Orthopedic Surgery Board Review MCQs: Adult Reconstruction, Trauma, & Spine | Part 199

Key Takeaway
This page offers Part 199 of an Orthopedic Surgery Board Review MCQ bank. It provides 100 high-yield, verified multiple-choice questions, mirroring OITE and AAOS exam formats. Designed for orthopedic surgeons and residents, its purpose is to aid comprehensive preparation for board certification exams.
About This Board Review Set
This is Part 199 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 199
This module focuses heavily on: Arthroplasty, Deformity, Foot, Fracture, Infection, Knee, Ligament.
Sample Questions from This Set
Sample Question 1: Figures 5a and 5b show the radiographs of an active 52-year-old man who has increasing knee pain and progressive varus deformity after undergoing total knee arthroplasty 7 years ago. Examination reveals a small effusion, but he has good mot...
Sample Question 2: A well-developed college football player reports swelling and a heaviness in the arm after lifting weights. Examination reveals that distal pulses are normal and equal in both arms. A venogram is shown in Figure 13. What is the most likely ...
Sample Question 3: A 16-year-old girl was involved in a motorcycle accident that resulted in a significant right tibial fracture with soft-tissue loss over the distal 4 cm of the anterior medial tibia. The patient has had two irrigations and debridements and ...
Sample Question 4: Kyphosis from a vertebral osteoporotic compression fracture often results in progressive kyphosis due to...
Sample Question 5: When making a comparison to autograft incorporation, the inflammatory process in allograft tissue anterior cruciate ligament (ACL) reconstruction...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figures 5a and 5b show the radiographs of an active 52-year-old man who has increasing knee pain and progressive varus deformity after undergoing total knee arthroplasty 7 years ago. Examination reveals a small effusion, but he has good motion and stability. What is the most likely diagnosis?
Explanation
REFERENCES: O’Rourke MR, Callaghan JJ, Goetz DG, et al: Osteolysis associated with a cemented modular posterior-cruciate-substituting total knee design. J Bone Joint Surg Am 2002;84:1362-1371.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 529-530.
Question 2
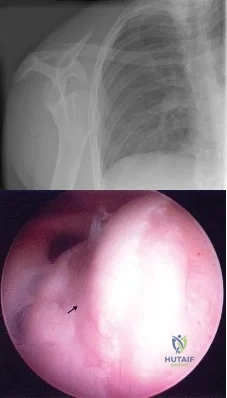
A well-developed college football player reports swelling and a heaviness in the arm after lifting weights. Examination reveals that distal pulses are normal and equal in both arms. A venogram is shown in Figure 13. What is the most likely cause of this condition?
Explanation
REFERENCES: Angle N, Gelabert HA, Farooq MM, et al: Safety and efficacy of early surgical decompression of the thoracic outlet for Paget-Schroetter syndrome. Ann Vasc Surg 2001;15:37-42.
Azakie A, McElhinney DB, Thompson RW, et al: Surgical management of subclavian-vein effort thrombosis as a result of thoracic outlet compression. J Vasc Surg 1998;28:777-786.
Question 3
A 16-year-old girl was involved in a motorcycle accident that resulted in a significant right tibial fracture with soft-tissue loss over the distal 4 cm of the anterior medial tibia. The patient has had two irrigations and debridements and recently had an intramedullary nail placed for the skeletal injury. Vacuum-assisted closure (VAC) has been used to cover the defect since the injury. The risk of infection developing in the tibia is
Explanation
REFERENCES: Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292.
Dedmond BT, Kortesis B, Punger K, et al: The use of negative-pressure wound therapy (NPWT) in the temporary treatment of soft-tissue injuries associated with high-energy open tibia shaft fractures. J Orthop Trauma 2007;21:11-17.
Herscovici D Jr, Sanders RW, Scaduto JM, et al: Vacuum-assisted wound closure (VAC therapy) for the management of patients with high-energy soft tissue injuries. J Orthop Trauma 2003;17:683-688.
Question 4
Kyphosis from a vertebral osteoporotic compression fracture often results in progressive kyphosis due to
Explanation
REFERENCES: Kayanja MM, Ferrara LA, Lieberman IH: Distribution of anterior cortical shear strain after a thoracic wedge compression fracture. Spine J 2004;4:76-87.
Kayanja MM, Togawa D, Lieberman IH: Biomechanical changes after the augmentation of experimental osteoporotic vertebral compression fractures in the cadaveric thoracic spine. Spine J 2005;5:55-63.
Kayanja MM, Schlenk R, Togawa D, et al: The biomechanics of 1, 2, and 3 levels of vertebral augmentation with polymethylmethacrylate in multilevel spinal segments. Spine 2006;31:769-774.
Kayanja M, Evans K, Milks R, et al: The mechanics of polymethylmethacrylate augmentation. Clin Orthop Relat Res 2006;443:124-130.
Question 5
When making a comparison to autograft incorporation, the inflammatory process in allograft tissue anterior cruciate ligament (ACL) reconstruction
Explanation
Question 6
A 29-year-old man reports severe knee instability and popliteal pain. History reveals that he had polio of the left lower extremity as a child and has been brace-free his entire life. Examination reveals that he walks with 40° of knee hyperextension and has a fixed ankle equinus deformity of 30° . He has no active motors about the knee or ankle. Which of the following methods will provide knee stability and pain relief?
Explanation
REFERENCE: Michael JW: Lower limb orthoses, in Goldberg B, Hsu JD (eds): Atlas of Orthoses and Assistive Devices. St Louis, MO, Mosby, 1997, pp 209-224.
Question 7
A 38-year-old woman is polytraumatized in a motor vehicle crash. She has multiple injuries including a unilateral femur fracture. The patient is felt to be borderline and, although she is currently stable, she could potentially deteriorate quickly. Which of the following parameters has been suggested as an indicator of which patients would benefit from damage control?
Explanation
Question 8
A 20-year-old football player has repeated episodes of heat cramps during summer training sessions. A deficiency of what electrolyte is most responsible for heat cramps?
Explanation
REFERENCES: Bergeron MF, Armstrong LE, Maresh CM: Fluid and electrolyte losses during tennis in the heat. Clin Sports Med 1995;14:23-32.
Halpern B: Fluid and electrolyte replacement in athletes. Sports Med Digest 1994;16:1-5.
Question 9
What nerve is most at risk during placement of the anterolateral portal in elbow arthroscopy?
Explanation
REFERENCES: O’Driscoll SW, Morrey BF: Elbow arthroscopy, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 21-34.
Field LD, Altchek DW, Warren RF, O’Brien SJ, Skyhar MJ, Wickiewicz TL: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Question 10
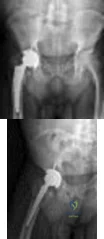
A 70-year-old man undergoes removal of an infected total hip arthroplasty (THA) and insertion of an articulating antibiotic-loaded spacer to treat a deep periprosthetic hip infection. While in a nursing home receiving intravenous antibiotics 3 weeks after surgery, the patient trips and falls. Examination reveals swelling in the mid and distal thigh, intact skin and neurovascular structures, and severe pain with knee or hip movement. Radiographs of the femur are shown in Figures 1 through 4. What is the most appropriate treatment for the fracture below the implant?
Explanation
This patient has a type C periprosthetic femoral fracture. The articulating spacer is not involved in the fracture, which is well distal to the implant. The most appropriate treatment is open reduction and internal fixation of the fracture. Traction is not appropriate for this fracture because the injury can be treated surgically despite the history of previous hip infection. Traction would also be needed for at least 5 weeks and would delay the surgical treatment of the periprosthetic fracture until the time of second-stage revision THA. The fracture is fairly distal, and revision to a longer antibiotic-loaded implant or uncemented stem is not suitable for this fracture pattern, because it extends well past the isthmus. A femoral stem in the distal fragment would provide little stability for the fracture. Removal of the articulating spacer and reimplantation using a long-stem fluted uncemented hip replacement is not appropriate, because it would be premature to reimplant the man's hip while he is still receiving treatment for a deep hip infection.
Question 11
Figure 9 shows a cross-sectional view of the spinal cord at the lower cervical level. Injury to the structure indicated by the black arrow will lead to what neurologic deficit?
Explanation
REFERENCES: Bohlman H, Ducker T, Levine A: Spine trauma in adults, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 911.
Northrup B: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, p 545.
Question 12
A 20-year-old patient has foot pain. A radiograph and T 1 -weighted MRI scan are shown in Figures 8a and 8b. A biopsy specimen is shown in Figure 8c. Treatment should consist of
Explanation
REFERENCES: Dahlin DC, Unni KK: Bone Tumors: General Aspects and Data on 8,542 Cases. Springfield, IL, Charles C. Thomas, 1986.
Gitelis S, Mallin BA, Piasecki P, Turner F: Intralesional excision compared with en bloc resection for giant cell tumor of bone. J Bone Joint Surg Am 1993;75:1648-1655.
Question 13
Radiographs of a pediatric patient reveal a suspected osteosarcoma of the distal femur. Additional staging studies should consist of
Explanation
REFERENCE: O’Reilly R, Link M, Fletcher B, et al: NCCN pediatric osteosarcoma practice guidelines: The National Comprehensive Cancer Network. Oncology (Huntingt) 1996;10:1799-1806, 1812.
Question 14
A 47-year-old woman has a painful bunion of the right foot, and shoe wear modifications have failed to provide relief. Examination reveals a severe hallux valgus with dorsal subluxation of the second toe. Radiographs are shown in Figures 14a and 14b. The most appropriate management should include
Explanation
REFERENCE: Mann RA, Rudicel S, Graves SC: Repair of hallux valgus with a distal soft-tissue procedure and proximal metatarsal osteotomy: A long-term follow-up. J Bone Joint Surg Am 1992;74:124-129.
Question 15
A 45-year-old female returns to your clinic with 10-weeks of severe pain that starts in her back and extends down her right leg to the top of her foot. On physical exam she has decreased sensation on the dorsal aspect of her foot and 4/5 strength in her EHL. She has a positive straight leg raise on the right. The remaining physical exam is unremarkable, including normal achilles and patellar reflexes bilaterally, no clonus, and a down-going Babinski sign. Her pain has not been relieved by NSAIDs, epidural steroids or physical therapy. Figure A is a sagittal MRI and figure B is a axial MRI through the L4/5 disc space. What is the best treatment option at this time? Review Topic

Explanation
Patients with paracentral herniated lumbar discs present with radicular pain affecting the traversing (caudal) nerve root. Unless the patient develops progressive neurologic decline, patients with herniated lumbar discs should undergo no less than 6 weeks of conservative treatment consisting of anti-inflammatory medications, rest and therapy. Most patients improve with nonoperative modalities. If appropriate conservative care fails, the correct surgical option is a unilateral microdiscectomy.
In the Spine Patient Outcomes Research Trial (SPORT) Weinstein et al. reported on the results of 501 patients with herniated lumbar discs who had failed at least six weeks of non-operative care. The patients were randomized to operative or nonoperative care, however there was a high amount of crossover between the two groups. Because of this, there was no difference reported between the two groups at final follow-up using an intent-to-treat analysis.
Weinstein et al., because of the flaws with the intent-to-treat analysis, also published an observational study on 528 patients who received surgery and 191 who received nonoperative care for a herniated lumbar disc. They reported that while both groups had an improvement from baseline, at two years, patients who elected to undergo surgery had significantly better outcomes than those who chose conservative care.
Lurie et al. reported the eight-year results from the observational group of the SPORT data, and found that the patients who underwent surgery continued to have statistically superior outcomes compared to those who underwent conservative care at long-term follow-up.
Figure A is a T2 sagittal MRI of the lumbar spine demonstrating a right sided L4/5 disc herniation, and Figure B is an axial image again demonstrating a paracentral L4/5 disc herniation.
Incorrect answers:
Question 16
A 72-year-old man with a history of Parkinson’s disease, stable coronary artery disease, and mild renal insufficiency is seen for hip arthroplasty. Which of the following is considered the most appropriate bearing of choice?
Explanation
REFERENCES: Bragdon CR, Greene ME, Freiberg AA, et al: Radiostereometric analysis comparison of wear of highly cross-linked polyethylene against 36- vs 28-mm femoral heads. J Arthroplasty 2007;22:125-129.
MacDonald SJ: Metal-on-metal total hip arthroplasty: The concerns. Clin Orthop Relat Res 2004;429:86- 93.
Question 17
Which of the following vertebrae has the smallest pedicle isthmic width in a nondeformity patient?
Explanation
REFERENCE: Ofiram E, Polly DW, Gilbert TJ Jr, et al: Is it safe to place pedicle screws in the lower thoracic spine than in the upper lumbar spine? Spine 2007;32:49-54.
Question 18
A 71-year-old woman undergoes a posterior lumbar decompression and fusion from L4-S1. Thirty-six hours after the procedure, she reports severe right-sided chest pain and shortness of breath. Doppler ultrasound reveals a clot proximal to the knee within the femoral vein. A large pulmonary embolus is confirmed by CT angiography. The next most appropriate step in management should consist of
Explanation
REFERENCES: Cain JE Jr, Major MR, Lauerman WC, et al: The morbidity of heparin therapy after development of pulmonary embolus in patients undergoing thoracolumbar or lumbar spinal fusion. Spine 1995;20:1600-1603.
Roberts AC: Venous imaging and inferior vena cava filters. Curr Opin Radiol 1992;4:88-96.
Becker DM, Philbrick JT, Selby JB: Inferior vena cava filters. Arch Intern Med
1992;152:1985-1994.
Question 19
Compared to metal-on-polyethylene total hip bearing surfaces, the debris particles generated by metal-on-metal articulations are
Explanation
metal-on-metal articulations in total hip arthroplasty are several orders of magnitude smaller
and may be up to 100 times more numerous than those found with metal-on-polyethylene articulations.
REFERENCES: Davies AP, Willert HG, Campbell PA, et al: An unusual lymphocytic perivascular infiltration in tissues around contemporary metal-on-metal joint replacements.
J Bone Joint Surg Am 2005;87:18-27.
Firkins PJ, Tipper JL, Saadatzadeh MR, et al: Quantitative analysis of wear and wear debris from metal-on-metal hip prostheses tested in a physiological hip joint simulator. Biomed Mater Eng 2001;11:143-157.
Question 20
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. Treatment should include

Explanation
Question 21
A 9-year-old child sustains a proximal tibial physeal fracture with a hyperextension mechanism. What structure is at most risk for serious injury?
Explanation
REFERENCE: Beaty JH, Kasser JR: Rockwood and Wilkins Fractures in Children. Philadelphia, PA, JB Lippincott, 2006, p 961.
Question 22
Figures 57a and 57b are the MRI scans of a 61-year-old man who is unable to elevate his dominant arm following a golf injury 24 hours ago. He has moderate pain during attempted arm elevation. Examination reveals significant spinati atrophy and he is only able to elevate his arm fully overhead while supine. The neurologic examination is normal. What is the next most appropriate step in management? Review Topic

Explanation
Question 23
Which of the following agents increases the risk for a nonunion following a posterior spinal fusion?
Explanation
REFERENCES: Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Martin GJ Jr, Boden SD, Titus L: Recombinant human bone morphogenetic protein-2 overcomes the inhibitory effect of ketorolac, a nonsteroidal anti-inflammatory drug (NSAID), on posterolateral lumbar intertransverse process spine fusion. Spine 1999;24:2188-2193.
Question 24
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity. Postoperative radiographs are shown in Figures 3 and 4. How does the plate function?

Explanation
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
Question 25
What is the most common maxillofacial/dental injury in ice hockey?
Explanation
displacement of the tooth from aleveolar support. A crown fracture is an incomplete loss or fracture of the tooth enamel without loss of the tooth. The other injuries (mandible fracture, lip laceration, tooth
avulsion, and temporomandibular contusion) occur but are not nearly as common.
REFERENCES: Lahti H, Sane J, Ylipaavalniemi P: Dental injuries in ice hockey games and training. Med Sci Sports Exerc 2002;34:400-402.
Minkoff J, Stecker S, Varlotta GP, et al: Ice hockey, in Fu FH, Stone DA (eds): Sports Injuries, ed 2.
Philadelphia, PA, 2001, pp 516-517.
Question 26
A 35-year-old man has profound deltoid weakness after sustaining a traumatic anterior shoulder dislocation 6 weeks ago. Electromyographic (EMG) studies confirm an axillary nerve injury. Follow-up examination at 3 months reveals no recovery of function. What is the best course of action?
Explanation
REFERENCES: Perlmutter GS: Axillary nerve injury. Clin Orthop 1999;368:28-36.
Artico M, Salvati M, D’Andrea V, et al: Isolated lesions of the axillary nerves: Surgical treatment and outcome in twelve cases. Neurosurgery 1991;29:697-700.
Vissar CP, Coene LN, Brand R, et al: The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery: A prospective clinical and EMG study. J Bone Joint Surg Br 1999;81:679-685.
Pasila M, Jarma H, Kiviluoto O, et al: Early complications of primary shoulder dislocations. Acta Orthop Scand 1978;49:260-263.
Question 27
With respect to femoral component design, stress relief osteopenia in the proximal femur following noncemented total hip arthroplasty appears to be most strongly influenced by the
Explanation
Question 28
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?
Explanation
REFERENCES: Robinson CM, Aderinto J: Posterior shoulder dislocations and
fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.
Cicak N: Posterior dislocation of the shoulder. J Bone Joint Surg Br 2004;86:324-332.
Question 29
A 78-year-old athletic woman has a history of severe back pain without antecedent trauma. She was in the emergency department 2 days ago with a T12 compression fracture. A dual x-ray absorptiometry (DEXA) scan performed earlier this year revealed a T-score of -2.8. Her condition may be attributable to
Explanation
The diagnosis is severe osteoporosis because this patient's T-score is lower than -2.5 on DEXA scan and her fragility fracture involves the T12 vertebra. Osteoporosis may be associated with polymorphisms of the COL1A1 gene. EXT1 is associated with multiple hereditary exostoses, and translocation X:18 is associated with synovial sarcoma. The gene p53 is associated with Li-Fraumeni syndrome and osteosarcoma.
RECOMMENDED READINGS
Masoodi TA, Alsaif MA, Al Shammari SA, Alhamdan AA. Evaluation and identification of damaged single nucleotide polymorphisms in COL1A1 gene involved in osteoporosis. Arch Med Sci. 2013 Oct 31;9(5):899-905. doi: 10.5114/aoms.2012.28598. Epub 2012 May 13.
PubMed PMID: 24273577. ? View Abstract at PubMed
Kurt-Sirin O, Yilmaz-Aydogan H, Uyar M, Seyhan MF, Isbir T, Can A. Combined effects of collagen type I alpha1 (COL1A1) Sp1 polymorphism and osteoporosis risk factors on bone mineral density in Turkish postmenopausal women. Gene. 2014 May 1;540(2):226-31. doi: 10.1016/j.gene.2014.02.028. Epub 2014 Feb 22. PubMed PMID: 24566004. ? View Abstract at PubMed
Question 30
A 22-year-old man sustained a shoulder dislocation while playing collegiate football at age 18. Since that time, he has dislocated the shoulder three more times despite physical therapy. His last dislocation occurred 4 weeks ago while sleeping. What is the most appropriate management for this patient? Review Topic
Explanation
Question 31
Figures below show the radiographs, MRI, and MR arthrogram obtained from a 25-year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy.When counseling patients who have a cam deformity, the orthopaedic surgeon should note that
Explanation
Question 32
Figures below demonstrate the radiographs obtained from a 56-year-old man with a 3-year history of right groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?
Explanation
Chronic opioid consumption prior to total joint arthroplasty has been associated with increased pain after surgery, increased opioid requirements, a slower recovery and longer hospital stay, and higher 90-day postoperative complications compared with patients not on chronic opioids preoperatively. Based on this information, Nguyen and associates performed a study in three patient groups that included 1) chronic opioid users who underwent no preoperative intervention, 2) chronic opioid users who were weaned down to 50% of their prior opioid regimen, and 3) patients who were not chronic opioid users. The authors found that the reduction of preoperative opioid use improved postoperative function, pain, and recovery and that the weaned group performed more like the opioid naive group than the chronic opioid user
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to surgery.
Question 33
Figures 1 and 2 are the radiograph and MRI scan of a 16-year-old boy who injured his right knee by a lateral side impact while playing football. The MRI indicates what structure was most likely injured?

Explanation
Question 34
Figure 242 is the anteroposterior radiograph of a 28-year-old man who underwent resection and reconstruction for an Ewing sarcoma. What is the most common functional deficit encountered during rehabilitation?
Explanation

Question 35
-A collegiate offensive football lineman has decreased bench-press strength and shoulder pain as off-season workouts begin. Examination revealed no atrophy, and deltoid and rotator cuff strength testing findings were normal. Translational testing was difficult to achieve because of his large size.Apprehension and relocation test findings were negative. An O’Brien’s active compression test result was negative. Jerk testing was positive on the affected side. Which diagnosis is most likely revealed on an MRI arthrogram?
Explanation
Question 36
A 35-year-old construction worker sustained a midshaft clavicle fracture that developed a hypertrophic nonunion. One year after the injury, it was internally fixed without bone graft. Four months after the surgery he was asymptomatic and he was released to full activity. Five months following surgery, the patient was digging a ditch and he felt pain in the clavicle. The 4-month and 5-month postoperative radiographs are shown in Figures 117a and 117b. What is the most likely cause of this failure? Review Topic
Explanation
Question 37
Figure 6 shows the radiograph of a 14-year-old baseball player who felt a pop and had an immediate onset of pain in his elbow after a hard throw from the outfield. The best course of action should be to
Explanation
REFERENCES: Case SL, Hennrikus WL: Surgical treatment of displaced medial epicondyle fractures in adolescent athletes. Am J Sports Med 1997;25:682-686.
Woods GW, Tullos HS: Elbow instability and medial epicondyle fractures. Am J Sports Med 1977;5:23-30.
Question 38
The patient undergoes right hip arthroscopy. During placement of a standard anterior portal, the 2 structures most at risk for iatrogenic injury are the
Explanation
The clinical scenario describes a young man with a painful hip joint related to femoroacetabular impingement (FAI) based on his history of pain with prolonged sitting and the examination findings of pain and limited internal rotation, flexion, and adduction. Plain radiographs confirm the diagnosis and show decreased head-neck offset or a CAM deformity. Epidemiologic studies have shown that the most common abnormal morphology is a combined CAM/pincer deformity. In isolated CAM deformities, the most consistent finding is separation between the acetabular cartilage and labrum. The “alpha angle” is the angle between the midline of the femoral neck and a line from the center of the femoral head to the point at which the femoral head becomes aspherical. It can be measured on either a lateral radiograph of the femoral neck or on an axial cut of cross-sectional imaging (a CT scan or MR image). It is used to quantify the degree of asphericity at the anterior head-neck junction. Cadaveric studies have
shown that placement of a standard anterior portal during hip arthroscopy is closest to the LFCN and femoral neurovascular bundle.
Question 39
Which of the following clinical scenarios represents an appropriate indication for convex hemiepiphysiodesis/hemiarthrodesis in the treatment of a child with a congenital spinal deformity?
Explanation
REFERENCE: Winter RB, Lonstein JE, Denis F, Sta-Ana de la Rosa H: Convex growth arrest for progressive congenital scoliosis due to hemivertebrae. J Pediatr Orthop 1988;8:633-638.
Question 40
An Asian 45-year-old man has bilateral upper extremity dysfunction. Figure 35a shows a T2-weighted sagittal MRI scan of the cervical spine, and Figure 35b shows a T2-weighted axial MRI scan at the level of the C3 vertebral body. What is the most likely pathologic process?
Explanation
REFERENCES: McAfee PC, Regan JJ, Bohlman HH: Cervical cord compression from ossification of the posterior longitudinal ligament in non-orientals. J Bone Joint Surg Br 1987;69:569-575.
Kricun R, Kricun ME: MRI and CT of the Spine. New York, NY, Raven Press, 1994,
pp 126-130.
Question 41
When performing a long fusion to the sacrum in an osteopenic patient in whom optimal sagittal balance is restored, which of the following is a benefit of extending the distal fixation to the pelvis, rather than the sacrum alone?
Explanation
REFERENCE: Hu SS, Berven SH, Bradford DS: Adult spinal deformity, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 465-477.
Question 42
Primary chondrosarcoma of bone most commonly occurs in which of the following locations?
Explanation
REFERENCES: Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Simon M, Springfield D, et al: Chondrosarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 276.
Question 43
- A 40-year old man has limited, painful motion in dorsiflexion at the metatarsophalangeal (MTP) joint of the right great toe, despite nonsurgical treatment. Radiographs show dorsal and medial osteophytes and minimal narrowing of the articular space. Treatment should consist of
Explanation
Question 44
What structure is considered the single most important soft-tissue restraint to anterior-posterior stability of the sternoclavicular joint?
Explanation
REFERENCES: Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Rockwood CA Jr, Matsen FA III, Jobe CM: Gross Anatomy of the Shoulder. Philadelphia, PA, WB Saunders, 1998.
Question 45
..First-line treatment recommendations include
Explanation
Ultrasound
MRI scan of the thigh
Chest CT scan and whole-body bone scan
Positron emission tomography (PET) scan
Presurgical radiation therapy
Marginal resection
Radical resection and postsurgical radiation
Transverse incision centered over the mass
Incision centered over the mass in line with long axis of limb
Sentinel node biopsy
Core needle biopsy
For each soft-tissue mass clinical scenario or question below, match the most appropriate next evaluation or treatment step listed above.
Question 46
What is the primary indication for performing an arthroscopic synovectomy on a patient with hemophilia that is the result of factor VIII deficiency? Review Topic
Explanation
Question 47
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits.The patient undergoes successful primary THA with a metal-on-metal bearing. At 1-year follow-up, she reports no pain and is highly satisfied with the procedure. However, 3 years after the index procedure, she reports atraumatic right hip pain that worsens with activities. Radiographs reveal the implants in good position with no sign of loosening or lysis. An initial laboratory evaluation reveals a normal sedimentation rate and C-reactive protein (CRP) level. The most appropriate next diagnostic step is

Explanation
metal-on-metal articulation is associated with excellent wear rates in vitro. Because it offers a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions—including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis after the possible transfer of metal ions across the placental barrier—make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.The work-up of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including the erythrocyte sedimentation rate, C-reactive protein (CRP) level, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging, including MRI with MARS, should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following a revision of failed metal-on-metal hip replacements.
Question 48
Which of the following statements best describes the anatomy of the sartorial branch of the saphenous nerve during medial meniscal repair?
Explanation
REFERENCES: Dunaway DJ, Steensen RN, Wiand W, et al: The sartorial branch of the saphenous nerve: Its anatomy at the joint line of the knee. Arthroscopy 2005;21:547-551.
Rodeo SA: Arthroscopic meniscal repair with use of the outside-in technique. Instr Course Lect 2000;49:195-206.
Question 49
Which of the following is considered an advantage of metal femoral heads compared with ceramic heads?
Explanation
REFERENCE: Cook SD: Materials consideration in total joint replacement, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 27-33.
Question 50
Figure 14 is a sagittal-cut MR image from the hindfoot of a 54-year-old woman who has had plantar heel pain for 3 months. There is no history of trauma. Her pain is worse when she rises and at the end of the day. Upon examination she has localizable tenderness over the plantar medial tubercle of the calcaneus. The Achilles is intact and nontender, and subtalar joint motion is full and painless. A Tinel test result is negative. What is the most likely diagnosis?

Explanation
Plantar fasciitis is inflammation of the plantar fascia at its insertion onto the medial calcaneus. The T2-weighted sagittal MR image reveals thickening of the plantar fascia with no evidence of a calcaneal stress fracture, coalition, or inflammation of the insertion of the Achilles tendon.
RECOMMENDED READINGS
Lareau CR, Sawyer GA, Wang JH, DiGiovanni CW. Plantar and medial heel pain: diagnosis and management. J Am Acad Orthop Surg. 2014 Jun;22(6):372-80. doi: 10.5435/JAAOS-22-06-
Question 51
A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time?
Explanation
REFERENCES: Findlay JM: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;39:210.
Dickman CA, Mamourian A, Sonntag VK, et al: Magnetic resonance imaging of the transverse atlantal ligament for the evaluation of atlantoaxial instability. J Neurosurgery 1991;75:221-227.
Question 52
Osteophyte formation at the posteromedial olecranon and olecranon articulation in high-caliber throwing athletes is most often the result of underlying
Explanation
REFERENCES: Conway JE, Jobe FW, Glousman RE, Pink M: Medial instability of the elbow in throwing athletes: Treatment by repair or reconstruction of the ulnar collateral ligament. J Bone Joint Surg Am 1992;74:67-83.
Wilson FD, Andrews, JR, Blackburn TA, McCluskey G: Valgus extension overload in the pitching elbow. Am J Sports Med 1983;11:83-88.
Question 53
Figures 163a through 163c show the radiograph and MRI scans of a 45-year-old woman with severe right arm pain. She has had symptoms for 6 months without resolution despite multiple nonsurgical treatments. Examination reveals weakness in the right triceps and wrist flexors with decreased sensation in the middle finger and a positive Spurling's sign. What is the most appropriate treatment for the patient's symptoms? Review Topic

Explanation
Question 54
What type of exercise is used early in the rehabilitation process to safely stimulate co-contraction of the scapular and rotator cuff muscles? Review Topic
Explanation
Question 55
Figure 10 shows the radiograph of an 18-year-old woman who sustained a spinal cord injury in a motor vehicle accident. Based on the radiographic findings, her injury is best described as
Explanation
REFERENCE: Allen BL Jr, Ferguson RL, Lehmann TR, O’Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
Question 56
Which of the following statements is true regarding the superomedial fragment of an intra-articular calcaneus fracture?

Explanation
Question 57
In a polytraumatized patient with a high lactate level, large base deficit, and pulmonary injury, what is the best initial treatment for a femoral shaft fracture?
Explanation
intramedullary nails in the acute setting is to be avoided because of the possibility of increasing the patient's morbidity. Plating is time consuming and leads to blood loss which should be avoided in the severely injured patient. Skeletal traction and supine positioning are detrimental in the trauma patient. Expedient external fixation, resuscitation, and later definitive treatment with an intramedullary nail is considered to be the best choice for the polytraumatized patient with a femoral shaft fracture.
Question 58
A 13-year-old boy was evaluated for leg length difference. His pelvis balanced when a 1-inch (2.54 cm) block was placed under his left foot. History revealed he had a left distal femur physeal fracture treated with casting at age 10. Radiographs show normal limb alignment, but his left distal femoral physis is closed and his left femur is 2.5 cm shorter than the right. All other physes are open. His bone age is equal to his chronologic age. What surgical treatments will best equalize his discrepancy? Review Topic
Explanation
Question 59
An 18-year-old man sustains an injury to his lateral ankle after being kicked while playing soccer. He reports persistent pain on the lateral ankle as well as a popping sensation with attempted ankle dorsiflexion and eversion. Which of the following structures anatomically restrains the retracted structure shown in Figure 12?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 81-89.
Sarrafian S: The Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 113-158.
Question 60
Figures 11a and 11b show the radiographs of a 50-year-old man who was struck by a car. Treatment should consist of
Explanation
REFERENCES: Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 97-108.
Asnis SE, Wanek-Sgaglione L: Intracapsular fractures of the femoral neck: Results of cannulated screw fixation. J Bone Joint Surg 1994;76A:1793-1803.
Question 61
Based on the current available best-evidence, what postoperative activities should be recommended for patients undergoing first-time lumbar diskectomy for disk herniation? Review Topic
Explanation
Ostelo et al., in a Cochrane review update, demonstrated that exercise programs starting 4 to 6 weeks after surgery in patients undergoing first-time lumbar diskectomy for disk herniation lead to a faster decrease in pain and disability than no rehabilitation. Additionally, high-intensity exercise programs seem to lead to a faster decrease in pain and disability than low-intensity programs.
Carragee et al., in a prospective review of 50 consecutive patients undergoing first-time lumbar diskectomy for disk herniation, demonstrated that lifting of postoperative activity restrictions after limited diskectomy allowed shortened sick leave without increased complications. He concluded that postoperative precautions in these patients may not be necessary.
Question 62
What is the most likely complication following treatment of the humeral shaft fracture shown in Figure 6?
Explanation
REFERENCES: Chapman JR, Henley MB, Agel J, et al: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
McCormack RG, Brien D, Buckley RE, et al: Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail: A prospective, randomised trial. J Bone Joint Surg Br 2000;82:336-339.
Question 63
Figures 80a and 80b are the radiographs of a 21-year-old football player who underwent anterior cruciate ligament (ACL) reconstruction with patellar tendon autograft 1 year ago. He reports mild stiffness in his knee. Upon examination, he has a negative Lachman test result, trace effusion, and range of motion from 0 to 85 degrees of knee flexion. Which factor is most contributory to his examination findings?
Explanation
Technical failure is the most common reason for ACL reconstruction failure. Tunnel position is the most frequent cause of technical failure. Malpositioning of the tunnel affects the length of the graft, causing either decreased range of motion or increased graft laxity. This patient has anterior and vertical placement of his femoral tunnel, which has been shown to cause stiffness in knee flexion. Although graft choice is an important factor when planning ACL reconstruction, overall outcomes with autograft tissues are fairly similar. Fixation of the graft at the femoral or tibial end is not as important as tunnel position. Fixing the graft in flexion can cause extension loss when isometry is not achieved, but this condition is not touched upon in this scenario.
CLINICAL SITUATION FOR QUESTIONS 81 THROUGH 84
Figures 81a through 81d are the MR images of a 25-year-old man with left knee pain after a motorcycle collision. He has palpable pedal pulses with an ankle-brachial index of 0.95. Neurologic examination findings of the injured extremity are normal.
Question 64
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of
Explanation
50 degrees) with multiple contiguous vertebral wedging and end plate irregularity, all consistent with the diagnosis of Scheuermann’s kyphosis. The patient is skeletally immature; therefore, there is the potential for progression of the kyphotic deformity. Extension bracing has shown efficacy in the treatment of Scheuermann’s kyphosis that measures 50 degrees to 74 degrees, and has actually reduced the curvature permanently in some patients. A thoracolumbosacral orthosis may be used if the apex of kyphosis is at T7 or lower. Indications for surgical treatment are controversial, but spinal fusion most likely should not be considered for a painless kyphosis measuring less than 75 degrees.
REFERENCES: Murray PM, Weinstein SL, Spratt KF: The natural history and long-term follow-up of Scheuermann kyphosis. J Bone Joint Surg Am 1993;75:236-248.
Wenger DR, Frick SL: Scheuermann kyphosis. Spine 1999;24:2630-2639.
Tribus CB: Scheuermann’s kyphosis in adolescents and adults: Diagnosis and management.
J Am Acad Orthop Surg 1998;6:36-43.
Question 65
Which Morton neuroma histology is most common?
Explanation
Morton neuroma is a compressive neuropathy of the interdigital nerves of the forefoot that most commonly is noted in the third web space. Perineural fibrosis is commonly noted on microscopic examination of resected tissue. This accounts for the relatively higher failure rate of neuroma decompression by transection of the intermetatarsal ligament as opposed to resection. Wallerian degeneration is seen following axonal transection in the distal part of the nerve. Distal axonopathy is degeneration of the axon and myelin and is associated with "stocking-glove" distribution neuropathy. Segmental demyelination is characterized by breakdown of myelin with an intact axon
and is associated with lead poisoning and hereditary sensory motor neuropathy.
RECOMMENDED READINGS
Akermark C, Crone H, Saartok T, Zuber Z. Plantar versus dorsal incision in the treatment of primary intermetatarsal Morton's neuroma. Foot Ankle Int. 2008 Feb;29(2):136-41. doi: 10.3113/FAI.2008.0136. PubMed PMID: 18315967.View Abstract at PubMed
Ha'Eri GB, Fornasier VL, Schatzker J. Morton's neuroma--pathogenesis and ultrastructure. Clin Orthop Relat Res. 1979 Jun;(141):256-9. PubMed PMID: 477115. View Abstract at PubMed
Graham CE, Graham DM. Morton's neuroma: a microscopic evaluation. Foot Ankle. 1984 Nov-Dec;5(3):150-3. PubMed PMID: 6519606. View Abstract at PubMed
Question 66
A 12-year-old boy reports limping and chronic knee pain that is now inhibiting his ability to participate in sports. Clinical examination and radiographs of the knee are normal. Additional evaluation should include Review Topic
Explanation
Question 67
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms? Review Topic

Explanation
Question 68
A 55-year-old man underwent cementless total hip arthroplasty for advanced painful osteoarthritis of the hip 2 years ago. The follow-up radiograph shown in Figure 30 shows
Explanation
REFERENCES: Engh CA, Massin P, Suthers KE: Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop 1990;257:107-128.
Vresilovic E, Hozack WJ, Rothman RH: Radiographic assessment of cementless femoral components: Correlation with intraoperative mechanical stability. J Arthroplasty 1994;9:137-141.
Question 69
Figure 109 is the radiograph of an 11-year-old boy who felt a snap in his right hip while jumping hurdles during track practice yesterday. He complains of pain to his right groin region and is walking with a limp. What physical examination test will cause the patient to experience the most discomfort?

Explanation
Question 70
A B C Figures 30a through 30c are the radiograph and MR images of a 54-year-old woman who has severe leg pain with walking. Her treatment has included 12 weeks of physical therapy, anti-inflammatory medications, and narcotic pain relievers, and she is interested in surgery. Minimally invasive transforaminal lumbar interbody fusion (MIS TLIF) is recommended. When compared with open TLIF, MIS TLIF is associated with

Explanation
MIS TLIF involves a steep learning curve but is associated with similar longterm outcomes as open TLIF, arguably comparable or possibly lower complication rates, and equivalent fusion rates. The major distinguishing feature comparing open to minimally invasive surgery for this and other spinal diagnoses has been shorter hospital stays.
RECOMMENDED READINGS
Peng CW, Yue WM, Poh SY, Yeo W, Tan SB. Clinical and radiological outcomes of minimally invasive versus open transforaminal lumbar interbody fusion. Spine (Phila Pa 1976). 2009 Jun 1;34(13):1385-9. doi: 10.1097/BRS.0b013e3181a4e3be. PubMed PMID: 19478658. View
Abstract at PubMed
Lee KH, Yue WM, Yeo W, Soeharno H, Tan SB. Clinical and radiological outcomes of open versus minimally invasive transforaminal lumbar interbody fusion. Eur Spine J. 2012 Nov;21(11):2265-70. doi: 10.1007/s00586-012-2281-4. Epub 2012 Mar 28. PubMed PMID:
Question 71
-If a physician elects to shorten a femur by 4 cm for traumatic bone loss treatment and places an intramedullary nail for fixation, which deformity will be created in the lower extremity?
Explanation

Question 72
The load versus deformation curve of the functional spinal unit (FSU) is made up of the neutral zone, the elastic zone, and the plastic zone. What is the plastic zone of the curve believed to represent?
Explanation
REFERENCES: Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 15-23.
Panjabi MM, White AA: Physical properties and functional biomechanics of the spine, in White AA, Panjabi MM: Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 1-83.
Question 73
Trabecular bone is remodeled through the formation of
Explanation
Question 74
Figure 1 shows a patient with an open tibia fracture who presents to the emergency department after a propeller injury in brackish water (river water and sea water). What is the most appropriate antibiotic coverage for this patient?

Explanation
soil-borne pathogens (clostridial species). Vancomycin is not indicated for coverage in marine environments, rather it is more commonly used for populations with a high prevalence of nosocomial infections. Sulfamethoxazole-trimethoprim is not used for open fracture coverage.
Question 75
Figure 17 is the radiograph of a 3-year-old girl who has shoulder pain after a fall. What is the best next step?
Explanation
Patients with a pathologic fracture of a unicameral bone cyst or simple bone cyst should first pursue nonsurgical treatment and 4 to 6 weeks of immobilization. Spontaneous healing occurs in fewer than 10% of patients, possibly due to cyst decompression. The most appropriate form of surgical treatment is controversial. Many substances have been injected with variable results. Injection with steroid, bone marrow, demineralized bone matrix, and calcium phosphate/calcium sulfate have been attempted. Curettage and bone grafting and
decompression have been attempted. Indications for treatment are based on cyst size, symptoms, and location. Unicameral bone cysts typically resolve as patients reach skeletal maturity.

CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 23
Figure 18 is the lateral radiograph of the lumbar spine of an 11-year-old boy who has had lower back pain for 2 months. There is no history of injury. He denies radiating pain to his legs, numbness, weakness, and bowel or bladder changes. His usual activities include soccer practices and games 3 to 5 times per week. He has used over-the-counter anti-inflammatory medications, but has had no other treatment.
Question 76
A 12½-year-old boy reports intermittent knee pain and limping that interferes with his ability to participate in sports. He actively participates in football, basketball, and baseball. He denies any history of injury. Examination shows full range of motion without effusion. Radiographs reveal an osteochondritis dissecans (OCD) lesion on the lateral aspect of the medial femoral condyle. MRI scans are shown in Figures 14a and 14b. Initial treatment should consist of Review Topic
Explanation
Cessation of sport activities for 4 to 6 months may allow healing of the lesion. Surgical treatment of juvenile OCD lesions is reserved for unstable lesions, patients
who have not shown radiographic evidence of healing and are still symptomatic after
6 months of nonsurgical management, or patients who are approaching skeletal maturity. Good results with stable in situ lesions that have failed to respond to nonsurgical management have been reported with both transarticular and retroarticular drilling. Results after excision alone are poor at 5-year follow-up, and it is unclear if microfracture will improve the long-term outcome. Mosaicplasty may be the next best option for patients who remain or become symptomatic after excision of the fragment and microfracture.
Wall et al. reviewed juvenile OCD. They state that JOCD has better potential for healing than adult OCD, but several series have shown up to a 50% failure to heal with nonsurgical techniques. The presence of a loose body is an indication for surgical fixation, drilling or regenerative procedures, depending on the presence/extent of subchondral bone sclerosis and the surgeon's experience.
Figure A and B are coronal MRI images showing a stable appearing JOCD lesion of the medial femoral condyle.
Incorrect
in the first
(SBQ13PE.9) A 6-year-old boy complains of a 'clunking' sensation in his left knee. He has no associated pain and denies trauma. He can elicit the sensation when moving his knee from flexion into full extension. He is otherwise healthy, with no birth or developmental issues. On examination, there is a palpable clunk felt over the anterior knee through range of motion. There is no obvious instability or tenderness and he had normal patellar tracking. An AP radiograph of the knee is shown in Figure A. What would be the most likely diagnosis? Review Topic

Agenesis of the anterior cruciate ligament
Thickened medial plica
Grade IV chondral flap
Pigmented villonodular synovitis
Abnormal meniscal morphology
This child presents with an asymptomatic click in the knee. It is associated with widening of the lateral joint space of the knee on X-ray. These features are highly suggestive of a discoid lateral meniscus in this age category.
The principal diagnostic feature of a discoid meniscus is the complaint of snapping or clicking in the knee. Children are usually asymptomatic. Although, less frequently, children may present with pain that is largely secondary to an underlying meniscal tear. MRI scans of the knee have show to have the greatest sensitivity for identifying discoid menisci. The presence of a contiguous central meniscus on three consecutive slices is usually indicative of the diagnosis. Treatment is mostly focused on conservative modalities. Surgical intervention is reserved for symptomatic cases with recurrent locking, swelling or persistent pain is present in older children.
Kramer et al. looked at the presentation of pediatric knee pain. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the discoid meniscus.
Figure A shows an AP radiograph of a pediatric knee. There is an increased lateral joint space suggestive of a discoid meniscus.
Illustrations A-C show an MRI of the knee with 3 consecutive coronal cuts showing an abnormal appearing discoid meniscus.
Incorrect Answers:
Question 77
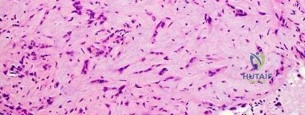
A 54-year-old woman reports worsening pain in her buttock, especially when sitting for long periods of time. She has occasional pain and paresthesias radiating down her posterior leg. She has no significant medical history. MRI scans are shown in Figures 15a and 15b and a biopsy specimen is shown in Figure 15c. What is the most likely diagnosis?
Explanation
REFERENCES: Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 1135-1136
Menendez LR: Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 251.
Question 78
A 61-year-old woman has increasing pain in her left great toe. She states that she has had discomfort for years but now has pain with all shoe wear. A radiograph is shown in Figure 35. To provide the most predictable pain-free result, treatment should consist of
Explanation
REFERENCES: Mann RA: Disorders of the first metatarsophalangeal joint. J Am Acad Orthop Surg 1995;3:34-43.
Coughlin MJ, Abdo RV: Arthrodesis of the first metatarsophalangeal joint with Vitallium plate fixation. Foot Ankle Int 1994;15:18-28.
Question 79
Which of the following genetic disorders has an X-linked recessive inheritance pattern?
Explanation
linked recessive disorders occur when a mutation occurs on the X chromosome that causes the phenotype to be expressed in males and in females who are homozygous for the gene mutation. These disorders are much more common in males since they only have one X chromosome. Other X-linked recessive disorders include: Duchenne muscular dystrophy, Becker's muscular dystrophy, Hunter's syndrome, and spondyloepiphyseal dysplasia (SED) tarda.
Vanderhave et al. reviewed the orthopaedic consideration in patients with hemophilia. Amongst other things, they discuss arthroplasty in patients with this condition. While they are at higher risk for stiffness and acute hemarthrosis following total knee arthroplasty, ~90-95% of patients have good or excellent results.
Illustration A shows how hemophilia is inherited through a punnett square. Illustration B shows how a weak clotting mechanism causes increased bleeding in patients with hemophilia.
Incorrect Answers:
Question 80
Figures 12a through 12e show the radiograph, MRI scans, and biopsy specimens of a 17-year-old boy. What is the most likely diagnosis?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999,
pp 247-263.
Question 81
Use of titanium elastic nailing for treatment of pediatric femur fractures is associated with a higher complication rate among
Explanation
Studies of titanium elastic nailing for femur fractures demonstrated a higher rate of complications, including angular deformity and construct failure, among patients weighing more than 50 kg (100 pounds). Other methods of fixation are recommended for these patients. Flexible nails are not commonly needed, but they also are not associated with a higher complication rate in children younger than age 6.5. Titanium elastic nailing works well in closed or minimally open transverse midshaft fractures, even in the setting of early or immediate weight bearing.

Video 8a
Video 8b
Question 82
The illustration shown in Figure 19 shows a Chamberlain line. What is the most likely diagnosis?
Explanation
REFERENCES: Wiesel SW, Rothman RH: Occipito-atlantal hypermobility.
Spine 1979;4:187-191.
Clark CR: The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 50-51.
Question 83
Decreased sun exposure leads to decreased bone health via what mechanism?
Explanation
Question 84
An 82-year-old man is seen in consultation after being admitted for a fall from ground level. There was no loss of consciousness and the patient recalls striking his head and sustaining a hyperextension-type injury to the cervical spine. Examination reveals an 8-cm head laceration with only mild axial neck tenderness. He has generalized weakness throughout the upper extremities and maintained motor function of the lower extremities. There are no obvious sensory deficits, and the bulbocavernous reflex and deep tendon reflexes are maintained. What is the most appropriate diagnosis at this time? Review Topic
Explanation
(SBQ13PE.25) A 7-year-old girl presents with a early onset scoliosis as seen in the PA radiograph in Figure A. Images do not demonstrate any vertebral anomalies. Physical exam shows normal neurologic function in her lower extremities. An MRI of the spinal axis should be obtained to rule out all of the following pathologies EXCEPT: Review Topic

Atlantoaxial rotatory instability
Syringomyelia
Spinal cord tumor
Dysraphism
Tethered cord
Early-onset scoliosis is associated with syringomyelia, spinal cord tumor, dysraphism, and tethered cord, and therefore they must be ruled out with a preoperative MRI. There is no association between early-onset scoliosis and atlantoaxial rotatory instability.
Early-onset scoliosis can be classified as idiopathic, neuromuscular, or congenital. For this patient without bony or neurologic abnormalities, it would likely be diagnosed as juvenile (bewteen ages 3 and 10 years) idiopathic scoliosis. Commonly associated spinal pathologies (even in patients with no radiographic or neurologic abnormalities) include syringomyelia, spinal cord tumor, dysraphism, tethered cord, and Arnold-Chiari malformation. Before considering any surgical intervention, such as a growing rod construct, these intra-spinal conditions must be ruled-out with an MRI of the spinal axis.
Gillingham et al. present a review of the etiology, diagnosis, and management of early-onset scoliosis. They cite other studies that demonstrated rates as high as 21% of patients with early-onset scoliosis and a normal neurologic exam having occult spinal pathology such as those mentioned above. They recommend MRI for patients with early-onset scoliosis measuring greater than 20° prior to any surgical intervention.
Figure A is a PA radiograph of a skeletally immature patient with a 90° right thoracic curve. Illustration A is an PA radiograph of the same patient after treatment with a growing-rod construct and correction of the scoliotic curve to 46°.
Incorrect Answers:
Question 85
What nerve is most likely to develop a traumatic neuroma following open reducation and internal fixation of a talar neck fracture via a posterolateral approach?
Explanation
REFERENCES: Swanson TV, Bray TJ, Holmes GB Jr: Fractures of the talar neck: A mechanical study of fixation. J Bone Joint Surg Am 1992;74:544-551.
Lawrence S, Botte M: The sural nerve of the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
Question 86
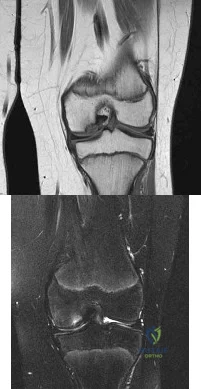
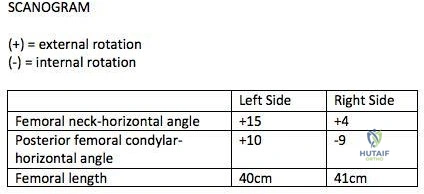
A 26-year-old male underwent statically locked intramedullary nail fixation for a comminuted left femur fracture. An early post-operative computed tomography (CT) scanogram was taken to check rotational alignment, as shown in Figure A. What would be the next best step in the management of this patient?
Explanation
>15 degrees and symptomatic. Therefore, the most appropriate next step would be to continue with postoperative observation and close follow-up.
The primary purpose of CT scanogram is to measure the angle of rotation of the femoral neck relative to the femoral condyle. To do this, the right and left femurs must be scanned together using a 5mm helical slice scanner at the hip and knee. The first slice should reveal the alignment of the femoral neck, so as to allow for measurement of the femoral neck-to-horizontal (FNH) angle. The second slice should reveal the alignment of the posterior femoral condyles. This allows measurement of the posterior condyle-to-horizontal (PCH) angle. Finally, to calculate the rotational alignment (RA), the FNH angle and PCH angles are subtracted (e.g., RA = FNH -PCH). Normal RA is usually +5 to +20 degrees, which is also referred to as 5 to 20 degrees of femoral anteversion.
Lindsey et al. reviewed femoral malrotation following intramedullary nail fixation. They showed the incidence of rotational malalignment was ~28%. Normal femoral neck anteversion (angle of the femoral neck relative to the transverse axis through the femoral condyles) is ~11-13°. However, they noted that some patients have up to 15° difference in rotation in native limbs. Therefore <15 degrees of rotational difference after fixation is considered acceptable.
Gugala et al. examined the long-term functional implications for patients with iatrogenic femoral malrotation following femoral intramedullary nail fixation. They
showed that patients can compensate for even significant femoral malrotation (up to 30 degrees) and tolerate it well. However, external femoral malrotation (more common) appears to be better compensated/tolerated than internal malrotation.
Figure A shows that the left femoral neck is externally rotated (ER) by 15° to the horizontal (ER15). The right femoral neck is externally rotated (ER) by 4° to the horizontal (ER4). The left distal fragment is ER10. The right distal fragment is internally rotated (IR) by 9°. Thus, left femur has a total (ER15)-(ER10)= (+15)-(+10)=(+5), and right femur has (ER4)-(IR9)= (+4)-(-9)=(+13) to the horizontal. Therefore, the difference is 8 degrees.
Incorrect Answers:
>15 degrees and symptomatic.
Question 87
Immobilization with a sling
Explanation
Radiographically Active Cyst (age 4 to 8 years old with pathologic fracture)
Align and immobilize
Observe for spontaneous healing
Reassess after 2 to 4 months and if recurrent, follow procedure for pathological fracture of radiographically active cysts described in the article above.
Question 88
What is the primary intracellular signaling mediator for bone morphogenetic protein (BMP) activity?
Explanation
REFERENCES: Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044.
Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Zuscik MJ, Drissi MH, Reynolds PR, et al: Molecular and cell biology in orthopaedics, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006,
in press.
Question 89
A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had increasing pain and elbow instability. There is no clinical evidence of infection, and radiographs show no new bony process. What is the best option for this patient?
Explanation
REFERENCES: Blaine TA, Adams R, Morrey BF: Total elbow arthroplasty after interposition arthroplasty for elbow arthritis. J Bone Joint Surg Am 2005;87;286-292.
Cheng SL, Morrey FB: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Question 90
A 17-year-old basketball player and pole vaulter who has had anterior knee pain for the past 18 months now reports a recent inability to jump. Based on the MRI scan shown in Figure 11, management should consist of Review Topic

Explanation
Question 91
A 40-year-old man fell 10 feet from a tree and sustained the closed isolated injury shown in Figures 35a and 35b. Management consists of splinting. At his 2-week follow-up visit, he clinically passes the wrinkle test. He agrees to open reduction and internal fixation. What is the best surgical approach to obtain anatomic reduction and limit wound dehiscence?
Explanation
REFERENCES: Borrelli J Jr, Lashgari C: Vascularity of the lateral calcaneal flap: A cadaveric injection study. J Orthop Trauma 1999;13:73-77.
Freeman BJC, Duff S, Allen PE, et al: The extended lateral approach to the hindfoot: An anatomical basis and surgical implications. J Bone Joint Surg Br 1998;80:139-142.
Zwipp H, Tscherne H, Wulker N: Osteosynthesis of dislocated intra-articular calcaneus fractures. Unfallchirurg 1988;91:507-515.
Question 92
Hip pain of month duration has developed in a year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. What is this patient's prognosis for infection resolution?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin- resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was
21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 93
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
REFERENCES: Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 94
..Further imaging shows pulmonary metastases without an obvious primary tumor of origin and an incomplete fracture of the right distal femur. A decision is made to surgically treat his distal femur fracture. What is the role of establishing a preoperative histologic diagnosis for this patient?
Explanation
t(X;18)(p11.2;q11.2)
t(11;22)(q24;q12)
t(1;3)(p36.3;q25)

Question 95
Thyroid hormone regulates skeletal growth at the physis by stimulation of
Explanation
REFERENCES: Ballock RT: Regulation of skeletal growth and maturation by thyroid hormone, in Buckwalter JA, Ehrlich MG, Sandell LJ, Trippel SB (eds): Skeletal Growth and Development: Clinical Issues and Basic Science Advances. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1998, pp 301-317.
Rosier RN, O’Keefe RJ, Reynolds PR, Hicks DG, Puzas JE: Expression and function of TGF-b= and PTHrP in the growth plate, in Buckwalter JA, Ehrlich MG, Sandell LJ, Trippel SB (eds): Skeletal Growth and Development: Clinical Issues and Basic Science Advances. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1998, pp 285-299.
Trippel SB: IGF-I and FGF-2 in growth plate regulation, in Buckwalter JA, Ehrlich MG, Sandell LJ, Trippel SB (eds): Skeletal Growth and Development: Clinical Issues and Basic Science Advances. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1998, pp 263-283.
Question 96
During the first 2 years of life, which of the following actions is most responsible for increasing structural stability of the physis?
Explanation
REFERENCES: Burkus J, Ogden J: Development of the distal femoral epiphysis: A microscopic morphological investigation of the zone of Ranvier. J Pediatr Orthop 1984;4:661-668.
Shapiro F, Holtrop ME, Glimcher MJ: Organization and cellular biology of the perichondrial ossification groove of Ranvier: A morphological study in rabbits. J Bone Joint Surg Am 1977;59:703-723.
Question 97
A 25-year-old man sustained the closed injury shown in Figures 22a and 22b. Examination reveals that this is an isolated injury, and he is hemodynamically stable. Treatment should consist of
Explanation
REFERENCES: Brumback RJ, Virkus WW: Intramedullary nailing of the femur: Reamed versus nonreamed. J Am Acad Orthop Surg 2000;8:83-90.
Brumback RJ, Ellison TS, Poka A, et al: Intramedullary nailing of femoral shaft fractures: Part III. Long-term effects of static interlocking fixation. J Bone Joint Surg Am 1992;74:106-112.
Question 98
Figure 4a shows the radiograph of a 20-year-old man who has an injury to the right shoulder. Figure 4b shows an arthroscopic view (posterior portal). The arrow points to a Review Topic
Explanation
Question 99
Figures below demonstrate the radiographs obtained from a 63-year-old man who had right total hip arthroplasty (THA) 4 months ago. Progressive stiffness began 2 months after surgery, and he now reports pain only after prolonged physical activity. His examination reveals a normal gait and painless range of motion with flexion of 70°, extension of 0°, internal rotation of 20°, external rotation of 20°, abduction of 10°, and adduction of 10°. His erythrocyte sedimentation rate and C-reactive protein level are within defined limits. Physical therapy has produced no benefit. What is the most appropriate next step?
Explanation
Question 100
An 82-year-old woman reports right buttock pain after a car trip. Laboratory studies show an erythrocyte sedimentation rate of 30 mm/h and WBC of 4,600/mm 3 . Figure 34a shows a plain AP radiograph of the pelvis, and Figure 34b shows a delayed technetium Tc 99m bone scan. Management should consist of
Explanation
REFERENCES: Newhouse KE, el-Khoury GY, Buckwalter JA: Occult sacral fractures in osteopenic patients. J Bone Joint Surg Am 1992;74:1472-1477.
Marmor L: Stress fracture of the pubic ramus simulating a loose total hip replacement. Clin Orthop 1976;121:103-104.
