Orthopedic Surgery Board Review MCQs: Hip, Shoulder, Elbow, Arthroplasty & Tumor | Part 87

Key Takeaway
This page offers Part 87 of a comprehensive, interactive MCQ set for orthopedic surgeons preparing for AAOS and OITE board certification exams. It features 100 high-yield, verified questions covering Arthroplasty, Elbow, Hip, and Shoulder, designed to simulate actual exam conditions and enhance critical medical knowledge for successful exam preparation.
About This Board Review Set
This is Part 87 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 87
This module focuses heavily on: Arthroplasty, Elbow, Hip, Ligament, Nerve, Shoulder, Tumor.
Sample Questions from This Set
Sample Question 1: Thedirectanterior(Smith-Peterson)approachtohiparthroplastyismostcommonlyassociatedwithinjurytowhatnerve?...
Sample Question 2: Figures 71a and 71b/ are the MR images of a 65-year-old man who dislocated his shoulder.What is his most likely chief symptom?...
Sample Question 3: Figures below show the radiographs obtained from an 86-year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgica...
Sample Question 4: A professional pitcher reports pain localized to the medial aspect of his throwing elbow. History reveals that he was pitching in a playoff game and heard and felt a pop in his elbow. MRI reveals a complete ulnar-sided avulsion of the media...
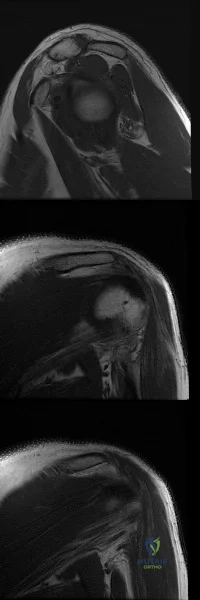
Sample Question 5: A 16-year-old girl has had painless swelling in her posterior left arm for the past 4 months. A radiograph, MRI scans, and an incisional biopsy specimen are shown in Figures 43a through 43d. What is the cytogenetic translocation most common...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The direct anterior (Smith-Peterson) approach to hip arthroplasty is most commonly associated with injury to what nerve?
Explanation
Some authors have reported the incidence of lateral femoral cutaneous nerve neuropraxia following hip arthroplasty with the direct anterior approach to be near 80%, but resolution of the sensory deficits has been observed in most patients over time. Femoral nerve palsy has been reported to occur in .64% to 2.3% direct lateral (Hardinge) and anterolateral (Watson-Jones) approaches, and the superior gluteal nerve may be injured with proximal extension of the abductor muscular dissection. The posterior approach has been reported to be associated with sciatic nerve injury, especially in cases of dysplasia. Pudendal nerve injury has not been reported with the anterior, anterolateral, direct lateral, or posterior approaches to hip
arthroplasty. It has been reported following hip arthroscopy and the use of a traction table, however.
Question 2
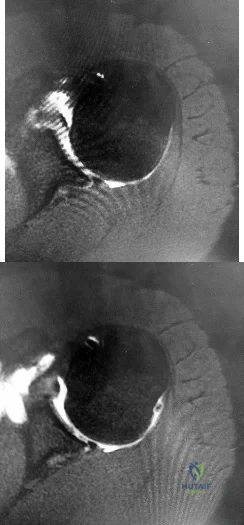
Figures 71a and 71b/ are the MR images of a 65-year-old man who dislocated his shoulder. What is his most likely chief symptom?
Explanation
This patient has a massive rotator cuff tear resulting in disruption of the transverse force couple between the subscapularis anteriorly and the infraspinatus and teres minor posteriorly. These muscles provide dynamic shoulder stability throughout active elevation. Loss of the force couple produces a pathologic increase in translation of the humeral head and decreased active abduction and external rotation, which results in difficulty raising an arm. The most common neurologic deficit after shoulder dislocation is isolated injury to the axillary nerve that supplies sensation to the lateral aspect of the shoulder, not the anterior aspect. Recurrent instability is uncommon unless there is a labral tear or massive subscapularis tear. The biceps muscle is not viewed in the MR images, and a complete proximal biceps tendon rupture would be uncommon in the setting of an anterior shoulder dislocation.

CLINICAL SITUATION FOR QUESTIONS 72 THROUGH 75
Figures 72a through 72e are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0 degrees
to 90 degrees and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted.
Question 3
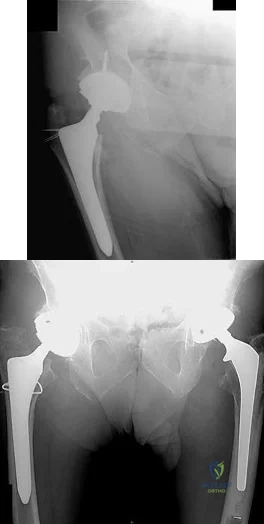
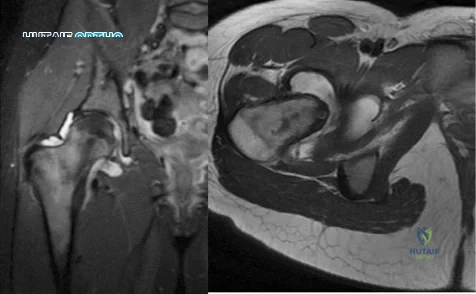
Figures below show the radiographs obtained from an 86-year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 4
A professional pitcher reports pain localized to the medial aspect of his throwing elbow. History reveals that he was pitching in a playoff game and heard and felt a pop in his elbow. MRI reveals a complete ulnar-sided avulsion of the medial collateral ligament (MCL). Examination reveals valgus instability and ulnar nerve involvement. What recommendations should be made based on the patient’s desire to return to sport? Review Topic
Explanation
stresses during the late cocking and acceleration phase of throwing can injure the anterior band of the MCL. Clinically, the injuries may present as chronic or acute, and a pop may be noted in the latter. Associated ulnar nerve involvement is common. Valgus instability is present in about 25% of patients. Patients typically are athletes who participate in throwing and have localized medial elbow pain and tenderness along the course of a ligament that extends from the medial epicondyle of the distal humerus to the sublime tubercle of the ulna. Surgical reconstruction is the procedure of choice in an athlete desiring a return to a high level of throwing.
Question 5
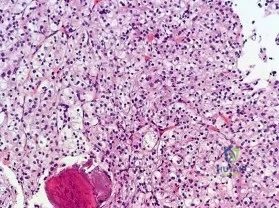
A 16-year-old girl has had painless swelling in her posterior left arm for the past 4 months. A radiograph, MRI scans, and an incisional biopsy specimen are shown in Figures 43a through 43d. What is the cytogenetic translocation most commonly associated with this tumor?
Explanation
REFERENCES: Kawai A, Woodruff J, Healey JH, et al: SYT-SSX gene fusion as a determinant of morphology and prognosis in synovial sarcoma. New Engl J Med 1998;338:153-160.
Sandberg AA: Cytogenetics and molecular genetics of bone and soft tissue tumors. Am J Med Genet 2002;115:189-193.
Question 6
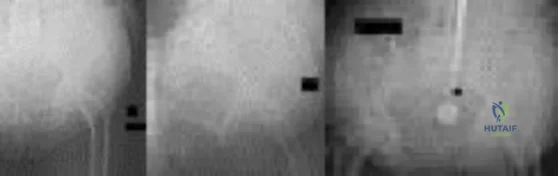
What is the most likely explanation for the change between the initial intraoperative radiograph (Figure 11a) and the radiograph taken 4 weeks after surgery (Figure 11b) in an 87-year-old man who underwent primary hip replacement for osteoarthritis?
Explanation
The image demonstrates subsidence of the femoral implant. The implant subsided because it did not have good initial stability. The tapered femoral implant was placed after initial preparation for an anatomic femoral stem. A limited, nondisplaced femoral neck fracture was encountered during the procedure and treated. Two advantages of tapered stems are the efficient transfer of stress to the proximal femur and the ability to accommodate some subsidence to achieve enhanced stability. Although subsidence of a tapered stem to a more stable position can produce a good result, quality of metaphyseal bone should be considered. Attention to surgical technique remains important to optimize component stability for biological fixation.
RECOMMENDED READINGS
Savory CG, Hamilton WG, Engh CA Sr, Della Valle CJ, Rosenberg AG, Galante JO. 15 Hip designs. In: Barrack RL, Booth RE Jr, Lonner JH, McCarthy JC, Mont MA, Rubash HE, eds. Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:345-368.
Blaha JD, Borus TA. Press-fit femoral components. In: Callaghan J, Rosenberg A, and Rubash H, eds The Adult Hip. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:1036-1043.
Question 7
Which of the following has been shown to have similar biochemical and clinical characteristics as iliac crest autograft?

Explanation
Hoegel et al found that the reamings had alkaline phospatase activity, indicating living osteoblasts. The amount of activity was independent of the reamer sizes and reamer design.
Frolke et al concluded that reaming debris supports callus building (healing) as much as conventional iliac crest bone grafting in an animal fracture gap model.
Question 8
A 17-year-old boy with left spastic hemiplegia secondary to cerebral palsy is being evaluated for persistent swan neck deformities of the affected hand. Splinting has been tried with some improvement, but the patient does not want to wear the splints any more. On physical examination, he demonstrates full extension of the metacarpophalangeal (MCP) joints, 30° of hyperextension of the proximal interphalangeal (PIP) joints, and flexion of the distal interphalangeal (DIP) joints when he attempts to actively extend his digits. He is able to initiate flexion at the PIP joints with his MCP joints held in neutral extension. He has equal PIP flexion when the MCP joints are extended and flexed. What is the most appropriate surgical treatment to address his swan neck deformity?
Explanation
This patient demonstrates full extension of the MCP joints when he actively extends his fingers, indicative of overpull of the extrinsic finger extensors. This clinical scenario can be corrected by a central slip tenotomy. A terminal tendon release is used to address a Boutonnière deformity. The patient does not demonstrate intrinsic tightness (equal PIP flexion while the MCP flexed and extended), therefore his swan neck would be unlikely to respond to intrinsic lengthening. Dorsal rerouting of the lateral bands is performed for a Boutonnière deformity. A central slip tenotomy would balance the extension forces between the PIP and DIP joints.
Question 9
…A 56-year-old podiatrist with a negative past medical history had anterior knee pain after an injury. His radiographs, CT scan, and T1-weighted sagittal and fat-saturated axial MR images are shown in Figures 15a through 15e, respectively. After arthroscopic partial medial menisectomy, the patient was turned to the prone position and an open posterior arthrotomy and excision was performed. Low-power and high-power hematoxylin and eosin stained histologic specimens are shown in Figures 15f and 15g, respectively. Based on the history, radiographs, CT scan, MRI scans, and histologic findings, what is the most likely diagnosis?
Explanation
Figures 16a and 16b are the right femur radiographs of a 59-year-old man who has severe pain in his right distal thigh and knee with no significant trauma and an inability to bear weight. Blood tests demonstrate anemia, serum protein electrophoresis/urine protein electrophoresis findings are negative, and electrolyte levels are within defined limits.


Question 10
An 8-year-old boy falls and injures his thumb. A radiograph is shown in Figure 23. Initial management should consist of
Explanation
REFERENCES: O’Brien ET: Part IV: Dislocations of hand and carpus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 429-431.
Bohart PC, Gelberman RH, Vardell RF, Solomon PB: Complex dislocations of the MCP joint. J Bone Joint Surg Am 1974;56:1459-1463.
Question 11
Compared with myodesis, osteomyoplasty offers which of the following advantages in transtibial amputation?
Explanation
theorized to enhance bony stability and increase end-bearing of the residual limb, and may enhance patient-perceived functional outcomes relative to myodesis. Fibular abduction is a known complication of traditional myodesis techniques, and is believed to represent syndesmotic instability. Osteomyoplasty requires additional surgical time and increased surgical morbidity, and because the success of the procedure is dependent on achieving bony union, early prosthetic fitting and immediate weight bearing are typically contraindicated.
Question 12
Which of the following radiographic findings indicates that the injury to the great toe shown in Figures 60a and 60b should be reducible by closed manipulation?

Explanation
Question 13
A 42-year-old woman is brought to the emergency department following a motor vehicle accident. She has sustained multiple injuries, and she is intubated and pharmacologically paralyzed. Sagittal cervical CT scans through the right cervical facets, the left cervical facets, and the midline are shown in Figures 12a through 12c, respectively. Definitive management of her cervical injury should consist of
Explanation
REFERENCES: Jackson RS, Banit DM, Rhyne AL III, et al: Upper cervical spine injuries.
J Am Acad Orthop Surg 2002;10:271-280.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 14
A 24-year-old woman who has hypotension, a head injury, and who experienced a poor response to resuscitation has been taken to the operating room for a splenectomy. Following abdominal surgery she remains unstable with increasing pulmonary respiratory pressures and decreasing oxygen saturation. She has a transverse mid-diaphyseal fracture of the tibia with a 4-cm laceration and soil-contaminated muscle in the wound. Based on these findings, management should consist of
Explanation
REFERENCES: Bosse MJ, Kellam JF: Orthopaedic management decisions in the multiple trauma patient, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 151-164.
Weresh MJ, Stover MD, Bosse MJ, Jeray K, Kellam JF: Pulmonary gas exchange during intramedullary fixation of femoral shaft fractures. J Trauma 1999;46:863-868.
Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 15
What is the most common causative bacteria in septic arthritis in children? Review Topic
Explanation
Question 16
Figure 36 shows the hip arthrogram of a newborn. Which of the following structures is enclosed by the circle?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA,
WB Saunders, 2002, vol 1, pp 532-533.
Severin E: Contribution to the knowledge of congenital dislocation of the hip joint.
Acta Chir Scand 1941;84:1.
Question 17
A 65-year-old woman presents with neck pain for 18 months. She has taken NSAIDs and undergone physical therapy without improvement. Over the past 6 months, she has also noticed progressive hand clumsiness and difficulty with gait. Sagittal and axial MRI images are shown in figures A and B, respectively. What is the most appropriate next step in management? Review Topic

Explanation
Cervical myelopathy is typically caused compression on the spinal cord and classically present with neck pain, parasthesias, clumsiness, gait imbalance, and/or urinary retention. Nonoperative management is reserved for patients without functional impairment. ACDF is the treatment of choice for focal compression from anterior disc-ostephyte changes. Posterior decompression is indicated in patients with multi-level disease. It is important to note in patients with significant kyphosis, the kyphosis must be reversed in order for decompression alone to be effective.
Hsu reviewed posterior decompression techniques in the cervical spine. They state that the choice of anterior versus posterior approach is determined based on sagittal spine alignment, extent and location of pathological involvement, and patient preference. They recommend laminectomy and fusion for cervical stenosis and kyphosis <10 degrees. The use of BMP-2 as an adjunct in the cervical spine is not recommended by the author.
Emery reviewed cervical spondylotic myelopathy and recommend nonoperative treatment in patients with minimal symptoms without pathologic reflexes or gait imbalances. They suggest that the preferred posterior techniques are now laminectomy and fusion or laminoplasty.
Figure A and B are sagittal and axial T2 MRI sequences showing a degenerative disc osteophyte complex at C5-C6 with resultant canal stenosis and cord compression. Illustration A is a lateral C spine radiograph in a patient who is status post ACDF at C5-C6.
Incorrect Answers:
Question 18
An 11-year-old girl is struck in the leg by a loaded sled while sledding and is seen in the emergency department; she is reporting severe knee pain. Radiographs are read as normal. Examination reveals that she is exquisitely tender over the proximal tibial physis. The neurovascular examination is normal. What is the next step in management?
Explanation
REFERENCES: McGuigan JA, O’Reilly MJ, Nixon JR: Popliteal arterial thrombosis resulting from disruption of the upper tibial epiphysis. Injury 1984;16:49-50.
Burkhart SS, Peterson HA: Fractures of the proximal tibial epiphysis. J Bone Joint Surg Am
1979;61:996- 1002.
Question 19
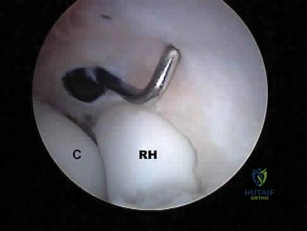
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50? Review Topic
Explanation
Question 20
A 28-year-old male sustains a midshaft fibula fracture after being kicked during a karate tournament and develops compartment syndrome isolated to the lateral compartment of his leg. If left untreated, which of the following sensory or motor deficits would be expected?

Explanation
Matsen et al discuss the poor results which can be a cause of late diagnosis and surgical decompression. They recommended compartment monitoring in equivocal cases as well as release of all four leg compartments when facing leg compartment syndrome. A diagram of a two-incision fasciotomy is shown in Illustration B.
Olson et al provide a review of compartment syndrome for the lower extremity. They discuss a variety of injuries and medical conditions may initiate acute compartment syndrome, including fractures, bleeding disorders, and other trauma. Although the diagnosis is primarily a clinical one, they also recommend supplementation with compartment pressure measurements in equivocal cases.
Question 21
A concussion diagnosis is made when there is
Explanation
Neurocognitive testing is a helpful tool in the management of concussions, but testing does not independently determine if an athlete has experienced a concussion or when he or she can return to play. Neuroimaging findings typically are normal in concussive injury. Loss of consciousness occurs in fewer than 10% of patients with concussions. A concussion diagnosis is difficult to determine because of the lack of objective clinical and/or imaging findings. In general, a concussion is a disturbance in brain function caused by a direct or indirect force to the head.

RESPONSES FOR QUESTIONS 26 THROUGH 31
Plain radiographs
CT scan
MRI
Arthrogram
Which imaging method listed above is most appropriate for definitive diagnosis and management of each clinical scenario described below?
Question 22
A 25-year-old male polytrauma patient undergoes initial temporary external fixation for a femoral shaft fracture. He is converted to a femoral nail at 7 days. This management can be expected to result in
Explanation
REFERENCES: Harwood PJ, Giannoudis PV, Probst C, et al: The risk of local infective complications after damage control procedures for femoral shaft fracture. J Orthop Trauma 2006;20:181-189.
Roberts CS, Pape HC, Jones AL, et al: Damage control orthopaedics: Evolving concepts in the treatment of patients who have sustained orthopaedic trauma. Instr Course Lect
2005;54:447-462.
Question 23
Longitudinal radioulnar dissociation, including Essex Lopresti fractures, requires disruption of the interosseous membrane (IOM). The interosseous membrane (IOM) consists of all of the following ligaments EXCEPT?

Explanation
The IOM bridges the radius and ulna and acts as a hinge for rotation of radius about ulna. The central portion is thickened, and forms the central band which is the most important ligament for IOM load distribution characteristics.
Noda et al, in a cadaver study, identified the precise anatomical insertions and attachment points of each of the 5 IOM components. They found the most distal and proximal ends of the radial origin of the central band were 53% and 64% of total radial length from the tip of the radial styloid, whereas those of the ulnar insertion were 29% and 44% of total ulnar length from the ulnar head.
Pfaeffle et al also performed a cadaveric biomechanical study applying compressive loads to specimens with IOMs that are intact, cut, or cut/reconstructed with flexor carpi radialis allografts. They found that reconstruction of the IOM can restore the normal load transfer chararcteristics and that the central band of the IOM is the most important portion of the IOM to be reconstructed.
Question 24
Figure 12 shows a lateral radiograph of the elbow. What is the most likely diagnosis?
Explanation
REFERENCE: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 132-133.
Keats TE, Anderson MW: Atlas of Normal Roentgen Variants That May Simulate Disease, ed 7. St Louis, MO, Mosby Inc, 2001, p 497.
Question 25
A surgeon contemplates performing a hemiarthroplasty (HA) or total hip arthroplasty (THA) for an active, community ambulating 70-year-old female with a displaced femoral neck fracture. Which of the following is true for these options?
Explanation
There are a few differences between THA and HA performed in the setting of displaced FNF. THA has a higher dislocation rate, greater blood loss, requires a larger exposure than HA, and the operation is longer. HA often requires reoperation because of progressive acetabular erosion. Patient outcomes and function are greater following THA than HA.
Florschultz et al. reviewed current management of FNF. They concluded that CRIF / ORIF is indicated for displaced femoral neck fractures in younger individuals, select active elderly, and medically unfit patients. HA is indicated for lower demand ambulatory older patients. THA is indicated for the active elderly and those with preexisting acetabular disease.
Avery et al. reviewed 7-10 year results of an RCT comparing THA with HA. More HA patients had died during follow-up. All surviving patients had polyethylene wear (THA) and acetabular erosion (HA). They concluded that there was lower mortality and a trend towards superior function in patients with a THA in the medium term.
Hedbeck et al. performed a RCT comparing HA and THA. At 4 years, there was improved function and quality of life with THA. They recommend THA in elderly, lucid patients with a displaced FNF.
Incorrect Answers:
Question 26
A 6-year-old Little League pitcher has had pain in the right elbow for the past 2 weeks. Examination reveals mild lateral elbow joint tenderness with full range of motion and no effusion or collateral laxity. A radiograph is shown in Figure 38. Initial management should consist of
Explanation
REFERENCES: Bauer M, Jonsson K, Josefsson PO, et al: Osteochondritis dissecans of the elbow: A long-term follow-up study. Clin Orthop 1992;284:156-160.
Takahara M, Ogino T, Sasaki I, et al: Long term outcome of osteochondritis dissecans of the humeral capitellum. Clin Orthop 1999;363:108-115.
Byrd JW, Jones KS: Arthroscopic surgery for isolated capitellar osteochondritis dissecans in adolescent baseball players: Minimum three-year follow-up. Am J Sports Med
2002;30:474-478.
Question 27
Figure 99 shows a dorsal approach for a midfoot arthrodesis following a Lisfranc injury in a 43-year-old woman. The base of the second metatarsal is labeled with the letter B. The interval used to create this exposure is
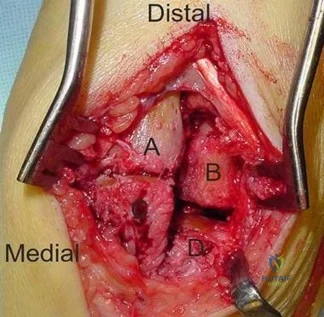
Explanation
The interval shown is between the extensor hallucis longus (left) and the extensor hallucis brevis (right), which is not an internervous plane because both are innervated by the deep peroneal nerve. The neurovascular bundle is under the extensor hallucis brevis muscle. Both
muscles are innervated by branches of the deep peroneal nerve. The superficial peroneal
Question 28
-Figures 14a through 14d are the radiographs and sagittal T1- and T2-weighted MRI scans of an otherwise healthy 10-year-old girl who has experienced 3 weeks of worsening pain with weight bearing and is now refusing to bear weight to either of her lower extremities. She denies any history of injury or trauma.She has not had any fevers or recent illnesses. She denies any numbness or parasthesias. She has had no bowel or bladder incontinence. In the emergency department she is afebrile and tender to palpation over the midlumbar spine. She has pain with hyperextension and flexion of her back. Her white blood cell count is 11.4 (reference range, 4.5-11.0 x109/L), erythrocyte sedimentation rate is 40 mm/h (reference range, 0-20 mm/h), and C-reactive protein is 2.6 mg/L (reference range, 0.08-3.1 mg/L). What is the most appropriate course of action at this time?

Explanation

Question 29
Metal-on-metal lumbar disk arthroplasty devices may generate cobalt and chromium ions into the serum of patients after implantation into the lumbar spine. Which of the following statements best represents the levels of the serum ion levels in these patients? Review Topic
Explanation
Question 30
A patient who underwent total knee arthroplasty 6 years ago now reports knee pain for the past 3 days following dental surgery. Cultures of the aspirate are positive for Staphylococcus epidermidis. Management should consist of
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 323-337.
Goldman RT, Scuderi GR, Insall JN: 2-stage reimplantation for infected total knee replacement. Clin Orthop 1996;331:118-124.
Question 31
Which of the following acetabular cup designs has shown the greatest survivorship at 10 years in patients younger than age 60 years?
Explanation
REFERENCES: Smith SE, Harris WH: Total hip arthroplasty performed with insertion of the femoral component with cement and the acetabular component without cement: Ten to thirteen-year study. J Bone Joint Surg Am 1997;79:1827-1833.
Pellicci PM, Tria AJ Jr, Garvin KL, (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 195-206.
Question 32
An 11-year-old boy reports the acute onset of elbow pain and swelling after pushing his brother. The patient's mother and a younger sibling have experienced numerous fractures. You note that the patient and his mother have blue sclera and normal-appearing teeth. A radiograph of the elbow is shown in Figure 60. This patient's disorder is most likely the result of Review Topic

Explanation
Type I is subclassified into the A type (absence of dentinogenesis imperfecta) and B type (presence of dentinogenesis imperfecta). These individuals have blue sclerae, and although the initial fracture usually occurs in the preschool years, it may occur at any age. Furthermore, olecranon apophyseal fractures that occur after relatively minor trauma have been associated with type I OI. Cells from individuals with type I OI largely demonstrate a quantitative defect of type I collagen; they synthesize and secrete about half the normal amount of type I procollagen. In this patient, there are no indications that the child has been subjected to abuse. Radiographs of the elbow show no evidence of osteopetrosis (due to abnormal osteoclast function) or rickets (due to a deficiency of vitamin D). Morquio syndrome (characterized by a defect of the enzyme N-Ac-Gal-6 sulfate sulfatase) is not associated with blue sclera.
Question 33
While performing a total shoulder arthroplasty, excessive retraction is placed on the "strap muscles" (short head of biceps and coracobrachialis). Neurovascular examination would reveal weakness of which of the following? Review Topic
Explanation
this area. Excessive traction on the musculocutaneous nerve could lead to a neurapraxia with resultant weakness of elbow flexion and forearm supinaton because of the loss of biceps function.
Question 34
A 17-year-old girl who initially presented as a child with multiple skeletal lesions, café-au-lait spots, and precocious puberty now has bone pain. A recent bone scan reveals multiple areas of increased scintigraphic uptake, including bilateral proximal femurs. A radiograph is shown in Figure 19. Besides activity modification, what is the next best line of treatment for decreasing her pain? Review Topic

Explanation
Question 35
A 22-year-old woman injured her ankle when she fell off a ladder. Radiographs reveal a displaced large posterior malleolus fracture of about 45% of the joint. What is the best definitive treatment?
Explanation
optimal function can be achieved. Open reduction and internal fixation allows this achievement. In cases where comminution exists, absolute stability may have to be sacrificed so as to not strip small comminuted bone fragments. Therefore, a bridging technique is worthwhile. External fixation can be used as a temporary technique until the soft tissues are more amenable to definitive fixation. Cast treatment is not indicated in adult forearm fractures. Locking nails for forearm use are not reamed. With regards to articular fractures, anatomic reduction and rigid stabilization are required to achieve the best results and allow for fracture healing. This environment also allows for the best chance of the cartilage repair process to form "hyaline-like" cartilage. Open reduction and internal fixation with absolute stability is the mainstay of treatment for partial articular fractures such as split depression tibial plateau fractures and posterior malleolus fractures involving greater than about 25% to 30% of the joint. The gold standard for the treatment of a closed femur fracture is a reamed intramedullary locked nail. Results are uniformly excellent. This can be done without stripping of the soft tissues such as in open reduction and internal fixation. External fixation can be used as a temporary device in patients in extremis for damage control reasons.Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr. Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am. 1986 Sep;68(7):1008-17. http://www.ncbi.nlm.nih.gov/pubmed/3745238')">View Abstract at PubMedJones DB Jr, Kakar S. Adult diaphyseal forearm fractures: intramedullary nail versus plate fixation. J Hand Surg Am. 2011 Jul;36(7):1216-9. Epub 2011 May
Question 36
Figures 163a through 163c show the radiograph and MRI scans of a 45-year-old woman with severe right arm pain. She has had symptoms for 6 months without resolution despite multiple nonsurgical treatments. Examination reveals weakness in the right triceps and wrist flexors with decreased sensation in the middle finger and a positive Spurling's sign. What is the most appropriate treatment for the patient's symptoms? Review Topic

Explanation
Question 37
In performing an opening wedge high tibial osteotomy at the tibial tubercle, the osteotome extends 5 mm posteriorly and centrally out of the bone as shown in Figures 17a and 17b. What is the first structure it enters?
Explanation
REFERENCES: Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3.
Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 422.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, plate 480.
Question 38
A 17-year-old boy underwent open reduction and internal fixation of a navicular fracture 5 days ago. A follow-up examination now reveals a tensely swollen foot with erythema and multiple skin bullae. The patient is febrile and has marked pain with palpation of the entire forefoot and hindfoot. What is the next step in management?
Explanation
REFERENCES: Ault MJ, Geiderman J, Sokolov R: Rapid identification of group A streptococcus as the cause of necrotizing fasciitis. Ann Emerg Med 1996;28:227-230.
McHenry CR, Piotrowski JJ, Pentrinic D, Malangoni MA: Determinants of mortality for necrotizing soft-tissue infections. Ann Surg 1995;221:558-563.
Question 39
A 40-year-old man sustains a scapular body fracture after an all-terrain vehicle accident. Which of the following is the most commonly associated injury?
Explanation
Question 40
Sacral fractures are most likely to be associated with neurologic deficits when they involve what portion of the sacrum?
Explanation
REFERENCES: Denis F, Davis S, Comfort T: Sacral fractures: An important problem.
A retrospective analysis of 236 cases. Clin Orthop Relat Res 1988;227:67-81.
Wood KB, Denis F: Fractures of the sacrum and coccyx, in Vacarro AR (ed): Fractures of the Cervical, Thoracic and Lumbar Spine. New York, NY, Marcel Dekker, 2003, pp 473-488.
Question 41
A displaced pediatric supracondylar humerus fracture is treated with closed manipulation and placement of 2 Kirschner wires placed from the lateral side. What would be the effect of adding a third pin from the lateral side? Review Topic
Explanation
Question 42
A 17-year-old football player continues to have discomfort after sustaining a blow to his midthigh during a game 8 weeks ago. A plain radiograph is shown in Figure 13. What is the most appropriate management?
Explanation
REFERENCES: Lipscomb AB, Thomas ED, Johnston RK: Treatment of myositis ossificans traumatica in athletes. Am J Sports Med 1976;4:111-120.
Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.
Ryan JB, Wheeler JH, Hopkins WJ, et al: Quadriceps contusions: West Point update. Am J Sports Med 1991;19:299-304.
Question 43
A 23-year-old man sustained an injury to his left foot when a forklift rolled over it at work. Examination reveals marked swelling of the midfoot and forefoot, with tenderness to palpation over the medial hindfoot and dorsomedial forefoot. The distal dorsalis pedis pulse is audible on Doppler examination, and his sensation is intact to touch. Radiographs are shown in Figures 33a and 33b. Management should consist of
Explanation
REFERENCES: Resch S, Stenstrom A: The treatment of tarsometatarsal injuries. Foot Ankle 1990;11:117-123.
Schenck RC Jr, Heckman JD: Fractures and dislocations of the forefoot: Operative and nonoperative treatment. J Am Acad Orthop Surg 1995;3:70-78.
Kuo RS, Tejwani NC, Digiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Question 44
Initial repair of the large U-shaped rotator cuff tear shown in Figure 12 consists of closing the tear side-to-side to take advantage of margin convergence. The most significant biomechanical consequence of this repair step results in
Explanation
REFERENCES: Burkhart SS: A stepwise approach to arthroscopic rotator cuff repair based on biomechanical principles. Arthroscopy 2000;16:82-90.
Burkhart SS, Athanasiou KA, Wirth MA: Margin convergence: A method of reducing strain in massive rotator cuff tears. Arthroscopy 1996;12:335-338.
Question 45
Collagen orientation is parallel to the joint surface in what articular cartilage zone?
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 498-499.
Mankin HJ, Mow VC, Buckwalter JA: Articular cartilage structure, composition, and function, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006,
in press.
Question 46
Figure 199 is the clinical photograph of a 68-year-old man with a history of atrial fibrillation who was treated with warfarin. Nine days after undergoing elective total hip arthroplasty, he has a swollen left thigh. His wound remains dry and he is afebrile. His erythrocyte sedimentation rate (ESR) is 25 mm/h (reference range [rr], 0-20 mm/h) and C-reactive protein (CRP) level is 6.1 mg/L (rr, 0.08-3.1 mg/L). Aspiration reveals 3246 white blood cells (WBCs)/µL with 47% polymorphonucleocytes. Treatment at this time should consist of
Explanation
This patient has a large postsurgical hematoma. Although his ESR and CRP level are elevated, they are not considered elevated given his recent surgery. Additionally, the hip aspiration reveals a synovial cell count lower than 10000 WBC/µL along with a low percentage of polymorphonucleocytes. Treatment at this time should consist of observation. The hematoma is likely attributable to postsurgical anticoagulation, considering his history of atrial fibrillation.
Question 47
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of
Explanation
REFERENCES: Teng AL, Pinzur MS, Lomasney L, et al: Functional outcome following anatomic restoration of the tarsal-metatarsal fracture dislocation. Foot Ankle Int
2002;23:922-926.
Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Question 48
What ligament is the primary restraint to applied valgus loading of the knee?
Explanation
REFERENCE: Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 767.
Question 49
Figure 8 shows the radiograph of a 76-year-old man who has knee pain and swelling. History reveals that he underwent total knee arthroplasty 18 years ago. What is the most likely diagnosis?
Explanation
REFERENCES: Kilgus DJ, Moreland JR, Finerman GA, et al: Catastrophic wear of tibial polyethylene inserts. Clin Orthop Relat Res 1991;273:223-231.
Vince KG: Why knees fail. J Arthroplasty 2003;18:39-44.
Question 50
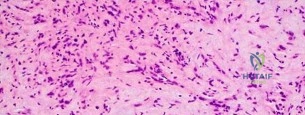
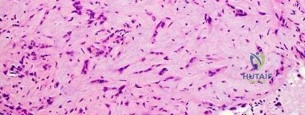
A 69-year-old woman reports a painful clicking in her right shoulder. A soft-tissue mass is palpated at the lower portion of the scapula. Based on the MRI scan and biopsy specimens shown in Figures 72a through 72c, what is the most likely diagnosis?
Explanation
REFERENCES: Vastamaki M: Elastofibroma scapulae. Clin Orthop Relat Res 2001;392:404-408.
Nielsen T, Sneppen O, Mykre-Jensen O, et al: Subscapular elastofribroma: A reactive pseudotumor. J Shoulder Elbow Surg 1996;5:209-213.
Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 286-289.
Question 51
- What is the usual mechanism of injury for the fracture shown in Figures 49a and 49b?

Explanation
Question 52
A 52-year-old, right hand dominant man comes for evaluation of right shoulder pain that has been intermittently bothering him for three months. The pain is worse with overhead activities. He denies any history of trauma. His range of forward elevation in the plane of the scapula is painful and is limited to 145 degrees, compared to 170 degrees on his unaffected side. A radiograph is shown in Figure A. He saw another orthopedist a month ago, who ordered an MRI, which showed a small, partial thickness supraspinatus tendon tear. He received a subacromial injection of lidocaine at that time which temporarily relieved 90 percent of the pain he felt with passive forward elevation of his shoulder past 90 degrees. Today he is requesting a subacromial injection of platelet rich plasma (PRP). You tell him that with regard to pain, function and range of motion, subacromial injection of PRP: Review Topic

Explanation
PRP injection.
Platelet rich plasma has been used for the treatment of chronic tendinopathy in different areas with mixed results. No benefit to patients with symptoms of subacromial impingement has been demonstrated for subacromial injection of PRP, when added to a standard therapy program.
Kesikburun et al. conducted a randomized controlled trial in which patients with rotator cuff tendinopathy or partial rotator cuff tears were randomized to receive ultrasound-guided subacromial injection of either PRP or lidocaine, followed by a standard six-week therapy program. The authors found no difference in pain, range of motion or validated outcome scores at one year follow up.
Hall et al. reviewed sports medicine applications for PRP. At that time (2009), with regard to PRP, they concluded that there was "little clinical evidence for its use."
Ketola et al. sought to determine the effectiveness of subacromial decompression for the treatment of subacromial impingement syndrome. They randomized 140 patients to a supervised exercise program or arthroscopic subacromial decompression followed by a supervised exercise program. They found no clinically important differences between the two groups at 24 months follow up.
Figure A shows a right shoulder radiograph without osseous pathology. Incorrect answers:
Question 53
A football player who injured his right lower extremity during a game could not get up and reported extreme pain. The initial sideline evaluation showed a probable anterior cruciate, posterior cruciate, and lateral collateral ligament rupture with a very unstable knee. He also reports pain in his ankle and is unable to dorsiflex the ankle. He has limited sensation over the dorsum of his foot. Examination reveals no swelling of the ankle and no pain with passive range of motion of the ankle. What is the most likely diagnosis? Review Topic
Explanation
Question 54
Which of the following post-reduction forearm fractures patterns may be treated non-operatively in an otherwise healthy 22-year old male?
Explanation
Even in the setting of minimal displacement, fractures involving the radial diaphysis, or both bones of the forearm, are at high risk of displacing further and progressing to malunion or nonunion. Given the potential for a resulting loss of forearm rotation, open reduction internal fixation is indicated for almost all adult diaphyseal radius and both bone fractures.
Schulte et al. review the management of both bone forearm fractures in adults. They review biomechanics, fixation techniques, outcomes and complications. They note that the goals of fixation in simple patterns are 'cortical opposition, compression, and restoration of forearm geometry.'
Anderson et al. treated 330 acute diaphyseal forearm fractures with compression plating from 1960 to 1970. At 4 months to 9 years follow up, they achieved a 97.9%
union rate for the radius and 96.3% union rate for the ulna.
Illustration A shows measurement of radial bow. A dotted line perpendicular to the line drawn from the radial tuberosity to the ulnar aspect of the distal radius can be used to measure radial bow when drawn at the point of maximum distance to the ulnar edge of the radius.
Incorrect answers:
Question 55
What does Dual Energy X-ray Absorptiometry (DEXA) testing, as a technique, measure?
Explanation
REFERENCES: Genant HK, Faulkner KG, Gluer CC: Measurement of bone mineral density: Current status. Am J Med 1991;91:49S-53S.
Genant HK, Engelke K, Fuerst T, et al: Review: Noninvasive assessment of bone mineral density and stature: State of the art. J Bone Miner Res 1996;11:707-730.
Engelke K, Gluer CC, Genant HK: Factors influencing short-term precision of dual X-ray bone absorptiometry (DXA) of spine and femur. Calcif Tissue Int 1995;56:19-25.
Question 56
What structure is considered the single most important soft-tissue restraint to anterior-posterior stability of the sternoclavicular joint?
Explanation
REFERENCES: Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Rockwood CA Jr, Matsen FA III, Jobe CM: Gross Anatomy of the Shoulder. Philadelphia, PA, WB Saunders, 1998.
Question 57
A 21-year-old male is brought to the emergency department after being involved in gang-related violence. A radiograph of his pelvis is shown in Figure A. The patient is hemodynamically stable. Which of the following imaging modalities is the next best step in evaluating this patient for the most common associated injury? Review Topic

Explanation
The incidence of GSW is increasing and it is the 2nd leading cause of death in young males in the US after motor vehicle accidents. The incidence of a GSW to the buttock is approximately 8% of all GSW to the extremities. Potential complications of pelvic and acetabular GSW include septic arthritis, enterocutaneous, enteroacetabular, and vesicoacetabular fistulas, infected nonunion, malunion, and injuries to the iliac vessels. The presence or absence of intra-abdominal injuries affects treatment and outcome.
Bartkiw et al. reviewed 2808 GSW and found 1235 associated fractures including 42 fractures of the hip and pelvis. Ten orthopaedic operative procedures were performed in 7 patients. Associated nonorthopaedic injuries included 15 small/large bowel perforations (36%), 7 vessel lacerations (17%), and 2 urogenital injuries (5%) that required surgery.
Najibi et al. reviewed 39 GSW to acetabulum. They found 32 simple and 7 associated fracture patterns. The most common simple and associated patterns were anterior column and both column, respectively. Bowel injuries were the most common associated injures (42%). Predictors of poor outcome include high-velocity missile, involvement of acetabular dome, abdominal injury, nerve injury, vascular injury, and male gender. Deep infection was associated with primary anastomosis of bowel injury and an associated fracture pattern.
Figure A shows a GSW to the right hip with acetabular fracture and visible bullet fragment.
Incorrect Answers:
Question 58
A 14-year-old boy has had knee pain for the past 2 months. He also has a low-grade fever of 101.3 degrees F (38.5 degrees C). Laboratory studies show a WBC count of 12,100/mm 3 and an erythrocyte sedimentation rate of 58/h. A biopsy specimen of a lesion in the distal femoral metaphysis is shown in Figure 38. What is the most appropriate treatment?
Explanation
REFERENCES: McCarthy JJ, Dormans JP, Kozin SH, et al: Musculoskeletal infections in children: Basic treatment principles and recent advancements. Instr Course Lect 2005;54:515-528.
Calhoun JH, Manring MM: Adult osteomyelitis. Infect Dis Clin North Am 2005;19:765-786.
Question 59
A 30-year-old man who participates in recreational sports reports the spontaneous onset of intermittent pain and swelling about the right knee. Examination reveals a 3+ effusion, with a range of motion of 10° to 60°. He has mild diffuse tenderness but no instability. MRI scans and an arthroscopic view are shown in Figures 39a through 39c. Management should consist of
Explanation
REFERENCES: Coolican MR, Dandy DJ: Arthroscopic management of synovial chondromatosis of the knee: findings and results in 18 cases. J Bone Joint Surg Br
1989;71:498-500.
Ogilvie-Harris DJ, Saleh K: Generalized synovial chondromatosis of the knee: A comparison
of removal of the loose bodies alone with arthroscopic synovectomy. Arthroscopy
1994;10:166-170.
Question 60
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. Which of the four muscles of the rotator cuff provides the most resistance to this patient's direction of instability?
Explanation
indicated. If a patient has excessive glenoid retroversion (not seen in this scenario with 5 degrees of retroversion), a posterior opening-wedge osteotomy is appropriate.
Question 61
A 45-year-old IV drug abuser has sternoclavicular (SC) joint pain for the past 2 weeks. He is afebrile and physical exam findings include point tenderness and swelling. He most likely has septic arthritis of the sternoclavicular joint. If so, what is the most likely infecting organism?

Explanation
According to the reference by Ross et al, Staphylococcus aureus accounts for 49% of infections. SC joint arthritis accounts for 1% of septic arthritis in the general population but 17% in the IV drug abuse population. Symptoms include spontaneous swelling with the appearance of joint subluxation and localized pain. These patients are not uncommonly afebrile.
Question 62
.What is the most appropriate treatment if instability is present at the time of evaluation?
Explanation

Question 63
Figure 46 shows the radiograph of an obese 12-year-old boy who has had left hip pain for the past 3 months. What is the best course of action?
Explanation
REFERENCES: Loder RT, Aronsson DD, Greenfield ML: The epidemiology of bilateral slipped capital femoral epiphysis: A study of children in Michigan. J Bone Joint Surg Am 1993;75:1141-1147.
Aronsson DD, Karol LA: Stable slipped capital femoral epiphysis: Evaluation and management. J Am Acad Orthop Surg 1996;4:173-181.
Hurley JM, Betz RR, Loder RT, Davidson RS, Alburger PD, Steel HH: Slipped capital femoral epiphysis: The prevalence of late contralateral slip. J Bone Joint Surg Am 1996;78:226-230.
Loder RT, Aronson DD, Dobbs MB, Weinstein SL: Slipped capital femoral epiphysis. J Bone Joint Surg Am 2000;82:1170-1188.
Question 64
A 30-year-old man has pain in the left arm after a motor vehicle accident. His neurovascular examination is intact, and radiographs are shown in Figures 25a and 25b. What is the best course of management?
Explanation
REFERENCES: Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Yokoyama K, Itoman M, Kobayashi A, et al: Functional outcomes of “floating elbow” injuries in adult patients. J Orthop Trauma 1998;12:284-290.
Question 65
A year-old man with a body mass index of 31 had a month gradual onset of right medial knee pain. Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
Explanation
According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Nonarthroplasty), level 1 evidence confirms that weight loss and exercise benefit patients with knee osteoarthritis. The other responses have either inclusive evidence (a valgus-directing brace) or no evidence to support their use (glucosamine 1,500 mg/day and chondroitin sulfate 800 mg/day as well as
arthroscopic debridement and lavage).
Question 66
Which of the following structures is predominantly composed of Type 1 collagen? Review Topic
Explanation
Type 1 collagen accounts for more than 90% of the total collagen content in the body. Type 1 collagen is found in bone, ligament, tendon, meniscus, annulus of intervertebral discs, skin, healed cartilage, scar tissue, and nerves.
Duthon et al present a review of the ACL and its histologic and mechanical properties. The ACL has a mean length of 32 mm and a width of 7-12 mm. They state that the ACL has a microstructure of collagen bundles of multiple types (mostly type I) and a matrix made of a network of proteins, glycoproteins, elastic systems, and glycosaminoglycans with multiple functional interactions.
Incorrect
1: Epithelial
2: L4 disc
Basement
Membrane is made up of Type
nucleus pulposus is composed of mostly Type
4 collagen.
2 collagen
4: Medial femoral condyle articular cartilage is comprised mostly of Type 2 collagen. 5: Dupuytren's contracture tissue is mostly Type 3 collagen.
Question 67
Figure 1 is an MRI scan of the right hip of a 19-year-old woman with a 6-month history of right groin pain. She was diagnosed with a stress fracture and was treated with 3 months of limited weight bearing. Figure 2 is a repeat MRI scan in which the edema pattern changed minimally but the pain worsened. Ibuprofen alleviates most of her pain. What is the best next step?
Explanation
cells, forms the nidus of the tumor, which is easily identified on CT scans.
Question 68
Which of the following areas of the vertebral segment has the highest ratio of cortical to cancellous bone? Review Topic
Explanation
Question 69
What structure provides the major blood supply to the humeral head?
Explanation
the major blood supply to the humeral head. The posterior circumflex humeral artery
supplies a much smaller portion of the proximal humerus. The nutrient humeral artery is the main blood supply for the humeral shaft. The thoracoacromial artery is primarily a muscular branch. The rotator cuff insertions contribute some blood supply to the tuberosities but not a major contribution.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Cushner MA, Friedman RJ: Osteonecrosis of the humeral head. J Am Acad Orthop Surg 1997;5:339-346.
Question 70
What spinal nerves in the cauda equina are primarily responsible for innervation of the bladder?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton-Century-Crofts, 1976, p 254.
Pick TP, Howden R (edS): Gray’s Anatomy. New York, NY, Bounty Books, 1977, p 1004.
Question 71
..Further imaging shows pulmonary metastases without an obvious primary tumor of origin and an incomplete fracture of the right distal femur. A decision is made to surgically treat his distal femur fracture. What is the role of establishing a preoperative histologic diagnosis for this patient?
Explanation
t(X;18)(p11.2;q11.2)
t(11;22)(q24;q12)
t(1;3)(p36.3;q25)

Question 72
A 14-year-old boy has had a 3-month history of low back pain with no known trauma. The pain is worse with activity and relieved by rest, although he does report difficulty with prolonged sitting in school. The patient was on the football team but stopped participating because of the back pain during football practice. He reports no history of radicular pain and denies any numbness, tingling, or weakness in the legs. Neurologic examination is normal. Back examination reveals slight tenderness over the lower back area but no swelling or skin defects. Strength testing is 5 over 5 in the lower extremities and the straight leg raise test is negative. Back range of motion is nearly full, but back extension is painful. The hamstrings are slightly tight. Initial radiographs, including AP, lateral and oblique views, are negative. What is the best test to determine the patient's diagnosis? Review Topic
Explanation
have no role in the evaluation of the patient who presents with classic spondylolysis-type symptoms. The most sensitive physical examination finding is pain with back extension. Oblique radiographs can be obtained, but they are not as sensitive or specific as a bone scan with SPECT. The patient does not have any signs of a disk problem; therefore, an evaluation of the disk is not helpful.
(SBQ13PE.79) A 17-year-old male American football lineman presents with low back pain of insidious onset that is somewhat worse with activity. He has no neurologic complaints, night pain or fevers. His symptoms have been present for a few years but this is the first time he has sought medical attention. What physical examination finding is most likely to be found in this clinical scenario? Review Topic
Popliteal angle of 5 degrees
Heel cord tightness
Increased femoral anteversion
Pain with lumbar extension in single leg stance
Numbness of the skin of the anterolateral calf and dorsum of the foot
The patient demographics and clinical presentation are consistent with lumbar spondylolysis. Pain with lumbar extension is the most common physical exam finding.
Office assessment of the patient with spondylolysis should note pertinent negatives that would signify other causes of back pain. The history is most commonly negative for neurologic symptoms such as weakness or numbness, although patients will occasionally have radicular pain. On exam, patients may have localized spasm or tenderness, step off (if there is spondylolisthesis), hamstring tightness. The most common finding is pain with lumbar extension.
McCleary et al. review the diagnosis and treatment of spondylolysis in athletes. They identify three types of patients with spondylolysis: (1) female dancer or gymnast who is hyperlordotic, with increased motion and flexibility, (2) male weightlifter or football player undergoing a growth spurt, with decreased motion and flexiblity, especially of the spinal erectors, and (3) a novice athlete undergoing vigorous preparation for a new sport, with poor core strength and flexibility.
Incorrect
Question 73
A 30-year-old patient has acetabular dysplasia and moderate secondary osteoarthrosis. Which of the following studies will best help predict the success of periacetabular osteotomy?
Explanation
REFERENCE: Murphy S, Deshmukh R: Periacetabular osteotomy: Preoperative radiographic predictors of outcome. Clin Orthop 2002;405:168-174.
Question 74
A patient with rheumatoid arthritis with both ankle and subtalar involvement was treated as shown in Figures 11a and 11b. What complication is unique to this type of fixation?
Explanation
REFERENCES: Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 236-237.
Thordarson DB, Chang D: Stress fractures and tibial cortical hypertrophy after tibiotalocalcaneal arthrodesis with an intramedullary nail. Foot Ankle Int 1999;20:497-500.
Hammett R, Hepple S, Forster B, et al: Tibiotalocalcaneal (hindfoot) arthrodesis by retrograde intramedullary nailing using a curved locking nail: The results of 52 procedures. Foot Ankle Int 2005;26:810-815.
Question 75
A 38-year-old woman has a lesion on her left foot that has increased in size over the past 6 months. The clinical photograph is shown in Figure 17a, and a photomicrograph of the biopsy specimen is shown in Figure 17b. What is the most likely diagnosis?
Explanation
REFERENCES: Hughes LE, Horgan K, Taylor BA, Laidler P: Malignant melanoma of the hand and foot: Diagnosis and management. Br J Surg 1985;72:811-815.
Fortin PT, Freiberg AA: Malignant melanoma of the foot and ankle. J Bone Joint Surg Am 1995;77:1396-1403.
Question 76
What structure is 7cm from the acromion and at greatest risk of injury during a deltoid splitting approach for a proximal humerus fracture?

Explanation
Based on the knowledge of the course of the axillary nerve, and potential complications regarding the
vascular supply to the humeral head with the delto-pectoral approach, some authors are suggesting deltoid-splitting approach to the proximal humerus for reduction and fixation of proximal humeral fractures.
Cetik et al evaluated 24 cadaver shoulders to better identify the course of the axillary nerve and identify the "safe zones" for deltoid-splitting incisions. They found the distance from the tip of the acromion to the axillary nerve varied depending on patient specific factors like arm length and they identified a "safe area" where dissection was free of injury to the axillary nerve (Illustrations A and B).
Question 77
Antegrade femoral nailing has an increased rate of which of the following when compared to retrograde femoral nailing?

Explanation
was significantly greater in the retrograde group. The referenced study by Winquist et al noted a 99.1% union rate with intramedullary nailing. The referenced study by Moed et al noted a 6% nonunion rate in non-reamed retrograde femoral nailing with nail dynamization at 6-12 weeks and early weightbearing.
Question 78
Posttraumatic physeal arrest is most common at which of the following locations?
Explanation
REFERENCES: Ecklund K, Jaramillo D: Patterns of premature physeal arrest: MR imaging of 111 children. AJR Am J Roentgenol 2002; 178:967-972.
YAtotoartanadQpyiQter GN: Physeal bridge resection. J Am Acad Orthop Surg 2005; 13:4

Figure 64a Figure 64b
Question 79
Figures A-C are images of a 37-year-old man who presents with isolated muscle atrophy due to a compressed nerve. Which of the following sequences correctly describes the pathway of this nerve through the brachial plexus, before it innervates the affected muscles?
Explanation
Quadrilateral space syndrome is a condition defined by axillary nerve, +/- posterior humeral circumflex artery compression in the quadrilateral space. It most commonly affects the dominant shoulder in overhead movement athletes (e.g. basketball players) or other throwing athletes. Physical examination may reveal weakness with the arm positioned in abduction and external rotation. In situations of long-standing compression, there may also be atrophy of the teres minor and deltoid muscle.
Chafik et al. dissected thirty-one cadaveric human shoulders to describe the neuromuscular anatomy of teres minor. They showed that the primary nerve branch to teres minor travelled in a fascial sling 44 mm medial to the muscular insertion. This
area may be the potential site of greatest compression and tethering of this nerve in patients with isolated teres minor atrophy.
Friend et al. performed a cadaveric dissection of nine shoulder specimens to look at the anatomical variability in course, length and branching pattern of both the teres minor nerve and the axillary nerve. These were compared to a case-based study of these two male patients with isolated atrophy of teres minor. They concluded that there is no good anatomical predictor of nerve compression outside the quadrilateral space as there is considerable anatomical variation in its origin and course, as well as potential site of compression.
Figure A-C are MRI images that show atrophy of the teres minor muscle and possibly deltoid muscle. The rotator cuff muscles are labeled in Illustration A. The teres minor muscle is labeled in Illustration B. Illustration C shows a diagram of the brachial plexus.
Incorrect
1:
This
describes
the
musculocutaneous
nerve.
3:
This
describes
the
suprascapular
nerve.
4:
This
describes
the
long thoracic
nerve.
Question 80
Your 25-year-old patient complains of anterior knee pain after retrograde femoral nailing for a diaphyseal fracture and asks you why you didn’t perform antegrade nailing as he has seen on the internet. You tell him that retrograde nailing is your preferred technique over antergrade nailing for diaphyseal femoral fractures because it has been shown to have?

Explanation
Question 81
A 9-year-old child has right groin pain after falling from a tree. Examination reveals that the right leg is held in external rotation, and there is significant pain with attempts at passive range of motion. Radiographs are shown in Figures 43a and 43b. Management should consist of
Explanation
REFERENCES: Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
Hughes LO, Beaty JH: Fractures of the head and neck of the femur in children. J Bone Joint Surg Am 1994;76:283-292.
Question 82
An 18-year-old patient sustains a comminuted left femoral fracture starting 6.5cm distal to the lesser trochanter. He undergoes antegrade femoral nailing in the supine position on a radiolucent table. Upon completion of proximal and distal interlocking, both patellae are positioned facing the ceiling and a lateral radiographs confirms that the posterior condyles of both limbs are aligned. On AP imaging of both femora, it is noted that the lesser trochanter of the left (injured) side is larger than the right (uninjured) side. Assuming symmetrical anteversion, the left femur has been nailed Review Topic
Explanation
Rotational malalignment is the most common complication of intramedullary nailing of a comminuted diaphyseal femoral fracture. The rotational profile of the lesser trochanter can be used to evaluate rotational alignment. The proximal femur is rotated until a neutral position is obtained as judged by the radiographic profile of the lesser trochanter. If the AP image shows a smaller lesser trochanter, there is IR of the LT. A larger LT indicates external rotation (ER) of the LT.
Jaarsma et al. describe CT imaging in determining rotational alignment. They note that the incidence of post-nailing malalignment > 10 ° is 40%, > 15 ° is 20-30%, and
> 20 ° is 16%. They also note that patients with ER deformities have more symptoms than those with IR deformities, and that small deformities <15 ° give rise to less complaints. This is because ER deformities lead to compensation with hip retroversion, which causes more symptoms than hip anteversion when compensating for IR deformities.
Incorrect Answers:
(SBQ12TR.37) A 44-year-old male presents with the isolated injury seen in Figure A after a motor vehicle accident and underwent the operative treatment seen in Figure B within 8 hours from the time of incident. Which of the following complications is this patient at highest risk of developing?

Pulmonary embolus
Periprosthetic fracture
Contralateral hip fracture
Osteonecrosis
Infection
This young male patient has sustained a displaced femoral neck fracture and underwent open reduction internal fixation with 3 cannulated screws. Based on the available options, the patient is most at risk of developing osteonecrosis of the femoral head.
Femoral neck fractures in young patients typically are the result of a high-energy trauma. Fracture displacement has been shown to disrupt vascular supply to the femoral head by interrupting retinacular vessels and ligament teres vascularization, as well as increasing intracapsular pressure, producing a tamponade effect. The incidence of osteonecrosis in patients younger than 60 years with displaced femoral neck fractures has been shown to be between 15-30%. Quality of reduction is one key factor that has been shown to influence outcomes postoperatively.
Loizou et al. prospectively studied 1,023 patients who sustained an intracapsular hip fracture that was treated with internal fixation using standard fixation modalities. They showed that osteonecrosis was less common for undisplaced (4.0%) than for displaced fractures (9.5%). The population at greatest risk were women younger than the age of 60 with displaced fractures.
Barnes et al. review subcapital hip fractures. They found that late segmental collapse was more common in displaced fractures in women younger than age 75 years than in those older than age 75 years treated with internal fixation.
Figure A shows a displaced, Garden 3/Pauwels I hip fracture. Figure B shows anatomical fixation with 3 cannulated screws.
Incorrect Answers:
Question 83
In Ewing’s sarcoma, neoplastic properties are thought to be related to a
Explanation
tumor cell proliferation include inactivation of tumor suppressor genes, or activation of proto-oncogenes.
REFERENCES: Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Pierz KA, Womer RB, Dormans JP: Pediatric bone tumors: Osteosarcoma Ewing’s sarcoma, and chondrosarcoma associated with multiple hereditary osteochondromatosis. J Pediatr Orthop 2001
;21:412- 418.
Question 84
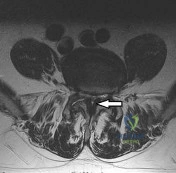
Figure 93 shows the axial T2-weighted MRI scan of the lumbar spine of a 70-year-old man. The arrow points to which of the following structures? Review Topic
Explanation
(SBQ12SP.14) A 36-year-old male presents with acute onset of right buttock and leg pain following lifting a heavy object. On physical exam he has weakness to knee extension, numbness over the medial malleolus, and a decreased patellar reflex. Which of the following would most likely explain this clinical presentation. Review Topic
Lumbar arachnoiditis
L4/L5 paracentral disc herniation
L3/L4 far lateral (foraminal) disc herniation
L4/L5 far lateral (foraminal) disc herniation
L5/S1 far lateral (foraminal) disc herniation
The clinical presentation is consistent with a L4 radiculopathy. A L4/L5 far lateral (foraminal) disc herniation would compress the exiting root (L4) and cause these symptoms.
The location of a prolapsed lumbar disc determines its symptoms. Central disc herniations may give rise to back pain or cauda equina syndrome. Paracentral disc herniations (90-95% of cases) affect the traversing nerve root. Far lateral disc herniations (5-10%) affect the exiting nerve root.
Gregory et al. summarize physical signs in lumbar disc herniation. They state that the straight-leg-raise is the most sensitive (73-98% sensitive) test and the crossed straight-leg-raise is the most specific (88-98% specific) test for lumbar disc herniation. Other specific tests include weak ankle dorsiflexion (89% specific), absent ankle reflex (89% specific), and calf wasting (94% specific, but a late finding).
Illustration A shows how a paracentral L4/L5 disc herniation affects the traversing L5 root, but a far lateral L4/L5 disc herniation affects the L4 root. Illustration B shows the dermatomal distribution of pain with root involvement from L3 to S1.
Incorrect Answers:
Question 85
Which of the following is the only nonreversible effect of anabolic steroids?
Explanation
Once anabolic steroids are stopped, muscle hypertrophy and training gains are quickly lost and the HDL/ LDL ratios return to their preexisting levels. Fortunately, the personality effects and the acute acne are reversible.
REFERENCES: Hartgens F, Kuipers H: Effects of androgenic-anabolic steroids in athletes. Sports Med 2004;34:513-554.
Evans NA: Current concepts in anabolic-androgenic steroids. Am J Sports Med 2004;32:534-542.
Question 86
A 16-year-old snowboarder has significant pain and is still unable to bear weight after sustaining a lateral ankle injury in a fall 1 week ago. Examination reveals swelling and tenderness in the sinus tarsi. AP, lateral, and mortise radiographs of the ankle are unremarkable. Management should consist of
Explanation
REFERENCES: Kirkpatrick DP, Hunter RE, Janes PC, Mastrangelo J, Nicholas RA: The snowboarder’s foot and ankle. Am J Sports Med 1998;26:271-277.
Ebraheim NA, Skie MC, Podeszwa DA, Jackson WT: Evaluation of process fractures of the talus using computed tomography. J Orthop Trauma 1994;8:332-337.
Question 87
A 10-year-old girl with a history of an obstetrical brachial plexus palsy has been referred for evaluation. Examination reveals a severe adduction internal rotation contracture of the shoulder and a mild flexion contracture of the elbow. Hand function is normal. Radiographs show mild glenohumeral joint incongruity. To achieve the best functional outcome, management should consist of
Explanation
REFERENCES: Jahnke AH Jr, Bovill DF, McCarroll HR Jr, James P, Ashley RK: Persistent brachial plexus birth palsies. J Pediatr Orthop 1991;11:533-537.
Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L’Episcopo transfers in obstetrical palsy: A retrospective review of 20 cases. J Pediatr Orthop 1990;10:442-444.
Goddard NJ, Fixsen JA: Rotation osteotomy of the humerus for birth injuries of the brachial plexus. J Bone Joint Surg Br 1984;66:257-259.
Question 88
A 12-year-old girl who plays softball has chronic lateral hindfoot aching pain that is aggravated by weight-bearing activity. She reports that the pain has recurred after initial improvement with cast immobilization, and it continues to limit her overall level of activity. Radiographs are seen in Figures 40a through 40c. What is the most appropriate surgical treatment?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 757-765.
Lemley F, Berlet G, Hill K, et al: Current concepts review: Tarsal coalition. Foot Ankle Int 2006;27:1163-1169.
Question 89
The medial collateral ligament complex of the elbow originates on what portion of the medial epicondyle?
Explanation
REFERENCE: O’Driscoll SW, Jaloszynski R, Morrey BF: Origin of the medial ulnar collateral ligament. J Hand Surg Am 1992;17:164-168.
Question 90
A 30-year-old woman injured the ring finger of her nondominant hand while playing baseball 5 weeks ago. She now reports pain and limited motion of the proximal interphalangeal (PIP) joint. A lateral fluoroscopy image is shown in Figure 36. Treatment of the PIP joint should consist of
Explanation
REFERENCES: Dionysian E, Eaton RG: The long-term outcome of volar plate arthroplasty of the proximal interphalangeal joint. J Hand Surg Am 2000;25:429-437.
Eaton RG, Malerich MM: Volar plate arthroplasty of the proximal interphalangeal joint: A review of ten years’ experience. J Hand Surg Am 1980;5:260-268.
Deitch MA, Kiefhaber TR, Comisar BR, et al: Dorsal fracture dislocations of the proximal interphalangeal joint: Surgical complications and long-term results. J Hand Surg Am 1999;24:914-923.
Question 91
03 What is the most common site of fracture because of osteolysis following cementless total hip arthroplasty with an extensively porus-coated femoral component?

Explanation

creates stress shielding. The force is seen through the femoral head into the stem and transfers to the bone at areas of
ingrowth and transmitted distally. As a result the part being skipped is the greater trochanter and leads to osteolysis by Wolf’s law and can result in fracture.

The osteolysis created about the acetabulum is due an inflammatory mechanism imparted on the wear debris from the bearing surfaces. This osteolysis rarely creates fractures.

The fractures about the stem are most commonly caused by the difference in modulus between the stem and bone back to this question next question
Question 92
A 17-year-old male soccer player sustains repeated lateral patellar dislocations refractory to physical therapy, bracing, and taping. After a workup including radiographs and MRI, the orthopaedic surgeon considers an isolated tibial tubercle osteotomy (TTO). He plans a 60-degree anteromedialization to address instability and to unload the patellofemoral joint. What is a relative contraindication to this procedure?
Explanation
TTO is a common treatment for patellofemoral instability. The angle of correction must be customized to each patient’s anatomy. For this patient, the orthopaedic surgeon plans an osteotomy that will both anteriorize and medialize the tubercle. This will consistently result in
a change of patellofemoral kinematics and contact pressures. Medialization decreases lateral and increases medial patellofemoral contact pressures, and anteriorization shifts contact pressures from distal to proximal. Significant anteriorization may not be desired in a patient with proximal patellar chondrosis unless a concomitant chondral procedure is performed as well. The patellar height (Caton-Deschamps ratio) is normal, precluding the need for distalization but not medialization. The TT-TG distance, at more than 20 mm, is a strong indication for osteotomy. The Q angle, although a less precise indicator of malalignment, is also elevated and would be considered an indication for osteotomy.

CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 41
A healthy, active 18-year-old man has acute-onset right knee pain and an inability to fully extend his knee following an attempt to stand from a seated position yesterday. He sustained a noncontact injury to his right knee while playing basketball 2 years ago and underwent primary anterior cruciate ligament (ACL) reconstruction with bone-patella-tendon-bone autograft and medial meniscus repair. He sustained another noncontact injury to the same knee 8 months later and underwent a revision ACL reconstruction using soft-tissue allograft and revision medial meniscus repair. He reports multiple episodes of “giving way” of his knee, but no pain prior to yesterday’s acute injury.
Question 93
The patient undergoes a mobile-bearing UKA. When compared to a fixed-bearing metal-backed unicompartmental arthroplasty, this procedure is associated with a
Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact ACL. The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph will allow the orthopaedic surgeon to determine the correction of the varus deformity and assess the lateral compartment. Inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared to other age groups, but survivorship is lower for UKA than TKA. No studies to date have shown differences in survivorship between fixed- or mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, and this occurs in fewer than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA is low. Arthritis progression may be faster for mobile-bearing UKAs than fixed-bearing UKAs.
The radiographs reveal a fracture of the extensively porous coated stem. This entity, although rare, is associated with higher risk for occurrence when thin stems are implanted in patients with thick cortices and there is a lack of proximal stable support for the prosthesis. Nonsurgical care likely would not help this patient. A triple-phase bone scan would not add any information that would change the treatment plan.
Question 94
A 60-year-old man who underwent left partial knee arthroplasty 6 months earlier was doing well until he experienced left knee pain and swelling for 4 weeks following a dental procedure. The left knee aspirate was bloody, with a white blood cell count of 8,000 and 70% neutrophils. Culture grew group B Streptococcus ( Granulicatella adiacens ), and serologies were elevated, with an erythrocyte sedimentation rate of 55 mm/h (reference range: 0 to 20 mm/h) and a C-reactive protein level of 24 mg/L (reference range: 0.08 to 3.1 mg/L). What is the best next step?
Explanation
This complication is best addressed with either a single-stage or two-stage total knee arthroplasty. A recent report suggests that a single-stage arthroplasty can be effective, although many surgeons would perform a two-stage procedure with an articulating or static spacer. Arthroscopic would be non-effective, especially given 4 weeks of symptoms. Resection arthroplasty without a spacer would leave an unstable and poorly functioning extremity. Knee fusion should be used as a salvage procedure.
Question 95
Figure 43 shows the lateral radiograph of a 12-year-old boy with mild osteogenesis imperfecta who injured his left elbow after pushing his brother. Treatment should consist of
Explanation
A displaced, isolated fracture of the apophysis of the olecranon is an unusual injury in a child. It has been suggested by several authors that children who have osteogenesis imperfecta may be especially prone to this injury. One study reported seven of these fractures occurring in five children who had the mild form of osteogenesis imperfecta (Sillence type IA). The authors of this study suggest that the diagnosis of osteogenesis imperfecta be considered in any child who has a displaced fracture of the apophysis of the olecranon, especially when the injury is associated with relatively minor trauma.
REFERENCES: Stott NS, Zionts LE: Displaced fractures of the apophysis of the olecranon in children who have osteogenesis imperfecta. J Bone Joint Surg Am 1993;75:1026-1033.
Gaddy BC, Strecker WB, Schoenecker PL: Surgical treatment of displaced olecranon fractures in children. J Pediatr Orthop 1997;17:321-324.
Dormans JP, Rang M: Fractures of the olecranon and radial neck in children. Orthop Clin North Am 1990;21:257-268.
Question 96
A patient with diabetic peripheral neuropathy undergoes a partial first ray amputation for a chronic ulcer beneath the first metatarsal head. The insertion of the anterior tibialis is preserved. The patient has 10 degrees of passive dorsiflexion at the ankle and no other foot deformities or ulcers. Which of the following is considered appropriate shoe wear for this patient?
Explanation
REFERENCES: Philbin TM, Leyes M, Sferra JJ, et al: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Pinzur MS, Dart HC: Pedorthic management of the diabetic foot. Foot Ankle Clin 2001;6:205-214.
Question 97
Genetic mutations that may result in the cervical abnormalities noted in the figures generally affect the
Explanation
The figures are characteristic of a child with Klippel-Feil syndrome (congenital cervical spine abnormalities) in association with congenital scoliosis in the upper thoracic spine and a right-sided Sprengel deformity (congenital elevation of the scapula). Sprengel deformity occurs in as many as 30% of children with Klippel-Feil syndrome. Other congenital conditions that are commonly associated with Klippel-Feil, and that should be screened for, include deafness in 30%, genitourinary abnormalities in 25% to 35%, and cardiovascular abnormalities in 4% to 29% of children with Klippel-Feil syndrome.
In Sprengel deformity, there is usually a tether called the omovertebral connection between the abnormally elevated scapula and the spinous processes in the upper thoracic region. This tether is most commonly bony but also may be cartilaginous or fibrous. Although there also may be abnormalities in the ribs, clavicle, or humerus, they are morphologic abnormalities only, not tethers.
Patients with Klippel-Feil syndrome should be discouraged from participating in contact or collision sports if they have a massive fusion of the cervical spine, any involvement of C2, or limited cervical motion. Fusions at 1 or 2 interspaces below C3 and normal cervical motion do not preclude participation in activities. A Sprengel deformity may limit abduction of the shoulder and normal racquet or throwing mechanics, but, in the absence of pain, is not a contraindication to attempted participation.
Klippel-Feil syndrome affects a heterogenous cohort of patients and different inheritance patterns have been seen, including autosomal-dominant and autosomal-recessive types, with varying levels of penetrance. The first human Klippel-Feil syndrome locus was identified on chromosome 8 and is called SGM1. Other candidates for mutations in Klippel-Feil include PAX genes and Notch pathway genes. In general, the involved genes help regulate the formation and segmentation of the vertebrae.
Between days 20 and 30 following conception, the paraxial mesoderm subdivides into segments called somites. As they mature, somites develop into 3 layers called the sclerotome, myotome, and dermatome. The sclerotome undergoes a process of resegmentation during which the caudal section from 1 somite joins with the rostral section of the immediately caudal somite to form the vertebral bodies. It is during the processes of segmentation and resegmentation that the abnormalities leading to Klippel-Feil syndrome occur. Gastrulation refers to the phase early in embryonic development when the single-layered blastula is reorganized into a trilaminar structure with 3 germ layers: the ectoderm, mesoderm, and endoderm. Neurulation refers to the process by which the notochord induces formation of the neural tube from the neural plate, forming the brain and spinal cord.

Question 98
Which of the following procedures is included in third-generation cement technique?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 181-193.
Maloney WJ, Hartford JM: The cemented femoral component, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, vol 2, pp 959-979.
Question 99
- The diagnostic distinction between a benign enchondroma and a low- grade intramedually chondrosarcoma is based primarily on the
Explanation
Question 100
What is the most appropriate next step in the work-up of a patient with the asymptomatic lesion shown in Figure 23?
Explanation
REFERENCES: Marks KE, Bauer TW: Fibrous tumors of bone. Orthop Clin North Am 1989;20:377-393.
Bullough PG, Walley J: Fibrous cortical defect and non-ossifying fibroma. Postgrad Med J 1965;41:672-676.
Skrede O: Non-osteogenic fibroma of bone. Acta Orthop Scand 1970;41:362-380.
