Orthopedic Board Review MCQs: Hip, Shoulder, Fracture & Deformity | Part 184

Key Takeaway
This page presents Part 184 of a comprehensive orthopedic board review. It offers 100 high-yield MCQs in OITE/AAOS format, focusing on Deformity, Fracture, Hip, and Shoulder. Designed for orthopedic surgeons preparing for their AAOS, ABOS, and OITE certification exams, it includes detailed explanations and two learning modes.
About This Board Review Set
This is Part 184 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 184
This module focuses heavily on: Deformity, Fracture, Hip, Shoulder.
Sample Questions from This Set
Sample Question 1: A 6 year-old-boy falls from his bunk bed and suffers the injury seen in Figures A and B. Upon presentation to the emergency room he is noted to have a pink hand with brisk capillary refill, but no palpable pulses. After closed reduction in ...
Sample Question 2: -Which of the following neurovascular structures is at greatest risk during the introduction of acetabular component fixation screws during total hip replacement?...
Sample Question 3: Factors contributing to an increased risk of hip fracture include reduced bone mineral density of the femoral neck, cognitive status of the individual, and...
Sample Question 4: A 35-year-old woman dislocated her right shoulder in a fall from a step stool several months ago. She now reports several painful recurrences. Examination reveals anterior and inferior apprehension that reproduces her symptoms. An MRI scan ...
Sample Question 5: Which of the following would be associated with the spinal deformity shown in Figures 79a and 79b? Review Topic...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
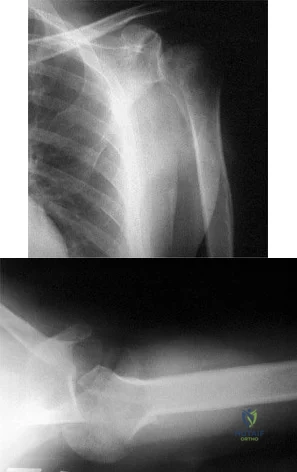
A 6 year-old-boy falls from his bunk bed and suffers the injury seen in Figures A and B. Upon presentation to the emergency room he is noted to have a pink hand with brisk capillary refill, but no palpable pulses. After closed reduction in the operating room and the procedure seen in Figures C and D, he remains well perfused, pulses are still not palpable, but triphasic pulses can be heard on doppler examination. What is the most appropriate course of action? Review Topic

Explanation
Pediatric supracondylar humerus fractures presenting with vascular compromise can present a challenge for clinical decision making. If the hand lacks adequate perfusion on presentation it requires emergent treatment with closed reduction and pinning. If perfusion does not return, then surgical exploration of the antecubital fossa is required. Treatment of the "pink pulseless hand" remains controversial. If the hand is well perfused but lacks palpable pulses then it should be expeditiously reduced and pinned. If the hand remains well perfused with triphasic doppler signals, no additional intervention is required. Recommendations vary if the hand is perfused, and pulses cannot be detected on palpation or doppler.
If there is a normal neurovascular exam on presentation, but abnormal after reduction and pinning, then one must consider that the reduction may have entrapped the brachial artery. If hardware removal and fracture re-displacement does not improve pulses/perfusion of the hand, or if the fracture can not be reduced without diminishing perfusion, then open reduction is indicated to evaluate the brachial artery.
Shah et al. present their preferred algorithm for treatment of a pink pulseless hand. They note that even with good clinical perfusion there may be a vascular injury or entrapment of the brachial artery. Thus they recommend if the hand is pink with no palpable pulse, perform a doppler exam. Triphasic doppler signals allow for observation, while abnormal or non-detectable doppler signals require surgical exploration. If an AIN or median nerve injury is present, exploration is considered. A diagram of their algorithm can be seen in Illustration A.
Weller et al. present a retrospective review of 1297 supracondylar humerus fractures. They had 20 patients (1.5%) with a pink pulseless hand with good doppler signals following closed reduction and fixation. These patients were treated with close observation. One patient developed inadequate perfusion nine hours after reduction and required vascular repair. The remaining 19 patients regained palpable pulses prior to discharge or prior to the first follow-up visit. They recommend observation despite non-palpable pulses as long as other signs of perfusion (capillary refill and doppler signals) suggest the hand is well perfused.
Figures A and B are AP and lateral radiographs of a type III supracondylar humerus fracture. Figures B and C demonstrate this fracture following closed reduction and percutaneous pinning with three lateral pins. Illustration A is a flow chart of a proposed decision making algorithm for a pink pulseless hand as presented by Shah et al.
Incorrect Answers:
reduction and fixation. Answer 2- Changing the pattern of fixation would only be indicated if the current construct did not provide stable fixation of the fracture. Answer 3- Following reduction and fixation of a supracondylar humerus fracture the most appropriate dressing is rigid long arm immobilization in a splint or cast. If there is concern for edema or perfusion then a cast should be bivalved. Answer 5- Surgical exploration of the antecubital fossa would be indicated if the hand had inadequate perfusion, or if the fracture could not be reduced and fixed without causing a notable decrease in pulses or perfusion.
Question 2
- Which of the following neurovascular structures is at greatest risk during the introduction of acetabular component fixation screws during total hip replacement?
Explanation
system they found that the posterior superior and posterior inferior quadrants of the acetabulum are the safest locations for screw placement because of better bone stock as well as less neurovascular structures as compared to the anterior quadrants.
Question 3
Factors contributing to an increased risk of hip fracture include reduced bone mineral density of the femoral neck, cognitive status of the individual, and
Explanation
Hayes and Myers noted that striking the ground in a stiff state with the trunk muscles contracted actually increased the peak impact force, whereas falling in a relaxed state actually reduced peak impact force. Flexion of the trunk at impact had no bearing on the impact force. Direction of the fall was important; falls to the side, not forward, were associated with an increased risk of hip fracture. Increased muscle activity about the hip is thought to be associated with spontaneous fractures of the hip and may actually account for up to 25% of hip fractures; however, it is not related to fractures resulting from a fall.
REFERENCE: Hayes WC, Myers ER: Biomechanical considerations of hip and spine fractures in osteoporotic bone, in Springfield D (ed): Instructional Course Lectures 46. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 431-438.
Question 4
A 35-year-old woman dislocated her right shoulder in a fall from a step stool several months ago. She now reports several painful recurrences. Examination reveals anterior and inferior apprehension that reproduces her symptoms. An MRI scan is shown in Figure 17. Management should consist of
Explanation
REFERENCES: Wolf EM, Cheng JC, Dickson K: Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Bokor DJ. Conboy VB. Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br
1999;81:93-96.
Coates MH, Breidahl W: Humeral avulsion of the anterior band of the inferior glenohumeral ligament with associated subscapularis bony avulsion in skeletally immature patients. Skeletal Radiol 2001;30:661-666.
Question 5
Which of the following would be associated with the spinal deformity shown in Figures 79a and 79b? Review Topic
Explanation
Question 6
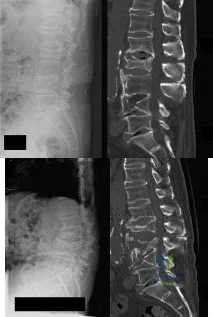
A 17-year-old girl is involved in a motor vehicle collision and sustains the injury shown in Figures 46a through 46c. She is neurologically intact in her bilateral lower extremities. Definitive treatment should consist of A B C

Explanation
The figures reveal a fracture-dislocation at L1-2. Proper treatment consists of posterior reduction, stabilization, and fusion 2 levels above and below the level of injury. Short-segment stabilization schemes do not stabilize the injury properly, and longer-segment constructs are not necessary. Anterior treatment is not indicated in fracture-dislocations.
RECOMMENDED READINGS
Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004 Nov-Dec;12(6):424-35. Review. PubMed PMID: 15615508. View Abstract at PubMed
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
Question 7
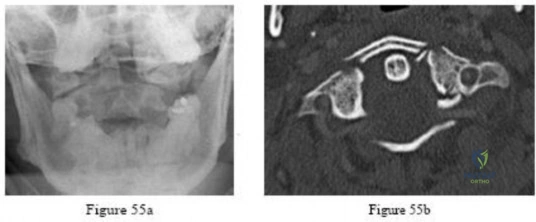
-Figures 55a and 55b are the radiograph and CT scan of a 61-year-old woman who has had neck pain after being involved in a high-speed motor vehicle collision. Examination reveals normal strength and sensation in both upper and lower extremities, normal rectal tone, and no other injuries. The C1-C2 lateral mass overhang measures 8.5 mm. What is the most appropriate treatment option?
Explanation

Question 8
When comparing the failure load of an evenly tensioned four-stranded hamstring tendon anterior cruciate ligament autograft to a 10-mm bone-patellar tendon-bone autograft, the hamstring graft will fail at a tension
Explanation
REFERENCES: Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA: Arthroscopic reconstruction of the anterior cruciate ligament: A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 1999;27:448-454.
Hamner DL, Brown CH Jr, Steiner ME, et al: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Noyes FR, Butler DL, Grood ES, et al: Biomechanical analysis of human ligament grafts used in knee-ligament repairs and reconstructions. J Bone Joint Surg Am 1984;66:344-352.
Question 9
A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient’s history is significant for smoking. The most immediate appropriate postoperative management for this patient should include
Explanation
REFERENCES: Sagi HC, Beutler W, Carroll E, et al: Airway complications associated with surgery on the anterior cervical spine. Spine 2002;27:949-953.
Epstein NE, Hollingsworth R, Nardi D, et al: Can airway complications following multilevel anterior cervical surgery be avoided? J Neurosurg 2001;94:185-188.
Emery SE, Smith MD, Bohlman HH: Upper-airway obstruction after multi-level cervical corpectomy for myelopathy. J Bone Joint Surg Am 1991;73:544-551.
Question 10
A 4-year-old girl who is undergoing chemotherapy for acute lymphocytic leukemia sustains a displaced fracture through an osteolytic lesion in the metaphysis of the distal femur as a result of a fall. Treatment should include
Explanation
Question 11
Examination of a 7-year-old boy reveals 20° of valgus following a lawn mower injury to the lateral femoral epiphysis. Treatment consists of total distal femoral epiphyseodesis and varus osteotomy. Following surgery, he has a limb-length discrepancy of 3 cm and 5° of genu valgum. Assuming that he undergoes no further treatment, the patient’s predicted limb-length discrepancy at maturity would be how many centimeters?
Explanation
REFERENCES: Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphyseodesis. J Pediatr Orthop 1996;16:173-179.
Westh RN, Menelaus MB: A simple calculation for the timing of epiphyseal arrest: A further report. J Bone Joint Surg Br 1981;63:117-119.
Question 12
A 26-year-old right hand-dominant man has had right shoulder pain for the past 6 months. History reveals that he was the starting pitcher for his high school team. Activity modification, physical therapy, cortisone injection, and anti-inflammatory drugs have failed to improve his symptoms. He has a positive O’Brien’s active compression test. What is the next most appropriate step in the diagnosis of this patient? Review Topic
Explanation
Question 13
What is the incidence and significance of anterior cruciate ligament laxity following tibial eminence fractures in skeletally immature individuals?
Explanation
REFERENCES: Willis R, Blokker C, Stall TM, et al: Long-term follow-up of anterior
eminence fractures. J Pediatr Orthop 1993;13:361-364.
Smith JB: Knee instability after fracture of the intercondylar eminence of the tibia.
J Pediatr Orthop 1984;4:462-464.
Question 14
A 72-year-old woman has had progressively increasing pain in the right knee for the past 6 months. She denies any trauma and has no pain in any other joints, but she notes occasional swelling in the knee and a catching sensation. Figures 31a and 31b show the plain radiographs and Figure 31c shows the MRI scan. Treatment should consist of
Explanation
REFERENCES: Lotke PA, Ecker ML: Osteonecrosis of the knee. J Bone Joint Surg Am 1988;70:470-473.
Ecker ML, Lotke PA: Osteonecrosis of the medial part of the tibial plateau. J Bone Joint Surg Am 1995;77:596-601.
Question 15
A 63-year-old man has had increasing left leg pain over the last several months. History reveals that he has had recurring cyclic pain in the leg for the past several years. Radiographs show an enlarged, sclerotic tibia, with thickened coarse trabeculae and varus bowing. What is the most appropriate management for this patient? Review Topic
Explanation
Question 16
In the absence of developmental dysplasia of the hip, what is the most common cause of osteoarthritis? Review Topic
Explanation
Question 17
Which of the following tissues has the highest maximum load to failure?
Explanation
REFERENCES: Woo SL, Hollis JM, Adams DJ, et al: Tensile properties of the human femur-anterior cruciate ligament-tibia complex: The effects of specimen age and orientation. Am J Sports Med 1991;19:217-225.
Staubli HU, Schatzmann L, Brunner P, et al: Quadriceps tendon and patellar ligament cryosectional anatomy and structural properties in young adults. Knee Surg Sports Traumatol Arthrosc 1996;4:100-110.
Wilson TW, Zafuta MP, Zobitz M: A biomechanical analysis of matched bone-patellar tendon-bone and doubled looped semitendinosus and gracilis tendon grafts. Am J Sports Med 1999;27:202-207.
Question 18
Lateral malleolus fractures can be treated with a variety of techniques, including posterior antiglide plating or lateral neutralization plating. What is an advantage of using lateral neutralization plating instead of posterior antiglide plating?

Explanation
Schaffer et al showed from a biomechanical standpoint that posterior antiglide plating was superior to lateral neutralization plating for distal fibula fracture fixation.
Weber et al reported a (30/70) 43% rate of plate removal secondary to peroneal discomfort. In addition, peroneal tendon lesions were found in 9 of the 30 patients.
Question 19
The MRI scan shown in Figure 24 reveals a right-sided herniated nucleus pulposus at L4-5 in a patient with pain in the right leg. Administration of a caudal epidural steroid injection provides immediate relief. Over the next week he notes generalized weakness of the lower extremities and has one episode of urinary incontinence. What is the next most appropriate step in management?
Explanation
REFERENCES: Knight JW, Cordingley JJ, Palazzo MG: Epidural abscess following epidural steroid and local anaesthetic injection. Anaesthesia 1997;52:576-578.
Abram SE, O’Connor TC: Complications associated with epidural steroid injections. Reg Anesth 1996;21:149-162.
Question 20
A 15-year-old boy falls from his bicycle and sustains an injury to his elbow. Prereduction radiographs are shown in Figure 12a. Closed reduction is performed without difficulty and postreduction radiographs are shown in Figure 12b. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Rasool MN: Dislocations of the elbow in children. J Bone Joint Surg Br 2004;86:1050-1058.
Beaty JH: Fractures and dislocations about the elbow in children. Instr Course Lect 1992;41:373-384.
Question 21
A 72-year-old woman was evaluated with an MRI scan for a shoulder mass that was confirmed to be a lipoma. Additional MRI findings included a 7-mm full-thickness tear of the supraspinatus tendon. Therefore, the patient was
Explanation
Question 22
A 16-year-old right-hand dominant male pitcher has had increasing pain in his dominant shoulder for the past 6 months without treatment. A coronal T2-weighted MRI scan is shown in Figure 80. What is the most appropriate treatment plan? Review Topic

Explanation
Question 23
Which of the following is associated with the use of large femoral heads in total hip arthroplasty?
Explanation
REFERENCES: Peters CL, McPherson E, Jackson JD, et al: Reduction in early dislocation rate with large-diameter femoral heads in primary total hip arthroplasty. J Arthroplasty 2007;22:140-144.
Inoue A, Asaumi K, Endo H, et al: Assessment of head wear more than ten years after total hip arthroplasty: 22- mm zirconia vs metal heads. Acta Med Okayama 2006;60:311-318.
Question 24
A 45-year-old man who has had recurrent pain and swelling of the left Achilles tendon insertion for the past 10 years reports that physical therapy and activity modification have provided relief in the past. He now has continued pain despite these efforts. He also reports occasional bouts of dysuria that he attributes to a history of prostatitis. He also notes recent eye irritation that he attributes to allergies. A lateral heel radiograph is shown in Figure 33. Which of the following laboratory studies would best aid in diagnosis?
Explanation
REFERENCE: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 560-650.
Question 25
What is the most common type of malalignment after intramedullary nailing of distal 1/3 tibia fractures?

Explanation
McKee et al randomized 85 patients undergoing intramedullary tibial nailing using manual traction with the leg draped free versus standard fracture table positioning and traction. They found that manual traction is an effective technique that can save a significant amount of time without sacrificing the quality of reduction or fixation of tibial shaft fractures.
Question 26
Deep posterior compartment
Explanation
The structures at risk are the anterior tibial artery and deep peroneal nerve in the anterior compartment, superficial peroneal nerve in the lateral compartment, sural nerve in the superficial posterior compartment, and posterior tibial nerve and posterior tibial and peroneal arteries and veins in the deep posterior compartment.
Question 27
A 15-year-old girl reports a 6-month history of activity-related knee pain and swelling. A radiograph, MRI scan, and biopsy specimen are shown in Figures 21a through 21c. What is the most likely diagnosis?
Explanation
REFERENCES: Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 295-313.
Lin PP, Thenappan A, Deavers MT, et al: Treatment and prognosis of chondroblastoma. Clin Orthop Relat Res 2005;438:103-109.
Question 28
Figures 4a and 4b show the radiographs of a 32-year-old man who has right groin pain with activity or prolonged standing. Which of the following factors would not prohibit consideration of acetabular liner exchange and grafting of the defects?
Explanation
REFERENCES: Maloney WJ, Herzwurm P, Paprosky W, Rubash HE, Engh CA: Treatment of pelvic osteolysis associated with a stable acetabular component inserted without cement as part of a total hip replacement. J Bone Joint Surg Am 1997;79:1628-1634.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 29
What complication is frequently associated with the Weil lesser metatarsal osteotomy (distal, oblique) in the treatment of claw toe deformities?
Explanation
REFERENCES: Trnka HJ, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int
2001;22:47-50.
Trnka HJ, Muhlbauer M, Zettl R, et al: Comparison of the results of the Weil and Helal osteotomies for the treatment of metatarsalgia secondary to dislocation of the lesser metatarsophalangeal joints. Foot Ankle Int 1999;20:72-79.
Question 30
Which of the following statements best describes the anatomic considerations of the popliteal artery posterior to the knee joint?
Explanation
90 degrees of flexion.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 151.
Anderson JE: Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-53.
Question 31
Figure 17 shows the radiograph of an 80-year-old woman who has left groin pain. She underwent a total hip arthroplasty 15 years ago and has no history of hip dislocation; however, she now reports that the pain results in functional impairment. Preoperative findings reveal that the component used has been discontinued, the locking mechanism is poor, and there is no replacement polyethylene available from the company. During surgery, the acetabular component is found to be well fixed, it is in satisfactory position, and adequate access can be obtained through the screw holes in the component to debride the osteolytic cavities. What is the best course of action for revision?
Explanation
REFERENCES: Maloney WJ: Socket retention: Staying in place. Orthopedics 2000;23:965-966.
Blaha JD: Well-fixed acetabular component retention or replacement: The whys and the wherefores. J Arthroplasty 2002;17:157-161.
Question 32
Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Agins HJ, Alcock NW, Bansal M, et al: Metallic wear in failed titanium-alloy total hip replacements: A histological and quantitative analysis. J Bone Joint Surg Am 1988;70:347-356.
Robinson RP, Lovell TP, Green TM, Bailey GA: Early femoral component loosening in DF-80 total hip arthroplasty. J Arthroplasty 1989;4:55-64.
Question 33
A 20-year-old elite college football player has ecchymosis, swelling, and pain on the lateral side of his foot after a game. Radiographs are shown in Figures 31a through 31c. Management should consist of
Explanation
REFERENCES: Glasgow MT, Naranja RJ Jr, Glasgow SG, et al: Analysis of failed surgical management of fractures of the base of the fifth metatarsal distal to the tuberosity: The Jones fracture. Foot Ankle Int 1996;17:449-457.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-252.
Question 34
When performing ankle arthroscopy through the anterolateral portal, what anatomic structure is at greatest risk?
Explanation
REFERENCES: Ferkel RD, Heath DD, Guhl JF: Neurological complications of ankle arthroscopy. Arthroscopy 1996;12:200-208.
Cooper PS, Murray TF Jr: Arthroscopy of the foot and ankle in the athlete. Clin Sports Med 1996;15:805-824.
Question 35
What do the T2-weighted, fat-saturated MRI scans shown in Figures 1 through 4 reveal?

Explanation
disruption of the ACL. The medial meniscus images show a disruption of normal meniscus morphology consistent with a bucket handle medial meniscus tear. Note the appearance on the sagittal MRI scan of what appears to be a second soft-tissue density in line with the PCL. This "double PCL" sign is highly indicative of a displaced medial meniscus tear rather than a displaced lateral meniscus tear.
Question 36
CLINICAL SITUATION Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. This knee injury is best described as a

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair, but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 37
What is the second most common primary bone malignancy in children?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 195.
Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 38
Which of the following is associated with increased fetal morbidity and mortality in acetabular fractures during pregnancy?
Explanation
Question 39
- A 25-yo man sustains the injury shown in Figures 29a and 29b as a result of high-speed trauma. Examination reveals diffuse weakness in the lower extremities that is slightly worse on the right side, and decreased rectal tone and sensation. A CT scan is shown in figures 29c and 29d. Definitive treatment of the injury to the spine is delayed because of a severe pulmonary contusion. At 15 days after the injury, the patient’s neurological status remains unchanged. Management should now consist of
Explanation
Question 40
A 23-year-old man is injured in a motorcycle accident and has a Glasgow Coma Scale (GCS) score of 10. His fiance arrives shortly after he does. He has an open, IIIc tibial fracture. The patient's parents are on the way but are not expected to arrive for some time. Who should be asked to provide informed consent?
Explanation
Question 41
Which of the following clinical tests is used to diagnose medial instability of the elbow? Review Topic
Explanation
Question 42
Intraoperative frozen section analysis reveals 10 neutrophils per high-power field and a positive gram stain result. What is the best next step?
Explanation
The radiograph reveals a rotator cuff dysfunction secondary to malpositioning of the humeral stem and a nonanatomic humeral head. Glenohumeral kinematics have been altered, resulting in damage to the rotator cuff, which in turn has led to impingement with the coracoacromial arch. This single radiograph reveals excessive humeral head height, “overstuffing” of the joint, and severe narrowing of the acromiohumeral interval. Osteolysis and implant loosening are not radiographically apparent. An orthogonal view (axillary lateral) would be necessary to evaluate for shoulder instability. A CT arthrogram is the most appropriate advanced imaging test in the setting of a retained shoulder arthroplasty to evaluate the integrity of the rotator cuff. An MRI evaluation would be obfuscated by artifact. Three-phase and indium-tagged white blood cell scans may be appropriate in the setting of an occult infection evaluation, but not as a test to evaluate rotator cuff injury.
In the absence of infection with rotator cuff compromise, the most appropriate procedure(s) during revision would involve humeral component explantation and conversion to rTSA Revision anatomic hemiarthroplasty may provide pain relief, but function may not appreciably change because of the unbalanced forced couples of the rotator cuff complex. Placement of a glenoid component in the setting of an irreparable rotator cuff tear is contraindicated because rapid glenoid loosening will occur due to eccentric loading during active shoulder motion. Resection arthroplasty should be reserved for recalcitrant cases of infection because this procedure does not provide functional improvement.
In the event that frozen section analysis and positive gram stain results indicate an infection, the treating surgeon should remove all components, perform a thorough debridement and irrigation of suspect tissue, implant an antibiotic spacer, and perform a second-stage reconstruction when deemed appropriate (in light of laboratory studies, repeat shoulder aspiration, frozen section analysis, and arthroscopic soft-tissue biopsy findings). Irrigation and debridement with primary exchange/conversion of components remains inferior to 2-stage reconstruction for infection eradication. Resection arthroplasty remains a salvage procedure for resistant cases that preclude reimplantation and generally is performed for symptom control and sepsis prevention.
RECOMMENDED READINGS
Bohsali KI, Wirth MA, Rockwood CA Jr. Complications of total shoulder arthroplasty. J Bone Joint Surg Am. 2006 Oct;88(10):2279-92. Review. PubMed PMID: 17015609. View Abstract at PubMed
Florschütz AV, Lane PD, Crosby LA. Infection after primary anatomic versus primary reverse total shoulder arthroplasty. J Shoulder Elbow Surg. 2015 Aug;24(8):1296-301. doi: 10.1016/j.jse.2014.12.036. Epub 2015 Feb 19. PubMed PMID: 25704211. View Abstract at PubMed
Padegimas EM, Maltenfort M, Ramsey ML, Williams GR, Parvizi J, Namdari S. Periprosthetic shoulder infection in the United States: incidence and economic burden. J Shoulder Elbow Surg. 2015 May;24(5):741-6. doi: 10.1016/j.jse.2014.11.044. Epub 2015 Jan 13. View Abstract at PubMed
Leung B, Horodyski M, Struk AM, Wright TW. Functional outcome of hemiarthroplasty compared with reverse total shoulder arthroplasty in the treatment of rotator cuff tear arthropathy. J Shoulder Elbow Surg. 2012 Mar;21(3):319-23. doi: 10.1016/j.jse.2011.05.023. Epub 2011 Aug 26. PubMed PMID: 21872496. View Abstract at PubMed
Iannotti JP, Spencer EE, Winter U, Deffenbaugh D, Williams G. Prosthetic positioning in total shoulder arthroplasty. J Shoulder Elbow Surg. 2005 Jan-Feb;14(1 Suppl S):111S-121S. PubMed PMID: 15726070. View Abstract at PubMed
Iannotti JP, Gabriel JP, Schneck SL, Evans BG, Misra S. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am. 1992 Apr;74(4):491-500. PubMed PMID: 1583043.View Abstract at PubMed
Grosso MJ, Frangiamore SJ, Ricchetti ET, Bauer TW, Iannotti JP. Sensitivity of frozen section histology for identifying Propionibacterium acnes infections in revision shoulder arthroplasty. J Bone Joint Surg Am. 2014 Mar 19;96(6):442-7. doi: 10.2106/JBJS.M.00258. View Abstract at PubMed
Question 43
A 6-year-old girl has the bilateral foot deformity shown in Figure 1. There is no family history of disease. Examination reveals fixed hindfoot equinus, and muscle function testing shows strong posterior tibial function, fair plus anterior tibial function, poor peroneal function, and strong gastrocnemius function. A Coleman block test shows a correctable hindfoot. Nerve conduction velocity studies show diminished function in the peroneal and ulnar nerves on both sides. Pathologic changes found in a sural nerve biopsy include “onion bulb” formation, and DNA testing confirms the presence of a mutation in the MPZ gene, consistent with hereditary motor sensory neuropathy type III (HMSN-III). What is the best course of action?
Explanation
REFERENCES: Wetmore RS, Drennan JC: Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 1989;71:417-422.
Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth. J Bone Joint Surg Br 1989;71:17-20.
Miller GM, Hsu JD, Hoffer MM, Rentfro R: Posterior tibial tendon transfer: A review of the literature and analysis of 74 procedures. J Pediatr Orthop 1982;2:363-370.
Question 44
Figures 75a and 75b are the radiographs after attempted reduction of an injury in a 9-year-old girl. Which anatomic structure is most likely to be interposed?
Explanation
The injury shown is a flexion-type supracondylar humerus fracture. The most commonly interposed anatomic structure is the ulnar nerve. The brachialis muscle is often interposed in extension-type fractures, as are the median nerve and radial artery. The radial nerve is at risk for entrapment in a humeral shaft fracture or distal third humeral fracture.

CLINICAL SITUATION FOR QUESTIONS 76 THROUGH 80
Figure 76 is the clinical photograph of an infant with foot deformities.
Question 45
Figure 7 shows the CT scan of a 22-year-old professional baseball pitcher who has had elbow pain for the past 6 months despite rest from throwing. Management should consist of Review Topic
Explanation
Question 46
Randomized controlled trials can be designed in several ways. Which of the following study designs refers to a randomized controlled trial in which two interventions are compared within the same study group?
Explanation
Question 47
Use of titanium elastic nailing for treatment of pediatric femur fractures is associated with a higher complication rate among
Explanation
Studies of titanium elastic nailing for femur fractures demonstrated a higher rate of complications, including angular deformity and construct failure, among patients weighing more than 50 kg (100 pounds). Other methods of fixation are recommended for these patients. Flexible nails are not commonly needed, but they also are not associated with a higher complication rate in children younger than age 6.5. Titanium elastic nailing works well in closed or minimally open transverse midshaft fractures, even in the setting of early or immediate weight bearing.

Video 8a
Video 8b
Question 48
What is the primary goal of the initial (acute) rehabilitation phase of an overhead athlete's shoulder?
Explanation
Question 49
Figures 42a and 42b show the radiographs of a 52-year-old man who sustained a fall from a motorcycle 6 months ago and now reports pain and stiffness in his left shoulder. What is the most reliable treatment to improve function and comfort of the shoulder? Review Topic
Explanation
Question 50
Which nerve is not included in a standard popliteal nerve block?
Explanation
A standard popliteal nerve block is performed with the patient prone. The injection aims for the area at, or close to, the peroneal and tibial nerves. The sural nerve branches distal to the injection site, so this nerve and the superficial peroneal, deep peroneal, and tibial nerves are covered with the injection. The saphenous nerve is in an anteromedial location at knee level and is not close enough to the area covered by the posterior injection to be included in the analgesic effect.
RECOMMENDED READINGS
Varitimidis SE, Venouziou AI, Dailiana ZH, Christou D, Dimitroulias A, Malizos KN. Triple nerve block at the knee for foot and ankle surgery performed by the surgeon: difficulties and efficiency. Foot Ankle Int. 2009 Sep;30(9):854-9. PubMed PMID: 19755069. View Abstract at PubMed
Hromádka R, Barták V, Popelka S, Jahoda D, Pokorný D, Sosna A. [Regional anaesthesia of the foot achieved from two cutaneous points of injection: an anatomical study]. Acta Chir Orthop Traumatol Cech. 2009 Apr;76(2):104-9. Czech. PubMed PMID: 19439129. View Abstract at PubMed
Tran D, Clemente A, Finlayson RJ. A review of approaches and techniques for lower extremity nerve blocks. Can J Anaesth. 2007 Nov;54(11):922-34. Review. PubMed PMID: 17975239. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 42 THROUGH 44

42A

B
Figures 42a and 42b are the radiographs of a 32-year-old man with an accessory navicular, pes planovalgus deformity, and an associated gastrocnemius contracture. He has been treated with custom orthotics and a physical therapy program for several years and has progressed to stage II posterior tibial tendon dysfunction (PTTD). This patient is now interested in surgery. Tendon reconstruction with bony procedure to correct alignment, medializing calcaneal osteotomy with lateral column lengthening, and a subtalar arthroereisis implant are discussed with the patient.
Question 51
An 18-year-old lacrosse player is diagnosed with infectious mononucleosis. What is the recommendation for return to play? Review Topic
Explanation
Question 52
Which of the following is an advantage of using blocking screws for tibial nailing?

Explanation
Krettek found that medial and lateral blocking screws can increase the primary stability of distal and proximal metaphyseal fractures after nailing and can be an effective tool for selected cases that exhibit malalignment and/or instability by decreasing mechanically measured deformation.
In a later clinical study, Krettek found that after using blocking screws, tibial healing was evident radiologically at a mean of 5.4 months with a decreased rate of malunions.
Ricci also found that blocking screws are effective to help obtain and maintain alignment of fractures of the proximal third of the tibial shaft treated with intramedullary nails.
Question 53
Which of the following tissues used for anterior cruciate ligament (ACL) reconstruction has the highest maximum load to failure?
Explanation
REFERENCES: Hamner DL, Brown CH Jr, Steiner ME, Hecker AT, Hayes WC: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Cooper DE, Deng XH, Burstein AL, Warren RF: The strength of the central third patellar tendon graft: A biomechanical study. Am J Sports Med 1993;21:8l8-823.
Brown CH Jr, Steiner ME, Carson EW: The use of hamstring tendons for anterior cruciate ligament reconstruction: Technique and results. Clin Sports Med 1993;12:723-756.
Engebretsen L, Lewis JL: Graft selection and biomechanical considerations in ACL reconstruction. Sports Med Arthroscopy Rev 1996;4:336-341.
Question 54
A 31-year-old man sustained an unstable closed left posterior hip dislocation in a motorcycle accident. A postreduction radiograph is shown in Figure 51a. 3-D CT scans are shown in Figures 51b and 51c. What is the optimal surgical approach that will allow for the most appropriate treatment?

Explanation
Question 55
Which of the following are considered characteristic features of degeneration of a disk?
Explanation
REFERENCES: Happey F, Weissman A, Naylor A: Polysaccharide content of the prolapsed nucleus pulposus of the human intervertebral disc. Nature 1961;192:868.
Naylor A, Shentall R: Biomechanical aspects of intervertebral discs in aging and disease, in Jayson M (ed): The Lumbar Spine and Back Pain. New York, NY, Grune and Stratton Inc, 1976, pp 317-326.
Watkins RG, Collis JS: Lumbar Discectomy and Laminectomy. Rockville, MD, Aspen, 1987, pp 2-3.
Question 56
A 23-year-old baseball pitcher who has diffuse pain along the posterior deltoid reports pain during late acceleration and follow-through. Examination of his arc of motion from external rotation to internal rotation at 90 degrees of shoulder abduction reveals a significant deficit in internal rotation when compared to the nonthrowing shoulder. Initial management should consist of
Explanation
REFERENCES: Kibler WB: Biomechanical analysis of the shoulder during tennis activities. Clin Sports Med 1995;14:79-85.
Jobe FW, Tibone JE, Jobe CM, Kvitne RS: The shoulder in sports, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 961-990.
Question 57
A 22-year-old swimmer underwent thermal capsulorrhaphy treatment for recurrent anterior subluxation. Following 3 weeks in a sling, an accelerated rehabilitation program allowed him to return to swimming in 3 1/2 months. While practicing the butterfly stroke, he sustained an anterior dislocation. He now continues to have symptoms of anterior instability and has elected to have further surgery. Surgical findings may include a
Explanation
REFERENCES: Abrams JS: Thermal capsulorrhaphy for instability of the shoulder: Concerns and applications of the heat probe. Instr Course Lect 2001;50:29-36.
Hecht P, Hayashi K, Lu Y, et al: Monopolar radiofrequency energy effects on joint capsular tissue: Potential treatment for joint instability. An in vivo mechanical, morphological, and biochemical study using an ovine model. Am J Sports Med 1999;27:761-771.
Question 58
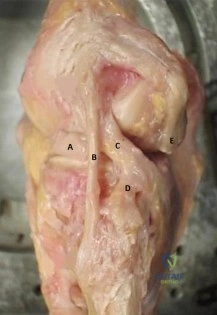
Figure A is the lateral view of a left knee cadaveric specimen that has the extensor mechanism removed. Which two structures labeled provide the most rotational stability in knee flexion? Review Topic
Explanation
extension.
The lateral knee is stabilized by 28 unique static and dynamic structures. These structures work in concert to resist varus gapping and rotational knee instability. The three primary stabilizers include the fibular or lateral collateral ligament (LCL), the popliteus tendon (PT) and the popliteofibular ligament (PFL). Injury to these ligaments results in increased forces seen on ACL and PCL ligament reconstruction grafts with combined posterolateral corner (PLC) injuries, which can result in graft failure if the PLC is not reconstructed as well.
James et al reviewed the anatomy and biomechanics of the lateral knee stabilizers, detailing the specific functional contributions of the individual structures. The LCL is the primary restraint to varus instability, the highest forces occurring at knee extension (0°-30°). The PT and PFL serve as restraints to rotational instability, the highest forces occurring at knee flexion (60°-90°).
LaPrade et al reviewed the anatomy and biomechanics of the medial knee stabilizers. The three key static stabilizers are the superficial medial collateral ligament (sMCL), the deep medial collateral ligament (dMCL), and the posterior oblique ligament (POL). The sMCL is the primary restraint to valgus instability (proximal sMCL) and secondary restraint to rotational instability (distal sMCL) at all knee flexion angles. The dMCL is a secondary restraint to valgus and rotational instability. The POL is the primary restraint to rotational instability.
Figure A depicts the lateral knee structures in a cadaver specimen (A = lateral meniscus, B = LCL, C = PT, D = PFL, E = lateral head of gastrocnemius). Illustration A is a labeled picture of the lateral knee structures. Illustration B is a table from James et al demonstrating the change in forces experienced by the different lateral stabilizers at varying degrees of knee flexion. You see the LCL resists rotation at 0°-30° (extension) while the PT and PFL resist rotation at 60°-90° (flexion).
Incorrect Responses:
Question 59
Figures 8a through 8d show the radiographs and CT scans of a 14-year-old girl who has a painful, rigid planovalgus foot. Management consisting of arch supports and anti-inflammatory drugs failed to provide relief. A below-knee walking cast resulted in pain resolution, but she now reports that the pain has recurred. Management should now consist of
Explanation
REFERENCES: Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Olney BW: Tarsal coalition, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 169-181.
Question 60
Radiating pain associated with a posterolateral thoracic disk herniation typically follows what pattern?
Explanation
REFERENCE: Skubic JW, Kostuik JP: Thoracic pain syndromes and thoracic disc herniation, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, pp 1443-1464.
Question 61
Figure 20 shows the radiograph of a 21-year-old college basketball player who jammed his left index finger on the rim. He reports pain and tenderness over the dorsum of the distal interphalangeal (DIP) joint. Examination reveals that he is unable to actively extend the DIP joint; however, the skin is intact. Management should consist of
Explanation
REFERENCES: Crawford GP: The molded polyethylene splint for mallet finger deformities.
J Hand Surg Am 1984;9:231-237.
Wehbe MA, Schneider LH: Mallet fractures. J Bone Joint Surg Am 1984;66:658-669.
Question 62
Figures below show the radiographs obtained from a 19-year-old woman with a 3-year history of progressive hip pain in the left groin with activity, which is unresponsive to activity modification and physical therapy. Examination reveals normal range of motion, with pain on anterior impingement testing. What treatment is associated with the best long-term results?

Explanation
This patient has symptomatic femoroacetabular impingement as well as clinical and radiographic signs of acetabular retroversion, including a cross-over sign, ischial spine sign, and posterior wall sign bilaterally. Good midterm to long-term outcomes have been reported with reverse (anteverting) Bernese periacetabular osteotomy (PAO). In patients with less retroversion, open or arthroscopic rim trimming with labral refixation have shown good short-term results, but longer-term results have yet to be fully delineated. Isolated hip arthroscopy and labral repair would not be indicated without addressing the retroversion deformity. Femoral varus rotational osteotomy plays no role in the treatment of this pathology. Open surgical dislocation with rim trimming could be considered in patients with less deformity, but some studies have shown inferior long-term results compared with reverse PAO.
Question 63
- A 50 year old man who has insulin-dependent diabetes mellitus with associated neuropathy has a stress fracture of the fourth metatarsal. Examination of the foot reveals acute swelling, warmth, and erythema; however, the patient reports very little pain. Treatment should include
Explanation
Question 64
Which of the following is associated with the use of bisphosphonates in the setting of metastatic breast cancer to the spine?
Explanation
REFERENCE: Body JJ: Breast cancer: Bisphosphonate therapy for metastatic bone disease. Clin Cancer Res 2006;12:6258s-6263s.
Question 65
A 28-year-old man was shot in the foot with a .22 caliber handgun approximately 2 hours ago. Examination reveals an entrance wound dorsally and a plantar exit wound. The foot is neurovascularly intact. Radiographs reveal a nondisplaced fracture of the third metatarsal. Soft-tissue management for this injury should consist of
Explanation
REFERENCES: Brettler D, Sedlin ED, Mendes DG: Conservative treatment of low velocity gunshot wounds. Clin Orthop 1979;140:26-31.
Hampton OD: The indications for debridement of gunshot bullet wounds of the extremities in civilian practice. J Trauma 1961;1:368-372.
Marcus NA, Blair WF, Shuck JM, Omer GE Jr: Low-velocity gunshot wounds to extremities. J Trauma 1980;20:1061-1064.
Question 66
Which of the following is considered a limitation of the Short Form 36 (SF-36) general health status instrument when applied to musculoskeletal conditions?
Explanation
Multilingual validated translations have been produced in addition to international population data sets. The survey can be patient self-administered via office visit, mail, or telephone. A bias of lower over upper extremity function with regard to outcome measures employing the SF-36 has been demonstrated. Limits on the detection of certain changes in quality of life status may impose ceiling and floor effects on analysis and interpretation.
Question 67
A 23-year-old otherwise healthy 6-ft, 4-in basketball player complains of pain in his knees. An examination reveals localized tenderness to palpation over the inferior pole of the patella. The patient notes a significant exacerbation of his pain when the examiner takes the knee from flexion to extension. Review Topic
Explanation
Question 68
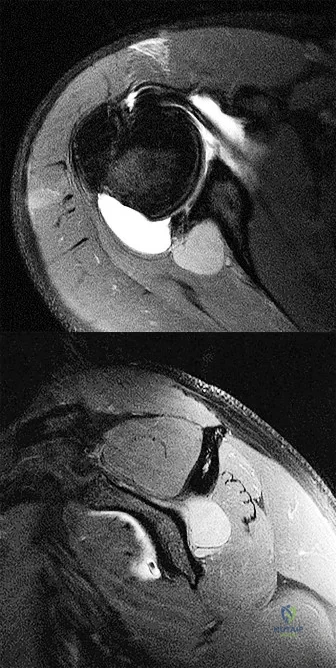
What is the most common associated pathology in patients who have suprascapular nerve entrapment secondary to ganglion cysts?
Explanation
REFERENCES: Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
Iannotti JP, Ramesey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Moore TP, Fritts HM, Quick DC, Buss DD: Suprascapular nerve entrapment caused by supraglenoid cyst compression. J Shoulder Elbow Surg 1997;6:455-462.
Question 69
A 29-year-old woman who underwent an anterior cruciate ligament (ACL) reconstruction 6 months ago now reports difficulty achieving full knee extension, and physical therapy fails to provide relief. The knee is stable on ligament testing. Figure 3 shows the findings at a repeat arthroscopy. Treatment should now include
Explanation
REFERENCES: Delince P, Krallis P, Descamps PY, et al: Different aspects of the cyclops lesion following anterior cruciate ligament reconstruction: A multifactorial etiopathogenesis. Arthroscopy 1998;14:869-876.
Fisher SE, Shelbourne KD: Arthroscopic treatment of symptomatic extension block complicating anterior cruciate ligament reconstruction. Am J Sports Med 1993;4:558-564.
Question 70
0 sustained a subcapital fracture of her hip. She is an avid tennis player, and history reveals no previous fractures. What is the most appropriate follow-up care? Review Topic
Explanation
Question 71
What is the most prevalent adverse event associated with allogeneic blood transfusion?
Explanation
REFERENCES: Aubuchon JP, Birkmeyer JD, Busch MP: Safety of the blood supply in the United States: Opportunities and controversies. Ann Intern Med 1997;127:904-909.
Popovsky MA, Whitaker B, Arnold NL: Severe outcomes of allogeneic and autologous blood donation: Frequency and characterization. Transfusion 1995;35:734-737.
Question 72
- A 13-year-old quarterback feels a “pop” in his knee while being tackled. Radiographs of the knee and results of a Lachman’s test are normal. Examination reveals tenderness over the distal femoral physis. To help confirm the diagnosis, management should first include
Explanation
Question 73
A 10-year-old girl is seen in the emergency department after being involved in a motor vehicle accident. She has right hip pain and is unable to bear weight. She has no neurovascular deficits and no other injuries. Radiographs reveal a posterior dislocation of the right hip without apparent fracture. The acetabulum appears to be developing normally. What is the best course of treatment? Review Topic
Explanation
Question 74
Kyphosis from a vertebral osteoporotic compression fracture often results in progressive kyphosis due to Review Topic
Explanation
Question 75
Figure 3 shows the radiographs of a 32-year-old man who fell 12 feet onto his outstretched arm and sustained a fracture-dislocation of the elbow. Initial management consisted of closed reduction of the dislocation. Surgical treatment should now include repair or reduction and fixation of the
Explanation
REFERENCES: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
O’Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF: The unstable elbow. Instr Course Lect 2001;50:89-102.
Question 76
Figures 1 through 4 are the wrist MR images of a 43-year-old right-hand-dominant bricklayer who reports gradually progressive left hand weakness for 4 months. He describes difficulty gripping objects, tying his shoes, and holding utensils. He denies any numbness, paresthesias, or a previous injury. An examination reveals intact sensation in a median, radial, and ulnar nerve distribution. He has atrophy of hand interossei and a positive Froment sign finding. He has no Tinel sign finding at the wrist or elbow and no exacerbation of symptoms with elbow hyperflexion. Electromyography shows signs of denervation in an ulnar nerve distribution distal to the wrist. What is the best next step?
Explanation
Question 77
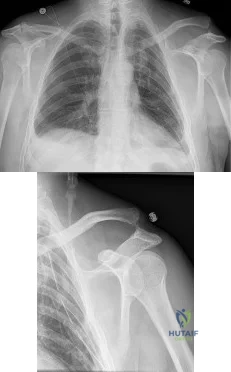
A 50-year-old man fell from a ladder onto his left shoulder and sustained the injury shown in the radiographs in Figures 71a and 71b. He underwent surgery with repair of the coracoclavicular ligaments and deltotrapezial fascia with coracoclavicular screw placement. Which of the following statements regarding postoperative complications is most accurate? Review Topic
Explanation
Question 78
If the site of the pathologic lesion is revealed in Figure 54f and not in Figure 54e after traumatic anterior shoulder dislocation, the mechanism of shoulder injury is likely
Explanation
For patients with anterior shoulder instability, most commonly, a Bankart lesion, or detachment of the anteroinferior labrum with the attached inferior glenohumeral ligament from the glenoid rim is found. A medialized anteroinferior capsulolabral attachment (ALPSA lesion) is a common finding in shoulders with chronic anterior instability. The anterior band of the inferior glenohumeral ligament is tightest with the arm in 90 degrees of abduction with the shoulder externally rotated, creating a “hammock” that supports the humeral head. At 45 degrees of shoulder
abduction, the capsuloligamentous components of the shoulder are at their loosest, resulting in the most total superior-inferior translation.
During traumatic anterior glenohumeral dislocation, associated injuries commonly occur. In a prospective database of 3633 patients who sustained a traumatic anterior glenohumeral dislocation, 13.5% had a neurologic deficit following reduction, the majority of which were injuries to the axillary nerve. The injuries typically were sensory but not motor deficits and resolved spontaneously over time. These isolated axillary nerve injuries were more common in young, athletic patients. Associated rotator cuff tears and greater tuberosity fractures are commonly associated with shoulder dislocation as well and are more common in patients 60 years of age and older.
Large, engaging posterior humeral head Hill-Sachs lesions are associated with increased rates of recurrent shoulder instability. At the time of surgical arthroscopy, the Hill-Sachs lesion should be assessed for engagement with the glenoid. In the absence of significant glenoid bone loss, some patients with engaging Hill-Sachs defects may be suitable for combined Bankart repair and Hill-Sachs remplissage at the time of surgery. When these procedures are combined, patients have an approximate 10-degree decreased shoulder external rotation with the arm at the side and in abduction when compared to the contralateral, uninjured shoulder. Rates of recurrent dislocation and return to sport are comparable to those for patients undergoing Bankart repair alone.
Humeral avulsion of the glenohumeral ligaments (HAGL) has become a well-recognized cause of recurrent shoulder instability and is reported in 1% to 9% of patients. HAGL lesions can occur in isolation or, more commonly, may be associated with other abnormalities such as a tear of the rotator cuff, Bankart lesion, Hill-Sachs deformity, or labral tear. Recurrence of shoulder instability is more likely to occur if there is failure to identify a HAGL lesion. HAGL lesions can result from trauma in the setting of combined hyperabduction and external rotation. This is in contrast to a Bankart lesion, which is a result of trauma when the shoulder is hyperabducted without substantial associated rotation.
RECOMMENDED READINGS
Warner JJ, Deng XH, Warren RF, Torzilli PA. Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med. 1992 Nov-Dec;20(6):675-85. PubMed PMID: 1456361. View Abstract at PubMed
Robinson CM, Shur N, Sharpe T, Ray A, Murray IR. Injuries associated with traumatic anterior glenohumeral dislocations. J Bone Joint Surg Am. 2012 Jan 4;94(1):18-26. doi: 10.2106/JBJS.J.01795. PubMed PMID: 22218378. View Abstract at PubMed
Visser CP, Coene LN, Brand R, Tavy DL. The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery. A prospective clinical and EMG study. J Bone Joint Surg Br. 1999 Jul;81(4):679-85. PubMed PMID: 10463745. View Abstract at PubMed
Boileau P, O'Shea K, Vargas P, Pinedo M, Old J, Zumstein M. Anatomical and functional results after arthroscopic Hill-Sachs remplissage. J Bone Joint Surg Am. 2012 Apr 4;94(7):618-26. doi: 10.2106/JBJS.K.00101. PubMed PMID: 22488618. View Abstract at PubMed
Bui-Mansfield LT, Banks KP, Taylor DC. Humeral avulsion of the glenohumeral ligaments: the HAGL lesion. Am J Sports Med. 2007 Nov;35(11):1960-6. Epub 2007 Apr 9. Review. PubMed PMID: 17420506. View Abstract at PubMed
Question 79
In the Lauge-Hansen classification system, a pronation-abduction ankle fracture has what characteristic fibular fracture pattern?

Explanation
Question 80
A 45-year-old tennis player undergoes surgery for chronic lateral epicondylitis. After returning to play, he notes increasing lateral elbow pain with mechanical catching and locking. Examination shows positive supine posterolateral rotatory instability. What ligament has been injured? Review Topic
Explanation
Question 81
What antithrombotic agent is a selective factor I0a inhibitor? Review Topic
Explanation
Question 82
Figure below depicts the radiograph obtained from a 30-year-old woman who began having more right than left hip pain during a recent pregnancy. Physical examination reveals increased range of motion with positive flexion abduction and external rotation and flexion adduction and internal rotation as well as pain with external logroll. Assessment of Figure below reveals
Explanation
Studies have demonstrated that pelvic inclination can dramatically affect the interpretation of radiographs in the dysplastic hip, with 9° of increased pelvic inclination leading to the presence of crossover signs and posterior wall signs. A distance of 30 mm to 50 mm from the sacrococcygeal junction to the pubis is often used to assess the adequacy of pelvic inclination on radiographs, although Siebenrock and associates determined the mean difference to be 32 mm in men and 47 mm in women. In this patient, the pelvic inclination is dramatically increased, leading to overestimation of acetabular retroversion.
Question 83
- A patient is in respiratory distress as a result of a high-speed motor vehicle accident. After emergent intubation, the arterial blood is poorly oxygenated, and examination shows left-sided tracheal deviation, absence of breath sounds on the right side and tympany on percussion over the right side of the chest. Management should include
Explanation
Question 84
An otherwise healthy 32-year-old man who underwent an uneventful L5-S1 lumbar microdiskectomy 6 weeks ago now reports increasing and severe back pain that awakens him from sleep. Examination reveals a benign-appearing wound, and the neurologic examination is normal. Laboratory studies show an erythrocyte sedimentation rate (ESR) of 90 mm/h and a WBC of 9,000/mm3. Plain radiographs are normal. What is the next most appropriate step in management?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 257-271.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 713-721.
Question 85
Figure 36 shows the hip arthrogram of a newborn. Which of the following structures is enclosed by the circle?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA,
WB Saunders, 2002, vol 1, pp 532-533.
Severin E: Contribution to the knowledge of congenital dislocation of the hip joint.
Acta Chir Scand 1941;84:1.
Question 86
Which of the following terms describe a rehabilitative exercise in which the foot is mobile and the motion of the knee is independent of hip and ankle motion?
Explanation
Question 87
When a structure like a long bone is under a bending load, its maximum stress is most dependent on what factor?
Explanation
REFERENCES: Hayes WC, Bouxsein ML: Biomechanics of cortical and trabecular bone: Implications for assessment of fracture risk, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 76-82.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 161-167.
Question 88
A sentinel event is defined as an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. What is the most common sentinel event related to spine surgery?
Explanation
REFERENCES: Wong DA, Watters WC III: To err is human: Quality and safety issues in spine care. Spine 2007;32:S2-S8.
Wong DA: Spinal surgery and patient safety: A systems approach. J Am Acad Orthop Surg 2006;14:226-232.
Question 89
A 56-year-old man who underwent a left total hip arthroplasty 8 years ago is seen following a fall from a standing height. A radiograph obtained at 2 years postoperatively is shown in Figure 55a and a current radiograph obtained in the emergency department is shown in Figure 55b. On further questioning, he reports pain in this thigh for the past 3 years that has been increasing in intensity. Appropriate management at this time includes which of the following?
Explanation
REFERENCES: Masri BA, Meek RM, Duncan CP: Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res 2004;420:80-95.
Springer BD, Berry DJ, Lewallen DB: Treatment of periprosthetic femoral fractures following total hip
arthroplasty with femoral component revision. J Bone Joint Surg Am 2003;85:2156-2162. Question 56
A 62-year-old woman who underwent a primary total knee arthroplasty under a combined spinal-epidural anesthetic presents 5 hours postoperatively with severe pain in the extremity that is unresponsive to narcotic pain medication. A tourniquet was used during the procedure. On examination, the patient is unable to dorsiflex or plantar flex the foot and the pulses appear to be asymmetric. What is the next most appropriate step in management?
Discontinuation of the epidural and serial neurologic exams
Loosening of the surgical bandages and elevation of the extremity
MRI of the spine to evaluate for an epidural hematoma
Return to the operating room for angiography and vascular bypass
Return to the operating room for angiography, vascular bypass, and four-compartment fasciotomy PREFERRED RESPONSE: 5
DISCUSSION: The patient has clinical evidence of vascular injury and compartment syndrome. An emergent
vascular consult and a return to the operating room for an angiogram and revascularization are needed. In these situations, thrombectomy alone is often not sufficient and a bypass is typically required. A four-compartment fasciotomy should be done following revascularization of the extremity.
REFERENCES: Calligaro KD, Dougherty MJ, Ryan S, et al: Acute arterial complications associated with total hip and knee arthroplasty. J Vase Surg 2003;38:1170-1177.
Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001;9:253-257.
Ninomiya JT, Dean JC, Goldberg VM: Injury to the popliteal artery and its anatomic location in total knee
arthroplasty. J Arthroplasty 1999;14:803-809.
Question 90
A 32-year-old man sustains a pilon fracture which is treated initially with a spanning external fixator, as shown in figure A. He is now 3 weeks from injury and skin swelling has subsided significantly. What is the most appropriate definitive treatment?

Explanation
OrthoCash 2020
Question 91
A 42-year-old woman sustains a closed posterior elbow dislocation. A closed reduction is performed, and the elbow appears stable under fluoroscopic examination. Initial treatment should consist of
Explanation
application of a hinged external fixator may be considered.
Question 92
A 5-year-old boy is seen in the emergency department with a 2-day history of refusing to walk. Examination shows that he has a temperature of 102.2 degrees F (39 degrees C) and limited range ot motion of the right hip. The AP pelvic radiograph is normal. The WBC count is normal but the C-reactive protein and erythrocyte sedimentation rate (ESR) are elevated. What is the next step in management?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2109-2113.
Abel MF (ed): Orthopaedic Knowlede Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 62-65.
Kocher MS, Mandiga R, Murphy JM, et al: A clinical practice guideline for treatment of septic arthritis
in children: Efficacy in improving process of care and effect on outcome of septic arthritis of the hip. J Bone Joint Surg Am 2003;85:994-999.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinica l prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 93
The gluteus maximus is innervated by which of the following nerves?
Explanation
REFERENCE: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 146-147.
Question 94
An 18-year-old female Marine Corps recruit enters basic training. Her enlistment history and physical examination showed that she was an elite high school cross country runner. What is her most significant risk factor for a femoral or pelvic stress fracture during basic training?
Explanation
12 menses. The referenced study did not find a statistically significant increase in risk of stress fracture in those recruits who had lesser menstrual irregularities in the year prior to recruit training, but there was a trend toward increased risk of stress fracture.
REFERENCES: Shaffer RA, Rauh MJ, Brodine SK, et al: Predictors of stress fracture susceptibility in young female recruits. Am J Sports Med 2006;34:108-115.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of
Orthopaedic Surgeons, 2004, pp 273-283.
Question 95
Figures 6a through 6d show the radiographs and biopsy specimens of an 8-year-old girl with leg pain. Management of the lesion should consist of
Explanation
REFERENCES: Wilson AJ, Kyriakos M, Ackerman LV: Chondromyxoid fibroma: Radiographic appearance in 38 cases and in a review of the literature. Radiology 1991;179:513-518.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 167-189.
Question 96
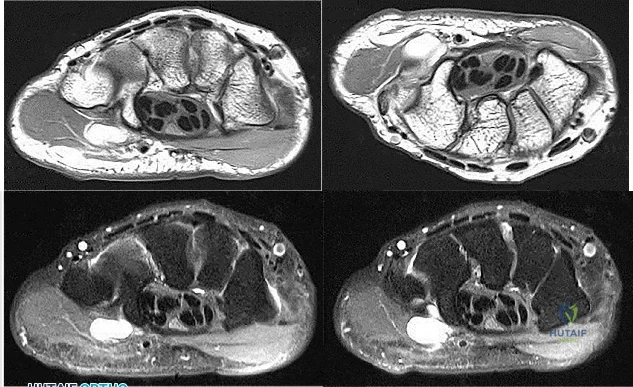
A 17-year-old presents with persistent left knee pain after a twisting injury during a soccer match 24 hours ago. On physical exam he has a mild effusion. He has tenderness to palpation on the medial joint line. Lachman test, anterior drawer test and posterior drawer test are attempted but limited secondary to pain. Dial test reveals a side-to-side external rotation difference of roughly 5 degrees. His MRI images are seen in Figures A-D. These findings would be most consistent with: Review Topic

Explanation
Many provocative tests have been described to aid in the diagnosis of meniscus tears.
The Apley test is performed with the patient prone, by axially loading the tibiofemoral joint at 90° of knee flexion. Pain with compression and external rotation (medial meniscus) or internal rotation (lateral meniscus) is considered positive.
The Ege's test is performed by having the patient squat with their knees maximally externally rotated or internally rotated. The test is positive when pain and/or a click is felt by the patient.
The McMurray test is performed by passively moving the knee from flexion to extension while externally or internally rotating the leg. A palpable click at the joint line with external rotation (medial meniscus) or internal rotation (lateral meniscus) is considered positive.
The Thessaly test is performed by supporting the patient as they internally or externally rotate their knee and body while keeping the foot planted, with the knee in 5° of flexion and then 20° of flexion. The test is positive when joint line pain and/or sense of locking/catching is experienced by the patient.
Ryzewicz et al. performed a systematic review of prospective cohort studies comparing magnetic resonance imaging (MRI) and clinical examination to arthroscopy in the diagnosis of meniscus tears. The Apley test, Ege's test, McMurray test and Thessaly test at 5° were shown have high specificity but low sensitivity. Joint line tenderness has a higher sensitivity, but lower specificity. The Thessaly test at 20° demonstrated the highest sensitivity and specificity, although there was only one available study evaluating this test.
Abdon et al. performed a prospective study looking at 68 clinical parameters to
determine which combinations of symptoms and signs indicated the presence of a meniscus tear. They found that joint-line tenderness and mechanical locking were predictive of a meniscus tear, while the McMurray sign did not prove valuable. Pain at rest, sick leave and medial patellar tenderness all negated the presence of a meniscus tear. The clinical accuracy in diagnosing meniscal tears was 61% in this study.
Figures A and B are T1 sagittal MR images demonstrating an intact anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL), respectively. Figures C and D are T2 coronal and sagittal MR images showing a complex tear of the posterior horn of the medial meniscus. Illustration A demonstrates the Ege's test. Illustration B shows the Thessaly test at 5° of flexion.
Incorrect
Question 97
Second impact syndrome (SIS) after head injury is characterized by which of the following?
Explanation
REFERENCES: Cantu RC: Second-impact syndrome. Clin Sports Med 1998;17:37-44.
Saunders RL, Harbaugh RE: Second impact in catastrophic contact-sports head trauma. JAMA 1984;252:538-539.
Stevenson KL, Adelson PD: Pediatric sports-related head injuries, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 781.
Question 98
A 19-year-old woman reports lower back pain following a motor vehicle accident. Radiographs obtained immediately after the accident and a bone scan obtained 4 weeks later are shown in Figures 25a through 25c. The patient asks questions regarding the cause, genetics, and natural history of her condition. She should be informed that the condition was
Explanation
REFERENCES: Lauerman WC, Cain JE: Isthmic spondylolisthesis in the adult. J Am Acad Orthop Surg 1996;4:201-208.
Hensinger RN: Spondylolysis and spondylolisthesis in children and adolescents. J Bone Joint Surg Am 1989;71:1098-1107.
Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
Fredrickson BE, Baker D, McHolik WJ, Yuan HA, Lubicky JP: The natural history of spondylolysis and spondylolisthesis. J Bone Joint Surg Am 1984;66:699-707.
Question 99
A 25-year-old professional baseball pitcher reports a 4-month history of gradually increasing medial elbow pain that occurs during the late cocking and acceleration phases of throwing. The pain occasionally refers distally along the ulnar aspect of the forearm. He denies any weakness; however, he notes occasional paresthesias. A nerve conduction velocity study demonstrates increased latency across the cubital tunnel. Management consisting of 6 weeks of rest and rehabilitation fails to provide relief as the symptoms returned when he resumed throwing. What is the best course of action?
Explanation
REFERENCES: Schickendantz MS: Diagnosis and treatment of elbow disorders in the overhead athlete. Hand Clin 2002;18:65-75.
Eaton RG, Crowe JF, Parkes JC III: Anterior transposition of the ulnar nerve using a non-compressing fasciodermal sling. J Bone Joint Surg Am 1980;62:820-825.
Question 100
Of the following clinical situations, which is most likely to lead to osteonecrosis associated with a slipped capital femoral epiphysis (SCFE)?
Explanation
REFERENCES: Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 2, pp 711-745.
