Orthopedic Surgery Board Review MCQs: Spine, Arthroplasty, Knee & Shoulder | Part 183

Key Takeaway
This page offers an interactive, high-yield Multiple-Choice Question (MCQ) set (Part 183) for orthopedic surgeons and residents. It features 100 verified questions in OITE/AAOS format, with clinical explanations, to aid in comprehensive board certification exam preparation.
About This Board Review Set
This is Part 183 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 183
This module focuses heavily on: Arthroplasty, Deformity, Knee, Shoulder, Spine.
Sample Questions from This Set
Sample Question 1: An active, right-handed 71-year-old woman fell on her left shoulder and sustained the injury shown in the radiographs in 52a and 52b and the CT scan in 52c. Management should consist of...
Sample Question 2: A 27-year-old professional soccer player sustained an injury to his cervical spine in a collision with another player. Initially he was diagnosed with a right C6 radiculopathy that resolved with rest, anti-inflammatory medications, and phys...
Sample Question 3: Increasing articular conformity of the tibial polyethylene insert of a fixed-bearing total knee arthroplasty (TKA) prosthesis will have which of the following biomechanical effects?...
Sample Question 4: A 29-year-old man who lifts weights states that he injured his left shoulder while performing a bench press 2 days ago. The following morning he noted ecchymosis and swelling in the left chest wall. Examination reveals ecchymosis and tender...
Sample Question 5: A 62-year-old man has cervical myelopathy with no evidence of cervical radiculopathy. MRI reveals stenosis at C4-5 and C5-6 with severe cord compression. Examination will most likely reveal which of the following findings?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
An active, right-handed 71-year-old woman fell on her left shoulder and sustained the injury shown in the radiographs in 52a and 52b and the CT scan in 52c. Management should consist of
Explanation

Question 2
A 27-year-old professional soccer player sustained an injury to his cervical spine in a collision with another player. Initially he was diagnosed with a right C6 radiculopathy that resolved with rest, anti-inflammatory medications, and physical therapy. Following a fall in a game, he noted a recurrence of neck pain without radicular signs or symptoms. Additional nonsurgical management over the past few months has failed to provide relief. A cervical MRI scan shows a right-sided C5-6 herniation without any evidence of disk disease at other cervical levels. The patient desires to continue his career as a professional soccer player. What treatment offers the best long-term option for return to play?
Explanation
contact sports. Therefore, anterior cervical fusion at C5-6 offers the best long-term option for return to play.
REFERENCES: Watkins RG: Cervical spine injuries in athletes, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 373-386.
Watkins RG: Neck injuries in football players. Clin Sports Med 1986;5:215-246.
Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Garvey T, Transfeldt EE, Malcolm JR, et al: Outcome of anterior cervical discectomy and fusion as perceived by patients treated for dominant axial-mechanical cervical spine pain. Spine 2002;27:1887-1895.
Question 3
Increasing articular conformity of the tibial polyethylene insert of a fixed-bearing total knee arthroplasty (TKA) prosthesis will have which of the following biomechanical effects?
Explanation
REFERENCES: D’Lima DD, Chen PC, Colwell CW Jr: Polyethylene contact stresses, articular congruity, and knee alignment. Clin Orthop 2001;392:232-238.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 265-274.
Question 4
A 29-year-old man who lifts weights states that he injured his left shoulder while performing a bench press 2 days ago. The following morning he noted ecchymosis and swelling in the left chest wall. Examination reveals ecchymosis and tenderness and deformity in the left anterior chest wall and axillary fold that is accentuated with resisted adduction of the arm. Passive range of motion beyond 90 degrees of forward flexion and 45 degrees of external rotation is extremely painful. Glenohumeral stability is difficult to assess because of severe guarding. Figure 29 shows an MRI scan. Management should consist of
Explanation
REFERENCES: Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Schepsis AA, Grafe MW, Jones HP, Lemos MJ: Rupture of the pectoralis major muscle: Outcome after repair of acute and chronic injuries. Am J Sports Med 2000;28:9-15.
Question 5
A 62-year-old man has cervical myelopathy with no evidence of cervical radiculopathy. MRI reveals stenosis at C4-5 and C5-6 with severe cord compression. Examination will most likely reveal which of the following findings?
Explanation
REFERENCES: Sachs BL: Differential diagnosis of neck pain, arm pain and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 741-742.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 673-680.
Question 6
The main arterial supply to the humeral head is provided by which of the following arteries?
Explanation
REFERENCES: Brooks CH, Revell WJ, Heatley FW: Vascularity of the humeral head after proximal humeral fractures: An anatomical cadaver study. J Bone Joint Surg Br 1993;75:132-136.
Gerber C, Schneeberger AG, Vinh TS: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 7
Which of the following best describes the mechanism of action of gentamycin?
Explanation
REFERENCE: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 217-236.
Question 8
Figure 1 is the right hand of a 65-year-old man with a history of hypertension and rheumatoid arthritis. He is taking immunosuppressive disease-modifying antirheumatic drugs (DMARDs) and is seen in the emergency department with rapid progression of erythema from his right thumb to his right arm during the last 12 hours. He is confused, lethargic, and has these vital signs: blood pressure 92/40, respiratory rate 45, temperature 39.7°C, pulse 135, and oxygen saturation 90% on 4 liters of oxygen by face mask. An examination of his right upper extremity reveals black bulla extending from the metacarpophalangeal down to the tip and no capillary refill at the pulp. Immediate treatment should consist of

Explanation
This patient has multiple criteria for necrotizing soft-tissue infection (NSTI, also known as necrotizing fasciitis) including rapidly progressive infection, black bulla, hypotension and hypoxia, and a history of immune compromise. Aggressive emergent debridement including the removal of all necrotic tissue and IV antibiotics can decrease morbidity and mortality. Not all patients will have such obvious NSTI findings. In less clear cases, a scoring system using laboratory values (the Laboratory Risk Indicator for Necrotizing Fasciitis) can help clarify the diagnosis. IV antibiotics are key to treatment as well, but any delay in surgical treatment can increase morbidity and mortality. The black bulla and necrotic-appearing thumb indicate that this infection is not confined to the flexor sheath, therefore irrigation of the tendon sheath alone would be insufficient treatment. Although the thumb is dysvascular, this is because of an infection, and revascularization is not indicated.
Question 9
The most common complication associated with corticosteroid injection for the treatment of interdigital neuroma is
Explanation
Interdigital neuromas represent perineural fibrosis of the intermetatarsal nerve most commonly seen in the second and third web spaces. The photographs depict a neuroma in the second web space, which is less common than in the third space. Its hypoechoic appearance is characteristic on ultrasound. PVNS occurs in joints. Lipomas are fatty tumors. A ganglion cyst can occasionally occur adjacent to a nerve, but it has a cystic appearance.
The most popular theory on the etiology of interdigital neuromas is compression neuropathy by the intermetatarsal ligament. The plantar approach for the resection of interdigital neuromas has become more popular, especially for recurrent neuromas. The major advantage is better visualization and access to the neuromas.
Infection and allergic reactions such as hives are rare after steroid injection. CRPS is not known to occur in this setting. Hammertoe formation can occur, especially after multiple steroid injections into an interdigital neuroma.
RECOMMENDED READINGS
Schon LC, Reed MA. Disorder of the nerves. In: Coughlin MJ, Saltzman CL, Anderson RB, eds. Mann's Surgery of the Foot and Ankle. 9th ed. Philadelphia, PA: Elsevier-Saunders; 2014:622-641.
Gauthier G. Thomas Morton's disease: a nerve entrapment syndrome. A new surgical technique. Clin Orthop Relat Res. 1979 Jul-Aug;(142):90-2. PubMed PMID: 498653. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 96 THROUGH 98
Figure 96 is the anteroposterior projection foot radiograph of a 35-year-old woman who is injured in a high-speed motorcycle collision. Her assessment reveals an isolated injury. Her pulses are palpable and her neuromotor examination is intact. There is tenting of skin with ecchymosis over the second metatarsal. The foot is extremely swollen but not tense. Passive toe range of motion is painless.

Question 10
A 28-year-old man reports an episode of buckling and giving-way of his right knee. Figure 54a and 54b show a radiograph and sagittal MRI scan. What is the most likely diagnosis? Review Topic

Explanation
Question 11
Figure 61 is the radiograph of a 34-year-old woman who was involved in a rollover motor vehicle accident. On arrival at the trauma center she is hypotensive and tachycardic. An abdominal CT scan reveals a spleen laceration. The patient remains hypotensive despite resuscitation and is taken to surgery for an emergent laparotomy and splenectomy. After surgery her delta base is -9 mmol/L. What is the most appropriate management of her pelvic ring injury? Review Topic

Explanation
(SBQ12TR.80) A 37-year-old male arrives to the trauma slot following a high-speed motorcycle crash. His Glasgow Coma score is 14 and his only orthopaedic injury is exhibited in Figure A. His current vital signs are a BP of 90/60, HR 120, and a lactate of 2.5 mMol/L. Other findings include a grade 1 splenic laceration and bilateral pulmonary contusions seen on chest radiograph. Which of the following has been suggested as an indication to perform damage control orthopedic care?

1 HR >110
Bilateral pulmonary contusions seen on chest radiograph
SBP = 90mmHg
Unilateral femur fracture
Lactate = 2.5 mMol/L
Pulmonary contusion severe enough to be diagnosed on chest radiograph alone is an indicator that the patient may benefit from damage control orthopaedics (DCO).
Despite the patient's overall stable nature, suffering pulmonary injury severe enough to be seen on x-ray alone suggests that temporary stabilization with staged definitive fixation may avoid potential morbidity.
Pape et al. review the evolution and balance of early total care (ETC) and DCO. Summarizing the literature, the authors report several standalone indicators that would justify DCO regardless of stable status. This includes: Injury Severity Score of greater than 40, Injury Severity Score of greater than 20 with chest trauma, multiple injuries with severe pelvic/abdominal trauma/ hemorrhagic shock, bilateral femoral fractures, pulmonary contusion noted on radiographs alone, hypothermia of less than 35 degrees C), and a head injury with an Abbreviated Injury Score of 3 or greater.
Figure A exhibits a right femoral shaft fracture. Illustration A exhibits a summarized table stating the criterion used to determine the condition of a polytrauma patient. (Table from Pape et al, PMID: 19726738)
Incorrect answers:
Question 12
A patient is scheduled to undergo total knee arthroplasty (TKA) following failure of nonsurgical management. History reveals that she underwent a patellectomy as a teenager as the result of a motor vehicle accident. Examination reveals normal ligamentous stability. For the most predictable outcome, which of the following implants should be used?
Explanation
ligament-sparing knee (P < 0.01). The patella functions to increase the lever arm of the extensor mechanism and to position the quadriceps tendon and the patellar ligament roughly parallel to the anterior cruciate ligament and posterior cruciate ligament, respectively. The patellar ligament thereby provides a strong reinforcing structure that functions to prevent excessive anterior translation of the femur during flexion of the knee. The absence of the patella results in the patellar ligament and the quadriceps tendon being relatively in line with one another. After a patellectomy, the resultant quadriceps force is no longer parallel to the posterior cruciate ligament. This results in loss of the reinforcing function of the patellar ligament. The authors believe this loss of reinforcing function may place increased stresses on the posterior cruciate ligament and posterior aspect of the capsule, which may result in stretching of these structures over time. They found a high rate of anteroposterior instability, a high prevalence of recurvatum, and a high rate of loss of full active extension compared with passive extension in the posterior cruciate ligament-sparing group, which supports their theory.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
Paletta GA Jr, Laskins RS: Total knee arthroplasty after a previous patellectomy. J Bone Joint Surg Am 1995;77:1708-1712.
Question 13
Figures 45a and 45b show the AP and lateral radiographs of a 15-year old patient who is undergoing surgery to add 3 cm of length to the femur. Based on the radiographic findings, what is the next most appropriate step in management?
Explanation
REFERENCES: Raney EM: Limb-length discrepancy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1519-1526.
Ilizarov GA: Pseudarthroses and defects of long tubular bones, in Transosseous Osteosynthesis: Theoretical and Clinical Aspects of the Regeneration and Growth of Tissue. Berlin, Springer-Verlag, 1992, p 453.
Question 14
Reconstruction of the injured structure is performed. After surgery, the patient initially notes limitation in motion, and later develops recurrent instability of the knee. Which factor most likely contributed to the development of instability?
Explanation
The anteromedial bundle originates on the anterior and proximal aspect of the lateral femoral condyle and inserts on the anteromedial aspect of the anterior cruciate ligament (ACL) footprint on the proximal tibia. The posterolateral bundle originates posterior and distal to 63 the anteromedial bundle and inserts on the posterolateral aspect of the tibial footprint. The fibers are parallel when the knee is in an extended position. As the knee moves into flexion,
the fibers of the anteromedial bundle rotate externally with respect to the posterolateral bundle. The anteromedial bundle is tensioned in both flexion and extension. The posteromedial bundle is tensioned in extension, but relaxes as the knee moves into flexion.
The lateral meniscus is more commonly injured with an acute injury to the ACL. The medial meniscus is injured more commonly when the ACL is chronically unstable.
The ACL is an intra-articular and intrasynovial structure. It is innervated by posterior articular branches from the tibial nerve. Innervation of the ACL involves several types of mechanoreceptors (Ruffini, Pacini, Golgi tendon, and free-nerve endings) that may contribute to proprioceptive function of the knee and modulation of quadriceps function.
Injury to the ACL is predominantly associated with instability to anterior translation of the tibia in extension. The ACL plays a secondary role to limit internal rotation of the tibia, and a loss of ACL stability is confirmed by the reduction of the tibia from a position of anterior translation and internal rotation (pivot shift). The radiographs demonstrate anterior placement of the femoral tunnel. The convex shape of the lateral femoral condyle can make it more difficult to visualize the anatomic femoral origin of the ACL. Failure to identify the
anatomic footprint can result in anterior placement of the femoral tunnel. Anterior ACL graft placement can result in its impingement against the posterior cruciate ligament and early limitation of knee flexion. Over time, impingement on the graft may result in stretching of the graft and recurrent knee instability symptoms.
RECOMMENDED READINGS
Duthon VB, Barea C, Abrassart S, Fasel JH, Fritschy D, Ménétrey J. Anatomy of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):204-13. Epub 2005 Oct 19. Review. PubMed PMID: 16235056. View Abstract at PubMed
Zantop T, Petersen W, Sekiya JK, Musahl V, Fu FH. Anterior cruciate ligament anatomy and function relating to anatomical reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006 Oct;14(10):982-92. Epub 2006 Aug 5. Review. PubMed PMID: 16897068. View Abstract at PubMed
Question 15
Percutaneous placement of a lateral proximal tibial locking plate that extends down to the distal third of the leg is associated with postoperative decreased sensation of which of the following distributions?

Explanation
Question 16
Figure 11 shows the anatomic dissection of the medial side of the knee joint after removal of the superficial fascia. The arrow is pointing to what structure?
Explanation
REFERENCES: Pagnani MJ, Warner JJ, O’Brien SJ, Warren RF: Anatomic considerations in harvesting the semitendinosus and gracilis tendons and a technique of harvest. Am J Sports Med 1993;21:565-571.
Warren LF, Marshall JL: The supporting structures and layers on the medial side of the knee: An anatomical analysis. J Bone Joint Surg Am 1979;61:56-62.
Question 17
A 57-year-old man reports right hip pain that has been progressive for the past several months. The pain is exacerbated by weight-bearing activities and improves somewhat with rest. A radiograph is shown in Figure 10a and a coronal T 1 -weighted MRI scan is shown in Figure 10b. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA,
WB Saunders, 2002, pp 3160-3162.
Sugano N: Osteonecrosis, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 877-887.
Question 18
Figure 28 shows an arthroscopic view of a right shoulder in the lateral position through a posterior portal. What is the area between structure B (biceps) and SS (subscapularis tendon)?
Explanation
REFERENCES: Selecky MT, Tibone JE, Yang BY, et al: Glenohumeral joint translation after arthroscopic thermal capsuloplasty of the rotator interval. J Shoulder Elbow Surg 2003;12:139-143.
Harryman DT, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
Question 19
A 9-year-old girl, who is an avid soccer player, has intermittent spontaneous snapping in her left knee that has worsened. There is no reported trauma or prior surgeries to her knee. Despite working with her trainer, she has developed anterior-based knee pain and lacks full extension. Her knee skin is unremarkable, but there is fullness to palpation on the lateral aspect of her knee. Her range of motion demonstrates a lack of 15° of terminal extension and ligamentous examination is unremarkable. Considering possible surgical treatments for this patient, what is the most appropriate surgical treatment?
Explanation
Question 20
A 22-year-old patient has had severe groin pain for many months and is unable to engage in any physical activity. The AP radiograph of the pelvis shows minimal arthritis. The lateral radiograph of the hip is shown in Figure 33a. An MR-arthrogram is shown in Figure 33b. What is the most appropriate treatment at this stage? Review Topic

Explanation
Question 21
A 4-year-old boy with arthrogryposis has little active motion of his knees or elbows. Both elbows are in full extension with good triceps strength, but he is unable to bring his hand to his face or feed himself. Management should consist of
Explanation
REFERENCES: Van Heest A, Waters PM, Simmons BP: Surgical treatment of arthrogrypsosis of the elbow. J Hand Surg Am 1998;23:1063-1070.
Caroll RE, Hill NA: Triceps transfer to restore elbow flexion: A study of fifteen patients with paralytic lesions and arthrogryposis. J Bone Joint Surg Am 1970;52:239-244.
Question 22
Which of the following is considered a risk factor for the development of low back pain?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 627-643.
Question 23
Excision of heterotopic bone about the forearm or elbow can be done with limited recurrence rates as early as which of the following after initial injury?

Explanation
The referenced study by McAuliffe et al is a retrospective review of heterotopic ossification (HO) about the elbow followed by 100 cGY (5 fractions over 1 week) of XRT as early as 3 months post-injury. They were able to achieve an average arc of motion > 100 degrees.
The other referenced study by Beingessner et al is a review of HO excision of the forearm. They found that excision and XRT, followed by 6 weeks of indomethacin, led to an increase of forearm motion from an average of 17 degrees to 136 degrees when the excision was done at 4 months post-injury.
Question 24
CLINICAL SITUATION Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities. What is the best next step in the patient’s evaluation?

Explanation
but she has not had any issues since the flap. She has abundant callus formation but the fracture line is still visible and unchanged on 2 sets of radiographs. The patient has persistent pain. The best initial evaluation is to ensure that there is no underlying infection with laboratory studies, including a complete blood count (CBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Nuclear medicine studies have questionable utility, but may be helpful if the inflammatory markers from laboratory studies come back elevated. A CT scan is not warranted because the sequential radiographs show persistent fracture lines and no changes. The patient has a hypertrophic nonunion. Originally, she had appropriate treatment and has shown the ability to make callus, thus her biologic capacity appears to be intact and bone grafting is not needed. The hypertrophic nature of her fracture nonunion indicates that she needs more stability. The best treatment for a hypertrophic nonunion of the tibia is exchange nailing. Based on successive radiographs and the lack of healing, observation is probably just delaying the inevitable. Plating with retention of the nail can be useful in recalcitrant long bone non-union, especially in the femur.
Question 25
A 65-year-old man has a painful mass of the middle finger. A clinical photograph, lateral radiograph, coronal MRI scan, and biopsy specimen are seen in Figures 20a through 20d. What is the most likely diagnosis?
Explanation
REFERENCES: Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 181-193.
Question 26
A 35-year-old man who is an avid weight lifter competing in local tournaments reports new onset pain and loss of motion in his dominant right shoulder. Examination reveals joint line tenderness, active elevation to 100 degrees, and external rotation to 10 degrees. His contralateral shoulder reveals 170 degrees forward elevation and 50 degrees external rotation. Radiographs are shown in Figures 46a and 46b. What is the next most appropriate step in management?
Explanation
REFERENCES: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.
Skedros JG, O’Rourke PJ, Zimmerman JM, et al: Alternatives to replacement arthroplasty for glenohumeral arthritis, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 485-499.
Question 27
A patient who has had neck pain radiating down the arm for the past 4 weeks reports that the pain was excruciating during the first week. Management consisting of anti-inflammatory drugs and physical therapy has decreased the neck and arm symptoms from 10/10 to 3/10. He remains neurologically intact. MRI and CT scans are shown in Figures 5a and 5b. The best course of action should be
Explanation
REFERENCES: Saal JS, Saal JA, Yurth EF: Nonoperative management of herniated cervical intervertebral disc with radiculopathy. Spine 1996;21:1877-1883.
Komori H, Shinomiya K, Nakai O, Yamaura I, Takeda S, Furuya K: The natural history of herniated nucleus pulposus with radiculopathy. Spine 1996;21:225-229.
Question 28
A 25-year-old man has had an insidious onset of left hip pain over the past 11 months. A radiograph, coronal MRI scan, and histopathologic specimens are seen in Figures 2a through 2d. What is the most likely diagnosis?
Explanation
REFERENCE: Sucato DJ, Rougraff B, McGrath BE, et al: Ewing’s sarcoma of the pelvis: Long-term survival and functional outcome. Clin Orthop 2000;373:193-201.
Question 29
What normal tissue has a low signal intensity (appears black) on both T1- and T2-weighted images?
Explanation
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 65-70.
Slucky AV, Potter HG: Use of magnetic resonance imaging in spinal trauma: Indications, techniques, and utility. J Am Acad Orthop Surg 1998;6:134-145.
Question 30
A 21-year-old professional ballet dancer reports a painful popping sensation over her right hip joint. Examination reveals that symptoms are reproduced with hip flexion and external rotation. Which of the following studies will best confirm the diagnosis?
Explanation
REFERENCES: Gruen GS, Scioscia TN, Lowenstein JE: The surgical treatment of internal snapping hip. Am J Sports Med 2002;30:607-613.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 139-153.
Question 31
A 35-year-old woman who runs long distance has had posterior calf tenderness for the past 3 months. A clinical photograph is shown in Figure 10a, and MRI scans are shown in Figures 10b and 10c. Management at this point should consist of
Explanation
REFERENCES: Alfredson H, Pietila T, Jansson P, Lorentzon R: Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med 1998;26:360-366.
Angermann P, Hougaard D: Chronic Achilles tendinopathy in athletic individuals: Results of nonsurgical treatment. Foot Ankle Int 1999;20:304-306.
Question 32
The term anorexia athletica refers to a problem whose criteria include all of the following, EXCEPT Review Topic
Explanation
Question 33
A 20-year-old football player has immediate pain in the midfoot and is unable to bear weight after an opposing player lands on the back of his plantar flexed foot. AP and lateral radiographs are shown in Figures 4a and 4b. Management should consist of
Explanation
REFERENCES: Bellabarba C, Sanders R: Dislocations of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 2, pp 1539-1558.
Murphy GA: Fractures and dislocations of the foot, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 9. St Louis, MO, Mosby, 1998, vol 2, pp 1956-1960.
Question 34
A 47-year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the aspiration and proceed to a revision TKA with possible augments on standby.
Question 35
A 10-month-old boy has an untreated developmental hip dislocation.
Explanation
Early radiographic findings of avascular necrosis (AVN) of the hip include sclerosis and a subchondral lucency. A common presentation of Legg-Calve-Perthes disease (idiopathic pediatric hip AVN) is intermittent pain in the thigh, groin, or knee with an examination localizing to the hip; a Trendelenburg gait or sign; and painful, restricted passive hip range of motion. AVN also may be observed in association with a slipped capital femoral epiphysis (SCFE). AVN risk is highest in the setting of an unstable SCFE (10%-60%); risk is 0% to 1.4% when the SCFE is stable. A multicenter review of the modified Dunn procedure for treatment of unstable SCFE noted an AVN rate of 26%.
The most common deformity associated with SCFE is proximal femoral varus, flexion, and external rotation leading to an abnormal femoral head-neck junction offset. This causes a loss of passive hip flexion and internal rotation and the phenomenon of obligate external
rotation with flexion. The residual deformity frequently results in femoroacetabular impingement. Labral tears also are associated with cam impingement secondary to underlying osseous abnormalities including abnormal femoral head-neck junction offset.
Endocrinopathies potentially are associated with SCFE because of hormone-related physeal changes and subsequent mechanical insufficiency of the proximal femoral physis. With renal osteodystrophy, the physeal widening results from secondary hyperparathyroidism and progressive proximal femoral deformity may develop. Optimal medical management of hyperparathyroidism is essential. Surgical stabilization via in situ fixation of the proximal femur is indicated when SCFE is diagnosed.
The proximal femoral epiphysis secondary ossification center commonly appears between the ages of 4 and 7 months. In the setting of developmental hip dislocation, the appearance of the secondary ossification center is commonly delayed. After closed or open reduction of developmental dysplasia of the hip, failure of the femoral head ossific nucleus to appear within 12 months following the reduction is a sign of proximal femoral growth disturbance and AVN.

Question 36
Figure 18a shows the initial lateral radiograph of a 6-year-old girl who sustained a fracture in a motor vehicle accident and was treated in a cast 1 year ago. She now has the valgus deformity seen in Figure 18b. Treatment should consist of
Explanation
REFERENCES: Cozen L: Knock-knee deformity in children: Congenital and acquired. Clin Orthop 1990;258:191-203.
Jackson DW, Cozen L: Genu valgum as a complication of proximal tibial metaphyseal fractures in children. J Bone Joint Surg Am 1971;53:1571-1578.
Brammar TJ, Rooker GD: Remodeling of valgus deformity secondary to proximal metaphyseal fracture of the tibia. Injury 1998;29:558-560.
Ogden JA, Ogden DA, Pugh L, et al: Tibia valga after proximal metaphyseal fractures in childhood: A normal biologic response. J Pediatr Orthop 1995;15:489-494.
Salter RB, Best TN: Pathogenesis of progressive valgus deformity following fractures of the proximal metaphyseal region of the tibia in young children. Instr Course Lect 1992;41:409-411.
Question 37
Figure 43 shows an arthroscopic view of the posteromedial compartment of a patient’s left knee using a 70-degree arthroscope placed through the intercondylar notch. The arrow is pointing to what structure?
Explanation
REFERENCES: Miller MD: Basic arthroscopic principles, in DeLee JC, Drez D Jr, Miller MD (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, Saunders, 2003, pp 224-237.
Gold DI, Schaner PJ, Sapega AA: The posteromedial portal in knee arthroscopy: An analysis of diagnostic and surgical utility. Arthoscopy 1995;11:139-145.
Question 38
An article in a leading orthopaedic journal describes a randomized controlled study comparing 2 popular and comparable surgical methods for fixation of hip fractures. Patients were randomized by a predetermined computer-generated list. There was approximately 20% crossover between treatment groups. Evaluation of study outcomes (clinical and radiographs) was performed by one of the surgeons participating in the study. Enrollment goals for appropriate power were achieved and final 1-year follow-up was obtained for 65% of patients. According to Oxford Group criteria, what is the appropriate level of evidence for this study? Review Topic
Explanation
Question 39
Figure 23 shows the postoperative radiograph of a patient who underwent an anterior cruciate ligament (ACL) reconstruction (with bone-patella tendon-bone autograft) that failed. He initially had loss of flexion postoperatively. What is the most likely cause of this failure? Review Topic

Explanation
Question 40
Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient? Review Topic

Explanation
Question 41
What is the most common bone tumor in the hand?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 103.
Kuur E, Hansen SL, Lindequist S: Treatment of solitary enchondromas in fingers. J Hand Surg Br 1989;14:109-112.
Question 42
Which of the following types of intra-articular pathology is associated with lateral meniscal cysts? Review Topic
Explanation
Question 43
Which of the following is a relative contraindication to performing laminoplasty in a patient with cervical myelopathy? Review Topic
Explanation
Question 44
An 18-year-old girl with quadriplegic cerebral palsy underwent posterior spinal fusion from T2 to the pelvis 3 weeks ago. She now has a low-grade fever and mild midline erythema in a 1-cm area from which there is slight clear yellowish drainage. What is the next most appropriate step in management?
Explanation
REFERENCES: Theiss SM, Lonstein JE, Winter RB: Wound infections in reconstructive spine surgery. Orthop Clin North Am 1996;27:105-110.
Richards BS: Delayed infections following posterior spinal instrumentation for the treatment of idiopathic scoliosis. J Bone Joint Surg Am 1995;77:524-529.
Question 45
Figures 94a and 94b show T1 sagittal and coronal MR images of the right shoulder of a 45-year-old woman. She has insidious onset of dull, aching right shoulder pain localized at the superior aspect of her shoulder. The nerve that supplies the atrophied muscle arises from the upper trunk from contributions of which nerve roots? A B
Explanation
The suprascapular nerve innervates the supraspinatus muscle. Patients with suprascapular neuropathy usually have insidious onset of dull, aching shoulder pain at the superior or posterior aspect of the shoulder. There can be several causes of nerve compression, and the nerve is susceptible to compression at the suprascapular and spinoglenoid notches. Extrinsic compression can be secondary to joint-related fluid filled cysts of soft-tissue masses. Traction neuropathy may occur as the result of excessive nerve excursion during athletic activity (usually overhead sports) or after a massive, retracted rotator cuff tear. The suprascapular nerve originates from the upper trunk from predominantly the C5 and C6 nerve roots, with an occasional contribution from the C4 nerve root.
RECOMMENDED READINGS
Boykin RE, Friedman DJ, Higgins LD, Warner JJ. Suprascapular neuropathy. J Bone Joint Surg Am. 2010 Oct 6;92(13):2348-64. doi: 10.2106/JBJS.I.01743. Review. 81
PubMed PMID: 20926731. View Abstract at PubMed
Piasecki DP, Romeo AA, Bach BR Jr, Nicholson GP. Suprascapular neuropathy. J Am Acad Orthop Surg. 2009 Nov;17(11):665-76. Review. PubMed PMID: 19880677 View Abstract at PubMed
Question 46
A 42-year-old woman who observes traditional Muslim practices is seen in your office accompanied by her physician husband to discuss possible elective bunion correction. In considering the treatment of this patient, what is one of the most important considerations?
Explanation
REFERENCE: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Question 47
A 42-year-old female with chronic discogenic back pain undergoes lumbar spine surgery via retroperitoneal approach. Figure A is the postoperative radiograph of her lumbar spine. Six weeks after the surgery the patient develops worsening low back pain. You obtain a radiograph of her lumbar spine, pictured in Figure B. What is the next best step in management? Review Topic

Explanation
Management of failed TDR is dictated by (1) patient symptoms and (2) radiographic implant position. Asymptomatic patients with implant subsidence without extrusion can be managed with close observation. Patients with persistent symptomatic back pain relating to facet joint or implant microinstability in the setting of an otherwise well-positioned TDR can be treated with posterior stabilization alone. Symptomatic patients with unacceptable implant position (i.e. complete dislodgement, fracture) require either revision arthroplasty or conversion to arthrodesis (anterior +/-
posterior).
Harrison et al. authored a report detailing a case of failed L5-S1 TDR with anterior dislocation of the polyethylene inlay and bilateral L5 pars fractures noted 2 weeks postoperatively. It is unclear whether the pars defect was missed following previous microdiscectomy, acquired during instrumentation, or acquired postoperatively due to abnormal endplate forces during rehabilitation. The patient underwent removal of TDR components and revision to anterior arthrodesis followed by percutaneous fixation of the bilateral L5 pars fractures.
Patel et al. published a review of the literature regarding revision lumbar TDR. Retroperitoneal revision procedures are complicated by higher risk of injury to vascular structures (16.7% versus 3.6% at primary surgery) and urogenital structures due to adhesions. Revision surgery should only be performed by surgeons familiar with the retroperitoneal approach to the spine. Alternative surgical approaches, such as the far lateral approach, should be considered to access the anterior spine at L4-L5 and above.
Madigan et al. reviewed the management of lumbar degenerative disc disease (DDD). They state that TDR is a motion-sparing surgical option designed to temper the problem of adjacent-segment disease. They report that long-term studies are limited, but point out that several short-term comparisons between TDR and ALIF show equivalent improvement in pain and function, equal complication rate, shorter hospitalization and lower rate of reoperation in the TDR group.
Figure A is a lateral radiograph of the lumbar spine showing L5-S1 total disc replacement. Figure B is a lateral radiograph of the lumbar spine showing L5-S1 total disc replacement with anterior dislocation of the polyethylene inlay.
Incorrect Responses:
Question 48
The parents of a 10-year-old boy with Down syndrome are seeking sports clearance for participation in the high jump at the Special Olympics. He is asymptomatic, and the neurologic examination is normal. The hips and patellae are clinically stable. Radiographs of the cervical spine in flexion and extension show a maximum atlanto-dens interval (ADI) of 6 mm. Based on these findings, what recommendation should be made?
Explanation
REFERENCES: Atlantoaxial instability in Down syndrome: Subject review. American Academy of Pediatrics Committee on Sports Medicine and Fitness. Pediatrics 1995;96:151-154.
Tredwell SJ, Newman DE, Lockitch G: Instability of the upper cervical spine in Down syndrome. J Pediatr Orthop 1990;10:602-606.
Segal LS, Drummond DS, Zanotti RM, et al: Complications of posterior arthrodesis of the cervical spine in patients who have Down syndrome. J Bone Joint Surg Am 1991;73:1547-1554.
Question 49
Patient outcome after open reduction and internal fixation of tibial plateau fractures shows that patients older than 50 years of age when compared to younger patients have
Explanation
Question 50
A B
Explanation
The radiographs reveal a tibial pilon fracture with an extruded and rotated anterior tibial fragment that lies deep to the anterior compartment neurovascular bundle, which contains the deep peroneal nerve. This nerve innervates the anterior compartment muscles and the extensor digitorum brevis and extensor hallucis brevis muscles and provides sensation to the dorsal aspect of the first interspace. An injury to the deep peroneal nerve at this level will only affect the innervation to the extensor digitorum brevis and extensor hallucis brevis muscles and the innervation of the first interspace. The superficial peroneal nerve innervates
the lateral compartment muscles above the level of this injury and innervates the dorsum of the foot. The medial forefoot is innervated by the saphenous nerve and the posterior tibial nerve innervates the posterior compartment muscles above the level of the injury. The sural nerve innervates the lateral foot and has no motor component, and the superficial peroneal nerve innervates the peroneus longus, which plantar flexes the first metatarsal above the level of the injury.
RECOMMENDED READINGS
Agur AM, Dalley AF, eds. Grant’s Atlas of Anatomy. 13th ed. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 2013:362-370.
Hoppenfeld S, de Boer P, Buckley R, eds. Surgical Exposures in Orthopaedics: The Anatomic Approach. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:625-673.
Question 51
A 17-year-old high school football player injures his right ankle during a game. Examination reveals swelling and a closed ankle deformity, with normal foot circulation and sensation. Radiographs are shown in Figures 10a and 10b. In addition to closed reduction, management should include
Explanation
REFERENCES: Browner BD, Jupiter JB, Levine AM, Trafton PG: Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 1887-1957.
Stiehl JB: Ankle fractures with diastasis. Instr Course Lect 1990;39:95-103.
Question 52
Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?
Explanation
REFERENCES: Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, Pa, Lippincott-Raven, 1998, pp 789-802.
Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
MacDonald SJ, Hersche O, Ganz R: Periacetabular osteotomy in the treatment of neurogenic acetabular dysplasia. J Bone Joint Surg Br 1999;81:975-978.
Question 53
Figures below show the radiographs obtained from a 79-year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. No evidence of infection is seen. What is the most appropriate treatment?

Explanation
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis, as shown in Figures 3 and 4. They also assist in obtaining correct limb alignment. Short metaphyseal-engaging stems are associated with failure rates that range between 16% and 29%. Cemented stems may be shorter than press-fit stems, because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.
Question 54
What is the primary goal of the initial (acute) rehabilitation phase of an overhead athlete’s shoulder?
Explanation
REFERENCES: Wilk KE, Meister K, Andrews JR: Current concepts in the rehabilitation of the overhead throwing athlete. Am J Sports Med 2002;30:136-151.
Wilk KE, Arrigo C: Current concepts in the rehabilitation of the athletic shoulder. J Orthop Sports Phys Ther 1993;18:365-378.
Question 55
A morbidly obese 80-year-old woman presents with back pain for 2 months. Sagittal T2-weighted, sagittal T1-weighted, coronal short tau inversion recovery (STIR) images are shown in Figures A through C, respectively. Which of the following statements is true of her diagnosis? Review Topic

Explanation
The MR signs suggestive of a benign, osteoporotic VCF include band-like low T1 signal, fluid sign, retropulsion of a vertebral bone fragment. Acute fractures show low signal on T1-weighted and high signal on T2-weighted and STIR images. The MR signs suggestive of malignant VCF include complete replacement of normal marrow signal, convex posterior vertebral border, pedicle involvement, focal paraspinal mass and epidural mass.
Kim et al. performed a literature review on management of the osteoporotic spine. They concluded that nonsurgical management should focus on pain control and maximizing function. Surgery remains controversial and should be reserved for those who fail nonoperative management. Surgical options include vertebroplasty, balloon tamp reduction, and decompression and instrumented fusion with structural graft and multiple fixation points.
Spivak et al. discussed percutaneous treatment of VCF. They recommend vertebroplasty for patients with unremitting pain and little deformity as it is less costly and does not require general anesthesia. They recommend kyphoplasty for cases with
greater vertebral collapse, especially subacute fractures where partial healing may hinder postural fracture reduction.
Figure A is a T2-weighted sagittal MR image showing a fluid-filled cleft ("fluid sign"). Figure B is a T1-weighted sagittal MR image showing loss of intensity (black) consistent with vertebral body edema. Figure C is a coronal STIR image showing the fluid-filled vertebral body cleft. An incidental renal cyst is noted. Illustration A shows different patterns of band-like signal abnormality on T1-weighted imaging. The black region represents low signal intensity (edema). Illustration B is a sagittal STIR image showing the MR fluid sign. Illustration C shows the band like signal abnormality on T1-weighted imaging. Illustration D shows metastatic disease with complete replacement of normal marrow intensity and diffuse convexity of the posterior vertebral border.
Incorrect
Question 56
An 18-year-old woman sustains a twisting injury of the knee while skiing. Figures 7a and 7b show the radiograph and coronal MRI scan of the knee. In addition to the injury shown, what is the most likely associated injury? Review Topic

Explanation
Question 57
A 58-year-old woman has a fracture through a metacarpal lesion after a motor vehicle accident. She denies any preinjury symptoms and the fracture heals uneventfully. Based on the radiograph and MRI scans shown in Figures 22a through 22c obtained following fracture healing, follow-up management should consist of
Explanation
REFERENCES: Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 213-228.
Marco RA, Gitelis S, Brebach GT, et al: Cartilage tumors: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:292-304.
Question 58
- Resurfacing the patella during a total knee replacement is strongly indicated when the diagnosis is
Explanation
Hence, chronic pain after TKA without resurfacing the patella was more common in knees affected by rheumatoid arthritis than in those affected by degenerative osteoarthritis. The authors of the study recommend that the patella be resurfaced when an unconstrained prosthesis is used in patients with a diagnosis of inflammatory arthritis and to a lesser degree osteoarthrosis.
Question 59
What preoperative factor correlates best with the outcome of rotator cuff repair?
Explanation
REFERENCES: Iannotti JP: Full-thickness rotator cuff tears: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
Iannotti JP, Bernot MP, Kuhlman JR, Kelley MJ, Williams GR: Postoperative assessment of shoulder function: A prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996;5:449-457.
Question 60
Figure 32 shows the radiograph of a laborer who jammed his thumb in a fall. Examination reveals pain at the base of the thumb and proximal thenar eminence region. Management should consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
Howard FM: Fracture of the basal joint of the thumb. Clin Orthop 1987;220:46-51.
Question 61
A 30-year-old farmer undergoes replantation of an above-the-elbow amputation. What form of management is most important following this surgery?
Explanation
REFERENCES: Wood MB: Replantations about the elbow, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1985, pp 472-480.
Goldner RD, Nunley JA: Replantation proximal to the wrist, in Wood MD (ed) Hand Clinics: Microsurgery. Philadelphia, PA, WB Saunders, 1992, pp 413-425.
Question 62
What is the most common malignancy involving the hand?
Explanation
REFERENCES: Fink JA, Akelman E: Nonmelanotic malignant skin tumors of the hand. Hand Clin 1995;11:255-264.
Fleegler EJ: Skin tumors, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 2184-2205.
Question 63
A healthy 27 year-old-male is brought into the emergency department after a fall from height. He has a suspected left C8-T1 nerve injury. Which of the following findings would most suggest a root avulsion injury rather than a brachial plexus injury at this level?
Explanation
Brachial plexus injuries are often classified as preganglionic vs. postganglionic injuries. Preganglionic injuries are typically avulsion injuries proximal to the dorsal root ganglion. Clinical features suggestive of lower root avulsion injury include a person falling from height clutching on object to save himself, Horner’s syndrome (drooping of the eyelid (ptosis), pupillary constriction (miosis) and anhidrosis), absence of a Tinel sign or tenderness to percussion in the neck, and a normal histamine test (C8-T1 sympathetic ganglion - intact triple response (redness, wheal, flare)).
Caporrino et al. reviewed 102 patients to assess the best modality (e.g. physical examination, MRI and nerve conduction studies [NCSs]) for diagnosing and localizing brachial plexus injuries. They found the best diagnostic performance with physical examination (sensitivity = 97.8%; specificity = 30.8%) and NCSs (sensitivity
= 98.9%; specificity = 23.1%). MRI had inferior performance for all measurements. They conclude that NCSs exhibited superior performance to MRI, and should be considered a more reliable supporting tool after detailed physical examination.
Incorrect Answers:
Question 64
A 79-year-old woman reports a history of left leg pain with walking. Her pain is exacerbated with walking and stair climbing, and her symptoms are improved by standing after she stops walking. Lumbar flexion does not provide any significant improvement of the symptoms and sitting does not significantly change symptoms. Her leg pain is worse at night and she obtains relief by hanging her leg over the side of the bed. The neurologic examination is essentially normal. Examination of the lower extremities demonstrates mild early trophic changes, and her pulses distally are palpable but are diminished bilaterally. Radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management?
Explanation
REFERENCES: Aufderheide TP: Peripheral arteriovascular disease, in Rosen P, Barkin R (eds): Emergency Medicine: Concepts and Clinical Practice, ed 4. St Louis, MO, Mosby, 1998,
pp 1826-1844.
Mirkovic S, Garfin SR: Spinal stenosis: History and physical examination. Instr Course Lect 1994;43:435-440.
Question 65
A young man sustains a lumbar strain in an on-the-job motor vehicle accident. Both he and his treating physician feel that he is capable of limited duty with appropriate restrictions shortly after the injury. What term best describes his work status?
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 131-137.
Question 66
The structure that runs just beneath the peroneal tubercle of the calcaneus is the
Explanation
The peroneal tubercle is often a good landmark at which to identify the peroneus longus tendon surgically, and a hypertrophic tubercle has been associated with peroneus longus tendinopathy. Both peroneal tendons curve anteriorly around the tip of the fibula, with the peroneal tubercle separating the 2 tendons at the level of the calcaneus. The peroneus brevis runs in front of the tubercle and the longus behind. The flexor hallucis longus runs through a fibro-osseus tunnel posterior to the hindfoot formed by the posterolateral (os trigonum) and posteromedial tubercle of the talus. The calcaneal fibular ligament attaches to the calcaneus below the posterior facet of the subtalar joint and deep to the peroneal tendons.
RECOMMENDED READINGS
Hyer CF, Dawson JM, Philbin TM, Berlet GC, Lee TH. The peroneal tubercle: description, classification, and relevance to peroneus longus tendon pathology. Foot Ankle Int. 2005 Nov;26(11):947-50. Pub PMID: 16309609.View Abstract at PubMed
Bruce WD, Christofersen MR, Phillips DL. Stenosing tenosynovitis and impingement
of the peroneal tendons associated with hypertrophy of the peroneal tubercle. Foot Ankle Int. 1999 Jul;20(7):464-7. PubMed PMID: 10437932.View Abstract at PubMed
Question 67
What dominant intracellular proteins become directly phosphorylated as a result of bone morphogenetic protein (BMP) binding to its receptors? Review Topic
Explanation
differentiation. Adenylate cyclase is a transmembrane protein that acts intracellularly to activate the G protein pathways. Myc is a proto-oncogene that encodes for a transcription factor involved in numerous cell-activation pathways, but is not directly phosphorylated by BMP receptor. ß-catenin is an intracellular molecule that plays a key role in the Wnt signaling pathway. This pathway is also involved in osteoblastic differentiation, but differs in target proteins within the cell.
Question 68
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. If the patient chooses surgical reconstruction, he should be advised that, when compared with a transtibial technique, the tibial inlay technique has been shown to provide

Explanation
appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used. Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
Question 69
Figures 29a and 29b show the radiograph and CT scan of a 48-year-old man who has diffuse spinal pain. What is the most likely diagnosis?
Explanation
REFERENCES: McCullough JA, Transfeldt EE: Macnab’s Backache, ed 3. Baltimore, MD, Williams and Wilkins, 1997, pp 190-194.
Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott, Williams and Wilkins, 2003, pp 141-151.
Question 70
Figure 26 shows the radiograph of a 48-year-old woman who has right arm pain and hematuria. A bone scan reveals increased uptake in the left ribs and thoracic spine. A needle biopsy specimen shows that the lesion is highly keratin positive and composed primarily of clear cells. What is the best course of action?
Explanation
REFERENCES: Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG: Methylmethacrylate as an adjunct in internal fixation of pathological fractures: Experience with three hundred and seventy-five cases. J Bone Joint Surg Am 1976;58:1047-1054.
Sun S, Lang EV: Bone metastases from renal cell carcinoma: Preoperative embolization. J Vasc Interv Radiol 1998;9:263-269.
Katzner M, Schvingt E: Operative treatment of bone metastases secondary to renal carcinoma: Basic research and treatment of renal cell carcinoma metastasis. Prog Clin Biol Res EORTC 1990;348:151-168.
Question 71
Preoperative chemotherapy and wide excision Tumoral calcinosis is a heritable condition that is characterized by periarticular metastatic calcification. Most patients are black, and the inheritance is usually autosomal recessive. Metastatic calcifications occur around joints and in the skin, marrow, teeth, and blood vessels. The periarticular masses may grow quite large and are attached to the fascia, but they are extra-articular. The masses may occur at the shoulder, hip, and elbow. Radiographically: The masses are composed of heavy, amorphous calcification in nodules. Laboratory:
Explanation
A 20-year-old woman has a large mass over the right hip. An anteroposterior and oblique radiographs are shown in Slides 1 and
Question 72
A 23-year-old professional baseball pitcher reports shoulder pain and decreased velocity while pitching. Physical examination reveals a side-to-side internal rotation deficit of 25 degrees. The O’Brien sign is negative; Neer and Hawkins signs are negative. Rotator cuff strength is full. Radiographs are unremarkable. What is the next step in management?
Explanation
REFERENCES: Wilk KE, Meister K, Andrews JR: Current concepts in rehabilitation of the overhead throwing athlete. Am J Sports Med 2002;30:136-151.
Myers JB, Laudner KG, Pasquale MR, et al: Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med 2006;34:385-391.
Question 73
In a statement put forth by AAOS, the role of the orthopaedic surgeon in the face of domestic and family abuse includes all of the following EXCEPT: Review Topic
Explanation
The statement put forth by the AAOS implores the orthopaedic surgeon to be aware of the integral components to identify, document, and care for minors, elders, and/or partners who are victims of domestic abuse.
Zilmer et al. in a JAAOS review and the basis for the AAOS statement emphasizes the ability to identify abuse, which includes, but is not limited to frequent/multiple injuries, temporal abnormalities in multiple injuries, frequent visits/utilization of the emergency department, and/or unusual injuries/fracture patterns not consistent with the clinical picture. Meticulous documentation is of paramount importance, in addition to communicating your concerns to the appropriate emergency department personnel.
Incorrect answers:
Question 74
Patient-specific instrumentation (PSI) reliably demonstrates which benefit over conventional intramedullary guidance systems?
Explanation
Cost is usually increased with PSI because the theoretical decreased number of surgical trays and shortened surgical time do not offset cost of presurgical imaging and extra cost associated with the necessary jigs. Studies do not demonstrate a reliable improvement in functional outcomes or coronal alignment when PSI is compared to standard instrumentation. Evidence reveals that PSI necessitates fewer trays than standard instrumentation.
Question 75
What is the predominant type of collagen in the tissue resulting from the surgical procedure shown in Figures 40a through 40c?
Explanation
REFERENCES: Magnussen RA, Dunn WR, Carey JL, et al: Treatment of focal articular cartilage defects in the knee: A systematic review. Clin Orthop Relat Res 2008;466:952-962.
Williams RJ III, Hamly HW: Microfracture: Indications, technique, and results. Instr Course Lect 2007;56:419-428.
Mithoefer K, Williams RJ III, Warren RF, et al: Chondral resurfacing of articular cartilage defects in the knee with the microfracture technique: Surgical technique. J Bone Joint Surg Am 2006;88:294-304.
Question 76
A researcher experimenting with limb patterning removes some tissue from 1 part of the limb bud (which we shall call Site A) and transplants it along the anteroposterior (AP) axis to create a mirror-hand duplication. Which of the following is true?
Explanation
The ZPA controls AP (radioulnar) growth. The signaling molecule is Shh, which is dose dependent. Higher Shh doses lead to posterior (ulnar) digits ulnar sided polydactyly. The extent of duplication is dose dependent (higher dose = more replication). Reduced Shh leads to loss of digits. Posterior elements (little finger/ulna) are formed EARLY prior to anterior elements which are formed LATE (radius/thumb). Disruption of AP patterning will result in loss of later forming elements (radius/thumb).
Al-Qattan et al. reviewed embryology of the upper limb. They summarized that embryology of the upper limb can be viewed in 2 distinct ways: the steps of limb development and the way that the limb is patterned along its 3 spatial axes. Cell signaling plays a major role in regulating growth and patterning of the vertebrate limbs. Signaling cell dysfunction results in congenital differences according to the affected signaling axis.
Illustration A shows an experiment to create ulnar dimelia by adding ZPA tissue to the anterior limb bud. The video shows development of the limb.
Incorrect Answers:
Question 77
A female cross-country runner has an insidious onset of right groin pain. Radiographs of the right hip reveal a tension-side stress fracture. History reveals that she was treated for a “foot” fracture 1 year ago. In addition to performing internal fixation of the femoral neck, which of the following should be obtained?
Explanation
REFERENCES: Bennell KL, Malcolm SA, Thomas SA, et al: Risk factors for stress fractures in track and field athletes: A twelve-month prospective study. Am J Sports Med 1996;24:810-818.
Barrow GW, Saha H: Menstrual irregularity and stress fractures in collegiate female distance runners. Am J Sports Med 1988;16:209-216.
Question 78
A middle-aged man sustains traumatic loss of the second, third, and fourth toes in a lawnmower accident. The wound is grossly contaminated with soil. Penicillin is added to his antibiotic regimen for coverage of what bacteria? Review Topic
Explanation
Question 79
A 17-year-old high school football player sustains a traumatic anterior shoulder dislocation, resulting in a small bony Bankart lesion and small Hill-Sachs lesion. The patient undergoes an arthroscopic Bankart repair with incorporation of the bone fragment and returns to play football the following year. He has a recurrent dislocation at football practice but decides to finish the football season before considering additional treatment. He sustains nine additional dislocations, with the last dislocation occurring while sleeping.What diagnostic test is most appropriate when planning revision surgery?
Explanation
more likely to have pain after surgery. Age and activity level are lesser influences on satisfaction.
Question 80
Figures 20a and 20b show the AP and lateral radiographs of a 62-year-old man who has had hip pain for the past 3 weeks. Figure 20c shows a CT scan of the abdomen and pelvis. A needle biopsy specimen is shown in Figure 20d. Preoperative management should include which of the following?
Explanation
REFERENCES: Chatziioannou AN, Johnson ME, Pneumaticos SG, et al: Preoperative embolization of bone metastases from renal cell carcinoma. Eur Radiol 2000;10:593-596.
Sun S, Lang EV: Bone metastases from renal cell carcinoma: Preoperative embolization. J Vasc Interv Radiol 1998;9:263-269.
Question 81
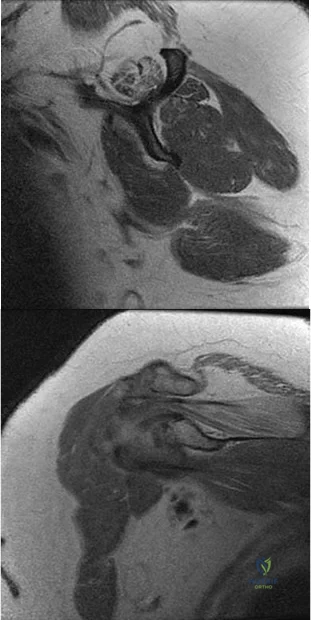
Figures 1 through 4 are the wrist MR images of a 43-year-old right-hand-dominant bricklayer who reports gradually progressive left hand weakness for 4 months. He describes difficulty gripping objects, tying his shoes, and holding utensils. He denies any numbness, paresthesias, or a previous injury. An examination reveals intact sensation in a median, radial, and ulnar nerve distribution. He has atrophy of hand interossei and a positive Froment sign finding. He has no Tinel sign finding at the wrist or elbow and no exacerbation of symptoms with elbow hyperflexion. Electromyography shows signs of denervation in an ulnar nerve distribution distal to the wrist. What is the best next step?
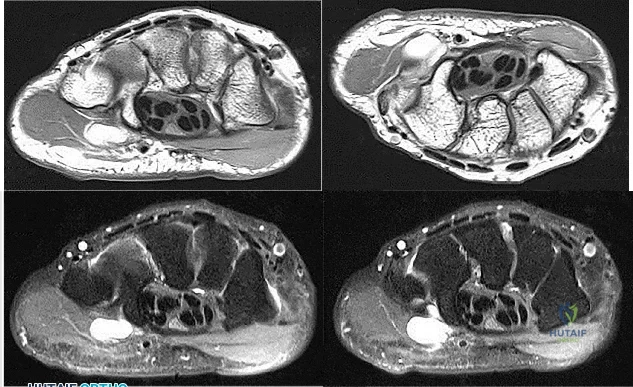
Explanation
Question 82
What is the most appropriate plating technique utilized for the medial malleolus fracture typically seen in a displaced supination-adduction ankle fracture?

Explanation
According to the referenced article by Toolan et al, placement of two horizontal (perpendicular to the fracture line) lag screws from medial to lateral are biomechanically the most important aspect of the construct whether a plate is used or not.
Question 83
Figures 113a and 113b are the radiographs of a 7-year-old girl who was evaluated for a visible elbow deformity by a foster parent. She thought the child fell, but her history was vague. On physical examination, a large prominence was seen over the posterolateral elbow, and the girl lacks the terminal 20 degrees of elbow extension. She has 75 degrees of elbow pronation and supination. She was nontender on examination. What is the most appropriate next treatment step? Review Topic

Explanation
Question 84
A 36-year-old woman is placed in a short arm cast for a nondisplaced extra-articular distal radius fracture. Seven weeks later she notes the sudden inability to extend her thumb. What is the most likely cause of her condition?
Explanation
REFERENCES: Skoff HD: Postfracture extensor pollicis longus tenosynovitis and tendon rupture: A scientific study and personal series. Am J Orthop 2003;32:245-247.
Bonatz E, Kramer TD, Masear VR: Rupture of the extensor pollicis longus tendon. Am J Orthop 1996;25:118-122.
Helal B, Chen SC, Iwegbu G: Rupture of the extensor pollicis longus tendon in undisplaced Colles’ type of fracture. Hand 1982;14:41-47.
Question 85
Osteonecrosis of the humeral head is a rare complication seen after dislocation of the glenohumeral joint in skeletally immature patients. When this complication is encountered, treatment should consist of
Explanation
REFERENCES: Pateder DB, Park HB, Chronopoulos E, et al: Humeral head osteonecrosis after anterior shoulder stabilization in an adolescent: A case report. J Bone Joint Surg Am 2004;86:2290-2293.
Wang P Jr, Koval KJ, Lehman W, et al: Salter-Harris type III fracture-dislocation of the proximal humerus. J Pediatr Orthop B 1997;6:219-222.
Question 86
A 25-year-old female presents to the emergency room for the fourth time in the last week. She has vague complaints of extremity pain. Physical examination by a male ER resident has been limited each visit because she is terrified of the pain that the clinician may cause. On physical examination, she is withdrawn and frightened. Regions of ecchymosis are noted throughout chest and abdomen. She has requested multiple radiographs, MRI and CT scans. Today's imaging (radiographs, MRI, CT scan) has been unrevealing. What is the most likely diagnosis? Review Topic
Explanation
Domestic violence or intimate partner violence can be in the form of mental or physical abuse, neglect or abandonment. Close to 25% of women will experience domestic violence. Risk factors include young age (19-29 years of age), females, pregnancy and lower socioeconomic status. Affected patients will have repeated visits to the emergency room, find reasons to stay in a treatment facility for an extended period of time and constantly seek approval of their partner.
Shields et al. reviewed factors influence outcome in treatment of patients affected by domestic violence. They found that positive outcomes were associated with interdisciplinary approaches to management. This included better history assessment, providing written documentation regarding intervention and better access to information on community resources.
Illustration A is a chart documenting the frequency of female domestic violence throughout the world as of 2012.
Incorrect Answers
Question 87
An increase in advanced glycation end-products (AGEs) is characteristic of which of the following clinical conditions and results in which pathologic process?
Explanation
AGEs are produced from spontaneous nonenzymatic glycation of proteins when sugars (glucose, fructose, ribose) react with lysine or arginine residues. Because of the low turnover, cartilage is susceptible to AGEs accumulation. The accumulation of AGEs has been thought to play a role in the development of OA of the knee and ankle.
Li et al. reviewed age-related changes in cartilage. They state that with aging, there is excessive collagen cross-linking increases cartilage stiffness, while shortening/degradation of aggrecan leads to loss of sugar side chains and water-binding ability, while increased levels of AGEs are associated with a decline in anabolic activity. There is also increased chondrocyte death and/or apoptosis.
Anderson et al. reviewed the relationship between osteoarthritis and aging. They state that knee cartilage thins with aging (especially on the femoral and patellar sides, suggesting a gradual loss of cartilage matrix. AGEs formation leads to modification of type II collagen by cross-linking of collagen molecules, increasing stiffness and brittleness and increasing susceptibility to fatigue failure.
Incorrect Answers:
Question 88
Which of the following is considered an advantage of the tibial inlay fixation compared to transtibial tunnel technique when used in posterior cruciate ligament reconstruction? Review Topic
Explanation
Question 89
Following preoperative chemotherapy, the percent of tumor necrosis has been shown to be of prognostic value for which of the following tumors?
Explanation
REFERENCES: Meyers PA, Heller G, Healey J, Huvos A, Lane J, Marcove R, et al: Chemotherapy for nonmetastatic osteogenic sarcoma: The Memorial Sloan- Kettering experience. J Clin Oncol 1992;10:5-15.
Wunder JS, Paulian G, Huvos AG, Heller G, Meyers PA, Healey JH: The histological response to chemotherapy as a predictor of the oncological outcome of operative treatment of Ewing sarcoma. J Bone Joint Surg Am 1998;80:1020-1033.
Question 90
A 50-year-old man with metastatic renal cell carcinoma has right hip pain. A radiograph and CT scan are shown in Figures 48a and 48b. The first step in management should consist of
Explanation
REFERENCES: Layalle I, Flandroy P, Trotteur G, Dondelinger RF: Arterial embolization of bone metastases: Is it worthwhile? J Belge Radiol 1998;81:223-225.
Chatziioannou AN, Johnson ME, Pneumaticos SG, Lawrence DD, Carrasco CH: Preoperative embolization of bone metastases from renal cell carcinoma. Eur Radiol 2000;10:593-596.
Question 91
A 46-year-old woman had an ankle fracture and ORIF 6 years ago. She had subsequent removal of some of the hardware, but her pain has persisted (Figures 44a and 44b).

Explanation
Patients younger than 40 years of age who have ankle arthritis pose an ongoing clinical challenge. Nonsurgical treatment should be maximized, although distraction arthroplasty can be used in an effort to delay the need for fusion.
One of the strongest indications for ankle arthroplasty is a preexisting hindfoot fusion with a goal to retain some ankle/hindfoot motion. Ankle fusion is perhaps the most predictable surgical treatment for a relatively young, active patient with ankle arthritis. Moreover, there are concerns regarding implant loosening when performing TAA in active patients.
Outcome after syndesmosis ORIF has been linked to the quality of the reduction at the index procedure. Syndesmotic malreduction that is severe necessitates osteotomy and revision ORIF.
RECOMMENDED READINGS
Sagi HC, Shah AR, Sanders RW. The functional consequence of syndesmotic joint malreduction at a minimum 2-year follow-up. J Orthop Trauma. 2012 Jul;26(7):439-43. doi: 10.1097/BOT.0b013e31822a526a. PubMed PMID: 22357084. View Abstract at PubMed
Smith NC, Beaman D, Rozbruch SR, Glazebrook MA. Evidence-based indications for distraction ankle arthroplasty. Foot Ankle Int. 2012 Aug;33(8):632-6. Review. View Abstract at PubMed
Kim BS, Knupp M, Zwicky L, Lee JW, Hintermann B. Total ankle replacement in association with hindfoot fusion: Outcome and complications. J Bone Joint Surg Br. 2010 Nov;92(11):1540-7. doi: 10.1302/0301-620X.92B11.24452. PubMed PMID: 21037349. View Abstract at PubMed
Daniels TR, Younger AS, Penner M, Wing K, Dryden PJ, Wong H, Glazebrook M. Intermediate-term results of total ankle replacement and ankle arthrodesis: a COFAS multicenter study. J Bone Joint Surg Am. 2014 Jan 15;96(2):135-42. doi: 10.2106/JBJS.L.01597. View Abstract at PubMed
Question 92
An 8-year-old sustains the injury shown in Figures A and B. Postoperative radiographs are shown in Figures C and D. After cast removal and in-office k-wire removal, elbow range of motion is found to be between 20-80 degrees of flexion. How soon after surgery is range of motion expected to be >90% of normal? Review Topic

Explanation
Displaced pediatric supracondylar elbow fractures are often treated with closed reduction and percutaneous pinning. Risk of stiffness is low considering the extra-articular nature of the injury. Utility of physical therapy to improve range of motion after operative treatment of this injury is not supported in the literature.
Zionts et al. retrospectively evaluated elbow stiffness after treatment for pediatric supracondylar fractures. Ninety-four percent of normal range of motion was restored by 6 months after the operative procedure. Further improvement occurs up to one-year postoperatively
Lee et al. surveyed 76 orthopaedic surgeons on their treatment of pediatric supracondaylar injuries. They noted that general orthopaedic surgeons used passive exercises to assist with elbow stiffness after operative management of pediatric supracondylar fractures. In contrast, pediatric orthopaedists used active range of motion to improve elbow motion.
Keppler et al. retrospectively reviewed patients who had sustained supracondaylar fractures to ascertain the effect of postoperative physical therapy. At one year follow up, there was no difference in motion between patients who had received physical therapy and those who had not.
Figures A and B demonstrate the AP and lateral radiographs of a pediatric supracondylar fracture. Figures C and D are the postoperative radiographs after closed reduction and percutaneous pinning of the elbow injury.
Incorrect Answers:
(SBQ13PE.13) A 17-month-old boy is referred to your clinic by his pediatrician for a workup of "bowed legs." The patient's mother states that she has other children that grew out of it by age 3 or 4. Examination of the patient reveals a child whose measurements reside in the 75% percentile for height and weight. His gait appears appropriate for a toddler without varus thrust. Supine measurements show 10-degrees of symmetric, bilateral genu varus. Appropriate workup includes: Review Topic
Longterm clinical and radiographic monitoring to plan for guided growth until skeletal maturity
X-rays today and at age 4 to assure resolution of his genu varum
Genetic screening for metabolic causes of Rickets
Vitamin D levels drawn today and weekly 50,000 IU vitamin D injections assuming the value is low
Clinical observation and follow up to monitor resolution of genu varum
This patient has physiologic genu varum or tibia vara, which is common in toddlers less than 2 years of age. The mainstay of treatment is simple observation, as there is predictable resolution of this alignment as children
There are numerous etiologies of genu varum in children. Most common in the children under age 2 is a predictable pattern of genu varum and internal torsion in the first year or so after beginning to walk. Persistence of genu varum, severe (>20 degrees) or worsening deformity, limb asymmetry or varus thrust gait, and low height and weight percentiles should trigger further workup with x-rays and metabolic or genetic screening. A family history of genu varum is non-specific, and in isolation, does not indicate heritable causes of genu varum.
Kling and Hensinger's review article highlights normal angular and torsional deviations in growing children, including genu varum and genu valgum as well as hip and hind foot deformities. They emphasize that understanding the natural history of these deformities in growing children helps the treating physician identify those who need more than simple observation of their malalignment.
Staheli et al. published normal values of rotational profile physical exam maneuvers (including thigh foot axis, transmalleolar axis, prone internal and external hip rotation) to better understand the predictable changes in different age groups.
Birch provides an update on current treatment of Blount's disease. He suggests further radiographic evaluation in ambulatory infants with asymmetric varus deformity or varus deformity that persists after age 18 months. If these findings are present, radiographs are recommended. If the X-rays reveal metaphyseal-diaphyseal angle
>16° on AP radiographs and confirm the diagnosis of infantile Blount disease, he recommends anti-varus long leg bracing during ambulation for patients aged <=3 years with progressive deformity, clear radiographic evidence of infantile Blount disease, or lateral thrust with ambulation.
Illustration A shows pathologic metaphyseal beaking common in Blount's disease. There are no pathognomonic x-ray findings in physiological bowing as presented in this question.
Incorrect Answers:
Question 93
Figure 38 shows the radiograph of a 75-year-old woman who has had right shoulder pain, difficulty sleeping on the affected arm, and difficulties performing activities of daily living for the past 6 weeks. Initial nonsurgical management includes analgesics, a subacromial cortisone injection, and gentle range-of-motion exercises. However, these modalities have failed to provide relief, and the patient reports that she is unable to elevate her arm. Her pain is worse and she would like the most reliable treatment method for pain relief and functional improvement. What is the best surgical treatment?
Explanation
REFERENCES: Favard L, Lautmann S, Sirveaux F, et al: Hemiarthroplasty versus reverse arthroplasty in the treatment of osteoarthritis with massive rotator cuff tear, in Walch G, Boileau P, Mole D (eds): 2000 Shoulder Prosthesis Two to Ten Year Follow-Up. Montpellier, France, Sauramps Medical, 2001, pp 261-268.
Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Werner CM, Steinmann PA, Gilbart M, et al: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 94
A 5-year-old girl sustains an isolated injury to the right shoulder area after falling off the monkey bars. Examination reveals intact neurovascular function in the extremity distally, but she is quite uncomfortable. An AP radiograph of the proximal humerus is shown in Figure 24. Her parents state that she is a very talented gymnast. Considering her age and potential athletic career, management should consist of
Explanation
REFERENCES: Martin RF: Fractures of the proximal humerus and humeral shaft, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994,
pp 144-148.
Sanders JO, Rockwood CA Jr, Curtis RJ: Fractures and dislocation of the humeral shaft and shoulder, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 937-939.
Question 95
Tumoral calcinosis Tumoral calcinosis is a heritable condition that is characterized by periarticular metastatic calcification. Most patients are black, and the inheritance is usually autosomal recessive. Metastatic calcifications occur around joints and in the skin, marrow, teeth, and blood vessels. The periarticular masses may grow quite large and are attached to the fascia, but they are extra-articular. The masses may occur at the shoulder, hip, and elbow. Radiographically: The masses are composed of heavy, amorphous calcification in nodules. Laboratory:
Explanation
A 20-year-old patient who is otherwise healthy has a soft mass over her hip. The mass has formed over the past 2 years. The radiographs are shown in Slides 1 and 2. Which of the following would be a common finding:
Question 96
When treating a proximal tibia fracture, the surgeon decides to (1) use blocking screws in the proximal fragment, and (2) pick the intramedullary nail based on the location of the Herzog curve. Which of the following combinations will best prevent the classic deformity associated with this fracture?
Explanation
Up to 58% of proximal tibial fractures are malaligned. Malalignment arises because the nail fits loosely in the wide metaphyses and cannot control alignment. Without close fit of the nail at the fracture site, the nail will not align the fracture independent of a stable reduction and careful nail path. Blocking screws serve to reduce the size of the proximal metaphyseal canal and guide final nail passage.
Stinner et al. discuss strategies in proximal tibial fracture nailing. They describe an accurate starting point (using the twin peaks AP view or fibular bisector AP view, and flat plateau lateral view). They emphasize fracture reduction prior to reaming and implant placement.
Hiesterman reviewed nailing of extra-articular proximal tibial fractures. Techniques described include blocking screws, unicortical plating, using a universal distractor, nailing in flexion/locking in extension, semiextended nailing (including percutaneous suprapatellar quads-splitting approaches), multiple proximal interlocking screws (>=3).
Illustration A shows placement of a coronal blocking screw. Illustration B shows placement of a sagittal blocking screw. Illustration C shows the effect of the Herzog curve. A more distal Herzog curve leads to a "wedge" effect and fracture displacement whereas a proximal Herzog curve contains the fracture. The "wedge" effect occurs as the nail is seated and impinges on the posterior cortex of the distal segment accentuating an apex anterior deformity because of the effective widening of the nail above the bend and posterior force on the distal segment to match the nail shape.
Incorrect Answers:
Question 97
At the time of arthroscopy, a 9-year-old boy was found to have a Watanabe type II discoid lateral meniscus. What is the most appropriate treatment? Review Topic
Explanation
Question 98
An 8-month-old infant has an infection of the fingertip as shown in Figure 22. If neglected, the anticipated path of ascending infection is the fingertip, the flexor sheath, and the
Explanation
REFERENCES: Peimer CA (ed): Surgery of the Hand and Upper Extremity: Acute and Chronic Sepsis. New York, NY, Mcgraw Hill, 1996, pp 1735-1741.
Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow and Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 445-446.
Question 99
A 45-year-old coach sustains a complete distal biceps tendon rupture at the elbow. Surgical repair is most indicated to Review Topic
Explanation
Question 100
What is the most frequent complication of both lateral closing wedge high tibial osteotomy and medial opening wedge osteotomy?
Explanation
REFERENCES: Scuderi GR, Windsor RE, Insall JN: Observations on patellar height after proximal tibial osteotomy. J Bone Joint Surg Am 1989;71:245-248.
Wright JM, Crockett HC, Slawski DP, et al: High tibial osteotomy. J Am Acad Orthop Surg 2005;13:279-289.
Hernigou P, Medevielle D, Debeyre J, et al: Proximal tibial osteotomy for osteoarthritis
with varus deformity: A ten to thirteen-year follow-up study. J Bone Joint Surg Am 1987;69:332-354.
Matthews LS, Goldstein SA, Malvitz TA, et al: Proximal tibial osteotomy: Factors that influence the duration of satisfactory function. Clin Orthop 1988;229:193-200.
Marti CB, Gautier E, Wachtl SW, et al: Accuracy of frontal and sagittal plane correction in open-wedge high tibial osteotomy. Arthroscopy 2004;20:366-372.
Marti RK, Verhigan RA, Kerkhoffs GM, et al: Proximal tibial varus osteotomy: Indications, technique, and five to twenty-one-year results. J Bone Joint Surg Am 2001;83:164-170.
Flierl S, Sabo D, Hornig K, et al: Open wedge high tibial osteotomy using fractioned drill osteotomy: A surgical modification that lowers the complication rate. Knee Surg Sports Traumatol Arthrosc 1996;4:149-153.
Billings A, Scott DF, Camargo MP, et al: High tibial osteotomy with a calibrated osteotomy guide, rigid internal fixation, and early motion: Long-term follow-up. J Bone Joint Surg Am 2000;82:70-79.
