Orthopedic Board Review MCQs: Trauma & Sports Medicine | Part 241

Key Takeaway
This page offers Part 241 of a high-yield Orthopedic Surgery Board Review MCQ bank, specifically for orthopedic surgeons and residents preparing for OITE/AAOS certification. It features 100 verified questions on fracture topics, designed to simulate exam conditions and enhance your board preparation effectively.
About This Board Review Set
This is Part 241 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 241
This module focuses heavily on: Fracture.
Sample Questions from This Set
Sample Question 1: What is the primary indication for performing an arthroscopic synovectomy on a patient with hemophilia that is the result of factor VIII deficiency? Review Topic...
Sample Question 2: -The World Health Organization Fracture Risk Assessment Tool (FRAX) calculates which fracture risk?...
Sample Question 3: A 25-year-old woman has lower leg pain during exercise without numbness, tingling, or weakness. The symptoms resolve by the following day. Compartment pressure measurements obtained 1 minute after exercise are shown in Figure 19a (Table 1)....
Sample Question 4: Figures 37a and 37b show the clinical photographs of a 43-year-old patient with type I diabetes mellitus who has a stump ulcer after undergoing successful transtibial amputation 1 year ago. Which of the following is considered the most pred...
Sample Question 5: A 34-year-old man underwent open reduction and internal fixation of a closed both bones forearm fracture 11 months ago. The radiographs shown in Figures 32a and 32b reveal a 3-mm gap and loose screws. What is the best treatment option?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What is the primary indication for performing an arthroscopic synovectomy on a patient with hemophilia that is the result of factor VIII deficiency? Review Topic
Explanation
Question 2
-The World Health Organization Fracture Risk Assessment Tool (FRAX) calculates which fracture risk?
Explanation
Question 3
A 25-year-old woman has lower leg pain during exercise without numbness, tingling, or weakness. The symptoms resolve by the following day. Compartment pressure measurements obtained 1 minute after exercise are shown in Figure 19a (Table 1). She undergoes anterior compartment fasciotomy with complete resolution of symptoms. Two years later, she has recurrent pain and tightness with exercise. Radiographs, a technetium bone scan, and noninvasive vascular study findings are normal. Compartment pressure measurements obtained 1 minute after exercise are shown in Figure 19b (Table 2). What is the most likely etiology for her recurrent symptoms?
Explanation
Exertional compartment syndrome involves an increase in compartment pressure caused by exercise or sports activity that restricts blood flow in the compartment, resulting in pain with continued activity. Compartment pressures of at least 15 mm Hg measured at rest, at least 30 mm Hg measured 1 minute after exercise, and at least 20 mm Hg measured 5 minutes after exercise are diagnostic. Surgical fasciotomy for exertional compartment syndrome is successful for the majority of patients, but recurrence rates as high as 20% have been reported. Scar formation within the fascial defect can result in recurrent symptoms and/or nerve entrapment, and recurrence is typically observed after an initial symptom-free period. In a series of 18 patients, recurrent symptoms occurred at a mean of 23.5 months after the index procedure. Other potential causes of recurrence include inadequate fascial release, failure to recognize involvement of other compartments, nerve compression, and misdiagnosis. Surgical complications after fasciotomy include hemorrhage leading to excessive fibrosis, neurovascular injury, and hematoma or seroma formation.
Question 4
Figures 37a and 37b show the clinical photographs of a 43-year-old patient with type I diabetes mellitus who has a stump ulcer after undergoing successful transtibial amputation 1 year ago. Which of the following is considered the most predictable method of healing the ulcer and preventing recurrent ulceration?
Explanation
REFERENCE: Hadden W, Marks R, Murdoch G, et al: Wedge resection of amputation stumps: A valuable salvage procedure. J Bone Joint Surg Br 1987;69:306-308.
Question 5
A 34-year-old man underwent open reduction and internal fixation of a closed both bones forearm fracture 11 months ago. The radiographs shown in Figures 32a and 32b reveal a 3-mm gap and loose screws. What is the best treatment option?
Explanation
REFERENCES: Ring D, Allende C, Jafarnia K, et al: Ununited diaphyseal forearm fractures with segmental defects: Plate fixation and autogenous cancellous bone-grafting. J Bone Joint Surg Am 2004;86:2440-2445.
Question 6
A college athlete on a scholarship has a medical condition that you feel presents a life-threatening risk to him with participation in athletics. Because of the gravity of this decision and the potential effect it can have on the student/athlete's future, the college asks for your guidance. As the team physician for the college, what is your ethical obligation?
Explanation
Question 7
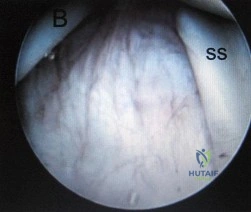
Figure 177 is an intra-articular photograph taken while viewing from the anterior superior portal during arthroscopy of a right shoulder. Which of the following findings identified at the time of surgery would be the most predictive for recurrence following arthroscopic repair of the demonstrated pathology? Review Topic

Explanation
Question 8
The primary purpose of obtaining the radiograph shown in Figure 9 is to assess
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Lequesne M, deSez S: Le faux profil du bassin: Nouvelle incidence radiographique pour l’etude de la hance. Son utilite dans les dysplasies et les differentes coxopathies. Rev Rhum Mal Osteoartic 1961;28:643.
Question 9
What is the most accurate description of the relationship between gender and knee loading during landing while playing basketball?
Explanation
REFERENCES: Hewett TE, Myer GD, Ford KR, et al: Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am J Sports Med 2005;33:492-501.
Ford KR, Meyer GD, Hewett TE: Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exer 2003;35:1745-1750.
Question 10
Acetabular reconstruction followed by external beam irradiation The plain radiographs show a purely lytic destructive lesion that is poorly marginated. The technetium bone scan does not show any major uptake. The computerized tomography scan shows purely lytic bone destruction with breakthrough of the cortical bone. Complete destruction of the cortical bone is suggestive of a malignancy. The magnetic resonance image shows a lesion that is homogenously low on T1-weighted images and high on T2-weighted images. Surgeons cannot make a definitive diagnosis based upon the radiographic features. The most common malignancies in this age group are:
Explanation
A 50-year-old woman has had severe hip pain for 4 months. Her plain radiographs (Slide 1), technetium bone scan (Slide 2), computerized tomography scan (Slide 3), and coronal T1- and T2-weighted magnetic resonance images (Slide 4) are presented. The most likely diagnosis based upon the radiographs would be:
Question 11
Venous thromboembolism may occur after total joint arthroplasty. The risk of this complication is elevated in patients with
Explanation
Obesity, a prior history of venous thromboembolism, and metabolic syndrome have all been associated with an increased risk of thromboembolism. A recent meta-analysis showed that diabetes had no significant relationship with venous thromboembolism following hip or knee arthroplasty. Tranexamic acid is an antifibrinolytic agent that has been shown to reduce blood loss substantially following hip and knee arthroplasty. It has also been shown to be safe in patients with severe medial comorbidities and a prior history of venous thromboembolism.
Question 12
Which of the following areas of the vertebral segment has the highest ratio of cortical to cancellous bone? Review Topic
Explanation
Question 13
A 36-year-old woman reports vague right shoulder pain. She denies any previous shoulder problems or any recent trauma. MRI scans are shown in Figures 81a and 81b. Weakness of which of the following is the most likely finding in her physical examination? Review Topic
Explanation
Question 14
A year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the
aspiration and proceed to a revision TKA with possible augments on standby.
Question 15
What is the structure indicated by the letter “A” in Figure A? Review Topic
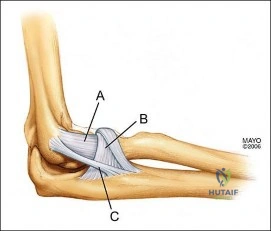
Explanation
Question 16
An 18-year-old boy has had pain in the right knee for the past 6 months. Examination reveals some fullness behind the knee but no significant palpable soft-tissue mass. There is no effusion, and he has full knee range of motion. The remainder of the examination is unremarkable. A radiograph and MRI scans are shown in Figures 33a through 33c, and biopsy specimens are shown in Figures 33d and 33e. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 20-21.
Unni KK, Dahlin DC, Beabout JW, Ivins JC: Parosteal osteogenic sarcoma. Cancer 1976;37:2466-2475.
Question 17
40A B Figures 40a and 40b are this patient's intraoperative arthroscopic images. The abnormality seen here illustrates which of the patient's clinical findings?
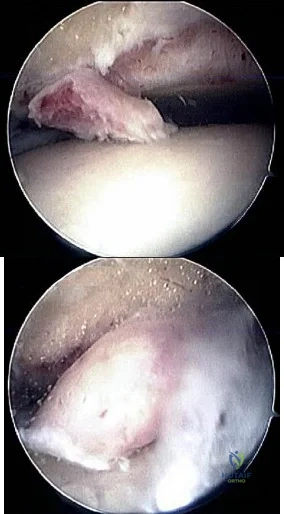
Explanation
Ankle sprains are the most common musculoskeletal injury; however, most of these sprains do not progress to chronic instability. Initial injuries are treated with RICE (rest, ice, compression, elevation), range of motion, weight bearing
as tolerated, and proprioceptive therapy. Lace-up ankle braces are most effective during the subacute period after a sprain. Structured physical therapy focused on proprioception is recommended for 6 weeks. Examination findings for ankle ligament instability are unreliable because of associated subtalar joint motion. Casting is not as effective as functional rehabilitation. Stress radiographs are recommended, but a clear pathologic range of measurements is not defined. Generalized ligament laxity can result in false-positive findings of instability; therefore, contralateral stress radiographs are often necessary for comparison. The difference in anterior drawer measurement between both ankles should not exceed 5mm. Likewise, the difference in talar tilt measurement between both ankles should be 5 or fewer degrees. Patients with mechanical symptoms, a joint effusion, or continued pain may have an intra-articular pathology such as a loose body or osteochondral lesion. Ankle instability can exist without ligamentous laxity. Symptoms of chronic instability can result from osteochondral lesions of talus, peroneal tendon pathology, loose bodies, anterior ankle impingement, and fracture nonunions. Although there is not sufficient evidence to recommend arthroscopy prior to all ligament reconstructions, arthroscopy is recommended when other pathology is suspected.
RECOMMENDED READINGS
Colville MR. Surgical treatment of the unstable ankle. J Am Acad Orthop Surg. 1998 Nov-Dec;6(6):368-77. Review. PubMed PMID: 9826420. View Abstract at PubMed
DiGiovanni CW, Brodsky A. Current concepts: lateral ankle instability. Foot Ankle Int. 2006 Oct;27(10):854-66. Review. PubMed PMID: 17054892. View Abstract at PubMed
Maffulli N, Ferran NA. Management of acute and chronic ankle instability. J Am Acad Orthop Surg. 2008 Oct;16(10):608-15. Review. PubMed PMID: 18832604. View Abstract at PubMed
Question 18
The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports, and the surgeon and rehabilitation team consider their request. Compared to nonaccelerated rehabilitation, patients who follow an early accelerated rehabilitation protocol experience
Explanation
The MR image shows bone bruises (“kissing contusions”) consistent with an ACL tear. During the ACL subluxation event, the posterolateral tibia plateau subluxes anteriorly, making contact with the mid portion of the lateral femoral condyle and resulting in this characteristic bone bruise pattern on MRI. Randomized clinical trials comparing early accelerated vs nonaccelerated rehabilitation programs have demonstrated no significant differences in longterm results with regard to function, reinjury, and successful return to play. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
Question 19
What is the most likely cause of recurrent symptoms following excision of a third web space neuroma?
Explanation
REFERENCES: Beskin JL: Recurrent interdigital neuromas, in Nunley JA, Pfeffer GB, Sanders RW, Trepman E (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 481-484.
Amis JA, Siverhus SW, Liwnicz BH: An anatomic basis for recurrence after Morton’s neuroma excision. Foot Ankle 1992;13:153-156.
Question 20
Figure 28 shows an arthroscopic view of a right shoulder in the lateral position through a posterior portal. What is the area between structure B (biceps) and SS (subscapularis tendon)? Review Topic
Explanation
Question 21
A non-communicative 16-year-old girl with spastic quadriplegic cerebral palsy and a 75-degree thoracolumbar scoliosis undergoes a successful posterior spinal fusion with instrumentation. What is the most predictable outcome of the surgical procedure?
Explanation
REFERENCES: Tsirikos Al, Lipton G, Chang WN, et al: Surgical correction of scoliosis in pediatric patients with cerebral palsy using the unit rod instrumentation. Spine 2008;33:1133-1140.
Cassidy C, Craig CL, Perry A, et al: A reassessment of spinal stabilization in severe cerebral palsy. J Pediatr Orthop 1994;14:731-739.
Question 22
The implant shown in Figures 47a and 47b is introduced submuscularly employing a minimally invasive technique. A percutaneous method of screw insertion is used distally. What nerve is most at risk?

Explanation
Question 23
An 18-year-old high school basketball player is being treated for Achilles tendinitis. What type of strengthening exercise has been shown to be helpful in the later phases of rehabilitation?
Explanation
All three types of these exercises have not been shown to benefit Achilles tendinitis as much as eccentric exercise.
REFERENCES: Jonsson P, Alfredson H, Sunding K, et al: New regimen for eccentric calf-muscle training in patients with chronic insertional Achilles tendinopathy: Results of a pilot study. Br J Sports Med
2008;42:746-749.
Maffulli N, Walley G, Say ana MK, et al: Eccentric calf muscle training in athletic patients with Achilles tendinopathy. Disabil Rehabil 2008;30:1677-1684.
Question 24
A patient with a grade 2 L5-S1 isthmic spondylolisthesis reports low back pain and bilateral lower extremity pain. Nonsurgical management has failed to provide relief, and the patient is now a candidate for surgical intervention. The
Explanation
Question 25
A 2-week-old infant has been referred for evaluation of nonmovement of the left hip. History reveals that the patient was delivered 6 weeks premature by cesarean section. Examination reveals no fever, and there is mild swelling of the thigh. Passive movement of the hip appears to elicit tenderness and very limited hip motion. A radiograph of the pelvis shows mild subluxation of the left hip. The next step in evaluation should consist of
Explanation
REFERENCES: Knudsen CJ, Hoffman EB: Neonatal osteomyelitis. J Bone Joint Surg Br 1990;72:846-851.
Morrissy RT: Bone and joint sepsis, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 579-624.
Question 26
Which of the following factors is most closely associated with early postoperative migration of “stand-alone” lumbar interbody fusion cages?
Explanation
REFERENCES: McAfee PC: Interbody fusion cages in reconstructive operations on the spine. J Bone Joint Surg Am 1999;81:859-880.
McAfee PC, Cunningham BW, Lee GA, et al: Revision strategies for salvaging or improving failed cylindrical cages. Spine 1999;24:2147-2153.
Question 27
A 26-year-old man is brought to the emergency department unresponsive and intubated after being found lying on the side of the road. He has a Glasgow Coma Scale score of 6. A chest tube has been inserted on the right side of the chest for a pneumothorax. An abdominal CT scan reveals a small liver laceration and minimal intraperitoneal hematoma. A pneumatic antishock garment (PASG) is on but not inflated. He has bilateral tibia fractures. A pelvic CT scan shows an anterior minimally displaced left sacral ala fracture and left superior and inferior rami fractures. He has received 2 L of saline solution and 4 units of blood but remains hemodynamically unstable. What is the next most appropriate step in management?
Explanation
REFERENCES: Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: Effective classification system and treatment protocols. J Trauma 1990;30:848-856.
Evers BM, Cryer HM, Miller FB: Pelvic fracture hemorrhage: Priorities in management. Arch Surg 1989;124:422-424.
Flint L, Babikian G, Anders M, Rodriguez J, Steinberg S: Definitive control of mortality from severe pelvic fracture. Ann Surg 1990;211:703-707.
Question 28
What is the most common presenting problem in patients with cauda equina syndrome? Review Topic
Explanation
Question 29
Which of the following regions in the growth plate is commonly affected in a Salter-Harris type II injury? Review Topic
Explanation
Question 30
A 14-year-old boy reports progressive right wrist pain. Radiographs are shown in Figure 3a, and a photomicrograph is shown in Figure 3b. What is the most likely diagnosis?
Explanation
REFERENCES: Lersundi A, Mankin HJ, Mourikis A, et al: Chondromyxoid fibroma: A rarely encountered and puzzling tumor. Clin Orthop Relat Res 2005;439:171-175.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 31
Based on the findings seen in the radiograph in Figure 26, emergent management should consist of
Explanation
REFERENCES: Isenberg J, Prokop A, Schellhammer F, et al: Palmar lunate dislocation. Unfallchirurg 2002;105:1133-1138.
Ruby LK: Fractures and dislocations of the carpus, in Browner BD, Jupiter JB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1367-1372.
Question 32
The spinal cord terminates as the conus medullaris at what vertebral level in adults? Review Topic 1 T12
Explanation
Question 33
Figure 10 shows patellar radiographs of a 68-year-old woman who underwent bilateral total knee arthroplasty 2 months ago. Following a recent fall onto the left side, she now reports anterior pain in the left knee. A CT scan shows that the femoral and tibial components are appropriately externally rotated and radiographs show acceptable axial alignment and no evidence of loosening. What is the most appropriate treatment option?
Explanation
If the components are determined to be in satisfactory position, soft-tissue procedures can be pursued. Lateral retinacular release is usually the first soft-tissue procedure used to improve patellofemoral mechanics. In this patient, the patellar fracture fragment is so small that it can be excised. Distal realignment is not usually used as the first line of treatment for patellar maltracking following TKA.
REFERENCES: Fehring TK, Christie MJ, Lavemia C, et al: Revision total knee arthroplasty: Planning, management, and controversies. Instr Course Lect 2008;57:341-363.
Patel J, Ries MD, Bozic KJ: Extensor mechanism complications after total knee arthroplasty. Instr Course Lect 2008;57:283-294.
Question 34
A 15-year-old high school soccer player collides with an opponent and is unconscious when the trainer arrives on the field. He is conscious within 15 seconds, breathing appropriately, and denies any headache, neck pain, or nausea. It is his first head injury. Provided that the athlete is free of symptoms, when should he be allowed to return to athletic activity?
Explanation
week period out of sport. The last week prior to return must be symptom-free and the athlete should not have symptoms in practice.
REFERENCES: Cantu RC: Return to play guidelines after a head injury. Clin Sports Med 1998;17:45-60.
Stevenson KL, Adelson PD: Pediatric sports-related head injuries, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 781.
Question 35
When performing elbow arthroscopy, it is often necessary to evaluate the posterior compartment. When entering the posterior compartment of the elbow, what are the two safest and most commonly used portals? Review Topic
Explanation
Question 36
Figures 42a and 42b show the radiographs of a 52-year-old man who sustained a fall from a motorcycle 6 months ago and now reports pain and stiffness in his left shoulder. What is the most reliable treatment to improve function and comfort of the shoulder?
Explanation
REFERENCES: Gerber C, Lambert SM: Allograft reconstruction of segmental defects of the humeral head for the treatment of chronic locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1996;78:376-382.
Spencer EE Jr, Brems JJ: A simple technique for management of locked posterior shoulder dislocations: Report of two cases. J Shoulder Elbow Surg 2005;14:650-652.
Sperling JW, Pring M, Antuna SA, et al: Shoulder arthroplasty for locked posterior dislocation of the shoulder. J Shoulder Elbow Surg 2004;13:522-527.
Hawkins RJ, Neer CS II, Pianta RM, et al: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
McLaughlin HL: Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;34:584-590.
Question 37
A 23-year-old male is involved in a motor vehicle accident and sustains a left open femur fracture, right open humeral shaft fracture, and an LC-II pelvic ring injury. Which of the following best describes the radiographic findings associated with this pelvic injury pattern using the Young-Burgess Classification system?

Explanation
Burgess et al discuss the effectiveness of a treatment protocol as determined by their pelvic injury classification and hemodynamic status. The injury classification system was based on lateral compression, anteroposterior compression, vertical shear, and combined mechanical injury types. They found that their classification-based treatment protocols reduce the morbidity and mortality related to pelvic ring disruption.
Tile discusses acute pelvic trauma and his classification system for pelvic injuries (ie. Types A, B, and C). He states that any classification system must be seen only as a general guide to treatment, and that the management of each patient requires careful, individualized decision making.
Incorrect
2:
This
describes
an
APC-II
injury
3:
This
describes
an
APC-III
injury
4:
This
describes
and
LC-I
injury
Question 38
A 52-year-old woman with a 2-year history of a flexible (stage II) adult-acquired flatfoot deformity has failed to respond to nonsurgical management consisting of immobilization, custom orthotics, nonsteroidal anti-inflammatory drugs, and physical therapy. The patient is unable to perform a single limb heel rise. Weight-bearing radiographs are shown in Figures 30a through 30c. What is the most appropriate surgical correction?
Explanation
REFERENCES: Greisberg J, Assal M, Hansen ST Jr, et al: Isolated medial column stabilization improves alignment in adult-acquired flatfoot. Clin Orthop Relat Res 2005;435:197-202.
Greisberg J, Hansen ST Jr, Sangeorzan BJ: Deformity and degeneration in the hindfoot and midfoot joints of the adult acquired flatfoot. Foot Ankle Int 2003;24:530-534.
Question 39
A 14-year-old girl has had mild pain and nail deformity of the great toe for the past 4 months. A radiograph is shown in Figure 50. What is the most likely etiology of the lesion?
Explanation
REFERENCES: Lokiec F, Ezra E, Krasin E, Keret D, Wientraub S: A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop 2001;21:76-79.
Letts M, Davidson D, Nizalik E: Subungual exostosis: Diagnosis and treatment in children. J Trauma 1998;44:346-349.
Davis DA, Cohen PR: Subungual exostosis: Case report and review of the literature. Pediatr Dermatol 1996;13:212-218.
Question 40
-Figure 162 is the CT scan of a 74-year-old woman who struck her head during a ground-level fall and has severe neck pain. Examination reveals normal strength and sensation in her upper and lower extremities.What is the most appropriate treatment option?

Explanation

Question 41
A 35-year-old man has had progressive right knee pain for the past 2 months. An AP radiograph, bone scan, MRI scan, and photomicrograph are shown in Figures 34a through 34d. What is the most appropriate treatment of this lesion?
Explanation
REFERENCES: Lackman RD, Hosalkar HS, Ogilvie CM, et al: Intralesional curettage for grades II and III giant cell tumors of bone. Clin Orthop Relat Res 2005;438:123-127.
Ward WG Sr, Li G III: Customized treatment algorithm for giant cell tumor of bone: Report of a series. Clin Orthop Relat Res 2002;397:259-270.
Question 42
A 39-year-old competitive cyclist sustains an injury to her left hip in a fall. Gadolinium arthrography, with an accompanying MRI scan, is shown in Figure 31. A cleft, or defect, identified by the arrow, indicates a detachment of the
Explanation
REFERENCES: Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieberman JM, Buly R: Acetabular labral tears: Evaluation with MR arthrography. Radiology 1996;200:231-235.
Czerny C, Hofmann S, Neuhold A, et al: Lesions of the acetabular labrum: Accuracy of MR imaging and MR arthrography in detection and staging. Radiology 1996;200:225-230.
Byrd JWT: Indications and contraindications, in Byrd JWT (ed): Operative Hip Arthroscopy. New York, NY, Thieme, 1998, pp 7-24.
Question 43
..A 60-year-old woman has a proximal femur fracture. A permeative, lytic defect is recognized at the fracture site. Appropriate imaging studies are performed and show no other lesions. What is the next treatment step?
Explanation
Question 44
A 65-year-old woman with rheumatoid arthritis is undergoing revision total knee arthroplasty (TKA) during which the medial collateral ligament (MCL) is damaged. Suture anchors are used to attempt primary repair, and a varus-valgus constrained insert also is used. Postsurgically she experiences instability that does not respond to bracing with a 3+ opening to valgus stress (Figure 120). What is the most appropriate surgical option?
Explanation
MCL repair or reconstruction may be considered in younger, more active patients, but this intervention is technically demanding and produces variable results. Rotating-hinge TKA is associated with good results in a number of small series that include cases performed with MCL insufficiency or absence. A rotating hinge is preferable over a fixed hinge because of decreased stresses on implants imposed by fixed-hinge devices.
Question 45
Figures 51a and 51b show subluxation of the
Explanation
REFERENCES: Rowland SA: Acute traumatic subluxation of the extensor carpi ulnaris tendon at the wrist. J Hand Surg Am 1986;11:809-811.
Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1026-1027.
Question 46
At revision, the stem is retained and a new head with a polyethylene bearing is selected. The best option for the head is
Explanation
Ceramic-on-ceramic is a controversial bearing surface typically reserved for younger patients such as this one. Some studies have suggested that the bearing is more expensive and does not really prolong the service life of the implant, although a recent meta-analysis of high-quality trials showed that there is a decreased revision rate with ceramic-on-ceramic, so its use may be justified. Complications of intraoperative bearing fracture and squeaking are more common than with conventional bearings, but pain and function scores are equivalent. Stripe wear associated with a vertical cup and morbid obesity are related to an increased risk for liner fracture. Concerns about head fractures with a new ceramic head and a damaged trunnion have led investigators to conclude that using a harder bearing than the initial bearing surface with a built-in titanium sleeve is probably the best solution when a stem is retained during revision surgery.

Question 47
-What is the most common metatarsal fracture in a 3-year-old?
Explanation
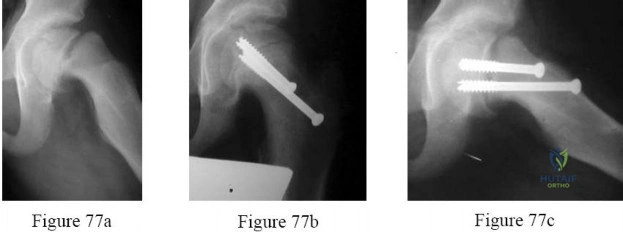
Figures 77a through 77c are the preoperative and postoperative radiographs of a 13-year-old boy who had sudden worsening of left hip pain following many months of mild pain. He was unable to walk because of his pain and underwent screw fixation.
Question 48
Which of the following patients with cerebral palsy is considered the ideal candidate for a selective dorsal rhizotomy?
Explanation
REFERENCES: Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29.
Renshaw TS, Green NE, Griffin PP, Root L: Cerebral palsy: Orthopaedic management. J Bone Joint Surg Am 1995;77:1590-1606.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 19-27.
Question 49
A child born with myelomeningocele is expected to be an ambulator with bracing. Examination by the consulting orthopaedic surgeon reveals rigid clubfeet in addition to the neurologic issues. Management should consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 65-78.
Kasser JE (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 503-514.
Question 50
A 48-year-old woman has knee pain that is worse with weight bearing. She reports no night pain or pain at rest. History reveals that she underwent total knee arthroplasty with cementless components 2 years ago. Examination reveals tenderness along the medial joint line. Figures 12a through 12c show radiographs and a bone scan. What is the most likely cause of the patient’s pain?
Explanation
REFERENCES: Fehring TK, Odum S, Griffin WL, Mason B, Nadaud M: Early failures of total knee arthroplasty. Clin Orthop 2001;392:315-318.
Fehring TK: Revision TJA corrects flexion extension gap imbalance. Orthop Today 2002;22:44.
Question 51
What is the mechanism of action of an intramuscular injection of botulinum type A toxin in reducing spasticitiy?
Explanation
REFERENCES: Koman LA, Mooney JF III, Smith B, Goodman A, Mulvaney T: Management of cerebral palsy with botulinum-A toxin: Preliminary investigation. J Pediatr Orthop 1993;13:489-495.
Brin MF: Botulinum toxin: Chemistry, pharmacology, toxicity, and immunology. Muscle Nerve Suppl 1997;6:S146-168.
Question 52
Figures 3a through 3c show the radiographs and bone scan of a patient who reports increasing pain associated with activity for the past several months. Laboratory studies show an erythrocyte sedimentation rate of 14 mm/h and a C-reactive protein level of 0.4. Aspiration is negative for infection. Management should consist of
Explanation
REFERENCES: Rand JA, Peterson LF, Bryan RS, Ilstrup DM: Revision total knee arthroplasty, in Anderson LD (ed): Instructional Course Lectures XXXV. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1986, pp 305-318.
Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 317-322.
Question 53
A 32-year-old man underwent a total medial meniscectomy 2 years ago. He now reports pain and recurrent swelling for the past 3 months. Work-up includes full standing hip-knee-ankle radiographs, standing AP radiographs of both knees in full extension, an axial view of the patellofemoral joint, and a 45-degree flexion AP radiograph. Contraindication to meniscus allograft transplantation includes which of the following? Review Topic
Explanation
Question 54
What muscles are responsible for the most common deformity after antegrade intramedullary nailing for a subtrochanteric femur fracture?

Explanation
The reference by French et al is a review on 45 patients with subtrochanteric fractures treated with cephalomedullary interlocked nailing. Based on femoral neck-shaft angle, 61% of the fractures were reduced in at least 5º varus. The authors attributed this malalignment to failure to counteract muscle forces acting on the proximal fragment, combined with the adducted position of the distal femur during portal creation.
The reference by Ricci et al is a report of 403 femoral shaft fractures treated with intramedullary nailing. Patients with proximal femoral shaft fractures were found to have the highest incidence of malalignment. The most common deformity in this group was varus, followed by procurvatum (or flexion).
Question 55
The AP radiograph of a 5-year-old boy shows a 20-degree left thoracic scoliosis. He was noted by his pediatrician to have asymmetry on a forward bend test. On examination he is neurologically intact except for decreased sensation on the lateral aspect of both flanks and to pinprick in both hands. He has no pain. What is the best initial step in treatment at this time? Review Topic
Explanation
Question 56
A 4-year-old boy with arthrogryposis has little active motion of his knees or elbows. Both elbows are in full extension with good triceps strength, but he is unable to bring his hand to his face or feed himself. Management should consist of
Explanation
REFERENCES: Van Heest A, Waters PM, Simmons BP: Surgical treatment of arthrogrypsosis of the elbow. J Hand Surg Am 1998;23:1063-1070.
Caroll RE, Hill NA: Triceps transfer to restore elbow flexion: A study of fifteen patients with paralytic lesions and arthrogryposis. J Bone Joint Surg Am 1970;52:239-244.
Question 57
2010 Pediatric Orthopaedic Examination Answer Book • 9 A 9-year-old girl has had bilateral knee and leg pain for the past 2 years. The family has noted increasing deformity in both lower extremities. She is less than the fifth percentile for height. Examination reveals bilateral femoral bowing, mild medial-lateral laxity of the knees, and the deformities shown in the radiograph seen in Figure 3. What is the most likely diagnosis?
Explanation
There is an asymmetry of the deformities that makes diastrophic dysplasia less likely.
REFERENCES: Goldberg MJ, Yassir W, Sadeghi-Nejad A: Clinical analysis of short stature. J Pediatr Orthop 2002;22:690-696.
Parmar VS, Stanitski DF, Stanitski CL: Interpretation of radiographs in a pediatric limb deformity practice: Do
radiologists contribute? J Pediatr Orthop 1999;19:732-734. Question 4
Patients with slipped capital femoral epiphysis are more likely to experience a delay in definitive diagnosis if they initially present to a physician reporting which of the following problems?
L Limp
Hip pain
Knee pain
Proximal thigh pain
Buttock pain
DISCUSSION: A delay in diagnosis of slipped capital femoral epiphysis (SCFE) can lead to significant worsening of the deformity or even progression from a stable to an unstable SCFE. Those patients that report knee pain as their primary complaint are most likely to experience significant delay. Other variables associated with this delay include Medicaid insurance and stable SCFE.
REFERENCES: Kocher MS, Bishop JA, Weed B, et al: Delay in diagnosis of slipped capital femoral epiphysis.
AL-Madena Copy
10 • American Academy of Orthopaedic Surgeons
Pediatrics 2004;113:e322-e325.
Rahme D, Comley A, Foster B, et al: Consequences of diagnostic delays in slipped capital femoral epiphysis. J Pediatr Orthop B 2006;15:93-97.
Question 58
Oxidation of polyethylene after sterilization occurs most rapidly when the implant undergoes
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Wright TM: Ultra-high molecular weight polyethylene, in Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 37-46.
Collier JP, Sutula LC, Currier BH, et al: Overview of polyethylene as a bearing material: Comparison of sterilization methods. Clin Orthop 1996;333:76-86.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 59
A 10-month-old infant has a deformity of the right foot. Radiographs, including simulated weight-bearing AP and lateral views and a maximum plantar flexion lateral view, are shown in Figures 57a through 57c. Initial management of the foot should consist of Review Topic

Explanation
Question 60
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?
Explanation
REFERENCES: Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809.
Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Pape HC, Auf’m’Kolk M, Puffrath T, et al: Primary intramedullary femur fixation in multiple trauma patients with associated lung contusion: A cause of posttraumatic ARDS? J Trauma 1993;34:540-548.
Question 61
A 6-year-old boy has had increasing pain and a mass in the suprapatellar region of the right femur for the past week. Examination of the mass reveals it may be firm, immobile, and tender to palpitation. The patient has no systemic symptoms. Laboratory studies show a WBC of 7000 per cubic millimeter, a hematocrit of 40%, and an erythrocyte sedimentation rate of 10 mm/hr. radiographs are normal. Figures 64a and 64b show saggital and axial T1-weighted MRI scans. Figure 64c shows frozen section pathology of the biopsy specimen. What is the most likely diagnosis?
Explanation
Question 62
The infection work-up is negative. What is the best next step?

Explanation
The cross-table lateral radiograph shows that the patient has decreased acetabular anteversion. She is likely impinging on her cup in flexion and levering the femoral component posteriorly. Given a well-fixed and well-aligned femoral component and a negative infection work-up, the preferred treatment is to revise the acetabulum with a goal of increasing acetabular anteversion to avoid prosthetic impingement. Conversion to a constrained or elevated rim liner is suboptimal in this setting, because the problem is impingement. Indications for a constrained liner are neuromuscular compromise, abductor deficiency, or instability despite well-fixed and well-placed components. Given her 5 of 5 abductor strength, gluteus medius repair is not indicated.
Question 63
Figures 1 and 2 are the radiographs of a 40-year-old woman who sustained a twisting injury to her lower extremity. What additional information or studies are important in determining treatment options?

Explanation
(SBQ12TR.24) In each of the following scenarios, atrophic fracture nonunion occurred after initial treatment with intramedullary nail fixation. Which scenario has shown to have the highest rate of osseous union if treated with exchange intramedullary nailing?
Oligotrophic nonunion of a comminuted humeral shaft fracture
Oligotrophic nonunion of a transverse humeral shaft fracture
Oligotrophic nonunion of an oblique distal femur fracture
Oligotrophic nonunion of a comminuted tibial shaft fracture
Oligotrophic nonunion of an oblique tibial shaft fracture
Reamed exchange nailing is recommended for the management of aseptic nonunions of noncomminuted tibial shaft fractures. Union rates have been reported between 76-96% in large studies.
Tibial exchange nailing promotes osseous bone healing of non-unions by providing biological and mechanical support. The biological support is provided by reaming the medullary canal. This increases periosteal blood flow and stimulates periosteal new-bone formation. The mechanical support is provided by a larger-diameter intramedullary nail, which increases the rigidity and strength of the nail.
Brinker et al. reviewed the concept of exchange nailing of nonunited long bone fractures. They showed that exchange nailing is the most successful in the treatment of nonunions following closed or open fractures without substantial bone loss. Aseptic, noncomminuted diaphyseal femoral and tibial shaft fractures showed the highest rates of union with exchange nailing, which were found to be 76-100% and 72-96%, respectively.
Illustration A shows a heterotrophic non-union of the tibia after intramedullary nailing. The patient was treated with exchange nailing with a larger nail. On the right shows a 4 month post-op radiograph after exchange nailing showing osseous union at the fracture site.
Incorrect Answers:
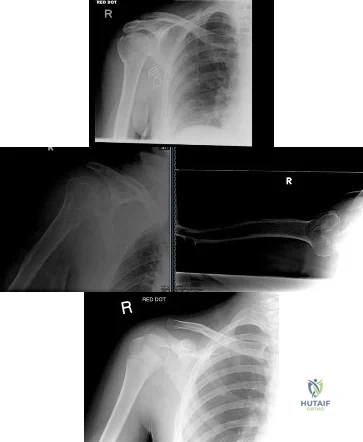
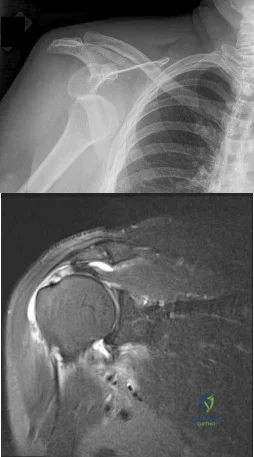
(SBQ12TR.79) A right-hand dominant female sustains a right proximal humerus fracture. The patient is provided a sling, and is recommended pendulum exercises with elbow range of motion to begin in 1 to 2 weeks. Which of the following would be an indication for surgical management?
Age greater than 70 years.
Fracture pattern in Figure A
Significant medical comorbidities.
Fracture pattern in Figure B
Fracture pattern in Figure C
The patient has been treated with non-operative management for her proximal humerus fracture. Operative management should be considered in patients with head splitting proximal humerus fractures and in those with dislocations that cannot be reduced.
Head splitting proximal humerus fractures should be treated with operative management. Open reduction internal fixation versus hemiarthroplasty are used to treat this type of fracture. Surgical management is also considered in proximal humerus fractures in young patients, in fractures where the greater tuberosity is
displaced >5 mm, and in proximal humerus fractures associated with humeral shaft fractures.
Koval et al. studied 104 patients with one-part proximal humerus fractures treated non-operatively, and found 80% with good or excellent results. They also found that 90% of patients treated non-operatively had either no or mild pain about the shoulder at follow-up.
Lefevre-Colau et al. performed a randomized prospective study on 74 patients with an impacted proximal humerus fracture. One group was treated with early mobilization of the shoulder (within 3 days after the fracture) while the other group was immobilized for 3 weeks followed by physiotherapy. They concluded that early mobilization was safe and allowed for quicker return to functional use of the affected limb.
Figure A shows an AP radiograph of a right minimally displaced greater tuberosity proximal humerus fracture. Figure B shows AP and axillary radiographs of a right head split proximal humerus fracture that is posteriorly dislocated. Figure C shows an AP radiograph of a right minimally displaced Salter Harris II proximal humerus fracture. Illustration A shows an AP radiograph of a left valgus impacted proximal humerus fracture with a greater tuberosity fragment displaced >5mm treated with ORIF.
Incorrect Answers:
Question 64
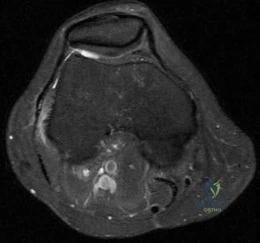
A 28-year-old man has left knee pain after a snow skiing accident. The MRI scan shown in Figure 47 reveals which of the following? Review Topic
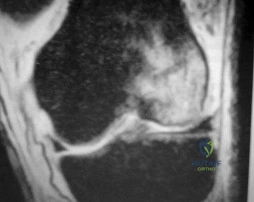
Explanation
Question 65
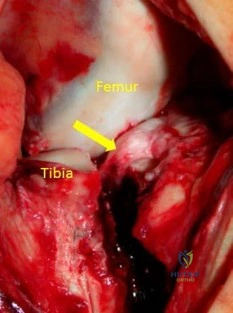
A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
Explanation
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
Question 66
Tendon fibroblasts detect applied strain through what mechanism?
Explanation
Question 67
-A 24-year-old collegiate pitcher has had increasing pain over his medial elbow for 3 months. He has point tenderness over his medial epicondyle and reproduction of his symptoms with a valgus stress test. What phase of the throwing cycle most likely will reproduce his symptoms?
Explanation
Question 68
A 37-year-old man pulled his hamstring playing softball 3 weeks ago. The patient had not noted any mass prior to his injury. MRI scans of the posterior thigh are shown in Figures 4a and 4b. Figure 4c shows the biopsy specimen from a needle biopsy. What is the most likely diagnosis?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 965-981.
Question 69
A 21-year-old man has had posterior neck discomfort for the past 6 months. A whole-body bone scan and a cervical single-photon emission CT reveal increased activity at the C7 spinous process. MRI reveals multifocal involvement of the spinous process lamina and facet of C7. A CT-directed needle biopsy reveals osteoblastoma. What is the best course of action?
Explanation
REFERENCES: Bridwell KH, Ogilvie JW: Primary tumors of the spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery. Philadelphia, PA, JB Lippincott, 1991, vol 2, pp 1143-1174.
Ozaki T, Liljenquist U, Hillmann A, et al: Osteoid osteoma and osteoblastoma of the spine: Experience with 22 patients. Clin Orthop 2002;397:394-402.
Question 70
A 25-year-old construction worker lands on his outstretched hand in a fall. The position of his wrist at the time of impact causes a force that leads to hyperextension, ulnar deviation, and intercarpal supination. Radiographs are shown in Figures 48a and 48b. Management should consist of
Explanation
REFERENCES: Kozin SH: Perilunate injuries: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:114-120.
Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J: Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-779.
Sotereanos DG, Mitsionis GJ, Ginnakopoulos PN, Tomaino MM, Herndon JH: Perilunate dislocation and fracture dislocation: A critical analysis of the volar-dorsal approach. J Hand Surg Am 1997;22:49-56.
Question 71
A 27-year-old woman sustained a bilateral C5-6 facet subluxation in a motor vehicle accident. Neurologic evaluation reveals normal motor, sensory, and reflex functions. She is awake, alert, and cooperative. Initial management should consist of
Explanation
REFERENCE: Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets: Case reports. J Bone Joint Surg Am 1991;73:1555-1560.
Question 72
In total knee arthroplasty, in vitro testing has shown that cross-linking can diminish the rate of polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
Explanation
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been shown to cause implant failure in the most recent clinical trials, but they remain the most important mechanical issues associated with current material processing methods.
Question 73
What is the most common benign bone tumor in childhood?
Explanation
REFERENCES: Aboulafia AJ, Kennon RE, Jelinek JS: Benign bone tumors of childhood. J Am Acad Orthop Surg 1999;7:377-388.
Biermann JS: Common benign lesions of bone in children and adolescents. J Pediatr Orthop 2002;22:268-273.
Question 74
Which of the following is an FDA approved adjunctive treatment for an acute open tibia fracture being treated with an intramedullary nail?
Explanation
Open tibial shaft fractures can present many treatment challenges. Although its use remains somewhat controversial, rhBMP-2 has been shown to have many positive effects when used to treat acute open tibia fractures. These benefits include accelerated early fracture healing, decreased rates of hardware failure, decreased need for subsequent bone grafting procedures, and decreased infection rates. rhBMP-2 does have FDA approval specifically for use in open tibia fractures being treated with an intramedullary nail.
Alt et al. present a comparison of patients with Grade III open tibia fractures treated
with un-reamed nails with or without rhBMP-2. They found significant decreases in need for secondary interventions such as bone grafting or nail exchange. Mean time to fracture healing was less in the rhBMP-2 group, but this difference was not statistically significant.
Govender et al. present a prospective randomized study of 450 patients with open tibia fractures treated with an intramedullary nail with or without rhBMP-2. They found statistically significant decreases in need for secondary intervention, hardware failure, and infection as well as faster wound healing and faster time to fracture union.
Wei et al. provide a meta analysis regarding use of rhBMP-2 in open tibia fractures. Due to decreased rates of secondary interventions they estimated a net savings of
$6,000 per case when rh-BMP2 was used. They found no significant difference in rates of infection, postoperative pain, hardware failure, or fracture healing at 20 weeks.
Incorrect answers:
Question 75
Which of the following factors is most likely to contribute to pseudarthrosis in a patient who has undergone a single-level anterior decompression and fusion procedure for the treatment of cervical radiculopathy? Review Topic
Explanation
diabetes mellitus, have been shown to significantly increase pseudarthrosis rates. The literature has been mixed with regard to fusion rates for allograft versus autograft, especially for one-level fusions; in that category, there is minimal, if any, difference. Similarly, several authors have shown higher rates of fusion with uninstrumented single-level rather than instrumented anterior cervical decompressions and fusions. The level (ie, cranial or caudal) of fusion and sagittal alignment have not been correlated with fusion rates.
Question 76
- An otherwise healthy 65-year-old man has had chronic pain in his prosthetic knee for the past 9 months. Repeated aspirations reveal a coagulase-negative staphylococcus infection. To eradicate the infection while maintaining the best possible joint function, management should consist of
Explanation
Present recommendations are to avoid a one-stage reconstruction in a patient in whom a glycocalyx elaborating microorganism has been isolated. In one study 52% of the isolates of S. epidermidis and 28% of the isolates of S. aureus elaborated glycocalyx. The microbiology laboratory can be asked to determine if the microorganisms elaborate glycocalyx. In the present case it should be assumed that the staphylococci elaborate glycocalyx and are resistant to antibiotics. A two-stage procedure is indicated for these reasons alone.
Antibiotic therapy alone has been used for a select group of patients who could not medically tolerate either a one-stage or a two-stage arthroplasty. The patient in this case is listed as otherwise healthy.
The decision to perform a resection arthroplasty as a definitive procedure without reimplantation is based on the bacteria’s resistance to antibiotics, quality of the local soft tissues, the complexity of the reconstruction, the patient’s refusal to have another operation, the patient’s overall health, or a combination of these factors. None of which appear to be present in this case.
Question 77
-Figure is the clinical photograph of a 70-year-old woman with squamous cell cancer on her thumb.Resection and reconstruction is planned and requires soft-tissue coverage. Thumb region coverage is best obtained with
Explanation

Question 78
Figure 33 shows the oblique radiograph of an 11-year-old boy who has a mild left flatfoot deformity. Examination reveals that subtalar motion is limited and painful. Despite casting for 6 weeks, the patient reports foot pain that limits participation in sport activities. A CT scan shows no subtalar joint abnormalities. Management should now include
Explanation
has been described for treatment of the peroneal spastic flatfoot without demonstrable
tarsal coalition.
REFERENCES: Gonzalez P, Kumar SJ: Calcaneonavicular coalition treated by resection and interposition of the extensor digitorum brevis muscle. J Bone Joint Surg Am 1990;72:71-77.
Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Luhmann SJ, Rich MM, Schoenecker PL: Painful idiopathic rigid flatfoot in children and adolescents. Foot Ankle Int 2000;21:59-66.
Question 79
A 25-year-old male involved in a motor vehicle accident sustains multiple injuries. He undergoes operative treatment for his humeral shaft fracture. Figures A and B show his preoperative and postoperative radiographs. The distal interlocks for this implant place which of the following nerves at risk?

Explanation
Rupp et al performed a cadaveric study with IM nails utilizing either lateral-to-medial or anterior-to-posterior distal interlocking screws. They showed that anterior-to-posterior screws placed the musculocutaneous nerve at high risk, while lateral-to-medial screws placed the radial nerve at high risk as it courses laterally distally along the humerus.
OrthoCash 2020
Question 80
A 12-year-old child falls from his bicycle and injures his right knee. Evaluation in the emergency department reveals knee effusion and pain with extremes of range of motion. Radiographs are shown in Figures 13a and 13b. Attempts at closed reduction are made and he is placed in a long leg cast with the knee flexed at 10 to 20 degrees. At follow-up, repeat radiographs continue to show anterior displacement of the fracture. What structure is most likely entrapped under the fragment?
Explanation
from Lowe and associates in JBJS 2002 where they found the lateral meniscus to be involved in blocking reduction. This was not thought due to entrapment of the lateral meniscus. Rather, with the anterior cruciate
ligament and lateral meniscus still being attached to the avulsed fracture fragment, they felt the two structures were pulling in opposite directions and therefore blocking reduction of the fragment.
REFERENCES: Falstie-Jensen S, Sondergard-Petersen PE: Incarceration of the meniscus in fractures of the intercondylar eminence of the tibia in children. Injury 1984;15:236-238.
Kocher MS, Micheli LJ, Gerbino P, et al: Tibial eminence fractures in children: Prevalence of meniscal entrapment. Am J Sports Med 2003;31:404-407.
Accousti WK, Willis RB: Tibial eminence fractures. Orthop Clin North Am 2003;34:365-375.
Lowe J, Chaimsky G, Freedman A, et al: The anatomy of tibial eminence fractures: arthroscopic observations following failed closed reduction. J Bone Joint Surg Am 2002;84:1933-1938.
Figure 14a Figure 14b Figure 14c Question 14
A 14-year-old boy underwent in situ screw fixation for a left slipped capital femoral epiphysis 8 months ago. He
noted 3 months of intermittent right hip pain but is presently asymptomatic. The last episode of pain was 2 days prior to this office visit. He reports that he has pain approximately once a week over the past 3 months. Examination of the right hip is normal, and includes pain-free internal rotation. Radiographs and an MRI scan are shown in Figures 14a through 14c. Treatment should consist of which of the following?
In situ screw fixation of the right hip
Physical therapy
Limitation of activities and return to the clinic if pain persists
Biopsy of the femoral neck lesion
Irrigation and debridement of the right hip PREFERRED RESPONSE: 1
DISCUSSION: The patient history is concerning for a pre-slip slipped capital femoral epiphysis (SCFE) of the right hip. In one study, nearly 40% of patients with SCFE had bilateral involvement, and of that 40%, half presented initially with a unilateral SCFE but had a subsequent SCFE on the contralateral limb. Radiographs are normal, but the MRI scan shows increased signal about the proximal femoral physis. Treatment should include prophylactic screw fixation of the right hip.
REFERENCES: Aronsson DD, Loder RT, Breur GJ, et al: Slipped capital femoral epiphysis: Current concepts. J Am Acad Orthop Surg 2006;14:666-679.
Loder RT, Aronson DD, Greenfield ML: The epidemiology of bilateral slipped capital femoral epiphysis: A study of children in Michigan. J Bone Joint Surg Am 1993;75:1141-1147.

Loder RT: Controversies in slipped capital femoral epiphysis. Orthop Clin North Am 2006;37:211-221, vii.
Figure 15a Figure 15b
Question 81
- A form of renal osteodystrophy that is characterized by pure osteomalacia is caused by
Explanation
Question 82
A 58-year-old woman who underwent a successful total hip replacement for degenerative arthritis 8 years ago reports groin pain for the past 6 months. A radiograph of the hip is shown in Figure 32. At revision, severe deficiency of the posterior column is noted. What reconstructive option would be most appropriate for the acetabulum?
Explanation
REFERENCES: Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
Berry DJ, Muller ME: Revision arthroplasty using an anti-protrusio cage for massive acetabular bone deficiency. J Bone Joint Surg Br 1992;74:711-715.
Question 83
Figure 54 is the lateral radiograph of a 55-year-old man who is evaluated for a 2-year history of pain and stiffness of his right metatarsophalangeal (MTP) joint. Upon examination he has dorsal bossing, severe crepitation, and pain with passive range of motion. There is pain with the "grind" test. Dorsiflexion is limited to 0 degrees. No sesamoid tenderness is present. What is the most appropriate surgical treatment?

Explanation
The radiograph reveals end-stage degenerative changes of the first MTP joint with a dorsal loose body. MTP arthritis and decreased joint dorsiflexion is referred to as hallux rigidus. A chevron bunionectomy is used to correct hallux valgus deformity without arthritis. The cheilectomy is used in lesser degrees of joint destruction. Resection of the proximal phalanx results in a floppy toe and is generally not recommended.
RECOMMENDED READINGS
McNeil DS, Baumhauer JF, Glazebrook MA. Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int. 2013 Jan;34(1):15-32. doi: 10.1177/1071100712460220. Review. PubMed PMID: 23386758.
View Abstract at PubMed
Deland JT, Williams BR. Surgical management of hallux rigidus. J Am Acad Orthop Surg. 2012 Jun;20(6):347-58. doi: 10.5435/JAAOS-20-06-347. Review. PubMed PMID: 22661564.
View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 55 THROUGH 58
Figures 55a and 55b are the anteroposterior and lateral radiographs of a 57-year-old man who fell off of a ladder 10 days ago and landed on his left foot. He is now unable to weight bear on the left. He has no history of trauma to this foot, and his medical history is unremarkable. Upon examination his left foot is swollen and tender. Pulses and sensation are intact.

A B
Question 84
A 45-year-old man sustained the injury seen in Figure 130a 6 weeks ago. He denies any prior injury to his shoulder. After treatment of the injury in the emergency department, he was noted to have significant weakness with empty can testing and external rotation at the side. He has full passive range of motion with forward flexion, abduction, and internal and external rotation, but has difficulty initiating abduction with his arm at his side. He has negative apprehension and relocation signs. A detailed neurologic examination shows no deficits. A coronal image from a follow-up MRI scan is seen in Figure 130b. Follow-up radiographs reveal no fractures. What is the most appropriate next step in his treatment? Review Topic
Explanation
Question 85
An 81-year-old man with severe low back pain reports right extensor hallucis longus and anterior tibialis weakness and difficulty urinating over the past 24 hours. He has a temperature of 101 degrees F (38.3 degrees C). MRI scans are shown in Figures 31a and 31b. Management should consist of
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 257-271.
Reihsaus E, Waldbaur H, Seeling W: Spinal epidural abscess: A meta-analysis of 915 patients. Neurosurg Rev 2000;23:175-204.
Question 86
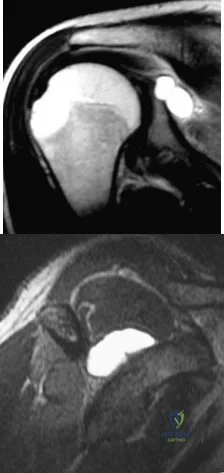
A 16-year-old right-hand dominant pitcher has had pain with throwing for the past 6 months but denies any history of trauma. Figures 9a and 9b show noncontrast MRI scans of the involved shoulder. What is the most likely diagnosis? Review Topic
Explanation
Question 87
Which of the following agents increases the risk for a nonunion following a posterior spinal fusion?
Explanation
REFERENCES: Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Martin GJ Jr, Boden SD, Titus L: Recombinant human bone morphogenetic protein-2 overcomes the inhibitory effect of ketorolac, a nonsteroidal anti-inflammatory drug (NSAID), on posterolateral lumbar intertransverse process spine fusion. Spine 1999;24:2188-2193.
Question 88
Spondyloepiphyseal dysplasia congenita and tarda, precocious osteoarthropathy, and Stickler syndrome are caused by a mutation in the gene coding for
Explanation
Question 89
Figure 23 shows the radiograph of a 7 year-old girl with a low thoracic-level myelomeningocele. She has a history of skin ulcers over the apex of the deformity, but her current skin condition is good. Management of the spinal deformity should consist of
Explanation
REFERENCES: Lindseth RE: Spine deformity in myelomeningocele. Instr Course Lect 1991;40:273-279.
Sharrard J, Drennan JC: Osteotomy excision of the spine for lumbar kyphosis in older children with myelomeningocele. J Bone Joint Surg Br 1972;54:50-60.
Question 90
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with prognosis in the setting of reaction to metal debris?
Explanation
Question 91
A 55-year-old patient with rheumatoid arthritis reports increasing elbow pain and swelling for the past 2 months. She underwent a cemented, semiconstrained elbow arthroplasty 8 years ago. Laboratory studies show a normal peripheral white blood cell count; however, the erythrocyte sedimentation rate and C-reactive protein level are elevated. Radiographs are shown in Figures 48a and 48b. Which of the following organisms is most difficult to eradicate? Review Topic

Explanation
Question 92
Which of the following forms of nonsurgical management is considered best for acute low back pain without radiculopathy?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
Helfgott SM: Sensible approach to low back pain. Bull Rheum Dis 2001;3:50.
Question 93
A 21-year-old woman with Marfan syndrome is seeking evaluation of her scoliosis. She reports no back or leg pain, and the neurologic examination is normal. Lateral and bending radiographs are shown in Figures 7a through 7e. Management should consist of
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 161-171.
Turi M, Johnston CE II, Richards BS: Anterior correction of idiopathic scoliosis using TSRH instrumentation. Spine 1993;18:417-422.
Moskowitz A, Trommanhauser S: Surgical and clinical results of scoliosis surgery using Zielke instrumentation. Spine 1993;18:2444-2451.
Question 94
Which of the following is the most stable construct for fixation of an unstable transforaminal sacral fractures?

Explanation
Question 95
What is the main biologic effect of aggrecan in cartilage? Review Topic
Explanation
Aggrecan is the predominant proteoglycan in cartilage. It contains a large number of negatively charged sequences that attract water called sulfated glycosaminoglycan (GAG) chains. Its the N-terminal globular domain of aggrecan that binds hyaluronan to form huge aggregates. Together with its chondroitin sulfate chains, they help to create a hydrophilic viscous gel that decreases the coefficient of friction as well as to help absorb compressive loads.
Ulrich-Vinthe et al. reviewed the biology of articular cartilage. They report that matrix metalloproteinases and aggrecanases play a major role in aggrecan degradation and their production is upregulated by mediators associated with joint inflammation and overloading.
Illustration A shows a depiction of the function of aggrecan in articular cartilage. In the relaxed state, the aggregates draw water into cartilage. With compressive loads, the water is displaced to cushion the load. Upon removal of the load, the water content is restored.
Incorrect Answers:
Question 96
Hip pain of month duration has developed in a year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. What is this patient's prognosis for infection resolution?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin- resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was
21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 97
A 21-year-old pregnant female arrives in the trauma bay with a closed head injury as well as an open ankle injury. During evaluation, what positioning is recommended to limit positional hypotension?

Explanation
reviews the appropriate physiological changes of pregnancy and covers the treatment of orthopedic trauma in the face of pregnancy.
Question 98
During an anterior retroperitoneal approach to the low lumbar spine, the iliac vessels are mobilized along the lateral side, allowing them to be retracted toward the midline. To gain adequate mobility of the common iliac vein for exposure of L5, it is important to identify which of the following structures?
Explanation
REFERENCE: Gray H: Anatomy of the Human Body. Philadelphia, PA, Lea & Febiger,
1918, 2000.
Question 99
A baseball player reports a dull pain in the posterior aspect of his throwing arm. Examination reveals decreased internal rotation and prominence of the inferomedial corner of the scapula. An MRI scan suggests a partial-thickness tear of the posterior supraspinatus tendon. Successful treatment would most likely include which of the following? Review Topic
Explanation
required, and capsulolabral imbrication is more consistent with the surgical treatment for multidirectional instability.
Question 100
What is the most common clinical presentation of a patient with a malignant bone tumor?
Explanation
REFERENCES: Buckwalter JA: Musculoskeletal neoplasms and disorders that resemble neoplasms, in Weinstein SL, Buckwalter JA (eds): Turek’s Orthopaedics: Principles and Their Application, ed 5. Philadelphia, PA, JB Lippincott, 1994, pp 290-295.
Mehlman CT, Crawford AH, McMath JA: Pediatric vertebral and spinal cord tumors: A retrospective study of musculoskeletal aspects of presentation, treatment, and complications. Orthopedics 1999;22:49-55.
