Orthopedic Board Review MCQs: Foot & Ankle, Spine, Sports Medicine | Part 203

Key Takeaway
This page presents Part 203 of a comprehensive, high-yield orthopedic surgery board review quiz. Authored by Dr. Mohammed Hutaif, it's meticulously designed for orthopedic residents and surgeons preparing for OITE/AAOS board certification. Featuring 100 verified multiple-choice questions on Foot, Knee, Nerve, and Tendon, this interactive resource offers both study and exam modes for optimal preparation.
About This Board Review Set
This is Part 203 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 203
This module focuses heavily on: Foot, Knee, Nerve, Tendon.
Sample Questions from This Set
Sample Question 1: You perform an ACL reconstruction with bone-patella tendon-bone (BTB) autograft and are explaining the postoperative rehabilitation protocol to your patient. Which of the following is associated with increased quadriceps volume and improved...
Sample Question 2: An otherwise healthy 45-year-old woman reports the onset of severe right leg pain. Figure 20a shows an axial MRI scan of the L4-5 level, and Figure 20b shows a sagittal view with the arrow at the L4-5 level. What nerve root is the most like...
Sample Question 3: A 44-year-old patient who has had a proximal first metatarsal osteotomy has recurrent pain and difficulty wearing many types of shoes. Radiographs show a large 1-2 intermetatarsal angle (IMA)....
Sample Question 4: -The stability of the longitudinal arch of the foot during standing with equal weight on both feet is due primarily to...
Sample Question 5: ABCFigures 62a through 62c are the MR images and CT scan of a 65-year-old man with a history of diabetes mellitus, hypertension, and smoking. He has a 6-week history of increasing midback pain, lower extremity pain, and weakness. What is th...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
You perform an ACL reconstruction with bone-patella tendon-bone (BTB) autograft and are explaining the postoperative rehabilitation protocol to your patient. Which of the following is associated with increased quadriceps volume and improved quadriceps strength at 1 year without a higher risk of knee instability? Review Topic
Explanation
Proper rehabilitation following ACL reconstruction is vital to a successful outcome. The cornerstone of ACL rehabilitation is range of motion, strengthening and functional exercises without risk of destabilizing the knee. There are a variety of rehabilitation protocols and recently an effort has been made to standardize the approach to postoperative ACL care. An accelerated protocol starting at 3 weeks postoperatively has been deemed safe and may enhance the speed and safety with which an athlete returns to play.
Kruse et al completed a meta-analysis of 29 Level I and II studies focused on the ACL rehabilitation process. The authors concluded that immediate postoperative weightbearing and knee range of motion 0-90 is safe. Early eccentric strengthening appears to accelerate and improve strength gains at 1 year as compared to delayed eccentric strengthening. Home-based rehabilitation programs can be as effective as formal physical therapy. Postoperative bracing and CPM use is neither necessary nor beneficial.
Van Grinsven et al conducted a systematic review of ACL rehabilitation programs and physical therapy modalities to develop an evidence-based rehabilitation protocol. The authors demonstrated that an accelerated protocol without postoperative bracing focused on reduction of pain, swelling and inflammation and regaining range of motion, strength and neuromuscular control has significant advantages and does not lead to stability problems.
Gerber et al performed a randomized trial comparing two accelerated postoperative rehabilitation protocols – early eccentric (ECC) rehabilitation versus traditional (TRAD) rehabilitation starting at 3 weeks. There were no significant differences in knee pain, effusion or stability. However, quadriceps strength, hopping distance and activity level improved by a significantly greater amount in the ECC group versus the TRAD group at 26 weeks postoperatively. In a separate analysis of these patients, quadriceps and gluteus muscle cross-sectional area and volume in ECC patients were more than twice those in the TRAD group.
Illustration A depicts two eccentric ergometers that can be used in postoperative ACL rehabilitation.
Incorrect Responses:
another Answer
type of brace,
2:
There
duration is
of
bracing or no bracing at all.
no
advantage
to
CPM
use.
Question 2
An otherwise healthy 45-year-old woman reports the onset of severe right leg pain. Figure 20a shows an axial MRI scan of the L4-5 level, and Figure 20b shows a sagittal view with the arrow at the L4-5 level. What nerve root is the most likely source of her pain?
Explanation
REFERENCES: McCulloch JA: Microdiscectomy, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 2, pp 1765-1783.
Hodges SD, Humphreys SC, Eck JC, Covington LA: The surgical treatment of far lateral L3-L4 and L4-L5 disc herniations: A modified technique and outcomes analysis of 25 patients. Spine 1999;24:1243-1246.
Question 3
A 44-year-old patient who has had a proximal first metatarsal osteotomy has recurrent pain and difficulty wearing many types of shoes. Radiographs show a large 1-2 intermetatarsal angle (IMA).
Explanation

Question 4
- The stability of the longitudinal arch of the foot during standing with equal weight on both feet is due primarily to
Explanation
Question 5
A B C Figures 62a through 62c are the MR images and CT scan of a 65-year-old man with a history of diabetes mellitus, hypertension, and smoking. He has a 6-week history of increasing midback pain, lower extremity pain, and weakness. What is the most likely diagnosis, and how should this diagnosis be confirmed?

Explanation
The sagittal T2-weighted and axial T2-weighted images show a lesion within the T8 vertebral body that involves the posterior elements. There is an associated epidural component that results in compression of the spinal cord. The sagittal reconstructed CT image shows a lytic lesion within the T8 vertebral body. This pattern of vertebral body involvement with preservation
of the adjacent disks and endplates in a 65-year-old patient is most compatible with a diagnosis of a tumor. The most likely tumor is a metastatic lesion. A CT-guided biopsy will confirm this diagnosis. Although thoracic tuberculosis does not typically cross the disk space, the lack of an anterior soft-tissue component decreases the likelihood of this diagnosis.
RECOMMENDED READINGS
Khanna AJ, Shindle MK, Wasserman BA, Gokaslan ZL, Gonzales RA, Buchowski JM, Riley LH 3rd. Use of magnetic resonance imaging in differentiating compartmental location of spinal tumors. Am J Orthop (Belle Mead NJ). 2005 Oct;34(10):472-6. Review. PubMed PMID: 16304794. View Abstract at PubMed
White AP, Kwon BK, Lindskog DM, Friedlaender GE, Grauer JN. Metastatic disease of the spine. J Am Acad Orthop Surg. 2006 Oct;14(11):587-98. Review. PubMed PMID: 17030592. View Abstract at PubMed
Question 6
Figures 7a through 7d show the radiographs and MRI scans of a 69-year-old woman with neck and upper extremity pain and progressive deformity of the cervical spine. What is the most likely diagnosis? Review Topic

Explanation
estimated to be between 11% and 47%. It can result in recurrent myelopathy if the spinal cord becomes draped over the kyphosis. In addition to the neurologic sequelae, the kyphosis itself can be a source of neck pain and deformity. Spondylolisthesis can develop, contributing to further cord compression. In this case, the patient had undergone a previous C4-5 anterior cervical diskectomy and fusion followed by a posterior laminectomy from C2 through C7, without fusion. This has resulted in severe kyphosis (i.e. postlaminectomy kyphosis) with grade II-III spondylolisthesis at C3-4 and a grade I spondylolisthesis at C2-3. While ankylosing spondylitis can also result in a chin-on-chest deformity secondary to ankylosis, there is no evidence of marginal syndesmophytes in the imaging studies to suggest this diagnosis. The occiput is hyperextended on C1 on the lateral upright radiograph to compensate for the kyphosis in an attempt to maintain horizontal gaze. This results in an unusual appearing relationship on the imaging studies. However, there is no widening of the distance between C1 and the occiput and no evidence of soft-tissue injury on the MRI scans to suggest an acute injury. C3-4 demonstrates an unstable spondylolisthesis and was never intended to be included in the C4-5 fusion. Klippel-Feil syndrome is the failure of segmentation of the cervical spine. The classic triad includes congenital fusion, low hairline, and a web neck.
Question 7
A football player who injured his right lower extremity during a game could not get up and reported extreme pain. The initial sideline evaluation showed a probable anterior cruciate, posterior cruciate, and lateral collateral ligament rupture with a very unstable knee. He also reports pain in his ankle and is unable to dorsiflex the ankle. He has limited sensation over the dorsum of his foot. Examination reveals no swelling of the ankle and no pain with passive range of motion of the ankle. What is the most likely diagnosis? Review Topic
Explanation
Question 8
Pelvic packing for a hemodynamically unstable patient with a pelvic ring fracture is best described by which of the following techniques?
Explanation
Question 9
Figures below depict the radiographs obtained from a 76-year-old woman with a painful total knee arthroplasty. She describes an uneventful recovery with no wound-healing issues and was pain free for the first 10 years. Although reporting no trauma or inciting event, she now describes pain in the entire knee that is most severe with her first few steps. She has begun to notice night pain and, more recently, constant swelling. What is the most appropriate work-up at this time?
Explanation
An evaluation of the painful total knee must be supported by an understanding of the potential etiologies of pain. They may include, aseptic loosening, infection, osteolysis, gap imbalance, referred pain, stiffness, and complex regional pain syndrome. In this case, the patient demonstrates start-up pain and had no prior history of infections. Her radiographs show subsidence of the tibia, indicating a loose prosthesis. Knowing that the prosthesis is already loose precludes the need for a bone scan. It is, however, important to rule out infection in this case; therefore, CRP and ESR testing is essential. Aspiration is also recommended when going into knee arthroplasty, and infection is a concern.
Question 10
Which of the following best characterizes bone mineralization?
Explanation
REFERENCES: Lian JB, Stein GS, Canalis E, et al: Bone formation: Osteoblast lineage cells, growth factors, matrix proteins, and the mineralization process, in Favus MJ (ed): Primer on Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 14-29.
Gehron RP, Boskey AL: The biochemistry of bone, in Marcus R, Feldman D, Kelsey J (eds): Osteoporosis. San Diego, CA, Academic Press, 1996, pp 95-184.
Question 11
A patient presents to the emergency department with the injury seen in Figure A. Which of the following is true about radial nerve palsies associated with isolated humeral shaft fractures after low velocity gunshot wounds?

Explanation
The majority of humeral shaft fractures are treated initially with a coaptation splint and then transitioned to a functional brace. Absolute surgical indications for operative management include: open fracture, brachial plexus injury, compartment syndrome, floating elbow, or vascular injury. A radial nerve palsy is not an indication for surgical management of an isolated humeral shaft fracture. Radial nerve injury from a low-velocity GSW is similar to that of blunt force trauma and thus, immediate exploration is not necessary. Instead, nerve function should be observed. Seventy percent of these nerve injuries will resolve spontaneously. Additionally, the patient should receive a short course of antibiotics as any low velocity GSW would be treated.
Guo et al retrospectively reviewed the electrophysiologic data for 40 radial nerve palsies caused by GSWs and blunt trauma. After characterizing the palsies by level of injury, completeness of nerve injury, and other associated nerves injured, they found there to be no difference in any of these variables between GSW induced radial nerve palsies and blunt trauma induced palsies.
Vaidya et al retrospectively reviewed the outcomes of 54 patients with humeral shaft fractures resulting from low velocity GSWs comparing operative and non-operative treatments. They found that patients receiving non-operative management did well and that 70% of radial nerve palsies in the non-operative treatment group resolved on
their own. They recommended non-operative treatment for the majority of isolated humeral shaft fractures resulting from civilian gunshot wounds.
Figure A is a radiograph of a humeral shaft fracture after a GSW. Illustration A is a radiograph of a humeral shaft fracture with a coaptation in place. Illustration B is an example of a functional brace.
Incorrect answers:
Question 12
Which of the following nerves travels with the deep palmar arch?
Explanation
REFERENCES: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 109.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 166-169.
Question 13
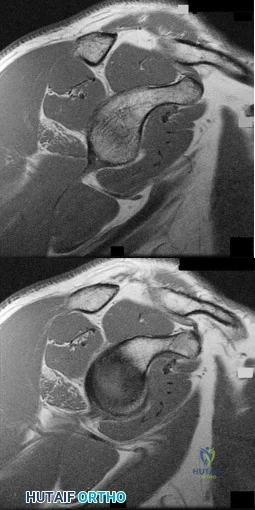
An 80-year-old man has had increasing shoulder pain for the past 4 months. He reports that it began with soreness and stiffness after chopping some wood. A coronal MRI scan is shown in Figure 16. Initial management should consist of
Explanation
REFERENCES: Rockwood CA Jr, Williams GR Jr, Burkhead WZ Jr: Debridement of degenerative, irreparable lesions of the rotator cuff. J Bone Joint Surg Am 1995;77:857-866.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 299-312.
Question 14
A 65-year-old man has a painful and often audible crepitus after undergoing a total knee arthroplasty 8 months ago. His symptoms are reproduced with active extension of about 30°. Examination reveals no effusion or localized tenderness, a stable knee, and a range of motion of 5° to 120°. Radiographs are shown in Figures 37a and 37b. Management should consist of
Explanation
REFERENCES: Beight JL, Yao B, Hozack WJ, Hearn SL, Booth RE Jr: The patellar “clunk” syndrome after posterior stabilized total knee arthroplasty. Clin Orthop 1994;299:139-142.
Lintner DM, Bocell JR, Tullos HS: Arthroscopic treatment of intra-articular fibrous bands after total knee arthroplasty: A follow-up note. Clin Orthop 1994;309:230-233.
Question 15
The thumb metacarpophalangeal (MCP) joint should be flexed to what degree to properly assess ligamentous stability?
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgery, 2002, pp 339-358.
Stener B: Displacement of the ruptured ulnar collateral ligament of the MP joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1962;44:869-879.
33 • American Academy of Orthopaedic Surgeons
Question 16
In a hypothetical study, an investigator uses pedometers to determine that the 20 women in his activity study averaged 2.1 million steps per year, whereas the 20 men averaged 1.8 million. The p-value for this difference was 0.09. Which of the following is a correct interpretation of the outcome of this study?
Explanation
Question 17
In addition to the radiographic features seen in Figures 49a and 49b, this patient will most likely have which of the following findings?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, p 1550.
Zaleske DJ: Metabolic and endocrine abnormalities, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 212-214.
Kaplan FS, August CS, Fallon MD, et al: Successful treatment of infantile malignant osteopetrosis by bone-marrow transplantation: A case report. J Bone Joint Surg Am 1988;70:617-623.
Question 18
Figures 43a and 43b show the T 1 - and T 2 -weighted MRI scans of a 78-year-old woman who reports the sudden atraumatic onset of well-localized medial knee pain. Pain is worse at night and also occurs with weight-bearing activity. What is the most likely diagnosis?
Explanation
REFERENCES: Soucacos PN, Berris AE, Xenakis TH, et al: Knee osteonecrosis: Distinguishing features in differential diagnosis, in Urbanik JR, Jones JD (eds): Osteonecrosis. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 413-424.
Ecker ML, Lotke PA: Osteonecrosis of the medial part of the tibial plateau. J Bone Joint Surg Am 1995;77:596-601.
Question 19
A 14-year-old boy sustains a right leg injury after being thrown from his motorcycle while racing. He reports diffuse right leg pain starting at his knee and proceeding distally to include his foot. After the injury the patient’s mother reports the tibia moving posteriorly then anteriorly while she was supporting the leg. In the emergency department 4 hours after injury, examination reveals a large knee effusion, firm compartments of the leg, a palpable posterior tibialis pulse with a warm, pink foot, and capillary refill of 2 seconds at the toes. His blood pressure is 100/50 mm Hg. Motor examination is intact, but there is decreased sensation in the dorsal first interspace and plantar aspect of the foot. Compartment pressure measurement reveals all four compartments with pressures of 33, 36, 33, and 38 mm Hg respectively. Radiographs are shown in Figure 59a and 59b. The remainder of the skeletal examination is normal. What is the optimal management for this injury?
Explanation
REFERENCE: Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, pp 1057-1061.
Question 20
Which factor is a contraindication to surgical treatment of a symptomatic CAM deformity?
Explanation
Multiple studies have confirmed that CAM or pincer anatomy is commonly present in asymptomatic hips. According to a large systematic review, CAM deformities are present in approximately one-third of asymptomatic hips in young adults, and the proportion was higher than 50% in the subgroup of athletes.
Ganz and associates proposed that femoral acetabular impingement is the root cause of osteoarthritis in the majority of nontraumatic, nondysplastic hips, and functional improvement with surgical correction of the deformity has been demonstrated. Despite the link between CAM deformity and hip osteoarthritis, a corresponding link between correction of the deformity and prevention of osteoarthritis has never been proven.
Results of CAM deformity correction, typically including repair of the degenerative labral tear, are much poorer when there is significant joint space loss. A typical joint space cutoff of 2 mm or less is used to recommend against hip preservation surgery.
Question 21
A patient reports a sudden recurrence of sciatica on her left side after undergoing a successful left L4-L5 diskectomy 15 months ago. Which of the following imaging modalities is most accurate in differentiating recurrence of the disk herniation from postoperative epidural scar tissue?
Explanation
cause of the encroachment. Answer #2 makes no sense. Answers #3 and #4 are incorrect because the MRI is now the standard imaging modality.
Question 22
Figure 61 is the radiograph of a 42-year-old man who falls from a roof and sustains a right calcaneus fracture. His hindfoot is moderately swollen without skin wrinkling and the skin is intact and viable. Neurologic examination findings are normal and the dorsalis pedis pulse is strong and palpable. What is the best treatment plan at this time?

Explanation
This patient has a displaced tuberosity of the calcaneus. A high rate of posterior skin breakdown is associated with these fracture types. The skin should be checked within 10 to 14 days when these fractures occur. The skin is swollen and not acutely at risk, so an immediate ORIF via an extensile lateral approach is not warranted. Immobilizing the ankle in a plantar-flexed position can take some tension off the posterior skin with this fracture type but should
not be definitive treatment. Splinting with repeat examination in 1 to 2 days is the preferred response because of the short follow-up for a repeat skin check. If the skin is at risk when a fracture of this type occurs, the ankle can be immobilized in plantar flexion to relieve tension on the skin. Immediate repair with either open or percutaneous techniques may be necessary if the skin remains at risk.
RECOMMENDED READINGS
Gardner MJ, Nork SE, Barei DP, Kramer PA, Sangeorzan BJ, Benirschke SK. Secondary soft tissue compromise in tongue-type calcaneus fractures. J Orthop Trauma. 2008 Aug;22(7):439-45. PubMed PMID: 18670282.View Abstract at PubMed
Schwartz AK, Brage ME, Laughlin RT, Stephen D. Foot injuries. In: Baumgartner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:453-468.
Question 23
Figure 16 shows the radiograph of a 23-year-old man who has severe right shoulder pain after his motorcyle hit a bridge guardrail. He is neurologically intact. Nonsurgical management will most likely result in
Explanation
REFERENCES: Egol KA, Connor PM, Karunakar MA, Sims SH, Bosse MJ, Kellam JF: The floating shoulder: Clinical and functional results. J Bone Joint Surg Am 2001;83:1188-1194.
Williams GR Jr, Naranja J, Klimkiewicz J, et al: The floating shoulder: A biomechanical basis for classification and management. J Bone Joint Surg Am 2001;83:1182-1187.
Edwards SG, Whittle AP, Wood GW: Nonoperative treatment of ipsilateral fractures of the scapular and clavicle. J Bone Joint Surg Am 2000;82:774-779.
Question 24
A 72-year-old man was involved in an automobile accident 4 weeks ago. Initially he noted pain about his nondominant left shoulder, which resolved within a few weeks after the accident. He now describes trouble with gripping and carrying items in his left hand. Radiographs are shown in Figures 20a through 20c. His signs and symptoms are the result of injury to which of the following ligaments?
Explanation
REFERENCES: Berger RA: The ligaments of the wrist: A current overview of anatomy with considerations of their potential functions. Hand Clin 1997;13:63-82.
Cohen MS, Taleisnik J: Direct ligamentous repair of scapholunate dissociation with capsulodesis augmentation. Tech Hand Up Extrem Surg 1998;2:18-24.
Question 25
A sagittal T1-weighted MRI scan of the knee joint is shown in Figure 23. What structure is identified by the arrow?
Explanation
REFERENCES: Gross ML, Grover JS, Bassett LW, Seeger LL, Finerman GA: Magnetic resonance imaging of the posterior cruciate ligament: Clinical use to improve diagnostic accuracy. Am J Sports Med 1992;20:732-737.
Sonin AH, Fitzgerald SW, Friedman H, Hoff FL, Hendrix RW, Rogers LF: Posterior cruciate ligament injury: MR imaging diagnosis and patterns of injury. Radiology 1994;190:455-458.
Question 26
A 30-year-old elite marathon runner reports chronic pain over the lateral aspect of the distal right leg and dysesthesia over the dorsum of the foot with active plantar flexion and inversion of the foot. Examination reveals a tender soft-tissue fullness approximately 10 cm proximal to the lateral malleolus. The pain is exacerbated by passive plantar flexion and inversion of the ankle. There is also a positive Tinel’s sign over the site of maximal tenderness. There is no motor weakness, and deep tendon reflexes are normal. Radiographs and MRI of the leg are normal. What is the next most appropriate step in management?
Explanation
REFERENCES: Styf J: Diagnosis of exercise-induced pain in the anterior aspect of the lower leg. Am J Sports Med 1988;16:165-169.
Sridhara CR, Izzo KL: Terminal sensory branches of the superficial peroneal nerve: An entrapment syndrome. Arch Phys Med Rehabil 1985;66:789-791.
Styf J: Entrapment of the superficial peroneal nerve: Diagnosis and results of decompression.
J Bone Joint Surg Br 1989;71:131-135.
Question 27
A 78-year-old woman undergoes an uneventful semiconstrained total elbow arthroplasty through a Bryan-Morrey approach. Her immediate postoperative management should include which of the following? Review Topic
Explanation
Question 28
A year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the
aspiration and proceed to a revision TKA with possible augments on standby.
Question 29
One week later, the patient develops recurrent hematoma with wound dehiscence (Figure 130). Treatment at this point should consist of
Explanation
Thigh swelling, bloody drainage, and the persistent need for postsurgical transfusion of PRBCs to maintain adequate hemoglobin and hematocrit levels indicates the presence of a substantial hematoma. Factors contributing to hematoma formation include the large dead space associated with a large soft-tissue pseudotumor, use of postsurgical pharmacologic DVT prophylaxis, higher American Society of Anesthesiologists (ASA) index, and substantial intrasurgical blood loss. Urgent surgical treatment of a postsurgical hematoma with persistent wound drainage is indicated to minimize risk for infection of the prosthetic components. Postsurgical hematoma may also be culture positive or represent early postsurgical infection. Irrigation and debridement should include exchange of the head and liner to provide access for debridement of the modular implant interfaces.
This patient has an infected revision THA with an open wound nearly 3 weeks after surgery. Irrigation and debridement with wound closure is appropriate for treatment of acute postsurgical infections. However, a high failure rate has been associated with this procedure and retention of the components, particularly in the setting of Staphylococcus aureus infection. A large, relatively poorly vascularized wound also increases risk for recurrent infection with retention of components. Treatment at this point to control infection necessitates removal of the prosthetic components. Because of the massive segmental proximal femoral bone loss, excision arthroplasty would result in a markedly shortened flail limb and considerable functional impairment. Removal of the components and insertion of an antibiotic cement spacer would allow wound closure and control of infection with the option of later second-stage reconstruction.

Question 30
A 7-year-old male is struck by a motor vehicle while crossing the street and suffers an open tibia fracture with a crush injury of the ipsilateral foot. After multiple attempts at limb salvage, the family and treating surgeon elect to proceed with a knee disarticulation. What complication of pediatric amputations is avoided with a knee disarticulation as opposed to a transtibial amputation?

Explanation
Krajbich reviews the management of pediatric patients with lower-limb deficiences and amputations. He advocates disarticulation as opposed to transosseous amputation when possible as bone overgrowth has not been observed in bone ends covered by articular cartilage.
O'neal et al retrospectively reviewed their rates of surgical revision for bone overgrowth in pediatric and adolescent amputees. The highest rates of revision were seen with metaphyseal-level amputations (50%) and with traumatic amputations (43%).
Benevenia et al reviewed their rates of overgrowth in skeletally immature transosseous amputees using an autogenous epiphyseal transplant from the amputated limb to cap the medullary canal. They found that only 1 of 10 patients undergoing amputation with this technique had complications due to bone overgrowth, compared with 6 of 7 patients undergoing traditional transosseous amputation.
Illustration A is a clinical photo of bone overgrowth eroding through the soft tissue in a transhumeral amputee. Illustration B demonstrates the radiographic appearance of bone overgrowth in a transtibial amputation.
Incorrect Answers:
Question 31
CLINICAL SITUATION Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. Initial surgical management should consist of

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair,
but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 32
A 45-year-old woman has had radiating pain in the medial ankle for the past 3 months. Examination reveals a small mass in the retromedial ankle region and a positive Tinel’s sign. An intraoperative photograph and a hematoxylin/eosin biopsy specimen are shown in Figures 24a and 24b. Treatment should consist of
Explanation
REFERENCES: Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Simon M, Springfield D: Surgery for the Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, pp 530-531.
Question 33
A 61-year-old man reports right hip pain and limited motion after undergoing total hip arthroplasty for posttraumatic arthritis 1 year ago. Figure 6 shows an AP radiograph of the pelvis. To improve motion and relieve pain, management should consist of
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Iorio R, Healy WL: Heterotopic ossification after total hip and total knee arthroplasty: Risk factors, prevention, and treatment. J Am Acad Orthop Surg 2002;10:409-416.
Question 34
A 28-year-old woman undergoes a closing-wedge high tibial osteotomy (HTO) for medial compartment overload after medial meniscectomy. Postsurgically, she reports improvement in her medial pain and resumes normal activities. About 9 months after her surgery, however, she reports burning pain in the front of her knee with running. Her examination reveals no joint line tenderness, mild pain with patellar compression, and limited patellar glides. What is the most likely cause of her symptoms?
Explanation
Question 35
Treatment of this fracture should consist of
Explanation
Varus posteromedial rotatory instability is a complex injury pattern that starts with varus stress resulting in a fracture of the anteromedial coronoid. The anterior MCL attaches to the sublime tubercle, which is part of the anteromedial coronoid facet. The posterior MCL attaches to the posterior medial aspect of the ulna. The radial collateral and lateral ulnar collateral attach to the ulna at the crista supinatoris. The bony landmark is the sublime tubercle; as noted above, the crista supinatoris is lateral on the ulna. The radial notch is also lateral and is the articulation between the proximal ulna and proximal radius. The anteromedial coronoid facet is part of the coronoid, which extends more lateral and anterior than the anteromedial facet. The anteromedial facet represents the critical weight-bearing portion of the ulnohumeral joint. Damage to this structure causes posteromedial subluxation that often results in severe progressive arthritis. The coronoid is the larger structure of which the anteromedial coronoid facet is a portion. The posteromedial coronoid facet does not appear to be critical in weight bearing. The radial notch is not associated with increased stress with weight bearing. The treatment of displaced fractures of this structure is open reduction and internal fixation utilizing buttress plating. Closed treatment is acceptable only for nondisplaced fractures with appropriate radiographic follow-up. Suture fixation is not advocated because of inadequate strength.
RECOMMENDED READINGS
Pollock JW, Brownhill J, Ferreira L, McDonald CP, Johnson J, King G. The effect of anteromedial facet fractures of the coronoid and lateral collateral ligament injury on elbow stability and kinematics. J Bone Joint Surg Am. 2009 Jun;91(6):1448-58. doi: 10.2106/JBJS.H.00222.
Sanchez-Sotelo J, O'Driscoll SW, Morrey BF. Anteromedial fracture of the coronoid process of the ulna. J Shoulder Elbow Surg. 2006 Sep-Oct;15(5):e5-8. Epub 2006 Jul 26. Erratum in: J Shoulder Elbow Surg. 2007 Jan-Feb;16(1):127. PubMed PMID: 16979044.
Question 36
A 14-year-old male soccer player was seen initially in the emergency room 1 week ago after an acute right hip injury during a soccer tournament. The patient reports that the hip pain has improved, but still requires crutches for long distance ambulation. His radiograph is seen in Figure A. What would be the next most appropriate step in management? Review Topic

Explanation
The diagnosis of an avulsion fracture of the anterior superior iliac spine is made on the basis of: 1. History (sudden contraction of the sartorial and tensor fasciae latae muscle), 2. Physical findings (tenderness over the anterior superior iliac spine [ASIS] and pain with straight-leg raise), 3. Patient's age (most commonly in adolescents or young adults), and 4. Radiographs (confirmed fracture on standard views of the pelvis). Treatment of these injuries is almost always conservative with crutches and progressive weight-bearing activities as tolerated. The relative indications for operative treatment include displacement of the fracture fragment > 3 cm or painful non-union.
White et al. defined two types of anterior superior iliac spine avulsion fractures. A sartorius avulsion fracture (Type 1) usually occurs when sprinting. The fracture fragment is usually small and displaced anteriorly. The tensor avulsion fracture (Type 2) usually occurs when twisting the trunk (e.g. swinging a bat). This fragment is usually larger than Type 1 fractures and more likely to be displaced laterally.
Holden et al. reviewed pediatric pelvic fractures. They state that avulsion fractures of the anterior superior iliac spine are usually low-energy injures, and are not associated with other life-threatening injuries. They do not require an extensive workup (e.g. CT scanning)
Figure A is an antero-posterior view of the pelvis with a small right-sided avulsion fracture of the anterior superior iliac spine.
Incorrect Answers:
Question 37
-The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports,and the surgeon and rehabilitation team consider their request. Compared to nonaccelerated rehabilitation,patients who follow an early accelerated rehabilitation protocol experience
Explanation
The Lachman test is the most sensitive examination for acute ACL injuries. ACL injury rates are higher in women than in men. This likely is attributable to anatomic differences (smaller notches, smaller ligaments, and different landing biomechanics). Lateral meniscal tears are more common than medial tears. The anterior drawer test is accentuated with 30 degrees of external rotation of the tibia. The MRI scan shows bone bruises consistent with an ACL tear. It is also always necessary to examine other structures of the knee in patients with ACL tears. All ligaments of the affected knee should be assessed.Lateral meniscal tears are frequently associated with ACL tears. Medial meniscal tears and posterolateral corner deficiency are also possible. Randomized clinical trials comparing an early accelerated vs nonaccelerated rehabilitation have demonstrated no significant differences in long-term results. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
Question 38
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure 5. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion?
Explanation
REFERENCES: Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947.
Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intra-articular distal humerus fractures in women older than age 65. J Orthop Trauma 2003;17:473-480.
Question 39
Which of the following descriptions is true regarding APC-II (anterior-posterior compression) pelvic injuries as classified by Young and Burgess?

Explanation
Burgess et al review the classifications of pelvic ring disruptions and their association with mortality. They concluded that APC injuries required more blood replacement and were related to death more often than lateral compression, vertical shear, or combined mechanism pelvic injuries.
Tile studied the anatomy of anterior to posterior pelvic ring injuries. Although the anterior structures, the symphysis pubis and the pubic rami, contribute to 40% to the stiffness of the pelvis, clinical and biomechanical studies have shown that the posterior sacroiliac complex is more important to pelvic-ring stability. The posterior sacroiliac ligamentous complex is more important to pelvic-ring stability than the anterior structures and therefore, the classification of pelvic fractures is based on the stability of the posterior lesion.
Question 40
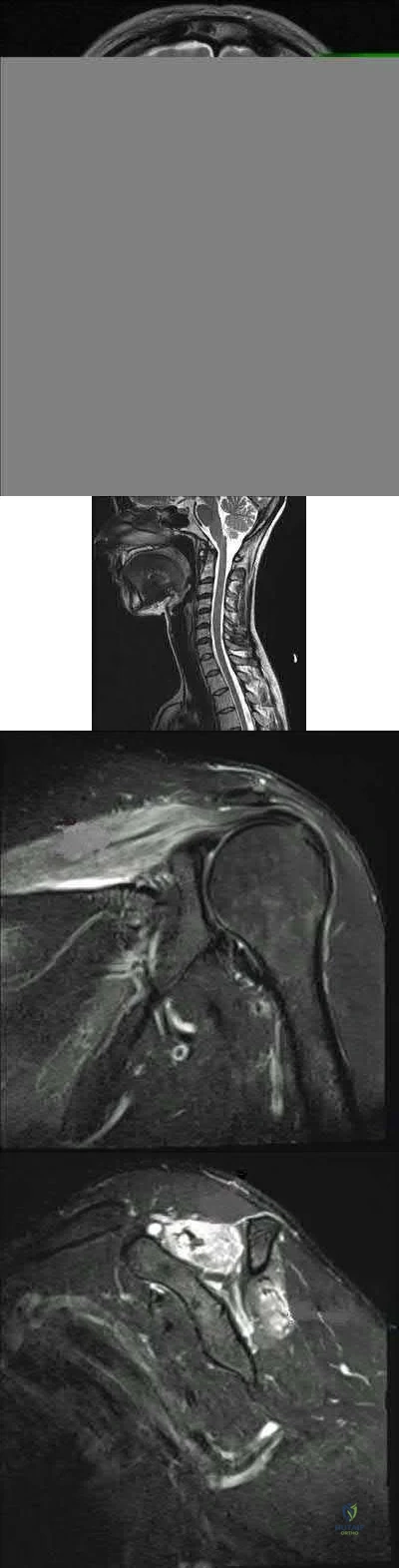
Figures 76a and 76b are the sagittal T1-weighted MRI scans of an active 27-year-old man who has had left dominant extremity shoulder pain and weakness for the past 5 months. He denies any history of a precipitating event but recalls that the pain began around the time he started lifting weights after a year off from lifting. Examination reveals full range of active and passive motion, negative Hawkins and Neer impingement signs, 5/5 abduction strength, 5/5 external rotation strength with arm adducted at his side, and a negative belly press, Gerber lift-off, and O'Brien's test. He does have weakness with resisted external rotation with the arm abducted to 90 degrees. Radiographs are unremarkable. An MRI arthrogram shows no rotator cuff tear or labral tears. What is the most likely diagnosis? Review Topic
Explanation
Question 41
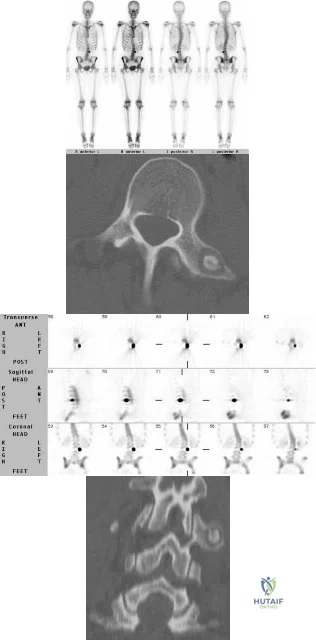
A 13-year-old premenarchal girl presents with back pain and scoliosis. Figures A through D are the bone scan, SPECT scan, axial and coronal images respectively. What is the most likely diagnosis? Review Topic
Explanation
patient
has
osteoid
osteoma
(OO).
OO and osteoblastoma (OB) of the spine commonly present in the 2nd decade of life. CT shows a low attenuation nidus with central mineralization and varying degrees of perinidal sclerosis. NSAIDS are thought to inhibit PGE 2 and PGI 2 produced within the nidus, and suppress perinidal edema arising from high levels of COX2 expression in neoplastic nidal osteoblasts.
Burn et al. reviewed pediatric OO and OB of the spine. OB is more likely to have neurological deficit because of spinal canal encroachment. Surgery involves complete resection. They recommend onlay fusion when the facet and pedicle have been resected, and instrumentation if resection of the vertebral body is carried out.
Jayakumar et al. discuss a case report of OO of the T6 vertebra that was treated successfully with NSAIDS alone. OOs of the spine are the most common cause of painful scoliosis in children and young adults. They caution against a non-operative course in patients with an immature skeleton, significant skeletal deformity or with a long delay before diagnosis.
Figures A and B are bone scan and SPECT scans respectively that demonstrate intense tracer uptake in the left transverse process of L3 characteristic of an osteoid osteoma. Dextroconvex scoliosis of the thoracic and levoconvex scoliosis of the lumbar spine is noted. Figures C and D are axial and coronal reconstructed CT images
showing show a lesion of the left transverse process of L3 with a dense "nidus" with surrounding lucency characteristic of osteoid osteoma. Illustration A is a table showing the characteristics of pediatric epidural spinal tumors.
Incorrect
Question 42
A 75-year-old female with a longstanding history of brachial plexus palsy 2 . A 63-year-old male with a 6 month history of shoulder pain and inability to abduct past 30 degrees

Explanation
A TSA involves replacement of the humeral head with a metal head and resurfacing of the glenoid to a cemented all-polyethylene surface. In order to achieve optimal results, patients must be selected carefully. Patients with an irreparable rotator cuff tear, non-functioning deltoid, inadequate glenoid bone stock and brachial plexopathy are poor candidates for TSA.
Edwards et al. conducted a multicenter randomized controlled trial to compare TSA versus hemiarthroplasty in patients with primary osteoarthritis of the shoulder. They found that TSA provided better scores for pain, mobility, and activity than hemiarthroplasty at 2 year follow-up. Boileau et al. followed 45 consecutive patients who underwent reverse TSA ( rTSA) for cuff tear arthropathy (CTA), post-traumatic arthritis, and failure of revision arthroplasty. After a mean follow-up of 40 months, they found that the reverse prosthesis improved function and was able to restore active elevation in patients with incongruent cuff-deficient shoulders. They also found that
the results were less predictable and complication and revision rates were higher in patients undergoing revision surgery as compared to those patients undergoing rTSA for CTA.
Illustrations A and B show the preoperative and postoperative x-rays of a patient with characteristic OA of the glenohumeral joint that was treated with TSA.
Incorrect Answers:

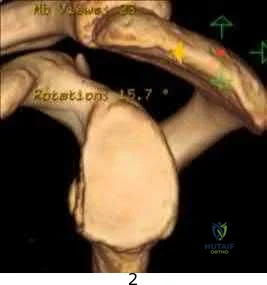
Figure A is a glenoid CT 3D reconstruction of a 26-year-old accountant who has recurrent shoulder instability. His first dislocation occurred after a fall while skiing. He has now sustained his third dislocation, which was reduced in the emergency department prior to being sent to your office. What is the most appropriate definitive treatment?
Immobilization in external rotation for 6 weeks Arthroscopic bony Bankart repair

Arthroscopic Remplissage procedure

Glenoid augmentation using coracoid transfer Glenoid augmentation using tricortical iliac crest graft
This patient has recurrent shoulder instability with a small bony defect of the anterior glenoid and no previous surgery. The most appropriate definitive management in this patient would be arthroscopic bony Bankart repair.
Older (>20 years old), recreational athletes with minor glenoid bone loss (<20 % of the glenoid surface area) may be treated with soft tissue stabilization procedures using suture anchors. Goals of this procedure include tightening and repairing the torn ligament and labrum to the glenoid.
Younger, contact sports athletes with large glenoid defect (>20%) may require bony augmentation type of procedures.
Lynch et al. review the clinical presentation, assessment and treatment algorithm for surgical management of bone loss associated with anterior shoulder instability. While defects larger than 25% of glenoid width should be managed with bony augmentation, they recommend soft-tissue stabilization in smaller defects.
Balg et al. analyzed 131 patients following Bankart procedure and identified following risk factors for failure: age <=20, competitive participation in contact sports, shoulder hyperlaxity, Hill-Sachs on AP radiograph, glenoid bone loss of contour on AP radiograph.
Using human cadaveric shoulders with various anterior glenoid defects sizes, The MOON Shoulder Group compared radiography, MRI and CT to determine the most reliable imaging modality for predicting bone loss. Three-dimensional CT, followed by regular CT were the most reliable and reproducible imaging modalities for predicting glenoid bone loss.
Figure A shows an en face sagittal 3D reconstruction of a glenoid with 10% surface area loss. Incorrect Answers:
A latissimus dorsi tendon transfer is a well established procedure for treatment of massive irreparable posterosuperior rotator cuff tears. All of the following factors have been shown to result in worse clinical outcomes after a transfer EXCEPT?

Nonsynergistic action of the transferred muscle Fatty atrophy of the supraspinatus and infraspinatus Deficiency of the subscapularis

Absence of the coracoacromial ligament Deltoid weakness
A latissimus dorsi tendon transfer can be utilized in patients with a massive, irreperable rotator cuff tear involving the supraspinatus and infraspinatus. It has been reported to relieve pain and improve function in a carefully selected patient population. Those patients with deficiency of the deltoid or subscapularis, nonsynergistic muscle action after transfer, or fatty infiltration of the posterosuperior cuff have worse clinical outcomes. Absence of the CA ligament may allow anterosuperior escape in RC deficient shoulders but has not been shown to lead to worse outcomes after a tendon transfer.
The paper by Warner, et. al demonstrated that poor tendon quality, stage 3/4 muscle fatty degeneration, and detachment of the deltoid insertion each had a statistically significant effect on the Constant score noting that salvage reconstruction of a previous cuff repair had more limited gains as compared to primary. The reference by Ianotti, et. al showed that synchronous in-phase contraction of the transferred latissimus dorsi is associated with a better clinical result while improved preoperative shoulder function and general strength also positively influence the clinical result.
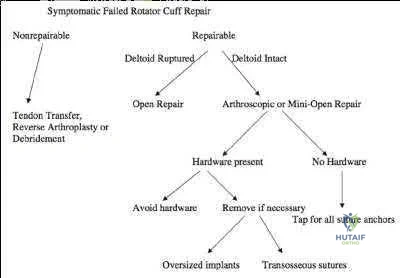
An active 68-year-old woman undergoes an uncomplicated rotator cuff repair with a double-row construct using biocomposite knotless anchors. At her two month follow up, she is noted to have increased shoulder pain, weakness and limited motion. Imaging reveals failure of the rotator cuff repair. What is the most likely mechanism of failure?

Anchor fatigue and breakage Anchor pull out from bone

Suture rupture secondary to anchor eyelet abrasion Suture pull out from the repaired tissue

Infection
Rotator cuff repair (RCR) failure most commonly occurs from a failure of the repaired tissue to heal with suture anchor pull out from the repaired tissue.
The overall complication rate of arthroscopic RCR is roughly 10%. Failed RCR most commonly results from failure to heal (19-94%) secondary to poor rotator cuff tissue, insufficient vascularity or poor bone quality. Other causes of RCR failure include surgical complications (deltoid disruption, infection, foreign body reaction, stiffness, neurologic injury), diagnostic errors (missed lesions of the rotator interval, long head of biceps or subscapularis tear), and technical errors (excessive tension due to lack of proper tissue mobilization, anchor pull out secondary to improper anchor placement).
George et al evaluated the causes of failed RCR and results of revision RCR. While results of revision RCR are inferior to primary RCR, arthroscopic repair yields > 60% good or excellent results. Risk factors for poor results following revision RCR include poor tissue quality, detachment of the deltoid origin and multiple previous surgeries.
Diduch et al reviewed the design and composition of various anchors used in arthroscopic shoulder surgery. Current advancements in the field include highstrength polyethylene sutures, new biocompatible anchor materials (PEEK, biocomposite) and modified designs including knotless systems. With improved strength of the current anchors and repair constructs, the most common mode of arthroscopic RCR failure is now related to tissue failure occurring at the tissue-anchor interface.
Cole et al discussed the different primary rotator cuff repair constructs, including single row, double row, transosseous and transosseous equivalent. The authors concluded that construct selection depends on tear acuity, size and tissue quality. For acute tears < 12mm in anteroposterior length, singlerow configuration likely has sufficient strength to maintain the repair and promote healing. For more chronic tears, poor tissue quality, or tears > 1215 mm in the anteroposterior dimension, the authors recommend double-row or transosseous-equivalent repair to better restore the anatomic footprint and provide optimal mechanical stability to achieve healing. Illustration A is an algorithm from George et al detailing the decision-making process when considering revision RCR for a symptomatic failed RCR.
Incorrect Responses
Biocomposite anchors exhibit high load-to-failure and result in fatigue failure less commonly than metal anchors.
A 32-year-old cross-training athlete awakens with severe left neck and shoulder pain after a day of intense upper body training. Aside from a recent viral illness, he is otherwise healthy. His pain improves, but two weeks later he notes significant left shoulder weakness. Examination reveals weakness of shoulder abduction, forward elevation and external rotation with the arm at his side. Radiographs are normal. Electromyography demonstrates 2+ positive sharp waves and fibrillations. Sensory nerve conduction studies show reduced amplitudes. MRI of the brain, cervical spine and shoulder are shown in Figures A-D, respectively. Which of the following is true of his prognosis?
Decompression will result in improved muscle strength and function.

The patient can expect a gradual return of muscle strength without long term functional deficits. Immunomodulators may decrease the number and severity of his relapses. 4 . Arthroscopic repair will result in the best functional outcomes given the patient's high activity level.
Question 43
In a patient who has undergone fusion with instrumentation from T4 to the sacrum for adult scoliosis, at which site is a pseudarthrosis most likely to be discovered?
Explanation
REFERENCES: Saer EH III, Winter RB, Lonstein JE: Long scoliosis fusion to the sacrum in adults with nonparalytic scoliosis: An improved method. Spine 1990;15;650-653.
Kostuik JP, Hall BB: Spinal fusions to the sacrum in adults with scoliosis. Spine
1983;8:489-500.
Balderston RA, Winter RB, Moe JH, et al: Fusion to the sacrum for nonparalytic scoliosis in the adult. Spine 1986;11:824-829.
Question 44
Based on the current available best-evidence, what postoperative activities should be recommended for patients undergoing first-time lumbar diskectomy for disk herniation? Review Topic
Explanation
Ostelo et al., in a Cochrane review update, demonstrated that exercise programs starting 4 to 6 weeks after surgery in patients undergoing first-time lumbar diskectomy for disk herniation lead to a faster decrease in pain and disability than no rehabilitation. Additionally, high-intensity exercise programs seem to lead to a faster decrease in pain and disability than low-intensity programs.
Carragee et al., in a prospective review of 50 consecutive patients undergoing first-time lumbar diskectomy for disk herniation, demonstrated that lifting of postoperative activity restrictions after limited diskectomy allowed shortened sick leave without increased complications. He concluded that postoperative precautions in these patients may not be necessary.
Question 45
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome? Review Topic

Explanation
Question 46
A 30-year-old patient has wrist pain. A radiograph and biopsy specimen are shown in Figures 34a and 34b. What is the most likely diagnosis?
Explanation
REFERENCES: Bieselker JL, Marcove RC, Huvos AG, Mike V: Aneurysmal bone cyst: A Clinico-pathologic study of 66 cases. Cancer 1973;26:615.
Martinez V, Sissons HA: A review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer 1988;61:2291.
Question 47
A 14-year-old girl has had progressive heel pain for the past several months. Based on the radiograph, MRI scan, and biopsy specimens shown in Figures 37a through 37d, treatment should include
Explanation
blood-filled spaces with bland fibrous connective tissue septa. The stroma has histiocytes, fibroblasts, scattered giant cells, hemosiderin, and occasional inflammatory cells. Treatment of these lesions consists of extended curettage, plus or minus the use of adjuvants (liquid nitrogen, phenol, argon beam coagulation), and finally filling the bone void (allograft or other bone substitute).
REFERENCES: Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
Ramirez AR, Stanton RP: Aneurysmal bone cyst in 29 children. J Pediatr Orthop 2002;22:533-539.
Question 48
A 73-year-old man is scheduled to have mature heterotopic bone resected from around his left total hip arthroplasty. The optimal management for prophylaxis against the return of heterotopic bone postoperatively is radiation therapy that consists of
Explanation
REFERENCES: Healy WL, Lo TC, DeSimone AA, Rask B, Pfeifer BA: Single-dose irradiation for the prevention of heterotopic ossification after total hip arthroplasty: A comparison of doses of five hundred and fifty and seven hundred centigray. J Bone Joint Surg Am 1995;77:590-595.
Pelligrini VD Jr, Gregoritch SJ: Preoperative irradiation for the prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Surg Am 1996;78:870-881.
Pelligrini VD Jr, Konski AA, Gastel JA, Rubin P, Evarts CM: Prevention of heterotopic ossification with irradiation after total hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
Question 49
A 6-year-old boy presents with a mass and a lucent lesion involving the tibial shaft as seen in Figure 17a. The mass is mildly tender to palpation. The bone scan is focally hot in the tibia. Biopsy specimens are shown in Figures 17b and 17c. What is the most likely diagnosis?
Explanation
REFERENCES: Campanacci M, Laus M: Osteofibrous dysplasia of the tibia and fibula. J Bone Joint Surg Am 1981;63:367-375.
McCaffery M, Letts M, Carpenter B, et al: Osteofibrous dysplasia: A review of the literature and presentation of an additional 3 cases. Am J Orthop 2003;32:479-486.
Question 50
Figure 11 shows the radiograph of a 2-year-old child with marked genu varum and tibial bowing. Based on these findings, what is the best initial course of action?

Explanation
Question 51
Figures 4a and 4b show the radiographs of a 53-year-old woman who was injured in a fall. After initial closed reduction, what is the preferred treatment for this fracture?
Explanation
REFERENCES: Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Pugh DM, Wild LM, Schemitsch EH, et al: Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. J Bone Joint Surg Am 2004;86:1122-1130.
Question 52
A patient undergoes the procedure shown in Figure A. This patient is most likely to be Review Topic
Explanation
In the pediatric population, arthroereisis is one option to restore the alignment of the hindfoot after talocalcaneal coalition. Hindfoot deformity correction is required because resection of the coalition alone will often increase the hindfoot valgus
deformity. The arthroereisis implant prevents this valgus collapse. Another alternative to correct the hindfoot valgus deformity is a calcaneal lateral column lengthening osteotomy.
Khoshbin et al. reviewed the long-term outcomes of coalition resection in 24 patients (32 coalitions). Resected talocalcaneal (TC) coalitions had less inversion/eversion postoperatively than resected calcaneonavicular (CN) coalitions but there was no difference in outcome scores. They obtained favorable results when even resecting talocalcaneal coalition with >50% involvement of the middle facet and hindfoot valgus angles >16 °, which were considered historical contraindications to resection.
Zaw et al. reviewed tarsal coalitions. Radiographic signs of CN coalition include the anteater sign (elongated anterior calcaneal process), decreased CN gap, reverse anteater sign (elongated lateral navicular) and hypoplastic lateral talar head. Radiographic signs of TC coalition include obliterated middle facet on a Harris view (osseous coalition), irregular cortices/dysplastic sustentaculum tali on a Harris view (nonosseous), C-sign on a lateral view, talar beaking, short talar neck with concave inferior surface, narrow posterior facet, and non-visibility of the middle facet.
Giannini et al. reviewed subtalar arthroereisis with coalition resection in 14 feet in patients aged 9-18 years. They achieved 57% excellent, 21% good and 21% fair results. Regarding pain, 86% had improvement and 14% had no change. Regarding ROM, 93% had improvement, and 7% had no change. Better scores were seen in patients <14 years.
Figure A shows the implantation of an arthroereisis implant in the sinus tarsi. Illustration A comprises coronal CT images of talocalcaneal coalition.
Incorrect Answers:
Question 53
A 7-year-old boy has had low back pain for the past 3 weeks. Radiographs reveal apparent disk space narrowing at L4-5. The patient is afebrile. Laboratory studies show a WBC count of 9,000/mmP3P and a C-reactive protein level of 10 mg/L. A lumbar MRI scan confirms the loss of disk height at L4-5 and reveals a small perivertebral abscess at that level. To achieve the most rapid improvement and to lessen the chances of recurrence, management should consist of Review Topic
Explanation
(SBQ12SP.92) A 36-year-old man presents to the emergency department after being involved in a motor vehicle collision. He is complaining of back pain and imaging shows the findings in Figure A. On neurological examination, he does not have any deficits. MRI shows approximately 25% canal encroachment and no evidence of injury to the posterior ligamentous complex. Which of the following is the most appropriate course in management? Review Topic

Strict bedrest for six weeks then progressive weightbearing
Ambulation as tolerated with or without a TLSO
Surgical decompression and anterior stabilization
Surgical decompression and posterior stabilization
Surgical decompression and combined anterior/posterior stabilization
The patient has a L1 burst fracture with minimal retropulsion of bony fragments in the spinal canal. In the absence of neurological deficits and injury to the PLC, the most appropriate treatment is ambulation as tolerated with or without a thoracolumbrosacral orthosis (TLSO).
Thoracolumbar burst fractures are typically caused by an axial load with flexion and commonly found in this location due to increased motion at these segments. With an intact posterior ligamentous complex (PLC) and no neural compromise, TLSO is the mainstay of treatment. If there is evidence of neurological deficit and/or PLC injury, decompression and fusion are indicated. The degree of acceptable kyphosis is controversial. The choice of anterior versus posterior approach is based on ease of decompression.
Vaccaro et al. introduced a new classification system for thoracolumbar injuries, TLICS, based on morphological appearance, integrity of the posterior ligamentous complex, and neurological status. They advocate use of the system for nonoperative versus operative decision making and communication between surgeons.
Bailey et al. completed a randomized, nonblinded controlled trial to determine the
efficacy of bracing for AO type A0-A3 thoracolumbar burst fractures. Both groups were encouraged to ambulate as tolerated and the no brace group had bending restrictions for 8 weeks. They found no difference in the Roland Morris Disability Questionnaire (RMDQ) score at 3 months after injury.
Figure A is sagittal CT scan of the lumbar spine showing a burst fracture of L1 with minimal retropulsion. Illustration A is the TLICS classification with score of 4 being the branch point for nonoperative versus operative management.
Incorrect Answers:
Question 54
What is the most common complication following metatarsal osteotomy for a bunion deformity in an adolescent?
Explanation
Physeal arrest of the first metatarsal-“While an open epiphysis cannot be considered an absolute contraindication to an osteotomy in either the proximal phalanx, or proximal first metatarsal, it is
important at surgery to determine the exact location of the metaphyseal epiphysis to avoid injury.” Pg. 307 Mann, Surgery of Foot and Ankle.
In studies performed by Blais et. Al. A females full foot growth is usually achieved by 14 years and at 12 years an average less than 1 cm of total foot growth remains with less than 50% of this growth at the proximal epiphysis. Males’ terminal growth expected at 16 years of age with 3cm left at 12 years and approximately 1.5 cm of metatarsal growth.
Most studies show recurrence of Hallux Valgus deformity after surgical correction in the juvenile as inordinately high.
Question 55
A patient who underwent a total knee arthroplasty for osteoarthritis 18 months ago now reports the sudden development of pain in the ipsilateral knee. Radiographs and examination of the knee are unremarkable. Aspiration of the synovial fluid 3 days later reveals a WBC count of 1,500/mm 3 . The cells consist of 30% neutrophils and 70% monocytes. Culture results will not be available for several days. The patient has not been on antibiotics prior to this point. Based on these findings, what is the most appropriate management?
Explanation
REFERENCES: Trampuz A, Hanssen AD, Osmon DR, et al: Synovial fluid leukocyte count and differential for the diagnosis of prosthetic knee infection. Am J Med 2004;117:556-562.
Mason JB, Fehring TK, Odum SM, et al: The value of white blood cell counts before revision total knee arthroplasty. J Arthroplasty 2003;18:1038-1043.
Kersey R, Benjamin J, Mason B: White blood cell counts and differential in synovial fluid of aseptically failed total knee arthroplasty. J Arthroplasty 2000;15:301-304.
Question 56
Figures 18a and 18b show the radiographs of a patient who has pain with walking. On careful questioning, it is determined that the discomfort occurs at push-off, or when the patient attempts to climb stairs. What nonsurgical option is most likely to ameliorate the symptoms?
Explanation
REFERENCES: Bono CM, Berberian WS: Orthotic devices: Degenerative disorders of the foot and ankle. Foot Ankle Clin 2001;6:329-340.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 58-63.
Question 57
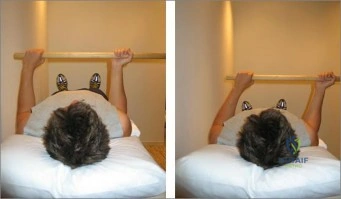
The right shoulder exercise seen in Figure A will put the LEAST amount of stretch on which structure? Review Topic
Explanation
External rotation shoulder wand exercises are commonly used for the treatment of adhesive capsulitis. Adhesive capsulitis is most commonly caused by contracture of the rotator interval. The rotator interval includes the anterior-superior capsule, superior glenohumeral ligament, coracohumeral ligament and long head biceps tendon. The structure most commonly contracted is the anterior-superior capsule, which limits external rotation when the arm is adducted.
Kuhn et al. showed that in the neutral position, each ligament except the posterior capsule significantly affected the torque required for external rotation. The greatest effect on resisting external rotation at 0 degrees of abduction was the entire inferior glenohumeral ligament > coracohumeral ligament > anterior band of the inferior glenohumeral ligament > superior and middle glenohumeral ligament.
Harryman et al. looked at the role of the rotator interval capsule in passive motion and stability of the shoulder. They found operative alteration of this capsular interval was found to affect flexion, extension, external rotation, and adduction of the humerus with respect to the scapula. Limitation of external motion was increased by operative imbrication of the rotator interval and decreased by sectioning of the rotator interval capsule.
Kim et al. reviewed shoulder MRIs to determine if abnormalities of the rotator interval were correlated with chronic shoulder instability. They found a significantly larger rotator interval height, rotator interval area, and rotator interval index in patients with chronic anterior shoulder instability compared to patients without instability.
Figure A shows a patient performing an exercise to increase right shoulder external rotation with a wand/stick. The right arm is fully adducted by her side, and her elbow flexed at 90 degrees.
Incorrect Answers:
Question 58
A 75-year-old man who is right-hand dominant has had a painful right shoulder for the past 6 months, with no improvement with nonsurgical management. Examination reveals an active motion of 60 degrees of forward flexion and abduction, with severe crepitus and pain. Radiographs reveal a high-riding humeral head with severe glenohumeral arthritic changes. What is the most appropriate treatment? Review Topic
Explanation
Question 59
The Cotton test evaluates which of the following structures?

Explanation
Question 60
A 58-year-old man with a 50-year history of osteomyelitis of the left tibia has a painful ulceration of the anterior lower limb. Figure 1 is the clinical photograph of the wound, which had purulent discharge and an unpleasant odor. Figures 2 and 3 are radiographs of the left tibia. A biopsy reveals malignant degeneration. What are the most likely findings?

Explanation
Question 61
Which of the following is the strongest contraindication for expansive open door laminoplasty for cervical myelopathy? Review Topic
Explanation
Open door laminoplasty allows decompression direct posterior decompression of the neural elements, as well as an indirect anterior decompression by allowing the cord to drift posteriorly. Posterior drift of the cord relies upon the presence of natural cervical lordosis. In the setting of kyphosis, the cord is tensioned ventrally over the vertebral bodies and discs, and does not have the redundancy to drift backward. Patients without lordosis would therefore be expected to show less post-operative improvement than those with normal cervical curvature.
Chiba et al. performed a retrospective review of patients treated with expansive open door laminoplasty for cervical spondylotic myelopathy (CSM) and ossification of the posterior longitudinal ligament (OPLL). They found that for patients with OPLL, cervical kyphosis was associated with lower recovery rates than those patients with pre-operative lordosis. The authors recommended against posterior decompression for CSM in the setting of OPLL with concomitant cervical kyphosis.
Suda et al. performed a retrospective review of 114 patients who underwent expansive
open door laminoplasty for cervical myelopathy in order to evaluate clinical outcomes and effects on cervical alignment. They found patients with C2-C7 kyphosis >13° had much lower rates of improvement compared with those patients with less kyphosis. The authors suggest an anterior decompression be used for patients with kyphosis greater than 13°, unless kyphotic correction was planned in addition to a laminoplasty.
Illustrations:
Illustration A demonstrates a lateral cervical spine x-ray which shows focal kyphosis at C4-5 and C5-6. Illustration B demonstrates the C7-sagittal vertical axis. Illustration C demonstrates the compression ratio.
Incorrect
<0.4 implies a poor prognosis.
Question 62
Compared with percutaneous pinning with Kirschner wires (K-wires), the treatment of metacarpal neck fractures with cannulated intramedullary screws is associated with
Explanation
In a biomechanical study, headless compression screws showed superior load to failure, higher three-point bending strength, and greater strength in axial loading compared with percutaneous K-wire fixation for metacarpal neck fractures. Headless compression screws provide greater initial stability to allow earlier motion in the postoperative period. No data comparing infection rates between the two methods of fixation are available; however, it is assumed that K-wires placed outside of the skin would have increased rates of infection. Neither fixation method would increase the time to healing.
Question 63
When comparing arthroscopic and open rotator cuff repairs, which of the following tears shows a decreased recurrent tear rate in the open versus the arthroscopic group? Review Topic
Explanation
Question 64
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. The surgical approach for definitive reduction and stabilization of this pattern is

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally
stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Question 65
A 68-year-old man underwent a primary total hip arthroplasty 2 years ago for a femoral neck fracture. His early postoperative course was unremarkable, but he notes some aching in the thigh since surgery. His symptoms have gotten worse over the last year, such that he now has activity-related thigh pain that limits his walking ability. An AP hip radiograph is shown in Figure 9. What is the most appropriate surgical management?
Explanation
There is a reactive radiolucent line around the fiber mesh portion of the implant, hypertrophy of the bone under the collar, and a pedestal formation at the distal tip of the implant, all of which indicate failure of bone ingrowth. If
bone ingrowth had occurred, there would be stress shielding of bone under the collar.
REFERENCES: Engh CA, Massin P, Suthers KE: Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop Relat Res 1990;257:107-128.
Lieberman JR, Huo MH, Schneider R, et al: Evaluation of painful hip arthroplasties: Are technetium bone scans necessary? J Bone Joint Surg Br 1993;75:475-478.
Vresilovic EJ, Hozack WJ, Rothman RH: Radiographic assessment of cementless femoral components: Correlation with intraoperative mechanical stability. J Arthroplasty 1994;9:137-141.
Question 66
An axial T 1 -weighted MRI scan of the pelvis is shown in Figure 13. The arrow is pointing to what muscle?
Explanation
REFERENCES: Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, Ogose A (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
Berquist TH: Pelvis, hips and thigh, in Berquist TH (ed): MRI of the Musculoskeletal System,
ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 210-238.
Question 67
A 36-year-old nurse has had redness, pain, and small vesicles on the pulp of her middle finger for the past 3 days. Management should consist of
Explanation
REFERENCES: Fowler JR: Viral Infections. Hand Clin 1989;5:613-627.
Jebsen PL: Infections of the fingertip: Paronychias and felons. Hand Clin 1998;14:547-555.
Question 68
A 22-year-old male cyclist was struck by a car. He complains of right knee pain and swelling, as well as reduced sensation and weakness in his right foot. His leg compartments are soft and not tender. Distal pulses in the extremity are palpable. Radiographs of the knee, as shown in Figures A and B, were taken after a closed reduction maneuver was performed. What would be the next best step in management of this patient?

Explanation
Fracture-dislocations of the knee must be suspected with all Schatzker type IV injuries as this fracture pattern is usually associated with high energy trauma. Identifying this injury should prompt a thorough assessment of the neurovascular structures across the knee. After closed reduction and emergent immobilization of the knee, ankle brachial indices (ABI) must be immediately performed. If <0.9, further vascular testing is warranted, such as MR or CT angiography.
Berkson et al. reviewed high energy tibia fractures. They state that Schatzker Type IV fractures typically requires more energy than corresponding lateral plateau fractures, due to denser bone on the medial side.
Chang et al. described an anatomic sub-classification of Schatzker IV fractures. They describe Group 1 fractures as classic medial unicondylar fractures. Group 2 fractures are complicated variants characterized by medial condyle fractures with lateral plateau extension. Usually these have articular impaction of the centroposterior lateral plateau.
Figures A and B show AP and lateral radiographs of the knee demonstrating a classic medial unicondylar Schatzker IV fracture. Note the anterior subluxation of the tibia in relation to the femur. Illustration A shows the multiple CT images of this fracture pattern.
Incorrect Answers:
Question 69
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Explanation
REFERENCE: Daftari TK, Whitesides TE Jr, Heller JG, et al: Nicotine on the revascularization of bone graft: An experimental study in rabbits. Spine 1994;19:904-911.
Question 70
The attachments of the transverse carpal ligament include which of the following structures?
Explanation
REFERENCES: Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 471-472.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 168-170.
Question 71
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. If present, what is the most likely complication after surgical treatment in this scenario?
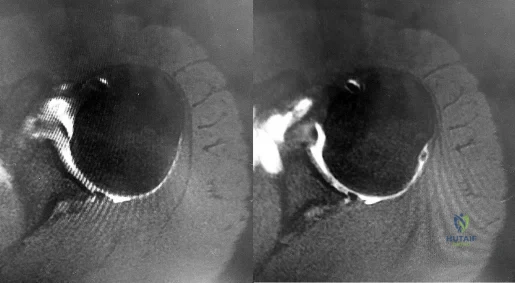
Explanation
and degenerative joint disease.
Question 72
A 19-year-old college pitcher reports posterior shoulder discomfort that started recently with pitching. He is able to throw with normal velocity and control, but his pain in the early acceleration phase of throwing is getting worse. Examination reveals symmetric rotator cuff strength and no increased anterior or posterior translation of either shoulder. He has some discomfort with his shoulder in abduction and external rotation. Supine range of motion of the right shoulder in 90 degrees of abduction reveals external rotation to 100 degrees and internal rotation to 25 degrees. His left shoulder has 95 degrees of external rotation and 45 degrees of internal rotation. He is not playing the next 2 weeks and requests some exercises that he can do on his own. Which of the following exercises will most likely improve his shoulder symptoms? Review Topic
Explanation
protraction, such as punches, and scapular retraction, such as row exercises, can all be helpful for the disabled throwing shoulder, but they will not restore the decreased internal rotation.
Question 73
Figures 17a and 17b show the AP and lateral radiographs of a 75-year-old woman who reports giving way and shifting of the knee, particularly when she is descending stairs or ambulating on level surfaces. History reveals a total knee replacement 5 years ago. Treatment should consist of
Explanation
REFERENCE: Pagnano MW, Cushner FD, Scott WN: Role of the posterior cruciate ligament in total knee arthroplasty. J Am Acad Orthop Surg 1998;6:176-187.
Question 74
A 60-year-old man reports increasing pain in his right foot with limited ankle dorsiflexion and anterior ankle pain after sustaining a fracture of the calcaneus in a fall several years ago. Bracing, nonsteroidal anti-inflammatory drugs, and cortisone injections have failed to provide significant relief. Radiographs are shown in Figures 19a and 19b. What is the next most appropriate step in management?
Explanation
REFERENCE: Robinson TF, Murphy GA: Arthrodesis as salvage for calcaneal avulsions. Foot Ankle Clin 2002;7:107-120.
Question 75
A 62-year-old woman with a bone mass density (BMD) T-score of -2.0 sustained a subcapital fracture of her hip. She is an avid tennis player, and history reveals no previous fractures. What is the most appropriate follow-up care?
Explanation
REFERENCE: Gardner MJ, Brophy RH, Demetrakopoulos D, et al: Interventions to improve osteoporosis treatment following hip fracture: A prospective, randomized trial. J Bone Joint Surg Am 2005;87:3-7.
Question 76
Figures 91a through 91c are the radiographs of a 10-year-old boy who has a 6-month history of progressive heel pain. The patient is a year-round soccer player and now experiences pain with most every step. What is the most appropriate management?

Explanation
Question 77
Acute redislocation of the glenohumeral joint is a complication that occurs following a first-time dislocation. This is most often seen with
Explanation
REFERENCES: Robinson CM, Kelly M, Wakefield AE: Redislocation of the shoulder during the first six weeks after a primary anterior dislocation: Risk factors and results of treatment.
J Bone Joint Surg Am 2002;84:1552-1559.
Bigliani LU, Newton PM, Steinmann SP, et al: Glenoid rim lesions associated with recurrent anterior dislocation of the shoulder. J Sports Med 1998;26:41-45.
Question 78
What is the most appropriate way to communicate instructions to a family when there is a language barrier?
Explanation
Ideally, professional medical interpreters should be used in situations involving language difficulties. Printed instructions are helpful, but, if there is a language barrier, these instructions cannot substitute for conversing and answering questions. Asking the child to translate (no matter how fluent he or she may be) is suboptimal. Nonmedical staff may not be fluent enough to adequately translate medical terms.

RESPONSES FOR QUESTIONS 14 THROUGH 16
Aspiration, cultures, surgical irrigation and debridement, and intravenous (IV) nafcillin
Aspiration, cultures, surgical irrigation and debridement, and IV vancomycin
Aspiration, cultures, Lyme serology, and oral amoxicillin
Biopsy, culture, curettage, bone graft, and possible internal fixation
Physical therapy, ibuprofen, and an antinuclear antibody test
Select the most appropriate treatment above to address each clinical scenario below.
Question 79
-Radiographs are shown in Figures 89a through 89c. What is the most likely diagnosis?
Explanation
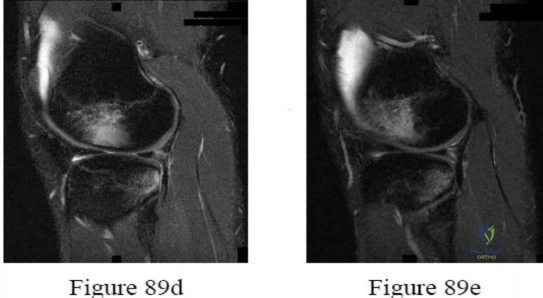
Question 80
006%-3.4 %. The typical skin flora includes staph and strep as well as P. acnes, which has a propensity for the shoulder. Because it is an anaerobic organism, cultures may only become positive after 7-21 days.
Explanation
A 47-year-old, healthy, active patient presents with a sub-acute, full-thickness supraspinatus tear. His physical examination reveals significant weakness and pain with abduction. There was no glenohumeral instability. Radiographs demonstrate a type 1 acromion. An MRI scan shows a crescent shaped tear with 2-cm of tendinous retraction and no tendinous fatty changes. A subacromial corticosteroid injection 6 weeks ago provided him with 24 hours of pain relief but no improvement in strength. What would be the most appropriate treatment option?
Repeat subacromial corticosteriod injection

Biological augmentation of rotator cuff with porcine small intestine xenograft Rotator cuff repair

Rotator cuff repair plus acromioplasty

Rotator cuff repair, remplissage procedure, bicep tenodesis and distal clavicle excision
This patient has an isolated supraspinatus rotator cuff tear with symptomatic weakness. The most appropriate treatment would be isolated rotator cuff repair.
The primary purpose of rotator cuff repair is to restore muscle function. Secondary outcomes include reduction of pain and prevention of irreversible cuff changes, specifically muscular atrophy. Non-operative treatment ( exercise, therapy and pain medications) are recommended for partial thickness tears. The indication of surgical repair includes, isolated supraspinatus weakness +/- pain
that correlates with MRI imaging of a respective full thickness tear. Routine acrominoplasty is not recommended in conjunction with rotator cuff repair, especially with no previous symptoms of impingement.
Pedowitz et al. developed clinical practice guidelines for the treatment of rotator cuff pathology. The strongest supporting evidence in current literature was given a grade of 'moderate' with four treatment recommendations. These were,
Exercise and non-steroidal anti-inflammatory drugs can be used to manage partial thickness tears,

Routine acromioplasty is not required the time of cuff repair,

Non-cross-linked, porcine small intestine submucosal xenograft patches should not be used to manage cuff tears, and

Surgeons can advise patients that workers' compensation status correlates with a less favorable outcome after rotator cuff surgery.
Illustration A shows the different shapes of rotator cuff tears. Incorrect Answers:
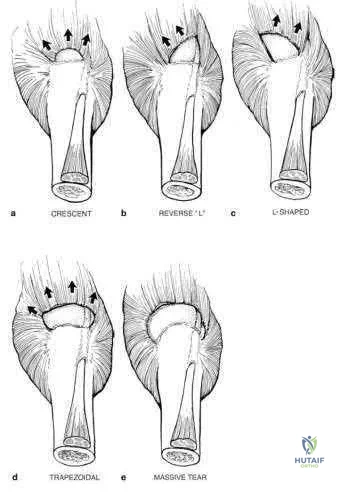
A 12-year-old baseball pitcher describes progressive worsening of medial elbow pain on
his throwing side. Examination reveals normal elbow range of motion. He is tender over the medial elbow to palpation. A dynamic ultrasound of his elbow shows no evidence of medial widening with valgus stress. His radiograph is shown in Figure A and an MRI is shown in Figure B. What is the most likely cause of his symptoms?

Displaced medial epicondyle avulsion fracture Medial apophysitis

Medial ulnar collateral ligament tear

Valgus extension overload with olecranon osteophytes Ulnar neuritis
The clinical presentation is consistent with Little League Elbow caused by medial apophysitis. Little League elbow is a general term explaining medial elbow pain in adolescent pitchers. The underlying pathology can include medial epicondyle stress fractures, avulsion fractures of the medial epicondyle, ulnar collateral ligament (UCL) injuries, or medial epicondyle apophysitis. In order to identify the underlying cause it is important to first rule out injury to the MCL by looking for medial widening on stress radiographs or dynamic ultrasound, or valgus instability on physical exam. Radiographs are useful to look for avulsion fractures or subtle physeal widening commonly seen with apophysitis.
Wei et al. obtained radiographs and magnetic resonance imaging on nine adolescent pitchers with a clinical diagnosis of Little League Elbow. They found radiographic findings in 4/9 and MRI findings in 6/9 patients. They emphasized that the MRI did not change management in any patients. Cain et al. review the different elbow conditions seen in throwing athletes. They emphasize the need to understand the underlying pathophysiology in order to treat and make appropriate changes to the biomechanics of the pitching technique.
Figure A shows an AP radiograph with slight widening of the apophysis, but no evidence of avulsion fracture. Figure B is an MRI which shows signal consistent with edema of the medial epicondyle apophysis.
Incorrect Answers:
The other responses are all typical throwing elbow conditions, but are much less common than apophysitis in the adolescent thrower.
What is the primary function of the structure labeled with an asterisk in Figure A?
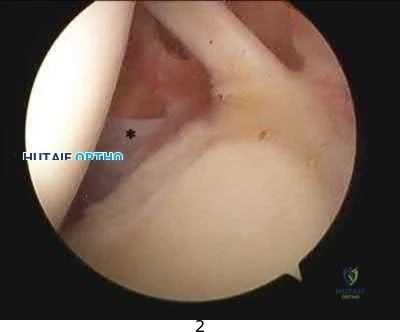
Prevents inferior translation of the humerus with the arm by the side Provides internal rotation of the humerus

Prevents anterior translation of the humerus with the arm in 45 degrees of abduction Prevents anterior translation of the humerus with the arm in 90 degrees of abduction Provides supination of the forearm and elbow flexion
The labeled structure is the middle glenohumeral ligament (MGHL) of the shoulder. The primary function of the MGHL is to prevent anterior translation of the humeral head with the arm in 45-60 degrees of abduction.
This structure originates from the glenoid labrum and inserts medial to the lesser tuberosity running obliquely across the subscapularis. The size of the structure may be variable and there are recognized normal anatomic variants ( including a cord like MGHL in the Buford complex). It is important to be able to recognize the MGHL and differentiate this from the subscapularis, IGHL, SGHL, and other intraarticular structures in the shoulder to be able to perform effective and precise arthroscopic procedures.
Burkhart et al. describe the function of the glenohumeral ligaments in anterior shoulder instability, noting that the MGHL provides a restraint to anterior translation with the arm in 45-60 degrees of abduction.
Wang et al. discuss microdamage to the inferior glenohumeral ligament from a basic science perspective, indicating that over time it may stretch and compromise it's function in restraining humeral translation.
Figure A is an arthroscopic image of the intraarticular structures of the shoulder with an asterisk on the MGHL.
Incorrect Answers (these are labeled on Illustration A, with the exception of the subscapularis which is difficult to visualize):

In which of the following clinical circumstances would it be appropriate to eccentrically ream the anterior glenoid?

year-old male undergoing a shoulder arthroplasty due to rotator cuff arthropathy 65-year-old female with a glenoid retroversion of 13-degrees undergoing shoulder arthroplasty

year-old female with humeral anteversion of 13-degrees undergoing shoulder arthroplasty

year-old female with glenoid retroversion of 25-degrees undergoing shoulder arthroplasty

year-old male with significant glenoid bone stock deficiency and severe osteoarthritis
The surgeon should consider eccentrically reaming the anterior glenoid when performing a total shoulder arthroplasty on a patient with a retroverted glenoid due to posterior deficiency associated with osteoarthritic changes which is most consistent with answer choice #2.
Normal version of the glenoid is 0-3 degrees of retroversion, but when doing a total shoulder the goal should be to place the glenoid component in neutral to slight anteversion. Reaming the anterior glenoid to neutral is a technique to be considered by the operative surgeon when presented with a patient undergoing total shoulder arthroplasty with a retroverted glenoid, as failure to perform this step increases the chance for glenoid loosening. If reaming down the anterior glenoid will take away too much bone stock (down to the coracoid process), one may consider bone grafting the posterior glenoid. To perform a total shoulder arthroplasty patients will need a functioning rotator cuff and appropriate glenoid bone stock.
Clavert et al. performed cadaveric analysis to simulate glenoid retroversion of greater than 15 degrees and found that retroversion to this degree cannot be safely corrected with eccentric anterior reaming when using a glenoid component with peripheral pegs due to penetration into the glenoid vault.
Nowak et al. used 3D-CT models of patients with advanced shoulder osteoarthritis with varying degrees of glenoid retroversion and simulated glenoid resurfacing. They found that smaller size glenoid components may allow for greater version correction when using in-line pegged components, as they would be less likely to result in peg penetration.
Illustration A shows >25 degrees of glenoid retroversion seen by axial radiograph of the shoulder in a patient with advanced osteoarthritis. In this case, anterior glenoid reaming is not the correct answer and a posterior glenoid allograft reconstruction would be appropriate.
Incorrect Answers:
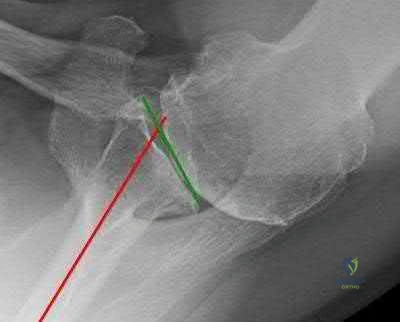
A 44-year-old left-hand dominant carpenter experienced immediate left elbow pain after trying to stop a heavy object from falling two days ago. Figure A shows a clinical image of the patient upon presentation. Physical exam shows full strength with wrist flexion, wrist extension, and pronation, but notable weakness with supination of the forearm. Sensory exam shows no deficits in the forearm or hand. There is a negative milking maneuver test and a positive hook test. Radiographs are shown in Figure B. What is the next most appropriate step in management?

Sling use as needed for comfort and progressive physical therapy Allograft reconstruction of the distal biceps tendon

Ulnar collateral ligament reconstruction Distal biceps tendon avulsion repair Brachioradialis and ECRB avulsion repair
Distal biceps tendon avulsion repair is the most appropriate next step in management.
Distal biceps tendon ruptures occur most commonly in middle-aged men and usually involve the dominant extremity. The mechanism of injury is usually a single traumatic event with eccentric force on the flexed elbow.
Sutton et al. authored a Level 5 review of distal biceps tendon ruptures. They discuss that nonsurgical management of distal biceps tears is appropriate in the low-demand or medically ill patient. Surgical repair improves elbow flexion strength by 30% and supination strength by 40% compared to nonoperative management.
O'Driscoll et al. conducted a Level 2 study examining the accuracy of the hook test for distal biceps rupture diagnosis. They found that the hook test was abnormal in 33 of 33 (100%) patients with complete biceps avulsions, and intact in 12 of 12 (100%) with partial detachments.
Figure A is a clinical image demonstrating ecchymosis in the distal arm and antecubital fossa. Figure B shows normal elbow radiographs. Illustration A shows a normal hook test with an intact distal biceps insertion.
Incorrect Answers:

Early reverse total shoulder designs (before the development of the Grammont-style prosthesis) had a high failure rate due to early loosening of the glenoid component. What biomechanical feature accounted for this problem?

Glenoid component did not have a neck Humeral component too horizontal Center of rotation too lateral

Center of rotation too anterior Center of rotation too inferior
Early reverse ball-and-socket designs failed because their center of rotation remained lateral to the scapula, which limited motion and produced excessive torque on the glenoid component, leading to early loosening. The first modern reverse prosthesis was designed by Paul Grammont. According to Boileau et al., Grammont's design "introduced 2 major innovations (1) a large glenoid hemisphere with no neck and (2) a small humeral cup almost horizontally oriented with a nonanatomic inclination of 155 degrees, covering less than half of the glenosphere. This design medializes the center of rotation compared to earlier versions which minimizes torque on the glenoid component. Furthermore, the humerus is lowered relative to the acromion, restoring and even increasing deltoid tension. The Grammont reverse prosthesis imposes a new biomechanical environment for the deltoid muscle to act, thus allowing it to compensate for the deficient rotator cuff muscles." According to Gerber, "moving the center of rotation more medial and distal as well as implanting a large glenoid hemisphere that articulates with a humeral cup in 155 degrees of valgus are the biomechanical keys to sometimes spectacular short- to midterm results".
Which of the following preoperative factors is a contraindication to total shoulder arthroplasty?

Passive external rotation less than 10 degrees Eccentric posterior glenoid erosion

A 2-cm full-thickness supraspinatus tendon tear Inflammatory arthritis

A preganglionic brachial plexus injury
A preganglionic brachial plexus palsy, otherwise known as a root avulsion injury, presents with a flail arm and has a poor prognosis for recovery of motor function. Patients with brachial plexus palsies are not candidates for total shoulder arthroplasty due to the substantial motor and sensory deficits associated with these injuries.
In contrast, patients with a preoperative loss of passive external rotation, posterior glenoid erosion, a reparable full-thickness rotator cuff tear isolated to the supraspinatus tendon, and inflammatory arthritis are not contraindicated for a total shoulder arthroplasty.
Iannotti et al. performed a Level I prospective study in 118 patients who underwent either a total shoulder arthroplasty or a shoulder hemiarthroplasty for primary osteoarthritis. The presence of a reparable full-thickness rotator cuff tear did not adversely affect outcomes in either group but rather provided better active external rotation in the cohort receiving total shoulder arthroplasties. The authors concluded that a reparable tear of supraspinatus is not a contraindication to the use of a glenoid component.
Norris et al. compared outcomes of total shoulder arthroplasty and hemiarthroplasty performed for primary osteoarthritis in 160 patients. There were no differences in postoperative pain, function, ASES scores, or range of motion between groups for patients with reparable rotator cuff tears. The authors concluded that minor thinning and small tears of the rotator cuff can be adequately addressed at the time of surgery without adversely affecting outcomes.
Illustration A is a cervical T2 axial MRI which shows a cervical root avulsion, a form of preganglionic brachial plexus injury. Notice the perineural hyperintensity.
Incorrect Answers:
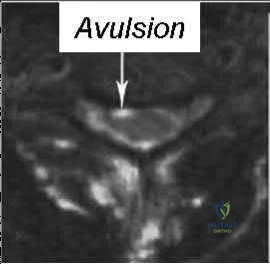
A 42-year-old male sustains a flail chest injury and subsequently undergoes operative stabilization of his chest wall. At first follow-up, the inferior angle of his ipsilateral scapula translates medially with any attempt at overhead activity. Injury to which of the following structures would cause this abnormality?

Spinal accessory nerve C8 and T1 nerve roots

Upper and lower subscapular nerves Thoracodorsal nerve

Long thoracic nerve
The clinical vignette describes medial scapular winging, which is seen after injury to the long thoracic nerve.
Medial scapular winging due to a long thoracic nerve palsy can be seen after repetitive stretching in athletes, with direct compression injury, or even iatrogenically during surgical procedures to the lateral thorax. Injury to the long thoracic nerve will eliminate the function of the serratus anterior,
which acts to protract the scapula laterally and upward and stabilize the vertebral border of scapula. This results in upper extremity weakness in forward elevation or abduction as the scapula is not stabilized against the thorax.
Meininger et al. report that lesions of the long thoracic nerve and spinal accessory nerves are the most common cause of scapular winging, although numerous underlying etiologies have been described. They report patients describe diffuse neck pain, shoulder girdle discomfort, upper back pain, and weakness with abduction and overhead activities. They also report that most cases are treated nonsurgically.
Wiater et al. review injuries to the spinal accessory nerve which causes dysfunction of the trapezius and subsequent lateral scapular winging. They note that the superficial course of the spinal accessory nerve in the posterior cervical triangle makes it susceptible to injury, and iatrogenic injury to the nerve after a surgical procedure is one of the most common causes of trapezius palsy. Most injuries are treated nonoperatively, but the Eden-Lange procedure, in which the insertions of the levator scapulae, rhomboideus minor, and rhomboideus major muscles are transferred, relieves pain, corrects deformity, and improves function in patients with irreparable injury to the spinal accessory nerve.
Illustration A shows a clinical photo of medial scapular winging, while illustration B shows a clinical photo of lateral scapular winging. Illustration C shows the long thoracic nerve during a rib fixation procedure, with the nerve sitting directly on top of the serratus anterior. The trapezius is overlying the scapula at the bottom of the photo, and the patient's head is to the right of the photo. Incorrect Answers:

A patient sustains a distal biceps brachii tendon rupture. If treated non-operatively, the greatest loss of strength would be seen with which activity?

Forearm supination Forearm pronation

Elbow flexion

Shoulder forward flexion Shoulder internal rotation
While both elbow flexion and forearm supination strength are affected, there is a greater percentage loss of supination strength. Patients may complain of weakness and fatigue with rotational activities such as using a screwdriver. The primary elbow flexor is actually the brachialis, and therefore less weakness in flexion is reported.
Patterson reviewed distal biceps ruptures and found nonsurgical treatments had 21 55% loss of supination strength and 8 36% loss of flexion strength.
Klonz reviewed anatomic and non-anatomic repairs and found better results with anatomic repairs with 91% return of supination strength and 96% return of flexion strength. Supination strength after nonanatomic repair did not improve in 4 of 8 patients (42%-56% of the uninjured arm).
A 27-year-old right hand dominant construction worker falls off a scaffold onto his outstretched arm. Figure A exhibits the radiograph taken at a local emergency room.
Following treatment, he is placed in a sling and follows up at your office two weeks later. He complains of a feeling that his arm is going to 'pop out'. Which specific physical examination finding is likely to be present?

Hornblower's Test Jobe's Test

Apprehension Sign with shoulder abducted and externally rotated Speed's Test

Kim's Test
The patient suffered a posterior shoulder dislocation, likely injuring the posterior capsule and/or labrum. Out of all the answer choices, Kim's test assesses posterior structures. Thus, Kim's test is the physical examination finding most likely to be present.
Posterior dislocations occur less frequently than anterior dislocations, and are often missed. Following closed reduction, persistent instability can occur, usually associated with posterior capsular or labral pathology. Posteriorly directed provocative maneuvers, such as the Kim test can be positive.
Robinson et al. performed an epidemiologic analysis on 120 posterior dislocations. Recurrent instability occurred at a rate of 17.7%. Risk factors for recurrent instability included age less than 40-years-old, dislocation during seizure, and a large reverse Hill-sachs (>1.5 cm3). Kim et al. describe the Kim lesion, a separation between the posteroinferior labrum and the articular cartilage without complete detachment of the labrum, which cause persistent posterior instability.
Figure A depicts a posterior dislocation on xray. Illustration A depicts the Kim test, which is performed by having the patient seated, arm at 90° abduction, followed by flexing the shoulder to 45° forward flexion while simultaneously applying axial load on the elbow and posterior-inferior force on the upper humerus. The test is positive when there is pain. Video 1 depicts the proper way to perform a Kim Test.
Incorrect answers:
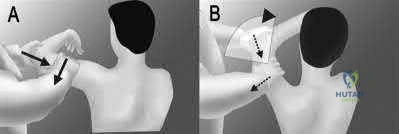
A 27-year-old male bodybuilder presents to the office with vague, deep shoulder pain and weakness with his bench press. His examination is somewhat difficult due to his large size, but no significant abnormal findings are noted. Radiographs are normal, and an MRI arthrogram is shown in Figure A. Which of the following is the most likely etiology of his complaints?

Pectoralis major rupture Supraspinatus partial thickness tear SLAP lesion

Tendonitis of the long head of the biceps Posterior labral tear
The clinical presentation and MRI are consistent with a Posterior labral tear.
Posterior labral tears are commonly seen in individuals that have repeated posteriorly-directed stress across their glenohumeral joint (football linemen, bodybuilders). These patients will often present with ill-described pain deep in their shoulder joint, along with decreases in shoulder strength. Focused shoulder examinations, such as the Jahnke Jerk Test or Push-pull test, can elicit pain from posterior labral tears; however, the sensitivity and specificity of these tests remain under question.
Mair et al. reviewed the outcome of posterior labral injuries in nine athletes who underwent arthroscopic repair with a bioabsorbable tack after failure of conservative management; all were
able to return to contact sports. They note that posteriorly applied forces can result in a shear-type vector that can cause posterior labral tears without capsular injury.
Bradley et al. reviewed 91 athletes with unidirectional recurrent posterior shoulder instability that were treated with an arthroscopic posterior capsulolabral reconstruction. They found that significant improvements in stability, pain, and function at a mean of 27 months postoperatively. Eightynine percent of the patients were able to return to their sport.
Figure A shows an axial MRI arthrogram of the shoulder with a posterior labral tear and an associated paralabral cyst. Illustration A is another axial shoulder MRI arthrogram cut showing a posterior labral tear (red arrow) and an associated paralabral cyst (yellow arrows).
Incorrect Answers:
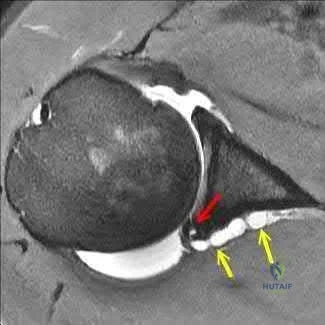
A patient sustains a full thickness tear of their teres minor. Which of the following test/signs would most likely be positive in this patient?

Jobe's test Belly press test

Internal rotation lag sign Hornblower's sign Hawkin's sign
Hornblower's test is completed by asking the patient to hold their shoulder in 90 degrees of abduction and 90 degrees of external rotation. The test is positive if the arm falls into internal rotation or they are unable to actively externally rotate against resistance. This suggests teres minor pathology.
There are various tests/signs used by clinicians to detect rotator cuff pathology. The teres minor is innervated by the axillary nerve and functions to externally rotate the humerus. The hornblower's test/sign has various descriptions, but all act to determine external rotation weakness. In addition to being sensitive and specific for teres minor pathology, it can also be positive with posterior supraspinatus tears.
Walch et al. review 54 patients that underwent repair of combined supraspinatus and infraspinatus rotator-cuff tears. They found that the hornblower's sign was highly sensitive and specific for irreparable degeneration of the teres minor, while the dropping-sign was highly sensitive and specific for irreparable degeneration of the infraspinatus.
Hertel et al. prospectively review 100 patients with painful shoulders and impingement syndrome. They compared various lag signs (ERLS-external rotation lag sign, IRLS-internal rotation lag sign, drop sign) to the Jobe and lift-off signs. The ERLS was less sensitive but more specific than the
Jobe sign for the supraspinatus/infraspinatus. The drop sign was the least sensitive but was as specific as the ERLS. The IRLS was as specific but more sensitive than the lift-off sign for subscapularis tears.
Illustration A shows another variation of the hornblower's sign as originally desbribed by Arthui et

positive if the patient is unable to do this without abducting the affected arm and demonstrates the difficulty in raising the hand to the mouth in the absence of external rotation of the shoulder. The video provided shows how to perform both variations of the hornblower's test.
Incorrect Answers:

Reverse total shoulder arthroplasty combined with latissimus dorsi transfer would be
most appropriate for which of the following patients?
year-old male with post-traumatic shoulder arthritis after a four-part proximal humerus fracture with no motor dysfunction

year-old male with grade 4 shoulder arthritis with severe deltoid muscle dysfunction secondary to a stroke

year-old female with significant rotator cuff arthropathy, a negative Hornblower sign and less than 5 degrees of external rotation lag

year-old female with pseudoparesis of anterior elevation and external rotation, narrowing of gleno-humeral joint and acetabularization of the acromion

year-old male with grade 4 shoulder arthritis and an isolated supraspinatus tear
Reverse total shoulder arthroplasty combined with latissimus dorsi transfer would be most appropriate in a patient with pseudoparesis of anterior elevation and external rotation, in the setting of shoulder arthritis (narrowing of glenohumeral joint and acetabularization of the acromion).
Combining a latissimus dorsi tendon transfers with reverse total shoulder arthroplasty (R-TSA) helps to restore control of active external rotation. Dysfunction with external rotation can be determined clinically with external rotation lag sign, a positive Hornblower's sign, and radiographically with fatty degeneration of the teres minor classified as stage 2 or greater according to the system of Goutallier et al. or Fuchs et al.
Gerber et al. found that R-TSA with combined lat dorsi transfer yielded minimal improvements in external rotation ROM (13 deg to 19 deg) compared to increases in shoulder ROM in flexion (94 deg to 137 deg) and abduction (87 deg to 145 deg), with this procedure.
Boileau et al. examined 17 consecutive patients treated with reverse shoulder arthroplasty and latissimus dorsi and teres major transfer (L'Episcopo). They found that external rotation increased from -21 degrees to 13 degrees (+34 degrees ). They recommend transferring both the LD and TM, rather than the LD alone as it results in better active external rotation.
Illustration A is a radiograph showing a right reverse total shoulder replacement. Illustration B shows a cadaveric image of the positioning of the latissimus dorsi tendon transfer prior to implantation of the reverse total shoulder components.
Incorrect Answers
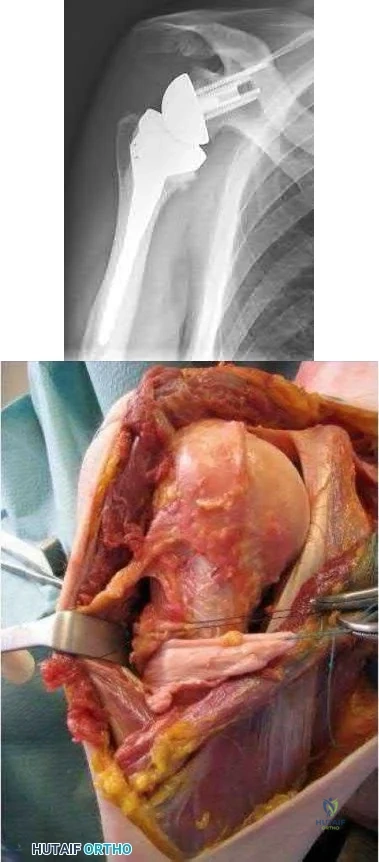
Figure A and B are MRI images of a 42-year-old male with symptoms of right shoulder neuropathy. If this patient has an abnormality detected on EMG and nerve conduction testing, which of the following nerves is most likely to be involved?
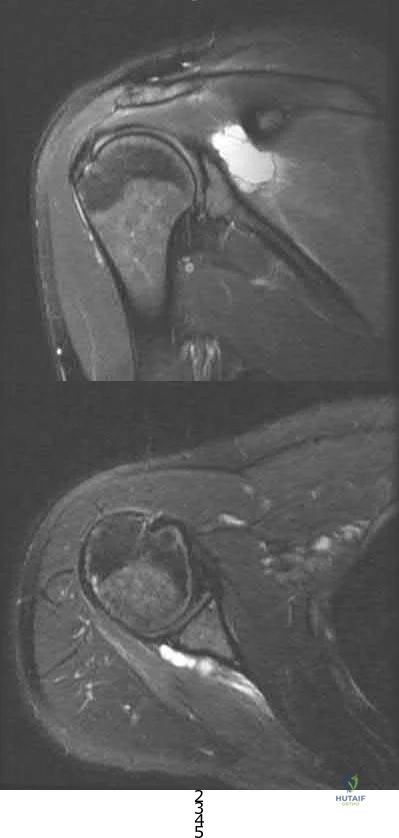
Subscapular nerve Axillary nerve Musculocutaneous nerve Suprascapular nerve Long thoracic nerve
This patient is presenting with suprascapular nerve compression secondary to a spinoglenoid cyst. Injuries of the posterior shoulder joint capsule or posterior-superior labrum can result in spinoglenoid cysts. They may lead to suprascapular nerve palsy.
Patients will present with characteristic findings of external rotation
( infraspinatus) weakness when the cyst is isolated in the spinoglenoid notch. If the cyst is located in the suprascapular notch, both external rotation weakness and abduction (supraspinatus) weakness will be present. Electromyography and MRI are the investigations of choice in depicting the etiology of this mononeuropathy.
Piatt et al. found posterosuperior labral tears in 65/73 patients who had spinoglenoid notch cysts. All patients presented with should pain and weakness. Patients undergoing surgical intervention by drainage or excision +/- arthroscopic labral repair had a better outcome than non-operative care.
Westerheide et al. reported fourteen patients who underwent arthroscopic decompression of ganglion cysts associated with suprascapular neuropathy. All patients had a labral tear intraoperatively with arthroscopic drainage and labral repair. There was not recurrence at an average of 51 months of followup.
Piasecki et al. reviewed suprascapular neuropathy. Causes include:nerve entrapment along this path, particularly at the vulnerable suprascapular and spinoglenoid notch, as well as extrinsic compression by soft-tissue masses.
Figures A is a coronal MRI showing a large hyperintense mass medial to the glenoid articulation. Figure B shows an axial MRI of the lesion posterior to the glenoid. Illustration A shows a diagram of the posterior right shoulder. The suprascapular nerve can be seen traveling through the spinoglenoid notch. Incorrect Answers:
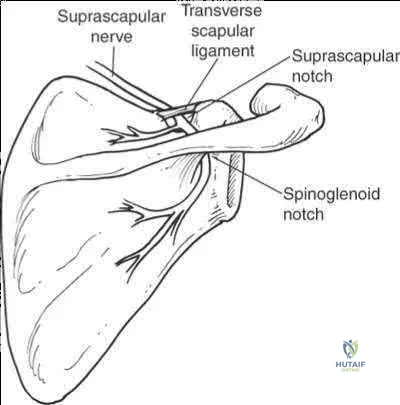
A 12-year-old right-hand-dominant pitcher presents with progressive right shoulder pain. He is now unable to pitch. He is tender to palpation over the lateral shoulder and has pain with rotation. An AP radiograph of the affected shoulder is shown in Figures A and a contralateral radiograph is shown in Figure B. What is the most likely diagnosis?
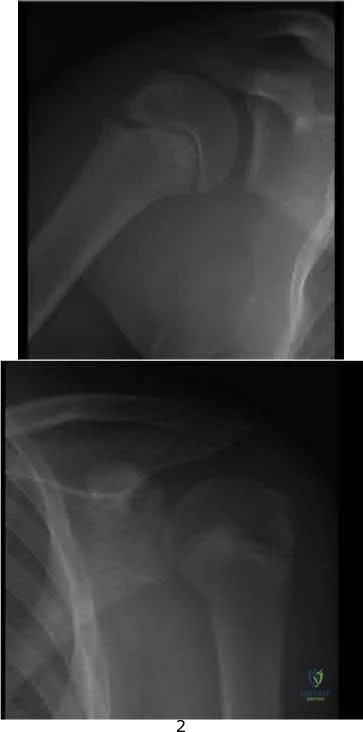
Septic arthritis of the shoulder SLAP tear
External impingement Internal impingement

proximal humerus. Patients may report a recent increase in pitching regimen. On examination, there is focal tenderness at the level of the physis. Treatment focuses on rest, physical therapy and a progressive throwing program. Pitching is often stopped for 2-3 months during rehabilitation.
Chen et al. review shoulder and elbow injuries in the young athlete. Little
Leaguer's shoulder results from epiphyseal lysis secondary to microtrauma. Pain over the anterolateral shoulder may be elicited on examination. The mainstay of treatment is 2-3 months of rest and return to pitching via a progressive throwing program.

Mcfarland et al. review techniques to prevent injuries in the throwing athletes. They note that overuse injures can be avoided when appropriate throwing mechanics are enforced and pitch counts are li
physeal widening noted especially when compared to the contralateral normal pediatric shoulder view seen in Figure B.
Incorrect Answers:
A 35-year-old carpenter has pain in the antecubital fossa that is worse with turning a screwdriver. He has undergone non-operative treatment for 6 months without relief. On physical examination his hook test is normal and there is pain and weakness with resisted supination. Radiographs are shown in Figures A-C. A MRI of the right elbow is shown in Figure D. The next most appropriate treatment is?

Exploration of the radial tunnel Superficial radial neurectomy

Detachment and repair of the biceps tendon Transfer of the biceps to the brachialis EMG with nerve conduction study
While complete trauamtic rupture of the distal biceps is more common, partial tears have been reported in the literature. The most common presentation is pain in the antecubital fossa worse with resisted supination.
Conservative management consists of NS

Transfer to the brachialis improves flexion strength but not supination.
Ramsey et al present a review article on distal biceps tendon injuries. They state that the most successful management of partial distal biceps tears that have failed conservative management is to surgically treat it like a complete rupture with release and surgical reattachment of the distal biceps to the radial tuberosity.
Figures A-C are normal radiographs of the elbow. Figure D is a crossreferenced axial and coronal T2 MRI that demonstrates increased signal and partial distal biceps tendon tearing. Illustration C shows the resected region of distal biceps tendon in the same patient and had an excellent functional outcome following distal biceps release and surgical reattachment with 2 double-loaded suture anchors.
Video V demonstrates The hook test for detecting complete distal biceps tendon avulsions.

A 49-year-old man sustains a dislocation of his left elbow that is successfully reduced and splinted. He misses his scheduled follow-up appointments and returns 6 weeks later. He is immediately enrolled in a course of vigorous physical therapy. At a repeat visit at 6 months, examination reveals that he lacks 40 degrees of elbow extension, and has flexion to 80 degrees. He is taken to the operating room for surgical release. Figures A and B are diagrams depicting the ligamentous attachments about the elbow. To restore elbow flexion, in addition to releasing the articular capsule, which ligament should be released?
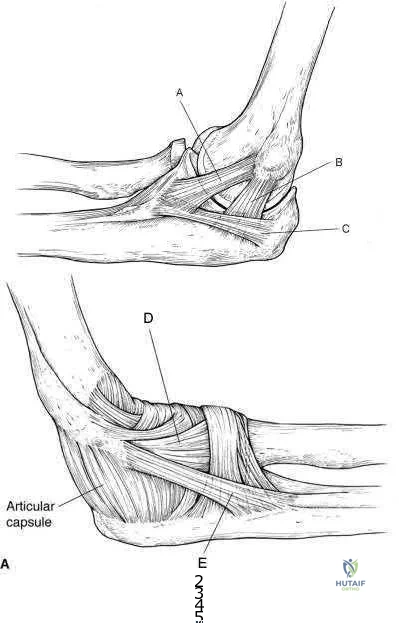
Ligament A Ligament B Ligament C Ligament D Ligament E
In addition to capsular release, the posterior band of the medial collateral ligament (MCL) should be released.
The posterior band of the MCL is attached dorsal to the axis of rotation and has greater variation in length. It increases in length by 9 mm between 60° and 120° of flexion. Posterior band contracture leads to loss of elbow flexion. In contrast, the anterior band of the MCL (AMCL) maintains a constant length ( isometric) throughout the entire arc of movement. Anterior capsule contracture leads to loss of extension.
Wada et al. treated 14 elbows with post traumatic contracture. Through a medial incision, the ulnar nerve was freed and the posterior band and posteromedial joint capsule were excised. Mean flexion increased from 89° preop to 127° postop. Anterior capsulectomy was performed for limited extension.
Morrey et al. studied structures providing stability about the elbow. They found that the anterior capsule stabilizes the elbow to varus-valgus stress in extension, not in flexion. The anterior band of the MCL is a primary stabilizer, especially in flexion.
Figures A and B are medial and lateral illustrations of the elbow, respectively, depicting the ligamentous attachments. Illustrations A and B are radiographs are 3D CT reconstruction images of the left elbow, respectively, showing heterotopic ossification around the posterior band of the MCL.
Incorrect Answers:

A 23-year-old male sustains a dislocation of his elbow that was successfully closed reduced in the emergency room. 3 months later, the patient presents with pain and a catching sensation in his elbow. On physical exam, he is noted to have a positive lateral pivot-shift test. Incompetence of which of the following ligaments in Figure A is most commonly associated with his condition?
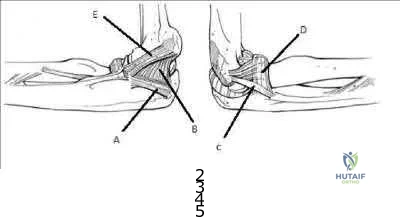
A B C D E
The patient is presenting with symptoms and physical exam consistent with posterolateral rotatory instability. Injury to the lateral ulnar collateral ligament
( LUCL), labeled C in Figure A, allows an abnormal external rotation
( supination) of the ulna on the humerus. This results in posterolateral rotatory instability. Posterolateral rotatory instability often presents as pain and recurrent clicking, snapping, clunking, or locking of the elbow. It should be noted that frank dislocations are not the most common presenting symptom. The physical exam is usually benign except for a positive lateral pivot-shift test or posterolateral rotatory drawer test. While injury to the LUCL is thought to be the primary pathology, other ligamentous stabilizers of the elbow may play a role.
Mehta et al. review posterolateral rotatory instability of the elbow. They state the instability usually results from an elbow dislocation with subsequent failure to heal of the ligamentous structures.
Patients with recurrent instability often require surgical intervention, as bracing is typically cumbersome and ineffective.
The video provided shows how to perform the lateral pivot-shift test. The patient is placed in the supine postion with forearm overhead and elbow extended. The elbow is then supinated with force and flexed to >40° while a valgus load applied. A positive result is palpable / visible clunk as the ulna and radius reduce suddenly. Illustration A shows the posterolateral rotatory drawer test.
External rotation and posterior forces are applied to the forearm attempting to sublux the radius posterior to the capitellum.
Incorrect Answers:
Figure A is the MR image of the left shoulder of an active 47year-old painter who has been experiencing shoulder pain for 9 months. In addition to the finding shown in Figure A, MRI examination of the intra-articular portion of the biceps tendon shows fraying greater than 50%. He has not obtained relief from an 8 month course of non-operative management including non-steroidal antiinflammatory medications, physical therapy and corticosteroid injection. What is the best next step in treatment?

New course of physical therapy

Activity shutdown with 6 weeks sling immobilization

Arthroscopic superior labrum anterior to posterior (SLAP) tear repair Arthroscopic debridement and possible biceps tenotomy versus tenodesis

Arthroscopic rotator cuff repair and acromioplasty
This patient has a Type II SLAP lesion. These should only rarely be repaired in patients older than 40 years of age. If a source of pain refractory to nonoperative management, biceps tenotomy or tenodesis should be considered.
SLAP repair for Type II SLAP lesions is a procedure that has enjoyed a high success rate in young patients. These are generally not indicated for repair in patients greater than 40 years of age due to high rate of stiffness postoperatively. A subset of patients continue to do poorly after SLAP repair. Poor range of motion and the development of post-surgical adhesive capsulitis is often an etiology for poor results. Arthrofibrosis recalcitrant to diligent therapy over many months can be treated with arthroscopic capsular release. This is predicated on failure of a dedicated course of physical therapy as part of a non-operative management course lasting greater than six months. As the propensity for stiffness increases with age, consideration should be treated with SLAP tear debridement and biceps tenotomy or tenodesis in patients greater than 40 years old. Tenotomy or tenodesis, however, can be effective at providing pain relief in the presence of proximal biceps tendon pathology.
Katz et al. reviewed 34 patients who presented to their group for management of failed SLAP repair. 50% were Worker's Compensation cases. The mean age at the time of initial SLAP repair was 43 years. They treated these patients conservatively initially followed by revision surgery in 21 cases. All completed a course of physical therapy initially. They concluded that once a patient has failed SLAP repair, there is a high chance of further conservative treatment failing. Although revision surgery improves outcomes, 32% will continue to have a "suboptimal" result. Holloway et al. reviewed 50 patients who underwent arthroscopic capsular release for adhesive capsulitis, comparing three groups: (1) post-surgical; (2) post-fracture; and (3) idiopathic adhesive capsulitis. All patients had completed supervised physical therapy and a home exercise program for at least one year. They concluded that arthroscopic capsular release improved range of motion equally for all three groups but patients in the post-surgical group had poorer subjective pain, function and satisfaction scores.
Figure A is an MRI showing a Type II SLAP tear. Illustration A shows the classification of SLAP lesions.
Incorrect Answers:
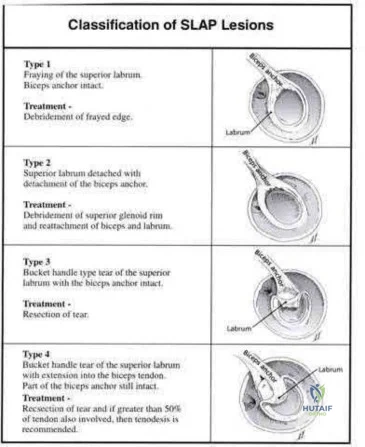
A 30-year-old man undergoes arthroscopic Bankart repair for recurrent anterior dislocation. He continues to experience instability postoperatively. Examination reveals a positive apprehension test. Radiographs of both shoulders are seen in Figure A. CT scan of his left shoulder is seen in Figure B. What is the best treatment option?
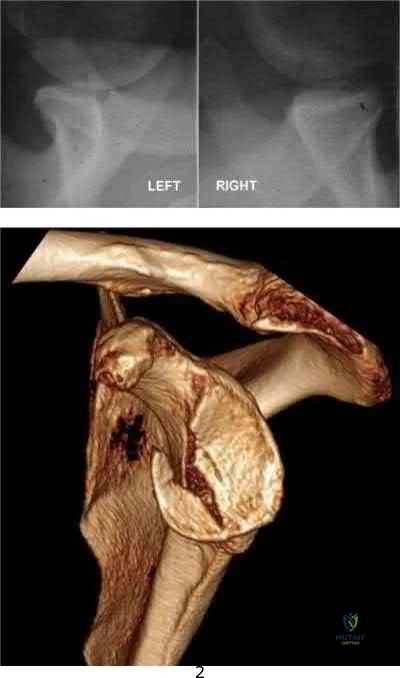
Bankart repair

Humeral head bone augmentation Remplissage

Coracoid autograft Connolly procedure
This patient has anterior glenoid bone deficiency (inverted pear glenoid) from a large bony Bankart lesion that was not adequately addressed in the index procedure. This is best treated with bony augmentation using the Latarjet vascularized coracoid transfer.
Patients with glenoid bone defects >20-30% have a high recurrence rate
(>60%) after Bankart repair alone. Bone grafting is necessary to offer containment. Autograft options include coracoid transfer (such as the Latarjet procedure which extends the articular arc and creates a conjoined tendon sling) and iliac crest bone grafting.
Burkhart et al. addressed glenohumeral bone defects. They advise that significant bone deficits cannot be adequately addressed via arthroscopic Bankart repair alone. The Latarjet transfer creates an extra-articular platform to extend the articular arc of the glenoid.
Hantes et al. assessed Latarjet repairs using CT. They found that there is almost complete repair of a 25% to 30% glenoid defect when using the Latarjet procedure.
Figure A comprises comparison Bernageau view glenoid profile radiographs of both shoulders.
Figure B is a 3D reconstruction CT with showing glenoid bone deficiency (inverted pear deformity) with a large bony Bankart lesion. Illustration A shows the method of obtaining a Bernageau glenoid profile view. Illustration B shows the "cliff sign" of anterior glenoid bone loss.
Illustration C depicts the Latarjet procedure. Illustration D depicts reduction in the articular arc with anterior glenoid loss.
Incorrect Answers:
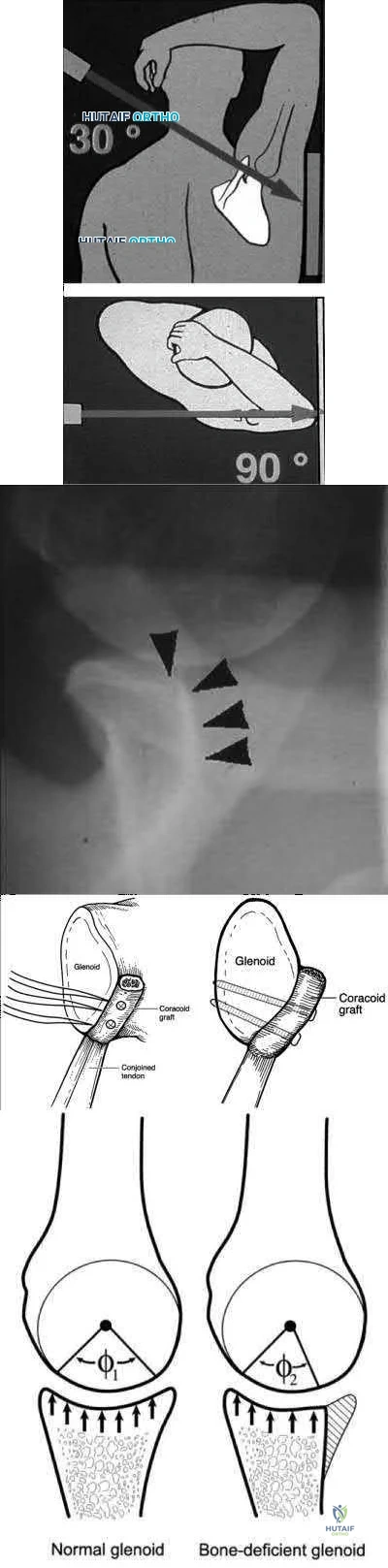
Figure A shows an arthroscopic picture of a 62-year-old male undergoing repair of a torn subscapularis tendon. In the image shown, G represents the glenoid, H represents the humeral head, and the dotted line represents the superolateral border of the subscapularis tendon. Which two ligaments form the structure marked with the asterisk?

Inferior and middle glenohumeral ligaments Middle and superior glenohumeral ligaments Coracohumeral and coracoacromial ligaments

Coracohumeral and superior glenohumeral ligaments Superior and inferior glenohumeral ligaments
The coracohumeral and superior glenohumeral ligaments form a complex that marks the superolateral margin of the subscapularis tendon.
In chronic or degenerative tears, the subscapularis will often retract medially and become scarred to the deltoid fascia. This makes identification difficult during arthroscopic repair. The coracohumeral and superior glenohumeral ligaments form a complex that inserts on the superolateral margin of the subscapularis. This "comma sign" can usually be identified during arthroscopic repair making identification of the subscapularis tendon an easier task.
Burkhart and Brady present surgical pearls for arthroscopic repairs of the subscapularis. Amongst other things, they state the subscapularis is almost always repairable with proper mobilization, but an Achilles tendon allograft or a subcoracoid pectoralis major transfer may be used for a severely degenerated subscapularis.
Lo and Burkhart describe the comma sign for repair of chronic subscapularis tears. They describe how the superior glenohumeral ligament/coracohumeral ligament complex and subscapularis tendon are intimately associated, and often tear off the humerus while remaining attached to each other. This complex, when torn, forms a "comma sign," that marks the superior and lateral margins of the subscapularis tendon.
Illustration A shows why the convergence of the superior glenohumeral and coracohumeral ligaments on the superolateral border of the subscapularis is referred to as the "comma sign." Incorrect Answers:
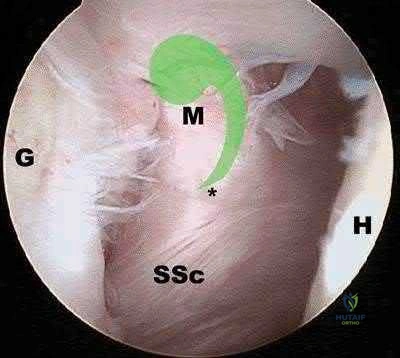
A 52-year-old man sustained the left elbow injury shown in Figure A while playing basketball 2.5 months ago. He underwent the procedure shown in Figure B. Post-operatively he was mobilized in a hinged brace. On examination today, his arc of elbow flexion is 75 degrees with loss of 45 degrees of full extension. His Disabilities of the Arm, Shoulder and Hand (DASH) Outcome Measure score is 45 points. What initial treatment option will likely provide the greatest improvement in this patients DASH score and functional range of motion?

Self-directed exercise therapy Supervised exercise therapy

Supervised exercise therapy with static progressive elbow splinting Continuous passive motion device

Closed manipulation under anesthesia
The clinical presentation is consistent with post-traumatic elbow stiffness following an elbow fracture-dislocation. Supervised exercise therapy with static elbow splinting over a 6 month period
has shown to have a significant improvement on DASH scores and functional range of motion (ROM) in patients with post-traumatic elbow stiffness.
Post-traumatic elbow stiffness is often difficult to manage. The ultimate goal of treatment is to restore a functional range of elbow motion (30° to 130°). Nonoperative modalities are considered the first-line of treatment. Aggressive physical therapy has traditionally been advocated. However, the use of static progressive elbow splinting with a turnbuckle, alongside aggressive physical therapy, has shown to provide better functional outcomes. Treatment is usually maintained over a period of 6-12 months. Surgery is considered when nonoperative therapy fails.
Doornberg et al. looked at a retrospective case series of 29 patients with posttraumatic elbow stiffness. They showed that static progressive splinting can help gain additional motion when standard exercises fail to produce additional improvements.
Lindenhovius et al. randomized sixty-six patients with post-traumatic elbow stiffness into static progressive elbow splint therapy or dynamic elbow splinting over a 12 month period. There was no significant difference in outcomes between treatment modalities. ROM increased by 40° vs. 39° at six months, respectively. DASH scores improved from 50 vs 45 at enrollment to 32 vs. 25 at six months, respectively.
Figure A shows a posterior elbow dislocation with an associated medial epicondyle fracture. Figure B shows ORIF of the fracture seen in Figure A. Illustration A shows a static progressive turnbuckle elbow splint used for posttraumatic elbow stiffness.
Incorrect Answers:
tissues, causing hemarthrosis and additional fibrosis in the joint.

A 25-year-old right-hand baseball pitcher presents with persistent shoulder pain for the past several months in his dominant throwing arm. On physical examination, he is found to have full arc of motion with the exception of an internal rotation deficit of 30 degrees compared to his contralateral side. He is asked to complete the exercise shown in the video in Figure V. This form of rehabilitation is meant to address pathology in which anatomic structure?

Superior glenohumeral ligament Middle glenohumeral ligament

Anterior band of the inferior glenohumeral ligament Superior band of the inferior glenohumeral ligament

Posterior band of the inferior glenohumeral ligament
tissues in patients demonstrating symptoms of internal impingement. The sleeper stretch helps to address posterior tightness and the only posterior structure listed in the responses is the posterior band of the inferior glenohumeral ligament (posterior IGHL).
Internal impingement is a significant cause of pain in throwing athletes. It results from impingement of the articular undersurface of the posterior supraspinatus against the posteriorsuperior glenoid.
This is thought to be secondary to tightness in the posterior soft tissues including the capsule and posterior band of the IGHL. The mainstay of non-operative management is posterior capsular stretching with the sleeper stretches and cross-body adduction stretches. Heyworth et al. review the etiology, diagnosis and management of internal impingement of the shoulder. They note that repetitive contact between greater tuberosity and glenoid rim posterosuperiorly lead to impingement of the posterior rotator cuff and labrum. This occurs when the arm is externally rotated and abducted.
Tyler et al. reviewed the effects of posterior capsular stretching on alleviating symptoms in patients with internal impingement. Twenty-

Figure V is a video that demonstrates the sleeper stretch to address tightness of the posterior soft tissues. The arm is forward flexed 90 degrees and the patient lies on his side in order to stabilize the scapula while the arm is internally rotated. Illustration A depicts the sleeper stretch.
Incorrect Answers:
not the focus of the sleeper stretch.
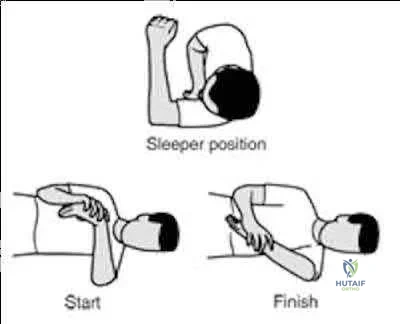
A 28-year-old professional baseball pitcher sustains a complete rupture of his ulnar collateral ligament. He is neurovascularly intact on exam. Which of the following surgical reconstruction techniques has been shown to result in the lowest complication rate and best patient outcome?

Splitting of flexor-pronator mass, figure-of-8 graft fixation. Splitting of flexor-pronator mass, docking graft fixation.

Splitting of flexor-pronator mass, docking graft fixation, ulnar nerve transposition. Detachment of flexor-pronator mass, figure-of-8 graft fixation, ulnar nerve transposition.

Detachment of flexor-pronator mass, docking graft fixation, ulnar nerve transposition.
Ulnar collateral ligament (UCL) reconstruction using a flexor-pronator musclesplitting approach and a docking graft fixation technique are associated with the lowest complication rate and best patient outcomes.
Vitale et al. performed a systematic review of retrospective cohort studies evaluating UCL reconstruction techniques in overhead athletes. They demonstrated that the flexor-pronator musclesplitting approach was associated with better outcomes than detachment of the flexorpronator mass, had a lower rate of postoperative ulnar neuropathy, and a lower overal complication rate. They also found fixation of the graft utilizing the docking technique was associated with better outcomes than the figure-of-8 technique. Abandoning the obligatory ulnar nerve transposition was associated with improved patient outcomes (89% vs. 75%) and a lower rate of postoperative ulnar neuropathy (4% vs. 9%).
Rettig et al performed a case series review of 31 overhead throwing athletes with ulnar collateral ligament injuries managed nonoperatively with 3 months rest followed by rehabilitation exercises. They concluded that 42% of athletes were able to return to their previous level of competition at an average of 6 months from diagnosis (earlier than reconstruction). The authors were unable to identify any patient-specific factors (duration of symptoms, age, acuity of onset) that would predict the success of nonoperative treatment.
Illustration A shows the figure-of-8 (Jobe) graft fixation technique. It is performed by passing the tendon graft through two bone tunnels in the medial epicondyle of the humerus and through one tunnel in the ulnar sublime tubercle. The graft is then sutured to itself in a figure-of-8 configuration. Illustration B shows the docking graft fixation technique. The graft is placed in a triangular configuration through a single humeral tunnel. The suture limbs are then brought out through two separate bone holes and tied over a bony bridge on the superior aspect of the medial epicondyle.
Incorrect Answers:
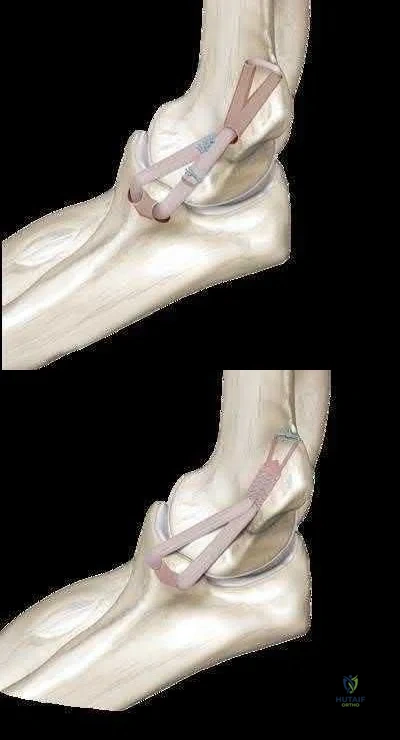
The right shoulder exercise seen in Figure A will put the LEAST amount of stretch on which structure?
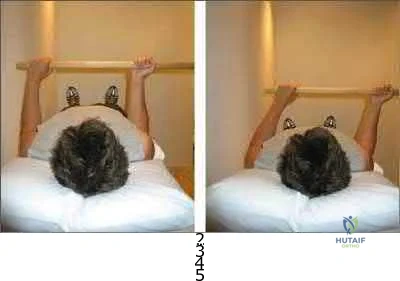
Inferior glenohumeral ligament Coracohumeral ligament Anterior-superior capsule Superior glenohumeral ligament Posterior capsule
Shoulder wand exercises, as shown in Figure A, are used to increase external range of motion of the shoulder. With the arm adducted and the elbow flexed, this exercise will put the LEAST amount of stretch on the posterior capsule.
External rotation shoulder wand exercises are commonly used for the treatment of adhesive capsulitis. Adhesive capsulitis is most commonly caused by contracture of the rotator interval. The rotator interval includes the anterior-superior capsule, superior glenohumeral ligament, coracohumeral ligament and long head biceps tendon. The structure most commonly contracted is the anterior-superior capsule, which limits external rotation when the arm is adducted. Kuhn et al. showed that in the neutral position, each ligament except the posterior capsule significantly affected the torque required for external rotation. The greatest effect on resisting external rotation at 0 degrees of abduction was the entire inferior glenohumeral ligament > coracohumeral ligament
> anterior band of the inferior glenohumeral ligament > superior and middle glenohumeral ligament.
Harryman et al. looked at the role of the rotator interval capsule in passive motion and stability of the shoulder. They found operative alteration of this capsular interval was found to affect flexion, extension, external rotation, and adduction of the humerus with respect to the scapula. Limitation of external motion was increased by operative imbrication of the rotator interval and decreased by sectioning of the rotator interval capsule.
Kim et al. reviewed shoulder MRIs to determine if abnormalities of the rotator interval were correlated with chronic shoulder instability. They found a significantly larger rotator interval height, rotator interval area, and rotator interval index in patients with chronic anterior shoulder instability compared to patients without instability.
Figure A shows a patient performing an exercise to increase right shoulder external rotation with a wand/stick. The right arm is fully adducted by her side, and her elbow flexed at 90 degrees.
Incorrect Answers:
) A 55-year-old male returns for followup 3 months after reverse shoulder arthroplasty. He reports limited function of his right shoulder but no antecedent trauma. A radiograph of his shoulder is shown in Figure A. All of the following variables are associated with this complication EXCEPT:

History of malunited proximal humerus fracture Proximal humeral bone loss

Failed primary arthroplasty Rheumatoid arthritis

Fixed preoperative glenohumeral dislocation
Rheumatoid arthritis is not associated with reverse shoulder arthroplasty (RSA) dislocation. RSA dislocation is a known complication of RSA. Risks include proximal humeral bone loss, chronic fracture sequelae with malunited/ununited tuberosities, failed previous arthroplasty, and fixed glenohumeral dislocation preoperatively. An irreparable subscapularis tears may be less of an issue with newer implant designs.
Trappey et al. studied instability and infection rates after RSA. They found that the rate of instability was similar in primary and revision surgery, but the rate of infection was higher in revision surgery. Instability was highest in the fracture sequelae group because of malunited tuberosities, contractures and proximal humeral bone loss.
Favre et al. examined the effect of component positioning on RSA stability.
They found that humeral version was more important than glenoid version. Stability is improved with the humerus in neutral or slight anterversion. They recommend avoiding retroversion >10deg. Edwards et al. examined subscapularis insufficiency and the risk of RSA dislocation. They found that of 138 RSA, all 7 dislocations occurred in patients with an irreparable subscapularis.
Dislocation was also more likely in patients with complex diagnoses, including proximal humeral nonunion, fixed dislocation, and failed prior arthroplasty.
Figure A shows reverse shoulder arthroplasty dislocation. Incorrect Answers:
) A 45-year-old man complains of chronic right shoulder pain. He has a history of chronic steroid use because of asthma. He recently completed a course of physical therapy
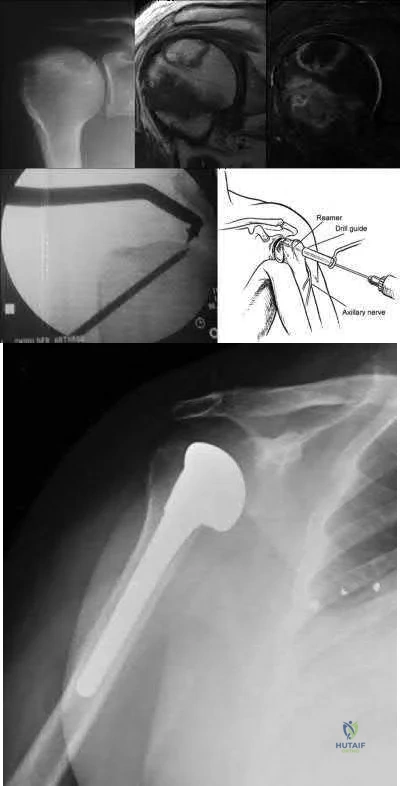
and has given up his job as a laborer in favor of a desk job. Examination reveals diminished shoulder abduction strength. A radiograph of his shoulder is shown in Figure A. Which of the following surgical treatment options (Figures B through F) is the most appropriate?

Figure B Figure C Figure D Figure E Figure F
This patient has early stage avascular necrosis (AVN) of the humeral head without subchondral collapse/flattening, likely related to chonic steroid use.
Core decompression is indicated.
Treatment of humeral head AVN is dependent on Cruess Stage. Precollapse stages (Stage I and II) may be treated by core decompression and joint preservation. Hemiarthroplasty is used for Stage III-IV disease. Total shoulder arthroplasty is used for Stage V disease. Resurfacing may be used for Stage III disease with focal chondral defects and sufficient remaining epiphyseal bone stock for fixation.
Harreld et al. reviewed humeral head AVN. They advocate attempting core decompression and arthroscopy for Stage III disease, and then tailoring resurfacing or replacement depending on defect size.
Smith et al. reviewed 31 hemiarthroplasties for steroid-related AVN (6 Stage III, 16 Stage IV, 5 Stage V). Unsatisfactory results were found in 45%. This was associated with glenoid cartilage wear over time. However, they still believed hemiarthroplasty was appropriate for younger active patients with stage III or stage IV disease.
LaPorte et al. performed core decompression for various stages of AVN.
Results were successful in 94%, 88%, 70% and 14% of Ficat-Arlet Stages I, II, III and IV humeral head AVN respectively, and more successful for nonsteroid related cases compared with steroidrelated cases. They recommend this treatment for Stages I-III.
Figure A comprises a radiograph showing Cruess Stage II disease ("snowcap" sign indicating sclerosis, preservation of the head contour and absence of subchondral collapse, left), a T1weighted
MRI (center) and T2-weighted fat saturated MRI (right) showing a variegated pattern of osteonecrosis, but with preservation of normal head contour. Figure B shows core decompression. Figure C shows hemiarthroplasty. Figure D shows reverse shoulder arthroplasty. Figure E shows resurfacing. Figure F shows total shoulder arthroplasty. Illustration A depicts the Cruess staging system. Illustration B shows a possible algorithm for management where they use the Ficat stages adapted from the hip.
Incorrect Answers:
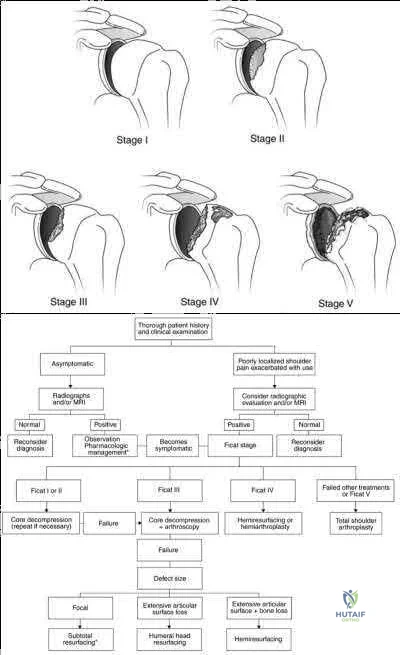
A 56-year-old otherwise healthy woman undergoes uncomplicated arthroscopic repair of a full-thickness rotator cuff tear. Prior to the procedure, the patient had attempted a long,
protracted course of physical therapy in an attempt to regain function without surgery. At her 10 day post-operative visit, she tearfully informs you that she cannot see her physical therapist because she has used up her 24-visit allotment for the year. She has 4 more weeks
until her insurance year turns over, and she does not have the financial means to pay out of pocket. What is the best next course of action?
Request a peer-to-peer review for authorization of additional visits or else the patient is likely to have a poor result

Provide a brief explanation and sheet of exercises for periscapular and cuff strengthening exercises using a resistance band

Test her range of motion and strength, and if limited, have her return weekly to your clinic for a guided home rehabilitation program

Explain to her that seeing a physical therapist during the first 6 weeks following cuff repair will not affect her range of motion one year removed from surgery

Give her a prophylactic corticosteroid injection to avoid early post-operative adhesive capsulitis
Early motion following rotator cuff repair has not been shown to impact range of motion and stiffness at one year post-operative clinical examinations.
Stiffness is a complication of protecting rotator cuff repairs from early re-tear with sling immobilization. However, with sling immobilization of up to 6 weeks, there is evidence of no increase in long-term stiffness. Accordingly, supervised physical therapy is not required in the first 6 weeks following arthroscopic rotator cuff repairs in order to obtain a good result.
Parsons et al. retrospectively reviewed 43 patients with full-thickness cuff tears who underwent a conservative early-postoperative protocol involving sling immobilization for 6 weeks with no formal therapy during that time. 10 /43 patient were characterized as stiff at their 6-week postoperative visit. At one year, there was no difference in the range of motion of the early stiff group compared to the non-stiff group.
Trenerry et al. collected prospective data on 209 consecutive patients undergoing primary rotator cuff repair. They found that patients in the stiffest quartile of range of motion testing at 6 weeks progressively regained range of motion by a post-operative visit at 72 weeks. The predictor of slowest recovery of early post-operative stiffness was found to be an internal rotation deficit with the patient reaching behind his or her back.
Incorrect Answers:
1: Early supervised physical therapy has not been shown to be essential to obtaining good motion post-operatively.
2 and 3: Strength testing and home strengthening programs in the early postoperative period would put the repair at risk for early failure.
5: Prophylactic corticosteroids are not indicated for prevention of postoperative stiffness, and furthermore, could theoretically interfere with healing.
A 62-year-old woman presents with chronic shoulder pain. On physical exam, she has anterior shoulder pain and her symptoms are reproduced with provocative testing of the biceps including supination against resistance and forward flexion of the shoulder against resistance. Internal and external rotation are painful, but her range of motion is intact. Shoulder radiograph and MRI images are shown in Figures A-E. Which of the following statements is true regarding the patient's condition?
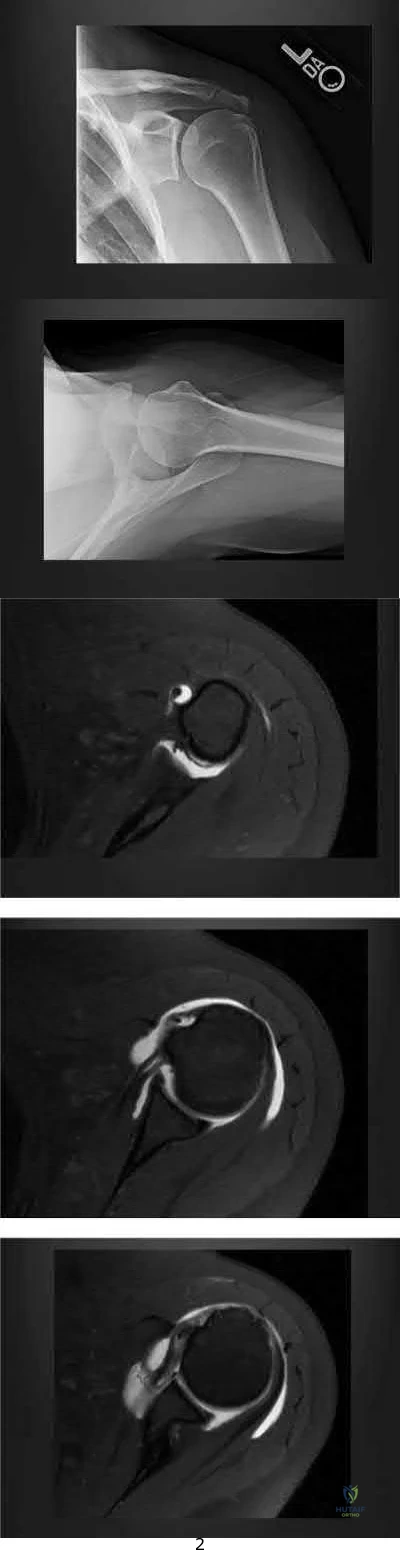
Her clinical examination is most consistent with a SLAP tear, which should be repaired. Her biceps pathology is due to her partial tearing of her subscapularis

She has isolated degenerative biceps tendonosis and an injection may cure her symptoms

She has end-stage rotator cuff arthropathy and should consider a reverse total shoulder arthroplasty

Her subacromial impingement is causing her biceps tendon sheath to be inflamed
The subscapularis tendon is the most important medial restraint to subluxation or dislocation of the long head of the biceps tendon (LHBT).
Anterior shoulder pain and positive provocative biceps clinical examination tests are common in patients with concomitant rotator cuff pathology. A consequence of subscapularis tendon tears -even partial tears - is that the LHBT can subluxate medially out of the intertubercular groove, as the subscapularis tendon is the most important restraint to medial instability of the LHBT. This instability can cause both pain and inflammation around the biceps tendon, leading to pain with resisted supination (Yergason's test) or resisted forward flexion (Speeds' test).
Walch et al. wrote a case series on 71 cases of biceps tendon instability. They found that dislocated LHBTs were associated with partial or complete subscapularis tears in 96% of cases.
Maier et al. published clinical results of treating acute traumatic medial LHBT instability with open repair of the subscapularis tendon and stabilization of the LHBT. They showed equivalent functional clinical outcomes to biceps tenotomy or tenodesis, with improved cosmesis and decreased muscle cramping.
Figures A and B show Grashey and axillary lateral views of the patient and demonstrate an os acromiale. Figures C, D, and E are axillary T2 MRI images. Figure C shows the tendon of the long head of the biceps in the distal aspect of the biceps grove. Moving proximally, Figure D shows the tendon subluxated onto the lesser tubercle and Figure E shows it fully dislocated medially.
Incorrect Answers:
A 78-year-old male presents to clinic 4 weeks after left total shoulder arthroplasty. He has not been wearing his sling and reports that he developed increased pain after slipping in the shower. He used the arm to catch himself from falling. On examination, he can flex the shoulder to 70 degrees, limited by pain. Active external rotation with arm at the side is 50 degrees and active internal rotation is 5 degrees. Passive external rotation is to 80 degrees. A radiograph of the left shoulder is shown below in Figure A. What other complaint is the patient most likely to have?

Pain with palpation of the bicipital groove Pain with palpation over the subdeltoid bursa Sensory loss over the lateral shoulder

Sensation of shoulder instability with external rotation Sensation of shoulder instability with internal rotation
The clinical presentation is consistent with a tear of the subscapularis, which is a well-described complication after total shoulder arthroplasty. The most likely additional complaint this patient will have is anterior shoulder instability, noticeable with external rotation of the shoulder.
Total shoulder arthroplasty is the preferred treatment for glenohumeral arthritis in patients with intact rotator cuff and good glenoid bone stock. The surgical approach involves detaching the subscapularis and capsule from the anterior humerus and dislocating the humeral head anteriorly. Post operatively, external rotation is limited to protect the subscapularis repair. If there is suspicion of a postoperative subscapularis tear, and ultrasound can be performed to confirm the diagnosis.
Miller et al. reported 7 cases of subscapularis tendon rupture after total shoulder arthroplasty, all of which were subsequently repaired. Decreased functional outcomes were observed in these patients, with lengthening techniques to address internal rotation contractures and prior surgery involving the subscapularis tendon as risk factors for rupture
Westoff et al. performed static and dynamic ultrasounds on 22 patients after total shoulder arthroplasty evaluating for numerous periarticular pathologies. The authors concluded that sonography is a useful tool for evaluation of periimplant tissues after TSA.
Figure A shows an intact left total shoulder arthroplasty without evidence of fracture, dislocation, or hardware loosening. Illustration A shows the incision for the subscapularis tendon during TSA. Incorrect Answers:
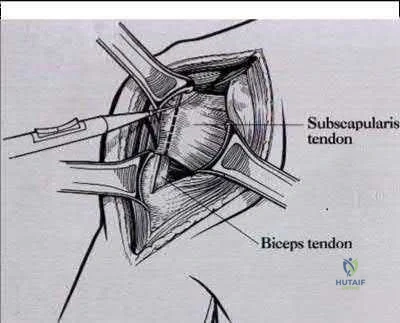
A 25-year-old lineman is referred to your office for a second opinion. 1 year ago, he underwent an arthroscopic procedure for shoulder instability. He complains of persistent sense of instability despite the surgery. Which of the following is a contraindication to revision arthroscopic labral repair for recurrent anterior glenohumeral instability?
Glenoid bone loss of 10%

Capsular attenuation from prior thermal capsulorraphy Anterior labral periosteal sleeve avulsion (ALSPA ) lesion Glenoid labral articular defect (GLAD) lesion

Combined Superior Labrum from Anterior to Posterior tear (SLAP) and recurrent Bankart lesion
Capsular attenuation or postthermal capsular necrosis from prior thermal capsulorraphy is a contraindicated to arthroscopic repair.
Thermal capsulorrhaphy utilizes heat generated by radiofrequency or laser ablation to cause capsular shrinkage in an effort to treat shoulder instability. However, high recurrence rates have been found, especially around two to three weeks after the index procedure, when the capsular tissue is the weakest. In the setting of recurrence following thermal capsulorrhaphy, open revision is recommended.
Creighton et al. reported on a series of 18 patients undergoing revision arthroscopic stabilization. Of the 18, 3 failed with recurrent instability, all with previous thermal capsulorrhaphy. Miniaci et al. reviewed the outcomes following thermal capsulorrhaphy noting high rates of recurrent instability, especially in the setting of initial treatment for multidirectional instability. Park et
al. reported on a series of 14 patients undergoing revision following thermal capsulorrhaphy. Ten out of 14 patients had signs of capsular thinning, insufficiency and attenuation.
Wong et al. surveyed 379 shoulder surgeons on the complications following thermal capsulorrhaphy. Capsular insufficiency and thinning were commonly associated with recurrent instability.
Hecht et al. performed thermal capsulorrhaphy and biomechanical analysis of the capsule in a sheep model. The authors found that the capsule was weakest at the 2-3 week post-operative timepoint, leading to the highest rate insufficiency, attenuation and mechanical failure at this time.
Incorrect answers:
A 47-year-old landscaper presents with worsening left shoulder pain and weakness. Three years ago, he injured the left shoulder in a fall and elected for nonoperative
management to minimize time off from work. Physical therapy was effective until 6 months ago when his shoulder function worsened to the point that he is now unable to work.

Examination of his active range of motion reveals forward elevation 120° with pain, abduction 100°, IR at neutral to T8 and ER at neutral 5°. He has a positive ER lag sign and Hornblower's sign. Belly press and lift-off tests are normal. A recent radiograph is shown in Figures A. MRI images are shown in Figures B and C. Which of the following is the best treatment option?
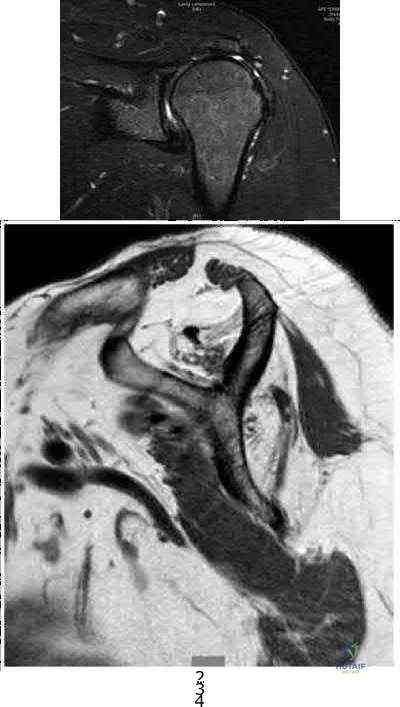
Continue physical therapy Latissimus dorsi transfer Arthroscopic rotator cuff repair Pectoralis major transfer

Reverse total shoulder arthroplasty
This patient has a chronic massive posterosuperior rotator cuff tear with marked atrophy, tendon retraction and loss of external rotation strength that is impacting his daily life. The best treatment option for this middle-aged laborer with an irreparable posterosuperior rotator cuff tear is a latissimus dorsi transfer to restore external rotation strength and motion.
Irreparable rotator cuff tears are marked by: (1) Superior displacement of the humeral head (AHI < 5-7mm), (2) Fatty infiltration of the rotator cuff muscles ( Goutallier stage 3-4), (3) Increased duration of the tendon tear and (4) Profound external rotation weakness. These findings are predictive of poorquality tissue and stiffness of the muscle-tendon unit, not amenable to primary repair. In this setting, a latissimus dorsi transfer can be utilized to restore shoulder strength, function and improve pain. Relative contraindications include subscapularis deficiency, deltoid deficiency, pseudoparalysis of the shoulder and advanced glenohumeral arthritis.
Gerber et al. performed a case series analysis of 67 patients with irreparable rotator cuff tears managed with latissimus dorsi transfer. Patients with an intact subscapularis demonstrated improvement in pain, range of motion and strength postoperatively, while no improvement was noted in patients with subscapularis deficiency. The authors conclude that latissimus dorsi transfer should not be performed in the setting of poor subscapularis function.
Iannotti et al. found that better clinical results following latissimus dorsi transfer were associated with: preserved active shoulder range of motion and strength (specifically forward elevation > 90° and external rotation > 20°), synchronous firing of the transferred latissimus dorsi muscle and male gender.
Figure A is an AP radiograph of the left shoulder with superior migration of the humeral head (AHI
< 5mm) and no evidence of glenohumeral arthritis. Figures B and C show a retracted posterosuperior rotator cuff tear and Goutallier stage 4 atrophy (more fat than muscle) of the supraspinatus, infraspinatus and teres minor, rendering this tear irreparable. Illustration A shows a latissimus dorsi transfer. The latissimus dorsi tendon is positioned over the top of the humeral head, covering most of the rotator cuff defect. The tendon is then secured to the subscapularis tendon edge and lesser tuberosity anteriorly, the remnant supraspinatus and infraspinatus tendons medially, and the greater tuberosity laterally.
Incorrect Answers:
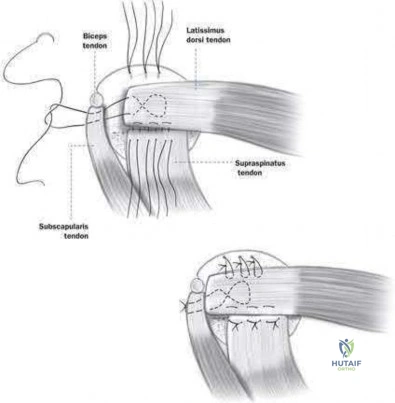
A collegiate swimmer develops medial winging of the scapula. If the EMG and nerve conduction studies are abnormal, the most likely nerve roots to be involved are?

C7, C8, T 1 C6, C7, C 8 C5, C6, C 7 C4, C5, C 6 C3, C4, C 5
Classic medial winging of the scapula is due to paralysis of the serratus anterior muscle which is supplied by the long thoracic nerve which holds the scapula to the chest wall and prevents the inferior angle of the scapula from migrating medially. It is innervated by the long thoracic nerve (C5, 6, 7).
Surgical treatment may include partial pec major transfer. Lateral winging may be caused by spinal accessory nerve palsy (CN XI, also ventral ramus C2,3,4). The nerve may be injured during neck surgery. This causes trapezius weakness, allowing the inferior pole of the scapula to migrate laterally. The modified Eden-Lange procedure may be used for this type of winging.
Gregg et al. describes paralysis of the serratus muscle in young athletes which they felt was due to repetitive traction. Full recovery usually occurs in an average of 9 months, and they recommend that surgical methods of treatment should be reserved for patients in whom function fails to return after a twoyear period.
Foo et al. describes a larger cohort of 20 patients again treated expectantly with observation and physical therapy. They reported consistent recovery but that it can take up to 2 years.
Illustration A shows a clinical photo of medial scapular winging. Illustration V is an instructional video of scapular winging. It begins with a clinical video of the condition.
A 62-year-old man complains of shoulder pain for 2 years. He has had 1 course of intra articular sodium hyaluronate and 6 weeks of physical therapy with little relief. Examination reveals diminished arm flexion and abduction secondary to pain. Radiographs of his shoulder are shown in Figures A and B. According to the American Academy of Orthopaedic Surgeons Clinical Practice Guidelines, what is the next best step?

Humeral head replacement arthroplasty Hemiarthroplasty and ream-and-run glenoid procedure

Cuff tear arthropathy (CTA) prosthesis

Total shoulder arthroplasty with a metal-backed cemented glenoid component Total shoulder arthroplasty with an all-polyethylene cemented glenoid component
This patient has end-stage glenohumeral osteoarthritis (GH OA). According to the AAOS CPG, total shoulder arthroplasty (TSA) is recommended using an allpolyethylene cemented glenoid component.
TSA is indicated for cases of end-stage GH OA. It is preferred to hemiarthroplasty. It is contraindicated in cases with insufficient glenoid bone stock (glenoid wear to the level of the coracoid), rotator cuff arthropathy or irreparable cuff tears and deltoid dysfunction. It provides good pain relief and has good survival at 10 years (>90%).
Radnay et al. performed a systematic review involving 1952 patients comparing TSA with humeral head replacement (HHR). They found that TSR provided greater pain relief, range of motion, patient satisfaction, and had lower revision rates. They recommend TSA over HHR for GH OA. Izquierdo et al. described the AAOS Clinical Practice Guidelines (CPG) regarding treatment of GH OA. This is summarized in Illustration A.
Figures A and B show end-stage GH OA with large osteophytes and subchondral sclerosis. There is significant glenoid wear and posterior subluxation (Walch B glenoid deformity). Illustration A is a table summarizing the AAOS CPG on treatment of GH OA. Illustration B shows a CTA humeral component. It is not paired with a glenoid component.
Incorrect Answers:
Metal-backed glenoids have higher rates of revision than all-polyethylene glenoids.
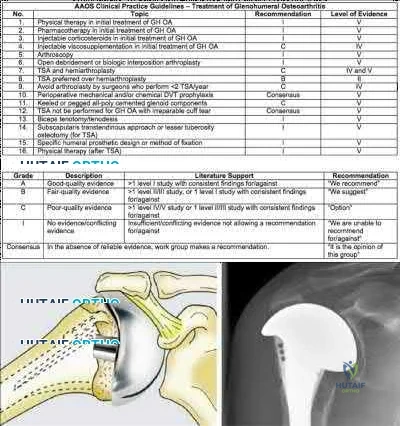
Posterior glenohumeral dislocations are as common as anterior dislocations in which of the following patient groups?
Football players

Marfan's syndrome patients Renal failure patients Epilepsy patients

Women
Millett et al and Robinson et al provide review articles on posterior shoulder dislocations, which are rare clinical entities that occur during seizures and electrocution (due to tetanic muscle contraction) or as a result of high energy trauma. Robinson et al noted that poor prognostic factors associated with posterior shoulder dislocation include late diagnosis, large bony defect of humeral head, associated proximal humerus fracture, and need for arthroplasty. In Gerber's series, posterior dislocations occurred with equal frequency to anterior in a cohort of epilepsy patients.
What nerve is injured most commonly during the superficial dissection when repairing a distal biceps rupture through a single incision anterior approach?

Medial antebrachial cutaneous nerve Lateral antebrachial cutaneous nerve Superficial radial nerve

Ulnar nerve

Posterior interosseous nerve
The lateral antebrachial cutaneous nerve (LABCN) is at risk during the superficial dissection when repairing a distal biceps rupture through a single incision anterior approach.
The LABCN is the terminal cutaneous branch of the musculocutaneous nerve, which supplies sensation to the volar-lateral aspect of the forearm. The LABCN pierces the deep fascia of the arm lateral to the musculotendinous junction of the distal biceps tendon after lying on top or piercing through the brachialis muscle. It exits the arm and lies in the subcutaneous tissues of the antecubital fossa. It is important to retract this nerve laterally during the approach to the distal biceps tendon.
Cohen describes the importance of identifying the LABCN during the superficial dissection as injury to this nerve is not uncommon (5-7%). Injury to the PIN (5 %) is devastating and occurs with retractor placement during the deep dissection and the use of suspensory fixation on the posterior cortex of the radius.
The review article by Ramsey et al covers the surgical anatomy and complications of biceps surgery, including injury to the LABCN.
Illustration A shows the LABCN relative to the anterolateral approach to the elbow which is commonly used to repair distal biceps avulsions. Illustration B shows the close proximity of the LABCN to the distal biceps in a human specimen.
Incorrect Responses:
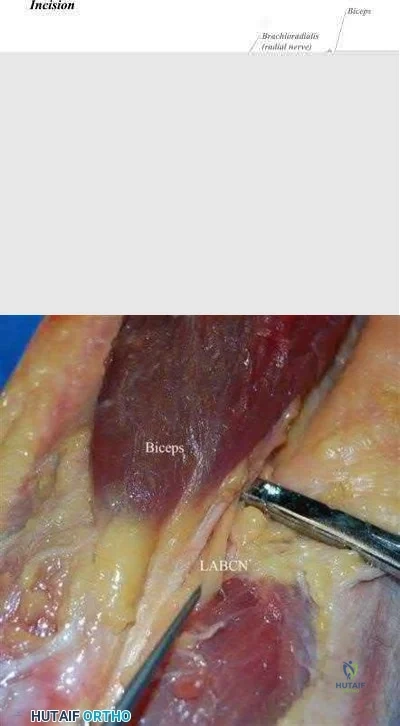
An MRI of the shoulder in a patient with chronic quadrilateral space syndrome is most likely to show which of the following?

Increased intra-capsular volume Loss of intra-capsular volume Fatty atrophy of the infraspinatus Fatty atrophy of the teres minor

Fatty atrophy of the latissimus dorsi
Quadrilateral space syndrome involves dysfunction of the axillary nerve, perhaps by entrapment or compression, resulting in the functional denervation of the teres minor.
The quadrilateral space is a potential space formed by the long head of the triceps medially, the humerus laterally, the teres minor above, and the teres major below. The axillary nerve and posterior circumflex humeral artery travel through this space.
The Sanders article describes the MRI appearance, which is that the muscle appears streaked with white on MRI and atrophied (See illustration A) consistent with fatty atrophy. Sanders group report this finding in 3% of shoulder MRIs. The posterior circumflex humeral artery also travels with the axillary nerve as it travels through this space. Loss of capsular volume on an arthrogram study is suggestive of adhesive capsulitis.
Illustration B is a diagram which shows the borders of the quadrilateral (or quadrangular) space.
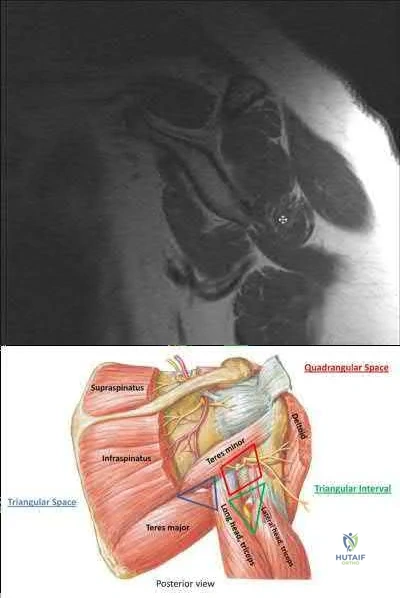
A 21-year-old collegiate volleyball player is noted to have weakness in external rotation and isolated atrophy of the infraspinatus on physical examination as seen in Figure A. An axial MRI image is shown in Figure B. This clinical condition is most likely caused by compression of the:
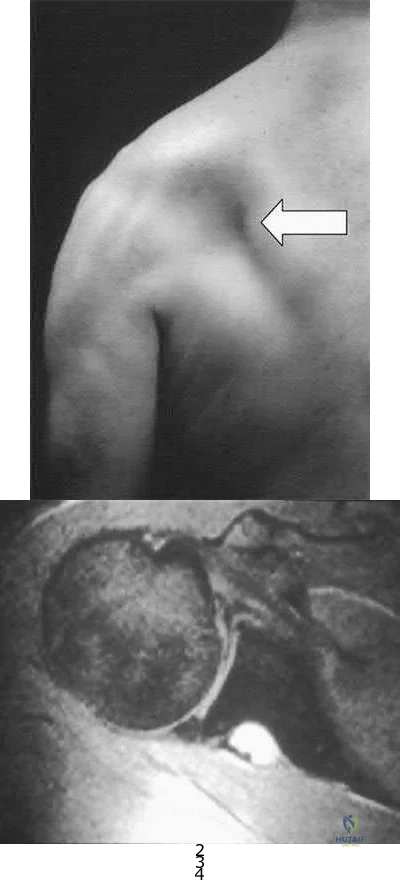
Axillary nerve at the triangular space Suprascapular nerve in the suprascapular notch Axillary nerve in the quadrangular space Suprascapular nerve in the spinoglenoid notch

Long thoracic nerve anterior to the scalenus and the first rib and posterior to the clavicle
The clinical presentation is consistent for a suprascapular neuropathy caused by compression of the suprascapular nerve by a cyst in the spinoglenoid notch.
The suprascapular nerve arises from the upper trunk of the brachial plexus with contributions from C5-6. It travels through the suprascapular notch of the scapula where it gives motor branches to the supraspinatus then around the spinoglenoid notch where it innervates the infraspinatus.
Compression of the nerve at the suprascapular notch will cause denervation and atrophy of both the supraspinatus and infraspinatus while compression at the spinoglenoid notch affects the infraspinatus in isolation. This is commonly seen in overhead athletes who sustain a SLAP tear and resultant spinoglenoid notch cyst as seen in the MRI. This will cause weakness and atrophy of the infraspinatus and can be noted both clinically and radiographically. Appropriate operative management is still not clear in the literature with some authors reporting a need for labral repair + cyst decompression and others reporting good outcomes with labral repair alone. Other cases have been treated with needle aspiration.
The cited reference by Cummins et al reviews the various causes, diagnosis, and treatment of suprascapular neuropathy.
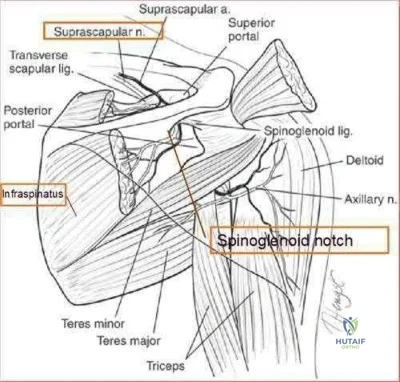
The reference by Martin et al is a retrospective study of the results of nonoperative treatment of suprascapular neuropathy in which 5 had excellent results and 7 had good results.
Which of the following provocative tests would most likely be positive in a patient with medial epicondylitis?

Resisted forearm pronation and wrist flexion with a clenched fist Resisted forearm supination and wrist extension with a clenched fist Dynamic valgus stress test

Milking maneuver Pinch grip test
A provocative test for medial epicondylitis can be elicited by applying resistance to a patient with their fist clenched, wrist flexed and pronated.
Medial epicondylitis is an overuse syndrome of the flexor-pronator mass. The pronator teres (PT) and flexor carpi radialis (FCR) are thought to be most affected with this condition. It is most common in the dominant arm and occurs with activities that require repetitive wrist flexion/forearm pronation. Patients are most tender over the origin of PT and FCR at the medial epicondyle.
Resisting a patient with their fist clenched, wrist flexed and pronated can cause worsening of their pain. This maneuver can be used as a provocative test for this condition.
Cain et al. reviewed elbow injuries in throwing athletes. They comment that the common flexorpronator muscle origin provides dynamic support to valgus stress in the throwing elbow, especially during early arm acceleration and help produce wrist flexion during ball release.
Amin et al. reviewed the evaluation and management of medial epicondylitis. They report that medial epicondylitis typically occurs in the fourth through sixth decades of life, the peak working years, and equally affects men and women. Physical therapy and rehabilitation is the main aspect of recovery from medial epicondylitis, once acute symptoms have been alleviated.
Illustration A shows a video of this provocative test for medial epicondylitis. Incorrect Answers:

A 72-year-old woman presents for follow-up after elbow surgery. Her radiographs are shown in Figures A and B. Which of the following pre-operative diagnoses is a relative contraindication to the use of this prosthesis design?

Acute intra-articular distal humerus fracture Malunited intra-articular distal humerus fracture Late-stage rheumatoid arthritis

Post-traumatic bony ankylosis Osteoarthritis
This patient has had an unconstrained total elbow arthroplasty (TEA).
Unconstrained TEA is least preferred for late-stage rheumatoid arthritis where there is significant capsuloligamentous instability and bony erosion.
Unconstrained (unlinked or resurfacing prosthesis) TEA depend on intact bony and ligamentous constraints for stability. These are appropriate for humeroulnar conditions with intact collateral ligaments and radiocapitellar articulation e.g. osteoarthritis, post-traumatic arthritis, intra-articular distal humerus fracture, and malunion of the distal humerus. Conditions with increased risk of

instability (ligamentous injury, rheumatoid arthritis) will benefit from a linked or semiconstrained prosthesis.
Mansat et al. reviewed the Coonrad-Morrey linked (semi-constrained) TEA implant in 70 patients after 5 years. They found that patients with inflammatory arthritis had higher function than those with traumatic conditions
( fractures, nonunions and post-traumatic arthritis). Survival rate was 98% and 91 % at 5 and 10 years, respectively. They concluded that this implant provided satisfactory treatment for different indications although radiolucent lines and bushing wear were a concern.
Hildebrand et al. reviewed the functional outcome of the Coonrad-Moorey prosthesis in 51 elbows after 50 months. The inflammatory arthritis group had higher performance scores than the traumatic/post-traumatic conditions group. Isometric extensor torque was found to be less than the nonoperated side. Radiolucency was noted in 11 elbows.
Figures A and B show an unconstrained TEA with radial head replacement. Illustration A shows more examples of unconstrained TEA. Illustration B shows a semiconstrained TEA. The arrow points to the anterior flange. Illustration C shows radiolucent lines around the stems. Illustration D shows severe bushing wear leading to locking mechanism failure. Illustration E is a table comparing linked and unlinked implants.
Incorrect Answers:

A professional baseball team has several pitchers with complaints of velocity loss with their pitches and shoulder pain of their dominant shoulders during spring training. Pitch counts are properly monitored. The average glenohumeral internal rotation deficit on the pitching staff is 45 degrees. The best intervention would be:
Pitchers throwing less fastballs and more changeups

Evaluate the pitchers elbows for ulnar collateral ligament acute ruptures. Increasing the weight training for the deltoid and latissimus dorsi muscles Focused stretches and therapies that address posterior capsular tightness Firing the general manager for finding pitchers that "lose their stuff"
Glenohumeral Internal Rotation Deficit (GIRD) is a phenomenon that occurs in baseball pitchers and is due to posterior capsular tightness. Treatment should begin with a therapy program addressing the pathologic posterior capsule.
GIRD is a phenomenon that is frequently found in high-level overhead throwing athletes, predominantly baseball pitchers. It is defined as the measured difference in internal rotation between the non-dominant arm and dominant arm. Worsening range of motion deficits are seen with increased repetitions, both over a single season and a career. GIRD > 25º is associated with development of shoulder pathologies or pain requiring periods of inactivity. Cessation of overhead throwing activities and initiation of a stretching program to address posterior capsular contractures is largely effective (90% in some series).
Burkhart et al. reviewed the conditions associated with high-level overhead throwing athletes shoulders, culminating in a theory of pathologic progression to "dead arm syndrome" (loss of velocity and effective pitching). Their theory attributes adaptive hyperexternal rotation (occurs during late-cocking / early acceleration phases of pitching) to lead to posterior-inferior capsular contracture and GIRD. Subsequent injuries to anterior structures - including SLAP lesions - would then occur.
Illustration A is a cartoon depiction of how to perform the sleeper stretch. This is a common component of a pitcher's maintenance stretching program.
Incorrect Answers:
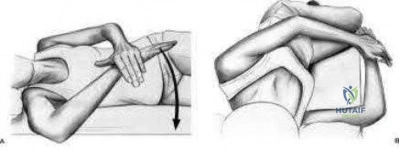
A 68-year-old man presents with severe right shoulder pain. He had a prolonged course of physical therapy and received several cortisone injections for his pain without improvement. Examination reveals pseudoparalysis of the right shoulder with a 20-degree external rotation lag with the shoulder adducted. With the shoulder placed in 90 degrees of abduction, he can actively externally rotate his shoulder. The patient was treated with a medialized reverse prosthesis shown in Figure A. Which of the following statement is true regarding this treatment option?

It is contraindicated in patients with shoulder pseudoparalysis

It can be used in patients with deltoid dysfunction when combined with latissimus dorsi transfer It shifts the center of rotation of the shoulder superior and lateral

The risk of scapular notching is increased with inferior placement of the glenoid component The risk of instability is increased with an irreparable subscapularis
The clinical presentation is consistent with a patient with pseudoparalysis that was treated with a reverse total shoulder arthroplasty (RTSA). The risk of postoperative instability is increased in patients with an irrepairable subscapularis when a medialized reverse prosthesis is used. Answers 1-4 are false statements.
RTSA is most commonly indicated for rotator cuff arthropathy. However, indications for use now include shoulder pseudoparalysis, anterosuperior escape of the humeral head, acute 3 or 4-part proximal humerus fractures, and greater tuberosity fracture nonunions. Contraindications to RTSA included deltoid dysfunction, insufficient glenoid bone stock, and bony deficiency of the acromion. Edwards et al. prospectively evaluated the risk of shoulder dislocation after reverse TSA. They found a significantly increased risk of dislocation (p=0.012) in patients with an irreparable subscapularis at time of surgery. There were no dislocations in the reparable group. Dislocations were more likely in patients with proximal humeral nonunions and failed prior arthroplasty. Mulieri et al. looked at the use of reverse TSA in patients with irreparable massive rotator cuff tears without evidence of glenohumeral arthritis. All outcomes were improved postoperatively, and they advocate
for reverse TSA in this subset of patients. Survivorship was over 90% at more than 4 years average follow up.
Boileau et al. evaluated the clinical outcomes of isolated biceps tenotomy/tenodesis in patients with massive rotator cuff tears and a biceps lesion. They found that the procedure can effectively treat pain and improve function in these patients. There was no difference in patients undergoing tenotomy versus tenodesis.
Figure A is a right shoulder radiograph status post RTSA with components in adequate position. Incorrect Answers:
Figure A shows immediate post-operative radiographs of a 75year-old patient with primary osteoarthritis. She presents 3 years later with increasing pain and weakness in the shoulder despite home physical therapy. Examination reveals limited active range of motion, with forward elevation of 80 degrees and external rotation of 50 degrees. Her deltoid function is intact. Repeat radiographs are seen in Figure B. Which treatment option would provide the best functional outcome for this patient?
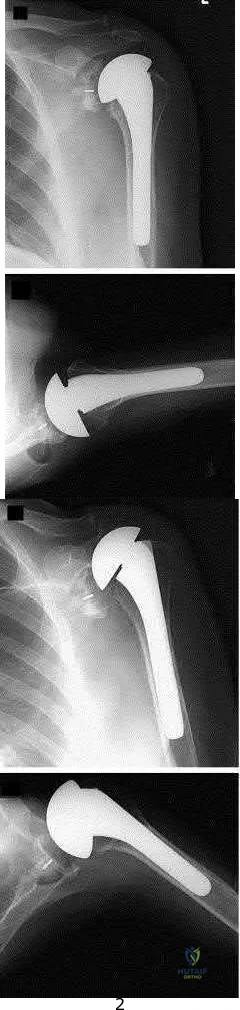
Open tendon transfer
Corticosteriod injection and supervised physical therapy

Open rotator cuff repair, subacromial decompression and distal clavical excision Revision to reverse shoulder arthroplasty

Revision to cuff arthropathy hemiarthroplasty
This patient presents with failed total shoulder arthroplasty. The best treatment option for functional outcome would be revision to reverse shoulder arthroplasty (rTSA).
RTSA is considered a viable treatment option for patients with failed shoulder arthroplasty. It allows for improved arm elevation and abduction in the setting of nonfunctional rotator cuff muscles, as seen in this example. Despite the expanding indications for rTSA, there are high complication rates in the revision setting. Complication rates for rTSA after failed shoulder arthroplasty have been reported to be between 11-36%. This procedure should, therefore, be performed by surgeons with extensive training in reconstructive shoulder arthroplasty.
Patel et al. retrospectively reviewed 31 patients (mean age, 68.7 years) who underwent rTSA for treatment of a failed shoulder arthroplasty. They found the greatest improvement with active forward elevation from 44° preoperatively to 108 ° postoperatively (P < .001). Complications occurred in 3 patients with periprosthetic fracture.
Hattrup et al. reviewed a series of 19 patients that underwent open rotator cuff repair after shoulder arthroplasty. Out of the 19 patients only 4 shoulders were successfully repaired. They concluded that successful rotator cuff repair after shoulder arthroplasty is possible but failure is more common. Figure A shows a left total shoulder arthroplasty that is well reduced in the glenoid. Figure B shows antero-superior escape of the prosthesis, indicative of a massive rotator cuff tear.
Incorrect Answers:
A 35-year-old man awoke following a night of heavy drinking with severe right shoulder pain and inability to raise his arm above his head. A radiograph from the emergency room is provided in Figure A. He was treated with a sling for a diagnosis of rotator cuff tear. Six weeks later, he complains of continued pain and difficulty using the arm. Which of the following is the next best step in management?

Physical therapy for range of motion followed by rotator cuff and deltoid strengthening exercises

Axillary radiograph of the shoulder

EMG to evaluate the suprascapular and axillary nerves Arthroscopic rotator cuff repair

Open subacromial decompression and latissimus dorsi transfer for massive cuff tear
The radiograph demonstrates overlap of the humeral head and glenoid suggesting shoulder dislocation. An Axillary radiograph is necessary to evaluate concentric reduction vs. dislocation of the shoulder. An example is provided in illustration A. Posterior shoulder dislocations can be easily be missed without the proper orthogonal views of the shoulder. Perron reviews the proper identification and emergency room care of posterior shoulder dislocation. Richardson found axillary radiographs to be more sensitive than trans-scapular radiographs for identifying posterior shoulder dislocations.

Recent randomized controlled trials comparing early passive range of motion to 6 weeks of immobilization after successful arthroscopic rotator cuff repair concluded that, compared to immobilization, early passive range of motion resulted in:
Higher Constant scores at 12 months

Increased rates of re-rupture as determined by ultrasound Equivalent functional outcomes

Less pain at 6 months

Inceased range of motion at 12 months
A series of high-quality RCTs have demonstrated that early passive range of motion has equivalent functional outcomes when compared to 6 weeks of immobilization after arthroscopic rotator cuff surgery.
Traditionally, most surgeons recommended early post-operative range of motion exercises for their patients in order to prevent adhesions and ultimately stiffness. However, recent evidence has found that there is no difference in the healing rate, range of motion or functional outcome between patients who undergo early versus delayed (i.e. initial 6 weeks of immobilization) passive range of motion exercises after arthroscopic rotator cuff repair.
Kim et al. conducted a randomized controlled trial comparing early passive range of motion vs. immobilization in 106 patients who underwent arthroscopic repair for full-thickness rotator cuff tears. They found that there was no clinically or statistically significant difference between the two groups in pain, healing or function.
Keener et al. also conducted a randomized controlled trial of 124 patients who were undergoing arthroscopic repair of a full-thickness rotator cuff tear and found no difference between early and delayed range of motion in healing and functional outcome.
Cuff & Pupello also compared early vs. delayed range of motion during the post-operative rehabilitation phase in a randomized controlled trial of 68 individuals undergoing arthroscopic rotator cuff repair and found no significant difference in range of motion or healing.
Incorrect Answers:
A 49-year-old male presents with right shoulder pain and weakness after undergoing open cervical lymph node biopsy approximately one year ago. A pertinent finding from the physical exam is seen in Figure A, with the patients arms by his side. Physical exam finding with the arms in a position of 90 degrees of forward elevation and 10 degrees of external rotation are shown in Figure B.
What nerve is most likely injured?

Long thoracic Suprascapular Spinal accessory Axillary Thoracodorsal
The patient is presenting with LATERAL scapular winging which is a result of injury to the spinal accessory nerve and resultant trapezius muscle palsy.
The spinal accessory nerve is fundamental to scapulothoracic function and essential for scapulohumeral rhythm. This nerve is vulnerable along its superficial course. The majority of injuries to the spinal accessory nerve are iatrogenic and occur secondary to head and neck surgery. There is often a marked delay in recognition and initiating treatment. Surgical treatment with the Eden-Lange transfer lateralizes the levator scapulae and rhomboids (transfer from medial border to lateral border)
Camp et al. reviewed the results of 111 patients who underwent operative management of a lesion to the spinal accessory nerve. They found that the majority (~80%) of injuries were sustained iatrogenically and that diagnosis was delayed for approximately 12 months.
Pikkarainen et al. reviewed the natural history of isolated serratus palsy. They found that symptoms mostly recover in 2 years, but at least one-fourth of the patients will have long-lasting symptoms, especially pain.
Figure A depicts a patient with lateral scapular winging. Figure B demonstrates physical exam of this patient with their arms in a position of 90 degrees of forward elevation and 10 degrees of external rotation. Illustration A highlights the difference between medial and lateral scapular winging. Illustration B depicts another example of a patient with lateral scapular winging.
Incorrect Answers:
An injury to the long thoracic nerve would result in serratus anterior palsy which would lead to MEDIAL scapular winging.

An injury to the suprascapular nerve would result in weakness and wasting of the supraspinatus and/or infraspinatus.
Question 81
A newborn girl is referred for evaluation of suspected hip instability. What information from her history would place her in the highest risk category?
Explanation
REFERENCES: Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Haynes RJ: Developmental dysplasia of the hip: Etiology, pathogenesis, and examination and physical findings in the newborn. Instr Course Lect 2001;50:535-540.
Question 82
Figures 1 and 2 are the right shoulder MRI scans of a 22-year-old right-handed professional male volleyball player with 4 months of right shoulder pain. The pain began insidiously and is exacerbated by overhead activities and hitting during games. He has maintained a daily program of shoulder stretching and strengthening exercises but has experienced a steady decline in function to the point of not being able to participate in volleyball. Examination reveals some mild atrophy at the posterior shoulder, full forward elevation, mild weakness of external rotation on the right shoulder, negative empty-can testing, positive O’Brien’s and negative apprehension. Surgical intervention would aim to resolve pathology related to which nerve?
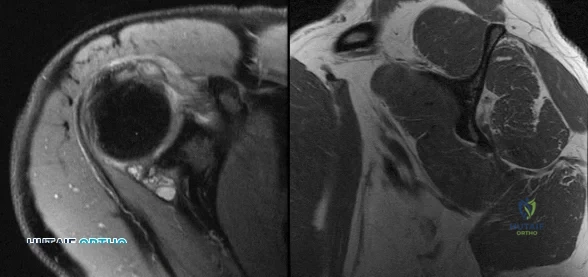
Explanation
Question 83
A 46-year-old woman has bilateral groin pain, with more severe pain on the left side than on the right side. Figures 44a and 44b show a radiograph and a T 1 -weighted MRI scan. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 3160-3162.
Epstein RE, Dalinka MK: Ischemic necrosis, in Stark DD, Bradley WG (eds): Magnetic Resonance Imaging, ed 3. St Louis, MO, Mosby, 1999, vol 2, pp 1023-1027.
Question 84
CLINICAL SITUATION Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities. What is the best next step in the patient’s evaluation?

Explanation
but she has not had any issues since the flap. She has abundant callus formation but the fracture line is still visible and unchanged on 2 sets of radiographs. The patient has persistent pain. The best initial evaluation is to ensure that there is no underlying infection with laboratory studies, including a complete blood count (CBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Nuclear medicine studies have questionable utility, but may be helpful if the inflammatory markers from laboratory studies come back elevated. A CT scan is not warranted because the sequential radiographs show persistent fracture lines and no changes. The patient has a hypertrophic nonunion. Originally, she had appropriate treatment and has shown the ability to make callus, thus her biologic capacity appears to be intact and bone grafting is not needed. The hypertrophic nature of her fracture nonunion indicates that she needs more stability. The best treatment for a hypertrophic nonunion of the tibia is exchange nailing. Based on successive radiographs and the lack of healing, observation is probably just delaying the inevitable. Plating with retention of the nail can be useful in recalcitrant long bone non-union, especially in the femur.
Question 85
Patients with tarsal tunnel syndrome are most likely to obtain a favorable outcome from decompression of the posterior tibial nerve if which of the following conditions is present?
Explanation
REFERENCES: Frey C, Kerr R: Magnetic resonance imaging and the evaluation of tarsal tunnel syndrome. Foot Ankle 1993;14:159-164.
Garrett AL: Poliomyelitis, in Nickel VL (ed): Orthopaedic Rehabilitation. New York, NY, Churchill Livingston, 1982, pp 449-458.
Pfeiffer WH, Cracchiolo A III: Clinical results after tarsal tunnel decompression. J Bone Joint Surg Am 1994;76:1222-1230.
Question 86
Figures 65a and 65b show the MRI scans of a 33-year-old man with severe left leg pain. He has had symptoms for 3 months with progressive worsening pain and function. Examination reveals ankle plantar-flexor weakness and diminished light touch sensation on the plantar surface of the foot. What treatment provides the best outcome? Review Topic
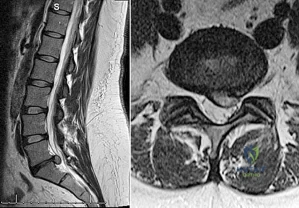
Explanation
Question 87
A 72-year-old woman falls onto her left hip after tripping over a curb during her daily 3-mile walk. An injury radiograph is shown in Figure A. What is the best long term solution?

Explanation
The aims of surgery for FNF in elderly patients are immediate pain relief, rapid mobilization, and low complications and revision. THA has best pain relief, fewer reoperations, best survivorship and is most cost-effective but has longer operative/anesthetic time, blood loss, higher infection rate, and potential instability compared with HA.
Healy and Iorio examined the optimal treatment for elderly FNF. They compared internal fixation (120 patients) with arthroplasty (HA, 43 patients; THA, 23 patients). There was no different in reoperation or mortality rates between the 2 groups, but arthroplasty was more cost effective, had independent living, and longer interval to reoperation/death. THA had less pain, better function, and lower rates of reoperation than HA, and was most cost-effective. They concluded that THA was the best treatment.
Yu et al. performed a meta-analysis of randomized controlled trials to determine whether THA or hemiarthroplasty (HA) was superior. They found that THA had lower risk of reoperation (RR = 0.53), higher risk of dislocation (RR = 1.99), and
higher functional scores at 1 and 4 years. There was no difference in mortality, infection and complication rates.
Figure A shows a displaced left femoral neck fracture. Incorrect Answers:
Question 88
Which of the following substances makes up the majority by weight of the extracellular matrix for articular cartilage?
Explanation
Question 89
Which of the following statements describing chordomas is false?
Explanation
REFERENCE: Casali PG, Stacchiotti S, Sangalli C, et al: Chordoma. Curr Opin Oncol 2007;19:367-370.
Question 90
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and
Explanation
REFERENCES: Botte MJ, Byrne TP, Abrams RA, et al: Halo skeletal fixation: Techniques of application and prevention of complications. J Am Acad Orthop Surg 1996;4:44-53.
Garfin SR, Botte MJ, Nickel VL: Complications in the use of the halo fixation device. J Bone Joint Surg Am 1987;69:954.
Question 91
Which of the following are considered appropriate nonsurgical bracing/orthotic options for a supple adult-acquired flatfoot deformity with forefoot abduction, secondary to posterior tibial tendon insufficiency?
Explanation
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Imhauser CW, Abidi NA, Frankel DZ, et al: Biomechanical evaluation of the efficacy of external stabilizers in conservative treatment of acquired flat foot deformity. Foot Ankle Int 2002;23:727-737.
Question 92
Which of the following is considered the lowest level that a standard thoracolumbosacral orthosis (TLSO) can immobilize?
Explanation
REFERENCES: White AA, Panjabi MM: Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 475-509.
Norton PL, Brown T: The immobilizing efficiency of back braces. J Bone Joint Surg Am 1957;39:111-139.
Question 93
Examination of a 25-year-old man who was injured in a motor vehicle accident reveals a fracture-dislocation of C5-6 with a Frankel B spinal cord injury. He also has a closed right femoral shaft fracture and a grade II open ipsilateral midshaft tibial fracture. Assessment of his vital signs reveals a pulse rate of 45/min, a blood pressure of 80/45 mm Hg, and respirations of 25/min. A general surgeon has assessed the abdomen, and a peritoneal lavage is negative. His clinical presentation is most consistent with what type of shock?
Explanation
REFERENCE: Sutton DC, Siveri CP, Cotler JM: Initial evaluation and management of the spinal injured patient, in Cotler JM, Simpson JM, An HS, et al (eds): Surgery of Spinal Trauma. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 113-126.
Question 94
A 56-year-old woman underwent a total knee arthroplasty 2 years ago and now has pain and swelling. Radiographs of her knee are unremarkable. Her C-reactive protein (CRP) level is 3.0 (reference range [rr], 0.08–3.1 mg/L), and her erythrocyte sedimentation rate (ESR) is 18 mm/h (rr, 0-20 mm/h). Aspiration of the knee reveals a white blood cell (WBC) count of 1200/mm3 with a differential of 30% neutrophils and 70% monocytes. Cultures will not be available for several days, and the patient has not been taking antibiotics. Based on these findings, the most appropriate next step is
Explanation
ESR and CRP level are recommended as starting points in the workup for the diagnosis or exclusion of periprosthetic joint infection (PJI). When both the ESR and CRP findings are within defined limits, PJI is unlikely. When both test findings are positive, PJI must be considered and further investigation is warranted. Clinicians need to be aware of other inflammatory conditions such as rheumatoid arthritis that can lead to elevation of inflammatory markers.
A high likelihood of infection is noted when the knee aspirate contains more than 2500 WBCs per high-powered field (HPF) with a differential count exceeding 60% neutrophils. Using these criteria, Mason demonstrated a sensitivity of 98% and a specificity of 95% for infection diagnosis.
For this patient, the inflammatory markers are within normal limits. The aspiration result is below 2500 WBC/HPF with a low percentage of neutrophils. The likelihood of infection is remote, and further nonsurgical treatment should not include antibiotics. There is no indication for surgery based upon the information presented.

Question 95
Figure 16a shows the radiograph of a 34-year-old woman who sustained a basicervical fracture of the femoral neck. The fracture was treated with a compression screw and side plate. Seven months postoperatively, she continues to have significant hip pain and cannot bear full weight on her hip. A recent radiograph is shown in Figure 16b. Management should now consist of
Explanation
REFERENCES: Marti RK, Schuller HM, Raaymakers EL: Intertrochanteric osteotomy for non-union of the femoral neck. J Bone Joint Surg Br 1989;71:782-787.
Ballmer FT, Ballmer PM, Baumgaertel F, et al: Pauwels osteotomy for nonunions of the femoral neck. Orthop Clin North Am 1990;21:759-767.
Question 96
From which artery does the princeps pollicis artery branch?
Explanation
The princeps pollicis artery can be located on the palmar aspect of the adductor pollicis and emerges into the subcutaneous tissue at the thumb metacarpophalangeal flexion crease. It branches from the radial artery just distal to the location of the deep palmar arch.
RECOMMENDED READINGS
Coleman SS, Anson B: Arterial patterns in the hand based on a study of 650 specimens. Surg Gynec Obstet 1961;4:409-424.
Ames EL, Bissonnette M, Acland R, Lister G, Firrell J. Arterial anatomy of the thumb. 78 J Hand Surg Br. 1993 Aug;18(4):427-36. PubMed PMID: 8409651. View Abstract at PubMed
Question 97
At the time of revision total knee arthroplasty, the surgeon is trialing the knee and finds that it extends fully and is stable in flexion with a 23-mm trial spacer; however, the patella is impinging on the polyethylene spacer. No augments were used on the femur or the tibia because the components fit well without them. What is the most appropriate action at this time?
Explanation
REFERENCES: Laskin RS: Joint line position restoration during revision total knee replacement. Clin Orthop Relat Res 2002;404:169-171.
Yoshii I, Whiteside LA, White SE, et al: Influence of prosthetic joint line position on knee kinematics and patellar position. J Arthroplasty 1991;6:169-177.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 123-145. Question 100
A 68-year-old woman is undergoing a cementless medial/lateral tapered femoral placement during a total hip arthroplasty and the surgeon notices a small crack forming in the anteromedial femoral neck with final implant insertion. The most appropriate management should include which of the following?
Placement of a cerclage cable around the femoral neck above the lesser trochanter
Removal of the implant, placement of a cable around the femoral neck above the lesser trochanter, and reinsertion of the implant
Removal of the press-fit implant and cementing of the same femoral stem
Final seating of the cementless femoral component without additional measures
Removal of the cementless femoral component and placement of a revision modular taper- fluted femoral stem
DISCUSSION: The recognized treatment of the proximal periprosthetic fracture is first to identify its extent and then to optimize the correction. Removing the implant seems logical to accomplish the identification. Several studies indicate that proximal cerclage wiring is adequate to create a “barrel hoop” stability of the proxima l femur. The postoperative management may also include protected weight bearing and periodic radiographs.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475503.
Warren PJ, Thompson P, Fletcher MD: Transfemoral implantation of the Wagner SL stem: The abolition of
subsidence and enhancement of osteotomy union rate using Dall-Miles cables. Arch Orthop Trauma Surg 2002;122:557-560.
Your Source for Lifelong Orthopaedic Learning
Question 98
Figure 10 shows the MRI scan of a 56-year-old woman with metastatic breast cancer who now reports progressive paraparesis. Her general health remains good. Treatment should consist of
Explanation
REFERENCE: Fardin DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 123-133.
Question 99
A 14-year-old boy has an asymptomatic mass on the right arm. MRI scans and biopsy specimens are shown in Figures 51a through 51d. Immunostaining is positive for desmin. Additional staging studies should include
Explanation
REFERENCES: Lawrence W, Jr., Hays DM, Heyn R, Tefft M, Crist W, Beltangady M, et al: Lymphatic metastases with childhood rhabdomyosarcoma: A report from the Intergroup Rhabdomyosarcoma Study. Cancer 1987;60:910-915.
Schleiermacher G, Peter M, Oberlin O, et al: Increased risk of systemic relapses associated with bone marrow micrometastasis and circulating tumor cells in localized ewing tumor. J Clin Oncol 2003;21:85-91.
Question 100
A 28-year-old woman has had pain in her hand and mild swelling of the little finger for the past 2 months. A radiograph is shown in Figure 41a, and the biopsy specimen is shown in Figures 41b and 41c. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 225.
McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 227.
