Orthopedic Board Review MCQs: Nerve, Upper Extremity & Pediatric Surgery Part 186

Key Takeaway
This page delivers Part 186 of a comprehensive Orthopedic Surgery Board Review. It features 100 high-yield, verified MCQs on Nerve topics, mirroring OITE and AAOS exam formats. Designed for orthopedic residents and surgeons, this interactive quiz offers essential board certification exam preparation.
About This Board Review Set
This is Part 186 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 186
This module focuses heavily on: Nerve.
Sample Questions from This Set
Sample Question 1: To adequately expose the volar plate of the proximal interphalangeal joint of the finger, which of following pulleys is typically incised?...
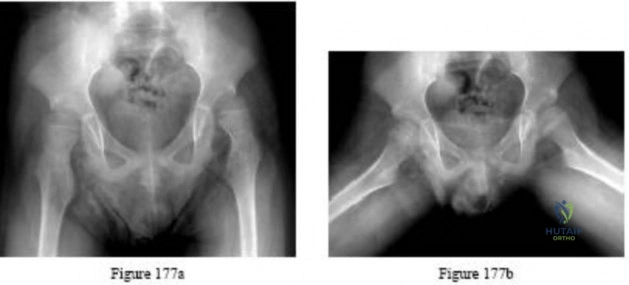
Sample Question 2: Figures 177a and 177b are the radiographs of a 7-year-old boy with spastic cerebral palsy. He has quadriparetic involvement and is unable to ambulate. He has very limited abduction, 30 degrees of flexion contractures, and pain on abduction....
Sample Question 3: -A patient undergoes an acute repair of a laceration of the median nerve in the antecubital fossa. A lack of functional recovery 6 months later is most likely due to...
Sample Question 4: What cell type causes the bone destruction in metastatic lesions?...
Sample Question 5: A 28-year-old man sustains the closed injury shown in Figures 3a through 3c after falling 8 feet while rock climbing. Management should consist of...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
To adequately expose the volar plate of the proximal interphalangeal joint of the finger, which of following pulleys is typically incised?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 176-186.
Strickland J: Flexor tendon-acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2,
pp 1853-1855.
Lin GT, Amadio PC, An KN, et al: Functional anatomy of the human digital flexor pulley system. J Hand Surg Am 1989;14:949-956.
Question 2
Figures 177a and 177b are the radiographs of a 7-year-old boy with spastic cerebral palsy. He has quadriparetic involvement and is unable to ambulate. He has very limited abduction, 30 degrees of flexion contractures, and pain on abduction. Bilateral varus osteotomies are scheduled with acetabular procedures to improve stability. Which type of acetabular osteotomy should be performed?
Explanation

Question 3
- A patient undergoes an acute repair of a laceration of the median nerve in the antecubital fossa. A lack of functional recovery 6 months later is most likely due to
Explanation
Functional recovery is generally complete after a crush injury because the basement membrane and endoneurium are left intact, and the damaged axons can regenerate within their original endoneurial tubes and reinnervate their original target organ. After a complete lesion to the nerve, however, functional recovery of movement is often quite poor. The loss of functional recovery probably is related to the failure of the axons to regenerate and the misdirection of regenerating axons, which leads to inappropriate innervation of denervated muscles. Inappropriate innervation is thought to result in a loss in the ability to accurately recruit individual muscles and motor units within a muscle, resulting in the loss of motor control.
Question 4
What cell type causes the bone destruction in metastatic lesions?
Explanation
REFERENCES: Cramer SF, Fried L, Carter KJ: The cellular basis of metastatic bone disease in patients with lung cancer. Cancer 1981;48:2649-2660.
Clohisy DR, Palkert D, Ramnaraine ML, Pekurovsky I, Oursler MJ: Human breast cancer induces osteoclast activation and increases the number of osteoclasts at sites of tumor osteolysis. J Orthop Res 1996;14:396-402.
Question 5
A 28-year-old man sustains the closed injury shown in Figures 3a through 3c after falling 8 feet while rock climbing. Management should consist of
Explanation
REFERENCES: Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp
1465-1518.
Grob D, Simpson LA, Weber BG, Bray T: Operative treatment of displaced talus fractures. Clin Orthop 1985;199:88-96.
Question 6
A patient sustained the injuries shown in the radiographs and clinical photograph seen in Figures 10a through 10c. The neurovascular examination is normal. The first step in emergent management of the extremity injuries should consist of
Explanation
REFERENCES: Sahin V, Karakas ES, Aksu S, et al: Traumatic dislocation and fracture-dislocation of the hip: A long-term follow-up study. J Trauma 2003;54:520-529.
Moed BR, WillsonCarr SE, Watson JT: Results of operative treatment of fractures of the posterior wall of the acetabulum. J Bone Joint Surg Am 2002;84:752-758.
Question 7
A 28-year-old woman has a moderate hallux valgus deformity and a prominence of the medial eminence. She can participate in all activities and reports that she could wear 3-inch heels in the past, but she now notes medial eminence pain even while wearing a soft leather flat shoe with a cushioned sole. She requests recommendations regarding surgical correction. Examination reveals a 1-2 intermetatarsal angle of 10 degrees. A clinical photograph and radiograph are shown in Figures 13a and 13b. What is the best course of action?
Explanation
REFERENCES: Chou LB, Mann RA, Casillas MM: Biplanar chevron osteotomy. Foot Ankle Int 1998;19:579-584.
Coughlin MJ: Roger A. Mann Award: Juvenile hallux valgus. Etiology and treatment. Foot Ankle Int 1995;16:682-697.
Pochatko DJ, Schlehr FJ, Murphey MD, Hamilton JJ: Distal chevron osteotomy with lateral release for treatment of hallux valgus deformity. Foot Ankle Int 1994;15:457-461.
Question 8
What is the most common site of metastases from a soft-tissue sarcoma?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 255-259.
Question 9
A 16-year-old girl injured her hip in a fall. Radiographs are shown in Figures 14a and 14b. She denies any history of pain prior to the fall and is currently asymptomatic. A bone scan, MRI scan, and biopsy specimens are shown in Figures 14c through 14f. What is the most likely diagnosis?
Explanation
REFERENCES: Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 30-43.
DiCaprio MR, Enneking WF: Fibrous dysplasia: Pathophysiology, evaluation, and treatment.
J Bone Joint Surg Am 2005;87:1848-1864.
Question 10
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with a prognosis if this patient is having a reaction to metal debris?
Explanation
Question 11
Figure 11 shows the anatomic dissection of the medial side of the knee joint after removal of the superficial fascia. The arrow is pointing to what structure?
Explanation
REFERENCES: Pagnani MJ, Warner JJ, O’Brien SJ, Warren RF: Anatomic considerations in harvesting the semitendinosus and gracilis tendons and a technique of harvest. Am J Sports Med 1993;21:565-571.
Warren LF, Marshall JL: The supporting structures and layers on the medial side of the knee: An anatomical analysis. J Bone Joint Surg Am 1979;61:56-62.
Question 12
Which of the following is the major blood supply to the heel pad?
Explanation
Question 13
Which of the following choices best describes the fracture pattern shown in Figures 2a through 2c?
Explanation
REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Matta J: Surgical treatment of acetabular fractures, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1009-1149.
Question 14
Which of the following procedures is considered most appropriate in patients with rheumatoid arthritis?
Explanation
REFERENCES: Granberry WM, Brewer EJ Jr: Early surgery in juvenile rheumatoid arthritis, in Calundruccio RA (ed): Instructional Course Lectures XXIII. St Louis, MO, CV Mosby, 1974, pp 32-37.
Stuchin SA, Johanson NA, Lachiewicz PF, Mont MA: Surgical management of inflammatory arthritis of the adult hip and knee, in Zuckerman JD (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-109.
Question 15
A 20-year-old college pitcher reports medial elbow pain after 3 innings of hard throwing. He recalls no injury and reports no pain with light throwing. The examination shown in the clinical photograph in Figure 48 reproduces the elbow pain. What is the most likely diagnosis?
Explanation
REFERENCES: Williams RJ III, Urquhart ER, Altchek DW: Medial collateral ligament tears in the throwing athlete. Instr Course Lect 2004;53:579-586.
Cain EL Jr, Dugas JR, Wolf RS, et al: Elbow injuries in throwing athletes: A current concepts review. Am J Sports Med 2003;31:621-635.
Question 16
What is the most common anatomic location for chondrosarcoma?
Explanation
REFERENCES: Marcove RC, Mike V, Hutter RV, et al: Chondrosarcoma of the pelvis and upper end of the femur: An analysis of factors influencing survival time in one hundred and thirteen cases. J Bone Joint Surg Am 1972;54:561-572.
Simon MA, Springfield DS, et al: Chondrosarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 276.
Question 17
Figure 15a shows the radiograph of a patient who has a chondrosarcoma of the acetabulum. Bone scans are shown in Figures 15b and 15c. Numerous soft subcutaneous masses are present. A clinical photograph of the hand is shown in Figure 15d. What is the most likely diagnosis?
Explanation
REFERENCES: Sun TC, Swee TC: Chondrosarcoma in Maffucci’s syndrome. J Bone Joint Surg Am 1985;67:1214-1219.
Schwartz HS, Zimmerman NB, Simon MA, et al: The malignant potential of enchondromatosis. J Bone Joint Surg Am 1987;69:269-274.
Began WB: Dyschondroplasia and hemangiomata (Maffucci’s syndrome). Arch Intern Med 1958;102:544.
Question 18
A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had
Explanation
Question 19
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
corrective osteotomy.
REFERENCES: O’Driscoll SW, Spinner RJ, McKee MD, et al: Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-1369.
Gurkan I, Bayrakci K, Tasbas B, et al: Posterior instability of the shoulder after supracondylar fractures recovered with cubitus varus deformity. J Pediatr Orthop 2002;22:198-202.
Spinner RJ, O’Driscoll SW, Davids JR, et al: Cubitus varus associated with dislocation of both the medial portion of the triceps and the ulnar nerve. J Hand Surg 1999;24:718-726.
Question 20
A 27-year-old man sustains a displaced femoral neck fracture and undergoes urgent open reduction internal fixation. What is the most prevalent complication after this injury?

Explanation
Haidukewych et al followed treatment of femoral neck fractures in young patients. They found almost 10% of displaced fractures were associated with the development of nonunion, where as 27% were associated with the development of osteonecrosis. Their results were influenced by fracture displacement and the quality of reduction. Varus malreduction most closely correlates with failure of fixation after reduction and cannulated screw fixation.
Swiontkowski reviews both the treatment and post operative complications in intracapsular hip fractures. In this Current Concept Review, the rate of AVN was discussed as being related to the pre-operative degree of displacement seen on radiographs.
Incorrect Responses:
Question 21
A patient who was involved in a motor vehicle accident 2 weeks ago now reports neck pain. Work-up reveals no evidence of nerve root involvement or acute radiographic abnormality. The patient appears to have a hyperextension soft-tissue injury of the neck (whiplash). What is the best course of treatment at this time?
Explanation
REFERENCES: Borchgrevink GE, Kaasa A, McDonagh D, Stiles TC, Haraldseth O, Lereim I: Acute treatment of whiplash neck injuries: A randomized trial during the first 14 days after a car accident. Spine 1998;23:25-31.
Mealy K, Brennan H, Fenelon GC: Early mobilization of acute whiplash injuries. Br Med J 1986;292:656-657.
Question 22
Figures 115a and 115b are the radiograph and intraoperative view of the femoral taper junction of a 68-year-old man who has left groin pain 8 years after undergoing total hip arthroplasty (THA). He has a mild limp and mild pain with active and passive range of motion. His erythrocyte sedimentation rate and C-reactive protein level are within defined limits. His serum cobalt level is 5.3 ppb and serum chromium level is 3.4 ppb. In addition to exchanging the acetabular insert, what is the best surgical procedure for this patient?
Explanation
This patient has symptomatic severe pelvic and femoral osteolysis occurring after a metal-on-metal bearing THA. Bearing surface wear and taper wear (corrosion) are debris sources contributing to osteolysis, and both sources should be addressed at surgery. Current recommendations are to not remove a stable cementless femoral component unless the taper is damaged so badly that a new ball will not lock on the taper. There have been reports of repeat local tissue reactions when a new cobalt chromium ball is placed on a taper with corrosion damage. The current recommendation is to minimize the amount of cobalt at the taper junction, and this can be done by avoiding a cobalt chromium ball in favor of a titanium taper sleeve on the damaged taper with a ceramic ball on the new sleeve. Use of a ceramic head on a previously used trunnion poses risk for fracture of the ceramic head.
Question 23
When posterior fusion with instrumentation to the sacrum is used to treat adult scoliosis, what instrumentation technique best increases the chance of a successful lumbosacral fusion?
Explanation
REFERENCES: Islam NC, Wood KB, Transfeldt EE, et al: Extension of fusions to the pelvis in idiopathic scoliosis. Spine 2001;26:166-173.
O’Brien N, et al: Sacral pelvic fixation and spinal deformity, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 601-614.
McCord DH, Cunningham BW, Shono Y, et al: Biomechanical analysis of lumbosacral fixation. Spine 1992;17:S235-S243.
Question 24
A healthy 70-year-old man has a swollen knee after undergoing a knee replacement 10 years ago. Aspiration of the knee reveals cloudy, viscous synovial fluid. Laboratory studies show an erythrocyte sedimentation rate of 10 mm/h and a C-reactive protein level of less than 0.5. What is the most likely diagnosis?
Explanation
REFERENCE: Barrack RL, Jennings RW, Wolfe MW, Bertot AJ: The value of preoperative aspiration before total knee revision. Clin Orthop 1997;345:8-16.
Question 25
A 30-year-old man who participates in recreational sports reports the spontaneous onset of intermittent pain and swelling about the right knee. Examination reveals a 3+ effusion, with a range of motion of 10° to 60°. He has mild diffuse tenderness but no instability. MRI scans and an arthroscopic view are shown in Figures 39a through 39c. Management should consist of
Explanation
REFERENCES: Coolican MR, Dandy DJ: Arthroscopic management of synovial chondromatosis of the knee: findings and results in 18 cases. J Bone Joint Surg Br
1989;71:498-500.
Ogilvie-Harris DJ, Saleh K: Generalized synovial chondromatosis of the knee: A comparison
of removal of the loose bodies alone with arthroscopic synovectomy. Arthroscopy
1994;10:166-170.
Question 26
All of the following are factors associated with transfer of patients to Level 1 trauma centers EXCEPT:

Explanation
Question 27
A 64-year-old man undergoes a primary total knee arthroplasty. Three months after surgery he reports persistent pain, weakness, and difficulty ambulating. Postoperative radiographs are shown in Figures 6a through 6c. What is the best course of action at this time?
Explanation
REFERENCES: Kelly MA: Extensor mechanism complications in total knee arthroplasty.
Instr Course Lect 2004;53:193-199.
Malkani AL, Karandikar N: Complications following total knee arthroplasty. Sem Arthroplasty 2003;14:203-214.
Norman AJ, Scott S, David GN (eds): Master Techniques in Knee Arthroplasty, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2003.
Question 28
A direct lateral (Hardinge) approach is used during total hip arthroplasty. The structure labeled A in Figure 7 is the
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 333-335.
Ramesh M, O’Byrne JM, McCarthy N, et al: Damage to the superior gluteal nerve after the Hardinge approach to the hip. J Bone Joint Surg Br 1996;78:903-906.
Question 29
A 71-year-old woman undergoes a posterior lumbar decompression and fusion from L4-S1. Thirty-six hours after the procedure, she reports severe right-sided chest pain and shortness of breath. Doppler ultrasound reveals a clot proximal to the knee within the femoral vein. A large pulmonary embolus is confirmed by CT angiography. The next most appropriate step in management should consist of
Explanation
REFERENCES: Cain JE Jr, Major MR, Lauerman WC, et al: The morbidity of heparin therapy after development of pulmonary embolus in patients undergoing thoracolumbar or lumbar spinal fusion. Spine 1995;20:1600-1603.
Roberts AC: Venous imaging and inferior vena cava filters. Curr Opin Radiol 1992;4:88-96.
Becker DM, Philbrick JT, Selby JB: Inferior vena cava filters. Arch Intern Med
1992;152:1985-1994.
Question 30
An 18-year-old woman sustains a twisting injury of the knee while skiing. Figures 7a and 7b show the radiograph and coronal MRI scan of the knee. In addition to the injury shown, what is the most likely associated injury?
Explanation
REFERENCES: Goldman AB, Pavlov H, Rubenstein D: The Segond fracture of the proximal tibia: A small avulsion that reflects major ligamentous damage. Am J Roentgenol 1988;151:1163-1167.
Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 31
A 51-year-old butcher has an 18-month history of recalcitrant medial elbow pain, which is affecting his occupational demands. He describes the pain as mainly anterior and distal to the medial epicondyle. His symptoms are exacerbated with resisted wrist flexion and forearm pronation. On examination, he is also found to have a positive Tinel's sign at the elbow with weakness of intrinsic strength. He has attempted physical therapy, activity modification, bracing, and anti-inflammatory medication without any significant improvement. Presurgical counseling should include the understanding that
Explanation
of pathologic tissue, release of the flexor carpi radialis - pronator teres origin, and/or repair of the flexor carpi radialis - pronator teres origin. Several authors have raised concern of the impact of concomitant ulnar neuropathy on results following surgical treatment for medial epicondylitis. Kurvers and Verhaar and Gabel and Morrey, among others, have reported a statistically significant association between concomitant ulnar neuropathy and worse outcomes following surgery. Most patients can anticipate a return to prior activity levels after surgery without any consistently reported loss of flexor/pronator strength. Prior corticosteroid injections
have not been found to impact results.
Question 32
A 13-year-old girl was riding on an all-terrain vehicle when the driver struck a tree. She sustained the injury shown in Figures 45a through 45d. This injury is best described as what type of acetabular fracture pattern?
Explanation
of displacement.
REFERENCES: Helfet DL, Beck M, Gautier E, et al: Surgical techniques for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 533-603.
Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 33
A 7-year-old girl has had a painful forearm for the past 2 months. Examination reveals fullness on the volar aspect of the forearm. Radiographs and an MRI scan are shown in Figures 42a through 42c. Biopsy specimens are shown in Figures 42d and 42e. What is the most likely diagnosis?
Explanation
REFERENCES: Garzon M: Hemangiomas: Update on classification, clinical presentation and associate anomalies. Cutis 2000;66:325-328.
Kurkcuoglu IC, Eroglu A, Karaoglanoglu N, et al: Soft tissue hemangioma is a common soft tissue neoplasm. Eur J Radiol 2004;49:179-181.
Question 34
Figure 13 shows the clinical photograph of a 66-year-old man who has had an increasingly painful right foot deformity for the past 3 years. Examination reveals that the subtalar joint is fixed in 15° of valgus, and forefoot supination can be corrected to 10° from neutral. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
REFERENCE: Mann RA: Flatfoot in adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 757-784.
Question 35
A 20-year-old woman sustained the closed injury shown in Figures 49a and 49b in a motor vehicle accident. Examination reveals that this is an isolated injury; however, she has a complete radial nerve palsy. Management should consist of
Explanation
REFERENCES: Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high-energy humeral shaft fractures. J Hand Surg Am 2004;29:144-147.
Foster RJ, Swiontkowski MF, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.
Question 36
Figure 19 shows an arthroscopic view from the anterior lateral portal of the knee looking into the suprapatella pouch. The use of an electrothermal device during this procedure most commonly causes significant postoperative complications by damaging which of the following structures?
Explanation
REFERENCES: Cash JD, Hughston JC: Treatment of acute patella dislocation. Am J Sports Med 1988;16:244-249.
Henry R, Goletz B, Williamson C: Lateral release in patello-femoral subluxation. Am J Sports Med 1986;14:121.
Question 37
Antibiotic-loaded bone cement prostheses, such as that shown in Figure 8, are best created by using which of the following methods?
Explanation
High-dose antibiotic-loaded bone cements are described as those containing greater than 1.0 g of antibiotic per 40 g of cement. Effective elution levels have been documented with 3.6 g tobramycin and 1.0 g vancomycin per 40 g of bone cement. This was documented by Penner and associates. Furthermore, it was shown that the combination of the two antibiotics in the bone cement improved the elution of both antibiotics.
REFERENCES: Hanssen AD, Spangehl MJ: Practical applications of antibiotic-loaded bone cement for treatment of infected joint replacements. Clin Orthop 2004;427:79-85.
Penner MJ, Masri BA, Duncan CP: Elution characteristics of vancomycin and tobramycin combined in acrylic bone-cement. J Arthroplasty 1996;11:939-944.
Question 38
A 22-year-old patient sustained a jamming injury to the right little finger. The lateral radiograph shown in Figure 18 reveals comminution of the base of the middle phalanx, with palmar and dorsal metaphyseal cortical involvement. The articular surface also is disrupted. Management should consist of
Explanation
REFERENCES: Stern PJ, Roman RJ, Kiefhaber TR, McDonough JJ: Pilon fractures of the proximal interphalangeal joint. J Hand Surg Am 1991;16:844-850.
Krakauer JD, Stern PJ: Hinged device for fractures involving the proximal interphalangeal joint. Clin Orthop 1996;327:29-37.
Question 39
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management? Review Topic
Explanation
Question 40
During percutaneous iliosacral screw placement for an unstable pelvic ring injury, use of the lateral sacral fluoroscopic image is critical to help avoid iatrogenic injury to what structure?

Explanation
In the 2000 reference by Routt et al, they state "a thorough knowledge of pelvic osseous anatomy, injury patterns, deformities, and their fluoroscopic correlations are mandatory for percutaneous pelvic fixation to be effective."
Illustration A shows a representative lateral sacral radiograph, with the major anatomic landmarks labeled. Safe SI screw insertion in the S1 body should be underneath the sacral ala line to minimize risk of a "in-out-in" screw that would come out in the area of the ala and injure the L5 nerve root that sits directly on top of this structure. Dysmorphic pelvic rings will often have a more vertical sacral line, or one that starts more inferiorly.
Question 41
A 52-year-old man has had back pain radiating to the left leg for the past 5 weeks. A radiograph, MRI scans, and biopsy specimens are shown in Figures 23a through 23f. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, vol 1, ch 8.
Question 42
A B
Explanation
The radiographs reveal a tibial pilon fracture with an extruded and rotated anterior tibial fragment that lies deep to the anterior compartment neurovascular bundle, which contains the deep peroneal nerve. This nerve innervates the anterior compartment muscles and the extensor digitorum brevis and extensor hallucis brevis muscles and provides sensation to the dorsal aspect of the first interspace. An injury to the deep peroneal nerve at this level will only affect the innervation to the extensor digitorum brevis and extensor hallucis brevis muscles and the innervation of the first interspace. The superficial peroneal nerve innervates
the lateral compartment muscles above the level of this injury and innervates the dorsum of the foot. The medial forefoot is innervated by the saphenous nerve and the posterior tibial nerve innervates the posterior compartment muscles above the level of the injury. The sural nerve innervates the lateral foot and has no motor component, and the superficial peroneal nerve innervates the peroneus longus, which plantar flexes the first metatarsal above the level of the injury.
RECOMMENDED READINGS
Agur AM, Dalley AF, eds. Grant’s Atlas of Anatomy. 13th ed. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 2013:362-370.
Hoppenfeld S, de Boer P, Buckley R, eds. Surgical Exposures in Orthopaedics: The Anatomic Approach. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:625-673.
Question 43
Figure 39 shows the AP radiograph of a 62-year-old man with degenerative osteoarthritis secondary to trauma. History reveals that he underwent total elbow arthroplasty 3 years ago. He continues to report instability and constant pain. A complete work-up, including aspiration and cultures, is negative. Treatment should consist of removal of the components and
Explanation
REFERENCES: Linscheid RL: Resurfacing elbow replacement arthroplasty: Rationale, technique and results, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 602-610.
Morrey BF, King GJ: Revision of failed total elbow arthroplasty, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 685-700.
Question 44
What structure is located immediately posterior to the capsule at the posterior cruciate ligament tibial insertion?
Explanation
tibial insertion, separated only by the posterior capsule of the knee. When performing
a posterior cruciate ligament reconstruction, this artery is at risk for injury during creation
of the tibial tunnel.
REFERENCES: Jackson DW, Proctor CS, Simon TM: Arthroscopic assisted PCL reconstruction: A technical note on potential neurovascular injury related to drill bit configuration. J Arthroscopy 1993;9:224-227.
Malek MM, Fanelli GC: Technique of arthroscopically assisted PCL reconstruction. Orthopedics 1993;16:961-966.
Question 45
A patient undergoes the procedure shown in Figure A. This patient is most likely to be Review Topic
Explanation
In the pediatric population, arthroereisis is one option to restore the alignment of the hindfoot after talocalcaneal coalition. Hindfoot deformity correction is required because resection of the coalition alone will often increase the hindfoot valgus
deformity. The arthroereisis implant prevents this valgus collapse. Another alternative to correct the hindfoot valgus deformity is a calcaneal lateral column lengthening osteotomy.
Khoshbin et al. reviewed the long-term outcomes of coalition resection in 24 patients (32 coalitions). Resected talocalcaneal (TC) coalitions had less inversion/eversion postoperatively than resected calcaneonavicular (CN) coalitions but there was no difference in outcome scores. They obtained favorable results when even resecting talocalcaneal coalition with >50% involvement of the middle facet and hindfoot valgus angles >16 °, which were considered historical contraindications to resection.
Zaw et al. reviewed tarsal coalitions. Radiographic signs of CN coalition include the anteater sign (elongated anterior calcaneal process), decreased CN gap, reverse anteater sign (elongated lateral navicular) and hypoplastic lateral talar head. Radiographic signs of TC coalition include obliterated middle facet on a Harris view (osseous coalition), irregular cortices/dysplastic sustentaculum tali on a Harris view (nonosseous), C-sign on a lateral view, talar beaking, short talar neck with concave inferior surface, narrow posterior facet, and non-visibility of the middle facet.
Giannini et al. reviewed subtalar arthroereisis with coalition resection in 14 feet in patients aged 9-18 years. They achieved 57% excellent, 21% good and 21% fair results. Regarding pain, 86% had improvement and 14% had no change. Regarding ROM, 93% had improvement, and 7% had no change. Better scores were seen in patients <14 years.
Figure A shows the implantation of an arthroereisis implant in the sinus tarsi. Illustration A comprises coronal CT images of talocalcaneal coalition.
Incorrect Answers:
Question 46
By which mechanism can a true aneurysm of the ulnar artery result?
Explanation
Question 47
A 27-year-old man was struck by a taxi cab and sustained comminuted right distal third tibia and fibula fractures; treatment consisted of placement of an intramedullary nail in the tibia the following morning. At his 6-month follow-up, he has clawing of all five toes. Examination reveals flexion deformities of the distal and proximal interphalangeal joints that are flexible with plantar flexion and rigid with dorsiflexion. Calluses are present on the dorsum and tip of the toes. Single heel rise is normal. He has a mild equinus contracture (relative to the left leg) that is not relieved with knee flexion. What is the most appropriate treatment option?
Explanation
REFERENCES: Feeny MS, Williams RL, Stephens MM: Selective lengthening of the proximal flexor tendon in the management of acquired claw toes. J Bone Joint Surg Br 2001;83:335-338.
Clawson DK: Claw toes following tibial fracture. Clin Orthop Relat Res 1974;103:47-48.
Question 48
A 3-year-old boy sustains a complete paralysis following a high thoracic spinal cord injury consistent with a SCIWORA-type injury (spinal cord injury without radiographic abnormality). Subsequent progressive spinal deformity will develop in what percent of patients with this injury?
Explanation
REFERENCES: Mayfield JK, Erkkila JC, Winter RB: Spine deformity subsequent to acquired childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-1411.
Lancourt JE, Dickson JH, Carter RE: Paralytic spinal deformity following traumatic spinal cord injury in children and adolescents. J Bone Joint Surg Am 1981;63:47-53.
Dearolf WW III, Betz RR, Vogel LC, Levin J, Clancy M, Steel HH: Scoliosis in pediatric spinal cord injured patients. J Pediatr Orthop 1990;10:214-218.
Question 49
The majority of severe cervical spine injuries occurring in contact sports evolve during axial loading and flexion of the cervical spine. At what minimum degree of flexion does axial loading place the cervical spine at risk during contact sports?
Explanation
REFERENCES: Thomas BE, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
Torg JS, Truex R Jr, Quedenfeld TC, Burstein A, Spealman A, Nichols C III: The National Football Head and Neck Injury Registry: Report and conclusions 1978. JAMA 1979;241:1477-1479.
Question 50
A 34-year-old man sustained a tibial fracture in a motorcycle accident. What perioperative variable is associated with the greatest relative risk for reoperation to achieve bone union?
Explanation
REFERENCE: Bhandari M, Tornetta P III, Sprague S, et al: Predictors of reoperation following operative management of fractures of the tibial shaft. J Orthop Trauma 2003;17:353-361.
Question 51
-While obtaining informed consent for a lateral closing-wedge osteotomy, what complication should be discussed with the patient as exclusive to this procedure and not encountered in medial opening-wedge osteotomy?
Explanation

Figure 56 is the MRI scan of a 15-year-old girl who had left knee pain after sustaining a noncontact twisting injury while playing soccer. She reported severe pain initially that has since improved. On examination, she had a large knee effusion with lateral joint line tenderness. Range of motion is from 5 degrees of extension to 70 degrees of flexion. She wishes to return to sports at her preinjury level of activity.
Question 52
Figure 1 is the radiograph of an 18-year-old, right hand-dominant man who has right side thumb pain after a tackle during a rugby game. Examination shows ecchymosis and swelling of the right thumb along with tenderness to palpation about the thumb CMC joint and metacarpal base. What ligament is holding the small fracture fragment in anatomical location to the trapezium?

Explanation
Bennett fractures are defined as intra-articular thumb metacarpal base fractures. The fracture is often caused by axial loading, and concomitant injuries to the thumb MCP joint and trapezium are common. The palmar ulnar aspect of the base of the metacarpal stays in place through its attachment to the trapezium by way of the anterior oblique ligament. The metacarpal shaft is displaced dorsally, proximally, and radially by the pull of the abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, and adductor pollicis brevis. These fractures are often considered unstable and are treated surgically.
Question 53
Figure 33 shows the MRI scan of a 55-year-old woman who has had a 6-week history of back and leg pain. Which of the following clinical scenarios is most consistent with the MRI scan findings at L4-L5?
Explanation
REFERENCE: McCullouch JA, Transfeldt EE: Macnab’s Backache, ed 3. Philadelphia, PA, Williams and Wilkins, 1997, pp 569-608.
Question 54
In total knee arthroplasty, in vitro testing has shown that cross-linking can diminish the rate of polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
Explanation
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been shown to cause implant failure in the most recent clinical trials, but they remain the most important mechanical issues associated with current material processing methods.
Question 55
Figure 5 is a T2-weighted MR image of a 26-year-old man who has had left leg pain for 3 months that has failed nonsurgical treatment. Surgical decompression is planned. Which approach would provide the most direct ability to perform surgical decompression?

Explanation
The MR image shows a far lateral disk herniation impinging on the exiting nerve root lateral to the exiting foramen. This is reached most directly with a far lateral (Wiltse) approach. This is a posterior paramedian approach that uses the interval between the paraspinal muscles (multifidus and longissimus) and arrives onto the facet joints. The intertransverse membrane can then be released, exposing the far lateral disk herniation. A posterior midline approach will allow easy access to the spinal canal, which is medial to the disk herniation, and will not allow for easy disk removal without the need for a facetectomy, which would destabilize the level. An anterior approach would not allow for access to the far lateral disk herniation, nor would a traditional retroperitoneal or newer transpsoas approach.
RECOMMENDED READINGS
Wiltse LL, Spencer CW. New uses and refinements of the paraspinal approach to the lumbar spine. Spine (Phila Pa 1976). 1988 Jun;13(6):696-706. PubMed PMID: 3175760. View Abstract at PubMed
Epstein NE. Evaluation of varied surgical approaches used in the management of 170 far-lateral lumbar disc herniations: indications and results. J Neurosurg. 1995 Oct;83(4):648-56. PubMed PMID: 7674015. View Abstract at PubMed
Question 56
An 8-year-old boy with moderate factor VIII hemophilia played kickball earlier in the day and now reports progressively severe groin pain and is unable to walk. Examination reveals marked paresthesias over the medial aspect of the distal tibia. What is the most likely diagnosis?
Explanation
REFERENCES: Greene WB: Diseases related to the hematopoietic system, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 379-426.
Gilbert MS, Radomisli TE: Therapeutic options in the management of hemophilic synovitis. Clin Orthop 1997;343:88-92.
Question 57
A 69-year-old patient with diabetes has had acute-onset back pain and difficulty with ambulation for several hours. Evaluation reveals a temperature of 38.3°C, a white blood cell (WBC) count of 14000/µL (reference range [rr], 4500-11000/µL), C-reactive protein (CRP) level of 120 mg/L (rr, 0.08-3.1 mg/L), erythrocyte sedimentation rate of 130 mm/h (rr, 0-20 mm/h), normal rectal examination findings, and normal sensation to light touch. Motor function testing of the lower extremities reveals 3/5 ankle dorsiflexion and 4/5 plantar flexion strength bilaterally. An MR image reveals a large epidural abscess from L1-5. What is the most appropriate treatment at this time?
Explanation
Epidural abscess is a serious and potentially disastrous condition. Although medical management is effective in some situations, surgical decompression is considered urgent with the presence of a neurological deficit. Medical management can be considered in the case of a neurologically intact patient, particularly when the microorganism has been identified. If medical management is chosen, careful observation and serial examination for neurologic deterioration is required. Surgical decompression is indicated if a patient's neurologic status worsens or if medical management failure is noted. Additionally, diabetes, a CRP level higher than 115 mg/L, WBC higher than 12500/µL , and bacteremia have proven predictive of medical treatment failure. This patient would be a better candidate for urgent surgical decompression and subsequent IV antibiotics than for medical management.
RECOMMENDED READINGS
Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.View Abstract at PubMed
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 58
An 18-year-old boxer sustained a blow to his right eye in a boxing match. Examination on the sideline reveals hyphema, reduced visual acuity and color vision, and a visual field cut. What is the next step in management? Review Topic
Explanation
Question 59
A patient undergoes cartilage implantation requiring amplification of donor cells. Which of the following statements best describes the transplants?
Explanation
REFERENCES: Brittberg M, Peterson L, Sjogren-Jansson E, et al: Articular cartilage engineering with autologous chondrocyte transplantation. J Bone Joint Surg Am
2003;85:109-115.
Caplan AI, Elyaderani M, Mochizuki Y, et al: Principles of cartilage repair and regeneration. Clin Orthop 1997;342:254-269.
Question 60
Figures 61a and 61b show the CT and MRI scans of a 40-year-old man who has hip pain. He undergoes total hip arthroplasty and curettage and cementation of the lesion as shown in Figure 61c. Histopathologic photomicrographs of the curettage specimen are shown in Figures 61d and 61e. What is the best course of treatment?
Explanation
REFERENCES: Weber KL, Pring ME, Sim FH: Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res 2002;397:19-28.
Pring ME, Weber KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642
Question 61
Figure 40 shows the radiograph of a 30-year-old woman who has a painful elbow. Examination reveals a deformed skull, multiple cafe-au-lait spots, and bone deformities. What is the most likely diagnosis?
Explanation
REFERENCES: Albright F, Butler AM, Hampton AO, et al: Syndrome characterized by osteitis fibrosa disseminata, areas of pigmentation and endocrine dysfunction with precocious puberty in females. N Engl J Med 1937;216:727-746.
Danon M, Robboy SJ, Kim S, Scully R, Crawford JD: Cushing syndrome, sexual precocity, and polyostotic fibrous dysplasia (Albright syndrome) in infancy. J Pediatr 1975;87:917-921.
Grabias SL, Campbell CJ: Fibrous dysplasia. Orthop Clin North Am 1977;8:771-783.
Question 62
If the patient had an isolated spine injury without neurologic deficit, the most appropriate next step would be
Explanation
The treatment of thoracolumbar burst fractures has evolved over the years. In the absence of a neurologic deficit or a posterior ligamentous complex injury, nonsurgical treatment is as effective as surgery. The degree of spinal canal compromise is not a risk factor for neurologic symptoms. Similarly, although kyphosis may be a marker of more significant injury, the degree of kyphosis does not correlate with chronic pain. In the setting of a burst fracture, MRI can be used to evaluate the integrity of the posterior ligamentous complex. Polytrauma may be considered a relative indication for surgical intervention in the setting of a stable burst fracture.
RECOMMENDED READINGS
Rechtine GR 2nd. Nonoperative management and treatment of spinal injuries. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S22-7; discussion S36. Review. PubMed PMID: 16685232. View Abstract at PubMed
Shen WJ, Shen YS. Nonsurgical treatment of three-column thoracolumbar junction burst fractures without neurologic deficit. Spine (Phila Pa 1976). 1999 Feb 15;24(4):412-5. PubMed PMID: 10065527. View Abstract at PubMed
Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. View Abstract at PubMed
Wood KB, Li W, Lebl DS, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014 Jan;14(1):145-64. doi: 10.1016/j.spinee.2012.10.041. Review. PubMed PMID: 24332321.View Abstract at PubMed
Question 63
Figures 1 and 2 show the radiographs obtained from a 68-year-old morbidly obese man who underwent left total hip replacement 7 years ago and did well, with no symptoms prior to the current presentation. He recently rose from a seated position and felt a pop in the hip, with immediate pain and inability to bear weight. Any pressure on the left foot now produces a painful, grinding sensation with loss of left hip stability. What is the best next step?

Explanation
The modular femoral stem has fractured. Changing the liner to a constrained design is not warranted at this time based on the information provided. Revision of the acetabular implant is appropriate because of the potential for damage to the existing cup from metal debris and femoral implant contact and to convert from a metal-on-metal articulation. Nonsurgical management would not provide pain relief or improvement; revision of the total hip arthroplasty is recommended. The implant failed in a short time, and retention of the femoral stem is not recommended because of the concern for failure with only a neck exchange. A dual-mobility bearing may be a good option if the surgeon plans to retain the acetabular component. Extended trochanteric osteotomy is a useful technique for the removal of a well-fixed femoral implant. In this patient, femoral stem removal without
osteotomy would be difficult due to the fracture of the implant’s femoral neck and the inability to gain purchase for extraction.
Question 64
The most appropriate treatment for this fracture is
Explanation
Tibial fractures are classified on the basis of their anatomical location and the status of the prosthesis fixation. Type I fractures involve the tibial plateau, type II fractures occur adjacent to the stem of the tibial component, type III fractures are distal to the tibial stem, and type IV fractures involve the tibial tubercle. Subclassifications include A with a well-fixed implant; B with a loose implant; and C, which occur intraoperatively.
Treatment of periprosthetic tibial fractures is based on the location of the fracture and the status of the component fixation. Types II or III fractures associated with prosthetic loosening or instability are best managed with revision arthroplasty, usually with a diaphyseal-engaging intramedullary tibial stem. Supplemental internal fixation may be necessary. Type III fractures with well-fixed and stable implants are treated using the standard principles of tibial fracture management.
Question 65
A 31-year-old woman has increasing pain and tightness in her right knee, with occasional stiffness and recurrent hemorrhagic effusions. MRI scans are shown in Figures 2a and 2b. What is the most likely diagnosis?
Explanation
REFERENCES: De Ponti A, Sansone V, Malchere M: Result of arthroscopic treatment of pigmented villonodular synovitis of the knee. Arthroscopy 2003;19:602-607.
Chin KR, Barr SJ, Winalski C, et al: Treatment of advanced primary and recurrent diffuse pigmented villonodular synovitis of the knee. J Bone Joint Surg Am 2002;84:2192-2202.
Bhimani MA, Wenz JF, Frassica FJ: Pigmented villonodular synovitis: Keys to early diagnosis. Clin Orthop 2001;386:197-202.
Question 66
5 standard deviations below young normals (< -2.5). The Z-score represents a comparison to age-matched normals.
Explanation
This patient has an impending subtrochanteric femur fracture and should be stabilized with cephalomedullary nailing.
Bisphosphonates have been shown to prevent osteoporotic fractures. They suppress osteoclastic recruitment and activity and induce apoptosis of osteoclasts. However, they have also been associated with subtrochanteric femur fractures. Cortical stress reactions in the form of lateral cortical thickening have been documented when radiographs were performed during the prodromal period preceding these fractures. If radiographs are obtained and demonstrate lateral cortical thickening in the presence of thigh pain, the entire femur should be stabilized with prophylactic cephalomedullary nailing to prevent fracture.
Shane et al. performed a review of atypical subtrochanteric and diaphyseal
femoral fractures. They report that long-term bisphosphonate use is associated with these injuries. Bisphosphonates localize in areas that are developing stress fractures and suppress intracortical remodeling. When bisphosphonate use has stopped, the risk of fracture decreases over time. They conclude that teriparatide may advance the healing of atypical femur fractures after surgical treatment.
Koh et al. studied the natural history of femoral stress lesions associated with bisphosphonate therapy. They determined certain features that predispose to complete stress fractures. They found all patients had thigh pain before fracture. They conclude that cortical stress reactions associated with prolonged antiresorptive therapy and the "dreaded black line" should be prophylactically stabilized to avoid a complete fracture.
Figure A is a radiograph of the proximal femur demonstrating lateral cortical thickening with the "dreaded black line." Illustration A is the same image with an arrow indicating the "dreaded black line."
Incorrect Answers:
Which of the following statements regarding bone mineral density (BMD) is true?
The 2017 American College of Rheumatology/American Association of Hip and Knee Surgeons Guideline for the Perioperative Management of Antirheumatic Medication states that hydroxychloroquine can be continued and etanercept
should be held for 2 weeks prior to undergoing total hip arthroplasty.
Patients with rheumatoid arthritis (RA) report high satisfaction following hip or knee replacement despite the higher rates of infection, dislocation, and readmission rates. Patients with RA may present on a variety of different biologic and nonbiologic medications used to control their systemic RA.
Optimal preoperative management of these immunosuppressant medications may help mitigate some of the risks of postoperative complications in RA patients.
Singh et al. reviewed the evidence surrounding the benefits and harms of various antirheumatic medications. They found evidence for traditional DMARDs, biologic agents, and nonbiologic agents in acute and established RA totaling 74 recommendations. They concluded that these recommendations are not prescriptions and that ultimate decision making should be patient- specific in a shared-decision
making process between the patient and physician.
Goodman et al. performed a multistep literature review on optimal antirheumatic medication management prior to joint replacement surgery. They were able to provide recommendations on when to continue, when to withhold, and when to restart these medications, and the optimal perioperative dosing of glucocorticoids. They concluded that these guidelines will help physicians manage antirheumatic medications at the time of elective THA or TKA.
Incorrect Answers:
An 83-year-old woman presents complaining of thigh pain. The pain has been progressing over the last few months. She denies any night chills or recent weight loss. She has smoked 1 pack per day for the last 40 years. Her current medications are alendronate and citalopram. Her current imaging is shown in Figure A. What is the next best step in treatment?
The patient is presenting with complex regional pain syndrome (CRPS) type 1 after a distal 1/3 tibial shaft fracture. The best diagnostic test for this is a thorough history and physical exam.
CRPS is a disorder of increased sympathetic activity in a region of prior trauma. Cases can be classified as type 1, where there is no demonstrable nerve damage, or type 2, where a specific nerve is affected. Patients will typically present with cool and mottled skin that atrophic and absent of hair. Many times the affected limb will be noticeably cooler than the contralateral side. In advanced stages, there will be joint contractures and extensive osteopenia on radiographs. Several diagnostic aids have been developed, but remain inadequate to diagnostic sensitivity compared to a thorough history and physical.
Shah et al. reviewed the diagnosis and treatment of CRPS. The authors reported that sweat quantification testing, skin thermography, and electromyography may be useful aids in diagnosis, but there is a lack of diagnostic sensitivity to make these tests reliable. The authors concluded that evidence suggests gabapentin, prazosin, propranolol, nifedipine, and mexiletine are the best medications for treatment.
Hogan et al. reviewed the diagnosis and treatment of CRPS. The authors reported that the most sensitive means for diagnosis is a good history and physical exam as there is no single test to confirm the diagnosis. The authors recommended a multidisciplinary team approach including pain specialists, physical therapists, and orthopedic surgeons as syndrome response to medications is variable.
Figures A and B demonstrate an AP and lateral radiograph of the right tibia and fibula with a distal 1/3 tibia fracture. Illustration A depicts that Lankford and Evans classification for CRPS.
Incorrect Answers:
A 72-year-old female with rheumatoid arthritis is scheduled to undergo total hip arthroplasty. She presents for her preoperative visit and asks about dosing of her antirheumatic medications. She currently takes etanercept weekly and hydroxychloroquine daily. Which of the following is the best dosing recommendation for her antirheumatic medications prior to surgery?
the entire right lower extremity, with sensitivity to cold temperatures. Physical exam demonstrates hyperesthesia of the extremity, thin and shiny appearing skin, cyanotic appearing with skin cool to the touch. What is the likely diagnosis and what is the best diagnostic test?
In a 5-year-old female without a history of trauma or rashes and with persistent oligoarthritis that improves during the day, the most likely diagnosis is juvenile idiopathic arthritis (JIA). Early-onset JIA is associated with chronic uveitis.
JIA is defined by the American College of Rheumatology as persistent arthritis and swelling in one or more joints for 6 weeks or longer in a patient younger than 16 years of age. It is a diagnosis of exclusion, usually entailing pattern recognition after a thorough history and physical exam. Serologic studies, including rheumatoid factor (RF), antinuclear antibody (ANA), and HLA-B27, may be helpful to rule out other etiologies (septic arthritis, systemic lupus erythematosus, rheumatic fever); however, these are neither sensitive nor specific. In patients with JIA, evaluation for possible uveitis by an ophthalmologist should be considered. Although this patient could have Lyme disease given the likely recent exposure to ticks during her camping trip, the lack of a rash, unresponsiveness to antibiotics, and polyarthritic nature make it less likely.
Arvikar et al. compared clinical features of systemic autoimmune arthritides to those of Lyme arthritis. They found that patients with Lyme arthritis usually had a clinical picture of monoarticular knee arthritis, whereas patients with systemic autoimmune arthritis manifested with polyarthritis. They concluded that systemic autoimmune arthritis with or without a history of Lyme disease should be treated with disease-modifying antirheumatic drugs (DMARDs).
Punaro et al. reviewed common rheumatologic conditions in children who may present to orthopaedic surgeons. For JIA, they reported a typical history of oligoarthritis for 6 weeks or more in a white female patient, with a peak onset between ages 1 and 3 years. Uveitis was typically chronic, bilateral, and asymptomatic. They concluded that while serologic tests were useful in
excluding other diagnoses, they were less useful in confirming JIA.
Incorrect Answers:
A 40-year-old patient sustains the injury in Figures A and B six months ago and underwent the appropriate fixation method. The patient is continuing to experience a tremendous amount of pain in
returning from summer camp. She denies any antecedent trauma, fevers, or rashes. Antibiotics prescribed by her primary care doctor have provided no significant relief, but she reports feeling better at
the end of the day. Labs reveal a negative rheumatoid factor. Which of the following is most commonly associated with her diagnosis?
The hardware shown in Figure A is a tension band plate. It is able to perform its function due to the Hueter-Volkmann Law.
Bones undergo continuous remodeling and turnover which are sensitive to the surrounding mechanical environment. Bone remodeling is governed by Wolff’s law, while the mechanical influence on longitudinal bone growth is controlled by the Hueter– Volkmann law. Wolff’s law relates to the adaptation of bone to its mechanical environment, and involves bone apposition stimulated by intermittent increased stress and bone resorption following reduced intermittent stress. The Hueter–Volkmann law relates to immature bone growth suppression through sustained compressive loading and growth acceleration by reduced loading or distraction.
Villemure et al. performed a review of growth plate mechanics and mechanobiology. They report that growth plates are sensitive to the surrounding mechanical environment. There are a number of clinical conditions of the skeleton that are thought to result from abnormal mechanical loading conditions influencing longitudinal growth prior to skeletal maturity, such as clubfoot (associated with limb position in utero), slipped capital femoral epiphysis, tibia vara, spondylolisthesis, and scoliosis.
Shabtai et al. performed a review of the limits of growth modulation using tension band plates in the lower extremities. Tension band plates have been found to be safe and effective at correcting pediatric frontal plane angular deformities. They found that the success rate for idiopathic cases nears 100%. The success rate for pathologic cases is lower and they have a higher complication rate. They conclude that tension band plates are a reasonable option for all but the most extreme frontal and sagittal plane deformities.
Figure A is a bilateral knee radiograph of a pediatric patient with tension band plates on the right tibia. Illustration A is a bilateral knee radiograph of the same pediatric patient.
The physis appears to have partially closed down and the angle of the screws has changed. One of the screws has broken which happens frequently.
Incorrect Answers:
A 5-year-old girl presents with an 8-week history of pain and swelling in the right knee, right shoulder, and left elbow after
Limb buds develop at 4 weeks and are first able to be visualized by transvaginal ultrasound at 8 weeks.
In a developing fetus, limb buds form at 26 days. The development of the limb is guided by a complex interaction of gene transcription factors and regulatory loops. The most important genes in limb development are sonic hedgehog (SHH), HOX genes, and WNT genes. Ultrasound evaluation is increasingly
being utilized to diagnose and guide treatment for developmental anomalies of a fetus. The limb buds of the fetus can be first seen at 8 weeks of gestation.
Krakow et al. reported on the prenatal diagnosis of fetal developmental dysplasias. They found that differentiating these disorders in the prenatal period can be challenging because they are rare and because many of the ultrasound findings are not necessarily pathognomic for a specific disorder.
Oetgen et al. authored a review on prenatal diagnosis of musculoskeletal conditions. They note that ultrasonography is a safe and cost-effective tool used to prenatally detect common musculoskeletal conditions such as clubfoot, skeletal dysplasias, limb-length discrepancies, spinal abnormalities, and hand and other upper extremity deformities.
Illustration A is a pictorial representation of limb bud formation Incorrect Answers:
The hardware shown in Figure A relies on which of the following principles to achieve its function?
Both Hemophilia A and B are inherited by X-linked recessive patterns. Hemophilia A is caused by factor VIII deficiency, whereas hemophilia B is caused by factor IX deficiency.
Factor VIII deficiency, also known as Hemophilia A, most commonly affects males due to the X-linked recessive inheritance pattern and occurs with a frequency of 1:5000 males. Factor IX deficiency, also known as hemophilia B, also only affects males due to X-linked recessive inheritance, with a frequency of 1:30000 males. Both disorders commonly present with recurrent spontaneous hemarthroses that affect large joints, typically the knee, leading to chronic synovitis and eventually joint destruction. Initial treatment involves factor replacement to within 60% normal, joint aspiration, and immobilization until the physical exam is normal. Treatment for chronic synovitis involves radiosynovectomy, open synovectomy, or arthroscopic synovectomy. End- stage joint destruction requires reconstructive surgery with aggressive factor replacement pre- and postoperatively.
Luck et al. performed a review on hemophilic arthropathy and recommended treatment options for hemophilic arthropathy. The authors recommend that infants get
primary prophylaxis with factor replacement prior to developing a "target" joint. In patients that experience a hemarthrosis, factor replacement with joint aspiration and immobilization until a normal physical exam are paramount for reducing chronic synovitis. Synovectomy, either arthroscopic or open, is recommended for chronic synovitis to reduce the progression of arthropathy. Then arthroplasty is reserved for end-stage joint destruction characteristic of recurrent synovitis.
Zingg et al. performed a retrospective review of 43 consecutive TKA in patients with hemophilic arthropathy. At 9.5 years follow-up there were two hematogenous infections, three revisions, 94% good-to-excellent patient- reported outcomes, and significantly increased ROM compared to preoperative examination. The authors concluded that TKA remains a successful option for end-stage arthropathy for hemophiliacs, but outcomes do not reach the level of non-hemophiliacs.
Journeycake et al. performed a retrospective review on 28 arthroscopic synovectomies performed on pediatric hemophiliac patients with chronic synovitis. At 5-years follow-up 76% of affected joints had stable or improved levels of function. The authors concluded that arthroscopic synovectomy provides a reliable means for limiting current hemorrhage in the affected joint and improving ROM.
Illustration A depicts a pedigree with an X-linked recessive inheritance pattern. Notice how only males are affected, but women can be carriers. Illustration B depicts the process by which recurrent hemarthroses leading to chronic synovitis and then arthropathy.
Incorrect Answers:
deficiency of von Willibrand factor; which assists in platelet adhesion. It is inherited in autosomal recessive pattern with the gene locus found on chromosome 12.
In terms of fetal limb bud development, which of the following is true?
Fluoroquinolones such as levofloxacin act by block DNA replication by inhibiting DNA gyrase.
Fluoroquinolone antibiotics are bactericidal, and their mechanism of action works through the inhibition of DNA gyrase. Side effects of fluoroquinolones include inhibition
of early fracture healing through toxic effects on chondrocytes and increased rates of tendinitis, with a special predilection for the Achilles tendon.
Levine et al. published a review on fluoroquinolones. They report that fluoroquinolones act by inhibiting DNA topoisomerases such as DNA gyrase (topoisomerase II). Due to increasing antibiotic resistance, their use is limited to specific clinical scenarios.
Additionally, their use in children is restricted due to a potential for growth disturbance and cartilage damage.
Perry et al. performed an experimental study on the inhibition of fracture healing by levofloxacin and trovafloxacin in rats. They found that experimental fractures systemically exposed to levofloxacin or trovafloxacin have diminished healing during the early stages of fracture repair. They, therefore, concluded that the administration of quinolones during early fracture repair may compromise fracture healing in humans.
Illustration A is an image illustrating the targets of the various antibiotic classes. Incorrect Answers:
Which of the following bleeding disorders is caused by an X- linked recessive mutation?
An isotonic muscle contraction is a muscle contraction with constant tension such as the upwards and downwards motions of a biceps curl.
The word “isotonic” is derived from two Greek words: “iso”, meaning “same”, and “tonikos” meaning “tension”. An isotonic muscle contraction is one during which the muscle maintains the same tension as it shortens. There are two types of isotonic contractions: concentric and eccentric. In a concentric isotonic contraction, the muscle shortens while contracting. In an eccentric isotonic contraction, the muscle lengthens during contraction.
Ashe et al. review exercise programs used in physical therapy. They report that muscle strengthening can be classified into isotonic, isometric, and isokinetic contractions.
Isotonic exercises involve the development of muscular force through range of motion or movement. Isokinetic exercises involve the force generation at a constant speed.
Isometric exercises involve the development of force without movement, as in tensing and holding a muscle
at a certain part of the range.
Illustration A is an image which illustrates the difference between isotonic and isometric contractions.
Incorrect Answers:
Which of the following correctly describes a class of antibiotics and its mechanism of action?
The third step in applying EBM is to appraise the evidence.
Evidence-based medicine (EBM) refers to an explicit process of using and evaluating information to make medical decisions. When applying EBM in practice, there are 5 steps that should be followed: 1) formulate an answerable question, 2) gather evidence, 3) appraise the evidence, 4)
implement the evidence, and 5) evaluate the process to determine the efficacy of the proposed treatment.
Bernstein published a review on EBM. He advocates for the use of a five-step process for sound decision making: formulate answerable questions, gather evidence, appraise the evidence, implement the valid evidence, and evaluate the process.
Spindler et al. published a review on reading and reviewing the orthopaedic literature. They focus on the third step of EBM: appraising the evidence. They report that systematic review assists the orthopaedic surgeon in interpreting study results and in understanding the relative validity of these results in the hierarchy of evidence.
Illustration A is a table listing the 5 steps of EBM.
Incorrect Answers:
4: Gathering evidence is the second step of EBM.
Which of the following activities describes an isotonic muscle contraction?
On average, physicians interrupt patients within 23 seconds of their interview.
The patient-physician interaction often begins with an initial "survey of problems" through an open-ended question designed to give the patient the freedom to speak and explain
their reason for seeking care. This is followed by a set of focused or closed-ended questions designed to elicit additional details and clarification. Unfortunately, physicians are often quick to interrupt or redirect patients prior to the completion of their reason for seeking care. This practice may lead to missed information, poor communication, and poor
patient satisfaction. Time constraints on physicians may contribute to this behavior. Marvel et al. looked at 264 patient-physician interviews by board-certified family practice physicians. They found patients' initial statement of concern were only complete 28% of the time with an average physician redirection
time of 23.1 seconds. They found patients only needed an additional 6 seconds to complete their statement of concern compared to those who were
redirected by the physician. They conclude that obtaining a complete patient agenda takes little time and can improve interview efficacy and increase data collection.
Incorrect Answers:
When applying evidence-based medicine (EBM) in practice, there are 5 steps that should be followed. Which of the following describes the third step?
For upper extremity surgery, the majority of narcotic pills prescribed by hand surgeons are not consumed by patients.
Patients in the United States are treated very aggressively for pain control. This is due, in part, to The Joint Commission, which has controversially identified pain as the "5th vital sign." An opioid epidemic has ensued which has been linked to a decreased the life expectancy in the United States for three consecutive years beginning in 2014. As a result, unused prescription pain medication following upper extremity surgery represents a liability for patients and surgeons. Following simple soft tissue surgeries (trigger finger, carpal tunnel, mass removal) patients typically only require pain
medication for 2-3 days, and there is no difference in pain control between narcotic or anti-inflammatory medication.
Stanek et al. implemented a standardized postoperative opioid prescription protocol for a group of academic hand surgeons. They found that the protocol decreased the opioid prescription size by 15%, prescription variability, and decreased refills. The authors recommend the development of specific prescription guidelines.
Rodgers et al. interviewed 250 patients after upper extremity surgery about opioid consumption. They reported that patients most frequently received 30 narcotic pills, which provided relief in 92% of cases. The authors found that patients undergoing bone procedures used on average 14 pills, most patients took medication for less than two days post-operatively, and the number of pills consumed on average was 10, with 19 pills unused. As a result, the authors advocated for more limited narcotic prescriptions post-operatively.
Weinheimer et al. randomized patients undergoing hand surgery to receive either Norco or acetaminophen/ibuprofen. They found no difference in time until patients were pain- free, average VAS scores, or the absolute number of those patients who were pain-free. They did find that the narcotic group experienced more adverse side effects (23% vs 3%), ultimately recommending for limiting narcotics post-operatively.
Incorrect answers:
During a new patient office visit, a physician asks an initial open- ended question to the patient. On average, how much time elapses before the physician redirects the patient's initial statement of concern?
The patient’s laboratory workup is likely to reveal hypovitaminosis D. Metabolic and endocrine abnormalities should be considered in patients who exhibit poor fracture healing, especially in those who lack history and exam findings suggestive of infection.
In addition to ruling out infection, a nonunion workup should include tests to identify metabolic and endocrine abnormalities. 25-hydroxyvitamin D3, synthesized from cholecalciferol in the liver, is the laboratory study of choice to determine vitamin D deficiency. Low vitamin D is a common, and easily treated, form of malnourishment in orthopedic trauma patients. Other important factors that can negatively impact fracture healing include protein malnourishment, diabetes mellitus, nicotine use, and HIV.
Warner et al. showed perioperative vitamin D deficiency correlated with
inferior clinical outcomes in patients who underwent operative fixation of ankle fractures. Of the 98 patients studied, 36 (37%) were found to be deficient in vitamin D (<20 ng/ml) and 31 (32%) were found to have a vitamin D insufficiency (> 20 ng/ml, <30 ng/ml). They concluded insufficient vitamin D may result in worse outcomes in orthopedic trauma patients recovering from fracture fixation.
Brinker et al. reviewed metabolic and endocrine abnormalities in 37 patients with nonunions. Inclusion criteria were: 1) an unexplained nonunion that occurred despite adequate reduction and stabilization; 2) history of multiple low-energy fractures with at
least one nonunion; or 3) a nonunion of a nondisplaced pubic rami or sacral ala fracture. Of the 37 patients who met screening criteria, 31 (84%) had metabolic or endocrine abnormalities. Vitamin D deficiency, discovered in 25 of 37 patients (68%), was the most common newly diagnosed abnormality. The authors conclude all patients with nonunion who meet their screening criteria should be referred to an endocrinologist.
Bishop et al. reviewed the assessment of compromised fracture healing and advocate for a metabolic and endocrine workup in the presence of nonunion. If an endocrinology consultation is unavailable, the initial laboratory screening should include 25- hydroxyvitamin D, calcium, thyroid-stimulation hormone, phosphorus, and alkaline phosphatase levels. They also emphasize that the presence of normal inflammatory markers does not exclude the possibility of infection, which should remain in consideration until fracture union and resolution of symptoms.
Incorrect Answers
However, the rate of infection is lower than hypovitaminosis D and both can occur simultaneously.
A hand surgeon plans on performing a carpal tunnel release on a healthy 45- year-old female. Which of the following is true regarding pain management for this case in the post-operative setting?
The ideal scenario to use the ANOVA test is when comparing parametric continuous data (i.e. BMI) for three or more groups.
In statistical analyses, data can be described as discrete (categorical, ordinal) or continuous. Discrete data are observations that can be expressed as categories such as gender, race, or disease status. Continuous data, such as age, are observations for which the difference between the numbers have meaning on a numerical scale. The ANOVA test is used to compare differences in mean values (i.e. continuous data) when there are more than two independent sample groups. When discrete data is compared in the setting of two or more independent sample groups, the chi-squared (parametric) or Fischer's exact test (non-parametric) may be utilized.
Kuhn et al. reviewed statistical tests when discrete data are analyzed. They reported that data may be either discrete (i.e. categorical) or continuous (i.e. age, BMI, height). They presented examples of tests used for discrete data including the chi-square test and Fischer's exact test. They emphasized the importance of scrutinizing the data presented prior to selecting a statistical test.
Greenfield et al. reviewed statistical tests when continuous data are analyzed. They reported that statistical tests for continuous data must be used if the outcome of interest is a comparison of sample means for data that are continuous (i.e. the height of populations). They discuss one-sample t-tests, independent two-sample t-tests, paired t- tests, and ANOVA.
Illustration A demonstrates an algorithm that is helpful in selecting the correct statistical test.
Incorrect Answers:
A 40-year-old Hispanic male presents with persistent pain seven months after open reduction internal fixation of a closed distal tibial fracture. His postoperative course was unremarkable and weight- bearing was resumed at six weeks. Exam reveals a well-healed incision with tenderness at the fracture site. There is no swelling or erythema. Radiographs demonstrate intact hardware and an oligotrophic nonunion. Laboratory workup is most likely to support which of the following interventions:
General anesthesia carries an increased risk of thromboembolism compared to spinal anesthesia. The remaining statements are false.
There have been multiple factors that demonstrate an increased risk of venous thromboembolism (VTE). Some of these risk factors include a previous VTE, obesity (BMI
> 30), surgery type (i.e. total joint arthroplasty),
hypercoagulable states (i.e. cancer, inheritable traits), myocardial infarction (MI), congestive heart failure, family history of VTE, hormone replacement therapy, elevated hormone conditions, varicose veins, and general anesthesia (increased risk compared to epidural/spinal anesthesia). Current AAOS guidelines recommend mechanical prophylaxis in all total hip and knee arthroplasty patients and chemoprophylaxis is recommended, but no optimal regimen is recommended. Chemical prophylaxis should be individualized for each patient and their risk factors.
Geerts et al. put forth their recommendations on the prevention of VTE from the American College of Chest Physicians in 2008. Some of the important points include aspirin not being recommended as a monotherapy (this recommendation was changed in 2012 and is now accepted as monotherapy), recommendation for mechanical prophylaxis, and recommendation for routine chemoprophylaxis for elective hip and knee arthroplasty for a minimum of 10 days.
Caprini et al. retrospectively reviewed 939 patients with either a DVT, PE, or PE and DVT and their treatment. They found that there was lower than anticipated use of low molecular weight heparin, insufficient bridging of patients to warfarin, and insufficient continuation of anticoagulation following hospitalization. They concluded that hospitals need to re-evaluate adherence to VTE treatment guidelines and develop strategies to optimize therapy.
Incorrect Answers:
An orthopedic surgery intern is preparing to perform statistical analyses for his research project. He presents to the department statistician inquiring about the Analysis of Variance (ANOVA) test. Which of the following below is the ideal scenario to use the ANOVA test?
While almost all patients undergoing major orthopaedic procedures receive VTE prophylaxis, this is often not within the ACCP post-operative VTE prophylaxis guidelines.
VTE events typically occur following hospital discharge, within the first 2 to 6 weeks following surgery. Risk is increased with major orthopaedic surgery due to greater soft tissue disruption, venous stasis from limb manipulation, and post-operative immobility. VTE following major orthopaedic hip and knee surgery represents not only a significant cause of postoperative morbidity and mortality but contributes a substantial economic burden. Prophylaxis is the single-most-important factor mitigating the risk of VTE. Therefore adherence to the AAOS and ACCP guidelines is recommended.
Friedman et al. evaluated compliance of physicians with American College of Chest Physicians (ACCP) post-operative VTE prophylaxis guidelines following TKA and THA. The authors found moderate compliance overall, with 47% of THA and 61% of TKA patients receiving appropriate prophylaxis in terms of type, duration, start time, and dose. Compliance with Warfarin use was the lowest, while that with low-molecular-weight heparin was significantly higher. They concluded that while almost all patients received prophylaxis, this was often not within the guidelines.
Oster et al. investigated the economic consequences of VTE following major orthopaedic hip or knee surgery. The authors found that 2.2% of patients developed clinically significant VTE, 62% after hospital discharge and that patients who developed in-hospital VTE had a significantly longer length of hospital stay and associated costs than those that did out-of-hospital and were later readmitted. They concluded that the economic impact of VTE was
substantial regardless of setting.
Incorrect answers:
Which of the following statements is true as it relates to the risk of thromboembolism?
Those utilizing opioids prior to elective hip and knee arthroplasty are at elevated risk of complications. Weaning opioids preoperatively has been shown to improve postoperative outcomes.
Nonoperative management of osteoarthritis (OA) is focused on reducing pain and limiting functional impairment with medications, physical therapy, activity modification, weight
loss, and intra-articular corticosteroid injections.
Pharmacologic management of OA includes NSAIDs and tramadol (per the AAOS CPGs). Opioids have been increasingly used for OA despite the lack of evidence behind their usage. Chronic opioid usage may improve OA-related pain but it has been associated with numerous adverse effects and worse musculoskeletal treatment outcomes.
Gaffney et al. in their review of perioperative pain management for hip and knee arthroplasty, describe the role of opioids, cryotherapy, acetaminophen, NSAIDs, tramadol, anticonvulsants, spinal analgesia, epidural analgesia, peripheral nerve blocks, and periarticular injections. They recommend IV dexamethasone on POD1, scheduled Tylenol, scheduled NSAIDs (Celebrex vs naproxen vs ketorolac), and PRN tramadol, oxycodone, or hydromorphone for breakthrough pain.
Nguyen et al. performed a retrospective matched cohort comparing patients undergoing hip or knee arthroplasty who were either opioid-naive, chronic opioid users, or chronic opioid users weaned of opioids preoperatively. They found that chronic opioid users who were able to reduce their preoperative opioid use by half prior to arthroplasty had outcomes (SF12 physical component and WOMAC) superior to those who were unable to decrease preoperative opioid use.
Sing et al. performed a retrospective review including 1263 patients undergoing primary THA or TKA, finding that patients who utilized opioids preoperatively had elevated postoperative pain, consumed a greater amount of morphine equivalents, walked fewer meters, had a longer postoperative length of stay, were more likely to be discharged to a care facility, and had 4-
5x greater 90d complications. They conclude that opioid users are a high-risk group.
Incorrect answers:
Which of the following is true regarding venous thromboembolism (VTE) following major orthopaedic hip or knee surgery?
This patient has developed CRPS following fixation of a distal radius fracture. All of the above are characteristics of CRPS except for decreased perfusion to the fingertips.
CRPS is divided into two general categories: Type I, occurring in the absence of a specific nerve injury, and Type II, resulting from presence of a specific nerve injury. The incidence is 6-26 cases per 100,000 person-years, mostly affecting females (4:1), and smokers. The International Association of the Study of Pain (IASP) has developed the Budapest Criteria for the diagnosis of CRPS. These include sensory (reports of hyperesthesia and/or allodynia), vasomotor (reports of temperature asymmetry and/or skin color changes and/or skin color asymmetry), sudomotor/edema (reports of edema and/or sweating changes and/or sweating asymmetry), and motor (reports of decreased ROM, weakness, or trophic changes to hair or nails) changes. Vitamin C following distal
radius fracture fixation has been suggested as preventative, though still somewhat controversial. Following development of CRPS, treatment includes psychotherapy, occupational therapy, sympathetic blockade, and antidepressants.
Birklein and Schlereth comprehensively review CRPS. The authors describe how after a trauma there is an abundance of inflammatory mediators which stimulate the peripheral nerves. In addition, the proinflammatory cytokine network stimulates bone cell and fibroblast proliferation and potentially endothelial dysfunction. They note that these molecular changes lead to autonomic disturbances and an overwhelming pain response.
Koh et al. also present a review of CRPS. The authors stress that CRPS is a clinical diagnosis and one of exclusion. They discuss that CRPS is best treated within a multidisciplinary team including orthopaedic surgeons, pain management, therapy, and psychological services. Early diagnosis is furthermore critical. Finally, the authors advocated vitamin C administration on the day of fracture as prophylaxis against CRPS.
Incorrect answers:
A 65-year old male with worsening right hip osteoarthritis has failed nonsurgical management and would like to proceed with total hip arthroplasty. He has consulted with a pain management specialist and is treating his pain with opioids. If he is able to successfully decrease the amount of opioids he takes preoperatively by 50%, what effect would that have on his postoperative functional outcome?
Etanercept is a biologic disease modifying anti-rheumatic drug (DMARD) which works by binding and inhibiting TNF-a, in effect suppressing the autoimmune response associated with rheumatoid arthritis (RA).
There are a number of DMARDs commonly used in the medical management of RA. TNF- a is a frequent target, given its pivotal role as one of the major cytokines driving the progression of RA. Etanercept is one example of a TNF-a inhibitor that is often used to treat RA, juvenile RA, psoriatic arthritis, and ankylosing spondylitis. Infliximab, adalimimab, golimumab are other
commonly used TNF-a inhibitors. Before initiating these medications, patients and physicians should be aware of the possibility of reactivation of latent tuberculosis as well
as increased rates of infection and lymphomas with long- term use.
Saleh et al. reviewed the perioperative management of RA patients. They note that patients that are maintained on etanercept perioperatively have a significantly increased rate of perioperative infection. The authors discuss recommendations that etanercept be held at least one half-life prior to surgery and in some instances up to 4-5 half-lives before surgery. They recommend restarting the medication at 2 weeks post-operatively so long as the surgical sites are healing uneventfully.
Nikiphorou et al. evaluated the impact of biologic agents on the surgical treatment of RA. The authors discussed that although rates of major joint replacements (THA/TKA) for osteoarthritis are increasing, the rates of THA/TKA for RA has been essentially unchanged over >10 years. They concluded that effective medical management of RA has led to fewer orthopedic surgeries being performed in the RA population.
Incorrect Answers:
A 60-year-old female underwent open reduction and internal fixation of a distal radius fracture 3 weeks ago. She returns to your clinic and appears anxious. She complains of pain and difficulty sleeping. When you remove her splint her entire hand and wrist are sensitive. You suspect that she has developed complex regional pain syndrome (CRPS). All of the following are common signs or symptoms of CRPS EXCEPT:
All of the statements listed above are true EXCEPT for answer 2 - BMP-2 is not FDA indicated for single-level posterolateral lumbar fusions.
Bone morphogenetic proteins are a member of the TGF-beta superfamily. It is an osteoinductive material that induces mesenchymal stems cells to differentiate into bone- forming osteoblasts. There has been an increasing amount of literature published around its use in long bone procedures, spinal procedures, and nonunions. Currently, the FDA indications for rhBMP-2 are acute open tibial shaft fractures treated within 14 days and single level ALIFs with a lumbar tapered fusion device.
Hsu et al. authored a systematic review including 6 articles on the cost- effectiveness of BMP-2 compared to iliac crest bone graft (ICBG) in lumbar and cervical arthrodesis procedures. They conclude that in lumbar arthrodesis procedures BMP-2 is only cost- effective when taking into account societal costs such as productivity and lost wages.
Carreon et al. performed a cost-utility analysis on an RCT that they performed comparing BMP-2 to ICBG in posterolateral lumbar fusions. There are more complications, increased need for additional treatment and revision surgery in patients over 60 years old receiving ICBG compared with rhBMP-2/ACS, which account for an increased cost utility for the ICBG group.
Glassman et al., in the paper that the aforementioned study worked off of, performed an RCT of rhBMP-2/ACS (Infuse bone graft) versus iliac crest bone
graft (ICBG) for lumbar spine fusion in patients over 60 years of age. They conclude that BMP-2 is a viable ICBG replacement in older patients in terms of safety, clinical efficacy, and cost-effectiveness.
Cheng et al. looked at the osteogenic activity of fourteen different BMPs on mesenchymal progenitor cells. They found BMP-2, 6, and 9 induced high levels of alkaline phosphatase activity in pluripotent stem cells. They conclude BMP-
2, 6, and 9 may play important roles in inducing osteoblast differentiation of mesenchymal stem cells.
Illustration A (Cheng et al.) is a figure demonstrating the distinct osteogenic activity of human BMPs. BMP-2, 6, and 9 are the most potent agents to induce osteoblast lineage differentiation of mesenchymal progenitor cells while most BMPs can promote the terminal differentiation of committed osteoblast precursors.
Incorrect answers:
Which of the following medications specifically target tumor necrosis factor alpha (TNF-a)?
Fretting corrosion results from the relative micromotion between two affixed materials placed under a load and is characterized by the formation of pits,
grooves, and oxide debris. This may be seen at modular junctions.
The process of fretting corrosion involves the physical disruption of the passivated layer at the junction of two materials due to friction caused by micromotion under pressure.
The increased surface roughness and release of metallic oxide debris may then, in turn, lead to other types of corrosion such as crevice corrosion. Fretting corrosion has been described at the head-neck junction in total hip arthroplasty, and the risk is increased with an increasing number of component interfaces.
Brown et al. describe fretting corrosion within the context of modular hip tapers. The authors note that while modularity increases versatility, this comes at the cost of interfacial corrosion which may result in both device failure as well as the release of metal ions with local soft tissue reactions. They conclude that longer neck extension was associated with increased fretting corrosion
and that this can potentially be mitigated by increasing the stability of the interface.
Goldberg et al. performed in vitro corrosion testing of modular hip tapers. The authors found that once fretting corrosion created an environment suitable for crevice corrosion, corrosion continued regardless of continued mechanical loading. They concluded that mechanical loading had a significant impact on initiating the corrosion process.
Incorrect Answers:
temperature cycling causing rapid expansion/contraction of the metal. This may be a consideration during the manufacturing process of implants but is not seen in vivo.
When considering using recombinant human BMP-2 in orthopaedic surgery, all of the following are true EXCEPT:
The null hypothesis in this randomized controlled trial is that there is no difference in cement penetration during TKA with or without tourniquet use. As there was significant crossover (tourniquet use in the "no tourniquet" cohort), accepting the null hypothesis when it is false would result in beta (type 2) error.
In hypothesis testing, the assertion that the observed findings did not occur by chance alone but rather occurred because of a true association between variables is confirmed or rejected. By convention, the null hypothesis suggests that there is no significant association between variables while the alternative hypothesis suggests that there is a significant association. Alpha (type 1) error occurs when the null hypothesis is rejected
when it is, in fact, true (false positive effect). Beta (type 2) error occurs when the null hypothesis is
accepted when it is, in fact, false (false negative effect).
Kocher et al. reviewed power analyses, statistical errors, and the concept of statistical power. They discuss that beta represents the chance of a type II error, while alpha represents the chance of a type I error, and that conventionally beta is set at 0.2 and alpha at 0.05. The authors recommended that when a study observes no difference, the power of the study, or (1 - beta), should be reported.
Lochner et al. investigated the rates of beta error in randomized controlled trials in orthopedic trauma. They reported a 90% beta error rate in these trials, which exceeds accepted standards. The authors recommended that future authors perform pre-study power and sample-size calculations to
reduce these rates.
Illustration A shows a Bayesian analysis table demonstrating the relationship between alpha, beta, and the null hypothesis.
Incorrect Answers:
Which of the following types of corrosion is defined by the formation of pits, grooves, and oxide debris due to the relative micromotion between two affixed materials placed under a load?
Tobramycin is an aminoglycoside that acts primarily by disrupting protein synthesis through irreversibly binding to 30S ribosomal subunit, leading to altered cell membrane permeability, disruption of the cell envelope, and eventual cell death.
Exchange nailing with an antibiotic-impregnated intramedullary nail is often implemented in the treatment of chronic osteomyelitis with septic tibial nonunion as it provides both fracture stabilization and antibiotic elution. Vancomycin and tobramycin are often added to the polymethylmethacrylate (PMMA) cement for broad-spectrum coverage.
Vancomycin disrupts cell-wall synthesis in a time-dependent manner by binding to the D- Ala-D-Ala terminal of the growing peptide. It is extremely effective in gram-positive bacteria, but ineffective against gram-negative bacilli due to its large size. Conversely, tobramycin is effective against gram-negative organisms, and works chiefly through the inhibition of bacterial protein synthesis by irreversibly binding to the 30S ribosomal subunit.
Jaeblon et al. reviews the contemporary use of PMMA in orthopaedic surgery. The authors discuss the utility of PMMA as a delivery vehicle for antibiotics, eluting from both the surface and pores of the cement as well as the microcracks within it, while simultaneously eliminating dead space. They conclude that tobramycin is popular because it comes in powder form, which is easy to mix, and because of its broad spectrum activity, which includes antipseudomonal coverage. Moreover, it has been shown to potentiate the elution of other antibiotics, such as vancomycin.
McNamara et al. reviews the mechanism of Vancomycin. The authors report how this antibiotic has increased in importance in the last decade due to the growing resistance of many gram-positive bacteria to β-lactam antibiotics. They discuss that vancomycin is a large, complex, tricyclic glycopeptide molecule that works primarily through disruption of the biosynthesis of peptidoglycan, the major structural polymer of the gram-positive
bacterial cell walls, through binding to the D-alanyl-D-alanine terminal of cell wall precursor units. The authors conclude that unlike penicillins and cephalosporins, cross- resistance with vancomycin does not develop, because vancomycin acts against different stages of cell wall synthesis and different specific targets.
Nana et al. discusses the high affinity of microorganisms to adhere to foreign materials commonly used in orthopedics, including cobalt-chromium, titanium, polyethylene, and PMMA cement through the formation of biofilms. The
authors report that S. aureus and S. epidermidis are the most common biofilm-forming bacteria found in orthopedics, and, when combined with P. aeruginosa, they represent nearly 75% of biofilm infections. They conclude that while no current guidelines exist for treating these infections, recent studies have shown that biofilm growth can be fully inhibited when PMMA is mixed with both daptomycin and gentamicin.
Figures A and B are the AP and lateral radiographs of an infected nonunion of a tibial shaft fracture treated initially with an intramedullary nail.
Figure C is an axial CT image illustrating the tibial fracture nonunion.
Incorrect Answers:
A randomized controlled trial is undertaken to investigate whether tourniquet use increases cement penetration during total knee arthroplasty. Approximately 40% of the patients that were initially randomized to the "no tourniquet" group had tourniquets placed intraoperatively due to difficulty with visualization. Intent- to- treat analysis was conducted and the results showed no difference in the rates of cement penetration. What statistical term best applies if these results are accepted at face value?
Sclerostin is a direct antagonist of the Wnt/β-catenin pathway and thus a key regulator of the formation of mineralized bone matrix and bone mass. Anti- sclerostin antibodies result in inactivation of sclerostin, thereby promoting the anabolic Wnt/β-catenin pathway and resulting in INCREASED bone density
Sclerostin is a glycoprotein encoded by the SOST gene and produced primarily by osteocytes. It acts as a negative regulator of bone mass by directly antagonizing Wnt binding to the LRP5/6 receptor, thereby leading to β-catenin degradation and reduction of Wnt-target gene expression. This results in anti- anabolic properties, including inhibition of osteoblastic differentiation, bone formation, and loss of inhibition of osteoblast and osteocyte apoptosis. Genetic mutations resulting in loss of function or decreased expression of SOST have been linked to endosteal hyperostosis, increased bone mass, and increased bone density (as with Van Buchem disease and sclerosteosis). As a result, new immunotherapies targeting sclerostin (such as Romosozumab and
Blosozumab) are being investigated for their utility toward treating osteoporosis and have shown promising results.
Recker et al. presented a double-blinded phase 2 randomized controlled trial of blosozumab in the treatment of low bone mineral density in postmenopausal women. The authors found that administration of the monoclonal antibody resulted in significant dose- dependent increases in bone mineral density at the spine and hip. The authors concluded that the anti-sclerostin antibody was effective in the treatment of low bone mineral density in postmenopausal women.
Illustration A is a comparison of the unsuppressed Wnt pathway (left) with the Wnt- antagonized pathways (right). Sclerostin binds the LRP5/6 receptor in the place of Wnt, leading to the release of the destruction complex and β-catenin degradation. In the absence of sclerostin, the β-catenin translates into the nucleus and promotes downstream transcription of Wnt target genes.
Incorrect Answers:
sclerostin lead to an under- or uninhibited Wnt/β-catenin pathway and thereby INCREASED bone mass, such as would be seen in Van Buchem disease or sclerosteosis.
Figures A through C are the radiographs and CT scan of a 33- year-old male who was treated 13-months ago for an open tibial shaft fracture. He has received several courses of intravenous antibiotics for chronic osteomyelitis. Despite continued treatment with IV antibiotics, his inflammatory markers remain elevated. The decision is made to proceed with irrigation and debridement, nail removal with exchange for a polymethylmethacrylate intramedullary nail with vancomycin and tobramycin. What is the primary mechanism of action of tobramycin?
Lubricin is a hyaluronic acid-binding proteoglycan found in synovial fluid that reduces the coefficient of friction between the surfaces of the joint.
Lubricin reduces the friction between the surfaces in the joint, leading to decreased shear forces transmitted to the hyaline cartilage. It is a glycoprotein that is produced by the chondrocytes in the superficial zone and is not a primary component of the extracellular matrix. A deficiency in lubricin has
been associated with early-onset arthritis.
Schumacher et al. first discovered what is now known to be "lubricin" by studying the superficial zone of bovine articular cartilage. The authors noted that the chondrocytes in this zone secreted this proteoglycan. In addition, they found that this molecule, or a very similar molecule, was present in synovial fluid and moreover could serve as a functional metabolic marker for chondrocytes of the superficial zone of articular cartilage.
Jay et al. analyzed the synovial fluid in both normal and lubricin-deficient samples and found that the subdiffusive and elastic behavior of synovial fluid, at physiological shear rates, was absent in fluid from a patient who lacked lubricin. They concluded that lubricin provided synovial fluid with an ability to dissipate strain energy induced by physiologic motion, which is a chondroprotective feature distinct from boundary lubrication.
Incorrect Answers:
osteoblastogenesis.
Which of the following is accurate regarding sclerostin?
In the days following an intra-articular injury, the following substances are produced, contributing to articular cartilage damage and the eventual formation of post-traumatic arthritis: IL-1ß, TNF-a, nitric oxide, matrix metalloproteinases, aggrecans, and damage-associated molecular patterns.
Immediately following an intra-articular fracture, there is mechanical damage and necrosis of articular cartilage. Traditionally, orthopaedic surgeons are
taught that the most critical factor in affecting the outcomes of these patients is the accuracy of the articular reduction and restoration of the mechanical alignment. However, even in expertly reduced fractures, some patients experience poor outcomes and develop progressive, debilitating osteoarthritis. More recently, researchers have looked at inflammatory events that may also contribute to arthritis and ways to modulate these events.
Olson et al. provide a review article on the role of cytokines in post-traumatic arthritis. They note that, despite accurate articular reductions, many patients go on to develop
arthritic changes, often indistinguishable from primary OA. While mechanical alignment and structural damage are sometimes responsible, the cascade of cytokines and other signaling molecules listed above serve to catalyze these intra-articular events; developing ways to blunt this inflammatory response is of great interest.
Lewis et al. examined the relationship of inflammatory and post-traumatic arthritis in a rodent model. Tibial plateau fractures were induced in C57BL/6 and MRL/MpJ "superhealer" mice, which were killed at different time-points. Synovial fluid was inspected post-mortem for cytokine analysis, as well as gross specimens, and it was determined that an association exists between joint tissue inflammation and the development and progression of post- traumatic arthritis in mice.
Figure A is an XR of a tibial plateau fracture. Figure B is an XR of a knee demonstrating post-traumatic arthritis. Illustration A is a table of several cytokines and their functions. Illustration B is a timeline of intra-articular pathogenic events following an injury. Illustration C is a diagram showing various cellular events and pathogenic mechanisms in the acute aftermath following an intra-articular injury.
Incorrect Answers:
blood vessels, IL-8 is chemotactic, BMP2 plays a role in the development of bone and cartilage, BMP5 plays a role in cartilage development, and M-CSF causes hematopoietic stem cells to differentiate into macrophages or other related cells.
A 45-year-old patient presents to your clinic for evaluation of knee pain. He has been told he has osteoarthritis and has significant pain with knee range of motion. Which of the following components of synovial fluid is most responsible for reducing the coefficient of friction in a native knee joint?
This player has sustained a tear of the medial collateral ligament (MCL). The MCL is a ligament which inserts indirectly into bone through Sharpey's fibers.
Ligaments can insert on bone either indirectly and directly. Indirect is the most common and is a fibrous insertion. The superficial fibers of the tendon insert into the periosteum, while the deep fibers insert directly into the bone. These
deep fibers are called Sharpey's fibers and are made of type I collagen. The direct insertion has both deep and superficial fiber insertions as well. Direct insertions are fibrocartilaginous and consist of four transitional zones of increasing stiffness that allow force dissipation.
Lu et al. performed a review to determine the functional attachments of soft tissue to bone. They report that a specialized interface, called an insertion site or enthesis, integrates
tendon or ligament to bone and serves to facilitate joint motion. Fibrous (indirect) insertions typically occur over large areas, presumably to distribute force and reduce stress, and are characterized by perforating mineralized collagen fibers.
Cole et al. performed a review of fixation of soft tissues to bone. They report that recreation of the enthesis relies on adequate biologic healing afforded by adequate initial fixation. The healing pattern associated with direct soft–tissue- to-bone repair, such as rotator cuff repair, is different from that associated
with fixation within bone tunnels (ex. ACL reconstruction). The process of tendon healing within osseous tunnels occurs over time.
Lui et al. performed a review of the biology and augmentation of tendon-bone insertion repair. They report that when a ligament runs parallel to the bone, like the MCL, the insertion is more likely to be indirect. When a ligament enters the bone perpendicularly, such as the ACL, the insertion is direct. Indirect insertions may be elevated off the bone without cutting the ligament itself while direct insertions require cutting the substance of the ligament to detach it.
Figure A is a T2-weighted, coronal MRI demonstrating a tear of the MCL. Illustration A is a polarized photomicrograph demonstrating Sharpey fibers, indicated by the white arrows. G represents tendon, while B represents bone (Liu et al.). Illustration B is a Safranin-O-staining photomicrograph of a direct tendon insertion site (Liu et al.).
Illustration C is an H&E photomicrograph of the same direct tendon insertion site (Liu et al.). B represents bone, CFC represents calcified fibrocartilage, UCFC represents uncalcified fibrocartilage, and T represents tendon.
Incorrect Answers:
A 32-year-old male sustains the injury shown in Figure A. He undergoes surgical fixation with subsequent removal of hardware. He does well for 10 years and then presents to your office with increasing left knee stiffness and pain for the last 6 months. He reports no constitutional symptoms or recent trauma. His physical exam is notable for well-healed incisions, a mild effusion, no ligamentous instability, and 5-100 degrees of range of motion. An XR is obtained and shown in Figure B. Which of the following correctly lists the cytokines produced following the initial injury that may contribute to the findings shown in Figure B and the patient's current symptoms?
imaging is shown in Figure A. Which of the following correctly classifies the injured structure and its indirect insertion into bone?
Hypertrophic nonunions are described as having abundant callous formation without bony bridging at the fracture site and rarely require an increase in bone biology to achieve fracture healing.
A nonunion is defined as a fracture that has not healed and has no further capacity to heal without further intervention. Nonunions are typically classified as hypertrophic, oligotrophic, and atrophic. Hypertrophic nonunions show clear
evidence of ability to heal without bridging of fracture gaps. Atrophic nonunions show no evidence of biologic healing and no bridging of fracture gaps. Oligotrophic nonunions tend to fall somewhere in between hypertrophic and atrophic nonunions with some evidence of biologic activity however incomplete healing. Understanding these characteristics allows for proper identification of the nonunion and selection of appropriate intervention with regard to increasing bone biology and fracture stability to achieve healing.
Bishop et al. review the diagnosis and assessment of delayed bone healing through a systematic approach to help surgeons determine appropriate interventions to achieve healing. They state biologic capacity, fracture stability, deformity, infection, and host status should all be considered closely prior to establishing a plan of management for a nonunion.
Babhulkar et al. reviewed 113 patients diagnosed and treated for nonunions including 61 hypertrophic and 52 atrophic nonunions. They found all patients healed with improved function and pain following treatment of their nonunions. They found residual problems related to joint stiffness, limb length
discrepancy, and angular deformity.
Illustration A shows a hypertrophic nonunion of a tibial shaft fracture treated nonoperatively. Illustration B shows an atrophic nonunion following open reduction internal fixation of a humeral shaft fracture.
Incorrect Answers:
A 20-year-old male collegiate football player sustained a knee injury. His
The arrow is pointing to the superficial zone of articular cartilage in Figure A. The superficial zone of articular cartilage has the highest content of collagen and the lowest content of proteoglycans relative to the other zones.
Normal articular cartilage can be divided into 3 zones and the tidemark based on the shape of the chondrocytes and the orientation of the type II collagen. The zones, in order from closest to the joint surface, are superficial zone, intermediate (transitional) zone, and deep zone. The superficial zone has the highest content of collagen and lowest content of proteoglycans of all the zones; in contrast, the deep zone has the lowest content of collagen and the highest content of proteoglycans. The intermediate zone has amounts of collagen and proteoglycans that reside between those found in the superficial and deep zones.
Ulrich-Vinther et al. reviewed the biology of articular cartilage. They noted three distinct zones of articular cartilage that are separated from the subchondral bone by the tidemark. The authors noted that tissue engineering approaches are being used in an effort to regenerate damaged articular cartilage due to injury or aging.
Jeffery et al. studied the three-dimensional architecture of bovine articular cartilage with scanning electron microscopy. They noted that the collagen was ordered in different morphologies in each zone of articular cartilage. The authors concluded that the three- dimensional organization of collagen is important when considering cartilage structure and function.
Illustration A demonstrates the zones of articular cartilage and their spacial relationship. Illustration B shows the relationship between collagen and proteoglycans
within articular cartilage.
Incorrect Answers:
While planning for revision of a failed open reduction internal fixation you are planning to increase mechanical stability across the fracture site. In addition to addressing stability, which of the following fracture scenarios is least likely to require additional bone biology in order to achieve healing?
A is characterized by:
PROMIS is a useful orthopaedic patient-reported outcomes measure (PROM) that can assess disease specific and general health questions, validated for use in foot and ankle, upper extremity, and spine patients.
Multiple tools have been developed to asses patient-reported outcomes, however, some of these are narrow in scope, cumbersome to administer, and less useful in orthopedics. PROMIS was developed by a team of NIH researchers to address these shortcomings. Domains include physical, mental, and social health. PROMIS utilizes computer adaptive testing software (CAT), allowing for fewer questions and more accurate measurements. Additionally, results are reported as T-scores, allowing for easy interpretation.
Brodke et al. provide an overview of PROMIS. They report that this tool was developed to be easy to administer and broad in scope, utilizing item response theory. This validated tool is reliable in assessing specific function of the upper and lower extremities, as well as underlying health traits.
McCormick et al. described PROM used in spine surgery. They reinforce that the benefit of PROM is to gather insight into subjective measures not typically captured in traditional research, looking at such factors as general health quality, function, and pain. The authors also note the importance of these tools as greater emphasis is placed on quality of care and patient experience.
Godil et al. studied instruments to accurately measure quality and outcomes in lumber spine surgical registries. They conducted a prospective cohort study of
58 patients undergoing TLIF for lumbar degenerative spondylolisthesis and administered several PROs. They concluded that the ODI was the best measure assessing pain and disability in lumbar surgery, citing its validity and responsiveness in measuring the effectiveness of lumbar fusion; EuroQOL-5D (EQ-5D) was found to be the best, the most valid, and responsive measure of improvement for health-related quality of life.
Illustration A is a chart depicting the main domains and subcategories analyzed with PROMIS.
Incorrect Answers:
The layer of articular cartilage that the arrow points to in Figure
As part of the World Health Organization (WHO) Surgical Safety Checklist, all of the answers listed are methods to prevent wrong-site surgery EXCEPT marking an "X" on the operative extremity. Patients should be marked unambiguously, with either a "yes" or the surgeon's initials in permanent marker, prior to induction of anesthesia.
The WHO developed the Surgical Safety Checklist in an effort to improve the safety of patients undergoing surgery. Implementation of this checklist has resulted in improved clinician safety attitudes, as well as decreased patient morbidity and mortality. A time-out or group huddle occurs prior to induction with the patient, prior to incision, and prior to the patient leaving the operating room; all team members have an opportunity to speak up and discuss any concerns during this process. The American Academy of Orthopaedic Surgeons suggest the following to prevent wrong-site surgery: Surgical team engagement, patient confirmation, signing the surgical site (in the visible
surgical field or inline with the planned incision) with a permanent marker with the patient's assistance, and utilizing separate time-outs in the case of separate surgical procedures/sites.
Haynes et al. looked at changes in safety attitude, morbidity, and mortality following implementation of the WHO Surgical Safety Checklist. They administered a survey pre- and post-intervention at 8 hospitals. Post- intervention, they found an overall improvement in safety attitudes and found that this was correlated with a reduction in post-operative complication rates.
Gillespie at al. reviewed the evidence of implementing a surgical safety checklist. They utilized a realist synthesis methodology in this study. They concluded that intervention methods and implementation strategies were not well described in the literature, surgical checklists appear to be more successful when physicians are leading their implementation, and that greater participation and ownership of safety checklists can be expected by physicians are actively engaged in their development and implementation.
Illustration A is the WHO Surgical Safety Checklist. Illustration B is an example of the correct way to mark a patient for a right shoulder surgery for a planned deltopectoral incision.
Incorrect Answers:
Which of the following instruments incorporates both general disease and disease-specific measures and has been validated for use in patients with spine, foot and ankle, and upper extremity conditions?
This patient has a catastrophic ceramic component failure and requires a thorough debridement and revision with a head and liner exchange.
Ceramic bearings in hip arthroplasty are recognized for their superior wear properties and low-friction. However, ceramics are also brittle, have a high modulus of elasticity, and are prone to fracture under certain circumstances. Catastrophic bearing failure is not as common in newer-generation ceramics, as first-generation products were more prone to failure due to flaws in the manufacturing process. Squeaking is a known complication of ceramic-on- ceramic bearings and may be associated with catastrophic failure. Obesity, trauma, and component malposition have been linked to failure, and revision procedures should address any component malposition.
Malem et al. describe a case report of a catastrophic ceramic-on-ceramic total hip replacement failure presenting as a squeaking hip. Within 5 years of her index surgery, the patient developed a painful, squeaking hip with a limited range of motion. At the time of revision, she was found to have a broken femoral head, black wear debris, and a completely worn acetabular component, suggesting that a squeaking ceramic-on-ceramic hip replacement may be a sign of catastrophic failure.
Stanat et al. provide a meta-analysis and review of squeaking in 3rd and 4th generation ceramic-on-ceramic total hip replacements. They conclude that the only significant patient- associated risk factor for squeaking was body mass index. In terms of implant type and surgical factors, they found that the presence of a Stryker Accolade stem was associated with an increased incidence of squeaking; cup version was not associated with a higher incidence of squeaking in their analysis.
Figure A is a radiograph demonstrating ceramic fracture and displacement of the femoral component in relation to the acetabular component; ceramic fragments are present around the femoral neck and cup. The partially radiolucent head is a tip-off to the older generation ceramics. Illustration A is an intra-operative photograph demonstrating a fractured ceramic femoral head. Illustration B is a revision of the hip in Figure A utilizing ceramic-on- ceramic components. Illustration C (Traina et al.) is a treatment algorithm when ceramic bearing failure is suspected.
Incorrect Answers:
All of the following can be done to improve patient safety and prevent wrong site surgery EXCEPT:
Nitrogen-containing bisphosphonates exert their action by inhibiting farnesyl pyrophosphate synthase.
Nitrogen-containing bisphosphonates inhibit osteoclasts which leads to increased bone mass and reduced bone turnover. They act on the cholesterol biosynthesis pathway enzyme, farnesyl pyrophosphate synthase. By inhibiting this enzyme in the osteoclast, they interfere with geranylgeranylation (attachment of the lipid to regulatory proteins), which causes osteoclast inactivation. Non-nitrogen containing bisphosphonates are metabolized in the cell to compounds that replace the terminal pyrophosphate moiety of ATP, forming a nonfunctional molecule that competes with ATP in the cellular energy metabolism. Due to this disruption in metabolism, the osteoclast
initiates apoptosis and dies, leading to an overall decrease in the breakdown of bone. Examples of nitrogen-containing bisphosphonates are alendronate, risedronate, pamidronate, and zolendronate. Examples of non-nitrogen containing bisphosphonates are tiludronate, clodronate, etidronate.
Reszka et al. performed a review of bisphosphonates. They report that they bind to the bone mineral, which localizes their action to the target tissue. They are rapidly cleared from the circulation via renal excretion, which minimizes exposure of all other organs.
They do not easily penetrate cell membranes, which reduces exposure to non-target tissues. They also report that alendronate and risedronate are the only pharmacologic agents shown to prevent spine and nonvertebral fractures associated with postmenopausal and glucocorticoid-induced osteoporosis.
Luo et al. performed a systematic review to determine the efficacy and safety of alendronate for adult AVN treatment. They found most studies suggested a positive short-term efficacy of alendronate treatment in reducing pain, improving articular function, slowing of bone collapse progression, and delaying the need for arthroplasty. There were no severe adverse effects associated with alendronate treatment observed and most of the included studies suggested the use of alendronate in early AVN with a small necrotic lesion to achieve better outcomes.
Illustration A (Reszka et al.) details the nitrogen and non-nitrogen containing bisphosphonates and their chemical structures. Illustration B is the mevalonate pathway, showing the action of a nitrogen-containing bisphosphonate.
Incorrect Answers:
A 60-year-old patient presents to clinic complaining of left hip squeaking and stiffness following a ceramic-on-ceramic total hip replacement five years earlier. Initially, he was extremely pleased with the operation, but these symptoms of squeaking and stiffness have developed fairly abruptly over the past 6 months. On physical exam, he has a well-healed incision, a 1 centimeter leg length discrepancy (left shorter than right), decreased hip flexion, and decreased internal rotation. A radiograph is shown in Figure A. C- reactive protein is 0.2 mg/dL (nl <0.9 mg/dL) and erythrocyte sedimentation rate is 5 mm/hr (nl 0-15 mm/hr). What would you recommend for this patient?
in the red box?
Aspirin inhibits the aggregation of platelets, which are shown in Figure C.
The coagulation cascade is a complex interaction of multiple clotting factors which ultimately leads to the aggregation of platelets to form a clot. The end result of the clotting cascade leads to the conversion of prothrombin to thrombin, causing the formation of fibrin and the subsequent aggregation of platelets in a clot. Aspirin irreversibly blocks the formation of thromboxane A2 in platelets, which inhibits platelet aggregation and thus the formation of a clot.
Hyers reviewed the mechanism of action of various anticoagulants and the pathophysiology of venous thromboembolism. He noted that while deep vein thrombosis and pulmonary embolism resulted in significant morbidity and mortality in the United States, novel anticoagulants have recently been developed that hold promise for new therapeutic options.
Brown pooled the results of 14 randomized controlled trials examining venous thromboembolism (VTE) rates. Their analysis showed that VTE rates were not significantly different when aspirin was used for anticoagulation compared with vitamin K antagonists or low molecular weight heparin (LMWH). The authors concluded that aspirin could be used for VTE prophylaxis after major orthopaedic surgery.
Figure A shows a plasma cell. Figure B shows a neutrophil. Figure C shows arrows pointing to platelets in a peripheral blood smear. Figure D features a basophil, and figure E shows an osteoclast. Illustration A shows the mechanism of action of aspirin.
Incorrect Answers:
A man with osteonecrosis of the hip is treated with a medication which inhibits the pathway shown in Figure A. Which of the following medications best matches this mechanism of action of the medication
Demineralized bone matrix (DBM) is both osteoconductive and osteoinductive.
DBM is made from the acidic extraction of bone matrix from allograft. It removes the minerals and leaves the collagenous and noncollagenous structure and proteins. It is osteoconductive and osteoinductive as it contains collagen, bone morphogenic proteins (BMPs), transforming growth factor-beta (TGF-β), and residual calcium. It does not contain mesenchymal precursor cells or impart structural support.
Ripamonti et al. performed a review of regenerative medicine and tissue engineering of bone. They report that the understanding of bone formation by autoinduction has been pivotal for setting the rules for tissue engineering. An extracellular matrix combined with TGF-β is capable of performing this task.
Grabowski et al. review bone graft and bone graft substitutes. They report that DBM is both osteoinductive and osteoconductive. DBM provides varying degrees of osteoconductive potential based on the carrier material chosen.
They also report that given the techniques used for demineralization are proprietary, the actual techniques are not published, and the process is not regulated. They conclude that the actual concentration of BMPs is varied when comparing various lots of the same preparation.
Figure A is a coronal CT slice demonstrating a depression fracture of the lateral tibial plateau.
Incorrect Answers:
Aspirin exerts its primary effect on which of the following cells (identified by black arrows)?
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 67
A 20-year-old athlete sustains a 2- x 3-cm grade IV chondral injury to the right knee. After failure of nonsurgical management, which of the following procedures would ensure the highest percentage of hyaline-like cartilage?
Explanation
REFERENCES: Brittberg M, Lindahl A, Nilsson A, et al: Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 1994;331:889-895.
Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 787-804.
Question 68
A 14-year-old girl has had mild pain and nail deformity of the great toe for the past 4 months. A radiograph is shown in Figure 50. What is the most likely etiology of the lesion?
Explanation
REFERENCES: Lokiec F, Ezra E, Krasin E, Keret D, Wientraub S: A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop 2001;21:76-79.
Letts M, Davidson D, Nizalik E: Subungual exostosis: Diagnosis and treatment in children. J Trauma 1998;44:346-349.
Davis DA, Cohen PR: Subungual exostosis: Case report and review of the literature. Pediatr Dermatol 1996;13:212-218.
Question 69
A 6-year-old boy has had increasing pain and a mass in the suprapatellar region of the right femur for the past week. Examination of the mass reveals it may be firm, immobile, and tender to palpitation. The patient has no systemic symptoms. Laboratory studies show a WBC of 7000 per cubic millimeter, a hematocrit of 40%, and an erythrocyte sedimentation rate of 10 mm/hr. radiographs are normal. Figures 64a and 64b show saggital and axial T1-weighted MRI scans. Figure 64c shows frozen section pathology of the biopsy specimen. What is the most likely diagnosis?
Explanation
Question 70
A 52-year-old woman who underwent cheilectomy 1 year ago for hallux rigidus now reports continued pain in the first metatarsophalangeal joint. She did not have any incision healing problems, and has not had any fevers, erythema, or drainage. Which of the following procedures will provide the best combination of pain relief and function?
Explanation
REFERENCES: Machacek F Jr, Easley ME, Gruber F, et al: Salvage of a failed Keller resection arthroplasty. J Bone Joint Surg Am 2004;86:1131-1138.
Myerson MS, Schon LC, McGuigan FX, et al: Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int
2000;21:297-306.
Question 71
A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient’s family reports that he is a Jehovah’s Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patient’s blood pressure becomes unstable. What is the most appropriate action?
Explanation
REFERENCES: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Jehovah’s Witnessess Official Web Site: Medical Care and Blood, 2008, http://www.watchtower.org/e/medical_care_and_blood.htm
Question 72
A 20-year-old girl reports a shoulder dislocation while reaching for a high shelf. Her history reveals multiple past dislocations with spontaneous reduction and no obvious traumatic event at onset. A photograph of her hand is shown in figure
Explanation
The first line of treatment for shoulder dislocations in patients with MDI should consist of physical therapy aimed at strengthening the rotator cuff and scapular stabilizers. For those who fail to respond to 3 to 6 months of nonsurgical treatment, surgical intervention can be considered with inferior capsular shift being the procedure of choice for multidirectional instability. Good results have been achieved with surgical procedures for posterior and multidirectional instability, but results have been less predictable than those achieved with procedures for traumatic anterior instability.
Ide et al. evaluated the results of an 8-week rehabilitation program with shoulder-strengthening exercises and a novel scapular-stabilizing shoulder orthosis in 46 patients with MDI. There was a significant increase in mean total scores on the modified Rowe grading system and mean torque of internal and external rotation with a normalization of mean external/internal torque ratios at the completion of the program. The authors concluded that shoulder strengthening exercises represent a
useful treatment option for patients with MDI.
Levine et al. reviewed treatments of multidirectional shoulder instability in athletes. Nonoperative management remains the initial treatment of choice. Open capsular shifts remain the operative treatment of choice, however, arthroscopic electrothermal capsulorrhaphy has become increasingly used as an alternative to an open approach.
Beasley et al. reviewed multidirectional instability in the shoulder of female athletes. The authors note that women tend to have greater ligamentous laxity than men and female athletes have a greater risk of converting laxity to symptomatic instability.
Figure A demonstrates metacarpophalangeal hyperextension, which is a sign of generalized ligamentous laxity.
Incorrect Answers:
Question 73
03 A 35 year old man sustains a dislocation of his dominant shoulder in a fall. The shoulder is reduced and placed in a sling, but returns 6 hours later with shoulder dislocated again, despite use of a sling. A CT scan is shown in figure 36. Management should now consist of
Explanation
back to this question go to explanation
Question 74
What do the T2-weighted, fat-saturated MRI scans shown in Figures 1 through 4 reveal?

Explanation
disruption of the ACL. The medial meniscus images show a disruption of normal meniscus morphology consistent with a bucket handle medial meniscus tear. Note the appearance on the sagittal MRI scan of what appears to be a second soft-tissue density in line with the PCL. This "double PCL" sign is highly indicative of a displaced medial meniscus tear rather than a displaced lateral meniscus tear.
Question 75
A 34-year-old man sustained a gunshot wound to the knee 18 months ago and was treated with bullet removal and a 10 day course of oral antibiotics. He now complains of 12 months duration of pain in the thigh and recent ulceration and drainage of the skin near the site of his gunshot wound. Physical exam is notable for a draining sinus tract, erythema and tenderness of the mid-thigh. He is afebrile. An MRI image of this patient is shown in Figure A. Which of the following is the most appropriate management?

Explanation
In the referenced article by Parsons and Strauss, the management of chronic osteomyelitis is reviewed.
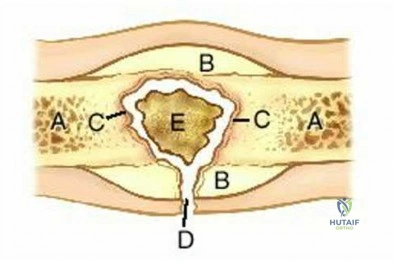
OrthoCash 2020
Question 76
After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office with continued pain 2 years after surgery. He describes instability, particularly when descending stairs. Upon examination, there is range of motion from 0 to 120 degrees with no extensor lag. The knee is stable to varus and valgus stress in extension, but there is flexion instability in both the anterior-posterior direction and in the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection workup is negative. What is the most appropriate surgical intervention at this time?
Explanation

Video 99 for reference
This patient has valgus knee alignment, and, after undergoing appropriate bone resections and soft-tissue balancing, has demonstrated a tight PCL on trial reduction as evidenced by lift-off of the trial insert as described by Scott and Chmell. The appropriate maneuver is PCL recession with partial release of tight (usually anterolateral) PCL fibers. However, for this patient, instability resulted in increased anterior translation. At this stage, the options are to convert to either a deeper-dish insert with increased sagittal conformity or a posterior stabilized insert. The only appropriate choice among the responses is use of an insert with increased sagittal conformity to prevent excessive anterior translation. Increasing the polyethylene could improve stability in flexion, but, considering there is good stability in extension, this likely would lead to an inability to achieve full extension. The patient’s valgus deformity, flexion contracture, correction with release of the iliotibial band, and posterolateral capsule predispose him to increased risk for peroneal nerve palsy. His symptoms at follow-up suggest knee flexion
instability with pain, swelling, and difficulty descending stairs. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant depending on the condition of the ligaments likely is needed to address his symptoms. The difference in extension vs flexion stability makes polyethylene exchange a poor option. There is no reason to believe a constrained rotating hinge design is necessary. Repeat use of a PCL-retaining insert is not recommended.
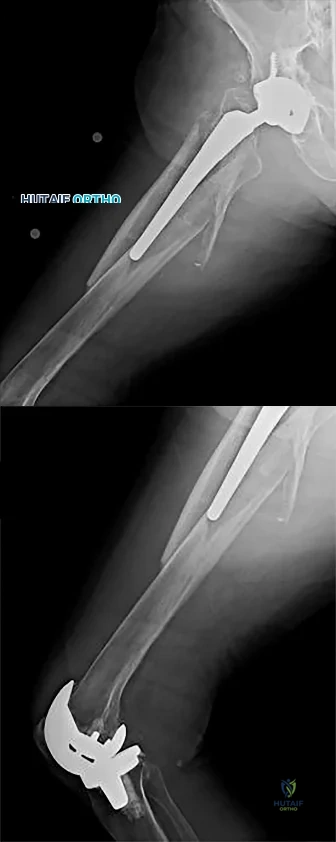
Question 77
A 70-year-old man who underwent an uncomplicated large rotator cuff repair 6 months ago is now seeking a second opinion regarding persistent pain and weakness in his shoulder. Examination reveals that his incision is well healed and unreactive. The surgical report suggests that the tendons were secured back to bone with sutures through the greater tuberosity. Figure 28 shows a radiograph that was obtained 1 week ago. What is the most likely diagnosis?
Explanation
REFERENCES: Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213.
Jost B, Pfirrmann CW, Gerber C, Switzerland Z: Clinical outcome after structural failure of rotator cuff repairs. J Bone Joint Surg Am 2000;82:304-314.
Question 78
A 56-year-old woman sustained the fracture shown in Figures 30a and 30b in a motor vehicle accident. What mechanism is most likely responsible for the injury? Review Topic
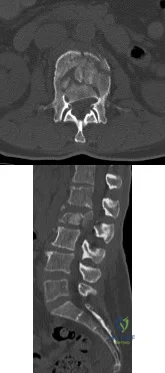
Explanation
Question 79
Which of the following findings helps to distinguish between stress fractures of the tibia and shin splints?
Explanation
After activity, pain persists longer with tibial stress fractures.
DISCUSSION: Anterior tibial pain can often be difficult to diagnose. A bone scan showing the tibial cortex in a diffuse, longitudinal orientation is consistent with shin splints compared to a more discreet, localized uptake more commonly seen with a stress fracture. Bone stress injuries are due to cyclical overuse of the bone. They are relatively common in athletes and military recruits but are also seem in otherwise healthy people who have recently started new or intensive physical activity. Diagnosis of bone stress injuries is based on the patient’s history of increased physical activity and on imaging findings.
The general symptom of a bone stress injury is stress-related pain. Bone stress injuries are difficult to diagnose based only on a clinical examination because the clinical symptoms may vary depending on the phase of the pathophysiological spectrum in the bone stress injury. Imaging studies are needed to ensure an early and exact diagnosis. If the diagnosis is made early, most bone stress injuries heal well without complications.
REFERENCES: Mubarak SJ, Gould RN, Lee YF, et al: The medial tibial stress syndrome: A cause of shin splints. Am J Sports Med 1982;10:201-205.
Knobloch K, Yoon U, Vogt PM: Acute and overuse injuries correlated to hours of training in master running athletes. Foot Ankle Int 2008:29:671-676.
Kiuru MJ, Pihlajamaki HK, Ahovuo JA: Bone stress injuries. Acta Radiol 2004;45:317-326.
Question 80
Figure 51 shows the radiograph of a 42-year-old construction worker who has pain and limited motion in his dominant elbow. Management consisting of nonsteroidal anti-inflammatory drugs and cortisone has failed to provide relief. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Gramstad GD, Galatz LM: Management of elbow osteoarthritis. J Bone Joint Surg Am 2006;88:421-430.
Steinmann SP, King GJ, Savoie FH III, et al: Arthroscopic treatment of the arthritic elbow.
J Bone Joint Surg Am 2005;87:2114-2121.
Question 81
Which of the following conditions precludes performing a tendon transfer?
Explanation
REFERENCES: Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. St Louis, MO, Mosby, 2003, pp 1283-1287.
Coughlin MJ, Mann RA: Disorders of tendons, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 786-861.
Question 82
-A 24-year-old collegiate pitcher has had increasing pain over his medial elbow for 3 months. He has point tenderness over his medial epicondyle and reproduction of his symptoms with a valgus stress test. What phase of the throwing cycle most likely will reproduce his symptoms?
Explanation
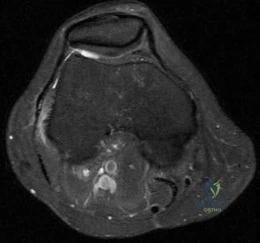
Question 83
Ten years after undergoing TKA, a 77-year-old woman experiences 2 weeks of pain, swelling, and erythema following a routine dental cleaning procedure (Figures 109a and 109b). Her erythrocyte sedimentation rate is 25 mm/h (reference range 0-20 mm/h), her C-reactive protein level is 1.7 mg/L (reference range, 0.08-3.1 mg/L), and alpha-defensin findings are negative.
Explanation
Managing complications following a failed TKA requires an understanding of the mode of failure and treatment principles. Generally, TKA can fail for the following reasons: infection, instability, aseptic loosening, stiffness, and extensor mechanism dysfunction.
Managing an infected TKA requires knowledge of the timing and circumstances surrounding the infected implant. Patients with acute infections (symptom duration of fewer than 3 weeks) are candidates for debridement and prosthesis retention. Chronic infections (symptoms lasting longer than 3 weeks and for more than 3 months from the time of index arthroplasty) should be treated with resection arthroplasty, parenteral antibiotics, and reimplantation surgery at a later date. Evaluation of possible acute infections should include aspiration, serology, and alpha-defensin.
Instability following TKA is a common cause of early failure and revision surgery. The etiology of instability can include overresection of the posterior condyles, collateral ligament insufficiency, and late rupture of the posterior cruciate ligament. Recognizing the cause of instability is critical to eventual successful revision. Typically, isolated polyethylene exchange is not effective or reliable to address instability. In many cases, component malrotation and ligament imbalance contribute to instability. Revision surgery focuses on restoration of the joint line, proper femoral and tibial component rotation, and restoration of the femur posterior condylar.
Component loosening and osteolysis are the common mechanisms of TKA failure. Prior to revision, concurrent infection must be ruled out as a source of failure. At the time of revision, proper fixation and rotation of the femoral and tibial components must be ensured. If the components are well fixed and rotated, successful isolated bearing exchange and bone grafting in the setting of osteolysis is possible. Isolated component exchanges also can be successfully performed, provided the remaining components are in an acceptable position. However, when in doubt, revision of both components generally yields more consistent results.
Stiffness following TKA can affect as many as 10% of patients following surgery. Depending on the timing and extent of arthrofibrosis, treatment options include manipulation under anesthesia or revision TKA. Manipulation typically is effective early during the postsurgical
course (for up to 4 months) and is most effective for loss of flexion. To address chronic stiffness and arthrofibrosis, revision TKA offers modest improvements in range of motion. Isolated polyethylene exchange has proven inconsistent in this setting, so revision of both components to ensure proper component rotation and joint line restoration offers the best chance to improve range of motion.
Extensor mechanism complications also can occur following TKA. Although the frequency is decreasing with improved component design and surgical techniques, periprosthetic patella fractures can occur. Treatment centers on the integrity of the extensor mechanism and fixation of the patellar component (if resurfaced). In general, if the extensor mechanism is intact, nonsurgical treatment is favored. Surgical treatment of periprosthetic patellar fractures following TKA has been associated with high complication rates and low healing rates.
Question 84
Cortical bone demonstrates viscoelastic behavior as its mechanical properties are sensitive to strain rate and duration of applied load. Regarding longitudinal strain in cortical bone, which of the following statements regarding this characteristic is true?
Explanation
For LOW strain rates typical of normal activity (physiological strain rates of <0.1/s), bone is ELASTIC and DUCTILE (increasing ultimate strain with increasing strain rate). There is a ductile-to-brittle transition with increasing strain rate from normal to
supranormal rates. For EXTREMELY HIGH supranormal strain rates (>0.1/s, high impact trauma), bone is VISCOELASTIC and BRITTLE (low ultimate strain with increasing strain rate). Bone also becomes stronger and stiffer (higher modulus, steeper slope of stress-strain plot) as strain rate increases. This viscoelastic property helps in damping muscle contracture.
Natali and Meroi reviewed studies examining mechanical properties of bone. Mechanical properties are correlated with moisture, deformation rate, density and region of bone. Mechanical adaptation of bone is affected by strain rate (rate at which bone is deformed), strain mode (tension, compression, shear), strain direction (direction of strain relative to bone surface), strain frequency (cycles/second), stimulus duration (period over which deformation cycles are applied), strain distribution (pattern of strain magnitude across bone section) and strain energy (energy stored during deformation).
Illustration A shows the mechanical properties of bone with increasing strain rates. Incorrect Answers:
increase. During normal activity, as strain rate increases, bone is more ductile. With high impact trauma, bone is more brittle.
Question 85
If the structure marked by the tip of the probe in Figure 94 is repaired to the bony glenoid with suture anchors during an arthroscopic stabilization procedure, what is the most likely result? Review Topic

Explanation
Question 86
Which of the following areas of the vertebral segment has the highest ratio of cortical to cancellous bone? Review Topic
Explanation
Question 87
A 32-year-old man underwent a total medial meniscectomy 2 years ago. He now reports pain and recurrent swelling for the past 3 months. Work-up includes full standing hip-knee-ankle radiographs, standing AP radiographs of both knees in full extension, an axial view of the patellofemoral joint, and a 45-degree flexion AP radiograph. Contraindication to meniscus allograft transplantation includes which of the following? Review Topic
Explanation
Question 88
A radiograph of a 27 month old child with bilateral genu valgum and internal tibial torsion shows the metaphyseal-diaphyseal angle of Levine and Drennen is 12 degrees on the right and 13 degrees on the left. Based on this finding, management should consist of
Explanation
Question 89
A 27-year-old woman reports the acute atraumatic onset of burning pain in her right shoulder followed a week later by significant weakness and the inability to abduct her shoulder. One week prior to this incident she had recovered from a flu-like syndrome. Examination reveals full passive motion of the shoulder and the inability to actively raise the arm. Sensation in the right upper extremity is normal. Cervical spine examination is normal. Radiographs of the shoulder and cervical spine are normal. What is the most likely diagnosis?
Explanation
REFERENCES: Turner JW, Parsonage MJ: Neuralgic amyotrophy (paralytic brachial neuritis). Lancet 1957;2:209-212.
Omer GE, Spinner M, Van Beek AL (eds): Management of Peripheral Nerve Problems, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 101-104.
Question 90
Wear of metal-on-metal articulations in total hip arthroplasty is characterized by which if the following findings?
Explanation
Orthopaedic Knowledge Update: Hip & Knee Reconstruction 2. Rosemont, IL, Americal Academy of Orthopaedic Surgeons, 2000, pp 25-34. Jazrawi L, Kummer FJ, Di Cesare PE: Alternative Bearing Surfaces for Total Joint Arthroplasty. J Am Acad Orthop Surg 1998;6:198-203
Which of the following findings is a predisposing factor for an acute lateral patellar dislocation?
Hypoplastic medial femoral condyle
Dysplastic vastus lateralis
Patella baja
Decreased Q angle
Excessive internal rotation of the femur
Most acute patellar dislocations occur during the second decade. Lateral dislocations are by far the most common direction of injury. Patients with abnormal patellofemoral mechanics sustain patellar dislocations with less trauma and soft tissue injury compared with normal subjects. Predisposing factors for dislocation include hypoplastic lateral femoral condyle, dysplastic vastus medialus obliqus (VMO), patella alta, contracted iliotibial band, tight lateral retinaculum, valgus knee deformity, increased Q angle, ligamentous laxity, lateral insertion of patellar tendon on tibia, excess internal rotation of the femur / external rotation of tibia, previous patellar dislocations and injury to medial patellofemoral ligament (MPFL). Some authors favor open exploration of the MPFL following arthroscopic examination for acute patella dislocations.
Braham S, Vrahas MS, Fu FH: Knee fractures in the athlete. Orthop Clin North Am 2002;33:566-574
Which of the following substances is labeled with technetium Tc 99m in a conventional bone scan?
calcium
phosphate
Alkaline phosphatase
Biphosphonate
Type I collagen
Item deleted 04.47
What is the preferred type of graft for skin loss of the palmar aspect of the hand?
Unmeshed split-thickness
Meshed split-thickness
Multiple pinch
Full-thickness
Full-thickness with attached subcutaneous fat
In general, soft tissue coverage in the hand should supply tissue that is thin, pliable, durable, and that allows for tendon gliding. The goal is to replace "like with like". Ideally, the reconstruction should allow for sensation, dynamic function, and restoration of form. Skin grafts are usually autografts and they are either splitthickness skin grafts (STSG) or full-thickness skin grafts (FTSG). Compared to STSG, full thickness grafts contract less, are more durable and flexible, and have better sensation. They are the preferred grafts for areas prone to shear and load such as fingertips, the palm, and areas over joints. STSG are better for dorsal hand wounds. STSG can be meshed or unmeshed. Meshed STSG have fewer problems with seromas, hematomas, and infections; therefore, they have better take. However, the appearance of unmeshed STSG is more aesthetically satisfying.
Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp470-492.
What ligament is attached to the displaced distal tibial articular fracture shown in Figures12a and 12b?
Anterior talofibular
Anterior tibiofibular
Posterior talofibular
Posterior tibiofibular
Calcaneofibular

Ankle (AP & lateral) x-rays show a non-displaced lateral malleolus fracture and a minimally displaced posterior malleolar fracture. Mortise is well preserved. No tibiotalar dislocation/subluxation. Medial malleolus seems intact. The injury to the posterior plafond component or
posterior malleolus is a posterolateral avulsion fracture resulting from the pull of the posterior-inferior tibiofibular ligament. If this fragment constitutes >25-30% of the plafond surface, and/or is displaced more than 2 mm, the fragment needs internal fixation. The origin of the posterior tibiofibular ligament is broad, covering most of the horizontal distal surface of the tibia. As the ligament fibers sweep laterally and distally to insert on the fibula they fit over the trochlea.
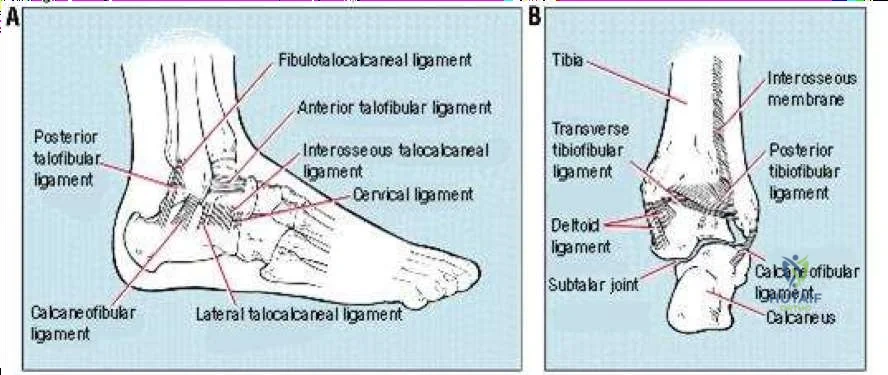
Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, Americal Academy of Orthopaedic Surgeons, 2000, pp 203-225
Michelson JD: Ankle fractures resulting from rotational injuries. J Am Acad Orthop Surg 2003;11:403-412
A 35-year-old man with ankylosing spondylitis has progressive sagittal plane imbalance, difficulty with horizontal gaze, and thigh fatigue with standing. Radiographs are shown in Figures 13a and 13b. Maximum correction of the sagittal decompensation can be accomplished at a single level by which of the following procedures?
Smith-Peterson osteotomy (posterior closing wedge hinging on the posterior longitudinal ligament)
Transpedicular wedge resection osteotomy
Combined anterior and posterior surgery
Anterior opening wedge osteotomy
Vertebral column resection
In the radiographs we have AP / lateral spinal xrays of a patient with known ankylosing spondylitis. Of note, there are bilateral total hip arthroplasties. There is marked thoracic kyphosis, and mild thoracolumbar scoliosis. No evidence of acute fx/ dislocations. Notice that the question specifically states… maximum correction of the sagittal decompensationcan be accomplished at a single levelby which of the following procedures? Surgical correction of the kyphosis deformity with osteotomy was first done in 1945. Since then, surgeons have tried several different approaches and techniques to correct the stiff kyphosis. The transpedicular wedge osteotomy was described by Thomasen (1985) for the correction of deformity secondary to ankylosing spondylitis. In this technique the spinous process of L2 and the upper part of L3 are removed; the laminae of the second and the upper part of the third lumbar vertebrae are also removed as well as the articular processes of L2-3 and the pedicles of L2. A wedge fracture is created on the posterior wall of the vertebral body of L2. Then, plates are fixed to the spinous processes of T12-L1 and L3-4. Thomasen osteotomy places the apex of correction anteriorly, serving to shorten the spine and avoid anterior column lengthening. Advantages include the prevention of neural compression by creation of a large, shared neural foramen through removal of the pedicles, limited stretch of anterior structures, and cancellous bone healing. This technique provides maximum correction of the deformity, and can be accomplished at a single level. You either know it, or you don’t.
Berven SH, Deriven V, Smith JA, Emami A, Hu SS, Bradford DS: Management of fixed sagittal plane deformity: Results of the transpedicular wedge osteotomy. Spine 2001;26:2036-2043.
Thomasen E: Vertebral osteotomy for correction of kyphosis in ankylosing spondylitis.
Clin Orthop 1985;194:142-152
Question 91
Based on the diagram shown in Figure 16, what muscle derives its innervation from the nerve identified by the letter “A”?
Explanation
REFERENCES: Moore K: Anatomy, ed 3. Philadelphia, PA, Williams and Wilkins, 1992.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, pp 400, 405, 407, 450.
Question 92
When an acute infection of a total elbow arthroplasty is managed with irrigation and debridement, which of the following organisms is associated with the highest risk of persistent infection?
Explanation
IV antibiotics.
REFERENCES: Yamaguchi K, Adams RA, Morrey BF: Infection after total elbow arthroplasty. J Bone Joint Surg Am 1998;80:481-491.
Schoifet SD, Morrey BF: Treatment of infection after total knee arthroplasty by debridement with retention of the components. J Bone Joint Surg Am 1990;72:1383-1390.
Question 93
Figures 21a through 21c show the radiographs of a 70-year-old woman who has persistent pain with activity after undergoing hip revision 6 months ago. Treatment should now consist of
Explanation
REFERENCES: Gill TJ, Sledge JB, Muller ME: The Burch-Schneider anti-protrusio cage in revision total hip arthroplasty: Indications, principles, and long-term results. J Bone Joint Surg Br 1998;80:946-953.
Sharkey PF, Hozack WJ, Callaghan JJ, et al: Acetabular fracture associated with cementless acetabular component insertion: A report of 13 cases. J Arthroplasty 1999;14:426-431.
Question 94
A 35-year-old man is brought to the emergency department following a motorcycle accident. He is breathing spontaneously and has a systolic blood pressure of 80 mm Hg, a pulse rate of 120/min, and a temperature of 98.6° F (37° C). Examination suggests an unstable pelvic fracture; AP radiographs confirm an open book injury with vertical displacement on the left side. Ultrasound evaluation of the abdomen is negative. Despite administration of 4 L of normal saline solution, he still has a systolic pressure of 90 mm Hg and a pulse rate of 110. Urine output has been about 20 mL since arrival 35 minutes ago. What is the next best course of action?
Explanation
REFERENCE: Mayo K, Kellam JK: Pelvic ring disruptions, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1052-1108.
Question 95
Figures 1 through 3 are the radiographs of a 65-year-old man who sustained a fracture from a fall. The patient elects open reduction and internal fixation of the distal radius. After plating the distal radius, the distal radioulnar joint (DRUJ) is examined and found to be unstable in both pronation and supination. What is the best next step?

Explanation
styloid fracture were found to increase risk for DRUJ instability. An ulnar styloid base fracture involves the insertion of the radioulnar ligaments and can cause DRUJ instability if displaced. If persistent instability is present after fixation of the ulnar styloid, DRUJ pinning is a reasonable option. Early ROM
The initial radiographs show a comminuted displaced distal radius fracture, along with a displaced fracture of the base of the ulnar styloid. The displacement is best seen on the oblique view. After reduction and fixation of the radius, DRUJ stability should be assessed. The majority of scenarios that involve this injury pattern will not be unstable because of the oblique band of the interosseous ligament. When DRUJ instability is present after fixation of the radius, reduction and fixation of the ulnar styloid fracture is the best option to provide stability of the distal radioulnar joint (DRUJ) (Figure below). A study by Lawton and associates revealed that all distal radius fractures complicated by DRUJ instability were accompanied by an ulnar styloid fracture. A fracture at the ulnar styloid’s base and substantial displacement of an ulnar
with splinting would not allow reduction or healing of the ulnar styloid and would result in persistent instability. Short-arm casting also would not allow stability of the DRUJ and would be a less reliable method with which to achieve healing of the ulnar styloid.
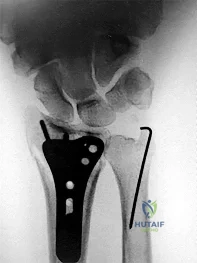
Question 96
Examination of a 12-year-old girl with a painful flatfoot deformity reveals tenderness in the region of the sinus tarsi and no appreciable subtalar motion. Radiographs are shown in Figures 48a through 48c. Two attempts to relieve her symptoms by cast immobilization fail to relieve the pain. Management should now consist of
Explanation
REFERENCES: Gonzalez P, Kumar SJ: Calcaneonavicular coalition treated by resection and interpostion of the extensor digitorum brevis muscle. J Bone Joint Surg Am 1990;72:71-77.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 211-218.
Question 97
A 13-year-old right-hand dominant pitcher was treated for Little League shoulder. What finding increases his risk of recurrence?
Explanation
rotator cuff weakness, and increased height have not been shown to correlate with recurrent symptoms.
Question 98
The main blood supply to the lateral two thirds of the talar body is provided by the
Explanation
REFERENCES: Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999,
pp 1465-1518.
Haliburton RA, Sullivan CR, Kelly PJ, et al: The extra-osseous and intra-osseous blood supply of the talus. J Bone Joint Surg Am 1958;40:1115-1120.
Question 99
A 35-year-old woman undergoes an L4-5 anterior fusion via a left retroperitoneal approach. Postoperative examination reveals that her right foot is cool and pale. Her neurologic examination is normal, and her pedal pulses are asymmetric. What is the most likely reason for the right foot finding?
Explanation
REFERENCES: Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, p1550.
Benzel EC (ed): Spine Surgery Techniques, Complication Avoidance and Management. New York, NY, Churchill Livingstone, 1999, p 190.
Question 100
A 79-year-old woman reports a history of left leg pain with walking. Her pain is exacerbated with walking and stair climbing, and her symptoms are improved by standing after she stops walking. Lumbar flexion does not provide any significant improvement of the symptoms and sitting does not significantly change symptoms. Her leg pain is worse at night and she obtains relief by hanging her leg over the side of the bed. The neurologic examination is essentially normal.
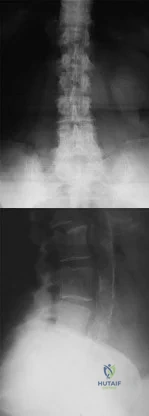
Explanation
