Orthopedic Surgery Board Review MCQs: Trauma & Arthroplasty | Part 249

Key Takeaway
This page presents Part 249 of a comprehensive Orthopedic Surgery Board Review MCQ set, ideal for residents and surgeons preparing for OITE and AAOS certification. Featuring 100 high-yield, verified questions on topics like Ankle, Knee, and Arthroplasty, it offers both study and exam modes for effective preparation.
About This Board Review Set
This is Part 249 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 249
This module focuses heavily on: Ankle, Arthroplasty, Fracture, Infection, Knee, Revision.
Sample Questions from This Set
Sample Question 1: A 50-year-old woman with a 2-part surgical neck proximal humerus fracture and metaphyseal comminution...
Sample Question 2: A 28-year-old man has left knee pain after a snow skiing accident. The MRI scan shown in Figure 47 reveals which of the following? Review Topic...
Sample Question 3: Ayear-oldmanhasadrainingsinusandrecurrentinfectionofhisrighttotalkneearthroplasty.Hehashadtwopriorrevisionsurgeriesaftertheprimaryprocedureandthreeothersurgeriesbeforehisinitial replacement,includingaproximaltibialosteotomyandsubsequenthard...
Sample Question 4: A 12-year-old boy with an ankle fracture undergoes closed reduction under sedation in the emergency department. Figure 27 shows a lateral radiograph of the ankle after two attempts at closed reduction. Based on these findings, treatment sho...
Sample Question 5: Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 50-year-old woman with a 2-part surgical neck proximal humerus fracture and metaphyseal comminution
Explanation
Proximal humerus fractures account for approximately 5% of all fractures, with incidence increasing to reflect an aging population and related osteoporosis. Treatment is dependent upon the mechanism of injury, the patient’s physiologic age and activity level, the fracture pattern, and rotator cuff integrity. Most of these injuries are nondisplaced or minimally displaced and are associated with a good overall prognosis with nonsurgical treatment and temporary impairment. A patient with a nondisplaced surgical neck fracture should be treated without surgery. K-wire stabilization, although technically difficult to achieve, is an option for compliant patients with 2-part, 3-part, and valgus-impacted 4-part fractures who have adequate bone stock. Valgus-impacted 4-part fractures pose reduced risk for osteonecrosis because of the preserved blood supply through the medial hinge, which allows for this technique. For displaced 2-part fractures accompanied by
metaphyseal comminution, K-wire fixation cannot provide adequate stability to initiate a graduated home exercise or outpatient physical therapy program. Formal open reduction with intramedullary or plate fixation in addition to bone grafting (fibular strut allograft) is the best surgical option for the clinical scenario involving a displaced surgical neck fracture with comminution. Osteosynthesis of 3-part fractures may be feasible for physiologically young and active patients without humeral head involvement and osteoporosis.
Current indications for primary hemiarthroplasty include most 4-part fractures, 3-part fractures and dislocations in elderly patients with osteoporotic bone, head-splitting articular segment fractures, and chronic anterior or posterior humeral head dislocations with more than 40% of articular surface involvement. Because of the intra-articular nature of this patient’s 4-part injury in this scenario, hemiarthroplasty with anatomic reconstruction of the greater and lesser tuberosities is most appropriate. Relative indications for hemiarthroplasty also include fractures with more than 20 degrees of varus, associated moderate to severe osteopenia, and revision surgery for failed osteosynthesis. Currently accepted indications for rTSA include scenarios in which the fracture pattern, level of comminution, bone quality, and rotator cuff deficiency preclude plate fixation or hemiarthroplasty. Scenarios involving 4-part fractures and associated rotator cuff tears and tuberosity comminution are best served with a reverse shoulder prosthesis. One of the positive attributes of this implant is the ability to achieve functional forward flexion and abduction regardless of tuberosity healing, position, and degree of comminution. Caution is warranted with this surgical technique because complication rates are higher than for hemiarthroplasty reconstruction. Acute, irreducible 2-part fracture-dislocations of the proximal humerus necessitate open reduction and internal fixation of the affected tuberosities (posterior, lesser tuberosity; anterior, greater tuberosity) through screw, anchor, and/or suture fixation. These fracture-dislocations can be managed with this technique because of the integrity of the vascular supply, which is maintained by the soft-tissue attachments to the intact tuberosities. Repeated attempts at a closed reduction in the 37-year-old with the posterior fracture-dislocation could result in neurovascular injury and myositis ossificans and should be avoided. Arthroplasty reconstruction in this scenario should not be the index procedure in light of concerns regarding implant survivorship in patients of this age and their assumed elevated activity levels.
RECOMMENDED READINGS
Harrison AK, Gruson KI, Zmistowski B, Keener J, Galatz L, Williams G, Parsons BO, Flatow EL. Intermediate outcomes following percutaneous fixation of proximal humeral fractures. J Bone Joint Surg Am. 2012 Jul 3;94(13):1223-8. doi: 10.2106/JBJS.J.01371. View Abstract at PubMed
Iannotti JP, Ramsey ML, Williams GR Jr, Warner JJ. Nonprosthetic management of proximal humeral fractures. Instr Course Lect. 2004;53:403-16. Review. View Abstract at PubMed
Mata-Fink A, Meinke M, Jones C, Kim B, Bell JE. Reverse shoulder arthroplasty for treatment of proximal humeral fractures in older adults: a systematic review. J Shoulder Elbow Surg. 2013 Dec;22(12):1737-48. doi: 10.1016/j.jse.2013.08.021. Review. View Abstract at PubMed
Jobin CM, Galdi B, Anakwenze OA, Ahmad CS, Levine WN. Reverse shoulder arthroplasty for the management of proximal humerus fractures. J Am Acad Orthop Surg. 2015 Mar;23(3):190-201. doi: 10.5435/JAAOS-D-13-00190. Epub 2015 Jan 28. Review. View Abstract at PubMed
Bae JH, Oh JK, Chon CS, Oh CW, Hwang JH, Yoon YC. The biomechanical performance of locking plate fixation with intramedullary fibular strut graft augmentation in the treatment of unstable fractures of the proximal humerus. J Bone Joint Surg Br. 2011 Jul;93(7):937-41. View Abstract at PubMed
Kontakis G, Koutras C, Tosounidis T, Giannoudis P. Early management of proximal humeral fractures with hemiarthroplasty: a systematic review. J Bone Joint Surg Br. 2008 Nov;90(11):1407-13. doi: 10.1302/0301-620X.90B11.21070. Review. PubMed PMID: 18978256. View Abstract at PubMed
Hertel R, Hempfing A, Stiehler M, Leunig M. Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus. J Shoulder Elbow Surg. 2004 Jul-Aug;13(4):427-33. PubMed PMID: 15220884. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 67 THROUGH 70
Figure 67 is the radiograph of a right-hand-dominant 70-year-old woman who arrives at the emergency department with acute left shoulder pain following a fall down a flight of stairs. She expresses acute diffuse left shoulder pain and swelling. Prior to her injury, she had full active painless shoulder range of motion.

Question 2
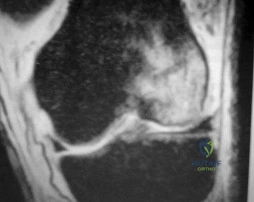
A 28-year-old man has left knee pain after a snow skiing accident. The MRI scan shown in Figure 47 reveals which of the following? Review Topic
Explanation
Question 3
A year-old man has a draining sinus and recurrent infection of his right total knee arthroplasty. He has had two prior revision surgeries after the primary procedure and three other surgeries before his initial replacement, including a proximal tibial osteotomy and subsequent hardware removal. On clinical examination, he has a draining sinus in the mid portion of his surgical scar and a range of motion of 5° to 85°. AP and lateral radiographs of the right knee are shown in below. During surgery, the femoral component is found to be grossly loose, but the tibial component is well fixed. What is the most appropriate extensile approach that would provide adequate exposure and aid in tibial component extraction?
Explanation
Extended tibial tubercle osteotomy is an extensile approach to revision total knee arthroplasty that affords excellent exposure and can facilitate removal of tibial sleeves and cones. This patient has had multiple surgeries, including a proximal tibial osteotomy, as well as poor range of motion, patella baja, and a well- fixed metaphyseal sleeve component. Classically, an extended tibial tubercle osteotomy provides outstanding exposure for component removal in the setting of prior high tibial osteotomy and patella baja. For this patient, it is important to recognize the patella baja on the radiographs, as well as the tibial sleeve. In many of these cases the osteotomy provides access to the sleeve to help with extraction, because the stem will not pull through the sleeve or detach from the tray to allow visualization of the sleeve. The extended medial parapatellar approach is just a long medial approach that typically yields good exposure
but would not help with the patella baja or extraction of the tibial sleeve. The quadriceps snip would give good exposure to the knee but would not aid in tibial component removal. Lastly, the medial epicondyle osteotomy could help with exposure and tensioning of the medial complex of the knee but would not help
with tibial component extraction.
Question 4
A 12-year-old boy with an ankle fracture undergoes closed reduction under sedation in the emergency department. Figure 27 shows a lateral radiograph of the ankle after two attempts at closed reduction. Based on these findings, treatment should now consist of Review Topic

Explanation
Question 5
Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?

Explanation
Bae et al reviewed thirty-six cases of compartment syndrome in 33 pediatric patients. Approximately 75% of these patients developed compartment syndrome in the setting of fracture. "They found pain, pallor, paresthesia, paralysis, and pulselessness were relatively unreliable signs and symptoms of compartment syndrome in these children. An increasing analgesia requirement in combination with other clinical signs, was a more sensitive indicator of compartment syndrome."
Whitesides et al summarizes the diagnosis and treatment of acute compartment syndrome. They emphasize the need for early diagnosis, as "muscles tolerate 4 hours of ischemia well, but by 6 hours the result is uncertain; after 8 hours, the damage is irreversible." They recommend fasciotomy be performed when tissue pressure rises past 20 mm Hg below diastolic pressure.
Question 6
Figures 34a and 34b show the clinical photographs of a 46-year-old woman who has a painful deformity of the second toe. Surgical treatment consisting of metatarsophalangeal capsulotomy and proximal interphalangeal joint resection arthroplasty resulted in satisfactory correction, but the toe remains unstable at the metatarsophalangeal joint. What is the next most appropriate step?
Explanation
REFERENCES: Coughlin MJ: Crossover second toe deformity. Foot Ankle 1987;8:29-39.
Thompson FM, Deland JT: Flexor tendon transfer for metatarsophalangeal instability of the second toe. Foot Ankle 1993;14:385-388.
Question 7
Well-differentiated liposarcomas never have chromosomal abnormalities. Liposarcomas account for approximately 10% to 15% of sarcomas. Some general statements about liposarcomas are listed below:
Explanation
Question 8
In children with moderate to severe osteogenesis imperfecta (OI), intravenous pamidronate therapy has been shown to increase the thickness of cortical bone. This occurs primarily as a consequence of
Explanation
REFERENCES: Zeitlin L, Fassier F, Glorieux FH: Modern approach to children with osteogenesis imperfecta. J Pediatr Orthop B 2003;12:77-87.
Falk MJ, Heeger S, Lynch KA, et al: Intravenous bisphosphonate therapy in children with osteogenesis imperfecta. Pediatrics 2003;111:573-578.
Glorieux FH, Bishop NJ, Plotkin H, et al: Cyclic administration of pamidronate in children with severe osteogenesis imperfecta. N Engl J Med 1998;339:947-952.
Question 9
Figures 25a and 25b show the clinical photographs of a 19-year-old baseball outfielder who has shoulder pain after sliding headfirst into second base. He reports pain while batting, sliding, and catching. Examination reveals a posterior prominence during midranges of forward elevation, which then disappears with a palpable clunk during terminal elevation and abduction. What is the most likely diagnosis?
Explanation
REFERENCES: Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Fiddian NJ, Kling RJ: The winged scapula. Clin Orthop 1984;185:228-236.
Question 10
The therapeutic effect of etanercept in the treatment of rheumatoid arthritis is primarily mediated through
Explanation
REFERENCES: Weinblatt ME, Kremer JM, Bankhurst AD, et al: A trial of etanercept, a recombinant tumor necrosis factor receptor: Fc fusion protein, in patients with rheumatoid arthritis receiving methotrexate. N Engl J Med 1999;340:253-259.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 489-530.
Question 11
A 19-year-old man who plays college volleyball undergoes a routine preparticipation physical examination. Figure 35 shows a posterior view of his dominant shoulder. An electromyogram shows that this is a chronic injury, and an MRI scan shows no abnormalities. The best course of action should be
Explanation
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Martin SD, Warren RF, Martin TL, Kennedy K, O’Brien SJ, Wickiewicz TL: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
Question 12
A 13-year-old baseball pitcher presents with worsening medial-sided elbow pain. He pitches 7 months out of the year, throws 85 pitches per game and plays in two games per week. His fastball speed is approximately 75mph. He regularly plays outfield once he has been relieved of pitching. Which of the following is most likely contributing to his elbow pain? Review Topic
Explanation
Little League elbow is a medial-sided overuse injury that occurs in the skeletally immature athlete. During execution of the baseball pitch, tremendous valgus and extension stresses occur at the elbow. Repetitive microtrauma can ultimately injure the medial epicondyle apophysis, ulnar collateral ligament or the flexor-pronator muscle mass. Limiting the number of pitches and innings played per game, as well as the number of months of competitive pitching per year, has been recommended to prevent these overuse injuries in the young athlete.
Olsen et al performed a case control study to determine risk factors associated with the development of shoulder and elbow injuries in adolescent baseball pitchers. Greater than 8 months of competitive pitching per year, more than 80 pitches per game and a fastball speed of greater than 85mph were all associated with increased risk of injury. Continued pitching despite arm fatigue and pain, being a starting pitcher, greater number of warm-up pitches, participating in showcases and regular use of NSAIDs were also associated with injury. The type of pitch (fastball, changeups and breaking balls) and continued play in a different position once being relieved was not associated with increased risk of injury.
Andrews et al authored a review article on ulnar collateral ligament injuries in throwing athletes. According to the USA Baseball Medical/Safety Advisory Committee, young baseball pitchers should avoid breaking pitches, such as curveballs and sliders, and avoid year-round baseball. A minimum of 3 months of complete rest from pitching per year is vital. Youth pitching coaches should be educated to ensure proper pitching mechanics are being reinforced.
Illustration A is a table depicting the recommended maximum number of pitches by age group.
Incorrect Answers:
Question 13
A 10-year-old boy who is active in soccer has had activity-related heel pain for the past 3 months. Examination reveals tenderness over the posterior heel and a tight Achilles tendon. Radiographs demonstrate a 2-cm cyst in the anterior body of the calcaneus. His physes have not closed. Based on these findings, what is the most appropriate management?
Explanation
REFERENCES: Ogden JA, Ganey TM, Hill JD, et al: Sever’s injury: A stress fracture of the immature calcaneal metaphysis. J Ped Orthop 2004;24:488-492.
Pogoda P, Priemel M, Linhart W, et al: Clinical relevance of calcaneal bone cysts: A study of 50 cysts in 47 patients. Clin Orthop Relat Res 2004;424:202-210.
Question 14
A 28-year-old woman has a moderate hallux valgus deformity and a prominence of the medial eminence. She can participate in all activities and reports that she could wear 3-inch heels in the past, but she now notes medial eminence pain even while wearing a soft leather flat shoe with a cushioned sole. She requests recommendations regarding surgical correction. Examination reveals a 1-2 intermetatarsal angle of 10 degrees. A clinical photograph and radiograph are shown in Figures 13a and 13b. What is the best course of action?
Explanation
REFERENCES: Chou LB, Mann RA, Casillas MM: Biplanar chevron osteotomy. Foot Ankle Int 1998;19:579-584.
Coughlin MJ: Roger A. Mann Award: Juvenile hallux valgus. Etiology and treatment. Foot Ankle Int 1995;16:682-697.
Pochatko DJ, Schlehr FJ, Murphey MD, Hamilton JJ: Distal chevron osteotomy with lateral release for treatment of hallux valgus deformity. Foot Ankle Int 1994;15:457-461.
Question 15
A 10-year-old girl reports activity-related bilateral arm pain. Examination reveals no soft-tissue masses in either arm, and she has full painless range of motion in both shoulders and elbows. The radiograph and bone scan are shown in Figures 20a and 20b, and biopsy specimens are shown in Figures 20c and 20d. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 118-119.
Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 197.
Question 16
A 13-year-old boy hyperextends his knee while playing basketball and reports a pop that is followed by a rapid effusion. A lateral radiograph is shown in Figure 4. Initial management consists of attempted reduction with extension, with no change in position of the fragment. What is the next most appropriate step in management?
Explanation
REFERENCES: Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60.
Mulhall KJ, Dowdall J, Grannell M, et al: Tibial spine fractures: An analysis of outcome in surgically treated type III injuries. Injury 1999;30:289-292.
Owens BD, Crane GK, Plante T, et al: Treatment of type III tibial intercondylar eminence fractures in skeletally immature athletes. Am J Orthop 2003;32:103-105.
Vocke AK, Vocke AR: Cartilaginous avulsion fracture of the tibial spine. Orthopedics 2002;25:1293-1294.
Question 17
Internal impingement is characterized by which of the following anatomic lesions? Review Topic
Explanation
Question 18
Which of the following findings is likely to be pathologic in a thin, well-conditioned endurance athlete?
Explanation
REFERENCES: Pelliccia A, Maron BJ, Culasso F, DiPaolo FM, et al: Clinical significance of abnormal electrocardiographic patterns in trained athletes. Circulation 2000;102:278-284.
Maron BJ, Thompson PD, Puffer JC, McGrew CA: Cardiovascular preparticipation screening of competitive athletes: A statement for health professionals from the Sudden Death Committee (Clinical Cardiology) and Congenital Cardiac Defects Committee (Cardiovascular Disease in the Young), American Heart Association. Circulation 1996;94:850-856.
Question 19
What is the most common bacteria cultured from dog and cat bites to the upper extremity?
Explanation
REFERENCE: Talan DA, Citron DM, Abrahamian FM, et al: Bacteriologic analysis of infected dog and cat bites. Emergency Medicine Animal Bite Infection Study Group. N Engl J Med 1999;340:85-92.
Question 20
An 11-year-old boy reports the acute onset of elbow pain and swelling after pushing his brother. The patient's mother and a younger sibling have experienced numerous fractures. You note that the patient and his mother have blue sclera and normal-appearing teeth. A radiograph of the elbow is shown in Figure 60. This patient's disorder is most likely the result of Review Topic

Explanation
Type I is subclassified into the A type (absence of dentinogenesis imperfecta) and B type (presence of dentinogenesis imperfecta). These individuals have blue sclerae, and although the initial fracture usually occurs in the preschool years, it may occur at any age. Furthermore, olecranon apophyseal fractures that occur after relatively minor trauma have been associated with type I OI. Cells from individuals with type I OI largely demonstrate a quantitative defect of type I collagen; they synthesize and secrete about half the normal amount of type I procollagen. In this patient, there are no indications that the child has been subjected to abuse. Radiographs of the elbow show no evidence of osteopetrosis (due to abnormal osteoclast function) or rickets (due to a deficiency of vitamin D). Morquio syndrome (characterized by a defect of the enzyme N-Ac-Gal-6 sulfate sulfatase) is not associated with blue sclera.
Question 21
What tendon has an intra-articular (instrasynovial) location in the knee joint?
Explanation
REFERENCES: Kimura M, Shirakura K, Hasegawa A, Kobayashi Y, Udagawa E: Anatomy and pathophysiology of the popliteal tendon area in the lateral meniscus: 1. Arthroscopic and anatomical investigation. Arthroscopy 1992;8:419-423.
Arnoczky SP, Skyhar MJ, Wickiewicz TL: Basic science of the knee, in McGinty JB (ed): Operative Arthroscopy. New York, NY, Raven Press, 1991, pp 155-182.
Question 22
4 mg/kg for 48 hours
Explanation
Question 23
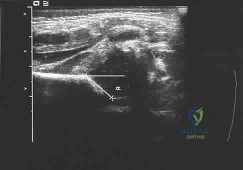
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management? Review Topic
Explanation
not reduced after 2 to 3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness.
Question 24
A 52-year-old man who was a former high school pitcher now reports loss of elbow flexion and extension with pain at the extremes of motion. Nonsurgical management has failed to provide relief. Examination reveals movement from 50 degrees to 110 degrees and is painful only at the limits of motion. A radiograph is shown in Figure 12. Treatment should consist of
Explanation
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Morrey BF: Primary degenerative arthritis of the elbow: Treatment by ulnohumeral arthroplasty. J Bone Joint Surg Br 1992;74:409-413.
Redden JF, Stanley D: Arthroscopic fenestration of the olecranon fossa in the treatment of osteoarthritis of the elbow. Arthroscopy 1993;9:14-16.
O’Driscoll SW: Elbow arthritis: Treatment options. J Am Acad Orthop Surg 1993;1:106-116.
Question 25
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has
Explanation
Question 26
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk?
Explanation
REFERENCES: Molnar GE, Gordon SU: Cerebral palsy: Predictive value of selected clinical signs for early prognostication of motor function. Arch Phys Med Rehabil 1976;57:153-158.
Wu YW, Day SM, Strauss DJ, et al: Prognosis for ambulation in cerebral palsy: A population-based study. Pediatrics 2004;114:1264-1271.
Question 27
Which of the following changes in the parameters of the gait cycle occurs in the transition from normal walking to running?
Explanation
Examination of a 5-year-old child who has fibular hemimelia reveals the foot has two rays and is stiff in equinus and valgus. The level of the foot is just proximal to the midshaft of the contralateral tibia, and the knee has full active flexion and extension, but slight valgus. Treatment should include
Amputation through the midshaft of the tibia
Correction of the foot deformity and lengthening with a ring fixator
Knee disarticulation
Ankle disarticulation
Ankle disarticulation and contralateral epiphyseodesis of the proximal tibia Answer: 4
Congenital absence of the fibula, also called fibula hemimelia, has several manifestations. These range from complete absence of the fibula with missing lateral rays of the foot (i.e. terminal longitudinal deficiency) to absence of only a portion of the fibula without foot involvement (i.e. intercalary longitudinal; deficiency). Congenital fibular deficiency usually occurs sporadically without a known cause. The child with complete absence of the fibula presents clinically with an anterolateral bow of the tibia, an equinovalgus deformity of the foot, and a tarsal coalition. The talotibial joint is usually malformed, with the fused talocalcaneus having a flat upper surface that articulates with the tibia in a valgus and equinus position. The foot may be missing one or two lateral rays. There is always significant shortening of the epsilateral femur. Treatment: There is a reasonable consensus that complete fibular hemimelia is best treated by performing an ankle disarticulation in early childhood and fitting a Syme-type prosthesis. Children with lesser (<5cm) at birth may be a candidate for lengthening procedures, but the exact indications and results of these procedures have not been well defined. Children with large discrepancies (>5cm) at birth and those with major foot deformities are better managed with amputation.
Question 28
A 38-year-old woman is polytraumatized in a motor vehicle crash. She has multiple injuries including a unilateral femur fracture. The patient is felt to be borderline and, although she is currently stable, she could potentially deteriorate quickly. Which of the following parameters has been suggested as an indicator of which patients would benefit from damage control?
Explanation
Question 29
A 51-year-old male truck driver has had progressive left hip pain for more than 2 years, and he reports that the pain has become severe in the past 9 months. He is now unable to work because of the pain. Examination reveals that range of motion of the hip is limited to 95 degrees of flexion, 0 degrees of internal rotation, and 20 degrees of external rotation. The plain radiograph, MRI scan, and intraoperative gross photographs are shown in Figures 9a through 9d. Management should consist of
Explanation
REFERENCE: Milgram JM: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801.
Question 30
Figure 1 is the clinical photograph of a 64-year-old man who crashed while riding his motorcycle. An examination reveals his long-finger metacarpophalangeal (MP) joint is stuck in extension. He cannot passively or actively flex at the MP joint. A hand radiograph is seen in Figure 2. Which interposed structure is preventing reduction?

Explanation
This patient has a dorsally dislocated MP joint. In these cases, the volar plate can be displaced dorsal to the metacarpal head, preventing reduction. Although early publications described a “noose effect” of the lumbrical and flexor tendons, the primary block to reduction is the volar plate. Simple MP dislocations can be reduced closed by flexing the wrist and then gently sliding the base of the proximal phalanx over the end of the metacarpal. Longitudinal traction on the finger will only incarcerate the volar plate further and should be avoided. Patients with complex dislocations that fail closed reduction require open
reduction.
Question 31
A 50-year-old patient underwent multiple debridements for an open radial shaft fracture with bone loss. The bed currently shows no evidence of infection but has a 14-cm diaphyseal bone defect. The most appropriate treatment includes open reduction and internal fixation along with
Explanation
A. clinical examination.
B. invasive pressure measurement.
C. arterial Doppler study.
D. MRI.
Compartment syndrome of the hand can result from a variety of factors, including a traumatic event such as crush injury, fracture, vascular insult, a high-pressure injection injury, or an insect or spider bite. The treatment involves decompressive fasciotomy of the involved compartments. The diagnosis of hand compartment syndrome is determined by history, examination, and objective testing. Patients experience pain out of proportion to the injury, along with swelling and tense skin. Pain may occur with passive motion of the metacarpophalangeal joints as the intrinsic muscles are stretched. Invasive intracompartmental pressures can be measured in the compartments of the hand but not in the fingers. Arterial Doppler studies assess arterial blood flow,
and an abnormality would be a late finding. 41
MRI would show edema of the hand and fingers, but the decision to perform surgical release is less likely made from the findings. The most appropriate method of determining the need for finger fasciotomy is the history and physical examination.
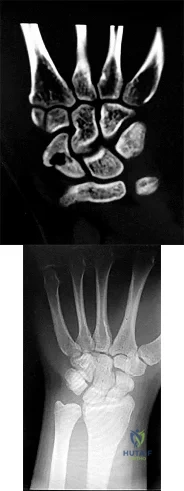
45- Figures 1 and 2 show the MRI studies of a 35-year-old manual laborer with persistent wrist pain despite immobilization. At the time of surgery, collapse of the capitate and arthritic changes of the midcarpal joint are noted. What is the most appropriate procedure for this condition?
A. Local vascularized bone graft
B. Proximal row carpectomy
C. Midcarpal fusion
D. Total wrist arthroplasty
The T1-weighted MRI reveals decreased signal that is consistent with avascular necrosis (AVN) of the capitate. Figure 2 demonstrates increased signal of the capitate consistent with edema. The etiology of AVN of the capitate may be related to trauma, abnormal interosseous vascular supply, and hypermobility. Surgical treatment is considered for patients who have had persistent symptoms despite immobilization. At the time of surgery, collapse of the capitate and arthritic changes would be treated most appropriately with a salvage procedure. A midcarpal fusion is a motion-preserving salvage procedure and is the most appropriate option given to address the pain associated with the midcarpal arthritic changes. The alternative options are not appropriate for this patient. Local vascularized bone grafts are considered for situations in which no evidence of capitate collapse or arthritis is observed.
Question 32
Figure 10 shows the radiograph of an active 75-year-old woman who reports severe leg pain after a fall. Management should consist of
Explanation
REFERENCES: Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242.
Montijo H, Ebert FR, Lennox DA: Treatment of proximal femur fractures associated with total hip arthroplasty. J Arthroplasty 1989;4:115-123.
Question 33
What is a known risk factor for lateral distal femoral locking plate failure when used for the fixation of comminuted extra-articular fractures?
Explanation
Implant failure is common in distal femur fractures stabilized with plate fixation. Contributors to failure include a short working length of the construct, plate-screw density more than 0.5 and short plate lengths. This will lead to failure as it causes increased strain on the plate over a short segment, and
does not allow enough motion at the fracture site to form bone for healing by secondary intention.
Ricci et al. reviewed 355 cases of distal femur plate fixation. 64 patients (19%) required reoperation to promote union, including 30 that had a planned staged bone grafting. Risk factors for proximal implant failure included open fracture, smoking, increased body mass index, and shorter plate length.
Kregor et al. reviewed 119 patients with distal femoral plate fixation. They found that 93% fractures healed without acute bone grafting. Complications included 5 losses of proximal fixation, 2 nonunions, and 3 acute infections.
Illustration A is an AP of the distal femur demonstrating a comminuted distal femur fracture which has failed fixation with a laterally based distal femur locking plate. It has undergone varus collapse which is a common mechanism of failure for these injuries. Illustration B is a series of AP radiographs of the distal femur of the same patient that was revised to an intramedullary retrograde nail. Illustration C and D show the concepts of plate length, plate-to-screw density and the working length of the plate.
Incorrect Answers:

OrthoCash 2020
Question 34
A 30-year-old patient has had severe left hip pain and difficulty ambulating, necessitating the use of a cane, for the past 6 months. A photomicrograph of the femoral head sectioned at the time of surgery is shown in Figure 31. What is the most likely diagnosis?
Explanation
REFERENCES: Basset LW, Mirra JM, Cracchiolo A III: Ischemic necrosis of the femoral head: Correlation between magnetic resonance imaging and histologic sections. Clin Orthop 1987;223:181-187.
Sugano N: Osteonecrosis, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopedics. St Louis, MO, Mosby, 2002, pp 878-887.
Question 35
Which of the following best describes the relationship of the anterior tibial artery and dorsalis pedis artery to the extensor hallucis longus (EHL) tendon as they progress from the level of the ankle to the dorsum of the foot?
Explanation
REFERENCES: Resch S: Functional anatomy and topography of the foot and ankle, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 1, pp 25-49.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Question 36
Which of the following properties apply to the human meniscus when compared with articular cartilage?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 3-23.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, AAOS, 1999, pp 349-354.
Question 37
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function. A pathognomonic radiographic feature of this injury is a

Explanation
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Question 38
A 79-year-old woman with a massive rotator cuff tear presents to the emergency department with pain and difficulty moving her arm 7 weeks after undergoing reverse TSA for a displaced 4-part proximal humerus fracture.
Explanation
The complication rate is high after surgical treatment of proximal humerus fractures, particularly in elderly patients with osteoporotic bone. In patients treated with ORIF, common complications include varus malunion (16%), avascular necrosis (10%), screw penetration (8%), and infection (4%). In cases involving a dislocation of the humeral head, avascular necrosis is more common. In patients treated with hemiarthroplasty or TSA, complications include component loosening, infection, and dislocation. TSA is associated with
glenoid loosening in patients with rotator cuff incompetence and should be avoided in these patients. Reverse TSA is a potential solution for this population. Dislocation and postoperative infection are potential complications after reverse TSA.
RECOMMENDED READINGS
Krappinger D, Bizzotto N, Riedmann S, Kammerlander C, Hengg C, Kralinger FS. Predicting failure after surgical fixation of proximal humerus fractures. Injury. 2011 Nov;42(11):1283-
Question 39
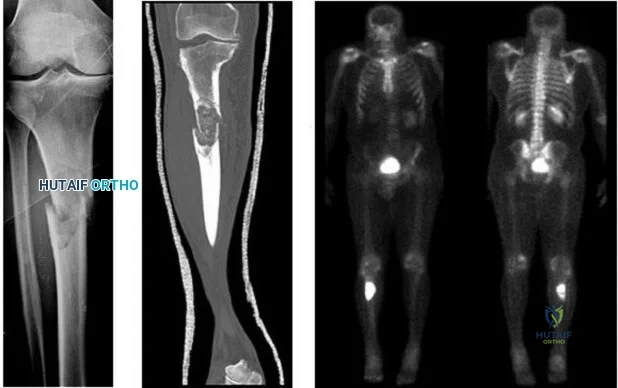
..Figures 107a through 107c are the radiograph, CT, and bone scan of a 68-year-old man. While walking, he collapsed and was unable to ambulate because of pain and deformity in his right leg. What is the most appropriate next step?
Explanation
Glomus tumor
Diffuse pigmented villonodular synovitis (PVNS)
Extra-abdominal fibromatosis
Schwannoma
Hemangioma
Please match the characteristics below to the condition listed above.
Question 40
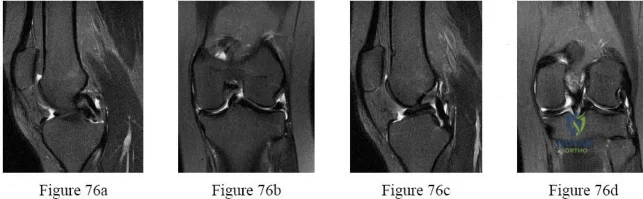
-What do the T2-weighted, fat-saturated MRI scans shown in Figures 76a through 76d reveal?
Explanation
Question 41
A 50-year-old man reports left shoulder pain and weakness after undergoing a lymph node biopsy in his neck 2 years ago. Examination reveals winging of the left scapula. Electromyography shows denervation of the trapezius. Surgical treatment for this condition involves Review Topic
Explanation
Question 42
The World Health Organization (WHO) developed specific criteria for osteoporosis in 1994 based on the T-score obtained by dual-energy absorptiometry (DEXA). The T-score represents the number of standard deviations that the individual's bone mineral density differs from the normal peak bone mass in young adults. Osteoporosis is defined as a T-score of 1 +2.5 or below. 2 -1.0 to -2.0.
Explanation
Question 43
A previously healthy 65-year-old woman has a closed fracture of the right clavicle after falling down the basement stairs. Examination reveals good capillary refill in the digits of her right hand. Radial and ulnar pulses are 1+ at the right wrist compared with 2+ on the opposite side. In the arteriogram shown in Figure 36, the arrow is pointing at which of the following arteries?
Explanation
REFERENCE: Radke HM: Arterial circulation of the upper extremity, in Strandness DE Jr (ed): Collateral Circulation in Clinical Surgery. Philadelphia, PA, WB Saunders, 1969, pp 294-307.
Question 44
In addition to radiographs of the primary lesion and chest, MRI of the primary lesion, and CT of the chest, staging studies for Ewing’s sarcoma should include which of the following?
Explanation
REFERENCES: Schleiermacher G, Peter M, Oberlin O, Philip T, Rubie H, Mechinaud F, et al: Increased risk of systemic relapses associated with bone marrow micrometastasis and circulating tumor cells in localized ewing tumor. J Clin Oncol 2003;21:85-91.
Daldrup-Link HE, Franzius C, Link TM, Laukamp D, Sciuk J, Jurgens H, et al: Whole-body MR imaging for detection of bone metastases in children and young adults: Comparison with skeletal scintigraphy and FDG PET. Am J Roentgenol 2001;177:229-236.
Question 45
A 22-year-old woman has had progressive upper extremity weakness for the past several years. History reveals no pain in her neck or shoulders. Examination reveals scapular winging of both shoulders and weakness in external rotation. She can abduct to only 120 degrees bilaterally, and there is mild supraspinatus weakness. She is otherwise neurologically intact with normal sensation and reflexes; however, she has difficulty whistling. A clinical photograph is shown in Figure 14. What is the most likely diagnosis?
Explanation
REFERENCES: Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Bunch WH, Siegel IM: Scapulothoracic arthrodesis in fascioscapulohumeral muscular dystrophy: Review of seventeen procedures with three to twenty-one-year follow-up. J Bone Joint Surg Am 1993;75:372-376.
Question 46
A 21-year-old man with neurofibromatosis and multiple cutaneous neurofibromas has a rapidly enlarging painless mass on his buttock. Examination reveals a nontender, well-defined 6- x 6-cm soft-tissue mass that is deep to the fascia. The best course of action should be to order
Explanation
REFERENCES: Demas BE, Heelan RT, Lane J, Marcove R, Hajdu S, Brennan MF: Soft-tissue sarcomas of the extremities: Comparison of MR and CT in determining the extent of disease. Am J Roentgenol 1988;150:615-620.
Kransdorf MJ, Jelinek JS, Moser RP Jr, et al: Soft-tissue masses: Diagnosis using MR imaging. Am J Roentgenol 1989;153:541-547.
Question 47
Figures 1 and 2 are the radiographs of a 17-year-old man who injured his wrist 6 months ago. He is experiencing pain and limited motion. What is the most effective treatment option?
Explanation
Figures 1 and 2 show a scaphoid nonunion with substantial bone resorption at the nonunion site. Cast immobilization and bracing with bone stimulator use would not be successful treatments at this point because the fracture is 6 months old and there is considerable bone resorption at the fracture site. Scaphoid excision with intercarpal fusion is an option to use only after bone-grafting procedures have failed or arthritis is present. Bone-grafting procedures using both vascularized and nonvascularized graft sources are associated with a high success rate that decreases with avascular necrosis of the proximal pole. If left untreated, scaphoid nonunions can progress to carpal collapse and degenerative arthritis.
Question 48
Varus intertrochanteric osteotomy for coxa valga commonly produces which of the following results?
Explanation
REFERENCE: Millis MB, Murphy SB, Poss R : Osteotomies about the hip for the prevention and treatment of osteoarthrosis. Instr Course Lect 1996;45:209-226.
Question 49
Botulinum toxin is used to treat vasospastic disorders of the hand such as the Raynaud phenomenon to improve digital perfusion and reduce pain. Botulinum toxin enables which transmitter to be unopposed, resulting in vasodilation?
Explanation
Nitric oxide is the only transmitter listed that is not inhibited by botulinum toxin. Substance P and glutamate are inhibited by botulinum toxin from release by pain nociceptors, thus reducing pain. Fonseca and associates have postulated that botulinum toxin inhibits the RhoA kinase pathway by blocking reactive oxygen species, which in turn does not allow actin/myosin to activate, thus preventing vasoconstriction of smooth muscle. Blocking the RhoA kinase pathway allows the action of nitric oxide to be unopposed, causing vasodilation. Nitric oxide is a potent vasodilator. Thus, botulinum toxin promotes nitric oxide activity to increase vasodilation.
Question 50
A 2-day-old infant has the hyperextended knee deformity shown in Figure 7. No other deformities are found on examination. A radiograph shows that the ossified portion of the proximal tibia is slightly anterior to that of the distal femur. Management should consist of
Explanation
REFERENCES: Ko JY, Shih CH, Wenger DR: Congenital dislocation of the knee. J Pediatr Orthop 1999;19:252-259.
Johnson E, Audell R, Oppenheim WL: Congenital dislocation of the knee. J Pediatr Orthop 1987;7:194-200.
Roy DR, Crawford AH: Percutaneous quadriceps recession: A technique for management of congenital hyperextension deformities of the knee in the neonate. J Pediatr Orthop
1989;9:717-719.
Question 51
Figure 45 shows the radiograph of a 2-year-old patient who has progressive lumbar scoliosis as the result of hemivertebra. Examination reveals no associated cutaneous lesions, and an MRI scan shows no associated intraspinal anomalies. Treatment should consist of
Explanation
REFERENCE: Callahan BC, Georgopoulos G, Eilert RE: Hemivertebral excision for congenital scoliosis. J Pediatr Orthop 1997;17:96-99.
Question 52
Figures 71a and 71b/ are the MR images of a 65-year-old man who dislocated his shoulder. What is his most likely chief symptom?
Explanation
This patient has a massive rotator cuff tear resulting in disruption of the transverse force couple between the subscapularis anteriorly and the infraspinatus and teres minor posteriorly. These muscles provide dynamic shoulder stability throughout active elevation. Loss of the force couple produces a pathologic increase in translation of the humeral head and decreased active abduction and external rotation, which results in difficulty raising an arm. The most common neurologic deficit after shoulder dislocation is isolated injury to the axillary nerve that supplies sensation to the lateral aspect of the shoulder, not the anterior aspect. Recurrent instability is uncommon unless there is a labral tear or massive subscapularis tear. The biceps muscle is not viewed in the MR images, and a complete proximal biceps tendon rupture would be uncommon in the setting of an anterior shoulder dislocation.

CLINICAL SITUATION FOR QUESTIONS 72 THROUGH 75
Figures 72a through 72e are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0 degrees
to 90 degrees and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted.
Question 53
When performing a posterior cruciate ligament reconstruction with a tibial inlay-type approach, what is the approximate anatomic distance of the popliteal artery from the screws used for fixation of the bone block?
Explanation
(range, 18.1 mm to 31.7 mm). Other approaches, such as the transtibial tunnel technique which involves drilling an anterior-posterior tunnel, have also been studied in cadavers. Matava and associates noted that increasing flexion reduces but does not completely eliminate the risk of arterial injury during arthroscopic posterior cruciate ligament reconstruction. However, this study did not use the small, medial utility incision recommended by Fanelli and associates, which creates an interval for the surgeon’s finger between the medial gastrocnemius and the posteromedial capsule so that any migration of the guidepin can be palpated and changed prior to any injury to the posterior neurovascular bundle.
REFERENCES: Matava MJ, Sethi NS, Totty WG: Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: Implications for posterior cruciate ligament reconstruction. Arthroscopy 2000;16:796-804.
Miller MD, Kline AJ, Gonzales J, et al: Vascular risk associated with posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. J Knee Surg 2002;15:137-140.
Johnson DH, Fanelli GC, Miller MD: PCL 2002: Indications, double-bundle versus inlay technique and revision surgery. Arthroscopy 2002;18:40-52.
Question 54
An otherwise healthy 70-year-old man has back and bilateral leg pain in an L5 distribution that is aggravated by standing more than 10 minutes or walking more than 100 feet. He has to sit to get relief. Neurologic and pulse examinations are normal. A radiograph and MRI scan are shown in Figures 4a and 4b. Treatment should consist of
Explanation
REFERENCES: Fischgrund JS, Mackay M, Herkowitz HN, et al: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-2812.
Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-808.
Question 55
- Which of the following conditions associated with a closed fracture of the clavicle indicates the need for open reduction and internal fixation?
Explanation
Question 56
Figure 30a is the anteroposterior radiograph of a 20-year-old woman with mild right groin pain and intermittent “catching” in the hip region. What is the most appropriate next step? tear
Explanation
Because this patient is young, substantial bilateral acetabular dysplasia is present, and the joint space is well preserved, periacetabular osteotomy is the treatment of choice (Figure 30b). Arthroscopic evaluation and treatment is insufficient to address the mechanical deformity. Although a hip injection can be diagnostically helpful, it would not alter the treatment plan in this scenario. The patient’s young age would make observation and subsequent THA less desirable. Femoral osteotomies also were performed to address rotational deformity.

Question 57
When performing the exposure for an anterior approach to the cervical spine, the surgical dissection should not enter the plane between the trachea and the esophagus and excessive retraction should be avoided to prevent injury to the
Explanation
REFERENCES: Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Patel CK, Fischgrund JS: Complications of anterior cervical spine surgery. Instr Course Lect 2003;52:465-469.
Question 58
A 14-year-old girl reports a 3-week history of anterior thigh pain and a palpable mass after sustaining a soccer-related injury. Examination reveals a tender, firm mass in the midportion of the rectus femoris. MRI scans are shown in Figures 39a through 39c. What is the most appropriate management?
Explanation
REFERENCES: Hughes C IV, Hasselman CT, Best TM, et al: Incomplete, intrasubstance strain injuries of the rectus femoris muscle. Am J Sports Med 1995;23:500-506.
Temple HT, Kuklo TR, Sweet DE, et al: Rectus femoris muscle tear appearing as a pseudotumor. Am J Sports Med 1998;26:544-548.
Question 59
What pharmacologic agents are preferred for the treatment of symptomatic active Paget’s disease?
Explanation
REFERENCE: Delman PD, Meunier PJ: The management of Paget’s disease. N Eng J Med 1997;336:558-566.
Question 60
Which of the following physical examination findings is most likely present in the condition producing the MRI findings shown in Figure 92?
Explanation
REFERENCES: Vellet AP, Marks PH, Fowler PJ, et al: Occult posttraumatic osteochondral lesions of the knee: Prevalence, classification, and short-term sequelae evaluated with MR imaging. Radiology 1991;178:271-276.
Cone R: Imaging sports-related injuries of the knee, in DeLee J, Drez D, Miller M (eds): DeLee & Drez’s Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 2, pp 1595-1652.
Question 61
A 7-year-old patient has had a painless limp for several months. Examination reveals pain and spasm with internal rotation, and abduction is limited to 10° on the involved side. Management consists of 1 week of bed rest and traction, followed by an arthrogram. A maximum abduction/internal rotation view is shown in Figure 40a, and abduction and adduction views are shown in Figures 40b and 40c. The studies are most consistent with
Explanation
REFERENCE: Reinker KA: Early diagnosis and treatment of hinge abduction in Legg-Perthes disease. J Pediatr Orthop 1996;16:3-9.
Question 62
A 77-year-old man with a history of mild renal insufficiency and atrial fibrillation on warfarin therapy is scheduled to undergo a left total hip arthroplasty. He previously underwent a right total hip arthroplasty with development of significant heterotopic bone that resulted in limitation of motion. What is the most appropriate form of prophylactic treatment to minimize the formation of heterotopic bone on his left hip?
Explanation
REFERENCES: Kolbl O, Knelles D, Barthel T, et al: Preoperative irradiation versus the use of nonsteroidal anti-inflammatory drugs for prevention of heterotopic ossification following total hip replacement: The results of a randomized trial. Int J Radiat Oncol Biol Phys 1998;42:397-401.
Pakos EE, Ioannidis JP: Radiotherapy vs nonsteroidal anti-inflammatory drugs for the prevention of heterotopic ossification after major hip surgery: A meta-analysis of randomized trials. Int J Radiat Oncol Biol Phys 2004;60:888-895.
Seegenschmiedt MH, Makoski HB, Micke O, et al: Radiation prophylaxis for heterotopic ossification about the hip joint: A multicenter study. Int J Radiat Oncol Biol Phys 2001 ;51:756-765.
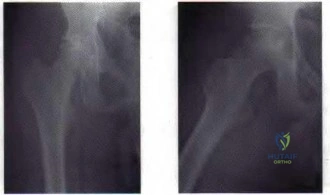
Figure 23 a Figure 23b
Question 63
Figure 1 is the radiograph of an 18-year-old, right hand-dominant man who has right side thumb pain after a tackle during a rugby game. Examination shows ecchymosis and swelling of the right thumb along with tenderness to palpation about the thumb CMC joint and metacarpal base. What ligament is holding the small fracture fragment in anatomical location to the trapezium?

Explanation
Bennett fractures are defined as intra-articular thumb metacarpal base fractures. The fracture is often caused by axial loading, and concomitant injuries to the thumb MCP joint and trapezium are common. The palmar ulnar aspect of the base of the metacarpal stays in place through its attachment to the trapezium by way of the anterior oblique ligament. The metacarpal shaft is displaced dorsally, proximally, and radially by the pull of the abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, and adductor pollicis brevis. These fractures are often considered unstable and are treated surgically.
Question 64
Figure 42 shows the radiograph of a patient with spinal muscular atrophy. Examination reveals good upper extremity function, and she can tie her shoes and propel a manual wheelchair. Posterior instrumentation and fusion may result in
Explanation
REFERENCES: Bentley G, Haddad F, Bull TM, Seingry D: The treatment of scoliosis in muscular dystrophy using modified Luque and Harrington-Luque instrumentation. J Bone Joint Surg Br 2001;83:22-28.
Furumasu J, Swank SM, Brown JC, Gilgoff I, Warath S, Zeller J: Functional activities in spinal muscular atrophy patients after spinal fusion. Spine 1989;14:771-775.
Granata C, Cervellati S, Ballestrazzi A, Corbascio M, Merlini L: Spine surgery in spinal muscular atrophy: Long-term results. Neuromuscul Disord 1993;3:207-215.
Question 65
Disadvantages of anterior-inferior plate fixation for acute clavicular fractures relative to superior plating include
Explanation
Question 66
A 41-year-old man is involved in a high-speed motor vehicle crash and sustains a closed femoral midshaft fracture and a unilateral pulmonary contusion with a hemothorax, requiring placement of a chest tube. He has an initial blood pressure of 90/50 mm Hg. After receiving two liters of crystalloid, he has a blood pressure of 115/70 mm Hg and a heart rate of 90 bpm. He has normal mentation and does not require ventilator support. An arterial blood gas reveals that his delta base is
Explanation
Question 67
- An 8-year-old girl has a supracondylar fracture of the distal humerus. Her neurovascular status is intact. Radiographs show hyperextension of 10 degrees of the distal fragment and an angle between the humeral shaft and capitellar physis (Baumann’s angle) of 88 degrees. Management should consist of
Explanation
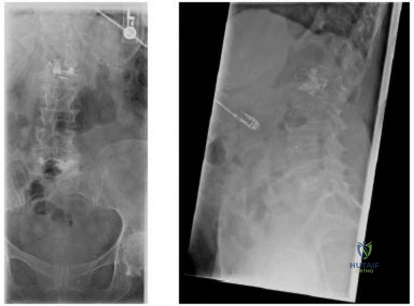
Question 68
A 78-year-old woman undergoes her third lumbar decompression and fusion from L3 to L5 without complication. On the morning of postoperative day 3, examination reveals painless, flaccid weakness of both lower extremities. She also has an absent bulbocavernous reflex and a mild saddle paresthesia. MRI scans of the lumbar spine are shown in Figures 26a and 26b. What is the most appropriate management at this time?
Explanation
REFERENCES: Yi S, Yoon do H, Kim KN, et al: Postoperative spinal epidural hematoma: Risk factor and clinical outcome. Yonsei Med J 2006;47:326-332.
Uribe J, Moza K, Jimenez O, et al: Delayed postoperative spinal epidural hematomas. Spine J 2003;3:125-129.
Question 69
The most appropriate treatment for this fracture is
Explanation
Tibial fractures are classified on the basis of their anatomical location and the status of the prosthesis fixation. Type I fractures involve the tibial plateau, type II fractures occur adjacent to the stem of the tibial component, type III fractures are distal to the tibial stem, and type IV fractures involve the tibial tubercle. Subclassifications include A with a well-fixed implant; B with a loose implant; and C, which occur intraoperatively.
Treatment of periprosthetic tibial fractures is based on the location of the fracture and the status of the component fixation. Types II or III fractures associated with prosthetic loosening or instability are best managed with revision arthroplasty, usually with a diaphyseal-engaging intramedullary tibial stem. Supplemental internal fixation may be necessary. Type III fractures with well-fixed and stable implants are treated using the standard principles of tibial fracture management.
Question 70
A 56-year-old man who tripped and fell out of his golf cart onto his right shoulder 4 days ago now reports mild pain while chipping. Examination reveals mild bruising over the lateral clavicle but good shoulder range of motion and strength. A radiograph is shown in Figure 9. Appropriate treatment at this time should include which of the following?

Explanation
Question 71
Which of the following statements is most accurate regarding undetected intraoperative surgical glove perforation?
Explanation
REFERENCES: Al-Habdan I, Sadat-Ali M: Glove perforation in pediatric orthopaedic practice. J Pediatr Orthop 2003;23:791-793.
Sadat-Ali M, Al-Othman A: Glove perforations in orthopaedic practice. Saudi Med J 1996;17:811-813.
Question 72
When comparing the overall outcomes of surgical versus nonsurgical treatment of stable thoracolumbar burst fractures in patients without neurologic injury, 5 years following injury, the principle differences lie in Review Topic
Explanation
Question 73
One of the serious potential complications of repair of distal biceps tendon ruptures is limited pronation and supination as a result of synostosis. What surgical approach and technique presents the highest risk for development of this complication?
Explanation
REFERENCE: Norris TR: Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, p 342.
Question 74
A 56-year-old woman underwent a total knee arthroplasty 2 years ago and now has pain and swelling. Radiographs of her knee are unremarkable. Her C-reactive protein (CRP) level is 3.0 (reference range [rr], 0.08–3.1 mg/L), and her erythrocyte sedimentation rate (ESR) is 18 mm/h (rr, 0-20 mm/h). Aspiration of the knee reveals a white blood cell (WBC) count of 1200/mm3 with a differential of 30% neutrophils and 70% monocytes. Cultures will not be available for several days, and the patient has not been taking antibiotics. Based on these findings, the most appropriate next step is
Explanation
ESR and CRP level are recommended as starting points in the workup for the diagnosis or exclusion of periprosthetic joint infection (PJI). When both the ESR and CRP findings are within defined limits, PJI is unlikely. When both test findings are positive, PJI must be considered and further investigation is warranted. Clinicians need to be aware of other inflammatory conditions such as rheumatoid arthritis that can lead to elevation of inflammatory markers.
A high likelihood of infection is noted when the knee aspirate contains more than 2500 WBCs per high-powered field (HPF) with a differential count exceeding 60% neutrophils. Using these criteria, Mason demonstrated a sensitivity of 98% and a specificity of 95% for infection diagnosis.
For this patient, the inflammatory markers are within normal limits. The aspiration result is below 2500 WBC/HPF with a low percentage of neutrophils. The likelihood of infection is remote, and further nonsurgical treatment should not include antibiotics. There is no indication for surgery based upon the information presented.

Question 75
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm P 3 P , an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
REFERENCES: Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Kocher MS, Zurakowski D, Kasser JR: Differentiating between septic arthritis and transient synovitis of the hip in children: An evidence-based clinical prediction algorithm. J Bone Joint Surg Am 1999;81:1662-1670.
Question 76
A 21-year-old woman is struck by a car and sustains a Gustillo IIIB fracture of the tibia. The wound was debrided and immobilized with an external fixator. Radiographs are shown in Figure A. The soft tissue defect was covered with a free flap. Her recovery was complicated by wound infection with Klebsiella pneumoniae and Escherichia coli. One month after her injury, she underwent intramedullary nailing and placement of an antibiotic spacer measuring 15cm in length. Radiographs are shown in Figure B. At the next stage of surgery 6 weeks later, the surgeon should plan to do all of the following:

Explanation
The Masquelet staged technique of induced membranes is an option for filling large bone defects up to 25cm in length. This technique protects against autograft resorption, stimulates mesenchymal cell-to-osteoblast differentiation, maintains graft position, and prevents soft tissue interposition. Cement impregnation achieves high local antibiotic concentration without risk of systemic toxicity.
Ashman et al. discussed the techniques of addressing bone defects. Options include:
(1) acute limb shortening (up to 4cm in the tibia and humerus, and 7cm in the femur);
(2) distraction osteogenesis for defects up to 10cm long (at 1mm/day with consolidation period of 5days per mm, or total treatment time of up to 60days/cm), (3) autograft (up to 25cm of vascularized fibula, or 3cm of nonvascularized iliac crest),
and (4) Masquelet technique.
Taylor et al. reviewed the induced membranes technique. They found that the membrane is well vascularized and composed of type I collagen with fibroblasts with an inner epithelial cell layer. There is a high concentration of VEGF, RUNX2 (CBFA1), TGFß1, and BMP2. The membrane is sutured over bone graft to create a closed pouch. When a nail is present, they note a second internal membrane around the nail, potentially increasing local vascularity and osteoinductive factor concentration.
Figure A shows a Gustillo IIIB tibia fracture with a large bone defect held in a temporizing external fixator. Figure B shows the same defect following intramedullary nailing and with a cement spacer placed circumferentially around the nail in the defect.
Incorrect Answers
Question 77
What significant structure is most at risk during a posterior approach of the Achilles tendon near its musculotendinous junction?
Explanation
REFERENCES: Webb J, Moorjani N, Radford M: Anatomy of the sural nerve and its relation to the Achilles tendon. Foot Ankle Int 2000;21:475-477.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Question 78
Figures A and B are post-operative radiographs of a 54-year-old female. In the first 6 months after this procedure, what is the most likely factor for functional impairment in this patient?
Explanation
Anterior knee pain is reported to be a common symptom following treatment of patellar fractures. A likely contributing factor to the anterior knee pain is scarring and tightness of the structures surrounding the knee, as well as patella maltracking due to quadricep/hamstring weakness and/or poor muscle synchrony. Other factors for anterior knee pain may include symptomatic hardware, which may be treated with removal of fixation after union has been achieved.
Lazaro et al. looked at the outcome data on thirty patients with isolated unilateral patellar fractures. Anterior knee pain during activities of daily living was experienced by twenty-four (80%) of the patients. The knee extensor mechanism on the injured side had deficits in strength (-41%), power (-47%), and endurance (-34%) as compared with the uninjured side.
Lebrun et al. reviewed a series of 40 operatively treated patella fractures and found that at over 6 years postoperatively, significant symptomatic complaints and functional deficits persisted based on validated outcome measures as well as objective physical evaluations. Removal of symptomatic fixation was required in 52% of the patients treated with osteosynthesis, whereas 38% of those with retained fixation self-reported implant-related pain at least some of the time.
Figure A and B show AP and lateral radiographs of a comminuted patella fracture treated with a tension band repair construct. The articular surface looks well reduced.
Incorrect Answers:
Question 79
A 25-year-old man is unresponsive at the scene of a high-speed motor vehicle accident and remains obtunded. Initial evaluation in the emergency department reveals a left-sided femoral shaft fracture and a right-sided humeral shaft fracture. The cervical spine remains immobilized in a semi-rigid cervical collar, and the initial AP and lateral radiographs obtained in the emergency department are unremarkable. What is the most appropriate management at this time? Review Topic
Explanation
Question 80
A patient falls off a roof and sustains the fracture shown in Figure 29. What is the most likely complication that results from injury to the structure that is located at the arrow?

Explanation
Question 81
-Figures a and b are the anteroposterior and lateral plain radiographs of a 45-year-old woman who had severe bilateral leg pain for 6 months. Figures 5c and 5d are her sagittal and axial T2-weighted MRI scans. After attempting nonsurgical treatment including physical therapy and epidural injections, she continued to experience persistent pain. What is the most appropriate treatment?

Explanation

Question 82
- A 30-year-old man underwent replantation of his dominant thumb at the metacarpophalangeal joint level 2 days ago. Since replantation, the temperature of the thumb has been between 87.8 F (31 C) and 93.2 F (34 C). The temperature is now 82.4 F (28 C), and there is brisk capillary refill and venous engorgement. Management at this time should include
Explanation
Question 83
The patient develops an inability to dorsiflex her foot 2 days after surgical intervention while she is sitting in a chair after physical therapy. Initial treatment should consist of
Explanation
Gamma irradiation produces free radicals. Although these free radicals can form cross-links with other polyethylene chains, the free radicals can also form a bond with oxygen, resulting in early oxidation. Gamma irradiation in air produces the highest risk for oxidized polyethylene, resulting in the highest risk for wear, delamination, and subsequent osteolysis.
This patient demonstrates severe periarticular osteolysis. When she is asymptomatic, this suggests the acetabular and femoral components remain well fixed to the bone. Consequently, she can be treated by removing the wear generator (polyethylene exchange), along with bone grafting of the osteolytic defect. Considering the extensive amount of osteolysis, observation for 1 year would not be appropriate.
The psoas is the anatomic structure that runs anterior to the acetabulum. The femoral neurovascular structures are at risk if the retractor is placed anterior and inferior to the psoas tendon.
The patient develops a foot drop 2 days after surgery. As a result, it can be assumed that the nerve was not injured directly during the surgical procedure. Although MR imaging or a CT scan may be indicated to identify an evolving hematoma, the immediate concern is to minimize pressure on the sciatic nerve. Tension on the nerve can be decreased by flexing the surgical knee and positioning the bed flat.
Question 84
A football player sustains a traumatic anterior inferior dislocation of the shoulder in the last game of the season. It is reduced 20 minutes later in the locker room. The patient is neurologically intact and has regained motion. If the patient undergoes arthroscopic evaluation, what finding is seen most consistently?
Explanation
REFERENCES: Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.
Bottoni CR, Wilckens JH, DeBerardino TM, et al: A prospective, randomized evaluation of arthroscopic stabilization versus nonoperative treatment in patients with acute, traumatic,
first-time shoulder dislocations. Am J Sports Med 2002;30:576-580.
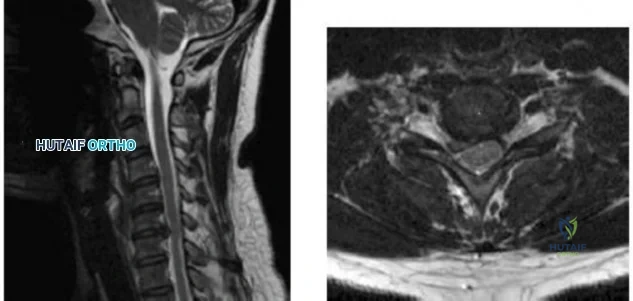
Question 85
-Figures a and b are the MRI scans of the cervical spine without contrast of a 38-year-old man with neck pain radiating into the right upper extremity for the past 4 weeks. He denies numbness or weakness.Examination was significant for reproduction of pain going down the right arm with neck extension and right lateral rotation. What is the next treatment step?
Explanation
Question 86
04 Which of the following laboratory studies is predictive of wound healing prior to performing a lower extremity amputation?
Explanation
(eliminates false positive predictions with using area under the Doppler waveform). Pressures less than 20 mm Hg are predictive of poor healing. Miller 505-6
back to this question next question
Question 87
Figure 44 shows the radiograph of an 11-year-old girl who has hip pain. Further diagnostic workup should include
Explanation
REFERENCES: Steel HH: Protrusio acetabuli: Its occurrence in the completely expressed Marfan syndrome and its musculoskeletal component and a procedure to arrest the course of protrusion in the growing pelvis. J Pediatr Orthop 1996;16:704-718.
Wenger DR, Ditkoff TJ, Herring JA, Mauldin DM: Protrusio acetabuli in Marfan’s syndrome. Clin Orthop 1980;147:134-138.
Question 88
Figure 35 shows the AP radiograph of a patient who underwent a previous upper tibial osteotomy (UTO). The patient may be at risk for which of the following during total knee arthroplasty (TKA)?
Explanation
REFERENCES: Parvizi J, Hanssen AD, Spangehl MJ: Total knee arthroplasty following proximal tibial osteotomy: Risk factors for failure. J Bone Joint Surg Am 2004;86:474-479.
Meding JB, Keating EM, Ritter MA, et al: Total knee arthroplasty after high tibial osteotomy: A comparison study in patients who had bilateral total knee replacement. J Bone Joint Surg Am 2000;82:1252-1259.
Question 89
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?
Explanation
REFERENCES: Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
McCarty DJ, Halverson PB, Carrera GF, Brewer BJ, Kozin F: Milwaukee shoulder: Association of microspheroids containing hydroxyapatite crystals, active collagenase, and neutral protease with rotator cuff defects. I: Clinical aspects. Arthritis Rheum 1981;24:464-473.
Question 90
- What is the primary immediate source of energy for muscle?
Explanation
Almost 90% of the total ATP formed by glucose metabolism is formed during oxidative phosphorylation. This is accomplished by a series of enzymatically catalyzed reactions in the mitochondria. When the body’s stores of carbohydrates decrease below normal, glucose can be formed from the breakdown of protein and fat via gluconeogenesis to yield more ATP.
Question 91
Resuscitation of a trauma patient who has been in hypovolemic shock is complete when which of the following has occurred?
Explanation
REFERENCES: Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: End point of resuscitation. J Trauma 2004;57:898-912.
Moore FA, McKinley BA, Moore EE, et al: Inflammation and the Host Response to Injury, a large-scale collaborative project: Patient-oriented research core--standard operating procedures for clinical care. III. Guidelines for shock resuscitation. J Trauma 2006;61:82-89.
Englehart MS, Schreiber MA: Measurement of acid-base resuscitation end points: Lactate, base deficit, bicarbonate or what? Curr Opin Crit Care 2006;12:569-574.
Question 92
What is the most common surgical cause of the foot deformity shown in Figure 9?
Explanation
REFERENCES: Donley BG: Acquired hallux varus. Foot Ankle Int 1997;18:586-592.
Myerson MS, Komenda GA: Results of hallux varus correction using an extensor brevis tenodesis. Foot Ankle Int 1996;17:21-27.
Question 93
Which of the following clinical scenarios represents an appropriate indication for convex hemiepiphysiodesis/hemiarthrodesis in the treatment of a child with a congenital spinal deformity?
Explanation
REFERENCE: Winter RB, Lonstein JE, Denis F, Sta-Ana de la Rosa H: Convex growth arrest for progressive congenital scoliosis due to hemivertebrae. J Pediatr Orthop 1988;8:633-638.
Question 94
When a Workers' Compensation patient recovers after an injury to a point that further restoration of function is no longer anticipated, he or she is said to have reached which of the following?
Explanation
Functional capacity evaluations (FCE) are based upon a theoretical model of comparing job demands to worker capabilities. The results of FCEs are often used to determine musculoskeletal capacity to return to work.
Strong et al. reported on the use of FCE in the Workers' Compensation system, and note how these FCE results are required by employers to determine the level of return to work of their employees. They also mention that the reports are frequently perceived with a negative tone. The employees reported a wider range of restrictions in their varied life roles than did the FCE reports, which deal more narrowly with work roles.
Pransky et al. reported that although FCE's are relied upon for determination of ability to perform physical work, several scientific, legal, and practical concerns persist. They note that test criteria often do not accurately reflect real-life job requirements or performance, and subjective evaluation remains common. They conclude that more research into predictive linking of FCE outcomes with occupational outcomes is necessary to determine their role in the Workers' Compensation system.
Incorrect Answers:
1: A functional capacity evaluation (FCE) is set of tests, practices and observations that are combined to determine the ability of the evaluated to function in a variety of circumstances (most often employment) in an objective manner. 3: Permanent disability is any lasting disability that results in a reduced earning capacity after maximum medical improvement is reached; this implies that MMI must be reached before this is determined. 4: Impairment rating is an objective data point obtained by a physician reviewing the patient's overall condition during a functional capacity evaluation. 5: This is the process a patient uses to tell their employer they want a personal physician to treat them for a work injury.
Question 95
A 5-month-old girl with arthrogryposis has a limb-length discrepancy. Examination and radiographs reveal unilateral hip dislocation. Management should consist of
Explanation
REFERENCES: Staheli LT, Chew DE, Elliot JS, Mosca VS: Management of hip dislocations in children with arthrogryposis. J Pediatr Orthop 1987;7:681-685.
Szoke G, Staheli LT, Jaffe K, Hall JG: Medial-approach open reduction of hip dislocation in amyoplasia-type arthrogryposis. J Pediatr Orthop 1996;16:127-130.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996.
Question 96
A 72-year-old woman who fell on her right shoulder while using a treadmill is now unable to elevate her right arm. An MRI scan is shown in Figure 7. What is the most likely diagnosis?
Explanation
REFERENCE: Gerber C, Myer DC, Schneeberger AG, et al: Effect of tendon release and delayed repair on the structure of the muscles of the rotator cuff: An experimental study in sheep. J Bone Joint Surg Am 2004;86:1973-1982.
Question 97
A 38-year-old woman with metastatic thyroid carcinoma has had increasing pain in the left hip for the past 3 months. An AP radiograph and coronal T 1 -weighted MRI scan are shown in Figures 28a and 28b. Management should consist of
Explanation
REFERENCES: Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Swanson KC, Pritchard DJ, Sim FH: Surgical treatment of metastatic disease of the femur. J Am Acad Orthop Surg 2000;8:56-65.
Clarke HD, Damron TA, Sim FH: Head and neck replacement endoprosthesis for pathologic proximal femoral lesions. Clin Orthop 1998;353:210-217.
Question 98
A 28-year-old woman fell on her right wrist while rollerblading 2 days ago. She was seen in the emergency department at the time of injury and was told she had a sprain. Examination now reveals dorsal tenderness in the proximal wrist but no snuffbox or ulnar tenderness. Standard wrist radiographs are normal. What is the next most appropriate step in management?
Explanation
REFERENCES: Walsh JJ, Berger RA, Cooney WP: Current status of scapholunate interosseous ligament injuries. J Am Acad Orthop Surg 2002;10:32-42.
Browner BD, Levine AM, Jupiter JB, et al (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1366-1367.
Question 99
- A 15-year-old girl has a thoracic kyphosis that causes mild pain. Examination reveals a sagittal curve measuring 55 degrees and wedging of the eighth through tenth vertebrae. The iliac apophyses are Risser 4. Management should include
Explanation
(2) with surgical fusion if >75o and Risser 3 or less, (3) with surgical fusion if >65o and Risser 4/5 if necessary or symptomatic. Posterior instrumentation, anterior release and interbody fusion is the treatment of choice for curves >75o, or those >55o on hyperextension. Other causes of kyphosis include trauma, infection, spondylitis, bone dysplasia, neoplasia, neurofibromatosis.
Question 100
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads? Review Topic
Explanation
