Orthopedic Board Prep MCQs: Fracture, Tendon & Tumor - Part 222

Key Takeaway
This page provides Part 222 of an interactive MCQ practice exam for orthopedic surgeons and residents preparing for OITE, ABOS, and AAOS board certifications. Featuring 100 high-yield questions on Fracture, Tendon, and Tumor, it offers rigorous preparation with detailed explanations and two learning modes.
About This Board Review Set
This is Part 222 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 222
This module focuses heavily on: Fracture, Tendon, Tumor.
Sample Questions from This Set
Sample Question 1: A woman with a neck and chest tumor has weakness in the biceps and paresthesias in the thumb. Brachioradialis and infraspinatus function are normal. The lesion is affecting which of the following structures?...
Sample Question 2: What are the five most common tumors that metastasize to bone?...
Sample Question 3: A 63-year-old woman is seen 10 weeks after sustaining a closed minimally displaced distal radius fracture. She has been in a short-arm cast and reports minimal pain but notes that she is having difficulty using her thumb. An extensor pollic...
Sample Question 4: A 35-year-old male sustains a closed tibial shaft fracture after falling from 12 feet. Which of the following measurements would be concerning for an evolving compartment syndrome?...
Sample Question 5: Figures 155a and 155b are the plain radiographs of a 17-year-old boy who recently noted painless swelling in his distal thigh. Examination reveals a firm, fixed, deep distal thigh mass. There is no associated tenderness. What is the best ne...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A woman with a neck and chest tumor has weakness in the biceps and paresthesias in the thumb. Brachioradialis and infraspinatus function are normal. The lesion is affecting which of the following structures?
Explanation
REFERENCE: Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995, p 334.
Question 2
What are the five most common tumors that metastasize to bone?
Explanation
REFERENCES: Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
CA, January/February 2000, vol 50, no. 1 (Cancer Statistics).
Question 3
A 63-year-old woman is seen 10 weeks after sustaining a closed minimally displaced distal radius fracture. She has been in a short-arm cast and reports minimal pain but notes that she is having difficulty using her thumb. An extensor pollicis longus (EPL) tendon rupture is suspected. Which examination finding would confirm lack of EPL function?
Explanation
As many as to 5% of patients with a nondisplaced distal radius fracture experience EPL rupture. The extensor pollicis brevis (EPB) tendon often attaches to the extensor hood and sometimes continues more distally, providing weak metacarpophalangeal extension even in the setting of EPL disruption. However, because of the vector of its pull, the EPB cannot extend the thumb dorsal to the plane of the palm. A positive Froment sign is noted when flexion of the thumb interphalangeal joint with an attempted key pinch is caused by adductor pollicis weakness from ulnar nerve dysfunction. Compression of the median nerve in the carpal tunnel affects the recurrent motor branch of the abductor pollicis brevis, leading to thenar atrophy. The flexor pollicis longus tendon (FPL) is intact so the patient would not have difficulty flexing the thumb with the palm flat.
Question 4
A 35-year-old male sustains a closed tibial shaft fracture after falling from 12 feet. Which of the following measurements would be concerning for an evolving compartment syndrome?

Explanation
Given the poor outcomes associated with missed compartment syndromes, it is important to obtain both clinical and objective data when determining if a patient needs fasciotomies. Determining if a patient needs fasciotomies in the operating room while a patient is under anesthesia is complicated by the fact that obtaining a clinical exam is impossible, and that the diastolic blood pressure may be falsely decreased compared to normal pre- or postoperative measurements. Currently, it is recommended that intraoperative compartment pressures be compared to preoperative diastolic blood pressures, with delta p < 30 indicating the need for fasciotomies.
Kakar et al. review the preoperative, intraoperative, and postoperative diastolic blood pressure (DBP) in 242 patients with a tibia fracture treated operatively. They found the mean DBP was 18 points lower in the operating room compared to the preoperative measurement. In addition, they found the difference between preoperative and postoperative diastolic blood pressures to be within 2 points, indicating the decrease seen intraoperatively is likely a spurious value induced by anesthetic.
McQueen and Court-Brown prospectively review 116 patients with tibia fractures that had continuous monitoring of their anterior compartment for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of
30 mmHg is a more reliable indicator of compartment syndrome.
Incorrect Answers:
Question 5
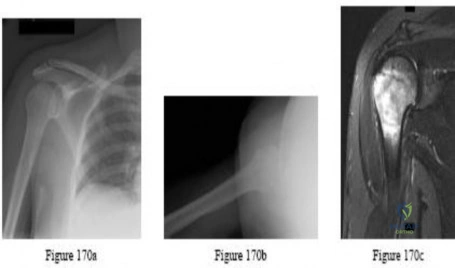
Figures 155a and 155b are the plain radiographs of a 17-year-old boy who recently noted painless swelling in his distal thigh. Examination reveals a firm, fixed, deep distal thigh mass. There is no associated tenderness. What is the best next treatment step?

Explanation
Question 6
The patient in Figure 55 is actively attempting to make a fist. This clinical scenario suggests which of the following anatomic lesions?
Explanation
REFERENCE: Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995, p 189.
Question 7
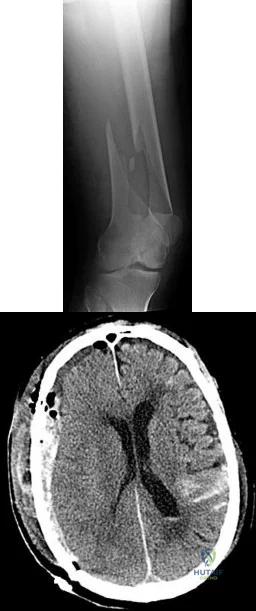
14A 14B An 18-year-old man was involved in an altercation during which he sustained the injuries shown in Figures 14a and 14b. His Glasgow Coma Scale (GCS) score is 11 (a GCS score of 9-12 indicates moderate head injury). The neurosurgeons elect to not place an intracranial pressure (ICP) monitor. The patient responds appropriately to stimuli and is hemodynamically stable. What is the most appropriate initial treatment?
Explanation
Although management of femoral shaft fractures in patients with head injuries remains controversial, most practitioners agree that "damage-control principles" are appropriate for patients with evolving head injuries. This patient has a subarachnoid hemorrhage and a decreased GCS but is responding appropriately. The best treatment is a damage-control approach for the femur that will cause minimal blood loss and allow the brain injury (and swelling) to equilibrate. External fixation can be performed expeditiously and with minimal blood loss, which will reduce further injury to the brain. Special attention should be paid to maintaining cerebral perfusion pressure higher than 70 mmHg. Admission to the intensive care unit is recommended for monitoring of this injury. Knee immobilizers are not tolerated well by young muscular men with femur shaft fractures. A GCS score of 11 or higher can be observed without ICP monitoring.
RECOMMENDED READINGS
Flierl MA, Stoneback JW, Beauchamp KM, Hak DJ, Morgan SJ, Smith WR, Stahel PF. Femur shaft fracture fixation in head-injured patients: when is the right time? J Orthop Trauma. 2010 Feb;24(2):107-14. PubMed PMID: 20101135. View Abstract at PubMed
Roberts CS, Pape HC, Jones AL, Malkani AL, Rodriguez JL, Giannoudis PV.Damage control orthopaedics: evolving concepts in the treatment of patients who have sustained orthopaedic trauma. Instr Course Lect. 2005;54:447-62. Review. PubMed PMID: 15948472. View Abstract at PubMed
Question 8
A 68-year-old woman with metastatic breast carcinoma is seen in the emergency department. She appears lethargic, and she reports abdominal pain, nausea, and constipation. An EKG reveals a shortened QT interval. The only physical finding on examination is diffuse hyporeflexia. What is the most appropriate step in management?
Explanation
REFERENCE: Stewart AF: Clinical practice: Hypercalcemia associated with cancer. N Engl J of Med 2005;352:373-379.
Question 9
The recurrent motor branch of the median nerve innervates which of the following muscles?
Explanation
REFERENCES: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 109.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 170.
Question 10
Figures 92a through 92c are the radiographs of a 34-year-old man with low-back pain and an inability to walk upright. What is the appropriate surgical treatment? A B C

Explanation
This patient has a marked fixed sagittal imbalance and a mild coronal imbalance. His fused sacroiliac joints indicate ankylosing spondylitis. Sufficient correction likely can be achieved with a pedicle subtraction osteotomy in the midlumbar spine. Smith-Petersen osteotomies necessitate flexibility of the anterior column, which is not associated with this diagnosis. Also, osteoclasis can result in vascular injuries. Vertebral column resection should not be needed in this case.
RECOMMENDED READINGS
Patel NM, Jenis LG. Inflammatory arthritis of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:339-349.
Kim KT, Suk KS, Cho YJ, Hong GP, Park BJ. Clinical outcome results of pedicle subtraction osteotomy in ankylosing spondylitis with kyphotic deformity. Spine (Phila Pa 1976). 2002 Mar 15;27(6):612-8. PubMed PMID: 11884909. View Abstract at PubMed
Question 11
A 2-year-old boy has been referred for musculoskeletal evaluation. Examination reveals shortened proximal limbs, hip and knee flexion contractures, an abducted thumb, and ear abnormalities. His parents are concerned about his deformed feet. What is the most common foot deformity associated with this patient’s diagnosis?
Explanation
REFERENCES: Ryoppy S, Poussa M, Merikanto J, Marttinen E, Kaitila I: Foot deformities in diastrophic dysplasia: An analysis of 102 patients. J Bone Joint Surg Br 1992;74:441-444.
Bussett GS: The osteochondrodysplasias, in Morrissy RT, Weinstein S (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, p 219.
Question 12
A 9-year-old boy has pain over the midfoot medially with activity. Based on the findings shown in Figures 26a and 26b, which of the following is considered the most effective short-term management?
Explanation
REFERENCES: Borges JL, Guile JT, Bowen JR: Köhler’s bone disease of the tarsal navicular.
J Pediatr Orthop 1995;15:596-598.
Williams GA, Cowell HR: Köhler’s disease of the tarsal navicular. Clin Orthop 1981;158:53-58.
Question 13
An 82-year-old man has had episodic right thigh pain after undergoing a total hip arthroplasty 10 years ago. Initial postoperative radiographs are shown in Figures 26a and 26b, and current radiographs are shown in Figures 26c and 26d. What is the most likely cause of his pain?
Explanation
REFERENCES: Engh CA, Massin P, Suthers KE: Roentgenographic assessment of biologic fixation of porous-surface femoral components. Clin Orthop Relat Res 1990;257:107-128.
Engh CA, Hooten JP, Zettl-Schaffer KF, et al: Evaluation of bone ingrowth in proximally and extensively porous-coated anatomic medullary locking prostheses retrieved at autopsy. J Bone Joint Surg Am 1995;77:903-910.
Question 14
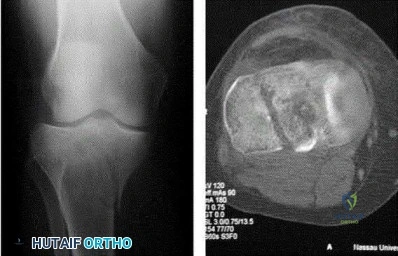
Figure 9 shows the radiograph of a 75-year-old woman who reports the sudden onset of disabling medial knee pain. What is the most likely diagnosis?
Explanation
REFERENCES: Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 413-418.
Insall JN, Windsor RE, Scott WN, Kelly MA, Aglietti P (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 609-634.
Question 15
A patient falls off a roof and sustains the fracture shown in Figure 29. What is the most likely complication that results from injury to the structure that is located at the arrow?

Explanation
Question 16
Patients with rheumatoid arthritis may exhibit an increase in viral load for which of the following viruses?
Explanation
REFERENCES: Callan MF: Epstein-Barr virus, arthritis, and the development of lymphoma in arthritis patients. Curr Opin Rheumatol 2004;16:399-405.
Baecklund E, Sundstrom C, Ekbom A, et al: Lymphoma subtypes in patients with rheumatoid arthritis: Increased proportion of diffuse large B cell lymphoma. Arthritis Rheum
2003;48:1543-1550.
Question 17
Metal-on-metal lumbar disk arthroplasty devices may generate cobalt and chromium ions into the serum of patients after implantation into the lumbar spine. Which of the following statements best represents the levels of the serum ion levels in these patients? Review Topic
Explanation
Question 18
A 6-year-old child has a fixed flexion deformity of the interphalangeal (IP) joint of the right thumb. The thumb is morphologically normal, with a nontender palpable nodule at the base of the metacarpophalangeal joint. Clinical photographs are shown in Figures 42a and 42b. Based on these findings, what is the treatment of choice?
Explanation
REFERENCES: Tan AH, Lam KS, Lee EH: The treatment outcome of trigger thumb in children. J Pediatric Orthop B 2002;11:256-259.
Slakey JB, Hennrikus WL: Acquired thumb flexion contracture in children: Congenital trigger thumb. J Bone Joint Surg Br 1996;78:481-483.
Herring JA: Disorders of the upper extremity: Thumb dysplasia, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, p 445.
Question 19
A 35-year-old man who is involved in an improvised explosive device attack is hit by a piece 57 of shrapnel. He has a solitary penetrating wound in his left tibia. Radiographs show no fracture. He has significant pain and his calf is grossly swollen. He has good sensation and palpable dorsalis pedis and tibialis posterior pulses. He has elevated pressure in all 4 compartments. When performing a 4-compartment fasciotomy using the 2-incision technique, which structure is at risk when opening the deep posterior compartment?
Explanation
Compartment syndrome is commonly seen in lower-extremity trauma, especially in blast injuries or high-energy trauma to the lower extremity. It is important to recall the neurovascular structures present in each of the 4 compartments. The posterior tibial artery is in the deep posterior compartment along with the tibial nerve, the peroneal artery and vein, and the posterior tibial vein. The lateral compartment contains the superficial peroneal nerve.
The anterior compartment contains the deep peroneal nerve and the anterior tibial artery and vein. The superficial posterior compartment does not have any neurovascular structures. The saphenous nerve is superficial.
RECOMMENDED READINGS
Thompson JC, ed. Netter’s Concise Atlas of Orthopaedic Anatomy. Teterboro: NJ: Icon Learning Systems; 2002.
Mubarak SJ, Owen CA. Double-incision fasciotomy of the leg for decompression in compartment syndromes. J Bone Joint Surg Am. 1977 Mar;59(2):184-7. PubMed PMID: 15455478.View Abstract at PubMed
Question 20
What is the average linear wear rate of a conventional, noncross-linked ultra-high molecular weight polyethylene liner used in total hip arthroplasty?
Explanation
REFERENCES: Callaghan JJ, Albright JC, Goetz DD, Olejniczak JP, Johnston RC: Charnley total hip arthroplasty with cement: Minimum twenty-five year follow-up. J Bone Joint Surg Am 2000;82:487-497.
Isaac GH, Wroblewski BM, Atkinson JR, Dowson D: A tribological study of retrieved hip prostheses. Clin Orthop 1992;276:115-125.
Question 21
The best candidate for a reverse total shoulder arthroplasty is a patient with rotator cuff tear arthropathy with Review Topic
Explanation
Question 22
Which soft-tissue sarcoma is most likely to develop lymphatic metastasis?
Explanation
Question 23
A 58-year-old man reports a 2-month onset of groin pain with no history of trauma. Examination reveals that range of motion of the hip is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 20. Treatment should consist of
Explanation
REFERENCES: Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Urbanski SR, de Lange EE, Eschenroeder HC Jr: Magnetic resonance imaging of transient osteoporosis of the hip: A case report. J Bone Joint Surg Am 1991;73:451-455.
Question 24
A 29-year-old woman reports dysesthesias and burning after undergoing bunion surgery that consisted of a proximal crescentic first metatarsal osteotomy 6 months ago. Examination reveals a positive Tinel’s sign at the proximal aspect of the healed incision. What injured nerve is responsible for her continued symptoms?
Explanation
REFERENCES: Kenzora JE: Sensory nerve neuromas: Leading to failed foot surgery. Foot Ankle 1986;7:110-117.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Question 25
The anterior approach to total hip arthroplasty requires dissection between which of the following muscle planes?
Explanation
DISCUSSION: The anterior approach to the hip joint involves identifying the plane between the tensor fascia lata and the sartorius muscles.
REFERENCES: Berger RA, Duwelius PJ: The two-incision minimally invasive total hip arthroplasty: Technique and results. Orthop Clin North Am 2004;35:163-172.
Matta JM, Shahrdar C, Ferguson T: Single-incision anterior approach for total hip arthroplasty on an orthopaedic table. Clin Orthop Relat Res 2005;441:115-124.
28 • American Academy of Orthopaedic Surgeons
Figure 3Id Figure 31e
Question 26
An 18-year-old man has had an enlarging mass in his hand for the past 3 months. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 54a through 54d. What is the most likely diagnosis?
Explanation
REFERENCES: Abramovici L, Steiner GC: Bizarre parosteal osteochondromatous proliferation (Nora’s lesion): A retrospective study of 12 cases, 2 arising in long bones. Hum Pathol 2002;33:1205-1210.
Nora FE, Dahlin DC, Beabout JW: Bizarre parosteal osteochondromatous proliferations of the hands and feet. Am J Surg Pathol 1983;7:245-250.
Question 27
When compared to smokers who do not quit, an improvement in the rate of lumbar fusion is seen in patients who cease smoking for at least how many months postoperatively? Review Topic
Explanation
Question 28
Figures 26a through 26c show the MRI scans of a 47-year-old man who underwent arthroscopic shoulder surgery 6 months ago and continues to have pain despite a prolonged course of rehabilitation. Management should now consist of Review Topic

Explanation
Question 29
An 8-year-old sustains the injury shown in Figures A and B. Postoperative radiographs are shown in Figures C and D. After cast removal and in-office k-wire removal, elbow range of motion is found to be between 20-80 degrees of flexion. How soon after surgery is range of motion expected to be >90% of normal? Review Topic

Explanation
Displaced pediatric supracondylar elbow fractures are often treated with closed reduction and percutaneous pinning. Risk of stiffness is low considering the extra-articular nature of the injury. Utility of physical therapy to improve range of motion after operative treatment of this injury is not supported in the literature.
Zionts et al. retrospectively evaluated elbow stiffness after treatment for pediatric supracondylar fractures. Ninety-four percent of normal range of motion was restored by 6 months after the operative procedure. Further improvement occurs up to one-year postoperatively
Lee et al. surveyed 76 orthopaedic surgeons on their treatment of pediatric supracondaylar injuries. They noted that general orthopaedic surgeons used passive exercises to assist with elbow stiffness after operative management of pediatric supracondylar fractures. In contrast, pediatric orthopaedists used active range of motion to improve elbow motion.
Keppler et al. retrospectively reviewed patients who had sustained supracondaylar fractures to ascertain the effect of postoperative physical therapy. At one year follow up, there was no difference in motion between patients who had received physical therapy and those who had not.
Figures A and B demonstrate the AP and lateral radiographs of a pediatric supracondylar fracture. Figures C and D are the postoperative radiographs after closed reduction and percutaneous pinning of the elbow injury.
Incorrect Answers:
(SBQ13PE.13) A 17-month-old boy is referred to your clinic by his pediatrician for a workup of "bowed legs." The patient's mother states that she has other children that grew out of it by age 3 or 4. Examination of the patient reveals a child whose measurements reside in the 75% percentile for height and weight. His gait appears appropriate for a toddler without varus thrust. Supine measurements show 10-degrees of symmetric, bilateral genu varus. Appropriate workup includes: Review Topic
Longterm clinical and radiographic monitoring to plan for guided growth until skeletal maturity
X-rays today and at age 4 to assure resolution of his genu varum
Genetic screening for metabolic causes of Rickets
Vitamin D levels drawn today and weekly 50,000 IU vitamin D injections assuming the value is low
Clinical observation and follow up to monitor resolution of genu varum
This patient has physiologic genu varum or tibia vara, which is common in toddlers less than 2 years of age. The mainstay of treatment is simple observation, as there is predictable resolution of this alignment as children
There are numerous etiologies of genu varum in children. Most common in the children under age 2 is a predictable pattern of genu varum and internal torsion in the first year or so after beginning to walk. Persistence of genu varum, severe (>20 degrees) or worsening deformity, limb asymmetry or varus thrust gait, and low height and weight percentiles should trigger further workup with x-rays and metabolic or genetic screening. A family history of genu varum is non-specific, and in isolation, does not indicate heritable causes of genu varum.
Kling and Hensinger's review article highlights normal angular and torsional deviations in growing children, including genu varum and genu valgum as well as hip and hind foot deformities. They emphasize that understanding the natural history of these deformities in growing children helps the treating physician identify those who need more than simple observation of their malalignment.
Staheli et al. published normal values of rotational profile physical exam maneuvers (including thigh foot axis, transmalleolar axis, prone internal and external hip rotation) to better understand the predictable changes in different age groups.
Birch provides an update on current treatment of Blount's disease. He suggests further radiographic evaluation in ambulatory infants with asymmetric varus deformity or varus deformity that persists after age 18 months. If these findings are present, radiographs are recommended. If the X-rays reveal metaphyseal-diaphyseal angle
>16° on AP radiographs and confirm the diagnosis of infantile Blount disease, he recommends anti-varus long leg bracing during ambulation for patients aged <=3 years with progressive deformity, clear radiographic evidence of infantile Blount disease, or lateral thrust with ambulation.
Illustration A shows pathologic metaphyseal beaking common in Blount's disease. There are no pathognomonic x-ray findings in physiological bowing as presented in this question.
Incorrect Answers:
Question 30
A previously healthy 65-year-old woman has a closed fracture of the right clavicle after falling down the basement stairs. Examination reveals good capillary refill in the digits of her right hand. Radial and ulnar pulses are 1+ at the right wrist compared with 2+ on the opposite side. In the arteriogram shown in Figure 36, the arrow is pointing at which of the following arteries?
Explanation
REFERENCE: Radke HM: Arterial circulation of the upper extremity, in Strandness DE Jr (ed): Collateral Circulation in Clinical Surgery. Philadelphia, PA, WB Saunders, 1969, pp 294-307.
Question 31
A 64-year-old woman with rheumatoid arthritis cannot fully extend her fingers actively at the metacarpophalangeal (MCP) level. Full passive extension is possible, but she cannot actively maintain that extension when her fingers are released. The MCP joints do extend when her wrist is passively flexed. What is the most likely cause of this problem?
Explanation
Loss of MCP extension is common in the setting of rheumatoid arthritis, but potential causes are varied. An understanding of various etiologies is needed to address the multiple facets of inflammatory arthropathy, for which causes include extensor tendon rupture, MCP joint flexion contracture/dislocation, subluxation of the extensor tendons at the MCP joint (sagittal band rupture), and posterior interosseous nerve (PIN) palsy. These causes are differentiated during an examination. Extensor tendon ruptures, as seen with caput ulnae syndrome (Vaughan-Jackson syndrome) allow for passive MCP extension, not active extension or the ability to maintain extension actively, and would not involve finger extension with passive flexion tenodesis of the wrist. Flexion contractures of the MCP joints, as may be seen in dislocations, would not allow active or passive motion. Subluxation of the extensor tendons at the MCP joints, as seen in attenuation of the sagittal bands, will usually preclude the initiation of active extension, but patients will be able to maintain extension of the MCP joints once they are placed in extension by the examiner. With a PIN palsy, no active extension or active hold is possible, but passive extension and tenodesis with wrist flexion are maintained. Synovitis of the elbow is the most likely cause of the PIN palsy. An extensor tenosynovitis or caput ulnae syndrome would not prohibit MCP extension unless the condition progressed to the point of causing other pathology.
Question 32
Figure 68 is the radiograph of a 33-year-old runner who recently decided to begin running barefoot on trails. Since his transition to running without shoes 3 months ago, he has been having pain in the second metatarsophalangeal (MTP) joint. He feels like he is walking on a stone, notes edema in the ball of his foot, and has started to see a deviation of the second toe. What is the most likely etiology of these symptoms and findings?

Explanation
Lesser-toe plantar plate injuries are becoming increasingly recognized. Patients typically have an increase in pain, a positive Lachman test result upon examination, and deviation of the MTP joint. On radiograph, MTP subluxation can be appreciated. Nonsurgical treatment with a metatarsal pad may be attempted. Many patients who have surgery will have a partial or full tear of the plantar plate. The repair necessitates reinsertion of the plantar plate to the base of the proximal phalanx.
RECOMMENDED READINGS
Doty JF, Coughlin MJ, Weil L Jr, Nery C. Etiology and management of lesser toe metatarsophalangeal joint instability. Foot Ankle Clin. 2014 Sep;19(3):385-405. doi: 10.1016/j.fcl.2014.06.013. Epub 2014 Jul 10. PubMed PMID: 25129351. View Abstract at PubMed
Nery C, Coughlin MJ, Baumfeld D, Raduan FC, Mann TS, Catena F. Prospective evaluation of protocol for surgical treatment of lesser MTP joint plantar plate tears. Foot Ankle Int. 2014 Sep;35(9):876-85. doi: 10.1177/1071100714539659. Epub 2014 Jun 23. PubMed PMID:
Question 33
A patient who underwent an L5-S1 hemilaminotomy and partial diskectomy for radiculopathy 3 weeks ago now reports increasing leg and back pain with radicular signs. An axial T2-weighted MRI scan is shown in Figure 97a, an axial T1-weighted MRI scan is shown in Figure 97b, and a contrast enhanced T1-weighted MRI scan is shown in Figure 97c. What is the most appropriate management for the patient's symptoms? Review Topic
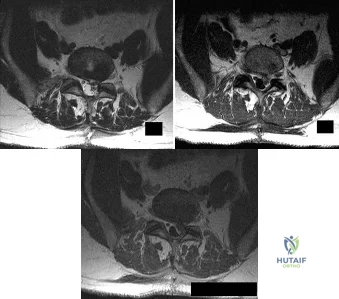
Explanation
Question 34
After performing an open distal clavicle excision and resecting 15 mm of distal clavicle, which potential concern for shoulder function could result?
Explanation
AC joint arthritis often is marked by pain along the anterior and superior aspects of the shoulder. It can occasionally radiate into the trapezius and the anterolateral neck region. A patient may have tenderness to palpation directly at the AC joint or pain with the cross-body adduction stress test and the O'Brien active compression test. During the cross-body adduction test, this patient has pain when the examiner lifts his arm in 90 degrees of forward flexion and maximally adducts it across his body. Although the cross-body adduction test is the most sensitive provocative test for AC joint osteoarthritis at 77%, the O’Brien active compression test has been shown to be most specific at 95%.
Physical therapy, rest, activity modification, and other nonsurgical treatments might not reverse osteoarthritis changes at the AC joint, but these interventions can often help improve pain, range of motion, and function. A corticosteroid injection into the AC joint may be an option if nonsurgical treatments do not work, although Wasserman and associates demonstrated that only 44% of AC joint injections accurately entered the joint.
Persistent pain is the most common complication following distal clavicle excision. Although the exact amount of distal clavicle that should be resected is a topic of debate, resection of 10 mm or more of the distal clavicle may lead to instability of the AC joint, especially if the AC capsule is sectioned.
Question 35
Patellofemoral arthroplasty is contraindicated in the presence of
Explanation
Any inflammatory disease, including crystalline arthropathy, is a contraindication for patellofemoral arthroplasty. Patellar tilt and dysplasia frequently occur in the setting of patellofemoral arthritis and do not constitute a contraindication to this procedure. Severe crepitus is common and frequently addressed with patellofemoral arthroplasty.

CLINICAL SITUATION FOR QUESTIONS 47 THROUGH 50
A 70-year-old woman has a 3-year history of gradually increasing diffuse and global right knee pain. Her main issues are difficulty with stairs, stiffness with prolonged sitting, and swelling. She has taken nonsteroidal anti-inflammatory medications and has received intra-articular steroid injections, all with decreasing efficacy. Her right knee examination reveals range of motion of 15 to 80 degrees with a fixed deformity to varus and valgus stress. Her symptoms are no longer manageable nonsurgically. Radiographs reveal a 30-degree mechanical axis deformity.
Question 36
The risk of progression with congenital kyphosis is greatest with which of the following?
Explanation
REFERENCES: McMaster MJ, Singh H: Natural history of congenital kyphosis and kyphoscoliosis: A study of one hundred and twelve patients. J Bone Joint Surg Am 1999;81:1367-1383.
Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, p 351.
AL-Madena Copy
Question 37
A right-handed 44-year-old construction worker reports pain and limited range of motion in his right elbow that has limited his ability to work for the past year. Examination reveals range of motion from 60 to 90 degrees, and he has pain at the extremes of flexion and extension. Pronation and supination are minimally restricted. Anti-inflammatory drugs have failed to provide relief. A radiograph is shown in Figure 8. Management should now consist of
Explanation
REFERENCES: Antuna SA, Morrey BF, Adams RA, et al: Ulnohumeral arthroplasty for primary degenerative arthritis of the elbow: Long-term outcome and complications. J Bone Joint Surg Am 2002;84:2168-2173.
Phillips NJ, Ali A, Stanley D: Treatment of primary degenerative arthritis of the elbow by ulnohumeral arthroplasty: A long-term follow-up. J Bone Joint Surg Br 2003;85:347-350.
Question 38
A 42 year-old-woman who underwent surgery for lumbar scoliosis 2 years ago now has fixed sagittal plane imbalance and severe back pain. Which of the following is considered a contraindication to isolated pedicle subtraction osteotomy for the treatment of iatrogenic flatback syndrome in this patient?
Explanation
REFERENCES: Potter BK, Lenke LG, Kuklo TR: Prevention and management of iatrogenic flatback deformity. J Bone Joint Surg Am 2004;86:1793-1808.
Bridwell KH, Lenke LG, Lewis SJ: Treatment of spinal stenosis and fixed sagittal imbalance. Clin Orthop 2001;384:35-44.
Question 39
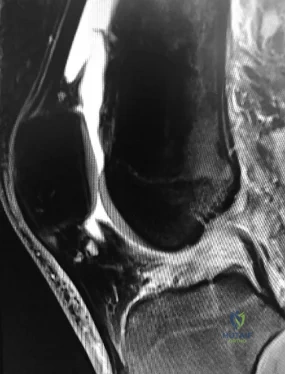
A 31-year-old woman has increasing pain and tightness in her right knee, with occasional stiffness and recurrent hemorrhagic effusions. MRI scans are shown in Figures 2a and 2b. What is the most likely diagnosis?
Explanation
REFERENCES: De Ponti A, Sansone V, Malchere M: Result of arthroscopic treatment of pigmented villonodular synovitis of the knee. Arthroscopy 2003;19:602-607.
Chin KR, Barr SJ, Winalski C, et al: Treatment of advanced primary and recurrent diffuse pigmented villonodular synovitis of the knee. J Bone Joint Surg Am 2002;84:2192-2202.
Bhimani MA, Wenz JF, Frassica FJ: Pigmented villonodular synovitis: Keys to early diagnosis. Clin Orthop 2001;386:197-202.
Question 40
A 29-year-old obese patient is transferred from an outside facility for the management of a closed-head injury and the fracture shown in Figure A. He presents to the trauma bay as a transient responder to blood products, and undergoes urgent pre-surgical angiography embolization. Surgery is performed within 8 hours from the time of injury. The patient develops a deep wound infection 1 week post-operatively. Which of the following factors would be considered the MOST statistically significant predictor for post-operative infection in this patient.

Explanation
Question 41
Which of the following is considered a potential advantage in prophylaxis for the prevention of deep venous thrombosis associated with the use of low-molecular weight heparin (LMWH) as compared with fixed-dose unfractionated heparin?
Explanation
REFERENCES: Colwell CW Jr, Spiro TE, Trowbridge AA: Use of enoxaparin, a low-molecular weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14.
Bara L, Billaud E, Kher A, Samama M: Increased anti-Xa bioavailability for a low-molecular weight heparin (PK 10169) compared with unfractionated heparin. Semin Thromb and Hemost 1985;11:316-317.
Paiement GD: Prevention and treatment of venous thromboembolic disease complications in primary hip arthroplasty patients, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 331-335.
Question 42
Figure 51 shows the radiograph of a 42-year-old construction worker who has pain and limited motion in his dominant elbow. Management consisting of nonsteroidal anti-inflammatory drugs and cortisone has failed to provide relief. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Gramstad GD, Galatz LM: Management of elbow osteoarthritis. J Bone Joint Surg Am 2006;88:421-430.
Steinmann SP, King GJ, Savoie FH III, et al: Arthroscopic treatment of the arthritic elbow.
J Bone Joint Surg Am 2005;87:2114-2121.
Question 43
Figure 46 shows the radiograph of a 65-year-old man who reports restricted range of motion and pain with sitting 18 months after undergoing right side revision total hip arthroplasty. What is the most appropriate management? L Intensive physiotherapy
Explanation
REFERENCES: Board TN, Karva A, Board RE, et al: The prophylaxis and treatment of heterotopic ossification following lower limb arthroplasty. J Bone Joint Surg Br 2007;89:434-440.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative
Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Question 44
Figures 20a through 20c show the radiographs of a 69-year-old woman who has severe pain in her dominant right arm after falling on the ice. History includes arthritis, hypertension, and heart disease. She is neurovascularly intact. Management should consist of
Explanation
REFERENCES: Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humeral fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
Morrey BF: Fractures of the distal humerus: Role of elbow replacement. Orthop Clin North Am 2001;31:145-155.
Question 45
When treating a proximal tibia fracture, the surgeon decides to (1) use blocking screws in the proximal fragment, and (2) pick the intramedullary nail based on the location of the Herzog curve. Which of the following combinations will best prevent the classic deformity associated with this fracture?
Explanation
Up to 58% of proximal tibial fractures are malaligned. Malalignment arises because the nail fits loosely in the wide metaphyses and cannot control alignment. Without close fit of the nail at the fracture site, the nail will not align the fracture independent of a stable reduction and careful nail path. Blocking screws serve to reduce the size of the proximal metaphyseal canal and guide final nail passage.
Stinner et al. discuss strategies in proximal tibial fracture nailing. They describe an accurate starting point (using the twin peaks AP view or fibular bisector AP view, and flat plateau lateral view). They emphasize fracture reduction prior to reaming and implant placement.
Hiesterman reviewed nailing of extra-articular proximal tibial fractures. Techniques described include blocking screws, unicortical plating, using a universal distractor, nailing in flexion/locking in extension, semiextended nailing (including percutaneous suprapatellar quads-splitting approaches), multiple proximal interlocking screws (>=3).
Illustration A shows placement of a coronal blocking screw. Illustration B shows placement of a sagittal blocking screw. Illustration C shows the effect of the Herzog curve. A more distal Herzog curve leads to a "wedge" effect and fracture displacement whereas a proximal Herzog curve contains the fracture. The "wedge" effect occurs as the nail is seated and impinges on the posterior cortex of the distal segment accentuating an apex anterior deformity because of the effective widening of the nail above the bend and posterior force on the distal segment to match the nail shape.
Incorrect Answers:
Question 46
A 32-year-old woman sustained an elbow dislocation, and management consisted of early range of motion. Examination at the 3-month followup appointment reveals that she has regained elbow motion but has a weak pinch. A clinical photograph is shown in Figure 21. What is the most likely diagnosis? Review Topic

Explanation
(SBQ12TR.54) A 37-year-old male cashier is shot in the leg. He sustains the injury shown in Figures A and B, and is subsequently taken to the operating room for intramedullary nailing. Figure C shows a radiograph of the nail starting point (*). What complication is most likely to result?

Varus malunion
Nonunion
Valgus malunion
Malrotation
Superficial peroneal nerve injury
This patient is presenting with a comminuted fracture of the proximal third of the tibia. He is appropriately undergoing intramedullary nail fixation, however, the start point illustrated in Figure C is too medial and often leads to a valgus malunion.
Intramedullary nail fixation is more technically demanding in proximal tibial fractures than diaphyseal fractures. The valgus deformity is due to imbalanced muscle forces on the proximal fragment, which are then accentuated by a start point that is too medial. An apex anterior (procurvatum) deformity can also occur and results from the pull of the patellar tendon or a posteriorly directed nail that deflects off the posterior tibial cortex and rotates the proximal fragment. The ideal starting point for proximal tibial fractures is slightly lateral to the medial aspect of the lateral tibial spine on a true AP x-ray and very proximal and just anterior to the anterior margin of the articular surface.
Nork et al. reported the results of intramedullary nailing of proximal tibial fractures with emphasis on techniques of reduction. Various techniques were found to be successful including attention to the proper starting point, the use of unicortical plates, and the use of a femoral distractor applied to the tibia.
Lowe et al. describe surgical techniques for complex proximal tibial fractures. They describe the extended leg position, use of a femoral distractor, temporary plate fixation, blocking (Poller) screws, and use of percutaneous clamps as means to achieve reduction during fixation.
Figure A and B show an AP and lateral radiograph of a comminuted extra-articular fracture through the proximal third of the tibia. Figure C demonstrates a start point that is too medial (represented by the asterisk) for intramedullary nail fixation. Illustration A and B show the ideal start point for intramedullary nail fixation of the tibia on AP and lateral radiographs.
Incorrect Answers:
Varus malunion is more likely to occur in midshaft tibia fractures with an intact fibula.
Nonunion after a proximal tibial fracture treated with intramedullary nailing is less common than malunion.
Malrotation occurs most commonly after IM nailing of fractures through the distal third of the tibia.
The superficial peroneal nerve is at risk during distal screw fixation using a LISS plating technique for fracture fixation.
Question 47
A 25-year-old semiprofessional football player sustains a hyperextension injury to the left foot. He is unable to bear weight. Examination reveals tenderness along the midfoot with swelling and plantar ecchymosis. Radiographs are negative. What is the next step in evaluation of this patient?
Explanation
REFERENCES: Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.
Hunt SA, Ropiak C, Tejwani NC: Lisfranc joint injuries: Diagnosis and treatment. Am J Orthop 2006;35:376-385.
Question 48
Figure 25 shows the radiograph of an 84-year-old woman who has pain and is unable to extend her knee. History reveals that she underwent total knee arthroplasty 8 years ago. Aspiration and studies for infection are negative. During revision surgery, management of the tibial bone loss should consist of
Explanation
REFERENCES: Mow CS, Wiedel JD: Structural allografting in revision total knee arthroplasty. J Arthroplasty 1996;11:235-241.
Engh GA, Herzwurm PJ, Parks NL: Treatment of major defects of bone with bulk allografts and stemmed components during total knee arthroplasty. J Bone Joint Surg Am 1997;79:1030-1039.
Clatworthy MG, Ballance J, Brick GW, et al: The use of structural allograft for uncontained defects in revision total knee arthroplasty: A minimum five-year review. J Bone Joint Surg Am 2001;83:404-411.
Question 49
A 35-year-old laborer who sustained a forefoot injury 10 years ago has returned to work but reports a progressively painful deformity of the hallux and continued midfoot pain that is aggravated by weight-bearing activities. Shoe wear modifications have failed to provide relief. Direct palpation reveals no pain at the first metatarsocuneiform joint. A radiograph is shown in Figure 11. What is the next most appropriate step in management?
Explanation
REFERENCES: Kitaoka HB, Patzer GL: Arthrodesis versus resection arthroplasty for failed hallux valgus operations. Clin Orthop 1998;347:208-214.
McGarvey WC, Braly WG: Bone graft in hindfoot arthrodesis: Allograft vs autograft. Orthopedics 1996;19:389-394.
Ouzounian TJ: Metatarsophalangeal arthrodesis for salvage of failed hallux valgus surgery. Foot Ankle Clin 1997;2:741-752.
Question 50
A 68-year-old woman who sustained a closed distal tibia fracture 2 years ago was initially treated with an external fixator across the ankle for 12 weeks, followed by intramedullary nailing of the fibula and lag screw fixation of the tibia. She continued to report persistent pain so she was treated with a brace and a bone stimulator. She now reports pain in her ankle. Examination reveals ankle range of motion of 8 degrees of dorsiflexion to 25 degrees of plantar flexion. She is neurovascularly intact. Current radiographs are shown in Figures 9a through 9c. What is the next most appropriate step in management?
Explanation
REFERENCES: Carpenter CA, Jupiter JB: Blade plate reconstruction of metaphyseal nonunion of the tibia. Clin Orthop 1996;332:23-28.
Lonner JH, Siliski JM, Jupiter JB, Lhowe DW: Posttraumatic nonunion of the proximal tibial metaphysis. Am J Orthop 1999;28:523-528.
Stevenson S: Enhancement of fracture healing with autogenous and allogeneic bone grafts. Clin Orthop 1998;355:S239-S246.
Wiss DA, Johnson DL, Miao M: Compression plating for non-union after failed external fixation of open tibial fractures. J Bone Joint Surg Am 1992;74:1279-1285.
Question 51
A 27-year-old man sustains a displaced femoral neck fracture and undergoes urgent open reduction internal fixation. What is the most prevalent complication after this injury?

Explanation
Haidukewych et al followed treatment of femoral neck fractures in young patients. They found almost 10% of displaced fractures were associated with the development of nonunion, where as 27% were associated with the development of osteonecrosis. Their results were influenced by fracture displacement and the quality of reduction. Varus malreduction most closely correlates with failure of fixation after reduction and cannulated screw fixation.
Swiontkowski reviews both the treatment and post operative complications in intracapsular hip fractures. In this Current Concept Review, the rate of AVN was discussed as being related to the pre-operative degree of displacement seen on radiographs.
Incorrect Responses:
Question 52
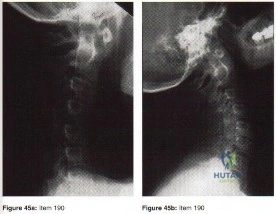
Explanation
In the context of viewing a lateral cervical spine to evaluate cranial setting, multiple lines can be used to assess anatomic relationships (i.e. McRae’s Chamberlin’s, or McGregor’s) McRae’s and Chamberlin’s use the foramen magnum as one land mark. Commonly, however, the margins of the foramen magnum are difficult to precisely identify. McGregor’s line connects the posterior margin of the hard palate to the most caudal point of the occiput and is easier to use. The tip of the odontoid should not project more than 4.5 mm above this line.
Anterior subluxation of more than 10-12 mm implies destruction of the entire ligamentous complex.
An atlantoaxial distance greater than 3.5mm is considered abnormal in an adult. The subaxial cervical spine is affected through involvement of the facets, interspinous ligaments, and intervertebral discs (spondylodiscitis). The initial site of destruction has been postulated to be through synovitis of the neurocentral joints with erosion of the adjacent disc and bone causing subluxation, or through primary facetal arthritis and ligamentous laxity causing secondary chronic discovertebraltrauma and destructive hypermobile segmentsis associated with disc destruction and toward the C2-C3 and C3-C4 segments, typically lack osteophytes, and often are at multiple levels, giving a stepladder appearance.
Question 53
An adult with a distal humeral fracture underwent open reduction and internal fixation. What is the most common postoperative complication?
Explanation
REFERENCES: Webb LX: Distal humerus fractures in adults. J Am Acad Orthop Surg 1996;4:336-344.
McKee MD, Wilson TL, Winston L, et al: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Question 54
At what age does the lateral epicondyle normally ossify in males?
Explanation
Question 55
Within the intervertebral disk, aggrecan is primarily responsible for: Review Topic
Explanation
Aggrecan, the most abundant proteoglycan within the intervertebral disk, is a hydrophillic molecule which helps attract and maintain water within the disc. This is important to maintain compressive strength. Early in life aggrecan has a high percentage of chondroitin sulfate chains. With aging this gradually changes to higher percentage of keratin sulfate. Other proteoglycans include decorin and versican. Decorin is believed to regulate cell cycles and influence fibrillogensis. Versican is a large extra-cellular matrix proteoglycan involved in cell adhesion and migration.
Roughley et al. provide a review of biologic changes within the intervertebral disc during development, maturation, and degeneration. They note that aggrecan works to maintain water content within the disc, thus improving its compressive strength. Aggrecan content decreases with age leading to a loss of compressive strength.
Illustration A shows the structure of aggrecan.
Incorrect answers:
Question 56
30%
Explanation
Initial assessment of a trauma patient should involve evaluation of airway, breathing and circulation. An average adult has approximately 5 L of circulating blood volume. Class III and IV hemorrhagic shock, approximated by loss of greater than 30% of blood volume, typically requires resuscitation with fluids and blood products. Lactate level (normal <2.5) is typically the most sensitive indicator of adequate perfusion.
According to ATLS guidelines, the emphasis of the initial assessment is to assume the worst injury and begin treatment before diagnosis. In cases of hemorrhagic shock, treatment involves aggressive resuscitation with crytalloid and/or blood products.
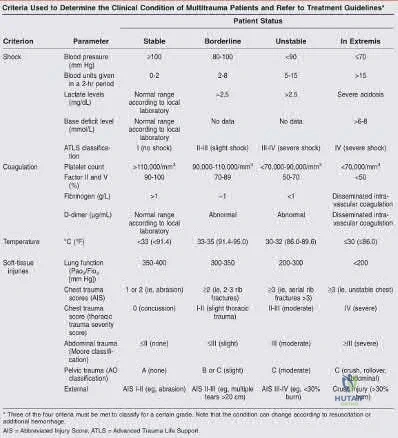
Illustration A is a chart showing the physiological changes associated with different levels of hemorrhagic shock
Incorrect Answers:
1: Blood loss of <15% typically leads to no changes in vital signs
2: Blood loss of 15-30% typically leads to heart rate >100 and diminished urine output
4, 5: Blood loss of greater than >40% typically leads to heart rate >140, decreased blood pressure and negligible urine output.

OrthoCash 2020
Which of the following fracture patterns would be most appropriately treated with open reduction and internal fixation with posteromedial and lateral plates via dual incisions?

The patient in Figure D has a bicondylar tibial plateau fracture with a posteromedial fracture fragment, which is an indication for lateral and posteromedial plating via dual incisions.
Bicondylar tibial plateau fractures are typically treated with open reduction internal fixation. Studies have shown that the posteromedial fragment is common in bicondylar tibial plateau fractures. Standard lateral implants do not gain adequate screw purchase in posteromedial bone. Posteromedial incisions using the interval between the semimembranosus and medial head of the gastrocnemius can be used to gain access to the fragment and provide exposure to place a posteromedial plate.
Barei et al. reviewed 57 OTA C-type bicondylar tibial plateau fractures, and found the presence of a posteromedial fragment in 74% of cases. They suggest
the use of alternate methods of fixation for the posteromedial fragment rather than lateral fixed-angle plates alone.
Higgins et al. reviewed 111 patients with bicondylar tibial plateaus that underwent CT scan evaluation. They found the incidence of a posteromedial fragment in 59% of the patients and on average accounted for 25% of the articular surface.
Barei et al. reviewed 83 patients treated with dual incisions for fixation of bicondylar tibial plateau fractures. They found deep infections in 8.4% of patients. Satisfactory articular reduction was found in 62% of patients, satisfactory coronal alignment in 91% of patients, satisfactory sagittal alignment in 72%, and satisfactory condylar width in 98%.
Figure A shows an AP and lateral radiograph of a split/depressed lateral tibial plateau fracture. Figure B shows an AP and lateral radiograph of a proximal third tibial shaft fracture with a proximal fibula fracture. Figure C shows an AP and lateral radiograph of a medial plateau fracture with articular depression. Figure D shows an AP and lateral radiograph of a bicondylar tibial plateau fracture. Figure E shows an AP and lateral radiograph of a tibial tubercle fracture in a tibia with open physes.
Incorrect Answers:
OrthoCash 2020
Figure A shows the radiographs of a 87-year-old patient after a fall from standing. He lives in a nursing home and uses a walker to transfer from bed to chair. His past medical history includes recurrent urinary tract infections, congestive heart failure, angina and diabetes. Which of the following factors is associated with the best postoperative outcome in this patient?

Immediate surgical intervention
Postoperative epidural analgesia
Postoperative antibiotics
Pre-operative medical optimization
Choosing total hip arthroplasty instead of hemiarthroplasty Corrent answer: 4
Geriatric patient with hip fractures tends to have a number of coexisting medical conditions that impact surgical risk. A successful pre-operative medical evaluation has the greatest impact on surgical outcomes in this patient population.
Patients with complex past medical histories are at great risk of complications with surgery. This helped to drive the formation of the ASA classification system as a way to score patients out of 5 based on their anesthetic and surgical risks. Patients with significant systemic disease (ASA III and IV) have shown to demonstrate poorer outcomes as compared to patients with less severe medical comorbidities (ASA I and II).
Egol et al. looked at factors that impact the outcomes of hip fractures in geriatric patients. They showed that cardiac and pulmonary complications were most frequent complications post-operatively. It was stated that early mobilization and pre-operative evaluations have the greatest impact on outcomes.
Parvizi et al. looked at the thirty-day mortality following hip arthroplasty for acute fracture. They reviewed a database of 7774 consecutive patients that underwent hip arthroplasty for the treatment of an acute fractures. The overall mortality was 2.4%. Risk factors were found to be cemented implants, female patients, elderly patients, and patients with cardiorespiratory comorbidities.
Roberts et al reviewed the 2015 AAOS Clinical Practice Guideline: Management of Hip Fractures in the Elderly. Although pre-operative medial optimization was not mentioned in this review, there is strong evidence to support an interdisciplinary care program for patients with hip fractures.
Figure A shows a displaced left femoral neck fracture. Incorrect Answers:
more than 24-48 hours and a higher 1-year mortality rate. However, In patients with with more than 3 medical comorbidities, medical optimization has a greater impact on post-operative outcomes than time to surgery.
OrthoCash 2020
A 36-year-old male sustains severe injuries as a result of a motor vehicle collision. After 5 days, the patient is stabilized and transferred to your facility for continued management. After obtaining appropriate imaging, including the images shown in Figures A, B and C the patient should be given which of the following mobility restrictions?

Touch-down weight bearing on the left lower extremity, non-weightbearing on the right lower extremity
Weight bearing as tolerated on the left lower extremity, non-weightbearing on the right lower extremity
Non-weight bearing on the left lower extremity, non-weightbearing on the right lower extremity
Touch-down weight bearing on the left lower extremity, weight bearing as tolerated on the right lower extremity
Weight bearing as tolerated on the left lower extremity, weight bearing as tolerated on the right lower extremity
Figures B and C shows a stable, impacted lateral compression (LC) type I injury, which can be treated with immediate mobilization without restrictions. The right lower extremity has a pilon fracture, which should be treated with non-weight bearing.
LC-I injuries are stable patterns, as they involve an impaction injury to the anterior sacrum, which has some inherent stability. In addition, the posterior sacro-iliac (SI) soft tissue structures remain intact, which provides critical stability during immediate mobilization.
The reference by Tile is a review article on the principles of management of these injuries, and he reviews how the Tile classification system is important to help determine surgical need and where the stabilization is required. For the stable LC-1 type injury, no fixation is required.
Incorrect Answers:
OrthoCash 2020
A 24-year-old male sustains the fracture dislocation shown in Figure A. How is this fracture pattern best classified?
Moore I
Moore II
Schatzker III
Schatzker V
OTA type 41B3 Corrent answer: 2
Figure A shows a Moore Type II fracture. Moore type II fractures consist of fractures involving the entire tibial condyle, where the fracture line begins in the opposite compartment and extends across the tibial eminence.
A number of classification systems are used to describe tibial plateau fractures. The main classification systems that are widely used include Schatzker, AO/OTA, Hohl and Moore. The Moore classification describes high energy fracture-subluxation injuries of the knee. This is thought to have clinical implications as the type of fracture pattern can indicate an associated soft-
tissue injury.
Moore retrospectively reviewed over a 1000 proximal tibia fractures to devise a classification systems based on the characteristic of five types of tibia plateau fracture patterns. He believed this system helped to better understand knee instability and concomitant soft-tissue injury. For example, Moore Type III fractures (rim avulsion) are associated with a high rate of neurovascular injury.
Figure A shows a fracture involving the entire tibial condyle. Illustration A shows a schematic diagram of the Moore classification (I - V). Illustration B shows a table that describes the Moore classification (I - V).
Incorrect Answers:

OrthoCash 2020
A 19-year-old male football player plants and twists his right lower extremity sustaining a spiral fracture of his distal third tibial shaft. Of the following images, which is most commonly associated with distal third spiral tibial shaft fractures.

The patient has a spiral distal tibial shaft fracture. Spiral distal tibial shaft fractures are commonly associated with intraarticular fracture extension, usually in the form of a posterior malleolus fracture.
Spiral distal third tibial shaft fractures need to be evaluated for intraarticular extension prior to operative management. As this can be missed on x-rays, a CT scan of the ankle is recommended to identify this associated injury. This is important when intramedullary fixation is used for definitive management, as nail insertion can displace a previously non displaced intraarticular fracture.
Anteroposterior screw fixation prior to nailing may be useful in these cases.
Boraiah et al. found that in 62 patients with spiral distal tibial fractures, 39% (24 patients) had a posterior malleolus fracture. They recommended CT evaluation of the ankle to prevent missed intraarticular fractures.
Hou et al. found a posterior malleolus fracture in 9.7% (28 out of 288 cases) of patients with tibial shaft fractures. They recommended CT or MRI evaluation of the ankle prior to surgery.
Figure A shows an axial CT scan of a right ankle with a posterior malleolus
fracture. Figure B shows an AP radiograph of a right ankle with a vertical medial malleolus fracture. Figure C shows a coronal CT scan of a right ankle with a Tillaux fracture. Figure D shows a sagittal CT scan of a right ankle with a comminuted talus fracture. Figure E shows a lateral radiograph of a right knee showing a knee dislocation. Illustration A shows an AP radiograph of a left distal third spiral/oblique tibial shaft fracture. Illustration B shows a lateral radiograph of a left distal third spiral/oblique tibial shaft fracture. Illustration C shows a sagittal CT of a distal third spiral/oblique tibial shaft fracture with a posterior malleolus fracture.
Incorrect Answers:

OrthoCash 2020
A 67-year-old female patient presents with increasing right hip/thigh pain over the past three months, which is now recalcitrant to anti-inflammatories. There is no history of trauma or constitutional symptoms. Her past medical history consists of hypertension, coronary artery disease, osteoporosis and gastric reflux. Physical examination reveals mild pain at the extremes of range of motion of the hip and a painful right sided limp. A radiograph of the right hip is seen in Figure
What would be the most appropriate treatment for this patient at this time?

Observation only
Referral to physiotherapy
MRI spine and hip
Total hip arthroplasty
Intramedullary femoral nail Corrent answer: 5
This osteoporotic female patient is presenting with subtrochanteric lateral cortical thickening and hip pain. This is consistent with an insufficiency fracture of the femur secondary to use of bisphosphonate medication for treatment of osteoporosis. The most appropriate treatment would be intramedullary femoral nail fixation.
Bisphosphonate medications have been shown to be associated with atypical (subtrochanteric) femur fractures. These patients often have prodromal hip pain and lateral cortical thickening on radiographs prior to fracture. In addition, there has shown to be a significantly increased risk of fracture in the presence of the “dreaded black line” that occurs at the site of thickening.
Lenart et al. examined a case series of patients using bisphosphonates for the treatment of osteoporosis. They identified 15 postmenopausal women who had
been receiving alendronate for a mean (±SD) of 5.4±2.7 years and who presented with atypical low-energy fractures. Cortical thickening was present in the contralateral femur in all the patients with this pattern.
Goh et al. retrospectively reviewed patients who had presented with a low-energy subtrochanteric fractures. They identified 13 women of whom nine were on long-term alendronate therapy. Five of these nine patients had prodromal pain in the affected hip in the months preceding the fall, and three demonstrated a stress reaction in the cortex in the contralateral femur.
Figure A shows a right hip radiograph with subtrochanteric lateral cortical thickening. There is mild arthritic changes in the hip. Illustration A shows a bone scan and radiographs of subtrochanteric lateral cortical thickening that resulted in fracture.
Incorrect Answers

OrthoCash 2020
A right-hand dominant female sustains a right proximal humerus fracture. The patient is provided a sling, and is recommended pendulum exercises with elbow range of motion to begin in 1 to 2
weeks. Which of the following would be an indication for surgical management?

Age greater than 70 years.
Fracture pattern in Figure A
Significant medical comorbidities.
Fracture pattern in Figure B
Fracture pattern in Figure C
The patient has been treated with non-operative management for her proximal humerus fracture. Operative management should be considered in patients with head splitting proximal humerus fractures and in those with dislocations that cannot be reduced.
Head splitting proximal humerus fractures should be treated with operative management. Open reduction internal fixation versus hemiarthroplasty are used to treat this type of fracture. Surgical management is also considered in proximal humerus fractures in young patients, in fractures where the greater tuberosity is displaced >5 mm, and in proximal humerus fractures associated with humeral shaft fractures.
Koval et al. studied 104 patients with one-part proximal humerus fractures treated non-operatively, and found 80% with good or excellent results. They also found that 90% of patients treated non-operatively had either no or mild pain about the shoulder at follow-up.
Lefevre-Colau et al. performed a randomized prospective study on 74 patients with an impacted proximal humerus fracture. One group was treated with early mobilization of the shoulder (within 3 days after the fracture) while the other group was immobilized for 3 weeks followed by physiotherapy. They concluded that early mobilization was safe and allowed for quicker return to functional use of the affected limb.
Figure A shows an AP radiograph of a right minimally displaced greater tuberosity proximal humerus fracture. Figure B shows AP and axillary radiographs of a right head split proximal humerus fracture that is posteriorly dislocated. Figure C shows an AP radiograph of a right minimally displaced Salter Harris II proximal humerus fracture. Illustration A shows an AP radiograph of a left valgus impacted proximal humerus fracture with a greater tuberosity fragment displaced >5mm treated with ORIF.
Incorrect Answers:

OrthoCash 2020
A 37-year-old male arrives to the trauma slot following a high-speed motorcycle crash. His Glasgow Coma score is 14 and his only orthopaedic injury is exhibited in Figure A. His current vital signs are a BP of 90/60, HR 120, and a lactate of 2.5 mMol/L. Other findings include a grade 1 splenic laceration and bilateral pulmonary contusions seen on chest radiograph. Which of the following has been suggested as an indication to perform damage control orthopedic care?

HR >110
Bilateral pulmonary contusions seen on chest radiograph
SBP = 90mmHg
Unilateral femur fracture
Lactate = 2.5 mMol/L
Pulmonary contusion severe enough to be diagnosed on chest radiograph alone is an indicator that the patient may benefit from damage control orthopaedics (DCO).
Despite the patient's overall stable nature, suffering pulmonary injury severe enough to be seen on x-ray alone suggests that temporary stabilization with staged definitive fixation may avoid potential morbidity.
Pape et al. review the evolution and balance of early total care (ETC) and DCO. Summarizing the literature, the authors report several standalone indicators that would justify DCO regardless of stable status. This includes: Injury Severity Score of greater than 40, Injury Severity Score of greater than 20 with chest trauma, multiple injuries with severe pelvic/abdominal trauma/ hemorrhagic shock, bilateral femoral fractures, pulmonary contusion noted on radiographs alone, hypothermia of less than 35 degrees C), and a head injury with an Abbreviated Injury Score of 3 or greater.
Figure A exhibits a right femoral shaft fracture. Illustration A exhibits a summarized table stating the criterion used to determine the condition of a polytrauma patient. (Table from Pape et al, PMID: 19726738)
Incorrect answers:
implement DCO.
OrthoCash 2020
A 24-year-old patient presents after a fall from the balcony of a third story building in which he landed on his feet. He reports lumbar back pain and numbness in his perineum region. Radiographs of his hips and pelvis are seen in Figure A, while CT images are shown in Figures B and C. How is this fracture pattern best classified?

Young-Burgess APC Type II
Young-Burgess LC Type I
"U" Type Spinopelvic Dissociation
Denis Zone-I
Denis Zone-II
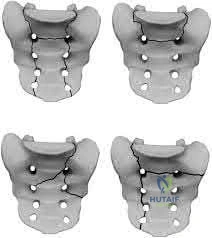
This patient has a Denis zone-III "U" Type Spinopelvic Dissociation of the sacrum.
The Denis classification system for sacral fractures is based on anatomical fracture zones. Zone-III fractures involve the spinal canal and have a high rate of associated neurologic injury. It is important to recognize bilateral sacral
fractures with a transverse component, as this often causes spinopelvic discontinuity and possible cauda equina. The lack of mechanical continuity between the spine and pelvis will most likely require reduction and fixation for initial stability. There may also be a need for sacral decompression with fixation mechanisms given the onset of neurologic symptoms.
Mehta et al. reviewed sacral fractures. They report that patients with a transverse sacral fracture involving more proximal sacral segments (S1, S2, or S3) tend to have a higher prevalence of bladder dysfunction than do those involving distal sacral segments (S4 or S5).
Schildhauer et al. report the best way to visualize Denis zone-III "U" type fractures is to obtain a lateral view of the sacrum or sagittal reformatted images with a CT scan. Standard pelvic radiographs often miss this injury.
Figure A shows an AP pelvis with suggestion of sacral irregularities. No fracture pattern can be indentified. Figures B and C show CT scan images showing a "U" Type fracture pattern with angulation and translational displacement of the cephalad and caudad parts of the sacrum. Illustration A shows examples of complex sacral Denis zone-III fractures.
Incorrect Answers:
OrthoCash 2020
A 55-year-old male presents with the radiographs seen in Figures A and B after falling off his bike. Physical examination reveals an isolated, closed elbow injury. His limb is neurovascularly intact. Which complication would be most likely with surgical fixation of this injury?

Ulnar neuropathy
Posterior interosseous nerve injury
Early loss of fixation
Elbow flexion contracture
Avascular necrosis
This patient is presenting with a comminuted capitellar and trochlear fracture. If treated with open reduction internal fixation, the most likely post-operative complication would be elbow stiffness or contracture.
An axial compression force transmitted by the radial head to the capitellum with the elbow in a semiflexed position can result in a shear fracture of the anterior portion of the capitellum. AP, lateral, and radiocapitellar radiographs are recommended to identify these injuries. The lateral X-ray may reveal the “double arc” sign, which represents extension of the capitellum fracture into the trochlea. Extension of the fracture into the trochlea has important implications into the surgical approach to these injuries.
Ruchelsman et al. retrospectively reviewed the outcomes of sixteen patients with capitellar fractures treated with open reduction internal fixation. They found the presence of greater flexion contractures at the time of follow-up in elbows with Type-IV capitellar fractures. All fractures healed, and no elbows had instability or weakness with fixation.
Ring et al. retrospectively reviewed the outcomes of twenty one distal humerus articular fractures that were reduced and stabilized with implants buried beneath the articular surface. Ten patients required a second operation: (6) release of an elbow contracture; (2) treatment of ulnar neuropathy; (1) removal of hardware; (1) early loss of fixation.
Figures A and B show AP and lateral radiographs of the elbow with a comminuted fracture of the capitellum and trochlea. Note the “double arc” sign on the lateral view. Illustrations A and B show open reduction internal fixation of the fracture. Note fixation with multiple interfragmentary screws.
Incorrect Answers:

OrthoCash 2020
Figure A shows a radiograph of a 30-year-old male who underwent fixation of a left leg injury just over two years ago. He presents with persistent pain and drainage from the distal wound despite 4 months of oral antibiotics. He has no systemic symptoms. He has a past medical history of Grave's disease and Irritable Bowel Syndrome. What would be the best management at this stage?

Chronic suppressive, culture-directed, antibiotic therapy
Above knee amputation
Endocrine consultation, irrigation and debridement, removal of hardware and negative-pressure wound therapy
Irrigation and debridement, removal of hardware, over-reaming medullary canal, external fixation and culture-directed antibiotics
Irrigation and debridement, retention of hardware, acute bone grafting and culture-directed antibiotics
This is a case of fracture nonunion in the setting of chronic osteomyelitis and infected hardware. The best treatment option available would be irrigation and debridement, removal of hardware, ring external fixator and culture directed antibiotics.
The management of infected nonunion in the setting of chronic osteomyelitis is technically demanding. The aims of treatment are to eradicate the infection and obtain bone union. Non-surgical options are largely unsuccessful in patients with draining chronic osteomyeltis in the setting of infected hardware and nonunion. Surgical options involve incision and debridement of necrotic tissue followed by reconstruction of bone and possible soft tissue (to provide
healthy viable coverage). The most common techniques are ringed fixator/circular frames, staged intramedullary device with or without external fixator, free tissue transfer, or radical debridement, bone grafting, and fixation.
Motsitsi et al. reviewed the management of infected nonunion of long bones. They suggest that the Ilizarov technique is regarded as a standard treatment in infected nonunion of the tibia. When there is bone defect after debridement, the bone can be shortened or treated with bone transport.
Egol et al look at a series of patients with chronic osteomyelitis. Limb salvage should be attempted in all patients. The presence of a chronic draining sinus requires surgical debridement and culture directed antibiotics. Infected hardware should be removed. A two-stage strategy is the best and well-proven treatment option.
Figure A shows a intramedullary nail in the left tibia. There is a moderate amount of bone loss at the fracture site with mixed sclerotic bone suggestive of osteomyelitis.
Incorrect Answers:
OrthoCash 2020
A 32-year-old male sustained the injury seen in Figure A after a motor vehicle accident. Which of the following factors is most predictive of mortality with this type of injury?

Fracture classification
Number of blood transfusions in the first 24 hours
Gender
Time to operative fixation
Use of pelvic binders Corrent answer: 2
The best predictors of mortality with pelvic ring fractures include older age and hemodynamic shock at presentation. The amount of blood transfused indicates the severity of hemodynamic instability.
Pelvic ring fractures are typically high energy, blunt injuries. The leading cause of mortality with these injuries is hemorrhage and hemodynamic instability.
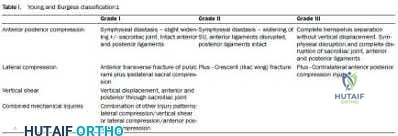
The most common source of hemorrhage include venous injury (80%), which is usually caused by a shearing injury of posterior thin walled venous plexus and bleeding cancellous bone. Other sources of hemorrhage include arterial injury (10-20%) from the superior gluteal artery (posterior ring injury, anterior posterior compression [APC] pattern), internal pudendal artery (anterior ring injury, lateral compression [LC] pattern) and obturator artery.
Smith et al. found fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased Injury Severity Scores (ISS) scores. Deaths were most commonly from exsanguination (<24 hours) or multiorgan failure (>24 hours).
Starr et al. demonstrated that age and shock on presentation were most predictive of mortality after pelvic ring injury.
Figure A shows a APC III pelvic fracture. Illustration A shows a table describing the Young-Burgress classification of pelvic ring fractures.
Incorrect Answers:
OrthoCash 2020
Figure A shows intraoperative radiographs of a 45-year-old patient with a left elbow injury. What would be the next most appropriate step in this patients care?

Early range of motion
Hinged elbow brace for 4 weeks
Repair lateral collateral ligament
Remove and upsize implant
Remove and downsize implant Corrent answer: 5
The intraoperative images are consistent with overstuffing of the ulnohumeral joint during a radial head replacement. The most appropriate next step would be removing and downsizing the implant.
Overstuffing the radiohumeral joint by >2.5 mm can significantly alter elbow kinematics. It has also shown to lead to pain and early joint disease. The most sensitive method to assess for overstuffing of the joint is by direct visualisation intra-operatively. This can be performed by visualising the lateral aspect of the ulnohumeral joint when the radial head is resected and comparing this to when the trial radial head is reduced in place. In comparison, radiographic asymmetry of the medial ulnohumeral joint has been shown to be less sensitive. Radiographic findings of incongruity of ulnohumeral joint only occurs when significant overlengthening of the radius occurs.
Frank et al. examined the effect of radial head thickness in seven cadaver specimens. They found that incongruity of the medial ulnohumeral joint would only become apparent radiographically after overlengthening of the radius by
>or=6 mm.
Doornberg et al. examined seventeen computed tomography scans of the elbow to investigate the height of the radial head relative to the lateral edge and central ridge of the coronoid process. They found that the radial head was on average only 0.9 mm more proximal than the lateral edge of the coronoid process.
Figure A shows intraoperative radiographs of a patient that has undergone a radial head arthroplasty. There is significant widening of the medial ulnohumeral joint on an AP radiograph as well as widening of the ulnohumeral joint on the lateral radiograph,
Incorrect Answers:
OrthoCash 2020
Aside from improving the intramedullary nail starting point in Figure A, the use of blocking screws could have been used at the time of fixation to prevent this post-operative deformity. What would have been the correct orientation of these screw(s) in the proximal fragment?

Medial only
Lateral only
Anterior and medial
Posterior and medial
Posterior and lateral Corrent answer: 5
The clinical presentation is consistent with a malunion of a proximal one-third tibia fracture with a valgus and procurvatum deformity. The correct orientation of Poller blocking screws to help prevent this malalignment would be in the posterior and lateral aspects of the metaphyseal fragment.
Insertion of the blocking screw lateral to the nail prevents valgus deformity, and insertion of the blocking screw posterior to the nail prevents apex anterior deformity. A more lateral starting point for nail insertion can also help to
prevent valgus deformity. The semiextended position of the knee for nail insertion also helps to eliminate the tendency for the fracture to flex, due to the avoidance of excessive knee flexion during the reduction.
Stedtfeld et al. describes the mechanical model for blocking screws. They state that two or more blocking screws can be placed in each plane (AP and lateral) alongside the nail to create a narrow canal for the nail. This allows for multiple points of fixation and realignment of the bone as the nail is passed.
Lindvall et al looked at a series of 56 extra-articular proximal tibial fractures treated with intramedullary nailing or percutaneous locked plating. Neither nailing or plating these fractures showed a distinct advantage in the overall outcomes. Apex anterior malreduction however was the most prevalent form of malreduction in both groups.
Lang et al. looked at a series of proximal third tibia fracture treated with intramedullary nailing. They reported that posterior tibial comminution will also contribute to apex anterior angulation. They states this occurs when the fracture hinges on the intact cortex anteriorly during nail insertion.
Figure A shows a proximal one third tibia fracture treated with an intramedullary nail. There is malreduction of the fracture with valgus and procurvatum deformity.
Incorrect Answers:
OrthoCash 2020
When evaluating a fracture dislocation of the elbow, a varus and posteromedial rotation mechanism of injury typically results in what injury pattern?
A fracture of the radial head requiring ORIF
A highly comminuted radial head fracture requiring radial head arthroplasty or resection
An MCL injury requiring repair
A type I avulsion fracture of the coronoid
An anteromedial coronoid fracture
A varus and posteromedial rotation mechanism of injury typically results in a fracture of the anteromedial facet of the coronoid which frequently requires reduction and fixation to restore stability.
A varus and posteromedial mechanism of injury about the elbow presents with an injury pattern distinctly different from other injury patterns. A key part of treating this injury pattern is recognizing a fracture of the anteromedial facet of the coronoid, which often requires reduction and fixation to restore stability about the elbow. It is important to recognize this during preoperative planning since this injury typically requires a medial approach.
Steinman presents a review article describing coronoid fracture patterns and their mechanisms of injury.
Doornberg and Ring present a level 4 review showing that coronoid fracture patterns and their required treatments are predictable based on mechanism of injury. Varus and posteromedial mechanisms were found to reliably create a fracture of the anteromedial facet of the coronoid, and were associated with sparing of the MCL and radial head.
Doornberg and Ring also presented a Level 3 review of anteromedial facet cornoid fractures. They found that they could not be adequately visualized and treated from a lateral approach, and that they typically required reduction and fixation to restore adequate stability to the elbow. This stresses the importance of recognizing this injury pattern during preoperative planning.
Illustrations A and B are AP and lateral radiographs of an elbow following a varus/posteromedial injury with an anteromedial coronoid facet fracture.
Illustration C is a diagram demonstrating fracture lines that create an anteromedial facet fracture fragment. This fracture can be subclassified into three subtypes [anteromedial rim (a), rim plus tip (b), and rim and tip plus the sublime tubercle (c)]
Incorrect answers:

OrthoCash 2020
A 26-year-old female presented to the emergency department with the injury seen in Figure A after an awkward fall while intoxicated. She undergoes closed reduction and repeat radiographs are seen in Figure B. After a normal physical examination, including ranging the hip from 0-90 degrees, which of the following options would be the next most appropriate step in management?

Femoral skeletal traction
CT scan
Hip spica cast application
Observation only
Serial neurovascular examinations Corrent answer: 2
This patient has presented with a posterior left hip dislocation. The next most appropriate step would be performing a post-reduction CT scan to assess for joint reduction and congruity, associated fractures, or loose bodies.
Hip dislocations occur most commonly in young patients with high energy trauma. They are usually classified as simple or complex, with complex dislocations being those with associated fractures of the acetabulum or proximal femur. Urgent close reduction should occur within 6 hours from the time of injury. Post reduction CT scans must be performed for all traumatic hip dislocations to look for fractures or impacted areas of the femoral head or acetabulum, as well as incongruent reductions and free intra-articular joint fragments.
Calkins et al. looked at measurements of the posterior acetabulum on CT scans (the Acetabular Fracture Index) after hip dislocations to evaluate for hip stability. Hips were found to be unstable if less than 34% of the remaining posterior acetabulum was present after dislocation. Hips with greater than 55% were stable. In between 34 and 55% were indeterminate.
Moed et al. found that posterior wall fractures involving less than 20% of the posterior wall were considered stable. Fractures involving more than 40%-50% were unstable, leaving a wide range of posterior wall fractures classified as indeterminate.
Figure A shows a left posterior hip dislocation. Figure B shows a reduced left hip with no obvious fracture. Illustration A shows an axial CT scan image of the left hip. There is no acetabular fracture identified.
Incorrect Answers:

OrthoCash 2020
A 40-year-old male sustained the injury seen in Figure A, and subsequently underwent the procedure shown in Figure B. One hour post-operatively he starts to complain of pain in the operative leg, and the pain is unchanged with active or passive stretch. The external dressing is released with little resolution of symptoms. His blood pressure is 115/78 mm Hg with compartment pressures in the leg measuring 31 to 35 mm Hg. His ABI index is 1.1 in the leg. What would be the next step in management?

MRI angiography of leg
Four-compartment fasciotomy
Follow-up examination the following day
Continued monitoring and serial examinations
EMG study
The patient is at risk for developing compartment syndrome of the leg. The next most appropriate step would be to support his systemic blood pressure and monitor compartment pressures.
A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam. An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) <30 mm Hg may help to confirm the necessity for fasciotomy. However, the treatment of early compartment syndrome should be to initially improve the limbs perfusion pressure gradient. This can be done by treating underlying factors such as hypotension, coagulopathy, or vascular compromise due to either a true vascular injury or artificially by external compression. Frequent reassessment is then critical to effectively manage these patients. If clinical
diagnosis persists despite these efforts, urgent fasciotomy would be considered.
McQueen looked at 116 patients with tibial diaphyseal fractures who had continuous monitoring of anterior compartment pressure for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of 30 mmHg is a more reliable indicator of compartment syndrome.
White et al. looked at 101 patients with tibial fractures with satisfactory Delta P measurements. THey found that patients with elevated intramuscular pressures >30 mm Hg after tibial fracture do not have a greater incidence of complications than those with low pressures, so long that Delta P <30 mm Hg.
Figure A shows a Shatzker V tibial plateau fracture. Figure B shows fixation of fracture seen in Figure A.
Incorrect Answers:
OrthoCash 2020
A 10-year-old girl suffers a displaced tibia fracture. Initial numbness over the dorsum of the the foot resolved following an anatomic closed reduction and placement in a long leg cast performed in the emergency room. The cast was placed with the the ankle dorsiflexed just above neutral to prevent equinus contracture and then the cast and padding was adequately bivalved. Overnight, the patient began experiencing recurrent numbness and paresthesias in her exposed toes and a slight increase in her pain at the fracture site. Your next best step would be:
Repeat closed reduction under conscious sedation
Selective compartment fasciotomies
External fixation and compartment monitoring
compartment fasciotomies with fracture fixation done emergently
Modify the cast to reposition the ankle into slight plantarflexion Corrent answer: 5
Circumferential casting with the ankle dorsiflexed can cause increased intracompartmental pressures in the leg. However, this patient's cast has been adequately bivalved during initial cast placement. Therefore, the next best step is cast modification to allow the ankle to assume an angle between neutral and 30 degrees of plantar flexion and further reducing the compartment pressure.
Tibia fractures are one of many common underlying etiologies for the development of compartment syndrome in the leg. Fracture reduction as well as eliminating circumferential dressings are important early preventative steps to take. Bivalving casts - including splitting the cast padding - is often indicated in fractures of long bones that are treated with initial casting. While casting patients in a plantigrade or dorsiflexed position reduces the risk of equinus contractures and holds the ankle mortise reduced, dorsiflexing the ankle has been shown to increase the intracompartmental pressures throughout the leg compartments.
Weiner et al. placed pressure monitors into the anterior and deep posterior compartments in healthy volunteers to measure the effects of casting on compartment pressures. They found that the intramuscular pressures were lowest with the ankle positioned between plantigrade and a resting plantar flexion position (0-37 degrees), and that bivalving the cast reduced the pressures 33-47%.
Illustration A shows the needle trajectories for compartment pressure monitoring in the leg. This should be performed within 5 cm of the fracture to get accurate peak pressures.
Incorrect Answers:
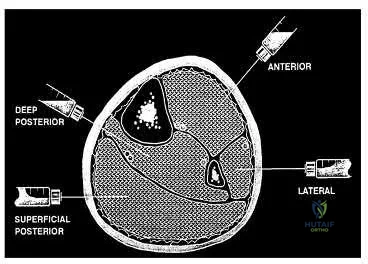
OrthoCash 2020
A 35-year-old male horseback rider was bucked into the air and then landed forcefully with his perineum on the saddlehorn of the saddle. At a one year follow-up, the only long term sequela of his injuries is erectile dysfunction. Which radiographic injury seen in Figures A-E is most commonly associated with this complication?

This patient has sustained a saddle-horn injury to the pelvis. An anterior posterior compression (APC) injury is the most common pelvic injury associated with this mechanism.
Saddle-horn injury to the pelvis occurs when a horseback rider is bucked into the air and then lands forcefully with his or her perineum on the saddlehorn of the saddle. The bony injury to the pelvis usually consists of a diastasis of the pubic symphysis with/without subsequent widening of the sacroiliac joints. The
majority of patients are able to return close to their pre-injury level of employment and activity after these injuries. However, sexual dysfunction is a common complication with this injury. Sexual dysfunction can be due to urethral, vascular, neurologic, and psychogenic injuries.
Collinge et al. looked at a series of male patients with injuries to the perineum after coming into contact with the saddle or saddle horn on a horse. Eighteen of the twenty patients were found to have sexual dysfunction at the time of the latest follow-up. A multi-disciplinary approach to these patients is needed when treating pelvic injuries.
Cannada et al. surveyed 71 women of childbearing age who had a pelvic fracture. She found that half the patients reported physical genitourinary complaints with 38 percent of women noting new onset pain with intercourse. In terms of psychological impact, they showed that 45 percent of patients answered affirmatively to decreased interest in intercourse and decreased orgasm frequency after the injury.
van Nieuwenhoven et al. describe three equestrians who suffered from straddle injuries with symphysis diastasis and rupture of sacroiliac ligaments after falls or kicks from horses. They show that these presumed low-energy injuries can cause extremely severe injuries to the pelvis itself and to the adjacent organs.
Figure A shows a Burgess APC Type II pelvic fracture. Figure B shows left ASIS avulsion fracture. Figure C shows a left hip dislocation. No pelvic fracture is identified. Figure D shows a subacute superior/inferior pubic rami fracture.
Figure E shows a right femoral neck fracture.
Incorrect Answers:
OrthoCash 2020
A 31-year-old male driver was involved in a high-speed motor vehicle accident. His injuries include a left subdural hematoma (Abbreviated Injury Score [AIS]=4), left segmental femur fracture (AIS=3), ruptured spleen (AIS=4), nasal fracture (AIS=2), fractured left ribs 4 to 7 (AIS=2), and a closed pelvic ring fracture (AIS=3). What is his Injury Severity Score (ISS)?
Question 57
An active 36-year-old woman with rheumatoid arthritis has continued forefoot discomfort despite the use of orthotics and shoe wear modifications. A radiograph and a clinical photograph are shown in Figures 26a and 26b. Treatment at this point should consist of
Explanation
REFERENCES: Ouzounian T: Rheumatoid arthritis of the foot & ankle, in Myerson MS (ed): Foot & Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 2, pp 1189-1204.
Mann RA, Thompson FM: Arthrodesis of the first metatarsophalangeal joint for hallux valgus in rheumatoid arthritis. J Bone Joint Surg Am 1984;66:687-692.
Coughlin MJ: Rheumatoid forefoot reconstruction: A long-term followup study. J Bone Joint Surg Am 2000;82:322-341.
Question 58
A 42-year-old woman has a history of nontraumatic ankle swelling with tenderness over the Achilles tendon and plantar fascia. She reports that while vacationing in Connecticut 2 months ago she noted the presence of a “red bull’s eye” rash. Management should consist of
Explanation
REFERENCES: Neu HC: A perspective on therapy of Lyme infection. Ann NY Acad Sci 1988;539:314-316.
Faller J, Thompson F, Hamilton W: Foot and ankle disorders resulting from Lyme disease. Foot Ankle 1991;11:236-238.
Question 59
Figures 32a and 32b show the radiographs of an active 13-year-old boy who has persistent left thigh pain and a limp despite a trial of protected weight bearing. Management should consist of
Explanation
REFERENCES: Walker RN, Green NE, Spindler KP: Stress fractures in skeletally immature patients. J Pediatr Orthop 1996;16:578-584.
Arata MA, Peterson HA, Dahlin DC: Pathological fractures through non-ossifying fibromas: Review of the Mayo Clinic experience. J Bone Joint Surg Am 1981;63:980-988.
Question 60
below depict the AP and lateral radiographs obtained from a year-old man with long-standing right knee osteoarthritis and pain that is unresponsive to nonsurgical treatment. The patient undergoes navigated cruciate-retaining right total knee arthroplasty. After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office reporting continued pain 2 years after surgery. He describes instability, particularly when descending stairs. On examination, range of motion of 0° to 120° is observed, with no extensor lag. Slope of the tibial component is 7°. The knee is stable to varus and valgus stress in extension, but flexion instability is present in both the anterior-posterior direction and the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection work-up is negative. What is the most appropriate surgical intervention at this time?
Explanation
The patient’s symptoms at follow-up—pain, swelling, and difficulty descending stairs—suggest knee flexion instability. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant (depending on the condition of the ligaments) likely is needed to address his symptoms. The difference in extension stability and flexion stability makes polyethylene exchange a poor option. A constrained rotating hinge design is not necessary. Repeat use of a PCL-retaining insert is not recommended. Tibial and femoral revision both are required. Correction of excessive slope will be attained with tibial revision, femoral component revision is required to convert to a PCL-substituting design. There is also an opportunity to increase posterior condylar offset if needed.
Question 61
…A 56-year-old podiatrist with a negative past medical history had anterior knee pain after an injury. His radiographs, CT scan, and T1-weighted sagittal and fat-saturated axial MR images are shown in Figures 15a through 15e, respectively. After arthroscopic partial medial menisectomy, the patient was turned to the prone position and an open posterior arthrotomy and excision was performed. Low-power and high-power hematoxylin and eosin stained histologic specimens are shown in Figures 15f and 15g, respectively. Based on the history, radiographs, CT scan, MRI scans, and histologic findings, what is the most likely diagnosis?
Explanation
Figures 16a and 16b are the right femur radiographs of a 59-year-old man who has severe pain in his right distal thigh and knee with no significant trauma and an inability to bear weight. Blood tests demonstrate anemia, serum protein electrophoresis/urine protein electrophoresis findings are negative, and electrolyte levels are within defined limits.


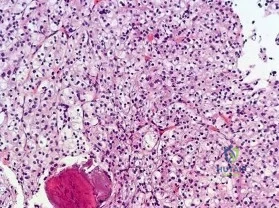
Question 62
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior-stabilized TKA without evidence of component loosening. What is the recommended treatment for this patient?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor
mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful total knee arthroplasty.
Question 63
A 40-year-old man who is an avid weight lifter has had chronic pain in the proximal anterior shoulder for the past year. He denies any history of trauma. Examination reveals tenderness at the intertubercular groove, a positive speed test, and a positive Neer impingement sign. Nonsurgical management has failed to provide relief, and he is now considering surgery. Arthroscopic findings in the glenohumeral joint are shown in Figure 31. Based on these findings, treatment should consist of
Explanation
REFERENCES: Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310.
Burkhead WZ, Arcand MA, Zeman C, et al: The biceps tendon, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1996.
Question 64
Figure 32 shows the radiograph of a laborer who jammed his thumb in a fall. Examination reveals pain at the base of the thumb and proximal thenar eminence region. Management should consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
Howard FM: Fracture of the basal joint of the thumb. Clin Orthop 1987;220:46-51.
Question 65
A 75-year-old woman reports persistent severe low back pain after lifting a bag of groceries 8 weeks ago. She denies the presence of any lower extremity pain, weakness, or other symptoms. AP and lateral lumbar spine radiographs are shown in Figures 47a and 47b. For further evaluation, what imaging study should be obtained next? Review Topic
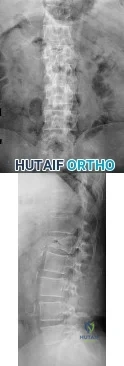
Explanation
Question 66
below demonstrate the radiographs obtained from a year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. A further work-up reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MRI with MARS. Revision THA is recommended. The most common complication following revision of a failed metal-on- metal hip arthroplasty is
Explanation
Question 67
On MRI, a nonsanguinous effusion has what appearance?
Explanation
REFERENCES: Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
White EM: Magnetic resonance imaging in synovial disorders and arthropathy of the knee. Magn Reson Imaging Clin N Am 1994;2:451-461.
Question 68
Examination of a 12-year-old girl with bilateral anterior knee pain reveals excessive femoral anteversion and excessive external tibial torsion. The patient has no patellofemoral instability. Nonsurgical management consisting of muscle strengthening and nonsteroidal medication has failed to relieve the patient’s pain. Treatment should now consist of
Explanation
REFERENCE: Delgado ED, Schoenecker PL, Rich MM, Capelli AM: Treatment of severe torsional malalignment syndrome. J Pediatr Orthop 1996;16:484-488.
Question 69
A 21-year-old female college athlete sustained a stress fracture of the fifth metatarsal 1 year ago which was treated successfully with surgical stabilization and she returned to normal activities. She now has a tension-sided femoral neck fracture. Along with surgical fixation of the fracture, what is the next step in management? Review Topic
Explanation
Question 70
Which modality has the broadest application for reduction of postsurgical transfusion?
Explanation
TXA is easy to administer, inexpensive, and safe for virtually all patients. Multiple studies have demonstrated transfusion rates lower than 3% for total knee arthroplasty and lower than 10% for total hip arthroplasty. Regional and hypotensive anesthesia effectively reduce transfusion; however, they cannot be used in as wide a range of patients as TXA. A reduced transfusion trigger must be considered along with patient symptoms when determining the need for transfusion.
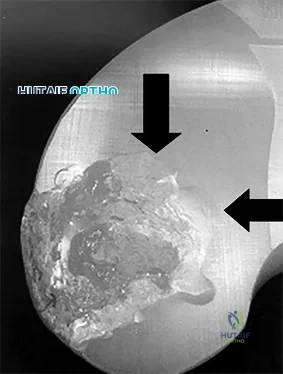
Question 71
Figures 9a through 9c are the preoperative radiographs and a T2-weighted MR image of a patient treated with surgery for spondylolisthesis and neuroforaminal stenosis. Figure 9d is the postsurgical radiograph. Interbody fusion offers which advantage over posterolateral fusion (PLF)? A B C D
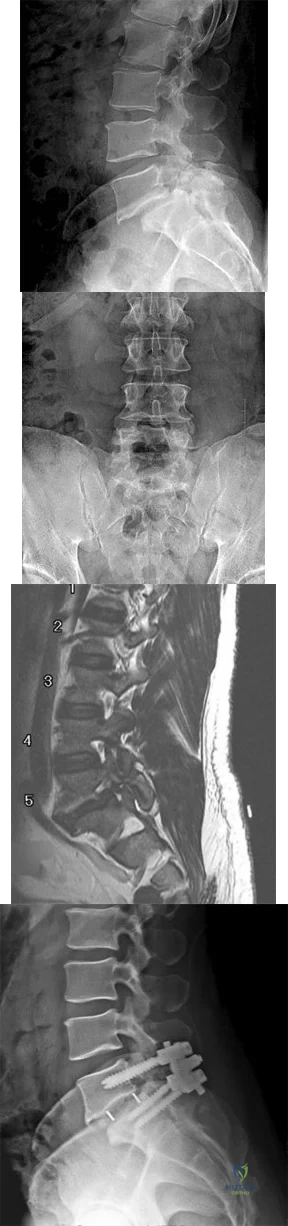
Explanation
Interbody fusion, when compared to PLF, is a predictor of more substantial blood loss. Multilevel posterior lumbar interbody fusion (PLIF) is an independent predictor of blood loss for posterior spine fusion. Some retrospective studies suggest that fusion rates are higher for transforaminal lumbar interbody fusion (TLIF) than PLF, but this finding has not been borne out in prospective studies. The main advantage of TLIF in the context of this question is restoration of neuroforaminal height, and many surgeons will consider TLIF or PLIF for that reason. The parasagittal MR image seen in Figure 9c shows neuroforaminal narrowing. The pre- and postsurgical radiographs show a difference in neuroforaminal height.
RECOMMENDED READINGS
DiPaola CP, Molinari RW. Posterior lumbar interbody fusion. J Am Acad Orthop Surg. 2008 Mar;16(3):130-9. Review. PubMed PMID: 18316711. View Abstract at PubMed
Eismont FJ, Norton RP, Hirsch BP. Surgical management of lumbar degenerative spondylolisthesis. J Am Acad Orthop Surg. 2014 Apr;22(4):203-13. doi: 10.5435/JAAOS-22-04-203. Review. PubMed PMID: 24668350. View Abstract at PubMed
McAfee PC, DeVine JG, Chaput CD, Prybis BG, Fedder IL, Cunningham BW, Farrell DJ, Hess SJ, Vigna FE. The indications for interbody fusion cages in the treatment of spondylolisthesis: analysis of 120 cases. Spine (Phila Pa 1976). 2005 Mar 15;30(6 Suppl):S60-5. PubMed PMID: 15767888. View Abstract at PubMed
RESPONSES FOR QUESTIONS 10 THROUGH 14
Postoperative deep surgical site infection
Proximal junctional kyphosis
Pedicle screw cut-out
Pseudarthrosis
Sagittal imbalance
Please match the scenario described below with the most likely complication listed above.
Question 72
A 22-year-old professional baseball pitcher has had pain in the axillary region of his dominant shoulder for the past several weeks. While throwing a pitch during a game, he notes a sharp pulling sensation with a “pop” in his shoulder. Examination the following day reveals tenderness along the posterior axillary fold and pain and weakness with resisted extension of the shoulder. What is the most likely cause of his symptoms?
Explanation
REFERENCES: Schickendantz MS, Ho CP, Keppler L, et al: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains and related injuries.
Magn Reson Imaging Clin N Am 1999;7:39-49.
Livesey JP, Brownson P, Wallace WA: Traumatic latissimus dorsi: Tendon rupture. J Shoulder Elbow Surg 2002;11:642-644.
Question 73
Figure 17 shows the radiograph of a 2-year-old girl who sustained a fracture of the femur in a fall while walking with her parents. History reveals that this is her third long bone fracture, having sustained a humerus fracture 1 year ago and a fracture of the opposite femur 9 months ago. There is no family history of any similar problem. Examination reveals distinctly blue sclerae, normal appearing teeth, and no skin lesions. What is the most likely cause of this patient’s disorder?
Explanation
REFERENCES: Kocher MS, Shapiro F: Osteogenesis imperfecta. J Am Acad Orthop Surg 1998;6:225-236.
Sillence DO, Senn A, Danks DM: Osteogenesis imperfecta: An expanding panorama of variants. Clin Orthop 1981;159:11-25.
Cole WG: Etiology and pathogenesis of heritable connective tissue diseases. J Pediatr Orthop 1993;13:392-403.
Question 74
Patients who have osteonecrosis of the humeral head and who have the best prognosis are those with which of the following conditions?
Explanation
REFERENCES: Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head.
J Shoulder Elbow Surg 2002;11:281-298.
Mansat P, Huser L, Mansat M, et al: Shoulder arthroplasty for atraumatic avascular necrosis of the humeral head: Nineteen shoulders followed up for a mean of seven years. J Shoulder Elbow Surg 2005;14:114-120.
Question 75
A 16-year-old ice hockey player is struck on the chest by the puck. He skates a few strides and then collapses. What is the most likely diagnosis?
Explanation
REFERENCES: Maron BJ, Strasburger JF, Kugler JD, Bell BM, Brodkey FD, Poliac LC: Survival following blunt chest impact-induced cardiac arrest during sports activities in young athletes. Am J Cardiol 1997;79:840-841.
Link MS, Maron BJ, Estes NAM III: Commotio cordis, in Estes NAM III, Salem DN, Wang PJ (eds): Sudden Cardiac Death in the Athlete. Armonk, NY, Futura, 1998, pp 515-528.
Question 76
What type of exercise is used early in the rehabilitation process to safely stimulate co-contraction of the scapular and rotator cuff muscles? Review Topic
Explanation
Question 77
A 45-year-old man reports severe discomfort following a twisting injury to his right ankle and foot. Plain radiographs are negative; however, the CT scans shown in Figures 39a and 39b reveal a fracture. Management should consist of
Explanation
REFERENCES: Heckman JD: Fractures and dislocations in the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2267-2405.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Question 78
A 20-year-old man has activity-related deep-seated shoulder pain in his dominant right shoulder. He has taken 3 months off training as a college javelin thrower, and management consisting of physical therapy has failed to provide relief. Shoulder arthroscopic views are shown in Figures 16a through 16c. What is the underlying association with this condition? Review Topic
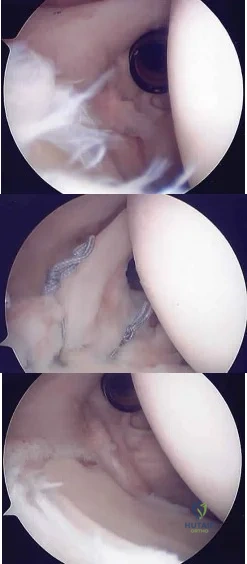
Explanation
Question 79
Which factor increases the success rate associated with all-inside lateral meniscal repair?
Explanation
Decreased patient age, neutral alignment, and a concomitant ACL tear are associated with improved success rates of meniscal repair. Meniscus tears on the contralateral side of the knee and articular cartilage defects are not associated with improved healing rates.
RESPONSES FOR QUESTIONS 5 THROUGH 6
Physical therapy and a home exercise program
Corticosteroid injection
Arthroscopic debridement
Microfracture
Osteochondral autograft transplantation (OAT)
Match the treatment above with the clinical scenario below
Question 80
Lumbar disk replacement has been shown to offer which of the following results?
Explanation
REFERENCES: Geisler FH, Blumenthal SL, Guyer RD, et al: Neurological complications of lumbar artificial disc replacement and comparison of clinical results with those related to lumbar arthrodesis in the literature. J Neurosurg Spine 2004;1:143-154.
Tropiano P, Huang RC, Girardi FP, et al: Lumbar total disc replacement: Seven to eleven-year follow-up. J Bone Joint Surg Am 2005;87:490-496.
Question 81
Figure 61 shows the radiograph of a 28-year-old professional football player who sustained a hyperextension injury to the great toe. He continued to play with pain and loss of push-off strength. What is the most likely diagnosis?

Explanation
Question 82
Figure 50 shows the cross table lateral radiograph of a 31-year-old paratrooper who has recalcitrant groin pain. The pain is worse after activities such as standing or sitting (driving). Examination reveals that pain can be reproduced by internal rotation of the leg with the hip and knee in 90 degrees of flexion. Extensive nonsurgical management has failed to provide relief. What is the treatment of choice? Review Topic

Explanation
Question 83
A patient with a transverse femur fracture undergoes statically locked antegrade intramedullary nailing. Postoperatively, the patient appears to have a
Explanation
Question 84
A 10-month-old infant has a deformity of the right foot. Radiographs, including simulated weight-bearing AP and lateral views and a maximum plantar flexion lateral view, are shown in Figures 57a through 57c. Initial management of the foot should consist of Review Topic

Explanation
Question 85
A 6-year-old boy presents with a mass and a lucent lesion involving the tibial shaft as seen in Figure 17a. The mass is mildly tender to palpation. The bone scan is focally hot in the tibia. Biopsy specimens are shown in Figures 17b and 17c. What is the most likely diagnosis?
Explanation
REFERENCES: Campanacci M, Laus M: Osteofibrous dysplasia of the tibia and fibula. J Bone Joint Surg Am 1981;63:367-375.
McCaffery M, Letts M, Carpenter B, et al: Osteofibrous dysplasia: A review of the literature and presentation of an additional 3 cases. Am J Orthop 2003;32:479-486.
Question 86
Which of the following methods best aids in diagnosis of an interdigital neuroma?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 145-147.
Bennett GL, Graham CE, Mauldin DM: Morton’s interdigital neuroma: A comprehensive treatment protocol. Foot Ankle Int 1995;16:760-763.
Question 87
Kinematic analysis of the medial and lateral menisci has demonstrated that the lateral meniscus has which of the following characteristics compared with the medial meniscus?
Explanation
REFERENCES: Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. New York, NY, Churchill Livingstone, 2001, vol 1, p 474.
Thompson WO, Thaete FL, Fu FH, et al: Tibial meniscal dynamics using 3D reconstructions
of MR images, in Proceedings of the Orthopaedic Research Society 1990;389.
Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy
of Orthopaedic Surgeons, 2005, pp 15-28.
Question 88
Figures 38a and 38b show the AP and lateral radiographs of a 12-year-old baseball pitcher who has pain in his right dominant elbow. Management should consist of
Explanation
REFERENCES: Cabanela ME, Morrey BF: Fractures of the olecranon, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 2000, pp 365-379.
Nuber GW, Diment MT: Olecranon stress fractures in throwers: A report of two cases and a review of the literature. Clin Orthop 1992;278:58-61.
Question 89
A 78-year-old woman reports a 1-week history of severe low back pain. She denies any trauma or recent falls. She is neurologically intact, and is able to ambulate, although she does require the use of a walker. Radiographs of the lumbar spine show a T11 compression fracture with a 20% loss of anterior column height. What is the most appropriate management at this time? Review Topic
Explanation
Question 90
During what phase of the throwing motion is the highest torque measured across the glenohumeral joint?
Explanation
REFERENCES: Jobe FW, Moynes DR, Tibone JE, Perry J: An EMG analysis of the shoulder in pitching: A second report. Am J Sports Med 1984;12:218-220.
Pappas AM, Zawacki RM, Sulliva TJ: Biomechanics of baseball pitching: A preliminary report. Am J Sports Med 1985;13:216-222.
Altcheck DW, Dines DM: Shoulder injuries in the throwing athlete. J Am Acad Orthop Surg 1995;3:159-165.
Question 91
The use of knee arthroscopy following total knee arthroplasty is most effective in treating which of the following conditions?
Explanation
REFERENCES: Lucas TS, DeLuca PF, Nazarian DG, et al: Arthroscopic treatment of patellar clunk. Clin Orthop 1999;367:226-229.
Takahashi M, Miyamoto S, Nagano A: Arthroscopic treatment of soft-tissue impingement under the patella after total knee arthroplasty. Arthroscopy 2002;18:E20.
Question 92
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals lumbar paraspinal spasm and a positive straight leg raising test. Deep tendon reflexes, motor strength, and sensation in the lower extremities are normal. Radiographic findings are normal. If symptoms persist for longer than a few weeks, what is the best course of action?
Explanation
REFERENCES: Epstein JA, Epstein NE, Marc J, et al: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Hashimoto K, Fujita K, et al: Lumbar disc herniation in children. J Pediatr Orthop
1990;10:394-396.
Question 93
Figure 12 shows a lateral radiograph of the elbow. What is the most likely diagnosis?
Explanation
REFERENCE: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 132-133.
Keats TE, Anderson MW: Atlas of Normal Roentgen Variants That May Simulate Disease, ed 7. St Louis, MO, Mosby Inc, 2001, p 497.
Question 94
What is the most important genetic element that distinguishes community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) from hospital-acquired MRSA? Review Topic
Explanation
encodes a penicillin-binding protein with a very low affinity for beta-lactam antibiotics, resulting in methicillin resistance. SCCmec mobile genetic units carry the mecA gene with additional genetic elements that together yield the multidrug-resistant strains found in healthcare environments. SCCmec type IV is specific to CA-MRSA and lacks these additional genetic elements, resulting in less multidrug resistance.
Question 95
below show the radiographs obtained from an year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 96
A 13-year-old gymnast has had recurrent right elbow pain for the past year. She denies any history of trauma. Rest and anti-inflammatory drugs have failed to provide relief. Examination reveals no localized tenderness and only slight loss of both flexion and extension (10 degrees). What is the most likely diagnosis?
Explanation
REFERENCES: Krijnen MR, Lim L, Willems WJ: Arthoscopic treatment of osteochondritis dissecans of the capitellum: Report of 5 female athletes. Arthroscopy 2003;19:210-214.
Schenck RC, Goodnight JM: Osteochondritis dissecans. J Bone Joint Surg Am 1996;3:439-456.
Question 97
- Posterior cruciate insufficiency diagnosed using the quadriceps active test is confirmed with tibial translation
Explanation
Question 98
A 42-year-old man with a history of renal cell carcinoma has progressive weakness in the lower extremities for the past 3 weeks. The patient desires intervention. A sagittal T 2 -weighted MRI scan is shown in Figure 9a, and a sagittal contrast enhanced T 1 -weighted MRI scan is shown in Figure 9b. He currently ambulates minimal distances with a walker. His life expectancy is 8 months. Treatment of the spine lesion should consist of
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 351-366.
White AP, Kwon BK, Lindskog DM, et al: Metastatic disease of the spine. J Am Acad Orthop Surg 2006;14:587-598.
Question 99
A 23-year-old male college quarterback presents with acute left shoulder pain after being tackled. A radiograph of the injury is shown in figure A. After successful closed reduction, what shoulder position should be avoided in order to minimize the risk of a repeat injury? Review Topic

Explanation
Shoulder stability is achieved through the both dynamic and static stabilizers. The static stabilizers include the bony morphology of the joint, glenoid labrum, capsule, and glenohumeral ligaments. The contributions of the glenohumeral ligaments to shoulder stability are dependent upon the position of the humerus relative to the glenoid. Posterior stability is afforded to the joint by the superior glenohumeral ligament (SGHL) and the posterior band of the inferior glenohumeral ligament (IGHL). The SGHL specifically is taught and provides posterior stability with the shoulder in flexion, adduction, and internal rotation.
Kim et. al. reviewed their experience treating 27 athletes diagnosed with traumatic posterior shoulder instability and treated with arthroscopic posterior labral repair and capsular shift. Most patients were found to have an incompletely stripped posterior capsulolabral complex. After arthroscopic repair and shift, all 26 of the 27 patients treated had improved shoulder function and objective scores, a stable shoulder, and were able to return to sport.
Millett et. al. reviewed posterior shoulder instability. They describe the static restraints of the posterior shoulder as the SGHL, posterior band of IGHL, and the coraohumeral ligament (CHL). The SGHL and CHL are both taught in the position of flexion, adduction, and internal rotation, whereas the posterior band of the IGHL is taught in abduction. They describe posterior instability occuring secondary to overhead sports due to repetitive microtrauma causing gradual capsular failure.
Figure A is an axillary radiograph of the left shoulder demonstrating a posterior dislocation and an engaging reverse Hill-Sachs lesion.
Incorrect Answers:
Question 100
Figures below represent the radiographs obtained from a 37-year-old man with severe right knee pain. He has a history of prior tibial osteotomy for adolescent tibia vara but notes residual bowing of his legs. On examination, he is 5'8" tall and weighs 322 pounds. He has a waddling gait with a bilateral varus thrust and 20° varus deformity of both legs. His right knee range of motion is 0° to 120° with a fixed varus deformity. What is the best next step?
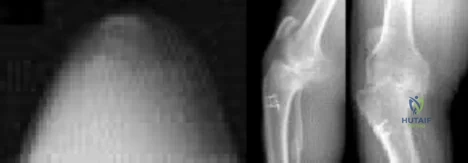
Explanation
This patient has severe, uncorrectable varus deformity and pain from end-stage osteoarthritis secondary to prior adolescent tibia vara. Although he is young to consider arthroplasty, this option is likely to give him the most functional limb, compared with arthrodesis with a long antegrade nail. During arthroplasty surgery, his knee will likely require extensive medial release to achieve anatomic limb alignment. Standard components in total knee arthroplasty likely would result in lateral instability, so this option is
not the best answer. The best choice is total knee arthroplasty with a constrained device, which adds constraint to the knee to provide balance.
