Orthopedic Board Prep MCQs: Arthroplasty, Deformity & Shoulder | Part 58

Key Takeaway
This page offers Part 58 of a comprehensive orthopedic surgery board review quiz, specifically designed for orthopedic residents and surgeons preparing for their OITE and AAOS/ABOS certification exams. It features 100 high-yield, verified multiple-choice questions focusing on Arthroplasty, Deformity, and Shoulder, complete with detailed explanations.
About This Board Review Set
This is Part 58 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 58
This module focuses heavily on: Arthroplasty, Deformity, Shoulder.
Sample Questions from This Set
Sample Question 1: Figure 39 shows the radiograph of a 4-month old infant who has been undergoing weekly casting since birth for a congenital equinovarus deformity. Management should now consist of...
Sample Question 2: A 72-year-old woman with diabetes mellitus who underwent a total shoulder arthroplasty for degenerative arthritis 5 years ago now reports the sudden onset of shoulder pain following recent hospitalization for pneumonia. Laboratory values sh...
Sample Question 3: A 66-year-old man has a high-grade angiosarcoma of the right tibia. A radiograph is shown in Figure 43. Treatment should consist of...
Sample Question 4: What condition favors pollicization in hypoplasia of the thumb?...
Sample Question 5: -A 15-year-old dancer who has had brief episodes of back pain over the past 2 years now reports a 3 month history of low back pain and a decreased tolerance for dance. Figure 22a-c show flexion and extension x-rays and CT scan. She reports ...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 39 shows the radiograph of a 4-month old infant who has been undergoing weekly casting since birth for a congenital equinovarus deformity. Management should now consist of
Explanation
REFERENCES: Lehman WB, Atar D: Complications in the management of talipes equinovarus, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992,
pp 135-136.
Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002,
pp 927-935.
Tachdjian MO: Pediatric Orthopedics, ed 2. Philadelphia, PA, WB Saunders, 1990,
pp 2461-2564.
Question 2
A 72-year-old woman with diabetes mellitus who underwent a total shoulder arthroplasty for degenerative arthritis 5 years ago now reports the sudden onset of shoulder pain following recent hospitalization for pneumonia. Laboratory values show a WBC count of 11,400/mm3 and an erythrocyte sedimentation rate of 52mm/h. What is the most appropriate action?
Explanation
REFERENCES: Matsen FA III, Rockwood CA Jr, Wirth MA, et al: Glenohumeral arthritis and its management, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 953-954.
Stinchfield FE, Bigliani LU, Neu HC, et al: Late hematogenous infection of total joint replacement. J Bone Joint Surg Am 1980;62:1345-1350.
Question 3
A 66-year-old man has a high-grade angiosarcoma of the right tibia. A radiograph is shown in Figure 43. Treatment should consist of
Explanation
REFERENCE: Simon MA, Springfield DA: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, ch 29.
Question 4
What condition favors pollicization in hypoplasia of the thumb?
Explanation
The decision to ablate and pollicize vs preserve and reconstruct is based on the stability of the carpometacarpal joint. A stable thumb is more easily used in prehension activities of grasping and pinching. All other responses are associated with surgical options for reconstruction of the thumb. The carpometacarpal joint is the “keystone” for thumb-to-hand attachment. Without a stable carpometacarpal joint, pollicization may be required. No other response necessitates pollicization.
RECOMMENDED READINGS
McCarroll HR. Congenital anomalies: a 25-year overview. J Hand Surg Am. 2000 Nov;25(6):1007-37. Review. PubMed PMID: 11119659. View Abstract at PubMed
Manske PR, Goldfarb CA. Congenital failure of formation of the upper limb. Hand Clin. 2009 May;25(2):157-70. doi: 10.1016/j.hcl.2008.10.005. Review. PubMed PMID: 19380058.View Abstract at PubMed
Question 5
- A 15-year-old dancer who has had brief episodes of back pain over the past 2 years now reports a 3 month history of low back pain and a decreased tolerance for dance. Figure 22a-c show flexion and extension x-rays and CT scan. She reports no leg pain, nor any bowel or bladder difficulties. Management should now consist of
Explanation
Question 6
A 22-year-old female collegiate javelin thrower has shoulder pain. She notes that her pain is primarily located in the posterior aspect of her shoulder, is exacerbated with throwing, and she experiences maximal tenderness in the extreme cocking phase of the throwing cycle. On examination, she reports deep posterior shoulder pain when the arm is abducted 90 degrees and maximally externally rotated to 110 degrees. This reproduces her symptoms precisely. Shoulder radiographs are normal. What is the most likely diagnosis? Review Topic
Explanation
Question 7
A 42-year-old woman underwent an instrumented posterior spinal fusion at L3-S1 with transforaminal lumbar interbody fusion. She had an excellent
Explanation
Question 8
Figures 25a through 25c show the radiographs, including a stress radiograph, of a 58-year-old woman who twisted her ankle on a step. She has no history of diabetes or vascular disease. Examination reveals a closed injury with moderate swelling about the ankle. Her neurologic examination is normal. She has a strong dorsalis pedis pulse and tenderness over the lateral malleolus and the medial side of her ankle. What is the most appropriate management? Review Topic

Explanation
Question 9
An otherwise healthy 25-year-old man sustained a wound with a 1-cm by 1.5-cm soft-tissue loss over the volar aspect of the middle phalanx of his middle finger. After appropriate debridement and irrigation, the flexor digitorum profundus tendon and neurovascular bundles are visible. The wound should be treated with a
Explanation
flap is ideal for small wounds on the volar aspect of digits. A thenar flap is suitable for tip injuries. A lateral arm flap will not reach the fingers. A Moberg flap is limited to distal injuries of the thumb.
REFERENCES: Kappel DA, Burech JG: The cross-finger flap: An established reconstructive procedure. Hand Clin 1985;1:677-683.
Lister GD: Skin flaps, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1741.
Question 10
A 54-year-old woman underwent prophylactic intramedullary fixation for an impending fracture of her right femur secondary to metastatic breast cancer. A bone scan revealed a second lesion in her inferior pubic ramus. Her oncologist has recommended that she receive the intravenous bisphosphonate, zoledronic acid, because the medication would
Explanation
REFERENCES: Mundy GR, Yoneda T: Bisphosphonates as anticancer drugs. N Engl J Med 1998;339:398-400.
Rosen LS, Gordon D, Kaminski M, et al: Zoledronic acid versus pamidronate in the treatment of skeletal metastases in patients with breast cancer or osteolytic lesions of multiple myeloma: A phase III, double-blind, comparative trial. Cancer J 2001;7:377-387.
Question 11
1 and 2 show the radiograph and CT obtained from a year-old woman who underwent right total hip replacement in She initially did well with no pain. She was last seen 7 years ago and was having mild hip pain at that time. She was found to have a supra-acetabular cyst on radiographs. She has had severe right hip pain for the past 9 months while using a walker for ambulation. The initial blood work reveals an estimated erythrocyte sedimentation rate of 32 mm/hr, a C-reactive protein level of 5 mg/L, a serum cobalt level of 4 µg/L, and a serum chromium level of 6 µg/L. Right hip aspiration is performed, revealing a white blood cell count of 139, 52% neutrophils, and a negative leukocyte esterase test. What is the best next step?
Explanation
The hip replacement was performed in 1995, during the period when the previous generation of polyethylene was utilized. This polyethylene was subjected to irradiation in air, with subsequent oxidation and consequent osteolysis after implantation. The mechanism of osteolysis begins with the uptake of polyethylene particles by macrophages, which then initiate an inflammatory cascade and the release of osteolytic factors. This cycle continues, with eventual implant loosening and failure. The imaging shows significant osteolysis and raises concern for pelvic discontinuity and acetabular implant failure. The surgical treatment consists of acetabular reconstruction. In this patient, concern exists for discontinuity based on the substantial amount of bone loss and nonsupportive anterior and posterior columns. This scenario requires complex acetabular revision using a custom triflange device, distraction with a jumbo acetabular component, or placement of a porous metal cup/cage construct with augmentation. The laboratory values are not consistent with infection or failure due to metal debris.
Question 12
A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 189-199.
Kwon BK, Vaccaro AR, Grauer JN, et al: Subaxial cervical spine trauma. J Am Acad Orthop Surg 2006;14:78-89.
Question 13
-A 37-year-old woman has a 2-month history of weakness in thumb and finger extension, but has normal radial deviation during extension of the wrist. An MRI scan of her forearm shows no abnormality. She does not recall any traumatic event. Needle electromyography findings show fibrillations and reduced
Explanation

Question 14
A 40-year-old female recreational basketball player notes pain deep within her shoulder that occurs with activity. Pain began insidiously 6 months previously. She has completed a physical therapy program, and an intra-articular corticosteroid injection provided excellent temporary relief. Physical examination shows symmetric range of motion of her shoulder. She has a positive O'Brien’s active compression test. There is no pain with cross-arm adduction or tenderness to palpation over the acromioclavicular joint. Resisted abduction is nonpainful and strong. MRI shows increased signal in the substance of the superior labrum, low-grade bursal surface fraying of the supraspinatus, and mild degenerative changes within the acromioclavicular joint. What is the best treatment option?
Explanation
Question 15
Up to what time frame are the risks minimized in anterior revision disk replacement surgery?
Explanation
REFERENCE: Tortolani JP, McAfee PC, Saiedy S: Failures of lumbar disc replacement. Sem Spine Surg 2006;18:78-86.
Question 16
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?
Explanation
REFERENCES: Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
McCarty DJ, Halverson PB, Carrera GF, Brewer BJ, Kozin F: Milwaukee shoulder: Association of microspheroids containing hydroxyapatite crystals, active collagenase, and neutral protease with rotator cuff defects. I: Clinical aspects. Arthritis Rheum 1981;24:464-473.
Question 17
Which gene correlates with severity of disease in spinal muscular atrophy (SMA)? Review Topic
Explanation
Question 18
Overgrowth of a limb in a patient with neurofibromatosis type 1 (NF1) is most likely associated with the presence of
Explanation
REFERENCES: Alman BA, Goldberg MJ: Syndromes of orthopaedic importance, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 287-338.
Greene WB: Neurofibromatosis type I, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1584-1588.
Question 19
An 11-year-old girl is struck in the leg by a loaded sled while sledding and is seen in the emergency department; she is reporting severe knee pain. Radiographs are read as normal. Examination reveals that she is exquisitely tender over the proximal tibial physis. The neurovascular examination is normal. What is the next step in management? Review Topic
Explanation
Question 20
When an acute infection of a total elbow arthroplasty is managed with irrigation and debridement, which of the following organisms is associated with the highest risk of persistent infection?
Explanation
IV antibiotics.
REFERENCES: Yamaguchi K, Adams RA, Morrey BF: Infection after total elbow arthroplasty. J Bone Joint Surg Am 1998;80:481-491.
Schoifet SD, Morrey BF: Treatment of infection after total knee arthroplasty by debridement with retention of the components. J Bone Joint Surg Am 1990;72:1383-1390.
Question 21
A 39-year-old male with chronic renal disease and type 2 diabetes mellitus fell 1 week ago after slipping on ice. He is unable to bear weight on the right lower extremity or perform active knee extension. He reports no prior history of knee pain or instability. Lachman, posterior drawer, posterolateral recurvatum testing are deferred secondary to patient's pain. He has a palpable dorsalis pedis pulse but does have neuropathy as determined by Semmes-Weinstein filament testing. His radiograph is shown in Figure A and MR images in Figures B and C. What is the most appropriate initial plan for management? Review Topic

Explanation
Primary surgical repair within 2 weeks of injury is recommended to prevent extensor mechanism contracture. Patellar tendon ruptures typically occur in patients younger than 40 years old. Most ruptures occur at the junction of the tendon and distal pole of the patella.
Matava et al. presents a level 5 review on patellar tendon ruptures and states that active knee extension is permitted at 3 weeks postoperatively. Non-weightbearing movement exercises like heel slides are encouraged. This can incorporate active knee flexion with passive extension. Alternatively, active knee flexion in the prone position with passive knee extension can be performed. Open chain strengthening exercises such as leg extensions are started later, as are weight bearing resistance exercises like squats, lunges and leg presses.
Volk et al. discuss potential complications and pitfalls of patients with the management of extensor mechanism injuries. They warn that complications can consist of misdiagnosis, delayed surgery, failed repair due to poor surgical planning of injury site, or wound infection.
Figure A demonstrates patella alta which in this case is indicative of complete patellar tendon rupture. Patella alta can be quantified by using the Insall-Salvati ratio (patellar tendon length / patellar bone length): PTL/PBL normal =1, >1.2 is patella alta, <0.8 is patella baja) with the knee flexed to 30 degrees. Figure B and C are sagittal T1 and T2 images showing complete patellar tendon rupture.
Incorrect answers:
Question 22
A 52-year-old woman with a 2-year history of a flexible (stage II) adult-acquired flatfoot deformity has failed to respond to nonsurgical management consisting of immobilization, custom orthotics, nonsteroidal anti-inflammatory drugs, and physical therapy. The patient is unable to perform a single limb heel rise. Weight-bearing radiographs are shown in Figures 30a through 30c. What is the most appropriate surgical correction?
Explanation
REFERENCES: Greisberg J, Assal M, Hansen ST Jr, et al: Isolated medial column stabilization improves alignment in adult-acquired flatfoot. Clin Orthop Relat Res 2005;435:197-202.
Greisberg J, Hansen ST Jr, Sangeorzan BJ: Deformity and degeneration in the hindfoot and midfoot joints of the adult acquired flatfoot. Foot Ankle Int 2003;24:530-534.
Question 23
Figure below depicts the radiograph obtained from a 52-year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?
Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 24
Figure 1 is the MR image of a high school soccer player who sustained a right knee injury during a game while making a cut toward the ball. He felt a pop and his leg gave way. During physical examination, as the knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a "clunk" within the knee. What is the most likely biomechanical basis for the "clunk"?

Explanation
Question 25
Type I collagen fibers in peripheral nerves are primarily responsible for which of the following?
Explanation
The COL1A1 gene produces a component of type I collagen, called the pro-alpha1(I) chain. This chain combines with another pro-alpha1(I) chain and also with a pro-alpha2(I) chain (produced by the COL1A2 gene) to make a molecule of type I procollagen. These triple-stranded, rope-like procollagen molecules must be processed by enzymes outside the cell. Once these molecules are processed, they arrange themselves into long, thin fibrils that cross-link to one another in the spaces around cells. The cross-links result in the formation of very strong mature type I collagen fibers.
Wong et al. provide a review of the basic science behind nerve healing and the recovery after nerve repair. They note the importance of minimizing additional surgical insult and careful handling of nerve tissue during repair to optimize outcomes.
Pertici et al. noted that autologous nerve implantation to bridge a long nerve gap presents the greatest regenerative performance in spite of substantial drawbacks. They were able to show improved nerve guided regrowth with a type I collagen matrix conduit as compared to a conduit made of a mix of type I and type III collagen.
Illustration A shows a diagram of type I collagen, showing the rope-like characteristics behind the tensile strength.
Incorrect Answers:
Question 26
Kinematic testing of patellofemoral motion demonstrates that malalignment that produces increased Q angle causes a shift of the patella laterally in the trochlear groove and is most pronounced during what phase of the flexion arc? Review Topic
Explanation
Question 27
82 • American Academy of Orthopaedic Surgeons A 12-year-old girl is seen for left ankle pain. Radiographs reveal osteochondritis dissecans (OCD) involving the talus. What should the parents be told regarding management?
Explanation
REFERENCES: Perumal V, Wall E, Babekir N: Juvenile osteochondritis dissecans of the talus. J Pediat Orthop 2007;27:821-825.
Letts M, Davidson D, Ahmer A: Osteochondritis dissecans of the talus in children. J Pediatr Orthop 2003;23:617-625.
Question 28
A 45-year-old man reports severe discomfort following a twisting injury to his right ankle and foot. Plain radiographs are negative; however, the CT scans shown in Figures 39a and 39b reveal a fracture. Management should consist of
Explanation
REFERENCES: Heckman JD: Fractures and dislocations in the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2267-2405.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Question 29
A 14-year-old boy has medial ankle pain, progressive unilateral flatfoot deformity, and pain with most activities of daily living. He denies any recent injury. His parents recall that at age 7 years he sustained an injury that was treated as a sprain. Examination reveals valgus deformity with painless, unrestricted passive motion of the ankle. He has grossly equal limb lengths. A radiograph of the affected ankle is shown in Figure 48a, and the contralateral ankle is shown in Figure 48b. Management should consist of
Explanation
REFERENCES: Thompson DM, Calhoun JH: Advanced techniques in foot and ankle reconstruction. Foot Ankle Clin 2000;5:417-442.
Ting AJ, Tarr RR, Sarmiento A, Wagner K, Resnick C: The role of subtalar motion and ankle contact pressure changes from angular deformities of the tibia. Foot Ankle 1987;7:290-299.
Tarr RR, Resnick CT, Wagner KS, Sarmiento A: Changes in tibiotalar joint contact areas following experimentally induced tibial angular deformities. Clin Orthop 1985;199:72-80.
Question 30
A research study is initiated on 500 patients undergoing total hip arthroplasty. The patients are followed and outcome is assessed according to body mass index (BMI). The effects of BMI on outcome should be reported as which of the following?
Explanation
Question 31
They found statistically significant decreases in need for secondary intervention, hardware failure, and infection as well as faster wound healing and faster time to fracture union.
Explanation
A 76-year old patient underwent partial foot amputation through the talonavicular and calcaneocuboid joints. Besides Achilles tendon lengthening, what additional procedure(s) may be required to prevent the most common post-operative deformity?
Posterior capsule release
Anterior tibialis transfer to the talar neck
Anterior tibialis transfer to cuboid
Flexor hallucis longus transfer to calcaneus
Peroneus brevis transfer to calcaneus Corrent answer: 2
Achilles tendon lengthening AND anterior tibialis transfer to the talar neck would be required to prevent equinovarus deformity.
Partial foot amputation through the talonavicular and calcaneocuboid joints is also known as the Chopart amputation. Chopart amputation alone is known to result in significant equinovarus deformity. This deformity results in excessive pressure on the anterior wound during gait, causing pain and wound complications. Transfer of the tibialis anterior tendon to talar neck will provide force, and muscle tone, that promotes ankle dorsiflexion. Lengthening of the Achilles tendon will also reduce the equinus moment force across the ankle joint.
Dillion et al. examined the gait patterns of partial foot amputees. They found that amputations proximal to the metatarsal heads compromised the normal propulsive function of the foot and ankle. The ideal level of amputation to maintain normal propulsive function was distal to the metatarsal heads (i.e., disarticulating the metatarsophalangeal (MTP) joint).
Illustration A is a lateral radiograph showing a Chopart amputation. Incorrect Answers:
prevent the equinovarus deformity.

OrthoCash 2020
A 32-year-old male is involved in a motor vehicle collision and sustains the injury seen in Figure A. What is the most common urological injury associated with this injury pattern?

Testicular torsion
Posterior urethral tear
Bladder denervation
Testicular rupture
Renal hematoma
The figure shows an anteroposterior pelvic ring injury. The most common urological injury with pelvic ring injuries remains the posterior urethral tear, followed by bladder rupture.
Watnik et al notes lower urinary tract (bladder to end of urethra) injuries in up to 25% of patients with this injury. He reports that when contaminated urine communicates with the anterior arch, the possibility of infection exists, and early repair of bladder disruptions with simultaneous anterior arch plating minimizes this risk.
Routt et al notes that even with simultaneous treatment of these injuries, complications are common (late stricture in 44%, impotence in 16%, delayed incontinence in 20% of females, anterior deep pelvic infection in 4%). Despite this, they report that early urological repairs are easily performed at the time of anterior pelvic open reduction and internal fixation.
OrthoCash 2020
A 26-year-old women, 31-weeks pregnant, presents to the emergency department with the injury shown in Figure A. She states the injury occurred while lifting a heavy vacuum five days ago. She suffers from chronic headaches and sleep disturbances. On inspection, there are multiple dorsal and volar bruising over her wrist and upper arm. She is neurologically intact. After closed reduction and immobilizing the arm, what would be the next best step in management of this patient?

Diagnostic wrist arthroscopy
Urgent MRI wrist
Skeletal survey radiographs
Request a consultation with social worker in the hospital
Urgent open reduction internal fixation Corrent answer: 4
This patient presents with classic features of domestic violence. The most appropriate next step would be consultation with a social worker at the hospital, assess for child and patient safety, and encouraging the patient to seek self-protection.
Factors suggestive of domestic violence in the patient include pregnancy, delayed presentation after injury, inconsistent history, multiple bruises and complaints of chronic headache/sleep disturbances. Victims frequently miss days of work and as a result are at risk for losing their jobs. Victims are also more likely to engage in high-risk behavior with sex, drugs, alcohol, smoking, and eating.
The AAOS published a document outlining the Orthopaedic Surgeon’s responsibilities in domestic and family violence. Musculoskeletal injuries that should raise a suspicion of a problem include (1) Multiple injuries/fractures; (2) Unusual patterns of injury/fracture; (3) Injuries/fractures of varying ages; (4)
Injuries/fractures inconsistent with or disproportional to the history; (5) Multiple injuries treated in different hospital emergency departments or by different providers.
Incorrect Answers:
OrthoCash 2020
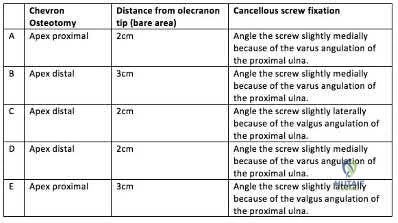
A 45-year-old man undergoes open reduction and internal fixation for a comminuted intra-articular humerus fracture . An olecranon osteotomy is performed and subsequently fixed with an intramedullary cancellous screw. Which of the following options in the table shown in Figure A best describes the characteristics of this osteotomy?
Question 32
A patient with Charcot-Marie-Tooth disease has a progressively rigid cavovarus foot deformity. The patient states that the pain is restricted to the forefoot, where rigid claw toe deformities have developed. Which of the following structures is primarily involved in creation of a claw toe deformity?
Explanation
REFERENCES: Keenan MA, Gorai AP, Smith CW, Garland DE: Intrinsic toe flexion deformity following correction of spastic equinovarus deformity in adults. Foot Ankle 1987;7:333-337.
Pichney GA, Derner R, Lauf E: Digital “V” arthrodesis. J Foot Ankle Surg 1993;32:473-479.
Mizel MS, Michelson JD: Nonsurgical treatment of monarticular nontraumatic synovitis of the second metatarsophalangeal joint. Foot Ankle Int 1997;18:424-426.
Question 33
A 34-year-old woman reports constant midlateral arm pain after sustaining minimal trauma to the shoulder. Radiographs and a biopsy specimen are shown in Figures 29a and 29b. What is the most likely diagnosis?
Explanation
REFERENCES: Campanacci M, Baldini N, Boriani S, et al: Giant cell tumor of bone. J Bone Joint Surg Am 1987;69:106-114.
Goldenberg RR, Campbell CJ, Bonfiglio M: Giant cell tumor of bone: An analysis of two hundred and eighteen cases. J Bone Joint Surg Am 1970;52:619-664.
Question 34
During a retroperitoneal approach to the L4-5 disk, what structure must be ligated to safely mobilize the common iliac vessels toward the midline from laterally and gain exposure?
Explanation
REFERENCES: Baker JK, Reardon PR, Reardon MJ, et al: Vascular injury in anterior lumbar surgery. Spine 1993;18:2227-2230.
Lewis WH: Gray’s Anatomy of the Human Body: The Veins of the Lower Extremity, Abdomen, and Pelvis, ed 20. Philadelphia, PA, Lea & Febiger, 2000.
Question 35
A 55-year-old man who works as a carpenter reports chronic right anterior shoulder pain and weakness. Examination reveals 90 degrees of external rotation (with the arm at the side) compared to 45 degrees on the left side. His lift-off examination is positive, along with a positive belly press finding. An MRI scan reveals a chronic, retracted atrophied subscapularis tendon. What is the most appropriate management of his shoulder pain and weakness? Review Topic
Explanation
Question 36
A 61-year-old woman with a long-standing history of rheumatoid arthritis reports progressive elbow pain for the past 12 months. She denies any recent trauma to the elbow; however, she notes increasing pain and decreased joint motion that are now compromising her function. Radiographs are shown in Figures 57a and 57b. What is the most appropriate treatment at this time? Review Topic

Explanation
Question 37
A farmer is seen in the emergency department after falling out of a hay loft onto the barn floor below. He is unable to bear weight. Exploration of a 0.5 cm laceration over the anterior tibia reveals bone. Radiographs reveal oblique displaced midshaft tibial and fibular fractures. Based on these findings, what is the most appropriate antibiotic prophylaxis?
Explanation
REFERENCES: Okike K, Bhattacharyya T: Trends in the management of open fractures: A critical analysis. J Bone Joint Surg Am 2006;88:2739-2748.
Holtom PD: Antibiotic prophylaxis: Current recommendations. J Am Acad Orthop Surg 2006:14:S98-S100.
Question 38
A 38-year-old man who is an avid runner reports a several month history of right hip pain. Based on the radiograph and cross-sectional CT scan shown in Figures 33a and 33b, what is the most likely diagnosis for the lesions seen on the femoral neck?
Explanation
REFERENCES: Pitt MJ, Graham AR, Shipman JH, et al: Herniation pit of the femoral neck. Am J Roentgenol 1982;138:1115-1121.
Daenen B, Preidler KW, Padmanabhan S, et al: Symptomatic herniation pits of the femoral neck: Anatomic and clinical study. Am J Roentgenol 1997;168:149-153.
Question 39
A 7-year-old boy has had low back pain for the past 3 weeks. Radiographs reveal apparent disk space narrowing at L4-5. The patient is afebrile. Laboratory studies show a WBC count of 9,000/mm P 3 P and a C-reactive protein level of 10 mg/L. A lumbar MRI scan confirms the loss of disk height at L4-5 and reveals a small perivertebral abscess at that level. To achieve the most rapid improvement and to lessen the chances of recurrence, management should consist of
Explanation
REFERENCES: Ring D, Johnston CE II, Wenger DR: Pyogenic infectious spondylitis in children: The convergence of discitis and vertebral osteomyelitis. J Pediatr Orthop
1995;15:652-660.
Crawford AH, Kucharzyk DW, Ruda R, et al: Diskitis in children. Clin Orthop 1991;266:70-79.
Question 40
A 13-year-old boy has a radiographically mild, clinically stable slipped capital femoral epiphysis (SCFE). What is the most appropriate treatment? Review Topic
Explanation
(SBQ13PE.46) What developmental milestones are likely to be present in a 30-month-old child? Review Topic
Hand dominance established
Hops on one foot
Heel-to-toe walk
Puts shoes on correct feet
Manages buttons
Hand dominance is usually established in the third year of life.
Normally, children younger than 2 years of age are ambidextrous. In some normal cases this persists after 2 years. Although there is some variability in this timing, strong hand preference in a younger child may be the result of a neurologic deficit.
Frankenburg et al. used the Denver Developmental Screening Test (DDST) to evaluate 1036 Denver area children from 2 to 6.4 years. The ages at which 25, 50, 75 and 90 percent of children could perform tasks were calculated to establish norms for the sample. The authors stress that the DDST is not an intelligence test, but rather a screening test to be used in clinical practice to determine whether a child's development is within the normal range.
Illustration
A
shows
the
DDST.
Incorrect
2:
Normal
for
Question 41
- Work-related injuries to the lower back are most often related to which of the following risk factors?
Explanation
Question 42
A 6-year-old sustains the injury shown in Figures A and B. The nerve most commonly affected by this fracture pattern innervates which of the following motor groups?

Explanation
The most common neurapraxia after pediatric extension-type supracondylar fractures involve the AIN. It supplies the FPL (thumb IP flexion), the pronator quadratus, and the FDP of the index/long fingers. Subsequently, patients are often unable to make an “a-ok” sign. Most of these neuropraxias resolve without complication. The ulnar nerve is most commonly implicated with flexion-type supracondylar fractures.
Abzug et al. review management of supracondylar fractures. They note that the AIN
is most commonly injured nerve in extension type supracondylar fractures. They note that nerve injuries often resolve within 6-12 weeks.
Babal et al. completed a meta-analysis to determine the risk of neurapraxia associated with pediatric supracondylar fractures. The rate of traumatic neurapraxia was 11.4% amongst 5000 patients. The AIN was affected 34.1% of the time. AIN neurapraxia was most common in extension type injuries.
Figures A and B show an AP and lateral radiographs of a displaced pediatric supracondylar fracture
Incorrect Answers
Question 43
A patient who sustained a cerebrovascular accident (CVA) 18 months ago has a long-standing spastic adduction contracture of the shoulder with a rigid block to passive external rotation. Significant hygiene problems exist with maceration and continued skin breakdown. Management should consist of
Explanation
REFERENCES: Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
McCollough NC III: Orthopaedic evaluation and treatment of the stroke patient. Instr Course Lect 1975;24:45-55.
Question 44
Clinical evidence suggests that grafts for replacing a torn anterior cruciate ligament often stretch after surgery. What is the most probable mechanism for this behavior?
Explanation
REFERENCES: Boorman RS, Thornton GM, Shrive NG, et al: Ligament grafts become more susceptible to creep within days after surgery. Acta Orthop Scand 2002;73:568-574.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 596-609.
Lu L, Kaufman KR, Yaszemski MJ: Biomechanics, in Einhorn TA, O’Keefe RJ,
Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 45
A 40-year-old unrestrained passenger reports chest wall pain after a motor vehicle accident. Which of the following structures is most important in preventing the injury shown in Figure 33?
Explanation
REFERENCES: Gilot GJ, Wirth MA, Rockwood CA: Injuries to the sternoclavicular joint, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott, Williams and Wilkins, 2006, vol 2, pp 1373-1374.
Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Question 46
Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with a 2-month history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?

Explanation
Question 47
During a posterior approach to the right Achilles tendon, the surgeon encounters a nerve running with the small saphenous vein as shown in Figure 22. This nerve innervates what part of the foot?
Explanation
REFERENCES: Aktan Ikiz ZA, Ucerler H, Bilge O: The anatomic features of the sural nerve with an emphasis on its clinical importance. Foot Ankle Int 2005;26:560-567.
Lawrence SJ, Botte MJ: The sural nerve in the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
Question 48
A 38-year-old woman fell from a ladder onto her right hip. The radiographs and CT scan are shown in Figures 52a through 52d. What is the best surgical approach for this fracture?
Explanation
REFERENCES: Letournel E: The treatment of acetabular fractures through the ilioinguinal approach. Clin Orthop Relat Res 1993;292:62-76.
Matta JM: Operative treatment of acetabular fractures through the ilioinguinal approach:
A 10-year perspective. Clin Orthop Relat Res 1994;305:10-19.
Question 49
Hip pain of 1-month duration has developed in a 72-year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. What is this patient's prognosis for infection resolution?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin- resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was
21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 50
During the early swing phase of the normal gait cycle, what lower extremity muscle is primarily contracting?
Explanation
REFERENCES: Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Wootten ME, Kadaba MP, Cochran GV: Dynamic electromyography II: Normal patterns during gait. J Orthop Res 1990;8:259-265.
Question 51
What pathology is most likely to result in failure of an arthroscopic Bankart repair?
Explanation
REFERENCES: Burkhart SS, De Beer JF: Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 2000;16:677-694.
Cole BJ, Romeo AA: Arthroscopic shoulder stabilization with suture anchors: Technique, technology, and pitfalls. Clin Orthop 2001;390:17-30.
Question 52
A 43-year-old man sustained a closed, intra-articular pilon fracture. It has now been 1 year since he underwent open reduction and internal fixation. Which of the following statements most accurately describes his perceived outcome?
Explanation
REFERENCE: Marsh JL, Weigel DP, Dirschl DR: Tibial plafond fractures: How do these ankles function over time? J Bone Joint Surg Am 2003;85:287-295.
Question 53
A 54-year-old woman undergoes an interposition arthroplasty that fails and requires conversion to a total elbow arthroplasty. She has progressive elbow pain and radiographic loosening. Erythrocyte sedimentation rate and C-reactive protein are normal. Joint aspiration is positive for Staphylococcus epidermidis. What surgical treatment would best optimize function and decrease risk of recurrence?
Explanation
is best reserved for low-demand or infirm patients.
Question 54
Which of the following provocative tests would most likely be positive in a patient with medial epicondylitis? Review Topic
Explanation
Medial epicondylitis is an overuse syndrome of the flexor-pronator mass. The pronator teres (PT) and flexor carpi radialis (FCR) are thought to be most affected with this condition. It is most common in the dominant arm and occurs with activities that require repetitive wrist flexion/forearm pronation. Patients are most tender over the origin of PT and FCR at the medial epicondyle. Resisting a patient with their fist clenched, wrist flexed and pronated can cause worsening of their pain. This maneuver can be used as a provocative test for this condition.
Cain et al. reviewed elbow injuries in throwing athletes. They comment that the common flexor-pronator muscle origin provides dynamic support to valgus stress in the throwing elbow, especially during early arm acceleration and help produce wrist flexion during ball release.
Amin et al. reviewed the evaluation and management of medial epicondylitis. They report that medial epicondylitis typically occurs in the fourth through sixth decades of life, the peak working years, and equally affects men and women. Physical therapy and rehabilitation is the main aspect of recovery from medial epicondylitis, once acute symptoms have been alleviated.
Illustration A shows a video of this provocative test for medial epicondylitis. Incorrect Answers:
Question 55
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of
Explanation
REFERENCES: Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 56
A 10-year-boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals no soft-tissue mass, and mild tenderness. Figures 33a and 33b show the plain radiograph and MRI scan, and the biopsy specimens are shown in Figures 33c and 33d. What is the most likely diagnosis?
Explanation
REFERENCE: Simon MA, Springfield DS, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-200.
Question 57
Figure 37 shows the clinical photograph of a 1-day-old infant who weighed 10.25 lb at birth. Examination reveals an absent right Moro reflex and limited active motion of the right shoulder, elbow, and wrist, but flexion of the fingers. Passive range of motion of the shoulder and elbow is normal. What is the most likely diagnosis?
Explanation
REFERENCES: Hoffer MM, Phipps GJ: Closed reduction and tendon transfer for treatment of dislocation of the glenohumeral joint secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:997-1001.
Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667.
Waters PM, Smith GR, Jaramillo D: Glenohumeral deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:668-677.
Question 58
A 45-year-old woman with stage II posterior tibial tendinitis has failed to respond to nonsurgical management. Recommended treatment now includes posterior tibial tendon debridement and medial calcaneal displacement osteotomy along with transfer of what tendon?
Explanation
REFERENCES: Sitler DF, Bell SJ: Soft tissue procedures. Foot Ankle Clin 2003;8:503-520.
Guyton GP, Jeng C, Krieger LE, et al: Flexor digitorum longus transfer and medial displacement calcaneal osteotomy for posterior tibial tendon dysfunction: A middle-term clinical follow-up. Foot Ankle Int 2001;22:627-632.
Question 59
A 58-year-old man presents to the clinic with 9 months of progressive right lower extremity pain. Over the past 4 months, he also notes a decreased ability to walk long distances due to pain, which is relieved by sitting down. Figure A and B
Explanation
Surgical management of lumbar stenosis typically consists of wide pedicle to pedicle decompression at the affected levels. Instrumention and fusion may be indicated if there is evidence of instability. Nonsurgical management typically involves oral medications, physical therapy, and corticosteroid injections
Weinstein et al. (2010, 2008), as part of the SPORT trial, found that surgical management of symptomatic lumbar stenosis with decompressive laminectomy resulted in greater improvement in pain, function, and satisfaction as compared to nonsurgical management. These advantages were maintained at both two and four years of follow up.
Figure A is a T2 sagittal MRI showing lumbar spinal stenosis from L1-L5, most prominent from L3-L5. Figure B is a T2 axial MRI showing severe stenosis at L4-L5 secondary to ligamentum flavum hypertrophy and facet arthropathy. Illustration A is an example of a one-level decompressive laminectomy.
Incorrect Answers:
mortality.
Question 60
Figure 20 shows the MRI scan of a 20-year-old athlete who has a painful shoulder. This pathology is most commonly seen in
Explanation
REFERENCES: Misamore GW, Facibene WA: Posterior capsulorrhaphy for the treatment of traumatic recurrent posterior subluxations of the shoulder in athletes. J Shoulder Elbow Surg 2000;9:403-408.
Mair SD, Zarzour RH, Speer KP: Posterior labral injury in contact athletes. Am J Sports Med 1998;26:753-758.
Question 61
The thickest bone in the occiput is located
Explanation
REFERENCES: Nadim Y, Lu J, Sabry FF, et al: Occipital screws in occipitocervical fusion and their relation to the venous sinuses: An anatomic and radiographic study. Orthopedics 2000;23:717-719.
Ebraheim N, Lu J, Biyani A, et al: An anatomic study of the thickness of the occipital bone: Implications for occipitocervical instrumentation. Spine 1996;21:1725-1729.
Question 62
A 32-year-old volleyball player has dull posterior shoulder pain. An examination reveals moderate external rotation weakness with his arm at his side, but normal strength on supraspinatus isolation. Deltoid and supraspinatus bulk appear normal, although there appears to be mild infraspinatus atrophy. Sensation is normal throughout the shoulder and shoulder girdle. What is the most likely diagnosis?
Explanation
This clinical scenario describes a patient with an isolated injury affecting the infraspinatus muscle. The anatomic location of such a lesion would be at the spinoglenoid notch, at which the suprascapular nerve may be compressed distal to its innervation of the supraspinatus but proximal to the infraspinatus innervation. A calcified transverse scapular ligament would also affect the suprascapular nerve but is proximal to the innervation of both muscles. Quadrilateral space syndrome would affect innervation of the deltoid (and teres minor). Parsonage-Turner syndrome is a more diffuse, and often severely painful, brachial plexus neuropathy.
Question 63
A 17-year-old basketball player and pole vaulter who has had anterior knee pain for the past 18 months now reports a recent inability to jump. Based on the MRI scan shown in Figure 11, management should consist of
Explanation
REFERENCES: Al-Duri ZA, Aichroth PM: Surgical aspects of patella tendonitis: Techniques and results. Am J Knee Surg 2001;14:43-50.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 218-219.
Question 64
A young, healthy male undergoes a distal biceps repair and sustains an iatrogenic nerve injury during the procedure. Which of the following clinical findings are most likely to be seen in this circumstance? Review Topic
Explanation
Distal biceps avulsions can be partial or complete. Indications for surgical management include young, healthy patients who do not wish to sacrifice function, as well as partial biceps avulsions that do not respond to conservative management. Repair of a distal biceps avulsion can be approached through either an anterior one-incision technique or a two-incision technique (Boyd-Anderson). The one-incision technique uses the interval between the brachioradialis (radial nerve) and pronator teres (median nerve), while the two-incision technique uses this same interval in addition to a second posterolateral elbow incision. The lateral antebrachial cutaneous nerve is the most common nerve injured during either approach.
Kelly et al. retrospectively reviewed 74 distal biceps tendon repairs, and found five sensory nerve paresthesias. The lateral antebrachial cutaneous nerve was most commonly injured, followed by the superficial radial nerve.
Cain et al. retrospectively reviewed 198 distal biceps tendon repairs, and found a 36% complication rate. Lateral antebrachial cutaneous nerve paresthesias were found in 26%, while radial sensory nerve paresthesias were found in 6%, and posterior interosseous nerve (PIN) injury in 4%.
Illustration A shows the close relationship between the lateral antebrachial cutaneous nerve (LABCN) and the distal biceps. Illustration B shows the sensory nerves of the upper extremity and their respective areas of innervation.
Incorrect Answers:
Question 65
Up to what time frame are the risks minimized in anterior revision disk replacement surgery? Review Topic
Explanation
Question 66
A 15-year-old diver has had persistent, activity-related low back pain for the past 2 months. He denies any history of trauma. Examination reveals that the pain is localized to the lumbosacral junction, and there are no radicular symptoms. The pain is worse with back extension. Neurologic examination is normal, as are AP, lateral, and oblique radiographs of the lumbosacral spine. Further evaluation should include
Explanation
REFERENCES: Congeni J, McCulloch J, Swanson K: Lumbar spondylolysis: A study of natural progression in athletes. Am J Sports Med 1997;25:248-253.
Harvey CJ, Richenberg JL, Saifuddin A, Wolman RL: The radiological investigation of lumbar spondylolysis. Clin Radiol 1998;53:723-728.
Question 67
Figure 53 is a coronal-cut CT scan of a 63-year-old woman who has a longstanding pes planus. She is seen for lateral ankle discomfort. Upon examination she is tender over the sinus tarsi and distal to the fibula. She has painless passive hindfoot eversion with 5/5 eversion strength. The most appropriate diagnosis is

Explanation
With the use of CT scans, adults with symptomatic flatfoot deformity have been noted to develop subluxation of the talocalcaneal joint with resulting lateral hindfoot pain. Impingement of the talus and calcaneus in the sinus tarsi and/or between the tip of the fibula and the calcaneus may occur. This impingement is known as lateral impaction syndrome. Hindfoot motion is painless; therefore, this patient does not have symptomatic subtalar arthritis. Middle facet and calcaneonavicular coalitions are not present (hindfoot motion is present).
RECOMMENDED READINGS
Malicky ES, Crary JL, Houghton MJ, Agel J, Hansen ST Jr, Sangeorzan BJ. Talocalcaneal and subfibular impingement in symptomatic flatfoot in adults. J Bone Joint Surg Am. 2002 Nov;84-A(11):2005-9. PubMed PMID: 12429762. ? View Abstract at PubMed
Ananthakrisnan D, Ching R, Tencer A, Hansen ST Jr, Sangeorzan BJ. Subluxation of the talocalcaneal joint in adults who have symptomatic flatfoot. J Bone Joint Surg Am. 1999 Aug;81(8):1147-54. PubMed PMID: 10466647. ?View Abstract at PubMed
Question 68
A 73-year-old man stepped off a street curb and felt a crack in his left hip. He is now unable to bear weight. A radiograph is shown in Figure 54a. Biopsy specimens are shown in Figures 54b and 54c. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 269.
Mercuri M, Picci P, Campanacci L, et al: Dedifferentiated chondrosarcoma. Skeletal Radiol 1995;24:409-416.
Question 69
Figure 40 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. Closed reduction is readily accomplished, and the elbow seems stable. Management should now consist of application of a splint for
Explanation
REFERENCES: Mehlhoff TL, Noble PC, Bennett JB, Tullos HS: Simple dislocation of the elbow in the adult: Results after closed treatment. J Bone Joint Surg Am 1988;70:244-249.
Linscheid RL, O’Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 441-452.
O’Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF: The unstable elbow. Instr Course Lect 2001;50:89-102.
Ross G, McDevitt ER, Chronister R, Ove PN: Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med 1999;27:308-311.
Question 70
-A 15-year-old boy underwent open reduction and internal fixation for a tibial tubercle fracture. The next morning he had dramatically increased pain, hypotension, ascending rash, and fever to 103°F. What is the most appropriate course of action?
Explanation

Question 71
Figure 53 shows the arteriogram of a 45-year-old man who has severe vasculitis. What do the findings show?
Explanation
REFERENCE: Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadephia, PA, Mosby-Year Book, 1998, p 110.
Question 72
-What leads to muscle hypertrophy?
Explanation

Question 73
A 36-year-old professional baseball player reports the acute onset of severe right groin pain while attempting to avoid being hit by a baseball while at bat. Examination reveals tenderness, soft-tissue swelling, and ecchymosis in the right groin extending over the medial thigh. MRI scans are shown in Figures 8a and 8b. Management should consist of
Explanation
REFERENCES: Gilmore J: Groin pain in the soccer athlete: Fact, fiction, and treatment. Clin Sports Med 1998;17:787-793.
Irshad K, Feldman LS, Lavoie C, et al: Operative management of “hockey groin syndrome”:
12 years of experience in National Hockey League players. Surgery 2001;130:759-766.
Question 74
A 32-year-old man presents to the emergency department with a humeral shaft fracture. He has wrist drop as well as impaired finger and thumb extension. Which motor function would be expected to recover last?

Explanation
Abrams et al detailed the order of innervation of the radial nerve and found the following order (proximal to distal): brachioradialis, extensor carpi radialis longus, supinator, extensor carpi radialis brevis, extensor digitorum communis, extensor carpi ulnaris, extensor digiti quinti, abductor policis longus, extensor policis longus, extensor policis brevis, and extensor indicis proprius.
Branovacki et al found a slightly different pattern: brachioradialis, extensor carpi radialis longus, superficial sensory, extensor carpi radialis brevis, supinator, extensor digitorum/extensor carpi ulnaris, extensor digiti minimi, abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus and extensor indicis proprius.
While both extensor digitorum and extensor indicis proprius extend the index finger MCP joint, only extensor indicis proprius hyperextends the index finger past neutral
Question 75
A 28-year-old hockey player has a shoulder deformity after being checked into the boards. Examination reveals that swelling has improved, but there is tenderness along the distal clavicle. Radiographs reveal a grade II acromioclavicular joint separation. Initial management should consist of
Explanation
REFERENCES: Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocation. Am J Sports Med 1995;23:324-331.
Question 76
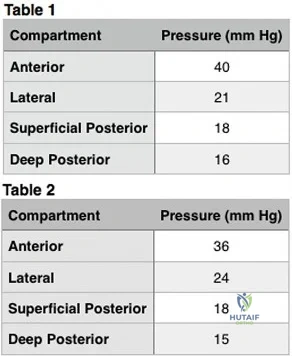
Which study is most useful for diagnosis of exertional compartment syndrome?
Explanation
The most sensitive study in the diagnosis of exertional compartment syndrome is intracompartmental pressures taken at rest (compared to pressures taken immediately after exercise). MRI often can reveal nonspecific muscle edema in exertional compartment syndrome, but this is usually not diagnostic. Arterial Doppler studies are usually unremarkable unless they are taken after exercise, in which case these findings may be abnormal.

CLINICAL SITUATION FOR QUESTIONS 48 THROUGH 50
Figures 48a through 48f reveal the radiographs and MR images of a 30-year-old man who has a 1-year history of atraumatic medial-sided left knee pain refractory to nonsurgical measures.
Question 77
Which of the following factors is associated with improved outcomes following surgery for hip fractures?
Explanation
Question 78
Figures 55a through 55c are the clinical photograph and radiographs of a 5-year-old boy who fell and injured his right elbow. His radial pulse is thready. Which neurologic deficit most commonly is associated with this injury?
Explanation
This injury is a type III supracondylar humerus fracture with posterolateral displacement. The area of ecchymosis is anteromedial, corresponding to the proximal spike of the humeral metaphysis. The brachial artery is likely tented over this spike, leading to diminished perfusion. The median nerve also resides in this area, and any neurological deficit is likely in its most vulnerable fibers, those of the anterior interosseous nerve (AIN). The AIN contains no sensory fibers, and its motor function involves flexion of both the thumb IP joint and the index distal IP joint.
First dorsal web space anesthesia and an inability to extend the fingers would indicate radial nerve neuropraxia, which would be more likely with posteromedially displaced fractures and lead to anterolateral ecchymosis. Finger abduction is controlled by the ulnar nerve, which most often is injured in flexion injuries and iatrogenically by medially placed pins.

Question 79
A 2-year-old boy has been referred for musculoskeletal evaluation. Examination reveals shortened proximal limbs, hip and knee flexion contractures, an abducted thumb, and ear abnormalities. His parents are concerned about his deformed feet. What is the most common foot deformity associated with this patient’s diagnosis?
Explanation
REFERENCES: Ryoppy S, Poussa M, Merikanto J, Marttinen E, Kaitila I: Foot deformities in diastrophic dysplasia: An analysis of 102 patients. J Bone Joint Surg Br 1992;74:441-444.
Bussett GS: The osteochondrodysplasias, in Morrissy RT, Weinstein S (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, p 219.
Question 80
The patient undergoes further testing and it is discovered that the lesion encompasses 70% of the joint. What is the best next treatment option?
Explanation
A tarsal coalition is an abnormal connection of 2 or more bones in the foot. Although tarsal coalitions are present at birth, children and adults typically do not show signs of the disorder until early adolescence or later. The exact incidence of the disorder is hard to determine; however, it is caused by a gene mutation that affects cells that produce the tarsal bones. The 2 most common locations for tarsal coalitions are between the calcaneus and the navicular or between the talus and the calcaneus. It is estimated that 1 out of every 100 people may have a tarsal coalition. In 50% of cases, both feet are affected. Tarsal coalitions are rarely discovered until symptoms arise. Symptoms may include stiff and painful feet, a rigid flatfoot, or increased pain or a limp with high-level activities. Upon examination, symptoms may include tenderness in the area of the coalition, loss of motion, rigid flat feet, and arthritic changes of the joint. Imaging studies begin with radiographs. A CT scan can provide bony detail for imaging tarsal coalitions and determining the extent of the coalition and any accompanying degenerative change. MRI can provide details of the soft tissues. Treatment includes nonsurgical care including rest, orthotics, a temporary boot or cast, and injections. Surgical options include resection with interposition of muscle or fatty tissue from another area of the body or fusions when large (exceeding 50% of the joint), more severe coalitions are encountered.
RECOMMENDED READINGS
Lemley F, Berlet G, Hill K, Philbin T, Isaac B, Lee T. Current concepts review: Tarsal coalition. Foot Ankle Int. 2006 Dec;27(12):1163-9. Review. PubMed PMID: 17207452. View Abstract at PubMed
Badgley CE. Coalition of the calcaneus and the navicular. Arch Surg. 1927;15:75-88. Conway JJ, Cowell HR. Tarsal coalition: clinical significance and roentgenographic demonstration. Radiology. 1969 Mar;92(4):799-811. PubMed PMID: 5767760. View Abstract at PubMed
Herzenberg JE, Goldner JL, Martinez S, Silverman PM. Computerized tomography of talocalcaneal tarsal coalition: a clinical and anatomic study. Foot Ankle. 1986 Jun;6(6):273-
Question 81
Figure 13 is the photograph of 18-month-old triplets with a lower-limb condition. What is the best initial treatment? Review Topic

Explanation
(SBQ13PE.56) A 22-month-old female is hospitalized with a fever and malaise. She is found to be bacteremic, and blood cultures grow methicillin-sensitive Staphylococcus aureus (MSSA). During her hospitalization, the pediatrician notices her arm is slightly swollen and appears painful to use. MRI is obtained and demonstrated in figure A. Which feature of the MRI suggests the need for surgical management? Review Topic

Brodie's Abscess
Osteomyelitis of the humeral metaphysis
Subperiosteal abscess of the humerus
Presence of subcutaneous air
High risk of proximal humeral growth arrest
This patient has osteomyelitis of the humerus with a large subperiosteal abscess. The presence of subperiosteal abscess necessitates surgical intervention for irrigation and debridement (I&D).
The diagnosis of acute osteomyelitis in children is made based upon a constellation of findings including pain, systemic signs of infection, elevated serum inflammatory markers, and imaging studies demonstrative of osseous infection. It is most commonly hematogenously spread to the metaphysis of immature bone, which is highly vascular prior to skeletal maturity. Treatment involves obtaining specimen for culture, empiric antibiotic treatment, and surgical irrigation and debridement of known abscesses. The end-point of treatment is return of pain-free functionality and the resolution of local/systemic signs of infection.
Conrad reviewed the management of acute hematogenous osteomyelitis and emphasized that surgical intervention in the presence of abscess can be both therapeutic and diagnostic: I&D can obtain culture and narrow the antibiotic plan.
Jones et. al. reviewed chronic pediatric osteomyelitis and report that surgery is the mainstay of treatment because removal of dead bone is essential for resolution of infection. This may be performed with sequestrectomy and curettage, with an emphasis on prevention of pathologic fracture, growth disturbances, bone loss, joint involvement, and permanent loss of function.
Figure A is a coronal STIR MRI image of the humerus demonstrating osteomyelitis
with extensive subperiosteal abscess.
Incorrect Answers:
Brodie's abscess is a type of subacute osteomyelitis which remains indolent and creates a focal intra-osseous abscess. This is not demonstrated in the clinical image.
The patient does have osteomyelitis of the humeral metaphysis, but this alone is not the indication for surgery. Uncomplicated osteomyelitis may be treated effectively with antibiotics alone.
Presence of subcutaneous air is suggestive of necrotizing fasciitis, which is a surgical emergency. The MRI however does not demonstrate this finding.
The infection and its surgical management both increase risk of injury to the proximal humeral physis and has the potential for growth arrest or angular deformity.
(SBQ13PE.3) Figure A demonstrates a physical examination maneuver in a 1 month old infant. What is this maneuver? Review Topic

Ortolani Test
Barlow Test
Galeazzi Sign
Patrick test
Teratologic Sign
Figure A shows a schematic image of the Ortalani test.
The Ortolani test, or Ortolani maneuver, is part of the physical examination for developmental dysplasia of the hip. It is used alongside the Barlow test to detect subluxated hips that are either reducible or irreducible. A positive sign is a distinctive 'clunk' which can be heard and felt as the femoral head relocates anteriorly into the acetabulum.
Guille et al. showed that the use of Pavlik harness has become the mainstay of initial treatment for the infant who has not yet begun to stand. If concentric reduction of the hip cannot be obtained, surgical reduction of the dislocated hip is the next step before they are able to stand.
Video V is a lecture discussing the hip examination of the infant. Incorrect Answers:
pressure on the knee, directing the force the femoral head posteriorly. A positive Barlow test would result in posterior subluxation/dislocation of the hip. Answer 3: Galeazzi test is performed by flexing an infant's knees in the supine position so that the ankles touch the buttocks. If the knees are not level then the test is positive, which indicates a potential congenital hip issue (e.g. DDH). Answer 4: Patrick or Faber test (flexion, abduction, external rotation) has been described both for stressing the SI joint and for isolating symptoms to the hip Answer 5: Teratologic dislocation of the hip is a term used to imply that the hip joint did not develop normally in utero, thus the hip is in a fixed dislocated position at birth.
Question 82
Figures 51a and 51b show the AP and lateral radiographs of the elbow of a 26-year-old man who fell. Closed reduction was performed in the emergency department, and management consisted of immobilization for 3 weeks prior to the initiation of motion. At 12 weeks after injury, he reports continued feelings of instability and catching in his elbow when using his arms to rise from a chair. Which of the following procedures needs to be performed, at a minimum, to reestablish stability of the elbow? Review Topic

Explanation
Question 83
Which of the following statements describing chordomas is false?
Explanation
REFERENCE: Casali PG, Stacchiotti S, Sangalli C, et al: Chordoma. Curr Opin Oncol 2007;19:367-370.
Question 84
Which of the following best describes a Bonferroni correction? Review Topic
Explanation
To perform a Bonferroni correction, divide the critical P value (alpha level) by the number of comparisons being made. For example, if 10 hypotheses are being tested, the new critical P value would be (alpha level)/10. The statistical power of the study is then calculated based on this modified P value.
Guyatt et al. discusses hypothesis testing and the role of alpha levels and P values. They report that the Bonferroni correction is derived from testing a dependent or independent hypotheses on a set of data and finding that the probability of a type I error is offset by testing each hypothesis at a statistical significance level divided by the number of times what it would be if only one hypothesis were tested.
Incorrect
1:
This
describes
Bayesian
analysis.
2:
This
describes
Hawthorne
effect.
3:
This
describes
Pearson
correlation.
Question 85
Figures 27a through 27c show the radiographs and CT scan of a 27-year-old man who sustained a low-velocity gunshot wound to the neck. He is quadriplegic (ASIA A), hemodynamically stable, and does not have drainage from his wound. After initial resuscitation and stabilization, the cervical spine and spinal cord injuries are best managed by
Explanation
REFERENCES: Bono CM, Heary RF: Gunshot wounds to the spine. Spine J 2004;4:230-240.
Punjabi MM, Jue JJ, Dvorak J, et al: Cervical spine kinematics and clinical instability, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005,
pp 55-87.
Question 86
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
Explanation
REFERENCES: Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its affects on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
Question 87
A 16-year-old female dancer has persistent posterior ankle pain, particularly after a vigorous dancing schedule. Examination reveals tenderness both posteromedially and posterolaterally. MRI scans are seen in Figures 44a and 44b. What is the most likely diagnosis?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont IL, American Academy of Orthopaedic Surgeons, 1998, pp 315-332.
Hamilton WG, Hamilton LH: Foot and ankle injuries in dancers, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1225-1256.
Question 88
A 9-year-old boy falls from a scooter and sustains the injury shown in the radiographs in Figure 26. After closed reduction and cast immobilization, what is the most likely complication that can result?
Explanation
REFERENCES: Vanheest A: Wrist deformities after fracture. Hand Clin 2006;22:113-120.
Cannata G, De Maio F, Mancini F, et al: Physeal fractures of the distal radius and ulna: Long-term prognosis. J Orthop Trauma 2003;17:172-179.
Ray TD, Tessler RH, Dell PC: Traumatic ulnar physeal arrest after distal forearm fractures in children. J Pediatr Orthop 1996;16:195-200.
Aminian A, Schoenecker PL: Premature closure of the distal radial physis after fracture of the distal radial metaphysis. J Pediatr Orthop 1995;15:495-498.
Question 89
Which of the following plain radiographic views of the shoulder best reveals a Hill-Sachs lesion of the humeral head?
Explanation

Question 90
A 16-year-old boy with osteochondritis dissecans of the capitellum has intermittent symptoms of catching and locking. Examination is unremarkable. Radiographs reveal a loose body anteriorly with a diameter of 10 mm. To remove the loose body, elbow arthroscopy is being considered. Which of the following procedures would minimize the risk of neurovascular complication during the procedure?
Explanation
REFERENCES: Lynch GJ, Meyers JF, Whipple TL, Caspari RB: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
O’Driscoll S: Loose bodies and synovial conditions, in Green D, Hotchkiss R, Pederson W (eds): Green’s Operative Hand Surgery. New York, NY, Churchill Livingstone, 1999, pp 235-249.
Question 91
For a patient with a type II odontoid fracture, which of the following factors best predicts the development of a nonunion with nonsurgical management? Review Topic
Explanation
Question 92
During a dual incision fasciotomy of the leg, the soleus is elevated from the tibia to allow access to which of the following compartments?

Explanation
Question 93
A 62-year-old man complains of shoulder pain for 2 years. He has had 1 course of intra-articular sodium hyaluronate and 6 weeks of physical therapy with little relief. Examination reveals diminished arm flexion and abduction secondary to pain. Radiographs of his shoulder are shown in Figures A and B. According to the American Academy of Orthopaedic Surgeons Clinical Practice Guidelines, what is the next best step? Review Topic

Explanation
TSA is indicated for cases of end-stage GH OA. It is preferred to hemiarthroplasty. It is contraindicated in cases with insufficient glenoid bone stock (glenoid wear to the level of the coracoid), rotator cuff arthropathy or irreparable cuff tears and deltoid dysfunction. It provides good pain relief and has good survival at 10 years (>90%).
Radnay et al. performed a systematic review involving 1952 patients comparing TSA with humeral head replacement (HHR). They found that TSR provided greater pain relief, range of motion, patient satisfaction, and had lower revision rates. They recommend TSA over HHR for GH OA.
Izquierdo et al. described the AAOS Clinical Practice Guidelines (CPG) regarding treatment of GH OA. This is summarized in Illustration A.
Figures A and B show end-stage GH OA with large osteophytes and subchondral sclerosis. There is significant glenoid wear and posterior subluxation (Walch B glenoid deformity). Illustration A is a table summarizing the AAOS CPG on treatment of GH OA. Illustration B shows a CTA humeral component. It is not paired with a glenoid component.
Incorrect Answers:
Question 94
A 14-year-old girl reports bilateral patellofemoral symptoms. Based on the radiograph and MRI scans shown in Figures 23a through 23d, what is the next most appropriate step in management of the lesion?
Explanation
REFERENCES: Dunham WK, Marcus NW, Enneking WF, et al: Developmental defects of the distal femoral metaphysis. J Bone Joint Surg Am 1980;62:801-806.
Verdonk PC, Verstraete K, Verdonk R: Distal femoral cortical irregularity in a 13-year old boy: A case report. Acta Orthop Belg 2003;69:377-381.
Question 95
Which of the following statements best describes the instantaneous axis of rotation (IAR) for the functional spinal unit? Review Topic
Explanation
Question 96
Which of the following statements best describes the kinematic behavior of the knee during motion from full extension to flexion?
Explanation
greater in the anterior-posterior direction (translates), resulting in more lateral translation, rollback, and medial pivoting.
REFERENCE: Churchill DL, Incavo SJ, Johnson CC, et al: The transepicondylar axis approximates the optimal flexion axis of the knee. Clin Orthop Relat Res 1998;356:111-118.
Figure 98c Question 98
A 71-year-old businessman reports medial knee pain recalcitrant to nonsurgical management.
Examination reveals that his body mass index (BMI) is 28 and he has a mild varus deformity with a range of
motion from 5 degrees to 130 degrees of flexion. Anterior drawer and Lachman’s test are negative. Radiographs are shown in Figures 98a through 98c. For cultural and religious reasons, he is concerned about maintaining his range of motion and kneeling ability. Which of the following options is best?
High tibial osteotomy
Unicompartmental knee arthroplasty
Cruciate-retaining total knee arthroplasty with a fixed bearing design
Posterior stabilized total knee arthroplasty with a fixed bearing design
Cruciate-sacrificing total knee arthroplasty with a rotating platform design PREFERRED RESPONSE: 2
DISCUSSION: Unicompartmental arthroplasty of the knee is associated with better range of motion than either total knee arthroplasty or high tibial osteotomy. In a prospective randomized trial of unicompartmental and total knee arthroplasty for patients with medial compartment osteoarthritis, patients with the unicompartmental prosthesis had better range of motion. The literature that compares range of motion in cruciate-retaining as opposed to posterior stabilized and fixed bearing as opposed to mobile- bearing total knees suggests relatively equivalent range of motion between these designs.
REFERENCES: Newman JH, Ackroyd CE, Shah NE: Unicompartmental or total knee replacement? Five- year results of a prospective randomized trial of 102 osteoarthritic knees with unicompartmental arthritis.
J Bone Joint Surg Br 1998;80:862-865.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 59-69.
Question 97
A 26-year-old woman sustained a nondisplaced femoral neck fracture and treatment consisted of use of percutaneous cannulated screws. At her 3-month follow-up visit, she reports hip pain and is unable to ambulate. A radiograph is shown in Figure 1. What is the next most appropriate treatment?
Explanation
REFERENCES: Hartford JM, Patel A, Powell J: Intertrochanteric osteotomy using a dynamic hip screw for femoral neck nonunion. J Orthop Trauma 2005;19:329-333.
Mathews V, Cabanela ME: Femoral neck nonunion treatment. Clin Orthop Relat Res 2004;419:57-64.
Question 98
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. Treatment should include

Explanation
Question 99
A 4-month-old infant is referred for evaluation of congenital scoliosis. The child has no congenital heart anomalies, and a renal ultrasound shows that he has one kidney. Examination reveals mild scoliosis and a large hairy patch on the child’s back. Neurologic evaluation is normal for his age. A clinical photograph and radiograph are shown in Figures 19a and 19b. Initial management should consist of Review Topic

Explanation
Question 100
Which of the following is true regarding changes in the vascularity of the adult intervertebral disc with age? Review Topic
Explanation
The intervertebral disc is composed of an outer structure called the annulus fibrosis and an inner structure called the nucleus pulposus. The annulus fibrosis is composed
of type 1 collagen, water, and proteoglycans. The inner nucleus pulposus is composed of type 2 collagen, water, and proteoglycans. Intervertebral discs are avascular with capillaries terminating at the end plates. The nucleus pulposus receives nutrition primarily through diffusion through blood vessels within the endplate.
Roberts et al. review the histology and pathology of the intervertebral disc. They note that at birth, the cartilagenous end plates have large vascular channels through them as well as vascular channels through the annulus. Soon after birth, these vascular channels close with none remaining at the end of the first decade of life. However, with age, more blood vessels grow into the disc from the outer annulus fibrosis in response to degenerative changes.
Illustration A is a diagram of the vascular supply in an adult intervertebral disc. Incorrect Answers:
