Orthopedic Board Review MCQs: Arthroplasty, Fracture, Hip & Ankle | Part 238
Key Takeaway
This page delivers Part 238 of an OITE & AAOS Orthopedic Board Review MCQ series. It provides 100 verified, high-yield questions for orthopedic residents and surgeons. Prepare for board certification by mastering clinical scenarios across Ankle, Arthroplasty, Fracture, and Hip in Study or Exam Mode.
About This Board Review Set
This is Part 238 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 238
This module focuses heavily on: Ankle, Arthroplasty, Fracture, Hip.
Sample Questions from This Set
Sample Question 1: Treatment of an atrophic nonunion of the radial diaphysis should include which of the following?...
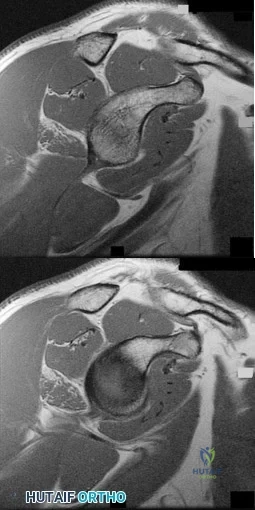
Sample Question 2: Figure 52 shows the MRI scan of a 28-year-old baseball pitcher. Examination will most likely reveal which of the following findings?...
Sample Question 3: A 22-year-old woman injured her ankle when she fell off a ladder. Radiographs reveal a displaced large posterior malleolus fracture of about 45% of the joint. What is the best definitive treatment?...
Sample Question 4: The need for postoperative allogeneic blood transfusions after total hip arthroplasty has been shown to be reduced when using...
Sample Question 5: Receptor activator of nuclear factor kappa b (RANKL) and macrophage colony stimulating factor (MCSF) signaling pathways are necessary for the formation of multinucleated osteoclasts that resorb bone. Which of the following cells are known t...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Treatment of an atrophic nonunion of the radial diaphysis should include which of the following?

Explanation
Question 2
Figure 52 shows the MRI scan of a 28-year-old baseball pitcher. Examination will most likely reveal which of the following findings?
Explanation
REFERENCES: Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Inokuchi W, Ogawa K, Horiuchi V: Magnetic resonance imaging of suprascapular nerve palsy.
J Shoulder Elbow Surg 1998;7:223-227.
Question 3
A 22-year-old woman injured her ankle when she fell off a ladder. Radiographs reveal a displaced large posterior malleolus fracture of about 45% of the joint. What is the best definitive treatment?
Explanation
optimal function can be achieved. Open reduction and internal fixation allows this achievement. In cases where comminution exists, absolute stability may have to be sacrificed so as to not strip small comminuted bone fragments. Therefore, a bridging technique is worthwhile. External fixation can be used as a temporary technique until the soft tissues are more amenable to definitive fixation. Cast treatment is not indicated in adult forearm fractures. Locking nails for forearm use are not reamed. With regards to articular fractures, anatomic reduction and rigid stabilization are required to achieve the best results and allow for fracture healing. This environment also allows for the best chance of the cartilage repair process to form "hyaline-like" cartilage. Open reduction and internal fixation with absolute stability is the mainstay of treatment for partial articular fractures such as split depression tibial plateau fractures and posterior malleolus fractures involving greater than about 25% to 30% of the joint. The gold standard for the treatment of a closed femur fracture is a reamed intramedullary locked nail. Results are uniformly excellent. This can be done without stripping of the soft tissues such as in open reduction and internal fixation. External fixation can be used as a temporary device in patients in extremis for damage control reasons.Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr. Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am. 1986 Sep;68(7):1008-17. http://www.ncbi.nlm.nih.gov/pubmed/3745238')">View Abstract at PubMedJones DB Jr, Kakar S. Adult diaphyseal forearm fractures: intramedullary nail versus plate fixation. J Hand Surg Am. 2011 Jul;36(7):1216-9. Epub 2011 May
Question 4
The need for postoperative allogeneic blood transfusions after total hip arthroplasty has been shown to be reduced when using
Explanation
(p < 0.001) after surgery.
REFERENCES: Waddell JP: Evidence-based orthopedics. J Bone Joint Surg Am 2001;83:788.
Feagan BG, Wang CJ, Kirkley A, et al: Erythropoietin with iron supplementation to prevent allogeneic blood transfusion in total hip joint arthroplasty: A randomized, controlled, trial. Ann Intern Med 2000;133:845-854.
Question 5
Receptor activator of nuclear factor kappa b (RANKL) and macrophage colony stimulating factor (MCSF) signaling pathways are necessary for the formation of multinucleated osteoclasts that resorb bone. Which of the following cells are known to produce RANKL?
Explanation
Question 6
Which of the following nerves is most commonly injured during ankle arthroscopy?
Explanation
REFERENCES: Ferkel RD, Heath DD, Guhl JF: Neurological complications of ankle arthroscopy. Arthroscopy 1996;12:200-208.
Barber CL, Click J, Britt BT: Complications of ankle arthroscopy. Foot Ankle 1990;10:263-266.
Question 7
A 70-year-old woman with a body mass index (BMI) of 34 and a history of hypercholesterolemia has elected to undergo total hip arthroplasty. Her son recently learned he has factor V Leiden following an episode of pulmonary embolism. What are this patient's risk factors for thromboembolic disease?
Explanation
Risk stratification is one of the most critical clinical evaluations to undertake before performing total joint arthroplasty. Many factors have been identified that increase the risk for venous thromboembolism (VTE) The major factors include previous VTE, obesity, type of surgery (such as total joint arthroplasty), hypercoagulable states, myocardial infarction, congestive heart failure, family history of VTE, and
hormone replacement therapy. Hypercholesterolemia is not a risk factor for thromboembolic disease.
Question 8
Which of the following conditions is associated with palmoplantar pustulosis?
Explanation
REFERENCES: Wirth MA, Rockwood CA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 608-609.
Sonozaki H, Azuma A, Okai K, et al: Clinical features of 22 cases with inter-sterno-costo-clavicular ossification: A new rheumatic syndrome. Arch Orthop Trauma Surg 1979;95:13-22.
Question 9
A 19-year-old football player is taken off the field because of fatigue. Examination reveals a rash shown in Figure A. Oral examination reveals findings shown in Figure B. Posterior cervical glands are palpable. A mass is palpable in the left upper quadrant. Which of the following is true regarding the most likely diagnosis? Review Topic

Explanation
IM is caused by the Epstein-Barr virus (EBV). Annual incidence is 1-3% in college freshmen. It is characterized by Hoagland's triad (fever, pharyngitis, lymphadenopathy). Some have rash and splenomegaly. Splenic rupture is rare (0.1-0.2% of patients). It is caused by sudden increase in portal venous pressure from a simple Valsalva maneuver or from external trauma. The risk of rupture is highest in the first 3 weeks of illness.
Putukian et al. reviewed IM and athletic participation. They recommend return to LIGHT activity after 3 weeks from symptom onset when the athlete is afebrile, has a good energy level, and does not have any significant associated abnormalities. They recommend returning to CONTACT sports after at least 3 weeks when the athlete has no remaining clinical symptoms, is afebrile, and has a normal energy level.
Jaworski et al. discussed infectious diseases in athletes. They state that splenic rupture occurs because of lymphocytic infiltration that distorts the support structure of the spleen, leading to fragility. They recommend return to light, non-contact activities once the athlete is afebrile and appropriately hydrated, fatigue has improved, and a minimum period of 3 weeks has passed from symptom onset.
Figure A shows a petechial rash, which can be seen in IM. Amoxicillin increases the risk of rash. Figure B shows unilateral exudative pharyngitis. The left tonsil is
covered
by
a
white
exudate/pseudomembrane.
Incorrect
Question 10
What vessel is marked with an asterisk in Figure 44?
Explanation
REFERENCES: Agur AM, Dalley AF (eds): Grant’s Atlas of Anatomy, ed 12. Philadelphia, PA, Lippincott Williams and Wilkins, 2008.
Uflacker R: Atlas of Vascular Anatomy: An Angiographic Approach, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006.
Question 11
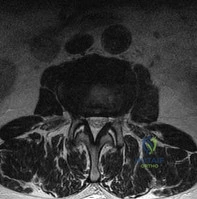
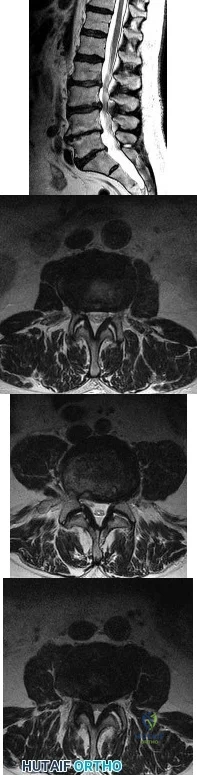
A 78-year-old man has a history of worsening bilateral calf pain with activity. MRI scans are shown in Figures 31a through 31d. His symptoms are not improved with forward flexion of the lumbar spine. His lower extremity pain is relieved when he sits or ceases activity. Which of the following tests would be most helpful in establishing a diagnosis? Review Topic
Explanation
Decreased range of motion and hip joint pain, especially in internal rotation and abduction, are common findings in patients with degenerative arthritis of the hip. While post-myelography CT has been found superior to MRI as a single study for the preoperative planning of decompression for lumbar spinal stenosis, it will not assist in differentiating vascular from neurogenic claudication.
Question 12
A right-handed 24-year-old woman underwent an arthroscopic Bankart repair for recurrent anterior dislocations 9 months ago. Despite extensive physical therapy for 8 months, the patient has very limited range of motion (elevation to 130 degrees and external rotation to 10 degrees with the arm at the side). Shoulder radiographs are normal. The next step in management should consist of
Explanation
REFERENCES: Warner JJ, Allen AA, Marks PH, Wong P: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
Harryman DT II, Matsen FA III, Sidles JA: Arthroscopic management of refractory shoulder stiffness. Arthroscopy 1997;13:133-147.
Question 13
Figure 50 shows the radiograph of a 26-year-old man who sustained an isolated open injury to his foot. Examination reveals no gross contamination in the wound. There is a palpable dorsalis pedis pulse and sensation is present on the dorsal and plantar aspects of the foot. Initial treatment should consist of wound debridement, antibiotics, and
Explanation
REFERENCES: Smith CS, Nork SE, Sangeorzan BJ: The extruded talus: Results of reimplantation. J Bone Joint Surg Am 2006;88:2418-2424.
Brewster NT, Maffulli N: Reimplantation of the totally extruded talus. J Orthop Trauma 1997;11:42-45.
Question 14
An 18-year-old gymnast has had a 1-year history of foot pain. Examination reveals medial midfoot tenderness without swelling. Non-weight-bearing in a cast for 6 weeks has failed to provide relief. An axial CT scan of the midfoot is shown in Figure 20. What is the optimal treatment for this condition?
Explanation
REFERENCES: Quirk RM: Stress fractures of the navicular. Foot Ankle Int 1998;19:494-496.
Saxena A, Fullem B, Hannaford D: Results of treatment of 22 navicular stress fractures and a new proposed radiographic classification system. J Foot Ankle Surg 2000;39:96-103.
Question 15
Bleeding is encountered while developing the internervous plane between the tensor fascia lata and the sartorius during the anterior approach to the hip. The most likely cause is injury to what artery?
Explanation
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 312.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 304.
Question 16
In an effort to reduce costs, a limited MRI sequence is planned to detect a possible occult hip fracture. What is the anticipated fracture signal?
Explanation
REFERENCES: Miller MD: Review of Orthopaedics, ed 3. Philadelphia PA, WB Saunders, 2000, p 116.
Guanche CA, Kozin SH, Levy AS, et al: The use of MRI in the diagnosis of occult hip fractures in the elderly: A preliminary review. Orthopedics 1994;17:327-330.
Question 17
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?
Explanation
REFERENCES: Lyons RP, Green A: Subscapularis tendon tears. J Am Acad Orthop Surg 2005;13:353-363.
Warner JJ, Higgins L, Parsons IM, et al: Diagnosis and treatment of anterosuperior rotator cuff tears. J Shoulder Elbow Surg 2001;10:37-46.
Question 18
When do most symptomatic thromboembolic events occur after total joint arthroplasty?
Explanation
Most clinical venous thromboembolism events occur between the second and sixth weeks after surgery. It is estimated that 10% of patients are readmitted to the hospital within the first 3 months after total hip or knee arthroplasties. Most pulmonary events on the day of surgery are related to fat embolism or cardiac events.
Question 19
..Staging studies show no other lesions and surgical treatment is planned; when should a biopsy be performed?
Explanation
Figures 117a through 117c are the radiographs and MRI scan of a 16-year-old boy who has had a persistent fullness in his thigh since being kicked while playing soccer 4 weeks ago. He states that initially the area was painful, but now all symptoms other than the mass have resolved.

Question 20
What are the optimal conditions for leaving the acetabular shell in place, replacing the acetabular liner, and grafting the osteolytic defect shown in Figure 39?
Explanation
REFERENCES: Ries MD: Complications in primary total hip arthroplasty: Avoidance and management. Wear. Instr Course Lect 2003;52:257-265.
Dumbleton JH, Manley MT, Edidin AA: A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J Arthroplasty 2002;17:649-661.
Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 175-180.
Question 21
Figures 1 and 2 show the radiograph and CT obtained from a 78-year-old woman who underwent right total hip replacement in 1995. She initially did well with no pain. She was last seen 7 years ago and was having mild hip pain at that time. She was found to have a supra-acetabular cyst on radiographs. She has had severe right hip pain for the past 9 months while using a walker for ambulation. The initial blood work reveals an estimated erythrocyte sedimentation rate of 32 mm/hr, a C-reactive protein level of 0.5 mg/L, a serum cobalt level of 0.4 µg/L, and a serum chromium level of 0.6 µg/L. Right hip aspiration is performed, revealing a white blood cell count of 139, 52% neutrophils, and a negative leukocyte esterase test. What is the best next step?
Explanation
The hip replacement was performed in 1995, during the period when the previous generation of polyethylene was utilized. This polyethylene was subjected to irradiation in air, with subsequent oxidation and consequent osteolysis after implantation. The mechanism of osteolysis begins with the uptake of polyethylene particles by macrophages, which then initiate an inflammatory cascade and the release of osteolytic factors. This cycle continues, with eventual implant loosening and failure. The imaging shows significant osteolysis and raises concern for pelvic discontinuity and acetabular implant failure. The surgical treatment consists of acetabular reconstruction. In this patient, concern exists for discontinuity based on the substantial amount of bone loss and nonsupportive anterior and posterior columns. This scenario requires complex acetabular revision using a custom triflange device, distraction with a jumbo acetabular component, or placement of a porous metal cup/cage construct with augmentation. The laboratory values are not consistent with infection or failure due to metal debris.
Question 22
At which joint do degenerative changes occur first in a patient with chronic, untreated scapholunate dissociation?
Explanation
Stage I of scapholunate advanced collapse (SLAC) is characterized by the presence of radioscaphoid arthritis. A predictable pattern exists of the progression of degenerative changes for SLAC wrist, including stage I (radial styloid involvement at the scaphoid fossa), stage II (scaphoid and entire scaphoid facet involvement), stage III (degeneration between the capitate and lunate), and stage IV (pancarpal involvement). The radiolunate joint is often spared.
Question 23
What approach should be chosen for the injury seen in Figure 67? Review Topic

Explanation
Innervates the medial aspect of the proximal thigh
Originates from the dorsal roots of L4-L5
Course runs medial to the femoral artery
Courses along the medial border of the psoas muscle
Courses under the inguinal ligament PREFERRED RESPONSE 5
Question 24
Which of the following procedures is considered most appropriate in patients with rheumatoid arthritis?
Explanation
REFERENCES: Granberry WM, Brewer EJ Jr: Early surgery in juvenile rheumatoid arthritis, in Calundruccio RA (ed): Instructional Course Lectures XXIII. St Louis, MO, CV Mosby, 1974, pp 32-37.
Stuchin SA, Johanson NA, Lachiewicz PF, Mont MA: Surgical management of inflammatory arthritis of the adult hip and knee, in Zuckerman JD (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-109.
Question 25
Figures 1 and 2 show the radiographs obtained from a 68-year-old morbidly obese man who underwent left total hip replacement 7 years ago and did well, with no symptoms prior to the current presentation. He recently rose from a seated position and felt a pop in the hip, with immediate pain and inability to bear weight. Any pressure on the left foot now produces a painful, grinding sensation with loss of left hip stability. What is the best next step?
Explanation
The modular femoral stem has fractured. Changing the liner to a constrained design is not warranted at this time based on the information provided. Revision of the acetabular implant is appropriate because of the potential for damage to the existing cup from metal debris and femoral implant contact and to convert from a metal-on-metal articulation. Nonsurgical management would not provide pain relief or improvement; revision of the total hip arthroplasty is recommended. The implant failed in a short time, and retention of the femoral stem is not recommended because of the concern for failure with only a neck exchange. A dual-mobility bearing may be a good option if the surgeon plans to retain the acetabular component. Extended trochanteric osteotomy is a useful technique for the removal of a well-fixed femoral implant. In this patient, femoral stem removal without
osteotomy would be difficult due to the fracture of the implant’s femoral neck and the
inability to gain purchase for extraction.
Question 26
Figure 8a shows the clinical photograph of an 83-year-old woman who has an enlarging left forearm mass. MRI scans are shown in Figures 8b and 8c. What is the next most appropriate step in management?
Explanation
REFERENCES: Damron TA, Beauchamp CP, Rougraff BT, et al: Soft-tissue lumps and bumps. Instr Course Lect 2004;53:625-637.
Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 27
Which of following is pathognomonic of intervertebral disk degeneration? Review Topic
Explanation
large proteoglycan molecules in
the nucleus pulposus is
pathognomonic
of intervertebral disk
(IVD) degeneration.
Degeneration of the intervertebral disk (IVD) is a major pathological process implicated in low back pain and is often considered a prerequisite for intervertebral disc herniation. While the pathophysiologic causes of IVD degeneration at the molecular level are not fully known, there are many physical and molecular changes that are known to contribute to the disease process. The most significant is loss of large proteoglycan molecules and decreased water content.
An et al. showed that large proteoglycans (PGs), such as aggrecan and versican, decrease in patients with intervertebral disk (IVD) degeneration.
Kepler et al. reviewed IVD degeneration. They report that degeneration leads to changes in the expression of matrix proteins, cytokines, and proteinases. They suggest treatment with gene therapy, such as Growth and Differentiation Factor-5 (GDF-5), may help to promote the healing of degenerated intervertebral disks.
Illustration A shows a cadaveric image of normal disk anatomy (left) and IVD degeneration (right)
Incorrect Answers:
Question 28
A 44-year-old man was involved in a low speed rear-end motor vehicle accident 4 weeks ago. He predominantly reports pain in the back of the neck, with occasional radiation into the trapezius region bilaterally. He denies any extremity pain. The pain has not changed in intensity, but is worse with neck range of motion. Cervical spine radiographs were negative for acute osseous trauma or instability. What is the next most appropriate step in management? Review Topic
Explanation
Question 29
A 35-year-old woman with type 1 diabetes mellitus has been treated for the past 2 years at a wound care center for persistent bilateral fifth metatarsal head ulcers. Management has consisted of shoe wear modifications, treatment with multiple enzymatic ointments, and a fifth metatarsal head resection on the left side. Physical examination reveals intact pulses, minimal ankle dorsiflexion, neutral hindfoot, and a persistent ulcer under the fifth metatarsal heads. What treatment will best help heal the ulcers?
Explanation
REFERENCES: Laughlin RT, Calhoun JH, Mader JT: The diabetic foot. J Am Acad Orthop Surg 1995;3:218-225.
Aronow MS, Diaz-Doran V, Sullivan RJ, et al: The effect of triceps surae contracture force on plantar foot pressure distribution. Foot Ankle Int 2006;27:43-52.
Question 30
Which of the following factors is associated with the highest rate of nonunion of a midshaft clavicle fracture?
Explanation
Clavicle fractures are often secondary to direct blows to the lateral aspect of the shoulder. Physical examination is important to ascertain the status of the
skin and neurovascular structures to help guide treatment management. Although most non-displaced middle 1/3 clavicle fractures may be treated successfully with conservative measures, the risk for non-union (1-5%) increases with increasing comminution, female gender, shortening greater than 2 cm and an advanced age of the patient.
Robinson et al. reviewed 581 patients treated non-operatively for midshaft clavicle fractures. A nonunion rate of 4.5 % was identified at 24 weeks after the injury. They identified four factors that contributed to non-union, including: female gender, lack of cortical apposition, comminution of the fracture fragments and advancing age.
Zlowdzki et al. reviewed 2144 clavicle fracture cases in a comprehensive meta-analysis. They report displacement as the highest risk factor for nonunion (15.1%) in nonoperatively treated clavicle fractures, and simple slings were favored over figure of 8 braces. They also report an 86% reduction in the nonunion rate when operative fixation is chosen over nonoperative treatment for displaced clavicle fractures.
Illustration A shows the presence of a non-union of a midshaft clavicle fracture. A video is provided that reviews management of clavicle injuries.
Incorrect Answers

OrthoCash 2020
Question 31
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms?
Explanation
A traumatic blow to the outstretched arm results in posterior glenohumeral forces. Labral detachment at the glenoid rim is common. Patients report slipping or pain with posteriorly directed pressure. Rarely do these patients have true dislocations that require reduction; however, recurrent episodes of subluxation or pain are not uncommon. Posterior repair has
been shown to be successful in the treatment of traumatic instability.
REFERENCES: Bottoni CR, Franks BR, Moore JH, et al: Operative stabilization of posterior shoulder instability. Am J Sports Med 2005;33:996-1002.
Williams RJ III, Strickland S, Cohen M, et al: Arthroscopic repair for traumatic posterior shoulder instability. Am J Sports Med 2003;31:203-209.
Kim SH, Ha KI, Park JH, et al: Arthroscopic posterior labral repair and capsular shift for traumatic unidirectional recurrent posterior subluxation of the shoulder. J Bone Joint Surg Am 2003;85:1479-1487.
Question 32
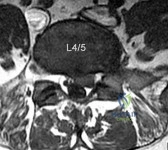
A 32-year-old male presents with left leg pain and weakness. An axial image from his MRI is shown in Figure A. Which of the following physical exam findings would be most consistent with this MRI finding. Review Topic
Explanation
radiculopathy.
While nerve root innervation shows some variability by patient, L5 is "characteristically" responsible for the sensation to the dorsal aspect of the foot, ankle dorsiflexion (tibialis anterior - along with L4), great toe extension (EHL), and hip abduction (gluteus medius).
Suri et al. reported on specific physical exam findings that significantly increased the likelihood of nerve root impingement at specific lumbar levels. They found: L2 was associated with decreased anterior thigh sensation. L3 was associated with a positive femoral stretch test. L4 was associated with a blunted patellar reflex, decreased medial ankle sensation or a positive crossed femoral stretch test. L5 was associated with was associated with decreased hip abductor strength.
Luri et al. reported 8-year follow up on the patients in the spine patient outcomes research trial who underwent surgical vs. conservative care for treatment of lumbar herniated disc. They found that patients who underwent surgical treatment had superior results that were maintained at 8 years compared to patients who underwent conservative management.
Figure A is an axial MRI at the L4/5 disc space that shows a left paracentral disc herniation compressing the descending L5 nerve root. Illustration A identifies the structures in the MRI image. Illustration B demonstrates the dermatome, reflex and motor function associated with the L4, L5 and S1 nerve root.
Incorrect Answers:
(SBQ13PE.102) An 26-year-old male presents to your office complaining of bilateral hip and low back pain. On physical examination, he has 10 degree bilateral hip flexion contractures. An AP pelvis radiograph is demonstrated in figure A. Which of the following findings is consistent with this patient's presentation? Review Topic

A positive flexion, adduction, internal rotation (FADDIR) test
A history of untreated slipped capital femoral epiphysis (SCFE)
A thrombophilia
Normal serum ESR and CRP
Positive Human Leukocyte Antigen B27 (HLA-B27)
The patient has large joint arthralgia and sacroiliac joint sclerosis on AP pelvis radiograph, which is consistent with ankylosing spondylitis. Patients with ankylosing spondylitis have positive Human Leukocyte Antigen B27 (HLA-B27).
Ankylosing spondylitis (AS) is a seronegative spondyloarthropathy that affects the axial skeleton as well as large joints including the hips and knees. The most common initial site of pain is the sacroiliac (SI) joint, and is demonstrated as sacroiliitis on pelvic radiograph. Hip involvement is common, and typically manifests as hip pain and flexion contracture. Serologic studies will be typically be negative for rheumatoid factor, but positive for HLA-B27 in 90% of patients.
Kubiak et. al. review orthopaedic management of AS. Common orthopaedic manifestations include SI joint pain, hip flexion contractures, and stiffness of the cervical and lumbar spine. They report that laboratory analysis of patients with active disease will typically demonstrate mild elevation of ESR, CRP, and WBC. Patients with chronic AS may demonstrate a normocytic anemia. If HLA-B27 is negative, a high clinical suspicion should still be maintained.
Gensler et al. review the different clinical conditions that compose of juvenile-onset spondyloarthritis. They report on the different spondyloarthritides includes ankylosing spondylitis, reactive arthritis, arthropathy associated with inflammatory bowel disease, and that associated with psoriasis. They emphasize that the appearance of sacroiliac joint and spinal disease in the form of ankylosing spondylitis usually takes 5–10 years after initial symptom presentation, and therefore, a definite diagnosis can take several years leading to a delay in diagnosis.
Figure A is an AP pelvis radiograph of a skeletally mature individual demonstrating sclerosis of the SI joint indicative of sacroiliitis. Illustration A shows a axial CT image of the patient in the stem. Sclerosis and bone erosion can be seen in the sacroiliac joint.
Incorrect Answers:
osteonecrosis Answer 3: A infarctions,
of
the
femoral
epiphysis.
thrombophilia may have
osseous manifestations such as bone
which
are
not
evident
on
this
image.
Question 33
Figures 71a and 71b/ are the MR images of a 65-year-old man who dislocated his shoulder. What is his most likely chief symptom?
Explanation
This patient has a massive rotator cuff tear resulting in disruption of the transverse force couple between the subscapularis anteriorly and the infraspinatus and teres minor posteriorly. These muscles provide dynamic shoulder stability throughout active elevation. Loss of the force couple produces a pathologic increase in translation of the humeral head and decreased active abduction and external rotation, which results in difficulty raising an arm. The most common neurologic deficit after shoulder dislocation is isolated injury to the axillary nerve that supplies sensation to the lateral aspect of the shoulder, not the anterior aspect. Recurrent instability is uncommon unless there is a labral tear or massive subscapularis tear. The biceps muscle is not viewed in the MR images, and a complete proximal biceps tendon rupture would be uncommon in the setting of an anterior shoulder dislocation.

CLINICAL SITUATION FOR QUESTIONS 72 THROUGH 75
Figures 72a through 72e are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0 degrees
to 90 degrees and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted.
Question 34
A 14-year-old boy has a midshaft fibular lesion. Biopsy results are consistent with Ewing’s sarcoma. Following induction chemotherapy, local control typically consists of
Explanation
REFERENCES: Nesbit ME Jr, Gehan EA, Burgert EO Jr, et al: Multimodal therapy for the management of primary, nonmetastatic Ewing’s sarcoma of bone: A long-term follow-up of the First Intergroup study. J Clin Oncol 1990;8:1664-1674.
Simon MA, Springfield DS, et al: Ewing’s Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 287-297.
Question 35
The condition shown in Figures 9a and 9b is most likely the result of

Explanation
Question 36
A healthy 2-year-old boy falls from a swing and sustains a displaced midshaft femoral fracture with 1 cm of shortening. What is the most appropriate treatment?
Explanation
DISCUSSION: For children between the ages of 1 and 6 years, closed reduction and early spica casting is recommended. In some instances, associated injuries or body habitus may preclude cast treatment. Pavlik harness treatment of femoral fractures is for infants younger than 1 year of age. Rarely is there an indication for traction. Internal fixation is reserved in general for children older than age 6 years or with confounding factors.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 271-280.
Flynn JM, Schwend RM: Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg 2004;12:347-359.
Figure 29a Figure 29b
Question 37
A 47-year-old woman with no history of trauma has had a painful, stiff shoulder for the past 3 months. Treatment consisting of subacromial injection and nonsteroidal anti-inflammatory drugs has been ineffective. Her active range of motion is painful and is limited to 90 degrees of abduction, 60 degrees of elevation, 30 degrees of external rotation, and internal rotation to the posterior superior iliac spine. Plain radiographs of the cervical spine and shoulder are normal. Management at this time should consist of
Explanation
Question 38
A 15-year-old boy reports a 2-day history of progressive left buttock pain and severe limping. He denies any history of trauma or radiation of the pain. He has an oral temperature of 100.4 degrees F (38 degrees C). Examination reveals that the lumbar spine and left hip have unguarded motion. The abdomen is nontender. There is moderate tenderness of the left sacroiliac region with no palpable swelling. Pain is elicited when the left lower extremity is placed in the figure-4 position (FABER test). Laboratory studies show a peripheral WBC count of 11,500/mmP3P (normal to 10,500/mmP3P) and an erythrocyte sedimentation rate of 38 mm/h (normal up to 20 mm/h). Radiographs of the pelvis, hips, and lumbar spine are normal. A nucleotide bone scan (posterior view) is shown in Figure 44. Initial management should consist of Review Topic

Explanation
Question 39
Figure 6 shows a sagittal oblique MRI scan. The arrow is pointing to what structure?
Explanation
REFERENCES: Clarke HD, Scott WN, Insall JN, et al: Anatomy, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 3-66.
Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 40
Epithelioid sarcoma most commonly occurs in which of the following anatomic locations?
Explanation
REFERENCES: Gupta TD, Chaudhuri P (eds): Tumors of the Soft Tissues, ed 2. Stamford, CT, Appleton and Lange, 1998, p 475.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St. Louis, MO, Mosby-Year Book, 1995, p 1074.
Question 41
Figures below show the radiographs obtained from a 79-year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. No evidence of infection is seen. What is the most appropriate treatment?

Explanation
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis, as shown in Figures 3 and 4. They also assist in obtaining correct limb alignment. Short metaphyseal-engaging stems are associated with failure rates that range between 16% and 29%. Cemented stems may be shorter than press-fit stems, because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.
Question 42
The comparative outcomes of needle aponeurotomy (NA) and collagenase Clostridium histolyticum (CCH) use in the treatment of Dupuytren contracture indicate that patients treated with CCH have
Explanation
A. Proximal row carpectomy
B. Vascularized bone graft
C. Radial shortening osteotomy
D. Capitate shortening osteotomy
Osteonecrosis of the capitate is a rare condition that presents with an insidious onset of dorsal wrist pain. When nonsurgical treatment fails to alleviate symptoms, surgical intervention is appropriate. When collapse of the capitate is present, partial excision of the capitate with interposition, partial wrist arthrodesis, or wrist denervation can be considered. In the absence of collapse, capitate-preserving options are available. Vascularized grafting is a mainstay of treatment. Grafting with distal radius vascularized grafts based on the 1,2 intercompartmental supraretinacular artery or the 4 + 5 extensor compartment artery and second metacarpal graft based on the first dorsal metacarpal artery have been described.
Question 43
A 57-year-old man involved in a motor vehicle accident sustains an injury to his right shoulder. A spot AP radiograph is shown in Figure 34. What is the next most appropriate step in the orthopaedic management of this patient? Review Topic

Explanation
Question 44
The thickest bone in the occiput is located
Explanation
REFERENCES: Nadim Y, Lu J, Sabry FF, et al: Occipital screws in occipitocervical fusion and their relation to the venous sinuses: An anatomic and radiographic study. Orthopedics 2000;23:717-719.
Ebraheim N, Lu J, Biyani A, et al: An anatomic study of the thickness of the occipital bone: Implications for occipitocervical instrumentation. Spine 1996;21:1725-1729.
Question 45
The spinal cord terminates as the conus medullaris at what vertebral level in adults? Review Topic 1 T12
Explanation
Question 46
In a pilon fracture, the Chaput fragment typically maintains soft tissue attachment via which of the following structures?

Explanation
Question 47
A 21-year-old man sustains multiple gunshot wounds to his right upper extremity. He can not extend his digits or his thumb but can extend and radially deviate his wrist. An injury to the radial nerve or one of its branches has most likely occurred at which of the following locations?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 53.
Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 428-429.
Question 48
What is the goal of surgical treatment in this scenario?
Explanation
This patient has a metastatic neuroendocrine tumor. Surgical treatment should prioritize palliation of her symptoms. She has high-grade spinal cord compression without neurologic signs or symptoms. Steroids are beneficial for patients with high-grade spinal cord compression caused by tumors, and these drugs should be administered in the acute setting. This patient was appropriately initially treated with conventional radiation. However, she is not a candidate for further radiation because of spinal cord tolerance limits and insufficient clearance between the tumor and spinal cord. Consequently, stereotactic radiation is not an option.
The goal of surgical treatment of this tumor should be palliation of her symptoms rather than cure. A costotransversectomy approach offers the advantage of ventral and dorsal spinal cord access, which is necessary in this case. A sternotomy or transthoracic approach would offer ventral access, but dorsal access would be less than optimal.
RECOMMENDED READINGS
Rose PS, Buchowski JM. Metastatic disease in the thoracic and lumbar spine: evaluation and management. J Am Acad Orthop Surg. 2011 Jan;19(1):37-48. Review. PubMed PMID: 21205766.View Abstract at PubMed
Rades D, Abrahm JL. The role of radiotherapy for metastatic epidural spinal cord compression. Nat Rev Clin Oncol. 2010 Oct;7(10):590-8. doi: 10.1038/nrclinonc.2010.137. Epub 2010 Aug
Question 49
The use of bisphosphonates in children with osteogenesis imperfecta is becoming more widely accepted as treatment to improve quality of life and to decrease the risks of fracture. What is the mechanism by which bisphosphonates work?
Explanation
Question 50
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the Review Topic
Explanation
Question 51
What is the heaviest weight that can be safely applied to the adult cervical spine via Gardner-Wells tong traction?
Explanation
REFERENCES: Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Anderson DG, Vacccaro AR, Gavin K: Cervical orthoses and cranioskeletal traction, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005,
pp 110-121.
Question 52
A young gymnast fell awkwardly onto an outstretched hand during a competition. At the time of impact, his forearm was positioned in supination. Axial and posterolateral forces were loaded along the forearm into the elbow and the elbow underwent a significant valgus thrust. What injury pattern is most likely to result from the combination of these forces at the elbow?
Explanation
The key features of a terrible triad injury include a radial head fracture, coronoid fracture, and dislocation of the elbow. Disruption of the lateral collateral ligament complex often concomitantly occurs. While restoration of the bony anatomy is important for static stability, the key primary stabilizer that needs to be addressed is the lateral collateral ligament complex. In acute injuries LCL repair may be possible. In chronic injury, LCL reconstruction would need to be considered.
O'Driscoll et al. 1991, examined 5 patients with recurrent posterolateral rotatory instability of the elbow. They showed that by applying supination of the forearm with a valgus moment and an axial compression force to the elbow while it is flexed from full extension, this can demonstrate posterolateral rotatory instability of the elbow. The elbow is reduced in full extension and must be subluxated as it is flexed in order to obtain a positive test result (a sudden reduction of the subluxation).
O'Driscoll et al. 1992 looked at a cadaveric study of the elbow. They showed that external rotation and valgus moments with axial forces resulted in posterior dislocations in 12 of the 13 specimens when the anterior medial collateral ligament (AMCL) remained intact. Clinically, it valgus stability in pronation is demonstrated, the AMCL can be assumed to be intact.
Illustration A and B shows radiographs of a terrible triad injury. There is posterolateral dislocation of the elbow with associated radial head fracture, coronoid fracture.
Incorrect Answers:
Question 53
A 46-year-old woman reports pain and a shortened appearance of her toe after undergoing a Keller resection arthroplasty 2 years ago for hallux rigidus. Examination reveals mild swelling and motion limited to 25 degrees at the metatarsophalangeal joint. Radiographs show large dorsal osteophytes on the first metatarsal head, 50% resection of the proximal phalanx, and complete loss of the metatarsophalangeal joint space. Which of the following is considered the most reliable procedure to improve her pain and the appearance of her toe?
Explanation
REFERENCES: Myerson MS, Schon LC, McGuigan FX, Oznur A:Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int 2000;21:297-306.
Mann RA, Coughlin MJ: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 252-253.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 293-303.
Question 54
Figure 7 shows the MRI scan of a 23-year-old competitive rugby player who has anterior ankle pain and swelling. He states that he has been playing for many years and has sprained his ankle several times. Examination will reveal what specific hallmark feature?
Explanation
REFERENCES: Ogilvie-Harris DJ, Mahomed N, Demaziere A: Anterior impingement of the ankle of the ankle treated by arthroscopic removal of bony spurs. J Bone Joint Surg Br 1993;75:437-440.
Cannon LB, Hackney RG: Anterior tibiotalar impingement associated with chronic ankle instability. J Foot Ankle Surg 2000;39:383-386.
Question 55
1 and 2 show the radiograph and CT obtained from a year-old woman who underwent right total hip replacement in She initially did well with no pain. She was last seen 7 years ago and was having mild hip pain at that time. She was found to have a supra-acetabular cyst on radiographs. She has had severe right hip pain for the past 9 months while using a walker for ambulation. The initial blood work reveals an estimated erythrocyte sedimentation rate of 32 mm/hr, a C-reactive protein level of 5 mg/L, a serum cobalt level of 4 µg/L, and a serum chromium level of 6 µg/L. Right hip aspiration is performed, revealing a white blood cell count of 139, 52% neutrophils, and a negative leukocyte esterase test. What is the best next step?
Explanation
The hip replacement was performed in 1995, during the period when the previous generation of polyethylene was utilized. This polyethylene was subjected to irradiation in air, with subsequent oxidation and consequent osteolysis after implantation. The mechanism of osteolysis begins with the uptake of polyethylene particles by macrophages, which then initiate an inflammatory cascade and the release of osteolytic factors. This cycle continues, with eventual implant loosening and failure. The imaging shows significant osteolysis and raises concern for pelvic discontinuity and acetabular implant failure. The surgical treatment consists of acetabular reconstruction. In this patient, concern exists for discontinuity based on the substantial amount of bone loss and nonsupportive anterior and posterior columns. This scenario requires complex acetabular revision using a custom triflange device, distraction with a jumbo acetabular component, or placement of a porous metal cup/cage construct with augmentation. The laboratory values are not consistent with infection or failure due to metal debris.
Question 56
A 20-year-old man with fascioscapulohumeral dystrophy has severe scapular winging of both shoulders. He can no longer abduct above 80 degrees, and it affects his activities of daily living. A clinical photograph is shown in Figure 26. Definitive management should consist of
Explanation
REFERENCES: Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Bunch WH, Siegel IM: Scapulothoracic arthrodesis in fascioscapulohumeral muscular dystrophy: Review of seventeen procedures with three to twenty-one-year follow-up. J Bone Joint Surg Am 1993;75:372-376.
Question 57
A 30-year-old woman sustained a nondisplaced unilateral facet fracture of C5 in a motor vehicle accident. She is neurologically intact and has no other injuries. Management should consist of
Explanation
REFERENCE: Clarke CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
Question 58
A 55-year-old man reports increasing weakness in his arms that has progressed to his lower limbs, resulting in frequent tripping and falling. Examination reveals weakness in shoulder abduction and external and internal rotation bilaterally. Fasciculation is noted. He also has weakness in elbow flexion and extension bilaterally, and his grip strength is diminished. An electromyogram and nerve conduction velocity studies show decreased amplitude of compound motor action potential, slightly slowed motor conduction velocity, and denervation signs with decreased recruitment in all extremities. The sensory study is normal. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: de Carvalho M, Johnsen B, Fuglsang-Frederiksen A: Medical technology assessment: Electrodiagnosis in motor neuron diseases and amyotrophic lateral sclerosis. Neurophysiol Clin 2001;31:341-348.
Daube JR: Electrodiagnostic studies in amyotrophic lateral sclerosis and other motor neuron disorders. Muscle Nerve 2000;23:1488-1502.
Troger M, Dengler R: The role of electromyography (EMG) in the diagnosis of ALS. Amyotroph Lateral Scler Other Motor Neuron Disord 2000;1:S33-S40.
Question 59
The essential lesion responsible for posterolateral rotatory instability of the elbow is disruption of the
Explanation
REFERENCES: O’Driscoll SW, Jupiter JB, King GJW, Hotchkiss RN, Morrey BF: The unstable elbow. J Bone Joint Surg Am 2000;82:724-738.
Olsen BS, Sojbjerg JO, Dalstra M, Sneppen O: Kinematics of the lateral constraints of the elbow. J Shoulder Elbow Surg 1996;5:333-341.
O’Driscoll SW, Morrey BF, Korinek S, An KN: Elbow subluxations and dislocation: A spectrum of instability. Clin Orthop 1992;280:186-197.
Question 60
A 39-year-old male with chronic renal disease and type 2 diabetes mellitus fell 1 week ago after slipping on ice. He is unable to bear weight on the right lower extremity or perform active knee extension. He reports no prior history of knee pain or instability. Lachman, posterior drawer, posterolateral recurvatum testing are deferred secondary to patient's pain. He has a palpable dorsalis pedis pulse but does have neuropathy as determined by Semmes-Weinstein filament testing. His radiograph is shown in Figure A and MR images in Figures B and C. What is the most appropriate initial plan for management? Review Topic

Explanation
Primary surgical repair within 2 weeks of injury is recommended to prevent extensor mechanism contracture. Patellar tendon ruptures typically occur in patients younger than 40 years old. Most ruptures occur at the junction of the tendon and distal pole of the patella.
Matava et al. presents a level 5 review on patellar tendon ruptures and states that active knee extension is permitted at 3 weeks postoperatively. Non-weightbearing movement exercises like heel slides are encouraged. This can incorporate active knee flexion with passive extension. Alternatively, active knee flexion in the prone position with passive knee extension can be performed. Open chain strengthening exercises such as leg extensions are started later, as are weight bearing resistance exercises like squats, lunges and leg presses.
Volk et al. discuss potential complications and pitfalls of patients with the management of extensor mechanism injuries. They warn that complications can consist of misdiagnosis, delayed surgery, failed repair due to poor surgical planning of injury site, or wound infection.
Figure A demonstrates patella alta which in this case is indicative of complete patellar tendon rupture. Patella alta can be quantified by using the Insall-Salvati ratio (patellar tendon length / patellar bone length): PTL/PBL normal =1, >1.2 is patella alta, <0.8 is patella baja) with the knee flexed to 30 degrees. Figure B and C are sagittal T1 and T2 images showing complete patellar tendon rupture.
Incorrect answers:
Question 61
Examination of a 6-year-old boy who sustained a displaced Salter-Harris type II fracture of the distal radius reveals 35 degrees of volar angulation. A satisfactory reduction is obtained with the aid of a hematoma block. At the 10-day follow-up examination, radiographs show loss of reduction and 35 degrees of volar angulation. Management should now consist of
Explanation
be damaged.
REFERENCES: Dimeglio A: Growth in pediatric orthopaedics, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 33-62.
Waters PM: Forearm and wrist fractures, in Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 251-258.
Question 62
Figure 36 shows the hip arthrogram of a newborn. Which of the following structures is enclosed by the circle?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA,
WB Saunders, 2002, vol 1, pp 532-533.
Severin E: Contribution to the knowledge of congenital dislocation of the hip joint.
Acta Chir Scand 1941;84:1.
Question 63
Figures 1 and 2 show the radiographs obtained from a 68-year-old morbidly obese man who underwent left total hip replacement 7 years ago and did well, with no symptoms prior to the current presentation. He recently rose from a seated position and felt a pop in the hip, with immediate pain and inability to bear weight. Any pressure on the left foot now produces a painful, grinding sensation with loss of left hip stability. What is the best next step?

Explanation
The modular femoral stem has fractured. Changing the liner to a constrained design is not warranted at this time based on the information provided. Revision of the acetabular implant is appropriate because of the potential for damage to the existing cup from metal debris and femoral implant contact and to convert from a metal-on-metal articulation. Nonsurgical management would not provide pain relief or improvement; revision of the total hip arthroplasty is recommended. The implant failed in a short time, and retention of the femoral stem is not recommended because of the concern for failure with only a neck exchange. A dual-mobility bearing may be a good option if the surgeon plans to retain the acetabular component. Extended trochanteric osteotomy is a useful technique for the removal of a well-fixed femoral implant. In this patient, femoral stem removal without
osteotomy would be difficult due to the fracture of the implant’s femoral neck and the inability to gain purchase for extraction.
Question 64
A young man sustains a lumbar strain in an on-the-job motor vehicle accident. Both he and his treating physician feel that he is capable of limited duty with appropriate restrictions shortly after the injury. What term best describes his work status?
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 131-137.
Question 65
Which of the following physical examination findings is most likely present in the condition producing the MRI findings shown in Figure 92?
Explanation
REFERENCES: Vellet AP, Marks PH, Fowler PJ, et al: Occult posttraumatic osteochondral lesions of the knee: Prevalence, classification, and short-term sequelae evaluated with MR imaging. Radiology 1991;178:271-276.
Cone R: Imaging sports-related injuries of the knee, in DeLee J, Drez D, Miller M (eds): DeLee & Drez’s Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 2, pp 1595-1652.
Question 66
Because of the ongoing pain and instability and the demonstration of radiographic instability when the ankle is stressed, what surgical procedure should be performed to restore stability to the ankle joint based on the CT findings?
Explanation
The fracture at the insertion of the AITFL into the fibula represents a syndesmosis injury. In some cases, a direct repair of the fracture will stabilize the syndesmosis, but in most cases this injury should most likely be reinforced by placing a screw or suture tensioning device across the syndesmosis for additional support.A Brostrom or allograft reconstruction is indicated for an ankle sprain involving the ATFL or CFL.Simply excising the fragment will leave the patient with an incompetent syndesmosis. Repairing the SPR with or without a groove deepening procedure is indicated if there is evidence of subluxated or dislocated peroneal tendons, which is not demonstrated on the CT scans. The bone has been avulsed off the fibula by the portion of the AITFL that attaches to the fibula, therefore indicating that there is a syndesmosis injury. Allograft lateral ligament reconstruction and excision of loose body/fracture fragment are incorrect procedures based on location. The deltoid is a medial structure and this fracture is lateral. The ATFL and CFL attach at the inferior margin of the fibula near the lateral process of the talus and calcaneus. A SPR avulsion would present as an avulsion off the lateral wall of the fibula, not superior and not into the syndesmotic space as shown on the CT scans.
Question 67
Figures 15a through 15c show the radiographs of a 23-year-old football player who was injured when another player fell on his flexed and planted foot. He reports severe pain in the midfoot with a feeling of numbness on the dorsum of the foot, and he is unable to bear weight on the limb. Examination reveals mild swelling. Management should consist of
Explanation
REFERENCES: Baxter DE: The Foot and Ankle in Sport, ed 1. St Louis, MO, Mosby, 1995,
pp 107-123.
Curtis MJ, Myerson M, Szura B: Tarsometatarsal joint injuries in the athlete. Am J Sports Med 1993;21:497-502.
Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Thompson MC, Mormino MA: Injury to the tarsometatarsal joint complex. J Am Acad Orthop Surg 2003;11:260-267.
Question 68
Standard guidelines necessitate the use of intraoperative neurophysiological monitoring for patients undergoing surgery for which condition?
Explanation
There are currently no official guidelines on the appropriate use of neuromonitoring in spine surgery. In general, use of neuromonitoring is at surgeon discretion and often is based on the surgeon's perceived risk for neurologic injury during surgery and medicolegal concerns. In most reports,
neuromonitoring is considered useful in cases of deformity correction, spinal cord decompression, instrumentation placement, and revision surgery. However, even for some of these cases, studies have shown limited benefits of neuromonitoring and substantial associated costs.
RECOMMENDED READINGS
Lall RR, Lall RR, Hauptman JS, Munoz C, Cybulski GR, Koski T, Ganju A, Fessler RG, Smith ZA. Intraoperative neurophysiological monitoring in spine surgery: indications, efficacy, and role of the preoperative checklist. Neurosurg Focus. 2012 Nov;33(5):E10. doi: 10.3171/2012.9.FOCUS12235. Review. PubMed PMID: 23116090. View Abstract at PubMed Peeling L, Hentschel S, Fox R, Hall H, Fourney DR. Intraoperative spinal cord and nerve root monitoring: a survey of Canadian spine surgeons. Can J Surg. 2010 Oct;53(5):324-8. PubMed PMID: 20858377. View Abstract at PubMed
Garces J, Berry JF, Valle-Giler EP, Sulaiman WA. Intraoperative neurophysiological monitoring for minimally invasive 1- and 2-level transforaminal lumbar interbody fusion: does it improve patient outcome? Ochsner J. 2014 Spring;14(1):57-61. PubMed PMID: 24688334. View Abstract at PubMed
Question 69
Figures 18a through 18c show injuries sustained by a 22-year-old woman after falling 45 feet while mountain climbing. After being airlifted to the nearest trauma center, her arterial blood gas was 7.21, pO2 84, pCO2 48, and delta base -11 mmol/L. Her Hgb is 8.7 and her resuscitation is ongoing. Based on this data, what would be the best management of her orthopaedic injuries?

Explanation
prolonged, invasive surgery. Upper extremity fractures are best managed acutely with splints in this clinical setting. Definitive fracture fixation should be delayed until the patient is adequately resuscitated.
Question 70
Figure below shows the abdominal radiograph obtained from a 70-year-old woman who experiences nausea and abdominal tightness 48 hours following left total knee arthroplasty performed under general anesthesia. She received 24 hours of cefazolin antibiotic prophylaxis and a patient-controlled analgesia narcotic pump for pain management. She has been receiving warfarin for thromboembolic prophylaxis. Her severe abdominal distension and markedly decreased bowel sounds are most likely secondary to the administration of
Explanation
The radiograph reveals severe intestinal dilatation, which has occurred as the result of acute colonic pseudo-obstruction and is associated with excessive narcotic administration following total joint arthroplasty. Anesthetic type, antibiotic administration, and warfarin have not been associated with this obstruction. Electrolyte imbalances such as hypokalemia have been associated with postsurgical acute colonic pseudo-obstruction.
Question 71
Spontaneous rupture of the extensor pollicis longus tendon is most frequently associated with which of the following scenarios?

Explanation
clinically satisfactory.
The referenced article by Gelb is a review of the etiology and treatment of this injury. He reviews the above discussion and findings.
Question 72
The images reveal T2-weighted MRI sequences with edema isolated to the infraspinatus. In the absence of a tear in the infraspinatus tendon, the edema is most likely due to compression of the suprascapular nerve in the spinoglenoid notch. As this pathology persists, progressive muscle atrophy and fatty infiltration can result. Compression of the suprascapular nerve in the suprascapular notch would have resulted in edema and weakness in both the supra- and infraspinatus muscles. Compression is commonly caused by cysts from the joint secondary to labral tears. A rotator cuff tear of the infraspinatus is not identified on these images, and there is no history of trauma provided. There is no evidence of an anteroinferior labral tear, nor would this be expected to result in external rotation weakness or MRI abnormality of the infraspinatus. Quadrilateral space syndrome results in compression of the axillary nerve, which supplies the teres minor. Correcr answer : C
Explanation
Figure 1 is the radiograph of a 12-year-old baseball player who has posterolateral elbow pain with throwing. The area of interest is designated by the black arrow. His range of motion and strength are full. No previous treatment has been provided. What is the most appropriate initial treatment?
Elbow arthroscopy with debridement
Immobilization and rest for 6 weeks
Corticosteroid injection
Open osteochondral autograft transfer
Osteochondritis dissecans of the capitellum is a painful condition that affects immature athletes who undergo repetitive compression of the radiocapitellar joint. Management is based primarily on the integrity of the articular cartilage surface and the stability of the lesion. Nonsurgical treatment is typically selected for patients
with early-grade, stable lesions, and it involves activity modification with cessation of sports participation. The duration of activity modification is dictated by symptoms, with 3 to 6 weeks of rest followed by return to sport in 3 to 6 months commonly used as a guideline. Strengthening and stretching exercises are commonly incorporated after the pain has subsided. Surgical intervention or corticosteroid injection would not be first-line treatment.
Figures 1 and 2 are the radiographs of a 69-year-old man with a history of treated prostate cancer and hemodialysis-dependent end- stage renal disease who presents to the emergency department with progressively worsening right shoulder pain and stiffness. Laboratory tests reveal a white blood cell count of 17,000, erythrocyte sedimentation rate, 75, and CRP, 10.1. He has a draining sinus located along the anterior shoulder. What is the best next step?
Question 73
A decrease in alkaline phosphatase would most likely be manifest in which metabolic disorder?
Explanation
TNSALP is found in osteoblasts and hydrolyzes inorganic phosphates, leading to an increase in serum phosphate levels, which helps to maintain physiologic levels. A decrease in this process impairs bone mineralization leading to rickets. In the perinatal period, hypophosphatasia and decreased mineralization leads to caput membraneceum, shortened limbs and respiratory failure. Childhood hypophosphatasia is marked by premature loss of deciduous teeth and rachitic deformities. Adult hypophosphatasia I is characterized by teeth and chest wall deformities (similar to adolescent hypophosphatasia) as well as recurrent metatarsal and femoral stress fractures.
Mornet reviewed hypophosphatasia and the alkaline phosphatase mutations. Screening for the 65 distinct mutation can aid in diagnosis and family counseling in severe forms.
Illustration A shows abnormal dentition found in hypophosphatasia. Illustration B shows widespread rachitic changes characteristic of hypophosphatasia.
Incorrect Answers:
Question 74
What is a risk factor for interdigital neuroma?
Explanation
The only proven risk factor for development of an interdigital neuroma is female gender, which likely is related to the use of fashionable shoes that force plantar flexion of the metatarsal heads and secondary hyperdorsiflexion of the metatarsophalangeal joints. The other factors listed have not been proven to cause interdigital neuroma, as well as mediolateral compression of the forefoot.
RECOMMENDED READINGS
Hill KJ. Peripheral nerve disorder. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:307-327.
Schon LC, Mann RA. Diseases of the nerves. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby-Elsevier; 2007:613-686.
Question 75
A sentinel event is defined as an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. What is the most common sentinel event related to spine surgery?
Explanation
REFERENCES: Wong DA, Watters WC III: To err is human: Quality and safety issues in spine care. Spine 2007;32:S2-S8.
Wong DA: Spinal surgery and patient safety: A systems approach. J Am Acad Orthop Surg 2006;14:226-232.
Question 76
- A patient sustains a closed dorsal dislocation of the proximal interphalangeal joint of the middle finger without an associated fracture. Closed treatment results in a cocentric stable reduction. The finger is not immobilized. Which of the following conditions may appear 1 year later?
Explanation

Examination of a 3-year-old boy who slammed his finger in a door 3 months ago reveals 0 to 40 degrees of proximal interphalangeal joint motion. Radiographs are shown in Figures 47a and 47b. Management should consist of
Volar osteotomy
Observation only
Flexor tenolysis
Volar plate arthoplasty
A hinged distraction external fixator
Subcondylar fractures of the proximal and middle phalynx occur at the neck of the phalynx, usually as a result of a crush injury, and almost exclusively in the pediatric age group. The distal fragment rotates dorsally and the degree of displacement may be misjudged if a true lateral is not obtained. If malunion occurs there is block to flexion. Subcondylar fossa reconstruction by removal of bone through a palmar approach removes this boney block.
Question 77
Figures 76a and 76b are the sagittal T1-weighted MRI scans of an active 27-year-old man who has had left dominant extremity shoulder pain and weakness for the past 5 months. He denies any history of a precipitating event but recalls that the pain began around the time he started lifting weights after a year off from lifting. Examination reveals full range of active and passive motion, negative Hawkins and Neer impingement signs, 5/5 abduction strength, 5/5 external rotation strength with arm adducted at his side, and a negative belly press, Gerber lift-off, and O'Brien's test. He does have weakness with resisted external rotation with the arm abducted to 90 degrees. Radiographs are unremarkable. An MRI arthrogram shows no rotator cuff tear or labral tears. What is the most likely diagnosis? Review Topic
Explanation
Question 78
Figures below demonstrate the radiographs obtained from a 63-year-old man who had right total hip arthroplasty (THA) 4 months ago. Progressive stiffness began 2 months after surgery, and he now reports pain only after prolonged physical activity. His examination reveals a normal gait and painless range of motion with flexion of 70°, extension of 0°, internal rotation of 20°, external rotation of 20°, abduction of 10°, and adduction of 10°. His erythrocyte sedimentation rate and C-reactive protein level are within defined limits. Physical therapy has produced no benefit. What is the most appropriate next step?
Explanation
7% of primary THA cases. Improvement in pain is expected within 6 months, and most patients will not need surgical treatment. Surgical excision may be warranted for symptomatic patients after full maturation of the HO, usually 6 to 18 months after the surgery. Patients can be followed with repeated serum alkaline phosphatase levels, which are elevated initially and should return to normal upon maturation of the HO. Alternatively, a bone scan can show decreased activity after the HO has matured. Twenty-five milligrams of indomethacin 3 times daily for 6 weeks or 1 dose of irradiation at 700 to 800 Gy is effective in the prevention of HO but not for the treatment of established HO.
Question 79
Figure 22 shows the radiograph of a 7-year-old boy who underwent retrograde elastic nailing of a femoral shaft fracture. What is the most common problem following this procedure?
Explanation
REFERENCES: Flynn JM, Luedtke LM, Ganley TJ, et al: Comparison of titanium elastic nails with traction and a spica cast to treat femoral fractures in children. J Bone Joint Surg Am 2004;86:770-777.
Flynn JM, Hresko T, Reynolds RA, et al: Titanium elastic nails for pediatric femur fractures: A multicenter study of early results with analysis of complications. J Pediatr Orthop 2001;21:4-8.
Ligier JN, Metaizeau JP, Prevot J, et al: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Question 80
A 44-year-old man sustains the injury shown in Figures 1 through 3. What is the most appropriate treatment?

Explanation
Reduction, either open or closed, with internal fixation (pinning) is the recommended treatment for the majority of these injuries. Closed reduction with pinning is most often performed for acute injuries. Open reduction with pinning is performed for those injuries that cannot be reduced by closed means or those with a delayed presentation. Four cases of successful closed reduction and splinting, all performed upon presentation in the emergency department, have been described by Storken and associates, but the authors note that their review of three prior reports uncovered cases of secondary dislocation, which required surgical stabilization. One of the dislocations occurred 4 months after the reduction. They assert that an indication for primary ORIF is a CMC dislocation associated with major fractures. Primary arthrodesis can be considered in cases with severe intra-articular comminution, but this procedure substantially limits the ability of the hand to increase and decrease the transverse metacarpal arch, which is an important functional movement. It can also lead to osteoarthritis of the triquetrohamate joint. Suspension arthroplasty has been described for old fracture-dislocations of the fifth CMC joint, using a partial slip of the extensor carpi ulnaris.








Question 81
What is the most common complication associated with the treatment of the distal biceps ruptures as shown in Figures 79a and 79b? Review Topic

Explanation
Question 82
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include
Explanation
REFERENCES: Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
Question 83
A right-handed 20-year-old college baseball pitcher has had a 6-month history of vague right elbow pain while pitching. Examination reveals full flexion of the elbow and a loss of only a few degrees of full extension. The elbow is stable, but palpation reveals tenderness over the olecranon. Plain radiographs are inconclusive. MRI and CT scans are shown in Figures 20a and 20b. Management should consist of
Explanation
REFERENCES: Azar FM, Wilk KE: Nonoperative treatment of the elbow in throwers. Oper Tech Sports Med 1996;4:91-99.
Griffin LY (ed): Orthopaedic Knowledge Uupdate: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 191-203.
Question 84
Which of the following pelvic injury types has the highest reported mortality rate?
Explanation

OrthoCash 2020
Question 85
What is the most common mechanism of injury that produces turf toe?
Explanation
REFERENCES: Clanton TO, Ford JJ: Turf toe injury. Clin Sports Med 1994;13:731-741.
Rodeo SA, O’Brien S, Warren RF, et al: Turf toe: An analysis of metatarsophalangeal joint sprains in professional football players. Am J Sports Med 1990;18:280-285.
Question 86
A 14-year-old girl has had mild pain and nail deformity of the great toe for the past 4 months. A radiograph is shown in Figure 50. What is the most likely etiology of the lesion?
Explanation
REFERENCES: Lokiec F, Ezra E, Krasin E, Keret D, Wientraub S: A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop 2001;21:76-79.
Letts M, Davidson D, Nizalik E: Subungual exostosis: Diagnosis and treatment in children. J Trauma 1998;44:346-349.
Davis DA, Cohen PR: Subungual exostosis: Case report and review of the literature. Pediatr Dermatol 1996;13:212-218.
Question 87
Figure 54 is the lateral radiograph of a 55-year-old man who is evaluated for a 2-year history of pain and stiffness of his right metatarsophalangeal (MTP) joint. Upon examination he has dorsal bossing, severe crepitation, and pain with passive range of motion. There is pain with the "grind" test. Dorsiflexion is limited to 0 degrees. No sesamoid tenderness is present. What is the most appropriate surgical treatment?

Explanation
The radiograph reveals end-stage degenerative changes of the first MTP joint with a dorsal loose body. MTP arthritis and decreased joint dorsiflexion is referred to as hallux rigidus. A chevron bunionectomy is used to correct hallux valgus deformity without arthritis. The cheilectomy is used in lesser degrees of joint destruction. Resection of the proximal phalanx results in a floppy toe and is generally not recommended.
RECOMMENDED READINGS
McNeil DS, Baumhauer JF, Glazebrook MA. Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int. 2013 Jan;34(1):15-32. doi: 10.1177/1071100712460220. Review. PubMed PMID: 23386758.
View Abstract at PubMed
Deland JT, Williams BR. Surgical management of hallux rigidus. J Am Acad Orthop Surg. 2012 Jun;20(6):347-58. doi: 10.5435/JAAOS-20-06-347. Review. PubMed PMID: 22661564.
View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 55 THROUGH 58
Figures 55a and 55b are the anteroposterior and lateral radiographs of a 57-year-old man who fell off of a ladder 10 days ago and landed on his left foot. He is now unable to weight bear on the left. He has no history of trauma to this foot, and his medical history is unremarkable. Upon examination his left foot is swollen and tender. Pulses and sensation are intact.

A B
Question 88
Immobilization with a sling
Explanation
Radiographically Active Cyst (age 4 to 8 years old with pathologic fracture)
Align and immobilize
Observe for spontaneous healing
Reassess after 2 to 4 months and if recurrent, follow procedure for pathological fracture of radiographically active cysts described in the article above.
Question 89
A previously asymptomatic 14-year-old girl sustained a twisting injury to her ankle. Radiographs are shown in Figures 2a and 2b. Management should consist of
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 69-75.
Biermann JS: Common benign lesions of bone in children and adolescents. J Pediatr Orthop 2002;22:268-273.
Question 90
A 70-year-old man has worn through his metal-backed patellar component and sustained damage to the femoral component. Following removal of the components and debridement of the metal-stained synovium, the surgeon finds that the thickness of the remaining patella is 10 mm. Treatment should now include
Explanation
REFERENCES: Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620.
Pagnano MW, Scuderi GR, Insall JN: Patellar component resection in revision and reimplantation total knee arthroplasty. Clin Orthop 1998;356:134-138.
Barrack RL, Matzkin E, Ingraham R, Engh G, Rorabeck C: Revision knee arthroplasty with patella replacement versus bony shell. Clin Orthop 1998;356:139-143.
Question 91
In a postganglionic brachial plexus lesion at Erb’s point (point of formation of the upper trunk by the C5 and C6 nerve roots), which of the following nerves will still function normally?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System: Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, pp 28-29.
Zimmerman NB, Weiland AJ: Assessment and monitoring of brachial plexus injury in the adult, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA,
JB Lippincott, 1991, vol 2, pp 1273-1283.
Question 92
A prospective randomized trial is conducted to test the efficacy of Vitamin C versus placebo in treating patients who develop chronic regional pain syndrome (CRPS) after distal radius fractures. At first follow-up, the rates of CRPS are 1% and 9% in the study and placebo group, respectively. Which statistical test is most appropriate to determine significance?
Explanation
Data can be classified as numerical (continuous) or categorical (proportional). Responses to such questions as "What is your major?" or Do you own a car?" are categorical because they yield data such as "biology" or "no." In contrast, responses to such questions as "How tall are you?" or "What is your G.P.A.?" are numerical. When comparing two independent means from numeric data, a t-test is performed. However, if categorical data is being compared, the chi-square test will determine if the proportions are really different.
Kocher et al. review basic clinical epidemiology and biostatistics relevant to orthopaedic surgery. Amongst other things, they describe that data can be summarized in terms of measures of central tendency, such as mean, median, and mode, and in
terms of measures of dispersion, such as range, standard deviation, and percentiles. Illustration A shows an algorithm for determining which test to use for varying data.
Incorrect Answers:
Question 93
Which of the following changes occur in the spinal cord and the spinal canal when the cervical spine moves from neutral to full flexion?
Explanation
REFERENCES: Breig A: Biomechanics of the Central Nervous System: Some Basic Normal and Pathologic Phenomena. Stockholm, Sweden, Almquist and Wiksell, 1960.
Ghanayem AJ, Zdeblick TA, Panjabi MM: Biomechanics of nonacute cervical spine trauma, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 103-105.
Question 94
Which of the following characteristics is seen in patients with osteochondritis dissecans of the elbow? Review Topic
Explanation
Question 95
A 25-year-old man sustains a left brachial plexus injury from a fall while rock climbing. Examination reveals poor intrinsic function of the hand, ptosis, and miosis. He is able to abduct and forward flex his shoulder with full strength. This combination of physical findings is most suggestive of what pattern of nerve injury?
Explanation
A preganglionic lesion occurs proximal to the spinal foramen, whereas a postganglionic lesion occurs distal to the spinal foramen in the root, trunk, division, cord, or branches of the brachial plexus. The Horner sign, which is characterized by miosis, ptosis, anhydrosis, and enophthalmos, results from an injury to the sympathetic ganglion, which lies in close proximity to the T1 root level. The presence of a Horner sign is highly suggestive of a T1 preganglionic injury. Other physical examination indicators of a preganglionic injury include atrophy of the parascapular muscles (injury to the dorsal rami of the cervical spinal nerve roots), winged scapula (injury to the long thoracic nerve) and hemidiaphragmatic paralysis (phrenic nerve injury). The lack of intrinsic hand function in this patient is also suggestive of an injury at the level of C8-T1. Preservation of shoulder abduction and forward flexion would not typically be seen with an injury to the C5-C6 roots or the upper trunk.
Question 96
important in patients with renal impairment, which is not typically seen in SCT.
Explanation
Level of evidence provides guidance to the study quality. It is used to assess therapeutic studies (as with this question), prognostic studies, diagnostic studies and economic or decision models. When determining the level of evidence, readers must critically appraise the study question, treatment, intervention and outcomes of the study design. Level-II therapeutic studies consist of well-designed prospective cohort studies, poor-quality randomized controlled trials (follow-up less than 80%) and systematic review of Level-II studies or non-homogenous Level-I studies.
Wright et al. provided an excellent summary of clinical research study level of evidence. This has been provided as Illustration A.
Illustration A shows a chart of level of evidence. There is a column for each type of study which corresponds to a row that outlines the level of evidence based on study
design.
Incorrect Answers:
Low serum phosphate and normal calcium levels are found in what common etiology of hereditary rickets?
X-linked hypophosphatemic
Vitamin D-dependent, type I
Vitamin D-dependent, type II
Autosomal dominant hypophosphatemic
Jansen's metaphyseal chondrodysplasia
Low serum phosphate and normal calcium levels are found in X-linked hypophosphatemic rickets.
X-linked hypophosphatemic rickets is the most common form of hereditary rickets. It is an X-linked dominant disorder which has been linked to the PHEX gene. Laboratory findings
of this disorder include low serum phosphate, normal serum calcium and 25 hydroxycholecalciferol levels, and inappropriately low 1,25-dihydroxyvitamin D3.
Carpenter et al. showed hypophosphatemic rickets was initially referred to as “vitamin D resistant rickets” due to its lack of response to therapeutic vitamin D. Current treatment with activated vitamin D metabolites (calcitriol or
alfacalcidol) and phosphate salts have been shown to help with this condition.
Illustration A shows an insufficiency fracture of the proximal tibia in an adult patient with X-linked hypophosphatemic rickets. A stress fracture on the medial tibia may be a presenting feature of untreated disease.
Incorrect Answers:
receptor (PTHR1).
A healthy patient undergoes routine pre-operative laboratory testing and is found to have a leukocyte count of 1.5 × 10(9) cells/L. When the historical records are examined, this is found to be the patients base-line level over a period of years. Which of the following statements is most likely to be true:
The patient is at a significantly higher risk of surgical infection
The patient is more likely to be of African than of European descent
The patient is more likely to be of European than of Middle Eastern descent
The patient is more likely to be a non-athlete than an athlete
The patient is more likely to be female than male
The clinical presentation is consistent with Benign Ethnic Neutropenia, a condition in which a patient has chronic, benign, inborn and lifelong absolute neutrophl count below population mean. This condition is found in the U.S. to be most common in African- Americans, some groups of Middle Eastern patients, males, children under 5 years old, and athletes compared to non- athletes.
A standardized level at present for abnormally low absolute neutrophil count (ANC) is below 1.5 x 10(9) cells/L, however this may not have clinical or scientific relevance as a cutoff point, particularly in the affected Ethnic groups. Fewer than 1% of all populations have absolute neutrophil count < 1.0 X 10(9) cells/L. Most patients in the affected ethnic groups with low ANC and no associated history or symptoms are not expected to have any increased risk of infection or adverse effect. Smoking was also associated with higher leukocyte and neutrophil counts but proportionately lower increase in African-American patients. One hypothesis for the increased prevalence of B.E.N. in patients of African descent is a theorized evolutionary protection against malaria, though
it remains unclear if this is causal or just correlative.
Haddy et al. provide an excellent scientific review of B.E.N. and emphasize the importance of recognizing this most common form of neutropenia.
Eichner et al. review B.E.N. in the setting of sports medicine and state the relative increase of these lab findings in athletes vs non-athletes.
Hsieh et al. provide an extensive cross-sectional population study focused on the prevalence of Benign Ethnic Neutropenia in the U.S. They reviewed 25,222 participants in the National Health and Nutrition Examination Survey 1yr of
age or older from 1999-2004, and detail the association of this condition with age, sex, ethnicity, and smoking status.
Denic et al. analyzed neutrophil count in a healthy Arab population in the U.A.E. and found low neutrophil counts in this population with a distribution suggestive, but not definitively, of an autosomal dominant inheritance. They also discuss the hypothesized association of B.E.N. and malaria infection.
Incorrect answers:
Question 97
The arrow in Figure 11 points toward a finding consistent with which of the following?
Explanation
REFERENCES: McLain R, Weinstein J (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 1173.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 674.
Question 98
What molecules have been shown to promote fibrosis during muscle injury?
Explanation
Question 99
A 78-year-old woman undergoes an uneventful semiconstrained total elbow arthroplasty through a Bryan-Morrey approach. Her immediate postoperative management should include which of the following? Review Topic
Explanation
Question 100
A 13-year-old gymnast has had recurrent right elbow pain for the past year. She denies any history of trauma. Rest and anti-inflammatory drugs have failed to provide relief. Examination reveals no localized tenderness and only slight loss of both flexion and extension (10 degrees). What is the most likely diagnosis?
Explanation
REFERENCES: Krijnen MR, Lim L, Willems WJ: Arthoscopic treatment of osteochondritis dissecans of the capitellum: Report of 5 female athletes. Arthroscopy 2003;19:210-214.
Schenck RC, Goodnight JM: Osteochondritis dissecans. J Bone Joint Surg Am 1996;3:439-456.
