Orthopedic Board Review MCQs: Arthroplasty, Deformity, Foot & Hip | Part 237

Key Takeaway
This page offers Part 237 of Dr. Hutaif's OITE/AAOS Orthopedic Surgery Board Review. It features 100 verified high-yield MCQs, formatted for board exams. Designed for orthopedic residents and surgeons, this quiz provides critical practice and in-depth explanations to master key topics like Arthroplasty, Deformity, Foot, and Hip for certification success.
About This Board Review Set
This is Part 237 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 237
This module focuses heavily on: Arthroplasty, Deformity, Foot, Hip.
Sample Questions from This Set
Sample Question 1: In X-linked hypophosphatemic rickets, the gene defect may be found in which of the following?...
Sample Question 2: A 23-year-old male reports a firm, immobile mass behind his tibia that creates pain when he walks long distances or uses stairs. He reports no night pain or constitutional symptoms. His WBC, LDH, and Alkaline phosphatase are normal. Radiogr...
Sample Question 3: A 30-year-old man has had a slowly enlarging mass on the plantar medial aspect of the foot for the past 6 months. The mass is now 1 cm in diameter, adherent to the plantar fascia, and painful with weightbearing. The overlying skin is mobile...
Sample Question 4: Two years ago, a 63-year-old man underwent right total hip arthroplasty (THA) with a modular femoral head-neck and neck-stem prosthesis (a photograph of the removed implantis shown in Figure 181). He now has increasing hip pain. Radiographs...
Sample Question 5: Figures 1 through 3 demonstrate the radiographs obtained from a 25-year-old man who injured his right,by punching a wall 3 weeks earlier. He notes pain and deformity about the ulnar aspect of his hand. The best treatment option is...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
In X-linked hypophosphatemic rickets, the gene defect may be found in which of the following?
Explanation
Question 2
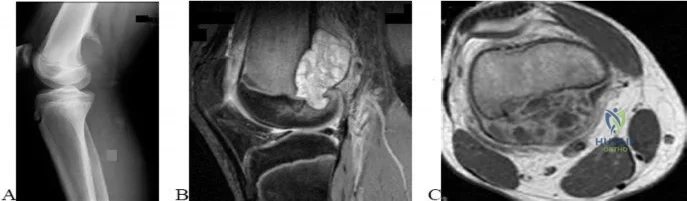
A 23-year-old male reports a firm, immobile mass behind his tibia that creates pain when he walks long distances or uses stairs. He reports no night pain or constitutional symptoms. His WBC, LDH, and Alkaline phosphatase are normal. Radiographs are shown in Figures A and B. A T1 MRI is shown in Figure C. What is the next most appropriate step in management?

Explanation
Osteochondromas are benign lesions, and therefore treatment is dictated by the severity of the symptoms they produce, the skeletal maturity of the patient, and concern for malignant transformation. If the symptoms are tolerable, excision is delayed until patient reaches skeletal maturity or for as long as possible due to increased risk of recurrence. In a more symptomatic skeletally immature patient, marginal excision is performed. Depending on the location, an additional concern for these patients is periarticular deformity or limb length inequality after removal. In skeletally mature patients, marginal excision is the treatment with very low risk of local recurrence. Concern for malignant transformation, found in less than 1% of patients, is an indication for wide resection.
Gitelis et al. discussed osteochondromas addressing general characteristics, presentation, and management options. Nonsurgical management is used in asymptomatic patients with no concern for malignant degeneration. Surgical excision is indicated in patients who have pain, interference with joint function, or impingement of the mass on neurovascular structures. These symptomatic tumors are usually treated with marginal resection, but there is the option of intralesional excision in skeletally mature patients. If there is concern for malignant degeneration, wide resection is performed for all patients.
Figure A and B are radiographs of an osteochondroma in which the cortex of the lesion and the underlying cortex are continuous. Figure C is a sagittal cut of a T1-weighted MRI image showing the high signal features of fatty marrow extending from the medullary canal of the tibia up into the bony stock of the pedunculated osteochondroma.
Incorrect Answers:
A 51-year-old female with known metastatic breast cancer presents with acute right thigh pain and inability to bear weight. A radiograph is shown in Figure A. A biopsy is performed that confirms metastatic breast cancer. What is the next step in management?

Local radiation therapy
Intramedullary nailing only
Intramedullary nailing and chemotherapy
Intramedullary nailing, radiation therapy to the tumor site, and chemotherapy
Intramedullary nailing, radiation therapy to the entire femur, and chemotherapy
This patient is presenting with biopsy proven metastatic breast cancer and a pathological fracture. The treatment in this situation is intramedullary nailing with postoperative radiation therapy to the entire femur and chemotherapy.
Due to the process of placing the intramedullary nail, the treating surgeon contaminates the ENTIRE femur with breast cancer. The surrounding area is already contaminated with tumor cells from the fracture, however. While the intramedullary nail will stabilize the pathological fracture, it does nothing to control the local progression of breast cancer in this patient's leg. Local radiotherapy will not only improve the local control of disease but it will palliate the patient's cancer related pain.
Weber et al review bone metastasis to the femur and propose valuable treatment pearls for clinical decision making and the biology which prevents cancer bearing bones to heal properly despite appropriate mechanical stabilization.
Swanson et al review the role of the orthopaedic surgeon in evaluating and treating metastatic bone disease, paying close attention to the necessity to obtain a tissue diagnosis in the event of presumed metastatic disease PRIOR to proceeding with any treatment plan.
All of the following locations are common sites for giant cell tumor of bone to occur EXCEPT?
Posterior elements of the spine
Distal femur
Sacrum
Distal radius
Proximal tibia
As reviewed by Robert Turcotte in the referenced article, the most common locations for giant cell tumor of bone to occur are about the distal femur/proximal tibia, distal radius, and the sacrum. The spine is an uncommon location for giant cell tumors, and when they occur, they usually occur in the vertebral body, not the posterior elements. In the axial skeleton, the sacrum is a common location for giant cell tumor of bone. Outside of the sacrum, giant
cell tumor of bone is characteristically an epiphyseal/metaphyseal lesion. As discussed in the in vitro study by Gortzak et al, treatment of giant cell tumor of bone includes aggressive intralesional curettage augmented with adjuvant treatment like hydrogen peroxide, argon beam, liquid nitrogen, or phenol. Due to the morbidity of the surgical treatment, and the less than perfect long term outcome, adjuvant therapy with an antibody against RANKL called denosumab is currently being investigated in multiple centers across North America as described by Thomas et al in their phase 2 study. Denosumab inhibits osteoclast mediated osteolysis and treatment is associated with improved bone stock and sclerosis of the GCT lesions. While denosumab doesn't obviate the need for surgical excision, the resulting surgical procedure is less extensive and early data may suggest a decreased risk of local recurrence.
While giant cell tumor of bone is a benign condition, there is a small chance for pulmonary seeding of giant cell metastases. This occurs in somewhere between 2-5% of patients with primary giant cells and occurs more often in patients with recurrent disease.
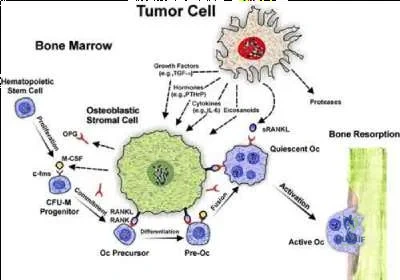
A 59-year-old female presents with a metastatic spinal tumor and has a lytic lesion in the T12 vertebral body. The process of bone resorption in her lytic lesion is mediated by
Direct resorption of bone by tumor cells
Neoangiogenesis of the vertebral body
Macrophage-mediated bony destruction
Tumor induced activation of osteoclasts
Necrosis of the vertebral body
Metastatic tumors are thought to induce osteolysis not by direct resorption of bone (remember only osteoclasts can destroy bone) but rather by releasing osteoclastogenic inflammatory cytokines.
Okeefe et al present a Level 5 review that states TNFa, RANKL, IL-1b, and IL-6 are osteoclastogenic inflammatory cytokins. Among these, RANKL is the most
notable and important cytokine. It binds to RANK, a surface receptor, and initiates osteoclastogenesis.
Goltzman presents a Level 5 review of the skeletal manifestations of malignancy. They report that by binding and neutralizing RANKL, osteoprotegrin (OPG) can diminish the production of functioning osteoclasts, and this factor has been shown to block bone resorption that is associated with malignancy.
Illustration A is a schematic representation of tumor-cell induced osteolysis.
Patients with which of the following conditions have the highest incidence of malignant tumor?
Single enchondroma
Single osteochondroma
Multiple hereditary exostosis
Ollier's disease
Maffucci's syndrome
Of all the listed cartilage lesions, patients with Maffucci's syndrome have the highest risk of malignant tumor - estimated to be 100% over the lifetime of the patient.
Single enchondromas and osteochondromas have a 1% risk of malignant transformation. Multiple hereditary exostosis patients have approximately a 10 % life time risk of malignant transformation. Ollier's disease is one of multiple enchondromas and carries a 30% risk of malignant transformation ( Illustration A) while Maffucci's syndrome is multiple enchondromas with hemangiomas (Illustration B). Maffucci's is also associated with a large number of other malignancies—particularly, pancreatic and hepatic adenocarcinoma, mesenchymal ovarian tumors, brain tumors such as glioma and astrocytoma, and various kinds of sarcomas.
While patients with enchondromas and osteochondromas do have a slight elevation in the risk for malignant transformation, it is not as great as those patients with Ollier's disease or Maffucci's syndrome. Distinguishing enchondromas from low grade chondrosarcomas can be done by looking at radiograph features such as the degree of endosteal scalloping on radiographs and the clinical presence of pain, both associated with low grade chondrosarcomas.
Ryzewicz et al review the diagnosis, pathology, and recommended treatment for patients with benign cartilage lesions. They recommend periodic follow-up even for the most benign lesions to track for malignant degeneration.

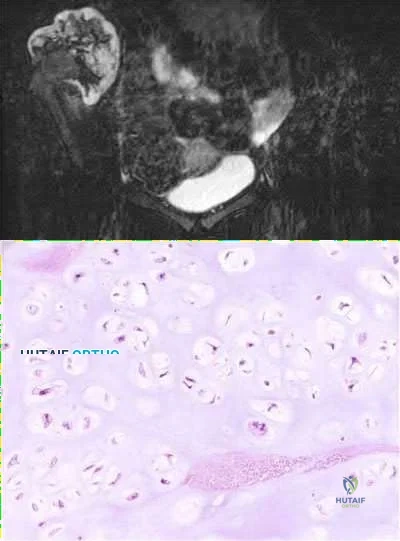
A 44-year-old male reports a mass at his right iliac crest that bothers him when he wears a belt. He denies constitutional symptoms
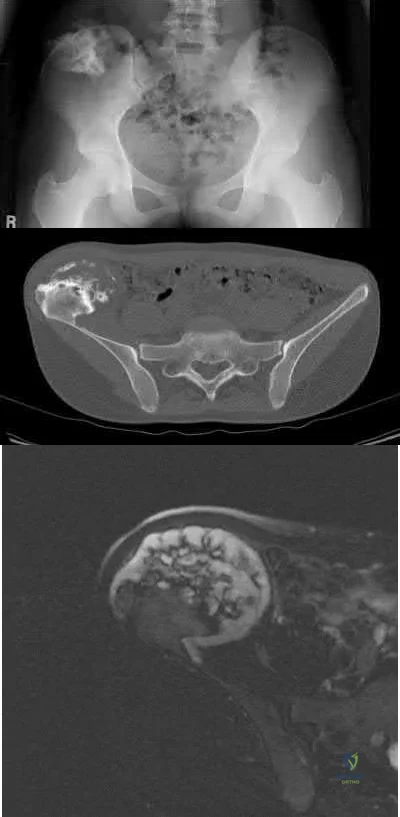
and has no bowel function disturbance. His ESR and CRP are normal. His chest CT is normal. Pelvis radiograph, CT, and MRI images are shown in Figures A-D. A biopsy is performed with histology shown in Figure E. What is the next most appropriate step in management?
Repeat CT scan in 3 months
Neoadjuvant radiation followed by marginal surgical resection followed by adjuvant chemotherapy 3 . Marginal surgical resection
Wide surgical resection
Neoadjuvant chemotherapy followed by marginal surgical resection followed by adjuvant chemotherapy
The history, imaging, and biopsy is consistent with chondrosarcoma and is appropriately treated with wide surgical resection. Chondrosarcoma is a malignant tumor of cartilaginous origin. It can be a primary lesion but may also develop from a preexisting cartilaginous lesion (e.g., osteochondroma, enchondroma). On plain radiographs, chondrosarcoma is typically visualized as a destructive, lytic lesion. Extension into surrounding soft tissues is frequently seen and delineated well on MRI. The characteristic chondroid matrix (rings
and arcs) can be seen on radiographs (70%), and better visualized by CT. The histology generally demonstrates enlarged, pleomorphic chondrocytes with multinucleated lacunae.
Level 4 evidence by Lee et al reviewed 227 patients with chondrosarcoma with an average follow-up of 6 years. They found that “patients who had had a resection with wide margins (margins extending outside the reactive zone) had a longer duration of survival than did those who had had a so-called marginal resection (margins extending outside the tumor but within the reactive zone) or an intralesional resection (margins within the lesion) (p < 0.04)."
Sixty Gy is a typical radiation dose for which of the following indications?
Prevention of post-operative heterotopic ossification
Neoadjuvant radiation therapy for a high-grade chondrosarcoma
Adjuvant radiation therapy for a high-grade osteosarcoma
Adjuvant radiation therapy for a soft-tissue sarcoma
Palliative therapy for a painful adenocarcinoma metastasis in the thoracic spine
Sixty Gy (or 6000 cGy) is a typical radiation dose for adjuvant radiation therapy for a soft-tissue sarcoma.
External beam radiotherapy plays a major role in the treatment of soft-tissue sarcomas following limb salvage surgery. Radiation doses can vary between 45 and 65 Gy. Any dose of XRT compromises wound healing, but especially those of 45 Gy (delayed healing) and 60 Gy (not expected to heal).
Incorrect Answers:
Question 3
A 30-year-old man has had a slowly enlarging mass on the plantar medial aspect of the foot for the past 6 months. The mass is now 1 cm in diameter, adherent to the plantar fascia, and painful with weightbearing. The overlying skin is mobile. Management at this time should consist of
Explanation
Question 4
Two years ago, a 63-year-old man underwent right total hip arthroplasty (THA) with a modular femoral head-neck and neck-stem prosthesis (a photograph of the removed implant is shown in Figure 181). He now has increasing hip pain. Radiographs reveal a stable hip arthroplasty and elevated serum cobalt and chromium levels. MR imaging is obtained, and, based on these findings, the patient’s hip is revised. Which corrosion type likely is responsible for this THA failure?
Explanation
Micromotion at the femoral head-neck or stem-neck junction can lead to fretting corrosion. Fretting corrosion is among the most common causes of failure in modular components. Modularity gives surgeons additional intraoperative flexibility but has resulted in corrosion-related failure and an implant recall. Although titanium and cobalt-chrome contain a protective surface oxide layer, continued micromotion at the modular junction may disrupt the protective layer, resulting in fretting corrosion. This may eventually lead to excessive metal ion formation and painful synovitis that necessitates a revision procedure. Galvanic corrosion is attributable to a mismatch in electrochemical gradients between dissimilar metals. Crevice or pitting corrosion occurs in fatigue cracks because of differences in oxygen tension.
Question 5
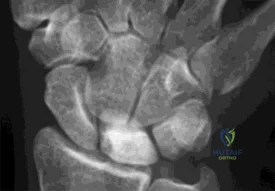
Figures 1 through 3 demonstrate the radiographs obtained from a 25-year-old man who injured his right, by punching a wall 3 weeks earlier. He notes pain and deformity about the ulnar aspect of his hand. The best treatment option is

Explanation
The initial radiographs reveal a fourth and fifth carpometacarpal (CMC) joint fracture dislocation. The injury is associated with a shear fracture of the dorsal rim of the hamate. Further assessment with CT might be helpful in fully evaluating the extent of injury. Extensor carpi ulnaris is a deforming force at the base of the fifth metacarpal. This unstable fracture dislocation could be treated with closed reduction and pinning if the patient presented within a few days of injury. However, because he presented in a delayed fashion (3 weeks after injury), open reduction with internal fixation was required (Figures 4 and 5). In the series by Zhang and associates, patients with fourth and fifth CMC fracture dislocations presenting in a delayed fashion and treated nonsurgically had suboptimal results. Therefore, closed reduction and casting are not appropriate. An arthrodesis and resection arthroplasty are salvage procedures considered for a painful arthritic joint and would less likely should not be considered for this acute injury.



Question 6
Figure 4a shows the radiograph of a 20-year-old man who has an injury to the right shoulder. Figure 4b shows an arthroscopic view (posterior portal). The arrow points to a Review Topic
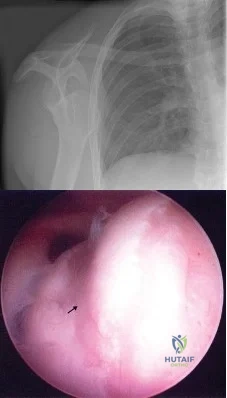
Explanation
Question 7
A 70-year-old man reports symptomatic medial knee pain that has become progressively worse during the past year. MRI reveals a complex, posterior horn medial meniscus tear with associated medial lateral and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable relief of symptoms?
Explanation
Total knee replacement is a well-established surgery for diffuse, symptomatic osteoarthritis of the knee joint, and its efficacy has been shown in many studies. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee, arthroscopy in the setting of existing osteoarthritis is efficacious for relieving the signs and symptoms of a torn meniscus but not for osteoarthritis. Likewise, in young and active patients, clinical outcomes show improvement after realignment osteotomy for single-compartment osteoarthritis. Unicondylar knee replacement is not indicated for tricompartmental disease of the knee.
Question 8
Which of the following is an advantage of computer-assisted navigation used to place medullary nail interlocking screws compared to a freehand techinque?

Explanation
Ricci et al compared two fluoroscopic navigation tracking technologies, optical and electromagnetic versus standard freehand fluoroscopic targeting, in a standardized foam block model for placement of interlocking screws. They found that fluoroscopy time (seconds) and number of fluoroscopy images were significantly less when using the computer-guided systems than for freehand-unguided insertion. Average distance of pin placement from the target in the foam blocks was significantly greater for controls than for each of the navigated systems.
Suhm et al performed a prospective controlled clinical study to compare fluoroscopic guidance with fluoroscopy-based surgical navigation for distal locking of intramedullary implants. The surgical navigation group showed increased procedure time, but equivalent precision with reduced radiation exposure. There was no significant difference in the technical reliability between both groups.
Question 9
Figures 1 through 3 show the radiograph and MR arthrograms obtained from a 25-year-old woman who has had right groin pain since joining the military 4 years ago. She has undergone treatment with NSAIDs, physical therapy, and activity modification. Examination reveals positive flexion abduction and external rotation, a positive external log roll, and increased range of motion. What is the most appropriate treatment?

Explanation
This patient has symptomatic hip dysplasia that has been recalcitrant to nonsurgical management. Radiographs reveal an upsloping sourcil (acetabular index of 18) and a lateral center edge angle of 14, with posterior uncovering. The MR arthrogram shows no definitive evidence of a labral tear. Appropriate surgical management would include periacetabular osteotomy. Viscosupplementation in the hip is controversial in the treatment of osteoarthritis and plays no role in the treatment of dysplasia. Hip arthroscopy with labral repair is controversial in mild hip dysplasia, with studies demonstrating between 60% and 77% good and excellent results, inferior to the results for hip arthroscopy in a femoroacetabular impingement cohort. In moderate to severe dysplasia, hip arthroscopy is not recommended. Because the acetabular cartilage is well maintained, total hip arthroplasty would not be recommended in this young and active patient.
Question 10
Genetic analysis has revealed a strong linkage between osteoarthritis in women with which of the following molecules?
Explanation
of over 400 families showed that type IX collagen is linked to development of OA in women. Mice with a type IX collagen gene deletion are also susceptible to early arthritis. Other genes, such as cartilage enzyme aggrecanase ADAMTS-5, have also been associated with OA.
Question 11
A patient reports hyperesthesia over the base of the thenar eminence following volar locked plating of a distal radius fracture. A standard volar approach of Henry was used. What is the most likely cause of the hyperesthesia?
Explanation
REFERENCES: Jupiter JB, Fernandez DL, Toh CL, et al: Operative treatment of volar intra-articular fractures of the distal end of the radius. J Bone Joint Surg Am 1996;78:1817-1828.
Hoppenfield S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, JB Lippincott, 1994, pp 156-176.
Question 12
Figure 6 shows a sagittal oblique MRI scan. The arrow is pointing to what structure?
Explanation
REFERENCES: Clarke HD, Scott WN, Insall JN, et al: Anatomy, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 3-66.
Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 13
Locked plating techniques have been shown to have biomechanical advantages over standard plating in which of the following scenarios?
Explanation
REFERENCES: Zlowodzki M, Williamson S, Cole PA, et al: Biomechanical evaluation of the less invasive stabilization system, angled blade plate, and retrograde intramedullary nail for the internal fixation of distal femur fractures. J Orthop Trauma 2004;18:494-502.
Comparison of the AO Locking Plate with the Standard Limited-Contact Dynamic Compression Plate (LC-DCP) for Fixation of Osteoporotic Humeral Shaft Fractures. David J. Hak, MD, MBA; Scott J. Hazelwood, PhD. OTA Book of Abstracts 2003.
Question 14
An 18-year-old woman injures her left knee playing soccer. At the time of anterior cruciate ligament (ACL) reconstruction, she was noted to have an irreparable posterior horn medial meniscus tear. Partial meniscectomy will have what primary effect? Review Topic
Explanation
Question 15
A paraplegic 32-year-old man was pulling himself up in bed by grasping the headboard rails when he felt a pop and immediate pain. A radiograph and CT scan are shown in Figures 2a and 2b. Based on these findings, management should consist of
Explanation
REFERENCES: Froimson AI: Fracture of the coracoid process of the scapula. J Bone Joint Surg Am 1978;60:710-711.
Gil JF, Haydar A: Isolated injury of the coracoid process: Case report. J Trauma
1991;31:1696-1697.
Question 16
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits.The patient undergoes successful primary THA with a metal-on-metal bearing. At 1-year follow-up, she reports no pain and is highly satisfied with the procedure. However, 3 years after the index procedure, she reports atraumatic right hip pain that worsens with activities. Radiographs reveal the implants in good position with no sign of loosening or lysis. An initial laboratory evaluation reveals a normal sedimentation rate and C-reactive protein (CRP) level. The most appropriate next diagnostic step is

Explanation
metal-on-metal articulation is associated with excellent wear rates in vitro. Because it offers a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions—including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis after the possible transfer of metal ions across the placental barrier—make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.The work-up of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including the erythrocyte sedimentation rate, C-reactive protein (CRP) level, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging, including MRI with MARS, should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following a revision of failed metal-on-metal hip replacements.
Question 17
A 10-year-old girl is seen in the emergency department after being involved in a motor vehicle accident. She has right hip pain and is unable to bear weight. She has no neurovascular deficits and no other injuries. Radiographs reveal a posterior dislocation of the right hip without apparent fracture. The acetabulum appears to be developing normally. What is the best course of treatment? Review Topic
Explanation
Question 18
A 63-year-old man has a feeling of generalized clumsiness in his arms and hands, difficulty buttoning his shirt, and gradually worsening gait instability. During examination, his neck is gently passively flexed to end range while he is seated. The patient describes an electric shock-like sensation that radiates down the spine and into the extremities. This describes which of the following? Review Topic
Explanation
Question 19
The direct anterior (Smith-Peterson) approach to hip arthroplasty is most commonly associated with injury to what nerve?
Explanation
Some authors have reported the incidence of lateral femoral cutaneous nerve neuropraxia following hip arthroplasty with the direct anterior approach to be near 80%, but resolution of the sensory deficits has been observed in most patients over time. Femoral nerve palsy has been reported to occur in .64% to 2.3% direct lateral (Hardinge) and anterolateral (Watson-Jones) approaches, and the superior gluteal nerve may be injured with proximal extension of the abductor muscular dissection. The posterior approach has been reported to be associated with sciatic nerve injury, especially in cases of dysplasia. Pudendal nerve injury has not been reported with the anterior, anterolateral, direct lateral, or posterior approaches to hip
arthroplasty. It has been reported following hip arthroscopy and the use of a traction table, however.
Question 20
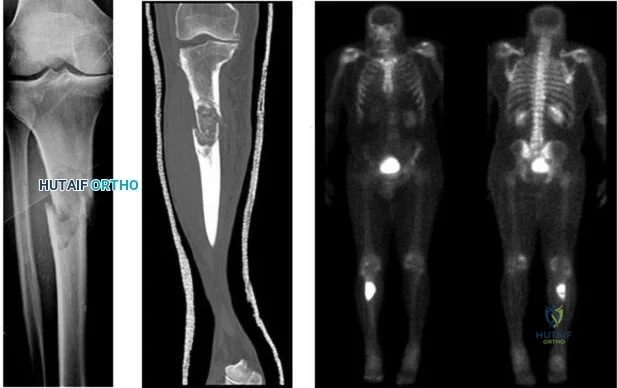
..A lateral radiograph (Figure 131a), sagittal short tau inversion recovery MRI scan (Figure 131b), and an axial T1 contrast MRI scan (Figure 131c) were performed on a 15-year-old boy who has injured his right knee twice during the last 5 months. He has a reduced range of motion of the knee and posterior thigh tenderness. A biopsy showed bland spindle cells, giant cells, and blood-filled spaces without endothelial lining. What is the most appropriate treatment?
Explanation

Figure 132 is the bone scan of a 73-year-old man who is referred from his family doctor with diffuse bone pain, fatigue, and right knee pain. Examination is notable for pain with motion about the right knee and mild hyporeflexia.
Question 21
In hybrid arthroplasty, the use of a polymethylmethacrylate (PMMA) precoated femoral component has been shown to result in
Explanation
REFERENCES: Sporer SM, Callaghan JJ, Olejniczak JP, Goetz DD, Johnston RC: The effects of surface roughness and polymethylmethacrylate precoating on the radiographic and clinical results of the Iowa hip prosthesis: A study of patients less than fifty years old. J Bone Joint Surg Am 1999;81:481-492.
Schulte KR, Callaghan JJ, Kelley SS, Johnston RC: The outcome of Charnley total hip arthroplasty with cement after a minimum twenty-year follow-up: The results of one surgeon. J Bone Joint Surg Am 1993;75:961-975.
Question 22
A 77-year-old woman underwent semiconstrained right total elbow arthroplasty 4 weeks ago through a Bryan-Morrey approach. Her recovery was uneventful until 2 days ago when she began her physical therapy session at an outpatient clinic. During resisted extension exercises, she felt a "pop" in her elbow, accompanied with pain and inability to extend her elbow against resistance. What is the most likely cause of her symptoms? Review Topic
Explanation
Question 23
Figures 42a through 42c show the MRI scans of a 56-year-old woman with progressively worsening low back and bilateral lower extremity pain. Based on these images, what muscle or muscle group would be expected to be weak on physical examination? Review Topic

Explanation
with L5-S1 spondylolisthesis. Many patients with spondylolisthesis report hamstring tightness; however, these structures are not usually weak. Quadriceps and tibialis anterior weakness is seen with L4 nerve root irritation. The gastrocnemius is generally weak in S1 nerve root syndromes.
Question 24
Figure 1 is the radiograph of a 22-year-old man who underwent an open reduction and pinning of a perilunate dislocation 10 weeks ago. The hardware has been removed. What is the best next step?
Explanation
Lunate or perilunate dislocations are usually treated with open reduction and internal fixation through a dorsal or combined dorsal and volar approach. A high index of suspicion is necessary when treating patients who sustain multiple trauma because as many as 25% of lunate or perilunate dislocations are missed initially. The radio dense appearance of the lunate seen in Figure 1 is an example of transient ischemia of the lunate that can occur following treatment of lunate and perilunate dislocations. It has been reported in up to 12.5% of cases. This usually is seen between 1 and 4 months post injury with a relative radio density of the lunate. This appearance of the lunate should not be over treated and usually is a benign self-limiting event. Surgery is not indicated at this time; the incorrect responses are treatment options for Kienbock disease. Treatment of the lunate or perilunate dislocation involves initial gentle closed reduction followed by open reduction, ligamentous and bone repair, and internal fixation. Median nerve dysfunction is common, and a simultaneous carpal tunnel release is often performed. Early treatment seems to produce better results, but good results have been reported when treatment is delayed for up to 6 months. The many questions regarding treatment of this problem involve the use of capsulodesis to supplement intercarpal ligament repair, repair/stabilization of the lunotriquetral interval vs no treatment of that articulation, and intercarpal fixation techniques. In delayed cases, proximal row carpectomy when the head of the capitate is intact and total wrist fusion if there are degenerative changes have been used. Chondral injuries are common, may not be recognized on radiographs, and may negatively affect longterm outcomes. Even when treatment is optimal, this injury is associated with a guarded prognosis and possible permanent partial loss of wrist motion and grip strength. At 10-year follow-up, radiographs will often demonstrate degenerative changes, but these changes do not always substantially negatively affect hand function.
Question 25
A surgeon is preparing a medial gastrocnemius rotational flap to cover a medial proximal tibia defect at the time of revision knee replacement surgery. To optimize coverage, the surgeon must optimally mobilize which artery?
Explanation
The medial sural arteries vascularize the gastrocnemius, plantaris, and soleus muscles proximally. They arise from the popliteal artery. If not adequately mobilized, a gastroc soleus flap can be devascularized.
RESPONSES FOR QUESTIONS 15 THROUGH 17
Semimembranosis release
Medial gastrocnemius release
Medial tibial plateau downsizing osteotomy
Iliotibial band pie crusting
Popliteus tendon release
Cruciate release of the capsule posterior lateral corner
Select the most appropriate release listed above to address each scenario described below.
Question 26
A 30-month-old boy underwent open reduction of his right hip to address developmental hip dysplasia. The reduction was performed through an anterior approach, and a shortening femoral osteotomy was not performed. Four months after surgery, hip radiographs reveal absence of ossification of the femoral epiphysis and fragmentation of the ossific nucleus. What is the likely cause of this complication?
Explanation
The incidence of pediatric hip dysplasia is approximately 1 per 100 live births, with hip dislocation present in 1 in 1000 births. Two surgical approaches primarily are used for surgical reduction in the dislocated pediatric hip: the modified medial approach as described by Weinstein and the
anterior Smith-Peterson approach. The Weinstein modification of the Ludloff approach exploits the interval between the pectineus muscle and the femoral neurovascular bundles rather than the interval between the pectineus and the adductor longus and brevis. The modified “bikini” anterior Smith-Peterson approach passes between the sartorius and tensor fascia lata superficially and between the rectus and gluteus medius during deep dissection.
When using the medial approach, the neurovascular bundle is particularly at risk, including the medial circumflex femoral vessels that supply blood to the femoral head ossific nucleus. Damage to this structure increases risk for osteonecrosis of the femoral head. Unlike the anterior approach, the medial approach does not allow for the performance of a capsulorrhaphy, poses higher risk for postprocedure redislocation, and is less useful in children of walking age. Identification of the ligamentum teres during deep dissection assists in localization of the true bony acetabulum.
The anatomic structure primarily at risk during the anterior approach is the lateral femoral cutaneous nerve. Excessive traction or transection of this structure will result in numbness in the proximal lateral thigh. This surgical approach allows for identifying and addressing all potential impediments to reduction: the redundant capsule, hypertrophic labrum, hypertrophic ligamentum teres, pulvinar, iliopsoas tendon, and transverse acetabular ligament. In older children who undergo open reduction with periacetabular osteotomy without a concomitant proximal femoral shortening osteotomy, reduction may be accompanied by increased pressure on the femoral head which, in turn, may result in secondary osteonecrosis of the femoral head.
RECOMMENDED READINGS
Karol LA. Developmental dysplasia of the hip. In: Song KM, ed. Orthopaedic Knowledge Update: Pediatrics 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2011:159-167.
Vitale MG, Skaggs DL. Developmental dysplasia of the hip from six months to four years of age. J Am Acad Orthop Surg. 2001 Nov-Dec;9(6):401-11. Review. PubMed PMID: 11730331. View Abstract at PubMed
Weinstein SL, Ponseti IV. Congenital dislocation of the hip. J Bone Joint Surg Am. 1979 Jan;61(1):119-
Question 27
During total knee arthroplasty using a posterior cruciate-retaining design, excessive tightness in flexion is noted, while the extension gap is felt to be balanced. Which of the following actions will effectively balance the knee?
Explanation
REFERENCE: Ayers DC, Dennis DA, Johanson NA, Pelligrini VD: Common complications of total knee arthroplasty. J Bone Joint Surg Am 1997;79:278-311.
Question 28
What measure of physiologic status best evaluates whether an injured patient is fully resuscitated and best predicts that perioperative complications will be minimized following definitive stabilization of long bone fractures?
Explanation
REFERENCES: Blow O, Magliore L, Claridge JA, et al: The golden hour and silver day: Detection and correction of occult hypoperfusion within 24 hours improves outcomes from major trauma. J Trauma 1999;47:964-977.
Crowl A, Young JS, Kahler DM, et al: Occult hypoperfusion is associated with increased morbidity in patients undergoing early femur fracture fixation. J Trauma 2000;48:260-267.
Shulman AM: Prediction of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:725-800.
Question 29
A “p value” of 4% (p=0.04) indicates that the
Explanation
The p value is the probability that the chance selection of patients might suggest a difference in treatment that was not real. Only with a small p value are we willing to believe that the observed difference in treatment is very likely real and not simply due to chance.
The confidence interval provides a measure of the magnitude of the possible difference between two groups of patients, regardless of whether or not the p value was small. This makes the confidence interval more informative than the p value when different treatments are compared. This is much beyond the scope of this review.
Question 30
Figures 17a and 17b show the AP and lateral radiographs of a 75-year-old woman who reports giving way and shifting of the knee, particularly when she is descending stairs or ambulating on level surfaces. History reveals a total knee replacement 5 years ago. Treatment should consist of
Explanation
REFERENCE: Pagnano MW, Cushner FD, Scott WN: Role of the posterior cruciate ligament in total knee arthroplasty. J Am Acad Orthop Surg 1998;6:176-187.
Question 31
Early postoperative infections following primary total hip arthroplasty are most likely caused by which organism?
Explanation
S aureus is the most common organism cultured in early (fewer than 4 weeks postoperative) periprosthetic infections. Methicillin-resistant S aureus is becoming a more common pathogen in certain patient populations. B hemolytic Streptococcus and some gram-negative infections can also be found in early postoperative infections. S epidermidis, S viridans, and P acnes are more commonly found in late (more
than 4 weeks postoperative) infections.
Question 32
A 3-year-old boy had been treated with serial casting for a right congenital idiopathic clubfoot deformity. The parents are concerned because the child now walks on the lateral border of the right foot. Examination shows that the foot passively achieves a plantigrade position with neutral heel valgus and ankle dorsiflexion to 15 degrees. The forefoot inverts during active ankle dorsiflexion. Mild residual metatarsus adductus is present. Management should now consist of
Explanation
REFERENCES: Kuo KN, Hennigan SP, Hastings ME: Anterior tibial tendon transfer in residual dynamic clubfoot deformity. J Pediatr Orthop 2001;21:35-41.
Garceau GJ: Anterior tibial tendon transfer for recurrent clubfoot. Clin Orthop 1972;84:61-65.
Miller GM, Hsu JD, Hoffer MM, et al: Posterior tibial tendon transfer: A review of the literature and analysis of 74 procedures. J Pediatr Orthop 1982;2:363-370.
Question 33
A 55-year-old woman has slowly increasing pain at the distal end of her little finger that is exacerbated by cold temperatures. She denies any history of trauma to her hands and is employed as a school teacher. The histology of the resected specimen is shown in Figure 71. What is the most likely diagnosis?
Explanation
REFERENCES: Zook EG, Brown RE: The perionychium, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 1353-1380.
McDermott EM, Weiss AP: Glomus tumors. J Hand Surg Am 2006;31:1397-1400.
Question 34
-A collegiate offensive football lineman has decreased bench-press strength and shoulder pain as off-season workouts begin. Examination revealed no atrophy, and deltoid and rotator cuff strength testing findings were normal. Translational testing was difficult to achieve because of his large size.Apprehension and relocation test findings were negative. An O’Brien’s active compression test result was negative. Jerk testing was positive on the affected side. Which diagnosis is most likely revealed on an MRI arthrogram?
Explanation
Question 35
A previously healthy 20-year-old male wrestler is seen for evaluation and treatment of draining sores of the forearm. Empiric treatment for cellulitis was started with oral clindamycin with improvement. Culture of the drainage reveals methicillin-resistant staphylococcus aureus (MRSA). Sensitivities at 48 hours demonstrate additional resistance to erythromycin and a positive D-zone test. Definitive antibiotic treatment until resolution should consist of which of the following? Review Topic
Explanation
any signs of systemic illness, an oral antibiotic regimen is appropriate. When culture results reveal resistance to erythromycin, then a D-zone test should be performed to check for inducible clindamycin resistance. The D-zone test is performed by plating the sample on an agar and placing antibiotic disks made of clindamycin and erythromycin on the agar. A zone of inhibition in the shape of the letter D is seen with an inducible strain. If the D-zone test is positive, then clindamycin should not be used because the strain of MRSA can become resistant to the treatment. Therefore, because of the positive D-zone test, the antibiotic should be changed to oral doxycycline. IV antibiotics are not indicated for this infection. Oral rifampin should never be used as a single agent as resistance rapidly develops.
Question 36
A 6-year-old boy presents to the emergency room after falling off a trampoline and landing on his elbow. Examination reveals good radial and ulnar pulses, and a warm, pink, sensate extremity. Radiographs are shown in Figures A and
Explanation
Pulselessness occurs 10-20% of the time following extension type supracondylar fractures. Most authors recommend observation of the pink, pulseless limb as in the majority of cases, vascular spasm will resolve in 12-24 hours and/or the collateral circulation will be adequate. Isolated nerve injuries are usually neuropraxia and can be observed. Pulseless hands with AIN or median nerve palsy warrant early exploration because of the high probability of arterial entrapment at the fracture site, or tethering.
Choi et al. performed a review of 1255 pediatric supracondylar fractures treated at a single institution. There were 33 pulseless fractures (2.6%). All 24 well perfused patients did well postoperatively without vascular repair, although 10 remained pulseless. Of the 9 poorly perfused patients, 4 underwent vascular repair and 2 developed compartment syndrome. They concluded that patients with poor perfusion were at increased risk of vascular repair and compartment syndrome.
Franklin et al. reviewed pediatric supracondylar fractures with neurovascular compromise. They recommend: (1) observation for 48h for the pulseless, well-perfused hand, (2) exploration if the pulse disappears after reduction, (3) exploration for pulseless hands with AIN/median nerve palsy, (4) delay of 8-21 hours did not increase the risk of complications.
Figures A and B are AP and lateral radiographs showing a Gartland type III supracondylar fracture of the humerus.
Incorrect Answers:
Question 37
A 15-year-old girl who plays high school basketball has had worsening forefoot pain and swelling that is aggravated by activity for the past 5 weeks. She denies any history of an injury. Examination reveals no deformities. A radiograph is shown in Figure 38. Initial management should consist of
Explanation
walking cast.
REFERENCE: Mann RA, Coughlin MJ: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 413-415.
Question 38
A 35-year-old man sustains a closed Monteggia fracture. Examination reveals that sensation, vascular status, and finger flexion are normal. When he extends his wrist, it deviates radially, and he is unable to extend his fingers or thumb. After reduction of the fracture, what is the next step in treatment for the extensor deficits of the thumb and fingers?
Explanation
REFERENCES: Jessing P: Monteggia lesions and their complicating nerve damage. Acta Orthop Scand 1975;46:601-609.
Stein F, Grabias SL, Deffer PA: Nerve injuries complicating Monteggia lesions. J Bone Joint Surg Am 1971;53:1432-1436.
Question 39
Compared with percutaneous pinning with Kirschner wires (K-wires), the treatment of metacarpal neck fractures with cannulated intramedullary screws is associated with
Explanation
In a biomechanical study, headless compression screws showed superior load to failure, higher three-point bending strength, and greater strength in axial loading compared with percutaneous K-wire fixation for metacarpal neck fractures. Headless compression screws provide greater initial stability to allow earlier motion in the postoperative period. No data comparing infection rates between the two methods of fixation are available; however, it is assumed that K-wires placed outside of the skin would have increased rates of infection. Neither fixation method would increase the time to healing.
Question 40
Which of the following correctly describes a physical or molecular change in the degenerative pathway of intervertebral disk disease? Review Topic
Explanation
There are many physical and molecular changes in the degenerative pathway of intervertebral disk disease. These include:
DECREASE: Synthesis of collagen types II and IX, nutritional transport, water content, absolute number of viable cells, proteoglycans and pH.
INCREASE: Synthesis of collagen types I and X, keratin sulfate-to-chondroitin sulfate ratio, lactate and degradative enzyme activity.
Kepler et al. reviewed intervertebral disk degeneration and emerging biologic treatments. They report treatment of IVD is challenging, as discs are avascular structures and the delivery of therapeutic proteins via the bloodstream is limited. Methods considered to enhance disk cellularity include in vitro expansion and subsequent reimplantation of disk tissue, mesenchymal stem cell (MSC) implantation, and injection of platelet-rich plasma (PRP) into the disk.
Illustration A is a non-exhaustive list of potential biological treatments for IVD (c. 2014)
Incorrect Answers:
(SBQ12SP.49) As part of his treatment plan for congenital scoliosis, a 7-year-old boy is placed into halo gravity traction using 10 pins, inserted into the thickest part of the skull, with a torque wrench to apply an insertional torque of 6 in-lb. After 1 week, he is noted to have developed a complication at one pin site. Which of following changes
in technique would have been recommended to reduce the impact of pin complications? Review Topic
Using more pins
Using fewer pins
Applying a higher insertional torque
Applying a lower insertional torque
Inserting pins by palpation without a torque wrench
The recommended insertional torque for halo application in preadolescent patients is
to 5 in-lb. The insertional torque used in this case was too high.
Halo application is performed in children for multiple conditions, most often stabilization for cervical spine trauma (as definitive treatment or in conjunction with operative management) and for traction as part of a larger treatment plan for severe curves in scoliosis. Due to reduced thickness of the pediatric skull, higher rate of pin site infections and skull puncture, and unreliability of many torque wrenches, current recommendations are to use a higher number of pins (8 to 12) with lower insertional torque (1 to 5 in-lb) in case pins need to be removed or exchanged.
Caird et al. conducted a retrospective review of 13 patients under 4 years old who had halo application for cervical trauma, arthrodesis, or scoliosis. They reported an average of 8 pins used per patient (range 6-12) and insertional torque of 2 to 4 in-lb. Nine patients (69%) suffered some complication, mostly pin site infection (6 cases), and so they conclude halo application is safe in toddlers, but ambulation should be limited.
Copley et al. performed a study manually comparing the accuracy at low settings of torque wrenches from 4 different manufacturers. They found that overall, the accuracy was within 10% of the intended torque in only 69.2% of all trials, and that Jerome and Mountz wrenches were more accurate than PMT and Bremer at the low settings recommended for pediatric patients.
Limpaphayom et al. looks at complication rates of using halo traction for correction of spinal deformity or immobilization. They found an overall complication rate of 53% (36/68), and 10% (7/68) of children required unanticipated surgery for treatment of these complications. The most common complication was pin-site infections, with 76% (13/17) of these resolving with oral antibiotics alone. Traction-related neurologic injuries that occurred were common, 31% (9/31) but all resolved with a decrease or removal of traction weight, with complete resolution occurring immediately in 4 of 9 events.
Incorrect Answers:
Question 41
A 27-year-old man now reports dorsiflexion and inversion weakness after an automobile collision 6 months ago in which compartment syndrome developed isolated to the anterior and deep posterior compartments. Examination reveals the development of a progressive cavovarus deformity, but the ankle and hindfoot remain flexible. In addition to Achilles tendon lengthening, which of the following procedures is most likely to improve the motor balance of his foot and ankle? Review Topic
Explanation
(SBQ12FA.1) Figure A is a radiograph of a healthy, independent 51-year-old male. He is treated with immediate open reduction internal fixation to prevent which of the following complications?

Fracture non-union
Avascular necrosis
Skin necrosis
Plantar flexion weakness
Ankle stiffness
Figure A shows an avulsion fracture of the calcaneal tuberosity. Immediate open reduction and internal fixation is required to prevent wound complications.
Displaced avulsion fractures of the calcaneal tuberosity should be managed urgently to prevent necrosis of the soft tissues overlying the heel. In these injuries, the Achilles tendon is securely attached to the fractured tuberosity. Urgent closed reduction and casting is usually not possible due to the power and proximal pull of the triceps surae. Surgical fixation is required. The best treatment modality is open reduction and bone-to-bone fixation with screws. Closed reduction and percutaneous pinning fixation is not strong enough to provide a stable fixation of the tuberosity.
Lui reported on avulsion fractures of the bony insertion of the Achilles tendon at the calcaneus. He stated that screw fixation alone is not sufficient for repair of these injuries. His technique involved two suture anchors used capture the small bone fragment to the calcaneus. This allowed for the pull of the triceps surae to be neutralized and early physical therapy.
Hess et al. looked at a case series of calcaneal tuberosity avulsion fractures that were
treated in a delayed fashion. All three patients with posterior tuberosity calcaneal avulsion fractures developed skin necrosis because of a delay in treatment.
Figure A shows a displaced posterior tuberosity calcaneal avulsion fracture. Illustration A shows skin breakdown overlying the posterior tuberosity calcaneal avulsion fracture.
Incorrect Answers:
Question 42
A 62-year-old man with a long history of ankylosing spondylitis has neck pain after lightly bumping his head on the wall. Examination reveals neck pain with any attempted motion; the neurologic examination is normal. Plain radiographs show extensive ankylosis of the cervical spine and kyphosis but no fracture. What is the next most appropriate step in management?
Explanation
REFERENCES: Brigham CD: Ankylosing spondylitis and seronegative spondyloarthropathies, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998,
pp 724-727.
McDowell GS, Cammisa FP, Eismont FJ: Hyperextension injuries of the cervical spine, in Levine AM, Eismont FJ, Garfin SR, Zigler JE (eds): Spine Trauma. Philadelphia, PA,
WB Saunders, 1998, pp 372-374.
Question 43
The comparative outcomes of needle aponeurotomy (NA) and collagenase Clostridium histolyticum (CCH) use in the treatment of Dupuytren contracture indicate that patients treated with CCH have
Explanation
A. Proximal row carpectomy
B. Vascularized bone graft
C. Radial shortening osteotomy
D. Capitate shortening osteotomy
Osteonecrosis of the capitate is a rare condition that presents with an insidious onset of dorsal wrist pain. When nonsurgical treatment fails to alleviate symptoms, surgical intervention is appropriate. When collapse of the capitate is present, partial excision of the capitate with interposition, partial wrist arthrodesis, or wrist denervation can be considered. In the absence of collapse, capitate-preserving options are available. Vascularized grafting is a mainstay of treatment. Grafting with distal radius vascularized grafts based on the 1,2 intercompartmental supraretinacular artery or the 4 + 5 extensor compartment artery and second metacarpal graft based on the first dorsal metacarpal artery have been described.
Question 44
Which of the following tumors is most likely to present with a pathologic fracture in a child?
Explanation
REFERENCES: Wilkins RM: Unicameral bone cysts. J Am Acad Orthop Surg 2000;8:217-224.
Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Hecht AC, Gebhardt MC: Diagnosis and treatment of unicameral and aneurysmal bone cysts in children. Curr Opin Pediatr 1998;10:87-94.
Question 45
..Figures 107a through 107c are the radiograph, CT, and bone scan of a 68-year-old man. While walking, he collapsed and was unable to ambulate because of pain and deformity in his right leg. What is the most appropriate next step?
Explanation
Glomus tumor
Diffuse pigmented villonodular synovitis (PVNS)
Extra-abdominal fibromatosis
Schwannoma
Hemangioma
Please match the characteristics below to the condition listed above.
Question 46
A 67-year-old woman undergoes a revision total shoulder arthroplasty for replacement of a loose glenoid component. Examination in the recovery room reveals absent voluntary deltoid and triceps contraction, weakness of wrist and thumb extension, and absent sensation in the palmar aspect of all fingertips and the radial forearm. The next most appropriate step in management should consist of
Explanation
REFERENCES: Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Lynch NM, Cofield RH, Silbert PL, Hermann RC: Neurologic complications after total shoulder arthroplasty. J Shoulder Elbow Surg 1996;5:53-61.
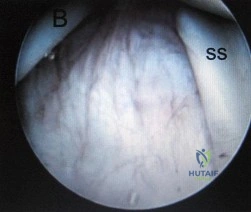
Question 47
Figure 28 shows an arthroscopic view of a right shoulder in the lateral position through a posterior portal. What is the area between structure B (biceps) and SS (subscapularis tendon)? Review Topic
Explanation
Question 48
A 21-year-old collegiate track athlete increased her training 4 months ago in anticipation of starting the season. Two months into her training program, she reported pain followed by a 1-month history of diffuse pain in the first metatarsophalangeal joint that was aggravated by weight bearing. A removable walker boot partially relieved the pain, and she was able to complete the season. Her pain has now returned; however, she denies any history of injury. Examination reveals tenderness over the medial sesamoid but no deformities. A radiograph and bone scan are shown in Figures 22a and 22b. What is the best treatment option at this time?
Explanation
REFERENCES: Sanders R: Fractures of the midfoot and forefoot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1601-1603.
Saxena A, Krisdakumtorn T: Return to activity after sesamoidectomy in athletically active individuals. Foot Ankle Int 2003;24:415-419.
Question 49
A 35-year-old runner has pain beneath the second metatarsophalangeal joint. He reports that he has significantly decreased his running distance since the onset of the pain. He denies any history of trauma or injury to the foot. A radiograph is shown in Figure 14. Initial management should consist of
Explanation
REFERENCES: Trepman E, Yeo SJ: Nonoperative treatment of metatarsophalangeal joint synovitis. Foot Ankle Int 1995;16:771-777.
Mizel MS, Michelson JD: Nonsurgical treatment of monarticular nontraumatic synovitis of the second metatarsophalangeal joint. Foot Ankle Int 1997;18:424-426.
Question 50
A newborn girl is referred for evaluation of suspected hip instability. What information from her history would place her in the highest risk category?
Explanation
REFERENCES: Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Haynes RJ: Developmental dysplasia of the hip: Etiology, pathogenesis, and examination and physical findings in the newborn. Instr Course Lect 2001;50:535-540.
Question 51
A 72-year-old female presents to the office 5 weeks after distal radius fracture surgery with the findings seen in Figure A. She performed daily cleansing with soap and water and dry dressings. Which of the following has been shown to decrease the risk of developing this complication?

Explanation
The risks of external fixation include cellulitis, pin-track drainage, osteomyelitis and pin loosening. The rate of complications is about 20%. Chlorhexidine gluconate has broad spectrum activity against gram-positive and negative bacteria by disrupting cell membranes. It is not affected by blood and has low skin irritancy. Studies show that simple pin-site care (showers, dry dressings) maintains a low infection rate.
Egol et al. performed a randomized trial examining external fixation pin tracts about the wrist. They compared (1) weekly dry dressings, (2) daily pin care with half normal saline (NS) and hydrogen peroxide (H2O2) and (3) chlorhexidine discs with weekly changes. They found pin-site complications in 19%, with no difference between the 3 groups. They do not recommend additional wound care beyond sterile dressings.
Stinner et al. performed a survey on the use of half-pins by the limb lengthening and reconstruction society. They found that most respondents preferred hydroxyapatite coating (81%) because of improved fixation and decreased loosening (less radiographic pin-tract rarefaction and greater extraction torque, which may lead to
lower infection rates). Most encouraged shower (60%) and washing solution (67%)(soap and water, peroxide or saline) for pin site care.
Figure A shows an external fixator around the wrist with cellulitis around the proximal half-pins.
Incorrect Answers
Question 52
- Following closed reduction for the injury shown in Figures 69a and 69b, treatment should consist of
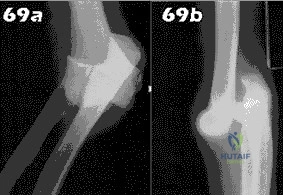
Explanation
Repair or reconstruction of the medial and lateral collateral ligaments-Acute dislocations can be reduced in supination and tested for valgus stability in pronation. Treatment is determined by the stability following reduction. When there are fractures, the principle is to fix the bones so that the only limitation is the ligaments and then to repair them if the elbow is not stable enough to permit early motion.
Immobilization for 14 days-The longer the immobilization had been, the larger the flexion contracture (p less than 0.001) and the more severe the symptoms of pain were. The results indicate that early active motion is the key factor in rehabilitation of the elbow after a dislocation. Simple dislocation of the elbow in the adult. Results after
closed treatment. Immobilization for 25 days- See above.
Question 53
Following reconstruction of the anterior cruciate ligament (ACL), which of the following rehabilitation exercises has the greatest potential to harm the graft?
Explanation
REFERENCES: Beynnon BD, Gleming BC, Johnson RL, Nichols CE, Renstrom PA, Pope MH: Anterior cruciate ligament strain behavior during rehabilitation exercises in vivo. Am J Sports Med 1995;23:24-34.
Beynnon BD, Johnson RJ, Fleming BC, Stankewaich CJ, Renstrom PA, Nichols CE: The strain behavior of the anterior cruciate ligament during squatting and active flexion-extension: A comparison of an open and a closed kinetic chain exercise. Am J Sports Med 1997;25:823-829.
Question 54
Figure 35 shows the lateral radiograph of a 15-year-old basketball player who felt a dramatic pop in his knee when landing after a lay-up. The patient reports that he cannot bear weight on the injured extremity. Management should consist of
Explanation
REFERENCES: Ogden JA, Tross RB, Murphy MJ: Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
Pape JM, Goulet JA, Hensinger RN: Compartment syndrome complicating tibial tubercle avulsion. Clin Orthop 1993;295:201-204.
Question 55
A 19-year-old man was in a motorcycle accident. He sustained a grade IIIB open tibia fracture with a wide zone of injury to the surrounding soft tissue and a closed-head injury. The patient was treated emergently with irrigation, debridement, and external fixation. What is the most accurate statement regarding long-term functional and financial outcomes?
Explanation
Lower Extremity Assessment Project data suggest that long-term functional outcomes and patient satisfaction at 7 years are equivalent between those
who undergo limb-salvage and primary amputations. Return to work is essentially the same between the 2 groups. The projected lifetime healthcare cost for patients treated with amputation is nearly 3 times higher than costs for those who are treated with limb-salvage procedures.
RECOMMENDED READINGS
Busse JW, Jacobs CL, Swiontkowski MF, Bosse MJ, Bhandari M; Evidence-Based Orthopaedic Trauma Working Group. Complex limb salvage or early amputation for severe lower-limb injury: a meta-analysis of observational studies. J Orthop Trauma. 2007 Jan;21(1):70-6. PubMed PMID: 17211275. View Abstract at PubMed
MacKenzie EJ, Jones AS, Bosse MJ, Castillo RC, Pollak AN, Webb LX, Swiontkowski MF, Kellam JF, Smith DG, Sanders RW, Jones AL, Starr AJ, McAndrew MP, Patterson BM, Burgess AR. Health-care costs associated with amputation or reconstruction of a limb-threatening injury. J Bone Joint Surg Am. 2007 Aug;89(8):1685-92. PubMed PMID: 17671005. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 85 THROUGH 88
Figures 85a and 85b are the plain radiographs of a 38-year-old man who fell off the roof of a 2-story house and sustained an isolated injury to his right knee. Examination reveals a swollen leg with a knee effusion. The skin is intact, but there are some abrasions and an obvious deformity. His neurovascular examination reveals active dorsiflexion and plantar flexion with some pain and symmetric palpable pulses

85A

B
Question 56
Anabolic steroid use has which of the following effects on serum lipoprotein levels?
Explanation
REFERENCES: Hartgens F, Rietjens G, Keizer HA, et al: Effects of androgenic-anabolic steroids on apolipoproteins and lipoprotein (a). Br J Sports Med 2004;38:253-259.
Blue JG, Lombardo JA: Steroids and steroid-like compounds. Clin Sports Med
1999;18:667-689.
Question 57
Hip pain of 1-month duration has developed in a 72-year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. The patient has a final culture that reveals methicillin-resistant Staphylococcus aureus (MRSA). If the attending physician recommends the two-stage protocol, including the use of an antibiotic-cement spacer, what is the most likely prognosis for this patient?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin- resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was
21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California
Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 58
Radiating pain associated with a posterolateral thoracic disk herniation typically follows what pattern?
Explanation
REFERENCE: Skubic JW, Kostuik JP: Thoracic pain syndromes and thoracic disc herniation, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, pp 1443-1464.
Question 59
A 66-year-old woman who previously underwent hemiarthroplasty 2 years ago for a fracture continues to have severe pain and loss of motion despite undergoing physical therapy. A radiograph is shown in Figure 2. What is the most likely reason that this patient has failed to improve her motion?
Explanation
REFERENCES: Bigliani LU, Flatow EL, McCluskey G, et al: Failed prosthetic replacement for displaced proximal humeral fractures. Orthop Trans 1991;15:747-748.
Boileau P, Krishnan SG, Tinsi L, et al: Tuberosity malposition and migration: Reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg 2002;11:401-412.
Tanner MW, Cofield RH: Prosthetic arthroplasty for fractures and fracture-dislocations of the proximal humerus. Clin Orthop Relat Res 1983;179:116-128.
Question 60
A 27-year-old man sustained a gunshot wound to the lumbar spine and undergoes an exploratory laparotomy. An injury to the cecum is identified and treated. Management should now include
Explanation
a 7-day course of broad-spectrum antibiotics. Fragment removal is not indicated.
REFERENCES: Roffi RP, Waters RL, Adkins RH: Gunshot wounds to the spine associated with a perforated viscus. Spine 1989;14:808-811.
Velmahoos GC, Demetriades D: Gunshot wounds of the spine: Should retained bullets be removed to prevent infection? Ann R Coll Surg Engl 1976;94:85-87.
Question 61
An elite football player has sustained a left knee injury during play. A dynamic imaging analysis is performed on the affected knee, which shows anterior shift and internal rotation of the tibia at low flexion angles. There is also some mild medial translation of the tibia at greater flexion angles. What structure(s) have most likely been injury? Review Topic
Explanation
The ACL is the primary restraint to anterior translation of the tibia relative to the femur. It also acts as secondary restraint to tibial rotation and varus/valgus rotation. ACL-deficient knees have been shown to have abnormal knee kinematics, which has been thought to contribute to the osteoarthritis that develops after injury.
DeFrate et al. examined the knee joint kinematics of 8 patients with unilateral anterior cruciate ligament rupture using in vivo imaging. They found significant anterior shift and internal rotation of the tibia at low flexion angles in ACL-deficient knees. They also noted some medial translation of the tibia between 15° and 90° of flexion.
Illustration A shows the effect of medial tibial translation on tibiofemoral contact in ACL-deficient knees. The medial translation of the tibia causes increased contact between the tibial spine and inner surface of the medial femoral condyle. This might be a contributing factor to the joint degeneration observed in ACL-deficient patients.
Incorrect Answers:
Question 62
Figures 26a through 26c show the MRI scans of a 47-year-old man who underwent arthroscopic shoulder surgery 6 months ago and continues to have pain despite a prolonged course of rehabilitation. Management should now consist of Review Topic

Explanation
Question 63
The patient in Figure 55 is actively attempting to make a fist. This clinical scenario suggests which of the following anatomic lesions?
Explanation
REFERENCE: Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995, p 189.
Question 64
Which of the following findings is considered the strongest indication for surgical treatment of a mallet fracture of the distal phalanx?
Explanation
REFERENCES: Green DP, Butler TE Jr: Fractures and dislocations in the hand, in Rockwood CA, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 621-623.
Light TR (ed): Hand Surgery Update 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 19-28.
Question 65
03 Figure 72 shows the radiograph of a 4 y/o girl who has a painless right Trendelenburg limp. Management should consist of
Explanation
(unlike their bilateral counterparts which generally do not need to be reduced). Open reduction is used to obtain absolute concentric reduction. In the dislocated hip reduced at age 15 mths or older, there is usually enough associated bony deformity, either femoral, acetabular, or both to require stabilizing osteotomy to maintain the concentric reduction. Femoral shortening is often necessary to relax soft tissues before a perfect reduction is possible in children > 2 y/o.
back to this question next question
Question 66
A 17-year-old high school track athlete has had progressive midfoot pain for the past 3 weeks that prevents him from running. Examination reveals pain over the tarsal navicular. Radiographs are normal, but a CT scan reveals a nondisplaced sagittally oriented fracture line. Management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Torg J, Pavlov H, Cooley LH, et al: Stress fractures of the tarsal navicular: A retrospective review of twenty-one cases. J Bone Joint Surg Am 1982;64:700-712.
Question 67
Which of the follow medications activates antithrombin III? Review Topic
Explanation
Heparin works by binding to and enhancing the ability of antithrombin III to inhibit factors IIa, III, Xa. It is metabolised by the liver. The risks associated with its use include bleeding and heparin induced thrombocytopenia (HIT). The reversal agent is protamine sulfate.
Brown et al. performed a pooled analysis of 14 randomized controlled trials (RCTs) on VTE rates. They showed that VTE rates with aspirin were not significantly different than the rates for vitamin K antagonists (VKA), low molecular weight heparins (LMWH), and pentasaccharides. They concluded that aspirin may be used for VTE prophylaxis after major orthopaedic surgery.
Murphy et al. reviewed VTE prophylaxis in pediatric patients. Using public health data over 10 years, 285 611 clinical encounters were reported as lower extremity orthopaedic trauma. The incidence of VTE events was 0.058 %. Adolescents and polytrauma patients with injuries of the femur/femoral neck, tibia/ankle, and pelvis are more commonly affected.
Roehrig et al. first examined the coagulation enzyme Factor Xa (FXa) as a target for antithrombotic therapy. This study contributed to the development of rivaroxaban, which is commonly used as an oral antithrombotic agent.
Illustration A shows the interaction between anticoagulant drugs and the coagulation cascade.
Incorrect Answers:
Question 68
A 10-year-old girl fell from her bike and now reports pain and swelling in the left knee and pain with weight bearing. Examination reveals a left knee effusion and pain with range of motion. A radiograph is shown in Figure 85. Treatment should consist of
Explanation
REFERENCES: Mah JY, Adili A, Otsuka NY, et al: Follow-up study of arthroscopic reduction and fixation of type III tibial-eminence fractures. J Pediatr Orthop 1998; 18:475-477.
McLennen JG: Lessons learned after second-look arthroscopy in type III fractures of the tibial spine. J Pediatr Orthop 1995;15:59-62.
Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
72 • American Academy of Orthopaedic Surgeons
Question 69
The preferred surgical approach to the elbow of a child with an irreducible type III supracondylar distal humerus fracture and pulseless extremity is through which of the following muscle intervals?
Explanation
REFERENCES: Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 115.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, p 119.
Question 70
A 75-year-old woman began a walking program 2 months after undergoing right total knee arthroplasty. She had to stop the program after 4 weeks because of hindfoot pain and ankle swelling. Radiographs are shown in Figures 42a and 42b. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA,
WB Saunders, 1995, p 2591.
Kearon C: Natural history of venous thromboembolism. Semin Vasc Med 2001;1:27-37.
Aldridge T: Diagnosing heel pain in adults. Am Fam Physician 2004;70;332-338.
Question 71
A 21-year-old male is brought to the emergency department after being involved in gang-related violence. A radiograph of his pelvis is shown in Figure A. The patient is hemodynamically stable. Which of the following imaging modalities is the next best step in evaluating this patient for the most common associated injury? Review Topic

Explanation
The incidence of GSW is increasing and it is the 2nd leading cause of death in young males in the US after motor vehicle accidents. The incidence of a GSW to the buttock is approximately 8% of all GSW to the extremities. Potential complications of pelvic and acetabular GSW include septic arthritis, enterocutaneous, enteroacetabular, and vesicoacetabular fistulas, infected nonunion, malunion, and injuries to the iliac vessels. The presence or absence of intra-abdominal injuries affects treatment and outcome.
Bartkiw et al. reviewed 2808 GSW and found 1235 associated fractures including 42 fractures of the hip and pelvis. Ten orthopaedic operative procedures were performed in 7 patients. Associated nonorthopaedic injuries included 15 small/large bowel perforations (36%), 7 vessel lacerations (17%), and 2 urogenital injuries (5%) that required surgery.
Najibi et al. reviewed 39 GSW to acetabulum. They found 32 simple and 7 associated fracture patterns. The most common simple and associated patterns were anterior column and both column, respectively. Bowel injuries were the most common associated injures (42%). Predictors of poor outcome include high-velocity missile, involvement of acetabular dome, abdominal injury, nerve injury, vascular injury, and male gender. Deep infection was associated with primary anastomosis of bowel injury and an associated fracture pattern.
Figure A shows a GSW to the right hip with acetabular fracture and visible bullet fragment.
Incorrect Answers:
Question 72
In Charcot-Marie-Tooth disease a progressive deformity develops in the foot. Which functional muscles predominate in deformity formation?
Explanation
REFERENCE: Herring JA (ed): Tachjians Pediatric Orthopedics, ed 3. Philadelphia, PA,
WB Saunders, 2002, vol 2, p 984.
Question 73
A 35-year-old woman began to train for a half marathon. After 8 weeks of increasing her mileage, what changes can you expect in her Achilles tendon?
Explanation
Question 74
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the Review Topic
Explanation
Question 75
Figures 20a and 20b are the radiographs of a 56-year-old woman who runs a horse farm. She has a 2-year history of increasing ankle pain and swelling without previous treatment. Which treatment is most appropriate at this time?
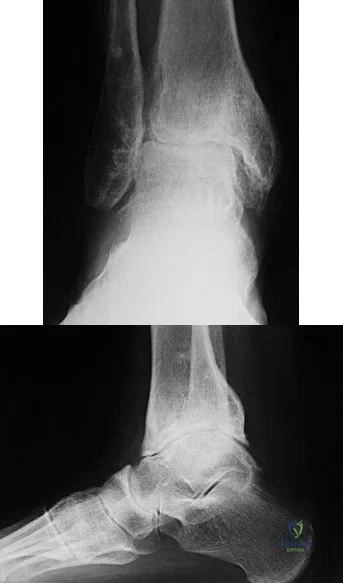
Explanation
This patient has end-stage ankle arthritis. A short course of NSAIDs may provide pain and inflammation relief. Bracing with either an ankle-foot orthosis or Arizona brace can reduce pain by offloading the ankle joint. Ankle fusion is a reliable procedure for treatment of end-stage ankle arthritis and is especially recommended for active people after it is determined that nonsurgical measures no longer provide adequate relief. Arthroscopic debridement and cheilectomy may be indicated for bony impingement and mild arthritis with little articular cartilage loss. The long-term results of ankle distraction arthroplasty are not yet well defined but likewise would be reserved for scenarios in which nonsurgical measures no longer provide adequate relief. The patient must be able to wear a thin-wire external fixator for 3 months.
RECOMMENDED READINGS
Abidi NA, Neufeld SK, Brage ME, Reese KA, Sabharwal S, Paley, D. Ankle arthritis. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:159-193.
Saltzman CL: Ankle arthritis, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle. Philadelphia, PA, Mosby Elsevier, 2007, vol 1, pp 929-932.
Question 76
An 8-month-old infant has an infection of the fingertip as shown in Figure 22. If neglected, the anticipated path of ascending infection is the fingertip, the flexor sheath, and the
Explanation
REFERENCES: Peimer CA (ed): Surgery of the Hand and Upper Extremity: Acute and Chronic Sepsis. New York, NY, Mcgraw Hill, 1996, pp 1735-1741.
Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow and Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 445-446.
Question 77
A 28-year-old woman who is an avid runner reports pain about the left hip with activities. Nonsurgical management has failed to provide relief. An MRI arthrogram is shown in Figure 47. What is the most likely diagnosis?
Explanation
REFERENCES: Guanche CA, Sikka RS: Acetabular labral tears with underlying chondralmalacia: A possible association with high-level running. Arthroscopy 2005;21:580-585.
McCarthy JC: The diagnosis and treatment of labral and chondral injuries. Instr Course Lect 2004;53:573-577.
Question 78
Deep venous thromboses are primarily composed of red blood cells and fibrin. What is fibrin?
Explanation
Question 79
A patient with deficient anteroinferior bone stock undergoes a Latarjet procedure that transfers a portion of the coracoid to the glenoid rim and secures it with two screws. After surgery, the patient reports numbness on the anterolateral forearm. To verify the diagnosis, what muscle should be tested for strength?
Explanation
REFERENCES: Ho E, Cofield RH, Balm MR, Hattrup SJ, Rowland CM: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270.
Boardman ND 3rd, Cofield RH: Neurologic complications of shoulder surgery. Clin Orthop 1999;368:44-53.
Allain J, Goutallier D, Glorion C: Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder. J Bone Joint Surg Am 1998;80:841-852.
Question 80
- A patient is in respiratory distress as a result of a high-speed motor vehicle accident. After emergent intubation, the arterial blood is poorly oxygenated, and examination shows left-sided tracheal deviation, absence of breath sounds on the right side and tympany on percussion over the right side of the chest. Management should include
Explanation
Question 81
Figure 1 is the T2 coronal MRI scan of a 52-year-old woman with a 6- month history of shoulder pain. She does not recall a history of trauma. Physical therapy is recommended. What is the most significant predictor of failure of nonoperative treatment?
Explanation
Question 82
In a patient who has undergone fusion with instrumentation from T4 to the sacrum for adult scoliosis, at which site is a pseudarthrosis most likely to be discovered?
Explanation
REFERENCES: Saer EH III, Winter RB, Lonstein JE: Long scoliosis fusion to the sacrum in adults with nonparalytic scoliosis: An improved method. Spine 1990;15;650-653.
Kostuik JP, Hall BB: Spinal fusions to the sacrum in adults with scoliosis. Spine
1983;8:489-500.
Balderston RA, Winter RB, Moe JH, et al: Fusion to the sacrum for nonparalytic scoliosis in the adult. Spine 1986;11:824-829.
Question 83
Figures 86a through 86c are the radiographs and biopsy specimen of a 14-year-old boy who has had left knee pain for 4 weeks. What is the most likely diagnosis?
Explanation
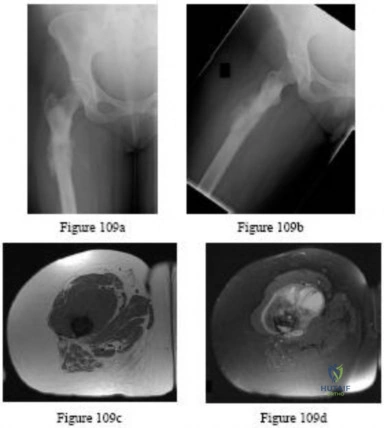
Question 84
Figures below show the radiographs obtained from a 79-year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. No evidence of infection is seen. What is the most appropriate treatment?

Explanation
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis, as shown in Figures 3 and 4. They also assist in obtaining correct limb alignment. Short metaphyseal-engaging stems are associated with failure rates that range between 16% and 29%. Cemented stems may be shorter than press-fit stems, because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.
Question 85
An year-old African American woman who lives in a large city is scheduled for total hip arthroplasty to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
Explanation
Demographic factors are associated with increased risk for MRSA colonization, so it is important to identify vulnerable patients. Female gender and advanced age reduce the risk for colonization, whereas African American race increases this risk. Urban environments do not influence MRSA colonization.
Question 86
-The Coleman block test is used to test for
Explanation

Question 87
Figures 9a through 9c are the preoperative radiographs and a T2-weighted MR image of a patient treated with surgery for spondylolisthesis and neuroforaminal stenosis. Figure 9d is the postsurgical radiograph. Interbody fusion offers which advantage over posterolateral fusion (PLF)? A B C D
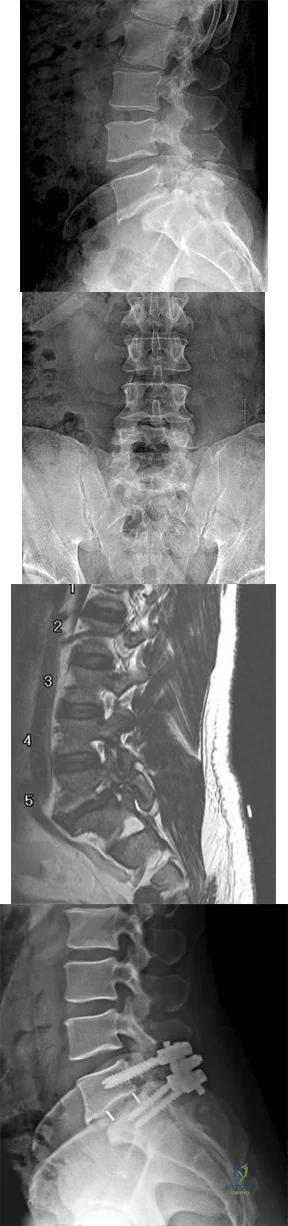
Explanation
Interbody fusion, when compared to PLF, is a predictor of more substantial blood loss. Multilevel posterior lumbar interbody fusion (PLIF) is an independent predictor of blood loss for posterior spine fusion. Some retrospective studies suggest that fusion rates are higher for transforaminal lumbar interbody fusion (TLIF) than PLF, but this finding has not been borne out in prospective studies. The main advantage of TLIF in the context of this question is restoration of neuroforaminal height, and many surgeons will consider TLIF or PLIF for that reason. The parasagittal MR image seen in Figure 9c shows neuroforaminal narrowing. The pre- and postsurgical radiographs show a difference in neuroforaminal height.
RECOMMENDED READINGS
DiPaola CP, Molinari RW. Posterior lumbar interbody fusion. J Am Acad Orthop Surg. 2008 Mar;16(3):130-9. Review. PubMed PMID: 18316711. View Abstract at PubMed
Eismont FJ, Norton RP, Hirsch BP. Surgical management of lumbar degenerative spondylolisthesis. J Am Acad Orthop Surg. 2014 Apr;22(4):203-13. doi: 10.5435/JAAOS-22-04-203. Review. PubMed PMID: 24668350. View Abstract at PubMed
McAfee PC, DeVine JG, Chaput CD, Prybis BG, Fedder IL, Cunningham BW, Farrell DJ, Hess SJ, Vigna FE. The indications for interbody fusion cages in the treatment of spondylolisthesis: analysis of 120 cases. Spine (Phila Pa 1976). 2005 Mar 15;30(6 Suppl):S60-5. PubMed PMID: 15767888. View Abstract at PubMed
RESPONSES FOR QUESTIONS 10 THROUGH 14
Postoperative deep surgical site infection
Proximal junctional kyphosis
Pedicle screw cut-out
Pseudarthrosis
Sagittal imbalance
Please match the scenario described below with the most likely complication listed above.
Question 88
Figure 62a and Figure 62b
Explanation
Figure 58 reveals a posttraumatic valgus deformity. Correction of valgus with lateral soft-tissue release places tension on the peroneal nerve, resulting in an increased risk for nerve palsy. Figures 59a (lateral view) and 59b (Merchant view) illustrate juvenile rheumatoid arthritis with tibiofibular fusion and lateral patellar dislocation. Chronic patellar dislocation is associated with contracture of the lateral retinacular soft tissues and increased risk for patellar subluxation or dislocation after TKA. Extensor mechanism realignment, possibly including tibial tubercle osteotomy and/or proximal soft-tissue realignment, may be required during TKA to centralize the extensor mechanism. Figures 60a (anteroposterior [AP] view) and 60b (lateral view) reveal a fused knee in full extension.
TKA after fusion is associated with multiple complications including skin necrosis, infection, and instability. The skin is contracted because of limited knee motion and has multiple scars (Figure 60c). Mobilization of the skin during and after knee arthroplasty can place excess tension on the soft tissues, resulting in skin necrosis and infection. Treatment consisting of prompt debridement and soft-tissue coverage, usually with medial gastrocnemius muscle transposition, is required. Figure 61 shows a knee with prior tibial tubercle fixation and marked patella infera. Shortening of the patellar ligament is associated with restricted knee motion. This may necessitate more extensile exposure using tibial tubercle osteotomy or rectus snip during TKA to obtain adequate surgical exposure. The inferior position of the patella can cause impingement between the patellar component and tibial insert, resulting in anterior knee pain. Restoring a more normal position of the patella may necessitate distal positioning of the femoral component as well as tibial tubercle osteotomy with proximal recession of the osteotomized tibial tubercle. Figures 62a (AP view of the distal femur) and 62b (AP view of the proximal femur) show a posttraumatic deformity with a large retained intramedullary rod. There is a varus distal femoral deformity that is not severe enough to necessitate extra-articular corrective osteotomy. However, intramedullary hardware precludes use of conventional intramedullary instrumentation, so computer navigation or patient-specific cutting guides will be necessary to orient the bone cuts and avoid implant malalignment.
Question 89
Which of the following muscle tendons inserts just lateral to the long head of biceps tendon on the proximal humerus?
Explanation
REFERENCE: Bal GK, Basamania CJ: Pectoralis major tendon ruptures: Diagnosis and treatment. Tech Shoulder Elbow Surg 2005;6:128-134.
Question 90
A 27-year-old woman sustained a bilateral C5-6 facet subluxation in a motor vehicle accident. Neurologic evaluation reveals normal motor, sensory, and reflex functions. She is awake, alert, and cooperative. Initial management should consist of
Explanation
REFERENCE: Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets: Case reports. J Bone Joint Surg Am 1991;73:1555-1560.
Question 91
Patients with ankylosing spondylitis undergoing total knee arthroplasty are likely to experience which of the following complications?
Explanation
REFERENCES: Parvizi J, Duffy GP, Trousdale RT: Total knee arthroplasty in patients with ankylosing spondylitis. J Bone Joint Surg Am 2001;83:1312-1316.
Fintersbush A, Amir D, Vatashki E, et al: Joint surgery in severe ankylosing spondylitis. Acta Orthop Scand 1988;59:491-496.
Question 92
Closed chain kinetic exercises are differentiated from open chain exercises by which of the following? Review Topic
Explanation
Question 93
The images reveal T2-weighted MRI sequences with edema isolated to the infraspinatus. In the absence of a tear in the infraspinatus tendon, the edema is most likely due to compression of the suprascapular nerve in the spinoglenoid notch. As this pathology persists, progressive muscle atrophy and fatty infiltration can result. Compression of the suprascapular nerve in the suprascapular notch would have resulted in edema and weakness in both the supra- and infraspinatus muscles. Compression is commonly caused by cysts from the joint secondary to labral tears. A rotator cuff tear of the infraspinatus is not identified on these images, and there is no history of trauma provided. There is no evidence of an anteroinferior labral tear, nor would this be expected to result in external rotation weakness or MRI abnormality of the infraspinatus. Quadrilateral space syndrome results in compression of the axillary nerve, which supplies the teres minor. Correcr answer : C 40- A 41-year-old right-hand-dominant man has been treated nonsurgically for right elbow arthritis. His radiographs reveal end-stage ulnohumeral arthritis with complete loss of the joint space. He reports pain during the mid-arc of elbow flexion and extension. During the last 8 years, he has attempted activity modification, medication, physical therapy, and multiple cortisone injections. His symptoms have progressed, resulting in constant pain, loss of a functional range of motion, and an inability to perform many activities of daily living. Secondary to his age and activity demands, he undergoes a soft-tissue interposition arthroplasty of his elbow with an Achilles allograft. Which presurgical finding correlates with elevated risk for postsurgical complications?
Explanation
A. Elbow arthroscopy with debridement
B. Immobilization and rest for 6 weeks
C. Corticosteroid injection
D. Open osteochondral autograft transfer
Osteochondritis dissecans of the capitellum is a painful condition that affects immature athletes who undergo repetitive compression of the radiocapitellar joint. Management is based primarily on the integrity of the articular cartilage surface and the stability of the lesion. Nonsurgical treatment is typically selected for patients
with early-grade, stable lesions, and it involves activity modification with cessation of sports participation. The duration of activity modification is dictated by symptoms, with 3 to 6 weeks of rest followed by return to sport in 3 to 6 months commonly used as a guideline. Strengthening and stretching exercises are commonly incorporated after the pain has subsided. Surgical intervention or corticosteroid injection would not be first-line treatment.
42- Figures 1 and 2 are the radiographs of a 69-year-old man with a history of treated prostate cancer and hemodialysis-dependent end- stage renal disease who presents to the emergency department with progressively worsening right shoulder pain and stiffness. Laboratory tests reveal a white blood cell count of 17,000, erythrocyte sedimentation rate, 75, and CRP, 10.1. He has a draining sinus located along the anterior shoulder. What is the best next step?
Question 94
Figures 2a and 2b show the clinical photograph and radiograph of a 16-year-old cheerleader who fell on her left lower extremity while performing a pyramid. Following adequate sedation, closed reduction is performed, but an incomplete reduction is noted. What structure is most likely preventing a reduction?
Explanation
REFERENCES: Pehlivan O, Akmaz I, Solakoglu C, et al: Medial peritalar dislocation. Arch Orthop Trauma Surg 2002;122:541-543.
Rivera F, Bertone C, De Martino M, et al: Pure dislocation of the ankle: Three case reports and literature review. Clin Orthop 2001;382:179-184.
Question 95
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5° of angulation. When the MCP joint is flexed 30°, a radially directed stress produces 45° of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
REFERENCES: Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint.
J Am Acad Orthop Surg 1997;5:224-229.
Question 96
Figure A shows the operative technique used during arthroscopic repair of 25-year-old male patient with vague shoulder pain. The glenoid rim was prepared using the drill bit insertion angles as shown. Three suture anchors, measuring 14mm in length were inserted 4-6 mm deep to the surface. What structure is at the highest risk with this technique? Review Topic
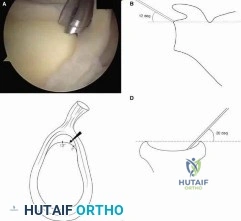
Explanation
At the scapular spine level, the suprascapular nerve is approximately 1.5-2.0 cm from the glenoid cortex. This places the nerve at risk of injury during shoulder surgery, and injuries have been described. Arthroscopic SLAP repair is known to be a safe and relatively simple procedure. However, deep drilling or anchor insertion from the anterior or anteriosuperior portal during SLAP repair can place the suprascapular nerve at risk of iatrogenic injury.
Morgan et al. performed a cadaveric study to compare the risk of injury to the suprascapular nerve during suture anchor placement in the glenoid when using an anterosuperior portal versus a rotator interval portal. Standard 3 × 14 mm suture anchors were placed in the glenoid rim (1 o’clock, 11 o’clock, and 10 o’clock positions for the right shoulder). They showed that the distance from the far-posterior anchor tip to the suprascapular nerve averaged 8 mm (range, 3.4 to 14 mm) for the anterosuperior portal and 2.1 mm (range, 0 to 5.5 mm) for the rotator interval portal (P = .001).
Koh et al. evaluated the risk of suprascapular nerve injury during the drilling and anchor insertion for anterior SLAP repair. They inserted 1 suture anchor
arthroscopically from the anterior portal at 00:30-1:00 o’clock in right shoulders (11-11:30 in left). Using a mean drill depth was 14.2 (±2.8) mm, all suture anchors perforated the glenoid wall and the tips were measured to be approx. 3.1 (±2.7) mm from the suprascapular nerve.
Figure A shows an arthroscopic view and corresponding schematic image of arthroscopic drill position for SLAP repair. Illustration A shows the close proximity of anchor tip to the suprascapular nerve, as the nerve nerve enters the supraspinatus fossa below the superior transverse scapular ligament and then enters the infraspinatus fossa between the neck of the scapula and base of the spine of the scapula.
Incorrect Answers:
(SBQ11UE.106) A 60 year-old diabetic man presents with increasing right shoulder pain and stiffness for 10 weeks. He works as a lawyer and has been treating the pain with non-steroidal anti-inflammatory drugs with little improvement. He had a previous injury to his right shoulder 15 years ago while playing hockey, but cannot recall any recent precipitants for this presentation. Physical examination shows significant reduction in right shoulder range of motion, with the greatest loss in external rotation. His MRI images are seen in Figures A-C. What would be the most appropriate treatment? Review Topic

Open supraspinatus cuff repair
Arthroscopic supraspinatus cuff repair
Reverse shoulder arthroplasty
Arthroscopic posterior capsular release
Physical therapy and medical management
The patient is presenting with right shoulder adhesive capsulitis. The most appropriate treatment at this time would be physical therapy and medical management (i.e., nonsteroidal anti-inflammatories +/- intra-articular steroid injections).
Adhesive capsulitis (aka frozen shoulder) is defined by pain and loss of both active and passive motion, especially loss of external rotation in comparison to the contralateral side. Risk factors include diabetes, thyroid disease, age, previous surgery and prolonged immobilization. Initial treatment options include NSAIDs, physical therapy, and intra-articular steroid injections. Surgical treatment is not commonly recommended, but may be used late in the course to address residual stiffness if extensive therapy has failed.
Griggs et al. prospectively reviewed seventy-five consecutive patients (seventy-seven shoulders) with adhesive capsulitis. They showed that 90 percent of the patients reported a satisfactory outcome with shoulder stretching exercises. However, male gender and diabetes mellitus were associated with worse motion at the final evaluation.
Hannafin et al. reviewed the treatment options for adhesive capsulitis. They suggest
that benign neglect, home-based and supervised physical therapy, and intra-articular corticosteroid injections should be considered in the early treatment of adhesive capsulitis. Duration of treatment should be considered for at least 3 months before more aggressive treatments are considered.
Levine et al. retrospectively reviewed the treatment and outcome of 234 patients with adhesive capsulitis. No significant difference was found for success of nonoperative treatment versus operative treatment or patient gender. With supervised treatment, most patients with adhesive capsulitis experience resolution with nonoperative measures in a relatively short period.
Figures A (Sagittal oblique T1 MRI), and Figure B (coronal oblique fat-saturated T2 MRI) show the anterior rotator cuff interval in the right shoulder demonstrate high-signal soft tissue thickening of the coracohumeral ligament (arrow). Figure C (Coronal oblique fat-saturated T2 MRI) demonstrates a thickened inferior glenohumeral ligament of the right shoulder.
Incorrect Answers:
Question 97
At the time of revision total knee arthroplasty, the surgeon is trialing the knee and finds that it extends fully and is stable in flexion with a 23-mm trial spacer; however, the patella is impinging on the polyethylene spacer. No augments were used on the femur or the tibia because the components fit well without them. What is the most appropriate action at this time?
Explanation
REFERENCES: Laskin RS: Joint line position restoration during revision total knee replacement. Clin Orthop Relat Res 2002;404:169-171.
Yoshii I, Whiteside LA, White SE, et al: Influence of prosthetic joint line position on knee kinematics and patellar position. J Arthroplasty 1991;6:169-177.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 123-145. Question 100
A 68-year-old woman is undergoing a cementless medial/lateral tapered femoral placement during a total hip arthroplasty and the surgeon notices a small crack forming in the anteromedial femoral neck with final implant insertion. The most appropriate management should include which of the following?
Placement of a cerclage cable around the femoral neck above the lesser trochanter
Removal of the implant, placement of a cable around the femoral neck above the lesser trochanter, and reinsertion of the implant
Removal of the press-fit implant and cementing of the same femoral stem
Final seating of the cementless femoral component without additional measures
Removal of the cementless femoral component and placement of a revision modular taper- fluted femoral stem
DISCUSSION: The recognized treatment of the proximal periprosthetic fracture is first to identify its extent and then to optimize the correction. Removing the implant seems logical to accomplish the identification. Several studies indicate that proximal cerclage wiring is adequate to create a “barrel hoop” stability of the proxima l femur. The postoperative management may also include protected weight bearing and periodic radiographs.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475503.
Warren PJ, Thompson P, Fletcher MD: Transfemoral implantation of the Wagner SL stem: The abolition of
subsidence and enhancement of osteotomy union rate using Dall-Miles cables. Arch Orthop Trauma Surg 2002;122:557-560.
Your Source for Lifelong Orthopaedic Learning
Question 98
A 16-year-old high school football player sustains an injury to the left hip. The avulsed fragment identified by the arrow in Figure 34 represents the origin of which of the following structures?
Explanation
REFERENCES: Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Mader TJ: Avulsion of the rectus femoris tendon: An unusual type of pelvic fracture. Pediatr Emerg Care 1990;6:198-199.
Question 99
A 21-year-old professional ballet dancer reports a painful popping sensation over her right hip joint. Examination reveals that symptoms are reproduced with hip flexion and external rotation. Which of the following studies will best confirm the diagnosis?
Explanation
REFERENCES: Gruen GS, Scioscia TN, Lowenstein JE: The surgical treatment of internal snapping hip. Am J Sports Med 2002;30:607-613.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 139-153.
Question 100
Figure 17 shows the clinical photograph of a 45-year-old female tennis player who has right arm pain and weakness with elevation after undergoing a cervical biopsy several months ago. The cause of her shoulder weakness is damage to the
Explanation
REFERENCES: Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Wright TA: Accessory spinal nerve injury. Clin Orthop 1975;109:15-18.
