Orthopedic Board Review MCQs: Deformity, Hip & Nerve Surgery | Part 173

Key Takeaway
This page offers Part 173 of a comprehensive Orthopedic Surgery Board Review MCQ bank by Dr. Mohammed Hutaif. It features 100 verified, high-yield questions, accurately modeled for OITE and AAOS/ABOS board certification exams. Designed for residents and surgeons, it provides critical exam preparation with detailed explanations covering Deformity, Hip, and Nerve topics.
About This Board Review Set
This is Part 173 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 173
This module focuses heavily on: Deformity, Hip, Nerve.
Sample Questions from This Set
Sample Question 1: A 16-year-old girl has had anterior leg pain and a mass for the past 8 months. Figures 2a and 2b show a radiograph and an H & E histologic specimen. Which of the following disorders is believed to be a precursor of this lesion?...
Sample Question 2: A 24-year-old man has bilateral hip pain. An examination and imaging studies (plain radiographs and MR imaging) confirm evidence of femoroacetabular impingement (FAI) with a CAM deformity in both hips. The patient mentions that he has a 19-...
Sample Question 3: 30%...
Sample Question 4: Haversian canals are found in the center of an osteon in compact bone. They contain blood vessels and nerves....
Sample Question 5: A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5° of angulation. When t...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 16-year-old girl has had anterior leg pain and a mass for the past 8 months. Figures 2a and 2b show a radiograph and an H & E histologic specimen. Which of the following disorders is believed to be a precursor of this lesion?
Explanation
REFERENCE: Springfield DS, Rosenberg AE, Mankin HJ, et al: Relationship between osteofibrous dysplasia and adamantinoma. Clin Orthop 1994;309:234-244.
Question 2
A 24-year-old man has bilateral hip pain. An examination and imaging studies (plain radiographs and MR imaging) confirm evidence of femoroacetabular impingement (FAI) with a CAM deformity in both hips. The patient mentions that he has a 19-year-old brother who has occasional hip pain. With respect to his brother’s pain, how should you counsel the patient?
Explanation
Evidence suggests that FAI is more common in siblings of patients with FAI, particularly those with a CAM deformity. It is unlikely this patient has well-established osteoarthritis, even in the presence of FAI.

CLINICAL SITUATION FOR QUESTIONS 145 THROUGH 147
Figures 145a and 145b are the radiographs of a 56-year-old man who has had persistent pain in his right groin since undergoing primary total hip surgery 11 months ago. His erythrocyte sedimentation rate (ESR) is 38 mm/h (reference range [rr], 0-20 mm/h) and C-reactive protein (CRP) level is 28 mg/L (rr, 0.08-3.1 mg/L). A hip aspiration performed while the patient was taking antibiotics demonstrated 3200 white blood cells/µL with no growth. Treatment should consist of
Question 3
30%
Explanation
Initial assessment of a trauma patient should involve evaluation of airway, breathing and circulation. An average adult has approximately 5 L of circulating blood volume. Class III and IV hemorrhagic shock, approximated by loss of greater than 30% of blood volume, typically requires resuscitation with fluids and blood products. Lactate level (normal <2.5) is typically the most sensitive indicator of adequate perfusion.
According to ATLS guidelines, the emphasis of the initial assessment is to assume the worst injury and begin treatment before diagnosis. In cases of hemorrhagic shock, treatment involves aggressive resuscitation with crytalloid and/or blood products.
Illustration A is a chart showing the physiological changes associated with different levels of hemorrhagic shock
Incorrect Answers:
1: Blood loss of <15% typically leads to no changes in vital signs
2: Blood loss of 15-30% typically leads to heart rate >100 and diminished urine output
4, 5: Blood loss of greater than >40% typically leads to heart rate >140, decreased blood pressure and negligible urine output.

OrthoCash 2020
Which of the following fracture patterns would be most appropriately treated with open reduction and internal fixation with posteromedial and lateral plates via dual incisions?

The patient in Figure D has a bicondylar tibial plateau fracture with a posteromedial fracture fragment, which is an indication for lateral and posteromedial plating via dual incisions.
Bicondylar tibial plateau fractures are typically treated with open reduction internal fixation. Studies have shown that the posteromedial fragment is common in bicondylar tibial plateau fractures. Standard lateral implants do not gain adequate screw purchase in posteromedial bone. Posteromedial incisions using the interval between the semimembranosus and medial head of the gastrocnemius can be used to gain access to the fragment and provide exposure to place a posteromedial plate.
Barei et al. reviewed 57 OTA C-type bicondylar tibial plateau fractures, and found the presence of a posteromedial fragment in 74% of cases. They suggest
the use of alternate methods of fixation for the posteromedial fragment rather than lateral fixed-angle plates alone.
Higgins et al. reviewed 111 patients with bicondylar tibial plateaus that underwent CT scan evaluation. They found the incidence of a posteromedial fragment in 59% of the patients and on average accounted for 25% of the articular surface.
Barei et al. reviewed 83 patients treated with dual incisions for fixation of bicondylar tibial plateau fractures. They found deep infections in 8.4% of patients. Satisfactory articular reduction was found in 62% of patients, satisfactory coronal alignment in 91% of patients, satisfactory sagittal alignment in 72%, and satisfactory condylar width in 98%.
Figure A shows an AP and lateral radiograph of a split/depressed lateral tibial plateau fracture. Figure B shows an AP and lateral radiograph of a proximal third tibial shaft fracture with a proximal fibula fracture. Figure C shows an AP and lateral radiograph of a medial plateau fracture with articular depression. Figure D shows an AP and lateral radiograph of a bicondylar tibial plateau fracture. Figure E shows an AP and lateral radiograph of a tibial tubercle fracture in a tibia with open physes.
Incorrect Answers:
OrthoCash 2020
Figure A shows the radiographs of a 87-year-old patient after a fall from standing. He lives in a nursing home and uses a walker to transfer from bed to chair. His past medical history includes recurrent urinary tract infections, congestive heart failure, angina and diabetes. Which of the following factors is associated with the best postoperative outcome in this patient?

Immediate surgical intervention
Postoperative epidural analgesia
Postoperative antibiotics
Pre-operative medical optimization
Choosing total hip arthroplasty instead of hemiarthroplasty Corrent answer: 4
Geriatric patient with hip fractures tends to have a number of coexisting medical conditions that impact surgical risk. A successful pre-operative medical evaluation has the greatest impact on surgical outcomes in this patient population.
Patients with complex past medical histories are at great risk of complications with surgery. This helped to drive the formation of the ASA classification system as a way to score patients out of 5 based on their anesthetic and surgical risks. Patients with significant systemic disease (ASA III and IV) have shown to demonstrate poorer outcomes as compared to patients with less severe medical comorbidities (ASA I and II).
Egol et al. looked at factors that impact the outcomes of hip fractures in geriatric patients. They showed that cardiac and pulmonary complications were most frequent complications post-operatively. It was stated that early mobilization and pre-operative evaluations have the greatest impact on outcomes.
Parvizi et al. looked at the thirty-day mortality following hip arthroplasty for acute fracture. They reviewed a database of 7774 consecutive patients that underwent hip arthroplasty for the treatment of an acute fractures. The overall mortality was 2.4%. Risk factors were found to be cemented implants, female patients, elderly patients, and patients with cardiorespiratory comorbidities.
Roberts et al reviewed the 2015 AAOS Clinical Practice Guideline: Management of Hip Fractures in the Elderly. Although pre-operative medial optimization was not mentioned in this review, there is strong evidence to support an interdisciplinary care program for patients with hip fractures.
Figure A shows a displaced left femoral neck fracture. Incorrect Answers:
more than 24-48 hours and a higher 1-year mortality rate. However, In patients with with more than 3 medical comorbidities, medical optimization has a greater impact on post-operative outcomes than time to surgery.
OrthoCash 2020
A 36-year-old male sustains severe injuries as a result of a motor vehicle collision. After 5 days, the patient is stabilized and transferred to your facility for continued management. After obtaining appropriate imaging, including the images shown in Figures A, B and C the patient should be given which of the following mobility restrictions?

Touch-down weight bearing on the left lower extremity, non-weightbearing on the right lower extremity
Weight bearing as tolerated on the left lower extremity, non-weightbearing on the right lower extremity
Non-weight bearing on the left lower extremity, non-weightbearing on the right lower extremity
Touch-down weight bearing on the left lower extremity, weight bearing as tolerated on the right lower extremity
Weight bearing as tolerated on the left lower extremity, weight bearing as tolerated on the right lower extremity
Figures B and C shows a stable, impacted lateral compression (LC) type I injury, which can be treated with immediate mobilization without restrictions. The right lower extremity has a pilon fracture, which should be treated with non-weight bearing.
LC-I injuries are stable patterns, as they involve an impaction injury to the anterior sacrum, which has some inherent stability. In addition, the posterior sacro-iliac (SI) soft tissue structures remain intact, which provides critical stability during immediate mobilization.
The reference by Tile is a review article on the principles of management of these injuries, and he reviews how the Tile classification system is important to help determine surgical need and where the stabilization is required. For the stable LC-1 type injury, no fixation is required.
Incorrect Answers:
OrthoCash 2020
A 24-year-old male sustains the fracture dislocation shown in Figure A. How is this fracture pattern best classified?
Moore I
Moore II
Schatzker III
Schatzker V
OTA type 41B3 Corrent answer: 2
Figure A shows a Moore Type II fracture. Moore type II fractures consist of fractures involving the entire tibial condyle, where the fracture line begins in the opposite compartment and extends across the tibial eminence.
A number of classification systems are used to describe tibial plateau fractures. The main classification systems that are widely used include Schatzker, AO/OTA, Hohl and Moore. The Moore classification describes high energy fracture-subluxation injuries of the knee. This is thought to have clinical implications as the type of fracture pattern can indicate an associated soft-
tissue injury.
Moore retrospectively reviewed over a 1000 proximal tibia fractures to devise a classification systems based on the characteristic of five types of tibia plateau fracture patterns. He believed this system helped to better understand knee instability and concomitant soft-tissue injury. For example, Moore Type III fractures (rim avulsion) are associated with a high rate of neurovascular injury.
Figure A shows a fracture involving the entire tibial condyle. Illustration A shows a schematic diagram of the Moore classification (I - V). Illustration B shows a table that describes the Moore classification (I - V).
Incorrect Answers:

OrthoCash 2020
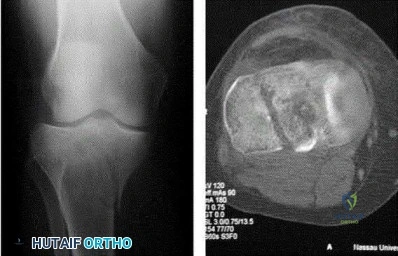
A 19-year-old male football player plants and twists his right lower extremity sustaining a spiral fracture of his distal third tibial shaft. Of the following images, which is most commonly associated with distal third spiral tibial shaft fractures.
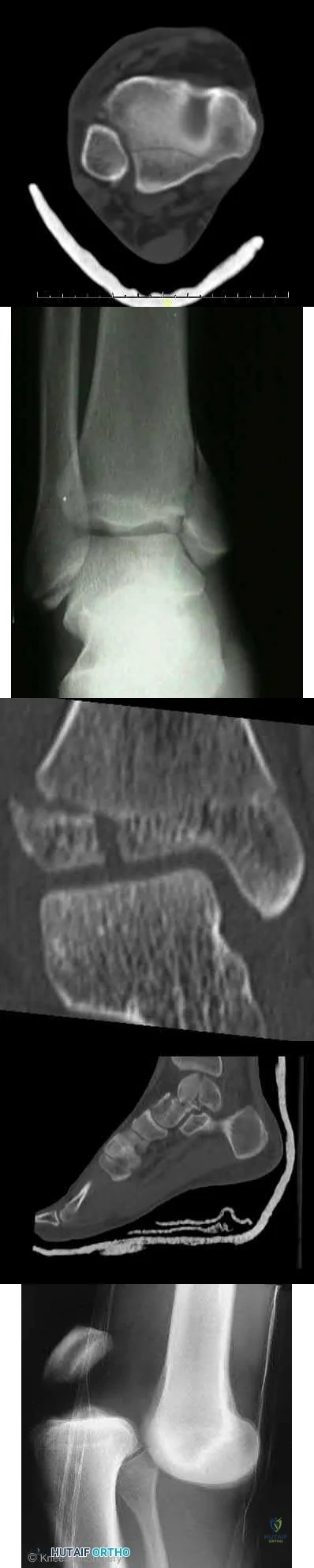
The patient has a spiral distal tibial shaft fracture. Spiral distal tibial shaft fractures are commonly associated with intraarticular fracture extension, usually in the form of a posterior malleolus fracture.
Spiral distal third tibial shaft fractures need to be evaluated for intraarticular extension prior to operative management. As this can be missed on x-rays, a CT scan of the ankle is recommended to identify this associated injury. This is important when intramedullary fixation is used for definitive management, as nail insertion can displace a previously non displaced intraarticular fracture.
Anteroposterior screw fixation prior to nailing may be useful in these cases.
Boraiah et al. found that in 62 patients with spiral distal tibial fractures, 39% (24 patients) had a posterior malleolus fracture. They recommended CT evaluation of the ankle to prevent missed intraarticular fractures.
Hou et al. found a posterior malleolus fracture in 9.7% (28 out of 288 cases) of patients with tibial shaft fractures. They recommended CT or MRI evaluation of the ankle prior to surgery.
Figure A shows an axial CT scan of a right ankle with a posterior malleolus
fracture. Figure B shows an AP radiograph of a right ankle with a vertical medial malleolus fracture. Figure C shows a coronal CT scan of a right ankle with a Tillaux fracture. Figure D shows a sagittal CT scan of a right ankle with a comminuted talus fracture. Figure E shows a lateral radiograph of a right knee showing a knee dislocation. Illustration A shows an AP radiograph of a left distal third spiral/oblique tibial shaft fracture. Illustration B shows a lateral radiograph of a left distal third spiral/oblique tibial shaft fracture. Illustration C shows a sagittal CT of a distal third spiral/oblique tibial shaft fracture with a posterior malleolus fracture.
Incorrect Answers:

OrthoCash 2020
A 67-year-old female patient presents with increasing right hip/thigh pain over the past three months, which is now recalcitrant to anti-inflammatories. There is no history of trauma or constitutional symptoms. Her past medical history consists of hypertension, coronary artery disease, osteoporosis and gastric reflux. Physical examination reveals mild pain at the extremes of range of motion of the hip and a painful right sided limp. A radiograph of the right hip is seen in Figure
What would be the most appropriate treatment for this patient at this time?

Observation only
Referral to physiotherapy
MRI spine and hip
Total hip arthroplasty
Intramedullary femoral nail Corrent answer: 5
This osteoporotic female patient is presenting with subtrochanteric lateral cortical thickening and hip pain. This is consistent with an insufficiency fracture of the femur secondary to use of bisphosphonate medication for treatment of osteoporosis. The most appropriate treatment would be intramedullary femoral nail fixation.
Bisphosphonate medications have been shown to be associated with atypical (subtrochanteric) femur fractures. These patients often have prodromal hip pain and lateral cortical thickening on radiographs prior to fracture. In addition, there has shown to be a significantly increased risk of fracture in the presence of the “dreaded black line” that occurs at the site of thickening.
Lenart et al. examined a case series of patients using bisphosphonates for the treatment of osteoporosis. They identified 15 postmenopausal women who had
been receiving alendronate for a mean (±SD) of 5.4±2.7 years and who presented with atypical low-energy fractures. Cortical thickening was present in the contralateral femur in all the patients with this pattern.
Goh et al. retrospectively reviewed patients who had presented with a low-energy subtrochanteric fractures. They identified 13 women of whom nine were on long-term alendronate therapy. Five of these nine patients had prodromal pain in the affected hip in the months preceding the fall, and three demonstrated a stress reaction in the cortex in the contralateral femur.
Figure A shows a right hip radiograph with subtrochanteric lateral cortical thickening. There is mild arthritic changes in the hip. Illustration A shows a bone scan and radiographs of subtrochanteric lateral cortical thickening that resulted in fracture.
Incorrect Answers

OrthoCash 2020
A right-hand dominant female sustains a right proximal humerus fracture. The patient is provided a sling, and is recommended pendulum exercises with elbow range of motion to begin in 1 to 2
weeks. Which of the following would be an indication for surgical management?

Age greater than 70 years.
Fracture pattern in Figure A
Significant medical comorbidities.
Fracture pattern in Figure B
Fracture pattern in Figure C
The patient has been treated with non-operative management for her proximal humerus fracture. Operative management should be considered in patients with head splitting proximal humerus fractures and in those with dislocations that cannot be reduced.
Head splitting proximal humerus fractures should be treated with operative management. Open reduction internal fixation versus hemiarthroplasty are used to treat this type of fracture. Surgical management is also considered in proximal humerus fractures in young patients, in fractures where the greater tuberosity is displaced >5 mm, and in proximal humerus fractures associated with humeral shaft fractures.
Koval et al. studied 104 patients with one-part proximal humerus fractures treated non-operatively, and found 80% with good or excellent results. They also found that 90% of patients treated non-operatively had either no or mild pain about the shoulder at follow-up.
Lefevre-Colau et al. performed a randomized prospective study on 74 patients with an impacted proximal humerus fracture. One group was treated with early mobilization of the shoulder (within 3 days after the fracture) while the other group was immobilized for 3 weeks followed by physiotherapy. They concluded that early mobilization was safe and allowed for quicker return to functional use of the affected limb.
Figure A shows an AP radiograph of a right minimally displaced greater tuberosity proximal humerus fracture. Figure B shows AP and axillary radiographs of a right head split proximal humerus fracture that is posteriorly dislocated. Figure C shows an AP radiograph of a right minimally displaced Salter Harris II proximal humerus fracture. Illustration A shows an AP radiograph of a left valgus impacted proximal humerus fracture with a greater tuberosity fragment displaced >5mm treated with ORIF.
Incorrect Answers:

OrthoCash 2020
A 37-year-old male arrives to the trauma slot following a high-speed motorcycle crash. His Glasgow Coma score is 14 and his only orthopaedic injury is exhibited in Figure A. His current vital signs are a BP of 90/60, HR 120, and a lactate of 2.5 mMol/L. Other findings include a grade 1 splenic laceration and bilateral pulmonary contusions seen on chest radiograph. Which of the following has been suggested as an indication to perform damage control orthopedic care?

HR >110
Bilateral pulmonary contusions seen on chest radiograph
SBP = 90mmHg
Unilateral femur fracture
Lactate = 2.5 mMol/L
Pulmonary contusion severe enough to be diagnosed on chest radiograph alone is an indicator that the patient may benefit from damage control orthopaedics (DCO).
Despite the patient's overall stable nature, suffering pulmonary injury severe enough to be seen on x-ray alone suggests that temporary stabilization with staged definitive fixation may avoid potential morbidity.
Pape et al. review the evolution and balance of early total care (ETC) and DCO. Summarizing the literature, the authors report several standalone indicators that would justify DCO regardless of stable status. This includes: Injury Severity Score of greater than 40, Injury Severity Score of greater than 20 with chest trauma, multiple injuries with severe pelvic/abdominal trauma/ hemorrhagic shock, bilateral femoral fractures, pulmonary contusion noted on radiographs alone, hypothermia of less than 35 degrees C), and a head injury with an Abbreviated Injury Score of 3 or greater.
Figure A exhibits a right femoral shaft fracture. Illustration A exhibits a summarized table stating the criterion used to determine the condition of a polytrauma patient. (Table from Pape et al, PMID: 19726738)
Incorrect answers:
implement DCO.

OrthoCash 2020
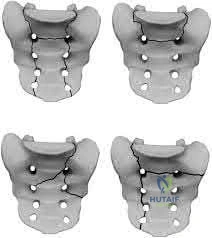
A 24-year-old patient presents after a fall from the balcony of a third story building in which he landed on his feet. He reports lumbar back pain and numbness in his perineum region. Radiographs of his hips and pelvis are seen in Figure A, while CT images are shown in Figures B and C. How is this fracture pattern best classified?

Young-Burgess APC Type II
Young-Burgess LC Type I
"U" Type Spinopelvic Dissociation
Denis Zone-I
Denis Zone-II
This patient has a Denis zone-III "U" Type Spinopelvic Dissociation of the sacrum.
The Denis classification system for sacral fractures is based on anatomical fracture zones. Zone-III fractures involve the spinal canal and have a high rate of associated neurologic injury. It is important to recognize bilateral sacral
fractures with a transverse component, as this often causes spinopelvic discontinuity and possible cauda equina. The lack of mechanical continuity between the spine and pelvis will most likely require reduction and fixation for initial stability. There may also be a need for sacral decompression with fixation mechanisms given the onset of neurologic symptoms.
Mehta et al. reviewed sacral fractures. They report that patients with a transverse sacral fracture involving more proximal sacral segments (S1, S2, or S3) tend to have a higher prevalence of bladder dysfunction than do those involving distal sacral segments (S4 or S5).
Schildhauer et al. report the best way to visualize Denis zone-III "U" type fractures is to obtain a lateral view of the sacrum or sagittal reformatted images with a CT scan. Standard pelvic radiographs often miss this injury.
Figure A shows an AP pelvis with suggestion of sacral irregularities. No fracture pattern can be indentified. Figures B and C show CT scan images showing a "U" Type fracture pattern with angulation and translational displacement of the cephalad and caudad parts of the sacrum. Illustration A shows examples of complex sacral Denis zone-III fractures.
Incorrect Answers:
OrthoCash 2020
A 55-year-old male presents with the radiographs seen in Figures A and B after falling off his bike. Physical examination reveals an isolated, closed elbow injury. His limb is neurovascularly intact. Which complication would be most likely with surgical fixation of this injury?

Ulnar neuropathy
Posterior interosseous nerve injury
Early loss of fixation
Elbow flexion contracture
Avascular necrosis
This patient is presenting with a comminuted capitellar and trochlear fracture. If treated with open reduction internal fixation, the most likely post-operative complication would be elbow stiffness or contracture.
An axial compression force transmitted by the radial head to the capitellum with the elbow in a semiflexed position can result in a shear fracture of the anterior portion of the capitellum. AP, lateral, and radiocapitellar radiographs are recommended to identify these injuries. The lateral X-ray may reveal the “double arc” sign, which represents extension of the capitellum fracture into the trochlea. Extension of the fracture into the trochlea has important implications into the surgical approach to these injuries.
Ruchelsman et al. retrospectively reviewed the outcomes of sixteen patients with capitellar fractures treated with open reduction internal fixation. They found the presence of greater flexion contractures at the time of follow-up in elbows with Type-IV capitellar fractures. All fractures healed, and no elbows had instability or weakness with fixation.
Ring et al. retrospectively reviewed the outcomes of twenty one distal humerus articular fractures that were reduced and stabilized with implants buried beneath the articular surface. Ten patients required a second operation: (6) release of an elbow contracture; (2) treatment of ulnar neuropathy; (1) removal of hardware; (1) early loss of fixation.
Figures A and B show AP and lateral radiographs of the elbow with a comminuted fracture of the capitellum and trochlea. Note the “double arc” sign on the lateral view. Illustrations A and B show open reduction internal fixation of the fracture. Note fixation with multiple interfragmentary screws.
Incorrect Answers:

OrthoCash 2020
Figure A shows a radiograph of a 30-year-old male who underwent fixation of a left leg injury just over two years ago. He presents with persistent pain and drainage from the distal wound despite 4 months of oral antibiotics. He has no systemic symptoms. He has a past medical history of Grave's disease and Irritable Bowel Syndrome. What would be the best management at this stage?

Chronic suppressive, culture-directed, antibiotic therapy
Above knee amputation
Endocrine consultation, irrigation and debridement, removal of hardware and negative-pressure wound therapy
Irrigation and debridement, removal of hardware, over-reaming medullary canal, external fixation and culture-directed antibiotics
Irrigation and debridement, retention of hardware, acute bone grafting and culture-directed antibiotics
This is a case of fracture nonunion in the setting of chronic osteomyelitis and infected hardware. The best treatment option available would be irrigation and debridement, removal of hardware, ring external fixator and culture directed antibiotics.
The management of infected nonunion in the setting of chronic osteomyelitis is technically demanding. The aims of treatment are to eradicate the infection and obtain bone union. Non-surgical options are largely unsuccessful in patients with draining chronic osteomyeltis in the setting of infected hardware and nonunion. Surgical options involve incision and debridement of necrotic tissue followed by reconstruction of bone and possible soft tissue (to provide
healthy viable coverage). The most common techniques are ringed fixator/circular frames, staged intramedullary device with or without external fixator, free tissue transfer, or radical debridement, bone grafting, and fixation.
Motsitsi et al. reviewed the management of infected nonunion of long bones. They suggest that the Ilizarov technique is regarded as a standard treatment in infected nonunion of the tibia. When there is bone defect after debridement, the bone can be shortened or treated with bone transport.
Egol et al look at a series of patients with chronic osteomyelitis. Limb salvage should be attempted in all patients. The presence of a chronic draining sinus requires surgical debridement and culture directed antibiotics. Infected hardware should be removed. A two-stage strategy is the best and well-proven treatment option.
Figure A shows a intramedullary nail in the left tibia. There is a moderate amount of bone loss at the fracture site with mixed sclerotic bone suggestive of osteomyelitis.
Incorrect Answers:
OrthoCash 2020
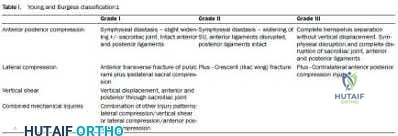
A 32-year-old male sustained the injury seen in Figure A after a motor vehicle accident. Which of the following factors is most predictive of mortality with this type of injury?

Fracture classification
Number of blood transfusions in the first 24 hours
Gender
Time to operative fixation
Use of pelvic binders Corrent answer: 2
The best predictors of mortality with pelvic ring fractures include older age and hemodynamic shock at presentation. The amount of blood transfused indicates the severity of hemodynamic instability.
Pelvic ring fractures are typically high energy, blunt injuries. The leading cause of mortality with these injuries is hemorrhage and hemodynamic instability.
The most common source of hemorrhage include venous injury (80%), which is usually caused by a shearing injury of posterior thin walled venous plexus and bleeding cancellous bone. Other sources of hemorrhage include arterial injury (10-20%) from the superior gluteal artery (posterior ring injury, anterior posterior compression [APC] pattern), internal pudendal artery (anterior ring injury, lateral compression [LC] pattern) and obturator artery.
Smith et al. found fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased Injury Severity Scores (ISS) scores. Deaths were most commonly from exsanguination (<24 hours) or multiorgan failure (>24 hours).
Starr et al. demonstrated that age and shock on presentation were most predictive of mortality after pelvic ring injury.
Figure A shows a APC III pelvic fracture. Illustration A shows a table describing the Young-Burgress classification of pelvic ring fractures.
Incorrect Answers:
OrthoCash 2020
Figure A shows intraoperative radiographs of a 45-year-old patient with a left elbow injury. What would be the next most appropriate step in this patients care?

Early range of motion
Hinged elbow brace for 4 weeks
Repair lateral collateral ligament
Remove and upsize implant
Remove and downsize implant Corrent answer: 5
The intraoperative images are consistent with overstuffing of the ulnohumeral joint during a radial head replacement. The most appropriate next step would be removing and downsizing the implant.
Overstuffing the radiohumeral joint by >2.5 mm can significantly alter elbow kinematics. It has also shown to lead to pain and early joint disease. The most sensitive method to assess for overstuffing of the joint is by direct visualisation intra-operatively. This can be performed by visualising the lateral aspect of the ulnohumeral joint when the radial head is resected and comparing this to when the trial radial head is reduced in place. In comparison, radiographic asymmetry of the medial ulnohumeral joint has been shown to be less sensitive. Radiographic findings of incongruity of ulnohumeral joint only occurs when significant overlengthening of the radius occurs.
Frank et al. examined the effect of radial head thickness in seven cadaver specimens. They found that incongruity of the medial ulnohumeral joint would only become apparent radiographically after overlengthening of the radius by
>or=6 mm.
Doornberg et al. examined seventeen computed tomography scans of the elbow to investigate the height of the radial head relative to the lateral edge and central ridge of the coronoid process. They found that the radial head was on average only 0.9 mm more proximal than the lateral edge of the coronoid process.
Figure A shows intraoperative radiographs of a patient that has undergone a radial head arthroplasty. There is significant widening of the medial ulnohumeral joint on an AP radiograph as well as widening of the ulnohumeral joint on the lateral radiograph,
Incorrect Answers:
OrthoCash 2020
Aside from improving the intramedullary nail starting point in Figure A, the use of blocking screws could have been used at the time of fixation to prevent this post-operative deformity. What would have been the correct orientation of these screw(s) in the proximal fragment?

Medial only
Lateral only
Anterior and medial
Posterior and medial
Posterior and lateral Corrent answer: 5
The clinical presentation is consistent with a malunion of a proximal one-third tibia fracture with a valgus and procurvatum deformity. The correct orientation of Poller blocking screws to help prevent this malalignment would be in the posterior and lateral aspects of the metaphyseal fragment.
Insertion of the blocking screw lateral to the nail prevents valgus deformity, and insertion of the blocking screw posterior to the nail prevents apex anterior deformity. A more lateral starting point for nail insertion can also help to
prevent valgus deformity. The semiextended position of the knee for nail insertion also helps to eliminate the tendency for the fracture to flex, due to the avoidance of excessive knee flexion during the reduction.
Stedtfeld et al. describes the mechanical model for blocking screws. They state that two or more blocking screws can be placed in each plane (AP and lateral) alongside the nail to create a narrow canal for the nail. This allows for multiple points of fixation and realignment of the bone as the nail is passed.
Lindvall et al looked at a series of 56 extra-articular proximal tibial fractures treated with intramedullary nailing or percutaneous locked plating. Neither nailing or plating these fractures showed a distinct advantage in the overall outcomes. Apex anterior malreduction however was the most prevalent form of malreduction in both groups.
Lang et al. looked at a series of proximal third tibia fracture treated with intramedullary nailing. They reported that posterior tibial comminution will also contribute to apex anterior angulation. They states this occurs when the fracture hinges on the intact cortex anteriorly during nail insertion.
Figure A shows a proximal one third tibia fracture treated with an intramedullary nail. There is malreduction of the fracture with valgus and procurvatum deformity.
Incorrect Answers:
OrthoCash 2020
When evaluating a fracture dislocation of the elbow, a varus and posteromedial rotation mechanism of injury typically results in what injury pattern?
A fracture of the radial head requiring ORIF
A highly comminuted radial head fracture requiring radial head arthroplasty or resection
An MCL injury requiring repair
A type I avulsion fracture of the coronoid
An anteromedial coronoid fracture
A varus and posteromedial rotation mechanism of injury typically results in a fracture of the anteromedial facet of the coronoid which frequently requires reduction and fixation to restore stability.
A varus and posteromedial mechanism of injury about the elbow presents with an injury pattern distinctly different from other injury patterns. A key part of treating this injury pattern is recognizing a fracture of the anteromedial facet of the coronoid, which often requires reduction and fixation to restore stability about the elbow. It is important to recognize this during preoperative planning since this injury typically requires a medial approach.
Steinman presents a review article describing coronoid fracture patterns and their mechanisms of injury.
Doornberg and Ring present a level 4 review showing that coronoid fracture patterns and their required treatments are predictable based on mechanism of injury. Varus and posteromedial mechanisms were found to reliably create a fracture of the anteromedial facet of the coronoid, and were associated with sparing of the MCL and radial head.
Doornberg and Ring also presented a Level 3 review of anteromedial facet cornoid fractures. They found that they could not be adequately visualized and treated from a lateral approach, and that they typically required reduction and fixation to restore adequate stability to the elbow. This stresses the importance of recognizing this injury pattern during preoperative planning.
Illustrations A and B are AP and lateral radiographs of an elbow following a varus/posteromedial injury with an anteromedial coronoid facet fracture.
Illustration C is a diagram demonstrating fracture lines that create an anteromedial facet fracture fragment. This fracture can be subclassified into three subtypes [anteromedial rim (a), rim plus tip (b), and rim and tip plus the sublime tubercle (c)]
Incorrect answers:

OrthoCash 2020
A 26-year-old female presented to the emergency department with the injury seen in Figure A after an awkward fall while intoxicated. She undergoes closed reduction and repeat radiographs are seen in Figure B. After a normal physical examination, including ranging the hip from 0-90 degrees, which of the following options would be the next most appropriate step in management?

Femoral skeletal traction
CT scan
Hip spica cast application
Observation only
Serial neurovascular examinations Corrent answer: 2
This patient has presented with a posterior left hip dislocation. The next most appropriate step would be performing a post-reduction CT scan to assess for joint reduction and congruity, associated fractures, or loose bodies.
Hip dislocations occur most commonly in young patients with high energy trauma. They are usually classified as simple or complex, with complex dislocations being those with associated fractures of the acetabulum or proximal femur. Urgent close reduction should occur within 6 hours from the time of injury. Post reduction CT scans must be performed for all traumatic hip dislocations to look for fractures or impacted areas of the femoral head or acetabulum, as well as incongruent reductions and free intra-articular joint fragments.
Calkins et al. looked at measurements of the posterior acetabulum on CT scans (the Acetabular Fracture Index) after hip dislocations to evaluate for hip stability. Hips were found to be unstable if less than 34% of the remaining posterior acetabulum was present after dislocation. Hips with greater than 55% were stable. In between 34 and 55% were indeterminate.
Moed et al. found that posterior wall fractures involving less than 20% of the posterior wall were considered stable. Fractures involving more than 40%-50% were unstable, leaving a wide range of posterior wall fractures classified as indeterminate.
Figure A shows a left posterior hip dislocation. Figure B shows a reduced left hip with no obvious fracture. Illustration A shows an axial CT scan image of the left hip. There is no acetabular fracture identified.
Incorrect Answers:

OrthoCash 2020
A 40-year-old male sustained the injury seen in Figure A, and subsequently underwent the procedure shown in Figure B. One hour post-operatively he starts to complain of pain in the operative leg, and the pain is unchanged with active or passive stretch. The external dressing is released with little resolution of symptoms. His blood pressure is 115/78 mm Hg with compartment pressures in the leg measuring 31 to 35 mm Hg. His ABI index is 1.1 in the leg. What would be the next step in management?

MRI angiography of leg
Four-compartment fasciotomy
Follow-up examination the following day
Continued monitoring and serial examinations
EMG study
The patient is at risk for developing compartment syndrome of the leg. The next most appropriate step would be to support his systemic blood pressure and monitor compartment pressures.
A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam. An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) <30 mm Hg may help to confirm the necessity for fasciotomy. However, the treatment of early compartment syndrome should be to initially improve the limbs perfusion pressure gradient. This can be done by treating underlying factors such as hypotension, coagulopathy, or vascular compromise due to either a true vascular injury or artificially by external compression. Frequent reassessment is then critical to effectively manage these patients. If clinical
diagnosis persists despite these efforts, urgent fasciotomy would be considered.
McQueen looked at 116 patients with tibial diaphyseal fractures who had continuous monitoring of anterior compartment pressure for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of 30 mmHg is a more reliable indicator of compartment syndrome.
White et al. looked at 101 patients with tibial fractures with satisfactory Delta P measurements. THey found that patients with elevated intramuscular pressures >30 mm Hg after tibial fracture do not have a greater incidence of complications than those with low pressures, so long that Delta P <30 mm Hg.
Figure A shows a Shatzker V tibial plateau fracture. Figure B shows fixation of fracture seen in Figure A.
Incorrect Answers:
OrthoCash 2020
A 10-year-old girl suffers a displaced tibia fracture. Initial numbness over the dorsum of the the foot resolved following an anatomic closed reduction and placement in a long leg cast performed in the emergency room. The cast was placed with the the ankle dorsiflexed just above neutral to prevent equinus contracture and then the cast and padding was adequately bivalved. Overnight, the patient began experiencing recurrent numbness and paresthesias in her exposed toes and a slight increase in her pain at the fracture site. Your next best step would be:
Repeat closed reduction under conscious sedation
Selective compartment fasciotomies
External fixation and compartment monitoring
compartment fasciotomies with fracture fixation done emergently
Modify the cast to reposition the ankle into slight plantarflexion Corrent answer: 5
Circumferential casting with the ankle dorsiflexed can cause increased intracompartmental pressures in the leg. However, this patient's cast has been adequately bivalved during initial cast placement. Therefore, the next best step is cast modification to allow the ankle to assume an angle between neutral and 30 degrees of plantar flexion and further reducing the compartment pressure.
Tibia fractures are one of many common underlying etiologies for the development of compartment syndrome in the leg. Fracture reduction as well as eliminating circumferential dressings are important early preventative steps to take. Bivalving casts - including splitting the cast padding - is often indicated in fractures of long bones that are treated with initial casting. While casting patients in a plantigrade or dorsiflexed position reduces the risk of equinus contractures and holds the ankle mortise reduced, dorsiflexing the ankle has been shown to increase the intracompartmental pressures throughout the leg compartments.
Weiner et al. placed pressure monitors into the anterior and deep posterior compartments in healthy volunteers to measure the effects of casting on compartment pressures. They found that the intramuscular pressures were lowest with the ankle positioned between plantigrade and a resting plantar flexion position (0-37 degrees), and that bivalving the cast reduced the pressures 33-47%.
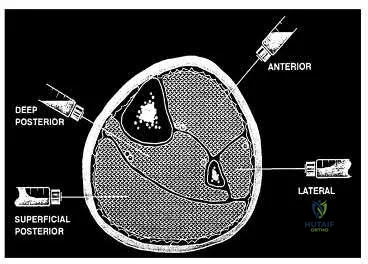
Illustration A shows the needle trajectories for compartment pressure monitoring in the leg. This should be performed within 5 cm of the fracture to get accurate peak pressures.
Incorrect Answers:
OrthoCash 2020
A 35-year-old male horseback rider was bucked into the air and then landed forcefully with his perineum on the saddlehorn of the saddle. At a one year follow-up, the only long term sequela of his injuries is erectile dysfunction. Which radiographic injury seen in Figures A-E is most commonly associated with this complication?

This patient has sustained a saddle-horn injury to the pelvis. An anterior posterior compression (APC) injury is the most common pelvic injury associated with this mechanism.
Saddle-horn injury to the pelvis occurs when a horseback rider is bucked into the air and then lands forcefully with his or her perineum on the saddlehorn of the saddle. The bony injury to the pelvis usually consists of a diastasis of the pubic symphysis with/without subsequent widening of the sacroiliac joints. The
majority of patients are able to return close to their pre-injury level of employment and activity after these injuries. However, sexual dysfunction is a common complication with this injury. Sexual dysfunction can be due to urethral, vascular, neurologic, and psychogenic injuries.
Collinge et al. looked at a series of male patients with injuries to the perineum after coming into contact with the saddle or saddle horn on a horse. Eighteen of the twenty patients were found to have sexual dysfunction at the time of the latest follow-up. A multi-disciplinary approach to these patients is needed when treating pelvic injuries.
Cannada et al. surveyed 71 women of childbearing age who had a pelvic fracture. She found that half the patients reported physical genitourinary complaints with 38 percent of women noting new onset pain with intercourse. In terms of psychological impact, they showed that 45 percent of patients answered affirmatively to decreased interest in intercourse and decreased orgasm frequency after the injury.
van Nieuwenhoven et al. describe three equestrians who suffered from straddle injuries with symphysis diastasis and rupture of sacroiliac ligaments after falls or kicks from horses. They show that these presumed low-energy injuries can cause extremely severe injuries to the pelvis itself and to the adjacent organs.
Figure A shows a Burgess APC Type II pelvic fracture. Figure B shows left ASIS avulsion fracture. Figure C shows a left hip dislocation. No pelvic fracture is identified. Figure D shows a subacute superior/inferior pubic rami fracture.
Figure E shows a right femoral neck fracture.
Incorrect Answers:
OrthoCash 2020
A 31-year-old male driver was involved in a high-speed motor vehicle accident. His injuries include a left subdural hematoma (Abbreviated Injury Score [AIS]=4), left segmental femur fracture (AIS=3), ruptured spleen (AIS=4), nasal fracture (AIS=2), fractured left ribs 4 to 7 (AIS=2), and a closed pelvic ring fracture (AIS=3). What is his Injury Severity Score (ISS)?
Question 4
Haversian canals are found in the center of an osteon in compact bone. They contain blood vessels and nerves.
Explanation
amputations have several options to optimize ambulation including solid, energy storing, and multi-axial prothesis.
Aaron et al. reviews the important considerations for patient specific prostheses and new developments on the horizon to maximize ambulation in prosthesis users.
Mesenchymal stem cells have the capacity to differentiate into all the following cell types EXCEPT?
Osteoclasts
Chondrocytes
Adipocytes
Osteoblasts
Fibroblasts
Mesenchymal stem cells are multipotent stem cells which retain the ability to self-renew and to form cells of the mesenchymal lineage. They can therefore form muscle, fat, tendon (made from fibroblasts), bone, cartilage, and the marrow stromal cells. Mesenchymal stem cells do not however form osteoclasts, which are formed from the monocyte lineage - from hematopoietic stem cells.
Caterson et al review the use of mesenchymal stem cells in tissue engineering and regeneration of musculoskeletal tissue.
A 60 year-old male was brought into the operating room for total hip replacement. Before making the incision, what precautionary procedure must be performed by the entire staff to minimize surgical error?
Mark the word "No" on the nonoperative extremities
Use intraoperative fluoroscopic imaging
Perform "timeout"
Have blood products ready in the operating room
Use the newest prosthesis
Surgical "timeout" is now part of the standard procedure which must be performed before starting surgery to minimize surgical error such as wrong site surgery.
Which of the following statements regarding articular cartilage is TRUE?
Cartilage is an isotropic material
Most of the water in articular cartilage exists in the deep layer next to the calcified cartilage
Cartilage only heals if the injury does not pass through the tidemark
Calcified cartilage is the only place that type IV collagen is found
Cartilage exhibits stress shielding of the solid matrix components
Cartilage exhibits significant stress shielding of the solid matrix components due to its high water content, the non-compressibility of water, and the structural organization of collagen and proteoglycans. Cartilage is composed of a permeable porous matrix and 65 to 80% of the total weight of articular cartilage is made up of water. A pressure gradient causes the water to flow through the porous-permeable solid matrix. Significant flow of fluid through the solid matrix requires high hydrodynamic pressures because of the low
permeability of the solid matrix.
The other answers are incorrect because cartilage is anisotropic, most of the water is located in the superficial layers, it only heals if the injury does pass through the tidemark, type X collagen is found in calcified cartilage and is thought to be involved in mineralization. Type IV collagen is found in the basal lamina.
A 38-year-old patient presents 6 months after intramedullary nailing of a distal third tibia fracture with symptoms consistent with complex regional pain syndrome. During the early stage of the disease he was treated with intermittent splinting, elevation and massage, contrast baths, and transcutaneous electrical nerve stimulation. Despite these modalities, he continues to have severe and debilitating symptoms. Which of the following treatment options is indicated as a second line of treatment?
Long leg cast immobilization for 3 months
Walking boot with non weight bearing for three months
Exchange nailing to stimulate healing response to the limb
Epidural spinal cord stimulator
Surgical sympathectomy of the affected limb
Complex regional pain syndrome is a chronic progressive disease of unknown etiology characterized by pain, swelling and skin changes. If nonoperative modalities fail, a surgical sympathectomy of the affected limb is indicated.
The first line of treatment is physical therapy including intermittent splinting, elevation and massage, contrast baths, and transcutaneous electrical nerve stimulation. Aggressive passive range-of-motion exercises should be avoided. If nonoperative modalites fail and symptoms remain severe, a surgical sympathectomy of the affected limb is indicated.
Keys to successful treatment include early clinical suspicion and treatment. Late CRPS is highly refractory to treatment and often results in permanent disability.
Two forms of Complex regional pain syndrome exist: 1) Reflex sympathetic dystrophy
- which does not demonstrate nerve lesions, and 2) Causalgia - which is associated with damage to peripheral nerves. Diagnostic criteria include:
Major criteria: intense and prolonged pain, swelling, stiffness, and discoloration (vasomotor disturbances).
Minor criteria: trophic changes, osseous demineralization, temperature changes, and palmar fibromatosis.
Tran et al present their systemic review of 41 RCTs of the research regarding treatment of CRPS. Their data suggest that only bisphosphonates offer clear medicinal benefits in the treatment of CRPS. Evidence regarding a beneficial effect of lumbar sympathetic blocks, gabapentin, and physical therapy is lacking. As such, these authors advocate for further study thru well-designed RCTs to better evaluate appropriate and effective treatment strategies.
You are planning an intramedullary nail to treat a geriatric patient with a peritrochanteric femur fracture. Which of the following preoperative considerations is correct regarding your implant?
The radius of curvature of an intramedullary nail is generally greater than the radius of curvature of the femur
Closed section nails have less stiffness than slotted nails
The medial/lateral nail starting point relative to the greater trochanter does not affect varus/valgus position in the fracture
The bending stiffness of your nail is proportional to the second power of the radius
Intramedullary nails allow for mostly direct intramembranous bone healing
The radius of curvature of an intramedullary nail is generally greater than the radius of curvature of the femur, which is why anterior distal femur
penetration is a known complication of intramedullary nailing procedures.
Egol et al. evaluated the radius of curvature of 948 femurs (474 matched pairs) and compared those data with current intramedullary nails. He found the average femoral anterior radius of curvature was 120 cm (± 36 cm)
whereas the radius of curvature of the intramedullary nails ranged from 186 to 300 cm.
The other answers are incorrect because closed section nails have more stiffness than slotted nails. The starting position on the greater trochanter greatly affects the post- operative varus/valgus of the fracture. Intramedullary nails allow for mostly indirect enchondral bone healing due to relative motion at the fracture site.
All of the following antibiotics function by interfering with protein synthesis by inhibiting ribosomes EXCEPT
gentamicin
tobramycin
vancomycin
erythromycin
linezolid
Gentamicin and tobramycin are aminoglycosides that function by inhibition of bacterial protein synthesis via irreversible binding to ribosomal subunits. Erythromycin functions by binding to the 50s subunit of the bacterial 70s rRNA complex and thereby inhibits protein synthesis. Linezolid binds to the 23s portion of the ribosomal subunit and inhibits protein synthesis. In contrast, Vancomycin acts by inhibiting proper cell wall synthesis and does not inhibit the ribosome.
The bending rigidity of the implant shown in Figure A is proportional to what power of the measured radius of the implant?
Question 5
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5° of angulation. When the MCP joint is flexed 30°, a radially directed stress produces 45° of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
REFERENCES: Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint.
J Am Acad Orthop Surg 1997;5:224-229.
Question 6
Figures 78a and 78b show the CT scans of a 22-year-old man with back pain after falling out of a tree. Examination reveals no palpable spinal step-offs, posterior spinal pain, and normal neurologic function in the lower extremities. Normal perineal sensation and normal rectal tone are present. What is the best management? Review Topic

Explanation
Question 7
Varus deformity after talar fractures is often seen due to collapse of the medial cortex. What artery supplies this portion of the talus?
Explanation
REFERENCES: Halibruton RA, Sullivan CR, Kelly PJ, et al: The extra-osseous and intra-osseous blood supply of the talus. J Bone Joint Surg Am 1958;40:1115.
Mulfinger GL, Trueta J: The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-167.
Question 8
Figures below show the radiographs obtained from a 90-year-old woman who is seen in the emergency department after a fall from a height. She has right hip and thigh pain and is unable to bear weight. Based on this patient's history and imaging, what is the best next step?
Explanation
Periprosthetic fracture is the third most common reason (after loosening and infection) for revision surgery after total hip arthroplasty (THA). Late periprosthetic fracture risk is 0.4% to 1.1% after primary
THA and 2.1% to 4% after revision THA. Risk factors for periprosthetic fracture include age over 70 years, decreasing bone mass, and loosening of implants and osteolysis. The risk of concomitant infection in the presence of a periprosthetic fracture is 11%, according to Chevillotte and associates. Obtaining presurgical aspiration or intrasurgical tissue for culture is recommended if concomitant infection is suspected.
Question 9
What is the most appropriate orthotic management for the lesion shown in Figure 6?
Explanation
REFERENCE: Rudicel SA: Intractable plantar keratoses, in Gould J (ed): Operative Foot Surgery. Philadelphia, PA, WB Saunders, 1994, p 70.
Question 10
Figures 70a and 70b show the sagittal MRI scan and axial CT of a patient who has decreased range of motion in the cervical spine. In which of the following directions would the cervical motion be most significantly limited?
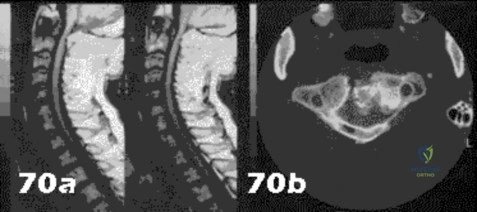
Explanation
Question 11
below show the clinical photograph and radiograph obtained from a year-old man who has deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?
Explanation
Figure 1 reveals an external rotation deformity of the right lower extremity. This deformity can have numerous causes, including extra-articular deformity. Figure 2 reveals a loose, subsided femoral component. Femoral stems typically subside into retroversion due to proximal femoral biomechanics, which cause a compensatory external rotation deformity. The combined findings from both images suggest an external rotation deformity most likely related to subsidence into retroversion.
Question 12
A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time? Review Topic

Explanation
(SBQ13PE.82) A renal ultrasound should be obtained in a patient with which of the following diagnoses? Review Topic
Congenital pseudoarthrosis of the clavicle
Accessory navicular
Congenital scoliosis
Charcot-Marie-Tooth Disease
Congenital curly toe
A renal ultrasound should be obtained in a patient with congenital scoliosis.
Congenitial scoliosis has a prevalence that is estimated at 1% to 4% in general population. It is associated with systemic anomalies in up to 61% of cases. The most common anomalies are cardiac defects, genitourinary defects and spinal cord malformations. As such, additional imaging of these systems should be considered in the initial work-up of these patients.
Ruf et al. retrospectively investigated 56 consecutive operative cases of congenital scoliosis. The average age at surgery was 9.9 years (1.5–17 years). There was one wound complication, 2 hardware failures, 1 revision and no neurological complications. They concluded that one-stage posterior hemivertebra resection and instrumentation was safe in this population.
Xu et al. examined the efficacy of selective partial hemivertebra excision via posterior-only approach in 17 adolescent patients with congenital kyphoscoliosis. There were no postoperative infections and no neurological complications. They concluded that this approach may be most successful in patients aged 9 to 14 years old, with the Risser sign grades from 0–3 and Cobb angles <60°.
Illustration A from Erol et al (UPOJ, Vol 15, 2002;37-42) shows a diagram of 'types' of congenital scoliosis based on the morphology of the vertebrae.
Incorrect Answers:
Question 13
A 12-year-old girl has had pain in her right knee for 1 month that started as activity-related and progressed to night pain. Radiographs are shown in Figures 16a and 16b, and a biopsy specimen is shown in Figure 16c. What is the recommended treatment?
Explanation
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 205.
Question 14
The skeletal muscle length-tension relationship for voluntary force generation is observed with which of the following biomechanical paradigms? Review Topic
Explanation
Question 15
A 22-year-old wrestler who underwent an open anterior shoulder reconstruction to repair a dislocated shoulder 6 months ago now reports shoulder pain after attempting a takedown. Examination reveals external rotation that is 15 degrees greater than the contralateral side. He has pain associated with abduction and external rotation but no apprehension. Which of the following tests would most likely reveal positive findings?
Explanation
REFERENCES: Gerber C, Krushell RJ: Isolated ruptures of the tendon of the subscapularis muscle: Clinical fractures in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Hawkins RJ, Bokor DJ: Clinical evaluation of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 149-177.
Question 16
When treating osteoporosis with alendronate, what is the most common side effect?
Explanation
REFERENCES: Marshall JK, Rainsford KD, James C, et al: A randomized controlled trial to assess alendoronate-associated injury of the upper gastrointestinal tract. Aliment Pharmacol Ther 2000;14:1451-1457.
Lane JM, Sandhu HS: Osteoporosis of the spine, in Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 227-234.
Question 17
Glenohumeral inferior stability in the adducted shoulder position is primarily a function of the
Explanation
REFERENCES: Warner JJ, Deng XH, Warren RF, Torzilli PA: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
Harryman DT II, Sidles JA, Harris SL, Matsen FA III: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
Question 18
Figures 9a and 9b show the radiographs of a 12-year-old girl who has had right hip pain for the past 4 months. She reports that the pain is so severe that she is unable to walk and is now using a wheelchair. Examination reveals pain with any attempted range of motion. Management should include
Explanation
REFERENCES: Springfield DS, Gebhardt MC: Bone and soft tissue tumors, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 507-518, 542-544.
Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002,
p 2030.
Question 19
Figures 18a through 18c show the clinical photograph, radiograph, and CT scan of a 21-year-old man who reports persistent pain after injuring his right shoulder 4 months ago. What is the most likely factor associated with this patient’s diagnosis?

Explanation
Question 20
An active 49-year-old woman who sustained a diaphyseal fracture of the clavicle 8 months ago now reports persistent shoulder pain with daily activities. An AP radiograph is shown in Figure 8. Management should consist of
Explanation
shown some healing response with callus formation, but these techniques are not successful
in an atrophic nonunion. The preferred technique for achieving union is open reduction and internal fixation with bone graft. Percutaneous fixation has no role in treatment of nonunions
of the clavicle.
REFERENCES: Boyer MI, Axelrod TS: Atrophic nonunion of the clavicle: Treatment by compression plating, lag-screw fixation and bone graft. J Bone Joint Surg Br 1997;79:301-303.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
Question 21
A 57-year-old woman with diabetes mellitus has purulent drainage from a lateral incision after undergoing open reduction and internal fixation of a displaced ankle fracture 10 days ago. Examination reveals moderate erythema and a foul odor coming from the wound. Cultures are obtained. What is the next most appropriate step in management?
Explanation
REFERENCES: Carragee EJ, Csongradi JJ, Bleck EE: Early complications in the operative treatment of ankle fractures: Influence of delay before operation. J Bone Joint Surg Br 1991;73:79-82.
Blotter RH, Connolly E, Wasan A, Chapman MW: Acute complications in the operative treatment of isolated ankle fractures in patients with diabetes mellitus. Foot Ankle Int 1999;20:687-694.
Question 22
What is the recommended treatment of a skeletally immature 12-year-old boy who has an anterior cruciate ligament-deficient knee?
Explanation
REFERENCES: Barry P: Anterior cruciate ligament injuries, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy. Philadelphia, Pa, WB Saunders, 1997, p 358.
McCarroll JR, Shelbourne KD, Porter DA, Rettig AC, Murray S: Patellar tendon graft reconstruction for midsubstance anterior cruciate ligament rupture in junior high school athletes: An algorithm for management. Am J Sports Med 1994;22:478-484.
Nottage WM, Matsuura PA: Management of complete traumatic anterior cruciate ligament tears in the skeletally immature patient: Current concepts and review of the literature. Arthroscopy 1994;10:569-573.
Stanitski CL: Anterior cruciate ligament injury in the skeletally immature patient: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:146-158.
Question 23
When an acute infection of a total elbow arthroplasty is managed with irrigation and debridement, which of the following organisms is associated with the highest risk of persistent infection?
Explanation
IV antibiotics.
REFERENCES: Yamaguchi K, Adams RA, Morrey BF: Infection after total elbow arthroplasty. J Bone Joint Surg Am 1998;80:481-491.
Schoifet SD, Morrey BF: Treatment of infection after total knee arthroplasty by debridement with retention of the components. J Bone Joint Surg Am 1990;72:1383-1390.
Question 24
Which of the following is considered a potential advantage in prophylaxis for the prevention of deep venous thrombosis associated with the use of low-molecular weight heparin (LMWH) as compared with fixed-dose unfractionated heparin?
Explanation
REFERENCES: Colwell CW Jr, Spiro TE, Trowbridge AA: Use of enoxaparin, a low-molecular weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14.
Bara L, Billaud E, Kher A, Samama M: Increased anti-Xa bioavailability for a low-molecular weight heparin (PK 10169) compared with unfractionated heparin. Semin Thromb and Hemost 1985;11:316-317.
Paiement GD: Prevention and treatment of venous thromboembolic disease complications in primary hip arthroplasty patients, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 331-335.
Question 25
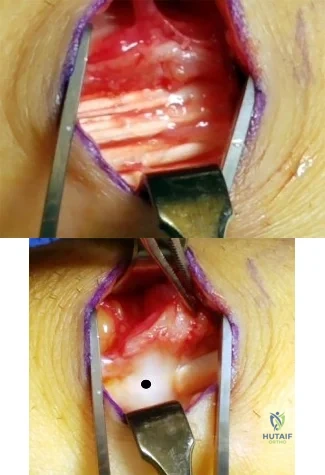
Figures 1 and 2 show the intraoperative photographs obtained during surgical treatment for de Quervain tendonitis. For orientation purposes, dorsal is at the top. Figure 1 is obtained just after the initial first extensor compartment release, and Figure 2 shows the floor of the first extensor compartment. If the structure marked by the black dot is not addressed, the most common postoperative problem would be
Explanation
The black dot identifies an accessory compartment of the extensor pollicis brevis (EPB) tendon. The incidence of accessory EPB compartment in patients undergoing surgical treatment for de Quervain syndrome ranges from 46% to 60%. Failure to release this compartment at the time of initial surgery can cause persistent postoperative pain. The patient would not experience altered sensation if this compartment were not released. Altered sensation would most commonly occur following injury to the dorsal radial sensory nerve branch during surgery. EPB tendon subluxation also would not occur should the accessory compartment not be released. For EPB tendon subluxation to occur, its own compartment would need to be released first. Finally, EPB tendon rupture would be an extremely uncommon complication of failure to release the accessory compartment.
Question 26
Optimal management of the injury shown in Figure 31 should include which of the following?
Explanation
REFERENCES: Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.
Sanders RW, Clare MP: Fractures of the calcaneus, in Bucholz RW, Heckman JD, Court-Brown C (eds): Rockwood and Green’s Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2293-2336.
Question 27
A 60-year-old woman with rheumatoid arthritis has atlanto-axial instability and basilar invagination. What MRI findings would suggest the need for cervical fusion?
Explanation
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, pp 700-701.
Monsey RB: Rheumatoid arthritis of the cervical spine. J Am Acad Orthop Surg
1997;5:240-248.
Bundschuh C, Modic MT, Kearney F, et al: Rheumatoid arthritis of the cervical spine: Surface-coil MR imaging. Am J Roentgenol 1988;151:181-187.
Question 28
Figure 35 is the MR image of an 18-year-old man who has had knee pain with running for 5 months. What is the most appropriate treatment?
Explanation
The MR image shows an osteochondritis dissecans (OCD), which is an acquired lesion of the subchondral bone. Patients with OCD initially report nonspecific pain and variable amounts of swelling. Initial radiographs help to identify the lesion and establish the physes status. MRI is useful for assessing potential for the lesion to heal with nonsurgical treatment. This lesion is unstable, considering the fluid line between the OCD and the underlying normal bone. Nonsurgical treatment is appropriate for small, stable lesions in patients with open physes and focuses on activity restriction for 3 to 9 months. Surgical treatment is necessary to address unstable or detached lesions. Stable lesions with intact articular cartilage can be treated with subchondral drilling to stimulate vascular ingrowth, with radiographic healing at an average of 4.4 months. Fixation is indicated for unstable or hinged lesions, and stabilization of the fragment can be achieved using a variety of implants through an arthroscopic or open approach. The fragment should be salvaged and the normal articular surface restored whenever possible.
Question 29
Which of the following nerves is most likely responsible for symptoms associated with plantar fasciitis?
Explanation
REFERENCE: Baxter DE, Pfeffer GB, Thigpen M: Chronic heel pain: Treatment rationale. Orthop Clin North Am 1989;20:563-569.
Question 30
What factor is associated with a high risk of developing pseudotumors after metal-on-metal hip resurfacing?
Explanation
Question 31
A 7-year-old boy has had chronic left leg pain that is worse at night but is not activity related. Use of nonsteroidal anti-inflammatory drugs for the past 6 months has failed to provide relief. A CBC count with differential, erythrocyte sedimentation rate, and C-reactive protein are within normal limits. Radiographs and a CT scan are shown in Figures 31a through 31c. Management should consist of
Explanation
REFERENCES: Donahue F, Ahmad A, Mnaymneh W, Pevsner NH: Osteoid osteoma: Computed tomography guided percutaneous excision. Clin Orthop 1999;366:191-196.
Rosenthal DI, Hornicek FJ, Wolfe MW, et al: Percutaneous radiofrequency coagulation of osteoid osteoma compared with operative treatment. J Bone Joint Surg Am 1998;80:815-821.
Question 32
A 63-year-old woman is seen 10 weeks after sustaining a closed minimally displaced distal radius fracture. She has been in a short-arm cast and reports minimal pain but notes that she is having difficulty using her thumb. An extensor pollicis longus (EPL) tendon rupture is suspected. Which examination finding would confirm lack of EPL function?
Explanation
As many as to 5% of patients with a nondisplaced distal radius fracture experience EPL rupture. The extensor pollicis brevis (EPB) tendon often attaches to the extensor hood and sometimes continues more distally, providing weak metacarpophalangeal extension even in the setting of EPL disruption. However, because of the vector of its pull, the EPB cannot extend the thumb dorsal to the plane of the palm. A positive Froment sign is noted when flexion of the thumb interphalangeal joint with an attempted key pinch is caused by adductor pollicis weakness from ulnar nerve dysfunction. Compression of the median nerve in the carpal tunnel affects the recurrent motor branch of the abductor pollicis brevis, leading to thenar atrophy. The flexor pollicis longus tendon (FPL) is intact so the patient would not have difficulty flexing the thumb with the palm flat.
Question 33
A 69-year-old woman has just undergone an uncomplicated total shoulder arthroplasty for glenohumeral osteoarthritis. A press-fit humeral stem and a cemented all-polyethylene glenoid component were placed. At this point, what is the postoperative rehabilitation plan?
Explanation
at 3 weeks risks tearing the subscapularis tendon repair. Active strengthening should not begin for 6 weeks postoperatively to allow the subscapularis tendon repair time to heal.
REFERENCES: Boardman ND III, Cofield RH, Bengston KA, et al: Rehabilitation after total shoulder arthroplasty. J Arthroplasty 2001;16:483-486.
Matsen FA III, Lippitt SB, Sidles JA, et al: Practical Evaluation and Management of the Shoulder. Philadelphia, PA, WB Saunders, 1994, pp 215-218.
Question 34
In patients undergoing elective hip or knee arthroplasty who are not at elevated risk (beyond the risk associated with the surgery) for venous thromboembolism or bleeding, using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism was assigned what grade of recommendation by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty?
Explanation
Using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism in patients undergoing elective hip or knee arthroplasty who are not at elevated risk beyond that of the surgery itself for venous thromboembolism or bleeding was given a moderate grade of
recommendation in the 2011 AAOS Clinical Practice Guideline referenced above.
Question 35
An 18-year-old man sustained closed humeral shaft and forearm fractures of his dominant arm in a motor vehicle accident. Neurovascular examination is intact, and his condition is stable. The best course of action for management of the injuries should be
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Bell MJ, Beachamp CG, Kellam JK, McMurtry RY: The results of plating humeral shaft fractures in patients with multiple injuries: The Sunnybrook experience. J Bone Joint Surg Br 1985;67:293-296.
Question 36
During the anterior approach for repair of a distal biceps tendon rupture, what structure, shown under the scissors in Figure 6, is at risk for injury?
Explanation
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Ramsey ML: Distal biceps tendon injuries: Diagnosis and management. J Am Acad Orthop Surg 1999;7:199-207.
Question 37
A 45-year-old woman has idiopathic scoliosis. Surgery is to include an anterior thoracic release through an open left thoracotomy. The thoracotomy will have what effect on the patient’s pulmonary function postoperatively?
Explanation
REFERENCES: Graham EJ, Lenke LG, Lowe TG, et al: Prospective pulmonary function evaluation following open thoracotomy for anterior spinal fusion in adolescent idiopathic scoliosis. Spine 2000;25:2319-2325.
Kishan S, Bastrom T, Betz RR, et al: Thoracoscopic scoliosis surgery affects pulmonary function less than thoracotomy at 2 years postsurgery. Spine 2007;32:453-458.
Question 38
A 52-year-old man sustained the left elbow injury shown in Figure A while playing basketball 2.5 months ago. He underwent the procedure shown in Figure B. Post-operatively he was mobilized in a hinged brace. On examination today, his arc of elbow flexion is 75 degrees with loss of 45 degrees of full extension. His Disabilities of the Arm, Shoulder and Hand (DASH) Outcome Measure score is 45 points. What initial treatment option will likely provide the greatest improvement in this patients DASH score and functional range of motion? Review Topic

Explanation
Post-traumatic elbow stiffness is often difficult to manage. The ultimate goal of treatment is to restore a functional range of elbow motion (30° to 130°). Nonoperative modalities are considered the first-line of treatment. Aggressive physical therapy has traditionally been advocated. However, the use of static progressive elbow splinting with a turnbuckle, alongside aggressive physical therapy, has shown to provide better functional outcomes. Treatment is usually maintained over a period of 6-12 months. Surgery is considered when nonoperative therapy fails.
Doornberg et al. looked at a retrospective case series of 29 patients with posttraumatic elbow stiffness. They showed that static progressive splinting can help gain additional motion when standard exercises fail to produce additional improvements.
Lindenhovius et al. randomized sixty-six patients with post-traumatic elbow stiffness into static progressive elbow splint therapy or dynamic elbow splinting over a 12 month period. There was no significant difference in outcomes between treatment modalities. ROM increased by 40° vs. 39° at six months, respectively. DASH scores improved from 50 vs 45 at enrollment to 32 vs. 25 at six months, respectively.
Figure A shows a posterior elbow dislocation with an associated medial epicondyle fracture. Figure B shows ORIF of the fracture seen in Figure A. Illustration A shows a static progressive turnbuckle elbow splint used for post-traumatic elbow stiffness.
Incorrect Answers:
Question 39
The most appropriate treatment for this fracture is
Explanation
Tibial fractures are classified on the basis of their anatomical location and the status of the prosthesis fixation. Type I fractures involve the tibial plateau, type II fractures occur adjacent to the stem of the tibial component, type III fractures are distal to the tibial stem, and type IV fractures involve the tibial tubercle. Subclassifications include A with a well-fixed implant; B with a loose implant; and C, which occur intraoperatively.
Treatment of periprosthetic tibial fractures is based on the location of the fracture and the status of the component fixation. Types II or III fractures associated with prosthetic loosening or instability are best managed with revision arthroplasty, usually with a diaphyseal-engaging intramedullary tibial stem. Supplemental internal fixation may be necessary. Type III fractures with well-fixed and stable implants are treated using the standard principles of tibial fracture management.
Question 40
Figures 92a through 92c are the radiographs of a 34-year-old man with low-back pain and an inability to walk upright. What is the appropriate surgical treatment? A B C

Explanation
This patient has a marked fixed sagittal imbalance and a mild coronal imbalance. His fused sacroiliac joints indicate ankylosing spondylitis. Sufficient correction likely can be achieved with a pedicle subtraction osteotomy in the midlumbar spine. Smith-Petersen osteotomies necessitate flexibility of the anterior column, which is not associated with this diagnosis. Also, osteoclasis can result in vascular injuries. Vertebral column resection should not be needed in this case.
RECOMMENDED READINGS
Patel NM, Jenis LG. Inflammatory arthritis of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:339-349.
Kim KT, Suk KS, Cho YJ, Hong GP, Park BJ. Clinical outcome results of pedicle subtraction osteotomy in ankylosing spondylitis with kyphotic deformity. Spine (Phila Pa 1976). 2002 Mar 15;27(6):612-8. PubMed PMID: 11884909. View Abstract at PubMed
Question 41
Which of the following conditions is typically associated with the ankle deformity shown in figure 14?
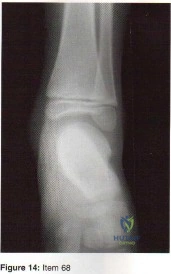
Explanation
Question 42
A 12-year-old boy with a family history of neurofibromatosis has anterolateral bowing of the left tibia. He has no pain and is ambulatory. Radiographs show a narrowed medullary canal but intact cortices. Treatment should consist of which of the following?
Explanation
REFERENCES: Vander Have KL, Hensinger RN, Caird M, et al: Congenital pseudarthrosis of the tibia.
J Am Acad Orthop Surg 2008;16:228-236.
Vitale MG, Guha A, Skaggs DL: Orthopaedic manifestations of neurofibromatosis in children: An update. Clin Orthop Relat Res 2002;401:107-118.
Question 43
A 41-year-old male underwent intramedullary nailing for a low-energy left femoral shaft fracture. At his follow-up appointment, he complains that his feet are pointing in opposite directions when walking. Using the imaging study shown in Figure A, which of the following represents this patient's left femur malalignment?
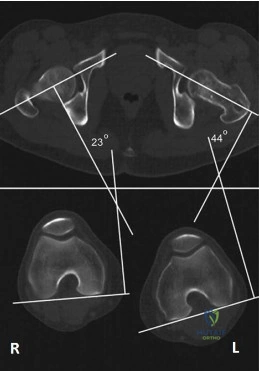
Explanation
Radiographic rotational malalignment after fixation of femoral shaft fractures may be measured by comparing the femoral anteversion of both femurs. This can be determined by measuring the angle between a line tangential to the dorsal bony contours of the femoral condyles and a line drawn through the axis of the femoral neck. Rotational differences of less than 10° are considered variations of normal.
Jaarsma et al. reviewed rotational malalignment after intramedullary nailing of femoral fractures. They report that rotational measurements by CT are superior to clinical assessment. They note a high incidence of malrotation after IM nailing of fractures. This has shown to be in the range 15% to 30%.
Figure A shows left femoral malrotation using CT-torsion measurements with axial cuts of the femoral neck and distal femoral condyles. Note the normal anteversion of the right femur (23 degrees; normal range 10-25).
Incorrect Answers:
Question 44
A 16-year-old high school football player has diffuse pain with attempted digital flexion after injuring the ring finger of the dominant hand 1 week ago. Examination reveals that he is unable to flex the distal interphalangeal joint. Management should consist of
Explanation
REFERENCES: Strickland JW: Flexor tendons: Acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 1851-1897.
Leddy JP: Avulsions of the flexor digitorum profundus. Hand Clin 1985;1:77-83.
Question 45
A 17-year-old high school athlete comes in with a 6-month history of right midfoot pain. She has been treated with cast immobilization, crutches, and physical therapy. She still has significant pain with activities and cannot participate in sports. Her radiograph is shown in Figure 93a, and MR images are shown in Figures 93b and 93c. What is the most appropriate 79 next step? A B C
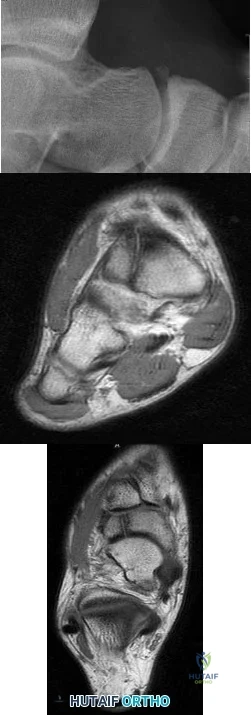
Explanation
RECOMMENDED READINGS
Lee S, Anderson RB. Stress fractures of the tarsal navicular. Foot Ankle Clin. 2004 Mar;9(1):85-104. Review. PubMed PMID: 15062216. View Abstract at PubMed
Anderson RB, Cohen BE. Stress fractures of the foot and ankle. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 2. 8th ed. Philadelphia, PA: Mosby; 2007:1590-1597.
Question 46
A 17-year-old boy who fell on a pitchfork in a barn 1 day ago now has a painful, swollen forearm. Examination reveals erythema, exquisite tenderness, and crepitus to palpation of the forearm. He has a pulse rate of 110/min and a blood pressure of 80/60 mm Hg. Radiographs show subcutaneous air and no fractures. Gram stain of wound drainage reveals a gram-positive bacillus. The next most appropriate step in management should consist of
Explanation
REFERENCES: Pellegrini VD, Evarts CM: Complications, in Rockwood CA Jr, Green DP (eds): Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, pp 365-370.
Gerding DN, Peterson LR: Infections caused by anaerobic bacteria, in Shulman ST, Phair JP, Peterson LR, Warren JR (eds): Infectious Diseases, ed 5. Philadelphia, PA, WB Saunders, 1997, pp 416-417.
Stephens DC: Myositis and fascitis, in Root RK (ed): Clinical Infectious Diseases, ed 1. Oxford, England, Oxford Press University, 1999, pp 769-770.
Question 47
Histologic studies of surgically resected tissue in lateral epicondylitis demonstrate which of the following findings? Review Topic
Explanation
Question 48
Following surgery for an ankle fracture, which of the following is considered the most important factor in achieving a satisfactory outcome? Review Topic
Explanation
Question 49
Lymphangioma
Explanation
Question 50
The lateral arm flap is based on what arterial supply?
Explanation
REFERENCES: Katsaros J, Tan E, Zoltie N: The use of the lateral arm flap in upper limb surgery. J Hand Surg 1991;16:598-604.
Katsaros J, Schusterman M, Beppu M, et al: The lateral upper arm flap: Anatomy and clinical applications. Ann Plast Surg 1984;12:489-499.
Question 51
A 23-year-old man who was the restrained driver in a car involved in a high-speed motor vehicle accident sustained the closed injury shown in Figures 32a through 32c. Which of the following factors has the greatest impact on the risk of osteonecrosis?
Explanation
REFERENCES: Lindvall E, Haidukewych G, Dipasquale T, et al: Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am 2004;86:2229-2234.
Vallier HA, Nork SE, Barei DP, et al: Talar neck fractures: Results and outcomes. J Bone Joint Surg Am 2004;86:1616-1624.
Question 52
Figures 1 and 2 are the radiographs of a 55-year-old woman homemaker with a 1-year history of insidious onset left wrist pain. She has failed conservative treatment and desires surgery. Her medical history is complicated by a smoking history of 1.5 packs of cigarettes per day. At the time of surgery her capitate articular surface is normal in appearance. The best procedure for her would be

Explanation
This patient has Lichtman stage 3B Kienbock disease. She is 55 years old and is a "low-demand" patient; however, she is a heavy smoker. Based on her condition and her current smoking status, salvage treatment that does not require bone healing such as a proximal row carpectomy is likely the best treatment option. A radial shortening osteotomy and a capitate shortening osteotomy may be helpful in offloading the lunate, but both procedures require bone healing and are better options in earlier stages of Kienbock disease. A scaphoid excision and four-corner fusion is typically performed for scapholunate advanced collapse or scaphoid nonunion advanced collapse wrist arthritis and would not be recommended in this scenario, as the lunate is avascular.
Question 53
In treating a lateral split-depression type tibial plateau fracture, which of the following adjuncts has been shown to have the least articular surface subsidence when used to fill the bony void?

Explanation
The referenced study by Russell et al noted a significantly increased rate of subsidence at 12 months with autograft as compared to calcium phosphate cement (in types I-VI).
The other referenced study by Lobenhoffer et al noted improved radiographic outcomes and earlier weightbearing with usage of calcium phosphate cement.
Question 54
A 27-year-old woman reports the acute atraumatic onset of burning pain in her right shoulder followed a week later by significant weakness and the inability to abduct her shoulder. One week prior to this incident she had recovered from a flu-like syndrome. Examination reveals full passive motion of the shoulder and the inability to actively raise the arm. Sensation in the right upper extremity is normal. Cervical spine examination is normal. Radiographs of the shoulder and cervical spine are normal. What is the most likely diagnosis?
Explanation
REFERENCES: Turner JW, Parsonage MJ: Neuralgic amyotrophy (paralytic brachial neuritis). Lancet 1957;2:209-212.
Omer GE, Spinner M, Van Beek AL (eds): Management of Peripheral Nerve Problems, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 101-104.
Question 55
Figure 14 shows a lateral radiograph of a knee joint. The bony structure indicated by the arrow is a sesamoid bone that resides in what tendon?
Explanation
REFERENCES: Anderson JE (ed): Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Wilkins, 1978, pp 4-69.
Weissman BNW, Sledge CB (ed): Orthopaedic Radiology. Philadelphia, PA, WB Saunders, 1986, p 514.
Question 56
The most common reason for proximal femur fracture fixation failure (Figure 15) is secondary to which common deformity?

Explanation
Malposition of a proximal lag screw may result in cut-out similar to that seen with a sliding hip screw. Varus malreduction also can result in implant failure. Studies have shown no difference in complication or healing rates when comparing short and long cephallomedullary nails.
RECOMMENDED READINGS
Kleweno C, Morgan J, Redshaw J, Harris M, Rodriguez E, Zurakowski D, Vrahas M, Appleton
P. Short versus Long Cephalomedullary Nails for the Treatment of Intertrochanteric Hip Fractures in Patients over 65 Years. J Orthop Trauma. 2013 Nov 13. [Epub ahead of print] PubMed PMID: 24231580.View Abstract at PubMed
Haidukewych GJ. Intertrochanteric fractures: ten tips to improve results. Instr Course Lect. 2010;59:503-9. Review. PubMed PMID: 20415401. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 16 THROUGH 20
A 23-year-old man sustains multiple injuries in a high-speed motor vehicle collision. Among his injuries are a right transverse-posterior wall acetabular fracture, a left open tibia fracture with compartment syndrome, and a right calcaneus fracture.
Question 57
Figure 1 is the MRI scan of a 35-year-old female soccer player who injured her knee during a game. Given the findings of the scan, physical examination is most likely to reveal
Explanation
Question 58
A 14-year-old patient has anterior knee pain. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 6a through 6e. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 18.
Question 59
A 67-year-old woman is seen in the emergency department after falling at home. Radiographs before and after treatment are shown in Figures 49a and

Explanation
Question 60
A 13-year-old boy has a radiographically mild, clinically stable slipped capital femoral epiphysis (SCFE). What is the most appropriate treatment? Review Topic
Explanation
(SBQ13PE.46) What developmental milestones are likely to be present in a 30-month-old child? Review Topic
Hand dominance established
Hops on one foot
Heel-to-toe walk
Puts shoes on correct feet
Manages buttons
Hand dominance is usually established in the third year of life.
Normally, children younger than 2 years of age are ambidextrous. In some normal cases this persists after 2 years. Although there is some variability in this timing, strong hand preference in a younger child may be the result of a neurologic deficit.
Frankenburg et al. used the Denver Developmental Screening Test (DDST) to evaluate 1036 Denver area children from 2 to 6.4 years. The ages at which 25, 50, 75 and 90 percent of children could perform tasks were calculated to establish norms for the sample. The authors stress that the DDST is not an intelligence test, but rather a screening test to be used in clinical practice to determine whether a child's development is within the normal range.
Illustration
A
shows
the
DDST.
Incorrect
2:
Normal
for
Question 61
Early postoperative infections following primary total hip arthroplasty are most likely caused by which organism?
Explanation
S aureus is the most common organism cultured in early (fewer than 4 weeks postoperative) periprosthetic infections. Methicillin-resistant S aureus is becoming a more common pathogen in certain patient populations. B hemolytic Streptococcus and some gram-negative infections can also be found in early postoperative infections. S epidermidis, S viridans, and P acnes are more commonly found in late (more than 4 weeks postoperative) infections.
Question 62
When counseling a patient with hypophosphatemic rickets, which of the following scenarios will always result in a child with the same disorder?
Explanation
REFERENCES: Evans GA, Arulanantham K, Gage JR: Primary hypophosphatemic rickets: Effect of oral phosphate and vitamin D on growth and surgical treatment. J Bone Joint Surg Am 1980;62:1130-1138.
Greene WB, Kahler SG: Hypophosphatemic rickets: Still misdiagnosed and inadequately treated. South Med J 1985;78:1179-1184.
Question 63
A 40-year-old female recreational basketball player notes pain deep within her shoulder that occurs with activity. Pain began insidiously 6 months previously. She has completed a physical therapy program, and an intra-articular corticosteroid injection provided excellent temporary relief. Physical examination shows symmetric range of motion of her shoulder. She has a positive O'Brien’s active compression test. There is no pain with cross-arm adduction or tenderness to palpation over the acromioclavicular joint. Resisted abduction is nonpainful and strong. MRI shows increased signal in the substance of the superior labrum, low-grade bursal surface fraying of the supraspinatus, and mild degenerative changes within the acromioclavicular joint. What is the best treatment option?
Explanation
Question 64
A 35-year-old man presents with mechanical knee pain after a fall. An arthroscopic picture taken during diagnostic arthroscopy is shown in Figure A. His surgeon considers treatment with Technique B and Technique C, which are shown in Figures B and C, respectively. Which of the following statement is true with respect to Technique B and C? Review Topic
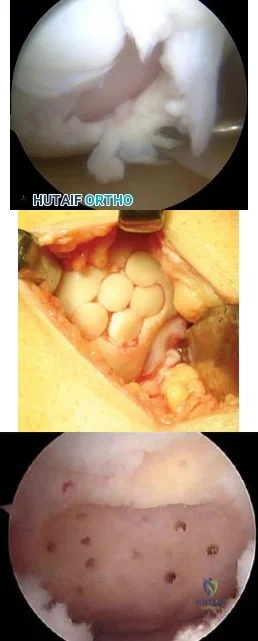
Explanation
The initial treatment for small articular cartilage defects is rest, NSAIDS and bracing. For larger defects (<2-4cm2), options include marrow stimulation procedures (abrasion chondroplasty, microfracture, osteochondral drilling) and autograft procedures (Mosaicplasty, a technique of osteochondral autograft transfer (OAT).
Alford et al. reviewed cartilage restoration. They defined a spectrum of treatment option ranging from (1) palliative (debridement/lavage), intended to reduce irritation
and inflammation, (2) reparative (marrow stimulation techniques), intended to recruit stem cells to proliferate fibrocartilage repair tissue, to (3) restorative (osteochondral grafting), designed to replace articular cartilage and subchondral bone as a single unit.
Magnussen et al. reviewed the treatment of cartilage defects in the knee. They compared autologous chondrocyte implantation (ACI), OATs, matrix-induced ACI, and microfracture. No one technique was superior to the rest. Outcomes for microfracture tended to be worse in larger lesions.
Figures A is an arthroscopic picture showing a grade IV chondral defect. Figure B shows microfracture. Figure C shows the multiple cylindrical plugs of mosaicplasty, a technique of osteochondral autograft transfer (OAT). Illustration A shows donor and recipient sites in mosaicplasty. Illustration B shows the spectrum of treatment options defined by Alford et al (MST = marrow stimulation; ACI = autologous chondrocyte implantation; OCG = osteochondral grafting with autograft/allograft).
Incorrect Answers:
Question 65
When treating a proximal tibia fracture, the surgeon decides to (1) use blocking screws in the proximal fragment, and (2) pick the intramedullary nail based on the location of the Herzog curve. Which of the following combinations will best prevent the classic deformity associated with this fracture?
Explanation
Up to 58% of proximal tibial fractures are malaligned. Malalignment arises because the nail fits loosely in the wide metaphyses and cannot control alignment. Without close fit of the nail at the fracture site, the nail will not align the fracture independent of a stable reduction and careful nail path. Blocking screws serve to reduce the size of the proximal metaphyseal canal and guide final nail passage.
Stinner et al. discuss strategies in proximal tibial fracture nailing. They describe an accurate starting point (using the twin peaks AP view or fibular bisector AP view, and flat plateau lateral view). They emphasize fracture reduction prior to reaming and implant placement.
Hiesterman reviewed nailing of extra-articular proximal tibial fractures. Techniques described include blocking screws, unicortical plating, using a universal distractor, nailing in flexion/locking in extension, semiextended nailing (including percutaneous suprapatellar quads-splitting approaches), multiple proximal interlocking screws (>=3).
Illustration A shows placement of a coronal blocking screw. Illustration B shows placement of a sagittal blocking screw. Illustration C shows the effect of the Herzog curve. A more distal Herzog curve leads to a "wedge" effect and fracture displacement whereas a proximal Herzog curve contains the fracture. The "wedge" effect occurs as the nail is seated and impinges on the posterior cortex of the distal segment accentuating an apex anterior deformity because of the effective widening of the nail above the bend and posterior force on the distal segment to match the nail shape.
Incorrect Answers:
Question 66
A 23-year-old woman has had vague left knee pain for the past 6 months. A radiograph and CT scan are shown in Figures 50a and 50b. What is the most likely diagnosis?
Explanation
REFERENCES: Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 185-196.
Okada K, Frassica FJ, Sim FH, Beabout JW, Bond JR, Unni KK: Parosteal osteosarcoma. A clinicopathological study. J Bone Joint Surg Am 1994;76:366-378.
Question 67
What cell type causes the bone destruction in metastatic lesions?
Explanation
REFERENCES: Cramer SF, Fried L, Carter KJ: The cellular basis of metastatic bone disease in patients with lung cancer. Cancer 1981;48:2649-2660.
Clohisy DR, Palkert D, Ramnaraine ML, Pekurovsky I, Oursler MJ: Human breast cancer induces osteoclast activation and increases the number of osteoclasts at sites of tumor osteolysis. J Orthop Res 1996;14:396-402.
Question 68
A defect in the gene coding for fibrillin-1 would lead to which diagnosis? Review Topic
Explanation
Marfan Syndrome is a genetic disorder of connective tissue typically caused by a mutation in the gene coding for the fibrillin-1 protein. Affected patients are typically very tall with long limbs and thin fingers and toes. Marfan Syndrome patients have many common features including ectopic lens, aortic root dilation, scoliosis, protrusio acetabuli, and ligamentous laxity.
Shirley et al. present a review of Marfan Syndrome with emphasis on the musculoskeletal manifestations including ligamentous laxity, protrusio acetabuli, and scoliosis. They note that scoliosis in these patients, when compared to those with idiopathic scoliosis, commonly progresses faster, is more resistant to bracing, and has a higher association with dural ectasia.
Dean presents a review of Marfan Syndrome and its underlying genetic cause of a mutation in fibrillin. They state that diagnosis can be made using the Ghent nosology (see Illustration A) which can diagnose or rule out the condition in 86% of patients. They caution using these criteria in young children as some features of Marfan Syndrome may not present until later ages.
Illustration A is a summary of the 2010 Revised Ghent nosology for diagnosing Marfan Syndrome.
Incorrect Answers:
Question 69
A 43-year-old woman has had pain in the left hip for the past 2 months. A radiograph, CT scan, MRI scan, and biopsy specimens are shown in Figures 16a through 16e. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra JM, Gold R, Downs J, Eckardt JJ: A new histologic approach to the differentiation of enchondroma and chondrosarcoma of the bones: A clinicopathologic analysis of 51 cases. Clin Orthop 1985;201:214-237.
Question 70
According to Musculoskeletal Infection Society (MSIS) guidelines, which set of patient laboratory study results fits the definition of chronic prosthetic joint infection?
Explanation
The MSIS definition of periprosthetic joint infection was updated in 2014 with two major and six minor criteria. The presence of one major criterion or three minor criteria is diagnostic for infection. The major criteria are two positive cultures with the same organism or a draining sinus tract. The current MSIS minor criteria are 1) an elevated ESR (more than 30 mm/hr) and CRP level (more than 10 mg/L), 2) an elevated synovial WBC count (more than 3,000 cells per/microliter), 3) an elevated synovial fluid polymorphonuclear count (more than 80%), 4) a positive histological analysis of periprosthetic tissue, and 5) a single positive culture.
Question 71
A 52-year-old man with a BMI of 40 and primary osteoarthritis undergoes total hip arthroplasty through a posterolateral approach. To retract the femur anteriorly when exposing the acetabulum, the surgeon places a sharp curved retractor over (anterior to) the anterior inferior iliac spine. Pulsatile bleeding is encountered. A branch of which artery has been injured?
Explanation
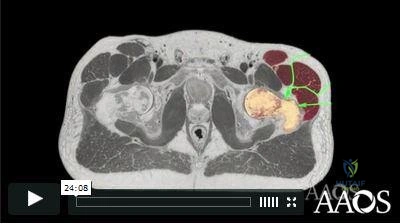
Video 182 for reference
The femoral artery crosses the hip joint anterior to the anterior hip capsule. The medial femoral circumflex artery enters the joint along the route of the obturator externus. The obturator artery enters the hip joint beneath the transverse acetabular ligament. The iliac circumflex vessel arises superior to the hip joint.

RESPONSES FOR QUESTIONS 183 THROUGH 188
For each clinical scenario described below, identify the corresponding anteroposterior pelvic radiographic image shown above.
Question 72
Which of the following structures is most commonly involved in lateral epicondylitis?
Explanation
REFERENCES: Nirschl RP: Elbow tendinosis/tennis elbow. Clin Sports Med 1992;11:851-870.
Regan W, Wold LE, Coonrad R, Morrey BF: Microscopic histopathology of chronic refractory lateral epicondylitis. Am J Sports Med 1992;20:746-749.
Question 73
Preventing "missed" femoral neck fractures associated with ipsilateral femoral shaft fractures is best achieved with
Explanation
Ipsilateral femoral neck and shaft fractures occur in up to 6% of femur fractures. A femoral neck fracture is often vertical and nondisplaced. A high degree of suspicion is necessary to avoid "missed" femoral neck fractures in patients with this condition. Although an examination and dedicated hip radiographs help to avoid missed injuries, a significant decrease in missed
injuries has been described with the use of thin-cut pelvic CT images. In patients who undergo trauma, a pelvic CT scan is often performed to assess for associated injuries and is easily reviewed to examine the femoral neck. Although MRI is advocated to identify isolated occult femoral neck fractures, CT has been described as the method of choice with which to identify ipsilateral femoral neck and shaft fractures in the trauma population. Currently, no literature supports the use of MRI in this population.
RECOMMENDED READINGS
Tornetta P 3rd, Kain MS, Creevy WR. Diagnosis of femoral neck fractures in patients with a femoral shaft fracture. Improvement with a standard protocol. J Bone Joint Surg Am. 2007 Jan;89(1):39-43. PubMed PMID: 17200308.View Abstract at PubMed
Kuhn KM, Agarwal A. Femoral fractures. In: Cannada LK, ed. Orthopaedic Knowledge Update
Question 74
A 5-year-old girl sustains an isolated injury to the right shoulder area after falling off the monkey bars. Examination reveals intact neurovascular function in the extremity distally, but she is quite uncomfortable. An AP radiograph of the proximal humerus is shown in Figure 24. Her parents state that she is a very talented gymnast. Considering her age and potential athletic career, management should consist of
Explanation
REFERENCES: Martin RF: Fractures of the proximal humerus and humeral shaft, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994,
pp 144-148.
Sanders JO, Rockwood CA Jr, Curtis RJ: Fractures and dislocation of the humeral shaft and shoulder, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 937-939.
Question 75
Which of the following factors has been shown to increase the risk of peroneal tendon pathology in patients who have undergone posterior plating of lateral malleolar fractures?
Explanation
Question 76
Figure 51 shows an arthroscopic view of the patellofemoral joint from an inferolateral portal. The arrow points to which of the following structures? Review Topic

Explanation
Question 77
Figure 11 shows the radiograph of a 3-year-old girl who sustained a proximal radius injury. Appropriate initial management should include
Explanation
REFERENCES: Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop
2000;20:7-14.
Radomisli TE, Rosen AL: Controversies regarding radial neck fractures in children. Clin Orthop 1998;353:30-39.
Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Surg Am 1999;81:1429-1433.
Gonzalez-Herranz P, Alvarez-Romera A, Burgos J, et al: Displaced radial neck fractures in children treated by closed intramedullary pinning (Metaizeau technique). J Pediatr Orthop 1997;17:325-331.
Question 78
A tall, thin 17-year-old basketball player and his parents request an evaluation of his flexible (hypermobile) pes planus/planovalgus foot deformities. As part of his evaluation, the orthopaedic surgeon notes pectus excavatum, disproportionately long arms, and scoliosis. In addition to providing treatment of his feet, what test or evaluation should the patient be referred for? Review Topic
Explanation
Question 79
A 70-year-old woman with a body mass index (BMI) of 34 and a history of hypercholesterolemia has elected to undergo total hip arthroplasty. Her son recently learned he has factor V Leiden following an episode of pulmonary embolism. What are this patient's risk factors for thromboembolic disease?
Explanation
Risk stratification is one of the most critical clinical evaluations to undertake before performing total joint arthroplasty. Many factors have been identified that increase the risk for venous thromboembolism (VTE) The major factors include previous VTE, obesity, type of surgery (such as total joint arthroplasty), hypercoagulable states, myocardial infarction, congestive heart failure, family history of VTE, and hormone replacement therapy. Hypercholesterolemia is not a risk factor for thromboembolic disease.
Question 80
A 70-year-old male with longstanding diabetic neuropathy sustains a fall down a flight of stairs and sustains the injury shown in Figures A and B. In the operating room, direct reduction of the fracture is performed. The syndesmosis is assessed and found to be intact. The fibula is fixed with a small fragment locking plate and the medial malleolus is fixed with screws. What is the next best step? Review Topic

Explanation
Diabetics with ankle fractures are prone to complications. Nonoperatively treated cases have up to a 50% incidence of skin breakdown in a cast. Surgically treated patients have up to 40% complication rate. Supplemental fixation can include include multiple syndesmotic screws, spanning external fixation, tibio-talar Steinmann pins, more rigid fibular plates, supplemental intramedulary fibular pinning. Weightbearing after surgery should be delayed (8-12weeks).
McCormack and Leith reviewed the complications in 26 diabetic ankle fractures. 19 patients had surgery. The incidence of complications was 42%. Two required amputation and died. None of the non-diabetic control group had complications. They concluded that in the older, diabetic patient with lower demands, especially if insulin-dependent, it may be preferable to accept a loss of reduction and malunion rather than risk the potentially devastating complications associated with operative intervention. If surgery is necessary, the results of this study provides a more accurate prognosis and allows for better discussion of surgical risks with the patient.
Roseunbaum et al polled AOFAS members on the treatment of diabetic ankle fractures. (1) For nondisplaced bimalleolar fracture with diabetic neuropathy, respondents preferred casting and nonweightbearing (NWB) for 8-12 weeks. (2) For Weber B fracture dislocation without neuropathy, without syndesmotic injury,
respondents preferred either 1/3 tubular or small fragment locking plates with syndesmotic screws and NWB for 8-12 weeks. (3) For bimalleolar fracture dislocation with neuropathy, without syndesmotic injury, respondents preferred small fragment locking plates with syndesmotic screws and NWB for 8-12 weeks.
Wukich and Kline reviewed the management of ankle fractures in diabetics. They found that neuropathy is more prevalent in patients with ankle fractures than without. They stress that 1% reduction in HbA1C results in 30% reduction in complication rate. Fracture healing is slower, callus is smaller, with less stiffness, tensile strength and collagen content. Amputation rate is up to 5% for patients treated operatively or nonoperatively. Complications are higher in patients with vasculopathy, neuropathy, or Charcot arthropathy.
Incorrect Answers:
Question 81
A year-old man who underwent left partial knee arthroplasty 6 months earlier was doing well until he experienced left knee pain and swelling for 4 weeks following a dental procedure. The left knee aspirate was bloody, with a white blood cell count of 8,000 and 70% neutrophils. Culture grew group B Streptococcus ( Granulicatella adiacens ), and serologies were elevated, with an erythrocyte sedimentation rate of 55 mm/h (reference range: 0 to 20 mm/h) and a C-reactive protein level of 24 mg/L (reference range: 08 to 1 mg/L). What is the best next step?
Explanation
This complication is best addressed with either a single-stage or two-stage total knee arthroplasty. A recent report suggests that a single-stage arthroplasty can be effective, although many surgeons would perform a two-stage procedure with an articulating or static spacer. Arthroscopic would be non-effective, especially given 4 weeks of symptoms. Resection arthroplasty without a spacer would leave an unstable and poorly functioning extremity. Knee fusion should be used as a salvage procedure.
ERGUIDE MCQ 401-450
ORTHOPEDICS HYPERGUIDE MCQ 351-400
ORTHOPEDICS HYPERGUIDE MCQ 301-350
ORTHOPEDICS HYPERGUIDE MCQ 251-300
ORTHOPEDICS HYPERGUIDE MCQ 201-250
ORTHOPEDICS HYPERGUIDE MCQ 151-200
ORTHOPEDICS HYPERGUIDE MCQ 101-150
FREE Orthopedics MCQS 2022 51-100
Orthopedics Hyperguide MCQ 1-50
Question 82
- A patient sustained a joint depression-type fracture of the calcaneus that healed despite lack of treatment. The loss of dorsiflexion the patient is now experiencing is most likely the result of
Explanation
Question 83
An 18-year-old female Marine Corps recruit enters basic training. Her enlistment history and physical examination showed that she was an elite high school cross country runner. What is her most significant risk factor for a femoral or pelvic stress fracture during basic training?
Explanation
12 menses. The referenced study did not find a statistically significant increase in risk of stress fracture in those recruits who had lesser menstrual irregularities in the year prior to recruit training, but there was a trend toward increased risk of stress fracture.
REFERENCES: Shaffer RA, Rauh MJ, Brodine SK, et al: Predictors of stress fracture susceptibility in young female recruits. Am J Sports Med 2006;34:108-115.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of
Orthopaedic Surgeons, 2004, pp 273-283.
Question 84
Tendons should have what ratio of matrix protein?
Explanation
Question 85
Osteopenia is defined by the World Health Organization (WHO) as a bone mineral density (BMD) that is
Explanation
The T-score represents a comparison to young normals or optimum peak density. The Z-score represents a comparison of BMD to age-matched normals. Measurements of bone mineral density (BMD) at various skeletal sites help in predicting fracture risk. Hip BMD best predicts fracture of the hip, as well as fractures at other sites.
REFERENCE: Kanis JA, Johnell O, Oden A, et al: Risk of hip fracture according to the World Health Organization criteria for osteopenia and osteoporosis. Bone 2000;27:585-590.
Question 86
A 21-year-old man who was injured in a snowboarding accident 18 months ago now reports wrist pain. An MRI scan is shown in Figure 37. Based on the image findings, what is the most likely diagnosis?
Explanation
REFERENCE: Perlik PC, Guilford WB: Magnetic resonance imaging to assess vascularity of scaphoid nonunions. J Hand Surg Am 1991;16:479-484.
Question 87
A 23-year-old woman with a history of bilateral recurrent ankle sprains, progressive cavovarus feet, and a family history of high arches and foot deformities is seen for evaluation. Management consisting of bracing and physical therapy has been poorly tolerated. Heel varus is partially corrected with a Coleman block. There are thick calluses under the first metatarsal heads. Sensation to touch and
Explanation
Question 88
What fibers of the anterior cruciate ligament tighten with extension of the knee? Review Topic
Explanation
Question 89
Six weeks after onset, what is the most clearly accepted indication for surgical management for lumbar disk herniation?
Explanation
REFERENCES: Rhee JM, Schaufele M, Abdu WA: Radiculopathy and the herniated lumbar disc: Controversies regarding pathophysiology and management. J Bone Joint Surg Am 2006;88:2070-2080.
Atlas SJ, Keller RB, Wu YA, et al: Long-term outcomes of surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: 10 year results from the Maine lumbar spine study. Spine 2005;30:927-935.
Question 90
In recurrent posterior shoulder instability, what is the recommended approach to the posterior capsule? Review Topic
Explanation
Question 91
Figure 3a is the initial radiograph of a 19-year-old man who sustained a closed clavicle fracture. Figures 3b and 3c show postoperative radiographs. If the patient had been treated nonsurgically, which of the following would most likely occur?
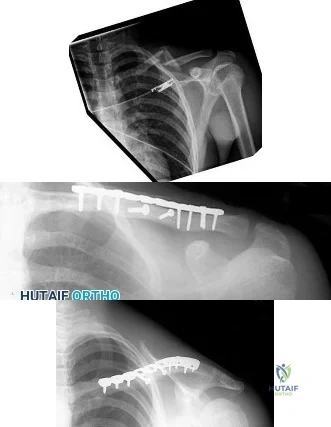
Explanation
Question 92
What type of brace is shown in Figures 22a and 22b?
Explanation
REFERENCES: Mehta JA, Brown C, Sargeant N: Charcot restraint orthotic walker. Foot Ankle Int 1998;19:619-623.
Morgan JM, Biehl WC III, Wagner FW Jr: Management of neuropathic arthropathy with the Charcot restraint orthotic walker. Clin Orthop 1993;296:58-63.
Question 93
A 15-year-old boy with a type I hereditary sensory motor neuropathy (Charcot-Marie-Tooth disease) reports recurrent ankle sprains and significant pain in the hindfoot and midfoot despite orthotic management. Examination reveals that he walks with a drop foot and has dynamic clawing of the toes. Clinical photographs of the left foot are shown in Figure 7. Management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 235-245.
Coleman SS: Complex Foot Deformities in Children. Philadelphia, Pa, Lea & Febiger, 1983, pp 147-165.
Thometz JG, Gould JS: Cavus deformity, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 94
Steroids are thought to prevent neurologic deterioration after traumatic spinal cord injury by which of the following mechanisms? Review Topic
Explanation
Question 95
A 22-year-old patient has had severe groin pain for many months and is unable to engage in any physical activity. The AP radiograph of the pelvis shows minimal arthritis. The lateral radiograph of the hip is shown in Figure 33a. An MR-arthrogram is shown in Figure 33b. What is the most appropriate treatment at this stage? Review Topic

Explanation
Question 96
Figure 10 shows patellar radiographs of a 68-year-old woman who underwent bilateral total knee arthroplasty 2 months ago. Following a recent fall onto the left side, she now reports anterior pain in the left knee. A CT scan shows that the femoral and tibial components are appropriately externally rotated and radiographs show acceptable axial alignment and no evidence of loosening. What is the most appropriate treatment option?
Explanation
If the components are determined to be in satisfactory position, soft-tissue procedures can be pursued. Lateral retinacular release is usually the first soft-tissue procedure used to improve patellofemoral mechanics. In this patient, the patellar fracture fragment is so small that it can be excised. Distal realignment is not usually used as the first line of treatment for patellar maltracking following TKA.
REFERENCES: Fehring TK, Christie MJ, Lavemia C, et al: Revision total knee arthroplasty: Planning, management, and controversies. Instr Course Lect 2008;57:341-363.
Patel J, Ries MD, Bozic KJ: Extensor mechanism complications after total knee arthroplasty. Instr Course Lect 2008;57:283-294.
Question 97
Figures 1 and 2 are intrasurgical photographs from the posterolateral viewing portal that were taken at the beginning and end of a right shoulder arthroscopic procedure performed on a 54-year-old man. This technique demonstrates superior results compared with traditional arthroscopic techniques when evaluating which outcome?
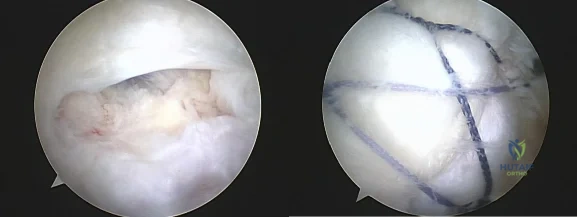
Explanation
Question 98
Risks associated with vertebral compression fractures in the elderly population can be defined by which of the following? Review Topic
Explanation
fractures are more likely to fall and are five times more likely to sustain subsequent fractures than individuals without such a fracture. Analysis of data from Medicare patients with a vertebral fracture had an overall mortality rate that was approximately twice that of the matched controls. The survival rates following a fracture diagnosis, as estimated with the Kaplan-Meier method, were 53.9%, 30.9%, and 10.5% at 3, 5, and 7 years, respectively which were significantly lower than the rates for the controls. The mortality risk following a fracture was greater for men than for women. The mortality risk was greater when the fracture occurred at a younger age. The adjusted hazard ratio was 1.8 compared to the non-fracture group
Question 99
A 23-year-old man cut the dorsal and ulnar aspects of his long finger on a table saw. The dorsal and ulnar skin over the middle phalanx is missing, with a 2-cm x 2-cm area of loss. There is a 50% loss of the extensor tendon (ulnar), and the remaining tendon has no tenosynovium. The physician should recommend irrigation and debridement and
Explanation
The patient has exposed bone and tendon and a partial tendon injury. The remaining radial tendon is satisfactory and no tendon repair is required. The exposed bone and tendon necessitate vascularized tissue coverage. A reversed cross-finger flap from the ring finger is suitable for coverage of the dorsal surface of an adjacent digit.
Question 100
A 10-year-old boy tripped as he was running down a hill, felt a painful pop in his right knee, and was unable to bear weight on the involved lower extremity. Examination reveals a tense effusion and an extensor lag of the right knee. Figures 36a and 36b show AP and lateral radiographs. Management should consist of
Explanation
The distal fragment can be much larger than it appears on the radiographs because it consists largely of cartilage.
REFERENCES: Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Grogan DP, Carey TP, Leffers D, et al: Avulsion fractures of the patella. J Pediatr Orthop 1990; 10:721 - 730. Question 37
When addressing a proximal intertrochanteric or subtrochanteric fracture in a juvenile with open growth plates, the arterial supply from what artery at the neck must be preserved?
Lateral femoral circumflex
Medial femoral circumflex
Superior gluteal
Inferior gluteal
Obturator
DISCUSSION: The medial femoral circumflex artery supplies blood to the femoral head. Its position along the posterior-superior femoral neck places this structure at risk with intramedullary nailing of the femur. Therefore, lateral entry through the greater trochanter is preferred when intramedullary fixation is performed.
REFERENCES: Gordon JE, Swenning TA, Burd TA, et al: Proximal femoral radiographic changes after lateral transtrochanteric intramedullary nail placement in children. J Bone Joint Surg Am 2003;85:1295- 1301.
Green NE, Swiontkowski MF: Skeletal Trauma in Children, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 419-424.
