Orthopedic Surgery Board Exam MCQs: Arthroplasty, Hip, Knee & Wrist | Part 17

Key Takeaway
This page offers Part 17 of a comprehensive Orthopedic Surgery Board Review MCQ bank. Designed for orthopedic surgeons and residents preparing for AAOS/ABOS and OITE exams, it features 100 high-yield, verified questions with detailed clinical explanations and interactive study/exam modes to optimize your board certification preparation.
About This Board Review Set
This is Part 17 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 17
This module focuses heavily on: Arthroplasty, Hip, Knee, Wrist.
Sample Questions from This Set
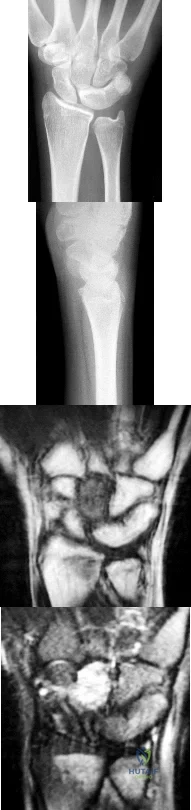
Sample Question 1: An 11-year-old girl has wrist pain. Figure 4a shows the radiograph, and Figures 4b and 4c show the low- and medium-power photomicrographs of a lesion in the distal radius. What is the most likely diagnosis?...
Sample Question 2: An otherwise healthy 33-year-old man who works in construction reports a 3-month history of knee pain. Radiographs are shown in Figures 9a and 9b. An axial T 1 -weighted MRI scan with contrast, an angiogram, and histologies are shown in Fig...
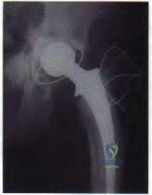
Sample Question 3: Which of the following abnormalities has been observed in a higher than expected frequency in patients with metal-on-metal hip bearings?...
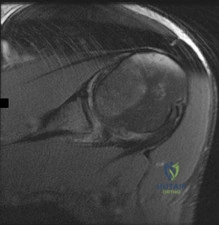
Sample Question 4: Which of the following is considered a reasonable goal for arthroplasty surgery in rotator cuff arthropathy?...
Sample Question 5: Figures 36a and 36b show the MRI scans of a 15-year-old girl who has had pain and recurrent hemarthrosis in the knee for the past year. Plain radiographs are normal. What is the most likely diagnosis?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
An 11-year-old girl has wrist pain. Figure 4a shows the radiograph, and Figures 4b and 4c show the low- and medium-power photomicrographs of a lesion in the distal radius. What is the most likely diagnosis?
Explanation
REFERENCES: Springfield DS, Gebhardt MC: Bone and soft tissue tumors, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 540-542.
Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, pp 1906-1909.
Question 2
An otherwise healthy 33-year-old man who works in construction reports a 3-month history of knee pain. Radiographs are shown in Figures 9a and 9b. An axial T 1 -weighted MRI scan with contrast, an angiogram, and histologies are shown in Figures 9c through 9f. What is the most likely diagnosis?
Explanation
REFERENCES: Sheth DS, Yasko AW, Raymond AK, et al: Conventional and dedifferentiated parosteal osteosarcoma: Diagnosis, treatment, and outcome. Cancer 1996;78:2136-2145.
Lewis VO, Gebhardt MC, Springfield DS: Parosteal osteosarcoma of the posterior aspect of the distal part of the femur: Oncological and functional results following a new resection technique. J Bone Joint Surg Am 2000;82:1083-1088.
Question 3
Which of the following abnormalities has been observed in a higher than expected frequency in patients with metal-on-metal hip bearings?
Explanation
REFERENCES: Dunstan E, Ladon D, Whittingham-Jones P, et al: Chromosomal aberrations in the peripheral blood of patients with metal-on-metal hip bearings. J Bone Joint Surg Am 2008;90:517-522. Ladon D, Doherty A, Newson R, et al: Changes in metal levels and chromosome aberrations in the peripheral blood of patients after metal-on-metal hip arthroplasty. J Arthroplasty 2004:19:78-83.
Visuri T, Pukkala E, Paavolainen P, et al: Cancer risk after metal on metal and polyethylene on metal total hip
arthroplasty. Clin Orthop Relat Res 1996:329:S280-S289. Question 61
A 73-year-old woman with a history of type II diabetes mellitus undergoes a total hip arthroplasty for osteoarthritis. She continues to have serosanguinous wound drainage from the midportion of the incision 12 days after surgery. What is the most appropriate treatment at this time?
Return to the operating room for debridement and irrigation with removal of all implants and immediate reimplantation
Return to the operating room for open debridement and irrigation, exchange of the polyethylene
insert, followed by appropriate antibiotics based on intraoperative culture results
Hip spica pressure dressing and a 2-week course of oral antibiotics
Hip aspiration for culture, followed by a 2-week course of appropriate IV antibiotics based on
culture results
Hip aspiration for culture, followed by a 6-week course of appropriate IV antibiotics based on culture results
DISCUSSION: This patient has an acute postoperative deep infection, with prolonged drainage at 12 days postoperatively. Even without other signs or symptoms of infection, the prolonged drainage this far out after surgery is concerning for an acute postoperative infection. The most appropriate treatment at this point is open debridement with retention of the implants. Modular parts, if present, are exchanged. Oral or IV antibiotics alone are generally inadequate to treat the infection, and this form of management alone would result in a missed opportunity to potentially cure the infection. Removal of all implants at this point is not required because early aggressive debridement within the first 2 weeks after surgery offers a reasonable outcome. After 4 to 6 weeks of symptoms, results of debridement are less favorable and removal of the implants is usually required.
REFERENCES: Crockarell JR, Hanssen AD, Osmon DR, et al: Treatment of infection with debridement and retention of the components following hip arthroplasty. J Bone Joint Surg Am 1998;80:1306-1313. Hanssen AD, Osmon DR: Assessment of patient selection criteria for treatment of the infected hip arthroplasty. Clin Orthop Relat Res 2000;381:91 -100.
Question 4
Which of the following is considered a reasonable goal for arthroplasty surgery in rotator cuff arthropathy?
Explanation
REFERENCES: Zeman CA, Arcand MA, Cantrell JS, Skedros JG, Burkhead WZ Jr: The rotator cuff-deficient arthritic shoulder: Diagnosis and surgical management. J Am Acad Orthop Surg 1998;6:337-348.
Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for the treatment of defects in the rotator cuff and the surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491.
Williams GR Jr, Rockwood CA Jr: Hemiarthroplasty in rotator cuff-deficient shoulders. J Shoulder Elbow Surg 1996;5:362-367.
Zuckerman JD, Scott AJ, Gallagher MA: Hemiarthroplasty for cuff tear arthropathy. J Shoulder Elbow Surg 2000;9:169-172.
Question 5
Figures 36a and 36b show the MRI scans of a 15-year-old girl who has had pain and recurrent hemarthrosis in the knee for the past year. Plain radiographs are normal. What is the most likely diagnosis?
Explanation
REFERENCE: Price NJ, Cundy PJ: Synovial hemangioma of the knee. J Pediatr Orthop 1997;17:74-77.
Question 6
The posterior cord of the brachial plexus terminates into what two main branches?
Explanation
REFERENCE: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 228-236.
Question 7
A healthy, active, independent 74-year-old woman fell and sustained the elbow injury shown in Figures 41a and 41b. Management should consist of
Explanation
REFERENCES: Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intra-articular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480.
Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humerus fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
Obremskey WT, Bhandari M, Dirschl DR, et al: Internal fixation versus arthroplasty of comminuted fractures of the distal humerus. J Orthop Trauma 2003;17:463-465.
Question 8
Which of the following cardiac conditions is considered an absolute contraindication to vigorous exercise?
Explanation
sudden death in young athletes. HCM phenotype becomes evident by age 13 to 14 years. Those at higher risk include individuals with cardiac symptoms, a family history of inherited cardiac disease, and those with a family history of premature sudden death. Echocardiography is useful for detecting structural heart disease, including the cardiomyopathies and valvular abnormalities. Trained adolescent athletes demonstrated greater absolute left ventricular wall thickness (LVWT) compared to controls. HCM should be considered in any trained adolescent male athlete with a LVWT of more than 12 mm (female of more than 11 mm) and a nondilated ventricle. Adolescent and adult athletes differ with respect to the range of LVWT measurements, as a manifestation of left ventricular hypertrophy (LVH). Differentiating LVH (“athlete’s heart”) from HCM involves looking at additional echocardiographic features. Sharma and associates reported that adolescents with HCM had a small or normal-sized left ventricle (less than 48 mm) chamber size, while those with LVH had a chamber size at the upper limits of normal (52 mm to 60 mm).
REFERENCES: Sharma S, Maron BJ, Whyte G, et al: Physiologic limits of left ventricular hypertrophy in elite junior athletes: Relevance to differential diagnosis of athlete’s heart and hypertrophic cardiomyopathy. J Am College Cardiol 2002;40:1431-1436.
Maron BJ, Spirito P, Wesley Y, et al: Development and progression of left ventricular hypertrophy in children with hypertrophic cardiomyopathy. N Engl J Med 1986;315:610-614.
Pelliccia A, Culasso F, Di Paolo FM, et al: Physiologic left ventricular cavity dilatation in elite athletes. Ann Intern Med 1999;130:23-31.
Question 9
A 69-year-old patient with diabetes has had acute-onset back pain and difficulty with ambulation for several hours. Evaluation reveals a temperature of 38.3°C, a white blood cell (WBC) count of 14000/µL (reference range [rr], 4500-11000/µL), C-reactive protein (CRP) level of 120 mg/L (rr, 0.08-3.1 mg/L), erythrocyte sedimentation rate of 130 mm/h (rr, 0-20 mm/h), normal rectal examination findings, and normal sensation to light touch. Motor function testing of the lower extremities reveals 3/5 ankle dorsiflexion and 4/5 plantar flexion strength bilaterally. An MR image reveals a large epidural abscess from L1-5. What is the most appropriate treatment at this time?
Explanation
Epidural abscess is a serious and potentially disastrous condition. Although medical management is effective in some situations, surgical decompression is considered urgent with the presence of a neurological deficit. Medical management can be considered in the case of a neurologically intact patient, particularly when the microorganism has been identified. If medical management is chosen, careful observation and serial examination for neurologic deterioration is required. Surgical decompression is indicated if a patient's neurologic status worsens or if medical management failure is noted. Additionally, diabetes, a CRP level higher than 115 mg/L, WBC higher than 12500/µL , and bacteremia have proven predictive of medical treatment failure. This patient would be a better candidate for urgent surgical decompression and subsequent IV antibiotics than for medical management.
RECOMMENDED READINGS
Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.View Abstract at PubMed
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 10
The patient subsequently requires split-thickness skin grafting over his lateral fasciotomy wound during soft-tissue reconstruction. In this setting, NPWT
Explanation
NPWT increases wound perfusion. The dressing may help decrease risk for wound infection, but will not do so by removing bacteria. It also helps to prevent wound contracture to improve the likelihood of primary wound closure. NPWT can help to improve tissue edema and will not elevate compartment pressure.
Hemorrhage is the most common major complication associated with NPWT. This risk is highest when NPWT is used in areas of major vessels and vessels that have been ligated and for patients undergoing anticoagulation therapy. Specialized white polyvinyl alcohol sponges are available to prevent adherence to vessels, exposed nerves, or exposed bone. NPWT should not be used directly over exposed major vessels. If major bleeding occurs, a return to the operating room for wound exploration is recommended.
Incisional NPWT is an effective treatment for persistent serous drainage. Wounds that drain persistently seal more quickly and pose lower risk for infection when incisional NPWT is used vs compressive dressings. Incisional NPWT has also demonstrated benefit when used on high-risk postsurgical wounds of the tibial plateau, pilon, and calcaneus. It has not been shown to contribute to increased risk for wound dehiscence or hematoma.
NPWT stabilizes the soft-tissue environment and does not necessitate frequent dressing changes. Despite this benefit, a delay of flap coverage after NPWT still poses higher risk for infection than early coverage. Consequently, flaps should not be delayed for long. NPWT promotes the formation of granulation
tissue and can be used over exposed bone, but it would not be expected to form granulation tissue over an exposed fracture site or hardware or promote fracture healing.
NPWT provides an excellent bolster for a skin graft and improves skin graft incorporation. It needs to be applied with nonadherent dressings to prevent adherence to the skin graft. NPWT is generally not used at skin grafting donor sites.
RECOMMENDED READINGS
Streubel PN, Stinner DJ, Obremskey WT. Use of negative-pressure wound therapy in orthopaedic trauma. J Am Acad Orthop Surg. 2012 Sep;20(9):564-74. doi: 10.5435/JAAOS-20-09-564. Review. PubMed PMID: 22941799.View Abstract at PubMed
Powell ET 4th. The role of negative pressure wound therapy with reticulated open cell foam in the treatment of war wounds. J Orthop Trauma. 2008 Nov-Dec;22(10 Suppl):S138-41. doi: 10.1097/BOT.0b013e318188e27d. Review. PubMed PMID: 19034160. View Abstract at PubMed
Question 11
A 45 year-old woman who has not reached menopause yet falls from a standing height and sustains a distal radius fracture. A DEXA scan reveals a T-score of -2.2. Which of the following treatments is indicated in this patient?
Explanation
Medications that are approved by the FDA for active treatment of osteoporosis: alendronate, risedronate, raloxifene, estrogen, calcitonin. These medications and preventative measures help to reduce fragility fractures by as much as 50%.
Freedman et al. performed a retrospective study that looked at a cohort of patients with fragility fractures and then looked at the type and frequency of osteoporosis related interventions. They found that only 60% of patients actually were either prescribed a medication, given a referral, or ordered additional workup (DEXA scan).
Schulman et al. reviewed a series of 80 female patients regarding osteoporosis and bone health, and found that the outpatient sports medicine office setting was an excellent opportunity to educate patients on these topics. The patients' post-education test scores increased significantly after a brief counseling session, and increases in daily calcium intake and exercise levels were also seen.
Question 12
When the iliac apophysis starts ossifying in the normal adolescent, growth of the sitting height or trunk height is characterized by
Explanation
REFERENCES: Anderson M, Hwang SC, Green WT: Growth of the normal trunk in boys and girls during the second decade of life: Related to age, maturity, and ossification of the iliac epiphyses. J Bone Joint Surg Am 1965;47:1554-1564.
Zaoussis AL, James JIP: The iliac apophysis and the evolution of curves in scoliosis. J Bone Joint Surg Br 1958;40:442-453.
Question 13
A 14-year-old male soccer player was seen initially in the emergency room 1 week ago after an acute right hip injury during a soccer tournament. The patient reports that the hip pain has improved, but still requires crutches for long distance ambulation. His radiograph is seen in Figure A. What would be the next most appropriate step in management? Review Topic

Explanation
The diagnosis of an avulsion fracture of the anterior superior iliac spine is made on the basis of: 1. History (sudden contraction of the sartorial and tensor fasciae latae muscle), 2. Physical findings (tenderness over the anterior superior iliac spine [ASIS] and pain with straight-leg raise), 3. Patient's age (most commonly in adolescents or young adults), and 4. Radiographs (confirmed fracture on standard views of the pelvis). Treatment of these injuries is almost always conservative with crutches and progressive weight-bearing activities as tolerated. The relative indications for operative treatment include displacement of the fracture fragment > 3 cm or painful non-union.
White et al. defined two types of anterior superior iliac spine avulsion fractures. A sartorius avulsion fracture (Type 1) usually occurs when sprinting. The fracture fragment is usually small and displaced anteriorly. The tensor avulsion fracture (Type 2) usually occurs when twisting the trunk (e.g. swinging a bat). This fragment is usually larger than Type 1 fractures and more likely to be displaced laterally.
Holden et al. reviewed pediatric pelvic fractures. They state that avulsion fractures of the anterior superior iliac spine are usually low-energy injures, and are not associated with other life-threatening injuries. They do not require an extensive workup (e.g. CT scanning)
Figure A is an antero-posterior view of the pelvis with a small right-sided avulsion fracture of the anterior superior iliac spine.
Incorrect Answers:
Question 14
Figure 1 is the MRI scan of a 19-year-old man who has an acute anterior shoulder dislocation. The bony fragment occupies 10% of the glenoid articular surface. What is the most appropriate treatment?
Explanation
Question 15
A 45-year-old man who is a smoker has a significant hemothorax and bilateral closed femoral fractures. On insertion of a chest tube, 1,100 mL of blood was returned. He has had 75 mL of chest tube output over the last 2 hours while being resuscitated in the ICU. His base deficit is now 2 and his urine output has been 3 mL/kg over the last hour. What is the next most appropriate step in management?
Explanation
REFERENCES: Nork SE, Agel J, Russell GV, et al: Mortality after reamed intramedullary nailing of bilateral femur fractures. Clin Orthop Relat Res 2003;415:272-278.
Pape HC, Zelle BA, Hildebrand F, et al: Reamed femoral nailing in sheep: Does irrigation and aspiration of intramedullary contents alter the systemic response? J Bone Joint Surg Am 2005;87:2515-2522.
Question 16
- Which of the following provides the most stable fixation for comminuted fractures of the posterior acetabular wall?
Explanation
According to Rockwood & Green and Browner & Jupiter the key to fixing these fractures is to re-establish a congruent articular surface. The other four distracters (i.e. cable, methylmethacrylate, multiple lag screws, and multiple K-wires) may achieve initial stability, but reduction will not be maintained. In addition, further studies show a higher incidence of mortality and complications with the use of lag screws and K-wires alone (Browner & Jupiter, Skeletal trauma, 1998)
Question 17
Which structure(s) is/are most at risk with surgical treatment of displaced clavicle fractures with ORIF?
Explanation
Complications associated with nonsurgical treatment of displaced midshaft clavicle fractures are uncommon. Although intrathoracic and local vascular complications have been reported with clavicle fracture, subclavian artery aneurysm and pneumothorax are rare. Malunion to some degree is inevitable with nonsurgical treatment of displaced clavicle fractures, but only about 9% of patients develop symptomatic malunion. Nonunion occurs in about 15% of patients.
Previously identified risk factors for nonunion of clavicle fractures include female gender, displacement exceeding 100%, comminution, and advanced age. Research demonstrates the strongest risk factors are smoking, comminution, and fracture displacement. Rate of nonunion in 1 study was approximately 13%. Murray and associates showed that by estimating the risk of nonunion using their model and operating only on fractures with at least a 40% chance of nonunion, they would only need to operate on 1.7 patients to prevent 1 nonunion (decreased from 7.5 procedures per nonunion if operating on all displaced midshaft fractures). This data could potentially be used to limit unnecessary procedures and decrease costs associated with treatment of clavicle fractures.
Hardware removal is the most common reason for revision surgery. Symptomatic malunion and supraclavicular nerve entrapment are rare after surgery. Nonunion is uncommon (in fewer than 2% of cases). The main reason for revision surgery is hardware removal to address local irritation/prominent hardware or infection.
An anatomical study demonstrated that in 97% of clavicles, 2 to 3 branches of the supraclavicular nerve were crossing the clavicle with wide location variability in the zone in which most clavicle fractures occur and surgery would take place. The subclavian vein and artery and brachial are rarely injured,
although there are case reports of injury to all either by the displaced fracture fragments or errant hardware.
RECOMMENDED READINGS
McKee RC, Whelan DB, Schemitsch EH, McKee MD. Operative versus nonoperative care of displaced midshaft clavicular fractures: a meta-analysis of randomized clinical trials. J Bone Joint Surg Am. 2012 Apr 18;94(8):675-84. doi: 10.2106/JBJS.J.01364. Review. PubMed PMID: 22419410.View Abstract at PubMed
Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am. 2004 Jul;86-A(7):1359-65. PubMed PMID: 15252081.View Abstract at PubMed
Murray IR, Foster CJ, Eros A, Robinson CM. Risk factors for nonunion after nonoperative treatment of displaced midshaft fractures of the clavicle. J Bone Joint Surg Am. 2013 Jul 3;95(13):1153-8. doi: 10.2106/JBJS.K.01275. PubMed PMID: 23824382.View Abstract at
PubMed
Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. J Bone Joint Surg Am. 2007 Jan;89(1):1-10. PubMed PMID: 17200303.View Abstract at PubMed
Nathe T, Tseng S, Yoo B. The anatomy of the supraclavicular nerve during surgical approach to the clavicular shaft. Clin Orthop Relat Res. 2011 Mar;469(3):890-4. doi: 10.1007/s11999-010-1608-x. Epub 2010 Oct 9. PubMed PMID: 20936387.View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 26 AND 27

A
B

C

D
Figures 26a through 26c are the radiographs of a 50-year-old athlete who sustained an injury to his right foot; the foot was plantar flexed and another player landed on the posterior aspect of his heel. After sustaining the injury he was unable to bear weight, and 3 days later he was seen in the emergency department because of persistent pain and tenderness over his midfoot.
Question 18
Figure 16 shows the lateral radiograph of a patient who is scheduled to undergo an anterior cruciate ligament (ACL) reconstruction. If the graft is tensioned at 20° of flexion and the femoral tunnel is created by passing a reamer over the guide wire marked “A,” the resulting ligament reconstruction will excessively
Explanation
REFERENCES: Daniel DM, Fritschy D: Anterior cruciate ligament injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 1994, pp 1313-1360.
Larson RL, Tailon M: Anterior cruciate ligament insufficiency: Principles of treatment. J Am Acad Orthop Surg 1994;2:26-35.
Question 19
What is the function of the rotator cuff during throwing?
Explanation
REFERENCES: Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
Abrams JS: Special shoulder problems in the throwing athlete: Pathology, diagnosis, and nonoperative management. Clin Sports Med 1991;10:839-861.
Question 20
…Figure 53 is the emergency department radiograph of a 7-year-old boy who has pain and is unwilling to use his right arm after a fall on the playground. What is the most appropriate initial treatment?
Explanation

Question 21
Atraumatic neuropathy of the suprascapular nerve usually occurs at what anatomic location?
Explanation
REFERENCES: Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Post M, Mayer J: Suprascapular nerve entrapment: Diagnosis and treatment. Clin Orthop 1987;223:126-136.
Question 22
Figures 3a and 3b show the current radiographs of a 58-year-old man who underwent total knee arthroplasty with a cruciate ligament sparing prosthesis 7 years ago. Examination reveals boggy synovitis and moderate pain, particularly anteriorly. Management should consist of
Explanation
REFERENCE: Brassard MF, Insall JN, Scuderi GR: Complications of total knee arthroplasty, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1801-1844.
Question 23
A 47-year-old man sustained a degloving injury over the pretibial surface and anterior ankle region in a motor vehicle accident. After debridement and irrigation, there is inadequate tissue for closure of the exposed anterior tibial tendon and tibia. Prior to definitive soft-tissue coverage, management should consist of
Explanation
REFERENCES: Webb LX: New techniques in wound management: Vacuum assisted wound closure. J Am Acad Orthop Surg 2002;10:303-311.
Clare MP, Fitzgibbons TC, McMullen ST, et al: Experience with the vacuum assisted closure negative pressure technique in the treatment of non-healing diabetic and dysvascular wounds. Foot Ankle Int 2002;23:896-901.
Question 24
A 20-year-old football player has repeated episodes of heat cramps during summer training sessions. A deficiency of what electrolyte is most responsible for heat cramps?
Explanation
REFERENCES: Bergeron MF, Armstrong LE, Maresh CM: Fluid and electrolyte losses during tennis in the heat. Clin Sports Med 1995;14:23-32.
Halpern B: Fluid and electrolyte replacement in athletes. Sports Med Digest 1994;16:1-5.
Question 25
Which of the following factors is responsible for causing the distal femur to pivot about a medial axis as the knee moves from full extension into early flexion?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 239-240.
Insall JN, Windsor RE, Scott WN, et al (eds): Surgery of the Knee, ed 2. New York, Churchill Livingstone, 1993, pp 1-13.
Question 26
A 62-year-old woman with a bone mass density (BMD) T-score of -2.0 sustained a subcapital fracture of her hip. She is an avid tennis player, and history reveals no previous fractures. What is the most appropriate follow-up care?
Explanation
REFERENCE: Gardner MJ, Brophy RH, Demetrakopoulos D, et al: Interventions to improve osteoporosis treatment following hip fracture: A prospective, randomized trial. J Bone Joint Surg Am 2005;87:3-7.
Question 27
A 23-year-old man who is a competitive overhead athlete has shoulder pain. Based on the pathology shown in Figure 47, what treatment option would yield the highest satisfaction and return to overhead sports?
Explanation
REFERENCES: Snyder SJ, Karzel RP, Del Pizzo W, et al: SLAP lesions of the shoulder. Arthroscopy 1990;6:274-279.
Altchek DW, Warren RF, Wickiewicz TL, et al: Arthroscopic labral debridement: A three-year follow-up study. Am J Sports Med 1992;20:702-706.
Question 28
A 15-year-old boy has a mass at the knee. Radiographs show an aggressive tumor involving the proximal tibia, and biopsy findings reveal a high-grade osteosarcoma. Staging studies show that the tumor impinges on the neurovascular bundle. The tumor enlarges during preoperative chemotherapy. Management should now consist of
Explanation
REFERENCES: Springfield D: Bone and soft-tissue tumors, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 423-468.
Question 29
Figure 48 shows the radiograph of a 17-year-old boy who sustained a gunshot wound to his forearm. There is a small entrance wound on the volar surface. The exit wound is dorsal and more than 15 cm in size, with loss of skin and an extensive amount of devitalized muscle hanging out of the wound. Vascular supply to the hand is excellent, the ulnar and median nerves are intact in the hand, but the radial sensory nerve function is absent. After repeated surgical debridements of the wound and bone, definitive treatment for the fracture would most likely be which of the following? Review Topic

Explanation
Question 30
A 22-year-old patient sustained a jamming injury to the right little finger. The lateral radiograph shown in Figure 18 reveals comminution of the base of the middle phalanx, with palmar and dorsal metaphyseal cortical involvement. The articular surface also is disrupted. Management should consist of
Explanation
REFERENCES: Stern PJ, Roman RJ, Kiefhaber TR, McDonough JJ: Pilon fractures of the proximal interphalangeal joint. J Hand Surg Am 1991;16:844-850.
Krakauer JD, Stern PJ: Hinged device for fractures involving the proximal interphalangeal joint. Clin Orthop 1996;327:29-37.
Question 31
What is the most common primary malignant bone or cartilage tumor in children?
Explanation
1 million children younger than age 15 years), and Ewing’s sarcoma is second (2.1 per
1 million children). Giant cell tumor and chondrosarcoma are rare in children. Osteochondroma is more common than any of the above tumors in children, but it is not malignant.
REFERENCES: Himelstein BP, Dormans JP: Malignant bone tumors of childhood. Pediatr Clin North Am 1996;43:967-984.
Pierz KA, Womer RB, Dormans JP: Pediatric bone tumors: Osteosarcoma, Ewing’s sarcoma, and chondrosarcoma associated with multiple hereditary osteochondromatosis. J Pediatr Orthop 2001;21:412-418.
Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence.
N Engl J Med 1999;341:342-352.
Question 32
Which radiographic abnormality most accurately serves as a predictor of ankle syndesmosis disruption?
Explanation
Normal syndesmotic relationships include a tibiofibular clear space smaller than 6 mm on both AP and mortise views. In a 1989 cadaveric study by Harper and Keller, a tibiofibular clear space exceeding 6 mm on both the AP and mortise views was the most reliable predictor of early syndesmotic widening. Tibiofibular overlap is measured 1 cm proximal to the plafond. Normal values exceed 6 mm or 42% of the width of the fibula on the AP view, or 1 mm on the mortise view. Proximal fibula fracture can occur in isolation without syndesmotic injury, frequently after direct trauma. The medial clear space is the distance between the lateral border of the medial malleolus and the medial border of the talus and is measured at the level of the talar dome. In the mortise view with the ankle in neutral dorsiflexion, the medial clear space should be equal to or smaller than the superior clear space between the talar dome and the tibial plafond. ?A normal medial clear space may be present with syndesmotic injury and consequently lacks sensitivity and specificity.
RECOMMENDED READINGS
Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. View Abstract at PubMed
Wuest TK. Injuries to the Distal Lower Extremity Syndesmosis. J Am Acad Orthop Surg. 1997 May;5(3):172-181. PubMed PMID: 10797219. View Abstract at PubMed
Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 40
A 41-year-old man sustained a twisting injury while running up stairs 4 weeks ago. He was treated in an ankle brace and has been bearing weight since the injury occurred. He has no history of ankle problems, but he now has ankle pain, swelling, and instability. The pain is aggravated by stairs, and the instability is worse on unlevel ground. Radiographs do not show a fracture.
Question 33
A 68-year-old man had a 3-year history of shoulder pain that failed to respond to nonsurgical management. Examination reveals forward elevation to 120 degrees and external rotation to 30 degrees. True AP and axillary radiographs and an axial CT scan are shown in Figures 1a through 1c. What management option would lead to the best long-term results? Review Topic

Explanation
Question 34
What is the most common short-term complication following femoral impaction grafting for revision total hip arthroplasty?
Explanation
REFERENCES: Mikhail MWE, Weidenhielm L, Jazrawi LM, et al: Collarless, polished, tapered stem failure. J Bone Joint Surg Am 2000;82:1513-1514.
Leopold SS, Rosenberg AG: Current status of impaction allografting for revision of a femoral component. Instr Course Lect 2000;49:111-118.
Question 35
A 21-year-old man is referred for evaluation of a lesion in the left proximal femur that was discovered when he was undergoing an upper gastrointestinal series. He reports no hip or thigh pain. Radiographs are shown in Figures 64a and 64b. What is the best course of action?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 87-102.
Rozencwaig R, Wilson MR, McFarland GB Jr: Melorheostosis. Am J Orthop 1997;26:83-89.
Question 36
A 4-year-old boy sustains the injury shown in Figures 10a and 10b as a result of being hit and dragged by a car. Wound closure is best accomplished by
Explanation
healing and survival of the underlying structures, prevent infection, and provide a durable and/or flexible cover. Furthermore, the standard cross-leg flap no longer is used because of significant problems with positioning and joint stiffness, and because it provides inadequate coverage material. For the various surfaces of the ankle and dorsum of the foot, very few local tissues are available to provide coverage when free skin grafting is insufficient. Thus, out of the possible answers, free rectus abdominis flap is the preferred response.
Question 37
- A patient sustains a closed dorsal dislocation of the proximal interphalangeal joint of the middle finger without an associated fracture. Closed treatment results in a cocentric stable reduction. The finger is not immobilized. Which of the following conditions may appear 1 year later?
Explanation

Examination of a 3-year-old boy who slammed his finger in a door 3 months ago reveals 0 to 40 degrees of proximal interphalangeal joint motion. Radiographs are shown in Figures 47a and 47b. Management should consist of
Volar osteotomy
Observation only
Flexor tenolysis
Volar plate arthoplasty
A hinged distraction external fixator
Subcondylar fractures of the proximal and middle phalynx occur at the neck of the phalynx, usually as a result of a crush injury, and almost exclusively in the pediatric age group. The distal fragment rotates dorsally and the degree of displacement may be misjudged if a true lateral is not obtained. If malunion occurs there is block to flexion. Subcondylar fossa reconstruction by removal of bone through a palmar approach removes this boney block.
Question 38
A 26-year-old football player develops tachycardia and hot, dry skin during a game. He is found to have a temperature of 41 degrees C, but is not sweating. Further examination reveals the player is not oriented to time or place, and he soon develops convulsions. Which of the following is the most important next step in treatment? Review Topic
Explanation
Heat stroke is a medical emergency with a high mortality rate. The hallmark features include central nervous system dysfunction and anhidrosis. Other symptoms include behavioral changes, such as confusion, disorientation, and staggering. Seizures and unconsciousness can also develop. The first modality of treatment is rapid reduction in temperature, which can be accomplished through ice water immersion, cooling blankets, or evaporative cooling methods including fans and cold water sprays. The goal in temperature reduction is 0.2 C per minute for a target temperature of 39 C.
Casa et al. reviewed current literature regarding the cause and care of exertional heat stroke. They stated that mortality from heat stroke remained significant, with the highest rates from sports existing between 2005 and 2009. They recommended accurate temperature assessment, prompt aggressive treatment using an efficient cooling modality (i.e. cold water or ice water immersion) prior to transport, and medically supervised return to play/duty as essential to preventing mortality.
Illustration A shows some of the visible differences between heat stroke and exhaustion, with the key discriminator being mental status changes present in heat stroke.
Incorrect Answers:
Question 39
A 45-year-old woman sustains an injury to her lower leg. Examination reveals that there is a deformity with no neurologic or vascular problems. The skin is intact. Radiographs are shown in Figures 46a and 46b. Which of the following factors would make closed management the least appropriate choice for this injury?
Explanation
REFERENCES: Trafton PG: Tibial shaft fractures, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 2153-2169.
Martinez A, Sarmiento A, Latta LL: Closed fractures of the proximal tibia treated with a functional brace. Clin Orthop 2003;417:293-302.
Question 40
Figures 1 through 4 are the radiographs and MR images of a healthy 21-year-old woman who has had persistent dorsal wrist pain despite immobilization and no history of trauma. The surgical procedure associated with the best prognosis in this scenario is
Explanation
This patient has osteonecrosis of the capitate. The MR images show evidence of osteonecrosis with decreased signal on the T1-weighted image. The radiographs are unremarkable, with the exception of lunotriquetral coalition, which does not necessitate treatment. The etiology of osteonecrosis of the capitate may be related to trauma, abnormal Interosseous vascular supply, and hypermobility. Surgery is an option for patients with persistent symptoms despite immobilization. Vascularized bone graft should be considered in this scenario because there is no evidence of capitate collapse or arthritic change about the wrist. Free and local vascularized bone grafts have produced satisfactory results. Capitate excision with interposition arthroplasty is indicated for patients with proximal pole capitate collapse. Total wrist fusion is a salvage procedure and would be considered if there were evidence of collapse and arthritic change. PRC would leave the capitate articulating with the radius and is not indicated.
Question 41
Figures 23a through 23h are the radiographs and MR images of a 32-year-old man with worsening left knee pain. A 3-foot hip-to-ankle radiograph shows a 13-degree varus knee deformity. The patient sustained a major left knee injury 5 years ago and a confirmed complete anterior cruciate ligament (ACL) tear. He managed this injury nonsurgically with a functional brace but experienced worsening pain. He was seen by an orthopaedic surgeon 18 months ago and a medial meniscus tear was diagnosed; the tear was treated with an arthroscopic partial medial meniscectomy. Since then, his knee has been giving way more often and he no longer feels safe working on a pitched roof. The patient received 6 months of formal physical therapy and was fitted for a new functional ACL brace, but he still has pain and instability symptoms. He believes he has exhausted his nonsurgical options and would like to undergo surgery. What is the most appropriate treatment at this time?
Explanation
Proximal tibial osteotomy is the most appropriate intervention to correct varus malalignment and to decrease stress on the ACL. In some cases, proximal tibial osteotomy alone may address both pain and instability, but, if instability persists, particularly in the setting in which instability can be dangerous, subsequent ACL reconstruction can further stabilize the knee with less stress on the graft after correction of malalignment. Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should only be performed at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL reconstruction alone is not indicated for this patient.
Question 42
Revision of failed hip resurfacing arthroplasty should involve
Explanation
Hip resurfacing offers several potential advantages over conventional total hip arthroplasty, particularly for patients younger than 75 years of age. This intervention can be
relatively bone conserving and is appropriate in settings involving proximal femoral deformity, precluding the use of a traditional femoral component. The use of hip resurfacing in osteonecrosis has been controversial, however. Although there are several reports of successful use of these implants to address osteonecrosis, concerns remain about extensive femoral head involvement (exceeding 40%) and ability to support the femoral head cap. Consequently, hip resurfacing is not recommended for patients with large femoral head lesions.
Evaluation of painful hip resurfacings requires a systematic approach. Radiographs can help surgeons assess implant position, loosening, or fractures. Serological studies including ESR, CRP, and serum cobalt and chromium levels can give clues as to whether infection, metallosis, or both are the underlying cause(s) of failure. Hip aspiration in the setting of metal-on-metal bearings necessitates a manual cell count and differential to avoid falsely elevated automated cell counts.
Revision of failed hip resurfacings should involve revisions of both the femoral and acetabular components. Although successful retention of the acetabular shell has been described, concerns remain regarding cup circumference mismatch, which can lead to suboptimal clearance between the new bearing surfaces.

Question 43
An 18-year-old man sustains an injury to the right brachial plexus after falling off his bicycle. Examination reveals no rhomboideus major or minor muscle function. This finding most likely indicates a preganglionic injury to which of the following nerve roots?
Explanation
REFERENCES: Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 23-28.
Millesi H: Brachial plexus injury in adults: Operative repair, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, JB Lippincott, 1991, vol 2, pp 1285-1301.
Question 44
Figures 85a through 85c are the sagittal and axial CT scans and sagittal T2 MR image of a 21-year-old man who was thrown from his motocross bike earlier in the day. He now has significant low-back pain; however, he is neurologically intact and has no trouble voiding urine. A standing plain radiograph obtained the next day is shown in Figure 85d. Treatment should involve A B C D

Explanation
Disruption of the posterior ligamentous complex is an important determinant of the stability of a burst fracture. This patient is neurologically intact and his MR images do not reveal posterior ligamentous complex (PLC) disruption. The standing radiograph confirms that overall alignment is acceptably and relatively preserved. Nonsurgical treatment with or without a brace is acceptable in this scenario; however, the patient should not be cleared to resume full activity until fracture healing, which may be as long as 3 months after the date of injury. Anterior or posterior surgery should be reserved for patients with PLC disruption, neurological injury, or, in some cases, multiple trauma.
RECOMMENDED READINGS
Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. View Abstract at PubMed
Vaccaro AR, Lehman RA Jr, Hurlbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Zeiller SC, Anderson DG, Bono CM, Stock GH, Brown AK, Kuklo T, Oner FC. A new classification of thoracolumbar injuries: the importance of injury morphology, the integrity of the posterior ligamentous complex, and neurologic status. Spine (Phila Pa 1976). 2005 Oct 15;30(20):2325-33. PubMed PMID: 16227897. View Abstract at PubMed
Vaccaro AR, Zeiller SC, Hulbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Lehman RA Jr, Anderson DG, Bono CM, Kuklo T, Oner FC. The thoracolumbar injury severity score: a proposed treatment algorithm. J Spinal Disord Tech. 2005 Jun;18(3):209-15. PubMed PMID: 15905761.View Abstract at PubMed
RESPONSES FOR QUESTIONS 86 THROUGH 89
Proximal junctional kyphosis (PJK)
Adjacent segment degeneration
Intraoperative neurological injury
Postsurgical wound infection
Please select the complication listed above that most commonly is associated with a clinical scenario described below.
Question 45
A 6-year-old boy is being treated for acute hematogeneous osteomyelitis of the distal femur with intravenous antibiotics. The best method to determine the success or failure of initial treatment is by serial evaluations of which of the following studies? Review Topic
Explanation
Question 46
A healthy 72-year-old woman is seen 14 days after cemented total knee arthroplasty. She reports increasing pain and swelling for the last 4 days accompanied by 4 days of wound drainage. Examination reveals that she is afebrile, and has erythema and moderate serosanguinous drainage from the wound. The knee is moderately swollen. Aspiration of the knee reveals no organisms on Gram stain. Culture results are expected back in 48 hours. Optimal management should consist of
Explanation
8 • American Academy of Orthopaedic Surgeons
DISCUSSION: Increased pain, swelling, erythema, and drainage 2 weeks removed from the primary arthroplasty are all signs of a probable infection. Erythrocyte sedimentation rate and C-reactive protein may not be helpful as they are elevated postoperatively even in the absence of infection. Even in the absence of infection, persistent wound drainage is an indication for surgical debridement to prevent subsequent infection. When a postoperative infection is easily recognized by clinical examination, there is no need to wait for a positive culture before proceeding with debridement.
REFERENCES: Weiss AP, Krackow KA: Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993;8:285-289.
Jaberi FM, Parvizi J, Haytmanek CT, et al: Procrastination of wound drainage and malnutrition affect the outcome of joint arthroplasty. Clin Orthop Relat Res 2008;466:1368-1371.
Insall JN, Windsor RE, Scott, WN: Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 959-964.
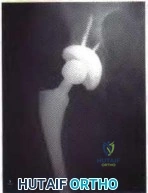
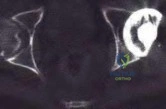
Figure 3a Figure 3b
Question 47
Which of the following is considered a disadvantage of knee disarticulation when compared with transfemoral amputation?
Explanation
disarticulation versus transfemoral amputation is the degree of trauma involving the soft tissue around the knee, as increased tissue trauma may lead to painful residual limbs and eventually the need for revision amputation at a higher level. If the residual limb of the knee disarticulation is unable to accommodate the distal-end weight bearing of the socket, then patients with a knee disarticulation may experience decreased levels of function compared with patients undergoing transfemoral amputation.
Question 48
A 3-year-old child is referred for evaluation of bowed legs. History reveals no dietary deficiencies; however, family history is significant for several members with bowed legs. Examination reveals genu varum, and the child is in the 5th percentile for height and weight. Laboratory studies show normal renal function, a normal calcium level, a decreased phosphate level, and an elevated alkaline phosphatase level. A plain radiograph of the lower extremities is shown in Figure 22. What is the most likely diagnosis?
Explanation
REFERENCES: Evans GA, Arulanantham K, Gage JR: Primary hypophosphatemic rickets: Effect of oral phosphate and vitamin D on growth and surgical treatment. J Bone Joint Surg Am 1980;62:1130-1138.
Loeffler RD Jr, Sherman FC: The effect of treatment on growth and deformity in hypophosphatemic vitamin D-resistant rickets. Clin Orthop 1982;162:4-10.
Loder RT, Johnston CE II: Infantile tibia vara. J Pediatr Orthop 1987;7:639-646.
Bassett GS, Scott CI: The osteochondrodysplasias, in Morrissy RT (ed): Pediatric Orthopaedics, ed 3. Philadelphia, Pa, JB Lippincott, 1990, vol 1, pp 91-142.
Question 49
Following surgery for an ankle fracture, which of the following is considered the most important factor in achieving a satisfactory outcome? Review Topic
Explanation
Question 50
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management?
Explanation
REFERENCES: Miller P, Kendrick D, Bentley E, et al: Cost effectiveness of lumbar spine radiographs in primary care patients with low back pain. Spine 2002;27:2291-2297.
Wong DA, Transfeldt E: Macnab’s Backache, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins 2007, pp 298-338.
Question 51
Which of the following regions in the growth plate is commonly affected in a Salter-Harris type II injury? Review Topic
Explanation
Question 52
According to Musculoskeletal Infection Society (MSIS) guidelines, which set of patient laboratory study results fits the definition of chronic prosthetic joint infection?
Explanation
The MSIS definition of periprosthetic joint infection was updated in 2014 with two major and six minor criteria. The presence of one major criterion or three minor criteria is diagnostic for infection. The major criteria are two positive cultures with the same organism or a draining sinus tract. The current MSIS minor criteria are 1) an elevated ESR (more than 30 mm/hr) and CRP level (more than 10 mg/L), 2) an elevated synovial WBC count (more than 3,000 cells per/microliter), 3) an elevated synovial fluid polymorphonuclear count (more than 80%), 4) a positive histological analysis of periprosthetic tissue, and 5) a single positive culture.
Question 53
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include
Explanation
REFERENCES: Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459.
Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
Skrzynski MC, Biermann JS, Montag A, Simon MA: Diagnostic accuracy and charge-savings of outpatient core needle biopsy compared with open biopsy of musculoskeletal tumors. J Bone Joint Surg Am 1996;78:644-649.
Question 54
50%
Explanation
Enneking et al. conducted both radiographic and histologic studies of sixteen massive retrieved human allografts four to sixty-five months after implantation. Analysis of the articular cartilage revealed no evidence that any chondrocytes had survived, even when the graft had been cryoprotected before it was preserved by freezing.
A 64-year-old woman with a longstanding history of rheumatoid arthritis complains of finger dysfunction for the past 6 months. Figure A displays her hand during active extension of all fingers. Figure B displays her hand maintaining her fingers extended following passive extension. What is the next most appropriate treatment for the ring finger?
Spiral oblique retinacular ligament reconstruction
Sagittal band reconstruction
Lateral band reconstruction
Central slip reconstruction
Triangular ligament and transverse retinacular ligament reconstruction
Sagittal band disruption is often associated with rheumatoid arthritis. When this patient attempts to actively extend the affected digit, the extensor tendon
subluxates ulnarly as a result of the sagittal band rupture, and is left with an extensor lag. If one passively extends the finger fully, the patient is able to maintain this position, as the tendon is intact.
Sagittal band reconstruction can be performed with Watson's technique of creating a distally based tendon graft harvested from the central third of the extensor tendon, passed deep to the intermetacarpal ligament and sutured back to itself. Illustration A depicts an intraoperative view of the tendon before reconstruction and Illustration B displays tendon following sagittal band reconstruction. Illustration C displays all of the anatomic locations
of the options listed above.
A splenectomy is performed in a 7-year-old boy following a motor vehicle accident. All of the following are recommended for long-term management EXCEPT:
Pneumococcal vaccination
Haemophilus influenza type B vaccination
Meningococcal group C vaccination
Lifelong prophylactic antibiotics
Hepatitis A vaccination
All of the responses are correct except the need for Hepatitis A vaccine. Hepatitis A is a virus with tropism for hepatocytes which causes infection from fecal-oral contaminated food/water, and shows no increased rate of either infectivity or morbidity in patients with hyposplenism.
Basic recommendations for splenectomized patients include:
All splenectomized patients and those with functional hyposplenism should receive pneumococcal immunization.
Patients not previously immunized should receive haemophilus influenza type B vaccine.
Patients not previously immunized should receive meningococcal group C conjugate vaccine.
Influenza immunization should be given.
Lifelong prophylactic antibiotics are still recommended (oral phenoxymethylpenicillin or erythromycin). This is seemingly despite lack of good data demonstrating a role for lifelong chemoprophylaxis and the acknowledgement that long-term compliance may be problematic.
Davies et al review the current level of evidence supporting these guidelines
for infection prevention in patients with hyposplenism. New to these guidelines are issues regarding occupational exposure and the use of the meningococcal group C and the seven-valent pneumococcal vaccine in non-immunized hyposplenic patients.
Gandhi et al evaluated their nonoperative management of blunt splenic injury in pediatric trauma care. They found compared to historical controls, children with blunt splenic injuries who were hemodynamically stable could be safely monitored with a protocol which required 4 days of inpatient care, 3 weeks of quiet home activities, and 3 months of light activity. This protocol seems to allow for safe return to unrestricted activity.
Incorrect Answer:
Ligaments attach to bone by both direct insertion and indirect insertion. Which of the following most accurately describes the order of the four transition zones of direct insertion?
Ligament > fibrocartilage > mineralized fibrocartilage > bone
Ligament > mineralized fibrocartilage > fibrocartilage > bone
Ligament > mineralized fibrocartilage > periosteum > bone
Ligament > Sharpey's fiber > periosteum > bone
Ligament > periosteum > fibrocartilage > bone
There are two types of tendon/ligament insertion into bone: direct and indirect insertion. The more common, indirect insertion, occurs when the superficial ligament fibers insert into the periosteum. Direct insertion of tendon/ligaments
into bone occurs through a transition of 4 distinct phases: 1) ligament, 2) fibrocartilage, 3) mineralized fibrocartilage, and 4) bone.
While flexing the elbow to perform a biceps curl, what type of muscle contraction is occuring?
Isometric
Isokinetic
Plyometric
Eccentric
Concentric
Concentric muscle contractions occur when a muscle shortens during contraction, as in the upward motion when performing a biceps curl. An eccentric contraction occurs when a muscle lengthens with contraction, as in the "negative" or lowering motion of a biceps curl. An example of an isometric (muscle contracts while maintaining constant length) contraction would be pushing against an immovable object. An example of an isokinetic (muscle has constant speed of contraction) occurs with specialized equipment like Cybex machines. Plyometric contractions occur when a muscle rapidly lengthens just prior to contraction - like during repetitive box jumping.
Woo and Buckwalter describe the mechanisms, barriers, and molecular processes involved in ligament and tendon injury and repair.
A 34-year-old laborer has her left foot crushed in a piece of farming equipment as shown in Figure A. All of the following are reasons for a poor outcome following a crush injury to the foot EXCEPT:
Workers compensation injury
Development of reflex sympathetic dystrophy (complex regional pain syndrome)
Delayed soft-tissue coverage in mangled extremities
Immediate skeletal stabilization
Ongoing litigation
This patient has a mangled extremity. Rigid skeletal stabilization is recommended to enhance soft-tissue healing.
Level 4 evidence from Myerson et al found that delayed soft-tissue coverage in mangled extremities correlated with poor outcome. Poor results also occurred
if treatment was not immediately initiated (immediate debridement shown in Illustration A), if patients subsequently had neuritis or reflex sympathetic dystrophy, or if patients were involved in ongoing workers' compensation and litigation. Neuroischemia following substantial soft-tissue injury likely plays a role in the development of chronic pain after crush injuries to the foot, either through direct trauma to the peripheral nerves or by intraneural or extraneural fibrosis. This trauma to the nerve may cause chronic neuritis, which then triggers a sympathetically mediated reflex sympathetic dystrophy (complex regional pain syndrome).
A 65-year-old man undergoes total knee replacement and is found to have deep vein thrombosis two days later. What molecule is
thought to be involved in this process when it is released during surgical dissection?
Prothrombin
RANKL
IL-1b
Thromboplastin
Factor XI Corrent answer: 4
Thromboplastin is also known more commonly as Tissue Factor (TF), which is involved in the Extrinsic Pathology of the coagulation cascade.
During surgical dissection, insults occur to the endothelial walls of blood vessels. There are three ways in which the body reacts to form a clot so that the patient does not bleed excessively. One is via vessel contraction, another is by collagen release, and a third is by tissue thromboplastin release. Thromboplastin release is part of the extrinsic coagulation pathway (see
Illustration A). Thromboplastin release activates Factor VII which activates Factor X which converts prothrombin to thrombin. Thrombin is the catalyst for converting fibrinogen to fibrin which induces clot formation. While this is useful for decreasing bleeding, it is the same mechanism by which a deep venous thrombosis (DVT) develops.
Which of the following materials has a Young's modulus of elasticity that is most similar to cortical bone
Titanium
Zirconia
Stainless steel
Ceramic (Al2O3)
Alloy (Co-Cr-Mo)
Of the materials listed Titanium has an elastic moduli closest to cortical bone. Titanium is extra-ordinarily light, strong, highly ductile, and corrosion resistant. Titanium is however very notch sensitive and has poor wear resistance.
Young Modulus of Elasticity is defined as the stiffness (ability to maintain
shape under external loading) of a material. On the stress vs. strain curve it is defined as the slope of the line in the elastic zone (see Illustration A). Young’s modulus is constant and different for each material. The relevant moduli (unit GPa) are approximated below:
Question 55
important in patients with renal impairment, which is not typically seen in SCT.
Explanation
Level of evidence provides guidance to the study quality. It is used to assess therapeutic studies (as with this question), prognostic studies, diagnostic studies and economic or decision models. When determining the level of evidence, readers must critically appraise the study question, treatment, intervention and outcomes of the study design. Level-II therapeutic studies consist of well-designed prospective cohort studies, poor-quality randomized controlled trials (follow-up less than 80%) and systematic review of Level-II studies or non-homogenous Level-I studies.
Wright et al. provided an excellent summary of clinical research study level of evidence. This has been provided as Illustration A.
Illustration A shows a chart of level of evidence. There is a column for each type of study which corresponds to a row that outlines the level of evidence based on study
design.
Incorrect Answers:
Low serum phosphate and normal calcium levels are found in what common etiology of hereditary rickets?
X-linked hypophosphatemic
Vitamin D-dependent, type I
Vitamin D-dependent, type II
Autosomal dominant hypophosphatemic
Jansen's metaphyseal chondrodysplasia
Low serum phosphate and normal calcium levels are found in X-linked hypophosphatemic rickets.
X-linked hypophosphatemic rickets is the most common form of hereditary rickets. It is an X-linked dominant disorder which has been linked to the PHEX gene. Laboratory findings
of this disorder include low serum phosphate, normal serum calcium and 25 hydroxycholecalciferol levels, and inappropriately low 1,25-dihydroxyvitamin D3.
Carpenter et al. showed hypophosphatemic rickets was initially referred to as “vitamin D resistant rickets” due to its lack of response to therapeutic vitamin D. Current treatment with activated vitamin D metabolites (calcitriol or
alfacalcidol) and phosphate salts have been shown to help with this condition.
Illustration A shows an insufficiency fracture of the proximal tibia in an adult patient with X-linked hypophosphatemic rickets. A stress fracture on the medial tibia may be a presenting feature of untreated disease.
Incorrect Answers:
receptor (PTHR1).
A healthy patient undergoes routine pre-operative laboratory testing and is found to have a leukocyte count of 1.5 × 10(9) cells/L. When the historical records are examined, this is found to be the patients base-line level over a period of years. Which of the following statements is most likely to be true:
The patient is at a significantly higher risk of surgical infection
The patient is more likely to be of African than of European descent
The patient is more likely to be of European than of Middle Eastern descent
The patient is more likely to be a non-athlete than an athlete
The patient is more likely to be female than male
The clinical presentation is consistent with Benign Ethnic Neutropenia, a condition in which a patient has chronic, benign, inborn and lifelong absolute neutrophl count below population mean. This condition is found in the U.S. to be most common in African- Americans, some groups of Middle Eastern patients, males, children under 5 years old, and athletes compared to non- athletes.
A standardized level at present for abnormally low absolute neutrophil count (ANC) is below 1.5 x 10(9) cells/L, however this may not have clinical or scientific relevance as a cutoff point, particularly in the affected Ethnic groups. Fewer than 1% of all populations have absolute neutrophil count < 1.0 X 10(9) cells/L. Most patients in the affected ethnic groups with low ANC and no associated history or symptoms are not expected to have any increased risk of infection or adverse effect. Smoking was also associated with higher leukocyte and neutrophil counts but proportionately lower increase in African-American patients. One hypothesis for the increased prevalence of B.E.N. in patients of African descent is a theorized evolutionary protection against malaria, though
it remains unclear if this is causal or just correlative.
Haddy et al. provide an excellent scientific review of B.E.N. and emphasize the importance of recognizing this most common form of neutropenia.
Eichner et al. review B.E.N. in the setting of sports medicine and state the relative increase of these lab findings in athletes vs non-athletes.
Hsieh et al. provide an extensive cross-sectional population study focused on the prevalence of Benign Ethnic Neutropenia in the U.S. They reviewed 25,222 participants in the National Health and Nutrition Examination Survey 1yr of
age or older from 1999-2004, and detail the association of this condition with age, sex, ethnicity, and smoking status.
Denic et al. analyzed neutrophil count in a healthy Arab population in the U.A.E. and found low neutrophil counts in this population with a distribution suggestive, but not definitively, of an autosomal dominant inheritance. They also discuss the hypothesized association of B.E.N. and malaria infection.
Incorrect answers:
Question 56
In a patient who has rheumatoid arthritis with acetabular protrusion, what is the best biomechanical position for the cup with respect to the preoperative center of rotation?
Explanation
REFERENCES: Crowninshield RD, Brand RA, Pedersen DR: A stress analysis of acetabular reconstruction in protrusio acetabuli. J Bone Joint Surg Am 1983;65:495-499.
Ranawat CS, Dorr LD, Inglis AE: Total hip arthroplasty in protrusio acetabuli of rheumatoid arthritis. J Bone Joint Surg Am 1980;62:1059-1065.
Question 57
What effect does deep freezing have on allograft tissue?
Explanation
REFERENCES: Shelton WR, Treacy SH, Dukes AD, Bomboy AL: Use of allografts in
knee reconstruction: I. Basic science aspects and current status. J Am Acad Orthop Surg 1998;6:165-168.
Caspari RB, Botherfield S, Horwitz RL, et al: HIV transmission via allograft organs and tissues. Sports Med Arthroscopy Rev 1993;1:42-46.
Question 58
Figure 3 shows the clinical photograph of a wrestler who has an acute mass in his ear. He does not wear protective headgear. The area is mildly tender and without erythema. Management should consist of
Explanation
REFERENCES: Kaufman BR, Heckler FR: Sports-related facial injuries. Clin Sports Med 1997;16:543-562.
Griffin CS: Wrestler’s ear: Pathophysiology and treatment. Ann Plastic Surg 1992;28:131-139.
Question 59
During preparation for the NCAA wrestling championships, a participant reports the development of vesicular lesions on his right chest wall that are mildly painful; however, they have not affected his ability to wrestle. How should this athlete be managed?
Explanation
hours before being allowed to participate. Also, all lesions must be dry and crusted and at least 120 hours of antiviral therapy should have been instituted.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 301-309.
Johnson R: Herpes Gladiatorium and other skin diseases. Clin Sports Med 2004;23:473-484.
Question 60
What radiographic measurement is best used to assess the adequacy of deformity correction for the patient shown in Figure 22?
Explanation
REFERENCES: Carroll K, Coleman S, Stevens PM: Coxa vara: Surgical outcomes of valgus osteotomies. J Pediatr Orthop 1997;17:220-224.
Cordes S, Dickens DR, Cole WG: Correction of coxa vara in childhood: The use of Pauwels’ Y-shaped osteotomy. J Bone Joint Surg Br 1991;73:3-6.
Question 61
Treatment should now include
Explanation
Extensive laminectomy in patients with degenerative spondylolisthesis does result in postoperative instability. In the study by White and Wiltse, further subluxation did occur in 66 percent of patients who were operated on for degenerative spondylolisthesis , whereas it was observed in only 2 percent of the spondylolisthesis or disc patients who did not have
spondylolisthesis postoperatively. The extent of decompression and facet removal must be limited in the patient with degenerative spondylolisthesis or a fusion of the transverse processes included as part of the treatment. Internal fixation devices have been used in these circumstances to prevent further subluxation while the fusion is consolidating. Wiltse outlined some guidelines for spinal fusion in spinal stenosis: (1) the patient who is less than sixty years old and had degenerative spondylolisthesis with a total loss of posterior stability due to removal of the articular processes (a one-level fusion of the transverse processes); (2) the patient who is less than fifty-five and had a midline decompression for degenerative spondylolisthesis with facet preservation; and
(3) the patient who is less than fifty years old with isthmic spondylolisthesis, if the posterior elements have been removed. Simple degenerative spinal stenosis seldom requires a fusion, even if all posterior stability has been lost. The problem with obtaining a successful spinal fusion is real and conditions are less than optimum in these instances.
Question 62
Figures 48a and 48b are the axial and sagittal T1-weighted MR images of the L4-5 disc level of a 38-year-old man. He is symptomatic from the pathology shown. A surgeon would expect the neurological findings to include

Explanation
The pathology shown in the MR images is a right-sided far lateral herniated nucleus pulposus at L4-5, which, if symptomatic, would cause a radiculopathy of the exiting root, L4. A more common posterolateral herniation at L4-5 would cause irritation of the traversing root, L5. The L4 root has a sensory distribution over the anterior thigh that extends along the anterior shin but does not tend to reach the toes. The motor distribution is to the quadriceps and anterior tibialis muscles, with the predominant reflex effect being the patella reflex. The L5 root has a sensory distribution to the first dorsal web space of the foot, motor distribution to the EHL, and no specific reflex.
RECOMMENDED READINGS
Standaert CJ, Herring SA, Sinclair JD. The patient history and physical examination: Cervical, thoracic, and lumbar. In: Herkowitz HN, Garfin SR, Eismont FJ, Bell GR, Balderston RA, eds. Rothman-Simeone The Spine. Vol 1. 5th ed. Philadelphia, PA: Saunders Elsevier; 2006:171-186.
Bono CM, Wisneski R, Garfin SR: Lumbar disc herniations. In: Herkowitz HN, Garfin SR, Eismont FJ, Bell GR, Balderston RA, eds. Rothman-Simeone The Spine. Vol 1. 5th ed. Philadelphia, PA: Saunders Elsevier; 2006:967-991.
Question 63
Figures 5a and 5b show the radiographs of an 11-year-old boy who felt a pop and immediate pain in his right knee as he was driving off his right leg to jam a basketball. Examination reveals that the knee is flexed, and the patient is unable to actively extend it or bear weight on that side. There is also a large effusion. Management should include
Explanation
REFERENCES: Heckman JD, Alkire CC: Distal patellar pole fractures: A proposed common mechanism of injury. Am J Sports Med 1984;12:424-428.
Tolo VT: Fractures and dislocations around the knee, in Green NE, Swiontkowski MF (eds): Skeletal Trauma in Children. Philadelphia, Pa, WB Saunders, 1994, vol 3, pp 380-382.
Question 64
A B Figures 60a and 60b are the postmyelography CT images of a 62-year-old man who has had low-back and bilateral lower-extremity pain. His pain began approximately 1 year ago and there was no precipitating event. The location of the pain is in the lower lumbar region in the midline and it radiates into the buttocks and thighs bilaterally. The pain is exacerbated by standing and walking and relieved by forward spine flexion. He reports no pain while sitting or lying supine. Upright radiographs demonstrate 4 mm of anterolisthesis of L4 on L5. What is the most appropriate surgical procedure?

Explanation
This patient radiographically has L4-5 degenerative stenosis and a low-grade spondylolisthesis. The axial images demonstrate a gap in the facet joint, more on the left than the right, which is highly suggestive of dynamic instability. Thus, this patient would most benefit from a laminectomy and fusion of L4-5. A microdiskectomy would not be helpful as this patient does not have a disk herniation. Patients undergoing posterior decompression alone experience an unacceptably high rate of recurrent stenosis and/or progression of spondylolisthesis. Early studies demonstrated that adding an intertransverse process fusion to posterior decompression significantly improved clinical outcomes. Anterior interbody fusion likely will not decompress the spinal canal sufficiently, though there is some thought that indirect decompression can be effective in some cases.
RECOMMENDED READINGS
Frymoyer JW. Degenerative Spondylolisthesis: Diagnosis and Treatment. J Am Acad Orthop Surg. 1994 Jan;2(1):9-15. PubMed PMID: 10708989. Majid K, Fischgrund JS. Degenerative lumbar spondylolisthesis: trends in management. J Am Acad Orthop Surg. 2008 Apr;16(4):208-15. Review. PubMed PMID: 18390483. View Abstract at PubMed
Carlisle E, Fischgrund JS. Lumbar spinal stenosis and degenerative spondylolisthesis. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006: 299-317.
Puschak TJ, Sasso RC. Spondylolysis-spondylolisthesis. In: Vaccaro AR, ed. Orthopaedic Knowledge Update 8. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:553-563.
Question 65
An obese 56-year-old woman with hypertension has had posterior heel pain for the past 6 months. She also notes some enlargement over the posterior aspect of the heel. Examination reproduces pain with palpation at the insertion of the Achilles tendon. A lateral radiograph is shown in Figure 45. What is the most likely diagnosis?
Explanation
REFERENCES: Schepsis AA, Wagner C, Leach RE: Surgical management of Achilles tendon overuse injuries: A long-term follow-up study. Am J Sports Med 1994;22:611-619.
Saltzman CL, Tearse DS: Achilles tendon injuries. J Am Acad Orthop Surg 1998;6:316-325.
Question 66
A 9-year-old boy falls from a scooter and sustains the injury shown in the radiographs in Figure 26. After closed reduction and cast immobilization, what is the most likely complication that can result? Review Topic

Explanation
Question 67
A healthy 64-year-old man just underwent an uncomplicated shoulder arthroplasty for severe glenohumeral osteoarthritis. Intraoperatively, 60 degrees of external rotation was obtained. Postoperatively, he starts on a range-of-motion program. What limitations are recommended?
Explanation
REFERENCES: Boardman ND III, Cofield RH, Bengston KA, et al: Rehabilitation after total shoulder arthroplasty. J Arthroplasty 2001;16:483-486.
Matsen FA III, Lippitt SB, Sidles JA, et al: Practical Evaluation and Management of the Shoulder. Philadelphia, PA, WB Saunders, 1994, pp 215-218.
Question 68
A 38-year-old woman with metastatic thyroid carcinoma has had increasing pain in the left hip for the past 3 months. An AP radiograph and coronal T 1 -weighted MRI scan are shown in Figures 28a and 28b. Management should consist of
Explanation
REFERENCES: Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Swanson KC, Pritchard DJ, Sim FH: Surgical treatment of metastatic disease of the femur. J Am Acad Orthop Surg 2000;8:56-65.
Clarke HD, Damron TA, Sim FH: Head and neck replacement endoprosthesis for pathologic proximal femoral lesions. Clin Orthop 1998;353:210-217.
Question 69
Which of the following factors is associated with the worst prognosis in soft-tissue sarcomas?
Explanation
REFERENCES: Collin C, Goobold J, Hadju SI, Brennan MF: Localized extremity soft tissue sarcoma: An analysis of factors affecting survival. J Clin Oncol 1987;5:601-612.
Eilber FC, Rosen G, Nelson SE, et al: High-grade extremity soft tissue sarcomas: Factors predictive of local recurrence and its effect on morbidity and mortality.
Ann Surg 2003;237:218-226.
Question 70
Among the options listed below, what is the best treatment for the complication shown in Figure 10c?
Explanation
Proximal femur fractures can be treated using a variety of implants including intramedullary nails, blade plates, and locking plates (now precontoured proximal femur plates). The comminution and lack of medial cortical support may predispose these fractures to nonunion.
The recent popularity of locking plates for proximal femur treatment has increased their use for this fracture; however, a disproportionately high rate of failure of these plates, including early implant failure with plate and screw breakage, cut out with varus collapse, and nonunion have been reported.?
Malreduction predisposes these fractures to failure. The initial postoperative radiographs do not reveal a varus malreduction because the tip of the greater trochanter is below the center of the femoral head.
Once failure occurs, the best fixation method among the options detailed is an intramedullary nail (second generation with screws into the femoral head) and restoration of alignment. THA is usually not recommended for treatment of subtrochanteric femur fractures in young patients.
RECOMMENDED READINGS
Wirtz C, Abbassi F, Evangelopoulos DS, Kohl S, Siebenrock KA, Krüger A. High failure rate of trochanteric fracture osteosynthesis with proximal femoral locking compression plate.
Injury. 2013 Jun;44(6):751-6. doi: 10.1016/j.injury.2013.02.020. Epub 2013 Mar 21. PubMed PMID: 23522837. View Abstract at PubMed
Floyd JC, O'Toole RV, Stall A, Forward DP, Nabili M, Shillingburg D, Hsieh A, Nascone JW. Biomechanical comparison of proximal locking plates and blade plates for the treatment of comminuted subtrochanteric femoral fractures. J Orthop Trauma. 2009 Oct;23(9):628-33. doi: 10.1097/BOT.0b013e3181b04835. PubMed PMID: 19897983. View Abstract at PubMed Glassner PJ, Tejwani NC. Failure of proximal femoral locking compression plate: a case series. J Orthop Trauma. 2011 Feb;25(2):76-83. doi: 10.1097/BOT.0b013e3181e31ccc.
PubMed PMID: 21245709. View Abstract at PubMed
Question 71
Figures 7a and 7b show the radiographs of a 51-year-old woman who injured her left leg after falling off a stepladder. Surgical reconstruction is performed with a compression screw and side plate; the postoperative radiograph is shown in Figure 7c. Following gradual progression of weight bearing, she reports that she slipped again and placed full weight on the extremity. She now notes a new onset of increased pain in her left thigh and hip region. Follow-up radiographs are shown in Figures 7d and 7e. Reconstruction should consist of
Explanation
REFERENCES: Bridle SH, Patel AD, Bircher M, Calvert PT: Fixation of intertrochanteric fractures of the femur: A randomized prospective comparison of a gamma nail and dynamic hip screw. J Bone Joint Surg Br 1991;73:330-334.
DeLee JC: Fractures and dislocations of the hip, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1659-1825.
Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Sanders RW, Regazzoni P: Treatment of subtrochanteric femur fractures using the dynamic condylar screw. J Orthop Trauma 1989;3:206-213.
Question 72
A B C D Figures 75a through 75d show the radiographs of an 85-year-old woman who fell from a step and sustained a right proximal femur fracture. Six months after surgery she has knee pain. What is the most likely cause of her pain?

Explanation
Three cases of anterior distal femoral cortex penetration during intramedullary nailing for subtrochanteric fractures were documented by Ostrum and Levy in a 2005 study. Case 1 involved a Zimmer (Warsaw, Indiana) M/DN antegrade femoral nail, Case 2 involved a Stryker (Mahwah, New Jersey) long-stem Gamma nail, and Case 3 a DePuy Synthes (West Chester, Pennsylvania) titanium femoral nail with spiral blade locking. The anterior Zimmer nail penetration resulted in a displaced supracondylar fracture, which subsequently required revision. The Gamma nail as well as the DePuy Synthes nail were left impaled through the distal femoral cortex, and the subtrochanteric fractures went on to union. The anteroposterior radius of curvature for the Zimmer, long Gamma, and DePuy Synthes nails is 257 cm, 300 cm, and 150 cm, respectively. It is estimated that the radius of curvature of the femoral diaphyseal canal is 114 to 120 cm. It appears that the difference in femoral anteroposterior bow between the bone and the implant is a contributing factor to distal femoral anterior cortex penetration in intramedullary nailing of subtrochanteric fractures. There is no evidence of osteoarthrosis on the radiographs. Although nonunion is possible, based on the radiographic findings it is more likely that this patient's pain is attributable to the curvature of the nail. The lateral image of the hip reveals an appropriate starting point for the device.
RECOMMENDED READINGS
Ostrum RF, Levy MS. Penetration of the distal femoral anterior cortex during intramedullary nailing for subtrochanteric fractures: a report of three cases. J Orthop Trauma. 2005 Oct;19(9):656-60. PubMed PMID: 16247312.View Abstract at PubMed
Egol KA, Chang EY, Cvitkovic J, Kummer FJ, Koval KJ. Mismatch of current intramedullary nails with the anterior bow of the femur. J Orthop Trauma. 2004 Aug;18(7):410-5. PubMed PMID: 15289685. View Abstract at PubMed
RESPONSES FOR QUESTIONS 76 THROUGH 78
- Nonsurgical treatment with closed reduction and immobilization
- Early mobilization with physical therapy initiated within 2 weeks
- Open reduction and internal fixation (ORIF) with locked implants
- Use of supplemental bone graft or substitutes
- Arthroplasty
- Workup for osteoporosis and counseling
Which intervention listed is most appropriate to address each scenario described?

76A B
Question 73
A 72-year-old man who underwent total shoulder arthroplasty 2 years ago slipped on ice and fell on his shoulder 3 weeks ago. Immediately after falling he was unable to elevate his arm. Motor examination reveals deltoid 5-/5, subscapularis 5-/5, external rotation 4-/5, and supraspinatus 2/5. Radiographs are shown in Figures 8a and 8b. What is the most likely diagnosis?
Explanation
REFERENCES: Hattrup SJ, Cofield RH, Cha SS: Rotator cuff repair after shoulder replacement. J Shoulder Elbow Surg 2006;15:78-83.
Sperling JW, Potter HG, Craig EV, et al: Magnetic resonance imaging of painful shoulder arthroplasty. J Shoulder Elbow Surg 2002;11:315-321.
Question 74
A 42-year-old woman reports that she has low back pain and had a transient loss of consciousness after falling off a horse. She denies having neck pain but notes that she was involved in a motor vehicle accident 2 years ago and had neck pain at that time. Examination reveals full range of motion of the neck and no localized tenderness. The neurologic examination is normal. A lateral radiograph of the cervical spine is obtained. Figures 41a and 41b show CT and MRI scans. What is the most likely diagnosis?
Explanation
REFERENCES: Schatzker J, Rorabeck CH, Waddell JP: Non-union of the odontoid process: An experimental investigation. Clin Orthop 1975;108:127-137.
Clark CR, White AA III: Fractures of the dens: A multicenter study. J Bone Joint Surg Am 1985;67:1340-1348.
Question 75
A 35-year-old man who is an avid weight lifter competing in local tournaments reports new onset pain and loss of motion in his dominant right shoulder. Examination reveals joint line tenderness, active elevation to 100 degrees, and external rotation to 10 degrees. His contralateral shoulder reveals 170 degrees forward elevation and 50 degrees external rotation. Radiographs are shown in Figures 46a and 46b. What is the next most appropriate step in management?
Explanation
REFERENCES: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.
Skedros JG, O’Rourke PJ, Zimmerman JM, et al: Alternatives to replacement arthroplasty for glenohumeral arthritis, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 485-499.
Question 76
Figures 7a through 7d show the radiographs and MRI scans of a 69-year-old woman with neck and upper extremity pain and progressive deformity of the cervical spine. What is the most likely diagnosis? Review Topic

Explanation
estimated to be between 11% and 47%. It can result in recurrent myelopathy if the spinal cord becomes draped over the kyphosis. In addition to the neurologic sequelae, the kyphosis itself can be a source of neck pain and deformity. Spondylolisthesis can develop, contributing to further cord compression. In this case, the patient had undergone a previous C4-5 anterior cervical diskectomy and fusion followed by a posterior laminectomy from C2 through C7, without fusion. This has resulted in severe kyphosis (i.e. postlaminectomy kyphosis) with grade II-III spondylolisthesis at C3-4 and a grade I spondylolisthesis at C2-3. While ankylosing spondylitis can also result in a chin-on-chest deformity secondary to ankylosis, there is no evidence of marginal syndesmophytes in the imaging studies to suggest this diagnosis. The occiput is hyperextended on C1 on the lateral upright radiograph to compensate for the kyphosis in an attempt to maintain horizontal gaze. This results in an unusual appearing relationship on the imaging studies. However, there is no widening of the distance between C1 and the occiput and no evidence of soft-tissue injury on the MRI scans to suggest an acute injury. C3-4 demonstrates an unstable spondylolisthesis and was never intended to be included in the C4-5 fusion. Klippel-Feil syndrome is the failure of segmentation of the cervical spine. The classic triad includes congenital fusion, low hairline, and a web neck.
Question 77
An 11-year-old basketball player reports that he felt a painful pop in the left knee when he stumbled while running. He is unable to bear weight on the extremity and cannot actively extend the knee against gravity. Examination reveals a large knee effusion. A lateral radiograph is shown in Figure 7. Management should consist of
Explanation
REFERENCES: Maguire JK, Canale ST: Fractures of the patella in children and adolescents.
J Pediatr Orthop 1993;13:567-571.
Grogan DP, Carey TP, Leffers D, et al: Avulsion fractures of the patella. J Pediatr Orthop 1990;10:721-730.
Question 78
A 21-year-old man has had posterior neck discomfort for the past 6 months. Radiographs, an MRI scan, and a photomicrograph of the biopsy specimen are shown in Figures 17a through 17d. What is the most likely diagnosis?
Explanation
REFERENCES: Bridwell KH, Ogilvie JW: Primary tumors of the spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery. Philadelphia, PA, JB Lippincott, 1991,
vol 2, pp 1143-1174.
Enneking WF: Musculoskeletal Tumor Surgery. New York, NY, Churchill Livingstone, 1983, pp 1043-1053.
Question 79
A 50-year-old man reports left shoulder pain and weakness after undergoing a lymph node biopsy in his neck 2 years ago. Examination reveals winging of the left scapula. Electromyography shows denervation of the trapezius. Surgical treatment for this condition involves
Explanation
REFERENCES: Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Langenskiold A, Ryoppy S: Treatment of paralysis of the trapezius muscle by Eden-Lange operation. Acta Orthop Scand 1973;44:383-388.
Romero J, Gerber C: Levator scapulae and rhomboid transfer for paralysis of trapezius: The Eden-Lange procedure. J Bone Joint Surg Br 2003;85:1141-1145.
Question 80
A 19-year-old man sustains a low-velocity gunshot wound to the forearm. What factor most strongly correlates with the development of compartment syndrome after this injury?
Explanation
REFERENCES: Moed BR, Fakhouri AJ: Compartment syndrome after low-velocity gunshot wounds to the forearm. J Orthop Trauma 1991;5:134-137.
Hahn M, Strauss E, Yang EC: Gunshot wounds to the forearm. Orthop Clin North Am 1995;26:85-93.
Question 81
After sustaining a muscle contusion injury, prolonged immobilization leads to Review Topic
Explanation
Question 82
What percentage of bone weight is collagen?
Explanation
Question 83
What is the second most common primary bone malignancy in children?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 195.
Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 84
Botulinum toxin is used to treat vasospastic disorders of the hand such as the Raynaud phenomenon to improve digital perfusion and reduce pain. Botulinum toxin enables which transmitter to be unopposed, resulting in vasodilation?
Explanation
Nitric oxide is the only transmitter listed that is not inhibited by botulinum toxin. Substance P and glutamate are inhibited by botulinum toxin from release by pain nociceptors, thus reducing pain. Fonseca and associates have postulated that botulinum toxin inhibits the RhoA kinase pathway by blocking reactive oxygen species, which in turn does not allow actin/myosin to activate, thus preventing vasoconstriction of smooth muscle. Blocking the RhoA kinase pathway allows the action of nitric oxide to be unopposed, causing vasodilation. Nitric oxide is a potent vasodilator. Thus, botulinum toxin promotes nitric oxide activity to increase vasodilation.
Question 85
You are interested in learning a new technique for minimally invasive total knee arthroplasty. The Keyhole Genuflex system seems appealing to you because the instrumentation comes with wireless controls. Which of the following represents an acceptable arrangement?
Explanation
REFERENCES: AAOS Standard of Professionalism -Orthopaedist -Industry Conflict of Interest (Adopted 4/18/07), Mandatory Standard numbers 6, 9, 12-15. http://www3.aaos.org/member/profcomp/SOPConflictsIndustry.pdf
The Orthopaedic Surgeon’s Relationship with Industry, in Guide to the Ethical Practice of Orthopaedic Surgery, ed 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007. http://www.aaos.org/about/papers/ethics/1204eth.asp
AdvaMed Code of Ethics on Interactions with Health Care Professionals 2005. http://www.advamed.org/MemberPortal/searchresults.htm?query=Advamed%20Code%20of%20Ethics%20on%20Interactions%20with%20Health%20Care%20Professionals%202005
Question 86
Up to what time frame are the risks minimized in anterior revision disk replacement surgery? Review Topic
Explanation
Question 87
- A physician who is currently in a fellowship program receives notification of a pending malpractice suit that refers to an incident that occurred 2 years ago when the physician was a resident. The physician would be insured if the residency program provided what type of insurance coverage?
Explanation
Question 88
A 22-year-old college football player reports shortness of breath and dyspnea after a tackle. Examination reveals tachypnea, tachycardia, the trachea is shifted to the right, and there are decreased breath sounds on the left lung fields. The first line of treatment on the field should be
Explanation
REFERENCES: Amaral JF: Thoracoabdominal injuries in the athlete. Clin Sports Med 1997;16:739-753.
Perron AD: Chest pain in athletes. Clin Sports Med 2003;22:37-50.
Question 89
A 40-year-old man who is an avid weight lifter has had chronic pain in the proximal anterior shoulder for the past year. He denies any history of trauma. Examination reveals tenderness at the intertubercular groove, a positive speed test, and a positive Neer impingement sign. Nonsurgical management has failed to provide relief, and he is now considering surgery. Arthroscopic findings in the glenohumeral joint are shown in Figure 31. Based on these findings, treatment should consist of
Explanation
REFERENCES: Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310.
Burkhead WZ, Arcand MA, Zeman C, et al: The biceps tendon, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1996.
Question 90
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function? Review Topic
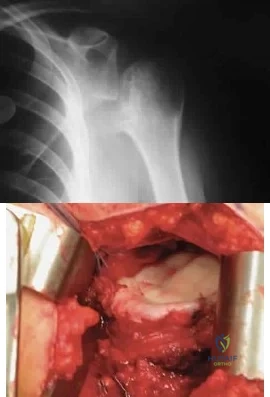
Explanation
Question 91
A 30-year-old elite marathon runner reports chronic pain over the lateral aspect of the distal right leg and dysesthesia over the dorsum of the foot with active plantar flexion and inversion of the foot. Examination reveals a tender soft-tissue fullness approximately 10 cm proximal to the lateral malleolus. The pain is exacerbated by passive plantar flexion and inversion of the ankle. There is also a positive Tinel’s sign over the site of maximal tenderness. There is no motor weakness, and deep tendon reflexes are normal. Radiographs and MRI of the leg are normal. What is the next most appropriate step in management?
Explanation
REFERENCES: Styf J: Diagnosis of exercise-induced pain in the anterior aspect of the lower leg. Am J Sports Med 1988;16:165-169.
Sridhara CR, Izzo KL: Terminal sensory branches of the superficial peroneal nerve: An entrapment syndrome. Arch Phys Med Rehabil 1985;66:789-791.
Styf J: Entrapment of the superficial peroneal nerve: Diagnosis and results of decompression.
J Bone Joint Surg Br 1989;71:131-135.
Question 92
A 74-year-old man has had worsening left shoulder pain for the past 3 years. Extensive nonsurgical management has provided only minimal relief. Examination reveals limitations in motion due to pain but good rotator cuff strength. Radiographs are shown in Figures 53a and 53b. What surgical procedure is most appropriate?
Explanation
REFERENCES: Bryant D, Litchfield R, Sandow M, et al: A comparison of pain, strength, range of motion, and functional outcomes after hemiarthroplasty and total shoulder arthroplasty in patients with osteoarthritis of the shoulder: A systemic review and meta-analysis. J Bone Joint Surg Am 2005;87:1947-1956.
Edwards TB, Kadakia NR, Boulahia A, et al: A comparison of hemiarthroplasty and total shoulder arthroplasty in the treatment of primary glenohumeral osteoarthritis: Results of a multicenter study. J Shoulder Elbow Surg 2003;12:207-213.
Gartsman GM, Roddey TS, Hammerman SM: Shoulder arthroplasty with or without resurfacing of the glenoid in patients who have osteoarthritis. J Bone Joint Surg Am 2000;82:26-34.
Question 93
A 65-year-old woman has severe pain and numbness in her hand. She notes frequent awakenings at nighttime and difficulty with fine tasks. She also has a history of cervical radiculopathy and notes intermittent pain in her upper arm and periscapular region. An examination reveals a positive Tinel sign over the midforearm and carpal tunnel. Electrodiagnostic testing shows a median nerve sensory distal latency of 3.8 ms (normal latency is 3.5 ms). Which intervention or test would best predict if carpal tunnel release would be successful in relieving this patient's symptoms?
Explanation
This patient demonstrates several upper extremity issues including possible carpal tunnel syndrome, cervical radiculopathy, and pronator syndrome. The electrodiagnostic testing is equivocal, and a corticosteroid carpal tunnel injection should be performed prior to surgical intervention to assess its effectiveness in eliminating the patient's symptoms. Positive response (meaning improvement in symptoms), after corticosteroid injection at the carpal tunnel correlates well with symptom relief following surgery. Trigger-point injections are not indicated for carpal tunnel syndrome. Ultrasound and carpal tunnel view radiograph can provide diagnostic information but would not be helpful in determining treatment in this specific case.
Question 94
A 46-year-old woman fell from her bicycle and sustained the injury shown in Figure 24. Which of the following ligaments has been disrupted?
Explanation
REFERENCES: Fukuda K, Craig EV, An KN, et al: Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Joint Surg Am 1986;68:434-439.
Bosworth B: Complete acromioclavicular dislocation. N Engl J Med 1949;241:221-225.
Question 95
What is the primary reason for including the ilium in the distal fixation of long instrumentation constructs in adult scoliosis? Review Topic
Explanation
Question 96
..Figures 3a and 3b are the radiographs of a 5-year-old child with midtibia swelling and no pain. What isthe most appropriate next step?
Explanation

Question 97
An 18-year-old boxer sustained a blow to his right eye in a boxing match. Examination on the sideline reveals hyphema, reduced visual acuity and color vision, and a visual field cut. What is the next step in management? Review Topic
Explanation
Question 98
What is the goal of surgical treatment in this scenario?
Explanation
This patient has a metastatic neuroendocrine tumor. Surgical treatment should prioritize palliation of her symptoms. She has high-grade spinal cord compression without neurologic signs or symptoms. Steroids are beneficial for patients with high-grade spinal cord compression caused by tumors, and these drugs should be administered in the acute setting. This patient was appropriately initially treated with conventional radiation. However, she is not a candidate for further radiation because of spinal cord tolerance limits and insufficient clearance between the tumor and spinal cord. Consequently, stereotactic radiation is not an option.
The goal of surgical treatment of this tumor should be palliation of her symptoms rather than cure. A costotransversectomy approach offers the advantage of ventral and dorsal spinal cord access, which is necessary in this case. A sternotomy or transthoracic approach would offer ventral access, but dorsal access would be less than optimal.
RECOMMENDED READINGS
Rose PS, Buchowski JM. Metastatic disease in the thoracic and lumbar spine: evaluation and management. J Am Acad Orthop Surg. 2011 Jan;19(1):37-48. Review. PubMed PMID: 21205766.View Abstract at PubMed
Rades D, Abrahm JL. The role of radiotherapy for metastatic epidural spinal cord compression. Nat Rev Clin Oncol. 2010 Oct;7(10):590-8. doi: 10.1038/nrclinonc.2010.137. Epub 2010 Aug
Question 99
Figures 3a and 3b show the inversion stress radiographs of a patient’s ankle. What is the most likely ligament injury pattern?
Explanation
REFERENCES: Harper MC: Stress radiographs in the diagnosis of lateral instability of the ankle and hindfoot. Foot Ankle 1992;13:435-438.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 39-54.
Question 100
A 31-year-old male sustains an ipsilateral displaced transverse acetabular fracture, pubic rami fractures, and a sacroiliac joint dislocation. What structure should be reduced and stabilized first?

Explanation
The referenced article by Matta reviewed 259 patients with acetabular fractures treated within 21 days of injury and found that the hip joint can be preserved and post-traumatic osteoarthrosis can be avoided if an anatomical reduction is achieved.
