Orthopedic Board Review MCQs: Shoulder, Elbow & Fracture | Part 109

Key Takeaway
This page offers Part 109 of a comprehensive Orthopedic Surgery Board Review MCQ bank. Authored by Dr. Hutaif, it features 100 high-yield questions modeled after OITE and AAOS exams. Designed for orthopedic residents and surgeons, it provides interactive study and exam modes with clinical explanations for rigorous board certification preparation.
About This Board Review Set
This is Part 109 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 109
This module focuses heavily on: Deformity, Elbow, Fracture, Shoulder.
Sample Questions from This Set
Sample Question 1: A 21-year-old hockey player who has recurrent shoulder subluxations undergoes an anterior capsulorrhaphy under general anesthesia, and an interscalene block is used to relieve postoperative pain. At the 1-week follow-up examination, he repo...
Sample Question 2: Autosomal dominant...
Sample Question 3: A 13-year-old baseball pitcher presents with worsening medial-sided elbow pain. He pitches 7 months out of the year, throws 85 pitches per game and plays in two games per week. His fastball speed is approximately 75mph. He regularly plays o...
Sample Question 4: -To maximally resist apex anterior angulation in the tibia, the pins of a unilateral external fixator should be oriented in which of the following planes?...
Sample Question 5: Intramedullary nailing of proximal tibial shaft fractures are technically demanding, and use of an extended medial parapatellar incision with a semiextended technique can prevent what common deformity at the fracture site?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 21-year-old hockey player who has recurrent shoulder subluxations undergoes an anterior capsulorrhaphy under general anesthesia, and an interscalene block is used to relieve postoperative pain. At the 1-week follow-up examination, he reports loss of sensation over the lateral region of the shoulder and is unable to actively contract the deltoid muscle. The remainder of the examination is normal. What is the best course of action at this time?
Explanation
REFERENCE: Ho E, Cofield RH, Balm MR, et al: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270.
Question 2
Autosomal dominant
Explanation
A patient presents with a hard leg mass and pain with activity. The anteroposterior and lateral radiographs are shown in Slide 1 and Slide 2. An axial computed tomography scan is shown in Slide 3. Which of the following tumor suppressor genes is most likely involved:
Question 3
A 13-year-old baseball pitcher presents with worsening medial-sided elbow pain. He pitches 7 months out of the year, throws 85 pitches per game and plays in two games per week. His fastball speed is approximately 75mph. He regularly plays outfield once he has been relieved of pitching. Which of the following is most likely contributing to his elbow pain? Review Topic
Explanation
Little League elbow is a medial-sided overuse injury that occurs in the skeletally immature athlete. During execution of the baseball pitch, tremendous valgus and extension stresses occur at the elbow. Repetitive microtrauma can ultimately injure the medial epicondyle apophysis, ulnar collateral ligament or the flexor-pronator muscle mass. Limiting the number of pitches and innings played per game, as well as the number of months of competitive pitching per year, has been recommended to prevent these overuse injuries in the young athlete.
Olsen et al performed a case control study to determine risk factors associated with the development of shoulder and elbow injuries in adolescent baseball pitchers. Greater than 8 months of competitive pitching per year, more than 80 pitches per game and a fastball speed of greater than 85mph were all associated with increased risk of injury. Continued pitching despite arm fatigue and pain, being a starting pitcher, greater number of warm-up pitches, participating in showcases and regular use of NSAIDs were also associated with injury. The type of pitch (fastball, changeups and breaking balls) and continued play in a different position once being relieved was not associated with increased risk of injury.
Andrews et al authored a review article on ulnar collateral ligament injuries in throwing athletes. According to the USA Baseball Medical/Safety Advisory Committee, young baseball pitchers should avoid breaking pitches, such as curveballs and sliders, and avoid year-round baseball. A minimum of 3 months of complete rest from pitching per year is vital. Youth pitching coaches should be educated to ensure proper pitching mechanics are being reinforced.
Illustration A is a table depicting the recommended maximum number of pitches by age group.
Incorrect Answers:
Question 4
- To maximally resist apex anterior angulation in the tibia, the pins of a unilateral external fixator should be oriented in which of the following planes?
Explanation
Question 5
Intramedullary nailing of proximal tibial shaft fractures are technically demanding, and use of an extended medial parapatellar incision with a semiextended technique can prevent what common deformity at the fracture site?

Explanation
Lang et al. reported in their study of 32 proximal third tibia fractures that 56% of the fractures had 5 degrees or more valgus angulation and 28% had 10 degrees or more valgus angulation. Angulation in the AP plane ranged from 0 degrees to 20 degrees, all of which was apex anterior. Nineteen (59%) fractures demonstrated 5 degrees or more angulation, and 7 (22%) fractures demonstrated 10 degrees of more angulation.
Tornetta advocates use of extended medial parapatellar incision with the leg in a semiextended position to allow for a more proximal and lateral starting point. This modified starting point forces the nail to overcome the tendency of the fracture to flex (apex anterior) and go into valgus.
Question 6
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured? Review Topic
Explanation
Question 7
Compared with percutaneous pinning with Kirschner wires (K-wires), the treatment of metacarpal neck fractures with cannulated intramedullary screws is associated with
Explanation
In a biomechanical study, headless compression screws showed superior load to failure, higher three-point bending strength, and greater strength in axial loading compared with percutaneous K-wire fixation for metacarpal neck fractures. Headless compression screws provide greater initial stability to allow earlier motion in the postoperative period. No data comparing infection rates between the two methods of fixation are available; however, it is assumed that K-wires placed outside of the skin would have increased rates of infection. Neither fixation method would increase the time to healing.
Question 8
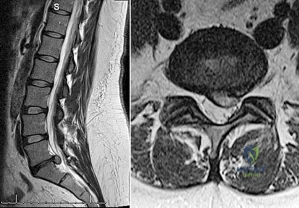
Which of the following changes occur in the spinal cord and the spinal canal when the cervical spine moves from neutral to full flexion?
Explanation
REFERENCES: Breig A: Biomechanics of the Central Nervous System: Some Basic Normal and Pathologic Phenomena. Stockholm, Sweden, Almquist and Wiksell, 1960.
Ghanayem AJ, Zdeblick TA, Panjabi MM: Biomechanics of nonacute cervical spine trauma, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 103-105.
Question 9
A 45-year-old right-hand dominant woman falls onto an outstretched left hand. Imaging shows a complex elbow dislocation. The postreduction CT scan demonstrates a reduced joint, comminuted radial head fracture, and type I coronoid fracture. Surgical intervention is recommended to address the involved structures. Which component of the intervention adds the most rotational stability?
Explanation
A. Improved longevity in comparison to the linked prosthesis
B. A significantly larger flexion-extension arc
C. A higher incidence of postsurgical instability
D. Lower frequency of ulnar nerve dysfunction
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
Question 10
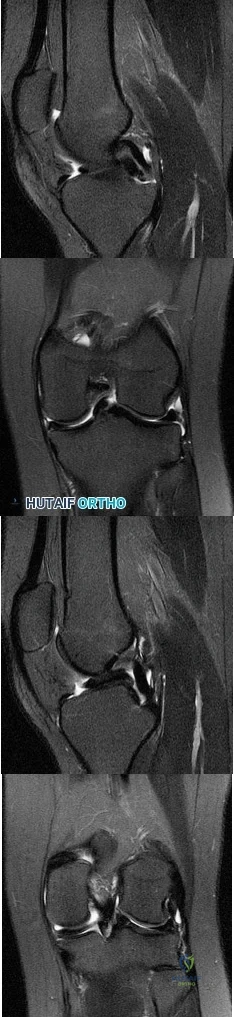
What do the T2-weighted, fat-saturated MRI scans shown in Figures 76a through 76d reveal? Review Topic
Explanation
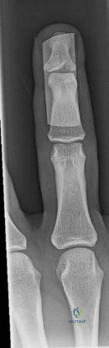
Question 11
The fracture seen in Figure 1 is most likely associated with injury to what ligamentous structure?
Explanation
A. Methicillin-resistant Staphylococcus aureus (MRSA)
B. Cutibacterium acnes
C. Enterococcus species
D. Staphylococcus epidermidis
C acnes is the most common organism recovered in prosthetic shoulder infections (33%), Coagulase-negative Staphylococcus is second (21%), Methicillin-sensitive S aureus (13%), and S epidermidis (10%). MRSA accounts for 5% and Enterococcus species, 1.5%.
Question 12
Which of the following cohorts of patients is at highest risk of a future anterior cruciate ligament (ACL) tear? Review Topic
Explanation
Question 13
-The center of rotation of the knee can be best described as
Explanation
Question 14
After performing a total hip arthroplasty through a posterolateral approach, an orthopaedic surgeon is unable to adequately externally rotate the leg and subsequently exposes the anterior capsule. When releasing the inferior aspect of the anterior capsule, pulsatile bleeding is encountered. A branch of which artery is most likely lacerated?
Explanation
Branches of the lateral femoral circumflex artery arise from the inferior aspect of the anterior hip capsule. They can be injured when removing the anterior capsule from any approach. The inferior gluteal artery supplies the gluteus maximus. The medial femoral circumflex artery enters the hip joint along the path of the obturator externus tendon. The femoral artery crosses the anterior hip joint in the superior-to-inferior direction and is located just medial to the hip joint.

Question 15
What is the most important muscle adaptation resulting from endurance training? Review Topic
Explanation
Question 16
A 10-year-old girl fell from her bike and now reports pain and swelling in the left knee and pain with weight bearing. Examination reveals a left knee effusion and pain with range of motion. A radiograph is shown in Figure 85. Treatment should consist of
Explanation
REFERENCES: Mah JY, Adili A, Otsuka NY, et al: Follow-up study of arthroscopic reduction and fixation of type III tibial-eminence fractures. J Pediatr Orthop 1998; 18:475-477.
McLennen JG: Lessons learned after second-look arthroscopy in type III fractures of the tibial spine. J Pediatr Orthop 1995;15:59-62.
Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
72 • American Academy of Orthopaedic Surgeons
Question 17
The posterior circumflex humeral artery and the axillary nerve usually lie in a space bordered superiorly by the
Explanation
REFERENCES: Rockwood CA Jr, Matsen FA III: The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, vol 1, pp 70-71.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, pp 401-402, 407.
Question 18
The use of elevated rim acetabular liners and long femoral necks may result in
Explanation
REFERENCES: Cobb TK, Morrey BF, Ilstrup DM: The elevated rim acetabular liner in total hip arthroplasty: Relationship to postoperative dislocation. J Bone Joint Surg Am 1996;78:80-86.
Urquhart AG, D’Lima DD, Venn-Watson E, Colwell CW Jr, Walker RH: Polyethylene wear after total hip arthroplasty: The effect of a modular femoral head with an extended flange-reinforced neck. J Bone Joint Surg Am 1998;80:1641-1647.
Question 19
A 27-year-old professional baseball pitcher who underwent arthroscopic olecranon debridement continues to have medial-sided elbow pain during late cocking. Physical examination reveals laxity and pain with valgus stress testing. What is the most likely cause of his pain? Review Topic
Explanation
Question 20
An 11-year-old boy stepped on a nail and sustained a puncture to the right forefoot 6 days ago. He was wearing tennis shoes at the time of injury. Treatment in the emergency department consisted of local debridement and tetanus prophylaxis; a radiograph was negative for foreign body, chondral defect, or fracture. He was discharged with a 3-day prescription of amoxicillin and clavulanate. The patient now has increasing pain and tenderness at the puncture site. What is the best course of action?
Explanation
REFERENCES: Riegler HP, Routson T: Complications of deep puncture wounds of the foot.
J Trauma 1979;19:18-22.
Green NE: Musculoskeletal infections in children: Part IV. Pseudomonas infections of the foot following puncture wounds. Instr Course Lect 1983;32:43-46.
Question 21
A 21-year-old man has mild but persistent aching pain in his left proximal thigh during impact loading activities. He denies pain at rest and has no other symptoms. Figures 34a through 34e show the radiographs and T1-weighted, T2-weighted, and gadolinium MRI scans of the left hip. What is the most likely diagnosis?
Explanation
REFERENCES: Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
May DA, Good RB, Smith DK, et al: MR imaging of musculoskeletal tumors and tumor mimickers with intravenous gadolinium: Experience with 242 patients. Skeletal Radiol 1997;26:2-15.
Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 4023-4034.
Question 22
A 14-year-old gymnast misses her dismount off of the uneven bars, hits the mat face first, and loses consciousness for about 15 seconds. She is dazed and confused for several minutes. She does not complain of pain; numbness; or weakness, and she is moving all extremities without deficit. The athlete and coach want to go back to competition that day. How should they be advised?
Explanation
symptoms with cognitive effort. They must be off of medications that could mask or alter concussion symptoms. Neurocognitive testing can be a helpful tool in determining brain function even after all symptoms of concussion have resolved. With a comparison baseline test, this evaluation, in conjunction with a physician's examination, may reduce risk for second impact syndrome. The athlete's clinical neurologic examination findings (cognitive, cranial nerve, balance testing) must return to baseline before resuming exercise. Research has shown that among youth athletes, it may take longer for tested functions to return to baseline (compared with the recovery rate in adult athletes). Brain MRI scan has no role in evaluating athletes for return to play in this situation.
Question 23
A 75-year-old woman began a walking program 2 months after undergoing right total knee arthroplasty. She had to stop the program after 4 weeks because of hindfoot pain and ankle swelling. Radiographs are shown in Figures 42a and 42b. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA,
WB Saunders, 1995, p 2591.
Kearon C: Natural history of venous thromboembolism. Semin Vasc Med 2001;1:27-37.
Aldridge T: Diagnosing heel pain in adults. Am Fam Physician 2004;70;332-338.
Question 24
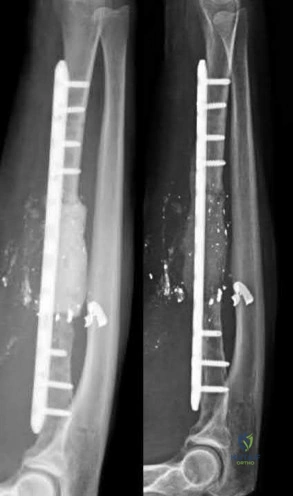
The authors found that all 9 patients went on to both clinical and radiographic union. They concluded that the Masquelet technique was successful in effectively reconstructing traumatic and posttraumatic bony defects in the forearm with a low incidence of complications.
Explanation
A 25-year-old male runs into a tree while going 45 mph on his motorcycle. He presents to your level 1 trauma hospital with the injuries shown in figures A through C. After closed reduction, which of the following is true with respect to treatment for this patient?

Heterotopic ossification is uncommon
Minifragment screws are sufficient for fracture fixation
Kocher-Langenbeck is the optimal surgical approach for this injury
Fragment excision leads to improved outcomes compared to open reduction and internal fixation
A 2 mm fragment step-off is considered the cut-off for non-surgical management
This patient has sustained a Pipkin II femoral head fracture with associated anterior hip dislocation. An open reduction with internal fixation of the femoral head fragments with direct visualization is indicated to restore stability and congruity of the hip joint. These fractures can be treated with mini-fragment screws with excellent reduction and purchase without risks of extensive chondral injury or screw prominence.
Femoral head fractures are uncommon injuries usually associated with hip dislocations. They are classified using the Pipkin Classification (Illustration B). While resection of small femoral head fracture fragments can be considered (Pipkin I) as sufficient and satisfactory treatment, this fragment is large and displaced and thus should be treated with ORIF for optimal results. Regarding the surgical approach, advocates for the direct anterior approach state direct access to the anterior portion of the femoral head with decreased overall complication rates. Other approaches, including surgical hip dislocation and Kocher-Langenbeck, are also useful depending on associated injuries (acetabulum fractures, etc.) and location of the head fragment. ORIF of these fractures can be performed with the use of countersunk mini-fragment screws, headless screws and even bioabsorbable pins to avoid prominence or extensive chondral injury.
Marecek et al. authored a review article on femoral head fractures. They described these injuries as being generally associated with hip dislocations and require prompt reduction. They noted that the surgical fixation of the femoral head is generally done through the direct anterior approach or via a surgical hip dislocation depending on associated injuries. The authors also discussed the importance of using mini-frag screws to avoid hardware prominence. They also noted that while heterotopic ossification is a common finding after the anterior approach for these injuries, it is rarely proven to be symptomatic.
Giannoudis et al. reviewed femoral head fractures focusing on management, complications and clinical results. They reported on 453 femoral head fractures in 450 patients. Regarding Pipkin Is, they noted that fragment excision gave better results compared to ORIF (p=0.07), while Pipkin IIs showed improved outcomes with ORIF. Regarding complications, they noted the following rates: wound infection (3%), sciatic nerve palsy (4%), AVN (11.9%), post-traumatic OA (20%) and HO (16.8%). They also noted the anterior approach was associated with promising long-term functional results and a lower incidence of major complication rates.
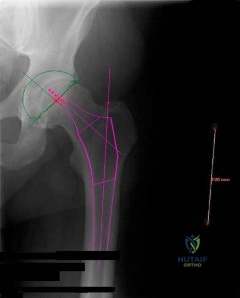
Figure A is an AP pelvis radiograph revealing a left hip dislocation with a large femoral head fracture extending into the weight-bearing zone of hip joint
(Pipkin II). Figures B and C are CT scan images revealing an anteriorly dislocated hip with a large femoral head fracture without associated acetabulum fractures. Illustration A is the post-op fluoroscopy showing ORIF of femoral head with multiple 2.7 cortical screws. Illustration B demonstrates the Pipkin classification for femoral head fractures.
Incorrect Answers:

Which of the following describes the most common organism cultured from septic olecranon bursitis?
Gram positive cocci in chains
Gram positive bacilli in branches
Gram positive cocci in pairs and clusters
Gram negative diplococci
Gram negative bacilli with thin rods Correct answer: 3
The most common cultured organism in the setting of septic olecranon bursitis is Staphylococcus aureus (S. aureus), appearing as gram positive cocci in pairs and clusters.
S. aureus is responsible organism in approximately 80% of cases of septic olecranon and prepatellar bursitis. Mixed flora is also common. Patient demographics in both conditions are similar, more commonly involving middle-aged males. Direct inoculation is presumed to be the primary culprit as opposed to hematogenous seeding, as blood supply to the bursal tissue is poor. Differentiating infectious from non-infectious bursitis can be challenging.
Aaron et al. provide a review article on the four most common types of bursitis: olecranon, prepatellar, trochanteric, and retrocalcaneal. They note that olecranon bursitis is the most common superficial bursitis, and that a careful history and physical exam can help differentiate infectious from noninfectious olecranon bursitis. The authors discuss one series of 46 patients demonstrating that a skin temperature overlying the affected bursa ≥2.2°C than the contralateral, unaffected bursa had a 100% sensitivity and 94% specificity in diagnosing a septic process.
Illustration A shows a patient with olecranon bursitis. Illustration B shows the classic gram stain for S. aureus (gram positive cocci in pairs and clusters).
Incorrect Answers:

During a trauma conference, a hand surgeon presents a case of a 25-year-old male who injured his elbow while roller skating. While describing the patient's radiographs, he reports that this injury is associated with valgus posterolateral rotatory instability. Which of the following images is most likely the patient's radiograph?

Posterolateral rotatory instability (PLRI) can result from a "terrible triad" fracture-dislocation pattern (seen in Figure E), classically involving a radial head fracture, coronoid tip or base fracture, and an elbow dislocation.
Terrible triad injuries typically occur with axial loading, supination, and a valgus directed force through the elbow. In comparison to PLRI which results from a terrible triad injury, posteromedial rotatory instability (PMRI) commonly results from an anteromedial coronoid facet fracture following a varus-directed force. These injuries also very frequently also have a lateral collateral ligament complex injury but often have no radial head fracture. PLRI is far more common than PMRI. Generally with a PLRI pattern, the lateral collateral ligament complex fails first, followed by injury to the anterior capsule or coronoid, and lastly the medial collateral ligament complex is affected. Nonoperative management is possible, but only indicated in small, non-displaced radial head fractures with small coronoid tip fractures. Typically, terrible triad injuries are addressed surgically with radial head fixation or arthroplasty, lateral collateral ligament repair, and, less commonly, coronoid fracture fixation or anterior capsule repair.
Ring et al. reviewed 56 patients who had been treated with an ORIF of the radial head at 48 months after injury. They found unsatisfactory outcomes for patients who had an ORIF of radial head fractures with greater than 3 articular fragments. The authors recommended ORIF of radial head fractures with 3 or few fragments.
Steinmann performed a review of coronoid process fractures. The author reports that with an anteromedial coronoid fracture, the anteroposterior (AP) radiograph of the elbow will demonstrate progressive narrowing of the joint space from lateral to medial. Dr. Steinmann concludes that an important determinant of stability is the involvement of the sublime tubercle (insertion point of the MCL), and that medial instability is likely with involvement of the sublime tubercle.
Mathew et al. review the anatomic, biomechanical, and operative principles of terrible triad injuries. The authors discuss that the primary goal of fixation is to stabilize the elbow and allow early range of motion. They underscore technical improvements and implant developments which have improved outcomes.
Figure A demonstrates a capitellum fracture. Figure B demonstrates an olecranon fracture.
Figure C demonstrates a displaced radial head fracture.
Figure D demonstrates an anteromedial facet coronoid fracture.
Figure E demonstrates a terrible triad injury with a radial head fracture,
coronoid tip fracture, and elbow subluxation.
Incorrect Answers:
A 32-year-old soccer player presents with severe right ankle pain and inability to bear weight after sustaining a slide-tackle injury during a game. Radiographs are shown in Figures A and B. Given the nature of his injury, he is taken for surgical reduction and fixation. Following medial malleolar fixation, the syndesmosis is addressed. All of the following are true regarding the most appropriate intraoperative technique for anatomic syndesmotic reduction EXCEPT:

The axis of the reduction clamp should parallel the anatomic trans-syndesmotic angle
The lateral tine of the clamp should be seated just posterior to the lateral malleolar ridge
The medial tine should be placed on the anterior third of the tibia on a true lateral fluoroscopic view of the ankle
The reduction clamp should be placed 1-2cm proximal to the tibial plafond
The surgeon should apply judicious compression under fluoroscopic visualization to avoid over-compression of the syndesmosis
When placing a clamp across the syndesmosis to facilitate reduction, the lateral tine should be placed directly on the lateral malleolar ridge. Placing the lateral tine either more anteriorly or posteriorly has been shown to result in sagittal malreduction from fibular translation.
Syndesmotic reduction has proven to be technically challenging, with reportedly greater than 50% of cases resulting in malreduction. Provisional reduction is most often attained via a pointed reduction clamp. Placement of the lateral tine is outlined above. The medial tine should be placed at the anatomic midportion of the medial tibia, which can be confirmed
fluoroscopically as the anterior third of the tibia on a true lateral view of the ankle. It is important to maintain the axis of the clamp parallel to the joint line and to the anatomic syndesmotic angle. The clamp should furthermore be maintained 1-2cm proximal to the mortise, at the level of the incisura, to avoid deformation or undue translation of the fibula. Lastly, over-compression of the syndesmosis has been demonstrated, though the clinical implications remain controversial.
Putnam et al. performed a radiographic analysis of the ideal orientation for placement of a syndesmotic reduction clamp. Based on the CT scans of uninjured adult ankles, the authors showed that the trans-syndesmotic axis could be most reliably paralleled by a reduction clamp by placing the lateral tine on the lateral malleolar ridge and the medial tine radiographically within the anterior third of the tibia, anatomically half-way between the anterior and posterior cortices. They further specified that the ideal location was within the central one-third of the distance from the anterior tibial cortex to the anterior fibular cortex.
Cosgrove et al. prospectively evaluated the effect of medial clamp tine positioning on the incidence of syndesmotic malreduction. The authors found that malreduction most often resulted from deviation of the clamp axis from the syndesmotic axis. With the clamp at 1-2cm proximal to the mortise and the lateral tine on the lateral malleolar ridge, the ideal position of the medial tine was within the anterior third of the tibia. The rate of sagittal malreduction increased substantially with increasingly posterior placement of the medial tine. The medial clamp position did not affect coronal plane malreduction.
Gardner et al. review the technical considerations in reduction and fixation of syndesmotic injuries. The authors stress careful positioning of the reduction clamp, advocating that the clamp should be placed from the lateral malleolar ridge to the center of the anteroposterior width of the medial tibia.
Additionally, they note that placement too proximal or distal results in coronal plane deformity of the fibula, and that over-compression of the syndesmosis is certainly possible.
Figure A is the AP radiograph of the left ankle demonstrating a displaced medial malleolar fracture and syndesmotic widening. Figure B is the lateral radiograph of the ipsilateral knee showing an associated proximal fibular fracture.
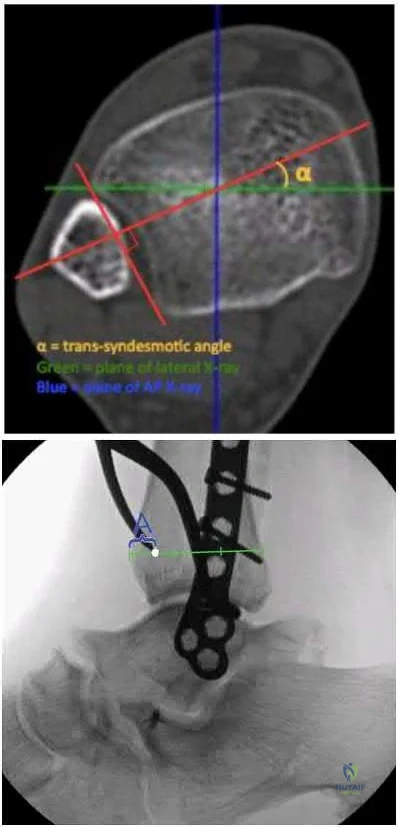
Illustration A shows the syndesmotic angle and anatomic trans-syndesmotic axis as compared to the AP and lateral fluoroscopic axes. Illustration B shows the ideal positioning of the medial tine within the anterior third of the tibia on a true lateral view of the ankle.
Incorrect answers:
A 45-year-old male injures his wrist during Live Action Role Play in Chicago two weeks ago. He underwent operative fixation by and presents to your clinic for his 2 week follow-up visit. You review his operative note in which the surgeon reports having to apply a volar
locking plate in a distal position to secure the difficult intra-articular fracture. The patient shows you the lateral film in Figure A. You remove his splint, he has no difficulty moving any fingers, very minimal pain, and is not taking any narcotic medication. How do you counsel him about his post-operative period?

The plate may need to removed once the fracture is healed to reduce the chance of flexor pollicis longus injury
The plate may need to removed once the fracture is healed to reduce the chance of flexor carpi radialis injury
The plate may need to removed once the fracture is healed to reduce the chance of flexor digitorum superficialis – index finger injury
The patient should undergo revision fixation as soon as possible
The plate is in appropriate position and will likely never need to be removed Correct answer: 1
This patient’s volar locking plate (VLP) is distal to the "watershed line", extending volarly beyond the most volar aspect of the distal radius. He is at greatest risk for an attritional rupture of the FPL.
A VLP placed this distal and volar is more likely to cause flexor tendon injury.
Up to 12% of all patients undergoing volar plate fixation will experience flexor tendon injury, and the FPL is the most common tendon associated with the VLP (57% of total flexor tendon ruptures). The average time from fixation to flexor tendon rupture has been cited at 9 months. To judge if a plate is volar to the watershed line, a plum line can be made in the proximal direction from the most volar edge of the distal radius. If a plate is volar to this (Soong) line, the patient is thought to be at a higher risk for flexor tendon injury. As a result, this patient should be followed closely and if pain with thumb flexion is present after 3 months, the surgeon should consider plate removal so long as the fracture is healed to reduce the chance of FPL rupture. Ruptured tendons require repair, grafting, or transfer with hardware removal.
Griffin and Chhabra comprehensively reviewed the risk factors and adverse events following VLP fixation of distal radius fractures, including flexor tendonitis and rupture. They found that risk factors for flexor tendon rupture following VLP fixation included plate placement distal to the watershed line and that PQ repair does not seem to affect flexor tendonitis.
Agnew et al. analyzed wrist MRIs to determine the relationship between the flexor tendons and the watershed line. They found that at 3mm proximal to the watershed line, the FPL and FDP to the index finger were 2.6 and 2.2mm anterior to the volar rim of the distal radius. The authors suggested that distally placed plates are incredibly close to the flexor tendons.
Chilelli et al. described 24 of 48 wrists which had VLP following distal radius fracture and went on to experiences loss of FPL flexion post-operatively. They found that FPL ROM generally returned after 52 days, however with an associated average loss of 11° in thumb IPJ ROM. The authors attribute this to stripping of FPL from the bone during the volar approach.
Soong et al. divided patients who underwent VLP fixation for distal radius fractures into three groups according to position of plate relative to a plum line extending proximally from the most volar and distal aspect of the distal radius: those with a VLP dorsal to the Soong line (grade 0), those with the VLP volar to the Soong line but proximal to the rim (grade 1), and those with a VLP volar to the Soong line and at or distal to rim (grade 2). Of the 73 cases reviewed, the authors reported three flexor tendon ruptures, two of which were grade 2 position. The authors concluded that both position of plate and type of plate were contributors to flexor tendon injury following VLP fixation.
Figure A is a lateral radiograph of the wrist demonstrating appropriate reduction and fixation but with the VLP volar to the "watershed" or Soong line.
Illustration A is a lateral radiograph with Soong's line drawn to show that this plate is too volar.
Incorrect Answers:

A 42-year-old construction worker sustains a crush injury to the hand at a job site. He has immediate pain and significant swelling, and is taken to the local emergency department for evaluation. Radiographs do not demonstrate any fracture or dislocation. On exam,
he experiences severe pain with passive motion at the metacarpal phalangeal joints and when the wrist is flexed and extended.
Otherwise he has intact sensation and appropriate capillary refill. What is the next best step in diagnosis or treatment?
Advanced imaging
Arterial Doppler
Admission for overnight observation
Surgical intervention
Pain control
This patient presents with compartment syndrome of the hand. A history and clinical exam are the best tools to identify the diagnosis, and the treatment consists of emergent fasciotomies.
Compartment syndrome of the hand may be secondary to trauma, burn, IV drug use, extravasation of IV fluids, or major limb revascularization. The diagnosis is usually made with pain out of proportion to exam, particularly with passive stretch of the digits. It is possible to have compartment syndrome without neurovascular changes (paresthesia, pallor, pulselessness), particularly earlier in the presentation. Compartment measurements may be obtained and are considered diagnostic with an absolute value greater than 30mmHg or when the compartment pressure is within 30mmHg of the patient's diastolic blood pressure. However pressure testing is not necessary in most cases, but may be particularly important in the patient who is obtunded, intubated, or who had a block, as the physical exam will be confounded. There are ten hand compartments: hypothenar, thenar, adductor pollicis, four dorsal interosseous, and three palmar interosseous; and emergent surgical release of all ten compartments is indicated.
Codding et al. comprehensively reviewed hand compartment syndrome. The authors identify the history and physical exam as the most critical aspect of the diagnosis. More specifically, they noted that pain with passive stretch of the MCPJ is the most sensitive clinical sign on physical exam. The authors conclude the short comings of the research on hand compartment syndrome, but note the potential morbidity of a missed diagnosis is so great that the threshold for surgical intervention should be very low.
Lipschitz et al. reviewed the measurement of compartment pressures in the hand. The authors discussed technical pearls including leveling the monitor at the level of the heart, using local analgesia on the skin only, inserting the needle perpendicular to the skin, and measuring all 10 hand compartments.
They noted that any measurement greater than 30mmHg or within 30mmHg of the diastolic blood pressure may be considered diagnostic.
Illustration A shows the standard incisions utilized to release all ten hand compartments. Incisions are generally placed directly overlaying the thenar musculature, hypothenar musculature, the carpal tunnel, and dorsally over the metacarpals. The radial and ulnar border of each metacarpal are incised through the dorsal incisions to release the interossei compartments.
Incorrect Answers:

A 60-year-old woman with a history of well-controlled diabetes and hypertension sustained a fall into a ditch yesterday and presents with persistent left ankle pain and deformity. The injury is closed, and the patient is neurovascularly intact. Injury films are shown in Figures A and B. An unsuccessful attempt at reduction in the emergency department with sedation was made. What is the cause of failure of closed reduction?

Subacute nature of fracture
Incarceration of the deltoid ligament
Incarceration of the fibula behind the posterolateral ridge of tibia
Entrapment of the flexor hallucis longus (FHL) tendon
Entrapment of the extensor digitorum brevis (EDB) Correct answer: 3
The patient has sustained a Bosworth fracture-dislocation, which is a fixed dislocation of the fractured fibula behind the posterolateral tibial ridge. These fractures are generally irreducible via a closed means and require open reduction.
The initial radiographs in this vignette reveal posterior subluxation of the talus and fibula without significant coronal plane deformity. This deformity should raise the suspicion of a Bosworth fracture-dislocation, especially if closed reduction is unsuccessful. Bosworth fracture-dislocations can often be associated with posterior malleolar fractures, specifically of the posterolateral rim of the distal tibia. These injuries often fail closed reduction, given the engagement of the fibula behind the posterolateral tibial ridge, and frequently require open reduction. In this situation, the most effective method to reduce the fracture is through a posterolateral approach. This is the same approach that can then be utilized for the fixation of the posterolateral fragment and fibula.
Delasotta et al. discussed a case presentation of a 24-year-old male with a Bosworth fracture-dislocation in which the anterior compartment musculature was interposed within the fracture site, impairing both closed and eventual open reduction of the injury. The authors go on to discuss how 3D CT reconstruction of the bone and soft tissues can aid in both the diagnosis and preoperative planning of such injuries. They also note that these injuries should be admitted for compartment and neurovascular checks and undergo urgent surgical treatment.
Gardner et al. performed a cadaveric study directly comparing fixation of posterior malleolar fractures to syndesmotic stabilization in a simulated stage IV pronation-external rotation injury. Compared with the intact specimens, the authors found that fixation of the posterior malleolus restored 70% of the native stiffness, but syndesmosis stabilization only restored 40%. The authors concluded that given the likely integrity of the posterior inferior tibiofibular ligament in the setting of posterior malleolar fractures, anatomic reduction and fixation may be more appropriate than syndesmotic stabilization and better suited to restore stability.
Switaj et al. retrospectively evaluated the incidence of posterior malleolar fractures and posterior pilon variants in a 270 patients with operatively treated ankle fractures. The authors noted a relative frequency of posterior malleolar fractures of 50% and that of the posterior pilon variants of 20% within the entire cohort. While they found no significant difference in frequency of posterior malleolar or posterior pilon variants with regard to either AO/OTA or Lauge-Hansen classification, patients with posterior pilon variants were significantly older.
Figure A and B show the AP and lateral views of an ankle revealing a lateral malleolar fracture with tibiotalar subluxation and posterior dislocation of the fibula with respect to the posterolateral ridge of the tibia, consistent with a
Bosworth fracture-dislocation.
Incorrect answers:
A 42-year-old male who works as a professional clown presents with severe ankle pain and gross deformity after tripping and falling over his props at a children’s birthday party. His radiograph is shown in Figure A. Following fixation of the medial and lateral malleolar fractures, the syndesmosis is assessed and is found to be persistently unstable. All of the following are true regarding posterior malleolar fixation EXCEPT:

Fixation of the posterior malleolus obviates the need for syndesmotic fixation in most cases
Fixation of the posterior malleolus remains biomechanically inferior to trans-articular syndesmotic fixation
Functional and radiographic outcomes following posterior malleolar fixation are at least equivalent if not superior to those following syndesmotic fixation
Non-anatomic fixation of the posterior malleolus will compromise syndesmotic fixation
The syndesmosis is often incompletely injured in the setting of a posterior malleolar fracture
Fixation of the posterior malleolus has been shown to be biomechanically superior to single-screw trans-articular syndesmotic fixation. Anatomic reduction and fixation will most often obviate the need for syndesmotic fixation, as the posterior inferior tibiofibular ligament (PITFL) is typically intact and attached to the fragment.
Posterior malleolar integrity is essential to ankle function and stability. The posterior malleolus not only contains the talus posteriorly but adds to articular congruity for tibiotalar load transfer and contributes to rotatory ankle stability through the PITFL. As a result, posterior malleolar fractures compromise these critical functions. Operative management is therefore aimed at containment of
the talus, restoration of articular congruity, reduction of the incisura, and restoring integrity to the syndesmosis. Functional and radiographic outcomes following posterior malleolar fixation have been shown to be at least equivalent to those following syndesmotic fixation.
Miller et al. compared the need for syndesmotic fixation in bi- and tri-malleolar ankle fractures following anatomic reduction and fixation in the prone position versus initial conservative management in the supine position. The authors found that fixation of the posterior malleolus obviated the need for syndesmotic fixation in 97.9% of cases, while nearly 25% of patients with no initial fixation required stabilization. They concluded that prone positioning and anatomic fixation of the posterior malleolus should be performed as this adequately restored syndesmotic stability in almost all cases.
Gardner et al. performed a radiographic evaluation of syndesmotic integrity in the setting of pronation-external rotation stage 4 ankle fractures with associated posterior malleolar fractures. Based on radiographs and MRI, no complete tears of the posterior-inferior tibiofibular ligament were evident. The fracture pattern was then simulated in cadavers, and posterior malleolar fixation restored 70% of the native stability while syndesmotic fixation alone restored only 40% of the native stability. The authors advocated for posterior malleolar fixation over syndesmotic stabilization.
Miller et al. prospectively compared the outcomes following posterior malleolar and syndesmotic fixation for unstable ankle fractures with partial syndesmotic injury. At a minimum one-year follow-up, the authors found that patients who had undergone open reduction with fixation of posterior malleolar fractures had no difference in outcomes as compared to those who underwent syndesmotic fixation. They concluded that not only was syndesmotic reduction maintained at final follow-up following posterior malleolar fixation, but that functional outcomes were at least equivalent to syndesmotic fixation.
Fitzpatrick et al. evaluated the impact of posterior malleolar fixation toward restoring syndesmotic stability in a cadaveric supination-external rotation stage 4 fracture model. The authors found that failure to fix or anatomically reduce posterior malleolar fragments resulted in non-anatomic translation of the fibula and ultimately in syndesmotic malreduction. They advocated for anatomic reduction and fixation of larger posterior malleolar fractures.
Figure A is an AP radiograph of the right ankle demonstrating a displaced trimalleolar ankle fracture with maintained relationship between the distal fibula and posterior malleolar fragment.
Incorrect Answers:
A 35-year-old morbidly obese female presents with global right ankle pain and significant swelling after a misstep over one of her cats on the stairs. She is unable to bear weight, but the skin is intact. Injury films are shown in Figures A through D. What is the internervous plane through which direct anatomic reduction and fixation of both fractures could best be achieved?



Question 25
A 16-year-old cheerleader reports an ache in the right shoulder and arm that is worse after activity. She denies any history of acute trauma. Examination reveals a positive sulcus sign and an AP glide test with a posterior and anterior apprehension sign. To confirm a diagnosis of multidirectional instability, which of the following imaging studies is most appropriate?
Explanation
REFERENCES: Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Warner JJ, Johnson D, Miller M, Caborn DN: Technique for selecting capsular tightness in repair of anterior-inferior shoulder instability. J Shoulder Elbow Surg 1995;4:352-364.
Question 26
Of the following signs or findings, which one is most consistent with the diagnosis of cervical radiculopathy? Review Topic
Explanation
Question 27
A year-old man has a draining sinus and recurrent infection of his right total knee arthroplasty. He has had two prior revision surgeries after the primary procedure and three other surgeries before his initial replacement, including a proximal tibial osteotomy and subsequent hardware removal. On clinical examination, he has a draining sinus in the mid portion of his surgical scar and a range of motion of 5° to 85°. AP and lateral radiographs of the right knee are shown in below. During surgery, the femoral component is found to be grossly loose, but the tibial component is well fixed. What is the most appropriate extensile approach that would provide adequate exposure and aid in tibial component extraction?
Explanation
Extended tibial tubercle osteotomy is an extensile approach to revision total knee arthroplasty that affords excellent exposure and can facilitate removal of tibial sleeves and cones. This patient has had multiple surgeries, including a proximal tibial osteotomy, as well as poor range of motion, patella baja, and a well- fixed metaphyseal sleeve component. Classically, an extended tibial tubercle osteotomy provides outstanding exposure for component removal in the setting of prior high tibial osteotomy and patella baja. For this patient, it is important to recognize the patella baja on the radiographs, as well as the tibial sleeve. In many of these cases the osteotomy provides access to the sleeve to help with extraction, because the stem will not pull through the sleeve or detach from the tray to allow visualization of the sleeve. The extended medial parapatellar approach is just a long medial approach that typically yields good exposure
but would not help with the patella baja or extraction of the tibial sleeve. The quadriceps snip would give good exposure to the knee but would not aid in tibial component removal. Lastly, the medial epicondyle osteotomy could help with exposure and tensioning of the medial complex of the knee but would not help
with tibial component extraction.
Question 28
The CT scan reveals a nondisplaced greater trochanteric fracture. The patient is now experiencing severe pain. What is the most appropriate treatment at this time?
Explanation
This patient presents with significant polyethylene wear, which can lead to both osteolysis and synovitis. However, synovitis usually manifests as a mild to moderate chronic ache, which should explain the discomfort. Although infection should always be ruled out with new-onset pain, no clinical parameters suggest acute hematogenous infection. Similarly, without any mention of back pain or neuropathy, radicular pain from the spine is unlikely. If this patient has a nondisplaced greater trochanteric fracture noted on MR imaging, the optimal immediate mode of treatment is to not rush into surgery despite the mild osteolysis. The patient’s severe pain is likely attributable to the nondisplaced greater trochanteric fracture rather than wear-induced synovitis, which typically presents as a mild to moderate ache. It is recommended to
allow the fracture to heal to avoid fracture displacement. Once the fracture is healed, a revision surgery with liner exchange can be recommended. Based on this clinical scenario, the acetabular component is within what is largely considered the “safe-zone” in THA. Despite this patient’s dislocations, the preferred treatment modality is to revise to a constrained liner. This patient had a well-functioning hip for longer than 15 years. Therefore, conversion to a constrained liner is the best treatment.
Question 29
A 7-year-old girl has had a painful forearm for the past 2 months. Examination reveals fullness on the volar aspect of the forearm. Radiographs and an MRI scan are shown in Figures 42a through 42c. Biopsy specimens are shown in Figures 42d and 42e. What is the most likely diagnosis?
Explanation
REFERENCES: Garzon M: Hemangiomas: Update on classification, clinical presentation and associate anomalies. Cutis 2000;66:325-328.
Kurkcuoglu IC, Eroglu A, Karaoglanoglu N, et al: Soft tissue hemangioma is a common soft tissue neoplasm. Eur J Radiol 2004;49:179-181.
Question 30
Figure 18a shows the clinical photograph of a 31-year-old man who has a slowly growing nodule on his right middle finger. It is minimally tender, and there is no erythema on examination. A biopsy specimen is shown in Figure 18b. What is the most likely diagnosis?
Explanation
REFERENCES: Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 1074.
Halling AC, Wollan PC, Pritchard DJ, et al: Epithelioid sarcoma: A clinicopathologic review of 55 cases. Mayo Clin Proc 1996;71:636-642.
Question 31
A 10-year-old boy reports a gradual onset of weakness; however, he is fully ambulatory. History reveals that he has a 17-year-old brother who has just stopped walking because of a similar condition. Laboratory studies show a creatine kinase level of 5,480 IU/L (normal 25 to 232 IU/L), and examination shows a slightly positive Gower sign. What is the most likely diagnosis?
Explanation
REFERENCES: Matsuo M: From molecular diagnosis to gene therapy. Brain Dev 1996;18:167-172.
Darras BT: Molecular genetics of Duchenne and Becker muscular dystrophy. J Pediatr 1990;117:1-15.
Gutmann DH, Fischbeck KH: Molecular biology of Duchenne and Becker’s muscular dystrophy: Clinical applications. Ann Neurol 1989;26:189-194.
Question 32
When elevating the arm, the ratio of scapulothoracic to glenohumeral motion over the total range of motion is best described as
Explanation
REFERENCES: Inman VT, Saunders JR, Abbott LC: Observations of the function of the shoulder joint. Clin Orthop 1996;330:3-12.
Freedman L, Munro RH: Abduction of the arm in the scapular plane: Scapular and glenohumeral movements. J Bone Joint Surg Am 1966;18:1503.
Question 33
- A 60-year-old man with no history of cancer has a destructive lesion in the proximal femur. He has a long history of tobacco use, but stopped smoking 5 years ago. A needle biopsy specimen of the lesion shows adenocarcinoma. Which of the following studies will most likely pinpoint the source of the primary tumor?
Explanation
Unlike skeletal metastasis of known origin - most often breast or prostate - a metastasis of unknown origin usually originates in the lung or kidney. In the present series, the most common occult primary site was the lung (63%) and the second most common was the kidney (10%).
Question 34
Which radiographic abnormality most accurately serves as a predictor of ankle syndesmosis disruption?
Explanation
Normal syndesmotic relationships include a tibiofibular clear space smaller than 6 mm on both AP and mortise views. In a 1989 cadaveric study by Harper and Keller, a tibiofibular clear space exceeding 6 mm on both the AP and mortise views was the most reliable predictor of early syndesmotic widening. Tibiofibular overlap is measured 1 cm proximal to the plafond. Normal values exceed 6 mm or 42% of the width of the fibula on the AP view, or 1 mm on the mortise view. Proximal fibula fracture can occur in isolation without syndesmotic injury, frequently after direct trauma. The medial clear space is the distance between the lateral border of the medial malleolus and the medial border of the talus and is measured at the level of the talar dome. In the mortise view with the ankle in neutral dorsiflexion, the medial clear space should be equal to or smaller than the superior clear space between the talar dome and the tibial plafond. ?A normal medial clear space may be present with syndesmotic injury and consequently lacks sensitivity and specificity.
RECOMMENDED READINGS
Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. View Abstract at PubMed
Wuest TK. Injuries to the Distal Lower Extremity Syndesmosis. J Am Acad Orthop Surg. 1997 May;5(3):172-181. PubMed PMID: 10797219. View Abstract at PubMed
Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 40
A 41-year-old man sustained a twisting injury while running up stairs 4 weeks ago. He was treated in an ankle brace and has been bearing weight since the injury occurred. He has no history of ankle problems, but he now has ankle pain, swelling, and instability. The pain is aggravated by stairs, and the instability is worse on unlevel ground. Radiographs do not show a fracture.
Question 35
A patient underwent a right hip arthroscopy, CAM resection, and labral repair while positioned supine on a fracture table with a perineal post. The leg was in traction for 4 hours, and no intrasurgical complications were noted. At the 2-week follow-up appointment, the patient was experiencing numbness and tingling in the perineum on the surgical side and noted pain predominantly while sitting. What is the likely cause of these symptoms?
Explanation
Although all of these responses are known complications related to hip arthroscopy, the symptoms of perineal numbness and pain associated with prolonged traction time indicate a compression injury to the pudendal nerve against the perineal post used to provide counter traction. Perineal numbness usually occurs on the surgical side, with pain in the area of the anus to the penis/clitoris. Pain is predominantly experienced while sitting, but is relieved when sitting on a toilet. Pain can be relieved with a diagnostic pudendal nerve block. This injury is not unique to hip arthroscopy; it also is described in the trauma literature. To prevent compression-type injuries, a well-padded post larger than 9 cm in diameter should be positioned against the medial thigh. Traction force should be kept to a minimum and the
extremity positioned in slight abduction. Continuous traction time should not exceed 2 hours, with intermittent traction used during prolonged procedures.

Question 36
Figure 69 is the radiograph of a 9-year-old who has posterior hindfoot pain while running. What is the most likely diagnosis?

Explanation
Sever disease is a traction apophysitis at the Achilles tendon insertion on the calcaneus. Plain radiographs may be unremarkable for this condition. Other osteochondroses of the foot include Kohler disease (tarsal navicular), Freiberg infraction (lesser metatarsal head), and Thiemann disease (great toe phalanx).
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Feldman DS. Osteochondrosis. In: Spivak JM, Di Cesare PE, Feldman Ds, et al, eds. Orthopaedic: A Study Guide. New York, NY: McGraw-Hill; 1999:765-766.
Schantz K, Rasmussen F. Thiemann's finger or toe disease. Follow-up of seven cases. Acta Orthop Scand. 1986 Feb;57(1):91-3. PubMed PMID: 3962642. View Abstract at PubMed
Question 37
A 24-year-old professional football player underwent surgery for a symptomatic cervical disk herniation with radiculopathy 9 months ago. A current radiograph is shown in Figure 17. He has normal neurologic findings, no pain, and full range of motion. A CT scan shows a solid fusion. When can he expect to return to play?
Explanation
REFERENCES: Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
Torg JS, Ramsey-Emrhein JA: Management guidelines for participation in collision activities with congenital, developmental, or post-injury lesions involving the cervical spine. Clin Sports Med 1997;16:501-530.
Question 38
Figures 65a and 65b show the MRI scans of a 33-year-old man with severe left leg pain. He has had symptoms for 3 months with progressive worsening pain and function. Examination reveals ankle plantar-flexor weakness and diminished light touch sensation on the plantar surface of the foot. What treatment provides the best outcome? Review Topic
Explanation
Question 39
A 24-year-old man reports the development of a foot drop following a knee dislocation 1 year ago. The common peroneal nerve was found to be in continuity at the time of surgical reconstruction of the posterolateral corner of the knee joint. He would like to eliminate the need for an ankle-foot orthosis. What is the best option to achieve elimination of the orthosis?
Explanation
REFERENCES: Pinzur MS, Kett N, Trilla M: Combined anteroposterior tibial tendon transfer in post-traumatic peroneal palsy. Foot Ankle 1988;8:27l-275.
Lipscomb P, Sanchez J: Anterior transplantation of the posterior tibial tendon for persistant palsy of the common peroneal nerve. J Bone Joint Surg Am 1961;43:60-66.
Question 40
What nerve is at greatest risk of harm from the portal shown in Figure 36?
Explanation
REFERENCES: Field LD, Altchek DW, Warren RF, O’Brien SJ, Skyhar MJ, Wickiewicz TL: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Papilion JD, Neff RS, Shall LM: Compression neuropathy of the radial nerve as a complication of elbow arthroscopy: A case report and review of the literature. Arthroscopy 1988;4:284-286.
Poehling GG, Whipple TL, Sisco L, Goldman B: Elbow arthroscopy: A new technique. Arthroscopy 1989;5:222-224.
Question 41
A 49-year-old man is seeking a second opinion for continued knee pain and swelling. He went to his primary doctor for swelling "on top of his knee," and he says his doctor drained some clear fluid. He noted that his condition improved for about 1 week before the swelling returned. He now has increasing pain and redness around his kneecap. Examination reveals significant swelling of his prepatellar bursa, with erythema over the bursa that extends to the surrounding skin. His temperature in the office is 101.7°F. What is the next step in treatment for this patient? Review Topic
Explanation
Question 42
A 55-year-old man reports increasing weakness in his arms that has progressed to his lower limbs, resulting in frequent tripping and falling. Examination reveals weakness in shoulder abduction and external and internal rotation bilaterally. Fasciculation is noted. He also has weakness in elbow flexion and extension bilaterally, and his grip strength is diminished. An electromyogram and nerve conduction velocity studies show decreased amplitude of compound motor action potential, slightly slowed motor conduction velocity, and denervation signs with decreased recruitment in all extremities. The sensory study is normal. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: de Carvalho M, Johnsen B, Fuglsang-Frederiksen A: Medical technology assessment: Electrodiagnosis in motor neuron diseases and amyotrophic lateral sclerosis. Neurophysiol Clin 2001;31:341-348.
Daube JR: Electrodiagnostic studies in amyotrophic lateral sclerosis and other motor neuron disorders. Muscle Nerve 2000;23:1488-1502.
Troger M, Dengler R: The role of electromyography (EMG) in the diagnosis of ALS. Amyotroph Lateral Scler Other Motor Neuron Disord 2000;1:S33-S40.
Question 43
Examination of an 18-year-old professional soccer player who was forcefully kicked across the shin while attempting a slide tackle reveals a marked effusion and limited motion of the knee. The tibia translates 12 mm posterior to the femoral condyles when the knee is held in 90 degrees of flexion. There is no posteromedial or posterolateral instability. Management should consist of
Explanation
REFERENCES: Miller MD, Bergfeld JA, Fowler PJ, Harner CD, Noyes FR: The posterior cruciate ligament injured knee: Principles of evaluation and treatment. Instr Course Lect 1999;48:199-207.
Posterior Cruciate Ligament Injuries in Principles and Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott, Williams and Wilkins, 2000.
Question 44
Figure 1 is the MRI scan of a 15-year-old boy who has had knee pain with running for 5 months. Radiographs show an osteochondritis dissecans (OCD) lesion of the medial femoral condyle. What is the most appropriate treatment?

Explanation
Question 45
When performing a flexor tendon repair of a digit other than the thumb, what structures of the flexor tendon sheath should be preserved?
Explanation
REFERENCES: Doyle JR: Anatomy of the finger flexor tendon sheath and pulley system.
J Hand Surg Am 1988;13:473-484.
Strickland JW: Flexor tendon injuries: I. Foundations of treatment. J Am Acad Orthop Surg 1995;3:44-54.
Question 46
An 8-year-old boy has had pain and swelling around the right knee for the past 4 weeks. He recalls bumping it about 4 weeks ago. He has no pain in other joints, and denies any fevers, chills, or other symptoms. A radiograph is shown in Figure 13. Laboratory studies show a WBC count of 9,700/mm P 3 P , an erythrocyte sedimentation rate of 18 mm/h, and a C-reactive protein level of 3.7 mg/L. What is the next most appropriate step in management?
Explanation
REFERENCES: Morrisy RT: Bone and joint sepsis, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 466-470.
Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis, and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Question 47
A 60-year-old right hand-dominant women fell on her outstretched arm and sustained an anterior shoulder dislocation. The shoulder is reduced in the emergency department and she is seen for follow-up 1 week later wearing a sling. Examination reveals that she has significant difficulty raising her arm in forward elevation and has excessive external rotation compared to the contralateral shoulder. What is the next most appropriate step in management?
Explanation
REFERENCES: Stayner LR, Cumming J, Andersen J, et al: Shoulder dislocations in patients older than 40 years of age. Orthop Clin North Am 2000;31:231-239.
Neviaser RJ, Neviaser TJ, Neviaser JS: Concurrent rupture of the rotator cuff and anterior dislocation of the shoulder in the older patient. J Bone Joint Surg Am 1988;70:1308-1311.
Question 48
A 23-year-old right-hand dominant professional baseball pitcher has right shoulder pain when releasing the ball. He has noticed his velocity has decreased over the past 2 months. Examination reveals supine abducted external rotation of 110 degrees compared to 100 degrees on the left side. His internal rotation is 30 degrees on the right compared to 70 degrees on the left side. Rotator cuff strength is normal. All other clinical tests are normal. MRI with contrast reveals no intra-articular lesions. What is the best course of treatment? Review Topic
Explanation
should then be followed by appropriate rotator cuff and scapular stabilization exercises. Only if this management fails to relieve the patient's symptoms should surgery be considered. This patient clearly does not need external rotation stretching given the fact that he has normal external rotation.
Question 49
Which of the following is considered the lowest level that a standard thoracolumbosacral orthosis (TLSO) can immobilize?
Explanation
REFERENCES: White AA, Panjabi MM: Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 475-509.
Norton PL, Brown T: The immobilizing efficiency of back braces. J Bone Joint Surg Am 1957;39:111-139.
Question 50
..A 75-year-old woman sustained a 4-part fracture dislocation of the proximal humerus with a comminuted humeral head. You decide to perform a reverse total shoulder replacement because of her age and activity level. This will be your first reverse total shoulder replacement. It is common practice in your hospital for an industry representative to be present when new implants are brought into the operating room. What information are you required to disclose?
Explanation
Arthroscopic or open debridement and capsular release
Interposition arthroplasty
Ulnohumeral arthrodesis
Linked total elbow arthroplasty (TEA)
Unlinked TEA
What surgical procedure listed above is most associated with the conditions defined below?
Question 51
Osteoarthritic cartilage is characterized by decreased
Explanation
Chondrocytes in OA are much more metabolically active than those of normal cartilage. Studies reveal measuring the levels of utilization on sulfate and H-glucosamine informing components of cartilage matrix. The amount of DNA also rises in OA cartilage most noticeable at the articular chondrocyte.
The synthesis of hyaluronate increases. Recent data suggests 1) hyaluronate that is synthesized is abnormal and, hence, does not allow aggregation; or 2) The excess synthesis is a response to a rapid degradation of synthesized product. This is in light of the fact that synthesis increases, yet concentration of hyaluronate decreases.
The correct answer is that proteoglycan content decreases. The synthesis of proteoglycan increases in OA, but due to the increased rate of breakdown of proteoglycan there is a net result of lowered proteoglycan content.
Question 52
- The diagnostic distinction between a benign enchondroma and a low- grade intramedually chondrosarcoma is based primarily on the
Explanation
Question 53
An extended head hemiarthroplasty (rotator cuff tear arthropathy head) has what theoretic advantage when compared to a standard hemiarthroplasty? Review Topic
Explanation
Question 54
A displaced pediatric supracondylar humerus fracture is treated with closed manipulation and placement of 2 Kirschner wires placed from the lateral side. What would be the effect of adding a third pin from the lateral side? Review Topic
Explanation
Question 55
He reports that he had no problems with the knee until 6 weeks ago when he noted the gradual onset of pain following a colonoscopy. Examination reveals a painful, swollen knee. Knee aspiration reveals a WBC count of 40,000/mm3. Management should consist of

Explanation
has been used successfully when the duration of symptoms is 3 weeks or less. Long-term suppressive antibiotics are most commonly used when the patient’s medical condition precludes further surgery. Delayed reimplantation has been shown to be superior to immediate reimplantation in multiple studies. Little data support the use of arthroscopic irrigation and debridement.
Question 56
A 17-year-old woman seen in the emergency department reports right knee pain and swelling that has progressively worsened over the past several weeks. Radiographs are shown in Figures 31a and 31b. What is the most likely diagnosis?
Explanation
REFERENCES: Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Question 57
Which of the following changes to heart rate, blood pressure, and bulbocavernosus reflex are typical of spinal shock?
Explanation
REFERENCE: Ditunno JF, Little JW, Tessler A, et al: Spinal shock revisited: A four-phase model. Spinal Cord 2004;42:383-395.
Question 58
A 54-year-old woman reports worsening pain in her buttock, especially when sitting for long periods of time. She has occasional pain and paresthesias radiating down her posterior leg. She has no significant medical history. MRI scans are shown in Figures 15a and 15b and a biopsy specimen is shown in Figure 15c. What is the most likely diagnosis?
Explanation
REFERENCES: Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 1135-1136
Menendez LR: Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 251.
Question 59
A 20-year-old-man sustained a scapular fracture after attempting to grab a beam as he fell through a ceiling at a job site 3 months ago. A clinical photograph is shown in Figure 36. He now reports pain in the anterior shoulder and difficulty with overhead activities. What nerve roots make up the involved peripheral nerve?
Explanation
REFERENCE: Leffert RD: Anatomy of the Brachial Plexus in Brachial Plexus Injuries. Churchill Livingstone, New York, NY, 1985.
Question 60
In Gustilo type III open tibial diaphyseal fractures, which of the following factors is associated with an increased risk of a poor functional outcome?
Explanation
(3 days or less from injury as compared to more than 3 days), and the timing of bone grafting after injury (within or after 3 months) did not impact the infection or union rates and had no effect on functional outcome. The LEAP study has shown at 7-year follow-up that patients who are definitively treated with external fixation have a significantly longer time to union, poorer functional outcomes, longer time to achieve full weight bearing, and more time in the hospital.
REFERENCES: Webb LX, Bosse MJ, Castillo RC, et al: Analysis of surgeon-controlled variables in the treatment of limb-threatening type-III open tibial diaphyseal fractures. J Bone Joint Surg Am 2007;89:923-928.
Question 61
An otherwise healthy 45-year-old man has a 3-cm subcutaneous mass on his anterior thigh that is presumed to be a lipoma. Removal of the mass is performed in the office of his primary care physician. Pathologic evaluation shows a high-grade malignant fibrous histiocytoma. Staging reveals no evidence of metastatic disease. Management at this time should consist of
Explanation
REFERENCES: Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173.
Giuliano AE, Eilber FR: The rationale for planned reoperation after unplanned total excision of soft-tissue sarcomas. J Clin Oncol 1985;3:1344-1348.
Lewis JJ, Leung D, Espat J, Woodruff JM, Brennan MF: Effect of resection in extremity soft tissue sarcoma. Ann Surg 2000;231:655-663.
Noria S, Davis A, Kardel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 62
A 21-year-old collegiate pitcher has had pain in his dominant shoulder for the past 3 months despite management consisting of rest, rehabilitation, and an analysis of throwing mechanics. An arthroscopic photograph from the posterior portal is shown in Figure 10. The biceps anchor to the bone was not detached to probing. Treatment of the lesion to the left of the cannula should consist of arthroscopic
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 261-270.
Snyder SJ, Banas MP, Karzel RP: An analysis of 140 injuries to the superior glenoid labrum. J Shoulder Elbow Surg 1995;4:243-248.
Question 63
When performing elbow arthroscopy, it is often necessary to evaluate the posterior compartment. When entering the posterior compartment of the elbow, what are the two safest and most commonly used portals?
Explanation
REFERENCES: Steinmann SP: Elbow arthroscopy. J Am Society of the Hand 2003 ;3:199-207.
Dodson CC, Nho SJ, Williams RJ III, et al: Elbow Arthroscopy. J Am Acad Orthop Surg 2008:16:574- 585.
Question 64
A 10-year-old girl who is Risser stage 0 has back deformity associated with neurofibromatosis type 1 (NF1). She has no back pain. Examination shows multiple cafe-au-lait nevi with normal lower extremity neurologic function and reflexes. Standing radiographs of the spine show a short 50-degree right thoracic scoliosis with a kyphotic deformity of 55 degrees (apex T8). A 10-degree progression in scoliosis has occurred during the past 1 year. There is no cervical deformity. MRI shows mild dural ectasia, primarily in the upper lumbar region. Management should consist of Review Topic
Explanation
Question 65
Which of the following is most frequently associated with heterotopic ossification about the shoulder?
Explanation
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, p 291.
Neer CS: Displaced proximal humerus fractures: Part II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
Question 66
-Ten or more years after severe polytrauma, premenopausal women, compared to men
Explanation
Question 67
Which of the following nerves is most likely responsible for symptoms associated with plantar fasciitis?
Explanation
REFERENCE: Baxter DE, Pfeffer GB, Thigpen M: Chronic heel pain: Treatment rationale. Orthop Clin North Am 1989;20:563-569.
Question 68
Closed chain kinetic exercises are differentiated from open chain exercises by which of the following? Review Topic
Explanation
Question 69
An 11-year-old boy has right shoulder pain and has been unwilling to use the arm after throwing a baseball in a Little League game 3 weeks ago. Examination reveals upper arm and shoulder tenderness with swelling. A radiograph and MRI scan are shown in Figures 27a and 27b. Management should consist of
Explanation
REFERENCES: Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 945-946.
Malawer MM: Tumors of the shoulder girdle: Techniques of resection and description of surgical classification. Orthop Clin North Am 1991;22:7-35.
Question 70
When an acute infection of a total elbow arthroplasty is managed with irrigation and debridement, which of the following organisms is associated with the highest risk of persistent infection?
Explanation
IV antibiotics.
REFERENCES: Yamaguchi K, Adams RA, Morrey BF: Infection after total elbow arthroplasty. J Bone Joint Surg Am 1998;80:481-491.
Schoifet SD, Morrey BF: Treatment of infection after total knee arthroplasty by debridement with retention of the components. J Bone Joint Surg Am 1990;72:1383-1390.
Question 71
A 21-year-old professional ballet dancer reports a painful popping sensation over her right hip joint. Examination reveals that symptoms are reproduced with hip flexion and external rotation. Which of the following studies will best confirm the diagnosis?
Explanation
REFERENCES: Gruen GS, Scioscia TN, Lowenstein JE: The surgical treatment of internal snapping hip. Am J Sports Med 2002;30:607-613.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 139-153.
Question 72
What is the most common cause of early failure for patellofemoral arthroplasty?
Explanation
REFERENCES: Lonner JH: Patellofemoral arthroplasty. J Am Acad Orthop Surg 2007;15:495-506. Argenson JN, Flecher X, Parratte S, et al: Patellofemoral arthroplasty: An update. Clin Orthop Relat Res 2005;440:50-53.

Question 73
An 8-year-old girl has had a painless enlarging mass of insidious onset in the left thigh for the past 3 weeks. Her mother denies any history of trauma, fever, or disease. Examination reveals a nontender, mobile mass in the left medial thigh. Her gait is normal. Figures 25a through 25d show the frog-lateral radiograph, the axial and coronal T1-weighted MRI scans, and the axial T2-weighted MRI scan. Biopsy results reveal a nonrhabdomyosarcoma soft-tissue sarcoma. The most appropriate treatment should consist of
Explanation
REFERENCES: Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby Year Book, 1995, p 757.
Gupta TD, Chaudhuri P (eds): Tumors of the Soft Tissues, ed 2. Stamford, CT, Appleton and Lange, 1998, p 605.
Question 74
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?
Explanation
REFERENCES: Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
O’Hara LJ, Marshall RW: Far lateral lumbar disc herniation: The key to the intertransverse approach. J Bone Joint Surg Br 1997;79:943-947.
Question 75
What molecules have been shown to promote fibrosis during muscle injury?
Explanation
Question 76
Figure 44 shows the AP radiograph of the hip of a patient who underwent screw fixation of the acetabulum. Which of the following structures is at least risk for injury during screw placement in the acetabular component?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 207-215.
Question 77
Figure 42 shows the sagittal T2-weighted MRI scan of a patient’s right knee. These findings are most commonly seen with a complete tear of the
Explanation
fluid in the soft tissues laterally. Additionally, there is a large bone bruise on the medial
femoral condyle. This combination indicates injury to the posterolateral complex. These injuries often have coexisting anterior and/or posterior cruciate ligament injuries. Failure to recognize the posterolateral corner injury can lead to failure of anterior or posterior cruciate ligament reconstructions.
REFERENCES: LaPrade RF, Gilbert TJ, Bollom TS, et al: The magnetic resonance imaging appearance of individual structures of the posterolateral knee: A prospective study of normal knees and knees with surgically verified grade III injuries. Am J Sports Med 2000;28:191-199.
Ross G, Chapman AW, Newberg AR, et al: Magnetic resonance imaging for the evaluation of acute posterolateral complex injuries of the knee. Am J Sports Med 1997;25:444-448.
Question 78
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
Explanation
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Question 79
A 22-year-old man has an acute spinal cord injury after a diving accident. Preliminary radiographs reveal bilateral jumped facets at C6-7. Neurologic examination shows an incomplete spinal cord injury consistent with an ASIA B impairment grade. The patient is otherwise hemodynamically stable with no other injuries. Attempts at closed high weight reduction with tong traction have so far been unsuccessful. What is the most appropriate management at this time? Review Topic
Explanation
Question 80
A researcher experimenting with limb patterning removes some tissue from 1 part of the limb bud (which we shall call Site A) and transplants it along the anteroposterior (AP) axis to create a mirror-hand duplication. Which of the following is true?
Explanation
The ZPA controls AP (radioulnar) growth. The signaling molecule is Shh, which is dose dependent. Higher Shh doses lead to posterior (ulnar) digits ulnar sided polydactyly. The extent of duplication is dose dependent (higher dose = more replication). Reduced Shh leads to loss of digits. Posterior elements (little finger/ulna) are formed EARLY prior to anterior elements which are formed LATE (radius/thumb). Disruption of AP patterning will result in loss of later forming elements (radius/thumb).
Al-Qattan et al. reviewed embryology of the upper limb. They summarized that embryology of the upper limb can be viewed in 2 distinct ways: the steps of limb development and the way that the limb is patterned along its 3 spatial axes. Cell signaling plays a major role in regulating growth and patterning of the vertebrate limbs. Signaling cell dysfunction results in congenital differences according to the affected signaling axis.
Illustration A shows an experiment to create ulnar dimelia by adding ZPA tissue to the anterior limb bud. The video shows development of the limb.
Incorrect Answers:
Question 81
A 17-year-old girl who initially presented as a child with multiple skeletal lesions, café-au-lait spots, and precocious puberty now has bone pain. A recent bone scan reveals multiple areas of increased scintigraphic uptake, including bilateral proximal femurs. A radiograph is shown in Figure 19. Besides activity modification, what is the next best line of treatment for decreasing her pain? Review Topic

Explanation
Question 82
A newborn has an anterolateral bow of the tibia and a duplication of the great toe. Which of the following conditions will develop as the infant grows?
Explanation
REFERENCE: Weaver KM, Henry GW, Reinker KA: Unilateral duplication of the great toe with anterolateral tibial bowing. J Pediatr Orthop 1996;16:73-77.
Question 83
03 A 28-year-old man who sustained the injury shown in Figure 31 is hemodynamically unstable. In addition to fluid resuscitation, the next most appropriate step in management should include
Explanation
Cook RE, Keating JF, Gillespie I: The role of angiography in the management of haemorrhage from major fractures of the pelvis. J Bone Joint Surg Br 2002;84:178-182.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp395-405.
back to this question next question
Question 84
A 7-year-old girl has pain and swelling of the right elbow after falling off her bicycle. Radiographs are shown in Figure 31. What is the most appropriate initial step in management?
Explanation
REFERENCES: Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425.
Attarian DE: Lateral condyle fractures: Missed diagnoses in pediatric elbow injuries. Mil Med 1990;155:433-434.
Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Badelon O, Bensahel H, Mazda K, et al: Lateral humeral condylar fractures in children: A report of 47 cases. J Pediatr Orthop 1988;8:31-34.
Question 85
Which of the following is considered a potential advantage of arthroscopic repair for anterior instability of the shoulder? Review Topic
Explanation
Question 86
Venous thromboembolism may occur after total joint arthroplasty. The risk of this complication is elevated in patients with
Explanation
Obesity, a prior history of venous thromboembolism, and metabolic syndrome have all been associated with an increased risk of thromboembolism. A recent meta-analysis showed that diabetes had no significant relationship with venous thromboembolism following hip or knee arthroplasty. Tranexamic acid is an antifibrinolytic agent that has been shown to reduce blood loss substantially following hip and knee arthroplasty. It has also been shown to be safe in patients with severe medial comorbidities and a prior history of venous thromboembolism.
Question 87
A 51-year-old plumber has a failed peroneus brevis tendon repair. He reports continued pain and swelling in the distal retrofibular area. MRI shows longitudinal tears of the peroneus longus and peroneus brevis. What is the surgical treatment of choice at this time?
Explanation
REFERENCES: Redfern D, Myerson M: The management of concomitant tears of the peroneus longus and brevis tendons. Foot Ankle Int 2004;25:695-707.
Borton DC, Lucas P, Jomha NM, et al: Operative reconstruction after transverse rupture of the tendons of both peroneus longus and brevis: Surgical reconstruction by transfer of the flexor digitorum longus tendon. J Bone Joint Surg Br 1998;80:781-784.
Question 88
The MRI scan of a patient with symptomatic shoulder pain reveals subacromial bursitis. What markers have been shown to be significant contributors to this pain? Review Topic
Explanation
Question 89
Figure 16 shows the MRI scan of a 43-year-old man who has had worsening low back pain for the past 4 months. What is the most likely diagnosis?
Explanation
REFERENCES: Boachie-Adjei O, Squillante RG: Tuberculosis of the spine. Orthop Clin North Am 1996;27:95-103.
Currier BL, Eismont FJ: Infections of the spine, in Rothman RH, Simeone FA (eds): The Spine. Philadelphia, PA, WB Saunders, 1992, p 2614.
Question 90
A 48-year-old woman has an open subtrochanteric femur fracture. No other injuries are reported. After thorough evaluation, it is determined that she will need emergent surgical fixation. The patient and family indicate that they are practicing Jehovah's witnesses and desire adherence to the religious standards with respect to blood product usage. The patient signs a valid advanced directive confirming these wishes. Which of the following would be considered acceptable treatment?
Explanation
Question 91
A 29-year-old woman reports dysesthesias and burning after undergoing bunion surgery that consisted of a proximal crescentic first metatarsal osteotomy 6 months ago. Examination reveals a positive Tinel’s sign at the proximal aspect of the healed incision. What injured nerve is responsible for her continued symptoms?
Explanation
REFERENCES: Kenzora JE: Sensory nerve neuromas: Leading to failed foot surgery. Foot Ankle 1986;7:110-117.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Question 92
A 19-year-old man was in a motorcycle accident. He sustained a grade IIIB open tibia fracture with a wide zone of injury to the surrounding soft tissue and a closed-head injury. The patient was treated emergently with irrigation, debridement, and external fixation. What is the most accurate statement regarding long-term functional and financial outcomes?
Explanation
Lower Extremity Assessment Project data suggest that long-term functional outcomes and patient satisfaction at 7 years are equivalent between those
who undergo limb-salvage and primary amputations. Return to work is essentially the same between the 2 groups. The projected lifetime healthcare cost for patients treated with amputation is nearly 3 times higher than costs for those who are treated with limb-salvage procedures.
RECOMMENDED READINGS
Busse JW, Jacobs CL, Swiontkowski MF, Bosse MJ, Bhandari M; Evidence-Based Orthopaedic Trauma Working Group. Complex limb salvage or early amputation for severe lower-limb injury: a meta-analysis of observational studies. J Orthop Trauma. 2007 Jan;21(1):70-6. PubMed PMID: 17211275. View Abstract at PubMed
MacKenzie EJ, Jones AS, Bosse MJ, Castillo RC, Pollak AN, Webb LX, Swiontkowski MF, Kellam JF, Smith DG, Sanders RW, Jones AL, Starr AJ, McAndrew MP, Patterson BM, Burgess AR. Health-care costs associated with amputation or reconstruction of a limb-threatening injury. J Bone Joint Surg Am. 2007 Aug;89(8):1685-92. PubMed PMID: 17671005. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 85 THROUGH 88
Figures 85a and 85b are the plain radiographs of a 38-year-old man who fell off the roof of a 2-story house and sustained an isolated injury to his right knee. Examination reveals a swollen leg with a knee effusion. The skin is intact, but there are some abrasions and an obvious deformity. His neurovascular examination reveals active dorsiflexion and plantar flexion with some pain and symmetric palpable pulses

85A

B
Question 93
Which medication or supplement is recommended to promote healing of atypical subtrochanteric fractures?
Explanation
Use of teriparatide in association with fracture fixation promotes healing because these fractures are associated with delayed healing. The other responses are not associated with healing of these fractures.
RECOMMENDED READINGS
Shane E, Burr D, Ebeling PR, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster D, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Koval K, Lane JM, McKiernan F, McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Sen HT, van der Meulen MC, Weinstein RS, Whyte M; American Society for Bone and Mineral Research. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2010 Nov;25(11):2267-94. doi: 10.1002/jbmr.253. Erratum in: J Bone Miner Res. 2011 Aug;26(8):1987. PubMed PMID: 20842676. View Abstract at PubMed
Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster DW, Ebeling PR, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Lane JM, McKiernan F,McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Howe TS, van der Meulen MC, Weinstein RS, Whyte MP. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American society for bone and mineral research. J Bone Miner Res. 2014 Jan;29(1):1-23. doi:10.1002/jbmr.1998. Epub 2013 Oct 1. PubMed PMID: 23712442. View Abstract at PubMed
Question 94
Which of the following statements regarding conus medullaris syndrome is most accurate?
Explanation
REFERENCES: Haher TR, Felmly WT, O’Brien M: Thoracic and lumbar fractures: Diagnosis and management, in Bridwell KH, Dewald RL, Hammerberg KW, et al (eds): The Textbook of Spinal Surgery, ed 2. New York, NY, Lippincott Williams & Wilkins, 1977, pp 1773-1778.
Reitman CA (ed): Management of Thoracolumbar Fractures. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 35-45.
Question 95
In total hip arthroplasty, increasing the perpendicular distance from the center line of the femur to the center of rotation of the femoral head (femoral offset) results in
Explanation
include an increased range of motion, better mechanical advantage for the abductors and decreased instability because of better soft tissue tension. According to Charnley,
increasing the femoral offset should improve the abductor lever arm which should decrease the abductor force required for walking, and therefore decrease the energy requirement for gait as well as the overall joint reactive force. The largest possible disadvantage of increasing the femoral offset is increasing the out of plane bending moment which puts stress on the prosthetic stem. Poly wear is a direct effect of surface area contact which is not changed with femoral Offset.
Question 96
Figures 10a and 10b show the radiographs of an athletic 9-year-old boy who has activity-related anterior knee pain with intact active knee extension. Examination reveals tenderness to palpation over the inferior pole of the patella. There is no effusion or ligamentous instability. Initial management should consist of
Explanation
REFERENCES: Stanitski CL: Anterior knee pain syndromes in the adolescent. J Bone Joint Surg Am 1993;75:1407-1416.
Stanitski CL: Anterior knee pain syndromes in the adolescent, in Schafer M (ed): Instructional Course Lectures 43. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1994, pp 211-220.
Question 97
Arthrodesis of which of the following joints has the greatest cumulative effect on midfoot/hindfoot motion?
Explanation
REFERENCES: Astion DJ, Deland JT, Otis JC, et al: Motion of the hindfoot after simulated arthrodesis. J Bone Joint Surg Am 1997;79:241-246.
Savory KM, Wülker N, Stukenborg C, et al: Biomechanics of the hindfoot joints in response to degenerative hindfoot arthrodeses. Clin Biomech 1998;13:62-70.
Question 98
...Figure 74 is the radiograph of an 11-year-old boy with pain in his left arm. Prognosis is most influenced by
Explanation

Question 99
What assay most directly assesses gene expression at the posttranslational level?
Explanation
REFERENCES: Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 19-76.
Question 100
A 69-year-old man has a painful slow-growing lesion of the distal phalanx of his thumb. History reveals that he has had chronic osteomyelitis of the thumb for the past 12 years. The radiograph and biopsy specimens are seen in Figures 9a through 9c. Treatment should consist of
Explanation
REFERENCES: Dell PC: Hand, in Simon MA, Springfield D (eds): Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 405-420.
McGrory JE, Pritchard DJ, Unni KK, Ilstrup D, Rowland CM: Malignant lesion arising in chronic osteomyelitis. Clin Orthop 1998;362:181-189.
