Orthopedic Board Review MCQs: Arthroplasty, Knee, Nerve, Shoulder & Trauma | Part 225

Key Takeaway
This page offers orthopedic surgeons and residents 100 high-yield, verified MCQs for AAOS/ABOS board certification. Modeled on OITE/AAOS exams, it provides interactive study and exam modes with detailed clinical explanations. Essential for comprehensive board review across key orthopedic topics.
About This Board Review Set
This is Part 225 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 225
This module focuses heavily on: Arthroplasty, Knee, Nerve, Shoulder, Trauma.
Sample Questions from This Set
Sample Question 1: Which of the following factors is associated with failure of arthroscopic excision of the distal clavicle?...
Sample Question 2: An otherwise healthy 45-year-old woman reports the onset of severe right leg pain. Figure 20a shows an axial MRI scan of the L4-5 level, and Figure 20b shows a sagittal view with the arrow at the L4-5 level. What nerve root is the most like...
Sample Question 3: A surgeon performs a minimally invasive total knee arthroplasty through a quadriceps-sparing approach using medial-to-lateral cutting jigs. When beginning therapy that afternoon, the patient can passively but not actively extend her knee, a...
Sample Question 4: If a surgeon inadvertently burrs through the midlateral wall of C5 during a anterior corpectomy, what structure is at greatest risk for injury?...
Sample Question 5: A 70-year-old man seen in the emergency department has had left shoulder pain and a fever of 101.5 degrees F (38.6 degrees C) for the past 3 days. He denies any history of trauma. Examination reveals tenderness anterosuperiorly and at the p...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following factors is associated with failure of arthroscopic excision of the distal clavicle?
Explanation
REFERENCE: Flatow EL, Duralde XA, Nicholson GP, Pollock RG, Bigliani LU: Arthroscopic resection of the distal clavicle with a superior approach. J Shoulder Elbow Surg 1995;4:41-50.
Question 2
An otherwise healthy 45-year-old woman reports the onset of severe right leg pain. Figure 20a shows an axial MRI scan of the L4-5 level, and Figure 20b shows a sagittal view with the arrow at the L4-5 level. What nerve root is the most likely source of her pain?
Explanation
REFERENCES: McCulloch JA: Microdiscectomy, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 2, pp 1765-1783.
Hodges SD, Humphreys SC, Eck JC, Covington LA: The surgical treatment of far lateral L3-L4 and L4-L5 disc herniations: A modified technique and outcomes analysis of 25 patients. Spine 1999;24:1243-1246.
Question 3
A surgeon performs a minimally invasive total knee arthroplasty through a quadriceps-sparing approach using medial-to-lateral cutting jigs. When beginning therapy that afternoon, the patient can passively but not actively extend her knee, although she has minimal knee pain. All regional blocks have been discontinued. What is the most likely reason for this finding?
Explanation
This patient lacks active knee extension. It is not attributable to the regional block because that block is no longer acting. The most likely cause is laceration of the patella tendon, which has been described during both large-incision surgery and minimally invasive surgery. However, this is reported with increased frequency during minimally invasive surgery. Quadriceps inhibition, avulsion of the quadriceps tendon, and femoral nerve palsy can cause lack of active extension, but these problems are less likely because the patient has minimal pain.
Question 4
If a surgeon inadvertently burrs through the midlateral wall of C5 during a anterior corpectomy, what structure is at greatest risk for injury?
Explanation
REFERENCES: Pfeifer BA, Freidberg SR, Jewell ER: Repair of injured vertebral artery in anterior cervical procedures. Spine 1994;19:1471-1474.
Gerszten PC, Welch WC, King JT: Quality of life assessment in patients undergoing nucleoplasty-based percutaneous discectomy. J Neurosurg Spine 2006;4:36-42.
Question 5
A 70-year-old man seen in the emergency department has had left shoulder pain and a fever of 101.5 degrees F (38.6 degrees C) for the past 3 days. He denies any history of trauma. Examination reveals tenderness anterosuperiorly and at the posterior glenohumeral joint line. He has very limited range of motion (passive and active). Laboratory studies show a WBC count of 12,000/mm 3 and an erythrocyte sedimentation rate of 48 mm/h. Initial management should consist of
Explanation
REFERENCES: Sawyer JR, Esterhai JL Jr: Shoulder infections, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997.
Leslie BM, Harris JM, Driscoll D: Septic arthritis of the shoulder in adults. J Bone Joint Surg Am 1989;71:1516-1522.
Question 6
A 56-year-old man who tripped and fell out of his golf cart onto his right shoulder 4 days ago now reports mild pain while chipping. Examination reveals mild bruising over the lateral clavicle but good shoulder range of motion and strength. A radiograph is shown in Figure 9. Appropriate treatment at this time should include which of the following?

Explanation
Question 7
What ligament is the primary stabilizer of the wrist following a proximal row carpectomy?
Explanation
REFERENCES: Stern PJ, Agabegi SS, Kiefhaber TR, et al: Proximal row carpectomy. J Bone Joint Surg Am 2005;87:166-174.
Wyrick JD: Proximal row carpectomy and intercarpal arthrodesis for the management of wrist arthritis. J Am Acad Orthop Surg 2003;11:227-281.
Question 8
A 65-year-old man has had “catching” in front of his knee since he had a total knee arthroplasty 9 months ago. Examination reveals a palpable and audible snap in the anterior aspect of the knee at about 40 degrees of flexion as the knee is being actively extended. A radiograph of the prosthetic knee will most likely show
Explanation
Pathologically, the clunk is produced by a suprapatellar fibrous nodule seen superior to the patellar component at re-operation. This nodule has been seen to catch in the intercondylar notch in primarily first generation TKAs. Current component designs have decreased this phenomenon through better engineering of femoral components. Treatment is by arthroscopic debridement or open arthroplasty resection. The nodule may be recurrent.
Question 9
A 2-year-old child is being evaluated for limb-length and girth discrepancy. As a newborn, the patient was large for gestational age and had hypoglycemia. Current examination shows enlargement of the entire right side of the body, including the right lower extremity and foot. The skin shows no abnormal markings, and the neurologic examination is normal. The spine appears normal. Radiographs confirm a 2-cm discrepancy in the lengths of the lower extremities. Additional imaging studies should include
Explanation
REFERENCES: DeBaun MR, Tucker MA: Risk of cancer during the first four years of life in children from The Beckwith-Wiedemann Syndrome Registry. J Pediatr 1998;132:398-400.
Ballock RT, Wiesner GL, Myers MT, et al: Hemihypertrophy concepts and controversies.
J Bone Joint Surg Am 1997;79:1731-1738.
Carpenter CT, Lester EL: Skeletal age determination in young children: Analysis of three regions of the hand/wrist film. J Pediatr Orthop 1993;13:76-79.
Question 10
When balancing gaps in the coronal plane, what structure preferentially impacts the flexion space more than the extension space?
Explanation
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point,
can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
Question 11
A 35-year-old carpenter sustained an injury to his dominant shoulder in a fall. He reports that he felt a sharp tearing sensation as he held on to a scaffold to keep from falling. Examination reveals swelling and ecchymosis down the upper arm, weakness to internal rotation, and deformity of the anterior axilla. He has good strength in external rotation and no apprehension with instability testing. Radiographs are normal. Management should consist of
Explanation
REFERENCES: Hanna CM, Glenny AB, Stanley SN, et al: Pectoralis major tears: Comparison of surgical and conservative treatment. Br J Sports Med 2001;35:202-206.
Connell DA, Potter HG, Sherman MF, et al: Injuries of the pectoralis major muscle: Evaluation with MR imaging. Radiology 1999;210:785-791.
Question 12
Figures A through C are the radiograph and CT scans of a 42-year-old man who sustained an injury to both of his ankles and underwent surgical repair 2 weeks prior to presentation to your office. One ankle is healing well. On the contralateral side, he reports pain and restricted ankle range of motion. Management should consist of
Explanation
Question 13
A 28-year-old woman has a moderate hallux valgus deformity and a prominence of the medial eminence. She can participate in all activities and reports that she could wear 3-inch heels in the past, but she now notes medial eminence pain even while wearing a soft leather flat shoe with a cushioned sole. She requests recommendations regarding surgical correction. Examination reveals a 1-2 intermetatarsal angle of 10 degrees. A clinical photograph and radiograph are shown in Figures 13a and 13b. What is the best course of action?
Explanation
REFERENCES: Chou LB, Mann RA, Casillas MM: Biplanar chevron osteotomy. Foot Ankle Int 1998;19:579-584.
Coughlin MJ: Roger A. Mann Award: Juvenile hallux valgus. Etiology and treatment. Foot Ankle Int 1995;16:682-697.
Pochatko DJ, Schlehr FJ, Murphey MD, Hamilton JJ: Distal chevron osteotomy with lateral release for treatment of hallux valgus deformity. Foot Ankle Int 1994;15:457-461.
Question 14
A patient has a humeral shaft fracture and is scheduled to undergo open reduction and internal fixation with a plate. What surgical approach will provide the greatest amount of exposure?
Explanation
REFERENCES: DeFranco MJ, Lawton JN: Radial nerve injuries associated with humeral fractures. J Hand Surg Am 2006;31:655-663.
Gerwin M, Hotchkiss RN, Weiland AJ: Alternative operative exposure of the posterior aspect of the humeral diaphysis with reference to the radial nerve. J Bone Joint Surg Am 1996;78:1690-1695.
Question 15
The lower extremity motor dysfunction in Charcot-Marie-Tooth disease most commonly involves which of the following muscles?
Explanation
REFERENCES: Mann RA, Missirian J: Pathophysiology of Charcot-Marie-Tooth disease. Clin Orthop 1988;234:221-228.
Tynan MC, Klenerman L, Helliwell TR, Edwards RH, Hayward M: Investigation of muscle imbalance in the leg in symptomatic forefoot pes cavus: A multidisciplinary study. Foot Ankle 1992;13:489-501.
Question 16
03 A 28-year-old man underwent surgical fixation for an intra-articular distal humeral fracture 8 weeks ago now reports progressively restricted elbow motion. Radiographs at the time of union are shown in Figures 13a and 13b. Management should now consist of
Explanation
delayed until the heterotopic ossification was “mature”. This was signified by a cold bone scan and normal serum alk phos, as well as a mature appearance on xray. It was thought that by waiting until the HO was mature, recurrence would be avoided. However, in the cited reference, out of the widely read Journal of Hand Surgery, the authors obtained good results with increased range of motion, resolution of cubital tunnel syndrome and no recurrence of contractures or loss of motion with excision of ectopic bone and elbow release that was performed once bony union of fracture was obtained. They also used a 5 day course of indomethacin post-op.
back to this question next question
Question 17
A 13-year-old gymnast presents with ongoing knee pain for the past few months. She tried conservative measures including kinesiotaping, physical therapy and rest. On physical exam, she has normal valgus alignment, negative patellar tilt and discomfort with resisted open chain knee extension. A representative radiographs are shown in Figure A-C. What is the most likely clinical diagnosis? Review Topic

Explanation
Evaluation of a patient with patellofemoral pain requires a physical examination and plain radiographs. Appropriate examination of all structures around the knee is critical to rule out other diagnoses. An MRI is useful for evaluating intra-articular or intra-osseous lesions, if clinical suspicion is suggestive of this. Treatment is predominantly conservative, with focus on low impact exercises that maximize aerobic conditioning.
Earl et al. review the epidemiology, etiology and management of patellofemoral syndrome. They note that there is no clear cause of this issue, although issues related to the quadriceps and dynamic malalignment may be contributory.
Outerbridge et al. describe overuse injuries in the young athletic patient. They provide an overview of diagnosis and management specific to this patient population.
Figures A, B and C show AP, lateral and merchant radiographs of a normal knee in a skeletally immature individual. No osseous abnormalities are identified.
Incorrect
Question 18
A 15-year-old girl has had a painful mass on the medial aspect of her left thigh for the past 5 years. The pain is present only when she is performing athletic activities and is completely relieved with rest. A radiograph and MRI scan are shown in Figures 29a and 29b. The patient and her parents would like to have the mass removed. What further diagnostic studies are required prior to considering surgical resection?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Murphey MD, Choi JJ, Kransdorf, MJ, et al: Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-1434.
Question 19
Which of the following is considered an advantage of arthroscopic distal clavicle excision compared with open distal clavicle excision?
Explanation
in 20 patients who underwent open distal clavicle excision that resulted in failure, 15 of those patients had a superior labral anterior posterior (SLAP) lesion. Of these 15 patients who had the lesion treated surgically, 9 went on to a good to excellent result after the surgery was performed arthroscopically. Fewer complications, lower infection rate, and decreased surgical time have not been documented in the literature. Arthroscopic technique sacrifices the inferior acromioclavicular ligament and preserves the superior acromioclavicular ligament.
REFERENCES: Berg EE, Ciullo JV: The SLAP lesion: A cause of failure after distal clavicle resection. Arthroscopy 1997;13:85-89.
Lemos MJ, Tolo ET: Complications of the treatment of acromioclavicular and sternoclavicular joint injuries, including instability. Clin Sports Med 2003;22:371-385.
Question 20
A 22-year-old college baseball pitcher reports the recent onset of anterior and posterosuperior shoulder pain in his throwing shoulder. Examination shows a 15-degree loss of internal rotation, tenderness over the coracoid, and a positive relocation test. Radiographs are normal, and an MRI scan without contrast shows no definitive lesions. A rehabilitation program is prescribed. Which of the following regimens should be initially employed? Review Topic
Explanation
Question 21
A 52-year-old woman has a 60-degree extensor lag following a right total knee arthroplasty performed 16 months ago. Since the time of her primary total knee arthroplasty she has undergone primary repair of a patellar tendon rupture that occurred after a fall 8 months ago. A lateral radiograph of the knee is shown in Figure 52. A CT scan obtained to determine component rotation showed that the femoral component is internally rotated 9 degrees and the tibial component is internally rotated 12 degrees. Appropriate management at this time should include
Explanation
Attempts at secondary repair have been associated with high failure rates whereas the use of an extensor mechanism allograft has been shown to more effectively restore active extension in a substantial percentage of patients. Important aspects of the technique include fully tensioning the graft in full extension and immobilization of the extremity for 6 to 8 weeks postoperatively to allow for graft healing. Nonsurgical management will not result in an acceptable outcome for a young patient, and attempted secondary repair is associated with a high rate of failure, even when augmented with local tissues. This patient has gross rotational
malalignment of the components and the surgeon faced with this problem should consider obtaining a CT scan to determine component rotation preoperatively.
REFERENCES: Burnett RS, Berger RA, Paprosky WG, et al: Extensor mechanism allograft reconstruction after total knee arthroplasty: A comparison of two techniques. J Bone Joint Surg Am 2004;86:2694-2699.
Nazarian DG, Booth RE: Extensor mechanism allografts in total knee arthroplasty. Clin Orthop Relat Res
1999;367-123-129. , „. H
AL-Madena Copy ^Lj-^M) <UjJlU

Question 22
Which laboratory findings would most support a diagnosis of prosthetic joint infection (PJI) in a hip or knee arthroplasty performed 3 weeks ago?
Explanation
The diagnosis of acute PJI is associated with different criteria than the diagnosis of a chronic PJI. There is no agreed-upon threshold for ESR during the acute period (6 weeks) following total joint arthroplasty. The CRP threshold is higher during the acute period (100 mg/L vs 10 mg/L for a chronic infection). The threshold for synovial fluid analysis for an acute PJI is 10000 cells/µL and more than 90% PMN neutrophils vs 3000 cells/µL and more than 80% PMN neutrophils for a chronic infection.

Question 23
A patient with Charcot-Marie-Tooth disease has a progressively rigid cavovarus foot deformity. The patient states that the pain is restricted to the forefoot, where rigid claw toe deformities have developed. Which of the following structures is primarily involved in creation of a claw toe deformity?
Explanation
REFERENCES: Keenan MA, Gorai AP, Smith CW, Garland DE: Intrinsic toe flexion deformity following correction of spastic equinovarus deformity in adults. Foot Ankle 1987;7:333-337.
Pichney GA, Derner R, Lauf E: Digital “V” arthrodesis. J Foot Ankle Surg 1993;32:473-479.
Mizel MS, Michelson JD: Nonsurgical treatment of monarticular nontraumatic synovitis of the second metatarsophalangeal joint. Foot Ankle Int 1997;18:424-426.
Question 24
An obese 62-year-old man reports a 10-year history of progressive flatfoot deformity and a 3-month history of a painful callus along the plantar medial midfoot that has not improved with custom shoe wear, pedorthics, and callus care. There is no hindfoot motion, but functional ankle motion remains. He does not have diabetes mellitus. Radiographs are shown in Figures 27a and 27b. What is the best surgical option at this point?
Explanation
REFERENCES: Johnson JE, Yu JR: Arthrodesis techniques in the management of Stage II and III acquired adult flatfoot deformity. Instr Course Lect 2006;55:531-542.
Pinney SJ, Lin SS: Current concept review: Acquired adult flatfoot deformity. Foot Ankle Int 2006;27:66-75.
Question 25
Which of the following agents increases the risk for a nonunion following a posterior spinal fusion?
Explanation
REFERENCES: Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Martin GJ Jr, Boden SD, Titus L: Recombinant human bone morphogenetic protein-2 overcomes the inhibitory effect of ketorolac, a nonsteroidal anti-inflammatory drug (NSAID), on posterolateral lumbar intertransverse process spine fusion. Spine 1999;24:2188-2193.
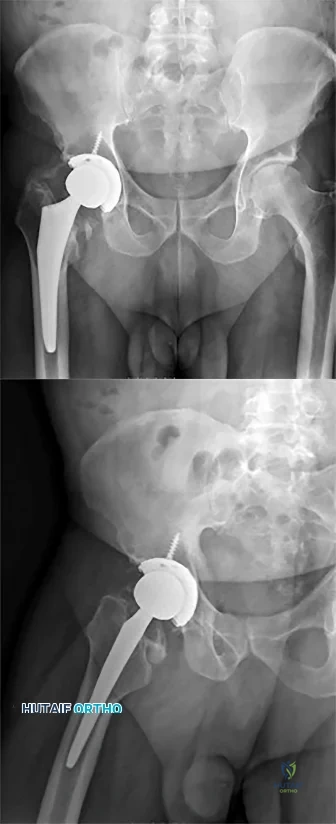
Question 26
below depicts the radiograph obtained from a year-old woman who began having more right than left hip pain during a recent pregnancy. Physical examination reveals increased range of motion with positive flexion abduction and external rotation and flexion adduction and internal rotation as well as pain with external logroll. Assessment of below reveals
Explanation
Studies have demonstrated that pelvic inclination can dramatically affect the interpretation of radiographs in the dysplastic hip, with 9° of increased pelvic inclination leading to the presence of crossover signs and posterior wall signs. A distance of 30 mm to 50 mm from the sacrococcygeal junction to the pubis is often used to assess the adequacy of pelvic inclination on radiographs, although Siebenrock and associates determined the mean difference to be 32 mm in men and 47 mm in women. In this patient, the pelvic inclination is dramatically increased, leading to overestimation of acetabular retroversion.
Question 27
During a Lisfranc (tarsometatarsal) amputation of the foot, which of the following is crucial to prevent the patient from having a supinated foot during gait.

Explanation
Illustration B depicts the level of a Lisfranc amputation of the foot. Incorrect Answers:
The posterior tibialis is the primary supinator of the foot, and releasing it would lead to an eversion deformity. The tibialis posterior tendon attachment to the bases of the second and third metatarsals will actually be released with this amputation, but the main attachment to the navicular preserved. 3-The anterior tibialis dorsiflexes and inverts the foot, but transferring it to the medial and middle cuneiforms would mimick its native function to dorsiflex and invert the foot. 4-A lengthened Achilles would lead to increased dorsiflexion, not supination. 5-Osteotomy of 2nd MT is crucial to preserve the medial cuneiform and midfoot stable.
Question 28
A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of
Explanation
REFERENCES: Rettig AC, Kollias SC: Internal fixation of acute stable scaphoid fractures in the athlete. Am J Sports Med 1996;24:182-186.
Rettig AC, Weidenbener EJ, Gloyeske R: Alternative management in midthird scaphoid fractures in the athlete. Am J Sports Med 1994;22:711-714.
Riester JN, Baker BE, Mosher JF, Lowe D: A review of scaphoid fracture healing in competitive athletes. Am J Sports Med 1985;13:159-161.
Question 29
-Which gene correlates with severity of disease in spinal muscular atrophy (SMA)?
Explanation
The other choices are not associated with spinal muscular atrophy.Defects in PMP22 are the cause of 70% to 80% of cases of Charcot-Marie-Tooth disease. Mutations in the dystrophin gene cause Duchenne muscular dystrophy.
Question 30
- A 10-year-old boy twisted his ankle while skateboarding and has pain and swelling around the lateral ankle just distal to the fibula. Radiographs are obtained and a lesion is identified in the distal tibia as seen in Figures 273a and 273b. Two weeks later he has no pain to palpation in the region and denies antecedent pain. What is the most appropriate treatment for this lesion?

Explanation

Question.1 .A 49-year-old weekend athlete has a 4-week history of pain in his unilateral plantar heel that is most severe for the first 20 steps upon arising in the morning. He has an area of maximal tenderness on the plantar medial aspect of the heel pad at the origin of the plantar fascia. He has only improved 30% after a 3-week course of physical therapy with toe intrinsic muscle strengthening and arch- and tendo-Achilles stretching. What is the best next treatment step?
Release the plantar fascia.
Inject the plantar fascia with platelet-rich plasma.
Prescribe a night splint and continue physical therapy.
Administer extracorporeal shockwave therapy to the heel.
Perform a series of 3 steroid injections into the plantar fascia.

Question.2 .Figures 16a and 16b are the radiographs of a 38-year-old carpenter with progressively worsening ankle pain; 14 years ago, he was involved in an all-terrain vehicle collision. Anti-inflammatory medication,corticosteroid injections, and bracing no longer effectively control his pain. The pain now interferes with his work and family responsibilities. Examination reveals an antalgic limp, varus deformity, limited ankle motion, limited eversion, and normal strength. Treatment should now consist of

ankle arthrodesis.
total ankle arthroplasty.
distal tibia osteotomy.
lateral ligament repair.
deltoid ligament release.
Question. 3 .A 48-year-old woman had total knee arthroplasty. She is unable to “lift her toes or ankle to her nose.”After 2 months of physical therapy, she has a slapping gait. What is the best next treatment step?
Ankle fusion
Ankle-foot orthosis
Sural nerve graft
Medial heel post
Laminectomy of L4/5
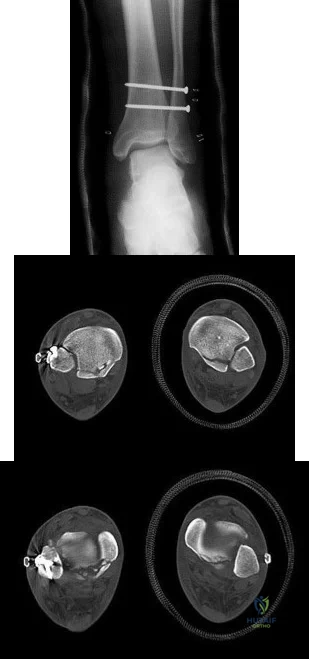
Question. 4 .Figures 46a through 46c are the CT scans of an 18-year-old who sustained an injury 3 weeks ago and now has ankle pain. Examination reveals an ankle effusion and painful range of motion. Recommended treatment should consist of
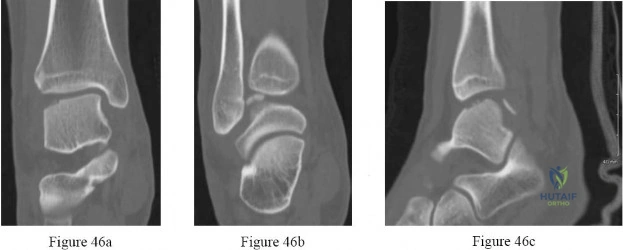
transtalar drilling.
fixation of the fragment.
osteochondral autograft.
weight bearing in a boot with early range of motion.
cast immobilization and nonweight-bearing activity for 6 weeks.
Question. 5 .A 47-year-old woman has a closed, displaced, Weber C bimalleolar ankle fracture. Past medical history includes diabetes mellitus for 7 years controlled with diet and an oral hypoglycemic agent. Semmes-Weinstein sensory testing reveals absence of sensation to the 5.07/10-gm monofilament on the plantar aspect of both feet. The skin is intact with 2+ pedal pulses. Treatment should include
open reduction with limited internal fixation.
closed reduction and application of an external fixator.
closed reduction and total contact cast immobilization.
retrograde intramedullary rod fixation with ankle fusion.
internal fixation and an extended period of immobilization.

Question. 6 .Figures 68a and 68b are the clinical photographs of a 55-year-old woman who had a right hindfoot fusion 3 years ago for a pes planovalgus deformity. Since the surgery, she has had lateral hindfoot pain and places most of the weight-bearing load on the lateral border of her foot when walking. What is the most likely cause of her symptoms?

Deltoid insufficiency
Excessive forefoot abduction
Residual heel valgus
Residual Achilles tendon contracture
Malposition of the transverse tarsal joint
Question 31
- Figures 59a and 59b show the plain radiographs, and Figures 59c and 59d show the CT scan of a 77-year-old woman who has had pain in her back and both buttocks for the past 6 months. She reports that the pain radiates down her right thigh and leg when she is standing. What is the most likely diagnosis?
Explanation
Question 32
A 23-year-old male is involved in a motor vehicle accident and sustains a left open femur fracture, right open humeral shaft fracture, and an LC-II pelvic ring injury. Which of the following best describes the radiographic findings associated with this pelvic injury pattern using the Young-Burgess Classification system?

Explanation
Burgess et al discuss the effectiveness of a treatment protocol as determined by their pelvic injury classification and hemodynamic status. The injury classification system was based on lateral compression, anteroposterior compression, vertical shear, and combined mechanical injury types. They found that their classification-based treatment protocols reduce the morbidity and mortality related to pelvic ring disruption.
Tile discusses acute pelvic trauma and his classification system for pelvic injuries (ie. Types A, B, and C). He states that any classification system must be seen only as a general guide to treatment, and that the management of each patient requires careful, individualized decision making.
Incorrect
2:
This
describes
an
APC-II
injury
3:
This
describes
an
APC-III
injury
4:
This
describes
and
LC-I
injury
Question 33
In the treatment of intra-articular calcaneal fractures, surgical reduction and fixation has been shown to have improved outcomes over nonoperative treatment in all of the following patient groups EXCEPT:

Explanation
Question 34
Figures 21a through 21c show the MRI scans of a 21-year-old football player who sustained a valgus knee injury while changing direction. Examination reveals swelling and tenderness along the medial aspect of the knee. There is a positive Lachman test, 3+ valgus laxity at 30 degrees, and 1+ valgus laxity at 0 degrees extension. The anterior drawer test is increased with the tibia in external rotation. The increase in the anterior drawer test with the tibia in external rotation is most likely the result of
Explanation
REFERENCES: Warren LA, Marshall JL, Girgis F: The prime static stabilizer of the medial side of the knee. J Bone Joint Surg Am 1974;56:665-674.
Indelicato PA: Injury to the medial capsuloligamentous complex of the knee, in Feagin J (ed): The Crucial Ligaments, ed 2. 1994, pp 351-360.
Question 35
03 Early failure of a unicompartmental knee arthroplasty that is the result of polyethylene wear is primarily caused by
Explanation
back to this question next question
Question 36
A cartilage water content increase is the hallmark of which osteoarthritis stage?
Explanation
Question 37
A 10-year-old child has leg discomfort with activity. A radiograph, bone scan, and biopsy specimen are shown in Figures 1a through 1c. What is the most likely diagnosis?
Explanation
REFERENCES: Harris WH, Dudley HR Jr, Barry RS: The natural history of fibrous dysplasia: An orthopaedic, pathological and roentgenographic study. J Bone Joint Surg Am 1962;44:207.
Campanacci M: Bone and Soft Tissue Tumors. Vienna, Austria, Springer-Verlag, 1990.
Question 38
When treating osteoporosis with alendronate, what is the most common side effect?
Explanation
REFERENCES: Marshall JK, Rainsford KD, James C, et al: A randomized controlled trial to assess alendoronate-associated injury of the upper gastrointestinal tract. Aliment Pharmacol Ther 2000;14:1451-1457.
Lane JM, Sandhu HS: Osteoporosis of the spine, in Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 227-234.
Question 39
An 18-month-old boy with obstetric brachial plexus palsy is being evaluated for limited right shoulder motion. Physical therapy for the past 6 months has failed to result in improvement of the contracture. Which of the following studies is necessary prior to any shoulder reconstruction? Review Topic
Explanation
Question 40
Figures 2a and 2b show the radiographs of a 72-year-old man with aseptic loosening of the tibial component of his total knee arthroplasty. Optimal management should include
Explanation
The insertions of the lateral ligaments are absent, thereby rendering the lateral side of the knee predictably unstable. Also, the large valgus deformity compromises the medial collateral ligament. The posterior cruciate ligament is also likely to be deficient with this much tibial bone destruction. The patient requires a posterior stabilized femoral component at the minimum, and possibly a constrained femoral component. Retention of the femoral component, even though it may be well-fixed, jeopardizes the outcome.
REFERENCES: Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 137-250.
Insall JN, Windsor RE, Scott WN, et al: (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 935-957.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 339-365.
Question 41
What is the most likely type of pathology seen in Figure 16?
Explanation
REFERENCES: McLain R, Weinstein J: Tumors of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1173.
Charlton OP, Martinez S, Gehweiler JA Jr: Pedicle thinning at the thoracolumbar junction: A normal variant. Am J Roentgenol 1980;134:825-826.
Question 42
A 20-year-old-man sustained a scapular fracture after attempting to grab a beam as he fell through a ceiling at a job site 3 months ago. A clinical photograph is shown in Figure 36. He now reports pain in the anterior shoulder and difficulty with overhead activities. What nerve roots make up the involved peripheral nerve?
Explanation
REFERENCE: Leffert RD: Anatomy of the Brachial Plexus in Brachial Plexus Injuries. Churchill Livingstone, New York, NY, 1985.
Question 43
A 62-year-old woman reports diffuse aches and pains of the hip and pelvis. She denies any significant trauma but does have a history of chronic anemia. Figure 17a shows a radiograph of the pelvis, and Figures 17b and 17c show T 2 -weighted MRI scans. What is the most likely diagnosis?
Explanation
REFERENCE: Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA,
WB Saunders, 2002, pp 2189-2216.
Question 44
A 41-year-old woman with diabetes mellitus fell onto her outstretched arm and sustained an injury to the right elbow. Radiographs are shown in Figures 53a and 53b. What is the most appropriate management?

Explanation
Question 45
Based on the findings seen at C5-6 in Figure 30, the most likely deficit for this patient will be weakness of the
Explanation
REFERENCE: Hoppenfeld S: Evaluation of nerve root lesions involving the upper extremity, in Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-23.
Question 46
A 27-year-old man sustains a Gustilo and Anderson type II open tibia fracture during a motorcycle accident. He had his full 3 doses of tetanus vaccination as an infant. He also had a tetanus booster vaccination 18 months ago when he began a new job. In addition to intravenous antibiotics, what tetanus prophylaxis should be administered?

Explanation
the past 5 years so he does not need an update of the vaccination or immune globulin. Illustration A is a concise table that can be used as an algorithm to provide appropriate tetanus prophylaxis.
Question 47
A 32-year-old woman has left second toe dactylitis (sausage toe). Radiographs show a “pencil in cup” distal interphalangeal joint deformity. Examination reveals that subtalar motion is markedly reduced. What is the most likely diagnosis?
Explanation
REFERENCES: Jahss MH: Disorders of the Foot and Ankle, ed 2. Philadelphia, PA,
WB Saunders, 1991, pp 1691-1693.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 172-173.
Question 48
What percentage of bone weight is collagen?
Explanation
Question 49
A high school football player asks you about an oral supplement that increases body mass and improves sprint times. He would like to use it to improve performance. What is the most likely agent?
Explanation
REFERENCES: McGuine TA, Sullivan JC, Bernhardt DT: Creatine supplementation in high school football players. Clin J Sports Med 2001 ;11:247-253.
Rawson ES, Gunn B, Clarkson PM: The effects of creatine supplementation on exercise-induced muscle damage. J Strength Cond Res 2001; 15:178-184.
Branch JD: Effect of creatine supplementation on body composition and performance: A meta-analysis.
Int J Sport Nutr Exerc Metab 2003;13:198-226.
Question 50
A number of potential complications are associated with the direct lateral approach to the lumbar spine; which complication is most common?
Explanation
Sofianos and associates examined the cases of 45 patients who underwent the lateral transpsoas approach and found that 18 of 45 patients (40%) experienced at least 1 complication. The most common complication was postsurgical weakness of the iliopsoas, which was an issue for 10 of 45 patients (22.2%). The second-most-common complication in this series was anterior thigh hypoesthesia. This occurred in 8 of 45 patients (17.8%). A series of 600 patients by Rodgers and associates noted that thigh pain and psoas weakness following a direct lateral approach to the lumbar spine were both "nearly universal" but almost "always transient."
RECOMMENDED READINGS
Sofianos DA, Briseño MR, Abrams J, Patel AA. Complications of the lateral transpsoas approach for lumbar interbody arthrodesis: a case series and literature review. Clin Orthop Relat Res. 2012 Jun;470(6):1621-32. doi: 10.1007/s11999-011-2088-3. Review. PubMed
PMID: 21948287.View Abstract at PubMed
Lee YP, Regev GJ, Chan J, Zhang B, Taylor W, Kim CW, Garfin SR. Evaluation of hip flexion strength following lateral lumbar interbody fusion. Spine J. 2013 Oct;13(10):1259-62. doi: 10.1016/j.spinee.2013.05.031. Epub 2013 Jul 12. PubMed PMID: 23856656. View Abstract at PubMed
Rodgers WB, Gerber EJ, Patterson J. Intraoperative and early postoperative complications in extreme lateral interbody fusion: an analysis of 600 cases. Spine (Phila Pa 1976). 2011 Jan 1;36(1):26-32. doi: 10.1097/BRS.0b013e3181e1040a. PubMed PMID: 21192221. View
Abstract at PubMed
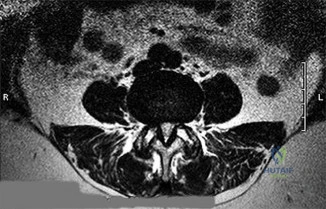
CLINICAL SITUATION FOR QUESTIONS 21 AND 22
Figures 21a through 21c are the preoperative lateral standing radiograph, axial T2-weighted MR image at L4-5, and supine sagittal MR image of a 45-year-old woman who has had back and leg pain for 2 years. Treatment had included nonsteroidal anti-inflammatory drugs, physical therapy, and epidural corticosteroid injections. Her pain limited her activities of daily living; she could walk only 1 to 2 blocks before her pain became intolerable.
21A

B

C
Question 51
Varus malalignment after a talar neck fracture with medial comminution causes a decrease in what motion?

Explanation
Herscovici et al review the appropriate management of complex ankle and hindfoot injuries in this instructional course lecture.
Daniels et al performed a cadaveric study where they osteotomized the talar neck and then studied ankle motion with and without removal of a medially based wedge of bone. They found that subtalar eversion was specifically decreased.
Sanders et al found that secondary reconstructive procedures following talar neck fractures were most commonly performed to treat subtalar arthritis or misalignment.
Question 52
A 45-year-old man sustains a low-velocity gunshot wound to the base of the right thumb. The open wound is allowed to heal by secondary intention, resulting in a contracture of the first web space. Clinical photographs are shown in Figures 49a through 49c. Treatment should now consist of
Explanation
REFERENCES: Buchler U, Frey HP: Retrograde posterior interosseous flap. J Hand Surg Am 1991;16:283-292.
Brunelli F, Valenti P, Dumontier C, et al: The posterior interosseous reverse flap: Experience with 113 flaps. Ann Plast Surg 2001;47:25-30.
Question 53
Anterior subluxation in a throwing athlete is most commonly the result of
Explanation
REFERENCES: Kvitne RS, Jobe FW: The diagnosis and treatment of anterior instability in the throwing athlete. Clin Orthop 1993;291:107-123.
Jobe FW, Tibone JE, Jobe CM, Kvitne RS: The shoulder in sports, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1999, pp 961-990.
Question 54
A 42-year-old man sustained a burst fracture at L2 in a motor vehicle accident. Examination reveals that he is neurologically intact. Figure 18 shows a cross-sectional CT scan through the fracture. If the fracture is managed nonsurgically for the next 2 years, the retained fragments can be expected to
Explanation
REFERENCES: Mumford J, Weinstein JN, Spratt KF, et al: Thoracolumbar burst fractures: The clinical efficacy and outcome of nonoperative management. Spine 1993;18:955-970.
Wood KB, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurologic deficit: A prospective, randomized study. J Bone Joint Surg Am 2003;85:773-781.
Question 55
.Figures 41a through 41c are the radiograph and MRI scans of a 76-year-old woman who has intractable left shoulder pain. She was given 2 cortisone injections and oral pain medication without experiencing lasting relief. Examination reveals 60 degrees of active forward elevation (120 degrees passively), 30 degrees of external rotation lag, and a positive Hornblower sign. Pain relief and improved functionality will most likely be achieved with

Explanation
Question 56
Figures 36a and 36b are the radiographs of a 79-year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. There is no evidence of infection. What is the most appropriate treatment?
Explanation
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis (Figures 36c and 36d). They also assist in obtaining correct limb alignment. Short metaphyseal-engaging stems are associated with failure rates between
16% and 29%. Cemented stems may be shorter than press-fit stems because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.
RESPONSES FOR QUESTIONS 37 THROUGH 40
Lateral femoral cutaneous nerve
Lateral femoral circumflex artery
Superior gluteal nerve
Superior gluteal artery
Sciatic nerve
Femoral artery
Femoral vein
Femoral nerve
Saphenous branch of the femoral nerve
Profunda femoris artery
Inferior gluteal nerve
Match each description below with the anatomic structure listed above.
Question 57
A 30-year-old patient reports chronic medial knee pain and swelling. Figure 9a shows an articular cartilage lesion observed during arthroscopy. The surgeon decides to treat the lesion with the microfracture technique seen in Figure 9b. A biopsy of the repaired tissue 1 year after treatment is likely to show which of the following findings?
Explanation
REFERENCES: Buckwalter JA, Mankin HJ: Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Instr Course Lect 1998;47:487-504.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 471-488.
Question 58
Figure 11 shows the radiograph of a 3-year-old girl who sustained a proximal radius injury. Appropriate initial management should include
Explanation
REFERENCES: Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop
2000;20:7-14.
Radomisli TE, Rosen AL: Controversies regarding radial neck fractures in children. Clin Orthop 1998;353:30-39.
Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Surg Am 1999;81:1429-1433.
Gonzalez-Herranz P, Alvarez-Romera A, Burgos J, et al: Displaced radial neck fractures in children treated by closed intramedullary pinning (Metaizeau technique). J Pediatr Orthop 1997;17:325-331.
Question 59
The orthosis shown in Figure 47 is commonly used for
Explanation
REFERENCE: Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 2, p 1185.
Question 60
A 42-year-old man has a symptomatic flatfoot deformity and walks with a slight limp after falling off a scaffold 9 months ago. He also reports that he has had difficulty returning to work. Orthotics have failed to provide relief. Current radiographs are shown in Figures 19a and 19b. To relieve his pain and return the patient to work, treatment should consist of
Explanation
REFERENCES: Komenda GA, Myerson MS, Biddinger KR: Results of arthrodesis of the tarsometatarsal joints after traumatic injury. J Bone Joint Surg Am 1996;78:1665-1676.
Sangeorzan BJ, Veith RG, Hansen ST Jr: Salvage of Lisfranc’s tarsometatarsal joint by arthrodesis. Foot Ankle 1990;10:193-200.
Question 61
Which of the following structures is most commonly involved in lateral epicondylitis?
Explanation
REFERENCES: Nirschl RP: Elbow tendinosis/tennis elbow. Clin Sports Med 1992;11:851-870.
Regan W, Wold LE, Coonrad R, Morrey BF: Microscopic histopathology of chronic refractory lateral epicondylitis. Am J Sports Med 1992;20:746-749.
Question 62
Which of the following clinical tests is used to diagnose medial instability of the elbow? Review Topic
Explanation
Question 63
A patient has right shoulder pain. Figure 1a shows a gadolinium-enhanced transverse MRI scan at the level of the coracoid. Figure 1b shows an arthroscopic view of the anterior structures from a posterior portal. These images reveal which of the following findings?
Explanation
REFERENCES: Gusmer PB, Potter HG, Schatz JA, et al: Labral injuries: Accuracy of detection with unenhanced MR imaging of the shoulder. Radiology 1996;200:519-524.
Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Williams MM, Snyder SJ, Buford D Jr: The Buford complex: The “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex. A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 64
A patient is scheduled to undergo total knee arthroplasty (TKA) following failure of nonsurgical management. History reveals that she underwent a patellectomy as a teenager as the result of a motor vehicle accident. Examination reveals normal ligamentous stability. For the most predictable outcome, which of the following implants should be used?
Explanation
ligament-sparing knee (P < 0.01). The patella functions to increase the lever arm of the extensor mechanism and to position the quadriceps tendon and the patellar ligament roughly parallel to the anterior cruciate ligament and posterior cruciate ligament, respectively. The patellar ligament thereby provides a strong reinforcing structure that functions to prevent excessive anterior translation of the femur during flexion of the knee. The absence of the patella results in the patellar ligament and the quadriceps tendon being relatively in line with one another. After a patellectomy, the resultant quadriceps force is no longer parallel to the posterior cruciate ligament. This results in loss of the reinforcing function of the patellar ligament. The authors believe this loss of reinforcing function may place increased stresses on the posterior cruciate ligament and posterior aspect of the capsule, which may result in stretching of these structures over time. They found a high rate of anteroposterior instability, a high prevalence of recurvatum, and a high rate of loss of full active extension compared with passive extension in the posterior cruciate ligament-sparing group, which supports their theory.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
Paletta GA Jr, Laskins RS: Total knee arthroplasty after a previous patellectomy. J Bone Joint Surg Am 1995;77:1708-1712.
Question 65
Figures 3a and 3b show the MRI scans of a patient with neck pain. What is the most likely diagnosis?
Explanation
REFERENCES: Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Funasaki H, Winter RB, Lonstein JB, et al: Pathophysiology of spinal deformities in neurofibromatosis: An analysis of seventy-one patients who had curves associated with dystrophic changes. J Bone Joint Surg Am 1994;76:692-700.
Question 66
A 59-year-old woman with a history of osteoporosis is involved in a high-speed motor vehicle accident, resulting in left hip pain and deformity. The initial radiograph from the trauma bay is shown in Figure 1. Postreduction CT is shown in Figures 2 through 4. What is the most appropriate definitive surgical treatment?
Explanation
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
Question 67
A 9-year-old girl reports the immediate onset of severe groin pain and the inability to walk after tripping on a curb. Examination reveals marked hip pain with passive range of motion. A radiograph is shown in Figure 21. Regardless of treatment, what is the most common complication following this injury?
Explanation
REFERENCES: Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Rhoad RC, Davidson RS, Heyman S, et al: Pretreatment bone scan in SCFE: A predictor of ischemia and avascular necrosis. J Pediatr Orthop 1999;19:164-168.
Question 68
Figure 17 is the radiograph of a 3-year-old girl who has shoulder pain after a fall. What is the best next step?
Explanation
Patients with a pathologic fracture of a unicameral bone cyst or simple bone cyst should first pursue nonsurgical treatment and 4 to 6 weeks of immobilization. Spontaneous healing occurs in fewer than 10% of patients, possibly due to cyst decompression. The most appropriate form of surgical treatment is controversial. Many substances have been injected with variable results. Injection with steroid, bone marrow, demineralized bone matrix, and calcium phosphate/calcium sulfate have been attempted. Curettage and bone grafting and
decompression have been attempted. Indications for treatment are based on cyst size, symptoms, and location. Unicameral bone cysts typically resolve as patients reach skeletal maturity.

CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 23
Figure 18 is the lateral radiograph of the lumbar spine of an 11-year-old boy who has had lower back pain for 2 months. There is no history of injury. He denies radiating pain to his legs, numbness, weakness, and bowel or bladder changes. His usual activities include soccer practices and games 3 to 5 times per week. He has used over-the-counter anti-inflammatory medications, but has had no other treatment.
Question 69
When comparing the failure load of an evenly tensioned four-stranded hamstring tendon anterior cruciate ligament autograft to a 10-mm bone-patellar tendon-bone autograft, the hamstring graft will fail at a tension
Explanation
REFERENCES: Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA: Arthroscopic reconstruction of the anterior cruciate ligament: A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 1999;27:448-454.
Hamner DL, Brown CH Jr, Steiner ME, et al: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Noyes FR, Butler DL, Grood ES, et al: Biomechanical analysis of human ligament grafts used in knee-ligament repairs and reconstructions. J Bone Joint Surg Am 1984;66:344-352.
Question 70
A 59-year-old active woman undergoes elective total hip replacement in which a posterior approach is used. She has minimal pain and is discharged to home 2 days after surgery. Four weeks later, she dislocates her hip while shaving her legs. She undergoes a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Explanation
First-time early dislocations are often treated successfully without revision surgery, especially when no component malalignment is present. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful but is usually reserved for patients with recurrent dislocations.
Question 71
Figures 1 and 2 show the radiographs obtained from a 68-year-old morbidly obese man who underwent left total hip replacement 7 years ago and did well, with no symptoms prior to the current presentation. He recently rose from a seated position and felt a pop in the hip, with immediate pain and inability to bear weight. Any pressure on the left foot now produces a painful, grinding sensation with loss of left hip stability. What is the best next step?

Explanation
The modular femoral stem has fractured. Changing the liner to a constrained design is not warranted at this time based on the information provided. Revision of the acetabular implant is appropriate because of the potential for damage to the existing cup from metal debris and femoral implant contact and to convert from a metal-on-metal articulation. Nonsurgical management would not provide pain relief or improvement; revision of the total hip arthroplasty is recommended. The implant failed in a short time, and retention of the femoral stem is not recommended because of the concern for failure with only a neck exchange. A dual-mobility bearing may be a good option if the surgeon plans to retain the acetabular component. Extended trochanteric osteotomy is a useful technique for the removal of a well-fixed femoral implant. In this patient, femoral stem removal without
osteotomy would be difficult due to the fracture of the implant’s femoral neck and the inability to gain purchase for extraction.
Question 72
The findings in Brown-Sequard syndrome include loss of which of the following? Review Topic
Explanation
Question 73
An 18-year-old man underwent open reduction and internal fixation of a tibial spine avulsion and a posterolateral corner repair. Two years later, he underwent lateral collateral ligament (LCL) and posterolateral corner reconstruction because of instability. Examination reveals a pronounced lateral varus knee thrust when ambulating. Varus stress in 30 degrees of flexion produces a 10-mm opening that is eliminated in extension. The Lachman’s test is 2 mm with a firm end point, and the posterior drawer test is negative. Standing radiographs show widening of the lateral joint space and a 5-degree mechanical varus alignment. What is the most effective course of treatment?
Explanation
REFERENCES: Naudie DD, Amendola A, Fowler PJ: Opening wedge high tibial osteotomy for symptomatic hyperextension-varus thrust. Am J Sports Med 2004;32:60-70.
Covey DC: Injuries of the posterolateral corner of the knee. J Bone Joint Surg Am
2001;83:106-118.
Question 74
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
Explanation
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Question 75
The strongest biomechanical construct for open reduction and internal fixation of a talar neck fracture uses what interval and entry point?
Explanation
REFERENCES: Swanson TV, Bray TJ, Homes GB Jr: Fractures of the talar neck: A mechanical study of fixation. J Bone Joint Surg Am 1992;74:544-551.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 37-38.
Question 76
A 15-year-old girl has left knee pain and an enlarging mass in the distal thigh. AP and lateral radiographs are shown in Figures 52a and 52b, and a biopsy specimen is shown in Figure 52c. What is the most likely diagnosis?
Explanation
REFERENCES: Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
Gibbs CP, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 77
273 In an athlete who has full, painless range of motion and a normal neurological examination, which of the following is considered an absolute contraindication to participation in a collision sport such as football?
Explanation
Thomas BE, et al. Cervical spine injuries in football players. J AM Acad Orthop Surg 1999;7:338-347
Torg JS et al: Neurapraxia of the cervical spinal with transientquadriplegia. JBJS Am 1986:68:1354-
Question 78
What is the major difference in outcome following open reduction and internal fixation (ORIF) of the tibial plafond at 2 to 5 days versus 10 to 20 days?
Explanation
REFERENCES: Sirkin M, Sanders R, DePasquale T, et al: A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 1999;13:78-84.
Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 79
Which of the following is considered an advantage of metal femoral heads compared with ceramic heads?
Explanation
REFERENCE: Cook SD: Materials consideration in total joint replacement, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 27-33.
Question 80
Bone morphogenetic proteins transduce intracellular signal through what class of cell surface receptor?
Explanation
Question 81
A tall, thin 17-year-old basketball player and his parents request an evaluation of his flexible (hypermobile) pes planus/planovalgus foot deformities. As part of his evaluation, the orthopaedic surgeon notes pectus excavatum, disproportionately long arms, and scoliosis. In addition to providing treatment of his feet, what test or evaluation should the patient be referred for? Review Topic
Explanation
Question 82
Surgical treatment for symptomatic disk herniations is associated with which of the following?
Explanation
REFERENCE: Weinstein JN, Lurie JD, Tosteson TD, et al: Surgical vs nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006;296:2451-2459.
Question 83
An elderly patient falls and sustains an extension injury to the neck that results in upper extremity weakness, spared perianal sensation, and lower extremity spasticity. These findings best describe what syndrome?
Explanation
motor function.
REFERENCES: Apple DF Jr: Spinal cord injury rehabilitation, in Rothman RH, Simeone FA (eds): The Spine, ed 3. Philadelphia, PA, WB Saunders, 1992, Chapter 31.
Leventhal MR: Fractures, dislocations and fracture-dislocations of spine, in Crenshaw AH (ed): Campbell’s Operative Orthopaedics, ed 8. St. Louis, MO, Mosby, 1992.
Question 84
271 Which of the following factors has been shown to contribute to poor results after anatomic reduction of posterior wall acetabulum fractures?
Explanation
Complications can include sciatic nerve injury (incidence, 3% to 18%), heterotopic ossification (7% to 20%), and osteonecrosis of the femoral head (5% to 8%). Despite the relative simplicity of this acetabular fracture, unsatisfactory outcomes after surgical repair of the posterior wall occur in at least 18% to 32% of cases, results that are worse than for most of the other more complex acetabular fracture patterns.
Moed BR, et al. Results of operative treatment of fractures of the posterior wall of the acetabulum. JBJS AM 2002:84:752-758
Matta JM: Fractures of the acetabulum: Accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. JBJS Am 1996;78:1632-1645
back to this question next question
Question 85
A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate Review Topic

Explanation
Question 86
A 63-year-old woman with a history of poliomyelitis has a fixed 30-degree equinus contracture of the ankle, rigid hindfoot valgus, and normal knee strength and stability. She reports persistent pain and has had several medial forefoot ulcerations despite a program of stretching, bracing, and custom footwear. What is the next most appropriate step in management?
Explanation
REFERENCES: Perry J, Fontaine JD, Mulroy S: Findings in post-poliomyelitis syndrome: Weakness of muscles of the calf as a source of late pain and fatigue of muscles of the thigh after poliomyelitis. J Bone Joint Surg Am 1995;77:1148-1153.
Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Question 87
A 16-year-old football player is participating in the second session of two-a-day preseason practices. He complains of dizziness and fatigue. He is brought to the sideline by the athletic trainer where examination demonstrates confusion and disorientation. Ambient temperature is 82°F. What would be the next most appropriate step in his treatment?
Explanation
Question 88
Figures below demonstrate the radiographs obtained from a 56-year-old man with a 3-year history of right groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?
Explanation
Chronic opioid consumption prior to total joint arthroplasty has been associated with increased pain after surgery, increased opioid requirements, a slower recovery and longer hospital stay, and higher 90-day postoperative complications compared with patients not on chronic opioids preoperatively. Based on this information, Nguyen and associates performed a study in three patient groups that included 1) chronic opioid users who underwent no preoperative intervention, 2) chronic opioid users who were weaned down to 50% of their prior opioid regimen, and 3) patients who were not chronic opioid users. The authors found that the reduction of preoperative opioid use improved postoperative function, pain, and recovery and that the weaned group performed more like the opioid naive group than the chronic opioid user
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to
surgery.
Question 89
..First-line treatment recommendations include
Explanation
Ultrasound
MRI scan of the thigh
Chest CT scan and whole-body bone scan
Positron emission tomography (PET) scan
Presurgical radiation therapy
Marginal resection
Radical resection and postsurgical radiation
Transverse incision centered over the mass
Incision centered over the mass in line with long axis of limb
Sentinel node biopsy
Core needle biopsy
For each soft-tissue mass clinical scenario or question below, match the most appropriate next evaluation or treatment step listed above.
Question 90
Figures 12a through 12e show the radiograph, MRI scans, and biopsy specimens of a 17-year-old boy. What is the most likely diagnosis?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999,
pp 247-263.
Question 91
What pathology is most likely to result in failure of an arthroscopic Bankart repair?
Explanation
REFERENCES: Burkhart SS, De Beer JF: Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 2000;16:677-694.
Cole BJ, Romeo AA: Arthroscopic shoulder stabilization with suture anchors: Technique, technology, and pitfalls. Clin Orthop 2001;390:17-30.
Question 92
A 15-year-old baseball pitcher who reports increasing pain in his right shoulder over the past 3 weeks states that the pain increases the more he pitches. Radiographs of both shoulders are shown in Figures 35a and 35b. What is the next most appropriate step in management?
Explanation
REFERENCES: Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in the adolescent baseball pitchers: A case report. J Bone Joint Surg Am 1985;67:495-496.
Cahill BR, Tullos HS, Fain RH: Little league shoulder: Lesions of the proximal humeral epiphyseal plate. J Sports Med 1974;2:150-152.
Question 93
A 67-year-old man who underwent humeral head arthroplasty for a four-part fracture 6 months ago reports that he is still unable to actively elevate his arm. Rehabilitation after surgery consisted of a sling with passive range-of-motion exercises for 2 weeks and then progressed to active-assisted and strengthening exercises at 3 weeks. Radiographs are shown in Figures 28a and 28b. What is the primary cause of his inability to elevate the arm?
Explanation
REFERENCES: Hartsock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humeral fractures. Orthop Clin North Am 1998;29:467-475.
Hughes M, Neer CS: Glenohumeral joint replacement and postoperative rehabilitation.
Phys Ther 1975;55:850-858.
Compito CA, Self EB, Bigliani LU: Arthroplasty and acute shoulder trauma. Clin Orthop 1994;307:27-36.
Question 94
Which of the following is a relative contraindication to performing laminoplasty in a patient with cervical myelopathy? Review Topic
Explanation
Question 95
The load versus deformation curve of the functional spinal unit (FSU) is made up of the neutral zone, the elastic zone, and the plastic zone. What is the plastic zone of the curve believed to represent?
Explanation
REFERENCES: Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 15-23.
Panjabi MM, White AA: Physical properties and functional biomechanics of the spine, in White AA, Panjabi MM: Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 1-83.
Question 96
Compared with surgically treated patients, patients with extra-articular distal third humeral shaft fractures that are treated nonsurgically with functional bracing can be expected to show which of the following findings?
Explanation
Question 97
What type of muscle contraction occurs while the muscle is lengthening?
Explanation
REFERENCES: Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000,
pp 12-13.
Lieber RL: Form and function of skeletal muscle, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 98
A 70-year-old woman is brought to the emergency department with a two-part greater tuberosity fracture with an anterior subcoracoid dislocation. One day after successful closed reduction, examination reveals marked swelling of the involved arm, forearm, and hand, as well as large amounts of “weeping” serous fluid but no obvious lacerations. The fingers are warm and pink, and the pulses are normal distally with good refill. Edema is present. There is no pain with passive and active motion of the elbow, wrist, and fingers. What is the next most appropriate step in management?
Explanation
REFERENCE: Killewich LA, Bedford GR, Black KW, et al: Diagnosis of deep venous thrombosis: A prospective study comparing duplex scanning to contrast venography.
Circulation 1989;79:810.
Question 99
Which of the following cannulated screw configurations used in the treatment of subcapital femoral neck fractures is optimal?

Explanation
Booth et al performed a cadaveric study comparing central versus calcar (cortical-adjacent) fixation. The results demonstrated significant improved stability, load, stiffness, and displacement in all tested parameters for the group with calcar-adjacent screw fixation.
Lindequist and Törnkvist performed a Level 4 study of 72 femoral neck fractures. They found that all 5 of their nonunions had screws placed greater than 3mm from the femoral calcar. Additionally, 16 of 18 fractures healed in the group of displaced fractures where both the fixating screws were placed within 3 mm from the femoral neck cortex.
Gurusamy et al performed a Level 4 study of 395 patients undergoing femoral neck fixation. They found a reduced spread of the screws on the lateral view was associated with an increased risk of nonunion of the fracture.
Illustration A depicts the optimal configuration of an inverted triangle with the single screw being inferior and all of the screws being cortical adjacent.
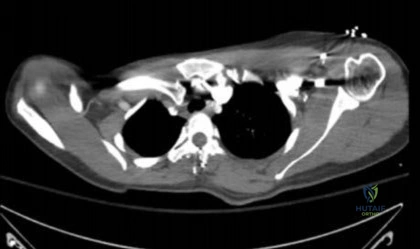
Question 100
This image represents the end stage of an uncompensated rotator cuff tear.
Explanation
Axillary lateral and anteroposterior (AP) images of the right shoulder (Figures 59c and 59d) reveal osteoarthrosis of the glenohumeral joint, which typically is not associated with significant rotator cuff pathology. An examination often shows limitations in range of motion, crepitance, and pain with motion. An AP radiographic image of the right shoulder (Figure 59b) reveals proximal humeral migration, which normally correlates with rotator cuff tear size. Tears extending into the infraspinatus tendon are associated with more humeral migration than is seen with isolated supraspinatus tears. Presenting complaints are usually of pain and weakness. Examination findings include subacromial crepitance and weakness during rotator cuff testing. Rarely, this may be associated with pseudoparalysis in large uncompensated rotator cuff tears. The CT image of the right shoulder (Figure 59a) shows superior migration of the humerus with respect to the glenoid surface and end-stage
degenerative changes at the glenohumeral joint. These changes are classified as rotator cuff arthropathy. Pain and weakness are common, as is the presence of pseudoparalysis and limited range of motion.
RECOMMENDED READINGS
Kelly JD Jr, Norris TR. Decision making in glenohumeral arthroplasty. J Arthroplasty. 2003 Jan;18(1):75-82. Review. PubMed PMID: 12555187. View Abstract at PubMed
Keener JD, Wei AS, Kim HM, Steger-May K, Yamaguchi K. Proximal humeral migration in shoulders with symptomatic and asymptomatic rotator cuff tears. J Bone Joint Surg Am. 2009 Jun;91(6):1405-13. doi: 10.2106/JBJS.H.00854. PubMed PMID:
