examining a patient with marked hyperreflexia, which of the following findings best suggests that the condition is not caused by a cerivcal spine pathology?
Explanation
REFERENCES: Montgomery DM, Brower RS: Cervical spondylotic myelopathy: Clinical syndrome and natural history. Orthop Clin North Am 1992;23:487-493.
Ono K, Ebara S, Fuji T, Yonenobu K, Fujiwara K, Yamashita K: Myelopathy hand: New clinical signs of cervical cord damage. J Bone Joint Surg Br 1987;69:215-219.
An HS, Simpson JM: Surgery of the Cervical Spine. Baltimore, MD, Williams and
Wilkins, 1994.
Question 61
Figures 78a and 78b show the CT scans of a 22-year-old man with back pain after falling out of a tree. Examination reveals no palpable spinal step-offs, posterior spinal pain, and normal neurologic function in the lower extremities. Normal perineal sensation and normal rectal tone are present. What is the best management? Review Topic

Explanation
Question 62
According to Musculoskeletal Infection Society (MSIS) guidelines, which set of patient laboratory study results fits the definition of chronic prosthetic joint infection?
Explanation
The MSIS definition of periprosthetic joint infection was updated in 2014 with two major and six minor criteria. The presence of one major criterion or three minor criteria is diagnostic for infection. The major criteria are two positive cultures with the same organism or a draining sinus tract. The current MSIS minor criteria are 1) an elevated ESR (more than 30 mm/hr) and CRP level (more than 10 mg/L), 2) an elevated synovial WBC count (more than 3,000 cells per/microliter), 3) an elevated synovial fluid polymorphonuclear count (more than 80%), 4) a positive histological analysis of periprosthetic tissue, and 5) a single positive culture.
Question 63
A 70-year-old healthy man had total knee arthroplasty 18 years ago, and it now is painful. Radiographs reveal aseptic loosening and the range of motion before surgery is 15 to 85 degrees. The strongest indication for performing a tibial tubercle osteotomy to aid in exposure in his knee would be
Explanation

Question 64
-Figures a through f are the radiograph, CT scan, MRI scan, and bone scan of a 28-year-old woman with a newly diagnosed breast carcinoma who underwent a bone scan for staging. She has no hip pain but a lesion is noted. What is the best next treatment step?
Explanation
Question 65
What is the most common complication associated with scalene regional anesthesia for shoulder procedures?
Explanation
REFERENCES: Weber SC, Jain R: Scalene regional anesthesia for shoulder surgery in a community setting: An assessment of risk. J Bone Joint Surg Am 2002;84:775-779.
Conn RA, Colfield RH, Byer DE, Lindstromberg JW: Interscalene block anesthesia for shoulder surgery. Clin Orthop 1987;216:94-98.
Question 66
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals that the knee is held in 45 degrees of flexion, and any attempt to actively or passively extend the knee produces pain and muscle spasms. A lateral radiograph is shown in Figure 4. What is the most likely diagnosis?
Explanation
REFERENCES: Houghton GR, Ackroyd CE: Sleeve fractures of the patella in children: A report of three cases. J Bone Joint Surg Br 1979;61:165-168.
Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Question 67
Patients with patellar clunk syndrome are best managed by which of the following methods?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 329.
Diduch DR, Scuderi GR, Scott WN, et al: The efficacy of arthroscopy following total knee replacement. Arthroscopy 1997;13:166-171.
Lucas TS, DeLuca PF, Nazarian DG, et al: Arthroscopic treatment of patellar clunk. Clin Orthop 1999;367:226-229.
Question 68
An 18-year-old collegiate basketball player has had a 3-month history of activity-related back pain. She describes isolated low back pain without radiation that increases with training and playing basketball. Her pain resolves with rest. Physical therapy for 6 weeks has failed to provide relief. An axial CT scan is shown in Figure 17a, and Figures 17b and 17c show sagittal CT reconstructions through the right and left lumbar facets, respectively. Further management should consist of which of the following?
Explanation
REFERENCES: Debnath UK, Freeman BJ, Grevitt MP, et al: Clinical outcome of symptomatic unilateral stress injuries of the lumbar pars interarticularis. Spine 2007;32:995-1000.
Bono CM: Low-back pain in athletes. J Bone Joint Surg Am 2004;86:382-396.
Question 69
A 75-year-old woman reports foot pain and states that her foot has become progressively “flatter” in the past 3 years. Custom inserts and physical therapy have failed to provide relief. Examination reveals a flexible hindfoot and mild heel cord contracture. The patient is able to perform a single limb heel rise. Weight-bearing radiographs are shown in Figures 21a through 21d. What is the most appropriate surgical management?
Explanation
REFERENCES: Toolan BC: Midfoot arthrodesis: Challenges and treatment alternatives. Foot Ankle Clin 2002;7:75-93.
Horton GA, Olney BW: Deformity correction and arthrodesis of the midfoot with a medial plate. Foot Ankle 1993;14:493-499.
Question 70
A left-handed 23-year-old man who fell 5 feet from a ladder onto his left elbow sustained the closed injury shown in Figure 26. Management should consist of
Explanation
REFERENCES: Hotchkiss RN: Fractures and dislocations of the elbow, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 929-1024.
Murphy DF, Greene WB, Gilbert JA, Dameron TB Jr: Displaced olecranon fractures in adults: Biomechanical analysis of fixation methods. Clin Orthop 1987;224:210-214.
Hume MC, Wiss DA: Olecranon fractures: A clinical and radiographic comparison of tension band wiring and plate fixation. Clin Orthop 1992;285:229-235.
Question 71
A 26-year-old man sustained an isolated injury to his left hip joint in a motor vehicle accident. Closed reduction was performed, and the postreduction radiograph is shown in Figure 29. Management should now consist of
Explanation
REFERENCES: Tile M, Olson SA: Decision making: Non operative and operative indications for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 496-532.
Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993, pp 337-339, p 507.
Question 72
A 26-year-old rugby player injured his foot when tackled from behind. Radiographs are seen in Figures 35a through 35c. What is the most appropriate treatment?
Explanation
REFERENCES: Chiodo CP, Myerson MS: Developments and advances in the diagnosis and treatment of injuries of the tarsometatarsal joint. Orthop Clin North Am 2001;32:11-20.
Hunt SA, Ropiak C, Tejwani NC: Lisfranc joint injuries: Diagnosis and treatment. Am J Orthop 2006;35:376-385.
Question 73
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include
Explanation
REFERENCE: Sabharwal S, Tredwell SJ, Beauchamp RD, Mackenzie WG, Jakubec DM, Cairns R: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 74
A 17-year-old male football player is seen 1 week after developing symptoms of infectious mononucleosis in the middle of the season. Examination reveals evidence of splenomegaly. He and his parents want to know if he can play in a game the following day. What is the most appropriate recommendation? Review Topic
Explanation
Question 75
Figures 57a and 57b are the MRI scans of a 61-year-old man who is unable to elevate his dominant arm following a golf injury 24 hours ago. He has moderate pain during attempted arm elevation. Examination reveals significant spinati atrophy and he is only able to elevate his arm fully overhead while supine. The neurologic examination is normal. What is the next most appropriate step in management? Review Topic

Explanation
Question 76
A 25-year-old woman returns for her first postoperative visit after arthroscopic thermal capsulorrhaphy for recurrent multidirectional instability. Examination reveals that the portals are healed, there is no swelling; and passive range of motion is within the normal range. However, she is unable to actively raise her arm. Shoulder radiographs are normal. What is the most likely cause of these findings? Review Topic
Explanation
Question 77
A year-old woman had a primary total hip arthroplasty 7 years ago that included a proximally coated titanium stem, a cobalt alloy femoral head, a titanium hemispherical acetabular component, and a polyethylene liner. She did well for 4 years but has now had two dislocations and reports pain and weakness around the left hip. She denies any fevers, chills, or constitutional symptoms. On examination, the patient walks well without any signs of an antalgic or Trendelenburg gait. Her abductor mechanism demonstrates good strength. Her erythrocyte sedimentation rate and C-reactive protein level are normal. On radiographs, all components appear well fixed and in good alignment. What is the most appropriate treatment at this time?
Explanation
Trunnionosis is a recently recognized complication following total hip arthroplasty and can occur when a cobalt alloy femoral head is used on a titanium alloy or cobalt alloy femoral stem. Patients often present with pain or swelling around the hip but at times can present with instability. Certain femoral stem designs have been associated with increased reports of trunnionosis. In a patient with a cobalt alloy femoral head who presents with instability, swelling, and weakness around the hip, the potential for trunnionosis and
an adverse local tissue reaction should be considered.
Question 78
A 32-year-old man underwent a total medial meniscectomy 2 years ago. He now reports pain and recurrent swelling for the past 3 months. Work-up includes full standing hip-knee-ankle radiographs, standing AP radiographs of both knees in full extension, an axial view of the patellofemoral joint, and a 45-degree flexion AP radiograph. Contraindication to meniscus allograft transplantation includes which of the following? Review Topic
Explanation
Question 79
03 What is the most common site of fracture because of osteolysis following cementless total hip arthroplasty with an extensively porus-coated femoral component?

Explanation

creates stress shielding. The force is seen through the femoral head into the stem and transfers to the bone at areas of
ingrowth and transmitted distally. As a result the part being skipped is the greater trochanter and leads to osteolysis by Wolf’s law and can result in fracture.

The osteolysis created about the acetabulum is due an inflammatory mechanism imparted on the wear debris from the bearing surfaces. This osteolysis rarely creates fractures.

The fractures about the stem are most commonly caused by the difference in modulus between the stem and bone back to this question next question
Question 80
Figure 11 shows the radiograph of a 26-year-old man with type I diabetes mellitus who was struck by a motor vehicle. What is the most common complication associated with this pelvic fracture?
Explanation
REFERENCES: Geerts WH, Code KI, Jay RM, et al: A prospective study of venous thromboembolism after major trauma. N Engl J Med 1994;331:1601-1606.
Steele N, Dodenhoff RM, Ward AJ, et al: Thromboprophylaxis in pelvic and acetabular trauma surgery: The role of early treatment with low-molecular-weight heparin. J Bone Joint Surg Br 2005;87:209-212.
Question 81
Which of the following factors has been shown to be the strongest predictor of screw cutout of a dynamic compression hip screw used for an intertrochanteric femur fracture?

Explanation
Baumgaertner et al reported that he had no screws cut out if the tip-apex distance was less than 25mm. Tip-apex distance was the strongest predictor of cutout. Increasing age of the patient, poor reduction, use of a high angle sideplate, and unstable fracture were weaker predictors of cutout.
Kyle et al demonstrated that obtaining an anatomic reduction when using a sliding hip screw with intertrochanteric fractures leads to the best radiographic and clinical outcomes.
Question 82
- Following closed reduction for the injury shown in Figures 69a and 69b, treatment should consist of
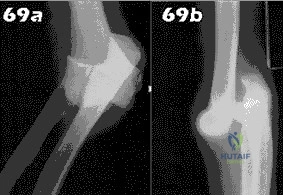
Explanation
Repair or reconstruction of the medial and lateral collateral ligaments-Acute dislocations can be reduced in supination and tested for valgus stability in pronation. Treatment is determined by the stability following reduction. When there are fractures, the principle is to fix the bones so that the only limitation is the ligaments and then to repair them if the elbow is not stable enough to permit early motion.
Immobilization for 14 days-The longer the immobilization had been, the larger the flexion contracture (p less than 0.001) and the more severe the symptoms of pain were. The results indicate that early active motion is the key factor in rehabilitation of the elbow after a dislocation. Simple dislocation of the elbow in the adult. Results after
closed treatment. Immobilization for 25 days- See above.
Question 83
A 47-year-old man comes for evaluation of his dominant right elbow, which has been bothering him with activity for the past 3 months, especially with activities requiring wrist extension. He is an active squash player and has been unable to continue this sport. Examination shows tenderness at the common extensor origin. What is the next best step? Review Topic
Explanation
Lateral epicondylitis is a common problem with numerous non-operative treatments available. There is little scientific evidence to support any of these treatments however and the quality of most reports is low and their conclusions limited by bias and/or study design. Tennis elbow often resolves with time regardless of which conservative treatment is chosen.
Coombes et al. randomized patients with unilateral tennis elbow to receive either (1) corticosteroid injection, (2) placebo injection, (3) corticosteroid injection plus physical therapy or (4) placebo injection plus physical therapy. They found that
corticosteroid resulted in worse clinical outcome and recurrence rate compared to placebo injection. Use of physical therapy did not produce any significant differences.
Dines et al. review the diagnosis and of tennis injuries, including lateral epicondylitis. Although they acknowledge that there is "no long term benefit with regard to tendon healing," they note that steroid injection may be useful to control acute symptoms.
Boyer et al. review the myths surrounding lateral epicondylitis. They note that despite widespread use, corticosteroid injection has repeatedly been shown to have no long term benefit. They conclude based on their review of the literature that if there is any benefit to steroid injection, it is of short duration, and in patients whose symptoms have been of short duration, without any previous treatment.
Incorrect answers:
Question 84
Figure 2 shows the lateral radiograph of an 8-year-old boy who sustained an acute injury to the elbow after falling down the stairs. Management should consist of
Explanation
REFERENCES: Murphy DF, Greene WB, Gilbert JA, Dameron TB Jr: Displaced olecranon fractures in adults: Biomechanical analysis of fixation methods. Clin Orthop 1987;224:210-214.
Chambers HG, Wilkins KE: Part IV: Fractures of the proximal radius and ulna, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 629-630.
Question 85
Figure 76 is the MR image of a 16-year-old high school football player who sustained a traumatic dominant shoulder dislocation during a game. On-field reduction was unsuccessful. The shoulder is reduced in the emergency department, and the player and his family followup in clinic. Which factor is most associated with failure of surgical treatment in this scenario?
Explanation
The MR image reveals a Bankart lesion. Arthroscopic Bankart repair failure likelihood is increased by numerous factors. Age, number of recurrences, and bony defects are most associated with failure of arthroscopic repair. Shoulder dominance, amount of periosteal
stripping, and difficulty of reduction do not correlate with increased recurrence risk following surgery.
CLINICAL SITUATION FOR QUESTIONS 77 THROUGH 79
A 17-year-old volleyball player has a 3-month history of gradually worsening right shoulder pain. She describes a vague sensation of her shoulder “popping out of place” and weakness associated with overhead activities. She has intermittent generalized paresthesias in her right upper extremity, and she has discontinued participation in sports as a result of her symptoms. Glenohumeral range of motion is symmetric bilaterally. Empty can test findings are negative with full strength of the supraspinatus. An active compression test is negative, and sulcus sign findings are positive. An anterior apprehension test produces pain that is unrelieved with a relocation test. A cervical spine examination is unremarkable.
Question 86
What measure of physiologic status best evaluates whether an injured patient is fully resuscitated and best predicts that perioperative complications will be minimized following definitive stabilization of long bone fractures?
Explanation
REFERENCES: Blow O, Magliore L, Claridge JA, et al: The golden hour and silver day: Detection and correction of occult hypoperfusion within 24 hours improves outcomes from major trauma. J Trauma 1999;47:964-977.
Crowl A, Young JS, Kahler DM, et al: Occult hypoperfusion is associated with increased morbidity in patients undergoing early femur fracture fixation. J Trauma 2000;48:260-267.
Shulman AM: Prediction of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:725-800.
Question 87
A 6-year-old boy has had increasing pain and a mass in the suprapatellar region of the right femur for the past week. Examination of the mass reveals it may be firm, immobile, and tender to palpitation. The patient has no systemic symptoms. Laboratory studies show a WBC of 7000 per cubic millimeter, a hematocrit of 40%, and an erythrocyte sedimentation rate of 10 mm/hr. radiographs are normal. Figures 64a and 64b show saggital and axial T1-weighted MRI scans. Figure 64c shows frozen section pathology of the biopsy specimen. What is the most likely diagnosis?
Explanation
Question 88
A college football player performs bicep curls as part of his weight lifting routine. During the flexion phase of the curl, what term defines the type of muscle contraction?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 89-125.
Evans WJ: Effects of exercise on senescent muscle. Clin Orthop 2002;403:S211-S220.
Question 89
Figures 13a and 13b show the MRI scans of a 70-year-old patient who has a posterior calf mass. Examination reveals that the mass extends to the midcalf level. A biopsy specimen reveals a high-grade soft-tissue sarcoma. Metastatic work-up shows no lesions. Management should consist of
Explanation
REFERENCES: Lindberg RD, Martin RG, Romsdahl MM, et al: Conservative surgery and post-operative radiotherapy in 300 adults with soft tissue sarcoma. Cancer 1981;47:2391-2397.
Sim FT, Frassica FS, Frassica DA: Soft tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Rosenberg SA, Tepper J, Glatstein E, et al: The treatment of soft-tissue sarcomas of the extremities: Prospective randomized evaluations of (1) limb sparing surgery plus radiation therapy compared with amputation and (2) The roll of adjuvant chemotherapy. Am Surg 1982;196:305-315.
Question 90
A 48-year-old man reports localized plantar forefoot pain. Examination reveals a discrete callus (intractable plantar keratosis) with well-localized tenderness beneath the second metatarsal head. The callus most likely lies beneath what structure?
Explanation
REFERENCES: Coughlin MJ, Mann RA: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 413-465.
Cracchiolo A: Surgical procedures of the lateral metatarsals, in Jahss MH (ed): Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991, pp 1269-1283.
Question 91
Which of the following studies is considered most sensitive in monitoring a therapeutic response in acute hematogenous osteomyelitis?
Explanation
REFERENCE: Unidia-Kallio L, et al: Serum c-reactive protein, ESR and WBC in acute hematogenous osteomyelitis in children. Pediatrics 1994;93:59-62.
Question 92
Figure 24 shows an axial MRI scan of the ankle. The arrowhead is pointing to what structure?
Explanation
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. New York, NY, Lippincott, 1993, pp 234-235.
Sammarco GJ: Peroneus longus tendon tears: Acute and chronic. Foot Ankle Int
1995;16:245-253.
Question 93
When balancing gaps in the coronal plane, what structure preferentially impacts the flexion space more than the extension space?
Explanation
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point,
can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
Question 94
Figures 36a and 36b show the MRI scans of a 15-year-old girl who has had pain and recurrent hemarthrosis in the knee for the past year. Plain radiographs are normal. What is the most likely diagnosis?
Explanation
REFERENCE: Price NJ, Cundy PJ: Synovial hemangioma of the knee. J Pediatr Orthop 1997;17:74-77.
Question 95
Which of the following increases radiation exposure to patients and personnel during surgery?
Explanation
REFERENCE: Wagner L, Archer B: Minimizing Risks from Fluoroscopic X-rays: A Credentialing Program for Anesthesiologists, Cardiologists, Surgeons, Radiologists, and Urologists, ed 3. The Woodlands, TX, Partners in Radiation Management, 2000.
Question 96
Which of the following articulation couplings shows the lowest coefficient of friction as tested in the laboratory?
Explanation
REFERENCES: Cuckler JM, Bearcroft J, Asgian CM: Femoral head technologies to reduce polyethylene wear in total hip arthroplasty. Clin Orthop 1995;317:57-63.
Sharkey PF, Hozack WJ, Dorr LD, Maloney WJ, Berry D: The bearing surface in total hip arthroplasty: Evolution or revolution, in Price CT (ed): Instructional Course Lectures 49. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 41-56.
Question 97
Figure 26 shows the radiograph of a 48-year-old woman who has right arm pain and hematuria. A bone scan reveals increased uptake in the left ribs and thoracic spine. A needle biopsy specimen shows that the lesion is highly keratin positive and composed primarily of clear cells. What is the best course of action?
Explanation
REFERENCES: Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG: Methylmethacrylate as an adjunct in internal fixation of pathological fractures: Experience with three hundred and seventy-five cases. J Bone Joint Surg Am 1976;58:1047-1054.
Sun S, Lang EV: Bone metastases from renal cell carcinoma: Preoperative embolization. J Vasc Interv Radiol 1998;9:263-269.
Katzner M, Schvingt E: Operative treatment of bone metastases secondary to renal carcinoma: Basic research and treatment of renal cell carcinoma metastasis. Prog Clin Biol Res EORTC 1990;348:151-168.
Question 98
During C1-C2 transarticular screw fixation, screw misplacement is most likely to result in injury to the
Explanation
REFERENCES: Mueller ME, Allgower M, et al: Manual of Internal Fixation, ed 3. New York, NY, Springer-Verlag, 1991, pp 634-636.
Gebhard JS, Schimmer RC, Jeanneret B: Safety and accuracy of transarticular screw fixation C1-C2 using an aiming device: An anatomic study. Spine 1998;23:2185-2189.
Question 99
Risk for vascular injury during transtibial drilling for reconstruction of this injury is increased by
Explanation
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, 1 major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading.
In Question 12, the scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-
producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag.
Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used. Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
Question 100
The clinical factors shown to most significantly predict the long-term outcome of Perthes disease of the hip include which of the following? Review Topic
Explanation
(SBQ13PE.87) A 4-week-old child is suspected to have classic arthrogryposis, also known as amyoplasia. Clinical examination and hip ultrasound reveal a unilateral, non-reducible, hip dislocation. What do you recommend to reduce the hip? Review Topic
Pavlik harness application
Semi-rigid abduction brace application
Skeletal traction
Early closed reduction and spica casting
Delayed open reduction with or without pelvic and femoral osteotomy
Delayed open reduction with or without pelvic and femoral osteotomy is recommended in the management of unilateral hip deformities associated with amyoplassia. This procedure should be performed at 6-9 months of age. In order to proceed with reduction, there must be a reasonable arc of flexion/extension and active movement of the lower limbs.
Amyoplasia is the most common recognizable form of arthrogryposis. It most commonly occurs as a sporadic symmetric contracture syndrome that is characterized by symmetrical limb involvement, normal to above-average intelligence, and often a midline facial hemangioma. Approximately 80% of children with amyoplasia will have involvement of the hip ranging from soft tissue contractures to unilateral or bilateral hip dislocations.
Bevan et al. reviewed arthrogryposis. They state that open hip reduction is recommended for the management of unilateral dislocation. There is more controversy with regard to the treatment of bilateral hip dislocations. Open reduction can be performed by a medial or anterolateral approach, with or without pelvic and
femoral osteotomy. This procedure is generally delayed for 6-9 months to facilitate the procedure.
Bernstein et al. also reviewed arthrogryposis. They state that the term 'arthrogryposis' encompasses a broad spectrum of diseases, all with the common phenotype of multiple congenital contractures.
Illustration A shows the characteristic features of an infant with severe arthrogryposis. Note the internal rotation of the shoulders, elbow and knee hyperextension, flexed and ulnarly deviated wrists, flexed finger, external rotation of hips and bilateral clubfeet.
Incorrect answers:
