OITE & ABOS Orthopedic MCQ Prep: Arthroplasty, Trauma & Knee - Part 208

Key Takeaway
This page provides Part 208 of a comprehensive OITE and AAOS Orthopedic Board Review quiz. Designed for orthopedic residents and surgeons, it features 100 verified, high-yield MCQs covering Arthroplasty, Fracture, Knee, Ligament, and Tendon. It's an essential tool for board certification exam preparation.
About This Board Review Set
This is Part 208 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 208
This module focuses heavily on: Arthroplasty, Fracture, Knee, Ligament, Tendon.
Sample Questions from This Set
Sample Question 1: A 25-year-old man sustained a head injury after being ejected from his car. Examination reveals a Glasgow Coma Scale score of 7 and a swollen right knee. Clinical examination shows that the knee is very unstable, suggesting tears of the med...
Sample Question 2: Figure 13 is the photograph of 18-month-old triplets with a lower-limb condition. What is the best initial treatment? Review Topic...
Sample Question 3: Injurytothepoplitealarteryduringtotalkneearthroplasty(TKA)ismostlikelytooccurwhenplacingasharpretractor...
Sample Question 4: A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?...
Sample Question 5: A 52-year-old woman has a 60-degree extensor lag following a right total knee arthroplasty performed 16 months ago. Since the time of her primary total knee arthroplasty she has undergone primary repair of a patellar tendon rupture that occ...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 25-year-old man sustained a head injury after being ejected from his car. Examination reveals a Glasgow Coma Scale score of 7 and a swollen right knee. Clinical examination shows that the knee is very unstable, suggesting tears of the medial collateral and anterior and posterior cruciate ligaments, as well as the posterior lateral corner. What is the most appropriate first step to rule out a vascular injury?
Explanation
REFERENCES: Miranda FE, Dennis JW, Veldenz HC, et al: Confirmation of the safety and accuracy of physical examination in the evaluation of knee dislocation for injury of the popliteal artery: A prospective study. J Trauma 2002;52:247-252.
Mills WJ, Barei DP, McNair P: The value of the ankle-brachial index for diagnosing arterial injury afterknee dislocation: A prospective study. J Trauma 2004;56:1261-1265.
Question 2
Figure 13 is the photograph of 18-month-old triplets with a lower-limb condition. What is the best initial treatment? Review Topic

Explanation
(SBQ13PE.56) A 22-month-old female is hospitalized with a fever and malaise. She is found to be bacteremic, and blood cultures grow methicillin-sensitive Staphylococcus aureus (MSSA). During her hospitalization, the pediatrician notices her arm is slightly swollen and appears painful to use. MRI is obtained and demonstrated in figure A. Which feature of the MRI suggests the need for surgical management? Review Topic

Brodie's Abscess
Osteomyelitis of the humeral metaphysis
Subperiosteal abscess of the humerus
Presence of subcutaneous air
High risk of proximal humeral growth arrest
This patient has osteomyelitis of the humerus with a large subperiosteal abscess. The presence of subperiosteal abscess necessitates surgical intervention for irrigation and debridement (I&D).
The diagnosis of acute osteomyelitis in children is made based upon a constellation of findings including pain, systemic signs of infection, elevated serum inflammatory markers, and imaging studies demonstrative of osseous infection. It is most commonly hematogenously spread to the metaphysis of immature bone, which is highly vascular prior to skeletal maturity. Treatment involves obtaining specimen for culture, empiric antibiotic treatment, and surgical irrigation and debridement of known abscesses. The end-point of treatment is return of pain-free functionality and the resolution of local/systemic signs of infection.
Conrad reviewed the management of acute hematogenous osteomyelitis and emphasized that surgical intervention in the presence of abscess can be both therapeutic and diagnostic: I&D can obtain culture and narrow the antibiotic plan.
Jones et. al. reviewed chronic pediatric osteomyelitis and report that surgery is the mainstay of treatment because removal of dead bone is essential for resolution of infection. This may be performed with sequestrectomy and curettage, with an emphasis on prevention of pathologic fracture, growth disturbances, bone loss, joint involvement, and permanent loss of function.
Figure A is a coronal STIR MRI image of the humerus demonstrating osteomyelitis
with extensive subperiosteal abscess.
Incorrect Answers:
Brodie's abscess is a type of subacute osteomyelitis which remains indolent and creates a focal intra-osseous abscess. This is not demonstrated in the clinical image.
The patient does have osteomyelitis of the humeral metaphysis, but this alone is not the indication for surgery. Uncomplicated osteomyelitis may be treated effectively with antibiotics alone.
Presence of subcutaneous air is suggestive of necrotizing fasciitis, which is a surgical emergency. The MRI however does not demonstrate this finding.
The infection and its surgical management both increase risk of injury to the proximal humeral physis and has the potential for growth arrest or angular deformity.
(SBQ13PE.3) Figure A demonstrates a physical examination maneuver in a 1 month old infant. What is this maneuver? Review Topic

Ortolani Test
Barlow Test
Galeazzi Sign
Patrick test
Teratologic Sign
Figure A shows a schematic image of the Ortalani test.
The Ortolani test, or Ortolani maneuver, is part of the physical examination for developmental dysplasia of the hip. It is used alongside the Barlow test to detect subluxated hips that are either reducible or irreducible. A positive sign is a distinctive 'clunk' which can be heard and felt as the femoral head relocates anteriorly into the acetabulum.
Guille et al. showed that the use of Pavlik harness has become the mainstay of initial treatment for the infant who has not yet begun to stand. If concentric reduction of the hip cannot be obtained, surgical reduction of the dislocated hip is the next step before they are able to stand.
Video V is a lecture discussing the hip examination of the infant. Incorrect Answers:
pressure on the knee, directing the force the femoral head posteriorly. A positive Barlow test would result in posterior subluxation/dislocation of the hip. Answer 3: Galeazzi test is performed by flexing an infant's knees in the supine position so that the ankles touch the buttocks. If the knees are not level then the test is positive, which indicates a potential congenital hip issue (e.g. DDH). Answer 4: Patrick or Faber test (flexion, abduction, external rotation) has been described both for stressing the SI joint and for isolating symptoms to the hip Answer 5: Teratologic dislocation of the hip is a term used to imply that the hip joint did not develop normally in utero, thus the hip is in a fixed dislocated position at birth.
Question 3
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
Explanation
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Question 4
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
Explanation
REFERENCES: Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its affects on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
Question 5
A 52-year-old woman has a 60-degree extensor lag following a right total knee arthroplasty performed 16 months ago. Since the time of her primary total knee arthroplasty she has undergone primary repair of a patellar tendon rupture that occurred after a fall 8 months ago. A lateral radiograph of the knee is shown in Figure 52. A CT scan obtained to determine component rotation showed that the femoral component is internally rotated 9 degrees and the tibial component is internally rotated 12 degrees. Appropriate management at this time should include
Explanation
Attempts at secondary repair have been associated with high failure rates whereas the use of an extensor mechanism allograft has been shown to more effectively restore active extension in a substantial percentage of patients. Important aspects of the technique include fully tensioning the graft in full extension and immobilization of the extremity for 6 to 8 weeks postoperatively to allow for graft healing. Nonsurgical management will not result in an acceptable outcome for a young patient, and attempted secondary repair is associated with a high rate of failure, even when augmented with local tissues. This patient has gross rotational
malalignment of the components and the surgeon faced with this problem should consider obtaining a CT scan to determine component rotation preoperatively.
REFERENCES: Burnett RS, Berger RA, Paprosky WG, et al: Extensor mechanism allograft reconstruction after total knee arthroplasty: A comparison of two techniques. J Bone Joint Surg Am 2004;86:2694-2699.
Nazarian DG, Booth RE: Extensor mechanism allografts in total knee arthroplasty. Clin Orthop Relat Res
1999;367-123-129. , „. H
AL-Madena Copy ^Lj-^M) <UjJlU

Question 6
A 6-year-old girl has the bilateral foot deformity shown in Figure 1. There is no family history of disease. Examination reveals fixed hindfoot equinus, and muscle function testing shows strong posterior tibial function, fair plus anterior tibial function, poor peroneal function, and strong gastrocnemius function. A Coleman block test shows a correctable hindfoot. Nerve conduction velocity studies show diminished function in the peroneal and ulnar nerves on both sides. Pathologic changes found in a sural nerve biopsy include “onion bulb” formation, and DNA testing confirms the presence of a mutation in the MPZ gene, consistent with hereditary motor sensory neuropathy type III (HMSN-III). What is the best course of action?
Explanation
REFERENCES: Wetmore RS, Drennan JC: Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 1989;71:417-422.
Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth. J Bone Joint Surg Br 1989;71:17-20.
Miller GM, Hsu JD, Hoffer MM, Rentfro R: Posterior tibial tendon transfer: A review of the literature and analysis of 74 procedures. J Pediatr Orthop 1982;2:363-370.
Question 7
Figures 56a through 56c are the lateral radiograph and MRI scans of a 32-year-old woman who reports a 3-week history of heel pain, tenderness, swelling, and onset following an increase in running activity. What is the most likely diagnosis?

Explanation
Question 8
03 5.
Explanation
The radiograph here shows the typical Paget’s lesion in the right iliac wing with mixed lytic and sclerotic areas.
Question 9
Figure 33 shows the MRI scan of a 55-year-old woman who has had a 6-week history of back and leg pain. Which of the following clinical scenarios is most consistent with the MRI scan findings at L4-L5?
Explanation
REFERENCE: McCullouch JA, Transfeldt EE: Macnab’s Backache, ed 3. Philadelphia, PA, Williams and Wilkins, 1997, pp 569-608.
Question 10
A patient has a painful metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with prognosis if this patient is having a reaction to metal debris?
Explanation
Painful MOM THA and taper corrosion can cause substantial damage to a patient's hip if left untreated. In this case, the workup for a painful MOM THA starts the same as a workup for a painful metal-on-polyethylene bearing couple. Infection must be ruled out in every case with a set of inflammatory markers. If these markers are remotely elevated, this is an indication for joint aspiration. In patients with metal debris, the pathology report often indicates too many cells to count or cellular debris. Metal ion levels do not seem to correlate with prognosis. There are well-functioning patients with high ion levels and poor-functioning patients with low ion levels. Advanced imaging with MARS MRI to evaluate for peritrochanteric fluid collection, a soft-tissue mass, or synovial/capsular hypertrophy will reveal signs of a metal reaction that indicate the need for a revision discussion. A CT scan can show more advanced bony destruction as an indicator of poor prognosis. These films can be used to determine the need for a structural graft or augments for reconstruction of bone loss attributable to metal debris.
Question 11
A 23-year-old man has had heel pain and fullness for the past several months. He reports that initially the pain was present only with activity, but more recently the pain has become constant. Figures 53a through 53d show a radiograph, a bone scan, and T2-weighted and gadolinium MRI scans. What is the most likely diagnosis?
Explanation
bone cyst.
REFERENCES: Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
Dorfman HD, Czerniak B: Bone Tumors. St Louis, MO, Mosby, 1998, pp 855-879.
Question 12
A patient who is an observant Jehovah’s Witness requires major surgery for scoliosis that will likely result in significant blood loss. Which of the following might the patient consider allowing the surgical team to use?
Explanation
REFERENCES: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
www.watchtower.org. Official Web Site of Jehovah’s Witnesses. Link verified as active as of August 8, 2008.
Question 13
A 24-year-old man is ejected from his motorcycle and sustains a significant hip injury. The fracture shown in Figures 64a through 64e is best described as what type of fracture?
Explanation
REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. New York, NY, Springer-Verlag, 1993, pp 115-140.
Beaule PE, Dorey FJ, Matta JM: Letournel classification of acetabular fractures: Assessment of interobserver and intraobserver reliability. J Bone Joint Surg Am 2003;85:1704-1709.
Question 14
- A healed fracture of the tibia that demonstrates 25 degrees apex posterior angulation and 28 degrees varus angulation on AP and lateral radiographs is most accurately described as a
Explanation
Question 15
In the nonsurgical management of posterior tibial tendon dysfunction with flexible deformity, a common strategy is to prescribe an ankle-foot orthosis or a University of California Biomechanics Laboratory (UCBL) orthosis with medial posting. A high patient satisfaction rating and favorable outcome with this nonsurgical management is most likely in which of the following situations?
Explanation
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Noll KH: The use of orthotic devices in adult acquired flatfoot deformity. Foot Ankle Clin 2001;6:25-36.
Question 16
A 40-year-old laborer sustains the injury shown in the radiograph and CT scan in Figures 56a and 56b. What is the most common complication associated with surgical intervention?
Explanation
REFERENCES: Sanders R: Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.
Sanders R, Fortin P, DiPasquale T, et al: Operative treatment in 120 displaced intra-articular calcaneal fractures: Results using a prognostic computed tomography scan classification. Clin Orthop Relat Res 1993;290:87-95.
Question 17
A 27-year-old male competitive soccer player reports a 1-year history of pain in the adductor region that has prevented him from playing. Examination reveals tenderness about the adductor attachment to the pelvis, and pain at the same site with resisted contraction of the adductors. There is no tenderness over the hip joint and no signs of a sports hernia. Radiographs are normal. MRI does not show any evidence of enthesopathy. What is the next best step in management?
Explanation
REFERENCES: Schilders E, Bismil Q, Robinson P, et al: Adductor-related groin pain in competitive athletes: Role of adductor enthesis, magnetic resonance imaging, and entheseal pubic cleft injections. J Bone Joint Surg Am 2007;89:2173-2178.
Robinson P, Barron DA, Parsons W, et al: Adductor-related groin pain in athletes: Correlation of MR imaging with clinical findings. Skelet Radiol 2004;33:451-457.
Question 18
Which of the following factors is most likely to contribute to pseudarthrosis in a patient who has undergone a single-level anterior decompression and fusion procedure for the treatment of cervical radiculopathy? Review Topic
Explanation
diabetes mellitus, have been shown to significantly increase pseudarthrosis rates. The literature has been mixed with regard to fusion rates for allograft versus autograft, especially for one-level fusions; in that category, there is minimal, if any, difference. Similarly, several authors have shown higher rates of fusion with uninstrumented single-level rather than instrumented anterior cervical decompressions and fusions. The level (ie, cranial or caudal) of fusion and sagittal alignment have not been correlated with fusion rates.
Question 19
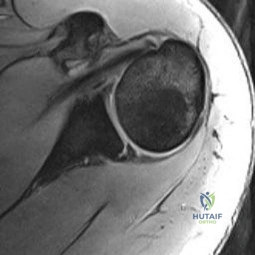
A 37-year-old man has left shoulder pain and weakness. Coronal T1- and axial T2-weighted MRI scans are shown in Figures 17a and 17b. The biopsy specimen is shown in Figure 17c. What is the most likely diagnosis?
Explanation
REFERENCES: Ferrick MR, Marzo JM: Suprascapular entrapment neuropathy and ganglion cysts about the shoulder. Orthopedics 1999;22:430-434.
Post M: Diagnosis and treatment of suprascapular nerve entrapment. Clin Orthop 1999;368:92-100.
Question 20
A 17-year-old quarterback reports shoulder pain localized over the anterior aspect of the shoulder that occurs during the follow through phase of throwing. The pain worsens toward the end of the game, but becomes asymptomatic the next day. He denies any pain during the cocking phase of throwing or during normal daily activities. Examination reveals a negative relocation test and a negative posterior load and shift test. Motion of the shoulder is normal. An MRI arthrogram is shown in Figure 75. Based on the history, examination, and MRI findings, what initial treatment should be recommended? Review Topic
Explanation
Question 21
A man who weighs 75 kg (165 pounds) is scheduled for elective total hip arthroplasty. He reports a history consistent with anaphylaxis from penicillin. Within 1 hour of the incision the patient should receive 1000 mg of
Explanation
Question 22
03 A patient with carpometacarpal joint arthritis of the thumb undergoes trapezium excision and interposition arthroplasty. One year after treatment, radiographs reveal that there has been 25% subsidence of the thumb metacarpal compared with its preoperative height. This degree of subsidence will have what effect on the surgical outcome?
Explanation
pinch stress causes a large amount of axial compressive force through the CMC joint. They also compared preoperative and postoperative functional measurements, including key pinch strength, tipto-tip pinch strength, grip strength, and thumb ROM. Their findings were that postoperatively the first metacarpal subsided 21% at rest (p=0.001). and it subsided another 10.5% during maximal lateral key pinch. Even with this degree of subsidence, the patients experienced increases in pinch strength and grip strength. Also, all patients except for one who had bony impingement reported that they were subjectively much better and more functional.
Lin et. al. also studied trapezium excision and interposition arthroplasty and found no significant differences between results in patients with varying degrees of subsidence. Thus, subsidence does not affect the results of interposition arthroplasty for basal thumb arthritis.
back to this question next question
Question 23
A 19-year-old rugby player has severe knee pain after being injured in a game 2 weeks ago. Examination reveals a knee effusion, limited motion, and increased 3+ Lachman’s test and anterior drawer. There is also increased external rotation at 30 degrees of knee flexion when the patient is placed in the prone position. Based on these findings, which of the following actions would most likely increase the risk of anterior cruciate ligament (ACL) reconstruction failure?
Explanation
REFERENCES: Veltri DM, Warren RF: Posterolateral instability of the knee. J Bone Joint Surg Am 1994;76:460-472.
Covey DC: Injuries of the posterolateral corner of the knee. J Bone Joint Surg Am
2001;83:106-118.
Question 24
Figure 46 shows the radiograph of a 65-year-old man who reports restricted range of motion and pain with sitting 18 months after undergoing right side revision total hip arthroplasty. What is the most appropriate management? L Intensive physiotherapy
Explanation
REFERENCES: Board TN, Karva A, Board RE, et al: The prophylaxis and treatment of heterotopic ossification following lower limb arthroplasty. J Bone Joint Surg Br 2007;89:434-440.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative
Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Question 25
A 22-year-old man has mild hip pain bilaterally and multiple skeletal lesions. Based on the pelvic radiograph shown in Figure 30, what is the inheritance pattern for his disorder?
Explanation
REFERENCES: Stieber JR, Dormans JP: Manifestations of hereditary multiple exostoses. J Am Acad Orthop Surg 2005;13:110-120.
Hilton MJ, Gutierrez L, Martinez DA, et al: EXT1 regulates chondrocyte proliferation and differentiation during endochondral bone development. Bone 2005;36:379-386.
Question 26
A 25-year old right-hand dominant professional baseball pitcher complains of posteromedial right elbow pain that is worsened by throwing. He also reports occasional paresthesias in his small and ring finger after lengthy bullpen sessions. On examination, he is tender along the medial olecranon and complains of pain when extending the elbow >- 20° of extension. He has negative valgus stress, moving valgus stress, and milking maneuver tests. He is stable to varus stress, chair rise, and lateral pivot shift tests. Radiographs reveal a small osteophyte along the posteromedial border of the olecranon. What is the most likely diagnosis?
Explanation
A. Lateral head of triceps (radial nerve) and brachialis
(musculocutaneous nerve)
B. Lateral head of the triceps (radial nerve) and biceps brachii
(musculocutaneous nerve)
C. Lateral brachialis (radial nerve) and medial brachialis
(musculocutaneous nerve)
D. Brachialis (musculocutaneous nerve) and coracobrachialis
(musculocutaneous nerve)
Question 27
Which intervention most effectively prevents surgical-site infections following spine surgery?
Explanation
The use of IV antibiotics for prophylaxis of surgical-site infection is supported by Level 1 evidence in spine surgery. It has been given a "B" recommendation by the North American Spine Society. The use of specific bathing solutions the day of surgery may be beneficial, but the evidence in spine surgery is lacking. Similarly, evidence for use of vancomycin (either topically or IV) is not supported by high-level studies, although retrospective and basic science studies support topical vancomycin use.
RECOMMENDED READINGS
Brown MD, Brookfield KF. A randomized study of closed wound suction drainage for extensive lumbar spine surgery. Spine (Phila Pa 1976). 2004 May 15;29(10):1066-8. PubMed PMID: 15131430. View Abstract at PubMed
Diab M, Smucny M, Dormans JP, Erickson MA, Ibrahim K, Lenke LG, Sucato DJ, Sanders JO. Use and outcomes of wound drain in spinal fusion for adolescent idiopathic scoliosis. Spine (Phila Pa 1976). 2012 May 15;37(11):966-73. doi: 10.1097/BRS.0b013e31823bbf0b.
PubMed PMID: 22037527. View Abstract at PubMed
Evaniew N, Khan M, Drew B, Peterson D, Bhandari M, Ghert M. Intrawound vancomycin to prevent infections after spine surgery: a systematic review and meta-analysis. Eur Spine J. 2014 May 18. [Epub ahead of print] PubMed PMID: 24838506. View Abstract at PubMed Rubinstein E, Findler G, Amit P, Shaked I. Perioperative prophylactic cephazolin in spinal surgery. A double-blind placebo-controlled trial. J Bone Joint Surg Br. 1994 Jan;76(1):99-
Question 28
below depicts the radiograph obtained from a year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing pain. What is the best current technique for total hip arthroplasty?
Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 29
-If a physician elects to shorten a femur by 4 cm for traumatic bone loss treatment and places an intramedullary nail for fixation, which deformity will be created in the lower extremity?
Explanation

Question 30
Figures 6a and 6b are the radiographs of a thin 23-year-old man who sustained a closed injury to his left arm in a fall. He has no other injuries and his

Explanation
Question 31
A 15-year-old boy with a type I hereditary sensory motor neuropathy (Charcot-Marie-Tooth disease) reports recurrent ankle sprains and significant pain in the hindfoot and midfoot despite orthotic management. Examination reveals that he walks with a drop foot and has dynamic clawing of the toes. Clinical photographs of the left foot are shown in Figure 7. Management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 235-245.
Coleman SS: Complex Foot Deformities in Children. Philadelphia, Pa, Lea & Febiger, 1983, pp 147-165.
Thometz JG, Gould JS: Cavus deformity, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 32
An 80-year-old man with a history of chronic obstructive pulmonary disease (COPD) and dementia is involved in a fall from standing height, striking his forehead. He is seen in the emergency department with predominantly mechanical neck pain but no obvious neurologic deficits. Radiographs reveal a nondisplaced type II odontoid fracture. What is the most appropriate treatment? Review Topic
Explanation
Question 33
A 70-year old woman undergoes revision total knee arthroplasty for tibial component aseptic loosening. She is concerned about recurrent loosening, and tibial stem fixation options during revision are reviewed. Figure below displays a radiograph of the revision technique used for this patient. What is the incidence of intraoperative tibial shaft fracture that is associated with this type of revision surgery?

Explanation
Using press-fit tibial stems during a hybrid revision total knee arthroplasty is associated with a 3% to 5% incidence of intraoperative tibial shaft fracture. Diaphyseal fixation of press-fit stems has the advantage of setting component alignment, dispersing forces on the proximal tibia, and offers excellent clinical results. The disadvantages include proximal and distal tibia anatomic mismatch and tibial shaft fracture. Cipriano and associates reported a tibial shaft fracture incidence of 4.9% in a series of 420 consecutive
knee revisions. All fractures healed with nonsurgical management, and none led to implant loosening. In this patient, it is important to recognize on the radiograph that this technique is a hybrid method of revision total knee arthroplasty, with cementation along the tibial tray and metaphysis and with press-fit fixation of the diaphyseal engaging stem. Then, it is important to know the risk and management of intraoperative diaphyseal tibial fractures. Cemented tibial stems are associated with a low rate of intraoperative fracture, because the implant is typically undersized to allow for an appropriate cement mantle. Option C is incorrect, because this revision is not cemented. Option A underestimates the incidence of fracture, whereas D overestimates the rate of fracture.
Question 34
Figures 1 through 3 show the MRI images and a radiograph obtained from a 31-year-old woman who has a 1-year history of diffuse right wrist pain that is gradually worsening. She denies fever or chills and also denies a history of injury. Her examination reveals no swelling, no erythema, an 80 degree arc of active wrist flexion and extension, and dorsal wrist tenderness. The most likely diagnosis is
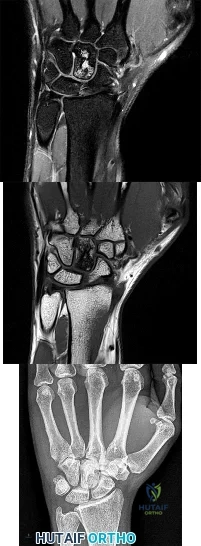
Explanation
Question 35
New painful paresthesias near the site of the incision after an ulnar nerve transposition is the result of injury to what nerve?
Explanation
REFERENCE: Dellon AL, Mackinnon SE: Injury to the medial antebrachial cutaneous nerve during cubital tunnel surgery. J Hand Surg Br 1985;10:33-36.
Question 36
-A 45-year-old woman sustained a fall from height and has the injury shown in Figures 135a and 135b.A 3-dimensional reconstruction CT scan is shown in Figure 135c. Joint-spanning external fixation is applied on the day of injury. Ten days later, her skin is acceptable for definitive fixation. What is the most appropriate type of fixation for her fracture?
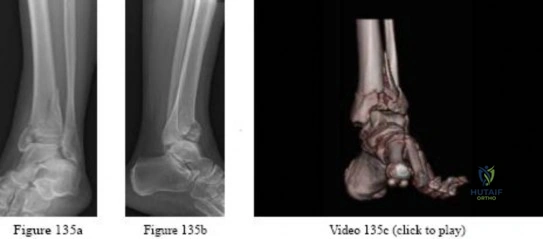
Explanation

Question 37
A 3-year old child from an isolated mountain area is evaluated for multiple medical problems, including vomiting, loss of appetite, polyuria, and failure to thrive. History reveals the child was normal at birth. The parents, who appear healthy, are second cousins and have two other children who are normal. The parents state that they know of another family member who died at age 6 years after a similar medical history. Radiographs of the lower extremities show bowing of the long bones with cupping and widening of the physes. What is the most likely diagnosis?
Explanation
hemolytic anemia, rhabdomyolysis, and hepatocellular injury that began during refeeding and resolved with treatment. The signs and symptoms, pathophysiology, and treatment of refeeding hypophosphatemia are reviewed.
Renal Osteodystrophy-Musculoskeletal complications in patients with chronic renal failure are common and may be related to the disease itself or to treatment. The altered metabolism in patients with chronic renal failure leads to renal osteodystrophy, which consists of osteomalacia and secondary hyperparathyroidism [1]. Erosive changes attributable to secondary hyperparathyroidism may be easily confused with rheumatoid arthritis, seronegative spondyloarthropathies, infection, or even malignancy.
Primary Hyperparathyroidism-Preferential involvement of cortical bone with apparent preservation of cancellous bone in primary hyperparathyroidism was confirmed by percutaneous bone biopsy. Over 80% of patients had a mean cortical width below the expected mean, whereas cancellous bone volume in over 80% of patients was above the expected mean.
Skeletal disease in primary hyperparathyroidism J Bone Miner Res 1989 Jun; 4(3):283-91
Nutritional vitamin D deficiency-Rickets, osteomalacia, and renal osteodystrophy are disorders of the mineralization of bone that result from a lack of available calcium, phosphorus, or both. The diseases that result from numerous mechanisms present with a symptom-sign-radiographic complex with such a high degree of stereotypy that laboratory investigation is often required to distinguish one form from another. The disorders in children, known as rickets, produce bowing and other deformities of the long bones and dwarfism. These disorders are principally related to the profound effect of the deficiency states on the epiphyseal plate; whereas the same disorders in adults produce an often severe osteopenia and pathologic fractures. Because of newer developments in our understanding of the factors affecting calcium-phosphorus
hemostasis and vitamin D metabolism, many of the children and Rickets, osteomalacia, and renal osteodystrophy.
Question 38
An axial T 1 -weighted MRI scan of the pelvis is shown in Figure 35. Which of the following structures is enclosed by the circle?
Explanation
REFERENCES: Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, et al (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
Berquist TH: Pelvis, hips and thigh, in Berquist TH (ed): MRI of the Musculoskeletal System,
ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 210-238.
Question 39
Which of the following illustrations shown in Figures 21a through 21e correctly shows the projection of the sacroiliac joint on the outer table of the ilium?
Explanation
REFERENCES: Waldrop JT, Ebraheim NA, Yeasting RA, Jackson WT: The location of the sacroiliac joint on the outer table of the posterior ilium. J Orthop Trauma 1993;7:510-513.
Xu R, Ebraheim NA, Yeasting RA, Jackson WT: Anatomic considerations for posterior iliac bone harvesting. Spine 1996;21:1017-1020.
Question 40
A 60-year-old woman with a history of osteoporosis fell from a standing height and sustained a supracondylar distal humerus fracture with an intercondylar extension. Which of the following plate constructs yields the highest stiffness for fixation of the fracture?
Explanation
Question 41
Which of the following is a true statement regarding thoracic disk herniations? Review Topic
Explanation
common in the lower third near the thoracolumbar region. Posterior laminectomy and disk excision has the highest rate of neurologic deterioration and is not recommended. Multiple studies have shown that herniated thoracic disks can be found at one or more levels in 40% of asymptomatic individuals.
Question 42
A 24-year-old woman who has hypotension, a head injury, and who experienced a poor response to resuscitation has been taken to the operating room for a splenectomy. Following abdominal surgery she remains unstable with increasing pulmonary respiratory pressures and decreasing oxygen saturation. She has a transverse mid-diaphyseal fracture of the tibia with a 4-cm laceration and soil-contaminated muscle in the wound. Based on these findings, management should consist of
Explanation
REFERENCES: Bosse MJ, Kellam JF: Orthopaedic management decisions in the multiple trauma patient, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 151-164.
Weresh MJ, Stover MD, Bosse MJ, Jeray K, Kellam JF: Pulmonary gas exchange during intramedullary fixation of femoral shaft fractures. J Trauma 1999;46:863-868.
Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 43
The clinical factors shown to most significantly predict the long-term outcome of Perthes disease of the hip include which of the following? Review Topic
Explanation
(SBQ13PE.87) A 4-week-old child is suspected to have classic arthrogryposis, also known as amyoplasia. Clinical examination and hip ultrasound reveal a unilateral, non-reducible, hip dislocation. What do you recommend to reduce the hip? Review Topic
Pavlik harness application
Semi-rigid abduction brace application
Skeletal traction
Early closed reduction and spica casting
Delayed open reduction with or without pelvic and femoral osteotomy
Delayed open reduction with or without pelvic and femoral osteotomy is recommended in the management of unilateral hip deformities associated with amyoplassia. This procedure should be performed at 6-9 months of age. In order to proceed with reduction, there must be a reasonable arc of flexion/extension and active movement of the lower limbs.
Amyoplasia is the most common recognizable form of arthrogryposis. It most commonly occurs as a sporadic symmetric contracture syndrome that is characterized by symmetrical limb involvement, normal to above-average intelligence, and often a midline facial hemangioma. Approximately 80% of children with amyoplasia will have involvement of the hip ranging from soft tissue contractures to unilateral or bilateral hip dislocations.
Bevan et al. reviewed arthrogryposis. They state that open hip reduction is recommended for the management of unilateral dislocation. There is more controversy with regard to the treatment of bilateral hip dislocations. Open reduction can be performed by a medial or anterolateral approach, with or without pelvic and
femoral osteotomy. This procedure is generally delayed for 6-9 months to facilitate the procedure.
Bernstein et al. also reviewed arthrogryposis. They state that the term 'arthrogryposis' encompasses a broad spectrum of diseases, all with the common phenotype of multiple congenital contractures.
Illustration A shows the characteristic features of an infant with severe arthrogryposis. Note the internal rotation of the shoulders, elbow and knee hyperextension, flexed and ulnarly deviated wrists, flexed finger, external rotation of hips and bilateral clubfeet.
Incorrect answers:
Question 44
Figures below show the radiographs obtained from a 79-year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. No evidence of infection is seen. What is the most appropriate treatment?

Explanation
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis, as shown in Figures 3 and 4. They also assist in obtaining correct limb alignment. Short metaphyseal-engaging stems are associated with failure rates that range between 16% and 29%. Cemented stems may be shorter than press-fit stems, because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.
Question 45
In the anterior cruciate ligament-deficient knee, what structure provides an important secondary restraint to anterior tibial translation? Review Topic
Explanation
Question 46
Which of the following therapies has a direct anabolic effect on bone?
Explanation
Question 47
Which of the following radiographic images is best for detecting anterior acetabular deficiency in the dysplastic hip?
Explanation
REFERENCES: Garbuz DS, Masri BA, Haddad F, et al: Clinical and radiographic assessment the young adult with symptomatic dysplasia. Clin Orthop Relat Res 2004;418:18-22.
Delauney S, Dussault RG, Kaplan PA, et al: Radiographic measurements of dysplastic adult hips. Skelelal Radiol 1997;26:75-81.
Question 48
A 56-year-old man has a chief complaint of leg weakness and inability to walk. Examination reveals 5 out of 5 motor strength in all lower extremity muscle groups tested and normal sensation to light touch in both lower extremities. The patient is slow in getting up from a seated position and has an unsteady wide-based

Explanation
Question 49
A 54-year-old woman with idiopathic carpal tunnel syndrome undergoes open carpal tunnel release with a flexor tenosynovectomy. The pathology from the tenosynovium is likely to show
Explanation
REFERENCES: Shum C, Parisien M, Strauch RJ, et al: The role of flexor tenosynovectomy in the operative treatment of carpal tunnel syndrome. J Bone Joint Surg Am 2002;84:221-225.
Fuchs PC, Nathan PA, Myers LD: Synovial histology in carpal tunnel syndrome. J Hand Surg Am 1991;16:753-758.
Kerr CD, Sybert DR, Albarracin NS: An analysis of the flexor synovium in idiopathic carpal tunnel syndrome: Report of 625 cases. J Hand Surg Am 1992;17:1028-1030.
Question 50
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5° of angulation. When the MCP joint is flexed 30°, a radially directed stress produces 45° of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
REFERENCES: Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint.
J Am Acad Orthop Surg 1997;5:224-229.
Question 51
Figure 1 points to the "tear drop" of the wrist. This radiographic landmark represents which anatomic portion of the wrist?

Explanation
Question 52
Sciatic nerve
Explanation
The principal thrombogenic stimulus leading to the production of venous thromboembolic disease during total hip arthroplasty occurs at which time:
Question 53
A 56-year-old man underwent right total shoulder arthroplasty 2 months ago. Recently while reaching with his shoulder in a flexed and adducted position, he noted shoulder pain and afterwards he could not externally rotate his arm. An axillary radiograph is shown in Figure 30. What is the most likely cause of this problem?
Explanation
REFERENCES: Cofield RH, Edgerton BC: Total shoulder arthroplasty: Complications and revision surgery. Instr Course Lect 1990;39:449-462.
Wirth MA, Rockwood CA Jr: Complications of total shoulder replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Question 54
Figure 34 shows the standing AP radiograph of a 2-year-old girl who has a left bowleg deformity. Her mother states that she first noticed the problem when the child began walking at age 10 months, and the deformity has worsened over the past 6 months. Examination reveals a definite lateral thrust of the knee during the stance phase of gait. Management should consist of
Explanation
REFERENCES: Zionts LE, Shean CJ: Brace treatment of early infantile tibia vara. J Pediatr Orthop 1998;18:102-109.
Richards BS, Katz DE, Sims JB: Effectiveness of brace treatment in early infantile Blount’s disease. J Pediatr Orthop 1998;18:374-380.
Raney EM, Topoleski TA, Yaghoubian R, Guidera KJ, Marshall JG: Orthotic treatment of infantile tibia vara. J Pediatr Orthop 1998;18:670-674.
Question 55
An 11-year-old boy sustained an ankle injury while playing football. Figure 20 shows an AP radiograph obtained the day of injury. Treatment should consist of
Explanation
REFERENCES: Cass JR, Peterson HA: Salter-Harris Type-IV injuries of the distal tibial epiphyseal growth plate, with emphasis on those involving the medial malleolus. J Bone Joint Surg Am 1983;65:1059-1070.
Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibia physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Question 56
A 46-year-old woman reports pain and a shortened appearance of her toe after undergoing a Keller resection arthroplasty 2 years ago for hallux rigidus. Examination reveals mild swelling and motion limited to 25 degrees at the metatarsophalangeal joint. Radiographs show large dorsal osteophytes on the first metatarsal head, 50% resection of the proximal phalanx, and complete loss of the metatarsophalangeal joint space. Which of the following is considered the most reliable procedure to improve her pain and the appearance of her toe?
Explanation
REFERENCES: Myerson MS, Schon LC, McGuigan FX, Oznur A:Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int 2000;21:297-306.
Mann RA, Coughlin MJ: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 252-253.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 293-303.
Question 57
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
REFERENCES: Apple DF: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 1130-1131.
Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 544-545.
Question 58
A 63-year-old woman has a femoral neck fracture. A biopsy specimen obtained from the fracture site at the time of her hemiarthroplasty reveals metastatic carcinoma. Seven days after surgery, she becomes confused and lethargic. Which of the following laboratory values is most likely implicated in the patient’s symptoms at this time?
Explanation
REFERENCES: Clohishy D: Management of skeletal metastasis in clinical orthopaedics, in Craig E (ed): Operative Orthopaedics. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 994-997.
Mundy GR: Hypercalcemia of malignancy revisited. J Clin Invest 1988;82:1-6.
Question 59
All of the following are advantages of supine over lateral positioning during intramedullary nailing of subtrochanteric femur fractures EXCEPT:

Explanation
Advantages of the supine position include: may help protect a potentially unstable spine, facilitates access to sites other than the injured femur, shorter setup time, rotational and angulatory deformities may be more easily appreciated. Disadvantages of the supine position include: starting point localization may be more difficult.
Question 60
A 9-year-old girl has had bilateral knee and leg pain for the past 2 years. The family has noted increasing deformity in both lower extremities. She is less than the fifth percentile for height. Examination reveals bilateral femoral bowing, mild medial-lateral laxity of the knees, and the deformities shown in the radiograph seen in Figure 3. What is the most likely diagnosis? Review Topic

Explanation
Question 61
Figures 150a through 150d are the radiographs and MR images of a 37-year-old woman who has a 3-month history of severe right hip pain. She does not recall any trauma prior to the pain onset and denies any past steroid exposure. She has 3 children and is not currently pregnant. The pain is located in her groin and the onset was sudden. The pain is refractory to anti-inflammatory medications. What is the most appropriate treatment?
Explanation
The patient’s MR images are consistent with transient hip osteoporosis. No signs suggest avascular necrosis. She has no joint narrowing. Transient osteoporosis of the hip is characterized by bone marrow edema in the femoral head and neck. This condition affects more men than women and is sometimes seen in the third trimester of pregnancy but can be seen in women who are not pregnant as well. This is a self-limiting condition, and the treatment is limited weight-bearing activity until the symptoms resolve. Core decompression is rarely used in these cases. There is no indication for arthroplasty or osteotomy in this scenario.
Question 62
CLINICAL SITUATION Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. Initial surgical management should consist of

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair,
but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 63
In infantile idiopathic scoliosis, which of the following factors suggests progression?
Explanation
REFERENCES: Mehta MH: The rib-vertebra angle in the early diagnosis between resolving and progressive infantile scoliosis. J Bone Joint Surg Br 1972;54:230-243.
Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, p 697.
Question 64
An otherwise healthy 45-year-old man has a 3-cm subcutaneous mass on his anterior thigh that is presumed to be a lipoma. Removal of the mass is performed in the office of his primary care physician. Pathologic evaluation shows a high-grade malignant fibrous histiocytoma. Staging reveals no evidence of metastatic disease. Management at this time should consist of
Explanation
REFERENCES: Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173.
Giuliano AE, Eilber FR: The rationale for planned reoperation after unplanned total excision of soft-tissue sarcomas. J Clin Oncol 1985;3:1344-1348.
Lewis JJ, Leung D, Espat J, Woodruff JM, Brennan MF: Effect of resection in extremity soft tissue sarcoma. Ann Surg 2000;231:655-663.
Noria S, Davis A, Kardel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 65
A 30-year-old man reports pain and weakness in his right arm. Examination reveals grade 4 strength in wrist flexion and elbow extension, decreased sensation over the middle finger, and decreased triceps reflex. These symptoms are most compatible with impingement on what spinal nerve root?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Upper Saddle River, NJ, Prentice Hall, 1976, p 125.
Lauerman WC, Goldsmith ME: Spine, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 353-378.
Question 66
Figure below depicts the radiograph obtained from a 52-year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?
Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 67
A 1-year-old infant has the hand deformities shown in Figure 40. What pathologic process is the most likely cause of these deformities?
Explanation
REFERENCE: Foulkes GD, Reinker K: Congenital constriction band syndrome: A seventy-year experience. J Pediatr Orthop 1994;14:242-248.
Question 68
A 32-year-old amateur bowler has progressive pain in the lateral aspect of the proximal forearm and elbow. Nonsurgical management consisting of a tennis elbow brace, nonsteroidal anti-inflammatory drugs, and activity modification has failed to provide relief. Examination reveals tenderness in the lateral aspect of the proximal forearm and exacerbation of symptoms with resisted finger extension. Radiographs of the elbow reveal no abnormalities. Which of the following studies will aid in diagnosis?
Explanation
REFERENCES: Eversmann WW Jr: Entrapment and compression neuropathies, in Green DP (ed): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingston, 1993, pp 1341-1385.
Sarhadi NS, Korday SN, Bainbridge LC: Radial tunnel syndrome: Diagnosis and management. J Hand Surg Br 1998;23:617-619.
Question 69
Based on the MR arthrogram of the elbow shown in Figure 8, which of the following structures is torn?
Explanation
MR arthrography provides improved sensitivity compared to conventional MRI, without contrast, for the detection of UCL pathology, particularly in the subacute or chronic setting. After the soft-tissue edema and joint fluid associated with the injury have resolved, the torn end of the ligament may lie in contact with its adjacent attachment and create a false-negative appearance. In this patient, a noncontrasted MR arthrogram showed no tear, yet the tear is apparent with intra-articular contrast and distention. MR arthrography of the elbow also may be useful in detecting intra-articular bodies or in evaluation for loose osteochondral fragments or flaps.
REFERENCES: Morrey BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128.
Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 200-210.
Question 70
A 16-year-old high school pitcher notes acute pain on the medial side of his elbow during a pitch. Examination that day reveals medial elbow tenderness, pain with valgus stress, mild swelling, and loss of extension. Plain radiographs show closed physes and no fracture. Which of the following diagnostic studies will best reveal his injury?
Explanation
REFERENCES: Timmerman LA, Andrews JR: Undersurface tear of the ulnar collateral ligament in baseball players: A newly recognized lesion. Am J Sports Med 1994;22:33-36.
Timmerman LA, Schwartz ML, Andrews JR: Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography: Evaluation of 25 baseball players with surgical confirmation. Am J Sports Med 1994;22:26-32.
Fritz RC, Stoller DW: The elbow, in Stoller DW (ed): Magnetic Resonance Imaging in Orthopedics and Sports Medicine, ed 2. Philadelphia, PA, Lippincott Raven, 1995, pp 743-849.
Question 71
Which of the following patients requires preoperative noninvasive cardiac testing?
Explanation
REFERENCES: Bushnell BD, Horton JK, McDonald MF, et al: Perioperative medical comorbidities in the orthopaedic patient. J Am Acad Orthop Surg 2008;16:216-227.
Auerback A, Goldman L: Assessing and reducing the cardiac risk of noncardiac surgery. Circulation 2006;113:1361-1376.
Fischgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 105-113.

Question 72
A 26-year-old man is brought to the emergency department unresponsive and intubated after being found lying on the side of the road. He has a Glasgow Coma Scale score of 6. A chest tube has been inserted on the right side of the chest for a pneumothorax. An abdominal CT scan reveals a small liver laceration and minimal intraperitoneal hematoma. A pneumatic antishock garment (PASG) is on but not inflated. He has bilateral tibia fractures. A pelvic CT scan shows an anterior minimally displaced left sacral ala fracture and left superior and inferior rami fractures. He has received 2 L of saline solution and 4 units of blood but remains hemodynamically unstable. What is the next most appropriate step in management?
Explanation
REFERENCES: Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: Effective classification system and treatment protocols. J Trauma 1990;30:848-856.
Evers BM, Cryer HM, Miller FB: Pelvic fracture hemorrhage: Priorities in management. Arch Surg 1989;124:422-424.
Flint L, Babikian G, Anders M, Rodriguez J, Steinberg S: Definitive control of mortality from severe pelvic fracture. Ann Surg 1990;211:703-707.
Question 73
A 55-year-old man who underwent total shoulder arthroplasty 10 years ago recently reports an increase in shoulder pain. Laboratory studies consisting of a white blood cell count, erythrocyte sedimentation rate, and C-reactive protein are all negative, as is joint aspiration. Radiographs are shown in Figures 95a and 95b. If all intraoperative frozen sections are negative, what is the appropriate treatment during revision surgery to provide pain relief and improved function? Review Topic
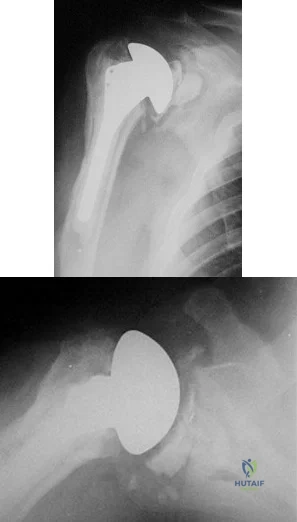
Explanation
Question 74
Which of the following is the most relevant clinical factor in the maturation assessment of an adolescent female athlete contemplating anterior cruciate ligament (ACL) reconstruction?
Explanation
REFERENCES: Micheli LJ, Foster TE: Acute knee injuries in the immature athlete. Instr Course Lect 1993;42:473-481.
Stanitski CL: Anterior cruciate ligament injury in the skeletally immature patient: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:146-158.
Fowler PJ: Anterior cruciate ligament injuries in the child, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2067-2074.
Question 75
Figures 74a through 74c are the postsurgical radiographs of a 74-year-old man who has stiffness in his right knee 8 weeks after undergoing elective right total knee arthroplasty (TKA). The surgery was performed for primary varus osteoarthritis and was uncomplicated. His range of motion is 5 to 80 degrees. What is the most appropriate next treatment step?
Explanation
Stiffness following TKA is a disabling complication. One option involves MUA, a valuable technique with which to increase range of motion after TKA for patients with stiff knees. A systematic review of the literature was performed to identify studies that reported the clinical outcomes and measured range of motion for patients undergoing MUA. Fourteen studies (913 patients) reported range of motion results following MUA at up to 10-year followup. The review demonstrated that MUA for a stiff primary TKA is an efficacious procedure to restore range of motion, and it carries a low complication rate. Early gains in motion were
reported to be maintained in the long term. A second review systematically evaluated the outcomes of 4 treatments for arthrofibrosis that develops subsequent to TKA (MUA, arthroscopic debridement, open surgical release, and revision TKA). This study showed that there were no significant differences in the Knee Society Score of the 4 treatment modalities. Although open surgical release resulted in the greatest increase in range of motion, there were methodological study limitations because the majority of the papers were case series, which decreased the quality of the evidence. Response 1 is correct because the TKA appears appropriately sized and is well aligned. Responses 2 and 3 are incorrect, considering the early time frame (8 weeks) from initial surgery. Although the patella is unresurfaced in the radiographs, there is no indication for revision TKA (even secondary patellar resurfacing) at this early juncture.
Question 76
Figures 46a through 46d are the injury radiographs and postsurgical open treatment radiographs of a 13-year-old girl who fell while on a trampoline and sustained an injury to her right-dominant elbow. The skin is closed and she has normal vascular and neurologic examination findings. Which complication most likely could occur as a result of this injury and treatment?
Explanation
This girl sustained a fracture dislocation of the elbow with a severely displaced and rotated radial neck fracture. Required treatment was open reduction and internal fixation (ORIF). Less severely displaced radial neck fractures can be treated with closed reduction, percutaneous pinning, or flexible nail manipulation. In this scenario, interposed capsular tissue and rotation of the radial head were indications for ORIF. ORIF is associated with a higher risk for poor
outcomes. Complications following ORIF of radial neck fractures in children include posterior interosseous neuropraxia, valgus angulation, premature closure of the radial head physis, AVN of the radial head, nonunion, and elbow stiffness. Stiffness is most common. Compartment syndrome, infection, and anterior interosseous nerve palsy are less common complications.

CLINICAL SITUATION FOR QUESTIONS 47 THROUGH 50
A 6-year-old boy arrives at the emergency department with forearm pain. Today he was picking up his backpack when he felt a pop in his forearm that resulted in the current injury. His history is significant for 6 other fractures treated nonsurgically. His mother states that she had 15 fractures during childhood but is healthy now. Both the boy and his mother have blue sclera. Figures 47a and 47b are the radiographs of his injured forearm.
Question 77
An infant is born with a mass that involves both the volar and dorsal compartments of the left arm. A clinical photograph and biopsy specimen are shown in Figures 41a and 41b. What is the best initial course of action?
Explanation
REFERENCE: Kurkchubasche AG, Halvorson EG, Forman EN, Terek RM, Ferguson WS: The role of preoperative chemotherapy in the treatment of infantile fibrosarcoma. J Pediatr Surgery 2000;35:880-883.
Question 78
A 45-year-old man who smokes reports the rapid onset of color changes and coolness in the fingers. Examination shows an abnormal Allen test. Plain radiographs of the hand and wrist are normal. Which of the following studies will best aid in diagnosis?
Explanation
REFERENCES: Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2288-2290.
Manske PR (ed): Hand Surgery Update. Rosemont, IL, American Society for Surgery of the Hand, 1994, pp 197-205.
Question 79
A professional baseball team has several pitchers with complaints of velocity loss with their pitches and shoulder pain of their dominant shoulders during spring training. Pitch counts are properly monitored. The average glenohumeral internal rotation deficit on the pitching staff is 45 degrees. The best intervention would be: Review Topic
Explanation
GIRD is a phenomenon that is frequently found in high-level overhead throwing athletes, predominantly baseball pitchers. It is defined as the measured difference in internal rotation between the non-dominant arm and dominant arm. Worsening range of motion deficits are seen with increased repetitions, both over a single season and a career. GIRD > 25º is associated with development of shoulder pathologies or pain requiring periods of inactivity. Cessation of overhead throwing activities and initiation of a stretching program to address posterior capsular contractures is largely effective (90% in some series).
Burkhart et al. reviewed the conditions associated with high-level overhead throwing athletes shoulders, culminating in a theory of pathologic progression to "dead arm syndrome" (loss of velocity and effective pitching). Their theory attributes adaptive hyperexternal rotation (occurs during late-cocking / early acceleration phases of pitching) to lead to posterior-inferior capsular contracture and GIRD. Subsequent injuries to anterior structures - including SLAP lesions - would then occur.
Illustration A is a cartoon depiction of how to perform the sleeper stretch. This is a common component of a pitcher's maintenance stretching program.
Incorrect Answers:
Question 80
An 8-year-old girl was treated for a Salter-Harris type I fracture of the right distal femur 2 years ago. Examination reveals symmetric knee flexion, extension, and frontal alignment compared to the contralateral knee. She has 1-cm of shortening of the right femur. History reveals that she has always been in the 50th percentile for height, and her skeletal age matches her chronologic age. Radiographs are shown in Figure 9. What is the expected consequence at maturity?
Explanation
REFERENCES: Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphysiodesis. J Pediatr Orthop 1996;16:173-179.
Moseley CF: Assessment and prediction in leg-length discrepancy. Instr Course Lect 1989;38:325-330.
Question 81
A 34-year- woman has pain at the base of the thumb that worsens é pinching activities. Nonsurgical treatment has failed to provide relief. Examination reveals that the basilar joint is hypermobile, tender and painful when stressed. A radiograph of the trapeziometacarpal joint shows normal contour with widening when compared with the opposite side. Management should consist of
Explanation
Question 82
A 35-year-old man has profound deltoid weakness after sustaining a traumatic anterior shoulder dislocation 6 weeks ago. Electromyographic (EMG) studies confirm an axillary nerve injury. Follow-up examination at 3 months reveals no recovery of function. What is the best course of action?
Explanation
REFERENCES: Perlmutter GS: Axillary nerve injury. Clin Orthop 1999;368:28-36.
Artico M, Salvati M, D’Andrea V, et al: Isolated lesions of the axillary nerves: Surgical treatment and outcome in twelve cases. Neurosurgery 1991;29:697-700.
Vissar CP, Coene LN, Brand R, et al: The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery: A prospective clinical and EMG study. J Bone Joint Surg Br 1999;81:679-685.
Pasila M, Jarma H, Kiviluoto O, et al: Early complications of primary shoulder dislocations. Acta Orthop Scand 1978;49:260-263.
Question 83
Figures 3a and 3b show the current radiographs of a 58-year-old man who underwent total knee arthroplasty with a cruciate ligament sparing prosthesis 7 years ago. Examination reveals boggy synovitis and moderate pain, particularly anteriorly. Management should consist of
Explanation
REFERENCE: Brassard MF, Insall JN, Scuderi GR: Complications of total knee arthroplasty, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1801-1844.
Question 84
A 45-year-old woman has had right wrist pain for the past 2 months. A radiograph, bone scan, and MRI scan are shown in Figures 66a through 66c, and a photomicrograph is shown in Figure 66d. What is the most likely diagnosis?
Explanation
REFERENCES: Cheng CY, Shih HN, Hsu KY, et al: Treatment of giant cell tumor of the distal radius. Clin Orthop Relat Res 2001;383:221-228.
Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 263-284.
Question 85
Which of the following tendons is the primary antagonist of the posterior tibialis tendon?
Explanation
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 550-551.
Mann RA: Biomechanics of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 2-36.
Question 86
Anterior approach
Explanation
The nerve most commonly injured in the posterior approach to the hip is the sciatic nerve. Overall injury prevalence is 1% to 2%. This nerve is more commonly injured in cases of hip dysplasia with excessive leg lengthening. The superior gluteal nerve is at highest risk with the direct lateral approach to the hip. This nerve courses in the gluteus medius muscle and is
at risk when splitting the muscle 5 cm proximal to the greater trochanter. The lateral femoral 73
cutaneous nerve is commonly damaged with anterior total hip replacement surgery. Neuropraxia has been reported in 81% of patients. The inferior gluteal nerve travels from the greater sciatic notch and enters the gluteus maximus muscle. It is at risk when the posterior approach to the hip is used.
RECOMMENDED READINGS
Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia.
PA: Lippincott Williams & Wilkins; 2003:365-453.
DeHart MM, Riley LH Jr. Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg. 1999 Mar-Apr;7(2):101-11. Review. PubMed PMID: 10217818. View Abstract at PubMed
Goulding K, Beaulé PE, Kim PR, Fazekas A. Incidence of lateral femoral cutaneous nerve neuropraxia after anterior approach hip arthroplasty. Clin Orthop Relat Res. 2010 Sep;468(9):2397-404. doi: 10.1007/s11999-010-1406-5. PubMed PMID:
Question 87
An active 68-year-old woman undergoes an uncomplicated rotator cuff repair with a double-row construct using biocomposite knotless anchors. At her two month follow up, she is noted to have increased shoulder pain, weakness and limited motion. Imaging reveals failure of the rotator cuff repair. What is the most likely mechanism of failure? Review Topic
Explanation
The overall complication rate of arthroscopic RCR is roughly 10%. Failed RCR most commonly results from failure to heal (19-94%) secondary to poor rotator cuff tissue, insufficient vascularity or poor bone quality. Other causes of RCR failure include surgical complications (deltoid disruption, infection, foreign body reaction, stiffness, neurologic injury), diagnostic errors (missed lesions of the rotator interval, long head of biceps or subscapularis tear), and technical errors (excessive tension due to lack of proper tissue mobilization, anchor pull out secondary to improper anchor placement).
George et al evaluated the causes of failed RCR and results of revision RCR. While results of revision RCR are inferior to primary RCR, arthroscopic repair yields > 60% good or excellent results. Risk factors for poor results following revision RCR include poor tissue quality, detachment of the deltoid origin and multiple previous surgeries.
Diduch et al reviewed the design and composition of various anchors used in arthroscopic shoulder surgery. Current advancements in the field include high-strength polyethylene sutures, new biocompatible anchor materials (PEEK, biocomposite) and modified designs including knotless systems. With improved strength of the current anchors and repair constructs, the most common mode of arthroscopic RCR failure is now related to tissue failure occurring at the tissue-anchor interface.
Cole et al discussed the different primary rotator cuff repair constructs, including single row, double row, transosseous and transosseous equivalent. The authors concluded that construct selection depends on tear acuity, size and tissue quality. For acute tears < 12mm in anteroposterior length, single-row configuration likely has sufficient strength to maintain the repair and promote healing. For more chronic tears, poor tissue quality, or tears > 12-15mm in the anteroposterior dimension, the authors recommend double-row or transosseous-equivalent repair to better restore the anatomic footprint and provide optimal mechanical stability to achieve healing.
Illustration A is an algorithm from George et al detailing the decision-making process when considering revision RCR for a symptomatic failed RCR.
Incorrect Responses
Question 88
When posterior fusion with instrumentation to the sacrum is used to treat adult scoliosis, what instrumentation technique best increases the chance of a successful lumbosacral fusion?
Explanation
REFERENCES: Islam NC, Wood KB, Transfeldt EE, et al: Extension of fusions to the pelvis in idiopathic scoliosis. Spine 2001;26:166-173.
O’Brien N, et al: Sacral pelvic fixation and spinal deformity, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 601-614.
McCord DH, Cunningham BW, Shono Y, et al: Biomechanical analysis of lumbosacral fixation. Spine 1992;17:S235-S243.
Question 89
A 62-year-old woman with a bone mass density (BMD) T-score of -2.0 sustained a subcapital fracture of her hip. She is an avid tennis player, and history reveals no previous fractures. What is the most appropriate follow-up care?
Explanation
REFERENCE: Gardner MJ, Brophy RH, Demetrakopoulos D, et al: Interventions to improve osteoporosis treatment following hip fracture: A prospective, randomized trial. J Bone Joint Surg Am 2005;87:3-7.
Question 90
Figure 36 shows the hip arthrogram of a newborn. Which of the following structures is enclosed by the circle?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA,
WB Saunders, 2002, vol 1, pp 532-533.
Severin E: Contribution to the knowledge of congenital dislocation of the hip joint.
Acta Chir Scand 1941;84:1.
Question 91
A 47-year-old woman has had a 1-month history of left hip and medial thigh pain that is exacerbated by sitting. Laboratory studies show a total protein level of 8.2 g/dL (normal 6.0 to 8.0) and an immunoglobulin G (IGG) level of 2,130 mg/dL (normal 562 to 1,835). A radiograph, CT scan, and biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 16.
Question 92
Histologic studies of surgically resected tissue in lateral epicondylitis demonstrate which of the following findings? Review Topic
Explanation
Question 93
A 75-year-old woman reports persistent severe low back pain after lifting a bag of groceries 8 weeks ago. She denies the presence of any lower extremity pain, weakness, or other symptoms. AP and lateral lumbar spine radiographs are shown in Figures 47a and 47b. For further evaluation, what imaging study should be obtained next? Review Topic
Explanation
Question 94
A 38-year-old left hand-dominant bodybuilder reports ecchymosis in the left axilla and anterior brachium after sustaining an injury while bench pressing 3 weeks ago. Coronal and axial MRI scans are shown in Figures 16a and 16b. What treatment method yields the best long-term results? Review Topic
Explanation
Question 95
Surgical treatment for symptomatic disk herniations is associated with which of the following?
Explanation
REFERENCE: Weinstein JN, Lurie JD, Tosteson TD, et al: Surgical vs nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006;296:2451-2459.
Question 96
Osteonecrosis of the humeral head is a rare complication seen after dislocation of the glenohumeral joint in skeletally immature patients. When this complication is encountered, treatment should consist of Review Topic
Explanation
Question 97
A 20-year-old collegiate pitcher has had a 5-month history of shoulder pain while throwing, decreased velocity, and difficulty with location of his pitches despite multiple attempts at rest. He reports no traumatic event. Examination with his throwing arm abducted at 90 degrees reveals external rotation to 110 degrees and internal rotation to 70 degrees when compared with his nonthrowing shoulder which has external rotation to 95 degrees and internal rotation to 85 degrees. He has a positive O'Brien's sign, positive modified Jobe's relocation test, full rotator cuff strength, no obvious muscular atrophy, and no scapular winging. Radiographs of the affected shoulder show no abnormalities. What is the next most appropriate step in management? Review Topic
Explanation
Question 98
A 52-year-old man who dislocated his dominant shoulder has it reduced in the emergency department and he is placed in a sling. At his 5-day followup evaluation, he reports that this is his first shoulder dislocation and that the pain is mostly gone but he notes difficulty using his arm overhead and away from his body. Examination reveals minimal pain with passive range of motion, a positive apprehension and relocation test, and 3/5 strength with the empty can test and external rotation at the side compared with 5/5 with those tests on the contralateral side. Cutaneous sensation over the lateral aspect of the shoulder is intact. Radiographs show the glenohumeral joint is reduced with no fractures or degenerative changes. What is the next step in management? Review Topic
Explanation
cuff tears following dislocation in young individuals warrants early surgical intervention. Delay of surgical repair for large, full-thickness tears may lead to irreversible changes, including atrophy and retraction of the tendon. As a result, clinical outcomes may be compromised. CT will demonstrate bony changes, but it is not as effective as MRI for soft-tissue pathology. While in the short term a sling for comfort might be helpful, 6 weeks of immobilization is unnecessary because recurrent instability is rarely an issue. Physical therapy can be beneficial but could potentially delay identification of an acute rotator cuff tear. In the event the MRI does not reveal a large, full-thickness rotator cuff tear, physical therapy would be an appropriate next step. There is no indication for urgent shoulder arthroscopy.
Question 99
A 35-year-old man has a brachial plexus injury affecting the lateral cord. He partially improves with observation and now has complete return of median nerve function and pectoral muscle function. What nerve transfer is most likely to restore the motor function he is lacking?
Explanation
The lateral cord of the brachial plexus gives off the lateral pectoral nerve, the musculocutaneous nerve, and then contributes to the median nerve. The patient has had recovery of function of these components except for the musculocutaneous nerve. The musculocutaneous nerve innervates the biceps and the brachialis, which provide elbow flexion. To restore motor function, a nerve transfer would have to provide reinnervation of the biceps and brachialis.
Question 100
A 24-year-old professional football player underwent surgery for a symptomatic cervical disk herniation with radiculopathy 9 months ago. A current radiograph is shown in Figure 17. He has normal neurologic findings, no pain, and full range of motion. A CT scan shows a solid fusion. When can he expect to return to play?
Explanation
REFERENCES: Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
Torg JS, Ramsey-Emrhein JA: Management guidelines for participation in collision activities with congenital, developmental, or post-injury lesions involving the cervical spine. Clin Sports Med 1997;16:501-530.
